

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 12/3060/03. The contractual start date was in March 2014. The final report began editorial review in January 2017 and was accepted for publication in June 2017. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Laurence Moore and Rona Campbell are Scientific Advisors to DECIPHer IMPACT, a not-for-profit organisation that licenses the ASSIST smoking prevention programme. Adam Fletcher, Rona Campbell, Matthew Hickman and Chris Bonell are members of the National Institute for Health Research Public Health Research Research Funding Board.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2017. This work was produced by White et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2017 Queen’s Printer and Controller of HMSO
Chapter 1 Background to the research
Definitions of illicit drug use and legislative framework governing use
Illicit drugs are those for which non-medical use is prohibited by international drug control treaties. 1 This includes plant-based substances (e.g. cannabis, cocaine, heroin) and synthetic substances such as amphetamine-like stimulants, novel psychoactive substances and prescription opioids. In the UK, illegal drugs are controlled substances defined in the 1971 Misuse of Drugs Act2 or determined to be capable of producing a psychoactive effect and not exempted by the 2016 Psychoactive Substances Act. 3 Glues, gases and aerosols (GGAs) also face restrictions on sales to those aged < 18 years under the Cigarette Lighter Refill (Safety) Regulations 19994 and Anti-social Behaviour Act 2003. 5 Henceforth, GGAs will be classified as illicit drugs.
The prevalence of illicit drug use in school-age adolescents
In the UK, over the past 10 years there has been a steady decline in the number of students aged 11–15 years in England who report ever having tried drugs, from 26% in 2004 to 15% in 2014. 6 In 2014, 10% of 11- to 15-year-olds had used drugs in the last year, a decrease from 18% in 2004. The proportion who have ever used drugs increases with age: in 2014, 6% of 11-year-old children reported having used drugs, which increased to 24% for 15-year-olds. 6 The proportion of children using drugs in the last month increases with age, reaching 12% in 15-year-olds. In total, 8% of 11- to 15-year-olds had tried cannabis, 6.8% had tried GGAs and 1% had tried cocaine, ecstasy and magic mushrooms. 6
Direct harms to health associated with illicit drug use
The latest Global Burden of Disease Study found that the risk factors for disability-adjusted life-years (DALYs) attributable to drug use disorders in young people had increased between 1990 and 2013. 7 One DALY represents the loss of the equivalent of 1 year of full health. Across 188 countries, drug use disorders were ranked 14th in the causes of DALYs in 10- to 14-year-olds; fifth in 15- to 19-year-olds (behind alcohol misuse, unsafe sex, iron deficiency and unsafe water), up from sixth in 1990; and second in 20- to 24-year-olds (behind alcohol misuse), up from fourth in 1990.
In the UK, the direct harms to health associated with drug use in school-age children are mainly attributable to cannabis and GGA use. Around 10% of cannabis users will become dependent on it8 and it is the primary reason for seeking specialist drug treatment in the UK in those aged < 18 years. 9 In 2014/15, 13,454 (73%) 11- to 18-year-olds receiving specialist drug treatment did so primarily for cannabis use. 9 The proportion of young people seeking treatment for cannabis use has been on an upwards trend since 2005/6 (from 55%, n = 9043). The median age at first treatment was 16 years. 9
A number of cohort studies have shown that regular cannabis users have lower attendance rates and are more likely to leave school10,11 and have a lower level of educational achievement. 12 In the Avon Longitudinal Study of Parents and Children (ALSPAC) birth cohort,13 lifetime cannabis use by 15 years of age was associated with a 2-point lower mathematics General Certificate of Secondary Education (GCSE) score, a 48% increased risk of not attaining five or more GCSEs and a threefold increased risk of leaving school, or having no qualifications, after adjusting for prior key stage 2 results, parental substance misuse, gender and concurrent drug and tobacco use. Stronger associations were found for weekly cannabis use. 13 This is consistent with case–control studies, which have found poorer verbal learning, memory and attention in those who regularly use cannabis than in those who do not. 14
Indirect harms of drug use for health
Illicit drug use may indirectly affect health by limiting opportunities for employment and educational attainment resulting in exclusion from school.
In the UK, in 2014/15 there were 607 (3% of all offences) proven offences (defined as a reprimand, warning, caution or conviction) that were drug related among 10- to 14-year-olds, increasing to 6922 cases (10.3%) in 15- to 17-year-olds. 15 There were 142 guilty verdicts delivered at courts attributable to drug offences among 10- to 14-year-olds (5.5% of all indictable offences), increasing to 2480 (17.2%) among 15- to 17-year-olds. 15 All offences and convictions are subject to disclosure to a potential employer under the Rehabilitation of Offenders Act 197416 if the role requires, such as when working with children or vulnerable adults, within law, health-care and pharmacy professions and in some senior management posts and when matters of national security are involved. The exact impact of drug convictions on employment is not known.
In 2014/15 there were 480 permanent (10%) and 7900 fixed-period (3.3%) drug- and alcohol-related exclusions in state-funded secondary schools in England. 17 These data do not disaggregate between illicit drug use and alcohol use.
Evidence on the effectiveness of school-based drug prevention
In response to a commissioning brief published by the National Institute for Health Research (NIHR) inviting applications to examine using peer support to prevent illicit drug uptake in young people (reference 12/3060), we conducted a scoping review of relevant systematic reviews and randomised controlled trials (RCTs). The effectiveness of school-based drug prevention has been examined in a 2014 Cochrane systematic review. 18 In this review, 51 RCTs of universal (i.e. provided to all) school-based prevention interventions were identified, with only two studies from the UK. The interventions reviewed showed, on average, no protective effect on drug use after 12 months. In terms of what types of interventions are effective, interventions that aim to increase knowledge did not lead to changes in drug use behaviour, whereas those aiming to increase social competences (i.e. teaching self-management, social skills, problem-solving, skills to resist media and interpersonal influences, how to cope with stress) or based on social influence theories (i.e. correcting overestimates of the prevalence of drug use, increasing awareness of media, peer and family influences, practising refusal skills) increased knowledge about drugs but had small and inconsistent effects on drug use at ≥ 12 months. The six studies that examined interventions using components from both social competence and influence approaches had a small beneficial effect on preventing cannabis use, but no effect on hard drug use (defined as heroin, cocaine or crack) after 12 months. The authors noted that many studies did not describe the randomisation method or account for clustering (non-independence between children in the same school) in their analyses, despite all being cluster RCTs (cRCTs). 18
A second systematic review examined the effectiveness of peer-led interventions to prevent tobacco, alcohol or illicit drug use in 11- to 21-year-olds. 19 Pooled data from the three school-based RCTs reporting a drug use outcome (976 students, 38 schools) suggested that peer-led interventions had a small protective effect on cannabis use at ≥ 12 months. One study in this review, the Towards No Drug Abuse Network (TND-Network) study, which involved nominated peers delivering lessons on drug use, found a small reduction in monthly cannabis use. 20 In a subgroup of students whose friends had already used substances (calculated as a composite of tobacco, alcohol, cannabis and cocaine use), an iatrogenic effect was found whereby monthly cannabis use slightly increased. Contamination was potentially an issue in this study, as classes rather than year groups or schools were allocated. Another school-based drug abuse prevention trial, the European Drug Addiction Prevention (EU-Dap) trial, reported no effect on drug use at 18 months in the peer-led intervention arm,21 but implementation of the intervention in this arm was poor, with only 8% of centres implementing all seven sessions and 71% not conducting any meetings at all.
These reviews identified a number of methodological weaknesses in the evidence base, including small sample sizes, contamination, inadequate reporting of randomisation and outcomes and a failure to account for clustering in cRCTs. 18 Interventions using a combination of social influence and social competence training have had small beneficial effects on knowledge and cannabis use at 12 months’ follow-up. 18 Two peer-led RCTs have shown a small beneficial effect of peer-led interventions on preventing and reducing cannabis use. 19 There were some limitations in the design of these interventions, including the iatrogenic effects in one peer-led study20 and low levels of implementation in another study. 21 This suggests that a more careful approach to intervention design and refinement is needed. In these reviews, no drug prevention interventions were implemented in a UK educational setting.
Rationale for the current study
The rationale for this study was to develop, refine and conduct a pilot cRCT of a new school-based peer-led drug prevention intervention. Specifically, in our study we aimed to adapt an existing, effective, peer-led smoking prevention intervention (ASSIST) that uses components of social influence and competence programmes to deliver information on illicit drug use from the UK national drug education website [see www.talktofrank.com (accessed 29 August 2017)].
ASSIST
The ASSIST intervention is an evidence-based, informal peer-led smoking prevention intervention based on diffusion of innovations theory22 that aims to diffuse and sustain non-smoking norms via secondary school students’ social networks in Year 8 (age 12–13 years). 23 It is part of the tobacco control plans of the Scottish24 and Welsh25 Governments and is recommended by the National Institute for Health and Care Excellence. 26 In the UK, > 120,000 students have taken part in the ASSIST intervention and an estimated 2200 young people have not taken up smoking because of ASSIST who otherwise would have done so. The five stages of ASSIST, as currently delivered, are listed in Table 1.
| Stage | Primary focus | Core tasks |
|---|---|---|
| 1 | Nomination of peer supporters |
|
| 2 | Recruitment of peer supporters |
|
| 3 | Training of peer supporters |
|
| 4 | Intervention period |
|
| 5 | Acknowledgement of peer supporters’ contribution |
|
Talk to FRANK
The Talk to FRANK website (see www.talktofrank.com) was set up by the UK Department of Health and the Home Office in 2003 to provide up-to-date, youth-friendly information and advice on the risks of illicit drug use. Between January and December 2014 there were 5.1 million visits to the FRANK website. 27 In 2013, 18% of 11- to 15-year-olds (increasing from 5% of 11-year-olds to 33% of 15-year-olds) reported that the website was a source of helpful information about drugs. 28 The FRANK website is the most commonly cited source of information by teachers (78%) for preparing lessons on drugs. 6
Information is provided using a number of interactive methods including videos showing the effects of specific drugs, regular updates on the legality and mechanism of effect of new drugs, an A-Z guide of drugs and a frequently asked questions (FAQs) section. Highly rated FAQs include those on the long-term effects of cannabis, the levels of drug use associated with dependence, criminal consequences and the half-life of specific drugs. FAQs are also tailored to young people, parents and health professionals. Support is offered through the website with instant messaging, live chat (available at specific times during the day), an online forum, a confidential 24-hour telephone service and an e-mail or text service. Trained advisors operate this free service and local help can also be found by entering a postcode.
CASE+
There was a previous attempt to adapt the ASSIST intervention to prevent cannabis use. An unpublished feasibility trial (CASE+) in six Scottish secondary schools found little change in intentions to use cannabis in 732 students aged 12–13 year over a 3-month follow-up (Munro A, Bloor M. A Feasibility Study for a Schools-based, Peer-led, Drugs Prevention Programme, Based on the ASSIST Programme: the Results. Centre for Drug Misuse Research Occasional Paper. Glasgow: University of Glasgow; 2009). The intervention included an extra day of education solely on cannabis use in addition to the 2 days of training on smoking in the ASSIST intervention. However, the study had several limitations: (1) no drug use data were collected, (2) 3 months’ follow-up is not long enough to ascertain a likely effect of the intervention over longer periods and (3) the intervention content was solely related to cannabis use.
The process evaluation indicated that, although implementation fidelity and acceptability to school staff was high, students were overwhelmed with the amount of information that they received in the extra day of training on cannabis. The peer supporters also rarely had conversations about cannabis but focused on smoking, because only a few students were experimenting with cannabis at age 12/13 years and there was sensitivity around discussing cannabis use as it is illegal. We decided to adapt the ASSIST model to deliver the information from the FRANK website rather than CASE+ as it has a database of information on illicit drugs and not just cannabis. The FRANK website has demonstrated a large number of hits per year and teachers and young people use it, such that it provides an accessible drug education resource that updates.
Study design
This study was conducted in three stages. Stage 1 involved the development of two new school-based peer-led drug prevention interventions: ASSIST + FRANK (+FRANK) and FRANK friends. Stage 2 involved the delivery of the interventions in one school each, conducting a process evaluation and using this information to refine the interventions. Stage 3 was a four-arm pilot cRCT (+FRANK, FRANK friends, ASSIST and usual practice) with an embedded process evaluation. The ASSIST arm was used to investigate any potential indirect effects of a smoking prevention intervention on drug use.
Aim and objectives
The overall aim of this study was to assess the feasibility, acceptability and fidelity of delivery of the +FRANK and FRANK friends interventions to inform a full-scale RCT.
The objectives were to:
-
refine the ASSIST logic model to drug prevention and develop the ASSIST + FRANK and FRANK friends interventions
-
test the feasibility of the +FRANK and FRANK friends interventions in one school each and
-
assess the acceptability of the intervention to trainers, students, parents and school staff and explore the barriers to and facilitators of implementation
-
explore the fidelity of intervention delivery by +FRANK and FRANK friends trainers and peer supporters
-
refine the interventions
-
-
conduct a pilot cRCT of the +FRANK and FRANK friends interventions to
-
assess the feasibility and acceptability of the refined interventions to trainers, students, parents and school staff
-
assess the fidelity of intervention delivery by trainers
-
compare the feasibility and acceptability of the interventions
-
assess trial recruitment and retention rates
-
pilot outcome measures
-
record the delivery costs and pilot methods for assessing cost-effectiveness
-
-
determine the design, structures, resources and partnerships necessary for a full-scale trial to take place.
Chapter 2 Methods
Design
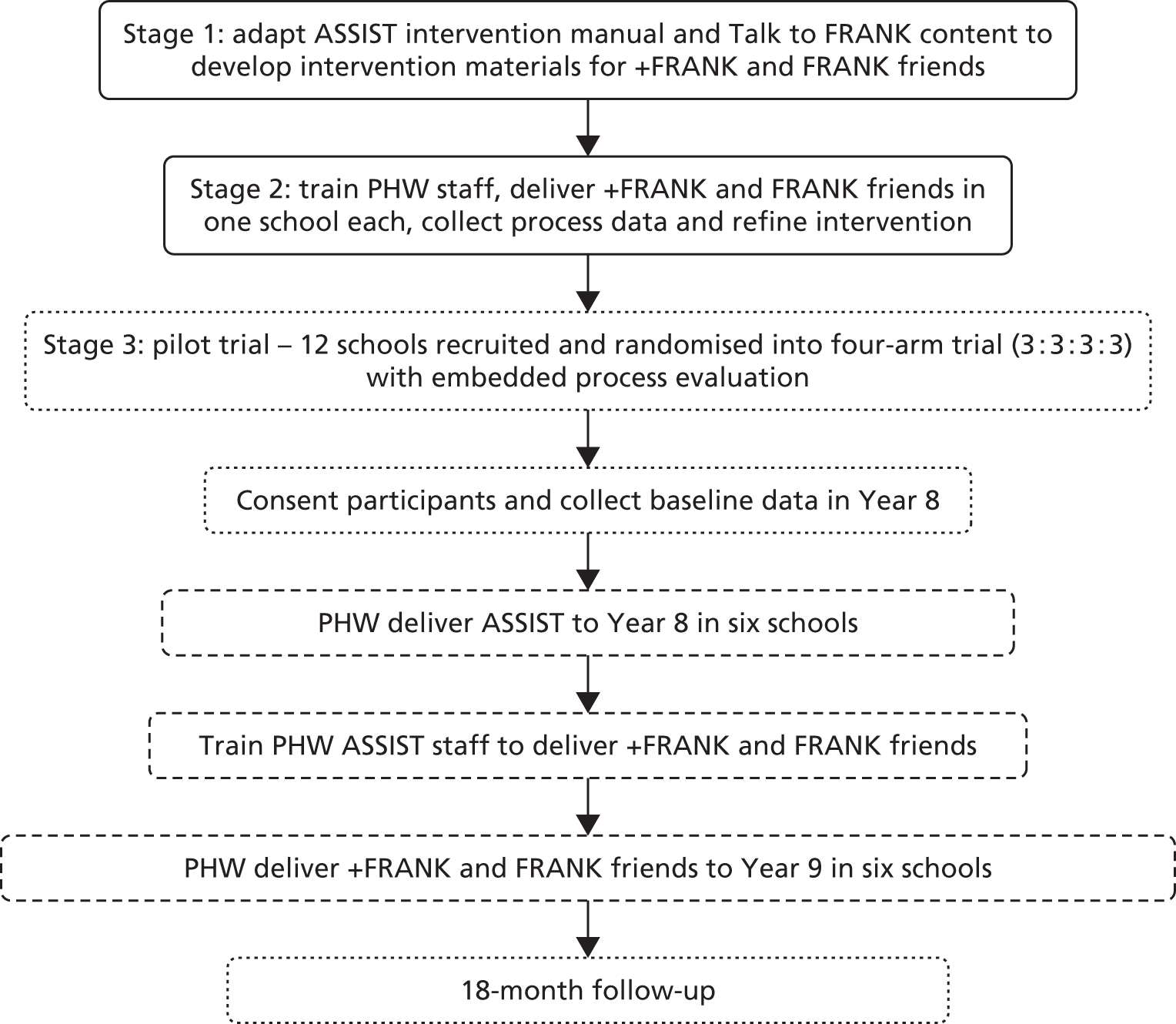
The three stages of the project are described in Figure 1.
FIGURE 1.
Study schema. Note: stages did not take place in chronological order. The ASSIST intervention was delivered in Year 8 and the baseline data collection for the pilot trial (stage 3) took place before the piloting of the +FRANK and FRANK friends interventions. Dashed lines indicate stages that were part of the pilot cRCT. PHW, Public Health Wales.
Setting
The study took place in seven local authorities in South Wales (Cardiff, Newport, Torfaen, Blaenau Gwent, Rhondda Cynon Taf, Merthyr Tydfil and Caerphilly). With a projected population of 1,155,800 in 2016, these local authorities represent 36.9% of the Welsh population. 29 Fourteen out of the 72 secondary schools across the seven local authorities participated. Two schools received one of the interventions each in stage 2. Twelve schools were involved in stage 3, the pilot cRCT.
Ethics approval and monitoring
The study was granted ethics approval by Cardiff University School of Social Sciences Research Ethics Committee (reference SREC/1103). NHS research and development (R&D) approval was also granted, as Public Health Wales (PHW) staff delivered the interventions (reference 2013PHW0015).
Trial monitoring
The ongoing conduct and progress of the study was monitored by an independently chaired Trial Steering Committee (TSC). The membership included independent scientific experts, representation from the Department of Health, policy leads for children and young people in PHW and a parent representative.
Interventions
We present here an outline of each intervention provided at the time of the submission of the proposal for funding. The content of the activities and the method of delivery had yet to be developed. Both interventions underwent revision during stages 1 and 2.
+FRANK: an informal peer-led drug prevention adjunct to ASSIST
+FRANK is an informal peer-led intervention to prevent drug use in UK Year 9 secondary school children. A summary of the +FRANK intervention is provided in Table 2.
| Stage | Primary focus | Core tasks |
|---|---|---|
| 1. | Re-engagement of ASSIST peer supporters |
|
| 2. | Recruitment |
|
| 3. | Training of peer supporters |
|
| 4 | Intervention period |
|
| 5 | Acknowledgement of peer supporters’ contribution |
|
FRANK friends: an informal peer-led drug prevention intervention
FRANK friends is a standalone informal peer-led intervention to prevent drug use in UK Year 9 secondary school children. It replicates the format of the ASSIST intervention in the peer nomination process, the 2 days of off-site training and the four face-to-face follow-up visits. The +FRANK intervention includes only 1 day of off-site training. The additional day of training in the FRANK friends intervention is mainly spent developing communication skills, which are covered in training for the ASSIST intervention. A summary of the FRANK friends intervention is provided in Table 3.
| Stage | Primary focus | Core tasks |
|---|---|---|
| 1. | Nomination of peer supporters |
|
| 2. | Recruitment |
|
| 3. | Training of peer supporters |
|
| 4 | Intervention period |
|
| 5 | Acknowledgement of peer supporters’ contribution |
|
Stage 1: development of the +FRANK and FRANK friends interventions
We used a three-phase multimethod framework to guide the adaptation of the ASSIST smoking prevention intervention to develop content, resources and delivery methods for the +FRANK and FRANK friends interventions (Figure 2). 30 The methods used at each stage allowed for integration of the scientific literature with key stakeholders’ knowledge and expertise. Key stakeholders included people with direct experience or knowledge of youth drug taking, recipients of the existing ASSIST smoking prevention intervention, intended recipients of the newly developed interventions and those who delivered any existing drug prevention interventions within the setting (i.e. schools) or who provided intervention resources (e.g. financing, staffing).
FIGURE 2.
Framework for intervention coproduction and prototyping. a, Stakeholders comprise those within or external to the delivery setting (e.g. school-based: school teachers, head teacher, contact teacher, head of year, receptionist, head of personal, social, health and economic education; national and local policy leads; and parents/guardians/carers.

Phase 1: evidence review and stakeholder consultation
Evidence review
We conducted a scoping review of systematic reviews and RCTs of school-based drug prevention. We also examined the latest population-based randomly sampled surveys on the prevalence of illicit drug use in school-age children in the UK.
Consultations with young people
We gathered multiple perspectives about drug use and existing drug education to tailor the intervention content to increase acceptability within the school context and population. Our aim was to maximise acceptability and reduce problems with implementation. This involved a range of methods.
Focus groups with young people
Six focus groups were conducted with 47 young people aged 13–15 years, who were purposively sampled from three schools, a youth centre and a student referral unit. A semistructured topic guide was used with broad open-ended questions relating to participatory task-based activities using resources based on the Talk to FRANK website.
Interviews with the ASSIST intervention delivery team
Interviews were conducted with five members of the PHW ASSIST delivery team.
Structured observations of current practice
Structured observations of all five stages of ASSIST intervention delivery were conducted (n = 8), as well as one observation of the ASSIST ‘Train the Trainers’ course.
Stakeholder consultation
A range of informal consultations was also conducted with young people and practitioners, one with five volunteers from a young people’s public involvement group aged 16–19 years; one with seven young people aged 13–15 years; one with five recipients of the ASSIST intervention aged 12–13 years; and nine individual consultations with health professionals working for drug agencies (n = 4), with young people (n = 4) or both (n = 1).
Audio recordings from interviews and focus groups were transcribed verbatim and analysed using thematic analysis. Researcher field notes from observations and informal consultations were combined with the data from the interviews and focus groups. An a priori coding framework focused on assessing the acceptability of the content and delivery of the intervention. An element of flexibility was maintained in coding such that data that did not fit the framework were also captured in an inductive manner. This approach to analysis has been described in detail elsewhere. 31 The findings from the analyses fed into the coproduction of intervention content during phase 2.
Phase 2: coproduction
An intervention development group (IDG) was established consisting of members of the research team and the PHW ASSIST delivery team. The PHW team had delivered the ASSIST intervention to > 350 schools over a period of 7 years and so had extensive experience of intervention delivery within schools. The aim of the IDG was to adapt the ASSIST intervention materials to deliver information from the Talk to FRANK website, informed by the findings from phase 1.
Coproduction of intervention content took the form of an action research cycle over a series of meetings of the IDG at which findings from stage 1 were considered, ideas were presented by all members, feedback on ideas was sought and refinements were made and presented again, until the final content was agreed. Five face-to-face meetings were held over the course of a 4-month period. These were supplemented by communications by e-mail when face-to-face meetings were not possible or when matters arose that required discussion between meetings.
Phase 3: prototyping
After a first draft of the +FRANK and FRANK friends interventions had been developed, the manuals and resources (e.g. fact sheets on the effects of cannabis on mental health) underwent expert review. Two experts were asked to examine key uncertainties identified during phases 1 and 2. The lead author of the ASSIST cRCT23 examined the fit of the activities with diffusion of innovations theory,22 on which the ASSIST intervention was based. The lead trainer of DECIPHer IMPACT (Bristol, UK), the company that licenses ASSIST, and reviewers examined the age appropriateness of the activities and the suitability of the timings and sequencing of activities.
Preliminary feedback on acceptability and feasibility was collected during training of the PHW intervention delivery staff. Training involved the delivery of the two interventions to the IDG. Feedback was also sought from ASSIST trainers at a DECIPHer IMPACT ‘Train the Trainer’ course. The interventions were also delivered to a young people’s public involvement group (aged 16–19 years). Feedback was sought from young people on each activity, with a particular emphasis on relevance for their age group and interest in and engagement with the content.
Stage 2: delivery and refinement of the +FRANK and FRANK friends interventions
The +FRANK and FRANK friends interventions were delivered in one school each. The aim was to conduct a detailed process evaluation examining the acceptability and feasibility of the intervention from the perspective of teachers [contact and school management team (SMT) members], peer supporters and trainers within the school context.
Figure 3 provides an overview of the process and methods used to refine the intervention content and delivery mechanism.
FIGURE 3.
Framework for refining the intervention content and delivery mechanism.

Public Health Wales identified eligible +FRANK schools for the initial feasibility testing as the schools were required to have received the ASSIST intervention in Year 8. Eligible FRANK friends schools were required to have not received the ASSIST intervention in Year 8. The order of invitation was not determined by any defined method. The interventions were delivered over two different terms because of a lack of capacity in the PHW team to deliver them concurrently. The +FRANK intervention was delivered first followed by the FRANK friends intervention. Information was collected to determine acceptability and feasibility to inform refinements to the intervention manuals and associated resources in preparation for the pilot trial. This involved a range of methods.
Structured observations, evaluation forms and interviews
Independent structured observations were undertaken by two researchers of all intervention activities, including recruitment, re-engagement, training and follow-up visits. Observation forms captured whether or not objectives for the sessions and learning outcomes for activities were met using a traffic light system. Green indicated that the activity had been fully delivered with all objectives met, amber indicated minor deviations in delivery and red highlighted that activity objectives had not been met. The timings of the activities delivered were also recorded along with notes on any deviations to the timetable and/or activity instructions. Trainers completed self-assessment forms following each delivery episode to capture their perceptions of the delivery for each aspect of intervention delivery and training.
Evaluation forms were completed by peer supporters and trainers at the end of the off-site training days and final follow-up visit. Interviews were conducted with peer supporters, trainers, contact teachers and members of the SMT after the last follow-up. Interviews with peer supporters were conducted individually, in pairs or in small groups, to suit the requirements of the school. Additional interviews were conducted with trainers and students after delivery in the two schools that took part in the initial feasibility testing.
Interviews were conducted with peer supporters using a semistructured topic guide to explore all parts of the interventions, particularly what did and did not work, with a view to identifying areas for potential refinement. Interviews with school staff explored the intervention delivery, methods and processes. Interviews with SMT members explored their awareness and understanding of the interventions, the information that they had received and their overall impressions of the intervention. Audio recordings of interviews were transcribed verbatim and anonymised at the point of transcription. This included removing personal names, school names and any other identifying information. Qualitative data analysis was facilitated by the use of NVivo 10 (QSR International, Warrington, UK), a qualitative data analysis software programme.
A framework analysis was employed. 32 A coding matrix was used to index and categorise data, with categories and themes being predetermined based on the research objectives (e.g. feasibility of delivery of the intervention components, acceptability of the intervention components to peer supporters) and with any unexpected themes identified being added. Data collected from the structured observations and self-assessments were organised in descriptive ‘chunks’ for each component/activity within the interventions. Identification of recurring and salient themes was examined against this framework. Two coders agreed on the framework and then referred to an additional two independent members of the research team to discuss/resolve any discrepancies and reach a consensus. To agree on refinements to intervention resources and delivery mechanisms, the results were shared with the Trial Management Group (TMG) and IDG.
Stage 3: external pilot cluster randomised controlled trial
The external pilot trial was a parallel, four-arm cRCT with school as the unit of randomisation. The investigator team, students and staff were unblinded and fieldworkers were blinded. The primary aim of the pilot trial was to assess the feasibility and acceptability of the intervention and trial methods and gather data to plan a future full-scale trial. This included estimating rates of eligibility, recruitment and retention at the 18-month follow-up, as well as the acceptability, reliability and rates of completion of pilot primary and secondary outcome measures.
Eligibility criteria and recruitment
The pilot trial was embedded within the 2014/15 delivery of the ASSIST intervention by PHW. As part of the Welsh Government’s Tobacco Control Action Plan, PHW was funded to deliver the ASSIST intervention to 50 schools a year. The Welsh Government provided PHW with a list of approximately 160 schools eligible for the ASSIST intervention out of the 220 secondary schools in Wales. The Welsh Government informed PHW that schools were selected on the basis of having a high percentage of children in receipt of free school meals (FSMs) and schools were in relatively deprived areas according to the Welsh Index of Multiple Deprivation (WIMD). 33 The Welsh Government did not provide the exact cut-off points applied for FSMs or the WIMD to exclude schools. From this list PHW recruited schools from the counties of Cardiff, Newport, Torfaen, Blaenau Gwent, Rhondda Cynon Taf, Merthyr Tydfil and Caerphilly, inviting those that had not received the ASSIST intervention in the past 2 years. Out of the 72 schools in these counties, 40 had not received the ASSIST intervention in the last 2 years and formed our sampling frame. These schools were sent a project information sheet, reply envelope and form asking them to contact PHW or the principal investigator if they wished to be involved in the study. Non-responders were followed up with a reminder and telephone call from the study manager (KM). All interested schools were visited by the study manager to discuss the study in more detail.
Consent
Head teachers signed a memorandum of understanding before taking part in the study describing the roles and responsibilities of both the intervention delivery and the research teams and the timeline of intervention delivery and assessments. Letters were sent to parents/guardians asking them to contact the school if they did not wish their child to participate in the trial. Parents who did not wish their child to participate were able to opt their child out of data collections. Written consent detailing the right to withdraw was sought from all participants. At all data collection points, age-appropriate information sheets were provided, together with a verbal explanation by researchers on the right to withdraw.
Sample size
As this was a pilot trial a power calculation was not required. The estimated sample size at baseline was 1440 students across 12 schools (n = 360 per arm), chosen to provide some information on variability within and between schools at baseline and follow-up. This sample was not anticipated to provide adequate power to detect a statistically significant difference across groups. However, the sample was used to indicate the likely response rates and permit estimates [with 95% confidence intervals (CIs)] of intraclass correlation coefficients (ICCs) of drug prevalence in anticipation of a larger cRCT. 34
Randomisation
Schools agreed to take part prior to randomisation. The study used an assignment ratio of 1 : 1 : 1 : 1. Allocation was conducted by the study statistician, blind to the identity of schools, and minimised on the median percentage of students in receipt of FSMs (below/above median) and median school size (below/above median) to balance the randomisation. Optimal allocation was used to carry out the randomisation. 35
Interventions
The +FRANK and FRANK friends interventions delivered in the external pilot cRCT are described in Tables 2 and 3, respectively. Delivery of the +FRANK and FRANK friends interventions occurred between September and November 2015. In the +FRANK arm, peer nomination was repeated to examine the proportion of students nominated in Year 8 who were renominated in Year 9.
Usual practice
Children participated in their usual personal, social, health and economic education (PSHE) lessons provided by the schools. All schools followed a national PSHE curriculum, which may include education on drug use and smoking.
Quantitative data collection process
The consent procedure and questionnaires were self-reported. All data were collected by fieldworkers. Questionnaires were completed in school halls or classrooms under examination conditions. Researchers, fieldworkers and dedicated school staff helped children with literacy problems and special educational needs. Baseline data collection took place between 17 September and 20 October 2014, prior to randomisation. Follow-up data collection took place 18 months later between 22 March and 5 May 2016. To increase response rates, additional collections were made for students who were absent. Schools were paid £300 for staff cover for the data collections after the 18-month follow-up.
Outcome measures
The main study outcomes were operationalised as progression criteria. Progression criteria were agreed by the TMG, TSC and NIHR Public Health Research (PHR) Research Funding Board. Assessment methods used a mix of quantitative and qualitative data. Table 4 shows the research questions that the progression criteria addressed, the data collection methods and the sources of data used.
| Research question | Progression criteria | Data collection method | Data examined |
|---|---|---|---|
| 1. Was it feasible to implement the +FRANK intervention in (at least) two out of three intervention schools? | ≥ 75% of Year 8 ASSIST peer supporters are recruited and retrained as +FRANK peer supporters in Year 9 | Attendance records | Percentage of students who completed ASSIST training in Year 8 attending the recruitment and training sessions for +FRANK |
| PHW staff delivered the +FRANK training in full in all three intervention schools | Structured observations of training and follow-up sessions | Number of predefined learning outcomes met at training and follow-up sessions | |
| Interviews with trainers | Facilitators of and barriers to delivering the intervention activities | ||
| 2. Was it feasible to implement the FRANK friends intervention in (at least) two out of three intervention schools? | ≥ 75% of Year 9 students nominated are recruited and trained as FRANK friends peer supporters | Attendance records | Percentage of students who were nominated to be FRANK friends peer supporters attending the recruitment and training sessions |
| PHW staff delivered the FRANK friends training in full in all three intervention schools | Structured observations of training and follow-up sessions | Number of predefined learning outcomes met at training and follow-up sessions | |
| Interviews with trainers | Facilitators of and barriers to delivering the intervention activities | ||
| 3. Was the intervention acceptable to students trained as +FRANK peer supporters? and 4. Was the intervention acceptable to students trained as FRANK friends peer supporters? | ≥ 75% of +FRANK and FRANK friends peer supporters report having at least one or more informal conversations with their peers at school about drug-related risks/harms |
|
|
| ≥ 75% of +FRANK and FRANK friends peer supporters report ongoing contact with PHW staff throughout the year through follow-up visits |
|
|
|
| 5. Was the +FRANK intervention acceptable to the majority of SMTs, other school staff and parents? and 6. Was the FRANK friends intervention acceptable to the majority of SMTs, other school staff and parents? |
|
|
|
|
|||
| 7. Were the trial design and methods acceptable and feasible? | Randomisation occurred as planned and was acceptable to SMTs | Interviews with SMT staff |
|
| A minimum of five out of six intervention schools and two out of three schools from the comparison arms participate in the 18-month follow-up | Study records |
|
|
| Student survey response rates are acceptable at baseline (80%+) and follow-up (75%+) | Attendance records |
|
Self-reported outcome measures
The self-report questionnaires included items to assess the anticipated primary outcome in a future full-scale trial, the lifetime prevalence of illicit drug use, using questions from the ALSPAC cohort. 36 At baseline, students were asked whether they had ever tried 10 drugs that had a > 1% prevalence in 13- to 14-year-olds in the 2013 Smoking, Drinking and Drug use survey,37 with an additional ‘other’ open response category. At follow-up an additional seven drugs were added. Street names were also provided for all drugs and a fictitious drug (semeron) was used to examine false responding. We also examined a number of potential secondary outcomes in this population: frequency of use of each drug in the past 12 months, last 30 days and last week; cannabis dependence using the Cannabis Abuse Screening Test (CAST);38,39 lifetime smoking and weekly smoking status (weekly defined as smoking at least one or more cigarette a week40); number of cigarettes smoked every day; nicotine dependence using the Fagerström Test for Nicotine Dependence (FTND)41 and Heaviness of Smoking Index (HSI);41,42 lifetime alcohol consumption; the frequency of heavy episodic alcohol use using the Adolescent Single Alcohol Question (A-SAQ), which is a modified version of the modified Single Alcohol Screening Questionnaire;43 and health-related quality of life, using the Child Health Utility-9 Dimensions (CHU-9D) measure. 44,45
Self-reported measures of intermediary factors
To examine the hypothesised mechanisms of action described in the logic models, we examined a number of intermediary factors. These included the perceived lifetime prevalence of drug use in Year 9, the frequency of drug offers, conversations with friends about drugs and visiting the Talk to FRANK website, ever having talked to a peer supporter about drugs, whether students would get help for themselves or a friend from the Talk to FRANK website if they had a problem and knowledge about drugs calculated as the number of correct answers from eight true or false questions about drugs (see Appendix 1, Table 16).
Statistical analysis
Statistical analyses were largely descriptive. The eligibility, recruitment and retention rates for schools and students were summarised using a Consolidated Standards of Reporting Trials (CONSORT) diagram (see Figure 7). 46,47 The data collected for trial participants were summarised by trial arm and combined across arms. To examine the acceptability of potential outcome measures the percentage of missing values are reported for all variables. Categorical variables were summarised using the percentage in each category. Numerical variables were summarised using the mean, standard deviation (SD) and a five-number summary (minimum, 25th percentile, median, 75th percentile, maximum). We present mean and median values to examine the shape of each distribution. We estimated the percentage of recanted responses, whereby individuals indicated having never used a drug at follow-up but indicated that they had used at baseline, as a measure of reliability. Comparisons were made between those who completed the study and those who dropped out of the study. ICCs were calculated. Exploratory effectiveness analyses using multilevel linear and logistic regression models adjusting for gender, age, FSM entitlement and residence with an adult in employment were conducted for indicative outcome and intermediary variables. We fitted an interaction term to examine effects in students who had and had not used drugs at baseline. If the ICC was < 1 × 10–8, a single-level model was used. All analyses used intention-to-treat populations.
Cost analysis
We estimated the cost of delivering the +FRANK and FRANK friends interventions. The cost and cost-effectiveness of the ASSIST intervention has been previously reported. 48 We aimed to provide preliminary evidence on the likely affordability of these interventions and also pilot methods of data collection. We focused on additional costs, over and above those of usual practice, that would be incurred by the public sector (i.e. PHW and schools/education authorities). We did not track or cost the resources used in development or the feasibility testing of the +FRANK or FRANK friends interventions (i.e. stages 1 and 2) as once manuals and resources are developed these are sunk costs. We also excluded the costs of the ‘Training the Trainers’ session as these are artificially high in a pilot trial setting where the training costs are spread over a small number of schools. However, it is important to recognise that some costs associated with updates to the intervention and PHW staff training, because of staff turnover, would be needed if the intervention is used routinely.
We recorded the time spent and other costs of administrating (e.g. contacting schools, arranging venues) and delivering (e.g. intervention days and follow-up sessions) the intervention. The cost of delivering the intervention was predominantly for room hire, catering, PHW staff time, transport costs and intervention consumables (e.g. text messaging service). PHW estimated unit costs for PHW staff time and transport, as well as expenses incurred for room hire, catering, student transport (i.e. coach hire) and consumables.
Process evaluation
The process evaluation examined the feasibility and acceptability of the two interventions from the perspectives of peer supporters, schoolteachers, intervention delivery staff, parents and a public health commissioner. Researcher notes were taken at each stage of intervention delivery, including the training of intervention delivery staff, nomination of peer supporters, training of peer supporters and post-intervention delivery (to assess objectives 3a–c; see Chapter 1).
Two staff members conducted structured observations to assess whether the defined learning outcomes of all intervention activities were met. Observations of the delivery of all intervention activities, across all sites, were made by two members of the research team to examine the fidelity of intervention delivery.
In each school, one member of the SMT plus the contact teacher, head of year or PSHE lead were interviewed. Post-intervention interviews were also conducted with a purposive sample of peer supporters in schools with the highest and lowest prevalence of drug use. All interviews were audio recorded, fully transcribed and anonymised and electronically stored on a secure server. Table 5 provides an outline of the methods used at each stage of the process evaluation in the external pilot, as well as the issues examined.
| Stage | Method | Issues examined |
|---|---|---|
| Recruitment and re-engagement of influential students | Record of participation | Response rates |
| Researcher observations | ||
| Trainer feedback form | ||
| Peer supporter training | Record of participation | Attendance/engagement |
| Researcher observations | Intervention fidelity | |
| Post-training evaluation form completed by peer supporters | Acceptability to peer supporters | |
| Interviews with trainers | Explore acceptability and feasibility of delivering the intervention training | |
| Follow-up visits | Record of participation | Retention rates/engagement |
| Researcher observations | Intervention fidelity | |
| Post-intervention evaluation form completed by peer supporters | Acceptability of content and role as a peer supporter | |
| Post intervention | Interviews with peer supporters | Acceptability of intervention content, delivery method and role of peer supporter |
| Interviews with teaching staff | Acceptability of intervention content and delivery method and feasibility of intervention delivery | |
| Interviews with trainers | Acceptability of intervention content and delivery method and feasibility of intervention delivery | |
| Interviews with parents | Acceptability of intervention content, delivery method and role of peer supporter |
Qualitative data analysis
Thematic analysis was employed in the qualitative analysis. 32 The deductive coding framework developed in stage 2 feasibility testing was adapted to examine the feasibility and acceptability of the intervention against progression criteria. We used a coding matrix to index and categorise data, with categories and themes being predetermined based on the research objectives (e.g. feasibility of delivery of the intervention components, acceptability of the intervention components to peer supporters), with flexibility maintained so that any unexpected themes identified from the data could also be added. A sample of six transcripts was coded and compared and regular data analysis meetings were held by the qualitative research team to discuss emerging themes and ensure consistency in coding. Analysis was conducted using NVivo 10 software to assist with the systematic coding of data to identify patterns in the narrative provided by teachers, peer supporters, students, parents and schools.
Changes to the protocol
There were no major changes to the protocol. 49 In the statistical analysis section we stated that we would adjust for baseline levels in the analysis of lifetime drug, smoking and alcohol use at the 18-month follow-up. However, we did not adjust for lifetime measures of use at baseline or conduct subgroup analyses in baseline users. This is because with lifetime measures adjustment creates a situation of perfect prediction. As baseline users can only remain users at 18 months, estimates for students who report lifetime use at baseline cannot be calculated. A request for a 3-month non-financial extension was granted towards the end of the study.
Chapter 3 Results
This chapter presents the results of the study, which are organised according to the three stages of the study: (1) development of the +FRANK and FRANK friends interventions, (2) feasibility testing of the +FRANK and FRANK friends interventions and (3) external pilot cRCT.
Stage 1: development of the +FRANK and FRANK friends interventions
The development process took 18 months and consisted of 42 activities (Figure 4 shows the frequency and timeline of each activity). The process was iterative and cumulative, with refinements made before proceeding to the next stage.
FIGURE 4.
Frequency and timeline of each activity in the development of the +FRANK and FRANK friends interventions. ALPHA, Advice Leading to Public Health Advancement.
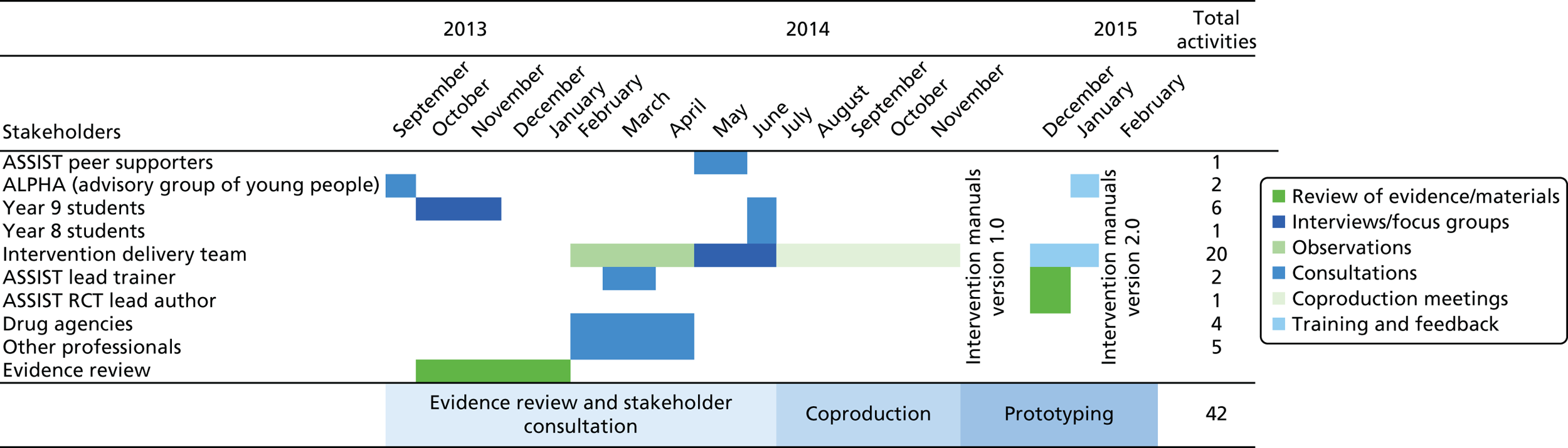
Table 6 summarises the results from stage 1.
| Activity | Objectives | Results |
|---|---|---|
| Phase 1: evidence review and stakeholder consultation | ||
| Evidence review | Identify target age group for the interventions and identify target drugs to focus the intervention content on |
|
| Consultation with young people’s involvement group | Explore thoughts about drug education in school, young people’s conversations about drugs with friends, awareness of Talk to FRANK and opinions of the website |
|
| Consultation with Year 9 students | Explore views about drug use in their age group and ideas about content for a drug prevention intervention |
|
| Focus groups with Year 9 students | Explore knowledge and risk perceptions of drug use and perceptions of drug use prevalence in their age group and the acceptability and age appropriateness of drug education messages on the Talk to FRANK website |
|
| Consultations with stakeholders (drug agencies and professionals who work with young people) | Explore awareness of drug education resources and support and views on appropriate content for a drug prevention intervention |
|
| Consultations with Year 8 recipients of the ASSIST intervention | Explore ideas about peer supporter training and content for a drug prevention intervention |
|
| Observations of current ASSIST practice | Identify aspects of the intervention that work well and could be adapted for use to deliver a drug prevention intervention and with a Year 9 population |
|
| Interviews with the intervention delivery team | Identify possible influences on intervention feasibility and acceptability, for example explore aspects of the ASSIST intervention that could be adapted to deliver a drug education intervention and for use with 13- to 14-year-olds, as well as those that might not lend themselves to adaptation |
|
| Phase 2: coproduction | ||
| Meetings of the IDG | Action research cycle of assessment, analysis, feedback and agreement on the core components of the intervention required to educate peer supporters on the harms of drug use and the skills required to communicate these to their peers |
|
| Phase 3: prototyping | ||
| Expert review of intervention materials | Identify potential problems or weaknesses in the intervention materials prior to piloting |
|
| Testing of intervention materials with young people | Delivery of the intervention. Identification of issues around the feasibility and acceptability of the newly developed intervention content |
|
| Training of the intervention delivery team | Simulation of intervention delivery. Identification of issues around the feasibility and acceptability of the intervention content |
|
Phase 1: evidence review and stakeholder consultation
In line with Medical Research Council (MRC) guidance on developing complex interventions,50 we reviewed the existing literature. Two systematic reviews of school-based drug prevention programmes found small effects on cannabis use in the short term. 18,19 Researchers working on one RCT noted evidence of poor implementation of interventions21 and, in another peer-led programme, evidence was found of iatrogenic effects20 (see Chapter 1, Evidence on the effectiveness of school-based drug prevention, for further details).
Population-based studies on the prevalence of drug use in secondary school-aged children in the UK have shown that the lifetime prevalence of any illegal drug use in England doubled from 6.8% to 12.4% and then to 23.1% from 13 to 14 to 15 years, respectively. 28 The lifetime prevalence of drug use was > 1% only for cannabis, GGAs, ecstasy, poppers, cocaine, ketamine, mephedrone and magic mushrooms. Cannabis had the highest lifetime prevalence, which increased from 2.7% to 7.5% and then 18.7% from age 13 to 14 to 15 years, respectively. GGA prevalence was 3.5%, 4.0% and 4.4% for 13-, 14- and 15-year-olds, respectively. No equivalent data were available in Wales. This informed our decision to deliver the intervention to UK Year 9 students (aged 13–14 years) and focus the intervention content on cannabis and GGA use.
Consultations with young people and practitioners in drug charities noted a local issue with steroid use in older age groups, which was not apparent in prevalence data as these were gathered in England and did not sample from Welsh schools. This led us to include information on steroids in the interventions.
The consultations and focus groups with young people suggested that 13- to 14-year-olds were relatively familiar with the potentially harmful effects of drugs on health:
Like we all know weed is bad, we all know what it does to you as well.
Young person 6
Young people were less familiar with the potential legal consequences of being caught in possession of an illegal drug in the UK:
When it says unlimited fine, does that mean the police can just charge you?
Young person 9
The familiarity of young people with the harmful effects of drugs on health prompted us to expand the focus to include the harms associated with drugs being illegal and therefore unregulated. These included the possibility of unexpected effects brought about by consuming an unknown compound, of unknown purity and dose. Other concerns that young people voiced included the potential harmful effects of drug use on family relationships, future education and employment:
I mean that’s your mum, that’s one of your parents, they put a roof over your head. If you get drove away from them you don’t get food for yourself, you don’t get a roof over your head, you’re out on the streets. You don’t have anyone to get you a meal or look after you ‘cause you’re on your own.
Young person 29
’Cause then you’re getting a criminal record that’s stopping you from getting a job and loads of stuff.
Young person 19
A number of factors that might influence the engagement of students during peer supporter training were found in both the interviews with the ASSIST delivery team and the independent observations by the research team of the delivery of the intervention. In particular, flexibility in delivering intervention activities to different groups and the need for engaging, interactive content were noted:
We work to the same objectives, but in terms of how we run some activities, we might change them a bit . . . with different groups you know, how they react to a certain activity you might change it round to help the running of it.
Trainer 2
Making sure that they’re interactive . . . so they’re up and about, they get moving around, break off activities, um, just making it as interactive as possible.
Trainer 6
Phase 2: coproduction
During coproduction, the IDG reflected on findings from stage 1 to adapt the content from the ASSIST intervention or develop new content. In interviews with the ASSIST team it was noted that it was important to provide peer supporters with interesting and memorable facts about smoking that they could use in conversations with their peers:
So if we can give them facts that sort of link into what they could be talking about with their friends, it makes it easier for these conversations to happen. In ASSIST, one of the facts they always remember, is that smoking could affect your ability to get an erection. That is the one that sticks with them, and you might not have done the training for 10 weeks, and they will still remember that.
Trainer 2
In ASSIST, we know that young people will leave knowing the ingredients of a cigarette, long-term, short-term health effects, is it guaranteed. We know that you’d go up to any young person that had done the training and you’d ask them how many ingredients are in a cigarette and they’d be able to tell you.
Trainer 2
This led us to adapt information from the Talk to FRANK website about the risks of drug use into memorable factual statements. These key statements were then used across several activities within the peer supporter training and were added to the peer supporter diaries as a reminder.
Phase 3: prototyping
Expert peer review, independent from the IDG, by the lead author of the ASSIST RCT23 and the lead trainer at DECIPHer IMPACT, was used to examine and address key areas of uncertainty. The feedback led to refinements in the timing of the intervention activities and the presentation of instructions in the intervention manual.
Feedback provided by the trainers at the end of the two training sessions indicated that the training was well received and that some of the issues that were raised at the end of the first training session, such as concerns about the need for an encyclopaedic knowledge of drugs, had been addressed during the second training session. This was achieved by providing additional drug education during the session along with the inclusion of a ‘new to trainers’ worksheet that trainers could use to demonstrate to peer supporters the difficulty of keeping track of new drugs and street names. Suggestions raised by trainers for improving activities were added to the intervention materials during refinement prior to stage 2. A final training session was delivered to run through the finalised intervention materials and schedules in advance of stage 2 delivery in two schools so that trainers could become more familiar with the running order of the +FRANK and FRANK friends training days and the resources required for carrying out the activities.
Stage 2: feasibility testing of the +FRANK and FRANK friends interventions
+FRANK intervention
Seven structured observations of delivery were completed for the +FRANK intervention, eight self-assessments were completed by the trainers and 14 +FRANK peer supporters completed an evaluation form at the end of the off-site training day. At the end of intervention delivery (i.e. after the final follow-up), 12 peer supporters completed evaluation forms. Interviews were also conducted after intervention delivery with six peer supporters, three trainers (at the end of the off-site training and the last follow-up), two of the contact teachers and two members of the SMT.
Recruitment
Of the 18 students invited to be retrained, 13 attended the re-recruitment meeting and 14 attended the off-site training day.
In total, 78% of Year 8 ASSIST peer supporters were recruited and retrained as +FRANK peer supporters in Year 9. Although only 13 students attended the recruitment session, one student who was absent was provided with details about the programme and was given an opportunity to attend the training via the contact teacher. The contact teacher stated that those who did not take part did so for a variety of reasons, including one peer supporter not wanting the responsibility, one not enjoying the ASSIST training, one having too many commitments and another being absent from school too frequently.
At the recruitment stage of the ASSIST intervention, if a nominated student or his or her parent/guardian did not want him or her to attend the off-site training, trainers worked down the ranked list of students with the most nominations and invited the student with the next highest number of nominations. With the +FRANK intervention it was not possible to substitute students because they must have trained as an ASSIST peer to be invited to take part in the intervention. This feature of the +FRANK intervention increases the risk that less than the required 17.5% of the year group are trained as peer supporters.
Acceptability of the +FRANK intervention to peer supporters
Peer supporters felt that the peer nomination process was an acceptable method of recruiting. They thought that students in receipt of the most nominations were more likely to be listened to.
Recruitment meeting
Most peer supporters noted that having previously participated in the ASSIST intervention was a positive influence when deciding whether or not to participate in the +FRANK intervention. Familiarity with the trainers and the peer supporter role encouraged students to become +FRANK peer supporters:
. . . ’cause I like I liked doing it last time and . . . I thought it would be good to do it again.
+FRANK school, peer supporter 5
A few peer supporters indicated that they would have benefited from receiving more information at the recruitment meeting, about what to expect and the content of the new programme:
I don’t know, made a bit more detail of what we were doing then maybe we like, we’d have more . . . we’d know whether we’d want to go or not.
+FRANK school, peer supporter 2
Training day
Most of the peer supporters and trainers reported that the +FRANK intervention activities delivered on the training day were acceptable. Some peer supporters noted that a lot of new information was provided, which could be challenging for some:
Loads of facts like, I can remember like parts of them, but I can’t remember which one goes where like.
+FRANK school, peer supporter 1
But maybe it sounds like you need ways of remembering some of that information?
Yeah . . . like writing it down and then just . . . like stick it in my bag so I can remember it.
Some trainers also noted that too much information was being delivered during the training sessions:
Yeah. And probably there was too much information there because I found they needed a lot of prompting for that activity. Some of the groups worked quite well and others, unless you were kind of stood there helping them with the activity they were kind of like what do I do.
Trainer 2
Some peer supporters compared the +FRANK training with their experiences of the ASSIST training, noting the lack in the +FRANK training of activities related to practising conversations about drugs and that they would have liked more opportunities for this:
And they did give us conversation skills like on the smoking course as well but they just didn’t really explain how to give on the information. And really I think that like . . . like I think what would have been cool is because on the smoking course we did like an acting thing and I think, even on the drug course or even on the smoking course as well we could have like acted like bringing up drugs in conversation. That would have been like a good thing.
+FRANK school, peer supporter 2
Peer supporter conversations and use of the diaries
Eleven out of 14 peer supporters returned their diaries. All 11 diaries noted at least one or more informal conversation. The majority of conversations were reported as being face-to-face and easy to initiate. Peer supporters felt that the diaries were helpful in providing a space to record their conversations and could also be referred to to remind themselves of facts and be shown to others:
They were like, good like easy to talk about, like it wasn’t like, like they always listened, like I had like my say, they had their say about it.
+FRANK school, peer supporter 1
Um, well obviously in the diaries you had lots of facts in there so if you forgot any while you were talking just take it out and read through it.
+FRANK school, peer supporter 3
Follow-up sessions
Twelve peer supporters attended the in-person follow-ups 1 and 4. Ten of the 14 peer supporters provided either an e-mail address or a mobile number for the e-follow-up sessions but students indicated that they tended not to use their e-mail. Of the peer supporters who provided contact details, five were e-mailed a task as part of the e-follow-up session. One peer supporter engaged with each of these e-follow-up sessions.
Structured observations, trainer self-evaluation forms and interviews with peer supporters and trainers suggested that there were a number of factors influencing the poor attendance at the e-follow-up sessions. First, there was uncertainty among the peer supporters about why their contact details were needed. One peer supporter noted that they were not allowed to provide their own mobile number so gave their parent’s. Others could not remember their number or forgot to complete the tasks. Second, the school did not provide students with a designated e-mail address and so there was no unified method of contacting students. Third, one teacher also noted that some students would not have permission from their parents to provide their e-mail address. Fourth, during observations of delivery by the research team it was noted that the collection of the details was rushed because of the timing of the follow-up session at the end of the school day. Fifth, the school also had a no homework policy, which meant that students were not familiar with completing tasks out of school. Finally, no text messages were sent by the PHW intervention delivery team because of technical problems with the messaging service. This came to light only after follow-up 4. Peer supporters indicated that they would have preferred to have someone to supervise a designated session for completing the e-follow-up tasks and to be able to work as a group, rather than being left to complete the e-follow-up by themselves:
I didn’t leave anything because I didn’t know my number and I couldn’t remember my e-mail address.
+FRANK school, peer supporter 4
So many of them haven’t got e-mail addresses . . . asking them for e-mail addresses, you’ll only get a handful, or they’ll use Mum’s or Dad’s, and it’s not always appropriate.
+FRANK school, teacher 2, SMT
Yeah if we like we all done it at the same time, ’cause like, no one would probably bother to do it, ’cause no one’s here telling us to actually do it.
+FRANK school, peer supporter 1
One peer supporter who completed the e-follow-up tasks indicated that they enjoyed using the website and was able to think and provide answers in their own time.
I enjoyed answering the questions and reading the information on the website . . . I didn’t feel put on the spot, I could answer in my own time.
+FRANK school, peer supporter 4
Fidelity of implementation
Of the 15 activities in the +FRANK training day, five were delivered in full, eight had minor deviations from the manual and two were not delivered at all. Observations highlighted the need to change the timing of some of the activities as well as amend some of the instructions for trainers, to indicate which tasks are essential and which are optional.
FRANK friends
Fifteen structured observations were made of delivery of the FRANK friends intervention, nine self-assessments were completed by the FRANK friends trainers and 26 FRANK friends peer supporters completed an evaluation form at the end of the second off-site training day. At the end of intervention delivery, 21 peer supporters completed evaluation forms. Interviews and focus groups were also conducted after intervention delivery with 20 peer supporters, five trainers (at the end of off-site training and the last follow-up), two contact teachers and two members of the SMT. Five focus groups were conducted in the FRANK friends school.
Recruitment
Of the 30 students invited to be peer supporters, 29 attended the recruitment meeting and 26 attended both off-site training days.
Acceptability of the FRANK friends intervention to peer supporters
The peer nomination process was perceived as inclusive and fair as it reflected the opinion of everyone in the year group.
It was a positive experience for peer supporters as they felt respected by their peers and believed that they were suitable for the role as they had a wide social network.
Recruitment meeting
Peer supporters mentioned that they were given sufficient and clear information about the study and the role of a peer supporter. They noted the informal and friendly setting of the recruitment meeting, which put them at ease to speak freely and decide whether or not to participate in the study:
It was sort of an introduction because if people didn’t feel like they were right for what they were doing or they didn’t – wouldn’t enjoy it then they could just leave, and I think that was important ’cause it’s a comfortable environment where you’re not forced to do anything.
FRANK friends school, peer supporter 1
Training days
In general, peer supporters enjoyed the 2-day training and were keen to increase their knowledge about drugs. Most of them felt that they had received the right amount of information. Some peer supporters commented that it was easy to learn and retain facts on drugs as the facts were short and relevant for their age:
. . . wasn’t complicated, long-worded facts that we’d easily forget about by the next day, it was like short facts that would stick in our mind and they clearly have from the training.
FRANK friends school, peer supporter 2
And the fact that we concentrated on the most likely ones for our age, it wasn’t like all loaded on us, it was just the three ones ones that we were probably gonna be dealing with.
FRANK friends school, peer supporter 3
Most peer supporters found the training on conversation skills particularly useful because it increased their confidence in initiating conversations with their peers. It also taught peer supporters ways to bring up drugs in conversations and respond to the reactions of their peers in different situations:
There was this one activity where we had like a piece of paper and it gave us a situation to talk to them about and like how we had to act so then we knew how to respond to what they were feeling like or what they were acting like.
FRANK friends school, focus group 3, peer supporter 15
However, a few supporters thought that the conversations felt forced and might not be practical in the real world:
. . . but I think the techniques that we got taught you couldn’t really do it in real life and like we were practising conversations, it just felt awkward and like forced.
FRANK friends school, peer supporter 5
Follow-up sessions
Attendance at the four in-person follow-up sessions ranged from 16 to 21 peer supporters out of the 26 who were trained. The content and duration of the follow-up sessions were acceptable to peer supporters. Peer supporters used the follow-up sessions to reinforce the knowledge that they had gained during training and also to obtain support around conversations from trainers and fellow peer supporters:
Some conversations like people didn’t think that the facts were true. But then like we spoke to the people [trainer] and they explained what we could do if that happened.
FRANK friends school, peer supporter 4
Peer supporters were required to visit the Talk to FRANK website to complete some activities in a couple of the follow-up sessions. The activity was well received by peer supporters as it was interactive and fun:
I think the video [health effects of cannabis] was very helpful as well because it’s, more people prefer to watch videos than be told all the time and if they wa, like watch that it was quite appealing to other people as well.
FRANK friends school, focus group 5, peer supporter 20
However, a few peer supporters mentioned that the follow-up sessions were less engaging than the 2-day training session and that that might have a negative impact on attendance:
I think some of the follow ups were quite, quite slow . . . I was just waiting for something . . . And I think less people started turning up and then it felt, it didn’t feel as special then.
FRANK friends school, focus group 1, peer supporter 9
Peer supporter conversations and use of the diaries
Twenty out of the 26 peer supporters returned their diary. All diaries noted at least one or more informal conversation. The majority of peer supporters recorded that they had had face-to-face conversations. This allowed peer supporters to gauge and respond to the reactions of their peers through reading their facial expressions and body language:
Face to face you can react like on the spot of what they’re thinking and what they’re looking like, so you can see if they’re look – if they’re looking scared or if they’re looking nervous then you can try and support them through whatever they’re going through.
FRANK friends school, peer supporter 3
Some peer supporters felt that text messages and social media were not an appropriate medium by which to communicate information about drugs:
It was easier to bring it into the conversation, whereas like when you’re [text] messaging them it comes out like of nowhere.
FRANK friends school, peer supporter 4
Peer supporters used the diaries in several ways, including to reflect on conversations that they had had and remind themselves of the facts that they had learned:
The diaries helped a lot because they could see how the conversations went and if they didn’t go well then we were able to write what didn’t go well and what did go well.
FRANK friends school, focus group 5, peer supporter 19
It had like the facts on, top five facts so we could always go back to there if we forgot to say something, to remember it so that was really good for reminding us.
FRANK friends school, focus group 5, peer supporter 19
Fidelity of implementation
In the FRANK friends training days, across the 25 activities, 13 were delivered in full, nine had minor deviations from the manual and three were not delivered at all.
Refinements to the +FRANK and FRANK friends interventions: what changed from stage 1
The outcomes of the process evaluation were presented to the TMG. The TMG then agreed some amendments to the +FRANK and FRANK friends interventions. Nearly all of the refinements were made to both the +FRANK intervention and the FRANK friends intervention as a result of the process evaluation undertaken at stage 2 (Table 7). Peer supporters were contacted by e-mail or text message after training with the contact details for the Talk to FRANK website and were sent updates when news items or new drugs were added to the website. Peer supporters were also sent reminders to have conversations and bring their diary to follow-up sessions. The training day agenda was reordered and the timings of activities were amended to accurately reflect the time recorded during observations. Activities deemed to be non-essential were changed to be ‘optional’ and could be delivered at the trainers’ discretion if time allowed.
| Intervention element | Refinements made |
|---|---|
| Recruitment meeting |
|
| Training day |
|
| Follow-up sessions |
|
Refinements unique to the +FRANK intervention included e-follow-up sessions 2 and 3 changing to in-person follow-up sessions in which trainers go into the school to deliver tasks. Follow-up session 4 was dropped and the content was covered in follow-up session 3.
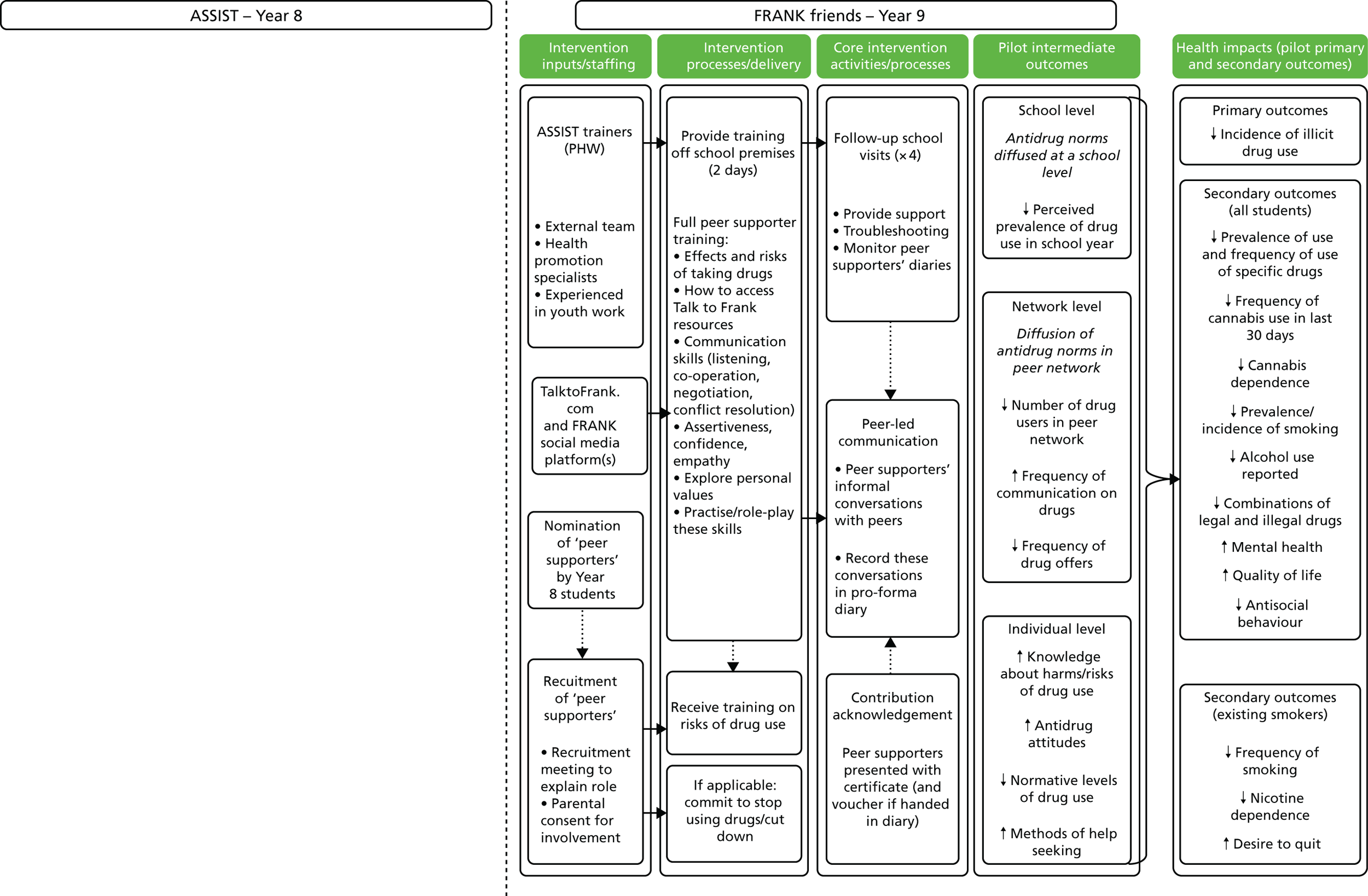
Figures 5 and 6 show the refined intervention logic models for the +FRANK and FRANK friends interventions, respectively.
FIGURE 5.
+FRANK logic model.
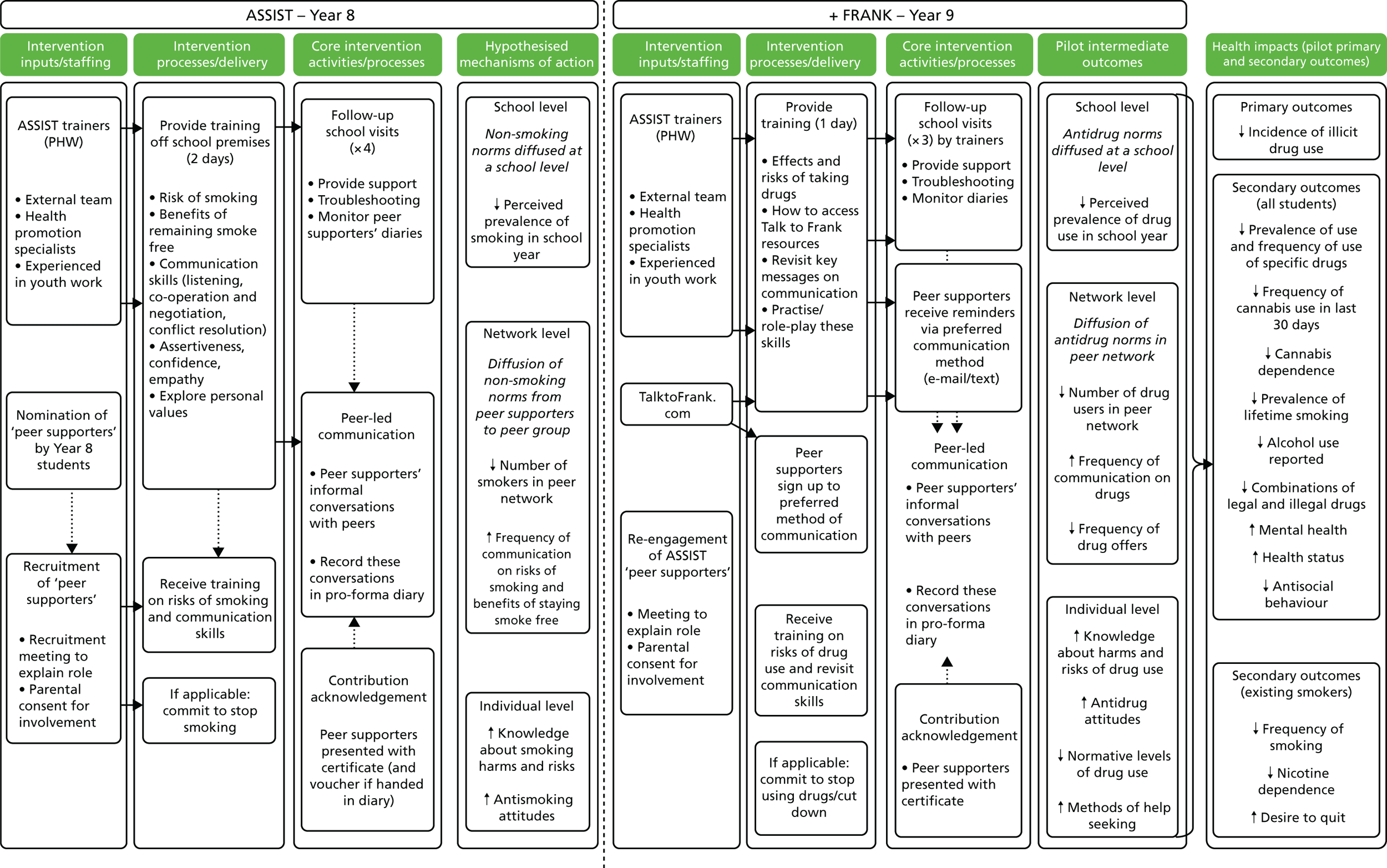
FIGURE 6.
FRANK friends logic model. The ASSIST intervention is not given as part of the FRANK friends intervention.
Stage 3: external pilot trial
The external pilot trial was a parallel-group, four-arm cRCT with school as the unit of randomisation.
Recruitment and retention
Forty schools were invited to take part in the external pilot cRCT (Figure 7). Because of delays in contracting and the requirement to deliver the intervention in the autumn 2014 term, we oversampled schools to reduce the time needed to recruit the required 12 schools. Eight schools declined to participate, with seven citing staff workload and another already having a smoking prevention intervention, Operation Smoke Storm,51 planned. Twelve schools did not return telephone or e-mail messages. Twenty schools responded that they were interested in participating. Two schools were unable to meet the study manager and the lead ASSIST trainer, one because of staff absence and the other not providing a reason. Eighteen schools were visited, with one unable to commit that year because of changes in staffing and one withdrawing as the amount of money offered to recompense for time was not considered to be enough. Two schools were recruited to take part in the feasibility testing of the interventions and two were held in reserve.
FIGURE 7.
Trial CONSORT diagram. a, Because of staff absence; b, because the amount of money offered to recompense for time was not considered to be enough; c, three students started home schooling between baseline and follow-up; d, one student was suspended from school during the follow-up data collection period.
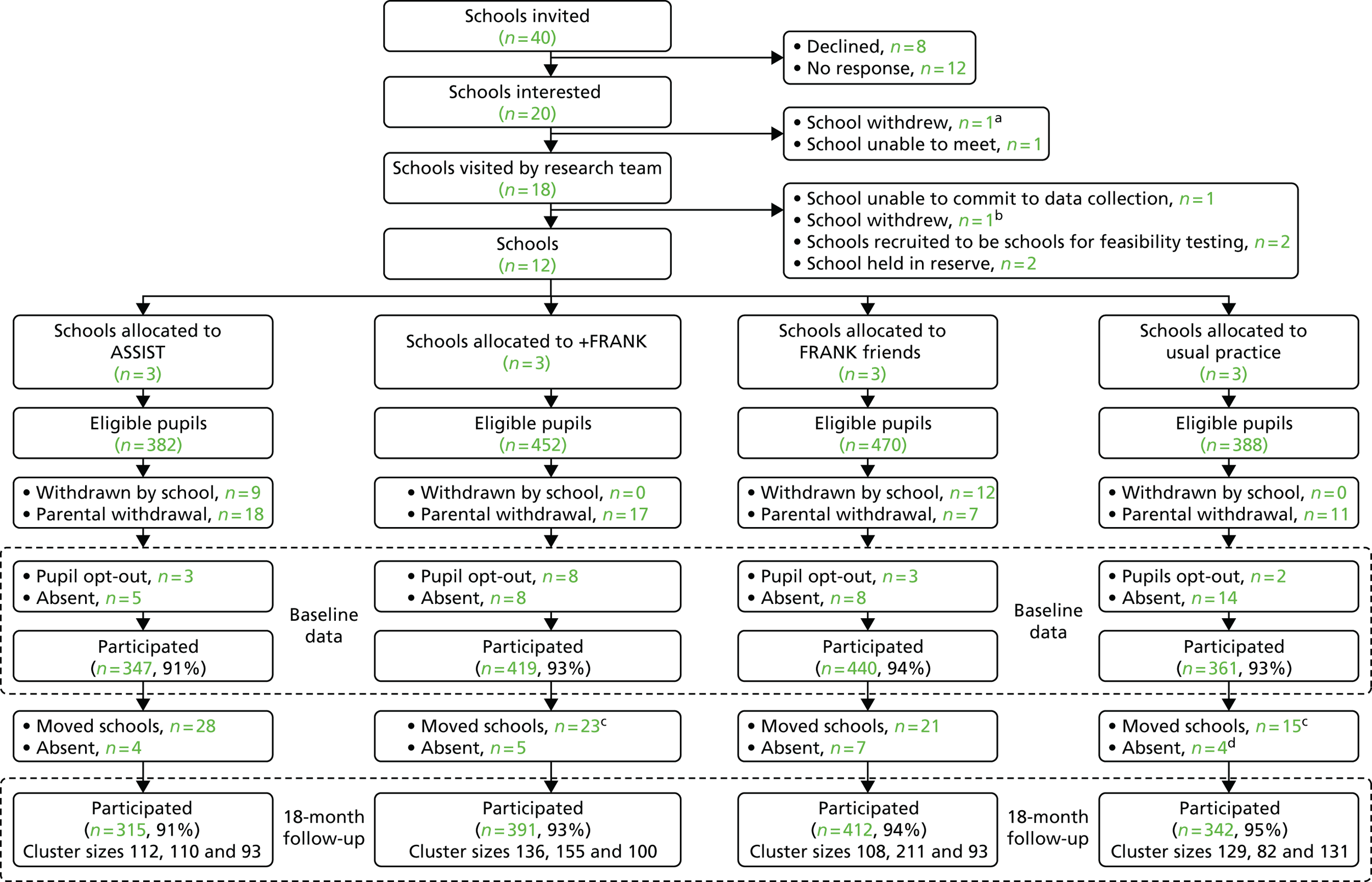
Twelve schools were randomised into the four trial arms, three to the ASSIST intervention, three to the +FRANK intervention, three to the FRANK friends intervention and three to the usual practice arm. There were 1692 students Year 8 aged 13–14 years across the 12 schools. Of these, 125 (7.4%) were withdrawn by the schools, were opted out by parents, opted out themselves or were not at school when the main or absentee surveys took place. This left 1567 students (92.6% of those eligible) who completed the baseline assessment, with 347 attending ASSIST schools, 419 attending +FRANK schools, 440 attending FRANK friends schools and 361 attending usual practice schools.
All schools allocated to the intervention arms received the intervention as planned. All 12 schools took part in the 18-month follow-up. Across the four arms, 107 students (6.8% of the baseline respondents) did not take part in the follow-up, with 84 moving school, 20 not being at school when the survey was administered and three starting home schooling. This left 1460 (93.2%) students who completed the 18-month follow-up, 315 (90.8%) in the ASSIST arm, 391 (93.3%) in the +FRANK arm, 412 (93.6%) in the FRANK friends arm and 342 (94.7%) in the usual practice arm.
Characteristics of trial participants at baseline
Categorical data
The categorical baseline characteristics and outcome measures for the trial participants are summarised in Tables 8 and 9, respectively.
| Variable | Baseline data: distribution over categories by trial arm (%) | ||||
|---|---|---|---|---|---|
| +FRANK (n = 419) | Usual practice (n = 361) | FRANK friends (n = 440) | ASSIST (n = 347) | Overall (n = 1567) | |
| Gender | |||||
| Missing | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Male | 52.5 | 50.7 | 51.1 | 54.5 | 52.1 |
| Ethnicity | |||||
| Missing | 1.4 | 0.6 | 0.7 | 1.2 | 1.0 |
| White British | 93.8 | 81.7 | 85.0 | 93.9 | 88.6 |
| White not British | 2.1 | 1.7 | 3.0 | 1.2 | 2.0 |
| Mixed race | 1.4 | 2.8 | 2.0 | 1.7 | 2.0 |
| Asian or Asian British | 0.5 | 7.8 | 7.0 | 1.2 | 4.1 |
| Black or black British | 0.2 | 2.5 | 0.7 | 0.3 | 0.9 |
| Other | 0.5 | 3.0 | 1.6 | 0.6 | 1.4 |
| Do you have FSMs? | |||||
| Missing | 3.6 | 1.7 | 1.6 | 2.6 | 2.4 |
| No | 66.6 | 72.3 | 71.8 | 73.5 | 70.9 |
| Yes | 22.2 | 18.0 | 20.2 | 17.6 | 19.7 |
| I don’t know | 7.6 | 8.0 | 6.4 | 6.3 | 7.1 |
| Are any of the adults you live with in full- or part-time work? | |||||
| Missing | 0.7 | 0.6 | 0.5 | 0.9 | 0.6 |
| No | 16.7 | 11.4 | 12.7 | 12.4 | 13.4 |
| Yes | 69.7 | 72.3 | 73.6 | 72.1 | 71.9 |
| I don’t know | 12.9 | 15.8 | 13.2 | 14.7 | 14.0 |
| What kind of house or flat do you live in? | |||||
| Missing | 0.5 | 1.1 | 1.1 | 0.9 | 0.9 |
| One rented from the council or a housing association | 16.0 | 11.1 | 12.3 | 9.5 | 12.4 |
| One rented from a landlord | 12.6 | 11.4 | 9.3 | 10.7 | 11.0 |
| One owned by your family (including one with a mortgage) | 44.9 | 49.9 | 55.9 | 54.8 | 51.3 |
| Other | 0.7 | 1.9 | 0.7 | 1.7 | 1.2 |
| I don’t know/not sure | 25.3 | 24.7 | 20.7 | 22.5 | 23.2 |
| How much do you have to spend for yourself each week? | |||||
| Missing | 1.4 | 1.9 | 1.4 | 1.7 | 1.6 |
| I don’t have any money to spend | 5.5 | 4.7 | 8.6 | 5.2 | 6.1 |
| < £5 | 17.2 | 19.7 | 20.0 | 17.9 | 18.7 |
| £5.00–9.99 | 33.9 | 28.8 | 31.4 | 35.2 | 32.3 |
| £10.00–14.99 | 21.7 | 19.4 | 16.4 | 15.0 | 18.2 |
| £15.00–19.99 | 11.0 | 10.0 | 8.4 | 13.3 | 10.5 |
| ≥ £20 | 9.3 | 15.5 | 13.9 | 11.8 | 12.6 |
| Variable | Baseline data: distribution over categories by trial arm (%) | ||||
|---|---|---|---|---|---|
| +FRANK (n = 419) | Usual practice (n = 361) | FRANK friends (n = 440) | ASSIST (n = 347) | Overall (n = 1567) | |
| Lifetime illicit drug use | |||||
| Missing | 4.1 | 1.9 | 0.9 | 1.4 | 2.1 |
| Yes | 2.6 | 6.4 | 4.5 | 3.2 | 4.1 |
| No | 93.3 | 91.7 | 94.5 | 95.4 | 93.7 |
| Lifetime cannabis use | |||||
| Missing | 3.1 | 0.3 | 0.5 | 0.6 | 1.1 |
| Yes | 1.7 | 3.9 | 2.5 | 1.7 | 2.4 |
| No | 95.2 | 95.8 | 97.0 | 97.7 | 96.4 |
| Lifetime GGA use | |||||
| Missing | 3.3 | 1.1 | 0.5 | 1.4 | 1.6 |
| Yes | 1.4 | 3.9 | 2.0 | 1.4 | 2.2 |
| No | 95.5 | 95.0 | 97.5 | 97.1 | 96.2 |
| CASTa | |||||
| Missing | 28.6 | 14.3 | 18.2 | 33.3 | 21.1 |
| Screened positive for dependency (score of ≥ 4) | 28.6 | 21.4 | 36.4 | 0.0 | 23.7 |
| Ever tried smoking, even if a puff? | |||||
| Missing | 6.2 | 4.2 | 4.5 | 5.2 | 5.0 |
| Yes | 11.0 | 10.8 | 10.7 | 6.6 | 9.9 |
| Weekly smoking statusb | |||||
| Missing | 6.2 | 4.2 | 4.5 | 5.2 | 5.0 |
| Yes | 0.5 | 0.3 | 1.1 | 0.3 | 0.6 |
| Ever consumed a whole alcoholic drink? | |||||
| Missing | 2.1 | 3.0 | 4.3 | 2.3 | 3.0 |
| Yes | 25.1 | 25.8 | 18.0 | 31.4 | 24.6 |
| A-SAQc | |||||
| Missing | 6.7 | 11.8 | 10.1 | 8.3 | 9.1 |
| Heavy episodic alcohol used | 28.6 | 37.6 | 32.9 | 21.1 | 29.5 |
There was an equal distribution of male and female participants across the trial arms, with 52.5%, 50.7%, 51.1% and 54.5% of male participants in the +FRANK, usual practice, FRANK friends and ASSIST arms, respectively. Ethnicity was evenly distributed, with very few non-white participants in each arm. About 20% of participants were in receipt of FSMs, with a slightly higher percentage in the +FRANK arm. The average percentage of students in receipt of FSMs in Wales is 17.5%. 52 Housing tenure and living with an employed adult were not evenly balanced. There was a higher percentage of students resident in social housing (16.0% vs. 11.1%, 12.3% and 9.5%) and living without an adult in employment (16.7% vs. 11.4%, 12.7% and 12.4%) in the +FRANK than in the usual practice, FRANK friends and ASSIST arms, respectively. Spending money was fairly evenly distributed, with 32.3% of students having between £5.00 and £9.99 to spend per week.
The indicative primary outcome in this study was the lifetime prevalence of illicit drug use. Overall, 4.1% of baseline respondents reported that they had ever tried drugs. There was an imbalance between the arms, with a slightly higher prevalence in the usual practice arm (6.4%) than in the FRANK friends (4.5%), ASSIST (3.2%) and +FRANK (2.6%) arms. This compares with 7% of 12-year-olds and 11% of 13-year-olds in the 2014 Smoking, Drinking and Drug Use survey. 6 The most commonly used drugs were cannabis (2.4%) and GGAs (2.2%), with all other drugs having a prevalence across all arms of < 1% (see Appendix 1, Table 18). Table 19 (see Appendix 1) shows the frequency of use of each drug in the past week, 30 days and 12 months. Of the 65 students who had ever tried drugs, 36.9% used cannabis in the past 12 months, 9.2% used cannabis in the past 30 days and 6.2% used cannabis in the last week. For GGAs, use in the past 12 months, 30 days and last week was 36.9%, 9.2% and 7.7%, respectively. Of the 38 students who had ever tried cannabis, 23.7% screened positive for dependency on the CAST. 38
Numerical variables
The mean age of participants was 12.6 years (SD 0.30 years) across all arms. Students who reported smoking at least one cigarette a week completed the FTND and HSI. Only 15 students reported smoking at least one cigarette a week and the median number of cigarettes smoked per week was 3.0 (interquartile range 1.03 to 35.0). Twelve participants completed all of the items on the FTND and HSI. There was some evidence of floor effects, with a median score of 0 on the HSI and 0.5 on the FTND. There was evidence of ceiling effects on the quality of life measure, the CHU-9D, with median and mean scores of 0.915 and 0.887, respectively, across all students (see Appendix 1, Table 22).
Missing data
There were very few missing responses. For questions on gender, FSM entitlement, parental employment and spending money, missing responses ranged between 0% and 2.5%, with no discernible difference across arms. In total, 2% of participants did not provide information on lifetime illicit drug use, with slightly more missing data in the +FRANK arm (4.1%) than in the other arms (usual practice 1.9%, FRANK friends 0.9%, ASSIST 1.4%). With regard to the CAST, 21% of responses were missing. In total, 5% of responses for ever having tried and weekly smoking, around 3% of responses for ever having consumed an alcoholic drink and 10% of responses on the A-SAQ were missing, with comparable numbers of missing data across the arms. Twelve out of 15 respondents who smoked one cigarette or more a week answered all questions on the FNTD and HSI. Finally, 11% of participants did not complete all items on the CHU-9D.
Characteristics of the outcome measures at the 18-month follow-up
Of the 107 students who did not take part at the 18-month follow-up, 14 (13.1%) reported lifetime illicit drug use at baseline. Of the 1460 students retained, 51 (3.5%) had used illicit drugs at baseline, suggesting that drug use was more common in students who did not take part at follow-up.
Categorical data
The indicative primary and secondary outcome measures collected at the 18-month follow-up are reported in Table 10. Across all trial participants the prevalence of illicit drug use was 11.6%. The lifetime prevalence of illicit drug use in the ASSIST (9.5%) and FRANK friends (9.7%) arms was similar, with a higher prevalence of use found in the +FRANK (15.1%) and usual practice (11.7%) arms. These differences between trial arms should be interpreted with caution. There was a wide variation in prevalence across schools, from 4.6% to 17.6%, and within arms, with prevalence ranging from 4.6% to 13.3% in the FRANK friends arm. There was an imbalance at baseline, with a higher level of socioeconomic disadvantage in the +FRANK arm. The ICC was 0.003 for lifetime prevalence of illicit drug use for the comparison between the usual practice arm and the FRANK friends arm and < 1 × 10–8 for the comparison between the usual practice arm and the +FRANK arm.
| Variable | 18-month follow-up data: distribution over categories by trial arm (%) | ||||
|---|---|---|---|---|---|
| +FRANK (n = 391) | Usual practice (n = 342) | FRANK friends (n = 412) | ASSIST (n = 315) | Overall (n = 1460) | |
| Lifetime illicit drug use | |||||
| Missing | 1.5 | 3.2 | 1.2 | 0.6 | 1.6 |
| Yes | 15.1 | 11.7 | 9.7 | 9.5 | 11.6 |
| No | 83.4 | 85.1 | 89.1 | 89.8 | 86.8 |
| Lifetime cannabis use | |||||
| Missing | 0.3 | 0.3 | 0.2 | 0.3 | 0.3 |
| Yes | 10.7 | 7.6 | 6.6 | 7.0 | 8.0 |
| No | 89.0 | 92.1 | 93.2 | 92.7 | 91.7 |
| Lifetime GGA use | |||||
| Missing | 0.0 | 0.6 | 0.2 | 0.3 | 0.3 |
| Yes | 5.4 | 3.2 | 2.9 | 4.4 | 4.0 |
| No | 94.6 | 96.2 | 96.8 | 95.2 | 95.8 |
| Lifetime use of legal highs | |||||
| Missing | 0.0 | 0.6 | 0.2 | 0.3 | 0.3 |
| Yes | 2.6 | 1.5 | 1.2 | 1.6 | 1.7 |
| No | 97.4 | 98.0 | 98.5 | 98.1 | 98.0 |
| Lifetime cocaine use | |||||
| Missing | 0.0 | 1.5 | 0.2 | 0.3 | 0.5 |
| Yes | 1.3 | 1.2 | 0.2 | 1.3 | 1.0 |
| No | 98.7 | 97.4 | 99.5 | 98.4 | 98.6 |
| CASTa | |||||
| Missing | 19.0 | 7.7 | 22.2 | 0.0 | 13.7 |
| Screened positive for dependency (score of ≥ 4) | 28.6 | 34.6 | 48.1 | 31.8 | 35.0 |
| Ever tried smoking, even if a puff? | |||||
| Missing | 2.6 | 4.4 | 1.0 | 2.2 | 2.5 |
| Yes | 28.1 | 24.9 | 19.2 | 23.8 | 23.9 |
| Weekly smoking statusb | |||||
| Missing | 2.6 | 4.4 | 1.0 | 2.2 | 2.5 |
| Yes | 3.6 | 2.6 | 1.7 | 1.6 | 2.4 |
| Ever consumed a whole alcoholic drink? | |||||
| Missing | 16.6 | 12.9 | 10.0 | 10.5 | 12.5 |
| Yes | 45.8 | 40.9 | 37.1 | 51.4 | 43.4 |
| A-SAQc | |||||
| Missing | 0.0 | 0.7 | 0.0 | 0.0 | 0.2 |
| Heavy episodic alcohol used | 40.2 | 50.7 | 36.6 | 35.8 | 40.5 |
The most commonly used drugs were, in rank order, cannabis (8.0%), GGAs (4.0%), legal highs (1.7%) and cocaine (1.0%). All other drugs had an overall prevalence of < 1% (see Appendix 1, Table 20). Of the 169 students who reported drug use, the majority of use had been in the past 12 months [cannabis 58.6%, GGA 19.5%, legal highs 11.5%, cocaine 5.9%) (see Appendix 1, Table 21). The use of cannabis (21.9%) in the last 30 days was more common than the use of GGAs (5.3%), legal highs (3.0%) and cocaine (2.4%) in the last 30 days, with cannabis (8.9%) and cocaine (1.2%) the only drugs that were used by > 1% of participants in the last week. Some students provided an illogical response for drug use over different periods, for example using in the last week but not in the last month, but this was rare, with only six students making this error. In total, 35% of the 117 students who ever reported trying cannabis screened positive for cannabis dependency.
Around one-quarter (23.9%) of students had tried smoking, with prevalence slightly higher in the +FRANK arm (28.1%) and lower in the FRANK friends arm (19.2%) than in the usual practice arm (24.9%) or ASSIST arm (23.8%). Weekly smoking was very rare, at 2.4% in the overall sample. With regard to the other outcome measures, the prevalence of consuming a whole alcoholic drink had nearly doubled since baseline, to 43.4% overall. Of those who had consumed a whole alcoholic drink, around 40.5% screened positive for heavy episodic alcohol consumption on the A-SAQ, with fewer screening positive in the ASSIST arm (35.8%) and more screening positive in the usual practice arm (50.7%).
The prevalence of the categorical intermediary variables outlined in the logic model are described in Appendix 1 (see Table 23). Overall, students’ perceived prevalence of drug use in their year was 52.3%; 26.5% had been offered drugs in the last year, 55.5% had had a conversation with a school friend about drugs; 10.3% had visited the Talk to FRANK website; 17.8% had talked to a peer supporter about the harms of drugs; and 37.9% said that they would get help for themselves or a friend from the Talk to FRANK website.
Numerical variables
A summary of the numerical indicative secondary outcome measures is shown in Table 11. The five-number summaries show a lot of variation within arms in the number of cigarettes smoked a week. Across the 54 students who reported smoking one cigarette a week, the number of cigarettes smoked per week ranged from 1 to 100, with a median of 6.0, a mean of 14.4 and a SD of 18.9. There was an imbalance between trial arms, with a median of 8.0 cigarettes a week in the FRANK friends arm, 4.0 in the usual practice arm, 6.5 in the +FRANK arm and 10.0 in the ASSIST arm. There were very low scores on the FTND and HSI measures of nicotine dependence. Overall, the median score on the HSI was 2.0 (range 0.0–9.0) and on the FTND was 0.0 (range 0.0–5.0), suggesting a very low level of dependence on nicotine, reflecting the small number of cigarettes smoked a day. There were very high scores across all students on the measure of quality of life, the CHU-9D, with a median and mean score of 0.888 and 0.865, respectively, out of a maximum of 1.
| Variable (potential scale range) | Trial arm | n | Missing (%) | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| FTND (0–10)a | +FRANK | 19 | 5.0 | 0.0 | 0.0 | 0.0 | 2.0 | 5.0 | 0.9 | 1.4 |
| Usual practice | 15 | 11.8 | 0.0 | 0.0 | 1.0 | 2.0 | 4.0 | 1.1 | 1.4 | |
| FRANK friends | 9 | 10.0 | 0.0 | 0.0 | 0.0 | 2.0 | 4.0 | 1.1 | 1.5 | |
| ASSIST | 6 | 14.3 | 0.0 | 0.0 | 0.0 | 0.0 | 2.0 | 0.3 | 0.8 | |
| Overall | 49 | 9.3 | 0.0 | 0.0 | 0.0 | 2.0 | 5.0 | 1.0 | 1.3 | |
| HSI (0-6)a | +FRANK | 16 | 20.0 | 0.0 | 0.5 | 2.0 | 3.5 | 9.0 | 2.3 | 2.4 |
| Usual practice | 15 | 11.8 | 0.0 | 1.0 | 2.0 | 4.0 | 6.0 | 2.5 | 1.9 | |
| FRANK friends | 9 | 10.0 | 0.0 | 0.0 | 2.0 | 3.0 | 6.0 | 2.0 | 2.3 | |
| ASSIST | 6 | 14.3 | 0.0 | 0.0 | 0.0 | 0.0 | 3.0 | 0.5 | 1.2 | |
| Overall | 46 | 14.8 | 0.0 | 0.0 | 2.0 | 3.0 | 9.0 | 2.1 | 2.1 | |
| Number of cigarettes smoked in an average weeka | +FRANK | 20 | 0.0 | 1.0 | 2.0 | 6.5 | 17.5 | 100.0 | 15.1 | 23.5 |
| Usual practice | 17 | 0.0 | 1.0 | 2.0 | 4.0 | 20.0 | 50.0 | 13.8 | 17.2 | |
| FRANK friends | 10 | 0.0 | 2.0 | 4.0 | 8.0 | 11.0 | 32.0 | 10.3 | 9.3 | |
| ASSIST | 7 | 0.0 | 1.0 | 1.0 | 10.0 | 42.0 | 50.0 | 19.4 | 20.9 | |
| Overall | 54 | 0.0 | 1.0 | 2.0 | 6.0 | 20.0 | 100.0 | 14.4 | 18.9 | |
| CHU-9D (0–1) | +FRANK | 391 | 7.4 | 0.4 | 0.8 | 0.9 | 0.9 | 1.0 | 0.9 | 0.1 |
| Usual practice | 342 | 5.8 | 0.3 | 0.8 | 0.9 | 1.0 | 1.0 | 0.9 | 0.1 | |
| FRANK friends | 412 | 6.3 | 0.3 | 0.8 | 0.9 | 1.0 | 1.0 | 0.9 | 0.1 | |
| ASSIST | 315 | 7.6 | 0.3 | 0.8 | 0.9 | 1.0 | 1.0 | 0.9 | 0.1 | |
| Overall | 1460 | 6.8 | 0.3 | 0.8 | 0.9 | 1.0 | 1.0 | 0.9 | 0.1 |
The prevalence of the numerical intermediary variables outlined in the logic model is described in Appendix 1 (see Table 24). Across all students, the perceived percentage of students who took drugs in their year group ranged from 0% to 100%, with a median of 5.0%, mean of 11.9% and SD of 16.2%. The knowledge about drugs score ranged from 1 to 8, with a median of 6.0, mean of 5.6 and SD of 1.3.
Missing data
At the 18-month follow-up, levels of missing data were low. For questions on lifetime illicit drug use, only 1.6% of students overall did not provide a response. Only four (0.3%) students overall did not provide data on lifetime cannabis, GGA and legal high use and seven (0.5%) did not provide data on cocaine use. There was a similar proportion of missing data across arms for drug use questions. Missing responses on the CAST were higher at 13.7%, probably because of the requirement to answer six questions. In total, 2.5% of students did not provide data on ever having tried and weekly smoking and around 12% of responses on ever having consumed an alcoholic drink were missing. Among those who had drunk a whole alcoholic drink, only one person did not answer the A-SAQ screening question. Among the 54 students who smoked one cigarette or more a week, 14.8% had missing data on the HSI and 9.3% had missing data on the FNTD. Around 7% had missing data on the CHU-9D.
Exploratory effectiveness analysis
We examined the effectiveness of the interventions on the indicative primary and secondary outcomes and intermediary variables (see Appendix 1, Tables 25–27). It was not possible to estimate effects for cannabis or GGA use in the past 30 days, cannabis dependency, weekly smoking status or ever having visited the Talk to FRANK website, as there were too few cases at baseline per arm.
The odds of lifetime drug use at the 18-month follow-up were marginally lower in the +FRANK arm than in the usual practice arm [n = 561, 12.4% vs. 13.4%; odds ratio (OR) 0.96, 95% CI 0.58 to 1.59]. The odds of lifetime drug use were lower in the FRANK friends arm than in the usual practice arm (n = 576, 9.3% vs. 13.4%; OR 0.70, 95% CI 0.39 to 1.24). The odds of lifetime drug use were also marginally lower in the ASSIST arm than in the usual practice arm (n = 497, 8.7% vs. 11.1%; OR 0.81, 95% CI 0.46 to 1.42). The overall direction of effects for the FRANK friends arm across the secondary outcomes and hypothesised intermediary variables indicated a potential positive effect; for the +FRANK and ASSIST arms the pattern was mixed.
In exploratory subgroup analyses, interaction terms indicated that the effects of the +FRANK and FRANK friends interventions were comparable in baseline lifetime drug users and baseline lifetime non-drug users (see Appendix 1, Table 28).
Reliability of measures of illicit drug use
We examined the possibility of false-positive responding by including a fictitious drug, semeron, in the measure of lifetime drug use. False-positive responding was very rare, with only two participants at baseline and three at follow-up saying that they had ever taken the fictitious drug.
We also examined the reliability of measures of lifetime drug use by calculating the proportion of lifetime drug use that was recanted, whereby baseline drug users responded that they had never used drugs at follow-up. Out of the 65 drug users at baseline, 27 (41.5%) recanted reports of lifetime use at follow-up. The level of recanting was 14.8% (n = 4) in the +FRANK arm and 29.6% (n = 8) in the FRANK friends arm, with levels of 48.2% (n = 13) in the usual practice arm and 7.4% (n = 2) in the ASSIST arm. There was a wide variation across sites and within arms; no recanting was found in five schools, one school each had one two, three and four cases, two schools had five cases and one school had seven cases. As two-thirds of lifetime drug use occurred after the baseline assessment, the removal of students who recanted had a minimal effect on drug use prevalence (removed 12.0%, not removed 11.6%). The low number of baseline users and students who recanted mean that these results should be interpreted with caution as small differences in absolute numbers can appear to be large differences in prevalence.
To further explore recanting we examined changes in other time-invariant variables. Between baseline and follow-up, the gender of seven students changed and 109 (7.0%) provided a different date of birth. After removing errors in the date of birth provided, including putting the date of the data collection or using an adjacent month but the correct date and year (e.g. 24 June 2002, 24 May 2002), 47 (3.0%) dates of birth changed between baseline and follow-up.
Assessment of costs
Intervention costs
The estimated cost of delivering the +FRANK intervention was approximately £1942 per school (Table 12) or £13.87 per student. The majority of the costs related to the time (estimated to be 3.5 working days) spent by the two intervention delivery staff members preparing for and delivering the intervention and follow-up sessions. The other substantial cost related to the hire of the venue, student transport and catering for the off-site training sessions. The estimated cost of delivering the FRANK friends intervention was approximately one-third higher, at £3041 per school (£20.69 per student; Table 13), reflecting some economies in training students to be peer supporters for both the ASSIST intervention and the +FRANK intervention. Tables 12 and 13 do not include the opportunity cost of the teacher accompanying students on the training day; some schools may decide to pay for supply teacher time to cover this absence.
| Resource item | Units | Cost (£) |
|---|---|---|
| Administration per school (3 hours of band 3 staff time, contacting schools, arranging venues, preparing materials) | 3 hours | 28.14 |
| Intervention delivery staff time per school (0.5 days of preparation + 0.5 days for day recruitment + 1 training day + 3 half-day follow ups = 3.5 days) | 26.25 hours | 333.64 |
| Senior intervention delivery staff time per school (0.5 days of preparation + 0.5 days for day recruitment + 1 training day + 3 half-day follow ups = 3.5 days) | 26.25 hours | 400.58 |
| Intervention delivery staff travel expenses per school for training days and follow-ups | 200 miles | 134.00 |
| Room hire, student transport and catering | ||
| School 1 | 1 day | 723.00 |
| School 2 | 1 day | 792.00 |
| School 3 | 1 day | 1119.00 |
| Average | 878 | |
| Consumables per school | ||
| Text messaging | 50.00 | |
| Training materials | 49.17 | |
| Printing | 68.27 | |
| Average total cost per school | 1941.80 | |
| Resource item | Units | Cost (£) |
|---|---|---|
| Administration per school (6 hours of band 3 staff time, contacting schools, arranging venues, preparing materials) | 6 hours | 56.28 |
| Intervention delivery staff time per school (0.5 days of preparation + 0.5 days for the survey + 0.5 days for recruitment + 2 training days + 4 half-day follow-ups = 5.5 days) | 41.3 hours | 524.29 |
| Senior intervention delivery staff time per school (0.5 days of preparation + 0.5 days for the survey + 0.5 days for recruitment + 2 training days + 4 half-day follow-ups = 5.5 days) | 41.3 hours | 630.24 |
| Intervention delivery staff travel expenses per school for training days and follow-ups | 400 miles | 268.00 |
| Room hire, student transport, catering | ||
| School 1 | 2 days | 1592.16 |
| School 2 | 2 days | 1244.00 |
| School 3 | 2 days | 1346.90 |
| Average | 1394.35 | |
| Consumables per school | ||
| Text messaging | 50.00 | |
| Training materials | 49.17 | |
| Printing | 68.27 | |
| Average total cost per school | 3040.60 | |
It is important to note that the +FRANK intervention, unlike the FRANK friends intervention, has the requirement that schools have already delivered the ASSIST intervention. As the ASSIST intervention has approximately the same cost as the FRANK friends intervention, delivery of the ASSIST intervention (£3041) + the FRANK intervention (£1942) would have an estimated cost per school of £4983.
Process evaluation
Quantitative and qualitative data were used to determine whether or not the progression criteria were met (see Table 4 for criteria). Quantitative data are presented first, followed by qualitative data, organised according to the progression criteria that they address.
Quantitative data
Tables 14 and 15 show that the progression criteria assessing the feasibility of implementing the +FRANK and FRANK friends interventions, respectively, were met.
| School ID | Total n invited to ASSIST training | Total n ASSIST trained | % trained | Total n peer supporters invited to +FRANK training | Total n peer supporters +FRANK trained | % trained |
|---|---|---|---|---|---|---|
| 1. ≥ 75% of Year 8 ASSIST peer supporters are recruited and retrained as +FRANK peer supporters in Year 9 | ||||||
| Site 3 | 28a | 17 | 61 | 15 | 14 | 93 |
| Site 4 | 28 | 25 | 89 | 25 | 23 | 92 |
| Site 6 | 22 | 22 | 100 | 22 | 20 | 91 |
| School ID | Recruitment meeting (%) | Training day (%) | Follow-up 1 (%) | Follow-up 2 (%) | Follow-up 3 (%) | Intervention delivered in full |
| 2. PHW staff delivered the +FRANK training in full in all three intervention schools | ||||||
| Site 3 | 100 (n = 3) | 100 (n = 20) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes |
| Site 4 | 100 (n = 3) | 100 (n = 20) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes |
| Site 6 | 100 (n = 3) | 100 (n = 20) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes |
| School ID | Total n peer supporters trained | Total n peer supporters who had at least one conversation | % reporting at least one conversation | |||
| 3a. ≥ 75% of +FRANK peer supporters report having at least one or more informal conversations with their peers at school about drug-related risks/harms | ||||||
| Site 3 | 14 | 14 | 100 | |||
| Site 4 | 23 | 22 | 96 | |||
| Site 6 | 20 | 16 | 80 | |||
| School ID | Total n peer supporters trained | Total n peer supporters who had at least one contact with PHW | % who had contact with PHW staff | |||
| 3b. ≥ 75% of +FRANK peer supporters report at least one contact with PHW staff, either during a follow-up visit or via e-mail, text or Facebook (Facebook Inc, Menlo Park, CA, USA) | ||||||
| Site 3 | 14 | 14 | 100 | |||
| Site 4 | 23 | 23 | 100 | |||
| Site 6 | 20 | 20 | 100 | |||
| School ID | Total n peer supporters invited | Total n peer supporters trained | % trained | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1. ≥ 75% of Year 9 students nominated are recruited and trained as FRANK friends peer supporters | ||||||||||
| Site 1 | 23 | 22 | 96 | |||||||
| Site 2 | 45 | 34 | 76 | |||||||
| Site 7 | 20 | 15 | 75 | |||||||
| School ID | Recruitment meeting (%) | Training day 1 (%) | Training day 2 (%) | Follow-up 1 (%) | Follow-up 2 (%) | Follow-up 3 (%) | Follow-up 4 (%) | Intervention delivered in full | ||
| 2. PHW staff deliver the FRANK friends training in full in all three intervention schools | ||||||||||
| Site 1 | 100 (n = 3) | 100 (n = 19) | 100 (n = 9) | 100 (n = 1) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes | ||
| Site 2 | 100 (n = 3) | 100 (n = 19) | 100 (n = 9) | 100 (n = 1) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes | ||
| Site 7 | 100 (n = 3) | 100 (n = 19) | 100 (n = 9) | 100 (n = 1) | 100 (n = 1) | 100 (n = 1) | 100 (n = 3) | Yes | ||
| School ID | Total n peer supporters trained | Total n peer supporters who had at least one conversation | % of peer supporters reporting at least one conversation | |||||||
| 3a. ≥ 75% of FRANK friends peer supporters report having at least one or more informal conversations with their peers at school about drug-related risks/harms | ||||||||||
| Site 1 | 22 | 22 | 100 | |||||||
| Site 2 | 34 | 27 | 82 | |||||||
| Site 7 | 15 | 15 | 100 | |||||||
| School ID | Total n peer supporters trained | Total n peer supporters who had at least one contact | % of peer supporters reporting at least one contact with PHW staff | |||||||
| 3b. ≥ 75% of FRANK friends peer supporters report ongoing contact with PHW staff throughout the year via a follow-up visit | ||||||||||
| Site 1 | 22 | 22 | 100 | |||||||
| Site 2 | 34 | 34 | 100 | |||||||
| Site 7 | 15 | 15 | 100 | |||||||
In the three +FRANK schools, we examined the percentage of Year 8 peer supporters who were renominated in Year 9. Of the 78 ASSIST Year 8 peer supporters, 50 (64.1%) were renominated, 24 (30.8%) were not and four (5.1%) were lost to follow-up by Year 9. This suggests that around one-third of students nominated as being the most influential by their peers in Year 9 were not trained in the +FRANK intervention.
Qualitative data
Interviews were conducted after intervention delivery was completed (i.e. after the last follow-up) with 66 participants across the three +FRANK and three FRANK friends schools. This included 36 peer supporters (19 in +FRANK schools), 11 members of the intervention delivery team (all worked on both interventions), eight parents (two from +FRANK schools), 10 school staff members (five from +FRANK schools) and a public health commissioner. Some of the peer supporter interviews were conducted as paired interviews. A similar number of interviews was conducted across each school. The characteristics of the participants who were interviewed are summarised in Appendix 1 (see Table 17).
Across the interviews a number of themes emerged, as detailed in the following sections.
Adaptation of the ASSIST peer-led approach to drug prevention and peer-led delivery
Peer supporters, parents, school staff and the public health commissioner found the peer-led approach acceptable. Peer supporters reported that it was beneficial to understand the possible harms and effects of drugs:
I think it’s really helpful and especially when we get to take part and then the feedback to our peers and it’s just really helpful for people and keeps them safe if they know the facts.
School 2, peer supporter 171
It’s a good role, because you can help people, educate people about drugs.
School 7, peer supporter 51
Parents were comfortable with their children taking on the role of a peer supporter and having informal conversations with their peers about the harms of drug use. One parent thought that students may find a peer-led drug prevention intervention more acceptable than other forms of drug education:
I broadly approve of both the method and the sort of the anti-drug message that the peer-to-peer, because clearly there is a gap in that respect, you know children would not tend to look at me for instance for information . . . you know, telling children that it’s not legal clearly is not working.
School 1, parent 1
The public health commissioner also noted the value of a peer-led approach to drug prevention:
Erm, well it’s not like anything I have come across previously because I think most of the ones that have been tried have either been you know what I call traditional educational packages, then delivered by teachers or others, or even peers because that is, you know peer education is something fundamentally different.
Public health commissioner
Peer nomination process
The peer nomination process was perceived as being acceptable to the majority of peer supporters, parents and teachers. Most peer supporters reported that being selected by their peers was a positive experience:
I was really flattered, when they said that we’ve been chosen by our friends and everything, I was really shocked and surprised, but flattered at the same time.
School 3, peer supporter 140
Peer supporters also noted that they thought being nominated by peers was more credible than if they had been selected by teachers for the role. A few peer supporters and teachers were surprised at the nomination of some individuals:
I think a few weren’t really suitable I thought.
OK, what made them not suitable? What was it about them?
Erm, some of them are like really naughty in school and they haven’t done much really, how can I explain it? Like they, they’re not very, erm, polite to people. So I was, I was really like taken aback when I seen that they were on there.
Of the peer supporters and teachers who were surprised about which students were nominated, all reported that these students behaved well during the off-site training. Teachers felt that the nomination process resulted in a good mix of students from across the year group, who might not have been selected by teachers:
I think that those students, you know for social reasons they are very engaging and they are confident and I think that’s what they look up to but sometimes that confidence comes not through sort of maybe academic but maybe because of their street cred. Erm and often I think perhaps we wouldn’t, as teachers, select them.
School 4, teacher 2, SMT
Off-site peer supporter training
Many of the peer supporters and teachers appreciated activities that encouraged the practising of conversations. Some commented on the particular benefits of practising conversations:
They [the trainers] would say that it is hard to have conversations, especially at our age, but they would manage to build your confidence up, and we even had like a little session where you kind of practised with one another, having a conversation. And that, it just made me feel that I could literally do anything.
School 6, peer supporter paired interview 1, peer supporters 67 and 52
Acceptability of having conversations about drugs
The majority of parents and teachers found it acceptable for the peer supporters to be disseminating information to their peers about the risks of drug use during informal conversations. Some teachers and peer supporters felt that students in this year group had not yet learned much about the harms of drug use and so this made the job easier as it would be something that they were interested in hearing about:
We have learned quite a lot about smoking over the years. But drugs is a bit, you know, it’s like untouched upon subject, like I’ve never, you know, been sat down and taught about drugs.
School 3, peer supporter paired interview 1, peer supporter 46
I think with the majority of my friends, erm, they haven’t tried drugs, and like me, they didn’t know a lot, so when I would come back and tell them a few facts, they would be really interested and I think that helped, because they wanted to know more . . . They were like really interested, didn’t know a lot, so when I was coming to tell them they were erm, kind of overjoyed that they were learning something different all the time.
School 6, peer supporter paired interview 1, peer supporters 67 and 52
The fact that drug use is less prevalent than smoking was discussed as being both a facilitator of and a barrier to having conversations about drugs. Some school staff felt that the illegality of drug use reduces its acceptability, but for others the illegality was seen as a facilitator of having conversations:
When you talk to them, yes, they had had conversations, and I wonder whether it’s a bit easier to talk about that, rather than smoking, because drugs is, you know, an illegal action, whereas quite a lot of people smoke, even if . . . at certain ages it’s usual, but it’s more acceptable to young people.
School 3, teacher 1, school contact
Some +FRANK peer supporters felt that the lack of drug use among their peers made it easier to broach the subject compared with smoking:
It was . . . I don’t know . . . it felt easier to do them on drugs instead of smoking, because it just felt like that, like . . . hardly anyone would be doing that.
School 4, peer supporter 15
Reducing barriers to initiating conversations
The fact that the training provided interesting and appropriately sized ‘facts’ to be used in conversations was valued by some peer supporters:
They told us facts that we can take into our conversations with other people . . . the facts was only small facts so it was easy to remember.
School 7, peer supporter 83
In general, peer supporters found that short, memorable facts were useful, especially for initiating conversations with their peers. Memorable facts mainly fell into two categories: first, shocking facts about potential health risks, which often focused on GGAs, and, second, those that contradicted commonly held myths about drugs, such as the prevalence of drug use in their age group or the addictive nature of cannabis:
With the glues, gases and aerosols, erm, they’re easy to get access to and I was completely shocked when I heard erm, the sudden sniffing death, that . . . that like literally blew me over. I think it really erm, stunned a lot of people.
School 3, peer supporter 140
It like surprised a lot of people . . . Like lots of people thought 15% was very low. I thought like a lot more people took drugs . . . 15%, that’s pretty low I think. It just like stuck in my brain like whoa this isn’t what I thought.
School 2, peer supporter 84
The one about one in 10 people get addicted to cannabis when they smoke it. So it’s like they know to not smoke it in case they do get addicted.
School 7, peer supporter 51
Face-to-face compared with electronic means of communication
Some peer supporters reported that having conversations face-to-face was easier, and more appropriate, than doing so by text message or social media. It was felt to be of particular importance when discussing such a sensitive topic because being able to read non-verbal cues helped with gauging the reactions of their peers to the conversation:
Also if you’re sat with the boys, straight away you can tell how they feel about the conversation. You can tell if they’re nervous, they’re surprised. By text, if they go ‘wow, I never knew that’, you don’t know, that could be sarcastic, that could be whatever.
School 2, peer supporter 89
The potential for misunderstandings to be caused when communicating by text message or social media was also of concern to peer supporters:
I think it was more easy to understand face to face. Me and some of my friends have had conversations about it on the phone. But I think if . . . if I was texting it, maybe they would take it the wrong way. Because you can read the text and think, oh, they’re having a go at me or something, so read it the wrong way. So I was afraid to do that. I think it was more easy and relevant to speak face to face with people instead. I think it’s easier to express your feelings face to face, because you can just come out with it, and it’s harder on social media.
School 3, peer supporter 140
Some peer supporters commented that it would be strange to start a conversation about drugs on social media as this is not what they use it for normally.
Follow-up sessions
Most peer supporters reported that the follow-up sessions were helpful for refreshing knowledge and prompted them to continue to have conversations with their peers:
And the follow-up sessions, what did you think of these?
Yeah just a good reminder, just with the time gaps in between, it just helped you refresh.
Recapping overall facts, so if you’d forgotten one, you’d be like oh yeah I had forgotten about that one and then use that in the next conversation and you’d remember it then.
Trainers were able to provide guidance during follow-up sessions on having conversations:
Like if you were stuck on conversations . . . they [trainers] were always there to like straight, help you straightway like so they were always there straightway.
School 4, peer supporter 61
Some peer supporters and teachers commented that the follow-up sessions were less engaging than the training day(s), partly because they were carried out at school:
I think they started to get boring towards the end really, towards the end, we didn’t really do anything to do with it really.
School 4, peer supporter 97
I know it’s not a lesson and the guys running it aren’t teachers, I do appreciate that . . . but just to stimulate and engage the kids . . . I just felt it could be a little bit more zippy in those follow-up sessions.
School 1, teacher 1, school contact and SMT
Trainers
All peer supporters perceived the trainers to be friendly and helpful. This increased peer supporters’ desire to engage with the intervention:
I think I liked it because they were friendly enough, and they were like more like people than other ones because they try to be like too serious and that can get really boring and you like don’t take notice.
School 1, peer supporter 34
All peer supporters reported that they felt comfortable raising issues or concerns with the trainers:
I think the . . . trainers . . . themselves were friendly and encouraging so we knew we could go to them at any time and it was very like secure.
School 1, peer supporter paired interview 1, peer supporter 70
The majority of peer supporters were also confident that trainers would be able to provide credible and accessible information:
I think they were knowledgeable because every time one of us asked them a question about a certain drug or something they’d have an answer straight away, they knew what they were saying.
School 7, peer supporter 99
Peer supporters from the +FRANK intervention were pleased to work with the trainers who they had worked with during the ASSIST intervention.
Well it was a good thing that we had [trainer] again because like we kind of already knew him and like his way of like doing the programme.
School 4, peer supporter 61
Usefulness of the Talk to FRANK website
Most of the peer supporters and trainers stated that the Talk to FRANK website was a useful resource to support their roles. Trainers used the website when they did not know the answer to a question. Most peer supporters found the website accessible in terms of layout and access from mobile phones, with age-appropriate content:
It wasn’t hard to understand either. That was straight forward as well. I think it’s really useful because if I don’t know any information and [my friends] ask me something, I could literally go on my phone, quickly type in Talk to FRANK website and I could go on there and even if I don’t know where to get the information, it’s clear to click on something, oh there’s the information they need and then tell them.
School 7, peer supporter 99
There was more facts on there, there was more names of drugs, there was personal experiences, so it was all helpful if you were still having the conversations.
School 4, peer supporter 61
Peer supporters also used the website if asked a question that they could not answer. The A-Z of drugs drop-down menu, which provided a glossary of drugs, was cited as being a useful feature when they were asked a question that they could not answer:
There’s loads of like different names of drugs isn’t it and they have like all the names on there, so it’s like if one person says to me what’s that, they can have a look and it tells you what it is like.
School 2, peer supporter 171
Peer supporters found the personal stories of drug misuse posted on the website useful:
Quite useful, because it has stories on there from people who’ve suffered from drug use.
School 4, peer supporter 97
Importance of contact teachers
All trainers noted the importance of having contact teachers who were supportive and who encouraged peer supporters to engage with the intervention, as well as being well organised:
He’s the teacher we always go to if you have a problem or something, we’re told to go to him . . . So yeah it’s good.
School 1, peer supporter paired interview 1, peer supporter 70
And you know, I had different people e-mailing me from the school, at different times, even communication within the school you know, with each other they didn’t know what each other were doing and I was kind of like the middle person at one point.
Trainer 1
One peer supporter did not feel well supported as the contact teacher was too busy. Another peer supporter stated that non-teaching staff should not take on the role of a contact teacher as they may not have the authority required and peer supporters may not listen to them.
Interaction between the school context and the intervention
Across schools there was variation in the commitment of contact teachers, support provided for peer supporters and the visibility and ease of organisation of the intervention. Most trainers and teachers stated that having the buy-in and commitment of the school, especially the SMT and contact teacher, was vital in ensuring that the intervention was implemented as planned:
Senior leadership need to buy into it and make sure that, you know, that the contact teacher is engaged, has the time to actually commit to the programme and gain an understanding of the programme erm and they need to be supporting it from a whole school approach so you know even form tutors should be saying in form tutoring, you know we’ve got students that have engaged in this, how’s it going, you know they should be encouraging it throughout the school rather than just in the 1-hour sessions that we book it in.
Trainer 2
Some teachers commented that members of school staff needed to champion the intervention for the students to take it seriously:
I think [the contact teacher] should be a member of staff who’s interested, and is willing to support the programme, and to keep supporting it as it goes through, I think that’s really important, because if you’re not positive yourself, you’re not going to give weight to the programme.
School 3, teacher 1, school contact
Unintended benefits of being a peer supporter
Many peer supporters, teachers and parents thought the peer supporter role brought broader benefits, including increased confidence and improved communication skills, which they linked to future career prospects and examination success:
Yes, yes, for future jobs, they can be more like . . . gives us the skills, like communication skills.
School 1, peer supporter 46
Did you get any feedback from your parents about what they thought?
I just told my mum about it and she said that’s good, really good on you. Like she was like for when you go to university and stuff.
My mum was pleased because she said it improved my confidence and she said like she can see and I’ve improved others.
Could help with different exams I guess in school, like the oral exam things and presentations in English.
School 1, teacher 1, school contact and SMT
Several teachers commented that nominated students would be more likely to become engaged in other activities within the school as they were recognised as having matured as a result of the additional peer supporter role:
Well now that they’re, they’re aware of the facts, they can take on a teacher role can’t they really they, they can make students aware. Or they can speak to their, their, you know, their um classes about it. They could give talks about it couldn’t they? You know, so when we’re doing, there’s usually a drug awareness week isn’t there. You could actually involve them. Within their form classes. Or even in the assembly.
School 7, teacher 2, SMT
Some of them [peer supporters] are already involved in other groups as well, er . . . you know, they have the option to join these groups or . . . for the School Council they’re nominated. So it could be that er . . . you know, some of them finding a . . . that haven’t been nominated before . . . That actually, they’ve got a voice and . . . And they could be sort of nominated in future for things like the School Council.
School 3, teacher 2, school contact
Comparing the +FRANK and FRANK friends interventions
In the +FRANK intervention, the intervention was delivered in Year 9 but peer supporters were those nominated in Year 8. Some peer supporters commented that they might not have been renominated if the nomination process was repeated, whereas others felt that they would have been. One teacher felt that friendship groups and those who were influential did not change between Year 8 and Year 9.
I think it doesn’t change greatly [from Year 8 to Year 9] and it doesn’t change greatly throughout school. Those people who are what we’d call ringleaders then, they tend to remain quite a force throughout the time.
School 4, teacher 2, SMT
In the +FRANK intervention the off-site training of peer supporters takes place over 1 day whereas in the ASSIST and FRANK friends interventions training takes place over 2 days. All of the trainers commented that they were pushed for time to cover all of the contents of the +FRANK intervention in 1 day, leading to them ‘rushing’ to deliver the full training (Trainer 2). As the +FRANK training was new to them they needed time to become familiar with the delivery, which may in part have accounted for this pressure, but an awareness of being observed to meet the learning objectives of the activities added extra pressure:
I think we really struggled for timing and fitting everything in and it seemed quite chaotic I suppose, we tried to make sure everything was covered and um I think we were all quite conscious of making sure that we were ticking the right boxes along the way as well.
Trainer 3
One trainer commented that the gap between the ASSIST intervention and the +FRANK intervention was potentially over a year and so peer supporters would have benefited from receiving a refresher session on conversation skills, which was not possible within a 1-day training course:
I just felt erm, yeah, there wasn’t enough time. I know they’ve already done day 2 of ASSIST but I did feel we could have spent a little more time on discussing the skills . . . Erm, you do need to have time to concentrate on the skills and recap all their communication skills and their teamwork . . . It’s not just about them learning about the facts.
Trainer 1
At one site, peer supporters would have liked the +FRANK training to have been carried out over 2 days:
Too much for 1 day, they should spread it out over 2 days.
School 4, peer supporter group interview 1, peer supporter 91
One trainer noted that peer supporters were disappointed that it was a 1-day training course rather than a 2-day course as in the ASSIST intervention. As a result, peer supporters were less engaged, which the trainer also felt could be because of the lack of novelty:
I think because they had 2 days’ training the year before, it was a little bit of a disappointment, erm, I know there were some at recruitment, we said actually just 1 day this time. You know you could see they were a bit like oh, I think that comes down to the fact that every kid wants 1 or 2 days off school and plus they knew what to expect this time around.
Trainer 1
Trainers noted that the 2 days of training in the FRANK friends intervention meant that they felt more relaxed as they had time to answer questions and had greater flexibility over the timings of the activities. The extra day of training gave trainers a ‘breathing space’ (trainer 1). They were also more experienced at delivering the training on drugs as the delivery of the +FRANK intervention preceded the delivery of the FRANK friends intervention.
There was no consistent message from trainers with regard to which intervention to roll out in the future. Two trainers felt that the FRANK friends intervention was better at securing student engagement and providing support than the +FRANK intervention:
Yeah, it’s been a bit of a mix but you know I would say if it was to be rolled out long term then probably FRANK friends is more effective in that it’s a new experience for the peer supporters to get the 2 days of training so they look at the skills and they get the facts, they get the four follow-ups but I think what is essential is that initial stage the school really understand what it is that they’re engaging on and you know that they support it from the offset.
Trainer 2
Another trainer found it hard to judge as the +FRANK and FRANK friends schools were very different:
Um I think, well it feels like, I think, it’s really hard to say which one I think um has worked the best +FRANK or FRANK friends. Because there’s a vast difference between um through FRANK friends schools.
Trainer 4
Modifications for future delivery
Three parents would have liked more detailed information or somewhere to refer to for more information:
Erm, I know, I know it was only a brief, brief letter, you know what I mean, er, it would have been nice some sort of website on there or something, because I didn’t see anything like that on there.
School 4, parent 1
Some teachers and students noted that there was a low level of awareness of the interventions in the schools. They suggested that in the future the intervention should be more widely publicised in schools:
Teachers weren’t educated on what we’re actually doing . . . There’s been a few times when it’s been like oh you guys, you’ve got FRANK. OK, well the teacher’s been like what’s FRANK?
OK, so there’s something here then about the way the school shares the information.
Trying to like tell the teachers. So like they’ve been chosen by their peers as influential members. Because I know that now that our head teacher gave us our certificates. I know that he knows now that our group is, you know, well behaved and influential. We might get asked to do other things. Which maybe we would fit the role of, so it would be nice if other teachers knew that too. So if they ever wanted something like that.
I do think with perhaps regards to what we’re doing in school is perhaps . . . embedding it a little bit more from a school perspective . . . I think you know so making sure there are regular erm, regular sort of erm announcements and notices to all of our learners that these learners are in school. Perhaps making sure we’ve got a display up and running because we did have a display up and running when they did erm the ASSIST course . . . So they know there are people they can go to for that support.
School 6, teacher 2, SMT
Chapter 4 Discussion
We have successfully developed two school-based peer-led interventions to prevent illicit drug use in young people aged 13–14 years. We used a three-stage design to coproduce the interventions with stakeholders, test their feasibility and refine them, before conducting an external pilot cRCT. This chapter presents the main findings of the study against our objectives and suggests modifications that should be incorporated into a fully powered cRCT.
Objective 1: adaptation of the ASSIST intervention to drug prevention and development of the +FRANK and FRANK friends interventions
In stage 1 we used a three-phase framework to adapt intervention materials from the ASSIST intervention to deliver information from the Talk to FRANK website to an older year group, as well as prototyping new content and delivery methods. The process took 18 months and consisted of 42 activities, including consultations with young people in Years 8 and 9, staff from drug charities who delivered drug education, health promotion specialists, ASSIST peer supporters, the lead author of the ASSIST RCT23 and a DECIPHer IMPACT trainer (which licenses and trains all ASSIST delivery staff). By doing so we were able to address any potential issues with the intervention content, delivery process and fit to the school context that might arise during implementation.
We conducted a scoping review of population-level prevalence studies on drug use in the UK and RCTs of peer-led drug prevention. The latest population-based prevalence study in the UK showed that the lifetime prevalence of any drug use more than doubled between 13 (11%) and 15 (24%) years of age. 6 This led us to target delivery to UK Year 9 students (aged 13–14 years). In this prevalence study, cannabis (13 years: 2.8%; 15 years: 15.8%) and GGAs (13 years: 3.7%; 15 years: 1.9%) had the highest lifetime prevalence in 13- to 15-year-olds. 6 At the age of 15 years, magic mushrooms, cocaine, speed, mephedrone and legal highs also had a prevalence of > 1%. 6 Consultation with local drug agencies suggested that there was a problem with steroid use in South Wales. We therefore chose to focus the interventions on these drugs, with the time devoted in the training of intervention delivery staff and peer supporters proportional to their lifetime prevalence.
The consultations with stakeholders led us to develop intervention activities focused on delivering information from the Talk to FRANK website on the risks of illicit drug use for short- and long-term health, the legal consequences of a caution or conviction for possession (e.g. restricted job and travel prospects), the potential impacts on educational performance, the risks of school suspensions and exclusions and the potential shame and stress caused to family members from drug use. We then used an iterative process of prototyping intervention materials through repeated delivery and interviews with trainers and peer supporters to identify problems and make amendments.
Objective 2: test the feasibility of the +FRANK and FRANK friends interventions
Assessing the acceptability of the +FRANK and FRANK friends interventions to trainers, students, parents and members of school staff and exploring the barriers to and facilitators of implementation
In stage 2 we conducted a process evaluation examining the delivery and receipt of the +FRANK and FRANK friends interventions in one school each. Two members of the research team made independent observations of all intervention activities, including follow-up sessions. In the +FRANK intervention we carried out seven observations, collected 34 evaluation forms and conducted 13 interviews with peer supporters and trainers. In the FRANK friends intervention, we carried out 15 observations, collected evaluation forms of the training from 47 peer supporters and trainers, conducted 29 interviews with peer supporters, trainers and teachers (including members of the SMT) and held five focus groups with peer supporters.
We assessed peer supporter attendance during the interventions. In the +FRANK school, 12 of the 14 peer supporters attended follow-up sessions 1 and 4, which were carried out in person. Only one peer supporter completed the e-follow-up sessions. In the FRANK friends school, between 16 and 21 of the 26 trained peer supporters attended the four follow-up sessions. Independent observations of intervention delivery and interviews with trainers found that some activities were too long, others were too short and the sequencing of activities could be improved.
Fidelity of delivery
In the +FRANK intervention, across the 15 activities, five were delivered in full, eight had minor deviations and two were not delivered at all. In the FRANK friends intervention, across the 25 activities, 13 were delivered in full, nine had minor deviations and three were not delivered at all. The observations suggested that some trainers had struggled to switch off from the coproduction stage.
Refining the interventions
The attendance records, interviews and structured observations led to changes in the +FRANK intervention. We removed the electronic follow-up sessions and dropped the final follow-up in which peer supporters received a certificate from the trainers. These were replaced with three face-to-face follow-ups. Other changes applied across both interventions, including changes in the content and sequencing of peer supporter training activities and highlighting in the instruction manual which activities were essential and which were optional. These barriers to delivery would not have been identified and the accompanying refinements would not have been made without this initial feasibility testing.
Objective 3: conduct an external pilot cluster randomised controlled trial of the +FRANK and FRANK friends interventions
In the stage 3 external pilot cRCT, all progression criteria for the +FRANK and FRANK friends interventions were met.
Assessing the feasibility and acceptability of the refined interventions to trainers, students, parents and school staff
The process evaluation involved 66 interviews with peer supporters, PHW intervention delivery staff, school staff including members of the SMT, PSHE leads and contact teachers and a commissioner of public health interventions. Independent structured observations of the delivery of all intervention activities (n = 195; n = 111 for the FRANK friends intervention) were made by two members of the research team.
In the +FRANK arm, 92% of the ASSIST peer supporters were recruited and retrained and 92% of the peer supporters reported at least one conversation and all reported a contact with intervention delivery staff. In the FRANK friends arm, 82% of the peer supporters were trained and 94% of the peer supporters reported at least one conversation and all reported a contact with intervention delivery staff. The success in meeting these criteria is likely to reflect that the ASSIST training materials that we adapted had been adequately tested and refined. Our study design also allowed for stakeholder concerns to be elicited and addressed before implementation.
The qualitative analysis suggested that most elements of the interventions were acceptable to students, teachers and parents:
-
School setting. Teachers and parents noted that schools were an acceptable environment to deliver drug education to young people. Trainers and teachers thought that involving someone from the SMT and having a committed contact teacher were needed to facilitate intervention delivery.
-
Peer nomination. The ASSIST peer nomination approach to intervention delivery was regarded as preferable and more credible by parents and the public health commissioner than didactic drug education in schools.
-
Peer supporter role. Peer supporters reported feeling comfortable having conversations about drugs with their school friends, particularly with regard to the risks of drug use for health,. They thought that the training on communication skills would help in oral examinations and with their future employment. Teachers reported that they thought that the peer supporter training had increased some students’ confidence and they had involved them in other school activities.
-
Follow-up sessions. Peer supporters noted that follow-up sessions were helpful and acted as a prompt to continue having conversations with peers. This may in part be because trainers were perceived to be friendly, credible and knowledgeable.
-
The Talk to FRANK website. The website was perceived positively, with peer supporters noting that it was easy to access (including by mobile phone) and to understand. In particular, the A-Z feature was cited as a commonly used feature when they were asked a question about a drug they did not know.
Assessing the fidelity of delivery of the interventions by trainers
All +FRANK and FRANK friends intervention activities (100%) were delivered as intended. This is a substantial improvement in meeting the essential learning objectives from that found for intervention delivery in stage 2. This may be attributed to amendments made to the intervention manuals, content, timings and sequencing based on requests by trainers and discussions by the IDG. Trainers are likely to have improved their knowledge of the materials and delivery and the questions that are commonly asked by students. Trainers’ awareness of being observed and scored may also have improved adherence.
Comparing the feasibility and acceptability of the +FRANK and FRANK friends interventions
The progression criteria relating to feasibility and acceptability were met for the +FRANK and FRANK friends interventions. However, the process evaluation indicated that the hypothesised intervention logic may not hold as well for the +FRANK intervention as for the FRANK friends intervention. In the +FRANK schools, students completed the peer nomination process in Year 8 and Year 9. Around one-third of the +FRANK peer supporters were not nominated as being the most influential by their peers in Year 9. This meant that other students who were perceived to be influential in Year 9 were not trained to be peer supporters. This is a potential barrier to the diffusion of the messages from the Talk to FRANK website as the intervention logic model for the ASSIST intervention is predicated on peers being perceived as influential and a sufficient proportion (17.5% in the ASSIST intervention) of these influential peers being trained.
Although we were able to re-recruit 92% of Year 8 ASSIST peer supporters to reprise their role as a +FRANK peer supporter in Year 9, the number of peer supporters available to train in the +FRANK intervention is limited by the number of ASSIST peer supporters. In the FRANK friends intervention, if a parent or student does not consent to attend training, the student with the next highest number of nominations is invited, thus maintaining an ideal 17.5% of the year group trained. In the +FRANK intervention this cannot occur and so a lower proportion of students may be trained. Consequently, the diffusion of information is reduced as there would be a smaller number of peer supporters relative to other students.
Trainers reported feeling rushed in terms of delivering the content in the +FRANK intervention as training took place over 1 day, whereas the FRANK friends training took place over 2 days and the trainers could spend more time on activities and answering questions. One trainer and two peer supporters mentioned that more training on communication skills was needed. One trainer also noted that +FRANK peer supporters were disappointed that training took place over only 1 day as they were expecting the training to last for 2 days, as in the ASSIST intervention.
For these reasons, we recommend that the FRANK friends intervention is taken forward to a full-scale trial.
Assessing trial recruitment and retention rates
Of the 40 schools invited to participate, 12 provided no response and eight declined to participate. Of the 12 who provided no response, it is not clear whether they would have participated. Of the 18 schools visited by the research team, only one withdrew and another could not commit to the data collections. Of the 16 remaining schools, 12 took part in the cRCT, two were kept in reserve and two were used in the stage 2 feasibility testing. Because of delays in the contracting process, we deliberately oversampled schools to be invited to ensure that 12 schools were recruited by the start of the school term. In any subsequent trial we would have a longer recruitment period and would anticipate a higher rate of recruitment.
The 12 schools recruited were randomised and retained at the 18-month follow-up. In total, 93% of eligible students were recruited at baseline and retained at the 18-month follow-up. The retention of schools might be attributed to the signing of a memorandum of understanding by a member of the SMT. The memorandum of understanding clearly laid out the timing of the intervention delivery and data collections. Schools were also paid to supervise data collections. The high recruitment and retention rates were probably the result of the recruitment and data collection processes that we had refined during other school-based studies. We monitored recruitment and retention rates and conducted multiple follow-up collections for absent students.
Pilot outcome measures
We found low rates of missing data for almost all variables. The highest rate of incomplete data (23%) was for the CAST measure of cannabis dependency at baseline. As the lifetime prevalence of cannabis use was only 2.4%, this represented eight people not completing the measure. This measure may not have been completed because of a combination of the measure requiring six responses, a need for clearer signposting in the filter questions or lack of comprehension. At follow-up, 13.7% of responses were missing on the CAST. This reduction in the proportion of missing responses on the CAST may be the result of changes made to the follow-up questionnaire to improve the filtering of cannabis users or improvements in understanding of the instructions. There was some evidence of floor effects for the measures of nicotine dependence, with median scores at baseline of 0 on the HSI and 0.5 on the FTND. At follow-up, the median score was 2.0 on the FTND and 0.0 on the HSI. This suggests that there may be limited value in assessing nicotine dependence in this age group in the UK as levels of dependency are low.
The prevalence of lifetime drug use at baseline was 4.1%. The most commonly used drugs were cannabis (2.4%) and GGAs (2.2%); all other drugs had a prevalence of < 1%. At the 18-month follow-up, the prevalence of lifetime drug use was 11.6%. The ICC for illicit drug prevalence at follow-up for the comparison between usual practice and the FRANK friends intervention was 0.003 and for the comparison between usual practice and the +FRANK intervention was < 1 × 10–8. These estimates suggest that, between 13 and 15 years of age, the prevalence of lifetime drug use nearly triples, which provides justification for our decision to deliver the interventions to this age group.
The most common drugs used were cannabis (8.0%), GGAs (4.0%), legal highs (1.7%) and cocaine (1%). Of those who used, the majority had done so in the past 12 months. Use of cannabis in the last 30 days (21.9%) was more common than use of GGA (5.3%) in the last 30 days, with cannabis (8.9%) and cocaine (1.2%) the only drugs that were used by > 1% of students in the last week. In total, 35% of the 117 students who reported ever trying cannabis screened positive for cannabis dependency. The pattern of lifetime prevalence of specific drugs, with cannabis and GGA being the most prevalent, replicates that found in the most recent population-based study in the UK. 6
The lifetime prevalence of illicit drug use at 18 months was 9.5% in the ASSIST arm, 9.7% in the FRANK friends arm, 15.1% in the +FRANK arm and 11.7% in the usual practice arm. There was an imbalance in baseline risk factors for drug use, with living without an adult in employment53 and in social housing54,55 more common in the +FRANK arm than in the other arms. This imbalance is likely to be attributable to the small number of schools per arm. In a larger full-scale trial, a larger number of schools would be randomised into each arm, thus reducing the potential for imbalances. As the sample size in this study was not determined by a formal power calculation but by convenience, effect sizes should be interpreted with caution as there is a risk of a type 2 error with underpowered comparisons. In an adequately powered trial we could be more confident that a sufficient number of students were included in the analysis to detect a difference across arms.
Of the 65 drug users at baseline, 27 (41.5%) recanted use in the follow-up survey. The recanting of lifetime drug use has been found in a number of prospective cohort studies. 56,57 The rate that we found was slightly lower than those recorded in other UK-based studies, such as the Belfast Youth Development Study (63.8% for 10 illicit drugs assessed at between 12 and 15 years of age),58 but higher than those in the ALSPAC birth cohort [14.4% cannabis, 25.2% other illicit drugs (cocaine, amphetamines, inhalants, sedatives, hallucinogens, opioids), assessed at between 14 and 18 years of age],59 although our survey was undertaken with students of a different age range. These studies found that recanting is less common in adolescents reporting higher levels of cannabis use. 58,59 As prevalence was lower in this study than in the previous studies, partly because of population-level declines in the prevalence of drug use,58,59 selection of a younger age group than in these analyses and a shorter follow-up period, we might expect higher rates of recanting in our study. Importantly, we found the highest rates of recanting in the usual practice arm, suggesting that this was not attributable to performance bias, in which participants change responses after exposure to the intervention.
It has been suggested that recanting is less likely to be the result of intentional distortion but rather the result of poor comprehension, forgetfulness or even carelessness. 56,57 Consistent with this suggestion, we found that between baseline and follow-up, seven students’ gender changed and 47 (3.0%) students changed their date of birth. An alternative explanation is that recanting may be logical. The perception by students of whether their use of a drug constituted ‘trying it’, or in the case of GGAs ‘to get high’, may change with age, comprehension and exposure to drug use. One suggestion for addressing the issue of recanting would be to use objective biomarkers of drug exposure. Unfortunately, objective measures of cannabis use have a poor sensitivity in population surveys, even for heavy daily users, over periods of > 3 months. 60,61 This would preclude identification of a significant proportion of lifetime cannabis use in our study as around 40% had not used cannabis in the past 12 months. This is in addition to other problems of using biomarkers of lifetime drug use, including there being no test currently available for all controlled substances if taken > 3 months ago and there being no test at all for novel psychoactive substances. These limitations are in addition to the likely pragmatic, methodological (e.g. response bias) and ethical (e.g. acceptability to students and parents) barriers to collecting hair samples on thousands of young people. For these reasons, self-report measures have recently been described as still representing the ‘gold standard’ in assessing the use of illicit drugs. 61
Recording the delivery costs and piloting methods for assessing cost-effectiveness
The interventions were developed and delivered at an affordable average cost per school. The estimated cost per school for the +FRANK intervention was £1942 (£13.87 per student) and for the FRANK friends intervention was £3041 (£20.69 per student). It is important to note that schools could not receive the +FRANK intervention alone as there is a requirement to receive the ASSIST intervention first. As the ASSIST intervention is of the same intensity as the FRANK friends intervention it has the same cost implications as the FRANK friends intervention. This means that the approximate costs of the ASSIST plus +FRANK interventions are those of the FRANK friends plus +FRANK interventions (£4983).
Assessments of the cost-effectiveness of school-based drug prevention interventions are relatively scarce. When economic evaluations have been performed, cost-effectiveness analyses are available only for studies conducted in the USA,62 and neither of the two peer-led programmes20,21 have examined cost-effectiveness. Our study provides preliminary information on the costs borne by the NHS, as public health services reside in the NHS in Wales. The study has demonstrated that it is feasible to conduct an economic evaluation alongside a pilot cRCT of a school-based intervention to prevent drug use. However, to fully judge the cost-effectiveness of the intervention the within-trial estimates of intervention costs, and the prevalence of drug use, would need to be extrapolated over the lifetime of participants. 63
Objective 4: determine the design, structures, resources and partnerships necessary for a full-scale trial to take place
For the definitive trial we propose a two-arm cRCT (randomisation at school level), with integrated economic and process evaluations. The hypothesis for the full-scale trial would be that the FRANK friends intervention is more effective and cost-effective at preventing illicit drug use in young people (aged 13–14 years) than a control condition of usual practice. The primary outcome would be lifetime illicit drug use. The secondary outcome measures would be all those used in the 18-month follow-up in the external pilot cRCT, except for the FTND41 and HSI. 41,42
Strengths and limitations
We collected both quantitative and qualitative data to assess the acceptability of the +FRANK and FRANK friends interventions and trial assessments and methods. This approach enabled triangulation of data to strengthen the internal and external validity of the findings. Focus group and interview data from teachers, students and parents enabled an in-depth exploration of their experiences and views of the interventions. This information was used in stages 1 and 2 to refine the intervention.
We used a robust qualitative methodology for data collection, analysis and reporting from a large sample, allowing detailed exploration of the core elements of the intervention and saturation of dominant themes. The students, teachers and parents who took part in the focus groups and interviews were, however, a self-selecting sample. Those who did not take part may have given different responses from those who did choose to participate. For example, the students who volunteered may have been those who were more receptive to information on the harms of drugs. Similarly, parents who were interviewed may have been more engaged in their child’s schooling than those who were not. However, teachers and students were forthcoming when discussing what they did not like about the interventions.
A further strength of the study was the contribution of key stakeholders to the delivery and implementation of the school-based drug prevention interventions. These stakeholders included students, ASSIST trainers, parents, teachers (SMT and other roles) and, in addition to young people who had received the ASSIST intervention, the lead trainer of ASSIST delivery staff, drug agency staff, older adolescents and a public health commissioner. The involvement and contribution of stakeholders was integral to the development, refinement and evaluation of the interventions.
Conclusions
The +FRANK and FRANK friends peer-led drug prevention interventions were acceptable to peer supporters, teachers and parents. It was feasible to conduct a cRCT of these interventions in a school setting with young people age 13–14 years. The process evaluation indicated that the FRANK friends intervention was preferred over the +FRANK intervention. Qualitative, quantitative and economic evidence suggests that there should be a follow-on full-scale cRCT of the FRANK friends intervention.
Acknowledgements
We would like to thank all of the participants. Particular thanks go to the PHW intervention delivery staff who helped develop the intervention: Mathew Taylor, Buddug James, Elizabeth McIntosh, Alwen Jones, Eiddan Harries, Shakira Leslie, Rebecca Williams and Gemma Cox.
Contributions of authors
James White (Senior Lecturer, Public Health) led the study and preparation of the report.
Jemma Hawkins (Research Fellow, Public Health) coproduced the intervention content, conducted the interviews and observations and wrote up the results for publication.
Kim Madden (Research Associate, Public Health) managed the trial, coproduced the intervention content and managed the process evaluation and wrote up the results for publication.
Aimee Grant (Research Fellow, Public Health) conducted the interviews and observations and wrote up the results for publication.
Vanessa Er (Research Associate, Public Health) analysed the qualitative data and wrote up the results for publication.
Lianna Angel (Data Manager, Trial Methodology) organised the data entry, drafted the CONSORT diagram and contributed to writing of the report.
Timothy Pickles (Research Associate, Statistics) carried out the statistical analysis and contributed to the writing of the report.
Mark Kelson (Research Fellow, Statistics) managed the statistical analysis and contributed to the writing of the report.
Adam Fletcher (Professor, Social Science and Health) contributed to the design of the interventions and research and provided expertise in qualitative data analysis in complex interventions.
Simon Murphy (Professor, Social Interventions and Health) contributed to the design of the interventions and research and provided expertise in process evaluations of complex interventions.
Luke Midgley (PhD student, Public Health) conducted the interviews and observations of intervention delivery and wrote up the results for publication.
Gemma Eccles (Undergraduate Student, Psychology) conducted the interviews and wrote up the results for publication.
Gemma Cox (Senior Public Health Practitioner, Public Health) contributed to the development of the interventions and wrote up the results for publication.
William Hollingworth (Professor, Health Economics) conducted the analysis on the costs of the interventions and contributed to the writing of the report.
Rona Campbell (Professor, Public Health Research) reviewed the intervention materials.
Matthew Hickman (Professor, Public Health and Epidemiology) reviewed the primary and secondary outcome measures and provided expertise in the assessment of illicit drug use and drug prevention.
Chris Bonell (Professor, Public Health Sociology) provided expertise in the evaluation of drug prevention interventions in schools, the epidemiology of school-level risk factors and process evaluations.
Laurence Moore (Director, MRC/CSO Social and Public Health Sciences Unit) provided expertise in the design and evaluation of complex public health improvement interventions.
Publication
Hawkins J, Madden K, Fletcher A, Midgley L, Grant A, Cox G, et al. Development of a framework for the co-production and prototyping of public health interventions. BMC Public Health 2017;17:689.
Data sharing statement
All available data can be obtained by contacting the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Babor T. Drug Policy and the Public Good. Oxford: Oxford University Press; 2010.
- Misuse of Drugs Act 1971. London: The Stationery Office; 1971.
- Psychoactive Substances Act 2016. London: The Stationery Office; 2016.
- The Cigarette Lighter Refill (Safety) Regulations 1999. London: The Stationery Office; 1999.
- Anti-social Behaviour Act 2003. London: The Stationery Office; 2003.
- Smoking Drinking and Drug Use among Young People in England – 2014. London: Health and Social Care Information Centre; 2015.
- Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, . GBD 2013 Risk Factors Collaborators . Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study. Lancet 2015;386:2287-323. https://doi.org/10.1016/S0140-6736(15)00128-2.
- Lopez-Quintero C, de los Cobos JP, Hasin DS, Okuda M, Wang S, Grant BF, et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug and Alcohol Depend 2011;115:120-30. https://doi.org/10.1016/j.drugalcdep.2010.11.004.
- Young People’s Statistics from the National Drug Treatment Monitoring System (NDTMS) 1 April 2014 to 31 March 2015. Manchester: Department of Health; 2016.
- Lynskey MT, Coffey C, Degenhardt L, Carlin JB, Patton G. A longitudinal study of the effects of adolescent cannabis use on high school completion. Addiction 2003;98:685-92. https://doi.org/10.1046/j.1360-0443.2003.00356.x.
- Roebuck MC, French MT, Dennis ML. Adolescent marijuana use and school attendance. Econ Educ Rev 2004;23:133-41. https://doi.org/10.1016/S0272-7757(03)00079-7.
- Horwood LJ, Fergusson DM, Hayatbakhsh MR, Najman JM, Coffey C, Patton GC, et al. Cannabis use and educational achievement: findings from three Australasian cohort studies. Drug Alcohol Depend 2010;110:247-53. https://doi.org/10.1016/j.drugalcdep.2010.03.008.
- Stiby AI, Hickman M, Munafè MR, Heron J, Yip VL, Macleod J. Adolescent cannabis and tobacco use and educational outcomes at age 16: birth cohort study. Addiction 2015;110:658-68. https://doi.org/10.1111/add.12827.
- Solowij N, Pesa N, Castle D, Murray RM, D’Souza DC. Marijuana and Madness. Cambridge: Cambridge University Press; 2012.
- Youth Justice Annual Statistics: 2014 to 2015. London: Ministry of Justice and Youth Justice Board for England and Wales; 2016.
- Rehabilitation of Offenders Act 1974. London: The Stationery Office; 1974.
- Statistics: Exclusions. London: Department for Education; 2016.
- Faggiano F, Minozzi S, Versino E, Buscemi D. Universal school-based prevention for illicit drug use. Cochrane Database Syst Rev 2013;12.
- MacArthur GJ, Harrison S, Caldwell DM, Hickman M, Campbell R. Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: a systematic review and meta-analysis. Addiction 2016;111:391-407. https://doi.org/10.1111/add.13224.
- Valente TW, Ritt-Olson A, Stacy A, Unger JB, Okamoto J, Sussman S. Peer acceleration: effects of a social network tailored substance abuse prevention program among high-risk adolescents. Addiction 2007;102:1804-15. https://doi.org/10.1111/j.1360-0443.2007.01992.x.
- Faggiano F, Vigna-Taglianti F, Burkhart G, Bohrn K, Cuomo L, Gregori D, et al. The effectiveness of a school-based substance abuse prevention program: 18-month follow-up of the EU-Dap cluster randomized controlled trial. Drug Alcohol Depend 2010;108:56-64. https://doi.org/10.1016/j.drugalcdep.2009.11.018.
- Rogers EM. Diffusion of Innovations. London: Simon and Schuster; 2010.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. https://doi.org/10.1016/S0140-6736(08)60692-3.
- Tobacco Control Strategy – Creating a Tobacco-Free Generation. Edinburgh: Scottish Government; 2013.
- Tobacco Control Action Plan for Wales. Cardiff: Welsh Government; 2012.
- School-based Interventions to Prevent the Uptake of Smoking among Children and Young People. Manchester: NICE; 2010.
- Drug Strategy Annual Review, 2014 to 2015. London: UK Home Office; n.d.; n.d.
- Smoking, Drinking and Drug Use among Young People in England – 2013. London: Health and Social Care Information Centre; 2015.
- Welsh Government . Local Authority Population Projections n.d. http://gov.wales/statistics-and-research/local-authority-population-projections/?lang=en (accessed 23 June 2016).
- Stokols D. Toward a science of transdisciplinary action research. Am J Community Psychol 2006;38:63-77. https://doi.org/10.1007/s10464-006-9060-5.
- Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods 2006;5:80-92. https://doi.org/10.1177/160940690600500107.
- Ritchie J, Lewis J, Nicholls CM, Ormston R. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage; 2013.
- Welsh Government . Welsh Index of Multiple Deprivation 2011 n.d. http://gov.wales/statistics-and-research/welsh-index-multiple-deprivation/?tab=previous&lang=en (accessed 12 September 2017).
- Austin PC. Estimating multilevel logistic regression models when the number of clusters is low: a comparison of different statistical software procedures. Int J Biostat 2010;6. https://doi.org/10.2202/1557-4679.1195.
- Carter BR, Hood K. Balance algorithm for cluster randomized trials. BMC Med Res Methodol 2008;8. https://doi.org/10.1186/1471-2288-8-65.
- University of Bristol . Life of a 16 + Teenager n.d. www.bristol.ac.uk/alspac/researchers/resources-available/data-details/questionnaires/documents/ques-922-life-of-a-16-plus-teenager.pdf.
- Fuller E, Hawkins V. Smoking. London: Health and Social Care Information Centre; 2014.
- Legleye S, Piontek D, Kraus L. Psychometric properties of the Cannabis Abuse Screening Test (CAST) in a French sample of adolescents. Drug Alcohol Depend 2011;113:229-35. https://doi.org/10.1016/j.drugalcdep.2010.08.011.
- Piontek D, Kraus L, Klempova D. Short scales to assess cannabis-related problems: a review of psychometric properties. Subst Abuse Treat Prev Policy 2008;3. https://doi.org/10.1186/1747-597X-3-25.
- Statistics on Smoking: England, 2013. London: Health and Social Care Information Centre; 2013.
- John U, Meyer C, Schumann A, Hapke U, Rumpf HJ, Adam C, et al. A short form of the Fagerström Test for Nicotine Dependence and the Heaviness of Smoking Index in two adult population samples. Addict Behav 2004;29:1207-12. https://doi.org/10.1016/j.addbeh.2004.03.019.
- Etter J-F. A comparison of the content, construct and predictive validity of the cigarette dependence scale and the Fagerström test for nicotine dependence. Drug and Alcohol Depend 2005;77:259-68. https://doi.org/10.1016/j.drugalcdep.2004.08.015.
- Kaner E, Bland M, Cassidy P, Coulton S, Deluca P, Drummond C, et al. Screening and brief interventions for hazardous and harmful alcohol use in primary care: a cluster randomised controlled trial protocol. BMC Public Health 2009;9. https://doi.org/10.1186/1471-2458-9-287.
- Stevens K. Assessing the performance of a new generic measure of health-related quality of life for children and refining it for use in health state valuation. Appl Health Econ Health Policy 2011;9:157-69. https://doi.org/10.2165/11587350-000000000-00000.
- Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 1996;276:637-9. https://doi.org/10.1001/jama.1996.03540080059030.
- Campbell MK, Elbourne DR, Altman DG. CONSORT group . CONSORT statement: extension to cluster randomised trials. BMJ 2004;328:702-8. https://doi.org/10.1136/bmj.328.7441.702.
- Hollingworth W, Cohen D, Hawkins J, Hughes RA, Moore LA, Holliday JC, et al. Reducing smoking in adolescents: cost-effectiveness results from the cluster randomized ASSIST (A Stop Smoking In Schools Trial). Nicotine Tob Res 2012;14:161-8. https://doi.org/10.1093/ntr/ntr155.
- White J, Moore L, Campbell R, Fletcher A, Bonell C, Murphy S, et al. Adapting and Piloting the ASSIST Model of Informal Peer-Led Intervention Delivery to the Talk to Frank Drug Prevention Programme in UK Secondary Schools (ASSIST + Frank): Intervention Development and a Pilot Trial 2014. https://njl-admin.nihr.ac.uk/document/download/2007574 (accessed 12 September 2017).
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance . Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Operation Smoke Storm . Interactive Education. Learning about Health n.d. www.operationsmokestorm.com/ (accessed 13 September 2016).
- Welsh Government . My Local School n.d. http://mylocalschool.wales.gov.uk/ (accessed 13 October 2016).
- McVie S, Norris P. Neighbourhood Effects on Youth Delinquency and Drug Use. Edinburgh: University of Edinburgh, Centre for Law and Society; 2006.
- Baumann M, Spitz E, Guillemin F, Ravaud J-F, Choquet M, Falissard B, et al. Associations of social and material deprivation with tobacco, alcohol, and psychotropic drug use, and gender: a population-based study. Int J Health Geogr 2007;6. https://doi.org/10.1186/1476-072X-6-50.
- Buu A, Dipiazza C, Wang J, Puttler LI, Fitzgerald HE, Zucker RA. Parent, family, and neighborhood effects on the development of child substance use and other psychopathology from preschool to the start of adulthood. J Stud Alcohol Drugs 2009;70:489-98. https://doi.org/10.15288/jsad.2009.70.489.
- Fendrich M, Rosenbaum DP. Recanting of substance use reports in a longitudinal prevention study. Drug Alcohol Depend 2003;70:241-53. https://doi.org/10.1016/S0376-8716(03)00010-3.
- Shillington AM, Reed MB, Clapp JD, Woodruff SI. Testing the length of time theory of recall decay: examining substance use report stability with 10 years of national longitudinal survey of youth data. Subst Use Misuse 2011;46:1105-12. https://doi.org/10.3109/10826084.2010.548436.
- Percy A, McAlister S, Higgins K, McCrystal P, Thornton M. Response consistency in young adolescents’ drug use self-reports: a recanting rate analysis. Addiction 2005;100:189-96. https://doi.org/10.1111/j.1360-0443.2004.00943.x.
- Taylor M, Sullivan J, Ring SM, Macleod J, Hickman M. Assessment of rates of recanting and hair testing as a biological measure of drug use in a general population sample of young people. Addiction 2016;112:477-85. https://doi.org/10.1111/add.13645.
- Gjerde H, Øiestad EL, Christophersen AS. Using biological samples in epidemiological research on drugs of abuse. Norsk Epidemiol 2011;21. https://doi.org/10.5324/nje.v21i1.1420.
- Taylor M, Lees R, Henderson G, Lingford-Hughes A, Macleod J, Sullivan J, et al. Comparison of cannabinoids in hair with self-reported cannabis consumption in heavy, light and non-cannabis users. Drug Alcohol Rev 2017;36:220-6. https://doi.org/10.1111/dar.12412.
- Caulkins JP, Rydell CP, Everingham SS, Chiesa J, Bushway S. An Ounce of Prevention, a Pound of Uncertainty: the Cost-Effectiveness of School-Based Drug Prevention Programs. Santa Monica, CA: RAND Corporation; 1999.
- Deogan C, Zarabi N, Stenström N, Högberg P, Skärstrand E, Manrique-Garcia E, et al. Cost-effectiveness of school-based prevention of cannabis use. Appl Health Econ Health Policy 2015;13:525-42. https://doi.org/10.1007/s40258-015-0175-4.
Appendix 1
| Have a go at answering whether you think the following statements are true or false (please mark an X in one box on every line) | True | False |
|---|---|---|
| 1. People under 18 cannot get arrested for possession of cannabis | ||
| 2. Cannabis is the main illegal drug that under 18s receive specialist drug treatment for | ||
| 3. Cannabis addiction occurs in about 10% of users | ||
| 4. A caution for a cannabis-related offence can stop you visiting the USA | ||
| 5. If a young person is caught with cannabis, their parent or guardian will be contacted by the police | ||
| 6. 60% of 16- to 24-year-olds have taken an illegal drug | ||
| 7. If a young person is caught with cannabis the school can permanently exclude them | ||
| 8. You can die the first time you sniff or inhale a GGA |
| Intervention | Group | Gender | n |
|---|---|---|---|
| Not applicable | Public Health Commissioner | 1 | |
| Both FRANK Friends and +FRANK | Intervention delivery trainer | Male | 2 |
| Female | 9 | ||
| FRANK Friends | Peer supporters | Male | 9 |
| Female | 8 | ||
| Parents | Male | 3 | |
| Female | 3 | ||
| School staff | School contact teacher | 3 | |
| SMT | 2 | ||
| +FRANK | Peer supporters | Male | 12 |
| Female | 7 | ||
| Parents | Male | 1 | |
| Female | 1 | ||
| School Staff | School contact teacher | 3 | |
| SMT | 2 |
| In your life have you ever tried . . . | Response | Trial arm | Total (N = 1567) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| +FRANK (N = 419) | Usual practice (N = 361) | FRANK friends (N = 440) | ASSIST (N = 347) | ||||||||
| n | % | n | % | n | % | n | % | n | % | ||
| Cannabis? | Missing | 13 | 3.1 | 1 | 0.3 | 2 | 0.5 | 2 | 0.6 | 18 | 1.1 |
| No | 399 | 95.2 | 346 | 95.8 | 427 | 97.0 | 339 | 97.7 | 1511 | 96.4 | |
| Yes | 7 | 1.7 | 14 | 3.9 | 11 | 2.5 | 6 | 1.7 | 38 | 2.4 | |
| Inhaling or sniffing GGAs to get ‘high’? | Missing | 13 | 3.1 | 4 | 1.1 | 2 | 0.5 | 5 | 1.4 | 24 | 1.5 |
| No | 399 | 95.2 | 343 | 95.0 | 429 | 97.5 | 337 | 97.1 | 1508 | 96.2 | |
| Yes | 7 | 1.7 | 14 | 3.9 | 9 | 2.0 | 5 | 1.4 | 35 | 2.2 | |
| Cocaine? | Missing | 12 | 2.9 | 4 | 1.1 | 2 | 0.5 | 3 | 0.9 | 21 | 1.3 |
| No | 406 | 96.9 | 354 | 98.1 | 435 | 98.9 | 342 | 98.6 | 1537 | 98.1 | |
| Yes | 1 | 0.2 | 3 | 0.8 | 3 | 0.7 | 2 | 0.6 | 9 | 0.6 | |
| Legal highs? | Missing | 12 | 2.9 | 5 | 1.4 | 3 | 0.7 | 3 | 0.9 | 23 | 1.5 |
| No | 406 | 96.9 | 353 | 97.8 | 434 | 98.6 | 342 | 98.6 | 1535 | 98.0 | |
| Yes | 1 | 0.2 | 3 | 0.8 | 3 | 0.7 | 2 | 0.6 | 9 | 0.6 | |
| Steroids? | Missing | 12 | 2.9 | 3 | 0.8 | 2 | 0.5 | 3 | 0.9 | 20 | 1.3 |
| No | 405 | 96.7 | 355 | 98.3 | 436 | 99.1 | 342 | 98.6 | 1538 | 98.1 | |
| Yes | 2 | 0.5 | 3 | 0.8 | 2 | 0.5 | 2 | 0.6 | 9 | 0.6 | |
| Ritalin? | Missing | 12 | 2.9 | 4 | 1.1 | 2 | 0.5 | 3 | 0.9 | 21 | 1.3 |
| No | 406 | 96.9 | 354 | 98.1 | 434 | 98.6 | 343 | 98.8 | 1537 | 98.1 | |
| Yes | 1 | 0.2 | 3 | 0.8 | 4 | 0.9 | 1 | 0.3 | 9 | 0.6 | |
| Amphetamines? | Missing | 13 | 3.1 | 4 | 1.1 | 2 | 0.5 | 3 | 0.9 | 22 | 1.4 |
| No | 404 | 96.4 | 353 | 97.8 | 437 | 99.3 | 343 | 98.8 | 1537 | 98.1 | |
| Yes | 2 | 0.5 | 4 | 1.1 | 1 | 0.2 | 1 | 0.3 | 8 | 0.5 | |
| Ecstasy? | Missing | 12 | 2.9 | 4 | 1.1 | 5 | 1.1 | 3 | 0.9 | 24 | 1.5 |
| No | 406 | 96.9 | 355 | 98.3 | 432 | 98.2 | 343 | 98.8 | 1536 | 98.0 | |
| Yes | 1 | 0.2 | 2 | 0.6 | 3 | 0.7 | 1 | 0.3 | 7 | 0.4 | |
| Mephedrone? | Missing | 12 | 2.9 | 4 | 1.1 | 2 | 0.5 | 2 | 0.6 | 20 | 1.3 |
| No | 407 | 97.1 | 354 | 98.1 | 436 | 99.1 | 343 | 98.8 | 1540 | 98.3 | |
| Yes | 0 | 0.0 | 3 | 0.8 | 2 | 0.5 | 2 | 0.6 | 7 | 0.4 | |
| Poppers? | Missing | 13 | 3.1 | 4 | 1.1 | 2 | 0.5 | 3 | 0.9 | 22 | 1.4 |
| No | 405 | 96.7 | 356 | 98.6 | 435 | 98.9 | 342 | 98.6 | 1538 | 98.1 | |
| Yes | 1 | 0.2 | 1 | 0.3 | 3 | 0.7 | 2 | 0.6 | 7 | 0.4 | |
| Semeron? | Missing | 13 | 3.1 | 3 | 0.8 | 2 | 0.5 | 4 | 1.2 | 22 | 1.4 |
| No | 406 | 96.9 | 358 | 99.2 | 437 | 99.3 | 342 | 98.6 | 1543 | 98.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Other drugs? | Missing | 10 | 2.4 | 1 | 0.3 | 2 | 0.5 | 2 | 0.6 | 15 | 1.0 |
| No | 409 | 97.6 | 360 | 99.7 | 437 | 99.3 | 345 | 99.4 | 1551 | 99.0 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Have you tried . . . | Response | Trial arm | Total (N = 1567) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| +FRANK (N = 419) | Usual practice (N = 361) | FRANK friends (N = 440) | ASSIST (N = 347) | ||||||||
| n | % | n | % | n | % | n | % | n | % | ||
| Inhaling or sniffing GGAs to get ‘high’ in the last week? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 10 | 2.9 | 43 | 2.7 |
| No | 401 | 95.7 | 348 | 96.4 | 434 | 98.6 | 336 | 96.8 | 1519 | 96.9 | |
| Yes | 0 | 0.0 | 3 | 0.8 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Inhaling or sniffing GGAs to get ‘high’ in the last 30 days? | Missing | 18 | 4.3 | 11 | 3.0 | 5 | 1.1 | 9 | 2.6 | 43 | 2.7 |
| No | 401 | 95.7 | 347 | 96.1 | 434 | 98.6 | 336 | 96.8 | 1518 | 96.9 | |
| Yes | 0 | 0.0 | 3 | 0.8 | 1 | 0.2 | 2 | 0.6 | 6 | 0.4 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Inhaling or sniffing GGAs to get ‘high’ in the last 12 months? | Missing | 17 | 4.1 | 10 | 2.8 | 4 | 0.9 | 7 | 2.0 | 38 | 2.4 |
| No | 397 | 94.7 | 344 | 95.3 | 428 | 97.3 | 334 | 96.3 | 1503 | 95.9 | |
| Yes | 5 | 1.2 | 7 | 1.9 | 8 | 1.8 | 6 | 1.7 | 26 | 1.7 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Cannabis in the last week? | Missing | 20 | 4.8 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 398 | 95.0 | 350 | 97.0 | 433 | 98.4 | 338 | 97.4 | 1519 | 96.9 | |
| Yes | 1 | 2 | 2 | 6 | 1 | 02 | 0 | 0.0 | 4 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Cannabis in the last 30 days? | Missing | 20 | 4.8 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 398 | 95.0 | 349 | 96.7 | 432 | 98.2 | 338 | 97.4 | 1517 | 96.8 | |
| Yes | 1 | 0.2 | 3 | 0.8 | 2 | 0.5 | 0 | 0.0 | 6 | 0.4 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Cannabis in the last 12 months? | Missing | 16 | 3.8 | 7 | 1.9 | 5 | 1.1 | 7 | 2.0 | 35 | 2.2 |
| No | 398 | 95.0 | 344 | 95.3 | 428 | 97.3 | 336 | 96.8 | 1506 | 96.1 | |
| Yes | 5 | 1.2 | 10 | 2.8 | 6 | 1.4 | 3 | 0.9 | 24 | 1.5 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Cocaine in the last week? | Missing | 19 | 4.5 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 400 | 95.5 | 352 | 97.5 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Cocaine in the last 30 days? | Missing | 19 | 4.5 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Cocaine in the last 12 months? | Missing | 18 | 4.3 | 10 | 2.8 | 4 | 0.9 | 8 | 2.3 | 40 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 337 | 97.1 | 1522 | 97.1 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 2 | 0.5 | 2 | 0.6 | 5 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Amphetamines in the last week? | Missing | 18 | 4.3 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 40 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 435 | 98.9 | 338 | 97.4 | 1525 | 97.3 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Amphetamines in the last 30 days? | Missing | 18 | 4.3 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 40 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 1 | 0.2 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Amphetamines in the last 12 months? | Missing | 18 | 4.3 | 9 | 2.5 | 4 | 0.9 | 8 | 2.3 | 39 | 2.5 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 1 | 0.2 | 1 | 0.3 | 2 | 0.5 | 0 | 0.0 | 4 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Legal highs in the last week? | Missing | 19 | 4.5 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Legal highs in the last 30 days? | Missing | 19 | 4.5 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Legal highs in the last 12 months? | Missing | 18 | 4.3 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 40 | 2.6 |
| No | 399 | 95.2 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1522 | 97.1 | |
| Yes | 2 | 0.5 | 1 | 0.3 | 0 | 0.0 | 1 | 0.3 | 4 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Ecstasy in the last week? | Missing | 18 | 4.3 | 11 | 3.0 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 401 | 95.7 | 350 | 97.0 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Ecstasy in the last 30 days? | Missing | 18 | 4.3 | 11 | 3.0 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 401 | 95.7 | 350 | 97.0 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Ecstasy in the last 12 months? | Missing | 18 | 4.3 | 11 | 3.0 | 5 | 1.1 | 8 | 2.3 | 42 | 2.7 |
| No | 400 | 95.5 | 350 | 97.0 | 433 | 98.4 | 338 | 97.4 | 1521 | 97.1 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Steroids in the last week? | Missing | 18 | 4.3 | 9 | 2.5 | 4 | 0.9 | 8 | 2.3 | 39 | 2.5 |
| No | 400 | 95.5 | 352 | 97.5 | 436 | 99.1 | 338 | 97.4 | 1526 | 97.4 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Steroids in the last 30 days? | Missing | 18 | 4.3 | 10 | 2.8 | 4 | 0.9 | 8 | 2.3 | 40 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 435 | 98.9 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Steroids in the last 12 months? | Missing | 18 | 4.3 | 10 | 2.8 | 4 | 0.9 | 8 | 2.3 | 40 | 2.6 |
| No | 400 | 95.5 | 350 | 97.0 | 435 | 98.9 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 1 | 0.2 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Poppers in the last week? | Missing | 18 | 4.3 | 9 | 2.5 | 4 | .9 | 8 | 2.3 | 39 | 2.5 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 337 | 97.1 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 2 | 0.5 | 2 | 0.6 | 4 | 0.3 | |
| Poppers in the last 30 days? | Missing | 18 | 4.3 | 9 | 2.5 | 4 | .9 | 8 | 2.3 | 39 | 2.5 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 337 | 97.1 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 2 | 0.5 | 2 | 0.6 | 4 | 0.3 | |
| Poppers in the last 12 months? | Missing | 18 | 4.3 | 9 | 2.5 | 4 | 0.9 | 8 | 2.3 | 39 | 2.5 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 337 | 97.1 | 1522 | 97.1 | |
| Yes | 1 | 0.2 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 2 | 0.5 | 2 | 0.6 | 4 | 0.3 | |
| Ritalin in the last week? | Missing | 18 | 4.3 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 40 | 2.6 |
| No | 401 | 95.7 | 352 | 97.5 | 434 | 98.6 | 338 | 97.4 | 1525 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Ritalin in the last 30 days? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Ritalin in the last 12 months? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 400 | 95.5 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Mephedrone in the last week? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Mephedrone in the last 30 days? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Mephedrone in the last 12 months? | Missing | 18 | 4.3 | 10 | 2.8 | 4 | 0.9 | 8 | 2.3 | 40 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Semeron in the last week? | Missing | 18 | 4.3 | 9 | 2.5 | 5 | 1.1 | 8 | 2.3 | 40 | 2.6 |
| No | 401 | 95.7 | 352 | 97.5 | 434 | 98.6 | 338 | 97.4 | 1525 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Semeron in the last 30 days? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 434 | 98.6 | 338 | 97.4 | 1524 | 97.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Semeron in the last 12 months? | Missing | 18 | 4.3 | 10 | 2.8 | 5 | 1.1 | 8 | 2.3 | 41 | 2.6 |
| No | 401 | 95.7 | 351 | 97.2 | 433 | 98.4 | 338 | 97.4 | 1523 | 97.2 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 2 | 0.1 | |
| Some other drug in the last week? | Missing | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| No | 418 | 99.8 | 361 | 100.0 | 440 | 100.0 | 347 | 100.0 | 1566 | 99.9 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Some other drug in the last 30 days? | Missing | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| No | 418 | 99.8 | 361 | 100.0 | 440 | 100.0 | 347 | 100.0 | 1566 | 99.9 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Some other drug in the last 12 months? | Missing | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| No | 418 | 99.8 | 361 | 100.0 | 440 | 100.0 | 347 | 100.0 | 1566 | 99.9 | |
| Yes | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| In your life have you ever tried . . . | Response | Trial arm | Total (N = 1460) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| +FRANK (N = 391) | Usual practice (N = 342) | FRANK friends (N = 412) | ASSIST (N = 315) | ||||||||
| n | % | n | % | n | % | n | % | n | % | ||
| Cannabis? | Missing | 1 | 0.3 | 1 | 0.3 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 348 | 89.0 | 315 | 92.1 | 384 | 93.2 | 292 | 92.7 | 1339 | 91.7 | |
| Yes | 42 | 10.7 | 26 | 7.6 | 27 | 6.6 | 22 | 7.0 | 117 | 8.0 | |
| Inhaling or sniffing GGAs to get ‘high’? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 370 | 94.6 | 329 | 96.2 | 399 | 96.8 | 300 | 95.2 | 1398 | 95.8 | |
| Yes | 21 | 5.4 | 11 | 3.2 | 12 | 2.9 | 14 | 4.4 | 58 | 4.0 | |
| Legal highs? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 381 | 97.4 | 335 | 98.0 | 406 | 98.5 | 309 | 98.1 | 1431 | 98.0 | |
| Yes | 10 | 2.6 | 5 | 1.5 | 5 | 1.2 | 5 | 1.6 | 25 | 1.7 | |
| Cocaine? | Missing | 0 | 0.0 | 5 | 1.5 | 1 | 0.2 | 1 | 0.3 | 7 | 0.5 |
| No | 386 | 98.7 | 333 | 97.4 | 410 | 99.5 | 310 | 98.4 | 1439 | 98.6 | |
| Yes | 5 | 1.3 | 4 | 1.2 | 1 | 0.2 | 4 | 1.3 | 14 | 1.0 | |
| Ecstasy? | Missing | 1 | 0.3 | 4 | 1.2 | 1 | 0.2 | 1 | 0.3 | 7 | 0.5 |
| No | 384 | 98.2 | 336 | 98.2 | 410 | 99.5 | 313 | 99.4 | 1443 | 98.8 | |
| Yes | 6 | 1.5 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 10 | 0.7 | |
| Tranquillisers? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 386 | 98.7 | 337 | 98.5 | 410 | 99.5 | 313 | 99.4 | 1446 | 99.0 | |
| Yes | 5 | 1.3 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 10 | 0.7 | |
| LSD? | Missing | 0 | 0.0 | 4 | 1.2 | 1 | 0.2 | 1 | 0.3 | 6 | 0.4 |
| No | 385 | 98.5 | 337 | 98.5 | 411 | 99.8 | 312 | 99.0 | 1445 | 99.0 | |
| Yes | 6 | 1.5 | 1 | 0.3 | 0 | 0.0 | 2 | 0.6 | 9 | 0.6 | |
| Amphetamines? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 387 | 99.0 | 338 | 98.8 | 410 | 99.5 | 313 | 99.4 | 1448 | 99.2 | |
| Yes | 4 | 1.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 8 | 0.5 | |
| Mephedrone? | Missing | 0 | 0.0 | 3 | 0.9 | 2 | 0.5 | 2 | 0.6 | 7 | 0.5 |
| No | 386 | 98.7 | 338 | 98.8 | 409 | 99.3 | 313 | 99.4 | 1446 | 99.0 | |
| Yes | 5 | 1.3 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 7 | 0.5 | |
| Steroids? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 388 | 99.2 | 338 | 98.8 | 411 | 99.8 | 312 | 99.0 | 1449 | 99.2 | |
| Yes | 3 | 0.8 | 2 | 0.6 | 0 | 0.0 | 2 | 0.6 | 7 | 0.5 | |
| Heroin? | Missing | 0 | 0.0 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 |
| No | 390 | 99.7 | 336 | 98.2 | 410 | 99.5 | 313 | 99.4 | 1449 | 99.2 | |
| Yes | 1 | 0.3 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 6 | 0.4 | |
| Magic mushrooms? | Missing | 2 | 0.5 | 6 | 1.8 | 5 | 1.2 | 2 | 0.6 | 15 | 1.0 |
| No | 386 | 98.7 | 333 | 97.4 | 407 | 98.8 | 313 | 99.4 | 1439 | 98.6 | |
| Yes | 3 | 0.8 | 3 | 0.9 | 0 | 0.0 | 0 | 0.0 | 6 | 0.4 | |
| Crack? | Missing | 1 | 0.3 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 6 | 0.4 |
| No | 388 | 99.2 | 336 | 98.2 | 411 | 99.8 | 314 | 99.7 | 1449 | 99.2 | |
| Yes | 2 | 0.5 | 3 | 0.9 | 0 | 0.0 | 0 | 0.0 | 5 | 0.3 | |
| Ketamine? | Missing | 0 | 0.0 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 |
| No | 388 | 99.2 | 337 | 98.5 | 411 | 99.8 | 314 | 99.7 | 1450 | 99.3 | |
| Yes | 3 | 0.8 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 5 | 0.3 | |
| Ritalin? | Missing | 0 | 0.0 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 |
| No | 389 | 99.5 | 337 | 98.5 | 410 | 99.5 | 314 | 99.7 | 1450 | 99.3 | |
| Yes | 2 | 0.5 | 2 | 0.6 | 1 | 0.2 | 0 | 0.0 | 5 | 0.3 | |
| Poppers? | Missing | 1 | 0.3 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 |
| No | 389 | 99.5 | 339 | 99.1 | 409 | 99.3 | 313 | 99.4 | 1450 | 99.3 | |
| Yes | 1 | 0.3 | 1 | 0.3 | 2 | 0.5 | 1 | 0.3 | 5 | 0.3 | |
| Methadone? | Missing | 0 | 0.0 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 |
| No | 389 | 99.5 | 337 | 98.5 | 411 | 99.8 | 314 | 99.7 | 1451 | 99.4 | |
| Yes | 2 | 0.5 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 4 | 0.3 | |
| Semeron? | Missing | 0 | 0.0 | 2 | 0.6 | 1 | 0.2 | 1 | 0.3 | 4 | 0.3 |
| No | 389 | 99.5 | 339 | 99.1 | 411 | 99.8 | 314 | 99.7 | 1453 | 99.5 | |
| Yes | 2 | 0.5 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 3 | 0.2 | |
| Have you tried . . . | Response | Trial arm | Total (N = 1460) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| +FRANK (N = 391) | Usual practice (N = 342) | FRANK friends (N = 412) | ASSIST (N = 315) | ||||||||
| n | % | n | % | n | % | n | % | n | % | ||
| Cannabis in the last week? | Missing | 22 | 5.6 | 21 | 6.1 | 10 | 2.4 | 10 | 3.2 | 63 | 4.3 |
| No | 362 | 92.6 | 316 | 92.4 | 397 | 96.4 | 299 | 94.9 | 1374 | 94.1 | |
| Yes | 5 | 1.3 | 4 | 1.2 | 2 | 0.5 | 5 | 1.6 | 16 | 1.1 | |
| Illogical | 2 | 0.5 | 1 | 0.3 | 3 | 0.7 | 1 | 0.3 | 7 | 0.5 | |
| Cannabis in the last 30 days? | Missing | 19 | 4.9 | 17 | 5.0 | 6 | 1.5 | 9 | 2.9 | 51 | 3.5 |
| No | 360 | 92.1 | 315 | 92.1 | 393 | 95.4 | 296 | 94.0 | 1364 | 93.4 | |
| Yes | 10 | 2.6 | 9 | 2.6 | 10 | 2.4 | 9 | 2.9 | 38 | 2.6 | |
| Illogical | 2 | 0.5 | 1 | 0.3 | 3 | 0.7 | 1 | 0.3 | 7 | 0.5 | |
| Cannabis in the last 12 months? | Missing | 9 | 2.3 | 12 | 3.5 | 4 | 1.0 | 4 | 1.3 | 29 | 2.0 |
| No | 344 | 88.0 | 308 | 90.1 | 383 | 93.0 | 289 | 91.7 | 1324 | 90.7 | |
| Yes | 36 | 9.2 | 21 | 6.1 | 22 | 5.3 | 21 | 6.7 | 100 | 6.8 | |
| Illogical | 2 | 0.5 | 1 | 0.3 | 3 | 0.7 | 1 | 0.3 | 7 | 0.5 | |
| Inhaling or sniffing GGAs to get ‘high’ in the last week? | Missing | 16 | 4.1 | 20 | 5.8 | 12 | 2.9 | 11 | 3.5 | 59 | 4.0 |
| No | 374 | 95.7 | 322 | 94.2 | 396 | 96.1 | 304 | 96.5 | 1396 | 95.6 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 1 | 0.3 | 0 | 0.0 | 3 | 0.7 | 0 | 0.0 | 4 | 0.3 | |
| Inhaling or sniffing GGAs to get ‘high’ in the last 30 days? | Missing | 15 | 3.8 | 19 | 5.6 | 14 | 3.4 | 10 | 3.2 | 58 | 4.0 |
| No | 371 | 94.9 | 320 | 93.6 | 394 | 95.6 | 304 | 96.5 | 1389 | 95.1 | |
| Yes | 4 | 1.0 | 3 | 0.9 | 1 | 0.2 | 1 | 0.3 | 9 | 0.6 | |
| Illogical | 1 | 0.3 | 0 | 0.0 | 3 | 0.7 | 0 | 0.0 | 4 | 0.3 | |
| Inhaling or sniffing GGAs to get ‘high’ in the last 12 months? | Missing | 12 | 3.1 | 18 | 5.3 | 12 | 2.9 | 8 | 2.5 | 50 | 3.4 |
| No | 364 | 93.1 | 319 | 93.3 | 390 | 94.7 | 299 | 94.9 | 1372 | 94.0 | |
| Yes | 14 | 3.6 | 5 | 1.5 | 7 | 1.7 | 8 | 2.5 | 34 | 2.3 | |
| Illogical | 1 | 0.3 | 0 | 0.0 | 3 | 0.7 | 0 | 0.0 | 4 | 0.3 | |
| Legal highs in the last week? | Missing | 19 | 4.9 | 19 | 5.6 | 15 | 3.6 | 12 | 3.8 | 65 | 4.5 |
| No | 371 | 94.9 | 323 | 94.4 | 397 | 96.4 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Legal highs in the last 30 days? | Missing | 20 | 5.1 | 18 | 5.3 | 16 | 3.9 | 11 | 3.5 | 65 | 4.5 |
| No | 370 | 94.6 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 1 | 0.3 | 3 | 0.9 | 0 | 0.0 | 1 | 0.3 | 5 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Legal highs in the last 12 months? | Missing | 19 | 4.9 | 18 | 5.3 | 14 | 3.4 | 10 | 3.2 | 61 | 4.2 |
| No | 367 | 93.9 | 318 | 93.0 | 393 | 95.4 | 301 | 95.6 | 1379 | 94.5 | |
| Yes | 5 | 1.3 | 6 | 1.8 | 5 | 1.2 | 4 | 1.3 | 20 | 1.4 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Cocaine in the last week? | Missing | 18 | 4.6 | 20 | 5.8 | 14 | 3.4 | 12 | 3.8 | 64 | 4.4 |
| No | 372 | 95.1 | 320 | 93.6 | 397 | 96.4 | 303 | 96.2 | 1392 | 95.3 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Cocaine in the last 30 days? | Missing | 18 | 4.6 | 20 | 5.8 | 15 | 3.6 | 10 | 3.2 | 63 | 4.3 |
| No | 372 | 95.1 | 320 | 93.6 | 396 | 96.1 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 1 | 0.2 | 2 | 0.6 | 4 | 0.3 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Cocaine in the last 12 months? | Missing | 18 | 4.6 | 20 | 5.8 | 15 | 3.6 | 10 | 3.2 | 63 | 4.3 |
| No | 370 | 94.6 | 319 | 93.3 | 395 | 95.9 | 301 | 95.6 | 1385 | 94.9 | |
| Yes | 2 | 0.5 | 2 | 0.6 | 2 | 0.5 | 4 | 1.3 | 10 | 0.7 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Steroids in the last week? | Missing | 20 | 5.1 | 17 | 5.0 | 15 | 3.6 | 12 | 3.8 | 64 | 4.4 |
| No | 371 | 94.9 | 322 | 94.2 | 397 | 96.4 | 303 | 96.2 | 1393 | 95.4 | |
| Yes | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Steroids in the last 30 days? | Missing | 19 | 4.9 | 18 | 5.3 | 16 | 3.9 | 12 | 3.8 | 65 | 4.5 |
| No | 371 | 94.9 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 1 | 0.3 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Steroids in the last 12 months? | Missing | 19 | 4.9 | 19 | 5.6 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 369 | 94.4 | 320 | 93.6 | 395 | 95.9 | 300 | 95.2 | 1384 | 94.8 | |
| Yes | 3 | 0.8 | 2 | 0.6 | 1 | 0.2 | 3 | 1.0 | 9 | 0.6 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Tranquillisers in the last week? | Missing | 20 | 5.1 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 67 | 4.6 |
| No | 370 | 94.6 | 322 | 94.2 | 396 | 96.1 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Tranquillisers in the last 30 days? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 11 | 3.5 | 66 | 4.5 |
| No | 370 | 94.6 | 322 | 94.2 | 395 | 95.9 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 2 | 0.5 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Tranquillisers in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 15 | 3.6 | 11 | 3.5 | 65 | 4.5 |
| No | 367 | 93.9 | 321 | 93.9 | 394 | 95.6 | 303 | 96.2 | 1385 | 94.9 | |
| Yes | 5 | 1.3 | 1 | 0.3 | 2 | 0.5 | 1 | 0.3 | 9 | 0.6 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Amphetamines in the last week? | Missing | 19 | 4.9 | 21 | 6.1 | 15 | 3.6 | 12 | 3.8 | 67 | 4.6 |
| No | 372 | 95.1 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1392 | 95.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Amphetamines in the last 30 days? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 13 | 4.1 | 67 | 4.6 |
| No | 371 | 94.9 | 321 | 93.9 | 395 | 95.9 | 302 | 95.9 | 1389 | 95.1 | |
| Yes | 2 | 0.5 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Amphetamines in the last 12 months? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 15 | 4.8 | 69 | 4.7 |
| No | 368 | 94.1 | 321 | 93.9 | 394 | 95.6 | 300 | 95.2 | 1383 | 94.7 | |
| Yes | 5 | 1.3 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 7 | 0.5 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 | |
| Heroin in the last week? | Missing | 17 | 4.3 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 64 | 4.4 |
| No | 373 | 95.4 | 321 | 93.9 | 397 | 96.4 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Heroin in the last 30 days? | Missing | 17 | 4.3 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 65 | 4.5 |
| No | 372 | 95.1 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1392 | 95.3 | |
| Yes | 2 | 0.5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Heroin in the last 12 months? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 370 | 94.6 | 321 | 93.9 | 395 | 95.9 | 301 | 95.6 | 1387 | 95.0 | |
| Yes | 3 | 0.8 | 0 | 0.0 | 1 | 0.2 | 2 | 0.6 | 6 | 0.4 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Ecstasy in the last week? | Missing | 19 | 4.9 | 21 | 6.1 | 15 | 3.6 | 12 | 3.8 | 67 | 4.6 |
| No | 372 | 95.1 | 319 | 93.3 | 396 | 96.1 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Ecstasy in the last 30 days? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 372 | 95.1 | 319 | 93.3 | 395 | 95.9 | 303 | 96.2 | 1389 | 95.1 | |
| Yes | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Ecstasy in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 13 | 4.1 | 68 | 4.7 |
| No | 370 | 94.6 | 319 | 93.3 | 394 | 95.6 | 302 | 95.9 | 1385 | 94.9 | |
| Yes | 2 | 0.5 | 2 | 0.6 | 1 | 0.2 | 0 | 0.0 | 5 | 0.3 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Ritalin in the last week? | Missing | 19 | 4.9 | 20 | 5.8 | 15 | 3.6 | 11 | 3.5 | 65 | 4.5 |
| No | 372 | 95.1 | 319 | 93.3 | 397 | 96.4 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Ritalin in the last 30 days? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 11 | 3.5 | 66 | 4.5 |
| No | 372 | 95.1 | 319 | 93.3 | 396 | 96.1 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Ritalin in the last 12 months? | Missing | 20 | 5.1 | 20 | 5.8 | 16 | 3.9 | 11 | 3.5 | 67 | 4.6 |
| No | 370 | 94.6 | 318 | 93.0 | 394 | 95.6 | 302 | 95.9 | 1384 | 94.8 | |
| Yes | 1 | 0.3 | 2 | 0.6 | 2 | 0.5 | 2 | 0.6 | 7 | 0.5 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| LSD in the last week? | Missing | 19 | 4.9 | 21 | 6.1 | 15 | 3.6 | 12 | 3.8 | 67 | 4.6 |
| No | 371 | 94.9 | 319 | 93.3 | 397 | 96.4 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| LSD in the last 30 days? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 371 | 94.9 | 319 | 93.3 | 396 | 96.1 | 303 | 96.2 | 1389 | 95.1 | |
| Yes | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| LSD in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 11 | 3.5 | 66 | 4.5 |
| No | 370 | 94.6 | 319 | 93.3 | 395 | 95.9 | 303 | 96.2 | 1387 | 95.0 | |
| Yes | 2 | 0.5 | 1 | 0.3 | 1 | 0.2 | 1 | 0.3 | 5 | 0.3 | |
| Illogical | 0 | 0.0 | 2 | 0.6 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Mephedrone in the last week? | Missing | 19 | 4.9 | 19 | 5.6 | 15 | 3.6 | 12 | 3.8 | 65 | 4.5 |
| No | 372 | 95.1 | 323 | 94.4 | 397 | 96.4 | 303 | 96.2 | 1395 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Mephedrone in the last 30 days? | Missing | 19 | 4.9 | 19 | 5.6 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 372 | 95.1 | 323 | 94.4 | 396 | 96.1 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Mephedrone in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 13 | 4.1 | 68 | 4.7 |
| No | 369 | 94.4 | 322 | 94.2 | 395 | 95.9 | 302 | 95.9 | 1388 | 95.1 | |
| Yes | 3 | 0.8 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 4 | 0.3 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Poppers in the last week? | Missing | 18 | 4.6 | 20 | 5.8 | 14 | 3.4 | 12 | 3.8 | 64 | 4.4 |
| No | 373 | 95.4 | 321 | 93.9 | 398 | 96.6 | 303 | 96.2 | 1395 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Poppers in the last 30 days? | Missing | 17 | 4.3 | 20 | 5.8 | 14 | 3.4 | 11 | 3.5 | 62 | 4.2 |
| No | 373 | 95.4 | 321 | 93.9 | 398 | 96.6 | 303 | 96.2 | 1395 | 95.5 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Poppers in the last 12 months? | Missing | 18 | 4.6 | 20 | 5.8 | 14 | 3.4 | 11 | 3.5 | 63 | 4.3 |
| No | 372 | 95.1 | 321 | 93.9 | 397 | 96.4 | 303 | 96.2 | 1393 | 95.4 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 1 | 0.2 | 1 | 0.3 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Crack in the last week? | Missing | 19 | 4.9 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 66 | 4.5 |
| No | 372 | 95.1 | 322 | 94.2 | 397 | 96.4 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Crack in the last 30 days? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 372 | 95.1 | 322 | 94.2 | 396 | 96.1 | 303 | 96.2 | 1393 | 95.4 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Crack in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 371 | 94.9 | 321 | 93.9 | 395 | 95.9 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 1 | 0.3 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Magic mushrooms in the last week? | Missing | 19 | 4.9 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 66 | 4.5 |
| No | 371 | 94.9 | 321 | 93.9 | 397 | 96.4 | 303 | 96.2 | 1392 | 95.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Magic mushrooms in the last 30 days? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 371 | 94.9 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Magic mushrooms in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 370 | 94.6 | 320 | 93.6 | 395 | 95.9 | 303 | 96.2 | 1388 | 95.1 | |
| Yes | 1 | 0.3 | 1 | 0.3 | 1 | 0.2 | 0 | 0.0 | 3 | 0.2 | |
| Illogical | 1 | 0.3 | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 | |
| Semeron in the last week? | Missing | 19 | 4.9 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 66 | 4.5 |
| No | 372 | 95.1 | 322 | 94.2 | 397 | 96.4 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Semeron in the last 30 days? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 372 | 95.1 | 322 | 94.2 | 396 | 96.1 | 303 | 96.2 | 1393 | 95.4 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Semeron in the last 12 months? | Missing | 19 | 4.9 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 371 | 94.9 | 322 | 94.2 | 395 | 95.9 | 303 | 96.2 | 1391 | 95.3 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Ketamine in the last week? | Missing | 18 | 4.6 | 20 | 5.8 | 15 | 3.6 | 12 | 3.8 | 65 | 4.5 |
| No | 373 | 95.4 | 322 | 94.2 | 397 | 96.4 | 303 | 96.2 | 1395 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Ketamine in the last 30 days? | Missing | 18 | 4.6 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 66 | 4.5 |
| No | 373 | 95.4 | 322 | 94.2 | 396 | 96.1 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Ketamine in the last 12 months? | Missing | 20 | 5.1 | 20 | 5.8 | 16 | 3.9 | 12 | 3.8 | 68 | 4.7 |
| No | 370 | 94.6 | 322 | 94.2 | 395 | 95.9 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Methadone in the last week? | Missing | 18 | 4.6 | 21 | 6.1 | 15 | 3.6 | 12 | 3.8 | 66 | 4.5 |
| No | 373 | 95.4 | 321 | 93.9 | 397 | 96.4 | 303 | 96.2 | 1394 | 95.5 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Methadone in the last 30 days? | Missing | 18 | 4.6 | 21 | 6.1 | 16 | 3.9 | 12 | 3.8 | 67 | 4.6 |
| No | 373 | 95.4 | 321 | 93.9 | 396 | 96.1 | 303 | 96.2 | 1393 | 95.4 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Methadone in the last 12 months? | Missing | 19 | 4.9 | 21 | 6.1 | 16 | 3.9 | 12 | 3.8 | 68 | 4.7 |
| No | 371 | 94.9 | 321 | 93.9 | 395 | 95.9 | 303 | 96.2 | 1390 | 95.2 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 2 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Some other drug in the last week? | Missing | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 |
| No | 390 | 99.7 | 342 | 100.0 | 412 | 100.0 | 315 | 100.0 | 1459 | 99.9 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Some other drug in the last 30 days? | Missing | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 |
| No | 390 | 99.7 | 342 | 100.0 | 412 | 100.0 | 315 | 100.0 | 1459 | 99.9 | |
| Yes | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Some other drug in the last 12 months? | Missing | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| No | 390 | 99.7 | 342 | 100.0 | 412 | 100.0 | 315 | 100.0 | 1459 | 99.9 | |
| Yes | 1 | 0.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | |
| Illogical | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Variable (potential scale range) | Trial arm | n | Missing (%) | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| FTND (0–10)a | +FRANK | 2 | 50.0 | 0.0 | 0.0 | 4.5 | 9.0 | 9.0 | 4.5 | 6.36 |
| Usual practice | 4 | 20.0 | 0.0 | 0.0 | 0.5 | 2.0 | 3.0 | 1.0 | 1.41 | |
| FRANK friends | 5 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 0.6 | 0.55 | |
| ASSIST | 1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | NA | |
| Overall | 12 | 20.0 | 0.0 | 0.0 | 0.5 | 1.0 | 9.0 | 1.3 | 2.57 | |
| HSI (0–6)a | +FRANK | 2 | 50.0 | 0.0 | 0.0 | 2.5 | 5.0 | 5.0 | 2.5 | 3.54 |
| Usual practice | 4 | 20.0 | 0.0 | 0.0 | 0.0 | 1.5 | 3.0 | 0.8 | 1.50 | |
| FRANK friends | 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.00 | |
| ASSIST | 1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | NA | |
| Overall | 12 | 20.0 | 0.0 | 0.0 | 0.0 | 0.0 | 5.0 | 0.7 | 1.61 | |
| Number of cigarettes smoked in an average weeka | +FRANK | 4 | 0.0 | 1.0 | 1.5 | 3.5 | 52.5 | 100.0 | 27.0 | 48.70 |
| Usual practice | 5 | 0.0 | 1.0 | 1.0 | 1.0 | 3.0 | 10.0 | 3.2 | 3.90 | |
| FRANK friends | 5 | 0.0 | 3.0 | 8.0 | 35.0 | 40.0 | 175.0 | 52.2 | 70.53 | |
| ASSIST | 1 | 0.0 | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 | NA | |
| Overall | 15 | 0.0 | 1.0 | 1.0 | 3.0 | 35.0 | 175.0 | 25.9 | 49.02 | |
| CHU-9D (0–1) | +FRANK | 419 | 10.3 | 0.426 | 0.802 | 0.878 | 0.931 | 1.000 | 0.858 | 0.105 |
| Usual practice | 361 | 8.2 | 0.326 | 0.826 | 0.897 | 0.952 | 1.000 | 0.870 | 0.109 | |
| FRANK friends | 440 | 10.9 | 0.326 | 0.812 | 0.886 | 0.952 | 1.000 | 0.863 | 0.105 | |
| ASSIST | 347 | 10.8 | 0.488 | 0.839 | 0.898 | 0.952 | 1.000 | 0.873 | 0.100 | |
| Overall | 1567 | 10.7 | 0.416 | 0.845 | 0.915 | 0.952 | 1.000 | 0.887 | 0.095 |
| Variable | 18-month follow-up data: distribution over categories by trial arm (%) | ||||
|---|---|---|---|---|---|
| +FRANK (n = 391) | Usual practice (n = 342) | FRANK friends (n = 412) | ASSIST (n = 315) | Overall (n = 1460) | |
| Perceived prevalence of lifetime drug use in year group | |||||
| Missing | 13.8 | 16.4 | 18.0 | 17.8 | 16.4 |
| Anyone in year group has tried | 58.3 | 58.2 | 41.3 | 53.0 | 52.3 |
| None | 27.9 | 25.4 | 40.8 | 29.2 | 31.2 |
| Drug offers in last year | |||||
| Missing | 1.8 | 0.6 | 1.7 | 1.0 | 1.3 |
| Any | 29.4 | 27.5 | 21.4 | 28.6 | 26.5 |
| None | 68.8 | 71.9 | 76.9 | 70.5 | 72.2 |
| Conversations with school friends about drugs | |||||
| Missing | 2.3 | 1.2 | 1.5 | 1.6 | 1.6 |
| Any | 57.0 | 55.0 | 59.7 | 48.9 | 55.5 |
| None | 40.7 | 43.9 | 38.8 | 49.5 | 42.8 |
| Ever visited the Talk to FRANK website? | |||||
| Missing | 3.3 | 3.2 | 2.7 | 1.9 | 2.8 |
| Yes | 13.0 | 1.5 | 15.3 | 9.8 | 10.3 |
| No | 83.6 | 95.3 | 82.0 | 88.3 | 86.9 |
| Ever talked to a peer supporter about the harms of taking drugs? | |||||
| Missing | 2.0 | 0.6 | 1.0 | 1.6 | 1.3 |
| Yes | 23.3 | 12.0 | 20.1 | 14.3 | 17.8 |
| No | 55.5 | 60.2 | 57.0 | 63.2 | 58.7 |
| Don’t know | 19.2 | 27.2 | 21.8 | 21.0 | 22.2 |
| Would you get help for yourself or a friend from the Talk to FRANK website you or he/she had a problem? | |||||
| Missing | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Yes | 35.8 | 36.3 | 44.4 | 33.7 | 37.9 |
| No | 64.2 | 63.7 | 55.6 | 66.3 | 62.1 |
| Variable (potential scale range) | Trial arm | n | Missing (%) | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived percentage of students in your year who take drugs (0–100%) | +FRANK | 385 | 1.5 | 0.0 | 2.0 | 5.0 | 20.0 | 80.0 | 13.3 | 16.1 |
| Usual practice | 336 | 1.8 | 0.0 | 1.0 | 5.0 | 17.5 | 100.0 | 12.2 | 16.6 | |
| FRANK friends | 402 | 2.4 | 0.0 | 1.0 | 5.0 | 15.0 | 100.0 | 12.2 | 17.4 | |
| ASSIST | 310 | 1.6 | 0.0 | 2.0 | 4.0 | 10.0 | 100.0 | 9.4 | 13.7 | |
| Overall | 1433 | 1.8 | 0.0 | 2.0 | 5.0 | 15.0 | 100.0 | 11.9 | 16.2 | |
| Knowledge about drugs score (1–8) | +FRANK | 362 | 7.4 | 2.0 | 5.0 | 6.0 | 7.0 | 8.0 | 5.6 | 1.3 |
| Usual practice | 324 | 5.3 | 2.0 | 5.0 | 6.0 | 6.0 | 8.0 | 5.5 | 1.3 | |
| FRANK friends | 387 | 6.1 | 2.0 | 5.0 | 6.0 | 7.0 | 8.0 | 5.7 | 1.4 | |
| ASSIST | 295 | 6.3 | 1.0 | 4.0 | 5.0 | 6.0 | 8.0 | 5.4 | 1.3 | |
| Overall | 1368 | 6.3 | 1.0 | 5.0 | 6.0 | 7.0 | 8.0 | 5.6 | 1.3 |
| Variable | ASSIST vs. usual practice (reference) | +FRANK vs. usual practice (reference) | FRANK friends vs. usual practice (reference) | +FRANK vs. ASSIST (reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | OR | 95% CI | n | OR | 95% CI | n | OR | 95% CI | n | OR | 95% CI | |
| Indicative primary outcome | ||||||||||||
| Lifetime illicit drug use | 497 | 0.81 | 0.46 to 1.42 | 561 | 0.96 | 0.58 to 1.59 | 576 | 0.70 | 0.39 to 1.24 | 550 | 1.21 | 0.71 to 2.08 |
| Indicative secondary outcomes | ||||||||||||
| Cannabis use in lifetime | 508 | 1.11 | 0.49 to 2.48 | 573 | 1.17 | 0.45 to 3.05 | 590 | 0.65 | 0.17 to 2.46 | 553 | 1.05 | 0.54 to 2.05 |
| Cannabis use in past 12 months | 486 | 1.40 | 0.66 to 2.97 | 541 | 1.41 | 0.60 to 3.34 | 570 | 0.82 | 0.33 to 2.06 | 529 | 0.94 | 0.42 to 2.09 |
| GGA use in lifetime | 507 | 1.59 | 0.62 to 4.08 | 573 | 1.66 | 0.71 to 3.86 | 589 | 0.87 | 0.31 to 2.44 | 554 | 1.13 | 0.51 to 2.50 |
| GGA use in past 12 months | 476 | 1.85 | 0.48 to 7.14 | 534 | 2.86 | 0.84 to 9.73 | 555 | 1.12 | 0.29 to 4.36 | 526 | 1.58 | 0.51 to 4.88 |
| Ever having tried smoking (even if a puff) | 497 | 1.18 | 0.69 to 2.01 | 559 | 1.10 | 0.64 to 1.90 | 583 | 0.65 | 0.32 to 1.29 | 540 | 0.93 | 0.59 to 1.46 |
| Ever having consumed a whole alcoholic drink | 454 | 1.50 | 0.74 to 3.02 | 497 | 1.26 | 0.71 to 2.23 | 530 | 0.75 | 0.35 to 1.58 | 481 | 0.82 | 0.57 to 1.19 |
| Engages in heavy episodic alcohol use (A-SAQ)b | 471 | 0.94 | 0.60 to 1.49 | 532 | 0.84 | 0.55 to 1.29 | 542 | 0.53 | 0.31 to 0.90 | 537 | 0.89 | 0.58 to 1.36 |
| Intermediary variables | ||||||||||||
| Perceived prevalence of lifetime drug use in year groupc | 333 | 1.14 | 0.70 to 1.84 | 369 | 0.98 | 0.49 to 1.96 | 382 | 0.43 | 0.14 to 1.27 | 350 | 0.84 | 0.46 to 1.54 |
| Any drug offers in last yeard | 502 | 1.41 | 0.92 to 2.17 | 568 | 1.09 | 0.57 to 2.09 | 582 | 0.78 | 0.44 to 1.41 | 546 | 0.72 | 0.36 to 1.45 |
| Any conversations with school friends about drugse | 495 | 0.82 | 0.57 to 1.18 | 554 | 1.25 | 0.89 to 1.77 | 569 | 1.38 | 0.98 to 1.94 | 535 | 1.53 | 1.07 to 2.18 |
| Ever visited Talk to FRANK websitef | 496 | 3.16 | 0.32 to 1.72 | 561 | 12.64 | 4.47 to 35.74 | 576 | 14.25 | 4.54 to 4.70 | 538 | 3.99 | 0.72 to 2.22 |
| Variable | ASSIST vs. usual practice (reference) | +FRANK vs. usual practice (reference) | FRANK friends vs. usual practice (reference) | +FRANK vs. ASSIST (reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Coefficient | 95% CI | n | Coefficient | 95% CI | n | Coefficient | 95% CI | n | Coefficient | 95% CI | |
| Intermediary variables | ||||||||||||
| Perceived percentage of students in your year who take drugs | 497 | –1.22 | –3.77 to 1.33 | 563 | 2.01 | –4.45 to 8.47 | 571 | –2.42 | –10.95 to 6.10 | 544 | 2.80 | –3.79 to 9.39 |
| Knowledge about drugs score | 448 | 0.01 | –0.33 to 0.36 | 493 | 0.09 | –0.13 to 0.31 | 513 | 0.32 | 0.03 to 0.62 | 485 | 0.11 | –0.17 to 0.39 |
| Variable | ASSIST vs. usual practice (reference) | +FRANK vs. usual practice (reference) | FRANK friends vs. usual practice (reference) | +FRANK vs. ASSIST (reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | RD | 95% CI | n | RD | 95% CI | n | RD | 95% CI | n | RD | 95% CI | |
| Indicative primary outcome | ||||||||||||
| Lifetime illicit drug use | 497 | –2.10 | –7.75 to 3.55 | 561 | –0.42 | –5.99 to 5.15 | 576 | –3.45 | –9.53 to 2.63 | 550 | 1.94 | –3.39 to 7.26 |
| Indicative secondary outcomes | ||||||||||||
| Cannabis use in lifetime | 508 | 0.48 | –5.22 to 6.19 | 573 | 1.01 | –6.19 to 8.20 | 590 | –1.13 | –9.31 to 7.04 | 553 | 0.44 | –4.50 to 5.38 |
| Cannabis use in past 12 months | 486 | 2.06 | –2.53 to 6.65 | 541 | 2.27 | –3.15 to 7.69 | 570 | -0.62 | –5.43 to 4.20 | 529 | –0.25 | –5.66 to 5.17 |
| GGA use in lifetime | 507 | 1.68 | –1.78 to 5.13 | 573 | 2.02 | –1.30 to 5.33 | 589 | –0.35 | –3.92 to 3.22 | 554 | 0.54 | –3.03 to 4.12 |
| GGA use in past 12 months | 476 | 1.20 | –1.46 to 3.87 | 534 | 2.68 | –0.49 to 5.85 | 555 | 0.17 | –1.94 to 2.28 | 526 | 1.31 | –2.30 to 4.92 |
| Ever having tried smoking (even if a puff) | 497 | 2.91 | –7.66 to 13.47 | 559 | 2.05 | –8.76 to 12.84 | 583 | –5.11 | –17.26 to 7.04 | 540 | –1.22 | –9.93 to 7.49 |
| Ever having consumed a whole alcoholic drink | 454 | 10.75 | –6.81 to 28.31 | 497 | 6.67 | –8.81 to 22.16 | 530 | –7.41 | –25.27 to 10.46 | 481 | –4.67 | –13.56 to 4.21 |
| Engages in heavy episodic alcohol use (A-SAQ)b | 471 | –0.92 | –8.22 to 6.37 | 532 | –2.88 | –9.97 to 4.21 | 542 | –8.74 | –17.20 to –0.29 | 537 | –1.90 | –8.83 to 5.02 |
| Intermediary variables | ||||||||||||
| Perceived prevalence of lifetime drug use in year groupc | 333 | 2.56 | –7.11 to 12.22 | 369 | 0.15 | –14.98 to 15.27 | 382 | –15.06 | –39.39 to 9.26 | 350 | –3.07 | –14.71 to 8.58 |
| Any drug offers in last yeard | 502 | 5.96 | –1.35 to 13.28 | 568 | 1.61 | –9.91 to 13.13 | 582 | –2.66 | –12.30 to 6.98 | 546 | –4.57 | –17.11 to 7.96 |
| Any conversations with school friends about drugse | 495 | –4.82 | –13.53 to 3.88 | 554 | 5.42 | –2.84 to 13.68 | 569 | 7.75 | –0.38 to 15.88 | 535 | 9.94 | 1.61 to 18.28 |
| Ever visited Talk to FRANK websitef | 496 | 4.87 | –5.45 to 15.19 | 561 | 14.63 | 10.19 to 19.07 | 576 | 14.79 | 8.24 to 21.34 | 538 | 9.28 | –1.67 to 20.22 |
| Variable | ASSIST vs. usual practice (reference) | +FRANK vs. usual practice (reference) | FRANK friends vs. usual practice (reference) | +FRANK vs. ASSIST (reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | OR | 95% CI | n | OR | 95% CI | n | OR | 95% CI | n | OR | 95% CI | |
| Indicative secondary outcomes | ||||||||||||
| Cannabis use in lifetime | 500 | 0.79 | 0.07 to 8.64 | 557 | 0.68 | 0.09 to 4.88 | 584 | 0.60 | 0.10 to 3.75 | 539 | 0.90 | 0.07 to 11.40 |
| Cannabis use in past 12 months | 485 | 2.61 | 0.07 to 4.42 | 538 | 2.10 | 0.22 to 9.88 | 568 | 1.07 | 0.15 to 7.57 | 527 | 1.14 | 0.03 to 41.82 |
| GGA use in lifetime | 499 | 5.65 | 0.33 to 97.86 | 557 | 1.42 | 0.12 to 6.83 | 583 | 1.55 | 0.12 to 0.41 | 540 | 0.25 | 0.02 to 4.05 |
| GGA use in past 12 months | 475 | 16.74 | 0.38 to 729.45 | 531 | 3.02 | 0.12 to 7.30 | 553 | 0.82 | 0.03 to 4.67 | 524 | 0.27 | 0.01 to 7.17 |
| Ever having tried smoking (even if a puff) | 489 | 0.54 | 0.05 to 5.78 | 543 | 0.75 | 0.11 to 5.34 | 577 | 0.75 | 0.14 to 4.15 | 526 | 1.55 | 0.12 to 20.06 |
| Ever having consumed a whole alcoholic drink | 446 | 0.27 | 0.01 to 5.03 | 484 | 0.27 | 0.03 to 2.75 | 524 | 0.30 | 0.04 to 2.30 | 470 | 1.20 | 0.06 to 23.52 |
| Engages in heavy episodic alcohol use (A-SAQ)b | 463 | 2.61 | 0.21 to 32.30 | 517 | 1.26 | 0.14 to 0.97 | 536 | 0.83 | 0.11 to 6.57 | 524 | 0.83 | 0.06 to 11.48 |
| Intermediary variables | ||||||||||||
| Perceived prevalence of lifetime drug use in year groupc | 489 | 0.60 | 0.04 to 9.36 | 357 | 0.08 | 0.01 to 1.42 | 378 | 0.50 | 0.02 to 0.27 | 521 | 0.31 | 0.02 to 4.71 |
| Any drug offers in last yeard | 583 | 2.87 | 0.25 to 32.94 | 552 | 1.14 | 0.14 to 9.13 | 576 | 1.37 | 0.21 to 8.83 | 607 | 0.32 | 0.02 to 5.96 |
| Any conversations with school friends about drugse | 487 | 2.57 | 0.20 to 33.16 | 538 | 0.31 | 0.04 to 2.39 | 563 | 1.27 | 0.23 to 7.04 | 521 | 0.11 | 0.01 to 2.00 |
| Ever visited Talk to FRANK websitef | 490 | 0.47 | 0.01 to 27.59 | 545 | 0.08 | < 0.01 to 2.21 | 570 | 0.13 | 0.01 to 2.60 | 526 | 0.05 | 0.01 to 2.03 |
List of abbreviations
- +FRANK
- ASSIST + FRANK
- A-SAQ
- Adolescent Single Alcohol Question
- ALSPAC
- Avon Longitudinal Study of Parents and Children
- CAST
- Cannabis Abuse Screening Test
- CHU-9D
- Child Health Utility-9 Dimensions
- CI
- confidence interval
- CONSORT
- Consolidated Standards of Reporting Trials
- cRCT
- cluster randomised controlled trial
- DALY
- disability-adjusted life-year
- FAQ
- frequently asked question
- FSM
- free school meal
- FTND
- Fagerström Test for Nicotine Dependence
- GCSE
- General Certificate of Secondary Education
- GGAs
- glues, gasses and aerosols
- HSI
- Heaviness of Smoking Index
- ICC
- intraclass correlation coefficient
- IDG
- intervention development group
- MRC
- Medical Research Council
- NIHR
- National Institute for Health Research
- OR
- odds ratio
- PHW
- Public Health Wales
- PSHE
- personal, social, health and economic education
- RCT
- randomised controlled trial
- SD
- standard deviation
- SMT
- school management team
- TMG
- Trial Management Group
- TSC
- Trial Steering Committee
- WIMD
- Welsh Index of Multiple Deprivation