
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 12/153/26. The contractual start date was in May 2014. The final report began editorial review in May 2016 and was accepted for publication in September 2016. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2017. This work was produced by Lohan et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Research aims and objectives
Introduction
This chapter details the aims and objectives of the research study, ethics approval, study relevant documents, Steering Group arrangements, stakeholder representation and public and patient involvement (PPI) in the research.
Aims and objectives
Primary aim
The aim of the study was to determine the value and feasibility of conducting an effectiveness trial of the If I Were Jack Relationship and Sexuality Education (RSE) intervention in post-primary schools.
Secondary objectives
The research aimed to achieve the following secondary objectives:
-
assess the acceptability of the intervention to schools (school principals and RSE teachers), male and female pupils and parents
-
identify optimal delivery structures and systems for the delivery of the resource in the classroom
-
establish participation rates and reach including equality of engagement across schools of different socioeconomic and religious types
-
assess trial recruitment and retention rates
-
assess variation in normal RSE practice across the participating schools
-
refine survey instruments as a result of cognitive interviews with male and female pupils
-
assess differences in outcomes for male and female pupils
-
identify potential effect sizes that might be detected in an effectiveness trial and estimate appropriate sample size for that trial
-
identify the costs of delivering If I Were Jack and pilot methods for assessing cost-effectiveness in a future trial.
Ethics approval
Ethics approval for the study was granted by the Research Ethics Committee of the School of Nursing and Midwifery, Queen’s University Belfast (QUB) (reference 04.02.02.V2).
Study protocol, participant letters of invitation, information leaflets, consent forms and data collection instruments
For the protocol (version 2), see or http://dx.doi.org/10.1016/j.ijer.2014.08.003.
For participant letters of invitation, information leaflets and consent forms, see Appendix 1.
For data collection instruments, see Appendix 2.
Protocol amendments
National Institute for Health Research (NIHR) Protocol version two changes (20 April 2015) included the following:
-
Updated version number.
-
Updated date of version.
-
Changed Clinicaltrials.gov registration number (NCT02092480) to an International Standard Randomised Controlled Trial Number (ISRCTN99459996).
-
Changed all references to seven schools to eight schools in the text and the flow chart.
-
Changed all references to three control schools to four control schools in the text and the flow chart.
-
Adjusted the sample size calculation from 630 to 720 to reflect the increased number of schools.
-
Added in a stratification subsection in section 5.b.
-
Added in a randomisation subsection in section 5.b.
-
Updated Appendix 3 (outcome measures) by removing the ‘Beliefs about Consequences’ outcome and the ‘London measure of unplanned pregnancy’ which occurred post pilot. These changes were due to low variability in responses and the low numbers of pregnancy, respectively. The newly developed Intention to Avoid Unintended Teenage Pregnancy (UTP) scale was added.
-
In this section Process evaluation, the following line was removed: ‘Inquire into teacher trainer’s views on the training materials for teachers’. This is because the researcher is delivering the teacher training.
-
Added the information video on YouTube (YouTube, LLC, San Bruno, CA, USA) to the Parents Information Evening section.
-
Changed the sample size estimate for parent focus groups from 25–95 to eight-20.
Stakeholder representatives, international advisory group, trial steering group and details of meetings
Stakeholder group
Ms Joanna Brown, RSE and Local Area Coordinator, Sexual Health Training Team, Belfast Health and Social Care Trust (BHSCT), Northern Ireland (NI), UK.
Dr Bernadette Cullen, Consultant in Public Health, Public Health Agency (PHA) of NI.
Ms Kathryn Gilbert, Curriculum and Assessment Programme Manager, Council for the Curriculum, Examinations and Assessment (CCEA), NI.
Dr Naresh Chada, Senior Medical Officer, Department of Health, Social Services and Public Safety (DHSSPS), NI.
Ms Janet Moore, DHSSPS.
International Advisory Group
Trial Steering Group
Professor Vivien Coates (Independent Member and Chairperson), Institute of Nursing and Health Research, School of Nursing, University of Ulster, NI.
Dr Suzanne Guerin (Independent Member), School of Psychology, University College Dublin, Ireland.
Dr Liam O’Hare (Member), Centre for Effective Education, School of Education, QUB.
Master Patrick Lynn (Independent Public Member/School Pupil).
Miss Chloe Templeton (Independent Public Member/School Pupil).
Dr Darrin Barr (Independent Public Member/School Principal).
Ms Grace McCarthy (Independent Public Member/School Teacher).
Ms Lisa Barr (Independent Public Member, Parent).
Dr Maria Lohan (Member and Chief Investigator), School of Nursing and Midwifery, QUB.
Dr Áine Aventin (Member), School of Nursing and Midwifery, QUB.
Dr Hannah-Rose Douglas (Independent Member), National Collaborating Centre for Women’s and Children’s Health, NI.
Trial Steering Group meetings
The Trial Steering Group met three times, on 9 October 2014, 11 May 2015 and 24 November 2015. For Trial Steering Group minutes see Appendix 4.
Public and patient involvement
The study was informed by several stakeholders:
-
Survey research with adolescents evaluating the If I Were Jack interactive film and a qualitative study with teachers. 1
-
In the intervention development phase (see Chapter 3), we convened a professional stakeholders’ group (see above) of senior representatives from key government departments [Health and Safety Executive, PHA, DHSSPS, CCEA (Belfast, UK), and Department of Education Ireland] who, alongside teachers and pupils, were involved in designing the intervention. 2
-
Prior to the pilot study for questionnaire development, we liaised with a young people’s research group. This was an ad hoc group comprising the young people from the Trial Steering Group and additional members of a Young People’s Advisory Group working on a similar study at QUB, in which Dr Lohan (Chief Investigator) was involved.
-
During the pilot study for questionnaire development (see Chapter 4).
-
During the feasibility trial through consultation with the Trial Steering Group, which included relevant independent and public lay membership (see above).
-
During the feasibility trial through process evaluation whereby we sought the views of teachers, pupils and parents regarding potential refinements to the intervention (see Chapter 7).
Chapter 2 Background and rationale for the study
Existing research: understanding unintended teenage pregnancy
Teenage pregnancy remains a worldwide public health concern. 3,4 The UK has the highest rate of adolescent pregnancy in Western Europe. 4 Although rates of teenage pregnancy have been gradually falling across the UK since 2002, the birth rate for girls aged under 20 years in England and Wales remains high, at 37.4 per 1000 in 2014. 5 In real terms, just under 26,000 women under the age of 20 years became pregnant in England and Wales in 2014 and approximately half of these pregnancies ended in legal abortion, reflecting the potentially unintended or unwanted nature of these conceptions. 6 The conception rate for Scotland was 37.7 per 1000 in 2013. 7 In NI, abortion is illegal and is considered lawful only in exceptional circumstances in which the life of the pregnant woman is at immediate risk or if there is a risk of serious injury to her physical or mental health. Reflecting this different legal framework, government targets around reducing teenage pregnancies in NI relate to births and not conceptions. In NI, the birth rate to teenage mothers per 1000 of the female population aged 13–19 years in 2014 was 10.3 per 1000 young women (a total of 839 births). 8 The rate for young women in the most deprived areas was nearly 30 per 1000. 9
Although the life course for teenage parents is not universally negative,10,11 the social disadvantage and exclusion that are linked to teenage pregnancy are considered problematic. 12 UTP can lead to considerable adverse health problems for teenagers and their infants, as well as generate enormous emotional, social and economic costs for adolescents, their families and society. 13 Although UTP is a complex phenomenon that cannot be prevented through RSE alone,14–20 high-quality RSE is an essential component in the process of reducing unintended pregnancy rates, as well as being a vital aspect of improving holistic sexual health and well-being. 21–27 Reflecting the importance of RSE, the governments of NI, England and Scotland all emphasise the policy importance of the reduction of teenage pregnancy rates via the implementation of RSE in schools as a key objective in current sexual health policies. 26–28
Unprotected sex during teenage years is well established as the main proximate behavioural determinant of teenage pregnancy and is a commonly measured behavioural outcome in studies examining the impact of RSE interventions on teenage pregnancy. 17,27,29 Research indicates that, although other behavioural determinants (such as frequency of sexual intercourse and number of sexual partners) are important, avoidance of unprotected sex via consistent use of contraception is central in explaining variation in levels of adolescent pregnancy. 22
A number of systematic reviews have identified the characteristics of effective RSE programmes that may have an impact on sexual risk-taking behaviours. 19,30–36 These include the use of theoretically based interventions targeting sexual and psychosocial mediating variables such as knowledge, attitudes, self-efficacy, intentions, perceptions of risk, and perceptions of peer norms which are linked to sexual behaviour change; the use of culturally-sensitive and gender-specific interventions; the use of interactive modalities that promote personal identification with the educational issues and engagement of young people; the use of skills-building components; the involvement of parents in the RSE process; and facilitating linkages with support services.
Evidence supporting a theory-based approach
Providing a theoretically informed foundation for sexual health education programmes is considered key to effectiveness because it ensures that the most important determinants of young people’s sexual behaviour are targeted. 22,32,34,37–39 The underpinning theoretical framework for the intervention used in this study combines the well-established theory of planned behaviour40,41 and recent updates to this theory,42,43 which focus on the individual behavioural antecedents of an unplanned pregnancy along with an understanding of the broader socioenvironmental factors (such as social class) and underlying values (such as religiosity and gender ideologies) associated with the occurrence of teenage pregnancy. 18 Interventions should target six psychosocial mechanisms that research indicates are related to a reduction in risk-taking behaviour: knowledge, skills, beliefs about consequences, social influences, beliefs about capabilities and intentions. 19,44,45
Evidence supporting the use of culturally relevant and gender-specific interventions
The World Health Organization (WHO),46,47 recent systematic reviews commissioned by the US-based National Campaign to Prevent Teen Pregnancy,48,49 and the NIHR,50 among others,1,22,51–54 recognise that adolescent men have a vital yet neglected role in reducing teenage pregnancies, and that there is a pressing need for RSE interventions designed especially for them.
In relation to cultural relevance, research suggests the need to engage with young people both empathetically and cognitively in order to increase the relevance of the issues being raised. 14,23,30,31,55 As Ingham and Hirst24 have noted, it is important to harness the potential for sex education to be keenly anticipated, especially by those who are less engaged in the wider school curriculum, a factor that was identified as a possible barrier to impact. 50
Evidence relating to socioeconomic position and inequalities
Research suggests that interventions targeting only schools in disadvantaged areas are insufficient for achieving population-level reductions in teenage pregnancy. 56,57
Evidence supporting the use of interactive computer-based interventions
Recent systematic reviews have shown the value of interactive-computer-based interventions,34,35,55 and a meta-analysis examining these reviews in relation to the theoretical mediators of safer sex36 concluded that they were successful in impacting knowledge, attitudes and self-efficacy relating to sexual health.
Evidence supporting the use of skills-building components
Reviews and trials of health promotion and educational interventions show that simply providing information does not lead to behaviour change and that instead it is necessary to support young people to develop their own communication skills in relation to preventing risky sexual behaviours. 14,17,19,21–23,30,34,47,58 A recent NIHR Health Technology Assessment systematic review19 of the effect of interventions aiming to encourage young people to adopt safer sexual behaviour found that school-based interventions that provide information and teach young people sexual health negotiation skills can bring about improvements in behaviour-mediating outcomes such as knowledge, attitudes and self-efficacy. The authors noted that these variables are no less valuable than behavioural variables because they provide young people with a solid foundation on which to make sexual decisions.
Evidence supporting the involvement of parents in Relationship and Sexuality Education
Although evidence suggests that schools are an important context for sex education,14,48,59 recent systematic reviews have also shown that programmes that reach beyond the classroom (including multifaceted approaches with a parental or community component) are more effective,19,25,60 particularly with adolescent men. 48 In particular, factors such as parental monitoring and supervision and familial communication have been associated with adolescent sexual behaviours. 61,62 Teenagers who can recall a parent communicating with them about sex are more likely to report delaying sexual debut and increased condom and contraceptive use. 63–65
Most parents do, however, recognise the importance of speaking to their children about sex and most would like more resources to help them in this regard. 66 Furthermore, many teenagers report parents as a primary source of information on sexual health matters. 67 The unprecedented growth in the use of online and mobile technology over the past few decades by people of all ages presents opportunities for increasing the reach (and decreasing the perceived embarrassment) of parental involvement in sex education. 68 More than 20 years ago, Miller et al. 66 found that a home-based video sex education intervention designed to make it easier for parents to talk to their teens about sex was effective in increasing the frequency of parent–teen communication regarding sexual topics. The use of ‘education entertainment’ for addressing health issues has become increasingly common since then69 and, in recent times, studies61,68,70 have demonstrated the importance of embracing such modalities as engaging adjuncts to school-based education.
Rationale for the feasibility trial
The study is justified on the following grounds.
Previous research by members of the study team
When we used an earlier version of this interactive video drama (IVD), a component of the intervention in this study (see Chapter 3) as part of a research project on teenage males and unintended pregnancy, 85% of a sample of male pupils in Ireland (n = 360) and 72% in Australia (n = 386) agreed or strongly agreed with the statement that it ‘helped me understand the effect an unplanned pregnancy would have on a guy like me’. In Ireland and Australia, 79% and 69%, respectively, agreed or strongly agreed that the IVD ‘made me realise that I should never get myself in that situation’. 71
The public health concern of teenage pregnancy and the potential reach of targeted school-based interventions to provide young people with a solid foundation on which to make sexual decisions
The core aim of the If I Were Jack intervention is to use an evidence-based process to allow schools to provide pupils with opportunities for exploring the issues surrounding teenage pregnancy and parenthood with reference to the individual, family, community and society. If it is acceptable and effective, it has the potential to be rolled out to large numbers of boys and girls attending schools across the UK and to be of benefit to several groups of people. In 2011/12 there were 24,251 pupils in Year 11 in the 216 mainstream post-primary schools in NI72 and 551,800 pupils in the 3268 state-funded secondary schools in England. 57 Pupils will benefit from an engaging educational resource. Parents will benefit from a process designed to involve and support them in communicating with their child. RSE teachers will benefit because the resource will provide them with a stimulus for engaging pupils in an immersive decision-making experience from the point of view of a teenage male, followed by guided classroom-based activities.
Teenage pregnancy is both an outcome of, and a contributor to, inequalities in health. 12 The aggregate projected spend for 2013–20 for treating both unintended pregnancy and sexually transmitted infections (STIs) (for all ages) across the UK is estimated to be between £84.4B and £127B. This is based on a projected spend of £11.4B of NHS costs as a result of unintended pregnancy and STI costs, and between £73B and £115.3B of wider public sector costs. 73 The NI government estimates the cost to the Exchequer of teenage pregnancies at £20,000 per teenage mother on the basis that a teenage pregnancy effectively withdraws the mother from the labour market (not in education, employment or training) for at least 18 months and accounting for unemployment benefits and administration, plus tax revenue forgone. 26 Our population-based approach is consistent with the evidence that universal interventions are necessary to achieve population-level reductions in teenage pregnancies. 56,74–76
This study will begin a process of robust evaluation that may also lead to the roll-out across the UK and international applications of the intervention
Internationally, policy-makers and researchers have called for scientifically evaluated school-based RSE interventions. 16,21–25,77,78 A successful feasibility would underpin the development of a UK-wide Phase III trial. The intervention has been designed specifically for use in NI, but it is based on international research regarding effective RSE interventions. Although the video drama features NI actors, there is no specific reference to NI in the video and we believe that it would have strong cultural resonance in the rest of the UK. Furthermore, although the accompanying materials make specific reference to the NI curriculum and legislation in NI governing termination of pregnancy, the costs of making changes to these references so that the materials could be used in contexts across the UK would be negligible.
The need to develop and evaluate age- and gender-specific Relationship and Sexuality Education resources
The need for gender-sensitive interventions to address teenage pregnancy has been highlighted as a global health need by the WHO46,47 and has been recommended in systematic reviews. 19,48,49 Addressing teenage males’ RSE is an important mechanism for promoting positive development and improving the lives of all young adults, especially those suffering the effects of various types of disadvantage. 48,51–53,79
A recent inspection by the Education and Training Inspectorate of RSE implementation in post-primary schools in NI identified the need for RSE resources for older adolescents, especially at Key Stage 4 (age 14+ years). 80 The absence of such resources is thought to be a demotivating factor, making RSE more difficult for some schools to implement. Internationally, there has also been demand for age-appropriate school-based RSE interventions. 16,21–25,77,78
We aim to initiate a process of robust scientific evaluation, which will ultimately produce generalisable findings especially relating to gender-specific interventions. The intervention we propose is gender-inclusive in terms of intent and impact and it can be used in mixed-sex classrooms, but is gender-specific in that it specifically targets the inclusion of adolescent men by developing an interactive film from a man’s point of view.
The strengths of the If I Were Jack intervention
The If I Were Jack intervention is grounded in empirical research on adolescent men’s attitudes to UTP; was developed in consultation with key health and education experts, pupils, teachers and parents; and is informed by the best available evidence regarding the development of classroom-based RSE interventions. It is predicted to impact on a number of behavioural and psychosocial mediating variables, which research suggests decrease sexual risk-taking behaviour. It uses an innovative combination of intervention components which address deficits in existing RSE interventions and aim to maximise potential impact.
The right place for this study
This research is necessary to address the deficit of research on high-quality RSE interventions in NI. Although RSE is mandatory in NI, its provision in schools is known to be underdeveloped and highly variable. 9,80–83 In addition, given that RSE in NI is underdeveloped, we are more likely to be able to test the efficacy of the intervention in NI as a prelude to a Phase III trial to test its effectiveness. In our preliminary research and in working through a partnership model to develop this study, we believe that we are in a strong position to overcome the problems in implementing RSE in NI and have already found the resource to be culturally sensitive and acceptable to statutory stakeholders and schools.
The educational and policy demands for such an intervention
The letters of support from across the health and educational sector of the UK (including, in NI, the Chief Medical Officer, PHA NI, DHSSPS and CCEA) identify the need for and support this study. Several stakeholder organisations are also offering in-kind contributions in terms of membership of a study stakeholder’s group along with a contribution of £20,000 co-funding from PHA. This stakeholder investment in this project attests to the widely held need to evaluate evidence-based, theory-informed RSE resources that clearly target boys as well as girls in relation to unintended pregnancy and improving sexual health and well-being.
Chapter 3 The intervention
Overview of the intervention
The If I Were Jack intervention2 is a classroom-based RSE resource intended for use by teenagers aged 14–15 years, based around a core component – a culturally sensitive interactive IVD to immerse young people in a hypothetical scenario of a week in the life of Jack, a teenager who has just found out that his girlfriend is pregnant. It is designed to be delivered by teachers over 4 weeks, and also incorporates communication with parents/guardians within the RSE process.
It is composed of a number of components:
-
the If I Were Jack IVD, which asks pupils to put themselves in Jack’s shoes and consider how they would feel and what they would do if they were Jack
-
classroom materials for teachers containing four detailed lesson plans with specific classroom-based and homework activities including group discussions, role-plays, worksheets and a parent–pupil exercise
-
a 60-minute face-to-face training session for teachers wishing to implement the intervention
-
a 60-minute information and discussion session for parents/guardians delivered by RSE teachers (also presented as a brief 6-minute YouTube video delivered by the principal investigator (PI) containing an overview of the key points, for those who were unable to attend)
-
detailed information brochures and factsheets about the intervention and UTP in general for schools, teachers, teacher trainers, young people and parents.
The IVD is interactive in that the film pauses throughout with questions that invite users to imagine being Jack. On individual computers, they watch Jack as he thinks about what his friends and parents might say, chats to his girlfriend and attends a pregnancy counselling session. The user answers questions about how they would think, feel and react in these situations and ultimately decide upon a pregnancy resolution option. Although targeted specifically at young men, through the presentation of the case scenario of an UTP from a teenage male’s point of view, it can also be used by young women and in mixed-sex classrooms. By asking both girls and boys to empathise with Jack and ask themselves how they would think and feel if they were in his situation, it is designed to make explicit the gender assumptions around roles and responsibilities for teenage pregnancy while opening them up for reflection and negotiation.
The face-to-face teacher training session lasted for 60 minutes and was mandatory for those delivering the intervention. It included an overview of the If I Were Jack feasibility trial and the components of the intervention, its underlying theory and key messages. Teachers were given a full demonstration of the IVD and detailed information on the accompanying activities and how they should be implemented. They were advised that they should stick as closely as possible to the implementation guidelines detailed in the ‘information for teachers’ booklet. However, as implementation processes were being piloted as part of the study, they were informed that they could vary implementation if necessary and were asked to record any variation in implementation in the implementation log booklets.
The development of the intervention was informed by empirical research on adolescent men’s attitudes to UTP and the best available evidence regarding the components of effective RSE interventions. It was designed to fit with the RSE curriculum by a team of researchers working with experts from the DHSSPS, PHA, and CCEA, as well as teacher trainers, teachers, parents and adolescents.
The intervention includes an innovative combination of different components, content and educational objectives which provide pupils with educational information and opportunities for communication with peers and parents, skills practice, reflection and anticipatory thinking (see Appendix 5). The design and development of the If I Were Jack intervention is detailed in full in Aventin et al. 2 and addresses identified deficits in existing RSE interventions. Additional intervention components, which are based around the IVD, include classroom materials, a comprehensive training session for teachers/RSE facilitators and an information and discussion session for parents. For the feasibility trial this information was also presented as a brief 6-minute YouTube video delivered by the PI containing an overview of the key points, for those who were unable to attend. Further information about the intervention, including excerpts from the film and feedback from end users regarding the acceptability of the IVD, is also available from the project website (see www.qub.ac.uk/IfIWereJack). 84
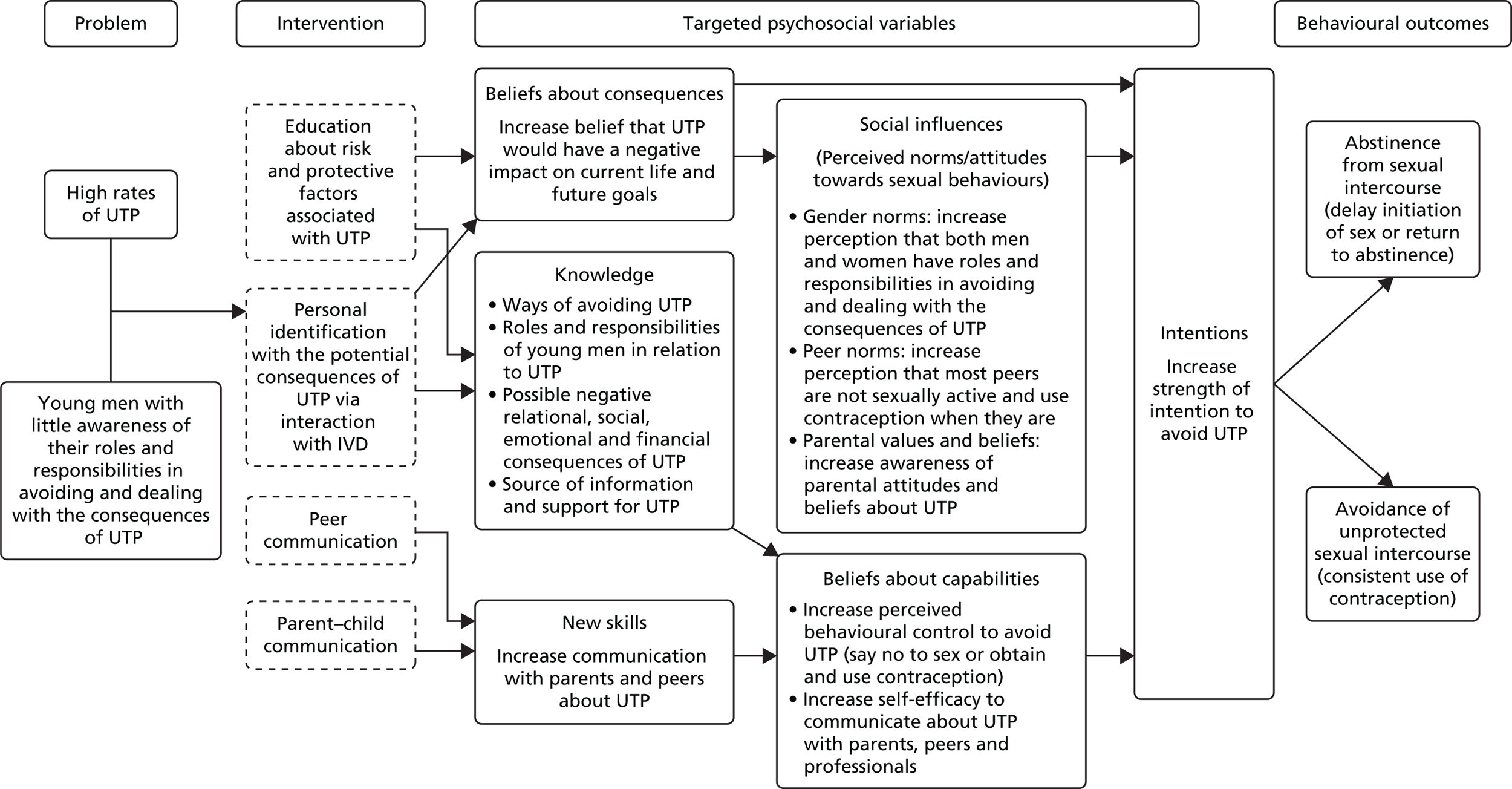
The intervention is designed to increase adolescents’ intentions to avoid an UTP by delaying sexual intercourse or consistently using contraception in sexual relationships. To achieve this impact, it targets six psychosocial mechanisms (see Appendix 5), which theory and research suggest are key to decreasing sexual risk-taking behaviour: (1) knowledge; (2) skills; (3) beliefs about consequences; (4) other sociocultural influences such as peer norms, gender norms and parental values and beliefs; (5) beliefs about capabilities; and (6) intentions. 40,85–87 The If I Were Jack theory of change model is detailed in Figure 1. The intervention aims to maximise potential impact by incorporating components, which some studies have indicated are key elements of effective RSE interventions (e.g. interactive media,34,35 peer discussion25,37 and parental involvement). 88 In brief, we hypothesise that by encouraging personal identification with the UTP scenario in the IVD, we engage pupils in an exercise of the imagination whereby they stop and think about the consequences that an UTP might have on their current life and future goals. This identification and reflection process is reinforced by providing knowledge about the risks and consequences of UTP and ways to avoid it and offering opportunities to practice communicating about UTP with peers and parents/guardians (activities that also increase awareness of peer norms and personal and familial values and beliefs about sexual behaviour and unintended pregnancy). We hypothesise that by targeting these psychosocial factors, we impact on teenagers’ sexual behaviour via pathways through their intention to avoid UTP.
FIGURE 1.
If I Were Jack theory of change model.
Methods
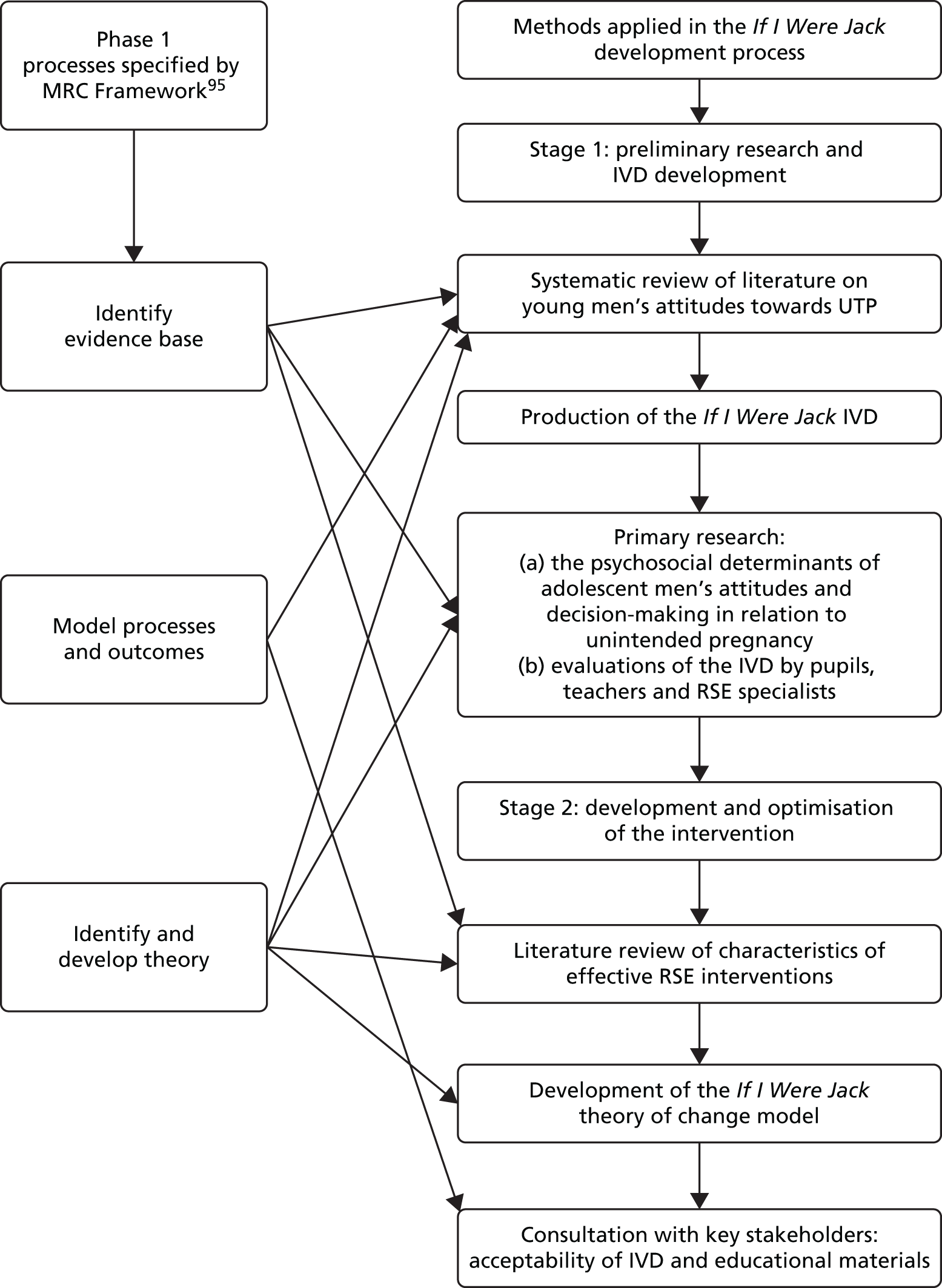
Development of the intervention was a two-stage process (Figure 2) informed by the Medical Research Council (MRC) Framework. 89 The process began with a systematic review of the literature on adolescent men and UTP. 90 Following this, a version of the IVD was developed as a data collection tool and used to develop the empirical evidence base on adolescent men’s attitudes and decision-making in relation to an UTP (see Chapter 2, Previous research by members of the study team). 1 Feedback from pupils, teachers and educational specialists indicated that this version of the IVD had potential to be redeveloped as part of an intervention. This resulted in stage 2 of the process, in which a further systematic review of the literature on the characteristics of effective RSE was conducted. The IVD was redeveloped, which involved the filming of a new Northern Irish version (for the purposes of cultural relevancy) and the development of additional intervention materials informed by the theory of change model depicted in Figure 1 and by consultation with stakeholders.
FIGURE 2.
The If I Were Jack development process.
Results
Stage 1: preliminary research and development of the interactive video drama
Systematic review
A systematic review of the literature on young men’s attitudes towards UTP and parenthood indicated a number of potential psychosocial influences on young men’s attitudes towards UTP and pregnancy outcome decisions. 90 These included social class, religiosity, gender identity, masculinity, the idealisation of pregnancy and parenthood, and attitudes and subjective norms regarding how significant others (such as parents, friends and partners) would expect them to behave in such a situation. The If I Were Jack intervention targets these psychosocial influences as key mechanisms.
The If I Were Jack IVD was inspired and modified (with permission) from a version used in an Australian study of adolescent men and pregnancy. 91 Irish and Northern Irish versions were filmed (to be more culturally and contextually relevant), informed by previous Irish research92 and in consultation with an expert advisory group and youth drama groups, first for use as a data collection tool in a study examining influences on young Irish men’s attitudes and decision-making in relation to a hypothetical UTP. 1 A significant change included the addition of a third pregnancy outcome choice, namely ‘adoption’, in addition to ‘keeping the baby’ and ‘abortion’. Evaluation supported the notion of developing it as an educational resource and offered suggestions for how it might be optimised for use in the classroom. 71 There was agreement among participants that it was authentic in its representation of a believable UTP scenario; engaging to users because of its interactive modality; unique in its representation of the male role in UTP and use of high-quality drama; easy to use; and held potential for inclusion within broader RSE curriculum. 71 Formative evaluation of the original Australian version indicated that the IVD had potential for achieving key educational and health promotion outcomes in relation to raising awareness around UTP in young men’s lives. 93 Further development and evaluation of the existing Northern Irish IVD into an educational intervention ensued in stage 2 of the production process.
Stage 2: development and optimisation of the intervention
Stage 2 focused on developing the intervention. This involved redevelopment of the IVD and design of accompanying classroom materials based on evidence regarding the characteristics of effective RSE interventions and theoretical understanding of the determinants of behavioural change. Also central to stage 2 was consultation in relation to the content (see Chapter 1, Public and patient involvement).
Identifying the evidence and modelling theory
A number of systematic reviews have identified the characteristics of RSE interventions that have been effective in changing sexual risk-taking behaviours. 19,30,33–35 The If I Were Jack intervention represents an innovative combination of these different elements. Providing a theoretically informed foundation for sexual health education programmes is considered key to effectiveness because it ensures that the most important determinants of young people’s sexual behaviour are targeted. 21,34,37 The If I Were Jack intervention is broadly based around the theory of planned behaviour40 but also draws on other psychosocial theories which emerged as important during the systematic review stage described above. The If I Were Jack theory of change model is depicted in Figure 1, the development of which (informed by Kirby et al. 94) included four steps:
-
identification and selection of the health goal (reduction of UTP rates)
-
identification and selection of important related behaviours (abstinence from sexual intercourse and avoidance of unprotected sexual intercourse)
-
identification and selection of important risk and protective factors (targeted psychosocial variables as indicated by theory and research)
-
identification and selection of intervention components (see below).
Developing the content and components
Educational outcomes were defined for each of the user groups (pupils, teachers, teacher trainers and parents) based on the targeted psychosocial variables detailed in the theory of change model (see Figure 1) and then considering possible activities that might help young people to achieve this outcome. An overview is provided in Appendix 5.
Refining the content in consultation
The draft IVD and educational materials were reviewed by a steering group and amended following feedback. Further consultation with relevant stakeholders – teachers, pupils and parents – regarding their acceptability was also undertaken. This is described in full in Aventin et al. 2 Notable refinements made as a result included the following.
Addressing the issue of abortion
Although the intervention is non-directive in terms of pregnancy outcome options, stakeholders were concerned that the mention of ‘abortion’ might negatively impact on uptake, in particular in schools that have an anti-abortion ethos. This issue was addressed by changing the order in which the pregnancy outcome options were displayed in the IVD; including information about the legal status of abortion (locally); and changing wording that might be interpreted as pro-abortion. In addition, teachers were reminded repeatedly during the teacher training session and in the classroom materials that they have the opportunity to state the school ethos and RSE policy and that the intervention allows for this flexibility.
Making it gender sensitive
Although the intervention was developed specifically for teenage males, preliminary research suggested that it would also be suitable for use by teenage women. The learning objective was to introduce the topic of UTP through the male perspective, arguably a fresh perspective, but to use this as a starting point to discuss both male and female perspectives and to explore similarities as well as differences. Thus, girls are also asked through this intervention to imagine ‘If I Were Jack’. Following consultation, additional amendments made to address this issue involved the addition of three questions to the IVD which referred to how the female character may be feeling (i.e. ‘If I were Jack, how do I think Emma would be feeling now?’). Such questions allowed for further exploration of the female partner’s perspective while retaining the focus of the exercise on the perspective of the male character.
Increasing credibility
Increasing the credibility of the intervention to gatekeepers (schools, teachers and parents) was achieved by developing a dedicated website for the intervention. The website includes, among other features, expert stakeholders’ and teachers’ audio- and video-recorded testimonies.
Increasing accessibility
The IVD was developed for the internet, adapting the previous version, which was delivered to the end user on digital versatile disc (DVD), and transforming it into the online environment.
Discussion
Effective RSE interventions require rigorous development processes and transparent reporting to ensure both substantive and process-related knowledge transfer. The design and development of the If I Were Jack intervention benefited from the guidance provided by the MRC framework for the development and evaluation of complex interventions87 and followed the recommended process of identifying the evidence base, identifying theory relating to the phenomenon of young men and UTP and modelling the processes and outcomes of implementing the intervention through preliminary research and consultation with key stakeholders. In applying the framework in the real world we learned lessons, which both complement and extend beyond the guidance that accompanies it, and gained practical insight into a development process that might be useful for others. Three key lessons are detailed in full in Aventin et al. 2 and are summarised below:
-
Know and involve your target population and engage their gatekeepers in addressing contextual complexities:
-
systematic reviews
-
primary research
-
development/adaptation of film script, storyboard and interactive questions
-
consultation
-
participation.
-
-
Know the behaviours you wish to target and model the process of change:
-
psychosocial theory
-
characteristics of effective interventions
-
logic modelling.
-
-
Look beyond development:
-
consider evaluation, implementations and knowledge transfer from the start.
-
Limitations
A recent systematic review of effective sexual health interventions19 indicated the importance of building connections with community-based sexual health services and providing longer-term programmes. The If I Were Jack intervention was unable to address such components owing to the strategy employed to develop and test an existing IVD. Such issues and other evidence-based components could be addressed in future development work.
As the If I Were Jack intervention strongly emphasises the potential negative consequences that having a child might have on a teenager’s current life or future goals, another potential limitation of the intervention is that it may have a possible negative impact on teenagers who have had, or are about to have, a child. It has the potential to reinforce or indeed instigate stigmatisation processes. Design features of the intervention aim to off-set this potential negative impact through the teacher training process, which emphasises the importance of reminding and discussing with pupils that the resource refers to UTP (i.e. a pregnancy that is unexpected and unwanted) rather than a teenage pregnancy in general, which for some young people can be a planned and positive experience. Pupils are also informed by the teachers and researchers involved that they can and should contact the school counsellor/pastoral care (PC) officer should they find any part of the intervention upsetting.
Conclusions
The If I Were Jack intervention is a unique, evidence-based, theory-informed intervention that to date has been found to be acceptable to statutory stakeholders, teachers, pupils and parents in diverse geographical and cultural settings (Ireland, NI and Australia). The intervention is based on existing evidence-based RSE programmes targeting UTP and includes key behaviour change techniques that are influential in changing sexual behaviour and incorporates sociological understandings of gender norms relating to pregnancy. The If I Were Jack intervention is the first to be documented in the scientific literature2 that specifically addresses teenage males and UTP.
Although the MRC guidelines89 suggest a very useful framework for conducting Phase I research, they provide little description of how this should proceed (relative to guidance provided on Phases II–IV). This effectively relegates the importance of this phase to considerations of summative evaluation, despite growing consensus that the development of conceptually based, acceptable interventions is of vital importance before proceeding to trial. This is compounded by a dearth of published literature reporting the development of complex interventions in practice. The result is an increased potential for misallocation of research labour and resources on what is already a costly and time-consuming process. More broadly, as the new mantra of knowledge translation spreads across the academic community there is ever more need to report intervention development processes and intervention components in detail for others seeking to bridge the gap between research and interventions. Reporting on these methodological processes has already directly inspired a research team to develop and evaluate a similar IVD-based educational resource on young people and marijuana use for British Columbia, Canada, entitled Cycles (University of British Columbia, Vancouver, BC, Canada). 95 Consequently, the model of intervention development reported in this report and elsewhere2 is presented not as an ideal, but as an exemplar that other researchers might utilise, modify and improve.
Chapter 4 Developing and evaluating the questionnaire
Introduction
The study endeavoured to conduct a qualitative and quantitative validation of a questionnaire developed for the study to ensure its reliability and acceptability to participants. The questionnaire incorporated validated questions from the Sexual Health And RElationships (SHARE) questionnaires18 and items from a number of standardised measures to provide broad estimates of effect size and the feasibility and acceptability of the questions. The measures were chosen because the constructs they measure map closely to the theoretical framework underpinning the intervention (theory of planned behaviour; see Chapter 3) and they are widely used measures with robust reliability and validity (see Appendix 6). The questionnaire also incorporated a measure of intention to avoid UTP, developed as part of the research process (see Feasibility study below). A prior intention in relation to development was that the questionnaire should aim to take no longer than 30 minutes to complete, as this is the average length of RSE lessons in NI. Effort was made to ensure that the study team consulted with the sexual health and education expert members of the project Stakeholders Group and end users who are members of the Trial Steering Group (see Chapter 1) regarding the acceptability of the questions in the long version of the instrument. The structure of the chapter will describe the following stages in development and evaluation.
Pilot study
Rationale
A key outcome of this study was to pilot test the feasibility, usability and acceptability of providing demographic data and answering questions measuring the proposed primary and secondary outcomes of a future Phase III trial (see Chapter 6), that is, sexual behaviour data, including engagement in sexual intercourse, contraception use and diagnosis of STIs; data regarding knowledge, attitude, skills and intentions relating to avoiding UTP; and data on socioeconomic status (SES). The pilot study was not intended to assess the design and usability of the format of the questionnaire itself.
Methods
Unlike the finalised version of the questionnaire (for the feasibility study), the pilot version was of a basic format using the SurveyMonkey™ (Palo Alto, CA, USA) platform as the feasibility trial website was still in design.
To pilot test the questionnaire prior to the beginning of the feasibility trial, a school was approached that had been identified as willing to use the questionnaire, through prior liaison, with 50–60 of their Year 11 students (male and female, aged 14–15 years), who had proactively volunteered. In order to facilitate completing the questionnaire online, the Year 11 students were spilt into two groups across two different computer rooms and a researcher and a Learning for Life and Work (LLW) curriculum teacher (see Appendix 7) were present at all times in both groups. The session lasted for 1 hour. The data were analysed quantitatively by use of descriptive statistics and analysis of the reliability and spread of the scales.
Qualitative analysis was also made possible via focus group methodology. Focus group interviews are used extensively within social sciences to elicit information, perceptions, beliefs and attitudes. The group dynamic allows for a more natural conversational style rather than a traditional rigid interview technique. Researchers often use this technique to engage the end user in instrument design. Pupils who had completed the questionnaire were asked to participate in the focus group session regarding the acceptability and feasibility of the questions. These interviews lasted for 25 minutes. The students gathered around in a circle and the discussion was audio-recorded to facilitate note taking at a later stage. To begin with, the researchers reminded the students of the purpose (i.e. to find out what they thought about the questionnaire and not to be afraid of giving their honest opinions). The researchers also went over some ground rules, following the Respect, Involvement, Confidentiality, Equality (RICE) rules below:
R: Respect for an individual’s contributions, which we can demonstrate by listening to one another’s views.
I: Involvement in the discussions and activities.
C: Confidentiality – we are not going to talk about our own personal/individual stories but we can talk about relationships in general.
E: Equality – we want to acknowledge that everyone’s experience and opinions are equally valid.
The questions asked during the course of the cognitive interviews are listed below.
-
Would you prefer to complete the questionnaire on the computer or on paper?
-
What did you think about the length of the questionnaire?
-
What did you find useful or interesting about the questionnaire?
-
What did you find difficult or confusing about the questionnaire?
-
Is there anything that you think should be removed from the questionnaire?
-
When you talk about these issues with your friends what terms do you tend to use?
-
I have some specific terms that I wanted to check your understanding of. Ask what would that mean to you? Do you think there are some people your age who would not understand what it meant?
For invitation letters, information sheets and consent forms for schools, teachers, parents/guardians and pupils regarding questionnaire development, see Appendix 2. For the focus group topic guide, see Appendix 3.
Results
The participating school was a grant-maintained integrated co-educational secondary school (which did not go on to be involved in the feasibility trial). The school was located in an urban area and 17.8% of its students were eligible for free school meals. In total, 38 students (mean age of 14.72 years) agreed to take part (in two rooms containing 22 and 16 pupils, respectively), provided parental consent and completed the questionnaire.
Quantitative analyses
The estimated time taken to complete the questionnaire was 40 minutes; the actual time taken was around 25 minutes, including time taken to log in. The first section contained sociodemographic questions. The sample of respondents comprised 55% male and 45% female students and was spilt between 14- and 15-year-olds (26% and 68%, respectively). All students completed these questions, although two incorrectly inputted the date of the pilot study instead of their date of birth. Owing to this error, the online questionnaire was developed to bring up an error message if the year of birth does not equate to a Year 11 student. Sixteen students skipped the question that asked them to write in their postcode. As this information is important for a check to ensure that questionnaires can be correctly linked across the trial and potentially used for gathering multiple deprivation score, it was necessary to keep this in but it was accompanied with more explanation as to why this information was being collected. One question asked about the educational achievement of the respondent’s mother and father (or guardian) and was broken down into six questions asking specifically about General Certificates of Secondary Education (GCSEs), Advanced levels (A levels), degrees, apprenticeships, diplomas or no qualifications. Five participants skipped these questions and 18 did not know the answer. It was therefore decided to incorporate these questions into a single item referring to highest achieved qualification.
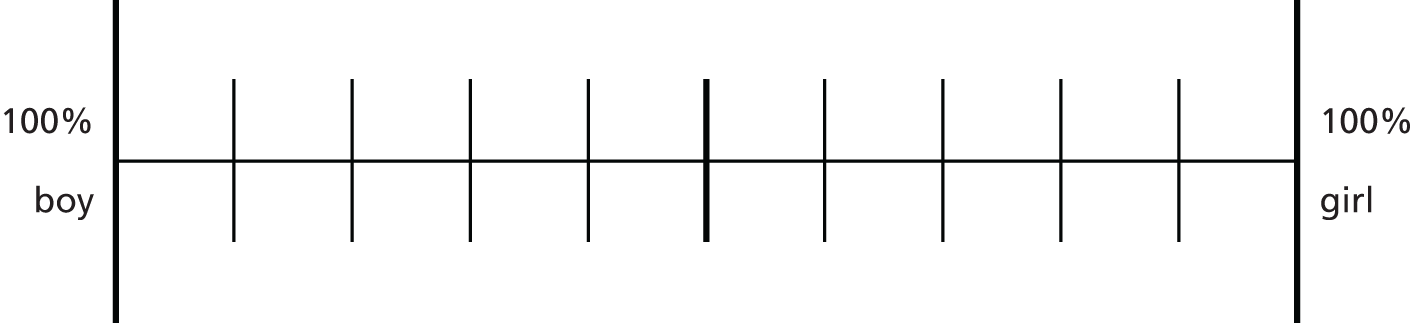
Owing to limited variation in responses received to the categorical tick box responses for the question ‘Whose responsibility is it to prevent unintended pregnancy?’, it was decided to change the response format of the question to the following visual analogue scale (Figure 3), with the following instructions: put an X on the line below to show how much responsibility you think boys and girls should have. For example, if you think that girls have more responsibility than boys, put an X on the line closer to girl; if you think that boys have more responsibility than girls, put an X on the line closer to boy; if you think that boys and girls should have equal responsibility, put an X in the middle of the line.
FIGURE 3.
Whose responsibility is it to prevent unintended pregnancy? A visual analogue scale.
Only 14% (five participants) of the sample said that they had experienced penetrative sex and only three answered the question regarding their age at which they first had sex, which was 15 years. When asked how many times they had had sex, two participants responded that they had had sex once; however, one participant said that they had had sex 30 times. It could be likely that they have been sexually active 30 times in the past but it could also be the case that this may have been an error and was perhaps meant to say ‘three’. To minimise this type of error and therefore to ensure that we could correctly interpret the data, it was decided to use fixed-category responses rather than free responses.
As the pilot study sought to determine participants’ level of comfort in answering potentially personal questions about a sensitive topic, the question ‘how comfortable do you feel in answering these questions?’ was added to the pilot questionnaire to assess this. Most participants felt comfortable answering all or most of the questions (n = 18), but some did report experiencing discomfort (n = 7).
Reliability and spread of pilot results
The decision to include or exclude scales or items was based on internal consistency (Cronbach’s alpha), and the overall variability of the data produced (standard deviation). Those values > 0.70 were considered acceptable (Table 1). The internal consistency for the Sexual Stereotyping scale did not meet the threshold; this measure was included because it produces a high degree of variability in the data. This was replaced by the Male Role Attitude scale instead, which can be used by both sexes. The attitude items were excluded owing to their unacceptable levels of internal consistency and low degree of variability.
| Measurement scales or knowledge items | Cronbach’s alpha | Number of items | Mean | Standard deviation |
|---|---|---|---|---|
| 1. Sexual Self-Efficacy | 0.922 | 13 | 110.8 | 11.7 |
| 2. Intentions to Avoid Teenage Pregnancy | 0.869 | 16 | 127.4 | 18.0 |
| 3a. Comfort Communicating about Sex (boys) | 0.812 | 6 | 84.0 | 25.7 |
| 3b. Comfort Communicating about Sex (girls) | 0.721 | 6 | 88.2 | 23.0 |
| 4. Costs of Unintended Pregnancy | 0.699 | 6 | 75.2 | 17.5 |
| 5. Sexual Stereotyping | 0.611 | 11 | 59.7 | 22.8 |
| 6. Attitudes | 0.364 | 4 | 56.5 | 4.4 |
The knowledge items (Table 2) employed a true/false response format rendering a check on internal consistency inadvisable. However, closer examination of the individual items revealed that some were producing ceiling effects, indicating that the questions were too obvious. A decision was made to exclude items 2, 4, 9 and 10 and to retain all other items.
| Knowledge items | True, n (%) | False, n (%) |
|---|---|---|
| 1. Washing the vagina after penetrative sex will help to prevent pregnancy (false) | 12 (31.6) | 25 (65.8) |
| 2. A girl cannot get pregnant the first time she has penetrative sex (false) | 7 (18.4) | 28 (73.7) |
| 3. A girl can get pregnant if the boy withdraws his penis (pulls out) before ejaculation (coming) (true) | 22 (57.9) | 15 (39.5) |
| 4. When a teenage boy and girl have a baby together, they will likely get married to each other eventually (false) | 7 (18.4) | 30 (78.9) |
| 5. Contraception (when used correctly) provides as much protection against pregnancy as not having sex (false) | 22 (57.9) | 15 (39.5) |
| 6. The rhythm method (only having sex during the few days before and after a woman’s period) is as safe as using a condom in preventing pregnancy (false) | 18 (47.4) | 18 (47.4) |
| 7. When teenagers have penetrative sex for the first time, the majority of them use condoms (false) | 14 (36.8) | 22 (57.9) |
| 8. Teenage males can seek advice from pregnancy counsellors (true) | 20 (52.6) | 16 (42.1) |
| 9. An advantage of using condoms is that they help prevent sexually transmitted diseases (true) | 33 (86.8) | 2 (5.3) |
| 10. An advantage of using condoms is that they can be bought in shops and chemists by either boys or girls (true) | 35 (92.1) | 1 (2.6) |
| 11. More than half of all teenagers in Northern Ireland have had penetrative sex by the time they are 16 (false) | 31 (81.6) | 5 (13.2) |
The Cost of Unintended Pregnancy scale had an acceptable level of internal consistency (α = 0.699; see Table 7); however, on account of the three-point Likert scale, it produced very little variability in participant responses (Table 3). A decision was made to exclude the scale on this basis.
| Costs of unintended pregnancy (α = 0.699) | Mean | Standard deviation |
|---|---|---|
| 1. Teenagers avoid pregnancy because their parents would not approve | 1.80 | 0.871 |
| 2. Teenagers avoid pregnancy because they are not ready to be a parent | 2.46 | 0.373 |
| 3. Teenagers avoid pregnancy because having to decide whether to keep the baby or not might be a very difficult decision | 2.31 | 0.398 |
| 4. Teenagers avoid pregnancy because having a baby might really change their life | 2.51 | 0.375 |
| 5. Teenagers avoid pregnancy because it might mess up their future plans for college, school or a career | 2.51 | 0.316 |
| 6. Teenagers avoid pregnancy because their friends would not approve | 1.32 | 0.771 |
Qualitative analysis
All 38 pupils who answered the questionnaire participated. The questions asked during the course of the cognitive interviews are listed below, along with the responses given by the students.
-
Would you prefer to complete the questionnaire on the computer or on paper?
In this pilot, all pupils completed the questionnaire using the online SurveyMonkey™ format. However, they were asked if they would prefer to do this on paper or computer. There was general agreement with the students that they would prefer to do this online, that it would be more confidential.
because once you click the button it is away
-
What did you think about the length of the questionnaire?
Most said it was too long. Others said:
‘too much reading’; ‘frustrating’; ‘it was all right’; ‘too personal’; ‘I thought it was all right’; ‘very detailed’; ‘too many details in some parts’.
One student noted that:
it was shorter than the other one we did.
-
What did you find useful or interesting about the questionnaire?
Responses to this varied:
‘not really’; ‘it was all interesting’; ‘it was useful’.
One student felt that the questionnaire would help give teenagers the opportunity to think through issues:
it’s a good mind set for teenagers – gives them an idea of what sex is actually like and what pregnancy can do. It can ruin your life if you want to have a scholarship or go to college or something like that.
As this was a pilot and not part of the trial, students were given an answer sheet to the true and false knowledge questions after they had finished. They really liked getting this information, although this would not be offered to students in the main trial.
-
What did you find difficult or confusing about the questionnaire?
The length of the questionnaire was mentioned as a disadvantage:
just the number of questions that kept coming up and up after every single question.
There was also confusion over the difference between likely and somewhat likely. Other comments made included:
‘some didn’t make sense’; ‘it was weird’.
It was not possible to clarify the meaning of these terms in either case but the researcher present thought that they were trying to say that they could not understand why some of the questions were part of a questionnaire about UTP.
-
Is there anything you think should be removed from the questionnaire?
Both groups agreed that asking for the postcode should be removed and queried why it was in there.
I don’t like giving my postcode.
Some pupils thought that the question ‘have you ever had sex’ should be removed. One pupil said this was too personal; however, this point of view did not garner much agreement from others. Another student felt that the question relating to family finance was also too personal to ask.
I didn’t understand why there were questions about your financial circumstances. Just the financial stuff is a bit personal.
Some said that the set up with everyone sitting so close made them feel uncomfortable and others said that they did not mind. They suggested that we could make it more private by asking them to do it at home (some said they would not feel comfortable doing this), one suggested a sheet of paper, talk to each pupil privately, interview them (others disagreed with this); do it on your phone.
-
When you talk about these issues with your friends what terms do you tend to use?
It was reported that they would not use the terminology in the questionnaire when talking with friends. The discussion then moved to a discussion of what terms they did not understand, which were stated to be ‘legal highs’, ‘sexual advance’ and ‘rubber Johnny’.
-
I have some specific terms that I wanted to check your understanding of. Ask what would that mean to you? Do you think there are some people your age who would not understand what it meant?
Feedback on participants understanding of key terms used is detailed in Table 4.
| Phrase for clarification | Student response to phrase | Altered phrase |
|---|---|---|
| ‘Future sexual encounter’ | No problem | – |
| ‘Resist peer influence’ | No problem | – |
| ‘In a relationship’ | No problem | – |
| ‘Sexual advance’ | Did not understand | Added a definition: can be used to describe an attempt by one person to gain sexual favour with another (also called ‘come on to’ or ‘pull’) |
| ‘A sexual encounter’ | No problem | – |
| ‘Feeling obliged to have sex’ | Did not understand | Changed to ‘feeling you have to’ |
| ‘Control your sex urges’ | No problem | – |
| ‘Peers’ | No problem | – |
| ‘Most women cannot be trusted’ | No problem | – |
| ‘dating relationship’ | Outdated | Changed to ‘boyfriend/girlfriend’ |
| ‘manipulate’ | Did not understand | Added a definition: to control or influence (a person or situation) cleverly or dishonestly |
| ‘highly regarded’ | Did not understand | Change |
| ‘easy/sexually easy’ | Had some problems | Added a definition: can mean someone who agrees to have sexual intercourse with others without difficulty |
| ‘multiple sexual partners’ | No problem | – |
| ‘sexually active’ | Did not understand | Added a definition: can be used to describe a person who participates in sexual intercourse |
| ‘sexual exploits’ | Did not understand | Added a definition: the people you have had sexual intercourse with in the past |
| ‘sexuality’ | Had some problems | Added a definition: can be used to describe a person’s sexuality or preference (e.g. whether you are sexually attracted to males, females, both males and females, or have never been attracted to anyone) |
| ‘Other drugs’ | Had difficulties thinking about other types of drugs | Added: ‘e.g. ecstasy, magic mushrooms, LSD, cocaine, heroin’ |
Observations made during questionnaire completion
Although there were two groups completing the questionnaire independently in different rooms, the two researchers administering the questionnaire observed similar issues. The major difficulty observed by both researchers was that friends sat side by side and many openly and audibly discussed their answers and the meanings of words/questions/response sets. This was even more of an issue in the group that had the least personal space. To combat this the possibility to play music via the internet to keep the students focused and minimise the opportunity for discussion was examined. Ultimately this would not be possible, owing to issues such as the selection of music, the availability of headphones in schools and the ability of the software. Emphasis was placed at the beginning of the questionnaire that this questionnaire addresses private and sensitive issues and that respondents should remember to respect each other’s privacy when completing the questionnaire and not to discuss their answers. Other issues that were noted during the observations were:
-
One female, in reference to the Intentions scale, said that she could not answer the questions because she felt that they were too personal. The researcher reminded her and the rest of the group that they could skip any questions they were uncomfortable answering. A decision was made to emphasise this more clearly in writing on the questionnaire and in the verbal introduction.
-
Some queried the Likert-scale responses on the Intentions scale:
What’s the difference between likely and somewhat likely?
-
Other questions or comments included:
‘what is penetrative sex?’; ‘what is a legal high?’; ‘what is contraception?’; ‘I don’t remember my post code’.
-
One male said that he did not have a father so should he put ‘not sure’ in response to the paternal education question. It was decided that the questionnaire employed in the feasibility trial should include a ‘not applicable’ option.
Summary of changes made to questionnaire for feasibility study
In conclusion, the Year 11 students who assisted with the pilot development stage of the questionnaire were mostly positive about their experiences in completing the questionnaire. Feedback on their understanding of key terms used was critical to ensure that future participants can understand what is being asked and also to enable reliable estimates of effects. A number of changes were made to the questionnaire in light of this work, which are summarised below.
-
changes made to terminology used
-
‘hover over’ definitions used on terms on the online questionnaire and a separate definitions page on the paper version of the questionnaire
-
response format from one questionnaire changed to a visual analogue scale
-
more description about a Likert scale and how to answer them
-
removed Cost of Unintended Pregnancy scale
-
the knowledge items two, four, nine and 10 were removed
-
changed ‘How many times have you had sex?’ question from free response to fixed-category tick boxes
-
included ‘not applicable’ option to question on paternal and maternal education?
-
greater explanation of why we are asking for postcodes
-
inserted reminders in the online questionnaire if any items are left blank unintentionally
-
validity checks for date of birth inserted into online questionnaire
-
explained why the questionnaire contains questions relating to parental education and finances
-
broke up how longer scales are displayed – no more than six questions per page
-
added progress bar to online version.
Feasibility study
Further exploration and analyses of how well the questionnaire performed after baseline data collection, after follow-up 1 (second data collection wave) and post trial after follow-up 2 (third wave of data collection) were conducted. The following sections detail this, in addition to any further proposed changes thought necessary to bring forward to a main trial.
Rationale
The aim was to further refine the survey instruments by assessing their acceptability and usability among the pupils now completing them within the setting of the feasibility study.
Methods
An electronic version of the questionnaire was developed post pilot and offered to the schools as an alternative to the use of paper-based questionnaires.
The data were analysed quantitatively following baseline data collection, by use of descriptive statistics and analysis of the reliability and spread of the scales. The research team also made minor amendments to the survey instruments to aid user understanding after each data collection wave; these changes were based on analysis of responses and qualitative experiences of watching the pupils complete them.
As with the pilot study, qualitative analysis was also made possible via focus group methodology. This was conducted post trial. Two separate focus groups were conducted within two of the control group schools. The focus groups were audio-recorded to ease transcription and lasted no longer than 45 minutes. Soft drinks and snacks were provided and the interviewer tried to create a relaxed atmosphere to facilitate a discussion in which everyone had a voice. The focus groups were timed to coincide with the end of data collection for the feasibility trial and occurred either directly after data collection or within a few days of this. This timing ensured that issues the participants may have had and the survey instrument itself would be fresh in their minds. Although they were already familiar, sample questionnaires were given out to all participants so that they could examine it in detail.
Participants were given an overview of what a focus group is as well as a topic guide (see Appendix 3). They were reminded that although they would be discussing the questionnaire, for example, whether the questions were easy or difficult, they would not be asked to discuss their own personal answers. For relevant invitation letters, information sheets and consent forms for schools, teachers, parents/guardians and pupils, see Appendix 2.
The focus group schedule (see Appendix 3) was divided into five topics: questionnaire instructions, questionnaire design, terminology used, individual questions and other issues.
Results
Quantitative analysis
Baseline data collection was conducted during December and November 2014 in eight schools with 831 pupils (mean age 14.45 years) completing the questionnaire across the eight participating schools. Three of the eight schools elected to use the electronic questionnaire at baseline data collection. The paper version of the questionnaire only was available for use at follow-up 1 and 2 data collection owing to technical software problems.
Analysis of demographic variables
Table 5 details the questions in the ‘about yourself’ and ‘your family’ sections. Within this section we tried to assess social class in a variety of ways. A surprisingly small percentage of pupils aspired to attend university or college upon leaving formal schooling, suggesting that the wording of this question might require amendment. The majority of girls and boys categorised themselves as heterosexual. There was a range of living arrangements reported and a wide range of responses to respondents families’ financial situation, although ‘average’ was the most common answer.
| Survey questions | Intervention | Control |
|---|---|---|
| Future aspirations, n (%) | ||
| At college/uni full-time | 63 (15.1) | 46 (11.4) |
| At college/uni and working part-time | 32 (7.7) | 54 (13.4) |
| Working full-time | 186 (44.7) | 180 (44.7) |
| Working part-time | 106 (25.5) | 90 (22.3) |
| On a training scheme | 15 (3.6) | 19 (4.7) |
| Unemployed | 4 (1) | 1 (0.3) |
| Other | 10 (2.4) | 13 (3.2) |
| Sexuality, n (%) | ||
| Female | ||
| I have never felt sexually attracted to anyone | 32 (18.3) | 24 (12.1) |
| Only to males, and never to females | 132 (75.4) | 165 (82.9) |
| More often to males and at least once to a female | 9 (5.1) | 8 (4.0) |
| About equally often to females and to males | 2 (1.1) | 2 (1.0) |
| More often to females and at least once to a male | – | – |
| Only to females, never to males | – | – |
| Male | ||
| I have never felt sexually attracted to anyone | 13 (5.9) | 6 (3.0) |
| Only to males, and never to females | 1 (0.5) | 1 (0.5) |
| More often to males and at least once to a female | – | 2 (1.0) |
| About equally often to females and to males | 1 (0.5) | 4 (2.0) |
| More often to females and at least once to a male | 1 (0.5) | 3 (1.5) |
| Only to females, never to males | 204 (92.7) | 184 (92.0) |
| Live with, n (%) | ||
| Both parents in same household | 272 (65.2) | 297 (72.4) |
| Mother only | 81 (19.4) | 65 (15.9) |
| Father only | 8 (1.9) | 7 (1.7) |
| Mother and partner or stepfather | 30 (7.2) | 28 (6.8) |
| Father and partner or stepmother | 9 (2.2) | 2 (0.5) |
| Grandparents only | 2 (0.5) | 1 (0.2) |
| Foster care | 1 (0.2) | 1 (0.2) |
| Others | 14 (3.4) | 9 (2.2) |
| Well off, n (%) | ||
| Not at all well off | 2 (0.48) | 2 (0.5) |
| Not very well off | 11 (2.7) | 30 (7.4) |
| Average | 198 (47.7) | 189 (46.9) |
| Well off | 147 (45.4) | 140 (34.7) |
| Very well off | 35 (8.4) | 18 (4.5) |
| I do not know | 22 (5.3) | 24 (6.0) |
Analysis of primary and secondary outcomes
Sixty pupils (7%) surveyed reported that they had had sex and the average age at which they had sex for the first time was 13.7 years in the intervention group and 14 years in the control group. In the ‘Age First Time’ question one pupil entered 20 and another entered 21. As these are impossible values given the age of the pupils filling in the questionnaire, they were excluded from the summary calculations for this question. Of those who reported ever having sex, the most common number of partners was one; however, 42% reported having had more than one partner. A complete breakdown of these responses can be viewed in Table 6.
| Survey questions | Intervention | Control |
|---|---|---|
| Ever had sex, n (%) | ||
| Yes | 35 (8.5) | 25 (6.4) |
| No | 376 (91.5) | 367 (93.6) |
| Age first time | 13.7 (0.184) n = 34 | 14 (0.096) n = 20 |
| How many people have you ever had sex with, n (%) | ||
| One | 20 (58.8) | 13 (54.2) |
| Between 2 and 5 | 7 (20.6) | 7 (29.2) |
| Between 6 and 10 | 4 (11.8) | 4 (16.7) |
| More than 10 | 3 (8.8) | – |
| Number of times had sex in past 6 months, n (%) | ||
| Once | 17 (53.1) | 5 (22.7) |
| Between 2 and 5 times | 11 (34.4) | 7 (31.8) |
| Between 6 and 10 times | 2 (6.3) | 5 (22.7) |
| Between 11 and 20 times | – | 1 (4.6) |
| More than 20 times | 2 (6.3) | 4 (18.2) |
| When last had sex, n (%) | ||
| < week ago | 5 (14.3) | 7 (29.2) |
| > week ago but < month ago | 9 (25.7) | 7 (29.2) |
| 1–6 months ago | 16 (45.7) | 7 (29.2) |
| > 6 months ago | 5 (14.3) | 3 (12.5) |
| Number of sexual partners in past 6 months (girls), n (%) | ||
| One | 5 (71.4) | 6 (85.7) |
| Between 2 and 5 | 2 (28.6) | 1 (14.3) |
| Between 6 and 10 | – | – |
| More than 10 | – | – |
| Number of sexual partners in last 6 months (boys), n (%) | ||
| One | 12 (60.0) | 9 (69.2) |
| Between 2 and 5 | 6 (30.0) | 2 (15.4) |
| Between 6 and 10 | – | 2 (15.4) |
| More than 10 | 2 (10.0) | – |
| Had sex when you did not want to in past 6 months, n (%) | ||
| Yes | 7 (21.9) | 7 (28.0) |
| No | 25 (78.1) | 18 (72.0) |
| Had sex when you did not want to in past 6 months (girls), n (%) | ||
| Yes | 1 (11.1) | – |
| No | 8 (88.9) | 7 (100) |
| Had sex when you did not want to in past 6 months (boys), n (%) | ||
| Yes | 6 (26.1) | 7 (38.9) |
| No | 17 (73.9) | 11 (61.1) |
Table 7 shows the responses to the contraception questions. Fewer than half of those participants who reported sexual activity (either in the intervention or control group) stated that they always used contraception (48%). Twenty-two pupils reported that they had been unprotected in the last sexual encounter they had had. They reported using a range of contraception types, the most common of which was condoms. Twenty-six (45%) reported that they had sex without using a condom at least once in the past 6 months.
| Survey questions | Intervention | Control |
|---|---|---|
| How often has sex been protected, n (%) | ||
| Never | 5 (14.7) | 3 (13) |
| Not very often | 4 (11.8) | 4 (17.4) |
| About half the time | 3 (8.8) | – |
| Most of the time | 3 (8.8) | 6 (26.1) |
| Always | 19 (55.9) | 10 (43.5) |
| Contraception used the last time you had sex, n (%) | ||
| None for me, do not know about partner | 8 (22.9) | 3 (12.0) |
| None for either of us | 5 (14.3) | 6 (24.0) |
| Yes | 22 (62.9) | 16 (64.0) |
| Type of contraception used the last time you had sexa | ||
| Pill, patch or vaginal ring | 5 | 5 |
| Condoms | 19 | 14 |
| Emergency contraceptive pill | 2 | 1 |
| Injection | 1 | – |
| Implant | – | – |
| Withdrawal method | 2 | – |
| Intrauterine device | – | – |
| Diaphragm/cap/spermicide | – | – |
| Natural family planning | – | 1 |
| Do not know name | – | – |
| Other | 1 | – |
| Number of times you had sex without a condom in past 6 months, n (%) | ||
| Never | 19 (57.6) | 13 (52.0) |
| Once | 4 (12.1) | 5 (20.0) |
| Between 2 and 5 times | 7 (21.2) | 4 (16.0) |
| Between 6 and 10 times | 2 (6.1) | 2 (8.0) |
| Between 11 and 20 times | 1 (3.0) | – |
| > 20 times | – | 1 (4.0) |
Table 8 lists the responses to questions regarding how easy or difficult participants would find accessing and using condoms. This question was asked to the entire sample. The majority of respondents felt that they would find it easy to suggest using condoms, but were not sure about how easily they would obtain condoms and how to use them correctly. However, these questions had a high rate of missing data (78 respondents either skipped or missed this question). This may be due to the fact that these questions were placed at the end of the questionnaire and therefore may have been missed due to time issues. Alternatively, respondents may have missed the fact that they were eligible to answer these questions, as they came directly after the sexual behaviour and pregnancy questions, which involved skipping instructions for those ineligible to complete them.
| Survey questions | Intervention | Control |
|---|---|---|
| Ease of getting condoms, n (%) | ||
| Very easy | 68 (18.0) | 54 (14.4) |
| Easy | 85 (22.5) | 77 (20.5) |
| Not sure | 144 (38.1) | 156 (41.6) |
| Difficult | 48 (12.7) | 51 (13.6) |
| Very difficult | 33 (8.7) | 37 (9.9) |
| Ease of suggesting condoms, n (%) | ||
| Very easy | 75 (20.0) | 69 (18.7) |
| Easy | 134 (35.6) | 133 (36.0) |
| Not sure | 133 (35.4) | 118 (32.0) |
| Difficult | 21 (5.6) | 29 (7.9) |
| Very difficult | 13 (3.5) | 20 (5.4) |
| Use a condom properly, n (%) | ||
| Very easy | 88 (23.4) | 59 (16.1%) |
| Easy | 102 (27.1) | 124 (33.9) |
| Not sure | 155 (41.2) | 151 (41.3) |
| Difficult | 17 (4.5) | 15 (4.1) |
| Very difficult | 14 (3.7) | 17 (4.6) |
Responses to the alcohol and drug questions are provided in Table 9. In total, 419 (50%) pupils admitted to drinking alcohol and 54 (6.5%) admitted to having used drugs. Sixty-eight pupils (representing almost 20% of our sample) reported being drunk at least two to three times a month over the previous 6-month period.
| Survey questions | Intervention | Control |
|---|---|---|
| Ever drunk alcohol, n (%) | ||
| Yes | 239 (57.2) | 180 (44.0) |
| No | 179 (42.8) | 229 (56.0) |
| How often have you got drunk in past 6 months, n (%) | ||
| Never | 111 (46.6) | 100 (55.9) |
| < once a month | 74 (31.1) | 65 (36.3) |
| 2–3 times a month | 31 (13.0) | 7 (3.9) |
| Once a week | 16 (6.7) | 6 (3.4) |
| > once a week | 6 (2.5) | 1 (0.6) |
| Ever taken drugs, n (%) | ||
| Yes | 33 (7.9) | 21 (5.2) |
| No | 386 (92.1) | 383 (94.8) |
Five questions were asked regarding reasons for delaying sex over the past 6 months, and responses are shown in Table 10. The majority of delayed sex was not due to contraception availability or alcohol or drug usage but rather to values. Many pupils felt that they should wait until they are older (n = 390) or that their parents would not approve (n = 291). Reponses were mixed about whether sex had been delayed due to not having the correct partner, with slightly more pupils saying that this was not a consideration in delaying sex. Almost 300 pupils skipped these questions entirely. Similar to the issue reported above in the condom questions, this question had a high rate of missing data. This may be due to the fact that these questions were placed at the end of the questionnaire and therefore may have been missed as a result of time issues. Alternatively, respondents may have missed the fact that they were eligible to answer these questions, as they came directly after the sexual behaviour and pregnancy questions, which involved skipping instructions for those ineligible to complete them.
| Survey questions | Intervention | Control |
|---|---|---|
| Delay sex because of no contraception, n (%) | ||
| Yes | 63 (24.1) | 55 (20.0) |
| No | 198 (75.9) | 220 (80.0) |
| Delay sex because parents would not approve, n (%) | ||
| Yes | 151 (55.3) | 140 (49.5) |
| No | 122 (44.7) | 143 (50.5) |
| Delay sex because under influence of alcohol/drugs, n (%) | ||
| Yes | 28 (10.6) | 27 (9.9) |
| No | 237 (89.4) | 247 (90.2) |
| Delay sex because believe you should be older, n (%) | ||
| Yes | 198 (67.4) | 192 (62.5) |
| No | 96 (32.7) | 115 (37.5) |
| Delay sex because was not with right partner, n (%) | ||
| Yes | 112 (43.8) | 96 (34.5) |
| No | 144 (56.3) | 182 (65.5) |
Table 11 contains information about the pregnancy-related questions. One boy in the sample reported that he had got a girl pregnant; eight others reported that they did not know. One girl in the sample reported that she had been pregnant. Both pregnancies had occurred within the previous 12 months and one of these was still in the pregnancy stage; the other pregnancy outcome was not reported. The female respondent admitted that she had not intended to get pregnant, whereas the male respondent said that he had intended to get his partner pregnant.
| Questions and responses | Intervention | Control |
|---|---|---|
| [Boys] Ever got a girl pregnant, n (%) | ||
| Yes | – | 1 (5.9) |
| No | 20 (76.9) | 14 (82.4) |
| Do not know | 6 (23.1) | 2 (11.8) |
| [Girls] Ever been pregnant, n (%) | ||
| Yes | 1 (12.5) | – |
| No | 7 (87.5) | 6 (100.0) |
| Do not know | – | – |
| How many months ago did you/she get pregnant, n | ||
| Less than 1 month ago | – | 1 |
| Between 2 and 5 months ago | – | – |
| Between 6 and 9 months ago | – | – |
| Between 10 and 12 months ago | 1 | – |
| More than 1 year ago | – | – |
| Do not know | – | – |
| What happened with pregnancy, n | ||
| Still pregnant | – | 1 |
| Miscarriage | – | – |
| An abortion | – | – |
| A baby | – | – |
| I do not know | – | – |
| Intended pregnancy (girls), n | ||
| I intended to get pregnant | – | – |
| My intentions kept changing | – | – |
| I did not intend to get pregnant | 1 | – |
| Intended pregnancy (boys), n | ||
| I intended for my partner to get pregnant | – | 1 |
| My intentions kept changing | – | – |
| I did not intend for my partner to get pregnant | – | – |
Visual analogue scale
A small percentage of respondents did not answer this question (5.2%). The majority of participants placed the responsibility on boys to prevent UTP in the 26–50% range (Table 12), although there was a spread of answers across all the possible quartiles. Based on this we did not make any amendments to the visual analogue scale for the first follow-up.
| Quartiles | Intervention (%) | Control (%) | Total (%) |
|---|---|---|---|
| 0–25% | 2.4 | 2.2 | 2.3 |
| 26–50% | 78.1 | 78.4 | 78.2 |
| 51–75% | 12.0 | 11.5 | 11.8 |
| 76–100% | 3.2 | 2.0 | 2.5 |
| Skipped question | 4.3 | 6.1 | 5.2 |
| Total | 100.0 | 100.0 | 100.0 |
Comfort completing the questionnaire
The majority of participants stated that they felt comfortable in answering most of all the questions in this questionnaire (80%, n = 608). A small number of participants (4%, n = 27) stated that they were uncomfortable in answering all of the questions asked. Again there was a high percentage of missing data for this question, potentially as a result of it being the last question.
Scale reliability and validity
Cronbach’s alpha is calculated as a measure of internal consistency/reliability for all scales. Overall, the reliability of the measures was satisfactory (Table 13).
| Scale | Completed, n | Mean | SD | Min. | Max. | Cronbach’s Alpha |
|---|---|---|---|---|---|---|
| Family Connectedness | 813 | 0.526 | ||||
| Intervention | 409 | 15.2 | 0.123 | 4 | 20 | |
| Control | 404 | 15 | 0.094 | 7 | 20 | |
| Comfort Communicating about Pregnancy | 756 | 0.576 | ||||
| Intervention | 385 | 5.4 | 0.153 | 2 | 8 | |
| Control | 371 | 5.4 | 0.107 | 2 | 8 | |
| Comfort Communicating about Contraception | 706 | 0.699 | ||||
| Intervention | 349 | 8.3 | 0.087 | 3 | 12 | |
| Control | 357 | 8.4 | 0.131 | 3 | 12 | |
| Sexual Self-Efficacy | 557 | 0.876 | ||||
| Intervention | 280 | 3 | 0.198 | 0 | 5 | |
| Control | 277 | 3.1 | 0.123 | 0 | 5 | |
| Male Role Attitudes | 682 | 0.729 | ||||
| Intervention | 341 | 18.9 | 0.836 | 8 | 32 | |
| Control | 341 | 19.4 | 0.244 | 8 | 32 | |
| Sexual Socialisation Total | 718 | 0.568 | ||||
| Intervention | 328 | 49.7 | 1.080 | 28 | 82 | |
| Control | 336 | 49.6 | 0.538 | 28 | 71 | |
| Sexual Socialisation Peer | 704 | 0.748 | ||||
| Intervention | 352 | 31.4 | 0.612 | 14 | 59 | |
| Control | 352 | 31.2 | 0.300 | 13 | 49 | |
| Sexual Socialisation Parent | 706 | 0.596 | ||||
| Intervention | 358 | 18.4 | 0.622 | 9 | 32 | |
| Control | 348 | 18.4 | 0.264 | 9 | 29 |
The Sexual Self-Efficacy scale, Male Role Attitudes scale and Sexual Socialisation Peer scale had high internal consistency (Cronbach’s alpha in excess of 0.7), Family Connectedness, Comfort Communicating about Pregnancy, Comfort Communicating about Contraception, Sexual Socialisation Total and the Sexual Socialisation Parent scales had satisfactory internal consistency (Cronbach’s alpha: 0.526–0.699). Overall, there was a high proportion of missing data for nearly all of the scales.
There are seven items assessing knowledge. The overall knowledge scores were roughly equal for both groups (n = 4.7 intervention group; n = 4.5 control group). The knowledge items (Table 14) employed a true/false response format, rendering a check on internal consistency inadvisable. The questions highlighted in bold in Table 14 are those for which the majority of respondents gave the incorrect answer. These results suggested that there were some items that could be dropped from the main trial questionnaire, such as the item ‘washing the vagina after penetrative sex will help to prevent pregnancy’, for which most respondents selected the correct answer.
| Knowledge item | True, n (%) | False, n (%) |
|---|---|---|
| Washing the vagina after penetrative sex will help to prevent pregnancy (false) | 50 (6) | 522 (63) |
| A girl can get pregnant if the boy withdraws his penis (pulls out) before ejaculation (coming) (true) | 348 (42) | 279 (34) |
| Contraception (when used correctly) provides as much protection against pregnancy as not having sex (false) | 261 (31) | 349 (42) |
| The rhythm method (only having sex during the few days before and after a woman’s period) is as safe as using a condom in preventing pregnancy (false) | 83 (10) | 363 (47) |
| When teenagers have penetrative sex for the first time , the majority of them use condoms (false) | 340 (41) | 201 (24) |
| Teenage males can seek advice from pregnancy counsellors (true) | 393 (47) | 101 (12) |
| More than half of all teenagers in Northern Ireland have had penetrative sex by the time they are 16 (false) | 382 (46) | 132 (16) |
Intentions to Avoid Teenage Unintended Pregnancy scale
An Intentions to Avoid Teenage Unintended Pregnancy scale (TUPS) was developed for inclusion in the questionnaire (see Pupil Questionnaire in Appendix 3). A related publication is in preparation for submission and is detailed in publications associated with the report in the Acknowledgements section. Each item in the TUPS was preceded by the stem ‘when thinking about future sexual encounters how likely is it that you would…’. All items were summed to produce a total score, which could range from 15 to 75, with higher scores indicating greater intentions to avoid UTP. Existing intention measures focused mainly on retrospective reports of women, whereas this scale was designed to be prospective, including both men and women. Content validity was established through basing scale items on the empirical literature and then testing these in the pilot study. After completing the 15 items of the TUPS all students took part in a discussion about the scale. Some expressed confusion over the terms used in the Likert scale (e.g. what was the difference between somewhat likely and extremely likely), while others felt that some of the questions were too personal. The five-point Likert scale comprised extremely unlikely = one, somewhat unlikely = two, unsure = three, somewhat likely = four, and extremely likely = five. The spread of descriptive statistics showed that the majority of pupils were able to use the scale in a sensible manner; therefore, no changes to the scale were deemed necessary. The subject matter of the scale means that several items seek information of a personal nature. All students were informed that if they felt uncomfortable answering any questions they could skip them. As this is ultimately a matter of personal opinion, no further action was taken. During the feasibility study construct validity of the TUPS was established by means of principal components analysis, which revealed three factors (contraceptive use, child–parent communication and controlling the timing of sex), spread across 12 items. Internal consistency of the 15-item tool as measured by Cronbach’s alpha was 0.798. The TUPS is a potentially useful measure of adolescents’ intentions to avoid UTP that has been psychometrically validated, and we would continue to incorporate its use moving forward to a full trial. The scale could be especially useful in assessing the impact of future interventions designed to prevent UTP in this population.
Analysis of socioeconomic status variables
Socioeconomic status was measured in the study using six different variables in order to determine the best measurement to use for a future Phase III trial. The different measurements used were postcode (also used as a back-up method to match questionnaires across the three time points), receipt of free school meals, mother’s highest level of education, father’s highest level of education, how well off the family is perceived to be and future aspirations. Table 15 shows the breakdown of the missing data and ‘don’t know’ responses for each variable across all three time points.
| Measure | Baseline, n (%) | Follow-up 1, n (%) | Follow-up 2, n (%) |
|---|---|---|---|
| Postcode | 28 (3) | ||
| Do you receive free school meals? | 33 (4) | 47 (7) | 10 (1) |
| What is your mother’s highest level of education? | 302 (36) | a | a |
| What is your father’s highest level of education? | 304 (37) | a | a |
| How well off is your family? | 62 (7) | 26 (4) | 18 (2) |
| What are your future aspirations? | 12 (1) | 12 (2) | 19 (2) |
Table 15 demonstrates that two of the SES measures (mother’s and father’s educational level) had unacceptably high levels of non-response. Those measures were not repeated in either of the follow-ups. Highest level of parental education is a commonly used proxy measure of SES in the literature, although based on the results from this feasibility study this measure would not be selected for use in the full trial. The other measures had smaller, more stable, levels of missing data across all three time points (ranging from 1% to 7%). The question ‘How well off is your family?’ did present some challenges to understanding (see Chapter 2); however, as the study progressed we modified the explanation for this question and consequently reduced the level of non-response down to 2% (from 7%). As such, the research team have increased confidence in the quality of responses received on this question. As SES is difficult to measure, prior to going forward to a future Phase III trial the research team would endeavour to conduct more qualitative research with a young people’s advisory group and a review of the literature to ascertain those measures that we should continue to use.
Summary of changes made to questionnaire for first follow-up data collection (5 months after baseline data collection)
-
Added ‘If there are any questions you do not understand, look at the list of definitions at the end of the questionnaire but please ask us if you need any help ‘ to the instructions.
-
Questions 4 (What is your ethnic background?), 5 (How religious do you think you are?) and 6 (What religion where you brought up with?) removed from the baseline questionnaire.
-
Question 7: changed to include ‘(By this we mean how well off your family is in terms of money)’.
-
Question 11: changed from ‘Have you ever drunk alcohol?’ to ‘Have you ever taken an alcoholic drink (not just a taste or a sip)?’.
-
Question 20: certain questions within changed from ‘For girls/boys only’ to ‘If you are a girl/boy’.
-
Question 21: changed font size and highlighted important instructions.
-
Question 22: removed ‘This section concerns beliefs about being a man.’ From the description.
-
Question 23: changed ‘ your degree of agreement/disagreement with’ to ‘how you feel about’.
-
Question 43: moved to the next page.
-
Moved Thank you message up to above Question 46.
-
Question 46: removed lines and shortened box size.
-
Added definitions page.
Summary of changes made to questionnaire for second follow-up data collection (9 months after baseline data collection)
-
Added NIHR logo.
-
Removed Participant identification number (ID) and Date completed from front cover.
-
Added ‘If there are any questions you do not understand, look at the list of definitions at the end of the questionnaire but please ask us if you need any help‘ to the instructions.
-
Questions 4 (What is your ethnic background?), 5 (How religious do you think you are?) and 6 (What religion where you brought up with?) removed from the follow-up questionnaire.
-
Question 7: changed to include ‘(By this we mean how well off your family is in terms of money)’.
-
Question 11: changed from ‘Have you ever drunk alcohol?’ to ‘Have you ever taken an alcoholic drink (not just a taste or a sip)?’.
-
Question 20: certain questions within changed from ‘For girls/boys only’ to ‘If you are a girl/boy’ and added ‘Boys & Girls’ to other questions.
-
Question 21: changed font size and highlighted important instructions.
-
Question 22: removed ‘This section concerns beliefs about being a man’ from the description.
-
Question 28: added additional option ‘not since June 2015’ as the first option.
-
Question 43: moved to the next page.
-
Moved Thank you message up to above Question 46.
-
Question 46: removed lines and shortened box size.
-
Added definitions page.
-
Changed all ‘Go to Q…’ references to ‘Go to Question…’.
-
Changed word search.
Qualitative data analysis
In total, 12 pupils participated (six in each group), each of whom had responded at least twice to the paper version of the questionnaire. The groups comprised both male (n = 4) and female pupils (n = 8).
Questionnaire instructions
Both focus groups began by reading the first page of the questionnaire, which contained the instructions to aid completion. The clarity of the instructions was then discussed and anything that had been missed out that really should be stated on this page was considered. Both groups felt that, overall, the instructions contained the right amount of information and were clear, with the exception of one statement. The troubling statement was ‘Don’t spend much time on any one question; make a choice and move to the next’. It was clear from the discussion that this was confusing and they felt that a statement like ‘if you are stuck on a question, move on to the next question and you can come back to that one later’ would be more clear. They felt that the instructions were reassuring, saying ‘that you don’t have to answer all of them if you don’t want to’. They also liked the pointer to the list of definitions that is at the back of the questionnaire and suggested that it should be highlighted more and perhaps put at the top of the page so that everyone will notice it. One participant suggested that there should be a pointer to the definitions at the top of every page such as, ‘if you have trouble with some of the definitions then see the definitions page at the back’.
One of the groups highlighted the fact that they did not actually read the instructions when they were completing the questionnaire, instead skipping on to the first question and that they thought that most others were the same. One stated ‘I didn’t even know they were there’. Someone else said ‘I knew they were there – but it’s probably only for people completing it first time’. Another felt that ‘you just really get on with the questions’ but that it was good to have the instructions just in case.
This highlights that the instructions need to be more visible and integrated within the questionnaire.
Questionnaire design
The focus groups then discussed the design and visual appeal of the questionnaire. They felt that printing the questionnaire in colour as opposed to black and white would not have any specific advantages and that it was fine the way it was. One person felt that it was off-putting at first because ‘it just looked like there was a lot but then you fly through it’. They felt like there should be more clear space as the sections were ‘a bit close together’.
Font type and size were deemed to be fine. The shading of alternative question lines was complimented as it ‘helps keep you on track with the questions’.
One of the focus groups noted a design element that impacted on the privacy of participants. They had noticed that if you reported having previously had sex that the last section contained a large number of questions that needed to be completed. Those reporting no sex did not have to complete this section. Therefore, this meant that you could work out who in the class had had sex.
One thing that maybe would be like embarrassing for someone who has had sex and doesn’t want their friends to know and then they are at it for an extra 10 minutes compared to everyone else.
This was seen as being obvious to spot, ‘It is really easy to see you can just look around you’.
In order to combat this the group discussed randomising the sections so that it would not be as obvious or add in dummy questions to keep everyone roughly to the same time. Overall, there is a need to space out the questionnaire and potentially consider randomising the questions within it to ensure privacy.
Terminology used
The conversations then moved on to discussing the specific terminology used within the questionnaire. To aid understanding and to minimise any potential embarrassment at having to ask questions because they may be ‘too embarrassing to ask’ or ‘they [classmates] might mock you for not knowing it’, a definitions list was provided along with the questionnaire after the initial baseline data collection. In the second round of data collection this definition list was provided as a separate sheet and in the final data collection round this was provided within the questionnaire, on the back page. Some of the focus group participants admitted that they did not ‘even know they were there’, whereas some did use this page and found it useful. Those who did not notice the list felt that it should be positioned at the start of the questionnaire where it would be visible and more people would know that it was there and that this would be preferable to having a separate sheet. One group disagreed and felt that it would be better as a separate sheet so that they could have it in front of them at all times and that it would save having to flick back and forth. However, both groups agreed that the definitions list needed better signposting. One participant suggested putting a reminder at the top of each questionnaire page to check the definitions page, whereas another felt that when a word is encountered for the first time that is in the definitions page then there should be a comment to say ‘go to page 15 or whatever for a definition’.
Each focus group spent time reading over the definitions contained in the list, the outcome of which was that they were pitched at the correct level. Comments were made such as ‘they are not big massive words; most people our age would understand most of them’.
They also liked how short the definitions were. The only definition with which participants had an issue was that of a legal high. It was felt that after reading the definition (which is a standard governmental definition) that ‘maybe some people might not understand what a legal high is’.
The participants were asked what their understanding was of the following specific terms (which are not included in the definition list): unprotected sex, penetrative sex, sex urges, sexual favour and unwanted sexual advance. They were able to describe unprotected sex as ‘sex without condoms’ and as sex with ‘no protection’.
The term penetrative sex had responses such as ‘don’t really know’, and, although participants understood the term when it was explained, it appears that it is not one they are used to hearing or thinking of. They were able to describe sex urges as ‘wanting to have sex; your desires – sexual’, but one group wanted this to be included in the definition list. No one was able to offer a definition of the term sexual favour. Unwanted sexual advance was explained as:
if someone tries something on but you didn’t want to; not wanting to have sex with someone even though they are trying to.
To revise the terminology used in the questionnaire, the focus groups highlighted that we need to increase signposting to the definitions, to add a few definitions to the list (such as sexual favour and sex urges) and to work on making a couple of the definitions clearer (such as legal highs).
Individual questions
For this section of the focus groups, the research team had highlighted 10 individual questions that they wanted to discuss, the focus group comments for each will be summarised below.
This question was rather controversial, and, although all the participants stated that they did complete this question, they were not happy at being asked to do it. They felt that it was ‘a bit suspicious so you would feel more comfortable if you knew why’ and that we should ‘write why you need this’.
There was a lot of difficultly expressed with this question. Although participants felt that it was ‘good to have options’ listed, the suggested options seemed confusing. First, they felt that an option for ‘have not decided yet’ was missing from the list, as ‘you don’t know what you are going to do yet so it is hard to just pick one answer’.
Several thought that the option for attending university part time was confusing as they did not think it was possible to do this. They did not have a clear understanding about what was meant by a training scheme. One asked ‘where would you put training to be a hairdresser?’
It was suggested that, although examples might be helpful, participants would have preferred fewer options such as attending college, attending university, working, unemployed and do not know.
Many of the focus group participants mentioned that this question caused them difficulty when completing the questionnaire:
I didn’t know how to fill this in.
It was clear that ‘well off’ was not a term that they were used to. One asked ‘is the question trying to ask you if your family has money?’ and someone else offered the explanation that the question was asking if ‘you have what you need and then you have more as well’.
The explanation that was added to the subsequent data collection was welcome but some participants still felt that we could explain this better, as the ‘new version still has well off in it so it could still be a bit tricky’.
They felt that people their age would probably find it hard to compare where they are at between the options given.
The focus group participants did not like this question and the majority stated that they were guessing the answer rather than ticking the ‘don’t know’ box. They felt that more examples of the options could be given. This was because they had difficulties understanding what certificates and diplomas were and whether or not a university degree was higher than each of these. They did all understand what an apprenticeship was.
There was a mixed reaction to the response categories in this Likert-scale questionnaire (Table 16).
| Questionnaire | Focus Group 1’s suggestion | Focus group 2’s suggestion |
|---|---|---|
| Extremely likely | Certain Definite |
Definitely |
| Somewhat likely | Possible | Probably |
| Not sure | – | – |
| Somewhat unlikely | Not likely | Probably not |
| Extremely unlikely | Never No way |
Never |
In the original questionnaire (applied in the pilot study), the question, ‘Have you ever drunk alcohol?’ was included. During data collection and analysis it was changed to ‘Have you ever taken an alcoholic drink (not just a taste or a sip)?’ to avoid confusion with drinking and being drunk. Both focus groups agreed that they preferred the new question wording and that is was best to avoid the word ‘drunk’.
It was felt that this question was clear, as it aimed to see who would be more responsible. Participants thought that the example sheet was very helpful and that integrating it into the questionnaire rather than using a separate sheet should be considered. One suggestion was that it would be nice to include a ‘don’t know’ box.
These questions contain questions for both boys and girls and then also separate questions for boys and girls. The groups agreed that it would be more helpful to ‘write the questions so anyone can fill them out’ by writing ‘boyfriend/girlfriend; partner’ instead of the current gender-specific options. Regarding the four-point Likert scale used they had difficulties between a little uncomfortable and somewhat uncomfortable because they look the same. They suggested changing ‘a little uncomfortable’ to ‘Quite uncomfortable’, ‘Somewhat uncomfortable’ to ‘Very uncomfortable’ and ‘Very uncomfortable’ to ‘Extremely uncomfortable’.
This question was deemed to be very confusing. One person realised that they had completed the question wrong, stating ‘I think I ticked this side when I ticked no as well’.
Several people thought that it overused the word ‘certain’. They did not like the ‘neither certain nor uncertain’ option and would prefer ‘don’t know’ instead. Someone pointed out that they expected ‘very certain’ to be the first option (currently the first option is ‘very uncertain’) as other questions started on very certain. One person was confused about the need for the uncertain options, as ‘if you tick yes why would you need uncertain?’
They wanted the instructions left at the beginning of the question even though no one admitted to reading them while they completed it. The idea of potentially changing the layout to have the ‘If yes’ questions underneath the ‘Could you do it?’ questions was welcomed as participants thought that this looked clearer.
This question, in its current format, contains a list of STIs and asks the respondent to tick what they have or have not been diagnosed with. Both focus groups preferred the new question format idea of just asking if you have had an STI and asking the respondent to write in what that was. They thought that people who ticked all the boxes were ‘just having a laugh’ or might have been ‘probably like thinking the question was asking them what they had heard of’.
Other issues
The final section of the focus group discussions gave the participants the opportunity to bring up any other issues that they may have had with the questionnaire. Some issues that arose were the different order of the Likert scales:
question 22 goes from strongly disagree to strongly agree but question 23 goes from strongly agree to strongly disagree.
They also preferred the agree/disagree Likert scales rather than uncertain/certain ones as they have fewer words and are more black and white:
dead on straight agree/disagree are better.
It was also noted that it was good the way you could just skip questions that did not apply rather than having to tick no. One group discussed the fact that there were not really any questions about the wider issues of dealing with UTP (e.g. did you know anyone this happened to? How would you feel if it happened to you? What would you do?). They felt that it ‘doesn’t really get to the point – it like kinda goes around it’.
Conclusions
In conclusion, these focus groups brought to light a number of interesting problems with the survey instrument, as well as some suggested changes that the research team could make to allow greater understanding for the target age group (Table 17).
| Section | Suggested change |
|---|---|
| Questionnaire instructions | Make instructions more visible |
| Better integrate definition list | |
| Questionnaire design | Space out the questionnaire |
| Randomise questions order | |
| Terminology used | Increase signposting to the definitions |
| Add definitions to the list (sexual favour and sex urges) | |
| Make a couple of the definitions clearer (legal highs) | |
| Individual questions | State why we are asking for participants’ postcodes |
| Change options for the leave school question | |
| Consider removing the perceived wealth/’well-off’ question | |
| Change wording of Likert responses in the Intentions scale | |
| Include a do not know box in the visual analogue scale | |
| Change layout of the Comfort Communicating scale | |
| Change wording of Likert responses in the Comfort Communicating scale | |
| Change layout of the Sexual Self-Efficacy scale | |
| Change the format of the STI question | |
| Other issues | Ensure standardisation of Likert-scale options throughout |
| Consider adding more questions regarding UTP |
Mode of administration: electronic versus paper based
Consenting pupils were tested using either a paper questionnaire or an online survey under exam conditions. When making arrangements to facilitate the testing, schools were given the option of how they would prefer to administer the questionnaire. Three schools agreed that they would prefer to use the online survey. Although using an electronic version of the questionnaire had numerous benefits (informed by use of the electronic SurveyMonkey™ online platform in the pilot study), including increased data completeness and the hover-over definitions, its use was discontinued after the first follow-up owing to technical difficulties. Only some pupils from two comparison schools were able to use this mode. During the baseline data collection there were numerous administrative difficulties in using the electronic questionnaire. All three schools had issues, including not being able to log-in and having timing out issues, and a significant number of participants in these classes had to transfer to using a paper questionnaire. For the first follow-up only one school of the original three was happy to try the electronic method again. The software developers were present throughout this data collection to troubleshoot problems and again the same issues occurred. After this session the data collected were not available on the server and these data were unfortunately lost. Owing to these issues, the research team was not confident that the electronic system was fit for purpose and its use was discontinued in order to ensure the safety of the collected data and to maintain positive relationships with both schools and participants who were frustrated with the software issues. In total, 2231 paper versions of the questionnaire were completed and 82 questionnaires were completed online (data from 11 of these were lost as a result of a technical error).
The online survey was able to record the length of time taken to complete the survey; this was recorded at 23 minutes and 45 seconds (range 8–43 minutes). Detailed time records were not available for those completing the questionnaire in paper format but the majority of pupils were able to complete the questionnaire within the constraints of one timetabled lesson.
Conclusions
The questionnaire has been significantly tested, revised and strengthened throughout both the pilot and feasibility study. The pilot was conducted using the SurveyMonkey™ platform as the software developers providing the electronic version were not able to provide a working copy in time to facilitate this. As such, the testing was mainly focused on the clarity of meaning and format of the questions posed as well as the definitions used. It also served to provide insight with regard to the ability and acceptability to conduct this research online in a classroom environment. After the pilot questionnaire and focus groups were completed, significant changes were made to the questionnaire both in terms of the definitions given and the wording of some questions. At this stage some questions and a scale were removed owing to limited variability in participant responses. Both paper questionnaires and an online electronic questionnaire were utilised during the feasibility study. Schools had a choice of which administration mode would be used and three schools selected to use the electronic questionnaire. Unfortunately, there were numerous issues at baseline in these three schools, including participants being unable to access the questionnaire online and being timed out. Many participants had to switch to using paper questionnaires. At the first follow-up, only one school agreed to use the online questionnaire as a result of these issues, and the software developers attended that session to troubleshoot problems. Unfortunately, the issues persisted and we were left with no usable data from that data collection session. It was then that the research team decided not to continue with the electronic version owing to its instability and to loss of data. Nevertheless, persevering with the paper questionnaire, minor amendments were made to questions to improve readability, removing questions that did not need to be asked at each time point, and a separate page containing definitions that mirrored those in the electronic version was produced. Based on cognitive interviews after the final data collection wave in the feasibility study, we determined that further changes were required. These included simplifying and standardising the Likert-scale options and increasing the privacy of the participant by ensuring that skipped sections would be replaced with an equivalent number of questions and randomising sections that would be incorporated into the questionnaire for a proposed future trial.
Chapter 5 Recruitment, randomisation, allocation and retention
Introduction
Feasibility trials offer unique opportunities to examine anticipated and unexpected challenges to successful recruitment and retention and to explore possible solutions suited to the particular context in which the trial is taking place. The present study aimed to (1) establish trial recruitment and retention rates to inform a larger effectiveness trial; (2) assess acceptability of participation, including equality of engagement in and across schools of different socioeconomic and religious types and schools allocated to the comparison group; and (3) identify optimal recruitment and retention strategies for a larger effectiveness trial.
We begin with a brief review of the literature on factors thought to influence participation in research and techniques reported to improve recruitment and retention in randomised controlled trials (RCTs) in general, and school-based health research in particular. We detail the anticipated challenges of recruitment and retention, the multilevel strategies used in the current study to recruit and retain schools, teachers, pupils and parents and their yield, as well as the challenges we encountered during the process. We conclude with lessons learned for a future full-scale trial.
Why is successful recruitment and retention important: a background literature review
Randomised controlled trials generally require large numbers of participants and follow-up over long time periods. Recruiting adequate numbers of participants and retaining them in the study for its entire duration, although challenging, is essential for ensuring internal and external validity and reducing bias that is introduced if certain groups of participants refuse participation or withdraw from the study.
However, participation rates in general have been decreasing over the past decades and it is increasingly difficult to recruit and retain participants to RCTs. 96 Fewer than one-third of publicly funded RCTs reach their recruitment targets within the specified time frame and more than half need to be extended owing to recruitment difficulties. 97 This can result in extended study duration, increased expenditure and findings that are not statistically accurate, because recruitment may be biased towards particular groups. 98 In worst case scenarios, insufficient recruitment or retention can result in a trial being stopped or a delay in the roll-out of an intervention with serious public health benefits. 99
Factors influencing recruitment and retention
It is widely recognised that the proliferation of research studies, marketing surveys and opinion polls over the past decades, and the resulting increase in the number of participation requests received by both individuals and sites, has led to a situation whereby increasing numbers of people refuse all (or all but the most immediately relevant) requests to take part in research. 100 Other factors thought to influence research participation include the characteristics and demographics of potential participants, factors related to the study design, and characteristics of the investigator(s). 101,102
Demographic factors that are associated with increased likelihood of participating in research include being younger, female, married, of higher SES, of higher educational attainment and in employment. 96,101,103 Factors relating to the study design include the length of time participants are expected to engage with the study, the potential burden placed on them, the treatment being offered, concern about allocation to the control group and the focus of the study (in particular whether or not it is sensitive/controversial). 98,101 The characteristics of the organisation responsible for the research and its representative investigators, particularly perceptions of their credibility, is also thought an important influencing factor. 98,104
In reference to school-based research, Pound et al. 104 found that perceptions of the social value of the study (i.e. value to students and the community and perceived benefits of taking part) and confidence in the organisation responsible for the research strongly influenced the decisions of school management to take part in a trial. Barriers to recruitment included the amount of effort involved for the school, interest in the project and commitment to other research. In a qualitative investigation of the views of school superintendents and principals, Befort et al. 105 found that school management was interested in research projects that (1) provide tangible benefits to their school; (2) are consistent with their academic mission; (3) are not burdensome; (4) do not take place during exam time or other busy periods; and (5) are credible and non-controversial.
Strategies to optimise recruitment and retention
In a recent systematic review of methods to improve recruitment to RCTs, Treweek et al. 98 concluded that effective interventions include telephone reminders to non-respondents; the use of opt-out rather than opt-in procedures; and open designs whereby participants know which treatment they are receiving in the trial. Over the years, others have reported that recruitment facilitators include engagement with the target population when developing the intervention and preparing participant information about the study;106 a personalised and culturally sensitive approach to participants;99,107 designing recruitment processes that are aimed towards clearly highlighting to potential participants the beneficial outcomes of taking part and addressing any barriers or perceived negative outcomes;108 providing research and implementation support by providing a dedicated research team contact;109 minimising the workload for participants by adapting trial processes so they are in line with usual ways of working at the site;109 providing financial or other incentives;29 and good communication and expressions of appreciation to site facilitators and participants. 108,109 Although some have suggested the value of using technology such as internet-based questionnaires110 and the use of video to provide trial information111–113 to improve recruitment, a recent systematic review98 concluded that their effect is not clear. At the very least, however, the use of video does have obvious benefits in terms of recruiting participants with low literacy levels. 114
A number of studies have reported recruitment and retention facilitators that are specific to schools. Lytle et al. 108 argue that an essential strategy is to adjust the recruitment process to suit the culture of each school and to plan to impact on a number of individual-, environmental- and behavioural-level factors. In addressing individual factors, they sought to help the school decision-makers recognise the importance of the research projects goals and objectives. They did this by emphasising the proximal and distal public health benefits of the programme intervention and highlighting the value and credibility of the programme using expert testimonials. In addition, they increased the primary decision-makers’ self-efficacy in being able to ‘sell’ the programme to implementers by offering to speak to implementers themselves. The researchers sought to influence environmental factors by ‘reducing external barriers to acceptance, enhancing social norms, and by committing future support to schools through training and materials provision’. 108 To achieve this they shared testimonials from participants who took part in the pilot trial, adjusting recruitment procedures to suit individual schools, providing a clear outline of roles and responsibilities of both school and research team members, facilitating discussion on the benefits and perceived barriers to taking part and providing external support (e.g. training, paying for substitute teachers), which would enhance implementation in intervention schools. Targeting behavioural factors, the team provided incentives in the form of training, research and intervention materials and support during implementation. For schools randomised to the control group, materials were provided at the end of the trial. In addition, providing refreshments at any meetings was seen to increase attendance as was sending personal thank you notes to all involved from the research team following such meetings. Obtaining ‘intention to act’ was operationalised in the recruitment process by asking individuals to sign a contract. Although these were not considered legally binding they were part of a behavioural process important for formalising the agreement. Lytle et al. 108 also imply that marketing techniques can be of value in recruiting for schools. For example, they sent a letter to schools saying that ‘only two more slots’ were available and used videos with end-user testimonials to increase credibility and perceived acceptability.
Aarons et al. 107 argue that it is essential to consider each participating school’s needs in planning intervention and data collection activities. They argue that it is essential to communicate to decision-makers at the recruitment stage that the research will not interrupt the ‘ebb and flow’ of the school. In particular, time and timing are important considerations for both recruitment and implementation planning in schools; although study deadlines must be met, this needs to be balanced with the school timetable. 107 Summer, Christmas and Easter closures as well as half-term breaks in autumn and winter must all be considered, along with school-specific staff development closures, public holidays and exam periods. Furthermore, the school curriculum is often overcrowded, with some schools less willing than others to remove pupils from exam subjects. In this regard, Befort et al. 105 suggest that, from the outset, researchers should be very clear about time commitments and how the study may be used to improve the school’s academic mission.
Financial incentives have been reported to be beneficial for recruiting and retaining both schools and pupils. 29 Harrington et al. 115 suggest that if schools are concerned about possible allocation to the control group (thereby depriving their pupils of a potentially beneficial intervention), a delayed treatment condition rather than no treatment may be an added incentive for schools to participate.
Potential barriers to and facilitators of successful recruitment and retention
Table 18 details potential barriers to and facilitators of successful recruitment and retention.
| Recruitment barriers | Recruitment facilitators | Retention barriers | Retention facilitators |
|---|---|---|---|
|
|
|
|
In conclusion, as outlined in Table 18, it was anticipated that a number of barriers to and facilitators of recruitment could impact on our ability to reach recruitment targets and retain participants in the study. In general, it was anticipated that key influences would be whether or not (1) the school was currently or recently involved in a research project; (2) school management, teachers and parents saw RSE as a priority subject and teenage pregnancy as a current concern; and (3) school management, teachers and parents perceived both the research project and intervention as credible, beneficial, compatible with their needs, ways of working and ethos, and not burdensome in terms of time and resources. Although the initial intervention design and development process sought to overcome potential intervention-level barriers (see Chapter 3), it was also anticipated that important research-level facilitators of recruitment and retention would include (1) approaching schools that were more likely to see RSE as a priority subject and teenage pregnancy as a current concern; (2) encouraging buy-in and intention to act by making roles and responsibilities clear from the outset, assigning a trial champion in each school and building positive relationships with all participants; and (3) providing token incentives, reimbursement of expenses and research support.
Recruitment targets in the current study
Schools
Initial and revised recruitment targets are described below. In 2013, there were 210 registered post-primary schools in NI. NI has a unique education system and post-primary schools can be broadly categorised as ‘secondary’ (n = 133) or ‘grammar’ (n = 68), with the latter using academic ability to select pupils. Various management structures also exist, with ‘controlled’ schools (n = 75) managed by one of the five NI Education and Library Boards and ‘voluntary’ and ‘maintained’ schools (n = 135) managed by a board of trustees. The Roman Catholic (RC) Church manages a significant number of voluntary (RC maintained) secondary (n = 68) and grammar (n = 29) schools. Although religion is not a criterion for attendance at NI schools, most pupils at controlled schools are from Protestant denominations and most of those attending RC maintained schools are Catholic. There are also a number of ‘integrated’ schools (n = 20), which aim to provide a religiously and culturally mixed environment.
Eight post-primary schools (five controlled secondary schools and three RC maintained secondary schools) in NI were excluded from target recruitment because they had < 30 Year 11 pupils and one was excluded because it was an Irish language school (secondary other maintained). The remainder of registered post-primary schools were included as targets for recruitment (Box 1).
In order to capture this diversity, and reflecting the aim to examine the acceptability of the intervention in different school types, the following seven schools were initially sought for recruitment: one integrated; one controlled grammar; one voluntary ‘other managed’ grammar; two voluntary RC grammars; and two schools of any type in deprived areas. Our preliminary research indicated potential challenges in recruiting RC schools owing to the fact that some may perceive an ‘abstinence-plus’ intervention such as If I Were Jack to be incompatible with the Catholic ethos. Conversely, it was anticipated that there may be greater uptake of the intervention in deprived areas where teenage birth rates are higher. For this reason two RC grammar schools and two schools in deprived areas were targeted for recruitment and one of each was randomly assigned to the comparison and intervention groups.
Controlled (48).
Controlled integrated (5).
Grant maintained integrated (15).
RC maintained (65).
Grammar (68)Controlled (17).
Voluntary: RC managed (29).
Voluntary: other managed (22).
Teachers and other school staff
One teacher who would act as main trial contact within each participating school was targeted for recruitment. This individual would be asked to work with the trial manager to co-ordinate baseline and follow-up data collection with pupils, to recruit teachers to deliver the intervention (if necessary) and to participate in an interview regarding their perceptions of taking part in the research and (if appropriate) current RSE provision in the school. In intervention schools, at least one teacher was targeted for recruitment to deliver the intervention to Year 11 pupils and to take part in an interview about their experiences of using the intervention. In addition, within each school at least one school administrator/secretary to support the research team and make contact with parents was targeted for recruitment. Although not an initial consideration, the need arose to recruit a school Information Technology (IT) technician who could support use of the interactive film in intervention schools and use of the online survey in all schools opting to use this method of data collection.
Pupils
The target population was all Year 11 pupils aged between 14 and 16 years in participating schools. Pupils were excluded if their parents/guardians withdrew them from the study, if they declined to take part or if they were unable to read the questionnaire owing to language difficulties (i.e. if English was not their first language). Pupils with reading difficulties and/or learning disabilities were included if they wanted to take part and if teachers thought that they would be able to understand and complete the questionnaire (with or without the aid of a teaching assistant or researcher reading the questionnaire aloud and explaining problematic words). Based on the average size of Year 11 in schools in 2011/12 (mean = 114; median = 113) and allowing for an 80% consent rate, it was estimated that approximately 730 pupils would be recruited to the study.
Parents
At least one parent or guardian of each participating Year 11 pupil in the intervention group was sought for recruitment to attend a 1-hour parents’ and guardians’ information and discussion session at their child’s school. Based on anecdotal evidence from teachers regarding difficulties engaging parents in non-academic activities, it was estimated that parent/guardian representatives of approximately 50% of Year 11 pupils would attend these sessions, which would result in around 200 participating parents.
Recruitment strategies
Recruitment took place over a 4-month period (May–June and September–October 2014), which allowed for no possibility of contact with potential participants during the summer break period (July and August). Schools were retained in the study for a period of 12 months from baseline data collection.
Although an aim of the study was to assess the relative importance of anticipated barriers to and facilitators of recruitment and retention, as well as other potential influencing factors, it was intended that the recruitment and retention strategies for the feasibility study would mimic best practice so that their value and feasibility in a full trial may be determined. The strategies employed to achieve this are described below.
Recruiting schools
Three strategies were used to recruit targeted schools: (1) RSE teacher training events; (2) personal introductions by members of advisory and steering groups; and (3) ‘cold-call’ invitation. Regardless of the strategy used, all principals [and, when applicable, the RSE co-ordinator or PC vice principal (VP)] were posted a formal letter of invitation and information sheet, which included detailed information on what would be involved on consenting to participate, including the estimates of required time and resources (see Appendices 2 and 3). This was followed, within 1 week of posting the letter, with a telephone call to the principal. In most instances, several more attempts to make contact with the principal and/or other contact (if suggested by the principal at first contact) were required before a decision on whether or not they would like to participate was made. In most cases the decision was made following a meeting with the principal or PC VP and, for the majority of schools, a teacher [such as the designated RSE co-ordinator, Head of Year 11, Head of LLW curriculum/personal development (PD), or Head of Religious Education (RE)]. During this meeting the research fellow described the intervention and the research study and explained what would be expected of the school, teachers, pupils and parents, should they agree to participate. In order to promote the credibility of the research project potential participants were told that the study was funded by the NIHR and the PHA NI and had received ethics approval from QUB. In order to promote the credibility of the intervention and impact perceptions of its potential benefits, the meeting also included the presentation of a 5-minute video of health and education experts talking about the resource and its potential benefits for use in the classroom and testimonials from teachers who had used the intervention during the pre-piloting development phase.
Strategy 1: recruitment at Relationship and Sexuality Education training events
This method was chosen as the primary recruitment strategy with the intention that it would optimise the potential to recruit schools that saw RSE as a priority subject and/or had an interest in developing their RSE curriculum. In addition, it was thought that the opportunity to promote the intervention and research process among key school stakeholders at a statutory funded training event and to address any concerns in situ would lead to positive perceptions of the credibility of the research team and benefits of involvement in the trial.
These day-long events, which take place approximately seven times annually, are funded by the PHA NI and facilitated by two Sexual Health Coordinators from the BHSCT’s Sexual Health Training Team. Although the content of the training varies, the sessions generally include subjects such as healthy relationships, STIs, contraception, childhood trauma, emotional intelligence, sexual orientation and RSE policy development. On average, representatives (usually the PC VP or RSE/LLW co-ordinator) from nine schools across NI attend each event following direct invitation from the facilitators. Attendance at the event is followed with a voluntary all-staff half-day RSE training session in each school. Over the 10 years that the events have been running, there has been total post-primary school attendance of between 40% and 100% across the five NI Education and Library Board areas. Schools that do attend report expectations that they will improve their provision of a statutory part of the curriculum. Those who do not attend report time pressures as the primary influencing factor.
On request to the facilitators we were invited to attend two of these events in April and October 2014 and to give a 30-minute recruitment presentation. A member of the research team introduced the intervention and provided an overview of the research. It included presentation of a 5-minute video of health and education experts talking about the resource and it potential benefits for use in the classroom and testimonials from teachers who had used the intervention during the pre-piloting development phase. Teachers in attendance were asked to provide their contact details if they were interested in receiving more information about the research.
Following the events schools were categorised according to school management type and deprivation proxy (indicated for the purposes of the current study by percentage of pupils at the school eligible for free school meals). The schools approached following these events were therefore selected on the basis of (1) their expressed interest and (2) their fit with recruitment criteria. Schools attending the event and meeting these criteria that declined to participate after initial contact were replaced by the next school from the list of all eligible schools attending the event.
Strategy 2: recruitment following introduction by steering and advisory group members
This strategy was used to contact five schools and as an aid to recruit the target of two RC grammar schools and one voluntary other managed grammar school, all of which were difficult to recruit, with low attendance of representatives at the RSE training events. An additional RC maintained secondary school was recruited this way when the recruitment target was adjusted. Only one RC grammar representative attended the RSE training events and, although three voluntary other managed representatives attended, all declined to take part. It was anticipated that this strategy would help to increase the perceived credibility of the trial and the possibility of arranging an initial meeting with school management.
In implementing this strategy, steering and advisory group members were asked if they had contacts in post-primary schools and if they would be willing to (1) suggest schools that might be amenable to receiving information about the research and/or (2) contact a representative of the school introducing the trial manager and seeking an expression of interest in receiving a letter of invitation from the research team. One steering group member directly contacted two voluntary other managed principals (by telephone) on behalf of the research team asking if they would be open to contact from the research team, and two other steering group members recommended (but did not introduce) two RC grammar schools that they thought might be amenable to participate. One advisory group member introduced the research team (via e-mail) to representatives in two RC grammar schools and one RC maintained school.
Strategy 3: recruitment through cold-call invitation
This strategy was used to contact five RC grammar schools and one voluntary other managed school that met the recruitment criteria but with which no contact had been established prior to sending the letter of invitation. Two of the RC grammar schools were recommended by steering group members. In addition to including the standard information sheet (which contained minimal information on the intervention), steering group members’ advised the inclusion of a flyer with promotional detail on the If I Were Jack intervention, testimonials from experts and end users and a link to the project website as well as a letter of invitation, which stated that there was ‘one place remaining’ for a RC grammar/voluntary other managed school.
Recruiting teachers and other school staff
The initial meeting between the trial manager and the school generally included either the principal or PC VP and a teacher who had attended the RSE training event or had responsibility for RSE/LLW. The main school contact following school consent to participate (the trial champion) was either the head of LLW and RSE co-ordinator (five schools); head of RE (one school); head of Year 11 (one school); or a senior teacher (one school).
Participating teachers who would deliver the intervention if randomised to the intervention group and/or facilitate delivery of the questionnaire at baseline and follow-up were identified by the principal/PC VP or trial champion prior to baseline data collection and randomisation. These teachers were then invited to attend a 30-minute meeting with the trial manager at the outset of the study. During this meeting they were provided with information sheets and the research was explained to them with the aid of Microsoft PowerPoint version 14 (Microsoft Corporation, Redmond, WA, USA) slides and a study flow chart. They were offered an opportunity to ask questions and consent to taking part in the research. In only two schools did the RSE co-ordinator attend this meeting, both of whom indicated that they had not yet identified other teachers to take part in the research. Both of these schools assigned teachers to facilitate the questionnaire data collection without any input from the researcher. One of these schools was later assigned to the intervention group, at which point an additional teacher was provided with an overview of the research during the teacher training session. In one school all members of the teaching staff were provided with an overview of the research during a staff training day. During the information sessions teachers were asked to consent to take part in an interview or focus group discussion and these were arranged with individual teachers or via the trial champion at the appropriate time. At the end of the study the trial champions in all schools were presented with a box of chocolates or bunch of flowers and an individualised thank you card from the research team.
At the initial meeting with school management the trial manager asked if she could be introduced to a school administrator who might help with administrative aspects of participation (i.e. provision of class lists, contact with parents, expenses). In five schools the trial manager was introduced to this person and in three schools contact only ever took place via e-mail or telephone. Following initial labelling and posting of information sheets and consent forms to parents, these individuals were presented with a small plant and note of thanks from the research team.
Although not initially anticipated, in some schools the trial manager had contact with the school’s IT technician. In intervention schools this involved liaison with the technician to ensure that pupils could access the If I Were Jack film and online resources and, in schools that opted to allow pupils to complete the questionnaire online, the IT technician was asked to test access to the survey and help with troubleshooting problems with this (see Chapter 7).
Recruiting pupils
After the school and teachers had consented to take part, parents/guardians of all Year 11 pupils were posted information sheets and given 2 weeks to withdraw their child from the study before the research was brought to the attention of pupils. During the teacher’s information session, the trial manager offered to spend a class period with pupils prior to data collection, during which the research would be explained in detail to them. All schools declined this offer stating that, owing to time constraints, it would be preferable to provide this information at the beginning of the baseline data collection session. Teachers were therefore provided with information sheets to distribute 1 week prior to baseline data collection to Year 11 pupils whose parents had not withdrawn them from the study. They were asked to encourage pupils to read the information sheet and inform them that they would have an opportunity to ask questions about it and decide whether or not they wanted to take part before completing the questionnaire the following week.
At the beginning of the baseline data collection sessions, either the trial manager or a trained research assistant spent 15 minutes explaining the research to pupils, giving them an opportunity to ask questions and asking them to complete a consent form indicating whether or not they wanted to take part. As a means of saying thank you to pupils for taking part in the study (and an incentive suggested by teachers), chocolates and sweets were provided to students after they had completed each questionnaire. Pupils who declined to participate or whose parents opted them out were supervised by a teacher in a separate classroom or the school library during data collection.
Participating teachers were asked to recruit volunteers from their class groups (six pupils minimum) to take part in a focus group discussion with a researcher (immediately following implementation in intervention schools and immediately following the 9-month follow-up in comparison schools). Pupils were provided with drinks and snacks during these sessions as an incentive for participating.
Recruiting parents
Parents or guardians of participating Year 11 pupils in the intervention group were invited via letter to participate in a 1-hour parents’ and guardians’ information and discussion session at their child’s school. At the request of the research team (and owing to a very small number of reply slips indicating attendance or non-attendance) a reminder text message was sent from the school to parents the day before the session. In three schools this session was managed and facilitated by a teacher and in one school (owing to teacher sick leave) by the PI. Schools were encouraged to run the event in the evening to facilitate attendance by working parents.
In an attempt to reach parents who did not attend the session, a 6-minute video for parents/guardians containing key messages was posted on YouTube. School administrators texted a link to the video to parents.
Parents who attended the parents’ session were invited to participate in a focus group discussion with a researcher immediately following the session if that suited them or to provide their contact details if they wished to take part at another time. In addition, the YouTube video provided contact details for any parents wishing to take part in a focus group.
Following implementation, parents of participating pupils were sent a text message containing a link to a short survey which asked parents for their views on the intervention.
Methods: how we evidenced our data on recruitment
Data collection consisted of three elements
-
Number of expressions of interest at RSE training days, invitation letters sent, responses received, telephone calls made, e-mails sent, participants declining participation and participants agreeing to take part in the study were all recorded in a database to allow the calculation of recruitment and retention rates and calculation of time taken for participants.
-
Time spent by the research team on recruitment activities, including delivery of recruitment presentations, preparation and posting of invitation letters, making follow-up telephone calls and sending e-mails to obtain expressions of interest, and arranging and conducting introductory meetings were recorded in researcher activity logs and used to estimate total time spent on recruitment activity.
-
Qualitative data were obtained from a combination of field notes, records of e-mail communication and contact notes following telephone conversations with participants who declined to participate, documented meetings with steering group members, and semistructured interviews with principals, VPs, teachers and parents recruited to the study.
Data analysis
To calculate recruitment and/or retention rates, a percentage was derived from the total number of invitations sent by school management type and the resulting number of schools, pupils and parents recruited.
To calculate the time associated with the various recruitment strategies and overall time spent on recruitment and retention activities, estimated time spent was totalled and divided by the number of schools, pupils and parents successfully recruited. This resulted in the total amount of time spent by the research team per school randomised.
Qualitative data were organised using NVivo 10 (QSR International, Warrington, UK) and analysed using a form of thematic analysis based on the six steps proposed by Braun and Clarke. 116 This involved moving between inductively derived codes emerging from the data and searching for data on pre-defined themes outlined in our topic guides. These inductively and deductively derived codes were analysed to form overarching themes.
Results
The Consolidated Standards of Reporting Trials (CONSORT) flow diagram is depicted in Figure 4.
FIGURE 4.
Consolidated Standards of Reporting Trials flow diagram.
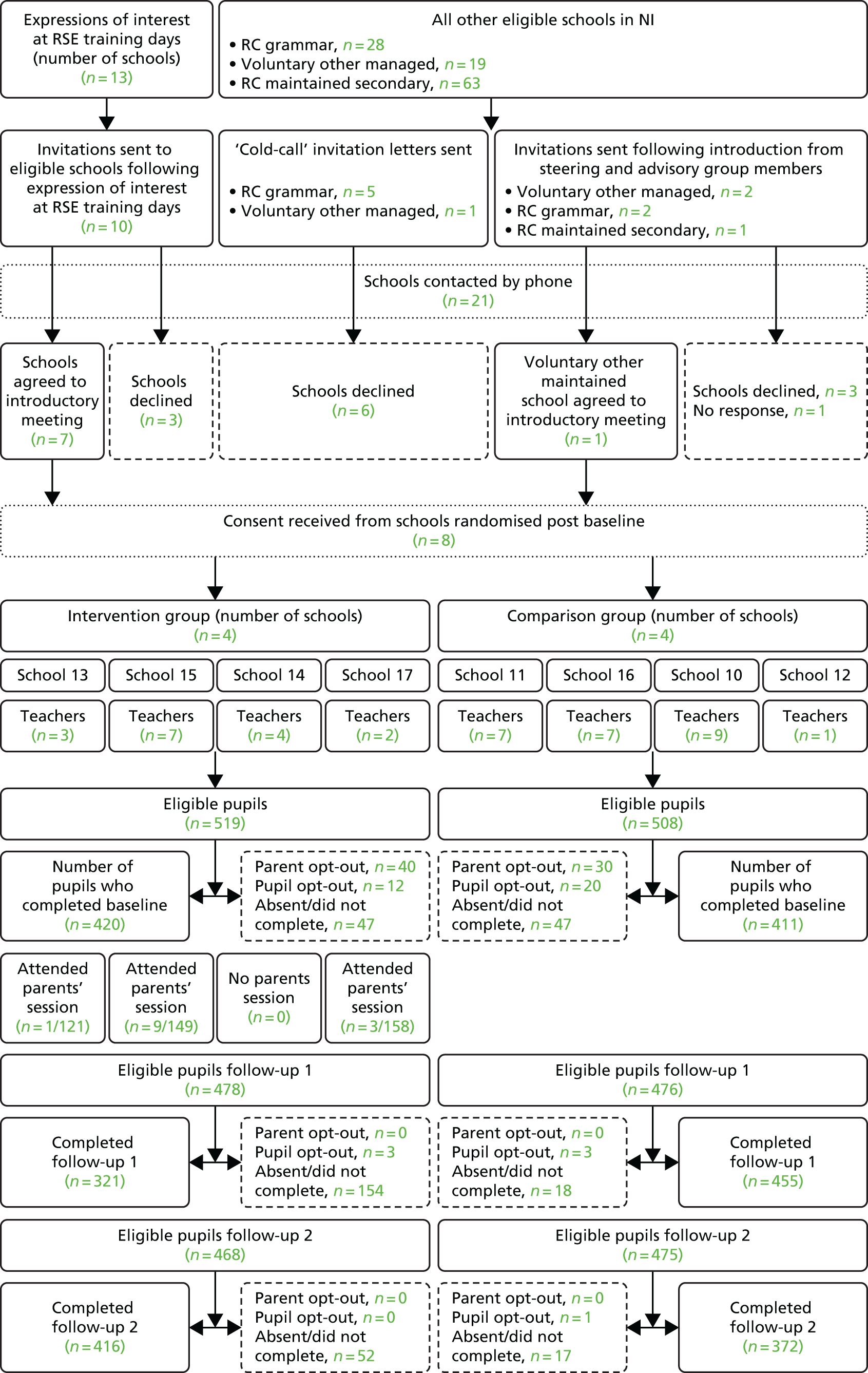
Randomisation and allocation
Schools were the unit of randomisation, with four randomly allocated to the intervention group and four to the control group. After baseline data collection, schools were randomised as pairs to ensure that one of each type was in the intervention arm. The schools were grouped into four pairs based on their school management type: secondary schools in deprived areas, Catholic schools, grammar schools and other types. This process was conducted by the Northern Ireland Clinical Trials Unit (NICTU), a UK Clinical Research Collaboration-registered clinical trials unit, overseen by the trial statistician, using a method of simple randomisation completed using NQuery version 3.0 software (Statsols, Cork, Ireland).
Recruitment of schools
In October 2014, following unsuccessful attempts to recruit a second RC grammar school, recruitment targets were revised to maintain the diversity of schools included in the study but to broaden the scope to include RC secondary schools that, despite being RC schools, are not as academically driven as RC grammar schools. The revised target was eight schools of the following types: two secondary schools of any management type in deprived areas, two controlled secondary schools, two RC maintained schools and two grammar schools.
A total of eight schools were recruited (see Figure 4). The over-recruitment of one additional school was the result of the yield from the final attempt to recruit RC schools of any type following difficulties recruiting RC grammar schools.
Invitations were sent to a number of RC maintained schools and two responded on the same day with a decision to take part. It seemed unwise, and possibly unethical, to contact schools about a study and not invite them to participate once they had expressed an interest in doing so. Recruitment of schools via RSE training events was by far the most successful strategy, leading to 70% of schools invited by this method (n = 7) being randomised into the study. Invitation following introduction by a steering or advisory group member led to the recruitment of one additional school (a 20% recruitment rate). Cold-call invitation was unsuccessful, with all six schools approached declining to take part.
Targets for recruiting schools of different socioeconomic and religious types were met, but required more intensive work to reach particular school types and adjustments to initial recruitment specifications in order to achieve the recruitment target within the specified timeframe. As illustrated in Table 19, our main challenge was in recruiting RC grammar schools (i.e. RC schools that use academic ability to select pupils) and voluntary other managed grammar schools (i.e. non-RC Church or privately funded schools that use academic ability to select pupils). Although the overall school recruitment rate was 38% (100% for integrated, controlled grammar and controlled secondary schools), the recruitment rate for RC maintained secondary, RC grammar and voluntary other managed grammars was 67%, 13% and 17%, respectively.
| School recruitment | Integrated | Controlled secondary | RC maintained secondary | Controlled grammar | Voluntary RC grammar | Voluntary other managed grammar | All |
|---|---|---|---|---|---|---|---|
| Number of schools contacted | 2 | 1 | 3 | 1 | 8 | 6 | 21 |
| Number of schools recruited | 2 | 1 | 2 | 1 | 1 | 1 | 8 |
| School recruitment rate (%) | 100 | 100 | 67 | 100 | 13 | 17 | 38 |
Between June and October 2014 one of eight RC grammar schools approached and one of six voluntary other managed schools approached was recruited. Faced with a recruitment deadline of the end of October it was decided to revise initial recruitment targets to recruit RC schools of any type rather than just RC grammars. One RC grammar and one RC maintained secondary in a deprived area had already been recruited, and so it was decided to recruit one additional RC school of any type in a non-deprived area, which could be paired with the RC grammar for randomisation. This was achieved by inviting schools from the list of those attending the RSE training events.
As outlined in Table 20, a total of 13 schools approached declined to participate in the study. All but one of these schools made this decision prior to meeting with the trial manager. The most common reason for non-participation (n = 4) was that having considered the information sheets, school management and/or the teacher responsible for delivering LLW considered that there was no time available within the current curriculum at Year 11 to deliver the intervention and take part in the research. Three schools also reported that they were already involved in another research project and could not accommodate a further study at that time. Two other schools indicated that owing to staff changes (maternity leave and a change in the LLW team) they did not think it was an appropriate time to take part. Two schools declined to take part without providing a reason. The PC VP and Head of RE of one RC grammar school met with the trial manager prior to making their decision as they were concerned that the intervention might not be compatible with their school ethos. Having expressed positive views that they felt it was in line with their ethos at the meeting, they later declined to take part having consulted with the school Chaplin who felt that the intervention was not in fact compatible with the school ethos. Although a number of schools mentioned at first contact that they did not have any issues with teenage pregnancy in their school, only one cited this as their primary reason for non-participation.
| Reasons for non-participation | Number of RC maintained secondary | Number voluntary RC grammar | Number voluntary other managed grammar | All school types |
|---|---|---|---|---|
| No space in LLW curriculum | 1 | 2 | 1 | 4 |
| Currently involved in other research | 2 | 1 | 3 | |
| Not a suitable time owing to staff changes | 1 | 1 | 2 | |
| Declined without providing reason | 2 | 2 | ||
| Intervention incompatible with ethos | 1 | 1 | ||
| Intervention incompatible with needs | 1 | 1 | ||
| All non-participants | 1 | 8 | 4 | 13 |
The schools that did participate in the research reported doing so for a number of reasons, primary among which was their desire to improve RSE provision for their pupils and their belief that the If I Were Jack resource would be of benefit to their pupils. Schools in deprived areas were particularly interested in taking part because of their current and past experiences of teenage pregnancy in the community.
Principals indicated that they were approached several times a week to take part in research, and, although all appreciated the potential benefits of research they were often too busy to respond to such requests. All agreed that direct face-to-face contact with them or a subject teacher was the optimal strategy:
If [an invitation] just comes as an e-mail there is a fair chance it’ll end up in the bin […] If it’s preceded by a phone call there is probably a better chance [it’ll be considered].
If you just send something in and it comes to me, it could go over my head. If you send it to my teacher or you engage somebody or you phone the school up and say ‘Could I come in to chat to the Principal?’ or ‘Could I come in to speak to somebody?’ rather than sending a letter, I think that’s the way to hook people in . . . Personal contact is key.
One principal summed up how she went about considering research participation:
We would regularly get asked for research, maybe three or four times a week, so the volume of research out there, I think, is immense, and the time restraints that that places, depending on the type of research and what the investigator is looking for, specifically, can impact whole school activity, so we need to be very careful in terms of what we select and the benefits that are going to be achieved to the students. But then, also, I do think we’ve a wider responsibility as educators to look outside the students sometimes and possibly to learn from the practice of research and contribute to it on a more holistic educational basis. So, it’s, for me, it’s trying to balance up the benefits of that.
Principals agreed that a number of considerations were important in helping them to make a decision about whether or not to take part. Central among these were the potential burden on pupils, especially those in exam classes, the burden on teachers and the credibility of the project:
Firstly, if there’s any credibility in what’s being done. Secondly, if it can be fitted in with minimum disruption. If it’s going to affect exam classes there’s almost no chance.
Principals were asked what kind of things do they consider before deciding whether or not to take part.
Well, the first thing I would look at is, is it in an area of interest that we can contribute to that is very specific to my school? Is it an area that the students can benefit from? So, with the Jack project, I felt it was a wee bit innovative and that there were potential useful resources from it. The [other] things that I look at are what are the time constraints and the commitment for the students and the staff?
Several principals noted that ‘Area Learning Communities’ or other head teacher forums such as the ‘Catholic Heads Association’, which were attended regularly by principals, might be possible venues for presenting research and recruiting schools. Others noted that buy-in from teachers was a must and that often a good way of reaching the principal is through a subject teacher.
So, sometimes, if a specific teacher in an area is going to drive it and sees it as very beneficial, is going to inform practice and that, they would come to me and they would sell the research if they are going to lead it. The difficulty for me is sometimes, if there’s not an original buy-in from staff, it can prove very difficult to manage . . . so if you get the hook through somebody else, if it’s a subject-specific area, that could be a driver for running it as well.
Sometimes I get e-mails from folks I’ve never met or have no connection with, so they haven’t really much hope of being successful. Mmm, it depends on how the approach is made and on the reason behind it [the research].
I suppose for me the best time to get me is either early in the morning, between eight and quarter to nine or later in the afternoon, sort of, between half past four and six. That would be times when I’m not out and about or engaging with kids or staff.
Principals especially did not want pupils in significant exam years to be disrupted with external research studies.
If you’re wanting to do it with Year 11 to 14, especially Year 11 and 12, there’s hardly a week goes by where they’re not involved in some kind of controlled assessment . . . I won’t take kids out of English and Maths or maybe even other GCSE subjects to do [research].
Principals also had an especially strong message for researchers in terms of taking some of the responsibility for the organisation of the research within the school, especially in terms of conducting the data collection.
[I would immediately decline to take part in research projects] that are going to be very time-consuming . . . or, where projects put the onus on the school – ‘Could you get us a group? Here’s the list – could you go away and do it, and when you’re finished, could you bring it back to us and I’ll pick it up from you?’ and you’re like ‘What?!’
Principals were asked how important monetary incentives, such as getting the If I Were Jack resource to use at the end might be in a future trial. They agreed that monetary incentives would be an important facilitator of participation:
Very important. They would be the enticement to get you involved. It sounds very mercenary and I don’t mean to be mercenary in this day and age, but if I’m going to . . . if it’s going to be time and energy with students and staff and commitment, and if the benefits are not solely related to students and staff and outcomes, then there’s got to be a reason why you would do it.
One principal in the control group suggested that having access to the resource was a more important incentive than money to them:
We now have access to the Jack resources. From our point of view that is probably more valuable . . . that’s probably a better incentive than money.
Reasons principals chose to participate are detailed in Table 21.
| Reasons for school participation | n (%) |
|---|---|
| Belief that the intervention would be useful to pupils | 8 (100) |
| Credibility of the intervention/research | 8 (100) |
| Desire to improve RSE provision within the school | 6 (75) |
| Compatibility of the intervention with pupil needs (teenage pregnancy a concern) | 5 (63) |
| Positive experiences with previous research | 1 (13) |
| Involvement in research perceived as beneficial for upcoming inspection | 1 (13) |
Schools took between 1 and 19 days (mean = 6 days) to confirm their decision. Two schools did not respond with a decision despite several attempts at contact. Allowing 1 week following postage of the introductory letter, this means that it took an average of 2 weeks to receive a participation decision from schools.
For an overview of the number of contacts made, outcome and time take taken to decide by schools approached see Appendix 8.
Recruitment of teachers
A total of 40 teachers were recruited across the eight participating schools (see Figure 4). One teacher later opted out of implementing the intervention owing to an extended period of sick leave. For school personnel involvement in a semistructured interview or focus group discussion regarding their experiences of taking part in the research (comparison and intervention) following the final follow-up see Chapter 7.
Recruitment of pupils, pupil opt-out and retention
Recruitment of 831 pupils to the study at baseline represents an overall pupil recruitment rate of 80.9%. Parental withdrawal of consent accounted for 6.8% of the loss (n = 70) and pupil opt-out for 3.1% (n = 32). Pupil absence or unavailability at baseline in combination with pupils who chose not to complete the questionnaire or who were unable to because they had not returned consent forms to the research team accounted for the remaining 9% of loss (n = 94). In one school a number of pupils indicated that they were unable to participate because they did not have sufficient English to understand the consent form.
In two schools, teachers had forgotten to distribute the information sheets to pupils. They also had not given them any indication that the school was taking part in the research or that data collection was scheduled for that day. Although the researchers made an effort to spend a little more time explaining the research in these two schools, given time constraints there was a limit to the amount of additional information that could be imparted to pupils at this juncture. There was a noticeable difference among pupils who had prior warning and a chance to read the information sheets, both in their questions to the researcher and their expressed satisfaction with taking part.
As detailed in Table 22, pupil participation also varied by school type, with the highest recruitment rates in the three RC schools (> 90%) and the controlled secondary school (92%). The lowest rates were in the controlled grammar school (55%) and one of the integrated schools (62%), both of which had high pupil absentee rates on the day of baseline data collection. The controlled grammar schools’ absentee numbers at baseline (n = 40) were accounted for by the fact that one class group were undergoing an observation for teacher training purposes and were not permitted to leave their class to take part, while the remaining pupils had to attend a sports event. In the integrated school the absences at baseline (n = 25) were accounted for by the fact that data collection took part first thing on a Monday morning when absences were usually higher. Trial champions were provided with questionnaires and consent forms for absent pupils and asked to return them on several occasions before the cut-off point of 23 January. Teachers reported an inability to find time to administer the questionnaires to pupils as the reason for not returning them.
| Controlled integrated | Grant maintained integrated | Controlled secondary | RC maintained secondary | Controlled grammar | Voluntary RC grammar | Voluntary other managed grammar | All | ||
|---|---|---|---|---|---|---|---|---|---|
| School ID | 10 | 13a | 14 | 11a | 15 | 12 | 16 | 17 | – |
| % pupils eligible for free school meals | 32.4 | 57.4 | 35.1 | 48.0 | 45.5 | 15.0 | 8.5 | 4.0 | – |
| Number of eligible pupils | 132 | 121 | 91 | 98 | 149 | 123 | 155 | 158 | 1027 |
| Number of parent/guardian withdrawals of consent | 12 | 11 | 2 | 2 | 9 | 10 | 6 | 18 | 70 |
| Number of pupils opting out | 17 | 10 | 0 | 2 | 2 | 1 | 0 | 0 | 32 |
| Number absent at baseline | 0 | 24 | 5 | 6 | 2 | 40 | 1 | 16 | 94 |
| Number recruited | 103 | 76 | 84 | 88 | 136 | 72 | 148 | 124 | 831 |
| Pupil recruitment rate (%) | 78.0 | 62.8 | 92.3 | 89.8 | 91.3 | 59.3 | 95.5 | 79.1 | 80.9 |
Pupil opt-out rates ranged from 0% to 13% across the schools, with the highest rates in both integrated schools (Table 22). Pupils were not asked to give a reason for non-participation. Observations indicated that pupil opt-outs tended to occur in friendship groups (i.e. it was rare for a single young person to opt out; instead, friendship pairs or groups tended to opt out together). In the school with the highest opt-out rate (n = 17), pupils had not been provided with the information sheet prior to the study and baseline data collection was scheduled by teachers to immediately follow an exam in a large exam hall, which made providing an overview of the study at a sufficiently loud volume for all students to hear very difficult. In the words of one of the attending teachers, decisions to opt out ‘spread like wildfire’.
In another of the schools a teacher told the trial manager after the baseline data collection session that she had had ‘around 25’ pupils outside the hall prior to the research team’s arrival saying that they did not want to take part. The teacher asked them to listen to the explanation of the study prior to deciding. Two pupils opted out following the overview of the study.
Pupil retention rates per school are detailed in Table 23.
| School ID | Follow-up 1 questionnaire | Follow-up 2 questionnaire | |
|---|---|---|---|
| Intervention | 13 | 51.3% drop | 9.2% drop |
| 15 | 46.3% drop | 8.1% drop | |
| 14 | 21.4% drop | 31.0% drop | |
| 17 | 8.9% increase | 6.5% increase | |
| Comparison | 11 | 3.4% increase | 2.3% drop |
| 16 | 3.4% drop | 2.3% drop | |
| 10 | 2.9% drop | 8.7% drop | |
| 12 | 12.5% drop | 11.1% drop |
In the intervention cluster pupil retention was 74.0% by follow-up 1 and 91.4% by follow-up 2. In the comparison cluster, pupil retention was 96.6% by follow-up 1 and 94.9% by follow-up 2. Pupil retention at trial level was 85.2% by follow-up 1 and 93.1% by follow-up 2. The lower follow-up at follow-up 1 was mostly because it occurred too near the holidays when pupils’ attendance had already started to drop off.
We originally aimed to recruit 80% of eligible children into the research trial (based on pupil ‘opt-in’ and allowing for ‘opt-out’ parental consent). Of the eight schools recruited, there were 1027 eligible pupils in Year 11 who could participate at baseline data collection. (For an overview of pupils responding to the questionnaire at each data collection time point, see Tables 28 and 29.) The proportion of eligible pupils (at baseline) who provided questionnaire data was 81% (for both the intervention and control group). At follow-up 1 data collection (allowing for loss of eligible pupils who had moved school or were now being home-schooled), these figures were 60% and 78%, respectively (the reason for this lower return is because we left data collection too close to the summer holidays and many of the pupils were already absent from class). At follow-up 2 data collection (allowing for loss of eligible pupils who had moved school), these figures were 76% and 77%, respectively. At each data collection time point (baseline, follow-up 1 and 2) 97% of pupils who completed the questionnaire answered the questions relating to the main composite primary outcome measure (see Chapter 6). At baseline, this involved 803 pupils and at follow-up 2 745 pupils (representing a reduction in numbers of 7%). Of the 803 pupils who answered the main composite primary outcome measure at baseline, 629 (22% drop-out) went on to answer the same questions at follow-up 1 data collection and 699 (13% drop-out) at follow-up 2 data collection (Tables 24 and 25).
| Data collection time point | Number of questionnaires answered | ||||||
|---|---|---|---|---|---|---|---|
| Baseline only | Baseline and follow-up 1 | Baseline and follow-up 2 | Baseline, follow-up 1 and follow-up 2 | Follow-up 1 only | Follow-up 2 only | Follow-up 1 and follow-up 2 | |
| Baseline | 39 | 48 | 126 | 618 | N/A | N/A | N/A |
| Follow-up 1 (5 month) | N/A | 48 | N/A | 618 | 6 | N/A | 26 |
| Follow-up 2 (9 month) | N/A | N/A | 126 | 618 | N/A | 2 | 26 |
| Data collection time point | Number of eligible pupils | Number of pupils responding to questionnaire | Number of pupils answering all questionnaire items related to the composite primary outcome measure | Number of pupils answering all questionnaire items related to the composite primary outcome measure at baseline and follow-up 1 | Number of pupils answering all questionnaire items related to the composite primary outcome measure at baseline and follow-up 2 |
|---|---|---|---|---|---|
| Baseline | 1027 | 831 | 803 | 629 | 699 |
| Follow-up 1 | 1024 | 698 | 676 | 629 | N/A |
| Follow-up 2 | 1013 | 772 | 772 | N/A | 699 |
The trial ended following successful completion of follow-up data collection with all pupils by 30 October 2015.
Recruitment of parents and parental opt-out
Recruitment of parents and guardians to attend the school-facilitated information and discussion session was extremely low, with an overall recruitment rate of 2.3% (i.e. 9 mothers and one father representing 10 different pupils) assuming potential recruitment of one representative parent or guardian for each eligible pupil in the three intervention schools that held the session (n = 428). All three schools chose to run the event in the late afternoon (two schools started at 15:30 and one at 16:30). Reasons for this early start included difficulties keeping the school open late for such an event and a lack of desire on the part of the teachers to stay late themselves. One school did not hold the parents event because the teacher who was responsible for organising and delivering it went on sick leave and failed to ‘catch up’ on organising it on her return 1 week later.
In the three schools that held the event, parental attendance was extremely low (between one and six parents/guardians attended). Based on experiences of similar events, teachers in two of the schools anticipated that attendance would be very low. One teacher said that ‘our parents are not very supportive of their children when it comes to things like this’.
In response to poor attendance at these sessions, recruitment targets were revised. A 6-minute information video was recorded which contained the key points from the information session. This was posted on a locked YouTube channel and parents were sent a link to access it via e-mail or text message. From parents who attended these sessions we aimed to recruit a total of 25 parents to take part in a focus group interview with a researcher. In order to capture the views of those who did not attend the information session or focus groups all parents/guardians were sent a link to a short online survey. It was estimated that 40% of parents would respond to this survey. Parents of pupils in the comparison group were not recruited to the study.
The information session video on the YouTube channel was viewed by 45 parents (12.5%, assuming potential recruitment of one representative parent or guardian for each eligible pupil in the three intervention schools alerted to the online video). Owing to an administrative error, parents in one school did not receive the information video but only a printed copy of the information sheet. This school (school ID 17) had the highest number of parental opt-outs.
In total, 29 parents responded to the parents’ survey, representing an 8.3% response rate [all parents whose children were eligible to receive the intervention (eligible pupils minus parental and pupil opt-outs) received the text alerting them to the survey]. In school 17 this figure was reduced to n = 21, owing to only one class being able to receive the intervention as a result of teacher sick leave. Of the responding parents, 22 indicated that they had not attended the information and discussion session (see Chapter 7).
See Chapter 7 for more information provided by parents who took part in a semistructured interview or focus group discussion following one of the information sessions.
As indicated in Table 25, parental withdrawal of consent rates ranged from 2% to 11% with the lowest rates in one of the RC maintained secondary schools and the controlled secondary (n = 2) and the highest in the voluntary other managed grammar (n = 18). Most parents did not include a reason, but of those who did (n = 16) reasons provided were variations of:
my child does not want to take part (n = 10)
I do not want my child to take part (n = 2)
my child wants to focus on his/her exam subjects (n = 1)
my child is busy with extra-curricular activities (n = 2)
my child has a learning disability so I do not think it is appropriate for him to take part (n = 1)
At the time of data collection teachers in four of the schools reported that some parents had been in contact with them because they were confused about whether or not to send back the withdrawal of consent form if they were happy for their child to take part. In the voluntary RC grammar school, five parents who had initially opted out contacted the school after their child had received the information sheet to say that they were now happy for their child to take part. Teachers theorised that this may have been at the request of the child but one teacher reported that a parent to whom she had spoken had previously thought that her child was being ‘singled out’ for participation in the study and when she realised everyone would be taking part she changed her mind.
Discussion
This study allowed analysis of anticipated and unexpected challenges to successful recruitment and retention to inform decisions regarding optimal recruitment and retention strategies for a future Phase III trial.
The study has demonstrated that using RSE training days is a powerful way of recruiting schools to sexual health trials and much more effective than cold-call invitation or approach following introduction. These events offered an opportunity to provide a clear overview of the research and its potential benefits to schools and pupils and, owing to the fact that recruitment presentations took place at statutory events, added to perceptions of its credibility, an important consideration in helping a study stand out from the numerous invitations received by schools. A future full trial should exploit this and other means of recruiting schools, by means of, for example, some of the suggestions made by participants, such as continued provision of and access to the resource. Should recruitment at such events not provide the total number of required schools, a future trial might also consider asking contacts at recruited schools to introduce them to colleagues at other schools who they know might be interested in taking part.
Recruitment targets for schools were met within the planned time frame following some adjustment to the initial sample stratification definitions. The overall recruitment rate of 38% was strongly impacted by the challenges we faced recruiting RC schools and voluntary other managed grammar schools. Although it was anticipated that recruiting RC schools might be difficult, an unexpected caveat was that it was not RC schools in general that were difficult to recruit, but RC grammar schools (recruitment rate: 13% in RC grammar compared with 67% in RC maintained secondary) and other academically focused grammar schools, in particular, voluntary other managed grammars (recruitment rate: 17%). The controlled grammar and voluntary other managed school recruited was strongly influenced by professional networks. The main reason that the sample was stratified in this way was so that the reach of the intervention could be examined, in particular, its acceptability in RC schools and schools in deprived areas. This stratification would, therefore, not be necessary for a future full trial. Had stratification not been done in this way, in order to recruit schools of different management types, recruitment rates would have been much higher and resources expended on recruitment activities would have been lower.
Although the interaction between religious ethos and intervention content is important, much more influential in terms of potential barriers to recruitment in the current study were perceptions of the relevance of the intervention for the pupils, burden on teachers and pupils and the schools’ current and prior involvement in other research. The majority of RC schools that declined to participate did so without knowing anything about the intervention aside from the fact that it was about teenage pregnancy. Similarly, the grammar schools in general who refused to take part indicated as primary reasons a lack of room in the curriculum (‘we do not have room for it or we already have a comprehensive RSE programme’) and a perceived lack of fit with pupil needs (‘we do not have any problems with teenage pregnancy’). We therefore propose that in a future full trial the sample is not stratified by school management type or deprivation, but, rather, that recruitment targets should seek to recruit all schools that express an interest in participating in the study. However, in order to ensure a representative sample, it is still important to ensure that a mix of schools is recruited to a full trial, including grammar and religious schools. We therefore suggest that targeted recruitment, which speaks to the needs of different school types, is vital. For example:
-
recruitment presentations and introductory literature should include information about the intervention and emphasise its academic relevance (fit with the statutory RSE curriculum) and innovative nature (targeted at teenage males), and provide more information on the persistent public health problem of teenage pregnancy, which transcends social class and remains problematic for teenagers and their families
-
introductory letters could be adapted so that, although all the key messages are included, the emphasis is adapted to different school types (e.g. the academic focus and innovative nature of the intervention is emphasised to grammar schools and so on). A clear outline of the content of the intervention and testimonials from pervious users in RC schools might encourage them to look at the intervention prior to deciding that it is not in line with their ethos.
The most common reasons provided for non-participation were a lack of space in the LLW curriculum and prior commitment to other research. Although the intervention was designed to be used within the LLW/PD curriculum, during the study two of the schools delivered it during ‘form’/PC and a third during RE classes because teachers felt that it was simpler to fit it within these classes for the purposes of the study. This was not emphasised to schools at the recruitment stage and should be during a full trial. School commitment to other research is an important issue and not something that we can impact greatly in the short term. Planning for a future trial should, however, be cognisant of the amount of invitations that schools receive to participate in research and include innovative ways of ensuring that the invitation actually reaches school decision-makers.
Reasons for schools choosing to participate included a keenness to get involved in more research, the fact that they had had positive experiences with previous research, the fact that the intervention was compatible with needs (teenage pregnancy a current concern for the school), the credibility of the intervention/research (word of mouth), and the fact that involvement in research was perceived as beneficial for upcoming inspections.
Pupil recruitment targets were met, with an overall pupil recruitment rate of 80.9%. Absentees who did not return completed questionnaires accounted for 9% of non-participants, and parental and pupil opt-outs accounted for the remaining 9.9% (6.8% and 3.1%, respectively). Of those parents (n = 16) who provided a reason why they had opted their child out, most said that their child did not want to take part or that they did not think their child had time to take part. Although the parental opt-out rate was satisfactory, a number of teachers indicated that they felt that some parents had misunderstood the withdrawal of the consent form and had returned it because this is what they usually do in order to allow their child to participate in such activities. Indeed, a number of parents wrote on the form that they found it confusing and several sent it back while also indicating that they were happy for their child to take part. A future trial might ensure that data collection documentation is clearer to parents, perhaps involving steering group members in ensuring clarity in this regard. In addition, parents might be given the option of contacting the research team or school co-ordinator via telephone for clarification prior to consenting.
Equally, although pupil opt-out rates were relatively low in the study, it was evident that most withdrew consent because of their dissatisfaction with the fact that they had not been pre-warned about the study or given time to consider whether or not they wanted to take part. In the school in which pupil opt-out was highest, baseline data collection took place immediately after an exam in a large hall (the acoustics of which made it difficult for all pupils to hear the information about the research). Although provided to teachers, pupils had not been given copies of the information sheet prior to data collection. A future trial should ensure that pupils are provided with adequate information about the research prior to data collection. As none of the schools took up the offer of the research fellow providing this on a separate occasion prior to data collection, this might be best achieved by creating a short video that teachers should show to pupils a week or so prior to data collection. Moreover, although data collection in a large hall saves on resources in terms of the numbers of research assistants needed to attend the data collection sessions, we found that, in most cases, it was not an appropriate option for recruitment or ensuring data quality. In two of the three schools that chose this option, pupils were more likely to chat to each other during completion. Furthermore, when pupils decided that they did not want to take part, this generally resulted in several pupils in the same physical area deciding not to take part and these pupils then caused disruption to those who were taking part. All follow-up data collection in the current study was conducted in small class groups (apart from in one school in which teacher control of the year group was exceptionally high). This is recommended for a future trial.
When large numbers of absentee questionnaires were left for teachers they struggled to return to them, indicating that it was difficult to find time to collect data from these pupils within the already busy school schedule. A future trial might attempt to minimise the number of absentees by ensuring that data collection does not take place at a time when absences are more likely (e.g. Monday mornings and Friday afternoons). Equally, when there are large numbers of absentees, researchers might offer to facilitate supervision and distribution of these at a particular time so as to encourage completion and ease the burden on the teacher.
Although the core part of this intervention is a teacher-delivered intervention to pupils, additional communication to involve parents also featured in the logic model of the intervention. We failed to reach the proposed target of recruiting one parent/guardian representative for 50% of participating pupils to attend the parents’ information and discussion session. Co-ordinators in all the intervention schools indicated that parents were difficult to engage in general (see Chapter 7). Some indicated that this was due to a lack of interest on the part of the parents, whereas others noted factors such as the distance parents lived from the school (in some rural schools as far as 30 miles) and possible difficulties they had with transport or child-minding for younger children or being unable to get time off work to attend. Often reported predictors of parental attendance include sociodemographic variables such as education and income level, which may be related to resources and ability to attend. 117–120 A future trial might consider providing parents with incentives in order to attend, including funds for travel or child-minding.
As with schools, researchers have found that parents who perceive that the programme may help address their children’s problems are more likely to engage. 117 Given the importance attached to ensuring that schools and parents are aware of the importance of speaking to their children about such issues, a future trial might consider developing a short video for parents to explain the significance of helping teenagers avoid teenage pregnancy and the impact that an UTP might have on their lives.
Alternatively, some teachers also suggested that the topic of teenage pregnancy might be a challenging one, especially in areas in which parents themselves had experienced an UTP. One teacher suggested that parents might have been afraid that teachers would ‘judge’ them if they came to the session and, in focus groups, several pupils indicated that their parents refused to do the parent/pupil homework exercise with them because they felt it would be ‘hypocritical’ to advise them about teenage pregnancy when they had been teenage parents themselves. This is unlikely to be a universal perception, however, and it is worth noting that one mother who attended a parents’ focus group said that the very reason she had attended was because she had experienced teenage pregnancy herself and she wanted to ensure her children waited until they were older. A future trial should ensure that the non-judgemental nature of the intervention in general and in the parents’ session in particular is communicated to parents. Another option, used by Harrington et al. 115 to recruit hard to reach populations, was explanatory telephone calls to parents to successfully increase participation. A future trial might consider this option.
In addition, cultural differences in attitudes towards sex education programmes, problems reading or comprehending the consent form, information sheet and letter of invitation may all have contributed to a lack of engagement. This may have been a particular problem in one school that has an ethnic minority population of 20%. A future trial should cost for translation services and might also involve ethnic minority parents in this process.
Although we had modest success with the YouTube video, it was in fact much more successful than inviting parents to attend the session. Haggerty et al. 120 compared attendance at a parenting workshop with participation in a self-administered version of the same programme. They found that older child age and higher levels of parent education strongly predicted engagement with the self-administered version of the intervention. A future trial might develop and examine the value of this methodology further, for example, by creating a more engaging video such as animation or similar.
The main reasons for participation were that schools were keen to get involved in more research, that they had had positive experiences with previous research, that the intervention was compatible with needs (teenage pregnancy was a current concern), the credibility of the intervention/research (word of mouth), and involvement in research was perceived as beneficial for upcoming inspection. It was agreed by principals that in a future trial, or trials in general, monetary incentives are important. However, monetary incentives would, they argued, work only in the context of the social value of the research itself and if the benefits to the participants had a positive impact on school recruitment. The small incentives provided to staff and pupils were, however, greatly appreciated. They were presented as a ‘thank you’ for time and effort and, as such, went some way towards helping maintain positive relationships with participants.
All schools were retained in the trial and the pupil retention rate was mainly attributed to the provision of clear information from the beginning and continuous contact with schools at meaningful points in time.
Conclusions
In relation to recruitment, the feasibility study demonstrated that our target aim of recruiting seven schools, four to the intervention arm and three to the control arm, was realistic and demonstrated that we could achieve our school recruitment target rate (target of 25%, achieved 37%). The study also demonstrated that it was feasible to recruit the full range of the most common types of schools in NI, namely in terms of the differing school management types, including faith-based schools, schools that are especially academically oriented and those that are not, and schools that are in socially deprived as well as socially affluent areas. This was important because we believe that this is the first RSE intervention trial to include faith-based schools in the UK and > 50% of schools in NI are faith-based schools. Nonetheless, we learned that the hardest schools to recruit for this trial were schools that were both faith based (RC) and high academic achieving schools. These are what are known as ‘Catholic Grammar Schools’ in NI.
Overall, we learned some valuable lessons about how to recruit for our next trial. RSE training days for teachers, facilitated by statutory agencies – in our case the PHA – were especially successful. In addition, in order to recruit schools across the socioeconomic and management spectrum, we recommend having tailored recruitment materials, for example tailored letters, that speak to the needs of different schools, and including testimonials from others, perhaps those drawn from a feasibility trial. Financial incentives and ensuring that the letters reach the decision-makers in schools are also important considerations for future recruitment strategies.
Pupil recruitment targets within the school were met (target of 80% pupil recruitment, achieved 80.1%). Approximately 9% of this was due to absentee pupils at baseline and 10% was due to refusal to consent to study. We aim to make parental opt-out consent processes clearer in the full effectiveness trial. Parental recruitment strategies to information evenings for intervention and follow-up focus groups failed very badly. Parental recruitment to the intervention (parental information sessions) failed, achieving only 2.3% of all parents/guardians. Consequently, recruitment of parents to focus group interviews also failed, as it was planned to recruit parents through the information session. Following more detailed research with parents and consultation on this topic, it has been decided to change the intervention component for parents to an online delivery method. Separate research funding has been obtained to deliver this change. We would still recommend pursuing a smaller amount of focus group interviews with parents in the next trial, but, overall, we shall rely more heavily on online survey data collection methods for parents. Recruitment of teachers for semistructured interviews within schools was unproblematic.
Randomisation processes proved successful, with no issues to report. Retention of schools was successful (100%) as was retention of pupils (93.1%). However, we learned the importance of developing a connection with the trial champion in schools and, in many cases, the school principal (head teacher) or VP, of staying in touch with schools and of not doing data collection with pupils too near the summer breaks when absenteeism is high.
Chapter 6 Quantitative results
Introduction
Unprotected sex during teenage years is well established as the main proximate behavioural determinant of teenage pregnancy and is a commonly measured behavioural outcome in studies examining the impact of RSE interventions on teenage pregnancy. 16,18,121–123 Studies indicate that, although other behavioural determinants (such as frequency of sexual intercourse and number of sexual partners) are important, avoidance of unprotected sex via consistent use of contraception is central in explaining variation in levels of teenage pregnancy. 22,124 A reduction in UTP rates would be the ideal primary outcome measure. However, the sample size would need to be very large in order to detect change in relation to this. In addition, teenage conception rates are not routinely collected in NI health and social care data, although teenage births are. In this study it was intended to pilot the acceptability of collecting a surrogate proximate behavioural determinant associated with UTP, namely having had unprotected sex, from pupils within schools within this age group (aged 14–15 years).
Secondary outcomes informed by our theory of change model (see Chapter 3) include knowledge, attitudes, skills and intentions relating to avoiding UTP. These short-term impacts are hypothesised to lead to increased intention to avoid UTP. 40,125–127 In this feasibility trial, data were collected using a number of standardised measures chosen because the constructs that they measure map closely to the theoretical framework underpinning the intervention (see Chapter 4). For these analyses, we were interested in how the results are differentiated between males and females and in relation to SES. In addition, to assist with the economic evaluation model to be used in a Phase III effectiveness trial, additional secondary outcomes were frequency of engagement in sexual intercourse, contraception use and diagnosis of STIs.
We have summarised the main quantitative findings of the study in a report format specifically tailored to the interests of both participating pupils and schools and are about to embark on disseminating this to participant schools (pending the return of the trial manager from maternity leave, as she has the strongest relationship with participating schools, and will deliver the reports in person). For both the pupil and school report, see Appendix 9.
For an overview of the integration of the quantitative component of the feasibility study, see Appendix 9.
Methods
The main purpose of the statistical analysis was to assess the feasibility and acceptability of the measures used. A detailed statistical analysis plan was written prior to analysis. The reporting and presentation of findings are in accordance with the CONSORT guidelines for cluster RCTs. 128 Primary analyses were on an intention-to-treat (ITT) basis, using all participants with complete data for baseline and follow-up, in the groups to which they were randomised. In intervention schools, all trial participants’ data were included in the analyses, regardless of the extent of their engagement with the programme. In all tables the means [standard deviations (SDs)] are presented for continuous variables and the overall mean is presented with standard error (SE) adjusted for the eight clusters (schools). Number (%) is presented for all categorical variables for those pupils who answered the questions. The p-values in the tables are indicative only and should not be interpreted as a definitive result. The 95% confidence intervals are more useful to interpret the data at this stage, to inform variance in the outcome results rather than the use of inferential statistics.
Appropriate descriptive summaries of baseline demographic and questionnaire data for pupils and from the two study groups were tabulated and descriptive summaries produced for baseline data at cluster level, where appropriate questionnaire data relating to pupil outcomes (at 5- and 9-month follow-up) were analysed using frequencies and descriptive statistics using Stata® 2013 (StataCorp LP, College Station, TX, USA) or IBM Statistical Product and Service Solutions Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY, USA). Differences between the trial groups for all the outcomes are reported using descriptive statistics. Factors that may influence outcomes such as sex (male/female), social class and religiosity were also explored.
Results
Baseline characteristics of participating pupils
In total, 831 Year 11 pupils aged between 14 and 16 years took part in the baseline evaluation. Just < 50% (49.5%) were female and just > 50% (50.5%) were male. Overall, 420 pupils were randomly allocated to the intervention group and 411 to the control group (see Chapter 5 for the randomisation process). Table 26 shows the breakdown of the sample by sex and group allocation.
| Sex | Intervention | Control | Total, n (%) |
|---|---|---|---|
| Female | 190 | 208 | 398 (47.9) |
| Male | 230 | 203 | 433 (52.1) |
| Total, n (%) | 420 (50.5) | 411 (49.5) | 831 (100) |
Table 27 shows the baseline demographic characteristics of the sample. This shows that the mean age was 14.4 years (SE = 0.019) in both the intervention and control groups. The ethnicity of the majority of participants was white (British/Irish) and the next largest group was Chinese (8% in total). For those whose ethnicity fell into the ‘other’ category, the most commonly cited ethnicity was Polish. In terms of religion, a wide range of religions was listed, with the most common being Christian, Atheist and Mormon. The most common religion in the sample was Catholic (n = 422, 50.8%). The second most common was Protestant (n = 307, 36.9%). The majority (41.6%) of pupils in the intervention group identified themselves as ‘not very religious’, whereas the control group (46.8%) most commonly identified themselves as ‘fairly religious’. Most of the pupils were not in receipt of free school meals; however, a slightly larger proportion in intervention schools were obtaining free school meals (16.4% vs. 10.6% in control schools). Here, we also present two measures of SES, one of which is based on parental highest level of education and one of which is based on children’s future educational aspirations (for further discussion on the issues encountered relating to a measure of SES, see Chapter 4).
| Characteristic | Intervention | Missing data | Control | Missing data |
|---|---|---|---|---|
| Mean age, years (SE) | 14.4 (0.019) | 14.5 (0.012) | ||
| Ethnicity, n (%) | 4 (1) | 4 (1) | ||
| White | 392 (93.3) | 391 (95.1) | ||
| Chinese | 2 (0.5) | 6 (1.5) | ||
| Irish Traveller | 3 (0.7) | 4 (1) | ||
| Other | 19 (4.5) | 6 (1.5) | ||
| Religiosity, n (%) | 2 (0.5) | 3 (0.7) | ||
| Very | 31 (7.4) | 45 (10.9) | ||
| Fairly | 155 (36.9) | 191 (46.5) | ||
| Not very | 174 (41.4) | 107 (26.0) | ||
| Not at all | 58 (13.8) | 65 (15.8) | ||
| Religion, n (%) | 2 (0.5) | 8 (1.9) | ||
| None | 25 (6.0) | 24 (5.8) | ||
| Catholic | 183 (43.6) | 239 (58.2) | ||
| Protestant | 181 (43.1) | 126 (30.7) | ||
| Muslim | 4 (1.0) | 1 (0.2) | ||
| Mixed | 7 (1.7) | 4 (1.0) | ||
| Other | 18 (4.3) | 9 (2.2) | ||
| Do you get free school meals?, n (%) | 1 (0.2) | 7 (1.7) | ||
| Yes | 135 (32.1) | 87 (21.2) | ||
| No | 264 (62.9) | 312 (75.9) | ||
| Do not know | 20 (4.8) | 5 (1.2) | ||
| Mother highest level of education, n (%) | 283 (67.4) | 268 (65.2) | ||
| Primary school | 3 (0.7) | 2 (0.5) | ||
| GCSE/O level or equivalent | 84 (20) | 95 (23.1) | ||
| A level or equivalent | 48 (11.4) | 44 (10.7) | ||
| Apprenticeship (e.g. plumber) | 2 (0.5) | 2 (0.5) | ||
| Certificate or diploma | 15 (1.9) | 18 (2.3) | ||
| University degree | 93 (11.6) | 112 (14.0) | ||
| None | 3 (0.4) | 1 (0.1) | ||
| Do not know | 147 (18.4) | 125 (15.6) | ||
| Not applicable | 3 (0.4) | 4 (0.5) | ||
| Father highest level of education, n (%) | 21 (5) | 7 (1.7) | ||
| Primary school | 8 (1.9) | 12 (2.9) | ||
| GCSE/O level or equivalent | 72 (17.1) | 106 (25.8) | ||
| A level or equivalent | 36 (8.6) | 29 (7.1) | ||
| Apprenticeship (e.g. plumber) | 26 (6.2) | 25 (6.1) | ||
| Certificate or diploma | 14 (3.3) | 15 (3.6) | ||
| University degree | 89 (21.2) | 74 (18.0) | ||
| None | 3 (0.7) | 9 (2.2) | ||
| Do not know | 149 (35.5) | 127 (30.9) | ||
| Not applicable | 2 (0.5) | 7 (1.7) | ||
| Future aspirations, n (%) | 4 (1.0) | 8 (1.9) | ||
| At college/uni full-time | 63 (15) | 46 (11.2) | ||
| At college/uni and working part-time | 32 (7.6) | 54 (13.1) | ||
| Working full-time | 186 (44.3) | 180 (43.8) | ||
| Working part-time | 106 (25.2) | 90 (21.9) | ||
| On a training scheme | 15 (3.6) | 19 (4.6) | ||
| Unemployed | 4 (1.0) | 1 (0.2) | ||
| Other | 10 (2.4) | 13 (3.2) | ||
| Sexuality, n (%) | 25 (6.0) | 12 (2.9) | ||
| I’ve never felt sexually attracted to anyone | 45 (10.7) | 30 (7.3) | ||
| Only to male, and never to females | 133 (31.7) | 166 (40.4) | ||
| More often to males and at least once to a female | 9 (2.1) | 10 (2.4) | ||
| About equally often to females and to males | 3 (0.7) | 6 (1.5) | ||
| More often to females and at least once to a male | 1 (0.2) | 3 (0.7) | ||
| Only to females, never to males | 204 (48.6) | 184 (44.8) |
Stopping rules/discontinuation criteria
The following were the trial stopping/discontinuation criteria as documented in the study protocol.
-
We shall monitor for harm by examining outcome data as soon as possible after each follow-up. If deterioration in scores indicated in the outcome measures in the intervention group are not matched by deterioration in scores in the control group, we would consider stopping the intervention.
Results
-
At follow-up 1 we found no evidence of harm and the ongoing process evaluation also indicated an overall positive evaluation among users.
-
Results at follow-up 1 (5 months post implementation) indicated that there was no significant difference between the two groups (intervention and control) at baseline for the primary outcome (abstinence or protected sex) (p = 0.45) or at 5-month follow-up (p = 0.80). However, the intervention group showed a small non-significant increase (improvement) in proportions across time of 0.6% compared with a worsening/deterioration of 2% in the control group. These results are noted in detail below in the reportage of the results of the primary outcome.
-
Thus the trial continued to completion to follow-up 2 and ended on completion of data collection by 30 October 2015.
Defining primary and secondary outcomes
Primary outcome
The surrogate measures (alternatives to the use of teenage pregnancy) used in this feasibility study to create the composite primary outcome measure were abstinence from sexual intercourse (delay in initiation of sex or return to abstinence) or avoidance of unprotected sexual intercourse (consistent correct use of contraception that does not include withdrawal or natural family planning). In this trial we used a number of questionnaire items to obtain this outcome (for the full questionnaire, see Appendix 3).
At baseline, follow-up 1 and follow-up 2, the delay of initiation of sex was determined using the following questionnaire item.
-
Have you ever experienced penetrative sex (penis–vagina) with another person?
-
Yes
-
No
-
At follow-up 1 data collection, a return to abstinence was determined using the following questionnaire item. If pupils responded more than 5 months ago, they had abstained since baseline. (In some schools follow-up 1 took place 6 months post baseline. If this was the case the question was changed to reflect this.)
-
When was the last time you had penetrative sex with someone?
-
Less than 1 week ago.
-
More than 1 week but less than 1 month ago.
-
1–4 months ago.
-
More than 5 months ago (when baseline data collection occurred).
-
At follow-up 2 data collection, a return to abstinence was determined using the following questionnaire item. If pupils responded that they had not had sex since June 2015, they had abstained for the past 4 months.
-
How many times have you had penetrative sex since you completed the last questionnaire in June 2015? (which was 4 months prior)
-
Not since June 2015.
-
Once.
-
Between two and five times.
-
Between six and 10 times.
-
Between 11 and 20 times.
-
More than 20 times.
-
Avoidance of unprotected sexual intercourse (consistent correct use of contraception that does not include withdrawal or natural family planning) was determined using the following two questionnaire items.
-
Thinking about ALL the times you have had sex EVER. How often were you or your partner protected against pregnancy? (Do not count the withdrawal method or emergency contraception – ‘the morning after pill’).
-
Never.
-
Not very often.
-
About half the time.
-
Most of the time.
-
Always.
-
-
The last time you had penetrative sex, did you or your partner use any form of contraception?
-
None for me, do not know about partner.
-
None for either of us.
-
Yes.
-
-
If yes, please tick all the contraceptives that you used the last time you had sex: Type:
-
Pill, patch or vaginal ring.
-
Condoms.
-
Emergency contraceptive pill.
-
Injection.
-
Implant.
-
Withdrawal method.
-
Intrauterine device.
-
Diaphragm/cap/spermicide.
-
Natural family planning.
-
Do not know name.
-
Other.
-
In the feasibility study, 91.5% of responding pupils in the four intervention schools and 93.6% of pupils in the four control schools reported that they had not yet had penetrative sex at baseline. At follow-up 1 this reduced to 91.3% and 89.4%, and at follow-up 2 to 84.1% and 87.5% for intervention schools and control schools, respectively. Pupil responses to the questionnaire items that were designed to determine abstinence are detailed in Table 28.
| Overall (schools combined) | Baseline | Follow-up 1 | Follow-up 2 | |||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| Have you ever experienced penetrative sex with another person? | ||||||
| Yes, n (%) | 35 (8.5) | 25 (6.4) | 26 (8.7) | 40 (10.6) | 59 (16.0) | 47 (12.5) |
| No, n (%) | 376 (91.5) | 367 (93.6) | 273 (91.3) | 338 (89.4) | 311 (84.1) | 328 (87.5) |
| When was the last time you had penetrative sex with someone? | ||||||
| More than 5 months ago (follow-up 1) | ||||||
| How many times have you had penetrative sex since you completed the last questionnaire in June 2015? | ||||||
| Not since June 2015 (follow-up 2) | ||||||
Sexually active respondents varied in their use of contraception/protection. Contraception types reported included the pill, patch or vaginal ring, condoms, emergency contraceptive pill, injection, implant, intrauterine devices, diaphragms/caps/spermicides, withdrawal and natural family planning. Condom use was the most common method of contraceptive used. Pupils reporting the withdrawal method and the natural family planning method (5% at baseline, 17% at follow-up 1, 5% at follow-up 2) were recorded into the results as not having used contraception (i.e. as having had unprotected sex). Pupil responses to withdrawal and natural family planning methods as forms of contraceptive are presented in Table 29.
| Method | Baseline | Follow-up 1 | Follow-up 2 | |||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| Withdrawal, n (%) | 2 (6.7) | 0 (0) | 2 (8.3) | 7 (12.1) | 0 (0) | 5 (12.5) |
| Natural, n (%) | 0 (0) | 1 (4.8) | 0 (0) | 2 (3.4) | 0 (0) | 0 (0) |
Contraceptive use components of the composite primary outcome are detailed in Table 30.
| Overall (schools combined) | Baseline | Follow-up 1 | Follow-up 2 | |||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| How often protected?, n (%) | ||||||
| Never | 5 (14.7) | 3 (13.0) | 5 (19.2) | 8 (20.0) | 15 (27.3) | 8 (19.1) |
| Not very often | 4 (11.8) | 4 (17.4) | 3 (11.5) | 9 (22.5) | 4 (7.3) | 1 (2.4) |
| About half the time | 3 (8.8) | 0 (0.0) | 1 (3.9) | 4 (10.0) | 3 (5.5) | 7 (16.7) |
| Most of the time | 3 (8.8) | 6 (26.1) | 2 (7.7) | 7 (17.5) | 12 (21.8) | 10 (23.8) |
| Always | 19 (55.9) | 10 (43.5) | 15 (57.7) | 12 (30.0) | 21 (38.2) | 16 (38.1) |
| Use of contraception when you last had sex?, n (%) | ||||||
| None for me, do not know about partner | 8 (22.9) | 3 (12.0) | 5 (19.2) | 4 (10.5) | 7 (13.7) | 4 (10.0) |
| None for either of us | 5 (14.3) | 6 (24.0) | 5 (19.2) | 8 (21.1) | 10 (19.6) | 9 (22.5) |
| Yes | 22 (62.9) | 16 (64.0) | 16 (61.5) | 26 (68.4) | 34 (66.7) | 27 (67.5) |
The primary composite outcome measure – abstinence or protected sex – is detailed in Table 31.
| Outcome measure | Intervention | Control | ||||
|---|---|---|---|---|---|---|
| Baseline (n = 411) | 5 months (n = 299) | 9 months (n = 370) | Baseline (n = 392) | 5 months (n = 377) | 9 months (n = 375) | |
| Abstinence or protected sex (yes), % | 96.8 | 97.7 | 96.2 | 97.7 | 97.4 | 97.3 |
| Change from baseline | 0.9% (improvement) | –0.6% (deterioration) | –0.3% (deterioration) | –0.4% (deterioration) | ||
| Abstinence or protected sex (yes), excluding withdrawal/natural family planning as unprotected, % (95% CI) | 96.4 (94.5 to 98.2) | 97.0 (95.1 to 98.9) | 94.6 (92.3 to 96.9) | 97.5 (95.9 to 99.0) | 95.5 (93.4 to 97.6) | 94.4 (95 92.1 to 96.7) |
| Change from baseline | 0.6% (improvement) | –1.8% (deterioration) | –2.0% (deterioration) | –3.1% (deterioration) | ||
There was no significant difference between the two groups at baseline for the composite outcome abstinence or protected sex including withdrawal/natural method (p = 0.45) or at 5- (p = 0.80) or 9-month follow-up (p = 0.91).
In the feasibility study, approximately 3% of our sample reported unprotected sex at baseline (3.6% intervention and 2.5% control) and approximately 5% reported unprotected sex at follow-up 2 (5.4% intervention and 5.6% control). This amounted to a 50% increase in unprotected sex by follow-up 2 in the intervention group (3.6% at baseline, rising to 5.4% at follow-up 2) compared with a more than doubling of unprotected sex by follow-up 2 in the control group (2.5% at baseline, rising to 5.6% at follow-up 2).
Subgroup analysis of primary outcome measure by gender
In the subgroup analysis of the primary outcome measure (Tables 32 and 33) by gender, there was an improvement in boys in the intervention arm (2.2% improvement at follow-up 1 and 0.5% improvement at follow-up 2) but a deterioration in females in the intervention arm was evident (1.3% deterioration at follow-up 1 and 4.4% deterioration at follow-up 2).
| Outcome measure | Intervention | Control | ||||
|---|---|---|---|---|---|---|
| Baseline (n = 186) | 5 months (n = 140) | 9 months (n = 182) | Baseline (n = 201) | 5 months (n = 195) | 9 months (n = 190) | |
| Abstinence or protected sex (yes), % (95% CI) | 98.4 (96.6 to 100.2) | 97.9 (95.5 to 100.3) | 96.1 (93.2 to 98.9) | 99.0 (97.6 to 100.4) | 98.5 (96.7 to 100.2) | 98.9 (97.4 to 100.4) |
| Change from baseline | 0.5% (deterioration) | 2.3% (deterioration) | 0.5% (deterioration) | 0.1% (deterioration) | ||
| Abstinence or protected sex (yes) excluding withdrawal/natural family planning as unprotected, % (95% CI) | 98.4 (96.6 to 100.2) | 97.1 (94.4 to 99.9) | 94.0 (90.5 to 97.4) | 99.0 (97.6 to 100.4) | 96.9 (94.5 to 99.3) | 94.2 (90.9 to 97.5) |
| Change from baseline | 1.3% (deterioration) | 4.4% (deterioration) | 2.1% (deterioration) | 4.8% (deterioration) | ||
| Outcome measure | Intervention | Control | ||||
|---|---|---|---|---|---|---|
| Baseline (n = 225) | 5 months (n = 159) | 9 months (n = 188) | Baseline (n = 191) | 5 months (n = 182) | 9 months (n = 185) | |
| Abstinence or protected sex (yes), % (95% CI) | 95.6 (92.9 to 98.2) | 97.5 (95.1 to 99.9) | 96.2 (93.5 to 99.0) | 96.3 (93.7 to 99.0) | 96.2 (93.4 to 98.9) | 95.7 (92.7 to 98.6) |
| Change from baseline | 1.9% (improvement) | 0.6% (improvement) | 0.1% (deterioration) | 0.6% (deterioration) | ||
| Abstinence or protected sex (yes) excluding withdrawal/natural family planning as unprotected, % (95% CI) | 94.7 (91.7 to 97.6) | 96.9 (94.1 to 99.6) | 95.2 (92.2 to 98.3) | 95.8 (93.0 to 98.7) | 94.0 (90.5 to 97.4) | 94.6 (91.3 to 97.9) |
| Change from baseline | 2.2% (improvement) | 0.5% (improvement) | 1.8% (deterioration) | 1.2% (deterioration) | ||
Secondary outcomes
The following secondary outcomes were drawn from the theoretical framework underpinning the intervention (theory of planned behaviour; see Chapter 3). To measure these outcomes we used some existing measures with robust reliability and validity (see Appendix 1). The baseline questionnaire is included in Appendix 2.
The first outcome chosen in this questionnaire was Knowledge. The purpose of this was to determine if pupils had increased knowledge about UTP. Knowledge scores represented the total score on the Knowledge scale (Q.15) and the sum of correct answers to the following questionnaire items:
Q.16 What is the legal age of consent (the age at which you can legally first have sex) in NI?
Q.17 Can you think of any health services, clinics or places you could visit if you wanted to get the following? Free Contraception; advice on sexual health (e.g. pregnancy, STIs).
Q.18 Can you think of any websites which provide information on sexual health, relationships and pregnancy?
The second outcome, Attitudes, aimed to determine if pupils:
-
had increased awareness that men and women have roles and responsibilities in avoiding UTP;
-
hold less stereotypical gender-related attitudes and have increased perception that most peers are not sexually active and use contraception when they are;
-
have increased perception that both parents (parent/child communication) and peers support abstinence and/or use of contraception.
Scores resulted from the incorporation of one questionnaire item (Q.19; Box 2), and the Comfort Communicating about Pregnancy scale (Q.20), the Comfort Communicating about Contraception scale (Q.20), the Male Role Attitudes scale (Q.22).
Put an X on the line below to show how much responsibility you think boys and girls should have. For example, if you think girls should have more responsibility than boys, put an X on the line closer to girl; if you think boys should have more responsibility than girls, put an X on the line closer to boy; If you think boys and girls should have equal responsibility, put an X in the middle of the line.
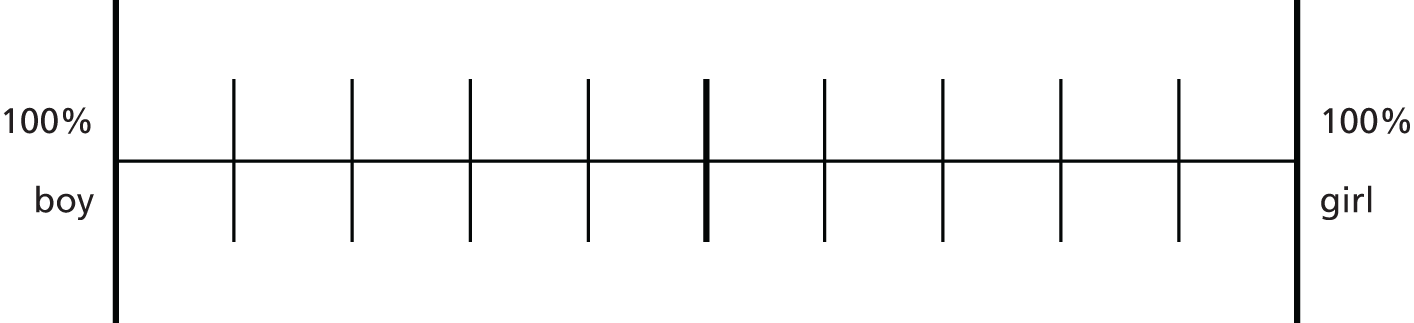
The third outcome, Skills, aimed to determine if pupils had increased self-efficacy in communicating about UTP and avoiding UTP. Scores resulted from the incorporation of the Sexual Self-Efficacy scale (Q.21) the Sexual Socialisation scale (Q.23), the Sexual Socialisation Peer subscale (Q.23) and Sexual Socialisation Parent subscale (Q.23).
The final outcome, Intentions, aimed to determine if pupils had higher anticipated regret about UTP and increased strength of intention to avoid UTP. For this construct, the questionnaire incorporated a measure of intention to avoid UTP, developed as part of the research process (see Chapter 4). Scores incorporated the Intentions scale, Intentions Self-Efficacy subscale, Intentions Attitudes subscale and the Intentions Norms subscale.
Descriptive statistics for the secondary outcomes are presented below (Tables 34–36). As the study was not powered to detect statistically significant differences between groups, we have not conducted mediation analysis or logistic regression to test the impact of these variables on the primary outcome measure.
| Outcome measure | Follow-up 1 | Follow-up 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | |
| Knowledge | ||||||||
| Knowledge | 0.81 ± 2.29 (n = 269) | 0.60 ± 2.09 (n = 356) | 0.21 (–0.14 to 0.55) | 0.24 | 1.03 ± 2.36 (n = 324) | 0.88 ± 2.16 (n = 370) | 0.15 (–0.19 to 0.48) | 0.39 |
| Attitudes | ||||||||
| Comfort communicating about pregnancy | 0.12 ± 1.62 (n = 251) | 0.06 ± 1.69 (n = 341) | 0.06 (–0.21 to 0.34) | 0.64 | 0.53 ± 1.58 (n = 322) | 0.57 ± 1.56 (n = 345) | –0.04 (–0.28 to 0.20) | 0.76 |
| Comfort communicating about contraception | 0.31 ± 2.02 (n = 229) | 0.23 ± 2.23 (n = 314) | 0.08 (–0.29 to 0.45) | 0.67 | 0.83 ± 2.21 (n = 275) | 0.87 ± 2.12 (n = 312) | –0.03 (–0.38 to 0.32) | 0.86 |
| Male role attitudes | –0.74 ± 3.42 (n = 220) | –0.19 ± 4.46 (n = 286) | –0.55 (–1.26 to 0.16) | 0.13 | –0.65 ± 3.71 (n = 263) | –1.52 ± 2.91 (n = 296) | 0.87 (0.32 to 1.42) | 0.002 |
| Skills | ||||||||
| Sexual self-efficacy | 0.18 ± 1.07 (n = 173) | 0.22 ± 1.16 (n = 219) | –0.04 (–0.26 to 0.19) | 0.74 | 0.25 ± 1.23 (n = 206) | 0.27 ± 1.19 (n = 236) | –0.01 (–0.24 to 0.22) | 0.92 |
| Sexual socialisation | 0.06 ± 7.62 (n = 203) | 0.84 ± 7.50 (n = 283) | –0.78 (–2.14 to 0.58) | 0.26 | 0.36 ± 7.81 (n = 255) | –0.48 ± 7.26 n = 294 | 0.84 (–0.43 to 2.10) | 0.19 |
| Sexual socialisation peer subscale | 0.17 ± 5.35 (n = 221) | 0.35 ± 5.41 (n = 308) | –0.18 (–1.11 to 0.75) | 0.70 | 0.38 ± 5.89 (n = 276) | 0.15 ± 5.64 (n = 317) | 0.23 (–0.70 to 1.16) | 0.62 |
| Sexual socialisation parent subscale | –0.61 ± 3.85 (n = 228) | 0.33 ± 3.77 (n = 306) | –0.39 (–1.04 to 0.26) | 0.24 | –0.02 ± 4.03 (n = 285) | –0.63 ± 3.54 (n = 312) | 0.61 (–0.001 to 1.22) | 0.05 |
| Intentions | ||||||||
| Intentions | 0.15 ± 6.93 (n = 216) | 0.67 ± 8.09 (n = 300) | –0.51 (–1.85 to 0.82) | 0.45 | 1.12 ± 7.93 (n = 261) | 1.68 ± 6.94 (n = 313) | –0.56 (–1.78 to 0.65) | 0.36 |
| Intentions self-efficacy subscale | 0.65 ± 3.17 (n = 239) | 0.39 ± 3.75 (n = 338) | 0.26 (–0.33 to 0.84) | 0.39 | 0.98 ± 3.63 (n = 296) | 0.87 ± 3.62 (n = 349) | 0.11 (–0.45 to 0.67) | 0.70 |
| Intentions attitudes subscale | –0.09 ± 2.25 (n = 251) | –0.16 ± 2.53 (n = 342) | 0.07 (–0.32 to 0.46) | 0.73 | 0.15 ± 2.25 (n = 312) | 0.07 ± 2.11 (n = 348) | 0.08 (–0.25 to 0.41) | 0.64 |
| Intentions norms subscale | –0.28 ± 4.22 (n = 249) | 0.14 ± 4.63 (n = 339) | –0.42 (–1.15 to 0.31) | 0.26 | 0.06 ± 4.62 (n = 301) | 0.68 ± 4.14 (n = 343) | –0.62 (–1.29 to 0.06) | 0.07 |
| Outcome measure | Follow-up 1 | Follow-up 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | |
| Knowledge | ||||||||
| Knowledge | 1.06 ± 2.40 (n = 125) | 0.70 ± 2.06 (n = 181) | 0.36 (–0.14 to 0.87) | 0.16 | 1.43 ± 2.29 (n = 157) | 1.04 ± 2.10 (n = 187) | 0.39 (–0.08 to 0.85) | 0.10 |
| Attitudes | ||||||||
| Comfort communicating about pregnancy | –0.03 ± 1.56 (n = 119) | 0.08 ± 1.63 (n = 179) | –0.11 (–0.48 to 0.26) | 0.56 | 0.48 ± 1.51 (n = 160) | 0.61 ± 1.55 (n = 180) | –0.12 (–0.45 to 0.20) | 0.46 |
| Comfort communicating about contraception | 0.10 ± 1.99 (n = 105) | 0.31 ± 2.17 (n = 160) | –0.21 (–0.73 to 0.31) | 0.43 | 0.80 ± 2.15 (n = 132) | 0.78 ± 2.03 (n = 156) | 0.01 (–0.47 to 0.50) | 0.96 |
| Male role attitudes | –1.03 ± 3.20 (n = 115) | –0.30 ± 4.07 (n = 142) | –0.73 (–1.65 to 0.18) | 0.12 | –1.02 ± 3.30 (n = 134) | –1.50 ± 2.62 (n = 147) | 0.47 (–0.22 to 1.17) | 0.18 |
| Skills | ||||||||
| Sexual self-efficacy | 0.23 ± 0.98 (n = 79) | 0.34 ± 1.17 (n = 100) | –0.11 (–0.44 to 0.21) | 0.49 | 0.38 ± 0.90 (n = 100) | 0.41 ± 1.01 (n = 108) | –0.03 (–0.30 to 0.23) | 0.79 |
| Sexual socialisation | –0.52 ± 8.20 (n = 93) | 0.45 ± 7.67 (n = 147) | –0.97 (–3.02 to 1.09) | 0.36 | 0.17 ± 7.92 (n = 120) | –0.72 ± 6.78 (n = 152) | 0.88 (–0.87 to 2.64) | 0.32 |
| Sexual socialisation peer subscale | –0.21 ± 5.69 (n = 101) | 0.15 ± 5.53 (n = 160) | –0.36 (–1.76 to 1.04) | 0.62 | 0.73 ± 5.80 (n = 135) | 0.17 ± 5.16 (n = 165) | 0.56 (–0.69 to 1.80) | 0.38 |
| Sexual socialisation parent subscale | –0.28 ± 4.11 (n = 105) | 0.11 ± 3.97 (n = 158) | –0.39 (–1.39 to 0.61) | 0.44 | –0.45 ± 4.03 (n = 132) | –0.85 ± 3.63 (n = 161) | 0.40 (–0.48 to 1.29) | 0.37 |
| Intentions | ||||||||
| Intentions | 0.34 ± 7.24 (n = 101) | 0.07 ± 7.68 (n = 153) | 0.26 (–1.63 to 2.16) | 0.78 | 1.01 ± 7.49 (n = 122) | 1.37 ± 6.44 (n = 161) | –0.36 (–1.99 to 1.28) | 0.67 |
| Intentions self-efficacy subscale | 0.50 ± 3.14 (n = 112) | –0.05 ± 3.25 (n = 169) | 0.55 (–0.22 to 1.32) | 0.16 | 0.83 ± 3.39 (n = 139) | 0.26 ± 3.22 (n = 174) | 0.58 (–0.16 to 1.31) | 0.13 |
| Intentions attitudes subscale | 0.24 ± 2.40 (n = 118) | –0.26 ± 2.67 (n = 175) | 0.49 (–0.11 to 1.09) | 0.11 | 0.23 ± 2.22 (n = 151) | 0.12 ± 2.16 (n = 181) | 0.10 (–0.37 to 0.58) | 0.67 |
| Intentions norms subscale | –0.28 ± 4.37 (n = 114) | 0.31 ± 4.65 (n = 173) | –0.59 (–1.67 to 0.48) | 0.28 | 0.09 ± 4.54 (n = 145) | 0.94 ± 4.06 (n = 177) | –0.85 (–1.79 to 0.10) | 0.08 |
| Outcome measure | Follow-up 1 | Follow-up 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | Intervention, Mean ± SD change | Control, Mean ± SD change | Difference mean change scores (95% CI) | p-value | |
| Knowledge | ||||||||
| Knowledge | 0.58 ± 2.18 (n = 144) | 0.50 ± 2.12 (n = 175) | 0.09 (–0.39 to 0.56) | 0.72 | 0.65 ± 2.37 (n = 167) | 0.72 ± 2.21 (n = 183) | –0.07 (–0.55 to 0.41) | 0.78 |
| Attitudes | ||||||||
| Comfort communicating about pregnancy | 0.27 ± 1.68 (n = 132) | 0.04 ± 1.77 (n = 162) | 0.23 (–0.17 to 0.63) | 0.26 | 0.57 ± 1.65 (n = 162) | 0.52 ± 1.57 (n = 165) | 0.05 (–0.30 to 0.40) | 0.77 |
| Comfort communicating about contraception | 0.49 ± 2.03 (n = 124) | 0.15 ± 2.29 (n = 154) | 0.34 (–0.18 to 0.86) | 0.19 | 0.87 ± 2.27 (n = 143) | 0.95 ± 2.21 (n = 156) | –0.08 (–0.59 to 0.43) | 0.75 |
| Male role attitudes | –0.41 ± 3.63 (n = 105) | –0.08 ± 4.82 (n = 144) | –0.33 (–1.44 to 0.77) | 0.55 | –0.26 ± 4.08 (n = 129) | –1.54 ± 3.18 (n = 149) | 1.27 (0.41 to 2.13) | 0.004 |
| Skills | ||||||||
| Sexual self-efficacy | 0.15 ± 1.13 (n = 94) | 0.12 ± 1.16 (n = 119) | 0.03 (–0.29 to 0.34) | 0.87 | 0.14 ± 1.48 (n = 106) | 0.14 ± 1.32 (n = 128) | 0.00 (–0.36 to 0.36) | 0.99 |
| Sexual socialisation | 0.55 ± 7.09 (n = 110) | 1.27 ± 7.31 (n = 136) | –0.72 (–2.54 to 1.11) | 0.44 | 0.53 ± 7.73 (n = 135) | –0.22 ± 7.76 (n = 142) | 0.75 (–1.08 to 2.58) | 0.42 |
| Sexual socialisation peer subscale | 0.48 ± 5.06 (n = 120) | 0.56 ± 5.29 (n = 148) | –0.08 (–1.33 to 1.18) | 0.90 | 0.05 ± 5.97 (n = 141) | 0.13 ± 6.13 (n = 152) | –0.08 (–1.47 to 1.32) | 0.92 |
| Sexual socialisation parent subscale | 0.12 ± 3.61 (n = 123) | 0.55 ± 3.53 (n = 148) | –0.43 (–1.29 to 0.43) | 0.32 | 0.35 ± 4.01 (n = 153) | –0.39 ± 3.43 (n = 151) | 0.74 (–0.10 to 1.58) | 0.09 |
| Intentions | ||||||||
| Intentions | –0.01 ± 6.68 (n = 115) | 1.29 ± 8.48 (n = 147) | –1.29 (–3.19 to 0.60) | 0.18 | 1.22 ± 8.32 (n = 139) | 2.02 ± 7.44 (n = 152) | –0.80 (–2.62 to 1.01) | 0.38 |
| Intentions self-efficacy subscale | 0.78 ± 3.21 (n = 127) | 0.83 ± 4.15 (n = 169) | –0.05 (–0.92 to 0.82) | 0.91 | 1.11 ± 3.83 (n = 157) | 1.48 ± 3.89 (n = 175) | –0.37 (–1.20 to 0.47) | 0.39 |
| Intentions attitudes subscale | –0.38 ± 2.08 (n = 133) | –0.06 ± 2.38 (n = 167) | –0.32 (–0.84 to 0.19) | 0.22 | 0.08 ± 2.27 (n = 161) | 0.02 ± 2.06 (n = 167) | 0.06 (–0.41 to 0.53) | 0.79 |
| Intentions norms subscale | –0.28 ± 4.10 (n = 135) | –0.05 ± 4.63 (n = 166) | –0.23 (–1.24 to 0.77) | 0.65 | 0.04 ± 4.71 (n = 156) | 0.40 ± 4.21 (n = 166) | –0.37 (–1.34 to 0.61) | 0.46 |
Compared with pupils in the control group, pupils in the intervention group had more of an increase in knowledge (Knowledge scale score) about UTP at follow-up 1 [0.21 (95% CI –0.14 to 0.55)] and at follow-up 2 [0.15 (95% CI –0.19 to 0.48)]. When asked about the legal age of consent (the age at which you can legally first have sex) in NI, 65.5% of respondents answered with the correct age of 16 years. Thirty-eight per cent of pupils correctly identified a health service, clinic or place where one could obtain free contraception [e.g. GP surgeries, Brook clinics (Brook Young People, Liverpool, UK)] and 40% were able to name a source of advice on sexual health (e.g. GP surgeries, sexual health clinics, internet). Pupils listed a wide variety of websites that provide information on sexual health, relationships and pregnancy. Eighty-nine per cent incorrectly (as determined by the research team) interpreted particular websites (e.g. named pornography sites) as sources of such information and 10.6% correctly identified websites that do provide such information.
At baseline, when asked whose responsibility it is to prevent UTP, 75.5% of pupils who responded to Q.19 attributed a 50 : 50 ratio of responsibility to boys and to girls. Less than 1% (0.6%) of responding pupils answered that it was only the boy’s responsibility to prevent UTP, and 0.7% answered that it was only the girl’s responsibility. At follow-up 1, 80.7% of pupils attributed a 50 : 50 ratio of responsibility to boys and girls, with 3.8% indicating that it was only the boy’s responsibility to prevent UTP and 0.2% that it was only the girl’s responsibility. At follow-up 2, 83.4% of pupils attributed a 50 : 50 ratio of responsibility to boys and girls, with 0.1% of responding pupils indicating that they thought it was only the boy’s or only the girl’s responsibility to prevent UTP. Both the intervention and control group demonstrated an improvement towards attributing an equal 50 : 50 ratio of responsibility over time, although the improvement was more pronounced in the intervention group (13.3% vs. 10.4% in the control group).
Scores on the Male Roles Attitudes scale at follow-up 1 indicated that pupils showed a decrease in stereotypical gender attitudes to the roles of males and females in society (e.g. men work and women care). This decrease in awareness was more evident in the intervention group [–0.55 (95% CI –1.26 to 0.16)]. At follow-up 2 pupils also had a decreased awareness of gender-specific roles, but on this occasion the decrease was more evident in the control group [0.87 (95% CI 0.32 to 1.42)] than in the intervention group, although see below that there was a sustained decrease of stereotypical gender attitudes among males in the intervention group.
Increased scores on the Comfort Communicating about Pregnancy scale indicated that more pupils in the intervention group than in the control group were comfortable communicating with parents and peers about avoiding UTP at follow-up 1 [0.06 (95% CI –0.21 to 0.34)] and follow-up 2 [–0.04 (95% CI –0.28 to 0.20)]. Similarly, scores on the Comfort Communicating about Contraception scale indicated that at follow-up 1 more pupils in the intervention group were more comfortable communicating with parents and peers about the use of contraception [0.08 (95% CI –0.29 to 0.45)]. However, at follow-up 2 more pupils in the control group were more comfortable communicating with parents and peers about the use of contraception [–0.03 (95% CI –0.38 to 0.32)].
In relation to sexual self-efficacy, pupils in the intervention group scored lower than those in the control group at both follow-up 1 [–0.04 (95% CI –0.26 to 0.19)] and follow-up 2 [–0.01 (95% CI –0.24 to 0.22)]. Scores on the Sexual Socialisation scale indicated that pupils scored better in the intervention group only at follow-up 2 [0.84 (95% CI –0.43 to 2.10)], as was the case with each Sexual Socialisation subscale: peer [0.23 (95% CI –0.70 to 1.16)]; parent [0.61 (95% CI –0.001 to 1.22)].
Looking at the Intentions scale as a whole, pupils scored higher in the control group at both follow-up 1 [–0.51 (95% CI –1.85 to 0.82)] and follow-up 2 [–0.56 (95% CI –1.78 to 0.65)]. When exploring the Intentions subscales, a difference was evident. Pupils in the intervention group scored higher at both follow-up 1 and at follow-up 2 for both the Intentions Self-Efficacy subscale [follow-up 1 0.26 (95% CI –0.33 to 0.84); follow-up 2 [0.11 (95% CI –0.45 to 0.67)] and the Intentions Attitudes subscale [follow-up 1 0.07 (95% CI –0.32 to 0.46); follow-up 2 [0.08 (95% CI –0.25 to 0.41)], whereas pupils in the control group scored higher at both follow-up 1 [–0.42 (95% CI –1.15 to 0.31)] and follow-up 2 [–0.62 (95% CI –1.29 to 0.06)] in relation to the Intentions Norms subscale.
Differences among male and female pupils in relation to secondary outcomes were also examined. Female pupils in the intervention group scored notably higher than their male counterparts in the Knowledge scale at both follow-up 1 and 2 [follow-up 1: female 0.36 (95% CI –0.14 to 0.87), male 0.09 (95% CI –0.39 to 0.56); follow-up 2: female 0.39 (95% CI –0.08 to 0.85), male –0.07 (95% CI –0.55 to 0.41)], the Intentions scale at follow-up 1 [follow-up 1: female 0.26 (95% CI –1.63 to 2.16), male –1.29 (95% CI –3.19 to 0.60)], the Intentions Self-Efficacy subscale [follow-up 1: female 0.55 (95% CI –0.22 to 1.32), male –0.05 (95% CI –0.92 to 0.82); follow-up 2: female 0.58 (95% CI –0.16 to 1.31), Male –0.37 (95% CI –1.20 to 0.47)] at both follow-up 1 and 2 and the Attitudes subscale [follow-up 1: female 0.49 (95% CI –0.11 to 1.09), male –0.32 (95% CI –0.84 to 0.19); follow-up 2: female 0.10 (95% CI –0.37 to 0.58), Male 0.06 (95% CI –0.41 to 0.53)] at both follow-up 1 and 2. Male pupils in the intervention group scored significantly higher on the Male Role Attitudes scale (p = 0.004) than male pupils in the control group at follow-up 2 and notably higher than their female counterparts in the intervention group [male 1.27 (95% CI 0.41 to 2.13), female 0.47 (95% CI –0.22 to 1.17)]. This was not evident at follow-up 1.
The total number of pupil participants who responded to the questionnaire at both baseline and follow-up 1 data collection was 666, and at both baseline and follow-up 2 data collection was 744 (see Chapter 5). The n values in the above table refer to the total number of participants who answered all the questionnaire items relative to the associated outcome measure at baseline, follow-up 1 and follow-up 2. Missing data can be deduced from this.
Secondary behavioural outcomes relating to the health economics evaluation model
Overall pupil responses (by treatment arm) to questions relating to secondary behavioural outcomes are detailed below in Table 37.
| Overall (schools combined) | Baseline | Follow-up 1 | Follow-up 2 | |||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| How many male partners have you had sex with in the past 6 months (or 5 months/follow-up 1, or 4 months/follow-up 2) (girls), n (%) | ||||||
| One | 5 (71.4) | 6 (85.7) | 10 (90.9) | 7 (77.8) | 19 (82.6) | 14 (87.5) |
| Between 2 and 5 | 2 (28.4) | 1 (14.3) | 1 (9.1) | 2 (22.2) | 3 (13.0) | 2 (12.5) |
| Between 6 and 10 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (4.4) | 0 (0.0) |
| More than 10 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (22.2) | 0 (0.0) | 0 (0.0) |
| How many female partners have you had sex with in the past 6 months (or 5 months/follow-up 1, or 4 months/follow-up 2) (boys), n (%) | ||||||
| One | 12 (60.0) | 9 (69.2) | 5 (62.5) | 9 (47.4) | 13 (61.9) | 13 (65.0) |
| Between 2 and 5 | 6 (30.0) | 2 (15.4) | 1 (12.5) | 6 (31.6) | 7 (33.3) | 5 (25.0) |
| Between 6 and 10 | 0 (0.0) | 2 (15.4) | 1 (12.5) | 0 (0.0) | 1 (4.8) | 1 (5.0) |
| More than 10 | 2 (10.0) | 0 (0.0) | 1 (12.5) | 4 (21.1) | 0 (0.0) | 1 (5.0) |
In the present feasibility study, respondents reported on having had STIs within the 6 months prior to baseline data collection, since follow-up 1 data collection, or since follow-up 2 data collection (Table 38). This question was poorly responded to, with 93.4% missing data at baseline, 91.3% missing data at follow-up 1 and 88.7% missing data at follow-up 2.
| STI | Baseline | Follow-up 1 | Follow-up 2 | |||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| Chlamydia | 1 | 1 | 2 | 1 | 1 | 5 |
| Genital warts | 0 | 2 | 3 | 0 | 1 | 4 |
| Herpes | 0 | 1 | 2 | 0 | 1 | 4 |
| Gonorrhoea | 0 | 2 | 2 | 0 | 1 | 4 |
| Pubic lice | 0 | 1 | 2 | 0 | 1 | 5 |
| Trichomonas | 0 | 1 | 2 | 0 | 1 | 4 |
| Syphilis | 0 | 1 | 2 | 0 | 1 | 4 |
| HIV | 0 | 2 | 2 | 0 | 1 | 4 |
| Hepatitis | 0 | 1 | 2 | 0 | 1 | 4 |
| Pelvic infection (girls) | 0 | 2 | 2 | 0 | 1 | 5 |
| Vaginal thrush (girls) | 0 | 1 | 2 | 0 | 1 | 4 |
| Cannot remember the name | 0 | 1 | 2 | 0 | 1 | 4 |
| None | 0 | 22 | 46 | 35 | 24 | 32 |
| Other | 0 | 0 | 3 | 0 | 0 | 0 |
| Total STIs | 1 | 16 | 28 | 1 | 12 | 51 |
| Missing data (%) | 93.4 | 91.3 | 88.7 | |||
Reported UTPs were very low. At baseline data collection, only one respondent (5.9%) in the control arm reported having intentionally gotten a girl pregnant within 1 month prior to baseline data collection, and six (23.1%) and two (11.8%) in the intervention and control arms, respectively, reported that they did not know if they had ever gotten a girl pregnant. Only one respondent (12.5%) in the intervention group reported having been unintentionally pregnant between 10 and 12 months ago. At follow-up 1 data collection, three (12%) respondents in the control arm and one (7.1%) in the intervention arm reported having gotten a girl pregnant without intent, while one (7.1%) and three (12.0%) in the intervention and control arms, respectively, reported that they did not know if they had ever gotten a girl pregnant. One (8.3%) female respondent reported not knowing if she had ever been pregnant at follow-up 1 data collection. At follow-up 2 data collection, two (6.9%) respondents in the intervention group reported having gotten a girl pregnant (one intentional and one unintentional) and one respondent (4.2%) in the control group reported having gotten a girl pregnant (also unintentional), while two respondents in the intervention group (6.9%) and one in the control group (4.2%) did not know if they had. One (3.7%) female respondent reported being unintentionally pregnant at follow-up 2 data collection and one (3.7%) reported not knowing if she had ever been pregnant.
At baseline data collection seven (21.9%) respondents in the intervention arm and seven (28.0%) in the control arm reported having had sex when they did not want to within the past 6 months. These figures were seven (14.9%) and four (10.3%), respectively, at follow-up 1, and two (8.3%) and six (16.2%), respectively, at follow-up 2.
Discussion and conclusion
In the feasibility study, approximately 3% of the sample reported unprotected sex at baseline (3.6% in the intervention and 2.5% in the control group) and approximately 5% reported unprotected sex at follow-up 2 (5.4% in the intervention and 5.6% in the control group). Although not significant, there was a 50% increase in unprotected sex (as determined by the composite primary outcome, abstinence or protected sex excluding withdrawal/natural family planning method) by follow-up 2 in the intervention group (3.6% at baseline, rising to 5.4% at follow-up 2) compared with a more than doubling of unprotected sex by follow-up 2 in the control group (2.5% at baseline, rising to 5.6% at follow-up 2). Drawing from robust representative epidemiological data of school-aged children across the UK (the WHO Health Behaviour in School-aged Children Survey GB, 2014)129 and the Young Persons’ Behaviour & Attitudes Survey 2013,130 it is known that between 25% and 33% of 15-year-olds are having sex. Looking more closely at the rates of unprotected sex for this age group, we can determine a rate of 2.8% reporting unprotected sex (overall in England, Wales, Scotland and NI) (sample, N = 7904 and n = 224 reporting unprotected sex). Therefore, the 1.3% difference (in change from baseline to follow-up 2) in unprotected sex between groups as found in the feasibility study could potentially have a significant impact on UTP rates. If such a finding were to hold true in a sufficiently powered trial, this would indicate that, for every 1000 pupils, 13 fewer would have unprotected sex during the follow-up period.
Owing to difficulties encountered in establishing a reliable and valid measure of SES (see Chapter 4), subgroup analysis by SES was not possible within this feasibility study as first intended. Subgroup analysis by gender was possible and revealed gender differences. In relation to the primary composite outcome there was an improvement in boys in the intervention arm but a deterioration in girls. Female pupils in the intervention arm scored notably higher in the Knowledge scale and in the Intentions Self-Efficacy and Attitudes subscales than their male counterparts. Interestingly, male pupils in the intervention group scored significantly higher than male pupils in the control group at follow-up 2 and notably higher than their female counterparts in the intervention group in the Male Role Attitudes scale. The Male Role Attitudes scale is essentially an analysis of emerging masculinities that are more gender equal versus the traditional gender-related views that men and women are unequal.
A number of additional secondary outcome measures (sexual frequency, contraceptive use and occurrence of STIs) were thought to be particularly relevant to informing a health economic evaluation. The feasibility of collecting these data was also explored. Although all three outcome measures were perceived as being feasible to collect, the occurrence of STIs was poorly responded to, with missing data in excess of 90%.
Chapter 7 Process evaluation
Introduction
The feasibility of delivering the intervention as part of an effectiveness trial was addressed by an embedded process evaluation. This allowed an examination of the school contexts, including current RSE provision, and the implementation and acceptability of the intervention among participants in the intervention group. An outline of the aims, objectives and methods employed for the qualitative component of the study is followed by an overview of findings relating to the contexts of participating schools and their current RSE provision and triangulated perceptions of the acceptability and feasibility of the intervention and research processes.
Aims and objectives
The aims of the process evaluation were to (1) assess the ways in which the intervention was implemented; (2) assess how it was received and how it could be further improved; and (3) collect details on the context of participating schools that might help to explain differences in perceptions of feasibility and acceptability.
The objectives of the qualitative component were to:
-
record the current policies on, and provision of, RSE in schools and to assess what RSE was delivered in schools during the feasibility trial
-
inquire into teachers’ experiences of using the intervention with pupils and parents/guardians (intervention group)
-
record pupils’ experiences of using the intervention at school and home (intervention group)
-
gain further information on implementation fidelity and teachers’, pupils’ and parents/guardians’ reactions through researcher observation
-
inquire into parents’/guardians’ reactions to their children using the intervention, as well as the barriers to and facilitators of their own participation
-
record participants’ experiences of taking part in the trial
-
obtain teachers’ views on the quality of the training session offered on the intervention
-
test the face validity of the quantitative instruments among pupils in the control group by conducting cognitive interviews on the topic of the questionnaire (see Chapter 4)
-
record experiences of recruiting schools, also paying attention to refusals (see Chapter 5)
-
record schools’ reactions to being assigned to control or intervention group (see Chapter 5 for randomisation and allocation).
Methods
A summary of the sample and data collection and analysis methods are outlined below. As illustrated in Figure 5, methods differed between the intervention and control groups. For interview and observation schedules, the parent’s survey and pupil comment sheet, see Appendix 3.
FIGURE 5.
Structure and key components of the If I Were Jack feasibility trial process evaluation.
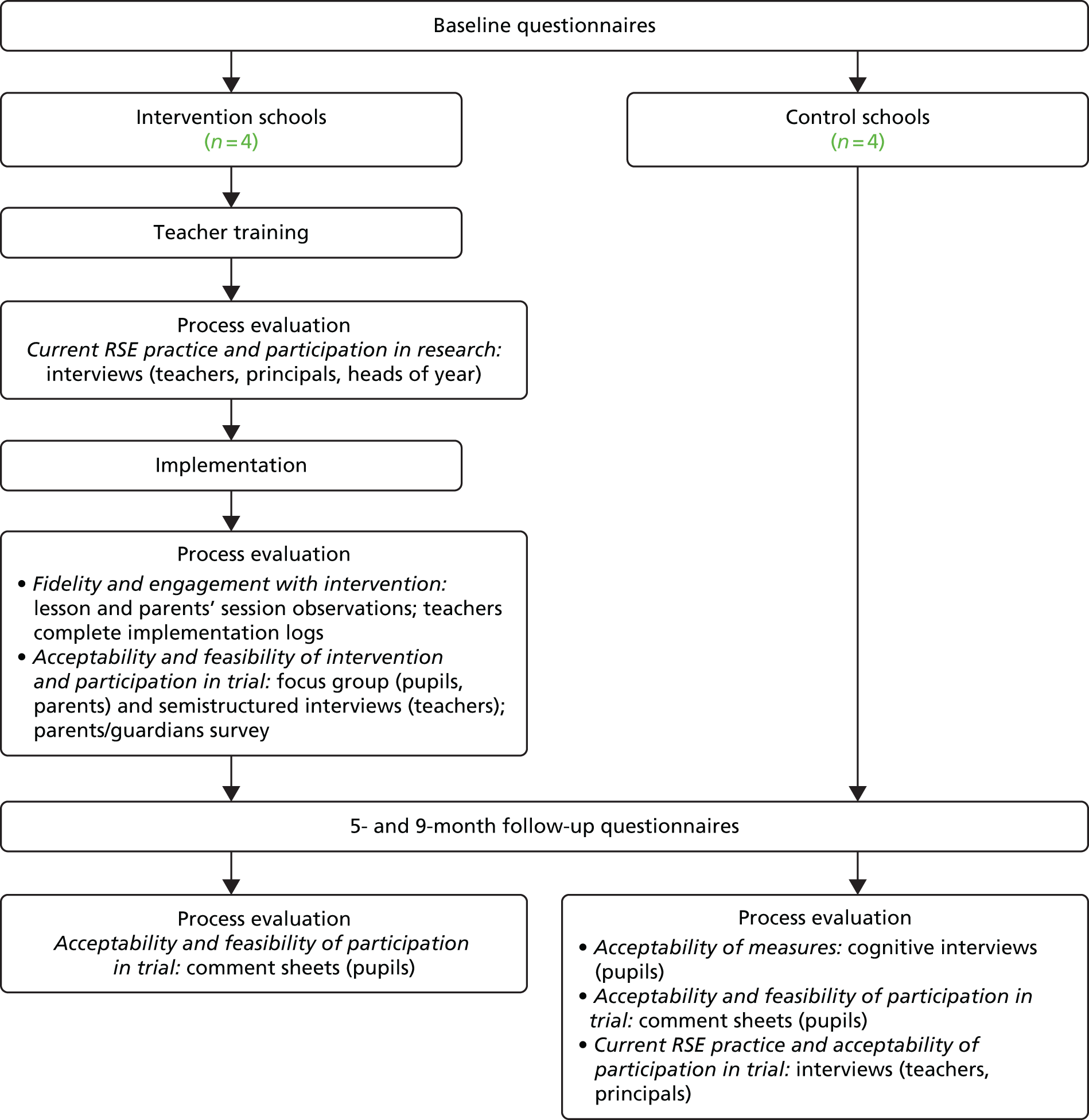
Data collection
In all participating schools data collection involved individual semistructured interviews/focus group discussions and a comment sheet regarding the ‘good and bad things’ about participating in the trial, which was delivered to pupils immediately following the final follow-up questionnaire. In addition, in intervention schools data were collected from structured observations of at least one lesson and one parent information and discussion session in each school, and a short online parent survey.
Intervention schools
-
RSE provision: semistructured interviews with teachers (RSE-coordinators, heads of Year 11, PC VPs)
-
the nature, quantity and quality of current RSE
-
facilitators of and barriers to teaching RSE.
-
-
Research participation: semistructured interviews with principals/heads of Year 11
-
perceptions of the conduct of research in schools in general and experiences of participation in the trial
-
barriers to and facilitators of research participation
-
engaging parents.
-
-
Feasibility and acceptability of the intervention and implementation process and taking part in the trial: individual interviews and focus group discussions with all teachers who delivered the intervention, focus group discussions with a sample of pupils who received the intervention and a sample of parents/guardians who attended the information and discussion sessions, comment sheets provided after last follow-up and an online questionnaire sent to all parents
-
strengths and weaknesses (perceptions) of the intervention materials
-
experiences of delivering/receiving the intervention
-
experiences of the teacher training session
-
experiences of facilitating the parents/guardians’ session
-
experiences of taking part in the trial
-
experiences of parent/pupil homework activity
-
suggested improvements for future trials
-
impressions of the information and discussion sessions
-
barriers to and facilitators of engaging parents in RSE
-
Control schools
-
RSE provision and participation in the trial: semistructured interviews with teachers (RSE co-ordinators, heads of Year 11)
-
the nature, quantity and quality of current RSE
-
facilitators of and barriers to teaching RSE in school
-
experiences of taking part in the trial.
-
-
Research participation: semistructured interviews with school principals/heads of Year 11
-
perceptions of the conduct of research in schools in general and experiences of participation in the trial
-
barriers to and facilitators of research participation
-
engaging parents.
-
-
Feasibility and acceptability of the questionnaire and taking part in the trial: focus group cognitive interviews with a sample of pupils from two of the four schools in the control group and comment sheets provided after last follow-up
-
overall impressions of the questionnaires
-
focus on questions/words/formatting that was hard/easy to understand
-
experiences of taking part in the trial and suggested improvements for future trials.
-
Data analysis
Following transcription of all audio-recorded interviews and removal of any identifying characteristics of specific schools and individuals, the data were analysed using a form of thematic analysis based on the six steps proposed by Braun and Clarke. 116 In summary, this follows well-established qualitative analysis practice of recording patterns and concepts that inductively emerged from the data and searching for data on pre-defined codes outlined in our topic guides and the literature on perceptions of RSE and UTP. These inductively and deductively derived codes were then entered in a codebook and grouped to form overarching themes. We used the qualitative software NVivo 10 to organise the data, and ensured methodological rigour by establishing credibility, transferability, dependability and confirmability using techniques suggested by Lincoln and Guba. 131 Two researchers independently coded segments of the transcripts and met to discuss and resolve any discrepancies. In schools in the control group, special attention was given to the specifics of analysing cognitive interviews. The feasibility of research methods was assessed by observation in intervention schools using structured schedules and through interviews with school staff and was subjected to the same analysis.
Findings
Sample
A total of 13 teachers across the four intervention schools delivered If I Were Jack. A total of 26 school personnel, 51 pupils and 10 parents took part in interviews or focus group discussions (across both the intervention and control schools).
Intervention schools
-
All teachers involved in delivering the intervention (n = 13).
-
School principals (n = 3), PCVPs (n = 1), heads of Year 11 (n = 1), and/or RSE co-ordinators (who did not deliver the intervention) (n = 1).
-
A sample of pupils from each class in each of the four schools that received the intervention (n = 39).
-
A sample of parents/guardians who attended information and discussion sessions to take part in focus group discussions (n = 10).
Control schools
-
Teachers designated as trial champions in each school (n = 4).
-
Heads of Year 11 (n = 1) and school principals (n = 2).
-
A sample of pupils from each class who took part in cognitive interviews in two of the four control schools (n = 12).
Data were also collected from structured observation of five lessons delivering the intervention and from 29 parents who responded to the online survey.
An overview of the context of participating schools, including a brief description of each school, is followed by an outline of existing RSE provision. The remainder of the section discusses results relating to the acceptability of the intervention and the feasibility of implementation and participation in the research.
The context of participating schools
As indicated in Table 39, of the eight schools that took part in the study, seven were located in urban areas and one in a rural area; five were secondary schools and three were grammar schools, with the former enrolling pupils regardless of academic ability and the latter accepting pupils with the highest marks in entrance exams. In terms of management type, three were controlled schools (i.e. managed by the Education Authority), two were RC maintained schools, two were voluntary (i.e. managed by a board of trustees) and one was grant maintained. Three schools were in affluent areas, with the percentage of pupils eligible for free school meals ranging from 4% to 15%, and five were in deprived areas, with the percentage of pupils eligible for free school meals ranging from 32% to 48%.
| School ID | Location | All pupils 2014/15 | Year 11 pupils 2014/15 | School type | Management type | All pupils eligible free school meals (%) | % religion per school | All pupils with SEN per school | Trial allocation |
|---|---|---|---|---|---|---|---|---|---|
| 10 | Urban | 667 | 141 | Secondary | Controlled integrated | 32.4 | P: 74.4 C: 5.9 O: 19.8 |
213 | Control |
| 11 | Rural | 610 | 98 | Secondary | Catholic maintained | 48 | Pa Ca Oa |
113 | Control |
| 12 | Urban | 815 | 122 | Grammar | Controlled | 15 | P: 62.7 C: 6.5 O: 30.5 |
82 | Control |
| 13 | Urban | 617 | 124 | Secondary | Grant maintained integrated | 57.4 | P: 50.4 C: 31.3 O: 18.3 |
268 | Intervention |
| 14 | Urban | 478 | 93 | Secondary | Controlled | 35.1 | Pa Ca O: 16.5 |
113 | Intervention |
| 15 | Urban | 882 | 153 | Secondary | Catholic maintained | 45.5 | Pa Ca O: 0.0 |
235 | Intervention |
| 16 | Urban | 1080 | 155 | Grammar | Voluntary Catholic | 8.5 | P: 0.0 C: 99.5 Oa |
33 | Control |
| 17 | Urban | 1077 | 158 | Grammar | Voluntary other managed | 4 | P: 62.7 C: 12.4 O: 25.0 |
53 | Intervention |
Relationships and sexuality education in participating schools
Three overarching themes emerged relating to the provision of RSE: (1) existing provision – content, frequency, co-ordination and delivery; (2) attitudes towards RSE; and (3) obstacles to and facilitators of quality RSE. In general, it emerged that provision was extremely variable across the eight schools and, in most cases, not seen as a priority subject, although those staff members tasked with co-ordinating RSE were all motivated to prompt changes in this regard. In some schools there was a clear sense of a considered, planned, well-structured RSE programme, while in others, provision was so haphazard that even the RSE team had difficulties articulating the content and frequency of provision. In most of the schools pupils remembered learning about reproduction in Biology but could recount few, if any, other instances in which teenage pregnancy was mentioned.
Theme 1: existing provision – content, frequency, co-ordination and delivery of Relationship and Sexuality Education
Representatives of all eight schools indicated that pupils were provided with some form of RSE. All reported having a written RSE policy. One school had published their policy on their website, three provided unpublished copies for analysis and three indicated that their policy was under redevelopment. The documents contained information on the school ethos, the morals, values and principles underpinning the policy, a general list of topics covered within the RSE programme and information on curriculum provision and delivery.
All eight schools provided most of their provision within the PD strand of the LLW curriculum (see Appendix 7), although subjects such as reproduction, relationships and sexuality were also reported to be covered in subjects such as Science, RE and Home Economics and also touched on in PC/form classes. In one school pupils received eight additional RSE lessons per year as part of their PC classes. All used the ‘Insync’ PD Programme developed by the CCEA (see Appendix 7) at Key Stage 3 (Years 8–10) but provision at Key Stage 4 (Years 11–13), for which there are no official curriculum materials, was highly variable (see Appendix 10).
Although most of the school representatives had received some training, either during their initial teacher training or by attending short courses and conferences post qualification, they agreed that the majority of those delivering the RSE content would not have received any training specific to the delivery of RSE. Some schools had planned external training for the near future, whereas others provided in-house training when possible.
Teachers in the RC schools described their general approach as one that focused on right information, right choices, loving relationships and always being in line with the RC Church’s teachings and ethos.
Our [current RSE] policy very much was based on the ACCORD [a voluntary organisation operating in NI that aims to promote a deeper understanding of Christian marriage, and to offer couples the means to safeguard and nourish their marriage and family relationships]. It’s supposed to cover sexuality, morality, ethics, values, personal . . . there’s a few general things there, where obviously throughout our whole curriculum are mentioned, status of family, sacredness of life, obviously confidential child protection issues, homosexuality . . . We are all for abstinence until you are within a healthy relationship.
When asked about how pupils are taught about birth control in biology and RE, teachers responded:
It’s really trying to avoid teenage pregnancies as well, pointing out to them, you know, that they know the risks, so that they’re not naive and silly and end up having a baby because they had no information. It’s all about making sure that they know the risks of pregnancy and when they’re older, knowing how to avoid it.
For content, frequency and delivery of RSE in participating schools, see Appendix 10. The information is based on self-report and the limitations of that are recognised. Teachers were vague as RSE content varies so much and many schools do not have a structured programme.
Theme 2: attitudes towards Relationship and Sexuality Education
In three schools, representatives gave the impression that, in general, RSE remained a sensitive, if not controversial, subject and that attitudes towards RSE among school staff were mostly negative, with many staff feeling uncomfortable, with some emphasis placed on the particular difficulties in engaging with the issue of homosexuality.
In both RC schools, teachers gave the impression that PC in general, and RSE in particular, were an important priority and generally accompanied by positive attitudes, and that academic focus did not take precedent.
In the controlled grammar school the Head of Year suggested that PC was seen as important, conceding, however, that RSE may not always be prioritised.
Teachers thought that pupils enjoyed the RSE provision but probably wanted more.
In all of the schools it was felt that attitudes towards RSE in the school were changing and most were anticipating further changes following new guidance on the provision of RSE from the Department of Education in 2015 (see Appendix 7).
When asked for their views on the quality of RSE provision in the school, most teachers were positive, but also agreed that it varied from teacher to teacher, with most agreeing that further improvements could be made.
I suppose what we’re doing is fairly good, I must admit. I think it’s very high quality but, like that, I think it does need to be evaluated, reviewed and made better, as we would do with any subject.
Theme 3: barriers to and facilitators of quality Relationship and Sexuality Education
Commonly mentioned barriers included negative attitudes and lack of motivation on the part of team members, a lack of time or priority afforded to RSE provision, an unavailability of up-to-date resources, financial constraints, discomfort among teachers and a lack of opportunities for training.
Facilitators included a strong, experienced team, supportive management and available resources. In some schools quality of provision was attributed to dedicated, experienced team members and a well-planned programme with a sound underpinning ethos.
In one school, the LLW teacher felt that an academic focus and conservative, perhaps naive, attitudes among staff members were detrimental to the provision of RSE.
It’s OK. It could be a lot better, and I think . . . there are elements of the natural conservatism, the elements of the focus being on academics because we’re the school that we are, versus the misconception that, because the kids are from the backgrounds they’re from and they’re at the school they’re at, they’re not getting up to this nonsense, as opposed to accepting that they are getting up to this nonsense.
Most schools mentioned having used an external organisation such as ‘Love for Life’ (Love for Life, Waringstown, UK). Some no longer used the service owing to financial constraints or decisions to manage their own RSE locally. A number of staff felt that RSE provision by external facilitators (as an adjunct to that provided in-house) has advantages for both staff and pupils.
Acceptability of the intervention
Although some pupils felt that the whole idea of RSE was embarrassing and awkward in relation to teachers and fellow classmates in general, when asked about their impressions of the intervention overall, most young people and teachers in intervention schools were positive and provided suggestions that they felt would help improve the various components.
Acceptability of the intervention
Two themes relating to the acceptability of the intervention emerged from pupil focus groups. These related to (1) the strengths and limitations of the core intervention and (2) personal lessons learned. The first theme concerned pupils’ views on the good and bad elements of the IVD and related activities, as well as suggestions about elements of the intervention that they felt should be changed. The second theme related to perceptions of actual or potential personal gain or loss as a result of using the intervention. Three themes relating to the acceptability of the intervention emerged from teacher interviews and focus groups. These themes related to the strengths and limitations of (1) the core intervention, (2) the teacher training session, and (3) the parents’ information and discussion session.
Strengths and limitations of the core intervention (film and accompanying activities)
Teachers agreed that pupils enjoyed and easily engaged with the IVD and, although there were variations across class groups, pupils interacted well with most of the accompanying activities. All participants agreed that the overall concept of the intervention was acceptable and, allowing for minor changes to some of the activities, most said that they would use it again.
Positive aspects included the fact that it was locally set, realistic, relatable, interesting, informative and helpful.
I think, as resources go, it’s one of the best I’ve seen out there because anything we have is quite ancient, dated or from, like . . . England, Australia . . . We’re very lucky to have a resource that is very current and set, you know, in the local area.
I think it’s actually a very good resource, and I think the fact that it’s coming from a boy’s point of view is unique and the pupils took to that well, you know, because they’re always hearing about teenage pregnancy always more geared from the girl’s point of view. So, I think they found that maybe kind of . . . made them more interested in it, just from the very start.
The most common complaint about the IVD from pupils, which was supported by some teachers, was that there were too many questions embedded within it, too many stop-starts and that some of the questions seemed repetitive or did not include the specific option that the pupil wanted to pick.
It would have been nice to have the whole film and then to go back to run through it, without the questions, because the questions, you were kind of . . . it took a long while just to get through them.
Some pupils thought that the film was outdated, a bit ‘cheesy’ and the behaviour of the actors within a bit ‘childish’ and in need of updating, whereas others said that updating the film was not necessary because, when they compared it with other resources they used in school, it seemed very contemporary. Some pupils attributed the outdated feel to the assumption that young people had not been involved in writing the script.
Although participants did not spontaneously mention the focus on the male protagonist’s perspective as a limitation, when prompted, all agreed that more focus on the female protagonist’s perspective would perhaps be helpful. One suggestion was that an activity focused on the girl’s perspective might be beneficial. Male and female participants also agreed, however, that the focus on the boy’s perspective was both acceptable and relevant to them.
It would be better if you could, like, go from, like, each side, each perspective, if they took, like, the girl and the boy. It would be better because you’d get a rounded perspective of what it would be like.
Some pupils were disappointed by the fact that the story did not have an ending and saw this as one of the biggest weaknesses of the film. Teachers reaffirmed this feeling among pupils.
The only thing that really annoyed me about it is they don’t actually tell you what she does with the baby at the end. Like everybody wanted to know!
Most teachers agreed that providing pupils with a worksheet to complete the ‘Pause: Fast Forward: Rewind’ activity worked best. Pupils agreed that they would prefer less written and more interactive or discussion activities, although some did say that they enjoyed the opportunity afforded them by the worksheets to think things out in private before discussion.
Regarding homework, the majority said that homework was a bad idea, mainly because they did not usually have homework for LLW, PC or RE, and teachers confirmed that homework was not a good idea because pupils resisted this as a result of not being accustomed to having homework in this context. Although some pupils said that they did the homework without difficulty, most said that they did not do it at all or that their teacher asked them to do it during the class period. Pupils from the grammar school weighed up the time involved in completing homework against other priorities.
Four of the 10 additional activities sparked particular conversation: (1) ‘If I had a baby’; (2) ‘Making a difficult decision’; (3) role-plays; and (4) the parents’ survey. There was general agreement that the ‘If I had a baby’ activity, which asks young people to compare their own schedule with that of a parent with a 6-month-old child, was enjoyable and for some even shocking.
Yeah. That was . . . that was probably one of the most effective because it was a real eye-opener. It was something that they talked about even after we’d done it, even the following week – ‘I couldn’t believe that . . .’ So, em, something like that, where there’s a comparison of their own life, I think really works.
In relation to the ‘Making a difficult decision’ activity, which asks young people to consider the pros and cons of keeping the baby, having the baby adopted or having an abortion for Jack, Emma and the baby, teachers noted, and many young people fed back, that they found the exercise difficult, particularly when trying to think of the pros of abortion for the baby.
I think they were embarrassed to say because this was like is there any pros for the baby with, for example, abortion. For some of them, they found it quite . . . well, they would say, ‘But how could there be a pro if they’re dead?’ and for them to say that out loud, some of them struggled to put that into words . . . It was as if we were nearly tricking them – ‘Is there a positive?!’
The role-play activity sparked a mixed reaction, with some young people saying that they loved it and others saying that it was ‘embarrassing’ and an opportunity for members of the class to ridicule those who ‘went to the top of the room’ to act out the parts. Although some teachers were adamant that their pupils would not engage in role-play, others felt that it was worth keeping in because some pupils enjoyed it and through watching others, those who will not participate can still benefit.
Finally, although some pupils appreciated the potential benefit, the parents’ survey was associated with predominantly negative views. The activity asked pupils to interview a parent/guardian (or other trusted adult) regarding their views of the If I Were Jack film. Although some young people said that they had never received the worksheet, others said that they consciously did not do it or ‘forgot’, with only a few girls admitting that they had completed it with their mother and one boy saying that he had done it with his older brother. The majority mentioned embarrassment and fear of awkwardness as primary reasons for avoiding the activity. In addition, many anticipated that bringing up such a subject had the potential to encourage further discussion from parents – the thought of which put off most pupils. For some pupils, the concern was less about embarrassment and more about their parents’ actual or perceived unwillingness to engage with them. Some pupils thought that it would better to do the activity with friends or a sibling.
I’m like close to my parents – I can tell them anything, but I wouldn’t do it. Like I don’t know . . . it’s weird. It’s weird talking to your parents, you know, especially when you’re like 15. Like sitting down and just be like, ‘Yeah, by the way, I learned about sex today’.
I got it, but my Mum said that she couldn’t fill it in because she would be hypocritical because she got pregnant at 17.
Teachers reported mixed views on the parent survey homework exercise, with many reporting that the majority of pupils chose to leave the material for the exercise behind and not even consider taking it home to discuss with parents. When asked if the teachers got a sense that this was the first time the pupils had discussed such matters, responses included:
Yes . . . One of the kids was like, ‘My dad was like really proud of me for going to him to tell him that this had happened! ‘And it was just like . . . because that had led into a conversation where his dad had said to him, ‘If this did happen to you, would you feel that you could come and ask me for advice and help?’ and he said, ‘Well, on the basis of this response, yes,’ and his dad was going, ‘Good, I’m really pleased – this is fantastic, because this is what I’m here for! OK, I’d kill you, but [laughing] . . . I would be angry at you, but it’s really good that you would come and speak to me about that’. So, there was a bit of sort of the kids going . . .’. My dad’s actually reasonable . . .’ do you know [laughing]?! There was some things like that, where they have this idea that their parents are terrifying, and actually, they just care, you know.
Regarding the controversial statements activity, teachers reported that most students enjoyed it:
Yeah, and then they got a little bit of feedback. But I just wandered around, without being too intrusive, letting them . . . It was interesting what they picked up on, what they chose, what was important . . . They got a laugh with some of them as well, you know, like ‘Should women shave their legs’ . . . I mean, they were really talking about it, instead of just sitting hoping that I wouldn’t come round. I was listening and they really were discussing, so that was good.
One teacher, however, did not do the controversial statements activity, as she felt that it would not work with her class group and was unrelated to the rest of the activities.
Teachers agreed the intervention could have been broader in scope.
I do think there could have been much more discussion on other things, you know, like if you do sleep around, there’s other things can happen, like STIs and all of that, and I really felt that was missing in it. I mean, I know you’re just talking about the consequences, but they’ve slept together, do you know, and they’re . . . so I just felt that we could have taken it a wee bit further in that regard.
Participants offered suggestions for minor changes to the intervention (see Appendix 11).
Personal lessons learned
The most commonly mentioned personal gain was that the intervention offered pupils more insight into the possible consequences of an UTP on their lives.
And realising you probably wouldn’t have a . . . like a career . . . Well, you would, like you’d probably get like a job that you wouldn’t really need much qualifications, but if you had a baby, you’d probably be less likely to go to university when you had to take care of a child.
For some, the intervention seemed to challenge existing beliefs, such as the following.
-
Babies are not hard work:
But people are always saying babies are worth it, they’re genuinely worth getting up at, you know, 4am.
-
Abortion is an option for some people:
I understand that it has to be put in because it is an option, but I do like think it’s really stupid, especially since it’s like allowed up to like 24 weeks or something I think it is, which that is technically murder because like it’s breathing, which is . . . But the boys were being really immature about that question, like saying stupid things like ‘Yeah, do that now’, and it annoyed like quite a lot of us.
-
Men have feelings and responsibilities when it comes to UTP:
Yeah, it was good to see how . . . because, usually, you focus on the girl, like how it would affect the girl, but there, you see . . . it isn’t affecting the guy physically at all, but it’s . . . like the moral implications of it, so how he’d think . . . what would be right, and usually you don’t think of that. Usually, guys are portrayed as just leaving.
In addition, some participants mentioned that there were advantages to putting yourself in Jack’s shoes and that the intervention had prompted them to consider teenage males’ roles and responsibilities.
I’d never thought about it that way, like from a guy’s point of view. It was all from a girl’s point of view, like going through that.
Strengths and weaknesses of the teacher training session
Although process evaluation findings indicated that teachers felt that they could implement the intervention with the help of the detailed ‘teacher’s information booklets’ and an online video, they were adamant that the training session was useful for them and suggested that, for the purposes of a future trial, the face-to-face training session should be retained.
Strengths and weaknesses of the parents/guardians’ information and discussion session
As noted in Chapter 5, recruitment of parents and guardians to attend the school-facilitated information and discussion session, to view the information session video on the YouTube channel and to respond to the parent’s online survey was extremely low. Twenty-nine parents/guardians responded to the online survey, with 22 indicating why they had not attended the information and discussion session (Table 40).
| Reason for not attending | n (%) |
|---|---|
| I was unable to attend owing to other commitments | 15 (68) |
| It was not at a suitable time of day | 4 (18) |
| I did not know about it | 2 (9) |
| I did not need information on how to talk to my child about avoiding teenage pregnancy | 1 (5) |
| I thought it might embarrassing | 1 (5) |
| It did not interest me | 1 (5) |
One mother wrote that her son had asked her not to attend:
My son was a little embarrassed by the subject matter being shown and discussed and requested that I did not attend.
Mothers and teachers attending focus group discussions shared speculations about why parents may not have attended and why the general experience of the teachers was that parents were difficult to engage in non-curricular activities in general. Reasons included that they were generally disinterested or apathetic, or that they did not feel the need to talk about such issues because they have already addressed them with their child or that they did not have time to attend owing to work commitments (as a result of the early timing of the event), or an unwillingness to give up other commitments, the distance from school and language barriers.
One teacher in the intervention group spoke of previous successes using short animations relating to online safety. Other teachers agreed that sending a link to a video via text message might reach more parents. Some teachers suggested alternative ways of engaging parents, including tagging on the session to other events that are more likely to be attended, such as parents’ evenings (when parents meet with their children’s teachers regarding progress).
Feasibility of implementation
Experiences of implementation
Three themes emerged relating to pupils’ experiences of implementation: (1) characteristics of the ideal implementer; (2) facilitators of and barriers to successful implementation; and (3) indications of fidelity.
Characteristics of the ideal implementer
Most pupils were happy with the fact that their teacher had delivered the intervention; however, when prompted they agreed that there were certain personal characteristics that made some teachers more suitable than others to deliver sexual health-related subjects. Commonly mentioned characteristics were a sense of humour, light-hearted, not too serious, someone who pupils respected, who was open and easy to talk to and who was encouraging. Many pupils thought that there was a general advantage of younger teachers, referring to them as being more relatable. Other interesting feedback included a desire for teachers not to react to what they were hearing and that it was thought that male pupils were more receptive to male implementers. One pupil expressed concern that your teacher might remember what you had said and make assumptions about you in future years to come. Pupils also differed according to whether or not they thought that the intervention should be delivered by someone internal or external.
Somebody that you didn’t know, it would be far easier to talk to them about it.
I think it’s better with one of your teachers because like you’re better talking to them because they understand you more, and I think you can trust them and open up to them better, where if it had have been just some random person comes in, I think you’d be more like ‘Should I tell them or should I not? Will you trust them or will you not?’ Like you feel uncomfortable . . .
One teacher implied that her ability to address embarrassment from the outset had facilitated implementation and engagement. One teacher also related how the fact that she had known the pupils for such a long time helped to alleviate any awkwardness.
Facilitators of and barriers to successful implementation
Most teachers noted the value of an ‘off the shelf’ resource that required little preparation, with the exception of reading for familiarisation and photocopying the materials needed. However, two teachers in one school thought that there was too much preparation involved, mainly because they felt that some of the activities were too repetitious or not appropriate for their particular students and needed to be supplemented with others that they sourced themselves. In general, teachers expressed a need to have flexibility in how they chose to use the resource, in a way that they felt would work best for their class group.
Although all four intervention schools attempted to watch the online film on individual computers with at least one class group, owing to technical difficulties relating to the school network, all but one school proceeded to show the film on an overhead projector. Although teachers saw the advantages of using individual computers, most agreed that showing the film on an overhead was less hassle and also had benefits for pupils with reading difficulties.
I think, when we were able to do it with the overhead, you could have a bigger control of the pace, so that one child hadn’t got nearly everything finished in one lesson, and you could add in wee bits where you felt . . . or it also allowed you to explore, if somebody said something totally off-the-wall, that you could stop and say ‘Let’s explore that – let’s think about it a wee bit more’.
Some pupils could see the advantages of using individual computers (‘Filling it in yourself, you do it at your own pace and it goes into your head better’), whereas others commented that the fact that the teacher could read and explain the text in the questions as an advantage (‘Everyone had different opinions for the answers . . . And like you could hear what everybody’s different opinions were, which is good.’).
A common problem was that there was not sufficient time, particularly for watching the film in schools with a 35-minute lesson. One teacher suggested that it would be better to show a section of film over three lessons and follow this with an activity. There was a mixed reaction from pupils to this suggestion, however:
It’s an easier flow, easier to understand, if it’s all in one go.
I just think it’s easier to understand because then, if you’re doing a bit at the time, it’s easier to kind of process and then you can think about the questions more, instead of just taking in the whole video. I think it’s just better, just easier to understand bit by bit . . .
One pupil felt that the whole intervention would have been best delivered all in one go over 1 day.
Teachers agreed that the intervention was targeted at the correct age group, but many felt that it could also be used with a younger year group, with most suggesting Year 10.
Some pupils and teachers reflected on the distraction caused by peers who did not take it seriously or were too ‘immature’ to contribute seriously to discussions. This was notably attributed to boys.
Pupils noted the importance of confidentiality, concerns that something said would end up on Facebook (Facebook, Inc., Menlo Park, CA, USA) the next day and were uncomfortable with the notion that teachers and fellow pupils may be trying to look at their answers.
Others reported that the intervention worked less well for more challenging class groups.
Fidelity of implementation of the protocol
As detailed above, teachers often felt the need to adapt the resource to their own class situation, or were logistically forced to adapt in the moment. In one school both teachers decided not to deliver lesson four. Although both teachers agreed that they felt the pupils had had enough of the intervention after three lessons, one conceded that a lack of time was also a factor. Some teachers noted that they took longer than expected to deliver the intervention and that some pupils missed out on some activities owing to interruptions such as closures as a result of heavy snow, bus strikes, fire drills and pupils being taken out of class for sports and music activities. Some teachers extended the lessons in order to ensure that the homework activities were completed within school time. One teacher decided to focus on one dilemma rather than the four provided in the pack. Some teachers felt that allowing small group discussion prior to whole group discussion worked best for their pupils.
One pupil suggested that his teacher had not implemented the intervention as instructed, suggesting that the pupils were sat down in front of the IVD without explanation, provided with the worksheets and left to their own devices to figure out what to do.
Most of the teachers said that they delivered all activities, even if they had to extend the number of periods in order to do so. In one school, however, the teachers decided to leave out various activities, including the scavenger hunt, the parental survey, the controversial statements activity and activities involving role-play.
Fieldworker reflections on data collecting in schools
The fieldworkers reported that the majority of data collection was carried out in accordance with protocol and that most schools and children were accommodating and happy to participate. When asked about any problems they encountered, three overarching themes emerged from their reflections. These were school environment, pupil issues and researcher issues. First, in relation to school environment, fieldworkers initially experienced difficulties with computers and online questionnaires and reverted to paper questionnaires. In addition, pupil proximity in classrooms during questionnaire completion was thought by some to be too close and to potentially compromise confidentiality. Although teachers were thought of as helpful during the initial stages, some thought that their continued presence in the classroom may have affected the children’s confidence to ask questions and seek help. In one school, examinations ran over time, which resulted in timing issues, and buses arrived to take children home before they could complete the questionnaire. Second, in relation to pupil issues, fieldworkers noted that a few were confused about the confidentiality of the study, some had difficulty describing their family circumstances within the questionnaire, and some struggled with the wording of questions and terms used. Third, in relation to researcher issues, a few fieldworkers commented on dealing with challenging behaviour in the classroom and the extra time required to clarify the process, define terms and provide additional support for individual pupils (see Appendix 13 for categorised raw data and themes).
Feasibility of participation in the trial
Pupil comment/feedback sheets
When the intervention was complete, pupils were asked for their views about their participation in the trial. They were asked to write down their thoughts on the ‘good things’ and ‘bad things’ about taking part via a student comment/feedback sheet (see Appendix 11). A content analysis was completed on some of the pupil responses; see Table 41 for details of the sample.
| School number | Total number of responses |
|---|---|
| 10 | 43 |
| 11 | 73 |
| 12 | 47 |
| 14 | 39 |
| 15 | 21 |
| 16 | 85 |
| 17 | 94 |
| Total: 7 schools | Total: 402 pupils |
Summarising the data
Absolute frequencies were used as a means to summarise the data (i.e. the number of times a statement or issue was found in the sample). The young people’s comments in relation to the ‘good things’ about taking part in the If I Were Jack trial focused on eight categories, whereas the ‘bad things’ about taking part focused on nine categories of data (see Appendix 13). These are presented hierarchically and suggest that, although the majority found taking part informative, interesting and/or relevant, which made them think more about the issues addressed, they thought that the questionnaire was too long and repetitive and therefore boring to complete. Most thought that missing formal class time and receiving sweets for their participation was good and those who thought missing class was a ‘bad thing’ focused on sport and games as opposed to missing out on more traditional subjects. In general, the questionnaire was considered easy to understand and to complete by most; however, there were a few who experienced confusion around the use of some terms and the question structure. In relation to the content of the questions, a lot of the young people thought that they were very personal, which made some feel uncomfortable. However, others felt comfortable with this and enjoyed the opportunity to share their views. Only two thought it awkward when parents became involved. For a lot of the young people some questions did not apply and confidentiality was questioned in terms of pupil proximity and completion time of the questionnaire. It was felt that those who were sexually active were easily spotted as they took longer to complete the questionnaire; likewise, those who were not sexually active required less time. Members of the research team who collected data in the schools were thought of as helpful and nice, and four young people commented that they were happy to help with research in general. The puzzles at the end were liked, although a few thought a prize should be awarded for completion of these.
Is there anything that you think we should change the next time we do research like this?
The young people were also asked to highlight areas for improvement. Fifty-one young people in the sample expressed their views and provided guidance on the way forward for this type of research (see Appendix 13). Some common issues emerged from their comments, which were themed accordingly. This resulted in four themes that described the young people’s views and suggestions in relation to (1) the relevance of the questions to their personal experiences; (2) the practicalities of completing the questionnaire; (3) issues around the ‘youth-friendliness’ of the questionnaire; and (4) the restrictive nature of the closed question format and how they would like an opportunity to better demonstrate their knowledge, morals and subjective opinions on the issues. Each theme is detailed below with a cluster of excerpts from the young people’s responses, which illustrate the essence of the theme.
-
Relevance
-
questions relate too much to a female aspect of a relationship/sexual encounter
-
make one just for boys and a different one for girls
-
have a greater range of questions, in particular for those who do not plan on having sexual relations until they are older
-
change the wording on questions, as they made me feel like I should have had these experiences before
-
put the option ‘hasn’t happened’ in some questions.
-
-
Practicalities
-
I would not like to do anything else about things like that because I do not like sharing my details with other people
-
put people further away from each other; make it more confidential
-
explain it more each time
-
spread out the tests more
-
make the questionnaire shorter
-
do not be as forward with the questions
-
I would not ask personal details such as postcode.
-
-
Youth-friendly
-
make it less formal, include some funny images or funny stories to make the person completing the questionnaire more comfortable and at ease
-
make it sound less complicated
-
change some questions so they are not as personal or about other people that you may know
-
rethink how questions are asked; some questions are hard to understand
-
word things better.
-
-
Subjective opinions
-
ask what the school says on pregnancy and how the school teaches students to avoid it
-
maybe educate us more on the outcomes of UTP so we have a better understanding
-
ask what your opinion of teenage pregnancy is and what are others’ opinions (e.g. peers, parents). What is your opinion of people who are sexually active at a young age?
-
have fewer multiple-choice questions so people can give their own opinion.
-
Teachers
Teachers were asked about their experiences of taking part in the research. One teacher in a comparison school was disappointed not to receive the resource. The designated trial champion in one school spoke about the interruptions to her own work owing to technology problems experienced by those delivering the intervention and the importance of support from the research team. In another (grammar) school in the control group, the trial champion indicated that, although it had been challenging to begin with, he had learned to deal with the organisation of data collection over the course of the year and had really valued help received from classroom assistants.
Several teachers felt that offering pupils the opportunity to opt out was not in line with their usual way of doing things and led to disruption.
I know that we had a significant number of pupils who were given the opt-out option. Ehh I’m not sure if I would give them that option. I can probably understand the reasons behind it but, ehh, that option to opt-out is easy and some of those pupils who opted out are the very pupils who you would want to get a response from.
Some teachers noted that pupils found it hard to understand the connection between the questionnaire and the resource.
The baseline questionnaire, I think [was confusing] for some pupils, because then, whenever . . . whenever they went to then do the resource, they felt, well, what had that got to do with . . . where was the connection? They didn’t see that there was a connection in there.
One principal felt that it would have been more convenient to allow pupils to complete the questionnaires online at a time that suited them. Teachers also noted the fact that those pupils who took part in the focus groups enjoyed ‘having their say’. The principal of one of the schools in the control group reflected on the inconvenience of taking part in two research studies at the same time but also noted that the If I Were Jack trial was well organised.
Discussion and conclusions
This feasibility trial implemented an embedded process evaluation. Existing provision (content, frequency, co-ordination and delivery) was assessed. In NI there is no official curriculum material targeted to Key Stage 4 (Years 11–13). Year 11s were the participating year group in this feasibility study, although there was a consensus among participating teachers that they would also like to use the intervention with Year 10. In general, it emerged that provision was extremely variable and not perceived as a priority subject. Some schools had well-structured RSE programmes, whereas others had difficulty articulating the RSE provision within the school. Pupils recalled little to no attention or emphasis placed on UTP.
Although RC schools described their approach as always in line with the RC Church’s teachings and ethos, this did not appear to alter the nature or attitude towards RSE provision compared with non-RC participating schools. Participating grammar schools, although academically focused, were not distinguishable in terms of their existing RSE provision. Teachers reported a general sense that RSE provision remained somewhat sensitive, controversial and that attitudes towards RSE were highly variable, with some reports of religious conservatism and homophobia, and that improvements could be made. Training and opportunities for training appeared to be all but absent since teachers had qualified.
Regarding the general acceptability of the intervention and participation in the trial, If I Were Jack was positively received, with pupils enjoying and engaging particularly well with the IVD, as well as with most of the accompanying materials. Most teachers reported a willingness to use the intervention again, and pupils and teachers were forthcoming in suggesting minor changes for improvement. Pupils and teachers were particularly enthusiastic about the local context of the IVD and the uniqueness of the fact that it was pitched from the teenage male perspective. Both male and female pupils felt that more focus on the girl’s perspective would be helpful. In a full trial we would consider incorporating more ‘If I Were Emma’ questions into the IVD and adding additional focus on girl’s perspective in accompanying activities. One school expressed disappointment not to have been allocated to the intervention arm.
There was a consensus that the homework component was not well received among both pupils and teachers due, in part, to an embedded tradition of RSE not being associated with homework, but, most notably, to pupils reporting parent’s actual or perceived unwillingness to engage with them. The ‘If I had a baby’ activity was very well received, with teachers reporting that pupils were still engaging with the context of the activity weeks later, attributing the fact that pupils could really compare to their own current lifestyle as the main trigger for conversation.
One notable area of negative feedback was with respect to the ‘Making a difficult decision’ activity, where one question asked pupils to consider the pros and cons of having the baby, having the baby adopted or having an abortion for Jack, Emma and the baby. The concept of considering pros for the baby in relation to abortion was not well received. As is often the case, engagement with role play was highly variable.
Teachers reported that should If I Were Jack become openly available, an online training video for teachers would suffice but they acknowledged the need for a researcher-led teacher training session in the context of a research trial so that issues such as fidelity and timing of the intervention could be adequately explained and reinforced. Moreover, our own observations of the variability of implementation encountered during the trial highlighted the absolute importance of appropriate training around issues such as those raised by the teacher. In a full trial we would, therefore, retain the face-to-face training session and we would also aim to reinforce the importance of relaxed and confident delivery and build confidence by allowing teachers the opportunity to consider the intervention in group settings with a longer training session being implicated.
Engagement with parents was particularly difficult during this feasibility study. The embedded process evaluation offered some insight into why this may have been the case. The most significant thing to emerge was that getting parents to attend a session dedicated to explaining the intervention was likely to be unobtainable for a variety of reasons, mainly because it was impossible to host such a session at a time that would be commonly accessible to all target parents.
Regarding the feasibility of implementation, pupils were generally responsive to the fact that teachers were the ones delivering the intervention. Pupils did emphasise that certain personal characteristics attributed to individual teachers stood out, such as having a sense of humour and being easy to talk to, in addition to younger teachers being more relatable.
In relation to facilitators of and barriers to successful implementation, teachers valued an ‘off the shelf’ resource, which required little preparation to deliver it. It was anticipated that ensuring 100% compliance in relation to fidelity of implementation to protocol would be almost impossible in relation to teachers. The process evaluation confirmed this to be the case. Teachers did report adaptations to the delivery of the intervention, often to meet the needs of their own particular class, or owing to logistical constraints. Field worker reflections confirmed that the majority of data collection took place in accordance with the protocol.
Regarding the feasibility of participation in the trial, pupil comment sheets revealed a few minor issues in relation to the content of the questionnaire, but also in relation to confidentiality, owing to close proximity in class when filling out the questionnaire. It was noted by pupils that they felt that those pupil participants who were sexually active were potentially identifiable owing to the fact that they had to complete more questions, thus taking more time to complete the questionnaire.
In conclusion, the general feedback evidenced by the process evaluation component of the feasibility study was that the If I Were Jack intervention proved acceptable to schools and to participating pupils. Moving forward to a Phase III effectiveness trial, the research team note the consensus on excluding the homework activities, but continue to reinforce the importance of the homework piece, and so will consider offering it as an option and not a necessity. Based on the above process evaluation and that associated with questionnaire development, minor changes to the questionnaire and classroom materials will be considered, in addition to minor logistical changes associated with data collection (i.e. avoiding exam and holiday periods). Only one substantial refinement in relation to the parental component was required, which was the replacement of the teacher led face-to-face information session for parents by online videos designed to deliver the intervention to parents/guardians into their home. Fidelity of implementation of the protocol will be reinforced in teacher training sessions. The refinements were completed in 2016.
Chapter 8 Economic analysis of the If I Were Jack intervention and the future modelling of its cost-effectiveness
Introduction
The overall aim of the economic component was to identify the costs of delivering the If I Were Jack intervention and to develop a framework for assessing cost-effectiveness in a future Phase III trial. The objectives of the analysis were:
-
to identify the relevant resources used in the set up and delivery of If I Were Jack and their associated costs
-
to qualitatively explore the opportunity costs of delivering the intervention
-
to explore alternative methods of delivering intervention training in a future trial
-
to identify the key parameters for a cost-effectiveness analysis in a future trial.
The structure of the chapter is based around these four objectives, and the methods and results for each objective are described within each section.
Identification of the relevant resources used in the set up and delivery of the If I Were Jack intervention and their associated costs
Methods
We calculated the economic cost of If I Were Jack according to the principle of opportunity cost. That is, when resources have alternative beneficial uses (i.e. an opportunity cost), it is important to represent this with some monetary value, regardless of whether the resources were directly purchased in the market place. A microcosting approach was taken from a public sector decision-maker perspective. Relevant costs were identified, measured and valued in monetary units using the 2013/14 price year. The identification of appropriate intervention costs was guided by a number of sources. These included the practical guide to costing behavioural interventions of Ritzwoller et al. 132 and methods used in other behavioural interventions such as the Diabetes Education and Self-Management for Ongoing and Newly Diagnosed (DESMOND) programme,133 A Stop Smoking In Schools Trial (ASSIST)134 and the First-aid Advice and Safety Training (FAST) parent programme. 135 In keeping with both ASSIST and FAST trials, costs were categorised according to the stage at which they were incurred in the research process: planning and preparation for delivery (stage 1) and delivery itself (stage 2).
Pre-start-up costs associated with the development of If I Were Jack were not included in the analysis (e.g. lesson plan development, designing of materials, DVD production2) as these are non-recurring costs that were incurred prior to the start of this study. Stage 1 costs in the If I Were Jack intervention covered recurring costs associated with printing the classroom materials for teachers, providing the DVD and the delivery of teacher training. As the identification of relevant resources occurred prior to the implementation of the intervention, the research team were able to record the resource use prospectively.
Stage 2 costs covered the costs associated with teacher time input for lesson preparation, printing/photocopying of worksheets and teaching, and administration time input for printing/photocopying of worksheets. Resource use was gathered prospectively via a specifically designed Teacher Resource Use Questionnaire (see Appendix 3). The questionnaire had two objectives:
-
to measure the resources actually used in the delivery of each component of If I Were Jack in terms of time input and materials
-
to establish what teaching activities may have been displaced in order to deliver If I Were Jack, or, indeed, if time was freed up as a result of the intervention being implemented.
These were intended to provide us with more information on the true opportunity cost of delivering the intervention.
The quantity of resource use at each stage was multiplied by unit costs at 2013/14 prices to estimate total costs, mean cost per teacher, mean cost per school and mean cost per student. In accordance with the principle of opportunity cost, the cost of teaching time was included, as this reflects the benefits to the children forgone as a result of If I Were Jack being taught instead of something else. The trainer in the trial was a post-doctoral research fellow employed by the university. Training took place at schools within the staff room, so no costs were associated with the training location. Teachers were supplied with the intervention materials by the research team. The grade of teacher delivering pupil and parent components of If I Were Jack varied; thus, we used the mid-scale point on the upper pay scale (UPS2; Department of Education Northern Ireland). 136 We assumed that a clerical officer at point 11 on the National Joint Council pay scale carried out the photocopying of classroom materials when the teachers did not. All staff costs included 24% for employers’ costs.
Results
Stage 1 resource use and costs
The key resources identified for the planning and preparation stage (stage 1) are presented in Table 42 along with their costs. The costs are based on the training of 16 teachers and the participation of 420 students at baseline in the intervention group.
| Resource use | Cost detailsa | Unit cost (£) | Number of units | Total cost (£) over four schools |
|---|---|---|---|---|
| Classroom materials (master copies) | First 10 copies £82.65 (£39.15 for each additional 10 copies) | 6.09 | 16 copies | 97.42 |
| Instructions for teachers | First 10 copies £46.76 (£8.70 for each additional 10 copies) | 2.77 | 16 copies | 44.37 |
| Parent and guardian discussion guide | First 10 copies £46.76 (£8.70 for each additional 10 copies) | 0.92 | 16 copies | 44.37 |
| Parent and guardian information sheet | Assume £0.10 per double-sided black and white page | 0.10 | 420 copies | 42.00 |
| DVD | £1 per copy for 300 copies (price changes depending on volume ordered) | 1.00 | 16 copies | 16.00 |
| Total cost of materials (£) | 244.16 | |||
| Training sessions | Four groups sessions and 1 individual session took place | N/A | 5 sessions | 0.00 |
| Teacher | Rate per hour = (salary + 24% employers cost)/195 days × 6.5 hours a day. Salary = UPS2 £35,801 | 35.02 | 16 | 560.39 |
| Disposable course materials [PowerPoint slides (Microsoft Corporation, Redmond, WA, USA)] | Assume £0.10 per double-sided black and white page, 6 pages | 0.30 | 16 copies | 4.80 |
| Location and associated cost (e.g. room hire) | All based in school classrooms/staff room | N/A | N/A | 0 |
| Food and refreshments | None provided | N/A | N/A | 0 |
| Total cost of training | 565.19 | |||
| Stage 1 planning and preparation for delivery subtotal | 809.35 | |||
Stage 2 resource use and costs
The key resources identified for the delivery of the classroom lessons and the information evening along with their costs are presented in Table 43. Two of the 16 teachers who were trained were not involved in the delivery of the intervention. Teachers delivered either the classroom component or the information evening. The costs are therefore presented as total costs and mean costs per teacher based on the responses from the Teacher Resource Use Questionnaire of the 12 teachers who delivered the classroom component and the two teachers who delivered the information evening.
| Description | Resource use | Cost details | Unit cost (£) | Total time (hours) | Total cost (£) | Mean (SD) cost per teacher (£) |
|---|---|---|---|---|---|---|
| Delivery of classroom intervention (n = 12) | ||||||
| Teaching time | Rate per hour = (salary + 24% employer’s cost)/(195 days × 6.5 hours a day). Salary = UPS2 £35.801 | 35.02/hour | 31.50 | 1103.13 | 91.93 (44.25) | |
| Preparation timea | 26.67 | 933.87 | 77.82 (62.15) | |||
| Other time | 2.67 | 93.39 | 7.78 (13.24) | |||
| Printing/copyinga of classroom materials by teacher | 2.33 | 81.71 | 6.81 (9.58) | |||
| Printing/copying of classroom materials by clerical officera | Mid point rate per hour = £7.93 + 24% employers cost = £9.83/hour | 9.83/hour | 5.29 | 65.58 | 5.47 (5.28) | |
| Classroom materials (printing/photocopying) | Assume £0.05 per single-sided black and white page, 20 sheets in total | 0.05 | – | 1154.00 | 96.17 (44.99) | |
| Delivery of information evening component (n = 2) | ||||||
| Teachers’ delivery time | As above | As above | 2.00 | 70.04 | 35.02 (0) | |
| Preparation time | 2.25 | 78.80 | 39.40 (6.19) | |||
| Other time | 3.00 | 105.06 | 52.53 (24.76) | |||
| Other staff timeb | Varied | 1.50 | 600.22 | 300.11 (417.47) | ||
| Printing/copying of classroom materials by clerical officer | As above | As above | 0.67 | 6.55 | 3.27 (2.32) | |
| Stage 2 delivery of intervention subtotal (n = 14) | 4292.34 | 357.18 (75.24)c | ||||
The total costs of the If I Were Jack intervention for the feasibility study are presented in Table 44. Stage 1 costs were apportioned to the teachers delivering the intervention. This allowed a cost per teacher and a cost per school to be calculated. Cost per pupil was calculated by dividing the total cost for each school by the number of pupils at that school participating at baseline. It can be seen that in the feasibility study the mean cost per school and per pupil after adjusting for school as the cluster was £1275.42 and £13.66, respectively.
| Description of costs | Cost (£) |
|---|---|
| Stage 1 planning and preparation for delivery | |
| Materials | 244.15 |
| Training | 565.19 |
| Stage 1: totala | 809.34 |
| Stage 2: delivery totalb | 4292.34 |
| Overall totalc | 5101.68 |
| Mean cost per teacher (SE)d | 364.41 (75.24) |
| Mean cost per school (SE)d | 1275.42 (341.32) |
| Mean cost per pupil (SE)d | 13.66 (4.51) |
A qualitative exploration of the opportunity costs of delivering the intervention
When resources are allocated to be used in a particular way, they are no longer available to be used in another way. As a result, any benefits that would have been received are forgone. The opportunity cost is the term used to reflect the value of the benefits that have been forgone. Although costing the resource use as detailed in objective 1 is a pragmatic approach to measuring this opportunity cost, we wanted to explore the potential sacrifices more directly via the teachers.
Methods
As stated previously, another objective of the Teacher Resource Use Questionnaire was to establish what teaching activities may have been displaced in order to deliver If I Were Jack, or, indeed, if time was freed up as a result of the intervention being implemented. Responses to the relevant questions were collated and summarised.
Results
Of the 14 teachers involved in the delivery of the intervention, 12 delivered the main classroom component and two delivered the parents’/guardians’ information evening component. In the feasibility study, no teacher delivered both.
When teachers were asked what they would normally have been doing during the time they spent being trained to deliver If I Were Jack, 11 of the 14 teachers responded. Ten out of the 11 teachers indicated that they would have been preparing for lessons and marking; two of these teachers specifically mentioned sex education lessons and two mentioned PC. One of the 11 teachers stated that they would have been doing personal study.
When asked what they would have been doing in the time they spent preparing to deliver the lessons, all 12 of the 14 teachers involved in delivering the lessons stated that they would have been preparing for other lessons. Two specified sex education lessons, two specified RE, two specified PC and one specified that the lesson would have been for the LLW module.
When asked what they would normally have been doing during the time they spent delivering the lessons for If I Were Jack, all 12 of the 14 teachers stated that they would have been delivering other lessons, six specified PC lessons, three specified sex education lessons, two specified RE lessons and one stated that they would have delivering a lesson from the LLW module.
Only two teachers delivered the parents’/guardians’ information session. When asked what they would normally have been doing during the time they spent preparing for this session, both responded that they would have been doing work-related activities. When asked what they would normally have been doing during the time they spent delivering the information session, one responded work-related activities and the other responded non-work/leisure activities.
All 14 teachers were asked if they felt that anything had been sacrificed which would have been of benefit to pupils because of the time spent using If I Were Jack. Thirteen teachers provided a response, with 11 stating ‘No’ and two stating ‘Yes’. Only one of the teachers who said yes provided more information to say ‘Some of the pupils did start to think how their lives would change – problems, parents’. On reflection, this information suggests that the teacher should have responded ‘No’ (i.e. nothing had been sacrificed). Indeed, it suggests that something had been gained in that, from the teacher’s perspective, the intervention had helped the pupils to think about the consequences of an unintended pregnancy in their lives.
The final question asked teachers if they felt that by using If I Were Jack they had saved time normally spent looking for RSE resources/planning RSE activities. Twelve of the 14 teachers provided a response: 11 said ‘Yes’ and nine of these provided further information. In general, the responses indicated that teachers felt that the resources were ‘effective’, ‘well-planned’ and ‘up-to-date’ and that they saved time that would have been spent searching for relevant activities and alternative sex education resources. The one teacher who did not think that the intervention had saved them time did not provide any further information.
Exploration of alternative methods of delivering intervention training in a future trial
In this feasibility study the intervention was delivered to four schools by a university researcher with a total of 16 teachers involved. Even with this relatively small number of schools and teachers, the organisation of teachers’ training sessions proved difficult. Principal barriers included identifying a time that suited both teachers at each school and the researcher delivering the training, and finding a suitable venue for the training within the school. These issues would only be exacerbated by increasing the number of schools and teachers, which would be required for a future Phase III trial. We also acknowledge that using a university researcher to deliver training on a large scale may not be realistic. Thus, using scenario analyses we explored alternative approaches to training for a future Phase III trial in order to estimate the financial impact of the alternatives.
Methods
We constructed realistic scenarios of alternative methods of delivering the training by varying the following parameters: the training venue, provision of teaching cover, mode of training delivery and the trainer. For each scenario we estimated the total costs for each stage of the intervention [i.e. stage 1 (planning and preparation for delivery) and stage 2 (delivery)]. Based on the feasibility study results at follow-up 1, it was estimated that 25 intervention schools, 100 teachers and 2625 pupils would be required in a Phase III trial. The cost of materials (stage 1) was therefore calculated by increasing the quantity of units from the feasibility study accordingly, and then multiplying the quantities by the unit costs observed in the feasibility study. Training costs were calculated based on the details specified in the scenario. Mean cost per teacher, mean cost per school and mean cost per pupil were also calculated for each scenario.
Scenario 1
In the feasibility study training was delivered over lunch breaks or in free periods. In scenario 1 we explored the financial impact of providing cover by a supply teacher for teachers to attend training delivered by a non-government-funded facilitator within their own school at an estimated rate of £250 for a half day. It was assumed that a half day (3.25 hours) of teaching cover would be required based on the recommendation of the National Association of Schoolmasters Union of Women Teachers, one of the largest teachers’ unions representing teachers across the UK.
Scenario 2
In scenario 2 we explored the financial impact of teachers attending group training sessions delivered by a non-government-funded facilitator in a hired venue such as a hotel. This method was recently employed with success in the Steps Towards Alcohol Misuse Prevention Programme (STAMPP) trial (ISRCTN47028486). We hypothesised the need to hire venues across the UK on six occasions for a Phase III trial. In common with scenario 1, this would require the provision of teaching cover for a half day. We used the hotel costs observed in STAMPP for a whole day of training (£25 per head) and divided this by two to obtain a half day training cost (£12.50 per head).
Scenario 3
Teachers’ views on future training approaches were gathered as part of the process evaluation (see Chapter 7). Feedback indicated that face-to-face training was potentially not necessary owing to the programme materials being so comprehensive. Therefore, in this scenario we explored the impact of delivering training via 25 separate 60-minute webinars. We assumed that teachers at each school connected to it as a group and not individually in their own time. It was also assumed that teaching cover would not be needed. We used the cost associated with the delivery of 25 separate 60-minute web conferences with audio via British Telecom (BT) Conferencing (BT Group plc, London, UK) for the public sector at a rate of 13 pence per minute (0.04 pence for audio, 0.09 pence for web) per connection (host and school). A total cost estimate of £390 was obtained via personal communication with a BT Accounts Manager.
Results
The results of the scenario analyses for a Phase III trial are also presented in Table 45. The highest teacher training costs were associated with the use of hotels to host the training events and a facilitator to deliver the training (scenario 1). The lowest costs were associated with the use of webinars delivered at a school level (scenario 3).
| Description of costs | Scenario 1: cost of teaching cover provided for training in schools delivered by a facilitator (£) | Scenario 2: cost of teaching cover provided for group training in hired venues delivered by a facilitator (£) | Scenario 3: cost of webinars delivered into schools (£) |
|---|---|---|---|
| Stage 1: planning and preparation for delivery | |||
| Materialsa | 1525.95 | 1525.95 | 1525.95 |
| Trainingb | 11,412.82 | 12,662.82 | 3922.41 |
| Stage 1: total | 19,188.77 | 15,688.77 | 5,448.36 |
| Stage 2 delivery: totalc | 30,659.57 | 30,659.57 | 30,659.57 |
| Overall total | 49,848.34 | 46,348.34 | 36,107.93 |
| Mean cost per teacher | 498.48 | 463.48 | 361.08 |
| Mean cost per school | 1993.93 | 1853.93 | 1444.32 |
| Mean cost per pupil | 18.99 | 17.66 | 13.76 |
Identifying the parameters for a cost-effectiveness analysis in a future trial
The aims of this section are to:
-
provide a framework for an economic model that would encompass the future impacts on costs and outcomes (both health and social outcomes) as a result of engagement with the If I Were Jack intervention
-
use this framework to outline needs and possible sources for data to populate any such model as may be constructed in the future.
The word ‘framework’ is important. What is presented is not an ‘economic model’ as such, and there has never been an intention within the current study to conduct a modelling exercise. Rather, it is the feasibility of conducting such an exercise that is being assessed and presented.
The framework: from trial outcomes to social outcomes
Owing to the social impacts of many interventions, especially public health interventions, extending beyond the life of any single randomised trial, it is often the case that funders and decision-makers are interested in ‘modelling’ what these future impacts – usually expressed in terms of costs (to reflect net resource impacts) and benefits (to reflect future impacts on health and other aspects of well-being) – might be. For the If I Were Jack intervention, we have attempted to map out the important events subsequent to engaging with If I Were Jack. This is presented in Figure 6, along with the consequent data needs and possible sources of such data. Some of the required data can be sourced from a trial, whereas other data would have to be sourced from elsewhere.
FIGURE 6.
Current and future impacts of If I Were Jack on costs and benefits. HRQoL, health-related quality of life.
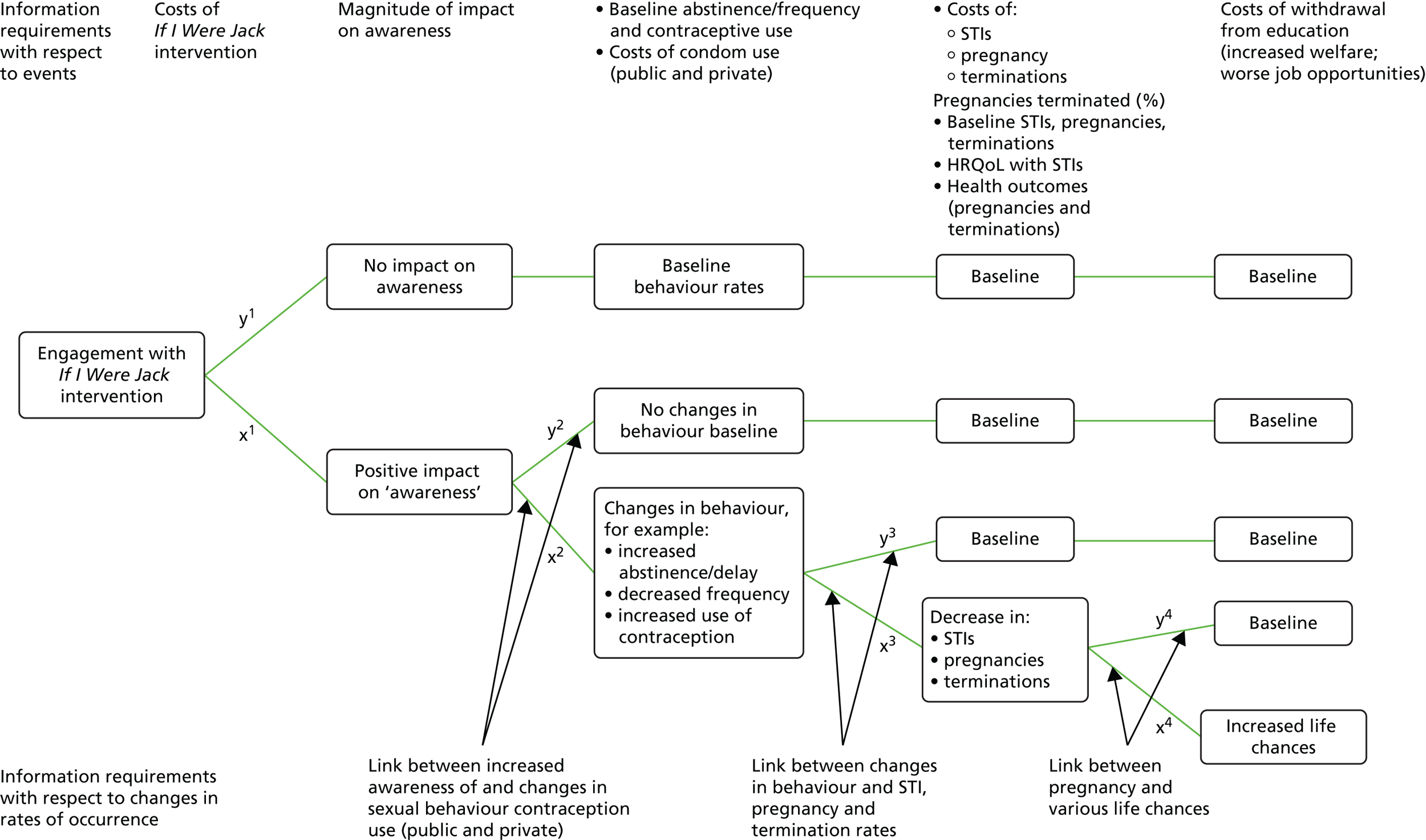
The framework in Figure 6 should be read from left to right and, thus, starts with a defined population that would engage with the intervention. The boxes represent events, or collections of events, that could have well-being and/or resource consequences. Data needs associated with the boxes are displayed at the top of the framework and labelled ‘Information requirements: events’. So, for example, all one would need to know at the stage of engaging with the intervention are the costs of the If I Were Jack intervention.
The lines between the boxes represent changes in rates at which the events might occur, and the data needs associated with these (at the bottom of Figure 6) are labelled ‘Information requirements: changes in rates of occurrence’. For these rates, ‘x’ and ‘y’ should always sum to 100, as they represent percentage amounts by which the original population, and subsequent sub-divisions of that population, is spread across the set of events occurring in the next stage of the framework. The subscripts on ‘x’ and ‘y’ simply represent the progressing stages to which our ‘x’ and ‘y’ values apply.
For example, an important secondary outcome from the trial is likely to be related to ‘awareness raising’. Awareness is regarded as an important secondary outcome because it is believed to mediate the primary behavioural outcome of safe sexual intercourse/no sexual intercourse. For a certain percentage of the targeted population (x1), awareness will be raised, whereas for a corresponding percentage (y1 = 100 – x1), there will be no such impact. Trial data would indicate what these percentages might be and, for any individual who is positively influenced, what the magnitude of the change in awareness might be. For those whose awareness is not raised, we might assume that they revert to baseline rates for future events as we move from left to right in Figure 6. These rates are merely indicated by the word ‘baseline’ (issues related to ‘baseline’ data are discussed below).
More positively, however, any raised awareness might subsequently lead to changes in behaviour. It is important to note that such changes might conventionally be seen as leading to greater abstinence and increased condom use. However, a more positive outlook might be to view increased awareness as leading to increased confidence with respect to decision-making about sex. This might lead to increased condom use, but is better expressed as leading to increased levels of contraceptive use. Alongside abstinence, we need also to think of ‘delay’ of sexual intercourse and ‘frequency’. For these, we would need to know how higher awareness relates to changes in contraceptive use, delay and frequency behaviours, that is, values for x2 and y2 – which could be obtained from a subsequent trial and for which there is an existing literature (see Chapter 3). 19,21–23,25
We would also require data on the costs of contraceptive use, including condom use. Once again, for those going down the ‘y2’ pathway, we might assume that they revert to baseline from that point onwards.
The fact that programme participants might feel more in control of their sexual behaviour and decision-making, of course, has value in and of itself. However, the next stage would also involve estimating the extent to which increased contraceptive use (and changes in delay and frequency) relates to more immediate (health) events. For each of these, a separate value of x3 (and, correspondingly, y3) would be required. These events would be as follows:
-
STIs, for which data would be obtainable from a trial as well as literature linking contraceptive use, delay and frequency changes to STI occurrences137,138
-
pregnancies before the age of 17 years25
-
terminations associated with pregnancies, for which we would require data on which to base an assumption about the continuation, and corresponding termination, rates.
For each of these, we would require data on costs (of a STI, a delivery and a termination) and we would have to make assumptions about what costs to include (e.g. do we go as far as counting the lifetime costs of a birth and what assumptions do we make about replacement; that is, does an early birth now replace another birth that might have happened later?). 139 We would also require data on health-related quality of life and other health outcomes associated with STIs, pregnancy and termination.
The final set of events in Figure 6 comes under the general heading of ‘life chances’. Once again, we would require estimates of the percentages x4 and y4; essentially, for what proportion of people are life chances negatively impacted by an early pregnancy? The impact of such an event is portrayed currently in terms of withdrawal from education and the consequent effects of that on increased welfare payments and worse job opportunities, for which we think there are data available from government sources in NI. On the basis that a teenage pregnancy effectively withdraws the mother from the labour market for at least 18 months, the DHSSPS estimates that the cost of a teenage pregnancy to the Exchequer (unemployment benefits and administration, plus tax revenue forgone) stands at £20,000 per mother. 26 In 2006, it was estimated that teenage pregnancy costs the NHS £63M per year. 140 In 2009–10, £26M was paid in benefits to teenage mothers on income support (England and Wales-based data). 141 Other adverse sexual health outcomes also cost the NHS large sums. For example, it is estimated that the UK spends between £700M and £1B per year treating STIs and their sequelae. 142,143
Other data needs: the ‘baseline’
Depending on the ‘level’ addressed by the modelling, and in order to address the issue of the ‘baseline’ for many of the variables, other requirements might be for NI-level data – for example, things like current rates of condom use and abstinence, and for STIs, age-specific pregnancies and associated terminations, as well as data on withdrawals from education.
Discussion and conclusions
The economic analysis provides a detailed breakdown of the recurring costs that were incurred in the planning, preparation and delivery of the If I Were Jack intervention in the feasibility study. The identification of potential resources prior to implementing the intervention allowed the data to be collected prospectively, thus maximising the accuracy of the estimates. The total cost to deliver the intervention was estimated to be £5101, equating to £1275 per school and £14 per pupil. The scenario analyses revealed that the inclusion of formalised teacher training sessions for a future trial could range from £14 per pupil when webinar-based training is used, to £19 per pupil if face-to-face training delivered by a facilitator within schools is adopted. Information gleaned from the process evaluation (see Chapter 7), however, suggested that face-to-face training may be more efficacious in engaging the teachers and generating better fidelity to protocol in terms of implementation. Thus, the cheapest option may not be the best approach for a future Phase III trial.
It must be highlighted that these estimates are based on the delivery of the intervention in a trial setting. If the intervention were to be mainstreamed, then other costs would need to be considered, including those associated with ‘train the trainer events’, updating the intervention materials, or making the interactive DVD region specific. Likewise, some aspects of the costs may decrease over time. The costs reported in the scenario analyses reflect the cost of introducing and delivering If I Were Jack on one occasion. In reality, once teachers have been trained they would not need to be retrained on an annual basis, requiring only, at most, refresher training. Therefore, the cost per pupil would fall when there is no staff turnover.
The overall conclusion that can be drawn from the qualitative exploration of the opportunity costs of delivering the intervention is that If I Were Jack ultimately saved teachers time, which would otherwise have been spent preparing for or delivering lessons within the same or related curriculum module. Perhaps most importantly, teachers did not feel that anything that would have been of benefit to pupils had been sacrificed because of the time spent using If I Were Jack. The methods of cost evaluation (questionnaires provided in advance and follow-up interviews) provided an additional insight into the implementation of RSE in schools (business as usual) and specifically this intervention. In a future trial, we would repeat data collection on cost estimates, to see if there are any changes over time and over space (the rest of the UK) and also because this analysis not only informs economic analysis but also the implementation of the intervention more broadly.
Finally, if an analysis of longer-term impacts beyond the life of a trial was required, we have provided a framework for how this might be approached and have assessed how trial data might inform parts of such a framework in combination with data gathered from published and other public sources.
Chapter 9 Summary and conclusion
Introduction
The purpose of this chapter is to summarise the main findings of the study. It will be structured in the following way. First, we begin by outlining some of the limitations of this study. Second, we summarise the findings in relation to the study aim and objectives. Third, we summarise the findings in relation to the prescribed progression criteria to a larger effectiveness trial. Finally, we summarise how these findings might add to the emerging literature relating to the evaluation of RSE interventions in schools along with suggestions for future research.
Study limitations
In this exploratory trial we assessed the feasibility and acceptability of an effectiveness trial of If I Were Jack. The study was therefore designed to generate learning that could inform the decision about whether or not to proceed with an effectiveness trial, and also – if a decision to proceed was made – learning in relation to optimising the design and implementation of an effectiveness trial. Nonetheless, although this study was a learning exercise, the study itself also has a number of limitations that should be borne in mind when interpreting the results presented in this report.
Systems for identifying schools
A total list of all eligible schools in NI was sought for this trial. However, we did not use this as part of our recruitment strategy. Instead, we presented the research at RSE training days for teachers and then created a convenience quota sample, based around the voluntary participation of schools that met our inclusion criteria. The advantage of this approach is that it proved to be an efficient and effective method of achieving a stratified sample of schools. The disadvantage is that the non-random nature of the selection of schools means that the data cannot be said to be representative of schools in NI. In a future trial, we would send an invitation letter to all eligible schools in the defined areas. In addition, we would use two networks to help with school recruitment in defined areas: the Wales School Health Research Network, which is a network of secondary schools across Wales and South West England led by the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement, Cardiff University, in a partnership with Public Health Wales and the Welsh Government; and the University College London Partners, School Health and Wellbeing Research Network. Although these networks do not encompass all schools in the relevant area, they will help the trial to extend its reach, while also being an efficient approach to recruitment.
Feasibility of collecting follow-up data in secondary schools at 12–14 months
We did not plan to conduct long-term follow-up of pupils of > 1 year (as would happen in a future effectiveness trial), as this would be unfeasibly costly for an exploratory trial and would cause unnecessary delay to the ultimate goal of an effectiveness trial.
Pupil recruitment rates
Pupil recruitment rates at baseline were just above our threshold of 80%. This rate was affected by 9% of absenteeism in schools and 10% of withdrawal from our study. We did not have good information on the characteristics of pupils who were not present on the day of baseline data collection. However, we learned valuable lessons about the reasons for parental and pupil withdrawal and how participant withdrawal might be averted in future trials through improved pupil information sessions and clearer information for parents.
Intervention acceptability to parents
We did not learn as much as we might have about this aspect of the study because we failed at the first fence, as it were, in terms of engaging parents with the parental information sessions. We did, however, begin to test our hypothesis that online delivery methods would work better with parents during a main trial and better understand some of the strategies for reaching parents online.
Delivery of an interactive video drama
Technical difficulties, mostly associated with school internet networks, also led to all but one school showing the IVD via overhead projector as opposed to on individual computers. Process evaluation findings revealed, however, that the use of overhead projectors was an acceptable means of delivery for both teachers and pupils, with most acknowledging that there were additional benefits to delivering the intervention in this way (i.e. ability to control the pace, an opportunity to stop and explain words or questions and being better for pupils with reading difficulties). In a future trial we would still encourage use of individual personal computers or tablets and we would seek to build in a mode of delivery into the memorandum of agreement. However, owing to the positive evaluation of the overhead projector modality, we would not exclude a school if this was the only feasible means of delivery.
Electronic data collection
We piloted the use of electronic data collection against data collection using traditional paper forms. Electronic data collection failed owing to technical difficulties caused primarily by a lack of competence on behalf of the company we hired to develop the online data collection tool. Following several investigations, the company concluded that the problems were due to conflicts with saving the data on a cloud server; however, they were unable to resolve the issues within the timeframe of the study. We therefore did not have an opportunity to thoroughly investigate the other advantages and disadvantages of electronic data collection. However, in schools in which online data collection did work, pupil and teacher feedback was positive.
Pupil confidentiality and independence while completing questionnaires
Although data collection was generally administered under ‘exam conditions’, with teachers remaining in the classroom and fieldworkers supervising data collection, the layout of many of the classrooms meant that pupils were in close proximity. Fieldworker observations suggested that, in some cases, pupil independence and confidentiality may have been compromised. It is difficult to say what effect this may have had on data quality but it provided valuable lessons for planning data collection in a main trial.
Missing data
We had high rates of missing data in relation to questions on STIs, which, we have surmised, was likely to be due to the fact that pupils ignored this question if they had not had a STI diagnosis. Although we would still use this question again as part of an overall health economics evaluation in a main trial, with prompts to reinforce relevance, caution needs to be applied to the results of this question in the current study.
Data linkage
We did not test the feasibility of conducting data linkage of our feasibility study data with health and social care records of teenage conceptions, because such data linkage is not possible in NI, owing to the fact that the NI health service does not collect conception data as part of health records. In a future effectiveness trial, we would ask participants if they would be happy to provide personal information to allow the research team to follow them up with questionnaires relating to fertility and sexual health in the future.
Generalisability of the acceptability of the intervention
This feasibility trial tells us only about the acceptability of this intervention in one country of the UK, namely NI. However, during the course of the feasibility trial we conducted a separate ‘transferability study’144,145 to assess the acceptability of the intervention in the other countries of the UK. Summary results are presented below (see Criteria for progression to main trial).
Generalisability of the trial methods across the UK
Although we did not test our methods UK wide, a thorough literature review on all aspects of our methods allows us to interpret applicability across the UK.
Fidelity to implementation of the protocol
Achieving total fidelity to implementation of the protocol is very difficult in schools-based research where skilled teachers are delivering the intervention. Although we recorded where teachers made adaptions to the intervention protocol, we did not link these data with pupil outcomes.
Intention to treat
Randomised controlled trials often suffer from two major complications – non-compliance and missing outcomes. 146 ITT is used as the most unbiased way of analysing a trial, and this was the statistical approach undertaken in this feasibility study. In order to assess the necessity and appropriateness of utilising the ITT approach, full reporting of any deviations from random allocation and missing response is essential, as reinforced in the CONSORT guidelines on the reporting of RCTs. 128,147 The ITT approach can be optimised if complete outcome data are available for all randomised subjects in order to determine the per-protocol population, defined as the subset of the ITT population who completed the study without any major protocol violations. In this feasibility study we were unable to determine which participating pupils randomly allocated to the intervention group were actually in receipt of the intervention. We assume that the percentage of compliance was high, because pupil attendance in class was consistently high throughout the intervention period, but we are unable to report on actual numbers. Moving forward to a Phase III effectiveness controlled RCT, potential solutions worth considering would be to insert a question at the beginning of the follow-up questionnaire to ascertain whether or not participants have viewed the IVD and participated in the other relevant intervention activities. Alternatively, pupils who have not been in receipt of the intervention post baseline could be instructed not to take the follow-up questionnaire.
Summary findings relating to study aims and objectives
Primary aim
The aim of the study was to determine the value and feasibility of conducting an effectiveness trial of the If I Were Jack RSE intervention in post-primary schools.
We now break down the main findings of the study under the study objectives.
Secondary objectives
To assess the acceptability of the intervention to schools (principals and RSE teachers), male and female pupils and parents.
The intervention proved to be acceptable to schools (principals and RSE teachers), as evidenced by the very favourable remarks by teachers and school principals right across all participating schools.
I think, as resources go, it’s one of the best I’ve seen out there because anything we have is quite ancient, dated or from, like . . . England, Australia . . . We’re very lucky to have a resource that is very current and set, you know, in the local area.
I think it’s actually a very good resource, and I think the fact that it’s coming from a boy’s point of view is unique and the pupils took to that well, you know, because they’re always hearing about teenage pregnancy always more geared from the girl’s point of view. So, I think they found that maybe kind of . . . made them more interested in it, just from the very start.
If I Were Jack was also an acceptable intervention for pupils, both male and female. Pupils commented on specific positives of the intervention and these included that it was ‘locally set’, ‘realistic’, ‘relatable’, ‘interesting’, ‘informative’ and ‘helpful’.
It didn’t give you one point of view, it gave you many, and it gave you the way that he was worried, and that she was worried. It didn’t show you everything would be fine.
Male
Like, if it was to happen to someone, it’s kind of a difficult situation to deal with and it shows you that. It’s almost like em . . . you get a first-hand experience of what would happen and it’s scary.
Female
In relation to parents, the low rate of parental/guardian withdrawal of children from the study (6.8%) suggests that the vast majority of the parents were happy for their child to participate in the intervention and the associated research. However, the results also suggest that parents were not willing to participate themselves in the intervention in the planned way (i.e. in a face-to-face information session about the intervention). Thus, a key change to the intervention, which we will undertake as a result of this feasibility trial, is to change the face-to-face information sessions to an online format. The parental component of the intervention will instead be delivered through three short (< 5 minute) online videos to parents. The links for these videos will be texted and/or e-mailed (with one additional reminder) by participating schools to all parents/guardians of the intervention year group on school communication lists. This electronic communication approach was successfully piloted in the feasibility study. Recent studies 68,69,148 demonstrate the importance of embracing such ‘education entertainment’ modalities as engaging adjuncts to school-based education. This refinement has been funded by the Health and Social Care Research and Development Office of Northern Ireland (HSC R&D). It was completed in 2016 and we would plan to pre-test this approach as part of a main trial.
Another secondary objective was to identify optimal delivery structures and systems for the delivery of the resource in the classroom. Teachers valued the fact that they considered If I Were Jack to be an ‘off-the-shelf’ product that required little preparation time, apart from some familiarisation with the content and photocopying. Teachers indicated that if the resource was being made more readily available outside the research environment, then teacher training could become accessible online, with a contact number to address any enquiries. They did, however, acknowledge that, in the context of participation in a research trial, a researcher-led session was essential to reinforce fidelity of implementation, etc. The evaluation also revealed that more time could have been dedicated to the teacher training session, as teachers reported a lack of time to address all questions.
Process evaluation indicated that there would be advantages to conservatively forewarning teachers of the time requirements of component elements of the intervention, thereby enabling forward planning (i.e. avoid using last lesson session of the day). One school had a 35-minute lesson time and struggled to complete the IVD and other accompanying activities within a single lesson, as hoped. Time-related issues were prevalent, with teachers reporting incidents such as examinations running over time and pupils being unable to complete questionnaires because school had ended for the day and they had to race off to catch their buses. Teachers valued the presence of the research team and the assistance made available through classroom assistants. Pupils valued incentives, such as sweets, but some suggested that a ‘contraceptive goody bag’ might be better.
Finally, in relation to the delivery of the intervention in the classroom, there was a consensus that pupils were receptive to teachers as deliverers of the intervention. However, process evaluation findings also revealed that some pupils had an aversion to engaging with parents in the homework activity, in addition to an actual or perceived perception that their parents would not be willing to engage in the homework activity with them. Although teachers reported that some students did undertake the homework activity, this was regarded by the teachers as an optional bonus, rather than a requirement. Thus, for a future trial we must consider the necessity of this ‘beyond classroom’ component to the overall logic model of the intervention.
As detailed above, technical difficulties meant that the questionnaire was delivered predominantly in paper form. Technical difficulties, mostly associated with school networks, also led to all but one school showing the IVD via overhead projector as opposed to online. Process evaluation revealed this was an acceptable method of delivery, with most teachers acknowledging that there were additional benefits to delivering in this way (i.e. control of pace, the opportunity to stop and explain, and being better for pupils with reading difficulties). In a future trial, we would still encourage use of individual personal computers or iPad (Apple Inc., Cupertino, CA, USA) computers, and we would seek to build in a mode of delivery into the memorandum of agreement. However, owing to this positive evaluation of overhead method, we would not exclude a school if this was the only feasible way of delivery.
A further secondary objective was to establish participation rates and reach, including equality of engagement across schools of different socioeconomic and religious types. The study demonstrated that it was feasible to recruit the full range of the most common types of schools in NI, namely schools with differing school management systems, including faith-based schools, schools that are especially academically oriented and those that are not, and schools that are in socially deprived as well as socially affluent areas. The inclusion of faith-based schools is important because we believe that this is the first RSE intervention trial to include faith-based schools in the UK and > 50% of schools in NI are faith based. Nonetheless, we also learned that the hardest schools to recruit for this trial were schools that were both faith based (i.e. RC) and high academic achieving schools. These are what are known as ‘Catholic Grammar Schools’ (RC Grammar) in NI. The overall recruitment rate for RC schools was 30%. However, the recruitment rate for RC grammar schools was 13%, while the recruitment rate was 67% in RC maintained secondary schools. The latter are RC schools for which the pupil’s entry selection is not dependent upon high academic achievement at 11 years of age. Thus, although the trial succeeded in recruiting a breadth of schools across crucial sociodemographic criteria, we are acutely aware that we also then need to reach potentially socially excluded groups of pupils within these schools, those students who are most likely to become a teenage father/mother (e.g. those from more deprived groups, those with low literacy, low attainment and poor school attendance, and those with learning disabilities), and we address this in the discussion below.
Another secondary objective aimed to assess trial recruitment and retention rates. In terms of school recruitment, the feasibility study demonstrated that our target aim of recruiting seven schools, four to the intervention arm and three to the control arm, was realistic and that we could achieve our school recruitment target rate (target = 25%, achieved 37%). In terms of pupil recruitment, the target was also met, with an overall pupil recruitment rate of 80.9%. Absentees who did not return completed questionnaires accounted for 9% of non-participants, and parental and pupil opt-outs accounted for the remaining 9.9% (6.8% and 3.1%, respectively). However, one conclusion of the trial has been a commitment to work with the trial steering group in the main trial to enhance clarity around the consent process for parents and guardians, as some indicated confusion regarding the opt-out form (assuming it was an opt-in form). Pupil information sessions also need to be better monitored by researchers to ensure that they follow protocol. We shall consider a short audio-visual presentation, which could be easily shown by teachers in addition to information sheets. In addition, we would try to avert data loss to pupil absenteeism by not conducting data collection on Monday mornings or Friday afternoons or in the weeks preceding holiday periods. In terms of parental recruitment, as reported above, we failed to adequately engage parents in the study (parental information sessions), recruiting only 2.3% of all parents/guardians. The recruitment of teachers for semistructured interviews within schools was unproblematic. Retention of schools was successful (100%) as was retention of pupils (93.1%).
We also aimed to assess variation in normal RSE practice across the participating schools. In this feasibility study, existing provision of RSE (content, frequency, co-ordination and delivery) was assessed. In NI there is no official curriculum material targeted to Key Stage 4 (Years 11–13). Year 11 was the participating year group in this feasibility study, although there was a consensus among participating teachers that they would also like to use the intervention with Year 10. In general it emerged that RSE provision was extremely variable and not perceived as a priority subject. Some schools had well-structured RSE programmes, whereas others had difficulty articulating the RSE provision within the school. Pupils recalled little to no attention or emphasis placed on UTP. All schools provided most of their RSE provision using the ‘Insync’ Personal Development programme, developed by CCEA, of the LLW statutory component of the NI curriculum. This programme was developed for Key Stage 3 to be targeted to Years 8–10 (see Appendix 7). Although RC schools described their approach as always in line with the RC Church’s teachings and ethos, this did not appear to alter the nature or attitude towards RSE provision compared with non-Catholic participating schools. Participating grammar schools, although academically focused, were not distinguishable in their existing RSE provision. Teachers reported a general sense that RSE provision remained somewhat sensitive and controversial and that attitudes towards RSE were highly variable, with some reports of religious conservatism and homophobia, and that improvements could be made. There was unanimous willingness to embrace new approaches and improve existing provision. Post-qualification training and opportunities for training for teachers appeared to be all but absent.
A further secondary objective was to refine the survey instruments as a result of cognitive interviews with male and female pupils. The pupil questionnaire has already undergone substantial redevelopment, as informed by the pilot and feasibility study (detailed in full in Chapter 4). Based on cognitive interviews (and other feedback mechanisms such as the pupil comment sheets and fieldworker observation sheets) after the final data collection in the feasibility study, we determined that further changes to the pupil questionnaire were required. These included simplifying and standardising the Likert-scale options and increasing the privacy of the participant by ensuring that skipped sections would be replaced with an equivalent number of questions and by randomising sections that would be incorporated into the questionnaire for a Phase III effectiveness trial. This was suggested by pupils so as to disguise who was answering what questions at any particular time point during data collection sessions, thereby negating any presumptions being made by fellow pupils about sexual activity and time taken to answer certain questions as a result. For an overview of the suggested changes to the questionnaire that emerged from the focus group activity see Table 17.
We also aimed to assess differences in outcomes for male and female pupils. In the subgroup analysis of the primary outcome measure by gender, there was an improvement in boys in the intervention arm (2.2% improvement at follow-up 1 and 0.5% improvement at follow-up 2), but a deterioration in females in the intervention arm was evident (1.3% deterioration at follow-up 1 and 4.4% deterioration at follow-up 2). Female pupils in the intervention group scored notably higher than their male counterparts in the Knowledge scale at both follow-ups 1 and 2; in the Intentions scale at follow-up 1; in the Intentions Self-Efficacy subscale at both follow-up 1 and 2; and in the Attitudes subscale at both follow-ups 1 and 2. Male pupils in the intervention group scored significantly higher (p = 0.004) than male pupils in the control group at follow-up 2 and notably higher than their female counterparts in the intervention group in the Male Role Attitudes scale (male 1.27, 95% CI 0.41 to 2.13; female 0.47, 95% CI –0.22 to 1.17). This was not evident at follow-up 1. The Male Role Attitudes scale is essentially an analysis of emerging masculinities that are more gender equal versus the traditional gender-related views that men and women are unequal.
The questionnaire also included a specific attitudinal question relating to whose responsibility it was to prevent an UTP, allowing for the balance of responsibility to be moved towards males or females. Both the intervention and control group demonstrated an improvement towards attributing an equal 50 : 50 ratio of responsibility over time, although the improvement was more pronounced in the intervention group (13.3% vs. 10.4% in the control group).
Another secondary objective was to identify potential effect sizes that might be detected in an effectiveness trial and estimate an appropriate sample size for that trial. The results of the feasibility study provided us with some useful parameters to calculate a sample size calculation for the main trial. To take this in sequence, we first report the effect size results in the feasibility trial. In the feasibility study, approximately 3% of our sample reported unprotected sex at baseline (3.6% in the intervention group and 2.5% in the control group) and approximately 5% reported unprotected sex at follow-up 2 (5.4% in the intervention group and 5.6% in the control group). This amounted to a 50% increase in unprotected sex by follow-up 2 in the intervention group (3.6% at baseline rising to 5.4% at follow-up 2) compared with a more than doubling of unprotected sex by follow-up 2 in the control group (2.5% at baseline rising to 5.6% at follow-up 2). We used this potential effect size to inform the sample size calculation for the main trial. The main trial will be powered to detect a 50% reduction in the incidence of unprotected sex (from an expected rate of 2.8% to 1.4%) by 15 years of age. A difference of 1.4% in unprotected sex has been shown to have a meaningful impact on pregnancy rates. 18,122,124,149 The between-group difference in the incidence of unprotected sex of 1.3% (95% CI 0.5% to 2.2%) by 9 months in our feasibility trial demonstrates that such an effect size is plausible and is consistent with effect sizes seen in the literature. 122 The study will take account of clustering. In the feasibility trial data the intraclass correlation coefficient (ICC) was 0.01. As pilot studies can provide imprecise estimates of ICCs,150 we re-estimated using ICCs from three sources: (1) the Randomized Intervention of PuPil-Led sex Education (RIPPLE) cluster RCT; (2) data from the WHO Health Behaviour in School-aged Children Survey GB;129 and (3) the Young Persons’ Behaviour and Attitudes Survey 2011. 9 The data from the WHO and Northern Ireland Statistics and Research Agency (NISRA) studies were combined. Both the RIPPLE and combined WHO and NISRA studies found an ICC of 0.004. In terms of our sample size calculation based on these data, first, based on the ICC of 0.01 (95% CI 0.01 to 0.04), and assuming 120 students per year group in school, and a 7% rate of attrition (based on the conservative attrition rate found in the feasibility study plus two additional schools), a trial involving 33 schools per group will provide 80% power at a 5% significance level. The power would rise to 93% if we used the alternative ICC of 0.004. Table 46 shows the sample size calculation based on the first ICC (0.01).
| Control | Intervention | Sample size per group | ICC (95% CI) | Cluster size | VIF | Multiply by VIF | Dropout rate | Inflated for dropouts | Divided by cluster size to give number of schools per group | Power |
|---|---|---|---|---|---|---|---|---|---|---|
| 2.8% | 1.4% | 1646 | 0.01 (0.01 to 0.04) | 120 | 2.19 | 3605 | 7% + two additional schools | 3876 | 33 | 80% |
The final secondary objective was to identify the costs of delivering If I Were Jack and generate methods for assessing cost-effectiveness in a future trial. The mean cost of delivering If I Were Jack per pupil after adjusting for school cluster was £13.66. The economic cost was calculated to include teacher and school costs according to the principle of opportunity cost and using a microcosting approach taken from a public-sector decision-maker perspective. Preparation for a future cost-effectiveness decision model that incorporates theories of behaviour change was also undertaken. The structure of the model is illustrated in Figure 6. In the main trial, this framework will be populated with data from future primary research, policy documents and published literature (see further elaboration under progression rules below).
Criteria for progression to main trial
The following issues were considered when deciding whether or not to develop a protocol for a Phase III trial:
-
The intervention is acceptable to schools (principals and RSE teachers), pupils and parents; can be feasibly implemented by teachers in schools in NI; and any indications of necessary further development do not exceed the PHA’s contribution of £20,000. If there is a consensus among school teachers that the If I Were Jack intervention would be of little value to other schools or if fundamental logistical problems in its delivery become evident and cannot be rectified, we would not proceed to trial.
The intervention is acceptable to schools as evidenced by positive evaluations from schools (principals and RSE teachers), pupils and parents. Participants suggested only minor amendments to the core intervention. However, participants did propose a significant refinement to the parental component of the intervention because we did not attract sufficient numbers of parents to attend information and discussion sessions in the schools. Arising from process evaluation findings and consultation with trial steering group members, we propose to transform this element of the intervention from teacher-led information sessions that parents are required to attend into three short, highly engaging videos, which would be accessed electronically by parents. We anticipate that the cost of this refinement will be approximately £20,000 in production costs. However, separate funding has been obtained for this change from the HSC R&D.
Furthermore, as we now anticipate UK-wide effectiveness, we have completed a ‘transferability study’144,145 of our intervention in Scotland, Wales and England with our collaborators. The transferability study was jointly funded through QUB and the Social and Public Health Sciences Unit of University of Glasgow and involved qualitative research on the suitability of the If I Were Jack intervention in three diverse schools and among key stakeholders in each of the other three countries of the UK. The results of this transferability study suggested that we should reshoot the interactive film for England and Wales using English actors, to enhance cultural sensitivity. In addition, in order to make both films identical and to take an opportunity to update computer-based technology and film, we would aim to reshoot the NI version for use in Scotland and Wales at the same time. In addition, the transferability study findings recommend that we make minor changes to the classroom materials to localise some of the references to services and increase compatibility with the respective RSE curricula of each of the nations where relevant. The cost of reshooting the film is estimated at £45,000. However, these costs would not be incurred if the main trial were to take place in NI only.
-
Recruitment, participation and retention rates are likely to be adequate for a main trial. We would expect high rates of recruitment, participation and retention. However, if we do not recruit at least 25% of schools approached, we would not proceed to trial. Moreover, if we experience > 25% of parents withdrawing their children from the study or > 25% of pupils refusing to participate, we shall not proceed to trial. Finally, in relation to retention, if < 85% of pupils complete the primary outcome measure at follow-up, we would not proceed to trial.
Recruitment of schools was successful. A total of eight schools, six principals, two VPs, 40 teachers, and 831 pupils were recruited at baseline. The overall recruitment rate was 38%. The recruitment rate of RC schools was 30%.
The pupil recruitment rate was 80.9%. Parental withdrawal of consent accounted for 6.8% of loss (n = 70) and pupil opt-out for 3.1% (n = 32). Pupil absence or unavailability at baseline with absentee questionnaires and consent form not returned to the research team accounted for the remaining 9.1% (n = 94).
Retention of schools: all schools have remained in the trial at follow-up 2.
Retention of pupils in relation to primary outcome measure was 93% at follow-up 2.
-
The potential effect sizes reported in the feasibility study indicate an achievable sample size (see sample size calculation of 66 schools reported above).
-
The survey instruments can be feasibly delivered to time in the recruited schools and show acceptable reliability and validity. The instruments showed high acceptability. The majority of participants stated that they felt comfortable in answering most of the questions in the questionnaire (80%, n = 608). Paper-based surveys worked much better than electronic methods. In a future trial, we would hire two fieldworkers per classroom in order to more ably assist pupils with learning difficulties.
We were able to collect data on all theoretically interesting mediating variables of knowledge, attitudes and self-efficacy to avoid a pregnancy and intentions to avoid a pregnancy. Overall, the reliability of the measures (scales) used to assess these variables was satisfactory. Cronbach’s alpha was calculated as a measure of internal consistency/reliability for all scales. The Male Role Attitudes, Sexual Socialisation Peer scale, Sexual Self-Efficacy scale and TUPS all had high internal consistency (Cronbach’s alpha in excess of 0.7); Family Connectedness, Comfort Communicating about Pregnancy, Comfort Communicating about Contraception, Sexual Socialisation Total and the Sexual Socialisation Parent scales had satisfactory internal consistency (Cronbach’s alpha: 0.526–0.699).
We also tested a number of questions for use in a future health economic cost–benefit analysis, relating to contraceptive use, numbers of partners and self-reported records of STI diagnoses. The question on STI diagnoses worked poorly insofar as there was an especially high rate of non-response for this question (88.7% of missing data at follow-up 2). Nonetheless, we believe that this is mostly because of the low rates of STI diagnoses among young people under 16 years of age and hence a perceived irrelevance. We shall consult with our young people on the steering group and a planned young people’s advisory group on a future trial to ascertain how best to position the relevance of this question on a future questionnaire.
-
An economic evaluation can be feasibly conducted as part of the main trial.
An economic evaluation can be feasibly conducted in a main trial as we have been able to achieve the groundwork for this in the feasibility trial. The aims of the economic component in the feasibility trial were to identify the costs of delivering If I Were Jack and to develop a framework for assessing cost-effectiveness in a future trial (see Figure 6). This was achieved by the following:
-
The identification of the relevant resources used in the set up and delivery of If I Were Jack and their associated costs was completed using a microcosting approach, from a public-sector decision-maker perspective. Relevant costs were identified, measured and valued in monetary units using the 2013/14 price year, guided by a recognised practical guide to costing behavioural interventions. 132 The mean cost per pupil for delivery of the intervention (including training of teachers) was calculated as £13.66.
-
The identification of parameters for a future cost-effectiveness decision model that incorporates theories of behaviour change is illustrated in Figure 6.
-
The aim of the economic evaluation in the main trial, and as proposed now to be a UK-wide trial, as noted above, is to describe the costs and consequences of implementing If I Were Jack in schools across all countries of the UK so as to provide information to decision-makers on the implications of rolling out the intervention further. Initially, we plan to conduct an analysis of the opportunity costs of implementing If I Were Jack in trial schools in Scotland, England and Wales. This will include the duration of time taken up by If I Were Jack in school from the perspective of the teacher and the impact on time spent on other important curricula activities compared with time spent on standard RSE. The aim of this will be to provide a measure of the opportunity cost to schools of implementing If I Were Jack compared with current RSE in control schools. The structure of the evaluation will follow NICE guidance for evaluating public health interventions151 and recent guidance published by Edwards et al. 152 on economic evaluations in public health. Costs will include the cost of implementing the intervention in schools including any training involved and the cost of current RSE in the control schools. We shall also collect information on health-care cost information in the intervention and control arms, including the costs of sexual health-related primary care attendances, costs of any STIs and cost of unintended pregnancies, although numbers of these are likely to be small. The cost of culturally adapting If I Were Jack to the different countries will also be reported, given that others may want to also adapt the intervention before rolling it out. Mean cost per pupil will be reported alongside consequences, including use of contraception, STIs and unintended pregnancies, which will be collected using questionnaires that are administered to pupils at baseline and follow-up. Costs will also be reported by country, given the different sexual health services provided and, hence, differential implications for health service costs by country.
Given that STIs and unintended pregnancies are likely to be rare but potentially high-impact events in this group, the long-terms costs and consequences will be modelled as part of the decision model described above in point 2 and shown in Figure 6. In addition to collecting information as part of the trial, we shall look to systematic reviews in the literature of evidence of the impact of digital interventions on sexual health behaviour in this population group, for example the review recently undertaken and published by Bailey et al. 55 We shall review the literature for any gaps in evidence identified. We shall undertake one-way, two-way and probabilistic sensitivity analyses of the results. Cost-effectiveness acceptability curves and cost-effectiveness planes will be reported. The model will have a 20-year time horizon, and discounting of future costs and benefits will comply with NICE guidance for evaluating public health interventions. 151
Summary findings relating to the evaluation of Relationship and Sexuality Education interventions in schools and future research
Thinking through implementation and evaluation from the outset of intervention design
In providing guidelines for the development and evaluation of complex interventions of this kind, the UK’s MRC89 recommend that high-quality evaluation is preceded by a systematic approach to intervention development. The iterative four-phase approach outlined in the MRC framework involves developmental work (referred to as ‘Phase I’ research), which includes identification of the evidence base, identification or development of theory relating to the phenomenon of interest and modelling of processes and outcomes to inform optimisation of the intervention prior to evaluation. However, in our view, although the MRC guidelines89 suggest a very useful framework for conducting Phase I research, they provide little description of how this should proceed (relative to guidance provided on Phases II–IV). This effectively relegates the importance of this phase to brief summaries in evaluation research, despite growing consensus that the development of conceptually based, acceptable interventions is of vital importance before proceeding to trial. This is compounded by a dearth of published literature reporting the development of complex interventions more broadly but, also, specific developmental process in relation to RSE interventions are scant in the literature (for exceptions, see Carswell et al. ,153 Kirby et al. ,94 McCarthy et al. 154 and Wight and Abraham155). The result is a paucity of models that might guide comparable research. In Chapter 3 we report the intervention design process in detail to hopefully guide other researchers in the design phases of comparable interventions.
We also offer the following observation in relation to the MRC guidelines. 89 The MRC guidelines do not indicate the importance of considering implementation during Phase I, despite the fact that this might alert the researcher to factors that may impact on successful implementation. In discussing Phase IV, the guidelines indicate that ‘successful implementation depends on changing behaviour – often of a wide range of people. This requires a scientific understanding of the behaviours that need to change, the factors maintaining current behaviour and barriers to and facilitators of change, and the expertise to develop strategies to achieve change based on this understanding’. 89 It seems likely many of these factors should be considered during the development phase, rather than post evaluation and this is the approach that we took during the study. The current study builds on the team’s Knowledge Translation Award from the Economic and Social Research Council (RES-189–25–0300),156 through which the intervention was initially developed and a ‘translation study’ offering insights into generating a culturally generalisable intervention across the UK. 144 It also follows foundational empirical groundwork generating understandings of adolescent males’ attitudes towards and decision-making in relation to teenage pregnancy. 1,90,93 A hallmark of this preparatory work has been meaningful consultation with all stakeholders, from pupils to senior policy-makers, ensuring that the If I Were Jack intervention can be sustainably implemented if proven to be effective. We would argue that an essential part of the design process involves thinking about and planning for all aspects of the research process that will follow – feasibility testing; evaluation; implementation, follow-up and monitoring.
The need for gender-sensitive interventions and gender analyses of Relationship and Sexuality Education interventions
The need for gender-sensitive interventions to address teenage pregnancy has been highlighted as a global health need by the WHO46,47 and recommended in systematic reviews of RSE education. 19,48,49,157 Boys have been especially neglected in educational interventions in relation to teenage pregnancy. 1,22,48,51–54 When they do receive RSE about pregnancy, it is often via programmes that are directed towards girls, although it is quite likely that males and females are affected differently by gender norms and values relating to pregnancy. 2 This is the first UK study of a gender-sensitive approach to prevent UTP and the first of its kind to specifically target teenage boys. Moreover, the study highlights the neglect of, and need for future research to report on, gender differences across the board in the evaluation of RSE interventions in order to better understand what works best for boys and girls. 157
The wider application of interactive video dramas in public health promotion and research
The appeal of the IVD as both a technological platform and a means of engaging young people in episodic thinking,158,159 which allows young people to think themselves into the future or into being a character, is perhaps noteworthy for future public health interventions. This original methodology was adapted from an earlier empirical project in which it was originally used as a tool for data collection. 1,160 The If I Were Jack IVD has already inspired other researchers to adapt this methodology into a comparable schools-based intervention, entitled Cycles, to address adolescents and marijuana use in British Columbia. 95,161 A further example is If I Were Nick – an internet-based smoking cessation intervention also directly inspired by If I Were Jack and collaboratively developed by Joan Bottorff and team with M Lohan as lead applicant. 162 The intervention is hosted on the national website of Quitnow Canada. 163 Part of the appeal of incorporating IVDs is the opportunity to involve the target audience in foundational arts-based research to script realistic characters with whom and settings with which they can identify. The end product IVD then helps to contextualise health promotion messages in their own lives. This ethnographically informed drama production, combined with the interactive computer component used in the creation of the IVD, is the approach that we shall now pursue with incarcerated young men in relation to a programme designed to prevent unintended pregnancy and prepare incarcerated young men for future parenthood in co-operation with our prison partners at Hydebank Wood Secure College, Northern Ireland Prison Service.
The tension between creating culturally sensitive and universal interventions
Creating drama productions, and ultimately interventions, with which all young people can identify and/or which are appealing to all young people in any target group is unrealistic. Research teams have to think carefully about whether they want to balance their intervention towards a subgroup (e.g. black and minority ethnic groups) or go for a broader universal approach, which will inevitably exclude some subgroups. In our research, we made a decision early on in the design stage (in consultation with our educational stakeholders and through script readings with young people in drama groups) to go for the middle ground, representing the majority population in NI. The main protagonist was white, upper working-class with an urban Belfast accent and living with both parents. The likability of the main protagonist proved to be central to creating a universal appeal. In this feasibility trial we learned that the addition of an audio track may be of benefit to those with literacy difficulties. In the transferability study, we learned that there was acceptable cultural translation between our NI version of If I Were Jack and the Scottish population. Pupils here recognised that Jack was not Scottish, but crucially he was also not clearly identifiable as Protestant or Catholic and there was no substantial difficulties with comprehension. However, in England and Wales, cultural identification with a Northern Irish character and the comprehensibility of the accent were substantial barriers. Thus, we have made a decision to reshoot an English version for use in England and Wales. This was regarded as acceptable in both North and South Wales. It is also envisaged that the cast for this new English version will be more multiethnic. However, we shall have to consult closely with young people again when recasting, as all relationships depicted in the movie will have to be authentic and plausible.
Therefore, our simple conclusions in this regard are as follows. Consult with the target audience throughout. Recognise that producing universal interventions will involve uncomfortable compromises, in terms of not being able to address all audience needs. Luckily, however, films are culturally understood to be stories about some people, and it is inevitable that they will have greater appeal to some audiences.
Recruitment strategies and inclusion of faith based schools
In many ways, our recruitment experiences and our research with schools inquiring into the best ways to approach and recruit schools in this study reinforces some of the lessons already available in the literature (see Table 18 for a summary). However, this study adds to the literature in the following ways. First, it suggests that the use of RSE training days for teachers is a very effective focal point for recruitment of schools for RSE research. In the UK countries, such as NI, Scotland and Wales, where there are national curricula for RSE and hence also statutory provision for training teachers, such training, we suggest, is a very efficient means of recruiting schools for trials of RSE interventions. Second, we would advocate for audio-visual information sheets for pupils. Based on our interviews with teachers and pupils, we suggest that if these are made readily available to teachers, it will enhance the information and consent procedures for pupils. Third, and perhaps most importantly, we believe that this is the first RSE intervention trial to include faith-based schools in the UK. Given that > 50% of schools in NI are RC, this was especially important in NI. Nonetheless, as the UK becomes increasingly multicultural, with the corresponding growth of other faith-based schools, we suggest that future RSE research should also seek to include minority religious schools. We suggest that recruitment of these schools could be enhanced by inclusion of these types of schools in the design of interventions and in tailoring recruitment invitation letters to these schools to assuage anticipated concerns.
Involving parents through schools in relation to Relationship and Sexuality Education interventions
Although evidence suggests that schools are an important context for sex education,14,22,48 recent systematic reviews have also shown that programmes that reach beyond the classroom can enhance effectiveness. 19,25,60 In particular, factors such as parental monitoring and supervision and familial communication have been associated with teenage sexual behaviours. 61,62 Teenagers who can recall a parent communicating with them about sex are more likely to report delaying sexual debut and increased condom and contraceptive use. 63–65 One element of the If I Were Jack theory of change involves increasing communication about UTP among parents and teens. First, the resource includes a homework task and materials to generate the communication from the child’s perspective. Second, it includes teacher-facilitated information sessions with parents. As detailed in this report, both of these aspects, and especially the parent information sessions were the least successful in terms of intervention implementation. This caused us to rethink this component based on follow-up research with parents, consultation with our trial steering group and further explorations of the literature during this study. In relation to the homework task, we have decided to keep this component but to recognise that it will not be implemented universally and we shall continue to monitor this as part of the process evaluation in a full trial. In relation to the teacher-facilitated information sessions, we shall change this to the form of three short online animations/films for parents and guardians which will be texted/e-mailed to parents directly from the schools. The primary purpose of these three short films is to inform parents/guardians of the resource being used in the classroom and the homework activity, and to guide them with information about the importance of communicating with their child about teenage pregnancy and sexual health, and hints and tips for doing so. Recent studies68,69 demonstrate the importance of embracing such ‘education entertainment’ modalities as engaging adjuncts to school-based education. This refinement has been funded by the HSC R&D. It was completed in 2016 and will be tested in the main trial. The broader point that this raises, however, is how best to include parents in school-based RSE interventions for pupils and this is a question that we believe requires further research.
Acknowledgements
The authors wish to give particular thanks to all participating schools, school principals and pupils who have made the research possible. We also wish to thank the Trial Steering Group (see Chapter 1), and the Stakeholder Group (see Chapter 1), in particular Ms Joanne Brown for her role in helping with the recruitment of schools.
Contributions of authors
Professor Maria Lohan (Acting Director of Research for the School of Nursing and Midwifery, QUB) co-designed the study and contributed to drafting of all chapters in the report.
Dr Áine Aventin (Research Fellow at the School of Nursing and Midwifery, QUB) co-designed the study, conducted and supervised all aspects of data collection, analysed all of the qualitative data and drafted the recruitment, process evaluation and intervention design chapters.
Dr Lisa Maguire (Research Fellow at the School of Medicine, Dentistry and Biomedical Sciences, QUB) co-designed the study, advising on methodological aspects, conducted the data collection and drafted the questionnaire design and quantitative results chapters.
Dr Rhonda Curran (Research Fellow at the School of Nursing and Midwifery, QUB) oversaw the compilation of this report, contributing to all of the chapters.
Mrs Clíona McDowell (Biostatistician at NICTU) conducted the statistical analysis for the quantitative results and contributed to the quantitative results chapter.
Dr Ashley Agus (Health Economist at NICTU) conducted the health economic costing component and drafted the health economics chapter.
Professor Cam Donaldson (Yunus Chairperson for Research in Social Business and Health, Glasgow Caledonian University) performed the health economic modelling component and drafted the health economics chapter.
Professor Mike Clarke (Professor/Director of MRC Methodology Hub at the School of Medicine, Dentistry and Biomedical Sciences, QUB) co-designed the study and advised on all methodological aspects of the study.
Dr Mark Linden (Lecturer at the School of Nursing and Midwifery, QUB) advised on psychometric aspects of questionnaire design and analysis and contributed to the questionnaire design chapter.
Dr Carmel Kelly (Nurse Consultant, South Eastern Trust and Lecturer at the School of Nursing and Midwifery, QUB) assisted in the analysis of all of the qualitative aspects of the process evaluation.
Dr Lisa McDaid (Programme Leader – Social Relationships and Health Improvement, MRC/Chief Scientist Office Social & Public Health Sciences Unit) advised on study design and execution and contributed to the literature review.
Dr Laura Dunne (Lecturer at the School of Education, QUB) advised on aspects of conducting data collection in schools.
Dr Peter O’Halloran (Lecturer, at the School of Nursing and Midwifery, QUB) contributed to the design of the intervention, the design of the feasibility study and the organisation of PPI.
Publications
Aventin Á, Lohan M. I’m all right, Jack. Every Child J 2013;3:38–43.
Aventin Á, Lohan M. You’re Wha. . .? Including young men in reproductive planning. Pract Midwife 2013;16:21–23.
Lohan M, Aventin Á, Maguire L, Clarke M, Linden M, McDaid L. Feasibility trial of a film-based educational intervention for increasing boys’ and girls’ intentions to avoid teenage pregnancy: Study protocol. Int J Edu Res 2014;68:35–45.
Aventin Á, Lohan M, O’Halloran P, Henderson M. Design and development of a film-based intervention about teenage men and unintended pregnancy: applying the Medical Research Council framework in practice. Eval Prog Plann 2015;49:19–30.
Aventin Á, Maguire L, Clarke M, Lohan M. Recruiting schools, adolescents and parents to a sexual-health trial: experiences, challenges and lessons learned from the Jack Trial (NCT02092480). Trials 2015;16(Suppl. 2):81.
Bottorff JL, Sarbit G, Oliffe JL, Kelly MT, Lohan M, Stolp S, et al. ‘If I Were Nick’: men’s responses to an interactive video drama series to support smoking cessation. J Med Internet Res 2015;17:e190.
The intervention described in the above article is based on the If I Were Jack methodology of interactive IVDs and was developed in relation to smoking cessation.
Lohan M, Aventin Á, Oliffe JL, Han CS, Bottorff JL. Knowledge translation in men’s health research: development and delivery of content for use online. J Med Internet Res 2015;17:e31.
Maguire L, Aventin Á, Lohan M, Clarke, M. What do young people really understand when completing questionnaires? Lessons learnt from developing a questionnaire to measure behavioural outcomes in a sexual health trial. Trials 2015;16(Suppl. 2):79.
Aventin Á, Lohan M, Maguire L, Clarke M. Recruiting faith-and non-faith-based schools, adolescents and parents to a cluster randomised sexual-health trial: experiences, challenges and lessons from the mixed-methods Jack Feasibility Trial. Trials 2016;17:365.
Data sharing statement
All data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Lohan M, Cruise S, O’Halloran P, Alderdice F, Hyde A. Adolescent men’s attitudes and decision-making in relation to an unplanned pregnancy. Responses to an interactive video drama. Soc Sci Med 2011;72:1507-14. http://dx.doi.org/10.1016/j.socscimed.2011.02.044.
- Aventin Á, Lohan M, O’Halloran P, Henderson M. Design and development of a film-based intervention about teenage men and unintended pregnancy: applying the Medical Research Council framework in practice. Eval Program Plann 2015;49:19-30. http://dx.doi.org/10.1016/j.evalprogplan.2014.11.003.
- Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 2011;84:478-85. http://dx.doi.org/10.1016/j.contraception.2011.07.013.
- Lawlor DA, Shaw M. Teenage pregnancy rates: high compared with where and when?. J R Soc Med 2004;97:121-3. https://doi.org/10.1258/jrsm.97.3.121.
- Statistical Bulletin: Births by Parents’ Characteristics in England and Wales 2014. Newport: Office for National Statistics; 2015.
- Conception Statistics in England and Wales 2010. Newport: Office for National Statistics; 2012.
- NHS Scotland . Teenage Pregnancy Year of Conception Ending 31 December 2013 2015. www.isdscotland.org/Health-Topics/Sexual-Health/Publications/2015-07-07/2015-07-07-TeenPreg-Report.pdf (accessed 8 September 2016).
- Births (Administrative Geographies) 1999–2014. Belfast: NISRA; 2015.
- Young Person’s Behaviour and Attitudes Survey 2011. Belfast: NISRA; 2011.
- Bonell C. Why is teenage pregnancy conceptualized as a social problem? A review of quantitative research from the USA and UK. Cult Health Sex 2004;6:255-72. http://dx.doi.org/10.1080/13691050310001643025.
- Duncan J, Beckford Jarrett S, Harvey K. Using estimation and projection package and Spectrum for Jamaica’s national HIV estimates and targets. Sex Transm Infect 2010;86:ii43-7. http://dx.doi.org/10.1136/sti.2010.044511.
- Harden A, Brunton G, Fletcher A, Oakley A. Teenage pregnancy and social disadvantage: systematic review integrating controlled trials and qualitative studies. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b4254.
- Savio Beers LA, Hollo RE. Approaching the adolescent-headed family: a review of teen parenting. Curr Probl Pediatr Adolesc Health Care 2009;39:216-33. http://dx.doi.org/10.1016/j.cppeds.2009.09.001.
- Wight D, Raab GM, Henderson M, Abraham C, Buston K, Hart G, et al. Limits of teacher delivered sex education: interim behavioural outcomes from randomised trial. BMJ 2002;324. https://doi.org/10.1136/bmj.324.7351.1430.
- Silva M. The effectiveness of school-based sex education programs in the promotion of abstinent behavior: a meta-analysis. Health Educ Res 2002;17:471-81. https://doi.org/10.1093/her/17.4.471.
- Stephenson JM, Oakley A, Johnson AM, Forrest S, Strange V, Charleston S, et al. A school-based randomized controlled trial of peer-led sex education in England. Control Clin Trials 2003;24:643-57. https://doi.org/10.1016/S0197-2456(03)00070-9.
- Fullerton D. Promoting Positive Adolescent Sexual Health & Preventing Teenage Pregnancy – A Review of Recent Effectiveness Research. Dublin: Crisis Pregnancy Programme; 2004.
- Henderson M, Wight D, Raab GM, Abraham C, Parkes A, Scott S, et al. Impact of a theoretically based sex education programme (SHARE) delivered by teachers on NHS registered conceptions and terminations: final results of cluster randomised trial. BMJ 2007;334. http://dx.doi.org/10.1136/bmj.39014.503692.55.
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13-19: a systematic review and economic evaluation. Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14070.
- Elliott L, Henderson M, Nixon C, Wight D. Has untargeted sexual health promotion for young people reached its limit? A quasi-experimental study. J Epidemiol Community Health 2013;67:398-404. http://dx.doi.org/10.1136/jech-2012-201034.
- Downing J, Jones L, Cook P, Bellis M. Prevention of Sexually Transmitted Infections (STIs): A Review of Reviews into the Effectiveness of Non-Clinical Interventions: Evidence Briefing Update. London: NICE; 2006.
- Swann C, Bowe K, McCormick G, Kosmin M. Teenage Pregnancy and Parenthood: A Review of Reviews. Evidence Briefing for Health Development Agency. London: Health Development Agency; 2003.
- Ellis S, Grey A. Prevention of Sexually Transmitted Infections (STIs): A Review of Reviews into the Effectiveness of Non-Clinical Interventions to Reduce the Risk of Sexual Transmission. Evidence Briefing for HDA. London: Health Development Agency; 2004.
- Ingham R, Hirst J, Aggleton P, Dennison C, Warwick I. Promoting Health and Wellbeing in Schools. London: Routledge; 2010.
- Oringanje C, Meremikwu MM, Eko H, Esu E, Meremikwu A, Ehiri JE. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev 2009;4. https://doi.org/10.1002/14651858.cd005215.pub2.
- Sexual Health Promotion: Strategy and Action Plan 2008–2013. Belfast: Department of Health, Social Services and Public Safety of Northern Ireland; 2008.
- The Sexual Health and Blood Borne Virus Framework 2011–15. Edinburgh: Scottish Government; 2011.
- A Framework for Sexual Health Improvement in England. London: Department of Health; 2013.
- Henderson M, Wight D, Nixon C, Hart G. Retaining young people in a longitudinal sexual health survey: a trial of strategies to maintain participation. BMC Med Res Methodol 2010;10. http://dx.doi.org/10.1186/1471-2288-10-9.
- Kirby D. Effective approaches to reducing adolescent unprotected sex, pregnancy, and childbearing. J Sex Res 2002;39:51-7. http://dx.doi.org/10.1080/00224490209552120.
- Kirby DB, Laris BA, Rolleri LA. Sex and HIV education programs: their impact on sexual behaviors of young people throughout the world. J Adolesc Health 2007;40:206-17. http://dx.doi.org/10.1016/j.jadohealth.2006.11.143.
- Kirby D. Emerging Answers: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted Diseases. Washington, DC: National Campaign to Prevent Teen and Unplanned Pregnancy; 2007.
- Robin L, Dittus P, Whitaker D, Crosby R, Ethier K, Mezoff J, et al. Behavioral interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: a decade in review. J Adolesc Health 2004;34:3-26. https://doi.org/10.1016/S1054-139X(03)00244-1.
- Bailey JV, Murray E, Rait G, Mercer CH, Morris RW, Peacock R, et al. Interactive computer-based interventions for sexual health promotion. Cochrane Database Syst Rev 2010;9. http://dx.doi.org/10.1002/14651858.CD006483.pub2.
- Guse K, Levine D, Martins S, Lira A, Gaarde J, Westmorland W, et al. Interventions using new digital media to improve adolescent sexual health: a systematic review. J Adolesc Health 2012;51:535-43. http://dx.doi.org/10.1016/j.jadohealth.2012.03.014.
- Noar SM, Pierce LB, Black HG. Can computer-mediated interventions change theoretical mediators of safer sex? A meta-analysis. Hum Commun Res 2010;36:261-97. https://doi.org/10.1111/j.1468-2958.2010.01376.x.
- Wight D, Abraham C, Scott S. Towards a psycho-social theoretical framework for sexual health promotion. Health Educ Res 1998;13:317-30. https://doi.org/10.1093/her/13.3.317-a.
- Jones L, Bates G, Downing J, Sumnall H, Bellis M. PSHE Secondary School Review: A Review of the Effectiveness and Cost Effectiveness of Personal Social and Health Education in Secondary Schools Focussing on Sex and Relationships and Alcohol Education for Young People Aged 11–19 years. Final Report. Liverpool: Liverpool John Moores University; 2009.
- Fullerton D, Butney L. An Overview of the Effectiveness of Sexual Health Improvement Interventions. Edinburgh: NHS Scotland; 2010.
- Ajzen I, Madden TJ. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J Exp Soc Psychol 1986;22:453-74. https://doi.org/10.1016/0022-1031(86)90045-4.
- Ajzen I. Attitudes, Personality and Behavior. Milton Keynes: Open University Press; 2005.
- Ajzen I, Lange PAM, Kruglanski AW, Higgins ET. Handbook of Theories of Social Psychology, Volume 1. London: Sage; 2012.
- Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health 2011;26:1113-27. http://dx.doi.org/10.1080/08870446.2011.613995.
- Philliber S, Kaye JW, Herrling S, West E. Preventing pregnancy and improving health care access among teenagers: an evaluation of the children’s aid society-carrera program. Perspect Sex Reprod Health 2002;34:244-51. https://doi.org/10.2307/3097823.
- Coyle K, Basen-Engquist K, Kirby D, Parcel G, Banspach S, Collins J, et al. Safer choices: reducing teen pregnancy, HIV, and STDs. Public Health Rep 2001;116:82-93. https://doi.org/10.1093/phr/116.S1.82.
- Evidence for Gender Responsive Actions to Prevent and Manage Adolescent Pregnancy. Copenhagen: WHO; 2011.
- Health Policy Framework Supporting Action Across Government and Society for Health and Well-Being. Copenhagen: WHO; 2012.
- Marsiglio W, Troccoli K. It’s a Guy Thing: Boys, Young Men, and Teen Pregnancy Prevention. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2006.
- Ries A, Sonenstein F, Troccoli K. It’s a Guy Thing: Boys, Young Men, and Teen Pregnancy Prevention. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2006.
- Merry SN, Stasiak K, Shepherd M, Frampton C, Fleming T, Lucassen MF. The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ 2012;344. http://dx.doi.org/10.1136/bmj.e2598.
- Smith LH, Guthrie BJ, Oakley DJ. Studying adolescent male sexuality: where are we?. J Youth Adolesc 2005;34:361-77. https://doi.org/10.1007/s10964-005-5762-5.
- In Their Own Right: Addressing the Sexual and Reproductive Health Needs of American Men. New York, NY: Alan Guttmacher Institute; 2002.
- Lindberg LD, Sonfield A, Gemmill A. Reassessing adolescent male sexual and reproductive health in the United States: research and recommendations. Am J Mens Health 2008;2:40-56. http://dx.doi.org/10.1177/1557988307309460.
- Gillespie K, Lohan M, Aventin A, Kelly C, Hyde A. Effective and Acceptable Sex Education for Teenage Men n.d.
- Bailey J, Mann S, Wayal S, Hunter R, Free C, Abraham C, et al. Sexual health promotion for young people delivered via digital media: a scoping review. Public Heal Res 2015;3.
- Kneale D, Fletcher A, Wiggins R, Bonell C. Distribution and determinants of risk of teenage motherhood in three British longitudinal studies: implications for targeted prevention interventions. J Epidemiol Community Health 2013;67:48-55. http://dx.doi.org/10.1136/jech-2011-200867.
- Schools, Pupils and their Characteristics. London: Department for Education; 2012.
- Hirst J. Developing sexual competence? Exploring strategies for the provision of effective sexualities and relationships education. Sex Educ 2008;8:399-413. https://doi.org/10.1080/14681810802433929.
- Wellings K, Nanchahal K, Macdowall W, McManus S, Erens B, Mercer CH, et al. Sexual behaviour in Britain: early heterosexual experience. Lancet 2001;358:1843-50. https://doi.org/10.1016/S0140-6736(01)06885-4.
- Gavin LE, Catalano RF, David-Ferdon C, Gloppen KM, Markham CM. A review of positive youth development programs that promote adolescent sexual and reproductive health. J Adolesc Heal 2010;46:75-91. https://doi.org/10.1016/j.jadohealth.2009.11.215.
- Guilamo-Ramos V, Jaccard J, Dittus P, Bouris AM. Parental expertise, trustworthiness, and accessibility: parent-adolescent communication and adolescent risk behavior. J Marriage Fam 2006;68:1229-46. https://doi.org/10.1111/j.1741-3737.2006.00325.x.
- Wight D, Fullerton D. A review of interventions with parents to promote the sexual health of their children. J Adolesc Health 2013;52:4-27. http://dx.doi.org/10.1016/j.jadohealth.2012.04.014.
- Akers AY, Holland CL, Bost J. Interventions to improve parental communication about sex: a systematic review. Pediatrics 2011;127:494-510. http://dx.doi.org/10.1542/peds.2010-2194.
- Hutchinson MK, Jemmott JB, Jemmott LS, Braverman P, Fong GT. The role of mother-daughter sexual risk communication in reducing sexual risk behaviors among urban adolescent females: a prospective study. J Adolesc Health 2003;33:98-107. https://doi.org/10.1016/S1054-139X(03)00183-6.
- Meschke LL, Bartholomae S, Zentall SR. Adolescent sexuality and parent-adolescent processes: promoting healthy teen choices. J Adolesc Health 2002;31:264-79. https://doi.org/10.1016/S1054-139X(02)00499-8.
- Miller BC, Norton MC, Jenson GO, Lee TR, Christopherson C, King PK. Impact evaluation of facts & feelings: a home-based video sex education curriculum. Fam Relat 1993;42:392-400. https://doi.org/10.2307/585339.
- Commendador KA. Parental influences on adolescent decision making and contraceptive use. Pediatr Nurs 2010;36:147-56.
- Guilamo-Ramos V, Lee JJ, Kantor LM, Levine DS, Baum S, Johnsen J. Potential for using online and mobile education with parents and adolescents to impact sexual and reproductive health. Prev Sci 2015;16:53-60. http://dx.doi.org/10.1007/s11121-014-0469-z.
- Papa MJ, Singhal A, Law S, Pant S, Sood S, Rogers EM, et al. Entertainment-education and social change: an analysis of parasocial interaction. J Commun 2000;50:31-55. https://doi.org/10.1111/j.1460-2466.2000.tb02862.x.
- Strasburger VC, Brown SS. Sex education in the 21st century. JAMA 2014;312:125-6. http://dx.doi.org/10.1001/jama.2014.4789.
- Lohan M, O’Halloran P, Cruise S, Alderdice F, Hyde A. If I Were Jack, Teenage Men’s Attitudes and Decision-Making in Relation to an Unintended Pregnancy. Final Report. Dublin: Health Services Executive (IRL) Crisis Pregnancy Programme; 2010.
- Schools and Pupils in Northern Ireland. Bangor: Department of Education Northern Ireland; 2012.
- Lucas S. Unprotected Nation The Financial and Economic Impacts of Restricted Contraceptive and Sexual Health Services. London: Family Planning Association and Brook; 2013.
- Wiggins M, Bonell C, Sawtell M, Austerberry H, Burchett H, Allen E, et al. Health outcomes of youth development programme in England: prospective matched comparison study. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b2534.
- Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, et al. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst Rev 2014;4. http://dx.doi.org/10.1002/14651858.CD008958.pub2.
- Dishion TJ, McCord J, Poulin F. When interventions harm. Peer groups and problem behavior. Am Psychol 1999;54:755-64. https://doi.org/10.1037/0003-066X.54.9.755.
- Stephenson J, Strange V, Allen E, Copas A, Johnson A, Bonell C, et al. The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England. PLOS Med 2008;5. http://dx.doi.org/10.1371/journal.pmed.0050224.
- Teenage Pregnancy Strategy for England and Wales – Beyond 2010. Nottingham: DCSF; 2010.
- Men’s Reproductive Health Curriculum. New York, NY: EngenderHealth; 2005.
- Report of an Evaluation of Relationships and Sexuality Education in Post Primary Schools. Bangor: Department of Education Northern Ireland; 2011.
- Schubotz D. Messed Up? Sexual Lifestyles of 16-Year Olds in Northern Ireland. Belfast: ARK; 2012.
- Rolston B, Schubotz D, Simpson A. Sex education in Northern Ireland schools: a critical evaluation. Sex Educ 2005;5:217-34. https://doi.org/10.1080/14681810500171409.
- Owen J, Carroll C, Cooke J, Formby E, Hayter M, Hirst J, et al. School-linked sexual health services for young people (SSHYP): a survey and systematic review concerning current models, effectiveness, cost-effectiveness and research opportunities. Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14300.
- Queen’s University Belfast . Young Men and Unintended Pregnancy: An Educational Resource n.d. www.qub.ac.uk/sites/IfIWereJack (accessed 24 June 2016).
- Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-37.
- Michie S, Johnston M, Abraham C, Francis J, Eccles M. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:1-15. https://doi.org/10.1007/s12160-013-9486-6.
- Rivis A, Sheeran P, Armitage CJ. Expanding the affective and normative components of the theory of planned behavior: a meta-analysis of anticipated affect and moral norms. J Appl Soc Psychol 2009;39:2985-3019. https://doi.org/10.1111/j.1559-1816.2009.00558.x.
- Grossman JM, Frye A, Charmaraman L, Erkut S. Family homework and school-based sex education: delaying early adolescents’ sexual behavior. J Sch Health 2013;83:810-17. http://dx.doi.org/10.1111/josh.12098.
- Developing and Evaluating Complex Interventions: New Guidance. London: MRC; 2008.
- Lohan M, Cruise S, O’Halloran P, Alderdice F, Hyde A. Adolescent men’s attitudes in relation to pregnancy and pregnancy outcomes: a systematic review of the literature from 1980-2009. J Adolesc Health 2010;47:327-45. http://dx.doi.org/10.1016/j.jadohealth.2010.05.005.
- Condon JT, Corkindale CJ, Russell A, Quinlivan JA. Processes and factors underlying adolescent males’ attitudes and decision-making in relation to an unplanned pregnancy. J Youth Adolesc 2006;35:423-34. https://doi.org/10.1007/s10964-005-9025-2.
- Hyde A, Howlett E, Brady D, Drennan J. The focus group method: insights from focus group interviews on sexual health with adolescents. Soc Sci Med 2005;61:2588-99. http://dx.doi.org/10.1016/j.socscimed.2005.04.040.
- Lohan M, Olivari MG, Corkindale C, Milani L, Confalonieri E, Cruise S, et al. Adolescent men’s pregnancy resolution choices in relation to an unintended pregnancy a comparative analysis of adolescent men in three countries. J Fam Issues 2013;34:1037-58. https://doi.org/10.1177/0192513X13484281.
- Kirby D, Coyle K, Alton F, Rolleri L, Robin L. Reducing Adolescent Sexual Risk: A Theoretical Guide for Developing and Adapting Curriculum-Based Programs. Scotts Valley, CA: ETR Associates; 2011.
- University of Victoria Centre for Addictions Research of BC n.d. www.uvic.ca/research/centres/carbc/publications/helping-schools/cycles/index.php (accessed 24 June 2016).
- Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol 2007;17:643-53. http://dx.doi.org/10.1016/j.annepidem.2007.03.013.
- Campbell NC, Murray E, Darbyshire J, Emery J, Farmer A, Griffiths F, et al. Designing and evaluating complex interventions to improve health care. BMJ 2007;334:455-9. http://dx.doi.org/10.1136/bmj.39108.379965.BE.
- Treweek S, Lockhart P, Pitkethly M, Cook JA, Kjeldstrom M, Johansen M, et al. Methods to improve recruitment to randomised controlled trials: Cochrane systematic review and meta-analysis. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2012-002360.
- Watson JM, Torgerson DJ. Increasing recruitment to randomised trials: a review of randomised controlled trials. BMC Med Res Methodol 2006;6. http://dx.doi.org/10.1186/1471-2288-6-34.
- Muehlenhard CL, Quackenbush DM, Davis CM, Yarber WL, Bauserman R, Scherer G, et al. Handbook of Sexuality-Related Measures. London: Sage; 2005.
- Patel MX, Doku V, Tennakoon L. Challenges in recruitment of research participants. Adv Psychiatr Treat 2003;9:229-38. https://doi.org/10.1192/apt.9.3.229.
- McDonald AM, Knight RC, Campbell MK, Entwistle VA, Grant AM, Cook JA, et al. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials 2006;7. http://dx.doi.org/10.1186/1745-6215-7-9.
- Dunn KM, Jordan K, Lacey RJ, Shapley M, Jinks C. Patterns of consent in epidemiologic research: evidence from over 25,000 responders. Am J Epidemiol 2004;159:1087-94. http://dx.doi.org/10.1093/aje/kwh141.
- Pound B, Riddell M, Byrnes G, Kelly H. Perception of social value predicts participation in school-based research. Aust N Z J Public Health 2000;24:543-5. https://doi.org/10.1111/j.1467-842X.2000.tb00508.x.
- Befort C, Lynch R, James RL, Carroll SL, Nollen N, Davis A. Perceived barriers and benefits to research participation among school administrators. J Sch Health 2008;78:581-6. http://dx.doi.org/10.1111/j.1746-1561.2008.00349.x.
- Thompson TP, Greaves CJ, Ayres R, Aveyard P, Warren FC, Byng R, et al. Lessons learned from recruiting socioeconomically disadvantaged smokers into a pilot randomized controlled trial to explore the role of Exercise Assisted Reduction then Stop (EARS) smoking. Trials 2015;16. http://dx.doi.org/10.1186/1745-6215-16-1.
- Aarons S, Rose A, Walker J, Lyles B, Jenkins R, Raine T. Enhancing recruitment and data quality in a junior high school-based teen pregnancy prevention study. Eval Program Plann 2001;24:277-85. https://doi.org/10.1016/S0149-7189(01)00019-2.
- Lytle LA, Johnson CC, Bachman K, Wambsgans K, Perry CL, Stone EJ, et al. Successful recruitment strategies for school-based health promotion: experiences from CATCH. J Sch Health 1994;64:405-9. https://doi.org/10.1111/j.1746-1561.1994.tb03261.x.
- Dickson S, Logan J, Hagen S, Stark D, Glazener C, McDonald AM, et al. Reflecting on the methodological challenges of recruiting to a United Kingdom-wide, multi-centre, randomised controlled trial in gynaecology outpatient settings. Trials 2013;14. http://dx.doi.org/10.1186/1745-6215-14-389.
- Litchfield J, Freeman J, Schou H, Elsley M, Fuller R, Chubb B. Is the future for clinical trials internet-based? A cluster randomized clinical trial. Clin Trials 2005;2:72-9. https://doi.org/10.1191/1740774505cn069oa.
- Llewellyn-Thomas HA, Thiel EC, Sem FW, Woermke DE. Presenting clinical trial information: a comparison of methods. Patient Educ Couns 1995;25:97-107. https://doi.org/10.1016/0738-3991(94)00705-Q.
- Caldwell PH, Hamilton S, Tan A, Craig JC. Strategies for increasing recruitment to randomised controlled trials: systematic review. PLOS Med 2010;7. http://dx.doi.org/10.1371/journal.pmed.1000368.
- Palmer BW, Lanouette NM, Jeste DV. Effectiveness of multimedia aids to enhance comprehension of research consent information: a systematic review. IRB 2012;34:1-15.
- Hendrickson SG. Video recruitment of non-English-speaking participants. West J Nurs Res 2007;29:232-42. http://dx.doi.org/10.1177/0193945906292558.
- Harrington KF, Binkley D, Reynolds KD, Duvall RC, Copeland JR, Franklin F, et al. Recruitment issues in school-based research: lessons learned from the High 5 Alabama Project. J Sch Health 1997;67:415-21. https://doi.org/10.1111/j.1746-1561.1997.tb01287.x.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Fleming CB, Mason WA, Haggerty KP, Thompson RW, Fernandez K, Casey-Goldstein M, et al. Predictors of participation in parenting workshops for improving adolescent behavioral and mental health: results from the common sense parenting trial. J Prim Prev 2015;36:105-18. http://dx.doi.org/10.1007/s10935-015-0386-3.
- Heinrichs N, Bertram H, Kuschel A, Hahlweg K. Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: barriers to research and program participation. Prev Sci 2005;6:275-86. https://doi.org/10.1007/s11121-005-0006-1.
- Whittaker KA, Cowley S. An effective programme is not enough: a review of factors associated with poor attendance and engagement with parenting support programmes. Child Soc 2012;26:138-49. https://doi.org/10.1111/j.1099-0860.2010.00333.x.
- Haggerty KP, MacKenzie EP, Skinner ML, Harachi TW, Catalano RF. Participation in ‘parents who care’: predicting program initiation and exposure in two different program formats. J Prim Prev 2006;27:47-65. https://doi.org/10.1007/s10935-005-0019-3.
- Elliott L, Raab G, Wight D, Henderson M, Martin C, Birch A, et al. Evaluation of Healthy Respect Phase Two: Final Report. Glasgow: NHS Health Scotland; 2010.
- Chin HB, Sipe TA, Elder R, Mercer SL, Chattopadhyay SK, Jacob V, et al. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: two systematic reviews for the Guide to Community Preventative Services. Am J Prev Med 2012;42:272-94. https://doi.org/10.1016/j.amepre.2011.11.006.
- Facts on American Teen’s Sexual and Reproductive Health. New York, NY: Alan Guttmacher Institute; 2016.
- Santelli JS, Lindberg LD, Finer LB, Singh S. Explaining recent declines in adolescent pregnancy in the United States: the contribution of abstinence and improved contraceptive use. Am J Public Health 2007;97:150-6. http://dx.doi.org/10.2105/AJPH.2006.089169.
- Abraham C, Henderson M, Der G. Cognitive impact of a research-based school sex education programme. Psychol Health 2004;19:689-703. https://doi.org/10.1080/08870440410001722921.
- Albarracín D, Johnson BT, Fishbein M, Muellerleile PA. Theories of reasoned action and planned behavior as models of condom use: a meta-analysis. Psychol Bull 2001;127:142-61. https://doi.org/10.1037/0033-2909.127.1.142.
- Montano DE, Kasprzyk D, Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research and Practice. San Francisco, CA: Jossey-Bass; 2008.
- Campbell MK, Piaggio G, Elbourne DR, Altman DG. CONSORT Group . Consort 2010 statement: extension to cluster randomised trials. BMJ 2012;345. http://dx.doi.org/10.1136/bmj.e5661.
- Inchley J, Currie D, Young T, Samdal O, Torsheim T, Augustson L, et al. Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey. Copenhagen: World Health Organization; 2016.
- Northern Ireland Statistics and Research Agency . Young Persons’ Behaviour &Amp; Attitudes Survey 2013 n.d. www.csu.nisra.gov.uk/YPBAS%202013%20Technical%20Report.pdf (accessed 24 April 2016).
- Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: Sage; 1985.
- Ritzwoller DP, Sukhanova A, Gaglio B, Glasgow RE. Costing behavioral interventions: a practical guide to enhance translation. Ann Behav Med 2009;37:218-27. http://dx.doi.org/10.1007/s12160-009-9088-5.
- Gillett M, Dallosso HM, Dixon S, Brennan A, Carey ME, Campbell MJ, et al. Delivering the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: cost effectiveness analysis. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c4093.
- Hollingworth W, Cohen D, Hawkins J, Hughes RA, Moore LA, Holliday JC, et al. Reducing smoking in adolescents: cost-effectiveness results from the cluster randomized ASSIST (A Stop Smoking In Schools Trial). Nicotine Tob Res 2012;14:161-8. http://dx.doi.org/10.1093/ntr/ntr155.
- Mytton J, Ingram J, Manns S, Stevens T, Mulvaney C, Blair P, et al. The feasibility of using a parenting programme for the prevention of unintentional home injuries in the under-fives: a cluster randomised controlled trial. Health Technol Assess 2014;18. http://dx.doi.org/10.3310/hta18030.
- Department for Education . Teachers’ Pay and Allowances from 1 September 2016 n.d. www.education-ni.gov.uk/sites/default/files/publications/education/DE%20Circular%202016-24%20Teachers%20Pay%20and%20Allowances%20from%201%20September%202016.PDF (accessed 24 April 2016).
- Sweat M, O’Donnell C, O’Donnell L. Cost-effectiveness of a brief video-based HIV intervention for African American and Latino sexually transmitted disease clinic clients. AIDS 2001;15:781-7. https://doi.org/10.1097/00002030-200104130-00014.
- Patton GC, Bond L, Carlin JB, Thomas L, Butler H, Glover S, et al. Promoting social inclusion in schools: a group-randomized trial of effects on student health risk behavior and well-being. Am J Public Health 2006;96:1582-7. http://dx.doi.org/10.2105/AJPH.2004.047399.
- Armstrong N, Donaldson C. The Economics of Sexual Health 2005. www.fpa.org.uk/sites/default/files/economics-of-sexual-health.pdf (accessed 8 September 2016).
- Teenage Pregnancy Next Steps: Guidance for Local Authorities and Primary Care Trusts on Effective Delivery of Local Strategies. Nottingham: Department for Education and Skills; 2006.
- Hansard Written Answers – Teenage Pregnancy. London; 2011.
- Focus on Prevention: HIV and Other Sexually Transmitted Infections in the United Kingdom; Annual Report. London: HPA; 2004.
- IAG’s Response to Government White Paper Choosing Health. London: Independent Advisory Group on Teenage Pregnacy; 2004.
- Boydell N, Turney C, Jamal F, Fletcher A, Young H, Bonnell C, et al. Transferability Study of the Acceptability and Feasibility of Implementation of If I Were Jack, a Gender Sensitive Educational Intervention Relating to Unintended Teenage Pregnancy in Scotland, England and Wales. Project Report. Belfast: Queen’s University Belfast; 2015.
- Wang S, Moss JR, Hiller JE. Applicability and transferability of interventions in evidence-based public health. Health Promot Int 2006;21:76-83. http://dx.doi.org/10.1093/heapro/dai025.
- Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res 2011;2:109-12. http://dx.doi.org/10.4103/2229-3485.83221.
- Hollis S, Campbell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ 1999;319:670-4. https://doi.org/10.1136/bmj.319.7211.670.
- Guilamo-Ramos V, Lee JJ, Jaccard J. Parent-adolescent communication about contraception and condom use. JAMA Pediatr 2016;170:14-6. http://dx.doi.org/10.1001/jamapediatrics.2015.3109.
- Parkes A, Wight D, Henderson M, Stephenson J, Strange V. Contraceptive method at first sexual intercourse and subsequent pregnancy risk: findings from a secondary analysis of 16-year-old girls from the RIPPLE and SHARE studies. J Adolesc Health 2009;44:55-63. http://dx.doi.org/10.1016/j.jadohealth.2008.06.006.
- Eldridge SM, Costelloe CE, Kahan BC, Lancaster GA, Kerry SM. How big should the pilot study for my cluster randomised trial be?. Stat Methods Med Res 2015;25:1039-56. https://doi.org/10.1177/0962280215588242.
- Methods for the Development of NICE Public Health Guidance. London: NICE; 2012.
- Edwards RT, Charles JM, Lloyd-Williams H. Public health economics: a systematic review of guidance for the economic evaluation of public health interventions and discussion of key methodological issues. BMC Public Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-1001.
- Carswell K, McCarthy O, Murray E, Bailey JV. Integrating psychological theory into the design of an online intervention for sexual health: the sexunzipped website. JMIR Res Protoc 2012;1. http://dx.doi.org/10.2196/resprot.2114.
- McCarthy O, Carswell K, Murray E, Free C, Stevenson F, Bailey JV. What young people want from a sexual health website: design and development of Sexunzipped. J Med Internet Res 2012;14. http://dx.doi.org/10.2196/jmir.2116.
- Wight D, Abraham C. From psycho-social theory to sustainable classroom practice: developing a research-based teacher-delivered sex education programme. Health Educ Res 2000;15:25-38. https://doi.org/10.1093/her/15.1.25.
- Lohan M, Henderson M, O’Halloran P. Teenage Men and Unintended Pregnancy: An Educational Resource: ESRC End of Award Report. Swindon: ESRC; 2013.
- Bennett SE, Assefi NP. School-based teenage pregnancy prevention programs: a systematic review of randomized controlled trials. J Adolesc Health 2005;36:72-81. https://doi.org/10.1016/j.jadohealth.2003.11.097.
- Schacter DL, Addis DR, Buckner RL. Episodic simulation of future events: concepts, data, and applications. Ann N Y Acad Sci 2008;1124:39-60. http://dx.doi.org/10.1196/annals.1440.001.
- Schacter DL, Benoit RG, De Brigard F, Szpunar KK. Episodic future thinking and episodic counterfactual thinking: intersections between memory and decisions. Neurobiol Learn Mem 2015;117:14-21. http://dx.doi.org/10.1016/j.nlm.2013.12.008.
- Corkindale CJ, Condon JT, Russell A, Quinlivan JA. Factors that adolescent males take into account in decisions about an unplanned pregnancy. J Adolesc 2009;32:995-1008. http://dx.doi.org/10.1016/j.adolescence.2008.08.008.
- Moffat BM, Haines-Saah RJ, Johnson JL. From didactic to dialogue: assessing the use of an innovative classroom resource to support decision-making about cannabis use. Drugs Educ Prev Policy 2017;24:85-9. https://doi.org/10.1080/09687637.2016.1206846.
- Bottorff JL, Sarbit G, Oliffe JL, Kelly MT, Lohan M, Stolp S, et al. ‘If I Were Nick’: Men’s Responses to an Interactive Video Drama Series to Support Smoking Cessation. J Med Internet Res 2015;17. http://dx.doi.org/10.2196/jmir.4491.
- Quitnow Canada . If I Were Nick n.d. www.men.quitnow.ca/tactics/nick (accessed 24 June 2016).
- Kirby D, Davis CM, Yarber WL, Bauserman R. Handbook of Sexuality-related Measures. London: Routledge; 2011.
- Lief HI, Fullard W, Devlin SJ. A new measure of adolescent sexuality: SKAT-A. J Sex Educ Ther 1990;16:79-91.
- Pleck JH, Sonenstein FL, Ku LC. Masculinity ideology: its impact on adolescent males’ heterosexual relationships. J Soc Iss 1993;49:11-29. https://doi.org/10.1111/j.1540-4560.1993.tb01166.x.
- Lottes I, Kuriloff P. Sexual socialization differences by gender, Greek membership, ethnicity and religious background. Psychol Women Q 1994;18:203-19. https://doi.org/10.1111/j.1471-6402.1994.tb00451.x.
- Rosenthal D, Moore S, Flynn I. Adolescent self-efficacy, self-esteem and sexual risk-taking. J Community Appl Soc Psychol 1991;1:77-88. https://doi.org/10.1002/casp.2450010203.
Appendix 1 Participant letters of invitation, information leaflets and consent forms
Appendix 2 Data collection instruments
Appendix 3 Minutes of Steering Group meetings 1, 2 and 3
Appendix 4 The intervention
If I Were Jack key components, content and educational objectives
| When | Component | Content | Educational Objectives |
|---|---|---|---|
| Pre intervention | Teacher training session (60 minutes, online video and discussion forum) |
|
By the end of the session teachers should:
|
| Pre intervention | Parent information and discussion session (60 minutes, teacher led) |
|
By the end of the session parents should:
|
| Week 1 | If I Were Jack overview and ground rules |
|
By the end of the lesson pupils should be able to:
|
| If I Were Jack IVD |
|
||
| Homework: ‘If I had a baby’ activity and If I Were Jack factsheet |
|
||
| Week 2 | Group discussion: ‘If I had a baby’ activity and If I Were Jack factsheet |
|
By the end of the lesson pupils should be able to:
|
| Group discussion: Pause: Fast Forward: Rewind activity |
|
||
| Homework: online scavenger hunt activity |
|
||
| Week 3 | Group discussion: online scavenger hunt |
|
By the end of the lesson pupils should be able to:
|
| Small group work and discussion: ‘Making a difficult decision’ |
|
||
| Small group work and discussion: ‘Dilemmas’ |
|
||
| Homework: parent/guardian survey |
|
||
| Week 4 | Group discussion: parent/guardian survey Group discussion: controversial statements |
|
By the end of the lesson pupils should be able to:
|
| Role-play activity |
|
||
| Wrap-up: complete my plan activity |
|
Components and targeted psychosocial variables of the intervention
| Targeted psychosocial variables | Related components of the intervention | |
|---|---|---|
| Knowledge | Knowledge of ways of avoiding unintended pregnancy | If I Were Jack factsheet Pause: Fast Forward: Rewind activity |
| Knowledge about sources of support for unintended pregnancy | If I Were Jack factsheet Online scavenger hunt Parent/guardian survey |
|
| Knowledge about the possible negative relational, social, emotional and financial consequences of unintended pregnancy | Modelling of consequences in the IVD If I Were Jack factsheet ‘Making a difficult decision’ activity Pause: Fast Forward: Rewind activity ‘If I had a baby’ activity Parent/guardian survey |
|
| Knowledge about the roles and responsibilities of teenage males in relation to unintended pregnancy | Modelling of male role in the IVD If I Were Jack factsheet All discussion activities |
|
| Skills | Communication skills to discuss unintended pregnancy with peers and parents | Modelling of verbal scripts in the IVD Role-play activity ‘Dilemmas’ activity ‘Controversial statements’ activity Parent/guardian survey |
| Sociocultural influences | New awareness of peer norms regarding sexual behaviour and unintended pregnancy | If I Were Jack factsheet All discussion activities |
| New awareness of the impact of gender norms and stereotypical beliefs that avoiding and dealing with the consequences of an unintended pregnancy is a woman’s responsibility | Modelling of gender norm activity in the IVD ‘Controversial statements’ discussion activity ‘Dilemmas’ activity |
|
| New awareness of parental attitudes, values and beliefs in relation to unintended pregnancy and unintended pregnancy outcomes | Consideration of personal attitudes, values and beliefs while engaging with the IVD ‘Making a difficult decision’ activity ‘Dilemmas’ activity ‘Controversial statements’ activity ‘My plan’ activity |
|
| Beliefs about behavioural control | Improved self-efficacy in ability to communicate about unintended pregnancy with parents, peers and professionals | Modelling of communication strategies and verbal scripts in the IVD All discussion activities Role-play activity Parent/guardian survey |
| Improved perceived behavioural control in avoiding unintended pregnancy | If I Were Jack Factsheet Pause: Fast Forward: Rewind activity Personal reflection while using the IVD and engaging in other activities |
|
| Beliefs about consequence | Anticipated regret about the negative impact of unintended pregnancy on current life and future goals | Modelling of consequences in the IVD If I Were Jack Factsheet ‘Making a difficult decision’ activity Pause: Fast Forward: Rewind activity ‘If I had a baby’ activity Parent/guardian survey Personal reflection while using the IVD and engaging in other activities |
| Intention | Increased intention to avoid unintended pregnancy | Personal reflection while using the IVD and engaging in other activities ‘My plan’ activity |
Appendix 5 Outcomes and outcome measures
| Component | Aim | Measurement |
|---|---|---|
| Knowledge | Increase knowledge about ways of avoiding unintended pregnancy; roles and responsibilities of young men in relation to unintended pregnancy; possible negative relational, social, emotional and financial consequences of unintended pregnancy; and sources of information and support for unintended pregnancy | Individual assessment. Total score on 10 knowledge items. Selected items from the Mathtech Knowledge Inventory164 and SKATA165 |
| Communication skills | Increase skills for communicating with parents and peers about avoiding unintended pregnancy | Comfort Communicating about Pregnancy scale (parents, peers and professionals). Selected items from the Mathtech Behaviour Inventory164 |
| Attitudes about unintended pregnancy | Increase anticipated regret about the consequences of unintended pregnancy on current life and future goals | Items from the newly developed TUPS |
| Social influences | Increase awareness of peer norms, stereotypical gender norms and parental attitudes and beliefs about teenage pregnancy Gender norms: increase perception that both men and women have roles and responsibilities in avoiding and dealing with the consequences of unintended pregnancy Peer norms: increase perception that most peers are not sexually active and use contraception when they are Parental values and beliefs: increase awareness of parental attitudes and beliefs about unintended pregnancy |
Male role gender norms: Male Role Attitudes scale166 and knowledge items relating to responsibility for avoiding pregnancy Peer norms: knowledge items about sexual behaviour/contraceptive use among peers and Sexual Socialisation instrument (Peer subscale)167 Parental values and beliefs: Sexual Socialisation instrument (Parent subscale)167 |
| Beliefs about capabilities | Increase perceived behavioural control to avoid unintended pregnancy (say no to sex or obtain and use contraception correctly) and increase self-efficacy to communicate about avoiding unintended pregnancy with parents, peers and professionals | Sexual Self-Efficacy scale using an adapted version of the Sexual Self-Efficacy scale168 |
| Intentions | Increase strength of intention to avoid UTP | TUPS (constructed by research team) |
| Sexual behaviour | Abstinence from sexual intercourse (delay initiation of sex or return to abstinence) or avoidance of unprotected sexual intercourse (consistent correct use of contraception) | Sexual behaviour items (ever had sexual intercourse; frequency of sexual intercourse; contraception use ever/at last intercourse). Items adapted from previous sexual health surveys121,153 |
| Pregnancy | Avoidance of unintended pregnancy | Ever pregnant |
Appendix 6 Relationship and Sexuality Education provision within the personal development strand of the Learning for Life and Work Northern Irish curriculum
This includes the ‘Insync’ PD programme developed by CCEA at Key Stage 3 (Years 8–10). Relationships and sexuality is one of 10 themes within the programme, which are as follows:
Theme 1 – Health and the Whole Person
Theme 2 – Feelings and Emotions
Theme 3 – Managing Influences and Making Decisions
Theme 4 – Self Concept
Theme 5 – Managing Change
Theme 6 – Morals, Values and Beliefs
Theme 7 – Learning About Learning
Theme 8 – Safety and Managing Risk
Theme 9 – Relationships and Sexuality
Theme 10 – Drugs Awareness.
For a programme overview for Year 8 see www.nicurriculum.org.uk/docs/key_stage_3/insync/yr8/teacher_notes/y8_overview.pdf, for Year 9 see www.nicurriculum.org.uk/docs/key_stage_3/insync/yr9/teacher_notes/y9_overview.pdf, and for Year 10 see www.nicurriculum.org.uk/docs/key_stage_3/insync/yr10/teacher_notes/y10_overview.pdf.
The statutory requirements for PD within the NI curriculum are accessible via http://ccea.org.uk/sites/default/files/docs/curriculum/area_of_learning/learning_life_work/pers_dev/ks3_personaldev.pdf.
The non-statutory guidance document for PD is accessible via http://ccea.org.uk/sites/default/files/docs/curriculum/area_of_learning/learning_life_work/pers_dev/ks3_pd_nonstat_guidance_Aug2011.pdf.
Updated guidance for RSE for post-primary schools, published in August 2015, is accessible via http://ccea.org.uk/sites/default/files/docs/curriculum/area_of_learning/pdmu/rse/RSE_Guidance_PostPrimary.pdf.
Appendix 7 Number of contacts, outcomes and time taken to decide by schools approached
| School type | Recruitment strategy | Number of contacts prior to decision | Time to decide after first contact | Outcome | Reason for outcome |
|---|---|---|---|---|---|
| May–June 2014 | |||||
| Controlled integrated | Head of LLW attended April RSE training day | 3 | 8 days | Agreed to participate | Intervention considered compatible with needs Keen to get involved with more research |
| Controlled grammar | Head of Year 11 attended April RSE training day | 9 | 15 days | Agreed to participate | Credibility of the intervention/research PC VP expressed initial hesitation until a colleague talked positively about the study at a training event |
| RC grammar | Advisory group member introduced | 6 | 19 days | Refusal | Intervention considered incompatible with school ethos |
| RC grammar | Cold-call approach | 5 | 11 days | Refusal | Already involved in other research |
| Grant maintained integrated | RSE co-ordinator attended April RSE training day | 2 | 1 day | Agreed to participate | Intervention considered compatible with needs |
| RC secondary | RSE co-ordinator attended April RSE training day | 2 | 2 days | Agreed to participate | Intervention considered compatible with needs Involvement in research considered evidence for development of RSE programme at upcoming inspection |
| Voluntary other managed | RSE co-ordinator attended April RSE training day | 5 | 9 days | Refusal | Inappropriate timing: LLW staff changes |
| Voluntary other managed | Cold-call approach | 4 | 2 days | Refusal | Already involved in other research |
| September–October 2014 | |||||
| RC grammar | Cold-call approach | 4 | 5 days | Refusal | Reason for refusal not communicated |
| RC grammar | Cold-call approach | 1 | 1 day | Refusal | Already involved in other research |
| RC grammar | Cold-call approach | 5 | 6 days | Refusal | No space for intervention in the Year 11 LLW curriculum |
| RC grammar | Cold-call approach | 2 | 4 days | Refusal | Reason for refusal not communicated |
| RC grammar | Advisory group member introduced | 1 | 1 day | Refusal | No space for intervention in the Year 11 LLW curriculum |
| RC grammar | Senior teacher attended October RSE training day | 2 | 2 days | Agreed to participate | Credibility of the research Intervention considered compatible with needs (resources for teenage males) |
| Voluntary other managed | Steering group member introduced | 5 | No response after final contact (15 days post first contact) | Non-response | All telephone contact via Principal’s PA. She said they usually had a ‘no research’ policy |
| Voluntary other managed | RSE co-ordinator attended October RSE training day | 1 | 1 day | Refusal | Inappropriate timing: No space for intervention in LLW curriculum and conflict with exams |
| Voluntary other managed | Teacher attended October RSE training day | 2 | 2 days | Refusal | Intervention considered incompatible with needs (‘no problems with teenage pregnancy’ and existing comprehensive RSE provided by external facilitators) |
| Voluntary other managed | Steering group member introduced | 4 | 18 days | Agreed to participate | Credibility of the research |
| Controlled secondary | Head of LLW attended April RSE training event | 1 | 1 day | Agreed to participate | Intervention considered compatible with needs (teenage pregnancy resources) |
| RC secondary | Advisory group member introduced | 1 | 2 days | Refusal | Inappropriate timing: no space for intervention in LLW curriculum |
| RC secondary | Teacher attended April RSE training day | 2 | 1 day | Agreed to participate | Intervention considered compatible with needs (teenage pregnancy resources) Positive experiences participating in past research |
Appendix 8 School and pupil report
Appendix 9 Connections between qualitative and quantitative components in meeting key objectives
| Objectives of the research | Qualitative component | Quantitative component |
|---|---|---|
| Assess the acceptability of the intervention to schools (principals and RSE teachers), pupils and parents | Single and focus group interviews will be conducted with these participants in intervention arm to assess how the intervention is received | Measured in terms of success of being implemented |
| Identify optimal delivery structures and systems for the delivery of the resource in the classroom | Single and focus group interviews will be conducted with teachers pupils and school principals | |
| Establish intervention participation rates and reach including equality of engagement across schools of different socioeconomic and religious types | Telephone interviews with schools that choose not to participate | Measured through sampling and recruitment procedures |
| Assess trial recruitment and retention rates | As above and obtaining information (where possible) for withdrawalsa | Measured through sampling and recruitment procedures |
| Assess variation in normal RSE practice across the participating schools | Obtained through an interview with all relevant RSE teachers in intervention and control arms and an examination of any materials they might offer us | |
| Refine survey instruments as a result of cognitive interviews with male and female pupils | Cognitive interviews with a sample of pupils in control arm | |
| Assess differences in outcomes for male and female pupils | Interviews with pupils may aid explanation | Measured through quantitative instruments |
| Identify potential effect sizes that might be detected in an effectiveness trial and estimate appropriate sample size for that trial | Measured through quantitative outcome measures at baseline and follow-up | |
| Identify the costs of delivering If I Were Jack and pilot methods for assessing cost-effectiveness in a future trial | Additional clarification will be sought in interviews with school principals and teachers | Measured using a template recommended by Ritzwoller et al.132 |
Appendix 10 Content, frequency and delivery of Relationship and Sexuality Education in participating schools
| Trial Allocation | Intervention schools | Control schools | ||||||
|---|---|---|---|---|---|---|---|---|
| School ID | 13 | 14 | 15 | 17 | 10 | 11 | 12 | 16 |
| Core RSE delivered in | PD (only offered at Key Stage 3 – years 8–10) plus additional sessions | PD | PC delivered by year form teachers plus PD | PD and PC (form classes) | PD (form classes) and ‘Preparing for Adult Life’ GCSE | PD and form classes. Also half-day provided by external facilitators in Years 8, 11 and 13 | PD delivered by form teachers | PD delivered by form teachers |
| Year 8 | 1 lesson RSE team Puberty talk |
8 lessons LLW team Relationships; self-esteem |
6–8 lessons PC Feelings and Emotions RSE 6 lessons LLW Self-concept, managing influences, making decisions |
4–6 lessons LLW team Gender and identity; relationships |
4–5 lessons PD | 3–4 lessons PC Increasing self-esteem and informed decision-making Half-day session ‘Love for Life’ |
4 lessons PD Girls only – puberty talk from nurse |
|
| Year 9 | 4–6 sessions LLW team Qualities of good relationships; peer pressure; staying safe online |
8 sessions LLW team Rejection, loss, bereavement |
6–8 sessions PC Managing change in relationships; feelings and emotions; relationships and sexuality LLW 7 lessons Morals, values and beliefs |
4–6 sessions LLW team Friendships; romantic relationships |
4–5 lessons PD | 3–4 lessons PC Content not reported |
4 lessons PD | |
| Year 10 | 4–6 lessons LLW team Relationships, pregnancy myths; contraception, STIs 1 lesson ‘Icebergs and Babies’ ‘Love for Life’ Implications of early sex; STIs; pregnancy as a consequence of early sex |
4 lessons LLW team Boyfriends and girlfriends; introduction to common STIs |
8 lessons PC Managing change – self awareness Feelings and emotions; – understanding feelings, thinking about behaviour, coping with feelings Relationships and sexuality; – the implications of sexual maturity (e.g. conception, teenage pregnancy, underage parenting) LLW 6–8 lessons Safety and managing risk |
4–6 lessons LLW team Dating Relationships; Consequences of sex; STIs; pregnancy; abortion; parenthood |
4–5 lessons PD | 3–4 lessons PC Increasing self-esteem and informed decision-making 6 lessons ‘Teen Star’ programme – the effect of the media on young people |
4 lessons PD | |
| Year 11 | LLW not offered at Key Stage 4 1 session Local Area Project: group work on safe choices, future aspirations, sexual health, assertiveness and communication |
4 lessons for pupils taking LLW GCSE Complete ‘Sex and Relationships Education’ booklet focus on qualities of good parents; relationships and relationship breakdown; contraception; STIs; myths of pregnancy |
6–8 lessons PC Relationships and Sexuality: (i) Dating – understanding the nature of relationships; (ii) Dating – sexual behaviour; sexuality and responsibility; STIs; teenage pregnancy and its consequences; myths of teenage pregnancy; homosexuality 4–5 sessions GCSE LLW Concept of self, managing emotions and reactions Recognising assessing and managing risk Understanding relationships and sexuality and the responsibilities of healthy relationships |
5 lessons LLW team; school nurse Pregnancy myths; contraception; STIs; sex and the law (Jack to replace above lessons for the one participating class group) |
LLW not offered at Key Stage 4 1 lesson (girls only) Family planning nurse from local health centre 6 lessons ‘Preparing for Adult Life’ Units on relationships; roles and responsibilities as parents |
3–4 lessons PC Increasing self-esteem and informed decision-making Half-day ‘Love for Life’ session |
4 lessons PD | |
| Year 12 | 6–10 lessons Parenting awareness module for pupils taking extra-curricular courses |
3 lessons LLW STIs, contraception |
GCSE LLW Development repeat students only Content as per Year 11 |
4–6 lessons LLW Definitions of ‘Sex’; Consequences of Sex – positive/negative; STIs; AIDS; Negotiating Sex; Sex and the Law/Sexuality |
Not reported | 3–4 lessons PC Increasing self-esteem and informed decision-making |
||
| Years 13/14 | 2 lessons Guest speakers from Action Cancer and the Rainbow Project (LGBT issues) |
None | 8 Lessons PC Relationships and Sexuality Sexuality and responsibility; explore a range of issues arising (e.g. social media, cyber bullying, CSE, alcohol and drugs use, sexual exploitation, independent living at university) |
4 lessons LLW team STIs; Nexus – talk given by outside agency; relationships – casual vs. serious; gender differences in attitudes to sexual relationships |
Not reported | Half day ‘Love for Life’ session in Year 13 | Knowledge is Power Quiz | |
| Received by current Year 11 group? | LLW/PD content and puberty talk only | Yes | Yes. Pregnancy activities at Year 11 replaced with Jack | Yes. Jack replaces those listed at Year 11 for one class group | Yes | Yes | ||
Appendix 11 Suggested changes to the intervention (pupils and teachers combined)
| Component | Description | Suggested changes |
|---|---|---|
| IVD | Film |
|
| Text within film. 27 questions with multiple-choice answer sets |
|
|
| Jack factsheet | Homework. Doubled-sided A4 sheet to read. Contains information on intervention, a ‘fact or fiction’ quiz focused on teenage pregnancy myths and website addresses |
|
| If I had a baby | Homework. Doubled-sided A4 worksheet. Pupils compare their schedule to that of a parent with a 6-month old baby and are asked to consider what they would miss most and how their current life and future goals might change if they had a baby |
|
| Pause: Fast Forward: Rewind | Teacher-led discussion about what happened in the film, what might happen next and how the situation might have been prevented |
|
| Online scavenger hunt | Homework. Single A4 sheet. Pupils access four websites to find the answers to four questions |
|
| Making a difficult decision | Single A4 worksheet. Small group work and whole class discussion of the pros and cons of pregnancy outcomes for Jack, Emma and baby |
|
| Dilemmas | Small group work. Pupils read dilemma e-mail and write a response |
|
| Parent survey | Homework. Pupil asks parent(s)/guardian(s) or other trusted adult to watch excerpt of film and answer three questions |
|
| Controversial statements | Whole group discussion. Individual pupils pick out statement and give their opinion |
|
| Role play | Small groups of pupils write script, act out and discuss as a whole group |
|
| My plan | Homework. Single A4 worksheet. Pupils answer four questions and consider how they will avoid UTP |
|
| Training | 60-minute face-to-face training session |
|
| Parents’ session | 60-minute information and discussion session for parents facilitated by teacher |
|
Appendix 12 Field worker reflections on data collection in schools
Themes
-
School environment: computer equipment, pupil proximity, teacher involvement, timing.
-
Pupil issues: confusion, confidentiality and legal issues, family circumstances.
-
Researcher issues: challenging behaviour, additional support.
(A) School environment
-
Computer equipment:
-
online questionnaire was very problematic – even with computer staff there for support
-
very frustrating for young people using it as they had to log on numerous times within a session and many lost answers that they had given
-
some pupils could not log on because they forgot their log-in details for the school system. They were not aware that they could use other pupils’ log-in details for that day
-
had to switch to paper because webpage either timed out or showed an error screen, in my group only 2 or 3 completed it online.
-
-
Pupil proximity:
-
computers were really close together, the room was only half full and everyone could have seen everyone else’s screens if they wanted to
-
classroom set-up was not ideal. Pupils were seated in five rows of long table, close to each other – this made it difficult for them to fill the questionnaire in privately, as well as ask any questions discretely if they were in the middle of the row
-
small class groups instead of large hall with paper copies appeared to work best for ensuring silence and ensuring instructions understood.
-
-
Teacher involvement:
-
teacher motivation/support for project made a difference to data collection
-
issue with those who decline to take part – teachers were unsure how to handle this, with some wanting us to force them to do it
-
had to ask the teacher to stay at the top of the room; although she was helpful at the initial demographic stage of the questionnaire (e.g. parents’ education, etc.), as the questions went on pupils were getting embarrassed and were afraid to raise their hands in case she came over and not me
-
contact teacher and another two teaching assistants were looking over pupils’ shoulders throughout (I assume these pupils had reading difficulties and they were helping them with the question)
-
chocolate/sweets well received – one school had issue with handing out chocolate products.
-
-
Timing:
-
we had to wait 30 minutes
-
needed some more time in schools to properly explain process, etc.
-
(B) Pupil issues
-
Confusion:
-
had to explain the section asking about the factors influencing decision to have/not have sex
-
contraception definition
-
problems with difference between penetrative sex and sexual encounter
-
found Likert scales example sheet confusing
-
misunderstanding of men’s roles – girls did not think/know if they should complete it
-
did not understand the term ‘contraception’
-
what does financially mean?
-
what does resist peer pressure mean?
-
do you have to do the word search?
-
what does intimacy mean?
-
I have had a sip of alcohol but not gone out drinking, does that count?
-
some pupils were confused over whether or not ‘contraception’ and ‘contraceptive’ were the same thing, and one pupil asked whether this just included condoms, or other contraceptive methods too
-
words that people asked for clarification on: seldom, financially, intimacy, somewhat, sexual advance.
-
-
Confidentiality and legal issues:
-
whether they could be arrested if they said they’d had sex
-
whether anyone would be told their answers (it seems like they really need the confidential stuff drilled into them)
-
why do you need to know my post code?
-
what if I write a fake post code?
-
pupils were really confused about confidentiality – then why is my name/barcode on this, this is not confidential.
-
-
Family circumstances
-
some pupils did not live with/were not in contact with one or both of their parents – they found some questions difficult to answer
-
how to judge how financially well off their family was (Q10)
-
many did not know the highest level of education their parents had completed (Q127 + Q13)
-
some pupils did not know a lot about their parents’ attitudes, and found it hard to judge these
-
lots of students did not understand the question about parents’ education level or income.
-
(C) Researcher issues
-
Challenging behaviour:
-
persistent talking to each other and looking at each other’s questionnaires
-
in the second school I visited the teachers made me aware that I was going to be working with a lower reading class who were known to have challenging behaviour. This made it very difficult to enforce exam conditions or keep the answers of the pupils private. They were shouting their answers across the room and looking at each other’s questionnaires, which was impossible to stop. It may have been useful to have spaced them out more
-
four young people in my group did not have a questionnaire pack because their parents had opted them out. Three of these young people were unaware that they were not to be included and when I asked if they would have liked to participate and complete the questionnaire each said yes they would
-
where researchers are in different rooms, spread out over a large building, everyone should have a contact number for everyone else, and keep their mobile phone on.
-
-
Additional support:
-
for one pupil I had to read the second half of the questionnaire and explain what each question/answer was
-
one student really struggled and simply did not understand the questions; I tried to help but she got really embarrassed and eventually ran out of time and had to get a bus.
-
Appendix 13 Pupil comments (post trial)
-
If you had not had sexual experience, flicking past questions made it obvious to other peers that you hadn’t.
-
Weren’t very many answers for people who haven’t had sex. It was also obvious to everyone who hasn’t had sex, who was taking part as they had to skip loads of pages, making noise and were done quicker.
-
Make it sound less complicated.
-
Less sex questions, also add Mr Krabs to the SpongeBob word search.
-
More questions about something other than contraception.
-
More alcohol and drugs questions.
-
Rethink how questions are asked. Some questions are hard to understand.
-
Word things better.
-
Don’t be as forward with the questions.
-
More questions, less personal.
-
Have a lot of variety of questions.
-
Only make us do the questionnaire once.
-
Make the questionnaire shorter.
-
I wouldn’t like to do anything else about things like that because I don’t like sharing my details with other people.
-
Make one just for boys and a different one for girls.
-
Couple of the questions’ structures.
-
Change some questions so they are not as personal or some about other people that you may know.
-
Shorten the length of the questionnaire.
-
Fewer multiple choice questions so people can give their own opinion.
-
Reduce questionnaire size to core questions so it is easier to finish in the period.
-
Fewer questions because a lot of them are irrelevant for people who don’t want to have sex at a young age.
-
Questions for those with partners and those without.
-
Instead of saying ‘would you . . . if under the influence of drink/drugs’. Give an option like ‘you wouldn’t be in this situation’.
-
In some questions the ‘not sure’ option wasn’t available so add that in.
-
Put people further away from each other, make it more confidential.
-
More sweets.
-
Greater range of questions, in particular for those who do not plan on having sexual relations until they are older. Change the wording on questions as they made me feel like I should have had these experiences before.
-
Have more questions for people who have not taken drugs or had sexual intercourse.
-
Remove the option ‘hasn’t happened’ in some questions.
-
Space people out more.
-
More inclusive questions – questions are mostly heterosexual and gendered (e.g. Question 20 ‘talking with partner about avoiding pregnancy’).
-
Change up questions a bit as it gets very boring doing the same thing three times.
-
Take in that people are Christians, etc., and want to wait till they are older and won’t drink and do drugs most likely.
-
Take into account people’s religious beliefs.
-
Spread out the tests more.
-
Tell us why we are doing the questionnaire.
-
One questionnaire as all of them were very similar.
-
Goodie bag filled with contraception.
-
Just keep doing what you’re doing.
-
Make it less formal, include some funny images or funny stories to make the person completing the questionnaire more comfortable and at ease.
-
Educate us more on the outcomes of an UTP so we have a better understanding.
-
More interactive.
-
Ask what the school says on UTP and how the school teaches students to avoid it.
-
Ask, what is your opinion on teenage pregnancy, what are others’ opinions (e.g. peers, parents). What is your opinion of people who are sexually active at a young age?
-
Fewer multiple choice questions so people can give their own opinion.
-
Make some questions easier to understand.
-
Talk more about sexual encounters.
-
There should be more emphasis on the drugs and alcohol.
-
Not involving a certain number for someone. Not asking for address and financial questions.
-
Not such personal questions.
-
Have an ‘I don’t do drugs, drink, never had sex’ tick box.
Categories and frequencies of responses
| Category | Question and response | Frequency (number) |
|---|---|---|
| Good things | ||
| 1 | It was informative/interesting/relevant/makes you think | 106 |
| 2 | Missing class | 81 |
| 3 | Sweets/chocolates | 71 |
| 4 | Easy to complete/understand as explanations were given | 63 |
| 5 | Confidential/comfortable/opportunity to tell the truth | 25 |
| 6 | The researchers were helpful/nice | 21 |
| 7 | Puzzle at the end | 7 |
| 8 | Helps with research | 4 |
| Bad things | ||
| 1 | Quite long/repetitive/boring | 112 |
| 2 | Some personal/awkward/embarrassing/uncomfortable questions | 88 |
| 3 | Some questions do not apply/irrelevant to some people (e.g. age/experience/different genders or sexualities) | 26 |
| 4 | Did not understand: confusing terms/questions/structure | 23 |
| 5 | Missing class/sport training | 20 |
| 6 | Confidentiality questioned: postcode/other pupils nearby – privacy | 15 |
| 7 | Have to read/write/think/need more time | 3 |
| 8 | Awkward when parents get involved | 2 |
| 9 | No prizes for crosswords | 2 |
List of abbreviations
- A level
- Advanced level
- ASSIST
- A Stop Smoking In Schools Trial
- BHSCT
- Belfast Health and Social Care Trust
- BT
- British Telecom
- CCEA
- Council for the Curriculum, Examinations and Assessment
- CONSORT
- Consolidated Standards of Reporting Trials
- DHSSPS
- Department of Health, Social Services and Public Safety
- DVD
- digital versatile disc
- FAST
- First-aid Advice and Safety Training
- GCSE
- General Certificate of Secondary Education
- HSC R&D
- Health and Social Care Research and Development Office of Northern Ireland
- ICC
- intraclass correlation coefficient
- ID
- identification number
- ISRCTN
- International Standard Randomised Controlled Trial Number
- IT
- Information Technology
- ITT
- intention to treat
- IVD
- interactive video drama
- LLW
- Learning for Life and Work
- MRC
- Medical Research Council
- NI
- Northern Ireland
- NICTU
- Northern Ireland Clinical Trials Unit
- NIHR
- National Institute for Health Research
- NISRA
- Northern Ireland Statistics and Research Agency
- PC
- pastoral care
- PD
- personal development
- PHA
- Public Health Agency
- PI
- principal investigator
- PPI
- public and patient involvement
- QUB
- Queen’s University Belfast
- RC
- Roman Catholic
- RCT
- randomised controlled trial
- RE
- Religious Education
- RIPPLE
- Randomized Intervention of Pupil-Led sex Education
- RSE
- Relationship and Sexuality Education
- SD
- standard deviation
- SE
- standard error
- SES
- socioeconomic status
- STAMPP
- Steps Towards Alcohol Misuse Prevention Programme
- STI
- sexually transmitted infection
- TUPS
- Intentions to Avoid Teenage Unintended Pregnancy scale
- UPS2
- upper pay scale
- UTP
- unintended teenage pregnancy
- VP
- vice principal
- WHO
- World Health Organization