

Notes
Article history
The contractual start date for this research was in April 2021. This article began editorial review in August 2023 and was accepted for publication in June 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Public Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Tweed et al. This work was produced by Tweed et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Tweed et al.
Background and introduction
Secondary data – used in this context to mean the use, reuse or novel combination of existing data sets – offer a number of potential advantages for research, intelligence and evaluation. 1,2 These include large population sizes, low cost and the opportunity to link to different sources of data at the individual, household or geographical level.
For public health purposes, these advantages are enhanced further when secondary data from non-health sources are made available for analysis or linkage. Individual and population health is determined by a complex interplay of social, political, environmental and economic factors, so to understand and intervene in this interplay (an endeavour often referred to as ‘healthy public policy’) requires data not only from health care but also from other policy sectors such as education, social care, housing, transport, welfare and justice. 3 For example, we can link data on exposures to policies in those areas (such as changes in the social security system) to data outcomes routinely measured in the health service, such as prescribing and hospitalisations.
To date, the potential of cross-sectoral secondary data sharing and linkage appears to be under-utilised. 4 A survey of health authorities in 29 European countries identified limited use of cross-sectoral data for routine public health activities. 5 As Mourby et al. put it, ‘despite their societal value, success stories in administrative data linkage for research remain the exception rather than the rule’. 6 Yet, evidence from the UK suggests an appetite to improve the quality and usage of routinely collected data among those working in public health practice and policy. 7–9
A number of jurisdictions, including Scotland, have sought to adopt a ‘whole-systems’ approach to public health. Definitions of ‘whole-systems’ approaches vary but typically include the application of theoretical perspectives from complexity and systems science to practical public health challenges; a commitment to partnership working; and ongoing learning and adaptation as circumstances change. 10–12 Such approaches conceptualise public health challenges as complex adaptive systems made up of multiple interacting components where intervention impacts may be unpredictable, far-reaching and non-linear. This model creates new opportunities and challenges for the use of evidence and, in particular, secondary data: for instance, it may heighten demand for data sharing between different organisations and sectors, and result in greater emphasis on the timeliness, breadth and spatiotemporal disaggregation of data.
Previous research on the use of secondary data has focused on healthcare data; technical and ethical challenges relating to data quality, security and public trust; and the perspectives of researchers or the public. 4,6,13–17 There is very little evidence examining cross-sectoral secondary data sharing and use, or the use of secondary data as part of whole-systems approaches to public health. The views of evidence users; the role played by secondary data as part of wider decision-making processes; and the institutional, cultural and political factors affecting data sharing and linkage are also not well documented. Other authors have identified a broader neglect of policy-makers’ views on the use of data and evidence, and a mismatch between the forms of evidence produced by academic researchers and the needs, preferences and constraints of decision-makers. 7,18–20
Aims and objectives
We aimed to work with stakeholders to identify practical ways that secondary data could be more effectively utilised across sectors to support whole-systems approaches to improving health and reducing health inequalities. To do so, we undertook a series of participatory workshops, which drew on two scoping reviews of existing literature and three real-world case studies of cross-sectoral secondary data sharing.
Methods
Context and scope
Scotland continues to face persistent challenges with entrenched social and health inequalities, many of which have worsened during the COVID-19 pandemic. 21 Scotland has a multilevel public health system encompassing multiple local authority and health board areas with diverse populations and geographies. 22 The integration of health and social care; the establishment of Community Planning Partnerships; and the development of Public Health Scotland (PHS) as a single agency for public health has created new opportunities for joint working across NHS public health, local authorities and other partners such as police and community organisations. 11 Following the agreement of six national public health priorities in 2018, the Scottish Government, the Convention of Scottish Local Authorities, and PHS committed to a ‘whole-systems approach’ to public health. 11 While Scotland has a strong track record in the use of linked healthcare data, progress in sharing and linkage of data from other sectors, such as social care, education and criminal justice, has been more challenging. 23 It therefore provides an ideal context in which to answer questions about secondary data access, use and value; to contribute to knowledge on translating results into impact on information systems, as well as to knowledge on data infrastructure and decision-making.
We therefore sought to understand the role of cross-sectoral data sharing and linkage in providing evidence for decision-making in this context, from the perspectives of key stakeholders.
Following discussion with our project advisory group (see Appendix 1), we refined our scope to focus only on (1) data sharing, linkage and use within the public and third sector: this reflects the additional nuance and complexity associated with data sharing with commercial entities and (2) data sharing for the purposes of research, intelligence and evaluation, excluding its use in guiding individual-level decisions about service and care provision.
Conceptual framework
In designing the project, we drew on systems science approaches to public health and interdisciplinary perspectives on the use of evidence in healthy public policy and practice. 12,18,24–26
Our rationale for rooting our conceptual approach in systems thinking was based on three factors characteristic of situations where systems perspectives can be helpful:27 (1) we aimed to achieve sustained change on a broad scale rather than a short-term specific goal; (2) efforts to date to address issues around cross-sectoral data sharing and linkage had met with mixed success, with continued uncertainty and diversity of views about the nature of the problem and appropriate solutions; and (3) the wider context in which data sharing was taking place was likely to be influential, including issues such as research funding trends, resource pressures in the public and third sector, and public attitudes to privacy and data protection. Moreover, our study was based within a jurisdiction (Scotland) which had committed to applying systems science perspectives to public health under the rubric of a ‘whole-systems approach’.
To incorporate systems thinking, we explicitly introduced relevant concepts early in participant workshops and revisited these throughout (for instance, emphasising our interest in the ‘big picture’ of messy connections between different parts of the system, and seeking to identify key bottlenecks and levers where effort might have a disproportionate impact). We used Kumu (www.kumu.io) – an online visualisation tool for concept and systems mapping – to capture outputs across the scoping review, case studies and workshops. Study activities and participant materials were tailored to reflect our recognition that varied definitions of ‘evidence’ compete with multiple other factors as part of decision-making for public health across multiple institutions (e.g. government, NHS, third sector) and levels (e.g. local authorities, community planning, health boards, devolved and national government). 7,24,26
Workshops
We held workshops to bring together people working in public health practice; in policy sectors potentially relevant to health; and in information governance, infrastructure and/or support for data and research; as well as a number of public representatives. Our intended outputs from workshops included: a visual representation reflecting diverse stakeholder perspectives of contribution of secondary data to decision-making for public health benefit; qualitative data on stakeholders’ understanding of barriers/facilitators/benefits/risks to cross-sectoral data sharing and linkage; and a consensus set of recommendations underpinned by a smaller number of guiding principles, which identify specific actions to develop optimal use of cross-sectoral secondary data for improving health and reducing inequalities.
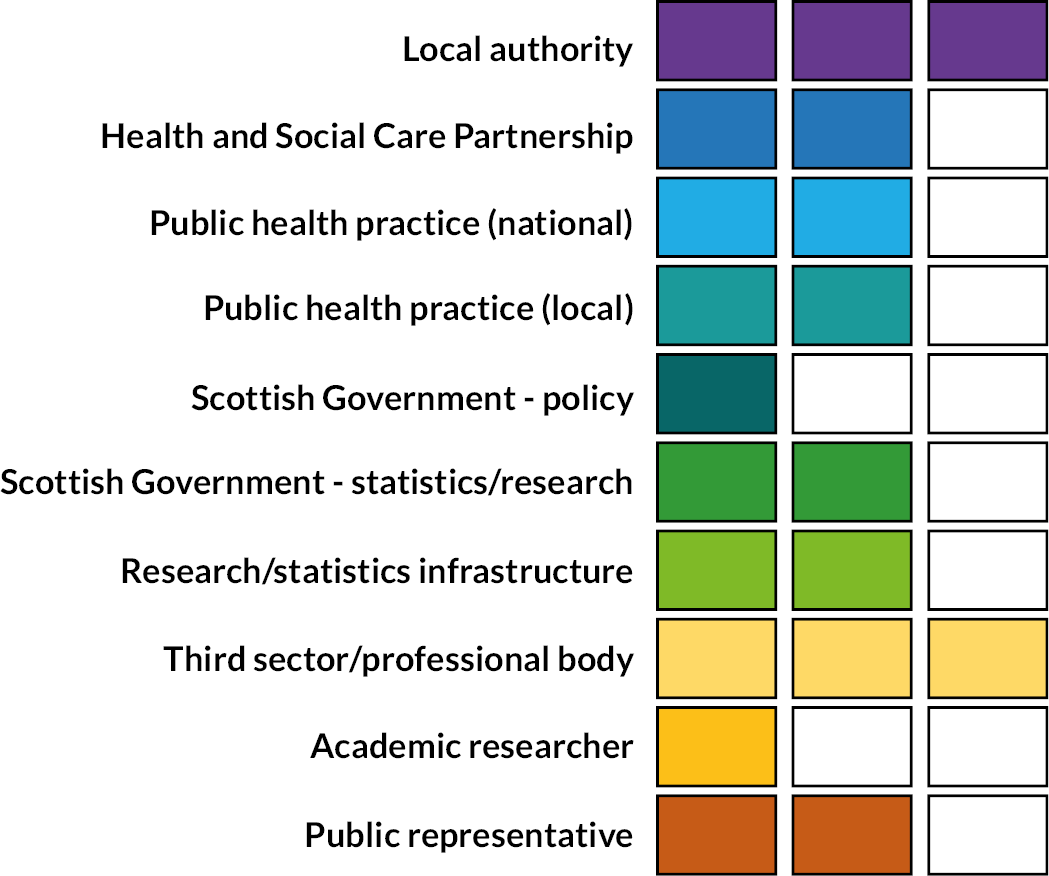
To identify potential attendees, we undertook a stakeholder mapping exercise with the project advisory group followed by a review of relevant organisational websites and advice from gatekeeper organisations such as Administrative Data Scotland. Participants were invited to attend via e-mail, with public representatives offered remuneration for time spent preparing and participating in workshops. A total of 39 invitations were issued, of which 20 individuals from 14 organisations (including 2 public representatives) consented to take part. Figure 1 illustrates the sample of stakeholders participating in the workshops: each box represents one individual.
FIGURE 1.
Workshop participants, by sector/role.
Workshops were intended to be sequential and cumulative, with the entire cohort of participants expected to attend all three. Due to the ongoing COVID-19 pandemic, workshops took place online between September and December 2021 using Microsoft Teams® (Microsoft Corporation, Redmond, WA, USA). 28 Using online meeting tools such as Microsoft Teams has been demonstrated to be an effective means for data collection through focus groups and workshops.
Each workshop lasted 3 hours and consisted of a mix of whole group and breakout room activities, including presentations, facilitated discussions and participatory tools such as live polling. Prior to each workshop, participants were invited to complete asynchronous online activities that provided background information for the workshop and used polls and free-text comments to gather additional data. Table 1 describes the purpose, content and format for each workshop.
| Workshop 1 | Workshop 2 | Workshop 3 |
|---|---|---|
| Objectives – shared with participants | ||
| To co-create a visual representation of how secondary data fit into wider decision-making processes so that we reach shared understanding of its potential contribution to public health practice and policy | To discuss key stages, challenges and successes of three cross-sectoral case studies so that we can identify transferable lessons from existing situations to inform overall recommendations | To develop a draft set of recommendations for action so that secondary data sharing and linkage across sectors can be used to best effect for improving health and reducing inequalities |
| Pre-session individual activities | ||
|
|
|
| Workshop activities as a group | ||
| Ideas generation – what would help you make better decisions in your current role? | Discussion of emerging findings from previous workshop and scoping review | Brainstorming recommendations, using the framework identified in the scoping review |
| Connecting and prioritising – how do these factors relate to each other, and what connections are most important? | Responses to case studies – what can we learn from these? | Refining and grouping recommendations – which ideas belong together, and how can we articulate them? |
| Relating to secondary data – how might secondary data sharing and linkage help address the challenges identified? | Relating case study responses to previous workshops and scoping reviews – where are the key challenges and what are their drivers? | Adding detail to the recommendations – impact/effort, organisations responsible, and timescales |
| Whole-group feedback | Whole-group feedback | Whole-group feedback |
Figure 2 illustrates the sequence of project activities, and their inter-relation.
FIGURE 2.
Flow of workshop activities in chronological order.
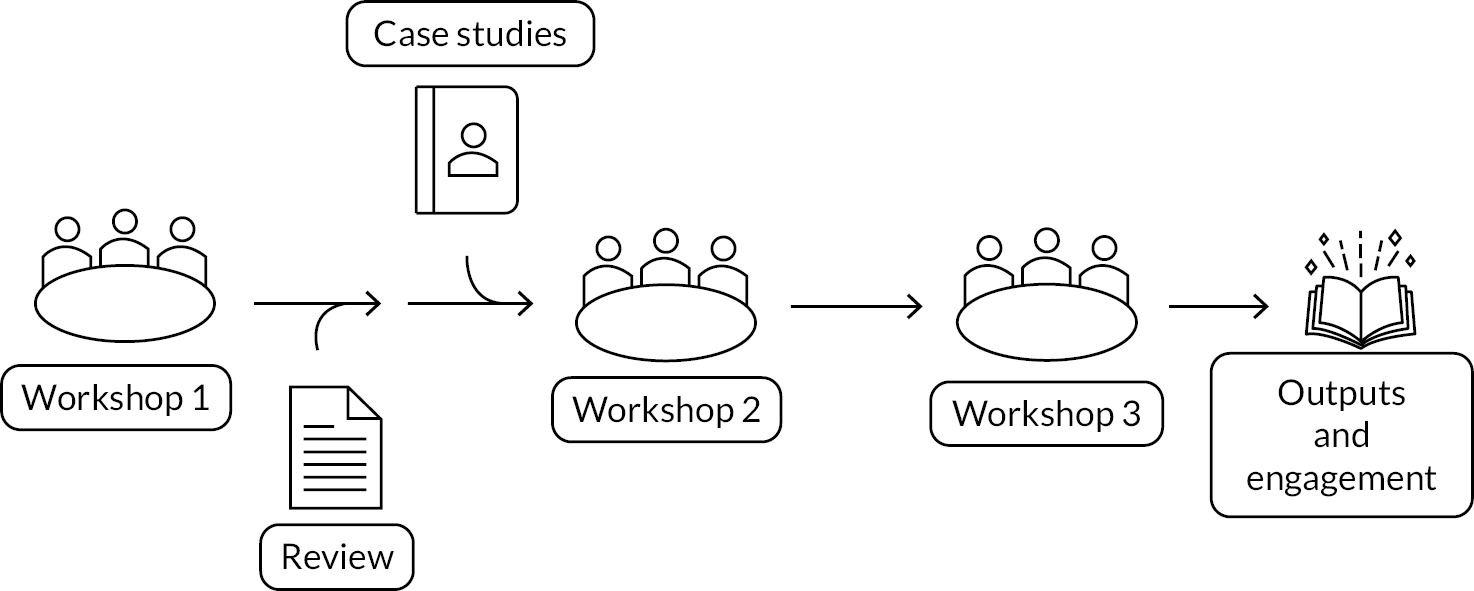
Workshop 1 introduced the project and invited participants to discuss their experience of decision-making in practice, and the actual and potential contribution of evidence from secondary data in this process, as part of facilitated break-out room discussions supported by the visual mapping tool Kumu. Workshop 2 began with a summary of feedback from the first workshop alongside a description of findings from the scoping reviews (see Scoping reviews), followed by breakout group sessions focusing on one of three case studies (see Case studies). These comprised a presentation on the case study by the lead investigator with an opportunity for questions and answers, then a facilitated discussion of the findings in the context of results from workshop 1 and the scoping reviews.
Workshop 3 started with a presentation of integrated findings from preceding workshops, the scoping reviews, and case studies, before moving on to interactive exercises to brainstorm and refine draft recommendations. Participants were invited to suggest initial recommendations using a framework based on the following themes, identified from the scoping reviews and earlier workshop discussions: features of data; technical; governance; legal and ethical; workforce; relational; political; institutional; and external factors. During this phase of the final workshop, participants worked in breakout rooms with the support of facilitators to first brainstorm initial ideas; then edit and refine them (e.g. clustering those which were similar); and finally discuss the impact and effort associated with each; assign them to relevant organisations; and propose appropriate time scales.
Following the workshops, draft recommendations were reviewed and edited by the project team for consistency and reducing duplication. The updated recommendations were circulated by e-mail to workshop participants for feedback, and discussed with a wider set of stakeholders (see Post-workshop engagement). A final set of recommendations was then agreed by the research team and approved by the project advisory group.
Scoping reviews
We undertook two scoping reviews to support discussions at the workshops: the first aimed to situate our project within the wider context of evidence use in decision-making for healthy public policy and practice, and the second aimed to understand existing evidence about barriers and facilitators affecting the use of secondary data in the UK context. We chose a scoping review approach given our interest in: understanding the broad ‘landscape’ of existing research; exploring concepts; and identifying potential theoretical or thematic frameworks for use in other elements of the project. 29–31
The research questions for the reviews were as follows:
-
What do existing scoping and systematic reviews say about how evidence is used in decision-making for public health practice and healthy public policy?
-
What are the barriers and facilitators at individual, organisational, and societal levels to the use of secondary data in decision-making for public health and healthy public policy in the UK?
Detailed search strategies and inclusion criteria are provided in the review protocol (see Report Supplementary Material 1); an example search strategy is provided in Appendix 2. For each review, we searched three bibliographic databases (MEDLINE, Scopus and the Social Science Citation Index) as well as websites of key organisations and asked our stakeholder advisory group to signpost any other relevant resources. With the support of an information specialist, we developed tailored search strategies for each bibliographic database, comprising terms relating to evidence (e.g. evidence, research, data, knowledge); the settings of interest (e.g. health policy, public health, public policy, health planning); and the article types of interest (i.e. systematic or scoping reviews, qualitative synthesis, or meta-ethnography). For question 2, our search strategy comprised terms relating to secondary data (e.g. secondary data, routine data, administrative data, data sharing); the settings of interest (as for question 1); and factors affecting utilisation (e.g. barriers, facilitators, challenges, support, obstacles).
Studies were eligible if they were published in English in the 10 years preceding the date of searches (June 2021); studies for question 1 additionally had to use systematic or scoping review methodologies, and those for question 2 had to be carried out in the UK (or for reviews, include studies carried out in the UK). Key terms used in inclusion/exclusion criteria were defined in the protocol, based on discussions with the project advisory group.
For each separate review, we screened retrieved citations based initially on the title and abstract and, for those found to be potentially relevant, the full text. An initial 25 titles and abstracts were screened for each review as part of pilot testing for the inclusion and exclusion criteria, and the remaining screening undertaken independently by 2 team members, with opportunities for discussion and feedback from other team members. A 10% sample of full texts was screened by two reviewers for each review, with the remainder of full-text screening undertaken independently by two team members. Data extraction was undertaken by one reviewer and checked by a second, using a structured template in Microsoft Excel. The findings of the two reviews were combined as part of the thematic analysis detailed in a subsequent section.
Case studies
Previous work has highlighted the value of case studies in understanding challenges for data sharing, and in sharing best practice: however, few case studies exist which deal with cross-sectoral data sharing and linkage. 4,17
In this project, we used three case studies of completed public health research projects using cross-sectoral data linkage to provide real-world examples for discussion by participants at the workshops. 32–35 Case study projects were selected on the basis of having attempted to undertake individual-level record linkage between health and non-health data sets for research aiming to inform healthy public policy. They were chosen to cover different policy sectors; data sets; geographies; funding models; and governance processes. The chosen projects are described in Table 2.
| Case study A | Case study B | Case study C | |
|---|---|---|---|
| Focus of research | Health outcomes of care-experienced children (Children’s Health in Care in Scotland project) | Health outcomes among people with overlapping experiences of homelessness, offending and substance use | Multimorbidity and unscheduled care among people receiving community social care |
| Study design | Cohort study using linked administrative data from health and non-health sources | ||
| Scope | Scotland-wide | Glasgow City Council area | Scotland-wide |
| Time period | 2009–10 to 2016 | 2010–1 to 2018–9 | 2010–1 to 2015–6 |
| Cohort size | ~ 650,000 individuals (including ~13,000 with care experience) | ~1 million individuals (including ~35,000 with ≥ 1 of the above experiences) | ~1.1 million individuals |
| Study aims | To provide first comprehensive national level evidence on the health of care experienced children in Scotland. | To describe health outcomes among people with the overlapping combination of adverse social and health experiences known as severe and multiple disadvantage, in order to identify opportunities for prevention and mitigation and to inform service planning and delivery. | To assess the relationship between multimorbidity and social care, and the association of multimorbidity and social care on unplanned admission to hospital. |
| Non-health data sets involved (sources) | Pupil Census (ScotXed, Scottish Government) Children’s Looked After Statistics (ScotXed, Scottish Government) |
HL1 applications for statutory homelessness support and Criminal Justice Social Work Reports (Glasgow City Health and Social Care Partnership) Prison records (Scottish Prison Service/Scottish Government) |
Recipients of social care (Scottish Social Care Survey) |
| Health data sets involved (sources) | Medication dispensing (Prescribing Information System) A&E attendances Hospitalisations (Scottish Morbidity Records) Birth and death registrations (National Records of Scotland) |
Dispensing for opioid dependence (Prescribing Information System) A&E attendances (Trak A&E) Hospitalisations (Scottish Morbidity Records) Birth and death registrations (National Records of Scotland) |
Medication dispensing (Prescribing Information System) Unscheduled care (Unscheduled Care Datamart) |
| Key references | Allik et al., 202132 | Tweed et al., 202334 | Henderson et al., 201933 Henderson et al., 202135 |
Project leads for each case study were included as co-investigators on this project in order to ensure alignment between the case studies and workshop planning. Data on the process and outcomes of each case study project were gathered using a proforma completed by the project lead and subsequent in-depth semistructured interviews (see Report Supplementary Material 2). Each case study lead facilitated a series of breakout room sessions on their project at the second workshop, comprising a presentation; question and answer session; and group discussion.
Post-workshop engagement
After the third workshop, a copy of the draft recommendations was circulated to all workshop participants with an invitation to provide further input, annotated in places to highlight areas which were incomplete or where consensus had not been reached.
We also sought feedback on the draft recommendations from a broader range of stakeholders, particularly those we had struggled to recruit to the workshops. The stakeholders we met with to discuss our emerging findings included the Scottish Government Data and Intelligence Network; the Integrated Joint Board Chairs and Vice-Chairs Network; the Digital Office for Scottish Local Government leadership team; and Research Data Scotland (RDS): further details are provided in Appendix 3, Table 6.
Analysis
We used thematic analysis throughout the study to analyse and interpret findings from the scoping reviews; case studies; and workshops. 36 Analysis of content generated by study activities took place on an ongoing and iterative basis, so that findings could be fed into workshop discussions and could inform the planning of subsequent activities. We used the web-based tool Kumu to facilitate thematic analysis, as well as to visualise findings and produce workshop materials for participants.
Analysis of findings from the scoping reviews identified a set of factors affecting the use of routine data, which were subsequently used to structure the interpretation of material from the case studies and participant discussions.
We sought to use participants’ original wording throughout the project and to be guided by their views and interpretations. This was felt to be especially important in developing the recommendations and accompanying detail (such as impact, effort, timescales and responsibilities): the research team aimed to edit recommendations only lightly to avoid repetition; where there was no input or no consensus on a particular point, we have noted this in the text and have made a clear distinction between participant views and commentary by the researchers, or broader stakeholders.
Public involvement
Our public involvement approach for this project comprised two main strands, reflecting the public’s role as the original source and owners of the data being discussed throughout the project. First, our project advisory group (see Appendix 1) included two public representatives, who contributed to shaping the design, delivery and dissemination of the study. Second, our workshop participants included two public representatives, who contributed to data collection and the development of recommendations. Recruitment of public representatives sought to reflect a range of perspectives, including those with experience of the issues featured in the case study projects (via lived experience networks supported by organisations which the case study leads had existing relationships, such as Homeless Network Scotland) and those with an interest in the use of data (via established public panels run by Administrative Data Research Scotland and the University of Glasgow). Public representatives were remunerated for their time preparing and attending meetings as per National Institute for Health and Care Research (NIHR) guidance and received support to participate in the form of briefings at the project start and informal check-ins and correspondence throughout the project.
Equality, diversity and inclusion
As part of this ‘research about research’, we considered equality, diversity and inclusion both in the substance of the research (i.e. ensuring that our research considered how secondary data could be used as part of efforts to address health inequalities, as well as overall population health) and the way it was conducted.
With regard to the first point, we ensured that ‘reducing inequalities’ was explicitly included as part of the study aim; emphasised health inequalities between diverse population groups as an important motivating factor for the research in our scene-setting with workshop participants; and selected case studies with an explicit focus on health inequalities. With regard to the second point, throughout the research, we opted to use person-first or other inclusive terminology when referring to different population groups and communities, especially in relation to our case studies (such as ‘people affected by homelessness’ or ‘care-experienced children and young people’). We sought to recruit public participants with lived experience of the issues covered by the case studies, although were only able to do this in one case, with the remaining public participants recruited from an existing public panel. We made a commitment in our recruitment materials to meeting participants’ accessibility needs to ensure their full participation in the workshop and asked all participants well in advance of the workshops to advise us of such measures. Measures taken included circulating papers and presentation slides in advance, and reviewing all presentation slides for accessibility. As our participants were primarily professional stakeholders and therefore selected based on existing roles, we were limited in our ability to select on the basis of diversity; however, we did seek to achieve diversity in gender, age and geographical location across Scotland. Our research team was also diverse in terms of gender and career stage, with consideration given to maximising development opportunities for less experienced staff (for instance, all of the co-investigators received facilitation training and opportunities; the project was jointly led between two researchers, one more junior and another more senior; and project staff were supported to develop applications for future research funding).
Results
In this section, we present a brief overview of the results from the scoping review and case studies before describing the findings from the workshops and the final set of recommendations for change. The study map, visualising themes identified from scoping reviews, case studies, and participant workshops, can be viewed at https://unlockingdata.kumu.io/unlocking-data-project-findings.
Scoping reviews
In the first scoping review, which examined previous literature reviews of how evidence is used in healthy public policy and practice, we identified 31 relevant studies from an initial pool of 1490 studies (see Appendix 2, Figures 4 and 5 for review flow charts and Appendix 2, Tables 4 and 5 for details of included studies).
We found that previous reviews of evidence use for healthy public policy generally fell into two groups: those examining evidence use in general terms18,37,38 and those which examined narrower questions about the use of specific types of evidence (e.g. economic evaluations) and/or in specific settings (e.g. for spatial planning and the built environment). We extracted data from both but weighted our synthesis and presentation towards the former.
In the second scoping review, which focused on primary research about barriers and facilitators to the use of secondary data in decision-making for healthy public policy and practice in the UK, we identified 29 relevant studies from an initial pool of 2456 studies, plus 2 studies from grey literature sources (see Appendix 2). Most studies in this review examined data use within health care, including economic evaluation and health technology assessment; post-approval monitoring of medications and devices; monitoring of provider performance; and surveillance systems. Fewer examples were evident of the sharing and use of secondary data beyond the healthcare system. Many of the studies retrieved were descriptive in nature, with limited critical reflection on processes of data access, utilisation, and impact: where challenges were discussed, the focus tended to be on technical aspects. Most existing case studies of secondary data use were descriptive in nature and positive in outlook, with little detail on the challenges encountered. Finally, most studies retrieved represented the perspective of researchers, with some examining public attitudes; very few investigated the views of evidence users from practice or policy.
We synthesised findings from the two reviews under the following key themes, derived inductively from the data: functions of evidence in practice; diverse understandings of what constitutes evidence; and factors influencing the use of evidence in decision-making, with a particular focus on secondary data. Findings from the last of these themes (factors influencing the use of evidence and data) were grouped into a set of key subthemes as follows: characteristics of data and evidence; technical; workforce; legal, ethical and governance; political and institutional; and external factors.
These themes and subheadings were then used to support the synthesis of findings from the case studies and workshops, and to guide participants in brainstorming and identifying recommendations.
Case studies
Case study materials used in the workshops – including linkage diagrams, timelines and presentation slides – are included in Report Supplementary Material 3. Here, we briefly summarise key themes from the case studies which formed the basis for discussions with participants at the workshops.
Common challenges encountered by these projects included: liaison with multiple different organisations, each with their own competing demands and priorities; difficulties identifying who had responsibility and authority for key decisions or clarifying existing permissions or conditions of use for relevant data sets; and sequential and interdependent governance processes which exacerbated delays. Governance processes were perceived as something of a ‘black box’, given uncertainty about the criteria for scrutiny and assessment, and unpredictable timelines. As all three of the studies were undertaking novel linkages, and some were using data sets not previously used for research, few meta-data were available in advance and unanticipated difficulties with data quality or completeness were common, often arising only once the data sets were made available and analysis underway. All studies were impacted by COVID-19 to some extent, most commonly due to additional pressures on data controllers and agencies responsible for data linkage and/or their prioritisation of other research projects focusing on COVID-19. For example, issues identified with one case study data set in March 2020 were not resolved until November/December 2020 due to staff re-assignment at data controller organisations. Most of the case study projects were required to substantially amend their initial plans as a result of these challenges, with negative knock-on impacts on the validity, generalisability and impact of the resulting work: for instance, because the findings were less timely, or for a more limited geographical area, than anticipated.
Facilitators identified by case study leads included existing relationships and networks with relevant organisations (such as data controllers); the availability of precedents as a basis for data sharing and linkage; support from those who had previously used and were familiar with the data sets; flexibility on the part of funding organisations; the ability to answer questions that would be difficult or impossible to address through other research methods; and where available, the skills and expertise of specialist data access co-ordinators. All projects enjoyed substantial goodwill and buy-in from external stakeholders and agencies, but case study leads suggested that the impact of this was limited by the wider systemic problems highlighted above.
Workshops
A total of 39 workshop invitations were issued, of which 20 individuals from 14 organisations (including 2 public representatives) consented to take part (see Figure 1). The participation rate at each workshop was as follows: 18/20 participants attended workshop 1, 15/20 participants attended workshop 2, and 17/20 participants attended workshop 3.
In our scene-setting discussions about decision-making, participants described significant challenges in trying to use evidence derived from cross-sectoral data sharing and linkage in their day-to-day work: these included organisation and cultural, as well as technical and ethical barriers.
We were looking at prevention in homelessness. But when we started to look at the streams of prevention, we realised that we would need data from so many different sources that it became impossible before we even started. So starting to look at stuff like poverty, and how often people were visiting doctors, and there was a whole cluster of information. But we realised that just trying to get any kind of data consent across such a broad church was almost impossible.
Participant, public/lived experience representative
Yeah, I just know within my own organisation it takes a lot to change the culture. So, you know, those legacy processes and just the way people have always done things. So, coming along and saying, right, okay, from now on all decisions are going to be evidence based, doesn’t really just happen overnight.
Participant, local government
In response to case studies, participants acknowledged that sharing and linkage of routine administrative data could offer unique benefits in terms of evidence for decision-making, especially where combined with other forms of evidence (such as qualitative research), although others highlighted the ways in which decision-making was shaped by what data were (easily) available, and how this might create biases or blind spots. At present, cross-sectoral data sharing and linkage are felt to be happening on an ad hoc basis, contingent on individual relationships.
I think one of the big challenges with secondary data is it’s often used because it’s what there is, rather than because it answers the question … So that’s about what we know we already can get our hands on, or what we know has been asked. There might be much, much better data available, but we don’t necessarily know who has it and who to ask.
Participant, local public health practice
I’ve got some brilliant examples of where we’re sharing secondary data and we are receiving secondary data and we support individual projects. But they’re very specific and they’re based on knowing the right person at the right time who had the same pattern for what you’re trying to achieve. So all the stars were aligned and it just worked.
Participant, local authority
COVID-19 was generally felt to have heightened awareness of the possibilities offered by data sharing and linkage, and to have changed perceptions regarding the balance of risks and benefits, resulting in some processes becoming much quicker. However, this was not universal and some processes remained time-consuming, with knock-on effects on public health decision-making:
I have learned that in times of crisis, public sector organisations seem to become less risk averse. Bureaucratic barriers have been broken down quickly and it would be helpful to maintain this in an appropriate way in respect of how we continue to do business moving forward.
Participant, local government
I’m aware of this project that’s looking at factors that might impact vulnerability to being a positive COVID-19 case, and it went through a fast track process. But by the time we got the decision, some of the restrictions have been eased. So we needed that data within, I’d say, like weeks or a month, but actually, we didn’t get the data until 5–6 months down the line and we didn’t get all the data for the research team. What was the point? That didn’t help with decision making. And if that decision, if that intelligence was available to decision makers within the month, then who knows what might have been the decisions about coming out of the lockdowns? We’ll never know now.
Participant, organisation supporting research
Several participants recognised that sharing and linkage of administrative data were less well-developed outside the healthcare system and that this posed challenges for research on the wider determinants of health:
I think the NHS has kind of spent a lot of time gathering data, and it’s now got, it’s had an infrastructure around ISD [Information Services Division] or whatever it is now for years. And I mean, there’s still areas of the NHS where it, you don’t have it so much like GPs. But like, I think it’s kind of like an example of where a lot of this stuff can be done. Whereas there are other factors, other areas of policy where data has just never been collected in a significant way in like … In [devolved policy sector] we’re starting it from scratch.
Participant, Scottish Government
Participants described duplication of effort as being common, and an appetite for a more co-ordinated and timely approach:
What we see at national level is that’s repeated, so you might have, say, [Health Board A] who’s dealing with getting a data-sharing agreement and they’ve got certain battles. And then we hear it from [Health Board B] as well and they have the same battles …. I think more and more we’re seeing that it should be the same process.
Participant, national public health agency
That, especially in a world which has shifted quite so much over the last couple of years, I’m now very sceptical, if you present me information from 2014, that it necessarily has any direct applicability to how the world is working right now.
Participant, local public health practice
While some technical challenges – such as interoperability of systems – were noted, participants also highlighted the over-riding importance of institutional, ethical, and political factors in determining whether cross-sectoral sharing and linkage took place. Resource and workforce constraints were particularly prominent, especially in the context of other demands and pressures on stakeholders:
It occurs to me that there’s a lot of, there is a division between the technical, which is, you know, just like methodologically can you do this? You know, do you have the legal consent and … But the much more squishier factor around, do you have trust? Do you have the relationships to be able to do this? Because you could have the technical skill and it could be legal, but you might just never get the institution to sign on to whatever it is you want to do.
Participant, Scottish Government
Just thinking about how the rise, elsewhere, of the Black Lives Matter agenda, for example, suddenly meant that finally, we were able to start saying actually, you know, it would be really very useful to be able to talk about ethnicity in the context of COVID vaccinations, use of services more generally … There’s a sudden shift, sometimes, in the political agenda or political environment that means that people are suddenly interested in a topic that they weren’t before. And that can suddenly plug or unplug things.
Participant, local public health practice
And it’s really difficult for IJBs [Integrated Joint Boards] to justify the recruitment or the expansion of data or analytical teams while we’re also cutting six social workers out of the system … So, it’s not that there’s not a desire to do the work or to be helpful or … it just starts to fall into the nice to do pile.
Participant, Health & Social Care Partnership
While there was discussion of potential risks associated with cross-sectoral data sharing and linkage, participants also highlighted that not acting also carried risks:
In my mind I was kind of like, well why bother; you’ve gone through that huge journey, we’re making it [the research] so difficult, why do people bother? And people bother because it matters. And so we have a moral obligation to find that story and act on it because keeping it separate is actually a failing on our part, was kind of my reflection, and the value of … you know, the data comes together to bring its full value I guess … Why would we have this data and this detail and not put it together and then do something about it?
Participant, National Public Health Agency
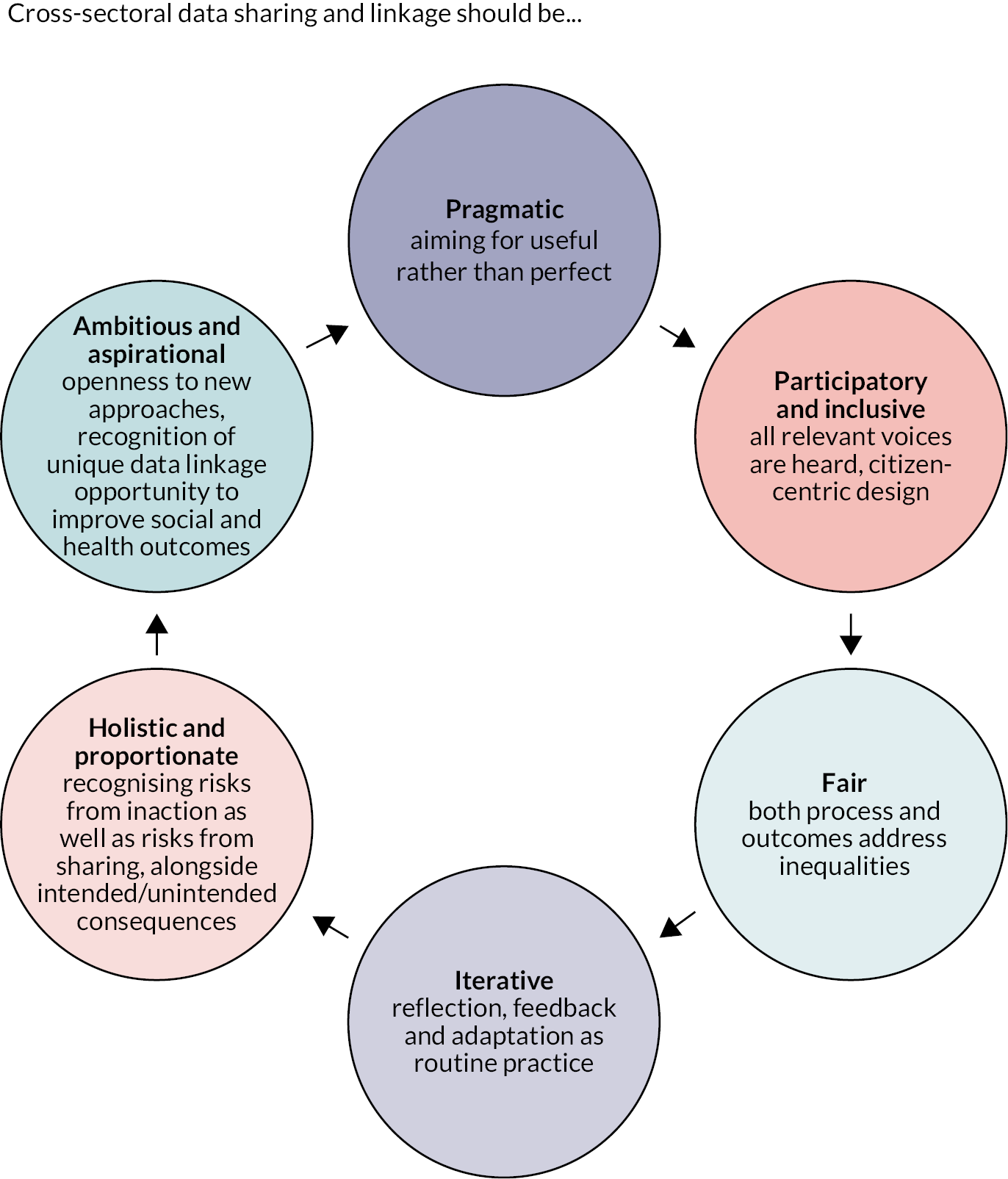
During workshops 1 and 2, participants began to identify key principles for cross-sectoral data sharing and linkage. We responded to this unexpected output by collating these suggestions into a set of six guiding principles, which were then further refined and validated during dedicated discussion time at the final workshop (Figure 3). The intention was that these serve as overarching principles that should guide cross-sectoral data sharing and linkage, alongside the detailed recommendations for action.
FIGURE 3.
Guiding principles for cross-sectoral data sharing and linkage identified by workshop participants.
During the final workshop, and as part of the post-workshop engagement, a set of recommendations was proposed and organised according to the themes identified in the scoping review (shown in Table 3).
| Ref | Recommendation |
|---|---|
| Governance | |
| A | Approaches to data sharing and linkage should be strategic rather than piecemeal, reflecting policy priorities and organisational missions, a long-term view, and which data are best suited to achieving the aim |
| B | Standardised data-sharing agreements and collaboration frameworks should be developed and agreed upon at the national level between key organisations to facilitate rapid and straightforward collaboration |
| C | Key data sets from multiple sectors should be available via a central repository acting as a ‘one-stop shop’ for sharing and linkage, with differing levels of governance according to sensitivity |
| D | There should be a focus on the creation, curation and rapid reuse of linked data sets that can be used many times for multiple different purposes |
| E | A cross-sectoral monitoring and evaluation framework should be agreed to measure the value and impacts of data sharing and linkage |
| F | Requirements from different governance panels for training and accreditation should be audited to identify and address potential areas of duplication |
| Characteristics of data | |
| G | Key data sets across multiple sectors should have mandatory data standards to ensure consistency and quality |
| H | To support ease of discoverability across different sectors, there should be a published list or register of key data sets (including details of what information they contain, standards for collection and curation, and how they can be accessed) |
| I | The possibility of a single ID number for individuals (as in Scandinavian countries) should be explored |
| Technical | |
| J | Investment in transformation of legacy systems which currently hinder integration and inter-operability |
| K | Technical solutions should avoid built-in obsolescence, as part of a long-term planning approach |
| Workforce | |
| L | Build capacity in related professional roles (e.g. in data curation, analysis, governance and public engagement) through a national public sector skills initiative |
| M | Ensure that data/analytical professional roles receive adequate resources and recognition, including clear career tracks enabling progression |
| N | Develop and disseminate training resources and guides on how to get started with data sharing and linkage |
| O | Integrate researchers and innovation leads into community planning throughout Scotland |
| Political and institutional | |
| P | Realising the benefits of cross-sectoral sharing and linkage requires senior leadership and commitment from across all organisations |
| Q | Greater engagement with politicians and policy-makers about the potential benefits of secure data sharing and linkage, and how it can be incorporated into planning and decision-making |
| R | Maximise expectations and incentives for policy-makers to collaborate with researchers, as part of a learning culture that seeks to make the best use of data for population health gain |
| S | Planning and investment in this area should be guided by long-term considerations as well as contingency planning for emergencies (such as future pandemics) |
| Working with and for the public | |
| T | Key population health measures and data sets should be identified at the point of policy/legislation development and co-produced with people living in communities of interest |
| U | A transparent, and wide-ranging public conversation about data sharing and linkage – including its purposes, processes, benefits and risks – is required |
Several recommendations are interlinked: for instance, recommendations A (a strategic rather than piecemeal approach to data sharing and linkage) and S (planning and investment should be guided by long-term considerations as well as contingency planning for future emergencies) both recognised that planning and investment in this area required a mix of proactive and reactive approaches in order to meet key strategic needs while maintaining flexibility to respond to unexpected contingencies.
Many recommendations were based on the scale-up or implementation of approaches which have been successful already, either within specific areas in Scotland or internationally: for instance, the Welsh Secure Anonymised Information Linkage (SAIL) databank was cited as an example of best practice for a ‘one-stop shop’ for key data sets from multiple sectors (recommendation C), while the Local Intelligence Support Teams (LIST) embedded into Health and Social Care Partnerships in Scotland were identified as a potential model for wider integration of research, intelligence, and innovation capacity with community planning structures with jurisdiction over the determinants of health (recommendation O).
Additional detail provided by participants on the likely impact and effort associated with individual recommendations, and the organisations responsible is included in the appendices (see Appendix 4, Table 7). Participants did not always reach consensus on the impact/effort status of the recommendations or on the organisations responsible; where this is the case, it is noted.
Discussion
Our findings offer an insight into the perspectives of evidence users working in policy and practice on how cross-sectoral data sharing can be used to best effect for improving public health, including a set of practical recommendations for change. Despite the complexity of the landscape in which decision-making takes place, workshop participants were able to generate broad consensus about the benefits of cross-sectoral data sharing and linkage, the necessity of change, the values which should guide that change, and the key next steps. The resulting recommendations span different aspects of the data sharing and linkage landscape, from technical and workforce considerations to public and political perceptions, governance, and institutional support: this reflects a sense that efforts on multiple fronts are required to address existing barriers and that no single change will suffice.
By incorporating perspectives from policy sectors and services beyond health care and foregrounding the views of evidence users rather than researchers or the public, the findings from our workshops represent an important addition to the existing literature on the use of routine data for public health. Many of the themes identified in our workshops coincide with this previous literature, such as the importance of trust; of resource constraints; and of cultures of evidence use. 4,6,15 However, the workshops also identified unique challenges for cross-sectoral data sharing and linkage relating to multiple actors and dependencies; interorganisational relationships and cultures; and different starting points for non-healthcare organisations in terms of data collection and sharing. Our findings also add to an emerging evidence base on the impact of COVID-19 on data sharing and linkage processes, and health research more generally,39–41 but offer a unique perspective by going beyond the healthcare system into sectors and organisations which impact the wider determinants of health.
Strengths and limitations
Our findings benefit from being informed by wider theoretical and empirical insights about evidence use in policy and practice, via the scoping reviews which underpinned the workshops and recommendation development, and by case studies of real-life challenges and impacts from projects which have undertaken cross-sectoral record linkage. The literature searches for the scoping review were conducted in June 2021, so there may be relevant material published since then that is not reflected in the review. Although uptake of invitations to participate in the workshops was reduced by workload pressures associated with the ongoing COVID-19 pandemic, workshops did include representation across all key sectors of interest and extensive post-workshop engagement with other key stakeholders provided additional opportunities to test and refine draft recommendations. Unsurprisingly, given this broad representation, we did not achieve consensus on every recommendation. Our findings were necessarily heavily informed by the Scottish context for public health and data sharing, but many of the themes and recommendations are of relevance to other jurisdictions with similar legal frameworks and data infrastructures. Our project did not examine in detail the resource implications of improved utilisation of secondary data across sectors, but the adequate investment is likely to be a key determinant of success alongside the proposals made by participants for strengthening governance, staffing, and infrastructure for data sharing.
There is increasing interest in secondary data sharing and linkage across a range of organisations and jurisdictions, partly spurred by evidence demands associated with the COVID-19 pandemic. However, many existing initiatives focus solely on healthcare data – such as the recent Goldacre Review in the UK – which may miss opportunities to understand and intervene on the wider determinants of health, including social, environmental, economic and commercial factors. 42 This is especially important in the context of ongoing and emerging challenges to public health, such as the cost-of-living increases observed in many European countries and worsening impacts of climate change. 43,44
Conclusions
This study adds to the existing literature by documenting the perspective of evidence users working in policy and practice on how cross-sectoral data sharing can be used to best effect for improving public health, including a set of practical recommendations for change. These recommendations span different aspects of the data sharing and linkage landscape, from technical and workforce considerations to public and political perceptions, governance, and institutional support: this reflects a sense that efforts on multiple fronts are required to address existing barriers and that no single change will suffice. To realise the potential value of cross-sectoral data sharing for informing healthy public policy and practice, we propose these recommendations should be considered in future strategies, guidance, and investment for data sharing by national and local governments; health and social care institutions; and other public bodies.
Additional information
CRediT contribution statement
Emily Tweed (https://orcid.org/0000-0001-6659-812X): Conceptualisation, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Visualisation, Writing – original draft, Writing – reviewing and editing.
Kristina Cimova (https://orcid.org/0000-0001-7747-9230): Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualisation, Writing – original draft, Writing – reviewing and editing.
Peter Craig (https://orcid.org/0000-0002-7653-5832): Conceptualisation, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – reviewing and editing.
Mirjam Allik (https://orcid.org/0000-0003-1674-3469): Funding acquisition, Investigation, Methodology, Writing – reviewing and editing.
Denise Brown (https://orcid.org/0000-0002-5195-5312): Funding acquisition, Investigation, Methodology, Writing – reviewing and editing.
Mhairi Campbell (https://orcid.org/0000-0002-4416-7270): Investigation, Methodology, Writing – reviewing and editing.
David Henderson (https://orcid.org/0000-0002-4411-8532): Funding acquisition, Investigation, Methodology, Writing – reviewing and editing.
Charlie Mayor (https://orcid.org/0000-0003-4729-3536): Funding acquisition, Investigation, Methodology, Writing – reviewing and editing.
Petra Meier (https://orcid.org/0000-0001-5354-1933): Methodology, Writing – reviewing and editing.
Nick Watson (https://orcid.org/0000-0002-0364-427X): Funding acquisition, Investigation, Methodology, Writing – reviewing and editing.
Valerie Wells: Methodology.
Lorna Dick: Project administration.
Acknowledgements
We would like to thank the following:
-
All of our workshop participants for their invaluable contributions;
-
Members of our advisory group (listed in Appendix 1), for their guidance throughout the project;
-
Valerie Wells, information specialist, for assistance with search strategies for the scoping review;
-
Lorna Dick, programme administrative assistant, for administrative support.
Data-sharing statement
De-identified transcripts from the workshops are archived with the UK Data Service’s ReShare repository (https://dx.doi.org/10.5255/UKDA-SN-856285) and are available on application via https://reshare.ukdataservice.ac.uk/. All other queries should be addressed to the corresponding author.
Ethics statement
Ethical approval for the study was granted by the University of Glasgow College of Social Sciences Research Ethics Committee (reference number 400200204; approval date 4 June 2021).
Information governance statement
The University of Glasgow is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, the University of Glasgow is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer here: www.gla.ac.uk/myglasgow/dpfoioffice/
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/KYTW2173.
Primary conflicts of interest: All authors except Kristina Cimova and Mhairi Campbell were co-investigators on the project and therefore received support for the present manuscript via the NIHR Public Health Research grant NIHR133585. Other support for the present manuscript included core funding for the Medical Research Council/Chief Scientist Office (MRC/CSO) Social and Public Health Sciences Unit (affecting Emily Tweed, Kristina Cimova, Peter Craig, Mirjam Allik, Mhairi Campbell, Denise Brown, and Petra Meier; MRC grant number MC_UU_00022/2 and CSO grant number SPHSU17). Other NIHR funding to authors included NIHR154243 (Peter Craig and Petra Meier); NIHR134801 (Peter Craig); NIHR131709 (Peter Craig); NIHR153474 (Emily Tweed and Petra Meier) and NIHR12/211/54 (Nicholas Watson). Petra Meier was a member of the NIHR Public Health Research programme’s Funding Board from 2018 to 2022. Emily Tweed was a member of the NIHR Public Health Research programme’s Prioritisation Committee from May 2022 to September 2023.
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the Public Health Research programme or the Department of Health and Social Care.
This article was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Other outputs from this project
Conference presentations
-
Society for Social Medicine and Population Health Annual Scientific Meeting 2022: poster presentation, ‘Unlocking data to inform public health policy and practice: decision-maker perspectives on the use of cross-sectoral data as part of a whole-systems approach’
-
International Population Data Linkage Network conference 2022: oral presentation, ‘Barriers and facilitators of cross-sectoral data linkage to inform healthy public policy and practice: lessons from three case study projects in Scotland’
Blogs
-
‘Finding the key to Unlocking Data’
-
‘Unlocking Data – using online workshops to develop recommendations for policy and practice’
Study registration
This study is registered as researchregistry6740.
Funding
This article presents independent research funded by the National Institute for Health and Care Research (NIHR) Public Health Research programme as award number NIHR133585.
This article reports on one component of the research award Unlocking data to inform public health policy and practice: decision-maker perspectives on the use of cross-sectoral data as part of a whole-systems approach. For more information about this research please view the award page (https://fundingawards.nihr.ac.uk/award/NIHR133585)
About this article
The contractual start date for this research was in April 2021. This article began editorial review in August 2023 and was accepted for publication in June 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Public Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Copyright
Copyright © 2024 Tweed et al. This work was produced by Tweed et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
List of abbreviations
- CSO
- Chief Scientist Office
- LIST
- Local Intelligence Support Teams
- MRC
- Medical Research Council
- NIHR
- National Institute for Health and Care Research
- PHS
- Public Health Scotland
- RDS
- Research Data Scotland
- SAIL
- Welsh Secure Anonymised Information Linkage
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/KYTW2173).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.
References
- Connelly R, Playford CJ, Gayle V, Dibben C. The role of administrative data in the big data revolution in social science research. Soc Sci Res 2016;59:1-12.
- McGrail KM, Jones K, Akbari A, Bennett TD, Boyd A, Carinci F, et al. A position statement on population data science: the science of data about people. Int J Popul Data Sci 2018;3.
- Academy of Medical Sciences . Improving the Health of the Public by 2040: Optimising the Research Environment for a Fairer, Healthier Future 2016.
- Wellcome Trust . Enabling Data Linkage to Maximise the Value of Public Health Research Data: Full Report 2015.
- Haneef R, Delnord M, Vernay M, Bauchet E, Gaidelyte R, Van Oyen H, et al. Innovative use of data sources: a cross-sectional study of data linkage and artificial intelligence practices across European countries. Arch Public Health 2020;78.
- Mourby MJ, Doidge J, Jones KH, Aidinlis S, Smith H, Bell J, et al. Health data linkage for UK public interest research: key obstacles and solutions. Int J Popul Data Sci 2019;4.
- Oliver KA, de Vocht F. Defining ‘evidence’ in public health: a survey of policymakers’ uses and preferences. Eur J Public Health 2017;27:112-7.
- Evans BA, Snooks H, Howson H, Davies M. How hard can it be to include research evidence and evaluation in local health policy implementation? Results from a mixed methods study. Implement Sci 2013;8.
- Cheetham M, Redgate S, van der Graaf P, Hunter R, Ritson L. Local Authority Champions of Research Project: A Report for the Health Foundation. Newcastle: Fuse; 2019.
- Stansfield J, South J, Mapplethorpe T. What are the elements of a whole system approach to community-centred public health? A qualitative study with public health leaders in England’s local authority areas. BMJ Open 2020;10.
- Public Health Scotland . Supporting Whole System Approaches n.d. www.publichealthscotland.scot/our-organisation/about-public-health-scotland/supporting-whole-system-approaches/ (accessed 1 October 2024).
- Carey G, Malbon E, Carey N, Joyce A, Crammond B, Carey A. Systems science and systems thinking for public health: a systematic review of the field. BMJ Open 2015;5.
- Harron K, Dibben C, Boyd J, Hjern A, Azimaee M, Barreto ML, et al. Challenges in administrative data linkage for research. Big Data Soc 2017;4.
- Sexton A, Shepherd E, Duke-Williams O, Eveleigh A. A balance of trust in the use of government administrative data. Arch Sci 2017;17:305-30.
- Lugg-Widger FV, Angel L, Cannings-John R, Hood K, Hughes K, Moody G, et al. Challenges in accessing routinely collected data from multiple providers in the UK for primary studies: managing the morass. Int J Popul Data Sci 2018;3.
- Deeny SR, Steventon A. Making sense of the shadows: priorities for creating a learning healthcare system based on routinely collected data. BMJ Qual Saf 2015;24:505-15.
- Jones KH, Heys S, Tingay KS, Jackson P, Dibben C. The good, the bad, the clunky: addressing challenges in using administrative data for research. Int J Popul Data Sci 2019;4.
- Oliver K, Innvar S, Lorenc T, Woodman J, Thomas J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv Res 2014;14.
- Petticrew M, Whitehead M, Macintyre SJ, Graham H, Egan M. Evidence for public health policy on inequalities: 1: the reality according to policymakers. J Epidemiol Community Health 2004;58:811-6.
- Chalmers I, Glasziou P. Avoidable waste in the production and reporting of research evidence. Lancet 2009;374:86-9.
- Scottish Public Health Observatory . Burden of Disease: Overview n.d. www.scotpho.org.uk/comparative-health/burden-of-disease/overview (accessed 1 October 2024).
- Scottish Government . 2015 Review of Public Health in Scotland: Strengthening the Function and Re-Focussing Action for a Healthier Scotland 2016.
- Walesby KE, Harrison JK, Russ TC. What big data could achieve in Scotland. J R Coll Physicians Edinb 2017;47:114-9.
- Oliver K, Lorenc T, Innvær S. New directions in evidence-based policy research: a critical analysis of the literature. Health Res Policy Syst 2014;12.
- Haynes A, Rychetnik L, Finegood D, Irving M, Freebairn L, Hawe P. Applying systems thinking to knowledge mobilisation in public health. Health Res Policy Syst 2020;18.
- Cairney P. The Politics of Evidence-Based Policy-Making. London: Palgrave; 2016.
- Egan M, McGill E, Penney T, Anderson de Cuevas R, Er V, Orton L, et al. NIHR SPHR Guidance on Systems Approaches to Local Public Health Evaluation. Part 1: Introducing Systems Thinking. London: National Institute for Health Research School for Public Health Research; 2019.
- Falter M, Arenas AA, Maples GW, Smith CT, Lamb LJ, Anderson MG, et al. Making room for Zoom in focus group methods: opportunities and challenges for novice researchers (during and beyond COVID-19). Forum Qualitative Sozialforschung Forum: Qual Soc Res 2022;23.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19-32.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5.
- Aromataris E, Munn Z. JBI Manual for Evidence Synthesis. 2020.
- Allik M, Brown D, Taylor Browne Lūka C, Macintyre C, Leyland AH, Henderson M. Cohort profile: the ‘Children’s Health in Care in Scotland’ (CHiCS) study – a longitudinal dataset to compare health outcomes for care experienced children and general population children. BMJ Open 2021;11.
- Henderson D, Burton JK, Lynch E, Clark D, Rintoul J, Bailey N. Data Resource Profile: the Scottish Social Care Survey (SCS) and the Scottish Care Home Census (SCHC). Int J Popul Data Sci 2019;4.
- Tweed EJ, Leyland AH, Morrison DS, Katikireddi SV. Co-occurring homelessness, justice involvement, opioid dependence and psychosis: a cross-sectoral data linkage study. Eur J Public Health 2023;33:249-56.
- Henderson DAG, Atherton I, McCowan C, Mercer SW, Bailey N. Linkage of national health and social care data: a cross-sectional study of multimorbidity and social care use in people aged over 65 years in Scotland. Age Ageing 2021;50:176-82.
- Braun V, Clarke V. APA Handbook of Research Methods in Psychology. 2012.
- Lorenc T, Tyner EF, Petticrew M, Duffy S, Martineau FP, Phillips G, et al. Cultures of evidence across policy sectors: systematic review of qualitative evidence. Eur J Public Health 2014;24:1041-7.
- Liverani M, Hawkins B, Parkhurst JO. Political and institutional influences on the use of evidence in public health policy. A systematic review. PLOS ONE 2013;8.
- Cosgriff CV, Ebner DK, Celi LA. Data sharing in the era of COVID-19. Lancet Digit Health 2020;2.
- Foraker RE, Lai AM, Kannampallil TG, Woeltje KF, Trolard AM, Payne PRO. Transmission dynamics: data sharing in the COVID-19 era. Learn Health Syst 2021;5.
- Moorthy V, Henao Restrepo AM, Preziosi MP, Swaminathan S. Data sharing for novel coronavirus (COVID-19). Bull World Health Organ 2020;98.
- MRC/CSO Social and Public Health Sciences Unit . ESRC Data Infrastructure Strategy Engagement Exercise. Consultation Response n.d. www.gla.ac.uk/media/Media_811021_smxx.docx (accessed 1 October 2024).
- The Lancet Public Health . The cost of living: an avoidable public health crisis. Lancet Public Health 2022;7.
- Howard S, Krishna G. How hot weather kills: the rising public health dangers of extreme heat. BMJ 2022;378.
- Bowrin K, Briere JB, Levy P, Millier A, Clay E, Toumi M. Cost-effectiveness analyses using real-world data: an overview of the literature. J Med Econ 2019;22:545-53.
- Boyko JA, Lavis JN, Abelson J, Dobbins M, Carter N. Deliberative dialogues as a mechanism for knowledge translation and exchange in health systems decision-making. Soc Sci Med 2012;75:1938-45.
- Chambers D, Wilson PM, Thompson CA, Hanbury A, Farley K, Light K. Maximizing the impact of systematic reviews in health care decision making: a systematic scoping review of knowledge-translation resources. Milbank Q 2011;89:131-56.
- Delnord M, Tille F, Abboud LA, Ivankovic D, Van Oyen H. How can we monitor the impact of national health information systems? Results from a scoping review. Eur J Public Health 2020;30:648-59.
- Farrer L, Marinetti C, Cavaco YK, Costongs C. Advocacy for health equity: a synthesis review. Milbank Q 2015;93:392-437.
- Greenhalgh C, Montgomery P. A systematic review of the barriers to and facilitators of the use of evidence by philanthropists when determining which charities (including health charities or programmes) to fund. Syst Rev 2020;9.
- Guindo LA, Wagner M, Baltussen R, Rindress D, van Til J, Kind P, et al. From efficacy to equity: literature review of decision criteria for resource allocation and healthcare decisionmaking. Cost Eff Resour Alloc 2012;10.
- Hannes K, Goedhuys J, Aertgeerts B. Obstacles to implementing evidence-based practice in Belgium: a context-specific qualitative evidence synthesis including findings from different health care disciplines. Acta Clin Belg 2012;67:99-107.
- Justo N, Espinoza MA, Ratto B, Nicholson M, Rosselli D, Ovcinnikova O, et al. Real-world evidence in healthcare decision making: global trends and case studies from Latin America. Value Health 2019;22:739-49.
- Kneale D, Rojas-García A, Raine R, Thomas J. The use of evidence in English local public health decision-making: a systematic scoping review. Implement Sci 2017;12.
- Koon AD, Windmeyer L, Bigdeli M, Charles J, El Jardali F, Uneke J, et al. A scoping review of the uses and institutionalisation of knowledge for health policy in low- and middle-income countries. Health Res Policy Syst 2020;18.
- Lawrence LM, Bishop A, Curran J. Integrated knowledge translation with public health policy makers: a scoping review. Healthc Policy 2019;14:55-77.
- Lemire M, Demers-Payette O, Jefferson-Falardeau J. Dissemination of performance information and continuous improvement: a narrative systematic review. J Health Organ Manag 2013;27:449-78.
- Masood S, Kothari A, Regan S. The use of research in public health policy: a systematic review. Evid Policy 2020;16:7-43.
- Moat KA, Lavis JN, Abelson J. How contexts and issues influence the use of policy-relevant research syntheses: a critical interpretive synthesis. Milbank Q 2013;91:604-48.
- Moore G, Redman S, Haines M, Todd A. What works to increase the use of research in population health policy and programmes: a review. Evid Policy 2011;7:277-305.
- Orton L, Lloyd-Williams F, Taylor-Robinson D, O’Flaherty M, Capewell S. The use of research evidence in public health decision making processes: systematic review. PLOS ONE 2011;6.
- Pineo H, Glonti K, Rutter H, Zimmermann N, Wilkinson P, Davies M. Use of urban health indicator tools by built environment policy- and decision-makers: a systematic review and narrative synthesis. J Urban Health 2019;97:436-7.
- Polisena J, Clifford T, Elshaug AG, Mitton C, Russell E, Skidmore B. Case studies that illustrate disinvestment and resource allocation decision-making processes in health care: a systematic review. Int J Technol Assess Health Care 2013;29:174-84.
- Quinn E, Huckel-Schneider C, Campbell D, Seale H, Milat AJ. How can knowledge exchange portals assist in knowledge management for evidence-informed decision making in public health?. BMC Public Health 2014;14.
- Salajan A, Tsolova S, Ciotti M, Suk JE. To what extent does evidence support decision making during infectious disease outbreaks? A scoping literature review. Evid Policy 2020;16:453-75.
- Sarkies MN, Bowles KA, Skinner EH, Haas R, Lane H, Haines TP. The effectiveness of research implementation strategies for promoting evidence-informed policy and management decisions in healthcare: a systematic review. Implement Sci 2017;12.
- Sebba J. An exploratory review of the role of research mediators in social science. Evid Policy 2013;9:391-408.
- Taylor-Phillips S, Stinton C, Ferrante Di Ruffano L, Seedat F, Clarke A, Deeks JJ. Association between use of systematic reviews and national policy recommendations on screening newborn babies for rare diseases: systematic review and meta-analysis. BMJ 2018;361.
- Tricco AC, Cardoso R, Thomas SM, Motiwala S, Sullivan S, Kealey MR, et al. Barriers and facilitators to uptake of systematic reviews by policy makers and health care managers: a scoping review. Implement Sci 2016;11.
- van Panhuis WG, Paul P, Emerson C, Grefenstette J, Wilder R, Herbst AJ, et al. A systematic review of barriers to data sharing in public health. BMC Public Health 2014;14.
- Zhao N, Koch-Weser S, Lischko A, Chung M. Knowledge translation strategies designed for public health decision-making settings: a scoping review. Int J Public Health 2020;65:1571-80. https://doi.org/10.1007/s00038-020-01506-z.
- Ainsworth J, Buchan I. Combining health data uses to ignite health system learning. Methods Inf Med 2015;54:479-87.
- Clark D, King A, Sharpe K, Connelly G, Elliott L, Macpherson LMD, et al. Linking routinely collected social work, education and health data to enable monitoring of the health and health care of school-aged children in state care (‘looked after children’) in Scotland: a national demonstration project. Public Health 2017;150:101-11.
- Cragg L, Williams S, van der Molen T, Thomas M, Correia de Sousa J, Chavannes NH. Fostering the exchange of real world data across different countries to answer primary care research questions: an UNLOCK study from the IPCRG. NPJ Prim Care Respir Med 2018;28.
- Dalton-Locke C, Thygesen JH, Werbeloff N, Osborn D, Killaspy H. Using de-identified electronic health records to research mental health supported housing services: a feasibility study. PLOS ONE 2020;15.
- Darby R, Lambert S, Matthews B, Wilson M, Gitmans K, Dallmeier-Tiessen S, et al. Enabling Scientific Data Sharing and Re-Use 2012:1-8. https://doi.org/10.1109/eScience.2012.6404476.
- Douglas A, Ward HJT, Bhopal R, Kirkpatrick T, Sayed-Rafiq A, Gruer L. SHELS researchers . Is the linkage of census and health data justified? Views from a public panel of the Scottish Health and Ethnicity Linkage study. J Public Health (Oxf) 2018;40:435-40.
- Gordon B, Barrett J, Fennessy C, Cake C, Milward A, Irwin C, et al. Development of a data utility framework to support effective health data curation. BMJ Health Care Inform 2021;28.
- Heeney C, Kerr SM. Balancing the local and the universal in maintaining ethical access to a genomics biobank. BMC Med Ethics 2017;18.
- Hill EM, Turner EL, Martin RM, Donovan JL. Let’s get the best quality research we can’: public awareness and acceptance of consent to use existing data in health research: a systematic review and qualitative study. BMC Med Res Methodol 2013;13.
- Hurt L, Ashfield-Watt P, Townson J, Heslop L, Copeland L, Atkinson MD, et al. Cohort profile: HealthWise Wales. A research register and population health data platform with linkage to National Health Service data sets in Wales. BMJ Open 2019;9.
- Knox S, Bhopal RS, Thomson CS, Millard A, Fraser A, Gruer L, et al. The challenge of using routinely collected data to compare hospital admission rates by ethnic group: a demonstration project in Scotland. J Public Health (Oxf) 2020;42:748-55.
- Leitmeyer KC, Espinosa L, Broberg EK, Struelens MJ. ECDC National Focal Points laboratory e-reporting survey group members, ECDC National Focal Points laboratory e-reporting survey group . Automated digital reporting of clinical laboratory information to national public health surveillance systems, results of a EU/EEA survey, 2018. Euro Surveill 2020;25.
- Meszaros J, Ho CH. Building trust and transparency? Challenges of the opt-out system and the secondary use of health data in England. Med Law Int 2019;19:159-81.
- Mukherjee M, Cresswell K, Sheikh A. Identifying strategies to overcome roadblocks to utilising near real-time healthcare and administrative data to create a Scotland-wide learning health system. Health Informatics J 2021;27.
- Neves AL, Poovendran D, Freise L, Ghafur S, Flott K, Darzi A, et al. Health care professionals’ perspectives on the secondary use of health records to improve quality and safety of care in England: qualitative study. J Med Internet Res 2019;21.
- Nienaber AI, Woodcock A, Liotopoulos FK. Sharing data – not with us! Distrust as decisive obstacle for public authorities to benefit from sharing economy. Front Psychol 2021;11.
- Oortwijn W, Sampietro-Colom L, Trowman R. How to deal with the inevitable: generating real-world data and using real-world evidence for HTA purposes – from theory to action. Int J Technol Assess Health Care 2019;35:346-50.
- Quinn A, Denney D, Hardwick N, Jalil R, Meek R. The feasibility and challenge of using administrative data: a case study of historical prisoner surveys. Int J Soc Res Methodol 2022;25:127-34.
- Ribeiro CDS, van Roode MY, Haringhuizen GB, Koopmans MP, Claassen E, van de Burgwal LHM. How ownership rights over microorganisms affect infectious disease control and innovation: a root-cause analysis of barriers to data sharing as experienced by key stakeholders. PLOS ONE 2018;13.
- Satinsky EN, Driessens C, Crepaz-Keay D, Kousoulis A. Mental health service users’ perceptions of data sharing and data protection: a qualitative report. J Innov Health Inform 2018;25:239-42.
- Slade SV, Davey CJ, Shickle D. Can data in optometric practice be used to provide an evidence base for ophthalmic public health?. Ophthalmic Physiol Opt 2016;36:503-11.
- Thew SL, Sutcliffe A, De Bruijn O, McNaught J, Procter R, Jarvis P, et al. Supporting creativity and appreciation of uncertainty in exploring geo-coded public health data. Methods Inf Med 2011;50:158-65.
- Warren LR, Clarke J, Arora S, Darzi A. Improving data sharing between acute hospitals in England: an overview of health record system distribution and retrospective observational analysis of inter-hospital transitions of care. BMJ Open 2019;9.
- Weir CJ, Heazell AEP, Whyte S, Norman JE. Evaluating improvement interventions using routine data to support a learning health system: research design, data access, analysis and reporting. BMJ Qual Saf 2020;29:696-700.
- Wistow J, Curtis S, Bone A. Implementing extreme weather event advice and guidance in English public health systems. J Public Health (Oxf) 2017;39:498-505.
- Heaven M, Lowe S. Data Linking Demonstration Project: Examining Fuel Poverty Using Home Energy Efficiency Data (HEED) and Routinely Collected Health Data. Cardiff: Welsh Government; 2013.
- McGinn L, Lowe S, Heaven M, Griffiths L. Supporting People Data Linking Feasibility Project: Research Report. Welsh Government; 2016.
Appendix 1 Advisory group membership
Our work was guided by an advisory group of 11 individuals from a range of organisations: we are indebted to them for their support. The following individuals were members of the project advisory group and provided consent to have their names included in the project report.
Sinead Brophy, Swansea University
Gordon McCorkindale, Public Representative
Iain McKay, Improvement Service
Nigel Mead, Public Representative
Amy Tilbrook, DataLoch, University of Edinburgh
Beatrix von Wissmann, NHS Greater Glasgow and Clyde
Neil White, Scottish Government
Appendix 2 Scoping reviews
Flow charts
FIGURE 4.
Flow chart for scoping review strand 1: what do existing scoping and systematic reviews say about how evidence is used in decision-making for public health practice and healthy public policy?
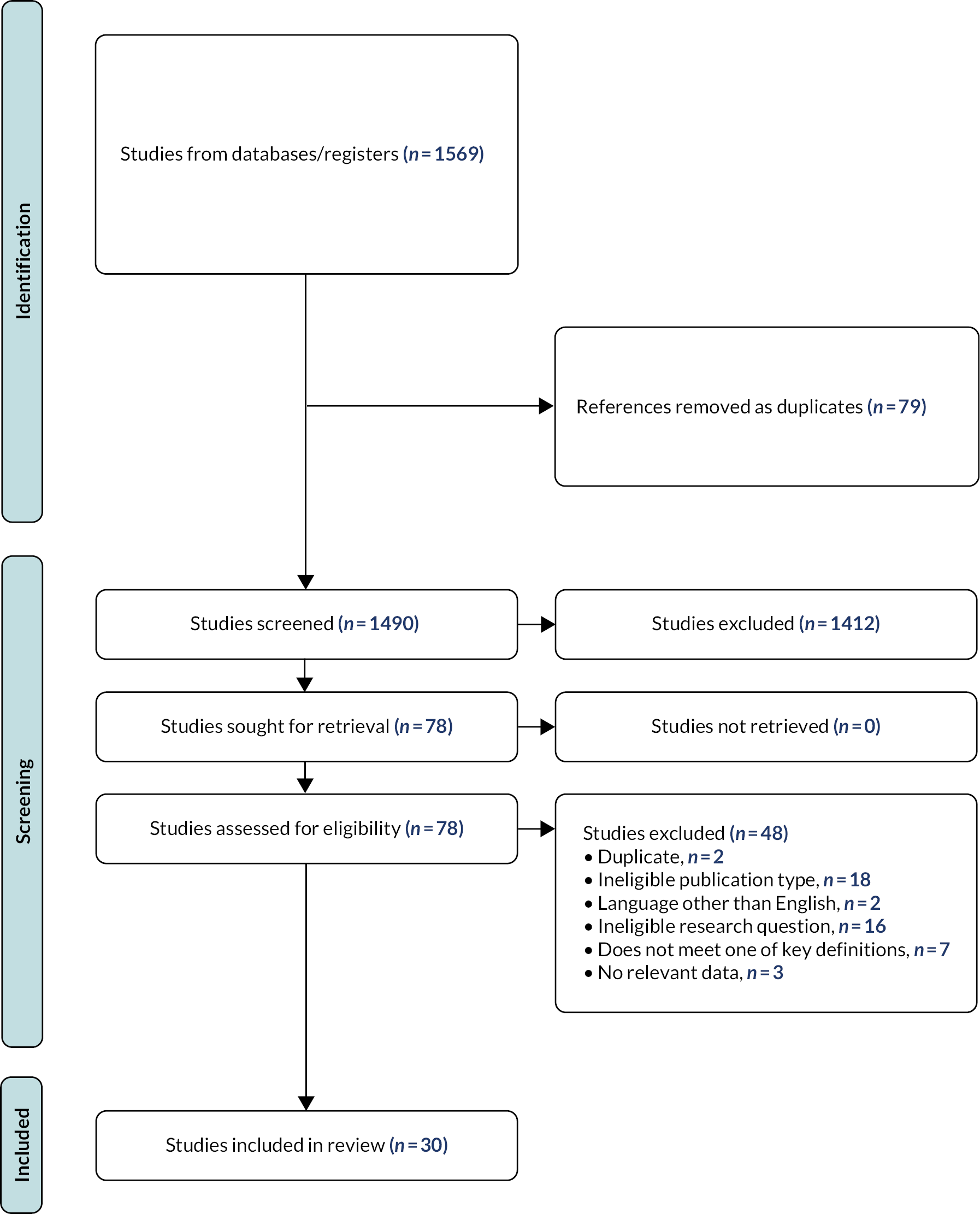
FIGURE 5.
Flow chart for scoping review strand 2: what are the barriers and facilitators at individual, organisational and societal level to the use of secondary data in decision-making for public health and healthy public policy in the UK?
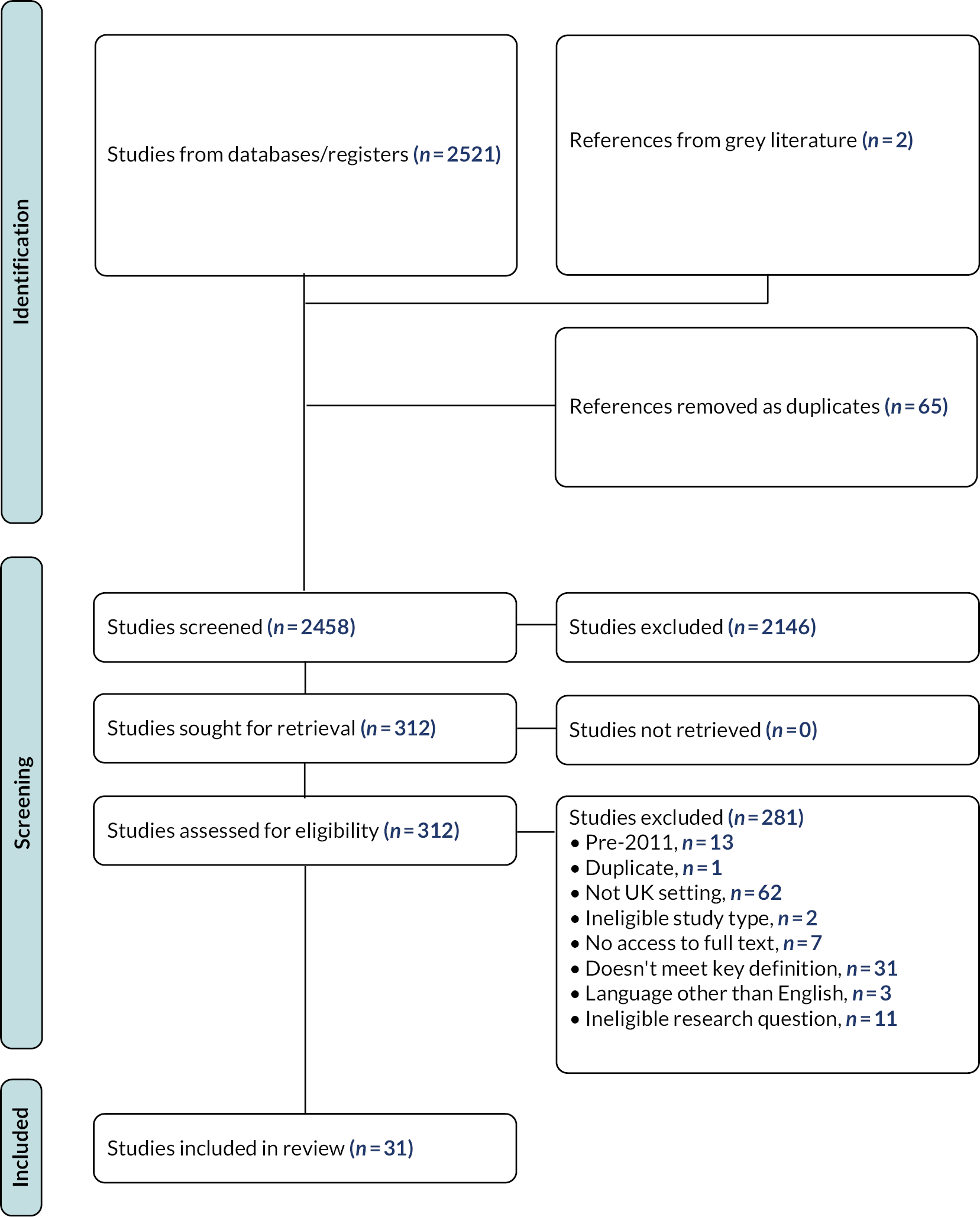
| First author | Year | Title | Journal | Reference |
|---|---|---|---|---|
| Bowrin, K. | 2019 | Cost-effectiveness analyses using real-world data: an overview of the literature | Journal of Medical Economics | 45 |
| Boyko, J.A. | 2012 | Deliberative dialogues as a mechanism for knowledge translation and exchange in health systems decision-making | Social Science and Medicine | 46 |
| Chambers, D. | 2011 | Maximising the impact of systematic reviews in health care decision making: a systematic scoping review of knowledge-translation resources | The Milbank Quarterly | 47 |
| Delnord, M. | 2020 | How can we monitor the impact of national health information systems? Results from a scoping review | European Journal of Public Health | 48 |
| Farrer, L. | 2015 | Advocacy for health equity: a synthesis review | The Milbank Quarterly | 49 |
| Greenhalgh, C. | 2020 | A systematic review of the barriers to and facilitators of the use of evidence by philanthropists when determining which charities (including health charities or programmes) to fund | Systematic Reviews | 50 |
| Guindo, L.A. | 2012 | From efficacy to equity: literature review of decision criteria for resource allocation and healthcare decision-making | Cost Effectiveness and Resource Allocation | 51 |
| Hannes, K. | 2012 | Obstacles to implementing evidence-based practice in Belgium: a context-specific qualitative evidence synthesis including findings from different healthcare disciplines | Acta Clinica Belgica | 52 |
| Justo, N. | 2019 | Real-world evidence in healthcare decision-making: Global trends and case studies from Latin America | Value in Health | 53 |
| Kneale, D. | 2017 | The use of evidence in English local public health decision-making: a systematic scoping review | Implementation Science: IS | 54 |
| Koon, A.D. | 2020 | A scoping review of the uses and institutionalisation of knowledge for health policy in low- and middle-income countries | Health Research Policy and Systems | 55 |
| Lawrence, L.M. | 2019 | Integrated knowledge translation with public health policy makers: a scoping review | Healthcare Policy | 56 |
| Lemire, M. | 2013 | Dissemination of performance information and continuous improvement: a narrative systematic review | Journal of Health Organization and Management | 57 |
| Liverani, M. | 2013 | Political and institutional influences on the use of evidence in public health policy. A systematic review | PLOS ONE | 38 |
| Lorenc, T. | 2014 | Cultures of evidence across policy sectors: systematic review of qualitative evidence | European Journal of Public Health | 37 |
| Masood, S. | 2020 | The use of research in public health policy: a systematic review | Evidence and Policy | 58 |
| Moat, K.A. | 2013 | How contexts and issues influence the use of policy-relevant research syntheses: a critical interpretive synthesis | The Milbank Quarterly | 59 |
| Moore, G. | 2011 | What works to increase the use of research in population health policy and programmes: a review | Evidence and Policy | 60 |
| Oliver, K. | 2014 | A systematic review of barriers to and facilitators of the use of evidence by policy-makers | BMC Health Services Research | 18 |
| Orton, L. | 2011 | The use of research evidence in public health decision-making processes: systematic review | PLOS ONE | 61 |
| Pineo, H. | 2019 | Use of urban health indicator tools by built environment policy- and decision-makers: a systematic review and narrative synthesis | Journal of Urban Health | 62 |
| Polisena, J. | 2013 | Case studies that illustrate disinvestment and resource allocation decision-making processes in health care: a systematic review | International Journal of Technology Assessment in Health Care | 63 |
| Quinn, E. | 2014 | How can knowledge exchange portals assist in knowledge management for evidence-informed decision making in public health? | BMC Public Health | 64 |
| Salajan, A. | 2020 | To what extent does evidence support decision making during infectious disease outbreaks? A scoping literature review | Evidence and Policy | 65 |
| Sarkies, M.N. | 2017 | The effectiveness of research implementation strategies for promoting evidence-informed policy and management decisions in health care: a systematic review | Implementation Science: IS | 66 |
| Sebba, J. | 2013 | An exploratory review of the role of research mediators in social science | Evidence and Policy | 67 |
| Taylor-Phillips, S. | 2018 | Association between use of systematic reviews and national policy recommendations on screening newborn babies for rare diseases: systematic review and meta-analysis | BMJ | 68 |
| Tricco, A. | 2016 | Barriers and facilitators to uptake of systematic reviews by policy makers and healthcare managers: a scoping review | Implementation Science: IS | 69 |
| van Panhuis, W. | 2014 | A systematic review of barriers to data sharing in public health | BMC Public Health | 70 |
| Zhao, N. | 2020 | Knowledge translation strategies designed for public health decision-making settings: a scoping review | International Journal of Public Health | 71 |
| First author | Year | Title | Journal | Reference |
|---|---|---|---|---|
| Ainsworth, J. | 2015 | Combining health data uses to ignite health system learning | Methods of Information in Medicine | 72 |
| Clark, D. | 2017 | Linking routinely collected social work, education and health data to enable monitoring of the health and health care of school-aged children in state care (‘looked after children’) in Scotland: a national demonstration project | Public Health | 73 |
| Cragg, L. | 2018 | Fostering the exchange of real-world data across different countries to answer Primary care research questions: an UNLOCK study from the IPCRG | NPJ Primary Care Respiratory Medicine | 74 |
| Dalton-Locke, C. | 2020 | Using de-identified electronic health records to research mental health supported housing services: a feasibility study | PLOS ONE | 75 |
| Darby, R. | 2012 | Enabling scientific data sharing and re-use | 76 | |
| Douglas, A. | 2018 | Is the linkage of census and health data justified? Views from a public panel of the Scottish Health and Ethnicity Linkage study | Journal of Public Health | 77 |
| Evans, B.A. | 2013 | How hard can it be to include research evidence and evaluation in local health policy implementation? Results from a mixed methods study | Implementation Science: IS | 8 |
| Gordon, B. | 2021 | Development of a data utility framework to support effective health data curation | BMJ Health and Care Informatics | 78 |
| Heeney, C. | 2017 | Balancing the local and the universal in maintaining ethical access to a genomics biobank | BMC Medical Ethics | 79 |
| Hill, E.M. | 2013 | ‘Let’s get the best quality research we can’: public awareness and acceptance of consent to use existing data in health research: a systematic review and qualitative study | BMC Medical Research Methodology | 80 |
| Hurt, L. | 2019 | Cohort profile: HealthWise Wales. A research register and population health data platform with linkage to National Health Service data sets in Wales | BMJ Open | 81 |
| Jones, K.H. | 2019 | The good, the bad, the clunky: Improving the use of administrative data for research | International Journal of Population Data Science | 17 |
| Knox, S. | 2020 | The challenge of using routinely collected data to compare hospital admission rates by ethnic group: a demonstration project in Scotland | Journal of Public Health | 82 |
| Leitmeyer, K.C. | 2020 | Automated digital reporting of clinical laboratory information to national public health surveillance systems, results of a EU/EEA survey, 2018 | Eurosurveillance | 83 |
| Lugg-Widger, F. | 2018 | Challenges in accessing routinely collected data from multiple providers in the UK for primary studies: managing the morass | International Journal of Population Data Science | 15 |
| Meszaros, J. | 2019 | Building trust and transparency? Challenges of the opt-out system and the secondary use of health data in England | Medical Law International | 84 |
| Mourby, M | 2019 | Health data linkage for UK public interest research: key obstacles and solutions | International Journal of Population Data Science | 6 |
| Mukherjee, M. | 2021 | Identifying strategies to overcome roadblocks to utilising near real-time health care and administrative data to create a Scotland-wide learning health system | Health Informatics Journal | 85 |
| Neves, A.L. | 2019 | Health care professionals’ perspectives on the secondary use of health records to improve quality and safety of care in England: qualitative study | Journal of Medical Internet Research | 86 |
| Nienaber, A.M.I. | 2021 | Sharing data – not with us! Distrust as decisive obstacle for public authorities to benefit from sharing economy | Frontiers in Psychology | 87 |
| Oortwijn, W. | 2019 | How to deal with the inevitable: generating real-world data and using real-world evidence for HTA purposes – from theory to action | International Journal of Technology Assessment in Health Care | 88 |
| Quinn, A. | 2020 | The feasibility and challenge of using administrative data: a case study of historical prisoner surveys | International Journal of Social Research Methodology | 89 |
| Ribeiro, C. | 2018 | How ownership rights over microorganisms affect infectious disease control and innovation: a root-cause analysis of barriers to data sharing as experienced by key stakeholders | PLOS ONE | 90 |
| Satinsky, E.N. | 2018 | Mental health service users’ perceptions of data sharing and data protection: a qualitative report | Journal of Innovation in Health Informatics | 91 |
| Slade, S.V. | 2016 | Can data in optometric practice be used to provide an evidence base for ophthalmic public health? | Ophthalmic and Physiological Optics | 92 |
| Thew, S.L. | 2011 | Supporting creativity and appreciation of uncertainty in exploring geo-coded public health data | Methods of Information in Medicine | 93 |
| Warren, L.R. | 2019 | Improving data sharing between acute hospitals in England: an overview of health record system distribution and retrospective observational analysis of inter-hospital transitions of care | BMJ Open | 94 |
| Weir, C.J. | 2020 | Evaluating improvement interventions using routine data to support a learning health system: research design, data access, analysis and reporting | BMJ Quality and Safety | 95 |
| Wistow, J. | 2017 | Implementing extreme weather event advice and guidance in English public health systems | Journal of Public Health | 96 |
| Grey literature sources | ||||
| Heaven, M. | 2013 | Data Linking Demonstration Project: Examining Fuel Poverty Using Home Energy Efficiency Data (HEED) and Routinely Collected Health Data | https://gov.wales/sites/default/files/statistics-and-research/2019-01/data-linking-demonstration-project-examining-fuel-poverty-using-home-energy-efficiency-data-and-routinely-collected-health-data.pdf | 97 |
| McGinn, L. | 2016 | Supporting People Data Linking Feasibility Project: Research Report | https://gov.wales/sites/default/files/statistics-and-research/2018-12/160310-supporting-people-data-linking-feasibility-study-final-en.pdf | 98 |
Appendix 3 Additional post-workshop engagment activities
| Forum | Description of audience |
|---|---|
| Scottish Government Data and Intelligence Network | Meeting of special interest group for those involved in data and intelligence across Scotland, with > 150 attendees |
| Integrated Joint Board Chairs and Vice-Chairs Network | Senior leadership from health and social care integration across Scotland, including local councillors with responsibility for this portfolio |
| Scottish Centre for Administrative Data Research | Interdisciplinary research centre for use and linkage of public sector data in Scotland |
| RDS | New partnership hosted by Scottish Government to promote and support the use of routine and linked data for research |
| PHS | Targeted engagement with PHS Data Protection Officer and Head of Health, Wellbeing and Social Care |
| Digital Office for Scottish Local Government leadership team | Collaboration between 30 councils in Scotland to drive digital innovation and transformation across local government |
Appendix 4 Additional detail on recommendations
| Key: | |||
|---|---|---|---|
| No consensus/not assigned (text = any indications provided by participants) | Low impact | Low effort | Short term |
| Medium impact | Medium effort | Medium term | |
| High impact | High effort | Long term | |
| Ref | Recommendation | Impact | Effort | Timing | Organisation(s) responsible | Notes |
|---|---|---|---|---|---|---|
| Governance | ||||||
| A | Approaches to data sharing and linkage should be strategic rather than piecemeal, reflecting policy priorities and organisational missions, a long-term view, and which data are best suited to achieving the aim | Short | National/devolved gov, NHS Scotland and boards, Local authorities, Health and Social Care Partnerships, organisations supporting research, third sector | This coincides with recommendation S, in recognising that planning and investment requires both long-term considerations as well as the strategic flexibility to respond to unexpected contingencies. It was noted that this required national leadership which transcended organisational boundaries. The key data sets identified through this process are referenced in subsequent recommendations; post-workshop engagement suggested that these should be understood as national assets, as a basis for political leadership and investment. | ||
| B | Standardised data sharing agreements and collaboration frameworks should be developed and agreed at national level between key organisations to facilitate rapid and straightforward collaboration | Weighted towards medium or high | Weighted towards medium | Organisations supporting research, national/devolved gov, NHS Scotland and boards, Local authorities, Health and Social Care Partnerships | Examples of similar cross-sectoral agreements do exist within Scotland, for instance between adjoining local authorities and their local territorial board, which could serve as a model – though it was acknowledged that achieving this at a national scale was a significant challenge. | |
| C | Key data sets from multiple sectors should be available via a central repository acting as a ‘one-stop shop’ for sharing and linkage, with differing levels of governance according to sensitivity | High | High | Medium | National/devolved governments | Examples from other countries such as Estonia, Denmark and Wales were noted here as potential models. |
| D | There should be a focus on the creation, curation and rapid reuse of linked data sets that can be used many times for multiple different purposes | Medium-high | Low-medium | Short-medium | National/devolved gov, organisations supporting research, third sector, other | |
| E | A cross-sectoral monitoring and evaluation framework should be agreed to measure the value and impacts of data sharing and linkage | Medium | Participants mentioned national/devolved governments, Health and Social Care Partnerships, and third sector – but also likely to require other organisations including NHS Scotland and boards and organisations supporting research | Demonstrating the impacts of data sharing and linkage through such a framework (to include both qualitative and quantitative work) was felt to be important to several other recommendations, including those relating to leadership and political commitments. Developing the framework would be a Scotland-wide task requiring appropriate consultation to ensure buy-in. | ||
| F | Requirements from different governance panels for training and accreditation should be audited to identify and address potential areas of duplication | Low | Low | Medium | Organisations supporting research, other | |
| Characteristics of data | ||||||
| G | Key data sets across multiple sectors should have mandatory data standards to ensure consistency and quality | Medium | Medium | Short | National/devolved gov, NHS Scotland and boards, Local authorities, Health and Social Care Partnerships, organisations supporting research, third sector | It was noted here that lessons could be learnt here from initiatives like UK Data Archive and SAIL in Wales, which might make this feasible in the shorter term. However, wider stakeholders recognised that standardisation can be resource-intensive and time-consuming (in contrast to the timescales suggested by participants) – hence the need to identify key data sets on a strategic basis (A) which should be prioritised in the first instance. |
| H | To support ease of discoverability across different sectors, there should be a published list or register of key data sets (including details of what information they contain, standards for collection and curation, and how they can be accessed) | High | High | Short-medium | National/devolved gov, NHS Scotland and boards, Local authorities, Health and Social Care Partnerships, organisations supporting research, third sector | It was noted that, as well as involvement of the organisations listed here, ownership of this resource was likely to be important – this need might be usefully met by a cross-sectoral partnership body like RDS. |
| I | The possibility of a single ID number for individuals (as in Scandinavian countries) should be explored | High | High | Not assigned by participants | Participants noted that this was among the changes likely to have the biggest impact but was also the most challenging to achieve, especially given the political and historical context around this debate in the UK. It was felt to require strong consensus and supporting ethical framework. Examples were cited from several other countries, and it was recognised that different models for governance and access were possible. External stakeholders were more circumspect about this prospect, highlighting recent or ongoing controversies over public sector data sharing and previous political efforts to introduce similar measures. It was felt that this recommendation sat apart from the others, in that if realised, many of the other proposals would be rendered unnecessary – but that it was perhaps the one least likely to be achieved. | |
| Technical | ||||||
| J | Investment in transformation of legacy systems which currently hinder integration and inter-operability | Medium | National/devolved governments | As an example, one participant cited the lack of automatic data quality tools in older systems. An advisory group member noted that this is particularly important for looking at trends over time and system dynamics. | ||
| K | Technical solutions should avoid built-in obsolescence, as part of a long-term planning approach | Not assigned by participants | One potential technical solution cited here was Scottish Government’s CloudFirst strategy. An advisory group member noted that if done at the design stage, this could achieve high impact for low effort. | |||
| Workforce | ||||||
| L | Build capacity in related professional roles (e.g. in data curation, analysis, governance and public engagement) through a national public sector skills initiative | High | Low | Short | National/devolved governments, other | It was noted that this should be wide-ranging and include careers advice at school as well as graduate levels. It was suggested that both generalist and specialist roles were required, as well as a greater understanding among potential evidence users. An advisory group member also noted that greater collaboration between these roles would be important. Timescales may be longer than suggested by participants. |
| M | Ensure that data/analytical professional roles receive adequate resource and recognition, including clear career tracks enabling progression | Short | National/devolved governments | Although this recommendation was not limited to academic roles, it was noted that academia could support this by recognising and rewarding work to build linkages or data infrastructure in similar ways to original research. | ||
| N | Develop and disseminate training resources and guides on how to get started with data sharing and linkage | Not assigned by participants | It was noted that there was a potential role here for mainstreaming and sharing existing tools (such as data accelerator programmes, or examples from the UK Data Archive). | |||
| O | Integrate researchers and innovation leads into community planning throughout Scotland | High | Low | Short | Participants mentioned LAs, HSCPs – but involvement of PHS, territorial NHS boards, and other community planning partners likely to be important | An initiative cited here as a positive example was the LIST embedded into Health and Social Care Partnerships but increasingly expanding into local authorities and community planning partnerships. |
| Political and institutional | ||||||
| P | Realising the benefits of cross-sectoral sharing and linkage requires senior leadership and commitment from across all organisations | High | Both high and low assigned | Short | National/devolved gov, NHS Scotland and boards, LA, HSCPs, organisations supporting research, third sector | It was noted that incentives would differ by organisations and that efforts should be tailored accordingly; the monitoring and evaluation framework proposed above (recommendation E) was felt to be important here in providing concrete evidence of impacts. National leadership in setting priorities and providing funding was suggested to be particularly important in surmounting differing priorities/remits across multiple organisations and the fact that benefits accrue in different sectors or over longer timescales than those where costs/efforts incurred. A strong ethical framework was also felt to be important to achieving improvements in social outcomes while avoiding adverse consequences. |
| Q | Greater engagement with politicians and policy-makers about the potential benefits of secure data sharing and linkage, and how it can be incorporated into planning and decision-making | Medium | Low | Not assigned by participants | Again, the monitoring and evaluation framework proposed above (recommendation E) was felt to be important here in providing concrete evidence of impacts – examples cited were insights into intervention effectiveness, population groups affected, rapid deployment, long-term consequences, and understanding causal chains. One example identified from the post-workshop stakeholder engagement was the use of secondary data in contribution analysis, as a means of pragmatic evaluation of policies and programmes. | |
| R | Maximise expectations and incentives for policy-makers to collaborate with researchers, as part of a learning culture that seeks to make best use of data for population health gain | High | Low | Medium | National/devolved governments, HSCPs | It was suggested that efforts in this respect could be targeted to those areas which are currently lacking evidence on which to base action, where the greatest policy impact might be achieved. |
| S | Planning and investment in this area should be guided by long-term considerations as well as contingency planning for emergencies (such as future pandemics) | Medium-high | Medium | National/devolved governments, HSCPs, third sector | This was suggested to be particularly salient at present. | |
| Working with and for the public | ||||||
| T | Key population health measures and data sets should be identified at the point of policy/legislation development and co-produced with people living in communities of interest | Medium | Medium | Not assigned by participants | Given the scale of this task, it was suggested that one initial approach would be to focus on new administrative data sets, requiring that they are designed and collected in a way that supports future linkage and which centres public engagement. | |
| U | A transparent and wide-ranging public conversation about data sharing and linkage – including its purposes, processes, benefits and risks – is required | Medium | Medium | Participants mentioned NHS Scotland and boards, LAs, HSCPs – but also likely to require national/devolved government and organisations supporting research | Again, it was suggested that the proposed monitoring and evaluation framework (recommendation E) would be helpful in informing this conversation. | |