

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 14/153/01. The contractual start date was in October 2015. The final report began editorial review in November 2017 and was accepted for publication in October 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Mike Clarke is currently a member of the National Institute for Health Research (NIHR) Health Technology Assessment General Board. Mark McCann has attended meetings and participated in activities with the Scottish Parliament Cross Party Group on Drugs and Alcohol, the Scottish Drugs Forum, Independence from Drugs and Alcohol Scotland and Addaction Springburn. He received grants from the Medical Research Council, Scottish Government Chief Scientist Office and the NIHR Public Health Research programme during the conduct of this study.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Higgins et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Background and introduction
The purpose of this study was to provide public health-related research evidence on novel psychoactive substances (NPSs). This chapter sets out the background and rationale for the study and the research questions that guided it.
This report is presented in eight chapters. The methodology of the study is presented in Chapter 2, followed by five results chapters, each detailing substantive findings as set out by our guiding research questions. In Chapter 8, we synthesise essential learning from all aspects of the study and present implications for policy and practice.
Research questions
The research project had 11 research questions:
-
What are the types and patterns of NPS use?
-
What are the developmental pathways into NPS use and are they different across types of NPSs?
-
Is there an association between NPS use and health and social outcomes?
-
What are the patterns of NPS use as they relate to the patterns of other substance use?
-
Why do individuals with similar sociodemographic profiles and illicit substance use differ in their decision to use or not use NPSs? What are the emerging factors that contribute to this decision to use or not use NPSs?
-
Does the drug-taking profile of a NPS user differ according to age, sex and social class and across traditional drug-using groups?
-
What are the harms associated with NPS use and how are these different from those of conventional illicit substances?
-
What are the appeals of NPSs and how are these the same as or different from those of traditional illicit substances?
-
What are the risks associated with NPS use and how are these different from those of traditional illicit substances?
-
What knowledge and experiences do NPS users have of treatment services for NPSs and how do these differ from their knowledge and experiences of services for other substances (licit and illicit)?
-
How can the research findings be integrated into a framework to inform existing service provision/policy formation and educational initiatives UK wide?
Background
The public health impact of substance misuse is a global challenge. 1,2 Contemporary data reflect an increasingly graduated and fractured drug scene. The old dichotomy between a relatively small number of highly problematic drug users and a more significant number of recreational and experimental users is changing to a more complex and dynamic picture,1,3 with NPSs contributing to this fragmentation. NPSs are synthetic alternatives to traditional illegal drugs. Compared with traditional drugs, NPSs are inexpensive, relatively easy to source and frequently more potent. There is no universally accepted legal definition of NPSs. The United Nations Office on Drugs and Crime (UNODC)2 uses the term and defines NPSs as:
[S]ubstances of abuse, either in a pure form or a preparation, that are not controlled by the 1961 Single Convention on Narcotic Drugs or the 1971 Convention on Psychotropic Substances, but which may pose a public health threat.
UNODC2
UNODC highlights that ‘new’ does not necessarily mean original formulations (several NPSs were first synthesised many decades ago) but substances that have recently become available on the market. 2
In the UK, the Advisory Council on the Misuse of Drugs (ACMD) defines NPSs as:
[P]sychoactive drugs which are not prohibited by the United Nations Single Convention on Narcotic Drugs or by the Misuse of Drugs Act 1971 and which people in the UK are seeking for intoxicant use.
ACMD4
The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) adopts a similar definition, although some substances that are controlled in the UK fall outside international control mechanisms, for example methoxetamine. 5
Over the past decade, first-, second- and third-generation NPSs have been increasingly referred to in policy and research documents6,7 and these substances have been appearing on the drugs market at an exceptional rate. By 2012, the number of NPSs outnumbered the total number of substances falling under international control. The overarching legal term ‘NPS’, with numerous substances grouped under this single heading, is now out of date and is of limited use when investigating differential patterns of use and harm. 8 Recognising the need for a more refined definition of NPSs, the EMCDDA subdivided the market into five categories:
-
‘legal highs’ – marketed at recreational users; could be purchased online and in headshops until 2016
-
research chemicals – marketed as being for scientific research purposes; sold readily online
-
food supplements – aimed at individuals seeking to enhance themselves physically or cognitively; available to buy online
-
designer drugs – manufactured illegally in laboratories and sold under the guise of illicit drugs [e.g. 3,4-methylenedioxy-methamphetamine (MDMA) and heroin]
-
medicines – sourced from patients or illegally purchased via the black drug market.
Novel psychoactive substances have been broadly categorised5,9 as ‘synthetic cannabinoid receptor agonists’ [e.g. JWH-018 (‘spice’)], ‘aminoindanes’ [e.g. 5,6-methylenedioxy-2-aminoindane (MDAI)], ‘synthetic cathinones’ (e.g. mephedrone), ‘tryptamines’ (e.g. 5-Meo-DPT), ‘ketamine- and phencyclidine-type substances’ (e.g. 4-MeO-PCP), ‘plant-based substances’ (e.g. khat), ‘piperazines’ (e.g. benzylpiperazine), ‘phenethylamines’ (e.g. Bromo-DragonFLY) and ‘other substances’ [e.g. dimethylamylamine (DMAA)]. 10
For this research, we too attempted to disentangle where possible the various NPSs (see Adley’s drugs wheel11 for further information).
Legislative context
Novel psychoactive substances present challenges for legislation and monitoring, researching and developing interventions. For many years in the UK under the usual system of drug control, individual drugs, or groups of drugs with similar chemical structures (‘generic definitions’), were placed under the Misuse of Drugs Act 1971,12 based on the assessment of likely harms to individuals and society. That system of drug control is a lengthy process, which involves evidence gathering and reviews undertaken by the ACMD. Based on this review, the ACMD makes a recommendation regarding whether or not to classify or schedule the drug, and what other approaches could be used (e.g. specific prevention, treatment and harm-reduction advice). In 2010, changes to this process were signalled when mephedrone, possibly the most commonly known NPS, was banned in circumstances that caused the ACMD and others to question if this decision was based on the best available evidence. 13 Shops and online retailers selling the drug labelled as plant food cleared their shelves prior to the ban. Since then, and because of the large increase in the number of NPSs identified,2 the UK Government decided that it needed new laws and approaches to NPSs. This resulted in the temporary class drug orders (TCDOs). These drug orders put substances/groups of substances under temporary control for up to 1 year after a rapid review. In 2014, an expert review was published detailing a new legislative approach to dealing with NPSs. Subsequently, a complete ban on ‘psychoactive’ products was introduced in May 2016; this approach met criticism from many experts. Prior to this, NPSs had been controlled for under the Misuse of Drugs Act 1971;12 however, it was not possible to continually update the legislative approach for classifying drugs at a pace matching their emergence onto the market14,15 and, therefore, a new approach was needed.
The Psychoactive Substances Act 2016 (PSA)16 defines a psychoactive substance as any substance that:
(a) is capable of producing a psychoactive effect in a person who consumes it, and (b) is not an exempted substance.
The PSA goes on to define a psychoactive effect as when a substance depresses or stimulates a person’s central nervous system and has an impact on the individual’s mental functioning or emotional state.
In passing the PSA, the UK Government adopted the policy approach implemented by the Government of Ireland, which introduced comparable legislation in 2010 called the Criminal Justice Psychoactive Substances Act 201017 in a context relevant to the present research.
The PSA focuses on penalising suppliers rather than consumers; indeed, those caught supplying NPSs could face a prison term of up to 7 years, and those being found in possession of NPSs for personal use are not criminalised. Nevertheless, many NPS users were highly critical of the legislation,18 as were other groups. 15 Particular concern was expressed over how a psychoactive effect was defined by the Home Office in the PSA.
The PSA definition is problematic given that any number of substances can fall within it, including flowers and incense. The ACMD highlighted this concern and produced an alternative version. They also warned that some form of revision would be needed to make the law enforceable. Furthermore, the association between the closure of headshops and reduction in use of NPSs is not supported by data from Ireland,3 where similar legislation has been in place for some time. As is the case in a prohibition context, it is likely that continued demand for NPSs will result in driving the substances underground, thus resulting in even less potential for quality control than existed pre legislative ban. This may lead to riskier patterns of sale and consumption, as again has happened in Ireland. 15
The EMCDDA’s analysis of the situation was that current practices needed to be continually modified if they were to address a drugs problem that was in a state of constant change. 19 In some European locations, including the UK, Ireland, Poland, Portugal and Austria, approaches to NPS control have been constructed on the basis of broad definitions of ‘psychoactivity’, with harmful outcomes not always being taken into consideration. 1–3
Any benefits, harms and unintended consequences, both short and long term, from the PSA and similar legislation will be evident only over a more extended period.
Market context
The marketing approach to NPSs was qualitatively different from that of other illegal drugs owing to the greater use of attractive packaging and branding. 20 According to Wallis,20 the effects of media attention on the NPS market are often counterproductive, leading to spikes in use. Interviews with key stakeholders (e.g. retailers, NPS innovators, enforcement professionals, policy-makers) suggested that the PSA was unlikely to affect the supply of NPSs through the internet/fast courier system. Reports in Northern Ireland after the legislation suggested that mephedrone availability was relatively unaffected, although drug purity had decreased. 21
Novel psychoactive substances also produced other innovations in the drug market. Shapiro5 noted that, serendipitously, the parallel growth of the internet was, for some, a very effective aid for producing and selling NPSs. On a global scale, users were able to interact and exchange knowledge about NPSs and their effects. In addition, it was evident that enterprising individuals had performed searches for patents relating to compounds that had been investigated by pharmaceutical companies but were no longer being pursued.
To avoid detection, encryption technology is reported to have been used when purchasing NPS drugs or their raw chemicals from Asia. 5 Retail order and shipment occurred from websites with payment through third parties [e.g. PayPal Holdings, Inc. (San Jose, CA, USA)]. Finally, the ‘dark web’ grew to house online black markets such as ‘Silk Road’; a high level of technical expertise was needed to access NPSs via this route using virtual currency (e.g. bitcoin). Despite NPSs being more readily available online, some evidence suggested that only a small proportion of NPS users obtain their drugs via online retailers. 22 Rather, NPS users often sourced from friends, dealers and headshops. Although they may not use the internet to purchase NPSs, many habitual internet users availed of the internet to research NPSs. O’Brien et al. 18 investigated the experiences of ‘cybernauts’ using an online survey (n = 183). Around 3 in 10 participants reported using NPSs within the previous week. Participants considered themselves to be knowledgeable consumers owing to their internet use; for example, the internet was the medium through which they gathered information about NPSs and, in turn, passed on their own experiences (e.g. harms experienced) to others.
Retailers have capitalised on the knowledge shared by these online communities and have even reported monitoring internet forums to gauge demand for different NPS types, adjusting their stock accordingly. 20 The relationship between NPSs and existing traditional markets is a highly complex one, and a temporal relationship between variations in the purity of traditional substances can be observed. 23 Other authors have documented the displacement effect of the various forms of NPSs. 24
Pharmacological context
From the pharmacological perspective, the level of innovation in the production of NPSs limits the knowledge of both the pharmacodynamics and the acute and chronic toxicity of these continually evolving substances. 25 Identifying individual substances bought via the internet or on the street is difficult. 26 Even when a new chemical is clearly and accurately identified, all too often there is little or no information on associated harms and suitable treatments. There is progress in studies aimed at assessing their pharmacology: individual pharmacodynamics and kinetics, toxicity profile, dependency risk and short- and longer-term threats to physical and mental well-being. 27,28
Furthermore, various NPSs are often ingested together or in conjunction with alcohol and/or other substances in an idiosyncratic way, adding uncertainties about the consequences of combined intake. 29 Synthetic cannabinoids (SCs) have also been examined in detail. 30
To assist in the identification of emergent NPSs, the Welsh Emerging Drugs and Identification of Novel Substances (WEDINOS) project was set up in September 2013. Prior to the blanket ban, results posted on submitted NPS samples have generated a reactive response, for example the invocation of procedures to also ban the next substance emerging from laboratories. Results from WEDINOS31 indicate how complicated the picture is, in that there is a cross-fertilisation between NPSs and other drugs leading to a more difficult screening and assessment process.
Against this backdrop of legislative, market and pharmacological challenges, we now examine the existing evidence base on the various NPSs as they relate to traditional drug use. This introduction is followed by a summary of available information on the assessment of NPS use in the light of potential interventions. Before we consider the extant literature, NPS contextual data (e.g. prevalence and death rates) are briefly summarised. A more detailed summary of NPS and other drug contextual data in UK regions is presented in Report Supplementary Material 1, Tables 31–38 and Figure 9.
Key messages from prevalence data
There is an incomplete picture of NPS use prevalence; nevertheless, available data indicate that NPS use is relatively low when compared with more frequently used illicit drugs (e.g. cannabis, powder cocaine, ecstasy), with NPS use tending to be higher in specific subgroups (SGs).
Data on general NPS use from nationally representative surveys are of course limited to recent years. In 2014/15, the prevalence of lifetime NPS use (mephedrone excluded) was 2% in Northern Ireland (Department of Health Northern Ireland)32 and Scotland (National Statistics Scotland)33 and 3% in England and Wales (Office for National Statistics). 34 There was a statistically significant reduction in the prevalence of NPS use in the previous year between 2010/11 and 2014/15 in two regions of Northern Ireland: South Eastern and Western Trusts (down by 1.4% and 1.1%, respectively, since 2010/11). 32 The estimate of the prevalence of lifetime NPS use for the UK from the European Commission22 survey was higher (10%) than in other UK national surveys, and was above the average prevalence rate for European countries (8%).
Data from UK misuse databases
The UK regional drug misuse databases provide an indication of recent drug use by problem users. Drug misuse databases in Northern Ireland and England/Wales report on a NPS category. In 2015/16 in Northern Ireland, 7% of service users with drug use problems reported NPS use [Northern Ireland Drug Misuse Database (NIDMD)]35 compared with 1.3% in England/Wales [National Drug Treatment Monitoring System (NDTMS)]. 36 A specific NPS category was not reported in Scotland [Scottish Drug Misuse Database (SDMD)]. In Northern Ireland, NPS use was much more frequently reported in the Western services than in any other areas. Weekly use was the most frequent form of use for those using NPSs, mephedrone, cocaine, speed, ecstasy and other stimulant drugs. The vast majority of users reported trying NPSs before the age of 25 years in Northern Ireland.
Deaths
In Northern Ireland, death by substances on death certificate statistics suggest that although deaths in which NPSs are implicated, are rare, they have become more common in recent years. 37 In 2015, deaths implicating NPSs were most frequent in Scotland (1.4 per 100,000),38 followed by Northern Ireland (0.9 per 100,000) and England/Wales (0.2 per 100,000). 39 In Scotland in 2015, the majority (77%) of the 74 deaths in which NPSs were implicated involved benzodiazepine NPS (e.g. etizolam). In research studies, deaths in which SCs, mephedrone and phenethylamines have been implicated have been reported. 40–44
Existing empirical evidence on novel psychoactive substances
Synchronous with the present study, Mdege et al. 45 were commissioned by the National Institute for Health Research (NIHR) to undertake an empirical and conceptual review of NPS to provide research recommendations. Focusing on the UK, their principal objective was to provide review evidence to be used in developing public health interventions targeting NPSs.
The study comprised a scoping review and narrative synthesis of evidence focusing on NPS use, associated harms and responses. Spanning the decade 2006–16, the authors examined Google (Google Inc., Mountain View, CA, USA) and relevant websites and online drug forums, and contacted experts on NPSs. Their research included primary and secondary studies detailing relevant research or discussion of key research. They also developed a UK-focused conceptual framework detailing an evidence-based public health approach to NPS use.
Using a scoping review, Mdege et al. 45 identified 995 articles, the majority of which examined the health-related adverse effects of NPS use at the individual level. They highlighted that the expanding literature on the NPS phenomenon is primarily clustered around four key areas:
-
Surveys and surveillance studies.
-
Qualitative work that focuses on the harms associated with use.
-
A limited number of systematic reviews centred on harms.
-
Literature that seeks to evaluate policy responses to the NPS phenomenon. There are also clinical guidelines based on the evidence, such as those of the Novel Psychoactive Treatment UK Network (NEPTUNE). 46 They conclude that the literature is characterised by being early in its stage of development and lacking in data to directly inform an evidence-informed public health response to NPSs. 45
Regarding survey data, there are 29 identified studies that assessed NPS use prevalence in the UK. The authors usefully summarised the findings of the prevalence studies in tabular form. These included results from the Crime Survey England and Wales (CSEW), the Scottish Crime and Justice Survey (SCJS), the All Ireland Prevalence Study (AIPS) and a range of additional European surveys and school-based surveys. They also included a useful summary of systematic reviews uncovered by study name, study population, NPS type and methodological characteristics. In the UK, nationally representative prevalence surveys have focused largely on mephedrone, with data on other NPSs much less developed. More detailed data covering motivations and patterns of use tend to be restricted to a small number of qualitative studies.
Age and sex trends
The prevalences of lifetime NPS use in young people [defined as people aged 11–15 years (in England and Wales) and 13–15 years (in Scotland)] in England and Wales (2.5%)47 and Scotland (2.0%)48 are comparable. In England, NPS prevalence was 10 times higher among 15-year-olds than among 11-year-olds (5.0% vs. 0.5%, respectively). 47 Similarly, in Scotland, 1% of 13-year-olds and 4% of 15-year-olds reported NPS use. 48 Although NPS use was marginally higher among males than among females in the Scottish Schools and Adolescent Lifestyle and Substance Use Survey (SALSUS) (2% vs. 1%, respectively),48 this pattern was not evident in the NHS Digital survey47 nor in the survey by the European Commission. 22 With a broader definition of young people (e.g. people aged 16–24 or 15–34 years), NPS use was around two to three times (4–7%) higher in younger than older adults across all UK regions. Some variations were possibly attributable to the use of different definitions of young people. 32–34
At-risk populations
Studies specifically designed to measure NPS prevalence have not examined SGs other than in standard demographic groups (e.g. age, sex). Research has highlighted higher prevalence rates among specific populations than at the wider population level, including people with eating disorders,49 mental health inpatients,50,51 men who have sex with men (MSM),52 prisoners,53 the homeless54 and club attendees. 55 Although these prevalence rates may not give precise prevalence estimates for these specific groups, they do indicate that these groups are more likely to use NPSs. Among those with eating disorders, patients with a history of self-harm and bingeing/purging were more likely to report NPS use. 49 Given the high prevalence of eating disorders in females, this factor may play more of a role in female NPS use initiation. A study of mental health patients – individuals who were younger, male and had a criminal record – reported higher rates of use. 50 Evidence suggests that mephedrone (41%) is the most popular NPS among club attendees, whereas lifetime prevalence for the use of other substances was less frequent [e.g. methylone, 11%; methylenedioxypyrovalerone (MDPV), 2%]. 55 Almost all mephedrone users (94%) reported use in the previous year and most (80%) reported using NPSs within the previous month. In a sample of patients at two sexual health clinics, Thurtle et al. ’s52 study revealed that monthly use was low (1.6%) in the total sample and particularly low in 16- to 24-year-olds (0.3%). However, among HIV-positive MSM, Chung et al. ’s56 case review found that 24% reported lifetime mephedrone use. Bourne et al. 57 describe reports of MSM in London using mephedrone in combination with gamma-hydroxybutyrate (GHB)/gamma-butyrolactone (GBL), using these ‘chemsex’ drugs during sex, often involving groups and adventurous sexual activity (e.g. ano-brachial intercourse).
Motivations for use
A systematic review focusing on international surveys of SC use found that motives for use are often centred around perceptions that SCs are safer than other non-cannabinoid illicit drugs and that it is easier to avoid detection in drug tests while still enjoying a ‘cannabis-like’ high. 40 Within the UK portion of the Global Drug Survey sample, Winstock et al. 55 found that motivations for the use of methoxetamine, relative to those for ketamine, were centred around easier access, less damage to kidneys or bladder and a preference for the drug’s effects. Users of mephedrone often report pleasant effects of the drug, such as euphoria and a sense of well-being. 21,58 Another study focused on salvia; users of this NPS sometimes experienced pleasant hallucinogenic effects. 59 Motives for use do appear to vary by population; for example, among prisoners, the main reasons for using SCs were to evade drug detection, to help pass time and for relaxation. 53 Among the homeless, NPSs are often viewed as being a less costly substitute for alcohol and other illicit drugs. 54
Adverse effects
In contrast to the limited body of research on motivations for NPS use, there has been more focus on the harmful impact of NPS use, as revealed in the recent review by Mdege et al. 45 Systematic review evidence suggests that frequent side effects of NPS include psychotic symptoms, behavioural changes (e.g. aggression) and physiological effects such as changes in blood pressure, pulse and temperature. 60
The adverse effects are further summarised here according to substance type.
Synthetic cannabinoids
Several systematic reviews have explicitly focused on the adverse effects of artificial cathinones. 40,61–64 Numerous side effects of SCs have been reported by these reviews, including physical (e.g. hypertension, seizures, palpitations, chest pain, tremors) and neuropsychiatric (e.g. aggression, suicidal thoughts, anxiety and psychosis) effects. Although SC use can lead to hospitalisation, people hospitalised because of SC use are usually released within 24 hours,40 with typical treatment including intravenous fluids, benzodiazepines and oxygen. 40,41
However, for patients who have more severe side effects of SCs (e.g. acute kidney injury, psychosis), hospitalisation can be as long as 2 weeks. Interestingly, more than half of prisoners in a study53 reported that they thought that spice was a more hazardous substance than cannabis, and that it was ‘fairly’ or ‘very’ addictive; they also mentioned that high prices in prison had got them into debt.
Mephedrone
Two studies21,58 examining the effects of mephedrone reported side effects similar to those of SCs, such as nasal damage associated with snorting, and challenging ‘comedowns’. In the study by Brookman,58 a cyclical association between crime and mephedrone was evident; specifically, violence often happened during the ‘buzz’ or comedown phase, after which they had to resort to crime to further fund their habit. Concerningly, many mephedrone users reported becoming violent when using the substance,58 and having to use other drugs, such as diazepam or cannabis, to deal with the comedown effects. Those using mephedrone in conjunction with GHB/GBL for sexual purposes regularly reported a negative impact on their relationship. Other issues included concerns over sexual selfishness and damage to employment and career prospects. 57
Salvia
One study59 focused on the effects of salvia; interestingly, not all users reported feeling any effects or even inconsistent effects. Lack of impact may be due to the short half-life of the drug.
Phenethylamines
Two systematic reviews42,43 have synthesised the research on phenethylamines effects; common side effects included agitation, tachycardia and hypertension. In the Suzuki et al. 43 review of patient case reports, as many as 4 in 10 patients required admission to an intensive care unit.
Bath salts
For bath salts, systematic review evidence suggests that the comedown effects can be similar to and, in some cases, more intense than those of other stimulants. 61
Evidence on prevention and intervention
The literature provides a useful summary of the research on, among other things, prevalence, motivations for use and adverse effects. Notable, however, is the absence of a knowledge base for the efficacy of any prevention/interventions for NPS use. To date, evidence has focused on providing guidance and advice on possible referral pathways and highlighting probable interventions. This is framed according to the symptomology, identified patterns of use, NPS class and specialist groups, including MSM and young people. To our knowledge, there are at present no completed or ongoing methodologically rigorous experiential trials or structured research evaluations of the effectiveness of pharmacological and/or psychosocial interventions for NPS use, either as a standalone drug of choice or within the unplanned or adjunctive drug context. 65
Chapter summary
This chapter set out the research questions of the present study in the context of existing evidence on NPSs. To accomplish that goal, we provided definitions of NPSs and summarised the legislative, market and pharmacological contexts of our work. Existing literature on a range of areas as they relate to the NPS phenomena was reviewed. This included reflections on current responses concerning interventions for the various NPSs as well as NPS vis-à-vis other substance use. Related to that effort, it became evident that there is a resounding need for more evidence within this area, which will help to articulate a clearer understanding of the complex nature of NPSs. The umbrella term ‘NPS’, used for legal purposes with multiple drugs grouped under this single heading, lacks utility for the practical purpose of exploring the markedly differential trajectories of use and harm. We seek in our findings to draw out a level of nuance that contributes to our grasp of the different categories of NPSs and their use by participants. In the research presented in the following chapters, we posit findings that can substantially contribute to the knowledge base on the use of NPSs, which constitute an ongoing public health challenge. We now present the methodology for the study, followed by our four substantive findings chapters.
Chapter 2 Methods
Design
The study used a three-phase mixed-methods design, as summarised in Figure 1.
FIGURE 1.
Study design.
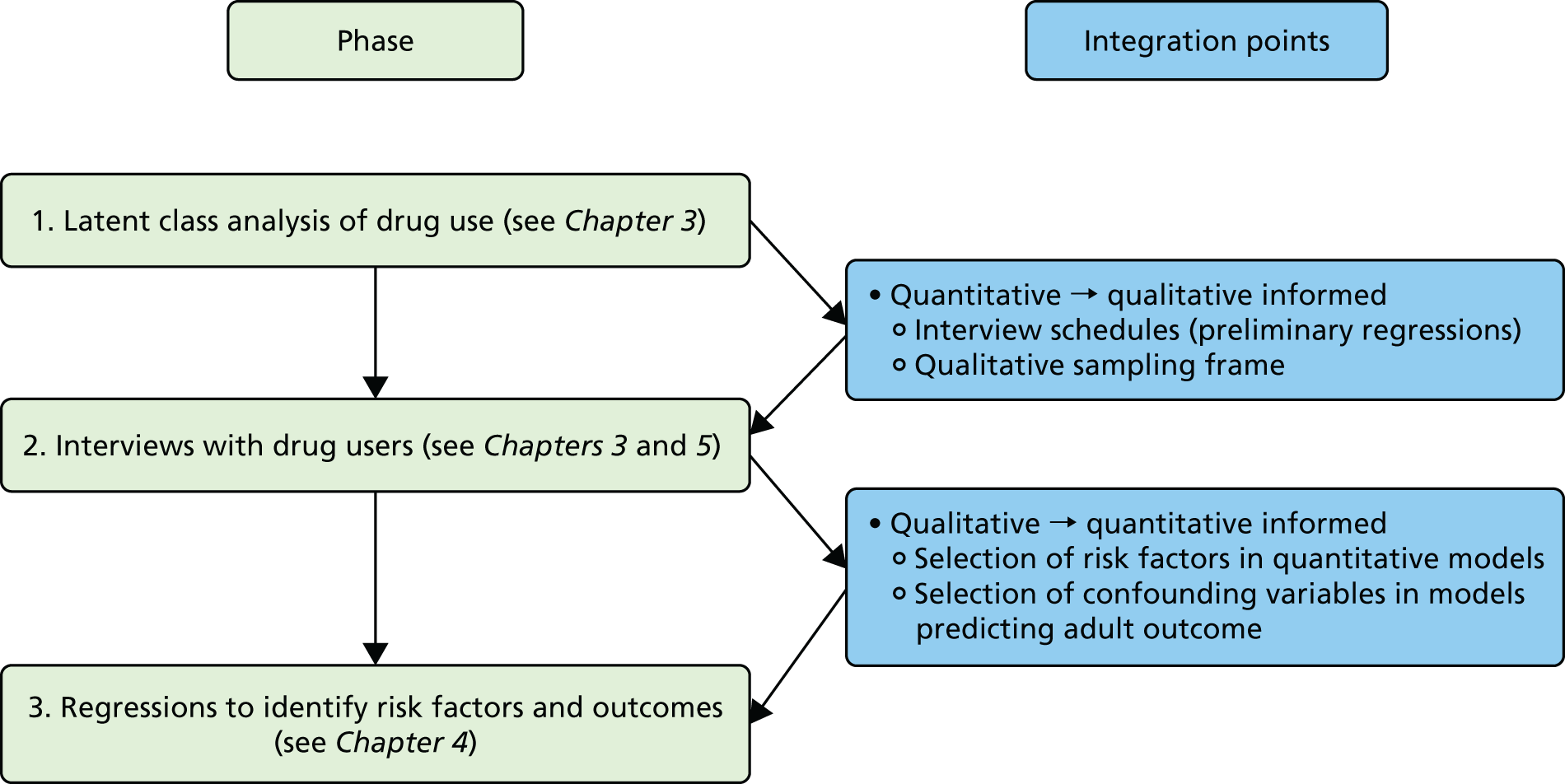
Phase 1 was a quantitative phase involving secondary data analysis of the Belfast Youth Development Study (BYDS) (see Secondary data source: Belfast Youth Development Study). A latent class analysis (LCA) using the 2039 BYDS participants who completed the ‘ever used’ drug questions at wave 7 (participants aged 21 years) was conducted to identify categories of drug use (including NPS use).
Phase 2 involved extensive qualitative analysis via narrative interviews of participants – sampled from BYDS, drug and alcohol service settings and prison – to explore trajectories of NPS use. NPS use did not emerge as a specific isolated class of drug use in phase 1 (see Chapter 3), which meant that robust conclusions could not be drawn about NPS use as distinct from other substance use through the quantitative analysis. By contrast, in phase 2 the narrative approach allowed rich data related specifically to NPS use to be obtained, allowing for highly detailed analysis of NPS use types. In addition, general risk factors related to polydrug use were identified.
In phase 3, the final quantitative phase, using the BYDS data set, the generalisability of the shared risk factor part of the model was tested, using the manual three-step approach66 to examine risk factors associated with latent class membership. In addition, adult outcomes (e.g. education, employment, health) associated with drug use were examined using weighted regressions. All analyses in this phase used multiple imputation to deal with missing data; extensive sensitivity tests were used to assess the quality of the multiple imputation models. Several integration analyses were built into the design to maximise the utility of the sequential mixed-methods design. Specifically, by integrating quantitative material with qualitative information, this allowed emerging findings to be further explored and cross-validated and later-phase methodologies to be refined.
Integration point 1
Following the completion of phase 1, the derived latent classes were used to inform a sampling frame for the qualitative analysis. This sampling frame was designed to allow the selection of participants from four groups who varied in terms of their NPS use pattern. The four sampling groups were (1) alcohol, (2) alcohol and tobacco (AT), (3) alcohol, tobacco and cannabis (ATC) and (4) polydrug. These specific groups were designed to help distinguish between factors related to NPS use and other drug use. In addition, preliminary regression analyses ran concurrent to qualitative data collection and identified key risk factors of drug use to be focused on in the phase 2 narrative interviews.
Integration point 2
The qualitative and quantitative team members selected variables from the BYDS longitudinal data sets to use in the phase 3 quantitative models assessing general risk factors and outcomes associated with drug use. Potential risk factors with the highest node frequencies were selected to be included in the quantitative models; subsequently, a process of aligning these risk factors with the BYDS variables was initiated. This was a dynamic and iterative process that continued until the team were content that optimal alignment between the risk factors and BYDS variables had been achieved.
Specific methodological details of each study phase are detailed in their respective results chapters.
Patient and public involvement
A professional liaison group (PLG) comprising key individuals from government, statutory sectors and community sectors and service users was formed. In addition, an international scientific advisory group (SAG) with membership from a range of key institutions in academia was set up. These groups were consulted at strategic points throughout the project and played an active role in the development of the project and interpretation of findings. For membership, see Acknowledgements. The research team also had regular contact with a local drug advocacy group [Belfast Experts by Experience (BEBE)]. This group provided valuable input at various stages throughout the study.
Secondary data source: Belfast Youth Development Study
This study used data from the BYDS, a longitudinal study of substance use during adolescence. The participants were young people who attended the target school year in post-primary schools in three locations across Northern Ireland. Schools were located in the Belfast conurbation, Ballymena and Downpatrick. The two townlands, Ballymena and Downpatrick, included rural catchment areas. The first data-collection wave took place in spring 2001, during the second part of the 2000–1 academic year; all pupils attending school year 8 in the schools that were taking part were invited to participate in the study. Parental consent was obtained by sending opt-out letters detailing the study for parents to return if they did not want their child to take part. In the following year (2002), data collection was repeated with the same methods for all pupils attending the successive school year 9 in participating schools. Data collection was repeated yearly until 2005 or school year 12 (participants aged 15–16 years).
The sampling strategy involved surveying all pupils in participating institutions from the targeted year group; therefore, cohort members entered and departed the study as they moved to or from participating schools. A number of schools participated in industrial action in years 4 and 5, and this led to lower completion rates in those years. Two further sweeps were carried out, one between the years 2006 and 2007; at this stage, some cohort members had left school, therefore the sampling strategy was adjusted to survey all participants for whom valid contact details had been provided. In addition, a number of schools and other educational institutions (including further education colleges and government training programmes, which were anticipated as destinations for school leavers from the original BYDS cohort) were invited to take part, and all pupils in these institutions were also surveyed. A seventh sweep of data collection was conducted between 2010 and 2011: all cohort members for whom contact details were available (n > 4000) were invited to participate through letters, e-mails, text messages or face-to-face contact. Cohort members were aged about 21 years at this stage. For more information on the BYDS, see Higgins et al. 67 and the Queen’s University Belfast (QUB) project webpage [www.qub.ac.uk/research-centres/darn/Projects (accessed 14 May 2019)].
The sample was further supplemented to include substance users recruited from carefully chosen sites (prisons, sexual health clinics and statutory and voluntary drug and alcohol services). The rationale for generating a further supplementary qualitative sample was threefold:
-
Elicit the most contemporary data available on the NPS phenomena (post PSA) and in the light of its fast-paced nature.
-
Maximise geographical coverage.
-
Seek locations with the potential for broad categories of user (e.g. prison, high-risk/complex users). This approach allowed us to capture a number of BYDS participants who were recorded in our data set as serving time in prison. We considered this expansion to cover prisons necessary as (1) our ongoing secondary data analysis showed a link between delinquency/criminality and polydrug use, (2) those in prison are a marginalised group who may not have engaged well with traditional drug and alcohol services, (3) the drivers of NPS use in prison are often unique to that environment (e.g. to avoid failing mandatory drug tests) and (4) our patient and public involvement (PPI) group discussions had indicated that the prison estate transcends geographical variation, thus maximising the opportunity to investigate the range in variations in types of NPSs. 40 Expanding our sample to include statutory and voluntary drug and alcohol services/sexual health clinics allowed us to broaden coverage to include high-risk, complex current users, who were uncommon in the BYDS sample.
The nature and extent of NPS use within the community derived from the BYDS sample, when complemented by knowledge gained from the prison estate, sexual health clinics and drug and alcohol services, provides a more robust and detailed evidence base to inform public health interventions. For this reason, the achieved sample was treated in a composite way. However, where relevant, our use of ‘setting codes’ in our analysis (see Analysis framework) was utilised to allow us to differentiate where experience was different according to site/setting.
Sample recruitment for the qualitative phase
The BYDS and supplementary sample participants were invited to take part in a narrative interview (see Belfast Youth Development Study sample and Supplementary sample for more detail on method) with two members of the research team, either on QUB premises or at a location more convenient to the participant (e.g. at a local community centre). The recruitment strategies for the BYDS, supplementary and prison samples were as follows.
Belfast Youth Development Study sample
Recruitment of BYDS participants commenced in March 2016. The sampling framework for the recruitment of BYDS participants was informed by the LCA of the BYDS data. Specifically, four groups were derived to take account of patterns of drug use as revealed by the LCA and to allow for detailed and controlled exploration of NPS use experiences. The four sampling groups were (1) alcohol; (2) alcohol, tobacco; (3) alcohol, tobacco, cannabis; and (4) polydrug. These groups were recontacted for their participation by two members of the team. Names and contact details of potential participants were provided by the study statistician in batches of 80 (20 from each of the four groups). Those responsible for recontacting were blinded to group status until each interview was completed. In previous BYDS surveys, young people were asked to provide their address, mobile phone number, house number and e-mail address. For some participants, all of this information was available; for others, partial information was available; and, for some, no information was provided from the last sweep. In the first instance, participant information sheets were posted to their home address and a week later each person was contacted by telephone. The recruitment process was designed to be as thorough as possible. Attempts were made to contact each potential participant by telephone on up to three occasions, over three different days and at three different times (i.e. morning, afternoon and evening). All details from call attempts and the result of any contact were recorded. For example, some phone numbers no longer worked, some young people were living abroad and some young people had moved house. On occasion, we were able to obtain new contact details from family members. In total, 25 participants were recruited from the BYDS.
The 25 participants recruited from the BYDS comprised 14 females and 11 males and all were aged 27–28 years at the time of interview. The majority were from the Greater Belfast area.
Supplementary sample
The process of recruiting individuals from the supplementary sample began in May 2016. With the help and guidance of local collaborators from the five Health and Social Care Trust areas, the research team compiled a database of statutory and voluntary drug and alcohol services as well as sexual health clinics across Northern Ireland. Contact with stakeholders was initiated with a phone call and followed up with an e-mail as well as postal delivery of study documentation (e.g. study leaflets/posters and information sheets). All but one service agreed to display posters to facilitate recruitment to the study. At this time, a study mobile phone was in use, and this proved beneficial in terms of recruitment for those in contact with drug and alcohol services, particularly in relation to the timing of calls but also in terms of flexibility regarding method of communication. We found that some respondents did not answer the phone to confirm interview attendance the day before the interview but did respond to a text message. The research team aimed to be as flexible as possible in relation to accommodating interviews for those in contact with drug and alcohol services while ensuring the safety of participants and the research team. The majority of interviews, particularly for those participants living in the Greater Belfast area, took place in an office at QUB; however, the research team did travel to community centres/public spaces closer to participants on request. It was necessary to monitor the number of interviews with participants recruited from specific services and also pay attention to demographics of the supplementary sample. Participants from this sample reported seeing the poster advertised in general practice surgeries, sheltered accommodation, hostels and youth drug and alcohol services and receiving information passed on by drug outreach workers. Follow-up contact was made with each service from which there was no uptake to ensure that posters were visibly displayed and confirm that lack of uptake was attributed to lack of interest as opposed to absent study information. Despite continued efforts, there was no uptake from sexual health clinics. The supplementary sample included a total of 36 participants (two participants participated in the interviews but were withdrawn and the interviews terminated once it became apparent that each was intoxicated). The majority of those recruited through services were male (n = 26). Participants’ ages ranged from 16 to 56 years, with the majority aged between 16 and 20 years.
Prison sample
In August 2016, the team was awarded additional resources to extend the study to include a sample from the three Her Majesty’s Prison (HMP) sites in Northern Ireland. This extension added value to the study and enabled us to learn more about NPS phenomena. Those in prison present as an even more marginalised group, some of whom will not have accessed/engaged well with traditional drug and alcohol services. Access to the three locations in the prison estate was granted separately by the governor in each setting. We secured the co-operation of the local drug and alcohol support service Alcohol and Drugs: Empowering People through Therapy (AD:EPT), which operates throughout all locations, to assist with study recruitment and arrangements for interviews. Recruitment strategies operated in broadly similar ways as the current study. Study recruitment posters were placed in communal areas of the prison and potential participants expressed their interest in taking part to the AD:EPT team. Recruitment posters outlined that researchers would be speaking to individuals who had ever used NPSs, thereby alleviating concerns around disclosure of present use by virtue of participation. AD:EPT staff would issue the study participant information sheet and co-ordinate arrangements with those who agreed to participate.
Total
In total, we completed 84 highly detailed life course narrative interviews across the sample sites:
-
BYDS sample (n = 25)
-
service sample (n = 34)
-
prison sample (n = 25)
-
site 1 (n = 15)
-
site 2 (n = 8)
-
site 3 (n = 2)
-
-
total (n = 84).
Life course perspective
The life course perspective, an effective methodological approach, was used to examine the trajectory of each participant’s drug taking. This affords the opportunity to understand the individual circumstances of respondents, as their trajectories can often be non-linear and highly varied. Importantly, it permits the location of drug use within the overall context of the participant’s life, that is, their experiences are about much more than the drugs they use. Risk and protective factors were used as a shared theoretical lens for the quantitative and qualitative data.
Loeber et al. 68 proposed that the presence of protective factors can predict low probability of substance use and other adverse outcomes. Longitudinal and other studies have identified a number of well-established individual, family, school and community risk factors that are associated with alcohol and drug use throughout the life course. 69–73 At an individual level, risk factors include attitudinal, biological, cognitive, developmental, personality, pharmacological and social factors. 74 For example, cognitive risk factors for substance use include a lack of knowledge about the risks of substance use as well as the viewpoint that substance use is ‘normal’ and that most people are substance users. Resilience may interact with such risk factors in a positive way by minimising their effects. 71 According to the self-medication hypothesis, effective regulation performs a key role in development of substance use. 75 Psychological characteristics related to substance use include low self-esteem, lack of assertiveness and poor self-control of behaviour. In addition, it is clear that there is a positive relationship between the importance of pharmacological risk factors and the frequency and quantity of substance use by an individual. As with the effects of traditional licit drugs use, the effects of NPS use are likely to vary owing to individuals’ neurochemical reactivity to drugs, putting some individuals at a considerably greater risk.
A number of factors at the level of the family are important in relation to attitudes towards substance use and behaviour. Genetics have a part to play in terms of the development of substance use disorders, social learning is crucial in terms of modelling behaviour and attitudes towards substance use, and parenting practices can be influential in terms of parenting style and family environment. In the same vein, family-level factors can serve in a protective capacity in preventing adolescent substance use, particularly through the use of parenting practices that centre round open communication, boundary setting, monitoring and nurturing. 73,76–78 Finally, at the school and community level, the degree to which an adolescent bonds with school and community are associated with substance use. 78–80 Students who are not engaged with school, and perform poorly academically, are more likely to use substances. Adolescents who feel isolated from or unsafe in their communities are more likely to use substances.
This was the perspective taken within the BYDS, and statistical data were utilised to model pathways in and out of substance use within the context of a wide range of variables at individual, family, school and community levels (see Higgins et al. 67), all underpinned by an integrated theoretical framework based on the risk and protective factors noted. So, too, is this conceptualisation evident in the life course perspective central to the qualitative narrative interviews conducted. In these interviews, we were able to focus on the individual’s substance use and their individual characteristics and agency not only at a single point in time but in the broader contexts of their family, school life and the community in which they lived. This life course approach allows for consideration of past episodes and future projections. In using this technique, we had capacity to identify moments of disruption, critical events or turning points that were important to individual’s drug careers. The ideas of a crossroads, bifurcation or ‘point of no return’ are constant in these biographical narratives, which are detailed further in subsequent chapters.
Narrative interviews
A narrative interview format was selected as optimal for accommodating a life course perspective to a participants’ substance use trajectory. The narrative interview is designed to encourage the participant to recount a significant event or period, in the wider context of their life history, and reconstruct the story from their own perspective. 81 The four stages of the narrative interview that we adopted were (1) substance use initiation, (2) main narration, (3) questioning phase and (4) concluding talk. 81
Interviews were completed with 84 participants and these were conducted in a dyad format (two interviewers per subject). The two-interviewer format has been utilised in circumstances where an interpreter is required or a cultural need is identified. In our case the rationale was twofold; from a pragmatic perspective the narrative method elicits significant amounts of information. Some narrative and/or non-narrative questions arose from what was said in the first interview. Given (1) the characteristics of the participants in the current study – a vulnerable population harder to reach and engage – and (2) the restrictions around access to some of the interview venues (e.g. prison), a decision was taken that in one sitting both interviewers could perform this ‘subsession’ function and gather as much detailed information as possible. This method was first trialled in our pilot and feedback was provided. The highly positive and detailed responses from participants, accompanied by endorsements of the method by our various gatekeepers, resulted in us adopting this method for all interviews. The method also successfully mitigated many of the issues that are presented by a lone-researcher format. The narrative interview was supplemented by a structured set of questions specifically relating to NPSs (see Appendix 1).
We were aware that ‘narratives are interactional accomplishments, not communicatively neutral artefacts’. 82 In recognition of this, we ensured rigour in analysing the data generated, attended to important issues of reflexivity and clearly explicated our overall method as detailed throughout. Shortly after conducting the interviews, the audio recordings and interview notes were reviewed. This information was used to document a basic memo for each participant. The accuracy of all transcripts was assessed against the audio recording and corrections were made where appropriate. Transcripts were analysed manually, as well as using NVivo 11 (QSR International, Warrington, UK) to support data organisation, coding, memo recording, notation of emerging themes, query running, etc. Structure was provided to the narratives by considering the data within the framework of risk and protective factors at individual, family, school and community levels (see Chapter 3 for further details).
Analysis framework
Our work required an integrated analytic approach, which necessitated both a deductive organising framework for code types (informed by our research questions and the quantitative findings) and a means to inductively develop codes. Previous researchers identified various code types. 83,84 Bradley et al. 85 documented an approach to data analysis that applied the principles of inductive reasoning while also employing predetermined code types to guide their data analysis and interpretation. These included (1) identifying key concept domains and essential dimensions of these concept domains, (2) relationship codes (identifying links between other concepts coded with conceptual codes), (3) participant perspective codes, which identify if the participant is positive, negative or indifferent about a particular experience or elements of an experience (e.g. a certain drug), (4) basic participant characteristic codes and (5) setting codes (basic information on specific sites).
In summary, Bradley et al. 85 posit that conceptual, relationship, perspective, participant characteristic and setting codes collectively express a structure appropriate for generation of three things: (1) taxonomy, (2) themes and (3) theory. They suggest that conceptual codes and subcodes facilitate the development of broad taxonomies. Relationship and perspective codes facilitate the development of themes and theory. Intersectional analyses with data coded for participant characteristics and setting codes can facilitate comparative analyses. We utilised a similar approach, which allowed us to generate the four-group taxonomy while also teasing out important themes and theory through our analysis.
Taxonomy development
The team utilised the five-code-type framework outlined in Analysis framework. Using the concurrent coding process across four team members, basic participant characteristic codes and setting codes (basic information on specific sites) were constructed and cross-checked across the team members. Characteristic codes included participants’ age, sex, relationship status, basic profile of drug use (ever use of traditional substances) and ever use of NPSs. Setting codes differentiated between samples (e.g. BYDS participants, those recruited from drug and alcohol services and those in prison). Setting codes also served to contextualise participants’ past and present environments and physical (e.g. growing up in care/varied familial structure), geographical (e.g. urban/rural and areas of social deprivation) and cultural (e.g. attitudes towards drug taking, normalised behaviour within peer and community setting) contexts.
After several checks and refinements, it was evident that in terms of ‘conceptual codes’ there was a range of factors driving groupings of certain respondents together. These broad groupings clearly dominated the data and affected how other subcodes and types of codes (e.g. relationship and perspective codes) operated in these groupings. After several team-wide assessments of the codes, we used them to construct a four-group taxonomy. A taxonomy is a system for classifying multifaceted, complex phenomena according to common conceptual domains and dimensions. A common language or taxonomy that distils complex information about groups of individuals into key components is paramount.
Our taxonomy identified key domains that were broad in nature. These included broad-based risk and protective factors at individual, family and community levels (guided also by quantitative analysis), detailed substance use repertoire and location of NPS in that context, patterns of use, primary motivations for substances used and critical incidents that resulted in either desistance or increased use. These conceptual codes defined key domains that characterised, for example, how the phenomenon of use in a ‘limited experimental’ way/‘contemporary regular’ way took shape, and differentiated them from one another. Conceptual subcodes helped to further define common dimensions in those key domains. One example was age as it interacted with market trends and availability; younger participants obviously reported greater exposure and access to NPSs during adolescence (with some initiating with NPSs), whereas older participants recounted early experiences with traditional drugs.
Key domains were also examined alongside multiple code types. For example, participant perspective was explored in conjunction with reported risk and protective factors from early years to present day (participant characteristics and setting codes) and relationships between exposure to risk, perception of risk and patterns of drug use/risk behaviour were noted. Participant perspective codes were also used, in terms of pleasure seeking as linked with certain taxonomy grouping (i.e. past recreationals and contemporary regulars). Furthermore, although persisters viewed severe intoxication from SCs as a positive side effect, contemporary regulars perceived these effects as highly negative.
Bradley et al. 85 noted that within each dimension there may be further subdimensions depending on the complexity of the inquiry. In our case, this meant further subdividing group 4, as detailed below. In essence, our taxonomy set out to describe a discrete set of axes or domains that characterised the multifaceted phenomena of NPS use. This was based on a conceptualisation that, over and above repertoire of drugs used, sex and so on, there was an overriding conceptual basis to why these taxonomy groupings were distinctive.
Intersectional analyses with data coded for participant characteristics and setting codes facilitated our comparative analyses as we finalised our coding framework. Biographical information on participants was reinforced by the use of our quantitative and qualitative data.
In the current study, we were keen to avoid simply pasting together data of two types; rather, we aimed to devise a system of data collection and analysis that followed a certain methodological logic, and one that met theoretical requirements, as dictated by the BYDS analysis, as outlined in Figure 1. A comparison of preliminary and emergent codes was back-coded to early transcripts to ensure coding consistency. This process was of considerable duration and the coding structure was considered finalised only at the point of theoretical saturation. 86–88 This is the point at which no new concepts emerge from reviewing of successive data from participants. Theoretical saturation took time to accomplish owing to diversity in our sample in terms of participant characteristics, perspectives and settings. Interviews ceased only when we were confident that data represented various NPSs from the perspective of the individual and reflected the multifaceted role that certain NPSs, and other substances, played in participants’ lives at different points in time.
The finalised code structure was then applied to the data delineated by taxonomy group and this approach (i.e. the five types of code) allowed us to generate themes by which to further analyse and facilitate theory development. The team met as a group to review any discrepancies (quantitative and qualitative) and resolved minor differences by negotiated consensus.
Themes evolved not only from the conceptual codes and subcodes, as in the case of our taxonomy group, but also from the relationship codes, which tagged data that linked concepts to each other. We recorded such linkages carefully within NVivo. We were able to conduct a comparative analysis of concepts coded in different taxonomy groups that were related to some extent by our basic setting codes. Through this comparison we attempted to assess whether or not certain concepts, relationships among concepts, or positive/negative perspectives were more apparent (as noted in the examples above) or were experienced/reported differently between taxonomy groups. This is evident in Chapters 3–7, where there is some exploration of setting codes, notably those in homeless accommodation or in prison settings.
Theory emphasises the nature of correlative or causal relationships and is used to explain phenomena. 89 We both deductively and inductively used theory within our study. For example, in our data, early-onset substance use was not linked to polydrug use trajectories after controlling for other influential variables. We attempted to be highly consistent in cataloguing relationships among concepts, using the constant comparison method to generate inductively conceptual codes and subcodes as well as relationship codes. Through its theoretical development, our study confirms much existing theoretical and empirical research but also suggests some new paradigms for understanding NPS as a deconstructed phenomenon.
Quantitative procedures
Latent class analysis
We conducted a LCA using data from the BYDS to identify the underlying patterns (or classes) of substance use based on student responses to questions on ‘ever use’ of the drug variables included in our data. These included alcohol, tobacco, cannabis, ecstasy, speed, lysergic acid diethylamide (LSD), cocaine, heroin, other pills, poppers and NPSs. The models were run in Mplus version 7 (Muthén & Muthén, Los Angeles, CA, USA) using maximum likelihood with 100 iterations and randomly generated start values. Model fit was assessed using Akaike information criterion (AIC), Bayesian information criterion (BIC), sample-size-adjusted Bayesian information criterion (ssaBIC), entropy, the Lo–Mendell–Rubin likelihood ratio test (LMR) and bootstrapped Lo–Mendell–Rubin likelihood ratio test (BLMR). Models with two to six classes were run and fit statistics for these models were compared. Subsequently, model estimates for both three- and four-class models were inspected, and the four-class solution was chosen as this provided more clearly distinguishable classes. A polydrug class emerged that was also characterised by NPS use (n = 214). The other three classes were ATC (n = 367), AT (n = 926) and alcohol (n = 532).
Examining risk factors and outcomes associated with drug use
The qualitative analysis, in conjunction with the professional advisory group (PAG) discussions, identified 16 risk factor themes associated with more problematic drug use. These themes were leaving home early, problems at school, leaving school early, parental substance use, family breakdown, bereavement/abuse, criminal justice system (CJS) contact, peer and partner risks, drug and alcohol service contact, sheltered accommodation, homelessness, kids, mental health problems, family mental health problems, early-onset drug and alcohol use, and personality. The themes identified from the qualitative analysis were mapped onto the BYDS variables using an alignment process. During this alignment process, the team identified BYDS variables that mapped onto the risk factor themes, checked the quality of alignment with the qualitative researchers and revised where appropriate.
Next, a series of models were run that looked at risk factors and outcomes associated with drug class. In these models, multiple imputation was used to handle missing data and extensive sensitivity testing was used to assess the extent to which our results change if the missing at random (MAR) assumption is incorrect by adjusting imputed data set estimates for the outcome variables upwards by 1–20% above that predicted by the imputation model. In the risk factors models, BYDS risk factor variables, as identified in the alignment process, were entered into LCAs at stage three of the manual three-step approach;66 in these models, polydrug was the reference class. Longitudinal risk factor variables were first modelled via growth curve analysis using robust maximum likelihood (MLR) estimation to derive initial status and slope parameters. Fit indices for all models indicated good fit. These intercept and slope parameters, instead of the original variables, were used in the analyses.
Subsequently, in the outcome models, adult outcomes associated with latent class membership were examined via weighted regression models. The outcomes examined included key domains such as mental health, drug and alcohol use, delinquency, education and employment. In these models, the risk factors that emerged as significant in the previous analyses were entered into the models as confounding variables. A full and detailed description of methods used in the quantitative models is included in Chapter 4.
Ethics and governance
Ethics approval for the quantitative component of the study (i.e. secondary analysis of BYDS data) was granted by the Research Ethics Committee, School of Social Sciences, Education and Social Work, QUB, in November 2015. Approval for the qualitative component with non-BYDS participants was granted from the Office for Research Ethics Committees Northern Ireland (ORECNI) in December 2015. Owing to using health and social care premises as participant identification centres, global governance was applied for and attained in March 2016. The extension for the study to include the three prisons in Northern Ireland as recruitment sites was approved by the NIHR in August 2016. Ethics approval and governance as well as security clearance were all in place by March 2017.
Quality control and qualitative research
The inclusion of the BYDS sample as well as a range of recruitment sites reduced selection bias inherent to recruitment from clinic populations alone. A purposive sampling strategy allowed for the inclusion of outliers and discovery of deviant cases. Data were then interrogated on the basis of corroboration while paying attention to negative cases. Secondary analysis of BYDS data, coupled with the collection and analysis of empirical data, allowed for triangulation in terms of answering the research questions.
Interview data were first coded by the same two researchers responsible for conducting the interviews, thus ensuring familiarity with the data and maximising efficiency in terms of time and cost. Both researchers read and independently coded the first five interviews using the coding framework generated from the research questions, adding new codes where necessary. Following independent coding, the two researchers collectively discussed and agreed decision-making around codes. Coding was then discussed among the wider team, as noted previously, and the coding frame was developed with continuous cross-checking of data among the researchers and the wider team, facilitating refinement throughout analysis and prior to interrogation of data during interpretation.
The involvement of the wider team in discussions around coding, refinement and development of themes ensured that the two researchers responsible for conducting the interviews and coding data were not hindered by familiarity and proximity to the data.
Detailed memo-keeping, from data collection through to interpretation, provided a visual audit trail of thought processes as the study progressed and facilitated researcher reflexivity.
Reflexivity emerges from the position that social researchers are part of the world they study90 and relates to the ways in which data might be shaped by researchers and the research process. The majority of the interviews were conducted by two female members of the research team. Both researchers were white, heterosexual, aged 30–35 years, had backgrounds in academia and had experience of working in the area of drug use and with vulnerable populations in non-clinical settings. At the beginning of each interview, researchers took time to offer refreshments and informally talk to participants in an attempt to put them at ease. The researchers introduced themselves and talked briefly about their job and research interests. Participants were given the opportunity to ask questions and raise any concerns about the interview. Post-interview feedback indicated that almost all participants reflected positively on the interview, stating that they felt comfortable and that researchers were non-judgemental about information divulged. In addition, younger participants mentioned that they expected the interview to be much more formal, but the fact that the researchers were informally dressed, friendly and relatively young put them at ease.
There were initial concerns that the presence of two researchers during each interview might tip the power balance and result in participants’ discomfort or unwillingness to open up. This was mitigated by ensuring that one researcher led the interview while the other asked questions only intermittently and on invitation from the lead interviewer so as not to disrupt the flow of the interview. Furthermore, two researchers present at each interview was beneficial to the data collection process for a number of reasons: first, in terms of rigour, having two people conduct the interview ensured exhaustive probing of the participant narrative (i.e. no relevant information was missed during the interview); second, in terms of researcher safety on campus, at community venues and in prisons; third, in terms of emotionality – biographical accounts regularly included sensitive information on adverse life experiences, for example abuse (physical, sexual, domestic), loss of family members/friends and experiences of homelessness. On occasion, participants became emotional during their narrative interview; for some this was the first time they had recounted these experiences. In a similar vein, emotionality was an issue for the researchers listening to an individual’s story. Researchers were very much in tune with how the other was dealing with the interview, and were on standby to take over questioning if necessary.
In terms of the research environment, interviews were conducted in a range of settings, including a private office on university premises, private offices in community centres (for participants that did not reside local to the university) and private rooms at each of the prison sites. The potential for the physical setting to have an impact on the data is acknowledged in each space. The university, as an institution, may have been perceived by some as oppressive, despite our intent and efforts to make participants feel as comfortable and at ease as possible. During the informal chat with participants (after the recording device was switched off), no participant expressed concerns about the interview venue. Community centres were generally chosen by participants for ease of access and so posed few issues in terms of interview dynamic and physical space. The prisons as venues for data collection might be considered to be the most problematic venues. One might imagine that prison itself is an oppressive environment wherein issues around substance use could not be discussed freely. A pilot interview was conducted in the prison prior to data collection. Following the interview, the participant was asked about his experience and his opinion on the content of the interview. Researchers received positive feedback and the participant highlighted that the prisoner development unit, where interviews were taking place, was a regular venue for individuals to work with the AD:EPT team and other teams in the prison, therefore discussing substance use in this environment was not an issue.
The strengths and limitations of the study are discussed in Chapter 8.
Chapter 3 Patterns of drug use
To map the patterns of drug use generally and as they relate to NPSs, we devised a twofold process.
First, we present a LCA and regression modelling of the BYDS data. These were used to classify different patterns of drug-taking behaviour in BYDS participants. Additional analyses using the latent class data to inform the subsequent qualitative analyses are also summarised. These additional analyses included provisional regression models to identify risk factors associated with types of drug-taking behaviour. The way in which the LCA informed the sampling frame for qualitative data collection and the integration of regression analyses to the qualitative component is also presented.
Second, using the narrative data we develop a taxonomy of use and discuss how four distinctive drug use typologies emerged. Characteristics of these groups and how they relate to the various NPSs used are presented, with a discussion of how the qualitative analysis informed the next stage of quantitative modelling. Specifically, the themes identified in the qualitative analysis were aligned with BYDS quantitative variables. These BYDS variables were then used as predictors of substance use in the quantitative models and are presented in Chapter 4.
Latent class analysis of the Belfast Youth Development Study
Determining the number of drug classes
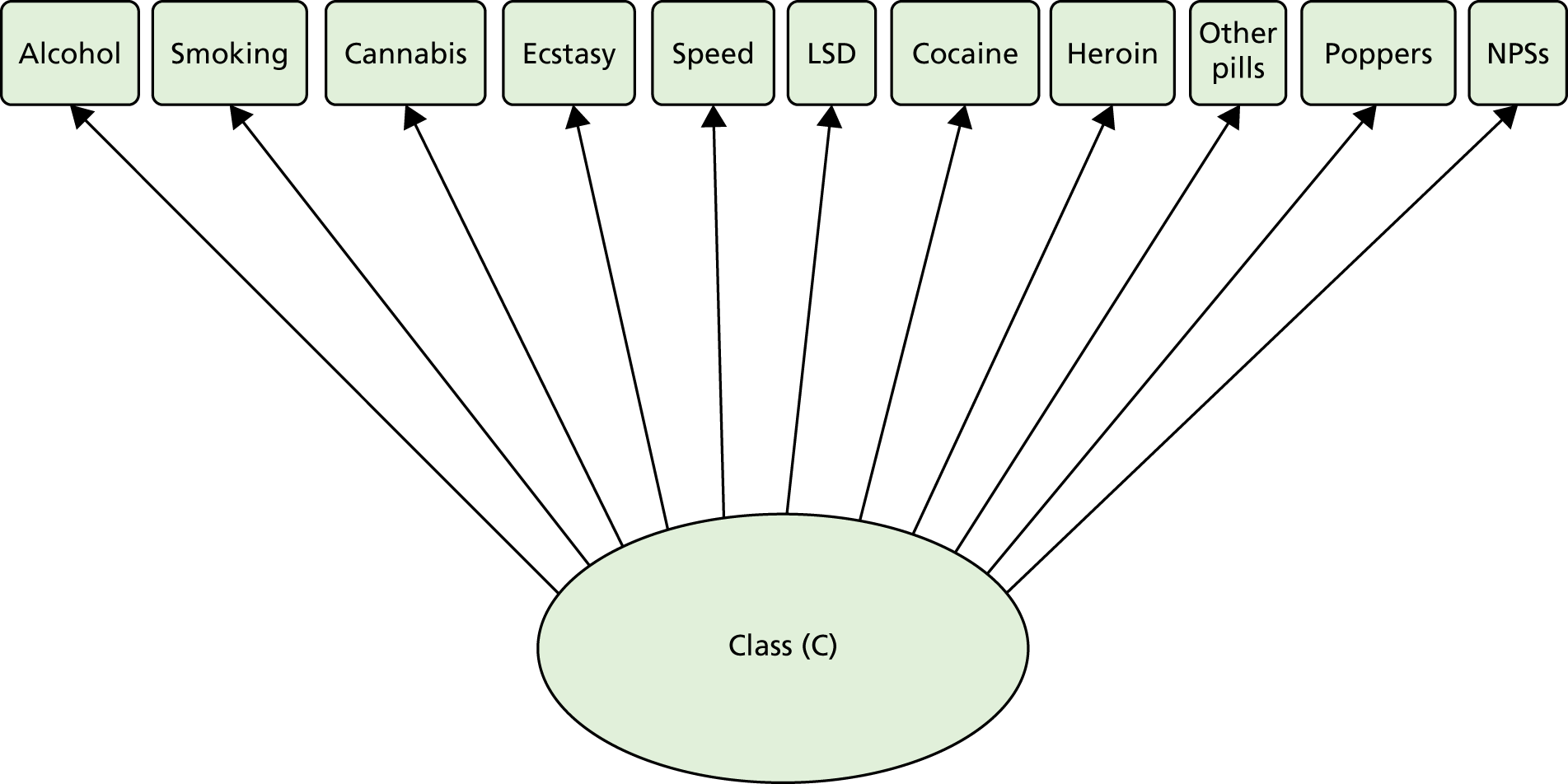
This study was a secondary analysis of data from the BYDS, a longitudinal study of substance use during adolescence (see Chapter 1 for more information). The data extraction plan was prepared and confirmed between October 2015 and November 2015 and then finalised in December 2015 through consultation with the knowledge exchange (KE) group. A draft analysis plan that addressed each of the research components was negotiated and completed by the team in January 2016 and a number of strategies were implemented over the next month to prepare the groundwork and data for the first stage of the analytical plan. We hypothesised in our application and follow-up responses that a number of homogeneous subpopulations would emerge in the data and would include a class of NPS users given the adequate numbers of NPS use in the sample. As depicted in Figure 2, the first stage of this strategy was to apply LCA to the data to identify the number and nature of classes based on ‘ever use’ of the drug variables included in our data. These included alcohol, tobacco, cannabis, ecstasy, speed, LSD, cocaine, heroin, other pills, poppers and NPSs. The actual questions used to assess drug-taking behaviour are shown in Appendix 2, Table 13.
FIGURE 2.
Representation of basic latent class structure: traditional and NPS drug use.
As is standard in LCA, models with two to six classes were estimated using MLR. 91 To help prevent solutions based on local maxima and reduce the risk of missing the model with the best fit, initially 100 random sets of starting values were specified, with 20 final-stage optimisations. The models were then compared in terms of relative fit by using information theory-based fit statistics (Table 1), namely the AIC, BIC and ssaBIC. For these three fit measures, lower values are representative of better model fit.
| Number of classes | Log-likelihood | Best H0 replicated | Number of parameters | AIC | BIC | ssaBIC | LMR (p-value) | BS-LRT (p-value) | Entropy |
|---|---|---|---|---|---|---|---|---|---|
| 1 | –7793.80 | N/A | 11 | 15,609.59 | 15,671.41 | 15,636.46 | N/A | N/A | N/A |
| 2 | –6039.21 | Yes | 23 | 12,124.41 | 12,253.68 | 12,180.60 | 3471.22 (< 0.001) | 3509.18 (< 0.001) | 0.89 |
| 3 | –5674.01 | Yes | 35 | 11,418.02 | 11,614.72 | 11,503.53 | 722.49 (< 0.001) | 730.39 (< 0.001) | 0.83 |
| 4 | –5612.82 | Yes | 47 | 11,319.64 | 11,583.79 | 11,434.47 | 121.05 (< 0.001) | 122.37 (< 0.001) | 0.77 |
| 5 | –5588.16 | Yes | 59 | 11,294.32 | 11,625.91 | 11,438.46 | 48.79 (0.010) | 49.33 (< 0.001) | 0.74 |
| 6 | –5576.52 | Yes | 71 | 11,295.03 | 11,694.07 | 11,468.49 | 23.04 (0.169) | 23.29 (0.143) | 0.76 |
The LMR and bootstrap likelihood ratio test were also used to compare models with increasing numbers of latent classes. Model estimates for both three- and four-class models were examined and the four-class solution was subsequently selected based on the interpretability of the results. After extensive exploratory modelling work we were able to determine that a four-class model was the best-fitting model according to the fit indices and information criteria; this provided us with unique and interpretable clusters of individuals with similar profiles within the latent SGs. Average latent class probabilities for most likely latent class membership are shown in Appendix 3, Table 14. Figure 3 shows that a four-class solution provides good cluster delineation (see Appendix 3, Table 15).
FIGURE 3.
Probability of substance use in each of the four latent classes identified in the BYDS data.
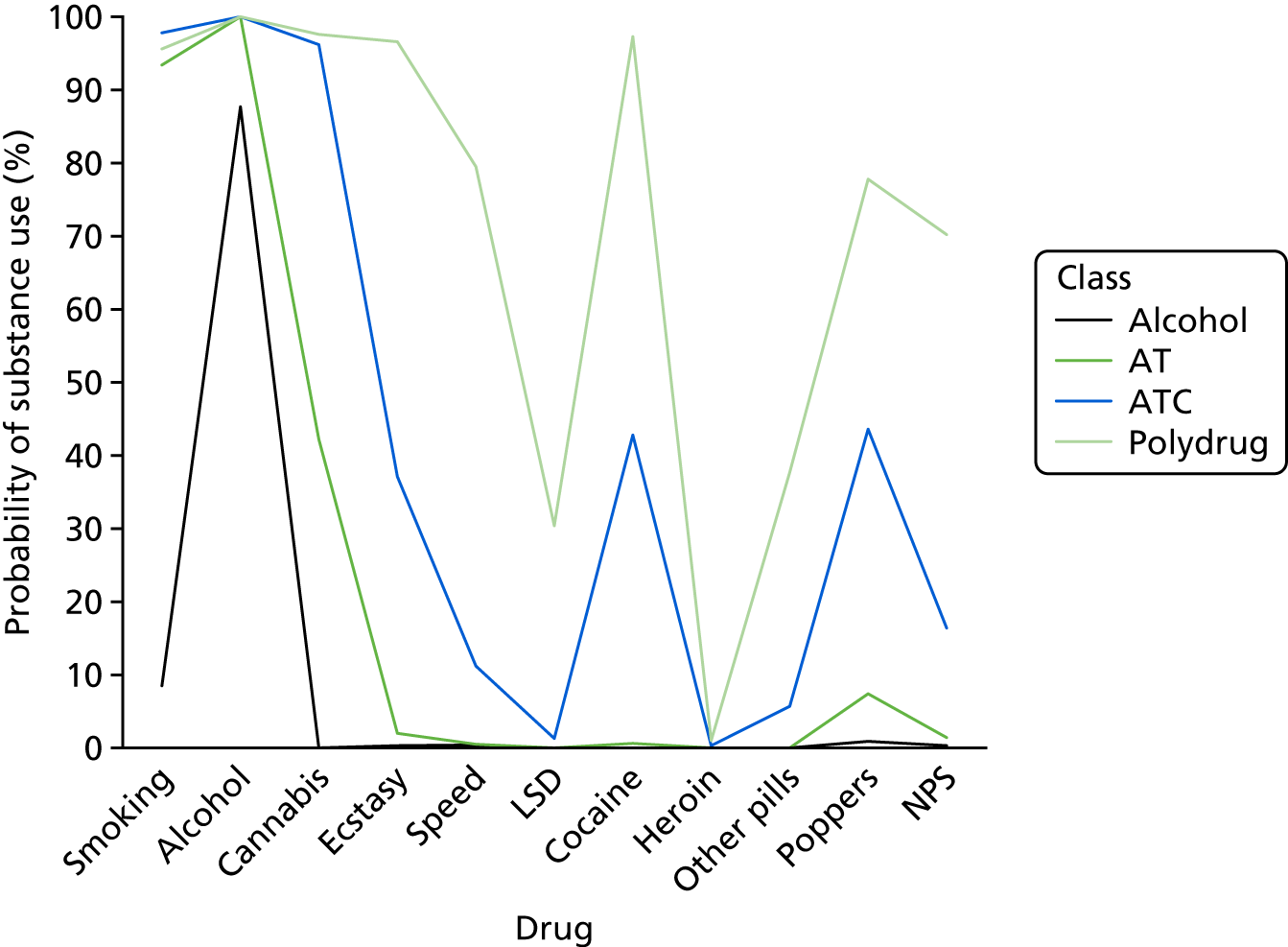
Therefore, a four-class solution was adopted in the present research to account for the different typologies of drug taking. The four classes of drug use identified were as follows:
-
Alcohol – high probability of alcohol use; a p-value of < 0.5 for all other substance use types.
-
AT – high probability of AT use; a p-value of < 0.5 for all other substance use types.
-
ATC – high probability of ATC use; average probability (p < 0.5) for all other substance use types. The probability of poppers (p = 0.44) and cocaine (p = 0.43) use, although a p-value of < 0.50, is noteworthy for this group.
-
Polydrug – high probability of alcohol, tobacco, cannabis, ecstasy, speed, cocaine, poppers and NPS use. Probability of a p-value of < 0.5 for all other substance types.
The percentage of participants reporting ever using drugs is shown by latent class in Table 2. The latent class probabilities for each substance type are shown by latent class in Appendix 3, Table 15. The sample sizes of the four latent classes were as follows: class 1 (alcohol; n = 532), class 2 (AT; n = 926), class 3 (ATC; n = 367) and class 4 (polydrug; n = 214).
| Class | Percentage of participants | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tobacco | Alcohol | Cannabis | Ecstasy | Speed | LSD | Cocaine | Heroin | Other pills | Poppers | NPS | |
| 1 (alcohol) | 0.9 | 87.5 | 0.0 | 0.4 | 0.4 | 0.0 | 0.8 | 0.0 | 0.0 | 1.4 | 0.4 |
| 2 (AT) | 97.1 | 100.0 | 42.0 | 1.4 | 0.3 | 0.0 | 0.4 | 0.0 | 0.0 | 3.4 | 1.0 |
| 3 (ATC) | 98.6 | 100.0 | 97.8 | 37.7 | 9.7 | 1.4 | 43.5 | 0.3 | 5.6 | 53.2 | 16.9 |
| 4 (polydrug) | 95.3 | 100.0 | 97.6 | 97.6 | 81.3 | 29.4 | 97.6 | 1.0 | 37.5 | 78.4 | 70.7 |
Predictors of drug use patterns (provisional analysis)
To inform the design of the qualitative analysis, predictors of latent class membership were examined using multinomial logistic regression. A backwards stepwise regression approach with Holm–Bonferroni corrections applied to adjust for multiple comparisons was used. In all models, sex and free school meal (FSM) status were controlled for. Separate models were fit to examine the relationship between latent class membership and family/relationships, school, leisure, friends’ substance use, drug abuse, delinquent/criminal acts and psychosis variables. All predictors in the models were binary coded (0 = no; 1 = yes). Polydrug users were the reference group in this analysis. This analysis is considered provisional and was designed solely to inform the content and structure of the interview schedules. The provisional results are presented in full in Report Supplementary Material 2, Tables 39–50. More refined models, which were built on the basis of the qualitative findings, are discussed in Chapter 4.
Informing the qualitative analysis
The aim of the qualitative component was to explore in detail the life experiences of drug users and, in particular, how NPS use related to their overall drug portfolio. If a unique NPS-only class had emerged from the LCA, the aim could have been achieved by sampling from this class. However, because this class did not emerge, an alternative sampling strategy was devised to examine NPS use qualitatively with adequate control for polydrug use. Sampling from only polydrug users would have made it difficult to distinguish between factors related to NPS use and those related to polydrug use. As shown in Table 2 and Appendix 3, Table 15, not all members of the polydrug group were NPS users. Therefore, in the qualitative analysis sampling, polydrug users were split into those who reported NPS use and those who did not. A small proportion of the class 3 (ATC) users reported using NPSs (see Table 2 and Appendix 3, Table 15). We wanted to explore this rare group of users further to shed light on why users who are more selective about substance use choose to try NPSs. Importantly, although the majority of ATC users did not use NPSs, the vast majority did report using cannabis. To distinguish between life experiences related to cannabis and to NPSs, individuals who reported using cannabis but not NPSs were also sampled from to serve as a comparator group.
In summary, to distinguish between factors related to NPS use and other drug use, sampling was based on four groups (Figure 4). Polydrug users were split into those who used NPSs and those who did not (polydrug and NPS users; polydrug users, no NPS). The ATC group (ATC and NPS users) were also sampled from, and a control group was formed of cannabis users who did not use NPSs (ATC no NPS). This allowed a distinction to be made in the analysis between NPS-specific experiences and those associated with cannabis. The specific criteria used to form the groups were as follows:
-
polydrug users and NPS – responded ‘yes’ to using mephedrone or legal highs; responded ‘yes’ to using all of the following: cigarettes, alcohol, cannabis, ecstasy, poppers and cocaine
-
polydrug users, no NPS – responded ‘yes’ to using cigarettes, alcohol, cannabis, ecstasy, poppers and cocaine
-
ATC and NPS – used mephedrone or legal highs, used cannabis; did not meet criteria for polydrug and NPSs
-
ATC user, no NPS – did not use mephedrone or legal highs, used cannabis; did not meet criteria for polydrug and no NPSs.
FIGURE 4.
Sampling strategy for the qualitative analysis.

Qualitative interviews with BYDS participants commenced using the sampling framework derived from the LCAs. As regression analyses ran concurrent to data collection, emerging significant variables in the multinomial logistic regressions were passed to the researchers conducting the interviews for additional probing, in case the themes emerged in the participant’s narrative.
Belfast Youth Development Study participants were selected and invited for interview based on the LCA and sampling framework presented in Figure 4. The qualitative sample was supplemented with individuals recruited from (1) drug and alcohol services and (2) the prison estates (see Chapter 2 for further information). Demographic information on the recruitment groups is shown in Table 3.
| Variable | Recruitment group | ||
|---|---|---|---|
| BYDS (N = 25) | Services (N = 34) | Prison (N = 25) | |
| Sex (n) | |||
| Male | 11 | 26 | 20 |
| Female | 14 | 8 | 5 |
| Age (years) | |||
| Range | 27–28 | 16–56 | 18–53 |
| Mean | 27 | 26 | 28 |
Based on the narrative data, and utilising our specific coding framework, we constructed a taxonomy of users (Table 4; see Chapter 2 for detail on construction). This allowed us to draw together the multiple lines of investigation. The rationale was that such data-driven classification would help us to identify subsets of participants.
| Group | Name |
|---|---|
| 1 | Limited experimentals |
| 2 | Past recreationals |
| 3 | Contemporary regulars |
| 4 | Dependents |
| SG1 | Generation NPS |
| SG2 | Availers |
| SG3 | Persisters |
| SG4 | Non-NPS users |
Following the development of the taxonomy groups, the data were interrogated using text searches and matrix code queries. This process of interrogation was to explore shared/differing characteristics in and across group taxonomies.
Group 4 (dependents) was by far the largest group and had variability, which from both a theoretical and empirical perspective necessitated subdivision into SGs.
The narratives provided dynamic data on the life cycle of participants’ use. For those who abstained from use or had never reported NPS use, data on motivations to resist/desist were also included. Table 5 provides detail on interview participants by group.
| Group | n | Sex, male/female | Source, BYDS/service/prison | Age (years) | |
|---|---|---|---|---|---|
| Range | Mean | ||||
| 1 | 8 | 3/5 | 5/3/0 | 19–27 | 24 |
| 2 | 14 | 5/9 | 11/3/0 | 17–28 | 26 |
| 3 | 10 | 5/5 | 7/2/1 | 16–28 | 25 |
| 4 | 52 | 44/8 | 2/26/24 | 17–56 | 28 |
| SG1 | 14 | 11/3 | 0/9/5 | 17–24 | 19 |
| SG2 | 15 | 14/1 | 2/6/7 | 19–50 | 32 |
| SG3 | 18 | 14/4 | 0/9/9 | 18–53 | 28 |
| SG4 | 5 | 5/0 | 0/2/3 | 34–56 | 42 |
As noted in Chapter 2, risk and protective factors were used as a shared theoretical lens between the quantitative and narrative data. To recap, longitudinal and other studies have identified a number of well-established individual, family, school and community risk factors that are associated with alcohol and drug use throughout the life course (see Chapter 2). 69–73 The overall larger BYDS research programme quantitatively examined these interactions in depth for a large number of respondents. 73 We do not lay claim to offering the same here. Rather, from a qualitative perspective the narratives articulate what these risks and protective factors looked like through the lived experiences of this group of participants. These are presented alongside information on the drug repertoires of the taxonomy groups (see Appendix 4 for detailed information).
Group 1: limited experimentals
Drug repertoire
The limited experimentals were participants who feature on the least severe end of the drug-using continuum. Members reported substance use that was generally limited to alcohol and cannabis; substances generally included alcohol and cannabis with one instance of experimenting with cocaine (n = 1) and poppers (n = 1). Although they had limited experience with substances, limited experimentals are nevertheless an important group to include as a comparison. Interestingly, none of those who fell into the limited experimentals group (n = 8) reported using any NPSs. All initiated with alcohol, with an average age at initiation of 15.6 years (range 13–18 years).
Moving beyond substance use profile, other shared characteristics for this group related to the risk and protective factors as described by participants; these emerged in the narrative interviews naturally, without prompting. Risk factors to experimental or opportunistic use of substances were evident in narrative accounts. Peer group pressure was important for both alcohol and drug use among this group. Noted, too, was the impact of changes in friendship groups, which resulted in exposure to different substance-using peers/acquaintances. Exposure to older drug-using peers was also noted. Half of the group mentioned some pressure to try substances at various times and set this alongside a sense of normalisation in the use of alcohol or cannabis among their peers. During adolescence, friends are crucial to a young person’s sense of belonging and drug-using behaviour. 92,93 Commensurate with transitional time points in the life course, key events such as going on a holiday with friends in late adolescence marked a period of excessive alcohol use and experimentation with other substances (n = 2). In addition, attending university and nights out with new peers while living away from home contributed to increased substance use (n = 2).
Protective factors
Given that this group had limited substance use experience, limited experimentals appear not to have been significantly affected by risk factors such as negative peer influences and traumatic critical incidents, possibly owing to some of the protective factors they highlighted. For example, when younger, limited experimentals were characterised by having family environments where parental monitoring and control were evident. Parental monitoring can limit substance use by allowing parents to intervene in situations where their child may be at risk. 94,95 The narrative interviews also revealed that limited experimentals expressed fear of getting caught using substances by their parents. One can speculate that the protective factors in place for traditional illicit drugs were also present for NPSs. The narrative interviews consistently indicated a strong influence by peers in both positive and negative ways. Indeed, the influence of peers as they relate to drug taking has been extensively documented in the literature. 96,97 From our narrative interviews, two-thirds of limited experimentals made note of group affiliation in a pro-social peer setting as protective factor, mitigating excessive substance use. Around half of participants in this group reflected that their peers did not use alcohol and/or drugs and that they generally did not have the opportunity to use substances extensively in their social environment. In essence, such positive peer influence was protective. 98–100
In a general sense, a normative developmental trajectory was evident and most participants in this group successfully transitioned to emerging adulthood101 and aged out of any significant substance use without intervention. This finding is consistent with the evidence from longitudinal studies that show that the vast majority of those who engage in delinquent behaviours as adolescents age out of these behaviours. 73,102 Positive role transitions,103,104 defined as changes in relationships, education, work and outlook on life, were evident in this group. Over half were in a romantic partnership and tended to report having a partner who did not use alcohol or drugs and disapproved of substance use. There was a clear sense of the influence of financial independence as respondents matured. They noted a desire to invest in a car or home and to avoid spending money on alcohol or drugs. Another influencing factor in this group appeared to stem from witnessing adverse consequences of substance use, such as seeing people in the community who have used substances, losing friends to substance use or having a family member who has a substance use problem.
Group 2: past recreationals
Drug repertoire
Past recreationals had wider drug repertoires than limited experimentals. Nevertheless, the past recreationals group featured participants whose substance use was still largely opportunistic and reasonably limited; almost all had aged out of these behaviours at the time of interview. Less than half reported NPS use and this was largely confined to use of mephedrone pre legislative ban. Use of NPSs by these respondents tended to be opportunistic in the same way that their use of traditional substances had been. The availability of mephedrone among those who reported use was a significant motive for use: none of those in this group actively sought out the substance; it was made available by a peer, thus resulting in experimentation. None reported mephedrone use following the ban in 2010 and only one member of the group reported using any stimulant-type NPSs that emerged following mephedrone [one participant had a single experience with ‘China White’ (local term used for a specific synthetic stimulant)]. Experiences with SCs were generally isolated incidents, with the exception of one participant who reported numerous experiences with ‘trippy’ (local term used for SCs) both in England and Northern Ireland. Pre-ban use among this group points to factors such as legality and/or availability of NPSs as influential. All past recreationals tended to initiate with alcohol earlier than the participants in the limited experimentals group, with the average age at initiation being 14.1 (range 11–16) years. Going to university was a risk factor for almost one-third of this group (4/14 participants), particularly for those who attended university outside Northern Ireland. This opportunity for leeway and lack of parental monitoring that university attendance offered was seen as key in terms of increased alcohol use and experimentation with drugs. When members of this group attended university the protective influence of parents was largely removed.
Risk factors
Parents were discussed as risk factors for four of the participants in this group (in terms of their substance use and lack of supervision); for the majority, parents were more of a protective influence. Being under the influence of alcohol was a risk factor to drug use for almost half of this group. Some studies have suggested that delaying and limiting alcohol use is important in preventing drug use in young people. 105 Almost one-third of this group (4/14 participants) made reference to peer pressure and engaging in alcohol or drug use to fit in. Romantic partners were a risk factor for some of this group in that having a partner who used drugs during teenage years resulted in participants’ use of drugs also. The role of partners in substance use has been well documented; according to the social development model, if there is a strong emotional bond with a partner this can have a negative or positive impact depending on the substance use habits of the partner. 106
Protective factors
Despite the wider drug repertoire, this group described many of the risk and protective processes described by the limited experimentals group. For example, half of the group (7/14 participants) described fear of disclosure to parents or ‘strict’ parenting as something that served as a protective factor when it came to drug use. In contrast with the parenting described by the limited experimentals group, the parenting described in the past recreationals group tended to protect by limiting rather than preventing substance use. Other important established protective factors were apparent in the form of involvement in sports while growing up. The positive effects of engagement in sports and other pro-social activity has been very well evidenced. 69 Interestingly, Iceland, which has experienced declines in substance use by children, has based its approach to substance use prevention in children on an evidence-based approach that specifically encourages uptake of sports and other activities. Having peers that had also aged out of drug use and/or having a romantic partner that had either aged out or was a non-user was highlighted as a protective influence and discussed by almost half of the sample (6/14 participants). Previous research has shown that behaviours such as substance use generally peak in adolescence,73,107 declining with biological and social maturity. 70 Being surrounded by fewer substance-using peers presents fewer opportunities for use, less peer pressure to use and greater stigma associated with use. In addition, Moffitt70 argues that as adolescents mature the consequences of substance use are no longer perceived as rewards but instead as punishments; typically at this stage important aspects of life such as family, work and community become a key deterrent to substance use. This was described without prompting in the narrative interviews of the past recreationals group; normal markers of successful assumption of adult roles were evident and served a protective role in late adolescence/early adulthood. Six participants made note of employment, financial responsibilities and changing priorities as indicators that marked a transition point in ageing out of the drug use process. Of those respondents in this group who had children (n = 4), all described their children as having a protective influence, and some of those who did not have children speculated that marriage and children would mark a transition point, including in other behaviour such as drinking and ‘going out’. Listening to stories from friends or parents or observing fewer health patterns of alcohol or substance use discouraged more chaotic patterns of consumption and therefore acted as a protective influence for almost one-third of this group (4/14 participants).
Group 3: contemporary regulars
Drug repertoire
The third group in our taxonomy, contemporary regulars, consisted of 10 participants. The average age of substance use initiation in this group was lower than in groups 1 (limited experimentals) and 2 (past recreationals): 13.5 (range 9–15) years. Alcohol was the primary substance with which this group initiated; however, cannabis, SCs and solvents were also reported as substances initially used. Half of the participants in the contemporary regulars group were single and half were in a relationship. Participants in this group generally had much wider repertoires than those in groups 1 and 2 (see Appendix 4). All the contemporary regulars reported alcohol and cannabis use and, in contrast to groups 1 and 2, all reported use of a novel psychoactive substance. All but two reported using ecstasy and all but one reported cocaine use. More experimental drug use is also observed among this group, with reports of ketamine and GHB use, for example, as well as NPSs beyond mephedrone [e.g. China White and MDMI (definition unknown; discussed as a novel psychoactive substance in narrative accounts]. This willingness to experiment with a wider range of substances is not observed in groups 1 or 2. Participants in the contemporary regulars group generally had much more extensive drug repertoires and lengthier drug careers than those in group 2. Importantly for some participants in this group, the primary driving force behind the transition from traditional illicit drugs to NPSs was market factors. We hypothesise that this group could be considered to be non-marginalised availers (SG2) because their transition to and from NPSs was a functional one. It is important to note that almost half of participants in this group highlighted their concern that the ‘moreish’ properties of mephedrone had created in them the potential to escalate from ‘recreational’ to ‘problem’ use.
Risk factors
Whereas being under the influence of alcohol was highlighted as a significant risk factor for group 2, the past recreationals group’s drug use was not accidental, opportunistic or a result of a lapse of judgement while under the influence of alcohol. As with groups 1 and 2, the narrative accounts of over half of this group included information on how their parents attempted to act in a protective capacity during their teenage years. However, rather than serving to lessen drug taking, it resulted in a shift towards concealing their drug use. This is interesting as the parental control was reported as having a protective effect by groups 1 and 2 and may be reflective of different attitudes and beliefs held by the groups. For example, Tilton-Weaver et al. 108 have theorised that negative peer influences could be reduced by parental monitoring, provided parents are viewed as legitimate authorities over friendships. 109 Alternatively, if youths feel controlled and intruded on this could lead to an escalation of delinquent behaviours such as substance use or increased orientation towards substance-using peers. 110,111
Protective factors
Reference to protective factors for the past recreationals group was centred around harm reduction as opposed to either preventing use (i.e. group 1) or limiting use (i.e. group 2). Decisions to use drugs appeared premeditated and informed and the protective influence of peers, in contrast to groups 1 and 2, was centred around harm reduction techniques for safer drug use – all contemporary regulars used drugs with peers and there are fewer references to non-using peers than in the other groups. Half of this group discussed the protective influence of peers in terms of offering advice/support to promote safer drug use. Furthermore, some participants in this group engaged in risk justification/neutralisation by either measuring the harms of drugs against the harms of alcohol or placing their more chaotic drug taking as a past feature of their drug career.
Although not always preventing drug taking, the protective influence of romantic partners who did not use drugs was still referred to by half of the past recreationals group. This influence resulted in some participants in this group abstaining and reporting signs of ageing out at the time of interview, whereas for others the influence of non-using romantic partners resulted in changes around the way participants used drugs, such as more infrequently, to a lesser extent or only on occasions when it could be concealed from non-using partners. One-third of the past recreationals group also discussed the protective influence of employment; this they presented as a measure of the functionality of their behaviour, that is, their drug use never resulted in them missing days from work.
Group 4: dependents
The dependents group, consisting of 52 participants, formed the largest group in our taxonomy. Dependents included individuals who self-reported dependency on one or more substance at some stage of their drug career. It is important to note that this was based on self-report of dependency and not verified independently by treatment data. However, in all narratives features of dependent use, for example in terms of tolerance and withdrawal, were noted.
The literature of drug dependency clearly evidences a sex disparity112 as well as reasons why females are less likely to report dependence. 113 We posit that female users were likely under-represented in this grouping and we are cognisant of the accumulating epidemiological clinical and qualitative research that suggests that what determines whether or not drug abuse and dependence develops or progresses further is often sex specific or sex sensitive. 112
Generally, the dependents group is characterised by having participants with more chaotic lives. Almost all were not in a relationship at the time of interview. The average age for substance use initiation was the earliest of the four groups, at 12.9 years (range 8–16 years). The majority initiated with alcohol (n = 36) and six participants initiated with cannabis. For a minority of the group it was not clear from their narratives which substance was used first; six participants reported synchronous onset with multiple substances, for example alcohol and cannabis, one participant reported using alcohol and mephedrone at the same age, one reported using alcohol and SCs at the same age, one reported using alcohol and ecstasy at the same age and one reported using cannabis and prescription medication at the same age.
Although all participants in the dependents group reported issues with dependency at some stage or another, patterns and levels of use within this group varied greatly. Some of the more established users reported long histories of drug use with multiple dependencies at various stages, whereas other, younger participants in this group reported dependency on a single substance [e.g. SCs, ‘synthetic’ acid/2,5-dimethoxy-4-iodophenethylamine (2C-I)]. Although all participants reported dependency, they were at very different points in their drug use career. Twenty-nine participants reported dependency on a single substance and 18 participants reported problems with multiple substances. Four participants from the dependents group reported never having used NPSs.
Subgroups
Given the significant variation in the dependents group in terms of participants’ dependency and relationship with NPSs, the group was subcategorised. SG1 comprised those for whom NPSs were their primary and only dependency. SG2 comprised those with dependency on a traditional illicit substance and for whom NPS served only to temporarily displace/substitute the traditional illicit substance (i.e. no dependency reported on NPSs). SG3 comprised individuals with multiple reported dependencies including dependency on NPSs.
Subgroup 1: generation new psychoactive substances
Drug repertoire
For SG1 (n = 14) the average age at initiation with any substance was 13.4 (range 11–16) years, with seven participants reporting alcohol as their first drug and two reporting cannabis as their first drug. For the other five participants it was not clear from their narrative which substance was used first; three reported using alcohol and cannabis at the same age, one reported using alcohol and mephedrone at the same age and one reported using alcohol and SCs at the same age.
Participants in group 4 were categorised into SG1 if their primary and only dependency was NPSs. The majority of the group (12/14 participants) had used SCs, with 11 participants reporting dependency on SCs. Five participants reported the use of mephedrone, with two reporting dependency. Three participants reported the use of other NPS powders, three reported the use of synthetic ecstasy (referred to as ‘herbal pills’) and one reported the use of NPS hallucinogens (e.g. 2C-I, 2C). The participant who mentioned using 2C, 2C-I reported dependency. For details of other substances, see Appendix 4.
Risk factors
When examining common characteristics of this group, peers stood out as the most common influential factor in terms of substance use, including NPS use. All participants reported that their friends used NPSs at the time of initiation. Watching friends and/or family using prior to first experience with NPSs served as a risk factor in this group. Community influences, including comments such as ‘everybody’s taking it’, and infiltration of NPSs into areas where young people lived and at sites where young people congregated were significant risk factors. Evidently the point in time at which NPSs emerged on the scene was significant given the age of participants in this group and the desire to experiment with substances. Notably, a proportion of participants in this group reported use, specifically of SCs, moving from social use with peers to use alone, which was an indicator of quick acceleration from experimental/social use to a more dependent pattern. The lack of knowledge about NPSs and naivety around what substances they were taking was a risk factor for this group, reflected in interchangeable terminology (e.g. ‘herbal’, legal highs, trippy) and elements of confusion when describing what they were using. Some reported not realising the signs of growing dependence on NPSs until they experienced withdrawal (e.g. sweating, vomiting, not being able to sleep, ‘craving the high’).
Early negative experiences with the education system was a predominant, common characteristic of this group. Seven participants in this SG were expelled from school/attended an alternative education programme. The remainder reported disengagement with education, with two participants leaving higher education as a result of their NPS use. Seven participants reported using substances in their school environment. Just as lack of school attachment is associated with substance use,114 so too are the reactions of the schools and employers reported here by the generation NPS group. Excluded from school, these children were removed from a relatively pro-social environment, leaving them with more free time in which to engage in substance use behaviour. 115
Going to live with other family members (commonly a grandparent) or leaving home as a result of other family issues, for example parental alcohol use, parental mental health problems and conflict between teen and parent, were also common. Parental substance use can lead to child substance use: the child observes and then imitates their parent’s behaviour. 116 In addition, in households where parents are problem users, there tends to be less routine, more conflict and fewer feelings of warmth and caring,117 further increasing the risk of substance use problems for their children. Indeed, lack of a structured environment was evident in the narratives: some participants reflected on hiding use from parents, yet it was clear that a number of parents were aware of substance use behaviour and did not seem to intervene effectively, either ignoring the behaviour or offering advice but with no sign of discipline or monitoring/control of behaviour. Parents splitting and conflict between parents were also factors for a significant number in this group. Parental separation has been found to be a key risk factor for early substance use, even after controlling for environmental and genetic factors. 118 A small proportion reported using NPSs with a partner and two out of the three females in the sample highlighted male partners as facilitators of their use in terms of initiating substance use. Eight of the sample reported that NPSs functioned for them as a means to achieve escapism, help with anxiety/depression and a distortion of reality.
Protective factors
In contrast to groups 1 (limited experimentals), 2 (past recreationals) and 3 (contemporary regulars), discussion of any kind of protective influence was rare in the narratives of this generation NPS group. Being aware of deaths in the community, effects of their use on family members and peers stopping use were all factors highlighted by those who sought help with their dependency or ceased use by their own accord.
Subgroup 2: availers
Drug repertoire
Participants reported dependency on one or more traditional illicit substance and no dependency on NPSs. NPSs were ‘availed’ of by this group when their drug of choice was not obtainable; thus, NPSs only temporarily displaced traditional drugs, much like those in the contemporary regulars group. The average age at initiation in this SG was 12.6 (range 8–15) years. In total, 12 participants initiated with alcohol, two with cannabis and one with alcohol and cannabis at the same age. In terms of drug-taking profile, participants in SG2 resembled those in group 3 in terms of willingness to experiment with a range of drugs; however, SG2 differed in that participants reported use of heroin, which group 3 participants did not, and were more likely to report use of prescription medication.
Risk factors
The majority of participants in SG2 discussed mental health issues in the context of their drug narratives. Issues associated with mental health included depression, anxiety, panic disorder and schizophrenia. One-third of the group reported self-harm and suicide attempts. Of course, there is a much more complex interplay of factors regarding dual diagnosis, particularly in relation to the extent to which mental health problems contribute to substance use and the degree to which substance use exacerbates mental health problems. 119 All participants in this group used substances with peers and, for many, peers increased risk in terms of initial access to drugs. Half of the group reported excessive use of alcohol during their drug careers. Most of this group reported limited engagement with education (n = 11); this ranged from lack of interest in school to expulsion and removal from mainstream education (n = 5). The majority of this group reported contact with the CJS, with contact largely related to drug-related offences, including possession, supply, crime to fund use and crime committed while under the influence. This crime and substance use nexus is believed to further escalate both behaviours, leading to more persistent offending and greater substance dependence. 120
Protective factors
This group was interesting in that almost half of the participants (n = 7) described the influence of parents as largely protective and many of them questioned their motivations for drug use and the trajectory of dependency that followed, although, given the multitude of risk factors identified in their narratives, it is perhaps unsurprising that this protective influence was not enough on its own to limit or prevent their substance use dependency. Some attributed decision-making around drug use to factors associated with personality, for example impulsivity and desire to take risks. However, most of those who reported stable upbringings also acknowledged that they self-medicated to cope with their mental health issues and/or reported experiencing the death of a close family member or friend during teenage years. Almost one-third of SG2 participants discussed employment in a protective capacity and, for those outside prison, they seemed, like contemporary regular group participants, to measure functionality in terms of not missing days at work as a result of substance use.
Subgroup 3: persisters
Drug repertoire
The persisters SG includes the most chronic substance users (n = 18). All participants in SG3 reported multiple dependencies, including dependency on NPSs. The average age at initiation in this group was 11.7 (range 10–16) years. A total of 12 initiated with alcohol, three with cannabis, two with alcohol and cannabis at the same age, one with alcohol and ecstasy at the same age and one with cannabis and prescription medicines at the same age.
Participants in this SG, as with those in SG1, initially believed that SCs offered a safer alternative to the traditional illicit drugs that they were using in a harmful way. Comorbidities and vulnerabilities among this group made the potent effects of SCs particularly appealing and so resulted in sustained use. This SG was particularly well placed to track the evolution of SCs over time. Ironically, legislation designed to reduce the harm of SCs was counterproductive and resulted in the development of more potent and particularly risky third-generation legal highs.
Risk factors
Almost all documented risk factors were at play for this group and included negative experiences at school, adverse life/childhood experiences, mental illness, contact with the CJS, complex family issues, social deprivation and homelessness. In terms of education, 17 participants in this group reported significant disengagement with education, including being expelled (n = 12). One anomaly was a male participant from our service-using sample who attended school (and is now at university) but reported problems throughout school as the school environment exacerbated his underlying anxiety problem leading to more excessive substance use at that age.
A large proportion of participants in this SG reported an unstable home environment while growing up. Ten participants reported that one or both parents used substances themselves and in three cases a parent was instrumental in facilitating substance use (selling, providing substances). There was clear evidence of a lack of parental monitoring owing to parental substance use and issues such as strained relationships in the home or other adverse experiences relating to family life. More than half of the participants in this SG disclosed adverse life/child experiences (e.g. around one-quarter mentioned physical or sexual abuse). Unfortunately, those who have experienced such abuse are more likely to suffer negative consequences from using drugs. 121 Five reported the death of a close family member and two reported the death of close friends.
Generally, having children was not a protective factor for this SG. Four participants had lost contact with their children/had children removed by social services, one of whom was regaining contact with his sons who are now adults. For the other three participants in this SG, substance use ceased/decreased during pregnancy/early years, but participants later resumed previous patterns of use.
For almost half of the participants in this SG, mental illness (anxiety, depression) was reported. Evidence of self-medication, in most cases through the use of SCs, was particularly highlighted by participants who had had adverse experiences or periods of homelessness.
As one might expect, all participants in this SG had contact with services at some stage. Five participants had contact with social services; for two this spanned more than two generations. Two participants reported being in care as a child. Consistent with the features of SG3, people who were in care as children tend to use drugs more regularly and use higher-class drugs than those who were not in care as children, making them a key group to monitor for substance use problems. 122,123
Seven participants in this group had experienced homelessness at some stage and three were residing in hostels at the time of interview. Homelessness did not emerge as a risk factor for any of the other groups or SGs and it is likely that the severity of SG3 participants’ drug dependency led to them losing their home and made it difficult to rehouse them; this may also have escalated their drug dependency, taking drugs in an effort to cope. 124,125
Contact with the CJS was common in this SG, with 15 participants reporting contact dating back to their early teens. Two of our female participants reported prostitution. There was evidence of contact with drug and alcohol services and multiple substance dependencies prior to NPS use for the majority of this SG.
Protective factors
The narratives of SG3 participants included references to risk factors; any kind of protective influence was lacking. For five participants in this SG, children were initially described as protective influences. These respondents reported abstaining from drugs when their children were born; however, the breakdown of relationships with significant others, or the removal of children from care, precipitated relapse. Nine participants described rebuffed efforts of family and friends to intervene and offer help and support. Several respondents reported creative, if unsuccessful, efforts by family and friends to assist in drawing attention to the effects of NPSs when participants were under the influence; for example, some participants were video recorded and the footage was shown to them when the participant was sober in a bid to deter them from future use. Employment was highlighted as protective for some in terms of either abstaining or reducing use, and job loss was described as a risk factor for relapse or returning to heavier drug use. Four of those from the prison sample highlighted prison itself as a protective influence and expressed concerns that they would return to using drugs on release.
Subgroup 4
Subgroup 4 did not report any use of NPSs while being dependent on other substances. They indicated that other substances were preferable and they chose not to use NPSs. The data on this group were very limited. Although this group was retained for transparency in the analysis, they are not reported on in detail.
Figure 5 summarises the risk and protective factors that emerged from the narratives by SG.
FIGURE 5.
Groups by repertoire and risk/protective factors. a, In comparison with other SGs in group 4.
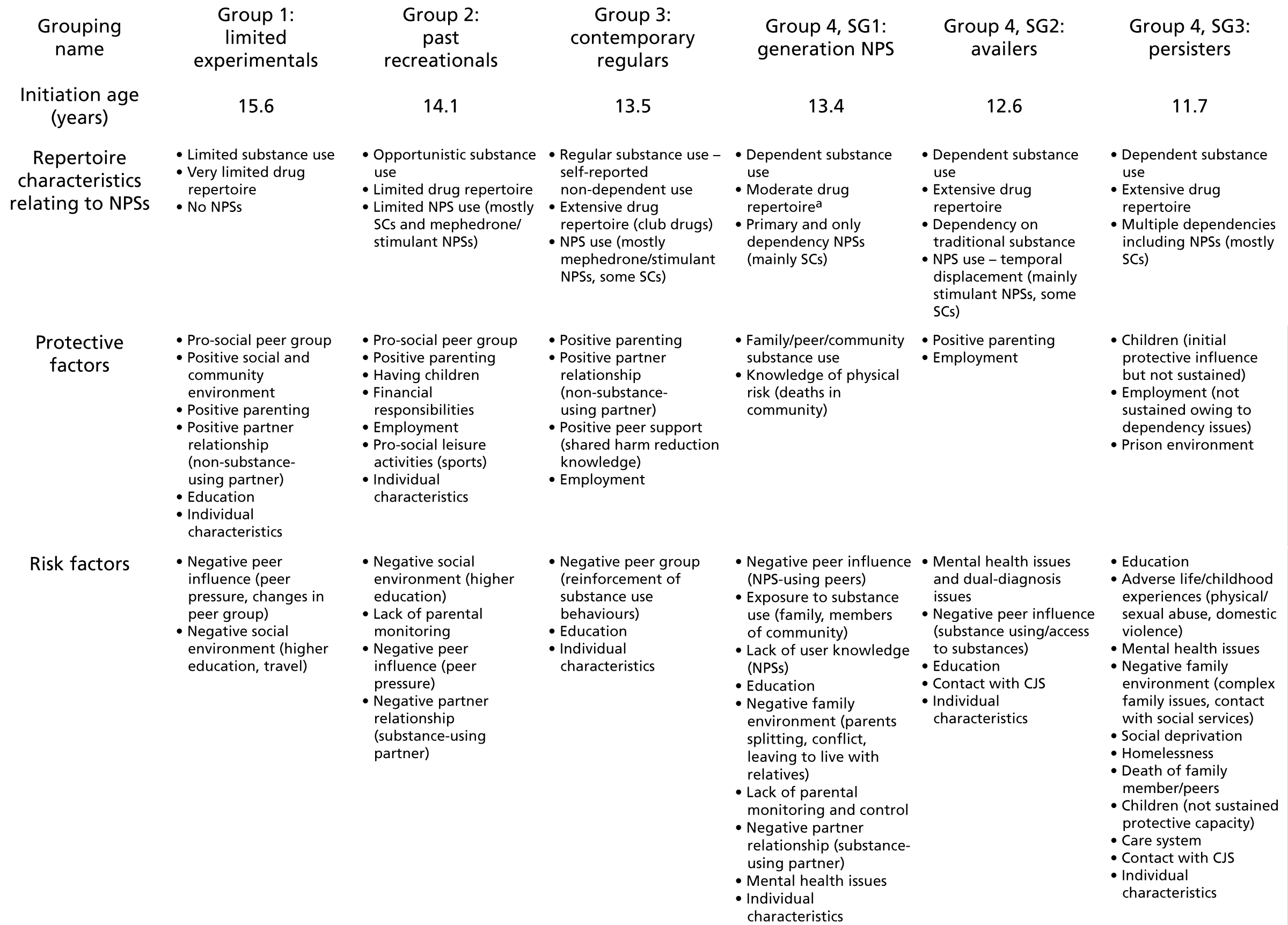
Chapter summary
The LCA revealed that only one class of substance use [class 4 (polydrug)] was characterised by NPS use. The multinomial regressions (see Appendix 5, Tables 18–20) showed that, based on the relative magnitude of effect sizes and number of significant differences between polydrug users and the other groups, there is a clear relationship between number of substances used and cumulative exposure to risk factors. In terms of exposure to drug-taking risk factors, polydrug users had the highest levels of exposure, followed by ATC users, then AT users, with the alcohol users showing the lowest levels of exposure.
The four-group taxonomy detailed patterns of substance use throughout our qualitative sample, ranging from those with very limited drug use repertoires to those reporting chronic use and dependency. Our data confirm the increasingly numerous messages from the literature that NPSs are best conceptualised as having a place within a polydrug use trajectory. As noted, commensurate with this hypothesis, our LCA did not generate a distinct NPS group, nor did it map neatly onto our qualitative group classifications. Rather, different NPSs made their way for different reasons and to different extents into the taxonomy groups 2–4.
Consistent with existing literature on trajectories of drug use, the taxonomy groups derived from the narratives clearly evidenced incrementally less favourable outcomes and multiple risks and adverse incidents as we progressed from group 1 to group 4. Common risks were early age at onset of substance use and length of substance use career. For example, age at onset progressively reduced as we moved through the taxonomy. The limited experimentals’ mean age at onset was 15.6 years, the past recreationals’ was 14 years, the contemporary regulars’ was 13 years and the dependents’ was 12.1 years. In addition, current and past extensiveness of substance behaviours appeared closely linked to early-life difficulties as reflected in the narratives (e.g. problems at school and the presence of criminal involvement in youth).
Dynamic changes such as important life events or ‘turning points’126 that can serve to protect or mitigate risks also showed a decreasing gradient as we moved through groups numerically. That is, such protective influences diminished rapidly by group to the extent that group 4 participants had few protective factors noted. Marriage, functional romantic relationships and a desire for financial security featured much more strongly in the narratives of the first two groups. Relationship breakdown, childhood in care, relapse or remission of physical and/or mental illness and bereavement appeared to have a firm influence on a person’s trajectory. The relative impact of these can be seen when looking across the four trajectories. Similarly clear was the cumulative effect of exposure to multiple adversity, which was very apparent in the female participants, especially the seven who fell into the dependent group. This summary of our groups through the narratives builds a picture of how risk factors were inter-related and tended to cluster together. For example, adverse childhood experiences appeared to be related to other family-level risk factors, for example poor parenting skills and parental substance use and mental illness.
A growing number of researchers are critical of too heavy a focus on risks at the expense of describing the specific pleasure and functions of specific drugs. 127,128 Whereas this chapter has focused on risk, the pursuit of pleasure as it relates to NPS use of varying types is discussed in Chapter 5.
Chapter 4 Longitudinal risk factors and outcomes associated with drug class membership
Risk factors associated with drug class membership
As reported in Chapter 3, 16 themes associated with more-problematic substance use were identified (Figure 6). The first 15 themes emerged directly from the qualitative analysis. When these themes were presented to the PAG for feedback, the group felt that these themes were in keeping with their professional experience. The PAG also felt that, based on their experiences of working with substance users, personality was often a key factor linked to problematic drug use. The qualitative transcripts were subsequently revisited, and the team concluded that these supported the PAG suggestion that personality is a key theme; specifically, impulsivity tended to characterise more problematic drug users.
FIGURE 6.
Themes associated with greater drug use dependency.
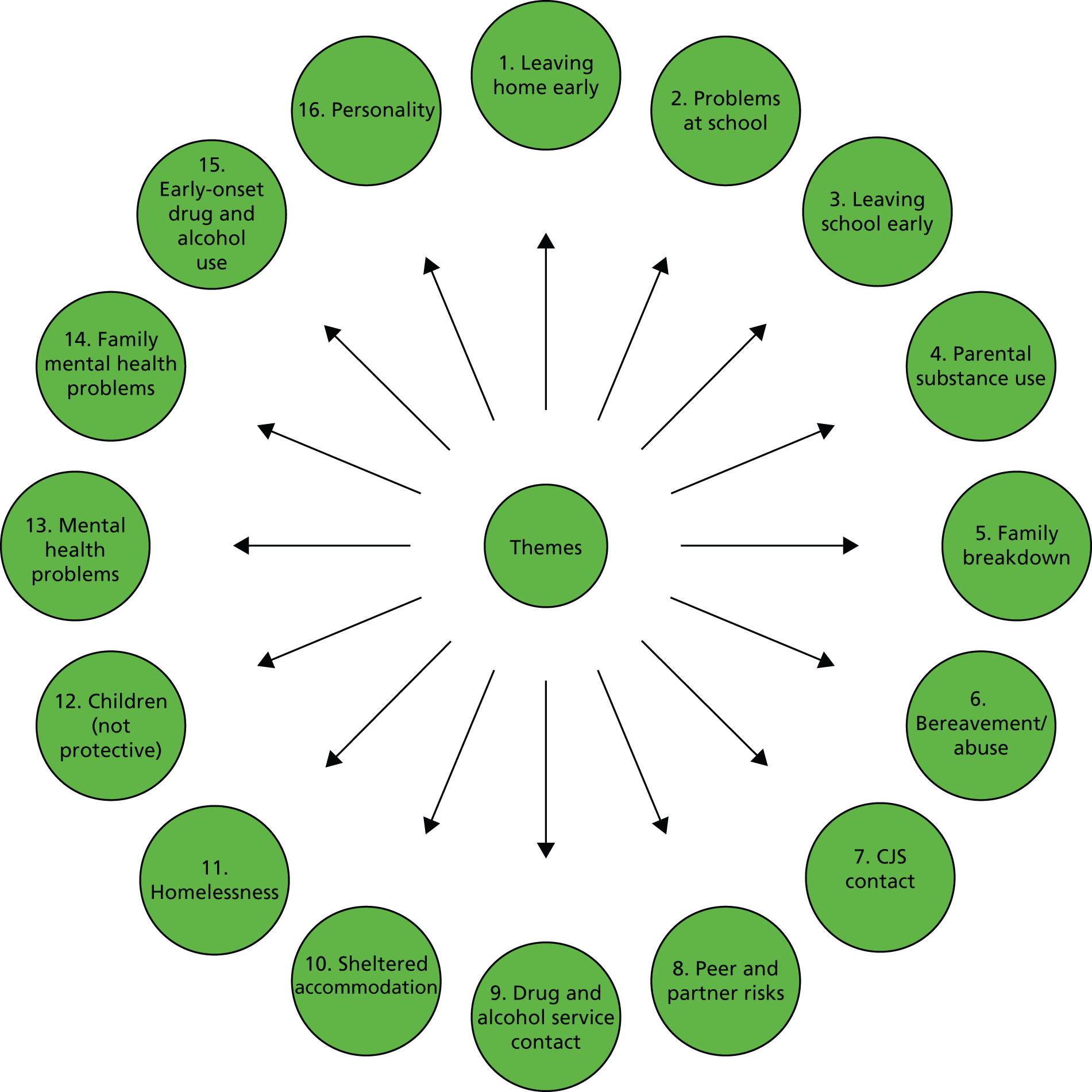
In keeping with the quantitative–qualitative–quantitative design of the research, in the third stage of the research quantitative modelling was used to assess the generalisability and relative importance of these themes using the quantitative BYDS data.
Selection of longitudinal risk factors based on the qualitative narratives
To assess if the identified themes were associated with more problematic drug/NPS use, BYDS variables were mapped onto these themes. The BYDS variables were then used to predict the latent classes identified in Chapter 3. The process of mapping BYDS variables to the themes is illustrated in Figure 7.
FIGURE 7.
Flow chart of the process of aligning BYDS variables with themes.
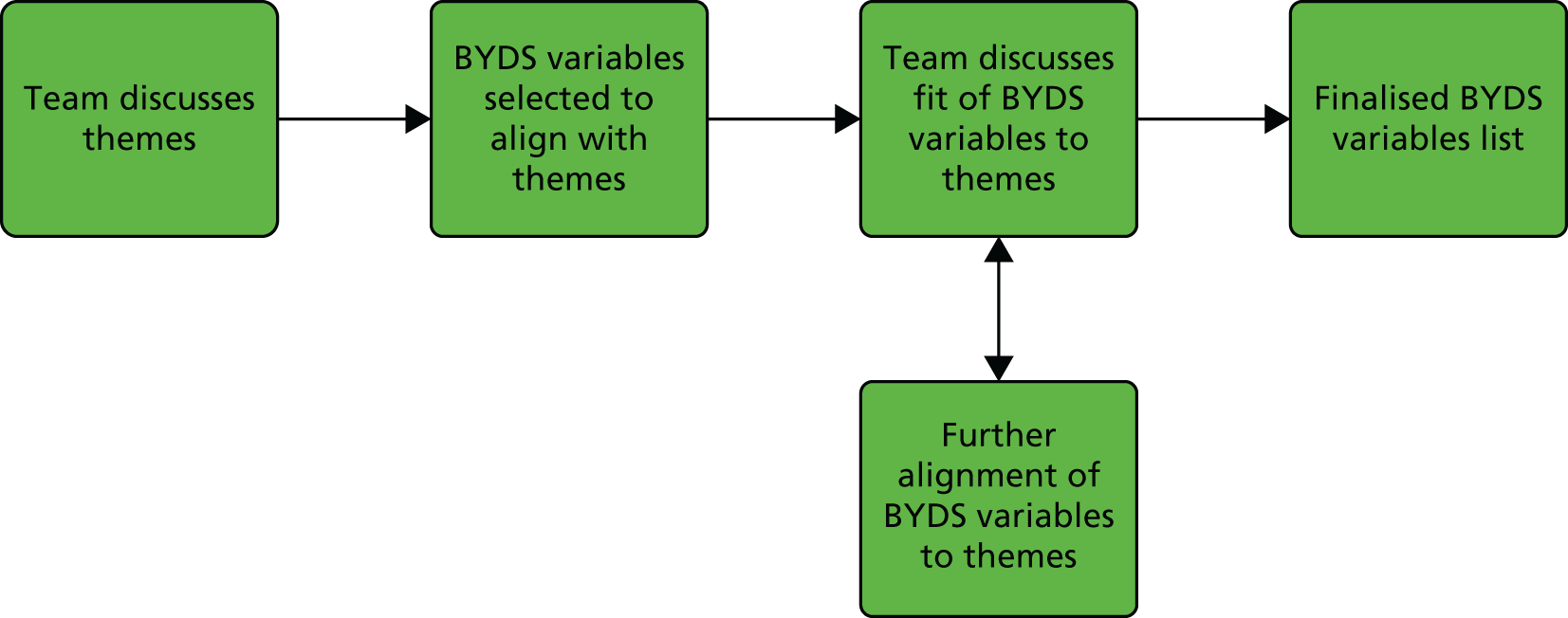
As Figure 7 shows, first the qualitative researchers briefed the project team on the 16 themes identified and their meaning, and the other team members asked follow-up questions to clarify the meaning of each theme.
Subsequently, the quantitative researcher reviewed the BYDS data sets to identify potential matches between BYDS variables and the risk factor themes. This review process involved searching the BYDS data files with key match terms, reading through the BYDS questionnaires, reviewing BYDS coverage documentation (for example, scales included in BYDS) and using project team knowledge of the data sets from previous BYDS analyses.
The variables identified were summarised in a document that was then discussed with the project team. The discussion highlighted that many of the variables fit well; however, for some themes the fit was less precise. Some variables were initially identified but excluded after discussion with the team because of poor fit (see Report Supplementary Material 3, Table 51). The qualitative researchers felt that these variables should be excluded because they were not representative of the detailed narratives from which the themes arose. Where poor fit to a theme occurred, further clarification was provided on the nature of the themes by the qualitative researchers and the review process of BYDS variables was repeated for those themes.
Several cycles of mapping the BYDS variables to the themes and cross-checking alignment with the team continued until the team was confident that it had maximised alignment between the BYDS variables and themes. The final set of BYDS variables identified as suitable predictors of problematic drug use are shown in Report Supplementary Material 3, Table 51.
The variables included and excluded via the matching process are as follows:
-
1. Leaving home early. In the BYDS data sets there was an indicator of who the participant currently lived with at waves 6 and 7. The measure at wave 6 (participants aged 16–17 years) was deemed more suitable because by wave 7 (age 21) it would not be unusual to live away from parents.
-
2. Problems at school/lack of enjoyment. From the range of school-related measures in the BYDS data sets, problems with ‘school commitment’, ‘school attachment’ and ‘being bullied’ were considered to be most reflective of this theme. Measures of school commitment and school attachment from waves 1 to 5 were available; however, only waves 2 to 5 were selected for inclusion in the present study as the response options at wave 1 were different.
-
3. Leaving school early. In wave 7 BYDS participants were asked at what age they finished school. However, it was impossible to tell if those who left at age 16 years had disengaged with education. For example, some may have gone on to study for Advanced level (A level) qualifications or National Vocational Qualifications (NVQs) at further education colleges. Indeed, many of those who reported leaving school at age 16 years reported getting A level qualifications. As participants were not specifically asked if they attended a further education college at age > 16 years it was decided that the BYDS data could not be used to derive an indicator of leaving school early. Having failed to obtain six or more General Certificates of Secondary Education (GCSEs) at A–C level (‘≥ 6 GCSEs’) was chosen as a suitable proxy indicator for early disengagement from school.
-
4, 5 and 14. Parental substance use, family breakdown/parents splitting and family mental health problems. Several themes related to family dysfunction emerged from the narratives, namely family breakdown, parental substance use and family mental health problems. Family breakdown, in the context of the narratives, refers to one or both parents moving out of the household. The BYDS participants were asked who they lived with at each wave while they were in compulsory post-primary education. A measure indicating if parents had moved out the house was computed from this (‘natural parent moved out’). Although living arrangements data are held for waves 1 to 5, it was decided to base this variable on change between waves 2 and 5; this was because of high levels of missingness for this variable at wave 1 (partly because some schools had not joined the sample by wave 1). The full BYDS data set did not hold measures of parental substance use and family mental health problems. There were some measures in the BYDS family survey, such as parental alcohol and cannabis use. However, the family survey only covered a small proportion of the BYDS full sample, making these variables unsuitable for the present analysis. Instead, two measures of family dysfunction were selected to closely align with these themes. The first was a measure of parental control129 and the second indicated if parents allowed their children to drink alcohol (‘unsupervised alcohol’). Unsupervised alcohol use was based on the wave 4 measure; prior to and after wave 4, unsupervised alcohol use was either very uncommon or very common. Parental monitoring129 and the inventory of parent and peer attachment130 were also considered as measures of these themes, but were considered not to align closely enough with the narratives.
-
6. Bereavement/loss/grief/abuse. BYDS contains several questions relating to online abuse. Surprisingly, online abuse did not arise as a theme in the narratives; rather, the abuse described by participants was face to face in nature. Physical abuse was measured by BYDS at waves 5, 6 and 7; for example, participants were asked if they had been a victim of a violent crime involving force or threat in the last 12 months. However, because the physical abuse questions related to the last 12 months as opposed to ‘ever’, this meant that coverage of physical abuse would have been too patchy to allow the compiling of a useful measure. At wave 5, participants were asked if they had lost one or both of their parents; this was selected as a measure of theme 6 (‘Death of parent/s’).
-
7. Contact with the CJS. Initially, BYDS questions such as ‘have you ever been in trouble with the police?’, ‘have you ever been arrested by the police?’, ‘have you ever had a formal warning at a police station?’ and ‘have you ever been to court for anything you did?’ were highlighted. These were considered by the team to align with the narratives, and consequently a measure of contact with the CJS was formed from these measures. The team felt that further measures related to this theme were needed to reflect the detailed delinquency experiences captured in the narratives. After further discussion and searches of the BYDS variables, it was also decided to include measures relating to loitering such as ‘hanging around on the street or in the park’. In addition, a measure of ‘delinquency’ in adolescence was selected.
-
8. Risks in terms of romantic partners and peers. Measures of peer and partner substance use in the BYDS data set cover a wide range of substances (e.g. cannabis, ecstasy, amphetamine and cocaine). The team felt that heroin did not feature in the narratives and therefore peer and partner heroin use was not considered to align with this theme. ‘Peer and partner cannabis, ecstasy/amphetamine and cocaine use’ was selected to represent this theme.
-
9. Contact with drug and alcohol services. Two indicators of contact with drug and alcohol services were identified: ‘have you gone to anyone for help with a drug problem?’ and ‘have you ever been in a treatment programme specifically related to drug use?’. It was decided to construct an indicator of contact with drug and alcohol services based on answers to these questions.
-
10 and 11. Sheltered accommodation and homelessness. The team chose not to include measures of these themes in the quantitative models as the narrative analysis revealed that this was more reflective of the service users’ part of the qualitative sample and less reflective of the BYDS participants in the qualitative sample.
-
12. Children (not a protective factor). Interestingly, having children did not appear to serve as a protective factor against drug dependency. At wave 7, participants were asked if they had had children and this was selected to measure and assess the generalisability of this theme.
-
13. Mental health problems. The BYDS data sets contain a wide range of mental health-related measures, including emotional subscales of the Strengths and Difficulties Questionnaire (SDQ);131 Moods and Feeling Questionnaire;132 Psychosis Screening Questionnaire (PSQ);133 self-harming behaviour and deliberate self-harm questions (derived from Hawton et al. 134) and the depressive symptoms scale. 135 It was decided that an early measure of mental health would be most suitable, ideally before the commencement of drug use problems that could have made mental health problems worse. In addition, as anxiety was highlighted as the main mental health issue emerging from the narratives, the selected scale needed to assess this. Subsequently, the emotional symptoms subscale at wave 1 was selected as the measure that most closely aligned to this theme.
-
15. Early-onset alcohol and drug use. In each wave, BYDS participants were asked if they had ever used alcohol and if they had ever been drunk. In choosing between ‘ever used alcohol’ and ‘ever been drunk’, frequencies were considered. Even at age 12 years, a large proportion of BYDS participants had tried at least a sip of alcohol and therefore the team decided to focus on the ‘ever been drunk’ variable. Other studies were reviewed to determine what cut-off points are typically used to define early-onset alcohol use. Cut-off points ranging from age 12 to 15 years are reported in the literature. 136–144 Of course, these studies represent a range of different countries and consequently a range of drinking norms. Therefore, international comparisons of early alcohol intoxication by age 13 years were considered;145 in international comparisons the UK had the highest percentage (24%) of young people who reported being intoxicated by age 13 years, with the exception of Denmark. The team felt that based on this it would make sense to classify early-onset alcohol use as those reporting having ever been drunk by wave 1 of the study. Using similar logic, the team decided to classify the early onset of cannabis use as having tried cannabis by wave 2; frequencies revealed that cannabis use by wave 1 was uncommon.
-
16. Personality. The BYDS data set included items from the International Personality Item Poll personality scales such as impulse control, emotional stability and risk taking. It was decided that impulse control was the personality dimension that emerged most strongly in the narratives.
The variables included and excluded as a result of the team discussions are summarised in Report Supplementary Material 2, Table 51. The coding of the included longitudinal predictor measures is detailed in Appendix 5.
Deriving initial status and growth measures for the longitudinal risk factors
Among the BYDS variables selected for the quantitative model, several were continuous variables measured at four or more waves: school attachment (waves 2–5), school commitment (waves 2–5), parental control (waves 2–5), hanging around on the street (waves 1–5) and hanging around in the park (waves 1–5). Growth models were fitted for these variables to compute intercepts and slopes for each individual. Intercepts were set to measure initial status, which was wave 1 or wave 2 depending on the earliest time point available for each variable, and slope provided a measure of change over time. Growth curve modelling involves the application of structural equation modelling methodology to the analysis of longitudinal data. The process involves fitting growth trajectories to the observed data (in Report Supplementary Material 3, Figure 21, deviations of the observed scores from each fitted trajectory are attributed to measurement error).
The growth models were fitted using MLR estimation. As recommended by Bollen and Curran,146 a variety of indices were used to assess fit for the growth models (see Report Supplementary Material 2, Table 52). The models had excellent fit according to all indices for school attachment, parental control and hanging around in the park. For the school commitment and hanging around on the street model, all indices with the exception of the chi-squared test suggest excellent model fit. In large samples, such as in the present research, chi-squared tests often lead to a rejection of the null hypothesis owing to an excess of statistical power. 146 It is therefore recommended to base model fit for large samples on a variety of indices including those not sensitive to sample size such as comparative fit index (CFI), Tucker–Lewis index (TLI) and root mean square error of approximation (RMSEA). These other indices suggest excellent model fit for the school commitment and hanging around on the street models. Quadratic models were fit for the school attachment, parental control, hanging around on the street and hanging around in the park models. A freed loading model provided the best fit for school commitment.
Mean intercept, slope and quadratic parameters are shown in Report Supplementary Material 2, Table 53, for each model, alongside their corresponding variances. The intercept and slope variances were significant for all models, with the exception of parental control, for which only the intercept variance was significant. As the slope variance for parental control was non-significant it was excluded from the variables to be included in the final quantitative model.
Analysis
The manual three-step approach66 was used to examine risk factors associated with latent class membership. Using this approach, class membership is treated as a latent variable, thus allowing individuals to be fractional members of all classes; this prevents issues such as incorrect estimates and standard errors (SEs). 147 Step 1 of this approach involved estimating the unconditional latent class model (see Chapter 3). In step 2, information derived from step 1 was added to the model, namely the most likely class membership variable and the logit values for misclassification error rates. Fixing the misclassification rates prevents class formation from being influenced by the covariates in the conditional models. Finally, in step 3 the predictor variables were entered into the model. In the present analysis the predictor variables were entered in eight blocks (family, peers, substance use history, school, delinquency, mental health/personality, partner, demographics). Blocks were entered based on the frequency they were reported as being related to polydrug/NPS use in the interviews, starting with the most frequently cited risk factors at step 1. Multiple imputation was used on the predictor variables to prevent listwise deletion of variables. School was included as a cluster variable to account for clustering of individuals in schools. All continuous predictor variables in the models were grand mean centred. In all models, polydrug was the reference class because NPS use was a defining feature of this class.
G*power 3.1 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) was used to compute logistic regression sensitivity z-tests (one tailed) at 80% power, with α set at 0.05. These showed that there was sufficient power to detect odds ratios (ORs) ranging from 1.30 for the smallest sample size (ATC vs. polydrug) to 1.20 for the largest sample size (AT vs. polydrug).
Results: longitudinal predictors of drug class
Descriptive statistics for the analysis variables by latent class are presented in Tables 6 and 7. Results from the manual three-step approach are shown in Tables 8–10 as ORs (see Appendix 5, Tables 18–20, for log-odds and SEs).
| Variable | Response | Class (%) | n | |||
|---|---|---|---|---|---|---|
| 1 (alcohol) | 2 (AT) | 3 (ATC) | 4 (polydrug) | |||
| Female | Yes | 62.5 | 64.6 | 56.6 | 49.8 | 1989 |
| FSM | 11.3 | 14.7 | 20.4 | 27.0 | 1843 | |
| Left home early | 4.1 | 4.6 | 6.2 | 7.1 | 1343 | |
| ≥ 6 GCSEs | 78.3 | 74.6 | 72.2 | 56.9 | 2009 | |
| Parent(s) dead | 1.8 | 3.2 | 3.1 | 5.4 | 1744 | |
| Trouble with police | 11.0 | 19.2 | 34.8 | 53.6 | 1697 | |
| Peers use cannabis | 23.3 | 48.4 | 79.3 | 92.2 | 1366 | |
| Peers use ecstasy | 11.3 | 23.2 | 43.8 | 78.3 | 1368 | |
| Peers use cocaine | 8.3 | 15.0 | 33.8 | 66.7 | 1367 | |
| Partner uses cannabis | 3.6 | 7.9 | 15.1 | 33.1 | 1255 | |
| Partner uses ecstasy | 1.7 | 4.0 | 4.9 | 23.5 | 1253 | |
| Partner uses cocaine | 2.2 | 3.1 | 2.9 | 28.1 | 1259 | |
| Sought help | 0.7 | 1.3 | 2.1 | 8.6 | 1744 | |
| Has child(ren) | 3.0 | 10.0 | 8.5 | 15.4 | 2015 | |
| Early alcohol use | 0.9 | 8.6 | 12.7 | 28.9 | 1252 | |
| Early cannabis use | 2.6 | 9.0 | 20.3 | 41.4 | 1610 | |
| Parent(s) moved out | 4.3 | 7.6 | 6.5 | 9.8 | 1534 | |
| Bullied | Not true | 89.9 | 88.9 | 88.1 | 92.7 | 1593 |
| Somewhat true | 8.0 | 8.7 | 9.4 | 4.3 | ||
| Certainly true | 2.2 | 2.4 | 2.5 | 3.0 | ||
| Parents allow drinking | No | 62.1 | 48.4 | 55.8 | 51.8 | 1564 |
| Yes, if supervised | 31.4 | 40.0 | 30.7 | 31.7 | ||
| Yes | 6.5 | 11.7 | 13.5 | 16.5 | ||
| Variable | Class, mean (SD) | n | |||
|---|---|---|---|---|---|
| 1 (alcohol) | 2 (AT) | 3 (ATC) | 4 (polydrug) | ||
| Emotional difficulties | 3.25 (2.24) | 3.19 (2.29) | 3.14 (2.18) | 2.95 (2.25) | 1418 |
| Impulsivity | 17.98 (7.68) | 20.35 (7.31) | 21.46 (7.19) | 22.03 (8.34) | 1717 |
| Delinquency | 1.21 (1.72) | 1.94 (2.17) | 2.89 (2.70) | 4.04 (2.99) | 1627 |
| School attachment (intercept) | 17.26 (3.74) | 15.91 (3.59) | 14.74 (3.69) | 13.64 (3.74) | 1871 |
| School commitment (intercept) | 14.25 (1.69) | 13.40 (2.12) | 12.75 (2.50) | 11.61 (2.96) | 1870 |
| School commitment (slope) | –0.25 (1.22) | –0.21 (1.62) | –0.25 (1.93) | –0.22 (2.23) | 1870 |
| Parental control (intercept) | 14.53 (3.03) | 13.54 (2.99) | 12.88 (3.08) | 12.08 (2.93) | 1872 |
| Hanging around on the street (intercept) | 1.34 (0.94) | 1.70 (0.90) | 2.00 (0.81) | 2.10 (0.74) | 1878 |
| Hanging around on the street (slope) | 0.05 (0.34) | 0.10 (0.32) | 0.17 (0.33) | 0.23 (0.30) | 1878 |
| Hanging around in the park (intercept) | 0.93 (0.54) | 1.06 (0.54) | 1.13 (0.59) | 1.15 (0.59) | 1878 |
| Hanging around in the park (slope) | –0.19 (0.23) | –0.18 (0.26) | –0.17 (0.28) | –0.21 (0.29) | 1878 |
| Variable | OR | |||||||
|---|---|---|---|---|---|---|---|---|
| Family | Peers | Substance use history | School | Delinquency | Mental health/personality | Partner | Demographics | |
| Parent(s) dead | 0.30* | 0.34 | 0.39 | 0.35 | 0.36 | 0.34 | 0.32 | 0.32 |
| Parent(s) moved out | 0.62 | 0.59 | 0.56 | 0.67 | 0.64 | 0.64 | 0.64 | 0.64 |
| Left home early | 0.51 | 0.63 | 0.58 | 0.63 | 0.57 | 0.55 | 0.59 | 0.66 |
| Parental drinking view | 0.63** | 0.68* | 0.69* | 0.73 | 0.69 | 0.73 | 0.70 | 0.70 |
| Parental control (intercept) | 1.31*** | 1.16** | 1.12* | 1.04 | 1.01 | 1.01 | 1.02 | 1.02 |
| Peers use cannabis | 0.10*** | 0.13*** | 0.15*** | 0.14*** | 0.14*** | 0.16** | 0.17** | |
| Peers use ecstasy | 0.18*** | 0.21** | 0.26** | 0.26** | 0.26** | 0.30* | 0.29* | |
| Peers use cocaine | 0.32** | 0.33** | 0.37* | 0.39* | 0.38* | 0.47 | 0.48 | |
| Bullied | 1.34 | 1.58 | 1.55 | 1.57 | 1.51 | 1.36 | 1.38 | |
| Early alcohol use | 0.09 | 0.09 | 0.11 | 0.11 | 0.13 | 0.16 | ||
| Early cannabis use | 0.20*** | 0.33* | 0.47 | 0.46 | 0.44 | 0.44 | ||
| Sought help | 0.84 | 1.13 | 1.22 | 1.31 | 2.18 | 2.77 | ||
| School attachment (intercept) | 1.05 | 1.03 | 1.03 | 1.02 | 1.02 | |||
| School commitment (intercept) | 1.77*** | 1.54*** | 1.49*** | 1.51*** | 1.49*** | |||
| School commitment (slope) | 1.72*** | 1.60*** | 1.58*** | 1.60*** | 1.57*** | |||
| ≥ 6 GCSEs | 0.71 | 0.72 | 0.75 | 0.72 | 0.67 | |||
| Delinquency | 0.86 | 0.86 | 0.85 | 0.86 | ||||
| Trouble with police | 0.61 | 0.61 | 0.56 | 0.57 | ||||
| Hanging around on the street (intercept) | 0.94 | 0.94 | 0.97 | 0.96 | ||||
| Hanging around on the street (slope) | 0.56 | 0.56 | 0.55 | 0.57 | ||||
| Hanging around in the park (intercept) | 1.00 | 1.01 | 0.90 | 0.86 | ||||
| Hanging around in the park (slope) | 2.32 | 2.39 | 2.29 | 2.39 | ||||
| Emotional difficulties | 1.05 | 1.08 | 1.07 | |||||
| Impulsivity | 0.99 | 1.00 | 1.00 | |||||
| Partner uses cannabis | 0.35 | 0.35 | ||||||
| Partner uses ecstasy | 0.87 | 0.85 | ||||||
| Partner uses cocaine | 0.57 | 0.57 | ||||||
| Female | 1.22 | |||||||
| FSM | 1.15 | |||||||
| Has child(ren) | 0.47 | |||||||
| Variable | OR | |||||||
|---|---|---|---|---|---|---|---|---|
| Family | Peers | Substance use history | School | Delinquency | Mental health/personality | Partner | Demographics | |
| Parent(s) dead | 0.60 | 0.60 | 0.66 | 0.61 | 0.73 | 0.73 | 0.68 | 0.71 |
| Parent(s) moved out | 1.02 | 1.08 | 1.06 | 1.12 | 0.99 | 0.97 | 0.96 | 0.90 |
| Left home early | 0.64 | 0.84 | 0.76 | 0.78 | 0.71 | 0.70 | 0.76 | 0.62 |
| Parental drinking view | 1.04 | 1.13 | 1.19 | 1.21 | 1.26 | 1.27 | 1.21 | 1.22 |
| Parental control (intercept) | 1.17*** | 1.06 | 1.04 | 1.00 | 1.00 | 0.99 | 1.01 | 0.99 |
| Peers use cannabis | 0.26** | 0.32* | 0.34* | 0.32* | 0.32* | 0.37 | 0.42 | |
| Peers use ecstasy | 0.25*** | 0.29** | 0.32* | 0.32* | 0.32* | 0.35* | 0.34* | |
| Peers use cocaine | 0.28*** | 0.29** | 0.32** | 0.32** | 0.31** | 0.41* | 0.38* | |
| Bullied | 1.32 | 1.49 | 1.46 | 1.51 | 1.46 | 1.32 | 1.40 | |
| Early alcohol use | 0.53 | 0.59 | 0.65 | 0.63 | 0.73 | 0.71 | ||
| Early cannabis use | 0.36*** | 0.43** | 0.52* | 0.52 | 0.50 | 0.50 | ||
| Sought help | 0.61 | 0.66 | 0.64 | 0.66 | 1.02 | 1.14 | ||
| School attachment (intercept) | 1.03 | 1.01 | 1.01 | 1.00 | 1.00 | |||
| School commitment (intercept) | 1.23** | 1.12 | 1.12 | 1.13 | 1.13 | |||
| School commitment (slope) | 1.25** | 1.17* | 1.19* | 1.20* | 1.20* | |||
| ≥ 6 GCSEs | 0.85 | 0.94 | 0.94 | 0.90 | 0.91 | |||
| Delinquency | 0.89 | 0.88 | 0.88 | 0.90 | ||||
| Trouble with police | 0.46** | 0.47* | 0.43* | 0.46* | ||||
| Hanging around on the street (intercept) | 1.23 | 1.23 | 1.28 | 1.22 | ||||
| Hanging around on the street (slope) | 0.51 | 0.51 | 0.51 | 0.49 | ||||
| Hanging around in the park (intercept) | 1.31 | 1.30 | 1.14 | 1.12 | ||||
| Hanging around in the park (slope) | 3.03* | 3.00* | 2.86* | 3.16* | ||||
| Emotional difficulties | 1.03 | 1.06 | 1.04 | |||||
| Impulsivity | 1.01 | 1.02 | 1.01 | |||||
| Partner uses cannabis | 0.53 | 0.46 | ||||||
| Partner uses ecstasy | 1.23 | 1.19 | ||||||
| Partner uses cocaine | 0.33 | 0.30 | ||||||
| Female | 1.70 | |||||||
| FSM | 1.05 | |||||||
| Has child(ren) | 1.63 | |||||||
| Variable | OR | |||||||
|---|---|---|---|---|---|---|---|---|
| Family | Peers | Substance use history | School | Delinquency | Mental health/personality | Partner | Demographics | |
| Parent(s) dead | 0.54 | 0.46 | 0.52 | 0.50 | 0.54 | 0.54 | 0.55 | 0.57 |
| Parent(s) moved out | 0.65 | 0.68 | 0.66 | 0.70 | 0.66 | 0.65 | 0.64 | 0.59 |
| Left home early | 0.79 | 1.00 | 0.92 | 1.03 | 0.98 | 0.97 | 1.01 | 0.99 |
| Parental drinking view | 0.78 | 0.78 | 0.82 | 0.81 | 0.85 | 0.85 | 0.80 | 0.81 |
| Parental control (intercept) | 1.07 | 1.03 | 1.00 | 0.99 | 1.01 | 1.01 | 1.02 | 1.01 |
| Peers use cannabis | 1.28 | 1.54 | 1.55 | 1.40 | 1.40 | 1.60 | 1.77 | |
| Peers use ecstasy | 0.31* | 0.35* | 0.38 | 0.37* | 0.37* | 0.41 | 0.40 | |
| Peers use cocaine | 0.45* | 0.45 | 0.48 | 0.46 | 0.46 | 0.64 | 0.61 | |
| Bullied | 1.51 | 1.70 | 1.70 | 1.75 | 1.72 | 1.58 | 1.65 | |
| Early alcohol use | 0.44* | 0.49* | 0.49 | 0.47 | 0.55 | 0.56 | ||
| Early cannabis use | 0.64 | 0.73 | 0.73 | 0.73 | 0.71 | 0.72 | ||
| Sought help | 0.46 | 0.53 | 0.50 | 0.51 | 0.76 | 0.82 | ||
| School attachment (intercept) | 0.99 | 0.98 | 0.98 | 0.97 | 0.97 | |||
| School commitment (intercept) | 1.13 | 1.11 | 1.12 | 1.12 | 1.13 | |||
| School commitment (slope) | 1.14 | 1.14 | 1.15 | 1.17 | 1.17 | |||
| ≥ 6 GCSEs | 1.30 | 1.39 | 1.40 | 1.32 | 1.34 | |||
| Delinquency | 0.95 | 0.94 | 0.94 | 0.97 | ||||
| Trouble with police | 0.82 | 0.83 | 0.74 | 0.79 | ||||
| Hanging around on the street (intercept) | 1.43 | 1.43 | 1.51 | 1.46 | ||||
| Hanging around on the street (slope) | 0.72 | 0.72 | 0.65 | 0.63 | ||||
| Hanging around in the park (intercept) | 1.28 | 1.26 | 1.09 | 1.06 | ||||
| Hanging around in the park (slope) | 2.53 | 2.53 | 2.44 | 2.66 | ||||
| Emotional difficulties | 1.03 | 1.06 | 1.03 | |||||
| Impulsivity | 1.01 | 1.02 | 1.02 | |||||
| Partner uses cannabis | 0.93 | 0.84 | ||||||
| Partner uses ecstasy | 0.73 | 0.67 | ||||||
| Partner uses cocaine | 0.17* | 0.16* | ||||||
| Female | 1.73 | |||||||
| FSM | 1.40 | |||||||
| Has child(ren) | 0.82 | |||||||
Alcohol versus polydrug
Relative to the polydrug users, participants in the alcohol group were less likely to have friends who take cannabis or ecstasy at age 17 years and have greater levels of school commitment at age 13 years. (A one-unit increase in school commitment slope was associated with a 0.45 increase in the relative log-odds of being in the alcohol group compared with the polydrug group.) In other words, as the general trend over time for school commitment is a decline, the alcohol group had lower levels of decline in school commitment over time. Although some of the family and substance use history variables were significant when first entered into the model, these were non-significant in the fully controlled model.
Alcohol and tobacco versus polydrug
Participants in the AT group were less likely to have friends who take cocaine or ecstasy at age 17 years and less likely to be in trouble with the police by age 14 years.
Participants in the AT group had less of a reduction in school commitment between the ages of 13 and 16 years than polydrug users.
A one-unit increase in hanging around in the park (slope) was associated with a 1.15 increase in the relative log-odds of being in the AT group compared with the polydrug group. The overall trend for hanging around in the park (slope) was negative (reduction in going to the park from age 13–16 years), which suggests that the AT group experienced less of a reduction in going to the park throughout adolescence.
Alcohol, tobacco and cannabis versus polydrug
The only significant difference between the ATC and polydrug groups was that participants in the ATC group were less likely to have a partner who used cocaine at age 17 years.
Adult outcomes associated with drug class
The next stage of analysis involved looking at adult outcomes (participants aged 21 years) associated with prior life course drug history. The adult outcomes investigated covered key aspects of adult life such as mental health, education, employment, offending, contact with the CJS and substance use. The outcome models were designed to incorporate key findings from the qualitative analysis. Specifically, risk factors that emerged from the narratives and were significant in the predictors of latent class membership analysis were included in the models. This meant that factors associated with later drug use were controlled for in the models. The coding of the longitudinal measures is detailed in Appendix 5.
Analysis
The four sets of drug class membership probabilities associated with the four latent classes were converted to logit scales. The logit variables for classes 1–3 were then entered into the model, thus allowing class 4 (polydrug) to serve as the reference group. This approach is designed to reduce bias in the regression coefficients, by using the drug class probabilities in the model rather than treating drug class as an exact observed variable. 147 Multiple imputation was used to handle missing data, and school-based clustering was adjusted for.
The distribution of means across different imputation sets was checked for variables in the models; there was no evidence of trending and estimates varied randomly. Extensive sensitivity analyses were conducted to assess the extent to which our results change if the MAR assumption is incorrect by adjusting imputed data set estimates for the outcome variables upwards by 1–20% above that predicted by the imputation model. The specific scenarios modelled for each outcome variable were:
-
Assume that the outcome is between 1% and 20% worse among those not observed than among those observed, conditional on all imputation predictor variables.
-
Assume that the outcome is between 1% and 10% worse for those with > 80% probability of being in the polydrug class.
-
Assume that the outcome is between 10% and 20% worse for those with > 80% probability of being in the polydrug class.
-
Assume that the outcome is between 1% and 10% worse among the unobserved ATC group than among the observed ATC group (for those with > 80% probability of being in the ATC class) and assume that the outcome is between 10% and 20% worse among the unobserved polydrug group than among the observed polydrug group (for those with > 80% probability of being in the polydrug class).
All sensitivity analyses had almost negligible influence on the model results, suggesting that the results are robust to deviations from the MAR assumption.
Imputation models were tested on the full BYDS cohort, that is, the 5809 participants who had taken part in at least one of the seven BYDS waves. However, as poor levels of imputation were achieved in these models, this analysis was not pursued further, and all modelling was restricted to the BYDS wave 7 sample.
Results
Descriptive statistics for the outcome measures by most probable drug class are presented in Tables 11 and 12. The linear and logistic regression results are presented in Appendix 5, Tables 21–31.
| Variable | Class, mean (SD) | n | |||
|---|---|---|---|---|---|
| 1 (alcohol) | 2 (AT) | 3 (ATC) | 4 (polydrug) | ||
| Depression | 3.26 (4.44) | 4.27 (5.15) | 5.43 (5.38) | 6.46 (5.71) | 1935 |
| Problem drinking | 5.28 (4.35) | 8.65 (4.68) | 11.80 (5.35) | 15.07 (6.24) | 1870 |
| Drug abuse | 0.07 (0.81) | 0.14 (0.76) | .60 (1.31) | 3.35 (4.13) | 1897 |
| Cannabis abuse | 0.00 (0.00) | 0.14 (0.85) | 1.08 (3.01) | 3.97 (5.66) | 1964 |
| Offending | 0.20 (0.54) | 0.34 (0.79) | 0.73 (1.23) | 1.41 (1.91) | 1843 |
| Variable | Class (%) | n | |||
|---|---|---|---|---|---|
| 1 (alcohol) | 2 (AT) | 3 (ATC) | 4 (polydrug) | ||
| NEET | 9.1 | 10.2 | 11.1 | 19.0 | 1995 |
| Psychosis | 5.8 | 7.7 | 14.6 | 23.1 | 1700 |
| Self-harm | 1.7 | 4.5 | 4.7 | 11.8 | 1980 |
| Medication | 5.0 | 5.7 | 8.2 | 8.8 | 1964 |
| Services | 12.4 | 15.1 | 18.5 | 20.9 | 1973 |
| Justice | 2.0 | 3.0 | 9.9 | 17.9 | 1943 |
After controlling for confounding variables, participants in the AT group were less likely to have poor adult outcomes than participants in the polydrug group across all areas examined, with the exception of being not in education, employment or training (NEET). Participants in the alcohol group were less likely to have poor adult outcomes than participants in the polydrug group across all areas examined, with the exception of being NEET and using medication or services for emotional or behavioural problems, when confounding variables were taken into account.
In the unadjusted models, the alcohol and ATC groups were less likely to be NEET; however, these differences were non-significant in the fully controlled models.
Both the adjusted and unadjusted models highlight that polydrug users are at greater risk of problematic behaviours related to drug use, cannabis use and offending.
Chapter 5 Key drivers for novel psychoactive substance use
Developing a clearer understanding of the complex drivers behind use and supply of NPSs is important to inform policy development. As discussed in the previous chapters, much evidence suggests that NPSs to a large extent follow existing polydrug use patterns. 148 However, Chapter 3 has already pointed towards the benefits of examining more specific considerations in those trajectories whereby nuance depending on drug repertoire and an interaction of risk and protective factors allows us to more clearly locate users in a graduated taxonomy. These groups are summarised in Figure 6.
In this chapter we discuss, in the context of a polydrug use repertoire, how types of NPSs are placed. Drivers for use range from those connected to issues of legality and evasion of detection in drug tests (according to various setting codes) to serving as a low-cost means to pleasure or as alternatives and/or adjuncts to traditional substances. We also discuss how their use intersects with key developments in the overall drug market vis-à-vis legislative bans (namely the amendment to the Misuse of Drugs Act 1971149 passed in 2010 and the Psychoactive Substances Act 201616). The relationship between NPSs and potency, quality and decisions for use is also discussed. Variance in the relative influence of these factors can be observed when discussed within the framework of the groups and where possible by particular NPSs. As noted in Chapters 3 and 4, within the data there was a predominance of discussion surrounding SCs and mephedrone, and this is reflected throughout.
Legal status
Although NPSs have never been legal for sale in terms of human consumption, the initial legal status of some substances was an influential driver for use for several respondents in our study. Legality served as a motivating factor for different reasons among different groups and for some was deemed more important than other factors. Respondents were clearly literate regarding the legislative context of NPSs and discussed the availability of various NPSs alongside policy, for example the availability of mephedrone was often observed before and after the 2010 ban. Interestingly, discussion surrounding the perceived legality of NPSs was particularly notable in the narratives of three distinct groups (past recreationals, generation NPSs and persisters), all for different reasons.
Cultural and contextual setting codes proved immanent in relation to attitudes to NPSs among certain groups. For past recreationals, legality was discussed in the context of availability and normalisation as well as source of availability (e.g. obtaining substances from a headshop in comparison with a street dealer):
Just whenever it was legal it was easy to get, it was very easy to get, a lot easier and a lot less risk, significantly less risk than trying to find a drug dealer.
1001
Another participant reflected on the interplay between legality and availability but highlighted that legality was not the driving force behind motivation for use:
I think if [mephedrone] had of been available the way that it was and been cocaine I probably would have taken it anyway, but I don’t think it would have been as available if it hadn’t of been legal if you know what I mean . . . I think if you are going to take stuff like that you are going to take it whether it’s legal or illegal.
1012
Legal status proved a conduit for crossover between scenes; that is, mephedrone emerged in scenes previously characterised only by AT use:
It was ridiculous – people were handing out grams of [mephedrone] for nothing, do you know what I mean, it was just everywhere. People were – you know, mates were buying it off the internet just to have at parties. You know, like £100 worth – getting X amount of grams, and that was going to do a party whatever night. It was a really weird drug – there were people taking it who wouldn’t have ever taken [ecstasy] or anything else.
1036
The legal status of mephedrone was not mentioned by anyone in the contemporary regulars group as a motivating factor in terms of use; rather, it was discussed in the context of increased availability and accessibility. In these cases, legality was not highlighted as a driving force but something that facilitated ease of access; however, this did not deter use post ban. Use ceased when availability declined and the quality of NPSs deteriorated, coinciding with the improving quality of traditional substances.
Among dependents, perceived legality around NPSs was most resonant for generation NPS and persisters. Generation NPS discussed the legal repercussions of possessing substances and the source of availability with regard to NPSs versus traditional substances:
You see we used to get told that if you had the herbal the police don’t have to take it off you, so we were like, ah that’s handier. So we thought we could walk about the town and smoke herbal. If the police were to say anything, this is herbal. But still got lifted [arrested] for it. I never got lifted but a lot of my friends got lifted and brought home.
1053
Although most of generation NPS accessed the substances from both headshops and street dealers, some participants discussed the transition from mephedrone to SCs following the ban. In these instances, perceptions around legal status drove decisions to switch substances:
That’s when I realised that I was severely addicted to mephedrone – and the day it was made illegal was the same day that I stopped taking it, because I didn’t want to go and find it off an illegal dealer. But the day I stopped sniffing mephedrone, I started smoking this thing called ‘magic’, ‘black magic smooth’ or something.
1054
For the persisters, it was evident from setting codes that NPS use served as a means to bypass drug screens. This was the case for those in contact with services and, perhaps most notably, for those in prison:
It was a way of taking it and bypassing the drug test, where now they test for it now so you know, I mean obviously they can’t test for everything because of all the new strains that’s coming out, when they couldn’t test for legal highs that would have been the way people was going, it’s like when people were turning from cannabis to heroin because it was less likely to be tested, they were turning from cannabis or heroin to legal highs because they weren’t going to get caught.
HMP1004
I mean that ‘Sky High’ stuff, I just had a bad whole time with it, it wasn’t what I thought it would be, because I did smoke stuff called, some legal weed called ‘herbal haze’, that was OK, and it wasn’t showing up on drug tests so I didn’t care, I was still getting stoned, I wasn’t collapsing, I wasn’t showing on a drug test, but I suppose they can put anything into them psychoactive substances.
HMP1005
Availability and accessibility
Availability of NPSs was a theme that cut across all groups in the taxonomy and proved more influential among specific groups as a driver for use. Availability proved instrumental in terms of motivations to use for the past recreationals. Use of NPSs was opportunistic in the same way as use of traditional illicit substances. Decisions to use or not to use NPSs in this group centred around what was available and presented to them by peers during the time at which they experimented with drugs. When discussing non-use of NPSs, one participant stated:
When I was coming up it was more like recreational drugs that were available like ecstasy and cocaine.
1009
One participant from this group who had used mephedrone reflected with regret on her use but framed it in the context of a scene wherein use was common owing to legality and availability:
When mephedrone came in, that was legal and that became popular, it was everywhere, I remember that it was everywhere and everybody was using that because it was legal at the time and we all would have dabbled in that unfortunately.
1012
Factors that were key in terms of availability for those in the past recreationals and generation NPS were the availability of NPSs and the ease with which participants were able to obtain the substances in comparison with traditional drugs. One participant reflected on the experience of accessing NPSs while studying in England:
You could have gone to the headshops and got them. They were dearer than buying them off the internet themselves. You could just so easily get it. You were in town, you were drinking in pubs in Liverpool and it was Saturday at 4 o’clock, then one of the lads would be like, ‘right, I’m away to [headshop] for a bag’.
1037
No-one from the past recreationals group reported accessing mephedrone post ban, nor did they access NPSs through street dealers. Substances were either sourced through headshops or provided through social supply from peers. In these instances, legality clearly played a part in accessibility.
For most of the contemporary regulars, NPSs were not availed of in an opportunistic way. Rather, contemporary regulars’ narratives tended to focus on the interface between availability and quality, specifically the declining quality and availability of traditional drugs and the subsequent transition from illicit stimulant drugs to NPSs, primarily mephedrone, when it was available. For most in this group, quality was as much of a driving force as was availability:
The only reason mephedrone really came on the scene was because the ecstasy had died out so they were trying to get something to replicate the effects of ecstasy so the mephedrone was there and now the ecstasy has come back in, the ecstasy is booming again now because it’s really good.
1008
So I took Es [ecstasy pills] then for quite a while and then they sort of started to fade out like I remember they were getting dearer and harder to get and then like the quality of them was getting worse and then you were hearing more and more stories in the news about people like dying and bad batches and stuff going about. Then what did I move on to . . . I think then meph[edrone] came on the scene as far as I know, at the time I think it was legal, ya know when it first came round, and everyone was getting it off the internet and stuff like that, it was just easy to get and that was for a couple of years.
1018
In terms of source of availability, unlike the past recreationals, the contemporary regulars reported self-sourcing NPSs and accessed mephedrone from both headshops and street dealers. A number of participants also reported sourcing mephedrone post ban in 2010, reinforcing the fact that the legal status merely mediated accessibility as opposed to influencing decisions to use.
For the availers, NPSs filled the gap in a similar fashion. However, rather than NPSs temporarily displacing traditional illicit drugs, they were perceived as more of a substitute/contingency plan when participants were unable to access their traditional illicit drug of choice:
There was one called Smoke, something Gold, a few different things I can’t remember the names of them all now, so I would try them all and once or twice when I couldn’t get any hash I would go down to the headshop and buy them because I really missed having a smoke.
1027
So if I couldn’t get the real thing, I would get the China White, which sometimes that would be quite regular . . . And as far as those herbal highs and stuff like that, I never bother with them because I can always get cannabis if I want to, it’s not a problem, so I don’t really see the point in getting . . . to be honest with you, I haven’t even tried it and I’ve heard very negative reports about it.
1032
For generation NPS, availability of substances (particularly SCs and mephedrone), in conjunction with the point of their drug career (i.e. stage of experimentation), was crucial in terms of motivations for use. In terms of cultural setting, SC use was described as normalised, as cannabis use was for previous generations:
Herbal’s been about for a long time but it only really blew up last year. Last year was when it all blew up, everybody started using it.
1046
The impact of the legislative ban on availability of NPSs was a focus in the narratives of generation NPS:
It’s [SC is] everywhere, always, but it got banned so it’s harder to get now, it only got banned about 2 or 3 months ago.
1044
Potency and quality
The quality and potency of NPSs emerged as influential in terms of motivations for use and decision-making; these factors varied across the groups for different reasons. For our contemporary regulars, it was the quality of mephedrone and the time at which it emerged on the market that proved most significant.
Evidence (primarily seizure data) suggests that NPSs such as mephedrone emerged on the scene at a time when the quality of illicit party drugs such as MDMA and cocaine were at an all-time low. This perceived lower quality and continued demand for these types of drugs, coupled with the emergence of a substance that was cheaper, more widely available, not controlled under existing drug law and more potent, made for a perfect storm:
Whenever the meph[edrone] came on the scene big time that totally took away the cocaine, nobody wanted to buy coke. Why would you go and buy £40 of rubbish cocaine that basically does nothing to you and is probably 2 or 3 per cent purity whenever you could go and buy a bag of mephedrone at the start for £10? It was a full gram, like a gram could keep you rocking for hours, give you the real high like you were taking ecstasy.
1008
Our persisters also commented on the quality of mephedrone in comparison with traditional stimulant drugs, as well as stimulant NPSs that preceded mephedrone:
The way the drug scene went there, all these legal highs came on the scene because all the good say good drugs, all them illegal ones had been about for ages and everyone that was doing it just all disappeared off the scene, like the mephedrone and all came out because all the ecstasy disappeared so people were looking [for] something that’s close to it so then that came on the scene.
1059
The ‘Gocaine’ was just crap after that, once the mephedrone was there it was better, obviously it was a lot stronger, different hit, better hit.
1020
In terms of SCs, the case was somewhat different in that motivations to use were more associated with potency as opposed to a quality issue with traditional drugs, such as cannabis. The potency of SCs appealed specifically to those in our most vulnerable group (generation NPS) and our most chronic dependent users (the persisters) (see Chapter 7 for more information). Although initially taken by surprise by the effects of the SCs, the persisters nevertheless went on to treat SCs as an important drug of choice in their repertoire as it provided the total block many of them required. This was particularly noticeable in the homeless community or for prisoners in long-term lockdown. For generation NPS this potency had appeal for the younger vulnerable participants in terms of value for money and effect.
Among the contemporary regulars in particular, there was a sense of a very market-literate group. These participants focused heavily on policy and legality in terms of traditional substances, NPSs and decriminalisation and regulation. They appeared very aware of the relationship between legality, quality and availability, as evidenced by this respondent:
I see like in Holland if you ask them can you get mephedrone, you know like they can get you ecstasy, they can get you cocaine, they can get you anything you want, it’s all the best of quality, everything is top quality. If you ask them what mephedrone is they’re like ‘meph[edrone], what’s that, it’s rubbish, it’s crap, why, what is this?’. They never had to take mephedrone because their ecstasy has always been good . . . they’ve never had to experiment because they can go to their coffee shops, buy their cannabis and they can take their ecstasy, don’t need to be going down routes of mephedrone, these silly legal highs.
1008
Cost
In a general sense, throughout the narratives, mention was made of the low cost of various NPSs when they first emerged. This was particularly evident in the case of mephedrone following its emergence, but did extend to comments on SCs also. Cost of NPSs as motivation for use was discussed to some degree by participants in all groups; however, other factors emerged as more influential in terms of decisions to use or not to use NPSs. For example, a small number of students from the past recreationals group described the low cost of mephedrone as a driver of their use during a time in their lives of limited funds and experimentation. Group 3, who were contemporary users, also discussed cost, but more in the context of cost and quality of mephedrone relative to cocaine.
Cost (mostly of SCs) as a driver for use was most often observed in the generation NPS and persisters SGs. Among the generation NPS SG, the relative value for money in comparison with cannabis was highlighted:
The reason why people sort of switched to herbal is because you get ridiculous amounts for your money and . . . because of the stronger buzz.
1048
The initial appeal of perceived cost-effectiveness resulted in unintended consequences for some in terms of toxicity (explored further in Chapter 6):
I went in to try and get served but they wouldn’t serve me because I wasn’t 18. I got a wee guy to go in and get me it and he went in and got me it and came back out, 3 grams for £15. I thought, ‘****, you’re paying £20 for nearly 1.5 [grams] of grass‘. I thought, ‘this is cheaper in money and you’re getting double the quantity‘. I said, ‘sweet‘. I tried it and I woke up in hospital.
HMP1022
Cost was not static and was closely linked to other market forces. Generation NPS observed the way in which cost of SCs increased following the ban. When asked if SCs were cheaper than cannabis, one participant stated:
It was but it’s not anymore because it’s banned now. It used to be £20 for 7 grams, pure cheaper like and all you needed was one or two bongs.
1044
Among those in the persisters SG, cost also emerged as a key factor in terms of motivation to use. Similar to generation NPS, participants in this SG compared NPSs (primarily SCs and mephedrone) with traditional drugs and opted for the most cost-effective option (lower cost + greater effect = preference for NPSs/SCs):
At that time I was like, ‘well, it’s [SC is] £10 down there and £15 for 2 grams, whereas it’s £25 for 2 grams of the proper stuff’, so I went down and I swapped over and I was just buying it every day and smoking it every day.
1020
[Mephedrone] was also cheaper, I mean, coke was like – you see, for the street stuff like, the proper stuff that’s been cut up like 90 times, cost about £40 a gram. This stuff is costing £10 – apparently give[s] you a far longer hit and all the rest of it, so . . . That’s why I tried it, you know what I mean?
HMP1017
Like those in generation NPS, the persisters focused on the increase in cost following the ban. Both groups were affected to some degree by the ban introduced via legislation (in 2010 and 2016) and the subsequent rise in cost:
You know they’ve put it [SCs] up to £20 a gram now for flip sake, it used to be £15 for 3 grams when it first came out, then it was £20, £25, £35 a few weeks back and now it’s back up to £20 a gram.
1021
Most participants from the prison sample discussed cost of NPSs outside the prison. Those who mentioned cost inside the prison observed inflated costs for all substances, including NPSs, in comparison with street prices:
On the street for cannabis grass you pay £10 a gram, in jail you[‘re] paying £50 a gram if not more sometimes.
HMP1040
The cost of NPSs was not cited as influential for motivations to use NPSs in the prison estate. The potency of SCs and lack of detection in some drug screen analysis proved more appealing than cost. It was suggested there was little variance in the cost of traditional drugs compared with NPSs:
I was smoking [SCs] one night and I was down on the drug test the next morning and I passed, it doesn’t pick it up like for grass. It would be the same price, a gram of grass would cost you in here the same as herbal but herbal would **** you up more so people would want that in here.
HMP1012
References to non-monetary exchanges for NPSs, prescription medication and traditional illicit substances were also noted in the prisons. One participant discussed increased availability of buprenorphine (Subutex, Indivior UK Ltd) and, when asked where NPSs sat in relation to it in terms of availability, stated:
It’s like anything, if you want it you can get it, if you were struggling in here and you were in a bad way, it’s like anything, you could go out there and ask for something and there might be nothing about but if you start offering money or tobacco, you know, ‘I’ve got a bit of tobacco here, I’ll give you tobacco for it’, people then would maybe start saying, ‘well, OK, there’s always something for sale if you want it’.
HMP1004
Pleasure
Pleasure emerged as a driving force for NPS use in the narratives of some participants across the groups. Pleasure and NPSs were discussed in different ways: for some, the pleasurable experiences were recounted in isolation; however, for more participants pleasure was juxtaposed with adversity.
Pleasure was highlighted as a key driving force for the contemporary regulars. In the other groups, some participants also discussed the pleasurable effects of mephedrone, particularly in relation to first/early episodes of use. One female participant from the past experimentals group reminisced about early pleasurable experiences with mephedrone:
[Mephedrone] was supposed to be a good copy of MDMA and I suppose it kind of was, it wasn’t perfect but like you got a nice buzz and you felt the rush of coming up and stuff then . . . well, it kept you awake, probably worse than MDMA, you couldn’t sleep for a wee while after, but it made you more talkative, more chatty, a lot less self-conscious, time sort of passed and you would not have necessarily noticed time pass because you were having so much fun like dancing and chatting and having a couple of drinks.
1001
Similarly, a female participant from the persisters SG recounted her initial experience with mephedrone as pleasurable, thus leading to more regular use:
I went to a party one night and they had meph[edrone] and I took a line of it and it made me, wow, not smacked but jaw swinging and all. I felt brilliant, I felt absolutely brilliant, really really brilliant, I loved it, so that became a habit at the weekends.
1019
One male recruited from the prison sample described the pleasure associated with cognitive function/access while under the influence of mephedrone:
Meth [edrone] is sort of similar like, you know, if you got a trip on it, you know, you’re loving it like, sort of thing . . . I know I’ll only use a certain percentage of my brain like, but I know if I take certain drugs it can unlock different parts of it, you know what I mean?
HMP1007
The same participant recounted an experience with mephedrone wherein he and his friends believed they had come close to figuring out the meaning of life. When probed further about his motives for using NPSs and other substances, he stated:
People say you jump out of aeroplane[s] and get this high like, you know what I mean? Blues release dopamine same [as] with any opiate . . . that receptor in the brain . . . that dopamine, that’s what gives you the desire to do whatever, ye know? It’s just the same as jumping out of a plane. It’s just the same as hitting a jump on a motorbike. I’m addicted to what the brain can do.
HMP1007
Some participants acknowledged the pleasurable aspect of taking NPSs, such as mephedrone; however, the pleasurable effects were often juxtaposed with the negative after-effects or more long-term negative perceived impact:
It’s probably the shitiest drug I can think of actually. I mean, it’s good, it’s fun, it gives you energy, you can – everyone’s laughing and smiling and partying. It was basically free at the time, I remember.
1036
I suppose you would be flying – the E [ecstasy] sort of effect – you would be flying off your head, you would be very much enjoying it, very talkative, good craic. You were up all night, you were partying for 48 hours on the stuff with hardly any drink. Obviously it wasn’t great afterwards, but at the time it was quite good fun. Yeah, I suppose that’s about it.
1037
I tried the legal highs and I liked the legal highs more than I liked any one of the other drugs because I was hallucinating. I felt better on the legal highs but the legal highs destroyed me, they destroyed me.
HMP1022
Comments about SCs and pleasure centred around reports of positive effects but described an overriding sense of negative outcome, so, again, pleasure was juxtaposed with adversity. When one participant was asked to describe the effects of SCs after the correct dosage was reached, he stated:
The best way to describe it is like a light bulb turns on in your head and the rays go out the ways. It is like going to heaven to be honest, if there was ever a description of it, it is the best feeling in the world. I know that’s why people go back, it’s the strongest high I’ve ever had anyway.
1030
The respondent finished his description, however, by stating:
Herbal wrecks you. You couldn’t care less about anything or anyone, even yourself really.
1030
Similarly, one female respondent from the dependents group spoke about SCs and stated:
You see the buzz you get off them, it’s brilliant, I love it, but it’s wild bad for your mental health like.
1049
When discussing pleasure and vaping SCs, one male participant from the dependents group stated:
It’s hard to describe, but it was just the best feeling I’ve ever had in my life to be honest, but I know how bad that is and what it turned me into. I would have lied, cheated, stole[n] probably to get it and that’s not me. I knew that turned me into a completely different person and I’m obviously really ashamed of myself.
1026
Chapter summary
The findings described in this chapter have addressed the ways in which NPSs emerged in participants’ drug use trajectories to fulfil a range of functions. Other authors have also attempted to highlight where NPSs occupy particular niches in the overall market. Corazza and Roman-Urrestarazu150 helpfully delineate four distinct ‘niches’ that they suggest NPSs have served over time. The first concerns those who avoid breaking the law by using new substances that are legal to use (at the time of using) and that induce effects similar to those of banned substances. The second niche use is avoidance of substance use detection, for example some prisoners use SCs to avoid failing routine drug tests. 151 Third, for some the prospect of a new and interesting experience will drive them to use NPSs. Historically, this can be likened to the situation in the 1980s when ecstasy came on the market and provided an experience different to that elicited by other stimulants such as cocaine. The fourth niche use of NPSs focuses more on the motivations of drug dealers, who may benefit from selling NPSs under the pretense that they are a traditional drug.
Our findings not only strongly resonate with but also add more advanced nuance to the niches as conceptualised by Corazza and Roman-Urrestarazu. 150 In addition to use for ‘skirting the law’,150 for example, we were able to add detail about how availability was mediated by legal status. Group 2, for example, ceased using as soon as legal routes of access were closed down. The relative importance of legal status by group was again incrementally less important as we moved through groups 1 to 4. In its place, other drivers surrounding potency and cost were important. Comments from the prison population and those in services confirmed the important function served by NPSs to evade drug tests. Despite a perception of safety, as implied by legality,150 more than half of the respondents purchased NPSs on the grounds of their pleasant effects (55.7%), good availability (45.7%), enhanced sociability (35.0%) and affordability (28.6%).
Chapter 6 Knowledge and harms of use
Deligianni et al. 152 assert that awareness of the effects of NPSs and, importantly, the potential health risks associated with the use of NPSs of various types is lacking. Recent survey data have indicated that UK user and non-user perceptions of NPS safety have so far not been enhanced or altered in the light of the PSA or recent research. The EMCDDA’s153 recent report also highlights that the impact of different methods of communicating the harms associated with NPSs is not well understood and calls for the development and strengthening of the evidence base relating to risk communication. There is also increasing debate about the role played by the media in elevating the profile of specific NPSs and their effects. 154 Data from the narrative interviews in our study concur that there is a confusing picture around potential harms of various NPSs.
Reference to any NPS type in the limited experimentals group was minimal. In terms of decision-making specific to NPSs, participants in this group indicated that they found the limited testing of such newer drugs off-putting:
I don’t know, maybe it is just different lifestyles now but also I am scared of everything particularly like taking something that isn’t tested and nobody knows what it is. I just wouldn’t be tempted by that at all, to try something that is just sort of the unknown.
1011
Interestingly, one participant reflected on the fact that NPSs were not available when she was growing up but equivocated on whether or not their legal status influenced her decision to use:
I think if we had have been at school and it was happening, because they’re called legal highs, I think probably that’s, I don’t know whether I would have taken them but I think I probably would have been more inclined to because they were called legal, like that they’re not quite as bad, but obviously they’re dangerous. I think I probably would have known that but maybe I would have done it because it wouldn’t have been as bad as taking actual drugs to me.
1039
For most in the limited experimentals group, knowledge and perception of consequences of NPS use was informed by hearsay or peer experience, as identified through relationships between cultural codes and perception of risk:
These drugs [NPSs] are a massive thing. As I say, I’ve lost friends and I’ve seen what it can do to people so it was never really a big thing for me, it never has been, I’ve no interest in it at all so I don’t, that’s pretty much it.
1007
A proportion of those in the past recreationals group reflected on NPS use generally during their narratives. Similar to the limited experimentals, a majority based their perceptions of NPSs (as a group of substances defined as being legal) on what they had heard from various sources (e.g. peers, media). From these sources participants attributed considerable ‘danger’ to NPS use as compared with traditional substances:
To be honest I would probably rather go out, if I was to make a logical decision now, I would probably look up some of my old friends and get something illegal, because I’ve seen in the papers about all this sort of stuff and it’s starting to get really, really dangerous and at least I know whenever I was using illegal drugs no one I knew personally or not even any of my friends had anyone . . . become seriously ill or die[d] through that drug use so I would probably.
1001
Some also felt that these newer drugs were linked to mental health issues and an increase in deaths:
The biggest risk I see and I have seen and, as I’ve said to you, I seen a kid die, I seen people commit suicide, it’s mental, it’s purely the mental thing with it, it fries people’s minds.
1009
Group 2 respondents (past recreationals) also highlighted that limited knowledge on the use and production of NPSs, again in general terms, would be a deterrent for use. Respondents also commented on the need for regulation and the classification of NPSs:
I think they’re [NPSs are] not for human consumption, in my mind. In my mind it’s like any drug, they should be regulated and made safe for humans, and if someone wants to get flying then that’s their prerogative – it wouldn’t be mine anymore, I haven’t done it in years or anything. Legal highs should be just classified like any other drug, you know? Drugs in my mind should be legalised under a very heavy governed regulations.
1037
For those who based their perception of NPSs on personal experience, feeling out of control was a common theme. Participants more often referred to specific substances here. These participants also reflected on feelings of paranoia and anxiety:
We were smoking and smoking [SCs] and usually it takes 15 minutes to kick in so I didn’t expect, so I was just sitting looking at my phone and I looked back up at your man and **** the eyes just went pure black and sunk into the back of his head. I was shaking and my hands were like that there and everything, and then everything started triangle-ing, it was herbal like, I don’t know what type, it was grass herbal, I don’t know what it was called though and everything became triangles . . . there’s this big ring of light around you and everything is black and that’s exactly how it felt, because I didn’t know my way around the place, it was my first night there and I was like, ‘how to **** am I getting back?’. It was paranoia setting in.
1042
In group 3 (the contemporary regulars) there was greater awareness among participants about NPSs and some sought out information to inform their decision-making around use. Again, participants more often referred to specific substances:
That very same guy, he called himself Dr Zee, [the] guy he was amazing, anything he says I basically trusted. Whenever I had seen that documentary [about mephedrone] I kind of felt a lot safer about taking mephedrone, felt 100% about taking it.
1008
Some in this group garnered any information available about NPSs, and when there was a lack of information on, for example, mephedrone and SCs, participants promoted a sense of caution among their peers, encouraging harm minimisation, as they would have done about any substance:
I think it was just at parties – ‘this is mephedrone, do you want to try some?’ – this is the effect. It’s not that people are pushing it on you, it’s being kind of generous. And it’s also, I’ve found, always that people are actually more cautionary about it. The thing is, like drugs to other people than you would normally expect, so for instance they would say, ‘these are the effects, this is how you could feel’, just to allow people the space to comprehend what they are going to expect so that when they do take it, it doesn’t result in them kind of being really freaked out by anything. So I found it always, every single drug I came across, it was always like with a gentle caution.
1036
Other harm reduction strategies were evident among this group, in this instance when using mephedrone:
But it was really sore on your nose whenever you’re sniffing it – wasn’t really sore, it never made me bleed or anything, but you could just tell there was a better way around taking it, and we started filling capsules with it, you know, you buy flu capsules in Tesco’s [Tesco plc, Welwyn Garden City]? . . . that there was a lot better way of taking it. You didn’t hurt your nose, you had a nice clean buzz whenever you were coming up on it.
1008
For several in this group there was an acknowledgement of the complexities surrounding the pharmacological properties of various NPSs alongside awareness that being legal or herbal did not imply safety:
Probably the fact that it was a synthetic, like it just put me off the idea of it. I was like, what does that even mean, it’s synthetic, like what’s in it, what chemicals are in? I knew that it was only legal because it was something to do with that particular molecular structure wasn’t illegal yet, like at the time when I was in New Zealand they were fighting to get it pushed through legislation to make that molecular structure illegal . . . It wasn’t legal because it was good for you or it was healthy or it wasn’t dangerous, it was legal because there was some, there was some loophole and people were exploiting it.
1017
Respondents in this group reflected on the physical harms and psychological symptoms of NPS use. For example, respondents noted cardiovascular issues and pain when using mephedrone:
Then that ‘M-CAT’ mephedrone was introduced . . . It was like a hit from MDMA but it didn’t last very long and it was everywhere, absolutely everywhere . . . You knew it was so wrong, and your heart would go and you would get pains in your left arm and things and you would think, ‘god, I’m actually going to have a heart attack here’.
1028
Psychological symptoms such as paranoia and anxiety were also a feature across accounts:
I remember one night I took it and this was a horrible experience for me . . . I started getting a paranoia attack. I kept getting convinced that people were behind my head doing wanker sign[s] behind my head, so I kept going like this here and that there, then one time I was looking behind my back and then I turned forward and then I was convinced that someone had cut my shoelaces with a pair of scissors. I know it sounds absolutely nuts but this was what was going on in my head at the time and like, literally I ended up leaving the house I was so convinced that people were doing things to me and this is why I hate meph[edrone], to this day I hate meph[edrone], I think it is a horrible, horrible substance that people should never go near, but like that night that was it, I swore off it from then on.
1022
Respondents in this group also demonstrated general awareness of the potential for harm of NPSs, again more generally, as compared with traditional illicit substances:
They are definitely [more risky]. Even with cocaine and stuff, like cocaine would just make you feel really, really buzzy, you know what I mean? But like it’s better than taking, I think, legal highs. Well, from the experience that I had with them anyway. And then ended up in hospital as well, twice in the same month because I took legal highs as well – I was drinking as well as I was taking them.
1051
A prevailing theme was the concept that certain types of NPSs ‘changed people’. Again, relating to mephedrone, increased levels of aggression were noted by several users:
I always thought people were talking about me. I remember chasing my boyfriend across the town and throwing my shoes at him and I’m not that kind of person, like I was getting really angry and I was like, ‘I’m going to turn out like my dad, my temper is horrendous’. I couldn’t control it and then I stopped doing that because it actually made me into such an evil person. I was throwing my drinks at him and everything. I couldn’t control what I was saying as well, it would just come out.
1015
Adverse experiences with certain NPSs did not put participants in this group off using traditional illicit substances, just the NPSs:
No, it’s not that I was scared to do any drug after that, it was just the legal.
1051
In group 4, SG1 (generation NPS), narratives tended to be more reflective of the effects, physical and psychological, of NPS use. This was mostly related to SC use:
Yeah, I was too used to grass, it wasn’t doing anything anymore, just leaving me hungry. I didn’t feel any good buzz of it and smoked legal highs and took and turned blue and my ma said to me, ‘if that doesn’t wise you up, nothing will’. I just kept smoking it . . . I’ve cramps in my stomach and all, like if I don’t get it I would . . . sweat like I’m sweating now . . . Just feel sweet, my stomach and all doesn’t be sore anymore, I be getting DTs [delirium tremens] . . . mood swings and all too.
1044
Experiencing and witnessing severe adverse effects of SCs was notable in this group, with reports of seizures, blackouts, dizziness, weakness, chest pain, palpitations and vomiting. The compulsion to continue use was evident despite these experiences:
There was a new blend, ‘Magic Dragon’, came out . . . One of my friends smoked a bomb of it . . . then dropped and had a seizure and sort of throwing up all over himself and all . . . Rang an ambulance and the security came down.
1046
There were references in this group, similar to those in group 3, of NPSs ‘changing people’. In the following instance, this concerned SCs:
It [SCs] just changes you as a person, changes your whole personality, it just . . . you would do stupid things all for a bag that size. I mean, stupid, stupid things that [you] never would’ve thought about doing.
1048
Given that NPSs were the primary and only substance of dependency in our generation NPS group, some participants reflected on the adverse effects experienced in periods of SC withdrawal:
Five days was the longest . . . was the whole withdrawal. The first 3 [days] were the hardest. After – the first to the third was some of the worst 3 days of my life. I was just lying in bed, aching with pain. If I moved I felt sick, if I breathed I felt sick, if I spoke my throat hurt and I felt sick, all I wanted to do was lie in bed and die . . . After 5 days, I didn’t really feel fresh but I felt done. After 2 weeks I felt clear, that was me, I was gone then. It was the first 3 days – phewww – crazy days.
1046
Related to the local Northern Ireland context, and identified in geographical, cultural and political codes, NPS use incurred paramilitary-style punishments for some participants. This was highlighted by a significant minority in the group:
I walked out, a man grabbed me so he did, dragged me up the entry and there was seven more men waiting there, and he said to me, ‘get on your knees’, and I goes, ‘no’ – and he pushed me . . . Then . . . they hit me with hammers, knuckle dusters, gave me a bad hiding [beating] first. Then they said they would shoot me here – that they’d put two bullets in my leg and see . . . one through there and one here [shows leg], straight through . . . That’s for taking legal highs in the area . . . I don’t think it’s teached me a lesson like, but I’d do the stuff over again.
HMP1018
With this group there was clear awareness of the issues linked to managing potency and dosage of NPSs:
I never let, you know, there are some eejits that I actually run about with who would spray up, have seven or eight sprays in a bomb of herbal, and that’s loads like – that’s die-on material. I’ve never, ever, ever let anybody pack me a bomb of herbal – always packed it myself – so I always control how much I’m taking. Regardless if it’s being passed about, I’ll always pack my own bomb, I’ll always roll my own joint, I don’t care what anybody else is. I have took smokes off other people’s joints that are packed and I have smoked very, very packed bombs like, that’s when I’ve had me bad trips, kind of put me to . . . you know what I mean?
1046
There also appeared to be a growing culture of sharing harm reduction advice in networks. As in group 3, several participants in this group drew on the risks with newer drugs and contextualised them with reference to traditional substances:
One hit from herbal – if I seen someone now who asks me, should I take herbal or why, the first thing I would just say, if you are going to take it, don’t take too much and take it on occasion.
1046
Similar observations were evident in the narratives of SG2, the availers, who attempted to mitigate risk of harm by careful dosage and testing potency. Consequences of use with this group also centred around physical and psychological harm (see Chapter 7 for more information specific to SCs):
Palpitations, nearly every one of them have give[n] me palpitations, which occasionally I get now and again with hash. My heart rate always speeds up on coke but occasionally you get palpitations, but every legal high I’ve done I’ve got palpitations and it’s kind of been uncomfortable, it’s been worrying, like a totally irregular heartbeat, it’s fluttering and then missing a beat and then fluttering and missing a beat. Just generally unpleasant.
1027
In SG4, the persisters, narratives recounted experience of use. As with generation NPS, this group reflected mostly on the potency and effects of SCs, with evidence of harm reduction information being passed around peers. Even our more experienced users reported unpredictable effects:
I laughed at them. They said, ‘be gentle on them’, and I says, ‘I’ve got big lungs, it takes a lot to knock me down’. I took it and I walked from about here to another 6 foot past the door and that was it, I can’t remember nothing. I remember going down on the wall, my knees wouldn’t hold me up, my hands still couldn’t hold me up, they weren’t operating properly, if you know what I mean, and I just slid down. I was sick a lot.
1021
In terms of harms experienced from use, the range was significant. Physical and social harms were evident and explored in this group in terms of the use of both mephedrone and SCs (see Chapter 7). With the use of SCs, the physical harms of use were reported both during use and in periods of withdrawal:
Sickness, diarrhoea, kidneys, I actually thought my kidneys were failing, like they were going in, people could feel it going in. Sure, you know, I lost all that. I’ve put it back on again and I’m raging. I lost two and a half stone . . . I thought I was dying. Physical, yes, most definitely physical pain all over my body, mostly inside here. I don’t know what part of your body is here.
1019
As well as sickness and vomiting reported as physical consequences of use, loss of appetite was also common with the use of SCs and mephedrone:
The powdered herbal stuff, very addictive, very addictive, and it was cause and effect of starvation as well, because at times there was maybe 2 or 3 days I was going without food and not even knowing it, you know, not even wanting to go without food. It’s just one of those things that you never thought of, you didn’t want to do, you never got hungry for some reason on the stuff, you never got hunger.
1020
There was also evidence of knowledge that some individuals used mephedrone to actively lose weight:
I had a friend and she was in England . . . and she got into I think it was meph[edrone] and like, she was a big girl . . . She done it to lose weight, that was her intention, to take it to lose weight. I was like, ‘be a normal person and go on a diet, don’t take drugs and like, because your jaw is hanging off you, you can’t eat, that’s not normal’. As I say, people take drugs for all kinds of reasons and that was her personal reason.
1007
In addition to weight loss with mephedrone, individuals reflected on sleep disturbance/insomnia and cognitive issues that affected their speech and concentration:
You see, to recover from that [mephedrone use], from all that, for about 6 to 8 months, it took me like . . . really . . . over a year like. Then my speech was all kind of messed up – kind of slurring words and all. Found it difficult to kind of figure out like simple words, you know, in a conversation? I was just kind of . . . mind completely blank. It started freaking me out like . . . a lot of really bad negative effects from it – probably still have effects from it now, to be honest with you. Concentration was gone for that whole time.
HMP1017
As identified through codes related to physical setting and use of NPSs, SCs were commonly used among the homeless population, both to induce sleep and ease the physical, social and psychological suffering often associated with living on the streets:
Yeah, the first time, but even now I could smoke it and go to sleep, I would smoke it and just fall asleep. Do you see when I was on the streets I would have a pipe next to me and take a pipe and then fall asleep because I couldn’t sleep on the street otherwise.
1015
The severity of adverse physical experiences of NPSs was evident with this group:
I ended up getting bowel problems. I ended up going to the doctor and he didn’t even know what mephedrone was, and I told him. It was something to do with the blood in the stomach, I can’t remember exactly what it was but my bowel wasn’t working right, just because I was taking so much of it. He said that’s what it probably was, but it didn’t stop me doing it, unfortunately.
1059
One participant also reflected on injecting mephedrone and experiencing physical harm at the injection site:
I said, ‘what’s that you are doing?’: I said, ‘heroin?’: And they go, ‘no, meph[edrone], kid’. I said, ‘**** it, give me a go at that’. I had a big black hole in my arm there and all because the meph[edrone] burns your arm, burns your skin away, and I didn’t realise . . . Then after that I sort of stopped it because the big hole in my arm it was disgusting and I just went, ‘ah, **** that’.
HMP1019
There were also numerous reports of mephedrone and SCs causing psychological harm with this group, predisposing people to outbursts of uncontrolled violence:
The first time I smoked it . . . they said I really flipped out, violent, punching staff, punching girls, punching boys. I don’t even remember it like. They were trying to lift me up the wall and I started being sick all round the hostel and they kicked me out the next day.
1021
On a very practical note, there was also a sense in this group of vulnerability to theft and other crimes while under the influence. This was particularly the case with those who experienced homelessness:
I always safely smoked it [SCs] because I didn’t want to be lying, because people were smoking it and they were falling asleep and people were stealing things out of their pockets and all, so I knew not to push myself that far.
1019
This group evidenced the most polydrug use of all groups, and the sheer number of substances used in harmful combinations was notable:
I took meph[edrone] one night actually, smoked herbal as well, seized out for about half an hour, foaming at the mouth and all, then some simultaneously of like, weed just, and that brought me round. I’m trying to think of any other dodgy experiences.
1030
Fluctuations in quality took even the most experienced users by surprise and resulted in medical treatment:
Someone I knew had it. I just took a few draws the first time and then that’s when . . . Then I got weaker stuff and that was alright, so [that] made me start smoking it, and then taking wee pipes of it, and then once the strong stuff came in again, that’s when I went back off it again. It was too strong because it was just knocking me out and I was waking up in hospital all the time – overdosing on it more or less, because I had methadone in me, you know what I mean? It was just knocking me clean out. Waking up and ambulance men and all around me. Just had enough of it, had enough because it was happening too often.
1058
Perception of risk among some participants was linked to the danger of mixing a range of NPSs with traditional substances (as noted previously), with potential risk of death. Users in this group also highlighted differences in the brands of SCs that they had used.
A lack of knowledge (linked to potency and unpredictability) and differences between obtaining online and obtaining from a street dealer were also evident:
I think that’s the problem these days, all these things are coming out and they’re so strong and people don’t know what they are and they’re taking them and that’s when stuff happens. It’s getting a bit more complicated with the amount of stuff coming out . . . When we were getting the 2C in the powder and stuff, we knew what it was because he was getting it off the dark web or whatever, so he knew what he was getting. When we were getting the 25I [2C-I-NBOMe] we didn’t know that’s what it was, we were just told it’s a trip, go head. So we done it, because from getting 2C-I and all that there it was a powder, so we thought it was something along those lines, but then when we found out what it was, it was like, hold on, we need to take a step back there. We must have rinsed it for about a year because it was cheap.
1059
Chapter summary
Recent data have indicated that a lack of knowledge on the various NPSs still exists and has not been enhanced despite the PSA or recent research. Media accounts, at times sensational, remain pivotal to information exchange. Our narrative data highlighted the mixed picture with regard to perceptions around safety and harms from use of various NPSs by respondents across our groupings. Linked to timing of onset, many of our respondents, irrespective of group, acknowledged a lack of information on the range of NPSs they were initially using. The inherent risks presented in these circumstances are significant. When mephedrone first emerged on the market in 2010, users tended to be mainly young and neophyte, non-marginalised experimenters. 153 We posit that the same appears to apply to some of our users in marginalised groups, who, although experienced polydrug users and even injectors, were taken by surprise by SCs. Recent assessments by the EMCDDA153 note the potential for further unintentional use of new synthetic opioids at a time when the distinction between the use of NPSs and illicit drugs may be diminishing. This, they note, raises public health concerns, and these concerns are shared by users who report fearing these substances.
Cultural context, in terms of exposure to and normalisation of NPSs, was associated with perceptions and experiences of risk, and was evident across all groups from the non-NPS users to those dependent on NPSs. Groups 1 and 2 reflected on safety in terms of risk of harm of using substances, including the potential physical and psychological effects of using substances and potential risk associated with the environment where substance use occurs. There was a general theme of wishing to remain in control of their behaviour, with respondents in group 2 reflecting on the significant effects of SCs and loss of control when under the influence. Decision-making was influenced by hearsay around effects (what participants have heard about people who use drugs through the media, peers and members of the community) and perceived risk. This was coupled with the scant information available on various NPSs and lack of testing. In group 3 there was evidence of the power of negative media stories as a means of information, which were for some the leverage needed to help them. Groups 3 and 4 drew on the physical, psychological and social harms associated with NPS use, and the emerging culture of harm reduction messages being passed on by peers themselves in user networks was evident. This was only possible once that wisdom had been experientially accrued over time. O’Brien et al. 18 found that, in an internet-based survey of ‘cybernauts’ (n = 183), participants considered themselves to be knowledgeable consumers, searching the web to gather knowledge about NPSs and pass on their own experiences (e.g. potential harms) to other NPS users. Retailers have capitalised on the knowledge shared by these online communities and have even reported monitoring internet forums for trends and adapting their stock accordingly. 20 The relationship between NPSs and existing traditional markets is a highly complex one, and a temporal relationship between variations in the purity of traditional substances can be observed. 23 Other authors have documented the displacement effect of the various forms of NPSs. 24
We have focused here on the harms as discussed by respondents but end with a word of caution with regard to how the media portray harms of use. Sumnall155 reported in The Guardian: ‘While the dangers of spice and other “novel psychoactive substances” are at the forefront of public consciousness, the numbers of people seeking treatment for their use are minuscule compared with those presenting with problems from using traditional cannabis’. Further, more detailed discussion on SCs now follows in Chapter 7.
Chapter 7 Synthetic cannabinoids
Synthetic cannabinoids account for the largest collective group of substances presently monitored by the European Union Early Warning System. 153 These drugs are designed to mimic the psychoactive effects of tetrahydrocannabinol (THC) and bind to the cannabinoid receptors in the body. Originally synthesised in the 1960s, reports suggest official detection of SCs in European drug markets around 2004. Emergence of SCs rapidly escalated from one product being monitored in 2008 to 169 products being monitored by December 2016. 153
With manufacture primarily taking place in China, SCs are generally imported to Europe in powder form, where they are sold in powder form or dissolved in solvents and sprayed onto (inert) plant material and prepared for distribution through drying, crushing and packaging. 156–160 Once prepared, SC products can be consumed through smoking rolled joints/pipes, vaping SC products161 and smoking SC-soaked paper. 162
Similar to SC brand names, the molecular structure of SCs has changed and evolved over the years, primarily to circumvent legislative control. Early variations of SCs are referred to as first-generation products and were not initially controlled under the Misuse of Drugs Act 1971. Following the introduction of legislation in 2010, second-generation SCs emerged and the cycle continued until the latest, third generation of SCs,163 controlled in 2016. The brand names under which SCs are sold are broad and diverse. Like other NPSs, SCs were originally available from street-based headshops, online vendors and street dealers. Research suggests that although legislation has reduced sales from high-street vendors, there is continued supply and demand from online vendors and street-based dealers. 15,41,164,165
Although often assumed to mimic the effects of THC in cannabis, SCs are much more potent and have enhanced affinity to bind fully to cannabinoid receptor type 1 (CB1) and cannabinoid receptor type 2 (CB2). THC in cannabis is only a partial agonist to the CB1 receptor. 166 Adverse effects of SCs include hypertension, seizures, palpitations, chest pain and tremors. Neuropsychiatric effects include aggression, suicidal thoughts, anxiety and psychosis. 45,167 Evidence demonstrates an unmistakable disparity in terms of side effects of THC in cannabis compared with SCs. In fact, Winstock et al. 168 note that an individual can be up to 30 times more at risk of requiring emergency care following SC use than cannabis use.
Research suggests that the appeal of SCs is now more evident among certain subpopulations, particularly those who are homeless, are incarcerated and/or suffer from mental illness. A recent study conducted by Van Hout and Hearne164 found that buyers in cryptomarkets expressed more interest in gamma-aminobutyric acid (GABA)-activating substances and stimulant and dissociative NPSs than SCs, with forum discussions focusing on the negative effects of SCs. Blackman and Bradley169 also note the shift from middle-class experimental users of SCs when the substances first emerged to only the most vulnerable and marginalised populations using SCs. This finding is supported by results from a US study wherein homelessness and mental illness were both prominent correlates of SC use. 170 Ralph et al. 54 also highlight prevalence of SC use among prisoners in England and cite avoiding detection as the primary motivation for use.
Existing guidance for the treatment of NPSs deals with the vast array of substances in a similar fashion to that for traditional illicit drugs, that is, according to presented needs and drug effect and based on the pharmacological category in which the substances fall. 46,171,172 These categories include depressants, stimulants and hallucinogens. SCs fall outside the remit of these categories in terms of clinical management, and so are considered separately. Interview data from the current study support evidence that SCs are entities worthy of separate and special consideration when dealing with the wider categories of NPSs. Data presented in this chapter generally offer support for existing evidence around the types of SCs, effects, perceptions and reported harms. 30,41 Findings substantially contribute to the sparse evidence base around serious adverse effects of SCs, motivations for use, drug use outcomes in less established substance users, withdrawal from SCs and the relationship between use of SCs and traditional illicit drugs, particularly heroin.
A recent systematic review of international trends of SC consumption suggests that use is generally not sustained and is confined to populations with previous extensive histories of substance use. 173 Data from the current study adds to the knowledge base as it evidences both sustained use of SCs and use that extends to populations not already engaged in more chronic patterns of substance use. Descriptions of use of SCs in our narratives yielded significant amounts of data and provided insights into the patterns of use. Where particularly relevant, data are presented with reference to taxonomy groups, otherwise they are presented by respondent identification number.
Patterns of use
In total, more than half of the sample (n = 46) reported lifetime use of SCs. Very experimental use of SCs (generally confined to isolated incidents) was observed among past recreationals and contemporary regulars as well as availers. More persistent and problematic use of SCs was noted among participants in our dependents group, notably in generation NPS and persisters.
Interview data indicate patterns of SC use that largely fall on either end of the drug use continuum, that is, use was either very experimental and generally an isolated incident or use was reported as dependent:
I was addicted to it four different times and I would say the last time was the hardest time to get off, that would have been just over a year ago, but every time you smoke it you do get hooked on it every time, it just gets worse and worse to quit.
HMP1020
I spent that £1600 just all on legal highs, and I was very addicted at that stage . . . smoking it, smoking it . . . Like, I was hooked from there onwards.
HMP1023
Very few participants reported use of SCs that was more sustained than experimental but not described in terms of problem use:
I didn’t really feel addicted to it [SCs] like, but if it was there I would’ve took it.
1057
For those who did report dependency on SCs, there was consensus that tolerance developed rapidly:
Herbal scared the **** life out of me whenever I started using it, but after a while my tolerance built up, started enjoying the buzz, started using it more. Then I got too high of a tolerance and started [to] dislike it but it sort of messed me mind up, so, I came off it and now, for the **** withdrawal, hairy, but I’m just very, I’m grateful for the fact that I was only using herbal for 3 months.
1046
Your tolerance, it’s pure quick too like, you don’t know, about 4 months in I didn’t have it 1 day and I just needed it and ever since then I haven’t stopped.
1044
I was only having two or three drags every time, then within the space of a few weeks I was up to smoking a one skinner and then I was smoking a two skinner, then when I wasn’t smoking I didn’t feel normal, everything kind of just got too much.
HMP1020
When the participant above was asked about the time frame after which he noticed not feeling ‘normal’, he stated:
I would say about 5 or 6 weeks.
HMP1020
Types and sources
The range of SCs reported by brand was diverse. Specific brands included but were not limited to ‘Doob’, ‘Magic Dragon’, ‘Clockwork Orange’, ‘Damnation’, ‘Hitman’ and ‘Sky High’. Participants also made reference to the range of flavours, in terms of flavourings added to mask the taste of the solvent used, including blueberry, strawberry and strawberry shortcake. Geographical setting codes highlighted regional variations in terms of the way SC products were understood and described. A number of our participants from a more rural part of Northern Ireland referred to SCs as ‘trippy’. The majority of those from the Greater Belfast area made reference to ‘herbal’ when discussing SCs; however, it was important to ascertain whether participants were referring to ‘smokeable herbal’ or ‘herbal powder/sniff’ (i.e. synthetic stimulants). Herbal cannabis was referred to as either cannabis or ‘grass’.
The primary route of administration of SCs reported was smoking in the same way as cannabis, that is, SCs added to tobacco in a rolled joint or smoked in a pipe/joint without adding tobacco. A number of participants from the prison sample also reported SCs in the form of soaked strips of paper smoked in a joint. One participant reported vaping SCs in the form of ‘C-Liquid’ using an e-cigarette. The majority of our participants sourced SCs from headshops prior to closure or from street dealers/friends of friends (social supply). In line with survey data, only a small proportion of those who used SCs reported purchasing them online.
Perceptions of synthetic cannabinoids: physical and psychological effects
Positive reported effects of SCs included a ‘heavy buzz’ and intense ‘stone’. Although some positive effects were reported, there was consensus that the experience of using SCs was not altogether a positive one. One participant noted the effects as simultaneously positive and negative and made reference to shame experienced following use:
It’s sort of like being stoned with a few extra things, if you, I don’t know, sometimes it just gives you a sore brain, it’s like somebody puts a pile of needles in there and it’s not great but most of the time when you smoke that first bong actually your brain lights up and everything is just so much better. But I don’t know, it doesn’t make you feel good if that makes any sense.
1030
From the early stages of data collection, contradictions between initial perceptions and subsequent experiences with SCs were evident. As noted from respondent characteristic coding and cross-group comparisons, both our younger participants and our more established substance users were under the impression that SCs carried with them less risk than traditional illicit drugs. SCs were initially assumed by both groups to be a legal substance that mimicked the effects of cannabis:
People always said it was like a substitute for cannabis, it’s just like grass and that’s what got a whole heap [of people] onto it, and before you know it, then it was flung everywhere, in schools, youth clubs, the whole lot. You couldn’t turn a corner without smelling it or seeing it. And . . . it was just weird. I seen what were happy and happy-go-lucky people change over a short while of time, all on this stuff . . . taking convulsions and heart palpitations and shit.
1048
I just wanted to see what it was like, but to me then, it was safe because it was called herbal, I thought it was good for you. I would rather smoke herbal than grass or ‘blow’, that’s how it starts.
1019
I thought you could treat herbal like cannabis and just keep it like normal.
1021
The reality for the majority, however, was that the effects were far from those of cannabis in terms of physical and psychological effects, both acute and long term.
One participant from generation NPS described his first encounter with SCs and the adverse physical effects experienced:
My wee cousin found it and he brought it down to me, he thought it was grass. I smoked the bong and he cleared and I just kept saying to myself, ‘I’m going to die’, and I just blanked out. I woke up and thought everything was sweet and I walked downstairs and my ma started shouting, ‘what to **** are you on?’ and all. I turned blue and there was white stuff coming out of my mouth and all, foaming at the mouth, then she was about to ring an ambulance but I came round to myself.
1044
When asked about the stage at which the participant became aware that he was not smoking cannabis, he stated:
Yeah, it felt like a whole different thing. Just hit you 5 seconds later and I knew straight away I was ****. It was scary. Now I can smoke that like I can smoke grass, doesn’t even barely do nothing anymore.
1044
Another young person from this group focused more on the adverse psychological effects following use:
There’s about four or five stages you go through whenever you take it. Some of them are good some of them are bad. First you feel all calm, you’re all OK and stuff, then the next minute you start feeling this really, really, really bad paranoia. You think everybody is just coming to get you, you know what I mean?
1051
Adverse psychological effects of SCs were also reported by more established substance users in the persisters SG:
I’ve been taking heroin for about 13 or 14 years but I had about 4 years clean there, but I went back on it the last 3 or 4 months there. It was more the herbal when I was out [of prison]. It’s really **** with my head big time. You would take your life in an instant coming off it and wouldn’t even think twice of doing it. It’s crazy. I don’t be suicidal or anything . . . I don’t know what it is – it’s not good at all.
HMP1021
In terms of chronic use, the effects of SCs are also described as very different from those of persistent cannabis use:
I believe it’s eating your insides, it’s affecting your kidneys and it’s affecting your bladder 110%. I’ve had to get tablets for my kidneys and my bladder and everything because of it. They can’t understand why, they don’t know what’s going on, they don’t know why I’m constantly needing to go to the toilet because everything seems alright. Herbal has ate my insides. I can feel it eating inside me, I can even feel my bones rattling, I can feel it.
1019
Commonly reported adverse physical and psychological effects of SC use included and were not limited to collapse, fits/seizures, blackouts, chest pain, palpitations, cardiac arrest, vomiting, loss of appetite, weight loss, disrupted sleep, stomach pain, sweating, self-harm, lack of awareness of behaviour, severe withdrawal, paranoia, anxiety, depression, psychosis, stress and memory loss.
Literature suggests that cardiac arrest following use of SCs is typically less common than acute adverse effects. 41 Although more participants reported acute adverse effects, almost one-quarter (n = 11) of those who reported lifetime use of SCs either experienced cardiac arrest themselves or knew someone who had experienced it following use of SCs:
My normal heart rate’s between 80 and 90. My heart rate was 178. They had to actually stop my heart and restart it again. I was actually dead. They had to restart my heart again, it was beating that fast, 178 or something it was. They actually had to stop my heart and restart it again . . . that was because of the herbal mixed with the methadone. So that’s what actually put me off it for good – it scared me like, big time, big time! They actually said to me, ‘you were in a body bag, you’re lucky you came around’, you know what I mean? It actually scared me something shocking like. I was in intensive care for 2 weeks. So, big time, I’ll never be near it again, never. That’s what I said to all the kids and all . . . ‘you don’t want to end up like me’, you know what I mean? They just don’t listen to you, they just don’t listen whatsoever.
1058
It’s lethal. My mate had a heart attack on it and he still couldn’t stop smoking it, because of it, and he has just got his heart fixed and he’s still smoking it.
HMP1007
Research indicates an association between chronic use of SCs and serious cognitive impairment in relation to concentration, attention and memory beyond the period of intoxication. 159,160,174,175 One of our younger SC users in the sample reflected on the lasting cognitive effects of SC use:
It’s just a mad hit you got off it. Like, there’s all sorts of crap in that stuff, chemicals and all. Like, you see my face, my skin, when I was smoking that stuff my skin used to always break out. It’s made my face bad now. It makes my memory – I don’t have good memory and all. I can’t read, I can’t really write or nothing, because of legal highs.
HMP1018
When asked about the period during which this change in cognitive function was observed, the respondent stated that it was over a period of 1 year and went on to say:
Yeah, I was in school – I don’t know how to add up. I used to be able to do it. Read, I can’t read anymore really. Like at night, when I sleep at night, I think I’m sleeping but I’m not. All mad stuff comes into my head. I need to watch like TV to keep my mind occupied, so I do. It just changed when I smoked different like brands of it.
HMP1018
There was consensus among those who reported issues of dependency with SCs that it was ‘worse’ than any other drug they had encountered. Furthermore, a small number of participants discussed the way in which the drug became known as ‘dirty’ and use, for some, carried with it shame:
When you’re smoking it . . . well, I don’t know if it’s the same for everyone else, but you’re seeing a wee bit of shame in yourself because you’re doing it, you’re smoking the dirtiest thing I’ve ever come across.
1030
Although some degree of normalisation of SC use was evident among generation NPS participants, stigmatisation of SC use and users was also observed. Perceptions of SCs changed as the number of drug-related deaths among young people increased and the media focused on SCs and ‘spice zombies’. One of our participants who transitioned from SCs to prescription medication stated:
You see like [friend’s name], then he ended up dying. I think that’s when it kind of hit a lot of people because he would have been really, really well known . . . So when all that happened I think it kind of calmed people down. I know you are going to get the general scumbags, they’re still going to take it [SCs].
1053
One participant expressed his frustration at being asked to leave the hostel he resided in at the time of interview because of his use of SCs. He suggested that SC users are more marginalised than injecting drug users in terms of harm reduction offered by services:
See, the heroin users, they get their needles and all changed. If they find needles in their room, the sharp box goes up.
1021
It is of interest that mephedrone was also perceived as a ‘dirty’ drug in terms of effect by users; however, those who used mephedrone did not reflect on use with shame.
Motivations for use
As highlighted previously, motivations for using SCs differed across the sample. For our established users and more vulnerable participants, SCs offered the desired effects (discussed in more detail in Relationship between synthetic cannabinoids and heroin). For younger members of our dependents SG generation NPS, initial motives for use centred primarily around availability, accessibility and normalisation of use among peer groups. It became clear that SCs for this peer group were as normalised as cannabis was for previous generations:
Well, we would have went in about 11 in the morning and then there was always someone that was like 19 and they would’ve done your drink run, and you would’ve paid them . . . for doing it. So, we would’ve done that there and then we would’ve went to like [to parks] . . . that was every Saturday – Friday and Saturday – we would’ve done it. And then when it got into the summer we started, everyone started smoking herbal. I don’t know, I think it was like, the first summer it was like a big thing, it’s like 5 years ago.
1053
Among the prison population, SCs were appealing in terms of lack of detection in routine drug screening tests:
I mean that Sky High stuff, I just had a whole bad time with it, it wasn’t what I thought it would be, because I did smoke some . . . legal weed called ‘herbal haze’, that was OK and it wasn’t showing up on drug tests, so I didn’t care. I was still getting stoned, I wasn’t collapsing, it wasn’t showing on a drug test, but I suppose they can put anything into them psychoactive substances . . . It doesn’t come up on a drug test, any other drug would come up on the drug test and you would get dropped to basic or sent to the block or something, like I was smoking it one night and I was down on the drug test the next morning and I passed. It doesn’t pick it up.
HMP1012
As indicated by the participant above, evading drug tests through the use of NPSs, reduced the chance of demotion from enhanced to basic allowance in terms of privileges in the prison. This excerpt demonstrates reproduction of risk through physical setting and drug policy.
The media have highlighted the use of ‘spice pigs’ in prison whereby vulnerable prisoners are recruited to sample new strains of SCs prior to distribution among the wider prison population. Our data captured a more sinister phenomenon wherein prisoners were offered SCs for free, but on the condition that they smoked a set amount, usually in excess and more for the entertainment of other prisoners rather than actually testing the effects of the drug:
The herbal cannabis in the jail, it’s something else. There was that much people were giving it away. People were actually only getting to smoke it if they would smoke a good amount on a bucket, so then other people could sit and laugh, laugh and have fun about what way these people were taking bad effects to it.
HMP1008
Quality
Distinctions were made in terms of SCs and perceived quality with regard to the presentation of the substance on purchase. SCs purchased from a street dealer in a sealed and branded bag were considered gold standard in terms of quality. This was the case both pre and post closure of headshops for those who primarily sourced SCs from dealers.
If you get it in a normal bag, someone has went out of their way to put it into this bag, whereas if you get the sealed bag you’re getting exactly what that boy bought off the internet.
1030
Then stuff like strawberry blends, strawberry shortcake, blueberry – that was all cheaper herbal that came in baggies. That stuff was a lot weaker – it was a lot, way, way, way, way more for your money. Everybody was trying to get the sealed bag stuff. The sealed bag stuff was the stronger stuff like. That was all the Sky High, the Magic Dragon and Doob, and all that.
1046
The use of brand names makes identification of SCs and assessment of harms difficult; however, there was consensus that Sky High was the most potent of all SCs. Despite the fact that participants may not have been well versed in the evolution of SCs from first-/second-generation to third-generation products, some of the more established SC users observed the changes across time and discussed the repercussions:
The herbal Sky High, it’s the only one that affects me. The orange one used to and then once Sky High was getting banned we sort of went around all different flavours to see what one is good, and there’s one pineapple [one] that would give you a giggly effect, you wouldn’t get that. If it was berry, you wouldn’t have as much mind stuff, if you know what I mean, you were too busy laughing at nothing.
1021
You see that Sky High, people are dropping with Sky High.
1049
The one that was the strongest was the Sky High.
HMP1018
Withdrawal from synthetic cannabinoids
A number of our participants discussed issues around physical and psychological symptoms of withdrawal experienced when ceasing regular SC use. Withdrawal was described in particularly unpleasant terms by all those who reported dependency issues with SCs:
It’s wild, wild addictive like. You see, whenever I was coming off that herbal, holy ****, I’m telling you, I was sweating and everything, I was at the toilet every morning being sick, couldn’t eat, couldn’t sleep, like I couldn’t sleep without it, couldn’t do stuff without it and I couldn’t move . . . I smoked legal highs and I want it more and more and more and more and more. I got addicted to it. It was getting to the stage, every morning I was being sick, you know, nothing was coming up and if I ate anything it was coming back up, if I drank anything it was coming back up – I was just . . . I don’t know . . . I was cold, I was shivering, I was sweating, just felt like I was dying when I was coming off it. It was just the hardest – it’s a nasty, nasty, nasty drug. It’s on our streets and it needs to be **** took off our streets – because I smoked it last night and I thought it was ‘green’, I thought it was grass . . . What the ****?
1049
There was consensus that symptoms of withdrawal were experienced within 1 to 2 days of ceasing use:
The next day. You see, if I woke up and I never had nothing and I drank nothing that day . . . I would be lying there in a ball, sweat beating off me.
1049
Although the period of withdrawal was described as particularly unpleasant and akin to withdrawal from opiates, symptoms reportedly subsided after several weeks. The following section, Relationship between synthetic cannabinoids and heroin, delves further into the complex relationship between the two substances. However, it was apparent that the SC effects and withdrawal played a role in terms of accelerated pathways to more problematic/severe substance use, particularly among our younger, generation NPS SG:
I managed to get off it [SCs] there about 3 months ago now. That was awful. It [was] literally like being in hell. Your skin is on fire, your head is just far gone, like even in the hospital, like I ended up over there, it was that bad, and I was clawing at the ground and trying to rip my hair out and all and they jabbed me with diazepam, like the strongest stuff they had, and I was still losing the plot, so it’s a lot stronger than anything else I’ve ever came across in my life, even the 4 years I was smoking grass, it was nothing on the 6 months of smoking herbal. It wrecked me. I’ve barely touched anything since, apart from the odd . . . joint or something, and I would have a wee smoke of it, but I’m not going out and buying drugs really, maybe the odd Class A, but I was never addicted to them anyway, it’s just for fun rather than fuelling my drug habit.
1030
Relationship between synthetic cannabinoids and heroin
Existing research on NPSs has described the transition from injecting traditional illicit drugs to injection of NPSs (e.g. from injecting heroin/crack cocaine to mephedrone/ethylphenidate) or the transition from smoking cannabis to smoking SCs. 176 Absent in the literature, however, is the way in which SCs relate to traditional illicit drugs other than cannabis, in particular heroin. Increased prevalence of SC use among vulnerable populations is documented in the literature; however, the complex dynamic of transitioning to and from SCs, motivations for transition, accelerated pathways and associated harms are explored to a lesser extent.
A significant proportion of those who reported SC use described the effects as equally or more harmful than heroin:
It’s basically heroin, the way it is. Obviously you’re not going to jag [inject] it but it’s just the worst thing on the street by far. It makes meph[edrone] look like fairy dust, in a good way, if you know what I mean? It’s wrecking people’s lives really, really badly . . . They don’t know enough about it to make an actual choice whether to smoke it or not. It just doesn’t seem that bad. Even when I first started smoking it, no one was, ‘ah, it’s really badly addictive’. I didn’t know it was addictive until I myself was addicted to it, then everybody just out of the blue started to tell me, ‘yeah, lad, that’s really bad’, and I was like, ‘now you tell me. It’s too late to go back now’. It made me not want to smoke weed anymore either, there’s no point. If you’re smoking legal highs weed isn’t going to work. It takes everything away from you.
1030
For some participants, developing lay knowledge around SCs and their opiate-like effects resulted in them being selected as drugs of choice. This was particularly evident among our vulnerable participants (homeless population and prison sample) in terms of escapism and passing time (on streets/in prison cell). For example, one prison participant stated:
Do you see, the screws, they lock us up all the time, they just say, ‘oh, no staff’, and you’re locked up all the time and, do you see, if you smoke a joint of herbal your time flies in because you be like goofing out and all and you’ll go to sleep. It’s **** mad.
HMP1012
Two of our participants who had experienced periods of homelessness stated:
When I was sitting in my sleeping bag I used to go like that [breathes in] and smoking pipes of it. It was just to feel numb, so I didn’t feel cold, I didn’t feel embarrassed, I didn’t feel anything, I felt no emotions at all, it’s just that’s what it used to do for me.
HMP1015
I can understand the homeless ones smoking it because it’s going to keep you warm at night, it’s going to make them sleep and they don’t feel the cold. It’s the same with the heroin, they take it to block it out so they’re not cold, so they can actually sleep and not be sitting up all night scared of getting attacked.
1019
For such vulnerable groups, use of SCs (in the same way as heroin) was functional and served as a means to ease the physical and psychological suffering associated with their situation and status as individuals living on the streets.
It was evident that the relationship between SCs and heroin was bidirectional as well as concurrent and both functional and instrumental. Some participants noted that they used SCs and heroin together, others stated that SCs led them on to heroin use, others used SCs to abstain from heroin and some used SCs or heroin to temporarily substitute the other. Although the interactions described in the following sections were reported by the minority of participants, the present study’s data contribute to a virtually non-existent evidence base on the relationship between SCs and heroin and so are deemed significant.
Simultaneous use of heroin and synthetic cannabinoids
The use of SCs in conjunction with heroin was observed by one participant to enhance the effects:
I know people that do take the heroin and the herbal at the same time and it’s all just to get that heavy hit.
HMP1008
Transition from synthetic cannabinoids to heroin
There were reports (albeit among the minority) of individuals transitioning from SCs to heroin. One participant recruited from the prison sample reported extensive use of heroin and following a period of pharmacological intervention reported use of only cannabis and diazepam. Despite her experience, this participant, like others in the persisters SG, was under the illusion that SCs resembled cannabis and therefore had limited reservations in terms of using during periods in which she could not access cannabis:
I was smoking grass when I first got out on licence and then came in here to finish my licence, got out and went to Belfast and there was no grass about, only herbal, so I said, ‘I’ll try that’, and that was it . . . I went back to smoking it [heroin] again because I had no herbal [SCs] one night and somebody went, ‘here, have a few lines, that will help you’. Me, like a dickhead, ‘yeah’, and it did help, so that was me back on it then.
HMP1021
For another participant, the transition from SCs to heroin occurred during a period of withdrawal from SCs:
I started smoking that herbal when I was about 21 or 20. That just went on for 5 years. I started smoking that stuff about 20. Yeah, it was brilliant at the start, ‘oh, this is strong stuff’, and then, do you see, as the years went on and I was still smoking it, and I got up one morning, my mate took the gear [heroin] beside me, I was being sick and going to the toilet and I said, ‘what to **** is wrong with me?’. I was only smoking it about 3 years, and he says, ‘you’re sitting there like a junkie’. I said, ‘what do you mean?’. And he goes, ‘do you see the way you get sick?’. He said, ‘do you see when I don’t have heroin, I just go like you’. I didn’t realise. Then I got a smoke of it and the sickness was away. That was me up and about and could do what I done. Then there was no herbal about one day and I went bought a bag of heroin and it just took the sickness away.
HMP1019
When reflecting on withdrawal from SCs in the physical setting of prison, the same participant stated:
I had to come in here and come off it and it wasn’t good, I was calling the nurses and the nurses were saying, ‘what’s wrong with you?’. And I said, ‘that herbal’. They were going, ‘there is nothing we can do’, because they don’t know, it’s like gear, when you’re sick on it they can’t really give you sub [Subutex] . . . because they don’t know what effects that will have . . . It’s just jail that I’ve took heroin, never outside.
HMP1019
Comparisons of withdrawal from SCs and withdrawal from heroin were made on a few occasions. One of our experienced drug users in group 4 (dependents) stated:
The withdrawal off it is the same as heroin. It starts here, goes to your sinuses. See, my taste and my smell, I lost it all. I lost all senses, all senses. It took me 8 weeks in the centre before I started coming around because I was going different colours every day and every day I was a different colour and different symptoms, sickness, diarrhoea, shaking, bleeding, going to kill people, fighting with each other.
1019
Some participants felt that coming off SCs was worse than coming off heroin, particularly in relation to managing the symptoms. One of our prison participants reflected on the timing of getting SCs:
It made you sick but, see, if you didn’t get your bag in time, even though you were sick in the morning, see, if you didn’t get it by a certain time, see, even if you smoked it you were still going to be sick. You had to get it by a specific time, your routine. See, if that was an hour late, you were **** all day like, you know? Every time you smoked it you would have been sick but still you had to smoke it . . . The withdrawal is worse than any drug on the planet like. It’s like a withdrawal from heroin with no substitute, the withdrawal with that. It’s the heaviest thing to come off. Your heart is literally beating out of your chest, your tongue and things you are saying . . . It’s just mad.
HMP1007
Transition from heroin to synthetic cannabinoids
A small number of participants reported shifting directly from heroin to SCs:
I started off on cannabis and then that led on to heavier drugs such as cocaine, speed and then opiates . . . That led me to heroin. That was the only thing that was blanking it all out for me. Then I ended up smoking it and then that wasn’t doing nothing, then I ended up using the ‘Pin’ [Klonopin] . . . Then, because I wanted to get off the heroin, to get my kids back, the only thing that made me get that feeling again was the herbal. So, it does basically – ruined my life as well, once I started smoking that, just, basically, it took it away for a wee while and then just basically started doing nothing after a while, just sent my head completely away. Started with hearing voices left, right and centre – started thinking people were looking at me when they weren’t and, just basically sent me head away big time.
1058
Interestingly, although this participant transitioned to SCs in a bid to abstain from heroin, the adverse psychological effects reported in terms of psychosis-like symptoms were described as much more severe than the side effects of heroin.
Heroin/synthetic cannabinoids: temporary displacement
A small number of participants appeared to use heroin and SC in something of a substitution capacity: when heroin was not available, SCs were utilised, and vice versa. One participant living in sheltered accommodation stated:
I used heroin in the hostel as well. It was just to substitute that [SCs]. It was the worst substitute I ever chose. I overdosed twice on that, once accident, second intentionally. Got my head together again, and then they kicked me out over Christmas and I sort of went using again heavily and then I’m up here now and I’m still trying to cut down.
1021
Chapter summary
It is clear from our findings that SCs are entities worthy of separate consideration when dealing with the wider categories of NPSs. On the whole, we offer further insight and corroboration for existing evidence on a range of issues. This includes analysis on SC types, effects, perceptions and reported harms. As highlighted, variations in potency across and within brands causes difficulty in terms of risk assessment and building knowledge around dosage, effect and risk of harm. We contend that our research substantially contributes to the sparse evidence base around SCs and serious adverse effects, motivations/outcomes for less established substance users, withdrawal and the relationship between SCs and traditional illicit drugs, particularly heroin. Interview data indicate patterns of SC use that largely fall on either end of the drug use continuum, that is, use was either very experimental and generally an isolated incident or use was reported as dependent. Our findings also highlighted the inherent risk posed by participants of being unaware of the effects of SCs. This was evident across both highly experienced and less experienced user groups. This was predicated on an assumption, even among experienced heroin users, that SCs were akin to cannabis. Some participants in our study indicated that their use of SCs had provided a transition back onto heroin for them. Other, less experienced users reflected on SCs’ role in providing an accelerated pathway to heroin use. Highlighted too was the sheer intensity of withdrawal from SCs against a backdrop of limited or no medical intervention to ameliorate the very significant symptoms of withdrawal.
Chapter 8 Key contributions to the evidence base and implications for policy and practice
Key contribution 1: novel psychoactive substances in polydrug use novel psychoactive substances groups
As expounded in the preceding sections of this report, our evidence supports the argument that NPSs are best conceptualised as having a place within a polydrug use trajectory. An important finding from our extensive statistical models based on longitudinal data confirmed that there was not a distinctive ‘NPS class’. The latent classes generated from the BYDS data also evidenced the difficulty of unpicking the relative importance of a range of risk and protective factors as they relate to substance use at a population level. However, in presenting our findings we have gone to considerable lengths to clearly differentiate within this overall NPS/polydrug use premise. We were fortunate to have the detail provided by narrative accounts to help us understand the subjective interplay of the range of risk and protective factors, drug repertoires, contexts, temporal relationships and so on as recounted in the lived experience of respondents. Furthermore, the importance of these factors in their narratives was evidenced by how people presented their story and how central to their account the risk and protective factors were. As presented in preceding chapters, analysis across taxonomy groups evidenced both shared patterns and, at times, rather clear distinctions in the nature, extent and balance of risk and protective factors inherent in accounts.
Conceptualising polydrug use
Polydrug use is broadly defined as ‘the use of more than one drug’,177 although such a generic definition means that a broad range of operational definitions could be derived for the purposes of research. The widening array of psychoactive substances, increased accessibility and a much greater sophistication in technical knowledge surrounding drug use has meant that the use of multiple substances has become more prevalent. 14,15 Existing evidence documents a myriad of reasons for mixing different traditional licit and illicit drugs during one consumption episode or indeed over a period of time. Some permutations have cumulative and/or complementary effects and may be combined to enhance the overall psychoactive experience. Counterbalancing the adverse effects of a substance can provide the motivation for taking an additional drug; known examples include utilising benzodiazepines to help assist with sleep post stimulant use. The sequential use of several drugs by an individual over time might reflect the substitution of one substance for another. This can be driven by market factors, such as cost or availability,178 or related to legality or trends in specific scenes. Well-known examples in this regard are users opting for cocaine instead of ecstasy, or GBL instead of GHB after GHB came under drug law control. Polydrug use can also be used to describe the tendency to use different substances in different settings or contexts, or simply reflect regular multisubstance use related to drug dependence.
Overall, the substance types that are used together depend not only on personal predilections but also on other factors noted such as local availability, specific scenes/fashion and, in the case of prescribed psychoactive medicines such as benzodiazepines, on local prescribing practices. 1,2 At a basic level, there is evidence in the literature that increases in the range of drugs available drives more polydrug use. 177 Others suggest that it also increases the social acceptability of taking various psychoactive substances together. 179 Over the past decade, there have been calls for further clarity in the definition of polydrug use to capture variations of experiences,180 motivations for polydrug use181 and environmental effects. 182 Polydrug use has been associated with ill health, mental health problems and social disadvantages and regarded as strongly stigmatised and marginalised behaviour. Some authors, in contrast, argue that the practice alludes to a new form of drug use competence, because experienced drug users intentionally and consciously aspire to produce, enhance or mediate certain effects. 183
Some studies have attempted to shed light on practices surrounding polydrug use. Examples include Kataja et al. ,184 who conducted interviews with 56 Finnish drug users with the specific purpose of gathering information on the use and mixing of multiple substances. Their findings posited that there were four key narrative types of polydrug use defined by different levels of risk evaluation and management: ‘social recreation’, ‘self-discovery’, ‘hustling’ and ‘addiction’. They hypothesised that these narrative types were reflections of social identities, formed by different layers of drug culture and individual risk-taking strategies, but acknowledge that polydrug use is a heterogeneous and diverse phenomenon.
Boeri et al. 185 explored forms of polydrug use in ecstasy users and provided insights on the motivations and settings of polydrug use. They suggested three primary categories: (1) separate polydrug use, (2) synergistic polydrug use including enhancing a high and/or coming down from one and (3) indiscriminate polydrug use. Klein183 suggests a three-part framework to help explain polydrug use: first, ‘maximisation of effect’; second, ‘economic or stretching’; and third, ‘sequenced combinations’.
Novel psychoactive substance groups
Through the lens of our taxonomy of groups, we contribute to this evidence base further by presenting empirical data and critical commentary on how various types of NPSs appeared to be located in and across a range of polydrug use trajectories. Building on the detail provided on groups presented in Chapter 3, we add to the analysis by anchoring the trajectory in a risk and protective framework as well as articulating drivers for their use. Knowledge, perceptions and experience of harm, as discussed in the preceding chapters, are also embedded. Inherent in this discussion is the recognition of the importance of a temporal dynamic, in that there are notable variations dependent on when users entered or returned to the market. Fluctuations in purity of other substances, in pricing and in levels of potency are all important background considerations and are drawn out where possible.
Limited experimentals
For the limited experimentals group, NPSs of any type did not feature, and we contend that the protective factors at play alongside minimal risk meant that participants did not use NPSs. Decisions not to use were deliberate, and there was a reasonable level of knowledge about NPSs. For example, some highlighted how limited testing of newer drugs, despite being legal, was a disincentive for use. Participants simply had no place for NPSs in their repertoire.
Past recreationals
The past recreationals’ use was largely of stimulant-type NPSs (e.g. mephedrone). Use was located in a constellation of alcohol, cannabis and cocaine and other stimulant-type substances. Use in this group was recreational in character, highly opportunistic and linked to legal status at the time; NPSs were also easily accessible from headshops. Participants in this group were on the less vulnerable end of the spectrum and characterised by having a wide range of protective factors at play. SCs featured only sporadically in this group and, in contrast to mephedrone use, use of SCs was one-off. Of note in this group was evidence that legal status provided a conduit for crossover between scenes; the low cost and wide availability of mephedrone was observed to encourage individuals to partake, even if they hitherto had not used illicit drugs. This group, however, demonstrated awareness of the complexities surrounding the pharmacological properties of various NPSs and an understanding that being ‘legal’ or ‘herbal’ did not imply safety.
Contemporary regulars
In the case of the contemporary regulars, it was possible to see a strong link between the clusters of drugs identified in respondents’ accounts. NPSs (mostly mephedrone) sat in a very experimental profile (ketamine and GHB as well as stimulant-type NPSs beyond mephedrone, e.g. China White and MDMI). SCs featured but were not as dominant a feature. Use of substances was important in the pursuit of adaptive personal goals in early adulthood, for example retaining social networks,186 finding romantic partners187 and discovering novel environmental stimuli. Use was generally characterised by stimulant-type substances and was linked to specific scenes (a range of regional dance, punk and MSM scenes). Ecstasy, cocaine and experimental use of substances such as ketamine and GHB were noted. Legality was not mentioned by anyone in this group as a driver for use. Rather, the primary force behind the transition from traditional illicit drugs to varying NPSs was market driven, that is, related to the availability/quality of other substances. Most notable here is the reduced quality of cocaine vis-à-vis the high quality of mephedrone. That said, almost half of participants in this group did report a concern that the ‘moreish’ properties of mephedrone had potential to escalate their own use, but none reported injecting behaviour. Discussion of protective factors for this group were in the realm of harm reduction (as opposed to either preventing or limiting use). Cautionary tales and passing on information about mephedrone and SCs were evidenced in accounts. Decisions to use drugs were highly premeditated and informed by an awareness of how to maximise effect and optimally sequence combinations, almost connoisseur-like, as discussed by Klein. 183 Where a lack of information existed on, for example, the mephedrone or SCs available, participants promoted a sense of caution among their peers, encouraging harm minimisation strategies.
Dependents
We further categorised the dependents group into four SGs (the fourth has minimal mention as NPSs were not taken by this group) with the aim being to provide a more detailed commentary on dependence through the lens of each. SG1 incorporated those participants for whom a novel psychoactive substance was their primary and only dependency. We contend that this group of respondents provide unique insight; while still within a polydrug use trajectory, they were the closest we came to having a distinct NPS class.
Subgroup 1: generation novel psychoactive substances
For participants in SG1, generation NPS, their primary and only dependency was a novel psychoactive substance, most probably a SC. The repertoire of this SG contrasts to those of the other SGs in that it was less diverse and no group members had used heroin. Rather, alcohol, cannabis and other prescription medication such as diazepam and pregabalin were more prominent. A conflation of circumstances appeared to facilitate NPS use in this SG. They included being vulnerable; significant risk factors noted in their accounts were early disengagement with school, poor parenting, negative peer influence and individual risks [undiagnosed attention deficit–hyperactivity disorder (ADHD) or impulsive personality]. They were young and neophyte, lacking in any user knowledge about effects and harms of NPSs. They were also influenced by perceptions of legality from which they inferred safety. The low cost of NPSs, availability and accessibility also featured. Being embedded in social scenes where NPS use was pervasive, in combination with the above, conspired to create substantial use and rapid dependence in this SG. SCs were key here and featured strongly in narrative accounts. In some cases, a trajectory of having used only alcohol through to dependence on SCs was noted. Peers stood out as the most common influential factor in terms of substance use generally and, by extension, NPS use. Moving from social use of SCs with peers to use alone was evidenced by the rapid acceleration from experimental/social use to dependent use. For this SG, timing of onset was linked to market dynamics. NPSs first hit the scene when these participants were highly social and ready to experiment with new substances in a market awash with low-cost, highly accessible substances. The evident naivety around what substances they were taking posed a significant risk to this SG. This was even reflected in interchangeable terminology (e.g. herbal, legal highs and trippy) and elements of confusion when describing what they were currently using. Some reported not realising that they were dependent on NPSs until they experienced withdrawal (e.g. sweating, vomiting, not being able to sleep, ‘craving the high’). Harms experienced through use of NPSs were noted by many and contextualised by the respondent themselves, by contrasting the experience with their use of a traditional substance, often cannabis. Narratives evidenced that over time participants started to witness severe adverse effects of SCs as well as adverse experiences of using NPSs themselves. For some, this served as a means to influence decisions to at least attempt to desist using. Adverse effects were significant, and there were reports of seizures, blackouts, dizziness, weakness, chest pain, palpitations and vomiting; perceptions of change in personality were also noted. As users built up experience of using over time, the SG appeared to learn more about managing potency and dosage of NPSs, and an emerging culture of sharing harm reduction advice in networks was also evidenced to some extent.
Driven by cost, there was evidence in this SG of ‘stretching’183 to make money go further. Participants observed the value for money offered by SCs in terms of quantity and effect, in comparison with cannabis. For these young and vulnerable participants, access to finances was often limited and so cost/value for money was an important driving force. All this reiterates the importance of attending to SCs within a comprehensive harm reduction framework. National health organisations and Health and Social Care Trusts may wish to consider the development of new guidelines and policy in relation to the management of SCs in a polydrug use context. Guidelines should be tailored to the needs of specific groups according to regional variations and for distinctive sectors, such as homeless and prison populations.
Subgroup 2: availers
The drug repertoire of this SG was interesting and, with the exception of heroin and reported dependency, ostensibly shared characteristics with group 3 (contemporary regulars). NPSs were ‘availed’ of by this SG when their drug of choice was not obtainable. In contrast to SG1, this SG reported dependency on traditional illicit substances and reported no issues around dependency with any NPSs. Also featured in this group was use of prescription medication. A clear and cumulative risk profile emerged here, with the majority noting individual-level risks including significant mental health issues in the context of their drug narratives. These included depression, anxiety, panic disorder and schizophrenia. Evidence of dual diagnosis was also evident in reported self-harm and suicide attempts. Early onset of problem alcohol use, negative peer influence, poor parenting, links to the CJS and reports of impulsivity and a propensity towards risk taking were also evident. Several respondents attempted to self-medicate as a means to achieve order and function in their lives. In contrast to the other SGs in this category, there was some evidence of users functioning in their day-to-day lives. Of note was that almost one-third of this SG discussed employment in a protective capacity and, for those outside the prison, like those in group 3, they seemed to measure functionality in terms of not missing days at work as a result of substance use.
There was a high level of user knowledge and wisdom among respondents in this SG. There was an assessment of safety built into modes of use and a sense that they sought to mitigate risk of harm by careful dosage and testing potency. Key drivers here were akin to those in group 3 in that NPSs entered the frame only when other substances were either not available or of insufficient quality. Perhaps the distinguishing variables here were the relative balance of protective factors evident in group 3 versus those in this SG. Both groups cited employment as protective influences; however, the availers discussed periods of non-employment and increased substance use that did not feature in the narratives of the contemporary regulars. The contemporary regulars also reported the protective influence of a non-using romantic partner in reducing substance use/increasing attempts to abstain, but this was not a marked feature in the narratives of the availers.
Subgroup 3: persisters
This final SG encompassed our most chronic and chaotic substance users. All reported multiple dependencies, including dependency on NPSs (mostly SCs and mephedrone). Complex, cumulative adverse experiences were noted by all. Several had experienced homelessness linked to their drug dependency. Early contact with the CJS was also common and for the females there was note of prostitution. Age at initiation with this SG was, for some, as young as 10 years. Atypical synchronous onset with multiple substances was evident, including the use of prescription medication alongside cannabis and alcohol. Despite being experienced users, a lack of knowledge about SCs in particular meant that, as was the case with those in SG1, they were taken by surprise by the effects, perceiving the descriptors of ‘legal’ and ‘herbal’ as inferring less harmful substances. Although legal status was not a driver for use here, it did operate to confer an erroneous message of safety. After the initial surprise, the myriad vulnerabilities among this group made the potent effects of SCs particularly appealing and so resulted in sustained use. Almost all known risk factors were at play for this group (with few protective factors noted): negative experiences at school, adverse life/childhood experiences, mental illness, contact with the CJS, complex family issues, social deprivation and homelessness. The majority made reference to trauma and abuse.
Perhaps unsurprisingly, the harms from use were substantial and linked to a lack of knowledge regarding potency and unpredictability as well as to differences in substances they obtained online versus a street dealer. There was also indication that SCs and mephedrone caused significant psychological harm and behaviour change. Common among respondents, as noted in Chapter 7, was major disruption of sleep and reports of aggression. This aggressive behaviour coincided with a reported increase in paranoia and anxiety, especially after using for several days. Note was made of outbursts of uncontrolled violence. In relation to withdrawal, SC users noted suicidal ideation owing to the severity of symptoms. There was an inherent understanding and acceptance in this SG of the harms incurred by mixing NPSs with traditional substances, up to and including fatal dosing. There was evidence in this group of injection of mephedrone, bringing with it the attendant harms associated with unsafe injecting practices. This included other effects such as the slow healing of wounds and/or injection-site injury. The frequency of injecting of mephedrone was also very high, compared for example with heroin.
For those who had stopped using, there was evidence that they could now reflect on the dangers of SC use. The unpredictability and variation in potency were key here. Users in this group provided detailed insights into the various brands they had used over time. Evidenced was the variability in potency across, but also within, SC brands and indicated by the presentation of the substance (e.g. sealed branded bag or clear zip-locked bag). There was a sense in this SG of vulnerability to theft and other crimes while under the influence of SCs; this was particularly the case for those who experienced homelessness.
The literature signals that predictors of NPS-specific dependence trajectories are not easy to unpick from polydrug use more generally. That said, trajectories for some different substances are related to their capacity to elicit physiological and/or psychological dependence. 2–5 Dependence tends to be associated with longer and more intense trajectories, for example in the case of heroin users. In this instance, it was clear that SCs played a major role in accelerating pathways to dependency for these participants, a significant minority of whom then entered the CJS and prison for reasons linked to their use. Addison et al. 188 noted that the intersections and associated harms of NPSs with other substances are unclear. The experience of this SG evidences the power of SCs in accelerating to dependent use. Note is also made of the potential of mephedrone to accelerate pathways to dependence and frequent daily injection. This has been evidenced across the literature.
Dependence has many underlying factors, particularly around what others have called compulsion (e.g. unplanned use) and ‘escalation’,6,7 and can differ across substances. Although all participants in group 4 reported issues with dependency, their patterns and levels of use of the range of NPSs varied between the SGs. Some of the more established users reported long histories of drug use with multiple dependencies, including NPSs at various stages, whereas other, younger, participants in generation NPS-reported dependency on a single new substance (e.g. a SC, mephedrone or 2C-I). The utility of constructs of dependence would need to be assessed with regard to longitudinal patterns of NPS use in a polydrug use framework. This is particularly relevant in the light of ‘compulsion’ as it relates to the SC/heroin dynamic as well as mephedrone, leading to a high frequency of injection in the case of one respondent.
In addition to significant differences in age at onset, other defining characteristics in patterns of use, as described in the narratives, were the differences observed across groups in terms of progression from one substance to another, the combined use and types of substance, and modes of consumption. An obvious example is the configuration of stimulant drugs evident in the repertoires of contemporary regulars and involving combined use of a very wide range of different substances evident through dance, punk and MSM scenes. The pattern of associations that were described by users in their narratives showed that, in some cases, substance use (e.g. in group 2, use of only one substance, usually alcohol/cannabis or a traditional stimulant) was linked with experimentation with a specific novel psychoactive substance rather than more regular use. Expanding repertoires across the groups rendered it more difficult to disentangle the order of drug onset in drug careers and, for some, there appeared to be synchronous onset of a range of substances. Several studies suggest that those who deviate from the typical pattern of drug use initiation are at higher risk of early onset of mood or anxiety disorders. 189 Further deviating from the gateway pattern appears to also be related to a higher likelihood of having comorbid mental health problems. 8,9 This was clearly notable in the persisters SG.
Key contribution 2: novel psychoactive substances as a snare for more problem use
Seminal work by Moffitt70 highlighted the potential of a range of snares that behaved like an accelerant for antisocial behaviour. Borrowing that concept, we posit that in a polydrug use pathway our data indicate that in some instances specific NPSs operated as a snare to more problematic patterns of use in a number of ways. First, branding SCs with the descriptors ‘legal’ and ‘herbal’ by marketers as an alternative to cannabis30 conferred a tacit message of safety, or at least minimal harm. When first introduced to the scene, the level of knowledge and user wisdom surrounding these substances was negligible for respondents in our sample. Perceiving similarities to cannabis and having little or no awareness of the signs of growing dependence resulted in the case of participants in generation NPS having accelerated pathways to dependent use. Ford et al. 30 noted the possibility that brain development in adolescence may render younger users more susceptible to the potential psychotic and/or pro-convulsant effects. From our data we also suggest that this may also extend to vulnerabilities to dependence.
Ralphs et al. 54 noted the highest prevalence and problematic use of NPSs, primarily SCs, among the same vulnerable groups that have traditionally been associated with problematic Class A substance use. Indeed, as was the case in our study, many dependent users of SCs referred to past problematic use of other substances, typically heroin. However, in our study, generation NPS participants clearly do not fit that overall assertion.
For those already reporting a dependency (the persisters), the effect of SCs still took them by surprise. Many continued with use owing to effects being perceived as either functional or pleasurable, even if they were unsuspected. The subsequent interchanging of SCs and heroin thereafter was noted in several accounts, as highlighted in Chapter 7. Introduction of the PSA has sought to ensure that NPSs are no longer legal to sell. However, in this vein, our PPI discussions did highlight the potential for users to continue to perceive NPSs as being of lesser harm as a consequence of no penalty being levied for those caught in possession (without intent to supply), in contrast to penalties surrounding other substances. Ensuring awareness that these substances are not akin to cannabis remains an important message to confer to users.
Second, in the case of mephedrone, when still ‘legal’, this novel psychoactive substance acted as a conduit for crossover between scenes, as indicated by the past recreationals, where NPSs were introduced to scenes where use had hitherto been limited. This offers a mechanism for exposure to alternative and potentially problematic scenes. In this vein, the ‘moreish’ properties of mephedrone were also noted by the contemporary regulars as having the potential to alter their patterns of use, this being the case even in very drug-wise experimenters. Injection of mephedrone, albeit limited in our sample, is also indicative of a potential for crossover in modes of use. In these cases, the number of daily injection episodes of mephedrone outstrip those for heroin. Such regular injection, and the properties of mephedrone described as almost corrosive, pose greater risk in terms of injection site injury. It is acknowledged that the numbers on which these assertions are based are relatively small; however, our PPI group fully supported the validity of the arguments presented.
Key contribution 3: suggested interventions/treatment modalities mapped onto our empirical findings
In constructing our taxonomy, we located various types of NPS use in a range of polydrug trajectories. A consideration of results categorised according to each of the four groupings raises a number of important issues for policy and practice. To date, the literature has focused on categorisation of treatment according to settings10,11,13 and avoided the now defunct notion of treatment aligned to specific NPS categories. Our suggestions here also build on the NEPTUNE guidance46 and draw on other extant literature to inform the framework of suggested interventions and treatment modalities, which is presented according to group classifications generated from the current research.
Education
It is considered important to provide young people with a balanced education and awareness framework that addresses risks and consequences associated with drug taking and emerging issues. Critical guidance from the ACMD5 highlights the need to cover NPSs in the school curriculum. However, it is also recognised that school-based prevention projects are not accepted universally as successful methods of relaying information on drugs to young people. 64 Educational data need to be delivered as part of a well-structured, thoughtfully balanced campaign, using evidence-based drug education programmes with a NPS component. These should take into account that decisions by young people to use substances are often based on factors other than educational messages. 190 For example, our research participants and the extant literature4–8 describe the negative and positive impact of peers on risk of NPS use. It is worthwhile for policy-makers to consider the creation of national drugs education programmes, which are culturally nuanced, and involve peer educators in the creation, delivery and evaluation of programmes that enable young people to resist peer pressure without damaging peer relationships. Our research indicates that education programmes that include access to and advice on harm reduction techniques for individuals who are using or at risk of polydrug/NPS use could be beneficial. Using informal and formal community networks, the information could be disseminated from a much more structured basis alongside the current peer-to-peer transfer of knowledge, which often relies on less informed and possibly outdated knowledge of harm reduction techniques.
Furthermore, the current findings highlight that negative experiences in the school system and disengagement from education were key contributory factors for individuals with the greatest problems relating to NPS and polydrug use. In a national US school population study,9 the authors posited that prevention and intervention efforts for NPS use should focus primarily on youth who were disengaged with or excluded from the school system, regardless of their polydrug use history. Future specific interventions for all young people who have been excluded from school should include both polydrug and NPS components, again employing a method of peer mentoring and peer education to fully engage the participants.
Public health
Public health models addressing the problems associated with drug misuse are wide and varied (e.g. owing to different definitions of public health). Generally speaking, public health interventions are designed to improve general health and population well-being. The concept is based on the notion that a large number of people at relatively low risk of poor health outcomes is a greater economic burden to society than a small number of people at relatively high risk. Mdege et al. 45 highlight that a dual public heath approach should be used to focus on both low- and high-risk populations. Using a different perspective on public health, the EMCDDA Trendspotter study191 considered a public health model as an approach that may be adapted to help those with problem NPS use. It is argued that as new drugs emerge onto the market they become embedded in the drug use repertoire and the cycle of new drugs continues with introduction of further new amalgams. To compound the issue, it is also understood that a growing number of drug users are increasingly aware of NPSs as adulterants of controlled drugs, that is, a purposeful blending of NPSs and older, more established drugs to induce a more intense and lengthier high. This was evident in the current study, where groups 3 and 4 demonstrated sophisticated knowledge of the effect intensity associated with different drug combinations alongside knowledge of specific harms associated with NPSs and, in particular, SC usage. Conversely, a number of established users (including injectors) expressed surprise at the strength and unintended effects of SCs and had difficulty anticipating the increasing complexity of SCs. There was also recognition of the toxic agents and additives in more traditional drugs, which in itself presents a public health concern in terms of assessment and treatment of new combinations, together with the growing concern regarding adulterants in the drug-using population.
The public health approach propounded by the EMCDDA is more suited to the needs of problematic users; they call for levels of integrated treatment provision that take account of housing, social care, homelessness and mental health services. 192 All these factors were alluded to by each of the SGs in group 4 (the dependents). The more holistic approach to treatment is not a new phenomenon, and neither is the call for a more integrative treatment system, which has been alluded to repeatedly in a number of documents that relate to the misuse of a range of culturally embedded drugs.
Harm reduction
Harm reduction was a topic referred to primarily by group 3 (contemporary regulars), in which it was reported that peer group members provided information and advice on specific substances, routes of administration that would provide the most intense experience and advice on how to avoid harmful consequences. However, previous knowledge of harm reduction techniques by already established drug users may not be enough to ensure their safety when taking NPSs. For example, lack of knowledge about drug interactions may create a high-risk situation for new users, who look to the more respected users in the peer group for experiential advice.
A number of participants discussed the complex relationship between heroin use and SCs. A small number reported moving from SCs to heroin owing to withdrawal, or as a result of an absence of heroin supply, whereas others progressed to using SCs alongside or after heroin use.
Injecting behaviours associated with heroin use and other injectable drugs, including NPSs, are highly correlated with a range of harms inducing soft tissue injury, abscesses, gangrene, sore or open wounds, bacterial infections and vein clotting. Results from some studies across Europe have indicated an increased rate of hepatitus C virus (HCV) and human immunodeficiency virus (HIV) transmission related to NPS usage,182,193–195 an increase that needs to be recognised and addressed via specifically tailored interventions. In Hungary, almost 70% of those attending low-threshold services were using SCs via injecting. 188 It is essential to consider results from some systematic reviews of evidence already published about the effectiveness of interventions with heroin and other intravenous drugs, and ascertain which treatment modalities may be best suited to the needs of NPS users at increased risk of infection from intravenous administration.
Treatment: working with novel psychoactive substances in the context of a polysubstance framework
Owing to the relatively recent emergence of NPSs there is currently limited evidence relating to the effectiveness of interventions for NPS-using populations. Undoubtedly it will take time to tailor and embed interventions for working with NPSs. Nevertheless, presently, there is consensus that intervention-level service providers should focus on adapting current drug interventions to meet the needs of the NPS-using population, rather than creating new pharmacological and psychosocial interventions. It is also noted that treatment must incorporate more extensive strategies. 181 Others have propounded that it is important to consider new intervention combinations to address the needs of NPS users [e.g. stigma, blood-borne viruses (BBVs), specific withdrawal symptoms]. 181,183,185,186 Findings from the current study underline that, for groups 1, 2 and 3, alcohol played a part in initiation of drug use, including NPSs, or accompanied the continued use of drugs. However, there is a lack of focus on treatment modalities for NPS users that consider alcohol use history; rather, treatment models have focused on either alcohol or polydrug use. NEPTUNE152 highlights that a substantial proportion of NPS use problems and behaviours are similar to those indicative of stimulant use and alcohol use. Similarly, for group 4, NPS use was also couched in a multisubstance use framework, and it is now widely recognised that we must take this into account when designing any treatment modality. The EMCDDA also advises that creating specific interventions for injecting NPS users may be beneficial, as the effects of newly formulated drugs or drug combinations are uncharted. 196
Several participants referred to NPS withdrawal symptoms; they reported that effects were on a continuum from moderate to severe, and a number of participants likened the withdrawal process to that of heroin. Unfortunately, there is little information available about the effectiveness of pharmacological interventions with NPSs, although Baja et al. 197 recommend the use of benzodiazepines for psychoses withdrawal in drug treatment settings as a result of mephedrone abuse. There are currently no specific substitute or maintenance pharmacological programmes available for people with problems related to chronic NPS usage. 64
According to Project NEPTUNE,152 psychosocial interventions should be used in direct response to the severity of the NPS problem and as a result of an assessment process that takes into account the service user’s health and other concomitant variables. Psychosocial interventions usually focus on behaviour change to attain desired outcomes198 and are provided in stepped care models that range from lower-intensity psychosocial and psychological interventions (PSIs), such as brief interventions, through to higher-intensity PSIs and residential treatment.
Cochrane reviews show that the evidence for successful PSIs for substance use disorders, including polydrug use, focuses on motivational interviewing, cognitive–behavioural therapy, contingency management and community reinforcement approaches. 199,200 Furthermore, individuals with higher severity and secondary use who have complex comorbidities will benefit from a combination of psychological treatment modalities that include relapse-prevention models as part of the treatment plan. 152
Solomon et al. 201 advise that, in the absence of research evidence to support the use of PSIs for NPS use, they should not be offered as a standalone therapy but should be used as an adjunct therapy alongside appropriate drug therapy as well as family, peer, community and psychiatric support. There is a universal recognition that research into the effectiveness of PSIs for NPS use as a primary or secondary drug of choice or as adulterants of controlled drugs should be conducted as matter of urgency to inform best practice and policy directives. 43,64,154,180,181,192,202–205
Immediate responders and emergency department services
Immediate responses are often required in some settings, including clubs, festivals and community and home environments, before individuals require treatment at hospital emergency departments. The European Drug Emergencies Network (EURODEN) provides guidance about when to call emergency services about drug use problems, a framework that is readily adaptable for use in situations in which someone becomes unwell because of NPSs. It provides guidance on indicators for concern related to levels of consciousness, significant agitation, seizures, breathing difficulties, heart rate and blood pressure. 187
In the emergency department setting, staff are usually guided by acute care management and practice protocols when dealing with patients who present with NPS-related problems, and often work to a symptomatic care framework, because in most cases NPS symptoms mirror those reported for other, more familiar drugs. 64 A number of participants reported a range of symptoms that required immediate response and attendance at primary care services, including extreme pain, cardiovascular issues, seizures, blackouts and kidney problems. The range of symptoms attested by the participants have been well documented in the recent literature, including from Project NEPTUNE33 and the EMCDDA. 206 Tracy et al. 172 outline possible responses to clinical care situations. The overview includes guidance on how to work with patients affected by incidental NPS use and serious harm related to chronic NPS use. The authors advise clinicians to make an assessment of mental state and presenting physical symptomology (particularly blood pressure, heart rate, temperature and level of consciousness). It is also vital to question the type of drug or NPSs used, the method and frequency of consumption and assess acute and chronic harms associated with use. The overall assessment and management of care should be underpinned by an ethos of empathy and a non-judgemental approach, as patients are likely to fear legal consequences of drug use or criticism from health and social care professionals. 34
Mental health and addiction services
A range of psychological harms were reported by all groups. Participants in groups 1 and 2 mentioned that these harms impeded or prevented their NPS use, whereas participants in groups 3 and 4 reported harms experienced as a direct result of their use. Significantly, comorbid mental health and substance use problems were reported by the more established users in group 4, consistent with previous research suggesting a high prevalence of co-existing substance use and mental health problems. 35,36 Currently, in the UK, both child and adult mental health teams are ill equipped to deal with co-existing substance use disorders owing to limited knowledge of NPS use in a polydrug use framework. Specific mental health teams primarily address specific comorbidities when there is a diagnosis of a severe and enduring mental health illness (SMI), such as schizophrenia. In addition, specialist addiction teams usually work with presentations of dual diagnosis, which primarily include anxiety and depression, and not SMIs. The situation is further compounded when individuals are ‘shunted’ between both services owing to their mental health diagnosis or as a result of the patients not being abstinent from substance use. NPS use increases the risk of psychotic symptomology, which has largely been reported as short term, but there are reports of growing instances when the psychotic episodes have become more persistent. 207 Individuals with higher mental health severity and who have complex comorbidities, including NPS use, would benefit from a combination of psychological treatment modalities that include relapse-prevention models as part of the treatment plan. 152
Finally, as noted in Dependents, those in the prison estate across group 4 reported more frequent lifetime drug use and a higher risk of significant harms than the general population. It is also recognised that the drug problems in prison have continued to increase, concerning both opioid use and, more recently, NPS use, which has emerged as a growing problem in prison settings in the UK and Europe. 208 Health intervention responses to NPSs have begun to emerge in some UK prisons, but provision remains limited and there is a lack of research on the nature and effectiveness of these developments in prison-based settings. 209 Public Health England210 published a toolkit that considers the management of NPSs in prisons and outlined the following as principles for treatment:
-
Prisons should accurately record prevalence use rates and side effects.
-
There should be an integrated multidisciplinary response to the situation in each custodial establishment.
-
Staff should respond to each case in a proportionate manner, taking into account the vulnerability of the prisoner who may be under the influence of NPSs.
-
Any health-care response should be based on presenting symptoms.
-
Where there are questions as regards capacity, staff should consult ‘consent to treatment’ guidance.
-
There is no specific pharmacological treatment for NPS use; treatment should be guided by the principles underlined in Project NEPTUNE,152 and significant changes in existing models of treatment should not be required.
Public Health England205 also highlighted models of good practice when working specifically with SCs and this included the use of observation cells, integrated staff and prisoner discussions that focus on response to SC use, drop-in clinics to facilitate access to PSIs, indications of the individual’s trajectory of drug use, use of specially tailored harm reduction advice, adoption of a ‘treat what you see’ approach to NPS interventions and engagement of prisoners as peer mentors to provide peer support.
The EMCDDA191 also indicated the importance of a health assessment, which should be conducted before the commencement of a sentence to identify needs associated with prior drug use, including NPS and polydrug use. Evidence also supports the use of opioid substitution treatment for those using opioids, via either intravenous or other routes of administration in prison. It is clear that treatment in the prison setting will reduce deaths and drug-injecting behaviours in prison, and individuals will also benefit from a continuum of care when they are released from custody. 64
Key contribution 4: messages for further research
A recent publication by the EMCDDA, Health and Social Responses to Drug Problems,8 includes comprehensive up-to-date information on responses to drug problems across Europe. This includes a section specifically on ‘the implications of novel psychoactive substances for policy and practice’.
The EMCDDA report acknowledges that understanding of patterns of novel psychoactive substance use remains poor and states that most information comes from populations and settings where problems have already occurred. Accordingly, the first major practical implication of the present research is that it provides much needed further empirical data on the lived experiences of NPS users across a range of settings, not just those in problem populations. Our study elicited data from users who did not consider their use problematic and provided comparison from some individuals who opted not to use at all, as well as those high-risk populations such as those in prison or homeless people.
Future research must generate improved epidemiological data on the extent of use, patterns of use and motivations for use, and how they evolve over time. This study has potential to immediately deliver findings to help inform the agenda of such large-scale epidemiological research by providing well-articulated nuanced accounts of how NPSs functioned in a range of polydrug use trajectories.
A further implication of our study derives from our finding on the uniqueness of the knowledge and information concerning SCs. Data point to a specific set of findings regarding the use of SCs that is not evidenced elsewhere in the literature. It was clear that the relationship between SCs and heroin was bidirectional as well as concurrent and both functional and instrumental. Highlighted too was the sheer intensity of withdrawal from SCs against a backdrop of limited or no medical intervention to ameliorate the very significant symptoms of withdrawal. In consequence, future research must focus on the symbiotic link between SCs and heroin use and how the administration of SCs is influenced by heroin use and vice versa. Furthermore, we must augment the evidence base on the withdrawal effects from SCs and adulterants to inform appropriate interventions and subsequently test their efficacy in practice.
Strengths and limitations of the study
A major strength of the study was its three-phased mixed-method design. Integration of qualitative and quantitative research paradigms is complex and our method was theoretically based and conceptually sound. The complementary integration of these co-existing and inter-related dimensions of the NPS phenomena led us to a more holistic understanding. Several integration analyses were built into the design to maximise the utility of the sequential mixed-methods design. Utilisation of the high-quality BYDS longitudinal data set was a clear asset in terms of its size and its capacity to add significant value.
For the qualitative component, we successfully recruited additional respondents across the selected sample locations and this permitted us to comprehensively answer the 11 research questions. The inclusion of several service sites, including a prison sample, allowed for a varied sample, maximising opportunities for a multiplicity of user perspectives to address our research questions. The objectives of purposive sampling were achieved, and as a result good coverage was obtained and the team concluded that thematic saturation had been reached. Benefit was obtained in the conduct and analysis of the study through the inclusion of team members who engage with the topic from different perspectives. This was augmented by a series of support groups with differing functions. The SAG comprised academic experts in the NPS area as well as methodological specialists. The PLG brought policy and practice knowledge and the service user perspective was achieved through regular updates with the BEBE, a service users forum. The research team comprised experts in both quantitative and qualitative research methods. Furthermore, the team included members with expertise in a wide variety of clinical backgrounds such as psychiatry, psychology and social work, thus improving the research by allowing multiple standpoints to influence all aspects of the research process (e.g. design, analysis and interpretation). Use of multiple viewpoints in the analysis and interpretation of the qualitative data acts as a form of multiple coding, thereby improving the validity of the findings.
The study was conducted during 2016/17. Given the fast-paced nature of NPSs, it is important to note that findings captured a particular point in time. They were also reflective of the sample generated. SGs such as MSM were not strongly represented in our sample. The PSA came into force during fieldwork and, although not particularly influential in our study, it may be influential for future work. It is also acknowledged that many of the data related to SCs and mephedrone.
The level of missing data for some of the BYDS analysis was a limitation. It is also important to note that the BYDS data were collected in 2011, so in a different context to narrative data collected. In addition, a primary constraint in any study based on self-report of drug use or any behaviour is the perceived inadequacy of other measures to triangulate within the analyses. The strength of the rapport during interviews, the reflective diaries and the time taken at the end of interviews to ensure acceptability to the participant all mitigated this to some extent. So too did the theoretical linkages back to the longitudinal data.
The present report provides an overview of what the qualitative findings tell us that is of relevance to our research questions. The richness and depth of the data set, however, allows for further important and theoretically driven analyses relating to the NPS phenomenon; these data will be presented in future research papers.
Finally, it is important to note that all our findings were shared, discussed and shaped in the various advisory fora noted. This included meetings with our SAG, several meetings of our PLG and with our service user group BEBE. The SAG supported the team by assisting us to locate and validate the findings in the current and emerging evidence base related to the various types of NPSs. How the various substances related to other substances in a polydrug use context was also shaped by the group. These discussions helped distil the key contributions of the project, which are reflected in the report. The PLG was instrumental in providing advice on how our findings could be shared with a common-sense logic that had application in the various policy and practice contexts (ranging from education through to immediate-responder settings). They informed and helped develop those sections of the report. The BEBE group too was highly engaged with the research, even before it commenced, helping us shape our submission, and engaged with the research through to publication. In terms of our findings, the BEBE group discussed with us our key hypothesis on several occasions throughout the production of the report. We amended some of the ordering and tenor of the text in the light of comments made by the group (one example was to make sure that we made it clear that the various drugs in the NPS umbrella were discussed in more detail in terms of their implications). The group noted the need to acknowledge that the focus of our findings was mostly around SCs and mephedrone and that there were other substances not covered. However, the BEBE group acknowledged the predominance of these within the Northern Ireland scene. We ensured that these limitations came across more strongly in the report as a result. All groups remain committed to further KE activity.
Acknowledgements
We are grateful to those individuals who participated in the interviews and shared their experiences with us. We are also grateful to the BEBE group, which provided valuable input at various stages of the project.
The team would like to sincerely thank members of the SAG and PLG for their attendance at meetings and teleconference calls and their very useful feedback on and input to the project findings and recommendations.
Scientific advisory group
Dr Caroline Chatwin, Professor Karen McElrath, Dr Russell Newcombe, Professor Harry Sumnall and Professor Marie Claire Van Hout.
Professional advisory group
Pauline Murnin, Gary Maxwell, Michael Foley, Clare Connolly, Dr Aisling Diamond, Victoria Creasy, Gary McMichael and Iain Cameron.
Contributions of authors
Kathryn Higgins, principal investigator, led the overall design of the study, contributed substantially to the analysis and led the writing of the report.
Nina O’Neill contributed significantly to the study design, jointly led the data collection and made a substantive contribution to the writing of the final report.
Leeanne O’Hara contributed significantly to the study design, jointly led the data collection and made a substantive contribution to the writing of the final report.
Julie-Ann Jordan led the secondary/quantitative analysis of the BYDS and made a substantive contribution to the writing of the final report.
Mark McCann contributed to the initial study design, contributed to the analysis plan and attended SAG meetings.
Tara O’Neill contributed to the first phase of the quantitative analysis.
Mike Clarke advised on all elements of the methodology and attended SAG meetings.
Tony O’Neill advised on the practice implications of the study, attended SAG meetings and contributed to the writing of the report.
Anne Campbell significantly contributed to writing of sections in the report relevant to treatment and practice and attended SAG and PLG meetings.
All authors were involved in this piece of research and all have approved the final version of the report.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- European Monitoring Centre for Drugs and Drug Addiction . European Drug Report 2017: Trends and Developments 2017.
- United Nations Office on Drugs and Crime (UNODC) . World Drug Report 2017 2017.
- European Monitoring Centre for Drugs and Drug Addiction . European Drug Report 2014: Trends and Developments 2014.
- Advisory Council on the Misuse of Drugs (ACMD) . Consideration of the Novel Psychoactive Substances (‘Legal Highs’) 2011.
- Shapiro H. NPS Come of Age: A UK Overview 2016. www.drugwise.org.uk/nps-come-of-age-a-uk-overview/ (accessed 10 June 2019).
- Measham F, Wood DM, Dargan PI, Moore K. The rise in legal highs: prevalence and patterns in the use of illegal drugs and first- and second-generation ‘legal highs’ in South London gay dance clubs. J Subst Use 2011;16:263-72. https://doi.org/10.3109/14659891.2011.594704.
- Shanks KG, Dahn T, Behonick G, Terrell A. Analysis of first and second generation legal highs for synthetic cannabinoids and synthetic stimulants by ultra-performance liquid chromatography and time of flight mass spectrometry. J Anal Toxicol 2012;36:360-71. https://doi.org/10.1093/jat/bks047.
- European Monitoring Centre for Drugs and Drug Addiction . Health and Social Responses to Drug Problems: A European Guide 2017.
- United Nations Office on Drugs and Crime (UNODC) . The Challenge of New Psychoactive Substances 2013.
- Chatwin C, Measham F, O’Brien K, Sumnall H. New drugs, new directions? Research priorities for new psychoactive substances and human enhancement drugs. Int J Drug Policy 2017;40:1-5. https://doi.org/10.1016/j.drugpo.2017.01.016.
- Adley M. The Drugs Wheel: A New Model for Substance Awareness 2017. www.thedrugswheel.com/downloads/TheDrugsWheel_2_0_5.pdf (accessed 30 October 2017).
- Great Britain . Misuse of Drugs Act 1971 1971.
- Sare J. How the media helped ban mephedrone. BMJ 2011;342. https://doi.org/10.1136/bmj.d1138.
- Sumnall HR, Evans-Brown M, McVeigh J. Social, policy, and public health perspectives on new psychoactive substances. Drug Test Anal 2011;3:515-23. https://doi.org/10.1002/dta.310.
- Stevens A, Fortson R, Measham F, Sumnall H. Legally flawed, scientifically problematic, potentially harmful: the UK Psychoactive Substance Bill. Int J Drug Policy 2015;26:1167-70. https://doi.org/10.1016/j.drugpo.2015.10.005.
- Great Britain . Psychoactive Substances Act 2016 2016.
- Great Britain . Criminal Justice Psychoactive Substances Act 2010 2010.
- O’Brien K, Chatwin C, Jenkins C, Measham F. New psychoactive substances and British drug policy: a view from the cyber-psychonauts. Drugs Educ Prev Policy 2015;22:217-23. https://doi.org/10.3109/09687637.2014.989959.
- European Monitoring Centre for Drugs and Drug Addiction . Europe’s Drugs Problem in ‘State of Flux’ 2013.
- Wallis L. Diffusion of New Psychoactive Substances: Understanding Population Motives, Harms and Intervention Needs n.d.
- O’Neill N. Mephedrone and Multiplicity: User Accounts of Effects and Harms. Contemp Drug Probl 2014;41:417-43. https://doi.org/10.1177/009145091404100307.
- European Commission . Young People and Drugs Report 2014 2014.
- Measham F, Moore K, Welch Z. Emerging Drug Trends in Lancashire: Night Club Surveys – Phase Three Report 2012.
- Martin J, Shenfield G. The hazards of rapid approval of new drugs. Aust Prescr 2016;39:2-3. https://doi.org/10.18773/austprescr.2016.005.
- Schifano F. Novel psychoactive substances (NPS): clinical and pharmacological issues. Drugs and Alcohol Today 2015;15:21-7. https://doi.org/10.1108/DAT-10-2014-0035.
- Sumnall H, Atkinson A, Begley E. Festival drug checking is here, but it now needs to be expanded across the country. The Conversation 2016. http://theconversation.com/festival-drug-checking-is-here-but-it-now-needs-to-be-expanded-across-the-country-63065 (accessed 31 May 2019).
- Baumeister D, Tojo LM, Tracy DK. Legal highs: staying on top of the flood of novel psychoactive substances. Ther Adv Psychopharmacol 2015;5:97-132. https://doi.org/10.1177/2045125314559539.
- Jones LE, Stewart A, Peters KL, McNaul M, Speers SJ, Fletcher NC, et al. Infrared and Raman screening of seized novel psychoactive substances: a large scale study of >200 samples. Analyst 2016;141:902-9. https://doi.org/10.1039/c5an02326b.
- Schifano F, Albanese A, Fergus S, Stair JL, Deluca P, Corazza O, et al. Mephedrone (4-methylmethcathinone; ‘meow meow’): chemical, pharmacological and clinical issues. Psychopharmacology 2011;214:593-602. https://doi.org/10.1007/s00213-010-2070-x.
- Ford BM, Tai S, Fantegrossi WE, Prather PL. Synthetic Pot: Not Your Grandfather’s Marijuana. Trends Pharmacol Sci 2017;38:257-76. https://doi.org/10.1016/j.tips.2016.12.003.
- WEDINOS . PHILTRE Annual Report 2014–15 2016. www.wedinos.org/resources/downloads/WN_Annual_Report_1415_final.pdf (accessed 1 October 2017).
- Department of Health Northern Ireland . All Ireland Drug Prevalence Survey 2014 15 2015.
- National Statistics Scotland . Scottish Crime and Justice Survey 2014 15: Drug Use 2016.
- Office for National Statistics . Drug Misuse: Findings From the 2014 to 2015 Crime Survey for England and Wales 2015.
- Department of Health Northern Ireland . Statistics from the NI [Northern Ireland] Drug Misuse Database: 1 April 2015–31 March 2016 2016.
- Public Health England (PHE) . Adult Substance Misuse Statistics from the National Drug Treatment Monitoring System (NDTMS): 1st April 2015 to 31st March 2016 2016.
- Northern Ireland Statistics and Research Agency . Drug Related and Drug Misuse Deaths 2006–2015 2015. www.nisra.gov.uk/publications/drug-related-and-drug-misuse-deaths-2006-2015 (accessed 30 October 2017).
- National Records of Scotland . Drug-Related Deaths in Scotland in 2015 2016.
- Office for National Statistics . Deaths Related to Drug Poisoning: England and Wales, 1993–2015 2016. www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsrelatedtodrugpoisoningenglandandwalesreferencetable/current (accessed 30 October 2017).
- Castaneto MS, Gorelick DA, Desrosiers NA, Hartman RL, Pirard S, Huestis MA. Synthetic cannabinoids: epidemiology, pharmacodynamics, and clinical implications. Drug Alcohol Depend 2014;144:12-41. https://doi.org/10.1016/j.drugalcdep.2014.08.005.
- Tait RJ, Caldicott D, Mountain D, Hill SL, Lenton S. A systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin Toxicol 2016;54:1-13. https://doi.org/10.3109/15563650.2015.1110590.
- Kyriakou C, Marinelli E, Frati P, Santurro A, Afxentiou M, Zaami S, et al. NBOMe: new potent hallucinogens – pharmacology, analytical methods, toxicities, fatalities: a review. Eur Rev Med Pharmacol Sci 2015;19:3270-81.
- Suzuki J, Dekker MA, Valenti ES, Arbelo Cruz FA, Correa AM, Poklis JL, et al. Toxicities associated with NBOMe ingestion-a novel class of potent hallucinogens: a review of the literature. Psychosomatics 2015;56:129-39. https://doi.org/10.1016/j.psym.2014.11.002.
- Busardò FP, Kyriakou C, Napoletano S, Marinelli E, Zaami S. Mephedrone related fatalities: a review. Eur Rev Med Pharmacol Sci 2015;19:3777-90.
- Mdege N, Meader N, Lloyd C, Parrott S, McCambridge J. The Novel Psychoactive Substance in the UK Project: empirical and conceptual review work to produce research recommendations. Public Health Research 2017;5. https://doi.org/10.3310/phr05040.
- Abdulrahim D, Bowden-Jones O. Guidance on the Management of Acute and Chronic Harms of Club Drugs and Novel Psychoactive Substances. London: NEPTUNE; 2015.
- NHS Digital . Smoking, Drinking, and Drug Use Among Young People in England in 2014 2015.
- NHS National Services Scotland . Scottish Schools Adolescent Lifestyle and Substance Use Survey (SALSUS): Drug Use Among 13 and 15 Year Olds in Scotland 2013 2014.
- Rhys Jones W, Masood M, Huke V, Reid F, Roche J, Patel M, et al. Novel psychoactive substance use, prescription drug abuse and internet drug purchasing in eating disorders. Res Adv Psychiatry 2016;3:33-4.
- Stanley JL, Mogford DV, Lawrence RJ, Lawrie SM. Use of novel psychoactive substances by inpatients on general adult psychiatric wards. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2015-009430.
- Moore AP, Lesser E. Legal highs, NPS, head shop drugs? Whatever you call them, we need to know more about prevalence. BJ Psych Bull 2015;39. https://doi.org/10.1192/pb.39.6.316a.
- Thurtle N, Dargan PI, Hunter LJ, Lovett C, White JA, Wood DM. A comparison of recreational drug use amongst sexual health clinic users in London with existing prevalence data. Int J STD AIDS 2016;27:1309-16. https://doi.org/10.1177/0956462415616056.
- Baker S. An Examination of the Reasons Why Prisoners Use Spice (Synthetic Cannabinoids) 2015.
- Ralphs R, Gray P, Norton A. New Psychoactive Substance Use in Manchester: Prevalence, Nature, Challenges and Responses. Manchester: Manchester Metropolitan University; 2017.
- Winstock AR, Mitcheson LR, Deluca P, Davey Z, Corazza O, Schifano F. Mephedrone, new kid for the chop?. Addiction 2011;106:154-61. https://doi.org/10.1111/j.1360-0443.2010.03130.x.
- Chung E, Waters L, Mercey D, Edwards S. High rates of recreational drug use (RDU) in HIV+ men who have sex with men (MSM) with sexually transmitted infections (STI). HIV Med 2014;15.
- Bourne A, Reid D, Hickson F, Torres-Rueda S, Steinberg P, Weatherburn P. ‘Chemsex’ and harm reduction need among gay men in South London. Int J Drug Policy 2015;26:1171-6. https://doi.org/10.1016/j.drugpo.2015.07.013.
- Brookman F. The Links Between Mephedrone Use, Violence and Other Harms in South Wales. Wales: Centre for Criminology, University of South Wales; 2014.
- Dalgarno P. Subjective effects of Salvia divinorum. J Psychoactive Drugs 2007;39:143-9. https://doi.org/10.1080/02791072.2007.10399872.
- Gray R, Bressington D, Hughes E, Ivanecka A. A systematic review of the effects of novel psychoactive substances ‘legal highs’ on people with severe mental illness. J Psychiatr Ment Health Nurs 2016;23:267-81. https://doi.org/10.1111/jpm.12297.
- Miotto K, Striebel J, Cho AK, Wang C. Clinical and pharmacological aspects of bath salt use: a review of the literature and case reports. Drug Alcohol Depend 2013;132:1-12. https://doi.org/10.1016/j.drugalcdep.2013.06.016.
- Brewer TL, Collins M. A review of clinical manifestations in adolescent and young adults after use of synthetic cannabinoids. J Spec Pediatr Nurs 2014;19:119-26. https://doi.org/10.1111/jspn.12057.
- Papanti D, Schifano F, Botteon G, Bertossi F, Mannix J, Vidoni D, et al. ‘Spiceophrenia’: a systematic overview of ‘spice’-related psychopathological issues and a case report. Hum Psychopharmacol 2013;28:379-89. https://doi.org/10.1002/hup.2312.
- Gunderson EW, Haughey HM, Ait-Daoud N, Joshi AS, Hart CL. ‘Spice’ and ‘K2’ herbal highs: a case series and systematic review of the clinical effects and biopsychosocial implications of synthetic cannabinoid use in humans. Am J Addict 2012;21:320-6. https://doi.org/10.1111/j.1521-0391.2012.00240.x.
- European Monitoring Centre for Drugs and Drug Addiction . Health Responses to New Psychoactive Substances 2016.
- Jeroen K. Vermunt . Latent class modeling with covariates: two improved three-step approaches. Polit Anal 2010;18:450-69. https://doi.org/10.1093/pan/mpq025.
- Higgins K, McLaughlin A, Perra O, McCartan C, McCann M, Percy A, et al. The Belfast Youth Development Study (BYDS): a prospective cohort study of the initiation, persistence and desistance of substance use from adolescence to adulthood in Northern Ireland. PLOS ONE 2018;13. https://doi.org/10.1371/journal.pone.0195192.
- Loeber R, Farrington DP, Stouthamer-Loeber M, White HR. Violence and Serious Theft: Development and Prediction from Childhood to Adulthood. Mahwah, NJ: Lawrence Erlbaum; 2008.
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull 1992;112:64-105. https://doi.org/10.1037/0033-2909.112.1.64.
- Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev 1993;100:674-701. https://doi.org/10.1037/0033-295X.100.4.674.
- Rutter M. Psychosocial resilience and protective mechanisms. Am J Orthopsychiatry 1987;57:316-31. https://doi.org/10.1111/j.1939-0025.1987.tb03541.x.
- Farrington DP, Ttofi MM, Bliesener T, Beelmann A, Stemmler M. Antisocial Behavior and Crime: Contributions of Developmental and Evaluation Research to Prevention and Intervention. Cambridge, MA: Hogrefe Publishing; 2011.
- Higgins K, Perra O, McCann M, McLaughlin A, McCartan C. Trajectories of Offending Behaviour in Northern Irish Adolescents. Belfast: Institute of Child Care Research; 2016.
- Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24. https://doi.org/10.1016/S0376-8716(99)00017-4.
- Khantzian EJ. The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Harv Rev Psychiatry 1997;4:231-44. https://doi.org/10.3109/10673229709030550.
- Farrington DP, Ttofi MM, Piquero AR. Risk, promotive, and protective factors in youth offending: results from the Cambridge study in delinquent development. J Crim Justice 2016;45:63-70. https://doi.org/10.1016/j.jcrimjus.2016.02.014.
- McCann M, Perra O, McLaughlin A, McCartan C, Higgins K. Assessing elements of a family approach to reduce adolescent drinking frequency: parent-adolescent relationship, knowledge management and keeping secrets. Addiction 2016;111:843-53. https://doi.org/10.1111/add.13258.
- Griffin KW, Botvin GJ. Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc Psychiatr Clin N Am 2010;19:505-26. https://doi.org/10.1016/j.chc.2010.03.005.
- Fletcher A, Bonell C, Hargreaves J. School effects on young people’s drug use: a systematic review of intervention and observational studies. J Adolesc Health 2008;42:209-20. https://doi.org/10.1016/j.jadohealth.2007.09.020.
- Perra O, Fletcher A, Bonell C, Higgins K, McCrystal P. School-related predictors of smoking, drinking and drug use: evidence from the Belfast Youth Development Study. J Adolesc 2012;35:315-24. https://doi.org/10.1016/j.adolescence.2011.08.009.
- Jovchelovitch S, Bauer MW, Bauer MW, Gaskell G. Qualitative Researching With Text, Image and Sound: A Practical Handbook. London: SAGE Publications Ltd; 2000.
- Holstein JA, Gubrium JF, Silverman D. Qualitative Research. London: SAGE Publications Ltd; 2016.
- Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual Sociol 1990;13:3-21. https://doi.org/10.1007/BF00988593.
- Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. London: SAGE Publications Ltd; 1994.
- Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res 2007;42:1758-72. https://doi.org/10.1111/j.1475-6773.2006.00684.x.
- Glaser B, Strauss A. Discovery of Grounded Theory. Hawthorne, NY: Aldine Publishing Co.; 1967.
- Glaser B. Basics of Grounded Theory. Mill Valley, CA: Sociology Press; 1992.
- Patton M. Qualitative Research and Evaluation Methods. Thousand Oaks, CA: SAGE Publications Ltd; 2002.
- Merton RK. On Theoretical Sociology: Five Essays, Old and New. New York, NY: Free Press; 1967.
- Hammersley M, Atkinson P. Ethnography. London: Routledge; 1995.
- Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equ Modeling 2007;14:535-69. https://doi.org/10.1080/10705510701575396.
- Brehm SS, Kassin S, Fein M. Social Psychology. Boston: Houghton Mifflin; 1999.
- Guxens M, Nebot M, Ariza C, Ochoa D. Factors associated with the onset of cannabis use: a systematic review of cohort studies. Gac Sanit 2007;21:252-60. https://doi.org/10.1157/13106812.
- Keijsers L, Frijns T, Branje SJ, Meeus W. Developmental links of adolescent disclosure, parental solicitation, and control with delinquency: moderation by parental support. Dev Psychol 2009;45:1314-27. https://doi.org/10.1037/a0016693.
- Kerr M, Stattin H, Burk WJ. A reinterpretation of parental monitoring in longitudinal perspective. J Res Adolesc 2010;20:39-64. https://doi.org/10.1111/j.1532-7795.2009.00623.x.
- Jeon KC, Goodson P. US adolescents’ friendship networks and health risk behaviors: a systematic review of studies using social network analysis and Add Health data. Peer J 2015;3. https://doi.org/10.7717/peerj.1052.
- Seo DC, Huang Y. Systematic review of social network analysis in adolescent cigarette smoking behavior. J Sch Health 2012;82:21-7. https://doi.org/10.1111/j.1746-1561.2011.00663.x.
- Boivin M, Dodge KA, Coie JD. Individual-group behavioral similarity and peer status in experimental play groups of boys: the social misfit revisited. J Pers Soc Psychol 1995;69:269-79. https://doi.org/10.1037/0022-3514.69.2.269.
- Chang L. The role of classroom norms in contextualizing the relations of children’s social behaviors to peer acceptance. Dev Psychol 2004;40:691-702. https://doi.org/10.1037/0012-1649.40.5.691.
- Stormshak EA, Bierman KL, Bruschi C, Dodge KA, Coie JD. The relation between behavior problems and peer preference in different classroom contexts. Conduct Problems Prevention Research Group. Child Dev 1999;70:169-82. https://doi.org/10.1111/1467-8624.00013.
- Arnett JJ. Adolescence and Emerging Adulthood: A Cultural Approach. Oxford Scholarship Online; 2001.
- Moffitt TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: follow-up at age 26 years. Dev Psychopathol 2002;14:179-207. https://doi.org/10.1017/S0954579402001104.
- Green MJ, Leyland AH, Sweeting H, Benzeval M. Causal effects of transitions to adult roles on early adult smoking and drinking: evidence from three cohorts. Soc Sci Med 2017;187:193-202. https://doi.org/10.1016/j.socscimed.2017.06.018.
- Allem JP, Sussman S, Soto DW, Baezconde-Garbanati L, Unger JB. Role transitions and substance use among Hispanic emerging adults: a longitudinal study using coarsened exact matching. Addict Behav 2016;58:95-9. https://doi.org/10.1016/j.addbeh.2016.02.032.
- Kirby T, Barry AE. Alcohol as a gateway drug: a study of US 12th graders. J Sch Health 2012;82:371-9. https://doi.org/10.1111/j.1746-1561.2012.00712.x.
- Fleming CB, White HR, Catalano RF. Romantic relationships and substance use in early adulthood: an examination of the influences of relationship type, partner substance use, and relationship quality. J Health Soc Behav 2010;51:153-67. https://doi.org/10.1177/0022146510368930.
- Farrington DP, Tonry M, Morris N. Crime and Justice: An Annual Review of Research. Chicago, IL: University of Chicago Press; 1986.
- Tilton-Weaver LC, Burk WJ, Kerr M, Stattin H. Can parental monitoring and peer management reduce the selection or influence of delinquent peers? Testing the question using a dynamic social network approach. Dev Psychol 2013;49:2057-70. https://doi.org/10.1037/a0031854.
- Smetana JG, Asquith P. Adolescents’ and parents’ conceptions of parental authority and personal autonomy. Child Dev 1994;65:1147-62. https://doi.org/10.2307/1131311.
- Goldstein SE, Davis-Kean PE, Eccles JS. Parents, peers, and problem behavior: a longitudinal investigation of the impact of relationship perceptions and characteristics on the development of adolescent problem behavior. Dev Psychol 2005;41:401-13. https://doi.org/10.1037/0012-1649.41.2.401.
- Kakihara F, Tilton-Weaver L, Kerr M, Stattin H. The relationship of parental control to youth adjustment: do youths’ feelings about their parents play a role?. J Youth Adolesc 2010;39:1442-56. https://doi.org/10.1007/s10964-009-9479-8.
- Tuchman E. Women and addiction: the importance of gender issues in substance abuse research. J Addict Dis 2010;29:127-38. https://doi.org/10.1080/10550881003684582.
- Green CA. Gender and use of substance abuse treatment services. Alcohol Res Health 2006;29:55-62.
- Bond L, Butler H, Thomas L, Carlin J, Glover S, Bowes G, et al. Social and school connectedness in early secondary school as predictors of late teenage substance use, mental health, and academic outcomes. J Adolesc Health 2007;40:357.e9-18. https://doi.org/10.1016/j.jadohealth.2006.10.013.
- Higgins K, O’Neill T, Jordan JA. Patterns of Offending in N. Ireland from Adolescence to Early Adulthood: Applying Research Findings to Inform Key Local Policy and Practice: Knowledge Exchange Report 2016.
- Bremner P, Burnett J, Nunney F, Ravat M, Mistral W. Young People Alcohol and Influences. York: Joseph Rowntree Foundation; 2011.
- Burke S, Schmied V, Montrose M. Parental Alcohol Misuse and the Impact on Children. Ashfield, NSW: NSW Department of Community Services; 2006.
- Waldron M, Grant JD, Bucholz KK, Lynskey MT, Slutske WS, Glowinski AL, et al. Parental separation and early substance involvement: results from children of alcoholic and cannabis dependent twins. Drug Alcohol Depend 2014;134:78-84. https://doi.org/10.1016/j.drugalcdep.2013.09.010.
- National Institute of Drug Abuse (NIDA) . Comorbidity: Addiction and Other Mental Illnesses 2010.
- Hammersley R, Marsland L, Reid M. Home Office Research Study 261: Substance Use by Young Offenders: The Impact of the Normalisation of Drug Use in the Early Years of the 21st Century. London: The Stationery Office; 2003.
- Liebschutz J, Savetsky JB, Saitz R, Horton NJ, Lloyd-Travaglini C, Samet JH. The relationship between sexual and physical abuse and substance abuse consequences. J Subst Abuse Treat 2002;22:121-8. https://doi.org/10.1016/S0740-5472(02)00220-9.
- Newburn T, Pearson G. The Place and Meaning of Drug Use in the Lives of Young People in Care. London: University of London; 2002.
- Ward J. Substance use among young people ‘looked after’ by social services. Drugs Educ Prev Policy 1998;5:257-67. https://doi.org/10.3109/09687639809034087.
- Didenko E, Pankratz N. Substance use: pathways to homelessness? Or a way of adapting to street life. BC’s Mental Health and Addictions J 2007;4:9-10.
- National Coalition for the Homeless . Substance Abuse and Homelessness 2009.
- Teruya C, Hser YI. Turning points in the life course: current findings and future directions in drug use research. Curr Drug Abuse Rev 2010;3:189-95. https://doi.org/10.2174/1874473711003030189.
- Aldridge J, Parker H, Measham F. Drug Trying and Drug Use Across Adolescence: A Longitudinal Study of Young People’s Drug Taking in Two Regions of Northern England. Report Prepared for the Home Office. 1999.
- Aldridge J, Measham F, Williams L. Illegal Leisure Revisited: Changing Patterns of Alcohol and Drug Use in Adolescents and Young Adults. London: Routledge; 2013.
- Kerr M, Stattin H. What parents know, how they know it, and several forms of adolescent adjustment: further support for a reinterpretation of monitoring. Dev Psychol 2000;36:366-80. https://doi.org/10.1037/0012-1649.36.3.366.
- Armsden GC, Greenberg MT. The inventory of parent and peer attachment: individual differences and their relationship to psychological well-being in adolescence. J Youth Adolesc 1987;16:427-54. https://doi.org/10.1007/BF02202939.
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry 1997;38:581-6. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
- Angold A, Costello EJ, Messer SC, Pickles A. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int J Methods Psychiatr Res 1995;5:237-49.
- Bebbington PE, Nayani T. The Psychosis Screening Questionnaire. Int J Meth Psych Res 1995;5:11-9. https://doi.org/10.1037/t30040-000.
- Hawton K, Rodham K, Evans E. By Their Own Young Hand: Deliberate Self-harm and Suicidal Ideas in Adolescents. London: Jessica Kingsley Publishers; 2016.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
- Donovan JE, Molina BS. Childhood risk factors for early-onset drinking. J Stud Alcohol Drugs 2011;72:741-51. https://doi.org/10.15288/jsad.2011.72.741.
- De Genna NM, Cornelius MD, Donovan JE. Risk factors for young adult substance use among women who were teenage mothers. Addict Behav 2009;34:463-70. https://doi.org/10.1016/j.addbeh.2008.12.014.
- Baumeister SE, Tossmann P. Association between early onset of cigarette, alcohol and cannabis use and later drug use patterns: an analysis of a survey in European metropolises. Eur Addict Res 2005;11:92-8. https://doi.org/10.1159/000083038.
- Bossarte RM, Swahn MH. Interactions between race/ethnicity and psychosocial correlates of preteen alcohol use initiation among seventh grade students in an urban setting. J Stud Alcohol Drugs 2008;69:660-5. https://doi.org/10.15288/jsad.2008.69.660.
- King KM, Chassin L. A prospective study of the effects of age of initiation of alcohol and drug use on young adult substance dependence. J Stud Alcohol Drugs 2007;68:256-65. https://doi.org/10.15288/jsad.2007.68.256.
- Hingson RW, Heeren T, Jamanka A, Howland J. Age of drinking onset and unintentional injury involvement after drinking. JAMA 2000;284:1527-33. https://doi.org/10.1001/jama.284.12.1527.
- McGue M, Iacono WG. The association of early adolescent problem behavior with adult psychopathology. Am J Psychiatry 2005;162:1118-24. https://doi.org/10.1176/appi.ajp.162.6.1118.
- Sartor CE, Lynskey MT, Bucholz KK, Madden PA, Martin NG, Heath AC. Timing of first alcohol use and alcohol dependence: evidence of common genetic influences. Addiction 2009;104:1512-18. https://doi.org/10.1111/j.1360-0443.2009.02648.x.
- Humphrey JA, Friedman J. The onset of drinking and intoxication among university students. J Stud Alcohol 1986;47:455-8. https://doi.org/10.15288/jsa.1986.47.455.
- Freise B, Grube JW. Youth Drinking Rates and Problems: A Comparison of European Countries and the United States. Berkeley, CA: Prevention Research Center, Pacific Institute for Research and Evaluation; 2005.
- Bollen KA, Curran PJ. Latent Curve Models. Hoboken, NJ: Wiley-Interscience; 2006.
- Clark S, Muthén B. Relating Latent Class Analysis Results to Variables Not Included in the Analysis. Los Angeles, CA: University of California; 2009.
- European Monitoring Centre for Drugs and Addiction . European Drug Report 2016 2016.
- Great Britain . Change to the Misuse of Drugs Act 1971 2013.
- Corazza O, Roman-Urrestarazu A. Novel Psychoactive Substances: Policy, Economics and Drug Regulation. Cham: Springer; 2017.
- Featherstone S. Spike nation. New York Times Magazine 2015.
- Deligianni E, Corkery JM, Schifano F, Lione LA. An international survey on the awareness, use, preference, and health perception of novel psychoactive substances (NPS). Hum Psychopharmacol 2017;32. https://doi.org/10.1002/hup.2581.
- European Monitoring Centre for Drugs and Drug Addiction . Synthetic Cannabinoids in Europe (Perspectives on Drugs) 2017.
- Nutt D. The ban on legal highs will only have one effect, more drug related deaths. The Guardian 2016. www.theguardian.com/commentisfree/2016/may/31/ban-legal-highs-drug-related-deaths-alcohol (accessed 30 October 2017).
- Sumnall H. Legal highs ban will fail to eradicate spice, warns government adviser. The Guardian 2016. www.theguardian.com/society/2016/jun/07/legal-highs-ban-fail-eradicate-spice-warns-government-adviser (accessed 10 June 2019).
- Kikura-Hanajiri R, Uchiyama N, Goda Y. Survey of current trends in the abuse of psychotropic substances and plants in Japan. Leg Med 2011;13:109-15. https://doi.org/10.1016/j.legalmed.2011.02.003.
- Musah RA, Domin MA, Cody RB, Lesiak AD, Dane AJ, Shepard JR. Direct analysis in real time mass spectrometry with collision-induced dissociation for structural analysis of synthetic cannabinoids. Rapid Commun Mass Spectrom 2012;26:2335-42. https://doi.org/10.1002/rcm.6354.
- Musah RA, Domin MA, Walling MA, Shepard JR. Rapid identification of synthetic cannabinoids in herbal samples via direct analysis in real time mass spectrometry. Rapid Commun Mass Spectrom 2012;26:1109-14. https://doi.org/10.1002/rcm.6205.
- Soussan C, Kjellgren A. The flip side of ‘Spice’: the adverse effects of synthetic cannabinoids as discussed on a Swedish internet forum. Nord Stud Alcohol Dr 2014;31. https://doi.org/10.2478/nsad-2014-0016.
- Van Hout MC, Hearne E. A Community Based Study of Synthetic Cannabinoid Use in Co. Monaghan, Ireland. Monaghan: Teach na Daoine Family Resource Centre; 2015.
- Lefever TW, Marusich JA, Thomas BF, Barrus DG, Peiper NC, Kevin RC, et al. Vaping synthetic cannabinoids: a novel preclinical model of e-cigarette use in mice. Subst Abuse 2017;11. https://doi.org/10.1177/1178221817701739.
- User Voice . Spice: The Bird Killer – What Prisoners Think About the Use of Spice and Other Legal Highs in Prison 2016. www.uservoice.org/wp-content/uploads/2016/05/User-Voice-Spice-The-Bird-Killer-Report-Low-Res.pdf (accessed 24 August 2016).
- Advisory Council on the Misuse of Drugs (ACMD) . ‘Third Generation’ Synthetic Cannabinoids 2014.
- Van Hout MC, Hearne E. New psychoactive substances (NPS) on cryptomarket fora: an exploratory study of characteristics of forum activity between NPS buyers and vendors. Int J Drug Policy 2017;40:102-10. https://doi.org/10.1016/j.drugpo.2016.11.007.
- Barnard M, Russell C, McKeganey N, Hamilton-Barclay T. The highs and lows of NPS/‘Legal High’ use: qualitative views from a UK online survey. Drugs Educ Prev Policy 2017;24:96-102. https://doi.org/10.1080/09687637.2016.1201046.
- Valento M, Lebin J. Emerging drugs of abuse: synthetic cannabinoids, phenylethylamines (2C Drugs) and synthetic cathinones. Clin Pediatr Emerg Med 2017;18:203-11. https://doi.org/10.1016/j.cpem.2017.07.009.
- Fattore L. Synthetic cannabinoids-further evidence supporting the relationship between cannabinoids and psychosis. Biol Psychiatry 2016;79:539-48. https://doi.org/10.1016/j.biopsych.2016.02.001.
- Winstock A, Lynskey M, Borschmann R, Waldron J. Risk of emergency medical treatment following consumption of cannabis or synthetic cannabinoids in a large global sample. J Psychopharmacol 2015;29:698-703. https://doi.org/10.1177/0269881115574493.
- Blackman S, Bradley R. From niche to stigma-headshops to prison: exploring the rise and fall of synthetic cannabinoid use among young adults. Int J Drug Policy 2017;40:70-7. https://doi.org/10.1016/j.drugpo.2016.10.015.
- Joseph AM, Manseau MW, Lalane M, Rajparia A, Lewis CF. Characteristics associated with synthetic cannabinoid use among patients treated in a public psychiatric emergency setting. Am J Drug Alcohol Abuse 2017;43:117-22. https://doi.org/10.1080/00952990.2016.1240799.
- Home Office . New Psychoactive Substances (NPS) Resource Pack 2015.
- Tracy DK, Wood DM, Baumeister D. Novel psychoactive substances: identifying and managing acute and chronic harmful use. BMJ 2017;356. https://doi.org/10.1136/bmj.i6814.
- Loeffler G, Delaney E, Hann M. International trends in spice use: prevalence, motivation for use, relationship to other substances, and perception of use and safety for synthetic cannabinoids. Brain Res Bull 2016;126:8-28. https://doi.org/10.1016/j.brainresbull.2016.04.013.
- Musshoff F, Madea B, Kernbach-Wighton G, Bicker W, Kneisel S, Hutter M, et al. Driving under the influence of synthetic cannabinoids (‘Spice’): a case series. Int J Legal Med 2014;128:59-64. https://doi.org/10.1007/s00414-013-0864-1.
- Zimmermann US, Winkelmann PR, Pilhatsch M, Nees JA, Spanagel R, Schulz K. Withdrawal phenomena and dependence syndrome after the consumption of ‘spice gold’. Dtsch Arztebl Int 2009;106:464-7. https://doi.org/10.3238/arztebl.2009.0464.
- MacLeod K, Pickering L, Gannon M, Greenwood S, Liddell D, Smith A, et al. Understanding the Patterns of Use, Motives, and Harms of New Psychoactive Substances in Scotland. Edinburgh: Scottish Government; 2016.
- European Monitoring Centre for Drugs and Drug Addiction . Annual Report on the State of the Drugs Problem in the European Union and Norway 2002.
- Boys A, Marsden J, Strang J. Understanding reasons for drug use amongst young people: a functional perspective. Health Educ Res 2001;16:457-69. https://doi.org/10.1093/her/16.4.457.
- Ives R, Ghelani P. Polydrug use (the use of drugs in combination): a brief review. Drug Educ Prev Polic 2006;13:225-32. https://doi.org/10.1080/09687630600655596.
- Schensul JJ, Convey M, Burkholder G. Challenges in measuring concurrency, agency and intentionality in polydrug research. Addict Behav 2005;30:571-4. https://doi.org/10.1016/j.addbeh.2004.05.022.
- Hansen D, Maycock B, Lower T. ‘Weddings, parties, anything . . .’, a qualitative analysis of ecstasy use in Perth, Western Australia. Int J Drug Policy 2001;12:181-99. https://doi.org/10.1016/S0955-3959(00)00075-X.
- Schifano F, Oyefeso A, Corkery J, Cobain K, Jambert-Gray R, Martinotti G, et al. Death rates from ecstasy (MDMA, MDA) and polydrug use in England and Wales 1996–2002. Hum Psychopharmacol 2003;18:519-24. https://doi.org/10.1002/hup.528.
- Klein A. Dr Axel Klein – ‘Everybody Is a Poly (Substance User)’ 2011. https://vimeo.com/80804708 (accessed 30 October 2017).
- Kataja K, Hakkarainen P, Vayrynen S. Risk-taking, control and social identities in narratives of Finnish polydrug users. Drug Educ Prev Polic 2017;35:1-10.
- Boeri M, Sterk C, Bahora M, Elifson K. Poly-drug use among ecstasy users: separate, synergistic, and indiscriminate patterns. J Drug Issues 2008;38:517-41. https://doi.org/10.1177/002204260803800207.
- Smirnov A, Najman JM, Hayatbakhsh R, Wells H, Legosz M, Kemp R. Young adults’ recreational social environment as a predictor of ecstasy use initiation: findings of a population-based prospective study. Addiction 2013;108:1809-17. https://doi.org/10.1111/add.12239.
- Hickson F, Bonell C, Weatherburn P, Reid D. Illicit drug use among men who have sex with men in England and Wales. Addict Res Theory 2010;18:14-22. https://doi.org/10.3109/16066350902770433.
- Addison M, Stockdale K, McGovern R, McGovern W, McKinnon I, Crowe L, et al. Exploring the intersections between novel psychoactive substances (NPS) and other substance use in a police custody suite setting in the north east of England. Drug Educ Prev Policy 2017;25:1-7. https://doi.org/10.1080/09687637.2017.1378620.
- Degenhardt L, Chiu WT, Conway K, Dierker L, Glantz M, Kalaydjian A, et al. Does the ‘gateway’ matter? Associations between the order of drug use initiation and the development of drug dependence in the National Comorbidity Study Replication. Psychol Med 2009;39:157-67. https://doi.org/10.1017/S0033291708003425.
- Reuter P, Pardo B. New psychoactive substances: Are there any good options for regulating new psychoactive substances?. Int J Drug Policy 2017;40:117-22. https://doi.org/10.1016/j.drugpo.2016.10.020.
- European Monitoring Centre for Drugs and Drug Addiction . High-Risk Drug Use and New Psychoactive Substances: Results from an EMCDDA Trendspotter Study 2017.
- Degenhardt L, Bruno R, Topp L. Is ecstasy a drug of dependence?. Drug Alcohol Depend 2010;107:1-10. https://doi.org/10.1016/j.drugalcdep.2009.09.009.
- Hser YI, Longshore D, Anglin MD. The life course perspective on drug use: a conceptual framework for understanding drug use trajectories. Eval Rev 2007;31:515-47. https://doi.org/10.1177/0193841X07307316.
- Hser YI, Evans E, Huang D, Brecht ML, Li L. Comparing the dynamic course of heroin, cocaine, and methamphetamine use over 10 years. Addict Behav 2008;33:1581-9. https://doi.org/10.1016/j.addbeh.2008.07.024.
- Hser YI, Huang D, Brecht ML, Li L, Evans E. Contrasting trajectories of heroin, cocaine, and methamphetamine use. J Addict Dis 2008;27:13-21. https://doi.org/10.1080/10550880802122554.
- European Monitoring Centre for Drugs and Drug Addiction . Best Practice Portal n.d. www.emcdda.europa.eu/best-practice (accessed 31 May 2019).
- Baja N, Mullen E, Wylie S. Dependence and psychosis with 4-methlmethcathinone (mephedrone) use: findings that shed new light on the possible pathogenesis of a disease or an adverse effect. BMJ 2010;6:327-30. https://doi.org/10.1136/bcr.02.2010.2780.
- Fletcher E, Tasker S, Easton P, Denvir L. New Psychoactive Substances Needs Assessment for Tayside 2014. Dundee: NHS Tayside, Angus Alcohol and Drugs Partnership, Alcohol and Drug Partnership Dundee City, Alcohol Drug Partnership Perth and Kinross; 2014.
- Nutt D, King LA, Saulsbury W, Blakemore C. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet 2007;369:1047-53. https://doi.org/10.1016/S0140-6736(07)60464-4.
- Scherbaum N, Schifano F, Bonnet U. New psychoactive substances (NPS) – a challenge for the addiction treatment services. Pharmacopsychiatry 2017;50:116-22. https://doi.org/10.1055/s-0043-102059.
- Solomon D, Grewal P, Taylor C, Solomon B. Managing misuse of novel psychoactive substances. Nurs Times 2014;110:12-5.
- Weinstein AM, Rosca P, Fattore L, London ED. Synthetic cathinone and cannabinoid designer drugs pose a major risk for public health. Front Psychiatry 2017;8. https://doi.org/10.3389/fpsyt.2017.00156.
- German CL, Fleckenstein AE, Hanson GR. Bath salts and synthetic cathinones: an emerging designer drug phenomenon. Life Sci 2014;97:2-8. https://doi.org/10.1016/j.lfs.2013.07.023.
- Tekulve K, Alexander A, Tormoehlen L. Seizures associated with synthetic cathinone exposures in the pediatric population. Pediatr Neurol 2014;51:67-70. https://doi.org/10.1016/j.pediatrneurol.2014.03.003.
- Pichini S, Rotolo MC, García J, Girona N, Leal L, García-Algar O, et al. Neonatal withdrawal syndrome after chronic maternal consumption of 4-methylethcathinone. Forensic Sci Int 2014;245:e33-5. https://doi.org/10.1016/j.forsciint.2014.10.027.
- European Monitoring Centre for Drugs and Drug Addiction . Policy and Practice Briefings: Responding to New Psychoactive Substances n.d. www.emcdda.europa.eu/best-practice/briefings/responding-new-psychoactive-substances (accessed 31 May 2019).
- European Monitoring Centre for Drugs and Drug Addiction . New Psychoactive Substances: An Update From the EU Early Warning System 2015.
- Macfarlane V, Christie G. Synthetic cannabinoid withdrawal: a new demand on detoxification services. Drug Alcohol Rev 2015;34:147-53. https://doi.org/10.1111/dar.12225.
- European Drug Emergencies Network (EURODEN) . Guidelines on When to Call the Emergency Services 112 for Unwell Recreational Drug Users 2015. www.emcdda.europa.eu/attachements.cfm/att_235696_EN_INT19_Euro-DEN%202015.pdf (accessed 10 June 2019).
- Public Health England (PHE) . New Psychoactive Substances in Prisons: A Toolkit for Staff 2015.
- Goldberg LR, Mervielde I, Deary I, De Fruyt F, Ostendorf F. Personality Psychology in Europe. Tilburg: Tilburg University Press; 1999.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999;282:1737-44. https://doi.org/10.1001/jama.282.18.1737.
- Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care. Geneva: World Health Organization; 2001.
- Gavin DR, Ross HE, Skinner HA. Diagnostic validity of the drug abuse screening test in the assessment of DSM-III drug disorders. Br J Addict 1989;84:301-7. https://doi.org/10.1111/j.1360-0443.1989.tb03463.x.
- Legleye S, Karila L, Beck F, Reynaud M. Validation of the CAST, a general population Cannabis Abuse Screening Test. J Subst Use 2007;12:233-42. https://doi.org/10.1080/14659890701476532.
Appendix 1 Interview schedule
Appendix 2 Belfast Youth Development Study drug use questions
| Question code | Question wording |
|---|---|
| qy754 | Have you ever tried cigarettes (even just once)? |
| qy761 | Have you ever drunk alcohol (even just once)? |
| qy777 | Have you ever tried CANNABIS (even just once)? |
| qy788 | Have you ever tried ECSTASY (even just once)? |
| qy798 | Have you ever tried SPEED (even just once)? |
| qy7108 | Have you ever tried LSD (even just once)? |
| qy7118 | Have you ever tried COCAINE (even just once)? |
| qy7128 | Have you ever tried HEROIN (even just once)? |
| qy7138 | Have you ever tried OTHER PILLS (even just once)? |
| qy7148 | Have you ever tried POPPERS (even just once)? |
| qy7157 | Have you ever used MEPHEDRONE? |
| qy7166 | Do you use any drugs called LEGAL HIGHS? |
Appendix 3 Latent class analysis probability tables
| Class | Count | Proportion (%) | Class (probability) | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| 1 | 532 | 26 | 0.93 | 0.07 | 0.00 | 0.00 |
| 2 | 926 | 45 | 0.05 | 0.88 | 0.07 | 0.00 |
| 3 | 367 | 18 | 0.00 | 0.14 | 0.82 | 0.04 |
| 4 | 214 | 11 | 0.00 | 0.00 | 0.10 | 0.90 |
| Total | 2039 | 100 | ||||
| Drug | Latent class (probability) | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| Tobacco | 0.085 | 0.934 | 0.978 | 0.956 |
| Alcohol | 0.877 | 1.000 | 1.000 | 1.000 |
| Cannabis | 0.000 | 0.422 | 0.962 | 0.976 |
| Ecstasy | 0.003 | 0.020 | 0.371 | 0.966 |
| Speed | 0.004 | 0.005 | 0.112 | 0.795 |
| LSD | 0.000 | 0.000 | 0.013 | 0.304 |
| Cocaine | 0.008 | 0.006 | 0.428 | 0.973 |
| Heroin | 0.000 | 0.000 | 0.003 | 0.010 |
| Other pills | 0.000 | 0.000 | 0.057 | 0.377 |
| Poppers | 0.009 | 0.074 | 0.436 | 0.778 |
| NPS | 0.003 | 0.014 | 0.164 | 0.702 |
Appendix 4 Sample characteristics
| ID | Age (years) | Sex | Recruitment group | Relationship status | Ever use of NPS | Drugs used | Qualitative group |
|---|---|---|---|---|---|---|---|
| 1002 | 27 | Male | BYDS | Married | No | Alcohol, cannabis | 1 |
| 1007 | 27 | Female | BYDS | In relationship | No | Alcohol, cannabis, cocaine | 1 |
| 1010 | 27 | Female | BYDS | Married | No | Alcohol, cannabis, poppers | 1 |
| 1011 | 27 | Female | BYDS | Single | No | Alcohol, cannabis | 1 |
| 1039 | 28 | Female | BYDS | Married | No | Alcohol | 1 |
| 1043 | 19 | Female | Services | Unassigned | No | Alcohol, cannabis | 1 |
| 1045 | 19 | Male | Services | Single | No | Alcohol, cannabis, cocaine | 1 |
| 1056 | 20 | Male | Services | Single | No | Alcohol | 1 |
| 1006 | 27 | Female | BYDS | In relationship | No | Alcohol, cannabis, cocaine | 2 |
| 1004 | 27 | Female | BYDS | In relationship | No | Alcohol, cannabis, cocaine, ecstasy | 2 |
| 1009 | 27 | Male | BYDS | In relationship | No | Alcohol, cannabis, cocaine, ecstasy | 2 |
| 1014 | 27 | Female | BYDS | Single | No | Alcohol, cannabis, ‘magic mushrooms’ | 2 |
| 1029 | 27 | Female | BYDS | Married | No | Alcohol, cannabis, cocaine, ecstasy | 2 |
| 1041 | 28 | Female | BYDS | In relationship | No | Alcohol, amphetamine, cannabis, cocaine, LSD, poppers | 2 |
| 1001 | 27 | Female | BYDS | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, MDMA, mephedrone | 2 |
| 1003 | 27 | Male | BYDS | Single | Yes | Alcohol, cannabis, magic mushrooms, ‘NPS hallucinogen’ | 2 |
| 1012 | 27 | Female | BYDS | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, mephedrone | 2 |
| 1013 | 28 | Male | BYDS | Single | Yes | Alcohol, cannabis, cocaine, ‘salvia’ | 2 |
| 1016 | 21 | Female | Services | Single | Yes | Alcohol, poppers, cannabis, SCs | 2 |
| 1037 | 28 | Male | BYDS | In relationship | Yes | Alcohol, cannabis, China White, cocaine, ecstasy, mephedrone | 2 |
| 1042 | 17 | Male | Services | Single | Yes | Alcohol, cannabis, ecstasy, SCs | 2 |
| 1052 | 21 | Female | Services | Single | Yes | Alcohol, cannabis, cocaine, SCs | 2 |
| 1036 | 28 | Male | BYDS | In relationship | Yes | Cannabis, cocaine, DMT, ecstasy, GHB, LSD, MDMA, mephedrone | 3 |
| 1005 | 27 | Male | BYDS | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, GHB, ‘herbal pills’, ketamine, LSD, MDMA, mephedrone, solvents | 3 |
| 1008 | 27 | Male | BYDS | In relationship | Yes | Alcohol, amphetamine, cannabis, China White, cocaine, ecstasy, herbal pills, ketamine, mephedrone, SCs | 3 |
| 1015 | 18 | Female | Services | In relationship | Yes | Alcohol, cannabis, cocaine, mephedrone, SCs | 3 |
| 1017 | 27 | Female | BYDS | In relationship | Yes | Alcohol, cannabis, SCs | 3 |
| 1018 | 27 | Female | BYDS | Single | Yes | Alcohol, amphetamine, cannabis, ecstasy, MDMA, mephedrone | 3 |
| 1028 | 28 | Female | BYDS | Single | Yes | Alcohol, cannabis, China White, cocaine, ecstasy, ketamine, magic mushrooms, MDMA, mephedrone, poppers, SCs | 3 |
| 1051 | 16 | Female | Services | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, LSD, MDMA, prescription medication, SCs, solvents | 3 |
| HMP1011 | 28 | Male | Prison 1 | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, mephedrone, SCs | 3 |
| 1022 | 27 | Male | BYDS | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, ketamine, MDMA, MDMI, mephedrone | 3 |
| 1053 | 19 | Female | Services | Single | Yes | Alcohol, cannabis, China White, cocaine, prescription medication, SCs, stimulant NPS (‘sniff’) | 4, 1 |
| 1044 | 18 | Male | Services | Unassigned | Yes | Alcohol, cannabis, cocaine, ecstasy, SCs, synthetic cocaine’ | 4, 1 |
| 1046 | 17 | Male | Services | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, MDMA, mephedrone, SCs | 4, 1 |
| 1047 | 17 | Male | Services | Single | Yes | Alcohol, cannabis, cocaine, MDMA, SCs | 4, 1 |
| 1048 | 17 | Male | Services | Single | Yes | Alcohol, cannabis, SCs | 4, 1 |
| 1049 | 18 | Female | Services | Single | Yes | Alcohol, cannabis, cocaine, herbal pills, mephedrone, prescription medication, SCs | 4, 1 |
| 1050 | 18 | Male | Services | Single | Yes | Alcohol, Cannabis, cocaine, ecstasy, herbal pills, LSD, morphine patches, ‘synthetic LSD’, 25I, 25e, 2C-B, SC powder | 4, 1 |
| 1054 | 24 | Male | Services | In relationship | Yes | Alcohol, cannabis, ecstasy, LSD, mephedrone, PCP, prescription medication, SCs | 4, 1 |
| 1055 | 18 | Male | Services | In relationship | Yes | Alcohol, SCs | 4, 1 |
| HMP1012 | 20 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, ketamine, mephedrone, prescription medication, SCs | 4, 1 |
| HMP1018 | 20 | Male | Prison 3 | Single | Yes | Alcohol, cocaine, herbal pills, prescription medication, SCs | 4, 1 |
| HMP1020 | 21 | Male | Prison 2 | Single | Yes | Alcohol, cannabis, SCs | 4, 1 |
| HMP1022 | 19 | Male | Prison 3 | In relationship | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, mephedrone, prescription medication, SCs | 4, 1 |
| HMP1024 | 20 | Female | Prison 3 | Single | Yes | Alcohol, cannabis, mephedrone, prescription medication, SCs | 4, 1 |
| 1025 | 27 | Male | BYDS | Single | Yes | Alcohol, cannabis, ecstasy, LSD, ketamine, MDMA, mephedrone | 4, 2 |
| 1027 | 48 | Male | Services | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, DMT, ecstasy, heroin, LSD, magic mushrooms, mephedrone, prescription medication, SCs, solvents | 4, 2 |
| 1032 | 50 | Male | Services | Single | Yes | Alcohol, amphetamine, barbiturates, cannabis, China White, cocaine, LSD, magic mushrooms | 4, 2 |
| 1034 | 34 | Male | Services | In relationship | Yes | Alcohol, amphetamine, cannabis, cocaine, ketamine, mephedrone, prescription medication, SCs | 4, 2 |
| 1038 | 27 | Male | BYDS | In relationship | Yes | Alcohol, cannabis, cocaine, magic mushrooms, MDMA, mephedrone | 4, 2 |
| 1040 | 28 | Male | Services | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, mephedrone, morphine patches, prescription pills, SCs | 4, 2 |
| 1057 | 19 | Male | Services | In relationship | Yes | Alcohol, cannabis, China White, cocaine, ecstasy, SCs | 4, 2 |
| 1061 pilot | 38 | Male | Services | In relationship | Yes | Alcohol, amphetamine, cannabis, China White, cocaine, ecstasy, LSD, herbal pills, heroin, prescription medication | 4, 2 |
| HMP1001 | 33 | Male | Prison 1 | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, herbal pills, prescription medication | 4, 2 |
| HMP1002 | 24 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, China White, cocaine, ecstasy, fentanyl, mephedrone, morphine, prescription medication | 4, 2 |
| HMP1009 | 35 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, fentanyl, mephedrone, prescription medication, SCs, solvents | 4, 2 |
| HMP1010 | 23 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, MDMA, mephedrone, methamphetamine, prescription medication | 4, 2 |
| HMP1014 | 37 | Male | Prison 1 | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, mephedrone, prescription medication, SCs | 4, 2 |
| HMP1016 | 30 | Male | Prison 1 | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, ketamine, MDMA, mephedrone, prescription medication | 4, 2 |
| HMP1025 | 33 | Female | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, heroin, LSD, methamphetamine, prescription medication, SCs | 4, 2 |
| 1019 | 42 | Female | Services | In relationship | Yes | Acid, alcohol, amphetamine, cannabis, cocaine, ecstasy, glue, LSD, speed, mephedrone, SCs, solvents | 4, 3 |
| 1021 | 37 | Male | Services | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, heroin, mephedrone, SCs | 4, 3 |
| 1026 | 24 | Male | Services | Single | Yes | Alcohol cannabis, cocaine, MDMA, mephedrone, SCs (C-Liquid), solvents, ‘synthetic MDMA’, ‘synthetic ketamine’, ‘synthetic LSD’, ‘synthetic cocaine’ | 4, 3 |
| 1030 | 20 | Male | Services | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, mephedrone, SCs herbal | 4, 3 |
| 1031 | 23 | Male | Services | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, mephedrone, prescription medication | 4, 3 |
| 1035 | 23 | Male | Services | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, herbal pills, heroin, LSD, MDMA, SCs | 4, 3 |
| 1058 | 27 | Male | Services | Single | Yes | Alcohol, amphetamine, cannabis, China White, cocaine, ecstasy, heroin, LSD, mephedrone, prescription medication, SCs | 4, 3 |
| 1059 | 30 | Male | Services | In relationship | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, herbal pills, heroin, ketamine, mephedrone, SCs | 4, 3 |
| 1020 | 26 | Male | Services | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, heroin, ketamine, LSD, mephedrone, ‘Polish Peeko’, prescription medication | 4, 3 |
| HMP1005 | 53 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, heroin, ecstasy, LSD, morphine, prescription medication, SCs, solvents, | 4, 3 |
| HMP1007 | 27 | Male | Prison 1 | Single | Yes | Alcohol, cannabis, cocaine, ecstasy, fentanyl, heroin, mephedrone, prescription medication, SCs, synthetic stimulants | 4, 3 |
| HMP1008 | 25 | Male | Prison 1 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, heroin, prescription medication, SCs | 4, 3 |
| HMP1013 | 24 | Female | Prison 3 | Single | Yes | Alcohol, amphetamine, cannabis, cocaine, ecstasy, heroin, mephedrone, morphine, prescription medication, SCs, morphine | 4, 3 |
| HMP1015 | 30 | Male | Prison 1 | Single | Yes | Alcohol, cannabis, cocaine, crack cocaine, heroin, prescription medication, SCs, ‘synthetic stimulants’ | 4, 3 |
| HMP1017 | 21 | Male | Prison 3 | Single | Yes | Acid, alcohol, buprenorphine and naloxone (Suboxone®, Indivior UK Ltd), cocaine, codeine, diazepam, ecstasy, MDMA, mephedrone, NRG, oxycontin, pregabalin (Lyrica®, Pfizer Inc.), SCs, Subutex, tramadol | 4, 3 |
| HMP1019 | 25 | Male | Prison 2 | In relationship | Yes | Alcohol, cannabis, cocaine, ecstasy, heroin, ketamine, mephedrone (injecting), prescription medication, SCs | 4, 3 |
| HMP1021 | 31 | Female | Prison 3 | Single | Yes | Alcohol, cannabis, cocaine, crack cocaine, fentanyl, herbal pills, heroin, mephedrone, methamphetamine, prescription medication, SCs | 4, 3 |
| HMP1023 | 18 | Female | Prison 3 | Single | Yes | Alcohol, cannabis, SCs | 4, 3 |
| 1033 | 48 | Male | Services | Divorced | No | Alcohol, methamphetamine | 4, 4 |
| 1060 | 56 | Male | Services | Single | No | Alcohol, cannabis, ecstasy, magic mushrooms | 4, 4 |
| HMP1003 | 35 | Male | Prison 1 | Single | No | Alcohol, cannabis, ecstasy, LSD, prescription medication, solvents | 4, 4 |
| HMP1004 | 34 | Male | Prison 1 | Single | No | Alcohol, anabolic steroids, cannabis, prescription medication | 4, 4 |
| HMP1006 | 38 | Male | Prison 1 | Single | No | Alcohol, cannabis | 4, 4 |
Appendix 5 Additional analysis details (longitudinal risk factors and outcomes associated with drug class membership analysis)
Coding of longitudinal predictor measures
The school attachment and school commitment scales used in the present research were formed via factor analysis in previous research. 73 Prior to computing scales, for the school attachment, school commitment, parental control, emotional difficulties and impulse control scales, expectation–maximisation (EM) was used to impute missing values where the respondent had completed at least one item on that scale in that wave. Separate EMs were computed for each scale at each time point, which allowed the other items from the same wave to be used as predictors in each model. Details of how all the BYDS model variables were coded are as follows (Table 16 contains all items).
| Measure | Wave(s) | Items |
|---|---|---|
| Left home early | 6 | Who do you currently live with? (response options: alone – away from the family home; with parent(s); with foster parents; with siblings – away from family home; with grandparents or other family members; with partner; with friends or flatmates) |
| School attachment | 2–5 |
I think going to school is a waste of time I never take school seriously I like school I am fed up with school I do not like the subjects I do I like my teachers I am always willing to help the teacher (Response options for all items: almost true; not very often true; sometimes true; often true; almost always or always true) |
| School commitment | 2–5 |
|
| Bullied | 4 | Other children or young people pick on me or bully me (response options: not true; somewhat true; certainly true) |
| ≥ 6 GCSEs | 7 | How many GCSE grades A–C do you have? (response options: 0; 1–2; 3–5; 6–9; > 10) |
| Parental control | 2–5 | See Kerr and Stattin129 for items and coding rules |
| Unsupervised alcohol | 4 | Do your parents allow you to drink alcohol? (response options: yes; yes, but only when I am with them; no) |
| Natural parent moved out | ? | Who lives with you in your home? (response options: mother; stepmother; grandmother; foster mother; father; stepfather; grandfather; foster father; I live in a children’s home; brothers; stepbrothers; foster brothers; sisters; stepsisters; foster sisters; other) |
| Death of parent(s) | 5 | Are either of your natural parents (mum or dad) dead? (response options: yes, mum; yes, dad; no) |
| Contact with police | 3 |
Ever been in trouble with the police? Ever been arrested by the police? Ever received a formal warning at the police station in front of your parents? Ever been in court for anything you did? (Response options for all items: yes; no) |
| Hanging around on the street | 1–5 | How often do you hang around on the street? (response options: more than once a week; once a week; once or twice a month; rarely or never) |
| Hanging around in the park | 1–5 | How often do you go to a park or playground? (response options: more than once a week; once a week; once or twice a month; rarely or never) |
| Delinquency | 2 | In the last 12 months, have you:
|
| Friends smoke cannabis | 6 | How many of your friends smoke cannabis? (response options: none; a few; most; all) |
| Friends use ecstasy or amphetamines | 6 | How many or your friends use ecstasy or amphetamines? (response options: none; a few; most; all) |
| Friends use cocaine | 6 | How many of your friends use cocaine? (response options: none; a few; most; all) |
| Partner smokes cannabis | 6 |
Have you had a girlfriend/boyfriend (or gone out with someone) in the last 12 months? Have you a girlfriend/boyfriend at the moment (someone you are currently going out with)? Does your current (or last) girlfriend/boyfriend do any of the following things? Smoke cannabis (Response options for all items: yes; no) |
| Partner uses ecstasy or amphetamines | 6 |
Have you had a girlfriend/boyfriend (or gone out with someone) in the last 12 months? Have you a girlfriend/boyfriend at the moment (someone you are currently going out with)? Does your current (or last) girlfriend/boyfriend do any of the following things? Use drugs such as ecstasy or amphetamines (Response options for all items: yes; no) |
| Partner uses cocaine | 6 |
Have you had a girlfriend/boyfriend (or gone out with someone) in the last 12 months? Have you a girlfriend/boyfriend at the moment (someone you are currently going out with)? Does your current (or last) girlfriend/boyfriend do any of the following things? Use cocaine (Response options for all items: yes; no) |
| Contact with drug and alcohol services | 7 |
Have you ever gone to anyone for help for a drug problem? Have you ever been involved in a treatment programme specifically related to drug use? (Response options for all items: yes; no) |
| Children | 7 | Do you have any children? (response options: yes; no) |
| Emotional difficulties | 1 |
|
| Early-onset alcohol use | 1 | Have you ever been drunk? (response options: yes; no) |
| Early-onset cannabis use | 2 | Have you ever tried cannabis even if it was just once? (response options: yes; no) |
| Impulsivity | 3 |
|
Left home early (wave 6)
This was derived from the wave 6 question ‘Who do you currently live with?’. This variable was coded 0 (no) if they were still living with a parent and coded 1 (yes) if they chose one of the other categories (alone – away from the family home; with foster parents; with siblings – away from family home; with grandparents or other family members; with partner; with friends or other flatmates).
School attachment (waves 2–5)
The school attachment scale at each wave comprised seven items: ‘I think going to school is a waste of time’; ‘I never take school seriously’; ‘I like school’; ‘I am fed up with school’; ‘I do not like the subjects I do’; ‘I like my teachers’; and ‘I am always willing to help the teacher’ (response options: almost true; not very often true; sometimes true; often true; and almost always or always true). Items were recoded to a scale of 0–4, with negative items recoded so that higher scores indicated greater levels of attachment across all items. Consequently, school attachment was measured on a scale of 0–28, with higher scores indicating greater levels of attachment. Internal consistency in each wave was good (α = 0.79–0.82).
School commitment (waves 2–5)
Four items formed the school commitment scale at each wave: ‘I am quiet at school and get on with my work’; ‘how many times have you bunked off class or skipped the whole day?’; ‘how many times have you been in trouble with the principal?’; ‘how many times have you been in detention?’. The response options for the first item were almost true; not very often true; sometimes true; often true; and almost always or always true. The response options for the other three items were 0; 1–2; 3–5; 6–9; > 10. Items were recoded on a scale of 0–4, with negative items recoded so that higher scores indicated greater levels of school commitment across all items. The school commitment items were summed to give a scale ranging from 0 to 16. Internal consistency in each wave was satisfactory (α = 0.61–0.62).
Bullied
This was based on the item ‘Other children or young people pick on me or bully me’ (response options: not true; somewhat true; certainly true). This variable was coded from 0 to 2, with higher values indicating greater levels of bullying.
Six or more GCSEs
The wave 7 item ‘How many GCSE grades A–C do you have?’ (response options: 0; 1-2; 3-5; 6-9; > 10) was used to form this measure. The resultant measure was binary coded to indicate if they had six or more GCSEs (0 = no; 1 = yes).
Parental control (waves 2–5)
This was assessed by Kerr and Stattin’s parental control scale. 129 This scale comprises five items (see Table 16). The items were coded 0–4, with higher scores indicating higher levels of parental control. The items were summed to form a scale ranging from 0 to 20. Internal consistency in each wave was good (α = 0.83–0.85)
Unsupervised alcohol
This was formed from the wave 4 question ‘Do your parents allow you to drink alcohol?’. The response options were no; yes, but only when I am with them; and yes. This variable was coded 0–2, with greater values representing fewer restrictions on alcohol use.
Natural parent moved out
This variable was coded 0 if neither natural parent had left the participant’s home between waves 2 and 5, and 1 if otherwise.
Death of parent(s)
At wave 5, participants were asked if one or both of their natural parents was dead. This measure was coded 0 if neither was dead at that point, and 1 if one or both parents were dead by wave 5.
Trouble with police (wave 3)
This variable indicated if the participants had had negative contact with the police by wave 3. If they said yes to one or more of the following, they were coded as having been in trouble with the police by wave 3 (code = 1): ‘ever been in trouble with the police?’; ‘ever received a formal warning at the police station in front of your parents?’; ‘ever been arrested by the police?’; ‘ever been in court for anything you did?’.
Hanging around on the street (waves 1–5)
This was assessed by the question ‘How often do you hang around on the street?’. The response options to this question were more than once a week; once a week; once or twice a month; and rarely or never. Responses to this item were coded 0–3, with higher scores indicating greater frequency of hanging around on the street.
Hanging around in the park (waves 1–5)
This was assessed by the question ‘How often do you go to a park or playground?’. The response options to this question were more than once a week; once a week; once or twice a month; and rarely or never. Responses to this item were coded 0–3, with higher scores indicating greater frequency of going to a park or playground.
Delinquency (wave 2)
This was formed from responses to 14 questions about delinquent acts such as stealing and weapon carrying (see Table 16 for full list); for each act the respondent indicated if they had committed that act in the last 12 months (yes = 1; no = 0). The scale was formed by summing responses to each delinquency question (scale range 0–14); higher scores indicate higher levels of delinquency.
Friends smoke cannabis (wave 6)
Participants were asked how many of their friends smoked cannabis at wave 6 (response options: none; a few; most; and all). This variable was coded as binary to indicate if they had any friends who smoked cannabis (yes = 1; no = 0).
Friends use ecstasy or amphetamines (wave 6)
Coding as per friends smoke cannabis (wave 6) variable.
Friends use cocaine (wave 6)
Coding as per friends smoke cannabis (wave 6) variable.
Partner smokes cannabis (wave 6)
At wave 6, respondents were asked if they had gone out with someone in the last 12 months or if they were going out with anyone at the moment. If they responded yes to either of these questions they were asked if their current or last girlfriend/boyfriend smoked cannabis. If they responded yes, the partner smokes cannabis variable was coded 1, otherwise the variable was coded 0. The variable was also coded 0 for those who were not going out with anyone at the moment and had not gone out with anyone in the last 12 months.
Partner uses ecstasy or amphetamines (wave 6)
Coding as per partner smokes cannabis (wave 6) variable.
Partner uses cocaine (wave 6)
Coding as per partner smokes cannabis (wave 6) variable.
Contact with drug and alcohol services (wave 7)
Wave 7 respondents were asked if they had ever gone to anyone for help with a drug problem or had been involved in a treatment programme specifically related to drug use. If they replied yes to either of these questions this variable was coded 1.
Children (wave 7)
Coded yes (1) if respondents indicated at wave 7 that they had children.
Emotional difficulties Strengths and Difficulties Questionnaire scale (wave 1)
This was formed from the SDQ emotional symptoms scale131 (see Table 16 for items). The five items were scored 0–2, with higher scores indicating greater emotional difficulties (scale range 0–10). Internal consistency on this scale was satisfactory (α = 0.64).
Early-onset alcohol use (wave 1)
Coded 1 (yes) if respondents said yes to ‘Have you ever been drunk?’ at wave 1.
Early-onset cannabis use (wave 2)
Coded 1 (yes) if respondents said yes to ‘Have you ever tried cannabis even if it was just once?’ at wave 2.
Impulse control (wave 3)
This was formed from the International Personality Item Pool personality scales211 (see Table 16 for items). The 11 items were scored 0–4 (reverse scoring for some items), with higher scores indicating greater impulsivity (scale range 0–44). Internal consistency on this scale was good (α = 0.79).
Coding of longitudinal outcome measures
The outcome variables were coded as follows (Table 17 contains all items).
| Measure | Wave | Items |
|---|---|---|
| Offending | 7 | Additional offending items at wave 7 (compared with predictor measures):
|
| Depression (PHQ-9) | 7 | See Spitzer et al.212 for items and coding rules |
| Excessive drinking (AUDIT) | 7 | See Babor et al.213 for items and coding rules |
| DAST | 7 | See Gavin et al.214 for items and coding rules |
| CAST | 7 | See Legleye et al.215 for items and coding rules |
| NEET | 7 |
Do you have a full-time job? Do you have a part-time job? Are you self-employed? Are you unemployed at present? Are you a student (either full or part time)? (Response options for all items: yes; no) |
| Psychosis | 7 | See Bebbington and Nayani133 for items and coding rules |
| Self-harm | 7 | Have you ever deliberately taken an overdose (e.g. of pills or other medication) or tried to harm yourself in some other way (such as cut yourself)? (response options: no; yes, once; yes, more than once) |
| Medication | 7 | In the last 12 months have you been prescribed any medication for a mental health, nervous, emotional, or behavioural problem? (response options: yes; no) |
| Services | 7 | In the last 12 months have you seen a GP, psychiatrist, psychologist or other mental health professional about any mental health, nervous, emotional or behavioural problem? (response options: yes; no) |
| Justice | 7 |
Are you currently on a ‘probation order’ or any other type of community sentence such as an ‘attendance centre order’, ‘reparation order’, ‘community responsibility order’ or ‘antisocial behaviour order (ASBO)’? Have you been summoned to appear in court? Have you ever been sent to a young offenders centre? (Response options for all items: yes; no) |
Depression
Measured using the Patient Health Questionnaire-9 items (PHQ-9). A total of 148 participants were asked if they had symptoms such as ‘little interest or pleasure in doing things’ or ‘feeling tired or having little energy’. Responses to items were on a four-point Likert scale with responses ranging from ‘not at all’ to ‘nearly every day’. The scale range was 0–27, with higher scores indicating greater levels of depressive symptoms. Internal reliability of the scale was excellent (α = 0.90).
Excessive drinking
The Alcohol Use Disorders Identification Test (AUDIT)213 10-item scale was used to measure problem drinking behaviour. Items on this scale cover areas such as hazardous alcohol use, dependence symptoms and harmful alcohol use. Each item is scored from 0 to 4, and the overall scale from 0 to 40, with higher scores indicating greater levels of problematic drinking. Cronbach’s alpha for the scale was 0.80.
Drug abuse
Assessed using the 20-item Drug Abuse Screening Test (DAST). 214 If participants answered no to the first item of this scale (‘have you abused any drug not including alcohol cigarettes or medicines given to you by your doctor in the last 12 months?’), they were given a score of 0 and did not have to answer the remaining 19 questions. Otherwise they answered the questions covering areas such as abusing more than one drug at a time, being able to stop using drugs and getting arrested for possession of drugs. Responses to items were coded yes (1) or no (0) and totalled to form a scale where higher scores indicate greater drug-related problems (scale range 0–20).
Cannabis abuse
The Cannabis Abuse Screening Test (CAST)215 is a six-item scale designed to measure cannabis abuse. Responses are on a five-point Likert scale ranging from never to very often (0–4). The items cover topics such as use before midday, memory problems when smoking cannabis and trying to reduce or stop cannabis without success. The total scale ranges from 0 to 24, with higher scores suggesting greater levels of cannabis use. Participants were asked to complete the CAST items only if they indicated that they had smoked cannabis in the last year, otherwise they were given a score of 0 on this scale and skipped the CAST items. The scale had excellent internal consistency (α = 0.90).
Offending
The offending scale was scored in the same way as the offending scale formed in the predictors’ analysis, except that two additional items were included in the scale. These additional items related to being involved in serious physical fights and group-based fights. The scale ranged from 0 to 16.
Not in employment, education or training
Participants were asked if they were employed (full time, part time or self-employed) or unemployed and if they were a student. Participants were classed as NEET if they were unemployed and did not report being a student (coded 1), otherwise they were coded as not NEET (0).
Psychosis
The PSQ133 was used to classify participants as either showing signs of psychosis (1) or not showing signs of psychosis (0).
Self-harm
If participants indicated that they had ever deliberately taken an overdose or tried to harm themselves, this was coded as 1.
Medication
This was coded 1 if the participant said they had been prescribed medication for a mental health, nervous, emotional or behavioural problem in the last 12 months.
Services
This was coded 1 if the participant said they had seen a general practitioner, psychiatrist, psychologist or other mental health professional about any mental health, nervous, emotional or behavioural problem in the last 12 months.
Justice
This was coded 1 if the participant reported being on a probation order, having ever been summoned to appear in court or having been sent to a young offenders centre.
| Variable | Family context | Peer substance use and relationships | Substance use history | Relationship with school | Delinquency | Mental health/personality | Partner substance use | Demographics |
|---|---|---|---|---|---|---|---|---|
| Parent(s) dead | –1.21 (0.58)* | –1.08 (0.65) | –0.95 (0.66) | –1.06 (0.64) | –1.01 (0.62) | –1.08 (0.62) | –1.14 (0.65) | –1.13 (0.65) |
| Parent(s) moved out | –0.48 (0.40) | –0.53 (0.54) | –0.58 (0.51) | –0.40 (0.53) | –0.44 (0.55) | –0.44 (0.56) | –0.44 (0.60) | –0.44 (0.62) |
| Left home early | –0.67 (0.50) | –0.47 (0.53) | –0.55 (0.52) | –0.47 (0.54) | –0.57 (0.54) | –0.59 (0.55) | –0.52 (0.57) | –0.41 (0.59) |
| Parental drinking view | –0.46 (0.15)** | –0.39 (0.17)* | –0.37 (0.18)* | –0.32 (0.18) | –0.37 (0.19) | –0.31 (0.19) | –0.36 (0.21) | –0.35 (0.21) |
| Parental control (intercept) | 0.27 (0.04)*** | 0.15 (0.05)** | 0.11 (0.05)* | 0.04 (0.05) | 0.01 (0.05) | 0.01 (0.05) | 0.02 (0.06) | 0.02 (0.06) |
| Peers use cannabis | –2.32 (0.46)*** | –2.05 (0.49)*** | –1.90 (0.51)*** | –2.00 (0.52)*** | –2.00 (0.52)*** | –1.82 (0.54)** | –1.76 (0.56)** | |
| Peers use ecstasy | –1.74 (0.46)*** | –1.55 (0.49)** | –1.34 (0.52)** | –1.33 (0.51)** | –1.33 (0.51)** | –1.22 (0.55)* | –1.24 (0.56)* | |
| Peers use cocaine | –1.14 (0.40)** | –1.12 (0.43)** | –0.99 (0.45)* | –0.94 (0.47)* | –0.96 (0.47)* | –0.75 (0.52) | –0.73 (0.52) | |
| Bullied | 0.29 (0.36) | 0.46 (0.40) | 0.44 (0.41) | 0.45 (0.44) | 0.41 (0.44) | 0.31 (0.47) | 0.32 (0.47) | |
| Early alcohol use | –2.46 (1.96) | –2.37 (2.13) | –2.22 (2.07) | –2.19 (2.05) | –2.01 (2.07) | –1.84 (1.85) | ||
| Early cannabis use | –1.61 (0.46)*** | –1.12 (0.49)* | –0.76 (0.50) | –0.78 (0.51) | –0.81 (0.52) | –0.82 (0.53) | ||
| Sought help | –0.17 (1.15) | 0.12 (1.20) | 0.20 (1.28) | 0.27 (1.26) | 0.78 (2.23) | 1.02 (1.29) | ||
| School attachment (intercept) | 0.05 (0.05) | 0.03 (0.05) | 0.03 (0.05) | 0.02 (0.05) | 0.02 (0.05) | |||
| School commitment (intercept) | 0.57 (0.10)*** | 0.43 (0.10)*** | 0.40 (0.10)*** | 0.41 (0.10)*** | 0.40 (0.11)*** | |||
| School commitment (slope) | 0.54 (0.12)*** | 0.47 (0.12)*** | 0.46 (0.12)*** | 0.47 (0.12)*** | 0.45 (0.12)*** | |||
| ≥ 6 GCSEs | –0.34 (0.27) | –0.33 (0.28) | –0.29 (0.28) | –0.33 (0.30) | –0.40 (0.31) | |||
| Delinquency | –0.15 (0.08) | –0.15 (0.08) | –0.16 (0.08) | –0.15 (0.09) | ||||
| Trouble with police | –0.50 (0.36) | –0.49 (0.37) | –0.58 (0.41) | –0.56 (0.40) | ||||
| Hanging around on the street (intercept) | –0.06 (0.20) | –0.06 (0.20) | –0.03 (0.20) | –0.04 (0.20) | ||||
| Hanging around on the street (slope) | –0.58 (0.48) | –0.58 (0.48) | –0.59 (0.52) | –0.56 (0.53) | ||||
| Hanging around in the park (intercept) | 0.00 (0.24) | 0.01 (0.24) | –0.13 (0.26) | –0.15 (0.26) | ||||
| Hanging around in the park (slope) | 0.84 (0.57) | 0.87 (0.57) | 0.83 (0.58) | 0.87 (0.57) | ||||
| Emotional difficulties | 0.05 (0.07) | 0.08 (0.07) | 0.07 (0.08) | |||||
| Impulsivity | –0.01 (0.02) | 0.00 (0.02) | 0.00 (0.03) | |||||
| Partner uses cannabis | –1.04 (0.61) | –1.06 (0.61) | ||||||
| Partner uses ecstasy | –0.14 (0.79) | –0.16 (0.78) | ||||||
| Partner uses cocaine | –0.56 (0.88) | –0.56 (0.87) | ||||||
| Female | 0.20 (0.29) | |||||||
| FSM | 0.14 (0.47) | |||||||
| Has child(ren) | –0.75 (0.57) |
| Variable | Family context | Peer substance use and relationships | Substance use history | Relationship with school | Delinquency | Mental health/personality | Partner substance use | Demographics |
|---|---|---|---|---|---|---|---|---|
| Parent(s) dead | –0.51 (0.42) | –0.51 (0.48) | –0.42 (0.48) | –0.50 (0.47) | –0.32 (0.45) | –0.32 (0.45) | –0.39 (0.48) | –0.34 (0.48) |
| Parent(s) moved out | 0.02 (0.32) | 0.08 (0.43) | 0.06 (0.42) | 0.11 (0.43) | –0.01 (0.48) | –0.03 (0.49) | –0.04 (0.53) | –0.11 (0.54) |
| Left home early | –0.45 (0.45) | –0.18 (0.51) | –0.28 (0.49) | –0.25 (0.52) | –0.34 (0.54) | –0.36 (0.55) | –0.28 (0.57) | –0.48 (0.62) |
| Parental drinking view | 0.04 (0.12) | 0.12 (0.15) | 0.17 (0.16) | 0.19 (0.16) | 0.23 (0.16) | 0.24 (0.17) | 0.19 (0.18) | 0.20 (0.19) |
| Parental control (intercept) | 0.16 (0.03)*** | 0.06 (0.04) | 0.04 (0.04) | 0.00 (0.05) | –0.00 (0.05) | –0.01 (0.05) | 0.01 (0.05) | –0.01 (0.06) |
| Peers use cannabis | –1.35 (0.44)** | –1.14 (0.46)* | –1.07 (0.48)* | –1.15 (0.49)* | –1.15 (0.49)* | –0.99 (0.51) | –0.86 (0.53) | |
| Peers use ecstasy | –1.40 (0.40)*** | –1.24 (0.43)** | –1.14 (0.46)* | –1.14 (0.46)* | –1.13 (0.46)* | –1.05 (0.49)* | –1.08 (0.49)* | |
| Peers use cocaine | –1.28 (0.35)*** | –1.23 (0.37)** | –1.14 (0.37)** | –1.15 (0.38)** | –1.16 (0.38)** | –0.89 (0.41)* | –0.97 (0.42)* | |
| Bullied | 0.28 (0.32) | 0.40 (0.36) | 0.38 (0.37) | 0.41 (0.39) | 0.38 (0.39) | 0.28 (0.41) | 0.34 (0.43) | |
| Early alcohol use | –0.63 (0.34) | –0.52 (0.34) | –0.43 (0.36) | –0.46 (0.38) | –0.32 (0.41) | –0.34 (0.42) | ||
| Early cannabis use | –1.02 (0.28)*** | –0.85 (0.31)** | –0.66 (0.33)* | –0.65 (0.33) | –0.70 (0.37) | –0.69 (0.38) | ||
| Sought help | –0.49 (0.59) | –0.42 (0.56) | –0.45 (0.56) | –0.42 (0.57) | 0.02 (0.61) | 0.13 (0.60) | ||
| School attachment (intercept) | 0.03 (0.04) | 0.01 (0.05) | 0.01 (0.05) | –0.00 (0.05) | –0.00 (0.05) | |||
| School commitment (intercept) | 0.21 (0.06)** | 0.11 (0.07) | 0.11 (0.07) | 0.12 (0.07) | 0.12 (0.07) | |||
| School commitment (slope) | 0.22 (0.07)** | 0.16 (0.08)* | 0.17 (0.08)* | 0.18 (0.08)* | 0.18 (0.09)* | |||
| ≥ 6 GCSEs | –0.16 (0.22) | –0.06 (0.24) | –0.06 (0.24) | –0.11 (0.27) | –0.09 (0.27) | |||
| Delinquency | –0.12 (0.07) | –0.13 (0.07) | –0.13 (0.07) | –0.11 (0.07) | ||||
| Trouble with police | –0.77 (0.30)** | –0.76 (0.30)* | –0.84 (0.33)* | –0.78 (0.33)* | ||||
| Hanging around on the street (intercept) | 0.21 (0.19) | 0.21 (0.19) | 0.25 (0.20) | 0.20 (0.20) | ||||
| Hanging around on the street (slope) | –0.67 (0.48) | –0.67 (0.48) | –0.68 (0.52) | –0.72 (0.52) | ||||
| Hanging around in the park (intercept) | 0.27 (0.21) | 0.26 (0.21) | 0.13 (0.24) | 0.11 (0.24) | ||||
| Hanging around in the park (slope) | 1.11 (0.46)* | 1.10 (0.46)* | 1.05 (0.49)* | 1.15 (0.49)* | ||||
| Emotional difficulties | 0.03 (0.06) | 0.06 (0.07) | 0.04 (0.07) | |||||
| Impulsivity | 0.01 (0.02) | 0.02 (0.02) | 0.01 (0.02) | |||||
| Partner uses cannabis | –0.64 (0.42) | –0.77 (0.44) | ||||||
| Partner uses ecstasy | 0.21 (0.63) | 0.17 (0.63) | ||||||
| Partner uses cocaine | –1.10 (0.63) | –1.19 (0.64) | ||||||
| Female | 0.53 (0.29) | |||||||
| FSM | 0.05 (0.30) | |||||||
| Has child(ren) | 0.49 (0.41) |
| Variable | Family context | Peer substance use and relationships | Substance use history | Relationship with school | Delinquency | Mental health/personality | Partner substance use | Demographics |
|---|---|---|---|---|---|---|---|---|
| Parent(s) dead | –0.61 (0.63) | –0.77 (0.65) | –0.66 (0.64) | –0.70 (0.63) | –0.62 (0.64) | –0.62 (0.66) | –0.60 (0.68) | –0.56 (0.69) |
| Parent(s) moved out | –0.43 (0.46) | –0.38 (0.48) | –0.42 (0.49) | –0.35 (0.49) | –0.41 (0.49) | –0.43 (0.50) | –0.45 (0.57) | –0.53 (0.59) |
| Left home early | –0.24 (0.55) | 0.00 (0.57) | –0.08 (0.57) | 0.03 (0.59) | –0.02 (0.61) | –0.03 (0.63) | 0.01 (0.66) | –0.01 (0.74) |
| Parental drinking view | –0.25 (0.18) | –0.25 (0.18) | –0.20 (0.19) | –0.21 (0.19) | –0.16 (0.20) | –0.16 (0.20) | –0.22 (0.21) | –0.21 (0.22) |
| Parental control (intercept) | 0.07 (0.04) | 0.03 (0.04) | 0.00 (0.05) | –0.01 (0.05) | 0.01 (0.05) | 0.01 (0.06) | 0.02 (0.06) | 0.01 (0.07) |
| Peers use cannabis | 0.25 (0.51) | 0.43 (0.55) | 0.44 (0.56) | 0.34 (0.57) | 0.34 (0.57) | 0.47 (0.59) | 0.57 (0.61) | |
| Peers use ecstasy | –1.16 (0.45)* | –1.04 (0.48)* | –0.98 (0.50) | –0.99 (0.50)* | –0.99 (0.50)* | –0.88 (0.54) | –0.91 (0.55) | |
| Peers use cocaine | –0.80 (0.38)* | –0.80 (0.41) | –0.73 (0.42) | –0.77 (0.42) | –0.77 (0.42) | –0.44 (0.43) | –0.49 (0.44) | |
| Bullied | 0.41 (0.35) | 0.53 (0.39) | 0.53 (0.40) | 0.56 (0.43) | 0.54 (0.42) | 0.46 (0.47) | 0.50 (0.48) | |
| Early alcohol use | –0.81 (0.37)* | –0.71 (0.36)* | –0.72 (0.39) | –0.75 (0.41) | –0.60 (0.42) | –0.58 (0.44) | ||
| Early cannabis use | –0.44 (0.32) | –0.32 (0.34) | –0.31 (0.37) | –0.31 (0.38) | –0.34 (0.42) | –0.33 (0.44) | ||
| Sought help | –0.77 (0.80) | –0.64 (0.86) | –0.69 (0.96) | –0.67 (0.98) | –0.28 (1.03) | –0.20 (1.11) | ||
| School attachment (intercept) | –0.01 (0.05) | –0.02 (0.05) | –0.02 (0.05) | –0.03 (0.06) | –0.03 (0.06) | |||
| School commitment (intercept) | 0.12 (0.07) | 0.10 (0.07) | 0.11 (0.07) | 0.11 (0.09) | 0.12 (0.09) | |||
| School commitment (slope) | 0.13 (0.09) | 0.13 (0.09) | 0.14 (0.09) | 0.16 (0.10) | 0.16 (0.10) | |||
| ≥ 6 GCSEs | 0.26 (0.31) | 0.33 (0.32) | 0.34 (0.33) | 0.28 (0.38) | 0.29 (0.37) | |||
| Delinquency | –0.05 (0.07) | –0.06 (0.07) | –0.06 (0.08) | –0.03 (0.08) | ||||
| Trouble with police | –0.20 (0.31) | –0.19 (0.32) | –0.30 (0.35) | –0.24 (0.36) | ||||
| Hanging around on the street (intercept) | 0.36 (0.23) | 0.36 (0.23) | 0.41 (0.24) | 0.38 (0.23) | ||||
| Hanging around on the street (slope) | –0.33 (0.51) | –0.33 (0.51) | –0.43 (0.57) | –0.47 (0.57) | ||||
| Hanging around in the park (intercept) | 0.25 (0.22) | 0.23 (0.22) | 0.09 (0.25) | 0.06 (0.25) | ||||
| Hanging around in the park (slope) | 0.93 (0.55) | 0.93 (0.55) | 0.89 (0.58) | 0.98 (0.56) | ||||
| Emotional difficulties | 0.03 (0.07) | 0.06 (0.07) | 0.03 (0.07) | |||||
| Impulsivity | 0.01 (0.02) | 0.02 (0.03) | 0.02 (0.03) | |||||
| Partner uses cannabis | –0.07 (0.44) | –0.17 (0.48) | ||||||
| Partner uses ecstasy | –0.32 (0.82) | –0.40 (0.83) | ||||||
| Partner uses cocaine | –1.76 (0.86)* | –1.84 (0.89)* | ||||||
| Female | 0.55 (0.32) | |||||||
| FSM | 0.34 (0.40) | |||||||
| Has child(ren) | –0.20 (0.50) |
| Model | Variable | Variable category | Coefficient | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | –0.12 | 0.03 | 0.000 |
| AT | –0.08 | 0.02 | 0.001 | ||
| ATC | 0.03 | 0.04 | 0.485 | ||
| Adjusted | Class | Alcohol | –0.09 | 0.04 | 0.013 |
| AT | –0.08 | 0.02 | 0.002 | ||
| ATC | 0.07 | 0.04 | 0.128 | ||
| FSM | Yes | –1.70 | 1.04 | 0.108 | |
| Class*FSM | Alcohol*yes | –0.14 | 0.09 | 0.113 | |
| AT*yes | 0.02 | 0.06 | 0.783 | ||
| ATC*yes | –0.25 | 0.11 | 0.033 | ||
| Sex | Female | 0.84 | 0.29 | 0.005 | |
| Peers use cannabis | Yes | 0.35 | 0.40 | 0.382 | |
| Peers use ecstasy | Yes | 1.11 | 0.51 | 0.038 | |
| Peers use cocaine | Yes | –0.81 | 0.53 | 0.138 | |
| Partner uses cocaine | Yes | 0.18 | 0.78 | 0.822 | |
| Trouble with police | Yes | 0.08 | 0.32 | 0.801 | |
| School commitment (intercept) | 0.21 | 0.09 | 0.018 | ||
| School commitment (slope) | 0.22 | 0.11 | 0.054 | ||
| Hanging around in the park (slope) | –0.37 | 0.50 | 0.467 | ||
| Model | Variable | Variable category | Coefficient | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | –0.39 | 0.04 | 0.000 |
| AT | –0.25 | 0.03 | 0.000 | ||
| ATC | 0.03 | 0.06 | 0.628 | ||
| Adjusted | Class | Alcohol | –0.34 | 0.05 | 0.000 |
| AT | –0.21 | 0.03 | 0.000 | ||
| ATC | 0.03 | 0.07 | 0.643 | ||
| FSM | Yes | 0.64 | 1.13 | 0.573 | |
| Class*FSM | Alcohol*yes | 0.11 | 0.10 | 0.287 | |
| AT*yes | 0.01 | 0.07 | 0.941 | ||
| ATC*yes | 0.01 | 0.12 | 0.963 | ||
| Sex | Female | –1.64 | 0.32 | 0.000 | |
| Peers use cannabis | Yes | 1.14 | 0.37 | 0.004 | |
| Peers use ecstasy | Yes | 0.18 | 0.47 | 0.705 | |
| Peers use cocaine | Yes | –0.18 | 0.48 | 0.708 | |
| Partner uses cocaine | Yes | 0.74 | 0.71 | 0.309 | |
| Trouble with police | Yes | –0.06 | 0.36 | 0.876 | |
| School commitment (intercept) | –0.18 | 0.09 | 0.061 | ||
| School commitment (slope) | –0.26 | 0.11 | 0.023 | ||
| Hanging around in the park (slope) | –0.11 | 0.42 | 0.804 | ||
| Model | Variable | Variable category | Coefficient | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | –0.17 | 0.02 | 0.000 |
| AT | –0.12 | 0.01 | 0.000 | ||
| ATC | –0.17 | 0.03 | 0.000 | ||
| Adjusted | Class | Alcohol | –0.12 | 0.02 | 0.000 |
| AT | –0.09 | 0.01 | 0.000 | ||
| ATC | –0.11 | 0.02 | 0.000 | ||
| FSM | Yes | –1.94 | 0.61 | 0.003 | |
| Class*FSM | Alcohol*yes | –0.16 | 0.06 | 0.006 | |
| AT*yes | –0.06 | 0.03 | 0.053 | ||
| ATC*yes | –0.24 | 0.08 | 0.003 | ||
| Sex | Female | –0.15 | 0.08 | 0.065 | |
| Peers use cannabis | Yes | 0.14 | 0.10 | 0.176 | |
| Peers use ecstasy | Yes | 0.04 | 0.14 | 0.777 | |
| Peers use cocaine | Yes | –0.13 | 0.17 | 0.428 | |
| Partner uses cocaine | Yes | 0.78 | 0.41 | 0.065 | |
| Trouble with police | Yes | 0.21 | 0.13 | 0.113 | |
| School commitment (intercept) | –0.04 | 0.03 | 0.251 | ||
| School commitment (slope) | –0.01 | 0.04 | 0.790 | ||
| Hanging around in the park (slope) | –0.24 | 0.17 | 0.178 | ||
| Model | Variable | Variable category | Coefficient | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | –0.19 | 0.03 | 0.000 |
| AT | –0.16 | 0.02 | 0.000 | ||
| ATC | –0.16 | 0.03 | 0.000 | ||
| Adjusted | Class | Alcohol | –0.14 | 0.02 | 0.000 |
| AT | –0.11 | 0.02 | 0.000 | ||
| ATC | –0.14 | 0.03 | 0.000 | ||
| FSM | Yes | –1.03 | 0.82 | 0.218 | |
| Class*FSM | Alcohol*yes | –0.14 | 0.08 | 0.091 | |
| AT*yes | –0.09 | 0.05 | 0.056 | ||
| ATC*yes | –0.12 | 0.10 | 0.242 | ||
| Sex | Female | –0.47 | 0.14 | 0.001 | |
| Peers use cannabis | Yes | 0.24 | 0.13 | 0.067 | |
| Peers use ecstasy | Yes | 0.21 | 0.25 | 0.407 | |
| Peers use cocaine | Yes | –0.28 | 0.30 | 0.354 | |
| Partner uses cocaine | Yes | –0.35 | 0.53 | 0.508 | |
| Trouble with police | Yes | 0.46 | 0.16 | 0.007 | |
| School commitment (intercept) | –0.10 | 0.05 | 0.064 | ||
| School commitment (slope) | –0.07 | 0.07 | 0.338 | ||
| Hanging around in the park (slope) | –0.18 | 0.33 | 0.587 | ||
| Model | Variable | Variable category | Coefficient | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | –0.06 | 0.01 | 0.000 |
| AT | –0.05 | 0.01 | 0.000 | ||
| ATC | –0.04 | 0.02 | 0.012 | ||
| Adjusted | Class | Alcohol | –0.05 | 0.01 | 0.000 |
| AT | –0.04 | 0.01 | 0.000 | ||
| ATC | –0.03 | 0.01 | 0.022 | ||
| FSM | Yes | –0.29 | 0.34 | 0.398 | |
| Class*FSM | Alcohol*yes | –0.02 | 0.03 | 0.448 | |
| AT*yes | –0.03 | 0.02 | 0.079 | ||
| ATC*yes | –0.04 | 0.04 | 0.326 | ||
| Sex | Female | –0.38 | 0.06 | 0.000 | |
| Peers use cannabis | Yes | 0.04 | 0.08 | 0.610 | |
| Peers use ecstasy | Yes | –0.08 | 0.11 | 0.489 | |
| Peers use cocaine | Yes | –0.12 | 0.13 | 0.378 | |
| Partner uses cocaine | Yes | 0.01 | 0.24 | 0.960 | |
| Trouble with police | Yes | 0.16 | 0.07 | 0.039 | |
| School commitment (intercept) | –0.04 | 0.02 | 0.069 | ||
| School commitment (slope) | –0.07 | 0.03 | 0.014 | ||
| Hanging around in the park (slope) | 0.03 | 0.10 | 0.787 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 0.93 | 0.02 | 0.000 |
| AT | 0.94 | 0.01 | 0.000 | ||
| ATC | 0.98 | 0.02 | 0.339 | ||
| Adjusted | Class | Alcohol | 0.93 | 0.03 | 0.006 |
| AT | 0.95 | 0.02 | 0.006 | ||
| ATC | 0.99 | 0.03 | 0.814 | ||
| FSM | Yes | 1.89 | 1.22 | 0.327 | |
| Class*FSM | Alcohol*yes | 1.05 | 0.06 | 0.361 | |
| AT*yes | 0.98 | 0.04 | 0.667 | ||
| ATC*yes | 0.94 | 0.06 | 0.349 | ||
| Sex | Female | 0.61 | 0.11 | 0.004 | |
| Peers use cannabis | Yes | 1.01 | 0.29 | 0.973 | |
| Peers use ecstasy | Yes | 0.91 | 0.27 | 0.739 | |
| Peers use cocaine | Yes | 0.94 | 0.36 | 0.876 | |
| Partner uses cocaine | Yes | 0.97 | 0.51 | 0.951 | |
| Trouble with police | Yes | 1.18 | 0.26 | 0.442 | |
| School commitment (intercept) | 0.95 | 0.06 | 0.396 | ||
| School commitment (slope) | 0.94 | 0.07 | 0.349 | ||
| Hanging around in the park (slope) | 0.89 | 0.30 | 0.724 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 0.92 | 0.03 | 0.004 |
| AT | 0.95 | 0.02 | 0.008 | ||
| ATC | 0.97 | 0.03 | 0.463 | ||
| Adjusted | Class | Alcohol | 0.90 | 0.04 | 0.009 |
| AT | 0.93 | 0.02 | 0.009 | ||
| ATC | 0.99 | 0.05 | 0.781 | ||
| FSM | Yes | 1.35 | 1.06 | 0.702 | |
| Class*FSM | Alcohol*yes | 1.00 | 0.07 | 0.957 | |
| AT*yes | 1.06 | 0.05 | 0.234 | ||
| ATC*yes | 0.93 | 0.08 | 0.361 | ||
| Sex | Female | 1.71 | 0.51 | 0.075 | |
| Peers use cannabis | Yes | 0.72 | 0.29 | 0.418 | |
| Peers use ecstasy | Yes | 1.44 | 0.61 | 0.391 | |
| Peers use cocaine | Yes | 0.39 | 0.20 | 0.073 | |
| Partner uses cocaine | Yes | 3.65 | 2.24 | 0.036 | |
| Trouble with police | Yes | 1.12 | 0.33 | 0.689 | |
| School commitment (intercept) | 1.11 | 0.08 | 0.165 | ||
| School commitment (slope) | 1.14 | 0.11 | 0.196 | ||
| Hanging around in the park (slope) | 1.34 | 0.59 | 0.510 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 1.00 | 0.02 | 0.882 |
| AT | 0.96 | 0.01 | 0.002 | ||
| ATC | 1.05 | 0.03 | 0.052 | ||
| Adjusted | Class | Alcohol | 1.01 | 0.03 | 0.762 |
| AT | 0.94 | 0.02 | 0.002 | ||
| ATC | 1.05 | 0.03 | 0.096 | ||
| FSM | Yes | 1.26 | 1.09 | 0.793 | |
| Class*FSM | Alcohol*yes | 0.96 | 0.07 | 0.596 | |
| AT*yes | 1.13 | 0.06 | 0.028 | ||
| ATC*yes | 1.00 | 0.10 | 0.972 | ||
| Sex | Female | 1.56 | 0.37 | 0.062 | |
| Peers use cannabis | Yes | 0.91 | 0.32 | 0.781 | |
| Peers use ecstasy | Yes | 1.90 | 0.71 | 0.084 | |
| Peers use cocaine | Yes | 0.63 | 0.27 | 0.283 | |
| Partner uses cocaine | Yes | 2.06 | 1.17 | 0.206 | |
| Trouble with police | Yes | 1.02 | 0.26 | 0.925 | |
| School commitment (intercept) | 1.09 | 0.07 | 0.176 | ||
| School commitment (slope) | 1.06 | 0.10 | 0.553 | ||
| Hanging around in the park (slope) | 1.16 | 0.38 | 0.643 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 0.99 | 0.01 | 0.341 |
| AT | 0.97 | 0.01 | 0.003 | ||
| ATC | 1.02 | 0.02 | 0.344 | ||
| Adjusted | Class | Alcohol | 0.99 | 0.02 | 0.724 |
| AT | 0.97 | 0.01 | 0.039 | ||
| ATC | 1.02 | 0.02 | 0.440 | ||
| FSM | Yes | 1.56 | 0.70 | 0.314 | |
| Class*FSM | Alcohol*yes | 1.00 | 0.04 | 0.967 | |
| AT*yes | 1.01 | 0.03 | 0.770 | ||
| ATC*yes | 1.00 | 0.05 | 0.953 | ||
| Sex | Female | 1.52 | 0.23 | 0.004 | |
| Peers use cannabis | Yes | 1.00 | 0.23 | 0.994 | |
| Peers use ecstasy | Yes | 1.17 | 0.29 | 0.546 | |
| Peers use cocaine | Yes | 1.09 | 0.26 | 0.710 | |
| Partner uses cocaine | Yes | 1.03 | 0.38 | 0.925 | |
| Trouble with police | Yes | 1.46 | 0.27 | 0.040 | |
| School commitment (intercept) | 1.03 | 0.05 | 0.553 | ||
| School commitment (slope) | 1.00 | 0.06 | 0.957 | ||
| Hanging around in the park (slope) | 1.28 | 0.34 | 0.346 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 0.90 | 0.02 | 0.000 |
| AT | 0.90 | 0.02 | 0.000 | ||
| ATC | 0.96 | 0.03 | 0.193 | ||
| Adjusted | Class | Alcohol | 0.92 | 0.03 | 0.017 |
| AT | 0.92 | 0.03 | 0.004 | ||
| ATC | 0.97 | 0.04 | 0.427 | ||
| FSM | Yes | 2.23 | 1.64 | 0.276 | |
| Class*FSM | Alcohol*yes | 1.06 | 0.06 | 0.293 | |
| AT*yes | 0.98 | 0.04 | 0.591 | ||
| ATC*yes | 1.00 | 0.07 | 0.983 | ||
| Sex | Female | 0.45 | 0.11 | 0.001 | |
| Peers use cannabis | Yes | 1.63 | 0.72 | 0.270 | |
| Peers use ecstasy | Yes | 0.39 | 0.15 | 0.016 | |
| Peers use cocaine | Yes | 1.58 | 0.68 | 0.291 | |
| Partner uses cocaine | Yes | 0.81 | 0.45 | 0.701 | |
| Trouble with police | Yes | 0.92 | 0.28 | 0.785 | |
| School commitment (intercept) | 0.75 | 0.04 | 0.000 | ||
| School commitment (slope) | 0.76 | 0.06 | 0.001 | ||
| Hanging around in the park (slope) | 0.92 | 0.35 | 0.832 | ||
| Model | Variable | Variable category | OR | SE | p-value |
|---|---|---|---|---|---|
| Unadjusted | Class | Alcohol | 0.96 | 0.02 | 0.049 |
| AT | 0.97 | 0.01 | 0.035 | ||
| ATC | 0.96 | 0.02 | 0.115 | ||
| Adjusted | Class | Alcohol | 0.98 | 0.03 | 0.596 |
| AT | 0.99 | 0.02 | 0.676 | ||
| ATC | 0.97 | 0.04 | 0.331 | ||
| FSM | Yes | 3.23 | 1.82 | 0.037 | |
| Class*FSM | Alcohol*yes | 1.01 | 0.05 | 0.881 | |
| AT*yes | 1.02 | 0.03 | 0.437 | ||
| ATC*yes | 1.00 | 0.07 | 0.995 | ||
| Sex | Female | 0.90 | 0.16 | 0.557 | |
| Peers use cannabis | Yes | 1.39 | 0.34 | 0.178 | |
| Peers use ecstasy | Yes | 0.79 | 0.27 | 0.481 | |
| Peers use cocaine | Yes | 1.05 | 0.38 | 0.884 | |
| Partner uses cocaine | Yes | 1.83 | 0.69 | 0.111 | |
| Trouble with police | Yes | 0.95 | 0.19 | 0.812 | |
| School commitment (intercept) | 0.89 | 0.05 | 0.022 | ||
| School commitment (slope) | 0.90 | 0.06 | 0.119 | ||
| Hanging around in the park (slope) | 0.68 | 0.20 | 0.197 | ||
List of abbreviations
- 25I
- 2,5-dimethoxy-4-iodophenethylamine
- 2C-I
- 2C-I-NBOMe
- A level
- Advanced level
- ACMD
- Advisory Council on the Misuse of Drugs
- AD:EPT
- Alcohol and Drugs: Empowering People through Therapy
- AIC
- Akaike information criterion
- AIPS
- All Ireland Prevalence Study
- AT
- alcohol and tobacco
- ATC
- alcohol, tobacco and cannabis
- AUDIT
- Alcohol Use Disorders Identification Test
- BBV
- blood-borne virus
- BEBE
- Belfast Experts by Experience
- BIC
- Bayesian information criterion
- BLMR
- bootstrapped Lo–Mendell–Rubin likelihood ratio test
- BYDS
- Belfast Youth Development Study
- CAST
- Cannabis Abuse Screening Test
- CB1
- cannabinoid receptor type 1
- CB2
- cannabinoid receptor type 2
- CFI
- comparative fit index
- CJS
- criminal justice system
- CSEW
- Crime Survey England and Wales
- DAST
- Drug Abuse Screening Test
- DMAA
- dimethylamylamine
- EM
- expectation–maximisation
- EMCDDA
- European Monitoring Centre for Drugs and Drug Addiction
- FSM
- free school meal
- GABA
- gamma-aminobutyric acid
- GBL
- gamma-butyrolactone
- GCSE
- General Certificate of Secondary Education
- GHB
- gamma-hydroxybutyrate
- HCV
- hepatitus C virus
- HIV
- human immunodeficiency virus
- HMP
- Her Majesty’s Prison
- KE
- knowledge exchange
- LCA
- latent class analysis
- LMR
- Lo–Mendell–Rubin likelihood ratio test
- LSD
- lysergic acid diethylamide
- MAR
- missing at random
- MDAI
- 5,6-methylenedioxy-2-aminoindane
- MDMA
- 3,4-methylenedioxy-methamphetamine
- MDMI
- definition unknown (discussed as a novel psychoactive substance in narrative accounts)
- MDPV
- methylenedioxypyrovalerone
- MLR
- robust maximum likelihood
- MSM
- men who have sex with men
- NDTMS
- National Drug Treatment Monitoring System
- NEET
- not in employment, education or training
- NEPTUNE
- Novel Psychoactive Treatment UK Network
- NIDMD
- Northern Ireland Drug Misuse Database
- NPS
- novel psychoactive substance
- NVQ
- National Vocational Qualification
- OR
- odds ratio
- ORECNI
- Office for Research Ethics Committees Northern Ireland
- PAG
- professional advisory group
- PHQ-9
- Patient Health Questionnaire-9 items
- PLG
- professional liason group
- PSA
- Psychoactive Substances Act 2016
- PSI
- psychosocial and psychological intervention
- PSQ
- Psychosis Screening Questionnaire
- QUB
- Queen’s University Belfast
- RMSEA
- root mean square error of approximation
- SAG
- scientific advisory group
- SC
- synthetic cannabinoid
- SCJS
- Scottish Crime and Justice Survey
- SDMD
- Scottish Drug Misuse Database
- SDQ
- Strengths and Difficulties Questionnaire
- SE
- standard error
- SG
- subgroup
- SMI
- severe and enduring mental health illness
- ssaBIC
- sample-size-adjusted Bayesian information criterion
- TCDO
- temporary class drug order
- THC
- tetrahydrocannabinol
- TLI
- Tucker–Lewis index
- UNODC
- United Nations Office on Drugs and Crime
- WEDINOS
- Welsh Emerging Drugs and Identification of Novel Substances