

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 13/42/02. The contractual start date was in July 2014. The final report began editorial review in November 2016 and was accepted for publication in March 2017. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Adam Fletcher, Graham Moore and Chris Bonell are members of the Public Health Research (PHR) Research Funding Board. Rona Campbell is a member of the PHR Research Funding Board, and reports grants from the University of Bristol during the conduct of the study and personal fees from DECIPHer Impact Limited, outside the submitted work. Note that the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer) and DECIPHer Impact Ltd are separate entities, the latter being a not-for-profit organisation.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2017. This work was produced by Fletcher et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2017 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Youth smoking: a public health priority
Smoking is a major cause of preventable illness, premature death and health inequalities in the UK. Preventing young people from taking up smoking is vital to maintain and accelerate recent declines in smoking rates. Although much research has been undertaken to develop and evaluate school-based prevention interventions targeting 11- to 15-year-olds,1 the General Lifestyle Survey Overview: A Report on the 2010 General Lifestyle Survey (GLS) illustrates that smoking continues to grow rapidly among older adolescents. 2 The GLS does not differentiate those in or out of education; however, with > 1.5 million British 16- to 18-year-olds now enrolled in further education (FE) courses, new smoking prevention interventions are required that target FE settings (e.g. general FE colleges, ‘sixth form’ colleges attached to secondary schools, etc.). 3 As well as being a period in life when smoking often begins, the transition to FE itself may also increase the risk of smoking as young people are exposed to new sources of peer influence and have more independence from their parents.
Health improvement in further education settings
Research evidence about smoking prevention interventions delivered in FE settings is sparse. Two recent systematic reviews of health improvement interventions in educational sites contain no reference to such studies in FE settings. 4,5 This finding supports calls from the National Institute for Health and Care Excellence for more evidence regarding smoking prevention interventions in secondary schools and in other youth settings such as FE institutions. 3 Furthermore, the failure of the two reviews4,5 to identify any cluster randomised controlled trials (RCTs) undertaken within FE settings highlights the lack of rigorous health improvement evaluation in this context to date.
A search of bibliographic databases undertaken in 2013 identified a further 14 relevant reports about smoking prevention and other health improvement interventions in FE settings. 6–19 Among these, six non-systematic literature and policy reviews reported increasing policy interest in health improvement interventions targeting young people within FE settings, but noted the absence of any evidence regarding appropriate or effective interventions in FE settings. 6,7,9,10,12,14 No examples of effective smoking prevention interventions delivered in this context were identified. Three studies evaluated single-session motivational interviewing interventions in English FE settings,8,11,17 finding that it is feasible to deliver brief interventions within FE settings. 11 These studies also found that motivational interviewing targeting high-risk students engaged in drug use may reduce their use of cigarettes, alcohol and drug use. 8 However, it was not an effective method for preventing the uptake of smoking among 16- to 19-year-olds in FE. 17 One quasi-experimental study of a multicomponent intervention combining health education, counselling and nicotine therapy in French vocational colleges was found to be effective in supporting smoking cessation. 19
Effective smoking prevention methods and approaches
With no evidence of effective smoking prevention methods or approaches in FE settings, the findings of five recent systematic reviews of smoking prevention interventions delivered in other educational and/or community contexts were identified and synthesised to inform the pilot intervention. 20–24 The reviews suggest that the following smoking prevention methods and approaches are effective: reducing the illicit sale of tobacco products to under-18s;20–23 initiating tobacco-free policies and environmental change;22 age-appropriate, interactive educational messages delivered via intensive, long-term mass media campaigns;21 and social competency and skills development interventions to support young people to resist peer influence. 24 A recent systematic review of school effects/environment interventions also found that initiating tobacco-free policies and environmental change can be effective, especially in permissive contexts,4 which is likely to be the case in some FE settings.
This evidence highlights the relevance of multilevel smoking prevention interventions and identifies a set of intervention methods and approaches that may underpin intervention efficacy:
-
restricting the availability of tobacco and opportunities for smoking
-
restructuring environmental contexts
-
educating and persuading young people about the harms of smoking and social norms via multiple methods and communication channels
-
modelling social/situational resistance skills.
Systematic reviews also consistently find that ‘multilevel’ interventions, which address both individual and environmental determinants of behaviour simultaneously, are most effective for improving young people’s health outcomes. 20,23,25,26 These interventions, which include ‘higher-level’ environmental components, also tend to be more cost-effective,27 and are less likely to generate inequalities than individually focused components alone. 28,29 However, if such interventions are to deliver major public health gains, they must also be feasible to deliver and sustain. 30
‘The Filter FE’ intervention design and logic model
‘The Filter FE’ intervention was co-designed by Action on Smoking and Health (ASH) Wales and the research team following a commissioned call from the National Institute for Health Research (NIHR) Public Health Research (PHR) programme in 2013. It is a smoking prevention intervention managed and delivered by trained staff working on ASH Wales’ ‘The Filter’ youth project, who apply existing staff training, social media and youth work resources in FE settings. Informed by the socioecological theory of health,31 and evidence of effective smoking prevention methods and approaches (summarised in Effective smoking prevention methods and approaches), Filter FE aimed to integrate multiple intervention activities within a multicomponent, multilevel intervention for FE settings.
The intervention design and hypothesised mechanisms are summarised in the logic model (Figure 1) and described in more detail in Chapter 2, Intervention components. In summary, five areas of synergistic activity were planned to augment any existing activities already undertaken in FE settings: (1) working with local shops to restrict the sale of tobacco to under-18s; (2) implementing tobacco-free campus policies; (3) training FE staff to deliver smoke-free messages; (4) publicising The Filter youth project’s online campaigns, advice and support services via FE websites and social media; and (5) on-site youth work activities to provide credible educational messages and promote social/situational resistance skills, as well as signposting cessation services. As described in the logic model (see Figure 1), it was hypothesised that these components would prevent the uptake of smoking via the restriction of the availability of tobacco; restructuring the institutional context to prevent smoking on site and promote non-smoking behaviour as normative; education and persuasion of young people regarding the harms of smoking and social norms via multiple interactive methods and channels of communications; and modelling social/situational self-efficacy and resistance skills.
FIGURE 1.
Intervention logic model. AUDIT-C, Alcohol Use Disorders Identification Test Consumption; EMCDDA, European Monitoring Centre for Drugs and Drug Addiction; EMQ, European Model Questionnaire; EQ-5D-5L, EuroQol-5 Dimensions, 5-level version; ESFA, European Smoking Prevention Framework Approach; HSI, Heaviness of Smoking Index; IT, information technology; ONS, Office for National Statistics; QoL, quality of life.

In order to enable scalability across different types of FE settings (including large institutions), as well as sustainability and fidelity, the intervention was designed so that it involved standardised processes and activities balanced with opportunities for a degree of local tailoring of activities. Some flexibility to allow for local adaptation can support universal adoption, institutional ownership and sustainable implementation of multiple activities. 32,33 The intervention was also designed to allow the ‘dose’ of staff training and youth work activities to vary according to the size of institutions.
Public involvement
As well as co-designing the pilot intervention, staff working on ASH Wales’ The Filter youth project were involved in designing all aspects of the pilot trial and process evaluation prior to bid submission. The research team also worked with the Involving Young People Officer based in the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement to organise two consultations with the Advice Leading to Public Health Advancement (ALPHA) youth group at the project development stage. ALPHA is a group of young people aged 14–21 years who advise researchers on intervention design, logic modelling and data collection methods by discussing and debating their views on the proposed research. Staff from Public Health Wales and FE teachers were also consulted on the intervention design, logic model and research strategy.
Three further consultation meetings with the ALPHA group took place post commissioning to enable the researchers to consult with young people during the project on recruitment and survey methods (e.g. advice on the design of publicity materials, information sheets and e-questionnaires), strategies for increasing retention/follow-up, and public engagement and knowledge exchange activities.
Study aim, objectives and research questions
The aim of the pilot trial was to evaluate the feasibility and acceptability of implementing and trialling a new multilevel smoking prevention intervention in FE settings. The study had three objectives.
The first objective was to assess whether or not prespecified feasibility and acceptability criteria were met, which were agreed with the NIHR Evaluation, Trials and Studies Coordinating Centre and Trial Steering Committee, and deemed necessary conditions for progressing to a Phase III trial. The progression criteria are listed in full in Chapter 2, Progression criteria. In order to meet this objective, data were collected and analysed to address the following research questions (RQs):
-
Did the intervention activities occur as planned in (at least) two out of three intervention settings?
-
Were the intervention activities delivered with high fidelity across all settings?
-
Was the intervention acceptable to the majority of FE managers, staff, students and the intervention delivery team?
-
Was randomisation acceptable to FE managers?
-
Did (at least) two out of three colleges from each of the intervention and control arms continue to participate in the study at the 1-year follow-up?
-
Do student survey response rates suggest that we could recruit and retain at least 70% of new students in both arms in a subsequent effectiveness trial?
The second objective was to explore the experiences of FE students, staff and the intervention delivery team to refine the intervention and study design prior to a potential Phase III trial. In order to meet this objective, data were collected and analysed to address the following RQs:
-
What are students’, college staff’s and intervention team members’ experiences of the intervention and views about its potential impacts on health?
-
What are the barriers to, and facilitators of, implementation and how do these vary according to college context and/or other factors?
-
Were there any unexpected consequences?
-
How acceptable were the data collection methods to students and staff, and do participants think that longer-term follow-up via e-mail or telephone interview would be feasible?
-
What resources and partnerships are necessary for a Phase III trial?
The third objective was to pilot primary, secondary and intermediate outcome measures and economic evaluation methods prior to a potential Phase III trial. It was not an objective of the pilot study to assess intervention effects nor was it powered to do so, but data were collected and analysed to address the following RQs:
-
Does the primary outcome measure (smoking weekly or more) have an acceptable completion rate, adequate validity and minimise floor/ceiling effects?
-
Do cotinine concentrations of saliva samples indicate any evidence of response bias between arms in self-reported smoking status?
-
Was it feasible and acceptable to measure all the secondary and intermediate outcomes of interest at baseline and follow-up?
-
Is it feasible to assess cost-effectiveness using a cost–utility analysis within a Phase III trial?
Chapter 2 Methods
In this section of the report we provide an overview of the study design, including the specific intervention components examined. Details are then provided of the sampling and recruitment of the FE settings and randomisation. We then describe the methods used to assess the ‘progression criteria’ (objective 1), explore participants’ experiences of the process of implementing and trialling the intervention (objective 2) and examine pilot trial outcomes (objective 3). Details of the pilot economic analysis and trial registration, governance and ethics are provided at the end of this chapter.
Study design: overview
A cluster randomised controlled pilot trial was undertaken in six FE settings in south-east Wales with allocation to the Filter FE intervention (three settings) or continuation of normal practice (three settings). In order to assess the feasibility and acceptability of delivering and trialling the intervention according to prespecified criteria (objective 1), we collected a range of quantitative and qualitative data via semistructured observations of the intervention delivery, interviews with FE college managers and the intervention team, and documentary evidence (e.g. college policies, intervention team records, etc.). The retention of FE settings and response rates were assessed using student survey data.
To explore participants’ experiences of implementing and trialling the Filter FE intervention (objective 2), data were collected via semistructured interviews with FE managers and the intervention team, focus groups with students and staff, as well as additional process and contextual data via observations of intervention settings, staff training and youth work activities.
Primary, secondary and intermediate (process) outcomes, and economic evaluation methods were also piloted in this study (objective 3). Surveys of new students enrolling at the participating FE settings in September 2014 (baseline) and September 2015 (1-year follow-up) were used to examine the pilot primary, secondary and economic outcome measures. Informed by the intervention logic model, multiple sources of data were also collected at baseline and follow-up to pilot intermediate (process) outcomes at multiple levels: the restriction of the availability of tobacco in local shops was assessed via ‘mystery shopper’ audits; changes to the institutional environment and policies were assessed via structured observations and analysis of college policy documents; and students’ knowledge, norms and social/situational self-efficacy and resistance skills were assessed via the student survey.
Intervention components
This section describes how each of the pilot intervention components were intended to be delivered, by whom, and their logic.
Prevention of the sale of tobacco to further education students aged < 18 years
To restrict availability locally, the intervention manager would map and contact all shops selling tobacco within 1 km of the intervention setting (i.e. within a 10-minute walk). Information letters would be distributed to these retailers to inform them that a new project (Filter FE) was taking place at their local FE institution, explain why reducing supply is an important component of prevention and remind them about the penalties for selling tobacco to under-18s. The letter focused only on sales of legal tobacco through the retailers. Posters, stickers and other materials would also be supplied for these shops to provide information to their customers about the legal age for purchasing tobacco products and the requirements to produce statutory identification to purchase tobacco.
Institutional policy review to promote a tobacco-free environment
To restrict opportunities for smoking and promote non-smoking as the norm via modifying the institutional context, the intervention manager would work with FE managers to review institutional policies using the tobacco-free campus guidance developed by ASH Australia. 34 This tool uses a three-stage process to promote a tobacco-free environment, including advice on advertising, the supply of tobacco and support services, as well as information on maintaining smoke-free public areas, buildings and vehicles. First, current policies and practices are reviewed using this tool to develop a new whole-campus tobacco-free policy. Second, the revised policies are implemented and launched. Third, policies are monitored, evaluated and updated/refined if required.
Further education staff training
To train staff to deliver smoke-free educational messages and support institutional change, training officers employed on The Filter youth project [accredited by the Young Men's Christian Association (YMCA) and Agored Cymru] would organise and deliver training sessions on site using modules and teaching resources developed and piloted by ASH Wales in schools and other youth settings. Interactive, 2-hour training workshops would be delivered to approximately 10 staff per session, with FE staff trained to integrate activities about smoking into their lesson plans and other routine work (e.g. via body mapping the health harms of smoking, exercises on how tobacco companies recruit young smokers). All staff attending these sessions would also be encouraged to champion new tobacco-free policies (see Institutional policy review to promote a tobacco-free environment) and intervene to prevent smoking on site. The number of sessions to be delivered would vary depending on the size of the FE setting to ensure that resources are distributed appropriately: one session to be delivered at smaller ‘sixth form’ sites (i.e. to reach a total of approximately 10 members of staff) and 2–4 sessions to be delivered at medium and large FE campuses, respectively (to reach up to 20–40 members of staff).
Social media
To educate and persuade students about the harms of smoking, social norms and the relevance of support services, The Filter youth project’s web and social media officers would work with staff and students to integrate it online social marketing campaigns, advice and support services (e.g. The Filter text/instant messaging services) with institutional websites and social media channels maintained by staff and/or students [e.g. the college Facebook (www.facebook.com; Facebook, Inc., Menlo Park, CA, USA) page, institutional Twitter (www.twitter.com; Twitter, Inc., San Francisco, CA, USA) feeds, Instagram (www.instagram.com; Facebook, Inc., Menlo Park, CA, USA), etc.]. As well as embedding information on each intervention setting’s home/index webpage, the web and social media officers would work with the college information technology staff and consult students to identify opportunities for publicising key information and messages via frequently accessed webpages/micro-sites (e.g. online learning portals, e-mail login pages).
Youth work activities
To educate and persuade students about the harms of smoking and model social/situational resistance skills, qualified youth workers from The Filter project would work with college staff and students to plan and deliver a range of youth work activities on site (e.g. smoke-free message film-making, graffiti walls and/or other arts-based activities). Youth workers would launch the project in the autumn term, and then work with staff and/or student groups to identify 5, 10 or 15 groups (depending on institutional size) of 10–20 students to take part in locally tailored group-based activities. As with the staff training, the numbers of sessions delivered would vary according to the FE setting’s size to ensure resources are distributed appropriately. These group-based youth work activities would be provided on site during college time and typically last 1–2 hours. Students would not be targeted based on their smoking status or any other characteristics, as the aim is to recruit as many newly enrolled students as possible. Information about online support/advice services would also be provided to current smokers, when appropriate.
Sampling and recruitment of further education settings
The following diversity and matching criteria were used to purposively sample six FE settings in south-east Wales: large FE college campuses (new intake of > 500 students) (n = 2), small FE college campuses (new intake of < 500 students) (n = 2) and ‘sixth form’ colleges attached to schools (n = 2).
Purposive sampling ensures a diversity in contexts at the intervention piloting stage so that a realist lens can be applied to address questions regarding not only what is feasible and acceptable in general, but also for whom and under what circumstances, and place much more emphasis on exploring potential mechanisms of action and how these may vary by context prior to large-scale RCTs. 35 To avoid contexts in which implementation may be less challenging (or atypical in other ways), private institutions, small sites (with < 100 students) and ‘sixth forms’ at schools where < 10% of students are entitled to free school meals were not included. To minimise the potential for contamination across arms, no more than one FE setting was recruited from any middle-layer super output area, nor were FE settings recruited in neighbouring middle-layer super output areas.
The intervention team identified and contacted school and FE managers in the summer term of 2014, with recruitment complete by July 2014. A total of 10 FE settings in south and mid-Wales were contacted by ASH Wales’ staff in May and June 2014. Those who first expressed an interest were visited by researchers between June and July 2014, until six FE settings had been recruited according to the sampling criteria, above. Participating FE settings are listed in Table 1 according to recruitment strata (pseudonyms).
| Sampling/randomisation strata | FE setting (pseudonyms) | Allocation | Estimated new students aged 16–18 years |
|---|---|---|---|
| Large FE college campuses (n = 2) | Valeside College | Intervention | 1027 |
| Middledale College | Control | 760 | |
| Small FE college campuses (n = 2) | Laurelton College | Intervention | 130 |
| Glynbel College | Control | 175 | |
| School ‘sixth form’ colleges (n = 2) | Athervale Sixth Form | Intervention | 110 |
| Afonwood Sixth Form | Control | 161 |
Randomisation
Colleges agreed to take part in the study prior to randomisation. This study used a 1 : 1 allocation ratio. Allocation to intervention and control arms was conducted by the study statistician and stratified by the size and type of FE settings. The three strata were large FE college campuses with a new intake of > 500 students, small FE college campuses with a new intake of < 500 students and sixth forms within secondary schools. Table 1 reports the outcome of the random allocation to trial arm by sampling strata, including the size of each FE setting’s new intake.
It was not possible for colleges, the intervention team and researchers to be blinded to allocation throughout the study. However, colleges were randomised after baseline data collection to ensure that all students, staff and researchers were blind at the time of the recruitment of colleges and baseline data collection.
Progression criteria
In line with Medical Research Council guidance,36 data collection during the pilot trial focused on assessing acceptability and feasibility, and allowing us to judge progress against the agreed criteria for progression to a subsequent trial of effectiveness and cost-effectiveness. The first objective was specifically to assess whether or not the criteria deemed necessary in order to progress to a larger cluster RCT were met (Box 1). These were agreed by the investigator team, the NIHR Evaluation, Trial and Studies Coordinating Centre and Trial Steering Committee prior to commencing the pilot trial as evidence of feasibility and acceptability of the intervention and trial methodology.
-
Did the intervention activities occur as planned in (at least) two out of three intervention settings? This will be assessed according to the extent to which the following intervention activities occurred:
-
tobacco retailers within 1 km of the FE setting were contacted in writing within 3 months of the start of the intervention
-
institutional policies and practices were reviewed, updated using the tobacco-free campus guidance, and changes communicated to staff and students within 6 months of the start of the intervention
-
a minimum of one, two or four staff training sessions were delivered as planned (according to institutional size), with a minimum of five staff attending each session
-
The Filter youth project’s web-based information, advice and support services were embedded on the FE institution’s homepage during the intervention and online information, advice and support services are promoted through at least one local social media channel maintained by staff and/or students (e.g. the college Facebook page, Twitter feed, etc.)
-
a minimum of 5, 10 or 15 youth work sessions were delivered as planned (according to institutional size) with a minimum of eight different students attending each session.
-
-
Were the intervention activities delivered with high fidelity across all settings?
-
Was the intervention acceptable to the majority of FE managers, staff, students and the intervention delivery team?
-
Was randomisation acceptable to FE managers?
-
Did (at least) two out of three colleges from each of the intervention and control arms continue to participate in the study at the 1-year follow-up?
-
Do student survey response rates suggest that we could recruit and retain at least 70% of new students in both arms in a subsequent effectiveness trial?
Data sources
In order to answer RQ 1 (see Box 1), quantitative and qualitative data were collected from multiple sources. To assess if tobacco retailers within 1 km of the FE setting were contacted in writing within 3 months of the start of the intervention, data collected via intervention team records were examined and cross-checked through interviews with the intervention team. To assess if institutional policies and practices were reviewed and updated using tobacco-free campus guidance, with changes communicated to staff and students within 6 months of the start of the intervention, data collected via intervention team checklists were examined and cross-checked with documentary analyses of college policies and structured observations of the FE environments at follow-up. To examine the fidelity and reach of staff training, data collected via intervention team checklists and semistructured observations of training were examined. Integration of ASH Wales’ The Filter online resources by intervention setting was assessed using intervention team checklists and cross-checked via semistructured observations of college websites and social media channels. To examine the implementation of youth work activities, data collected via intervention team checklists were examined and cross-checked in interviews with FE managers.
In order to answer RQ 2 (see Box 1), semistructured observations of staff training sessions (n = 1 per intervention setting) and group-based youth work sessions (n = 1 per intervention setting) were used to assess fidelity of delivery of those components across settings and the fidelity of other intervention components (activities aiming to prevent the sale of tobacco to under-18s in shops near the intervention site, institutional policy review and revision, social media integration) were examined via intervention team checklists and interviews with the intervention team and FE managers. To answer RQ 3 (see Box 1), intervention acceptability and whether or not this was reported by the majority of participants, was assessed via data from semistructured interviews with FE managers and the intervention team, and student and staff focus groups. Data from semistructured interviews with FE managers were used to examine RQ 4 (see Box 1). In order to answer RQs 5 and 6 (see Box 1), the retention of FE settings and response rates were assessed using student survey data.
Data analysis methods
The quantitative and qualitative data collected to answer RQs 1–6 were managed and analysed separately. For example, the standardised checklist data from the mystery shopper, environmental observation and policy audits were collated and analysed in Microsoft Excel® 2013 (Microsoft Corporation, Redmond, WA, USA), whereas data from focus groups and interviews were analysed using NVivo version 10 (QSR International, Warrington, UK). The emergent results from each data source were shared and discussed among the research team. Individual results were collated according to a framework derived from key RQs and relevant progression criteria to ensure that data from all sources were used when pertinent to answer the RQs, and to facilitate triangulation. When data from one source contradicted data from another source, this was noted and discussed.
Evaluating participants’ experiences of the process
In addition to examining intervention delivery according to prespecified criteria (objective 1), a second objective was to explore student, staff and intervention team experiences of implementing and trialling the intervention, and how this varied in different FE contexts, in order to refine the intervention and trial methods. RQs 7–11 addressed this objective (Box 2).
-
What are students’, college staff’s and intervention team members’ experiences of the intervention and views about its potential impacts on health?
-
What are the barriers to, and facilitators of, implementation and how do these vary according to college context and/or other factors?
-
Were there any unexpected consequences?
-
How acceptable were the data collection methods to students and staff, and do participants think that longer-term follow-up via e-mail or telephone interview would be feasible?
-
What resources and partnerships are necessary for a Phase III trial?
To answer RQs 7–11, multiple sources of qualitative data collected via semistructured observations, semistructured interviews and focus groups were analysed to explore student, staff and intervention delivery team experiences in depth, and how and why these varied.
Qualitative process data
Semistructured interviews and focus groups were conducted with a range of stakeholders to explore in detail the process of planning, implementing and receiving the intervention. Table 2 summarises the process evaluation data collected at each FE site. Each method of data collection is described in more detail below.
| Trial arm and FE setting | Data collection method (n) | ||||
|---|---|---|---|---|---|
| Semistructured observations of | Student focus groups | Staff focus groups | FE manager/staff interviews | ||
| Staff training sessions (total delivered) | Youth work sessions (total delivered) | ||||
| Intervention arm | |||||
| Valeside College (large FE college campus) | 1 (1) | 1 (10) | 5 | 2 | 1 |
| Laurelton College (small FE college campus) | 1 (1) | 1 (2) | 4 | 2 | 1 |
| Athervale Sixth Form (school sixth form college) | 1 (1) | 1 (3) | 2 | 1 | 1 |
| Comparison arm | |||||
| Middledale College (large FE college campus) | N/A (0) | N/A (0) | N/A | N/A | 1 |
| Glynbel College (small FE college campus) | N/A (0) | N/A (0) | N/A | N/A | 1 |
| Afonwood sixth form (school sixth form college) | N/A (0) | N/A (0) | N/A | N/A | 0 |
Semistructured observations
Semistructured observations of staff training and youth work sessions were conducted to provide contextual detail on the delivery, and receipt, of the intervention and to provide data on potential barriers to, and facilitators of, implementation. Observations focused on the way in which sessions were delivered, the content and activities included, and the way in which they were received by staff and young people. Semistructured observations (of staff training and youth work sessions) were recorded on templates devised a priori, documenting the content of sessions, the number and types of participants, and the dynamics among the group, allowing for observation of intervention acceptability and fidelity.
Whenever possible, the same researcher conducted the observations, interviews and focus groups in each FE setting, and observations of staff training and youth work sessions were carried out before focus groups to maximise the opportunity to respond to issues that arose from observations and preliminary analyses in focus groups and interviews. This depth of fieldworker immersion and data triangulation enabled unexpected and emergent issues [e.g. attitudes and beliefs around electronic cigarettes (e-cigarettes)] to be tested and clarified.
One staff training session in each of the three intervention sites was observed between April and June 2015. Sessions lasted a maximum of 2 hours. A total of 28 members of staff attended the three sessions observed (Table 3). Participants included both teaching and support staff.
| Intervention setting | Participants (n) | ||
|---|---|---|---|
| Total | Teaching staff | Support staff | |
| Valeside College (large FE college campus) | 6 | 0 | 6 |
| Laurelton college (small FE college campus) | 9 | 0 | 9 |
| Athervale Sixth Form (school sixth form college) | 13 | 10 | 3 |
Three observations of youth work sessions were undertaken, one in each intervention site, between March and May 2015. The largest observed group had 22 students, the smallest had six participants; a member of teaching staff sat in on each of the observed sessions (Table 4). It is not known what proportion of participants identified as smokers, as it was not the intention to target students based on smoking status.
| Intervention setting | Participants (n) | Teachers present (n) | ||
|---|---|---|---|---|
| Total | Female | Male | ||
| Valeside College (large FE college campus) | 8 | 4 | 4 | 1 |
| Laurelton College (small FE college campus) | 6 | 0 | 6 | 1 |
| Athervale Sixth Form (school sixth form college) | 22 | 16 | 6 | 1 |
Focus groups with students and staff
Focus groups were conducted with students and staff at all the intervention settings to explore their views on student smoking norms and behaviour; their awareness and/or experiences of participation in Filter FE project activities at their college, including their views on how successfully each component was implemented and barriers to implementation; their perceived impact of the intervention activities on student and staff smoking norms, and behaviours at their college; and the acceptability and feasibility of recruiting and collecting multiple waves of e-survey data from students. Focus groups with students were chosen for both pragmatic and methodological reasons. First, focus groups allowed us to quickly capture a range of views from a relatively largely number of students (n = 69 in all focus groups). Second, we wished to gain insights into students’ shared (or contested) understandings of the smoking culture within FE settings; focus groups were, therefore, the most appropriate method.
The number of student focus groups varied according to the size of the college (see Table 2). The aim was to recruit six student focus groups (three smokers groups, three non-smokers groups) at the large FE college campus, four in the medium-sized college campus and two in the sixth form college. This was almost achieved: in the large FE college, five student focus groups were taken, with four and two undertaken as planned in the other intervention colleges. FE managers recruited students to attend the focus groups. They were asked to recruit both students who identified as smokers and those who identified non-smokers, from a range of courses. In practice, it was difficult to purposively sample and stratify students into groups by smoking status as some young people identified as non-smokers but revealed that they smoke (e.g. ‘social smoking’) during the focus group; other groups were mixed because the students were recruited through friendship groups or through a convenience sample of one tutor group. Although managers were briefed about how to recruit students, this mode of recruitment meant that there was potential for students to come along without a clear understanding of the purpose of the focus groups. We were therefore careful to provide a clear introduction before each focus group started, allowing participants to withdraw if they wished.
Student focus groups took place between April and June 2015. Most were in June 2016, and were conducted only after all intervention activities were completed at the site. A total of 69 students participated in the focus groups, of whom 31 were female (45%) and 18 explicitly identified themselves as smokers (26%); some additional participants identified as non-smokers but during the focus group discussion revealed they sometimes smoked. The smallest focus group had two students and the largest had 13 participants. The focus groups included part-time and full-time students from a range of courses, including Advanced level (A-level), Business and Technology Education Council (BTEC) and vocational students. Student focus groups lasted between 40 and 80 minutes, and were all conducted in private rooms at the intervention college sites using topic guides. Topic guides covered their views on student smoking norms and behaviours; awareness of and participation in The Filter FE project; how successfully each component was implemented and why implementation may have been limited; perceived impact on student and staff smoking norms behaviours; and the acceptability and feasibility of recruiting and data collection methods piloted. All participants were provided with a £10 ‘Love2shop’ voucher for taking part in the focus groups.
We conducted two staff focus groups at the two larger intervention sites: one focus group with staff who had received training from The Filter team as part of the intervention, one with staff who had not. Only one staff focus group took place at Athervale Sixth Form because of the smaller number of students and staff based there. We aimed to include approximately eight staff in each focus group but, in practice, it was difficult to recruit staff to attend the focus groups, especially those who had not attended the training. In total, 19 staff participated across the five focus groups (including eight staff trained by The Filter team); the size of focus groups ranged from two to six participants. Focus groups were conducted in private rooms on each site using semistructured topic guides that covered the same broad areas as the one used in the student focus group (see above paragraph). Participating staff represented a range of teaching, management and support positions within each setting.
Semistructured interviews with further education managers
Semistructured interviews were conducted with FE managers at both intervention and control sites to explore their experiences of participating in a trial, including the acceptability of randomisation and data collection methods; perceived benefits and challenges of the Filter FE intervention on student and/or staff smoking behaviours; and, at intervention sites, managers’ experiences of implementation in their college context, including activities completed/not completed and barriers to, and facilitators of, implementation. Interviews were used as FE managers were the person (or in the case of one paired-interview, people) who could offer the best insight into their experience of participating in the research.
A member of the management staff at each of the six participating FE settings was recruited to participate in a semistructured interview at the end of the intervention. Interviews were conducted with FE managers at both intervention and control sites between June 2015 and February 2016, after the completion of the intervention. One (control) FE manager declined to participate in the interview. One interview was face to face with two staff members who had been working jointly as the lead FE manager for the study and four interviews were conducted over the telephone at the participants’ request. This may have affected the data collected as the face-to-face interview was longer and the interviewees and interviewer had an established rapport. However, the telephone interviews were conducted by two experienced qualitative researchers (one was the researcher who conducted the face-to-face interview) and we ensured that all data were included in the analysis and contributed to the findings. We were careful to provide prompts to aid the recall of managers who were interviewed. The time between recruitment to the study and the interviews may have affected some interviewees’ accounts and led to difficulties in recall, although two of the interviewees were particularly keen to provide feedback about the recruitment process and the early stages of the study, suggesting that the interviewees had time to reflect on the process even if they could not remember fine details. Interviews lasted between 20 and 60 minutes. Topic guides included questions and prompts regarding our a priori progression criteria, their experiences of being involved in the pilot RCT and of planning, implementing and receiving the intervention (if they were an intervention site).
Semistructured interviews with the intervention team
Semistructured interviews were conducted with the intervention team to explore their experiences of implementing the intervention; facilitators of, and barriers to, implementation; potential changes to be made to the intervention; and their experience of delivering the Filter FE within a trial context. Two of these interviews were conducted before the end of the intervention because the members of staff were leaving the organisation. Recruitment to these interviews was based on whether or not the individual had been involved in intervention implementation and aimed to encompass a range of different staff roles (project managers, staff trainers, youth workers and social media team members); researchers recruited these staff directly.
Interviews were conducted with six members of the intervention delivery team between April and September 2015. All interviews were conducted face to face; five of the six interviews were conducted in private rooms in the ASH Wales offices and one was conducted in a private space at an intervention site after a staff training session. Interviews lasted between 30 and 60 minutes. The interview topic guides covered their experiences of implementing The Filter in FE settings; facilitators of, and barriers to, implementation; what they would change about the intervention if they could; and their experience of delivering the intervention within a trial context.
Data analysis methods
Qualitative data collected via focus groups and semistructured interviews were transcribed verbatim and entered into NVivo software to aid data management and analysis. Qualitative data were analysed using techniques associated with thematic content analysis and grounded theory. Transcripts were initially divided into four groups to assist manageability: student focus groups, staff focus groups, FE manager interviews and intervention team members. First, one of the research team (MW) read each of the groups of transcripts to familiarise herself with the data. All transcripts for each group were then reread and coded line by line to identify emergent themes, and an initial coding framework was developed to identify key themes and subthemes. The coding framework included both deductive codes, derived from key RQs and relevant progression criteria, and inductive codes, identifying other relevant themes emerging from the data (e.g. e-cigarette use in FE settings). Micky Willmott and a second researcher (RL) independently applied this coding framework to three transcripts, then met to discuss and further refine the coding framework. The final agreed coding framework was applied to all subsequent manuscripts by Micky Willmott, noting and discussing any substantial additions or modifications with the research team, as necessary. The way in which themes inter-related and how they varied between different groups and contexts was carefully scrutinised throughout the analysis process and recorded using detailed memos.
The quotations presented in the report were selected because they best illustrate the common and/or interesting ideas and themes emerging from the data. These were discussed and agreed among the research team. When contradictory data were identified (e.g. the difference between school sixth forms and colleges, or when some students identified that they felt that they had been bullied into smoking), these are noted in the report.
Observation records of staff training and youth work sessions were analysed separately from interview and focus group data by Micky Willmott, with NVivo used to support cross-checking and data triangulation. Records were coded line by line, then grouped according to whether they related to the framework described above or inductive, emergent themes.
Most of the qualitative data collected for the process evaluation were collected by experienced qualitative researchers who were independent of the trial management or baseline data collection. Although this added an additional layer of contacts for FE managers to liaise with, it meant that the researchers had minimal knowledge or preconceptions about the sites. The researchers were all white professionals (three female and one male), which reflected the predominant ethnicity in FE sites. They had little knowledge of the areas in which the FE sites are based, and all were English, not Welsh or Welsh speakers, which may have had an impact on how the students and staff responded to them in focus groups. Researchers shared their reflections on data collection to aid analysis and an interpretative approach.
Pilot outcome measures
The final objective was to pilot primary, secondary and intermediate outcome measures and economic evaluation methods. The pilot cluster RCT design enabled a range of outcome measures and data collection methods (student surveys, policy audits, environmental observations and mystery shopper visits) to be piloted at baseline (September 2014) and at the 1-year follow-up (September 2015) to answer RQs 12–15 (Box 3).
-
Does the primary outcome measure (smoking weekly or more) have an acceptable completion rate, adequate validity and minimise floor/ceiling effects?
-
Do cotinine concentrations of saliva samples indicate any evidence of response bias between arms in self-reported smoking status?
-
Was it feasible and acceptable to measure all the secondary and intermediate outcomes of interest at baseline and follow-up?
-
Is it feasible to assess cost-effectiveness using a cost–utility analysis within a Phase III trial?
The pilot outcomes are described first in Pilot primary and secondary outcome measures and Pilot intermediate outcome measures, followed by a description of the data sources used to operationalise these measures to assess change at the student, college and community levels (see Data sources). These pilot outcomes are also summarised in the intervention logic model (see Figure 1). Finally, the methods for analysing the student survey data and other quantitative data sources are described in Statistical analyses.
Pilot primary and secondary outcome measures
All the pilot primary and secondary outcome measure data were collected via student surveys at baseline and at the 1-year follow-up, which are described in more detail later (see Data sources).
The pilot primary outcome was prevalence of weekly smoking (defined as smoking at least one cigarette weekly or more) at the 1-year follow-up, which was assessed using an item adapted from the GLS. 2 Students were asked: ‘Do you smoke cigarettes at all nowadays?’ and given four response options: ‘Yes, every day’, ‘Yes, at least once a week’, ‘Yes, occasionally but less than once a week’ and ‘No, never’. Those who responded ‘Yes, every day’ or ‘Yes, at least once a week’ were considered weekly smokers.
The pilot secondary outcomes were lifetime smoking, using the Office for National Statistics (ONS) GLS item;2 use of cannabis in the past 30 days and frequent cannabis use (four or more times in the past 30 days), using the European Monitoring Centre for Drugs and Drug Addiction European Model Questionnaire items;37 high-risk alcohol use, using the Alcohol Use Disorders Identification Test Consumption (AUDIT-C) measure;38 and health-related quality of life, using the EuroQol-5 Dimensions, 5-level version (EQ-5D-5L) measure. 39
The following three measures were additional pilot secondary outcomes at follow-up for baseline smokers only: self-report smoking cessation, using the ONS GLS item;2 number of cigarettes smoked per week, using the ONS GLS item;2 and nicotine dependence as measured using the Heaviness of Smoking Index (HSI). 40
Pilot intermediate outcome measures
As illustrated in the intervention logic model (see Figure 1), it was hypothesised that the intervention components would prevent the uptake of smoking through triggering changes at the individual (student), college and community levels. For this reason, intermediate outcome variables were piloted at each of these three levels by collecting a range of additional quantitative process data at baseline and at the 1-year follow-up via college policy audits, environmental observations and mystery shopper visits, as well as via the student surveys at each site.
At the individual level, baseline and follow-up student surveys assessed self-reported changes over time to attitudinal and knowledge-based precursors to smoking, including perceived prevalence of smoking (i.e. perceived norms), by adapting NatCen items;41 social and situational self-efficacy and skills, using the European Smoking Prevention Framework Approach (ESFA) items;42,43 and awareness of The Filter project.
At the institutional level, two measures of college environmental change were piloted. First, progress towards a tobacco-free environment, determined via an audit of FE college policies and structured observations at both intervention and comparison settings pre and post intervention. Second, staff commitment to smoking prevention and delivery of smoke-free messages, assessed via student survey items at follow-up.
At the community level, the availability of tobacco to students aged < 18 years from local retailers was assessed via a pre- and post-intervention mystery shopper audit of retailers within 1 km of intervention and comparison sites and items on the student follow-up survey.
Data sources
Quantitative data were collected at baseline (September 2014) and follow-up (September 2015) via the following methods: student surveys, college policy audits, structured observations of the college environment and mystery shopper visits. These methods are described in detail in turn below. All baseline data collection was completed prior to randomisation (October 2014). The investigator team was unblinded to allocation at follow-up, but all fieldworkers remained blinded throughout the study.
Student surveys
Students were eligible to participate at baseline if they were aged between 16 and 18 years on 1 September 2014 and had enrolled into FE studies in the 2014–15 academic year (i.e. they were new FE students, aged 16–18 years). Students who were older or younger than 16–18 years and completed the survey were excluded from analyses.
As this was a pilot trial, a power calculation was not required. The estimated sample size at baseline of 2500 students in six FE settings was chosen to provide some information on variability within and between settings at baseline and follow-up. This sample was chosen to indicate the likely response rates and permit estimates [with 95% confidence intervals (CIs)] and intracluster correlations (ICCs) of weekly smoking prevalence in advance of a potential effectiveness trial involving a larger number of clusters (colleges) and students.
At baseline and follow-up, the consent form and survey were completed using an e-questionnaire for ease of delivery and completion in all areas of college, including social spaces without desk access, with paper copies available if necessary (e.g. requested by student, because of technical problems, etc.). Use of incentives is considered fair recompense for time in work with young people. 44 Here, student participation was incentivised via prize draws for an iPad (Apple Inc., Cupertino, CA, USA) and shopping vouchers at both baseline and follow-up.
In the first week of September 2014 (i.e. the first week of the new term), students at each participating FE setting that used an e-mail system (four out of six institutions) were contacted directly via their new e-mail account and asked to complete the baseline survey directly via a weblink, they were also sent a reminder e-mail 3 weeks later. Those students who did not complete the survey online directly via this e-mail link, or who attended an institution without a student e-mail system, were given multiple opportunities to complete the e-questionnaire on site during September 2014 via: (1) timetabled classroom periods dedicated to survey completion, in which students used either college computers, their own devices (laptop, tablet computer or smartphone) or Google Nexus tablet computers (Google Inc., Mountain View, CA, USA) provided by the fieldworkers; or (2) informal data collection sessions (using Google Nexus tablet computers and/or quick layered response codes) in common areas at break periods. Hard copies were available as a backup (e.g. if the internet connection was too slow or could not be accessed temporarily) and were entered online once fieldworkers returned to the office. All baseline collection occurred between 1 and 30 September 2014. Detailed contact information (name, personal e-mail and mobile phone number) was collected at baseline to help track students who left or were on work-based placements at follow-up.
The 1-year follow-up took place when students had begun the next college year in September 2015 and used the same methods (i.e. e-mails to all students with a college e-mail account, classroom sessions, informal data collection sessions in common areas). To increase response rates, participants were also telephoned up to three times in September 2015 to collect follow-up survey data. All follow-up data collection occurred between 1 and 30 September 2015. Participants who left college or were unable to be contacted were lost to the trial at follow-up.
After the follow-up survey, all students were contacted and asked to provide a saliva sample in order to examine the reliability and validity of the self-reported smoking outcome via cotinine and anabasine testing. However, it was not feasible to recruit sufficient students to provide these samples, despite the use of £10 vouchers as incentives, and we do not report the results of this validation substudy here.
College policy audits
Institutional policies were obtained in September 2014 (baseline) and September 2015 (follow-up). Researchers requested all relevant tobacco policy documents directly from the management teams at each participating FE setting. Data were extracted into an online pro forma to capture the following information about each setting:
-
whether the institution has a specific tobacco policy in place or if tobacco use is covered in other institutional policies
-
the date of the policy and how often reviewed
-
whether or not students and/or staff are allowed to smoke or use e-cigarettes on site according to current policy
-
whether or not college policies make provisions for cessation services and other ‘quit resources’ on site
-
other details, including whether or not careers events, funding and financial connections are covered by existing institutional policies.
Structured observations of the college environment
One researcher completed a structured observation of each college environment (n = 6) at baseline and follow-up using a tablet computer. These observations aimed to assess student and staff practices (e.g. smoking outside of designated areas, where e-cigarettes are used, etc.) and the extent to which the physical environment at each site communicated tobacco-free messages (e.g. through signage) and/or supported institutional policies (e.g. directed people to designated smoking areas off site). Photographs were also taken on the tablet computers to illustrate the information recorded in the observational schedule.
Mystery shopper visits
Tobacco availability to students aged < 18 years was assessed at baseline and follow-up using a mystery shopper audit of all retailers within 1 km (i.e. within a 10-minute walk) of all six participating FE sites. These were the shops that were in the target area for intervention. The aim of the visits was to assess whether or not local shops were compliant with the restriction of tobacco sales to under-18-year-olds at baseline and/or follow-up, and to explore differences over time overall and by arm. The protocol for the mystery shopper activity was developed with input from Caerphilly Trading Standards officers in line with best practice guidance for test purchasing methods.
Mystery shopper exercises were carried out by two young people aged 17 years (one in 2014, one in 2015) who were (1) aged < 18 years and (2) not students at any of the sites included in the study. At both baseline and follow-up the mystery shoppers were male. The shoppers were accompanied by an adult fieldworker, who remained outside the shops and out of sight. The shopper entered the shop and asked to purchase cigarettes while the fieldworkers waited outside. They then completed an online, standardised checklist with the fieldworkers that covered type of shop visited, whether or not they were able to purchase cigarettes and the presence of age restriction warning posters or materials in the shop. There was one instance at baseline (none at follow-up) in which the shopper was unable to recall whether or not there was additional signage in the store regarding smoking or age restrictions.
A total of 18 shops were followed up at both baseline and follow-up; seven shops were also visited only once (either baseline or follow-up) because of closure or because their identity could not be verified at follow-up (e.g. name changed). In Chapter 3 we therefore report the results when data are available for shops at both baseline and follow-up (n = 18).
Statistical analyses
The primary aim of the pilot trial was to assess feasibility and acceptability, and gather data to plan a future definitive trial. This included estimating rates of eligibility, recruitment, retention at the 1-year follow-up, as well as the acceptability, reliability and rates of completion of pilot primary and secondary outcome measures.
The eligibility, recruitment and retention rates for colleges and students are summarised using a Consolidated Standards of Reporting Trials diagram (see Figure 2). The data collected for trial participants were summarised by trial arm and combined across arms. The aim was to examine the acceptability of potential primary and secondary outcome measures for a future trial, as well as describing the baseline characteristics of participants. The percentage of missing values was reported for all variables. Categorical variables were summarised using the percentage in each category. Numeric variables are summarised with the mean, standard deviation (SD) and a five-number summary (minimum, 25th centile, median, 75th centile, maximum). We present mean and median values to examine the shape of each distribution. All analyses used intention-to-treat populations.
We used chi-squared and t-tests to examine differences between students who did and did not provide data at baseline and follow-up. Cronbach’s alpha was calculated to examine the internal consistency of measures. Multilevel logistic regression models adjusting for baseline weekly smoking status, age, gender, residence with an employed adult, ethnicity and educational attainment [five or more General Certificate of Secondary Education (GCSE) at A*–C] were used to conduct exploratory effectiveness analyses. All statistical analyses were conducted with Stata® version 13 (StataCorp LP, College Station, TX, USA).
Data from the mystery shopper, policy audit and environmental observations were collated and analysed using Excel spreadsheets. For the mystery shopper survey, shops visited at both baseline and follow-up were matched in the spreadsheet and the data for each survey item (e.g. whether or not cigarettes were successfully purchased) compared. For each site, items on the policy audit were compared at baseline and follow-up, with differences between intervention and comparison sites scrutinised. Similarly, environmental observation items were compared between intervention and control site, noting any changes between baseline and follow-up.
Economic analysis
We piloted a brief health service use survey for student completion and the EQ-5D-5L (pilot secondary outcome) to record preference-based health-related quality of life. 39 These measures were piloted because it was anticipated that, if feasible to collect data from students in these settings, they could be used in any subsequent Phase III trial to measure any short-term impact of smoking on health-care use and/or health-related quality of life.
Trial registration, governance and ethics
The study was funded by the NIHR PHR programme (13/42/02). The trial protocol was registered with Current Controlled Trials (ISRCTN19563136). The study was overseen by a Trial Steering Committee, comprising an independent chairperson (Professor Paul Aveyard, University of Oxford) and three other independent members (Professor Angela Harden, University of East London; Professor Rob Anderson, University of Exeter; and Dr Julie Bishop, Public Health Wales). The Trial Steering Committee met every 6 months throughout the study (three times in total) to examine the methods proposed and monitor data for quality and completeness. With the agreement of the Trial Steering Committee and NIHR PHR co-ordinating centre, a separate Data Monitoring and Ethics Committee was not established because this was a pilot trial with no interim analysis.
The study was approved by the Cardiff University School of Social Sciences Research Ethics Committee prior to recruitment and data collection commencing. The validation substudy (saliva testing) was approved by the School of Medicine Research Ethics Committee, liaising with Cardiff University Human Tissue Act managers as necessary. The pilot trial protocol was approved by the South East Wales Trials Unit and the Trial Steering Committee.
Chapter 3 Results
In this section of the report, we first describe the student response rates at baseline and follow-up and the characteristics of the students participating in the study. The findings related to the primary objective are then presented, which was to assess the prespecified ‘progression criteria’ considered to represent evidence of feasibility and acceptability of the intervention and trial methodology. We then present student, staff and facilitators’ experiences of the intervention and trial process. Finally, we report the quantitative data analyses examining the pilot primary and secondary outcomes, including the pilot economic outcome measure and the pilot intermediate outcome measures.
Description of pilot trial sample
Six colleges were assessed as being eligible to participate in the trial and participated in the study, including random allocation (three intervention and three control; Figure 2). Colleges could not always know or provide exact ages of enrolled students before data collection, which is discussed further in Chapter 4.
FIGURE 2.
The Consolidated Standards of Reporting Trials diagram.
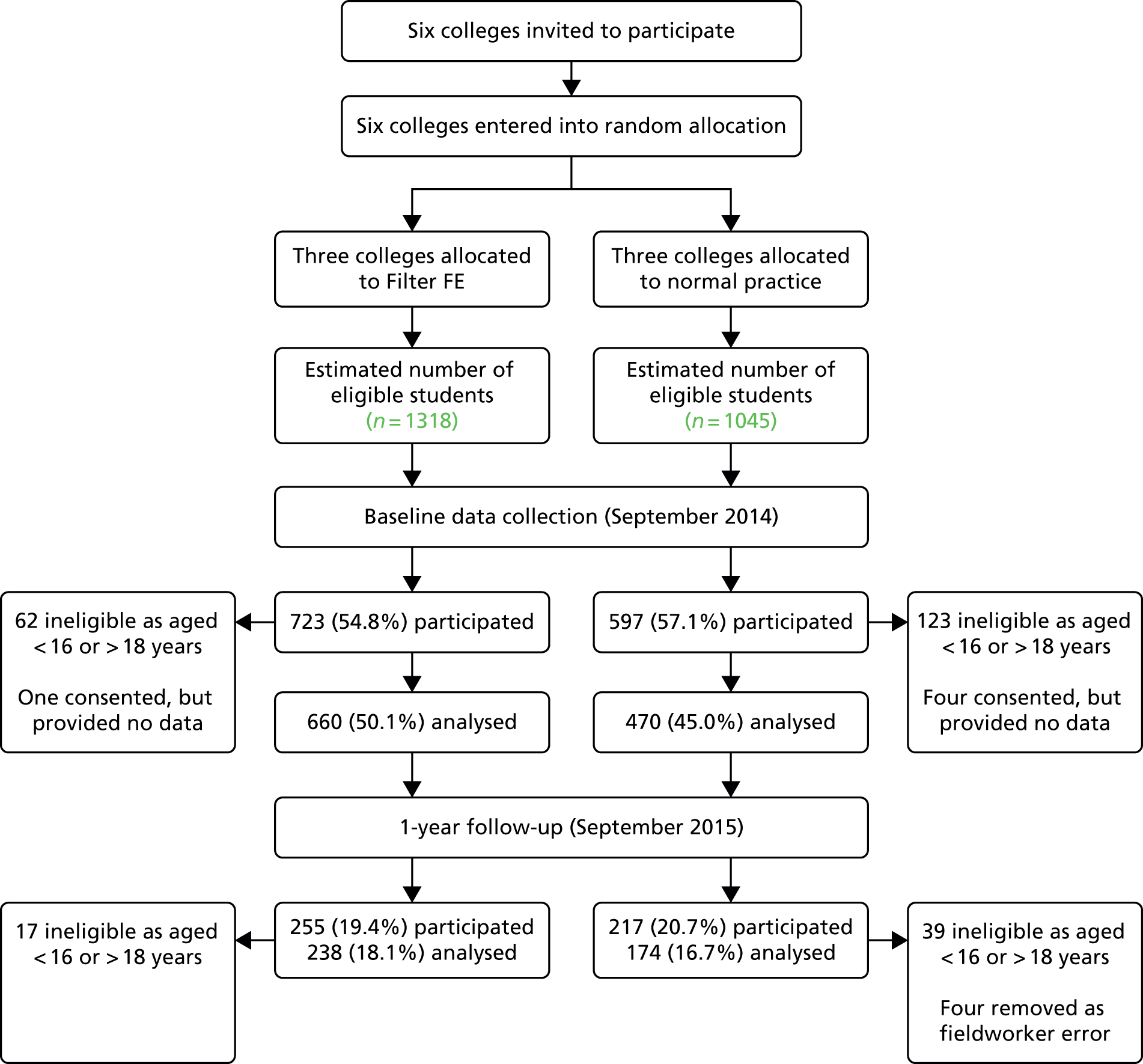
Flow of participants in the pilot trial
Of the target population of 2363 students at baseline, 1320 (55.8%) participated in baseline data collection. Of those 1320 participants, five students (0.4%) provided consent information but did not answer any questions on the survey and 185 (14.0%) were ineligible because they were aged < 16 years or > 18 years. Of those excluded as a result of age, around half (49.7%) were aged ≥ 21 years. The remaining 1130 students, 470 in the control arm and 660 in the intervention arm, equated to a baseline response rate of 47.8% based on the estimated total population of new students aged 16–18 years at these college campuses.
At the 1-year follow-up, 472 (35.7%) baseline respondents participated in the repeat survey. Fifty-six of these participants (12.0%) were students who were ineligible to take part in this study at baseline because they were aged < 16 years or > 18 years. Four participants’ responses were removed because of concerns about the quality of data collected on 1 day at one site, based on fieldworker reports (Laurelton College). Out of the 2363 potentially eligible students at baseline, 412 (17.4%) students who were eligible to participate provided valid survey data at baseline and at the 1-year follow-up. This comprised 238 students in the intervention arm and 174 students in the control arm.
Student characteristics
The categorical baseline characteristics for eligible and non-eligible participants are summarised and compared in Table 5.
| Variable | Baseline data: distribution over categories by eligibility, %a | |
|---|---|---|
| Eligible (aged 16–18 years) (n = 1130) | Not eligible (aged < 16 or > 18 years) (n = 185) | |
| Gender | ||
| Missing | 0 | 0 |
| Male | 37.1 | 38.9 |
| Ethnicity | ||
| Missing | 0.1 | 0 |
| White British | 92.8 | 91.4 |
| White not British | 0.9 | 2.7 |
| Mixed race | 3.1 | 1.1 |
| Asian or Asian British | 0.9 | 1.6 |
| Black or black British | 1.2 | 1.1 |
| Other | 1.1 | 2.2 |
| Is the adult you live with in paid work? | ||
| Missing | 2.7 | 34.5 |
| Yes | 76.8 | 46.0 |
| No | 14.2 | 15.1 |
| Not sure | 6.4 | 4.3 |
| Studying full or part time? | ||
| Missing | 1.3 | 2.7 |
| Full time | 95.3 | 85.4 |
| Part time | 3.5 | 11.9 |
| Working full or part time? | ||
| Missing | 1.5 | 3.2 |
| Full time | 6.7 | 12.4 |
| Part time | 26.4 | 27.6 |
| I do not work | 65.4 | 56.8 |
| Do you have five or more GCSEs? | ||
| Missing | 0.9 | 2.2 |
| Yes | 74.0 | 51.9 |
| No | 19.0 | 33.0 |
| Not sure | 6.1 | 13.0 |
| Qualification(s) studying at college | ||
| Missing | 1.2 | 2.7 |
| AS/A level | 34.5 | 8.11 |
| BTEC | 32.9 | 29.7 |
| Access level course | 7.4 | 12.4 |
| GCSE | 5.1 | 7.0 |
| Other vocational award, certificate or diploma | 4.1 | 4.9 |
| Welsh Baccalaureate | 0.4 | 0 |
| Other | 5.7 | 15.1 |
| Apprenticeship | 1.4 | 3.7 |
| Essential skills | 2.4 | 5.4 |
| HNC | 0.2 | 0.5 |
| HND | 0.4 | 2.3 |
| NVQ | 4.4 | 8.2 |
The eligible participants (i.e. those aged 16–18 years) who completed the baseline survey were predominantly female (62.9%), white British (92.8%), living with an adult in paid work (76.8%), studying full time (95.3%) and had five or more GCSEs (74%). They were enrolled on a wide range of courses, although the two most common FE pathways reported by participants at baseline were AS (Advanced Subsidiary level)/A-level courses (34.5%) and BTEC courses (32.9%).
The distribution of gender was similar in eligible and non-eligible participants. Ethnic group was evenly distributed across the two groups (eligible and non-eligible participants), with few non-white participants. Non-eligible participants were more likely than eligible participants to study part time, have a full-time job and be studying for an access level course, but less likely to have five or more GCSEs and study AS/A levels.
The categorical baseline characteristics of eligible participants by trial arm are summarised in Table 6. Gender was not evenly distributed across the trial arms: the control group comprised 44.7% males and the intervention group 31.8% males. Participants in the control group were older than intervention group students, with 15.1% of participants at control sites aged 18 years, compared with just 8.2% at intervention sites. Ethnicity was evenly distributed, with very few non-white participants in either arm. Control group participants were more likely to study part time and live with an adult in paid work, but less likely to have five or more GCSEs, and be studying for AS/A-levels than intervention group participants.
| Variable | Baseline data: distribution of categories by trial arm, % | ||
|---|---|---|---|
| Control (n = 470) | Intervention (n = 660) | Overall (N = 1130) | |
| Gender | |||
| Missing | 0 | 0 | 0 |
| Male | 44.7 | 31.8 | 37.1 |
| Age (years) | |||
| Missing | 0 | 0 | 0 |
| 16 | 60.4 | 69.1 | 65.3 |
| 17 | 24.5 | 22.7 | 23.4 |
| 18 | 15.1 | 8.2 | 11.0 |
| Ethnicity | |||
| Missing | 0.2 | 0 | 0.1 |
| White British | 91.3 | 93.9 | 92.8 |
| White not British | 0.4 | 1.2 | 0.9 |
| Mixed race | 2.6 | 3.5 | 3.1 |
| Asian or Asian British | 1.5 | 0.5 | 0.9 |
| Black or black British | 2.6 | 0.2 | 1.2 |
| Other | 1.5 | 0.8 | 1.1 |
| Is the adult you live with in paid work? | |||
| Missing | 4.1 | 1.7 | 2.7 |
| Yes | 68.9 | 82.4 | 76.8 |
| No | 18.7 | 10.9 | 14.2 |
| Not sure | 8.3 | 5.0 | 6.4 |
| Studying full or part time? | |||
| Missing | 0.9 | 1.5 | 1.3 |
| Full time | 93.4 | 96.7 | 95.3 |
| Part time | 5.7 | 1.8 | 3.5 |
| Working full or part time? | |||
| Missing | 1.3 | 1.7 | 1.5 |
| Full time | 7.7 | 6.1 | 6.7 |
| Part time | 23.8 | 28.2 | 26.4 |
| I do not work | 67.2 | 64.1 | 65.4 |
| Do you have five or more GCSEs? | |||
| Missing | 1.1 | 0.8 | 0.9 |
| Yes | 63.0 | 81.8 | 74.0 |
| No | 26.4 | 13.8 | 19.0 |
| Not sure | 9.6 | 3.6 | 6.1 |
| Qualification(s) studying at college | |||
| Missing | 1.7 | 0.8 | 1.2 |
| AS/A-level | 24.8 | 41.4 | 34.5 |
| BTEC | 30.4 | 34.7 | 32.9 |
| Access level course | 7.2 | 7.6 | 7.4 |
| GCSE | 8.3 | 2.9 | 5.1 |
| Other vocational award, certificate or diploma | 5.3 | 3.2 | 4.1 |
| Welsh Baccalaureate | 0.6 | 0.2 | 0.4 |
| Other | 8.5 | 3.6 | 5.7 |
| Apprenticeship | 1.5 | 1.4 | 1.4 |
| Essential skills | 3.8 | 1.4 | 2.4 |
| HNC | 0 | 0.3 | 0.2 |
| HND | 0.2 | 0.5 | 0.4 |
| NVQ | 7.4 | 2.3 | 4.4 |
Progression criteria assessment
The first objective was to assess if prespecified feasibility and acceptability criteria were met to determine whether or not to progress to a larger, Phase III trial to examine effectiveness (RQs 1–6). Intervention feasibility and acceptability addresses RQs 1–3: did the intervention activities occur as planned in (at least) two out of three intervention settings?; were the intervention activities delivered with high fidelity across all settings?; and was the intervention acceptable to the majority of FE managers, staff, students and the intervention delivery team? The questions regarding the acceptability and feasibility of trial methods (RQs 4–6) are then addressed in Trial feasibility and acceptability.
Intervention feasibility and acceptability
First, each of the five intervention components is considered in turn to understand whether or not they were delivered as planned (RQ 1) and with high fidelity across multiple settings (RQ 2). At the end of this section, the question of overall acceptability is addressed briefly (RQ 3) prior to presenting participants’ views in more detail in Process evaluation: participants’ experiences.
Prevention of the sale of tobacco in local shops
With the aim of restricting the local availability of tobacco at each intervention setting, the Filter FE intervention included a community-level component targeting local retailers. The aim was for the intervention manager to contact all shops selling tobacco within 1 km of the intervention setting (i.e. within a 10-minute walk). This component was intended to be delivered immediately post randomisation (early October 2014) via letters sent to these retailers to inform them that a new smoking prevention project (The Filter FE) was taking place at their local FE institution. Posters, stickers and other materials about The Filter and ASH Wales were also to be distributed to these shops to provide additional information to them and their customers about the legal age for purchasing tobacco products and the requirements to produce statutory identification to purchase tobacco. Owing to the location of the intervention settings in rural and suburban areas, in total there were only five shops within 1 km of all the intervention sites; one rural site had no tobacco retailers within 1 km (Laurelton College).
The results indicate that the criteria for RQs 1 and 2 were not met for this component at any of the three intervention sites. Despite the low number of retailers, the intervention team checklists were not recorded consistently and intervention team members reported that resources were not sent out to these retailers as planned. Various factors appeared to contribute to this, but the most common factors appeared to be the relatively short time available to identify and work with local community settings, as well as poor management of intervention implementation. There was also no evidence of changes in practices from the mystery shopper audit at follow-up in September 2015. In two out of the three shops close to intervention sites that were audited by a mystery shopper at baseline and follow-up, it was possible to buy cigarettes at follow-up but not at baseline (i.e. local availability of tobacco to students aged < 18 years may have increased; the findings of mystery shopper audit are reported in Pilot intermediate outcome measures). There was some observational evidence that age restriction signage increased in local shops between baseline and follow-up, although this was consistent across shops in both intervention and control arms.
Policy review to promote a tobacco-free environment
Five policies were audited and recorded at baseline. In one (control) site, Afonwood School, there was no written policy, but if students were caught smoking on site, a letter was sent to their guardian (a copy of the letter was obtained). With the aim of restricting opportunities for smoking and promoting non-smoking as the norm at each intervention setting, it was intended that the intervention manager would develop new whole-campus tobacco-free policies with each intervention setting. This component was intended to be delivered immediately post randomisation (early October 2014) by the intervention manager who would work with FE managers at each intervention setting to review their institutional policies using the tobacco-free campus guidance developed by ASH Australia. 34
Overall, there was little evidence that the intervention delivery team worked with intervention sites to support the introduction or modification of smoking policies. As with the prevention work targeting local shops (above), the intervention team checklists were not recorded consistently and intervention team members reported that this intervention component was not implemented as planned, again because of the short run-in time and poor management of the intervention implementation. The ASH Australia three-stage tobacco-free campus guidance was not used as intended at any site.
Analysis of institutional policy documents at follow-up found limited evidence of changes made to policies: at one intervention site the smoking policy was amended to include e-cigarettes, but both smoking and e-cigarettes were still permitted in designated ‘smoking areas’; fieldworker notes at one intervention setting recorded that one college had adopted a ‘campus-wide no smoking policy’ between baseline and follow-up but there was no written policy and it was not possible to attribute any changes directly to this intervention component. At the end of the intervention, none of the available school/college policies explicitly addressed issues (such as tobacco industry sponsorship, funding and gifts or tobacco advertising and sales on site), which are suggested in the ASH Australia guidance.
Further education staff training
It was intended that a minimum of one, two or four staff training sessions would be delivered at the intervention settings, proportionate to institutional size. Staff training was delivered at all intervention sites by experienced training officers employed by ASH Wales on The Filter youth project. However, in practice, the number of sessions delivered was driven by demand in each site and only three sessions were delivered in total, one in each site (i.e. lower than intended at the two FE college campuses). All sessions were attended by at least six staff, with a total of 28 staff attending overall, who were observed to be engaged and interested in the topics. At Valeside College, the large FE campus in the intervention arm, attendance was lowest (six people); a second training session had been arranged but was cancelled because of a lack of staff interest. ASH Wales staff used its own standard evaluation forms at the end of each staff training. However, these did not collect additional information we required (e.g. staff role, previous training, contact with students, etc.) and, therefore, were not collated or used in the analysis.
The content of the training was agreed between intervention sites and the intervention delivery team as planned, drawing on the different teaching resources developed and piloted by ASH Wales in schools and other youth settings for The Filter youth project. All of the FE settings chose the staff training resources developed by ASH Wales on e-cigarettes, and these sessions covered the same topics using the same combination of Microsoft PowerPoint® 2013 (Microsoft Corporation, Redmond, WA, USA) presentation, group exercises and discussion with high fidelity across all settings.
Social media
Observations of the college websites provided evidence that links to The Filter social marketing campaigns, and its advice and support services (e.g. The Filter text/instant messaging services), had been publicised on the institutional websites as planned. The intervention team also reported some use of college social media channels to provide more information about The Filter services and its smoking prevention messages (e.g. via retweeting on Twitter or sharing on Facebook). However, the intervention team member responsible for social media also reported it was challenging to engage the colleges: they did not have clear systems and structures for using social media, and did not appear to want to publicise smoking prevention messages. None of the three intervention sites embedded information on their home/index webpage or other frequently accessed webpages/microsites (e.g. online learning portals, e-mail login pages), as intended. Site staff also needed repeated prompting to share information about the intervention on social media.
Youth work activities
It was intended that 5, 10 or 15 groups (depending on institutional size) of 10–20 students would take part in 2-hour sessions provided on site during school/college time. Youth work sessions were delivered in each of the intervention sites, with a total of 15 youth work sessions delivered overall: 10 at the largest college, two at the other college and three in the school sixth form. A total of 190 students were reached across the three sites. The number of students who participated in each session varied significantly, from 4 to 40. The number of participants per session was highest in the school sixth form sessions, in which 80 students attended in total across the three sessions. Although planned to begin in the autumn term (October–December 2014), all the youth work activities took place in the spring and summer terms 2015.
Sessions were organised and run by facilitators from the intervention delivery team as planned, using The Filter youth work resources to educate and persuade students about the harms of smoking and model social/situational resistance skills. Facilitators agreed the content and length of sessions with staff at each intervention site and there was no evidence that young people were consulted at any school/college or involved in the design of activities.
In two of the three observed sessions, students worked in small groups to create smoke-free health promotion campaigns, then presented their ideas and voted on them at the end; the other session was a more general workshop that the facilitator said was intended to enable participants to explore how perceptions of smoking have changed over time. Participants did not appear to be engaged in the two sessions in which they developed a smoke-free message campaign, some students in the other observed session were reported to be engaged by some of the shorter, more interactive activities.
Was the intervention acceptable to the majority of further education managers, staff, students and the intervention delivery team?
In summary, low levels of acceptability were reported by the majority of participants at each pilot setting, meaning that the criteria for RQ 3 were not met. One major barrier to acceptability was the perception among FE staff and students that FE is ‘too late’ for smoking prevention interventions: current smokers reported disengagement and may benefit more from access to cessation services; and non-smokers do not want to be ‘bombarded’ with more educational messages about smoking in post-16 settings.
Another key barrier appeared to be the institutional cultures of FE settings, which promotes autonomy and student responsibility that, in turn, limits the willingness of staff to intervene on issues such as smoking and students’ engagement with such activities. Smoking prevention is not a priority for FE managers and staff, which further limits the acceptability of a multicomponent smoking prevention intervention such as this, although they did support external health agencies’ involvement in FE settings. The intervention team also found that the proposed smoking prevention activities were significantly less acceptable in college settings than in schools and other youth settings for these reasons (see Attitudes towards smoking in the further education context).
Participants’ views are presented in more detail in Process evaluation: participants’ experiences to explore these sources of unacceptability in more depth, in the wider context of student attitudes towards smoking and institutional culture, and alongside other barriers to implementation.
Trial feasibility and acceptability
This section addresses the progression criteria relating to trial methods and RQs 4–6: was randomisation acceptable to FE managers?; did (at least) two out of three colleges from each of the intervention and control arms continue to participate in the study at the 1-year follow-up?; and do student survey response rates suggest that we could recruit and retain at least 70% of new students in both arms in a subsequent effectiveness trial?
Interviews identified that randomisation was acceptable to FE managers. Recruitment and baseline surveys took place as planned, with all six FE settings retained at the 1-year follow-up. No college manager objected to the use of randomisation to intervention and comparison groups.
Recruitment and retention of students was challenging, despite the use of the multiple methods and incentives. Student survey response rates in this study did not suggest that it would be feasible to recruit and retain at least 70% of new students to a cluster RCT in FE settings without further methodological work.
The target population of 2363 enrolled students comprises some ineligible students as a result of settings having incomplete enrolment data on students aged > 18 years, and is therefore the incorrect denominator. In September 2014, 1320 students out of an estimated total sample of 2363 participated in the baseline survey. Of these 14.0% (n = 185) were ineligible as they were aged < 16 years or > 18 years and five students provided no data, leaving a baseline sample of 1130 (47.8%). Although this equates to a response rate of < 50%, the number of potentially eligible students at baseline (n = 2363) was provided by each institution and overestimates the actual number of new students aged 16–18 years in that setting and, therefore, underestimates the true response rate. If data on the number of eligible students were available, the correct denominator could be used and the baseline response rate would be higher.
In September 2015, 412 eligible students completed the follow-up survey (36.5% of baseline respondents; 17.4% of all potentially eligible students at baseline), which is significantly below the target response rate of 70%.
Process evaluation: participants’ experiences
Our second objective was to explore participants’ experiences of the intervention and pilot trial methods (RQs 7–10). We conducted semistructured observations of staff training sessions and youth work sessions delivered by The Filter team, focus groups with students and staff at each intervention site, and interviews with FE managers at intervention and control sites and The Filter staff who managed and delivered the intervention to obtain their views on the barriers to, and facilitators of, implementation. This section reports the results of analyses of these data to address RQs 7–10. It is divided into four subsections: Attitudes towards smoking in the further education context reports common student and staff views about smoking and transitions to FE, and how these interrelate, to understand the societal and institutional context in which The Filter FE intervention was being piloted; Barriers to acceptability and implementation builds on these analyses to report the key barriers to implementation, including the sources of unacceptability, of smoking prevention activities in this context; Implementation of intervention components and contextual variation describes participants’ experiences of each of the five intervention components separately; and Research methods: feasibility and acceptability reports the acceptability and feasibility of the trial design and research methods.
Attitudes towards smoking in the further education context
During focus groups and interviews, FE students and staff reported their attitudes towards smoking, and the extent to which they perceived the uptake of smoking to be a problem for this age group and/or whether or not prevention is a priority for FE settings to address. These focus groups therefore provided rich contextual data to understand the environment and systems within which the planned intervention activities were piloted. Through understanding these FE settings, and student and staff norms about smoking, we are able to more fully theorise the sources of unacceptability and other barriers to implementation described in Barriers to acceptability and implementation.
The importance of the principles of freedom, personal responsibility and self-determination in FE settings was a recurring theme emerging across focus groups with both students and staff at all sites. Participants often explained this by contrasting FE settings with more constraining school environments, where staff are considered to be ‘stricter’.
Three cross-cutting themes emerged that exemplified this desire for freedom, personal responsibility and self-determination, as well as the power of wider societal norms about smoking, to limit the acceptability and feasibility of smoking prevention activities in the context of FE settings. These cross-cutting themes, described below, are:
-
the hegemony of anti-smoking norms
-
the FE transition and liminal identities
-
smoking as an individual choice in FE.
The hegemony of anti-smoking norms
Anti-smoking attitudes were common among FE students and staff, including college managers. Participants were aware of the health harms of smoking, felt these were universally understood and agreed with the smoking ban in public places. Reflecting on national trends in smoking rates and attitudes about smoking in public, students realised that smoking was now much less socially acceptable. For example, one student explained:
Back in the olden days, it’s just everyone used to smoke didn’t they, and they used to think it was normal.
Athervale School, student focus group
The minority of students who smoked were typically guarded about their smoking status and felt that people made negative judgements about them specifically because they smoked. For example, one student stated:
I’ve met loads of people that smoke that aren’t as bad as you think they are. [. . .] People are stereotypical about smokers. Because they think they’re, they’re doing it because they want to look cool and stuff, but it’s nothing to do with that really.
Laurelton College, student focus group
Both non-smokers and smokers frequently used words like ‘dirty’, ‘smelly’, ‘stink’ and ‘disgusting’ to refer to smoking. One group of non-smoking students at Athervale School said the taste and smell was ‘disgusting’ and ‘gross’; another non-smoking student from Valeside College said, ‘I just find it pointless’. A staff member felt that FE students now frequently commented explicitly to each other about the smell, saying that:
If someone comes in and they’ve been smoking, they’ll pass a comment as well, you know, if it’s other students, they’ll say ‘Oh go away, you stink!’, you know [. . .] Because there’s less people smoking so it’s more noticeable.
Valeside College, staff focus group
Smokers also reported this process and how they felt judged by some non-smokers at their college:
I don’t like the, not the snobbiness but the, kind of ‘oh it’s a disgusting, filthy thing’ [. . .] because it’s an addiction isn’t it? But we don’t force anybody to smoke, we don’t say ‘yeah, oh you should smoke, why not’.
Valeside College, student focus group
Students who smoked occasionally – ‘socially’ – also appeared not to want to identify themselves as ‘smokers’ for this reason:
I don’t know if I’d, like when I fill in forms I don’t know if I consider myself a smoker, because I do when I drink, but I don’t know, about half one [. . .] My friends always joke and say that I am. Which I guess I am because I do smoke, I suppose, if you do smoke sometimes I guess you are down as being a smoker, so.
Valeside College, student focus group
Staff were also aware of the negative connotations of being a ‘smoker’ and described attempting to explain to students on some courses (e.g. health and social care) that this would likely be the case for them in their future workplaces.
The further education transition and liminal identities
Reflecting the power of these social norms about smoking, students also perceived smoking as a behaviour that brings particular responsibilities and requires them to show ‘respect’ for others, particularly children. Through sensitivity to social norms, and in the context of recent bans on smoking in public, the transition into FE enabled some students to demonstrate how they are responsible adults and, thus, differentiate themselves from (school) children. For example, one student explained:
I think everyone just respects the fact that some people don’t smoke and don’t want smoke in their face like, so it’s just that respect. It’s like if I’m walking down the street and there’s a woman and her kid in a pram or something walking by and I’m smoking, I’ll cross the street because I don’t want to blow that in the kid’s face like. It’s just out of respect ‘cos if they don’t smoke then, they shouldn’t have to have second-hand smoke.
Valeside College, student focus group
Although many of the students who identified as smokers (not social smokers) stated that they began smoking at a relatively young age, they still emphasised consideration for the welfare of non-smokers, particularly children, and supported bans on smoking in public. This suggests that during transition to FE, attitudes and actions relating to smoking helped to signify students’ co-occurring transition to adulthood and self-determination. This was also demonstrated in several participants’ indications that they would not buy tobacco for younger students, but may sell on to those in year 10 or 11 (aged 14–16 years) – ‘if I know them but not people in like year seven and eight [aged 11–13 years] and that’ – reflecting their own experience of commencing smoking in year 10 or 11.
The liminal status resulting from transition was further apparent in the characterisation of children and younger students as others. For example, when discussing e-cigarettes, students cited concern over the potential for e-cigarettes to act as a gateway to using tobacco, particularly for children. As one student put it:
Someone will use e-cigarettes as a start off before actually smoking properly, especially younger children tend to have them and then move on to the actual cigarettes.
Valeside College, student focus group
As well as acknowledging their responsibilities to protect younger people, students saw themselves as potential role models to children, typically differentiating themselves from children who have little autonomy and require protection from the effects of smoking.
Staff discussions of student smoking behaviour reflected this perception of students in transition and illustrated a sense of responsibility to help students negotiate this while respecting their personal decision-making and nurturing their autonomy. As one staff member explained:
It’s their choice to smoke. Now, either we can give them the messages about not smoking, but you know, we’re not, we don’t preach to them about not smoking, our main message to them is if you’re going to smoke, from my point of view, it’s making sure that they do it in the correct way, smoking the correct things, not illegal substances, and they’re in the right places. As long as they’re doing that, we, we’re off their back really.
Laurelton College, staff focus group
Both students and staff also discussed smoking as something young people can do to rebel, to assert their autonomy, especially in the face of opposition from authority figures. One student who smoked articulated this as:
It’s the trying to push people to stop that tends to make them think, no, balls to you.
Valeside College, student focus group
This resistance was expected to further limit how receptive students may be to advice and education in this context. As one staff member described:
I think it’s just, they’ve hit that particular age and, and as I said, the adult in them is trying to come out and they do not, they’re not receptive.
Laurelton College, staff focus group
Recognition of the liminal nature of their current status meant that students were also anticipating impending transitions, for example starting higher education or entering work, which affected their views about their future patterns of smoking. When asked, most non-smokers did not think that they would start to smoke in the future and most current smokers did not believe they would continue smoking into their twenties, suggesting associations between smoking and perceived life stage.
Smoking as an individual choice in further education
A recurrent theme was that smoking and quitting are choices that individuals make. As one student explained, smoking is ‘their choice’, with staff also reflecting this dominant view of autonomy and personal responsibility as embedded in FE. A staff member at Laurelton College explained:
As long as people are informed of what they’re doing. You know, they’ve got the information. That’s their choice.
Laurelton College, staff focus group
This meant that, in recognition of wider societal anti-smoking norms, students typically talked in terms of deciding to smoke as a ‘bad’ choice or not to smoke as a ‘good’ choice. For example, one student described with admiration how a friend chose not to smoke even when other friends did:
He turned round and said he didn’t like it at all. He just didn’t do it. And walked away from them. It’s a good choice isn’t it?
Valeside College, student focus group
Consistent with their belief that smoking is a choice, students and staff framed discussions about perceptions and behaviours relating to smoking in the context of rationally weighing up information on risk and deciding if this information was perceived as reliable and trustworthy. Students (and staff) frequently described what influences their smoking behaviour, including financial considerations, peer and family behaviour.
Reflecting the enhanced autonomy of the life stage, staff also believed that increased financial independence was significant in student decisions to spend money on smoking if they wanted to:
There’s an economic factor as well, because if you’re a student who’s suddenly getting your own EMA [Education Maintenance Allowance] and getting 30 quid a week, all of a sudden you can afford to go and buy that packet of cigarettes. It might last you 2 weeks, it might last you a day, but you’ve actually got the money and the buying power, whereas you might not have had that when you were 15.
Laurelton College, staff focus group
This further contributed to the sense that smoking was an individual choice in FE, in which decisions to smoke are made through a rational, consumer framework of weighing information about costs, personal preferences and risks to their health and image.
Some students and staff did recognise wider influences beyond the individual’s knowledge and attitudes, particularly peer pressure and the home environment. However, these ‘social things’ were seen as influences occurring earlier in the life course:
[Smoking] it’s a social thing and I don’t know many people who smoke so, I think that’s, I, my parents smoke, my mum and my dad, but I think it’s just, I don’t know, my mates don’t smoke so, I’ve never really got that urge to social smoke with my mates so. I think it’s just who you’ve associated yourself with really.
Valeside College, student focus group
Of all the students who smoked, only two perceived that they had been bullied into smoking by their peers, contrasting with the presentation of smoking as a personal decision. However, both students explained that this had happened when they were ‘younger’, in secondary school, when other students ‘forced’ them to smoke. One explained:
Truthfully I got bullied into it when I was younger. When I was like 11. I think it was 11 like. Smoking was, you just think you’re cool as well don’t you, in front of your mates and stuff, but no, not really. I don’t like doing it.
Laurelton College, student focus group
Students refuted the suggestion that they were still subject to such peer pressure in FE and typically perceived that they could now resist peer influences. In keeping with the perception of smoking as a personal choice, students and staff were also firmly convinced that cessation is primarily a matter of self-control. As one student who smoked explained:
If you want to give up you need will, you need willpower. And I just haven’t got any. At all.
Valeside College, student focus group
This viewpoint was also shared by non-smokers:
Chances are though a lot of people who smoke they have no intention of quitting so you can’t really help them, if they don’t want to help themselves.
Athervale, student focus group
Finally, although ‘stress’ was recognised as contributing to smoking and as limiting chances of cessation, students and staff did not consider FE environments to be particularly stressful.
Summary
This section has described the key themes arising from the discussions with FE students and staff regarding smoking in the context of transition into FE settings. These analyses illuminate the importance of self-determination for young people at this stage in their life, particularly in how this manifests and is rehearsed by FE students, and is accommodated in institutional processes during this transitional period. With these themes in mind, the next section describes the barriers to acceptability, and implementation of, The Filter FE intervention.
Barriers to acceptability and implementation
As described above (see Intervention feasibility and acceptability), the intervention was not implemented as planned. This section describes the key barriers to implementation in two categories: first, the intervention message and aims; and, second, wider challenges associated implementing interventions in FE settings.
Intervention message and aims
Key challenges in implementation were rooted in low levels of acceptability of a smoking prevention intervention in FE settings that, as described in Attitudes towards smoking in the further education context, emphasise personal responsibility, autonomy and individual choice. This institutional culture limits the potential and willingness to implement The Filter FE intervention as planned, as well as limiting students’ engagement with the activities that occurred.
Smoking was not a priority issue for staff or the students who they worked with. Overall, low levels of acceptability were reported by the majority of students and staff at all sites, including a perception that FE is ‘too late’ for smoking prevention intervention. It was suggested that current smokers would disengage and may benefit more from access to cessation services, whereas non-smokers do not want to be ‘bombarded’ with more educational messages about smoking.
These factors led the intervention team to identify that proposed smoking prevention activities were significantly less acceptable to students in FE settings than schools and other youth settings. Intervention staff also perceived that smoking was not seen as an issue, by staff or students, in FE colleges when compared with schools, potentially relating to differential exposure. One member of The Filter team suggested that:
I think schools do buy into it more because you are there from nine to three, aren’t you . . . so if you’re smoking, it’s very present on a school campus. If you’re in and out for FE, you can come and go as you choose, can’t you? Sixth form, you’ve got that freedom . . . so actually, even if you’re a smoker, the FE tutors might not see smoking on campus to be a massive issue because most people might be going down the local café . . . park, whatever, to have a fag . . . where it’s much more present . . . even if it’s round the shed or whatever . . . do you know what I mean? . . . It’s easier to hide in an FE setting.
Intervention team member
The data also illustrated staff receptivity to input from an outside agency, particularly on e-cigarettes, about which they felt they had little knowledge. All students (both smokers and non-smokers) reported having sufficient information about smoking tobacco and its effects on health, leading to some reluctance to engage in further repeated and unnecessary discussion. In contrast, many staff and students were uncertain how to evaluate the health risks of e-cigarettes, with discussions about e-cigarettes further illustrating the frames they felt that they and others used to make decisions about smoking. For example:
There’ve been no long-term studies [of e-cigarettes]. Nobody knows, you know, and you’re back into a situation of where we were 50 years ago when people thought smoking was fine, you know, and really healthy for you. But, are we going to say in 10 years down the road, oh my gosh, look what e-cigarettes have done to our kids growing up, they shouldn’t have had them for whatever reason.
Athervale School, staff focus group
Nevertheless, there were positive aspects of the intervention, including FE managers and staff welcoming the flexibility (e.g. they could choose the topic of the staff training). As one FE manager explained:
I’m always looking to work, you know with external people and whatever they can bring in to us training wise, we’ll always welcome that.
Laurelton College, FE manager
It was evident from interviews and focus groups with staff at FE colleges that they, like school staff, have a strong sense of a duty of care, albeit this could manifest in different ways (see Policy review to promote a tobacco-free environment on site policy). As one FE manager explained:
Post-16 [FE students] get glossed over sometimes on support work, you know, from outside agencies um, and, you know, they’re people and students who you can have a big impact on.
Athervale School, FE manager
Implementing interventions in further education settings
Although the opportunity to work with outside agencies to deliver an intervention was welcomed (see Intervention message and aims), there were several cross-cutting challenges to implementing a complex multicomponent intervention that are specific to a FE context. These centre on management and communication systems, intervention timing, timetabling and the nature of courses in FE.
In terms of management and communication, it was difficult for the implementation team to identify who to contact in each institution, with one FE manager commenting that ‘every organisation is structured differently’ (Middledale College, FE manager). This meant that, unlike schools where it might be possible to directly approach the personal, social and health education co-ordinator, the team found it difficult to identify who to contact as ‘they’ve all got different tiers’ (ID team member 3). However, one intervention team member went on to say that it was easier to identify who is in charge of social media in FE colleges than in schools, because of the presence of dedicated information technology staff:
I think colleges have specific people, whereas [school] sixth forms don’t have like a digital media officer, they have a member of staff who likes tweeting so they kind of tend to put them on it. Whereas in the colleges, they’ll have like one or two people who do the website and the social media, so they’re employed people to do it.
ID team member 3
The intervention delivery team members who required direct contact with students and staff (for youth work and staff training) also struggled to organise convenient times for delivery of sessions as sites required a long lead time to plan such sessions into their timetable. This was compounded by weaknesses in intervention management. For example, a lack of planning and organisation was observed. The intervention manager also had limited experience of working in FE settings and experienced high staff turnover in his own team during this pilot study.
In terms of the youth work sessions, one FE manager explained that, although it might seem an appropriate activity for tutorial time, the ‘pressure on our tutors and the timetabling is, is really quite immense now’ (Valeside College, FE manager), meaning that existing pastoral sessions with tutors are already struggling to accommodate all requirements. They went on to explain:
There’s now only going to be group tutorials, there’s going to be only five of those a year, and one of those sessions will be health and well-being, that would include smoking, but it also includes things like mental health and other things like that.
Valeside College, FE manager
Moreover, the nature of courses and timing of examinations mean that the academic year is quite truncated, so the opportunities for intervention are fewer than might be expected. As the Athervale School FE manager explained, the window of opportunity to intervene lasts only from ‘September to the Easter time, so it’s actually quite a short period of time to do work with students. It’s only 16 weeks’. They went on to describe their frustration at the organisation of sessions, explaining that with the pressures on students’ timetables, activities needed to be planned at least a term in advance.
As a result of the difficulty FE managers experienced in releasing staff and students, intervention team members were sometimes presented with smaller groups than they had anticipated, prompting changes to the delivery style of the session. Lack of prior information on group composition also meant they were also unable to anticipate the appropriate level to pitch the youth work sessions, as one intervention delivery team member described:
I don’t think the students are a problem, like. But it’s also then tailoring to the right level, because you have, some college students are in college ‘cos they can’t do A-levels, but it’s us knowing beforehand what kind of level we’re targeting the work at as well.
ID team member 3
Implementation was also problematic in colleges because of the diverse courses offered, with some students absent from campus for extended periods of the academic year on work placement, or attending college only on day release from their workplace. As one FE manager described:
Most of our courses will have some kind of placement element to them, so the target that the research was on, we might have, if you got 150 students in that campus, there are probably only 80 students on the campus on that given day.
Laurelton College, FE manager
Time pressures and competing priorities made it similarly difficult for intervention staff and FE managers to arrange the staff training. Indeed, time restrictions appeared to be a factor in choosing the sessions; staff were interested in e-cigarettes but it was also one of the shorter training sessions on offer. One of the intervention delivery team members explained the challenges in setting up the staff training:
It’s been quite hard getting the colleges to organise the sessions [. . .] we did quite detailed attachments in an e-mail about the different programmes they [FE managers] can pick from, we made it very clear that we can be very flexible on times and how many people we have. Um, and we found, I probably found that part hard, just because the contact was quite sporadic and actually it was, there were issues with the, probably all three colleges, there were issues with getting them to actually, get, take it, take the training up, which we were surprised at because we thought, well, they’d agreed to it and, it’s something for free, for them.
ID team member 1
The FE managers also reported time pressures as having an impact on participation. As one FE manager said: ‘it was physically impossible you know, to get all of those staff in there from 9.00 until 5.00’ (Laurelton College, FE manager). Another explained that they were keen to be involved but that they were incredibly time poor:
I think generally students and staff want to be involved, and want to have a go at doing things, it’s just a question of their, their time is split in so many different ways, and their priority and focus has to be on teaching, so if they’re missing another lesson from another subject, they become more hesitant, reticent, to do that, yeah?
Athervale School, FE manager
Further education managers suggested potential options for accommodating staff training, for example using inset days, but, as these are planned up to 1 year in advance, there were some doubts that smoking would be seen as a priority for such events.
Summary
A key challenge to student and staff engagement was a perception that the messages and aim of the intervention were occurring ‘too late’ to address smoking behaviour. This, combined with institutional cultures of FE settings that promote autonomy and student responsibility, meant that the willingness of staff to intervene on issues such as smoking, as well as students’ engagement with such activities, was further limited. Although staff welcomed work with external agencies and perceived a need for interventions targeting FE students, there are significant challenges to implementing interventions in FE settings relating to the heterogeneity of these institutions, the diverse courses and timetables being delivered, and the short windows of opportunity available for intervention.
Implementation of intervention components and contextual variation
As well as considering the acceptability and feasibility of each intervention component, analysis of qualitative data led us to question the relevance of the components of the intervention. This primarily related to if the approach (smoking prevention) was perceived as pertinent in this setting and among this population, and whether or not all the five intervention components were needed. This section discusses the perceived relevance of each intervention component in turn, then describes participants’ views about the impact, reach and awareness of the intervention overall. No significant unexpected consequences of the intervention were reported or observed.
Prevention of the sale of tobacco to further education students aged < 18 years
Shops near to the intervention sites were generally understood by students, staff and FE managers to be strict about sales practices at baseline (i.e. limited potential for this component to trigger changes). However, students had no trouble obtaining tobacco, which suggests that the focus of this component on preventing the supply of tobacco from shops near FE settings was misdirected. Some students did report purchasing from shops on the way to or from school/college but most commonly they would obtain tobacco from friends old enough to legitimately purchase it and/or from family members (particularly parents). One student described their father buying cigarettes for them because:
My dad says he’d rather me smoke in front of him than behind his back so that he knows what I’m smoking.
Laurelton College, student focus group
Students also reported sharing and selling tobacco products among themselves, with one stating that:
If one of us haven’t got fags, like our, like our friends are like that, come on, you can have one, sort of thing like. So no-one goes without.
Valeside College, student focus group
This notion of reciprocity relates to the main reasons cited by students and staff for students smoking: it is a source of identity and social bonding. Most students who smoked said that they had been asked to either buy tobacco for younger students or to sell some to them. However, as noted above (see Attitudes towards smoking in the further education context), students developed their own ethical framework for judging whether or not to do this. When students did go into shops to purchase cigarettes, they indicated that they were not deterred now that products are not visible to choose, with one student saying:
We know all the prices off by heart.
Athervale School, student focus group
Staff were also aware of alternative access routes to tobacco, with one commenting: ‘there’s always loopholes – they can always get it if they want it’ (Valeside College, staff focus group). Staff most frequently perceived that student access to tobacco was through their social networks rather than directly from shops. As one staff member said:
Very, very few students actually go and buy cigarettes or tobacco. It’s, it’s, somebody’s been on holiday or somebody’s selling stuff you know, that grey market . . .
Laurelton College, staff focus group
Indeed, staff and students were aware of various illicit supply modes employed by students, with some suggestion that students were uninterested in the ethics of buying potentially counterfeit products as a result of more sensitivity to price. For example:
They don’t care. Because again, it’s this thing, of the relevance to the young people. If they go to a shop and spend, I don’t know, £10, £15 whatever a pouch of tobacco is, but they can go and buy it off him down the road for £5, £6, well which one are they going to do? They’re going for the £5, £6 one.
Laurelton College, staff focus group
Staff in this focus group were not inclined to report students for using fake products, but might mention to students the potential dangers of using non-regulated products. Similarly, in the school sixth form (but neither of the intervention colleges) staff and students were aware of students selling single cigarettes to others for 50p. Staff described this awareness as:
You overhear things ‘do you know who’s selling roll ups’ or ‘so and so’s selling’.
Athervale School, staff focus group
However, this practice was unchallenged because ‘you’d have all the abuse and everything else and then when it went further, nothing would get done’. This was supported by a colleague, who added that it could also ‘impact into your lessons as well if you teach them’. They rationalised this approach by saying they would only act if they ‘actually physically see it’ and:
You’re not allowed to search a child’s bag or anything, so it creates a huge commotion doesn’t it, if you, it has to involve everybody, it goes like right up the chain. [. . .] but when you think, you know, it’s trivial really isn’t it at the end of the day? A cigarette. You know, for all the commotion. I know it isn’t, but it is, in a day, if you know what I mean.
Athervale School, staff focus group
Students were aware that staff were unlikely to try to intervene when sixth form students were selling to younger students, with one stating that it ‘would be quite hard to stop’ this trade. This was further discussed:
They have no proof that you did do it anyway, so they can’t do anything about it.
Unless they’re with the cameras, but they can’t.
So it’s quite hard to stop that kind of like, people passing tobacco.
No, because if there was more cameras, people would just leave anyway, and they’ll just like go somewhere else where there’s a blind spot, they will.
Athervale School, student focus group
Policy review to promote a tobacco-free environment
All intervention sites had a policy on smoking before the intervention commenced, reflecting wider societal anti-smoking norms and systemic requirements. Of all the five Filter FE intervention components, the issue of institutional policy on smoking generated most discussion among staff and students in focus groups. Below, we first discuss FE managers’ perceptions of the relevance of this intervention component and its poor implementation as a result of weaknesses in intervention management and delivery. Second, we go on to discuss staff’s and students’ responses to institutional policies on smoking, including perceptions of acceptability, as well as strengths and weaknesses of current policies.
There was low awareness of the planned policy review activities but acknowledgement that other intervention activities had influenced institutional policy processes. For example, one FE manager indicated that staff training on e-cigarettes ‘led that into the cognisance, oh we need to think about this’, in terms of how to incorporate them into site policy. The same FE manager also noted that:
One of the researchers said about no smoking signs not being in schools, and actually it wasn’t something that we’d thought about. I can’t say that we’ve had any direct outcome, but it’s something that we’ve [the senior management team] got up for discussion again, and to have a look at.
Athervale School, FE manager
This same manager said it ‘definitely’ would have been useful to have feedback about their policy and ‘the right way to do it’. Another intervention site manager said that they had e-mailed their policy to the intervention delivery team and described the background to their desire to carry out a review, saying:
There was consultation done by senior management in this college about 5 years ago and they wanted to ban smoking on campus altogether, but there was huge backlash to that, so then they obviously introduced designated smoking areas, which has never kind of settled, there is always people for smoking shelters and there are people against, but that’s why I thought to get an external body in, it would be interesting to get view and some extra training on that as well. [. . .] We haven’t changed the policy, um, we didn’t really come back with anything there from ASH.
Laurelton College, FE manager
Similarly, a manager at one of the control sites indicated their hope that, if they were part of the intervention, they would have received support on developing a smoking policy:
We don’t have a smoking policy, that was one of the things that I was hoping, if we did have the intervention, that we might have had a bit of, you know, a bit of input with that, that’s one of the things I was hoping, and that’s why, you know, one of the other reasons why I thought it might be useful to, to get involved.
Middledale College, FE manager
Knowledge of institutional policies was good among staff and students. The intervention sixth form was part of a school that had a site no smoking policy and, in both the intervention colleges, there were already established policies permitting smoking only in designated smoking areas on campus. Both control colleges had the same rule, although it was only formulated as written policy in one college. In all intervention sites, policies treated e-cigarettes in the same way as tobacco. One control college did not have any institutional rules about e-cigarettes and the other had recently added e-cigarettes to the smoking policy requiring students to vape in designated smoking areas after recognising the issue around the campus. (However, the FE manager indicated that this change was unrelated to their participation in the Filter project.) There was evidence that, despite being considered the same as tobacco in policies, the products are considered differently by students, who may perceive that it is acceptable to use them indoors as an alternative to smoking outside. As one school staff member said:
I have caught a few. Like if I go in someone’s classroom, like lunchtimes and stuff, like ‘what are you doing?’, ‘Oh, sorry miss’. So they do try and use them, saves them going outside.
Athervale School, staff focus group
The college policies of smoking only in designated areas were generally well accepted among staff and students, and attitudes to areas demonstrated the ubiquity of anti-smoking norms (see Attitudes towards smoking in the further education context), with some students commenting on the unsightliness and smelliness of the shelters. On the whole, college staff perceived that having a designated area was a pragmatic solution because, whether or not there was provision for them to smoke, ‘they’d find somewhere. So either it’s controlled to an extent’ (Laurelton College, staff focus group). Although staff and students perceived that people mostly adhered to the smoking policy, they also noted that many students smoked just outside the campus boundaries. One student described how ‘they’ll be like outside the gates, which is quite annoying when you’re walking past and that’s what you can smell’ (Valeside College, student focus group). A staff member at another college described how:
You see the buses arriving in the morning, and they don’t walk to the smoking shelter, they’re lighting up as they’re getting off the bus and smoking, walking towards the smoking [shelter], even though they’re not supposed to do it.
Laurelton College, staff focus group
In contrast to the general adherence to, and acceptance of, smoking only in designated areas in the colleges, the sixth form policy of prohibiting smoking on site was not well accepted by students. As one student explained, the prohibition of smoking for sixth formers left students who wish to smoke in a difficult position: ‘we’re not allowed out of school but then we’re not allowed to smoke in school, so where are we supposed to go?’ (Athervale School, student focus group). Students perceived that the school policy did not correspond with their desire for autonomy (see Attitudes towards smoking in the further education context) and liked the idea of designated smoking areas, saying that: ‘Like up the college they’ve got a bus stop which is a smoking area [. . .] That’s the thing I like about college’ (Athervale School, student focus group). Staff at the colleges were aware of this and recounted how school students were attracted to college because of the more liberal approach, with the smoking policy being a manifestation of this increased autonomy:
We used to take school groups around, they’d come for a visit to the college, and, so we’d show them round outside, and that used to be one of the first questions a schoolchild would ask, are you allowed to smoke in college? [laughter] [. . .] because it’s, we don’t have uniform, they, it was a freer environment.
Valeside College, staff focus group
School sixth form students who wished to smoke did so wherever they could without getting caught. One non-smoking student smoke said students smoke ‘wherever there’s no cameras’, with another qualifying, ‘or teachers’ (Athervale School, student focus group). It was widely known among school sixth form students that staff have ‘like a rota like, certain like, you certain time like an hour where different teachers will go outside and like chase up the smokers’ (Athervale School, student focus group). School sixth form students explained how staff pursue them up the rugby field to move them away from school buildings. When staff were not on duty, students smoked wherever they liked, as one student described: ‘if they’re not on duty, we’ll just sit on the steps’ (Athervale School, student focus group). The school staff described their response to finding sixth form students smoking and their discomfort in addressing it, saying that:
You’re not going to stop them, so I think it’s better that they’re in sort of one area, it’s not really a designated, because we don’t have smoking, but, technically we do. And I think we have to acknowledge that we do, and, you know, it, it’s just, a consistent problem and it’s these hardened smokers really, isn’t it?
Athervale School, staff focus group
Staff and students recognised that informal smoking areas exist on the school campus, despite an established system of sanctions for smoking (letters sent home to parents, followed by exclusion). However, students and staff all said they did not know anyone who had been excluded from school for smoking, ‘even though it’s school policy’ (Athervale School, staff focus group). Staff and students at the school sixth form stated that the legal status of sixth form students was different from that of younger students, meaning they were sanctioned differently. One (non-smoking) student explained: ‘The people in our year and the year above, though, the teachers are more laid back about it because, we’re old enough’, with their fellow student adding, ‘And we don’t legally have to be here either, so, that’s why they’re not so concerned about us’ (Athervale School, student focus group). This differed among some students who smoked, who suggested that they are concerned about being caught smoking because, unlike younger students for whom school is compulsory, ‘They could just kick us out for good, so I think the younger years are not that like worried, but us, yeah’ (Athervale School, student focus group).
In contrast, college students were unaware of the sanctions that might be applied if they were caught smoking outside the designated areas. Although the FE manager at one control site indicated that ‘there is staff on monitor because our students are quite sneaky [laughs] they will smoke in inappropriate areas’ (Glynbel College, FE manager), staff at the intervention colleges reported fewer problems with enforcing the designated smoking area policy. Staff at one college explained that the introduction of this policy had made a big difference:
I think we used to have a bigger problem last year, where they were smoking just about everywhere, and you know, it was part of our job to tell them, not here, but yeah, we don’t see them smoking in the wrong places so much these days, not in my experience anyway.
Laurelton College, staff focus group
At all intervention sites there were a few staff who smoked and it was evident from observations and focus groups that, at college, staff used the designated smoking areas although some reported smoking in their cars to avoid using the shelters because they felt that ‘they don’t want to be mingling with students when they’re having a quiet cigarette. They don’t want to socially mix with them’ (Laurelton College, staff focus group). Similarly, school sixth form students were aware that staff who smoked went off campus in their cars to smoke, even though this was forbidden for students. One FE manager suggested that it was not appropriate for staff to use designated smoking areas because:
Teachers should be like role models I think. You know and be helping to advocate stop smoking and things like that, but yet they are out there with the students.
Glynbel College, FE manager
Reflecting their sensitivity to the denormalisation of smoking (see Attitudes towards smoking in the further education context), staff and students were aware that smoking outside campus could detrimentally impact the institution’s reputation. One staff member from the small college indicated that students smoking just off premises ‘would look quite bad for the college’ and that this had influenced a recent decision not to move to a no smoking campus (Laurelton College, staff focus group), instead maintaining designated shelters on campus where smoking was less visible to the wider community. As one school student explained, concern to keep student smoking out of the public gaze (students were aware that the school declares itself to be a no smoking school) puts staff in a difficult position when enforcing the no smoking policy:
They try and like get you off the school grounds, [but] they don’t like people smoking at the shop because it still looks bad like a bunch of school girls like smoking at the top.
Athervale School, student focus group
Staff invoked their professional duty of care to students when discussing the pros and cons of their institution’s smoking policy. For example, staff discussed how the college had considered implementing a no smoking policy across all campuses but did not because ‘they thought the students would then go onto the main road’ (Laurelton College, staff focus group), which would not be safe. Similarly, school sixth form staff justified their attempts to contain sixth form students smoking in informal smoking areas, saying:
We have to usher them [students], sort of, to a certain area, but we can’t send them off the premises, because obviously they’re under our care aren’t they? So it becomes a bit of a problem.
Athervale School, staff focus group
Few staff or students expressed opposition to designated smoking areas, which seemed to help limit smoking on college campuses by reinforcing the denormalisation of smoking. However, the location of the designated smoking area was important in terms of whether or not it was used, by whom, and how acceptable it was perceived to be by smokers and non-smokers alike. For example, the FE manager at one of the control colleges described how the smoking shelter was near the campus crèche and that parents were concerned about this (Glynbel College, FE manager). Moreover, some staff and students felt that they may generate unintended consequences by providing new social spaces and areas where smoking is normalised. For example, some students who did not smoke indicated that they sometimes go to the smoking shelter to be with their friends and were equivocal about if this led to them smoking. However, students who smoked suggested that it might encourage non-smokers, saying:
They’re taking in second-hand smoke aren’t they? So they’re also getting some sort of nicotine in their system, at the same time.
Laurelton College, student focus group
Similarly, staff felt that forcing students to use the smoking shelters might normalise smoking and lead them to increase consumption. As one staff member described:
What I’ve noticed is, for example, the students before they came to college were having probably one or two fags a day, because they’re mixing with smokers who probably go more regularly, they start picking up the more regular group, so, because it’s like, they go to smoking shelters more often. When they’re in the smoking shelters, oh do you know what, I can smell your cigarette, give me a cigarette please. So, it, they probably, start smoking more.
Laurelton College, staff focus group
Staff indicated that the social aspect of designated smoking areas could be problematic for students in other ways, through forcing groups of students together who might not otherwise mix. As one explained:
The less confident students and they’re being put into a mixed, especially the middle shelter there, there could be 50, 60 students there. And they’re starting to feel anxious about going to the smoking shelter, so what happens then is they stand off themselves in a small little place, or their own little huddle, and then they’re having, you know, the tellings off, the causes for concern, for not using the smoking shelter, but they get more anxious about using the smoking shelter as well.
Laurelton College, staff focus group
Indeed, some students indicated avoidance of smoking in the designated areas because they did not want to associate with the groups there, moving to locations just off campus instead. As one group of students described, they smoke in the park because ‘it’s the closest’ for them and, even though there is a shelter nearby, ‘it’s always full of like [. . .] irritating people’, who are ‘childish’ (Valeside College, student focus group).
Staff training
The premise of staff training was to support staff in talking to students about smoking. The content of each session was determined by staff interest and focused on e-cigarettes, as this was deemed a priority for staff at each intervention setting. There was no specific training on illegal sales of tobacco, although this did come up in discussion. Interviews with FE managers suggest that the aim was not clearly understood, as one manager indicated:
What’s the aim of the staff training then? So they get trained on, yesterday it was the e-cig[arette]s. Is it for them then to go out to students and talk to them and deliver something on that as well then, or?
Valeside College, FE manager
The same intervention team member delivered all staff sessions, with content broadly the same in each session, although with adaptations according to the numbers in each group (most of the staff training sessions were smaller than the facilitator had anticipated).
Staff who were trained found the sessions very informative and the training acceptable. They particularly enjoyed learning in an interactive way on an issue that they felt they had a knowledge gap. As one FE manager summarised:
The training session was really, really useful, and thoroughly of value and, you know, the heads of year still talked about that, and what they’ve learnt from, particularly about e-cigarettes [. . .] they were thoroughly, enjoyed the way that it was delivered. You know and it was very interactive and hands on, and example, a lot of up to date, factual knowledge, um, and it was also done in a way, you know, that they could test their own knowledge.
Athervale School, FE manager
However, despite being well received, attendance at the sessions was low, with all sites experiencing difficulties in releasing staff (especially teaching staff) for training. Staff who attended the training were often those in support roles, as they had more flexible timetables than those with direct teaching or supervisory roles. As the manager at the smaller college noted:
I think we had about 10 in there in the end, about nine or 10, which is a good group and I mean the training was good, don’t get me wrong, but we did struggle to be able to release those 10 staff.
Laurelton College, FE manager
The trainer noted that this is a common issue: ‘It’s not just the FE, it’s generally when we do training. It can be a problem get, releasing staff to come along to training’ (ID team member 1), further remarking that, in some sites, she was allocated only a 1.5-hour slot for the training when the session would ideally be 2 hours long.
Although the training was well received and perceived as increasing knowledge, it is unclear whether or not staff expected it to facilitate talking to students about smoking. As one staff member said:
The training is definitely useful, you know, but it’s more for us about kind of signposting to the professional people, but we do need some knowledge on it.
Laurelton College, staff focus group
The FE manager at the same college explained anticipating that staff would use the training ‘if a student came in with a particular query on an e-cigarette or a concern, we use that knowledge then’ (Laurelton College, FE manager). However, it was clear that although they found it interesting, staff felt that there were still a lot of unknown issues around e-cigarettes:
I’ve got to be honest, I thought the e-cig[arette] was, in some ways interesting, to know a little bit more about it, but the message was quite vague because we don’t know enough about it.
Laurelton College, staff focus group
Similarly, in discussions about illegal sales of tobacco, staff felt that it was not their place to question students about it, one saying: ‘I don’t think it’s our, our place for us to question’, and another explaining that:
If you see a student who’s got illegal tobacco, which you would deem to be safe, I’d think, oh fair play, you’re students, you’re getting it cheaper. The same as you wearing a fake t-shirt and carrying a fake handbag. You know, what would you do? Do you report them to the police? I wouldn’t.
Laurelton College, staff focus group
Students also questioned the appropriateness of staff talking to them about smoking, reflecting the prevailing culture in FE of fostering self-determination and autonomy (see Intervention feasibility and acceptability). Students indicated that it might seem patronising or invasive:
They’re all, like, they’re older aren’t they, and like most of the people here are over 18 so, like it’s just telling a grown up not to do something. It’s a bit weird isn’t it?
Valeside College, student focus group
I don’t see the point, you know, because if you smoke then they know you smoke already, and then they’re going to come in try and start lecturing you on smoking, and they already know you smoke, then you’re going to get wound up and argue back and that.
Laurelton College, student focus group
Staff reported that, as well as reminding students to smoke in designated areas (in sites that have such policies), they tend to talk opportunistically to students about smoking but are wary of ‘preaching’ to them about smoking and encouraging them to quit. They suggested that such messages might be more effective coming from another young person (youth worker or another student). As one staff member suggested:
They’re used to us just like telling ‘em what to do, you know, reinforcing different things, I mean if it comes from somebody else, it’d be a bit more strong, I suppose. There’s only so much information they can take from a tutor, I suppose . . .
Valeside College, staff focus group
Another staff member explained how staff are concerned to develop and retain trust with students, with concerns that talking about smoking might threaten this, and suggesting that staff perceive smoking as a less-serious risk to students than other issues that may present:
When we’re dealing with students and it’s confidentiality, because that’s a big thing with us, because if, if they don’t get that, that bond with us, they’re not going to interact with us, or trust us, so you know, it’s, I’ve had more than one to say that I didn’t want his or her parents knowing that they smoke. I have to respect that, otherwise I’ve lost that trust, so they won’t come back to you, to iron out anything else, so rightly or wrongly, we, we sort of, don’t mention it to parents.
Laurelton College, staff focus group
Students corroborated that staff take the chance to speak informally with them about smoking and did not seem hostile to this, appreciating that the staff were trying to be helpful. As one student described:
There’s a kid in my class who constantly has to have a fag all the time, every break, doesn’t he, [name]? Every break. So the teachers joke about it, but they never like, obviously, because it’s more of a friendly thing, they’re not, because this is obviously to try and promote them saying anti-smoking. They do say, they don’t like smoking. [. . .] They do make an effort to make that known that it’s Stoptober and there is help and everything.
Valeside College, student focus group
Despite these concerns, staff indicated little time for pastoral work with students and that, although tutorials might seem like a potential opportunity to intervene, they actually presented little opportunity for any discretionary activities. Staff at one college whose role is to provide support to students felt that teaching staff might be resistant to training because of existing demands on their time, saying:
If you said to staff, right, you’ve got to have this training, because you’ve got to deliver this in your personal tutorial, that’s not going to go down very well is it?
Laurelton College, staff focus group
Youth work
As the content of the youth work activities was agreed by the intervention delivery team with each site, the content of sessions varied. Two sessions were delivered: one focused on developing a ‘no smoking’ campaign and the other looked at the role of advertising in promoting smoking. Neither focused specifically on illegal tobacco supply or use. Activities were delivered by two different facilitators and the same facilitator did not do all the sessions at each site. The quality and style of facilitation between sessions was observed to differ, with observers noting that one of the two facilitators provided little guidance or feedback on the tasks and did not seem to try to engage those students who were not actively participating. The other facilitator had difficulty maintaining the interest of the participants in one of the two sessions that they were observed to lead (the smoke-free campaign session), but was more successful in generating rapport with students in the other session. The different experiences of facilitators may also reflect participants’ lack of interest in the content of the sessions on smoke free campaigns.
Students felt that youth work sessions would not change their behaviour and that there were issues about who the sessions were targeted at, and why. Both students and staff felt that it was difficult to identify a target audience for which youth work sessions would be relevant and appropriate, as reflected in the observations of these sessions. Participants did not seem engaged in the two sessions in which they developed a smoke-free message campaign and were heard to make comments such as, ‘I don’t even want to be here’ and ‘Can we go now?’, with the facilitator remarking afterwards that they felt that the participants did not want to be there. However, moments of better engagement were reported, for example during a discussion of the risks of passive smoking and the session on perceptions of smoking over time, with students appearing genuinely interested by some of the photographs, videos and adverts the facilitator used to stimulate discussion. They responded well to the facilitator’s questions and, with a little encouragement, most were willing to talk as a whole group.
Some students found the youth work repetitive and felt that sessions would be more effective if delivered to younger students (e.g. those in year 9). As one explained, ‘sometimes they learn, they teach us stuff that we already know’ (Athervale School, student focus group). Students who identified as non-smokers felt that the sessions were not relevant to them, whereas smokers’ responses ranged from being quite hostile, because they felt that smoking is their choice, to interested but not affected by the content. As one group of students indicated:
It was quite effective. It did, does make you think a bit, but unless you’re actually thinking about quitting, before doing the training, then I suppose, it won’t really make you quit.
Yeah, we went out straight away for a fag didn’t we?
Yeah. [laughs] As soon as the training finished. We all went out for a fag!
Laurelton College, student focus group
Similarly, a staff member indicated that they were not sure of how generic sessions to both smokers and non-smokers would work, for staff or students. They said:
If you go into, what is it, year 6, primary school, right. There’s a, there’s a chance that not many of them will smoke, so you’re talking mainly to a group of non-smokers so you’re catching them early. If you go into tutorial session with us, you could have, you can have smokers and non-smokers. And it would be the same in staff training. In the training we were in we were all non-smokers, so we’re all kind of nodding our heads and agreeing, if there was a smoker in there, he’d probably be quite defensive and would be giving bigger arguments. And it would be the same in a tutorial session. You’re going to have the non-smokers who would go, yeah, agree, and then you’ve got the non-smokers who would just be challenging.
Laurelton College, staff focus group
Unlike the staff training, which did not require much adaption for FE settings, The Filter team made some changes to their youth work sessions in anticipation of the slightly older age group in FE. As one member of the intervention said, ‘[the sessions are] still all interactive that they can get involved with but it was more like, to try and get discussion as well.’ They went on to contrast their experience in schools with their recent experiences in FE, describing how:
In an FE setting, if there’s less young people then it can . . . they can be, like steer the session more themselves, like go with like what they’re interested in rather than just giving them activities that they don’t want to do anyway. So like, a lot of them in [Valeside College] talked about e-cigarettes. So then it was more like tailored towards that.
Intervention team member 2
The youth worker who delivered the sessions at the small college felt that the activities based around developing a smoking campaign ‘got a bit stagnant towards the end’, describing how ‘It was a new session so it was, you know, you try it out – sometimes it works, sometimes it doesn’t’ (intervention team member 4).
However, the flexibility of the sessions was problematic for FE managers when trying to recruit staff to engage their students with the sessions. As the manager at the large college noted, ‘I think the, the aim of it, of the session was a little bit woolly I think’, although they were able to describe the content of the sessions, saying:
The sessions were about marketing wasn’t it? And it was about young people’s attitudes towards smoking and what it influences them regarding, is it peer pressure, is it what they see in the papers or on television, that kind of thing.
Valeside College, FE manager
The sixth form youth work activities consisted of three consecutive sessions with the same class of students, whereas in the colleges there were one-off sessions with different groups, consisting of between five and 15 students. There were issues of continuity of attendance in the school sixth form, with the youth worker who ran sessions in both the school sixth form and the large college suggesting that they might have structured the sessions differently if they had multiple opportunities to engage with the same group of students. The youth worker felt that the sessions in the school sixth forms had been more ‘challenging’ (intervention team member 2) compared with those in the large college, where students had seemed to be more engaged. They speculated as to the reasons for this, saying it might be because there was a smaller group in the college and also:
I think [it was] ‘cos it was their PSE [personal, social education] lesson and I think they’d been told to come for a smoking workshop, so that doesn’t really go down well anyway [laughs] and I think a lot of them had, I don’t know whether it was the time of the year, a lot of them wanted to do like course work and but the teacher made them come in to the session. But then I guess it was different to their usual classes in the college as well, so don’t know, it’s hard to tell really.
She went on to add that the students ‘seemed a lot more mature in [Valeside] college as well [laughs]’. The other youth worker also delivered sessions in the large college (n = 5) and similarly felt that the sessions had been well received by students. In contrast to the facilitator’s impression, though, the FE manager at the school sixth form felt the training had:
Made them [students] think about whether they were going to carry on smoking, it was certainly raising their awareness with them. Whether they had actually any impact and they stopped smoking, I really couldn’t say.
Athervale School, FE manager
In the large college there was a teacher present who participated and the youth worker felt that this would have also helped the session run more smoothly in the school sixth form.
One control FE manager perceived their participation in the Filter research project had highlighted the issue of student smoking with staff, resulting in additional lessons ‘to raise awareness or just discussions and debates with students in the classroom’ (Glynbel College, FE manager).
Social media
It appeared that FE settings were reluctant to give smoking prevention messages prominence online, and at one of the sites the website was not adequate or active enough to be used. The intervention delivery team member responsible for this component of the intervention sent one tweet and a Facebook message to each intervention site each week, but very few posts were retweeted or shared without prompting. They stated:
With Facebook there just wasn’t the engagement there. Um, on Twitter it was a lot better, um, so I think there was probably about 12 posts again, something around that, and the majority of the FEs did retweet the ones that I directly tweeted them.
Intervention team member
Most students said that, although they access social media (e.g. Twitter, Facebook, Instagram), they do not really engage with messages from third parties on these forums and tend to ignore unsolicited/non-personalised messages unless they are already interested in what is being advertised. As one student indicated:
I just don’t think people would really pay attention to it [information]. I think there’s more interesting things you’d rather like I think.
Valeside College, student focus group
Another student from the same college explained:
It’s got to be your choice that is, some people will just go straight past, whereas if you’ve got it in your head that you want to quit you’re going to think, oh yeah, I’ll click on that and have a look, so. It depends on the person really.
Valeside College, student focus group
Students reported gathering a lot of information from social media but that it needed to be carefully targeted and age appropriate. They indicated that unwelcome messages could make them ‘switch off’ completely. As one staff member said, this was similar to students feeling badgered by their parents:
If you’re using things like Twitter, it’s got to be the right message and probably not too often, because I, I’ve got various Twitter accounts and there’s certain accounts that keep on popping up and you just, do you know what, I’m bored. So you just unfollow. So if the message is coming constantly, and you’re bombarding these messages, just click unfollow and then you’ve lost them straightaway. So it needs to be relevant and . . .
Just desensitises you again.
Yeah.
It’s just like, oh, whatever, whatever, isn’t it? You know.
The more you tell, the more parents tell teenagers what to do.
Yeah.
The less likely they are to do it anyway.
Laurelton College, staff focus group
Similarly, FE managers were cautious about inundating students with messages, while also feeling that the intervention messages should have been more obvious around campus. As one said: ‘people are just inundated with information and it’s just too much, you’ve got to be careful as to what you do get across’ (Valeside College, FE manager). The FE manager at one intervention site indicated they had retweeted messages from Filter and ASH Wales a couple of times, and some information had been included on the intranet, but they had not engaged much with social media. Students had very little awareness of any social media messages from ASH Wales and stated that they rarely, if ever, access the school or college website. Those who had seen something online had seen it in the youth work session.
In one discussion among college staff, they indicated that they thought social media messages needed to be carefully applied, as it might prompt students to smoke more. They speculated that:
It’s done on social media and it’s flashed at them, it makes them think they want a cigarette then? It sorts of brings it to their attention. If you don’t bring it to their attention, they’re fine getting on with things. The moment you bring it to their attention, it’s like ‘Right, I want one now’. So that can have a bit of an adverse effect.
Valeside College, staff focus group
Perceived impact and awareness of the intervention
Overall, the intervention had limited reach to staff and students. Very low levels of awareness of The Filter youth project and ASH Wales among staff and students reflect the weaknesses and challenges with implementation described above.
As the manager at Valeside College commented, ‘I don’t think they would have been aware of the project, because we, you know, we haven’t been, pushing it, pushing it, pushing it’. A few students in the intervention school sixth form had heard of The Filter project through having received other outreach youth work the previous year. FE managers could not recall all the intervention components, with one saying: ‘I’m going to struggle to answer questions about the intervention’ (Laurelton College, FE manager).
Some students participating in focus groups could recall participating in youth work sessions, and staff recalled receiving training. All students and staff were already aware of their site smoking policy, reflecting awareness of changing social norms around smoking and non-smoking normalised in practice (see Attitudes towards smoking in the further education context). As one student put it:
Obviously [I’ve] seen the signs and that obviously that’s a normal thing. And obviously that’s our generation, and I’m sure back in the day they wouldn’t have had those signs. Um, there are smoke-free signs in college isn’t there? That say no smoking?
Valeside College, student focus group
Staff and students seemed most engaged when discussing issues relating to the site policy on tobacco, although there was little input from the intervention delivery team on this. Staff who received training seemed to enjoy the sessions and found them informative. Student reactions to the youth work were mixed, although staff felt that they might have appreciated the sessions ‘because they do enjoy that kind of tutorial stuff. It gets them out of their own boring lessons’. However, they doubted the impact of the sessions, saying: ‘I don’t think it would have put anyone off smoking’ (Laurelton College, FE manager). Another FE manager concurred, stating that:
The youth work sessions, you know. With, without a doubt, um, you know, I think are really, really important [. . .] in an ideal world I would have liked to have done more youth work sessions. [. . .] just to get the message, just to get, just to get more students, and make them aware of the project, and make them aware of what you’re trying to achieve.
Valeside College, FE manager
The core message of the intervention (smoking prevention) was not clearly communicated; some students assumed that the intervention was ‘anti-smoking’ and smokers were not receptive to this. Similarly, students who were non-smokers felt that it was not necessary for them to be bombarded with this message. Students and staff felt that smoking prevention messages might be too late for this population group, but that improved smoking cessation support could be helpful. As one FE manager summarised:
To be honest, if by 16 they haven’t started yet, I don’t, I know they come to college then, I suppose they see, they may get new friends who do smoke, but they’re probably going to be trying it a lot younger than 16. Um, but maybe to prevent smoking but to also assist with quitting as well.
Valeside College, FE manager
Summary
This section has described in detail how each of the intervention components was received by staff and students. It shows that, despite a willingness to engage in an intervention in FE, including via policy change at the institutional level (as reported in Barriers to acceptability and implementation), the reach and impact on students and staff in terms of awareness of the intervention was very limited. In the light of the analyses presented in Intervention feasibility and acceptability, which indicate that smoking is largely denormalised among the FE population and that students and staff value freedom, personal responsibility and self-determination, it is perhaps unsurprising that core components of this intervention, such as staff training and youth working, were not perceived as relevant and necessary in the FE setting.
Research methods: feasibility and acceptability
This section focuses on RQ 10: how acceptable were the data collection methods to students and staff, and do participants think longer-term follow-up via e-mail or telephone interview would be feasible? First, we present FE managers’ perceptions of the randomisation and recruitment processes. Then we describe the acceptability and feasibility of the survey data collection methods used at baseline and follow-up in this pilot study.
Randomisation and recruitment
Further education managers stated that they were satisfied with the trial recruitment process (most were approached by e-mail by the intervention delivery team). Agreement to participate had usually been contingent on senior management approval, although one manager noted that it had been delegated to them, saying:
This just sort of fell into my lap a bit, but it’s not, it’s not, you know, I guess I was the nearest person to, you know, to sort of pick it up.
Middledale College, FE manager
In the smaller control college, students were involved in the decision regarding whether or not to participate, and according to the FE manager they had ‘a good input from the students, they were all excited about it’ (Glynbel College, FE manager).
Further education managers perceived the randomisation process as fair and acceptable. Some expressed disappointment that they were not in the intervention arm, but said that this possibility did not affect their decision to join the trial. A manager from a control site summarised the tenor of managers’ feelings about randomisation, saying:
Our students could only benefit and if they, if we weren’t chosen then things sort of stayed more or less, that’s what I thought at the time anyway, I thought that, you know, there was no harm done then.
Middledale College, FE manager
Further education managers had few reservations about getting involved in the study, although some had been concerned about the time commitment required. One manager described their reservations about which campus of the college was selected for randomisation and, after being asked to suggest a small campus, stated that they ‘didn’t think that we chose the right campus in all honesty’ because they knew that there were not many smokers on the small campus and also because the campus was located in a very rural area. There were no shops ‘within a 3-mile radius’, which they felt would therefore render redundant any intervention with shopkeepers about access to tobacco (Laurelton College, FE manager).
Further education managers reported several motivations for participating in the study. Primarily, managers were keen to work with other organisations, and for some it was part of their role to foster links with external agencies. One manager suggested that the reputation of these organisations was important:
When you got professional bodies like the Filter team and ASH, if they can come in and offer something different, we’ll always take that.
Laurelton College, FE manager
The same manager indicated that they had felt that it would be good for students to see the university at work, saying:
We are happy to support the university, it was good to work with the uni[versity] and us. You know, it created awareness of the university as well for our students.
Laurelton College, FE manager
Managers were also motivated by potential benefits for students, with most perceiving that smoking was an issue among their students:
My interest was in, you know, providing support um, and information to our staff and students about smoking. Because it is an issue.
Valeside College, FE manager
Another reason for participating in the study was that they might learn as an organisation. As one manager explained, ‘I thought it would benefit the students in the school, and that we might get some feedback from it that would allow us to, um, further support the students’ (Athervale School, FE manager). One of the managers at a control site indicated that they were disappointed not to be involved because they thought it might help them to develop their site policy on smoking.
Acceptability of the survey data collection methods
On the whole, surveys were an acceptable form of data collection and, although longer-term follow-up by telephone or e-mail was perceived as acceptable, both students and staff felt that it was unlikely to be feasible. However, there was some indication of fatigue among students about completing surveys, particularly on smoking. For example, one student said that:
People ain’t going to be willing because the smokers then probably find it offensive, and then they’re not willing to help people like yourselves like this then are they? Because they think ah, they’re just trying to offend us. So why should we help.
Laurelton College, student focus group
There was no strong preference among students for completing the surveys online or on paper, although online (including via mobile phone) was perceived as most convenient.
Accessing students to complete surveys was challenging. FE managers had concerns about data protection and it was not possible to share student e-mail addresses so that the surveys could be sent directly to them, so students were asked to complete the survey at freshers’ fairs. This was acceptable to both students and staff, although, as one FE manager put it, ‘The timing probably wasn’t brilliant for us because September/October is people really settling into their courses’ (Laurelton College, FE manager). Moreover, this system made it harder to trace students for the follow-up survey as they were approached at random. Indeed, after an initial registration period at the start of each academic year, students may move to different campuses or courses, or may attend the site only sporadically or on particular days (e.g. they may have started a work placement). As one FE manager explained:
Our learners tend, full-time learners tend to be in 3 days a week, and they could be any 3 days of 5, so, you know, come in on a Monday, not everybody’s going to be in on a Monday, not everybody, do you see what I mean? So it’s from that sort of point of view, it’s a very flexible provision, and um, and therefore you may not always get, you know, the responses, and it might, it just might mean that researchers need to come a bit more often to those sort of organisations or campuses really.
Middledale College, FE manager
For the follow-up survey, students were approached in public spaces on campuses. A few students indicated that they did not like being disturbed on their breaks to complete the follow-up survey (e.g. Valeside College, student focus group). Staff and students suggested that students might be asked to complete the survey in their tutor groups, although students indicated that they might then feel obliged to complete it. For example, one sixth form student said: ‘if you’re told to do it in a lesson like fill out this questionnaire please, you will’ (Athervale School, student focus group). However, students did not seem to mind this, saying: ‘It’s less of a chore then do you know what I mean?’ (Valeside College, student focus group).
Students and staff felt using personal e-mails would be the best way to follow-up students, but all acknowledged that few students check e-mails. Many students said using telephone or text message to contact them would be acceptable. For example, one student said:
I’m fine with anything. I’m easy, but obviously you’ve got to think as well. Phone numbers might change in a year or 2. Because my phone number’s changed three times last year, because I was upgrading my contract.
Valeside College, student focus group
However, one FE manager indicated that even now, when they try to contact students via telephone, ‘they won’t answer if it’s a withheld [number]’ (Glynbel College, FE manager). Another FE manager reiterated the difficulty in following up with students over time, stating that:
To be honest at the start at the year they were all very keen and they want to do that, but doing the follow-up and doing the evaluation they were less keen.
Athervale School, FE manager
Students had mixed views on the use of incentives (win an iPad, ‘Love2shop’ vouchers) to encourage them to complete the survey. Although they did not believe it undermined the credibility of the survey, they had differing views about whether or not it would be an effective inducement. One student said, ‘it was that they offered prizes, that’s the only reason I did it really’ (Laurelton College, student focus group). Staff also seemed to think that incentives would be helpful, as one staff member said, ‘They’re not going to do it for nothing’ (Laurelton College, staff focus group). On the other hand, some students felt that if the researcher was friendly, introduced themselves and made you feel comfortable, then ‘that would be fine’ (Valeside College, student focus group). A student at a different site indicated that:
I don’t think you should offer anything. To be quite honest. It’s like, if they want to fill it out, they will, and then if they don’t, then don’t it.
Laurelton College, student focus group
The shopping vouchers, in particular, were seen as acceptable and appropriate incentives. Some students felt that the prize of an iPad was too valuable for them to have a realistic chance of winning it and that more, smaller, prizes such as shopping vouchers, would be more effective. Students were cynical about their chances of winning prizes, comparing it with incentives they see on television and online. They felt that incentives did not motivate them to participate because:
Everybody thinks it’s a fix though when people, say like oh, take this survey and you’re going to get a prize. Everyone thinks it’s a fix, so you don’t actually think you’re going to win.
Athervale School, student focus group
Students needed to feel that they had a chance of winning for incentives to work, and were sceptical about the incentives because they had not heard who had won the iPad at baseline. One group of students suggested that it should be clear that there would be one prize per site so that they would know who had won. Alternative incentives suggested included smoking cessation advice: ‘free help stopping stuff’ (Valeside College, student focus group).
Summary
Overall, the FE managers were supportive of the research, including the use of randomisation, and they were keen to engage with external agencies to deliver interventions to students. However, FE settings are not often engaged in trials and may therefore require additional support and information to ensure that the research process is clear. Digital survey methods and use of incentives are likely to be the most effective methods for surveying students at multiple time points in this context, but more methodological work is required to understand how to work with organisational settings in which barriers to identification of appropriate sampling frames exist. More effective approaches to initial organisational process mapping would improve recruitment and retention rates if further research were to be conducted in this setting.
Pilot primary and secondary outcomes
The third objective of this study was to pilot primary, secondary and intermediate outcome measures and economic evaluation methods and measures. It was not an objective of the pilot study to assess intervention effects and the study was not designed or powered to do so. The response rates, prevalence and distribution by arm are reported for the pilot primary and secondary outcomes at baseline (see Missing data, prevalence and distribution by arm at baseline) and follow-up (see Missing data, prevalence and distribution by arm at follow-up). This section concludes by assessing the feasibility of assessing cost-effectiveness using a cost–utility analysis based on the EQ-5D-5L (see Feasibility of assessing cost-effectiveness)
Missing data, prevalence and distribution by arm at baseline
Pilot primary and secondary outcome measures at baseline are reported in Tables 7 (categorical data) and 8 (numerical data), by arm and overall.
| Variable | Baseline data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 470) | Intervention (n = 660) | Overall (N = 1130) | |
| Ever tried smoking, even if a puff? | |||
| Missing | 1.1 | 1.4 | 1.2 |
| Yes | 54.0 | 52.3 | 53.2 |
| Do you smoke at all nowadays? | |||
| Missing | 1.1 | 1.4 | 1.2 |
| Yes, every day | 20.6 | 14.9 | 17.3 |
| Yes, at least once a week | 3.0 | 3.6 | 3.4 |
| Yes, occasionally but not once a week | 6.8 | 8.8 | 8.0 |
| No, never | 68.5 | 71.4 | 70.2 |
| Weekly smoking status | |||
| Missing | 1.1 | 1.4 | 1.2 |
| Weekly smoker | 23.6 | 18.5 | 20.6 |
| Ever smoked cannabis? | |||
| Missing | 1.5 | 1.8 | 1.7 |
| Yes | 26.2 | 28.2 | 27.4 |
| Smoked cannabis in past 30 days?a | |||
| Missing | 0 | 0 | 0 |
| Yes | 43.1 | 40.9 | 41.8 |
| Smoked cannabis on ≥ 4 days in last 30 days?b | |||
| Missing | 0 | 0 | 0 |
| Yes | 60.4 | 48.7 | 53.5 |
| AUDIT-C | |||
| Missing | 1.1 | 2.0 | 1.6 |
| Hazardous drinker (scoring ≥ 2)c | 64.5 | 70.9 | 68.2 |
| Hazardous drinker (scoring ≥ 5)c | 36.4 | 38.5 | 37.6 |
| Variable (potential scale range) | Trial arm | n | Baseline data: demographic characteristics and outcomes by trial arm (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Missing | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD | |||
| AUDIT-C (0–12) | Control | 465 | 1.1 | 0.0 | 0.0 | 3.0 | 6.0 | 11.0 | 3.4 | 2.9 |
| Intervention | 647 | 2.0 | 0.0 | 1.0 | 4.0 | 6.0 | 11.0 | 3.6 | 2.7 | |
| Overall | 1112 | 1.6 | 0.0 | 1.0 | 3.0 | 6.0 | 11.0 | 3.5 | 2.8 | |
| Number of cigarettes per daya (0–100) | Control | 111 | 7.2 | 0.0 | 5.0 | 10.0 | 16.0 | 50.0 | 12.1 | 8.4 |
| Intervention | 122 | 2.5 | 0.0 | 5.0 | 10.0 | 15.0 | 35.0 | 10.5 | 6.5 | |
| Overall | 233 | 4.7 | 0.0 | 5.0 | 10.0 | 15.0 | 50.0 | 10.7 | 7.6 | |
| HSIa (0–6) | Control | 111 | 7.2 | 0.0 | 0.0 | 2.0 | 3.0 | 5.0 | 1.8 | 1.6 |
| Intervention | 122 | 2.5 | 0.0 | 0.0 | 1.0 | 3.0 | 5.0 | 1.6 | 1.5 | |
| Overall | 233 | 4.7 | 0.0 | 0.0 | 2.0 | 3.0 | 5.0 | 1.7 | 1.5 | |
Missing data
There were few missing values with the percentage of missing responses being < 2% for all but four questions: living with an adult in paid work, spending money each week, number of cigarettes per day and the heaviness of smoking (as measured using the HSI). Across these variables there were more missing data in control than in intervention arm participants. For living with an adult in paid work, the percentage of missing responses in the control arm was 4.1% and in the intervention arm was 1.7%. The percentage of missing data for spending money each week was not equally distributed across arms (control, 11.3%; intervention, 5.9%). For the number of cigarettes per day and the HSI, the percentage of missing data was 7.2% in the control arm and 2.5% in the intervention arm.
Prevalence and distribution by arm
The indicative primary outcome in this study was the prevalence of weekly smoking, which was 20.6% (n = 233) for all participants (95% CI 18.4% to 23.1%). There was a greater percentage of weekly smokers in the control arm than in the intervention arm [23.6% (n = 111) vs. 18.5% (n = 122)] (Table 9). This compares with 20.0% of 16- to 19-year-olds in the 2010 GLS. 2 Twenty-one per cent of control arm and 14.9% of intervention arm participants smoked every day. Around one-quarter of participants in each arm had ever smoked cannabis. Out of those who had ever tried cannabis, 43.1% of control and 40.9% of intervention group participants had smoked cannabis in the past 30 days. There were more control group participants who had smoked cannabis on ≥ 4 of the last 30 days (control, 60.4%; intervention, 48.7%). The majority of participants screened positive for hazardous levels of alcohol consumption using the ≥ 2 cut-off point on the AUDIT-C validated in adolescents45 (overall 68.2%); slightly more screened positive in the intervention group than in the control group (70.9% vs. 64.5%). The percentage screening positive using the ≥ 5 cut-off point, validated in adults,38 was evenly distributed across arms (control, 36.4%; intervention, 38.5%).
| Variable | 1-year follow-up data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 174) | Intervention (n = 238) | Overall (N = 412) | |
| Ever tried smoking, even if a puff? | |||
| Missing | 0.6 | 0.8 | 0.7 |
| Yes | 60.3 | 55.9 | 57.7 |
| Do you smoke at all nowadays? | |||
| Missing | 1.2 | 0.8 | 0.9 |
| Yes, every day | 16.7 | 13.0 | 17.3 |
| Yes, at least once a week | 4.6 | 1.3 | 3.4 |
| Yes, occasionally but not once a week | 6.9 | 7.6 | 8.0 |
| No, never | 70.7 | 77.3 | 70.2 |
| Weekly smoking status | |||
| Missing | 1.2 | 0.8 | 0.9 |
| Weekly smoker | 21.3 | 14.3 | 17.2 |
| Ever smoked cannabis? | |||
| Missing | 1.2 | 0.8 | 1.0 |
| Yes | 21.8 | 26.1 | 24.3 |
| Smoked cannabis in the past 30 days?a | |||
| Missing | 0 | 0 | 0 |
| Yes | 44.7 | 32.3 | 37.0 |
| Smoked cannabis for ≥ 4 days in last 30 days?b | |||
| Missing | 0 | 0 | 0 |
| Yes | 88.2 | 85.0 | 86.5 |
| AUDIT-C | |||
| Missing | 0 | 0 | 0 |
| Hazardous drinker (scoring ≥ 2)c | 71.3 | 77.3 | 74.8 |
| Hazardous drinker (scoring ≥ 5)c | 36.2 | 37.4 | 36.9 |
The ICC suggested there was a moderate level of clustering at baseline in weekly smoking status (ICC 0.03, 95% CI 0.00 to 0.08), lifetime smoking status (ICC 0.02, 95% CI 0.00 to 0.10) and screening positive for hazardous levels of alcohol consumption using the ≥ 2 cut-off point on the AUDIT-C (ICC 0.02, 95% CI 0.00 to 0.21). The ICCs for the use of cannabis in the last 30 days (ICC 0.12, 95% CI 0.03 to 0.39) and more than four times in the last 30 days (ICC 0.12, 95% CI 0.02 to 0.54) were larger. In contrast, there was very little clustering in lifetime cannabis use (ICC < 0.00001). There was a moderate level of internal consistency across items in the HSI (α = 0.50) and AUDIT-C (α = 0.65).
The distribution of numeric baseline variables for control and intervention group participants are summarised in Table 8. The five-number summaries show a wide range of values reported on the AUDIT-C, for the number of cigarettes per day and the HSI, with little difference across study arms. Median scores on the AUDIT-C (control, 3.0; intervention, 4.0), number of cigarettes per day (control, 10.0; intervention, 10.0) and HSI (control, 2.0; intervention, 1.0) were very similar across arms.
Missing data, prevalence and distribution by arm at follow-up
The characteristics of eligible and non-eligible participants according to the pilot primary and secondary outcome measures at follow-up are reported in Tables 9 (categorical data) and 10 (numerical data), by arm and overall.
Missing data
As at baseline, there were few missing values, with the percentage of missing responses for the pilot primary and secondary outcome item typically only 1–2%. Students who provided data at baseline and follow-up had a slightly lower prevalence of weekly smoking (16.7% vs. 22.8%; p = 0.03) and lifetime cannabis use (23.5% vs. 29.5%; p = 0.02) than students who provided data only at baseline. No meaningful difference was found on any demographic characteristic or other secondary outcomes.
Prevalence and distribution by arm
Across all participants the prevalence of weekly smoking was 17.2% (95% CI 13.9% to 21.2%). There was imbalance in prevalence, with more weekly smokers in the control arm (21.3%) than in the intervention arm (14.3%). The percentage of participants who smoked every day was slightly higher in the control arm than in the intervention group (control, 16.7%; intervention, 13.0%), as was the proportion smoking at least once per week (control. 4.6%; intervention, 1.3%).
Around one-quarter of participants had ever smoked cannabis, slightly more in the intervention group (26.1%) than in the control group (21.8%). Of those who had ever tried cannabis, 44.7% of control and 32.3% of intervention group participants had smoked cannabis in the past 30 days. The percentage of control and intervention group participants who had smoked cannabis on ≥ 4 of the last 30 days was similar (control, 88.2%; intervention, 85.0%). Seventy-five per cent of participants screened positive for hazardous levels of alcohol consumption at follow-up, using the ≥ 2 cut-off point on the AUDIT-C, with slightly more screening positive in the intervention group than in the control group (77.3% vs. 71.3%). The percentage screening positive using the ≥ 5 cut-off point validated in adults was similar in both arms (control, 36.2%; intervention, 37.4%).
The distribution of numeric outcomes for control and intervention group participants is summarised in Table 10. Across groups, the median AUDIT-C score was 4.0, number of cigarettes per week was 10.0 and the HSI score was 2.0. The five-number summaries suggest that there was a large range of scores on the AUDIT-C (0–11), number of cigarettes (0–30 per day) and HSI (0–5), and all had relatively large SDs. There was little variation across the intervention and control arms for medians on the AUDIT-C (control, 3.5; intervention, 4.0) and HSI (control, 2.0; intervention, 2.0), and participants in the intervention arm smoked slightly more cigarettes than those in the control arm (control, 8.0; intervention, 10.0). No formal comparisons were carried out, so any differences must be interpreted with caution.
| Variable (potential scale range) | Trial arm | n | 1-year follow-up data by trial arm (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Missing | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD | |||
| AUDIT-C (0–12) | Control | 174 | 0.0 | 0.0 | 1.0 | 3.5 | 6.0 | 11.0 | 3.6 | 2.6 |
| Intervention | 238 | 0.0 | 0.0 | 2.0 | 4.0 | 6.0 | 10.0 | 3.7 | 2.5 | |
| Overall | 412 | 0.0 | 0.0 | 1.0 | 4.0 | 6.0 | 11.0 | 3.6 | 2.6 | |
| Number of cigarettes per daya (0–100) | Control | 37 | 0.0 | 0.0 | 5.0 | 8.0 | 13.0 | 30.0 | 10.1 | 7.3 |
| Intervention | 34 | 0.0 | 0.0 | 6.2 | 10.0 | 15.0 | 25.0 | 10.9 | 6.2 | |
| Overall | 71 | 0.0 | 0.0 | 5.0 | 10.0 | 15.0 | 30.0 | 10.5 | 6.8 | |
| HSIa (0–6) | Control | 37 | 0.0 | 0.0 | 0.0 | 2.0 | 3.0 | 4.0 | 1.6 | 1.3 |
| Intervention | 34 | 0.0 | 0.0 | 0.0 | 2.0 | 3.0 | 4.0 | 1.6 | 1.6 | |
| Overall | 71 | 0.0 | 0.0 | 0.0 | 2.0 | 3.0 | 5.0 | 1.6 | 1.6 | |
There was a high level of clustering in weekly smoking status (ICC 0.08, 95% CI 0.00 to 0.21) and the use of cannabis in the last 30 days (ICC 0.11, 95% CI 0.01 to 0.60) at the 1-year follow-up. In contrast, there was very little clustering in lifetime smoking status (ICC 0.01, 95% CI 0.00 to 0.19), lifetime cannabis use (ICC < 0.00001) and use of cannabis more than four times in the last 30 days (ICC < 0.00001). The internal consistency across items in the HSI (α = 0.17) was poor and in the AUDIT-C (α = 0.58) was moderate.
Twenty per cent of students (n = 233) were weekly smokers at baseline. A number of smokers were lost to follow-up, such that baseline prevalence of weekly smoking among those who remained in the study at follow-up was 16.8% (n = 69). Of these weekly smokers, 18 (5.3%) were no longer weekly smokers at follow-up. There was no discernible difference by arm, with 7.4% (n = 10) in the control and 4.0% (n = 8) in the intervention arm not classified as a weekly smoker at follow-up. Of the 336 students who were not a weekly smoker at baseline and had data at follow-up, 21 (6.3%) were classified as a weekly smoker at follow-up. The difference in weekly smoking uptake was slightly higher in the control (8.9%, n = 12) than in the intervention arm (4.5%, n = 9).
Exploratory multilevel logistic regression models adjusting for baseline weekly smoking status, age, gender, residence with an employed adult, ethnicity and educational attainment (≥ 5 GCSEs at A*–C) indicated that there was very little difference in the risk of weekly smoking at follow-up between the intervention and control students (odds ratio 0.93, 95% CI 0.23 to 3.76).
To examine the reliability of reporting on having ever smoked, we calculated the percentage of participants who recanted. This is when participants provide an illogical permutation of responses. We used responses to the question, ‘Have you EVER tried smoking a cigarette, even if it was only a puff or two?’. Participants who recanted were those at baseline who said they had ever smoked and then at the 1-year follow-up said they had never smoked. Of the 412 participants, 206 (50.0%) at baseline and 238 (57.7%) at the 1-year follow-up had ever tried smoking. Out of the baseline ever smokers, 17 (8.3%) recanted by responding that they had never smoked at the 1-year follow-up.
Feasibility of assessing cost-effectiveness
EuroQol-5 Dimensions, 5-level version items and health service use at baseline
Participants were requested to tick one box that best describes their health today across five domains: mobility, self-care, usual activities (e.g. work, study, housework, family or leisure activities), pain/discomfort and anxiety/depression. Table 11 shows the distribution of responses to each item at baseline. They were then asked to put a cross on a line to indicate how good or bad their health is on a scale ranging from 0 (worst health you can image) to 100 (best health you can image). Table 12 shows the distribution of responses for each numerical item.
| Variable | Baseline data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 470) | Intervention (n = 660) | Overall (N = 1130) | |
| Mobility | |||
| Missing | 3.6 | 3.2 | 3.4 |
| I have no problems in walking about | 88.7 | 91.1 | 90.1 |
| I have slight problems in walking about | 5.1 | 4.5 | 4.8 |
| I have moderate problems in walking about | 1.5 | 0.6 | 1.0 |
| I have severe problems in walking about | 0.4 | 0.2 | 0.3 |
| I am unable to walk about | 0.6 | 0.5 | 0.5 |
| Self-care | |||
| Missing | 3.6 | 3.5 | 3.5 |
| I have no problems washing or dressing myself | 92.8 | 94.4 | 93.7 |
| I have slight problems washing or dressing myself | 1.7 | 1.1 | 1.3 |
| I have moderate problems washing or dressing myself | 0.6 | 0.7 | 0.7 |
| I have severe problems washing or dressing myself | 0.9 | 0 | 0.4 |
| I am unable to wash or dress myself | 0.4 | 0.3 | 0.4 |
| Usual activities | |||
| Missing | 3.8 | 3.8 | 3.8 |
| I have no problems doing my usual activities | 85.3 | 88.5 | 87.2 |
| I have slight problems doing my usual activities | 7.7 | 5.2 | 6.2 |
| I have moderate problems doing my usual activities | 2.3 | 1.8 | 2.0 |
| I have severe problems doing my usual activities | 0.4 | 0.5 | 0.4 |
| I am unable to do my usual activities | 0.4 | 0.3 | 0.4 |
| Pain/discomfort | |||
| Missing | 4.3 | 3.5 | 3.8 |
| I have no pain or discomfort | 75.3 | 72.6 | 73.7 |
| I have slight pain or discomfort | 13.4 | 18.9 | 16.6 |
| I have moderate pain or discomfort | 4.0 | 3.9 | 4.0 |
| I have severe pain or discomfort | 2.8 | 0.8 | 1.6 |
| I have extreme pain or discomfort | 0.2 | 0.3 | 0.3 |
| Anxiety/depression | |||
| Missing | 4.0 | 3.6 | 3.8 |
| I am not anxious or depressed | 69.8 | 60.6 | 64.4 |
| I am slightly anxious or depressed | 14.0 | 18.9 | 16.9 |
| I am moderately anxious or depressed | 6.4 | 11.7 | 9.5 |
| I am severely anxious or depressed | 3.6 | 4.1 | 3.9 |
| I am extremely anxious or depressed | 2.1 | 1.1 | 1.5 |
| During the last 30 days, have you visited a doctor or nurse? | |||
| Missing | 1.7 | 2.6 | 2.2 |
| Yes | 17.0 | 22.6 | 20.3 |
| During the last 30 days, have you been admitted to hospital? | |||
| Missing | 2.3 | 2.6 | 2.5 |
| Yes | 4.3 | 5.8 | 5.1 |
| How many nights admitted to hospital in last 30 days?a | |||
| Missing | 0 | 0 | 0 |
| Day case | 65.0 | 65.8 | 65.5 |
| 1 | 25.0 | 18.4 | 20.7 |
| 2 | 0 | 2.6 | 1.7 |
| ≥ 3 | 10.0 | 13.2 | 12.1 |
| Variable (potential scale range) | Trial arm | n | Baseline data: characteristics by trial arm (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Missing | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD | |||
| How good or bad is your health TODAY? [0 (worst you can imagine) to 100 (best you can image)] | Control | 449 | 4.5 | 0.0 | 72.0 | 85.0 | 96.0 | 100.0 | 80.0 | 21.5 |
| Intervention | 639 | 3.2 | 6.0 | 75.0 | 87.0 | 95.0 | 100.0 | 81.8 | 17.5 | |
| Overall | 1081 | 4.4 | 0.0 | 74.0 | 87.0 | 95.0 | 100.0 | 81.1 | 19.3 | |
| How many visits to a doctor or nurse in last 30 days? (0–6)a | Control | 78 | 2.5 | 1.0 | 1.0 | 2.0 | 3.0 | 5.0 | 1.9 | 1.1 |
| Intervention | 148 | 0.7 | 1.0 | 1.0 | 1.0 | 2.0 | 6.0 | 1.6 | 1.0 | |
| Overall | 226 | 1.3 | 1.0 | 1.0 | 1.0 | 2.0 | 6.0 | 1.7 | 1.0 | |
| EQ-5D-5L index score (–1.0 to 1.0) | Control | 470 | 0.0 | –0.3 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 |
| Intervention | 660 | 0.0 | 0.1 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 | |
| Overall | 1130 | 0.0 | –0.3 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 | |
Health service use over the last 30 days was defined as going to see a doctor or nurse about a health problem, excluding visits for contraceptive advice. For those who had visited a doctor or nurse, they were asked on how many occasions. Hospital admittance was also assessed over the last 30 days. Those who reported being admitted to hospital were asked whether it was for day care or the number of nights. Table 11 shows that around one-fifth of participants had visited a doctor and 5% had been admitted to hospital.
EuroQol-5 Dimensions, 5-level version items and health service use at follow-up
Participants were asked to repeat the EQ-5D-5L and health service use questions at follow-up. As at baseline, they were asked to tick one box that best describes their health on the day of survey over five domains: mobility, self-care, usual activities (e.g. work, study/housework, family or leisure activities), pain/discomfort and anxiety/depression. Table 13 shows distribution of responses to each item at follow-up. As with the baseline survey, participants were also asked to put a cross on a line to indicate how good or bad their health is on a rating scale from 0 (worst health you can imagine) to 100 (best health you can imagine). Table 14 shows the distribution of numerical responses and reported use of health services at follow-up for those respondents who indicated that they had visited a doctor or nurse over the last 30 days. The control group mean at follow-up was 1.8 visits (SD 1.3 visits), the intervention group mean at follow-up was 1.7 visits (SD 1.1 visits). The means for the EQ-5D-5L index score in the control and intervention group were both 0.9 (SD 0.1).
| Variable | 1-year follow-up data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 174) | Intervention (n = 238) | Overall (N = 412) | |
| Mobility | |||
| Missing | 2.9 | 0.8 | 1.7 |
| I have no problems in walking about | 90.8 | 93.3 | 92.2 |
| I have slight problems in walking about | 4.0 | 3.4 | 3.6 |
| I have moderate problems in walking about | 2.3 | 1.3 | 1.7 |
| I have severe problems in walking about | 0 | 0.8 | 0.5 |
| I am unable to walk about | 0 | 0.4 | 0.2 |
| Self-care | |||
| Missing | 2.9 | 0.8 | 1.7 |
| I have no problems washing or dressing myself | 93.7 | 96.6 | 95.4 |
| I have slight problems washing or dressing myself | 1.7 | 0.4 | 1.0 |
| I have moderate problems washing or dressing myself | 1.2 | 1.7 | 1.5 |
| I have severe problems washing or dressing myself | 0.6 | 0.4 | 0.5 |
| I am unable to wash or dress myself | 0 | 0 | 0 |
| Usual activities | |||
| Missing | 2.9 | 0.8 | 1.7 |
| I have no problems doing my usual activities | 90.8 | 90.8 | 90.8 |
| I have slight problems doing my usual activities | 3.5 | 6.3 | 5.1 |
| I have moderate problems doing my usual activities | 2.9 | 0.8 | 1.7 |
| I have severe problems doing my usual activities | 0 | 0.8 | 0.5 |
| I am unable to do my usual activities | 0 | 0.4 | 0.2 |
| Pain/discomfort | |||
| Missing | 3.5 | 0.8 | 1.9 |
| I have no pain or discomfort | 79.9 | 80.3 | 80.1 |
| I have slight pain or discomfort | 11.5 | 13.9 | 12.9 |
| I have moderate pain or discomfort | 4.0 | 3.8 | 3.9 |
| I have severe pain or discomfort | 1.2 | 0.8 | 1.0 |
| I have extreme pain or discomfort | 0 | 0.4 | 0.2 |
| Anxiety/depression | |||
| Missing | 2.9 | 1.3 | 1.9 |
| I am not anxious or depressed | 74.7 | 64.3 | 68.7 |
| I am slightly anxious or depressed | 8.6 | 17.2 | 13.6 |
| I am moderately anxious or depressed | 6.3 | 13.5 | 10.4 |
| I am severely anxious or depressed | 5.8 | 3.4 | 4.4 |
| I am extremely anxious or depressed | 1.7 | 0.4 | 0.9 |
| During the last 30 days, have you visited a doctor or nurse? | |||
| Missing | 3.5 | 0.8 | 1.9 |
| Yes | 23.6 | 23.1 | 23.3 |
| During the last 30 days, have you been admitted to hospital? | |||
| Missing | 2.9 | 0.8 | 1.7 |
| Yes | 6.9 | 5.0 | 5.8 |
| How many nights admitted to hospital in last 30 days?a | |||
| Missing | 0 | 0 | 0 |
| Day case | 83.3 | 83.3 | 83.3 |
| 1 | 8.3 | 8.3 | 8.3 |
| 2 | 8.3 | 8.3 | 8.3 |
| ≥ 3 | 0 | 0 | 0 |
| Variable (potential scale range) | Trial arm | n | 1-year follow-up data: characteristics by trial arm (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Missing | Minimum | 25th centile | Median | 75th centile | Maximum | Mean | SD | |||
| How good or bad is your health TODAY? [0 (worst you can imagine) to 100 (best you can image)] | Control | 168 | 3.0 | 10.0 | 70.1 | 84.0 | 90.1 | 100.0 | 80.5 | 16.5 |
| Intervention | 236 | 0.8 | 8.0 | 75.0 | 85.0 | 93.1 | 100.0 | 83.0 | 14.3 | |
| Overall | 404 | 1.9 | 8.0 | 75.0 | 85.0 | 92.0 | 100.0 | 82.0 | 15.3 | |
| How many visits to a doctor or nurse in last 30 days?a (0–6) | Control | 41 | 0 | 1.0 | 1.0 | 1.0 | 2.0 | 6.0 | 1.8 | 1.3 |
| Intervention | 55 | 0 | 1.0 | 1.0 | 1.0 | 2.0 | 5.0 | 1.7 | 1.1 | |
| Overall | 96 | 0 | 1.0 | 1.0 | 1.0 | 2.0 | 6.0 | 1.8 | 1.2 | |
| EQ-5D-5L index score (–1.0 to 1.0) | Control | 174 | 0.0 | 0.3 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 |
| Intervention | 238 | 0.0 | 0.1 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 | |
| Overall | 412 | 0.0 | 0.1 | 0.9 | 1.0 | 1.0 | 1.0 | 0.9 | 0.1 | |
Pilot intermediate (outcome) measures
Participants were asked to complete items addressing attitudinal and knowledge-based precursors to smoking, including perceived prevalence of smoking (perceived norms), at baseline. The aim was to explore potential changes in these individual-level characteristics that were targeted via the intervention and explicit in the logic model. NatCen attitudinal scales41 and ESFA items assessing social and situational self-efficacy and skills42,43 were used in this study. Table 15 shows the distribution of responses by arm at baseline.
| Variable | Baseline data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 470) | Intervention (n = 660) | Overall (N = 1130) | |
| People of my age smoke because it helps them to relax | |||
| Missing | 2.3 | 2.9 | 2.7 |
| True | 60.0 | 61.8 | 61.1 |
| False | 37.7 | 35.3 | 36.3 |
| People of my age smoke because they are addicted to tobacco | |||
| Missing | 2.6 | 2.7 | 2.7 |
| True | 77.8 | 77.3 | 77.5 |
| False | 19.6 | 20.0 | 19.8 |
| People of my age smoke because they believe it helps them to stay slim | |||
| Missing | 3.2 | 3.0 | 3.1 |
| True | 27.0 | 27.3 | 27.2 |
| False | 69.8 | 69.7 | 69.7 |
| People of my age smoke because it helps them with stress in their life | |||
| Missing | 3.0 | 3.0 | 3.0 |
| True | 77.7 | 77.3 | 77.4 |
| False | 19.4 | 19.7 | 19.6 |
| People of my age smoke to look cool in front of their friends | |||
| Missing | 2.6 | 2.7 | 2.7 |
| True | 77.2 | 77.7 | 77.5 |
| False | 20.2 | 19.6 | 19.8 |
| People of my age smoke because they find it exciting to break the rules | |||
| Missing | 3.0 | 3.0 | 3.0 |
| True | 52.6 | 52.6 | 52.6 |
| False | 44.5 | 44.4 | 44.4 |
| People of my age smoke because their friends pressure them into it | |||
| Missing | 2.6 | 3.0 | 2.8 |
| True | 74.0 | 72.1 | 72.9 |
| False | 23.4 | 24.9 | 24.3 |
| People of my age smoke because it gives them a good feeling | |||
| Missing | 3.0 | 3.3 | 3.2 |
| True | 66.2 | 63.2 | 64.4 |
| False | 30.9 | 33.5 | 32.4 |
| Have you ever felt pressure to smoke from your best friend? | |||
| Missing | 2.6 | 3.0 | 2.8 |
| Often | 3.6 | 1.5 | 2.4 |
| Sometimes | 13.0 | 10.2 | 11.3 |
| Never | 77.5 | 81.1 | 79.6 |
| I do not have one/any | 3.4 | 4.2 | 3.9 |
| Have you ever felt pressure to smoke from other friends? | |||
| Missing | 3.0 | 3.2 | 3.1 |
| Often | 4.3 | 2.1 | 3.0 |
| Sometimes | 20.4 | 18.0 | 19.0 |
| Never | 69.8 | 73.5 | 72.0 |
| I do not have one/any | 2.6 | 3.2 | 2.9 |
Participants completed a follow-up survey on attitudinal and knowledge-based precursors to smoking, including perceived prevalence of smoking (perceived norms). The survey tool was adapted from NatCen items41 social and situational self-efficacy and skills, using the ESFA items. 42,43 At follow-up, the survey incorporated questions on institutional-level influences, including awareness of college practices on smoking and The Filter project. It also considered community-level data to understand participant experience of tobacco purchasing and local retailer behaviour. Table 16 shows distribution of responses by arm at follow-up. Table 16 illustrates that a majority of students who attempted to purchase tobacco were able to do so. Only 5.1% of students were aware of The Filter project at follow-up, although this was higher in the intervention group (7.1%) than in the control group (2.9%).
| Variable | 1-year follow-up data: distribution over categories by trial arm (%) | ||
|---|---|---|---|
| Control (n = 174) | Intervention (n = 238) | Overall (N = 412) | |
| Individual level | |||
| People of my age smoke because it helps them to relax | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 63.8 | 73.1 | 69.2 |
| False | 33.3 | 26.1 | 29.1 |
| People of my age smoke because they are addicted to tobacco | |||
| Missing | 3.5 | 0.8 | 1.9 |
| True | 77.0 | 83.6 | 80.8 |
| False | 19.5 | 15.6 | 17.2 |
| People of my age smoke because they believe it helps them to stay slim | |||
| Missing | 2.9 | 1.3 | 1.9 |
| True | 28.7 | 28.2 | 28.4 |
| False | 68.4 | 70.6 | 70.0 |
| People of my age smoke because it helps them with stress in their life | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 80.5 | 86.6 | 84.0 |
| False | 16.7 | 12.6 | 14.3 |
| People of my age smoke to look cool in front of their friends | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 81.0 | 80.7 | 80.8 |
| False | 16.1 | 18.5 | 17.5 |
| People of my age smoke because they find it exciting to break the rules | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 60.9 | 60.0 | 59.2 |
| False | 36.2 | 41.2 | 39.1 |
| People of my age smoke because their friends pressure them into it | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 71.8 | 71.9 | 71.8 |
| False | 25.3 | 27.3 | 26.5 |
| People of my age smoke because it gives them a good feeling | |||
| Missing | 2.9 | 0.8 | 1.7 |
| True | 60.3 | 71.0 | 66.5 |
| False | 36.8 | 28.2 | 31.8 |
| Have you ever felt pressure to smoke from your best friend? | |||
| Missing | 2.9 | 1.3 | 1.9 |
| Often | 3.5 | 1.7 | 2.4 |
| Sometimes | 13.2 | 10.1 | 11.4 |
| Never | 78.2 | 84.8 | 82.0 |
| I do not have one/any | 2.3 | 2.1 | 2.2 |
| Have you ever felt pressure to smoke from other friends? | |||
| Missing | 2.9 | 1.3 | 1.9 |
| Often | 3.5 | 2.5 | 2.9 |
| Sometimes | 16.1 | 14.3 | 15.1 |
| Never | 76.4 | 80.7 | 78.9 |
| I do not have one/any | 1.2 | 1.3 | 1.2 |
| Institutional level | |||
| Do you ever see students smoking at your college? | |||
| Missing | 1.7 | 0.8 | 1.2 |
| Never | 6.3 | 1.3 | 3.4 |
| Once or twice a year | 2.3 | 0.8 | 1.5 |
| Yes, every month | 1.7 | 0.0 | 0.7 |
| Yes, every week | 9.2 | 6.3 | 7.5 |
| Yes, daily | 78.7 | 90.8 | 85.7 |
| Do you think your college could do more to prevent or restrict smoking to certain areas on site? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 54.6 | 47.5 | 50.5 |
| No | 27.0 | 33.6 | 30.8 |
| Not sure | 16.1 | 18.1 | 17.2 |
| Does your college have a designated smoking area for students to smoke? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 68.9 | 76.5 | 73.3 |
| No | 23.6 | 15.6 | 18.9 |
| Not sure | 5.2 | 7.1 | 6.3 |
| Do you ever see staff smoking at your college? | |||
| Missing | 2.9 | 0.8 | 1.7 |
| Never | 47.7 | 62.2 | 56.1 |
| Once or twice a year | 8.6 | 8.4 | 8.5 |
| Yes, every month | 4.0 | 2.9 | 3.4 |
| Yes, every week | 14.9 | 9.7 | 11.9 |
| Yes, daily | 21.8 | 16.0 | 18.5 |
| Do you think that the staff at your college are concerned about students smoking? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 40.2 | 38.7 | 39.3 |
| No | 33.3 | 37.4 | 35.7 |
| Not sure | 24.1 | 23.1 | 23.5 |
| Do you think that the staff at your college are working to prevent students from taking up smoking? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 44.3 | 31.9 | 37.1 |
| No | 28.2 | 44.9 | 37.8 |
| Not sure | 25.3 | 22.3 | 23.5 |
| Do staff ever warn students about the health risks of smoking? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 62.1 | 60.1 | 60.9 |
| No | 24.1 | 26.5 | 25.5 |
| Not sure | 11.5 | 12.6 | 12.1 |
| Do most staff appear confident when discussing a smoking-related issue with students? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 60.3 | 60.9 | 60.7 |
| No | 8.1 | 10.8 | 9.2 |
| Not sure | 29.3 | 28.2 | 28.6 |
| Do staff encourage students to use e-cigarettes to help them smoke less at college? | |||
| Missing | 2.3 | 0.8 | 1.5 |
| Yes | 12.1 | 5.9 | 8.5 |
| No | 58.1 | 65.6 | 62.4 |
| Not sure | 27.6 | 27.7 | 27.7 |
| Have you heard of The Filter youth project? | |||
| Missing | 4.0 | 0.8 | 2.2 |
| Yes | 2.9 | 7.1 | 5.3 |
| No | 86.8 | 87.4 | 87.1 |
| Not sure | 6.3 | 4.6 | 5.3 |
| Community level | |||
| In the past year have you ever gone into a shop near your college to buy cigarettes or tobacco? (This includes buying for somebody else) | |||
| Missing | 1.7 | 0.8 | |
| Yes | 14.4 | 12.2 | |
| No | 83.9 | 87.0 | |
| The last time you went into a shop near your college to buy tobacco or cigarettes, what happened?a | |||
| Missing | 0.0 | 0.0 | |
| I bought some cigarettes | 96.0 | 93.1 | |
| They refused to sell me cigarettes | 4.0 | 6.9 | |
Chapter 4 Discussion
This section starts by considering the limitations of this study. First, the limitations of the recruitment methods and measures used to survey students about smoking and other health outcomes are discussed, including sampling and retention problems. Second, other practical and methodological limitations are discussed, including problems identified with the focus group data collection methods and the deviations from the study protocol. The discussion then focuses on key results from the process evaluation, before consideration of generalisability and the implications of findings for intervention development in FE settings and future research are discussed. The final section reports conclusions and recommendations.
Limitations
Student survey limitations
Although data indicate acceptability of survey methods to participants, with very low levels of missing data at both baseline and follow-up, the utility of this survey approach was compromised by issues of access and recruitment highlighted in Chapter 3, Research methods: feasibility and acceptability. A key limitation with the survey methods was that establishing accurate data on total eligible sample size at each college at baseline was problematic because of a lack of accurate, up-to-date enrolment data. These issues were especially prevalent in large FE settings as a result of students enrolling, in principle, prior to September, but not registering at the start of term; students deferring or dropping out in early September; inclusion of students who study across multiple campuses but whose primary campus is not the study site; and the inclusion of some students aged > 18 years as a result of incomplete information at enrolment. This meant that the number of potentially eligible students provided by colleges included some students who were either aged < 16 years or > 18 years and are, therefore, ineligible.
As accurate information on the number of students aged between 16 and 18 years who were attending colleges was not available, the denominator included ineligible participants and response rates would have been higher if they were not included. Ineligible participants were older, worked part time and were more likely to be classified as a weekly smoker than those who were eligible. Initial data provided by colleges did not – and could not – account for changes attributable to early exit by students or course changes. Although the intervention was specifically aimed at new students, commencement of the study at the start of the academic year emerged as problematic for student engagement, as staff did not yet know students or tutor group composition. Beginning the study further into the academic year would not likely have aided recruitment, with many students out on work placements and attending sporadically once courses are fully under way.
Although response rates reported at baseline are underestimates, overall the response and retention rates in this study would be too low to power a cluster RCT design aiming to assess effectiveness, and it is uncertain whether or not those students undertaking the survey are representative of the student body as a whole. Attendance patterns further impacted data collection as students are not in set places and at set times, meaning no fixed data collection points, with researchers instead relying on passing traffic. Although access to tutor groups would appear to present a partial solution to these issues, lack of access to these groups was common.
Respondents in the intervention and control groups were not equivalent at baseline in terms of age or gender, which may have impacted outcomes if baseline smoking attitudes and behaviour differed. The trial arms were not well balanced for the indicative primary and secondary outcome measures at baseline or follow-up. This imbalance is not unusual given that there were few clusters and heterogeneity between clusters, and would not be considered a risk in a larger cluster RCT assessing effectiveness.
Although baseline survey participation rates were reasonable, the research experienced high levels of attrition between baseline and follow-up. Thirty-six per cent of baseline respondents completed the 1-year follow-up survey, constituting 17% of potentially eligible participants. This low response at follow-up should be considered in interpreting results and, for future research, analysis of characteristics of non-responders at follow-up is recommended to understand how this may be better addressed.
Response rates at follow-up were impacted by a lack of effective channels to contact students, including limited access to personal e-mail, and student reluctance to respond to unsolicited telephone calls. Although it may have seemed reasonable to surmise that FE students would constitute a seemingly captive audience similar to that in schools, in practice this was not the case. The identification of multiple problems in recruitment and retention was evident in follow-up response rates, which indicate a lack of feasibility for retention in this setting. Although it was assumed that existing social media channels would be a useful tool for promotion of – and retention in – the trial, in practice, levels of engagement with these channels were low. It cannot be established whether this is typical of FE settings or specific to these sample sites, suggesting that this should be considered for future research through pre-intervention discussion with staff and students.
In relation to selection of survey tools, both the EQ-5D-5L scale and the health service use measures had limitations that should be considered for future research. As the age group under investigation generally has low engagement with health services and, because of the limited timescale of the study, it may have been unrealistic to expect change when rates of smoking-related health problems are likely to be low compared with older smokers. This further suggests that the EQ-5D-5L would not be sensitive enough to pick up changes to health or quality of life over a time scale this short, and it is recommended for future work in this area that other, purpose-built scales are developed that are more sensitive to likely health impacts among this age group.
Limitations with other data collection methods
There are some limitations in our assessment of student and staff views on acceptability associated with sampling and recruitment to focus groups. The process of gathering students and staff members together for focus groups proved time-consuming and challenging. It is uncertain how representative focus group participants were of the wider staff and student populations, and there was limited time to explore this in detail. No socioeconomic information about the student participants in focus groups was obtained. Difficulties in securing staff time away from routine practice impacted both focus group participation and attendance at staff training, which was delivered under target levels as a result of limited demand by sites. This was attributed by staff to pressures on time and may have been further impacted by the lack of clarity on intervention content indicated in qualitative data obtained from the process evaluation.
Stratification to student focus groups by smoking characteristics was particularly challenging, not least because a key finding of this study (see Chapter 3, Attitudes towards smoking in the further education context) indicates that many FE students who smoke were reluctant to define themselves as ‘smokers’. Although some people who were regular smokers clearly defined themselves as such, the grouping of ‘non-smokers’ was, in practice, divided into those who did not smoke at all and those who were occasional, or ‘social’ smokers.
Mystery shopper activities were inconsistently delivered and recorded, with variation in how the same shops were classified at baseline and follow-up; for example, some shops that had been classified as convenience stores at baseline were classified as confectionery, tobacconist, newsagents at follow-up, and vice versa. This suggests that the definition of some shop types was not clear and further guidance was required. The data for shops classified as convenience stores or confectionery, tobacconist, newsagents are therefore presented together in Chapter 3. Variance also occurred in how the mystery shopper survey was completed between baseline and follow-up, even when the accompanying fieldworker had remained the same. In particular, the dates and times of visits were not precisely recorded at follow-up (only afternoon/evening stated, rather than the exact time).
The retailer elements of the study were also impacted by the locations of participating sites and, particularly, the lack of retailers in close proximity to colleges, which may have affected consistency of staff interaction with shops. The combined limitations of implementation and access mean that the impact of the intervention on local sales practices, particularly underage sales to students aged 16–17 years, cannot be fully assessed at this time. Future interventions that aim to incorporate a retailer behaviour element should consider this prior to implementation.
Intervention staff checklists were poorly completed throughout the project, which partly reflects high staff turnover within some small, voluntary sector teams such as this. This turnover further impacted FE staff engagement, with frustrations expressed at the number of intervention staff involved and the lack of a consistent point of contact. For future intervention delivery in this setting, the utilisation of permanently contracted staff, if available, should be considered. Implementation may be supported by earlier engagement with FE settings to tailor and deliver the intervention with college managers and other staff.
No major problems were encountered in securing access to conduct observations in the intervention sites; however, fieldworkers at the larger sites reported difficulties in ensuring that all locations had been checked thoroughly to identify if messages were consistent and all possible data were collected. The same researcher did not always complete the baseline and follow-up observations at each site, so differences between baseline and follow-up data may be because of observer bias. More detailed observations could be obtained if fieldworkers were familiar with the site and can visit more than once and at different times of the day to observe smoking behaviours. A more structured survey to monitor sites at baseline and follow-up might provide more accurate detail about changes over time. The use of a tablet computer to input the online survey on site worked well in most cases, although data from one site did not upload properly, so the fieldworker completed the survey from memory.
Deviations from the protocol
The only major deviation from the protocol was that post-follow-up saliva testing (cotinine and anabasine tests) did not go ahead as planned because the research team was unable to recruit students to provide these samples. This means that the validity of self-reported smoker status could not be verified in this study. For future research in this setting, prior exploration of the acceptability of saliva sample collection and testing should be undertaken with students to identify new methods of recruitment and better incentives that may improve participation.
The study protocol also included plans for economic analyses to include an assessment of the costs of the intervention based on reports of the resources used by ASH Wales’ staff and FE colleges. Within this, key interventional resources were considered to include intervention staff time (intervention manager, training and education officers, web and social media officers, youth workers), as well as training event and youth workshop travel and resources, and other consumables relating to the delivery of the project. However, it was not possible to do these planned economic analyses based on the costs of staff time and other intervention expenses because we did not receive these data from the intervention team.
Key results and generalisability
Acceptability
This section considers key findings from the process evaluation, including the influence of non-interventionist institutional cultures identified at participating sites and the perceptions of acceptability of intervention components.
Although the study was not powered to detect adverse intervention effects, these were considered in analysis of qualitative data, with no unintended harms to student participants or staff identified. The acceptability of the intervention to FE colleges suggests little risk of disruption to practice. However, lack of delivery of the policy review component, and staff disappointment with this, may have affected the relationships between colleges and research teams, with implications for future participation in similar trials.
A significant barrier to acceptability of intervention content, and the willingness of staff to fully engage, relates to culture within the FE sector, particularly large colleges, in which personal choice and freedom are highly valued and the voluntary nature of attendance is recognised. Both staff and students strongly valued the transitional nature of FE as an environment in which development from youth to adulthood occurs, with corresponding emphasis on personal responsibility, including for one’s own smoking behaviour. This was evident in the contrast between support for formal smoke-free norms as embodied in policy in FE settings, including approval for smokers to be regulated and restricted to approved territories, and the informal tolerance exhibited in staff attitudes to challenging smoking behaviour and intervening with young adult choices.
Although this finding reflects perceptions commonly found in higher education settings of students as adults free to pursue their own choices, in contrast with higher education, students in FE settings may not have the same legal status. As it is illegal to sell tobacco to those aged < 18 years, this suggests scope to query the non-interventionist stance commonly expressed. Further research would aid understanding of how to balance the necessary emphasis on students’ transitional and developmental needs and the legal framework FE settings operate in. Cross-cultural comparisons with educational systems in which attendance to the age of 18 years is compulsory may also aid understanding of the role of voluntary participation in FE as a contributor to the development of more permissive environments.
This cultural difference between school and FE was also evident in the view that FE may be ‘too late’ for prevention activities, suggesting a need to further explore smoking cessation in this context. Students and staff suggested that they had ‘heard it all before’ and were well enough informed on smoking harms, especially non-smokers who did not want to engage with seemingly irrelevant information. The lack of acceptability of content was evident in low engagement with youth work sessions focused on development of smoke-free message campaigns, which were felt to be more relevant to younger age groups, suggesting a more nuanced approach could be needed in this setting. This was recognised by the intervention team and contrasted with previous experience of delivery in school settings. However, challenging the limited acceptability for prevention in the setting may be important in light of evidence that 60% of adult smokers commence regular smoking after the age of 16 years, suggesting an unmet need for prevention after compulsory education. Further exploration of prevention delivery in post-16 settings should consider what might constitute acceptable intervention content to target audiences.
Data suggest high acceptability among FE staff for intervention activities focused on smoking policy review and development but, as a result of intervention management issues, policies were not reviewed as intended. Randomisation was acceptable to FE managers, who also perceived added value in participation through engagement with external organisations and student exposure to higher education research. Staff also indicated acceptability of the training component of the intervention, particularly when they perceived existing knowledge gaps, such as with e-cigarettes. However, this was not matched by perceived likelihood of utilising content in discussing smoking with students, reflecting the lack of support for interventionist approaches that contrast with the emphasis on personal responsibility.
The intervention team found FE settings challenging and not conducive to smoking prevention activities compared with other educational settings (e.g. they reported significant differences between the prevailing culture of FE colleges in this study and schools where they had worked), which was observed as impacting student engagement. They also noted limitations in terms of access to target populations in FE settings attributable to existing organisational behaviours and activities.
Reach
Data indicate low levels of engagement with social media channels used for message dissemination, reflecting a possible misperception in intervention development, as well as institutional barriers, including college variations in the level of staff engagement in social media channels. Although students reported routinely accessing social media, this did not seem to include use of formal college websites and social media channels, suggesting overestimation of the likely impact of this approach. This finding is significant for future intervention delivery in this setting, including informing recruitment and retention strategies that may aim to utilise social media.
A further limitation of the intervention – and the logic model – emerged from process data, in which students frequently reported obtaining tobacco from peers and family rather than local retailers, suggesting targeting local retailer practice was likely to have limited effect. The majority of students who tried to purchase cigarettes were able to do so successfully at follow-up, suggesting limited penetration of community-level activities. The majority of students were unaware of The Filter project at follow-up, suggesting limited impact of awareness-raising activities supporting roll-out, such as social media promotion, as discussed above.
The identification of ‘informal’ supply chains in this study has implications for targeting of any future interventions, and further research would help to identify whether this supply was primarily taking tobacco products from inside the home or proxy purchasing (someone aged > 18 years purchasing tobacco products for someone aged < 18 years). Despite the legal age for tobacco purchasing increasing from 16 to 18 years in the UK in 2007, the law on illegality of proxy purchasing was only implemented in October 2015 after follow-up analysis. It is important to note that retailer behaviour in any future interventions may be differentially impacted by any enforcement activity associated with this legal change.
Implications
Overall, the lack of support for the intervention, combined with institutional factors that impacted delivery, such as short run-in, FE timetabling and systems, and poor intervention management, meant that The Filter FE was not acceptable or feasible at any of the pilot sites at this time. However, it cannot be concluded from this research that individual components of the intervention could not transfer to FE settings effectively if some of the key implementation issues identified were addressed in future studies.
This research has identified multiple factors that suggest that these FE settings were not conducive contexts for the delivery of prevention interventions. The prevailing non-interventionist ethos evident in FE colleges – more so than school-based sixth forms – suggests a different approach is required in such large, transitional environments to increase acceptability. However, although findings from the process evaluation appear to strongly support resistance to prevention messages, interpretation of the validity of other intervention components should be assessed in light of implementation issues, such as those impacting the assessment of retailer practices. Although not successful in this study, staff willingness to engage on policy-related matters may also suggest that this component would benefit from further investigation and reassessment of impact. It is also noted that FE managers were keen to work with universities and outside agencies, particularly when knowledge gaps are perceived, as with e-cigarettes, suggesting coproduction in future intervention development to identify issues and approaches deemed pertinent. Although smoking prevention was not a receptive message for this population, interest was further expressed in access to smoking cessation (i.e. not accessed via general practitioner or health services, services that do not need transport to get to), as well as policy support for colleges, suggesting scope for future work.
This research illustrates the variations within this sector that make generalising from results problematic. The diversity of the sector, in terms of mix of socioeconomic groups, vocational and academic courses, and the settings students are exposed to, including workplaces, requires further enquiry to inform current knowledge on the impact of FE on health behaviours in young people. Exploratory analysis of organisational features, drawing on research into university culture and processes, could inform future intervention development. The lack of homogeneity across FE illustrates the necessity of flexibility in intervention development and delivery.
Overall, the limitations to data collection methods, combined with the limited implementation of some components, means that the potential impacts of smoking prevention activities across multiple levels (student, college, community) remain hard to interpret. Findings are most robust at the level of individual influence, with this research increasing understanding of issues of reach and acceptability for individuals in these settings. Organisationally, the process evaluation has highlighted important procedural and attitudinal influences on on-site intervention components. Questions have been raised regarding the role of organisational processes and norms on implementation of prevention interventions, which can be considered for future development work and delivery. At the level of community effects, implementation issues relating to retailer engagement and monitoring mean that little can be asserted about the retailer component of the intervention. Although a socioecological approach presented challenges in terms of the range and complexity of intervention components involved, such a broad exploration was beneficial in highlighting the range of issues impacting smoking behaviour and intervention delivery in this setting.
Conclusions and recommendations for further research
The principal conclusion and recommendation of this report is for no further evaluation of this smoking prevention intervention in FE settings without consideration of how to address the issues identified in implementation of intervention components and acceptability of this type of intervention. However, even if some practical delivery constraints could be overcome in future interventions, issues of acceptability and reach may still occur in this setting due to relatively deep-rooted cultural and procedural constraints reported. The process evaluation data revealed how institutional cultures within FE settings limit the acceptability of prevention activities for smoking, although it is recommended that this be investigated across a broader range of FE schools and colleges, including those in denser urban areas and with other sociodemographics. It is also recommended that more information on socioeconomic status be captured for future studies in FE settings to better understand potential contextual influences and barriers.
We would recommend that other pilot trials and process evaluations of pilot interventions adopt a mixed-methods, socioecological approach. Although there were various limitations with our data collection methods, these were partially counteracted by the use of multiple data sources to aid triangulation and fieldworker immersion to enhance depth of understanding, as well as robust review methods among the staff team. This included development of a framework for assessing individual results against RQs and group discussion of identified contradiction in the data. The strength of multiple data collection was further enhanced by the adoption of a socioecological lens, which ensured consideration of influences across individual, institutional and community levels. This ensured that data saturation was probably reached, with some inductive themes emerging via the data that could be researched further (e.g. peer influence and the role of institutional culture).
Staff and student views suggest that smoking cessation activities may be appropriate and acceptable in this setting, and it is suggested that these should be a focus for further intervention development research. Should further research and development take place in FE colleges, key considerations would include timing of engagement and intervention delivery of smoking cessation activities. Overall, this study suggests that there will be greater value in smoking cessation intervention activities than smoking prevention activities. This is because of the relatively low numbers of students who reported taking up smoking in the first year of their FE courses combined with the low levels of acceptability regarding prevention messages in this context.
It was feasible to recruit, randomise and retain FE settings within a cluster RCT design. FE managers valued the opportunity to be involved in health research, particularly the input of external agencies and the additional resources provided, and accepted randomisation. However, further methodological work is recommended to improve student recruitment and retention rates prior to any larger RCTs being conducted in this setting. Problems with identification of the baseline population would suggest potential delivery later in the academic year when the student population has stabilised. However, differences between school- and college-based FE settings are important, with more vocational colleges likely to have more sporadic campus attendance than more academic settings, suggesting a need for novel approaches to student engagement and recruitment.
Finally, this study benefited from extensive patient and public involvement with young people through the Advice Leading to Public Health Advancement (ALPHA) youth group. We would recommend further patient and public involvement with young people to help steer more successful evaluation design and develop trial methods in future research. For example, young people should be consulted prior to new research to develop new interventions targeting cessation as well as prevention, or new research to develop methods for recruiting and retaining more young people in FE settings.
Acknowledgements
The work was undertaken with the support of The Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement, a UK Clinical Research Collaboration PHR Centre of Excellence. Joint funding (MR/KO232331/1) from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the Welsh Government and the Wellcome Trust, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged.
Contributions of authors
Adam Fletcher planned and managed the project, including management of baseline survey collection, and led on development of data collection tools, the synthesis of quantitative and qualitative data sources to assess progression criteria, and reporting.
Micky Willmott led on the analysis and write-up of qualitative data, and contributed towards to the synthesis of quantitative and qualitative data sources to assess progression criteria, and report drafting.
Rebecca Langford managed the process evaluation, led on the collection and analysis of the qualitative data, consultation with young people and write-up of process evaluation findings.
James White conducted the statistical analysis, led on the drafting of the statistical findings sections and contributed to drafting other sections of the report.
Ria Poole managed the collection and analysis of follow-up survey data and contributed towards report drafting.
Rachel Brown provided support to the team on drafting and editing the report.
Honor Young contributed to the collection of baseline and follow-up survey data, and commented on report drafts.
Graham Moore contributed to project planning, advised on pilot outcomes and commented on report drafts.
Simon Murphy contributed to project planning and commented on report drafts.
Julia Townson contributed to project planning and commented on report drafts.
William Hollingworth advised on the economic evaluation and commented on report drafts.
Rona Campbell contributed to project planning and commented on report drafts.
Chris Bonell supported the design of the process evaluation and contributed to project planning and report drafting.
Data sharing statement
We shall make data available to the scientific community with as few restrictions as feasible. Please contact the corresponding author if you would like to access the data.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Backinger CL, Fagan P, Matthews E, Grana R. Adolescent and young adult tobacco prevention and cessation: current status and future directions. Tob Control 2003;12:46-53. https://doi.org/10.1136/tc.12.suppl_4.iv46.
- General Lifestyle Survey Overview: A Report on the 2010 General Lifestyle Survey. Newport: ONS; 2010.
- School-based Interventions to Prevent Smoking. NICE Public Health Guidance 23. London: NICE; 2010.
- Bonell C, Jamal F, Harden A, Wells H, Parry W, Fletcher A, et al. Systematic review of the effects of schools and school environment interventions on health: evidence mapping and synthesis. Public Health Res 2013;1.
- Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, et al. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst Rev 2014;4. https://doi.org/10.1002/14651858.CD008958.pub2.
- O’Donnell T, Gray G. The Health Promoting College. London: Health Education Authority; 1993.
- James K. Health Promoting College for 16–19 Year Old Learners. London: Department of Health; 2003.
- McCambridge J, Strang J. The efficacy of single-session motivational interviewing in reducing drug consumption and perceptions of drug-related risk and harm among young people: results from a multi-site cluster randomized trial. Addiction 2004;99:39-52. https://doi.org/10.1111/j.1360-0443.2004.00564.x.
- Drury C, Doherty S. An Audit of Healthy School Programmes Working With Colleges in England. Preston: Healthy Settings Development Unit, University of Central Lancashire; 2005.
- Doherty S, Dooris M. The healthy settings approach: the growing interest within colleges and universities. Educ Health 2006;24:42-3.
- Newbery N, McCambridge J, Strang J. Let’s talk about drugs: pilot study of a community-level drug prevention intervention based on motivational interviewing principles. Health Educ J 2007;107:276-89. https://doi.org/10.1108/09654280710742573.
- Slym RL, Day M, McCambridge J. National survey of drugs and alcohol provisions within further education colleges in England in 2006. Drugs Educ Prev Polic 2007;14:193-204. https://doi.org/10.1080/09687630601132702.
- Twardzicki M. Challenging stigma around mental illness and promoting social inclusion using the performing arts. J R Soc Promot Health 2008;128:68-72. https://doi.org/10.1177/1466424007087804.
- Warwick I, Statham J, Aggleton P. Healthy and Health Promoting Colleges: Identifying an Evidence Base. London: Thomas Coram Research Unit, Institute of Education, University of London; 2008.
- Warwick I, Maxwell C, Statham J, Aggleton P, Simon A. Supporting mental health and emotional well-being among younger students in further education. JFHE 2008;32:1-13. https://doi.org/10.1080/03098770701560331.
- Richards C. How Useful Are Bounded Online Chat Rooms As a Source of Pastoral Support in a Sixth-Form College 2009.
- McCambridge J, Hunt C, Jenkins RJ, Strang J. Cluster randomised trial of the effectiveness of motivational interviewing for universal prevention. Drug Alcohol Depend 2011;114:177-84. https://doi.org/10.1016/j.drugalcdep.2010.07.028.
- Audrey S, Langford R. Dying to get out: young drivers, safety and social inequity. Inj Prev 2014;20:1-6. https://doi.org/10.1136/injuryprev-2013-040756.
- Minary L, Cambon L, Martini H, Wirth N, Acouetey DS, Thouvenot F, et al. Efficacy of a smoking cessation program in a population of adolescent smokers in vocational schools: a public health evaluative controlled study. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-149.
- Stead LF, Lancaster T. Interventions for preventing tobacco sales to minors. Cochrane Database Syst Rev 2008;1.
- Brinn MP, Carson KV, Estermann AJ, Chang AB, Smith BJ. Mass media interventions for preventing smoking in young people. Cochrane Database Syst Rev 2010;11. https://doi.org/10.1002/14651858.CD001006.pub2.
- Hopkins DP, Razi S, Leeks KD, Priya Kalra G, Chattopadhyay SK, Soler RE. Task Force on Community Preventive Services . Smokefree policies to reduce tobacco use. A systematic review. Am J Prev Med 2010;38:275-89. https://doi.org/10.1016/j.amepre.2009.10.029.
- Carson KV, Brinn MP, Labiszewski NA, Esterman AJ, Chang AB, Smith BJ. Community interventions for preventing smoking in young people. Cochrane Database Sys Rev 2011;7. https://doi.org/10.1002/14651858.CD001291.pub2.
- Thomas RE, McLellan J, Perera R. School-based programmes for preventing smoking. Cochrane Database Syst Rev 2013;4. https://doi.org/10.1002/14651858.CD001293.pub3.
- Oude Luttikhuis H, Baur L, Jansen H, Shrewsbury VA, O’Malley C, Stolk RP, et al. Interventions for treating obesity in children. Cochrane Database Syst Rev 2009;1. https://doi.org/10.1002/14651858.CD001872.pub2.
- Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-119.
- Chokshi DA, Farley TA. The cost-effectiveness of environmental approaches to disease prevention. N Engl J Med 2012;367:295-7. https://doi.org/10.1056/NEJMp1206268.
- White M, Adams J, Heywood P, Babones SJ. Social Inequality and Public Health. Bristol: Policy Press; 2012.
- Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health 2013;67:190-3. https://doi.org/10.1136/jech-2012-201257.
- Glasgow RE, Lichtenstein E, Marcus AC. Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am J Public Health 2003;93:1261-7. https://doi.org/10.2105/AJPH.93.8.1261.
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q 1988;15:351-77. https://doi.org/10.1177/109019818801500401.
- Durlak JA, DuPre EP. Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol 2008;41:327-50. https://doi.org/10.1007/s10464-008-9165-0.
- Hawe P, Shiell A, Riley T. Theorising interventions as events in systems. Am J Community Psychol 2009;43:267-76. https://doi.org/10.1007/s10464-009-9229-9.
- Australia Guidance for a Tobacco Free Campus: Why We Should Make Campuses Tobacco Free and How to Do It. Sydney, NSW: ASH Australia; 2009.
- Fletcher A, Jamal F, Moore G, Evans R, Murphy S, Bonell C. Realist complex intervention science: applying realist principles across all phases of the MRC framework for developing and evaluating complex interventions. Evaluation 2016;22:286-303. https://doi.org/10.1177/1356389016652743.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Handbook for Surveys on Drug Use among the General Population. Lisbon: EMCDDA; 2002.
- Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med 1998;158:1789-95. https://doi.org/10.1001/archinte.158.16.1789.
- Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20:1727-36. https://doi.org/10.1007/s11136-011-9903-x.
- Borland R, Yong HH, O’Connor RJ, Hyland A, Thompson ME. The reliability and predictive validity of the Heaviness of Smoking Index and its two components: findings from the International Tobacco Control Four Country study. Nicotine Tob Res 2010;12:S45-50. https://doi.org/10.1093/ntr/ntq038.
- Fuller E. Survey of Smoking, Drinking and Drug Use among Young People in England in 2013. London: NatCen; 2013.
- de Vries H, Mudde A, Kremers S, Wetzels J, Uiters E, Ariza C, et al. The European Smoking Prevention Framework Approach (ESFA): short-term effects. Health Educ Res 2003;18:649-63. https://doi.org/10.1093/her/cyg033.
- de Vries H, Dijk F, Wetzels J, Mudde A, Kremers S, Ariza C, et al. The European Smoking prevention Framework Approach (ESFA): effects after 24 and 30 months. Health Educ Res 2006;21:116-32. https://doi.org/10.1093/her/cyh048.
- Hill M, Greene S, Hogan D. Researching Children’s Experience. London: Sage Publications; 2005.
- Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res 2003;27:67-73. https://doi.org/10.1111/j.1530-0277.2003.tb02723.x.
List of abbreviations
- A level
- Advanced level
- ALPHA
- Advice Leading to Public Health Advancement
- AS level
- Advanced Subsidiary level
- ASH
- Action on Smoking and Health
- AUDIT-C
- Alcohol Use Disorders Identification Test Consumption
- BTEC
- Business and Technology Education Council
- CI
- confidence interval
- e-cigarette
- electronic cigarette
- EQ-5D-5L
- EuroQol-5 Dimensions, 5-level version
- ESFA
- European Smoking Prevention Framework Approach
- FE
- further education
- GCSE
- General Certificate of Secondary Education
- GLS
- General Lifestyle Survey Overview: A Report on the 2010 General Lifestyle Survey
- HSI
- Heaviness of Smoking Index
- ICC
- intracluster correlation
- NIHR
- National Institute for Health Research
- ONS
- Office for National Statistics
- PHR
- Public Health Research
- RCT
- randomised controlled trial
- RQ
- research question
- SD
- standard deviation