

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 15/181/01. The contractual start date was in January 2017. The final report began editorial review in September 2021 and was accepted for publication in May 2022. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2023 Lohan et al. This work was produced by Lohan et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2023 Lohan et al.
Chapter 1 Introduction
Structure of this report
This report presents the findings from a cluster randomised controlled trial (RCT) evaluation of the If I Were Jack programme. This chapter provides the background for the study and a description of the programme. Patient and public involvement (PPI) in the study is described in Chapter 2. The major focus of the PPI involvement was in relation to the optimisation of the programme that occurred within this study prior to the trial. The methodology for the trial and process evaluation is outlined in Chapter 3. The results of the recruitment and data collection processes are outlined in Chapter 4. The quantitative findings from the trial regarding the impact of the programme on student outcomes are reported in Chapter 5, and the findings from the accompanying qualitative process study are set out in Chapter 6. Chapter 7 details findings of the economic evaluation, and key issues and conclusions emerging from the findings are set out in Chapter 8.
The public health problem addressed: reducing unintended teenage pregnancy and promoting positive sexual health
Relationship and sexuality education (RSE) for young people is a challenging, complex, controversial and critical worldwide public health issue. High-quality comprehensive RSE for young people is not only essential to achieving better health and health care for adolescents, but is also key to ensuring women’s rights, gender equality, and sound demographic and economic development for future generations. As such, high-quality RSE addresses three 2030 sustainable development goals: to ensure quality education, gender equality, and good health and well-being. 1,2
Although teenage pregnancy is not universally negative,1 reducing teenage pregnancy has the potential to reduce a myriad of negative medical outcomes, such as low birthweight and undernutrition, as well as the negative consequences for educational and social well-being of young people and their babies over the life course globally. 2–6 Teenage pregnancy is widely understood as not just a cause, but also a consequence, of under-privilege, which is why addressing teenage pregnancy through developing young people’s agency to improve their own lives is so important.
The UK still has the highest rate of teenage pregnancy in Western Europe. 7–9 Despite the fact that conception rates for women aged < 18 years have been falling (halving in the last decade), the rate in England and Wales in 2018 was 16.8 per 1000 population. 10,11 Approximately 25,000 teenage women become pregnant in England and Wales annually, and approximately half of these pregnancies end in legal abortion. 12 The teenage pregnancy rate in Scotland was 30.2 per 1000 in 2017. 13 In Northern Ireland (NI), abortion was illegal until October 201914,15 and was considered lawful only in exceptional circumstances in which the life of the pregnant woman was at immediate risk, or if there was a risk of serious injury to her physical or mental health. Reflecting the different legal framework (pre October 2019), government targets around reducing teenage pregnancies in NI relate to births and not conceptions. In NI, the birth rate to teenage mothers per 1000 young women aged 13–19 years was 11.3 in 2013. 16 In the same year, the teenage birth rate in the most deprived areas was 23.0 per 1000, nearly six times that of the least deprived areas (3.9 per 1000). 17
Preventing unintended conceptions implies preventing unprotected sex. Drawing from robust representative epidemiological data of school-aged children across the UK18 and the Young Persons’ Behaviour and Attitudes Survey NI,19 it is known that between 25% and 33% of 15-year-olds are having sex, with an associated rate of 2.8% reporting unprotected sex. Changing practices of unprotected sex and unintended pregnancy is complex, and cannot be achieved through RSE alone. 20–26 However, high-quality comprehensive RSE is an essential component in the process of reducing unintended pregnancy rates, as well as being a vital aspect of improving holistic sexual health and well-being. 27–33 The UK governments emphasise the policy importance of the implementation of RSE in schools in decreasing conception rates for those aged < 18 years and the promotion of positive sexual health among teenagers. 34–36
Current status of relationships and sexuality education
The current status of RSE provision in schools in the UK is as follows: educational policy, including relationship and sexuality education, is devolved to the nations of the UK. Hence, the terminology to describe the education young people receive relating to sex and relationships varies in each nation as follows. RSE guidance in NI is predominantly structured under the personal development (PD) strand of the Learning for Life and Work curriculum. In England, sex and relationship education (SRE) is provided under the umbrella term personal, social, health and economic education (PSHE). Pupils in Scotland receive relationships, sexual health and parenthood education as part of their Curriculum for Excellence framework. In Wales, SRE forms one of the six Areas of Learning Experience. For the purposes of uniformity in this report, the appellation RSE is applied UK-wide. In England and Wales, RSE is currently undergoing significant reform. England introduced compulsory RSE in 2020, post data collection for this trial,37 and Wales is set to do so in 2022/3. 38 In England, however, parents will still be able to opt out their children when the topic of sex is being discussed. NI and Scotland have statutory guidance on what should be taught, although this is not compulsory, and many schools follow their own guidance or ethos concerning how the curriculum is delivered. 39,40 Therefore, throughout the UK there is no uniform guidance for the curriculum, and, where guidance exists, it is open to interpretation by schools in terms of how it should be implemented.
The If I Were Jack programme
Brief description
If I Were Jack is an evidence-based, theory-informed, user-endorsed intervention designed to engage especially with teenage boys and intended to increase both teenage boys’ and teenage girls’ intentions to avoid an unplanned pregnancy and to promote positive sexual health. In addition, it fits with a comprehensive approach to relationship and sexuality education. 41 If I Were Jack is a classroom-based RSE resource intended for use by teenagers aged 14–15 years. A specific aim of the intervention is to open up for scrutiny the gender norms that typically situate the issue of a teenage pregnancy as a woman’s problem, to also encourage males to share sexual and reproductive responsibility.
How it was developed
It has been designed, developed and piloted in Ireland, South Australia, NI and the remainder of the UK over 12 years by a team based at Queen’s University Belfast (QUB; Belfast, UK) led by Professor Maria Lohan and in consultation with pupils, teachers, sex education specialists and governments’ education and health promotion departments. 41 Further cultural adaptation initiatives are under way, one being led by Dr Sarah Skeen (Stellenbosch University; Stellenbosch, South Africa) and Dr Áine Aventin (QUB) in South Africa and Lesotho, and one being led by Professor Alejandra López Gómez (Universidad de la República; Montevideo, Uruguay).
Some key stages in the development of If I Were Jack as used in this study are as follows:
-
The development of an earlier version of the interactive video drama (IVD) of If I Were Jack, for the purposes of researching adolescent men’s views on teenage pregnancy and pregnancy resolution options in schools only. 42,43 The If I Were Jack IVD was directly inspired by, and closely based on, If I Were Ben – an original IVD used by Carolyn Corkindale and team at Flinders University (Adelaide, SA, Australia) for the purposes of similar research.
-
The development of the If I Were Jack RSE resource. In response to positive feedback and demand from schools that viewed the IVD, the QUB team redeveloped the IVD and developed an accompanying RSE programme (four to six classes) for NI and Ireland (two versions) through funding from the Economic and Social Research Council (ESRC) of the UK (RES-189-25-0300). Intervention development occurred in close consultation with young people, teachers, RSE experts and statutory policy stakeholders in Departments of Health and Education in Ireland and NI, in close examination of the evidence on the most acceptable and effective RSE components, and in line with Medical Research Council (MRC) guidelines for the development of complex interventions. 41
-
A feasibility trial, process evaluation and health economic evaluation (ISRCTN99459996) of the If I Were Jack RSE resource in NI and a transferability study in England, Scotland and Wales44,45 funded by the National Institute for Health and Care Research (NIHR) Public Health Research programme (15/181/01). The primary results of this stage were as follows –
-
Recruitment of schools was successful across a broad range of school types including faith-based schools (target 25%, achieved 38%).
-
No schools withdrew during the year-long trial, and pupil retention was good (target 85%, achieved 93%).
-
The process and transferability evaluations showed the intervention to be acceptable to schools, pupils and teachers, and that it could be feasibly implemented with some straightforward enhancements, including remaking a version of the IVD with English actors for an England/Wales audience and increasing the ethnic mix of actors.
-
The cost of delivery per pupil was calculated to be £13.66, and behavioural change effects showed promise.
-
The programme was also separately implemented and evaluated in Ireland through a qualitative mixed-methods study46 in a maximum variation sample of schools, where again the acceptability and feasibility of implementation were demonstrated –
-
Redevelopment of the parental component of the intervention. 47 The parental component was changed from a face-to-face to an online component, and student–parent homework exercises were retained in response to results of the above feasibility trial, in a separate study funded by the Public Health Agency of Northern Ireland.
-
The JACK trial – current study to include optimisation of intervention to update materials and make it more suitable for use in England, Scotland and Wales, and UK-wide effectiveness trial with process and health economic evaluation. 48
-
Underpinning research on parents and young people with highest needs. Alongside the above development of the intervention and the underpinning research with young people, the lead principal investigator (PI) has been involved in related studies49–51 researching parents’ experiences of talking to their pre-adolescent and adolescent children about relationships and sexuality, and researching RSE needs of especially vulnerable groups of young people, notably young people in care. 52,53
Intervention components
The intervention components available on the project webpage, www.ifiwerejack.com/ (accessed 20 October 2022), include:
-
A culturally sensitive computer-based IVD to immerse young people in a hypothetical scenario of a week in the life of Jack, a teenager who has just found out that his girlfriend is unexpectedly pregnant. The If I Were Jack interactive film asks pupils to put themselves in Jack’s situation and consider how they would feel and what they would do if they were Jack. (The film is interactive in the sense that it requires viewers to respond about how they would think or act as the narrative develops, but the film does not change in response to these choices.)
-
Classroom materials for teachers containing detailed lesson plans with specific classroom-based and homework activities designed to build pupils’ skills to (1) obtain necessary information and (2) develop communication skills with peers and trusted adults. Teachers can deliver the intervention to pupils during four 50- to 60-minute or six 35- to 45-minute weekly classes.
-
Ninety-minute training session for teachers implementing the intervention.
-
Two short animated films to engage parents/guardians and help/encourage them to have a conversation with their teenager about avoiding unintended pregnancy.
-
Detailed information brochures, letters for schools, letters for parents about the intervention and factsheets and wallet cards about unintended teenage pregnancy (UTP) in general for schools, teachers, teacher trainers, young people and parents/guardians.
The Template for Intervention Description and Replication (TIDieR) checklist54 is used to describe the intervention in more detail, and this longer description of the intervention is available in Report Supplementary Material 1.
Theory of change and how it is hypothesised to work
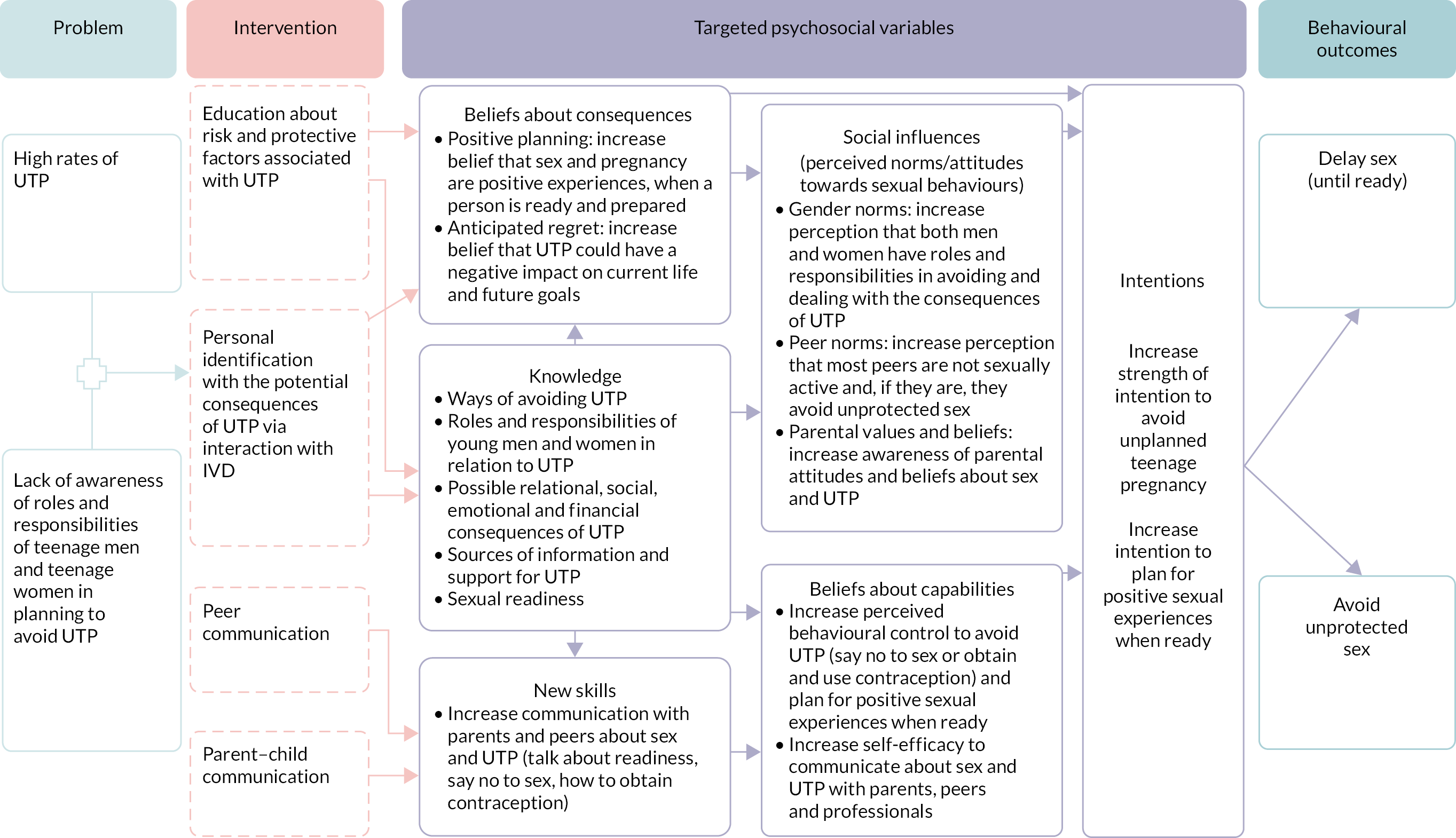
Presented in Figure 1 is the theory of change logic model of the intervention. Described on the left is the core public health problem: the relatively high rates of teenage pregnancy, as noted above. In addition, the public health need to engage young men as well as young women in addressing teenage pregnancy is stated. In brief, we hypothesise that by encouraging personal identification with the UTP scenario in the IVD, we engage pupils in an exercise of the imagination whereby they stop and think about the consequences that a UTP might have on their current life and future goals. This identification and reflection process is reinforced by providing knowledge about the risks and consequences of a UTP and ways to avoid it, and offering opportunities to practise communicating about UTP with peers and parents/guardians (activities that also increase awareness of peer norms, personal and familial values, and beliefs about sexual behaviour and unintended pregnancy). We hypothesise that by targeting these psychosocial factors, as well as inviting scrutiny and critical thinking in relation to wider social norms (gender norms and class norms), we can have an impact on teenagers’ sexual behaviour via pathways through their intention to avoid a UTP. The behavioural outcomes we seek to achieve are delaying sex until young people feel prepared and avoidance of unprotected sex.
FIGURE 1.
Theory of change logic model of the intervention.
Evidence supporting intervention components and theory of change
The characteristics of effective RSE programmes that help to increase their impact on sexual risk-taking behaviours have been précised in a number of systematic reviews. 25,55–62 These impactful characteristics include the use of theoretically based interventions targeting sexual and psychosocial mediating variables such as knowledge, attitudes, self-efficacy, intentions, perceptions of risk and perceptions of peer norms that are linked to sexual behaviour change; the use of culturally sensitive and gender-sensitive interventions; the use of interactive modalities that promote personal identification with the educational issues and engagement of young people; the use of skills-building components; the involvement of parents in the RSE process; and facilitating linkages with support services. The If I Were Jack intervention represents an innovative combination of all these different elements and is therefore predicted to decrease young people’s sexual risk-taking behaviour in relation to avoiding teenage pregnancy. The evidence for each of the components is further broken down below.
Evidence supporting a theory-based approach
Providing a theoretically informed foundation is considered key to the effectiveness of sexual health education programmes, ensuring that the most important determinants of young people’s sexual behaviour are targeted. 28,57,59,63–65 Early exploratory work for the design of the intervention is reported elsewhere. 41 The underpinning theoretical framework for this intervention combines the theory of planned behaviour,66,67 to address key psychosocial determinants of sexual behaviour, and gender-transformative programming, to address the broader context of promoting positive masculinities and addressing gender inequalities. 68,69
The use of theory of planned behaviour in If I Were Jack
The theory of planned behaviour largely focuses on individual-level behavioural antecedents of a particular behaviour of an unplanned pregnancy. The If I Were Jack intervention has been designed to increase teenagers’ intentions to avoid an unplanned pregnancy by delaying sexual intercourse until ready or avoiding unprotected sex by use of modern contraception. With these behaviours in mind, the intervention targets six psychosocial mechanisms, which research indicates are related to a reduction in risk-taking behaviour. These are: knowledge, skills, beliefs about consequences, social influences, beliefs about capabilities and intentions25,70,71 (see Figure 1). Each of the activities included in the intervention is designed to specifically target one or more of these psychosocial mechanisms, such as activities that provide pupils with educational information and opportunities for discussion, skills practise, reflection and anticipatory thinking.
Later critiques of the theory of planned behaviour bring an understanding of the broader socioenvironmental factors and underlying values that influence behaviours, such as religiosity and gender ideologies associated with teenage pregnancy. 24,67 Although these normative values are not addressed at a societal level in this intervention, they are addressed through young people’s agency. Through intervention activities, young people are invited to think critically about social class, religious and gender norms that may influence their thoughts and behaviours on this topic – hence especially the importance of gender-transformative theory.
If I Were Jack is also informed by gender-transformative programming
A gender-transformative approach was first developed by Geeta Rao Gupta68 in the context of the human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) epidemic, and has since gained traction as a means to improve health and well-being in sexual and reproductive health and rights (SRHR) and health and development policy more generally. 69,72–75 The World Health Organization (WHO) defines gender-transformative approaches as those ‘that address the causes of gender-based health inequities through approaches that challenge and redress harmful and unequal gender norms, roles, and power relations that privilege men over women’69 (Gender Mainstreaming for Health Managers: A Practical Approach. Geneva: World Health Organization; 2011. Licence: CC BY-NC-SA 3.0 IGO).
Over the past decade in the RSE evidence base, the need for gender-sensitive interventions to address teenage pregnancy has been highlighted as a global health need by WHO76–78 and recommended in systematic reviews of RSE education. 25,79–81 By gender sensitive, it is meant that RSE should seek optimal ways to engage both young men and young women and to address gender norms, roles and relations that may lead to generating healthy and enjoyable relationships and positive sexual and reproductive health over their lifespan. In addition, the language of gender-transformative theory that explicitly challenges gender inequalities has been part of the WHO guideline82 on preventing adolescent pregnancy in developing counties since 2011, specifically in relation to the engagement of men and boys. More recently, the WHO83 recommendations on adolescent SRHR state that ‘building equitable gender norms through comprehensive sex education can contribute to preventing gender-based violence and to promoting joint decision making on contraception in couples’ (WHO Recommendations on Adolescent Sexual and Reproductive Health and Rights. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.). The United Nations Population Fund also emphasises a focus on gender and empowerment outcomes consistent with a gender-transformative approach,84 as does the most recent agenda-setting document in the field: the Guttmacher–Lancet Commission on Sexual and Reproductive Health and Rights. 85 A further term used in the scientific literature by Haberland and Rogow86 is an ‘empowerment approach to Comprehensive Sex Education (CSE)’, to refer to programmes that emphasise gender/power versus those that do not. Their review states that comprehensive sex education (CSE) is most effective when it highlights a gender/power perspective. 86 Finally, engaging men and boys in a gender-transformative approach is also embedded in an ‘enabling environment’: an ecological framework to improve adolescent sexual and reproductive health –
These approaches promote alternative norms and understandings of masculinity and behaviors in intimate relationships that involve mutual respect and equitable decision making, sharing responsibilities for reproductive health (e.g., condom use), and the greater involvement of men as fathers and caregivers. 87
Reproduced with permission from Svanemyr et al. 87 This article is available under the Creative Commons CC-BY-NC-ND license and permits non-commercial use of the work as published, without adaptation or alteration provided the work is fully attributed. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
Hence, collectively across the literature with reference to a gender-sensitive, gender-transformative or empowerment approach to CSE, the need to develop RSE interventions that successfully engage adolescent women and adolescent men, and that address unequal gender dynamics in intimate relationships, has been expressed.
The If I Were Jack programme is designed to be both gender sensitive and gender transformative. It is gender sensitive as per the WHO definition, in that it is designed to include and engage young men on this topic alongside young women. It is gender transformative in that it addresses the negative gender norms and attitudes that place the burden of responsibility for preventing and dealing with the impacts of a teenage pregnancy on young women. It encourages communication and behavioural skills among young men and young women to enable them to prevent a teenage pregnancy and to know how to seek help. If I Were Jack acknowledges sexual pleasure and sexual intimacy in young people’s lives and asks young people to consider for themselves the balances between sexual pleasure and sexual responsibility in a gender-equitable manner. In addition, the programme seeks to address deficits in sex education for young men, particularly with respect to teenage pregnancy, that have been identified in the scientific literature, and that disadvantage adolescent men as well as adolescent women. 28,42,79,87–93
Evidence supporting the use of culturally relevant interventions
The resource includes an interactive computer-based modality incorporating drama and film. This is informed by research suggesting the need to engage with young people both empathetically and cognitively to convey the relevance of the issues being raised. 29,56,59,63,94 The feasibility trial and process evaluation44,45 demonstrated that the use of locally produced contemporary drama (in the IVD) made sex education more enjoyable and engaging for pupils. It is important to harness the potential for sex education to be enjoyed, especially by those who are less engaged in the wider school curriculum,30,95,96 a factor that was identified as a possible barrier to impact. 25 The feasibility trial44,45 also showed that the ability of users to identify with the key characters in the IVD, along with the overall tailored nature of the intervention in terms of linking in with local services, was central to its appeal and acceptability to pupils.
Evidence supporting the use of interactive computer-based interventions
The value of interactive computer-based interventions has been demonstrated in systematic reviews,59,60,97 particularly tailored, video-based interventions intended to elicit behaviour change. 98 A meta-analysis examining these reviews in relation to the theoretical mediators of safer sex61 concluded that they were successful in affecting knowledge, attitudes and self-efficacy relating to sexual health. Wearing headphones and sitting at individual computers, each participant is invited to answer questions on how he/she would feel and act as the drama unfolds.
Evidence supporting the use of skills-building components
Simply providing information does not lead to behaviour change; rather, young people must be supported to develop their own communication skills in relation to preventing risky sexual behaviours. 8,25,27–29,57,59,63,65,77,99,100 If I Were Jack emphasises the need for active participation and deliberation by the users so as to increase self-awareness and encourage ‘stop-and-think’ strategies in relationships. A further specific aim of the resource is to desensitise the discussion of sexual and reproductive topics through practising explicit ‘verbal scripts’63 for such conversations between young men and women.
Evidence supporting the involvement of parents in relationship and sexuality education
Although evidence suggests that schools are an important context for sex education,63,101,102 a number of systematic reviews have also shown that programmes that reach beyond the classroom can enhance effectiveness. 25,31,103 In particular, factors such as parental monitoring and supervision and familial communication have been associated with teenage sexual behaviours. 104,105 Parents are often a primary source of information about sex for adolescents,106 and teenagers who can recall a parent communicating with them about sex are more likely to report delaying sexual debut, and increased condom and contraceptive use. 107–109 One element of the If I Were Jack theory of change involves increasing self-efficacy in communicating about teenage pregnancy among parents and teens. This is built into the resource through home-based resources intended to generate communication and through short animated films for parents and guardians. This component informs parents of the resources and information about communicating about teenage pregnancy, including hints and tips about how to do so. Learning from the feasibility trial,44,45 in which parental attendance at information sessions was low (2.3%), the parental materials were redeveloped as animated films and provided online. Recent studies110–112 demonstrate the potential of embracing such ‘education entertainment’ or ‘edutainment’ modalities as engaging adjuncts to school-based education.
Importance of comprehensive relationship and sexuality education despite limitations of impact on health outcomes
Above, we have described the evidence for the programme characteristics of high-quality comprehensive RSE. Before we embark on describing the aims, objectives and results of this study, it is important to also sound a note of caution in terms of the limitations of comprehensive RSE alone in impacting on complex health behaviours, such as preventing unprotected sex and consequently preventing teenage pregnancy and reducing sexually transmitted infections (STIs). Another significant motivator for this study, however, was the importance of CSE as an international human right of young people and as an expressed need by young people.
By way of definition, CSE teaches about abstinence as part of the foundation for avoiding STIs and unintended pregnancy, and also teaches about condoms and contraception to reduce the risk of unintended pregnancy and of infection with STIs, including HIV. It also teaches interpersonal and communication skills and helps young people explore their own values, goals and options. 113 The United Nations Educational, Scientific and Cultural Organization (UNESCO) specifies that CSE should be scientifically accurate, incremental, curriculum based, based on a human rights approach, based on gender equality, culturally relevant and contextually appropriate, transformative, and able to aid the development of life skills needed to support healthy choices. 33 This can be contrasted with the abstinence-only-until-marriage (AOUM) approach. The AOUM approach teaches abstinence as the only morally correct option of sexual expression for teenagers. It usually censors information about contraception and condoms for the prevention of STIs and unintended pregnancy. 113 If I Were Jack is part of CSE.
First, we acknowledge that two large cluster RCTs of CSE programmes24,114 in the UK did not show a significant effect on health outcomes. The SHARE (Sexual Health and Relationships Education) programme, trialled in Scotland, did not reduce conceptions or terminations by the age of 20 in comparison with conventional provision. 24 The Randomised Intervention of PuPil-Led sex Education (RIPPLE) trial was a peer-led sex education programme conducted in south-east England. The final results showed that the programme was not associated with change in teenage abortions but may have led to fewer teenage births. 114
Second, overall reviews of evidence have also detailed the limitations of CSE alone in affecting health outcomes, although they can have important impacts on knowledge, attitudes and skills. A NIHR-funded systematic review25 of the effect of interventions aiming to encourage young people to adopt safer sexual behaviour found that school-based interventions that provide information and teach young people sexual health negotiation skills can bring about improvements in behaviour-mediating outcomes such as knowledge, attitudes and self-efficacy but did not find significant effects on health outcomes. The review noted that these variables are, however, no less valuable than behavioural health outcome variables because they provide young people with a solid foundation on which to make sexual decisions. Similar findings have been noted in other reviews115–117> and meta-analyses, some of which are undertaken by organisations opposed to the implementation of CSE118,119 and favouring AOUM approaches. However, the AOUM approach not only has been found to be scientifically ineffective in helping adolescents to delay intercourse, but also is regarded as ethically flawed in terms of denying young people rights to information, endangering gender stereotypes and marginalising sexual minority youth. 120
Thus, despite some limitations noted in the scientific evidence for CSE alone in having an impact on ultimate health outcomes, such as teenage conceptions and teenage pregnancy terminations, the United Nations33 and WHO conclude from the evidence that ‘CSE can help adolescents to develop knowledge and understanding; positive values, including respect for gender equality, diversity and human rights; and attitudes and skills that contribute to safe, healthy and positive relationships’83 (WHO Recommendations on Adolescent Sexual and Reproductive Health and Rights. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.). As the NIHR review also stated, these skills are no less important and reflect a holistic approach to RSE. 121–123
Moreover, young people have a right to high-quality comprehensive RSE. The United Nations Convention on the Rights of the Child,124 Articles 24 (health and health services) and 34 (sexual exploitation), stipulate that governments must provide education on health and well-being to enable children to protect their health, as well as implementing measures to protect children from sexual exploitation or violence. 124
Flowing from these fundamental rights, international human rights standards require that governments guarantee the rights of adolescents to health, life, education and non-discrimination by providing them with CSE in primary and secondary schools that is scientifically accurate and objective, and free of prejudice and discrimination. 125
The Committee on the Rights of the Child has further indicated that nation states should equip adolescents with relevant information in relation to contraception and avoidance of unintended pregnancy and STIs, including HIV/AIDS. 126
The right to sexual and reproductive health is also protected under the ‘right to the highest attainable standard of physical and mental health (https://www.refworld.org/docid/4538838d0.html; accessed 16 June 2020), enshrined in Article 12 of the International Covenant on Economic, Social and Cultural Rights. 127 Finally, the right information and education to promote SRHR is also linked to the United Nations Sustainable Development Goals (targets 3.7 and 5.6). 128
However, few countries follow human rights standards129 and include CSE curricula to be part of the mandatory school curriculum, or implement and sustain large-scale CSE programmes. 83 Hence, the Guttmacher–Lancet Commission on Sexual and Reproductive Health and Rights85 recognises the need for all countries to establish national curricula for comprehensive sexuality education based on evidence and drawing from international technical guidance such as that provided by the international policy community. 33 Furthermore, the Commission noted that, to be comprehensive, sex education must include strategies to increase gender equality and holistic health more broadly.
Finally, comprehensive RSE is also not just a right but a need, as expressed by young people themselves,41,45,96,130–133 and human rights standards state that the curricula should be developed with young people’s input, such as in the case of If I Were Jack (described more fully in the next chapter). With that balance of views on scientific evidence and children’s rights in mind, we now describe the aims and objectives of this study.
Aims and objectives of the JACK trial
The overall aim was to carry out the first UK-wide cluster RCT of a comprehensive relationship and sexuality education intervention using a gender-transformative approach to specifically engage with young men and young women to address teenage pregnancy and promote positive sexual health.
The objectives of the study were to:
-
assess the effectiveness of the intervention in preventing unprotected sex at 15 years of age among teenage boys and girls in a cluster RCT across the UK
-
assess the impact of the intervention on secondary outcome measures of knowledge, attitudes, skills and intentions to avoid teenage pregnancy, as well as additional behavioural outcomes of engagement in sexual intercourse, contraception use and STIs
-
examine any differential impacts for teenage boys and girls as well as for different socioeconomic groups and nations of the UK
-
conduct an economic evaluation of the intervention compared with current practice
-
conduct a process evaluation, examining reasons for participation and non-participation; intervention delivery and fidelity in intervention schools; RSE provision in all participating schools; and self-reported perceptions of effectiveness and moderating influences in intervention schools among a sample of pupils, teachers and school principals and parents.
The full protocol for this trial was published in June 2018,48 and the protocol and any updates to the protocol (described in Chapter 3, Deviations and rationale) can be found at the NIHR Evaluation, Trials and Studies website.
Chapter 2 Patient and public involvement
Introduction
Engagement of stakeholders, including policy-makers and commissioners, as well as teachers, young people and parents, has been central throughout this study. The purpose was to ensure that stakeholders’ views and opinions were used to inform key aspects of the intervention optimisation (stage 1 of this study), as well as study design processes, data collection procedures and dissemination. We begin this chapter with an overview of stakeholder involvement and then move to a fuller description of the process and results of stakeholder involvement as part of stage 1 of this study: intervention refinement and optimisation.
Overview of purpose and mechanisms of stakeholder engagement
The purpose and mechanisms of stakeholder engagement were as follows.
Intervention refinement and optimisation
-
During the intervention refinement and optimisation phase, (stage 1 of this study), we convened and consulted with a JACK trial Stakeholder Advisory Committee (SAC) (see Report Supplementary Material 2) consisting of senior representatives from key government departments and non-government organisations involved in RSE policy-making across the whole of the UK, including the Belfast Health and Social Care Trust (BHSCT; Belfast, UK), the Rainbow Project (Belfast, UK), Education Scotland (Livingston, UK), the Council for the Curriculum, Examinations and Assessment (Belfast, UK), the Personal, Social and Health Education Association (PSHEA; London, UK), NHS Glasgow (Glasgow, UK), Public Health Wales (Cardiff, UK), teachers and young people.
-
During the intervention refinement and optimisation phase, we also convened and consulted with a UK-wide Young Person’s Advisory Group (YPAG) (see below) on the refinement and acceptability of the intervention materials and processes.
Informing trial methodology
-
Throughout the study, consultations were held with the Trial Steering Committee (TSC) (see Report Supplementary Material 2). The TSC met four times: 13 March 2017, 22 February 2018, 16 May 2019 and 16 April 2021. The collective members of the international TSC included independent public members such as young people, parents, teachers and school principals; policy advisors to Public Health England (London, UK); experts in trial methodologies; and school-based RCT experts.
-
In addition, we engaged young people in the refinement of the trial outcome measure questionnaire. Representatives from the project YPAG, as well as young people who served on the TSC, provided feedback on the questionnaire that resulted in minor changes to the wording of some questions.
Implications of interim findings and dissemination
-
Members of the TSC, especially young person members, were consulted on the production of posters (see Report Supplementary Material 2) to thank schools for their involvement and provide an interim summary of findings.
-
The 2019 SAC meeting took the form of a ‘6 Nations’ Relationships and Sexuality Education Symposium held at QUB [with additional funding from QUB and EuroSocial (Madrid, Spain)]. In addition to members of the SAC, the event was attended by international experts from Departments of Health and Education across the four nations of the UK and from Ireland and delegates from the Ministry for Health in Uruguay. Dr Chandra Mouli from the WHO and Ineke van der Vlugt from Rutgers International, the Netherlands, also participated.
-
The symposium involved short presentations from each nation (including interim results of the JACK trial) and round table policy discussions on RSE and related sexual health policies.
-
The TSC met in April 2021 to consider the final findings of the study.
Stakeholder involvement in stage 1: intervention refinement and optimisation
Background and rationale
As reported in Chapter 1, in 2014/15 we conducted a cluster randomised controlled feasibility trial of the If I Were Jack intervention in eight schools in NI. In addition to the feasibility trial, and in preparation for the current UK-wide trial reported here, we also conducted a transferability study in nine schools in Wales, England and Scotland. The following research questions were addressed in the transferability study:
-
Was the intervention acceptable to schools and RSE curricula in other parts of the UK?
-
Would students and teachers in other parts of the UK find the intervention useful?
-
Could students in England, Wales or Scotland understand and relate to Jack and Emma as they appeared in the NI film?
-
Were there changes they would like to see to the classroom materials and film itself?
Together, the findings of the feasibility trial and transferability study indicated that, in all four UK nations, students, school staff and RSE experts welcomed and enjoyed the intervention. However, they also made some suggestions for improvements to the film, classroom materials, teacher training and parental components to make the resource materials relevant for use in their nations. We therefore sought to implement these and other changes in consultation with stakeholder groups, prior to commencing a full UK-wide trial. (Refinements to the parental components were conducted as part of a separate study in 2016, funded by the Public Health Agency for Northern Ireland.) This was achieved, as described below, during stage 1 of the current study.
Aim and objectives
Aim
-
To refine and optimise the If I Were Jack intervention for target populations in England, Scotland and Wales prior to a UK-wide RCT.
Objectives
Stage 1 of the current study involved a 12-month (January–December 2017) intervention refinement and optimisation process. This stage had the following objectives:
-
to convene a UK-wide SAC composed of RSE specialists and statutory stakeholders and YPAGs in each nation to inform refinement of the intervention and continue to build implementation capacity over the longer term
-
to produce updated and culturally refined versions of the If I Were Jack IVD – one for Scotland and NI using Northern Irish accents and one for Wales and England using English accents, both set in a UK urban setting and closely based on the original script and storyboarding
-
to refine classroom materials to match lesson-plan outcomes to learning outcomes of RSE curricula of the four nations where relevant (Scotland and Wales) and insert local information resources
-
to test the refined intervention in three schools based in England, Scotland and Wales judged against ‘stop/go’ criteria and deliver results to NIHR before progressing to stage 2.
Methods
Intervention refinement and optimisation was achieved via an iterative process involving consultation with stakeholders, including experts and YPAG members and a pilot study in England, Scotland and Wales. Table 1 summarises the key tasks and timeline of stage 1.
| Intervention refinement and optimisation tasks | Stage 1, year 1, January–December 2017 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| January | February | March | April | May | June | July | August | September | October | November | December | |
| Tendering and procurement (films) | ✓ | ✓ | ✓ | |||||||||
| Recruit YPAG and SAC | ✓ | |||||||||||
| YPAG consultations | ✓ | ✓ | ||||||||||
| Stakeholder group consultations | ✓ | ✓ | ✓ | |||||||||
| Produce refined versions of interactive films | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Produce refined intervention materials | ✓ | ✓ | ✓ | |||||||||
| Pilot study in England, Scotland and Wales | ✓ | ✓ | ||||||||||
| Further minor refinements to intervention materials | ✓ | |||||||||||
| Phase 1: report to NIHR | ✓ | |||||||||||
| Phase 2: stop/go decision | ✓ | |||||||||||
Consultation on refinements to the interactive video drama
Our UK-wide YPAG was composed of 12 young people, aged 14–16 years, six male and six female, three from each of NI, Wales, Scotland and England. The young people were recruited via the project team’s network with pre-established community youth groups.
Young Person’s Advisory Group residential, Cardiff, April 2017
We held a 2-day residential workshop in Cardiff in April 2017, to discuss refinements to the If I Were Jack IVD. Three youth workers accompanied the Northern Irish, Scottish and English young people on the journey to Cardiff. Two film producers from Morrow Communications Ltd (Belfast, UK), which was commissioned to produce the new IVDs, also attended the workshop. The workshop was led by experienced youth advisory group facilitators from the Centre for Development, Evaluation, Complexity and Implementation in Public Health Improvement at Cardiff University (Cardiff, UK). It included six structured sessions over 2 days involving interactive focus groups, workshops and debates designed to promote discussion among, and feedback from, the young people. The sessions addressed the following: (1) identifying problems with the IVDs and film scripts, and (2) suggesting changes that would maximise the relevance and acceptability of the films for young people across the UK. YPAG members met again via videoconference in August 2020 to consult on draft versions of the films.
Consultation on refinements to intervention materials
In June 2017, members of the research team engaged in a 1-day workshop in London with the SAC from the four nations (see Aims and objectives of the JACK trial). This consultation focused on refinements to the non-film-based intervention inputs, activities and materials, including teacher training materials, student activities and materials, and proposed intervention delivery processes.
Stakeholders provided feedback, relevant to their representative nations, on the following:
-
sexual health services for young people including online information and local services
-
the RSE curriculum and potential positioning of the intervention within it and identification of existing similar interventions
-
delivery processes, including proposed length of sessions and identification of potential challenges
-
detailed comments on proposed teacher, student and parent activities.
Members of the SAC provided follow-up comments and feedback via e-mail on the refined versions of the intervention materials during July and August 2017. Draft digital and hard-copy versions of the intervention materials were prepared in October 2017 for use during the pilot study.
Feedback from the YPAG and SAC was collated and, along with findings from the feasibility and transferability studies, informed amendments to the script and film storyboard as outlined in the results section below.
Intervention optimisation: pilot study
In November and December 2017, the refined intervention was piloted in three schools, one each in Wales, Scotland and England. Teachers were trained to deliver the intervention by members of the research team, and students and teachers completed short surveys regarding their views on the intervention. Teachers who delivered the programme also took part in circa 30-minute semistructured interviews with members of the research team.
Results
Intervention refinements: films
The primary recommendations of the YPAG in relation to the IVD were (1) technology and music (e.g. add more generic background music and include texts on screen rather than on a particular mobile phone); (2) fashion (e.g. sportswear instead of jeans, updated hairstyles); (3) language (e.g. use of slang and occasional swear words to make interactions more informal and realistic); (4) filming locations and scenarios (e.g. pros and cons list at home not in a café); and (5) cultural representations (e.g. include more actors from ethnic minority/non-white backgrounds and include mixed-sex friendship groups). The young people also examined the film’s scripts in detail and recommended changes to the language used. A full report of the YPAG methods and outcomes is available in Report Supplementary Material 2.
The team worked with the film production company (Morrow Communications) to cast and produce two versions of the film (one for Scotland and NI casting actors with NI accents, and one for Wales and England casting actors with English accents). YPAG members met again via videoconference in August 2017 to consult on draft versions of the films and minor amendments were made at this stage following their recommendations. These minor amendments related to slight changes to the questions that appear in the IVD and inserting a space between the various parents’ reactions in the films. The young people were overwhelmingly positive about the revised versions.
Intervention refinements: materials
As well as the provision of nation-specific information noted above, the SAC offered the following key recommendations on refinements to the intervention materials:
-
Owing to the variability in relation to sexual health services, sexual health and RSE terminology and the provision of RSE across the nations, separate sets of materials would be required for each nation.
-
Stakeholders encouraged the use of more ‘sex-positive’ language in the materials, for example changing references to ‘abstinence’ to ‘sex when ready’.
-
Stakeholders encouraged the inclusion of activities and amendment of language that would make the materials more relevant to the lesbian, gay, bisexual, transgender, and questioning (or queer) (LGBTQ+) communities.
Pilot study results
In November and December 2017, the refined intervention was successfully piloted in three schools, one each in Wales, Scotland and England. Teachers were trained to deliver the intervention by members of the research team, and students and teachers completed short surveys regarding their views on the intervention. Teachers who delivered the programme also took part in circa 30-minute semistructured interviews with researchers. As outlined in Table 2, survey findings relating to the films were used to inform the stage 2 progression rules. Findings relating to the non-film intervention components (i.e. teacher resources and student activities) informed further minor refinements to the classroom activities and teacher training materials but were not part of the progression criteria.
| Progression rules | Pilot study findings | Stop/go decision | ||
|---|---|---|---|---|
| England | Scotland | Wales | ||
| At least 60% of students view the entire film | 93% of 43 participating students viewed the entire film | 100% of 34 participating students viewed the entire film | 100% of 56 participating students viewed the entire film | Go |
| At least 80% of students who view the entire film find the accents clear and understandable | 88% of 43 students found the accents ‘clear and understandable’ | 85% of 34 students found the accents ‘clear and understandable’ | 100% of 56 students found the accents ‘clear and understandable’ | Go |
| At least 80% of teachers report that they would be happy to use the If I Were Jack film again | 100% of two teachers said that they would use the film again | 100% of two teachers said that they would use the film again | 100% of two teachers said that they would use the film again | Go |
Conclusion
The involvement of stakeholders has been a key method of ensuring the quality and acceptability of the intervention and trial methods. Stakeholder voices and opinions informed intervention development and optimisation, study design processes and dissemination. The dedicated intervention refinement phase and pilot study allowed optimisation of the intervention materials prior to progressing to the stage 2 trial. Close consultation with stakeholders throughout was key to the success of stage 1 of the project and laid solid stakeholder-informed foundations on which to build and implement processes and procedures for stage 2 of the study. All resulting materials were made available on the If I Were Jack website post trial.
Chapter 3 Methodology
Study design
The JACK trial was a Phase III134 multicentre, parallel-group, cluster RCT with two treatment groups: the If I Were Jack intervention versus schools’ usual RSE provision. Schools were the unit of randomisation, with a 1 : 1 allocation. An embedded process evaluation and economic evaluation were conducted (economic evaluation methods are detailed in Chapter 7). The trial protocol was published. 48
Ethics approval and research governance
The trial was conducted in line with the ESRC Framework for Research Ethics and received a full ethics review by the School of Nursing and Midwifery (QUB) Research Ethics Committee in July 2017 (Ref: 11.MLohan.05.17.M6.V1), which independently assessed our compliance with the ESRC Framework. This approval covered data collection in each partner site. A trial steering group was convened to oversee the trial (see Report Supplementary Material 3). QUB acted as the main sponsor of the research and ensured that governance and indemnity procedures were in place. The project was registered on the Human Subject Projects database in QUB and prospectively registered in an international register of trials (ISRCTN99459996).
Participants
The study sought to recruit schools in the four nations of the UK, and to recruit teachers and pupils within these schools. Parents were also recruited but participated only in the process evaluation.
Inclusion criteria for schools
The whole of NI was included, but, for reasons of practicality, convenience and cost, geographical restrictions were put in place for England (Greater London area), Scotland (five specified local authority areas) and Wales (South Wales). All secondary schools with over 30 pupils in Year 11 (NI), Year 10 (England and Wales) and S3 (Scotland) were eligible to participate. The detailed recruitment strategy can be found in Report Supplementary Material 3.
Further inclusion criteria were as follows:
-
Schools had to be able to send e-mail or text messages containing a link to the video to parents of their pupils. Prior feasibility and transferability studies suggested that this would exclude a very small proportion of schools.
-
Faith-based schools were not excluded in any UK region.
The exclusion criteria were as follows:
-
Independent private, special and Irish/Welsh-medium and Scottish Gaelic schools were excluded. This exclusion criterion did not exclude schools that have an embedded Irish/Welsh-medium component.
-
Schools with < 30 pupils in the target year group (Year 11 in NI, S3 in Scotland and Year 10 in England and Wales) were excluded.
-
Schools that had already participated in the feasibility (n = 8, NI), transferability (n = 3, England; n = 3, Scotland; n = 3, Wales) and pilot studies (n = 1, England; n = 1, Scotland; n = 1, Wales) involving the If I Were Jack intervention in preparation for the Phase III study were also excluded.
Inclusion criteria for teachers
Teachers who were responsible for the delivery of RSE to pupils in Year 11 in NI, S3 in Scotland and Year 10 in England and Wales during the 2018/2019 academic year were eligible for the study.
Inclusion criteria for pupils
All pupils entering Year 11 in NI, S3 in Scotland and Year 10 in England and Wales (mean age 14 years across all nations) in 2018/19 in eligible schools were eligible for the study. Students with mild learning difficulties or poor English were supported to complete the questionnaire by trained fieldworkers.
Inclusion criteria for parents
All parents in intervention schools were eligible for inclusion in the study.
Recruitment procedure
Sampling frame
A sampling frame of Department of Education listed schools for each nation of the UK and defined the socioeconomic status of schools [based on eligibility for free school meals (FSM) as indicated by the School Meal Census] was used. In each nation, eligible schools were stratified into two levels according to FSM (schools above and below the median national percentage of FSM for all eligible schools, rank ordered randomly). In NI, 14 schools were randomly selected from the above-median stratum and 10 from the below-median stratum (total 24), and in England, Scotland and Wales eight schools were randomly selected from the above-median stratum and six from the below-median stratum (to give a total of 14). The decision to select slightly more schools from the above median national percentage of FSM stratum was to allow for even random allocation of schools to trial groups and to reflect research that indicates that public health need for addressing adolescent unintended pregnancy is greater in areas of higher social deprivation. 18,135
Recruitment of schools
Main study recruitment took place over a 6-month period (February–June and to end-September 2018), with a break during the summer period (July and August). Where possible, schools were approached via a relevant senior manager in the schools (e.g. senior teacher or deputy head in charge of pastoral care, identified with the help of the School Health Research Network in Wales, the School Health and Wellbeing Research Network in London, and local professional networks in Scotland and NI). In Scotland, permission was obtained from each local authority (typically by approaching the Director of Education) prior to commencing recruitment. Any school that declined to participate was replaced by a randomly selected school in the same stratum. A multifaceted approach to recruitment of schools was employed and consisted of an e-mail with attachments including a promotional leaflet, an invitation letter and an information sheet.
To promote school retention, schools were provided with £1000 on completion of baseline and follow-up measures. Schools that decided to participate were invited to consent by signing a memorandum of understanding (MoU), and were asked to nominate a main point of contact (a trial champion teacher, who was typically a teacher with responsibility for RSE delivery or governance) within the school to deal with future correspondence between the research team and the school. No stopping guidelines were put in place for this study; any and all schools and students who agreed to take part were included. The full school recruitment strategy is detailed in Report Supplementary Material 3.
Recruitment of teachers
Trial champion teachers then identified teachers responsible for RSE delivery to the relevant year groups during the 2018/2019 academic year, and researchers delivered an information session and provided the school letter and information sheet, MoU and consent form (see Report Supplementary Material 3 for examples of each).
Recruitment of pupils
Schools posted to parents/guardians an information sheet and an opt-out consent form for their child’s participation in the trial research (see Report Supplementary Material 3), with prepaid response envelopes and a return deadline. Researchers collated a list of parents/guardians who opted their child out of participation and returned this to teachers. At least 1 week prior to baseline data collection, pupils attended a short information session delivered by a member of the research team, which included an animated video. Pupils were provided with pupil information sheets (see Report Supplementary Material 3) and given an opportunity to ask questions prior to deciding whether or not to participate. Only eligible pupils whose parents/guardians did not opt out of providing consent for them to participate attended.
Recruitment of parents
Schools texted/e-mailed parents of all participating pupils in intervention schools a short online survey asking for their views on the parents’ videos and parent/pupil homework exercise. A maximum of two texts/e-mails were sent to parents (the original message and link to survey and one reminder). At the end of the survey, respondents were asked to provide their contact details if they would like to be approached to take part in a parents’ focus group discussion in the event that their school was selected as a case-study school.
Informed consent
Written, informed consent for random allocation was obtained from a member of the school senior leadership team, and from students, parents, teachers and intervention delivery staff for data collection. Parents were also informed about the trial and offered the opportunity to withdraw their child from the trial (although not the intervention).
Particular attention was paid to enhancing the process of informed consent for students within a school environment through the following measures:
-
Information and informed consent forms were administered and collected by the research team. Although teachers may have been present during this process, it was emphasised to pupils that their participation in the study was voluntary and that, should they decline to participate, they would have the opportunity to continue with independent study during data collection periods.
-
The research team also produced a short animation video informed by the pupil members of the TSG to convey what the study involved and their right to consent, as well as their right to withdraw their consent at any time without giving any reasons. This was shown to pupils in schools prior to asking for written informed consent.
Randomisation, concealment and blinding
When the recruitment quota for schools had been filled prior to baseline data collection, schools within each nation and socioeconomic stratum were randomly allocated (1 : 1 concealed allocation) to a trial group by an independent Northern Ireland Clinical Trials Unit (NICTU) statistician. The statistician produced eight randomisation schedules (using unique identifiers for schools), one for each FSM stratum for each nation, using random permuted blocks of mixed size, generated using Dotmatics nQuery Advisor 7.0 (San Diego, CA, USA). The NICTU was not involved with recruitment and released the randomisation code only when all schools were recruited and baseline data collection was completed, ensuring allocation concealment.
The statistician sent teacher trainers the allocation schedule for all schools. The teacher trainers were part of the intervention delivery team, and independent of the external research team. School allocation was communicated to each school by the nation-specific teacher trainer following baseline data collection within the school. Research teams were unaware of school allocation until after schools were informed of their allocation. (In a trial of this type, it was not possible to blind participants to allocation.) At randomisation, the NICTU Trial Statistician also randomly selected two intervention group schools from each nation as case-study schools for the process evaluation (see Process evaluation methods).
Treatment group allocation
Intervention
In schools that were randomly allocated to the intervention group, pupils in the relevant year group received the If I Were Jack programme.
Usual RSE provision
The schools in the control group did not receive the If I Were Jack programme but continued with the regular RSE curriculum and usual classroom activity. Schools in the control group were placed on a waiting list to receive the programme in 2020 following completion of the final follow-up survey.
Data collection and management
Data management
A Data Management Protocol (see Report Supplementary Material 3) was developed detailing the procedures to be followed in recording, storing and sharing project data. Survey data were provided to NICTU in the form of Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA) documents, sent by password-protected e-mail by an external scanning company. Working files were created for each of the four locations: England, NI, Scotland and Wales. Validation checks were carried out on these data sets as per Data Management Guidelines and, when complete, four master data sets were created for analysis. Data sharing between sites was facilitated via a university-secure, password-protected Dropbox™ (Dropbox Inc., San Francisco, CA, USA) account.
Data retention/archiving
All data will be retained by QUB for a minimum of 5 years after completion of the final report (stored on a secure server, protected against unauthorised access by user authentication and a firewall). All hardcopy materials (other than pupil questionnaires) will also be stored by each partner institution for a minimum of 5 years after completion of the final report, in secure storage with restricted access, and accessible to the PI, if needed, on request. The data will be archived by year 10 in the UK Data Archive, located in the University of Essex (Colchester, UK).
Data collection
Baseline
At baseline (prior to commencement of intervention delivery), fieldworkers administered paper-based questionnaires to participating pupils, which they completed during the school day under exam conditions. Teachers were asked to stay at the front of the room to maintain order while also alleviating pupils’ concerns that teachers could see their answers. Fieldworkers supported pupils requiring extra help and ensured that questionnaires were completed confidentially.
Follow-up
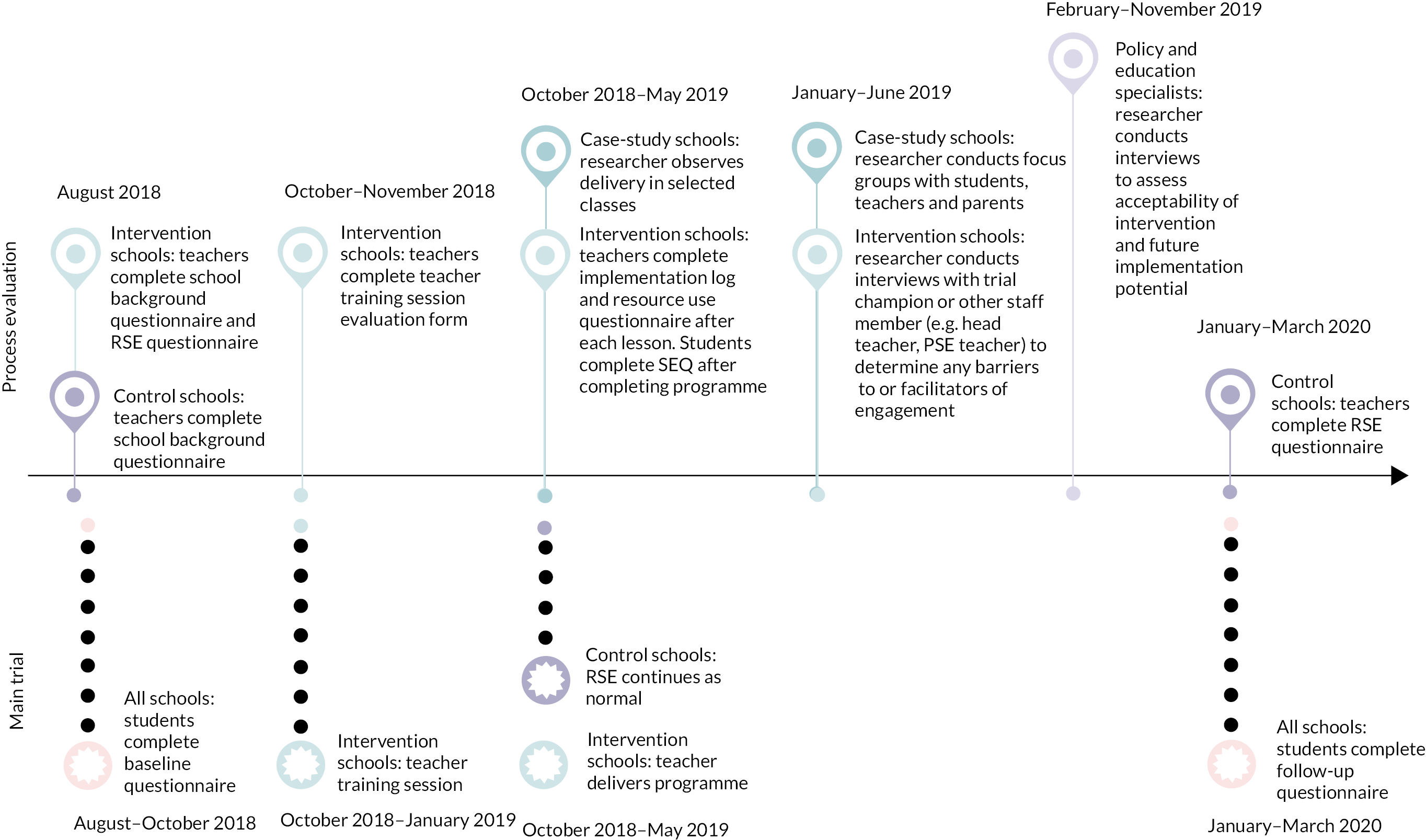
Participating pupils were in the study for approximately 18 months, and completed follow-up questionnaires between 12 and 14 months post intervention using procedures identical to those employed at baseline. The data collection timeline is shown in Figure 2.
FIGURE 2.
Data collection timeline. PSE, Personal and Social Education.
Outcomes and measures
The outcomes measured in this trial are based on the logic model (see Figure 1) and described in Table 3. A full copy of the baseline questionnaire is available in Report Supplementary Material 3.
| Component | Aim | Measurement |
|---|---|---|
| Knowledge | Increase knowledge about ways of avoiding unintended pregnancy; roles and responsibilities of young men in relation to unintended pregnancy; possible negative relational, social, emotional and financial consequences of unintended pregnancy; and sources of information and support for unintended pregnancy | Individual assessment. Selected items from the Mathtech Knowledge Inventory136,137 |
| Communication skills | Increase skills for communicating with parents and peers about avoiding unintended pregnancy | Comfort communicating about pregnancy scale (parents, peers and professionals). Selected items from the Mathtech Behaviour Inventory136,137 |
| Attitudes about unintended pregnancy | Increase anticipated regret about the consequences of unintended pregnancy on current life and future goals | Items from the intentions to avoid teenage unintended pregnancy scale developed and psychometrically tested in our feasibility trial44 |
| Social influences | Increase awareness of peer norms, stereotypical gender norms and parental attitudes and beliefs about teenage pregnancy Gender norms: increase perception that both men and women have roles and responsibilities in avoiding and dealing with the consequences of unintended pregnancy Peer norms: increase perception that most peers are not sexually active and use contraception when they are Parental values and beliefs: increase awareness of parental attitudes and beliefs about unintended pregnancy |
Male role gender norms: Male Role Attitudes Scale139 and knowledge items relating to responsibility for avoiding pregnancy Peer norms: knowledge items about sexual behaviour/contraceptive use among peers and sexual socialisation instrument (peer subscale)140 Parental values and beliefs: sexual socialisation instrument (parent subscale)140 |
| Beliefs about capabilities | Increase perceived behavioural control to avoid unintended pregnancy (say no to sex or obtain and use contraception correctly) and increase self-efficacy to communicate about avoiding unintended pregnancy with parents, peers and professionals | Sexual Self-efficacy Scale using an adapted version of the Sexual Self-efficacy Scale141,142 |
| Intentions | Increase strength of intention to avoid unintended pregnancy | Teenage unintended pregnancy scale44 |
| Sexual behaviour | Abstinence from sexual intercourse (delay initiation of sex or return to abstinence) or avoidance of unprotected sexual intercourse (consistent correct use of contraception) | Sexual behaviour items (ever had sexual intercourse, frequency of sexual intercourse, contraception use ever/at last intercourse). Items adapted from previous sexual health surveys143,144 |
| Pregnancy | Avoidance of unintended pregnancy | Ever pregnant |
Primary outcome
The primary outcome was self-reported avoidance of unprotected sex at last sexual encounter, defined as sexual abstinence or use of contraception (barrier or hormonal) at last sex, as measured by items on a paper-based questionnaire at baseline and again between 12 and 14 months later.
Analysis of the primary outcome, avoidance of unprotected sex, was undertaken with the whole study analysis population and included those not yet sexually active, alongside those who were. The unprotected sex category combined respondents who reported no contraception or unreliable contraception at last sex. Avoidance of unprotected sex combined all those who remained sexually abstinent and those who used reliable contraception at last sex.
Figure 3 shows how the primary outcome was determined. Three questions were used to determine if students were sexually active, The first question was ‘Have you ever had sex (penis-in-vagina)?’ If the answer was ‘no’, this was coded ‘0’ (no unprotected sex). If the answer was ‘yes’, the student was directed to the next question: ‘Last time you had sex did you use contraception?’. If the answer to this question was ‘no’, the response was coded 1. If the answer was ‘yes’, the student’s response to a third question was used as a check on use of reliable (barrier or hormonal) contraception. If participants answered ‘yes’ to the question ‘[l]ast time you had sex, did you or your partner use withdrawal (pulling out before ejaculating/cuming) or natural family planning/rhythm method (only having sex at certain times of the month)?’, their response was coded 1. If they answered, ‘no’, their response was coded ‘0’. A binary outcome was derived, with a score of 0 indicating not having had unprotected sex or never having had sex and a score of 1 indicating having unprotected sex.
Secondary outcomes
Secondary outcomes were 12- to 14-month impacts on knowledge, attitudes, skills and intentions to avoid teenage pregnancy, as well as sexual behaviours. Table 3 outlines the questionnaire components of the key secondary outcomes we were assessing, consistent with our logic model, provided in Chapter 1 (see also an early design paper). 41 Secondary outcomes were assessed using a number of standardised measures as follows. Knowledge was measured by items selected from the Mathtech Knowledge Inventory and Sexual Knowledge and Attitudes Test for Adolescents. 136–138 This measure included items relating to knowledge of safe contraceptive methods, how to access contraception and the age of sexual consent. Attitudes were measured by the male-role attitudes scale. 139 This scale was included to examine change in gender attitudes (masculinities) more generally in society and was not specifically related to teenage pregnancy. Higher scores indicate endorsement of traditional male-role stereotypes. Skills were measured through the Comfort Communicating Scale137 and the Sexual Self-efficacy Scale. 141 The Comfort Communicating Scale specifically looked at communication between peers, parents and health professionals around avoiding pregnancy. The Sexual Self-efficacy Scale measured one’s perceived ability to have protected consensual sex when ready. It included items relating to communicating consent, sexual preferences and sexual readiness. Intentions to avoid an unintended pregnancy were assessed using an ‘intentions to avoid a teenage pregnancy scale’, developed and psychometrically tested in the Phase II feasibility trial. 44 This measure was based on the concepts of sexual competence145 to include subscores on contraception (intentions to know about, discuss and use contraception effectively); willingness (intentions to have sex when both partners have communicated willingness and consent); readiness (intentions to weigh up when they are ready to begin a sexual relationship); norms (intentions to avoid peer pressure to have sex); and attitudes (intentions to be prepared and share responsibility for contraception with a partner). The items that make up each scale, as well as the internal validity of the scales used as part of the questionnaire, are described in Report Supplementary Material 3.
Secondary behavioural outcomes were assessed using the following questions:
-
Have you ever had sex without using any contraception?
-
The last time you had sex, was any form of contraception used?
Subgroup analyses
Informed by the intervention theory of change model and research design (see Figure 1), the effect of the intervention on the primary outcome for the following prespecified subgroups was examined: those reporting having had unprotected sex at baseline or not (as an especially high-risk group), nation (Wales, England, Scotland, NI), sex and socioeconomic status as measured by the Family Affluence Scale. 157 Finally, we also looked at subgroup variation by ethnic group.
Post hoc exploratory analyses
Three exploratory post hoc analyses were conducted after reviewing the primary outcome analyses. These were conducted to separately analyse the component questions used to identify the primary outcome of avoidance of unprotected sex: sexual abstinence (Have you ever had sex with another person?) and use of reliable contraception at last sex (Last time you had sex, did you use contraception? Last time you had sex, did you or your partner use withdrawal or natural family planning/rhythm method?). We also examined sex differences in use of reliable contraception.
Sample size
This trial was powered to detect a 50% reduction in the incidence of unprotected sex (from an expected rate of 2.8% to 1.4%) by 15 years of age. A difference of 1.3% in unprotected sex has been shown to have a meaningful impact on pregnancy rates. 24,146–148 The between-group difference in the incidence of unprotected sex of 1.3% [95% confidence interval (CI) 0.5% to 2.2%] by 9 months in our feasibility trial149 demonstrated that such an effect size is plausible and is consistent with effect sizes seen in the literature. 146 This study was designed to also take account of clustering. In the feasibility trial data, the intraclass correlation coefficient (ICC) was 0.01. 44 As pilot studies can provide imprecise estimates of ICCs,150 we re-estimated using ICCs from three sources: (1) the RIPPLE cluster RCT,148 (2) the WHO Health Behaviour in School-aged Children Survey (HBSC) GB18 and (3) the Young Persons’ Behaviour and Attitudes Survey 2011. 151 The data from the WHO and Northern Ireland Statistics and Research Agency (NISRA) studies were combined. Both the RIPPLE and combined WHO and NISRA studies found an ICC of 0.004. Based on (1) the ICC of 0.01 (95% CI 0.01 to 0.04), and assuming 120 students per year group in school, and (2) a 7% rate of attrition (based on the conservative attrition rate found in the feasibility study plus two additional schools), the sample size calculation showed that a trial involving 33 schools per group would provide 80% power at a 5% significance level. The alternative ICC of 0.004 was calculated to provide 93% power.
Statistical analysis
Statistical analysis (primary and secondary outcomes)
Primary analysis (at 12–14-months’ follow-up)
The primary effectiveness analysis was on an intention-to-treat basis, using a multilevel logistic regression model (two levels: pupils nested within schools) adjusting for the baseline outcome and stratification variables. 152
Subgroup analysis (at 12–14 months’ follow-up)
Multilevel logistic regression was used with interaction terms (treatment group by subgroup) for each of the above pre-specified subgroups. Owing to the low power and number of interactions being tested, the results of the subgroup analysis are reported using 99% CIs.
Missing data
Sensitivity analyses including imputed follow-up data based on the worst-performing school (in relation to detected incidence of unprotected sex) and best-performing school (where students did not have unprotected sex) at baseline were conducted for schools that did not collect follow-up data.
The scales captured as secondary outcomes for this trial generally had two types of missing data: (1) complete missing data (i.e. because the student was not present in school when the data were collected); and (2) partial missing data, where the student had completed some but not all items of the questionnaire. N is reported for each outcome to show the level of complete missing data for each outcome. The analysis population includes those for whom complete data at both baseline and follow-up were available. Partial missing data for the Male Role Attitudes Scale,139 Comfort Communicating136,137 and Intentions Scale44 was dealt with by averaging the responses of the questions answered, standardised on a scale of 0 to 1 then multiplying by 100 to derive a score for all students who completed some of the questionnaire.
Data linkage
This study did not undertake any data linkage with Health and Social Care or NHS records, given that data on conception rates are not available in NI and that data for sexual health-related services across the UK are not readily available as part of routinely collected data, owing to patient privacy requirements.
Process evaluation methods
Aims and research design
The overall aim of the process evaluation was to understand the implementation of the intervention as well as its acceptability and perceived effectiveness to pupils, teachers, parents and RSE stakeholders. The research design of the process evaluation was informed by realist approaches to the evaluation of interventions134,153 as well as Medical Research Council (MRC) guidance154 that process evaluations should consider the context, implementation and mechanisms of the impact of interventions. Multiple methods were utilised with a triangulated design.
Recruitment and sampling
Schools and participants included in the process evaluation were first recruited to the trial via the methods and ethical procedures outlined above. All study schools were included in the process evaluation. In addition, more in-depth study was conducted in eight case-study schools in the intervention group. These were selected as follows: at randomisation the NICTU Trial Statistician randomly selected two schools in the intervention group from each nation to be case-study schools and informed the schools.
Data collection
Table 4 outlines total data collection and the purpose of each item of data collection. Below are further details on each of these data collection items.
| Data source | Key focus area/purpose |
|---|---|
| All schools | |
| School background questionnaire | School structure, sociodemographic profiling, and experience of UTP |
| RSE questionnaire | Extant RSE provision |
| Fieldworker perception form | What worked well and what did not in relation to data collection; any other relevant observations |
| Intervention schools | |
| Parent/guardian online survey | The parent’s/guardian’s engagement with, and opinion of, animations and homework session; whether or not their child discussed programme with them |
| Parent/guardian data analytics | Website viewing statistics of the parental component for the implementation period obtained using Google Analytics (Google Inc., Mountain View, CA, USA) |
| Teacher implementation log | Recorded activities delivered in each lesson to assess each school’s fidelity to programme guidance |
| Semistructured trial champion/principal/head teacher interviews | Perceived barriers to and facilitators of successful implementation and engagement with different components of the intervention |
| Student engagement questionnaire | Programme delivery, parental participation, quality of teaching and perceptions of their engagement in the programme |
| Case-study schools (in addition to data collection outlined above in intervention schools) | |
| Lesson observations (lead fieldworker observation form) | Measuring teacher fidelity to implementation protocol and pupil engagement |
| Teacher focus groups | Perceived barriers to and facilitators of successful implementation and engagement with different components of the intervention |
| Pupil focus groups | Perceived barriers to and facilitators of successful implementation and engagement with different components of the intervention |
| Parent focus groups | Assess parental engagement and evaluation of the intervention |
| Education/policy specialists | |
| Education/policy specialist interviews | Current context of RSE policy and practices and perceptions of how these might influence programme uptake; acceptability of intervention and future implementation potential |
| Teacher trainers | |
| Audio-/video-recordings of teacher training | Check fidelity of teacher training in randomly selected intervention schools |
| Teacher trainer telephone interviews | Issues relating to delivery of training on school-by-school basis; perceptions of quality of training materials and how training was received by teachers |
Data collection, location and purpose
All study schools
Prior to intervention implementation, both intervention and control schools completed a school background questionnaire to gain an understanding of the broader school context (see Report Supplementary Material 3). Intervention and control schools also completed a questionnaire about their extant RSE provision (see Report Supplementary Material 3).
Intervention schools
Fidelity of delivery and evaluation. All intervention schools received a teacher training session. Teacher trainers were asked to audio-record a random sample of four sessions (six in NI). The research team used an online random number generator to select sessions and informed trainers. Teacher training satisfaction surveys (see Report Supplementary Material 3) and sealable envelopes were distributed to all teachers by the trainer at the end of sessions. Teachers were not asked to record their names on these surveys.
Teacher implementation logs were delivered to teachers during teacher training. These were designed to be filled out by each teacher at the end of each session or at the end of the programme (see Report Supplementary Material 3).
In intervention schools, researchers conducted audio-recorded interviews on an encrypted device with trial champion teachers or a teacher nominated by the trial champion teacher. Interviews were conducted during or at the end of the school day, by researchers from each nation, in school facilities or by telephone.
Student engagement questionnaires (SEQs) (see Report Supplementary Material 3) were distributed by teachers to all intervention school pupils after programme implementation, and returned to researchers.
A link and invitation to complete a short online survey was texted or e-mailed by schools to the primary parent/carer contact of all participating students (n ≈ 4097 potential parent participants). Information sheets and parent factsheets were available in English, Polish, Urdu, Punjabi, Arabic, Bengali and Mandarin. Parents who completed the survey were entered into a prize draw for £500. Trial champion teacher enquiries led to doubts that the link had been sent by some schools, but this remained difficult to confirm. Google Analytics (Google Inc., Mountain View, CA, USA) provided viewing statistics of the parental component of the website during the implementation period.
Intervention case-study schools
Focus group interviews were conducted by researchers with the school trial champion teacher and teachers who had delivered the programme, sometimes also including year heads or heads of pastoral care (see Report Supplementary Material 3).
Teachers who delivered the intervention invited pupils to volunteer to participate in focus group interviews, one per case-study school, through the use of an information and consent form (see Report Supplementary Material 3). Teachers were encouraged to include diversity in terms of sex, academic and behavioural records, and sociodemographic background (topic guide available in Report Supplementary Material 3).
Parents’ views were sought in semistructured interviews. Parents were recruited via school requests for volunteers from case-study schools and respondents to the online survey.
Researchers conducted classroom observations on between two and eight If I Were Jack lessons in each case-study school Researchers liaised with trial champion teachers to determine the school’s chosen programme delivery route to ensure observation of as many different programme exercises as possible by a variety of teachers.
External participants: teacher trainers and policy specialists
Teacher trainers
Researchers conducted short telephone interviews (see Report Supplementary Material 3) with one teacher trainer per nation.
Policy specialists
Policy specialists involved in the development of RSE policies or curricula in each of the four nations were identified by the research team and approached via e-mail or telephone call, providing an information and consent form (see Report Supplementary Material 3). Researchers conducted audio-recorded interviews largely by telephone (topic guide available in Report Supplementary Material 3).
Data analysis
All audio files were transferred securely to QUB and transcribed verbatim (interviews and focus groups) or typed up by researchers (observational field notes and other secondary source data). Data were organised using NVivo 12 (QSR International, Warrington, UK) software and analysed systematically and thematically based on the six steps proposed by Braun and Clarke155 to enable identification and analysis of patterns within the data by moving iteratively between theoretical understandings and the new data.
Methodological rigour was ensured by establishing credibility, transferability, dependability and confirmability using techniques suggested by Lincoln and Guba. 156 These inductively and deductively derived codes were first compiled as a code book and then applied to the data. These codes as applied to the data were discussed with the researchers from each of the four nations to check the validity of emerging themes and bring out some of the complexity in the data. All transcripts were independently coded by two members of the research team (10% coded by seven members). Meaningful quotations from participants were extracted to support and exemplify identified themes/subthemes. The data were analysed to form overarching themes emerging from each of the participant groups outlined above and also across these groups, but in all cases paying attention to deviant data. Open-ended questions from the SEQ and parent survey were transferred to NVivo 12 and thematically coded as per other qualitative data.
Implementation fidelity data were entered into Excel files in each site and transferred to QUB for summary descriptions. Data from the parents’ survey and SEQ were imported into Excel and SPSS 27.0 (Statistical Product and Service Solutions; SPSS Inc., Chicago, IL, USA) and tabulated as summary statistics. Descriptive data analysis was conducted to identify general patterns in the data.
FIGURE 3.
Flow diagram showing how the primary outcome was assessed. 0, Avoided unprotected sex; 1, unprotected sex.
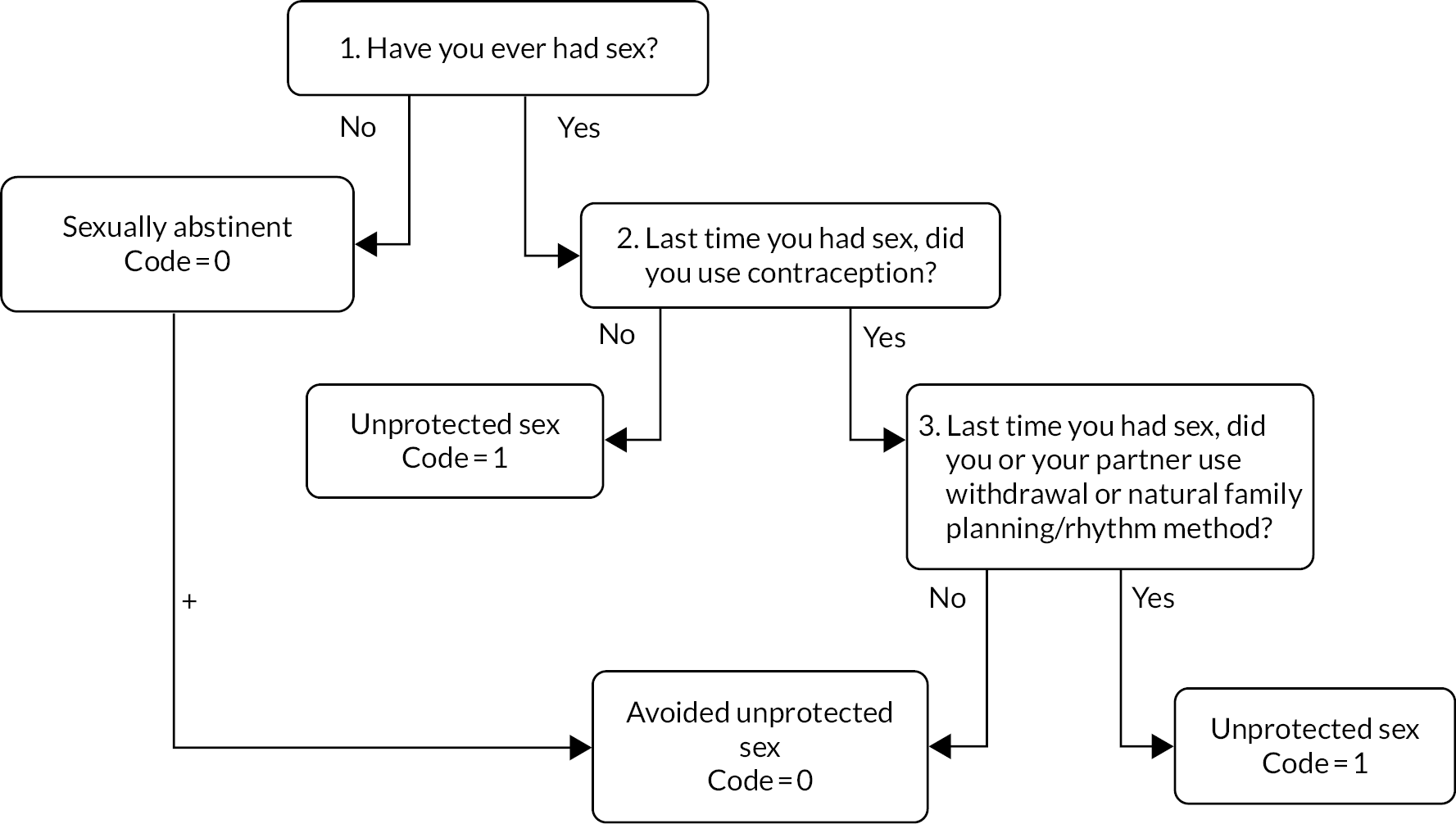
Deviations and rationale
The protocol for this evaluation was published in June 2018 and amended in August 2019. It is available at the NIHR Evaluation, Trials and Studies website (https://www.southampton.ac.uk/netscc/index.page; accessed 20 June 2022). The original aims and objectives of the evaluation have not altered, and the overall approach to the research design in relation to the cluster randomised trial, the process evaluation and the cost-effectiveness evaluation has also remained unchanged. A small number of minor deviations to the original protocol published in June 2018 have been made, and these are detailed below.
Minor changes to recruitment timing
The published protocol stated that the school recruitment period would run from February to June 2018. However, to recruit the full number of schools, this was extended slightly, and school recruitment took place over a 6-month period (February–June and to end-September 2018), with a break during the summer period (July and August).
Minor changes to intervention implementation
Our published protocol stated that:
As part of intervention implementation there will be a standardised 60 min training session for RSE teachers implementing the intervention. The training session will adhere to a predefined teacher-trainer protocol and will be delivered in schools by nation-specific established statutory and non-statutory RSE coordinators who normally provide RSE teacher training in schools.
Reproduced with permission from Lohan et al. 48 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/.
We encountered difficulties in using RSE co-ordinators who normally provide RSE in schools in Scotland and England. In Scotland, Education Scotland was unable to provide us with this teacher trainer resource. In England, the non-statutory facilitator did not complete training in two of the six schools in the intervention group. To address both these issues, the project team appointed external teacher trainers. These teacher trainers were trained in the same way as all other teacher trainers, as per protocol. The fidelity of the teacher training offered by the replacement teacher trainers was also assessed along with all other teacher trainers as part of trial methodology.
Minor changes to data collection
There was a change in timing in the collection of teacher implementation logs and teacher resource use questionnaires. We had planned to collect these data following implementation. However, teacher time and workload made it difficult to accommodate this. As a compromise, and to avoid the risk of retrieving no data, flexibility on timing of receipt was introduced and it was agreed that, at a minimum, a single implementation log/teacher resource use questionnaire would be completed on behalf of a given school.
In addition, it was not possible to arrange and collect focus group data from parents as specified in the original protocol. Parental engagement limited opportunities to conduct focus groups, and, therefore, individual face-to-face and telephone interviews were held in place of these.
Minor additions to data collection
In addition to the published aims, a SEQ was also added post protocol to the process evaluation in all intervention schools (see Report Supplementary Material 3). The SEQ was distributed by teachers to pupil participants in the intervention group in 32 schools (n = 3179 pupils) across the four nations of the UK on completion of the intervention. The SEQ included questions on pupil demographics and implementation factors (delivery length/mode, parental participation and teaching quality) and included a six-item SEQ (which showed good reliability and validity with a Cronbach’s alpha = 0.85). It also included three open-ended SEQ questions, which asked pupils for their opinions on the IVD as well as their most and least favourite programme activities, and their reasoning.
Minor additions to secondary outcomes
In the protocol, we include an examination of secondary behavioural outcomes, but these are not clearly specified. At the point of the statistical analysis plan, prior to study analysis, we specified the following secondary behavioural outcomes as relevant to trial analysis: (1) Have you ever had sex without using any contraception? (2) The last time you had sex, was any form of contraception used?
Minor changes to analysis plan/analysis principles
The published protocol48 stated that individual-level socioeconomic status was measured by the ‘highest qualification level of parents’. However, this was a drafting error. It was not intended to use this measure for two reasons. First, it was found to be unreliable in the feasibility trial owing to a large number of missing data. Second, it was predicted to be unreliable owing to the non-standardisation of educational terms for highest school qualification [e.g. Advanced Levels (A-Levels) and Scottish Highers]. This was replaced with the Family Affluence scale157 [number of family holidays during the past 12 months, family computer(s), ownership of a family car and ownership of a dishwasher]. The data were analysed in terms of three tertiles: low, medium and high. Other measures also included were pupils’ highest educational aspirations and age expected to leave school.
The first stage in mediation analysis required investigation of the effect of the intervention on each of the five measured mediators (i.e. knowledge, attitudes, sexual self-efficacy, intentions and behaviour). This was shown in the secondary outcomes analysis, in which the intervention was shown to have a significant effect on one or more mediator (i.e. intentions, knowledge and sexual self-efficacy and behaviour). The second stage of mediation analysis is only conducted if the intervention has been shown to affect both one or more of the mediators (first stage of mediation analysis) and the primary outcome. As the intervention did not prove effectiveness on the primary outcome (i.e. having had unprotected sex), the statistical analysis team deemed that it was not appropriate to explore whether or not mediators explain the effect of the intervention on the primary outcome.
Chapter 4 Results 1: recruitment and data collection results
Aims
The purpose of this chapter is to report the recruitment and data collection achieved in the cluster RCT and in the process evaluation. We also report attrition at a cluster and individual level, and the reasons for withdrawal.
School recruitment
A total of 803 schools were initially identified from educational authority records in each of the four nations as being eligible for participation based on inclusion criteria. These criteria included schools in defined geographic areas, as set out in the recruitment protocol (see Chapter 3). Independent, private schools, special schools, Irish-/Welsh-medium and Scottish Gaelic schools (but not those with an embedded Irish-/Welsh-medium component) and schools with < 30 pupils per year group (year 11 in NI, S3 in Scotland and year 10 in England and Wales) were excluded. Schools involved in previous studies involving the If I Were Jack intervention (n = 15) were also not eligible to participate in the current study. Eligible schools were stratified by socioeconomic status based on eligibility for FSM, resulting in two lists identifying schools above and below the nation-level median percentage of pupils eligible for FSM. These lists were then sent to NICTU and shuffled randomly before schools were approached (see Report Supplementary Material 3 for recruitment protocol). From these lists, 263 schools were contacted (172 in the above the median FSM stratum and 91 in the below the median stratum) and 66 were recruited, giving an overall recruitment rate of 25%. Rates of recruitment by nation were 29% NI, 11% England, 60% Scotland and 40% Wales. Reasons for recruitment and failure to recruit are discussed in the process evaluation results (see Chapter 7).
Pupil recruitment
All pupils from the target year group in recruited schools were eligible to participate in the trial. The 66 schools recruited to the trial had a total of 10,500 eligible pupils, of whom 8216 (78.2%) consented to participate in the trial.
Flow of participants in the trial
Consolidated Standards of Reporting Trials diagram
In total, 66 schools (n = 8216 pupils) were recruited to the JACK trial, with 33 (n = 4100 pupils) allocated to the intervention group and 33 (n = 4116 pupils) allocated to the usual RSE practice control group. The Consolidated Standards of Reporting Trials (CONSORT) flow diagram is shown in Figure 4, summarising school eligibility, number approached, recruitment and randomisation, and retention through the trial, along with median cluster size. Figure 4 additionally reports the number of schools that declined to participate prior to randomisation and withdrew following randomisation (n = 1) or were lost to follow-up (n = 3). It also reports the number of pupils who opted out of participation within schools and those lost to follow-up. Losses to follow-up at the school and pupil level are discussed further below.
FIGURE 4.
The CONSORT extension for cluster trials 2012 flow diagram (nation breakdown included). a, Sites were allocated to intervention or control post baseline data collection. E, England; S, Scotland; W, Wales.

Losses to follow-up
School-level attrition from trial
Retention at school level was generally strong. However, four recruited schools (n = 533, pupils; 6.5% of pupils enrolled in the trial) that completed baseline surveys were lost to follow-up (three in the intervention group and one in the control group):
-
The first school withdrew prior to implementation [intervention group, England, 134 pupils (1.6%), all girls, in above median FSM stratum (34% of pupils in receipt of FSM) and non-faith based]. Withdrawal reasons were teachers’ reluctance to engage with teacher training and additional commitments associated with being ‘a case-study school’ involving observations and interviews.
-
The second school withdrew after implementation of intervention but before follow-up surveys were conducted [control group, Wales, 139 pupils (1.7%), co-educational, in above median FSM stratum (28.6% pupils in receipt of FSM), non-faith based]. Withdrawal reasons cited were ‘other commitments with year 11 at this time’.
-
The final two schools withdrew owing to the COVID-19 pandemic lockdown measures. The UK lockdown (from March 2020) led to school closures, making it impossible to visit and collect survey data from two schools. Both schools were in the intervention group and had implemented the programme. One school was in NI [164 pupils (2.0%), co-educational, in above median FSM stratum (20% of pupils in receipt of FSM), faith based] and the other school was in Scotland [96 pupils (1.2%), co-educational, in the below median FSM stratum (6% of pupils in receipt of FSM), non-faith based].
Pupil-level attrition from trial
A total of 441 pupils (4.2% of eligible pupils) were opted out of participation in the research by parents before baseline data collection. A total of 8216 pupils (n = 4100, intervention group; n = 4116, control group) completed baseline assessments, and 6561 (n = 3201, intervention group; n = 3360, control group) completed follow-up assessments. Therefore, 1655 pupils (20.1% of pupils enrolled in the trial) were lost to follow-up at this stage. The primary reason accounting for the 20.1% loss to follow-up from baseline to follow-up was pupil absence or pupils having left the school (n = 1088; 65.7% of losses to follow-up). Other reasons for loss to follow-up were school withdrawal (n = 273; 16.5%), school closures due to the COVID-19 pandemic (n = 260; 15.7%) and pupil opt-out (n = 34; 2.1%).
Risk of bias
Losses to follow-up
Losses to follow-up were assessed to determine any potential risk of bias. Specifically, we queried whether loss to follow-up was higher in schools in some locations or depending on eligibility for FSM and whether or not the school was faith based. We also assessed whether or not there were differences in losses to follow-up between the two trial groups.
The rate of loss to follow-up was lowest in Wales (15.8%) and similar across the other three nations (approximately 22%). There was very little difference in loss to follow-up in relation to the proportion of pupils eligible for FSM in schools (below the nation-level median, 20.3%; above, 20.1%), and loss to follow-up for faith-based and non-faith-based schools was almost identical (approximately 37%). There was only a small difference in relation to parent opt-out (at the point of recruitment) for faith-based (13.2%) and non-faith-based schools (10.7%). Differences in losses to follow-up for the intervention (n = 899; 21.9%) and control groups (n = 756; 18.4%) were also small.
Baseline comparability
Participant characteristics
A summary of demographic characteristics and descriptive statistics of the randomised groups is presented in Table 5. The two groups were very similar in terms of sex, sexual identity, ethnicity, socioeconomic status and educational aspirations. The number of pupils who reported having no religion or who identified as not at all religious was slightly higher in the intervention group and the number of pupils who identified as Catholic was higher in the control group.
| Characteristic | Intervention group (N = 4100) | Control group (N = 4116) | Total (N = 8216) |
|---|---|---|---|
| Sex, n (%) | |||
| Male | 1980 (48.3) | 2121 (51.5) | 4101 (49.9) |
| Female | 2120 (51.7) | 1994 (48.5) | 4114 (50.1) |
| Age in years, mean (SD) | 14.5 (0.4) | 14.5 (0.4) | 14.5 (0.4) |
| Ever had sex with another person, n (%) | |||
| Yes | 234 (5.9) | 251 (6.3) | 485 (6.1) |
| No | 3767 (94.2) | 3743 (93.7) | 7510 (93.9) |
| Sexual identity, n (%) 8124 | |||
| Heterosexual/straight | 3652 (90.1) | 3722 (91.5) | 7374 (90.8) |
| Gay/homosexual/bisexual | 219 (5.4) | 175 (4.3) | 394 (4.8) |
| Not sure/prefer not to say/other | 183 (4.5) | 173 (4.2) | 356 (4.4) |
| Ethnicity, n (%) | |||
| White | 3114 (76.5) | 3079 (75.5) | 6193 (76.0) |
| Asian, Asian British/Irish | 475 (11.7) | 326 (8.0) | 801 (9.8) |
| Black African, black Caribbean, black British/Irish | 255 (6.3) | 369 (9.0) | 624 (7.7) |
| Mixed/multiple ethnic backgrounds | 155 (3.8) | 180 (4.4) | 335 (4.1) |
| Other | 71 (1.7) | 126 (3.1) | 197 (2.4) |
| Religion, n (%) | |||
| No religion | 1643 (41.0) | 1327 (33.0) | 2970 (37.0) |
| Catholic | 743 (18.5) | 1074 (26.7) | 1817 (22.6) |
| Protestant | 997 (24.9) | 1089 (27.1) | 2086 (26.0) |
| Buddhist | 11 (0.3) | 20 (0.5) | 31 (0.4) |
| Jewish | 13 (0.3) | 6 (0.2) | 19 (0.2) |
| Muslim | 417 (10.4) | 362 (9.0) | 779 (9.7) |
| Sikh | 25 (0.6) | 32 (0.8) | 57 (0.7) |
| Other | 162 (4.0) | 108 (2.7) | 270 (3.4) |
| Religiosity, n (%) | |||
| Very religious | 260 (6.4) | 324 (8.0) | 584 (7.2) |
| Fairly religious | 1053 (25.9) | 1175 (28.8) | 2228 (27.3) |
| Not very religious | 1043 (25.6) | 1140 (28.0) | 2183 (26.8) |
| Not at all religious | 1717 (42.2) | 1439 (35.3) | 3156 (38.7) |
| Socioeconomic status | |||
| Cluster level, n (%) | |||
| Schools above FSM median | 20 (60.6) | 19 (57.6) | 39 (59.1) |
| Schools below FSM median | 13 (39.4) | 14 (42.4) | 27 (40.9) |
| Individual level 8164 | |||
| Family affluence scale, mean (SD) | 6.1 (1.9) | 6.1 (1.9) | |
| Low tertile, n (%) | 1495 (36.7) | 1445 (35.3) | 2940 (36.0) |
| Medium tertile, n (%) | 1617 (39.7) | 1656 (40.5) | 3273 (40.1) |
| High tertile, n (%) | 963 (23.6) | 988 (24.2) | 1951 (23.9) |
| Educational aspirations, n (%) | |||
| Expected age leaving school (years) | |||
| 16 | 756 (18.5) | 702 (17.2) | 1458 (17.9) |
| 18 | 2372 (58.2) | 2474 (60.5) | 4846 (59.3) |
| I don’t know yet | 949 (23.3) | 914 (22.4) | 1863 (22.8) |
| Aspiration on leaving school | |||
| Getting or trying to get a job | 811 (20.4) | 829 (20.7) | 1640 (20.5) |
| Be in a job training scheme or apprenticeship | 330 (8.3) | 383 (9.6) | 713 (8.9) |
| Be at university | 1893 (47.6) | 2022 (50.5) | 3915 (49.0) |
| Be at a further education college (studying for a trade/job) | 784 (19.7) | 623 (15.6) | 1407 (17.6) |
| Be a full-time mum or a dad | 15 (0.4) | 11 (0.3) | 26 (0.3) |
| Other | 147 (3.7) | 139 (3.5) | 286 (3.6) |
School characteristics
The 66 schools recruited to join the trial had diverse contextual characteristics, an overview of which is presented in Table 6. Schools that later withdrew are identified in the table. In summary, of the 66 schools recruited to the trial, 59 were co-educational schools and seven were single-sex schools (four all-girls and three all-boys). Six of the single-sex schools were retained in the trial; one of the all-girls schools was lost owing to pandemic measures. Fifteen of the 66 schools were faith based, 13 of which were Catholic denomination. Two faith-based schools (one Protestant, one Catholic) were lost to follow-up. Of the 66 schools, 39 were in the above-median FSM stratum and 27 were in the below-median FSM stratum. The range in the number of pupils eligible for FSM in schools was as low as 2% in the lowest school and 52% in the highest school.
| Region | Schools per trial allocation (n) | Single-sex/mixed-sex schools (n) | Faith-based schools (n) | Range of percentage of pupils eligible for FSM (%) |
|---|---|---|---|---|
| NI | Intervention: 11 | Co-ed: 8 All-boys: 1 All-girls: 2 |
6 (6 Catholic) | 7–52 |
| Control: 12 | Co-ed: 11 All-boys: 1 |
5 (5 Catholic) | 7–44 | |
| England | Intervention: 6 | Co-ed: 4 All-boys: 1 All-girls: 1 |
0 | 2–38 |
| Control: 7 | Co-ed: 7 | 2 (1 Catholic; 1 Protestant) | 3–26 | |
| Scotland | Intervention: 6 | Co-ed: 6 | 0 | 7–28 |
| Control: 7 | Co-ed: 7 | 0 | 5–32 | |
| Wales | Intervention: 7 | Co-ed: 7 | 0 | 9–44 |
| Control: 6 | Co-ed: 6 | 1 (1 Protestant) | 8–32 | |
| Intervention total | Intervention: 30 | Co-ed: 25 All-boys: 2 All-girls: 3 |
6 (6 Catholic) | 2–52 |
| Control total | Control: 32 | Co-ed: 31 All-boys: 1 |
8 (6 Catholic; 2 Protestant) | 3–44 |
Process evaluation
In this section, we report the data collection achieved in the process evaluation and outline the removal of process evaluation data collected from schools that withdrew from the trial.
Data collection achieved
Published aims of the process evaluation are detailed in Chapter 6, with targets for triangulated data collection, including questionnaires, interviews and focus group interviews, detailed in Table 7.
| Who completed | Data source | Data collecteda,b | Intended totala | Reason for missing data |
|---|---|---|---|---|
| All schools | School background questionnaire | 58 schools | 62 schools | Schools unable to return before closure due to COVID-19 |
| RSE questionnaire (baseline) | 55 schools | 62 schools | Schools unable to return before closure due to COVID-19 | |
| Intervention schools | Parent/guardian online survey | 134 | N/A | N/A |
| Teacher implementation log | 29 intervention schools | 30 intervention schools | One school (S12S) was unable to return these prior to closure because of COVID-19 | |
| Trial champion/principal/head teacher interviews | 30 intervention schools | 30 intervention schools | N/A | |
| CS schools | Observations | 8 CS schools | 8 CS schools | N/A |
| Teacher focus groups | 8 CS schools | 8 CS schools | N/A | |
| Pupil focus groups | 8 CS schools | 8 CS schools | N/A | |
| Parent focus groups | 6 (5 interviews in CS schools plus interviews in 1 non-CS school) | 8 CS schools | Recruitment of parents for focus groups was challenging and not possible in all CS schools despite repeated efforts from trial team. Alternative interviews were conducted in non-CS school with strong relationship with parents | |
| Fieldworkers | Fieldworker perception form | Baseline: 66 schools Follow-up: 60 schools |
Baseline: 66 schools Follow-up: 62 schools |
In 2 schools (S20S and S15NI) fieldworkers did not return perception forms at follow-up |
| Education/policy specialists | Education/policy specialist interviews | 11 | 4–8 | N/A |
In addition to the published aims, a SEQ was also added post protocol in all intervention schools (see Supplementary Material 3). See Chapter 3 for a discussion of changes to protocol. Pupils completed a total of 3179 SEQs (Table 8). One school (S12S) was unable to return these prior to closure because of COVID-19.
| Participant type | Data source | Study group | Participants (n) |
|---|---|---|---|
| Schools | All school data | Intervention | 30 |
| All school data | Control | 32 | |
| Parents | Online survey | Intervention | 134 (2 male) |
| Individual semistructured interviews | Intervention case study (and some additional interviews in schools with strong relationships with parents) | 10 (1 male) | |
| Web analytics (unique visits to parent resources section of website) | Intervention | 1123 | |
| Students | SEQ | Intervention | 3179 (47% male) |
| Focus groups (case-study schools) | Intervention case study | 8 groups (n = 58) | |
| Teachers | Focus groups (case-study schools) | Intervention-case study | 8 groups (n = 31) |
| Semistructured interviews with trial champions/principals/head teachers | Intervention | Individual interviews: 29 (n = 29) Paired interviews: 5 (n = 10) Total teacher participants: (n = 39) |
|
| Teacher implementation log | Intervention | 128 | |
| RSE questionnaire | Intervention | 29 | |
| RSE questionnaire | Control | 26 | |
| School background questionnaire | Intervention | 29 | |
| School background questionnaire | Control | 30 | |
| Observations: students/teachers | Classroom observations (case-study schools) | Intervention case study | 35 observations in 8 schools |
| RSE policy experts | Semistructured interviews | N/A | 11 |
Trial and process evaluation missing data owing to Covid-19 measures
Data collection of certain process evaluation data sources was also affected by school closures resulting from COVID-19 and as such led to further missing data (Table 9).
| Data source | Number schools unable to return data because of COVID-19 |
|---|---|
| Trial follow-up survey | 2 (2 intervention schools) |
| School background questionnaire | 4 (2 intervention schools, 2 control schools) |
| RSE questionnaire | 7 (1 intervention school, 6 control schools) |
| Teacher implementation log | 1 intervention school |
| SEQ | 1 intervention school |
Chapter 5 Results 2: trial results
Baseline data
The values for the primary outcome and secondary outcomes at baseline are summarised in Table 10. There were no notable differences between the intervention and control groups in relation to the primary or secondary outcomes at baseline. There were also no differences between the two groups in relation to missing data at baseline.
| Outcomes | Intervention group (N = 4100) | Control group (N = 4116) | ||
|---|---|---|---|---|
| Primary | ||||
| Avoidance of unprotected sex, n (%) | 3836 (96.14) | 3808 (95.49) | ||
| Secondary outcomes | n | Mean (SD) | n | Mean (SD) |
| Knowledge | ||||
| Knowledge score | 4100 | 4.13 (1.92) | 4116 | 4.19 (1.90) |
| Attitudes | ||||
| Male-Roles Attitudes score | 3871 | 17.78 (4.19) | 3879 | 18.13 (4.22) |
| Skills | ||||
| Comfort Communicating | 3958 | 7.78 (1.85) | 3944 | 7.93 (1.83) |
| Sexual Self-efficacy score | 3958 | 3.17 (0.47) | 3945 | 3.19 (0.47) |
| Intentions to avoid a teenage pregnancy | ||||
| Intentions total score | 3974 | 49.01 (9.11) | 3981 | 49.42 (8.65) |
| Intentions contraception subscale score | 3935 | 19.82 (4.09) | 3946 | 20.05 (3.96) |
| Intentions willingness subscale score | 3957 | 12.93 (2.13) | 3972 | 12.96 (2.10) |
| Intentions time subscale score | 3912 | 4.20 (0.81) | 3939 | 4.20 (0.82) |
| Intentions readiness subscale score | 3914 | 8.69 (1.64) | 3934 | 8.76 (1.60) |
| Intentions norms subscale score | 3921 | 21.25 (3.80) | 3946 | 21.33 (3.73) |
| Intentions attitudes subscale score | 3904 | 11.72 (2.45) | 3936 | 11.79 (2.45) |
| Secondary outcomes: behavioural, n (%) a | ||||
| Ever had sex without using any contraception | 101 (45.09) | 108 (43.72) | ||
| Last time had sex, no form of contraception used | 69 (34.67) | 75 (35.55) | ||
Primary outcome
The primary and secondary outcomes are summarised in Table 11.
| Outcomes | N | Intervention group, n (%) | N | Control group, n (%) | aOR (95% CI)a | p-value | ICC |
|---|---|---|---|---|---|---|---|
| Primary | n (%) | n (%) | |||||
| Avoidance of unprotected sex | 3057 | 2648 (86.6) | 3203 | 2768 (86.4) | 0.85 (0.58 to 1.26) | 0.42 | 0.118 |
| Secondary | Mean change from baseline (SD) | Mean change from baseline (SD) | Adjusted mean difference (95% CI) a | ||||
| Knowledge score | 3198 | 1.09 (1.92) | 3358 | 0.87 (1.90) | 0.18 (0.024 to 0.34) | 0.02 | 0.030 |
| Male-Roles Attitudes score | 2999 | –0.35 (4.16) | 3146 | –0.26 (4.07) | –0.33 (–0.64 to –0.02) | 0.04 | 0.019 |
| Comfort Communicating score | 3053 | 0.50 (1.92) | 3186 | 0.37 (1.98) | 0.003 (–0.11 to 0.12) | 0.95 | 0.009 |
| Sexual Self-efficacy score | 3063 | 0.13 (0.45) | 3202 | 0.09 (0.48) | 0.021 (–0.003 to 0.05) | 0.08 | 0.004 |
| Intentions to avoid a teenage pregnancy | |||||||
| Total score | 3075 | 2.49 (8.80) | 3228 | 1.72 (8.75) | 0.61 (0.16 to 1.07) | 0.01 | 0.008 |
| Contraception subscale score | 3043 | 1.48 (4.20) | 3190 | 1.01 (4.11) | 0.34 (0.15 to 0.54) | < 0.001 | 0.005 |
| Willingness subscale score | 3061 | 0.36 (2.15) | 3215 | 0.33 (2.23) | 0.015 (–0.11 to 0.14) | 0.81 | 0.008 |
| Time subscale score | 3021 | 0.036 (0.95) | 3184 | 0.055 (0.97) | –0.025 (–0.075 to 0.026) | 0.34 | 0.006 |
| Readiness subscale score | 3023 | 0.24 (1.75) | 3180 | 0.14 (1.72) | 0.050 (–0.041 to 0.14) | 0.28 | 0.008 |
| Norms subscale score | 3034 | 0.79 (3.97) | 3193 | 0.54 (3.96) | 0.24 (0.012 to 0.47) | 0.039 | 0.010 |
| Attitudes subscale score | 3020 | 0.61 (2.69) | 3179 | 0.27 (2.66) | 0.31 (0.18 to 0.44) | < 0.001 | 0.004 |
| Secondary: behavioural | n (%) | n (%) | aOR (95% CI)a | ||||
| Ever had sex without using any contraception | 686 | 292 (42.57) | 324 (44.38) | 0.66 (0.40 to 1.09) | 0.10 | 0.008 | |
| Last time had sex, no form of contraception used | 174 (27.53) | 218 (32.88) | 0.55 (0.31 to 0.97) | 0.04 | 0.000 | ||
The number of young people in intervention schools who avoided unprotected sex (sexual abstinence or use of reliable contraception at last sex) was 2648 (86.6%), compared with 2768 (86.4%) in control schools [adjusted OR (aOR) 0.85, 95% CI 0.58 to 1.26; p = 0.42]. An exploratory post hoc analysis showed no effect on self-reported sexual abstinence at 12–14 months [2407 (78.30%) in the intervention group and 2511 (78.25%) in the control group; aOR 0.85, 95% CI 0.58 to 1.24; p = 0.39]. However, the exploratory post hoc analysis also showed that students in the intervention group were more likely than those in the control group to report using reliable contraception at last sex [42/106 (39.62%) in the intervention group vs. 29/110 (26.36%) in the control group; aOR 0.52, 95% CI 0.29 to 0.92; p = 0.025).
Secondary outcomes
Students in intervention schools were more knowledgeable about safe methods of contraception and avoiding unintended pregnancy [mean difference (MD) 0.18, 95% CI 0.024 to 0.34; p = 0.02], had improved attitudes towards progressive male gender roles (MD –0.33, 95% CI –0.64 to –0.02; p = 0.04) and had stronger intentions to avoid an unintended pregnancy (MD 0.61, 95% CI 0.16 to 1.07; p = 0.01) than students in control schools. There was no statistically significant difference in sexual self-efficacy or comfort communicating about avoiding unintended pregnancy.
Intentions to avoid unintended pregnancy included subscores on contraception, willingness, timeliness, readiness, norms and attitudes. Although the results indicate no effect of the intervention on the intentions subscales of willingness (MD 0.015, 95% CI –0.11 to 0.14; p = 0.81), timeliness (MD –0.025, 95% CI –0.075 to 0.026; p = 0.34) or readiness (MD 0.050, 95% CI –0.041 to 0.14; p = 0.28), students in the intervention schools had stronger intentions to use effective contraception (contraception subscale: MD 0.34, 95% CI 0.15 to 0.54; p < 0.001), to avoid peer pressure to have a sexual relationship (norms subscale: MD 0.24, 95% CI 0.012 to 0.47; p = 0.039) and not to have sex until ready and be prepared and to share responsibility for contraception with a partner (attitudes subscale: MD 0.31 95% CI 0.18 to 0.44; p < 0.001).
There were no differences between the intervention and control groups at the 12- to 14-month follow-up in relation to the number of students who reported ever having sex without contraception (intervention 42.57% vs. control 44.38%; OR 0.66, 95% CI 0.40 to 1.09; p = 0.10. However, at follow-up, students in the control group were more likely than those in the intervention group to report no use of contraception at last sex (intervention group 27.53% vs. control group 32.88%; OR 0.55, 95% CI 0.31 to 0.97; p = 0.04).
Subgroup analysis
The results of the subgroup analyses are summarised in Table 12. An exploratory post hoc subgroup analysis was conducted to look specifically at the effect of the intervention for those who were sexually active at baseline (average age 14 years). Among those sexually active at baseline, the proportion of students who had had unprotected sex by the 12- to 14-month follow-up was lower in intervention schools than in the control schools (49.38% vs. 60.92%; p for interaction = 0.06). The CIs in the adjusted analysis indicate benefit for nearly all who were sexually active at baseline (OR 0.56, 99% CI 0.29 to 1.09). Narrowing this down to look at the subgroup who had had unprotected sex by baseline, the results also favour the intervention but are not statistically significant (OR 0.64, 99% CI 0.28 to 1.46; p = 0.27).
| N | Intervention, n (%) | N | Control, n (%) | Adjusted OR (99% CI) | Interaction p-valuea | |
|---|---|---|---|---|---|---|
| Sexually active at baselineb | ||||||
| Yes | 154 | 80 (49.38) | 171 | 106 (60.92) | 0.56 (0.29 to 1.09) | 0.06 |
| No | 2903 | 330 (11.4) | 3032 | 332 (11.0) | 0.89 (0.53 to 1.51) | |
| Having had unprotected sex at baseline | ||||||
| Yes | 107 | 65 (60.75) | 124 | 82 (66.13) | 0.64 (0.28 to 1.46) | 0.27 |
| No | 2950 | 344 (11.66) | 3079 | 353 (11.46) | 0.87 (0.52 to 1.47) | |
| Nationc | ||||||
| NI | 689 | 113 (15.94) | 976 | 174 (17.40) | 0.78 (0.41 to 1.51) | 0.05 |
| Scotland | 626 | 96 (14.95) | 527 | 108 (19.67) | 0.76 (0.45 to 1.28) | |
| England | 734 | 28 (3.74) | 942 | 87 (9.01) | 0.46 (0.18 to 1.13) | |
| Wales | 1008 | 188 (18.22) | 758 | 94 (12.13) | 1.68 (0.72 to 3.91) | |
| Family affluence scale | ||||||
| Low tertile | 1113 | 143 (12.6) | 1081 | 140 (12.6) | 0.83 (0.46 to 1.47) | 0.60 |
| Medium tertile | 1193 | 149 (12.1) | 1298 | 181 (13.6) | 0.80 (0.46 to 1.41) | |
| High tertile | 742 | 132 (17.4) | 813 | 140 (16.8) | 0.97 (0.52 to 1.81) | |
| Sexc | ||||||
| Male | 1475 | 219 (14.38) | 1658 | 250 (14.65) | 0.84 (0.49 to 1.42) | 0.81 |
| Female | 1582 | 206 (12.80) | 1545 | 213 (13.46) | 0.87 (0.49 to 1.56) | |
| Ethnicity | ||||||
| Whitee | 2351 | 394 (16.34) | 2370 | 408 (16.78) | 0.86 (0.58 to 1.27) | 0.16 |
| Asian | 369 | 8 (2.13) | 279 | 5 (1.78) | 1.43 (0.31 to 6.55) | |
| Black | 169 | 12 (6.82) | 302 | 16 (5.16) | 1.69 (0.55 to 5.21) | |
| Otherf | 149 | 8 (5.33) | 238 | 30 (12.10) | 0.43 (0.11 to 1.65) | |
Other subgroup analyses focused on sociodemographic characteristics and their effect on the primary outcome results. In relation to nation, there was evidence that the intervention decreased the rates of unprotected sex in NI, Scotland and England. The p-value for the test for interaction (0.05) indicates evidence of a difference in the effectiveness of the intervention between nations. The CIs in the adjusted analysis indicate benefit for nearly all participants in England (OR 0.46, 99% CI 0.18 to 1.13). In Wales, the direction of the effect of the intervention differed from that of the other nations but the CIs were especially wide and indicate no significant difference between the intervention and control groups in Wales (OR 1.68, 99% CI 0.72 to 3.91).
There were no differential effects of the intervention on the primary outcome according to participant socioeconomic status, as measured by the Family Affluence Scale (p = 0.60), participant sex (p = 0.81) or participant ethnicity (p = 0.16).
Sensitivity analyses and missing data
Standardised scores were calculated for the Male Role Attitudes Scale, Comfort Communicating Scale, and Intentions (including subscales) to deal with partial missing data arising because students responded to some but not all questions (see Chapter 4). The results of the secondary analyses (based on the standardised scores) for these scales suggest that the intervention was effective in increasing adolescents’ intentions to say no to sex until ready (MD 1.26, 95% CI 0.026 to 2.49; p = 0.045), which was not observed in the main analysis reported above. The results for the other scales were similar to those reported in the main analysis.
Follow-up data were not available for four schools (three intervention and one control; see Chapter 4). The sensitivity analyses made different assumptions on the best- and worst-case scenarios. The best-case scenario assumed that none of the students in the intervention schools had unprotected sex but that 13% of students in control schools did. The worst-case scenario assumed that none of the students in the control school had unprotected sex but that 13% of students in the intervention schools did. The rate of 13% was based on the school with highest rate of unprotected sex at baseline.
The results of the sensitivity analysis are presented in Table 13. In the best-case scenario, at the 12- to 14-month follow-up, fewer students in the intervention school than in control schools reported unprotected sex (12.05% vs. 14.53%, OR 0.59, 95% CI 0.34 to 1.03; p = 0.06). In the adjusted worst-case scenario, a slightly higher number of students in the intervention schools had unprotected sex than those in control schools (14.92% vs. 13.49%, OR 1.39, 95% CI 0.71 to 2.71; p = 0.34).
| Primary outcome | Intervention, n (%) | Control, n (%) | Adjusted OR (95% CI);a p-value | ICC |
|---|---|---|---|---|
| Best case | ||||
| Yes | 425 (12.05) | 481 (14.53) | 0.59 (0.34 to 1.03); 0.06 | 0.21 |
| No | 3103 (88.0) | 2829 (85.5) | ||
| Worst case | 0.31 | |||
| Yes | 475 (14.92) | 463 (13.49) | 1.39 (0.71 to 2.71); 0.34 | |
| No | 2709 (85.08) | 2968 (86.51) | ||
Serious adverse events
This was a low-risk study; therefore, no data monitoring was required. No adverse events were observed or reported.
Chapter 6 Results: process evaluation
Aims
The published aims48 of the process evaluation were informed by realist approaches to the evaluation of interventions134,153 as well as by MRC guidance154 for process evaluations to consider the context, implementation and mechanisms of the impact of interventions. Our aims were as follows:
-
Context
-
Examine reasons for school participation and non-participation to inform the risk of bias in the trial as well as the long-term sustainability of the implementation of the intervention.
-
-
Implementation
-
Examine intervention delivery and fidelity in the context of overall RSE provision in intervention schools.
-
Assess RSE provision in control schools and potential contamination caused by any changes to provision that could be due to participation in the trial.
-
-
Mechanisms of impact
-
Explore self-reported perceptions of effectiveness and moderating influences in intervention schools among a sample of students, teachers and school principals/head teachers and parents.
-
Below, we address each of these aims, in turn detailing the data sources used to address each section, namely context, implementation and mechanisms of impact.
Context
Reasons for participation
As described in Chapter 3, a total of 258 eligible secondary schools across the UK were randomly selected and approached to participate in the study. Of the schools retained in the trial (62/66), the majority (n = 56) provided for students in co-educational settings. The all-boys schools were situated in NI (n = 2) and England (n = 1) and the all-girls schools in NI (n = 2) and England (n = 1). The majority of the 14 faith-based schools were situated in NI (n = 11). Scotland reported no faith-based schools in their sample and England and Wales had two and one, respectively. All these schools were Christian denominations. The widely utilised student socioeconomic indicator of percentage of students in a school entitled to FSM was applied in this study. The percentage of children eligible for FSM in the included schools ranged from as low as 2% to as high as 52%. The median was 22.29%.
A summary of reasons for participation and non-participation is provided in Table 14. Data sources for this section were:
-
researchers’ notes of telephone calls or written correspondence with schools
-
interviews (n = 29 individual interviews and n = 5 paired interviews) with school trial champions and school principals/head teachers (total, n = 39 participants)
-
school background questionnaires (n = 59) with school trial champions and school principals/head teachers
-
interviews with policy and education specialists (n = 11).
| Main reasons given for participation | Main reasons given for not participating |
|---|---|
| Quality novel resource Need to address RSE/holistic education Gap in male focus Teacher training Financial incentive |
Research saturation or other commitments RSE provision already in place Too busy to commit to surveys and/or this RSE programme delivery Non-alignment with school ethos |
Table 15 explains what the identifiers used alongside illustrative quotes in this chapter mean.
| Participant type (participant type code) | Example participant number (participant number code) | Example school number, nation (school ID code) | Example ID code |
|---|---|---|---|
| School (S) | N/A | 15, England (15E) | S15E |
| Teacher (T) | 1 (01) | 11, NI (11NI) | T0111NI |
| Parent (P) | 1 (01) | 12, Wales (12W) | P0112W |
| Student (PU) | 1 (01) | 12, Scotland (12S) | PU0112S |
| Student – SEQ | 1 (01) | 11, England (11E) | SEQ0111E |
| Policy specialist (PS) | 1 (01) | No school number, NI (NI) | PS01NI |
| Researcher observation (RO) | N/A | 23, England (23E) | RO23E |
Quality, novel resource, supportive of teacher skill development
Head teachers and trial champions across all nations and school contexts identified the lack of resources as the principal barrier to the quality provision of RSE. Universally, school staff talked about cuts to their budgets, which meant that they were less able to afford to bring in external experts to teach this subject. As a result, teachers often felt that they were left to their own devices to ‘cobble something together’ (T0119E) in terms of developing their own RSE provision:
[Teachers] create their own resources by taking bits from everywhere e.g. YouTube [YouTube, LLC, San Bruno, CA, USA] videos etc. They find they need to tailor resources to their students’ needs and to strike the right tone. A lot of the downloadable resources and lesson plans from the internet or organisations are poor quality.
T0122W
The If I Were Jack resource was reported as addressing teachers’ needs to have a current, relevant and high-quality programme to support teacher skill development:
With the level that our boys are at, you need to be giving them something that isn’t just sort of pulled together off the internet or someone’s sat there and gone, ‘Oh, could you just put something together for this?’ . . . To have something [If I Were Jack] that was so structured and had really, really clear, obvious outcomes, and actually had sort of different levels to it where you could push the levels of discussion, I think was really important because you could easily, with this subject, just cover the bare minimum and actually not really get them thinking a lot.
T0119E
Schools welcomed a place on the JACK trial because they viewed the programme as a novel and tested resource that would provide students with valuable information about sexual health:
We like to try the sort of new cutting-edge ways of delivering different parts of our curriculum. It fits in really well.
T0123W
If I Were Jack was received as a high-quality, ‘off-the-shelf’ (T0115E) resource, making it particularly attractive to teachers because of the inclusion of full lesson plans, classroom activities and comprehensive, step-by-step instructions for delivery:
The lessons were provided, the focus was there, the learning intentions were there.
T0117NI
Seeing something that was ready made that we could use was great . . . yeah, brilliant!
T0116W
Other motivators to take part reported by teachers included their overall impressions of the resource’s ‘novel use of interactive video drama’ (T0113NI) and the programme’s flexible delivery options, meaning that it would fit with their timetables:
. . . a nice enough short programme that doesn’t totally disrupt your teaching of your curriculum.
T0113NI
It looked like a no-brainer, as far as we were concerned . . . It’s a great resource, it really is, and we are always looking for good resources.
T0119E
Recognising the need to address relationships and sexuality education in school/holistic education
There were three layers to the acceptance by schools of the need and desire to address/improve RSE provision. First was a growing push by educational authorities to address RSE, exemplified by changes in legislation to mandatory RSE provision in schools in England in 202037 and, concurrently, schools’ own recognition of this need. Second, but equally important, was a desire by schools to meet the more holistic pastoral support needs of students within education, especially among socially deprived communities. Third, some schools recognised the specific need to address prevention of teenage pregnancy and closely related sexual health and well-being matters.
The changing RSE legislative landscape was highlighted particularly in schools in England:
Well, it’s because it’s statutory, isn’t it, as of this September? So, I know that that was something that was important, the fact that we’re going to have to be doing it.
T0119E
However, the pressure from educational authorities to improve was evident across the UK:
One of our targets this year was to renovate our [RSE] resources, and that’s one of the areas, the kind of teenage pregnancy and parenthood thing, that we felt we weren’t hitting the right note with it, so we thought it was a perfect time to try something new.
T0111S
School staff also earnestly conveyed to researchers that addressing RSE was important to them because a holistic approach to education was their overarching educational goal:
We are fairly, yeah, bohemian for a grammar school . . . some of the other grammar schools, certainly in this area, push, we regard push their kids too far to get better grades and to the detriment of their all-round health. Whereas, we certainly don’t do that.
T0119E
The importance of a holistic approach to education was especially emphasised in schools in areas of high social deprivation, where holistic education was regarded as essential to supporting students’ broader social and emotional needs. Concerns over poor student mental health and well-being were expressed, including the need for formal support in schools for students in the context of deprived local communities affected by unemployment, crime and high rates of substance use, alcoholism and domestic violence:
It’s a really, really, really high area for social deprivation, and we’re surrounded by, you know, quite difficult housing estates. . . . So, parents are facing a lot of financial challenges. We’ve got parents with all kinds of mental health issues and drug issues and alcohol issues, and our kids come in from a background of that, some of them.
T0115NI
Addressing RSE was seen as an essential part of this holistic approach to education
I think, because educating them in lots of different ways. We do lots around, em, consent, healthy relationships, what healthy sexual relationships look like, em, about coercive control in relationships. So, I think this was just another part of that, for us, em. And then it comes back to our positive relationship . . . So, that is the reason that we wanted to be involved in it, from a, ‘this is how it can change your future’.
T0122W
This need for a holistic approach incorporating CSE was also recognised by several Catholic schools recruited to the trial in NI especially:
We are a Catholic grammar school and we’re very aware of the Catholic Church’s teachings with regard to sexuality and sexual relationships. Yet, at the same time, we’re very aware . . . we have a duty of care to our young people and that is our priority . . . our approach to reflect how society is changing, and we’re very willing to do that, you know . . . under the umbrella of the Catholic ethos of strong morals and values.
T0127NI
Furthermore, for some schools, albeit not as many, the issue of adolescent pregnancy was thought to be especially relevant, and schools again emphasised that providing education on safe sex was part of their role in educating young people:
We had about five girls, all within the same year group, at various stages, had become pregnant . . . and we just felt that maybe we needed to revisit, eh, around the areas of safe sex . . . So, it came at a good time for us, whenever we heard about this pilot programme.
T0120NI
Addressing the gap in male focus
Teachers in several schools commented that they were drawn to participation in the trial by the gender element of the resource. Several teachers and school principals noted that boys’ roles and responsibilities were being neglected, especially in relation to teenage pregnancy, and the resource was regarded as filling a gap in provision in RSE:
Even the title, ‘Jack’, and the emphasis on the boy, and not just the girl, in the pregnancy, was really, em, good, and that was new because I think any of the programmes I’ve looked at in the past, it was generally looking from the focus of the female in the relationship, on how her life was changing, whereas I think we got a very good balance here, and I think that brought it really well up to date.
T0124NI
Teachers understood and liked that the programme was also challenging harmful masculinities that have an impact on boys and girls:
It’s looking at it from a boy’s point of view . . . Lots of our children, the boys have got quite a dominant . . . em, I’m going to say controlling sort of opinion, you know, that they’ve been brought up in an environment where the man has been in control, you know, and it’s hard to break that mould because, and the women . . . some of the girls, in some relationships we deal with, they’re quite happy with that, you know, and you have to say, ‘Well, that is not [a healthy relationship]’.
T0119W
Teachers in both co-educational and single-sex schools felt that the resource would strike a positive note in terms of focusing on young men’s viewpoints:
We thought it was important. We really liked the idea that the focus of the project is from a boy’s perspective, and . . . certainly, from teaching in an all-boys’ school, that was a real big draw for me, getting involved in the project.
T0112NI
Overall, the resource’s gender focus was viewed as especially novel and a common reason offered by teachers for joining the trial. Students’ perspectives on this are discussed further below.
Teacher training and support
The offer of teacher training in the resource was a further hook to becoming involved. The demand for teacher training arose from the perceived lack of teacher training in RSE, a near universally expressed view in interviews with teachers and policy specialists:
I didn’t feel terribly comfortable beforehand teaching it [RSE]. This is not my subject area.
T0129NI
Hence the opportunity to have teacher training as part of the JACK trial was regarded as useful not only for this resource but also as a way to help some schools develop or model further RSE teacher training:
I think, with [RSE], becoming statutory, sort of following that sort of framework [in the JACK trial] with training the staff beforehand, understanding what they need to do and what could be expected. It’s definitely a framework that we would use so we can implement it across the other relationship and sex education stuff for the other things that we’ll be teaching in future.
T0112E
Financial incentive
Teachers were asked during interviews if the £1000 incentive offered to schools for taking part in the study influenced their decision to join. The majority stressed that they would have joined the trial without it owing to their positive appraisal of If I Were Jack as a high-quality and much needed resource:
No, the money never came into it. For us, it was what can we do to best equip our children to make the right choices in what they’re doing, and . . . going back to contraception, STIs, em, positive, healthy relationships, and try and get them to understand that, if they are going to enter into a relationship like that, then contraception is the responsibility of both people, not just one.
T0122W
It’s £1000. Just a nice bonus. If it wasn’t there, we still would have done it because . . . It’s about the topic and what the students would get out of it and, ultimately, what we would get out of it with being given quality resources.
T0117NI
However, a minority did acknowledge it was a motivating factor, particularly against a backdrop of increasing challenges related to managing a school budget:
You will take any extra funding you can get.
T0123W
The financial incentive worked in terms of trial champion teachers recruiting senior management to come on board to join the trial:
[The money] didn’t impact me . . . because I wanted to do it and I liked the whole look of it. But . . . it was a good thing to get then senior management to jump on-board with it. That was a good . . . flag to wave and say, ‘look’. So, that was a good thing just to make sure that the whole school jumped on board, yeah.
T0134NI
Equally, internally in schools it worked for school management to bring teachers on board with them, both as a means of acknowledging their workload and as an opportunity to finance additional support for their departments:
I possibly would [have joined without the money], but it definitely was something that was [useful] because I was able to offer those teachers – you know, if I hadn’t had it . . . I might have panicked about giving those teachers extra work, and, definitely, they might be more likely to turn round and say, ‘No . . . I just can’t do it’, and I would have listened to them, you know.
T0115NI
It certainly gives us the option of buying in a whole load of other resources . . . that’s massive for us.
T0111S
Overall, although teachers in several schools reported that they would have joined the study without the offer of the incentive, many commented that it was a welcome bonus, particularly in terms of alleviating tight budgets. It was also cited by teachers as a powerful, domino-style recruitment aid for persuading colleagues or senior management to join.
Reasons for non-participation
Of the 258 schools approached with information and offers to participate in the trial, 192 were not recruited. The majority of these schools (n = 119) did not respond to any communication attempts from researchers. The rest of the schools (n = 73) declined to take part. The main reasons in the order of importance for refusal to participate, drawn from researchers’ notes on correspondence with schools, were as follows:
-
research saturation or other commitments
-
RSE provision already in place
-
too busy to commit to surveys and/or programme delivery
-
non-alignment with school religious ethos (in some faith-based schools only).
As these were brief notes from telephone conversations, we do not have extensive data to offer on these reasons.
Implementation fidelity
This section reports on intervention implementation fidelity to cover all aspects of implementation as follows:
-
Implementation of teacher training – assessed through a random selection of audio-recordings of the teacher training.
-
Implementation in the classroom – in terms of both the structure of the programme and content – assessed through 35 observations in classrooms in eight case-study schools; 128 teacher implementation logs; 29 individual interviews; five paired interviews (n = 10 participants); eight focus group interviews (n = 31 participants) with teachers; and eight focus group interviews with students (n = 58) in case-study schools.
-
Implementation of the parental component – assessed through an online survey with parents (n = 134 returned) and a SEQ (n = 3179).
Fidelity of implementation of teacher training delivery
In all intervention schools, teacher trainers delivered training to teachers prior to programme implementation (n = 14 teacher trainers: one in Scotland, two in NI, two in England and nine in Wales). Training in Wales was delivered by the Healthy Schools co-ordinators (Public Health Wales staff). All teacher trainers were trained in a face-to-face, 2-hour session with the JACK trial team prior to delivering teacher training. This included the provision of the teacher classroom activity manual.
Fidelity to the teacher training protocol was assessed in 50% of the schools across the four sites through 16 audio-recordings (including one video-recording) made by trainers. As described in Chapter 4, a fidelity checklist was used to assess the fidelity of teacher training. Each session was scored out of a possible maximum of 49 points and structured under nine sections to cover all aspects of the programme. Percentage scores were graded as < 50% = low, 50–70% = medium, and > 70% = high, as detailed in Table 16.
| Site | Number of trainers | Number of schools audio assessed | Average fidelity percentage | Fidelity grading |
|---|---|---|---|---|
| NI | 2 | 6 (including one video) | 100 | High |
| England | 2 | 4 | 61 | Medium |
| Scotland | 1 | 4 | 99 | High |
| Wales | 9 | 2 | 71 | High |
| Total UK | 14 | 16 | 83 | High |
Trainers in NI (100%), Scotland (99%) and Wales (71%) demonstrated ‘high’ fidelity. Only England demonstrated ‘medium’ fidelity (61%). Here, the contracted teacher trainer had delivered training in four out of six schools before researchers identified issues with low fidelity (average 26%). As teachers had already begun delivering the intervention in these schools, we did not deem it possible to offer further teacher training in these schools. A replacement trainer completed training in two remaining schools, with consequent audio-recordings assessed as ‘high’, increasing the overall grading to ‘medium’.
Some teachers who received ‘low’-fidelity training reported that certain activities were not covered, and that they felt unprepared when they encountered exercises seen as more challenging to deliver. These teachers still described the training as ‘good’, but felt that it had focused on factors such as accessing materials ‘rather than . . . the real content that you need them to understand and this is how to deliver it and this is how to talk about it’ (T0123E). Conversely, teachers trained by the replacement trainer suggested that they had had a more positive experience, and were aware of the importance of fidelity:
It was a forum to ask questions as well, and by making you go through it page by page, bit by bit by bit, it did make you really read it properly.
T0215E
Teacher perceptions of the training were generally positive. For some, the comprehensiveness of the training was a considerable advantage that meant that, ‘[w]e all left very clear as to what we had to do’ (T0320NI). For others, clarity over the research and the programme’s origin and objectives appeared to strengthen engagement:
It was good to put a face behind training because sometimes whenever you go to training, or, sure, whenever you get a programme, you know, you don’t know who has made the programme or what the purpose of the programme was. Well, at least we, you know, could say that this was research.
T0125NI
In summary, fidelity of teacher training, although it varied by nation, was generally high, with a minority of schools receiving training that did not adhere closely to the protocol.
Fidelity of implementation in the classroom
Approximately 168 teachers delivered the resource in the 30 intervention schools that completed the trial across the UK (Table 17).
| Nation | |||||
|---|---|---|---|---|---|
| NI | England | Scotland | Wales | Total UK | |
| Number of teachers | 36 | 46 | 31 | 55 | 168 |
Delivery-time models
The intervention was programmed to include four delivery-time models (see options A-D, Table 18) to reflect the different ways classes are organised and the different ways in which RSE is typically structured across the four nations of the UK.
| Intervention schools (n = 30) | Option A (50- to 60-minute lessons × 4) (n) | Option B (35- to 45-minute lessons × 6) (n) | Option C (2 half-days) (n) | Option D (1 full day) (n) | Combination |
|---|---|---|---|---|---|
| NI (n = 11) | 4 | 2 | 0 | 0 | 5 |
| England (n = 6) | 3 | 2 | 1 | 0 | 0 |
| Scotland (n = 6) | 2 | 2 | 0 | 0 | 2 |
| Wales (n = 7) | 5 | 0 | 0 | 2 | 0 |
| Total (N = 32) | 14 | 6 | 1 | 2 | 7 |
Most popular was option A. Almost half of the schools delivered over four lessons of 50–60 minutes. Six schools chose option B (six lessons of 35–45 minutes). All Scottish schools had 50-minute lesson periods, and those choosing option B reported providing six (and sometimes more) 50-minute lessons. Combinations of options (seven schools) could vary between classes in the same school, and were generally due to unforeseen difficulties rather than design. Six schools reported disjointed implementation and delayed completion. Most delays were a few weeks. However, one teacher in a school in Wales reported taking 5 months to complete the intervention owing to a series of mitigating events in the school. Reasons given for delays in all nations included inspections, conflicting curriculum priorities, staff illness or bereavement and temporary closure.
Delivery of classroom intervention activities
Teachers reported delivering an average of 83% of intervention activities across all sites (Table 19). Teachers in NI reported the highest delivery rate (88%), followed by Wales (85%), England (80%) and Scotland (78%). Most activities were delivered at least 80% of the time. The IVD had the highest delivery rate (99%) and the parent survey the lowest (38%) (see Table 19). Wallet cards, which signposted students to sources of information and support, had the next poorest delivery rate (75%).
| Resource activity | Nation (%) | Total UKa (%) | |||
|---|---|---|---|---|---|
| NI | England | Scotland | Wales | ||
| 1: intro (not asked for in TIL) | – | – | – | – | – |
| 2: ground rules | 93 | 88 | 91 | 100 | 94 |
| 3: IVD | 98 | 100 | 100 | 100 | 99 |
| 4: pause, fast-forward, rewind | 98 | 88 | 88 | 89 | 91 |
| 5: what about Emma? | 95 | 88 | 72 | 92 | 87 |
| 6: if I had to look after a baby | 88 | 94 | 75 | 94 | 87 |
| 7: fact or fiction? | 88 | 88 | 75 | 89 | 85 |
| 8: Jack wallet card | 84 | 65 | 53 | 86 | 75 |
| 9: Jack forum dilemmas | 86 | 82 | 72 | 92 | 83 |
| 10: online scavenger hunt | 84 | 59 | 91 | 94 | 85 |
| 11: homework parent survey | 40 | 53 | 34 | 33 | 38 |
| 12: staying safe scenarios | 98 | 76 | 94 | 92 | 92 |
| 13: controversial statements | 95 | 82 | 84 | 89 | 89 |
| 14: my plan | 95 | 71 | 91 | 50 | 78 |
| Total activities delivered | 88 | 80 | 78 | 85 | 83 |
Overall, data shown in Tables 19 and 20 suggest that, while certain activities were not delivered to high fidelity, overall fidelity of delivery of classroom materials was high. However, it must be emphasised that fidelity of implementation in the classroom is based on teacher self-report (in interviews and implementation logs). In addition, not all teachers who delivered all or part of the programme returned an implementation log. We know that at least one teacher attended teacher training and was meant to deliver the programme but chose not to do so and did not return an implementation log. Information from the trial champion at this school allowed this to be taken into account and added to fidelity figures. However, it is possible that teachers in other schools similarly chose not to deliver part of or all of the programme to their classes, and that their disengagement, for whatever reason, with the programme and/or the research may have also led to them not returning an implementation log. Consequently, the teacher implementation logs should be understood to represent a picture of teachers who may have been most engaged with the programme and research.
| School ID | Classes for which a TIL was returneda (n) | Maximum total activities (classes delivering × 13 activities) (n) | Activities completed (n) | % activities completed | Fidelity rating (high/medium/low) |
|---|---|---|---|---|---|
| S12NI | 5 | 65 | 42 | 65 | Medium |
| S13NI | 5 | 65 | 58 | 89 | High |
| S15NI | 2 | 26 | 25 | 96 | High |
| S17NI | 4 | 52 | 50 | 96 | High |
| S20NI | 3 | 39 | 34 | 87 | High |
| S24NI | 7 | 91 | 81 | 89 | High |
| S25NI | 2 | 26 | 26 | 100 | High |
| S27NI | 5 | 65 | 64 | 98 | High |
| S29NI | 4 | 52 | 45 | 87 | High |
| S32NI | 1 | 13 | 10 | 77 | High |
| S34NI | 5 | 65 | 56 | 86 | High |
| S11S | 5 | 65 | 62 | 95 | High |
| S12Sb | |||||
| S18S | 10 | 130 | 87 | 67 | Medium |
| S19S | 4 | 52 | 43 | 83 | High |
| S21S | 7 | 91 | 79 | 87 | High |
| S24S | 6 | 78 | 55 | 71 | Medium |
| S12W | 8 | 104 | 91 | 88 | High |
| S14W | 3 | 39 | 32 | 82 | High |
| S16W | 5 | 65 | 51 | 78 | High |
| S17W | 8 | 104 | 83 | 80 | High |
| S19W | 6 | 78 | 71 | 91 | High |
| S22W | 2 | 26 | 21 | 81 | High |
| S23W | 4 | 52 | 47 | 90 | High |
| S11E | 3 | 39 | 29 | 74 | Medium |
| S12E | 7 | 91 | 79 | 87 | High |
| S15E | 4 | 52 | 48 | 92 | High |
| S19E | 1 | 13 | 3 | 23 | Low |
| S20E | 1 | 13 | 11 | 85 | High |
| S23E | 1 | 13 | 6 | 46 | Low |
Reasons for deviations from intervention delivery fidelity
The primary reasons reported by teachers for deviations in intervention delivery fidelity were insufficient time, perceived clash with school ethos and inadequate computer facilities. Implementation fidelity was also more generally affected by teacher creativity: teachers changing/adapting materials to the perceived needs of students. Each of these points will be briefly elaborated, with data, below.
Although many teachers reported that the classroom activity manual was useful for timing activities, many also reported that delivering all activities within time frames was challenging. Time spent ‘settling students’ (T0216W), dealing with behavioural issues and delivering lessons to students of mixed abilities could mean rushing activities to cover material within time slots, and some activities would ‘overlap’ (T0312S) into succeeding lessons.
One teacher explained her decision to deviate from prescribed timings to suit the needs of her students:
I couldn’t have followed [the protocol] bit by bit. There was just no chance . . . We had open discussions, and then, once they started talking . . . they couldn’t stop. So I deviated a wee bit . . . to suit their special needs, to include them all.
T0329NI
The issue of special education needs (SEN) students struggling to understand material was commonly reported to be a main reason for classes ending before all activities could be completed, as time was spent on more simplified explanations of the tasks and materials to classes of students with mixed abilities. Having classroom assistants present was reported by teachers as greatly assisting delivery. In two schools, teachers delivering to classes with students with significant additional learning needs reported adding extra lessons as several students needed more time to digest content and key messages. However, most who reported partial completion were unable to provide more classes and subsequently left activities unfinished or left them out altogether.
A perceived clash of the programme with the school ethos also had an impact on implementation in schools that had volunteered for the trial. In one faith-based (Protestant) school, the teacher did not deliver the programme to his class within that school. The trial champion cited non-alignment of messages with this teacher’s moral values as the main factor. More commonly, a perceived clash with school ethos affected the delivery of a single component, namely the wallet cards with signposting to local/national external sexual and reproductive health services. In response to PPI involvement and especially the voice of schools during the optimisation phase, two versions of the wallet cards were available: one which gave a wide variety of voluntary and statutory services, and one which was restricted to statutory services, such as NHS Choices.
Despite this choice, one trial champion in a faith-based school indicated that apprehension around parental reaction had prompted his decision not to issue wallet cards of either description, stating that school staff felt unable to endorse all website content:
Can we stand by everything that was on all the websites? And the answer was we couldn’t be sure that everything on there was something we could say, and so it was to keep parents happier, to avoid issues with that down the line.
T0129NI
In another school, four out of seven teachers who delivered the programme reported distributing wallet cards, whereas the remaining three in the same school did not, stating that this was owing to material not fitting with the school ethos, highlighting that there were at times disjointed approaches to RSE within individual schools.
Finally, the issue of deficits in school’s computing suites also affected delivery, especially the online scavenger hunt. In one school, a researcher observing the online scavenger hunt lesson commented on how a combination of poor behaviour, an unprepared teacher and disruption due to computer issues impacted on the delivery of the lesson:
The classroom was so loud and chaotic, I looked around and couldn’t see a single student doing any work. The teacher was half-yelling/half-begging the students to log in and those who did couldn’t progress because they didn’t know what to do and other students had no initiative or were totally unwilling to listen.
RO23E
Teachers reported adding in additional content, motivated by teachers’ intentions to improve absorption of key messages for students. Mostly teachers reported making changes to make the material more attuned for SEN students. For example, one teacher reported a small change to the open-ended closing scene of the IVD (designed to encourage students to think through how it could end) to reassure a student with SEN:
Especially with the autistic children, they need to have an ending . . . For one of mine in particular, that was a very big struggle for him. He needed that closure. So, in the end, I just whispered an ending.
T0429NI
Others reported delivering paper-based activities verbally or in smaller chunks for mixed-ability classes to increase absorption of knowledge and key messages:
For children with special educational needs, they [worksheets] were very bulky at times . . . Too much on a page and you lost them and they couldn’t follow where you were. So, we didn’t use the worksheets as much as we could have because they just couldn’t do it. They preferred to [do it] verbally, which is very typical of a lot of our special needs.
T0329NI
A small number of teachers reported adding websites not on the recommended list, feeling that these provided additional sources of information and support that students could avail of, particularly from relevant local services. Students in one school, where STIs among students were a concern for staff, reported being shown images of STI-infected genitals. However, this was not part of the intervention programme nor recorded in this school’s teacher implementation logs (TILs).
Researcher observations also attested to widespread use of teacher independence and creativity in using the intervention. Some of these were reported as enhancing discussion in the classroom; for example, in relation to popular activity 6, ‘If I had to look after a baby’, some teachers spoke of their own experiences, such as the added stresses of twins or a colicky baby, or shared versus single parenthood, to emphasise messages and enhance relationships with students. However, some of this teacher independence was also noted as having a negative effect on students’ ability to consider and discuss. For example, one teacher insisted that a consensus should be formed among the students when discussing issues:
The teacher insisted that pupils working in groups should all come up with the same answer and she did not want different ones. In this respect discussion was not encouraged and personal opinion not validated.
RO29NI
In two observations, researchers observed teachers walking around the classroom and reading students’ responses over their shoulders and/or collecting and commenting on these.
Summary
Overall, in relation to classroom implementation fidelity, data drawn from teacher self-reports (interviews and implementation logs) suggest relatively high fidelity to protocol. However, classroom observations in 8 of the 30 schools suggests that fidelity was lower. Hence, we acknowledge the strengths and limitations of capturing implementation of fidelity through these methods and our overall understanding of this. Reasons for deviation in delivering classroom components were insufficient time, perceived clash with school ethos and inadequate computer facilities. Implementation fidelity was also more generally affected by teacher creativity. Implementation fidelity regarding distributing wallet cards might be improved by greater emphasis on this in teacher training and the school’s permission that these could be distributed. Implementation improvement in relation to the online scavenger hunt might be gained by asking students to use their digital devices rather than school computers, while emphasising the critical guidance on sites in advance.
Fidelity of implementation of parental component
The parental component of the intervention was composed of two parts:
-
A URL link texted/e-mailed by the school to parents bringing them to a website with online animated films and material for parents/guardians on the topic, information for parents to tell them the intervention was happening in schools and opportunities for parents to participate with their child in the intervention.
-
A homework activity brought home by the student to do with a parent/guardian/trusted adult. This activity was designed from the outset as an optional activity in response to feedback from schools in our prior research. 44
Overall, implementation of both these components was low.
Implementation fidelity for digital parental materials
The total potential number of parents/guardians that could have been reached was circa 4097. Website analytics indicated 1123 unique visits to ‘parent resources’ web pages during implementation, signifying that around 27% of parents visited these on one or occasion more. Analytics showed that, when visiting the website, 380 (9%) viewed the shorter animated film, 288 (7%) the longer animation and 658 (16%) the interactive film excerpt.
As noted in Chapter 4, an online survey to obtain feedback on the parental component was texted or e-mailed by schools to a primary parent/carer contact of participating students (n = ≈ 4097), and 3% of these were returned (n = 134, 2 male). One reason for the low response rate may be the failure of some schools to send out the text (50% of intervention schools were able to confirm they sent the text). Survey findings (Table 21) indicated that, of 134 respondents, 50% had watched the short animated ‘hook’ feature, 45% the longer animated instructional feature and 42% the interactive film excerpt. Although 4% of respondents said that they did not watch the films because they were not interested, most said they did not know about them (68%), forgot (14%), or did not have time (11%).
| Survey item | Yes (n) | No (n) | Not sure (n) |
|---|---|---|---|
| Parent watched shorter animated film for parents | 50% (67) | 50% (67) | – |
| Parent watched longer animated film for parents | 45% (60) | 55% (74) | – |
| Parent watched If I Were Jack interactive film excerpt | 42% (56) | 58% (78) | – |
| Parent completed homework exercise with their child | 34% (46) | 55% (73) | 11% (15) |
Implementation fidelity for the parent–student homework communication exercise
The above online digital materials were intended to prepare parents for an optional parent–student communication exercise assigned by teachers. This involved students completing a ‘survey’ worksheet by asking a parent/carer or trusted adult to watch or read the script of the interactive film excerpt and then answer three questions about what they would think and do if they were Jack or Emma’s parent/carer. Teachers were instructed to assign the homework exercise to students, informing them that, although they recommended that they complete the exercise, it was not compulsory.
Across the four sites, an implementation rate of 38% was reported in TILs for the homework exercise, ranging from 33% in Wales to 53% in England. A similar proportion of parent survey respondents (34%) said that they had completed the exercise with their child (see Table 21). However, the SEQ responses (n = 3179) revealed that only 13% of students (n = 403) said they had completed the task with their parents. Student-reported implementation varied by nation: 17% in NI, 11% in England and Wales, and 10% in Scotland. Differences in completion rates by sex of student were evident, with an independent t-test showing significantly more females reporting completion than males [t(2955) = 2.5; p = 0.011].
Explanations for low implementation of parental component
Explanations for the low implementation of this component were sought out in interviews with teachers, parents, students and RSE experts. Teachers indicated that non-completion of the exercise was mostly due to student refusal and/or reluctance at school or teacher level. Some schools and teachers decided to omit the activity from the outset to avoid parent controversy, whereas some said they did not set it because of student discomfort.
We’re facing . . . the sort of post-Birmingham backlash. So, a number of our Muslim parents are writing me letters and are wanting their children withdrawn from RSE.
T0115E
I think the majority of parents aren’t comfortable talking about these things, you know, with their kids, and when you speak to the kids, they say there is no way they would discuss this with their parents.
T0111S
Parents also reported reluctance to engage in the homework activity because of the awkwardness of speaking to their children about sex, including fears about appropriateness, religious and cultural barriers, and their own lack of knowledge:
A girl I know, she’s Christian, and I said my daughter was doing the [JACK] trial and she nearly didn’t speak to me for a week! . . . She doesn’t think it is appropriate that a 15-year-old should know all about those different things.
P0129NI
And a lot of the time, the parents have had bad experiences of education, so the kids are actually more educated than the parents and [kids] don’t feel comfortable in talking about it because they feel that they’ve got to explain things to their parents.
T0314W
One RSE expert noted the difficulties engaging parents in general, particularly when parents have not been encouraged to begin having conversations regarding relationships and sexuality with their children during the early years:
Trying to involve parents in these kinds of subjects and activities . . . I’ve found it difficult, on a number of levels. My opinion would be to get in early.
PS02W
As for students, the vast majority said that it felt uncomfortable or ‘awkward’ to raise these issues with parents, suggesting that it was better to allow these conversations to occur naturally:
Like if I get homework, I do it obviously, but then, ‘Go home and talk to your parents about it’, and I was just a bit, yeah, ‘I’m not doing that’. I can’t go up to my mum and just mention it at the dinner table!
Female, PU0112S
In interviews, parents shared some suggestions for improving fidelity, such as compulsory homework exercises and more regular school contact with parents about RSE:
A wee overview, you know, just like through e-mail, because then you can say, ‘Oh, you had this today – tell me about that.’
P0434NI
Relationships and sexuality education policy experts and teachers also noted that if RSE teacher training and support for teachers could be improved, the resulting rise in confidence would have a knock-on effect in terms of engaging parents:
[Teachers might think] ‘I don’t feel comfortable with dealing with it, I haven’t had the training’ . . . They don’t want to open a can of worms, they’re afraid . . . they won’t get the backing from their own management. Or . . . parents might complain.
PS03NI
Summary
In summary, fidelity for the parental components of the programme was lower than for other programme elements and reported completion levels varied across participant types. Parents, students, teachers and RSE experts reported multiple obstacles to parental component fidelity. However, a level of parental engagement with parental components is clear, and it is likely that targeted materials increased engagement.
Relationships and sexuality education provision in control schools
As outlined in Chapter 1, heterogeneity in RSE provision across UK schools is high. This section addresses the question of what the RSE provision in control schools was and a summary of changes to provision as a result of agreement to take part in the JACK trial. Data for this section are drawn from RSE control school questionnaires (completed by 26/32 control schools). In addition, we add a brief comparative analysis of RSE provision in control and intervention schools (the latter prior to intervention of If I Were Jack) based on identical RSE provision and identical analyses.
Assessment of provision in control schools
Relationships and sexuality education control school questionnaires were analysed to determine the approach to RSE and identify any reported changes to provision that could have been due to participation in the trial. Responses were analysed using an assessment tool (see Appendix 1), informed by the Whole School RSE Audit tool developed by the National Children’s Bureau for the Sex Education Forum (2020). 206 Criteria were organised into three categories: RSE quality, RSE quantity, and RSE governance and broader pastoral care. Examples of quality criteria included teacher training and confidence to deliver RSE. Examples of quantity criteria included time being clearly allocated for RSE. Examples of criteria relating to RSE governance and broader pastoral care included the presence of a written RSE policy or ethos. Schools received ratings for each of these categories and for their RSE provision overall. The ‘quality’ category was judged to be the most crucial and was consequently double-weighted within the overall score (Table 22).
| ID | Qualitya | Quantity | RSE governance and pastoral context | Overalla | ||||
|---|---|---|---|---|---|---|---|---|
| Score (%) | Rating | Score (%) | Rating | Score (%) | Rating | Score (%) | Rating | |
| S11NI | 30 | Low | 63 | Medium | 50 | Medium | 38 | Low |
| S16NI | 37 | Low | 38 | Low | 29 | Low | 35 | Low |
| S18NI | 37 | Low | 63 | Medium | 38 | Low | 39 | Low |
| S19NI | 83 | High | 75 | High | 67 | Medium | 78 | High |
| S21NI | 80 | High | 75 | High | 71 | Medium | 77 | High |
| S22NI | 20 | Low | 0 | Low | 13 | Low | 16 | Low |
| S26NI | 53 | Medium | 75 | High | 21 | Low | 47 | Low |
| S28NI | 57 | Medium | 75 | High | 38 | Low | 53 | Medium |
| S30NI | 53 | Medium | 75 | High | 63 | Medium | 58 | Medium |
| S33NI | 20 | Low | 0 | Low | 17 | Low | 17 | Low |
| S35NI | 30 | Low | 13 | Low | 8 | Low | 23 | Low |
| S14S | 27 | Low | 38 | Low | 33 | Low | 29 | Low |
| S16S | 62 | Medium | 75 | High | 64 | Medium | 63 | Medium |
| S17S | 77 | High | 63 | Medium | 71 | Medium | 74 | Medium |
| S23S | 54 | Medium | 75 | High | 41 | Low | 52 | Medium |
| S11W | 38 | Low | 50 | Medium | 23 | Low | 35 | Low |
| S15W | 93 | High | 75 | High | 96 | High | 92 | High |
| S13W | 40 | Low | 13 | Low | 25 | Low | 34 | Low |
| S24W | 70 | Medium | 63 | Medium | 63 | Medium | 67 | Medium |
| S13E | 40 | Low | 25 | Low | 29 | Low | 36 | Low |
| S14E | 43 | Low | 75 | High | 21 | Low | 40 | Low |
| S17E | 67 | Medium | 50 | Medium | 29 | Low | 55 | Medium |
| S18E | 62 | Medium | 50 | Medium | 64 | Medium | 61 | Medium |
| S18E | 62 | Medium | 50 | Medium | 64 | Medium | 61 | Medium |
| S21E | 40 | Low | 25 | Low | 42 | Low | 39 | Low |
| S22E | 42 | Low | 50 | Medium | 18 | Low | 37 | Low |
| S25E | 42 | Low | 38 | Low | 32 | Low | 39 | Low |
The majority of control schools (15/26) received ‘low’ ratings for their overall RSE provision, with eight receiving ‘medium’ ratings, and only three receiving ‘high’ ratings. Schools tended to score highest for RSE quantity, with nine schools receiving ‘high’ quantity ratings and eight receiving ‘medium’ quantity ratings. Schools scored lowest overall on RSE governance and broader pastoral care, for which only one school received a ‘high’ rating and eight a ‘medium’. Although the majority of control schools (17/26) reported having a written RSE policy or ethos, this was only one of the criteria used to assess this aspect. Finally, in relation to quality, only four schools received a ‘high’ rating and eight a ‘medium’.
More generally, apart from this scoring of school RSE provision, further insights were obtained regarding the delivery of RSE in control schools. First, control schools, in common with intervention schools, reported using a variety of delivery mechanisms for RSE, including through timetabled PSHE or PD or through other curriculum subjects, most commonly science and religion. Some schools used drop-down days, targeted talks, and health and well-being weeks to cover RSE. Nineteen out of 32 control schools reported that external agencies such as specialist organisations, health or education authorities and police services were involved. Some reported working ‘in tandem’ (T0115W) with these, whereas others reported that their RSE was ‘led by external providers’ (T0113W). However, every control school reported that teachers delivered at least some RSE, often ‘form teachers’, PD or PSHE teachers, or teachers of other subjects, such as science or religion. Only in four schools was school nurse involvement in delivery noted. Fifteen schools reported that staff who delivered RSE had received some training. However, just as in the majority of intervention schools, responses suggested that this was rarely sufficient, with even teachers who had received training describing lack of confidence, and stating that ‘teachers don’t feel equipped with the correct language’ (T0118S). One school described lack of training as ‘a big area of weakness’ (T0123S).
Changes to provision and potential contamination
No schools reported changes to RSE provision as a result of participation in the trial. However, five of the control schools described ongoing attempts to develop and update provision, with some describing previous resources as ‘outdated’ (T0117S). More broadly, most schools reported at least some recent changes in their approach to RSE. In general, there was an increased awareness of the need for relationship and sexuality education in schools owing to greater societal awareness of how questions of sexuality and intimate relationships are relevant to adolescent lives. There was ‘slightly more opportunity for debate . . . Children are much freer to talk now’ (T0128NI). There was also increased awareness owing to external (state) guidance (T0116S, T0114E), namely the PSHE review in Scotland (2019)36 and the introduction of statutory RSE in England (2020). 37
Comparison of control and intervention schools
It is further interesting to look at overall differences in RSE provision between control and intervention schools prior to the implementation of If I Were Jack in the intervention schools. RSE provision in control schools was assessed using the same methods that had been used in intervention schools. 206 The results shown in Table 23 show that schools in both the control and intervention groups were broadly comparable/equal in terms of the distribution of schools categorised as having high, medium or low provision of RSE outside If I Were Jack.
| RSE in school context | Number of intervention schools | Number of control schools |
|---|---|---|
| High provision | 3 | 3 |
| Medium provision | 7 | 8 |
| Low provision | 19 | 15 |
| Not available | 5 | 6 |
| Total | 32 | 32 |
Summary
In summary, RSE provision in control schools was regarded as of low to medium quality when judged against a tool designed to capture best practice. No schools reported changes to provision as a result of participation in the trial, but five schools reported updating their provision and most control schools made small ongoing changes to the provision of RSE. The quality of RSE provision in control and intervention schools overall (outside the provision of If I Were Jack) was broadly comparable with the majority of schools in both groups rated as low to medium provision.
Mechanisms of impact
In this section, we refer to the underpinning theory of change of the intervention based on social cognitive theory (theory of planned behaviour) along with gender transformative theory (which challenges gender inequalities) as discussed in Chapter 1. Based on the logic model, we focus on the end users’ self-perceptions of effectiveness in relation to some of the key active programming mechanisms of If I Were Jack. These are:
-
engaging boys and gender transformation
-
knowledge acquisition
-
enhanced communication skills
-
intentions for behaviour change in relation to avoiding unprotected sex (delaying sexual intercourse/practising safe sex).
By breaking it down in this way we offer a better sense of what was perceived to have worked best for whom, as well as an overall sense of perceived effectiveness.
The data for this section are drawn from:
-
teacher and trial champion interviews (n = 29 individual interviews and n = 5 paired interviews, total n = 39 participants)
-
teacher focus groups (eight groups, n = 31)
-
student focus groups (eight groups, n = 58)
-
SEQs (n = 3179).
Engaging males and gender transformation
For both students and teachers, the programme’s gendered focus was considered a key strength. However, it was also regarded by some as creating a tension between male and female perspectives. Although for some this was negative, for the most part this tension was regarded as positive and the active spark for critical thinking on gendered roles in preventing unintended pregnancy and promoting positive sexual health. Below we examine, first, data on the aspect of engaging males and, second, the data on gender transformation.
Engaging males
Students, both male and female, reported that the programme had engaged boys and encouraged consideration of male perspectives:
. . . the boy as well because they have to go through and tell everybody that obviously they’re going to be a dad.
Female, PU0112S
I think it should be on both sides, like, you know, I think, em, it is good to focus on their [boys’] side as well.
Female, PU0116W
It’s not just one person’s, it’s both responsibilities on things.
Male, PU0216W
. . . it’s both the people who are responsible really.
Male, PU0123E
Teachers sometimes reported being ‘pleasantly surprised’ at this perceived uncharacteristic engagement from male students (T0212S). One teacher stated, that it ‘[opened] up so many conversations and it, from a unique angle, I think it just really gets them thinking’ (T0116 W). Teachers reported that this encouraged female students to consider male classmates’ views and the ‘emotional impact [of UTP] on the boy as well as the girl’ (T0221S).
This aspect was also noted by students and perceived as generating empathy with how others (both male and female) may experience an unintended pregnancy:
If you were in that position and you were a boy, you wouldn’t know all like your girlfriend would be thinking, and that would definitely help.
Female, PU0129NI
It was good that Jack put, em, like Emma first, instead of putting himself first, thought about her and like what she’s going to do with the baby.
Male, PU0229NI
However, there was also a sense from some of the students and teachers that the programme at times overshadowed female perspectives. Some female students felt that insufficient detail had been provided on female perspectives: ‘we didn’t really hear much from her [Emma], like what she was going through’ (Female, PU0212S). Some reported struggling to engage with the programme for this reason: ‘like, I’m not a man . . . I ain’t going to get a girl pregnant any time soon’ (Female, PU0316W).
Others described how initial scepticism from girls (‘What’s the point in this then, Sir? . . . It’s all about the boy’s point of view’, TO222W) had led to useful discussion and, later, a sense of the programme’s relevance for female perspectives: ‘there was sort of like a turning point for them “this is to do with us [girls] as well” ’ (T0222W).
Gender transformation
Next we consider if this perceived enhanced engagement and empathy of males was also regarded as a trigger to challenge gender stereotypes and gender inequalities.
Teachers observed that the concept of shared responsibility with regard to timing of pregnancy and parenting, vocally supported by girls, had ‘sparked the debate’ (T0320NI), which caused male students to reconsider their perspectives:
That was definitely a key message that was delivered, that it’s everybody’s role, it’s everybody’s responsibility.
T0220NI
It was very much like, not making it too in your face but, if you’re in a relationship, this is an issue, an issue that you have to face together.
T0412S
Increased awareness of concept of shared responsibility for preventing unintended pregnancy was confirmed by male students:
It’s good. They need to know that they have, they have some responsibility like . . . they can’t just run away, run away from it, you know what I mean?
Male, PU0120NI
More broadly, students stated that the programme provoked them to challenge gender stereotypes in relation to readiness for sex and roles and responsibilities for preventing pregnancy. For example, one group recalled the challenging of gender stereotypes during a discussion on readiness for sex:
Female:
Male (1):
Male (2):
Female, PU0220NI; Male, PU0120NI; Male, PU0320NI
Students stated that it also challenged stereotypes in relation to females carrying condoms:
There was one about, em, was it ‘Is it slutty that a girl is carrying a condom?’ . . . I brought up the point that she just maybe doesn’t want to become pregnant and that’s just a safety precaution – that’s not anything strange. That’s literally just — that’s being sensible if the male is an idiot.
Male, PU0416W
Teachers also thought that messages went beyond stereotypes around practising safe sex to gender equality and responsibility for parenting more broadly:
Some of the boys, who are a bit blasé and bombastic even about it, if they’re like that in front of their friends, I’m certain that some of them would have gone away and started to think about things in a slightly different way, you know, and even if it’s just planted a seed of ‘Oh, I need to think about women differently’ or ‘Oh, I need to think about this situation differently’.
T0316W
However, both teachers and students also highlighted limitations to the ability of a programme such as this to significantly challenge gender stereotypes. This was for a mixture of reasons. Some students felt that for the programme to have been effective, a certain level of receptiveness to its messages had to pre-exist:
Anybody who was going to leave the kid or was just going to leave her to her own devices, I don’t think that changed their minds on that.
Male, PU0216W
Some male and female students felt males are males, and they are not going to ‘change’ in response to a programme like this:
Let’s be honest, boys just want to have a sex with a girl don’t they? . . . Some of them might think differently after using the programme. But some of them won’t care.
Male, PU0114W
Some thought that the programme activities might act to even embed stereotypes either because of the way they were framed or because of a lack of sufficient time or student, or indeed teacher, confidence, to challenge these in discussion:
Some people put really stupid things for their answers, and then there was no sort of like, ‘Oh no, you [shouldn’t be] doing that’, it was just moving straight on, and if they actually believed that, then there was nothing to sort of tell them, no, you don’t want to be doing that, you want to be doing something else.
Male, PU0416W
The teachers, despite agreeing that the controversial statements exercise was one of the strongest exercises, suggested that completing this activity earlier in the programme would allow such messages to be addressed and learning to be ‘threaded through’ the rest of the lessons (T0323E).
In summary, the gender focus of the programme was regarded as a key strength by both teachers and students for generating engagement, ‘sparking the debate’ and as a ‘unique angle’ to both question and understand gendered perspectives. It created a learning opportunity for male and female students to challenge unequal gender relations in relation to sexual freedoms, reproductive responsibility and gender equality more broadly. However, limitations of this approach were the potential to de-emphasise female perspectives and overshadow these through male perspectives. Furthermore, other limitations in the programme were its small scale in the face of societal gender norms and the lack of time within the programme activities to sufficiently disrupt gender norms and practices.
Knowledge acquisition
Students and teachers perceived the programme to have increased students’ factual knowledge and practical skills in gaining knowledge, to have addressed misconceptions, and to have improved understanding of the impact and options available following an unintended pregnancy, as well as understanding of personal risk.
New knowledge and practical skills for acquiring knowledge
Students described how activities had led to gaining new information. Areas of reported increases in knowledge included contraception and condoms (Female, SEQ3615E; Male, SEQ0116W), and ‘different characteristics about teenage pregnancy and sex’ (Male, PU0320NI).
Some recounted how the programme had challenged myths that they had previously believed:
Female:
Female:
Female, PU0529NI; Female, PU0129NI
However, not all agreed, with one all-boys’ group describing finding some misconceptions addressed by the programme as ‘kind of ridiculous, like you wouldn’t really believe them’ (Male, PU0419E).
Teachers commonly perceived that the programme had been ‘an eye-opener’ (T0119W). In addition, teachers perceived the programme to have addressed ‘myths’ (T0216 W) on subjects such as the fallibility of the withdrawal method: ‘A lot of the boys said, “But it’s OK if you withdraw”. No. You know, and I think they were like, “What, it’s not?” ’ (T0119W).
However, teachers also noted that not all students agreed that myths had been dispelled. Teachers thought this was more true for males, who often regard themselves as more informed, than for females. Teachers discussed how some male students ‘literally convinced themselves’ that they had already known information before the programme, but disputed this: ‘The boys certainly had that attitude that, “Well, you didn’t teach us anything that we didn’t know”. I doubt that’s true’ (T0219E).
Students considered lessons containing practical information impactful, as this could be used to protect themselves and make informed choices. They described how learning ‘where we could get help and where we could go for contraception and other things’ was ‘very helpful’ (Female, SEQ9217W). Others reported that they ‘never knew you could just show up to the sex clinic place’, particularly without parental consent (Male, PU0312S).
This was confirmed by teachers who reported noticing students ‘lift their heads’ (T0420NI) to take in information, such as types of contraception and how to obtain it. Such elements were perceived by teachers to have been particularly impactful for students: ‘Mine were like “We didn’t know a lot of that” ’ (T0319E). Another echoed the sentiment that the programme had left a lasting practical impact on students: ‘They definitely left, to me, knowing they had a lot more information to make responsible decisions with regard to sex’ (T0420NI).
Students reported that activities incorporating finding answers online had provided them with skills to seek information independently ‘ourselves’ (Female, SEQ6927NI), and ‘gave us information whilst teaching us how to find more in the future’ (Male, SEQ7019E). Reported barriers included navigation issues and ‘blocked’ sites (Female, SEQ0927NI), limited website utility and getting ‘side-tracked’ by other content (Male, PU0216W).
Teachers felt that it had been particularly effective in signposting students to resources where they could access reliable information independently rather than relying on friends: ‘[i]t was very much a wee bit of independent research and . . . any questions were answered’ (T0117NI). Another noted that, although it was impossible to know if students had done further research, they had accepted programme wallet cards: ‘there wasn’t too many left on the floor, which is always a good sign [laughing]!’ (T0112NI).
Unintended pregnancy: options, impact and personal risk
The programme was perceived by students to have effectively communicated information about ‘where to get help if I needed it’ (Female, SEQ0727NI), and options available to a young person facing an unintended pregnancy. Some males reported learning that they could speak to a crisis pregnancy counsellor: ‘just showing that that was like an option that you could have . . . it was quite useful to know that you could go and do that’ (Male, PU0219E).
Some students reported struggling to relate to the IVD characters, seeing them as too ‘robotic’ (Male, PU0416W), or insufficiently distressed: ‘[s]he didn’t seem [that stressed]. Like, if that was me personally, I would be like, this is the end of the world’ (Female, PU0223E). However, generally the participatory and character-focused nature of the programme was seen to have been effective in helping young people understand the realities of UTP. Students felt that messages had encouraged ‘mature’ engagement with the topic (Female, PU0129NI), and sympathetic engagement with the characters’ challenging experiences, showing: ‘what people actually go through, like people who are like getting beat up inside, you know, about having a baby’ (Male, PU0329NI).
Reflecting this, one teacher reported that the programme had been ‘genuinely relevant’ to her students’ lives, and its recognition of them as potentially sexually active had been key to ensuring engagement:
They saw it as something that really, really spoke to them. I also wonder if maybe we’re guilty sometimes of infantilising them a little bit, and because we treated them with a mature topic, in a mature way, they responded.
T0112S
In terms of drawbacks of the programme in this regard, apart from the aforementioned perceived implausibility of some of the myths challenged, generic limitations of internet searches, perhaps more significantly across a number of focus groups students perceived more attention was required on LGBTQ+ issues. One student who identified themselves as gay described the programme as ‘really focusing on straight people’ (gender not recorded, PU0121S). Teachers were encouraged to acknowledge this limitation from the very outset of the programme, but nonetheless it was important to the students to also express this.
Some students expressed negative views on the programme, perceiving it to be ‘extremely centred around straight people, heteronormativity, and very uncomfortable’ (gender missing, SEQ0711E). Others felt that the programme was not relevant to them, and that there was already sufficient information on the issue of UTP:
It’s stereotypical and doesn’t inform us on anything but heterosexual sex . . . there is enough info on teen pregnancy.
Female, SEQ9418S
However, there were also examples of LGBTQ+ students reporting enjoying the programme or feeling that it was covered important issues, despite the perceived reduced relevance of the issue of pregnancy. One student expressed very positive perceptions on the IVD and found activities involving internet research and information on STIs ‘very good [and] useful to me’, but reported reduced personal relevance over the focus on pregnancy: ‘I’m gay so I don’t think I’d really ever be affected directly by something like that’ (Male, SEQ10819E).
In summary, teachers and students mostly reported that gaining knowledge, and gaining skills to acquire knowledge, in relation to relationships and sexuality and the relevant ways the knowledge was presented, were key mechanisms of the programme’s effectiveness. A key limitation of this relevance, however, was in relation to the heteronormative focus of the intervention and, to a lesser extent, the focus on teenage pregnancy in limiting opportunities for all students to benefit.
Communication and skills
Students and teachers often reported perceiving the programme to have improved students’ ability to communicate on the subject. Sharing of perspectives and consideration of IVD characters’ experiences were perceived to have increased empathy.
Empathy and opportunities for practising communication
First and foremost, the programme seemed to have provided an opportunity for the students to think through the situation themselves and communicate with others in their classroom setting, including among those who might normally be hesitant to communicate. Students reported finding it useful to see the thought processes the main character went through before discussing his situation with others:
His thought process and how he kind of talked things out and how he communicated with others to try and solve the issue that he had, and it was kind of like a first-hand thing because . . . he’s literally saying his thoughts out loud, and it’s like as if you’re thinking with him and making the decisions with him.
Male, PU0119E
They kind of got interactive . . . after the video, they were more confident.
Female, PU0429NI
Especially hearing other people say their opinion, it made them like, ‘oh, I’ll just say mine’.
Female, PU0129NI
Teachers agreed that the approach had facilitated shared reflection on issues:
It really got them communicating and talking about things and seeing things.
T0314W
At the beginning . . . just the word ‘sex’ sort of makes everybody laugh, and by the end of it, they were having really positive conversations.
T0319E
Nonetheless, some students reported some challenges to engaging different groups of students in discussion, owing to ‘general disruption’ (Male, PU0320NI) and mobile phone use.
Second, both teachers and students reported that the programme developed the young people’s communication skills in listening, and in challenging and widening perspectives:
It did get people thinking . . . like some people were saying that some girls do wear certain clothes and then other people kind of gave them more of a different perspective and then they kind of like changed their mind and stuff. It was good.
Female, PU0529NI
Where we have got a range of different races and cultures and faiths, it worked really nicely . . . with our British values as well in order to be able to, you know, take on board what people say and . . . be respectful to other people’s viewpoints.
T0112E
Finally, in this regard, an enhanced sense of communication skills from the programme was perceived by students and teachers to equip students with a greater ability to communicate about personal issues and well-being more generally. Teachers highlighted the importance of the programme in creating open environments for discussing concerns in school settings, focusing on wider cultural change and teacher approachability: ‘we create a culture of “we’re prepared to discuss things” ’ (T0111S). Others agreed that the programme had highlighted the importance of communication more widely for students around sex, pregnancy and other risks:
[opening] their mind to the fact that they have to have discussions, regardless of whether it was just one night or whatever
T0321S
Male:
Female:
T0129NI; T0229NI
Even though we finished it . . . 5 weeks ago, the kids are still talking about ‘If I Were Jack’.
T0312S
Students also acknowledged that they had a stronger sense of their own ability to communicate on sexuality:
Male:
Female:
Male, PU0120NI; Female, PU0420NI
However, indications of barriers to ongoing communication were also present in the data. Some male students still agreed that young men were less likely to talk about it than young women, putting this down at times to ‘immaturity’ (Male, PU0329NI). Another group reported that discouragement from discussion after primary school RSE had continued to influence them: ‘we were told like not to talk about it outside of class and stuff like that . . . I think it just kind of carried on’ (Female, PU0221S).
In summary, a key strength of the programme was teacher and student perceptions that the programme had raised their ability to communicate on relationships and sexuality both within the classroom and beyond it, with enduring effects. Participants reported that it raised their competence to listen, appreciate other perspectives and challenge ideas. However, the potential for this impact to last beyond the support of the intervention or to override gendered stereotypes/behaviour was also questioned.
Perceived effectiveness in terms of intentions for behaviour change
Teachers were hesitant to draw conclusions on whether behavioural changes had occurred as a result of the programme so soon after implementation: it was ‘early days’ (T0123W). Others anticipated that behavioural change would be a slow process: ‘not something like flicking on a switch. It’s going to take time for that to seep in’ (T0124NI). In addition, some students were sceptical about the likelihood that the programme would effect behavioural change: ‘no boy or girl will listen to that or change what they will do’ (Female, SEQ12818S). However, more commonly, students and teachers perceived the programme to have triggered realisations surrounding risk, which, combined with practical knowledge, was already creating the foundations to delay sex and childbearing until they were ready and to avoid unprotected sex.
Delaying sex
A number of students and teachers focused on how the programme had highlighted the importance of feeling personally ready for sex:
It taught me that I should be careful when having sex and have it when you’re ready.
Female, SEQ16812E
It was well explained why it’s better not to have sex until you feel ready.
Male, SEQ5717NI
I think, in every lesson, there was an opportunity for me to say that, ‘remember this is meant to be a positive experience’.
T0420NI
Students and teachers considered programme statistics useful to challenging peer norms that underage sex (< 16 years of age) was widespread:
Lower, far lower than we thought.
Male, PU0120NI
To know that it’s not [more people] . . . that’s good, because a lot of people feel under pressure.
Female, PU0429NI
Students and teachers described especial pressure on males to have sex: ‘like a lad thing’ (Female, PU0429NI). A male student reported how the programme had encouraged him to rethink beliefs drawn from claims of his vocal peers:
I hear loads of stories . . . and you’re like, ‘oh, that’s loads’, but then if you round, like see how many of my friends around me haven’t lost it, so.
Male, PU0229NI
Some students and teachers considered females more likely to experience pressure to have sex from male partners and that female empowerment to delay sex would be enhanced as a result of the programme. Teachers observed that the confidence of girls to decline unwanted sex had been strengthened by the knowledge that their male classmates had also received this information, and that they no longer ‘felt they were the only one saying no’ (T0320NI). This teacher observation was also acknowledged by a male student in a focus group:
More guys are thinking about [sex] way more than girls, so if they think, ‘oh, fine, I’ll just wait until my girlfriend’s ready’, then it might be better for both of us in the long term.
Male, PU0229NI
Safer sex
The most common theme here was a greater sense among students, confirmed by teachers, that the students had an opportunity to take in the messages in a way that made sense to them, plan their behaviour and plan to have safe sex. There was a strong sense across the data with students and teachers that the resource was perceived as effective in this regard:
It gives you a chance to discuss what you, how you would respond in that situation.
Male, PU0120NI
Female:
Male:
Female, PU0212S; Male, PU0312S
Male:
Male:
Female:
Male, PU0312S; Male, PU0412S; Female, PU0112S
Made me think deeply on pregnancy and the choices I make in the future.
Female, SEQ3220E
Others added that information on STIs as well as pregnancy had helped them consider how to stay safe as they: ‘[didn’t] want to catch something’ (Male, PU0329NI).
Although some teachers reported that some male students initially distanced themselves from the suggestion that such strategies were relevant to them, after targeted explanations, teachers observed them to be more open to learning:
They did understand, ‘if I’m prepared for this and if I’m clued in, I’ll make a better decision, you know, or things maybe will go, will go more positively’.
T0420NI
Many teachers reported that the ‘If I had to look after a baby vs. Saturday schedule task’ was particularly helpful in reinforcing the message of delaying childbirth until one was ready. Teachers offered as evidence of effect their observations of students after class visiting recommended websites on their mobile phones and noting practical information, and suggested that this indicated intentions to make use of these resources, as well as using school resources. One teacher observed more use of school-based resources.
Female:
Male:
T0412S; T0212S
Another teacher also speculated about wider impacts: ‘[w]e have had, sort of on the back of this, a lot of boys going to see her [the school health and well-being lead]’, with it having ‘sparked more awareness, definitely’ of sexual health and well-being as an issue within the wider school environment (T0117W).
In summary, participants perceived the programme to have triggered realisations around relationships and sex, which, combined with practical knowledge, were already creating the foundations to avoid unprotected sex and delay sex and childbearing until they were ready. Teachers and students reported that students were actively seeking out information to help them to be informed and had greater confidence to think about relationships and sex. However, despite these benefits, teachers and students also recognised that behaviour change is generally the product of cumulative actions, rather than the outcome of a single programme, and that time would tell.
Summary and conclusion
This chapter was structured to answer focused questions of the process evaluation as defined in our study protocol. 48
First, we asked why schools chose to participate or declined to participate in the trial. The data demonstrated the primary reasons for participation were an acknowledgement by schools that If I Were Jack was a high-quality, novel resource; a recognised need by schools to address RSE/holistic pastoral education; recognition that there was a gap in current materials in relation to engaging males; the opportunity for teacher training that could have wider benefits for future RSE programmes; and the financial incentive. The main reasons for not participating were research saturation or other commitments, a perception that there was adequate RSE provision already in place, and the additional time commitment required by the trial to co-operate with the research components and/or programme delivery.
Second, we asked whether or not the intervention was delivered with fidelity. The data demonstrated that the teacher training and classroom activities were generally delivered with high to medium fidelity, with some exceptions, but that the parental component, an optional element, was delivered with low fidelity. We noted, however, the potential for a high risk of bias in measuring implementation fidelity of the classroom-based activities on teacher self-reports in implementation logs, some of which was picked up through data triangulation with classroom observations, student focus groups and SEQs. Gathering data through implementation logs was problematic.
Relatedly, we sought understanding for the reasons for high and low implementation, especially of classroom activities and the parental component. High fidelity to classroom implementation was enhanced by teacher training and the manualised and user-friendly nature of the programme, following years of prior optimisation with teachers. The primary reasons reported by teachers for deviations in intervention delivery fidelity were insufficient time, perceived clash with school ethos and inadequate computer facilities. Implementation fidelity was also more generally impacted by teacher creativity, that is teachers changing/adapting materials to the perceived needs of students, including SEN students. Low fidelity to implementation of the parental component was explained by parents in terms of not receiving the material and embarrassment or fear of raising these issues with their child. Teachers reported barriers to implementation owing to student refusal and/or reluctance at school or teacher level to engage with parents on these issues. Students said it would be embarrassing and awkward. A proposed solution to mitigating these barriers was normalising these conversations between parents and school at an earlier stage in education, with continuity on the topic throughout all stages; in other words, avoiding the ‘big talk’ with schools and parents at age 11/12 years.
Third, we asked about the nature of RSE delivered in control schools and whether or not this had changed owing to participation in the trial as a marker of risk of bias. Judged against assessment criteria informed by a best practice tool of RSE implementation in the UK (Sex Education Forum, 2020),206 most control schools (n = 15) received ‘low’ ratings for their overall RSE provision, with eight receiving ‘medium’ ratings and only three receiving ‘high’ ratings. There was no indication that the direction of RSE had substantially changed as result of participation in the trial. There was also broad comparability in the quality of RSE provision in both control and intervention groups outside the provision of If I Were Jack. On the whole, the quality of RSE provision in both groups was rated as ‘low’ to ‘medium’.
Fourth, we asked about the perceptions of effectiveness of the intervention, from the perspectives of both teachers and students, especially probing key theory-driven programming mechanisms as depicted in the intervention logic model. The data demonstrated that the gender focus of the intervention, the engagement of males and the generation of empathy and understanding of both male and female perspectives was a key strength of the programme: ‘[i]t really got them communicating and talking about things and seeing things’ (T0314W). Potential limitations to effectiveness relating to this mechanism were a perception that the programme could overshadow female perspectives and an acknowledgement that a short programme may be insufficient to challenge deeply embedded gendered ideas around sexuality.
The data demonstrated that the intervention was an opportunity to gain new knowledge on sex and relationships as well as acquiring skills of where and how to find information and support. According to teachers, it ‘lifted heads’ and was an ‘eye opener’ (T0124NI). Students reported that learning where they could get ‘contraception and other things’ was ‘very helpful’ as well as learning ‘where you could get help if you need it’, and for males especially, ‘it was quite useful to know that you could go and do that’ (T0124NI). A key limitation in the programme to generating knowledge acquisition was its strong heteronormative bias and focus on teenage pregnancy, although some LGBTQ+ students thought that the programme was nonetheless relevant.
Teacher and student perceptions that the programme provided an opportunity to learn and practise communication skills were especially evident in the data. Teachers and students both noted increased confidence among students to communicate with peers about sex and relationships. According to one teacher, ‘we treated them with a mature topic, in a mature way, [and] they responded’ (T0112S). The interactive video seemed to be an especially important trigger for generating communication skills on relationships and sexuality in the classroom. This was because the IVD was regarded as centring the importance of young people’s thoughts and ideas, thereby laying the groundwork and building confidence for young people in the classroom to pick up and continue the conversation. There was a strong sense that these communication skills would endure, although limitations to this were also noted.
Finally, the perceived impact of effecting behavioural change, especially in terms of delaying sex until one is ready and practising safe sex, was considered. Teachers and students tended not to ‘over-promise’ the programme’s potential impact on behaviours: ‘it’s like early days’ (T0115E). However, there were ample data to suggest that the programme provided an opportunity to think about and plan sexual behaviours in ways that were positive and healthy, in terms of both the messages that teachers conveyed [‘I think, in every lesson, there was an opportunity for me to say that, “remember this is meant to be a positive experience” ’ (T0420NI)] and the messages that students recounted for themselves {‘[m]ore guys are thinking about [sex] way more than girls, so if they think, “oh, fine, I’ll just wait until my girlfriend’s ready”, then it might be better for both of us in the long term’ (Male, PU0229NI)}.
In the final discussion chapter, the process evaluation data, the trial data and health economics data will be considered in the round to draw together the final conclusions of the study.
Chapter 7 Results: economic evaluation
Aim
The aim of the economic evaluation was to describe the costs and consequences of implementing If I Were Jack in UK schools to provide information to decision-makers on the implications of rolling out the intervention further. Two analyses were conducted:
-
Within-trial economic analysis. The aim of this analysis was to calculate the cost of teacher time to deliver If I Were Jack compared with current RSE provision (and hence the opportunity cost) based on teacher-completed resource use questionnaires. Descriptive statistics for sexual health-related health-care resource use and costs, and inputs to the model based on participant-completed data, were also calculated.
-
Decision analytic model. The aim of this analysis was to report the long-term cost and consequences of If I Were Jack based on a decision model, with input data collected from the trial in addition to relevant data from the published literature.
Methods
Within-trial analysis
For the within-trial economic evaluation, the main outcomes were the students’ self-reported health-care resource use related to STI services used in the last 6 months at baseline and since baseline (covering approximately the last 12 months) at follow-up and teacher resource use in delivery of the intervention. Further details on the methods for data collection are in Chapter 3. The student self-reported health-care resource use data included number of visits to sexual health clinics, number of school nurse appointments, number of general practitioner (GP) and GP nurse visits, number of free condoms received and number of condoms bought, number of emergency contraception pills purchased and other contraception methods accessed, and number of pregnancy and STI tests obtained (see Appendix 2).
The teacher resource use questionnaire included time spent on lesson and photocopy preparation, time and type of other inputs used (e.g. discussion and/or equipment), and lesson delivery time (see Appendix 2).
Costs of the If I Were Jack intervention
The cost of If I Were Jack was based on the opportunity cost of teachers delivering the intervention and the cost of adapting the intervention for different groups. The first was calculated from the time spent preparing and delivering the intervention multiplied by the average hourly wage of a secondary school teacher as reported by the Office for National Statistics (ONS). 158 This was divided by the number of students in each school, randomised to the intervention group, to calculate the total opportunity cost per student.
It is possible, though, that this time could have been spent delivering other RSE activities, and the effectiveness of these was assessed in the control group. A questionnaire was circulated to control schools to collect information on the resources required to deliver standard RSE. Costs were calculated using a similar methodology to costing the If I Were Jack intervention.
The If I Were Jack resources were adapted for the four different nations to make them more culturally relevant (i.e. the original resource was re-filmed and updated for NI and Scotland and remade with English actors for England and Wales). We included the cost of adapting the If I Were Jack resources given that it is likely that these resources will need to be updated over time to reduce the risk of them appearing dated. Based on the finances from the trial we report the total cost of updating the materials as well as an upper and lower estimate of the cost per student to update the materials, with the upper estimate being the greatest possible cost per student to update the materials if only the same number of students as those randomised to the intervention accessed it, and the lower estimate being the lowest possible cost per student if all of the students aged 14 in the country accessed the intervention.
Sexual health related service resource use and costs
Descriptive statistics for the percentage of students and mean number of contacts for self-reported health service use were reported for students in the control and intervention groups. Resource use for each student was multiplied by unit costs from published sources (Table 24). Both unadjusted and adjusted mean cost per student at follow-up were reported for the control and intervention groups, the latter obtained after adjusting for baseline resource use and stratification variables using clustering as a random effect. The 95% CIs were calculated based on bootstrapped bias-corrected methods.
| Resource | Cost (£) | Reference |
|---|---|---|
| Sexual health consultation in clinic | 120 | PSSRU159 |
| Sexual health advice from school nurse | 11 | PSSRU159 |
| Sexual health advice from GP | 34 | PSSRU159 |
| Sexual health advice from GP nurse | 12 | NICE160 |
| Condom (assumed three condoms per pack) | 2 | Boots161 |
| Other contraception (average cost of different contraceptives indicated by the students in the trial) | 7.16 | Boots161 |
| Pregnancy test | 4 | Boots161 |
| STI test | 16.50 | NICE160 |
| Emergency contraception | 30 | Boots161 |
Missing data
We assumed that data were missing at random (MAR). In line with published guidance on handling missing data in RCTs,162 and specifically in cost-effectiveness analysis alongside a RCT,163 our main analysis was a complete-case analysis. A sensitivity analysis using multiple imputation by chained equation (MICE) was conducted to test the robustness of the MAR assumption. 164 The MICE approach included a multilevel imputation method to account for clustering. Age and sex were included in the model as predictors of missingness in addition to the stratification variables and baseline costs. Estimates were derived using 20 imputations, and 95% CIs were calculated based on bootstrapped bias-corrected methods over a total of 10,000 iterations for each imputed data set.
Cost–consequences and decision model inputs
For consequences and relevant inputs to the decision model, we reported instances of unprotected sex (i.e. no contraceptive use at last sex), ever had sex, pregnancy tests, contraception use, STIs and testing for STIs. Unadjusted and adjusted (adjusting for stratification variables and baseline) ORs were reported for the intervention compared with control for unprotected sex, ever had sex, pregnancy tests and testing for STIs. Further subgroup analyses for contraception type and specific STIs were not possible owing to small participant numbers.
Long-term decision model
We designed a behaviour change-based decision model67 aimed at assessing the long-term cost-effectiveness of the If I Were Jack intervention versus RSE. The model was populated using evidence collected from the trial and published literature on different types of outcomes that are directly and indirectly related to pregnancies and STIs among young people. When no trial data were available, assumptions were made from pre-existing data and expert input. The model had a 20-year time horizon and calculated the expected costs and consequences for a hypothetical cohort of patients with similar characteristics to those enrolled in the trial. Twenty years was thought to be sufficient to capture the long-term benefits. People’s sexual behaviour changes when they are in their late 30s,166 and hence we did not model beyond this time-point. Both deterministic and probabilistic sensitivity analyses (PSAs) were conducted to assess the robustness of the results to alternative modelling assumptions. The long-term decision analysis model was conducted in R version 4.0.3 (The R Foundation for Statistical Computing, Vienna, Austria).
Design
A conceptual model developed to evaluate the long-term costs and consequences of the intervention, which incorporated theories of behaviour change, is illustrated in Figure 5. Reading from left to right, we started with the target population (young people aged < 16 years) who engaged with the If I Were Jack intervention and experienced an increase in the levels of the cognitive outcomes in topics related to sexual health (knowledge, attitude and skills). We hypothesised a change in the behaviour outcomes with an increase in the number of people who delayed vaginal sexual intercourse (abstinence), an increase in the instances of protected sex for those sexually active and a decrease in the instances of unprotected sex. This, in turn, led to a decrease in the number of unintended pregnancies and STIs in the target population.
FIGURE 5.
Health economic conceptual model of the If I Were Jack intervention.

Population
The target population was young people in post-primary schools in the UK, under 16 years of age, within the general population. An intervention that encourages the use of contraceptives is unlikely to prevent young people who hope to become pregnant from endeavouring to become pregnant. The model therefore assumes that the intervention is aimed at teenagers who want to prevent pregnancy.
Outcomes
The outcomes were reported in terms of the output of a cost–benefit or return on investment (ROI) analysis, whereby both costs and benefits are measured in monetary units. The ‘benefits’ were the cost savings that result from averted pregnancies. The ‘cost’ was the total amount of public money currently being spent for preventing pregnancies and STIs among young people.
Perspective
The analysis took a public sector perspective, which included costs incurred by the public sector. The analysis was presented with and without the inclusion of government-funded benefits. We reported aggregated costs by public sector (education, health care, welfare).
Modelling the health consequences of behavioural change
An extensive literature search and consultation with experts was conducted to identify quantitative evidence about the different elements (cognitive, behavioural and biological) of the theory of change behaviour that could be used to inform the final structure of the model for the target population. However, because no evidence was found about how variations in the cognitive outcomes could be converted into changes in the behavioural and biological outcomes, the structure of the model shown in Figure 5 was modified and focused on how changes in behavioural outcomes were translated into changes in biological outcomes. Specifically, the updated model assumed that the behavioural change targeted by the intervention will result in a delay in sexual debut and/or increase of contraception use. The analysis focused on how any changes in these behavioural outcomes affected the number of pregnancies and cases of STIs.
Modelling the number of pregnancies
To estimate the number of pregnancies averted, we used a mathematical model to define how different types of contraceptive methods were translated into cases of pregnancy:
The total number of pregnancies (Y) depended on the number of sexually active females in each group of the study (Nf), the probability of becoming pregnant within 1 year without contraception (L), the percentage of students using condoms (gcon), pill/patch/ring (gpil), emergency pill (geme), injection (ginj), diaphragm/cap/spermicide (gdia), implant (gimp), intrauterine device (giud), withdrawal (gwit) or no contraception (gnoc), and the contraceptive failure rates for each contraceptive class (Kcon, Kpil, Keme, Kinj, Kdia, Kimp, Kiud, Kwit). Evidence on the failure rates was taken from the ROI analysis of improving access to contraception in the UK. 165 The failure rate was defined as the percentage of women experiencing unintended pregnancy within 1 year of typical use of that contraceptive method. The rates of contraception use were taken from responses to the follow-up questionnaire in the If I Were Jack trial. The impact that social disadvantage may have on the number of unplanned pregnancies was accounted for based on evidence from the third National Survey of Sexual Attitudes and Lifestyles (NATSAL)166 and the proportion of pupils receiving FSM, collected from the trial. 167 A sensitivity analysis was conducted to assess the impact that variations in the area-level deprivation effect and failure rates of the contraceptive methods may have on the final results.
The proportion of sexually active males and females aged < 16 years was estimated using the answers to the HBSC surveys for England,168 Wales169 and Scotland170 and the Young Life and Times171 (YLT) survey for NI. We took this frequency to be an approximation of the proportion of sexually active females and males in the target population in each country. We used National Office of Statistics (NOS) data about the population estimates of females and number of births by age in 2017 in England, Wales, Scotland and NI to obtain the total number of sexually active females in the target population in each country. 16,172–174 We then combined these data with the evidence from the answers to the NATSAL-3 survey166 to obtain estimates of the number of sexually active females in three different age groups: 11–13 years, 14 years and 15 years.
There were no directly measured data for the probability of becoming pregnant within 1 year without contraceptive use in the UK. For the US, evidence from the published literature was available to first calculate the 1-month pregnancy probability and convert this into a 1-year probability. 175 This evidence was adapted in the literature using data from the HBSC surveys for England, Wales and Scotland and the 2011 YLT survey for NI. We used the available evidence on the conceptions and population of females, baseline condom use and annual condom failure rate to derive an estimate of L for each country in the UK among young people aged < 16 years. 16,168–173,176 We included in the model different types of outcomes associated with the number of pregnancies averted using the structure shown in Figure 6.
FIGURE 6.
Model structure for the outcome associated with the number of pregnancies averted.

The probability of becoming pregnant in the target population was expressed, following conception, in terms of the probability of females giving birth, terminating the pregnancy, miscarrying or having an ectopic pregnancy or a stillbirth. The probability of birth, abortion, miscarriage/ectopic pregnancy/stillbirth was based on national government statistics for England, Wales and Scotland. 16,170–174 For NI, the model uses the information about the number of abortions in England and Wales for NI residents. 177 The probability of miscarriage/ectopic pregnancy/stillbirth is based on Hospital Episode Statistics (HES) data collected by the Information Centre for Health and Social Care. 178
Modelling the number of sexually transmitted infections
The number of infections of each type of STI for each individual was modelled using a discrete event simulation approach based on an individual (or agent) multi-STI model. 179 The model estimated the number of STI cases averted for HIV and also for chlamydia, gonorrhoea and genital warts, according to the risk of infection as shown above and the proportion of sexually active individuals who received the intervention.
Sexual behaviour
Evidence about the frequency of vaginal sexual intercourse, number of sexual partners and proportions of sexually active teenagers using condoms for vaginal sexual intercourse was taken from the trial. Evidence about the effectiveness of condoms for protecting against STIs and reducing heterosexual HIV transmission was estimated based on evidence from the literature. 180–188 For genital warts, we used the evidence from a longitudinal study on young people,189 while a Cochrane systematic review estimated the reduction in HIV incidence due to condom use. 190
Benefit and cost outcomes
Monetising quality of life and other non-cost benefits
Utility scores were not assigned to teenage conceptions owing to a lack of evidence from the literature, difficulty in reaching a consensus around the valuation of pregnancies carried to term and those that are not, and the fact that it is not by any means certain that pregnancy as a health state generally diminishes health-related quality of life. 191,192 However, the model could explore the cost-effectiveness of reduced conceptions by young people based on willingness-to-pay criteria. The utilities associated with various STI outcomes were estimated using the evidence from the published literature. 193–195 We used these values to assign the utility weights to each type of STI considered, which were then used to calculate the quality-adjusted life-years (QALYs) gained from the reduction in cases of chlamydia, gonorrhoea, genital warts and HIV. The QALYs gained from reduction in each STI was calculated by multiplying the cases averted by (1 – utility for STI) multiplied by (1 – proportion treated for STI).
Costs
The costs incorporated within the health economic model included:
-
the costs from the trial for the intervention and control group
-
contraception methods and maternity costs
-
abortion and miscarriage costs
-
costs for the treatment of very low-birthweight babies
-
costs for the testing and treatment of STIs and their health consequences
-
government-funded benefits
-
medium- and long-term loss of earnings due to teenage pregnancy.
The health-care cost perspective includes costs 1–5 above, with the wider cost analysis including costs 1–7. The costs associated with the resource use collected in the trial are described in Within-trial analysis above. The average costs of birth, abortion and miscarriage/ectopic pregnancy/stillbirth were taken from the NHS reference costs. 196 The cost of pre-school and primary school education for children was also considered in the analysis, under the assumption that the government would maintain funding at current levels. 197 While we recognise there are variations in school age start and costs across the four nations, the figure for England was used. The mean per-pupil funding was taken from the analysis of the Institute for Fiscal Studies (IFS), with pre-school costs incurred only at ages 3 and 4 years and primary school costs incurred from the age of 5. 198 The cost of treatment of STIs was based on the health economic model developed for the National Institute for Health and Care Excellence (NICE) SRE public health guidance176 and expert guidance. Treatment for chlamydia is assumed to require doxycycline 100 mg twice per day for 1 week and azithromycin 1 g followed by 500 mg daily for the next 2 days. Given that first-line treatment for chlamydia is frequently provided outside specialist care, the model assumes that treatment is offered 50% of the time in GP practices and 50% in genitourinary medicine (GUM) clinics. A sensitivity analysis to assess the impact on the results of assuming that treatment for chlamydia is always provided in GUM clinics is also explored. Treatment for gonorrhoea is assumed to require ceftriaxone 1-g intramuscular (IM) injection in GUM clinics, whereas treatment for genital warts was assumed to require one dose of imiquimod and a GP consultation. An average cost of HIV treatment per year was estimated based on the sum of the average cost of care for HIV patients and the average cost of drug treatment. The costs of benefit payments were also included within the model as they were costs incurred by the public sector, which represent real resource savings if the child that might otherwise eventuate had not been conceived. Evidence on different types of benefit payments (child benefits, child tax credits, income support and housing benefits) for the target population was taken from published sources, such as the Teenage Pregnancy Strategy report199 and governmental sources. 200,201
Finally, when calculating the number of pregnancies and births averted through the use of contraception, it is generally not correct to assume that all of these births, if avoided today, would not have occurred later as a planned birth. 176 Evidence from the USA National Survey of Family Growth suggests that 60% of unplanned births are mistimed and 40% of births would have otherwise never occurred. 202 The full direct and indirect costs of birth can only be considered for those 40% of unplanned births that would have not occurred later. For the remaining 60% of births that are mistimed, the cost averted by contraception was the cost of incurring expenditure at an earlier point than otherwise would have occurred later. We calculated the cost of a mistimed birth (MB) as
where B is the cost of a birth, r is the discount rate and d is the number of years by which the birth would have been delayed (taken as 2 years in the literature203). Given that the proportion of MBs was based on US data, we varied this in sensitivity analysis to assess its impact on the results.
Sensitivity analysis
A number of deterministic sensitivity analyses (DSAs) and PSAs were undertaken to assess the impact on the results of key parameters and assumptions in the model. Under each scenario, each parameter was varied either separately in a deterministic way (DSA) or simultaneously using probability distributions (PSA) over a large number of iterations of the model.
Cost-effectiveness analysis
We calculated the mean incremental total cost of If I Were Jack compared with standard RSE practice for (1) cost per pregnancy averted, (2) cost per STI averted and (3) cost per QALY gained over a 20-year time period under a health-care (excluding government-funded benefits and lost earnings) and wider cost perspective (including government-funded benefits and lost earnings).
All costs and consequences after 12 months were discounted at an annual rate of 3.5% in line with NICE guidance to capture time preferences for costs and consequences. 204 All costs are reported in 2019/2020 Great British pounds.
Results
The cost of training and teacher time delivering If I Were Jack
The cost of If I Were Jack was based on the opportunity cost of teachers delivering the intervention. The data were collected via questionnaires from a total of 96 teachers across 30 intervention schools. Estimates for the lesson duration were obtained by taking the average time required for each type of lesson: type A (50–60 minutes), type B (35–45 minutes) and type C (drop-down day/two half-days. Estimates of the overall time spent and associated cost were then derived by summing up the estimates computed for each lesson type and dividing by the total number of students in the If I Were Jack group (Table 25). For comparison, standard RSE costs £4.42 per student (see Appendix 2, Table 49).
| Resource use | n (%) | Time (minutes), mean (SD) | Costs (£), mean (SD) |
|---|---|---|---|
| Lesson preparation | 87 (0.91) | 109 (84) | 44 (34) |
| Photocopy preparation | 63 (0.66) | 36 (51) | 35 (82) |
| Other input (e.g. discussion) | 63 (0.66) | 78 (114) | 31 (45) |
| Other input (e.g. equipment) | 50 (0.52) | – | 77 (74) |
| Overall preparation | 92 (0.96) | 187 (172) | 139 (133) |
| Lesson delivery | 94 (0.98) | 262 (89) | 104 (36) |
| Total | 94 (0.98) | 438 (229) | 240 (153) |
| Treatment cost per student | – | – | 5.48 |
Completion of the health-care resource use questionnaires
Of the 8216 students enrolled in the trial (4100 in the intervention group and 4116 in the control group), a total of 7734 (94%) and 6561 (80%) completed health resource use questionnaires at baseline and follow-up, respectively. Overall, a total of 6519 (79%) students provided complete responses, with a slightly higher completion rate in the intervention group (81%) than in the control group (77%).
Sexual health resource use and costs
Each type of sexual health resource use was summarised in terms of number and proportion of observations, means and standard deviations (SDs) (Table 26). Given the large number of students who did not use any resources, summary statistics related to the resource use questionnaire data were reported only for students who used the resources. Cost data were summarised in terms of means and SDs for all students because the average costs in the economic evaluation should be calculated based on all participants (Table 27). The mean adjusted difference of If I Were Jack minus standard RSE for health-care resource use costs only is –£2.33 (95% CI –£6.73 to £2.07) per student, adjusting for stratification variables (proportion of FSM and country) using a random intercept model to account for clustering (students within schools).
| Resource | Baseline | Follow-up | ||
|---|---|---|---|---|
| Control group (N = 4100) | Intervention group (N = 4116) | Control group (N = 3178) | Intervention group (N = 3341) | |
| Sexual health clinic | ||||
| n (%) | 58 (1.4) | 57 (1.4) | 150 (4.7) | 113 (3.4) |
| Mean (SD) | 1.67 (1.05) | 2.29 (2.53) | 2.11 (1.70) | 2.07 (1.82) |
| School nurse | ||||
| n (%) | 256 (6.2) | 271 (6.6) | 105 (3.3) | 131 (3.9) |
| Mean (SD) | 1.57 (1.05) | 1.61 (0.93) | 1.8 (1.24) | 1.63 (1.06) |
| GP | ||||
| n (%) | 62 (1.5) | 81 (2.0) | 138 (4.3) | 141 (4.2) |
| Mean (SD) | 1.53 (0.95) | 1.81 (1.64) | 1.67 (1.34) | 1.38 (0.80) |
| GP nurse | ||||
| n (%) | 40 (1.0) | 41 (1.0) | 55 (1.7) | 79 (2.4) |
| Mean (SD) | 1.25 (0.54) | 1.80 (1.71) | 1.64 (1.22) | 1.71 (2.05) |
| Free condoms | ||||
| n (%) | 256 (6.2) | 395 (9.6) | 434 (13.7) | 427 (12.8) |
| Mean (SD) | 2.56 (4.67) | 3.29 (5.31) | 2.93 (3.96) | 3.26 (4.67) |
| Bought condoms | ||||
| n (%) | 103 (2.5) | 155 (3.8) | 299 (9.4) | 395 (11.8) |
| Mean (SD) | 4.17 (7.24) | 3.92 (7.87) | 3.35 (4.81) | 3.38 (4.80) |
| Other contraception | ||||
| n (%) | 53 (1.3) | 75 (1.8) | 214 (6.7) | 218 (6.5) |
| Mean (SD) | 1.77 (1.92) | 1.75 (1.44) | 2.03 (2.13) | 2.12 (2.28) |
| Pregnancy test | ||||
| n (%) | 33 (0.8) | 50 (1.2) | 85 (2.7) | 87 (2.6) |
| Mean (SD) | 1.67 (1.08) | 1.30 (0.84) | 1.48 (0.87) | 2.05 (3.14) |
| STI test | ||||
| n (%) | 23 (0.6) | 33 (0.8) | 50 (1.6) | 55 (1.6) |
| Mean (SD) | 1.52 (0.99) | 2.55 (3.09) | 1.50 (0.84) | 2.22 (3.60) |
| Emergency contraception | ||||
| n (%) | 18 (0.4) | 25 (0.6) | 78 (2.5) | 96 (2.9) |
| Mean (SD) | 2.17 (2.96) | 1.76 (2.24) | 1.31 (0.84) | 1.98 (2.35) |
| Resource | Baseline | Follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control group, mean (SD) | Intervention group, mean (SD) | Control group, mean (SD) | Intervention group, mean (SD) | |||||
| Sexual health clinic | 2.992 (28.71) | 4.030 (49.16) | 12.352 (70.71) | 8.764 (61.43) | ||||
| School nurse | 1.146 (5.23) | 1.240 (5.26) | 0.681 (4.40) | 0.734 (4.26) | ||||
| GP | 0.832 (7.69) | 1.284 (11.88) | 2.552 (15.21) | 2.054 (11.14) | ||||
| GP nurse | 0.154 (1.65) | 0.228 (3.03) | 0.353 (3.26) | 0.505 (4.99) | ||||
| Free condoms | 0.336 (2.70) | 0.665 (3.91) | 0.833 (3.62) | 0.869 (4.06) | ||||
| Bought condoms | 0.219 (2.69) | 0.310 (3.47) | 0.657 (3.61) | 0.725 (3.77) | ||||
| Other contraception | 0.173 (2.16) | 0.241 (2.23) | 1.019 (5.49) | 1.035 (5.73) | ||||
| Pregnancy test | 0.056 (0.73) | 0.066 (0.70) | 0.164 (1.13) | 0.221 (2.44) | ||||
| STI test | 0.148 (2.28) | 0.354 (6.00) | 0.403 (3.59) | 0.623 (9.03) | ||||
| Emergency contraception | 0.299 (7.32) | 0.338 (6.74) | 0.997 (7.36) | 1.765 (15.74) | ||||
| Total costs | Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI |
| 5.49 (33.98) | 4.30 to 6.67 | 7.40 (59.53) | 5.38 to 9.42 | 18.33 (78.08) | 15.61 to 21.05 | 14.09 (63.54) | 11.94 to 16.25 | |
Within-trial total costs
For each student, the total costs were computed as the sum of the costs of delivering the If I Were Jack intervention, obtained from the teacher-completed resource use questionnaires, and the costs of the health-care resource use, obtained from the student-completed questionnaires. The total mean incremental cost of the intervention compared with standard RSE was £2.83 (95% CI –£2.64 to £8.29) per student. The adjusted mean total cost per student at follow-up obtained from the complete cases was £22.59 (95% CI £16.27 to £28.88) for the intervention and £19.78 (95% CI £13.59 to £25.96) for standard RSE. The adjusted analysis controlled for baseline total costs and stratification variables (proportion of FSM and nation) using a random intercept model to account for clustering (students within schools). The 95% CIs were calculated based on bootstrapped bias-corrected methods over a total of 10,000 iterations.
For the MICE sensitivity analysis with 20 imputed data sets, the total mean incremental cost per student of If I Were Jack compared with standard RSE was £1.81 (95% CI –£7.67 to £4.04).
We also included information on the cost of adapting the intervention to different groups, or updating it over time. The direct costs of making an adapted version for England/Wales with new video production was £35,000, to include all interactive video production and production of adapted online resource materials. Divided by the number of young people randomised to the intervention in England (n = 1071) and Wales (n = 1160), the cost per student was £15.69, which represents the upper estimate of the cost per student to adapt the intervention. If the intervention was rolled out to all young people 14 years of age in England (664,025 in 2020) and Wales (35,967 in 2020),173 the cost per student would be £0.05. The direct costs of making changes to the online resource materials for Scotland was £1000, or £1.15 per student if divided by the number of students randomised to the intervention in Scotland (n = 866), or £0.02 per student if rolled out to all students aged 14 in Scotland (57,487 in 2020).
Consequences and decision model inputs
The comparative results between the two trial groups in terms of unadjusted ORs at each time point and aORs at follow-up are reported in Table 28. Separate ORs between the groups are reported by time point (baseline and follow-up) for key outcome variables, including ever had unprotected sex, ever had sex and having a pregnancy or STI test. All aORs were computed after controlling for the corresponding baseline outcome values and stratification factors.
| Consequences | Baseline (n = 7734) OR (95% CI) | Follow-up (n = 6561) OR (95% CI) | Adjusted (n = 6519) OR (95% CI) |
|---|---|---|---|
| Ever had unprotected sex | 0.849 (0.682 to 1.106) | 0.959 (0.832 to 1.105) | 0.845 (0.625 to 1.142) |
| Ever had sex | 0.926 (0.771 to 1.113) | 0.980 (0.871 to 1.103) | 0.839 (0.622 to 1.131) |
| Testing for pregnancy | 1.519 (0.976 to 2.362) | 0.975 (0.719 to 1.319) | 0.952 (0.629 to 1.440) |
| Testing for STIs | 1.431 (0.839 to 2.442) | 1.046 (0.711 to 1.540) | 0.960 (0.619 to 1.488) |
Summary statistics for different types of consequences (by type of contraception and STI) at follow-up are reported in Table 29. Total number of cases and proportions for each type of contraception method [pill, condom, emergency pill, injection, implant, intrauterine device (IUD), diaphragm/cap/spermicide, other, none] and STI [chlamydia, genital warts, herpes, gonorrhoea, pubic lice, trichomonas, syphilis, HIV, hepatitis, pelvic inflammatory disease (PID), other] are separately reported for the intervention and control groups, as well as for all individuals in the study.
| Consequences | Trial group, n (%) | ||
|---|---|---|---|
| Control (N = 688) | Intervention (N = 733) | Total (N = 1421) | |
| Type of contraception | |||
| Pill | 188 (27.3) | 193 (26.3) | 381 (26.8) |
| Condom | 380 (55.2) | 402 (54.8) | 782 (55.0) |
| Emergency pill | 34 (4.9) | 21 (2.9) | 55 (3.9) |
| Injection | 32 (4.7) | 11 (1.5) | 43 (3.0) |
| Implant | 57 (8.3) | 39 (5.3) | 96 (6.8) |
| IUD | 6 (0.9) | 4 (0.5) | 10 (0.7) |
| Diaphragm/cap/spermicide | 1 (0.1) | 1 (0.1) | 2 (0.1) |
| Other | 6 (0.9) | 4 (0.5) | 10 (0.7) |
| None | 126 (18.3) | 164 (22.4) | 290 (20.4) |
| Type of STI | |||
| Chlamydia | 3 (0.4) | 11 (1.5) | 14 (1.0) |
| Genital warts | 3 (0.4) | 5 (0.7) | 8 (0.6) |
| Herpes | 2 (0.3) | 7 (1.0) | 9 (0.6) |
| Gonorrhoea | 5 (0.7) | 7 (1.0) | 12 (0.8) |
| Pubic lice | 2 (0.3) | 7 (1.0) | 9 (0.6) |
| Trichomonas | 2 (0.3) | 5 (0.7) | 7 (0.5) |
| Syphilis | 4 (0.6) | 7 (1.0) | 11 (0.8) |
| HIV | 3 (0.4) | 7 (1.0) | 10 (0.7) |
| Hepatitis | 2 (0.3) | 6 (0.8) | 8 (0.6) |
| PID | 2 (0.3) | 5 (0.7) | 7 (0.5) |
| Other | 2 (0.3) | 4 (0.5) | 6 (0.4) |
Long-term decision model
Over 20 years, per 100,000 young people receiving If I Were Jack compared with those receiving standard RSE, If I Were Jack resulted in 379 fewer unintended pregnancies, 680 fewer STIs and 10 additional QALYs at a cost saving of £969,876 (excluding government-funded benefits), or a cost saving of £9.70 per young person who received the intervention (Table 30). Table 31 reports the overall and treatment-specific base-case discounted (at 3.5%) cost estimates from the model disaggregated into the different cost components, and Figure 7 shows the total number of unintended pregnancies, split between number of abortions, miscarriage and births, and the total number of STIs, by STI type. The majority of cost savings, excluding benefits, were due to costs associated with birth avoided. This is as a result of the reduction in unintended pregnancies.
| Results | Control group | Intervention group | Averted outcomes/incremental costs |
|---|---|---|---|
| Unintended pregnancies, n | 2531 | 2152 | 379 |
| STIs, n | 1853 | 1173 | 680 |
| Discounted | |||
| QALYs loss | 28 | 18 | 10 |
| Total costs, £ (without benefits) | £20,459,742 | £19,470,336 | –£989,406 |
| Total costs, £ (with benefits and lost earnings) | £191,457,170 | £166,111,565 | –£25,345,605 |
| Cost components | Control (£) | Intervention (£) | Incremental (£) |
|---|---|---|---|
| Contraception costs | 4,832,457 | 5,982,093 | 1,145,703 |
| Pregnancy costs | 600,064 | 596,131 | –3933 |
| Abortion costs | 987,846 | 842,759 | –145,087 |
| Miscarriage/ectopic pregnancy/stillbirth costs | 99,396 | 81,888 | –17,507 |
| STI treatment | 270,122 | 172,520 | –97,602 |
| Birth costs | 13,669,857 | 11,794,945 | –1,874,912 |
| State benefits and lost earnings | 170,997,429 | 146,641,228 | –24,356,201 |
FIGURE 7.
Total number of teenage (< 16 years) unintended pregnancies and STIs per 100,000 young people over a time horizon of 20 years for standard RSE compared with the If I Were Jack intervention. (a) Unintended pregnancies; (b) STIs.
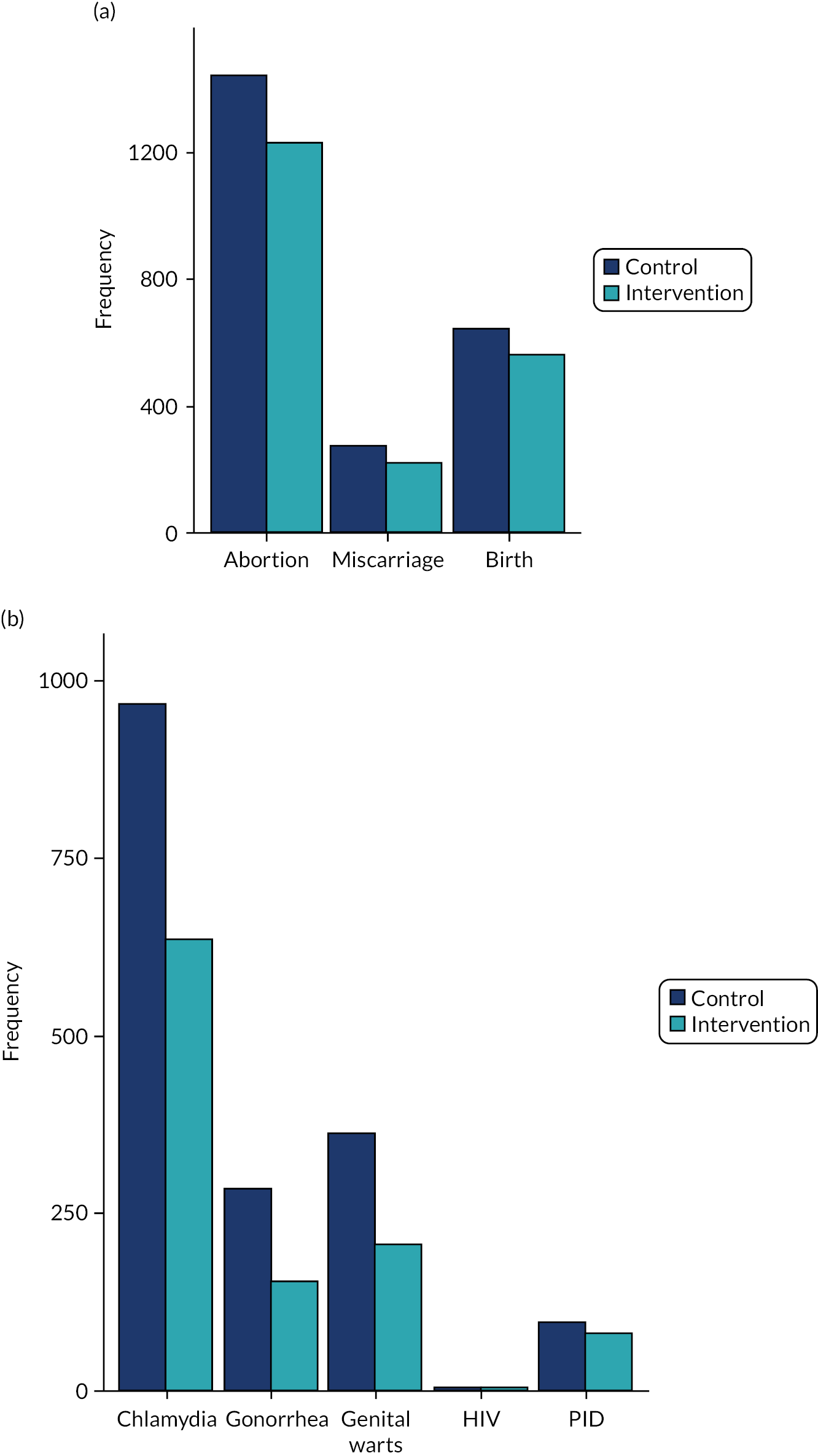
The largest gap was observed in the number of unintended pregnancies that resulted in abortions (1447 in the control group vs. 1229 in the intervention group), followed by births (644 in the control group vs. 559 in the intervention group) and miscarriages (272 in the control group vs. 220 in the intervention group). Similar trends were observed for most types of STIs, with the number of chlamydia cases being associated with the largest discrepancy between the two interventions (1090 in the control group vs. 635 in the intervention group), followed by genital warts (363 in the control group vs. 227 in the intervention group). Relatively small differences were observed in the cases of gonorrhoea (165 in the control group vs. 153 in the intervention group) and PID (females only; 94 in the control group vs. 80 in the intervention group), and no substantial difference was observed in the number of HIV cases (around 1 for both groups).
When nation-specific values were included in the model, including country-specific effects from the trial, the largest cost savings and greatest benefits were seen in England (see Appendix 2, Table 45).
Deterministic sensitivity analysis
The results of the one- and two-way sensitivity analyses testing low and high extremes in values for failure rates (the probability of an unintended pregnancy) for condoms and withdrawal, STI prevalence and transmission rates are reported in Appendix 2, Tables 46–48. In all scenarios, the If I Were Jack intervention exceeded standard RSE in that it resulted in better outcomes for a lower cost, except under the extreme scenario in which the failure rate of condoms was halved (from 18% in the base-case scenario to 9%), with a total number of 178 averted pregnancies (compared with the 379 in the base-case scenario) and an incremental total cost of £1,131,487 (excluding benefits and lost earnings). Detailed information about the results of the model under a selection of scenarios explored in the DSA is provided in Appendix 2, Tables 46, 47 (one-way sensitivity analysis) and 48 (two-way sensitivity analysis).
Probabilistic sensitivity analysis
Tables 32 and 33 show the results from the PSA, in which the model parameters were randomly varied by drawing their values from associated probability distributions (see Appendix 2, Table 44, for detailed information about the choice of the distributions and parameter variations). In Table 32, 95% bootstrapped CIs for the total number of unintended pregnancies, STIs and QALYs and associated costs (either excluding or including government-funded benefits) by treatment group are reported alongside estimates obtained in the base-case analysis. In addition, 95% bootstrapped CIs obtained under the PSA for the averted results for each type of outcome and incremental costs between the two groups are reported and compared with corresponding base-case estimates. In Table 33, total cost results obtained under the PSA reported by type of cost component, namely the costs related to contraception, pregnancy, abortion, miscarriage/ectopic pregnancy/stillbirth, STI treatment, birth, and government-funded benefits and lost earnings. For a £20,000 and £30,000 cost-effectiveness threshold per QALY gained there is, respectively, a 96% and 99% probability that the If I Were Jack intervention is cost-effective compared with standard RSE.
| Outcome | n (95% CI) | Total costs without benefits, £ (95% CI) | Total costs with benefits, £ (95% CI) | |||
|---|---|---|---|---|---|---|
| Control | Intervention | Control | Intervention | Control | Intervention | |
| Unintended pregnancies | 2,531 (2461 to 3100) | 2152 (2078 to 2716) | 20,459,742 (18,687,125 to 24,591,145) | 19,470,336 (17,003,319 to 22,175,576) | 191,457,170 (140,548,595 to 217,430,076) | 166,111,565 (134,884,491 to 171,019,049) |
| STIs | 1853 (1106 to 3400) | 1173 (412 to 2467) | ||||
| QALYs loss | 28 (19 to 45) | 18 (14 to 30) | ||||
| Averted outcomes/incremental costs | ||||||
| Unintended pregnancies | 379 (231 to 477) | –989,406 (–1,559,545 to –382,949) | –25,345,605 (–47,857,741 to 5,438,251) | |||
| STIs | 680 (189 to 1467) | |||||
| QALYs | 10 (5 to 16) | |||||
| Cost components | Control, estimate (£, 95% CI) | Intervention, estimate (£, 95% CI) | Incremental, estimate (£, 95% CI) |
|---|---|---|---|
| Discounted | |||
| Contraception costs | 4,832,457 (4,645,046 to 5,045,220) | 5,982,093 (5,791,743 to 6,190,293) | 1,145,703 (1,126,841 to 1,216,578) |
| Pregnancy costs | 600,064 (506,366 to 716,344) | 596,131 (480,238 to 703,678) | –3933 (–50,181 to 42,480) |
| Abortion costs | 987,846 (825,467 to 1,139,093) | 842,759 (747,888 to 947,512) | –145,087 (–214,646 to –60,854) |
| Miscarriage/ectopic pregnancy/stillbirth costs | 99,396 (73,811 to 141,232) | 81,888 (54,695 to 104,823) | –17,507 (–36,428 to –2,020) |
| STI treatment | 270,122 (149,359 to 693,619) | 172,520 (132,954 to 486,693) | –97,602 (–207,776 to 150) |
| Birth costs | 13,885,602 (11,576,613 to 16,041,941) | 11,928,685 (9,454,455 to 13,888,264) | –1,956,917 (–3,299,170 to –413,975) |
| Government-funded benefits and lost earningsa | 170,997,429 (156,208,678 to 183,834,114) | 146,641,228 (140,286,029 to 153,431,931) | –24,356,201 (–32,711,305 to –15,922,648) |
Incremental results obtained from the PSA, quantifying the impact of sampling uncertainty on base-case estimates, are graphically summarised in Figure 8 using separate cost-effectiveness planes for each type of outcome: pregnancies averted, STIs averted and QALYs gained. The majority of iterations (97.5% for pregnancies, 96.6% for STIs and 95.7% for QALYs) were located in the south-east quadrant as the If I Were Jack intervention resulted in better outcomes for a lower cost.
Probabilistic sensitivity analysis: cost-effectiveness planes
FIGURE 8.
Cost-effectiveness planes for the expected number of averted outcomes (unintended pregnancies, STIs and QALY losses) and the total costs increment (health service cost perspective) between the two treatment groups. Estimates are obtained based on a total of 1000 iterations for the PSA.
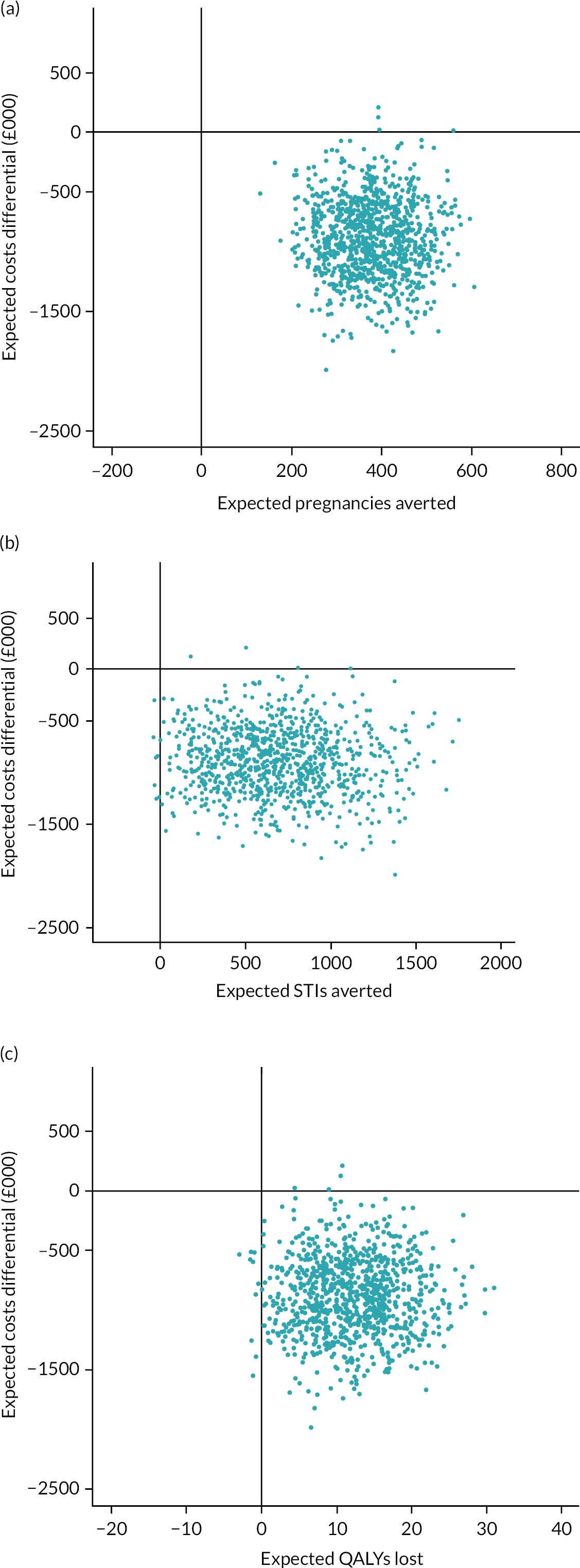
Chapter 8 Discussion
Primary and secondary results
The primary analysis found no significant differences between the intervention and control groups in relation to self-reported avoidance of unprotected sex, measured as a combination of sexual abstinence or use of reliable contraception at last sex. However, a post hoc exploratory analysis of these questions separately showed that the intervention was effective in increasing the use of reliable contraception at last sex for those who already were, or became, sexually active by the time of follow-up. There were no significant differences in rates of sexual abstinence between the intervention or control groups at the 12- to 14-month follow-up.
The If I Were Jack intervention led to significant improvements in a number of important secondary outcomes relating to our theory of change, notably knowledge, attitudes towards male gender roles and intentions to avoid an unintended pregnancy. There were also small and statistically non-significant improvements in sexual self-efficacy and comfort communicating about avoiding unintended pregnancy.
Significant improvements in knowledge included improved knowledge of reliable contraceptive methods, how to access contraception and the legal age of consent. Students in intervention schools had stronger intentions to avoid UTP. This included stronger intentions to use reliable contraception, avoid peer pressure to have sexual intercourse, not to have sex until ready and be prepared to share responsibility for contraception with a partner.
An additional planned sociodemographic subgroup analysis showed no significant differences between males and females in relation to the primary outcome. There were also no significant differences in relation to ethnicity, nation of the UK where delivery took place or socioeconomic status, as measured by the family affluence scale.
Intervention cost and cost-effectiveness
The costs for If I Were Jack fall within the ‘very low cost’ category (< £80 per student per year) for school-based interventions according to the Education Endowment Foundation guidance. 205 Taking account of staff time for training, lesson planning and delivery, in addition to health resource use, the If I Were Jack intervention cost less than £3 more per student than standard RSE.
The health economic analysis showed that If Were Jack is likely to be cost-effective when projected over a 20-year time horizon. Those in the intervention group were more likely to use reliable forms of contraception at last sex. This observed difference showed that, compared with standard RSE, the If I Were Jack intervention is likely to be cost-effective, as it would result in 379 (95% CI 231 to 477) fewer unintended pregnancies, 680 (95% CI 189 to 1647) fewer STIs and 10 (95% CI 5 to 16) QALYs gained per 100,000 young people for a cost saving of £9.89 (95% CI £3.83 to £15.60) per young person who receives it, with the majority of the cost savings related to health care. Approximately 96% of iterations are in the south-east quadrant of the cost-effectiveness plane, in that If I Were Jack results in better outcomes for a lower cost.
Process evaluation
The following issues were addressed: reasons for school participation; intervention delivery and fidelity in the context of overall RSE provision in intervention schools; RSE provision in control schools and potential contamination caused by any changes to provision that could be due to participation in the trial; and perceptions of effectiveness, especially relating to perceptions of the mechanisms of effectiveness at play in the intervention among students, teachers and school principals/head teachers.
Reasons for participation
The primary reasons for participation in the trial were an acknowledgement by schools that If I Were Jack is a high-quality, novel resource; a recognised need by schools to address RSE/holistic pastoral education; recognition that there is a gap in current materials in relation to engaging males; the opportunity for teacher training that could have wider benefits for future RSE programmes; and, lastly, the financial incentive. The main reasons for not participating were research saturation or other commitments, a perception that there was adequate RSE provision already in place, and the additional time commitment required by the trial to co-operate with the research components and/or programme delivery.
Relationship and sexuality education provision in control schools
The quality of RSE provision in both control and intervention groups, prior to the provision of If I Were Jack, was similar. On the whole, the quality of RSE provision in both groups was rated as low to medium when judged against assessment criteria of a best practice tool of RSE implementation in the UK (Sex Education Forum, 2020). 206 The comparability of low- to medium-quality provision in the intervention and control groups was consistent across all four nations, despite the fact the statutory requirements for RSE vary across the nations. There was no indication that the direction of RSE had substantially changed in the control schools as result of participation in the trial.
Intervention delivery and fidelity
The teacher training and classroom activities were generally delivered with medium to high fidelity, but the parental component, an optional element, was rarely delivered. The primary reasons reported by teachers for intervention delivery fidelity was the manualised programme and the downloadable classroom materials coupled with some flexibility in how it could be delivered. The primary reasons reported by teachers for deviations in intervention delivery fidelity were insufficient time, perceived clash with school ethos and inadequate computer facilities. Parents reported not receiving the materials and embarrassment or fear of having conversations about sex with their child. Teachers also noted student refusal and/or reluctance at a school or teacher level to engage with parents on RSE. Students who did not participate in parental element said that it would be embarrassing and awkward.
Perceptions of effectiveness/mechanisms of effectiveness
Students and teachers thought that the intervention was an opportunity to gain new knowledge on sex and relationships as well as acquiring skills in terms of where and how to find information and support. According to teachers, the intervention ‘lifted heads’ and was an ‘eye opener’ (T0121S). Students reported that learning where they could get ‘contraception and other things’ was ‘very helpful’, as was learning ‘where you could get help if you need it’, and for males knowing how to access support was largely received as ‘new information’ for them (T0121S). Teachers and students both noted increased confidence of students to communicate with peers about sex and relationships. The culturally specific interactive video seemed to be an especially enjoyable and important trigger for generating communication skills on relationships and sexuality in the classroom. It appeared to lay the groundwork and build confidence for young people in the classroom so that they could pick up and continue the conversation. The gender focus of the intervention, the engagement of males, and the generation of empathy and understanding of both male and female perspectives were regarded as key strengths of the programme. Potential limitations relating to this mechanism were a perception that the programme could overshadow female perspectives and an acknowledgement that a short programme may be insufficient to challenge deeply embedded gendered ideas around sexuality. A further limitation was the heteronormative bias of the intervention in focusing on adolescent pregnancy.
Interpretation of the study findings in the light of previous research
Overall, the results relating to the primary and secondary outcomes are consistent with two systematic reviews of systematic reviews of school-based RSE in high-income countries. 207,208 These reviews of reviews indicate that, overall, school-based RSE interventions demonstrate effectiveness in enhancing knowledge, skills and intentions, but do not demonstrate efficacy in relation to biological outcomes such as reducing adolescent pregnancy and HIV, or behavioural outcomes such as reductions in unprotected sex. While emphasising the importance of the psychosocial outcomes, these reviews also suggest that the absence of a clear pattern of effectiveness in relation to biological and behavioural outcomes is because rates of engagement in sexual intercourse and rates of HIV and pregnancy are low among adolescents aged < 16 years in high-income countries. Denford et al. 196 suggest that interventions could nevertheless be generating positive changes in sexual behaviours that are not yet manifest. The positive effects observed for the psychosocial secondary outcomes in our study (i.e. knowledge, attitudes towards male gender norms and intentions to avoid unintended pregnancy) support this argument, as these outcomes relate to mechanisms that research28,56–61,63,94 shows are linked to a reduction in risk-taking behaviour once young people are sexually active. Consistent with this theory of change, we found that evidence of positive behavioural change to avoid unprotected sex through use of reliable contraception was manifest among those who were sexually active (at baseline) or became sexually active (at follow-up). This suggests that the intervention was having a positive effect on one of the key behavioural changes of the intervention logic model, namely sexual readiness, with evidence that young people in the intervention group were more adequately prepared for this transition in life, whereas there was no evidence that the intervention increased rates of sexual initiation among young people. This finding in the present study is important, as previous high-quality systematic reviews31,209 report that few school-based interventions in high-income countries are effective in increasing contraceptive use or condom use at last sexual intercourse among young people who are sexually active, and none of the previous UK-based randomised trials of RSE interventions had demonstrated effectiveness on this outcome. 148 A US-based study demonstrated the effectiveness of an after-schools-based intervention (CAS-Carrera)70 in reducing unprotected sex at last sex among those who were sexually active. However, this study found significant effects for females only, whereas our study found that the intervention was equally effective for males and females who were sexually active, suggesting the importance of male engagement.
The positive impact on gender role attitudes with a significant shift in the intervention group towards more gender-equitable roles is consistent with Haberland and Rogow’s86 systematic review, which reported that HIV and sexuality programmes that addressed gender or power were more effective than programmes that did not. Gender inequity is widely regarded in the literature as contributing especially to deficits in girls’ SRHR but also to inequalities among boys. 75,84,85 In some studies, gender attitudes are measured among males using only the gender-equitable men’s scale. 210 It is clear from the qualitative data that the gender focus of the If I Were Jack intervention was explicit to participants. Specifically, the process evaluation results provide evidence that the gendered focus on generating critical gender awareness and male responsibility was seen as being one of the most innovative, stimulating and enjoyable elements of the intervention. In the trial results, significant positive changes in the intervention group were identified in relation to intentions to share responsibility (among males and females) to use contraception to prevent unintended pregnancy.
Our finding of significant improvements in young people’s intentions to avoid unintended pregnancy, which includes their perceived ability to share responsibility for contraceptive decision-making with a partner and communicate consent for sexual intercourse, sexual readiness and sexual preferences regarding timing, are important impacts because they address a neglected research area of considering young people’s sexual desires and preferences as part of healthy relationships in RSE. 208 Although RSE specialists have called for the inclusion of a discourse of pleasure to enhance a more holistic view of sexual well-being and other aspects of positive sexuality,211,212 the inclusion of the measurements of these outcomes are ‘conspicuous by their absence’ in randomised trials of sex education. 208
The process evaluation provided valuable insights on what RSE is wanted and what is needed and implementable in the classroom, including in faith-based schools in the UK. The JACK trial confirms that young people want comprehensive, positive, inclusive and skills-based learning to enhance their ability to develop healthy, positive relationships throughout their lives, delivered using interactive, participatory, learner-centred or critical thinking approaches. 130,208,213–217 The results also confirm teachers’ need for high-quality, evidence-informed RSE resource materials with manualised programming that are implementable in the classroom and are designed to enable participatory and critical learning. 217–220 Adding to this, both student and teacher perspectives emphasise the need to enhance teacher training and the skill set of teachers in delivering school-based RSE.
Strengths and limitations of the study
We undertook a well-conducted, large cluster RCT of an intervention proven feasibility, which was developed with very substantial user co-design. During this study, and prior to trial commencement, we undertook a further optimisation of the intervention to enhance its cultural salience across the four nations of the UK through PPI. We brought together a YPAG from the four nations of the UK in a weekend residential event to advise on all aspects of the production of two new IVDs, one using actors from NI (for use in NI and Scotland) and one using actors from England (for use in England and Wales). Further consultation on all aspects of the intervention and key aspects of study design were continued with the YPAG and a RSE expert stakeholders group, again from across all of the UK, as well as PPI membership of TSC throughout the trial. RSE experts’ feedback suggested that the opportunity to learn from other RSE experts across the whole of the UK, as well as invited international experts from WHO and Rutgers, Netherlands, was a key dividend of their partnership on this trial. 221
The trial was undertaken in a group of schools that were ethnically, culturally, and socioeconomically diverse. Uniquely, in a trial of a RSE intervention, we included schools in the four nations of the UK and included schools that were faith-based (although they were all Christian) as well as those that were not. It is also one of the few trials that has disaggregated the results by sex146 and included an analysis of how the intervention might promote more equitable gender relationships.
Participating schools were representative of the 263 schools initially approached and only four schools were lost to follow-up, two of which were a result of school closures during the COVID-19 pandemic lockdown measures. Our follow-up was lengthy to allow time both for intervention effects to develop and to capture the largest number of students before the school leaving age of 16 years. Although a longer follow-up period would have afforded a greater possibility of capturing intervention effects, especially once students reach the legal age of sexual consent (16 years in the UK), it is very difficult to collect data once students leave school. (In the UK, students may leave school at age 16 or continue until age 18 years.) The follow-up period of 12–14 months also allowed for investigation of persistence of intervention effects after the end of the facilitated intervention. Student participation was high and parental withdrawal of students was low. Our outcome research team and intervention team remained independent throughout the trial, and blinding of lead researchers was maintained. Outcomes were assessed using age-appropriate validated instruments. Although self-report outcomes can be open to recall bias, baseline data were collected before randomisation, instruments were used with standardised recall periods and actions at the school level are very unlikely to have biased reporting between intervention and control groups. Although some studies222 have included age of sexual debut as a secondary outcome, owing to concerns expressed by the reviewing research ethics committee relating to responsibilities to report sexual intercourse under the age of 13 years in the UK, age at sexual debut was not included.
Our data are subject to a number of limitations. Our trial was carried out in a randomly selected sample of the whole of NI, the south of Wales, urban and peri-urban areas of the south-east of England and central Scotland only. Our process evaluation did not identify any factors that might suggest that implementation or effects would be different in schools in other areas, given the level of diversity included, but we do not claim that the findings are generalised to all parts of the UK.
The ICC in the current study was much larger (0.12) than expected (0.01), based on our feasibility study44 and previous research in this area. 18,148 The sample size was also reduced as a result of losses to follow-up, including the loss of two schools due to COVID-19-related closures. Therefore, the study may have been underpowered. Although missing data can introduce bias, our data were analysed using an intention-to-treat approach, and sensitivity analyses to account for missing data led to little or no change in our conclusions. Missing data can probably be attributed to the sensitivity of sex research among any population, but especially among young people who are not yet at the legal age of sexual consent.
The large number of secondary outcomes investigated necessitated multiple statistical testing. However, to mitigate this, we tested only pre-specified secondary outcomes and subgroup analyses (which were reported using 99% CIs). The subgroup analyses were likely to have been underpowered. Although providing the most useful data for the majority of outcomes, student self-report is not without limitations. Specifically, it is not feasible to validate young people’s self-report of sexual activity with an objective measure, and self-reports therefore offer the best method of assessing sexual activity. 223 However, as is standard in measures of sexual activity, we provided definitions for sexual activities and terminology to aid comprehension, and student questionnaires were administered under exam conditions to enhance confidentiality of responses. 146 All the secondary outcomes were based on validated measures.
Our process evaluation was both broad, in collecting data from all schools, and deep, in exploring some processes in randomly selected case-study intervention schools in each of the four nations alongside a SEQ in all intervention schools. Although response rates for process data collection were generally high, there were two areas of data collection, the teacher implementation logs capturing delivery of implementation and surveys of parents, that had lower response rates. In relation to TILs, our triangulated data collection approach (of interviews with students, teachers and trial champions) meant that we were still able to assess acceptability and fidelity of the intervention in most schools.
The economic evaluation also had some limitations. The costs and outcomes associated with school-based public health interventions fall across multiple government bodies. 224 Outcomes such as QALYs, which are generally recommended for economic evaluations of health-care interventions in the UK, may not be the most relevant outcome of interest when the costs fall on the education sector. To address this limitation, we reported on a range of different outcomes in our analysis. Costs are reported separately to allow different decision-makers to determine the relative cost-effectiveness of the intervention on health, education and social welfare. We have included government-funded benefits, sometimes referred to as ‘transfer costs’, as, although they are complex to include and it is generally recommended that they be excluded from economic evaluations as they are cost neutral to society,225 they are a key component of the cost of unintended pregnancies and have been included in previous165 ROI analyses of contraception effectiveness. They are also likely to be of interest to some decision-makers who might consider keeping government-funded benefits to a minimum, an important political outcome. Finally, a key outcome that we are interested in, unintended pregnancy, is a rare outcome in the target age group, with costs that occur over a longer time horizon. To address this, we used decision modelling to extrapolate the hypothesised impact of reducing instances of unprotected sex on unintended pregnancies. One of the shortcomings of this approach is that the model was based on a range of assumptions. However, we attempted to address this by subjecting the model to a range of probabilistic and deterministic sensitivity tests.
Conclusion
The need for RSE to engage with young men to promote positive sexual health for all and challenge the gender inequalities that underlie young women’s generally poorer sexual health outcomes (especially in relation to sexual violence, adolescent pregnancy and STIs) is widely endorsed by the WHO83 and UNESCO33 among others. 75,84,85 To our knowledge, the JACK trial is the first randomised trial, health economic and process evaluation of a school-based RSE intervention using a gender-transformative approach to especially engage young men, as well as young women, and promote joint responsibility in preventing teenage pregnancy (by delaying sex until ready or through use of effective contraceptives) and promoting positive sexual health and relationships. To our knowledge, the JACK trial is also the first UK-wide trial of school-based RSE in which it was demonstrated that it was possible to recruit and retain faith-based schools in a trial of a comprehensive RSE. Although the intervention did not reduce the rate of unprotected sex overall (through a combination of either sexual abstinence or use of reliable contraception), positive effects were observed in the sexually active population at follow-up, and especially among those whose sexual debut was early (sexually active at baseline, median age 14 years), as well as for those who became sexually active by the follow-up time point. These results are particularly promising, as they indicate that this relatively low dose intervention is most effective for groups at higher risk of unintended pregnancy owing to earlier sexual debut and is likely to reflect the particular relevance of contraceptive use in those who already were, or became, sexually active by the 12- to 14-month follow-up. The intervention therefore showed evidence of having an impact one of its key behavioural outcomes, that of sexual readiness, while not increasing rates of sexual initiation. Furthermore, If I Were Jack was effective in equipping all young people (whether sexually active or not) with the knowledge, attitudes and intentions required for safe and pleasurable relationships now and in the future.
The health economic analysis showed that, based on a 20-year time horizon, the If I Were Jack intervention is likely to be cost-effective, as it would result in fewer unintended pregnancies and STIs and a QALY gain for a cost saving of £9.89 per young person who receives the If I Were Jack intervention compared with standard RSE, with the majority of the cost savings related to health care. It is a low-dose, low-cost intervention with the cost per student falling well below the Educational Endowment Fund threshold for ‘very low-cost’ interventions. The school-based method of delivery in If I Were Jack provides a universal and efficient way of promoting sexual health and pregnancy prevention owing to the potential population-level reach, and school delivery providing as a sustainable platform for delivery.
Implications for decision-makers and practice
The year 2020 marked the 25th anniversary of the Cairo International Conference on Population and Development (ICPD) and Beijing Platform for Action Women’s Rights, which fundamentally shifted thinking on sexual and reproductive health towards the need to address gender inequalities that disproportionately affect girls and women’s sexual and reproductive health. Equally, it drew attention to the need to engage men and boys in addressing gender inequalities and to engage with men and boys as reproductive agents in their own right. However, the lack of intentional male engagement along with a focus on addressing gender inequalities within RSE, a key starting place in achieving these aims, has been highlighted as an important gap by UNESCO,226 the WHO,83 United Nations Population Fund84 and the European Society of Experts on Sex Education in their International Guidance on Sexuality Education,212 and again noted in the latest systematic review of reviews of RSE programme evaluations. 208
Closer to home, in 2021, a governmental agency [Office for Standards in Education, Children’s Services and Skills (Ofsted)] inspection of schools in England227 illuminated the gendered nature of deficits in sexual and reproductive health. The report found that 60% of young women in schools experienced contact forms of sexual harassment, compared with 25% of males. In relation to non-contact forms of sexual harassment, such as unwanted or inappropriate sexual comments, the report found that 90% of young women in schools experienced this, compared with 75% of males.
The Ofsted report227 recommends comprehensive RSE as a fundamental building block to addressing this problem in schools and specifically recommends improved teacher training in RSE. However, an important lesson from the JACK trial to add to this recommendation, and which builds on decades of practitioner learning encompassed in the ICPD conference and Beijing Platform for Women’s Rights resolutions, is that RSE programming should not be gender neutral and assume it will equally engage with males as well as females, or gender blind in relation to addressing gender inequalities. 228
The problems highlighted by the Ofsted report227 illuminate the urgent need to address problematic masculinities in school cultures in high-income countries such as the UK. To be successful in doing so, RSE should intentionally and positively engage with young men as well as young women in addressing gender inequalities in sexual and reproductive health. As one young female pupil in the Ofsted report was quoted as saying: ‘it should not be our responsibility to educate boys’ (contains public sector information licensed under the Open Government Licence v3.0).
The JACK trial provides practitioners and programmers with an acceptable, feasible and cost-effective gender-transformative programme. This programme invites young people to engage in young men’s perspectives while equally inviting young people to challenge the unequal gender norms associated with male sexual desire and female reproductive responsibility. It encourages communication and behavioural skills among young men and young women to prevent a teenage pregnancy and to know how to seek help. If I Were Jack acknowledges sexual pleasure and sexual intimacy in young people’s lives and asks young people to consider for themselves the balances between sexual pleasure and sexual responsibility in a gender-equitable manner. In addition, the programme seeks to address deficits in sex education for young men, particularly with respect to teenage pregnancy, identified in the scientific literature, which disadvantages adolescent men as well as adolescent women. 28,42,46,79,87–92
If I Were Jack is, however, a brief intervention of a low dose not designed to address all RSE needs. Although this study has demonstrated the added value of even such a brief intervention, in terms of increased knowledge and gender-equitable attitudes among young people for healthy and positive intimate relationships as well as a reduction of unprotected sex among young people who are already sexually active, perhaps the greater added value is the rigorous testing of intentional male engagement and gender-transformative components, which could be incorporated more broadly into RSE programming. Recognising that access to RSE is a human right under United Nations Rights of the Child124 and optimally delivered as other subjects are, over the whole school year across all year groups, in an age-appropriate manner,83,85,212,226 arguably the added value to advancing RSE practice in this trial is in demonstrating how and why male engagement and gender-transformative programming is important. 228
We recognise too, however, that more work could be done to enhance the gender-transformative components of the If I Were Jack intervention. Notably, the intervention could also be enhanced through components that challenge hegemonic heterosexuality to more holistically address gender inequalities that relate to LGBTQ+ young people as part of RSE and provide a broader range of knowledge, skills and access to services. Nonetheless, this study could provide an important reference point for practitioners to incorporate intentional engagement of young men and gender-transformative components in RSE that could be extended in new ways.
Implications for research
Although our study included schools with diverse socioeconomic characteristics, the study was conducted within the context of a high-income country and is not necessarily generalisable outside this context. We have plans under way to develop and trial adaptations of the If I Were Jack intervention in South America and Southern Africa, taking learning from the current study into account. We would also recommend that the feasibility and effectiveness of gender-transformative interventions should be explored further in trials across a range of diverse contexts and, in particular, low- and middle-income countries. In addition, given the promising results of this brief, gender-transformative intervention, designed to especially engage with males, we would recommend research that could test the integration of the intervention components, or similar components, as part of broader comprehensive RSE curricula. It is important too that we extend research on RSE beyond schools to research how best to meet the needs of those who have missed out on this education. Members of the team have co-designed and implemented an RSE intervention based on If I Were Jack, specifically for young offenders in custodial settings in Northern Ireland and Scotland, with promising results so far. 229
Although our study shows that it is feasible to recruit and maintain faith-based schools to a RSE intervention, all of the faith-based schools in the current study were Christian, which limits the generalisability of the study to non-Christian faith-based schools. Therefore, we would also recommend that future studies seek to recruit a diverse range of faith-based schools alongside non-faith-based schools (where applicable) to better understand the feasibility, acceptability and effectiveness of school-based RSE interventions in faith-based schools. We suggest (depending on context and prevalence of faith-based schools within each context) that this can be best achieved through active engagement with faith-based schools during the design or adaptation of the intervention to achieve early dialogue on acceptability.
We did not undertake any data linkage as part of the current study, which means that it is not possible to assess the longer-term impacts of the If I Were Jack intervention on the study outcomes or in relation to rates of unintended pregnancies, as such data are not routinely collected in NI. We recommend that future studies explore the feasibility of anonymous data linkage with routine data (if available) to explore the longer-term effects of interventions.
As highlighted by Oringanje et al. (2016),31 and as evidenced in the literature, there is a lot of variation in the way some behavioural outcomes related to sexual activity are reported in RSE intervention studies. This can make it difficult to estimate ICCs, and thus the required sample size for cluster RCTs, in this area. The ICC in this study was much larger (0.12) than expected (0.01), despite the estimates being based on our own feasibility study27 and previous research in this area. 28,29 In addition, few RCTs of RSE interventions pre-specify primary and secondary outcomes, opening the door to the possibility of outcome switching, hampering the quality of sample size calculations and study interpretation in the field. We have highlighted this with the hope of informing other researchers in planning and designing future studies.
The use of TILs to capture teachers’ implementation of the programme was not as successful in the current study as we had hoped. Given the importance of implementation data to the process evaluation, we would recommend that there should be a distinct financial incentive (for example a £100 voucher) built into trials for collecting this information from individual teachers in each school. This would offset the low response rate by individual teachers and the disproportionate effort by the research team in trying to collect these responses.
The low parental participation observed in our study is a common finding in the experimental research literature on RSE. 146 However, the results of the process evaluation suggest that a significant proportion of parents may not have received programme materials from their child’s school, which makes it difficult to draw definite conclusions about parental engagement in the current study. We recommend that future studies include training for teachers and school staff in relation to building confidence to engage with parents around RSE. Future studies might also consider closer liaison with schools to ensure that information is communicated to parents to invite their participation in the research. Although the use of digital media to engage parents in this study did increase participation when compared with our earlier feasibility trial,48 there is a need to further explore opportunities and mechanisms to improve parental engagement in RSE.
Further work is required to evaluate the suitability of different health economic outcomes for inclusion in economic evaluations of sexual health interventions aimed at young people. Extrapolating outcomes over longer-time horizons will capture a wider range of cost and outcomes, but is subject to a wide range of uncertainty.
Acknowledgements
We are indebted to the pupils, teachers and school principals/head teachers from schools in NI, England, Scotland and Wales who participated in the study, giving so generously of their time and sharing their experiences with us. There was a designated ‘trial champion’ teacher in each school with whom the research team closely liaised and who gave invaluable support to the trial study team. Included in our thanks to participants are the RSE experts from the four nations of the UK who contributed important insights into RSE provision and future directions. We are also grateful to the administrative and support staff in all the schools who provided valuable support to facilitate the research.
We would like to acknowledge the advice and support received from the chairperson of the TSC, Professor Vivien Coates (Florence Nightingale Foundation Chair in Nursing, University of Ulster), along with all the members of TSC. The scientific members were Dr Cary Roseth (Michigan State University), Alison Hadley OBE (University of Bedfordshire), and Professors Michelle McKinley and Sarah Miller (QUB). The educational professional members were Dr Darrin Barr (school principal), Maire Thompson (school principal) and Grace McCarthy (teacher), who guided us with their advice. The pupil representatives were Dylan O’Neill (parent), Iman Zatari (pupil) and Kian Wilson (pupil). All provided valuable assistance to us throughout the study.
We are also very grateful to those involved in the new production of the If I Were Jack IVD for this study. Thanks to the producers and directors at Morrow Communications and to the whole cast and crew. In addition, our appreciation goes to Peter Gee of Cardiff University (Lead, the ALPHA young people’s research advisory group), who facilitated a 2-day residential consultation with young people to advise on all aspects of the production, and to the 12 young people involved from each of the nations of the UK.
We also express sincere gratitude to the members of the Trial Stakeholder Advisory Committee, who provided valuable advice on comprehensive RSE across the whole of the UK. The membership was Joanna Brown (BHSCT), Kathryn Gilbert (The Council for the Curriculum, Examinations & Assessment), Drs Louise Herron and Barbara Porter (The Public Health Agency), Michael McCarten (The Rainbow Project), Dr Julie Bishop (Public Health Wales), Wendy Ostler (Healthy Schools Wales), Elaine McCormack (NHS Greater Glasgow and Clyde), Suzanne Hargreaves (Education Scotland), Felicity Sung (Scottish Government), Christina McMellon (City of Edinburgh Council), Alison Hadley OBE, Jonny Hunt (Going Off the Rails, England), Lisa Hallgarten (Sex Education Forum, London), Dr Amy Booth (Barnsley Council, England) and Jonathan Baggaley (PSHEA, England).
In addition, we would like to express our appreciation in thanking a number of people who helped towards the successful completion of the study. Dr Eimear Ruane-McAteer, Dr Kim Appleton, Dr Florian Tomini, Dr Michelle Templeton, Dr Rhonda Curran and Jaele Rollins were involved for a period of the study and made valuable contributions to it. Dr Lisa Maguire and Professor Adam Fletcher contributed to early-stage proposal development. Mr Paul Doherty was the NI Clinical Trials Unit manager for the study.
Finally, we would like to thank the Ethics Committee at the School of Nursing and Midwifery, QUB, chaired by Dr Oliver Perra, to whom we are grateful for guiding the study’s ethics approval process.
Ethics approval
Ethics approval for the study was granted by the Research Ethics Committee of the School of Nursing and Midwifery, Queen’s University Belfast in July 2017 (reference number 11.MLohan.05.17.M6.V1).
This trial was registered with the ISRCTN (reference number 99459996).
Funding
Queen’s University Belfast agreed to act as sponsor for the research.
Contributions of authors
Maria Lohan (https://orcid.org/0000-0003-3525-1283) (Professor of Social Science and Health) was the chief investigator. She conceptualised the study and led design of the study, the research and writing of the manuscript. She conducted the trial’s progress review, including staff and resources, and ensured that the trial was administered in a financially responsible manner.
Kathryn Gillespie (https://orcid.org/0000-0001-5272-392X) (Research Fellow) was the lead researcher on the process evaluation data analysis and write-up. She contributed to data collection and to trial data interpretation and write-up.
Emily Warren (https://orcid.org/0000-0002-9117-844X), Ruth Lewis (https://orcid.org/0000-0002-6768-6188), Kelly Buckley (https://orcid.org/0000-0002-8862-3776), Theresa McShane (https://orcid.org/0000-0003-1284-1272) and Linda Adara (https://orcid.org/0000-0002-0015-3942) (Research Fellows) led school recruitment and study data collection, and contributed to process evaluation study design, data analysis and writing of the manuscript.
Áine Aventin (https://orcid.org/0000-0001-5849-0506) (Lecturer, Sexual and Reproductive Health, Co-investigator) was trial manager (year 1) and had day-to-day responsibility for the conduct of the trial and the operations of the research team in year 1. She also contributed to the conceptualisation and design of the study, optimisation of the intervention, process evaluation data analysis and writing of the manuscript.
Aisling Gough (https://orcid.org/0000-0002-4201-7316) (Research Fellow) and Susan Lagdon (https://orcid.org/0000-0003-0477-2297) [Lecturer, Psychology (Mental Health)] were trial managers during years 3 and 4 and year 2, respectively. During this time they had day-to-day responsibility for the conduct of the trial and the operations of the research team. They contributed to data collection and writing of the manuscript.
Aoibheann Brennan-Wilson (https://orcid.org/0000-0002-6652-6238) (Research Fellow) was closely involved in interpretation of the trial data and the writing of the manuscript.
Lisa McDaid (https://orcid.org/0000-0002-7711-8723) (Professor of Social Science and Health, Co-investigator) contributed to the conceptualisation and design of the study, led the Scotland study team, contributed to trial and process evaluation data interpretation, and contributed to writing of the manuscript.
Rebecca French (https://orcid.org/0000-0002-1962-5022) (Associate Professor of Sexual and Reproductive Health Research, Co-investigator) contributed to the conceptualisation and design of the study, led the England study team, contributed to trial and process evaluation data interpretation and writing of the manuscript.
Honor Young (https://orcid.org/0000-0003-0664-4002) (Senior Lecturer, Co-investigator) contributed to the conceptualisation and design of the study, led the Wales study team, contributed to the intervention optimisation, trial and process evaluation data interpretation, and writing of the manuscript.
Clíona McDowell (https://orcid.org/0000-0002-7644-7197) (Head of Statistics, NI Clinical Trials Unit, Co-investigator) led on the design of the statistical analysis plan and statistical analysis and contributed to the writing of the manuscript.
Danielle Logan (https://orcid.org/0000-0002-3932-3654) (Biostatistician) and Sorcha Toase (https://orcid.org/0000-0003-1799-5588) (Biostatistician) contributed to statistical analysis and to writing of the manuscript.
Rachael M Hunter (https://orcid.org/0000-0002-7447-8934) (Associate Professor – Health Economics, Head of the Health Economics Analysis and Research Methods Team, Priment Clinical Trials Unit, University College London, Co-investigator) and Andrea Gabrio (https://orcid.org/0000-0002-7650-4534) (Assistant Professor in Statistics) designed and conducted the health economic analysis.
Mike Clarke (https://orcid.org/0000-0002-2926-7257) (Professor and Director of Northern Ireland Clinical Trials Unit, Co-investigator) contributed to the conceptualisation and design of the study and trial data interpretation, and contributed to the writing of the manuscript.
Liam O’Hare (https://orcid.org/0000-0002-4453-2880) (Principal Research Fellow, Co-investigator) contributed to conceptualisation and design of the study and to the trial and process evaluation data interpretation, and contributed to the writing of the manuscript.
Chris Bonell (https://orcid.org/0000-0002-6253-6498) (Professor, Public Health Sociology, Co-investigator) contributed to the conceptualisation and design of the study and trial data interpretation, and contributed to the writing of the manuscript.
Julia V Bailey (https://orcid.org/0000-0002-5001-0122) (Associate Professor in Primary Care, Co-investigator) contributed to the conceptualisation and design of the study and intervention optimisation and to the writing of the manuscript.
James White (https://orcid.org/0000-0001-8371-8453) (Reader in Population Health, Co-investigator) contributed to the conceptualisation and design of the study, development of sample size calculation and recruitment strategy, statistical analysis plan, trial data interpretation and writing of the manuscript.
All co-authors (except Aisling Gough, who was unavailable) approved final manuscript.
Publications
Lohan M. Engaging Boys and Addressing Masculinities in Comprehensive Sex Education Reaps Benefits for Both Adolescent Boys and Girls: Results from the JACK Trial. 2022. URL: http://www.srhm.org/news/engaging-boys-and-addressing-masculinities-in-comprehensive-sex-education-reaps-benefits-for-both-adolescent-boys-and-girls-results-from-the-jack-trial/ (accessed 13 December 2022).
Lohan M, Brennan-Wilson A, Hunter R, Gabrio A, McDaid L, Young H, et al. Effects of gender transformative relationships and sexuality education to reduce adolescent pregnancy (the JACK trial): a cluster-randomised trial. Lancet 2022;7:e626–37.
Aventin Á, Gough A, McShane T, Gillespie K, O’Hare L, Young H, et al. Engaging parents in digital sexual and reproductive health education: evidence from the JACK trial. Reprod Health 2020;17:132.
Lohan M, Aventin Á, Clarke M, Curran RM, Maguire L, Hunter R, et al. JACK trial protocol: a phase III multicentre cluster randomised controlled trial of a school-based relationship and sexuality education intervention focusing on young male perspectives. BMJ Open 2018;8:e022128.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Any intention to use or share project data for purposes other than those outlined in the JACK trial project protocol or the JACK trial Data Management Protocol must be approved by the PI and Trial Management Group (consisting of representatives from all partner sites). Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- Bonell C. Why is teenage pregnancy conceptualized as a social problem? A review of quantitative research from the USA and UK. Cult Health Sex 2004;6:255-72. https://doi.org/10.1080/13691050310001643025.
- Kneale D, Fletcher A, Wiggins R, Bonell C. Distribution and determinants of risk of teenage motherhood in three British longitudinal studies: implications for targeted prevention interventions. J Epidemiol Community Health 2013;67:48-55. https://doi.org/10.1136/jech-2011-200867.
- Ashcraft A, Fernández-Val I, Lang K. The consequences of teenage childbearing: consistent estimates when abortion makes miscarriage nonrandom. Econ J 2013;123:875-90. https://doi.org/10.1111/ecoj.12005.
- Fletcher JM, Wolfe BL. Education and labor market consequences of teenage childbearing: evidence using the timing of pregnancy outcomes and community fixed effects. J Hum Resour n.d.;44:303-25. https://doi.org/10.1353/jhr.2009.0026.
- Savio Beers LA, Hollo RE. Approaching the adolescent-headed family: a review of teen parenting. Curr Probl Pediatr Adolesc Health Care 2009;39:216-33. https://doi.org/10.1016/j.cppeds.2009.09.001.
- Francesconi M. Adult outcomes for children of teenage mothers. Scand J Econ 2008;110:93-117. https://doi.org/10.1111/j.1467-9442.2008.00526.x.
- Lawlor DA, Shaw M. Teenage pregnancy rates: high compared with where and when?. J R Soc Med 2004;97:121-3. https://doi.org/10.1258/jrsm.97.3.121.
- Avery L, Lazdane G. What do we know about sexual and reproductive health of adolescents in Europe?. Eur J Contracept Reprod Heal Care 2008;13:58-70. https://doi.org/10.1080/13625180701617621.
- United Nations Statistics Division . Statistics and Indicators on Women and Men: Table 2.B – Indicators on Childbearing n.d. unstats.un.org/unsd/demographic/products/indwm/table2b.htm (accessed 14 May 2020).
- Office for National Statistics . Conceptions in England and Wales: 2018 n.d. www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/conceptionandfertilityrates/bulletins/conceptionstatistics/2018 (accessed 14 May 2020).
- Office for National Statistics . Births by Parents’ Characteristics in England and Wales, 2014 n.d. www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/birthsbyparentscharacteristicsinenglandandwales/2014 (accessed 14 May 2020).
- Office for National Statistics . Conceptions in England and Wales: 2013 n.d. www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/conceptionandfertilityrates/bulletins/conceptionstatistics/2015-02-24 (accessed 14 May 2020).
- NHS Scotland . Teenage Pregnancy: Year of Conception, Ending 31 December 2017. A National Statistics Publication for Scotland 2019. www.isdscotland.org/Health-Topics/Sexual-Health/Publications/2019-07-02/2019-07-02-TeenPreg-Report.pdf (accessed 6 May 2020).
- Her Majesty’s Government . A New Legal Framework for Abortion Services in Northern Ireland: Implementation of the Legal Duty Under Section 9 of the Northern Ireland (Executive Formation Etc) Act 2019: UK Government Consultation Response 2020. assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/875380/FINAL_Government_response_-_Northern_Ireland_abortion_framework.pdf (accessed 5 May 2020).
- Dyer C. Abortion in Northern Ireland is decriminalised. BMJ 2019;367. https://doi.org/10.1136/bmj.l6145.
- Northern Ireland Statistics and Research Agency (NISRA) . Births (Administrative Geographies) 1999–2014 n.d. www.ninis2.nisra.gov.uk/public/PivotGrid.aspx?ds=10390%26lh=73%26yn=1999-2019%26sk=74%26sn=Population%26yearfilter= (accessed 2 July 2021).
- Department of Health . NI Health and Social Care Inequalities Monitoring System (HSCIMS) – Health Inequalities in Northern Ireland: Key Facts 2015 2015.
- Inchley J, Currie D, Young T, Samdal O, Torsheim T, Auguston L, et al. Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013 2014 Survey 2016. https://apps.who.int/iris/handle/10665/326320 (accessed 6 December 2019).
- Northern Ireland Statistics & Research Agency (NISRA) . Young Person’s Behaviour and Attitudes Survey 2013 2013.
- Wight D, Raab GM, Henderson M, Abraham C, Buston K, Hart G, et al. Limits of teacher delivered sex education: interim behavioural outcomes from randomised trial. BMJ 2002;324. https://doi.org/10.1136/bmj.324.7351.1430.
- Silva M. The effectiveness of school-based sex education programs in the promotion of abstinent behavior: a meta-analysis. Health Educ Res 2002;17:471-81. https://doi.org/10.1093/her/17.4.471.
- Stephenson JM, Oakley A, Johnson AM, Forrest S, Strange V, Charleston S, et al. A school-based randomized controlled trial of peer-led sex education in England. Control Clin Trials 2003;24:643-57. https://doi.org/10.1016/S0197-2456(03)00070-9.
- Fullerton D. Promoting Positive Adolescent Sexual Health & Preventing Teenage Pregnancy: A Review of Recent Effectiveness Research. Dublin: Crisis Pregnancy Agency; 2004.
- Henderson M, Wight D, Raab GM, Abraham C, Parkes A, Scott S, et al. Impact of a theoretically based sex education programme (SHARE) delivered by teachers on NHS registered conceptions and terminations: final results of cluster randomised trial. BMJ 2007;334. https://doi.org/10.1136/bmj.39014.503692.55.
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation. Health Technol Assess 2010;14. https://doi.org/10.3310/hta14070.
- Elliott L, Henderson M, Nixon C, Wight D. Has untargeted sexual health promotion for young people reached its limit? A quasi-experimental study. J Epidemiol Community Health 2013;67:398-404. https://doi.org/10.1136/jech-2012-201034.
- Downing J, Jones L, Cook PA, Bellis MA. Prevention of Sexually Transmitted Infections (STIs): a Review of Reviews into the Effectiveness of Non-Clinical Interventions. Evidence Briefing Update. Liverpool: Centre for Public Health; 2006.
- Swann C, Bowe K, McCormick G, Kosmin M. Teenage Pregnancy and Parenthood: A Review of Reviews. Evidence Briefing. London: Health Development Agency; 2003.
- Ellis S, Grey A. Prevention of Sexually Transmitted Infections (STIs): A Review of Reviews Into the Effectiveness of Non-Clinical Interventions to Reduce the Risk of Sexual Transmission. Evidence Briefing. London: Health Development Agency; 2004.
- Ingham R, Hirst J. Promoting Health and Wellbeing in Schools. London: Routledge; 2010.
- Oringanje C, Meremikwu MM, Eko H, Esu E, Meremikwu A, Ehiri JE. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev 2009;4. https://doi.org/10.1002/14651858.CD005215.pub2.
- Mason-Jones AJ, Sinclair D, Mathews C, Kagee A, Hillman A, Lombard C. School-based interventions for preventing HIV, sexually transmitted infections, and pregnancy in adolescents. Cochrane Database Syst Rev 2016;11. https://doi.org/10.1002/14651858.CD006417.pub3.
- United Nations Educational, Scientific and Cultural Organisation (UNESCO) . International Technical Guidance on Sexuality Education: An Evidence-Informed Approach for Schools, Teachers and Health Educators 2009. unesdoc.unesco.org/ark:/48223/pf0000183281 (accessed 14 May 2020).
- National Institute for Health and Care Excellence (NICE) . Reducing Sexually Transmitted Infections 2022.
- Department of Health Social, Services and Public Safety . Sexual Health Promotion: Strategy and Action Plan 2008–2013 2008.
- Scottish Government . Pregnancy and Parenthood in Young People Strategy 2016–2026 2016.
- Department for Education . Relationships Education, Relationships and Sex Education, and Personal, Social Health and Economic Education 2017.
- Welsh Government . The Future of the Sex and Relationships Education Curriculum in Wales Recommendations of the Sex and Relationships Education Expert Panel 2017. gov.wales/sites/default/files/publications/2018-03/the-future-of-the-sex-and-relationships-education-curriculum-in-wales.pdf (accessed 14 May 2020).
- Council for the Curriculum, Examinations and Assessment . Relationships and Sexuality Education Guidance An Update for Post-Primary Schools 2019. ccea.org.uk/downloads/docs/ccea-asset/Curriculum/Relationships and Sexuality Education Guidance An Update for Post-Primary Schools.pdf (accessed 14 May 2020).
- Scottish Government . Conduct of Relationships, Sexual Health and Parenthood Education in Schools 2014. www.gov.scot/binaries/content/documents/govscot/publications/advice-and-guidance/2014/12/conduct-relationships-sexual-health-parenthood-education-schools/documents/00465948-pdf/00465948-pdf/govscot%3Adocument/00465948.pdf (accessed 14 May 2020).
- Aventin Á, Lohan M, O’Halloran P, Henderson M. Design and development of a film-based intervention about teenage men and unintended pregnancy: applying the Medical Research Council framework in practice. Eval Program Plann 2015;49:19-30. https://doi.org/10.1016/j.evalprogplan.2014.11.003.
- Lohan M, Cruise S, O’Halloran P, Alderdice F, Hyde A. Adolescent men’s attitudes and decision-making in relation to an unplanned pregnancy. Responses to an interactive video drama. Soc Sci Med 2011;72:1507-14. https://doi.org/10.1016/j.socscimed.2011.02.044.
- Lohan M, Olivari MG, Corkindale C, Milani L, Confalonieri E, Cruise S, et al. Adolescent men’s pregnancy resolution choices in relation to an unintended pregnancy: a comparative analysis of adolescent men in three countries. J Fam Issues 2013;34:1037-58. https://doi.org/10.1177/0192513X13484281.
- Lohan M, Aventin Á, Maguire L, Curran R, McDowell C, Agus A, et al. Increasing boys’ and girls’ intentions to avoid teenage pregnancy: a cluster randomised controlled feasibility trial of an interactive video drama-based intervention in post-primary schools in Northern Ireland. Public Health Res 2017;5:1-344. https://doi.org/10.3310/phr05010.
- Lohan M, Aventin Á, Clarke M, Curran RM, McDowell C, Agus A, et al. Can teenage men be targeted to prevent teenage pregnancy? A feasibility cluster randomised controlled intervention trial in schools. Prev Sci 2018;19:1079-90. https://doi.org/10.1007/s11121-018-0928-z.
- Gillespie K, Lohan M, Aventin Á, Kelly C, Hyde A. An Evaluation of the If I Were Jack Educational Resources in Post-Primary Schools With Regard to the Relationship and Sexuality Education Requirements of Teenage Men 2018.
- Aventin Á, Gough A, McShane T, Gillespie K, O’Hare L, Young H, et al. Engaging parents in digital sexual and reproductive health education: evidence from the JACK trial. Reprod Health 2020;17. https://doi.org/10.1186/s12978-020-00975-y.
- Lohan M, Aventin Á, Clarke M, Curran RM, Maguire L, Hunter R, et al. JACK trial protocol: a phase III multicentre cluster randomised controlled trial of a school-based relationship and sexuality education intervention focusing on young male perspectives. BMJ Open 2018;8. https://doi.org/10.1136/bmjopen-2018-022128.
- Hyde A, Drennan J, Howlett E, Carney M, Butler M, Lohan M. Parents’ constructions of the sexual self-presentation and sexual conduct of adolescents: discourses of gendering and protecting. Cult Health Sex 2012;14:895-909. https://doi.org/10.1080/13691058.2012.708944.
- Hyde A, Drennan J, Butler M, Howlett E, Carney M, Lohan M. Parents’ constructions of communication with their children about safer sex. J Clin Nurs 2013;22:3438-46. https://doi.org/10.1111/jocn.12367.
- Hyde A, Carney M, Drennan J, Butler M, Lohan M, Howlett E. The silent treatment: parents’ narratives of sexuality education with young people. Cult Health Sex 2010;12:359-71. https://doi.org/10.1080/13691050903514455.
- Hyde A, Fullerton D, McKeown C, Lohan M, Dunne L, Macdonald G. Doing relationships and sexuality education with young people in state care. Health Educ J 2017;76:194-205. https://doi.org/10.1177/0017896916655181.
- Hyde A, Fullerton D, Lohan M, Dunne L, Macdonald G. The role of knowledge in the contraceptive behaviour of sexually active young people in state care. Sex Reprod Healthc 2016;8:37-41. https://doi.org/10.1016/j.srhc.2016.02.001.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Kirby D, Laris B, Rolleri L. Sex and HIV Education Programs for Youth: Their Impact and Important Characteristics. Scotts Valley, CA: ETR Associates; 2006.
- Kirby D. Effective approaches to reducing adolescent unprotected sex, pregnancy, and childbearing. J Sex Res 2002;39:51-7. https://doi.org/10.1080/00224490209552120.
- Kirby D. Emerging answers: research findings on programs to reduce teen pregnancy and sexually transmitted diseases. Am J Heal Educ 2007;32:348-55. https://doi.org/10.1080/19325037.2001.10603497.
- Robin L, Dittus P, Whitaker D, Crosby R, Ethier K, Mezoff J, et al. Behavioral interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: a decade in review. J Adolesc Health 2004;34:3-26. https://doi.org/10.1016/S1054-139X(03)00244-1.
- Bailey JV, Murray E, Rait G, Mercer CH, Morris RW, Peacock R, et al. Interactive computer-based interventions for sexual health promotion. Cochrane Database Syst Rev 2010;9. https://doi.org/10.1002/14651858.CD006483.pub2.
- Guse K, Levine D, Martins S, Lira A, Gaarde J, Westmorland W, et al. Interventions using new digital media to improve adolescent sexual health: a systematic review. J Adolesc Health 2012;51:535-43. https://doi.org/10.1016/j.jadohealth.2012.03.014.
- Noar SM, Pierce LB, Black HG. Can computer-mediated interventions change theoretical mediators of safer sex? A meta-analysis. Hum Commun Res 2010;36:261-97. https://doi.org/10.1111/j.1468-2958.2010.01376.x.
- Shackleton N, Jamal F, Viner RM, Dickson K, Patton G, Bonell C. School-based interventions going beyond health education to promote adolescent health: systematic review of reviews. J Adolesc Health 2016;58:382-96. https://doi.org/10.1016/j.jadohealth.2015.12.017.
- Wight D, Abraham C, Scott S. Towards a psycho-social theoretical framework for sexual health promotion. Health Educ Res 1998;13:317-30. https://doi.org/10.1093/her/13.3.317-a.
- Jones L, Bates G, Downing J, Sumnall H, Bellis M. A Review of the Effectiveness and Cost Effectiveness of Personal Social and Health Education in Secondary Schools Focussing on Sex and Relationships and Alcohol Education for Young People Aged 11–19 Years. Final Report 2009.
- Fullerton D, Butney L. An Overview of the Effectiveness of Sexual Health Improvement Interventions. Edinburgh: NHS Scotland; 2010.
- Ajzen I, Madden TJ. Prediction of goal-directed behavior: attitudes, intentions, and perceived behavioral control. J Exp Soc Psychol 1986;22:453-74. https://doi.org/10.1016/0022-1031(86)90045-4.
- Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health 2011;26:1113-27. https://doi.org/10.1080/08870446.2011.613995.
- Gupta GR. Gender, sexuality, and HIV/AIDS: the what, the why, and the how. Can HIV AIDS Policy Law Rev 2000;5:86-93.
- World Health Organisation (WHO) . Gender Mainstreaming for Health Managers: A Practical Approach. Participant’s Notes 2011.
- Philliber S, Kaye JW, Herrling S, West E. Preventing pregnancy and improving health care access among teenagers: an evaluation of the Children’s Aid Society–Carrera program. Perspect Sex Reprod Health 2002;34:244-51. https://doi.org/10.2307/3097823.
- Coyle K, Basen-Engquist K, Kirby D, Parcel G, Banspach S, Collins J, et al. Safer choices: reducing teen pregnancy, HIV, and STDs. Public Health Rep 2001;116:82-93. https://doi.org/10.1093/phr/116.S1.82.
- Greaves L, Pederson A, Poole N. Making it Better: Gender-Transformative Health Promotion. Ontario: Canadian Scholars’ Press Inc.; 2014.
- Foreign, Commonwealth and Development Office (FCDO) Programme Partnership Arrangement (PPA) Learning Partnership Gender Group . A Theory of Change on Gender Equality &Amp; Women’s and Girls’ Empowerment 2015.
- Ruane-McAteer E, Amin A, Hanratty J, Lynn F, Corbijn van Willenswaard K, Reid E, et al. Interventions addressing men, masculinities and gender equality in sexual and reproductive health and rights: an evidence and gap map and systematic review of reviews. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2019-001634.
- Ruane-McAteer E, Gillespie K, Amin A, Aventin Á, Robinson M, Hanratty J, et al. Gender-transformative programming with men and boys to improve sexual and reproductive health and rights: a systematic review of intervention studies. BMJ Glob Health 2020;5. https://doi.org/10.1136/bmjgh-2020-002997.
- World Health Organisation (WHO) Regional Office for Europe . Evidence for Gender Responsive Actions to Prevent and Manage Adolescent Pregnancy: Young People’s Health As a Whole-of-Society Response 2011.
- World Health Organisation (WHO) Regional Office for Europe . Health 2020: A European Policy Framework Supporting Action Across Government and Society for Health and Well-Being 2013.
- Santa Maria D, Rafferty J, Lau M, Guilamo-Ramos V, Tebb K, Chadi N, et al. Advocating for adolescent and young adult male sexual and reproductive health: a position statement from the Society for Adolescent Health and Medicine. J Adolesc Health 2018;63:657-61. https://doi.org/10.1016/j.jadohealth.2018.08.007.
- It’s a Guy Thing: Boys, Young Men, and Teen Pregnancy Prevention. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2006.
- Ries A, Sonenstein F. It’s a Guy Thing: Boys, Young Men, and Teen Pregnancy Prevention. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2006.
- Bennett SE, Assefi NP. School-based teenage pregnancy prevention programs: a systematic review of randomized controlled trials. J Adolesc Health 2005;36:72-81. https://doi.org/10.1016/j.jadohealth.2003.11.097.
- World Health Organisation (WHO) . Preventing Early Pregnancy and Poor Reproductive Outcomes Among Adolescents in Developing Countries 2011.
- World Health Organisation (WHO) . WHO Recommendations on Adolescent Sexual and Reproductive Health and Rights 2018. https://apps.who.int/iris/bitstream/handle/10665/275374/9789241514606-eng.pdf?ua=1 (accessed 16 June 2020).
- United Nations Population Fund (UNFPA) . The Evaluation of Comprehensive Sexuality Education Programmes: A Focus on the Gender and Empowerment Outcomes 2015. www.unfpa.org/sites/default/files/pub-pdf/UNFPAEvaluationWEB4.pdf (accessed 6 June 2020).
- Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, et al. Accelerate progress–sexual and reproductive health and rights for all: report of the Guttmacher–Lancet Commission. Lancet 2018;391:2642-92. https://doi.org/10.1016/S0140-6736(18)30293-9.
- Haberland N, Rogow D. Sexuality education: emerging trends in evidence and practice. J Adolesc Health 2015;56:15-21. https://doi.org/10.1016/j.jadohealth.2014.08.013.
- Svanemyr J, Amin A, Robles OJ, Greene ME. Creating an enabling environment for adolescent sexual and reproductive health: a framework and promising approaches. J Adolesc Health 2015;56:7-14. https://doi.org/10.1016/j.jadohealth.2014.09.011.
- Schalet AT, Santelli JS, Russell ST, Halpern CT, Miller SA, Pickering SS, et al. Invited commentary: broadening the evidence for adolescent sexual and reproductive health and education in the United States. J Youth Adolesc 2014;43:1595-610. https://doi.org/10.1007/s10964-014-0178-8.
- Jaramillo N, Buhi ER, Elder JP, Corliss HL. Associations between sex education and contraceptive use among heterosexually active, adolescent males in the united states. J Adolesc Health 2017;60:534-40. https://doi.org/10.1016/j.jadohealth.2016.11.025.
- Smith LH, Guthrie BJ, Oakley DJ. Studying adolescent male sexuality: where are we?. J Youth Adolesc 2005;34:361-77. https://doi.org/10.1007/s10964-005-5762-5.
- The Alan Guttmacher Institute . In Their Own Right: Addressing the Sexual and Reproductive Health Needs of American Men 2002.
- Lindberg LD, Sonfield A, Gemmill A. Reassessing adolescent male sexual and reproductive health in the United States: research and recommendations. Am J Mens Health 2008;2:40-56. https://doi.org/10.1177/1557988307309460.
- Gillespie K. An Evaluation of the If I Were Jack Educational Resources in Post-Primary Schools With Regard to the Relationship and Sexuality Education Requirements of Teenage Men 2019.
- Kirby DB, Laris BA, Rolleri LA. Sex and HIV education programs: their impact on sexual behaviors of young people throughout the world. J Adolesc Health 2007;40:206-17. https://doi.org/10.1016/j.jadohealth.2006.11.143.
- Pound P, Denford S, Shucksmith J, Tanton C, Johnson AM, Owen J, et al. What is best practice in sex and relationship education? A synthesis of evidence, including stakeholders’ views. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-014791.
- Pound P, Langford R, Campbell R. What do young people think about their school-based sex and relationship education? A qualitative synthesis of young people’s views and experiences. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2016-011329.
- Bailey J, Mann S, Wayal S, Hunter R, Free C, Abraham C, et al. Sexual health promotion for young people delivered via digital media: a scoping review. Public Health Res 2015;3. https://doi.org/10.3310/phr03130.
- Tuong W, Larsen ER, Armstrong AW. Videos to influence: a systematic review of effectiveness of video-based education in modifying health behaviors. J Behav Med 2014;37:218-33. https://doi.org/10.1007/s10865-012-9480-7.
- Aranda K, Coleman L, Sherriff NS, Cocking C, Zeeman L, Cunningham L. Listening for commissioning: a participatory study exploring young people’s experiences, views and preferences of school-based sexual health and school nursing. J Clin Nurs 2018;27:375-85. https://doi.org/10.1111/jocn.13936.
- Claussen C. Men engaging boys in healthy masculinity through school-based sexual health education. Sex Educ 2019;19:115-29. https://doi.org/10.1080/14681811.2018.1506914.
- Marsiglio W. It’s a Guy Thing: Boys, Young Men, and Teen Pregnancy Prevention. Washington, DC: National Campaign to Prevent Teen Pregnancy; 2006.
- Wellings K, Nanchahal K, Macdowall W, McManus S, Erens B, Mercer CH, et al. Sexual behaviour in Britain: early heterosexual experience. Lancet 2001;358:1843-50. https://doi.org/10.1016/S0140-6736(01)06885-4.
- Gavin LE, Catalano RF, David-Ferdon C, Gloppen KM, Markham CM. A review of positive youth development programs that promote adolescent sexual and reproductive health. J Adolesc Health 2010;46:75-91. https://doi.org/10.1016/j.jadohealth.2009.11.215.
- Guilamo-Ramos V, Jaccard J, Dittus P, Bouris AM. Parental expertise, trustworthiness, and accessibility: parent-adolescent communication and adolescent risk behavior. J Marriage Fam 2006;68:1229-46. https://doi.org/10.1111/j.1741-3737.2006.00325.x.
- Wight D, Fullerton D. A review of interventions with parents to promote the sexual health of their children. J Adolesc Health 2013;52:4-27. https://doi.org/10.1016/j.jadohealth.2012.04.014.
- D’Cruz J, Santa Maria D, Dube S, Markham C, McLaughlin J, Wilkerson JM, et al. Promoting parent–child sexual health dialogue with an intergenerational game: parent and youth perspectives. Games Health J 2015;4:113-22. https://doi.org/10.1089/g4h.2014.0080.
- Akers AY, Holland CL, Bost J. Interventions to improve parental communication about sex: a systematic review. Pediatrics 2011;127:494-510. https://doi.org/10.1542/peds.2010-2194.
- Hutchinson MK, Jemmott JB, Jemmott LS, Braverman P, Fong GT. The role of mother-daughter sexual risk communication in reducing sexual risk behaviors among urban adolescent females: a prospective study. J Adolesc Health 2003;33:98-107. https://doi.org/10.1016/S1054-139X(03)00183-6.
- Meschke LL, Bartholomae S, Zentall SR. Adolescent sexuality and parent-adolescent processes: promoting healthy teen choices. J Adolesc Health 2002;31:264-79. https://doi.org/10.1016/S1054-139X(02)00499-8.
- Guilamo-Ramos V, Lee JJ, Kantor LM, Levine DS, Baum S, Johnsen J. Potential for using online and mobile education with parents and adolescents to impact sexual and reproductive health. Prev Sci 2015;16:53-60. https://doi.org/10.1007/s11121-014-0469-z.
- Papa MJ, Singhal A, Law S, Pant S, Sood S, Rogers EM, et al. Entertainment-education and social change: an analysis of parasocial interaction, social learning, collective efficacy, and paradoxical communication. J Commun 2000;50:31-55. https://doi.org/10.1111/j.1460-2466.2000.tb02862.x.
- Guilamo-Ramos V, Lee JJ, Jaccard J. Parent-adolescent communication about contraception and condom use. JAMA Pediatr 2015;170:1-3. https://doi.org/10.1001/jamapediatrics.2015.3109.
- Advocates for Youth . Sex Education Programs: Definitions &Amp; Point-by-Point Comparison 2009. advocatesforyouth.org/resources/fact-sheets/sex-education-programs-definitions-and-point-by-point-comparison/ (accessed 16 June 2020).
- Stephenson J, Strange V, Allen E, Copas A, Johnson A, Bonell C, et al. The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England. PLOS Med 2008;5. https://doi.org/10.1371/journal.pmed.0050224.
- Sabia JJ. Does sex education affect adolescent sexual behaviors and health?. J Policy Anal Manag 2006;25:783-802. https://doi.org/10.1002/pam.20208.
- Lou JH, Chen SH. Relationships among sexual knowledge, sexual attitudes, and safe sex behaviour among adolescents: a structural equation model. Int J Nurs Stud 2009;46:1595-603. https://doi.org/10.1016/j.ijnurstu.2009.05.017.
- Lopez LM, Bernholc A, Chen M, Tolley EE. School-based interventions for improving contraceptive use in adolescents. Cochrane Database Syst Rev 2016;6. https://doi.org/10.1002/14651858.CD012249.
- Weed SE, Ericksen IH. Re-examining the evidence for comprehensive sex education in schools: a global research review. Issues Law Med 2019;34:161-82.
- Weed SE, Ericksen IH. Re-Examining The Evidence: School-Based Comprehensive Sex Education in the United States. Salt Lake City, UT: The Institute for Research & Evaluation; 2017.
- Santelli JS, Kantor LM, Grilo SA, Speizer IS, Lindberg LD, Heitel J, et al. Abstinence-only-until-marriage: an updated review of U.S. policies and programs and their impact. J Adolesc Health 2017;61:273-80. https://doi.org/10.1016/j.jadohealth.2017.05.031.
- Morris RW. Research and evaluation in sexuality education: an allegorical exploration of complexities and possibilities. Sex Educ 2005;5:405-22. https://doi.org/10.1080/14681810500278501.
- World Health Organisation (WHO) Regional Office for Europe, Bundeszentrale für gesundheitliche Aufklärung (BZgA) . Standards for Sexuality Education in Europe: Guidance for Implementation 2013. www.fissonline.it/pdf/Guidance%20for%20implementation.pdf (accessed 16 June 2020).
- United Nations Population Fund (UNFPA) . UNFPA Operational Guidance for Comprehensive Sexuality Education: A Focus on Human Rights and Gender 2014. www.unfpa.org/sites/default/files/pub-pdf/UNFPA_OperationalGuidance_WEB3_0.pdf (accessed 16 June 2020).
- United Nation’s Children Fund (UNICEF) . A Summary of the UN Convention on the Rights of the Child 2019. downloads.unicef.org.uk/wp-content/uploads/2019/10/UNCRC_summary-1_1.pdf?_ga=2.71392275.1615898456.1591972779-902228205.1591972779 (accessed 16 June 2020).
- Office of the High Commissioner for Human Rights (OHCHR) . CESCR General Comment No. 3: The Nature of States Parties’ Obligations (Art. 2, Para. 1, of the Covenant) 1990. www.refworld.org/pdfid/4538838e10.pdf (accessed 16 June 2020).
- UN Committee on the Rights of the Child (CRC) . General Comment No. 4 (2003). Adolescent Health and Development in the Context of the Convention on the Rights of the Child 2003. docstore.ohchr.org/SelfServices/FilesHandler.ashx?enc=6QkG1d%2FPPRiCAqhKb7yhsiQql8gX5Zxh0cQqSRzx6ZfAICbDzm5DUreYo1tlYOkZcPE%2BQh98dgWJaknr%2BF7jm9%2BkvHmi4ctJTvJ1CPTUqN7%2F4K3R8rTOQIXpWvhMbx0f (accessed 16 June 2020).
- United Nations Committee on Economic Social and Cultural Rights (CESCR) . General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12) 2000. www.refworld.org/docid/4538838d0.html (accessed 16 June 2020).
- United Nations (UN) General Assembly . Transforming Our World: The 2030 Agenda for Sustainable Development 2015. www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1%26Lang=E (accessed 10 September 2021).
- United Nations Committee on the Rights of the Child (CRC) . General Comment No. 20 (2016) On The Implementation Of The Rights Of The Child During Adolescence 2016. www.refworld.org/docid/589dad3d4.html (accessed 16 June 2020).
- Allen L. ‘Say everything’: exploring young people’s suggestions for improving sexuality education. Sex Educ 2005;5:389-404. https://doi.org/10.1080/14681810500278493.
- Unis BD, Sällström C. Adolescents’ conceptions of learning and education about sex and relationships. Am J Sex Educ 2020;15:25-52. https://doi.org/10.1080/15546128.2019.1617816.
- Leung H, Shek DTL, Leung E, Shek EYW. Development of contextually-relevant sexuality education: lessons from a comprehensive review of adolescent sexuality education across cultures. Int J Environ Res Public Health 2019;16. https://doi.org/10.3390/ijerph16040621.
- Sex Education Forum . Young People’s RSE Poll 2018 2018. www.sexeducationforum.org.uk/sites/default/files/field/attachment/Young people%27s RSE poll 2018.pdf (accessed 18 June 2020).
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Harden A, Brunton G, Fletcher A, Oakley A. Teenage pregnancy and social disadvantage: systematic review integrating controlled trials and qualitative studies. BMJ 2009;339. https://doi.org/10.1136/bmj.b4254.
- Kirby D. Sexuality Education: An Evaluation of Programs and Their Effects 1984.
- Kirby D. Handbook of Sexuality-Related Measures. London: Routledge; 2011.
- Fullard W, Johnston D, Lief H. Handbook of Sexuality-Related Measures. London: SAGE Publications Ltd; 2005.
- Pleck JH, Sonenstein FL, Ku LC. Masculinity ideology: its impact on adolescent males’ heterosexual relationships. J Soc Issues 1993;49:11-29. https://doi.org/10.1111/j.1540-4560.1993.tb01166.x.
- Lottes IL, Kuriloff PJ. Sexual socialization differences by gender, Greek membership, ethnicity, and religious background. Psychol Women Q 1994;18:203-19. https://doi.org/10.1111/j.1471-6402.1994.tb00451.x.
- Quinn-Nilas C, Milhausen RR, Breuer R, Bailey J, Pavlou M, DiClemente RJ, et al. Validation of the sexual communication self-efficacy scale. Health Educ Behav 2016;43:165-71. https://doi.org/10.1177/1090198115598986.
- Rosenthal D, Moore S, Flynn I. Adolescent self-efficacy, self-esteem and sexual risk-taking. J Community Appl Soc Psychol 1991;1:77-88. https://doi.org/10.1002/casp.2450010203.
- Elliott L, Raab G, Wight D, Henderson M, Martin C, Birch A, et al. Evaluation of Healthy Respect Phase Two: Final Report March 2010 2010. www.healthscotland.com/uploads/documents/12159-HealthyRespectEvaluationReport_3342.pdf (accessed 20 April 2020).
- Carswell K, McCarthy O, Murray E, Bailey JV. Integrating psychological theory into the design of an online intervention for sexual health: the Sexunzipped website. JMIR Res Protoc 2012;1. https://doi.org/10.2196/resprot.2114.
- Palmer MJ, Clarke L, Ploubidis GB, Mercer CH, Gibson LJ, Johnson AM, et al. Is ‘sexual competence’ at first heterosexual intercourse associated with subsequent sexual health status?. J Sex Res 2017;54:91-104. https://doi.org/10.1080/00224499.2015.1134424.
- Chin HB, Sipe TA, Elder R, Mercer SL, Chattopadhyay SK, Jacob V, et al. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: two systematic reviews for the Guide to Community Preventive Services. Am J Prev Med 2012;42:272-94. https://doi.org/10.1016/j.amepre.2011.11.006.
- Santelli JS, Lindberg LD, Finer LB, Singh S. Explaining recent declines in adolescent pregnancy in the United States: the contribution of abstinence and improved contraceptive use. Am J Public Health 2007;97:150-6. https://doi.org/10.2105/AJPH.2006.089169.
- Parkes A, Wight D, Henderson M, Stephenson J, Strange V. Contraceptive method at first sexual intercourse and subsequent pregnancy risk: findings from a secondary analysis of 16-year-old girls from the RIPPLE and SHARE studies. J Adolesc Health 2009;44:55-63. https://doi.org/10.1016/j.jadohealth.2008.06.006.
- Lohan M, Aventin A, Maguire L, Clarke M, Linden M, McDaid L. Feasibility trial of a film-based educational intervention for increasing boys’ and girls’ intentions to avoid teenage pregnancy: study protocol. Int J Educ Res 2014;68:35-4. https://doi.org/10.1016/j.ijer.2014.08.003.
- Eldridge SM, Costelloe CE, Kahan BC, Lancaster GA, Kerry SM. How big should the pilot study for my cluster randomised trial be?. Stat Methods Med Res 2016;25:1039-56. https://doi.org/10.1177/0962280215588242.
- Northern Ireland Statistics and Research Agency (NISRA) . Young Person’s Behaviour and Attitudes Survey 2011 2011.
- Kahan BC, Jairath V, Doré CJ, Morris TP. The risks and rewards of covariate adjustment in randomized trials: an assessment of 12 outcomes from 8 studies. Trials 2014;15. https://doi.org/10.1186/1745-6215-15-139.
- May C. Towards a general theory of implementation. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-18.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE Publications Ltd; 1985.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res 2006;78:473-87. https://doi.org/10.1007/s11205-005-1607-6.
- Office for National Statistics . Earning and Hours Worked, Occupation by Four-Digit SOC: ASHE Table 14 2020.
- Curtis L, Burns A. Unit Costs of Health and Social Care 2018.
- Earnshaw J, Gavin L. NICE guide to the methods of technology appraisal. PharmacoEconomics 2008;26:725-27. https://doi.org/10.2165/00019053-200826090-00002.
- Boots 2019. www.boots.com (accessed 2 July 2021).
- White IR, Horton NJ, Carpenter J, Pocock SJ. Strategy for intention to treat analysis in randomised trials with missing outcome data. BMJ 2011;342. https://doi.org/10.1136/bmj.d40.
- Faria R, Gomes M, Epstein D, White IR. A guide to handling missing data in cost-effectiveness analysis conducted within randomised controlled trials. PharmacoEconomics 2014;32:1157-70. https://doi.org/10.1007/s40273-014-0193-3.
- van Buuren S. Flexible Imputation of Missing Data. Boca Raton, FL: CRC Press; 2018.
- Public Health England . Contraception: Economic Analysis Estimation of the Return on Investment (ROI) for Publicly Funded Contraception in England 2018. assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/730292/contraception_return_on_investment_report.pdf (accessed 14 May 2020).
- Wellings K, Jones KG, Mercer CH, Tanton C, Clifton S, Datta J, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet 2013;382:1807-16. https://doi.org/10.1016/S0140-6736(13)62071-1.
- Henderson M, Ecob R, Wight D, Abraham C. What explains between-school differences in rates of smoking?. BMC Public Health 2008;8. https://doi.org/10.1186/1471-2458-8-218.
- Brooks F, Magnusson J, Klemera E, Chester K, Spencer N, Smeeton N. HBSC England National Report. Health Behaviour in School-Aged Children (HBSC): World Health Organisation Collaborative Cross National Study 2015.
- Welsh Government Social Research . 2013/14/Health/Behaviour/in/School-Aged/Children./(HBSC)/Wales:/Key/Findings 2014.
- Currie C, Levin K, Todd J. HBSC National Team . HBSC Scotland National Report. Health Behaviour in School-Aged Children: World Health Organisation Collaborative Cross-National Study (HBSC) 2008.
- Schubotz D. Messed Up? Sexual Lifestyles of 16 Year Olds in Northern Ireland. Belfast: Access Research Knowledge; 2011.
- Office for National Statistics . Conceptions in England and Wales: 2017 n.d. www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/conceptionandfertilityrates/bulletins/conceptionstatistics/2017 (accessed 13 December 2019).
- Office for National Statistics . Population Estimates for UK, England and Wales, Scotland and Northern Ireland: Mid-2017 n.d. www.ons.gov.uk/releases/populationestimatesforukenglandandwalesscotlandandnorthernirelandmid2017 (accessed 13 December 2019).
- Public Health Scotland . Births in Scottish Hospitals: Maternity and Births n.d. www.isdscotland.org/Health-Topics/Maternity-and-Births/Births/ (accessed 13 December 2019).
- Wang LY, Davis M, Robin L, Collins J, Coyle K, Baumler E. Economic evaluation of Safer Choices: a school-based human immunodeficiency virus, other sexually transmitted diseases, and pregnancy prevention program. Arch Pediatr Adolesc Med 2000;154:1017-24. https://doi.org/10.1001/archpedi.154.10.1017.
- Nherera L, Jacklin P. A Model to Assess the Cost-Effectiveness of Sex and Relationship Education (SRE) Developed for NICE Public Health Guidance on Personal, Social, Health and Economic (PSHE) Education. London: National Collaborating Centre for Women’s and Children’s Health, National Institute for Health and Care Excellence; 2009.
- Office for National Statistics . Abortion Statistics for England and Wales: 2018 n.d. www.gov.uk/government/statistics/abortion-statistics-for-england-and-wales-2018 (accessed 13 December 2019).
- NHS Digital. NHS Maternity Statistics – England, 2010–2011: NHS maternity statistics table n.d. https://digital.nhs.uk/data-and-information/publications/statistical/nhs-maternity-statistics/2010-11 (accessed 31 October 2022).
- Sailer FD. Development of a Multi Sexually Transmitted Infections Modelling Software 2021.
- Health Protection Agency . Diagnoses and Rates of Selected STIs Seen at UK GUM Clinics by Country and Age Group: 2002–6 2007. www.gov.uk/government/organisations/health-protection-agency (accessed 13 December 2019).
- Lewis J, White PJ. Changes in chlamydia prevalence and duration of infection estimated from testing and diagnosis rates in England: a model-based analysis using surveillance data, 2000–15. Lancet Public Health 2018;3:e271-78. https://doi.org/10.1016/S2468-2667(18)30071-9.
- Sonnenberg P, Clifton S, Beddows S, Field N, Soldan K, Tanton C, et al. Prevalence, risk factors, and uptake of interventions for sexually transmitted infections in Britain: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal). Lancet 2013;382:1795-806. https://doi.org/10.1016/S0140-6736(13)61947-9.
- Turner KM, Adams EJ, Lamontagne DS, Emmett L, Baster K, Edmunds WJ. Modelling the effectiveness of chlamydia screening in England. Sex Transm Infect 2006;82:496-502. https://doi.org/10.1136/sti.2005.019067.
- Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al. Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection. Health Technol Assess 2007;11. https://doi.org/10.3310/hta11080.
- LaMontagne DS, Fenton KA, Randall S, Anderson S, Carter P. Establishing the National Chlamydia Screening Programme in England: results from the first full year of screening. Sex Transm Infect 2004;80:335-41.
- Town K, Furegato M, Field N, Hughes G. Estimating gonorrhoea prevalence in young heterosexual men and women attending community-based sexual health services to inform decisions on gonorrhoea testing. Epidemiol Infect 2017;145:1682-7. https://doi.org/10.1017/S0950268817000024.
- Brunham RC, Plummer FA. A general model of sexually transmitted disease epidemiology and its implications for control. Med Clin North Am 1990;74:1339-52. https://doi.org/10.1016/S0025-7125(16)30484-9.
- Rothenberg R, Potterat JJ, Koplan JP. The algebra of condoms and abstinence. Sex Transm Dis 2005;32:252-4. https://doi.org/10.1097/01.olq.0000158495.66446.44.
- Howell-Jones R, de Silva N, Akpan M, Oakeshott P, Carder C, Coupland L, et al. Prevalence of human papillomavirus (HPV) infections in sexually active adolescents and young women in England, prior to widespread HPV immunisation. Vaccine 2012;30:3867-75.
- Weller S, Davis K. Condom effectiveness in reducing heterosexual HIV transmission. Cochrane Database Syst Rev 2002;1. https://doi.org/10.1002/14651858.CD003255.
- Goldhaber-Fiebert JD, Brandeau ML. Evaluating cost-effectiveness of interventions that affect fertility and childbearing: how health effects are measured matters. Med Decis Making 2015;35:818-46. https://doi.org/10.1177/0272989X15583845.
- Schwarz EB, Smith R, Steinauer J, Reeves MF, Caughey AB. Measuring the effects of unintended pregnancy on women’s quality of life. Contraception 2008;78:204-10. https://doi.org/10.1016/j.contraception.2008.04.120.
- Hu D, Hook EW, Goldie SJ. Screening for Chlamydia trachomatis in women 15 to 29 years of age: a cost-effectiveness analysis. Ann Intern Med 2004;141:501-13. https://doi.org/10.7326/0003-4819-141-7-200410050-00006.
- Insinga RP, Dasbach EJ, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States. Clin Infect Dis 2003;36:1397-403. https://doi.org/10.1086/375074.
- Maclean CC, Stringer JS. Potential cost-effectiveness of maternal and infant antiretroviral interventions to prevent mother-to-child transmission during breast-feeding. J Acquir Immune Defic Syndr 2005;38:570-7. https://doi.org/10.1097/01.qai.0000142919.51570.88.
- NHS England . 2019/20/National/Schedule/of/NHS/Costs/2019/20/V2 n.d. www.england.nhs.uk/publication/2019-20-national-cost-collection-data-publication/ (accessed 31 October 2022).
- Belfield D, Crawford C, Sibieta L. Long-Run Comparisons of Spending per Pupil Across Different Stages of Education. London: Institute for Fiscal Studies; 2018.
- Licchetta M, Stelmach M. Fiscal Sustainability Analytical Paper: Fiscal Sustainability and Public Spending on Health. London: Office for Budget Responsibility; 2016.
- Wellings K, Wilkinson P, Gundy C, Kane R, Lachowycz K, Jacklin P, et al. Teenage Pregnancy Strategy Evaluation: Fina Report Synthesis 2005.
- Office for National Statistics . Annual Survey of Hours and Earnings 2017. www.ons.gov.uk/surveys/informationforbusinesses/businesssurveys/annualsurveyofhoursandearningsashe (accessed 13 December 2019).
- Lucas S. Unprotected Nation: The Financial and Economic Impacts of Restricted Contraceptive and Sexual Health Services. London: Brook, FPA; 2013.
- Chandra A, Martinez GM, Mosher WD, Abma JC, Jones J. Fertility, family planning, and reproductive health of U.S. women: data from the 2002 National Survey of Family Growth. Vital Health Stat 23 2005;25:1-160. https://doi.org/10.1037/e414702008-001.
- Montouchet C, Trussell J. Unintended pregnancies in England in 2010: costs to the National Health Service (NHS). Contraception 2013;87:149-53. https://doi.org/10.1016/j.contraception.2012.06.008.
- National Institute for Health and Care Excellence (NICE) . Guide to the Technology Appraisal and Highly Specialised Technologies Appeal Process 2014.
- Education Endowment Foundation . Sutton Trust-Education Endowment Foundation Teaching and Learning Toolkit 2018. https://educationendowmentfoundation.org.uk/public/files/Toolkit/Toolkit_Manual_2018.pdf (accessed 10 September 2021).
- National Children’s Bureau . Whole School RSE Audit Tool – Interactive n.d. www.sexeducationforum.org.uk/resources/advice-guidance/whole-school-rse-audit-tool-interactive (accessed 26 November 2020).
- Denford S, Abraham C, Campbell R, Busse H. A comprehensive review of reviews of school-based interventions to improve sexual-health. Health Psychol Rev 2017;11:33-52. https://doi.org/10.1080/17437199.2016.1240625.
- Lameiras-Fernández M, Martínez-Román R, Carrera-Fernández MV, Rodríguez-Castro Y. Sex education in the spotlight: what is working? systematic review. Int J Environ Res Public Health 2021;18. https://doi.org/10.3390/ijerph18052555.
- Mirzazadeh A, Biggs MA, Viitanen A, Horvath H, Wang LY, Dunville R, et al. Do school-based programs prevent HIV and other sexually transmitted infections in adolescents? A systematic review and meta-analysis. Prev Sci 2018;19:490-506. https://doi.org/10.1007/s11121-017-0830-0.
- Pulerwitz J, Barker G. Measuring attitudes toward gender norms among young men in Brazil: development and psychometric evaluation of the GEM scale. Men Masc 2007;10. https://doi.org/10.1177/1097184X06298778.
- Koepsel ER. The power in pleasure: practical implementation of pleasure in sex education classrooms. J Sex Educ 2016;11:205-65. https://doi.org/10.1080/15546128.2016.1209451.
- Ketting E, Friele M, Michielsen K. On behalf of European Expert Group on Sexuality Education . Evaluation of holistic sexuality education: a European expert group consensus agreement. Eur J Contracept Reprod Health Care 2016;21:68-80. https://doi.org/10.3109/13625187.2015.1050715.
- Patterson SP, Hilton S, Flowers P, McDaid LM. What are the barriers and challenges faced by adolescents when searching for sexual health information on the internet? Implications for policy and practice from a qualitative study. Sex Transm Infect 2019;95:462-7. https://doi.org/10.1136/sextrans-2018-053710.
- Goldfarb ES, Lieberman LD. Three decades of research: the case for comprehensive sex education. J Adolesc Health 2021;68:13-27. https://doi.org/10.1016/j.jadohealth.2020.07.036.
- Gardner EA. Abstinence-only sex education: college students’ evaluations and responses. Am J Sex Educ 2015;10:125-39. https://doi.org/10.1080/15546128.2015.1015760.
- Lindberg LD, Maddow-Zimet I, Boonstra H. Changes in Adolescents’ Receipt of Sex Education, 2006–2013. J Adolesc Health 2016;58:621-7. https://doi.org/10.1016/j.jadohealth.2016.02.004.
- Forrest S, Strange V, Oakley A. RIPPLE Study Team . What do young people want from sex education? The results of a needs assessment from a peer-led sex education programme. Cult Health Sex 2004;6:337-54. https://doi.org/10.1080/13691050310001645050.
- Burns S, Hendriks J. Sexuality and relationship education training to primary and secondary school teachers: an evaluation of provision in Western Australia. Sex Educ 2018;18:672-88. https://doi.org/10.1080/14681811.2018.1459535.
- Hilton GLS. Listening to the Boys: English boys’ views on the desirable characteristics of teachers of sex education. Sex Educ 2003;3:33-45. https://doi.org/10.1080/1468181032000052144.
- Helmer J, Senior K, Davison B, Vodic A. Improving sexual health for young people: making sexuality education a priority. Sex Educ 2015;15:158-71. https://doi.org/10.1080/14681811.2014.989201.
- Queen's University Belfast n.d. www.qub.ac.uk/sites/if-i-were-jack/6NationsRSESymposium/ (accessed 3 November 2022).
- Patton GC, Bond L, Carlin JB, Thomas L, Butler H, Glover S, et al. Promoting social inclusion in schools: a group-randomized trial of effects on student health risk behavior and well-being. Am J Public Health 2006;96:1582-7. https://doi.org/10.2105/AJPH.2004.047399.
- Brener ND, Billy JO, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health 2003;33:436-57. https://doi.org/10.1016/S1054-139X(03)00052-1.
- Oosterhoff M, Bosma H, Van Schayck OCP, Evers SMAA, Dirksen CD, Joore MA. A systematic review on economic evaluations of school-based lifestyle interventions targeting weight-related behaviours among 4–12 year olds: issues and ways forward. Prev Med 2018;114:115-22. https://doi.org/10.1016/j.ypmed.2018.06.015.
- Frisman L, Rosenheck R. How transfer payments are treated in cost-effectiveness and cost-benefit analyses. Adm Policy Ment Health 1996;23:533-46. https://doi.org/10.1007/BF02108689.
- United Nations Educational, Scientific and Cultural Organization . International Technical Guidance on Sexuality Education: An Evidence-Informed Approach – Revised Edition 2018. https://unesdoc.unesco.org/ark:/48223/pf0000260770 (accessed 16 June 2020).
- HM Government . Review of Sexual Abuse in Schools and Colleges n.d. https://www.gov.uk/government/publications/review-of-sexual-abuse-in-schools-and-colleges/review-of-sexual-abuse-in-schools-and-colleges (accessed 10 September 2021).
- Lohan M, Brennan-Wilson A, Hunter R, Gabrio A, McDaid L, Young H, et al. Effects of gender-transformative relationships and sexuality education to reduce adolescent pregnancy (the JACK trial): a cluster-randomised trial. Lancet 2022;7:E626-37. https://doi.org/10.1016/S2468-2667(22)00117-7.
- Robinson M, Templeton M, Kelly C, Buston K, Hunt K, Lohan M. Addressing sexual and reproductive health and rights with men in prisons: co-production and feasibility testing of a relationship, sexuality and future fatherhood education programme [published online ahead of print 18 July 2022]. Int J Prison Health 2022.
- Johnson A. National Survey of Sexual Attitudes and Lifestyles, 2010–2012 n.d. https://beta.ukdataservice.ac.uk/datacatalogue/studies/study?id=7799 (accessed 14 May 2020).
- Pilgrim H, Payne N, Chilcott J, Blank L, Guillaume L, Baxter S. Modelling the Cost-Effectiveness of Interventions to Encourage Young People, Especially Socially Disadvantaged Young People, to use Contraceptives and Contraceptive Services. Sheffield: School of Health and Related Research, University of Sheffield; 2010.
- Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J, Melbye M. Maternal age and fetal loss: population based register linkage study. BMJ 2000;320:1708-12. https://doi.org/10.1136/bmj.320.7251.1708.
- Social Exclusion Unit . Teenage Pregnancy 1999.
- Chen XK, Wen SW, Fleming N, Demissie K, Rhoads GG, Walker M. Teenage pregnancy and adverse birth outcomes: a large population based retrospective cohort study. Int J Epidemiol 2007;36:368-73. https://doi.org/10.1093/ije/dyl284.
- Chevalier A, Viitanen TK. The long-run labour market consequences of teenage motherhood in Britain. J Popul Econ 2003;16:323-43. https://doi.org/10.1007/s001480200125.
- Ermiisch J, Pevalin DJ. Who Has a Child As a Teenager? 2003.
- Neale B, Clayton CL. Understanding Families Over Time: Research and Policy. London: Palgrave Macmillan; 2014.
- Neale B, Davies L. Becoming a young breadwinner? The education, employment and training trajectories of young fathers. Soc Policy Soc 2016;15:85-98. https://doi.org/10.1017/S1474746415000512.
- Walker I, Goodman A, Kaplan G. Understanding the Effects of Early Motherhood in Britain: The Effects on Mothers 2004.
- Marvin-Dowle K, Kilner K, Burley VJ, Soltani H. Impact of adolescent age on maternal and neonatal outcomes in the Born in Bradford cohort. BMJ Open 2018;8. https://doi.org/10.1136/bmjopen-2017-016258.
- UK Collaborative Group for HIV and STI Surveillance . Testing Times: HIV and Other Sexually Transmitted Infections in the United Kingdom 2007.
- Jit M, Vyse A, Borrow R, Pebody R, Soldan K, Miller E. Prevalence of human papillomavirus antibodies in young female subjects in England. Br J Cancer 2007;97:989-91. https://doi.org/10.1038/sj.bjc.6603955.
- Sonnenberg P, Tanton C, Mesher D, King E, Beddows S, Field N, et al. Epidemiology of genital warts in the British population: implications for HPV vaccination programmes. Sex Transm Infect 2019;95:386-90. https://doi.org/10.1136/sextrans-2018-053786.
- Fisher M, Benn P, Evans B, Pozniak A, Jones M, Maclean S, et al. UK Guideline for the use of post-exposure prophylaxis for HIV following sexual exposure. Int J STD AIDS 2006;17:81-92. https://doi.org/10.1258/095646206775455829.
- Pilcher CD, Tien HC, Eron JJ, Vernazza PL, Leu SY, Stewart PW, et al. Brief but efficient: acute HIV infection and the sexual transmission of HIV. J Infect Dis 2004;189:1785-92. https://doi.org/10.1086/386333.
- Cohen MS, Gay CL. Treatment to prevent transmission of HIV-1. Clin Infect Dis 2010;50:S85-S95. https://doi.org/10.1086/651478.
- Pinkerton SD, Holtgrave DR, Jemmott JB. Economic evaluation of HIV risk reduction intervention in African-American male adolescents. J Acquir Immune Defic Syndr 2000;25:164-72. https://doi.org/10.1097/00042560-200010010-00011.
- Winer RL, Hughes JP, Feng Q, O’Reilly S, Kiviat NB, Holmes KK, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med 2006;354:2645-54. https://doi.org/10.1056/NEJMoa053284.
- National Institute for Health and Care Excellence (NICE) . Ectopic Pregnancy and Miscarriage: Diagnosis and Initial Management 2019. https://www.nice.org.uk/guidance/ng126 (accessed 14 May 2020).
- Department of Health and Social Care . Abortion Statistics, England and Wales: 2019 2020. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/891405/abortion-statistics-commentary-2019.pdf (accessed 31 October 2022).
- Pilgrim H, Payne N, Chilcott J, Blank L, Guillaume L, Baxter S. Modelling the Cost-Effectiveness of Interventions to Encourage Young People, Especially Socially Disadvantaged Young People, to Use Contraceptives and Contraceptive Services 2010. http://www.academia.edu/22970385/Modelling_the_cost_effectiveness_of_interventions_to_encourage_young_people_especially_socially_disadvantaged_young_people_to_use_contraceptives_and_ (accessed 3 November 2022).
- Department for Work and Pensions . Quarterly Benefits Summary: Data to May 2017 n.d. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/659423/dwp-quarterly-benefit-stats-summary-november-2017.pdf (accessed 14 May 2020).
- Thomas CM, Cameron S. Can we reduce costs and prevent more unintended pregnancies? A cost of illness and cost-effectiveness study comparing two methods of EHC. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2013-003815.
- Joint Formulary Committee . British National Formulary 2017. https://bnf.nice.org.uk/.
Appendix 1 Process evaluation results
Control school relationship and sexuality education provision assessment tool
| School ID: | Met, partially met, not met, CT | |
|---|---|---|
| Subcategory | Assessment question | |
| Quality | ||
| Attitude and overall provision | Do school responses suggest a positive attitude towards delivering high-quality RSE provision, and that RSE has a high priority among staff who deliver or organise? | |
| Is RSE a clear/identifiable part of the curriculum with timetabled lessons? | ||
| Content | Do school responses suggest that RSE covers sufficient topics and information? | |
| Do school responses suggest that it also addresses skills, values, and attitudes? | ||
| Does RSE cover availability of and access to local health/support services? | ||
| Parents | Are parents given information about the school approach to RSE? | |
| Are parents given support to be involved in RSE? | ||
| Responsive to pupil needs | Does the school respond to pupil needs and new issues where relevant? | |
| Do pupils have an opportunity to comment on their RSE provision? Is their view positive? | ||
| Do school responses suggest that RSE addresses and supports diversity among individuals and in sex and relationships? Does it include content on LGBT+/gender issues and support equality? | ||
| Facilitator | If teachers deliver RSE, are they trained? | |
| If teachers deliver RSE, are they supported, confident, and happy to do so? | ||
| If external facilitators deliver RSE, is this high quality and of sufficient breadth of topic and opinion? | ||
| If external facilitators deliver RSE, do responses suggest that this is a substitute for the school dealing with RSE or does this supplement other provision? | ||
| Materials | Is there a clear and consistent approach to which RSE resources are used with the school? Do school responses suggest that the resources used are appropriate? Are these modified to meet pupils’ needs? |
|
| Quality categorisation | Met: Partially met: Not met/CT: |
|
| Quantity | ||
| Quantity and sufficiency | Do school responses suggest that time is clearly identified and allocated for RSE? | |
| Is this sufficient? | ||
| Is RSE provision regular across school years or is it limited? If RSE is delivered through drop-down days, do school responses suggest that this is a substitute for the school timetabling regular RSE? |
||
| Do pupils have a view on quantity? | ||
| Quantity categorisation | Met: Partially met: Not met/CT: |
|
| RSE governance and broader pastoral context | ||
| RSE governance | Is there a written RSE policy/ethos or equivalent? Was there appropriate consultation where relevant? |
|
| Is RSE provision regularly reviewed? | ||
| Is there a designated person/team to oversee and develop RSE? | ||
| Do school responses suggest that RSE has a high priority? Within the school among senior staff? Among the wider school body? As reflected by resource allocation? |
||
| Broader pastoral care context | Do school responses suggest that pastoral care has a high priority? Within the school among senior staff? Among the wider school body? As reflected by resource allocation? |
|
| Does the school respond to pupil needs and new issues where relevant? Do pupils have a say in reviewing pastoral support? |
||
| Do school responses suggest that equality is part of the school culture? | ||
| Is there a clear pastoral care system in place? | ||
| Are health/support services available within or linked to the school? | ||
| Do school responses suggest that teachers are competent and confident in a pastoral role? | ||
| Do responses suggest that the use of external facilitators is a substitute for the school addressing this aspect of pastoral care, or does this supplement other provision? | ||
| Parents | Does the school have a strong relationship with parents? | |
| RSE governance and broader pastoral context categorisation | Met: Partially met: Not met/CT: |
|
Activity 11: If I Were Jack homework survey
Appendix 2 Economic evaluation results
Modelling the health consequences of behavioural change
The baseline probability of becoming pregnant without contraception is derived from the available evidence in the literature. The procedure used to identify the base-case value for this parameter is described in the following text.
The proportion of sexually active males and females aged < 16 years was estimated using the answers to the HBSC surveys for England, Wales and Scotland168–170,230 and the YLT survey for NI. 171 We take this frequency to be an approximation of the proportion of sexually active females and males in the target population in each country, which is shown in Table 34.
| Country | Females | Males |
|---|---|---|
| 1st vaginal intercourse (%) | 1st vaginal intercourse (%) | |
| England and Wales | 24 | 19 |
| Scotland | 27 | 24 |
| NI | 28 | 23 |
In addition to these data, we used national official statistics about the population estimates of females and number of births by age in 2017 in England, Wales, Scotland and NI172–174 to obtain the total number of sexually active females in the target population in each country. We then combined these data with the evidence from the answers to the NATSAL-3 survey,230 about the age when respondents (aged 20–24 years) first had vaginal intercourse, to obtain estimates of the number of sexually active females in three different age groups: 11–13 years, 14 years and 15 years. The data to obtain this estimate are shown in Table 35.
| Country | Age (years) | Female population (n) | Sexually active female population (n) | Births (n) |
|---|---|---|---|---|
| England and Wales | 11–13 | 976,860 | 3907 | 128 |
| 14 | 307,789 | 3693 | 674 | |
| 15 | 302,881 | 7269 | 2019 | |
| Scotland | 11–13 | 82,044 | 369 | 16 |
| 14 | 26,234 | 354 | 49 | |
| 15 | 26,116 | 705 | 178 | |
| NI | 11–13 | 33,567 | 157 | 3 |
| 14 | 10,887 | 152 | 15 | |
| 15 | 10,877 | 304 | 58 |
There are no directly measured data for the probability of becoming pregnant within 1 year without contraceptive use in the UK. For the US, evidence from the published literature is available to first calculate the 1-month pregnancy probability and convert this into a 1-year probability,175 which may overestimate pregnancy risk. This evidence was adapted in the literature using data from about the HBSC surveys for England, Wales and Scotland168–170,230 and the 2011 YLT survey for NI. 171 We used the available evidence on the conceptions and population of females, baseline condom use and annual condom failure rate to derive an estimate of L for each country in the UK among the teenagers aged < 16 years. 176 Age-specific rates are used to avoid overestimation based on the failure rates of 15-year-old teenagers, whereas 2017 country-specific population data (see Table 35) were used to derive the base-case values for L among teenage females aged < 16 years, which are reported in Table 36.
| Parameter | Parameter value | Source |
|---|---|---|
| Probability of becoming pregnant within 1 year without using contraceptives: aged 11–13 years (England and Wales) | 1.9% | 168,170,172,173,230 |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 14 years (England and Wales) | 10.9% | |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 15 years (England and Wales) | 16.6% | |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 11–13 years (Scotland) | 2.5% | 168,169,172,173 |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 14 years (Scotland) | 8.3% | |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 15 years (Scotland) | 15.1% | |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 11–13 years (NI) | 1.1% | 168,171–173 |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 14 years (NI) | 5.8% | |
| Probability of becoming pregnant within 1 year without using contraceptives: aged 15 years (NI) | 11.4% | |
| Baseline condom use: aged < 16 years (England and Wales) | 57% | 170,230 |
| Baseline condom use: aged < 16 years (Scotland) | 58% | 169 |
| Baseline condom use: aged < 16 years (NI) | 57% | 171 |
| Average condom failure rate | 18% | 165 |
| Average pill/patch/ring failure rate | 11% | |
| Average emergency pill failure rate | 9% | |
| Average injection failure rate | 6% | |
| Average diaphragm/cap/spermicide failure rate | 12% | |
| Average implant failure rate | 0.1% | |
| Average IUD failure rate | 0.5% | |
| Average withdrawal contraception failure rate | 22% |
It is important within any health economic analysis to compare the additional costs and benefits associated with an intervention. A pregnancy may result in a birth, an abortion or a miscarriage/ectopic pregnancy/stillbirth. The consequences of each of these outcomes need to be estimated in terms of costs and benefits. We therefore follow the approach used in the literature176,231 and include in the model the outcomes associated with the number of pregnancies averted.
The probability of birth, abortion, miscarriage/ectopic pregnancy/stillbirth is based on national government statistics for England, Wales and Scotland. 172,174 For NI, since abortion was not legal and official data were not available at the time of writing, the model uses the information about the number of abortions in England and Wales for NI residents. 173 This is likely to be an underestimate of the true value of the number of abortions for NI, and sensitivity analysis will be carried out to assess the impact of variations of this estimate on the results. The probability of miscarriage/ectopic pregnancy/stillbirth is reported by HES data collected by the Information Centre for Health and Social Care. 172–174,178 This suggests that 8.5% of all pregnancies result in miscarriage/ectopic pregnancy/stillbirth; however, this is not separated by age. One study was identified that reports outcomes of pregnancy by age and suggests that about 6% of all pregnancies of women aged < 20 years end in miscarriage, ectopic pregnancy or stillbirth. 232 This analysis was based within Denmark; however, it seems consistent with the UK HES data. It should be noted that these miscarriage statistics are based on the number of hospital stays and not all miscarriages require a hospital stay, meaning that the proportion of pregnancies ending in miscarriage, ectopic pregnancy or stillbirth may be underestimated. The impact of this on the model results is tested within a one-way sensitivity analysis. The probabilities of each outcome following conception are shown in Table 37.
| Age at conception (< 16 years) | Probability of abortion (%) | Probability of birth (%) | Probability of miscarriage/ectopic pregnancy/stillbirth (%) |
|---|---|---|---|
| England and Wales | 59.4 | 34.2 | 6.4 |
| Scotland | 55.1 | 38.5 | 6.4 |
| NI | 50 | 43.6 | 6.4 |
A pregnancy may result in a birth, an abortion, a miscarriage, an ectopic pregnancy or a stillbirth. The consequences of each of these outcomes need to be estimated in terms of costs and benefits. There are numerous negative outcomes typically associated with a teenage pregnancy. First, young age at pregnancy is associated with a greater likelihood of abortion. 172,233,234 Second, if the pregnancy is continued, there might be a greater risk of having a very low-birthweight baby. Finally, there are longer-term negative outcomes for the mother, the father and the child typically associated with a teenage birth. 235,236 These include lower education, poorer employment status and an increased risk of a female child becoming a teenage mother herself.
The evidence from two UK-specific reports about the financial and economic impact of teenage pregnancy suggests that about 43% of teenage mothers have no qualifications. 199,233 Based on this evidence, an estimate was derived about the medium-term negative impacts on earnings in the UK for teenage mothers who fail to gain qualifications. Focusing on vocational qualification, the estimated annual levels of earnings disparity between young workers with qualifications versus young workers with no qualifications lie between £2771 (Level 2 qualifications – CSE/GCSE or equivalent) and £3447 (Level 3 qualifications – AS/A-levels or equivalent). In addition, estimates about the long-term economic impacts of teenage pregnancy in terms of the potential scale of the motherhood penalty in the UK for non-teenage mothers were derived based on the average earnings for women in age groups 22–29 years, 30–39 years and 40–49 years, where the potential size of the gap is estimated to lie between 5% and 10% of earnings. 201 Given the average level of earnings in each age group, the size of the gap is estimated to be in the order of £990–1980 per annum for a woman in her 20s, rising to £1223–2445 for a woman in her 40s. 201 The medium- and long-term cost outcomes associated with teenage pregnancy that are included in the model are shown in Table 43.
Three articles235,237,238 were identified within the literature, assessing outcomes for the father of a child born to a teenage mother. Evidence from two237,238 of these, which were based on a longitudinal study of young fathers in the UK, indicates that parenthood may lead young fathers towards a low-skilled labour trajectory, especially for those living in a social deprivation status. However, this was a qualitative study, and no impact on the long-term economic outcomes of young fatherhood was captured. Evidence from the third235 article suggests that becoming a young father (< 23 years) is not associated with substantial long-term negative outcomes, although this study does not control for unobservable characteristics. Given the limited and poor quality of the evidence found in the literature, no negative impact on the father has been incorporated into the model. The review identified one study6 comparing the long-term outcomes of children born to teenage mothers with those of children born to older mothers. This study suggests that children of teenage mothers have a slightly lower chance of high educational attainment, greater risks of inactivity and teenage childbearing, and a higher probability of lower earnings. However, this study did not adequately control for unobservable characteristics, which may influence the child’s outcomes, and hence it may overestimate the negative outcomes associated with a teenage birth. Given that other studies235,239 found that accounting for unobserved family background typically mitigates the estimated consequences of early childbearing, the model takes a conservative approach and does not incorporate any long-term negative implications of a teenage birth on the child.
Finally, from the perspective of the state, young age at motherhood is typically associated with an increase in claims for means-tested benefits. 165 Based on the evidence retrieved from the literature,176 the model assumes that 90% of teenage mothers will receive income support and associated benefits, which include child tax credits. In addition to the long-term outcomes of a teenage birth, we identified a study240 using UK-based cohort data that considers the impact of teenage birth on immediate birth outcomes, including very low birthweight. This study suggests that the probability of women who aged< 16 years having a very low-birthweight baby (< 1500 g) is 0.016. The parameters associated with the outcomes of a teenage birth are shown in Table 38.
| Parameter | Parameter value (%) | Source |
|---|---|---|
| Range for the potential size of the earnings gap between teenage and non-teenage mothers | 5–10 | 201 |
| Probability of having no qualifications after having a baby for a woman aged < 16 years | 43 | 201 |
| Probability of receiving income support and associated benefits for a woman aged < 16 years | 90 | 176 |
| Probability of very low-birthweight baby for a woman aged < 16 years | 1.6 | 240 |
Modelling the number of sexually transmitted infections
The STI model implemented in the analysis consists of several interacting submodels for each STI. All submodels are connected with the same sexual network to enable transmission and co-infection.
The model estimates the number of STI cases averted for HIV and also for chlamydia, gonorrhoea and genital warts, according to the risk of infection as shown below and the proportion of sexually active individuals who receive the intervention. The data and assumptions used to derive the model parameters are presented in the following sections.
Sexually transmitted infection epidemiology
We separately report the epidemiology data that are used to inform the parameters of the model for each type of STI included: chlamydia, gonorrhoea, genital warts and HIV. We decided that it was not realistic to include syphilis or genital herpes in the model. This is because of their relatively lower incidence and the paucity of reliable data on the epidemiology of these STIs for the target population. Based on the same considerations, other economic evaluations in the literature that modelled STIs among young adolescents did not attempt to model the effectiveness of preventing these types of STIs either. 25,176,179,231
Chlamydia
The Department of Health and Social Care in England reports evidence about the screening for chlamydia in sexually active young men and women attending a range of health-care services, including general practice and family planning clinics. The prevalence of chlamydia in England in 2006–7 in the 16–19 years age group was 10.0% among men and 12.1% among women; the corresponding figures for those aged < 16 years were 1.5% and 7.5%, respectively. 180 A recent study29 implemented a method that synthesised data on chlamydia testing and diagnosis with information on care-seeking behaviour and infection history to derive estimates for the prevalence of chlamydia in England in male and female teenagers from 2000 to 2015. According to this study, the most recent and best population-based estimates for chlamydia prevalence in England come from the NATSAL-3 survey. 181 We therefore used this evidence to inform our estimates for the prevalence of chlamydia in the model. We then used an estimate of the per-episode transmission probability of 0.11, which was obtained based on the transmission probability per relationship of 68%. 179 In a similar way to other works in the literature, we estimated the per-episode transmission probability to be 0.11, assuming that the infection would be transmitted within 10 sexual episodes per relationship. 183,184
Gonorrhoea
The prevalence of gonorrhoea was estimated for south-east London as part of the English National Chlamydia Screening Programme. 180 However, the prevalence in London is typically higher than for the rest of the UK. A recent study185 estimated the prevalence of gonorrhoea in heterosexual men and women aged 15–24 years attending specialist and community-based sexual health services in England. To estimate the prevalence within the younger age group, we assumed the same relationship between age groups in the incident data, that is the prevalence in the UK for under-16-year-olds of 0.027% and 0.14% for males and females, respectively. 186 Based on the evidence from the literature, we assumed that the transmission probability per relationship for gonorrhoea is 50%. 187,188 We then estimated a per-episode transmission probability of 0.07 based on 10 sexual episodes per relationship in the same way as for chlamydia.
Genital warts
Genital warts are caused by the human papillomavirus (HPV), and 90% of cases of genital warts are attributable to HPV 6, HPV 11, HPV 16 and HPV 18. 189 The majority of infections are acquired through heterosexual sex, and the highest rates are among young people. 241 A study242 of antibodies to four types of HPV in UK (HPV 16, HPV 18, HPV 6 and HPV 11) showed that the prevalence of HPV 6 and HPV 11 was 6.5% and 14% for females aged < 16 and 16–19 years, respectively. The prevalence of HPV 16 and HPV 18 was similar to that of 6 and 11. Based on previous evidence,241 about 10% of HPV infections lead to the development of genital warts; therefore, we assumed in the model that the prevalence of genital warts was one-tenth the prevalence of HPV 6 and HPV 11. The prevalence among males was estimated from female prevalence by using the same relationship between males and females as seen for incidence. Thus, the prevalence was estimated to be 0.1% and 0.53% among males aged > 16 years and < 16 years, respectively. These prevalence estimates for the teenagers are in line with those reported from a recent study, which provides estimates for the prevalence of reported history of genital warts over different time periods by age in the UK (England/Wales) population, equal to 0.2% and 0.7% for the males and females, respectively. 243 As reported in a study of HPV epidemiology,189 we assumed that the transmission probability per relationship for genital warts was 65%. We estimated a per-episode transmission probability of 0.1 based on 10 sexual episodes per relationship in the same way as for chlamydia and gonorrhoea.
Human immunodeficiency virus
The prevalence of diagnosed HIV infection is typically higher among London residents than among those in the rest of the UK. 241 Following the approaches found in the literature,25 we used the number of adults between the ages of 15 and 59 years in the UK to estimate the average HIV prevalence in the 16–19 years age group to be 0.26% for men and 0.12% for women. There are no data on the prevalence of HIV for adolescents. We assumed prevalence for the > 16 years age group to be half that of adult prevalence175 corresponding to 0.13% for males and 0.06% for females. The < 16 years age group has been used as a starting point as, although some of the students will be 16 years at follow-up, our starting point for the model is when the young adults receive the intervention or not. Using the evidence from the British Association for Sexual Health and HIV guidelines244 for post-exposure prophylaxis after sexual exposure to HIV, a systematic literature review reported the risk of HIV transmission following an exposure from a known HIV-positive individual to be 0.1% for vaginal intercourse. Evidence from other studies shows that the probability of transmission increases to about 0.5% in the acute phase of the infection, when viral load is high. 245,246 Using the estimates from these studies and an average transmission probability estimate over 1 year, we assumed a mean transmission probability of 0.15% per sexual episode. 231
Based on the evidence from the literature, it is also assumed that, if chlamydia and gonorrhoea are left untreated, there is a 25% and 15% probability of contracting PID, respectively. 176 An estimate is also provided for the proportions of people who are treated for chlamydia, gonorrhoea or genital warts (90%) and PID or HIV (100%). 231 A summary of the base-case parameter values for the STIs is shown in Tables 39 and 40.
Sexual behaviour
Evidence about the effectiveness of condoms for protecting against STIs was taken from the available literature. The effectiveness of condoms in reducing heterosexual HIV transmission was estimated to be 90%, based on evidence from the literature. 247 For genital warts, we used the evidence from a longitudinal study on young people,248 which suggested that consistent use of male condoms reduced the risk of genital HPV transmission by 70%. A Cochrane systematic review25 estimated that consistent use of condoms results in an 80% reduction in HIV incidence, and the authors also noted that there was insufficient evidence to estimate the effectiveness of condoms in preventing other STIs. We therefore assumed that condom effectiveness was 80% for HIV, 70% for genital warts and 90% for chlamydia and gonorrhoea. A summary of the base-case values for the parameters related to sexual behaviours in the target population is shown in Table 41.
Benefit and cost outcomes of pregnancies and sexually transmitted infections averted
Health-related quality of life
NICE’s preferred measure for economic evaluation is the QALY, which facilitates a comparison of cost-effectiveness across health interventions that may differ in terms of their impact on the various dimensions of health. However, not all outcomes of interest were assigned a QALY weight, and therefore the modelling also facilitated a cost–consequences approach, with all the changes in model outcomes (the consequences) reported together with the net costs. In particular, we did not assign any QALYs to teenage conceptions for various reasons. First, there is limited evidence around how miscarriage and abortion affects the quality of life of the parents. 191,249 Second, the valuation of abortion may depend on ethical and religious views, and hence it would not be possible to reach a consensus around the valuation of an abortion. 192 Finally, other authors do not consider it appropriate to assign a utility weight to pregnancy. 176,231 Indeed, pregnancy is not a disease, and it is not by any means certain that pregnancy as a health state generally diminishes health-related quality of life. Many women choose to become pregnant in their lifetime, suggesting that, for them at least, the perceived benefits outweigh the costs. However, the model can explore the cost-effectiveness of reduced teenage conceptions based on willingness-to-pay criteria.
The utilities associated with various STI outcomes were estimated using the evidence from the published literature. 176 We used these values to assign the utility weights to each type of STI considered, which were then used to calculate the QALYs gained from the reduction in cases of chlamydia, gonorrhoea, genital warts and HIV. The QALYs gained from reduction of each type of STI were calculated by multiplying the cases averted by (1 – utility for STI) multiplied by (1 – proportion treated for that STI). This allowed the model to adopt NICE’s preferred approach with an incremental cost-per-QALY result. The specific utility values associated with the STI outcomes are reported in Table 42.
Costs
The average costs of birth, abortion and miscarriage/ectopic pregnancy/stillbirth were taken from the NHS reference costs. 196 Based on the evidence from the literature, the model also assumed that 1% of abortions are not funded by the NHS. 250 The costs of providing NHS care to children as they age were also included (primary care, secondary care and medications). The Office for Budget Responsibility has estimated annual per capita health spending by age of the child. 197 The cost of preschool and primary school education for children was also considered in the analysis, under the assumption that the government would maintain the funding levels at the current level. The mean per-pupil funding was taken from the analysis of the IFS, which estimates a mean cost of £1635 per preschool place and £4900 per primary school place. 198 Preschool costs are incurred only at ages 3 and 4 years, whereas primary school costs are incurred from the age of 5 years.
The cost of treatment of STIs was based on the health economic model developed for the NICE SRE public health guidance176 and expert guidance. Treatment for chlamydia was assumed to require doxycycline 100 mg twice per day for 1 week and azithromycin 1 g followed by 500 mg daily for the next 2 days. Given that first-line treatment for chlamydia is often provided outside specialist care, the models assumed that treatment is carried out 50% of the time in GP practices and 50% in GUM clinics. A sensitivity analysis to assess the impact on the results of assuming that treatment for chlamydia is always carried out in GUM clinics is also explored. Treatment for gonorrhoea was assumed to require ceftriaxone 1-g IM injection in GUM clinics, whereas treatment for genital warts was assumed to require one dose of imiquimod and a GP consultation. An average cost for HIV treatment per year was estimated based on the sum of the average cost of care for HIV patients and the average cost of drug treatment. 176
The costs of benefit payments were also included within the model, as they are costs incurred by the public sector that represent real resource savings if the baby that might otherwise eventuate were not conceived. We assumed that 90% of all teenager mothers within the model will receive income support, based on evidence within the Teenage Pregnancy Strategy,199 and hence that 90% of all teenage mothers will also receive associated benefits (housing benefit, child benefits and child tax credits). Claims of benefits were assumed to begin at the birth of the child, as evidence suggests that 90% of teenage mothers have moved out of their family home within 1 year of childbirth. 251 In the case of the 10% of people who do not receive income support, the model assumed that they will claim child benefits.
Child benefit is a regular payment from the government to help with the cost of raising a child. The child benefit entitlement is £20.70 per week for the first child in a family and £13.70 for subsequent children, up to a maximum of two further children. To estimate the cost savings for averted births, we estimated the birth number of the child not born because of the averted birth (i.e. the first or second child). Based on cohort fertility and population data from the ONS,200 and assuming that the distribution of averted births among our study population would be the same, it was estimated that 50.7% of averted births, were they to occur, would be in women with no children currently, and so they would be the first child in the household, and 15.1% of the births would be in women who already have one child, so these families would receive the award for a second child in the family. 165
Child tax credit is an annual benefit from the government to help with the cost of raising a child. As with child benefit, to estimate the cost savings attributable to not having to pay child tax credit for averted births, we had to estimate the birth number of the child not born because of the averted birth. From this, we could estimate that 50.7% of averted births, were they to occur, would be in women with no children currently, and so they would be the first child in the household (and the benefit received would be the ‘family element’ and ‘child element’) whereas 15.1% of averted births would occur in females who already have a child, and, therefore, the additional money received would be only the ‘child element’. 165
Income support is a benefit available for lone parents of low income, until their child reaches the age of 5 years. The benefit is not dependent on the number of children: only the first child of a single female would result in a new payment. A total of 50.7% of females aged 15–44 years are currently childless, and for this proportion of the averted births the child would be the first child in the family. From the Department for Work and Pensions,252 it was estimated that the average weekly award is £71.33 for a lone parent aged ≥ 18 years and £57.90 for a person aged 16–17 years. These values, multiplied by the number of averted live births and the percentage of teenage mothers who claim income support, give an estimate of the associated cost savings.
Housing benefit is paid to those on low incomes or claiming benefits to help cover the cost of rent. Although eligibility is not dependent on having children, households with children tend to receive higher benefits, as the value of the benefit received is dependent on household circumstances. The average weekly cost of housing benefit is £95.77, whereas the mean weekly increase in benefit payments for single females with children (compared to those without children) is £12.05. 165
All costs and associated parameters are shown in Table 43.
| Parameter | Parameter value (£) | Source |
|---|---|---|
| Average NHS abortion cost | 714 | 196 |
| Average NHS miscarriage/ectopic pregnancy/stillbirth cost | 653 | |
| Average NHS ectopic pregnancy cost | 1228 | |
| Average NHS stillbirth cost | 3765 | |
| Maternity care costs (costs of antenatal care, hospital delivery, postnatal care, neonatal care) | 5735 | 253 (uplifted to 2019) |
| Treatment of very low-birthweight child | 3354 | 196 |
| Azithromycin | 2.21 | 254 |
| Imiquimod | 48.60 | |
| Doxycycline | 1.10 | |
| Ceftriaxone | 9.58 | |
| GP consultation | 42.80 | 159 |
| GUM clinic visit | 116 | |
| Annual treatment cost of HIV | 18,667 | 176 (uplifted to 2019) |
| Cost of PID | 3795 | |
| Mean per capita health-care spending by age of the child (years) | ||
| 0 | 2800 | 165 |
| 1 | 2800 | |
| 2 | 2700 | |
| 3 | 2500 | |
| 4 | 2300 | |
| 5 | 2100 | |
| 6 | 1900 | |
| 7 | 1600 | |
| 8 | 1500 | |
| 9 | 1300 | |
| Average annual preschool cost per pupil | 1635 | 165 |
| Average annual primary school cost per pupil | 4900 | |
| Weekly entitlement of child benefits for a first child | 20.70 | |
| Weekly entitlement of child benefits for a second child | 13.70 | |
| Income support weekly award | ||
| < 16 years | 0 | 165,199,252 |
| 16–17 years | 57.90 | |
| > 17 years | 71.33 | |
| Child tax credit (family element) | 548 | |
| Child tax credit (child element) | 2780 | |
| Weekly average cost of housing benefit | 95.77 | |
| Average weekly increase in claim costs for single females with children | 12.05 | |
| Mean annual earnings for women aged 22–29 years | 19,800 | 201 |
| Mean annual earnings for women aged 30–39 years | 24,298 | |
| Mean annual earnings for women aged 40–49 years | 24,452 | |
| Medium-term earnings gap between young workers with and without qualifications | 2771 (Level 2) – 3447 (Level 3) | 206 |
| Long-term motherhood earnings gap between teenager and non-teenager mothers (age 22–29 years) | 990 (5% gap) 1980 (10% gap) | 201 |
| Potential motherhood earnings gap between teenager and non-teenager mothers (age 30–39 years) | 1215 (5% gap) 2430 (10% gap) | |
| Potential motherhood earnings gap between teenager and non-teenager mothers (age 40–49 years) | 1223 (5% gap) 2445 (10% gap) | |
Table 44 summarises all information related to the choice of all model parameters in the base-case and PSA scenarios, including parameter values, distributions and references.
| Parameter | Value | Distribution (95% CI) | Source | |
|---|---|---|---|---|
| Number of pregnancies | ||||
| Probability of becoming pregnant within 1 year without using contraceptives (England and Wales) | ||||
| Aged 11–13 years | 1.9% | Fixed but dependent on proportion of baseline condom use | 168,170,172,173,230 | |
| Aged 14 years | 10.9% | |||
| Aged 15 years | 16.6% | |||
| Probability of becoming pregnant within 1 year without using contraceptives (Scotland) | ||||
| Aged 11–13 years | 2.5% | Fixed but dependent on proportion of baseline condom use | 168,169,172,173 | |
| Aged 14 years | 8.3% | |||
| Aged 15 years | 15.1% | |||
| Probability of becoming pregnant within 1 year without using contraceptives (NI) | ||||
| Aged 11–13 years | 1.1% | Fixed but dependent on proportion of baseline condom use | 168,171–173 | |
| Aged 14 years | 5.8% | |||
| Aged 15 years | 11.4% | |||
| Baseline condom use | ||||
| England and Wales | 57% | Beta (30% to 80%) | 169 | |
| Scotland | 58% | Beta (30% to 80%) | 171 | |
| NI | 57% | Beta (30% to 80%) | 172 | |
| Failure rate | ||||
| Condom | 18% | Doubled | 165 | |
| Pill | 11% | Doubled | ||
| Injection | 6% | Doubled | ||
| Emergency pill | 9% | Doubled | ||
| Diaphragm/cap/spermicide | 12% | Doubled | ||
| Implant | 0.1% | Fixed | ||
| IUD | 0.5% | Fixed | ||
| Withdrawal | 22% | Doubled | ||
| Additional chance of having an unplanned pregnancy for people in most deprived areas | 28% | Beta (20% to 36%) | 167 | |
| Outcomes of pregnancies | ||||
| Probability of very low-birthweight baby for a woman aged < 16 years | 1.6% | Fixed | 240 | |
| Range for the potential size of the earnings gap between teenage and non-teenage mothers | 5% | Doubled | 201 | |
| Probability of having no qualifications after having a baby for a woman aged < 16 years | 43% | Fixed | 199 | |
| Probability of receiving income support and associated benefits for a woman aged < 16 years | 90% | Fixed | 199 | |
| Probability of abortion | ||||
| Non-NHS abortion (< 20 years) | 1% | Fixed | 250 | |
| England and Wales | 59.4% | Fixed but dependent on probability of miscarriage | 173–176 | |
| Scotland | 55.1% | |||
| NI | 50% | Beta (45% to 55%) | ||
| Probability of birth | ||||
| England and Wales | 34.2% | Fixed but dependent on probability of miscarriage | 173–176 | |
| Scotland | 38.5% | |||
| NI | 34.2% | Beta (24% to 44%) | ||
| Probability of miscarriage/ectopic pregnancy/stillbirth | ||||
| England and Wales | 6.4% | Beta (4% to 9%) | 232 | |
| Scotland | 6.4% | |||
| NI | 6.4% | |||
| STI parameters | ||||
| Males | Females | Fixed | 175,180,185,186,241 | |
| Prevalence of chlamydia | 0.5% | 4.7% | ||
| Prevalence of gonorrhoea | 0.027% | 0.14% | ||
| Prevalence of genital warts | 0.2% | 0.7% | ||
| Prevalence of HIV | 0.13% | 0.06% | ||
| Transmission rate of chlamydia | 0.11% | 179,187–189,243,245,246 | ||
| Transmission rate of gonorrhoea | 0.07% | |||
| Transmission rate of genital warts | 0.1% | |||
| Transmission rate of HIV | 0.0015% | |||
| Condom failure rate for all modelled STIs | 16% | |||
| Annual acts of vaginal sexual intercourse if sexually active (< 16 years) | 20 | Fixed | 176 | |
| Sexual partners per year (< 16 years) | 2 | Fixed | ||
| Condom use at last intercourse | 18% | Fixed | ||
| Condom effectiveness: HIV | 80% | Fixed | 247 | |
| Condom effectiveness: chlamydia and gonorrhoea | 90% | |||
| Condom effectiveness: genital warts | 70% | Fixed | 248 | |
| Utilities associated with the outcomes of STIs | ||||
| Chlamydia | 0.90 | Fixed | 249 | |
| Gonorrhoea | 1.00 | Fixed | 249 | |
| Genital warts | 0.91 | Fixed | 191 | |
| PID | 0.65 | Fixed | 249 | |
| HIV | 0.66 | Fixed | 192 | |
| Costs and associated parameters | ||||
| Average NHS abortion cost | £714 | Fixed | 196 | |
| Average NHS miscarriage cost | £653 | |||
| Average NHS ectopic pregnancy cost | £1228 | |||
| Average NHS stillbirth cost | £3765 | |||
| Maternity care costs (costs of antenatal care, hospital delivery, postnatal, neonatal care) | £5735 | 176 (uplifted to 2019) | ||
| Treatment of very low-birthweight child | £3354 | 196 | ||
| Azithromycin | £9.64 | Fixed | 254 | |
| Imiquimod | £48.60 | |||
| Doctor consultation | £42.80 | 159 | ||
| Annual treatment cost of HIV | £18,667 | 176 (uplifted to 2019) | ||
| Cost of PID | £3795 | |||
| Probability of treatment for chlamydia, gonorrhoea and genital warts | 90% | Beta (75%, 98%) | 176 | |
| Probability of treatment for HIV | 100% | Fixed | ||
| Probability of contracting PID if chlamydia untreated | 25% | Fixed | ||
| Probability of contracting PID if gonorrhoea untreated | 15% | Fixed | ||
| Mean per capita health-care spending by age of the child (years) | ||||
| 0 | £2800 | Fixed | 165 | |
| 1 | £2800 | |||
| 2 | £2700 | |||
| 3 | £2500 | |||
| 4 | £2300 | |||
| 5 | £2100 | |||
| 6 | £1900 | |||
| 7 | £1600 | |||
| 8 | £1500 | |||
| 9 | £1300 | |||
| Average annual preschool cost per pupil | £1635 | Fixed | 165 | |
| Average annual primary school cost per pupil | £4900 | |||
| Weekly entitlement of child benefits for a first child | £20.70 | Fixed | 165 | |
| Weekly entitlement of child benefits for a second child | £13.70 | |||
| Percentage of teen mothers receiving income support | 90% | Beta (60% to 99%) | 176 | |
| Income support weekly award | ||||
| < 16-years | £0 | Fixed | 165 | |
| 16–17 years | £57.90 | |||
| > 17 years | £71.33 | |||
| Child tax credit (family element) | £548 | Fixed | ||
| Child tax credit (child element) | £2780 | |||
| Weekly average cost of housing benefit | £95.77 | |||
| Average weekly increase in claim costs for single females with children | £12.05 | |||
| Mean annual earnings for women aged 22–29 years | £19,800 | Fixed | 200 | |
| Mean annual earnings for women aged 30–39 years | £24,298 | |||
| Mean annual earnings for women aged 40–49 years | £24,452 | |||
| Medium-term earnings gap between young workers with and without qualifications | £2771 (Level 2) – £3447 (Level 3) | Fixed | 201 | |
| Long-term motherhood earnings gap between teenager and non-teenager mothers (aged 22–29 years) | £990 (5% gap) £1980 (10% gap) |
|||
| Potential motherhood earnings gap between teenager and non-teenager mothers (aged 30–39 years) | £1215 (5% gap) £2430 (10% gap) |
|||
| Potential motherhood earnings gap between teenager and non-teenager mothers (aged 40–49 years) | £1223 (5% gap) £2445 (10% gap) |
|||
Model results
Country-specific results from base-case analysis
| Results | England | Wales | Scotland | NI | ||||
|---|---|---|---|---|---|---|---|---|
| Control | Intervention | Control | Intervention | Control | Intervention | Control | Intervention | |
| Unintended pregnancies, n | 2096 | 1756 | 199 | 182 | 185 | 167 | 121 | 116 |
| Averted unintended pregnancies, n | 340 | 17 | 18 | 5 | ||||
| STIs, n | 991 | 667 | 220 | 194 | 367 | 137 | 276 | 174 |
| Averted STIs, n | 324 | 126 | 130 | 102 | ||||
| Discounted | ||||||||
| QALYs lost | 16 | 11 | 3 | 2 | 6 | 2 | 3 | 2 |
| Averted QALYs lost | 5 | 1 | 4 | 1 | ||||
| Costs (without benefits), £ | 16,722,286 | 15,812,763 | 1,049,749 | 1,026,941 | 1,658,866 | 1,613,633 | 1,028,841 | 1,016,999 |
| Incremental costs (without benefits), £ | –909,523 | –22,808 | –45,233 | –11,842 | ||||
| Costs (with benefits), £ | 155,083,447 | 134,421,416 | 9,492,460 | 8,986,543 | 16,456,606 | 12,833,012 | 10,424,657 | 9,870,594 |
| Incremental costs (with benefits) | –£20,662,031 | –£505,917 | –£3,623,594 | –£554,063 | ||||
One-way sensitivity analysis results
| Averted outcomes/incremental costs | Failure condom (low = 9%) | Failure condom (high = 36%) | Failure withdrawal (low = 11%) | Failure withdrawal (high = 44%) |
|---|---|---|---|---|
| Total unintended pregnancies, n | 178 | 473 | 297 | 546 |
| Total costs (without benefits), £ | 1,131,487 | –2,469,381 | –88,077 | –5,171,471 |
| Total costs (with benefits), £ | –5,681,037 | –60,419,546 | –20,293,063 | –66,910,008 |
| Averted outcome/incremental costs | Prevalence (low) | Prevalence (high) | Transmission (low) | Transmission (high) |
|---|---|---|---|---|
| Total STIs, n | 306 | 1226 | 378 | 914 |
| Total QALYs lost, n | 5 | 21 | 6 | 15 |
| Total costs (without benefits), £ | –220,925 | –3,658,914 | –371,291 | –2,333,984 |
| Total costs (with benefits), £ | –6,300,043 | –101,258,497 | –10,444,206 | –61,227,019 |
| Averted outcomes/incremental costs | Transmission and failure withdrawal | Failure condom and condom effectiveness | ||
|---|---|---|---|---|
| LB | UB | LB | UB | |
| Total unintended pregnancies, n | 297 | 546 | 345 | 392 |
| Total STIs, n | 378 | 914 | 526 | 709 |
| Total QALYs lost, n | 6 | 7 | 10 | 15 |
| Total costs (without benefits), £ | –748,177 | –3,387,687 | –840,633 | –3,112,522 |
| Total costs (with benefits), £ | –17,832,709 | –54,922,644 | –8,461,138 | –30,856,684 |
The cost of delivering relationship and sexuality education activities in the control group
The cost of delivering RSE activities in the control group is calculated by identifying the number of teachers in a year group that teach RSE and the number of sexual health lessons taught to estimate the hours per year spent on activities that may be broadly similar to If I Were Jack. This is multiplied by the cost per hour of a teacher (£23.98) as reported by the ONS and divided by the number of students in the control schools to calculate the cost per student. This will be used for comparative purposes only, as If I Were Jack is likely to only make up a component of RSE in the intervention school. Data on teacher resource use and number of sexual health lessons are summarised in Table 49. These data were collected via questionnaires from a total of 26 control schools. Estimates for the number of lessons in a school year are obtained by taking the minimum/average/maximum number of lessons in a school year provided by each school.
| Resource use (N = 26 schools) | Number, mean (SD) | Costs (£), mean (SD) |
|---|---|---|
| Lessons | ||
| Minimum | 5.08 (7.9) | 491 (738) |
| Average | 7 (8.67) | 688 (798) |
| Maximum | 8.21 (7.98) | 791 (566) |
| Other resource costs (materials + consultancy) | – | 9.80 (7.53) |
| Total costs | ||
| Minimum | – | 501 (739) |
| Average | – | 697 (799) |
| Maximum | – | 801 (567) |
| Cost per student | ||
| Minimum | – | 3.18 |
| Average | – | 4.42 |
| Maximum | – | 5.10 |
List of abbreviations
- AIDS
- acquired immunodeficiency syndrome
- aOR
- adjusted odds ratio
- AOUM
- abstinence only until marriage
- BHSCT
- Belfast Health and Social Care Trust
- CI
- confidence interval
- CONSORT
- Consolidated Standards of Reporting Trials
- CSE
- comprehensive sex education
- DSA
- deterministic sensitivity analysis
- ESRC
- Economic and Social Research Council
- FSM
- free school meals
- GP
- general practitioner
- GUM
- genitourinary medicine
- HBSC
- Health Behaviour in School-aged Children
- HES
- Hospital Episode Statistics
- HIV
- human immunodeficiency virus
- HPV
- human papillomavirus
- ICC
- intraclass correlation coefficient
- ICPD
- International Conference on Population and Development
- IFS
- Institute for Fiscal Studies
- IM
- intramuscular
- IUD
- intrauterine device
- IVD
- interactive video drama
- LGBTQ+
- lesbian, gay, bisexual, transgender and questioning (or queer)
- MAR
- missing at random
- MB
- mistimed birth
- MD
- mean difference
- MICE
- multiple imputation by chained equation
- MoU
- Memorandum of Understanding
- MRC
- Medical Research Council
- NATSAL
- National Survey of Sexual Attitudes and Lifestyles
- NI
- Northern Ireland
- NICE
- National Institute for Health and Care Excellence
- NICTU
- Northern Ireland Clinical Trials Unit
- NIHR
- National Institute for Health and Care Research
- NISRA
- Northern Ireland Statistics and Research Agency
- Ofsted
- Office for Standards in Education, Children’s services and Skills
- ONS
- Office for National Statistics
- PD
- personal development
- PI
- principal investigator
- PID
- pelvic inflammatory disease
- PPI
- patient and public involvement
- PSA
- probabilistic sensitivity analysis
- PSHE
- personal, social, health and economic education
- PSHEA
- Personal, Social and Health Education Association
- QALY
- quality-adjusted life-year
- QUB
- Queen’s University Belfast
- RCT
- randomised controlled trial
- RIPPLE
- Randomised Intervention of PuPil-Led sex Education
- ROI
- return on investment
- RSE
- relationship and sexuality education
- SAC
- Stakeholder Advisory Committee
- SD
- standard deviation
- SEN
- special education needs
- SEQ
- student engagement questionnaire
- SHARE
- Sexual Health and Relationships Education
- SRE
- sex and relationship education
- SRHR
- sexual and reproductive health and rights
- STI
- sexually transmitted infection
- TSC
- Trial Steering Committee
- UTP
- unintended teenage pregnancy
- WHO
- World Health Organization
- YLT
- Young Life and Times
- YPAG
- Young Person’s Advisory Group
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/YWXQ8757).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.