

Notes
Article history
The contractual start date for this research was in April 2021. This article began editorial review in June 2023 and was accepted for publication in March 2024. The authors have been wholly responsible for all data collection, analysis and interpretation and for writing up their work. The Health and Social Care Delivery Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article. This article was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Permissions
Copyright statement
Copyright © 2024 Jago et al. This work was produced by Jago et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Jago et al.
SYNOPSIS
Introduction
This synopsis details the work of the Active-6 study. Active-6 is a repeated cross-sectional natural experiment, which explores child and parent/carer physical activity pre and post SARS-CoV-2 coronavirus disease (COVID-19) national lockdowns. Full details of the proposed study, including rationale, research design and analysis plans are available in the protocol which is available on the NIHR website. 1
Rationale for research and background
Physical activity is associated with many health benefits for children and adults, including reduced risk of obesity and improved cardiovascular health, health-related quality of life and cognitive and mental health. 2,3 Physical activity tends to track from childhood into adulthood, so ensuring that children engage in regular physical activity is essential for their current and future health. 4,5 The UK Chief Medical Officers recommend that all children and young people should accumulate an average of an hour or more of moderate to vigorous intensity physical activity (MVPA) per day. This is physical activity that raises the heart rate and makes children slightly hot, slightly sweaty and slightly out of breath. However, longitudinal data collected pre-pandemic between 2012 and 2018 observed that MVPA decreases by 2.2 minutes per weekday per year throughout primary school and that, by the age of 11 years, only 41% of children met the hour per day recommendation, down from 61% at age 6 years. 6 On average, girls participate in less physical activity than boys,7,8 and differences in physical activity patterns by family socioeconomic position have also been identified. 9
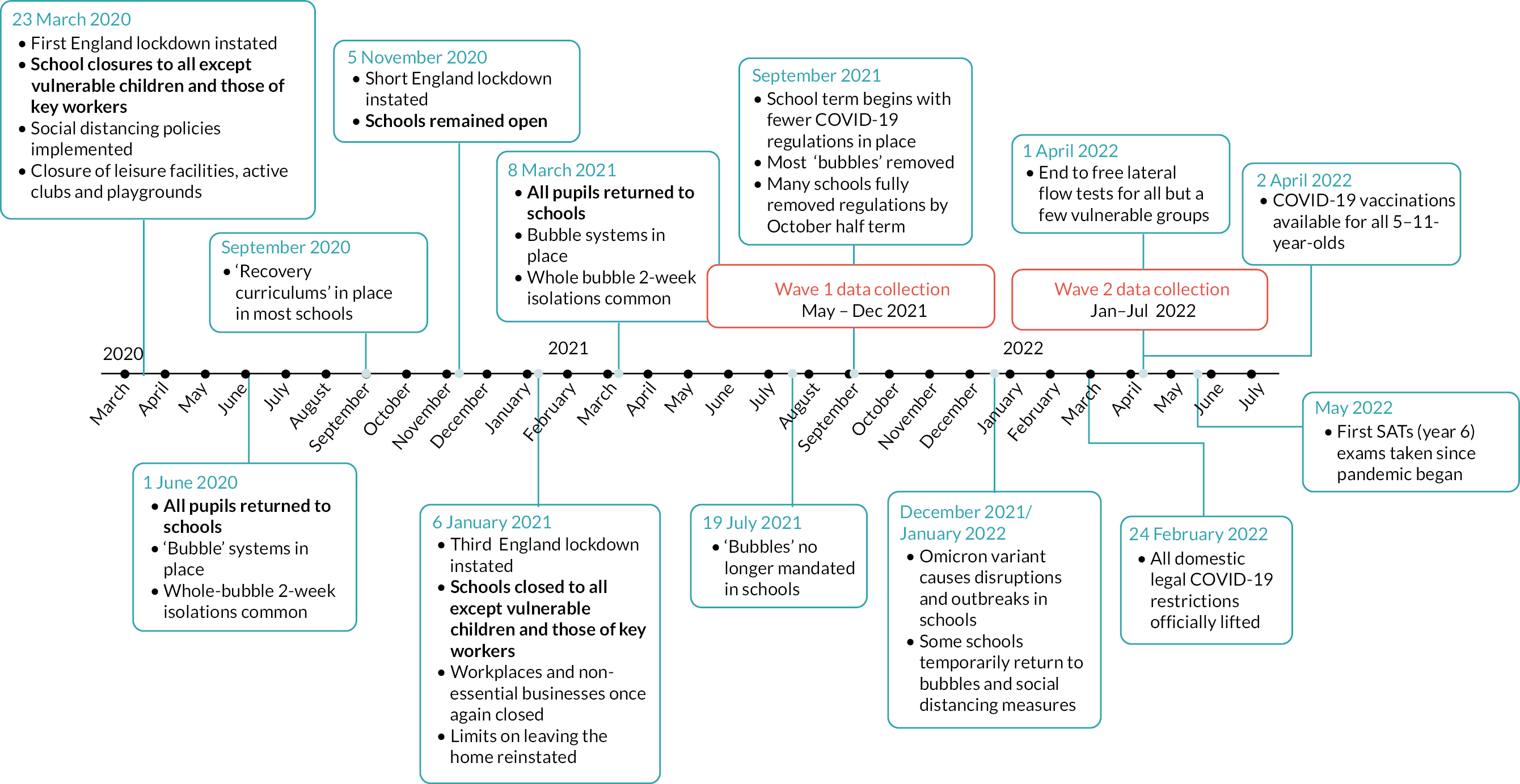
The COVID-19 pandemic and the associated social changes had a marked impact on physical activity patterns for adults and children around the world, as various lockdowns and social distancing measures were enacted throughout 2020–2. In England, national lockdowns occurred in March–May 2020, November 2020 and January–March 2021, including school closures and restrictions on access to leisure and sports centres and playgrounds. From March 2021, various social distancing measures remained and responded to fluctuating levels of COVID-19 and emerging variants, until February 2022 when all legal COVID-19 restrictions in England were lifted. The timeline in Figure 1 outlines these changes. These restrictions likely impacted physical activity among parents and children during their enforcement, but the extent to which the pandemic and restrictions had a longer-term effect on parent/carer and children’s physical activity is unclear. Evaluating these effects is therefore warranted to provide evidence to inform policy and practice to ensure that any adverse effects on physical activity are addressed on a population level.
FIGURE 1.
Timeline of COVID-19 policies in England. SATs, standard assessment tasks.
The Active-6 study sought to measure the impact of the pandemic on accelerometer-measured physical activity among year 6 children (aged 10–11 years) and their parents/carers in England following the final lockdown (January–March 2021). Using a baseline dataset collected in 2017/18, we sought to measure MVPA among year 6 children from the same schools to identify changes in the short-term period after the final lockdown had been lifted (May–December 2021), and if that change was maintained in the medium term (January–July 2022), indicating a more lasting change in activity levels. We also collected questionnaire data from both children and their parents/carers related to the type of activities in which they engage, health-related quality of life, household finances and well-being. We undertook qualitative data collection with parents, children and school staff to explain changes observed in quantitative analyses. Data related to school curriculum and extracurricular physical activity provision were collected from school staff, as well as an audit of school facilities. Our findings were then combined to provide rapid feedback to local and national policy-makers so that any negative impacts could be considered and addressed.
Objectives
The Active-6 study had seven interlinked objectives, reproduced from the study protocol:1
-
To assess the short-term effect of the COVID-19 pandemic on the weekday MVPA of year 6 children by comparing data from 2021 (wave 1) to data sampled from the same schools in 2017/18 (wave 0). Assess whether effects differ by socioeconomic position and/or gender.
-
To determine if there are differences between the physical activity and sedentary behaviour of year 6 children and their parents when compared with data sampled from the same schools in 2017/18 (wave 0) for the following secondary outcomes in 2021 (wave 1):
-
parent accelerometer-measured weekday minutes of weekday MVPA
-
child accelerometer-measured weekend minutes of MVPA
-
parent accelerometer-measured weekend minutes of MVPA
-
child accelerometer-measured weekday sedentary minutes
-
child accelerometer-measured weekend sedentary minutes
-
parent accelerometer-measured weekday sedentary minutes
-
parent accelerometer-measured weekend sedentary minutes.
-
-
To assess the medium-term effects of the COVID-19 pandemic on the primary and secondary outcomes listed in objectives 1 and 2 with data sampled from the same schools in 2022 (wave 2).
-
To examine the extent to which differences in total volume of physical activity and sedentary time in both 2021 (wave 1) and 2022 (wave 2) are explained by the variation in the frequency that the child is active, child physical activity enjoyment and motivation, mode of travel to school, child screen time, after-school club attendance, parent physical activity motivation and self-efficacy.
-
To examine the specific impact of school walking, cycling and play provision, curriculum physical activity, school grounds and school physical activity policies on differences in physical activity.
-
To produce rapid interim reports from the project to UK policy-makers to inform the development of effective strategies to increase physical activity in groups who may have been disproportionately affected by changes due to COVID-19.
-
To understand the implications of COVID-19 on the time and resources allocated to physical activity by schools and households by addressing four subaims:
-
To describe the implications of COVID-19 on household finances and spending on extracurricular physical activities.
-
To describe changes in the allocation of school budgets to physical activity before and after COVID-19 and explore the reallocation of time between academic activities and physical activity.
-
To assess the economic implications and affordability of potential mitigation strategies for schools and families.
-
To explore the associations between measures of health-related quality of life and capabilities in children and adults and examine the possible impact of inequalities.
-
-
To use qualitative methods to further explore changes in physical activity during COVID-19, including factors that influenced activity during this time, and potential solutions to mitigate long-term negative impact on physical activity.
Methods for data collection and analysis
Detailed methods are provided in the study protocol. 1 Specific study methods and analyses are published in detail elsewhere, summarised in the overview of synopsis papers (Table 1) and signposted in the relevant discussion sections.
| Paper no. | Title | Objective | Authors | Year | Journal | DOI |
|---|---|---|---|---|---|---|
| P1 | Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment | 1, 2 and 5 | Salway R, Foster C, de Vocht F, Tibbetts B, Emm-Collison L, House D, et al.10 | 2022 | Int J Behav Nutr Phys Act | https://doi.org/10.1186/s12966-022-01290-4 |
| P2 | A multi-perspective qualitative exploration of the reasons for changes in the physical activity among 10–11-year-old children following the easing of the COVID-19 lockdown in the UK in 2021 | 5, 7 | Walker R, House D, Emm-Collison L, Salway R, Tibbitts B, Sansum K, et al.11 | 2022 | Int J Behav Nutr Phys Act | https://doi.org/10.1186/s12966-022-01356-3 |
| P3 | Screen-viewing behaviours of children before and after the 2020–1 COVID-19 lockdowns in the UK: a mixed methods study | 4, 5 and 7 | Salway R, Walker R, Sansum K, House D, Emm-Collison L, Reid T, et al.12 | 2023 | BMC Public Health | https://doi.org/10.1186/s12889-023-14976-6 |
| P4 | Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: a natural experiment | 3, 5 | Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al.13 | 2023 | Int J Behav Nutr Phys Act | https://doi.org/10.1186/s12966-023-01441-1 |
| P5 | The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK | 7 | Walker R, House D, Salway R, Emm-Collison L, Hollander LE, Sansum K, et al.14 | 2023 | BMC Public Health | https://doi.org/10.1186/s12889-023-16021-y |
| P6 | Comparison of children’s physical activity profiles before and after COVID-19 lockdowns: a latent profile analysis | 4 | Salway R, de Vocht F, Emm-Collison L, Sansum K, House D, Walker R, et al.15 | 2023 | PLOS ONE | https://doi.org/10.1371/journal.pone.0289344 |
| P7 | The status of active after-school clubs among primary school children in England (UK) after the COVD-19 lockdowns: implications for policy and practice | 4, 5, 6 and 7 | Walker R, Salway R, House D, Emm-Collison L, Breheny K, Sansum K, et al.16 | 2023 | Int J Behav Nutr Phys Act | https://doi.org/10.1186/s12966-023-01499-x |
| P8 | The impact of the COVID-19 pandemic on the physical activity environment in English primary schools: a multi-perspective qualitative analysis | 6 and 7 | House D, Walker R, Salway R, Emm-Collison L, Breheny K, Sansum K, et al.17 | 2023 | Public Health Res | https://doi.org/10.3310/KLML4701 |
| P9 | Exploring parents’ physical activity motivation during the COVID-19 pandemic: a mixed methods study from a self-determination theory perspective | 4 | Emm-Collison L, Walker R, Salway R, House D, Sansum K, Breheny K, et al.18 | 2023 | Public Health Res | https://doi.org/10.3310/KPKW8220 |
| P10 | School-level variation in children’s moderate to vigorous intensity physical activity before and after COVID-19: a multilevel model analysis | 4 | Salway R, House D, Walker R, Emm-Collison L, Breheny K, Sansum K, et al.19 | Public Health Res | https://doi.org/10.3310/WQJK9893 | |
| P11 | Quality of life, capability wellbeing, financial strain and physical activity in the short and medium term COVID 19 post-lockdown phases in the UK: a repeated cross-sectional study | 5, 6 | Breheny K, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al.20 | Public Health Res | https://doi.org/10.3310/LYJG6305 |
Mixed-methods data were collected in two waves. Wave 1 quantitative data collection took place between May 2021 to December 2021 when lockdowns had finished but some COVID-19 mitigation policies were still in place in schools and across society and provided data on the short-term impacts of the COVID-19 lockdowns on physical activity and associated behaviours. Wave 2 took place between January and July 2022 when most restrictions had been removed, to provide data on the medium-term impact (Figure 1). Wave 1 qualitative data was collected between August and December 2021 and wave 2 between February and July 2022 and provided insights and explanation into any observed changes in MVPA.
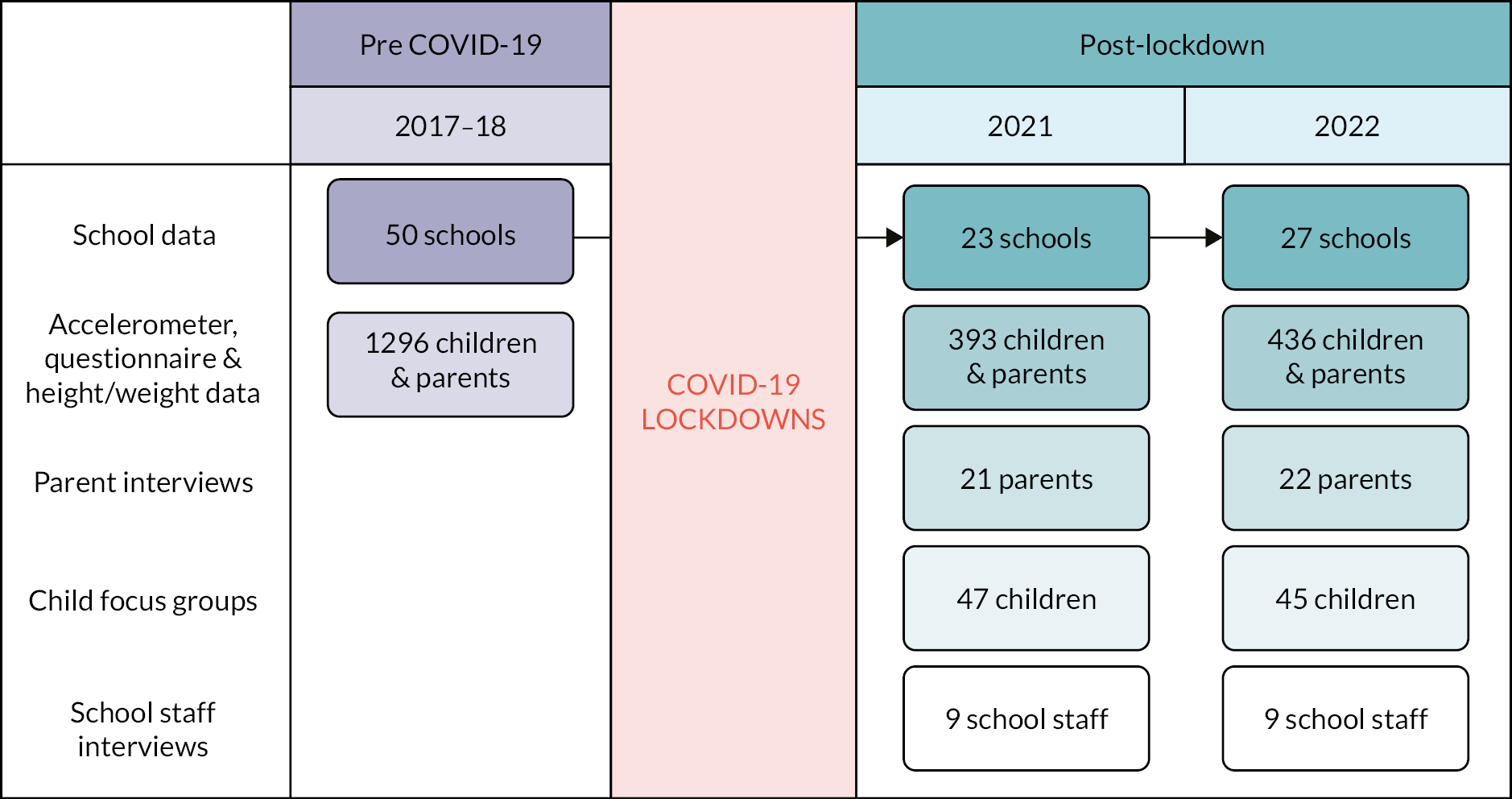
To provide baseline comparator accelerometer and questionnaire data, all participants were recruited from schools in the wider Bristol area (England) that had previously participated in B-Proact1v, a longitudinal cohort study. Both waves of Active-6 quantitative data (wave 1 n = 393; wave 2 n = 436) were compared with data from similar year 6 children and parents/carers from the third phase of the B-Proact1V study between March 2017 and June 2018, which we will refer to as wave 0 (n = 1296). 6 Participants at wave 0 provided written consent/assent, and online consent/assent was provided at waves 1 and 2. Figure 2 provides summary of data collection waves and participants, and Appendix 1 contains details on recruitment and consent processes.
FIGURE 2.
Data collected across all waves.
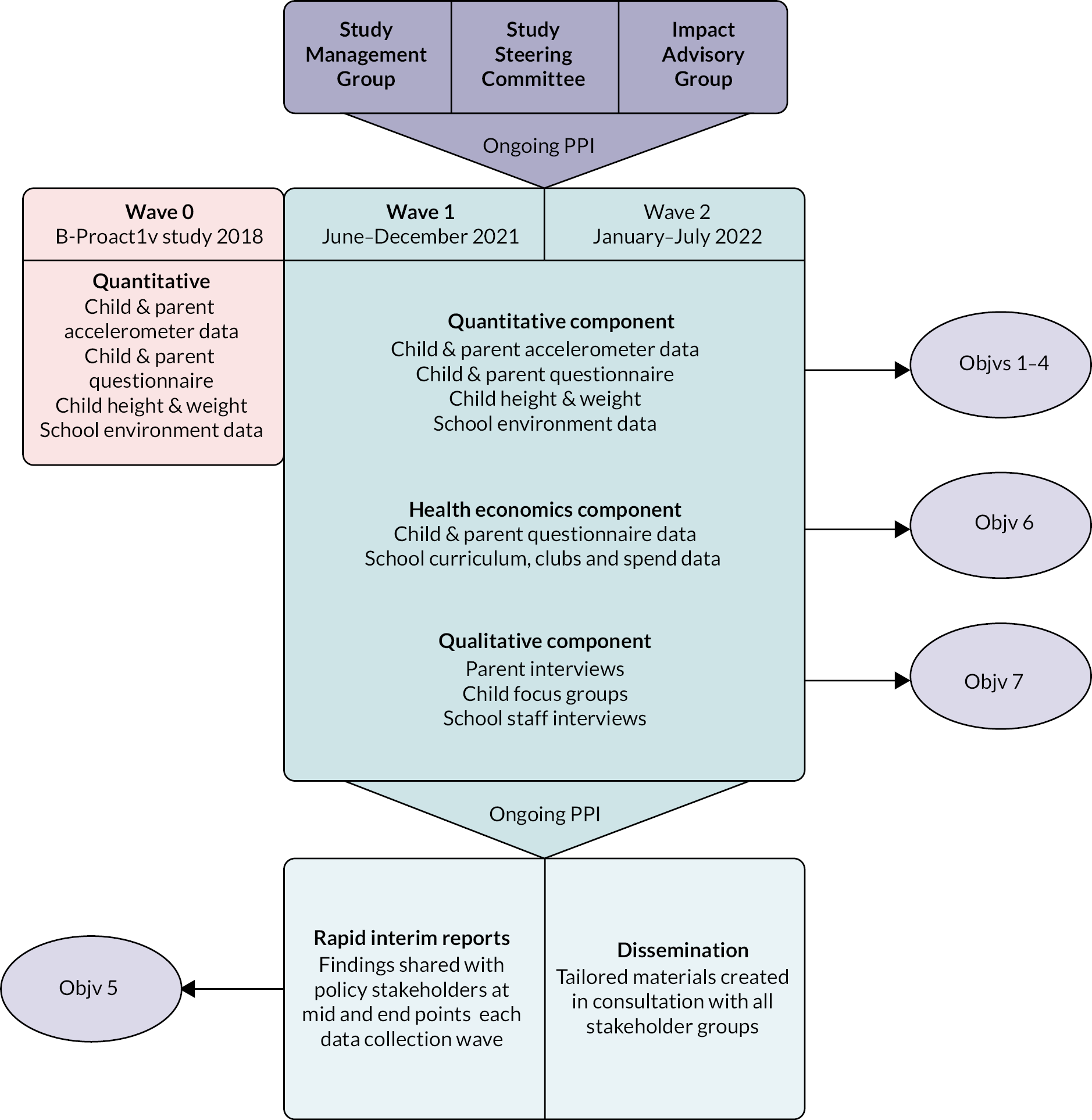
The study has three main components, summarised in Figure 3, and further detailed in Appendix 2.
FIGURE 3.
Diagram of study components. Objv, objective; PPI, patient and public involvement.
Quantitative component
At each time point, participating children and a parent or carer wore a waist-worn ActiGraph wGT3X-BT accelerometer (Actigraph LLC, Pensacola, FL, USA). Participants were asked to wear accelerometers during waking hours for five consecutive days in wave 0, including two weekend days, and for seven consecutive days in waves 1 and 2. Analysis of weekday accelerometer data was restricted to participants who provided at least two valid weekdays of data, and weekend accelerometer data for those who provided at least one valid weekend day of data, defined as at least 500 minutes of data, after excluding intervals of ≥ 60 minutes of zero counts allowing up to 2 minutes of interruptions. Further details have been reported elsewhere. 1,10 In all waves, child height and weight data were collected where possible however, particularly in wave 1, this was limited due to COVID-19 social distancing measures and remote data collection in many schools.
As well as accelerometer data and child measurement data, we collected questionnaire data from parents/carers and children that included demographic data, parent/carer characteristics, mode of travel to and from school, types of physical activity they participate in, parent/carer expenditure on child clubs (waves 1 and 2 only), parent/carer and child screen viewing, and motivation, perceived physical activity ability and health aspiration scales. To capture the school physical activity environment and how this may have changed across the study due to fluctuating social distancing restrictions, we collected data on school physical activity policies, use of physical activity in the curriculum, active after-school club provision and spend (waves 1 and 2 only) and the school built environment. A detailed table of variables collected can be found in Appendix 3.
Health economics component
Parent/carer and child questionnaires at waves 1 and 2 included questions to measure family economic situation and well-being. Parents were asked to report their health-related quality of life and capability well-being using validated questionnaires: the EuroQol 5-dimension (EQ-5D-5L) questionnaire and ICEpop CAPability measure for Adults (ICECAP-A). Children were asked to self-report their health-related quality of life using the Child Health Utility 9 Dimension (CHU9D) questionnaire, and the impact of COVID-19 on their capability well-being was assessed using questions employed in the Birmingham CONTRAST study (Short and long term impacts of Covid-19 on Older childreN’s healTh-Related behAviours, learning and wellbeing Study), which examined the impact of COVID-19 in children and young people. 21 Data on parent spending on after-school physical activity provision and other extra-curricular activities (e.g. community activities and academic tutoring) were collected using a questionnaire used in a previous study. 22 The Family Economic Strain Scale (FESS)23 was used to collect data on household finances. A detailed table of variables collected can be found in Appendix 3.
Qualitative component
Each wave of data collection consisted of in-depth semistructured interviews with parents/carers and school staff, and focus groups with year 6 children to identify the perceived impacts of the pandemic on child and parent physical activity. The parent interviews and focus groups in wave 1 covered changes in physical activity and screen time, with a focus on during lockdowns and when schools reopened. The school staff interviews explored the different approaches schools have taken to promote physical activity before and after the COVID-19 lockdowns and school closures, and the opportunities and challenges of those. In wave 2, qualitative research built upon wave 1 quantitative and qualitative findings where parents and school staff were asked about lasting changes in physical activity, screen time and the school environment. All topic guides can be found in Report Supplementary Material 1.
Oversight and management
The Active-6 study had three oversight and management groups. A study management group consisting of all co-applicants, study research staff and a parent/carer member met monthly to discuss progress, study design, problems and solutions and ethical issues. An independent study steering committee, consisting of an independent chair plus three independent members, including a parent/carer representative, met on four occasions throughout the study to offer guidance. And an impact advisory group of key stakeholders in policy and practice met six times over the study to disseminate rapid interim findings and to provide guidance and insight from the field.
Overview of papers synthesised in synopsis
Table 1 provides details of all papers that have been published from the Active-6 study, how they link to study objectives and publication status at time of publication.
Principal findings
Child physical activity and screen viewing in the short-term recovery phase of the COVID-19 pandemic
This section summarises wave 1 child accelerometer data (Paper 1), wave 1 qualitative data (Paper 2) and wave 1 screen-viewing data (Paper 3). Full details of the methods and findings can be found in those papers (Table 1) and cover objectives 1, 2, 4, 5 and 7.
March 2020 to April 2021: periods of lockdowns and restrictions (Paper 2)
Parents’ and children’s initial response to the first COVID-19 lockdown was characterised by feelings of novelty as families’ usual responsibilities for work and school subsided. This led to increased motivation for well-being and physical activities both among families and within schools. However, this novelty was short lived. The reinstatement of lockdowns and restrictions in winter 2020–21 caused many to feel frustrated, turning the initial feelings of novelty into tedium and low motivation. As the restrictions were prolonged, academic and vocational responsibilities and pressures gradually returned, creating a period that was described as the most challenging and inactive of the pandemic. The extent that children could access physical activity facilities in their local and home environment influenced their physical activity. In particular, greater access to green space and facilities within the home was an important factor that participants linked to more rural communities and greater economic affluence. Children without access to facilities quickly began to dislike the limited physical activities available to them, especially in the later stages of the lockdowns, which led to disengagement from physical activity. Life under COVID-19 lockdowns and restrictions also led to an increased importance of the parent in their child’s physical activity, as children were no longer able to be active through social activities and having fun with friends. The school day, where children were previously active during breaktimes and physical education (PE) lessons, at after-school clubs and with active travel, was for most pupils conducted in isolation within the home. Consequently, parental encouragement and availability to support their child’s physical activity became more influential during this period. Increased screen-viewing behaviour was also suggested during periods of COVID-19 lockdown and restrictions, with a sense that screen-viewing behaviour was unavoidable during these periods. Many aspects of children’s lives transitioned to screen-viewing activities, as families were unable to leave their homes for large periods of the day, and these became children’s medium of entertainment, education, socialising, childcare and forms of physical activity.
April 2021 to December 2021: the short-term recovery phase following lockdowns and restrictions (Papers 1 and 2)
Accelerometer-measured children’s physical activity found that children’s daily MVPA was on average around 7–8 minutes lower in the short term after the COVID-19 lockdowns than before the pandemic, on both weekdays and weekends (Paper 1). This 8-minute difference is broadly comparable to the decline that would have previously been expected to occur over a 3-year period during primary school; that is, their activity levels were those we would have expected of 13- to 14-year-olds. In addition, sedentary time was higher than pre-pandemic by 15–25 minutes per day (Paper 1). Although both girls and children from lower socioeconomic backgrounds were less likely to engage in MVPA both before and after lockdowns, there was no evidence that the 8-minute drop differed between groups (Paper 1). Qualitative analysis explored the reasons for this drop in MVPA (Paper 2). Children experienced emotional overwhelm and physical fatigue during the return to a lifestyle which more closely represented that of a pre-pandemic normality, particularly during the return to school in September 2021. This transition was more physically and emotionally demanding than the secluded and sedentary lockdown lifestyle. Apprehension and worry about COVID-19 were apparent in many children who also found it emotionally challenging when the number of people they interacted with on a daily basis greatly increased. These feelings of emotional overwhelm and fatigue at times manifested as social conflict and/or withdrawal, which impacted active play, led to some avoidance of active clubs and reduced enjoyment of physical activities.
Child screen viewing (Paper 3)
The reported reliance on screen viewing during lockdowns and the observed rise in sedentary time post-lockdown reflect a change in behaviour. We asked parents about their child’s screen viewing and they reported that, by December 2021, total leisure screen viewing was higher by 11% on weekdays compared with pre-COVID and by 8% at weekends. This difference equates to roughly 12–15 minutes per day and was larger among girls and children from lower socioeconomic backgrounds. We also saw a change in the types of screen viewing that children engaged in, with a shift in the balance between TV and non-TV screen viewing. There was a sharp rise of 70–80% in the time spent watching TV (including on-demand and streaming services), compared with before the pandemic. Described as an ‘addiction’ by participants, qualitative data also suggested screen-viewing behaviours increased in the period immediately post-lockdowns compared with pre-COVID-19. This stemmed from the increased exposure to and unavoidable screen viewing during periods of lockdown that led to habitualisation. This drew children away from activities they had previously enjoyed, such as active play. However, age-related and/or societal changes may also have contributed to these changes. Due to increased levels of habitualised screen viewing, parents played a key role in setting limitations on their child’s screen-viewing behaviour when they struggled to self-regulate. Organising activities outside the home was one means of breaking habitualised screen-viewing behaviour; however, many parents were not able to support the associated financial and time costs of these activities.
Child physical activity in the medium-term recovery period of the COVID-19 pandemic
This section summarises the change over time across all waves for child accelerometer data (Paper 4) and wave 2 qualitative data (Paper 5). Full details of the methods and findings can be found in those papers (Table 1) and cover objectives 3, 5 and 7.
Accelerometer-measured child physical activity (Paper 4)
Quantitative analysis found that after the short-term drop of 8 minutes seen in 2021, by 2022, children’s MVPA was on average similar to pre-pandemic times. However, the difference in MVPA between what we would have predicted based on pre-pandemic data and what we observed post-lockdown varied substantially over the full year June 2021–July 2022. The pre- and post-lockdown gap in MVPA was widest during the winter months when MVPA is typically lower, and only returned to pre-pandemic levels by May/June 2022. Moreover, this recovery was susceptible to COVID-19 outbreaks in this age group, such as those in December/January 2021/22 and again in February/March 2022. Thus, although children’s MVPA returned to pre-pandemic levels a year after lockdowns were ended, this recovery was precarious and sensitive to temporary disruptions in physical activity provision. Finally, despite the recovery in average MVPA in the medium-term, average weekday sedentary time remained higher than pre-pandemic by 13 minutes per day on average, and the majority of 10- to 11-year-old children (59%) still did not meet physical activity recommendations.
The ‘new normal’ for child physical activity (Paper 5)
In 2022, a ‘new normal’ for children’s physical activity was suggested to have emerged, characterised by an increased dependence on structured and organised physical activity, such as active clubs, and a decrease in unstructured and spontaneous physical activities. This change in activity patterns stemmed from the continuation of habits formed under COVID-19 lockdowns and restrictions. Time spent within the home post-lockdown continued to reflect the lifestyle of lockdown, such as increased screen time, and activities outside the home needed to be planned and prebooked, negatively impacting spontaneous physical activity opportunities. Lockdown habits within the wider context of health, including those related to sleep patterns and diet, were also suggested to have continued and negatively impacted physical activity. However, although many children had returned to pre-pandemic levels of physical activity, a differential impact was suggested among girls and children with lower socioeconomic position, who may be at risk of lower physical activity levels in the wake of the pandemic. These were suggested to stem from the complex, multifaceted barriers (outlined below) to attending organised activities, which have become the new normal for children’s physical activity.
Qualitative results highlighted the impact of missed developmental experiences among children. A key aspect of this related to interrupted social skills development, particularly in terms of children’s social confidence and ability to connect and harmoniously interact with others and may have discouraged active play. Children’s resilience skills, described as a crucial emotional skill for children, were also interrupted, with some reporting difficulties coping with physical discomfort brought on by physical activity. In addition, physical skills among children were also interrupted, reflected in decreases in time-based school athletics competitions and children’s swimming capabilities. As a result, a persisting sense of tiredness and fatigue among children discouraged them from physical activity. A perceived lasting impact of the pandemic on the mental health of children and their parents was also discussed, such as an increased requirement for and use of mental health support in schools. Families who were experiencing mental health challenges were thought to face elevated barriers to engaging their child in physical activity. For example, encouraging children to leave the home could require significant effort by the parent when children were uncooperative. Mental health challenges were seen as reciprocal with sedentary behaviours, which negatively impacted mental health and led to increased sedentary behaviours.
Understanding the new normal: child activity profiles and active club participation
This section summarises the findings of further analysis of child accelerometer data from all waves to explore child activity profiles (Paper 6), and qualitative, questionnaire, and cost data from waves 1 and 2 on active clubs (Paper 7). Full details of the methods and findings can be found in those papers (Table 1) and covers objectives 4, 5, 6 and 7.
The analysis in the previous section gives a picture of average MVPA change over time, and qualitative insights into why these changes took place (Papers 4 and 5). However, it was important to go beyond these analyses to explore the impact of the COVID-19 lockdowns on child physical activity in more detail. Specifically, we wanted to explore changes in typical patterns of child activity since the lockdowns to understand how physical activity has changed for different kinds of children, and movement between these groups (Paper 6). Additionally, recognising the importance of structured physical activity in the post-lockdown new normal, we wanted to look at changes to active club participation, cost and location (Paper 7).
Identifying children’s activity profiles (Paper 6)
We undertook analyses to explore the complex association between physical activity and sedentary time, to see whether there are specific groups of children who are most likely to be inactive post-lockdown, beyond the average patterns. We identified six ‘activity profiles’ for children that reflected different patterns of MVPA and sedentary time, ranging from a highly active profile, with high MVPA and low sedentary time especially at weekends, to a sedentary and inactive profile, with very low levels of MVPA and high sedentary time. We found that the profiles themselves had changed before and after COVID-19 lockdowns, with a pre-pandemic group, characterised by higher MVPA, replaced by a group characterised by a mix of MVPA and light activity, a pattern similar to that seen among younger children pre COVID-19. The proportions of children in each profile also changed, with more children in the least active profiles and fewer in the most active profiles, especially in the short-term recovery phase. In particular, by 2022, the largest profile was the sedentary and inactive, with over one-quarter (27%) of children in this group compared with 19% pre-pandemic. We also found that gender and socioeconomic gaps had widened. Only 18% of the most active profiles were girls compared with 30% before COVID-19, while in the least active profiles, the proportion of girls increased from 69% to 74%. We also saw socioeconomic differences, with the existing gap in the inactive profile widening from 63% from households with lower educational qualifications to 84%, and a new emerging socioeconomic disparity in the most active group, with fewer children from households with lower educational qualifications. These findings indicate changes in post-lockdown children’s physical activity, in terms of who is being active and how, and it is important to understand these further to develop new strategies to increase children’s physical activity and tackle inequalities.
The role of active clubs (Paper 7)
As qualitative analysis suggested a shift in child activity from unstructured play towards more structured physical activities, we undertook analysis on the role of school- and community-based active clubs in the post-lockdown ‘new normal’. This took a mixed-methods approach, combining quantitative data from children on club attendance, from parents on expenditure on clubs and from schools on active club provision, with qualitative data from all three groups. While total active club participation among children was similar before and after lockdowns, there was a rise in participation in school-based active clubs (43% of children participated in at least one school-based club in wave 0 compared to 50% in wave 2) and a corresponding drop in community-based active clubs (80% of children participated in at least one community-based club in wave 0 and 74% in wave 2). Qualitative analysis highlighted that the increased cost of living and fallout of the COVID-19 pandemic were mechanisms behind this possible shift from community- to school-based active clubs. It found that community-based active clubs were seen as a luxury that many were unable to afford due to their increased cost and requirement for parent time and support; 45% of parents said their child would attend more community clubs if they were cheaper. These findings were echoed in our cost analysis, with median costs per session of £6.67 for community-based active clubs and £3.88 for school-based active clubs, with 50% of school-based active clubs free to attend. Lower participation in community clubs created challenges to organising competitions and offered less opportunity for club-based friendships that had previously motivated children to attend, affecting the quality of experience of attending these clubs. Adults were also volunteering less at community-based active clubs due to decreased availability and increased work pressures. Subsequently, children from families with lower educational qualifications, and/or those experiencing increased economic strain, were particularly impacted and participated in fewer active clubs.
Despite increasing active club provision, many schools were struggling to meet the increased demand for active clubs. School-based active club provision largely relied on school staff volunteering their time, which has become more challenging due to an increasingly pressured school environment. As a result, many schools tried to ensure that as many children as possible had some access to active clubs by rotating children through waiting lists or with different children attending on different days. We found that those children attending school-based active clubs were attending fewer clubs per week than before the pandemic, with those attending on three or more days decreasing from 19% in wave 0 to 10% in wave 2, which could be a result of such policies. Funding sources, such as the PE and Sport Premium, were a key component of affordable school-based active club provision, with 62% partially or wholly subsidised to parents.
Gender differences continued in the medium-term post-lockdown, with similar percentages of girls and boys participating in school-based active clubs but fewer girls participating in community-based active clubs. Parents of girls reported a larger total expenditure on community-based active clubs than parents of boys (median average £12 for boys and £15 for girls), despite girls attending fewer clubs. This may be attributed to the gendered nature of club attendance and the associated costs, as clubs boys typically attend such as football and rugby are cheaper to run than those typically attended by girls, such as gymnastics. As discussed above, cost is a key barrier to active club participation in the context of the cost-of-living crisis and fallout of the COVID-19 pandemic, so may contribute to the gendered patterns in MVPA.
The role of schools
This section summarises qualitative data on changes to the school physical activity environment (Paper 8) and any school-level variation in MVPA outcomes (Paper 10). Full details of the methods and findings can be found in those papers (Table 1) and cover objectives 4, 6 and 7.
The primary school environment is a significant context for child physical activity. The structured nature of a school day regulates obesogenic behaviours24–28 and, for some children, school days are where they have greatest opportunity to engage in diverse physical activities, with around 15% of the total variability in child MVPA attributable to school-level factors. 29 In 2020 and 2021, English schools closed to most children on several occasions to mitigate the spread of COVID-19. When schools reopened, COVID-19 social distancing policies were in place for several months, which impacted schools’ physical activity environments, such as policies on sanitation of equipment, how much space children had access to, how active play could be supported and active travel.
Changes to the school physical activity environment (Paper 8)
We undertook analysis of all qualitative data across both waves to understand the changes to school physical activity environments that took place, how these were experienced by staff and pupils and if/how these were retained. Returning to the ‘in-person’ school rhythm in September 2020 was seen to increase child physical activity after the first lockdown and school closure. During this first term children’s well-being activities, including physical activity, were prioritised through recovery curriculums which were implemented to even out the detrimental physical, social and emotional impacts of lockdown. However, by September 2021, after another school closure and ongoing issues with pupils following guidance to self-isolate following infection with COVID-19, school staff described exceptional pressure to ‘catch up’ on lost learning. PE competed with core subjects for time, staffing issues (including ongoing COVID-19 infection and self-isolation) led to insufficient playground support staff and extracurricular clubs were reliant on scarce teaching staff time. Schools reported an uneven impact of lockdowns and COVID-19 measures on schools and their pupils, with the post-lockdown physical activity environment characterised by variation. COVID-19 social distancing policies have been retained to varying degrees within schools, at times in the interests of pupils and at others in the interests of the over-pressured school. School physical activity culture has also been impacted, with some schools unable to prioritise physical activity due to the post-lockdown pressures described above, while others strengthened their physical activity culture having understood its benefits to pupils through the pandemic. Importantly the pandemic, school closures and ongoing disruptions have had an uneven impact on children’s physical activity. School staff observed that children who were already inclined to physical activity have returned to their activities. Conversely, staff described greater challenges in getting less active children active post lockdowns, creating greater polarisation between active and inactive children.
Between-school differences in MVPA (Paper 10)
Exploring post-lockdown changes in the between-school differences in MVPA can help to determine quantitatively if the role that schools play has changed since the pandemic and can identify which school-level factors, such as environment, policies or sociodemographics, are associated with MVPA. Understanding these school factors is essential in understanding first why changes to children’s physical activity took place; second, which environmental and school factors impact on child physical activity post-COVID-19 lockdowns; and third, the opportunity to influence these to promote physical activity in schools going forward.
The quantitative data showed that while schools differed from each other in terms of average child MVPA, they all showed the same overall pattern of a drop in average MVPA in 2021 followed by a recovery in 2022. A reduction in the proportion of school-level variation in 2021 suggested that, in the short term, difference in physical activity between children was mainly due to unobserved individual factors, with the importance of schools re-established by 2022. Important school-level factors both pre and post lockdowns were the existence of a cycle training policy, the proportion of children in the year using active travel to school, and the average number of active after-school clubs attended in the year group, all of which had a positive association with MVPA, and whether PE lessons were often compromised due to lack of space. These factors increased in importance post lockdowns, accounting for nearly three-quarters (72%) of the school-level variation in 2022, compared with 22% pre COVID-19 (corresponding to 9% and 3% of the total variation in MVPA). Moreover, the relative importance of these factors has changed, with high average club attendance and compromised PE space becoming important in 2022, and active travel less of a contributor. Thus, while schools remain important, we have seen a change in the way in which schools affect children’s physical activity, with the increased role of active after-school clubs supporting other Active-6 findings.
Parent/carer physical activity and household well-being across the pandemic
This section summarises the parent accelerometer data across both waves (Paper 4), questionnaire and interview data on parents’ physical activity motivation across both waves (Paper 9) and household health, well-being and financial strain data across both waves (Paper 11). Full details of the methods and findings can be found in those papers (Table 1) and cover objectives 3, 4, 6 and 7.
We collected data on parent/carer physical activity, including accelerometer-measured MVPA, to provide information on household contexts. Health-related quality-of-life measures added to our evidence base for any changes in physical activity behaviour post lockdowns and allowed us to examine any associations with household finances and inequalities. The financial strain measure was included to understand the financial impact of COVID-19 on families, and which would potentially build into the narrative around solutions to increase physical activity (if needed) which must be mindful of the economic climate. We were also interested in the impact of the lockdowns on parent/carer motivation for physical activity.
Parent/carer physical activity and motivation (Papers 4 and 9)
Parent/carer physical activity has followed a very different pattern to children over the course of the pandemic (Paper 4). In the short-term post lockdown, there was no difference in MVPA on either weekdays or weekends, compared to pre-pandemic. However, by 2022 parents’ weekend MVPA was higher than before the lockdowns by 8 minutes. There was no difference in sedentary time at either point post lockdown.
To understand this observed pattern in MVPA, we undertook a mixed-methods analysis to explore how the lockdowns impacted parent/carer physical activity motivation (Paper 9). Framed within self-determination theory, the findings suggest that autonomous motivation, especially enjoyment and the importance for mental and physical well-being, was a key driver in keeping parents active during lockdowns, and remains important for physical activity post lockdown, with introjected regulation potentially playing an increased role. Interviews with parents highlighted the important role that motivation played in their physical activity engagement throughout the COVID-19 lockdowns and in the months following the easing of restrictions, offering explanation for the continuity of parent/carer MVPA we observed.
The qualitative findings also provide valuable insight into how the lockdowns impacted on parent/carer motivation through supporting, or thwarting, the basic psychological needs of autonomy, competence and relatedness. Whereas discussions of the lockdown impact on autonomy and competence were mixed and in many cases positive, crucially there appear to be enduring negative impacts on aspects of relatedness, particularly feeling connected to others, that must be addressed to support parent/carer motivation to be physically active and to maintain their well-being.
Health-related quality of life, capability well-being and family financial strain (Paper 11)
Given the observed changes in child physical activity, we explored whether there were related changes in parent/carer and child health-related quality of life, capability well-being and family financial strain in the short and medium terms after the COVID-19 lockdowns. We found no differences between the short- and medium-term (waves 1 and 2) adult or child health-related quality of life or capability well-being measures on average. However, family financial strain was slightly worse in wave 2 compared with wave 1. When health-related quality of life and capability well-being were explored alongside family financial strain, children in families experiencing most financial strain had notably poorer health-related quality of life, and parents’ health-related quality of life and capability well-being decreased as financial strain worsened. This finding is of interest in the context of the ‘new normal’ for children’s physical activity, as some families may be less able to participate in organised active clubs due to financial strain.
Discussion
Contribution to existing knowledge
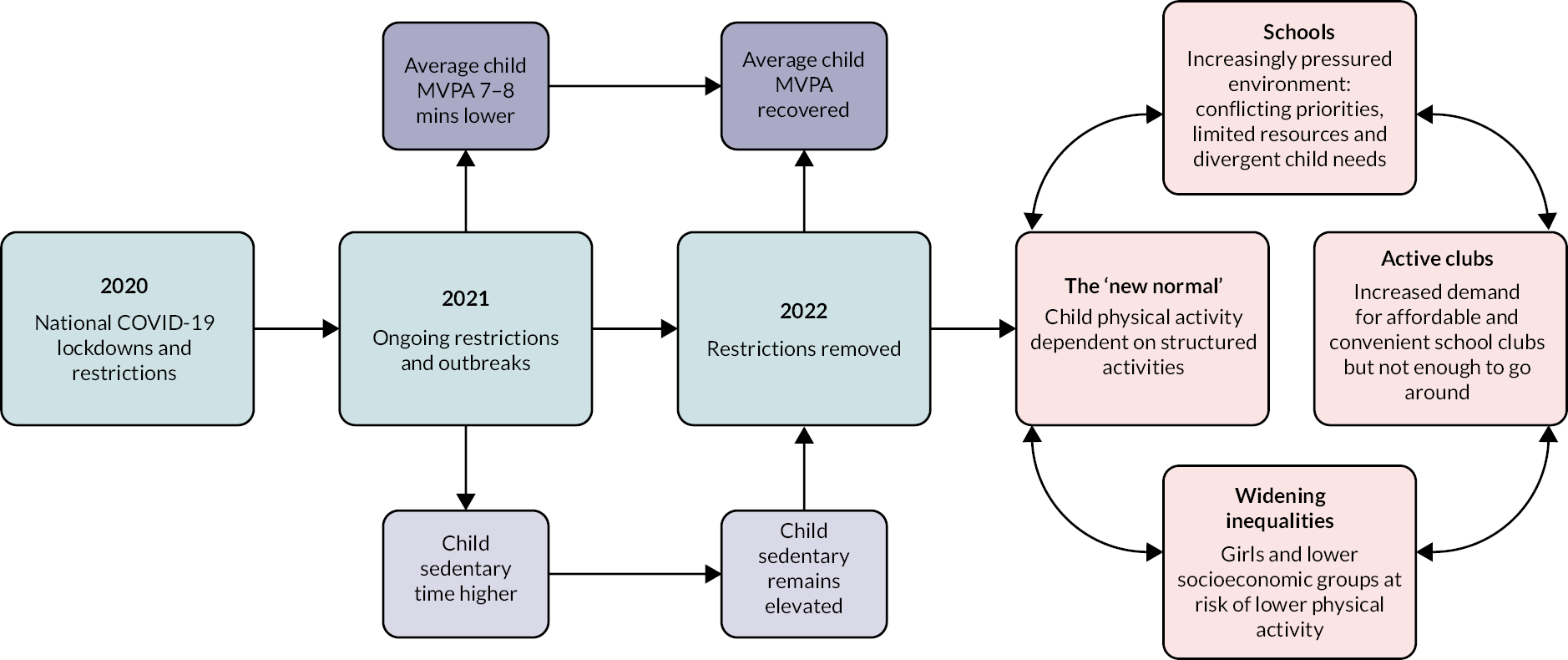
The findings of Active-6 make several valuable contributions to existing knowledge, providing layered and multiperspective insight into how the COVID-19 lockdowns impacted child and parent/carer physical activity in the short and medium terms (Figure 4).
FIGURE 4.
Summary of Active-6 key findings. MVPA, moderate to vigorous intensity physical activity.
It was expected that prolonged lockdowns would have a negative impact on child and adult physical activity, and studies undertaken during the lockdowns have evidenced this,30–33 but of greater importance is how behaviour was impacted in the longer term once lockdowns and restrictions were removed, as society recovered from the pandemic. Active-6 has found that it has taken a year since lockdowns were lifted for children’s MVPA to recover to pre-pandemic levels, and weekday sedentary behaviour remains elevated. But the fluctuations in MVPA we observed over the course of the study suggest that the recovery in children’s MVPA may be susceptible to temporary disruptions to physical activity provision, such as school closures. To our knowledge, this is the first peer-reviewed research to explore this in a UK context. Our data are broadly consistent with Sport England’s 2022 Active Lives Survey, which suggested that average activity levels had returned to pre-pandemic levels among children. 7 However, our study provides novel insight into the short- and medium-term impact of the lockdowns and restrictions in England using accelerometer-measured physical activity, rather than relying on self-report methods, such as those in the Active Lives survey.
Despite an overall recovery in levels of physical activity among children to their pre-pandemic levels, we found that still only 41% of children were meeting physical activity guidelines, and that the way in which children are active has changed. We have termed this the ‘new normal’ for children’s physical activity, characterised by a reliance on structured activities such as active clubs. This finding contributes to existing knowledge by providing unique insight into post-lockdown physical activity patterns among children in the UK. In our evaluation of the current status of active club participation among children, financial pressures were driving a shift from community-based to school-based clubs where children are physically active. Furthermore, schools were at times struggling to meet this increased demand, and the quality of community clubs may also be impacted by lower attendance. These findings add novel and timely insight into the post-lockdown challenges to children’s participation in physical activity and provide specific recommendations to address disparities and promote physical activity.
We have found that the post-lockdown school environment is highly pressured, impacting the extent to which schools can support and encourage child physical activity. Research shows schools are important contexts for child physical activity,27,34 so strategies sensitive to the post-lockdown school environment are needed to support schools to enable child physical activity and future research is needed to further explore the impact of post-lockdown changes on physical activity environments in schools, particularly over the longer-term, as schools continue to adapt post lockdowns. 35 However, our analysis highlights the importance of relatively simple changes, such as ensuring that PE is prioritised even when space is an issue, a cycle training scheme, a strong active club environment and, to a lesser extent, encouraging active travel to school where possible, which could potentially reduce post-lockdown differences between schools.
Across the range of our studies and analyses we found that the detrimental impact of the COVID-19 lockdowns has been worse for those least active, girls and lower socioeconomic families, evidencing a widening of socioeconomic inequalities. Socioeconomic health inequalities is a key public health issue in the UK; 35.6% of premature deaths are attributable to socioeconomic inequality36 We know that physical activity is a habit established in childhood for life and that it is beneficial for lifelong physical and mental health life. 2–5 Therefore, supporting more children from lower socioeconomic households to meet physical activity guidelines can therefore help address socioeconomic health inequalities. The Active-6 project provides unique insight into the post-lockdown challenges facing children from lower socioeconomic households, which has been identified in Sport England’s Active Lives Survey 2022. 7 Namely, cost-related barriers are creating challenges to participating in the new normal for children’s physical activity, which is exacerbating pre-existing disparities. However, due to sampling limitations, we feel that further research is warranted that explores physical activity among children from lower socioeconomic households.
We observed gender disparities in physical activity, with girls being less active than boys. Before the pandemic, there was clear evidence that girls participated in less physical activity than boys in the UK,8 which has continued following the pandemic. 7 Our results suggest that extended interruptions to physical activity during periods of lockdowns and restrictions impacted girls’ perceptions of self and physical activity. Recent reports echo the challenges of these negative perceptions among girls. 37 Subsequently, when combined with increased costs for girls community-based active clubs, these may be barriers to participation in the physical activity new normal for children. Thus, there is a need to promote physical activity among girls, and perhaps especially girls from lower socioeconomic groups.
Take home messages
-
After a short-term drop, average children’s physical activity recovered to pre-pandemic levels, but this recovery took nearly a year after the lockdowns and may be susceptible to future disruptions to physical activity, such as school closures and stay-at-home orders.
-
Most children are more sedentary than before the pandemic and 59% of 10- to 11-year-old children do not meet physical activity guidelines. There is a pressing need to promote and support physical activity in children.
-
Some groups have been more adversely impacted, particularly families with lower socioeconomic position, girls and children who were less active before the pandemic. Our findings suggest a widening gap and growing inequalities.
-
Strategies to support child physical activity must recognise how it has changed, with the ‘new normal’ suggesting there should be a stronger focus on access to structured activities, especially for those groups who typically engage in less activity.
Strengths and weaknesses of the study
The key strength of this study is that child physical activity post-COVID-19 lockdowns was measured through independent data collection and analysis methods (quantitative and qualitative) and then combined into one narrative that provides nuance and depth to our understanding. Collecting accelerometer-measured physical activity was a particular strength, as other major studies rely on self-report data, which are subject to social desirability and recall bias. 7 Additionally, this study used baseline data collected before the pandemic, rather than relying on recall, and the collection of two additional post-lockdown waves of data, to measure change over time. These data came from the same schools and the same-aged children, which reduced school-level variability in estimates. Active-6 collected data in the post-lockdown recovery phase of the pandemic to focus on the longer-term impacts of COVID-19 and implications for policy and practice beyond immediate restrictions. We applied novel statistical techniques to model change over time and account for important factors that influence differences, such as seasonality. Our qualitative data gathered multiple perspectives of parents, children and school staff to triangulate perspectives. Again, two waves of this data enabled us to note and observe any changes over time and provide explanation for the device-measured changes we observed. Lastly, our mixed-methods design means accelerometer and questionnaire data are supported and enhanced by the qualitative study, and vice versa.
This study does, however, have weaknesses. The natural experiment design means that it is possible that observed differences are due to factors that have changed between 2017/18 and 2021/22 other than COVID-19 and associated lockdowns. Our sample is biased towards households with higher educational qualifications, with only 40% of our families from non-graduate households. Therefore, we can generalise to some extent but not explore socioeconomic factors in detail. Finally, the adult sample of our study is not typical of adults as a whole. These are specifically parents/carers of 10- to 11-year-old children between the ages of 35–49 years and, importantly, 75% of our adult sample is female, so these data mainly represent the experiences of mothers. These sample biases must be considered when interpreting the study findings and suggest that future research to target low socioeconomic families and fathers could be warranted.
Challenges faced and limitations
The major challenge this study faced was undertaking participant recruitment and data collection through primary schools during the COVID-19 pandemic, when social distancing restrictions and case numbers fluctuated. Protocols had to be flexible to both virtual and in-person study briefings and data collection, with child height and weight data, particularly in wave 1, at times not possible to collect due to social distancing guidelines. The purpose of this study was to provide rapid insight on the impact of the pandemic on child physical activity and, as such, recruitment and data collection began as soon as possible. This prevented taking time for deeper school community engagement, and this, combined with an uneven impact of the pandemic, may have limited participation of schools and families.
Patient and public involvement
Engaging members of the wider communities of Active-6 has been of central importance to this study. We embedded patient and public involvement (PPI) at every step to improve the study outcomes and created dissemination materials that were useful and relevant to each audience. PPI, therefore, took place throughout the study, but was of particular importance in designing the specifics of data collection and creating resources to share our findings. PPI input has been invaluable, improving data collection protocols and materials and the content, design and channels for dissemination. This section on PPI, therefore, can be read and understood in conjunction with the following section on dissemination. Below we outline PPI undertaken with key stakeholder groups.
Parents
Parent members have sat on the study oversight groups – the study management group and study steering committee – and have shaped and steered the day-to-day management of the study, provided feedback on draft materials including interview guides, protocols and school feedback materials and contributed to publications.
Schools and children
We have worked closely with school staff and children to provide two-way dialogue on data collection processes and study findings. We ran two PPI sessions with children, which explored reflections on wave 1 data collection processes to build upon in wave 2 and provided feedback on several relevant dissemination materials. Year 6 teachers and senior leadership team staff were consulted on data collection processes and all school or classroom-focused materials we have produced.
Policy
At the outset of the study, an impact advisory group (IAG) was established, drawing advisors from a variety of local and national organisations working to promote children’s physical activity, including Department for Health and Social Care, Office for Health Improvement and Disparities, Sport England, Public Health Scotland, Active Scotland and Public Health Wales. Support from many of these organisations was established during the grant application process and the aim of this group was to share rapid findings for feedback and dialogue between the Active-6 team and policy colleagues as the study developed and the findings emerged. Members of the IAG advised the study team on relevant dissemination materials and channels, both in the IAG meetings and through targeted conversations with members about dissemination in their particular field. Several suggestions for dissemination materials and channels emerged from these conversations.
Practitioners
Senior staff from local club providers and national charity and third-sector organisations such as Wesport, Active Gloucestershire, Bristol Sport Foundation and the Youth Sport Trust sat on the IAG and contributed the perspective of child sport and physical activity providers on the data collection, interim findings and dissemination materials. A PPI session was run with on-the-ground club provider staff to review and improve the specific dissemination materials tailored to the practitioner audience. We additionally had a representative from the local authority public health team as co-applicant on the study and who sat on the study management group, providing a unique and valuable perspective on study decision-making.
Dissemination
Providing rapid feedback to policy and practitioner colleagues was a study objective, which we did through our IAG at mid and end points of each data collection wave. This took the study findings directly to those they impact upon in a timely manner and provided dialogue on the data collection and analysis while it was taking place.
Beyond this, our dissemination strategy aimed to share relevant and useful materials in a variety of formats to all study stakeholder groups. The key stakeholder groups identified for our study were policy, schools, active club and sports commissioners and providers, parents and children and academics. With their input, we designed tailored materials for each of these stakeholder groups and identified channels for dissemination.
Two outputs have been central to our dissemination plan and are designed for all stakeholder groups and to encourage engagement with further study resources. These are the ‘Active-6 hub’ and a study animation. We worked with Actify, a social enterprise that hosts an online platform of physical activity digital content, to produce these. The animation provides a very general overview of the study and findings, and then signposts to the hub, which is designed for different stakeholder groups to easily navigate to relevant study materials that provide further findings or offer recommendations to increase child physical activity.
Below, we outline the additional specific materials and resources produced to disseminate Active-6 findings to each stakeholder group and the channels through which we did this, and how the animation and hub was shared with these groups.
Policy
We worked with PolicyBristol to produce a policy briefing that identifies key findings from the study and a list of policy recommendations that can support children’s physical activity. The briefing was disseminated to a comprehensive list of contacts and stakeholders beyond the members of our IAG, including Members of Parliament, Peers and Councillors who sit on relevant all-party parliamentary groups or with relevant portfolios. Additionally, PPI and consultation with IAG members told us policy colleagues were keen for a slide deck of study findings. Both the policy briefing and the slide deck were launched with the IAG at a final study meeting in September 2023.
We have worked to present findings and content directly with policy partners in their spaces and to their audiences. We submitted evidence to the Prevention Inquiry for the Health and Social Care Select Committee to explore how to improve child physical activity since COVID-19 lockdowns. Professor Jago presented study findings at the Youth Sport Trust annual conference, the UK’s leading charity working to improve young people’s education and development through sport and play, where he was one of four speakers in the room with the aim to bring together policy-makers, academics and insight specialists to share the latest evidence on children’s activity and school sport. Locally, we presented findings to the NHS Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group via their Research Showcase Seminar, to the Office for Health Improvement and Disparities’ South West Children’s Healthy Weight and Physical Activity community of practice meeting at the Southwest Public Health Conference 2023, which convenes regional academics and practitioners, and Active-6 was featured as a case study in the 2022/23 Director of Public Health Report for Bristol City Council, which was presented to the Bristol Health and Wellbeing Board and the Bristol City Council Cabinet.
To focus dissemination in the areas and communities that participated in the study, we worked to share study findings to the relevant teams in the four local authorities in which the study took place. Colleagues in these local authorities have shared tailored summaries of the study’s key messages via newsletters and bulletins across public health, children and young people and education teams. This summary was also shared through the local authorities to primary school head teachers, so that the study reached primary school decision-makers and senior leadership team members.
Primary schools
The primary school environment is an important context for children’s physical activity and school staff a key audience for our findings. In addition to dissemination to senior leadership team members in the wider Bristol area described above, we wanted to maintain communication with the Active-6 schools so we produced and disseminated a classroom poster suggesting ‘4 things we can do to get active’, which had input from year 6 children and teaching staff. This poster was printed for study schools as children and staff felt this would be a useful presence in the classroom to remind them of the importance of activity and movement in the school day. We also shared the animation with study schools, and primary school staff told us that within schools the animation was a useful tool for engagement with physical activity post-lockdowns that can be watched in key stage 2 assembly and classrooms (with a class discussion), and shared with wider school and academy communities via their communication platforms.
We wanted the Active-6 schools to be able to engage with their data, so we shared school-level aggregated data on MVPA and sedentary time on weekdays and weekends for children and parents after each wave of data collection. We did this via tailored A2-sized posters which were printed for each study school and an electronic PDF copy was also shared with parents and families via school mailing lists or newsletters. We created two lesson plans (with input from study year 6 teachers), which we shared with these posters, exploring different themes around physical activity that were relevant to the key stage 2 science and maths curriculums. These materials were well received, with examples of staff feedback such as:
I have sent the data to share in our newsletter and shared the lesson plan so that it can be used in Upper KS2 as we think about active travel and healthy schools.
Year 6 teacher
It is good to see the feedback to understand more about how exercise habits have changed in recent years.
Year 6 teacher
[The resources are] absolutely brilliant and will help to back-up and inform what we do
PE coordinator
Beyond study and local primary schools, it was essential to communicate our findings with PE teachers at a national scale. We worked with the Youth Sport Trust (YST), whose main audience base is PE teachers, to collaborate and share findings. Active-6 papers are included in the YST ‘knowledge bank’, evidence is included in their 2023 PE and School Sport report, and we shared study findings in a post for the YST blog. We have written an article for PE Matters, the official journal for the Association for Physical Education, the membership organisation for PE teachers in the UK (Autumn 2023 issue), and Professor Jago shared findings in an analysis piece in the Times Education Supplement, to reach a wider teaching and school staff body.
Club providers
After consulting with club provider members of our IAG, we identified the need for a summary of findings and implications tailored to providers who deliver active clubs at schools and in the community. With input from staff who run clubs in primary schools, we created a one-page PDF provider summary and shared it through local networks of club commissioners and providers.
This summary was also an appropriate format for schools, particularly PE teachers and senior leadership team members, so was also disseminated via the local authority networks and channels.
Families/general public
The families that took part in Active-6 are a particular group with which we undertook steps to engage and share study findings. We shared the animation and hub directly with all Active-6 families via e-mail.
When key study papers were published we worked on a media release to share their findings with the general public and industry. These successful in gaining media traction and Active-6 findings have been covered by over 20 news outlets including nationally in The Times, The Guardian, the BBC, and internationally in France, the USA and India. We have worked to enhance the publication of key study papers by publishing blog posts in relevant partner blogs and online media in order to provide a plain language and accessible summary of the key messages. We published a thought leadership piece in The Conversation on the wave 1 accelerometer data, the blog for the Youth Sport Trust mentioned above sharing the findings on the ‘new normal’, and a post on our findings on club participation post-lockdown on We Can Move’s blog. Finally, we provide a plain language summary of each academic paper we publish on the Active-6 hub, with a link to the full paper.
Academics
To disseminate our findings to academic audiences we have 11 study papers in various stages of publication, outlined in Table 1, and have been accepted to presented findings at several relevant conferences. This included the Scottish Physical Activity Research Connections conference 2023, which brings together a network of physical activity researchers as well as policy-makers and practitioners.
Equality, diversity and inclusion
To maximise precision of the primary outcome, the schools invited to participate in Active-6 were 50 state primary schools which completed phase 3 of the pre-COVID B Proact1v study. These were a mixture of urban, suburban and rural schools, drawn from all five Indices of Multiple Deprivation (IMD) quintiles and of different sizes covering four local authorities in the Bristol area. The 28 schools that took part in Active-6 were broadly representative of these schools. 19 All children enrolled in year 6 in participating schools were eligible to take part. We did not employ stratified sampling to boost any specific demographic groups. Participating children were roughly equally split by gender, and were drawn from all IMD deciles, although there were more participants from higher socioeconomic backgrounds at all time points, especially in the post-lockdown data collection. The sample had low ethnic diversity, with only 8% from non-white backgrounds, slightly lower than the study area as a whole (12% estimated from 2021 Census). Participating adults were all parents/carers of 10- to 11-year-old children and were predominantly aged 35–49 years. The large majority (75%) were female; to increase participation rates we did not target parent/carers by gender. 14
In the qualitative study, there was more scope to shape and monitor recruitment, where certain study schools and groups were targeted to increase their inclusion. However, inclusion and representation of diverse ethnic backgrounds, lower socioeconomic status groups and male parents is limited, in part due to the challenges of conducting research during a pandemic and ongoing school and family disruptions and in part due to the relatively small quantitative sample from which to draw from. 11,14
In the study team, we were able to support the University of Bristol’s Widening Participation Research Summer Internship scheme, which provides promising undergraduate students from underrepresented backgrounds with hands-on research experience to encourage postgraduate study and/or a career in research. Our intern supported all aspects of Active-6 work and made a valuable contribution to the study.
Impact and learning
Further dissemination
As described above, our dissemination plan has been underway alongside the publication of study papers. We build on work to date and continue discussions and dissemination that ensure the outcomes of our research are taken forward by stakeholders.
Many of the key ideas that have emerged from this project are being taken forward in a UK Research and Innovation-funded project called PASSPORT, which seeks to develop a context-specific intervention for primary school physical activity. 35 We intend to continue our IAG into the PASSPORT study to continue the useful and engaged dialogue we have had in Active-6.
Impact
Findings from the study that have been published to date have had some impact in the general public, study schools, policy-makers and practitioners. Longer term, we are hoping to see the impact of the dissemination of the study findings. The study findings and implications can be brought into key policy agendas and decisions in the areas of child physical activity and schools. We have set up search and track functions on Overton, a policy database, to track any policy impact.
Lessons learned for future research
The Active-6 study has provided lessons to draw on for both research design and the focus of future studies in the field. Working with schools particularly through the challenge of COVID-19 has been informative, and we have learned that successful schools-based research depends on close collaboration between a school and the research team and recognising the specific and unique context and needs of each school and school community. 35 The findings of Active-6 are building a picture of an uneven impact of the pandemic on child physical activity, with certain groups of children more adversely affected and at risk of long-term health consequences of low physical activity. In Active-6, we identified a need for future research to undertake careful recruitment of under-represented groups, particularly schools with higher deprivation indicators and the families from these schools in turn, through long-term engagement and relationship building in schools.
The PASSPORT study seeks to explore and evaluate a context-specific model for child physical activity interventions in English primary schools, building on these reflections.
Implications for decision-makers
-
Policy and programmes to support children’s physical activity must be sensitive to the ‘new normal’ for child activity, which relies on organised activities such as clubs, with particular demand for convenient and affordable school-based clubs.
-
Primary schools need additional resources to provide a wide range of active clubs for all abilities.
-
Targeted support is needed for girls and children/schools from more disadvantaged communities, whose physical activity was more adversely affected by the lockdown.
-
There is a need to build on current initiatives to maximise the use of school facilities outside of school hours to increase children’s physical activity at scale cost-effectively.
-
Community and sports organisations need financial support to deliver convenient and affordable community-based clubs that all families can access.
Research recommendations
-
There is a need to develop new ways to work in partnership with schools to design bespoke physical activity programmes that can be delivered at the school site.
-
There is a need to develop new ways to help girls and children from lower-income households to be physically active.
-
There is a need to find the most effective means of maximising existing school resources such as extended school provision (after-school clubs) and physical resources (equipment) to promote physical activity outside of curriculum time.
Conclusions
COVID-19 lockdowns impacted child physical activity, it took almost a year of no restrictions for this to recover, and sedentary time remains high. Despite this recovery, 59% of children do not meet activity guidelines. There is a new normal to child physical activity that relies on structured activities, and some children and families may face challenges to taking part in the new normal. Strategies are needed to increase child physical activity for all.
Additional information
Contributions of authors
Russell Jago (https://orcid.org/0000-0002-3394-0176) was the principal investigator, oversaw all aspects of study design and interpretation, and edited the synopsis for intellectual content.
Danielle House (https://orcid.org/0000-0001-6171-9922) was the study manager, oversaw the management of data collection and study administration, and led the writing of the synopsis.
Ruth Salway (https://orcid.org/0000-0002-3242-3951) was the statistician for the study, developed and analysed all statistical elements of the study, and contributed to all aspects of the synopsis.
Robert Walker (https://orcid.org/0000-0001-9901-5285) was the qualitative lead for the study, developed and analysed all qualitative elements of the study and contributed to all aspects of the synopsis.
Lydia Emm-Collison (https://orcid.org/0000-0002-5493-3223) was a steering group member, developed the qualitative elements of the study, oversaw data collected in wave 0, led the writing of the parent motivation section of the synopsis and edited the synopsis for intellectual content.
Kate Sansum (https://orcid.org/0000-0003-3392-6750) was a fieldworker, conducted wave 2 data collection and edited the synopsis for intellectual content.
Katie Breheny (https://orcid.org/0000-0001-6886-4049) was the health economist for the study, developed the health economics elements of the study, led the writing of the health economics section of the synopsis and edited the synopsis for intellectual content.
Sarah Churchward (https://orcid.org/0009-0007-7765-3682) was a steering group member, contributed in a PPI capacity throughout the project and edited the synopsis for intellectual content.
Joanna G Williams (https://orcid.org/0000-0002-4737-1760) was a steering group member and edited the synopsis for intellectual content.
William Hollingworth (https://orcid.org/0000-0002-0840-6254) was a steering group member and edited the synopsis for intellectual content.
Frank de Vocht (https://orcid.org/0000-0003-3631-627X) was a steering group member and edited the synopsis for intellectual content.
Acknowledgements
A special thanks to the Active-6 schools, the school staff, child participants and parents/carers for their involvement in the study.
Thanks also to previous team members, Professor Charlie Foster, who was co-applicant, and in the study management group; Byron Tibbetts, who was project manager from April to December 2021; Tom Reid, who was fieldworker from April 2021 to January 2022; Lara Hollander, who helped to develop the wave 2 qualitative frameworks; Christine O’Shea, who was summer intern in 2022; and Tabitha Pring, who was a casual fieldworker for wave 2 data collection.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Ethics statement
Ethical approval was gained from the School of Policy Studies Ethics Committee at the University of Bristol, UK (Ref SPSREC/20-21/150)] on 9 March 2021. The project was listed on the Research Registry.
Information governance statement
The University of Bristol is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, the University of Bristol is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer here (www.bristol.ac.uk/secretary/data-protection/).
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/WYHT5821.
Primary conflicts of interest: Russell Jago, Katie Breheny, Frank de Vocht and William Hollingworth are partly funded by the National Institute for Health Research (NIHR) Applied Research Collaboration West (NIHR ARC West) at University Hospitals Bristol NHS Foundation Trust and the University of Bristol. Russell Jago is partly funded by the National Institute for Health and Care Research Bristol Biomedical Research Centre, and was a member of the PHR Prioritisation Group from 11 October 2019 to 12 October 2021, and a member of the PHR Research Funding Board from 1 June 2014 to 12 October 2021. Frank de Vocht has been on the NIHR Public Health Research Funding Board since 8 October 2019. William Hollingworth was a member of the HTA Clinical Evaluation and Trials Committee from 1 July 2016 to 31 March 2021.
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the PHR programme or the Department of Health and Social Care.
This synopsis was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Publications
Salway R, Foster C, de Vocht F, Tibbitts B, Emm-Collison L, House D, et al. Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment. Int J Behav Nutr Phys Act 2022;19:51. https://doi.org/10.1186/s12966-022-01290-4
Walker R, House D, Emm-Collison L, Salway R, Tibbitts B, Sansum K, et al. A multi-perspective qualitative exploration of the reasons for changes in the physical activity among 10–11-year-old children following the easing of the COVID-19 lockdown in the UK in 2021. Int J Behav Nutr Phys Act 2022;19:114. https://doi.org/10.1186/s12966-022-01356-3
Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary: a natural experiment. Int J Behav Nutr Phys Act 2023;20:42. https://doi.org/10.1186/s12966-023-01441-1
Salway R, Walker R, Sansum K, House D, Emm-Collison L, Reid T, et al. Screen-viewing behaviours of children before and after the 2020-21 COVID-19 lockdowns in the UK: a mixed methods study. BMC Public Health 2023;23:116. https://doi.org/10.1186/s12889-023-14976-6
Walker R, House D, Salway R, Emm-Collison L, Hollander L, Sansum K, et al. The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK. BMC Public Health 2023;23:1432. https://doi.org/10.1186/s12889-023-16021-y
Emm-Collison L, Walker R, Salway R, House D, Sansum K, Breheny K, et al. Exploring parents’ physical activity motivation during the COVID-19 pandemic: a mixed methods study from a self-determination theory perspective. Public Health Res 2024;27 March:1–35 [published online ahead of print] https://doi.org/10.3310/KPKW8220
Salway R, de Vocht F, Emm-Collison L, Sansum L, House D, Walker R, et al. Comparison of children’s physical activity profiles before and after COVID-19 lockdowns: a latent profile analysis. PLOS One 2023;18(11):e0289344. https://doi.org/10.1371/journal.pone.0289344
Walker R, Salway R House D, Emm-Collison L, Breheny K, Sansum K, et al. The status of active after-school clubs among primary school children in England (UK) after the COVD-19 lockdowns: implications for policy and practice. Int J Behav Nutr Phys Act 2023;20:120. https://doi.org/10.1186/s12966-023-01499-x
House D, Walker R, Salway R, Emm-Collison L, Breheny K, Sansum K, et al. The impact of the COVID-19 pandemic on the physical activity environment in English primary schools: a multi-perspective qualitative analysis. Public Health Res 2024;7 Feb:1–37. [published online ahead of print] https://doi.org/10.3310/KLML4701
Breheny K, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Quality of life, capability wellbeing, financial strain and physical activity in the short and medium term COVID 19 post-lockdown phases in the UK: a repeated cross-sectional study. Public Health Res (under review). https://doi.org/10.3310/LYJG6305
Salway R, House D, Walker R, Emm-Collison L, Breheny K, Sansum K, et al. School-level variation in children’s moderate to vigorous intensity physical activity before and after COVID-19: a multilevel model analysis. Public Health Res (under review). https://doi.org/10.3310/WQJK9893
Study registration
This study is registered as research registry (project 6646).
Funding
This article presents independent research funded by the National Institute for Health and Care Research (NIHR) Public Health Research programme as award number NIHR131847.
This synopsis reports on one component of the research award Assessing the impact of COVID-19 on the physical activity of 10–11-year-old children and their parents: Active-6 a mixed-methods study. For more information about this research please view the award page (https://www.fundingawards.nihr.ac.uk/award/10.3310/NIHR131847).
About this synopsis
The contractual start date for this research was in April 2021. This article began editorial review in June 2023 and was accepted for publication in March 2024. The authors have been wholly responsible for all data collection, analysis and interpretation and for writing up their work. The Health and Social Care Delivery Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article. This article was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
This synopsis was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Copyright
Copyright © 2024 Jago et al. This work was produced by Jago et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/WYHT5821).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.
List of abbreviations
- BMI
- body mass index
- CHU9D
- Child Health Utility 9 Dimension
- COVID-19
- coronavirus disease
- EQ-5D-5L
- EuroQol-5 Dimensions, five-level version
- FESS
- Family Economic Strain Scale
- HRQoL
- health-related quality-of-life
- ICECAP-A
- ICEpop CAPability measure for Adults
- IMD
- Indices of Multiple Deprivation
- MVPA
- moderate to vigorous intensity physical activity
- PE
- physical education
- YST
- Youth Sport Trust
References
- Jago R, Foster C, Williams J, de Vocht F, Hollingworth W. Protocol for Assessing the Impact of COVID-19 on the Physical Activity of Year 6 Children and Their Parents: Identifying Scalable Actions to Mitigate Adverse Impacts &Amp; Provide Rapid Evidence to Policy Makers (ACTIVE-6) 2021. https://fundingawards.nihr.ac.uk/award/NIHR131847 (accessed 3 October 2023).
- Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med 2020;54:1451-62. https://doi.org./10.1136/bjsports-2020-102955.
- Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. Int J Behav Nutr Phys Act 2020;17. https://doi.org./10.1186/s12966-020-01037-z.
- Telama R. Tracking of physical activity from childhood to adulthood: a review. Obes Facts 2009;2:187-95. https://doi.org./10.1159/000222244.
- Telama R, Yang X, Leskinen E, Kankaanpaa A, Hirvensalo M, Tammelin T, et al. Tracking of physical activity from early childhood through youth into adulthood. Med Sci Sports Exerc 2014;46:955-62. https://doi.org./10.1249/MSS.0000000000000181.
- Jago R, Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA. Association of BMI category with change in children’s physical activity between ages 6 and 11 years: a longitudinal study. Int J Obes (Lond) 2020;44:104-13. https://doi.org./10.1038/s41366-019-0459-0.
- Sport England . Active Lives Children and Young People Survey Coronavirus (COVID-19) Report: Mid-May to Late-July 2020 (the Summer Term) 2021.
- Sims J, Milton K, Foster C, Scarborough P. A profile of children’s physical activity data from the 2012 and 2015 health survey for England. BMC Public Health 2022;22. https://doi.org./10.1186/s12889-022-14150-4.
- Owen KB, Nau T, Reece LJ, Bellew W, Rose C, Bauman A, et al. Fair play? Participation equity in organised sport and physical activity among children and adolescents in high income countries: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 2022;19. https://doi.org./10.1186/s12966-022-01263-7.
- Salway R, Foster C, de Vocht F, Tibbitts B, Emm-Collison L, House D, et al. Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment. Int J Behav Nutr Phys Act 2022;19. https://doi.org./10.1186/s12966-022-01290-4.
- Walker R, House D, Emm-Collison L, Salway R, Tibbitts B, Sansum K, et al. A multi-perspective qualitative exploration of the reasons for changes in the physical activity among 10–11-year-old children following the easing of the COVID-19 lockdown in the UK in 2021. Int J Behav Nutr Phys Act 2022;19. https://doi.org./10.1186/s12966-022-01356-3.
- Salway R, Walker R, Sansum K, House D, Emm-Collison L, Reid T, et al. Screen-viewing behaviours of children before and after the 2020-21 COVID-19 lockdowns in the UK: a mixed methods study. BMC Public Health 2023;23. https://doi.org./10.1186/s12889-023-14976-6.
- Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: a natural experiment. Int J Behav Nutr Phys Act 2023;20. https://doi.org./10.1186/s12966-023-01441-1.
- Walker R, House D, Salway R, Emm-Collison L, Hollander LE, Sansum K, et al. The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK. BMC Public Health 2023;23. https://doi.org./10.1186/s12889-023-16021-y.
- Salway R, de Vocht F, Emm-Collison L, Sansum K, House D, Walker R, et al. Comparison of children’s physical activity profiles before and after COVID-19 lockdowns: a latent profile analysis. PLOS ONE 2023;18. https://doi.org/10.1371/journal.pone.0289344.
- Walker R, Salway R, House D, Emm-Collison L, Breheny K, Sansum K, et al. The status of active after-school clubs among primary school children in England (UK) after the COVD-19 lockdowns: implications for policy and practice. Int J Behav Nutr Phys Act 2023;20. https://doi.org/10.1186/s12966-023-01499-x.
- House D, Walker R, Salway R, Emm-Collison L, Breheny K, Sansum K, et al. The impact of the COVID-19 pandemic on the physical activity environment in English primary schools: a multi-perspective qualitative analysis. Public Health Res 2024. https://doi.org/10.3310/KLML4701.
- Emm-Collison L, Walker R, Salway R, House D, Sansum K, Breheny K, et al. Exploring parents’ physical activity motivation during the COVID-19 pandemic: a mixed methods study from a self-determination theory perspective. Public Health Res. https://doi.org/10.3310/KPKW8220.
- Salway R, House D, Walker R, Emm-Collison L, Breheny K, Sansum K, et al. School-level variation in children’s moderate to vigorous intensity physical activity before and after COVID-19: a multilevel model analysis. Public Health Res 2024. https://doi.org/10.3310/WQJK9893.
- Breheny K, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Quality of life, capability wellbeing, financial strain and physical activity in the short and medium term COVID 19 post-lockdown phases in the UK: a repeated cross-sectional study. Public Health Res 2024. https://doi.org/10.3310/LYJG6305.
- Husbands S, Mitchell PM, Floredin I, Peters TJ, Kinghorn P, Byford S, et al. The Children and Young People Quality of Life Study: A protocol for the qualitative development of attributes for capability well-being measures for use in health economic evaluation with children and young people. Wellcome Open Res 2022;7. https://doi.org./10.12688/wellcomeopenres.17801.1.
- Jago R, Tibbitts B, Porter A, Sanderson E, Bird E, Powell JE, et al. A revised teaching assistant-led extracurricular physical activity programme for 8- to 10-year-olds: the Action 3:30R feasibility cluster RCT. Public Health Res 2019;7:1-128. https://doi.org/10.3310/phr07190.
- Hilton JM, Devall EL. The Family Economic Strain Scale: development and evaluation of the instrument with single- and two-parent families. J Family Econ Issues 1997;18:247-71.
- Faulkner G, Zeglen L, Leatherdale S, Manske S, Stone M. The relationship between school physical activity policy and objectively measured physical activity of elementary school students: a multilevel model analysis. Arch Public Health 2014;72. https://doi.org./10.1186/2049-3258-72-20.
- Harvey A, Faulkner G, Giangregorio L, Leatherdale ST. An examination of school- and student-level characteristics associated with the likelihood of students’ meeting the Canadian physical activity guidelines in the COMPASS study. Can J Public Health 2017;108:e348-54. https://doi.org./10.17269/cjph.108.5925.
- Brazendale K, Beets MW, Armstrong B, Weaver RG, Hunt ET, Pate RR, et al. International Children’s Accelerometry Database (ICAD) Collaborators . Children’s moderate-to-vigorous physical activity on weekdays versus weekend days: a multi-country analysis. Int J Behav Nutr Phys Act 2021;18. https://doi.org./10.1186/s12966-021-01095-x.
- Brazendale K, Beets MW, Weaver RG, Pate RR, Turner-McGrievy GM, Kaczynski AT, et al. Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. Int J Behav Nutr Phys Act 2017;14. https://doi.org./10.1186/s12966-017-0555-2.
- Olds T, Maher C, Dumuid D. Life on holidays: differences in activity composition between school and holiday periods in Australian children. BMC Public Health 2019;19. https://doi.org./10.1186/s12889-019-6765-6.
- Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA, Jago R. A multilevel analysis of neighbourhood, school, friend and individual-level variation in primary school children’s physical activity. Int J Environ Res Public Health 2019;16. https://doi.org./10.3390/ijerph16244889.
- Rossi L, Behme N, Breuer C. Physical activity of children and adolescents during the COVID-19 pandemic – A scoping review. Int J Environ Res Public Health 2021;18. https://doi.org./10.3390/ijerph182111440.
- Kharel M, Sakamoto JL, Carandang RR, Ulambayar S, Shibanuma A, Yarotskaya E, et al. Impact of COVID-19 pandemic lockdown on movement behaviours of children and adolescents: a systematic review. BMJ Glob Health 2022;7. https://doi.org./10.1136/bmjgh-2021-007190.
- Neville RD, Lakes KD, Hopkins WG, Tarantino G, Draper CE, Beck R, et al. Global changes in child and adolescent physical activity during the COVID-19 pandemic: a systematic review and meta-analysis. JAMA Pediatr 2022;176:886-94. https://doi.org./10.1001/jamapediatrics.2022.2313.
- Stockwell S, Trott M, Tully M, Shin J, Barnett Y, Butler L, et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: a systematic review. BMJ Open Sport Exerc Med 2021;7. https://doi.org./10.1136/bmjsem-2020-000960.
- Fairclough SJ, Beighle A, Erwin H, Ridgers ND. School day segmented physical activity patterns of high and low active children. BMC Public Health 2012;12. https://doi.org./10.1186/1471-2458-12-406.
- Jago R, Salway R, House D, Beets M, Lubans DR, Woods C, et al. Rethinking children’s physical activity interventions at school: a new context-specific approach. Front Public Health 2023;11. https://doi.org./10.3389/fpubh.2023.1149883.
- Lewer D, Jayatunga W, Aldridge RW, Edge C, Marmot M, Story A, et al. Premature mortality attributable to socioeconomic inequality in England between 2003 and 2018: an observational study. Lancet Public Health 2020;5:e33-41. https://doi.org./10.1016/s2468-2667(19)30219-1.
- Women in Sport . Sport, Stereotypes and Stolen Dreams: Why Girls Still Feel They Don’t Belong in Sport 2023. https://womeninsport.org/resource/sport-stereotypes-and-stolen-dreams (accessed 2 April 2024).
Appendix 1 Recruitment and consent processes
The Active-6 study was able to recruit from the pool of 50 schools that participated in the final wave of the B-Proact1v study in 2017/18. All 50 schools were approached and invited to participate in wave 1 and again in wave 2. Each participating school signed a school study agreement outlining a key contact at the school and the broad expectations from each party.
Families were recruited from schools via briefings, undertaken by study researchers, to all year 6 pupils at the school. These were either virtual or in-person dependent on COVID-19 cases, policies and mitigation. During these briefings researchers explained why we were doing the study, why their school was participating, the data collection processes, the incentive/thank you gift participants would be given and answered any questions from the pupils and staff.
The day of the briefing a link to sign up to the study, along with participant information, was sent to all year 6 parents/carers via the school office. Families were given a week to sign up, with a reminder e-mail sent out after some days. Consent for the study was provided online via REDCap® (REDcap Consortium, Nashville, TN, USA), and both parents/carers and the children completed this form (consent and assent, respectively). Consent to be potentially contacted about a parent interview at a future date was also included at this stage, as well as yes/no parent consent for their child to take part in possible future focus groups. If consent to these was given, and if that parent or child was selected for an interview or focus group, opting out once contacted was of course possible. Additional oral consent for parent interviews was obtained at the start of the interview, and written child assent to participate in a focus group on the day.
Appendix 2 Details of study components
Parts of this section have been reproduced with permission from Jago et al. ,13 Breheny et al. ,20 and Walker et al. 14 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Quantitative component
Research aims
This component sought to measure the impact of the COVID-19 lockdowns on children’s and their parent/carer’s MVPA and sedentary time in the short and medium terms. We also sought to understand particular factors that might influence this impact.
Methods for data collection and analysis
Accelerometer and questionnaire data were collected from 393 children aged 10–11 years and their parents from 23 schools in wave 1 (June–December 2021) and 436 children and parents from 27 schools in wave 2 (January–July 2022). These were compared to a pre-COVID-19 comparator group (March 2017–May 2018) of 1296 children and parents in the same schools. Mean minutes of accelerometer-measured MVPA and sedentary time were derived for week and weekend days and compared across waves via linear multilevel models. We analysed the date of data collection as a time series, to explore temporal patterns via generalised additive mixed models. We gathered child and parent questionnaire data and school data to explore factors that might influence or explain changes in MVPA.
Limitations
Active-6 is a natural experiment and uses a before-and-after design, where the only available controls are historical. Therefore any differences may be due to other factors rather than COVID-19, especially if these differ over time. Although pre-pandemic data have suggested that children’s MVPA is relatively stable over time and our analysis takes into account seasonal differences, we cannot rule out longer-term secular changes. Our data suggest that there are likely to be differences in adaptations post pandemic by gender and socioeconomic position; however, the sample is not powered to explicitly test for such differences.
Key findings
After an initial drop in 2021, children’s MVPA returned to pre-pandemic levels by July 2022, while sedentary time remained higher. Parents’ MVPA was not affected in 2021 and increased in 2022, especially at weekends. The recovery in children’s physical activity is precarious and potentially susceptible to future COVID-19 outbreaks or changes in provision, and so robust measures to protect against future disruptions are needed. Furthermore, many children are still inactive, with only 41% meeting UK physical activity guidelines, so there is still a need to increase children’s physical activity.
Interrelationships with other parts of the award
As a mixed-methods study, the quantitative, health economics and qualitative components add greater depth of insight and analysis. The quantitative component provides a larger general data set to observe any changes and trends, complemented by the qualitative component that explores experiences and possible explanations for any observed changes.
Health economics component
Research aims
This component explores differences in health-related quality of life and well-being over time after the COVID-19 lockdowns had been lifted. Specifically, how health-related quality of life, capability well-being and family financial strain changed after the lockdowns, the relationship between these outcomes, and whether physical activity had any mediating effect on differences in health-related quality of life and capability well-being.
Methods for data collection and analysis
Cross-sectional data were collected in May–December 2021 (wave 1) and January–July 2022 (wave 2). Children (aged 10–11 years) and their parent/carer were recruited from 23 and 27 schools in each wave, respectively, and completed validated questionnaires measuring health-related quality of life (adults: EQ-5D-5L, children: CHU9D), capability well-being (adults: ICECAP-A) and family financial strain (adults: FESS). Children also completed questions on capability well-being. Mixed-effects regression models, adjusted for gender, age group (adults only), IMD and highest household education, were used to explore differences in health-related quality of life and capability well-being between waves. In addition, the moderating effect of financial strain, and the mediating effect of MVPA on health-related quality of life and capability well-being were explored.
Limitations
Pre-COVID-19 data on health-related quality of life were not collected, so analysis was limited to post lockdown only. Participating parents were predominantly female and participation was lower among lower socioeconomic groups, limiting our ability to explore inequalities.
Key findings
There were no differences in health-related quality of life (EQ-5D, CHU9D) and capability well-being (ICECAP-A) scores between waves, but financial strain was worse in wave 2 compared with wave 1 (FESS score difference 1.14 adjusted 95% CI 0.15: 2.12). Increased financial strain was associated with lower (worse) EQ-5D-5L, CHU9D and ICECAP-A scores. There was no evidence of a mediating effect of MVPA.
Interrelationships with other parts of the award
As a mixed-methods study, the quantitative, health economics and qualitative components add greater depth of insight and analysis. The health economics component provides a different perspective to the general quantitative component by exploring the specific aspect of health-related quality of life and well-being.
Qualitative component
Research aims
This component aimed to provide in-depth analysis of how the pandemic and lockdowns shaped children’s physical activity patterns in the short- and medium-term periods following lockdowns. We also aimed to identify any new challenges to engaging children in physical activity and ideas to mitigate these.
Methods for data collection and analysis
Data were collected in 2021 and 2022 with one-to-one interviews with school staff (N = 18) and parents (N = 43), and 12 child focus groups (N = 92) and analysed using the framework method.
Limitations
Participants were predominantly white British, active and from higher socioeconomic groups, although additional steps were taken to recruit participants from more diverse backgrounds, such as targeted recruitment and purposive sampling of children. We were therefore unable to explore socioeconomic issues in-depth.
Key findings
Periods of lockdown and severe restriction limited children’s activity. In 2021, following the easing of restrictions, emotional overwhelm and physical fatigue among children stemming from a sedentary and socially isolated life in lockdown were key contributors to the decreased moderate to vigorous physical activity and increased sedentary behaviour that was observed in the quantitative component. In 2022, we found a new normal for children’s physical activity, characterised by increased dependence on structured and organised physical activities, such as active clubs, and less on unstructured and spontaneous physical activities, such as physical play. While this may suit many children, girls and children from lower socioeconomic households face barriers to participating in the new normal.
Interrelationships with other parts of the award
As a mixed-methods study, the quantitative, health economics and qualitative components add greater depth of insight and analysis. The qualitative component has provided useful and complementary data to explore and understand the changes observed in the quantitative component.
Appendix 3 Quantitative variables
| Variable | Notes |
|---|---|
| Demographic data (parent reported) | |
| Child gender | |
| Child age | |
| Highest educational qualification in household | |
| IMD decile (from postcode) | IMD 2015 for wave 0; IMD 2019 for waves 1 and 2 |
| Parent gender | |
| Parent age group | |
| Parent ethnicity | |
| Child measurement data | |
| Child height | Measurement data not collected for some schools in waves 1 and 2 |
| Child weight | |
| Child body mass index (BMI) | |
| Child BMI z-score | Based on UK 1990 reference curves |
| Child BMI weight category | |
| Parent/carer characteristics | |
| Parent height (self-reported) | |
| Parent height (self-reported) | |
| Parent BMI | |
| Parent BMI category | |
| Employment status | |
| Relationship of parent/carer to child | |
| Number of children | |
| Child accelerometer data | |
| Number of valid days of weekday data | Wave 0: accelerometer worn for 5 days including weekend |
| Average weekday daily minutes sedentary time | Wave 1 and 2: accelerometer worn for 7 days including weekend |
| Average weekday daily minutes light activity | |
| Average weekday daily minutes MVPA | |
| Average weekday daily minutes accelerometer wear time | |
| Number of valid days of weekend data | |
| Average weekend daily minutes sedentary time | |
| Average weekend daily minutes light activity | |
| Average weekend daily minutes MVPA | |
| Average weekend daily minutes accelerometer wear time | |
| Child meets physical activity guidelines | Daily average of at least 60 minutes MVPA |
| Parent accelerometer data | |
| Number of valid days of weekday data | Wave 0: accelerometer worn for 5 days including weekend |
| Average weekday daily minutes sedentary time | Wave 1 and 2: accelerometer worn for 7 days including weekend |
| Average weekday daily minutes light activity | |
| Average weekday daily minutes MVPA | |
| Average weekday daily minutes accelerometer wear time | |
| Number of valid days of weekend data | |
| Average weekend daily minutes sedentary time | |
| Average weekend daily minutes light activity | |
| Average weekend daily minutes MVPA | |
| Average weekend daily minutes accelerometer wear time | |
| Parent meets physical activity guidelines | |
| Child active travel (child reported) | |
| Usual mode of travel to school | |
| Usual mode of travel from school | |
| Child types of physical activity (child reported) | |
| Frequency child attends sports club at school | |
| Frequency child attends sports club in the community | |
| Frequency child plays outside home | |
| Frequency child plays inside home/garden | |
| Frequency child is active with family | Not collected in wave 0 |
| Frequency child is active with siblings | |
| Days on which child attends an active after-school club at their school | |
| Parental expenditure | |
| Weekly expenditure on community sports clubs | Not collected in wave 0 |
| Weekly expenditure on academic tuition | |
| Weekly expenditure on community programmes/music etc. | |
| Would attend more clubs if they were cheaper | |
| Screen-viewing data | |
| Child minutes of weekday TV viewing (parent reported) | |
| Child minutes of weekday total leisure screen viewing (parent reported) | Wave 0: sum of games consoles, computer and phone |
| Child minutes of weekday schoolwork screen viewing (parent reported) | Not collected in wave 0 |
| Child minutes of weekend TV viewing (parent reported) | |
| Child minutes of weekend total leisure screen viewing (parent reported) | Wave 0: sum of games consoles, computer and phone |
| Parent minutes of weekday TV viewing | |
| Parent minutes of weekday total leisure screen viewing | Wave 0: sum of games consoles, computer and phone |
| Parent minutes of weekend TV viewing | |
| Parent minutes of weekend total leisure screen viewing | Wave 0: sum of games consoles, computer and phone |
| Child has access to PC at home (child reported) | |
| Child has access to games console at home (child reported) | |
| Child has access to phone/tablet at home (child reported) | |
| Health-related quality-of-life (HRQoL) measures | |
| Parent HRQoL (EQ-5D) | Not collected in wave 0 |
| Parent health scale (EQ-5D visual analogue scale) | |
| Parent capability well-being (ICECAP-A) | |
| Family financial strain (FESS) | |
| Family income compared to other families | |
| Child HRQoL (CHU9D) | |
| Child capability well-being questions | |
| Motivation etc. | |
| Parent motivation to be physically active (Behavioural Regulation in Exercise Questionnaire) | |
| Child motivation to be physically active | |
| Child physical activity perceived ability scale | |
| Parental health aspiration index | |
| School physical activity policies (school based) | |
| Policy on PE guidelines | |
| Policy on time spent in physical activity | |
| Active travel policy | |
| Cycle training offered | |
| School crossing patrol employed | |
| Staff continuing professional development on promotion of physical activity | |
| Staff facilities to promote physical activity | |
| PE budget | |
| Physical activity in the school curriculum (school based) | |
| Use of physical activity in non-PE subjects | |
| Physical activity breaks in addition to break/lunch time | |
| How often PE cancelled/withheld for academic reasons | |
| How often PE is compromised due to lack of space | |
| Rules about access to open space/equipment | |
| School active after-school clubs (school based) | |
| Club name and description | Not collected in wave 0 |
| Number of children attending | |
| Cost to school | |
| Cost to parents | |
| How club is funded | |
| Whether club is subsidised | |
| School built environment (school based) | |
| Walking and cycling provision (e.g. cycle lanes, traffic calming, pedestrian crossings, road safety signs) | |
| Play provision (e.g. playground markings, climbing walls, sand pits, play equipment) | |
| Sport provision (e.g. pitches, courts, hoops and nets) | |
| Other facilities (e.g. allotments, drinking fountains, outdoor learning space) | |
| School grounds (e.g. sloped site, suitability for sport or play) | |
| Aesthetics (e.g. trees, planted beds, murals, well-maintained grounds) | |