
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 11/3005/07. The contractual start date was in January 2013. The final report began editorial review in July 2016 and was accepted for publication in December 2016. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
David Ogilvie, Richard Prins, Andy Jones, Hilary Thomson and Shona Hilton report additional funding from the Medical Research Council. David Ogilvie, Louise Foley, Richard Prins and Andy Jones report additional funding from the UK Clinical Research Collaboration. Andy Jones is a member of the Research Funding Board of the National Institute for Health Research (NIHR) Public Health Research programme. Nanette Mutrie reports additional funding from the NIHR.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2017. This work was produced by Ogilvie et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Urban regeneration and public health
A variety of urban regeneration initiatives have been pursued in recent decades, often driven by a view that promoting economic growth is key to improving the health and prosperity of deprived urban populations. Urban regeneration refers to myriad activities, including housing improvements, broader changes to neighbourhood public spaces and other forms of inward investment. 1 The case for such interventions is consistent with a social ecological model of health in which economic conditions, as well as physical and social environments, are seen as important influences on the health and well-being of individuals and populations. 2–4 Research indicates that some forms of urban regeneration do indeed have the potential to improve the well-being of local residents. 5–7 However, the evidence that such initiatives have produced the economic or population health outcomes claimed for them in practice is far from conclusive, and different aspects of urban regeneration may have different effects. 8,9 Urban regeneration in deprived neighbourhoods may have further implications for health inequalities, as deprivation is itself associated with poorer health and well-being. 10,11 Previous regeneration projects have been associated with modest improvements in socioeconomic outcomes, but the effects were not larger than corresponding national trends. 8
Urban mobility, transport infrastructure and public health
One specific approach to improving access to employment, education and other opportunities involves increasing people’s mobility. However, the societal costs attributable to traffic congestion, poor air quality, physical inactivity, injuries, noise and other impacts of motor transport in English urban areas have been estimated at £40B per annum. 12 Furthermore, the benefits and harms of a pattern of mobility dominated by motor transport are inequitably distributed. Serious injuries to child cyclists and pedestrians are three and four times more frequent, respectively, in the most deprived areas of England than in the least deprived, and people without cars make fewer trips than those with cars, but travel 50% further on foot. 13,14 Less affluent groups or areas are therefore disadvantaged in terms of overall mobility and injury risk, although they may gain benefits from additional physical activity as a result.
Physical activity is important for health and well-being, and can help to prevent a wide range of non-communicable diseases,15 whereas sedentary behaviour is associated, independently of physical activity, with both cardiovascular and all-cause mortality. 16–18 Physical inactivity and sedentary behaviour are particularly prevalent in more affluent countries; the UK data included in a recent global study suggest that 63% of the population is physically inactive,19 and other data suggest that British adults sit for an average of 5.5 hours per day. 20
Recently, research and policy attention has been drawn to the potential of active travel (walking or cycling for transport) to contribute to daily physical activity and to promote good health. 21–23 Active travel can become a habitual, sustainable part of everyday life, as well as having important co-benefits such as helping to limit carbon emissions through reduced reliance on motorised transport. 24 In tandem, reducing car use has been identified as an important policy objective because of the relationship between motor vehicle use and poor health via physical inactivity, air pollution and injuries from road traffic accidents. 25–27 Reducing car use has also been promoted on equity grounds. People from lower socioeconomic backgrounds are less likely to have access to motor vehicles, but deprived areas bear a disproportionate burden of traffic-related injuries and air pollution. 28 A population shift towards more sustainable transport offers a potentially winning combination of an increase in physical activity coupled with reductions in traffic congestion and use of fossil fuels, and is therefore increasingly regarded as desirable on public health, environmental and equity grounds. 29
Physical activity and sedentary behaviour are partly shaped by local physical environmental conditions, such as the availability of recreational facilities and infrastructural design. 4,30 Although cross-sectional studies indicate associations between features of the built environment and both physical activity31,32 and sedentary behaviour,33 there is little longitudinal evidence to show whether and how changing the environment changes these behaviours. In particular, in a series of systematic reviews, we have shown a lack of good evidence from intervention studies as regards how to achieve this;34–36 National Institute for Health and Care Excellence (NICE) guidance has drawn particular attention to a lack of robust controlled longitudinal studies of the behavioural impacts of environmental changes,37,38 and a House of Lords report has identified a specific need for more evidence on the effects of interventions on car use. 39
One particularly contentious type of intervention is the construction of new major roads. On the one hand, infrastructure projects of this kind may improve mobility, including improving (road) access to more distant recreational amenities, which may facilitate their use for physical activity40 and may contribute to the economic revival of local communities. On the other hand, they have the potential to degrade the local environment, contributing to a process of ‘deprivation amplification’41 in vulnerable communities and widening existing inequalities. Exposure to roads and traffic has been shown to contribute to noise disturbance and severance, whereby residents are separated from the amenities that they use (such as shops and parks) or their interpersonal networks and social contacts are disrupted. 42–44 Other studies indicate an association between noise disturbance from traffic45 or living in industrial areas characterised by noise disturbance and air pollution46 and poorer quality of life or well-being. Furthermore, providing new or improved major roads has been shown to increase traffic47 and may contribute to making sedentary travel by car a more attractive option,26 and more traffic in local streets may make it less safe and attractive for people to be physically active outdoors, thereby promoting increases in other more sedentary activities. 48 In contrast, a growing body of evidence suggests that changes to the environment such as traffic calming, charging road users and constructing routes for walking or cycling can be effective in promoting active travel. 37,49,50
Egan et al. 51 showed in a systematic review that new major roads in urban areas are associated with noise disturbance and severance effects. However, that review found no evidence for the effects on physical activity or health inequalities, and little evidence to support a common assertion that new roads reduce the incidence of injuries. In the decade since that systematic review was completed, we are not aware of any new longitudinal studies examining the effects of motorways on physical activity, sedentary behaviour or well-being in local residents.
The extension of the M74 motorway in Glasgow
The intersection between urban mobility, transport infrastructure and public health is exemplified in Glasgow, a conurbation characterised by extremes of affluence and deprivation.
A longstanding project to extend the 1960s urban motorway network was resurrected by the new Scottish Government following devolution in 1999. The new motorway was intended to relieve congestion on the M8, an existing motorway built in the 1960s, which traverses the city centre. It also formed part of a wider strategic initiative to regenerate the ‘Clyde Gateway’ area, and changes in the local built environment were not limited to motorway construction. As described in more detail in Chapter 2, Characterising the environmental changes and refining the study design, the core of the intervention comprised the construction of a new 5-mile, six-lane section of motorway, which is mostly elevated above ground and runs through a predominantly urban, deprived area of south-east Glasgow. This was associated with a variety of changes to the urban built environment, including the insertion of highly visible viaducts and embankments, as well as junctions and slip roads intersecting with local streets in residential areas; the realignment of feeder roads; and the redevelopment of former open space, the demolition of old housing stock and the construction of a new residential development on a brownfield site adjacent to one of the new motorway junctions.
Numerous health-related claims were made for and against the new motorway. It was claimed that the new motorway would relieve congestion, improve conditions for pedestrians and cyclists on local streets, reduce traffic noise and bring new local employment opportunities, helping to regenerate some of the most deprived and least healthy urban communities in Europe. Objectors claimed that the new motorway would largely benefit freight traffic and workers and other motorists from outside the local area, and would encourage car use, degrade the quality of the local environment, and reduce the safety and attractiveness of local routes for pedestrians and cyclists. We summarised these issues into contrasting narratives and articulated them as two equally valid, competing, testable, overarching hypotheses about the effects of the intervention, expressed in the form of vignettes of two alternative extreme cases, a ‘virtuous spiral’ and a ‘vicious spiral’ (Table 1). 52,53
| Virtuous spiral | Vicious spiral |
|---|---|
| The opening of the motorway encourages inward investment to the area, providing new local opportunities for work | The opening of the motorway displaces some local businesses, whose employees now have to travel further to work, and gives easier access between the motorway network and the local area |
| Traffic on local roads is reduced, which makes conditions more pleasant for pedestrians and cyclists, and encourages people to spend more time out and about on local streets | This increases traffic on local roads and encourages local people to travel further and by car, not just for work but also for shopping and leisure |
| Local businesses thrive | At the same time, the motorway and its junctions degrade the local environment, making conditions less pleasant or safe for people in their homes and for pedestrians and cyclists |
| People perceive the local environment to have more positive attributes | The combination of fewer people out and about on local streets and the tendency to travel further afield to amenities leads to a decline in local shops and other amenities, which reinforces the decline in the attractiveness of the area and the car-bound exodus in search of alternatives |
| Any noise or air pollution produced by the motorway is not noticed against the background of existing urban conditions | |
| The well-being of local people and opportunities for physical activity both increase |
An independent Public Local Inquiry (PLI) in 2003 considered the arguments for and against the construction project. The inquirers concluded that the claimed benefits were likely to be ‘ephemeral’ and that the new motorway ‘would be very likely to have very serious undesirable results’ for local communities, and, therefore, recommended against the proposal. 54 With this advice having been overruled by the government of the day, construction began in 2008 and the motorway was finally completed and opened to traffic on 28 June 2011 at an eventual cost of approximately £800M. The intervention was funded by a public-sector partnership comprising Transport Scotland, Glasgow City Council, South Lanarkshire Council and Renfrewshire Council, and was delivered by Interlink M74 Joint Venture, a consortium of civil engineering contractors.
The new motorway runs between Tradeston (close to Glasgow city centre) and Cambuslang (on the south-east edge of the city), passing through or adjacent to several established residential areas such as Govanhill, Toryglen and Rutherglen: some homes are < 50 m from the carriageway (Figure 1). The most affected neighbourhoods are among the most deprived in the UK, reflecting a local history of rapid deindustrialisation in the late twentieth century. Car ownership is low, and part of the route lies in the Shettleston constituency, which at the time of construction had the lowest life expectancy for males in Scotland (68.2 years): > 7 years below the national average.
FIGURE 1.
Route of the M74 extension. Contains Ordnance Survey data © Crown Copyright and database right 2016.

Rationale and approach for the study
The opening of the M74 extension presented an opportunity to examine the health impacts of a new major road infrastructure in a natural experimental study, using the developing situation in Glasgow to understand more about the positive and negative effects of the changes to the urban landscape from which more general lessons could be learned for the planning and implementation of future initiatives. In anticipation of the planned motorway extension, a baseline cross-sectional study was carried out in 2005. This study included a postal survey of travel and physical activity behaviour, neighbourhood perceptions and general health and well-being in adult residents of the intervention area, and two matched control areas in Glasgow and a preliminary qualitative interview study. Contact was maintained with the original study participants by means of annual mailings, and the baseline study produced a Doctor of Philosophy thesis,55 four scientific publications,52,56–58 and hypotheses and research methods to inform the follow-up study described in this report. Key baseline findings included the observations that access to local amenities was the most significant quantitative local environmental correlate of active travel;57 that the new motorway might cause inequitable psychological or physical severance of routes to those amenities, for example by reducing the perceived safety of walking routes to local shops;58 and that people might not use local walking routes or destinations such as parks and shops if these were considered undesirable, unsafe or ‘not for them’. 58 The follow-up study built on our previously collected baseline data to examine if and how a major set of changes to the urban environment affected key aspects of the health and health-related behaviour of the local population.
It is not easy to parse urban regeneration ‘interventions’ into their components and establish causal relationships with behaviour or health, because such interventions are typically both complex and ill-suited to evaluation using randomised study designs. However, they can be seen as natural experiments, that is, interventions that are not designed for research purposes but that can nevertheless be used to evaluate the population health impacts of environmental or policy changes over time. 59 Interventions of this kind are often not primarily intended to improve health, although health-related claims were implicit in the case of the M74 extension and subsequently aired explicitly by both proponents and opponents of the project (see Table 1). The indirect or implicit nature of these health effects poses a problem if evaluation research is understood in simple terms of ‘what works?’ or, in other words, whether or not an intervention has achieved its stated aims and objectives. In this context, it may be at least as important for public health researchers to focus on investigating indirect or unintended effects on aspects of health and well-being of particular interest. No research study could conceivably evaluate effects across all possible domains identified in the public discourse about the motorway. We therefore chose to focus on the comparatively under-researched questions of the effects of this type of major change to the urban landscape on active travel, physical activity, sedentary behaviour, road traffic accidents and well-being, while acknowledging the potential importance of other effects – notably on employment and the economy – that were beyond the scope of our study.
Main research questions
The aims of the study were to address the following primary research questions:
-
What are the individual, household and population impacts of a major change in the urban built environment on travel and activity patterns, road traffic accidents and well-being?
-
How are these impacts distributed between different socioeconomic groups?
The study also aimed to address the following secondary research questions:
-
What environmental changes have occurred in practice?
-
How are the effects of the environmental changes experienced by local residents?
-
How are any changes in behaviour or well-being mediated and enacted at individual and household levels?
This report
This report summarises a considerable body of research, some of which has already been published – or submitted or prepared for publication – in other open-access academic journals, and to which an extensive study team has contributed in various ways (see Acknowledgements). Further details of the methods and results of the various analyses summarised in the report can be found in these publications, which are referred to in the text and are available via the Centre for Diet and Research Activity (CEDAR) study website (www.cedar.iph.cam.ac.uk/research/directory/traffic-health-glasgow). 60
Chapter 2 Study design and methods
Introduction
In this chapter, we describe the development of our final study design and methods. We begin by describing the key geographical areas, populations and outcomes of interest, after which we outline our specific study objectives and overall study design. We then describe the methods and results of a series of activities to characterise the specific environmental changes that had been proposed and that actually occurred, along with discussions and interviews with relevant stakeholders to develop a preliminary understanding of issues currently of concern in local communities, including views about the motorway’s environmental and economic impacts. Together, these activities laid the groundwork for the final, realised study design. The remainder of the chapter is devoted to describing the sampling and data collection methods, the derivation of variables and the overall approach to analysis.
Overall research design
In this section we describe the population and outcomes of interest, the study objectives and the overarching study design and logic model.
Study population and outcomes
To address the questions outlined in Chapter 1, Main research questions, we conducted a mixed-method longitudinal study with the elements outlined in Table 2.
| Study design element | Operationalisation |
|---|---|
| Population | Householders living close to the route of a new urban motorway |
| Intervention | Construction of a new urban motorway |
| Comparator | Householders not living close to the route of a new urban motorway |
| Primary outcomes | (1) Walking for transport, (2) cycling for transport, (3) car use and (4) MVPA within the neighbourhood |
| Secondary outcomes | (1) Road traffic casualties, (2) perceptions of the neighbourhood environment, (3) well-being and (4) overall MVPA |
We combined this with the analysis of routinely available population data on road traffic accidents and travel behaviour.
Objectives
The objectives of the study were:
-
to characterise the context, content and implementation of the intervention by means of an environmental survey
-
to follow up a cohort of residents of the intervention and control areas had who previously responded to a postal survey at baseline [2005; time point 1 (T1)]
-
to draw new repeat cross-sectional samples of residents of the intervention and control areas for a postal survey at follow-up [2013; time point 2 (T2)]
-
to objectively measure the travel and activity patterns of a subsample of survey participants
-
to estimate changes and differences in the primary and secondary outcome measures between the intervention and control areas, and by level of exposure to environmental changes within those areas
-
to examine the extent to which any changes in outcomes were mediated by changes in perceptions of the neighbourhood environment
-
to examine the extent to which any changes in behavioural outcomes were associated with changes in well-being
-
to interview a further subsample of participants to elicit how the effects of the environmental changes were experienced by local residents and how any changes in behaviour or well-being were mediated and enacted at individual and household level
-
to examine changes in the incidence and sociospatial distribution of road traffic accidents on the road network
-
to explore trends and spatial variation in travel behaviour using existing national population data sets
-
to examine the extent to which the results of the different analyses supported either of the two competing overall hypotheses regarding the cumulative effects of the intervention (see Table 1).
Study design
The study used a combination of quantitative [cohort, cross-sectional, repeat cross-sectional and interrupted time series (ITS)] and qualitative (documentary analysis and interview) research methods to evaluate both individual- and population-level changes in health and health-related behaviour, and to develop a more in-depth understanding of how these changes were experienced and brought about.
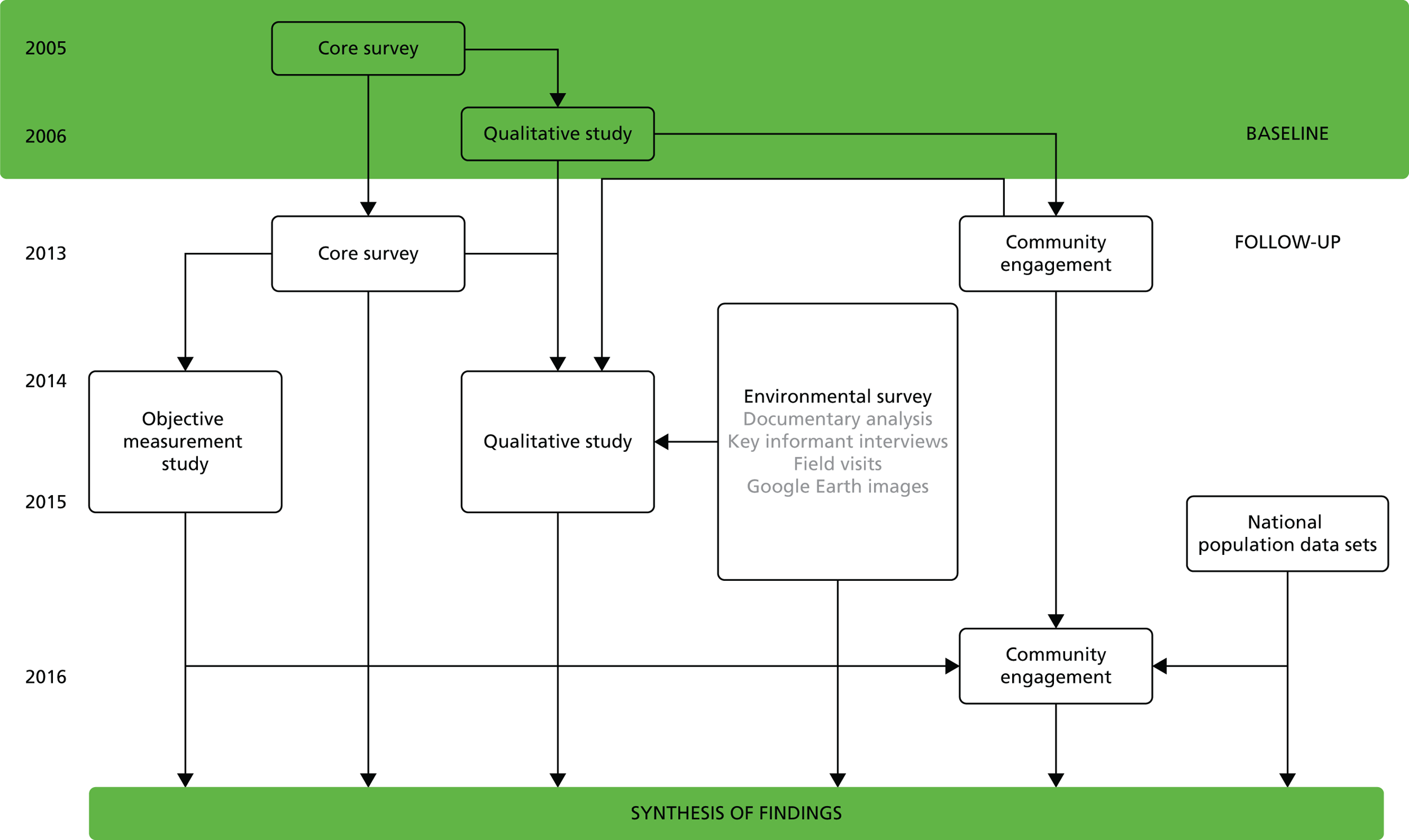
The study comprised six main components (Figure 2):
-
an environmental survey consisting of documentary analysis, interviews with key informants, field visits and use of Google Earth (Google Inc., Mountain View, CA, USA) images (objective 1)
-
core surveys of local study areas to compare changes in neighbourhood perceptions, travel behaviour, physical activity and well-being in the intervention and control areas by means of combined cohort and repeat cross-sectional follow-up surveys of local residents (objectives 2, 3, 5, 6 and 11)
-
an objective measurement study of a subsample of core survey participants to quantify any differences in physical activity between intervention and control areas (objectives 4, 5, 6 and 11)
-
a qualitative study of a subsample of core survey participants to elucidate their experiences of environmental changes and the mechanisms through which these may have influenced behaviour (objectives 7, 8 and 11)
-
an analysis of existing national population data sets to evaluate the impact of the intervention on road traffic casualties and to describe concurrent regional and national trends in travel behaviour (objectives 9–11)
-
running alongside all other components, a programme of community engagement to help shape the final study design, elicit a wider range of accounts and develop a shared understanding and interpretation of the emerging findings (objective 11).
FIGURE 2.
Study components.
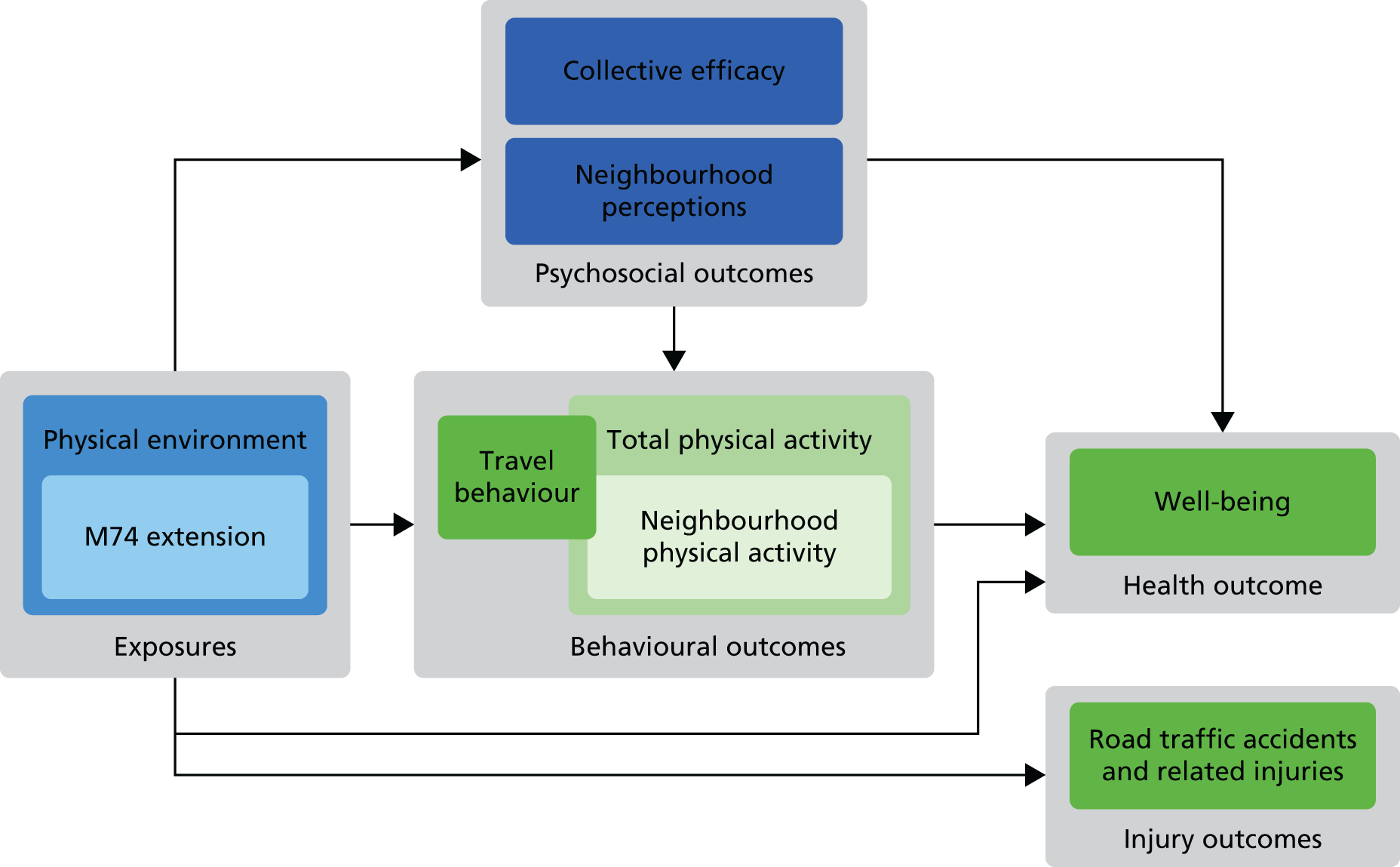
Logic model
As discussed in Chapter 1, we summarised the contrasting narratives about the motorway into vignettes describing two competing overarching hypotheses about the effects of the intervention. In order to operationalise the relationships of interest and refine our analytical priorities, these were further developed into an overarching logic model describing the main putative causal relationships to be investigated at follow-up (Figure 3).
FIGURE 3.
Overarching logic model.
Study areas
At baseline, three local study areas were defined: the ‘M74 corridor’ intervention area (South) and two control areas, one of which surrounded the existing M8 and M80 motorways (East) and one of which had no comparable major road infrastructure (North) (Figure 4). These study areas were carefully and iteratively delineated at baseline using spatially referenced Census and transport infrastructure data combined with field visits to ensure similar aggregate socioeconomic characteristics and broadly similar topographical and urban morphological characteristics apart from their proximity to urban motorway infrastructure (Table 3). 55 Baseline analysis confirmed no significant differences between the achieved survey samples in these three areas on any socioeconomic or behavioural summary measures apart from a minor difference of borderline statistical significance (p = 0.053) in the distribution of housing tenure. 57 All three study areas extend from inner mixed-use districts close to the city centre to residential suburbs, contain major arterial roads other than motorways and contain a mixture of housing stock including traditional high-density tenements, high-rise flats and new housing developments.
FIGURE 4.
Study areas for the core survey. Contains Ordnance Survey data © Crown Copyright and database right 2016.
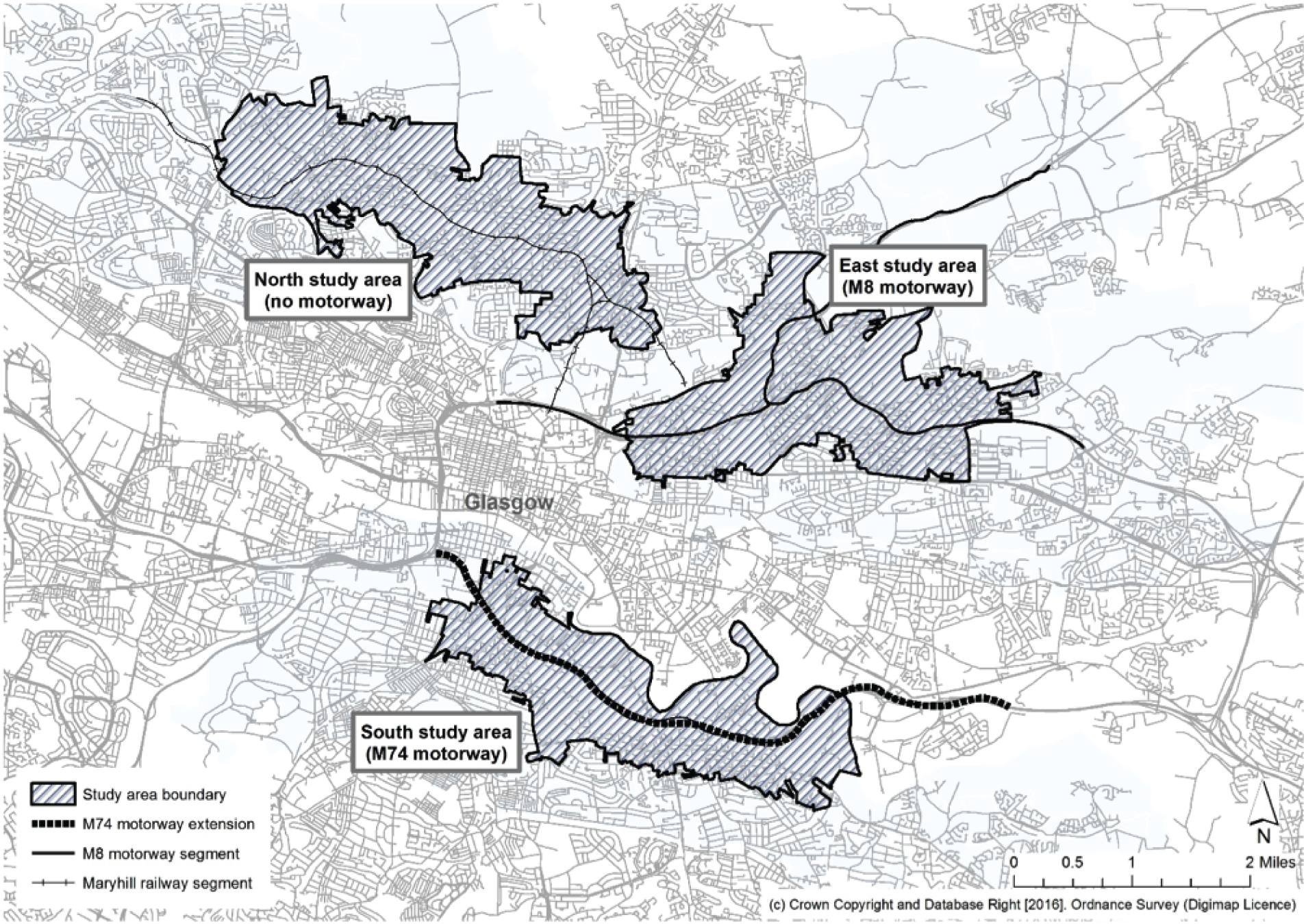
| Study area | Definition |
|---|---|
| South | A set of Census output areas encroaching within 500 m of the proposed route of the new M74 motorway |
| East | A set of Census output areas encroaching within 500 m of the routes of the existing M8 and M80 motorways |
| North | A set of Census output areas encroaching within 500 m of the route of the railway between Cowlairs and Maryhill and not encroaching within 500 m of the route of any existing or proposed motorway |
Characterising the environmental changes and refining the study design
In this section, we describe the environmental survey and preliminary community engagement (components 1 and 6 of the study design described in Overall research design), in which we aimed to understand more about the context, content and implementation of the intervention, thus addressing research question 3. This process consisted of (1) a documentary analysis; (2) preliminary community and stakeholder engagement, leading to (3) a series of in-depth interviews with key informants; and (4) field visits combined with the analysis of current and historic aerial imagery in the public domain. This information informed the final study design, outlined in the remainder of this chapter.
Documentary analysis
During the pre-construction planning and consultation phase, two key public documents outlined the proposal for the M74 extension and described its potential effects. The first of these, the Environmental Impact Assessment (EIA), was published in December 2003. 61 This document, led by proponents of the scheme within the Scottish Executive, outlined the plans for the new motorway and detailed the hypothesised positive and negative impacts on traffic flows, the environment and the community in the immediate area. After a significant number of objections to the compulsory purchase orders for land required for the scheme, and general public protest, an independent PLI was conducted by a senior planner within the Scottish Executive. The second key document, the report of findings from the inquiry, was published in March 2005. 54
To analyse and compare these two documents, the hypothesised impacts of the new motorway were organised according to the categories defined by the EIA and broadly used by the subsequent PLI (Table 4). As described in Chapter 1, Rationale and approach for the study, the study was limited to examining selected impacts of living near a new urban motorway. Further work on the environmental survey was therefore focused on the categories of impact that were most relevant and feasible for our study:
-
land use and landscape appraisal
-
visual impacts
-
noise and vibration
-
pedestrian and other community effects
-
economic effects.
| Impact | Explanation |
|---|---|
| Planning policy | Alignment of the new motorway with published transport or other policy aims (e.g. road construction, public transport, economic development, social justice) |
| Land use | Original land uses in the area lost to motorway construction (e.g. green space, wildlife corridors, industrial, residential) and the impact of these changes in land use |
| Geology, soil and contaminated land | Impacts on the environment resulting from the disturbance during motorway construction of land previously contaminated by industry |
| Water quality and drainage | Impacts on water quality attributable to road runoff or flooding, and proposed drainage systems |
| Ecology and nature conservation | Destruction of animal or plant habitats and the impact on local biodiversity and endangered species |
| Landscape appraisal | Temporary and permanent impacts on the character of the area through which the new motorway passes |
| Visual impacts | The visual effect of the new motorway, given that it is elevated above the townscape for much of its length |
| Cultural heritage | Destruction or demolition of sites of archaeological and cultural interest close to the new motorway |
| Disruption owing to construction | Impacts limited to the construction period, including traffic disruption, noise and vibration |
| Noise and vibration | Impacts related to ongoing traffic noise from the new motorway, mainly for nearby residential properties |
| Air quality | Impacts on air quality from dust and pollutants from the new motorway |
| Pedestrian and other community effects | Impacts on community journeys made by pedestrians and cyclists including severance effects attributable to increased traffic and the need to cross slip roads and junctions |
| Vehicle travellers | Impacts on travel time and stress for drivers on the new motorway |
Where a distinction was made between impacts predicted in the short term (e.g. 1 year) and in the long term (e.g. 15 years), our documentary analysis focused on the short-term impacts because these were more congruent with the time frame of our study, which examined impacts approximately 2 years after the opening of the new motorway. Although disruption attributable to the construction period was potentially relevant to our study, we had no way of verifying such impacts because we were unable to collect data during construction and, therefore, did not explore this category of impact further in the documentary analysis. Effects on vehicle travellers were important, in that changes in travel times may have influenced travel decisions. However, the measurement of traffic flows was beyond the scope of our study and was therefore not explored further in the documentary analysis. The potential economic effects of the new motorway were mostly explored with reference to the PLI, because this topic was not covered in detail in the EIA.
The two documents examined projected impacts in a number of key local areas in the M74 extension corridor (Figure 5).
FIGURE 5.
Key local areas in the M74 corridor. Contains Ordnance Survey data © Crown Copyright and database right 2016.

Findings from documentary analysis
Land use and landscape appraisal
The EIA emphasised a general pattern of potential adverse effects on residents at the western end of the development (notably in Tradeston and Eglinton), the demolition of existing commercial and industrial sites through the middle of the development, and the loss of green space, particularly in Auchenshuggle Woodland, at the eastern end of the development. The PLI described the majority of potential adverse impacts on townscapes as being concentrated in four residential areas: Eglinton, Toryglen, Rutherglen and Farme Cross. These residential areas would bear a combination of effects, including community severance, visual intrusion and noise.
Visual impacts
The projected visual impacts were considerable, as the new motorway is elevated above the townscape for much of its length. The EIA predicted adverse visual impacts in varying degrees across the entire development, with the most substantial occurring in Eglinton and Rutherglen and where the motorway crossed the River Clyde. In the long term, some potential beneficial impacts were described, whereby new planting associated with the scheme would replace existing views of derelict land or industrial estates.
Noise and vibration
The EIA assumed that a number of mitigation strategies would be in place to combat noise and vibration from the motorway, including low-noise road surfacing and noise barriers. Despite the mitigation strategies, the EIA predicted ongoing major adverse noise impacts in Toryglen. Modest positive benefits were predicted on certain streets in Eglinton and Rutherglen because of forecast traffic reductions on these streets. The PLI further commented that the River Clyde walkway and cycleway had not been included in the noise assessment presented in the EIA. However, this semi-rural area was remote from main roads, and the construction of the new motorway across the River Clyde could therefore result in significant adverse noise impacts.
Pedestrian and other community effects
The EIA described an existing north–south divide between communities on either side of the West Coast Mainline railway. The EIA summarised key intercommunity pedestrian journeys and identified the routes used to undertake these journeys. Rutherglen and Govanhill were identified as two communities attracting inward journeys from neighbouring communities because of their high concentration of facilities. These journeys would often, but not always, involve crossing the railway line.
The new motorway follows the West Coast Mainline for much of its length and, therefore, crosses existing roads that provide important north–south pedestrian linkages between the communities on either side. Although it does not physically sever any of these links, because crossing points such as underpasses are provided, pedestrians are nevertheless now required to pass over or under the new motorway.
The main proposed adverse severance effects on pedestrian journeys were at the site of the new junctions, because of the need to cross the new slip roads and increased traffic on these roads. This would be particularly salient for those with mobility difficulties. The EIA also proposed some severance relating to reluctance to use the new underpasses owing to unpleasantness or safety concerns, which would be heightened at night. However, beneficial effects on pedestrian journeys were projected on certain streets, particularly in Rutherglen, because of a forecast reduction of traffic on these streets.
The PLI agreed that these severance effects would occur and predicted that they would be substantially more serious than outlined in the EIA, to the extent that they would ‘devastate communities’ on either side of the M74. In particular, travel between Farme Cross and Rutherglen was identified as a key community journey on which severance effects would occur. In addition, pedestrian journeys on local streets would become more difficult and hazardous because of increased traffic flow on slip roads.
The PLI further explored the wider effects of M74 construction on social inclusion and environmental justice, which were not covered in the EIA. The PLI noted that, owing to a comparatively low level of car ownership, the motorway would be of limited use to the local population. Increased provision for car users would undermine the provision of public transport options, leaving those without cars ultimately more disadvantaged. Those who did own cars might subsequently travel further afield to access facilities, which would undermine local community facilities and further increase inequalities. The PLI criticised the use of public funds for the scheme, commenting that they might have been better spent on public transport and direct assistance for disadvantaged communities.
Economic effects
One of the key objectives of the motorway was to stimulate wider economic regeneration in the local area. Although this was mentioned only briefly in the EIA, the PLI examined the proposed economic benefits of the M74 construction. The key potential benefits identified were short-term employment during construction, time savings for vehicle journeys, cost savings from reduced vehicle accidents and associated injuries, the redevelopment of nearby vacant or derelict sites near the new motorway and the provision of new local jobs at these sites. However, the PLI highlighted the uncertainty of these effects on long-term economic regeneration, and identified potential adverse effects on the local economy, whereby loss of employment or income would arise from the demolition of existing industrial and commercial sites.
Discussion
The primary purpose of the M74 extension was to relieve traffic congestion on other motorways and main roads, particularly the M8 motorway. Both the EIA and the PLI agreed that it was likely to produce an initial reduction in traffic congestion, amounting to an average 5- to 10-minute reduction in journey time during peak periods. However, the documents differed in their prediction of the longevity of these effects. The EIA predicted that beneficial effects would remain until 2020 and beyond, whereas the PLI described a gradual erosion of these benefits owing to increasing traffic and increasing attractiveness of car journeys. Although the measurement of traffic flows was beyond the scope of our study, projected impacts of this kind were nonetheless important because they had been used to justify the construction of the new motorway on the assumption that the beneficial effects on congestion would outweigh the considerable drawbacks for those living nearby identified in both documents.
For the most part, the EIA and PLI were in agreement on the nature and scale of both positive and negative probable impacts of the new motorway on the landscape, visual and noise effects, and severance in the local area. The PLI identified additional potential positive and negative effects on the local economy. However, the EIA and the PLI fundamentally disagreed on whether or not the long-term benefits on traffic and congestion were sustainable and, therefore, on whether the benefits of the new motorway would outweigh the harms. The PLI concluded that the distribution of benefits and drawbacks was both unequal and inequitable, that the claimed benefits were likely to be ‘ephemeral’ and that the new motorway ‘would be very likely to have very serious undesirable results’ for local communities. 54
Preliminary community and stakeholder engagement
A complementary programme of community and stakeholder engagement ran alongside the study. This was brokered by the Glasgow Centre for Population Health (GCPH) and the Scottish Community Development Centre (SCDC), which are established centres working with community organisations in Glasgow. Between March and May 2013, initial contact was made with 18 key organisations in the M74 corridor, the interests of which may have been affected by the new motorway. These included local housing associations, development trusts, community councils, residents’ associations and public-sector development agencies. Organisations were invited to comment on whether or not any issues associated with the new motorway were of importance to local communities, and, if so, what these issues were. The process and outcomes of subsequent community and stakeholder engagement in the study are described in Chapter 8.
Findings from preliminary community and stakeholder engagement
For most of the organisations approached, the agenda had moved on and the M74 extension was not seen as an issue of concern, although in several cases organisations reported that they had originally been opposed to the development. A single community organisation in Eglinton that owned housing stock directly overshadowed by the new motorway reported ongoing issues with noise, dirt and deterioration in neighbourhood quality. In contrast, for several of the organisations the new motorway was regarded as having had a beneficial effect on neighbourhood quality, particularly where it acted as a bypass for streets that were previously congested (e.g. in Rutherglen town centre). In addition, a number of the organisations saw it as having facilitated other developments, each of which may have had a positive or negative effect on local quality of life and opportunities, particularly for employment. These included the development of the site for the 2014 Commonwealth Games and other industrial, commercial and housing developments near the new motorway.
Interviews with key informants
The interviews with key informants were intended to provide an overview of the environmental, economic and social impact of the new motorway. Informants were recruited purposively, based on their involvement with the local groups identified through the preliminary community engagement described in the previous section in combination with snowball sampling. Informants represented a variety of organisations, including local development groups, local community councils, local housing associations, local charities, organisations involved in the planning and development of the motorway and an anti-M74 protest group [Joint Action against M74 (JAM74)].
Between March 2014 and April 2015, information sheets and invitations were either e-mailed or posted to key informants’ organisations and followed up by either e-mail or telephone call. In cases in which an individual informant had already been identified by initial community engagement work, that informant remained the contact for that group. Twenty-five invitations were sent and 12 key informants consented to take part.
Key informant interviews were carried out using a semistructured format, based on a topic guide that could be applied flexibly to informants’ varying roles and levels of involvement with the local area. As key informants held a variety of roles, some were able to give an overview of issues, whereas others addressed local changes in more specific detail. Interviews were conducted in a variety of locations depending on the informants’ preferences, including their homes, places of work, cafés and the offices of the Medical Research Office/Chief Scientist Office (MRC/CSO) Social and Public Health Sciences Unit. All but one were recorded using a digital voice recorder and transcribed verbatim. One participant declined to be recorded; their interview was attended by two researchers, of whom one conducted the interview and the other wrote notes that formed the material for subsequent analysis. These key informant interviews were much more specifically focused on the M74 than the main programme of qualitative research with local residents described in Chapter 7. The topic guide focused on a number of themes, including the impacts of the physical structure of the motorway and associated engineering features, and its wider economic impacts (see Appendix 1).
Walkalong interviews, in which an interviewer and participant conduct their interview while walking through a particular space, were not originally envisaged as a method for interviewing key informants. However, two key informants suggested that they would be better able to address the main themes of their interview by showing their local area as well as describing it. We therefore conducted walkalong interviews with these two participants. More information on this method can be found in Evaluating the intervention.
Findings from interviews with key informants
Key informants were asked about their views on the environmental impacts of the motorway in general, as well as specific physical changes related to the structure of the motorway itself, including slip roads, embankments, junctions, viaducts and underpasses. Overall, views on the environmental impact of the motorway were mixed, with some key informants feeling that the motorway had been detrimental to the local environment and others feeling that it was a valuable part of local environmental regeneration. Specific impacts are discussed in more detail below.
Environmental impacts
Key informants’ views on the visual impact of the extension ranged between negative (‘ugly’ and ‘aesthetically, I think it’s awful’) and neutral (‘it’s had a reasonably minimal impact’). Perceptions of visual impact appeared to be related primarily to two factors: (1) how the new motorway looked in contrast to what had been there before; and (2) whether or not a particular section of the new motorway was elevated. A number of respondents mentioned that the new motorway sympathetically followed the existing line of the railway and was built on predominantly post-industrial, vacant or otherwise unattractive land, and therefore did not detract from a previously picturesque landscape. Others, however, felt that the motorway had visually ‘carved up’ the residential land and had added another unattractive feature to an already post-industrial residential landscape.
I mean, it’s not great to suddenly have these enormous concrete structures, particularly the flyovers. But on the other side, a lot of the land is now being developed as a result, you know, and wasteland versus, I suppose, not magnificent architecture but something happening as opposed to wasteland I think is good.
Key informant, local development trust
In areas where the motorway was elevated, key informants were more likely to describe negative visual impacts and, in particular, several of them drew attention to areas where they felt this visual disturbance was most acute, namely around Eglinton Street and Devon Street, and around the junction at Tradeston. In areas where the motorway was not elevated, however, key informants were more likely to describe visual disturbance as minimal.
Perceptions of pollution from noise and fumes were also related to whether or not the motorway was elevated and whether or not it was perceived to have diverted traffic away from local streets. A number of key informants felt that the new motorway had been highly successful in achieving the latter in certain areas, to the benefit of local people; however, there was less consensus about whether or not this had occurred in Govanhill. In streets such as London Road that were described as having experienced a significant decrease in traffic, the area was described as now being ‘lighter and more open’ as well as more appealing and safer for active travel. In other areas such as Rutherglen, some key informants drew attention to a recent Friends of the Earth report publicised in the media, indicating high levels of pollution in Rutherglen Main Street:
I think most damaging of all is the area around Rutherglen. I mean, it’s obviously not criminal in a legal sense but I think what was done there was very, very poor. [. . .] I mean, it’s an urban motorway – but it’s very, very close to the community of Rutherglen and now people are wringing their hands about the air quality in the Main Street. Well, you know, it’s stating the bleeding obvious.
Key informant, local community council
There seemed to be a lack of consensus around whether the motorway had reduced pollution in these areas by diverting traffic from (some) local streets or if pollution from traffic had merely been shifted to the motorway, which was sufficiently close to these areas to be a cause for concern. Several key informants called for detailed evidence on pollution to be gathered as a key indicator in evaluating the motorway’s impact. In addition, key informants discussed existing contaminated land related to the area’s industrial past. Several key informants felt that the construction of the M74 extension had been instrumental in ‘capping’ and covering up a number of pieces of land contaminated with industrial waste, whereas others had concerns that industrial wastes in the soil had been disturbed by the building process.
In terms of noise, negative impacts on the tranquillity of natural green spaces were described by several key informants, with particular reference to Malls Mire woodland in Toryglen (which is directly adjacent to the motorway) and Auchenshuggle Woodland to the east of Glasgow (through which the motorway runs; see Figure 5). However, the new motorway was also credited by one key informant with having being instrumental in creating the necessary accessibility to secure funding for a major new green space development, the Cuningar Loop.
Other aspects of the new motorway discussed by key informants included underpasses, which were described alternately as being ‘clean, modern . . . reasonably well lit’ or as being bare, unused spaces. Key informants discussed ideas for improving these spaces with interest, describing plans for urban parks, art works or well-planted green spaces. Existing planting along the new motorway was described as a positive aesthetic development by some, and as insufficient by others.
Although the majority of key informants agreed that the motorway had reduced journey times for car users, a few described the new motorway junctions as problematic, for example Polmadie junction near Govanhill, which was described as causing tailbacks in the local area at peak commuting times. Features such as slip roads were described as being mostly well designed, but with some problematic areas where traffic was required to filter abruptly into fewer lanes, causing tailbacks.
Key informants also described changes in both residential and industrial land use as a result of the new motorway. They discussed the removal of older housing stock as being related to the new motorway both directly (having been demolished to make way for the route) and indirectly (forming part of a broader regeneration plan). The creation of new housing (including the athletes’ village for the Commonwealth Games) was also discussed, with some key informants stating that the new motorway might attract new people (‘commuters’) and others stating that it might make journeys shorter for existing commuters. The attraction of new commuters to the area was described by one resident as having uncertain implications for community cohesion.
They also described a number of changes in industrial land use that they perceived to be related to the new motorway. Many of these were considered to be positive, for example the removal of an old processing plant [‘getting that bit of quite industrial stuff off their doorstep was quite nice’ (key informant, local development trust)] and the aesthetic overhaul undertaken by some companies that now found their premises directly overlooked by passing traffic. Other changes received a more mixed reception, such as a new recycling centre and incinerator, which was described by one key informant as facilitating the importation of waste from other areas [‘they’ve built it . . . right next to Govanhill ‘cos no one gives a shit about Govanhill’ (key informant, local development trust)]. Generally, several respondents felt that these new industrial developments were positive for the local economy, but others expressed concerns about encouraging more industrial development (reindustrialisation) in residential areas.
Economic impacts
The majority of key informants viewed the M74 extension as forming part of a package of economic regeneration that intertwined with other initiatives, including those associated with the Clyde Gateway development company and the Commonwealth Games. The new motorway was credited by some with making the area more accessible and therefore more attractive to investors, and one key informant considered it a factor that had helped their organisation to ‘ride out’ the recession. Several developments were described as already either in place or under construction, including new offices and the recycling facility mentioned previously. For the most part, key informants acknowledged the beneficial potential of these developments for local jobs, but some mentioned that this potential had yet to be realised. Others questioned the investment in road transport, wondering if a similar level of investment in active travel or public transport might have been preferable. It was acknowledged that the economic downturn, as well as a perception of instability that may have accompanied the Scottish independence referendum in 2014, may have contributed to slower than projected economic investment along the motorway corridor, and that a longer evaluation timeline might be needed to capture these potential benefits.
Competing changes
Key informants were also asked about any other changes that might have diminished, intensified, complicated or otherwise altered the effects of the new motorway on the local area. In addition to the changes referred to above, respondents also mentioned recent welfare reforms, initiatives encouraging local people to cycle and changes to the configuration of local streets.
Field visits and analysis of aerial imagery
In 2013, a member of the study team examined various aspects of the motorway infrastructure using Google Street View. In 2014, another member of the study team undertook several field visits to inspect the motorway and its relationship with the wider cityscape. Examples are shown in Figures 6–9.
FIGURE 6.
M74 extension crossing the Tradeston area on a viaduct. Photograph © Amy Nimegeer and reproduced with permission.

FIGURE 7.
M74 extension crossing the Eglinton area on a viaduct. Photograph © Amy Nimegeer and reproduced with permission.

FIGURE 8.
Noise barriers along the M74 extension at Rutherglen. Photograph © Amy Nimegeer and reproduced with permission.

FIGURE 9.
Underpass beneath the M74 extension at Rutherglen. Photograph © Amy Nimegeer and reproduced with permission.

The new motorway formed one component of a wider strategic initiative to regenerate the local area. We therefore wished to identify other concurrent major changes in the built environment. We developed bespoke software to display side-by-side aerial images of the same location taken at different times, using the Google Earth time slider function. The software allowed the operator to zoom the images and move them in tandem, comparing them in order to identify areas of difference and delineate each area with a polygon. The changes identifiable using this method included the construction or demolition of buildings, and the loss or gain of green space (Figure 10).
FIGURE 10.
Example of environmental change identified by comparing aerial images. (a) 2015; and (b) 2005. Source: Google Earth.


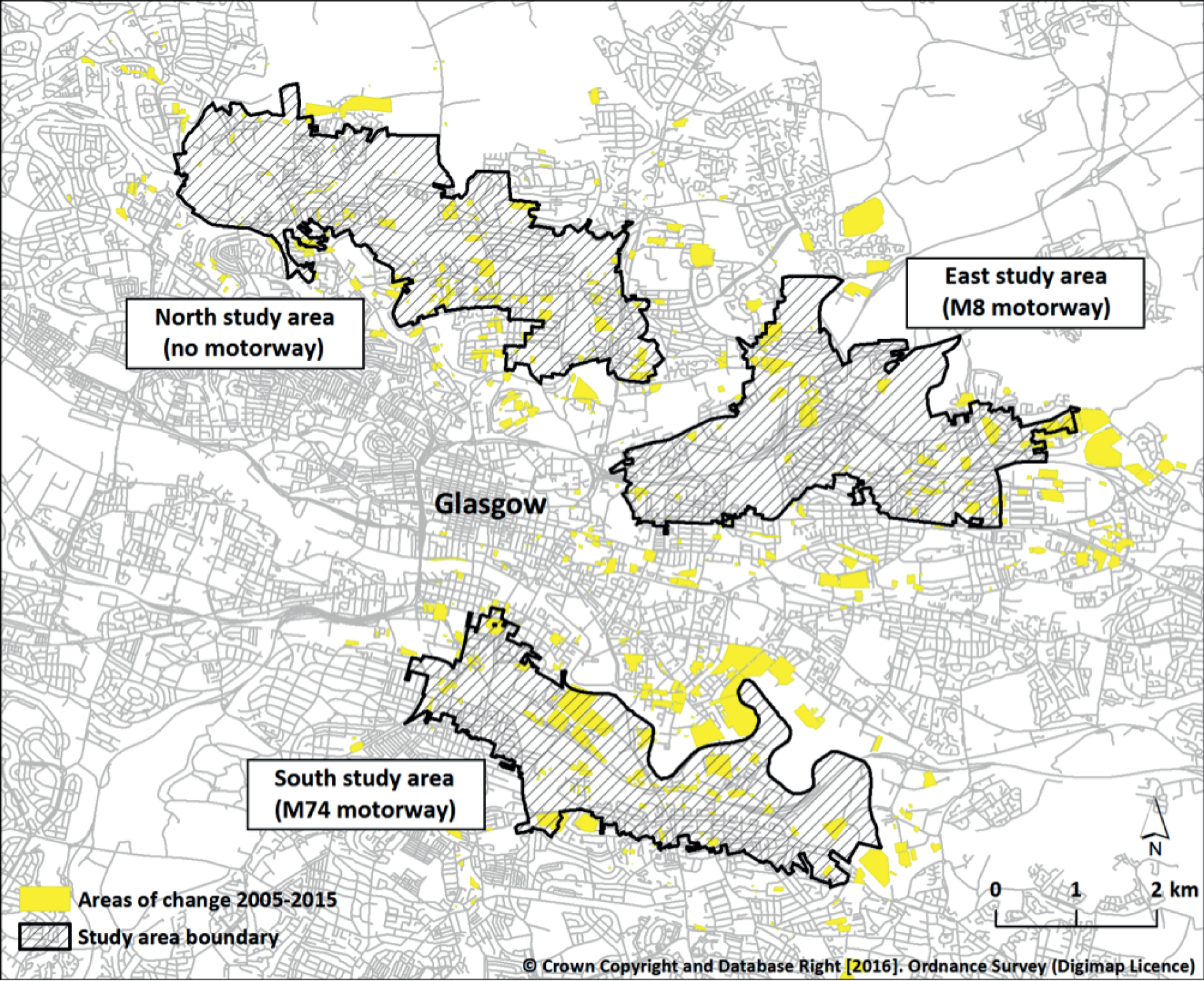
We used this method to identify (but not to characterise) all visible changes occurring between 2005 and 2015 in each of the three study areas and extending to approximately 1 km beyond their boundaries (Figure 11). As expected, large changes had occurred in the South study area during this time, but substantial changes were also identified in the other two areas.
FIGURE 11.
Areas of change within and surrounding the study areas. Contains Ordnance Survey data © Crown Copyright and database right 2016.
Evaluating the intervention
The information from the environmental survey further crystallised the relationships and outcomes of interest and contributed to shaping the final design of the study, particularly the qualitative fieldwork and analysis. In this section we describe the final study design in terms of the sampling and collection of data from participants, the derivation of variables and the overall approach to analysis.
Participant sampling
Core survey
Inclusion criteria
At baseline (2005; T1), eligible participants were adults aged ≥ 16 years residing in one of the three study areas, who responded to a postal survey delivered to their home address. If more than one householder was eligible, the individual with the most recent birthday was asked to complete the survey. At follow-up (2013; T2), eligible participants were (1) those who had responded to the postal survey at baseline, had not moved out of the UK, and responded to a subsequent postal survey at follow-up; or (2) adults aged ≥ 16 years residing in one of the three study areas, who responded to a postal survey delivered to their home address.
Recruitment
At both time points, eligible unit postcodes (the smallest unit of postal geography in the UK, corresponding to approximately 15 addresses on average) were identified for each of the three study areas. A random sample of 3000 private residential addresses in each area – 9000 in total – was drawn using the Royal Mail Postcode Address File. A survey pack was posted to each of these households, addressed to the householder. Participants were given the option to return a consent form giving permission to be contacted again in the future. Contact with these participants was maintained via yearly mailings between 2005 and 2012. At follow-up, a further 3000 postal surveys were issued in each study area. The recipients comprised all those baseline participants who could still be contacted, including those who had moved between or out of the study areas but not out of the UK, together with a newly drawn random sample of households to bring the total up to 3000 in each area. All follow-up participants were given the option to return a consent form giving permission to be contacted again for the objective measurement or qualitative substudies.
We followed evidence-based practice to maximise responses to the postal survey. 62 Potential participants were sent a notification postcard, which was followed by the survey 1 week later. The survey packs were posted in the first week of October at both time points, to account for potential seasonal variation in responses, and a repeat survey pack was sent to all non-responders approximately 1 month later. All mailings were staggered over multiple days to ensure that surveys were received and completed on a variety of days of the week. Responses received > 3 months after the first mailing were excluded from analysis.
Data collection
Core questionnaire
The core questionnaire collected information relating to demographic and socioeconomic characteristics and the main outcomes of interest: perceptions of the neighbourhood environment, travel behaviour, physical activity and sedentary behaviour, and well-being. In particular, it incorporated the following at both time points:
-
A 1-day travel record, adapted from similar instruments used in the Scottish Household Survey (SHS)63 and the National Travel Survey. 64 For each journey made the previous day, participants reported the purpose, the mode(s) of transport used and the time spent using each mode. Both single and multimodal journeys could be reported. Participants were asked not to report journeys made in the course of work, or purely for recreation.
-
The short form of the International Physical Activity Questionnaire (IPAQ), an extensively validated instrument in which participants estimated the number of days and the average daily duration of walking, moderate and vigorous physical activity, as well as the average daily time spent sitting, in the previous 7 days. 65
-
The Short Form 8 Health Survey (SF-8) scale, an extensively validated eight-item instrument assessing health-related quality of life in the previous 4 weeks. 66
-
A 14-item instrument assessing perceptions of the conduciveness of the neighbourhood environment for physical activity, developed for the study and assessed for its factor structure and test–retest reliability at baseline. 56
At follow-up, the following items were added to the core questionnaire:
-
The short version of the Warwick–Edinburgh Mental Well-being Scale (SWEMWBS), a seven-item instrument assessing positive mental well-being in the previous 2 weeks. The original long version of the instrument has been shown to have acceptable psychometric properties. 67,68
-
A nine-item instrument adapted from Sampson et al. 69 to assess collective efficacy, defined as the norms and networks that enable collective action and comprising informal social control (the willingness of community members to look out for each other and intervene where necessary) and social cohesion (feelings of belonging, shared values and mutual trust).
The full questionnaire issued at follow-up is reproduced in Appendix 2.
Objective measurement study
At follow-up, all core survey participants who had provided consent for recontact, and who currently lived in one of the three study areas, were eligible to take part in the objective measurement study. Information about this study and an invitation to take part was posted to these potential participants in a rolling recruitment exercise between October 2014 and July 2015. Those who responded were then contacted to agree a start date for their monitoring. Once this had been confirmed, participants were mailed an accelerometer [Actigraph GT3X+ (Actigraph, Pensacola, Florida, USA)] and global positioning system (GPS) receiver [Qstarz BT Q 1000XT (Qstarz International Co, Taipei, Taiwan)] attached to an elastic belt, along with written instructions for their use, a log sheet and a consent form.
The Actigraph GT3X+ is a small, lightweight triaxial waveform accelerometer. It detects normal human motion and rejects motion from other sources. It measures acceleration at a user-specified rate of between 30 and 100 Hz, and stores raw, unaccumulated data. Depending on the sampling rate, it has a battery life of 16–31 days and can store 12–43 days’ worth of data in on-board memory. The GT3X+ provides detailed information about the intensity, frequency and duration of activity and has been extensively validated in both laboratory and free-living conditions. However, it has well-documented limitations for assessing water-based activities or those dominated by upper body movement. 70
The Qstarz BT Q 1000XT data logger uses signals from satellites to determine the spatial co-ordinates (i.e. latitude and longitude) of participants at 5-second intervals. It is the size of a match box, has a battery life of 24–48 hours in normal use, can store up to 10 days’ worth of data in on-board memory and does not suffer from the loss of satellite signal when in a vehicle or under tree canopy that affects some alternative GPS devices.
Participants completed a 7-day protocol of accelerometer and GPS monitoring. They were asked to wear the two devices on an elastic waistband on the right hip during waking hours for 7 days, removing them only for bathing, showering and swimming. Participants used the log sheet to record times at which the devices were removed and reattached, and the reasons for removal. They were asked to switch off the GPS receiver while it was not being worn, and to recharge the batteries overnight.
At the end of the monitoring period, a field worker organised a face-to-face meeting with the participant at their home, workplace or other mutually convenient location. At this meeting they retrieved the devices, and collected and checked the completeness of the log sheet and consent form. Alternatively, participants could elect to return their devices and study documents by post. Following the retrieval and download of devices, participants received a thank-you letter containing a summary of their own activity data. During download, accelerometer data were scanned to identify participants who had completed less than four 10-hour days of monitoring. Those whose devices had recorded less than this quantity of data were offered the opportunity to rewear the devices for a further 7-day period.
Qualitative study
At follow-up, core survey participants who had provided consent for recontact and who lived in the South study area within 400 m of the M74 extension formed the sampling frame for the qualitative study. This substudy aimed to elicit how the effects of the environmental changes were experienced by local residents and how any changes in behaviour or well-being were mediated and enacted at individual and household level. A pilot study was conducted prior to the main period of data collection.
Pilot qualitative study
An initial review of methods for collecting qualitative spatial data revealed several methods that showed promise. We piloted two of these methods, namely photovoice and walkalong interviews, between March and August 2014 to assess whether either or both would be suitable for our needs and acceptable to our participants. Each participant in the pilot study undertook an initial semistructured interview and was then given the option of a second interview, which could be either photovoice or walkalong. As the initial interviews were held indoors, the second interviews were intended to provide additional insight into specific features of the outdoor built environment that participants viewed as key to their neighbourhood experience, as well as giving insight into their typical journeys through their local area.
For the pilot study, batched quota sampling was employed in a rolling recruitment exercise to achieve a sample that reflected a variety of characteristics, including area and duration of residence and distance from the new motorway, age, sex, socioeconomic status, presence or absence of impaired mobility, car ownership and household composition. Information about this study and an invitation to take part was posted to these potential participants, and followed up with a telephone call or e-mail to confirm willingness to participate and to arrange an initial interview. Willingness to participate in a second interview was established at the initial interview; the second interview was arranged either at that time, or by a subsequent telephone call if the participant wanted more time to make their decision. Consent forms were completed by participants immediately before each interview, except in the case of photovoice interviews, in which case consent was sought prior to the participant receiving their camera or taking their photographs.
In order to investigate participants’ perceptions, experiences and uses of their local neighbourhood in general, the initial interview followed a semistructured format using a topic guide (see Appendix 3). This included questions about residents’ perceptions of the local area as a place to live, their feelings towards the area, the activities they undertook in the local area and the extent to which any of these had changed. If a participant did not mention the M74 extension, the researcher raised the issue – but only at the end of the interview – in order to better understand the relative importance of the motorway and other sources of change in the lives of the participants. Interviews took place, depending on participants’ preferences, in homes, the offices of the MRC/CSO Social and Public Health Sciences Unit or in other (public) places. All interviews were recorded using a digital voice recorder and transcribed verbatim, and field notes were written in all cases.
Walkalong interviews were intended to illustrate a typical journey made by a participant, to consider more deeply the features of the local built environment (including the motorway) that affected their experience of place and to observe their interactions with their environment, including the microdecisions made as part of everyday journeys. This method proved unpopular, however, with only one participant in the pilot study opting to take part. Their walkalong interview followed a very loosely semistructured format, falling somewhere between Carpiano’s71 semistructured question-based approach and Kusenbach’s purely participant-led discussion. 72 Prior to the walkalong interview, the researcher re-examined the transcript of the initial interview and noted key topics and potential follow-up questions. The walking route was negotiated between researcher and participant based on the initial interview, and the participant was prompted to vocalise whatever came to their mind while moving through the neighbourhood and acting as a guide to the researcher, describing anything they viewed as particularly ‘bad’ or ‘good’ about the environment. If conversation faltered, the researcher introduced questions or prompts based on the previous interview (e.g. ‘in your interview you said . . . tell me more about that’). At key points when the participant made specific reference to a physical feature, additional photographs were taken by the researcher. The interview was recorded using a digital voice recorder and transcribed verbatim, and a wrist-worn GPS receiver was used by the researcher to record the route and waypoints. Walkalong interviews with key informants (see Interviews with key informants) followed a similar structure in that the participant selected the route and used environmental interactions to illustrate and stimulate their discussions; given the absence of a prior semistructured interview in these cases, the walkalong discussion was more closely based on the predetermined topic guide.
Photovoice interviews, like walkalong interviews, were used to further investigate how participants interpreted and interacted with their surroundings. The subjects of potential photographs were discussed between participant and researcher at the end of their initial interview. Most participants chose to photograph a typical journey, or to further illustrate points made during their initial interview, on the understanding that they would take additional photographs if they encountered anything else that they would like to raise with the researcher. They were given the choice of either using their own digital camera or smartphone, or using a disposable camera and posting it back to the researcher. There are currently no legal restrictions on taking photographs in public places, including photographs of people. 73 However, participants were instructed to take other people’s wishes for privacy into consideration, to refrain from taking photos of children (other than their own children) and to avoid taking close-ups of people’s faces. The photographs were developed by the researcher (if necessary) and formed the basis of the discussion for the second interview. This began with the researcher asking the participant to sort their photographs into their preferred order and then discuss each in turn. Participants linked their photographs together through different narratives (e.g. a journey, a theme such as traffic or a contrast such as ‘new vs. old’) and organised them into groups or a narrative flow based on the order in which they were taken. As with all other interviews, the photovoice interview was recorded and transcribed verbatim, and a digital copy of all photographs was kept for reference. Participants retained the copyright of their photographs, but as part of the consent process they were asked to give permission for their photographs to be used to illustrate the findings of the research (as in this report).
Main qualitative study
The main qualitative study fieldwork was conducted from September 2014 to April 2015, having been deferred to avoid collecting data around the time of the Commonwealth Games (23 July to 3 August 2014). Recruitment and data collection followed similar procedures to those used in the pilot study, with two important exceptions. First, following the pilot study we concluded that the walkalong method had proven too unpopular and time-consuming to be continued and therefore limited the main study design to an initial semistructured interview with each participant, followed by the option of a follow-on photovoice interview. Second, it became clear in the pilot study that most participants coming forward lived in one of two main areas, Govanhill and Rutherglen, and that experiences of the new motorway differed between these areas. We therefore decided to focus on these two areas as qualitative case studies and accordingly limited recruitment for the main study to participants living within 400 m of the M74 extension in either of these two areas.
Existing national population data sets
STATS19
Data from STATS19,74 a detailed data set of road traffic accidents, were obtained for the period 1997–2014 from the UK Department for Transport. STATS19 contains routinely collected information about all road traffic accidents in the UK that have resulted in a casualty and have been reported to the police. Detailed data are provided about each accident including the date, the casualty severity and the precise co-ordinates of the location. Each accident can be linked to a more detailed data set describing the type of road user (pedestrian, driver, passenger or cyclist) and to more information on the accident and the casualty. Multiple casualties can be assigned to each accident. The casualty severity of each accident is pre-classified using the following definitions: slight, an accident in which at least one person is slightly injured but no one is killed or seriously injured; serious, one in which at least one person is seriously injured but no one is killed; and fatal, one in which at least one person is killed. To increase the sample size of accidents available for analysis, we expanded the boundaries of the South, East and North study areas using 1000-m buffers rather than the 500-m buffers originally used to define these areas (see Overall research design and Chapter 5, Introduction). We also used the larger area covered by Glasgow City Council and its surrounding local authorities as a reference area for these analyses, partly because the intervention area spanned two local authority areas (Glasgow City and South Lanarkshire) and partly to provide a mixture of urban and rural areas, and varied designs and densities of road networks for comparison.
Scottish Household Survey
Travel diary data were obtained from the complete SHS63 data set for the whole of Scotland from 2009 to 2013. The SHS is a nationally representative rolling cross-sectional survey of adults aged ≥ 16 years selected from a geographically representative cluster-random sample of households. 63 Face-to-face interviews were conducted and participants completed a travel diary detailing all journeys completed during the previous day, including the origin, destination and purpose of each journey, and the mode of transport used on each stage of each journey. The distance of each journey was calculated by Transport Scotland in a geographical information system (GIS) using the straight-line distance between the origin and destination.
Incentives and feedback for participants
For the core survey, participants were entered into a £50 prize draw (at baseline) or received a £5 voucher (at follow-up). At follow-up, those who participated in the objective measurement study received a second £5 voucher, and those who participated in the qualitative study received an additional £10 voucher for each interview conducted.
Derivation of key variables
In this section, we describe the derivation of the key variables used in our quantitative analyses.
Travel behaviour
Core survey
We excluded the travel records of participants who returned a completely blank record, reported not having been at home on the day in question, returned a record so implausible that they appeared to have misunderstood the question or returned non-numeric values (such as ticks) instead of minutes values. However, we retained records in which participants had reported no journeys but had completed other parts of the record (e.g. specifying the day of the week), treating these as a positive indication of ‘no travel’ rather than as missing data on travel behaviour. Participants were instructed to report neither journeys made in the course of work (such as driving a bus or making deliveries), because these were not personal travel, nor those made purely for recreation (such as going for a bike ride) rather than to get from place to place, because recreational physical activity of this kind was captured in the physical activity questionnaire. If such journeys were reported, they were deleted from the travel behaviour record. Time spent using each mode of transport was summed and used to derive the following variables:
-
total travel time (minutes/day)
-
bus travel time (minutes/day)
-
car travel time (minutes/day)
-
walking time (minutes/day).
Summary variables were not derived for time spent on the train or using a bicycle, because fewer than 6% of participants at follow-up reported using these modes of transport.
Scottish Household Survey
Data for the period 2009–10 were pooled to represent the pre-intervention condition before the opening of the new motorway, data for 2012–13 were pooled to represent the post-intervention condition and data for 2011 were disregarded owing to the fact that the new motorway was opened midway through that year. Each travel diary recorded in the relevant years was parsed into individual journeys and then into individual journey stages. For example, the sequence ‘walked to bus stop, travelled on bus, and walked to destination’ describes one journey comprising three stages. To maximise the available sample size, we used journey stage as the unit of analysis. Each stage of each journey, regardless of its length or purpose, was classified as ‘active’ if it had been walked or cycled. The origin and destination of each stage was assigned to a Scottish Intermediate Zone following a system that classifies addresses into geographical polygons forming groups of approximately 4000 residents that respect physical boundaries and natural communities, have a regular shape and contain households with similar social characteristics. 75 As with the analysis of accidents described above, an expanded (1000-m) buffer was used to define the three study areas for analysis of the SHS travel diary data, and journey stages were assigned to one of the three study areas if the whole or the majority of the Intermediate Zone polygon containing either the origin or destination fell within the relevant expanded buffer. For the South study area, the River Clyde was used as a natural northern boundary when selecting the Intermediate Zones for analysis because it forms a natural barrier to walking and cycling journeys. This is consistent with the original delineation of the South study area (Figure 12).
FIGURE 12.
Intermediate Zones assigned to expanded study areas for analysis of SHS travel diary data. Contains Ordnance Survey data © Crown Copyright and database right 2016.
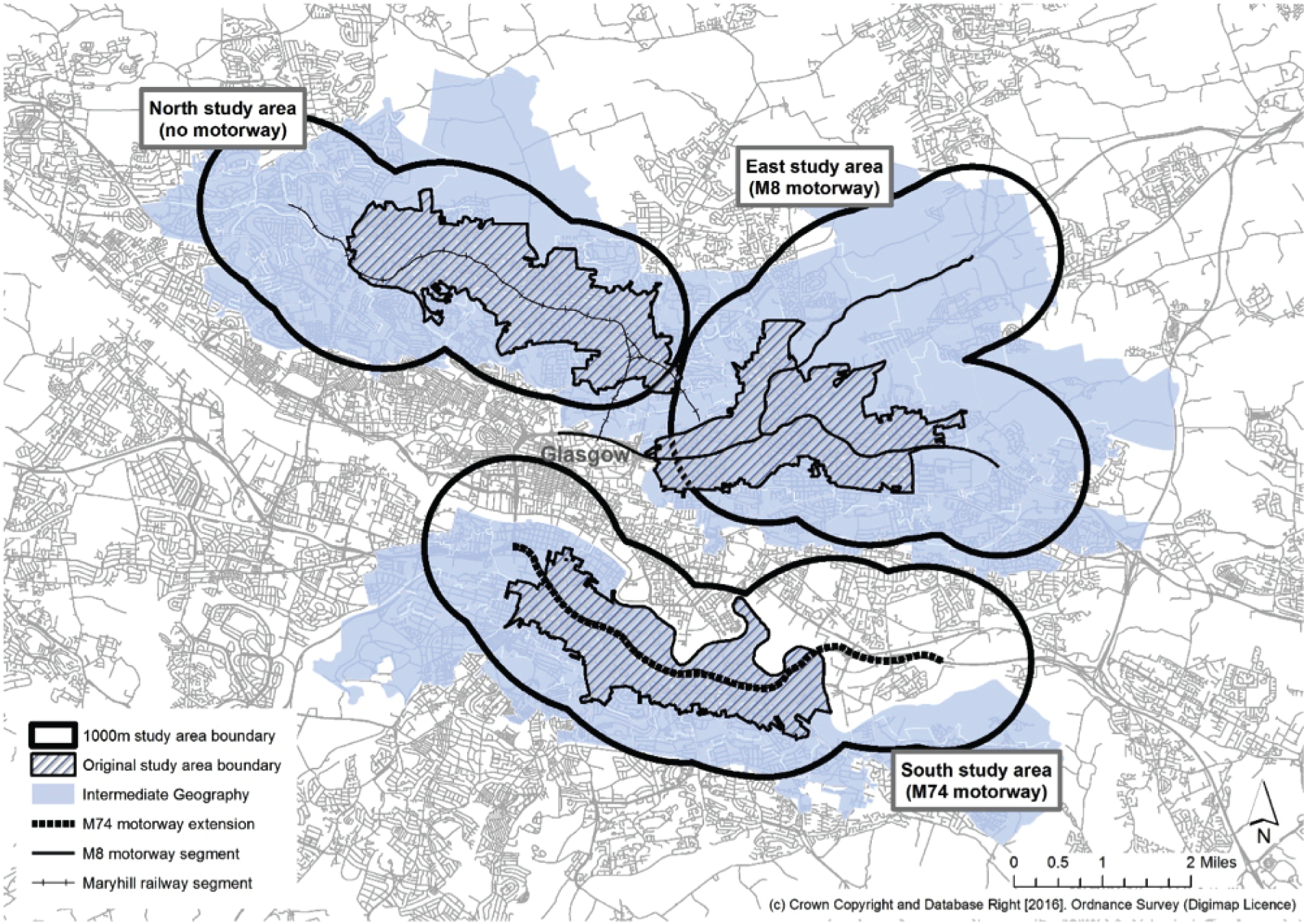
Physical activity and sedentary behaviour
Self-reported physical activity and sedentary behaviour
Following standard IPAQ data cleaning procedures,76 we excluded from analysis those respondents who had reported > 16 hours of physical activity per day and those who had missing or inconsistent data on the frequency or duration of sitting, walking, moderate activity or vigorous activity. Durations of activity of < 10 minutes were recoded to zero, and durations of > 180 minutes were recoded to 180 minutes. For walking, moderate activity and vigorous activity, participants’ estimates of the average number of minutes of activity per day were multiplied by the weekly frequency to derive the weekly minutes of activity. Weekly minutes of moderate activity and vigorous activity were then summed. This produced the following variables:
-
sitting (minutes/day)
-
walking (minutes/week)
-
moderate-to-vigorous physical activity (MVPA) (minutes/week).
Objectively measured physical activity and sedentary behaviour
We implemented standard rules to identify non-wear, valid days and valid records in the accelerometer data. Ninety minutes of continuous zeros were treated as evidence of non-wear, and a valid day was defined as one that contained a minimum of 600 minutes (10 hours) of wear time. A valid record was defined as one that contained a minimum of 4 and a maximum of 7 valid days. Records containing < 4 valid days of data were excluded, and those containing > 7 valid days were truncated to the first 7 days. For valid days in valid records only, cut-off points used in the National Health and Nutrition Examination Survey77–79 were applied to derive the following variables:
-
sedentary time (minutes/day)
-
light physical activity (minutes/day)
-
MVPA (minutes/day).
Objectively measured physical activity and sedentary behaviour within the neighbourhood
Software was written in Java version 8 (Oracle Corporation, Redwood Shores, California, USA) to match accelerometry data points to the closest recorded GPS location based on their date and time stamps. Data points with more than a 30-second difference between devices, and those recorded within 30 seconds of the GPS receiver being switched on, were excluded. Location spikes (artefactual, unfeasibly rapid changes in location) were identified and excluded. Indoor data points were not specifically excluded because the GPS data loggers were able to receive a signal most, but not all, of the time when indoors.
The merged data were projected into a GIS. An 800-m pedestrian network buffer was constructed around the weighted population centroid of the unit postcode for each participant’s home address, and activity within this buffer was identified using the same National Health and Nutrition Examination Survey cut-off points as above, generating the following variables:
-
neighbourhood sedentary time (minutes/day)
-
neighbourhood light physical activity (minutes/day)
-
neighbourhood MVPA (minutes/day).
Indicators of well-being
Physical and mental well-being
From the SF-8 responses, physical component summary of the SF-8 (PCS-8) scores and mental component summary of the SF-8 (MCS-8) scores were derived using a standard norm-based scoring method. 66 SWEMWBS responses were summed to produce a raw total score, which was then transformed into a metric score using standard procedures. 67 For both the SF-8 and the SWEMWBS, higher scores reflected higher well-being.
Exposure to the intervention
We used multiple ways of describing exposure to the intervention, as we hypothesised that different types of exposure would be more or less important for different outcomes. 80
Areal measure of exposure
As described in Evaluating the intervention, survey participants were sampled from three local study areas: an area surrounding the new M74 motorway (South); an area surrounding the established M8 motorway, which was built in the 1960s (East); and an area containing no comparable motorway infrastructure (North) (see Figure 4).
Individual measures of exposure
Using a GIS, we calculated the distance in metres from the weighted population centroid of the unit postcode for each participant’s home address (1) in a straight line to the nearest motorway infrastructure, and (2) by road network to the nearest motorway junction. Depending on the study area, the nearest motorway may have been the new M74 extension or the existing M8 motorway. We hypothesised that the effect of a unit change in distance would be greater among those living closer to motorway infrastructure. We therefore transformed these individual exposures using the negative natural logarithm to produce a measure of proximity, in which higher values represented greater exposure. We considered the straight-line distance to be the most appropriate exposure measure for the analysis of effects on well-being, because the experience of some of the hypothesised influences of the intervention on well-being (such as noise and vibration) was likely to depend on direct proximity. However, we considered the road network distance to be the most appropriate exposure measure for the analysis of effects on travel behaviour and physical activity, because these were more likely to depend on the routes available for people to follow.
Secondary measures of exposure
As described in Characterising the environmental changes and refining the study design, we used bespoke software to identify changes in the built environment using time-stamped aerial images. Polygons denoting the areas of change were then projected into a GIS, and the area in square metres of each change polygon was calculated. Using the GIS, we constructed an 800-m pedestrian network buffer around the weighted population centroid of the unit postcode for each participant’s home address, and identified the proportion of the area within that buffer that had changed. This gave an indication of the general amount of change occurring in the neighbourhood (an ‘upheaval index’), whereby higher values represented a greater amount of change (Figure 13). Examples of neighbourhoods experiencing different amounts of change can be found in Figure 14.
FIGURE 13.
Areas of change within participants’ neighbourhoods. Contains Ordnance Survey data © Crown Copyright and database right 2016.
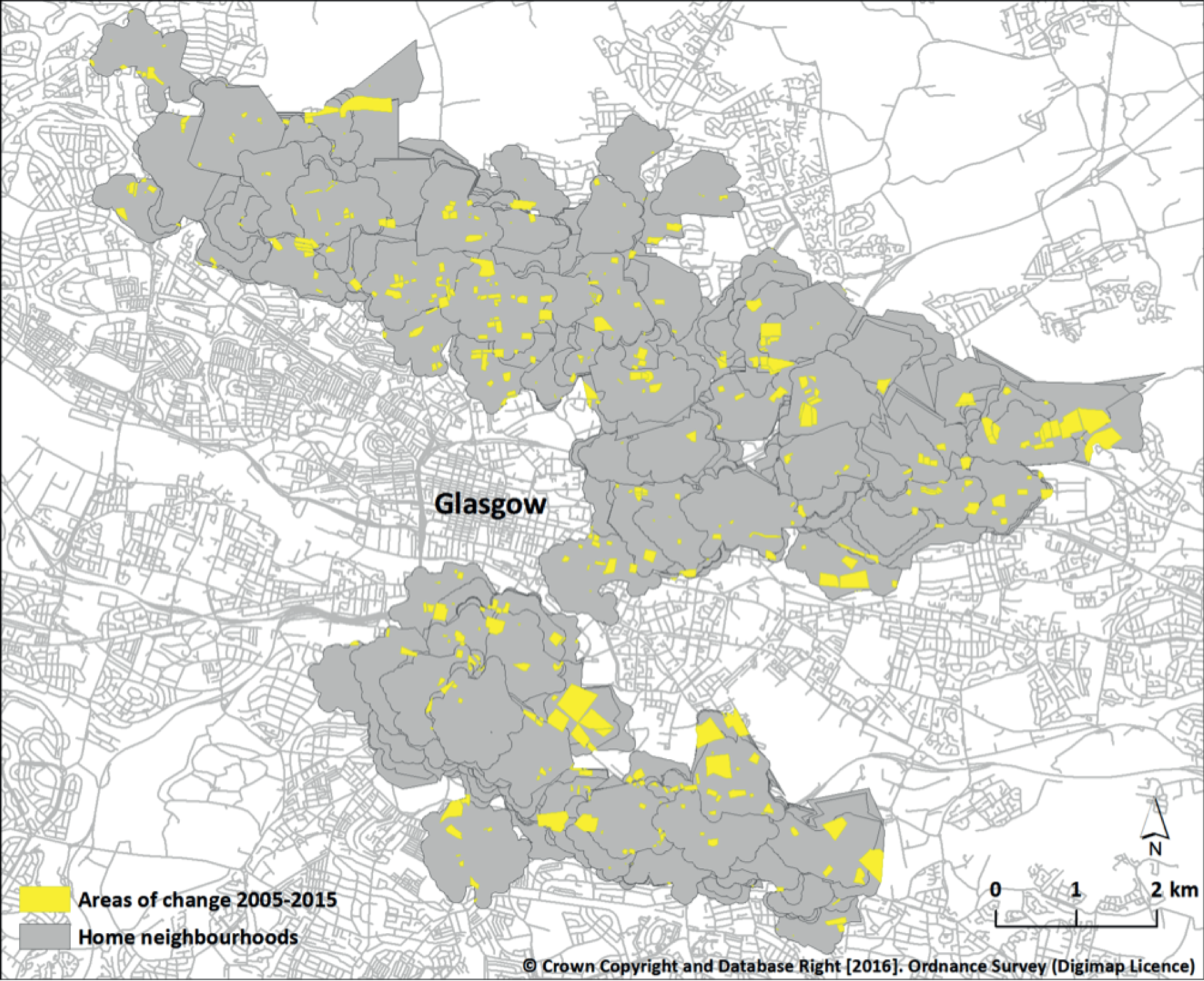
FIGURE 14.
Examples of neighbourhoods experiencing different levels of upheaval. (a) 1%; (b) 5%; and (c) 10% of the local built environment changed between 2005 and 2015. Contains Ordnance Survey data © Crown Copyright and database right 2016.
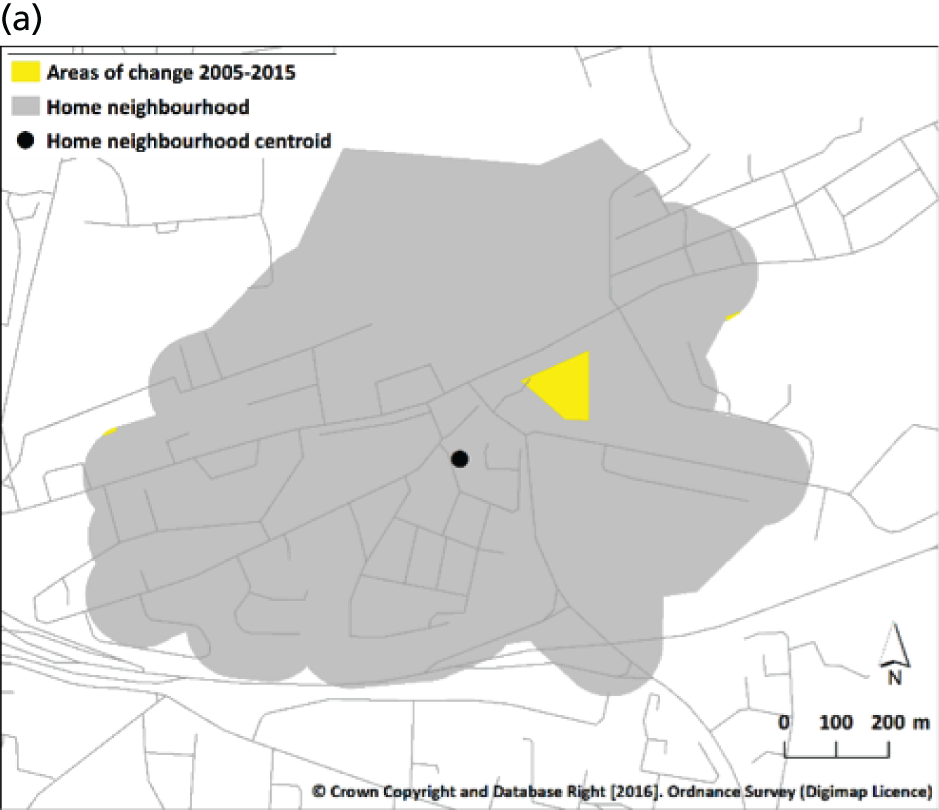


Other environmental variables
Perceptions of the neighbourhood environment
Perceptions of the conduciveness of the environment for physical activity were measured on a five-point scale. The values for the seven negatively worded items were reverse coded such that a positive value represented a ‘positive’ perception. Each of the 14 items, along with the three factors identified using principal components analysis at baseline,56 was used individually in analysis and no overall summary measure was derived (Table 5).
| Item | Factor |
|---|---|
| It is pleasant to walk | Safe and pleasant surroundings (Factor 1) |
| There is a park within walking distance | Convenience for walking (Factor 3) |
| There is convenient public transport | Low traffic (Factor 2) |
| There are convenient routes for cycling | |
| It is safe to walk after dark | Safe and pleasant surroundings (Factor 1) |
| There is little traffic | Low traffic (Factor 2) |
| It is safe to cross the road | |
| The surroundings are unattractive | Safe and pleasant surroundings (Factor 1) |
| There is little green space | Convenience for walking (Factor 3) |
| The nearest shops are too far to walk to | Convenience for walking (Factor 3) |
| There are no convenient routes for walking | Convenience for walking (Factor 3) |
| People are likely to be attacked | Safe and pleasant surroundings (Factor 1) |
| There is a lot of traffic noise | Low traffic (Factor 2) |
| The roads are dangerous for cyclists | Low traffic (Factor 2) |
Perceptions of collective efficacy were measured using nine items, each assessed using a five-point scale. A summary measure was calculated by taking the mean value of the responses to all nine items (Box 1).
People around here are willing to help their neighbours.
This is a close-knit neighbourhood.
People in this neighbourhood can be trusted.
People in this neighbourhood generally get along with each other.
People in this neighbourhood share the same values.
If a group of neighbourhood children was skipping school and hanging out on a street corner, how likely is it that your neighbours would do something about it?
If some children were spray-painting on a local building, how likely is it that your neighbours would do something about it?
If there was a fight in front of your house and someone was being beaten or threatened, how likely is it that your neighbours would break it up?
If a child was showing disrespect to an adult, how likely is it that people in your neighbourhood would tell off or scold that child?
Overall approach to analysis
Sample size estimation
The study was designed to detect changes in the key primary behavioural outcomes (travel behaviour and physical activity) and the most important secondary outcome (the incidence of road traffic accidents). Sample size estimations for natural experimental studies of this kind are complex and involve a large number of assumptions.
The distributional statistics of the primary travel behaviour outcomes in the baseline sample can be found in Table 6. 57 Applying these mean values and standard deviations (SDs) to the simplest situation of a comparison between two groups, a cross-sectional sample of 400 participants per study area at each time point (a target that was exceeded at baseline) was expected to allow the detection with 95% confidence and 80% power of an increase of 5 minutes per day in walking for transport from baseline to follow-up within one study area, or a cross-sectional difference of 2 minutes per day in cycling for transport or 5 minutes per day in walking for transport between intervention and control areas at follow-up. These differences are of a similar magnitude to the estimated effect sizes for interventions, and the differences in walking between ‘high-’ and ‘low-walkable’ neighbourhoods in observational studies synthesised in previous systematic reviews. 35,81 The availability of two control areas, and the potential to compare longitudinal changes between study areas using a combination of cohort and repeat cross-sectional analyses, increased the power of the study to detect smaller changes.
| Outcome | Mean | SD | Median | IQR | Range |
|---|---|---|---|---|---|
| Walking time (minutes/day) | 19.2 | 27.8 | 10.0 | 30.0 | 0–205 |
| Cycling time (minutes/day) | 0.7 | 7.3 | 0.0 | 0.0 | 0–130 |
| Car travel time (minutes/day) | 24.4 | 40.8 | 0.0 | 40.0 | 0–510 |
For physical activity, assuming a baseline (control) mean value for accelerometer-derived MVPA of 10 minutes per day and a SD of 7 minutes per day,82,83 86 participants per group were required to detect a difference of 3 minutes per day in MVPA between intervention and control areas.
For ITS analysis, it is not generally considered feasible to perform a conventional sample size estimation. 84 However, a minimum of 50 time points is recommended for ITS regression models with autoregressive integrated moving average (ARIMA) errors, to enable cyclical trends in the pre-intervention series to be adequately modelled. 85 The STATS19 accident data set contained 216 monthly data points from 1997 to 2014 and therefore substantially exceeded this minimum recommendation. 74
Analysis of core survey and objective measurement data
Many different quantitative analyses are summarised in this report. Further details of specific analyses can be found in subsequent chapters and in the relevant publications, but our general approach was to use multivariable regression modelling to estimate adjusted associations between dependent (‘outcome’) and independent (‘exposure’) variables. No missing data were imputed. Most analyses involved the use of linear, generalised linear, two-part or logistic regression to model continuous, skewed continuous or binary outcomes, respectively. We built up these models in stages by progressively adjusting them for various sets of individual, household, geographic and other covariates that were hypothesised to be potential confounders of the relationships of interest. Some models were stratified by pre-specified effect modifiers, for example the presence of a chronic condition and perceived financial strain in the case of the relationship between motorway exposure and well-being. Where significant relationships were found between exposure and outcome, we investigated potential mediation using the Baron and Kenny method. 86 All analyses were carried out using Stata® version 13 (StataCorp LP, College Station, TX, USA).
STATS19 analysis
Changes in the secular trend in road traffic accidents were analysed using ARIMA ITS models. Candidate models that fit the pre-intervention response variable were identified. An appropriate transfer function was then identified and applied according to whether the impact of the intervention appeared to take the form of an abrupt permanent change, a gradual permanent change or an abrupt temporary change. The analysis was stratified by study area, and differences in changes between areas were assessed to identify a potential intervention effect. Changes in accident frequency were then stratified by type of road user by linking to the casualty data set. Finally, we examined the sociospatial distribution of accidents and changes in that distribution. All analyses were carried out using Stata version 14 except where stated otherwise.
Scottish Household Survey analysis
We described and compared trends in summary measures of travel behaviour in the three study areas and the region as a whole, testing for differences in changes over time between areas and for interactions between study area and time period. All analyses were carried out using Stata version 14.
Qualitative analysis
All recorded interviews with key informants and residents were transcribed verbatim by a transcription service. Transcripts were then checked against the recordings and analysed thematically by one researcher with the assistance of NVivo version 10 software (QSR International, Warrington, UK). A handful of transcripts from the resident interviews (both the pilot and the main study) and the key informant interviews were double coded by two additional researchers to validate the initial interpretation of the data. An iterative process of analysis was used to code segments of transcripts, to extract related segments, to identify and group themes and to identify patterns and negative cases using the method of constant comparison. Field notes were also drawn on to allow information not captured in the recordings and transcripts to inform the analysis. The coding of segments and the identification of themes was non-exclusive, such that one excerpt of talk could be categorised under more than one theme. Initially, higher-order themes were predominantly derived from the topic guide. Lower-order themes emerging from the data elicited in the interviews could often be meaningfully grouped under one of the higher-order themes, but some spanned more than one of these or proved not to be closely related to any of the a priori constructs described in the topic guide, thereby necessitating the creation of new themes. Overarching themes developed during the final stages of analysis then spanned various combinations of the previously identified themes. The initial broad coding framework was discussed with the study team after the pilot study.
The aims of the initial analysis differed between the study of key informants and the study of residents. With the resident interviews, the aim was to better understand how the participants perceived, experienced and used their neighbourhood, whether this had changed and what part (if any) the new motorway had played in this change. With the key informant interviews, the analysis aimed to understand the key environmental changes occurring in the local areas as a result of the new motorway. An analysis of these data sets was therefore carried out separately to begin with and was later integrated in pursuit of a more holistic picture of neighbourhood change associated with the M74 extension. Although we did not use the approach of framework analysis as such, in working across these somewhat different data sets we used a framework matrix of key topics to help understand and integrate the important similarities and differences. The thematic analysis itself followed five steps: (1) immersion in the data (re-reading the transcripts while listening to the recordings); (2) annotating transcripts according to key emerging topics and ideas; (3) initial coding based on repeated topics from transcripts; (4) amalgamating codes into themes using NVivo (which also allowed us to identify the changes that residents prioritised, and what they regarded as the key drivers of change); and (5) applying theoretical lenses to the understanding and interpretation of the data. Emerging spatially referenced data (including areas that respondents chose to avoid) were also plotted in a GIS to visualise patterns of use and disuse as well as the meanings that respondents ascribed to different features of the built environment.
Synthesis of findings
In order to synthesise findings from each strand of analysis into a coherent overall interpretation, we drew on the concepts of two approaches described in the social science evaluation literature: pattern matching and causal process observation. Pattern matching entails the specification of an a priori theoretical pattern, which is then compared with the pattern of findings – importantly, not to individual ‘results’ in isolation – that emerge from subsequent empirical data. 87 To the extent that the theorised and observed patterns match or corroborate, the underlying theory can be supported. A key feature of pattern matching is that, as the complexity of the matched pattern increases, this strengthens the basis for causal inference as it becomes less plausible that alternative theories could explain the same pattern. In this study, we sought to examine the extent to which the results of different analyses (using different types of data, different outcome measures, different spatial levels of analysis and different types of comparison) were consistent with the pattern of relationships summarised in the vignettes of the hypothesised ‘virtuous’ and ‘vicious’ spirals described in Table 1.
Causal process observations are insights into context, process or mechanism that may complement a more statistical or correlational approach to causal inference by shedding light on how variables are related. 88 In this study, we applied this concept by using our in-depth qualitative data about particular cases (individuals, locations or case study areas) to elaborate our understanding of the more general relationships (or lack of relationships) observed in the quantitative data.
Ethics approval
The core survey was approved by the University of Glasgow Faculty of Medicine Ethics Committee at baseline (reference FM01304) and by the University of Glasgow Social Sciences Ethics Committee at follow-up (reference 400120077). In addition, the objective measurement study (reference 400130157) and the qualitative study (reference 400130156) received separate ethics approval from the latter committee at follow-up.
For the core survey, return of the questionnaire to the study team was taken as implied consent for the data to be used. This was considered appropriate because participants were free to consider the study information in their own time, which minimised the possibility of coercion. For the objective measurement study, participants provided written informed consent when their devices were retrieved; for the qualitative study, participants provided written informed consent prior to each interview. These various approaches to consent all received ethics approval.
Approval for use of SHS travel diary data for the purposes of this study was granted by the Scottish Government (reference A10776862). STATS19 data are made available for use by the Department of Transport without requiring formal approval. 74
Chapter 3 Descriptive characteristics of participant samples
Introduction
In this chapter we present the descriptive characteristics of participants in various parts of the study. Self-selection bias is a well-documented research phenomenon and, although we were able to recruit a heterogeneous core survey sample in terms of age, sex, health and various indicators of socioeconomic status, we make no claim that our sample is representative of the entire population of the local areas. The longitudinal cohort and the subsamples taking part in the objective measurement and qualitative studies were subject to further selection processes, and we therefore investigated the extent to which these participants differed from the overall core survey sample.
To complement our primary data collection, we analysed data from two other existing sources. The SHS is a nationally representative survey of Scottish adults, and we examined the similarities and differences between the SHS and core survey samples used in the analyses on travel behaviour. We also analysed data on road traffic accidents from the STATS19 data set,74 in which accidents are linked to detailed information about location, severity and type of road user but in which the sociodemographic characteristics of the people involved are not recorded.
Core survey
A total of 1345 and 1343 completed surveys were returned at baseline (2005; T1) and follow-up (2013; T2), respectively. After accounting for survey packs that were returned as undeliverable by the Royal Mail (Royal Mail Group Ltd, London, UK; 676 addresses at baseline and 509 at follow-up), the response rate was similar at both time points: 1345/(9000–676) = 16.1% at baseline and 1343/(9000–509) = 15.8% at follow-up. The longitudinal cohort comprised 365 participants who returned surveys at both time points. The remaining 980 (baseline) and 978 (follow-up) participants together formed the repeat cross-sectional sample.
Descriptive characteristics of the longitudinal cohort and repeat cross-sectional sample can be found in Table 7. At baseline, our sample contained more women than men and participants were aged 49–50 years on average. Approximately half of the sample were working, half owned a home and half owned a car, with slightly higher proportions of home and car ownership in the longitudinal cohort.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |||||
| n | % | n | % | n | % | n | % | |
| Age (years), mean (SD) | 360 | 50.4 (13.6) | 363 | 58.5 (13.6) | 962 | 48.8 (18.3) | 970 | 52.6 (16.5) |
| Male | 361 | 43.5 | 363 | 44.4 | 970 | 37.1 | 972 | 42.8 |
| Home ownership | 360 | 61.1 | 363 | 62.5 | 965 | 47.9 | 971 | 49.6 |
| Car ownership | 361 | 58.5 | 362 | 60.5 | 951 | 48.8 | 969 | 53.4 |
| Workinga | 359 | 58.5 | 364 | 48.1 | 961 | 48.3 | 972 | 48.3 |
| With chronic condition | 360 | 38.9 | 361 | 47.9 | 955 | 39.0 | 964 | 43.9 |
| Perceived financial strain | 361 | 361 | 955 | 950 | ||||
| Quite comfortably off | 11.9 | 12.5 | 4.9 | 5.2 | ||||
| Can manage without difficulty | 20.2 | 24.4 | 24.0 | 20.5 | ||||
| Have to be careful with money | 52.9 | 47.1 | 51.9 | 52.4 | ||||
| Find it a strain to get by | 15.0 | 16.1 | 19.2 | 21.9 | ||||
| Years lived in local area, mean (SD) | 365 | 18.3 (15.3) | 362 | 24.9 (16.6) | 980 | 18.2 (18.0) | 965 | 19.0 (17.4) |
In the longitudinal cohort, the changes in sociodemographic characteristics over time were consistent with the increase in the age of participants over the duration of the study. In the repeat cross-sectional sample, there were higher proportions of men, car owners and people with a chronic condition at follow-up than at baseline. In addition, the follow-up sample was on average significantly older than the baseline sample.
Cohort participants differed from the rest of the baseline sample in several important ways. On average, they were more likely to be men, to be employed, to own a home, to own a car and to describe themselves as being in a secure financial position. However, cohort participants did not differ from other baseline participants on average with regard to age, presence of a chronic condition or the duration for which they had lived in the local area.
In the longitudinal cohort, there were no significant sociodemographic differences between study areas at either time point. In the repeat cross-sectional sample, there were no significant sociodemographic differences between study areas at baseline. 57 At follow-up, however, participants in the North study area were, on average, significantly older, and those in the South perceived significantly less financial strain and had lived in the local area for less time than those in the other study areas.
Objective measurement study
Of the 988 potentially eligible participants, 196 (19.8%) returned a minimum of 4 valid days of accelerometry data with a corresponding GPS file containing some data (Figure 15).
FIGURE 15.
Flow of participants through the objective measurement study.

Descriptive characteristics of the objective measurement study sample can be found in Table 8. Participants had a mean age of 54 years and 55% were women. More than 60% were working, > 60% owned a home and > 60% owned a car.
| Variable | Objective measurement sample (n = 196), T2 | |
|---|---|---|
| n | % | |
| Age (years), mean (SD) | 194 | 54.0 (13.1) |
| Male | 195 | 44.6 |
| Home ownership | 195 | 65.1 |
| Car ownership | 196 | 63.3 |
| Workinga | 196 | 61.7 |
| With chronic condition | 194 | 35.1 |
| Perceived financial strain | 195 | |
| Quite comfortably off | 12.8 | |
| Can manage without difficulty | 26.2 | |
| Have to be careful with money | 44.1 | |
| Find it a strain to get by | 16.9 | |
| Years lived in local area, mean (SD) | 196 | 19.1 (16.0) |
Those taking part in the objective measurement study differed from the rest of the follow-up sample in several important ways. On average, they were more likely to be employed, to be home and car owners, and to describe themselves as being in a secure financial position and less likely to have a chronic condition. They were also more likely than the rest of the follow-up sample to have reported participating in walking and MVPA in their core survey. However, they did not differ from other follow-up participants on average in relation to age, sex or the duration for which they had lived in the local area.
Qualitative study
In total, 112 of the survey participants who had consented to recontact lived within the qualitative case study areas. All of these were invited to take part, and this resulted in 30 interviews (27% response rate): nine in the pilot study and 21 in the main study. Participants were evenly split between Govanhill and Rutherglen, the two case study neighbourhoods (15 from each). All participants undertook an initial semistructured interview and 13 also undertook a follow-on interview, of which 12 were photovoice interviews and the other was a walkalong interviews. One participant who completed a qualitative interview at follow-up had also taken part in the baseline qualitative interview study. 58
Further descriptive characteristics of the qualitative study participants can be found in Table 9. Two-thirds of participants were women, and most were in middle or late-middle age. More than half were working, more than half owned a home and more than half owned a car.
| Variable | Qualitative sample (N = 30), T2 (n) |
|---|---|
| Age (years) | |
| 20–35 | 4 |
| 36–50 | 10 |
| 51–65 | 9 |
| 65+ | 7 |
| Male | 11 |
| Owns a home | 18 |
| Owns a car | 16 |
| Workinga | 20 |
| Has a chronic condition | 11 |
| Perceived financial strain | |
| Quite comfortably off | 4 |
| Can manage without difficulty | 4 |
| Have to be careful with money | 19 |
| Find it a strain to get by | 3 |
| Years lived in local area | |
| 0–10 | 12 |
| > 10–20 | 9 |
| > 20–30 | 4 |
| ≥ 30 | 5 |
Although it was not appropriate to conduct formal statistical tests on a sample of this size, some differences were apparent between the qualitative subsample and the rest of the follow-up sample. There were fewer men and fewer people with a chronic condition, and more home owners and people in work in the qualitative substudy than in the follow-up sample as a whole.
Existing national population data sets
STATS19
A total of 78,919 road traffic accidents were recorded in Glasgow City and surrounding authorities between 1997 and 2014. A total of 13,595 of these resulted in serious injury or death. The total numbers for the South, East and North study areas were 10,167, 3832 and 3956, respectively. The annual count fell in each study area from 1997 to 2014. For all accidents, the annual count fell by 50.7% in the South (from 758 to 374), by 49.3% in the East (from 292 to 148) and by 50.5% in the North (from 315 to 156). For serious and fatal accidents, the annual count fell by 57.4% in the South (from 195 to 55), by 71.4% in the East (from 70 to 20) and by 68.6% in the North (from 70 to 22) (Table 10).
| Year | Glasgow City and surrounding local authorities | South | East | North | ||||
|---|---|---|---|---|---|---|---|---|
| All | Serious and fatal | All | Serious and fatal | All | Serious and fatal | All | Serious and fatal | |
| 1997 | 5901 | 1223 | 758 | 129 | 292 | 70 | 315 | 70 |
| 1998 | 5956 | 1229 | 708 | 123 | 300 | 68 | 312 | 73 |
| 1999 | 5469 | 1174 | 685 | 131 | 241 | 49 | 268 | 63 |
| 2000 | 5429 | 1030 | 680 | 84 | 258 | 52 | 285 | 46 |
| 2001 | 5198 | 947 | 665 | 111 | 233 | 44 | 274 | 52 |
| 2002 | 5024 | 912 | 665 | 103 | 243 | 43 | 266 | 47 |
| 2003 | 4951 | 861 | 660 | 97 | 233 | 41 | 242 | 48 |
| 2004 | 4865 | 707 | 650 | 80 | 234 | 31 | 256 | 34 |
| 2005 | 4613 | 629 | 614 | 68 | 232 | 32 | 239 | 43 |
| 2006 | 4504 | 725 | 615 | 107 | 209 | 32 | 226 | 30 |
| 2007 | 4279 | 621 | 535 | 68 | 200 | 23 | 198 | 31 |
| 2008 | 3885 | 713 | 496 | 91 | 208 | 34 | 208 | 46 |
| 2009 | 3620 | 584 | 459 | 61 | 203 | 31 | 149 | 20 |
| 2010 | 3283 | 515 | 424 | 63 | 175 | 26 | 147 | 28 |
| 2011 | 3234 | 463 | 417 | 57 | 133 | 15 | 155 | 28 |
| 2012 | 3061 | 467 | 400 | 60 | 155 | 31 | 141 | 23 |
| 2013 | 2733 | 368 | 362 | 48 | 135 | 23 | 119 | 15 |
| 2014 | 2914 | 427 | 374 | 55 | 148 | 20 | 156 | 22 |
The annual numbers of casualties are shown in Table 11. The numbers of casualties do not match the numbers of accidents because some accidents result in multiple casualties. As with accidents, the annual numbers of casualties of all types fell from 1997 to 2014 in the region as a whole, and in each of the three study areas.
| Year | Glasgow City and surrounding authorities | South | East | North | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Driver or rider | Passenger | Pedestrian | Driver or rider | Passenger | Pedestrian | Driver or rider | Passenger | Pedestrian | Driver or rider | Passenger | Pedestrian | |
| 1997 | 3554 | 2435 | 1844 | 387 | 317 | 267 | 149 | 99 | 134 | 151 | 112 | 122 |
| 1998 | 3741 | 2524 | 1767 | 384 | 292 | 220 | 159 | 138 | 107 | 167 | 112 | 114 |
| 1999 | 3455 | 2207 | 1622 | 353 | 265 | 252 | 141 | 100 | 76 | 140 | 74 | 105 |
| 2000 | 3402 | 2225 | 1598 | 352 | 246 | 256 | 158 | 110 | 74 | 137 | 101 | 109 |
| 2001 | 3360 | 2080 | 1478 | 373 | 263 | 235 | 137 | 96 | 68 | 147 | 100 | 98 |
| 2002 | 3244 | 1935 | 1438 | 336 | 246 | 265 | 152 | 79 | 74 | 145 | 104 | 100 |
| 2003 | 3212 | 1961 | 1374 | 351 | 255 | 227 | 143 | 92 | 74 | 125 | 81 | 93 |
| 2004 | 3163 | 1912 | 1318 | 335 | 263 | 215 | 169 | 89 | 57 | 130 | 92 | 88 |
| 2005 | 2909 | 1762 | 1322 | 330 | 253 | 206 | 152 | 84 | 60 | 137 | 68 | 84 |
| 2006 | 2913 | 1687 | 1242 | 319 | 224 | 214 | 142 | 66 | 50 | 114 | 62 | 89 |
| 2007 | 2806 | 1501 | 1172 | 285 | 161 | 197 | 145 | 78 | 44 | 103 | 56 | 74 |
| 2008 | 2475 | 1308 | 1106 | 275 | 170 | 166 | 130 | 69 | 59 | 120 | 67 | 78 |
| 2009 | 2474 | 1187 | 915 | 268 | 160 | 149 | 135 | 72 | 44 | 91 | 50 | 41 |
| 2010 | 2232 | 1153 | 842 | 245 | 178 | 132 | 130 | 67 | 43 | 89 | 37 | 44 |
| 2011 | 2223 | 1123 | 800 | 239 | 165 | 139 | 94 | 49 | 26 | 95 | 47 | 43 |
| 2012 | 2163 | 1021 | 784 | 258 | 104 | 132 | 114 | 70 | 32 | 94 | 41 | 47 |
| 2013 | 1903 | 854 | 692 | 225 | 112 | 117 | 90 | 46 | 37 | 78 | 30 | 43 |
| 2014 | 2108 | 895 | 724 | 236 | 117 | 129 | 105 | 58 | 38 | 93 | 41 | 53 |
Scottish Household Survey
A total of 3706 and 4205 individual travel diaries were completed by SHS participants in Glasgow City and surrounding local authorities during the periods 2009–10 and 2012–13, respectively. The numbers of individual journey stages recorded were 9777 (2009–10) and 11,684 (2012–13), respectively. Each participant was assigned to a study area based on the Scottish Intermediate Zone containing their home address (see Chapter 2, Derivation of key variables). The numbers of journey stages recorded in the South, East and North study areas were 434, 477 and 541, respectively in 2009–10, and these increased to 543, 560 and 593, respectively, in 2012–13.
Descriptive characteristics of the SHS travel diary sample can be found in Table 12. At both time points, there were more women than men, the 45- to-59-year age group contributed more participants than any other and most participants were working or studying.
| Time period | 2009–10 (n) | 2012–13 (n) | ||||||
|---|---|---|---|---|---|---|---|---|
| Area | Glasgow and surrounding authorities | South | East | North | Glasgow and surrounding authorities | South | East | North |
| Age (years) | ||||||||
| 16–24 | 328 | 20 | 15 | 25 | 373 | 17 | 19 | 19 |
| 25–34 | 570 | 43 | 47 | 43 | 636 | 47 | 32 | 44 |
| 35–44 | 711 | 39 | 43 | 43 | 707 | 38 | 36 | 37 |
| 45–59 | 970 | 49 | 57 | 58 | 1180 | 57 | 57 | 59 |
| 60–74 | 805 | 44 | 35 | 53 | 934 | 36 | 48 | 51 |
| 75+ | 322 | 16 | 20 | 17 | 374 | 7 | 13 | 24 |
| Sex | ||||||||
| Male | 1627 | 95 | 84 | 107 | 1874 | 97 | 81 | 107 |
| Female | 2079 | 116 | 133 | 132 | 2331 | 105 | 124 | 127 |
| Current economic status | ||||||||
| Employed/education/training | 2079 | 118 | 122 | 139 | 2399 | 132 | 111 | 132 |
| Unemployed and seeking work | 211 | 4 | 19 | 12 | 256 | 16 | 13 | 14 |
| Unable to work owing to sickness | 226 | 13 | 14 | 10 | 219 | 6 | 17 | 12 |
| Retired | 962 | 55 | 47 | 59 | 1103 | 36 | 52 | 58 |
| Other | 228 | 21 | 15 | 19 | 228 | 12 | 12 | 18 |
| How is your health in general? | ||||||||
| Very good | 1302 | 80 | 75 | 95 | 1480 | 68 | 62 | 90 |
| Good | 1330 | 72 | 75 | 81 | 1574 | 93 | 74 | 82 |
| Fair | 824 | 46 | 51 | 49 | 864 | 35 | 48 | 45 |
| Bad/very bad | 242 | 13 | 16 | 14 | 287 | 6 | 21 | 17 |
| Number of journey stages by study area | ||||||||
| Stages | 9777 | 435 | 477 | 541 | 11,684 | 543 | 560 | 593 |
| Mean number of stages (range) | 2.1 (1–14) | 1.9 (1–8) | 2.0 (1–8) | 2.2 (1–10) | 2.2 (1–10) | 2.2 (1–10) | 2.3 (1–9) | 2.1 (1–10) |
Comparison of the Scottish Household Survey and core survey samples
There were more women than men in both the baseline and follow-up core survey samples and in the SHS travel diary samples. In 2009–10, 44% of SHS respondents in Glasgow City and surrounding local authorities were men. Similar proportions were found in the SHS samples for all three study areas and at follow-up in 2012–13, as well as in the longitudinal cohort (44%) and repeat cross-sectional samples (37% at T1 and 43% at T2) for the core survey. The mean ages of the various core survey samples ranged from 49 to 59 years, and this range matches the 45- to 59-years age group that contributed the largest share of participants in the SHS sample. However, in general those in employment, education or training formed a greater proportion of the SHS samples (56–57%) than of the core survey samples (48–59%).
Conclusion
We recruited a total of approximately 2300 adults across the baseline and follow-up surveys in combination, providing a sample with considerable heterogeneity for a number of important sociodemographic characteristics and subsamples for the more detailed objective measurement and qualitative studies. We supplemented our primary data collection with routinely collected data on nearly 80,000 accidents from the STATS19 data set74 and on > 21,000 journey stages made by nearly 8000 adults from the SHS travel diary data set.
Chapter 4 Changes in activity patterns
Introduction
In the preceding chapters we outlined the justification for exploring the effect of motorway exposure on a limited set of health-related outcomes, described how these outcomes were measured, outlined the principles of our analyses and summarised the descriptive characteristics of our study samples. In this chapter, we report our analyses of the relationships between motorway exposure and changes in travel, physical activity and sedentary behaviour, using the core survey, SHS travel diary and objective measurement data. This combination of analyses was intended to buffer the methodological and inferential limitations of each individual approach, as well as to provide more nuanced information on particular aspects of the relationships in question. For example, the objective activity monitoring substudy was cross-sectional, limiting the scope for causal inference, but was less prone to the social desirability and recall biases associated with the self-reporting of physical activity. Conversely, the core survey and SHS travel diary data allowed us to examine changes in activity patterns over time, strengthening the basis for causal inference, but were limited by the self-reported behavioural data. We thereby aimed to use the three approaches in combination to provide a degree of triangulation and to strengthen the overall case for causal inference. 89
Non-normal distributions are a common statistical challenge when modelling travel and physical activity variables, often because of a high number of zero counts in the data. We used a combination of generalised linear models (GLMs), logistic model and two-part regression models to accommodate the skewness of our outcome variables. Two-part models have seldom been used in this field of public health intervention research, despite offering a good conceptual and methodological fit for this type of data and an efficient way of combining analytical options.
Patterns of behaviour and change over time in the core survey data
In this section, we describe patterns of travel, physical activity and sedentary behaviour at T1 (2005) and T2 (2013) using core survey data. We then examine the relationship between motorway exposure and change in these behaviours, using both areal and individual measures of exposure based on study area of residence and individual proximity to the motorway, respectively.
Patterns of travel behaviour
Using the criteria described in Chapter 2, Evaluating the intervention, 1141 and 1206 travel records were found to be suitable for analysis at baseline and follow-up, respectively. A total of 71 and 92 ineligible journeys were removed at baseline and follow-up, respectively.
Patterns of travel behaviour in the longitudinal cohort and repeat cross-sectional sample can be found in Table 13. At both time points, car and walking were the most frequently reported modes of transport, with approximately half of the sample reporting using them at T1, and one-third reporting using them at T2. The proportions of participants reporting any travel, and using any particular mode of transport, were, on average, significantly lower at follow-up than at baseline. For example, 91% and 85% of longitudinal and repeat cross-sectional participants, respectively, reported any travel at T1, and these proportions fell to 69% and 65%, respectively, at T2. Among those who travelled, however, the average daily time spent travelling or using a particular mode of transport was fairly consistent over time.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |||||
| n | % | n | % | n | % | n | % | |
| Percentage who travelled | 285 | 90.5 | 285 | 68.8 | 830 | 84.8 | 877 | 65.0 |
| Travel time if travelled (minutes/day), mean (SD) | 258 | 76.1 (52.3) | 196 | 75.1 (81.5) | 704 | 67.1 (50.9) | 570 | 67.4 (57.8) |
| Percentage who used the bus | 285 | 31.9 | 285 | 21.1 | 830 | 31.7 | 877 | 23.3 |
| Bus time if used the bus (minutes/day), mean (SD) | 91 | 52.4 (44.9) | 60 | 47.4 (35.0) | 263 | 42.2 (36.8) | 204 | 49.5 (53.4) |
| Percentage who used the car | 285 | 52.6 | 285 | 41.8 | 830 | 44.3 | 877 | 34.5 |
| Car time if used the car (minutes/day), mean (SD) | 150 | 53.0 (43.0) | 119 | 50.1 (46.4) | 368 | 50.2 (47.4) | 303 | 49.3 (44.3) |
| Percentage who walked | 285 | 56.5 | 285 | 36.1 | 830 | 53.1 | 877 | 33.1 |
| Walking time if walked (minutes/day), mean (SD) | 161 | 35.3 (27.1) | 103 | 37.7 (27.7) | 441 | 35.3 (30.2) | 290 | 34.7 (30.1) |
Table 14 presents unadjusted summary measures of travel behaviour by study area. It shows few large differences between areas, apart from a higher likelihood of using the bus among cohort study participants living in the East.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |||||
| n | % | n | % | n | % | n | % | |
| Percentage who travelled | ||||||||
| Total | 285 | 90.5 | 285 | 68.8 | 830 | 84.8 | 877 | 65.0 |
| South | 97 | 89.7 | 97 | 72.2 | 278 | 83.1 | 271 | 66.8 |
| East | 87 | 94.3 | 87 | 70.1 | 267 | 86.9 | 300 | 67.0 |
| North | 101 | 88.1 | 101 | 64.4 | 285 | 84.6 | 306 | 61.4 |
| Travel time if travelled (minutes/day), mean (SD) | ||||||||
| Total | 258 | 76.1 (52.3) | 196 | 75.1 (81.5) | 704 | 67.1 (50.9) | 570 | 67.4 (57.8) |
| South | 87 | 76.6 (56.7) | 70 | 62.2 (41.2) | 231 | 71.9 (59.9) | 181 | 66.1 (61.5) |
| East | 82 | 76.5 (47.4) | 61 | 80.3 (65.3) | 232 | 62.7 (40.4) | 201 | 68.9 (58.8) |
| North | 89 | 75.3 (52.7) | 65 | 83.9 (118.8) | 241 | 66.7 (50.3) | 188 | 67.1 (53.1) |
| Percentage who used the bus | ||||||||
| Total | 285 | 31.9 | 285 | 21.1 | 830 | 31.7 | 877 | 23.3 |
| South | 97 | 27.8 | 97 | 17.5 | 278 | 29.9 | 271 | 21.4 |
| East | 87 | 41.4 | 87 | 32.2 | 267 | 34.1 | 300 | 27.3 |
| North | 101 | 27.7 | 101 | 14.9 | 285 | 31.2 | 306 | 20.9 |
| Bus time if used the bus (minutes/day), mean (SD) | ||||||||
| Total | 91 | 52.4 (44.9) | 60 | 47.4 (35.0) | 263 | 42.2 (36.8) | 204 | 49.5 (53.4) |
| South | 27 | 46.0 (41.4) | 17 | 47.1 (35.3) | 83 | 45.8 (42.5) | 58 | 45.4 (43.5) |
| East | 36 | 62.0 (48.1) | 28 | 47.6 (38.3) | 91 | 36.8 (28.2) | 82 | 53.7 (54.0) |
| North | 28 | 46.1 (43.0) | 15 | 47.2 (30.1) | 89 | 44.3 (38.5) | 64 | 48.0 (60.7) |
| Percentage who used the car | ||||||||
| Total | 285 | 52.6 | 285 | 41.8 | 830 | 44.3 | 877 | 34.6 |
| South | 97 | 55.7 | 97 | 45.4 | 278 | 41.7 | 271 | 36.2 |
| East | 87 | 43.7 | 87 | 36.8 | 267 | 46.1 | 300 | 33.3 |
| North | 101 | 57.4 | 101 | 42.6 | 285 | 45.3 | 306 | 34.3 |
| Car time if used the car (minutes/day), mean (SD) | ||||||||
| Total | 150 | 53.0 (43.0) | 119 | 50.1 (46.4) | 368 | 50.2 (47.4) | 303 | 49.3 (44.3) |
| South | 54 | 52.1 (40.4) | 44 | 46.6 (37.1) | 116 | 56.0 (63.2) | 98 | 47.7 (50.9) |
| East | 38 | 54.9 (40.5) | 32 | 53.3 (59.3) | 123 | 47.0 (35.4) | 100 | 48.6 (41.9) |
| North | 58 | 52.7 (47.5) | 43 | 51.4 (44.8) | 129 | 48.0 (40.3) | 105 | 51.5 (39.9) |
| Percentage who walked | ||||||||
| Total | 285 | 56.5 | 285 | 36.1 | 830 | 53.1 | 877 | 33.1 |
| South | 97 | 57.7 | 97 | 35.1 | 278 | 56.1 | 271 | 35.4 |
| East | 87 | 58.6 | 87 | 41.4 | 267 | 51.7 | 300 | 32.7 |
| North | 101 | 53.5 | 101 | 32.7 | 285 | 51.6 | 306 | 31.4 |
| Walking time if walked (minutes/day), mean (SD) | ||||||||
| Total | 161 | 35.3 (27.1) | 103 | 37.7 (27.7) | 441 | 35.3 (30.2) | 290 | 34.7 (30.1) |
| South | 56 | 37.0 (27.1) | 34 | 35.9 (29.0) | 156 | 36.8 (31.4) | 96 | 35.1 (34.1) |
| East | 51 | 32.9 (25.8) | 36 | 41.5 (28.9) | 138 | 35.4 (27.5) | 98 | 35.2 (27.6) |
| North | 54 | 35.8 (28.5) | 33 | 35.6 (25.1) | 147 | 33.5 (31.4) | 96 | 33.6 (28.4) |
Patterns of physical activity and sedentary behaviour
Using the criteria described in Chapter 2, Evaluating the intervention, 958 and 1029 records were found to be suitable for the analysis of MVPA, 1050 and 1095 records for the analysis of walking, and 917 and 984 records for the analysis of sitting time, at baseline and follow-up, respectively.
Patterns of physical activity and sedentary behaviour in the longitudinal cohort and repeat cross-sectional sample can be found in Table 15. The proportions of participants reporting walking and MVPA were fairly consistent between time points, with > 80% of the sample at each time point reporting some walking and more than two-thirds reporting some MVPA. Similarly, self-reported sedentary behaviour was fairly consistent over time, at an average of approximately 380 minutes (6.3 hours) per day. In the repeat cross-sectional sample, however, among those who reported any walking, the average time spent doing so was lower at follow-up than at baseline (355 vs. 410 minutes/week; p = 0.008).
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |||||
| n | % | n | % | n | % | n | % | |
| Percentage who walked | 297 | 87.9 | 302 | 84.1 | 753 | 81.4 | 793 | 82.0 |
| Walking time if walked (minutes/week), mean (SD) | 261 | 375.6 (352.6) | 254 | 393.2 (363.7) | 613 | 410.3 (392.9) | 650 | 355.1 (346.3) |
| Percentage who participated in MVPA | 264 | 74.6 | 280 | 73.2 | 694 | 65.4 | 749 | 70.2 |
| MVPA time if participated in MVPA (minutes/week), mean (SD) | 197 | 527.8 (508.6) | 205 | 550.9 (505.7) | 454 | 569.8 (506.2) | 526 | 513.9 (447.6) |
| Sedentary time (minutes/day), mean (SD) | 268 | 388.3 (234.8) | 273 | 383.4 (236.1) | 649 | 380.6 (247.6) | 711 | 380.7 (239.5) |
Table 16 presents unadjusted summary measures of physical activity and sedentary behaviour by study area. It shows no large differences between areas at either time point.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | ||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |||||
| n | % | n | % | n | % | n | % | |
| Percentage who walked | ||||||||
| Total | 297 | 87.9 | 302 | 84.1 | 753 | 81.4 | 793 | 82.0 |
| South | 104 | 89.4 | 107 | 83.2 | 246 | 84.6 | 244 | 85.7 |
| East | 89 | 86.5 | 89 | 83.2 | 238 | 79.4 | 273 | 79.9 |
| North | 104 | 87.5 | 106 | 85.6 | 269 | 80.3 | 276 | 80.8 |
| Walking time if walked (minutes/week), mean (SD) | ||||||||
| Total | 261 | 375.6 (352.6) | 254 | 393.2 (363.7) | 613 | 410.3 (392.9) | 650 | 355.1 (346.3) |
| South | 93 | 382.2 (353.0) | 89 | 362.4 (326.6) | 208 | 395.2 (405.6) | 209 | 356.7 (337.3) |
| East | 77 | 352.1 (334.4) | 74 | 438.4 (395.3) | 189 | 410.0 (395.1) | 218 | 361.2 (352.5) |
| North | 91 | 388.7 (369.8) | 91 | 386.5 (371.8) | 216 | 425.0 (379.6) | 223 | 347.7 (350.0) |
| Percentage who participated in MVPA | ||||||||
| Total | 264 | 74.6 | 280 | 73.2 | 694 | 65.4 | 749 | 70.2 |
| South | 92 | 76.1 | 97 | 72.2 | 231 | 63.6 | 232 | 72.0 |
| East | 80 | 73.8 | 82 | 68.3 | 228 | 70.6 | 258 | 70.5 |
| North | 92 | 73.9 | 101 | 78.2 | 235 | 62.1 | 259 | 68.3 |
| MVPA time if participated in MVPA (minutes/week), mean (SD) | ||||||||
| Total | 197 | 527.8 (508.6) | 205 | 550.9 (505.7) | 454 | 569.8 (506.2) | 526 | 513.9 (447.6) |
| South | 70 | 545.1 (492.1) | 70 | 517.1 (430.9) | 147 | 577.8 (540.7) | 167 | 490.9 (439.6) |
| East | 59 | 535.5 (507.5) | 56 | 564.1 (436.3) | 161 | 561.9 (448.0) | 182 | 521.7 (458.2) |
| North | 68 | 503.5 (532.3) | 79 | 571.5 (607.3) | 146 | 570.4 (533.4) | 177 | 527.7 (445.6) |
| Sedentary time (minutes/day), mean (SD) | ||||||||
| Total | 268 | 388.3 (234.8) | 273 | 383.4 (236.1) | 649 | 380.6 (247.6) | 711 | 380.7 (239.5) |
| South | 105 | 387.5 (228.1) | 96 | 396.1 (250.7) | 217 | 388.7 (258.2) | 229 | 404.5 (249.4) |
| East | 76 | 373.6 (257.3) | 78 | 401.2 (230.6) | 198 | 369.0 (237.4) | 247 | 375.7 (239.4) |
| North | 87 | 402.0 (224.0) | 99 | 357.1 (225.7) | 234 | 382.9 (246.8) | 235 | 362.9 (228.5) |
Relationships with environmental exposures
Analytical strategy
To understand the relationship between exposure to a motorway and changes in travel, physical activity and sedentary behaviours, we undertook two main sets of analyses. The first examined changes within participants over time in the longitudinal cohort. The second examined changes within the population over time in the repeat cross-sectional sample, with each participant contributing data at one of the two time points.
Preliminary exploration indicated that the assumptions of linear regression could not be satisfied for modelling the travel behaviour, MVPA or walking outcomes because of non-linearity and skewness. For these outcomes, we therefore used two-part models to model the relationships in two stages. 92 The first stage modelled the likelihood of reporting a given behaviour, such as using the car (yes/no) or undertaking any MVPA (yes/no). The second stage modelled the quantity of the behaviour, but only among those who reported it (e.g. time spent using the car among those who used the car, or time spent in MVPA among those who reported any participation). For the first stage we used a logit regression. For the second stage we used a GLM with a gamma family and log link, because the distribution of these outcomes remained skewed even after removing the zero values. When using two-part models, it is important that zeros are genuine, that is, that they reflect people truly not engaging in the behaviour rather than simply not responding to the question. For the travel variables, removing participants who returned a blank travel record was intended to satisfy this criterion (see Chapter 2, Derivation of key variables); for the physical activity variables, because the zero values were positively reported by the participants, we were satisfied that they did not merely reflect non-response. Sitting time was normally distributed and is not readily conceptualised as a two-part process. It was therefore modelled using linear regression.
From the travel record, we assessed the relationships of (1) study area and (2) individual-level exposure stratified by study area, with (1) travel and travel time, (2) bus use and bus travel time, (3) car use and car travel time and (4) walking and walking time. From the IPAQ, we assessed the relationships of (1) study area and (2) individual-level exposure stratified by study area, with (1) walking participation and walking time, (2) MVPA participation and time spent in MVPA and (3) sitting time. For all outcomes, the final models were adjusted for age, sex, home ownership, car ownership, working status and years lived in the local area. In the longitudinal analyses we also adjusted for the baseline value of the outcome of the model in question. In the repeat cross-sectional analyses we added a variable indicating time point, whereby the coefficient for the interaction between time point and exposure gave an indication of the population shift in the outcome over time. For all analyses using study area as the exposure, we used the North study area (no motorway) as the reference category. Finally, in the longitudinal analyses of travel variables using individual-level exposure stratified by study area, we carried out only the first (logit) stage of the two-part model because of the small number of non-zero values available for the second stage.
Results
Longitudinal analyses of travel behaviour
The results of the multivariable two-part regression models are displayed in Table 17. Compared with those in the North study area, cohort participants in the South were significantly more likely to undertake travel by any mode at follow-up [odds ratio (OR) 2.1, 95% confidence interval (CI) 1.0 to 4.2], and cohort participants in the East were significantly more likely to use the bus at follow-up (OR 2.4, 95% CI 1.1 to 5.2). However, there were no differences between study areas for either time spent travelling in general, or time spent using any mode of transport in particular.
| Exposure | Any travel | Bus | Car | Walking | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | n | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | n | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | n | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | |
| Area: South (reference: North) | 277 | 2.1 (1.0 to 4.2) | 0.8 (0.5 to 1.1) | 277 | 1.3 (0.6 to 3.0) | 1.0 (0.6 to 1.7) | 277 | 1.4 (0.7 to 2.7) | 0.9 (0.6 to 1.3) | 277 | 1.2 (0.6 to 2.3) | 0.9 (0.6 to 1.4) |
| Proximity within South study area | 91 | 4.7 (1.1 to 19.7) | – | 91 | 2.1 (0.3 to 13.1) | – | 91 | 2.3 (0.7 to 8.1) | – | 91 | 2.0 (0.5 to 7.6) | – |
| Area: East (reference: North) | 277 | 1.8 (0.9 to 3.6) | 1.0 (0.7 to 1.5) | 277 | 2.4 (1.1 to 5.2) | 1.1 (0.7 to 1.7) | 277 | 1.1 (0.6 to 2.2) | 1.0 (0.7 to 1.6) | 277 | 1.6 (0.8 to 3.1) | 1.4 (1.0 to 2.0) |
| Proximity within East study area | 83 | 1.6 (0.6 to 3.9) | – | 83 | 1.3 (0.6 to 3.0) | – | 83 | 1.2 (0.5 to 3.0) | – | 1.7 (0.8 to 3.6) | – | |
Within the South study area, participants living closer to a motorway junction were more likely to use a car and to undertake travel by any mode at follow-up than those living further away, but only the finding for any travel remained statistically significant in the maximally adjusted model (OR 4.7, 95% CI 1.1 to 19.7).
Repeat cross-sectional analyses of travel behaviour
The results of the multivariable two-part regression models are displayed in Table 18. There were no significant differences between study areas for either likelihood of, or time spent using, any or all modes of transport. Within the South study area, however, participants living closer to a motorway access point were more likely to use a car at follow-up than those living further away (OR 3.4, 95% CI 1.1 to 10.7).
| Exposure | Any travel | Bus | Car | Walking | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Obs | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | Obs | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | Obs | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | Obs | Yes/no, OR (95% CI) | Minutes/day, IRR (95% CI) | |
| Area: South (reference: North) | 1655 | 1.0 (0.5 to 1.9) | 0.9 (0.7 to 1.1) | 1655 | 1.0 (0.6 to 1.8) | 0.9 (0.6 to 1.3) | 1655 | 1.1 (0.6 to 2.0) | 0.7 (0.5 to 1.0) | 1655 | 0.8 (0.5 to 1.4) | 0.9 (0.7 to 1.3) |
| Proximity within South study area | 534 | 0.8 (0.3 to 2.7) | 1.3 (0.9 to 2.1) | 534 | 0.9 (0.3 to 2.4) | 1.9 (0.8 to 4.3) | 534 | 3.4 (1.1 to 10.7) | 1.1 (0.5 to 2.3) | 534 | 1.1 (0.5 to 2.7) | 1.2 (0.7 to 2.0) |
| Area: East (reference: North) | 1655 | 0.9 (0.4 to 1.6) | 1.1 (0.9 to 1.3) | 1655 | 1.2 (0.7 to 2.1) | 1.3 (0.9 to 2.0) | 1655 | 0.8 (0.4 to 1.5) | 1.0 (0.7 to 1.3) | 1655 | 0.9 (0.6 to 1.5) | 1.0 (0.7 to 1.4) |
| Proximity within East study area | 548 | 0.7 (0.3 to 1.8) | 1.1 (0.5 to 1.5) | 548 | 0.8 (0.4 to 1.7) | 0.8 (0.5 to 1.2) | 548 | 1.0 (0.4 to 2.3) | 1.4 (0.9 to 2.2) | 548 | 0.7 (0.3 to 1.5) | 1.4 (0.8 to 2.3) |
Longitudinal analyses of physical activity and sedentary behaviour
The results of the multivariable two-part and linear regression models are displayed in Table 19. Compared with those in the North study area, cohort participants in the East were significantly less likely to report participation in MVPA at follow-up (OR 0.4, 95% CI 0.2 to 0.9). This significant association was mirrored by a similar (albeit non-significant) relationship in the South study area (OR 0.6, 95% CI 0.3 to 1.4).
| Exposure | Walking | MVPA | Sedentary behaviour | |||||
|---|---|---|---|---|---|---|---|---|
| n | Yes/no, OR (95% CI) | Minutes/week, IRR (95% CI) | n | Yes/no, OR (95% CI) | Minutes/week, IRR (95% CI) | n | Minutes/day, β (95% CI) | |
| Area: South (reference: North) | 248 | 0.7 (0.2 to 1.9) | 0.8 (0.6 to 1.1) | 214 | 0.6 (0.3 to 1.4) | 0.9 (0.7 to 1.3) | 215 | 52.5 (–15.7 to 120.6) |
| Proximity within South study area | 88 | 1.5 (0.2 to 9.7) | 1.3 (0.9 to 1.9) | 70 | 2.4 (0.5 to 11.7) | 1.3 (0.8 to 2.1) | 81 | –40.2 (–125.4 to 45.1) |
| Area: East (reference: North) | 248 | 0.6 (0.2 to 1.7) | 1.1 (0.8 to 1.5) | 214 | 0.4 (0.2 to 0.9) | 0.9 (0.6 to 1.3) | 215 | 39.4 (–33.5 to 112.3) |
| Proximity within East study area | 69 | 1.6 (0.3 to 7.5) | 1.0 (0.7 to 1.5) | 59 | 0.3 (0.1 to 1.0) | 0.8 (0.5 to 1.3) | 59 | 59.4 (–26.9 to 145.7) |
Within the East study area, participants living closer to a motorway junction were less likely to report participation in MVPA at follow-up than those living further away (OR 0.3, 95% CI 0.1 to 1.0). Among those who reported any MVPA, no associations between time spent in MVPA and motorway exposure were found. No statistically significant differences in outcomes were found for walking or for sedentary behaviour.
Repeat cross-sectional analyses of physical activity and sedentary behaviour
The results of the multivariable two-part and linear regression models are displayed in Table 20. There were no statistically significant differences in outcomes in the repeat-cross sectional analyses. However, some of the outcomes were similarly patterned by study area as in the cohort analyses. Compared with the North, in the South and East study areas the odds of participating in walking and MVPA decreased over time, whereas time spent in sedentary behaviour increased.
| Exposure | Walking | MVPA | Sedentary behaviour | |||||
|---|---|---|---|---|---|---|---|---|
| Obs | Yes/no, OR (95% CI) | Minutes/week, IRR (95% CI) | Obs | Yes/no, OR (95% CI) | Minutes/week, IRR (95% CI) | Obs | Minutes/day, β (95% CI) | |
| Area: South (reference: North) | 1499 | 1.0 (0.5 to 1.9) | 1.1 (0.8 to 1.4) | 1412 | 1.0 (0.5 to 1.7) | 0.9 (0.7 to 1.3) | 1318 | 20.7 (–42.6 to 84.0) |
| Proximity within South study area | 475 | 0.5 (0.1 to 1.7) | 0.9 (0.6 to 1.4) | 450 | 0.4 (0.1 to 1.1) | 0.9 (0.5 to 1.4) | 431 | 38.7 (–73.5 to 150.8) |
| Area: East (reference: North) | 1499 | 1.0 (0.5 to 1.9) | 1.1 (0.8 to 1.4) | 1412 | 0.7 (0.4 to 1.2) | 1.0 (0.8 to 1.3) | 1318 | 16.2 (–47.3 to 79.7) |
| Proximity within East study area | 495 | 1.5 (0.6 to 3.8) | 1.4 (1.0 to 2.1) | 474 | 1.1 (0.4 to 2.5) | 1.4 (0.9 to 2.0) | 432 | 35.9 (–53.0 to 124.7) |
Patterns of behaviour and change over time in the Scottish Household Survey data
In this section we describe changes between 2009–10 and 2012–13 in the proportion of journey stages reported in the SHS travel diary data that were walked or cycled. We then examine the relationship between motorway exposure and changes in active travel using an areal definition of exposure similar to the study areas described in Chapter 2, Overall research design, using the wider city region of Glasgow City and surrounding local authorities as a reference group.
Patterns of travel behaviour
The proportions of journey stages made by active modes of transport are shown in Table 21. All areas experienced small increases in this proportion from 2009–10 to 2012–13 (from approximately 21% to 24%) and there was little variation between areas in this respect. The wider region of Glasgow and surrounding authorities had a smaller proportion of active journey stages in 2009–10, and also experienced a smaller increase over time compared with the South, East and North study areas. This may reflect the much larger (and in parts rural) area covered by the wider region.
| Time period | Area, % (n) | |||
|---|---|---|---|---|
| Glasgow and surrounding authorities | South | East | North | |
| 2009–10 | 18.1 (1766) | 21.8 (95) | 21.4 (102) | 20.9 (113) |
| 2012–13 | 19.8 (2309) | 23.6 (128) | 24.6 (138) | 22.9 (136) |
Relationships with environmental exposures
Analytical strategy
To understand the relationship between motorway exposure and change in active travel behaviour, we took journey stage as the unit of analysis and used multinomial logistic regression to model the likelihood of a stage being active by regressing a binary outcome variable for each stage (active or not active) on the explanatory variables including study area of residence, time period (2009–10 or 2012–13) and, later, the interaction of area and time period. The wider region comprising Glasgow City and surrounding local authorities was used as the reference category in these analyses. Models were first estimated without covariates and then adjusted for age, sex, health status and employment status, all of which were dichotomised because of the comparatively small sample size of journey stages available for analysis in each study area. The models also took account of the clustering of journey stages within individuals.
The analyses were then repeated after weighting to correct for differences in selection probabilities between areas of Scotland, households of different sizes and the days on which people were available for interview. Weights were calculated by the SHS94 and provided within the extracted data set. The application of weighting made no substantial difference to the main findings, but a comparison with 2011 Census data95 showed that it had improved the representation of the 16- to 24-years age group. The weighted analyses are therefore presented in this report.
Two sensitivity analyses were performed. First, we examined the effect of using a smaller reference area limited to Glasgow City, which excluded the surrounding local authority areas of North and South Lanarkshire, Renfrewshire and East Renfrewshire, and East and West Dunbartonshire. Second, we examined the effect of excluding journey stages of certain lengths, on the grounds that these may have provided less opportunity for switching mode of transport and some previous studies have applied similar exclusion criteria. 96 In contrast to the main analysis, (a), which included all stages regardless of distance, these sensitivity analyses were limited to (b) stages > 0.5 km (for shorter stages, it might be reasonable to assume that they could only be walked or cycled), (c) stages < 5 km (for longer stages, it might be reasonable to assume that they would be walked or cycled only by enthusiasts) and (d) stages > 0.5 km and < 5 km (i.e. incorporating both criteria).
Results
The results of the multinomial logistic regression models are displayed in Table 22. In the South (M74 motorway) and East (M8 motorway) study areas, the relative risks of a stage being made by an active mode of transport were similar at both time points in both unadjusted and adjusted models. In the North, however, the relative risk of an active stage was significantly higher than in the reference area in 2012–13 [adjusted relative risk ratio (RRR) 1.79, 95% CI 1.22 to 2.56].
| Time period | 2009–10 | 2012–13 | ||
|---|---|---|---|---|
| RRR (95% CI) | p-value | RRR (95% CI) | p-value | |
| Unadjusted | ||||
| Area | ||||
| Glasgow and surrounding authorities | Reference | |||
| South | 1.26 (0.88 to 1.80) | 0.209 | 1.37 (0.96 to 1.96) | 0.081 |
| East | 1.39 (0.96 to 2.02) | 0.078 | 1.24 (0.87 to 1.77) | 0.240 |
| North | 1.26 (0.86 to 1.85) | 0.228 | 1.77 (1.22 to 2.56) | 0.003 |
| Adjusted | ||||
| Area | ||||
| Glasgow and surrounding authorities | Reference | |||
| South | 1.29 (0.88 to 1.88) | 0.193 | 1.37 (0.95 to 1.99) | 0.092 |
| East | 1.38 (0.93 to 2.05) | 0.108 | 1.13 (0.79 to 1.62) | 0.513 |
| North | 1.33 (0.14 to 1.95) | 0.136 | 1.79 (1.22 to 2.60) | 0.003 |
Tests for interactions between study area and time period showed an increased odds of active travel in journeys made in the South and North study areas in 2012–13 compared with those made in the reference area of Glasgow City and surrounding local authorities in 2009–10 (Table 23).
| Area | 2009–10 | 2012–13 | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | p-value | Lower 95% CI | Upper 95% CI | OR | p-value | Lower 95% CI | Upper 95% CI | |
| Glasgow and surrounding authorities | Reference | 1.16 | 0.076 | 0.99 | 1.36 | |||
| South | 1.29 | 0.181 | 0.89 | 1.89 | 1.60 | 0.015 | 1.11 | 2.34 |
| East | 1.38 | 0.108 | 0.93 | 2.05 | 1.32 | 0.146 | 0.91 | 1.91 |
| North | 1.34 | 0.133 | 0.91 | 1.95 | 2.07 | < 0.001 | 1.40 | 3.05 |
This pattern of results suggests that the proportion of journey stages made using active modes of transport may have increased in the years following the opening of the M74 extension in both intervention (South) and control (North) study areas compared with in the region as a whole. However, because this increase was, if anything, greater in the North than in the South, it is unlikely to be attributable to the new motorway in the South.
The sensitivity analyses made no substantial difference to the findings (see Appendix 4). For further details, see Olsen et al. 93
Patterns of behaviour in the objective measurement data
In this section, we describe the sedentary behaviour, light physical activity and MVPA recorded in the objective measurement study at T2 (2013), and examine the relationships between these behaviours (both in total, and within participants’ neighbourhoods) and both areal and individual measures of motorway exposure.
Patterns of physical activity and sedentary behaviour
Using the criteria described in Chapter 2, Evaluating the intervention, 196 records were suitable for analysis. However, three participants, despite providing some GPS data, did not provide adequate data to allow for the derivation of summary measures of activity in their neighbourhood, which reduced the sample available for those analyses to 193.
Patterns of physical activity and sedentary behaviour are summarised in Table 24. Participants included in these analyses provided nearly 7 days of data on average, wearing their accelerometers for an average of 861 minutes (approximately 14 hours) per day and recording a valid location on their GPS receiver for an average of 561 minutes (approximately 9 hours) per day. Most participants exceeded the minimum recommended daily quantity of MVPA, with an average of 45 minutes per day in the sample as a whole. About half of all light physical activity, and one-third of MVPA, occurred within the 800-m pedestrian network buffer used to define each participant’s home neighbourhood.
| Variable | n | Mean (SD) |
|---|---|---|
| Number of valid days | 196 | 6.7 (0.7) |
| Accelerometer wear (minutes/day) | 196 | 860.8 (74.6) |
| GPS provides a valid location (minutes/day) | 196 | 561.4 (216.8) |
| Total light physical activity (minutes/day) | 196 | 77.5 (31.2) |
| Total MVPA (minutes/day) | 196 | 44.7 (30.5) |
| Total sedentary time (minutes/day) | 196 | 658.4 (83.6) |
| Neighbourhood light physical activity (minutes/day) | 193 | 35.4 (22.3) |
| Neighbourhood MVPA (minutes/day) | 193 | 15.0 (13.8) |
There were no large differences in unadjusted summary measures of physical activity or sedentary behaviour between study areas (Table 25).
| Variable | Total | South | East | North | ||||
|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
| Total light physical activity (minutes/day) | 196 | 77.5 (31.2) | 59 | 74.1 (25.9) | 58 | 75.4 (30.4) | 79 | 81.7 (35.0) |
| Total MVPA (minutes/day) | 196 | 44.7 (30.5) | 59 | 44.6 (25.5) | 58 | 48.6 (35.6) | 79 | 41.8 (29.9) |
| Total sedentary time (minutes/day) | 196 | 658.4 (83.6) | 59 | 673.1 (69.5) | 58 | 655.7 (90.9) | 79 | 649.4 (87.2) |
| Neighbourhood light physical activity (minutes/day) | 193 | 35.4 (22.3) | 58 | 34.5 (22.7) | 57 | 33.0 (18.7) | 78 | 37.9 (24.4) |
| Neighbourhood MVPA (minutes/day) | 193 | 15.0 (13.8) | 58 | 15.2 (13.1) | 57 | 14.8 (14.9) | 78 | 15.0 (13.7) |
Relationships with environmental exposures
Analytical strategy
To investigate the relationships between motorway exposure and total and neighbourhood physical activity and sedentary behaviour, we conducted a series of cross-sectional regression analyses using both areal and individual measures of exposure.
Preliminary exploration indicated that the assumptions of linear regression could not be satisfied for either light physical activity or MVPA because of skewness. These outcomes were therefore modelled using GLMs with a gamma family and log link. Sedentary time was normally distributed and was therefore modelled using linear regression.
We assessed the relationships of (1) study area and (2) individual-level exposure stratified by study area, with (1) total sedentary behaviour, (2) total light physical activity, (3) total MVPA, (4) neighbourhood light physical activity and (5) neighbourhood MVPA. For all outcomes, the final models were adjusted for age, sex, home ownership, car ownership, working status, years lived in the local area and accelerometer wear time. Models for the neighbourhood-specific outcomes were also adjusted for the total value of the outcome in question; for example, the model for neighbourhood MVPA was adjusted for total MVPA. For all analyses using study area as the exposure, we used the North study area (no motorway) as the reference category. We conducted sensitivity analyses for the neighbourhood-specific models to investigate the effect of using two alternative buffer sizes to define the neighbourhoods, 400 m and 1600 m.
Results
The results of the multivariable GLM and linear regression models for total physical activity and sedentary behaviour are displayed in Table 26. There were no significant differences between areas, or by motorway proximity, for any of the outcomes.
| Exposure | n | Model 1 | n | Model 2 | n | Model 3 |
|---|---|---|---|---|---|---|
| Outcome: total light physical activity (minutes/day), IRR (95% CI) | ||||||
| Area: South (reference: North) | 196 | 0.9 (0.8 to 1.0) | 194 | 0.9 (0.8 to 1.0) | 194 | 0.9 (0.8 to 1.0) |
| Proximity within South study area | 58 | 1.1 (0.9 to 1.3) | 58 | 1.1 (0.9 to 1.3) | 58 | 1.0 (0.8 to 1.3) |
| Area: East (reference: North) | 196 | 0.9 (0.8 to 1.1) | 194 | 0.9 (0.8 to 1.1) | 194 | 0.9 (0.8 to 1.1) |
| Proximity within East study area | 58 | 0.9 (0.7 to 1.2) | 56 | 1.0 (0.8 to 1.2) | 56 | 1.0 (0.7 to 1.3) |
| Outcome: total MVPA (minutes/day), IRR (95% CI) | ||||||
| Area: South (reference: North) | 196 | 1.1 (0.8 to 1.3) | 194 | 1.0 (0.8 to 1.3) | 194 | 1.0 (0.8 to 1.3) |
| Proximity within South study area | 58 | 0.9 (0.7 to 1.3) | 58 | 1.1 (0.8 to 1.5) | 58 | 1.0 (0.7 to 1.4) |
| Area: East (reference: North) | 196 | 1.2 (0.9 to 1.5) | 194 | 1.1 (0.9 to 1.4) | 194 | 1.2 (0.9 to 1.5) |
| Proximity within East study area | 58 | 1.0 (0.6 to 1.6) | 56 | 1.0 (0.6 to 1.6) | 56 | 1.1 (0.6 to 1.8) |
| Outcome: total sedentary time (minutes/day), β coefficient (95% CI) | ||||||
| Area: South (reference: North) | 196 | 23.7 (–4.6 to 52.0) | 194 | 25.6 (–2.4 to 53.6) | 194 | 12.8 (–9.5 to 35.0) |
| Proximity within South study area | 58 | 24.5 (–15.5 to 64.6) | 58 | 14.8 (–26.5 to 56.0) | 58 | –13.6 (–47.5 to 20.2) |
| Area: East (reference: North) | 196 | 6.3 (–22.1 to 34.8) | 194 | 2.4 (–25.9 to 30.7) | 194 | 1.9 (–20.4 to 24.1) |
| Proximity within East study area | 58 | –36.7 (–92.9 to 19.6) | 56 | –48.5 (–102.6 to 5.5) | 56 | 2.5 (–46.4 to 51.5) |
The results of the multivariable GLM regression models for neighbourhood physical activity are displayed in Table 27. There were no significant differences between areas, or by motorway proximity, for any of the outcomes.
| Exposure | n | Model 1 | n | Model 2 | n | Model 3 |
|---|---|---|---|---|---|---|
| Outcome: neighbourhood light physical activity (minutes/day), IRR (95% CI) | ||||||
| Area: South (reference: North) | 193 | 0.9 (0.7 to 1.1) | 191 | 0.9 (0.7 to 1.1) | 191 | 1.0 (0.9 to 1.1) |
| Proximity within South study area | 57 | 1.0 (0.7 to 1.5) | 57 | 1.0 (0.7 to 1.4) | 57 | 1.2 (0.9 to 1.7) |
| Area: East (reference: North) | 193 | 0.9 (0.7 to 1.1) | 191 | 0.9 (0.7 to 1.1) | 191 | 1.0 (0.8 to 1.2) |
| Proximity within East study area | 57 | 1.0 (0.7 to 1.4) | 55 | 1.0 (0.7 to 1.4) | 55 | 1.2 (0.8 to 1.7) |
| Outcome: neighbourhood MVPA (minutes/day), IRR (95% CI) | ||||||
| Area: South (reference: North) | 193 | 1.0 (0.7 to 1.4) | 191 | 1.0 (0.7 to 1.3) | 191 | 1.0 (0.8 to 1.2) |
| Proximity within South study area | 57 | 0.8 (0.5 to 1.2) | 57 | 0.9 (0.6 to 1.4) | 57 | 1.2 (0.8 to 1.7) |
| Area: East (reference: North) | 193 | 1.0 (0.7 to 1.4) | 191 | 1.0 (0.7 to 1.4) | 191 | 0.9 (0.7 to 1.1) |
| Proximity within East study area | 57 | 1.3 (0.6 to 2.5) | 55 | 1.3 (0.7 to 2.5) | 55 | 1.3 (0.8 to 2.0) |
The sensitivity analyses using different buffer sizes did not materially alter these findings (data not shown).
Conclusion
We found some evidence from the core survey that the new motorway promoted travel generally, and car use more specifically, among those living nearby. Ultimately, this might be expected to disadvantage the half of our sample who did not own a car and to reinforce existing socioeconomic inequalities. Contrary to claims made by both advocates and opponents in advance of its construction, we found no clear evidence linking the new motorway with either an increase or a decrease in active travel, in the analyses of either the core survey or the SHS travel diary data. Given the lack of any such clear effect on active travel, we did not pursue the further moderation or mediation analyses for these outcomes envisaged in the original study design. We found weaker evidence for a possible effect of motorway exposure on physical activity or sedentary behaviour. From the core survey, we found that physical activity participation was reduced over time in the area containing an existing motorway, but we found no effects on time spent in physical activity in the analyses of either the core survey or the objective measurement data. This may indicate that the effects of motorway exposure on physical activity are complex and evolve over time.
Chapter 5 Changes in road traffic accidents
Introduction
In the preceding chapter, we summarised our analyses of the relationships between motorway exposure and changes in activity patterns. In this chapter, we report our investigation of the effect of the new motorway on trends in road traffic accidents and resulting injuries, and the clustering of accidents by neighbourhood level of deprivation. As with the SHS analyses reported in Chapter 4, Patterns of behaviour and change over time in the Scottish Household Survey data, for these analyses we defined larger boundaries for the three study areas than those used for the core survey analyses and described in Chapter 2, Overall research design. These extended study areas – defined using 1000-m buffers around the same motorway and railway infrastructure – provided a greater number of incident cases in the models stratified by study area, thus improving the overall power and fit of the analyses. Figure 16 displays both the original study boundaries defined at the time of the baseline study55 and the new boundaries used for the analyses reported in this chapter. Each accident was assigned to a study area based on the precise co-ordinates provided in the STATS19 data set. 74 As shown in Table 9, the annual numbers of accidents, and of serious and fatal accidents, fell in all three study areas between 1997 and 2014.
FIGURE 16.
Expanded study areas for accident analysis. Contains Ordnance Survey data © Crown Copyright and database right 2016.
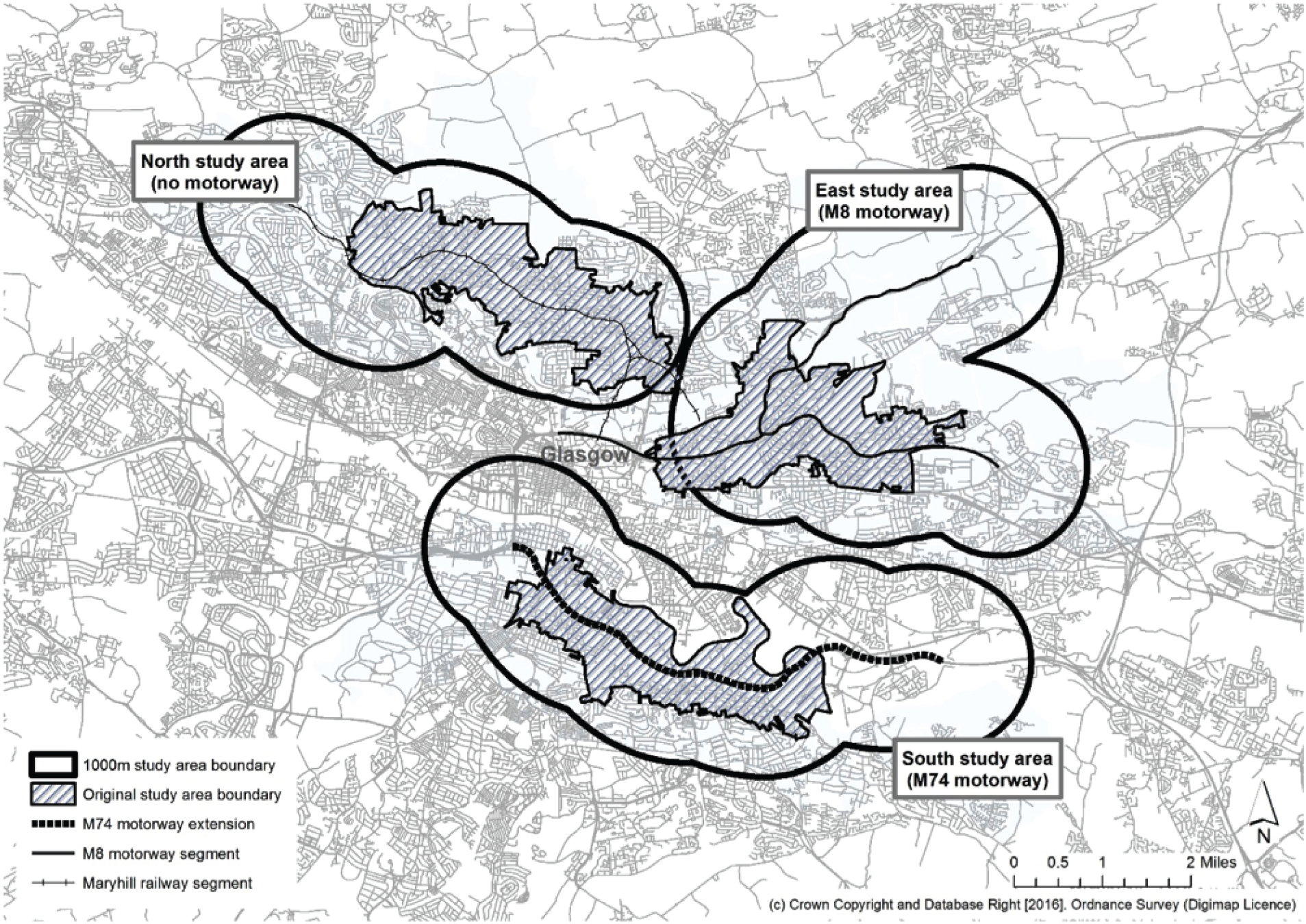
Patterns of accidents and injuries and changes over time
In this section, we describe the monthly and annual trends in road traffic accidents and related injuries in Glasgow City and surrounding local authorities as a whole and in each of our study areas.
The overall trends in monthly accident count are shown as time series plots for all accidents for the period 1997–2014 (Figure 17). All three study areas, as well as Glasgow City and surrounding local authorities as a whole, experienced a decreasing trend in monthly accident count over this period. The vertical lines indicate the months in which construction of the new motorway began (A: June 2008) and in which the new motorway was opened (B: June 2011).
FIGURE 17.
Trends in monthly accident counts, 1997–2014. (a) Glasgow and surrounding authorities; (b) south study area (M74 motorway); (c) east study area (M8 motorway); and (d) north study area (no motorway). Vertical green lines indicate the months in which construction of the new motorway began (A: June 2008) and in which the new motorway was opened (B: June 2011).
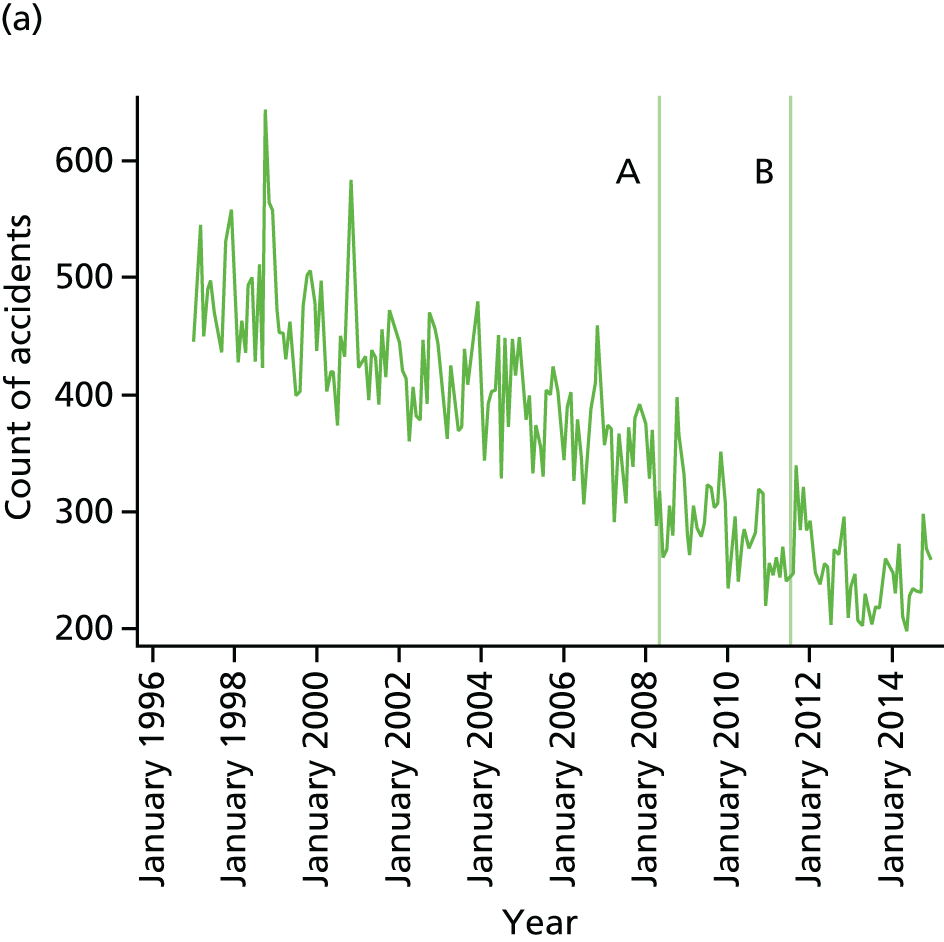
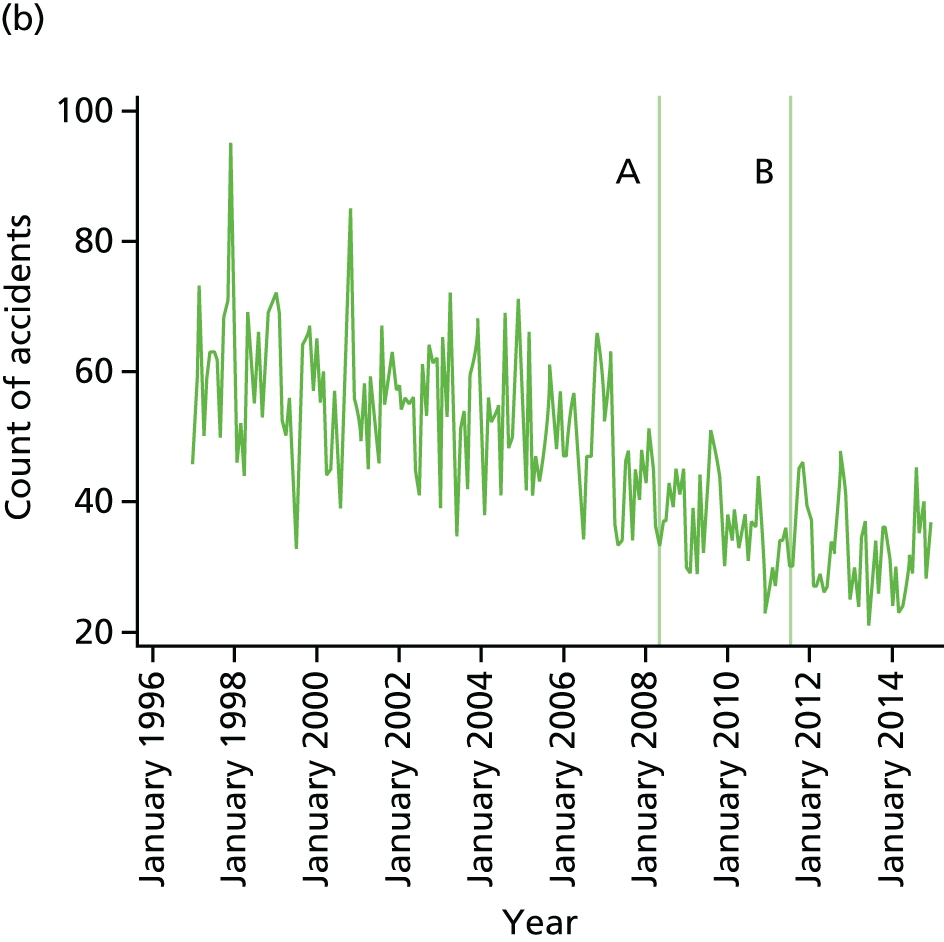
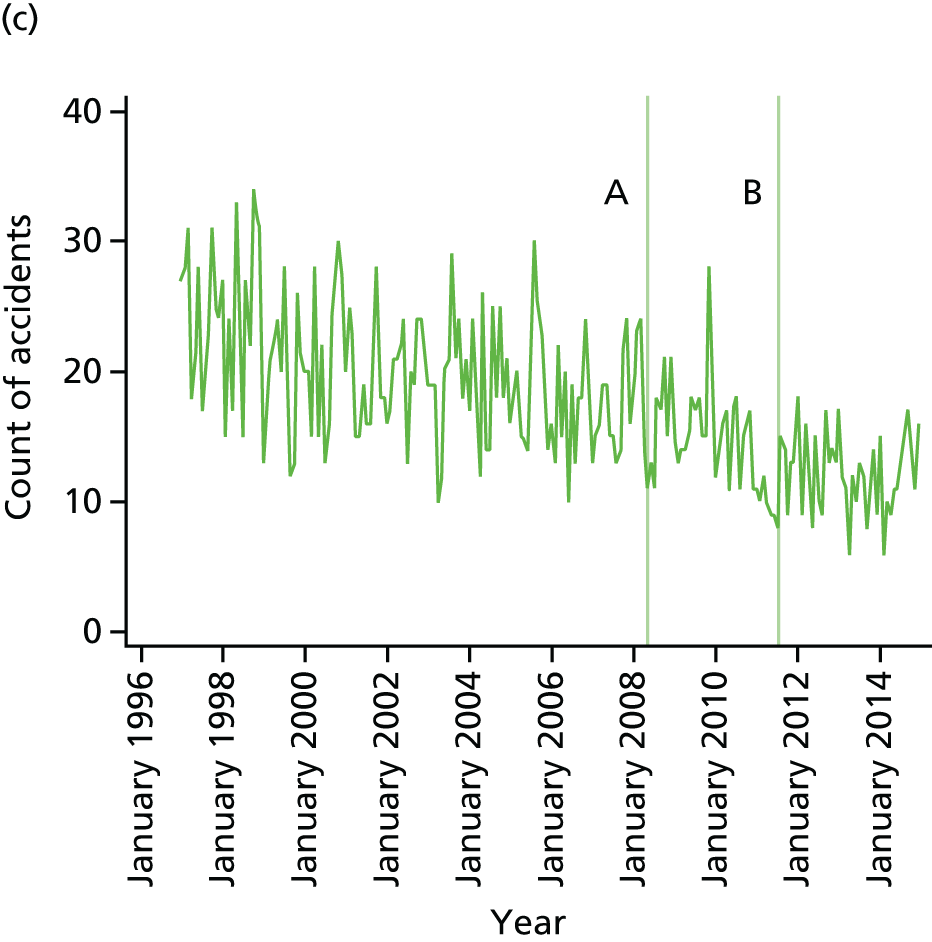
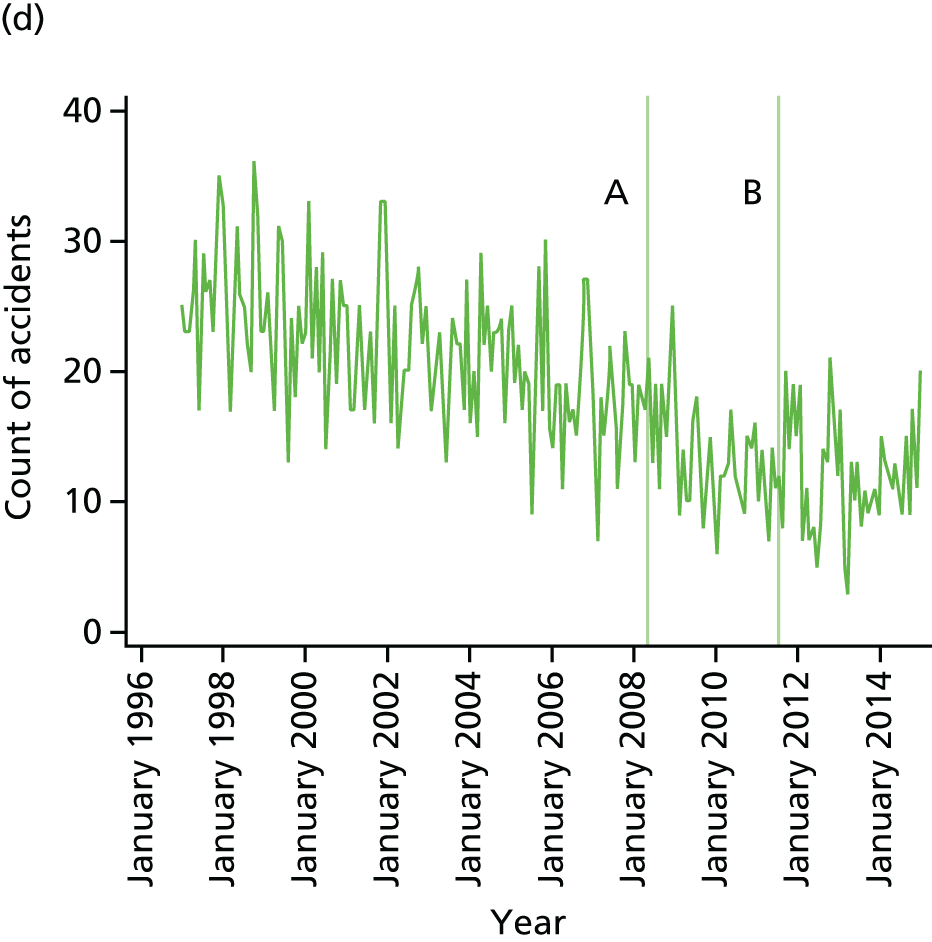
Relationships with environmental exposures
In this section, we examine the relationships between motorway exposure and changes in the trend of accident counts, using the areal measure of exposure described above.
Analytical strategy
Interrupted time series regression models with ARIMA errors were fitted to the monthly accident count data to test whether or not there had been a change in the secular trends of accidents during the construction of the new motorway or following its opening. 97,98 Individual models were fitted to each study area and data series. Log transformations and differencing were applied to the data to achieve time series that were normally distributed and stationary in both level and variance. For series in which there were months with a zero count of accidents, such as those limited to serious and fatal accidents in a single study area, the series were transformed using an inverse hyperbolic sine function. 99 To take account of the non-independent nature of the series, autocorrelation functions and partial autocorrelation functions of each model were used to identify seasonality and guide the initial model building. Detailed residual diagnostics were used to obtain a model with more accurate coefficient estimates. Outliers were identified following visual inspection of the initial models (p < 0.05); dummy variables for these outliers were then included and the models were re-estimated. The Akaike information criterion (AIC) was used to broadly assess model fit and to guide choices between competing models, with a lower AIC value indicating an improved fit. 100 The AIC was also used to assess whether or not removing outliers improved overall fit.
Definition of the intervention effect
The most appropriate way of modelling intervention effects in interrupted ARIMA time series models can be guided by the AIC criterion, or based on the anticipated impact of an intervention,101 as described in Chapter 1, The extension of the M74 motorway in Glasgow.
Motorway construction began in June 2008 and continued until the opening of the motorway 3 years later. During the construction period different local streets were closed and subject to diversions at different times, and these changes may have increased the risk of accidents as drivers, pedestrians and cyclists travelled unfamiliar routes. We therefore modelled the impact of the entire construction period as one intervention, hypothesising that it would take the form of an abrupt and temporary intervention effect lasting for the full duration of the construction phase. In contrast, we hypothesised that use of the new motorway would increase gradually following its opening, and therefore modelled the impact of the opening as a ramp intervention effect that was assumed to be both gradual and permanent. 102 Although opening on a specific date might be regarded as an abrupt step event, in practice changes in human behaviour, daily routines and other adjustments to new infrastructure often take months or years to become fully embedded. 49,103 By way of sensitivity analyses, we also modelled the series using step (‘abrupt permanent’), ramp (‘ongoing gradual’) and ramp-and-step (‘gradual’ then ‘permanent’) functions that reflected alternative ways of theorising the impact of the opening of the new motorway. These made no material difference to the overall results or goodness-of-fit of the models. In addition, we found no change in the variance of the series during the construction period or following the opening, and no change in the seasonal variance of the series when explored using a seasonal decomposition procedure based on loess [analysed using R version 0.98.1103 (The R Foundation for Statistical Computing, Vienna, Austria)]. 104
Traffic counts
The causes of road traffic accidents are multifactorial, and there is mixed evidence for whether or not an increase in traffic volume is associated with an increase in accidents or whether or not traffic count data should be included as a denominator in accident time series models. 105,106 We investigated the possibility of doing the latter, and extracted traffic count data from the Department of Transport, Transport Scotland and Glasgow City Council for this purpose. Data from all three sources turned out to be derived from counter locations that had changed after the opening of the new motorway, which made it impossible to make an unbiased assessment of temporal trends in traffic counts on local streets. However, the available data suggested no substantive change in the overall spatiotemporal distribution of traffic counts in Glasgow. Taking both observations into account, we therefore elected to apply the time series models to the accident count data only. 107–109 An evaluation conducted for Transport Scotland 16 weeks after the opening of the new motorway identified small decreases in traffic for some local streets, increases in traffic on the main feeder roads for the new motorway and ‘satisfactory’ traffic flow on the new motorway itself. 110
Results
Table 28 presents the results from the ITS models for (1) all accidents and (2) serious and fatal accidents only. There was a significant downwards trend in the monthly count of all accidents in each of the study areas over the period 1997–2014.
| Study area | Outcome | All accidents | Serious and fatal accidents | ||||
|---|---|---|---|---|---|---|---|
| Series | Parameter | Estimate (95% CI) | p-value | Parameter | Estimate (95% CI) | p-value | |
| Glasgow and surrounding local authorities | Change in series for full study period | Log ar(7 9 10 12) sarima(0,1,0,12) | –0.042 | < 0.0001 | Log ar(1 7 12) sarima(0,1,0,12) | –0.074 | < 0.0001 |
| (–0.054 to –0.030) | (–0.107 to –0.041) | ||||||
| Change in series during construction | –0.066 | < 0.0001 | 0.046 | 0.337 | |||
| (–0.098 to –0.035) | (–0.048 to 0.139) | ||||||
| Change in series following opening | –0.001 | 0.295 | 0.0027 | 0.385 | |||
| (–0.003 to 0.001) | (–0.003 to 0.009) | ||||||
| South | Change in series for full study period | Log ar(1 12 13) sarima(0,1,0,12) | –0.041 | 0.003 | Log ma(1 12) sarima(0,1,0,12) | –0.088 | < 0.0001 |
| (–0.069 to –0.014) | (–0.125 to –0.063) | ||||||
| Change in series during construction | –0.026 | 0.558 | –0.082 | 0.705 | |||
| (–0.116 to 0.063) | (–0.451 to 0.299) | ||||||
| Change in series following opening | –0.001 | 0.951 | –0.003 | 0.67 | |||
| (–0.006 to 0.006) | (–0.017 to 0.011) | ||||||
| East | Change in series for full study period | Log ar(1 12) sarima(0,1,0,12) | –0.053 | 0.001 | Log ma(12) sarima(0,1,0,12) | –0.119 | < 0.0001 |
| (–0.083 to –0.022) | (–0.163 to –0.075) | ||||||
| Change in series during construction | 0.065 | 0.264 | –0.044 | 0.831 | |||
| (–0.049 to 0.179) | (–0.446 to 0.358) | ||||||
| Change in series following opening | 0.005 | 0.142 | 0.012 | 0.255 | |||
| (–0.002 to 0.013) | (–0.008 to 0.032) | ||||||
| North | Change in series for full study period | Log ar(11) sarima(0,1,1,12) | –0.054 | 0.002 | Log ma(12) sarima(0,1,0,12) | –0.074 | < 0.0001 |
| (–0.088 to –0.019) | (–0.115 to –0.033) | ||||||
| Change in series during construction | –0.353 | 0.029 | –0.08 | 0.722 | |||
| (–0.669 to –0.037) | (–0.521 to 0.361) | ||||||
| Change in series following opening | –0.029 | < 0.0001 | 0.0001 | 0.994 | |||
| (–0.043 to –0.016) | (–0.024 to 0.024) | ||||||
Impact of the construction period for the new motorway
During the construction period, Glasgow and surrounding authorities in general, and the North study area in particular, experienced a small but significant decrease in the temporal accident trend when the intervention was modelled as a 3-year step effect. There was no such change in the South or East study areas.
Impact of the opening of the new motorway
The opening of the new motorway was not associated with any discernible change in the already decreasing temporal trend of accidents in the South or East study areas, or in Glasgow and surrounding authorities as a whole. However, the North (which contained no motorway) did experience a significant further decrease in monthly accident count following the opening of the M74 extension.
Serious and fatal accidents
There was no significant change in the temporal trend in serious and fatal accidents in any of the study areas, either during the construction of the M74 extension or following its opening.
Casualty types
Each accident can result in multiple casualties if more than one vehicle or road user is involved. Road users are pre-classified in the STATS19 data set as a pedestrian, a driver or rider, or a passenger. 74 Changes in the absolute counts of casualties for each category of road user were too small for time series models. Instead, we pooled serious and fatal casualties – the casualties of most public health importance – in two 3-year periods (1997–9 and 2012–14), and used analysis of variance and pairwise comparisons between study areas to compare changes in the proportions of all serious and fatal casualties attributed to each category of road user.
All three study areas experienced reductions in the number of casualties for pedestrians, drivers or riders, and passengers from 1997–9 to 2012–14 (Table 29). We found no significant differences between areas for drivers or riders, or for passengers. The reduction in pedestrian casualties was smaller in the South than in the East and North study areas, and significantly smaller than in Glasgow and the surrounding authorities as a whole (95% CI 0.016 to 0.158; t = 3.25, p = 0.007). However, because this difference was observed over the time period between 1997–9 and 2012–14, it may very well have been attributable to factors other than the new motorway. Casualty numbers were too small to permit meaningful exploration of differences in counts between single years.
| Study area | Pedestrian | Driver or rider | Passenger | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1997–9 | 2012–14 | % change | 1997–9 | 2012–14 | % change | 1997–9 | 2012–14 | % change | |
| Glasgow and surrounding authorities | 1703 | 571 | –66.5 | 1504 | 585 | –61.1 | 863 | 208 | –75.9 |
| South | 210 | 101 | –51.9 | 121 | 61 | –49.6 | 79 | 17 | –78.5 |
| East | 111 | 39 | –64.9 | 54 | 28 | –48.1 | 32 | 11 | –65.6 |
| North | 122 | 38 | –68.9 | 59 | 19 | –67.8 | 33 | 5 | –84.8 |
| ANOVA: p = 0.013, F = 3.60 a | ANOVA: p = 0.157, F = 1.74 | ANOVA: p = 0.535, F = 0.73 | |||||||
Changes in the sociospatial distribution of accidents
We also investigated whether or not the new motorway was associated with any change in the spatial patterning of accidents between more and less deprived neighbourhoods. Road traffic accidents typically occur in geographical clusters,112 and a major change to the local road network could have produced a change in this clustering. We used Poisson-based continuous scan statistics113 to detect spatial clusters of numbers of accidents. Each accident that occurred in Glasgow City or the surrounding local authorities was included in analysis and assigned a 2014 Scottish Index of Multiple Deprivation (SIMD) score114 based on the data zone (the smallest area of Scottish statistical geography) in which it occurred. We examined associations between accidents and deprivation, temporal changes in these associations, and changes in the locations of accident clusters and the socioeconomic patterning of clustered and non-clustered accidents. One-third (7682 of 22,724) of all accidents occurred in the most deprived data zones in Glasgow (those in the lowest quintile of the national SIMD distribution) and this proportion changed little over time. Most clusters of accidents were located in the city centre. Clusters of accidents were more likely than non-clustered accidents to be found in more deprived areas, with mean SIMD scores of 31.9 (n = 294) and 28.5 (n = 2908) for clustered and non-clustered accidents, respectively (p = 0.002). This pattern also remained consistent over time, and the spatial-temporal analysis detected no significant changes in the spatial distribution of clusters between 2009 and 2014. These results suggest that the opening of the M74 extension had no discernible impact on the sociospatial clustering of accidents.
Conclusions
In keeping with other recent studies in the UK,115,116 we observed a downwards trend in road traffic accidents between 1997 and 2014 in each of the study areas, and in Glasgow and the surrounding authorities as a whole. We found no evidence of either an increase or a decrease in this downwards trend that could be attributed to the M74 extension. The North study area did show further decreases in the downwards trajectory of accident incidence, both during the construction of the new motorway and after its opening. However, no such change was observed in the region as a whole, in the South study area surrounding the new M74 motorway or in the East study area surrounding the existing M8 motorway. If the effect observed in the North was causally attributable to the new motorway, it would most likely have been observed first and most strongly in the area surrounding the new motorway, and, second, on other major roads in the city that would have experienced a significant change in traffic flow. Neither of these effects were apparent, and the limited traffic count data available suggested that the M74 extension has had little impact on trends in the number of vehicles travelling in the city as a whole. The North study area contained a local transformational regeneration zone involving new housing, community facilities and improvements to green space from 2010 onwards. 117 It also benefited from the reopening of a disused railway line, improvements to pedestrian and cycle paths to the city centre and the introduction of new bus lanes. These and other factors beyond the scope of our study may have contributed to the additional decrease in accidents observed in the North study area.
Chapter 6 Changes in well-being
Introduction
In the preceding chapters, we summarised our findings on the relationships between motorway exposure and changes in activity patterns and road traffic accidents. In this chapter, we investigate the effects of motorway exposure on well-being. Of all of the analyses reported so far, the main analysis reported in this chapter is the one that provides the strongest evidence of an intervention effect. We therefore considerably extended this set of analyses to include explorations of how changes in well-being were distributed in the population, of the extent to which more general neighbourhood upheaval was associated with differences or changes in well-being, and of the extent to which effects on well-being were mediated by differences or changes in people’s perceptions of their neighbourhood. These complementary analyses provided a more detailed understanding of the relationships, and permitted a degree of triangulation to strengthen the overall case for causal inference.
Patterns of well-being and change over time
In this section, we describe patterns of well-being at T1 (2005) and T2 (2013) using the core survey data. We then examine the relationship between motorway exposure and (changes in) well-being using both areal and individual exposure measures, including tests for effect modification to investigate the extent to which the effects varied between groups of participants. We then introduce an additional exposure measure representing neighbourhood upheaval to the analysis and examine the relationships between well-being and neighbourhood upheaval, both in its own right and in combination with exposure to motorway infrastructure.
Patterns of well-being
Patterns of mental and physical well-being in the longitudinal cohort, the repeat cross-sectional sample and the full follow-up sample can be found in Table 30. In all samples, and at all time points, average well-being measured using the SF-8 was lower than in the general US population in which the instrument was developed, which has mean PCS-8 and MCS-8 scores of 49. 66 The Warwick–Edinburgh Mental Well-being Scale was administered in the 2012 Scottish Health Survey and a mean score of 50 was reported,118 but comparable population estimates for the short version are not available. In both longitudinal and repeat cross-sectional samples, physical (but not mental) well-being was significantly lower at follow-up (when participants were older on average) than at baseline.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | Full T2 sample (N = 1343) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | T2 | ||||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
| SWEMWBS | N/A | N/A | 1318 | 21.9 (4.1) | ||||||
| PCS-8 | 352 | 47.4 (11.0) | 360 | 45.9 (11.7) | 935 | 46.8 (11.8) | 960 | 45.3 (12.1) | ||
| MCS-8 | 352 | 45.5 (11.1) | 360 | 46.4 (11.1) | 935 | 43.8 (11.6) | 960 | 44.4 (12.1) | ||
Table 31 presents unadjusted summary measures of well-being by study area. There were no large differences between study areas at either time point.
| Variable | Longitudinal cohort (N = 365) | Repeat cross-sectional sample (T1, N = 980; T2, N = 978) | Full T2 sample (N = 1343) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | T2 | ||||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
| SWEMWBS | ||||||||||
| Total | N/A | N/A | N/A | N/A | 1318 | 21.9 (4.1) | ||||
| South | 423 | 22.0 (4.1) | ||||||||
| East | 439 | 21.8 (4.1) | ||||||||
| North | 456 | 21.9 (4.0) | ||||||||
| PCS-8 | ||||||||||
| Total | 352 | 47.4 (11.0) | 360 | 45.9 (11.7) | 935 | 46.8 (11.8) | 960 | 45.3 (12.1) | ||
| South | 122 | 47.7 (11.2) | 123 | 46.7 (11.9) | 305 | 47.0 (12.1) | 300 | 46.2 (12.1) | ||
| East | 105 | 46.7 (11.1) | 111 | 44.7 (12.0) | 307 | 46.7 (11.6) | 327 | 45.0 (11.9) | ||
| North | 125 | 47.5 (10.8) | 126 | 46.2 (11.2) | 323 | 46.7 (11.7) | 333 | 44.9 (12.5) | ||
| MCS-8 | ||||||||||
| Total | 352 | 45.5 (11.1) | 360 | 46.4 (11.1) | 935 | 43.8 (11.6) | 960 | 44.4 (12.1) | ||
| South | 122 | 46.4 (11.1) | 123 | 47.1 (11.5) | 305 | 43.9 (11.6) | 300 | 44.1 (11.8) | ||
| East | 105 | 44.7 (10.6) | 111 | 46.4 (9.7) | 307 | 43.2 (11.7) | 327 | 44.0 (12.7) | ||
| North | 125 | 45.2 (11.6) | 126 | 45.7 (11.9) | 323 | 44.3 (11.6) | 333 | 45.1 (11.7) | ||
Relationships with environmental exposures
Analytical strategy
To understand the relationships between motorway exposure and well-being, we undertook three main sets of analyses. The first examined changes within participants over time in the longitudinal cohort. The second examined changes within the population over time in the repeat cross-sectional sample, in which each participant contributed data at one of the two time points. The third examined cross-sectional relationships in the full follow-up sample, to allow for the use of the SWEMWBS data that had not been collected at baseline.
Using linear regression models, we assessed the relationships of (1) study area and (2) individual-level exposure (straight-line distance from home to the nearest motorway) stratified by study area with (1) PCS-8, (2) MCS-8 and (3) SWEMWBS score. For all outcomes, the final models were adjusted for age, sex, home ownership, car ownership, working status, perceived financial strain, presence of a chronic condition and years lived in the local area. In the longitudinal analyses we also adjusted for the baseline value of the outcome of the model in question. In the repeat cross-sectional analyses we added a variable indicating time point, whereby the coefficient of the interaction between time point and exposure gave an indication of the population shift in the outcome over time. For all analyses using study area as the exposure, we used the North study area (no motorway) as the reference category. As a final step, we tested all maximally adjusted models for interactions with perceived financial strain and presence of a chronic condition, which we hypothesised could act as effect modifiers (moderators). In models using individual exposure stratified by study area, interactions were tested only in the South and East study areas (i.e. those areas with a motorway).
Following the main analyses described above, we undertook a further supplementary analysis to investigate the relationships between neighbourhood upheaval and well-being. This consisted of two sets of analyses. The first examined changes within participants over time in the longitudinal cohort. The second examined cross-sectional relationships in the full follow-up sample. Using linear regression models, we assessed the relationship of individual-level exposure to neighbourhood upheaval with (1) PCS-8, (2) MCS-8 and (3) SWEMWBS score. Models were adjusted for the same set of covariates as described for the main analyses above. We then tested all maximally adjusted models for an interaction with study area.
Results
Longitudinal analysis of associations between motorway exposure and the Short Form 8 Health Survey
The results of the multivariable linear regression models are shown in Table 32. There were no significant differences between study areas for either the physical (PCS-8) or mental (PCS-8) component summary scores of the SF-8. In the South and East study areas, participants living closer to a motorway experienced reduced mental well-being (MCS-8) over time compared with those living further away. In the South, this finding remained statistically significant in the maximally adjusted model (beta coefficient –3.6, 95% CI –6.6 to –0.7).
| Exposure | β coefficient (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| n | Model 1 | n | Model 2 | n | Model 3 | n | Model 4 | |
| Outcome: PCS-8 | ||||||||
| Area: South (reference: North) | 348 | 0.0 (–2.2 to 2.2) | 346 | 0.4 (–1.8 to 2.6) | 336 | 0.5 (–1.8 to 2.8) | 336 | 0.5 (–1.6 to 2.6) |
| Proximity within South study area | 116 | –0.9 (–3.7 to 1.9) | 115 | –0.4 (–3.2 to 2.5) | 110 | –0.9 (–4.0 to 2.3) | 110 | –0.5 (–3.3 to 2.4) |
| Area: East (reference: North) | 348 | –0.8 (–3.1 to 1.5) | 346 | –0.7 (–2.9 to 1.6) | 336 | –1.1 (–3.4 to 1.2) | 336 | –0.7 (–2.9 to 1.4) |
| Proximity within East study area | 103 | –0.3 (–2.8 to 2.3) | 103 | 0.1 (–2.6 to 2.7) | 100 | 0.4 (–2.4 to 3.2) | 100 | 0.0 (–2.6 to 2.6) |
| Outcome: MCS-8 | ||||||||
| Area: South (reference: North) | 348 | –0.1 (–2.7 to 2.5) | 346 | 0.0 (–2.6 to 2.6) | 336 | 0.3 (–2.3 to 2.9) | 336 | 0.7 (–1.6 to 3.0) |
| Proximity within South study area | 116 | –3.2 (–6.4 to –0.1) | 115 | –3.6 (–6.8 to –0.5) | 110 | –3.9 (–7.2 to –0.6) | 110 | –3.6 (–6.6 to –0.7) |
| Area: East (reference: North) | 348 | 0.8 (–1.9 to 3.5) | 346 | 0.7 (–2.0 to 3.4) | 336 | 0.5 (–2.2 to 3.2) | 336 | 0.8 (–1.6 to 3.1) |
| Proximity within East study area | 103 | –3.5 (–6.7 to –0.3) | 103 | –2.9 (–6.2 to 0.5) | 100 | –1.2 (–4.6 to 2.2) | 100 | 0.2 (–2.5 to 2.9) |
Repeat cross-sectional analysis of associations between motorway exposure and the Short Form 8 Health Survey
The results of the multivariable linear regression models are displayed in Table 33. There were no significant differences between study areas for either the PCS-8 or MCS-8 scores. In the South, physical well-being (PCS-8) reduced over time in people living closer to the motorway compared with those living further away, but this was not statistically significant in the maximally adjusted model. In the East, a borderline significant (p = 0.06) interaction by chronic condition was found for mental well-being (MCS-8). In this area, stratified analysis indicated a reduction in MCS-8 over time among participants with a chronic condition living closer to the motorway compared with those living further away (beta coefficient –3.7, 95% CI –8.3 to 0.9).
| Exposure | Beta coefficient (95% CI) | |||||
|---|---|---|---|---|---|---|
| n | Model 1 | n | Model 2 | n | Model 3 | |
| Outcome: PCS-8 | ||||||
| Area: South (reference: North) | 1895 | 1.0 (–1.7 to 3.6) | 1870 | 0.2 (–2.2 to 2.6) | 1778 | –0.2 (–2.0 to 1.7) |
| Proximity within South study area | 604 | –6.0 (–10.6 to –1.5) | 593 | –5.2 (–9.4 to –0.9) | 571 | –1.5 (–4.8 to 1.7) |
| Area: East (reference: North) | 1895 | 0.1 (–2.6 to 2.7) | 1870 | –0.5 (–2.9 to 1.9) | 1778 | –0.8 (–2.6 to 1.0) |
| Proximity within East study area | 634 | 2.1 (–1.0 to 5.2) | 628 | 0.7 (–2.0 to 3.4) | 591 | 1.5 (–0.7 to 3.6) |
| Outcome: MCS-8 | ||||||
| Area: South (reference: North) | 1895 | –0.6 (–3.2 to 2.0) | 1870 | –0.6 (–3.3 to 2.0) | 1778 | –0.8 (–3.1 to 1.5) |
| Proximity within South study area | 604 | –3.3 (–7.8 to 1.1) | 593 | –3.7 (–8.2 to 0.8) | 571 | 1.4 (–2.6 to 5.4) |
| Area: East (reference: North) | 1895 | 0.0 (–2.6 to 2.6) | 1870 | –0.1 (–2.7 to 2.5) | 1778 | 0.5 (–1.8 to 2.8) |
| Proximity within East study area | 634 | –1.3 (–4.5 to 1.9) | 628 | –1.6 (–4.9 to 1.6) | 591 | –0.7 (3.5 to 2.1) |
Cross-sectional analysis of associations between motorway exposure and the short version of the Warwick–Edinburgh Mental Well-Being scale
The results of the multivariable linear regression models are displayed in Table 34. There were no significant differences in well-being between study areas. In the South and East study areas, participants living closer to a motorway had poorer well-being (as measured using the SWEMWBS) than those living further away; however, these findings were not statistically significant in the maximally adjusted models. A significant interaction (p = 0.011) by chronic condition was found in the East. In this area, stratified analysis indicated that participants with a chronic condition living closer to the motorway had significantly poorer well-being than those living further away (beta coefficient –1.1, 95% CI –2.0 to –0.3).
| Exposure | Outcome: SWEMWBS score, beta coefficient (95% CI) | |||||
|---|---|---|---|---|---|---|
| n | Model 1 | n | Model 2 | n | Model 3 | |
| Area: South (reference: North) | 1318 | 0.1 (–0.4 to 0.7) | 1310 | 0.1 (–0.4 to 0.7) | 1253 | 0.0 (–0.5 to 0.5) |
| Proximity within South study area | 419 | –1.0 (–1.8 to –0.2) | 418 | –1.0 (–1.8 to –0.2) | 404 | –0.1 (–0.9 to 0.7) |
| Area: East (reference: North) | 1318 | –0.2 (–0.7 to 0.4) | 1310 | –0.2 (–0.7 to 0.4) | 1253 | 0.0 (–0.5 to 0.5) |
| Proximity within East study area | 437 | –0.8 (–1.4 to –0.1) | 433 | –0.8 (–1.4 to –0.1) | 411 | –0.4 (–1.0 to 0.2) |
Longitudinal analysis of associations between neighbourhood upheaval and the Short Form 8 Health Survey
The results of the multivariable linear regression models are displayed in Table 35. Participants living in areas with a greater amount of change in the built environment in their neighbourhood experienced reduced mental (MCS-8 –0.16, 95% CI –0.31 to –0.02) and physical (PCS-8 –0.13, 95% CI –0.26 to 0.00) well-being over time compared with those living in neighbourhoods with less change. The association with mental well-being was significant and with physical well-being was of borderline significance (p = 0.051) in maximally adjusted models. Although these coefficients may appear comparatively small, they represent estimates of the difference in well-being between participants living in neighbourhoods that differed in upheaval by a single percentage point. It may be more meaningful to compare neighbourhoods that differ by a larger ‘dose’ of upheaval, for example 5% or 10% (see Figure 14). For these comparisons, the estimated differences in mental well-being are –0.8 and –1.6 MCS-8 units, respectively. For mental well-being, borderline significant (p = 0.052) and significant (p = 0.048) interactions were found by study area for the South and East, respectively. Stratified analysis indicated that participants in the South exposed to greater upheaval experienced reduced mental well-being (MCS-8 –0.18, 95% CI –0.34 to –0.02) over time compared with those exposed to less upheaval. A larger effect was found in stratified analyses in the East, but this was not significant (MCS-8 –0.34, 95% CI –0.79 to 0.12).
| Exposure | n | Model 1,β coefficient (95% CI) | n | Model 2,β coefficient (95% CI) | n | Model 3,β coefficient (95% CI) | n | Model 4,β coefficient (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Outcome: PCS-8 | ||||||||
| Percentage change to built environment in neighbourhood | 326 | –0.10 (–0.23 to 0.04) | 324 | –0.10 (–0.23 to 0.04) | 314 | –0.10(–0.25 to 0.04) | 314 | –0.13 (–0.26 to 0.00)a |
| Outcome: MCS-8 | ||||||||
| Percentage change to built environment in neighbourhood | 326 | –0.13 (–0.30 to 0.04) | 324 | –0.12 (–0.28 to 0.05) | 314 | –0.17 (–0.33 to 0.00) | 314 | –0.16 (–0.31 to –0.02) |
Cross-sectional analysis of associations between neighbourhood upheaval and the Short Form 8 Health Survey summary scores
The results of the multivariable linear regression models are displayed in Table 36. There were no significant differences in well-being between participants living in areas with a greater amount of built environment change and those living in areas with less change.
| Exposure | Outcome: SWEMWBS score, beta coefficient (95% CI) | |||||
|---|---|---|---|---|---|---|
| n | Model 1 | n | Model 2 | n | Model 3 | |
| Percentage change to built environment in neighbourhood | 1296 | –0.03 (–0.06 to 0.00) | 1288 | –0.03 (–0.06 to 0.01) | 1231 | –0.01 (–0.04 to 0.02) |
Relationships with changes in perceptions of the physical and social environment
In this section, we describe neighbourhood perceptions at T1 (2005) and T2 (2013) reported in our core survey. As described in Chapter 2, Evaluating the intervention, perceptions of the physical environment of the neighbourhood were measured at baseline and follow-up, whereas collective efficacy – a measure of the social environment – was measured at follow-up only. We report the relationship between motorway exposure and neighbourhood perceptions, using both areal and individual measures of exposure. We go on to report the extent to which changes in these perceptions mediated the reduction in mental well-being over time associated with motorway exposure in the main well-being analysis.
Analytical strategy
We calculated descriptive statistics for neighbourhood perceptions at follow-up using the full T2 sample. We used t-tests to test for differences between study areas. We then calculated descriptive statistics for change over time in perceptions of the physical neighbourhood (both individual items and the factors derived from them) in the longitudinal cohort.
We undertook two sets of analysis, both limited to participants living in the South and East study areas (the areas with a motorway). The first set of analyses used the full sample recruited from the South and East study areas at follow-up (n = 750). Linear regression analyses, adjusted for the same set of covariates as in the main analyses, were used to test the cross-sectional associations of proximity to a motorway with neighbourhood perceptions and collective efficacy, stratified by study area.
The second set of analyses used the cohort sample living in the South and East study areas (n = 209). Mediation analyses were conducted following the method of Baron and Kenny86 (Figure 18), adjusted for the same set of covariates as the main analyses and stratified by study area. The exposure (X) was proximity to a motorway. Mediators (M) were changes in perceptions of the neighbourhood (either items or the factors derived from them). The outcome (Y) was change in mental well-being (MCS-8). We conducted single mediator models, with a Sobel–Goodman test to assess the significance of the mediation effect.
FIGURE 18.
Baron and Kenny mediation analysis. Adapted from Baron R, Kenny D. The moderator–mediator distinction in social psychological research: conceptual, strategic, and statistical considerations, J Personal Social Psychol, 51, 1173–82, 1986, published by the American Psychological Association. 86

Results
Cross-sectional analysis of associations between motorway exposure and neighbourhood perceptions
Descriptive statistics for the neighbourhood perceptions in the full follow-up sample can be found in Table 37, stratified by study area. For most of the items relating to the physical environment, the average response was close to or greater (more favourable) than the midpoint of the scale (zero). The main exceptions were the items relating to traffic volume and noise and the danger of cycling, for which the mean responses were negative (unfavourable) in all three study areas. Average perceptions of the convenience of public transport differed significantly between all three study areas, with those in the North falling between those in the South (most favourable) and those in the East (least favourable). Average perceptions of collective efficacy were more favourable in the South than in the East, and vice versa for proximity to green space. Average perceptions of proximity to a park were more favourable in the South than in the North, and vice versa for traffic noise and the likelihood of being attacked.
| Perceptions of the physical environmenta | South | East | North | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | |
| Pleasantness for walking | 424 | 0.51 | 1.13 | 437 | 0.61 | 0.96 | 451 | 0.54 | 1.00 |
| Proximity to parkb | 423 | 1.22 | 0.93 | 438 | 1.21 | 1.06 | 455 | 0.95 | 1.17 |
| Public transportb,c,d | 423 | 1.41 | 0.76 | 436 | 0.86 | 1.16 | 457 | 1.11 | 0.99 |
| Routes for cyclingc | 418 | –0.10 | 1.11 | 431 | –0.18 | 1.07 | 451 | –0.02 | 1.10 |
| Safety walking after dark | 421 | –0.04 | 1.20 | 433 | 0.01 | 1.06 | 458 | 0.02 | 1.06 |
| Traffic volumec | 419 | –0.79 | 1.09 | 432 | –0.61 | 1.16 | 454 | –0.59 | 1.17 |
| Safety crossing road | 421 | 0.53 | 1.06 | 436 | 0.52 | 1.05 | 453 | 0.41 | 1.08 |
| Attractiveness | 422 | 0.23 | 1.19 | 435 | 0.22 | 1.14 | 456 | 0.28 | 1.14 |
| Green spacec,d | 418 | 0.18 | 1.21 | 431 | 0.42 | 1.18 | 454 | 0.36 | 1.19 |
| Proximity to shops | 418 | 0.99 | 1.15 | 433 | 0.92 | 1.13 | 453 | 0.87 | 1.08 |
| Routes for walking | 421 | 0.64 | 1.06 | 434 | 0.60 | 1.06 | 451 | 0.62 | 0.98 |
| Likelihood of attackc | 416 | 0.15 | 1.16 | 433 | 0.27 | 1.04 | 452 | 0.34 | 1.05 |
| Traffic noiseb,c | 422 | –0.35 | 1.25 | 430 | –0.36 | 1.23 | 456 | –0.03 | 1.29 |
| Road safety for cyclists | 415 | –0.51 | 1.09 | 434 | –0.37 | 1.09 | 455 | –0.48 | 1.09 |
| Collective efficacyd,e | 417 | 2.79 | 0.85 | 434 | 2.68 | 0.80 | 446 | 2.69 | 0.77 |
The results of the multivariable linear regression models are displayed in Appendix 5. In general, the relationships between the items and factors reflecting neighbourhood perceptions and proximity to a motorway in the South or East study areas were not significant. In the South, proximity to a motorway was negatively associated with access to a park (–0.32, 95% CI –0.52 to –0.12) and positively associated with the convenience of public transport (0.27, 95% CI 0.09 to 0.44), whereas in the East, the association with the convenience of public transport was in the opposite (negative) direction (–0.27, 95% CI –0.46 to –0.09). Overall, therefore, we found slight evidence that perceptions of the environment were more negative among those living closer to a motorway than among those living further away.
Longitudinal mediation analysis
Unadjusted changes in perceptions of the physical environment by study area in the longitudinal cohort can be found in Table 38. In the sample as a whole, there were small favourable changes in perceptions of the safety and pleasantness of walking over time. Only a few significant differences between study areas were observed, namely that positive changes in the perceived safety of walking, the risk of being attacked and the factor labelled safe and pleasant surroundings (factor 1, which included both of the individual items listed) were more pronounced in the East than in the South.
| Change in physical environment perceptions | South | East | North | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | |
| It is pleasant to walk | 124 | 0.32 | 1.13 | 112 | 0.35 | 0.97 | 125 | 0.56 | 1.21 |
| There is a park within walking distance | 123 | 0.07 | 1.03 | 112 | 0.07 | 1.14 | 125 | 0.12 | 1.32 |
| There is convenient public transport | 123 | 0.19 | 1.01 | 112 | 0.13 | 1.25 | 125 | 0.24 | 1.10 |
| There are convenient routes for cycling | 122 | 0.34 | 1.48 | 109 | 0.30 | 1.10 | 124 | 0.13 | 1.37 |
| It is safe to walk after darka | 121 | 0.04 | 1.29 | 111 | 0.55 | 1.07 | 124 | 0.31 | 1.18 |
| There is little traffic | 120 | 0.41 | 1.15 | 112 | 0.31 | 1.18 | 124 | 0.33 | 1.23 |
| It is safe to cross the road | 122 | 0.25 | 1.19 | 112 | 0.39 | 1.17 | 124 | 0.52 | 1.27 |
| The surroundings are unattractive | 122 | 0.10 | 1.39 | 112 | 0.22 | 1.31 | 124 | 0.34 | 1.45 |
| There is little green space | 121 | 0.12 | 1.59 | 112 | 0.37 | 1.42 | 123 | 0.08 | 1.50 |
| The nearest shops are too far to walk to | 121 | –0.14 | 1.37 | 111 | 0.12 | 1.29 | 123 | 0.07 | 1.35 |
| There are no convenient routes for walking | 123 | 0.15 | 1.38 | 112 | 0.30 | 1.28 | 123 | 0.18 | 1.34 |
| People are likely to be attackeda | 120 | 0.21 | 1.24 | 111 | 0.56 | 1.09 | 123 | 0.37 | 1.10 |
| There is a lot of traffic noise | 123 | 0.49 | 1.39 | 109 | 0.20 | 1.02 | 124 | 0.32 | 1.23 |
| The roads are dangerous for cyclists | 121 | 0.17 | 1.16 | 111 | 0.30 | 1.12 | 125 | 0.06 | 1.34 |
| Safe and pleasant surroundings (factor 1)a | 117 | 0.66 | 3.48 | 110 | 1.67 | 2.81 | 121 | 1.60 | 3.42 |
| Low traffic (factor 2) | 116 | 0.90 | 2.88 | 108 | 0.66 | 2.54 | 122 | 0.48 | 2.94 |
| Convenience for walking (factor 3) | 116 | 0.29 | 2.85 | 111 | 0.86 | 2.73 | 120 | 0.44 | 2.89 |
The mediation analysis found no evidence that changes in neighbourhood perceptions mediated the association between proximity to a motorway and change in mental well-being in either the South or the East study areas (see Appendix 6).
Conclusion
We found some evidence that living near to the new M74 motorway substantially worsened local residents’ mental well-being. In the area surrounding the existing M8 motorway, the negative association with mental well-being was concentrated among those with chronic conditions, which suggests the potential for exposures of this kind to exacerbate existing health inequalities and to contribute to poorer health outcomes. In addition, exposure to general upheaval in the built environment of the neighbourhood was associated with reductions in well-being, particularly among those living in the area surrounding the new motorway. Although living near a motorway was associated with poorer well-being, the perceptions of the neighbourhood measured in this study were not strongly associated with proximity to a motorway, and changes in these perceptions did not appear to mediate the effect on well-being.
Chapter 7 Understanding the changes
Introduction
In previous chapters, we examined the relationships between motorway exposure and activity patterns, road traffic accidents and well-being using quantitative research methods. In this chapter, we focus on the use of qualitative methods, drawing on material from the interviews with a subset of local residents (volunteers drawn from the survey sample) and with other key informants to develop an explanation of how the environmental changes and their effects were understood, experienced and interpreted in the area surrounding the new motorway. As outlined in Chapter 2, Evaluating the intervention, for both sets of interview data we undertook a thematic analysis and coded data using non-exclusive thematic codes based on both a priori and emerging concepts (Figures 19 and 20).
FIGURE 19.
Code-to-theory model for interviews with residents.
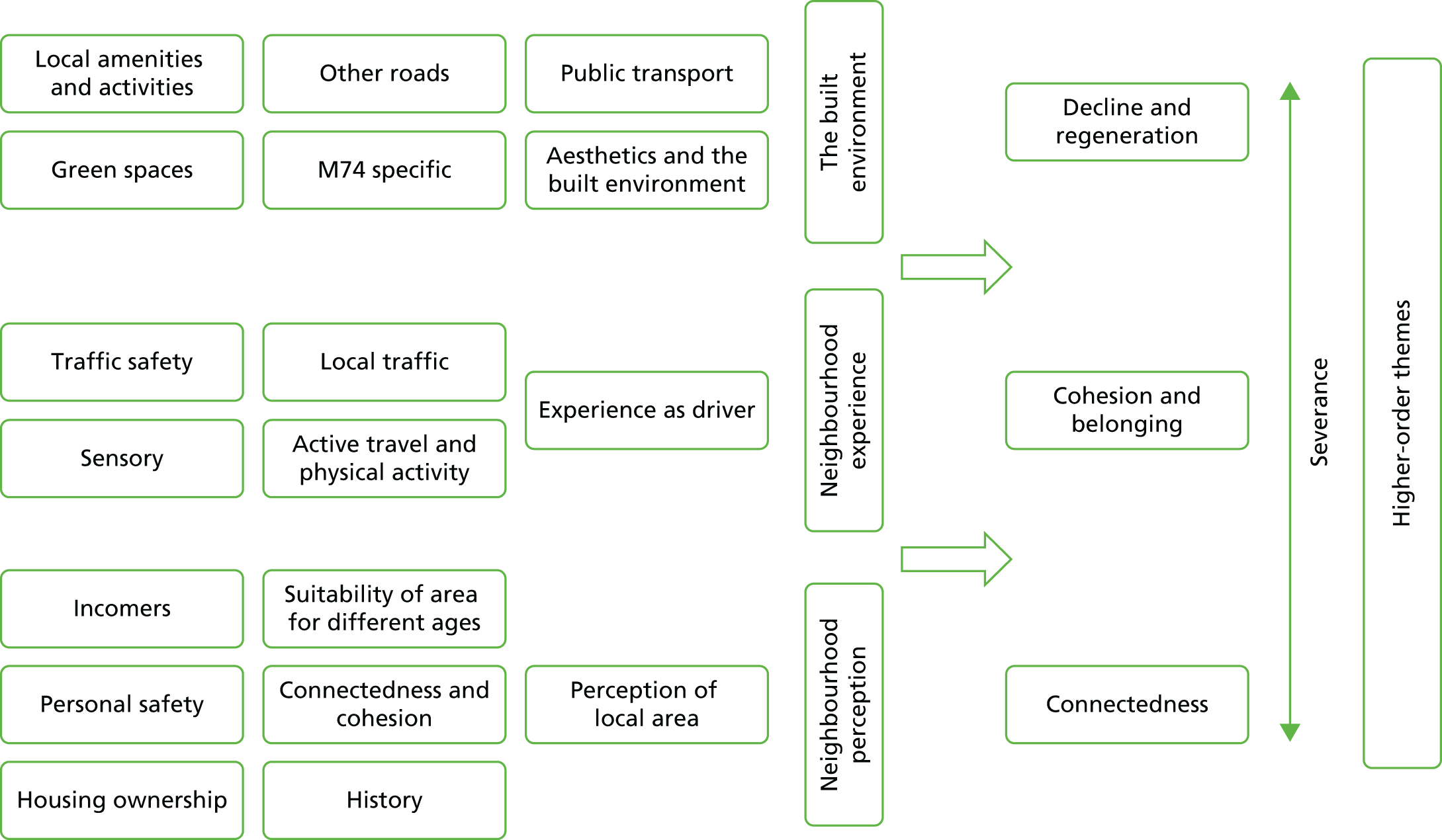
FIGURE 20.
Code-to-theory model for interviews with key informants.

These initial themes were then gathered into thematic groups relating to physical changes and experiential changes. As expected, key informant interviews were more likely to take a broader view of the impacts of the new motorway (e.g. how local change fit into a wider picture of environmental and economic change), whereas resident interviews tended to focus more on personal experiences of the local area. Analysis of the resident interviews therefore focused on how the issues represented in the themes were perceived by individuals, and how those issues had changed for them over time. In the analysis of the key informant interviews, we placed more emphasis on understanding their and their organisations’ roles in relation to the local area, and on understanding change at the community level. For overlapping topic areas of direct relevance to our main research questions (e.g. the direct impacts of the new motorway, connectivity and severance, active travel, community cohesion, and regeneration and decline) we collated data from both key informant and resident interviews into a matrix to investigate areas of overlapping and diverging opinion, and to provide a more holistic understanding of change. This was not framework analysis as such, but it was a way of combining two sets of data gathered using slightly different methods. Such charting has been shown to be a rigorous and effective way of representing complex qualitative data sets. 120
For the purposes of this chapter, we have divided our findings into explorations of physical changes in the local environment (including, but not limited to, the new motorway); changes in people’s perceptions and experiences of the local area; economic impacts of the new motorway; and the role of the notion of severance in understanding the changes that have taken place.
Our findings revealed heterogeneous responses to, and experiences of, changes in the neighbourhood in general as well the new motorway in particular. In the resident interviews, we did not introduce the topic of the new motorway until the end of the interview (if necessary). Instead, we tried to gain a sense of all the local changes considered important by the participant, building a picture of the neighbourhood-level system of change and where the M74 extension fit within that. Both the resident and key informant samples included people with markedly different attitudes towards the new motorway both before and after its construction, with some being opposed:
Aesthetically, I think it’s awful. It really is. I mean, especially if you’re coming in, you know, fae [from] sort o’ [south west of the motorway] an’ there’s . . . it just never looked finished really. An’ I remember both o’ us, ‘cos I drive in wi’ my wife, talking aboot it and saying you know ‘it’s running past some folks’ windows’, you know? . . . And it just darkened doon whole swathes o’ streets and stuff. So, you know, it really did cut a swathe right through.
Key informant, local community association
Others, however, were in favour:
[The motorway is] actually fantastic . . . My husband’s family come from [the] Rutherglen [other neighbouring community] area. Originally [neighbouring community] but they’re all now sort of in the bit between sort of Cambuslang and Rutherglen now. So . . . you used to have to drive round and drive through Rutherglen, it used to take so long. Now you can just go down to [nearest junction], whip up onto the motorway and straight back off. I mean it’s literally one or two junctions. But it makes a huge amount of different just for that short distance.
Woman aged 36–50 years living in Govanhill
Others were indifferent:
But see wi’ not being a driver? It makes no difference to me at all it being there. I cannae [cannot] remember what it was like before it was there, if you know what I mean? . . . So, it’s not made any impact on me whatsoever.
Woman aged 36–50 years living in Rutherglen
And others sill held mixed views, recognising both positive contributions and drawbacks:
[I]t’s a necessary evil, I suppose. It does make it, make commuting a lot quicker an’ going tae the airport and going south sort o’ thing, it makes that a lot quicker for people, yeah. And it does relieve the traffic in the Main Street.
Man aged 51–65 years living in Rutherglen
We shall explore potential reasons for these varying opinions in more detail, but in broad terms they seemed to be related to a number of factors, including proximity of dwelling to the motorway, car ownership, level of confidence in using busy multilane roads, duration of residence, degree of dispersal of both social networks and employment, and feelings of attachment to the local area. For many residents, the introduction of the motorway (several years before the interviews were conducted) was secondary to other more pressing social concerns in the local area. Particularly in Govanhill, these social issues, notably changing neighbourhood demographics as a result of in-migration and changing perceptions of personal safety in public spaces, had a greater bearing on their attitudes and actions than did the new motorway.
Changes to the physical environment
In this section, we describe participants’ perceptions of changes to the physical (built and natural) environment. Although some of these changes were associated by participants with the new motorway, many were not. We hoped that by gaining a picture of wider neighbourhood change and its significance to participants in this way, we would better understand the relative importance of the new motorway and its associated changes for local communities.
The M74 extension and associated physical changes
Participants discussed a number of features related to the M74 extension including the carriageway itself, its viaducts, underpasses, embankments, slip roads, junctions and planted verges, and its integrated pedestrian infrastructure. The physical structure itself evoked mixed feelings:
So, yeah, so from that perspective the M7 – I’m pro the M74 is what I’m trying to say . . . I think like whereas before you just had a big patch of wasteland, now you’ve got a nice shimmering motorway.
Man aged 20–35 years living in Govanhill
It’s less aesthetically pleasing.
Key informant, local advocacy group
Some participants drew attention to the imposing nature of the structure, with some describing it as either ‘impressive’ or ‘ugly’, whereas others felt that they had grown so accustomed to it that it now seemed as if it had ‘always been there’. For one respondent, this familiarisation was attributed to the long construction period:
It took such a long time to build it that it just gradually came, so it didn’t just suddenly appear overnight, it took time, so you’re just, just used to it now.
Man aged 36–50 years living in Rutherglen
For another respondent, it reflected to the large amount of change to which local residents had become accustomed:
I think folk are just used tae seeing huge swathes o’ . . . there’s no’ that sense and nobody complains aboot [change], you know? I just think people have got used tae change happening.
Key informant, local community association
For the most part, participants considered the underpasses to be well thought out, open and relatively well lit:
[It is l]it up an’ things like that so it’s . . . quite safe-looking. Like, you wouldn’t feel paranoid walking under it an’ that sort o’ thing so it’s . . . the motorway’s not really affected access to things as well. They’ve thought it out really well.
Woman aged 20–35 years living in Rutherglen
However, one participant living in Rutherglen felt that her new local underpass made her evening commute marginally darker.
Some participants praised the efforts to plant greenery on the motorway embankments:
I think there was an improvement because the landscaping and bits and pieces that they had done did certainly improve the outlook – and the new bridges and the work they done on the bridges kinda did actually genuinely brighten up that area. And most of the land, as I says, having been going in and out of Govanhill from kinda early seventies, most of the land was lying derelict, anyway.
Man aged 51–65 years living in Govanhill
However, others were less convinced about the choice of planting, given that broad-leaved trees shed their leaves for much of the year:
Well the screening planting that I’ve seen isn’t dense. It’s more of a . . . aesthetic planting than screening ‘cos it’s not anywhere near dense enough and layered enough to perform anything that you would want from screening and also the species choice. I mean if you choose broad-leaved trees they drop their leaves in the winter. Actually it’s the winter when the motorway’s loudest because that’s when the road is wettest and tyres on wet tarmac make a lot more noise than tyres on dry tarmac.
Key informant, local greenspace organisation
In addition, some key informants questioned who was responsible for the upkeep of these planted areas.
Other physical elements of the structure that were discussed by both residents and key informants included slip roads and junctions. For the most part, these were mentioned in the context of problematic traffic flow, which was thought to be related to poor design or planning and was particularly troublesome around peak commuting times. One junction near Govanhill in particular was mentioned several times as being problematic. New slip roads were also identified as challenging where participants considered that lanes ended in an abrupt and unsafe manner:
They haven’t designed the slip roads properly, in a sense that you’ve kind of going . . . if you want to kind of go straight on, if you’re coming in this direction here and you want to go straight on, they’ve kind of designed the slip road onto the M74 as you kinda got to kick and get onto it . . . what that’s meant is that three lanes are filtered into two lanes and that causes tailbacks either way . . . you often see a snarl up of traffic there and a snarl up of traffic there.
Key informant, local housing association
Most of the new motorway is elevated, but at one point near Govanhill it passes beneath a pre-existing arterial road. This creates very different effects at different places (Figures 21 and 22).
FIGURE 21.
(a) Elevated sections of the M74 extension; (b) elevated sections of the M74 extension close to housing in Laurieston; and (c) elevated sections of the M74 extension in Rutherglen. Photographs © Amy Nimegeer and reproduced with permission.



FIGURE 22.
M74 extension passing beneath an existing street in Govanhill. Photograph © study participant and reproduced with permission.

One particularly successful and much praised aspect of the new infrastructure was a new pedestrian overpass in Govanhill, which was considered by all who commented on it to have been well thought out and to represent a significant improvement over the existing pedestrian bridges over the railway line. Cycling infrastructure, however, was not as highly praised (for more detail, see Active travel).
Other local streets
The M74 extension did not occur in a ‘vacuum’. Within the time period of interest to the study, residents reported changes to the design and surface of local streets (e.g. widening of pavements, appearance of pot holes or resurfacing), traffic calming measures and other, ongoing, local transport projects. For example, a one-way system was implemented on some residential streets in Govanhill. Some regarded this as funnelling traffic onto Aikenhead Road (a main arterial road) and causing tailbacks, whereas others saw it as making local streets safer for children to play in. More than one participant discussed changes to the layout of Aikenhead Road, citing it as a possible contributor to poorer traffic flow and increased stress for local drivers (Figure 23). Such concurrent structural changes made disentangling the impacts of the M74 extension a challenge not only for researchers, but also for local residents.
FIGURE 23.
Reconfiguration of Aikenhead Road. (a) In 2015 (red line); and (b) in 2005. Source: Google Earth.


Local amenities
Residents and key informants discussed changes to local amenities including shops, schools, health facilities and green spaces. These were considered by residents to be important spaces for connecting with other local people (both casually and intentionally) and were central to conceptualisations of their neighbourhoods as healthy or desirable spaces. Shops in particular emerged as important local meeting places, imbued with the additional symbolic value of representing the character of the local area. In both Govanhill and Rutherglen, participants described concerns about a decline in the quality of their local high-street shops that was unrelated to the opening of the new motorway. In Rutherglen, several residents expressed concern that what had once been a unique, vibrant shopping area that reflected the town’s distinctive status as a royal burgh had been overtaken in recent years by betting shops, pound shops and charity shops (Figure 24):
The shopping area, the Main Street in Rutherglen has deteriorated . . . I mean, when you look at it an’ it’s all the bookies and the . . . I think there’s a pawn shop. Of course, I mean, they’re supplying a need . . . but . . . that is to the detriment of people.
Woman aged 65+ years living in Rutherglen
FIGURE 24.
Changing high-street shops in Rutherglen. Photograph © study participant and reproduced with permission.

Several residents expressed concern that the changing shops broadcast an unfavourable presentation of Rutherglen to outsiders as a community in decline. Similarly in Govanhill, several residents mentioned concerns about declining high-street shops, but with a slightly different emphasis reflecting recent demographic changes. A number of local shops now specialised in ‘ethnic’ clothing and foodstuffs. For some, this change in the nature of the local shops was indicative of a decline in traditional local culture:
[I]t’s not nice seeing so many closed shops, or shops being taken over by ethnic groups and things, you know?
Woman aged 51–65 years living in Govanhill
However, for others it was something to be celebrated, giving Govanhill a unique and multicultural character:
It’s a very diverse area. There’s quite a high, a high population of immigrants there. But that’s kind of translated into lots of interesting shops and things like that.
Man aged 20–35 years living in Govanhill
Although these changes to local shopping areas caused consternation, they were attributed by participants not to the opening of the new motorway, but rather to wider economic or social factors including rising car use. Some Govanhill residents had initially worried that the new motorway would cause people to bypass the local shopping area centred on Victoria Road. When this did not come to pass, however, they made their peace with the motorway and its presence:
I thought [the motorway] would destroy what’s left of the shops in Govanhill. I thought they were, be gone . . . so, I was very strongly against the motorway being built . . .
What do you think it was that kind of changed your mind about like . . .?
I think that it was, we didn’t become a ghost town and I think that’s the reason why.
Man aged 36–50 years living in Govanhill
One significant change for both communities was the opening of new ‘big box’ supermarkets nearby. Given the importance placed by residents on their local shops, it was perhaps surprising that these supermarkets were almost universally praised as beneficial to the local area, and were also described as frequent destinations for active travel (mirroring the findings of the baseline study57). One participant also described how cashiers in their local supermarket took care to remember the names of customers, particularly those perceived as being lonely and in need of connection.
Public transport
As might be expected in areas of comparatively low car ownership, public transport was important for residents of both areas. For the most part, residents considered both Govanhill and Rutherglen to be very well served by bus and rail services. However, recent changes to bus timetables and to the locations of bus stops had caused difficulties for some people with impaired mobility:
There used to be a bus stop in the middle and they seem to have taken it away at this side walking down towards [neighbouring road]. There is one in the middle at the opposite side but it is really quite a long walk. There’s no bus stop. I don’t mind walking but it’s for likes o’ the elderly, you know.
Woman aged 51–65 years living in Rutherglen
They moved bus stops and it’s – it passes the 101. Used to stop outside the bookies but now they’ve taken it up to the cash and carry so it’s quite a wee walk back for me and it’s a bad pavement and a bad road and a big kerb, so that’s awkward for me.
Woman aged 65+ years living in Govanhill
Particularly in Govanhill, these changes were described as having led to more hazardous walks to the bus stop, and longer and more convoluted journeys. In Rutherglen, however, refurbishment of the railway station was viewed very positively by local people. Although residents did not associate these changes to public transport with the opening of the new motorway, for key informants the new motorway was seen as part of a wider investment programme of which the causes and effects were difficult to disentangle. For example, Clyde Gateway – a regeneration company tasked with the physical, social and economic development of the east end of Glasgow – was inextricably linked with the new motorway in the minds of some key informants, who therefore thought that some other regeneration activities such as refurbishment of railway stations would not have occurred without the impetus of the investment in the M74 extension. For many local residents, however, investment in some local refurbishments was regarded as not necessarily for their benefit. On the contrary, many of them considered these changes to have been made for the benefit of people attending the Commonwealth Games in 2014, to present an attractive version of Glasgow to the wider world:
Yeah, just as well we had the Commonwealth Games or it would have still have been the way it was, you know? There’s no way in God’s creation, would I use that railway station, you know, but I would use it now if I had to, you know? But I wouldn’t have used it before, because it was too lonely and too isolated, you know? It was quite scary. But they’ve got it really nice, really. They’ve made a big difference to the place.
Woman aged 51–65 years living in Rutherglen
One of the things we got done was [the main road] outside my house got resurfaced. This is great, and like everything like that was getting done with the Commonwealth Games, you know, people were being so negative. I’m like, ‘Why are you being negative? We’re getting the road resurfaced. And it’s great’.
Woman aged 36–50 years living in Govanhill
These two quotations illustrate how local people may have benefited from changes even if those were perceived to have been mainly intended to benefit others. Other material suggests differences between those who benefited from changes and those who incurred the harms, raising questions of social justice (see Severance and connectivity).
Aesthetics
Other physical changes described by local residents included the demolition and construction of residential and commercial properties. Although no single building stood out in this respect, discussion of the razing of older buildings did draw attention to the rich historical background of the two case study communities, which was often prized by older residents and seemed to be central to their feelings of connection to place. However, residents also described a decline in the cleanliness and upkeep of buildings and street areas [including common spaces, closes (communal entrances), facades and front gardens]. For residents, this was most commonly associated with changing local demographics. The in-migration of people perceived as not sharing tacit local values relating to property upkeep, owing to either cultural differences or delinquency, and the rise of absentee landlords renting properties on a short-term basis to people with no local roots or connections, were frequently cited as causes of the decline in local aesthetic upkeep:
[. . .] the appearance of certain streets that’s really – you walk along and, you know, there’s rubbish out the front and there’s, you know, old prams that are just lying in the street or shopping trolleys, you know . . . I don’t remember it being, you know, as bad to be honest . . . you know, as I say about 10 years ago, probably about 10 or 11, maybe 12 – that’s when I did start realising you can see like, you know, certain windows ‘cos you would look and go that’s not curtains in the window, that’s linen sheet up there, you know, and the colour of windows, you know, and when the house looks manky, that close looks terrible, you know?
Woman aged 36–50 years living in Govanhill
Changes in local experience
One of the ways in which changes to the urban built environment may influence health and well-being is by altering how residents perceive, experience or interact with local amenities and people. 44 In this section, we consider the findings of our qualitative research in relation to the perceptions and experiences of the neighbourhoods.
Traffic
For many local residents, a significant factor influencing their feelings towards the new motorway was the extent to which they believed that it had affected levels of traffic on their local streets, or the extent to which their perceptions of these changes matched their prior expectations. Perceptions of whether or not traffic on local streets had changed were mixed:
Well I thought it would make a big difference but . . . I don’t see a great deal o’ difference because the traffic’s still just much the same oot here as it always was.
Man aged 65+ years living in Govanhill
It’s reduced the amount of traffic or lorries, big traffic, big trucks an’ things like that going along the Main Street. It’s certainly reduced all that.
Man aged 51–65 years living in Rutherglen
At the first we said, ‘well look, it’s taken a’ the traffic away, that’s great’. But they’ve sneaked back in again, you know, withoot anybody noticing. But it was a good thing. We were always for it. Away back when we stayed in wur [our] other hoose you got a lot of campaigners saying ‘no’ to this. I said, ‘Aye, I want it’. I wanted it a’ [all] the time, you know?
Man aged 51–65 years living in Rutherglen
On the whole, residents in Rutherglen were more likely than their Govanhill counterparts to report a definite decrease in traffic on local main roads. This conforms with the expectations set out in the EIA for the new motorway. 61 Residents in Govanhill were more likely to report that traffic had remained the same or increased, particularly those living on main roads, or to say that they were not sure. Key informants consistently identified London Road – a main arterial road, outside the qualitative case study neighbourhoods but linked with the new motorway – as one on which traffic had significantly decreased:
2 or 3 years ago before the extension was built it was really sometimes quite tricky even to, as a pedestrian, to get across London Road from one side to the other.
Key informant, local housing association
As mentioned above, however, residents attributed changes in traffic levels to different causes, for example:
And do you think that, since the motorway has come in, have you noticed any change in your local traffic?
No. No. As I said, they’ve changed the local traffic ’cos they’ve messed about wi’ all the roads an’ blocked off streets an’ shoving bus lanes in an’ . . .
So other changes have had more of an impact than that?
Yeah, definitely.
Man aged 51–65 years living in Govanhill
Noise and air pollution
Two key elements of experiential change described by participants were those of noise and pollution. Perhaps unsurprisingly, these were heavily intertwined with discussions of traffic and the M74 extension, and perceptions of noise and air pollution were related to perceptions of local traffic levels and the proximity of people’s dwellings to the motorway. In most cases, participants who perceived local traffic to have decreased also considered their exposure to noise to have decreased. However, a handful of participants acknowledged a decrease in local traffic but still believed that their exposure to pollution may have increased because of their proximity to the new motorway. A number of residents and key informants drew particular attention to the possibility that people living in extreme proximity to the motorway, for example in Devon Street or close to the junction with the M8 motorway, might experience particularly severe impacts. Discussions about pollution were manifested in three main ways. The first involved descriptions of an increase in settled particulates or grime on windows or in houses, which was quite commonly described in both Govanhill and Rutherglen:
[. . .] you have tae wash your windows a little more frequently ‘cos o’ the fumes and what-have-you.
Man aged 51–65 years living in Rutherglen
Where we are, now we run along [a main road] which we have noticed the smog, and the dirt and the dust, impossible to keep windows clean ‘cos the back of our flat goes onto [the main road] so you’ve got all the motor traffic there. So that’s quite difficult to cope with at times.
Woman aged 36–50 years living in Govanhill
The second, less frequent way involved health effects such as asthma and wheezing:
So if you open your windows you can notice it?
Yeah. Mm hmm.
OK. And you can – what can you smell it, or . . .?
It’s no’ smelling like, like congested, I speak (wheeze) like – [gestures to her chest]
In your chest?
Mm hmm.
Woman aged 36–50 years living in Govanhill
The third involved fumes:
So how has that changed that walk for you?
It just makes it a little bit more noisier and, obviously, pollution from the petrol fumes o’ the thingmy makes it a little bit . . . well, that’s changed it. There’s more pollution and things like that as well.
Man aged 51–65 years living in Rutherglen
For participants, therefore, pollution perceived to be attributable to the new motorway was something that could affect them both inside and outside their homes. During the course of the qualitative fieldwork, Friends of the Earth (London, UK) published an analysis of pollution in 2014, which identified Rutherglen High Street as one of 13 sites in Scotland to exceed the European Union’s legal limit for nitrogen dioxide and also reported that particulate matter of a diameter of ≤ 10 microns had increased between 2013 and 2014. 121 This story received news coverage, and a handful of participants were aware of it (see Chapter 2, Characterising the environmental changes and refining the study design):
[. . .] you’ll know that Rutherglen Main Street has some of the worst air quality in Scotland. There’s been quite a lot of press reporting on that recently.
Key informant, local community council
It took away some of the traffic but not all of it, so the Main Street’s still very heavily used, you see cars backed up all the time. So, I guess that causes a lot of pollution. In fact I’m sure it was Rutherglen Main Street came up pretty bad recently in a pollution survey.
Woman aged 36–50 years living in Rutherglen
Both residents and key informants referred to ground contamination in both Rutherglen and Govanhill, a legacy of their heavy industrial history. For some participants, their greatest concern about pollution from the motorway was that the construction might have disturbed land contaminated with chromium from former chemical works:
But they obviously were aware of the toxic waste . . . It’s just under [former site of works] and there is . . . well . . . I mean, it’s too late now. I mean, the M74’s there. My concern and always has been is with the dust, prevailing wind . . . driving it over.
Woman aged 65+ years living in Rutherglen
For more than one key informant, however, building the new motorway on contaminated land was a way of making the land useful again by ‘capping’ the contaminants, and the project provided an impetus to decontaminate sites in a way that would not otherwise have been economically viable. It should be noted that the chromium contamination of land in Rutherglen had been the subject of a health impact assessment before the motorway was built and was, in fact, the main health impact considered therein. 122 This pre-existing, historically rooted understanding of the local communities as post-industrial ‘polluted places’ may have coloured local perceptions of the impacts of the new motorway.
People’s experiences of noise were also variable. For some, the new motorway had led to a perceptible increase in noise, even intruding on their enjoyment of their outdoor spaces and reducing their desire to open windows at home, whereas others felt that it had had little perceptible impact and were in fact impressed at the low levels of noise they experienced. These differences were not always attributable to how close people lived to the new motorway, and may also have been related to individual habits and sensitivity to noise:
And it is quite noisy if you . . . open a window and it’s, you can hear it, and you if you go out in the garden before that came in it was really, really peaceful here . . . occasionally a train would pass but even then it was so low down there are so many trees. But the motorway’s a different thing. The noise of a motorway is really loud, isn’t it? And it seemed to just be humming in your head all the time, you’re sitting like that, and you go, ‘God, I wish that would stop’.
Woman aged 65+ years living in Govanhill
No. I can’t [hear the traffic from here], no. In all honesty, I can’t. But maybe people who stay [live] . . . there’s [street] there. They may hear it because they’re nearer. Where I am, I mean, it used tae be you could . . . even the railway, you could only hear the, or feel the slight . . . not a lot of tremor but you knew the railway was there. But you can’t hear the traffic.
Woman aged 65+ years living in Rutherglen
Some participants took pains to describe the difference between the noise from the existing railway line and the noise from the motorway. For some, the noise from the railway line was greater and, being intermittent, was harder to ignore:
It’s strange, because the railway line’s there, we used to notice vibrations when the heavy freight went by. You know, we had a couple o’ display cabinets and if they weren’t set up properly, you could hear the glass kinda chinking inside – but we never noticed that. It wasn’t, the lorries or anything like that, weren’t aware of anything like that wae [with] the vehicles.
Man aged 51–65 years living in Govanhill
Traffic noise was also discussed in relation to green space, which is discussed at greater length below (see Severance and connectivity).
Active travel
In the qualitative study participants described both positive and negative aspects of their experience of active travel, some of which related to the motorway and some of which related to other factors including health, the weather and the seasons.
As previously mentioned, several residents drew attention to integrated pedestrian infrastructure that was built as part of the M74 extension. For the most part, this was characterised in positive ways. In areas where the motorway was elevated, underpass areas were considered by many to be well-lit, wide (therefore allowing people to pass without invading each other’s personal space) and relatively secure. In particular, participants praised a new pedestrian overbridge in Govanhill. This replaced a previous crossing over the railway line, which was considered to be dark, narrow and unsafe to the extent that participants actively avoided using it. In contrast, the new pedestrian overbridge was described as open, light and secure, contrary to the fears expressed by some participants in the baseline interview study that such crossings would be more frightening and might deter walkers. 58 However, cycling infrastructure around the M74 extension was less widely appreciated. It was described as disjointed, with cycle lanes that began and ended abruptly, requiring cyclists to enter and exit the traffic on main roads in a way that felt unsafe:
Also the access at one of the junctions – well, certainly I don’t know about all of the junctions but certainly one of the junctions – yes, junction 2, it has – when the whole road system was changed with the slip roads and so on, provision for cycling was incorporated into that. But it’s one of these classic examples where you come up to it, the cycle infrastructure starts, you get up beyond the junction and the cycle infrastructure stops. So it’s – it’s good in the sense that it made provision. Because if you, you know, build these things to start with it’s better than retro-fitting them.
Key informant, local community council
Similarly, changes in traffic flows had changed people’s experiences of cycling in both Govanhill and Rutherglen:
So [junction] is the main junction that I would use. As a cyclist going through there, the cycle routes kind of cross over each other, so that’s . . . and you can’t get through, where there used to be a bike lane you can’t get through, where there used to be a bike lane there isn’t one now. So yeah, that’s changed and that’s definitely more dangerous ‘cos the density of traffic has increased.
Key informant, local greenspace organisation
In key informant interviews, it was noted that residents in one community to the north of the motorway expressed concern about the safety of their children walking to school, owing to an increase in traffic around the motorway slip roads. In Rutherglen, however, a decrease in traffic on the main street was perceived to have had the unexpected side effect of more cars being parked on the street. Together with existing cycling infrastructure that was regarded as confusing, in that it comprised a mixture of dedicated and shared-use routes, this constituted a worsening of the obstacles to cycling, which were perceived as a potential deterrent for inexperienced cyclists:
It makes it difficult for [new cyclists]. It’s not smooth to get from A to B. You’re getting off your bike, you’re walking it across. That’s if you’re doing what the sign tells you to do. On this stretch here that’s picture three, where I had the altercation. ‘Do you know . . .’ . . . someone shouting at me, ‘Do you know it’s illegal to cycle on the pavement?’ ‘Well, yeah I do, but not when it’s shared use it’s not’. I know that. But somebody that’s just started cycling might be a bit more intimidated about it.
Woman aged 36–50 years living in Rutherglen
In other words, the impacts of the new motorway combined with other factors in sometimes unexpected ways to produce changes in the local experience of active travel.
Some participants who perceived local traffic to have decreased (whether or not this was held to be associated with the new motorway) considered this to have benefited local people’s capacity and inclination to use active modes of transport:
I think the motorway certainly would’ve changed the character because we don’t get as much through traffic now, as you’ll see from that. And that’s changed the character, if you like, and it’s much easier tae get out and about and crossing roads and things like that. Much, much easier.
Man aged 51–65 years living in Rutherglen
For others, however, the presence of the motorway – despite being unlikely to change, deter or reroute active journeys – was described as affecting the quality of the active travel experience:
It’s a pretty busy road a’ [all] the way out that, depending on the time o’ day again. But it wouldn’t stop me. It wouldn’t stop me. Now, going that way, you’re going away from it . . .
So it’s more just that it’s changed the, sort of, experience of walking?
Yeah, it’s really . . . aye, visually it’s, you can see it, you’re aware of it more. Although sometimes it’s subconsciously, you’re no’ even thinking aboot it, but you know it’s there. You know it’s there.
Man aged 51–65 years living in Rutherglen
Such change in the quality of the experience may have the potential to erode the likelihood that people would make active journeys in future when an alternative was available.
Many participants cited work and other ‘utility’ journeys as their main reasons for active travel. Local high-street shops, ‘big box’ supermarkets nearby and green spaces emerged as important destinations. Beyond their immediate areas, some people also described recently developed pedestrian infrastructure, for example on the Clyde Walkway and in Glasgow Green, as places they enjoyed frequenting.
Aside from any effects attributable to the motorway, one factor emerged as being of major importance to local residents in determining active travel: their perceptions of personal safety. This was mentioned by people living in Rutherglen, who referred to crime related to drug and alcohol use and to an existing pedestrian underpass that was considered unsafe (Figure 25), which was also mentioned by participants in the baseline study,58 but it was a more dominant concern in Govanhill.
FIGURE 25.
View inside an existing pedestrian underpass in Rutherglen. Photograph © study participant; reproduced with permission.
Numerous participants from Govanhill described a decline in their perceived personal safety over the study period, which they associated mainly with incomers to the local area, along with changes in patterns of tenancy (see Aesthetics and the built environment) and, to a lesser extent, with drugs, alcohol and unoccupied young people:
I couldn’t exactly say when I did notice that ‘cos there’s certain, you know, streets I didn’t walk down just for the fact I didn’t have to walk down thae [those] streets. And it wasn’t because I went ‘I’m not walking down there’, just because I didn’t, you know, to get there I knew well, I can go that way, that’s quicker going, you know, cutting down that street . . . But one time I didn’t give it a thought walking down places whereas the last – definitely the last 5 years I just went ‘That’s it, I’m going in the car’.
Woman aged 36–50 years living in Govanhill
This change in perceived safety led the participant in question to avoid particular streets, and to make more journeys by car that she would previously have walked. Another resident in Govanhill described how she would rather have her children play video games at home, where they were safe, than allow them to play outside unsupervised:
I don’t ask my children [to] go outside because I’m scared.
Woman aged 36–50 years living in Govanhill
These perceptions of declining neighbourhood safety, and of the causes of that decline, had implications for community cohesion and the potential for local people to form neighbourhood relationships (see Severance and connectivity).
Economic impacts
Although the potential for local economic development emerged as a key issue in most of the key informant interviews, it was rarely mentioned in resident interviews. Residents tended not to describe any benefits of the new motorway for the local economy as such. Instead, they tended to mention greater convenience, or reductions in travel time, for driving. Key informants, however, were naturally more likely to consider the wider impacts of the new motorway and regarded its economic impact as a key beneficial outcome. The increased connectivity provided by the new motorway had been expected to attract businesses into the M74 corridor, and our data suggest that, to some extent, these expectations were in the early stages of being realised. It was clear from key informants that local economic development had been temporarily impeded by the recession that began in 2008, and some observed that many of the potential economic benefits might take some time to be fully realised. Business developments in the Rutherglen Low Carbon Zone and at other locations along the M74 corridor have been developed in conjunction with Clyde Gateway, an organisation charged with revitalising some of Glasgow’s most deprived communities. For many key informants, the work of Clyde Gateway and the M74 extension were inextricably linked:
One of the key driving forces behind the M74 extension was the promise of an economic spin-off in terms of jobs and investment . . . the three junctions that were built, in particular, you know, 2A, 2 and 1A, as they’re now known, are in the heart of the Clyde Gateway area. This allowed the area to be opened up for future redevelopment, primarily driven by the private sector pump primed by the public sector in terms of Clyde Gateway being a partnership between two local authorities, Scottish Enterprise, with funding from the government. And the idea being that these three junctions open up what was hitherto a difficult and complex area to navigate your way to and navigate your way around.
Key informant, local regeneration company
I think in terms of the [M]74, what it has done is opened up the accessibility and has, along with the Commonwealth Games, really allowed the local authority to consider the economic potential of sites which previously were locked or very poorly accessed by the existing network or were perceived to be in the wrong location for investment.
Key informant, local planning department
. . . obviously like the Clyde Gateway stuff over in Dalmarnock, Rutherglen edge, down towards Shawfield and stuff there’s like the new National Cycle Route, and new bridges and all that kind o’ stuff . . . although these things are kind of interconnected ‘cos I think like the Clyde Gateway was very much closely linked with the [M]74 extension, but it was also about regenerating Dalmarnock and the Commonwealth Games and all of that stuff as well, so it’s not a direct, necessarily a direct impact of the [M]74, it’s a contributing factor so, yeah, there probably has been. How that also fits in kind of a national framework of promoting sustainable transport, I don’t know. Would that stuff just have happened anyway?
Key informant, local development trust
For another key informant, however, the type of development being attracted appeared to be predominantly industrial. This potential reindustrialisation of the area was not necessarily compatible with improving the area as a place to live:
Now obviously the M74 was mostly passing through built-up urban areas already or derelict wasteland, so . . . I think Clyde Gateway have built quite a lot of industrial units. Toryglen has now got a cement works in amongst everything else. So joyful . . . o there’s a whole load of commercial and industrial units that have sprung up at the back of Toryglen and one of them is a cement works which is not attractive. When are cement works ever attractive? So yeah, that area feels more industrial and I expect it’s been a similar story along the route from various other places.
Key informant, local advocacy group
Some respondents also speculated that the majority of the economic benefits of the new motorway might be felt by those outside the local area.
Severance and connectivity
Despite being widely used in transport literature, severance is a term that can encompass a variety of definitions. According to Anciaes,123 it is sometimes used to denote a broad, ‘ball-of-wax’ concept that encompasses any dividing impacts related to transport infrastructure and at other times is used to refer solely to the effects of traffic itself, with physical infrastructure considered to exert a distinct ‘barrier effect’. For some scholars and planners, severance may relate to the impact of a new road on existing routes for journeys, but it can also encompass more abstract conceptualisations of ‘severing’ such as the rending of social relationships. Several typologies of severance exist, including Guo et al. ’s124 categorisation of effects into either static (physical obstruction) or dynamic (indirect or inconsistent severing). Clark et al. ,125 however, distinguish between physical severance (that which physically impedes movement) and psychological severance (that which creates a perception of division). One particularly comprehensive typology is that proposed by James et al. ,126 who suggest eight categories of transport-related severance. These are temporary physical barriers (traffic), permanent physical barriers (roads or other infrastructure), omission barriers (failure to provide adequate pedestrian crossings or similar), time barriers (e.g. if infrastructure is less traversable at night or in inclement weather), legal barriers (prohibition of certain forms of transport, e.g. of pedestrians on motorways), quality barriers (poor lighting or surfaces), attitudinal barriers (e.g. fear of safety) and information barriers (lack of information or knowledge about how to use facilities). These dimensions of severance can be used to consider the range of ways in which local people may feel themselves to be either physically or psychologically impeded in their movements because of transport infrastructure. Although there is little direct evidence regarding the link between severance and mental or physical health outcomes, previous research does suggest that severance may contribute to reduced social interactions and active travel. 44
In this chapter so far, a number of factors relating to the new motorway itself, as well as to wider systems of change taking place in the case study areas, have been shown to contribute to a complex picture of what may be described as severance and connectivity. Rather than an unambiguous severing effect of the new motorway, participants described the M74 extension as, by turns, a force for both connection and severance. In particular, it was seen as promoting active travel and connectedness (through improved pedestrian infrastructure and a perception of reduced traffic) in some areas and for some people, but as a severing force for others (through a perception of increased traffic and more challenging conditions for cycling). In addition, one resident living very close to the new motorway echoed the fears of some of the participants in the baseline study58 by describing the psychologically severing experience of feeling hemmed in by roads on all sides:
[This photograph] shows the same view, the same road. It just goes straight along there, straight down south. And then that way is heading into the city to join up wi’ the rest o’ the [M]74 an’ the M8 an’ all that kind o’ stuff . . . no matter what way you turn you’re getting it, you know? You go that way, as I say, you get that view, and then if you go down that way and go left down that way you’re gonnae get that view.
Man aged 51–65 years living in Rutherglen
One key informant, however, expressed an interesting and somewhat divergent perspective on the idea of severance and gaze. This was a view – also anticipated in the EIA for the project61 – that the M74 extension had, to some extent, ‘put Rutherglen on the map’ because a large number of drivers would now see it both signposted from the motorway and in direct view from the elevated carriageway.
As less is known about the social dimension of severance, it is worth paying attention to how that theme emerged from our data. Two core aspects of severance relate to social networks and community cohesion: one is created by cutting residents off from local amenities such as shops and the other is created by cutting them off (either psychologically or physically) from their local social contacts. In respect of amenities, our participants described the new motorway as having both a severing and a connecting effect. For example, a number of residents with cars described the motorway as connecting them with work and leisure facilities:
I use it, I think, pretty much every day to go to my work in [another area of Glasgow], to go and visit family in [a neighbouring area], to go to [a theme park], to go to [large regional shopping centres]. So it’s perfect for me, really.
Woman aged 20–35 years living in Rutherglen
For those without a car (or who avoided the motorway by preference) and who did not describe having dispersed social networks, the new motorway was described as having either a neutral [‘it makes no difference to me at all’ (woman aged 36–50 years living in Rutherglen)] or a negative impact on connectivity:
Yeah, yeah. Oh yeah. You used to just drive up tae the [supermarket] in 10 minutes. But since [the motorway opened], no. Even the light sequence is wrong, so it is. So, no it’s completely, for people who don’t use the motorway it is, it’s a bit o’ a nuisance.
Woman aged 36–50 years living in Govanhill
More interesting, perhaps, was the emerging importance of social places in the community where community members could interact and connect with each other. These included green spaces, social clubs, school gates, churches and local shops (Figures 26 and 27).
FIGURE 26.
Places where people interact in Rutherglen. (a) Shops on Main Street; and (b) the newly renovated Town Hall. Photographs © study participants; reproduced with permission.


FIGURE 27.
Local parks. (a) A small park in Rutherglen; and (b) Govanhill Park. Photographs © study participants; reproduced with permission.


Such interactions had implications for residents beyond the idea of friendly neighbourliness: being a ‘known face’ in the area was associated by some with greater feelings of local safety, and places where such contact occurred were therefore perceived as having local importance. It was noted above that residents felt more accepting of the motorway if they understood that their local shops would not be affected. Residents described green spaces as of particular importance in their communities, because those living in flats tended not to have a back garden or yard in which children could play safely. In general, green spaces were conceptualised as places where residents of neighbouring communities could interact and overcome social barriers. Such places are often referred to in the community development literature as third places. 127 One key informant had this to say about their local green space:
[Part of our role is] to help use these [woodlands] to improve community cohesion, break down barriers between . . . you know, social barriers that people have, through the delivery of social programmes and events.
Key informant, local greenspace organisation
However, the site in question was described as having been particularly affected by air and noise pollution and visual disruption from the new motorway nearby. Parks were seen as important places that facilitated the integration of children through play, including those from different cultural backgrounds, although they were also sometimes described as places where ‘unsafe’ activities such as teen drinking might occur, particularly after dark (see Figure 27):
So Govanhill Park is a nice area and it’s got the courts there as well. So it is regularly used . . . I think with the schools [close by] as well, that they are so multicultural, there’s a lot of multicultural mixing in the park as well, so you’ll often see not just the kids but the parents as well, so I think that’s been great for the community that part.
Woman aged 36–50 years living in Govanhill
Understanding severance and connectivity as they relate to a transport infrastructure project is complicated because they are embedded within a wider local system. In this chapter, we have tried to understand something of this wider context, examining severance in relation to the motorway in particular, as well as in relation to other physical and social factors. We have shown that both severing and connecting aspects of the new motorway had a spatial dimension (depending on the neighbourhood of residence and proximity to the motorway), a temporal dimension (e.g. the greater volume of traffic at certain times of day) and an individual dimension (related to people’s gender, health, mobility and length of residence, among other factors). In the case of the M74 extension, the spatial aspect was further complicated by the presence of an existing line of incomplete severance, the West Coast Main Line railway, parallel to the route of the new motorway. This makes it difficult to ascertain whether or not mitigation measures such as new footbridges would have had the same impact on connectivity if they had not been replacements for existing infrastructure.
Existing definitions of severance consider the physical or psychological separation of people from community assets or other people through a barrier effect. They tend not to consider the severance that may occur when new transport infrastructure, or another type of change, threatens these third places where community cohesion is created – as exemplified by our participants who expressed concerns about the impact of the new motorway on the character of local shopping streets or green spaces. The role of urban green spaces in enabling both social connection and restoration is well documented. 128,129 Our key informants described the disruptive effects of both the physical structure of the new motorway and the resulting traffic noise on the experience of using these potentially ‘restorative’ third places as particularly negative:
I have spoken with some of the people, you know, volunteers and local residents who have been coming here for a lot longer than me, you know, before the motorway was built and they’ve all said ‘Yeah, you used to be able to sit here and you could hear nothing’ . . . it was a real tranquil place where you could escape the city without going out to the countryside. Remember the demographic of the area that we’re in? We’re in a very deprived area . . . People that live round here don’t have the opportunities to engage with natural heritage in the way that people in more affluent areas do . . . Places like this are really, really important for people to experience natural heritage, to experience wildlife. So if that is compromised in any way, it’s the people that live around . . . that get affected.
Key informant, local green space organisation
Severance of this type was thus considered to be an issue of social justice, although – as discussed above – the new motorway was by no means the only factor affecting local third places, and our participants also discussed the influence of the recession on the sustainability of local shops, feelings of personal safety related to crime, alcohol and drug use, and changes in culture related to the arrival of incomers. Our findings therefore contribute to identifying and investigating a form of severance that appears to have been little studied to date.
Conclusion
Qualitative interviews conducted at baseline in 2005, when the new motorway was planned but not yet under construction, had elicited diverging views about its probable impacts. In the follow-up interviews described here, we found evidence of similarly mixed attitudes and experiences. Our sample reported both positive changes (improved pedestrian infrastructure, decreased local traffic, decreased noise, greater connectivity and improved quality of active travel) and negative changes (increased local traffic, increased air and noise pollution, severance, poorer quality of active travel and, in a minority of cases, poorer health) that they directly attributed to the new motorway. Some participants described positive changes, some negative and some both, whereas others seemed indifferent to the new motorway or described no related changes. Many described the new infrastructure for pedestrians to cross the motorway as lighter, more open and more secure than expected. Participants described how the physical structure of the M74 extension, as well as related changes in noise, traffic on local streets and other aspects of the physical environment, affected active travel in both negative and positive ways. Where participants perceived the motorway as having a direct impact on active travel, it was most frequently on the quality or experience of active travel rather than the frequency, route or duration of journeys. Perceptions of personal safety were often of greater concern to local residents, and were more likely to lead to changes in how, where and when people walked or cycled in their local area. We found that local experiences of severance were complex and associated with a number of factors, both related and unrelated to the new motorway. For those with access to a motor vehicle and with more dispersed social networks, the new motorway often facilitated their connections with amenities and people. In contrast, those whose social networks were more local, and who either lacked access to a vehicle or chose not to use the new motorway, sometimes found it to be a severing force, either physically or psychologically. There was also some evidence that the new motorway may have contributed to further severance by a hitherto little-explored mechanism involving disrupting local places of connection, such as local shops and green spaces. Overall, however, the qualitative evidence suggested that social factors such as community cohesion and safety were of greater significance to the majority of local people. Whether or not this would also be true in communities with different socioeconomic profiles, or those that lacked an industrial history or an existing line of severance in the form of a main railway line, remains an open question.
Chapter 8 Community and stakeholder engagement
Introduction
In this chapter, we extend the description of the programme of community and stakeholder engagement that we conducted as part of the study and introduced in Chapter 2, Characterising the environmental changes and refining the study design. We sought to ensure that our research questions were of relevance, both to local communities and to potential users of our evidence in the policy and practice sectors; that community members were collaborating partners, in a variety of ways; and that our findings thereby had the potential to stimulate action and change in the interests of the communities involved. Our engagement activities were concentrated at two key stages of the project. The first phase involved an initial scoping of community issues and perceptions with key informants from community organisations, described in detail in Chapter 2. This informed the refinement of our study design, particularly for the qualitative fieldwork and analysis, and generated an initial sample of key informants for subsequent interviews. The second phase, described in this chapter, involved sharing our preliminary findings with local communities and other stakeholders: partly to enable a ‘ground truthing’ of our overall interpretation of those findings, and partly to stimulate further discussion about opportunities and challenges facing those communities. Both elements were conducted in partnership with the SCDC and brokered by the GCPH.
Planning
Once emerging findings from the study were available, we planned a series of events in early 2016. These were originally envisaged as three structured half-day events to be held at community facilities in Rutherglen, Govanhill and the Gorbals – three communities adjacent to the motorway, two of which formed the case studies for the qualitative analyses described in Chapter 7. The aim was to bring together representatives of local organisations, as well as study participants and local residents, to consider and discuss the findings. We sent targeted invitations to local community representatives and to local residents who had taken part in our qualitative and objective measurement substudies, and supplemented these with mail-drop invitations in the local area. However, in light of the poor response to these invitations, we changed our plan and organised a ‘pop-up’ event in each of the three areas instead. These informal events were intended to engage local people and elicit their views by taking the findings to them, rather than expecting them to attend a more formal event. We also conducted an additional event in a sheltered housing complex in the Gorbals, one of the residential buildings closest to the new motorway, in which several residents had expressed interest in attending one of the originally envisaged events. To complement these informal community events, we organised a structured, formal half-day event with a particular focus on stakeholders. We invited representatives from relevant local and national organisations, as well participants from our qualitative and objective measurement substudies. The event was also promoted and cascaded through existing SCDC and GCPH networks.
Community events
In this section, we describe the four informal community events that took place between March and May 2016. The first took place at a sheltered housing complex in the Gorbals, which is overshadowed by the motorway; the second at a shopping centre in Rutherglen; the third at a community hall in the Gorbals; and the last on a main shopping street in Govanhill.
Sheltered housing event
This event took place in the common room of the housing complex and was attended by five residents. Two had homes that faced directly onto the new motorway; these were the only residents present who had lived in the complex before, during and after the construction of the new motorway. The other three had homes facing away from the motorway and had lived there only after the motorway was opened. The room was set up with a large map of the area on a table, and sticky notes and pens for annotation.
The two residents with homes facing the motorway highlighted stark problems with noise, vibration and air pollution that began during the construction period and continued after the motorway was opened. They described having to constantly clean their windows and spectacles because of the build-up of dirt, suffering from ongoing eye problems and being unable to open their windows because of the noise and air pollution. They also described sleep deprivation owing to motorway maintenance activities occurring at night. Although the three residents in homes facing away from the motorway also identified local problems with air and noise pollution, they were less sure that the new motorway was the main cause of these and were either indifferent or positive towards it overall. All the residents described increases in local traffic and in heavy goods vehicles using local streets; this was attributed to the motorway as well as to other changes in street layouts and the locations of bus stops. One resident who owned a car felt that the motorway helped her to get around, and others who did not own cars described the motorway as enabling family members to visit them more easily. Residents described difficulties in walking on uneven pavements and a lack of local amenities within walking distance, as well as changes to bus routes that paradoxically made it easier to reach amenities further away than to reach those nearby. Finally, although residents could highlight local road traffic accident hotspots, none felt that the motorway had affected the frequency of accidents.
Rutherglen event
This event took place in a busy shopping centre, frequented by local people as well as those from surrounding neighbourhoods. We set up a banner describing the purpose of the study and directing passers-by to the researchers if they were interested in talking about it. A large map of the area was set up on a table, with sticky notes and pens available for annotation (Figure 28). In total, there were 18 visits to the stand over several hours.
FIGURE 28.
Community engagement event in Rutherglen. Photograph © Amy Nimegeer; reproduced with permission.

Overall, attendees expressed positive, negative and neutral views regarding the motorway. The most consistently expressed view was that the motorway had significantly improved conditions for car users, allowing them faster and more convenient access to surrounding areas and amenities. As at the first event, some residents raised issues of environmental blight relating to noise and vibration from the motorway: one described being unable to open her back window because of the noise, and another described cracks forming in houses nearby. There were conflicting views about whether traffic on Rutherglen Main Street had increased or decreased, but some people felt that a reduction in traffic congestion had improved the local environment. Other comments received included observations that cars and lorries were infringing on cycle lanes on local streets and that public transport provision in the area had decreased, but it was not clear whether or not these were thought to be attributable to the M74 extension.
Gorbals event
This event took place in a community hall, as part of a local lunchtime event, which provided activities for adults and children and a free lunch. We set up a stand comprising the banner, map, sticky notes and pens as described above, and spoke with nine people who lived or worked in the Gorbals.
As at the second event, attendees expressed positive, negative and indifferent views about the motorway. However, unlike at the second event, where discussion focused on the benefits for car users, the discussion at this third event particularly highlighted health and social harms, with four of the attendees having been involved in protests against the plan to build the new motorway. Two mentioned that the PLI had strongly recommended against building the new motorway, but this advice had been rejected and construction had proceeded regardless. The motorway had been built through an area of comparatively low car ownership, where people were less likely than those living in other areas to benefit directly from using it. However, another resident expressed a contrasting narrative to the effect that the new motorway had helped to increase investment in the Gorbals because the area was now more accessible. Two attendees described motorway-related respiratory problems in children or grandchildren, with one child’s asthma having apparently remitted after they moved further away from the motorway. However, others suggested that the effect of the new motorway in reducing local congestion may have reduced exposure to fumes, because cars were now moving more quickly through the area rather than idling.
Govanhill event
This event took place outdoors on a main shopping street in Govanhill, which is frequented by local people and has a steady stream of foot traffic. It was not possible to set up a table or a map as at the previous events, so the stand consisted of only the study banner, and the research team simply spoke with passers-by. In total, there were seven visits to the stand over several hours.
As at the Rutherglen event, the conversation was dominated by discussion of the effects of the motorway on traffic and congestion. Those who had a car and used the motorway felt that it had reduced journey times and improved accessibility. However, some described congestion on local roads because of reconfigurations of local streets to accommodate a new motorway junction. Those who did not use the motorway expressed indifference overall, but some had concerns about the introduction of paid parking on the shopping street, which they felt had precipitated a decline in the quality of shops. Several attendees expressed the opinion that Govanhill was an area that was steadily going downhill, as a result of the in-migration of poorer, less skilled migrants and the out-migration of wealthier and more highly educated people. These changes were of greater importance to residents than any changes attributable to the motorway.
Stakeholder event
In this section, we describe the formal half-day stakeholder event that took place in May 2016 at a venue in Glasgow city centre. In total, there were 30 attendees: six local residents or study participants and 24 stakeholders from organisations including Transport Scotland, Glasgow City Council and the NHS, as well as members of local universities, housing organisations and advocacy groups. Attendees were seated during an initial plenary presentation that outlined the emerging findings from the study and were then given the opportunity to move around three interactive stands focusing on the findings of the core survey, qualitative study and analysis of road traffic accidents in more detail. Discussion around relevant themes from these interactive stands is summarised below.
Travel and physical activity
Most attendees thought that the motorway had benefited car users. However, some felt that the improved opportunity to connect to more remote destinations came at the expense of local destinations. In addition, the new motorway was perceived to have reduced the attractiveness of other modes of transport for longer journeys, such as using the train to get to Edinburgh. Several attendees described traffic problems at motorway junctions following changes in local street configurations and traffic management problems where slip roads met local streets. The result had been increased traffic congestion on local streets and worse conditions for cyclists and pedestrians. Other, more general, traffic issues raised were those of declining public transport provision in the Gorbals, the loss of free car parking on the main shopping street in Govanhill and the generally poor quality of cycling infrastructure, all of which were issues raised at the previous community events.
Well-being
Among the local residents attending the event were a family who lived close to the new motorway. Their accounts of air and noise pollution were strikingly similar to those elicited at the first event at the sheltered housing complex. During motorway construction, piling caused structural damage to their flat and cracked nearby pavements. Even after construction was completed, the family described constant traffic noise and vibration during the day, and noise from maintenance activities at night, which disrupted their sleep. They also described breathing difficulties, which they related to increased air pollution and being unable to sit outside on their balcony.
Communities and regeneration
Some attendees felt that the motorway had created a clear visual and psychological barrier between areas, making some areas inaccessible and disrupting local social networks. Conversely, one attendee felt that the motorway had opened up views of the cityscape for those driving on it (a form of ‘reverse severance’), echoing a perspective mentioned in Chapter 7, Changes in local experience. Attendees also raised wider issues relating to social and environmental justice and inequalities. The benefits experienced by some were not thought to justify the considerable expense of the new motorway, and people of lower socioeconomic status and those with impaired mobility were seen as experiencing more harms than benefits. The new motorway was also seen as bolstering the wider economy (e.g. improving access for multinational corporations) at the expense of the local economy and small businesses. There was also more general discussion about overall decline or regeneration in local communities. Govanhill and the Gorbals were both seen as becoming ‘ghettoised’ by a combination of poorer, less skilled migrants and absentee landlords, with new estates gradually becoming slums and the social fabric of communities becoming degraded. However, this was seen as a problem that predated the new motorway. It was also suggested that although the Gorbals was benefiting from active investment and regeneration, Govanhill seemed to be languishing – a view that had also been expressed at previous events.
Road traffic accidents
Some attendees expressed the opinion that traffic had noticeably increased in areas around the M74 extension, and that it was therefore surprising that this had not been translated into more accidents. However, other attendees felt that there had been little impact on local traffic and were therefore unsurprised at the lack of change in the frequency of accidents. It was agreed that the effect of the motorway on accidents might change if congestion were to increase in future.
Contribution to interpretation
In this section, we discuss the contribution of all five community and stakeholder engagement events to furthering our understanding of the study findings outlined in Chapters 4–7.
An almost unanimous view across all these events was that the new motorway had been a favourable development for car users, allowing for faster and more convenient journeys. This aligns with the finding from the core survey that car use was increased among those living near the new motorway (see Chapter 4, Patterns of behaviour and change over time in the core survey data). It also aligns with separate assessments conducted by Transport Scotland that found marked reductions in traffic flows and journey times across parts of the motorway network. 110,130,131 However, some attendees questioned the fairness of improving amenity for car users, in light of the comparatively low car ownership among local residents.
Other modes of transport, such as active travel and bus use, were less commonly raised. There were mixed opinions on whether amenity for these had improved or declined, although many felt that local cycle infrastructure was poor. There was also a lack of clarity on whether or not any changes in amenity were directly attributable to the motorway. For active travel in particular, this is consistent with findings from the core survey and SHS analyses (see Chapter 4, Patterns of behaviour and change over time in the core survey data and Patterns of behaviour and change over time in the Scottish Household Survey data) and the qualitative substudy (see Chapter 7, Changes in local experience). The community engagement events further elaborated a theme of tensions between different types of vehicles and road users (cars, lorries, buses, bicycles and pedestrians) in sharing road space, particularly on busy roads.
At the informal community events, there was little discussion of road traffic accidents, which is perhaps unsurprising given our finding that the new motorway was not associated with either an increase or a decrease in accidents (see Chapter 5, Relationships with environmental exposures). When asked directly about this, most attendees could identify local accident hotspots but these were never attributed to the new motorway. At the formal event, there were mixed opinions on whether local traffic had increased or decreased, and therefore mixed expectations in respect of how this was likely to affect accidents.
Although strong negative effects of the new motorway on well-being were found in our core survey analyses (see Chapter 6, Patterns of well-being and change over time), well-being as such was not directly mentioned by attendees at the engagement events. However, a variety of hypothesised contributors to poor health and well-being, including visual disturbance, air pollution, noise, vibration and sleep deprivation were frequently raised by residents, suggesting that these impacts may have been more tangible to them than a more abstract notion of well-being. In core survey analyses, individual residential proximity to the motorway appeared to be more closely related to well-being outcomes than study area of residence. This was borne out in the community engagement events, at which it became apparent that proximity to the motorway seemed to be important in terms of the experience of air pollution, noise, vibration and visual disturbance. Even among residents of the sheltered housing extremely close to the new motorway, there seemed to be an indication of a dose–response relationship in that those directly facing the motorway experienced more negative effects than those living slightly further away and not facing it.
The engagement events reaffirmed the finding from the qualitative substudy that the motorway acted as a connecting force for car users (see Chapter 7, Changes in local experience). However, they introduced a further nuance in that non-car users could also benefit if people in their social network were more able to connect to them via the motorway (e.g. residents of the sheltered housing who described reduced journey times for family members visiting them). Conversely, car users described an experience of severance if they were not comfortable driving on motorways, or if they experienced motorway-related congestion on local streets.
At the engagement events, the visual disturbance described by residents living close to the new motorway was consistent with descriptions of feeling ‘hemmed in’ that were made in qualitative interviews (see Chapter 7, Changes in local experience), and with the wider literature on severance. However, the accounts of extreme proximity elicited at the engagement events produced an additional nuance related to severance: for those living very close to the motorway, it was not the experience of living in their community that was most affected by the new motorway, but the experience of being in their own home. For people in this situation, leaving their homes and moving around the local area actually lessened the adverse effects of the new motorway, which suggests that more established ways of conceptualising severance may not apply to them in the same way. The community and stakeholder engagement programme was the only part of the study in which first-hand narratives of living in extreme proximity to the new motorway arose, adding to and complementing our main programmes of qualitative and quantitative data collection and analysis. It became clear through this programme that although the new motorway was no longer a dominant issue for residents in general, for those living in extreme proximity to it, it was, and is likely to continue to be, a significant cause for concern.
Finally, physical activity was not discussed at all at the informal community events, and only briefly at the formal stakeholder event, even though we found some evidence of a possible effect of motorway exposure on physical activity in the core survey (see Chapter 4, Patterns of behaviour and change over time in the core survey data). This suggests that physical activity was either not an outcome of particular interest to residents or stakeholders, or not closely linked in their minds with the new motorway.
Conclusion
In total, nearly 70 people participated in one of the five community and stakeholder engagement events, providing opinions about the motorway and insight into life in the local area. In general, residents attending the informal events were most concerned with immediate local impacts of the motorway on traffic congestion, noise and pollution. However, the lived experience seemed to differ between areas, with the Rutherglen event highlighting benefits for car users, the Gorbals event introducing negative impacts on health and well-being, and the Govanhill event suggesting that the new motorway was less important than wider social issues in the area. At the formal event, social justice was prominent among the issues of concern to stakeholders. It was clear that perspectives on the new motorway differed between areas, groups and individuals, ranging over a spectrum from the strongly positive to the neutral or indifferent, to the strongly negative. Attendees at the community engagement events also described having personally experienced a mixture of positive and negative effects, as well as acknowledging that the benefits experienced by some may have been achieved at the cost of harms experienced by others.
Chapter 9 Discussion
Introduction
The opening of the M74 motorway extension presented an opportunity to examine the health impacts of new major road infrastructure in a natural experimental study. We used the developing situation in Glasgow to understand more about the positive and negative effects of a major change in the urban built environment from which more general lessons might be learned for the planning and implementation of future initiatives in transport planning and urban regeneration. In this mixed-method controlled before-and-after study, we used a combination of quantitative and qualitative research methods to evaluate changes in travel and activity patterns, road traffic accidents and well-being associated with the new motorway, and to investigate mechanisms and processes linking these outcomes with changes in the physical and social environment. In this chapter, we begin by summarising the principal findings of the study. We go on to discuss the contributions and implications of our findings for four aspects of public health science: (1) the estimation of causal effects; (2) the explanation of causal effects; (3) the testing of more generalisable causal hypotheses; and (4) the implications of the findings for policy and practice. We then summarise the conceptual and methodological challenges we faced in designing and conducting the study, the strengths and limitations of the ways in which we addressed these, the contributions of the study to methodological investigation and development, and the implications of our findings and experience for future research. Our discussion is necessarily focused on a few selected issues arising from the large body of research summarised in the report. Further discussion of many of the more specific or technical issues can be found in the relevant publications (see Acknowledgements).
Principal findings
Changes in travel and activity patterns
After adjustment for multiple individual and household confounders as well as baseline travel behaviour, participants in our cohort survey living in the South study area surrounding the new motorway were about twice as likely as those in the North (where there was no motorway) to report travel by any mode of transport at follow-up. Within the South study area, participants living closer to a motorway junction were more likely to report travel by any mode (in the cohort analysis) and to report using a car (in the repeat cross-sectional analysis) at follow-up than those living further away. The finding on car use, in particular, was consistent with views elicited in community engagement to the effect that the new motorway had considerably improved the speed and convenience of car journeys.
The SHS data showed that the proportion of journey stages that were walked or cycled increased slightly over time in all three study areas. 63 This is an encouraging finding for public health in its own right, but there was no evidence that the rate of change was significantly different between the intervention and control areas. In contrast, our core survey data showed that the average daily quantity of active travel reported by participants decreased over time in all three areas, although this may have been an artefact of measurement as much as a reflection of a real decline. Neither area- nor individual-level exposure to the intervention was associated with either the likelihood or the quantity of active travel at follow-up in the core survey, corroborating the SHS findings.
In analogous analyses, cohort participants living in the East study area (surrounding the existing M8 motorway) were about half as likely as those in the North to report participating in any physical activity at follow-up, and those living closer to a motorway junction in the East were more likely to report a reduction in physical activity participation than those living further away. However, analysis of georeferenced accelerometer data collected in a subsample of survey participants in all three study areas at follow-up found that neither area- nor individual-level exposure to the intervention was associated with physical activity, either overall or within neighbourhood pedestrian network buffers of various sizes.
Qualitative interviews elicited a variety of personal and social factors related to physical activity, consistent with previous research. More particularly, participants described how the physical structure of the new motorway itself, as well as related changes in traffic, noise and other aspects of their surroundings, affected active travel in both positive and negative ways. Where the motorway was seen as having a direct impact, this was most often described as affecting the quality or experience of active travel rather than the frequency, duration or routes of journeys. In contrast, perceptions of personal safety were more often linked with making changes in the frequency, route or mode of active journeys. Although the divergence of views about the motorway previously elicited at baseline was reinforced, most participants at follow-up described the new pedestrian infrastructure for crossing the motorway as lighter, more open and more secure than expected.
Local residents experienced changes to connectivity that they associated with the new motorway and other factors. Broadly, those with dispersed social networks viewed the motorway as facilitating connections with amenities and people in other places. However, those whose networks were more localised, and who lacked either access to a car or confidence in using the motorway, sometimes found it be a cause of severance: physically, psychologically or through its impact on local sites of connection. More than the motorway infrastructure itself, social factors including community cohesion and perceptions of personal safety were viewed as primary causes of local severance.
Changes in road traffic accidents
The annual incidence of road traffic accidents in Glasgow City and surrounding local authorities fell by about half between 1997 and 2014. A similar reduction was observed in all three local study areas, and our analyses found no significant differences in temporal trends between study areas that could be attributed to either the construction or the opening of the new motorway. The reduction was greatest in the North study area, a pattern that appears unlikely to be attributable to the new motorway and that may reflect a variety of other factors outside the scope of this particular study. There was a social gradient in the location of accidents, and the opening of the new motorway had little impact on the spatial clustering of accidents.
Qualitative accounts of travel in the local area revealed several mechanisms that may have prevented the realisation of the claimed reduction in accidents. Local residents described new hazards, including the merging of lanes of traffic, vehicles travelling at high speeds on slip roads and altered layouts of existing streets close to the new motorway junctions. These may have contributed to the danger of crossing roads, particularly for pedestrians with impaired mobility.
Changes in well-being
Participants in our cohort survey living closer to the new motorway experienced significantly reduced mental well-being over time compared with those living further away, and in both a repeat cross-sectional analysis and a cross-sectional analysis we found evidence of an interaction whereby participants with a chronic condition living closer to the existing M8 motorway experienced a greater decrement in well-being than those living further away. In these analyses, proximity was modelled as the negative natural logarithm of the straight-line distance from home to the nearest motorway. Therefore, the average reduction in mental well-being per unit of proximity observed in these analyses – approximately 3.5 units on the MCS-8 scale – can be interpreted as the average difference between a participant living approximately 100 m from a motorway and one living 300 m away; or between a participant living 300 m away and one living 800 m away. These point estimates for the effect size on mental well-being are consistent with effects of ‘population significance’. They are similar in magnitude to those found in a clinical population experiencing reduced overall quality of life in a previous validation study (3.3 units). 66 In a general population, they are comparable to the difference between 18- to 24-year-olds and 45- to 49-year-olds (2.6 units) or between people not completing high school and graduates of tertiary education (4.2 units), and greater than that between those with a chronic physical condition and those without (2.0 units). 66 In a cohort analysis, reductions in both mental and physical well-being were also associated with an ‘upheaval index’ representing the proportion of land use in the immediate neighbourhood that had changed, particularly in the South study area. A difference of 10 percentage points in this upheaval index was associated with an estimated 1.6-unit difference in MCS-8: a difference of similar magnitude to that between people with a chronic physical condition and those without (2.0 units).
At follow-up, perceptions of both the social (collective efficacy) and physical environment of neighbourhoods were slightly more negative among those living closer to a motorway, but these differences were mostly not significant; and in the cohort analysis, there was no statistical evidence that changes in these perceptions mediated the changes in well-being associated with motorway exposure. Qualitative accounts elucidated the industrial history and character of the area, longstanding concerns about pollution and – for some – narratives of decline and powerlessness in local communities, suggesting a degree of acceptance of – or resignation to – the more recent changes brought about by the motorway. Nevertheless, the community engagement events elicited striking accounts of stark visual, noise, dust and other forms of disturbance, and their impacts on sleep, respiratory health and other contributors to well-being, although these were limited to those living in extreme proximity to the new motorway (see Explaining the effects of the intervention).
Principal contributions and implications of the study
In reflecting on the meaning of our evaluative findings, it is important to bear in mind two aspects of the way in which the study was conceptualised. The first is that we did not set out to evaluate whether the new motorway was ‘effective’ in any overall or comprehensive sense, and certainly not to evaluate its value for money. Although similar transport projects exist around the world and more are planned, constructing a new motorway in an urban area is only one of many specific ways in which central or local government might seek to improve infrastructure to promote mobility, to catalyse economic regeneration or to change people’s living environments. Instead, we took the opportunity presented by this natural experiment to investigate a more specific set of research questions focused on linking environmental change with travel and physical activity behaviour change, road traffic accidents and well-being in local communities. The second is that, in common with all natural experimental studies, we were not able to control the assignment or nature of the intervention, other concurrent activities or other potential confounding factors in the areas, populations and individuals concerned. 59 We therefore sought to build an evidential case for causal inference using multiple sources of data and types of analysis. 132 With these considerations in mind, in this section we discuss the meaning of our findings as they relate to the complementary scientific goals of causal estimation, causal explanation and more generalisable causal inference to inform policy and practice. We begin by drawing together the evidence from our various quantitative analyses that enables us to estimate the size of any changes in the outcomes of interest in the study that might be attributed to the intervention.
Estimating the effects of the intervention
Quantitative outcomes with stronger evidence of a causal relationship
Well-being
The evidence from this study suggests an unequivocally negative overall impact of the intervention on well-being. We found some evidence that living near to either a newly constructed or an established urban motorway worsened mental well-being, and we found no evidence to suggest any positive effects on well-being. The negative impacts were most pronounced in longitudinal cohort participants living near to the M74 extension. The pattern of findings across the South study area containing the new M74 motorway and the East study area containing the existing M8 motorway suggests how a population may respond and adapt to this type of major change to the urban environment over time. Although the worsening of well-being appeared to be broadly distributed across the population in the short term, it was more pronounced among those exposed to a higher degree of neighbourhood upheaval and became more concentrated in those with poorer health in the longer term.
These findings are consistent with previous cross-sectional studies suggesting a link between traffic noise disturbance and lower well-being. 45,46 In particular, one study found an average difference in mental well-being of 4.2 units (assessed using the Short Form questionnaire-36 items) between those experiencing and not experiencing this form of disturbance. 45 However, our findings are inconsistent with evaluations of other types of urban regeneration initiatives in the UK, which have found either no change or modest improvements in well-being. 5,6,133 In particular, a recent quasi-experimental study of neighbourhood renewal in multiple areas of Glasgow (none of which was included in our study areas) found a significant net increase in average mental well-being of 4.3 units (measured using Short Form questionnaire-12 items, another derivative of the Short Form questionnaire-36 items scale) attributable to higher versus lower levels of investment over 5 years, coupled with a significant net decrease in decline in physical well-being of 3.9 units (i.e. a beneficial effect). 134 Although our more general measure of neighbourhood ‘upheaval’ bears some relation to the changes investigated in that study, the housing improvements and social support initiatives that comprised the GoWell intervention programme could be expected to have different effects from the new motorway that we studied. 135
Travel and car use
Against a backdrop of a decrease in travel in our study cohort over time, we found some evidence that the new motorway promoted relative increases in travel generally, and car use more specifically, among those living nearby. These outcomes may be regarded as desirable for population health and welfare in one sense (greater mobility) and undesirable in another (greater use of motor vehicles). The increased likelihood of travel among those living in the general area of the new motorway, and more specifically in those living closer to a motorway junction, in cohort analyses suggests that this mobility impact of the new motorway may have been particularly pronounced in a group that was already wealthier and more mobile than the general local population. The new motorway also appeared to promote car use in the population living closer to a junction. Ultimately, this pattern of outcomes would be expected to increase the relative disadvantage experienced by the half of our sample who did not own a car.
It was beyond the scope of our study to measure changes in traffic flow, but Transport Scotland data (collected 1, 4 and 12 months after the opening of the new motorway) indicate marked reductions in traffic flows on both the existing M8 motorway and the local street networks (except for streets leading to the new motorway junctions, on which traffic increased). It is therefore not surprising that a major piece of transport infrastructure designed to improve the efficiency of motor vehicle journeys may have promoted travel and car use, as predicted in the findings of the PLI. There is little comparative public health evaluation literature on this particular topic, as highlighted in NICE guidance published in 2008 and updated in 2014. 37,38 However, our findings do mirror previous research showing two types of converse relationship: first, that reducing highway capacity can lead to the disappearance of motor vehicle traffic,136 and, second, that creating new infrastructure for active travel can lead to an increase in walking and cycling. 49,50
Quantitative outcomes with weaker or absent evidence of a causal relationship
Active travel and physical activity
We found some evidence for a reduction in physical activity participation in cohort participants living in the area surrounding the existing M8 motorway, among whom greater proximity to the motorway also predicted a reduced likelihood of participation over time. Apart from this, many of the associations that we found were weak and not statistically significant, and we found no significant effect on time spent in physical activity using either self-reported or objectively measured data. Notably, we found no clear evidence of either an increase or a decrease in active travel attributable to the new motorway, in either our own survey data or in those of the SHS. 63 In summary, therefore, our findings suggest a neutral effect of the new motorway on active travel, and a negative effect – if any – of motorway infrastructure on physical activity in the longer term.
With no similar previous studies available, direct comparisons with the existing literature are not straightforward. 51,137 However, exposure to road traffic noise has been found to be associated with less time spent outdoors, less physical activity and (albeit weakly) a higher prevalence of overweight, and routes away from traffic noise may be perceived to be more attractive for cycling. 138–142 However, a cross-country ecological comparison has shown an inverse relationship between the presence of motorways and the national prevalence of overweight and obesity. 143 That relationship may be confounded by the fact that motorway infrastructure reflects national economic prosperity, and therefore does not necessarily contradict our finding suggesting that more proximate exposure to motorway infrastructure may be associated with less healthy behaviour patterns. The stronger associations with physical activity found in the area surrounding the existing M8 motorway suggest the possibility of a non-linear temporal dose–response relationship, whereby any physical activity impacts of the new motorway may take > 2 years to emerge. A similar pattern was observed in the iConnect study of new walking and cycling routes elsewhere in the UK, in which significant effects on physical activity were observed after 2 years but not after 1 year. 49
Road traffic accidents
We found no clear evidence that either the construction or the opening of the new motorway altered the already declining incidence of road traffic accidents in the local area. Although we did observe a significant decrease in the temporal trend in the North study area following the opening of the M74 extension, this is unlikely to be attributable to the new motorway for two reasons. First, no such significant change was observed in the region as a whole or in the study areas surrounding the new or existing motorways. If the observed association were causal, it would most probably have been observed first and most strongly in the area surrounding the new motorway. Second, the limited traffic count data available suggest that the opening of the new motorway had little impact on trends in the number of vehicles travelling in the city as a whole.
Other UK analyses have also reported a significant decline in road traffic accidents over recent years. 115,116 This is likely to reflect trends in a number of factors that influence the epidemiology of accidents, including road and vehicle design and driver behaviour. However, we did not find any recent studies of the impact of new major road infrastructure in particular on accidents that materially altered the findings of a previous systematic review. 51 A summary of before-and-after studies of new motorways in Western Europe and North America has suggested an average reduction of between 7% and 9%, whereas a North American study of increasing the number and width of lanes on existing motorways found no effect on the number of accidents. 144,145
Summary of quantitative causal estimates
In this controlled before-and-after study of the impacts of building an urban motorway and associated infrastructure, we found comparatively strong evidence for a harmful effect on the well-being (particularly the mental well-being) of local communities, and of an increase in travel (particularly in car use). Although the risk of residual confounding cannot be eliminated in a natural experimental study of this kind, these findings were robust to adjustment for multiple individual and household confounders and were corroborated in different analyses. We found weaker evidence of a decline in physical activity participation over the long term, and no evidence of an overall increase or decrease in either the quantity of active travel or the incidence of road traffic casualties. Although these latter findings may indicate truly null effects, they may also reflect the average of diverging positive and negative effects in different groups, a limited statistical power to detect changes in certain outcomes, owing either to comparatively small numbers of cases (e.g. of cycle journeys or of casualties among more vulnerable road users) or to measurement error, or a combination of these factors. In particular, estimates of overall physical activity and sedentary time derived from self-reported measures are subject to substantial measurement error, and our analysis may simply have been unable to detect the signal of an intervention effect against the background noise of this measurement error.
Overall, therefore, in these quantitative estimates of causal effects we found stronger evidence for negative health impacts than for positive health impacts. We found no clear evidence to support either the claims or the counter-claims made prior to motorway construction about its probable impacts on active travel or injuries from road traffic accidents, but the balance of the evidence pointed more convincingly towards negative aggregate impacts – notably on well-being, for which the findings appear to be unequivocally negative overall. The increase in travel and car use observed in the South study area may also be attributable to the new motorway and may be considered either a beneficial or a harmful outcome depending on the perspective taken. However, any benefit in terms of an increase in mobility and consequent access to people and places is likely to have been distributed and experienced unequally and inequitably in the local population, with the costs being disproportionately borne by those less able to benefit.
Explaining the effects of the intervention
Although estimating effect sizes forms an important part of causal inference in natural experimental research, it is also – and, some would argue, equally – important to investigate potential explanations linking interventions with their observed effects, or lack of effects. 89 In this section we draw on insights from our qualitative research in particular, and from our qualitative and quantitative findings in combination, with two main aims. The first is to strengthen – where appropriate – the causal interpretation of the main outcome analyses discussed above, which can never be entirely free from the threat of residual confounding. The second is to investigate the extent to which the findings of this study may be generalisable.
Changes in well-being
A decline in average mental well-being was the outcome most convincingly associated with motorway exposure in our main outcome analyses, at both area and individual level. Although mediation analyses did not identify any convincing statistical evidence that this change in well-being was explained by changes or differences in perceptions of the physical or social environment the neighbourhood, over-reliance on this approach to identifying mechanisms has been questioned in the methodological literature, and it has been argued that factors can participate in causal mechanisms without being mediators in the statistical sense. 146 We can apply the concept of the causal process observation in using our qualitative data to elaborate our understanding of this relationship in respect of three aspects of this natural experiment: (1) the background to, or context of, the intervention; (2) the nature of the intervention and its effects; and (3) the concurrent changes in the study areas. 88
Qualitative accounts elucidated the industrial history and character of the area in which the new motorway was constructed. In this historical and geographical context, for some people, issues such as noise and other sources of pollution were not only long-standing concerns but were also somewhat integral to the character of their locality. Similarly, the physical changes embodied by the new motorway could be seen as entirely consistent with the history and development of the area over the long term, echoing previous infrastructure projects ranging from the West Coast Main Line railway in the nineteenth century to the Glasgow Road dual carriageway in Rutherglen in the last part of the twentieth century. Against this background, the new infrastructure may simply not have registered as a strong signal against the background noise of the area, in either a literal or a metaphorical sense. As we have shown in research in other parts of the UK, the differing effects of apparently similar infrastructural interventions in different areas are plausibly explained by the extent to which the intervention introduces a meaningful difference from the baseline conditions in each area. 147 This explanation appears even more plausible in light of the narratives of decline and powerlessness elicited from some participants. For these people, the new motorway could be seen as just another ‘thing being done’ to their communities, eliciting active protest from some, but perhaps eliciting acceptance or resignation from a larger number (and more unequivocal approval from others).
A second prominent theme in our qualitative research – mirroring the expectations of the new motorway expressed by participants in our baseline qualitative interviews in 200658 – was the divergence of people’s experiences and responses to the changes around them. This heterogeneity may both explain the lack of statistical association for some of the hypothesised relationships in the quantitative analyses and illustrate, through the causal process observations provided by some of the more extreme cases, some of the mechanisms by which well-being might be impaired. It is clear, for example, that changes in traffic disturbance varied from street to street, and not simply as a function of distance from the motorway. We found only weak evidence that perceptions of the physical environment worsened with greater proximity to the new motorway, and no statistical evidence that these perceptions mediated the observed decline in well-being; however, these statistical findings stand in stark contrast to the vivid accounts of multiple forms of disturbance given by some people living close to the new motorway, particularly at our community engagement events. Although no one would claim that those more extreme accounts were representative of residents of the area as a whole – and even those people describing substantially negative experiences were willing to admit to some advantages of the new motorway, such as convenience of access – this does not invalidate their contribution to describing a plausible causal process by which living closer to a motorway may contribute to a worsening of well-being over time. 88
It is clear from other qualitative evidence that changes in the social environment that were not adequately captured in the measure of collective efficacy included in our core survey may have influenced both the activity patterns and the well-being of local residents (see the next section). However, taken together, the quantitative and qualitative evidence suggests that those concurrent social changes are unlikely to provide the entire explanation for the decline in well-being associated with motorway exposure. The mediation analyses used in this study were subject to a number of limitations relating to the selection and measurement of the mediators and the sample size available for analysis, in addition to the ongoing debate about the practice and interpretation of such analyses mentioned above. 146 The decline in well-being was associated with individual proximity to the motorway, as well as with residence in the general area, and was also associated with a measure of general (physical) upheaval in the local area. Both of these observations strongly suggest that physical changes in the localities concerned were also important in the ‘causal recipe’ for worsening well-being.
Changes in travel and activity patterns
Although local residents clearly described changes to local transport infrastructure and their effects on connections relevant to their lives, we found little statistical evidence of any shifts in active travel or physical activity behaviours, particularly in the South study area. We can use qualitative causal process observations to explore these relationships further, in the same way as well-being.
In respect of active travel, perhaps the most important qualitative observation about the background to the intervention is that the new motorway was constructed parallel to, and mostly very close to, an existing plane of severance in the form of the West Coast Main Line railway. Many local journeys in the vicinity of the new motorway were therefore already significantly constrained by the limited points at which the railway could be crossed, and the introduction of an additional barrier in the form of the motorway did not necessarily make this situation worse. Indeed, for some people, the new pedestrian infrastructure built to cross the combined barriers of the motorway and railway line represented a material improvement on what was there before. In other words, the new motorway was not seen as having a uniformly negative impact on people’s ability or willingness to walk to local destinations, and where the design of new infrastructure contributed to perceptions of greater personal safety (see below) it was valued. Rather than affecting the frequency, duration or routes of local pedestrian or cyclist journeys, the motorway was more often seen in qualitative interviews as affecting the quality or experience of active travel, sometimes for better and sometimes for worse. This highlights one of the limitations of an approach to evaluation that prioritises quantitative analyses of ‘primary outcomes’ over other forms of evaluative insight. It identifies a way in which new infrastructure can have an effect on an outcome of interest that is not captured in a simple estimate of the quantity of a ‘behaviour’, but may nevertheless be crucial in shaping how that ‘behaviour’ is understood and practised by local people. It also underlines the observation (made above) that an overall ‘null’ effect may reflect the activation of a mixture of beneficial and harmful causal processes,148 in this case, for example, where a new pedestrian overbridge with improved lighting and sightlines may be perceived as safer in one sense, whereas crossing the road in the vicinity of a new motorway junction may be perceived as less safe in another.
As well as finding evidence for both an increase and a decrease in severance in its more traditional, physical sense, our qualitative research also elicited evidence of processes connecting or severing people into less obvious ways. At the local scale, our participants described the importance of ‘third places of connection’ whose amenity value was – in some cases – affected by the new motorway. These included shops and green spaces, which were among the most important destinations for local walking and cycling journeys identified in the baseline survey. 57 Mirroring the effects on the quality of active travel described above, it was not that people could no longer physically reach these third places, but, rather, it was suggested that the geographically specific interactions and relationships they helped to cultivate might be adversely affected. This was particularly the case for green space, and it is noteworthy that access to green space was the one perceived attribute of the physical environment that was rated significantly worse by those living closer to the new motorway. Access to green space is associated with reduced mortality; this relationship is likely to reflect a variety of potential restorative benefits and does not appear to be explained simply by people using local green space to be more physically active. 129,149 It may be particularly important in a comparatively deprived urban environment in which many households have no access to a garden of their own. 150 On a larger scale, the motorway was described in both qualitative interviews and community engagement events as improving connectivity for those who had more dispersed social networks and had (or were connected to others who had) access to a car. Enhancing mobility in this way might be expected to benefit the health and well-being of some people, for example by strengthening their social networks or giving them easier access to places to be active and other amenities. Indeed, previous research in Scotland has shown how having access to a car can provide an individual with some ‘protection’ against the disadvantage of living in an area poorly served with local amenities. 40 However, in a conurbation with a comparatively low prevalence of car ownership, it is obvious that such benefits are likely to be inequitably distributed.
For many of our participants living in the area surrounding the new motorway, perceptions of personal safety played a larger role in shaping their local activity patterns than did the infrastructural changes associated with the motorway itself, and these perceptions were in turn related to more profound social and cultural changes in their localities relating to crime, drug and alcohol use, increasing aspirations of car ownership and changes in community composition following inward migration. These themes were not a major focus of this study, and a detailed analysis of migration in particular was considered and excluded from the scope of the study design in the process of its development with the Research Funding Board. However, the prominence of these narratives in our qualitative data, reinforced in the community engagement events, suggests – at the very least – a need to consider how a physical infrastructure project might interact with such social processes. Most obviously, perhaps, when a community is experiencing significant social change it may be particularly in need of neutral third places of connection. These may enable different sociodemographic groups to become more familiar with each other’s presence and to develop a sense of belonging to, and feeling safe in, the area – as in the example, given by some of our participants, of children playing together in public open spaces.
Changes in road traffic accidents
Another theme that emerged from our qualitative research concerned the changes in the economic context between the early 2000s, when the new motorway was planned, and the early 2010s, when it was opened. The recession following the financial crash of 2008 is likely to have exacerbated what some participants perceived as an ongoing narrative of decline in their local areas, illustrated, for example, by changes in the composition of shops in local high streets. Of course, the new motorway was envisaged as part of a wider package of regeneration intended to counter such local economic disadvantage, but our data highlight ways in which the nature of the complete intervention as delivered – and the ways in which local road users engaged with it – may have contributed to a lack of quantifiable reduction in accidents and injuries. Before the motorway was constructed, for example, it was understood – at least informally – that its opening would pave the way for additional measures to calm traffic on local streets, such as speed tables or 20 mph (30 km/h) speed limits. In the event, however, it would appear that few of these evidence-based measures to reduce traffic speed and injury risk were implemented, and this may at least partly explain why the intervention did not achieve some of its claimed benefits in terms of promoting active travel and reducing casualties. Our study participants and other informants also described several aspects of the new road infrastructure that may have contributed further to this problem, including the hazards of merging lanes of traffic, vehicles travelling at high speeds on slip roads and altered layouts of existing streets close to the new motorway junctions. These may have contributed to the danger of crossing roads, particularly for pedestrians with impaired mobility, although we do not have direct evidence for this. There were, however, other concurrent changes in the city as a whole that may have contributed to the general downwards trend in accidents and increase in active travel noted in the routinely collected data sets that we used. These include changes in bus and rail service networks, the introduction of new bus lanes, and improvements to some walking and cycling routes.
Testing more generalisable causal hypotheses
We now turn to the potential contribution of our findings on causal estimation and causal explanation to more generalisable causal inference. It is an inescapable reality of this type of place-based natural experimental study that we cannot assume that effects we have observed in selected neighbourhoods in Glasgow would necessarily be replicated elsewhere in Scotland, the UK or further afield. Indeed, no single intervention study in this, or any other, field of applied public health research is likely to be capable of supporting ‘generalisability’ in that narrow sense. On the contrary, the only way to generate such inferences is by combining evidence from multiple studies. To that end, our findings begin to corroborate and extend those of other studies in showing the ways in which the behaviour, well-being and health of populations may respond to changes in the built environment, and will in time be accumulated with those of other current and future studies in a programme of evidence synthesis that lies beyond the scope of this report. In this section, we therefore focus on drawing together the various strands of this research project to assess the degree of causal support they offer for the overarching hypotheses that motivated the study and were outlined in Chapter 1 of the report. 87
We articulated the potential effects of the new motorway using two contrasting overarching vignettes of a ‘virtuous’ and a ‘vicious’ spiral (see Table 1). Mapping our findings against the key propositions of each vignette, we find – perhaps unsurprisingly – a mixture of confirmatory and disconfirmatory evidence on both sides. In respect of the ‘virtuous spiral’ hypothesis, other published data suggest that traffic on local roads has indeed been reduced, but we found only partial qualitative evidence that this had made conditions more pleasant for pedestrians and cyclists (at certain locations), and no evidence that people perceived their local environment in a more positive light or spent more time out and about in it as a result. We found divergent evidence about perceptions of noise and air pollution, with some people clearly experiencing marked adverse effects in this regard and others – as predicted – not noticing these changes against the background conditions of their urban surroundings. We found no evidence for an increase in either well-being or physical activity and comparatively strong evidence for a harmful effect on mental well-being. In respect of the ‘vicious spiral’ hypothesis, we found qualitative evidence that traffic had increased on some local streets and comparatively strong evidence that local people were more likely to travel – and by car – than they would have been in the absence of the new motorway. This and other qualitative evidence also provides some preliminary support for the predicted ‘car-bound exodus’ from ‘declining’ local areas. We found some support for the predicted degradation of the local environment making conditions less pleasant or safe for pedestrians and cyclists, but only for some people and not in our quantitative analyses.
Given the mixture of confirmatory and disconfirmatory evidence for either the ‘virtuous’ or the ‘vicious’ spiral, we went on to address the challenge of synthesising causal inferences from across this body of findings by taking a ‘pragmatic pluralist’ approach to the ‘ragged evidence’ of the natural experimental study. In so doing, we sought to match patterns of outcomes with patterns predicted by the intervention theory imperfectly captured in these vignettes, searching not for support for a singular overarching hypothesis, but rather for the least implausible explanation of the conditions that may be required to produce or prevent the outcomes of interest. 53,87,132,151
Turning first to the ‘virtuous’ spiral, although we did find some (mostly qualitative) evidence for beneficial impacts, our analysis suggests that the realisation of these benefits may depend on a mixture of individual, social and environmental factors in the causal recipe. The qualitative data suggest that more neutral or disinterested responses may be more likely where new infrastructure, and perceived associated pollution, is consistent with existing local narratives of place (as post-industrial or scenic and natural; as polluted or clean; or as a characterised by change or stability) or in areas where residents perceive themselves as having low collective efficacy. 152,153 In addition, local impacts of new transport infrastructure may be superseded by other more immediately pressing concerns, for example in areas of high perceived crime or significant change in social composition. Beneficial outcomes may be more likely where new urban transport infrastructure ameliorates, or at least does not exacerbate, the severance of residents from people and places nearby; where complementary actions are taken to ‘lock in’ early benefits, for example by calming or diverting traffic; where the intervention enhances the connectedness of people’s social life worlds, rather than disrupting them; and where associated pedestrian infrastructure minimises pre-existing negative social factors such as fear of crime. For those with more dispersed social networks and the means to travel by car, this last mechanism may be evoked by improving the major road network, and the journeys those people make further afield could contribute to their physical activity, prosperity and well-being. However, there are other social and environmental arguments in favour of encouraging more localised activity patterns, and the more ‘hypermobile’ society that is facilitated by policies that favour motor vehicle use may have very considerable opportunity costs. 154,155
Those opportunity costs are exemplified in the ‘vicious’ spiral, which can now be described in terms of a plausible causal recipe for adverse, inequitable impacts. Harmful outcomes may be more likely where the infrastructure further divides local communities: not only in the tangible sense of introducing physical obstacles to local journeys, but also in the way it partitions local people into those who gain and those who lose. Where people perceive their community to be in decline, or otherwise changing in ways that make them feel uncomfortable, and where they lack the means to benefit from the improved transport network themselves – or the means or autonomy to relocate to a more pleasant environment – this type of urban redevelopment may further erode a declining stock of social capital and sense of efficacy among more disadvantaged local residents and increase the relative burden of ill-health in those people. Even if investment in new major road infrastructure can be shown to bring wider economic benefits and is justified – as are many public health interventions – on utilitarian grounds, the question remains whether or not alternative ways of investing the same money might have produced more equitable and sustainable benefits for local people.
Ultimately, rather than conceptualising the new motorway as a complex set of inter-related and highly specific changes to the built environment – new carriageways, viaducts, slip roads, pedestrian crossings and the like – it may be more meaningful, both for understanding causal mechanisms and for drawing lessons for policy and practice, to shift analytical attention away from the surface form of the intervention towards its underlying function. 156 In this case, our evidence points to two critical functions – connecting and separating – that constitute two sides of the same coin and are both evoked by the same intervention in different ways for different people. Following a pragmatic pluralist, pattern-matching approach rather than a binary hypothesis-testing approach to causal inference, the overarching hypothesis with which our data are most consistent is that new transport infrastructure is more likely to benefit more people when it connects people with their social and physical surroundings – broadly defined – more than it separates them, and when people are protected from its harmful environmental impact by distance or other effective mitigation measures.
Interpretation for public health policy and practice
Living near to a new motorway was associated with a substantial worsening of local residents’ mental well-being, particularly for those exposed to a greater degree of upheaval in their immediate surroundings. Sources of pollution such as major roads and industrial sites are already disproportionately located in or near to more disadvantaged neighbourhoods, and our findings indicate a clear potential for such disadvantage to be amplified by further disrupting such neighbourhoods with new major road infrastructure. The additional concentration of this disadvantage among those with a chronic condition living near an existing motorway shows how one form of disadvantage (environmental) may be compounded over time by another (health), thereby contributing to worse clinical outcomes among those whose health is already impaired and who lack the means or autonomy to move house. This type of inequitable and harmful health impact, and its implications for the costs of health and social care, should be considered in the appraisal of proposals for future infrastructural investment, particularly in areas characterised by high levels of social housing, material deprivation and ill health.
Although we found little clear quantitative evidence for effects on active travel, physical activity or sedentary behaviour 2 years after the motorway was opened, that is not to say that the effects of building new major road infrastructure or its implications for policy and practice are neutral in this respect. The new motorway appeared to promote travel in general and car use in particular among those living nearby. Particularly in a country such as Scotland in which car ownership and use are strongly socioeconomically patterned, this direction of effect is liable to reinforce existing inequalities in access to amenities and opportunities, and runs counter to the stated objectives of national transport and health policies in Scotland, England and numerous other countries. The appraisal of proposals for future infrastructural investment should consider a wider range of options than the two considered in the PLI for the M74 extension, namely either to build it or not to build it. A more wide-ranging option appraisal might have explored the comparative environmental, health, social and transport benefits and costs of alternative uses of the resources, and this might have led to a different decision. Similar considerations apply, with perhaps greater urgency, in (mostly lower- and middle-income) countries and regions currently going through a ‘motorisation transition’ involving the rapid construction or expansion of highway networks.
Our findings complement those of a previous systematic review in suggesting that policy-makers cannot necessarily appeal to a probable reduction in the incidence of road traffic accidents to justify the construction of new major roads. 51 It may be taken for granted that such projects alone will reduce casualties, as was argued prior to the construction of the M74 extension, but we found no evidence that any such benefit had been achieved by 2014.
In summary, there is currently little clear public health evidence to guide decisions about investing in expensive urban regeneration projects of this kind. In terms of well-being, motorway construction appeared to be more harmful than helpful to local communities. We acknowledge that more time may be required for some benefits, such as economic revival (which we have not assessed directly), to be fully realised and to produce a more indirect positive impact on well-being. Nevertheless, it cannot be assumed that the benefits of regeneration will necessarily outweigh the harms of the physical and social impacts of the new infrastructure on local communities. In an area with an existing motorway, those with chronic conditions experienced the greatest adverse effect on well-being. This implies that transport projects of this kind may entrench existing health inequalities in an already vulnerable population. From a social justice perspective, there did not appear to be a fair distribution of benefits afforded by the motorway compared with its associated burdens among those living nearby, particularly for those without access to a car. Although the specific impact of environmental changes of this kind might very well be experienced differently in communities lacking an industrial history or an existing plane of severance, our findings clearly indicate a more general implication for policy and practice, namely that some of the overall health and social gains claimed for this type of investment either may not be achieved or may be achieved for some at the expense of others.
Patient and public involvement
As discussed in Chapter 2, Preliminary community and stakeholder engagement, and Chapter 8, we had a complementary programme of public involvement running alongside the study, in which we aimed to engage with a variety of stakeholders at key stages of the research process.
In the first phase, local community organisations were invited to comment on whether or not issues associated with the motorway were of concern. The motorway was not a hot topic, but respondents highlighted its role in facilitating wider neighbourhood regeneration. This initial engagement gave us a sense of what was important to communities, helped us to build relationships and raised awareness of the study among local stakeholders. It informed the design of the study, particularly the qualitative research, which explored the motorway in the context of wider changes in the physical or social environment.
In the second phase, a series of community events were organised to share and discuss emerging study findings. Four informal ‘pop-up’ events were conducted in local spaces including a shopping centre and a community hall. Passers-by were invited to discuss the study with researchers. In addition, a formal stakeholder-focused event was conducted, using interactive methods including a talking wall and a world café. Attendees included representatives from government, community groups and local residents. At all community events, researchers and attendees reflected on study findings, worked together to interpret findings and discussed wider opportunities and challenges facing local communities. This ‘ground-truthing’ process significantly contributed to the overall interpretation of the study, discussed further in Chapter 8, Contribution to interpretation.
Challenges, strengths, limitations and methodological contributions of the study
Challenges of the study
We faced a number of challenges in the design and execution of this study. We have chosen to highlight four of these here because they illustrate some of the difficulties inherent in natural experimental studies in public health intervention research. Although some of these issues were raised in a study design paper published in 2006,52 shortly after the baseline study began, they have become more widely discussed in the public health literature in the intervening decade, particularly in – and following – the guidance published by the MRC in 2011. 59
The first challenge was that of designing a tractable and independent public health study of an apparently simple, but in practice complex and highly contextual (and politicised), intervention in the urban environment. The public discourse about the proposal to extend the M74 motorway elicited many possible outcomes and pathways to those outcomes, some of which might be expected to take many years to develop and all of which might be worthy of evaluation in their own right. We acknowledge that we could have set out to evaluate the impact of the project in a more all-encompassing way, but instead we chose to focus our evaluative resources on a more limited – and more tractable – set of research questions that we could address within the context of a larger research programme and portfolio of related studies. We worked hard to maintain scientific independence and objectivity throughout the study, from the delineation of the main competing hypotheses onwards. When the study was originally conceived, the principal investigator lived not far from the boundary of one of the study areas, and the familiarity of several members of the research team with the local context was undoubtedly helpful in formulating the study design, achieving rapport with study participants and interpreting their accounts. However, any public health researcher living in the vicinity would naturally be expected to have their own attitudes and beliefs about the controversial topic of the study. We therefore ensured that survey materials at both baseline and follow-up were presented in terms of a general survey on ‘traffic and health’ without any reference to the new motorway, that the follow-up qualitative fieldwork was conducted by a researcher with no local connection; that the topic of the new motorway was allowed to arise naturally in the course of interviews, rather than being presented as their main purpose; that participants were encouraged to discuss both positive and negative impacts of the new motorway; and that minority opinions were identified and reported.
The remaining challenges were more methodological or technical in nature. The second challenge was that of defining exposure, both to the new motorway itself – the intervention of central interest to the study – and to related changes to the environment. Although simple area-based exposure measures are commonly used in natural experimental research, in this study our decision to augment these with individual measures a priori was vindicated by the finding that the latter measures proved to be more convincingly related to some of the outcomes. 157 Graded exposure measures of this kind have also been used in other recent natural experimental studies in this field, but the optimal definition of exposure for a given study is likely to vary according to the particular combination of intervention, study design and outcome in question and, therefore, to require careful thought in all cases. 80 The third challenge was that of delineating a comparison area or areas, in order to provide some evidence of what might have been expected to happen under a counterfactual scenario of no substantial change to the environment. Comparatively well-balanced study areas and samples were achieved at baseline as a result of painstaking work, but it is simply unrealistic to imagine that all important attributes of an area and its residents – including its road network, its topography and its history – could be precisely ‘matched’ in any number of control areas. Rather than seeking corroboration between comparisons of outcomes with multiple external control areas, we chose to use individual measures of exposure within our study areas as an additional basis for controlled comparisons, and to rely as much on causal explanation as on causal estimation as a way of investigating the evidence for causal inference. However, this corroborative approach threw up a fourth challenge: that of reconciling differences in outcomes between analyses using different samples and exposure measures. We did not expect perfect agreement in this respect, but our experience highlights the importance of thinking carefully about the different ways in which interventions may lead to outcomes in individuals and in populations, and about the complementary strengths, limitations and meanings of different analyses in this respect.
In the following sections, we briefly discuss our responses to these four challenges in terms of their implications for the strengths and limitations of the study and for future research, most which have been described elsewhere in the report but which are summarised here for the sake of completeness.
Strengths of the study
This is one of few intervention studies to have examined how changes in the environment influence changes in health and well-being, particularly with a focus on active living in a comparatively deprived population. It thereby adds to a small but growing body of evidence for the effects of changing the built environment on patterns of travel behaviour, physical activity, accidents and well-being, as called for in recent reviews arising from the policy, practice and research communities alike. 38,44,158 More specifically, it is the first study to have evaluated the effect of a new motorway on physical activity and sedentary behaviour, and it makes a particular contribution to our understanding of the impacts of new major road infrastructure by investigating changes in multiple related outcomes at both individual and population level.
We used two extensively validated instruments to capture changes and differences in various aspects of well-being, and assessed overall physical activity using the short IPAQ, which, although admittedly not ideal for detecting change in the time spent in different activities, has been widely used around the world and has comparable criterion validity to that of any other physical activity questionnaire of similar length. Although our measures of travel behaviour were not formally validated, our own survey instrument was closely based on that used in the National Travel Survey,64 and in both our own data and the SHS data63 we were able to disaggregate travel to the level of the mode of transport used for each stage of a journey. This enabled us to ascertain, for example, walking or cycling as part of a longer journey. Among other things, our study illustrates the potential value of using routinely collected data in the evaluation of natural experiments, most obviously in respect of the police STATS19 accident data,74 but also in respect of the SHS travel diary data set that we analysed. 63 This included > 20,000 journey stages reported by nearly 8000 people in the west of Scotland, collected as part of an ongoing repeat cross-sectional survey of a large, random, representative national sample of households, which we were able to analyse at minimal marginal cost.
Ours is among the first studies to have evaluated the effects of any environmental change on this range of outcomes using robust quasi-experimental methods, as outlined in research recommendations from NICE. 37 We collected original survey data from 2323 local residents, supplemented with detailed activity measurement in a subsample of 196 and qualitative fieldwork in a subsample of 30 (as well as 12 other key informants), along with analysis of 78,919 road traffic accidents and 7911 travel diaries from other routinely collected data sets. We investigated how the outcomes were associated with multiple measures of exposure, objectively defined at both area and individual level using a GIS. We made comparisons both between and within areas, in both longitudinal and repeat cross-sectional analyses, combining these different quantitative analytical approaches with each other and with qualitative research methods to offset the limitations of each approach and corroborate findings where appropriate. We controlled for a set of potential confounders in all models. A further strength of our modelling strategy lies in the use of two-part models for travel and activity outcomes that were not normally distributed. Despite their good theoretical and statistical fit and efficiency in combining analytical options, such models have seldom been used in this field to date. The ARIMA procedure used in our time series analyses provided a rigorous way of assessing impacts on accidents that are measured using count data. Like all statistical models, these analyses depended on assumptions about the form of the relationship between the intervention and its effects, but sensitivity analyses – in which key parameters of the time-series and other statistical models used in the study were altered – suggested that the main findings were not sensitive to these assumptions. Finally, the study provides a rich data set that constitutes a valuable platform for further analyses, about which potential collaborators can find out more at our data sharing portal. 159
Limitations of the study
It was not feasible to collect data relating to the main outcomes of the study throughout the period of motorway construction over a longer follow-up period, or with more detailed consideration of people who had moved into and out of the study areas. It is possible that – with additional funding – extending data collection in any of these ways might have revealed additional short-term impacts, the maintenance (or otherwise) of effects observed at 2-year follow-up or the emergence of other impacts in the longer term. Neither was it feasible to study the full range of potential impacts identified in public discourse, either before or after the motorway was constructed. In particular, we acknowledge the importance attributed to noise, air pollution and wider economic impacts by participants in our community engagement activities, which we were not able to assess directly in our own research. The evidence of impacts that we have elicited despite these limitations indicates the value of seeking to replicate our longitudinal analyses in larger samples with a longer duration of follow-up where possible, particularly in situations in which outcomes might be ascertained using routinely collected surveillance and population survey data.
We extracted data on road traffic accidents from the STATS19 portal74 and, although these data are widely used in research, they have known limitations. Chief among these are that they rely on accidents being reported to the police, and on the accuracy of police officers in reporting their exact locations. However, systematic differences or changes in the accuracy of reporting between study areas appear unlikely, particularly given that a single police force covers the region. Other limitations of our data include the collection of only 1 day of travel data for each participant at each time point, which provide estimates of activity with greater variance than those derived from longer (e.g. weekly) periods of measurement, the reliance on simple self-reported measures for estimating changes in travel, physical activity and sedentary behaviour over time and the reliance of the mediation analyses on self-reported measures of both the social and physical environment of neighbourhoods that may not have captured the mechanisms of most importance in mediating the outcomes of interest. The analysis of SHS travel data was subject to two additional limitations. First, journey distance in that data set is based on the straight-line distance between two points, rather than the inevitably longer real distance along the road and path network. Second, in the interests of data protection, participants in those analyses were assigned to study areas according to their area of residence, rather than to the more precise location given by their full unit postcode.
We chose to include a repeat cross-sectional design because we anticipated considerable attrition of the cohort over time, and this was confirmed, with approximately 70% of the original baseline sample lost in the 8 years that elapsed before follow-up. Together with the comparatively low response rate of approximately 16% at each time point, this represents an important limitation on the extent to which the survey data could be considered representative of the local population. The response and attrition rates were comparable to those of similar natural experimental studies in similar settings,6,49,160 and the repeat cross-sectional design was chosen to offset the anticipated attrition in particular. Nevertheless, the combination of large variances in some of the outcome measures, the comparatively small cohort sample, and the comparatively small number of pedestrian and cyclist casualties all contributed to limiting the statistical power of the study to detect some effects, although it is equally plausible that the lack of significant findings for those outcomes may reflect a true absence of associations. The scope of the qualitative study of residents was also limited by the achieved sample size of 30 participants. Although this does not necessarily threaten the validity of the inferences, it is possible that further themes may have been elicited and explored if more people had taken part.
A final limitation is the possibility of residual confounding, either because of an unmeasured confounder that may have been unequally distributed in the study population at baseline, or because of other regeneration projects or concurrent changes in the built environment, such as the wider Clyde Gateway initiative and the 2014 Commonwealth Games. This is a core and unavoidable challenge of this type of natural experimental research, and is complicated by the fact that the effects of a given ‘intervention’ may depend on its being related to those other changes rather than being observed merely as a result of ‘contamination’ by them. We sought to minimise the impact of potential residual confounding by carefully delineating the study areas to ensure the comparability of the samples and settings, by adjusting the analyses for multiple sociodemographic covariates, and by comparing the results of complementary analyses with different strengths and limitations. We did find some sociodemographic differences between the follow-up samples in the three study areas, despite the considerable care taken to balance the samples at baseline. Even with randomisation, perfect balance is not always achieved, and in this case it certainly remains possible that other actions taken in some neighbourhoods may have directly or indirectly influenced local patterns of activity and well-being. To take one example, we observed an unanticipated finding of an increased likelihood of bus use over time in cohort participants living in the East study area. It seemed unlikely that this outcome, observed between 2005 and 2013, could be causally attributed to a motorway built in the 1960s and more likely that it might reflect concurrent improvements to local bus services. An initial scoping exercise indicated that public transport improvements had taken place in the area, but the scale of work required to comprehensively assess and quantify this additional time-varying exposure was beyond the scope of the current study. Nevertheless, our study does represent a methodological advance on the uncontrolled or poorly controlled studies typical of previous research in this field, and other aspects of its conceptualisation and design provide a degree of complementary support for the causal inferences made.
Methodological investigation and development
Although methodological research was not the primary aim of this study, its design, evolution and execution over more than a decade have provided considerable methodological learning that may be of more general value to the field. We have shown how exposure to a particular physical environmental change may be characterised and analysed using a combination of area- and individual-level measures. We have also devised a novel measure of more general physical environmental change, which we have described as an upheaval index, and we have developed and demonstrated a method for computing this using aerial imagery in the public domain. We have applied both quantitative and qualitative research methods that are comparatively little used in this field, notably two-part regression models and the spatial method of photovoice interviews, adapting these to the particular needs of a natural experimental evaluation and illustrating ways in which they might be useful in future studies. We have sought to respond to a number of insights from critical scholarship as it relates to evaluation research, as exemplified by our use of vignettes to capture overarching research hypotheses linking multiple outcomes and mechanisms, and our use of the notion of pattern matching as a way of synthesising evidence for and against competing hypotheses. 53,87 We do not claim to have done more than scratch the surface of the problem of making sense of complex evaluation data in this way, but we hope that our efforts will contribute to a more general movement towards more thoughtful and ultimately generalisable public health intervention research. Finally, we have tried to embrace the perspectives of local communities in the research design in a meaningful way, partly in helping to shape our qualitative fieldwork but also – and perhaps more significantly – in contributing qualitative causal process observations to our understanding of intervention mechanisms (see Explaining the effects of the intervention), ‘ground-truthing’ our emerging findings and seeking to produce a credible interpretation of those findings, thereby feeding into a wider discussion about how research may be used by and be useful for communities.
Implications for future research
Some of our observational findings suggest further corroborative or explanatory research in their own right. For example, future research could explore regional variation and inequalities in travel behaviour in order to provide more understanding of whether or not the background changes that we observed in active travel in Glasgow are comparable to those in other urban areas in the UK and beyond, whether or not they could make more detailed use of the georeferenced activity data that we have collected to further investigate the phenomenon of severance in relation to ‘third places’ of connection, or whether or not they could use the objective measurement of air quality, respiratory function, sleep and other clinical measures to investigate the epidemiological and spatial distribution of adverse health effects of exposure to motorways. However, perhaps the most important implication of our study is that the health and social impacts of urban infrastructural projects, and how those impacts are distributed in the population, should not be taken for granted and cannot necessarily be inferred from the claims or predictions made to justify such initiatives in the first place. This implies a need for greater evaluative scrutiny of future investments of this kind, with research resources being allocated to those natural experimental opportunities with the greatest potential to reduce scientific uncertainty about outcomes and mechanisms. There are few rigorous evaluations of the effects of environmental change on most of the outcomes we have studied, particularly well-being, and replication of these findings is required. In natural experimental research, however, such replication is unlikely to involve multiple studies of exactly the same intervention. Instead, it will require multiple studies between which it will be possible to synthesise the effects of altering the same general characteristics of the environment in different contexts. This pursuit of more generalisable causal inference is complicated by the expectation of non-linear effects and the inter-relationships of multiple outcomes of importance for population health, among many other challenges. Simulation modelling offers one approach to investigating hypothesised complex and non-linear effects in systems,161 but this is likely to be useful only in tandem with further ‘practice-based evidence’ based on the empirical evaluation of the effects of actual changes in the real world. 158 In particular, more detailed exploration of the different ways in which people interpret and interact with their physical and social environments, and how these change in response to interventions and other exogenous factors, could help to advance our understanding of the ways in which policy, planning and practice do or do not ‘work’ in this respect. The combination of qualitative and georeferenced physical activity data collected in this study provide one rich resource for exploring this further using quantitative and qualitative methods in combination, but the ultimate aim of being able to make more generalisable causal statements is likely to entail the accumulation of multiple studies over time.
Conclusion
In this controlled before-and-after study of the impacts of building a new urban motorway and associated infrastructure, we found comparatively strong evidence for a harmful effect on the well-being (particularly the mental well-being) of local communities and of an increase in travel (particularly in car use). The findings also suggest that, on balance, 2–3 years after the completion of the motorway, the public health benefits claimed for it in terms of walking, cycling and road traffic casualties had not been realised. We acknowledge that more time may be required for some more ‘upstream’ benefits, such as economic revival and new employment opportunities (which we have not assessed directly), to be fully realised and to produce a more indirect positive impact on the health and well-being of the local population. Nevertheless, the study has highlighted the potential for infrastructural interventions of this kind to add further burdens to already disadvantaged communities, to entrench or exacerbate existing social inequalities in health and to contribute to poorer health outcomes among those living with chronic conditions. The health and social impacts of urban infrastructural projects of this kind should be more fully taken into account in future policy and planning.
Acknowledgements
Contributions of authors
David Ogilvie (Programme Leader in Physical Activity and Public Health, MRC Epidemiology Unit and CEDAR) led the design and execution of the study, led all baseline study analyses and publications, oversaw all subsequent study analyses and publications, and led the preparation of the final report.
Louise Foley (Career Development Fellow, MRC Epidemiology Unit and CEDAR) was the co-ordinator and lead quantitative researcher for the follow-up study, led multiple study analyses and publications and contributed to others, and co-ordinated the preparation of the final report, leading the preparation of sections and contributing to all sections.
Amy Nimegeer (Research Associate, MRC/CSO Social and Public Health Sciences Unit) was the lead qualitative researcher on the study, led multiple study analyses and publications and contributed to others, and led the preparation of sections of the final report and contributed to all sections.
Jonathan R Olsen (Research Associate, Institute of Health and Well-being, University of Glasgow) led multiple study analyses and publications relating to national population data sets and contributed to others, and led the preparation of sections of the final report and contributed to all sections.
Richard Mitchell (Professor of Health and Environment, Head of Public Health and Co-Director of the Centre for Research on Environment, Society and Health, Institute of Health and Well-being, University of Glasgow) contributed to the design, execution and oversight of the study in general, and oversaw some study analyses and publications and contributed to others.
Hilary Thomson (Senior Investigator Scientist, MRC/CSO Social and Public Health Sciences Unit) contributed to the design, execution and oversight of the study in general, oversaw the management of study fieldwork, and contributed to multiple study analyses and publications.
Fiona Crawford (Consultant in Public Health, NHS Greater Glasgow & Clyde) contributed to the design, execution and oversight of the study in general, led the community and stakeholder engagement programme, and contributed to multiple study analyses and publications.
Richard Prins (Career Development Fellow, MRC Epidemiology Unit and CEDAR) led multiple study analyses and one publication and contributed to others.
Shona Hilton (Deputy Director and Programme Leader in Informing Healthy Public Policy, MRC/CSO Social and Public Health Sciences Unit) contributed to the design, execution and oversight of the study in general, and oversaw some study analyses and publications and contributed to others.
Andy Jones (Professor of Public Health, Norwich Medical School) contributed to the design, execution and oversight of the study in general, and oversaw some study analyses and contributed to others.
David Humphreys (Associate Professor of Evidence-Based Social Intervention and Policy Evaluation Research Fellow, Department of Social Policy and Innovation, University of Oxford) contributed to the design, execution and oversight of the study in general, and contributed to multiple study analyses and publications.
Shannon Sahlqvist (Senior Lecturer, School of Exercise and Nutrition, Deakin University) contributed to the design, execution and oversight of the study in general, and contributed to multiple study analyses and publications.
Nanette Mutrie (Professor of Physical Activity for Health and Director of the Physical Activity for Health Research Centre, University of Edinburgh) contributed to the design, execution and oversight of the study in general, and contributed to multiple study analyses and publications.
All authors contributed to the design of the final report and approved the final version.
Wider contributions
This report represents an original summary and synthesis of a large body of research, most of which has already been published – or submitted or prepared for publication – in more detail in other open-access academic journals. Emma Coombes and Daniel Mackay each contributed to one or more of these analyses or publications.
Mark Petticrew and Stephen Platt contributed to the design, execution and oversight of the baseline phase of the study, which was supported by a MRC Special Training Fellowship in Health of the Public Research (award number G106/1203). Lyndal Bond and Simon Griffin contributed to the design of the follow-up study.
The authors thank the study participants, many of whom contributed to multiple parts of the study in multiple years; staff from the MRC/CSO Social and Public Health Sciences Unit survey office and data management teams, in particular Kate Campbell, Catherine Ferrell, John Gibbons, Elaine Hindle, Sally Stewart, Matthew Tolan and David Walker; Gillian Fergie and Chris Patterson from the MRC/CSO Social and Public Health Sciences Unit for assisting with the qualitative study; Stuart Hashagen and staff from the Scottish Community Development Centre and the Glasgow Centre for Population Health, in particular Carol Frame, Lizzie Leman and Catherine Tabbner, who carried out the community and stakeholder engagement programme on behalf of the study team; Stephen Sharp, for statistical advice; Dan Hayman, for developing the software used to compare Google Earth aerial images; and Steven Cummins, Jillian Anable and Sally Haw, for their guidance and support as members of the independent study steering committee.
Publications
Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Evaluating health effects of transport interventions: methodologic case study. Am J Prev Med 2006;31:118–26.
Ogilvie D. Shifting Towards Healthier Transport? From Systematic Review to Primary Research. PhD thesis. Glasgow: University of Glasgow, 2007. http://theses.gla.ac.uk/78
Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Perceived characteristics of the environment associated with active travel: development and testing of a new scale. Int J Behav Nutr Phys Act 2008;5:32.
Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Personal and environmental correlates of active travel and physical activity in a deprived urban population. Int J Behav Nutr Phys Act 2008;5:43.
Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Shoe leather epidemiology: active travel and transport infrastructure in the urban landscape. Int J Behav Nutr Phys Act 2010;7:43.
Olsen J, Mitchell R, Mackay D, Humphreys D, Ogilvie D, on behalf of the M74 study team. Effects of new urban motorway infrastructure on road traffic accidents in the local area: a retrospective longitudinal study in Scotland. J Epidemiol Community Health 2016;70:1088–95.
Foley L, Prins R, Crawford F, Humphreys D, Mitchell R, Sahlqvist S, et al. Effects of living near an urban motorway on the wellbeing of local residents in deprived areas: natural experimental study. PLOS ONE 2017;12:e0174882. DOI: 10.1371/journal.pone.0174882
Olsen J, Mitchell R, Ogilvie D, on behalf of the M74 study team. Effects of new motorway infrastructure on active travel in the local population: a retrospective repeat cross-sectional study in Glasgow, Scotland. Int J Behav Nutr Phys Act 2016;13:77.
Foley L, Prins R, Crawford F, Sahlqvist S, Ogilvie D, on behalf of the M74 study team. Effects of living near a new urban motorway on the travel behaviour of local residents in deprived areas: evidence from a natural experimental study. Health Place 2017;43:57.
Foley L, Prins R, Crawford F, Humphreys D, Mitchell R, Sahlqvist S, Thomson H, Ogilvie D, on behalf of the M74 study team. Effects of living near an urban motorway on the well-being of local residents in deprived areas: natural experimental study. PLOS ONE 2017; in press.
Under review
Olsen J, Foley L, Ogilvie D, Mitchell R, Mutrie N, on behalf of the M74 study team. Population levels of, and inequalities in, active travel: a national, retrospective, cross-sectional study of adults in Scotland. Under review.
Prins R, Foley L, Mutrie N, Ogilvie D, on behalf of the M74 study team. Effects of urban motorways on physical activity and sedentary behaviour in local residents: a natural experimental study. Under review.
In preparation
Foley L, Coombes E, Humphreys D, Jones A, Mitchell R, Ogilvie D, on behalf of the M74 study team. Effects of exposure to change in the neighbourhood built environment on the wellbeing of local residents in deprived areas: natural experimental study. In preparation.
Nimegeer A, Hilton S, Thomson H, Foley L, Ogilvie D, on behalf of the M74 study team. Perceptions of the effects of a new urban motorway on active travel: qualitative evidence from a natural experimental study. In preparation.
Nimegeer A, Hilton S, Thomson H, Foley L, Ogilvie D, on behalf of the M74 study team. Severance and connectivity in the wake of a new motorway: qualitative evidence from a natural experimental study. In preparation.
Olsen J, Mitchell R, Ogilvie D, on behalf of the M74 study team. Spatial-temporal trends in road traffic accident clusters and the impact of new transport infrastructure; a retrospective longitudinal natural experiment, Scotland, UK. In preparation.
Data sharing statement
The data set used in this study is managed by the MRC Epidemiology Unit at the University of Cambridge. The access policy for sharing is based on the MRC Policy and Guidance on Sharing of Research Data from Population and Patient Studies. All data sharing must meet the terms of existing participants’ consent and study ethics approvals. The authors’ Data Access and Sharing Policy defines the principles and processes for accessing and sharing our data. They welcome proposals for projects and aim to make data as widely available as possible while safeguarding the privacy of our participants, protecting confidential data and maintaining the reputations of our studies and participants. All data sharing is dependent on the project being approved by the study team, a data sharing agreement being in place with the University of Cambridge and resources being available to support the request. For further information, please refer to the MRC Epidemiology Unit data sharing portal at http://epi-meta.medschl.cam.ac.uk.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Kearns A, Tannahill C, Bond L. Regeneration and health: conceptualising the connections. J Urban Regeneration Renewal 2009;3:56-7.
- Jackson RJ. The impact of the built environment on health: an emerging field. Am J Public Health 2003;93:1382-4. https://doi.org/10.2105/AJPH.93.9.1382.
- Evans GW. The built environment and mental health. J Urban Health 2003;80:536-55. http://dx.doi.org/10.1093/jurban/jtg063.
- Sallis JF, Cervero RB, Ascher W, Henderson KA, Kraft MK, Kerr J. An ecological approach to creating active living communities. Annu Rev Public Health 2006;27:297-322. http://dx.doi.org/10.1146/annurev.publhealth.27.021405.102100.
- Batty E, Beatty C, Foden F, Lawless P, Pearson S, Wilson I. The New Deal for Communities Experience: A Final Assessment. London: Department for Communities and Local Government; 2010.
- Egan M, Katikireddi SV, Kearns A, Tannahill C, Kalacs M, Bond L. Health effects of neighborhood demolition and housing improvement: a prospective controlled study of 2 natural experiments in urban renewal. Am J Public Health 2013;103:e47-53. http://dx.doi.org/10.2105/AJPH.2013.301275.
- Thomson H, Thomas S, Sellström E, Petticrew M. Housing improvements for health and associated socio-economic outcomes: a systematic review. Campbell Syst Rev 2013;9. https://doi.org/10.4073/csr.2013.2.
- Thomson H, Atkinson R, Petticrew M, Kearns A. Do urban regeneration programmes improve public health and reduce health inequalities? A synthesis of the evidence from UK policy and practice (1980–2004). J Epidemiol Community Health 2006;60:108-15. https://doi.org/10.1136/jech.2005.038885.
- Thomson H. A dose of realism for healthy urban policy: lessons from area-based initiatives in the UK. J Epidemiol Community Health 2008;62:932-6. http://dx.doi.org/10.1136/jech.2007.068775.
- Breeze E, Jones DA, Wilkinson P, Bulpitt CJ, Grundy C, Latif AM, et al. Area deprivation, social class, and quality of life among people aged 75 years and over in Britain. Int J Epidemiol 2005;34:276-83. https://doi.org/10.1093/ije/dyh328.
- Erdem Ö, Prins RG, Voorham TA, van Lenthe FJ, Burdorf A. Structural neighbourhood conditions, social cohesion and psychological distress in the Netherlands. Eur J Public Health 2015;25:995-1001. http://dx.doi.org/10.1093/eurpub/ckv120.
- An Analysis of Urban Transport. London: Cabinet Office; 2009.
- Edwards P, Green J, Lachowycz K, Grundy C, Roberts I. Serious injuries in children: variation by area deprivation and settlement type. Arch Dis Child 2008;93:485-9. http://dx.doi.org/10.1136/adc.2007.116541.
- Transport Statistics Bulletin: National Travel Survey 2005. London: Office for National Statistics; 2006.
- Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Lancet Physical Activity Series Working Group . Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380:219-29. http://dx.doi.org/10.1016/S0140-6736(12)61031-9.
- Ford ES, Caspersen CJ. Sedentary behaviour and cardiovascular disease: a review of prospective studies. Int J Epidemiol 2012;41:1338-53. http://dx.doi.org/10.1093/ije/dys078.
- van der Ploeg HP, Chey T, Korda RJ, Banks E, Bauman A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch Intern Med 2012;172:494-500. http://dx.doi.org/10.1001/archinternmed.2011.2174.
- Bauman A, Chau J, Ding D, Bennie J. Too much sitting and cardio-metabolic risk: an update of epidemiological evidence. Curr Cardiovasc Risk Rep 2013;7:293-8. https://doi.org/10.1007/s12170-013-0316-y.
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Lancet Physical Activity Series Working Group . Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 2012;380:247-57. http://dx.doi.org/10.1016/S0140-6736(12)60646-1.
- Bennie JA, Chau JY, van der Ploeg HP, Stamatakis E, Do A, Bauman A. The prevalence and correlates of sitting in European adults – a comparison of 32 Eurobarometer-participating countries. Int J Behav Nutr Phys Act 2013;10. http://dx.doi.org/10.1186/1479-5868-10-107.
- Sahlqvist S, Goodman A, Cooper AR, Ogilvie D. iConnect consortium. Change in active travel and changes in recreational and total physical activity in adults: longitudinal findings from the iConnect study. Int J Behav Nutr Phys Act 2013;10. http://dx.doi.org/10.1186/1479-5868-10-28.
- Kelly P, Kahlmeier S, Götschi T, Orsini N, Richards J, Roberts N, et al. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int J Behav Nutr Phys Act 2014;11. http://dx.doi.org/10.1186/s12966-014-0132-x.
- Foley L, Panter J, Heinen E, Prins R, Ogilvie D. Changes in active commuting and changes in physical activity in adults: a cohort study. Int J Behav Nutr Phys Act 2015;12. http://dx.doi.org/10.1186/s12966-015-0323-0.
- Sallis JF, Spoon C, Cavill N, Engelberg JK, Gebel K, Parker M, et al. Co-benefits of designing communities for active living: an exploration of literature. Int J Behav Nutr Phys Act 2015;12. http://dx.doi.org/10.1186/s12966-015-0188-2.
- Woodcock J, Banister D, Edwards P, Prentice AM, Roberts I. Energy and transport. Lancet 2007;370:1078-88. https://doi.org/10.1016/S0140-6736(07)61254-9.
- Healthy Transport = Healthy Lives. London: British Medical Association; 2012.
- Sugiyama T, Wijndaele K, Koohsari MJ, Tanamas SK, Dunstan DW, Owen N. Adverse associations of car time with markers of cardio-metabolic risk. Prev Med 2016;83:26-30. http://dx.doi.org/10.1016/j.ypmed.2015.11.029.
- Fairness in a Car-Dependent Society. London: SDC; 2011.
- Woodcock J, Edwards P, Tonne C, Armstrong BG, Ashiru O, Banister D, et al. Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport. Lancet 2009;374:1930-43. http://dx.doi.org/10.1016/S0140-6736(09)61714-1.
- Kremers SP, de Bruijn GJ, Visscher TL, van Mechelen W, de Vries NK, Brug J. Environmental influences on energy balance-related behaviors: a dual-process view. Int J Behav Nutr Phys Act 2006;3. https://doi.org/10.1186/1479-5868-3-9.
- Saelens BE, Handy SL. Built environment correlates of walking: a review. Med Sci Sports Exerc 2008;40:550-66. http://dx.doi.org/10.1249/MSS.0b013e31817c67a4.
- Sallis JF, Cerin E, Conway TL, Adams MA, Frank LD, Pratt M, et al. Physical activity in relation to urban environments in 14 cities worldwide: a cross-sectional study. Lancet 2016;387:2207-17. http://dx.doi.org/10.1016/S0140-6736(15)01284-2.
- Koohsari MJ, Sugiyama T, Sahlqvist S, Mavoa S, Hadgraft N, Owen N. Neighborhood environmental attributes and adults’ sedentary behaviors: review and research agenda. Prev Med 2015;77:141-9. http://dx.doi.org/10.1016/j.ypmed.2015.05.027.
- Ogilvie D, Egan M, Hamilton V, Petticrew M. Promoting walking and cycling as an alternative to using cars: systematic review. BMJ 2004;329. http://dx.doi.org/10.1136/bmj.38216.714560.55.
- Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, et al. Scottish Physical Activity Research Collaboration . Interventions to promote walking: systematic review. BMJ 2007;334. https://doi.org/10.1136/bmj.39198.722720.BE.
- Yang L, Sahlqvist S, McMinn A, Griffin SJ, Ogilvie D. Interventions to promote cycling: systematic review. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c5293.
- Physical Activity and the Environment: Guidance on the Promotion and Creation of Physical Environments that Support Increased Levels of Physical Activity. London: NICE; 2008.
- Physical Activity and the Environment: Evidence Update April 2014. London: NICE; 2014.
- Behaviour Change. London: The Stationery Office; 2011.
- Ferguson NS, Lamb KE, Wang Y, Ogilvie D, Ellaway A. Access to recreational physical activities by car and bus: an assessment of socio-spatial inequalities in mainland Scotland. PLOS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0055638.
- Macintyre S, Maciver S, Sooman A. Area, class and health: should we be focusing on places or people?. J Soc Policy 1993;22:213-34. https://doi.org/10.1017/S0047279400019310.
- Appleyard D, Gerson MS, Lintell M. Livable Streets. Berkeley, CA: University of California Press; 1981.
- Hart J. Driven to Excess – Impacts of Motor Vehicle Traffic on Residential Quality of Life in Bristol, UK. Bristol: University of the West of England; 2008.
- Mindell J, Karlsen S. Community severance and health: what do we actually know?. J Urban Health 2012;89:232-46. http://dx.doi.org/10.1007/s11524-011-9637-7.
- Dratva J, Zemp E, Felber Dietrich D, Bridevaux PO, Rochat T, Schindler C, et al. Impact of road traffic noise annoyance on health-related quality of life: results from a population-based study. Qual Life Res 2010;19:37-46. http://dx.doi.org/10.1007/s11136-009-9571-2.
- Marques S, Lima M. Living in grey areas: industrial activity and psychological health. J Environ Psychol 2011;31:314-22. https://doi.org/10.1016/j.jenvp.2010.12.002.
- Trunk Roads and the Generation of Traffic. London: Department of Transport; 1994.
- Ding D, Sugiyama T, Winkler E, Cerin E, Wijndaele K, Owen N. Correlates of change in adults’ television viewing time: a four-year follow-up study. Med Sci Sports Exerc 2012;44:1287-92. http://dx.doi.org/10.1249/MSS.0b013e31824ba87e.
- Goodman A, Sahlqvist S, Ogilvie D. iConnect Consortium. New walking and cycling routes and increased physical activity: one- and 2-year findings from the UK iConnect Study. Am J Public Health 2014;104:e38-46. http://dx.doi.org/10.2105/AJPH.2014.302059.
- Panter J, Heinen E, Mackett R, Ogilvie D. Impact of new transport infrastructure on walking, cycling, and physical activity. Am J Prev Med 2016;50:e45-53. http://dx.doi.org/10.1016/j.amepre.2015.09.021.
- Egan M, Petticrew M, Ogilvie D, Hamilton V. New roads and human health: a systematic review. Am J Public Health 2003;93:1463-71. https://doi.org/10.2105/AJPH.93.9.1463.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Evaluating health effects of transport interventions methodologic case study. Am J Prev Med 2006;31:118-26. https://doi.org/10.1016/j.amepre.2006.03.030.
- Hawe P. Lessons from complex interventions to improve health. Annu Rev Public Health 2015;36:307-23. http://dx.doi.org/10.1146/annurev-publhealth-031912-114421.
- Hickman R. Roads (Scotland) Act 1984; Acquisition of Land (Authorisation Procedure) (Scotland) Act 1947. M74 Special Road (Fullarton Road to west of Kingston Bridge) Orders. Report of Public Local Inquiry Into Objections. Edinburgh: Inquiry Reporters Unit, Scottish Executive; 2004.
- Ogilvie D. Shifting Towards Healthier Transport? From Systematic Review to Primary Research 2007.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Perceived characteristics of the environment associated with active travel: development and testing of a new scale. Int J Behav Nutr Phys Act 2008;5. http://dx.doi.org/10.1186/1479-5868-5-32.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Personal and environmental correlates of active travel and physical activity in a deprived urban population. Int J Behav Nutr Phys Act 2008;5. https://doi.org/10.1186/1479-5868-5-43.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Shoe leather epidemiology: active travel and transport infrastructure in the urban landscape. Int J Behav Nutr Phys Act 2010;7. http://dx.doi.org/10.1186/1479-5868-7-43.
- Craig P, Cooper C, Gunnell D, Haw S, Lawson K, Macintyre S, et al. Using natural experiments to evaluate population health interventions: new Medical Research Council guidance. J Epidemiol Community Health 2012;66:1182-6. http://dx.doi.org/10.1136/jech-2011-200375.
- Centre for Diet and Activity Research . Traffic and Health in Glasgow n.d. www.cedar.iph.cam.ac.uk/research/directory/traffic-health-glasgow (accessed 20 February 2017).
- The M74 Completion: Environmental Statement. Edinburgh: Scottish Executive; 2003.
- Edwards P, Roberts I, Clarke M, Diguiseppi C, Wentz R, Kwan I, et al. Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst Rev 2009;3. https://doi.org/10.1002/14651858.mr000008.pub4.
- Scottish Executive . Scottish Household Survey n.d. www.gov.scot/Topics/Statistics/16002/ (accessed 3 April 2017).
- Department for Transport . National Travel Survey Statistics 2013. www.gov.uk/government/collections/national-travel-survey-statistics (accessed 5 May 2016).
- Craig C, Marshall A, Sjöström M, Bauman A, Booth M, Ainsworth B, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381-9. https://doi.org/10.1249/01.MSS.0000078924.61453.FB.
- Ware J, Kosinski M, Dewey J, Gandek B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8™ Health Survey. Lincoln, RI: QualityMetric Incorporated; 2001.
- Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick–Edinburgh Mental Well-being Scale (WEMWBS): a Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual Life Outcomes 2009;7. http://dx.doi.org/10.1186/1477-7525-7-15.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: a multilevel study of collective efficacy. Science 1997;277:918-24. https://doi.org/10.1126/science.277.5328.918.
- Plasqui G, Westerterp KR. Physical activity assessment with accelerometers: an evaluation against doubly labeled water. Obesity 2007;15:2371-9. https://doi.org/10.1038/oby.2007.281.
- Carpiano RM. Come take a walk with me: the ‘go-along’ interview as a novel method for studying the implications of place for health and well-being. Health Place 2009;15:263-72. http://dx.doi.org/10.1016/j.healthplace.2008.05.003.
- Kusenbach M. Street phenomenology: the go-along as ethnographic research tool. Ethnography 2003;4:455-85. https://doi.org/10.1177/146613810343007.
- Hansard . House of Lords: 16 July 2008, Column 1239 n.d. www.publications.parliament.uk/pa/ld200708/ldhansrd/text/80716-0001.htm (accessed 30 June 2016).
- Department for Transport . STATS19 n.d. https://data.gov.uk/dataset/road-accidents-safety-data (accessed 29 March 2016).
- Scottish Government . Scottish Neighbourhood Statistics: Intermediate Geography Background Information n.d. www.gov.scot/Publications/2005/02/20732/53083 (accessed 30 June 2016).
- Karolinska Institute . IPAQ: International Physical Activity Questionnaire n.d. www.ipaq.ki.se/ (accessed 26 April 2006).
- Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, et al. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol 2008;167:875-81. http://dx.doi.org/10.1093/aje/kwm390.
- Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40:181-8. http://dx.doi.org/10.1249/mss.0b013e31815a51b3.
- Tudor-Locke C, Brashear MM, Johnson WD, Katzmarzyk PT. Accelerometer profiles of physical activity and inactivity in normal weight, overweight, and obese U.S. men and women. Int J Behav Nutr Phys Act 2010;7. http://dx.doi.org/10.1186/1479-5868-7-60.
- Humphreys DK, Panter J, Sahlqvist S, Goodman A, Ogilvie D. Changing the environment to improve population health: a framework for considering exposure in natural experimental studies. J Epidemiol Community Health 2016;70:941-6. http://dx.doi.org/10.1136/jech-2015-206381.
- Saelens BE, Sallis JF, Frank LD. Environmental correlates of walking and cycling: findings from the transportation, urban design, and planning literatures. Ann Behav Med 2003;25:80-91. https://doi.org/10.1207/S15324796ABM2502_03.
- Health Survey for England 2008: Physical Activity and Fitness: Summary of Key Findings. Leeds: Health and Social Care Information Centre; 2009.
- Sisson SB, Tudor-Locke C. Comparison of cyclists’ and motorists’ utilitarian physical activity at an urban university. Prev Med 2008;46:77-9. https://doi.org/10.1016/j.ypmed.2007.07.004.
- Gottman J. Time-Series Analysis: A Comprehensive Introduction for Social Scientists. Cambridge: Cambridge University Press; 1981.
- Zhang F, Wagner AK, Soumerai SB, Ross-Degnan D. Methods for estimating confidence intervals in interrupted time series analyses of health interventions. J Clin Epidemiol 2009;62:143-8. http://dx.doi.org/10.1016/j.jclinepi.2008.08.007.
- Baron R, Kenny D. The moderator–mediator distinction in social psychological research: conceptual, strategic, and statistical considerations. J Personal Social Psychol 1986;51:1173-82. https://doi.org/10.1037/0022-3514.51.6.1173.
- Trochim W. Outcome pattern matching and program theory. Eval Program Plann 1989;12:355-66. https://doi.org/10.1016/0149-7189(89)90052-9.
- Dunning T, Dunning T. Natural Experiments in the Social Sciences: A Design-Based Approach. Cambridge: Cambridge University Press; 2012.
- Victora CG, Habicht JP, Bryce J. Evidence-based public health: moving beyond randomized trials. Am J Public Health 2004;94:400-5. https://doi.org/10.2105/AJPH.94.3.400.
- Foley L, Prins R, Crawford F, Sahlqvist S, Ogilvie D. behalf of the M74 study team . Effects of living near a new urban motorway on the travel behaviour of local residents in deprived areas: evidence from a natural experimental study. Health Place 2017;43:57-65. https://doi.org/10.1016/j.healthplace.2016.11.008.
- Prins R, Foley L, Mutrie N, Ogilvie D. behalf of the M74 study team . Effects of Urban Motorways on Physical Activity and Sedentary Behaviour in Local Residents: A Natural Experimental Study n.d.
- Cragg J. Some statistical models for limited dependent variables with application to the demand for durable goods. Econometrica 1971;39:829-44. https://doi.org/10.2307/1909582.
- Olsen JR, Mitchell R, Ogilvie D. M74 study team . Effects of new motorway infrastructure on active travel in the local population: a retrospective repeat cross-sectional study in Glasgow, Scotland. Int J Behav Nutr Phys Act 2016;13. http://dx.doi.org/10.1186/s12966-016-0403-9.
- Transport Scotland . Scottish Household Survey: Appendix: Notes and Definitions n.d. www.transport.gov.scot/statistics/j285661-33.htm (accessed 3 May 2016).
- Office for National Statistics . 2011 Census n.d. www.ons.gov.uk/census/2011census (accessed 7 June 2016).
- Rind E, Shortt N, Mitchell R, Richardson EA, Pearce J. Are income-related differences in active travel associated with physical environmental characteristics? A multi-level ecological approach. Int J Behav Nutr Phys Act 2015;12. http://dx.doi.org/10.1186/s12966-015-0217-1.
- Tsay R. Regression models with time series errors. J Am Stat Assoc 1984;79:118-24. https://doi.org/10.1080/01621459.1984.10477073.
- Hyndman R. The ARIMAX Model Muddle n.d. www.robjhyndman.com/hyndsight/arimax (accessed 6 October 2015).
- Moss C, Shonkwiler J. Estimating yield distributions with a stochastic trend and nonnormal errors. Am J Agric Econ 1993;75:1056-62. https://doi.org/10.2307/1243993.
- Bozdogan H. Model selection and Akaike’s information criterion (AIC): the general theory and its analytical extensions. Psychometrika 1987;52:345-70. https://doi.org/10.1007/BF02294361.
- Grundy C, Steinbach R, Edwards P, Green J, Armstrong B, Wilkinson P. Effect of 20 mph traffic speed zones on road injuries in London, 1986–2006: controlled interrupted time series analysis. BMJ 2009;339. https://doi.org/10.1136/bmj.b4469.
- McCleary R, Hay R. Applied Time Series Analysis for the Social Sciences. Beverly Hills, CA: Sage; 1980.
- Fujii S, Taniguchi A. Determinants of the effectiveness of travel feedback programs – a review of communicative mobility management measures for changing travel behaviour in Japan. Transport Pol 2006;13:339-48. https://doi.org/10.1016/j.tranpol.2005.12.007.
- Cleveland R, Cleveland W, McRae J, Terpenning I. STL: a seasonal-trend decomposition procedure based on loess. J Off Stat 1990;6:3-73.
- Aljanahi AA, Rhodes AH, Metcalfe AV. Speed, speed limits and road traffic accidents under free flow conditions. Accid Anal Prev 1999;31:161-8. https://doi.org/10.1016/S0001-4575(98)00058-X.
- Anastasopoulos PCh, Mannering FL. A note on modeling vehicle accident frequencies with random-parameters count models. Accid Anal Prev 2009;41:153-9. http://dx.doi.org/10.1016/j.aap.2008.10.005.
- Bernat DH, Maldonado-Molina M, Hyland A, Wagenaar AC. Effects of smoke-free laws on alcohol-related car crashes in California and New York: time series analyses from 1982 to 2008. Am J Public Health 2013;103:214-20. http://dx.doi.org/10.2105/AJPH.2012.300906.
- López-Ruiz M, Martínez JM, Pérez K, Novoa AM, Tobías A, Benavides FG. Impact of road safety interventions on traffic-related occupational injuries in Spain, 2004–2010. Accid Anal Prev 2014;66:114-19. http://dx.doi.org/10.1016/j.aap.2014.01.012.
- Bahadorimonfared A, Soori H, Mehrabi Y, Delpisheh A, Esmaili A, Salehi M, et al. Trends of fatal road traffic injuries in Iran (2004–2011). PLOS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0065198.
- M74 Completion Scheme Post-Project Evaluation Study: Sixteen Weeks After Opening Review. Glasgow: Transport Scotland; 2012.
- Olsen JR, Mitchell R, Mackay DF, Humphreys DK, Ogilvie D. M74 study team . Effects of new urban motorway infrastructure on road traffic accidents in the local area: a retrospective longitudinal study in Scotland. J Epidemiol Community Health 2016;70:1088-95. http://dx.doi.org/10.1136/jech-2016-207378.
- Slaughter DR, Williams N, Wall SP, Glass NE, Simon R, Todd SR, et al. A community traffic safety analysis of pedestrian and bicyclist injuries based on the catchment area of a trauma center. J Trauma Acute Care Surg 2014;76:1103-10. http://dx.doi.org/10.1097/TA.0000000000000176.
- Ball K, Jeffery RW, Crawford DA, Roberts RJ, Salmon J, Timperio AF. Mismatch between perceived and objective measures of physical activity environments. Prev Med 2008;47:294-8. http://dx.doi.org/10.1016/j.ypmed.2008.05.001.
- Scottish Government . SIMD: Background and Methodology n.d. www.gov.scot/Topics/Statistics/SIMD/BackgroundMethodology (accessed 30 June 2016).
- Lyons RA, Ward H, Brunt H, Macey S, Thoreau R, Bodger OG, et al. Using multiple datasets to understand trends in serious road traffic casualties. Accid Anal Prev 2008;40:1406-10. http://dx.doi.org/10.1016/j.aap.2008.03.011.
- Reported Road Casualties in Great Britain: Main Results 2014. London: HMSO; 2015.
- Glasgow City Council . Transformational Regeneration Areas (TRAs) 2013 n.d. https://glasgow.gov.uk/index.aspx?articleid=10910 (accessed 7 December 2015).
- The Scottish Health Survey – Main Report. Edinburgh: Scottish Government; 2013.
- Foley L, Prins R, Crawford F, Humphreys D, Mitchell R, Sahlqvist S, et al. Effects of living near an urban motorway on the well-being of local residents in deprived areas: natural experimental study. PLOS ONE 2017;12. https://doi.org/10.1371/journal.pone.0174882.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. http://dx.doi.org/10.1186/1471-2288-13-117.
- Friends of the Earth . Revealed: Scotland’s Most Polluted Streets n.d. www.foe-scotland.org.uk/air-pollution-streets-2014 (accessed 20 February 2017).
- Searl A. Health Impact Assessment of Air Quality Impacts of the Construction and Operation of the Proposed Completion of M74 in Southern Glasgow. Edinburgh: Institute of Occupational Medicine Consulting; 2003.
- Anciaes P. Measuring community severance for transport policy and project appraisal. Transac Built Environ 2013;130:559-70. https://doi.org/10.2495/UT130451.
- Guo X, Black J, Dunne M. Crossing pedestrians and dynamic severance on main roads. Road Transport Res 2001;10:84-98.
- Clark J, Hutton B, Burnett N, Hathaway A, Harrison A. The Appraisal of Comunity Severance. Crowthorne, Berkshire: Transport Research Laboratory; 1991.
- James E, Millington A, Tomlinson P. Understanding Community Severance Part 1: Views of Practitioners and Communities. Crowthorne: Transport Research Laboratory; 2005.
- Oldenburg R. The Great Good Place: Cafes, Coffee Shops, Community Centers, Beauty Parlors, General Stores, Bars, Hangouts, and How They Get You Through the Day. New York, NY: Paragon House; 1989.
- Maas J, van Dillen SM, Verheij RA, Groenewegen PP. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009;15:586-95. http://dx.doi.org/10.1016/j.healthplace.2008.09.006.
- Mitchell R, Popham F. Effect of exposure to natural environment on health inequalities: an observational population study. Lancet 2008;372:1655-60. http://dx.doi.org/10.1016/S0140-6736(08)61689-X.
- M74 Completion Scheme Post-Project Evaluation Study: Four Weeks After Opening Review. Glasgow: Transport Scotland; 2012.
- Scottish Trunk Road Infrastructure Project Evaluation (STRIPE): M74 Completion Scheme: One Year After Opening Evaluation. Glasgow: Transport Scotland; 2015.
- Vandenbroucke JP, Broadbent A, Pearce N. Causality and causal inference in epidemiology: the need for a pluralistic approach. Int J Epidemiol 2016;45:1776-86. https://doi.org/10.1093/ije/dyv341.
- Kearns A, Petticrew M, Mason P, Whitley E. SHARP Survey Findings: Mental Health and Well-being Outcomes. Edinburgh: Scottish Government Social Research; 2008.
- Egan M, Kearns A, Katikireddi SV, Curl A, Lawson K, Tannahill C. Proportionate universalism in practice? A quasi-experimental study (GoWell) of a UK neighbourhood renewal programme’s impact on health inequalities. Soc Sci Med 2016;152:41-9. http://dx.doi.org/10.1016/j.socscimed.2016.01.026.
- GoWell n.d. www.gowellonline.com/ (accessed 23 March 2017).
- Cairns S, Hass-Klau C, Goodwin P. Traffic Impact of Highway Capacity Reductions: Assessment of the Evidence. London: Landor; 1998.
- Lopez RP, Hynes HP. Obesity, physical activity, and the urban environment: public health research needs. Environ Health 2006;5. https://doi.org/10.1186/1476-069X-5-25.
- Ohrström E. Longitudinal surveys on effects of changes in road traffic noise-annoyance, activity disturbances, and psycho-social well-being. J Acoust Soc Am 2004;115:719-29. https://doi.org/10.1121/1.1639333.
- Foraster M, Eze IC, Vienneau D, Brink M, Cajochen C, Caviezel S, et al. Long-term transportation noise annoyance is associated with subsequent lower levels of physical activity. Environ Int 2016;91:341-9. https://doi.org/10.1016/j.envint.2016.03.011.
- Christensen JS, Raaschou-Nielsen O, Tjønneland A, Nordsborg RB, Jensen SS, Sørensen TI, et al. Long-term exposure to residential traffic noise and changes in body weight and waist circumference: a cohort study. Environ Res 2015;143:154-61. http://dx.doi.org/10.1016/j.envres.2015.10.007.
- Oftedal B, Krog NH, Pyko A, Eriksson C, Graff-Iversen S, Haugen M, et al. Road traffic noise and markers of obesity – a population-based study. Environ Res 2015;138:144-53. http://dx.doi.org/10.1016/j.envres.2015.01.011.
- Winters M, Davidson G, Kao D, Teschke K. Motivators and deterrents of bicycling: comparing influences on decisions to ride. Transportation 2011;38:153-68. https://doi.org/10.1007/s11116-010-9284-y.
- Rabin BA, Boehmer TK, Brownson RC. Cross-national comparison of environmental and policy correlates of obesity in Europe. Eur J Public Health 2007;17:53-61. https://doi.org/10.1093/eurpub/ckl073.
- Elvik R, Vaa T, Erke A, Srensen M. The Handbook of Road Safety Measures. Bingley: Emerald Group; 2009.
- Noland RB. Traffic fatalities and injuries: the effect of changes in infrastructure and other trends. Accid Anal Prev 2003;35:599-611. https://doi.org/10.1016/S0001-4575(02)00040-4.
- VanderWeele TJ. Mediation and mechanism. Eur J Epidemiol 2009;24:217-24. http://dx.doi.org/10.1007/s10654-009-9331-1.
- Sahlqvist S, Goodman A, Jones T, Powell J, Song Y, Ogilvie D. iConnect consortium. Mechanisms underpinning use of new walking and cycling infrastructure in different contexts: mixed-method analysis. Int J Behav Nutr Phys Act 2015;12. http://dx.doi.org/10.1186/s12966-015-0185-5.
- Prins RG, Panter J, Heinen E, Griffin SJ, Ogilvie DB. Causal pathways linking environmental change with health behaviour change: natural experimental study of new transport infrastructure and cycling to work. Prev Med 2016;87:175-82. http://dx.doi.org/10.1016/j.ypmed.2016.02.042.
- Bodicoat DH, O’Donovan G, Dalton AM, Gray LJ, Yates T, Edwardson C, et al. The association between neighbourhood greenspace and type 2 diabetes in a large cross-sectional study. BMJ Open 2014;4. http://dx.doi.org/10.1136/bmjopen-2014-006076.
- Ward Thompson C, Roe J, Aspinall P, Mitchell R, Clow A, Miller D. More green space is linked to less stress in deprived communities: evidence from salivary cortisol patterns. Landscape Urban Plann 2012;105:221-9. https://doi.org/10.1016/j.landurbplan.2011.12.015.
- Green J, Roberts H, Petticrew M, Steinbach R, Goodman A, Jones A, et al. Integrating quasi-experimental and inductive designs in evaluation: a case study of the impact of free bus travel on public health. Evaluation 2015;21:391-406. https://doi.org/10.1177/1356389015605205.
- Devine-Wright P. Rethinking NIMBYism: the role of place attachment and place identity in explaining place-protective action. J Community Appl Soc Psychol 2009;19:426-41. https://doi.org/10.1002/casp.1004.
- Mihaylov N, Perkins D, Manzo L, Devine-Wright P. Place Attachment: Advances in Theory, Methods and Applications. Abingdon: Routledge; 2014.
- Illich I. Energy and Equity. New York, NY: Harper & Row; 1974.
- Pratt M, Sarmiento OL, Montes F, Ogilvie D, Marcus BH, Perez LG, et al. Lancet Physical Activity Series Working Group . The implications of megatrends in information and communication technology and transportation for changes in global physical activity. Lancet 2012;380:282-93. http://dx.doi.org/10.1016/S0140-6736(12)60736-3.
- Hawe P, Shiell A, Riley T. Complex interventions: how ‘out of control’ can a randomised controlled trial be?. BMJ 2004;328:1561-3. https://doi.org/10.1136/bmj.328.7455.1561.
- Hooper P, Giles-Corti B, Knuiman M. Evaluating the implementation and active living impacts of a state government planning policy designed to create walkable neighborhoods in Perth, Western Australia. Am J Health Promot 2014;28:5-18. http://dx.doi.org/10.4278/ajhp.130503-QUAN-226.
- Reis RS, Salvo D, Ogilvie D, Lambert EV, Goenka S, Brownson RC. Lancet Physical Activity Series 2 Executive Committee . Scaling up physical activity interventions worldwide: stepping up to larger and smarter approaches to get people moving. Lancet 2016;388:1337-48. http://dx.doi.org/10.1016/S0140-6736(16)30728-0.
- University of Cambridge . MRC Epidemiology Unit: Data Sharing n.d. http://epi-meta.medschl.cam.ac.uk (accessed 23 March 2017).
- Cummins S, Petticrew M, Higgins C, Findlay A, Sparks L. Large scale food retailing as an intervention for diet and health: quasi-experimental evaluation of a natural experiment. J Epidemiol Community Health 2005;59:1035-40. https://doi.org/10.1136/jech.2004.029843.
- Diez Roux AV. Complex systems thinking and current impasses in health disparities research. Am J Public Health 2011;101:1627-34. http://dx.doi.org/10.2105/AJPH.2011.300149.
Appendix 1 Topic guide for key informant interviews
What do you think are the most important environmental changes related to the M74 extension?
Respondents may also be asked to identify changes on a map of the study area, provided by the researcher.
M74 itself
-
Noise.
-
Visual impact.
-
Pollution.
-
Impact on traffic flow.
Associated building features
-
Viaducts.
-
Embankments.
-
Slip roads.
-
Underpasses: lighting, artwork (severance).
-
Junctions: crossings, safety (severance).
-
Planting.
-
New building, development of open space (wider economic effects).
-
Changes to industrial real estate.
-
Changes to residential areas.
-
Change to green space.
-
Changes to the landscape/character of the areas it passes through.
Appendix 2 Core survey questionnaire
Appendix 3 Topic guide for resident interviews
For the purpose of this interview, ‘local area’ will be suggested, as it was in the survey, as being within half a mile of the participant’s house, or about 10 minutes’ walk, unless the participant defines it in another way.
Experiences and perceptions of the local area
Experiences and perceptions of neighbourhood
-
The local area as a place to live (general).
-
The local area as a healthy space.
-
Access to amenities.
-
Suitability for children and families.
-
Suitability for teenagers.
-
Suitability for older people.
-
Feelings of safety (general).
-
Feelings of safety and noise (traffic related).
-
Feelings of connectedness to other neighbourhoods.
Changes in experience and perceptions of neighbourhood
-
Has respondent’s experience of living in the local area changed? If so, how?
-
Have respondent’s perceptions of or feelings towards the local area changed? If so, how?
-
Why does respondent feel that these changes have come about?
-
Have changes in the physical environment influenced how the respondent experiences and perceives the local area? If so, which specific physical changes?
Use of the local area
Use, travel and activity within the local area
-
Types of activity undertaken in local area (social, work, visiting friends, shopping, exercise, etc.).
-
How often these activities are undertaken.
-
Types of travel within local area (how do participants get around?).
-
Does this include active travel (e.g. travelling to shops, work, to visit friends)?
-
How often does active travel occur?
Changes in use of the local area
-
Have types of activity undertaken in local area changed recently? If so, how?
-
Has active travel changed, increased or decreased? If so, how?
-
Do respondents feel any more or less comfortable travelling on foot or by cycle in local area than they used to? If so, describe.
-
Explanation for changes: why do they think changes have occurred?
-
Have changes in the physical environment influenced how respondent uses the local area? If so, which specific physical changes?
If it has not been mentioned yet at this stage, explicitly ask about the impact of the M74 extension.
Appendix 4 Sensitivity analysis of associations between motorway exposure and likelihood of active travel in Scottish Household Survey sample
| Area | All stages regardless of distance travelled, RRR (p-value) | Only journey stages of > 0.5 km, RRR (p-value) | Only journey stages of < 5 km, RRR (p-value) | Only journey stages of > 0.5 km and < 5 km, RRR (p-value) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||||
| 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | 2009–10 | 2012–13 | |
| Ref: Glasgow and surrounding authorities | ||||||||||||||||
| South | 1.3 (0.209); n: 420 | 1.4 (0.081); n: 533 | 1.3 (0.193); n: 420 | 1.4 (0.092); n: 533 | 1.2 (0.514); n: 348 | 1.4 (0.144); n: 467 | 1.2 (0.433); n: 348 | 1.3 (0.215); n: 467 | 1.1 (0.793); n: 305 | 1.2 (0.273); n: 386 | 1.1 (0.740); n: 305 | 1.2 (0.346); n: 386 | 0.9 (0.859); n: 233 | 1.2 (0.427); n: 320 | 1.0 (0.950); n: 233 | 1.1 (0.659); n: 320 |
| East | 1.4 (0.078); n: 468 | 1.2 (0.240); n: 543 | 1.4 (0.108); n: 468 | 1.1 (0.513); n: 543 | 1.5 (0.083); n: 401 | 1.1 (0.529); n: 474 | 1.5 (0.071); n: 401 | 1.0 (0.878); n: 401 | 1.2 (0.362); n: 334 | 1.2 (0.335); n: 384 | 1.2 (0.437); n: 334 | 1.2 (0.469); n: 384 | 1.3 (0.290); n: 267 | 1.1 (0.702); n: 315 | 1.3 (0.279); n: 267 | 1.1 (0.825); n: 315 |
| North | 1.3 (0.228); n: 533 | 1.8 (0.003); n: 581 | 1.3 (0.136); n: 533 | 1.8 (0.003); n: 581 | 1.3 (0.274); n: 467 | 1.8 (0.006); n: 507 | 1.4 (0.164); n: 467 | 1.8 (0.006); n: 507 | 1.1 (0.564); n: 382 | 1.5 (0.047); n: 442 | 1.2 (0.413); n: 382 | 1.5 (0.030); n: 442 | 1.1 (0.595); n: 316 | 1.5 (0.080); n: 368 | 1.2 (0.460); n: 316 | 1.6 (0.054); n: 368 |
| Ref: Glasgow city | ||||||||||||||||
| South | 1.2 (0.316); n: 288 | 1.2 (0.482); n: 348 | 1.4 (0.190); n: 288 | 1.2 (0.468); n: 348 | 1.0 (0.993); n: 229 | 1.1 (0.699); n: 301 | 1.1 (0.681); n: 229 | 1.1 (0.770); n: 301 | 1.0 (0.881); n: 218 | 1.0 (0.967); n: 250 | 1.0 (0.901); n: 218 | 1.0 (0.894); n: 250 | 0.8 (0.304); n: 159 | 0.9 (0.801); n: 203 | 0.8 (0.518); n: 159 | 0.9 (0.593); n: 203 |
| East | 1.1 (0.615); n: 458 | 0.9 (0.745); n: 530 | 1.1 (0.557); n: 458 | 0.8 (0.356); n: 530 | 1.1 (0.685); n: 391 | 0.8 (0.422); n: 465 | 1.2 (0.422); n: 391 | 0.8 (0.261); n: 465 | 0.9 (0.638); n: 326 | 0.8 (0.427); n: 371 | 0.9 (0.681); n: 326 | 0.8 (0.287); n: 371 | 0.9 (0.653); n: 259 | 0.7 (0.190); n: 306 | 1.0 (0.940); n: 259 | 0.7 (0.210); n: 306 |
| North | 1.0 (0.984); n: 496 | 1.3 (0.143); n: 519 | 1.1 (0.725); n: 496 | 1.3 (0.192); n: 519 | 0.9 (0.814); n: 434 | 1.3 (0.194); n: 449 | 1.0 (0.845); n: 434 | 1.3 (0.210); n: 449 | 0.8 (0.438); n: 355 | 1.0 (0.891); n: 394 | 0.9 (0.651); n: 355 | 1.0 (0.891); n: 394 | 0.8 (0.308); n: 293 | 1.0 (0.967); n: 324 | 0.9 (0.514); n: 293 | 1.0 (0.865); n: 324 |
Appendix 5 Cross-sectional associations between motorway exposure and neighbourhood perceptions at follow-up
| Physical environment perceptions | South (n = 371) | East (n = 379) | ||
|---|---|---|---|---|
| Beta coefficient (95% CI) | R 2 | Beta coefficient (95% CI) | R 2 | |
| It is pleasant to walk | –0.18 (–0.43 to 0.07) | 0.09 | –0.06 (–0.21 to 0.10) | 0.05 |
| There is a park within walking distance | –0.32 (–0.52 to –0.12) | 0.08 | –0.06 (–0.23 to 0.12) | 0.06 |
| There is convenient public transport | 0.27 (0.09 to 0.44) | 0.03 | –0.27 (–0.46 to –0.09) | 0.12 |
| There are convenient routes for cycling | 0.23 (–0.01 to 0.05) | 0.03 | 0.03 (–0.15 to 0.21) | 0.02 |
| It is safe to walk after dark | –0.15 (–0.41 to 0.11) | 0.09 | –0.11 (–0.28 to 0.06) | 0.09 |
| There is little traffic | –0.01 (–0.24 to 0.22) | 0.05 | –0.04 (–0.23 to 0.15) | 0.03 |
| It is safe to cross the road | –0.02 (–0.25 to 0.21) | 0.07 | –0.01 (–0.19 to 0.16) | 0.03 |
| The surroundings are unattractive | –0.12 (–0.38 to 0.14) | 0.06 | –0.07 (–0.25 to 0.11) | 0.10 |
| There is little green space | –0.06 (–0.32 to 0.20) | 0.05 | –0.05 (–0.25 to 0.14) | 0.05 |
| The nearest shops are too far to walk to | 0.08 (–0.15 to 0.32) | 0.11 | –0.13 (–0.31 to 0.05) | 0.08 |
| There are no convenient routes for walking | 0.05 (–0.17 to 0.28) | 0.06 | –0.11 (–0.29 to 0.06) | 0.07 |
| People are likely to be attacked | –0.15 (–0.40 to 0.10) | 0.08 | –0.04 (–0.21 to 0.12) | 0.07 |
| There is a lot of traffic noise | –0.24 (–0.51 to 0.03) | 0.08 | –0.19 (–0.39 to 0.01) | 0.03 |
| The roads are dangerous for cyclists | 0.11 (–0.13 to 0.35) | 0.05 | –0.09 (–0.27 to 0.09) | 0.02 |
| Safe and pleasant surroundings (factor 1) | –0.60 (–1.40 to 0.21) | 0.10 | –0.28 (–0.77 to 0.21) | 0.12 |
| Low traffic (factor 2) | –0.41 (–1.01 to 0.19) | 0.06 | –0.05 (–0.54 to 0.45) | 0.02 |
| Convenience for walking (factor 3) | –0.24 (–0.79 to 0.30) | 0.14 | –0.36 (–0.82 to 0.11) | 0.09 |
| Collective efficacy | 0.09 (–0.09 to 0.28) | 0.09 | 0.01 (–0.12 to 0.13) | 0.06 |
Appendix 6 Mediation of relationship between motorway exposure and mental well-being by neighbourhood perceptions
| Change in perceptions of physical environment | n | A coefficient (SE) | p-value | B coefficient (SE) | p-value | Total effect (SE) | p-value | Direct effect (SE) | p-value | Sobel p-value |
|---|---|---|---|---|---|---|---|---|---|---|
| South | ||||||||||
| It is pleasant to walk | 109 | –0.35 (0.20) | 0.08 | 1.12 (0.73) | 0.12 | –3.55 (1.46) | 0.02 | –3.16 (1.48) | 0.03 | 0.25 |
| There is a park within walking distance | 109 | –0.14 (0.16) | 0.40 | 1.73 (0.90) | 0.054 | –3.67 (1.49) | 0.01 | –3.43 (1.47) | 0.02 | 0.44 |
| There is convenient public transport | 109 | 0.01 (0.15) | 0.97 | –0.87 (0.87) | 0.31 | –3.74 (1.49) | 0.01 | –3.73 (1.49) | 0.01 | 0.97 |
| There are convenient routes for cycling | 108 | 0.04 (0.25) | 0.87 | 0.98 (0.61) | 0.11 | –3.53 (1.50) | 0.02 | –3.57 (1.49) | 0.02 | 0.87 |
| It is safe to walk after dark | 107 | –0.13 (0.21) | 0.54 | 0.38 (0.73) | 0.61 | –3.58 (1.48) | 0.02 | –3.53 (1.49) | 0.02 | 0.69 |
| There is little traffic | 106 | 0.13 (0.20) | 0.52 | 0.15 (0.79) | 0.84 | –3.60 (1.51) | 0.02 | –3.62 (1.52) | 0.02 | 0.85 |
| It is safe to cross the road | 107 | 0.07 (0.20) | 0.72 | –0.37 (0.79) | 0.63 | –3.66 (1.50) | 0.01 | –3.63 (1.50) | 0.02 | 0.77 |
| The surroundings are unattractive | 108 | –0.59 (0.22) | 0.01 | –0.98 (0.69) | 0.15 | –3.70 (1.50) | 0.01 | –4.28 (1.54) | 0.01 | 0.21 |
| There is little green space | 106 | –0.12 (0.27) | 0.64 | –1.31 (0.56) | 0.02 | –3.46 (1.49) | 0.01 | –3.62 (1.46) | 0.02 | 0.65 |
| The nearest shops are too far to walk to | 108 | –0.21 (0.24) | 0.37 | –0.16 (0.65) | 0.80 | –3.68 (1.51) | 0.01 | –3.71 (1.52) | 0.01 | 0.81 |
| There are no convenient routes for walking | 108 | –0.32 (0.24) | 0.18 | 0.11 (0.63) | 0.87 | –3.63 (1.50) | 0.02 | –3.59 (1.52) | 0.02 | 0.86 |
| People are likely to be attacked | 107 | –0.21 (0.21) | 0.31 | –0.18 (0.75) | 0.81 | –3.66 (1.50) | 0.01 | –3.70 (1.52) | 0.01 | 0.81 |
| There is a lot of traffic noise | 109 | –0.38 (0.23) | 0.10 | 0.63 (0.63) | 0.32 | –3.55 (1.46) | 0.02 | –3.31 (1.48) | 0.03 | 0.40 |
| The roads are dangerous for cyclists | 107 | 0.02 (0.20) | 0.94 | –0.17 (0.75) | 0.82 | –3.49 (1.48) | 0.02 | –3.49 (1.49) | 0.02 | 0.94 |
| Safe and pleasant surroundings (factor 1) | 104 | –1.23 (0.57) | 0.03 | –0.00 (0.28) | 1.00 | –3.54 (1.51) | 0.02 | –3.54 (1.56) | 0.02 | 1.00 |
| Low traffic (factor 2) | 104 | –0.23 (0.49) | 0.63 | 0.32 (0.32) | 0.32 | –3.50 (1.51) | 0.02 | –3.42 (1.51) | 0.02 | 0.67 |
| Convenience for walking (factor 3) | 104 | –0.75 (0.47) | 0.11 | –0.35 (0.33) | 0.30 | –3.44 (1.52) | 0.02 | –3.70 (1.53) | 0.02 | 0.38 |
| East | ||||||||||
| It is pleasant to walk | 100 | 0.15 (0.15) | 0.32 | 0.41 (0.97) | 0.67 | 0.10 (1.35) | 0.93 | 0.04 (1.37) | 0.97 | 0.70 |
| There is a park within walking distance | 100 | 0.31 (0.17) | 0.07 | 1.39 (0.85) | 0.10 | 0.10 (1.35) | 0.93 | –0.32 (1.37) | 0.81 | 0.22 |
| There is convenient public transport | 100 | 0.29 (0.19) | 0.12 | 0.20 (0.77) | 0.51 | 0.10 (1.35) | 0.94 | –0.04 (1.38) | 0.97 | 0.55 |
| There are convenient routes for cycling | 99 | –0.12 (0.18) | 0.50 | 0.74 (0.91) | 0.36 | 0.10 (1.34) | 0.94 | 0.19 (1.35) | 0.89 | 0.59 |
| It is safe to walk after dark | 99 | 0.07 (0.17) | 0.66 | 0.58 (0.86) | 0.50 | 0.24 (1.36) | 0.86 | 0.19 (1.36) | 0.89 | 0.71 |
| There is little traffic | 100 | –0.02 (0.19) | 0.91 | –0.99 (0.76) | 0.20 | 0.10 (1.35) | 0.94 | 0.08 (1.35) | 0.95 | 0.91 |
| It is safe to cross the road | 100 | –0.27 (0.19) | 0.15 | –0.26 (0.78) | 0.73 | 0.10 (1.35) | 0.94 | 0.03 (1.38) | 0.98 | 0.74 |
| The surroundings are unattractive | 100 | –0.06 (0.19) | 0.77 | 0.81 (0.76) | 0.28 | 0.10 (1.35) | 0.94 | 0.15 (1.35) | 0.91 | 0.78 |
| There is little green space | 100 | –0.02 (0.23) | 0.94 | 0.00 (0.62) | 1.00 | 0.10 (1.35) | 0.94 | 0.10 (1.36) | 0.94 | 1.00 |
| The nearest shops are too far to walk to | 100 | 0.28 (0.20) | 0.16 | 0.74 (0.74) | 0.31 | 0.10 (1.35) | 0.94 | –0.10 (1.37) | 0.94 | 0.41 |
| There are no convenient routes for walking | 100 | 0.04 (0.19) | 0.82 | 0.06 (0.75) | 0.94 | 0.10 (1.35) | 0.94 | 0.10 (1.36) | 0.94 | 0.94 |
| People are likely to be attacked | 99 | 0.02 (0.17) | 0.89 | 2.27 (0.82) | 0.01 | 0.09 (1.36) | 0.94 | 0.04 (1.31) | 0.97 | 0.89 |
| There is a lot of traffic noise | 99 | –0.11 (0.15) | 0.50 | 1.65 (0.92) | 0.07 | 0.07 (1.36) | 0.96 | 0.24 (1.35) | 0.86 | 0.52 |
| The roads are dangerous for cyclists | 99 | –0.10 (0.18) | 0.57 | 0.61 (0.78) | 0.44 | 0.10 (1.34) | 0.94 | 0.16 (1.35) | 0.90 | 0.65 |
| Safe and pleasant surroundings (factor 1) | 98 | 0.17 (0.40) | 0.68 | 0.79 (0.35) | 0.02 | 0.23 (1.36) | 0.87 | 0.10 (1.33) | 0.94 | 0.69 |
| Low traffic (factor 2) | 98 | –0.52 (0.40) | 0.19 | –0.03 (0.36) | 0.93 | 0.06 (1.34) | 0.96 | 0.05 (1.36) | 0.97 | 0.93 |
| Convenience for walking (factor 3) | 100 | 0.61 (0.41) | 0.14 | 0.42 (0.35) | 0.23 | 0.10 (1.35) | 0.94 | –0.15 (1.36) | 0.91 | 0.35 |
List of abbreviations
- AIC
- Akaike information criterion
- ARIMA
- autoregressive integrated moving average
- CEDAR
- Centre for Diet and Activity Research
- CI
- confidence interval
- CSO
- Chief Scientist Office
- EIA
- Environmental Impact Assessment
- GCPH
- Glasgow Centre for Population Health
- GIS
- geographical information system
- GLM
- generalised linear model
- GPS
- global positioning system
- IPAQ
- International Physical Activity Questionnaire
- ITS
- interrupted time series
- MCS-8
- mental component summary of the Short Form 8 Health Survey
- MRC
- Medical Research Council
- MVPA
- moderate-to-vigorous physical activity
- NICE
- National Institute for Health and Care Excellence
- OR
- odds ratio
- PCS-8
- physical component summary of the Short Form 8 Health Survey
- PLI
- Public Local Inquiry
- RRR
- relative risk ratio
- SCDC
- Scottish Community Development Centre
- SD
- standard deviation
- SF-8
- Short Form 8 Health Survey
- SHS
- Scottish Household Survey
- SIMD
- Scottish Index of Multiple Deprivation
- SWEMWBS
- short version of the Warwick–Edinburgh Mental Well-being Scale
- T1
- time point 1
- T2
- time point 2