

Notes
Article history
The research reported in this issue of the journal was funded by the HSDR programme or one of its preceding programmes as project number 16/52/21. The contractual start date was in January 2018. The final report began editorial review in July 2020 and was accepted for publication in January 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HSDR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2022. This work was produced by Marshall et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2022 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Context: rethinking how research influences practice
Managers and clinicians in the NHS, as in all health-care systems, are under growing pressure to improve and redesign services in a way that both optimises health outcomes and controls costs. The research community has great potential to contribute to this process, by producing and disseminating evidence on a variety of aspects of service organisation and care delivery. And yet, the disconnect between, on the one side, the theory and empirical evidence underpinning how best to design and deliver high-quality health services and, on the other side, what actually happens in practice has challenged policy-makers, academics and practitioners for several decades.
How people respond to this challenge depends on whether they perceive the problem to be how academic knowledge is conveyed from researchers to practitioners (‘knowledge transfer’), or the fundamental nature of knowledge and how it is produced (‘knowledge co-production’). 1–4
Knowledge transfer
When framed as a knowledge transfer problem, researchers are seen as having expert knowledge that needs to be transmitted to decision-makers in the health service in an accessible and timely fashion. 5 Knowledge is perceived as a relatively tangible, bounded and moveable ‘product’, whereas the decision-making process is likely to be seen as time-limited, linear and rational. Research evidence, regarded as the most valid and reproducible form of knowledge, is ‘pushed’ from the research community, through guidelines or evidence summaries, or ‘pulled’ by practitioners who are (or should be) well informed about the benefits of using research evidence.
The emergence of sophisticated informatics and communication technologies in recent years, and their use by the National Institute for Health and Care Excellence (NICE) and others, has helped to reinforce a view that the knowledge transfer model is the most appropriate way of closing the so-called ‘know–do gap’. 6 This may be a reasonable assumption in situations in which scientific knowledge is fairly unambiguous, easy to interpret and largely uncontested, such as is often the case (relatively speaking) for much of the clinical evidence underpinning the practice of evidence-based medicine. The transfer approach is more troublesome in the field of health services improvement or service redesign, where the issues that research attempts to address are more complex and the nature of the social science evidence is more contested. 7
Knowledge co-production
This recognition of the limitations of the knowledge transfer model has resulted in a reframing of the integration of research and practice, as requiring different approaches to the nature of evidence, its production and use, and the complexities of the challenges faced by care systems. 3,8
Rather than being separate processes, the production and utilisation of research evidence are seen to merge as complex, iterative and situated social processes. 9–12 That is, knowledge is created, understood, adapted, used and reiterated in the context in which it is needed, and through partnership between different actors.
Furthermore, decision-making by practitioners is regarded more as a situated, social and evolving process than as a one-off, rationally determined event. 6,11 Rather than research evidence needing to be fed into this in a linear and methodical way from outside, the emphasis becomes one of the integration of empirical evidence with other forms of knowledge in situ, including practical knowledge about how to improve and redesign services, and user knowledge about the experience of care services.
This integration is seen as a situated social process based on productive ongoing relationships, effective systems and conducive organisational cultures and contexts. 13–16 Increasingly, the literature in this area embraces a ‘complex adaptive systems’ way of understanding the world, as a means of understanding how actors have to overcome social and epistemic boundaries to helpfully facilitate knowledge processes. 17–19
Such a reframing suggests that the relationship between research producers and research users should focus on the ‘co-production’ of knowledge, rather than merely its transfer. 2,3,20–23 Co-production models of knowledge mobilisation are based on the assumption that knowledge created by researchers often needs to be adapted in some way if it is to be useful. Indeed, for knowledge to have influence, all participants need to be involved in its creation and use. 24 Researchers, using the scientific method as their predominant way of knowing, are not seen to have a monopoly on expert knowledge. Instead, they need to be willing to negotiate actively their forms of knowledge with others (‘a meeting of experts’, e.g. experts in research evidence and experts in improving health services), to recognise and act on power differentials in who dictates how knowledge is defined, and to adopt a more pluralistic orientation to knowledge to achieve change. 25,26
Broadly defined as joint working between people who or groups that have traditionally been separated into categories of user and producer, the term ‘co-production’ came to prominence in the 1970s27 and has gained much currency in public service discourse since. 28,29 When applied in health services research, it is increasingly used as a term to describe the co-production of research-informed knowledge through the engagement of policy-makers and practitioners with researchers. 30–33
However, the increasing popularity of the principle of co-production in public services comes on the basis of promising, but far from complete, evidence. 29,34–36 The literature highlights a range of dilemmas and challenges that need to be explored more fully; for example, is it desirable or feasible to bring researchers and practitioners more closely together, or might the logistical challenges and potentially greater costs than traditional approaches outweigh the benefits?32,37,38 What are the challenges of reconciling divergent or even incommensurate epistemologies?39 Should greater attention be paid to the political and social dimensions of co-production (e.g. the different interests, power and expectations of the parties)?30,31,39,40 Might co-production lead to a narrowing of focus towards problem-solving dimensions of research use,41 instead of encouraging important broader perspectives?23 Should the boundaries between researchers and practitioners be firmly drawn, or are there advantages in flexibility and in the blurring of boundaries?9,21 In what ways can researchers and service users get involved in the co-production of service redesign or improvement?42–44 And can health-care research that is co-produced in one location be translated effectively to other settings?32
The challenges posed by these questions have been exposed by the growing range of new initiatives that seek greater interactivity over research (and, by extension, knowledge co-production in some form) that have emerged in the NHS over the past two decades,17,45–47 as well as in the in the health systems of Canada,48,49 Australia50 and the USA. 51,52
Embedding researchers to encourage co-production
Many different terms and models have been used to describe approaches to research use that seek greater engagement and sustained interactivity, including knowledge brokers,53–60 NHS management fellows,12 Health Foundation improvement science fellows, National Institute for Health Research (NIHR) knowledge mobilisation research fellows, and researchers-in-residence. 61–65 What many of these models have in common is a desire to ‘embed’ researchers in service settings, for significant periods of time, to secure the sorts of sustained interaction thought necessary to promote knowledge co-production. Yet much of the literature is unclear about the relationship between knowledge co-production as a generic concept, ‘brokerage’ (the process by which knowledge is shared across boundaries) and ‘embeddedness’ (whereby researchers are, to a variable extent, located within practitioner teams).
Moreover, other aspects of the schemes that have emerged are highly variable and usually not well described. For example, schemes may vary markedly on the individuals involved (e.g. researchers, health professionals, managers, service users), the degree of close interaction or embeddedness of individuals (e.g. physical locations, contractual arrangements), the nature and degree of co-production sought (calling into question complex issues of epistemology and power) and the types of activities that take place (e.g. the balance between the brokering in of external knowledge and the co-creation of new knowledge in situ). These different models are emerging largely independent of each other, with little evidence of shared learning and only a very few examples of formal evaluation. What has been published mostly comprises descriptions of isolated initiatives, but little in the way of deep analysis and interpretation, and even less in terms of practical guidance.
Both the literature and current practice, therefore, highlight a rich research agenda around embedding researchers as a means to knowledge co-production and, hence, better research use. This includes a clear need to develop a better theoretical and empirical basis for such schemes in the NHS, and the need for evidence-informed practical guidance to support implementation of embedded co-production in practice. 32,38 This project addresses these gaps.
Research aims and objectives
The Embedded project aimed to increase the influence of health services research on decisions about the improvement and redesign of NHS services by:
-
developing insights and understanding about the nature, challenges and effectiveness of co-production initiatives in which researchers are embedded in service settings
-
producing practical guidance on the design and implementation of embedded models of co-production for managers and clinicians in the NHS, their academic partners and people who use services.
In addressing these aims, the project focused on the following specific objectives:
-
to review the theoretical and empirical health services, management and organisational literature relevant to embedded research initiatives and knowledge co-production, and identify the relationship(s) between the two (workstream 1)
-
to gather examples of embedded models in operation around the UK’s health services and public health sectors, focusing on examples where embeddedness and co-production co-exist, and to describe the features of these models, including their history, context, participants, scale, scope and content (workstream 2)
-
to undertake in-depth case studies in four of the examples identified, to understand their mechanisms, effectiveness and challenges (workstream 3)
-
to provide resources aimed at assisting in the recruitment of embedded researchers, alongside recommendations and guidance for their training and development, customisable for the different ways in which embedded co-production may be framed and specified, to allow those interested in developing and using such approaches to understand the design choices they face (workstream 4).
Overall study design
In this section, we set out the overall research strategy governing the four workstreams. Detailed descriptions of the research methods used for the three research-based workstreams (workstreams 1–3) are provided in Chapters 2–5. The activities underpinning workstream 4 (engagement, dissemination and influencing) were ongoing throughout the project, and are described here briefly, with specific outputs emerging from this work covered in Chapters 6 and 7. All appropriate research ethics and research governance permissions were obtained, with approval letters reproduced on the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)].
Workstream 1 used two separate narrative literature reviews to identify and describe the principles and practices of knowledge co-production and of embedded research initiatives. The results were used to develop practical frameworks for understanding knowledge co-production and embedded research; these are described in Chapters 2 and 3, respectively.
Workstream 2 identified and described the breadth and scope of embedded researcher initiatives operating in health settings across the UK and how these were designed to enable knowledge co-production. The results were used to further develop the frameworks of knowledge co-production and embedded research from workstream 1 and to identify candidate case studies for further in-depth examination in workstream 3 (see Chapters 4 and 5). Taken together, the results of workstreams 1 and 2 were used to inform development of an initial framework for planning embedded researcher initiatives that enable knowledge co-production (elaborated on in Chapter 6).
Workstream 3 built on the work undertaken in the first two workstreams by conducting four in-depth case studies to develop a deep understanding of how embedded models of knowledge co-production actually work in practice. The cases and methods of data gathering are detailed in Chapter 4, and the cross-case analysis is displayed in Chapter 5. Drawing on these insights, the implications for scheme design and an enhanced practical framework are set out in Chapter 6.
Workstream 4 used a range of approaches to engage stakeholders with the findings of the project, including developing, testing and disseminating practical guidance for managers, clinicians and academics. This work drew on all the emerging insights and outputs from workstreams 1–3. The processes deployed are described in the next section, and the practical outputs, tools and resources that emerged from that process are set out in Chapters 6 and 7.
Engaging and influencing (workstream 4 activities)
Throughout the project, considerable attention was given towards engaging with and influencing those already embarked on developing embedded research initiatives and those who might be interested in doing so. We aimed to engage with stakeholders to help shape our programme of work and to guide us in the production of useful materials, tools and resources for that community. This work addressed the objectives of workstream 4, namely that, as a consequence of undertaking the project, we wanted to see the following:
-
organisations already engaged in embedding researchers making fuller use of the evidence-based guidance, person specifications, training templates and training resources that we produced to optimise the effectiveness of their work
-
organisations that have not yet considered embedding and/or co-production models stimulated to explore their potential use in improving decisions that affect service delivery
-
future work commissioned to explore the effectiveness, cost and value of embedded research initiatives, focusing on those having the greatest potential to improve services.
Approach to engaging and influencing
The fundamental premise of this research is that knowledge needs to be produced in and through relationships with those who are going to use it (the rationale that underpins both embedded research and knowledge co-production). This, therefore, was also the approach that we took to knowledge creation in this research project. Hence, engaging and influencing key stakeholders were core elements of the proposal.
The principles underpinning our approach were aligned to the theory and practice of co-production models of knowledge mobilisation and to the principles of participatory research. 17,46,66 To that end, the influencing plan was co-produced by practitioners, service users and academics, and used approaches that focus on social interaction, as well as more traditional academic approaches to dissemination.
Audiences and actions
We identified three target audiences that we considered most likely to benefit from the new insights and the associated tools and resources. The primary audience was NHS and local government leaders, both managers and clinicians, whose provider and commissioning decisions could potentially be improved by making better use of health services research evidence.
The secondary target audience comprised the applied research and associated implementation communities, such as members of NIHR Applied Research Collaborations (ARCs) [formerly known as Collaborations for Leadership in Applied Health Research and Care (CLAHRCs)] and Academic Health Science Networks (AHSNs). The twofold aim here was both to encourage actors in these initiatives to explore the benefits and risks of engaging in embedded models of knowledge co-production and embedded research, and to contribute theoretical and empirical knowledge to the field.
The third target audience comprised front-line staff and service users; their interaction with embedded researchers are at the heart of the model. Helping those who want to access and use applied health research to see more clearly how the structural arrangements for the creation of that research affect its use is key.
The Embedded project team had extensive personal and professional networks in the field of NHS service management and knowledge mobilisation, in the UK and internationally. We used the team’s wider local and national networks in local health economies, ARCs/CLAHRCs, AHSNs and higher-education institutions to ensure that the outputs of the project had maximum impact.
A range of actions were devised to engage and influence these audiences.
Workshops
We hosted two participatory workshops during the study, each of which enabled us to co-produce practical outputs (see Chapters 6 and 7) and raise the profile of the project with target audiences.
Workshop 1 co-produced a framework of design options for embedded researcher initiatives and visual representations of the findings from the literature reviews (workstream 1) and the scoping exercise (workstream 2). Details of the design, attendees, process and outcomes are laid out in Chapter 6.
Workshop 2 co-produced a shared understanding and a clear narrative of the case study findings. Details of the design, attendees, process and outcomes are covered in Chapter 4.
A third planned workshop was precluded from taking place because of the COVID-19 crisis. This would have co-produced practical guidance and tools and resources for the design and implementation of embedded models. These goals were met instead by tapping into professional networks and through social media interactions, and by using data gathered from workshop 2.
Tools and resources
Working in partnership with the relevant stakeholders, we co-produced the following resources for use by health service and academic organisations to encourage and support the practical implementation of the learning from workstreams 1–3:
-
an animation to describe the role of embedded researchers in an engaging and accessible way
-
detailed guidance on the design and implementation of coherent embedded co-production models of knowledge mobilisation, presented in the form of webinars and interactive virtual workshops
-
job descriptions and person specifications to support recruitment to new embedded research posts
-
a description of the knowledge, skills and attitudes required of embedded researchers, and the different career pathways that could be pursued
-
guidance for the training and support of embedded researchers, together with resources that could be used by co-production knowledge mobilisers
-
an outline of how embedded researchers might prepare for their role and how organisations could create a conducive environment for them to thrive.
Additional information on each of these outputs is presented in Chapters 6 and 7, where we integrate the research findings from workstreams 1–3 with the engagement activities of workstream 4. The recruitment resource pack detailed in Chapter 7 can be found on the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)]. Practical outputs are also documented on the project’s Embedded Research website. 67
Network
In the original application, we proposed identifying and supporting embedded researcher learning sets that we were aware had been established in a number of locations across the country. As part of our scoping work, we discovered that these networks were often short lived or only partially active. When we discussed the desirability of greater peer support at our first workshop, the participants expressed considerable enthusiasm to establish a self-managed and lightly facilitated network to allow researchers to support and learn from each other.
At the request of the participants, and with their express permission, a network was established, first using a Google Group (Google Inc., Mountain View, CA, USA) and then a WhatsApp (Facebook, Inc., Menlo Park, CA, USA) group. We hoped that the group would provide a peer support resource for those involved in embedded research and a rich opportunity for the research team to get members’ input into our practical frameworks, emerging learning and influencing activities. Observations made through this network influenced the materials and tools created (presented in Chapters 6 and 7, and showcased on the project website). 67
Publications and presentations
To engage public sector leaders, senior clinicians and service managers, accessible audience-appropriate articles were prepared for the Health Service Journal and Local Government Chronicle. The emerging findings were also presented at national and international conferences and seminars, with more detailed reporting in academic journals (see Acknowledgements for a full list of publications and presentations). Through these means, we accumulated resources for the project website67 and prompted interest in and conversations about the emerging programme of work.
Social media
Working with our communications and influencing partner, Kaleidoscope Health and Care (London, UK), we established a website, Embedded Research,67 published regular blogs and set up an Embedded project Twitter account (@_embedded) (Twitter, Inc., San Francisco, CA, USA). In addition, we produced a series of webinars exploring key issues relating to embedded research (www.embeddedresearch.org.uk/resources/webinars/) and we designed an animation to popularise the key messages for audiences not yet familiar with embedded research. 67 The website and associated resources are described more fully in Chapters 6 and 7.
Patient and public involvement
Although progress is being made in involving patients and the public in the provision of their clinical care, in the broader issues of health service improvement and service redesign, patient and public involvement (PPI) has proved considerably more challenging. Experience-based co-design is a rare example of a specific methodology that brings service users and staff together to develop simple solutions to improve patients’ experiences of care. 68 However, moving the agenda from highly tangible but tightly bounded initiatives, such as experience-based co-design, to broader issues, such as how patients and the public can assist in ensuring research-based knowledge is used more effectively, has proved to be somewhat problematic. 69 The following approach has been gaining traction more recently in some jurisdictions (e.g. the USA and Canada): putting patients and service users at the heart of research teams, using patients as active partners and participants to ensure the relevance and applicability of applied research findings. 70 Nonetheless, despite these pockets of innovation, the field of knowledge mobilisation, in general, appears to have not yet been successful in finding a place for the patient voice. 3,4,71
We used the literature review and empirical work in this study to examine this challenge, with the aim of exploring and describing in detail examples of good practice in involving patients and the public in embedded knowledge co-production initiatives. As the subsequent chapters will show, embedded research initiatives involve patients to a varied extent and use diverse models. It was notable, however, that embedded scheme specifications rarely considered PPI in any depth, and the PPI that did occur was seen largely at the level of embedded research projects, but not usually at the level of the overarching embedded research initiative.
In addition to examining and conceptualising the role of patients and the public in embedded research, we specifically also wanted to make a practical difference. To achieve this, we wanted to seize the opportunity to involve patients and the public more substantively in knowledge co-production and to understand how to make an effective case for greater user involvement in this field. In our design of the project, we conceptualised patients as the main beneficiaries of a more evidence-informed health system. Indeed, we thought that patients, both existing and potential, should be central because it is primarily they who are disadvantaged when research-based knowledge is not used by health professionals and managers.
To that end, we framed the effective co-production of knowledge as being dependent on a number of different relationships. The primary focus for this research was on how researchers can build effective relationships with practitioners to co-produce knowledge and improve services, but we saw service users as a key element of the context in which these relationships are enacted, as stakeholders and as important motivators for change. The patient and public voice was therefore included from the early design stage of the proposal.
Our patient and public collaborators included a funded consultant (RP) with great experience as a PPI advisor to NIHR and as a member of the NIHR knowledge mobilisation research fellowship selection panel, who took on the explicit responsibility of challenging any tendency for service-centricity in the design and delivery of the proposal. In addition, the service co-applicants and collaborators were chosen for their commitment to PPI and their extensive contacts with patient groups, including user advisory groups that had been established specifically for knowledge mobilisation initiatives run by ARCs/CLAHRCs and AHSNs and within specific knowledge mobilisation roles. We also established a project PPI group comprising three additional lay members, two of whom already worked closely with the lead for workstream 2 and the other with the lead of workstream 4. We return to these issues in Chapter 8 to distil the learning from across workstreams on the role and potential of greater PPI.
Structure of the report
The remainder of this report is structured as follows.
Chapter 2 presents the methods and findings of a focused literature review of knowledge co-production, drawing from writings on health care as well as in more diverse fields. What emerges is a practical framework of different types of knowledge co-production, from relatively orthodox views of collaborative knowledge creation and use, to more radical conceptions of the capacity of co-production to upend existing assumptions and to challenge established patterns of power. This provides an account of the first part of workstream 1.
Chapter 3 presents the methods and findings of a focused literature review of embedded research schemes (the second part of workstream 1) and the scoping review of extant schemes in UK health-care settings (workstream 2). The findings are brought together to provide a framework for understanding the key features of embedded research initiatives.
Chapters 4 and 5 present the findings from our intensive case studies of different types of embedded research initiatives in which knowledge co-production was a feature (workstream 3). Chapter 4 describes the methods of data gathering and provides accessible accounts of each of the initiatives studied (with additional detail on both methods and cases contained in associated supplementary materials). Chapter 5 details the analytic approach to cross-case analysis and thematic analysis, building on the domains identified and elaborated in workstreams 1 and 2.
Chapters 6 and 7 integrate the understanding that emerges from Chapters 2–5 into a series of practical tools and resources aimed at helping the design, analysis and management of embedded knowledge co-production initiatives. Chapter 6 also notes the contributions and outputs derived from the engagement strategy run through workstream 4. Chapter 7 presents the recruitment resource pack in detail.
Finally, Chapter 8 situates and reflects on this work in the wider research literature and contemporary policy and practice concerns. It also considers the role, implications and potential for PPI in such schemes, and offers directions for further research.
Chapter 2 Exploring ideas of knowledge co-production
Introduction
As outlined in Chapter 1, the organisation and delivery of health and social care services require multiple forms of knowledge and expertise drawn from a wide range of sources. 33,72 Service managers and health service researchers increasingly recognise the limitations of producing research separately from the sites where this knowledge will be applied. 66,73,74 What was previously interpreted as a knowledge ‘pipeline’ problem,75 a knowledge ‘gap’76 or a knowledge ‘transfer’ issue77 is now increasingly reconceptualised as a need for collaborative knowledge creation in context,65,78,79 or ‘knowledge co-production’, in short.
Knowledge co-production comes laden with a variety of positive expectations. 80,81 In the context of embedded research, there can be an easy assumption that co-production is integral or even ‘naturally’ occurring. Against this, we begin to see concerns voiced about a potential ‘dark side’. 82 Some suggest that knowledge co-production, undertaken without caution, can smuggle in hidden interests and disguised power relations, potentially outweighing any proposed benefits with unacknowledged risks. 38 Critiques also focus on the overly instrumental and normative nature of much co-production literature (and practice), both within and outside health care. 83
Ideas of knowledge co-production are germane to any understanding of embedded research, but there remains a lack of clear conceptual underpinning or any precise formulation as to how these ideas may play out in practice. One persistent challenge is the differing assumptions, expectations and frames of reference that collaborators bring with them, and the ways in which these influence methods of working together. 84 There is a need to unpack what is meant by knowledge co-production, to develop greater conceptual clarity and an appropriate language for discussing its components and varied manifestations. This narrative literature review, the first of two in workstream 1, set out to address this issue.
Methods
We conducted a narrative literature review, to ‘synthesise representative literature on a topic in an integrated way such that new frameworks and perspectives on the topic are generated’,85 carrying out a framework analysis of the academic literature on knowledge co-production. The scope of the review was literature exploring a direct collaboration of academic researchers and non-academic stakeholders aimed at generating new knowledge.
Assembling the published literature
To gather a wide array of perspectives, we collected literature that featured theoretical or conceptual discussion of knowledge co-production, including reports of co-productive research activities incorporating reflective and theoretical insights into knowledge co-production, and editorial/review articles in which the main focus was knowledge co-production.
We conducted systematic searches of the Web of Science™ Core Collection™ (Clarivate Analytics, Philadelphia, PA, USA) in March 2018. The search terms and strategy are set out in Table 1. Because we wanted to bring together insights from a wide range of health, science and social science fields, we did not limit this search by discipline or by year, although the earliest article that satisfied our inclusion criteria was from 2003.
| Domain | Details |
|---|---|
| Search terms |
[Co-produc* or coproduc*] AND [knowledge* or research*] AND [(concept* near/3 (model* or framework*)) or theor*] [Co-produc* or coproduc*] AND [knowledge* or research*] refined by review/editorial |
| Article type | Reports of knowledge co-production projects and activities, including theoretical content, reviews and editorials of knowledge co-production |
| People/actors | Academic researchers and non-academics in direct collaboration |
| Content | Theoretical or conceptual discussion of knowledge co-production |
Screening the search results, we removed sources in which knowledge co-production between academic researchers and non-academics was not the principal or main topic. We therefore excluded writings on value and service delivery co-production, public service co-production and other kinds of collaborative co-production not involving researchers working with non-academics, or an explicit concern to make knowledge.
Other relevant articles identified through the reading and networks of the project team were subject to the same process of formal inclusion/exclusion. The numbers of articles screened, removed and included are shown in Figure 1.
FIGURE 1.
Flow chart of literature-gathering and screening.

The articles included for analysis are listed in full in Report Supplementary Material 1. As well as articles from health and directly health-related disciplines (n = 24), we reviewed articles from management studies (n = 15), environmental science (n = 15), sociology and social policy (n = 9), sustainability studies (n = 8), ecology (n = 5), human geography (n = 3), communication studies (n = 2), and one each from humanitarian and disaster studies, engineering, psychology and genomics. Source articles dated from 2003 to 2018.
Analysing the data
The framework analysis technique is well established for analysing large bodies of literature subsequent to searching, screening and preliminary reading. 86–88 This approach was appropriate because of its flexibility (allowing us to interrogate sources from diverse disciplines); its capacity for ongoing modification and revision in response to data reading, re-reading and re-interpretation; and its orientation towards descriptive understanding rather than prediction or normative goals. 89 Framework analysis facilitates an iterative, team-based approach to analysis, giving increased confidence that the categories and themes discerned have stability and interpretive utility.
An initial interpretive reading conducted by one member of the team (BR) aimed to discern and label groups of concepts occurring within and across the source articles. For instance, writers might report concerns around institutional politics, or the difficult emotions of perturbed professional identities, without necessarily using the words politics, identity or emotions.
The review team (BR, VW, HD and TT), which had access to the full set of sources as well as the evolving analytic categories, then discussed this working set of conceptual labels, or domains, for their face validity, coherence, completeness and overlaps, and made modifications as agreed. A closer re-reading of source articles was then conducted to see if the conceptual categories emerging provided a sufficient framework for interpreting the data. This second reading allowed us to identify additional content that would not fit easily into the domains, and to refine or develop further domains and, more significantly, subthemes within domains.
In discussions across the whole project team, it became evident that differing perspectives on knowledge co-production created tensions within each domain. We recorded and labelled these tensions and grouped them together into connected accounts of meaning.
What emerged was a set of five conceptual domains overlaid with a continuum of perspectives from the conventional to the radical. A conventional view of knowledge-making would see the boundaries between different knowledges and different roles largely maintained, with the goal of worthwhile but incremental change. A more radical approach would see boundaries more thoroughly dissolved, in pursuit of a more substantial overhaul of priorities and possibilities.
Given our goal of creating a language of shared meaning that would make knowledge co-production easier to discuss, we sought categories that were defined and coherent enough to allow for shared understanding, broad enough to encompass the messiness of divergent practices, and flexible enough to allow ongoing debate and refinement. The structured reading we lay out is not the only one available, but it has survived repeated interrogation across the wider project team of knowledgeable, diversely experienced collaborators, and through presentations at various professional events.
Findings in outline
The key findings were that there are five key conceptual domains in knowledge co-production; that, in each domain, there is a continuous spectrum of differing perspectives; and that each domain comprises two subthemes, also characterised by a spectrum of perspectives.
Five domains of meaning
Meanings and perspectives in knowledge co-production can be located, understood and compared within five related domains of meaning: politics, knowledge, identity, space–time and aesthetics:
-
The politics domain brings to the surface those negotiated and meaning-laden processes (among large and small groups, and individuals) that in conventional knowledge production are obscured or unspoken.
-
The knowledge domain concerns implications around the tangible product that co-producing parties reach for – what is this knowledge, and what is it for?
-
The identity domain allows a close examination of people who co-produce knowledge – what makes them who they are, individually and collectively?
-
The space–time domain concerns the physical processes and happenings of knowledge co-production. More than just a practical question of ‘where and when’, it involves different configurations and enactments of collaboration.
-
The aesthetic domain makes visible aspects of knowledge co-production experience and expression that may seem intangible and subjective, but that are highly significant – human likes and dislikes, and emotions that escape easy expression but are fundamental to collaboration.
These five domains mark out a conceptual space in which to consider the complex interplay of diverse ideas and understandings involved in knowledge co-production.
Spectrums within domains
In each domain we found that, underlying any superficially isolated points of opposition and difference, there were subtle variations of thinking that merge and separate, creating a spectrum of interpretations and actions. These range from non-collaborative or reservedly collaborative approaches that leave existing boundaries relatively unchallenged (we term these ‘conventional’ research or ‘provisional’ co-production), to approaches that challenge or unravel such boundaries in pursuit of more disruptive and substantial change (what we term ‘committed’ or ‘radical’ knowledge co-production). This spectrum is set out in Figure 2.
FIGURE 2.
Styles of knowledge co-production.

The extremes of this spectrum (conventional and radical) serve as idealised anchor points for clear thinking, but also reflect knowledge-making processes actually (in some cases) performed. Rather than a barrier or problematic void between them, there is a rich space of variation among subtly different approaches. Real-life knowledge co-production mostly happens in this intermediate space. To guard against binary thinking, we included a middle category of moderate co-production, which models a roughly equal balance and interplay between ideals.
These labels proved useful to unpack, interrogate and lay out subtle contrasts within domains, but should not be thought of as overly rigid or proscriptive. Labelled marker points do not indicate static types of knowledge co-production, but dynamic approximations, signposts that we have settled on after repeated interrogations of the literature and discussions among the team.
Subthemes within domains
In further exploring and categorising the themes in the literature, we identified two subthemes within each domain:
-
politics includes ideological and transactional politics
-
knowledge includes the substantive product and output of collaboration, and is also something that exists and has nature in itself
-
identities includes both the roles fulfilled by individuals and the way in which those individuals are less or more socially intertwined
-
space–time incorporates time and space as distinct physical dimensions that can be configured in a variety of ways, according to how they are realised and occupied in collaborations
-
aesthetics includes the preferences and affinities of people and groups involved in knowledge co-production, and the valuation and influence of emotions in collaborative proceedings.
In the subsequent section, we summarise each domain and subtheme, giving examples from the literature. These discussions are encapsulated graphically in Figure 3, and also in Table 2).
Findings in detail
Domain 1: politics
The politics domain incorporates ideologies of research, ranging from the apolitical (conventional co-production: politics seen as separate from knowledge-making) to the emancipatory (radical co-production: knowledge-making as a tool for social justice and structural change). Intermediate points are the utilitarian (provisional co-production: knowledge for instrumental application), the engaged (moderate co-production: research and practice/policy substantially shape each other) and the transformative (committed co-production: sustained micro- and meso-level change is part of the programme).
This domain also incorporates the instrumental politics of transactions, the often mundane institutional politics of co-producing knowledge. Attitudes across that subthematic spectrum range from politics as pollution (conventional), through politics as necessary (provisional) or valuable (moderate), to politics as essence (committed), and politics as all-encompassing (radical).
Politics as ideology
Diverse authors have observed the contrast between politically provocative styles and more functional styles of knowledge co-production. Orr and Bennett31 (social policy context) distinguish between co-production ‘based on a critique of the status quo’ and the de-politicised ‘anodyne’ use of co-production terminology in service of established interests, ‘not necessarily advancing the broader interest or public welfare’. Similarly, Lövbrand (climate science context)90 identifies:
. . . tension between the critical/reflexive ambition built into the co-production idiom, and the more utilitarian interpretation of the term. Whereas the former sets out to expose and interrogate the ontological assumptions underpinning public policy, the latter seeks to be useful by responding to the knowledge needs of societal decision-makers.
Analytically, one could accentuate the mutual distinctiveness of these positions. 91 In the narratives we reviewed, however, we found instability and equivocation between utilitarian and critical co-production styles. ‘Useful’ forms of knowledge co-production do not necessarily preclude more thoroughgoing change. Co-production with a stated transformative intent, meanwhile, often also carries slower-moving and locally specific change processes. Both understandings frequently pertain within projects, and between collaborators in how they see the value of a project developing; hence the value of exploring intermediate points along a spectrum. Dynamic exchange between intermediate points softens the edges of opposition between extremes.
Transactional politics
Alongside ideological politics, we have the prosaic politics of social interactions between institutions, organisations, policy bodies, academic disciplines, professions and service user groups. Negotiating the intricate mechanics of such transactions is necessary to secure and maintain a productive connection between stakeholders. 92,93 Hewison et al. 37 report an initiative that aspired to full engagement with non-academic collaborators,94 but whereby mutually incompatible policies and pressures on employees in the collaborating institutions made this impossible in practice. Subsequently, McCabe et al. 23 developed a typology among ‘contextual factors of partnerships’ in which collaborative structures determine what kinds of knowledge gains can practically be made.
Although the transactional politics of collaboration are usually difficult and demanding, this is sometimes seen as productive and valuable in itself. 95 Klenk and Meehan’s96 critique (environmental science context) of imperatives towards ‘integration’ of stakeholder contributions, which they argue neutralises the critical value of non-academic perspectives, advocates that disparate, incompatible voices should be protected. Such contributions imply a committed disposition in which transactional politics hold the value of co-production, contrasted with a more provisional disposition in which they are a barrier to be negotiated to arrive at expected knowledge products, amalgamation of perspectives, and effective knowledge use.
To be clear, the value of a politics lens on knowledge co-production is not in theoretically settling the political-or-otherwise status of research knowledge. 97 What differentiates styles of knowledge co-production is where the different stakeholders draw the boundaries between knowledge production and politics. Do they encourage a restricted, instrumental political engagement towards a foreseeable output? Do they confidently pursue a political re-ordering of knowledge processes and hierarchies? Or is there some hybrid of these? Whichever they choose, the collaborative political process is made visible, conscious and deliberate, instead of being kept below the threshold of awareness. 21,98 Politics becomes intentionally woven together, in contestable ways, with knowledge.
Domain 2: knowledge
The knowledge domain incorporates perspectives on the outputs of knowledge co-production, and implied positions on the nature of knowledge. Beyond being a pure commodity made for truth’s sake (conventional co-production), knowledge can have utility, transfer and ‘impact’ potential (provisional co-production). Or knowledge can be something through which people become inclusively engaged in social life (moderate co-production), or through which they gain new productive capacities (committed co-production). Knowledge may even enable actors to become empowered (radical co-production). Accordingly, knowledge has different kinds of existence: as an object in itself; as something exchanged or negotiated among those who hold it; as something held communally by ever-changing collections of people; or finally, as a constitutive property of a wider collective group, in a deeper, ongoing and embodied sense.
Output/product
A common framing in knowledge co-production literature is the agenda for research impact,92,95,99,100 reflecting a utilitarian impulse to show use-value and policy relevance. 101 Antonacopoulou102 upheld this view of co-produced knowledge, inviting researchers to pursue delivery that had an impact, explicitly turning away from political preoccupations (a provisional approach). In contrast, Pain et al. 103 (human geography context) critically explored the tensions between impact as an issue of economic accountability and as a matter of social responsibility – both inescapably political concerns. They advocated co-production as a way to ensure socially equitable and ‘radically transformative’ knowledge outputs. 103
Capacity-building (committed) and empowerment (radical style) are also common framings in the literature,40,104–106 whereas others speak of engagement, engaged scholarship and inclusion (a moderate style). 24,107,108 Each of these indicates a subtly different narrative of who and what knowledge is for.
Nature of knowledge
Associated with this array of output purposes are implicit understandings on the nature of knowledge itself, frequently presented through metaphor.
For Rycroft-Malone et al. ,33 the first move of health-care knowledge co-production is to challenge ‘pipeline’ conceptualisations of knowledge, knowledge transfer, implementation, the gap, and the ‘two communities’ model of knowledge production and use. 21 A pipeline conceptualisation imagines knowledge as a thing that must originate on the outside and be transported to the context where it is applied, or as Kitson and Harvey109 see it:
. . . the process by which knowledge moves from where it was first created and refined to where it has to get to in order to make an impact.
To sustain a ‘gap’ conceptualisation, these two places must be different, with knowledge travelling as an object package from one to the other. To discuss knowledge implementation techniques in terms of the success or failure of their transfer to the point of use109,110 is to retain a conventional sense of knowledge as a commodity that exists autonomously and is delivered post production to people and places without altering its nature.
Radical knowledge co-production, rejecting the object-and-transfer conceptualisation, imagines knowledge instead as a valued attribute of people located in time and place, a process performed and embodied, a presence that empowers and includes, a pervasive energy in movement and change, and a collective and communal good. In short, knowledge as a positive mode of human being. 111 For Kothari and Wathen,112 this understanding:
. . . is not just about knowing but encompasses ways of being and relating . . . making space for an additional ‘value-added’ communal perspective.
Between these idealisations is a middle ground of ambivalent metaphors. The idea of knowledge exchange, for example, imagines collaborators each contributing a genre of object-like knowledge to a sharing process that simultaneously creates knowledge anew, collectively. 18 Some emphasise tension in this dialogue, a ‘balancing act between imposing control’ (provisional) and ‘opening up a plurality of voices’ (committed). 113
When knowledge is said to be negotiated in co-production,114 a knowledge object again precedes the interaction, which results in a more diffusely social knowledge (moderate style). However, when there is any seeking of shared wisdom and ‘integrated or transformational understanding’ (committed style – Schuttenberg and Guth115), there is also the possibility of troublesome conflict and re-assertion of power status (provisional),98,114 felt as a ‘need to exercise a stronger voice’. 115
These tensions are political, not merely between related actors, but between perceiving knowledge as an object property held individually, unequal but shared and received, or an elusive and transient presence realised through communion. Terms such as impact, negotiation, exchange and transformation carry variable meanings in the literature, suggesting a range of tangled understandings that might be disaggregated, given the right tools for dialogue.
Domain 3: identity
Politics experienced at the individual level can be conceptualised through identity, both in terms of the roles that participants occupy, and by acknowledging individual feelings, affinities and sensibilities.
We found that roles in co-production might be separate and securely fixed (conventional style), or they might fit together as complementary and negotiable where they meet (provisional style, in which case conflict is more likely found to be counterproductive). Sometimes there is an expectation that roles naturally overlap (moderate style), interfere and contradict (committed style), or disintegrate and multiply (radical style), in which cases conflict may be naturalised and valued as significant.
The individuals involved might be thought by nature to be autonomous, or connected to each other in singular, transactional ways; they might be more interwoven and interdependent; or, in the extreme cases, less clearly separable from each other in terms of the multiple knowledge roles they embody.
In this domain, it is useful to hold in mind some typical characters in narratives of knowledge co-production. The basic players are academic researchers (whose accounts are usually of central interest for academic writers and audiences, even under committed and radical modes of co-production) and non-academic stakeholders, such as (health) professionals, policy-makers and service users (whose accounts rarely surface in enduring forms). Recurring figures include non-academics who gain skills and empowerment from involvement in research,116 researchers who skilfully ‘surf the boundary between ways of knowing’96 and ‘critical friends’. 117,118 ‘Critical friends’ implies researchers who are aligned with non-academic institutions, but remain able to be critical, or non-academics who develop an expert voice and agency in knowledge production by virtue of their insider status. 119
Role
This spectrum spans the ways in which people are understood to occupy their socially designated roles.
If those roles are thought of as naturally ordered, given and fixed to individuals, it indicates a conventional or provisional style in which one simply ‘is’ an academic or non-academic, and remains unproblematically so. If roles become partly negotiable, this typifies moderate co-production. In committed or radical styles, roles become performances, contingently (re)made by people and subject to ongoing change; possibilities arise of people disconnecting from rigidly defined roles, crossing role boundaries and enacting multiple performances, actively and creatively. In recognising an underlying common humanness at this end of the spectrum, researchers can, as Greenhalgh et al. 95 note:
. . . view research as a creative endeavour, with strong links to design and the human imagination . . . [placing] individual experience at the heart of this creative design effort.
Klenk and Wyatt120 (environmental-economics context) similarly advocate ‘engagement with partners that is creative and transformative rather than mainly informative’, suggesting experimentation with role boundaries, and scepticism of pre-conceived roles and duties.
Fenge et al. 121 (health and social care context) describe knowledge co-production ‘involving lay people, volunteers, service users and carers in scholarly writing and dissemination’, exploring how academia can embrace the expertise of these non-academics. Usually this suggests a single identity, such as a patient, professional or health-care policy-maker, that serves as a warrant for involvement, but becomes plural as collaborators contribute, not just information, but part of their personhood to knowledge-making. 122
Almost always, original role markers remain meaningful. The truly radical possibility is to abandon them entirely and see all collaborators as people originally equal, communally connected through their shared interest.
Individuals
Collaborative work can place demands on individuals. We see this reflected in O’Hare et al. ’s118 interest in ‘coping strategies’ for critical tensions, Orr and Bennett’s123 reflections on their ‘at times disturbing and debilitating’ experiences of co-production, and Vindrola-Padros et al. ’s65 account of researcher-in-residence strategies for facing challenges to their professional identity. This implies an individual consciousness that is separable from the role a participant occupies and is able to reflect on competing demands.
For researchers, knowledge co-production brings perceived risks, such as dominance by particular stakeholders, eroded independence and credibility, interpersonal conflict, burnout and stress, and damaged careers. 82 These threats relate to the individual status of the researcher, which, under the individualistic model of personal worth dominant in academic research, is vulnerable.
For non-academics, collaboration is largely expected to be an edifying and empowering process. By challenging the individualistic academic culture and directly confronting knowledge inequalities and cultural boundaries, it could be seen to ‘democratise knowledge’. 124 But such a framing, although notionally moving non-academic individuals into positions of power, may also place considerable responsibilities and expectations on them.
Underlying such anxieties are equivocations over the nature of people as reflexive individuals. If people are thought to be comfortable as autonomous beings (conventional style) then provisional or moderate ways can be found to account for their connections, but more committed or radical approaches are problematic. If the natural state of people is thought to be as communal, interconnected and multiply oriented beings, then the challenges of more radical co-production may be considered worthwhile and intrinsically valuable for the way they decentre individualistic orthodoxies.
This ontology of individuals meshes with an ontology of roles as fixed and stable (if restrictive) at one extreme, or mutable and multiple (allowing for creativity, if sometimes disorienting) at the other. The space between has possibilities for dialogue and the ongoing reconstruction of roles, and of the reshaping of the identities of the individuals occupying those roles.
Domain 4: space–time
Time and space are highly visible points of interest in knowledge co-production literature. Conventionally, time is imagined in a linear way, with knowledge first produced, then moved into policy or practice settings; provisional arrangements may be made around a variable but linear process of production and dissemination. Moving along this spectrum, time can enfold different collaborative stages that repeat and overlap or become more consciously iterative. In the radical ideal, ongoing production and ongoing application are in a mutually constitutive continuous cycle of renewal.
Space may be strictly divided between separate research and practice locations, or attention may be given to in-between, liminal meeting points where institutions begin to overlap. A blurring of boundaries and conscious challenging of spatial designations characterise more committed and radical forms of co-production.
Time
Time is crucially important in knowledge co-production. With non-academic contributors, time is usually prioritised by their primary identities (as managers, practitioners, etc.); negotiation is often necessary to divert that time towards knowledge collaboration. Co-ordinating the schedules of diverse stakeholders for meetings is a basic difficulty. 37 Supposing collaborators are brought together in a timely way, writers often emphasise the long time required to nurture collaboration: time invested in building trusting relationships and accumulating confidence among collaborators, and time taken to agree and implement knowledge-making plans, with the implication that the added value of outputs should correspond to added time inputs. Lehmann and Gilson125 speak on behalf of many co-producing researchers:
We spent an awful lot of time in meetings, formal and informal, big and small, in cycles of conversations to plan and implement strands of work, reflect on their outcomes and replan.
These cycles of conversations allude to a characteristic aspect of committed and radical styles: the iterative nature of knowledge co-production, in which different stages of the research process overlap more than in orthodox research – ‘planning, execution, dissemination and implementation are not separate and linear phases but interwoven’. 95
This contrasts also with provisional co-production in which consultations at specific points punctuate the path of knowledge into practice. A moderate style of co-production signifies ambiguity and overlap between pre-made knowledge being moved into application, and an ongoing process of making and modifying knowledge at the same time as ‘using’ it. 107
Space
In the conventional ideal, a ‘gap’8,78 envisages a one-way flow of knowledge in space from sites of production to adoption and routine use. In the radical ideal, knowledge attaches to communities in places, so is made just as it is inhabited and enacted, in a closed, reflexively aware loop. In between these extremes are a range of possibilities for co-production embedded in space and place.
Ideas about the in-between spaces that separate and connect institutions are ever present in knowledge co-production. These liminal interstices are valuable, for example, in creating ‘a shared space where multiple communities can come together’,23 and where collaborators are ‘able to challenge ideas and existing policies or entrenched beliefs’126 in ways otherwise not possible.
Rather than refer directly to specific physical sites important for knowledge co-production, writers sometimes evoked space through social-psychological metaphors. They wrote of space beyond hierarchies and boundaries; indeterminate social space; permeable space;114 exploratory space;79 nurturing, safe and inclusive space;127 space ‘both embedded in and insulated from research and practice’ and spaces ‘open, autonomous, unpredictable, dynamic, reflexive, and shared’;128 and spaces of ‘dialogic co-inquiry’ and the ‘cramped’ space of co-production. 40
Across the intermediate spectrum of spatial designations, these metaphors range from those that look for liminal gaps between original single-purpose spaces (provisional), those that bring different purposes to coincide and overlap in one space (moderate), and those that challenge and blur the boundaries between spaces (committed).
All of these pragmatically repurpose and reinterpret the physicality of extant institutions, whereas, in radical knowledge co-production, there is an acknowledged political awareness in the redefining of spaces. Bremer and Funtowicz129 draw on the political geography of Doreen Massey to highlight this awareness of distinct narratives of space that ‘coexist, meet up, affect each other, come into conflict or cooperation’. For many collaborative purposes, however, a language of spanning and blurring boundaries, temporarily displacing orthodox routines and interactions, and flexibly redrawing the borders between institutions – a metaphorical language of space – is found sufficient.
Domain 5: aesthetics
Knowledge co-production involves an aesthetics of attitudes, dispositions and emotional attunement that resonates across domains. Preferences for simplicity, rigidity and predictability in more conventional forms merge into a tolerance and interest in social complexity in intermediate forms of knowledge co-production. Beyond this, there is a positive solicitation of emergent outcomes, and an attraction to collective knowledge states that cannot be foreseen (implied in more radical approaches).
Alongside this, we find different valuations and language around emotions. Emotions can be marginalised, or a manageable complication to knowledge mobilisation and application; can be a complementary and useful form of rationality; or can be of foundational value in themselves as part of knowledge-making processes. At the radical extreme, the emotion/rationality distinction disappears, as communal production becomes shared, embodied and affect infused.
Preferences
Preferences, affinities and aversions in co-production writing are easily detected in the literature we reviewed, although not always so openly acknowledged. Our interpretation brings these recurring themes into open conversation. For instance, appreciative considerations of multifaceted, evolving connections between co-producing individuals and institutions suggest an ethic of connectedness and mutual responsibility between academia and other social sectors. 130 This leads away from a simple schema of entities with isolated purposes towards complexity of social patterns and trajectories. 131 A complex system is more likely to appear untidy, or messy, and lead to outcomes that are unforeseeable or not predictable, and is often thought to be more valuable for that.
Borg et al. ,132 writing on ‘valuing uncertainty’, tell of attempts to explore multifaceted realities through complex processes that ‘can be intense, unpredictable and at times rather chaotic’. Interest in complexity,21,133,134 in messiness105,135 and tolerance of messiness,33 in plurality and mutability136 and unpredictability95,128 is woven through narratives of knowledge co-production. These tropes create a graded succession, from knowledge transfer that is accountable and predictable (provisional), knowledge exchange that is attentive to complexity (moderate), and co-productions seeking creativity and social innovation (committed). Radical intentions are signalled by a challenge and subversion of orthodox constructions and a scepticism of norms conventionally made to appear simple, in which messy boundary work is moved backstage, out of view. 137,138
Emotions
Human actors embedded in messy realities may not be well placed to grasp and govern their situations in the manner of singular purposive and rational minds holding unitary object knowledge. They must find ways to create collective wisdom, drawing on diverse sources and expressions of connectedness to the world,139 indicating the importance of the ‘more-than-rational’. 139 Orientation to emotional knowledge and things known instinctively through experience,140 as well as attention to shared feelings and affect,141 are often active in knowledge co-production.
One example of emotionally rich language is the motif of ‘nurture’ common in this literature, whether used appreciatively102,112 or sceptically. 38 ‘Trust’ is also usually cited as a foundational condition of successful partnership. 142–144 The nature and conditions of this trust may suggest a strategic management and positive use of emotion, for example when Jagosh et al. 116 carefully engaged community members ‘who were already known to be knowledgeable, sincere, compassionate, and understanding’, so that others would ‘feel safe participating’. In other cases, emotional currents are detectable as forces motivating co-production. For instance, when Klenk et al. 145 envisage knowledge practices that ‘move and affect not only present concerns but also future solutions’, hope is a foundational emotion for energising the project.
Attunement to emotional knowledge does not imply positive emotional states. More often than being joyous, the emotional relations of knowledge co-production are fraught and difficult. What distinguishes styles of co-production is the extent to which emotions are given legitimacy in juxtaposition with rational object knowledge. In moderate styles of co-production, emotions and rationality are imagined to complement one another in working towards consensus or productive difference. In committed knowledge co-production, emotions may be foregrounded as sources of knowledge, emphasising the human and creative processes of project design. In radical knowledge production, mirroring the collapse of a knowledge–politics binary, the dichotomy of reason and emotion is more unstable. Rational and affective streams of consciousness are woven together into a thinking–feeling fabric of being.
Representing the conceptual framework
To visualise the five-domain framework, we created a diagram (Figure 3) in which co-production styles appear as concentric circles, and domains and subthemes as pairs of ellipses arranged around a central locus. An arrangement with conventional research on the outside and radical co-production at the centre evokes the impression of distancing and separateness in the conventional style, and of closeness and intensity in radical co-production. The ellipses representing each subtheme convey a dynamic sense of motion, we hope, as projects and collaborators may fluctuate between possibilities.
FIGURE 3.
Domains and subthemes of knowledge co-production.
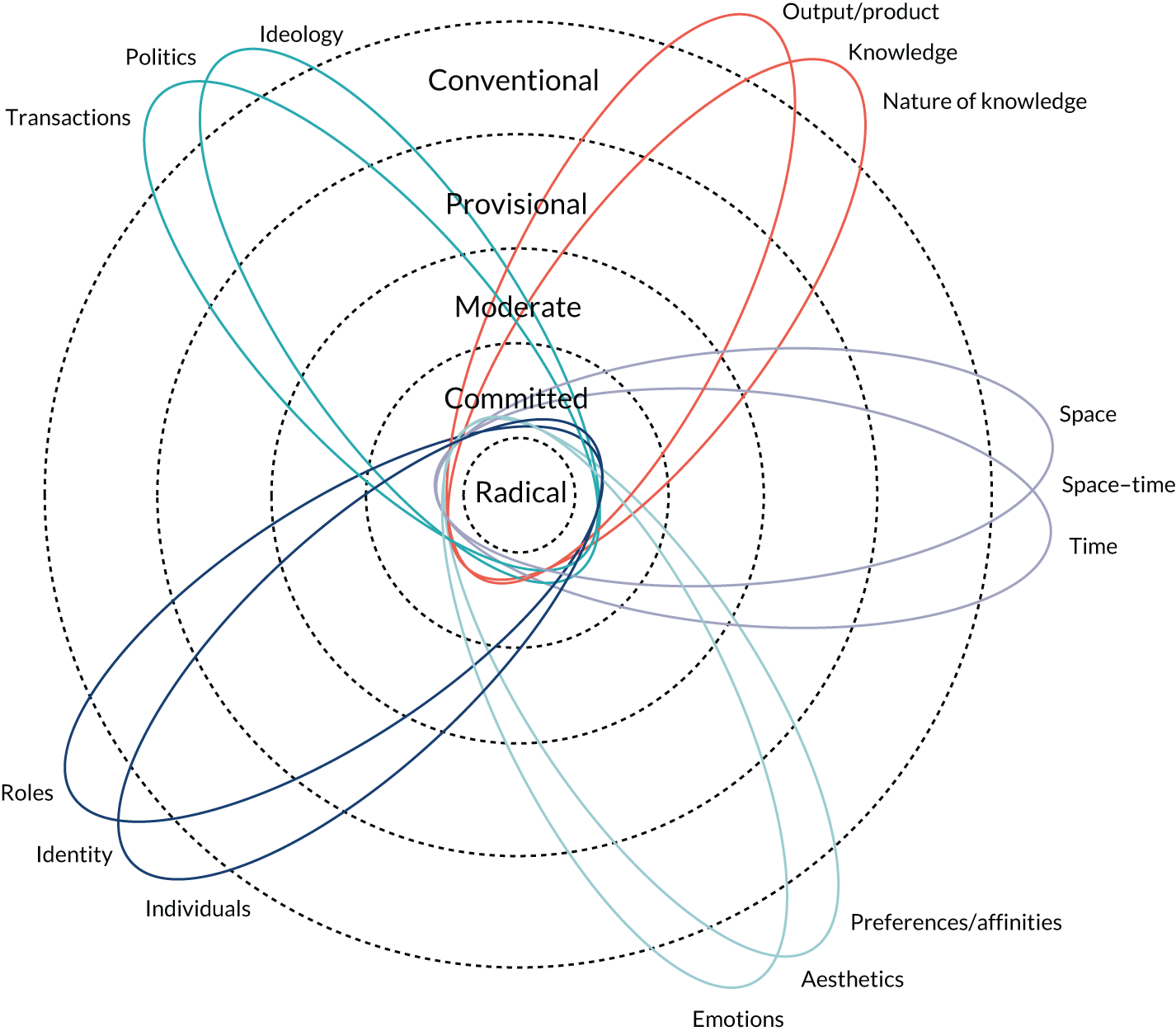
Table 2 characterises each marker point along the subthematic spectrums with a word or two, creating a grid of possibilities for co-production projects that can be read horizontally (to see progression across spectrums) or vertically (to see the properties of each style). Gradations in shading suggest the idea of blending between styles. A perspective that is in some ways committed, for example, could be, in other ways, radical or moderate, but is less likely provisional or conventional, if our domains are a sound analysis of thinking around co-production. However, all approaches are legitimate; dissonance between aspects of a project may indicate tension and dysfunctionality, but may also reflect different goals and intentions co-existing within a project, or changes in a project’s character over time. To emphasise, we propose these labels of recurring patterns to be descriptive, not normative.
| Spectrum | Style of knowledge co-production characterised as | ||||
|---|---|---|---|---|---|
| Conventional | Provisional | Moderate | Committed | Radical | |
| Politics spectrums | |||||
| Ideology is | Apolitical | Utilitarian | Engaged | Transformative | Emancipatory |
| Transactional politics are | Pollution | Necessary | Valuable | Essential/essence | All-encompassing |
| Knowledge spectrums | |||||
| Output/product is | Pure knowledge | Application, impact | Engagement, inclusivity | Process, capacity | Empowerment |
| The nature of knowledge is | Object | Transactional | Negotiated, exchanged | Communal | Embodied being |
| Identity spectrums | |||||
| Roles are | Separate, fixed | Complementary | Consensual, negotiable | Conflictual, problematic | Unstable, multiple |
| Individuals are | Autonomous | Connected | Interwoven | Communitarian | Inseparable |
| Space–time spectrums | |||||
| Time is | Linear | Variable-linear | Overlapping | Iterative | Cyclical |
| Space is | Separate | Liminal | Overlapping | Blurred | Contestable, politicised |
| Aesthetic spectrums | |||||
| Preferences are | Simple | Predictable | Complex | Emergent | Unforeseeable, subverted |
| Emotions are | Marginal | Manageable | Informative | Foundational | Ubiquitous |
Concluding remarks
Through our narrative literature review and detailed framework analysis, we have offered some conceptual categories, language and metaphors for articulating and disaggregating knowledge co-production aims and processes. These were derived from academic literature on knowledge co-production from a wide range of fields and traditions. We have provided a theoretically rich, yet robust and pragmatic, way of understanding and talking about the different aspects of knowledge co-production.
Conceptually, the framework explores five domains of meaning seen repeatedly in the literature, each with two distinct subthemes. Representing these on a spectrum, from more conventional knowledge production (shared subsequent to being created) to more committed or radical co-production, has allowed us to see the variegated nature of co-production possibilities. Should this way of mapping the field take hold, there is the possibility of greater depth and nuance to conceptual conversations, and more precision in theoretically informed empirical explorations of co-production practices.
More practically, the framework provides a coherent and consistent language for surfacing assumptions, sharing perspectives and making sense of difference. Therefore, we hope that knowledge collaborators, such as those embarking on embedded research initiatives, will use the framework to articulate their views on shared projects, both at inception and as they evolve. Primarily, we hope they will use it to identify their own and each other’s positions, to better communicate around and organise projects, and hence to be more successful in delivering those projects to meet various goals and outputs.
Of course, such a process may be as revealing of dissonance and divergence as alignment. For example, any specific project may have aspects that suggest different points on different spectrums at the same time. Sometimes such differences could promote productive tensions; at other times they may be sources of conflict and misunderstanding. Moreover, dynamic change, not static positioning, is to be expected: projects may shift between points on the various spectrums over time. The language and labels we have presented may thus be useful for analysing coherence or incongruence, and for articulating and examining dynamic shifts.
Through this review work, we have revealed the considerable complexity, nuance and contestability of simple ideas of knowledge co-production. But we have done so in a way that provides a practical framework for interrogating the idea and translating its aims and methods into practice. The second part of workstream 1 (and the second literature review) moves, in turn, to unpack ideas of embedded research practice (see Chapter 3). In this way (through these two reviews combined), we can get a better conceptual grasp of the diverse models of embedded knowledge co-production that lie at the heart of this project. The nature and findings from that second literature review are presented next.
Chapter 3 Exploring ideas of embeddedness
Text throughout this chapter has been reproduced with permission from Ward et al. 146 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Introduction
As noted in Chapter 1, and in line with the growing interest in knowledge co-production explored in Chapter 2, there has been a recent surge of interest in embedded approaches to research, particularly within health care. These have tended to focus on developing more productive ongoing relationships and increased social interaction between researchers and those in organisations. Examples include the incorporation of evidence-generating organisations into the wider health service delivery system,147,148 research–practice partnerships149 and local participatory research initiatives. 150
An increasingly popular form of embedded research involves physically locating researchers in non-academic organisations. In this incarnation, embeddedness refers to researchers being ‘in residence’ in the organisation,47,151 and ‘research’ is used to denote at least three things: the knowledge and expertise that researchers bring with them, the research-based knowledge that they broker into the organisation, and the new insights that are developed from data gathered and interpreted in situ. The negotiation of expertise, the contextualising of external knowledge and the co-production of new understandings are often key tenets of this type of initiative, leading to its comparison with the notion of ‘engaged scholarship’. 65,152,153 This is perceived to lead to greater organisational ownership of the knowledge being produced, ultimately leading to its incorporation into the work of the organisation. 65,154
A growing literature has started to highlight the multiple challenges that face embedded researchers and those with whom they work. 155,156 These include the challenges of establishing and maintaining relationships in the face of busy work schedules and tightly controlled service delivery spaces, defining and adapting the scope of the knowledge production work being undertaken, and maintaining an academic identity. 65 The literature has also started to highlight the aspects of an embedded research initiative that facilitate change, including trusting relationships, shared-decision-making, clear communication about the focus and function of the embedded researcher’s role and negotiating the different understandings that those in the organisation may have of the researcher’s role. 152
This growing literature largely focuses on descriptions of individual initiatives and/or the experiences of embedded researchers themselves, taking only an overview of the principles of embedded research. Reading across this literature, there are signs that embedded research initiatives are expressed and conducted very differently. However, there has been relatively little in the way of analysis of this diversity. This has resulted in a lack of understanding about what initiatives look like in practice, how and why they are designed as they are, and the implications of different variants. Workstreams 1 and 2 aimed to address such gaps.
Here we present the results of the second literature review carried out under workstream 1, identifying and analysing the published literature on embedded research initiatives as they have been put into operation. These findings are then combined with the scoping work of workstream 2, which sought to identify and analyse extant embedded schemes in health-related settings in the UK. In combing insights from the published literature and practical UK experience in health care, we have been able to outline 10 themes that encapsulate the key features of embedded research initiatives. These form a practical framework to understand the design features of embedded research initiatives.
Methods
This work comprised three parts spread across workstreams 1 and 2. The first was a review of the theoretical and empirical literatures on embedded research across different disciplines and settings. The articles included for analysis are listed in full in Report Supplementary Material 2. The second was a scoping exercise of embedded research initiatives in operation specifically in health settings across the UK. The third was a co-production workshop with embedded researchers and their managers. The literature review and scoping exercise ran in parallel, being mutually informative; the workshop was an integral part of the engagement strategy (workstream 4) and allowed refinement and some face validation of the emergent findings.
Assembling the published literature
For our review of the embedded research literature, we used a modified CLUSTER (Citations, Lead authors, Unpublished materials, Google Scholar, Theories, Early examples and Related projects) method. 157 This approach to systematic reviews of complex interventions was developed as a way of providing both contextual thickness (an adequate description of the intervention and its context) and conceptual richness (the theoretical and conceptual development that explains how an intervention is supposed to work). The developers of the method argue that this level of detail is unlikely to be present in a single publication, but may be present in a ‘cluster’ of related publications and materials. We reasoned that this method would help us better understand the intent, structures and processes underpinning embedded research initiatives. The aspects of the method that we used are outlined in Figure 4, adapted from Booth et al. 157
FIGURE 4.
Aspects of the CLUSTER method used in our study. This figure was created using the logic and approach as laid out in Booth et al. 157 Pearl citation, a key paper on an identifiable initiative that acts as a retrieval point for related outputs that may help to explicate theory or understand context; cluster search, a systematic attempt using a variety of search techniques to identify papers or other research outputs that relate to a pearl citation.
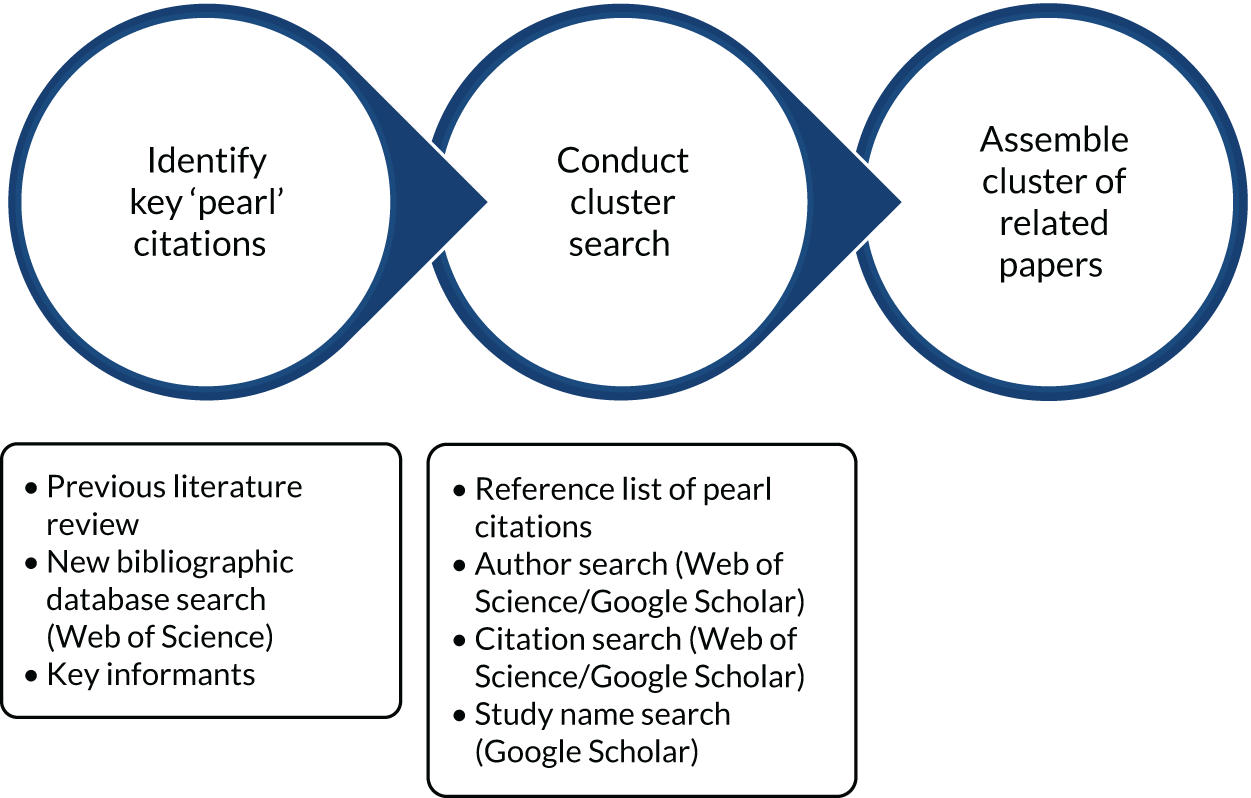
We began by assembling a database of 45 potential ‘pearl’ citations (papers focusing on an identifiable embedded research initiative; see Figure 4) from different disciplines including education, health and urban development. These citations were sourced from a review conducted by members of the wider team in 2015,158 from database searches between that review and January 2018, and through personal contact with key informants.
We discarded those citations that did not focus on a specific embedded research initiative, and then grouped together those that focused on the same initiative and/or involved the same authors. This resulted in 26 distinct ‘clusters’ of papers. We then used forwards and backwards citation-tracing and author searches to identify related materials to add depth to each cluster. This resulted in a total of 47 papers across the 26 clusters.
Scoping extant schemes in health and health care
For our scoping exercise (workstream 2), we focused on embedded research initiatives in operation in health settings across the UK. These settings included public, private and voluntary sector organisations with a role to play in commissioning and/or delivering health services. We used our network of contacts; requests via mailing lists such as the NHS Contact, Help, Advice and Information Network (CHAIN); and posts on Twitter to identify potential embedded research initiatives. We kept the definition broad at this stage to capture initiatives described as embedded and researchers who defined themselves as embedded.
We identified a total of 90 potential embedded research initiatives. We then used three criteria to determine which were of most interest and relevance to this study. These focused on identity (were the researchers in the initiative trained and/or experienced in research and were they seen as a researcher by those in the health setting?), knowledge production (was the initiative designed to produce knowledge that would have direct relevance and application to the organisation?) and immersion (were the researchers physically located in the health setting for a significant portion of their working week?). These enabled us to narrow our focus to 45 initiatives, a summary of which can be seen in Tables 3 and 4.
| UK location | Health service setting | Duration | Employment arrangements |
|---|---|---|---|
|
|
|
|
| Initiative ID (anonymised) | Setting | Scale | Time frame | Location |
|---|---|---|---|---|
| Alliston | Community | Project | 12–24 months | South East |
| Amhurst | Community | Project | ≥ 5 years | Yorkshire |
| Athelmer | Multiple | Portfolio | ≥ 5 years | Wales |
| Barrington | Acute | Portfolio | ≥ 5 years | Midlands |
| Battleford | Primary | Portfolio | 2–4 years | South West |
| Bayfield | Community | Portfolio | ≥ 5 years | North East |
| Bonnyville | Acute | Portfolio | ≥ 5 years | Midlands |
| Bridgetown | Multiple | Portfolio | 2–4 years | Scotland |
| Broderick | Acute | Portfolio | ≥ 5 years | South East |
| Chipman | Community | Portfolio | 12–24 months | South East |
| Coaldale | Community | Project | 2–4 years | South East |
| Coxheath | Acute | Portfolio | ≥ 5 years | South East |
| Crofton | Community | Portfolio | 2–4 years | East |
| Dawson | Community | Project | 12–24 months | South East |
| Evansville | Acute | Portfolio | 2–4 years | South East |
| Ferland | Acute | Portfolio | 2–4 years | Midlands |
| Finmoore | Primary | Portfolio | 2–4 years | Wales |
| Fruitvale | Acute | Portfolio | 2–4 years | South East |
| Fulford | Community | Portfolio | ≥ 5 years | Midlands |
| Gardenton | Community | Portfolio | 2–4 years | Midlands |
| Garrick | Multiple | Portfolio | 2–4 years | Scotland |
| Geraldton | Multiple | Portfolio | Up to 12 months | Wales |
| Glenburnie | Primary | Project | 12–24 months | North West |
| Glidden | Community | Portfolio | 2–4 years | South East |
| Goderich | Community | Portfolio | 2–4 years | North East |
| Goldpines | Primary | Project | 12–24 months | South East |
| Greenway | Multiple | Portfolio | 2–4 years | South East |
| Hillmond | Acute | Project | 12–24 months | Yorkshire |
| Kisbey | Multiple | Portfolio | 2–4 years | Midlands |
| Lawrencetown | Primary | Project | Up to 12 months | South East |
| Oakburn | Community | Project | 12–24 months | Midlands |
| Pinebluff | Community | Project | 12–24 months | South East |
| Porter | Primary | Portfolio | ≥ 5 years | Midlands |
| Reaburn | Acute | Portfolio | 2–4 years | South East |
| Retlaw | Acute | Portfolio | 2–4 years | South West |
| Rockland | Acute | Portfolio | 2–4 years | East |
| Rosetown | Primary | Project | 2–4 years | South East |
| Sherwood Park | Acute | Project | 12–24 months | South East |
| Silverdale | Primary | Portfolio | Up to 12 months | South West |
| St Thomas | Acute | Portfolio | 12–24 months | North East |
| Streetsville | Community | Portfolio | ≥ 5 years | South West |
| Summerside | Community | Portfolio | 2–4 years | Wales |
| Usk | Community | Portfolio | ≥ 5 years | South West |
| Waterford | Acute | Portfolio | 2–4 years | Midlands |
| Weedon | Primary | Project | ≥ 5 years | South West |
For each initiative, we gathered publicly available information if possible (e.g. from websites). Each initiative was asked to share internal documents including role descriptions, strategy documents and reports. In this way, we constructed a database of documentation on each of these schemes (a total of 236 source items). To deepen our understanding of the varying types of initiatives, we also conducted telephone interviews with individuals from 12 initiatives, selected on the basis of diversity, taking into account their setting, longevity, structural features and overall purpose. When possible, we interviewed both an embedded researcher and the manager or instigator of the initiative, conducting 17 interviews in total. Interviews focused on adding depth to our understanding of the intent, structure and processes associated with embedded research initiatives, with the interview guide being developed from the evolving literature analysis.
Analysing the assembled materials
We used an inductive and iterative analysis process to bring together the embedded research literature and scoping materials. We began with a detailed reading of the clusters identified during the literature review, concentrating on extracting definitions, concepts and working theories associated with each cluster. Through ongoing discussion between team members, we developed provisional and emergent themes. Next, we applied these themes to materials gathered during the scoping exercise, using them to produce detailed analytical descriptions of each initiative. During this process, we sometimes identified additional themes or merged or disaggregated others (going back to the literature clusters as necessary), until the analytic descriptions gradually stabilised. Finally, we coded the interview data using the same themes, while being alert to the identification of further themes or destabilisation of existing ones. Throughout the analysis process, we compared and discussed the coded materials and descriptions, with repeated and intensive discussion across a core group (VW, TT, BR and HD) and broader sense-testing across the whole project team. Over time, we settled on a set of 10 themes, and a finer-grained set of subthemes, that seemed to represent the key features of embedded research initiatives.
Testing the emergent findings with embedded research actors
The third and final part of this study involved testing and validating the themes and putting them into an overarching framework. We held a day-long co-production workshop with embedded researchers and their managers (n = 18) that made use of a range of creative activities and was facilitated by an experienced team of researchers in design and health (see Acknowledgements). Activities included commenting and adding thoughts to postcards representing each of the themes, discussing the relative priority of each theme, and building physical metaphor models of the themes and their interconnections. Workshop participants confirmed and validated the importance and relevance of all 10 themes and suggested ways of linking the themes in a single metaphor for an embedded research initiative. This was used subsequently to derive practical guidance and web-based tools and resources for those designing or analysing embedded initiatives (see Chapters 6 and 7).
Findings
The themes and subthemes are summarised in Table 5, grouped into three categories: intent, structure and processes. Although there are some overlaps, resonances and implications that run across the themes, they have proved robust in conversations within and beyond the research team, and have survived repeated testing against the source materials.
| Category | Theme | Subthemes |
|---|---|---|
| Intent | Intended outcomes | Knowledge outcomes |
| Capacity outcomes | ||
| Reputational outcomes | ||
| Power dynamics | Control | |
| Contribution | ||
| Gain | ||
| Intended effect on power dynamics | ||
| Structure | Scale | Scale of work |
| Timescale | ||
| Team size and composition | ||
| Involvement | Who is involved | |
| Scale and location of involvement | ||
| Type of involvement | ||
| Involvement mechanisms | ||
| Proximity | Location | |
| Intensity | ||
| Visibility | ||
| Belonging | Boundary management | |
| Contractual arrangements | ||
| Informal arrangements | ||
| Process | Functional activities | Range of activities |
| Purpose of activities | ||
| Training and support for activities | ||
| Skill and expertise | Topic specific | |
| Methodological | ||
| Interpersonal | ||
| Relational roles | Level of interdependence | |
| Relational stance | ||
| Type of input | ||
| Learning mechanisms | Performance monitoring | |
| Formal evaluation | ||
| Informal learning and reflection |
In the following sections, we describe each theme and associated subthemes in some detail, providing evidence from the various source materials (specific initiatives have been disguised by using coded names; see Table 4 for brief information on each initiative).
The intent of embedded research initiatives
Across the data, we were able to identify two themes relating to the underlying intent of embedded research initiatives: the intended outcomes and the nature of the power dynamics. The first of these is often to the fore in discussions about embedded research, whereas the latter often remains obscured. These are now explored in turn.
Intended outcomes
The primary explicit focus, or intent, for many initiatives was to produce knowledge that would be beneficial within the health-care organisation. This knowledge included both local insights (generated through local service evaluation, service improvement or practice development activities) and more generalisable knowledge (generated through larger-scale, formalised research activities and aimed at wider peer-reviewed promulgation). Some initiatives aimed to produce both forms of knowledge across a portfolio of different projects:
We just call it research with a big R or research with a small r. So, research with a big R is probably funded . . . The small-r stuff is more clinician generated . . . I don’t see it as a hierarchy, I almost see it as a journey, a pathway.
Embedded researcher, Crofton
Many initiatives also intended to bring about outcomes related to the capacity and capability of the individuals and organisations involved. These included the capacity to produce knowledge, to deliver services and to generate income:
The RiR [researcher-in-residence] role supports scale-up and spread of good practice, in order to share benefits of activity improvements.
Finmoore documents
The role is expected to result in:
The building of a culture in the locality which values the contribution of participatory evaluation of complex improvement programmes.
The building of local capacity and capability for critical evaluation.
Goldpines documents
Interestingly, the focus of such capacity-building activity was predominantly on the health service setting, rather than the academics and their organisations.
Some initiatives focused additionally on the reputational benefits of embedded research. 159 These included access to and involvement in large-scale change or research projects, the number of publications arising from an initiative, and increased or continuing funding for research and/or service delivery (which could stem from being seen to be involved in an initiative or from the knowledge being generated by an initiative):
They have used every bit [of evidence] that we’ve generated, and all of the documents that we’ve produced sit proudly in the CEO’s [chief executive officer’s] office and they’re given out at all of the events. So they do really value this as a, almost like a commodity . . . It raises the profile of the organisation.
Embedded research manager, Streetsville
Power dynamics
As with many schemes that focus on the persistent gap between research and practice, embedded research initiatives often addressed power dynamics, sometimes explicitly and proactively or, perhaps more often, implicitly and reactively. Duggan155 speaks to this tension when he cites Cheek:160 ‘Taking money from a sponsor is not a neutral activity; it links the researcher and research inexorably with the values of that funder.’. From our reading of the source materials, two aspects of power (who and what) seemed to be attached to three different facets of the initiative (control, contribution and gain). The concerns, then, were often about who is in control of the initiative, and what aspects of it are they in control of; who contributes to the initiative, and what do they contribute; and who benefits or gains from the initiative, and what are these benefits?
The first part (i.e. who is in control, contributes and gains?) tended to be reflected in the structural arrangements of an initiative, but was rarely discussed openly by our interviewees or in the literature. Those involved in initiatives appeared to be more cognisant of the second part of these power-related subthemes (i.e. what is being controlled, contributed and gained):
Successful research–practice partnerships require co-contribution of resources if the partnerships are to endure . . . financial and in-kind contributions made by both parties . . . demonstrated commitment to the partnership and the value of its outcomes.
Wolfenden et al. 149
A further way in which power dynamics played out was in relation to the intended effect of the initiative on the traditional roles ascribed to academia and practice, whereby academics were conceived as knowledge producers, and practitioners as knowledge consumers. Many initiatives sought to influence not only these epistemic positions, but also those found in health-care practice itself (e.g. between different groups of health-care professionals):
One of the things that I’ve ended up being is this kind of weirdly passionate advocate revolutionary on behalf of nurses – because I just think that they’re treated like shit basically. And clinical teams talk a big game about being this great high-functioning team, but they don’t really mean it – they don’t really treat nurses’ perspectives or admin[istrators’] perspectives, or anyone who’s not a consultant’s perspective as [being as] valid as their own. And I’ve ended up fighting for that.
Embedded researcher, Broderick
Or as Cunliffe and Scaratti153 noted:
While the Board might have invited the researchers in as ‘experts’, the researchers were keen to renegotiate that power relationship by acknowledging the expertise and situated knowledge of all participants.
However, actively disrupting power dynamics was rarely the explicit intention of initiatives. Although some sought to challenge power dynamics by bringing epistemic differences and other inequalities into focus, others sought to rebalance them by blurring roles and boundaries (e.g. by involving health-care staff in collecting and analysing data). Still others sought to maintain or bolster traditional roles and relationships, or simply left these unaddressed. In fact, many of our interviewees were reluctant to discuss power dynamics, or explicitly downplayed their relevance, and often seemed to have given these concerns little or no consideration:
The main driver especially for my managers is just improving clinical services . . . I don’t think [the power dynamics] really comes into anyone’s thought processes.
Embedded researcher, Barrington
Our workshop participants, in contrast, suggested that power dynamics were an emotive and often painful issue for those involved in embedded research initiatives, using words such as ‘emotion fuelled’, ‘tension’ and ‘frustrating’ when reflecting on this theme. Such feelings were also evident in the literature, such as when Hackett and Rhoten161 reflect on their ability (or lack thereof) to speak of their findings. Further discussion revealed that it was precisely when power dynamics were hidden or unacknowledged that significant disruption and frustration were experienced by those involved in the initiative.
The structure of embedded research initiatives
As outlined in Tables 3 and 4, the on-the-ground initiatives that we identified were located in different institutional settings and structured in diverse ways; such structural diversity was also seen in the literature. We were able to draw out four themes that represented the various structural features of embedded research initiatives: scale, involvement, proximity and belonging.
Scale
The scale at which embedded research initiatives were operating was a notable structural feature across the data. This comprised the scale of the work undertaken, the timescale of the initiative, and the size and composition of the embedded research team.
Early examples of embedded research initiatives in health-care settings tended to be relatively small in scale and short lived,151 often focusing on well-defined projects such as service evaluations. 64 Although we found examples of such single-focus, time-limited initiatives, many of those uncovered more recently had wider interests and/or a much longer time frame (over one-quarter had endured for ≥ 5 years; see Table 3). Moreover, some initiatives comprised a portfolio of defined projects, whereas others were more emergent:
This document will not establish the scope of the work and specific project areas . . . This may enable the role to be deployed in a range of settings, meeting the demands and needs of front-line services.
Finmoore documents
Much of the embedded research literature focuses on the challenges associated with performing the role of an embedded researcher and the need for ongoing support and mentoring. 63,155,156 Many of these observations stem from initiatives comprising an individual researcher working in a health services setting. Although our scoping exercise found examples of such initiatives, it also identified instances of embedded teams of researchers. 162,163 Our workshop participants suggested that multidisciplinary embedded research teams were particularly important for addressing the complex issues and problems that face health-care organisations.
Involvement
Another important structural feature of embedded research was the involvement of various actors within the initiative. We sought to establish whether or not embedded research initiatives involved people other than those researchers and health service staff working within them (e.g. going wider to include patients and members of the public) and, if so, how their involvement was facilitated and managed. From this, we developed four subthemes: who is involved in the embedded research initiative, the scale and location of their involvement, the activities they are involved in and the mechanisms for their involvement.
Relatively few initiatives were clear about the involvement of patients and members of the public in their work, and published accounts sometimes point to dissonance between intended and actual patient involvement. 64,150,153 Of those that did discuss this aspect, the majority limited involvement to the specific knowledge work being undertaken in the initiative (e.g. a well-bounded service evaluation or improvement project), rather than involving people in the design or operation of the embedded research initiative itself:
We recruited a service user partner to the evaluation team . . . If I’m going to be honest, I don’t think I would describe her as being involved in my role – more on the project.
Embedded researcher, Goldpines
Although rarely involving patients and members of the public, some initiatives did involve a wider range of stakeholders in activities, such as advisory groups. As with patients and members of the public, however, activities were also more likely to relate to the work being undertaken by the embedded researchers, rather than the conceptualisation or conduct of the initiative as a whole.
Proximity
Given the focus on researcher immersion as one selection criterion for initiatives, and the importance placed on this in the literature, we identified researcher proximity as a key structural feature. We did, however, identify three somewhat distinct ways in which immersion or proximity could play out in practice: through physical location, intensity and visibility.
Although seen as a key enabler of embedded research, the physical location of the researcher varied across initiatives and was not always a straightforward decision for many. Initiatives that comprised a portfolio of projects, or were more emergent in nature, faced decisions about where and with whom the researchers should be located, what spaces they would have access to and whether they would be working at a single location or across multiple spaces:
I am evaluating the [area-wide multispecialty] programme, a partnership of six organisations representing health, social and voluntary care . . . Challenges include: where am I embedded? In a team? Or in the space between strategy and delivery?
Goldpines documents
The intensity of contact between the researcher and those in the health-care setting was also variable across initiatives. Although documents from many initiatives showed a clear expectation about the proportion of researcher time to be spent in the health-care setting, these proportions ranged from 20% to 100%. Regardless of these documented expectations, the intensity of contact between researchers and those in the health-care setting tended to vary over time, with researchers often reporting a need for greater intensity towards the start of an initiative as relationships were being formed and expectations agreed.
The visibility of the researcher(s) was related both to their physical location and to the intensity of contact, but was not merely the result of these structural features. Visibility was instead more nuanced, and spoke to the profile of the researcher(s) and their embedded research work and the extent to which they were known and well regarded within the health-care organisation and further afield:
My role has changed quite a bit, so I’m becoming more visible . . . a lot of introductions from more senior members of staff.
Embedded researcher, Crofton
Visibility, then, is a function of the informal, relational work carried out by the researcher and the formal, structural features of an initiative, as well as the import or impact of their activities.
Belonging
Embedded research initiatives can be thought of as a mechanism for bringing together the worlds of research and practice. As such, we identified a number of structural features related to belonging (or otherwise) to these different worlds, and how this was facilitated in embedded research initiatives.
Both the literature and the people we interviewed emphasised the often precarious nature of working in an embedded role, and the sense of liminality that could arise from the need to work across (and between) multiple boundaries. 156,164,165 These included the epistemic and functional boundaries between academia and health-care settings, and those that arose between different organisations, professions, teams and priorities in each of those settings:
If I’m really honest, this has tested me to breaking point almost, because it’s not easy. The university were interested, then they weren’t, and then they were – I don’t belong to the teaching fraternity, I don’t belong to the research fraternity.
Embedded researcher, Finmoore
Embedded research initiatives often made use of a variety of formal, contractual arrangements to enable researchers to belong to the worlds of research and practice and to manage the boundaries between these. Contrary to earlier literature on embedded research,158 the embedded research initiatives we uncovered rarely made use of joint contracts of employment between academic and health service organisations (see Table 3). Instead, expectations and agreements about how researchers would formally belong to these settings were often documented in a memorandum of understanding (MoU), a funding agreement and job descriptions:
This MoU defines the relationship between the parties and sets out roles and responsibilities within this; it sets out how the group will be governed, the duration of the arrangement, principles of working together and agreed terms and conditions.
Garrick documents
In addition to formal, contractual arrangements, initiatives also made use of a range of more informal arrangements to enable researchers to belong to different worlds. These included support networks, mentors and champions. Although some initiatives built such arrangements into their structures, it was often researchers themselves who created these, or sought them out and nurtured them:
There were times when I started that I felt a bit isolated from academia . . .. And other than [my manager] I was the only person with a PhD [Doctor of Philosophy], so yeah, I did find that a bit isolating; so that’s why I went out and asked the senior lecturer at [university] to be my academic mentor, and they have agreed that I can go and sit in their department.
Embedded researcher, Summerside
Researchers who were wholly located and employed in a health-care setting and lacked formal, contractual links with academia often sought to maintain a connection by participating in academic activities such as conferences. These researchers highlighted the importance of being given permission and encouragement to engage in these activities:
I think it’s really, really important that I make sure I keep those links with academia . . . I think that’s one of the biggest challenges, that if I left and someone else took up this post, I think that they would have to somehow find that academic support . . .. It doesn’t come naturally with this, you have to find it yourself.
Embedded researcher, Bonnyville
The many and varied structural aspects discussed above often get ‘baked in’ as embedded research initiatives become established. More fluidly expressed, however, are the processes by which such initiatives operate, and it is to these that we now turn.
The processes of embedded research initiatives
Just as the embedded research initiatives we identified were structured in different ways, they also made use of a wide range of processes. We were able to categorise these into four themes that represented the ways in which initiatives played out day to day: functional activities, researcher skill and expertise, relational roles and learning mechanisms.
Functional activities
We found that a wide range of actions were being undertaken within embedded research initiatives, and that researchers were often expected to carry out a plethora of different activities. 166 These included relational activities (such as attending meetings and facilitating relationships), knowledge-creation activities (such as collecting and analysing data), educational activities (such as facilitating a journal club and arranging seminars) and project management activities (such as planning, managing and leading individual projects). In practice, although job descriptions suggested that likely activities were relatively tightly defined, many interviewees suggested that they were instead fluid and emergent, with new opportunities presenting themselves throughout the initiative:
[The researcher] was attached to long-term conditions group, which was a group that had many, many challenges and many problems, and constant changing of leads. Once she was sitting in on this group, [initially] she couldn’t figure out what she was going to do that was going to be helpful for them.
Embedded research manager, Battleford
The literature and the data from extant schemes suggested that there was a tendency for those leading initiatives to be overambitious about the activities that researchers should carry out. 162 This could lead to ‘role strain’ and contribute to difficulties in managing boundaries. Our interviewees and workshop participants suggested that focusing on the purpose of activities was an important way of combating this.
The ‘training and support’ subtheme was informed especially by discussions with our workshop participants and with some interviewees. They suggested that training and support would enable researchers to carry out the range of activities required by an embedded research initiative and that this should be considered at the design stage of the initiative. We found relatively few examples of such training and support for functional activities being provided to embedded researchers, although some researchers accessed these via their informal arrangements for belonging:
Embedded brokers benefited from allies, champions and ‘chaperones’ located throughout the host organisations, who . . . developed the brokers’ skills and knowledge in research (management fellows) or commissioning (researchers-in-residence).
Wye et al. 162
Researcher skill and expertise
The necessary skills and expertise of embedded researchers were a frequent preoccupation across the literature and the initiatives we identified; these came in three broad types: topic-specific skills and expertise, methodological skills and expertise, and interpersonal skills and expertise.
Topic-specific skills related to the particular clinical or practice-related issue that the embedded research initiative focused on, such as diabetes, neurorehabilitation or childhood obesity. Although many initiatives sought researchers with such specific content knowledge, some (particularly those working at larger scales, comprising a portfolio of projects or a team of embedded researchers) prioritised other, more generic, forms of skill and expertise:
Because we’ve got such a diverse trust, we have to not be too precious about what subject area we work in. However, I think we all have our own expertise in terms of skill set rather than subject.
Embedded researcher, Crofton
Methodological skills supported the ways in which knowledge was created within the initiative, and included the skills needed to define and refine the focus of the knowledge-creation activity, how to collect and analyse data and how to produce knowledge of different kinds. In many initiatives, this type of research ‘know-how’ was seen as particularly valuable, over and above any topic-specific skills and expertise. 166
Interpersonal skills and expertise were seen as highly valuable across the initiatives we identified. All role descriptions for embedded researchers required a range of interpersonal skills. These included facilitation skills, communication skills, relationship-building skills and emotional intelligence, and chimed with the emphasis in much of the literature on the social skills and dispositions of embedded researchers:151,154
And I think in essence, that sense of genuinely brokering is being able to . . . have a meaningful dialogue.
Embedded researcher, Finmoore
Researcher expertise and skill often then received explicit attention in embedded research initiatives. But how the different types of expertise and the softer interpersonal skills were channelled depended, in part, on the relational roles envisaged in the particular embedded initiative.
Relational roles
Although all embedded research initiatives aimed to bring research and practice into a closer relationship, we found that the type of role that researchers might play demonstrated a number of characteristics. These were the level of interdependence between researcher and health organisation, their relational stance and the type of input each provides.
Researchers in the initiatives we identified had varying levels of interdependence with the organisation in which they were embedded. This was expressed in the extent to which they viewed themselves (or were viewed by others) as insiders or outsiders in the health setting, the degree of flexibility and control they had over their work (including disseminating findings) and the extent to which they were able to access spaces (literal and figurative) within the health organisation. Their level of interdependence was often related to (and reflected in) contractual and informal arrangements for belonging, and was closely tied to power dynamics. Although we identified varying levels of interdependence across the initiatives, the challenge of managing the boundary between insider and outsider was a common theme:
Occupying these different spaces with people at various levels meant that I was forced to adopt multiple positions. This meant that I sometimes felt like an outsider, at other times, an insider, while sometimes both or neither simultaneously . . . This constant shifting and flux was unsettling.
Rowley156
Researchers adopted a variety of relational stances towards the health setting in which they were embedded and towards those working in it. The literature frequently highlights the role of an embedded researcher as a ‘critical friend’ and the importance of maintaining a critical stance towards the health setting. 151,158 This is usually related to the maintenance of academic professional identity that depends on a researcher’s ability to maintain a critical distance. 65 Researchers working in some initiatives, however, adopted roles as advocates and supporters, seeking to produce knowledge and operate in ways that would support, rather than challenge, the organisation. These choices were strongly related to the underlying intent of the initiative:
A critical friend needs to be, first of all, a friend. And it’s easy to assume the role of a critical friend where actually your voice is seen as the voice of an outsider. And in reality, it doesn’t have weight, because you’re seen as someone from the outside looking in and guiding, and instructing, and criticising, and telling. Whereas if you’re fundamentally part of the team, and you’re seen to be part of them when they’re in the trenches, you’re there with them . . . and that’s why you’ve got to get the right person because it’s not every researcher who can be an embedded researcher.
Embedded research manager, Summerside
The types of input provided by embedded researchers also varied across initiatives. Some researchers provided the health organisation with a fresh pair of eyes and a new way of seeing things, bringing insights that could help to catalyse change. 152 Other researchers provided an additional pair of hands, producing knowledge and evidence to drive the organisation’s processes and activities. Still others focused on providing specialist or expert advice (methodological or topic specific) in a more hands-off fashion. In line with our observations about functional activities, many initiatives also expected more than one type of input from researchers.
Learning mechanisms
Embedded research initiatives made use of a variety of mechanisms to assess how things were going and whether they were achieving their intended outcomes.
Those wholly based in NHS or other health service organisations tended to make use of performance monitoring mechanisms, including key performance indicators and annual performance reviews (typically for the embedded researchers). These mechanisms seemed to be used because they fitted into wider organisational governance arrangements that often focused on maintaining funding levels and controlling resource allocation:
I have to report my team’s work quite frequently to the board of trustees through my CEO.
Embedded research manager, Streetsville
Initiatives that were funded or controlled by organisations with a strong research focus (e.g. university departments, national research funders, academic–practice partnerships) tended to make use of formal evaluations. These were usually focused on producing an in-depth understanding of how and why the initiative was (or was not) working and made use of formal evaluation methodologies. Both summative and formative approaches were used, and these often resulted in academic publications (a literature that we have drawn on heavily as part of this work):
Research methods were applied to understand, inform, adapt and assess [the KM (knowledge mobilisation) team’s] impact. This paper draws on multiple sources including brokers’ logs, reflective essays and exit interviews; whole team workshops; and independent evaluations of the KM team.
Wye et al. 162
Some initiatives made use of more informal mechanisms for learning and reflection. These were usually understood to be developmental and formative in nature. Informal mechanisms included group or individual supervision, team meetings, workshops and learning sets. The main participants in such activities tended to be embedded researchers themselves, however, and there was relatively little involvement from those leading or managing the initiative.
Concluding remarks
The work described in this chapter (primarily the second literature review of workstream 1 and the scoping study of workstream 2, but also drawing on some of the engagement activities of workstream 4) provides a detailed and grounded analysis of embedded research initiatives, both as they are conceptualised and articulated in the academic literature and as they are playing out in UK health-related settings.
The underpinning logic of these schemes (outlined in Chapter 1) lies in a wide literature developed over decades,167,168 one that sees effective knowledge production and ‘research use’ as a social, situated and contextually mediated process. 4,9 In that sense, embedded research initiatives have a robust and persuasive logic that underpins their conception. They are, however, diversely enacted and much in need of more systematic and evaluative enquiry.
Through this work, we have drawn out and described 10 major themes with multiple subthemes, grouped under the categories of intent, structure and processes of embedded research initiatives. Each of these was clearly seen, but variably expressed, in both the wider literature and the data sources that we gathered about extant health-related schemes. Each theme exposed a degree of complexity and nuance that often remained hidden when proponents (or critics) talked of embedded research as though it were clearly understood and homogeneous. The themes have necessarily been presented as discrete categories, but overlaps and interconnections were legion.
To date, the literature on embedded research has tended to focus on individual initiatives and (especially) on the experiences of embedded researchers. We have lacked both descriptive and evaluative comparisons of embedded research initiatives. One reason for this was the absence of transparent, detailed and consistent reporting of initiatives. When reviewing the literature, for instance, we found scant description of the functional activities performed by embedded researchers, how belonging was managed and facilitated, or how various actors (beyond the researchers) were involved. Those involved in initiatives, however, had much to say about these and other aspects during e-mail exchanges, in interviews and in our workshop. This lack of detail in the published literature made it difficult to adequately compare initiatives and begin to understand how they worked and whether or not they were effective. We suggest that our themes could inform the reporting of initiatives at both an individual and collective level to enable further description and evaluation. For example, the themes naturally lend themselves to the assembly of categories of ‘similarly designed’ embedded research initiatives, thus contributing to the emergence of scheme typologies.
In sum then, the literature review and associated scoping work (workstreams 1 and 2) showed that embedded research initiatives come in a wide variety of shapes and forms. Despite being varied in terms of their intent, structure and processes, we were able to identify 10 themes that characterise their features, and then disaggregate these themes to reveal further layers of nuance. Making use of these themes is likely to bring about much needed clarity and transparency both within and between initiatives, enabling further in-depth understanding and comparison of the potential value of embedded research.
Subsequent ‘drilling down’ in specific schemes (the case studies explored in workstream 3) was able to use and build on this framework. That work is described in Chapters 4 and 5. Additional work through our engagement strategy (workstream 4) allowed these themes, and the insights gained from the case studies, to be further developed into visual metaphors and practical resources to aid dialogue about the design and management of embedded research initiatives. That practitioner-facing work is elaborated on in Chapters 6 and 7.
Chapter 4 Embedding in practice: the case accounts
Introduction
This and the following chapter present the research activities and findings of workstream 3. Informed by the findings of preceding workstreams, this involved in-depth qualitative research with four purposively selected ‘cases’ of embedded research, with the objective of understanding the contribution such initiatives make to the co-production and translation of research into practice. The reporting here and in Chapter 5 (and with methods further elaborated in Report Supplementary Material 3) makes use of the reporting guidelines of COnsolidated criteria for REporting Qualitative research (COREQ)169 to set out what was done. In this opening part of the analysis, we focus on ‘telling the story’ of each initiative, drawing attention to their key features, backstories and trajectories; Chapter 5 develops the analysis across the cases, looking for repeated patterns that speak to similarity and differences in the themes surfaced in the earlier workstreams. Thus, this chapter focuses more on description, whereas Chapter 5 takes a more analytic slant; the findings are separated in this way to ensure that the overall account does not become unmanageable, and to allow a clear focus on both the particularities of individual cases and the analytic insights that can be gleaned by looking across the cases.
As shown in Chapter 3, embedded research initiatives can vary considerably in terms of intent, structure and processes. This in-depth work was designed to investigate how such factors, together with other unanticipated issues, might shape how the embedded initiatives were formed, how they contributed to the co-production of knowledge and how they supported the translation and use of knowledge in the organisation and delivery of care.
The specific research objectives addressed in workstream 3 were as follows:
-
purposively select four exemplar embedded research initiatives reflecting anticipated typographical differences (e.g. in their affiliations, project characteristics, relational networks and funding)
-
describe the embedded researchers’ career histories, motivations and networks of research (university) and practice (NHS) partners, including changes over time in relationships, tasks and activities, and pattern of interactions
-
understand how embedded researchers, and members of their networks, mediate different forms of knowledge and cultural and social boundaries to promote co-production
-
appraise the contribution of embedded researchers and their networks to knowledge co-production, including detailed examples in selected NHS settings.
The conceptual framing for this work drew on a growing body of research (introduced in Chapter 1 and explored in depth in Chapters 2 and 3) that examines how co-production activities can help mediate and overcome a variety of well-documented social, cultural, organisational and epistemic boundaries. For example, there is strong evidence that research producers and research users are often decoupled or disconnected because of institutionalised knowledge boundaries. 170 These include differences in the syntactic nature of knowledge (words or terminology), the semantic nature of knowledge (meanings and assumptions) and the pragmatic nature of knowledge (its purposes and intent).
It has been shown that such differences can significantly retard the translation and application of research knowledge in health and care settings,171 but that a number of interventions and strategies can mediate these factors and boundaries, from knowledge brokers to co-design methodologies. Embedded research initiatives represent one prominent strategy for mediating such barriers. Although recognising that knowledge co-production comes in many guises (see Chapter 2) and that embedded research initiatives themselves can take many forms (see Chapter 3), this part of the project was designed to explore in depth the mechanisms employed and the dynamics that unfold.
Overview of study methods
A detailed account of the research methodology for workstream 3, the case selection process, exact methods and the extent of the data gathered can be found in Appendix 3. Here, we simply give an overview of the research strategy to contextualise and frame the subsequent findings.
Sampling and selection
Workstream 3 involved qualitative comparative case studies of four purposively selected examples of embedded research, although, as we show, one of these comprised additional subcases (multiple embedded researchers). Qualitative case study research affords depth, providing descriptive and explanatory understanding of any given case. Cases can be selected for a range of reasons: from the discovery or exploration of unique situations, the examination of comparative aspects or search for replicative logics, through to more conventional forms of representative sampling. 172–174
Sampling here aimed to identify and select examples of embedded initiatives that were likely to co-produce knowledge, while also taking into account key differences in their configuration that might explain how and why co-production varies (see Chapter 2). Selection was informed by the learning from workstreams 1 and 2, especially the national review of current initiatives, the emerging understanding of knowledge co-production (see Chapter 2) and the thematic summary of the design considerations and operational features of embedded research initiatives (see Chapter 3).
Through a robust and independent review process with additional moderation (detailed in Appendix 3), four cases were identified, reflecting differences in approach, outcomes, setting, scale, employment, maturity and location, as set out in Table 6. These sites were selected to explore anticipated variations in approach, outcomes, settings, scale, employment, maturity and location, with these considerations being informed by the design choices and operational features developed in workstream 2.
| Initiative ID and researcher(s) | Approach to knowledge | Primary outcome | Secondary outcome | Other outcomes | Setting | Scale | Employment | Duration (years) | Maturity | Location |
|---|---|---|---|---|---|---|---|---|---|---|
| Bridgetown: Anna, previously Jill | Moderate co-production | Capability/capacity | Formal academic knowledge | Local practice insights | Multiple | Portfolio | Joint | > 4 | Emerging | Scotland |
| Coxheath: Jane | Committed co-production | Local practice insights | Capability/capacity | Formal academic knowledge, prestige/credibility | Acute | Portfolio | Joint | > 8 | Established | South East |
| Porter: Rachel, Bev, Katrina, Karla and Victoria | Moderate co-production | Capability/capacity | Formal academic knowledge | Prestige/credibility, local practice insights | Primary | Portfolio | NHS | > 10 | Established | Midlands |
| Evansville: Bella and Tim | Provisional co-production | Formal academic knowledge | Local practice insights | – | Acute | Portfolio | University | 4 | Ended | South East |
Preliminary discussions with key gatekeepers signposted us to important individuals and groups involved with each initiative. We also used a ‘partner identification tool’ (see Appendix 1, Figure 13) to identify additional stakeholders for each initiative. Ultimately, we sought to identify those practitioners, managers, commissioners and patients who, in different ways, supported, worked with and interacted with the embedded researcher. Appendix 2, Table 19, offers an overview of the participants from each site. After appropriate ethics and research governance permissions [see the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)], these people were contacted by e-mail and invited to participate in the study. The invitation to participate, including details of the project and use of data, and the consent form can be found on the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)].
Data collection
We used a range of qualitative research methods to collect and analyse data, including semistructured interviews, focused observation and reflective diaries. In practical terms, these were organised with each participating case through a series of site visits over a 12-month period with the intention of studying changes over time. For the more geographically remote sites, on-site data-gathering took place over two discrete periods, each of 2–3 days’ duration, supplemented by multiple and various physically distanced interactions (telephone and e-mail). One site was more local to the research team, making multiple day-long visits possible. In total, each site received around 7–10 days of observation.
The initial site visit involved introducing the research to key study partners, carrying out the initial interviews with the embedded researcher and key partners, observing aspects of day-to-day practice and observing one or more planned meetings. On subsequent visits, we conducted follow-up interviews with the embedded researcher and additional partners (identified through the use of the partner identification tool; see Partner identification tool), and we carried out additional observations and shadowing of embedded research activities.
Between visits, additional short telephone interviews were carried out with each embedded researcher to discuss ongoing and planned embedded research activities. The research methods are detailed in the following paragraphs and elaborated on in Appendix 3, with major data extracts in Report Supplementary Material 3.
We recorded 46 formal interviews with 31 participants across the four case study sites. Interviews were usually one to one; some were completed face to face, others over the telephone (see Appendix 3, Table 19). Participants included embedded researchers and members of their wider network, identified through use of the partner identification tool and a broader ‘snowballing’ approach. We also completed extensive informal interviews as part of the periods of observation. The observations took place at three case study sites (Evansville had already concluded), and included observing a variety of specific events and more generalised shadowing of the embedded researchers in their roles (specific details of which can be found in Report Supplementary Material 4). Further details on each of these modes of data gathering now follow.
Interviews
Semistructured qualitative interviews were the primary method of data collection for workstream 3 and followed two topic guides, the first for embedded researchers (see Appendix 4, Table 21), the second for other stakeholders (see Appendix 5, Table 22). These were designed to explore participants’ views and experiences of their embedded research initiative, focusing on key stages and activities in the development and function of each initiative, investigating the contribution of key people, meetings or activities, and discussing participants’ views about the types of knowledge or evidence co-produced and how it becomes translated into practice. Interviews were then coded (see Appendix 6, Table 23).
Partner identification tool
Data collection also made use of less common techniques, derived from stakeholder analysis and social network analysis,175 to facilitate discussion with individual embedded researchers about the key contacts or people they engaged with in their activities.
This partner identification tool (see Appendix 1) prompted participants first to identify people they engaged with on a given issue or activity, to think about the quality or frequency of each relationship, and to consider ways in which these people might be categorised. The use of this tool in workstream 3 served two key purposes: to assist the team in identifying potential participants related to the work of each embedded researcher, and to understand each participant’s reflections or views of these relationships.
Observations
Each site visit included focused observations of the embedded researchers (except at Evansville, which had ended as an active initiative). The primary purpose of these observations was to deepen our insight into the embedded researchers’ activities ‘at work’, including the types of activities carried out and the relationships developed. They included observations of project meetings, staff consultations, training workshops and research seminars. We also shadowed the individual embedded researchers on their day-to-day activities.
Diaries
Given that site visits could take place several months apart, the study design made use of reflective diaries (voice-recorded) to enable embedded researchers to capture reflections on their work. This provided data in its own right and informed subsequent interviews. We produced a short guide, outlining the purpose of the diary method. It asked the embedded researchers to describe their activities and tasks, the types of knowledge utilised, the relationships involved, and any challenges or issues faced. A flexible, semistructured approach was adopted from the outset.
Despite our best efforts to facilitate diary completion, the researchers, in general, found the diaries somewhat difficult to engage with, owing to the high level of demands of their day-to-day work. Engagement was partial and somewhat superficial, and we recognised that the data from the diaries were likely to be of rather limited use. What this lost from our study was some of the immediacy and fine-grained detail of the day-to-day activities, the tensions and emotions from living embedded work; we therefore needed to rely more on retrospective reflections gathered through interviews, on-site conversations and e-mail communication.
Data analysis
We designed a co-production workshop with the aim of testing preliminary ideas and themes to develop a shared understanding of the in-depth case study findings. The workshop was attended by embedded researchers from three of the four cases and members of their wider teams; other colleagues from the embedded network (and some who attended the first workshop) also attended. Workshop 2 was facilitated by Kaleidoscope Health and Care colleagues (see Acknowledgements). The event was thought-provoking and engaging, and we gathered extensive feedback. These outputs were particularly helpful for the workstream-3 analysis and also fed into the work of workstream 4.
The initial (descriptive) account for each case is presented in the following section. Further details of the analytic strategy, together with significant data extracts, can be found in Report Supplementary Material 3. Through descriptive overviews of each embedded initiative, we sought to show how and why embedded researchers developed their roles, what activities they undertook to co-produce and translate knowledge, what types of relationships they developed and the boundaries they negotiated, and what types of impact they made on translating knowledge into everyday practice. For each case, we looked at the:
-
backstory to the initiative, including when it was established and the organisational context, such as employment positions
-
rationale and specifications for establishing the initiative – its strategic reason
-
features of the embedded researcher, such as their professional background and experience
-
key relationships the embedded researcher developed or used in their work, including those in university and NHS contexts
-
PPI built in to the initiative
-
embedded activities that reflected the particular rationale and specification
-
achievements and challenges that characterised the initiative.
In the next section, we outline the findings case by case under each of these headings, before exploring in more detail the diversity and range of experience for each of the descriptive categories.
Findings 1: case-by-case overview
This section provides a brief narrative account of each case, summarised in Table 7 using the seven basic features listed in the previous section. (The subsequent section will illustrate in greater depth the full diversity of experience across the cases.) The four cases have been anonymised and given pseudonyms: Bridgetown, Coxheath, Porter and Evansville.
| Feature | Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|---|
| Backstory | Established in 2015. Initiative across multiple settings with one researcher (university contract plus honorary NHS appointment). Funding was shared between the university and the NHS trust | Established in 2011. Hospital-based initiative with one researcher (university contract/honorary NHS). Funding was shared between the university and the NHS trust | Operating in some form for well over a decade. Community-based initiatives with five researchers (various contractual arrangements). This initiative received research council funding (i.e. external) | Established in 2014; now ended. Hospital-based initiative with initial research team of two, expanded to four part-time researchers and a health economist (university employed/honorary NHS contracts). Various sources of funding (internal, university support, funding via local clinical research network) |
| Rationale and specification | Culture change through capacity- and capability-building (local and strategic level) | Integrated working, practice development, plus research capability | Multipurpose, to lead and promote evidence-based practices | Research-informed improvement in clinical care/service delivery |
| Embedded researcher(s) | Anna: occupational therapist, motivated to ‘bridge the practice/academic gap’. Previous role-holder was Jill, employed to build research capacity and capability | Jane: international nursing academic with interest in leadership, practice development | Rachel, Bev, Katrina, Karla and Victoria: clinical research-related backgrounds, with shared interest in applied projects | Team included Bella (anthropology) and Tim (health economics) |
| Key relationships | Clinical and academic line managers, plus front-line stakeholders (largely inside NHS) | Multiple stakeholders across multiple care and research/charity domains | Various management configurations, front-line contact (NHS), informal academic | Senior steering group, strong academic involvement, front-line staff/managers (NHS) |
| PPI | Formal PPI accessed for external projects; assisted front-line clinicians with PPI arrangements | Project-specific PPI sought (internal, external and charity networks used) | Role dependent. Project-specific PPI when appropriate (internal/external) | Specific embedded PPI group set up for broad role involvement and for specific projects |
| Embedded activities | Scoping current landscape/research culture, building networks | Networking, research support, dissemination/translation, strategic work | Traditional research, service evaluation, quality improvement and capacity-building | Multiple projects across the hospital including research design and implementation |
| Achievements and challenges | Positive staff feedback. Challenges related to existing poor perceptions of research | Practice improvements. Challenges centred on making strategic contributions and crossing barriers | Sustainability. Varied challenges (workload, funding), emphasising the need for senior support | Legacy (PhD students, etc.), effective dissemination, value of the role and ‘buy-in’ |
Bridgetown
Bridgetown is a hospital-based initiative in Scotland that was formed through collaboration between an NHS trust and its local university. At the time of the study, the embedded researcher (Anna) had a joint appointment with both organisations and, in broad terms, was engaged in providing academic and professional input to a portfolio of service-facing research and improvement activities. She had a particular interest in implementation science and knowledge mobilisation theory. As Anna’s role was in its infancy, her time was spent mapping out the research culture and building relationships. Her early findings suggested a commonplace fear among front-line staff relating to academia and research; however, she was already beginning to receive positive feedback regarding her role, from the NHS trust in particular.
Coxheath
Coxheath is an acute hospital-based embedded initiative located in the South East, formed through a collaboration between an NHS trust and a local university. The initiative was well established (in excess of 8 years) and focused primarily on the role and activities of one embedded researcher, Jane, who had a joint appointment with both the trust and the university. Her role encompassed various work related to practice development, implementation and evaluation. Jane had established a broad network with multiple stakeholders, inside clinical practice, in academia and elsewhere: her collaborative relationships were at both a national and an international level. The impact of Jane’s work – and as such, the initiative – was far-reaching; however, Jane felt that her role had not yet been used as effectively at a strategic level as it might have been.
Porter
Porter represented a relatively distinctive case study. Rather than involving a single researcher, it comprised five embedded researchers working across four initiatives or areas of activity in an NHS trust specialising in community and mental health services. Together, these initiatives represented an embedded research portfolio that was nominally led by Carol, who, as the trust’s head of research and development (R&D), was responsible for some aspects of the embedded research initiative and acted as the trust’s primary link with the local universities and research ecosystem.
The five embedded researchers worked on different initiatives across the trust’s clinical divisions, typically with direct line management within the relevant division. Some of these roles could perhaps be interpreted more as traditional clinical research or quality improvement posts, rather than as embedded researchers seeking to co-produce knowledge. However, the participants and the oversight lead (Carol) did construe them as embedded researchers. The researchers faced individual challenges in their roles, but there was a shared sense of achievement relating to the sustainability of the initiative.
Evansville
This initiative was located in a large acute hospital trust and was funded for 3 years from April 2014; it has now ended and, for the purposes of this study, represented a mature and concluded initiative. Over its course, the initiative was characterised by a number of different configurations as the embedded team worked on different applied research projects, each requiring a slightly different working model. As the funding was not extended for this initiative, sustainability and legacy were relevant concerns. Despite the lack of ongoing funding, there was still a sense of enduring impacts relating to the research capacity-building undertaken, with ongoing developmental research projects and relationships.
Findings 2: comparative case descriptions
The chapter now works through a comparative analysis of each of the main descriptive dimensions outlined in Findings 1: case-by-case overview. The purpose here is to look closer at each case to develop analytic and explanatory understanding about how and why each case differs, and what implications these differences have for the co-production and translation of knowledge. We take as our organising framework the features listed in column 1 of Table 7. A full analytical description of each case study can also be found in Report Supplementary Material 3.
Backstory
Here we focus on understanding the history of the initiatives, taking into account the broader context from which they developed, such as funding arrangements, primary location and current (active) status (Table 8). Clearly, the background of each initiative is closely linked to its intended purpose and specifications, as discussed subsequently, but the history is also relevant to its trajectory, priorities and activities, making its inclusion important.
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Current initiative based on a previous joint role (Jill) supporting research capacity among front-line clinicians (in which relationships, expectations and governance arrangements between partners were clarified). Current embedded researcher, Anna, employed full time by the university, seconded to the NHS hospital trust | This well-established initiative was/is constructed around the work of a single embedded researcher, Jane. The specifications of her joint appointment by acute NHS hospital trust (honorary contract) and local university (main contract) developed over a long, diverse career in nursing | A complex initiative situated in a community health trust, Porter involves a total of five embedded researchers working across different arms of the organisation. Roles, accountability and the nature of each researcher vary. Despite this, all researcher roles are well established | The only one of the four initiatives to have ended, Evansville comprised a team of embedded researchers from a range of disciplines. The team was employed by the university with honorary contracts at the hospital trust to work on various projects relating to health services research. The initiative was funded for 3 years |
An important background issue relates to the history of collaboration between different partners, especially university and NHS organisations or leaders. These vary from highly developed institutional partnerships, often in the form of clinical academic departments, to less developed collaborations often relying more on personal connections between key individuals in each organisation. Linked to this, it could be suggested that the wider environment of applied health research, in particular translational health research, also conditions the development of each initiative, for example when there are connections with other professional research and training pathways or NIHR infrastructure.
A further consideration is the extent to which the initiative was led or shaped by one partner organisation more than another, or if it represented a ‘marriage of equals’. Certainly, one initiative (Porter) had been championed by a research-active leader based in an NHS hospital trust who then nurtured connections with university partners to further develop the initiative and its specifications.
Each initiative’s contextual background was reflected in notable practical differences in configurations, such as contractual arrangements, funding, line management and accountability. Some embedded researchers were employed solely by the trust or university with honorary status in the second institution, and these arrangements seemed to matter for subsequent relationships.
Each initiative told a different story regarding its funding. For some, the original funding was ongoing; in others, the source of funding had changed over time; and in one (Evansville), it had ended. Porter offered insight into some of these challenges and the associated negotiation, sometimes ongoing, involved. Two of its researchers, Rachel and Victoria, saw significant changes in funding throughout the course of their roles, which unsurprisingly created anxiety and uncertainty for them. For many of the researchers, contractual arrangements and sources of funding were split across different organisations; line management and accountability were therefore sometimes shared and came with competing ideals in relation to the purpose of the initiative. Researchers often had to juggle expectations in response.
The study found that each initiative had been devised, designed and established at a particular time to address a set of specific and locally significant issues that had been identified by one or two strategic partners. In all cases, however, the focus and significance of issues evolved over time, influenced by changing organisational priorities and expectations and by the experiences and expertise of all parties. As such, the more developed or ‘mature’ initiatives – those with a longer history – often had a clearer, more evolved sense of purpose. Bridgetown was a prominent example of this, whereby the experiences of the initial embedded researcher, Jill, had provided lessons for the current, ongoing initiative and her successor, Anna. Anna’s role was specifically designed to reduce the risk of the challenges Jill had faced, relating to the overall objectives, degree of impact and practical issues such as workload.
In terms of promoting the development of embedded research, each case had one or two ‘champions’ who strongly advocated the need and potential of the embedded approach. For example, the chief nurse at Coxheath (at the time of role construction) engaged with constructing a dual role and collaborative working across the university and her local hospital. In Porter, all five embedded researchers described how one or two senior people had helped get their roles off the ground and sustained them, alongside the background support of Carol (head of R&D at the trust). Embedded initiatives appear to need an advocate or champion operating at a relatively high or strategic level, who can ‘see the big picture’ and influence organisational and interorganisational decision-making, leverage necessary resources and legitimise the risk of investment.
Rationale and design specifications
To understand the rationale and specifications of each initiative, we examined their aims and intended purposes as linked to their particular background (Table 9). This analysis was informed by the findings of workstream 1, specifically the differentiation of initiatives according to their approach towards co-production (i.e. from the more conventional to the more radical; see Chapter 2). We also observed how the intent and purpose of each initiative changed over time.
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Moderate approach to co-production: to support research capacity development, but also facilitate broader culture change. Anna’s role differs from that of Jill (previous incumbent): it now takes a more strategic outlook, aligning with organisational priorities, bringing evidence to decision-making and influencing broader culture change | Committed approach to co-production: Jane’s work supports practice development across both organisations. As part of this, her role focuses on transformation effectiveness and innovation, and seeks to grow capacity and capability in other areas. The aim is to influence and network, forming links between practice and academia | Moderate approach to co-production: Porter has a long history of exploiting opportunities to bring research into practice. The ultimate goal of this current initiative is to promote evidence-based practice, using research that helps to improve patient and staff outcomes and experience | Provisional approach to co-production: the embedded team was constructed to undertake rigorous and systematic health services research close to service delivery. This research was driven by the challenges facing the trust, with the aim that findings and new insights would subsequently inform practice, improve service delivery and shape overall trust performance |
Across the four cases, there were significant and stark differences in how each embedded initiative was specified in terms of purpose. This revealed important differences in how ‘embedded research’ as a broader concept or construct was seen by the wider health-care and health research communities. Initiatives were intended to address markedly different issues, such as:
-
capacity and capability development (organisational or professional) (e.g. Bridgetown, Coxheath)
-
professional development for nursing and allied health professional (AHP) staff [e.g. Bridgetown, Porter (Victoria and Rachel)]
-
research development (design, planning and management) (e.g. Coxheath, Evansville)
-
research translation and use (dissemination and mobilisation) [e.g. Coxheath, Bridgetown, Porter (Victoria)]
-
applied (co-produced) research projects (e.g. Coxheath)
-
service improvement projects (e.g. Porter, Evansville)
-
service evaluation [e.g. Porter (Katrina and Bev)].
In all cases, there was no single or sustained purpose; rather, each initiative addressed multiple purposes that matured and developed over time. The experiences and interests of the embedded researcher(s) could have an important bearing on how these aims and purposes evolved, especially as they could bring new ideas to the initiative or mediate between the strategic priorities of multiple organisations. We found, for example, that the Coxheath initiative was shaped by the embedded researcher’s passion and commitment to professional development and co-creation. There was, however, arguably less scope for the researcher to influence the initiative’s rationale and direction when working as part of a team or with less organisational or strategic involvement. For example, some researchers at Porter, particularly those with bounded roles in service improvement, appeared to have very little influence over the purpose or direction of their role.
Although the explicit rationale and design specification of each initiative differed (through job specifications, descriptions and other documentation), there were also evident similarities in, for example, the translation of evidence into practice; empowering of front-line staff; transformation of the research culture; and, ultimately, the aim of improvements to service delivery.
Importantly, there was no single or shared understanding of the purpose of embedded research initiatives, a finding that echoed the conclusions of workstreams 1 and 2 (see Chapters 2 and 3). In each of the case studies, the embedding was designed and evolved against the backdrop of a particular institutional context to address certain strategic or operational priorities for research, research use, staff development and service improvement. However, the precise configuration or specification of these purposes varied according to the influence of key partners in the background and design, and the experiences of key stakeholders in the operation and maturation of the initiative. Significantly, embedded research could mean different things to different groups, and one of the roles of the embedded researcher could be to mediate and reconcile these differences in their own work.
The embedded researcher
As the previous sections suggest, embedded research initiatives are, in many ways, defined or differentiated by the embedded researcher(s), who, in many ways, provide the tangible focus and actionable work of the initiative (Table 10). We investigated each researcher in terms of their professional background, career and history; motivations and aspirations for undertaking the role; perceived skills, strengths and qualities; and understanding of the purpose and significance of embedded research.
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| An occupational therapist by training, Anna completed a PhD relating to professional decision-making theory. Post her PhD she worked in a variety of roles including in the voluntary and university sectors. Anna returned to health-care research and worked on projects before this clinical academic post. She described herself now as a clinical academic with an interest in implementation science and knowledge mobilisation | Jane was an internationally renowned nursing scholar and leader. Her career had involved various clinical roles, academic and leadership positions, and charity work. Jane described a passion for transformational and compassionate leadership, co-production, co-creation and practice development. She had worked ‘across’ organisations with an interdisciplinary approach for many years before this formal joint appointment | Rachel, Bev, Katrina, Karla and Victoria came to their roles with an array of backgrounds and skill sets, although with no existing clinical roles or affiliations. Instead, previous careers related to research (with and without PhD completion). There was a shared sense of motivation relating to applied health-related research and service/quality improvement that aimed to influence and improve practice for front-line clinicians and the patient experience | Team member skills were drawn from anthropology (Bella) and qualitative and quantitative methodologies and health economics (Tim). Bella’s experience offered a particularly helpful focus for data collection. She had spent significant time working as a health services researcher, and the applied and integrated focus of the Evansville initiative appealed to her. Although this initiative had ended, Bella remained in contact and offered support |
Embedded researchers in the four cases held a variety of formal titles. Anna from Bridgetown was an AHP research lead and university lecturer – clinical academic. Jane, at Coxheath, was a university professor of practice development, research and innovation and an NHS trust research centre co-director. At Porter, Rachel was an NHS trust senior research associate and university honorary fellow; Bev and Katrina were service evaluation and research associates at their NHS trust; Karla was an NHS trust service evaluation analyst; and Victoria was a university associate professor of communication in mental health, an NHS research consultant and an NHS and associate research lead. Finally, Bella from Evansville was an embedded researcher team member and anthropologist.
The embedded researchers thus varied in a number of key areas or dimensions that provided important points of comparison and shaped how their initiatives functioned. These included the following:
-
clinical or non-clinical background, affording different levels of understanding of clinical practice, culture and care organisations or health (or other academic) research environments and priorities
-
specialism, in terms of their area of professional (e.g. nursing, AHP) or research expertise (e.g. clinical, social science, translational)
-
level and type of qualification, especially whether or not the embedded research was trained to doctoral level in an area relevant to applied health or translational research
-
motivation, relating to their personal interests and commitment to embedded research and knowledge co-production, especially the perceived benefits to organisational and professional partners.
There appeared to be a marked difference between ‘traditional’ academic researchers in embedded roles and embedded researchers with a professional clinical background who had subsequently trained to doctoral level in an area of applied health research. The latter background gave the researcher a dual and combined understanding of two relatively distinct areas of practice, with relatively high levels of credibility in both domains (through professional and doctoral qualifications). Therefore, they seemed more qualified and legitimate to work across the boundaries of research and practice than those who might have primary qualifications in only one area.
Porter was a particularly interesting example in terms of diversity. Here, one initiative housed a mixture of professional backgrounds. For example, one researcher had a psychology background and a PhD in family therapy, and another had degree-level qualifications and experience in pharmaceutical research. These individuals’ backgrounds held a relevance both for their own embedded roles and for the initiative more broadly: the former influencing a broader, interdisciplinary network and contributing to organisational and strategic priorities, whereas the latter carried out work largely bounded within a specific clinical context.
Perhaps most interestingly, despite the significant diversity between researchers, we found similarities in the embedded researchers’ motivations in undertaking the role. There was a strong shared sense of the potential for research to provide tangible and applied ‘real-world’ change in the design and delivery of health services, and to improve patients’ experience of this care. This motivation was also relevant for those supporting the initiatives, particularly initiatives based in clinical practice.
Relationships
Key to the role of the embedded researcher is the ability to develop, use and broker relationships within and across the research and practice boundaries. We therefore investigated each embedded researcher’s patterns or networks of relationships, and how they understood these networks as informing and supporting their activities. To do this, we used the partner identification tool (see Partner identification tool and Appendix 1) in conjunction with qualitative interviews. The tool helped participants think about, identify, appraise (in terms of frequency or quality) and categorise (as NHS, university, other) their relationships.
The study found that interpersonal relationships, and the strength of these relationships, were fundamental to how the initiative was configured and functioned. Key contacts (Table 11) were seen as fundamental for each initiative’s success and sustainability, and also played an important role in securing and maintaining funding. As noted previously, such ‘champions’ offered sponsorship, endorsement and a degree of protection for the researchers and for their initiatives more broadly. These individual champions spanned clinical settings and university, although examples of the former were more widely noted. Champions tended to be those in senior management roles with associated status and power, with the ability to ‘open doors’, fight the researcher’s corner and ensure that they had ‘a seat at the table’.
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Anna’s role was in its early stages and she was still working to develop relationships and networks. Her immediate contacts (and line managers) were AHP directors and specialty leads, plus her academic mentors (Jill, her predecessor, and the head of school). She also had wider academic collaborators and was developing relationships with front-line AHPs | Jane worked with the university’s research centre director, and the trust’s director of operations/quality; these were also her direct lines of accountability. She also worked closely with front-line staff, various academics, students, and members of the trust’s human resources team. She had extensive relationships with local and national partners, such as Health Education England, and with charities | Each team member had different line management and front-line working relationships. Relationships with two local universities were largely informal (except for Victoria who held a joint role). Carol (head of R&D at the trust) acted as a gatekeeper to the researchers, although their individual links to her were minimal in terms of formal accountability | The team worked closely with three senior academics who offered significant support, and they also built relationships with senior NHS managers. Most relationships were between embedded team members and front-line clinicians (and their direct management); as projects were assigned, they worked to develop relationships and access |
The diversity and scope of the researchers’ networks and intrinsic relationships differed greatly. These networks can be seen most clearly in the completed partner identification tools for each embedded researcher depicted in Figures 5–11 [note that Bev and Katrina at Porter (see Figure 8) completed their partner identification tool together].
FIGURE 5.
Embedded researcher key partners: Bridgetown – Anna.
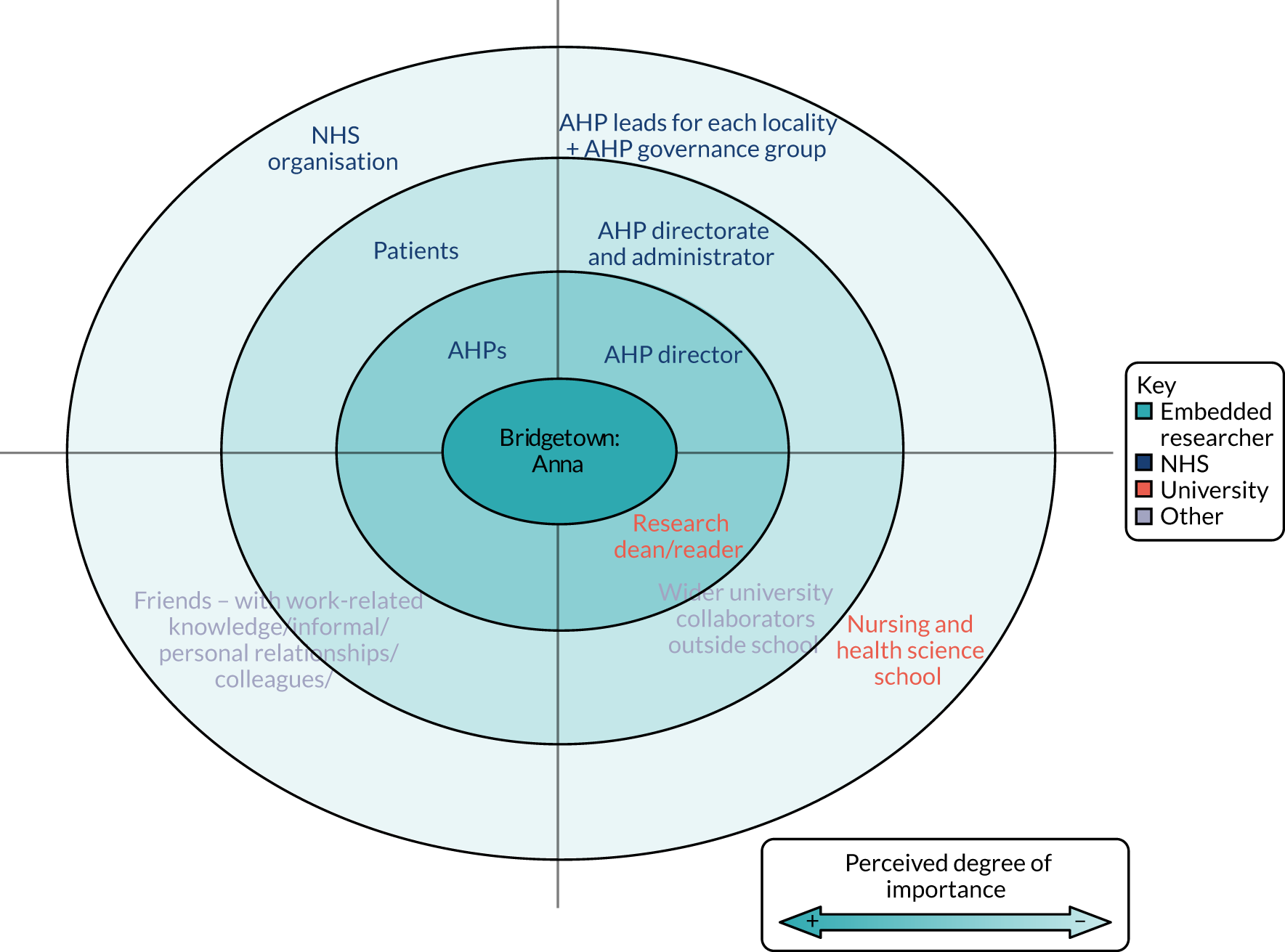
FIGURE 6.
Embedded researcher key partners: Coxheath – Jane. HEE, Health Education England; HR, human resources.
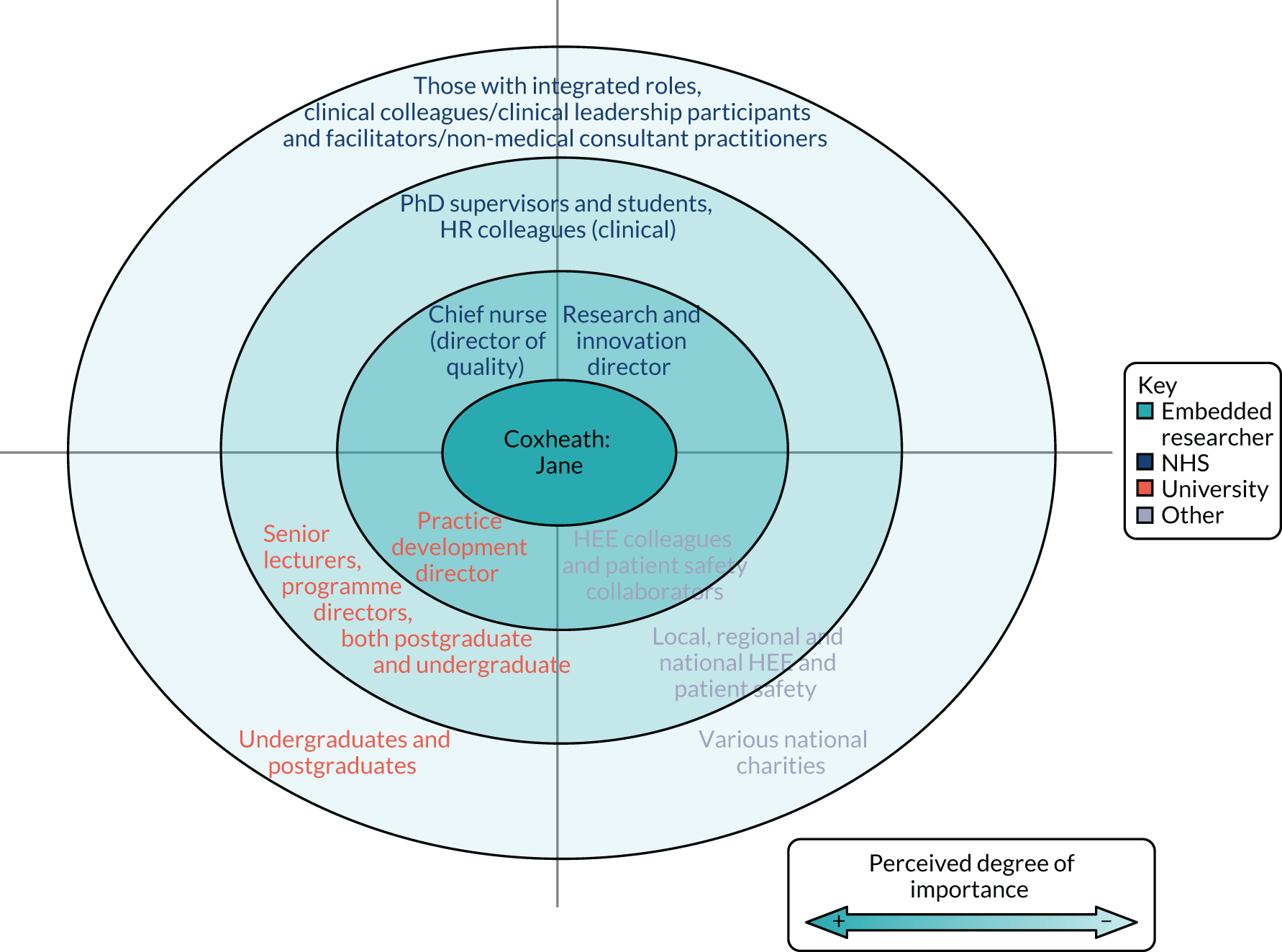
FIGURE 7.
Embedded researcher key partners: Porter – Rachel.

FIGURE 8.
Embedded researcher key partners: Porter – Bev and Katrina.

FIGURE 9.
Embedded researcher key partners: Porter – Karla. QI, quality improvement.
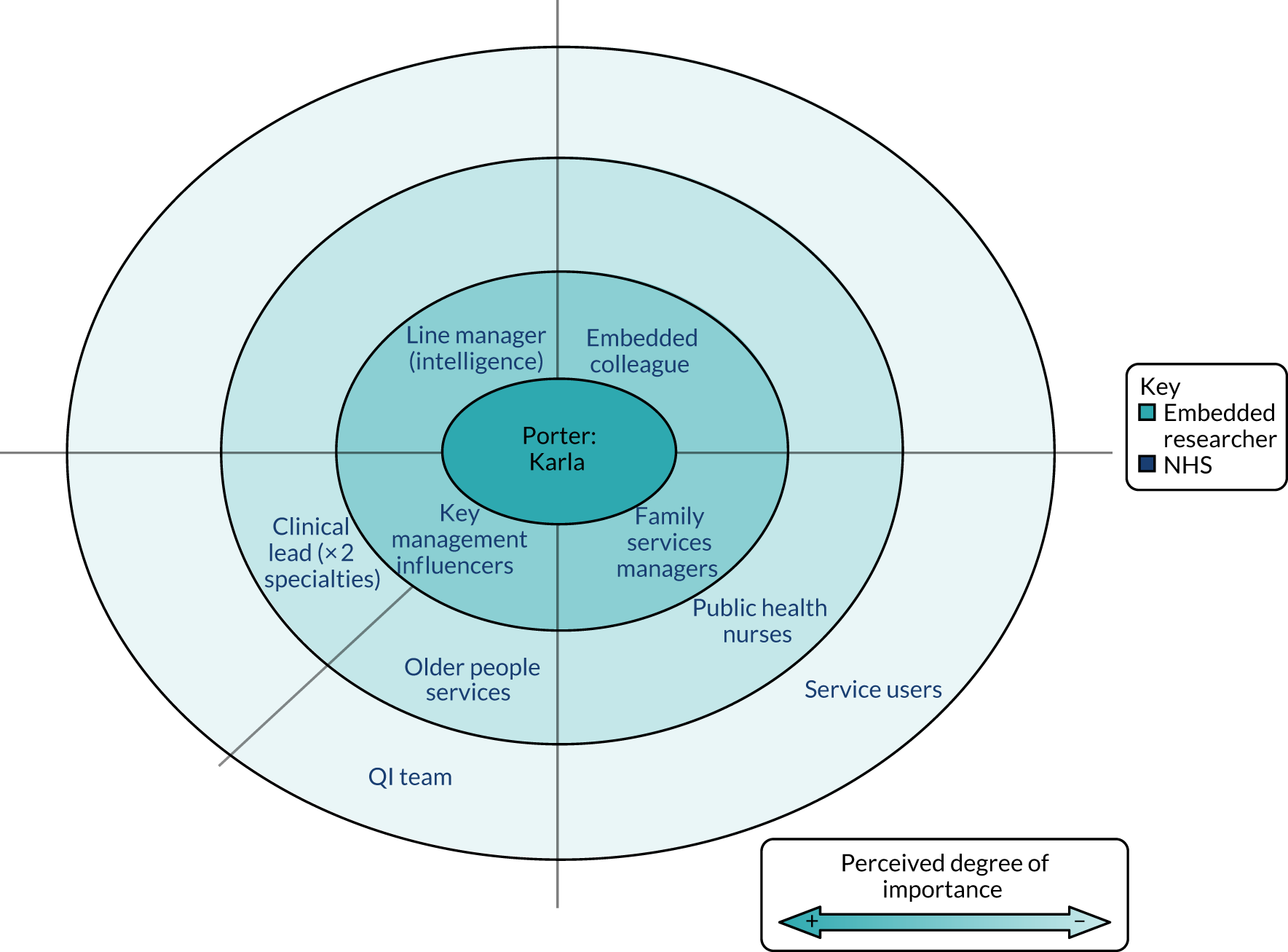
FIGURE 10.
Embedded researcher key partners: Porter – Victoria. CAMHS, child and adolescent mental health services; QI, quality improvement.
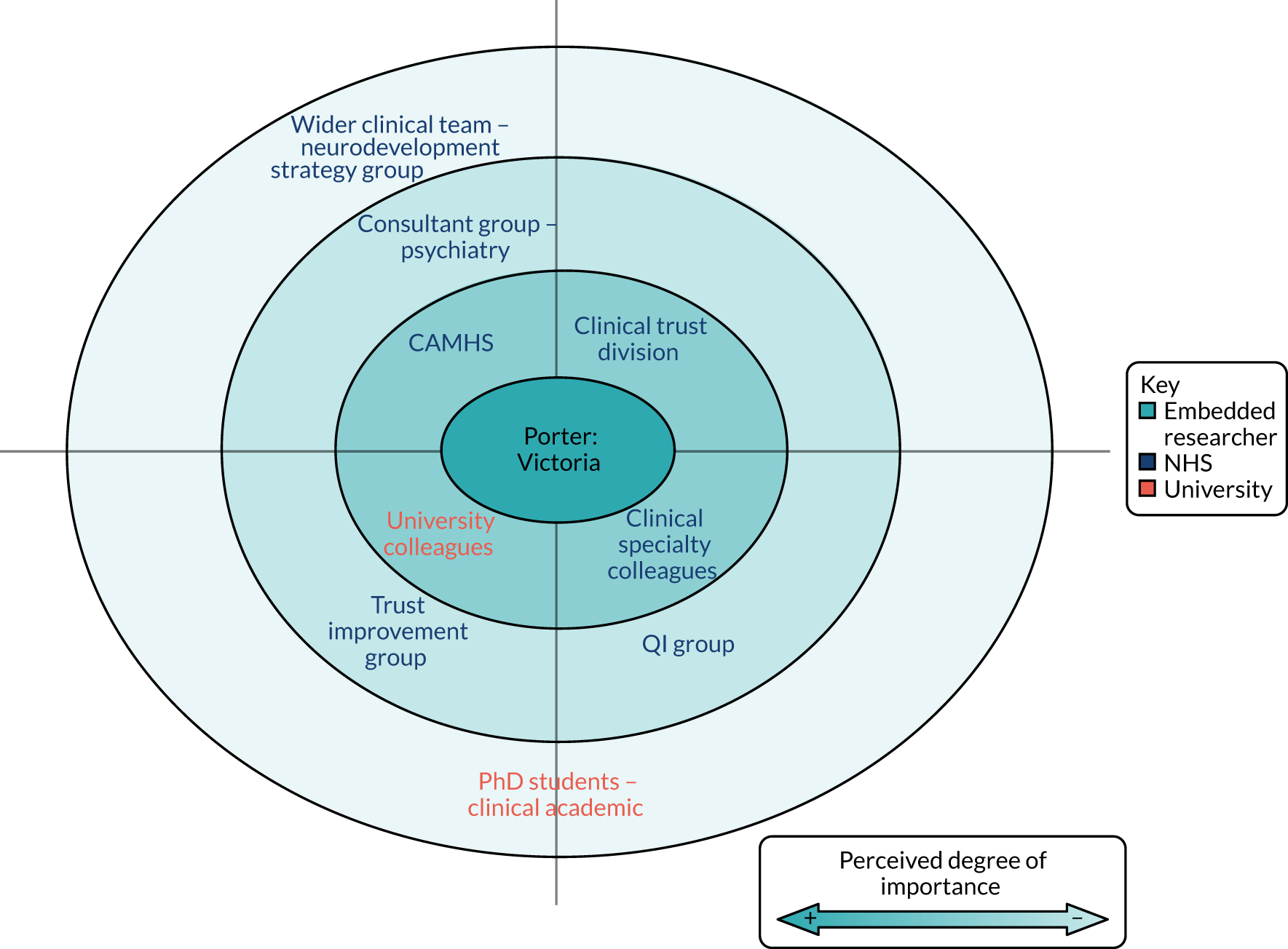
FIGURE 11.
Embedded researcher key partners: Evansville – Bella.
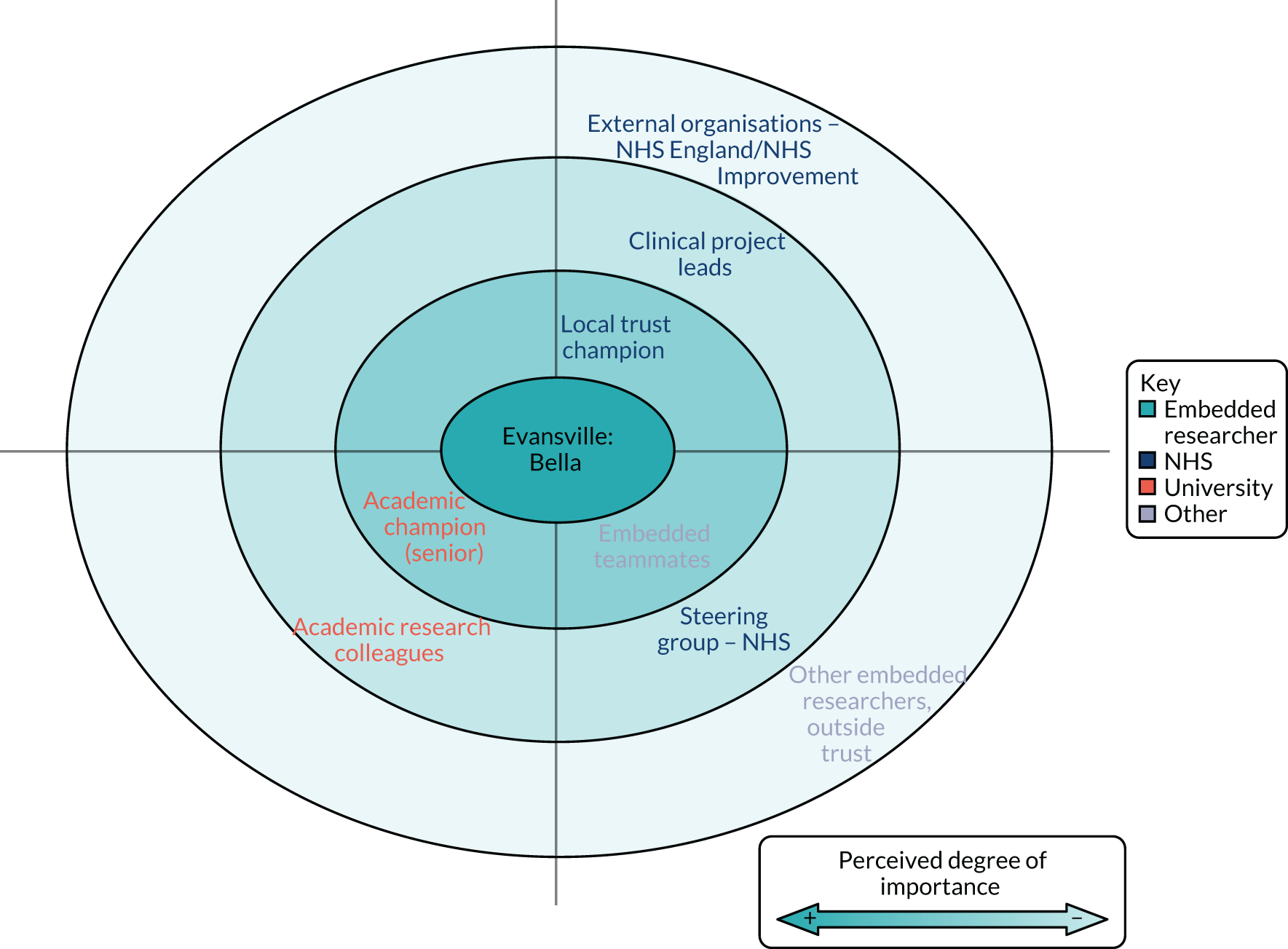
As the completed tools show, all embedded researchers had developed relationships across university and NHS organisational boundaries, but it was also clear that some relationships were weighted towards one more than the other, often depending on their background and contractual location or home. Given the focus and intent of all the embedded researcher initiatives (largely, research-informed service improvement), relationships within the NHS (especially NHS trusts) were seen as especially important. Moreover, some of the researchers at Porter (Bev and Katrina in particular) had very few academic relationships and infrequent contact with academia because of the ‘service evaluation’ nature of their work. As a result, university contacts were informal and based largely on involvement with previous treatment trials in their clinical setting. In comparison, but also at Porter, Victoria had strong, formal (contractual) relationships with both practice and academia. Again, the intent and purpose of her role was relevant: it was much more flexible, diverse and targeted at a broader organisational and strategic level.
In addition, some embedded researchers had large local, regional, national and international networks, involving a range of different stakeholders and collaborators. These could be drawn on to enrich the work of the embedded research (in terms of new or different ideas) and also to spread learning beyond the local initiative.
Overall, our research found (albeit to varying degrees and reflecting their particular backgrounds and contexts) that the embedded researchers acted as relational conduits or brokers within and between different communities to support the (co-)production, dissemination and utilisation of research to address particular strategic and operational purposes (see Embedded activities).
Most significantly, relationships with senior actors, within either or both the NHS and university sectors, were seen as particularly important for the success of each initiative. In broadly similar ways (but varying according to the level and experience of the embedded researchers), these relationships provided:
-
clarity and assurance about the embedded role and initiative (intent and purpose)
-
ongoing mentorship, support and guidance (for academic and/or clinical development)
-
sponsorship or buy-in for embedded research initiatives with third-party groups or organisations, by ‘opening doors’ and ‘providing air cover’
-
additional support and assurance around contractual and funding matters.
Researchers, then, were embedded, not just in service-related settings, but in dense and diverse networks across multiple institutions. Creating, maintaining and navigating these networks was clearly a major part of their day-to-day activities.
Patient and public involvement
The level of engagement with formal PPI groups in the embedded initiatives was variable, as were the structures and mechanisms that underpinned this involvement (Table 12).
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Anna was working to understand the organisational research culture, rather than working on individual, specific projects; general PPI was not sought in this sense. She saw her role as teaching others to engage meaningfully with PPI in their own research, and had a good relationship with the trust lead for PPI. Externally funded, co-applicant projects that Anna was involved with drew on the participation of patients and relatives (using e.g. NIHR INVOLVE) | Jane’s co-creation design methodologies involved PPI when appropriate (e.g. in co-design workshops and evaluation events). She emphasised the value of multiple stakeholder contributions, including the patient voice. Depending on the project, Jane also used formal PPI opportunities through external funders for her work on specific, larger research projects, as well as internal or trust-level service user networks and charity representatives | PPI engagement varied across the different roles. Examples included department-level PPI groups and access to trust-wide R&D PPI. PPI tended to be tied to specific projects undertaken by the researcher, rather than to the actual role or agenda of the researcher. In addition, those researchers involved in research capacity-building assisted in PPI when appropriate when mentoring clinicians | This initiative offered an example of PPI tied to the broad embedded research (team) agenda, rather than to individual projects. This was through the original set-up of a PPI advisory group by the embedded research team. The group advised on all project stages, from framing initial research questions through to how findings would be disseminated. Members of the PPI group attended the embedded steering group alongside senior trust members, thus linking both groups |
This finding only illuminates further the level of diversity (in intent, structures and processes) across the case studies, especially in terms of stakeholder involvement. Often this relates to the nature of the embedded researcher and the distinction between an explicit embedded researcher team (e.g. Evansville) and a single embedded researcher working on various, individual projects (e.g. Coxheath). As an example of the latter, as noted in Table 12, PPI at Bridgetown was not relevant for Anna’s broad embedded role, but was relevant for external projects [e.g. through INVOLVE at the NIHR: see www.invo.org.uk (accessed 3 March 2021)] and also in terms of her capacity-building work, whereby Anna pointed clinical staff towards more effective PPI in their own work.
It is important to note that experiences of PPI were shared only sparingly during the interviews and observation periods, although specific questioning by e-mail did elicit useful additional data. An analysis of the relational dimension for the PPI activity set out in Table 12 is offered in Chapter 5.
Embedded activities
The embedded researchers took part in a variety of activities and tasks commensurate with the prescribed intent and specification of their initiatives; so some activities in those initiatives oriented towards capacity development differed from those more concerned with service improvement. We observed striking differences in relation to the diversity and variability of these activities between initiatives, as outlined in Table 13.
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Activities included mapping out the existing NHS organisational research landscape and culture, and relationship- and network-building. This included mentorship, educational activities and events, and funding applications | A wide breadth of activities included networking (inside and outside the organisation), mentorship, research strategy contribution and management, dissemination, and the facilitation of numerous workshops, events and learning opportunities | Individual researchers undertook activities relating to the particular trust directorate and role. This included ‘traditional’ research, service evaluation work, capacity- and capability-building, and also contributions to the trust-wide quality improvement agenda | An array of research activities included research design, guidance, dissemination and write-up. Projects included addressing overcrowding in the emergency department and evaluation of various initiatives to improve care quality |
Detailed examples of the spectrum of activities in each of the case study sites are given in Report Supplementary Material 3, but, in brief, these comprised different mixes of the following:
-
capacity development – supporting and reviewing funding applications (e.g. master’s degrees or PhDs); methods training; assisting with individual projects (research design and implementation); mentorship, support and encouragement; relationship-building; signposting
-
improvement – service evaluation (information collation, report writing and dissemination), quality improvement (e.g. individual project support and supporting broad organisational agenda), supporting clinical colleagues with involvement in improvement work
-
research development and use – writing for publication (academic and practice audiences); grant applications; presentations (e.g. at conferences, events); networking and building opportunities for collaboration; implementation and dissemination.
As with other aspects, the embedded activities often evolved over time. In some cases, this change of focus was less visible or perhaps even intended. For example, as the research team at Evansville became established and relationships with front-line staff grew, the researchers found that their involvement in capacity and capability activities also developed and became more prominent. This had implications for their workload (as their role and work related to ongoing health services projects). The success of this ‘extra’ work left a void in some areas when the initiative ended.
Activities associated with more ‘traditional’ and ‘original’ research were also diverse, again relating to the overarching purpose of the initiative, but also the individual role. For some, contact with research in this sense was in building site capacity for randomised controlled trials. For others, they took part in funding applications, publications and various dissemination activities, offering a further example of contrast between roles in different initiatives.
The level of activity relating to strategic involvement and influence was also an important observation when examining the embedded researcher’s role: their strategic ‘voice’ either directly or indirectly was variable. For some, attending senior management team meetings was an explicit part of their role, for others their ‘attendance’ was indirectly through line managers and key strategic-level contacts. Some researchers undertook no activities outside their clinical specialty or department. In the main, the potential to engage embedded researchers in strategic activities was not always thought to have been fully realised.
Achievements and challenges
Embedded researchers and identified stakeholders were asked to reflect on the achievements and challenges of the initiative. There were stark differences in responses both within and between case study sites, suggesting differences in the perceptions, expectations and assumptions of participants. In other words, it was not easy to list achievements that were universally recognised or agreed on; rather, each local stakeholder group saw particular benefits and achievements, but also challenges, with each initiative (Table 14).
| Bridgetown | Coxheath | Porter | Evansville |
|---|---|---|---|
| Anna’s role had extensive support at a managerial level. The challenge in her role related to the existing research culture. She saw research as inaccessible to practitioners; for example, research papers were ‘pushed onto practice’ rather than trying to ‘create something that’s useful and accessible’. Anna noted how many clinicians feared research and how her role helped to challenge and change these ideas | Jane’s success was extensive and related to various applied research projects, publications and raising the trust’s profile. Jane’s influence and work were extensive and far-reaching. Challenges related to strategic relationships and values. Jane described extensively ‘siloed working’ and the challenges she faced working across multiple boundaries and organisational barriers | Investment in research roles was evident throughout the history of the initiative. The challenges varied between researchers: Victoria, for example, juggled two roles and sets of expectations. Rachel experienced many challenges relating to initial role funding. There was, however, a shared sense of the critical importance of senior ‘buy-in’ and support for the roles, to ensure sustainability | As this initiative has now finished (due to the end of funding), many of the challenges raised related to sustainability and effective dissemination of findings (to show the value of the role). In addition, the emphasis placed on the individual embedded researchers to ensure success was noted as a challenge, particularly when these members moved on |
Despite the diversity of intentions and processes among the different initiatives, we were able to collate insights into some possible criteria for assessing and measuring success. Key areas where the nature of success might be explored include:
-
capacity development – positive staff feedback; clinicians engaging in further research training and seeking out support (e.g. workshops, enquiries, e-mails); clinicians applying for grants, further research education (e.g. master’s degrees, PhDs, scholarships); front-line staff presenting at conferences and other events
-
improvement – tangible outputs such as report writing at departmental level (achieving deadlines), meeting the requirements of governance (relating to improvement involvement), interest and engagement with improvement initiatives from front-line staff, changes to practice based on findings
-
research development and use – grant applications (number and quality), publications (number and quality), uptake of findings in practice (impact case studies), international collaborations (and uptake of findings outside own organisation, nationally and/or internationally).
Importantly, the degree and nature of achievement of each initiative reflected, in part, their maturity. For example, one embedded researcher had been in post for only 12 months, limiting the scope or reach of their achievements, but also making more noticeable the significance of their impact in such a short time, especially in terms of building new relationships and networks around the role. In comparison, another long-established multiresearcher initiative showed individual role achievements (largely service improvement) and a broader sense of longevity.
Given the challenges of measuring success or achievements, it seemed that, when initiatives were more narrowly defined in their specific activities or goals, stakeholders were more able to comment on their relative success in delivering within an agreed time frame. Similarly, and again noting ambiguity, roles that were less bounded (in terms of focus, activities and scope) were often victims of their own success, and personal capacity became problematic. This was less challenging in roles bound by the requirements and focus of a specific project, service or department. Conversely, those with more ambitious or ambiguous aims, such as capacity-building or cultural change, could be seen and assessed in less concrete ways, with the likelihood of disagreement among stakeholder groups as to the level of success attained.
Concluding remarks
This chapter has presented the methods and data sources used in the four intensive case studies explored in workstream 3. In this initial analysis, we focused on ‘telling the story’ of each initiative, drawing attention to their key features, backstories and trajectories. Some interim conclusions are drawn here from the analysis, but the main discussion, in the light of the other strands of work in the project and the extant literature, and the drawing of conclusions for future scheme development take place in Chapter 8.
The over-riding conclusion from this descriptive analysis is that there is no single model or specification for embedded research, an issue also highlighted by the literature reviews of workstream 1 and the scoping work of workstream 2 (see Chapter 3). Although there may be general understandings of what an embedded initiative might involve or hope to achieve, they are interpreted, translated and enacted in different ways in local contexts. These variations reflect important historical and contextual factors relevant to each case. For example, the particular contextual priorities and pressures facing partner organisations at any given time are likely to shape how the initiative is framed and specified. Equally, the relative investment, funding or commitment to the initiative by different partners also directs the intention and specifications towards certain purposes over others.
Therefore, an embedded research initiative developed in a community hospital with relatively diffuse and limited involvement of university partners is likely to be different from an initiative created through a long-established university–NHS partnership to address specific improvement or capacity development issues. Moreover, as was evident in the trajectory of Bridgetown, where the initiative morphed as the embedded researcher changed (from Jill to Anna), initiatives themselves can shift focus and goals over time. History, context and emerging contingencies, especially in terms of funding and local service priorities, shape the rationale and specifications of any initiative.
Equally, initiatives vary according to the type (and number) of embedded researchers involved. Important variations can be seen in the embedded researchers’ professional backgrounds and their academic and professional qualifications, as well as their contractual and funding arrangements. That said, all the embedded researchers in our cases seemed motivated (albeit in slightly different ways) to close the gap between research and practice, by bringing research expertise closer to or within front-line clinical practice.
Key to each embedded researchers’ activities in closing this gap was the development and use of relationships across university–NHS boundaries. To varying degrees, embedded researchers represented, not just research capacity, but knowledge-brokering capacity. Where they varied was in what knowledge they brokered, whom they brokered between, and how they viewed the nature of knowledge or evidence. All the embedded researchers in these initiatives employed collaborative approaches to knowledge creation, with some embodying the more committed approaches to knowledge co-production explored in Chapter 2.
Success in any given initiative was often hard to define and was, in part, determined by the clarity with which the initiative was specified, for example whether or not it had bounded goals and explicit deliverable outcomes. Achievements could more easily be discerned in the form of successful processes, networks and relationships, and only sometimes in the shape of improved services. Challenges abounded across all the schemes, which suggested that the successful implementation and sustaining of embedded research is difficult. However, many of our participants (embedded researchers and wider stakeholders) spoke with enthusiasm of the potential and benefits of working in these ways.
A fuller discussion of these findings in the context of the literature can be found in Chapter 8. In Chapter 5, we turn to a deeper cross-case analysis of the four initiatives introduced here, to tease out the features and dynamics of embedded research.
Chapter 5 Embedding in practice: cross-case analysis
Introduction
Chapter 4 presented case-by-case accounts of each of the embedded initiatives studied in depth in workstream 3. The four case study sites (Bridgetown, Coxheath, Porter and Evansville) were introduced, as were their embedded researchers (see Table 10). This chapter presents a more thorough cross-case comparison of these four initiatives, informed by the analytic discoveries of workstreams 1 and 2. Specifically, the analysis is guided by the idea that embedded initiatives can vary across three main dimensions: their intent, their structures and their processes (see Chapter 3).
Methods and analysis
The methods of data-gathering in the four case studies were set out in Chapter 4 (and are elaborated on further in Appendix 3). The data analysis for the cross-case examination outlined here took an interpretative and abductive approach to explore the themes and dynamics in the cases, using the structure developed from the literature review and scoping analysis laid out in Chapter 3. An abductive approach seeks to combine inductive (grounded) data analysis with elements of more deductive (proposition-driven) analysis, with the goal of fostering close empirical–theoretical dialogue and, ultimately, proposition (theory) refinement. 174 Following Corbin and Strauss176 and Clarke et al. ,177 standard coding processes are used to generate empirically induced codes and concepts, which are then systematically related back to the concepts and theories derived from the literature, to confirm, clarify and challenge these thematic concepts as a basis for empirically informed theoretical elaboration.
Presentation of findings
In presenting the cross-case analysis, we use the 10 subthemes identified in Chapter 3 that encapsulate the domains of attention required in designing and describing embedded research initiatives.
These subthemes are arranged under the three headings of ‘intent’, ‘structures’ and ‘processes’, and these overarching categories provide the ordering for the findings presented here, with subthemes as follows:
-
intent – intended outcomes, power dynamics
-
structures – scale, involvement, proximity, belonging
-
processes – functional activities, skills and expertise, relational roles, learning mechanisms.
The names and basic contours of the four cases were laid out in Chapter 4 (see Table 7). The individual embedded researchers are also described in Chapter 4, and cross-referencing to Table 10 and the full list of interviewees, including other stakeholders, in Appendix 2 will be necessary to make sense of the findings presented here. Fuller case accounts, with extensive data, are presented in Report Supplementary Material 3.
Findings 1: cross-case variations in intent
Intended outcomes
Analysing and comparing the case studies in terms of their intended outcomes demonstrated considerable variation between initiatives, and showed that the intended purpose and outcomes of a given initiative are likely to change over time. In all cases, there were important, but often subtle, changes in emphasis between producing knowledge, building capacity and enhancing reputation, which reflected broader transitions in the strategic priorities of NHS organisations and the evolving expertise of the embedded researchers.
Different partner organisations (NHS and university) and key actors (the embedded researcher, line managers, front-line staff) could hold divergent expectations about the purpose and intent of the initiatives. This was a potential source of tension as the researchers tried to meet the expected and preferred outcomes of various parties.
A strong example of this was when embedded researchers faced competing intentions from academic and clinical practice, in terms of which type of outputs were valued: research publications for university assessment or service-facing development outputs. In cases where the researcher had two sets of competing expectations and outputs, they sometimes found creative means to meet multiple requirements at the same event, for example raising the clinical trust profile while presenting to a wholly academic audience:
So, in terms of your week then, 2 days here, 3 days there, does it look like that in practice?
No [chuckling], no, because I would have only been doing that if I was rigid about it; because the reality is, that there’s always things going on in both organisations that you need to be at, and some of those events actually benefit both organisations and that’s great . . . it makes me happy because that way I can do a bit of both jobs in one afternoon . . . For example, I’m going up to [place] to present to [academic conference] in November. That really benefits the trust – I shall, you know, put the trust banner on my presentation, and it’s all kind of clinically relevant research, but I can also count that as academic work because it’s research, and research is part of my academic job as well . . . So, it has a double benefit.
It sounds like there’s still two sets of priorities then?
Oh yeah, very different sets of priorities as well.
For senior NHS managers, the over-riding intention, in many cases, was capacity-building, specifically capacity-building that influenced patient care directly and delivered ‘real cultural change’. The researchers themselves shared similar intentions and were motivated by the potential to grow a research culture, change perceptions of research and ultimately improve staff and patient experience.
In this sense, there was sometimes a sense of superiority associated with the intentions of the embedded researcher, who had different expectations of their work to that of more ‘traditional’ academics:
I don’t want to be a full-time ivory tower academic [who] does research that’s philosophical or abstract or metaphysical or any of those kind of things. I wanted to do research that had some applied meaning, that would mean something to children and families.
Victoria, embedded researcher, Porter
The evolving and sometimes competing intentions and motivations of initiatives could put pressure on the embedded researcher, with practical implications for workload and their personal capacity. Anna, the embedded researcher at Bridgetown, was aware of this from the outset, particularly in relation to the work associated with research capacity-building (a strong intention underpinning her NHS support network). She had learned from her predecessor, Jill, that, to influence large-scale change, her approach would need to adapt:
One of the things I learned from Jill’s experience of having done a similar role before, running grant-raising groups . . . [you develop] one or two people who go on to have great careers, but they have great careers from an academic standpoint so they, they move over, they cross that boundary . . . So it doesn’t break down the boundary, it just helps one or two people cross over, as opposed to changing the system and how it works and dismantling the boundary or creating different boundaries.
Anna, embedded researcher, Bridgetown
Addressing and balancing multiple intended outcomes was central to these embedded research initiatives. Moreover, what was intended was not always explicit, fixed or even realistic, and the embedded researchers needed to pay close attention to the evolving discourses among partners and to be prepared to flex as appropriate.
Power dynamics
We observed how embedded researchers occupied an arguably unique space between clinical practice and academia. This often meant that the researcher must work across, and sometimes against, existing ‘silos’.
One of many implications of this was the distribution, and sometimes redistribution, of power and control, both for themselves and others. In some examples, such as those noted in the previous section, this redistribution of power and control was intentional; one aim of capacity-building was seen to be for front-line staff to gain more power and control to bring about change in services. There was a general sense that this change in dynamic was needed, although its far-reaching implications were possibly not always fully understood by those endorsing it, and, despite this widespread drive to empower front-line staff, researchers felt that organisational structures were not always ready for this change.
Jane in Coxheath, an experienced embedded researcher, offered her insights into ‘speaking truth to power’ – in this instance, that meaningful culture change (and power shifts) were unobtainable, being restricted by leadership styles and values:
There’s no sign-up from the executive team, and the executive teams themselves don’t have the shared values . . . I try and help the organisation to recognise what they’ve got to do to support our front-line teams . . . If you look at [name] report, the [name] report culture is the most frequent work, but they’re talking about organisational culture, not microsystems and I don’t think our chief exec[utive] understands the difference or why one is more important than the other.
And the interplay between them?
Yeah, the interplay between . . . I don’t feel there’s anybody else supporting the microsystems side, so I have to exaggerate their importance to get people to listen.
You’re saying things that people necessarily don’t want to hear?
Yeah, you’re speaking the truth to power?
‘Speaking truth to power’, in some form, was an established part of the embedded researchers’ role, and the respondents all shared their varied experiences of being a ‘critical friend’. This required a strong interpersonal skill set, contextual understanding and sometimes diplomacy (see Skills and expertise). It also required the embedded researcher to maintain professional objectivity and avoid ‘capture’ by the settings in which they were embedded.
For example, projects undertaken by the Evansville team regularly involved feeding back findings to senior NHS stakeholders. The tensions involved here were intensified for the researchers when findings were perceived as unexpected and sometimes uncomfortable. In these instances, the researchers shared how crucial it was to have senior support from outside the clinical setting, namely a senior academic to whom they could ‘diffuse’ responsibility when situations became difficult to manage:
I think that’s one of the big things around being an embedded researcher . . . all those relationships, but you need to constantly remind yourself that, you know, you are there to do a particular job. You are not like any other staff member within that organisation, you’re there as a researcher, and there is that kind of academic layer to the work that you’re doing, where you need to maintain that critical point really.
Bella, embedded researcher, Evansville
Of course, power was not always addressed directly or raised overtly in the interviews and conversations during site observations. Nevertheless, issues of power – implicit, unspoken, frequently unacknowledged – ran through the data and are touched on in subsequent sections, especially those concerning proximity, belonging and relational roles. In that sense, power, like ideas of identity and boundaries (straddling, crossing, breaching or maintaining), suffused and cut across many of the meaning categories created in the review and scoping work of Chapter 3.
Findings 2: cross-case variations in structures
Scale
The scale of the initiatives ranged from a single embedded researcher to an embedded team of up to five. Some schemes were bounded and time limited; others were more open, emergent and evolving. There were differences in terms of configuration too; for example, the Coxheath initiative was primarily configured and constructed around Jane as an individual, whereas Evansville was configured around an evolving portfolio of projects. Porter was different again, with an overarching strategic priority and focus to the configuration aimed at building research capacity and capability. The descriptive accounts in Chapter 4 outlined some of these differences in more depth.
Despite these differences, there was a sense that, in their timescales and overall life cycles, initiatives had identifiable stages of development: initially an incubation period, followed by formalisation and then a developmental stage, and finally (for fixed-term projects) a conclusion.
In the incubation period, relating to a specific individual, group or intention/idea, the initiative would begin to grow and the foundations would be laid, including the building of important relationships, ‘buy-in’ and extensive discussions over many months or even years. In Bridgetown, for example, this growth started under an earlier role-holder, Jill, developing the intentions of the role and identifying the key academic and practice stakeholders.
The initiative would then be formalised to a certain degree with role specification(s) and appointment(s) to address a given issue or project. This would include many practical considerations and arrangements, surrounding contracts and lines of reporting. At Porter, this phase in Victoria’s role offered helpful insight into the complexities of funding and contractual arrangements, in line with various expectations and intentions of the role:
I was in post for a very long time before I started to work out exactly what I was supposed to be doing, which was . . . kind of typical of the way these structures work; and to some extent, I was involved in writing my own job description . . . I’m employed by one of the directorates, not by the trust per se . . . so, I’m not actually affiliated with the R&D department . . . That made it even more complicated. [It’s] one contract with the university, that the trust buys out for 2 days a week, so it was set up as a university post, with trust partnership. So, the trust pay the university my salary for 2 days a week.
Victoria, embedded researcher, Porter
A developmental period would then follow. During this, the embedded researcher would demonstrate their potential and the role would grow; often the details of the role (particularly in terms of the nature of the work) would change and evolve in line with various expectations and demands. In many instances, the role undertaken would be different from that proposed and the overall workload larger than anticipated. Karla’s main duties in Porter related to service evaluation, but, as her role grew, she also became heavily involved in the trust’s quality improvement strategy: extra work that was not part of her original role.
In some instances, the initiative would then come to an end, as in the case of Evansville, where funding stopped at the end of its fixed timescale. Even so, there could be a degree of influence ‘left behind’ by the completed projects, in terms of increased research awareness, cultural change and service improvement. Bella, formerly at Evansville, said she was still contacted by members of the NHS trust for advice and support.
Many initiatives however – like three of the four studied here – would be funded indefinitely, with the embedded researchers on permanent contracts. As a result, the timescale of individual projects and activities would become important, rather than the duration of the overall initiative. Maintaining researcher objectivity over such longer timescales might become a concern. Scale and longevity, then, would sometimes be planned from inception, and, at other times, would emerge contingent on local circumstances.
Involvement
The teams surrounding the initiatives tended to be relatively small, compromising largely line managers and senior academic support, before branching outward to team members. Each initiative and embedded researcher had a distinct configuration or network of relationships. The partner identification tool used in the interviews helped us to identify those involved with the initiative (rather than the projects/work undertaken by the researcher in this instance), and how intrinsic their involvement was. The schematics drawn from use of that tool are displayed in Figure 5.
Each researcher identified two or three key contacts, often those to whom they reported directly or indirectly and who they felt had fundamental involvement with their work. These individuals often held senior positions in either the academic institution or the NHS, and the embedded researcher often described being ‘accountable’ to these individuals. In line with this seniority, such key contacts usually provided the embedded researcher with a degree of protection and a voice at a senior or strategic level. They were often important in ensuring funding and also access to other areas of the organisation, setting the tone from a senior level. There was universal agreement that, without these individuals and their ‘buy-in’, the embedded roles would be unsustainable.
Moving out from the centre of the partner identification tool, the individuals and groups came from a variety of sectors. Unsurprisingly, other members of the NHS team, often clinical specialties and/or professional group members (managers and department leads), were seen as important. In addition, relationships with members of the trust R&D teams were quite often seen as necessary. Again, these individuals brought access to front-line staff and their knowledge or expertise around each specific clinical context.
Academic colleagues were also identified here, showing collaborative relationships. The degree of importance placed on these formal and informal academic connections differed depending on each role. In some cases, senior academics (at dean or professorial level) were responsible for line management, but many of the academic relationships were with peers and brought shared research interests, support and a critical friend for the embedded researcher. In most instances, these relationships had been built over many years and their involvement and inclusion were of mutual benefit. Karla (Porter) offered her experience of the involvement she shared with colleague Victoria (also embedded at Porter):
So another person that I . . . have quite a bit of contact with, but I don’t know, I don’t know how to put her in terms of influence, is [Victoria] . . . Talking to her, she spans across the trust and [place]. So yeah, I suppose she’s, she’s very much like a partner, partner in crime, I guess.
So, between us we run the quality improvement group for the directorate . . . She was brought in as the strategic lead to basically get research on people’s agendas. So she is, in terms of the pecking order, very high up within the organisation, and it was her job to integrate research into people’s day jobs . . .
I’d say [she provides] peer support to be honest, because we meet every couple of months, and we just chew the fat about life in the different organisations and things . . . Because [Victoria] is still quite active in actually doing research, doing evaluation. So, it’s kind of peer support, that she’s done a PhD, I’ve done a PhD, and there aren’t many of us, what are we doing with that now? So, with that one it is more peer support, I guess, and thinking about and talking about the development of the quality improvement agenda.
Karla, embedded researcher, Porter
Other sectors involved with the embedded initiatives included non-profit organisations and wider collaborators including national and international partners (e.g. NHS England and NHS Improvement). In these instances, the embedded initiative might provide consultancy or informal input to other organisations or agencies. Students were also frequently included in the identification tool, their involvement relating to shared interests, capacity- and capability-building, and mentorship.
It is also important to note the involvement of patients. Although patients were noted infrequently during the completion of the partner identification tools, the motivation to improve their experience and the care they received was reiterated often by the embedded researchers and those supporting the initiatives. In terms of formal PPI, the researchers shared diverse experiences, largely related to the nature of their role and the projects in which they were involved.
Generally speaking, PPI was undertaken for specific projects for which it was perceived as relevant, and was accessed through existing PPI groups; this included internal, trust-level service user networks, charity PPI groups (relating to specialism or illness) and national PPI representation through schemes such as NIHR INVOLVE. Other experiences relating to PPI were shared through research capacity-building work; in these examples, the embedded researchers were encouraging and supporting others to employ PPI effectively. Evansville was the only case study to set up a designated PPI panel in relation to the initiative and the role of the embedded researchers more broadly. Despite this variability and the sometimes less tangible examples of patient involvement in initiatives, their inclusion (directly and indirectly) was viewed as fundamental by the embedded researchers.
The networks of involvement then were very specific and bespoke to each initiative and often to each individual embedded researcher. Although some connections were tight (e.g. to line managers and scheme champions), others were loose and informal, forming and reforming as needs were identified and projects developed. In most cases, PPI was limited to projects rather than being linked to the overarching strategic goals of the embedded initiative. In few cases did it seem that the connections described had been fully constructed or specified at scheme inception; instead, they emerged contingently as the schemes evolved.
Proximity
Each initiative varied in terms of how its relationships and activities afforded contact and proximity with different groups. In more obvious ways, this related to where embedded researchers and research activities were physically located. Researchers at Porter were generally located within the NHS organisation, with allocated desk space, whereas researchers at Coxheath, Bridgetown and Evansville had multiple desks (as did Victoria, the only researcher at Porter with a dual contract). Irrespective of desk space, there was a sense that work location was changeable and flexible:
I have to live my life with a pair of trainers and a rucksack, because I’m never in one building long enough to just be able to settle, I have to, I run round [location] – you know, I walk up to [location A] . . . and [location B] site is right over the other side of the city and I walk there; and the university campus is all spread out over here, and in 1 day I can be in four or five different buildings.
Victoria, embedded researcher, Porter
Much of the movement between locations was done in a conscious attempt to be more visible. There was a shared sense among researchers that physical visibility, particularly within the NHS organisation, was crucial to the success of their work. Visibility was seen as intrinsic to informal relationship-building, and generated opportunities to reduce the gap between practice and academia. Karla, at Porter, said she spent most of her time at one main location, ‘the main base [because] I like to be in the thick of things’, and went on to link this to perceptions of ‘embeddedness’:
Through writing these narrative reports I’ve started to get a really, really good understanding of the service . . . I’m visible as well, people have got to know me so people will then contact me and say, ‘oh’, you know, ‘you can you help me with this’. And actually, if I was just a name, people wouldn’t necessarily feel confident to do that . . . I think part of the embeddedness as well is actually like physical proximity . . . their hub is sat sort of probably where that couple are over there [about 5 m away], they’re that close to where I am, so quite often I’ll sort of go over and introduce myself, talk to them, work with them, so it’s sort of getting to know them as well.
Karla, embedded researcher, Porter
Embedded researchers in these case studies generally prized close proximity to the organisations in which they were embedded, but often had to work with great flexibility and agility across multiple sites and settings. Being physically co-located and ‘being seen’ were literal manifestations of the metaphorical need to close gaps between research and practice and required considerable effort.
Belonging
All the initiatives brought to the fore the importance of social, cultural and knowledge boundaries, and the degrees to which actors shared particular ways of thinking, values and norms, and a sense of belonging by virtue of their professional socialisation or organisational affiliation.
Much of the hidden or unseen work of the embedded researcher involved working across and mediating the tensions between these boundaries. At the same time, however, this created certain role ambiguities for the researchers themselves. As discussed previously, the original intention of the role could evolve, resulting in researchers taking on different areas of work. In Porter, Karla’s contracted work related to narrative report writing for local service evaluation, but her role had since grown unexpectedly and she was now also heavily involved in setting up a local, trust-wide quality improvement initiative. This ambiguity of role was experienced across all of the case studies and, in some instances, had significant implications for the number of hours worked, with few boundaries in place to limit this:
Technically [I] devote 16 hours [per week] to [the trust], but the reality is I do a bit at home on top, because you can’t squeeze it into 16 hours, that’s a nonsense . . . The other 24 hours then are university hours, but again, it’s impossible to fit my university job into 24 hours . . . I do an awful lot of the evening work, an awful lot of weekend work, a lot of juggling between posts, and a lot, wherever possible, [of] double-weighting, to try and make up some of the shortfall, because I work about 80 hours a week.
The problem is that both organisations [need you] to do the job properly, and I can’t bear not to, [and I] haven’t got enough time to do either job properly unless I put in extra hours.
Karla, embedded researcher, Porter
All of the embedded researchers therefore struggled with role and identity ambiguity relating to their sense of professional self, that is whether they were clinicians or academics (or both), whether they were aligned with the needs of the university or NHS (or both), and how they cultivated relationships with front-line staff or those facing the real-world need for research and evidence.
Each embedded researcher found their own paths to navigate these tensions of belonging, and appeared to find creative ways of resolving, or at least reconciling, multiple competing roles, in turn starting to forge new or distinct identities and belonging. They often found support, and a sense of that belonging, in informal relationships: they spoke at length about these relationships, which were often with other people in hybrid or similarly uncommon roles. These relationships, and even friendships, offered a sense of grounding, and opportunities to work through common problems or difficult experiences. Notably, the workshops and formation of the ‘embedded network’ that formed part of this project (see Chapters 1 and 6) seemed to demonstrate the emergence of a distinct occupational identity or sense of belonging around the embedded researcher role itself; for example, the researchers of Bridgetown and Coxheath came to see that they had much in common.
In summary, then, belonging across multiple sites, roles and identities posed specific challenges and additional work burdens. These were often actively managed, more informally than formally, but still left considerable unaddressed challenges and needs.
Findings 3: cross-case variations in processes
Functional activities
There were substantial variations in the nature of the work undertaken by the embedded researchers and in the scale of that work. The purpose of those activities also differed to some degree. Activities and projects included service evaluation, local and regional quality improvement, and small-scale research projects (often as part of research capacity- and capability-building). In those instances, much of the work was undertaken with a smaller, more local team. In some cases, the embedded researcher might even work one to one with an individual to support or guide a specific project.
Timescale similarly depended on the nature of the work. The heavily weighted service evaluation roles were structured around report deadlines (often annual and with accompanying interim reports). Other work, such as that relating to quality improvement, might be more flexible in its time frame and be part of larger, ongoing agendas or change programmes that took place over many years.
Researchers spoke little of formal training associated with their activities. In Porter, Bev and Katrina’s activities related largely to service evaluation, although they were also involved in recruiting for large-scale clinical trials (for which their service was often a patient recruitment site):
So, we’ll do an annual report on inpatient outcomes, outpatient outcomes, which we then share with the team, look at our outcomes, see what we need to be doing better, if we can do anything differently. So, we use that in conjunction with patient experience questionnaires . . . We’ll look at [them] and say ‘is there any way that we can improve on that?’.
Katrina, embedded researcher, Porter
Our bread and butter is service evaluation, so we’re getting outcome data for our service – that’s, that is what we have to do on a daily basis, but in conjunction with that, we do have other projects going on.
Bev, embedded researcher, Porter
For insight into the sheer range of activities undertaken by the embedded researchers, we can explore the work of Jane (Coxheath) and, to varying degrees, that of Anna (Bridgetown), Bella (Evansville) and Rachel and Victoria (both at Porter). To differing degrees, all five were involved in leading more ‘traditional’, original research, including funding applications, conference presentations and publications. Jane offered the most powerful example, with a helpful contextual insight into her activities and workload. Her work often related to relatively large, regional and national research projects, many of which she had secured funding for and that had been ongoing for months or years:
So, the work in the university, there’s two projects, but they’re not always primary research and they’ve been building on, or implementing or impact-based research . . . I’m now leading the work for Health Education England [relating to the] workforce transformation type agenda . . . that’s by July. The second piece of work is for [organisation name], so they want us to help them to develop a . . . career development framework for their mainly nursing staff at this stage, for health-care support workers across hospices . . . in the trust . . .
Two big things I’m working on, one is a single capability framework across the whole system . . . and then I’ve got three priorities, which is emergency department, general ward and children’s to apply that to, so that’s really important and hopefully will link to an IT [information technology] set-up that can be used . . . by Health Education England.
Then the other thing is . . . [a] collaborative research study across the trust to . . . and then I’ve got the ongoing stuff with the clinical leadership programme and the support of the consultant practitioners . . . There’s a conference that we’ve got in June . . .
Jane, embedded researcher, Coxheath
In short, the portfolios of functional activities of these embedded researchers were often sprawling, diverse and sometimes unmanageable, with variable (and often negligible) amounts of formal training. The activities frequently reflected a large span of scale: from local improvement projects to regional or even national initiatives; from the local, informal and unfunded, to generic knowledge generation from funded formal research.
Skills and expertise
As with the portfolio of functional activities, the skills and expertise needed by embedded researchers were many and diverse. The range described tended, in part, to reflect career backgrounds, local initiative specifications and evolving relationships with wider stakeholders.
However, common skill sets were identified, not only by the embedded researchers, but by members of their wider networks. Notably, there was considerable agreement across the varying levels of seniority; for example, managers largely noted the same necessary skills identified by junior members of the team, such as doctoral students. These skill sets could be summarised as follows:
-
possessing expertise and in-depth research knowledge
-
making research and research processes accessible
-
forming complex networks, connections and collaborations
-
building strong relationships and trust
-
harnessing the knowledge and potential in others
-
working across hierarchies
-
being committed and driven, with great stamina.
Unsurprisingly, research expertise and in-depth research knowledge were seen as central to the embedded researcher role. This assumption was shared across almost all participants in the case studies. Embedded researchers themselves naturally saw this as important, and central to their ability to adapt to new areas of research, specialties and topics. Crucially, their research knowledge gave credibility to their role:
I think that’s where the current knowledge, the current skills, the links, the experience, the knowledge and the credibility comes from; that’s what the clinical teams need, because . . . she’s not just a clinician giving advice on research, she is an active researcher giving advice on research.
So, there’s respect for that?
Absolutely, and I think that whilst my focus and priority is on that advice that she gives, I fully get and accept and desperately think we need that half-and-half split because she needs to be a currently credible researcher to give, to give the value to that research advice.
Making research and research processes accessible was also seen as fundamental to the embedded role – particularly when working to change perceptions of research and subsequently build research capacity and capability in the NHS organisation. Research was often seen as ‘out of reach’ for many clinicians and managers, and, in some instances, was deemed irrelevant. The embedded researchers’ ability to change these perceptions was seen as a necessary strength:
You said you called [embedded researcher] an ‘ally’, can you tell me a bit more about that?
[The research governance teams] are gatekeepers, and the process that you have to go through is very daunting, and the form that I’ve just sort of tried to fill out . . . it’s not the easiest of forms to do. So feeling like you’re on your own again, a barrier that you’ve got to overcome, whereas [name], well she definitely is on my side, because she had e-mailed a quick reply, I was reading it one time, she said ‘Be careful how you word such-and-such or this will happen’, and she helped us a lot, you know. So she’s always there, sort of watching that I don’t trip myself up.
The ability to form complex networks, connections and collaborations was at the heart of the embedded role. Arguably, this work sometimes received too little weight or acknowledgement relative to its importance (and relative to the more concrete and more obvious research skills). The term ‘bridging’ was used, as was ‘conduit’; however, these suggest the forming of a connection between two parties: the reality is that many of the embedded researchers were at the centre of complex webs of relationships and networks:
I can connect those people because I know what’s going on . . . [before] there just hasn’t been the forum to bring people together . . . to make those connections for people . . . I kind of feel like I’m a bit of a matchmaker essentially, because I’m kind of going round getting all this information, putting it in, and then kind of regurgitating it out in a sort of useful manner.
Karla, embedded researcher, Porter
The ability to build strong relationships and trust was key to maintaining these complex networks, connections and collaborations. There was a strong sense throughout the data that the embedded researchers were seen (and certainly aspired to be seen) as trustworthy and genuine, with no hidden agenda:
People trust her, they’re not wary of her, they believe that she’s going to be there tomorrow and have that feeling about, you know, that solidarity. And I think I’ve got the ability to give people that feeling because I’m an experienced researcher and a nurse, erm, but [embedded researcher] has it . . . So, I think there’s a level of trust . . .
You know, there are barriers that she doesn’t have to go over because she naturally lives with those barriers. Are you with what I’m saying? It’s like she’s already inside the pen, she lives inside the pen.
Peggy, nursing professor and NHS director, Porter
The skill to harness the knowledge and potential in others linked to some of the preceding skills (e.g. building relationships and making research accessible). Drawing out the potential in others and challenging their thinking (with care) were skills that embedded researchers displayed often. This related to the empowerment of others, not just those in junior positions, but also those working in senior management and leadership roles:
So, in establishing all of my ideas, my thinking, I went and sat with [embedded researcher] and we looked at the ideas, and what I was saying, and we, we had a conversation and she was able to support that conversation, that then helped me . . . articulate and reflect on my vision and then develop my thinking, such that I was able to make the pitch for a Darzi Fellow[ship].
Violet, collaborating general practitioner, Coxheath
As the quotation above demonstrates, working across hierarchies was an additional interpersonal skill strongly valued by the embedded researchers and by their wider teams. The ability to work with a variety of individuals, with differing roles and seniority, was important for success. Within this, there was the necessary ability to adapt their approach and communication to differing levels and audiences, so that the embedded researcher was seen as credible, relatable and personable:
With [embedded researcher] they know that she’s there, she was part of them, she has that ownership, that belonging. She recognises their significance; she has that continuity that’s really important . . . and before the post she’s in now really because she was embedded even when she worked for [university] – she was embedded in there. So, it’s been over time, exactly, that she’s known now, and she’s understood . . . And she can talk to people at a whole range of levels and she has that ability as well.
Peggy, nursing professor and NHS director, Porter
What has run across the range of skills and expertise noted so far has been the need for embedded researchers to be committed and driven, with great stamina. These characteristics were seen as crucial, largely as a result of the extensive challenges associated with the embedded role (including role creation, development, workload and competing expectations, alongside the cultural and strategic barriers). There was a sense that the embedded researchers needed to be strong, resilient, adaptable and committed to their role. This was voiced by many of the embedded researchers, especially Anna, Jane, Victoria and Karen:
It’s very time-consuming, and having anything that’s a split sort of role it is exhausting. It’s always more than the sum of its parts really, so it is very dependent on someone who has the energy and the drive and the vision to see something – that’s, you know, that’s not so much the norm.
Karen, associate dean of research, Bridgetown
Overall, there was broad agreement about the wide and diverse skills needed, but the degree to which each skill was important varied according to how the initiative was configured, particularly when looking at strategic involvement and the need for methodological expertise. For example, those roles that included a high proportion of service evaluation required fewer formal methods training and strategic interpersonal skills – these skills were much more relevant for initiatives that required ‘speaking truth to power’ and working across strategic organisational barriers at senior levels. The soft skills of effective communication and relationship-building, however, were always in demand.
Relational roles
The themes described in Findings 3: cross-case variations in processes show the relevance to embedded initiatives of effective communication and relationship-building. This was seen as a fundamental quality and skill of the researcher: the ability to build and sustain relationships, work across hierarchies (by being relatable and adaptable), harness skill and potential in others, and build trust were all crucial and could be described as skill in creative mediation:
Jane’s very approachable; she doesn’t make you feel stupid, she listens, she’s an active listener and then she helps you assimilate it. So . . . her communication skills are brilliant . . . and obviously the knowledge is there.
Sally, former chief nurse, Coxheath
Diplomacy and negotiation formed a large part of this relational work and were also necessary for managing conflict and balancing competing agendas, expectations and priorities.
The key influences on the nature of the embedded researchers’ relational roles were their professional background and, most crucially, the functional contribution expected of them. For example, three embedded researchers in Porter, Katrina, Bev and Karla, whose roles focused largely on service evaluation, spent less time negotiating agendas and experiencing conflict through different priorities. The boundaries and nature of their work were more tightly and clearly defined from the outset. By comparison, Jane in Coxheath was senior in both her past and current roles, and her work had far fewer boundaries and an ever-expanding remit. Within this work, she had to juggle an array of conflicts, perceptions and agendas. As a result, her extensive experience in creative mediation – the ability to relate to others and work across rigid professional and philosophical boundaries and hierarchies – was much more relevant to the success of her role.
Being accessible and relatable was universally seen as important. The researchers had to ensure that they were not ‘too academic’ in their approach, particularly if they were to make research ‘accessible’ (and change perceptions of research). All of the embedded researchers needed this ability, arguably because there was often a sense of unattainability attached to the term ‘research’, rather than a problem with any of the specific processes in ‘doing’ research (i.e. the term itself is intimidating to many people).
Additional relational aspects of the embedded researchers’ roles were covered in Belonging and Skills and expertise.
Learning mechanisms
As noted in Chapter 4 on the formal evaluation and performance monitoring of embedded initiatives, success was seen as largely challenging to measure, partly because of the ambiguity of roles, but also because of the complexity of the work being completed. There was, therefore, variation in terms of achievement and what was subsequently learnt about what was, or was not, achieved.
For work such as service evaluation reports and specific quality improvement projects, the outputs were relatively easy to monitor and evaluate. Similarly, there were individual research projects that had clear aims or objectives and tangible outputs on completion, such as publications. Such achievements were, by nature, more explicit and therefore easier to ‘see’, making it easier to recognise, in the first instance, and learn from them. Jane in Coxheath and Victoria in Porter, for example, published widely and often attended conferences. These achievements were easier to identify, and learning how to make these accomplishments was relatively straightforward.
Less easy to acknowledge, monitor and learn from, however, were projects around research capacity and capability growth. Often there was no baseline of existing understanding or culture. At the same time, measuring cultural change, particularly when it related to changes in perception and engagement, was, by nature, difficult. Much of the work associated with culture change is subtle and even invisible. Subsequent achievements can be difficult to identify and acknowledge, and subtle small-scale changes are likely to be missed.
Anna in Bridgetown was working to establish a baseline of research activity (as shared by a member of her management team, Gillian) to try to mitigate some of these challenges and offer a starting point from which achievement could be measured:
The first instance would be about how we get people being that, as I say, research active.
Is that quite difficult to measure?
Absolutely, absolutely . . . That has been quite challenging because we don’t have a baseline to work from, so it’s not something that is routinely gathered, and so it’s . . . a piece of work for [Anna]; she’s been getting ethical approval . . . to do a survey with all the staff . . . It’s a formal piece of research.
As a case study that had ended, Evansville showed that learning could be carried over into new initiatives through the accumulated experience of the embedded researcher (Bella). Bella said one initial goal of the embedded research role had been to disseminate findings beyond the immediate team, to ‘create a kind of a research or an evaluation mindset within the [whole] organisation’:
Many times, [people were] just looking at their daily practice, their work, they’re not considering types of evidence out there, they’re not thinking about evaluating what they’re doing, they’re not thinking about quality improvement. So, part of a deal for our team was, you know, to show them different ways in which they could do that.
Bella, embedded researcher, Evansville
It was only when the role was redesigned, however, that the team started sharing its findings widely every 2 months, ‘even . . . emerging findings’:
Our findings [now] are going to different implementation groups across the trusts, it’s not just going to three or four teams, they’re being presented at their group executive level in 2 weeks. So . . . the chief exec[utive] knows exactly what we’re doing, and they know what’s coming out of our evaluation so . . . We learned from that, I think, and now we’re really careful not just to focus on data . . . but actually to be able to use this formative design a bit more practically. So, I think that was one of the big issues we had on the team and one of the reasons why I don’t think we [i.e. the original embedded initiative] were funded beyond the 4 years.
Bella, embedded researcher, Evansville
Learning within the embedded research initiatives proved difficult then, not least because of the frequent lack of clarity over intentions and the emerging nature of many of the activities. Formative learning was clearly prioritised, alongside the necessary informal support systems for the embedded researchers. Summative learning was less in evidence, notwithstanding the varied governance and accountability mechanisms that played a role in shaping the overall work programmes and the day-to-day activities.
Concluding remarks
This chapter has dug deeper into the data from the four intensive case studies conducted in workstream 3. This cross-case analysis complements the case descriptions of Chapter 4, looking at the attributes and dynamics of these diverse schemes. Using the structured framework laid out in Chapter 3, and the account of knowledge co-production derived from a wide literature summarised in Chapter 2, we have drawn insights from the messy real-world experience of embedded research. As with Chapter 4, only interim conclusions are drawn here, with the main discussion of implications for future scheme development to be found in Chapters 6 and 8.
The analysis in this chapter was arranged under the broad domains of ‘intents’, ‘structures’ and ‘processes’, further broken down into their constituent themes as laid out in Chapter 3. Of course, there is much interplay and linkage between these domains and themes, and so boundaries between them should not be taken as firm or fixed. Nevertheless, this heuristic allows some degree of order to be placed on what otherwise would be a confusing mass of data.
In terms of intent, our in-depth study amply illustrated that there was often no singular or fixed intent to the schemes; rather, purposes evolved and flexed to reflect the priorities of key partners. Intentions were often shaped around building applicable knowledge (collaboratively, if not always co-productively) for the betterment of front-line services, often alongside the creation of new capacities and capabilities. Often discernible, if not always overt, was a desire to reshape patterns of power, especially the relations between academic and service partners, and sometimes also between different professions in the service settings. Intrinsic to this were ideas around the (re)negotiation of knowledge and the capacity of research to inform what counted as knowledge in context.
The structures created to support embedded research involved various practical configurations, but all had to pay attention to the scale of activity envisaged, the nature of the partners involved, and the importance for the researchers of presence and visibility in service settings. These important and relevant features, in turn, created tensions and dilemmas for the embedded researchers over identities and belonging. It was clear that such tensions, ambiguity and unsettlement were in play for many of the embedded researchers for much of the time. Managing these contradictions and tensions was a major preoccupation, drawing attention to the need for deft supervisory arrangements, careful mentoring and supportive networks.
The incredibly varied range of functional activities for many of these embedded researchers highlighted the complex processes that needed to be ‘designed in’ to embedded research schemes, and the extraordinary array of necessary skills and expertise needed to function effectively. The range of skills and styles we observed to be active in embedded research also suggests that these kinds of projects rarely settle on a single recognisable type of knowledge co-production, but fluctuate between (or sometimes blend) different approaches, sometimes more conventional, sometimes more committed. Nurturing and shaping the relational roles through which knowledge was brought to the fore and used mattered at least as much as, if not more than, standard research or project management skills in this context. Finally, given the often ambiguous and shifting nature of scheme goals, it was unsurprising that learning mechanisms, although much needed, often seemed underdeveloped.
Taken together then, the insights derived from these in-depth case studies suggest many areas of potential discussion, development and learning for stakeholders in embedded research, and it is to these issues that we now turn. Chapter 6 will move away from close-up examination of the dynamics of specific embedded cases to bring together the lessons from all four workstreams and introduce a design framework for the specification, management and assessment of embedded research initiatives. Sitting alongside this, a suite of tools, resources and supporting materials will then be described more fully in Chapter 7.
Chapter 6 Designing and supporting embedded research
Text throughout this chapter has been reproduced with permission from Ward et al. 178 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Introduction
Despite becoming an increasingly popular strategy, designing and managing the embedded co-production of knowledge is far from straightforward. As we saw in Chapters 3 and 4, initiatives can come in a wide variety of shapes and sizes and are usually both complex and emergent in nature. 158 Moreover, the nature of knowledge co-production itself is complex and multifaceted, as explored in Chapter 2. Dilemmas and challenges include the types of co-production sought, the extent to which researchers should be embedded in the organisational setting, how to manage boundaries and the (sometimes conflicting) interests of different parties, and how best to respond to the knowledge needs of organisations grappling with complex and changing hinterlands. 65,155,156
Consequentially, as we saw in the previous chapters, those involved in initiatives can struggle to consider and fully articulate the range of issues that are germane or the design options that are open to them. This, in turn, can lead to tensions within initiatives due to, for example, the differing (and often unexamined) expectations of those involved, the difficulty of evaluating and demonstrating the value of initiatives (especially to those investing time and/or money), the need to respond to changing internal staffing and external influences, and the difficulty of reconciling diverse and potentially discordant aspects of an initiative. 65,162
In this and the following chapter, we begin to integrate the findings from the research-based workstreams 1–3 into a design framework, supporting metaphors, and tools and resources to aid the design, analysis and management of embedded research initiatives. The framework is based on the extensive research reported in Chapters 2–5, work that enabled us to tease apart and map the various features of embedded co-production initiatives. It also draws on the extensive engagement and influencing activities of workstream 4, to focus on the practical manifestations of the programme of research. We present the design framework in the form of a ‘landscape map’ with accompanying materials, including a series of reflective questions. Other outputs and outcomes from the range of engagement activities deployed in workstream 4 (and outlined in Chapter 1) are also covered here and in the following chapter, to give a fully rounded picture of the contributions we have made to supporting the embedded co-production of knowledge. We conclude this chapter by drawing on our experiences of being involved in embedded research initiatives to discuss the potential utility and value of the materials for initiating and sustaining embedded research initiatives.
Approaches and methods
In this section, we describe the approaches and methods used to create the portfolio of tools, resources and supporting materials that emerged from this project. First, we explain how we developed the design framework for embedded research initiatives, drawing heavily on the research reported in Chapters 3–5. Then we revisit the engaging and influencing activities (workstream 4, outlined in Chapter 1) to show how these activities led to a wide range of supporting materials that promote and support the development of embedded research initiatives.
Developing the design framework
As documented in Chapters 2–5, the supporting research comprised a wide review of literatures on knowledge co-production and on embedded research (workstream 1), a scoping exercise of embedded research initiatives in health settings across the UK (workstream 2), and a co-production workshop with embedded researchers and their managers (part of workstream 4). This was followed by more detailed exploration of four ongoing initiatives, including about 50 in-depth interviews and an additional workshop with follow-up discussions to validate our thinking and create and refine the supporting materials (workstream 3).
The features of embedded co-production
As described in Chapter 3, our research identified 10 themes representing the common concerns of an embedded research initiative, and these were grouped under three categories relating to the underlying intent, structure and processes involved in an initiative. From each of these main themes, we then identified a number of additional subthemes that teased out the various aspects of each feature (see Table 5); their underlying rationales and evidence can be traced in Chapter 3.
Given the ongoing uncertainty about the link between what embedded research initiatives do and their outcomes, the features described should not be viewed prescriptively. Instead, they are descriptions of the conceptual and operational components that characterise embedded initiatives – areas that require focused attention and detailed articulation. Importantly, each feature illustrates the complexity and nuance of embedded research that sometimes fails to be acknowledged, disaggregated or given due regard. This led us to think of the features as a common language for describing, discussing, planning and managing initiatives, a set of tools and resources for more thorough and reflective analysis – and with greater specificity – than is usually the case.
Co-producing a basic design framework
Having identified the 10 features (and associated subthemes) from our literature review and empirical work, we held a day-long co-design workshop with embedded researchers and their managers (n = 18). The purpose of the workshop was twofold. First, we aimed to test, validate and (if necessary) amend the features. Second, we aimed to understand how best to communicate the features and work them into a practical framework for those designing or becoming involved in an embedded research initiative.
The workshop made use of a range of creative activities and was facilitated by an experienced team of researchers in design and health care (see Acknowledgements). The workshop began with participants adding comments and questions to postcards that depicted each of the 10 features with a simple icon (e.g. a location icon for proximity, a house for belonging). These thoughts were then discussed in small groups before being summarised and fed back to the rest of the group. Small groups also discussed and fed back whether or not some features were more of a priority than others. Insights that emerged during this part of the workshop included the emergent and often underarticulated nature of intended outcomes; the central (yet usually hidden) nature of power dynamics; the sense of ‘homelessness’ often felt by embedded researchers; the need to consider when and where to involve others in an initiative; the idea of proximity as a journey as much as a set of locations; and the need to manage expectations about researcher skills, expertise, roles and activities.
The next section of the workshop focused on visualising the features. Participants worked individually and then in small groups to produce physical models as three-dimensional metaphors of the features, before turning these into two-dimensional pictures. The aim was to give participants the time and space to explore and make sense of the features in different ways, and to develop insights about how they could best be communicated and shared with others involved in embedded research initiatives. Recurring metaphors drew on the natural world (e.g. trees, ferns, ponds, waves, soil), with many participants focusing on ideas of growth, tending and nurturing.
Other activities during the workshop included a discussion about formulating a network to support those in embedded researcher roles (informed by insights about the potential loneliness and ‘homelessness’ of embedded researchers) and a discussion about how to share the insights from our research and workshop (participants’ strong preference was for materials to be shared via a website and in open-access publications).
Visualising the framework and devising supporting materials
Although the workshop validated the features our research had identified, provided some powerful metaphors to describe those features and coalesced a group of people involved in embedded research, we still needed to develop the features into a practical framework to support the design, analysis and management of embedded research initiatives.
This additional work comprised three main activities: first, working with a professional illustrator to develop a single visual representation of the features; second, developing a series of reflective questions to help unpack the features and subthemes; and, third, providing a rich and evidence-rooted explanation of the themes and subthemes that would allow interested parties to track back to the published and grey literature.
To develop the visual representation of the major themes, we shared photographs and materials from the co-design workshop with a professional illustrator (see Acknowledgements) before holding a number of telephone and e-mail discussions. These focused on how adequately to represent the features in a coherent single image that captured both our research findings and the insights from participants at the co-design workshop. Between interactions with the illustrator, we discussed draft illustrations and metaphors with members of the wider team and sought further feedback from some of the workshop participants.
To support this visual re-working of the framework, we also developed a series of reflective questions for each theme, and we constructed more detailed and technical accounts of the themes and subthemes, drawing on our wide range of study materials. These additional materials drew on extensive discussions with members of our wider team and workshop participants, and, collectively, they provided material that was easy for potential stakeholders in embedded research initiatives to understand. All of these materials are freely available at the Embedded Research website. 67
Developing other supporting materials
Throughout the project, considerable attention was paid to engaging and influencing activities (workstream 4; see Chapter 1 for an outline of its approach, audience and actions). Activities ran in parallel with workstreams 1–3, drawing on and contributing to those research activities.
A project website was constructed at an early stage,67 and a series of webinars was run to create interest and drive web traffic. As research-based materials (such as the design framework) became available, these were converted to web resources and released for wider community commentary. The collaborative workshops programmed into the lifetime of the project created opportunities for the co-production of resources, which, in turn, were used to enhance the resources section of the website. The planned workshop that could not run because of COVID-19 restrictions was replaced with podcast interviews with other members of the team to provide a readily accessible record of the thinking behind the design framework. Articles in widely read practitioner journals (Health Service Journal, Local Government Chronicle) created additional interest, spread the core messages from the research, drove further website traffic and created additional useful discussions that fed back into the creation of supporting materials. Blogs and an active Twitter account (@_embedded) offered further channels to stimulate interest, and allowed followers to engage with the supporting materials under development.
Outputs: tools and resources for embedded research
The varied activities outlined in the preceding section produced a wide range of resources for those interested in developing embedded co-production to draw on. The translation of our research output (the core features of embedded research initiatives) into these resources was seen as essential if this work was to have wider influence and we were to work in ways that were sympathetic to an engaged, inclusive and co-productive orientation to knowledge. In this section, we explore the outputs created by these processes in collaboration with, and usually co-productively with, wider partners.
Because our workshop participants, and our own research and practical experience, had alerted us to the often emergent and dynamic nature of embedded research initiatives, the potentially complex relationships between the features, and the limited evidence to date on the outcomes of initiatives, we did not seek to create a prescriptive or instructional manual for embedded research initiatives. Instead, the materials were designed to provide a structured way of engaging with the complexities, nuance and choices involved in designing and developing an embedded research initiative.
So, although considerable work went into developing, sharing and validating these outputs, we do not regard them as definitive: their nature will remain provisional, their uses conditional and contextually contingent, and the contribution they make to the design and management of schemes necessarily partial. It remains our hope, however, that they will provide useful guidance.
Three groups of outputs are presented in this chapter and in Chapter 7: first, the design framework, its visual representation and its supporting metaphors; second, the set of interrogatory questions intended to build dialogical engagement with the framework; and, third (in Chapter 7), a suite of materials for those considering employing an embedded researcher or blended research and service team. Thus, those interested in learning more about embedded research can have an easy introduction and then ‘drill down’ into the nuance, substance and evidence for each theme (see the Embedded Research website67).
These three groups allow engagement in a multilayered way. The first uses the metaphor of the garden to introduce concepts of complexity, multifacetedness and interconnectivity. Then individual aspects of the garden (the themes and subthemes) can be explored both as metaphors and dialogically through questions such as those set out in Table 15. Finally, these web resources contain click-throughs to other resources such as more detailed expositions of the themes linked to the literature, published papers, case studies, job-related resources, an animation and the opportunity to join a network of like-minded practitioners in embedded research.
The design framework: an illustrated metaphor
The visual landscape seen in Figure 12 represents the features of an embedded research initiative. Drawing on the insights of the participants at workshop 1, we selected a garden as an overarching metaphor to represent the growing, emergent nature of embedded research initiatives and the active work that individuals and organisations need to put into planning and maintaining such initiatives.
FIGURE 12.
A visual landscape of the features of an embedded research initiative.
Each theme is represented as a separate area in the garden, with relevant visual metaphors as follows:
-
Intended outcomes are represented by the range of desirable produce emerging from the garden as a whole.
-
Power dynamics are seen as a river flowing through the whole space, with the scope both to power initiatives (the water wheel) and also (implicitly) to overwhelm (e.g. by flooding).
-
Scale is hinted at by the idea of a wood containing trees of different size, species and maturity.
-
Involvement uses ideas of the hive (honeybees) to suggest that collective engagement is needed to produce more than individuals can alone.
-
Proximity hints at ideas of distinct choices (the signpost), purposeful navigation (the map) and boundaries to be negotiated (the fence).
-
Belonging is represented by both a summer house (a structural space for belonging) and a picnic (reflecting informal social spaces for belonging).
-
Functional activities suggests the range of activities needed for success, their interconnectedness, ideas of investment for the future, and the toil sometimes involved in the tasks.
-
Researcher skill and expertise are represented by gardening equipment and tools.
-
Relational roles playfully suggests that actors from very different backgrounds and abilities may need to find ways to get along.
-
Learning mechanisms points towards growth (the baby birds), maturity and stillness (the wise heron) and calm reflection (seen here literally but intended metaphorically).
Questions for engaging with the framework
The integrated nature of the overarching metaphor in Figure 12 illustrates the complex interconnectivity of all its aspects, yet disaggregating the overall picture into its constituent parts also has value in teasing out distinct design components and ensuring focused discussion. Table 15 shows each of these aspects in turn and lists a series of questions designed to prompt contemplation and discussion of each feature. These questions can be used alongside the visual landscape to prompt further enquiry, articulation and discussion of key design and/or management issues at the outset and again as initiatives unfold.
| Feature or theme | Questions for consideration |
|---|---|
| Intended outcomes |
|
| Power dynamics |
|
| Scale |
|
| Involvement |
|
| Proximity |
|
| Belonging |
|
| Functional activities |
|
| Skill and expertise |
|
| Relational roles |
|
| Learning mechanisms |
|
Clearly, the questions laid out in Table 15 do not present the last word on how to explore the themes. As new or extant collaborations grapple with the concerns laid out, new ways of digging deeper will emerge appropriate to the specific initiative under scrutiny. To aid this, the framework on the Embedded Research website67 contains click-throughs to other resources, to which we now turn.
Other supporting materials from workstream 4
The design framework described above lies at the centre of a suite of practice-focused materials that aim to assist in the exploration of embedded forms of knowledge co-production. Other resources developed across the team included:
-
An animation to provide a visually attractive and engaging view of the possibilities.
-
Real-world case studies to showcase possible manifestations of embedded strategies.
-
A network of interested actors through which views and resources can be exchanged.
-
A ‘recruitment resources pack’ containing sample job adverts, job description and person specification, which can be adapted and adopted for different circumstances. The pack also includes guidance and training resources, to help the collaborating institutions consider what will make for a successful and sustainable initiative.
Given the practical nature and the target audience for the recruitment resources pack (specifically, managers, clinicians and potential embedded researchers), the recruitment resources are presented separately from the other supporting materials in Chapter 7.
Animated introduction to embeddedness
As the limitations of knowledge transfer approaches became evident, there was a need to be able to explain the nature and (potential) advantages of more co-productive approaches, such as those embraced by the term ‘embedded research’. The animation we created is designed to stimulate discussions on how embedded research is viewed alongside more traditional research methods. It asks viewers to consider how we better align academic and non-academic perspectives, to ensure that academic outputs are useful to the service and that the service outlines real-world problems for the academic community to help solve. It is intended as a resource to enable teams to consider whether or not there are models other than traditional research that may provide a more useful approach for them.
In addition, we hope that it will help to build the credibility of embedded researchers who are already in post, and support them to be accepted into the research world. Our intention is for the animation to be provocative in order to drive discussion and enable people to think more broadly about research approaches. We believe that it will interest all three of our target audience groups: NHS and local government leaders, the academic community, and front-line staff and service users.
Real-world exemplars
Real-world exemplars of embedded research initiatives are presented on the website in multimedia format, including webinars and documentation. These introduce some of the diverse manifestations of embedded co-production, allowing those interested in pursuing this approach to better understand the challenges and benefits. These examples also highlight the great variability of approaches, suggesting that there is no simple template, thus reinforcing the use of the design framework as a guide for discussions and design decisions, rather than a prescription.
Networked activities
The research proposal envisaged the creation of a network or community for embedded researchers, and the subsequent work confirmed its relevance: one of the themes identified through the literature review, and validated further through the case studies, spoke to how lonely the embedded researcher role could be. Moreover, the tension between belonging to an academic world while being embedded in a service organisation was highlighted.
This could imply an easy opportunity to create a peer network to offer support to people who may feel isolated in their roles. Our experience in this project, however, demonstrated something rather different.
When we discussed the desirability of greater peer support at the first workshop, the participants expressed considerable enthusiasm for establishing a self-managed and lightly facilitated network to allow researchers to support and learn from each other. A network was established, but, despite the initial enthusiasm, activity in the group was limited. The project team experimented with various communication tools (e-mail lists, a Google Group, WhatsApp groups), but, despite prompting within these resources, subsequent communications traffic remained generally light.
From these experiences, and analyses of the interactions through our website, actors in this domain appear to coalesce around specific activities, rather than as peers wanting to connect more broadly. This may be reflective of the diverse models of embedded research initiatives, and the very different specific subject matter people are working on; that is, the potential for common ground could be rather more limited than might first be thought. It also suggests that engagement and connecting activities across this domain may need to be more actively managed and resourced.
In contrast, we successfully connected with existing bodies, such as the AHSN network and the ARC network, to involve them in planning the resources we were developing, commenting on emerging artefacts and improving their knowledge of embedded research models. Colleagues from these networks participated in our various workshops and publicised our work widely in their own geographic and virtual networks. Project team members also attended AHSN and ARC implementation events to speak about the potential of embedded research to deliver improved outcomes and impact.
Reflecting on the tools and resources developed
As researchers and leaders of embedded research initiatives, we had seen that interest in developing this approach was increasing in both the UK and overseas. In UK health and related services alone, we identified almost 50 such schemes (see Chapter 3), and enquiries of interest in the approach from people in health service settings showed no sign of slowing.
Many of those contacting us cited their frustration with the often limited utility and impact of academic research, their desire for better situated and ‘useful’ knowledge to help them address service delivery issues, and their desire for closer interactions with researchers. But, although they recognised the promise of embedded research in addressing some of these issues, they were often unclear about the possible components of an embedded initiative, or how to go about designing a programme to meet their particular needs. This was compounded by the largely ad hoc and somewhat opaque nature of many of the initiatives that had been developed by others. We were told that this made it difficult to see exactly how existing schemes had been designed and developed, for what purposes, and with what obstacles and success.
Recognising these challenges, we extended our research in workstreams 1–3 (on the common core components of embedded co-production and the microdynamics of implementation) to create a multilayered practical framework to guide those designing, managing or analysing embedded research initiatives. That work has been described in this chapter, augmented by an account of the range of practical tools and resources that we have co-developed. The framework, scheme-related resources and associated web-based tools are now available on open access. 67
Next, we will discuss the potential for such tools to address common concerns over embedded research initiatives.
Published experience, as well as our own extensive interactions with embedded research teams, highlighted the need for open dialogue and discussion, both at scheme inception and as part of ongoing scheme development and management. 162,166 This included the need for a common understanding, agreed goals and a bespoke design that fitted the local context and met the needs and ambitions of those involved. The framework we developed provides a structured way of encouraging such shared understandings, and a means of drawing on the experience of others (through the detailed linkages in deeper layers of the framework).
Used as part of an ongoing dialogue, the framework has the potential to deepen shared understandings, highlight divergent assumptions and reveal potential (and often hidden) tensions in the design options being taken.
None of the core components identified in the framework is simple or straightforward, and many will be context dependent, or even contested by the divergent actors involved in embedded research schemes. A willingness to invest the time necessary to properly explore and negotiate ideas and expectations across the components may be advantageous, as could be a willingness to return and review these issues as schemes bed in. There is also a need for those involved to know and understand what they are getting into, and to be alert to the potential risks (and not just benefits) at different levels. This might include, for example, articulating the career risks for researchers associated with not following a traditional academic route: embedded research is often not well aligned to the norms or incentives of academia, and is demanding of time and skills. It might also cover the extensive commitment needed from key players on the service side to help navigate local politics and competing priorities within operational settings. Use of the framework and exploratory questions might usefully extend and deepen discussions in these and other areas.
In similar fashion, the practice-related artefacts co-created as part of this project offer starting points for local discussion and adaptation. Although drawing on items that are (or have been) in use, we can expect considerable extension and diversification of these materials over time. It is expected that the Embedded Research website67 will be hosted and maintained, at least in the medium term, by the Research Unit for Research Utilisation at the University of St Andrews (co-investigators VW and HD are co-directors of this unit). 179 The Embedded Research website67 will act as a repository for the tools, resources and materials developed as part of this project, with the potential to expand the materials held as the field matures.
As the ideas explored in this project spread and evolve, there will be a need for further evaluation of such schemes: for the purposes of learning and adaptation, for development of specific schemes over time (initiatives are often emergent and not rigorously defined at the outset), for comparison between initiatives of differing designs, and as a means to build a business case for further initiatives and investment.
There is also a conspicuous need for more rigorous and evaluative research on the process and outcomes of such schemes, so that more prescriptive advice can be given to those wishing to invest scarce resources. The framework and theoretical underpinnings reported here and previously have the potential to provide a common language and structured means of engagement with all these concerns, and the practical tools and resources developed have the potential to expedite scheme development.
This chapter has provided an account of the processes and outcomes that integrated insights from the research presented in Chapters 2–5 with some of components of the engaging and influencing work of workstream 4. In Chapter 7, we present the recruitment resource pack, which we hope will be practically useful to the embedded researchers, managers and clinicians who wish to design and deliver an embedded research scheme in their locality.
Chapter 7 Recruitment resource pack
Introduction
It was clear from the literature and the case study work that getting the right people into embedded researcher posts is a considerable challenge. Recognising this, we sought to provide some helpful materials to underpin the recruitment process. Drawing on the documentary resources gathered in the scoping exercise (workstream 2), and in dialogue with our study participants and members of our embedded research network, we prepared a recruitment resource pack, whose contents are presented in full in this chapter. The pack itself is available on the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)], and an editable version can be downloaded from the Embedded Project website. 67
In doing so, the team reviewed a range of job descriptions from extant schemes and used these, together with the emerging insights from the research, to create the necessary components to support recruitment. The pack contains a sample (customisable) job description and person specification for embedded research positions. The development of these incorporated the learning from the literature reviews (see Chapters 2 and 3) and the case studies (see Chapters 4 and 5), drawing in what embedded researchers and service people involved in embedded research initiatives indicated were important in terms of attitudes, skills and knowledge.
Guidance on possible approaches to recruitment and interview panel composition are also provided. These are quite generic, recognising that embedded roles could be hosted by many different organisations with different recruitment processes (e.g. see the diverse cases described in Chapter 4). These resources are supported by additional information for embedded researchers on how to prepare for their role if successfully appointed, and information for organisations on how to create a conducive environment for embedded researchers to thrive and the embedded research model to be sustained. These job-related resources could be used both by organisations looking to set up an embedded research initiative and by researchers considering an embedded research role as a career move.
The sample job descriptions and person specifications are intended to be used alongside the design framework (described in Chapter 6) to enable local teams to consider their project/team establishment and staffing as appropriate for their setting. By working through the framework, it is expected that the team will have a greater understanding of the social and organisational constructs under which their embedded research initiative will need to operate, and can thus adjust the sample job descriptions and person specifications accordingly. It is also expected that, if these resources are customised to support local constructs and contexts, then communication across partnerships will be stronger, leading to more robust local arrangements.
It was apparent from many directions, including the literature, our scoping work, the workshops and the embedded network, that, notwithstanding some common underpinnings, the actual manifestations of embedded research were very varied. For this reason, the recruitment resources noted previously and suggestions for access to training and development support were designed as broad guidance, rather than prescriptive ‘must-dos’. Training and development needs should be factored in when planning an embedded research programme or by funders seeking to seed new initiatives; however, delivery of this will be determined by both the specific programme of research and the individual researchers’ development needs. The training resources noted in the pack discuss the range of models of employment to promote sustainable embedded initiatives (e.g. shared funding models) and address the skills needed to gain and sustain funding. It was clear from many discussions that there was a risk of ‘career suicide’ for researchers unless they were strongly connected to and supported by (often through contractual arrangements) a local university setting, so these arrangements need careful thought.
The resource pack contains an introduction that sets out the background to the pack and its aims, and four sections:
-
embedded researchers – who and what are they (an overview of the embedded research role)
-
questions to consider when designing an embedded research initiative
-
helping an embedded research project to thrive
-
resources (materials to support the recruitment, training and development of the embedded researcher).
The rest of this chapter sets out the contents of these four sections.
Embedded researchers: who and what are they?
The resource pack groups the skill sets found among embedded researchers into four themes: functional activities, researcher skills and expertise, relational roles and learning mechanisms. Organisations should consider which of these is most relevant, but should bear all in mind, even if some elements of the programme have not yet been nailed down. As the findings set out in earlier chapters show, the changeable nature of embedded research programmes means that any areas of ambiguity may result in tension later down the line, particularly if expectations or accountabilities are not clear.
Functional activities
Embedded researchers must be comfortable with a broad portfolio of work, and a variety of activities within that work. Examples that we found included building relationships; collecting and analysing data; facilitating educational activities; participating in meetings; and having the project management skills to plan, manage and lead their own work.
No matter how well written the job description is, these activities are often quite fluid and will evolve with the piece of work. An embedded researcher needs to be comfortable with this emergent nature. Recruiting managers should consider how to foster any training and development opportunities to help develop some of these skills in a newly recruited researcher.
Researcher skills and expertise
Researcher skills and expertise can be defined into three broad categories:
-
Topic-specific skills relate to any clinical or practice-related issue that the embedded research initiative might focus on (e.g. diabetes, neurorehabilitation or childhood obesity). Not all embedded initiatives will require topic-specific skills, but it is worth identifying early if a specialism will be an important contributor to a researcher’s success in the programme.
-
Methodological skills relate to the research ‘know-how’ of the embedded researcher. They include the ability to define and refine the focus of the knowledge-creation activity, to collect and analyse data, and to produce knowledge of different kinds.
-
Interpersonal skills and expertise include the facilitation skills, communication skills, relationship-building skills and emotional intelligence necessary in programmes that are complex, have multiple stakeholders and rely on being able to build relationships quickly.
Relational roles
Embedded researchers will play different roles in different organisations, depending on the subject of their research. Some researchers may offer a fresh pair of eyes and a new way of seeing things. Others might provide an additional pair of hands, producing knowledge and evidence to drive the organisation’s processes and activities. They could also offer specialist or expert advice. They may do just one of these things, or all three, at different stages of the programme. An embedded researcher can also be a ‘critical friend’, so maintaining a critical stance towards the health setting is important.
A number of relational factors will therefore contribute to a project’s success, including the extent to which embedded researchers view themselves (or are viewed by others) as insiders or outsiders in the health setting, the degree of flexibility and control they have over their work (including disseminating findings), and the extent to which they are able to access spaces within the health organisation.
Relatively simple logistical arrangements, such as the employing organisation, and how easily researchers are able to access space within a health organisation can affect these relational factors, and should therefore be considered in designing the programme of work.
Learning mechanisms
Embedded research initiatives use a variety of mechanisms to learn how things are going and whether or not they are achieving their intended outcomes. Ambiguity about the aims and objectives of an embedded programme will make this measurement hard.
The NHS and other health service organisations tend to use performance monitoring mechanisms including key performance indicators and annual performance reviews, whereas programmes that are funded and/or controlled by organisations with a strong research focus tend to make use of formal evaluations.
Other programmes may use more informal mechanisms for learning and reflection, such as group or individual supervision, team meetings, workshops and learning sets.
Depending on the programme of work, the embedded researcher will need to be comfortable with the arrangements for tracking progress, and will play a key part in ensuring that this progress is tracked.
Questions to consider when designing an embedded research initiative
This part of the resource pack contains a series of prompts to help in the design of an embedded research programme, and to help create the optimal conditions for a researcher to thrive and the programme succeed. It directs users to the Embedded Research website67 to understand the background that informs the questions. The questions are grouped by theme and are set out in Table 15.
Helping an embedded researcher thrive
This section of the resource pack underscores the finding that clarity of arrangements for an embedded research programme, such as the nature of the research, how it is funded, and even logistic details, such as line management or where a person will sit, can make the difference between a highly effective programme and one that fails to flourish.
Common tensions during a project can arise from issues such as differing expectations of the researcher role or a piece of work; lack of clarity about how success will be evaluated, and what represents value for money for its funders; and a sense of loneliness or lack of belonging for the researcher, who may be perceived as an outsider by both the academic and health organisations they are working in.
This section works in conjunction with the prompts in the Resources section of the pack, and sets out a ‘handy checklist’ of ‘absolute must-dos’ before advertising a position. (Those who find their project design needs more work are pointed to the Embedded Research website67 for help with designing an embedded research programme.)
The list is grouped by topic and takes the form of a series of questions, as follows.
Aims and objectives
Are you as clear as you can be about the aims and objectives of the piece of research? Do you understand the purpose of your piece of work, and is that understanding shared across all partners? Do you know how you intend to measure performance over the course of the work?
Sponsorship
There will potentially be a tension between academic and service needs. Is there a senior individual in each area of work who can sponsor the embedded researcher to ensure that this is a positive tension?
Management
Do you have a clear understanding of, and clear agreement for, the management of this individual, particularly if it will be a joint appointment or their post will be jointly funded by more than one organisation or funding stream? Are you clear on the logistics of a joint appointment: who will offer performance feedback, support and coaching, not only to meet the programme’s objectives, but also to support the academic career of the researcher? Will the researcher have sustainable employment in the long term, and which employer should they best be employed by so they can ‘speak truth to power’ if the research results are not as expected?
Belonging
How will you support the researcher to become part of their teams in each organisation in which they work? How will you support them in their handover between teams?
Scope and boundaries
Do you have a clear idea of the scope of the work and the activities that you want the researcher to carry out? Are you clear about the accountabilities within the role, and the expectations you have of the researcher and the piece of work? Is a blended team more suitable to what you want to achieve than an individual researcher?
Introduction and support
How will you introduce the researcher to, and integrate them with, the team? Embedded researchers often have to walk a difficult line between gaining the trust of the team and remaining objective about their research; how will you support them in this? They must blend the worlds of academia and delivery, which can leave them feeling that they do not quite fit in either; what support can you offer? This will be instrumental in helping the embedded researcher to thrive.
Training and development
Embedded researchers need to possess a number of skills and often navigate complicated organisational and professional situations. For an individual to thrive in this role, how can you support their ongoing professional development? (A more detailed list of the types of training that might help an embedded researcher to thrive can be found in the next section, with information on some providers.)
Resources
This part of the pack contains resources to help organisations to recruit an embedded researcher, including a generic job description and person specification, two draft advertisements, and guidance on developing a training and personal development plan for the successful applicant. These resources are open source, and can be downloaded from the resources section of the Embedded Research website. 67
Job description
Sitting in front of a blank piece of paper to write a job description can be both daunting and time-consuming. The resources pack contains a ‘long-hand’ job description (Box 1), based on a review of a number of examples from embedded researchers already working in programmes of research. Guidance notes are included in italics in square brackets.
Employing organisation 1 (employment contract): [name here].
Employing organisation 2 (honorary contract): [name here].
Role descriptor: Embedded researcher.
Remuneration: [range on appropriate pay scale].
Responsible to: The researcher’s employment contract will be with [employing organisation 1] and an honorary contract may be held with [employing organisation 2]. There will be an assigned workplace in both settings and responsibility to both organisations.
[This is an example of useful language. In our experience, these jobs are normally organised as a joint contract; the researcher’s employment contract may be with the university and an honorary contract held in a specified department of the local authority, NHS trust, care or voluntary sector organisation. As a minimum, we recommend clarity as to which organisations are involved and who holds day-to-day responsibility for the researcher. An organisational chart may help illustrate the researcher’s lines of accountability.]
Job summaryThe embedded researcher will work in close partnership with colleagues in the university and [insert name of trust, council or voluntary sector partner] and carry out qualitative research within [organisation] in collaboration with others. The researcher will add value to the organisation through applied research that makes a difference to service delivery.
The role is flexible and responds to the need of the organisation where the research is taking place.
The postholder may be supporting people to make choices about how the research needs to be conducted. They will work on site with the delivery partners in [insert location of trust, care or voluntary sector organisation] and an academic base will be physically located in the [insert location of base at academic institution].
The postholder will foster collaborations with individuals and groups that are central to the research studies and topics that are pertinent at the time for the organisation. These may include clinicians, service users and managers.
The postholder will facilitate partnerships between academia and service colleagues to combine knowledge in order to improve [insert service specialty] design and/or delivery.
[Each embedded research role is unique and will be shaped by the organisations involved. The following are important common components that are likely to feature in most roles.]
Work with local partners to ensure that service/system transformation is catalysed using applied research.
Facilitate collaboration and networking that engages and supports activities that contribute to the research.
Undertake and disseminate research.
Develop and maintain effective working relationships with a diverse range of internal and external stakeholders.
Work closely with [insert name of local AHSN and ARC as appropriate if links have been established], one of 15 Academic Health Science Networks and/or Applied Research Collaborations in England and the main vehicles for delivering work requiring partnerships between health and care partners and academic institutions.
Key working relationships[These are some of the frequently occurring relationships encountered during the Embedded project. They vary according to programme and not all will be relevant to the work being set up.]
Clinicians, for example AHPs, doctors, nurses.
Service users/patients.
Carers/guardians.
Service managers.
Local government colleagues.
Integrated care systems colleagues.
Academic colleagues, for example research dean, reader, clinical academics.
External advisors.
Academic lead for the research programme.
Service lead for the research programme.
Academic team colleagues.
Service team colleagues.
Research and innovation director.
Methodologists and statisticians.
Clinical project leads.
Research governance, ethics and R&D teams.
Main duties and responsibilities Research strategy and deliveryThe researcher will:
-
develop an agreed research agenda with the employing organisation/system, under the direction of academic and service line managers
-
carry out research as part of [team], under the direction of academic line manager
-
support others to develop their research/evaluation skills, building research capability and culture within the organisation more broadly
-
co-produce a research programme/design a programme of work, etc.
-
liaise closely with other members of the team and staff at [organisation] to contribute to the success of the work of the team
-
review the relevant literatures, depending on the topic of the research undertaken
-
identify and contextualise significant, complex and sensitive issues related to service delivery, which are part of the research programme
-
develop proposals for external research grant funding, under the direction of academic and service line managers and in collaboration with appropriate [organisation] staff to ensure that appropriate ethics clearance and research governance approvals are obtained for all empirical research activity
-
develop qualitative research instruments
-
lead on/contribute to the analysis of qualitative data
-
plan and roll out clinically driven research
-
lead on/assist in the delivery of dissemination activities
-
draft/support drafting of progress reports as required by the principal investigator
-
lead on/contribute to drafting papers for publication
-
contribute to presenting findings to different audiences and attend relevant conferences
-
liaise with the relevant administrative team for the support of the project
-
report progress to Professor [name] and the relevant steering group.
The researcher will:
-
build networks with numerous individuals and groups to contribute to and influence organisational and research strategy
-
nurture effective strategic partnerships to identify changes in the health and care system that may be the topic for applied research
-
liaise with health/social care/third-sector [delete or add as appropriate] stakeholders on key issues and to understand their work in the context of the research programme.
The researcher will:
-
add value to the organisation through applied research that makes a difference to service delivery
-
foster close working relations with academic colleagues and service colleagues
-
build and support the professional and personal development of others (both individuals and teams)
-
act as an advisor and facilitator for organisations that are part of the research study (this could include public health, social care, NHS, local government, charities)
-
ensure confidentiality on all matters and information obtained during the course of employment.
The researcher will be competent in using a range of methods to conduct/disseminate the research and develop the service, such as:
-
capacity- and capability-building
-
service evaluation
-
quality improvement activities
-
training/guiding clinicians/managers through the different stages of the research process, and then on to publication
-
gaining insights from local practice
-
sharing formal academic knowledge
-
producing knowledge.
The researcher will be committed to their own personal career development and learning and will:
-
participate in educational activities as appropriate to the stage of their career
-
be expected to carry out their own informal learning and reflection to shape their future practice.
This job description is intended as a starting point – organisations are encouraged to adapt it to fit their programme of research and context. An editable version of the job description is on the Embedded Research website. 67
Person specification
The person specification in Table 16 is a basis to work from, designed to be a helpful tool rather than the definitive answer. Each category is classified as essential or desirable, but these classifications should be changed as required for the specific role.
| Category | Classification |
|---|---|
| Knowledge/understanding of | |
| The complex inter-relationships in organisations and how to work with these across various interfaces (primary/secondary care; public health/clinical care; commissioning/providers, health/social care) | Essential |
| How to change a research culture from an optional extra to part of core service delivery | Desirable |
| Skills/abilities | |
| Ability to quickly absorb new information and research new topics/build a network to support a requested research programme | Essential |
| Knowledge of a range of research methodologies so that these can be adapted and applied to the service | Essential |
| Strategic thinking to see beyond a presenting situation to underlying causes and research topics | Essential |
| A methodical and accurate approach to work with attention to detail and a willingness to adapt and innovate | Essential |
| The highest ethical and professional standards in health service practice, research and education | Essential |
| Qualifications/certification | |
| PhD in health service research/social sciences | Desirable |
| Master’s in health service research-related area | Essential |
| Experience | |
| Working closely with the health trust/council/voluntary partners and applying academic expertise to help solve practical problems | Essential |
| Working across organisational boundaries | Essential |
| Working with clinical trials units | Desirable |
| Forming complex networks, connections and collaborations | Essential |
| Continuous and audience-relevant dissemination of knowledge | Desirable |
| Acting as a translator and facilitator for others, enabling accessibility and potential | Essential |
| Conducting high-quality academic research | Essential |
| Co-creation and co-production of research studies | Essential |
| Line-managing junior staff and/or research supervision | Desirable |
| Using theory in practical situations | Essential |
| Engaging and managing a wide range of stakeholder groups | Essential |
| Working both independently and collaboratively | Essential |
| Supervising junior staff | Desirable |
| Track record of | |
| Gaining successful research grant funding from external bodies | Desirable |
| Publication in relevant peer-reviewed journals | Essential |
| Publication in sector-relevant publications | Desirable |
| Delivering projects on time and within budget | Essential |
| Finding creative means to meet multiple requirements | Desirable |
| Personal skills and abilities | |
| Ability to act as a ‘critical friend’ and offer a different perspective | Essential |
| Ability to build capacity and capability and increase credibility of health and care research | Essential |
| Communication | |
| Excellent interpersonal, oral and written communication skills | Essential |
| The ability to communicate information in a useful, accessible way | Essential |
| The ability to write reports clearly and quickly | Essential |
| Aptitude | |
| Resilient and committed to this way of working | Essential |
| Diplomacy and positivity to support relationships with a range of colleagues | Essential |
| Outward-facing and enjoy working with different groups of people, to develop ideas and methods | Essential |
| Desire to use academic expertise in a practical way | Essential |
| Ability to live with ambiguity relating to sense of professional self, that is clinician or academic | Essential |
| Highly self-motivated and hard-working | Essential |
| Commitment to continuous professional development | Essential |
Job advertisements
This section of the resources pack contains text for two draft job advertisements (see Boxes 2 and 3) that could be used to recruit an embedded researcher. Organisations may, however, prefer to write their own advertisement, tailored to their organisation.
We are looking for an Embedded Researcher to support applied research and make a difference to changing our research culture from an optional extra to part of core service delivery.
The successful candidate will need to be a researcher with a track record of working with the NHS and/or local government and/or voluntary sector. They will need to be independent, resilient and innovative and have exceptional influencing skills and experience of developing funding applications for high-quality research in close collaboration with health/care/voluntary [delete as appropriate] staff and managers. They will be a critical companion, diplomatically challenging staff assumptions and ideas and answering their questions with a sensitive approach.
Being ‘embedded’ in the service setting increases the potential for well-designed research, applied directly to the context in which solutions will be adopted, to facilitate successful implementation and improve health and care for service users. This model allows researchers and health and care staff to understand and value each other’s roles, knowledge and approaches and to develop their complementary skills. The team will undertake research of value both to [insert organisation title] and the wider health and care sector.
This is a fantastic opportunity for a highly applied health services or social science researcher to make a practical contribution to improving service user/patient care. The embedded researcher’s role is both to mobilise established evidence and to create new knowledge through pragmatic evaluation.
The role is wide-ranging, and the successful applicant will be expected to negotiate their contribution to the research initiative once in post and to agree a role with the partners that is both ambitious and achievable. This is likely to include the following roles:
-
working with and alongside a range of people across organisational boundaries
-
focusing on knowledge and bringing people from completely different disciplines and backgrounds together
-
being the supportive facilitator between research and practice, making research more accessible to staff as a topic and showing them how they can either use existing research and evidence or actually create research and evidence themselves.
For an informal discussion about the post, please contact [insert name of recruiting manager].
Applications should be completed by [insert link/submission information].
The closing date for applications is [insert closing date].
Ever felt you want to do something more . . . applied? Wondered how you could combine your passion for research with the operational knowledge of those working in health service delivery to make stuff . . . better? Perhaps it felt like you could do more to translate theory into practice? Well, we’ve got some good news for you – we’re setting up an embedded research programme, and we’re looking to recruit our embedded researcher.
Don’t worry if you don’t know a lot about embedded research as an approach – we hadn’t heard of it either until we saw this video [hyperlink to animation]. But when we did, the lightbulb switched on and we realised that this was the thing we had been looking for – a chance to bring research to the frontline and to make a real impact, straight away.
But we need to be up front with you: embedded researchers are a rare breed. Some would say unicorn rare. They’re passionate about research, having devoted their early career to perfecting their technical skills in research methodology and funding applications. But they also love working with a diverse group of people. They’re brilliant at communicating, and often act as the (diplomatic) critical friend to the services they work with.
Most importantly of all, they care about improving things. They want to bring the rigour of research to the messy world of service delivery and make a difference, to the patients, to the staff and to the system.
If you’re reading this and thinking ‘This sounds interesting’, then it’s almost certainly worth picking up the phone and calling us to learn more. You may surprise yourself and discover that you’re actually a unicorn and you didn’t even know it.
Applications procedureFor an informal discussion about the post, please contact [insert name of recruiting manager].
Applications should be completed by [insert link/submission information].
The closing date for applications is [insert closing date].
Interview process
As these roles can be complex, with posts often funded from two or more organisations, the selection process needs to consider the needs of all funding organisations. This section sets out five suggested steps:
-
Invite representation from all funding bodies to be involved in the selection process. This could start with joint agreement of the design of the research (see Helping an embedded researcher thrive for questions to help with these discussions) followed by the development of an agreed job description and person specification. At this point, line management for the position should be agreed.
-
If numbers allow, a representative from each funding organisation should be involved in the interview panel, allowing for appropriate gender and ethnicity representation on the panel.
-
The person taking line management responsibility for the position should ideally chair the interview panel and ensure clarity on the employing organisation. The approach to line management and sponsorship from other funding organisations should be explained to interviewees. This will help foster a sense of belonging from the outset.
-
Consider involving a public/patient representative on the panel, to again foster the importance of this from the outset.
-
Develop interview questions based on the agreed job specification, to ensure a focus on testing against essential criteria, particularly interpersonal and communication skills.
Training and development programme
As discussed previously in this chapter, embedded researchers need a portfolio of skills to be successful in their role. These skills and personal attributes should form part of the continuous professional development of these individuals. This section of the resource pack contains suggestions for this process.
Many embedded researchers will be hosted by more than one organisation, as the bringing together of research and practice in a single role often means joint funding. Organisations should therefore:
-
ensure that performance and development needs are discussed regularly with the individual researcher by both organisations they work in, that is the academic and service organisation
-
produce a shared development plan that is owned by the researcher and recognised by both organisations.
The resource pack offers a list of suggested core development activities and some optional additional activities, drawn from the research and case studies in workstreams 1–3. The list is not exhaustive and is intended as a list of options that could form part of a researcher’s ongoing development, alongside other personally identified development needs.
This training may be delivered by a variety of sources; some suggestions are listed in the final section of the pack: ‘Useful organisations and further resources’.
Core skills development
-
Communication and listening skills.
-
Presentation skills.
-
Personal resilience.
-
Service evaluation.
-
Quality improvement activities.
-
PPI techniques.
-
Budget management.
-
Developing networks across boundaries.
-
Research programme-specific knowledge (e.g. integrating care systems, building a nursing research network).
-
Writing and submitting research grant applications.
-
Writing for a variety of journals: academic and service journals.
Optional activities
-
Action learning set facilitation.
-
Coaching tools and techniques.
Useful organisations and further resources
Finally, the resource pack contains links to organisations and further resources. These include sector-level bodies, such as the NHS Leadership Academy, The King’s Fund, the Local Government Association, the National Council for Voluntary Organisations, and Universities UK, and resources for networking with similar professionals through Health Education England Library and Knowledge Services.
Dissemination plan
The tools and resources described in this chapter, underpinned by the theory, evidence and conceptual frameworks described in Chapters 2–6, have resulted in a rich legacy from the Embedded project. This section summarises how this legacy will be maintained and developed.
The Embedded research website
The Embedded research website,67 developed in partnership with the Kaleidoscope Health and Care team, is the principal and enduring source of information for anyone wanting to consider and use the learning arising from the Embedded project. The website will be maintained by the University of St Andrews Research Unit for Research Utilisation team, which, over many years, has developed a significant international reputation for its work on knowledge mobilisation.
Most importantly, in terms of making a practical contribution to supporting embedded research in practice, the website67 hosts the tools and resources developed in workstream 4 and outlined in this chapter: job descriptions and person specifications for embedded researchers, advice about how best to recruit embedded researchers, and guidance to help new embedded researchers and their host organisations prepare for carrying out embedded research initiatives. These resources are available in a format that allows them to be downloaded and customised by those who want to use them.
The website also provides access to this final report, publications arising from the project in peer-reviewed and professional or trade journals, the framework developed empirically from workstreams 1–3, an animation introducing embedded research to new audiences, and podcasts and a range of webinars and blogs developed by the research team and our partners. New information and practical resources can be added to the website, adding value to the current content.
Twitter activity
The project Twitter account, @_embedded, which, as of 11 December 2020, has 325 followers, will remain operational and is a useful way of disseminating new learning and information about future events.
Publications
Eight papers have been, or are in the process of being, produced by the Embedded team (see Publications). Six of these are aimed at academic audiences and have been/will be published in high-quality peer-reviewed journals (three of which will be open access); two are targeted at practitioners and have been published in professional or trade publications.
Presentations and wider influencing
The Embedded team has presented the study’s findings at a large number of conferences, seminars and interactive ‘melting pots’, as summarised in Acknowledgements. During the COVID-19 crisis, many of these presentations were delivered online; links to the recordings, if available, are accessible on the Embedded research website. 67 In addition, the senior members of the Embedded team fulfil a range of leadership roles in the academic and health and care sectors and, in these roles, will continue to promote the insights about embedded research gained from this project.
Concluding remarks
This chapter has presented in detail one of the key outcomes of the Embedded project: the embedded researcher resource pack. It is hoped that this will prove a flexible and useful resource for any organisations wishing to embark on embedded research. It is a rich resource, informed by research and drawn from the findings of other workstreams in the project, that should help address the challenges of developing and implementing an embedded research initiative, from the initial conceptualisation and goal-setting, to the recruitment of suitable candidates, and the support necessary once in position for the researcher and the project to thrive.
Collaboration and dialogue were important features of the resource pack’s development, resulting in a dynamic resource that reflects the real-world experiences of embedded researchers and those that work with them. In combining sets of questions and prompts with ready-made elements, such as job advertisements and person specifications that can be tailored to need or used ‘off the peg’ as preferred, the aim has been to create a dynamic and adaptable resource. A portable document format (PDF) of the pack can be printed out from the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 22 March 2021)], or an editable version can be downloaded from the Embedded research website. 67
We now turn to the final chapter, bringing together what has been learned in the course of the Embedded project before presenting a discussion on the findings and pointing the way forward for further research in this area.
Chapter 8 Integration, discussion and conclusions
Introduction
Research and researchers represent a rich source of empirical, theoretical and methodological knowledge that can help health and care organisations with some of their most pressing challenges. There is, however, a persistent and well-documented disconnect between such research-informed knowledge and the arrangements for everyday care. Addressing this has challenged policy-makers, academics and practitioners for several decades. 180 As a result, many parts of the health service are perhaps not as informed by up-to-date research-based knowledge as they might be, and there are many, as yet unanswered, questions that could be addressed by careful study.
In many health systems, considerable money and effort have been invested in the creation, synthesis and promulgation of clinical effectiveness evidence (e.g. through NICE guidelines), but health services research is far broader than this. It encompasses, for example, quantitative and qualitative data on health needs, evidence on the lived experience of health conditions and the care provided, and theoretical and empirical insights into the costs and consequences of particular ways of organising and delivering services. This diversity of topics, methods and theory, alongside the often contextualised nature of interpretation, makes the ready translation and transfer of knowledge from health services research especially problematic.
In consequence, many strategies have been developed to try to improve the connect between health services research (in all its diversity) and the health system, or components thereof. This project, Embedded, has explored, in depth, one of these approaches: the embedding of experienced researchers in service teams for sustained periods, with the explicit goal of creating new and actionable knowledge in context. Central to this is the locating of embodied research expertise in close physical proximity to the sites of action for research-informed knowledge (‘researchers-in-residence’).
In this concluding chapter, we first locate the embedded approach in the context of other strategies aimed at increasing the usefulness of health-related research (and the literatures surrounding these), and we outline the arguments underpinning the embedded approach specifically. We then revisit the aims and objectives of this project, noting progress towards those goals and any areas of deviation from our original plans. Subsequent sections reflect on the findings from this programme of work, highlighting the key insights and contributions, before drawing out some of the implications for future developments in embedded research. In outlining the contributions of this work, we have been guided by the framework for reporting new knowledge about how to improve health care, Standards for QUality Improvement Reporting Excellence 2.0 (SQUIRE 2.0). 181 The importance of PPI is also brought to the fore, together with an analysis of its often rather limited application in embedded research initiatives to date. Hence, we make some suggestions for more active involvement in the embedded schemes of the future.
We begin by exploring the range of approaches used to address the knowledge–practice gap that emphasise closer engagement between research and service actors, before homing in on the rationale for embedded research: knowledge co-production.
Promoting better research and better research use
Making best use of health services research is about getting the right research done (work that focuses on service-relevant issues) and getting the research that is available to have influence and impact through changes to services for the improvement of care. Both of these require close collaboration with service personnel and service users if they are to be achieved.
Many approaches to these challenges have been explored (Box 4). Some have been about strengthening practitioners’ research skills, building local research capacity and developing greater research awareness. 182,183 Others use brokers or intermediaries to bridge the worlds of research and practice, realising that active processes of facilitation work better than passive dissemination. 3,182 More recently, we have seen initiatives putting patients and service users at the heart of research teams,70,184 and the development of research–practice partnerships, which can exist in many guises. 183,185 Finally, taking the idea of ‘sustained interactivity’ further,9 we find initiatives that seek to ‘embed’ researchers in service settings, where they can broker external research-related knowledge, create and co-produce new knowledge in situ and build the capacities to negotiate and apply such knowledge to improve care. 158,184,186
Many structural innovations have emerged as a means of addressing the disconnect between research and practice, including:
-
Embedding research skills – research awareness has long been a part of the professional clinician’s repertoire, and many initiatives have sought to bolster research skills in the clinical setting by, for example, support for clinician–researcher hybrid roles. 173
-
Brokering expert knowledge – a variety of agencies and individuals have emerged that actively seek to facilitate the importation of research findings and evidence summaries into the care setting. 3,173
-
Developing locality-based R&D units – locally situated collaborative research infrastructures can help support better targeted applied research and undertake brokering activities. 176
-
Supporting research–practice partnerships – sustained collaborative partnerships between academic institutions and service delivery organisations can allow shared problem-solving and greater receptivity towards research findings. 174
-
Creating learning health systems – building analytic capacity into service teams so that they can access and apply evidence and better exploit insights from routine data has been promoted to spur care transformation. 175,177
-
Bringing patients centre stage – using patients as active partners and participants in research teams has a strong and growing tradition in ensuring the relevance and applicability of applied research findings. 70
-
Embedding researchers for knowledge co-production – situating experienced researchers in service settings as active members of the service team is a relatively novel, yet growing, approach to addressing the research–practice disconnect. 158,175
Although each of these models attempts to mobilise knowledge by closing the gap between the researcher and practitioner communities, there are also many differences, for example the individuals involved (e.g. researchers, health professionals, managers, service users); the nature of the interactions and the settings where these take place; the nature and extent of collaboration, and the type of activities that support this; and the character of the boundaries that need to be bridged (cultural, organisational and epistemic). Each of these can vary hugely, and their details are rarely well described in accounts of various models.
Partnerships are central to most of these models, but the structures and mechanisms for promoting and supporting such partnerships can also vary. Dimensions of effective research partnerships that have been highlighted in the literature include a sharing of power and influence within the partnership, relationships based on strategic programmes rather than individual projects, the desirability of working on common areas of interest, the need for early demonstrable advantage to the partners to justify their efforts, the importance of demonstrating a genuine commitment to partnership over time, the importance of researchers valuing a broad notion of ‘knowledge’ and ‘evidence’, and the need for practitioners to value scientific evidence. 187–192
Much of the supporting literature57,193 has focused on the attributes needed for partnership roles and on the consequences for individual post-holders. Building on this, reviews by Bullock et al. 12 and Phipps and Morton194 have considered the characteristics and capacities of individuals who seem to be effective at working in partnerships across the academic–practitioner boundary. These include good communication and negotiation skills, flexibility, the ability to engender trust, entrepreneurship, creativity, and a sensitivity to context.
Overall, many different models for better connecting research and practice through partnerships have emerged, and there is a need to deeper explore how these are put into operation and their potential. What has been published to date mostly comprises descriptions of specific initiatives or wish lists for the personal attributes of their protagonists, but little in the way of support for more structured analysis across schemes or practical guidance about set-up and management. There is a clear need, therefore, to develop better theoretical and empirical underpinnings for the different models, and to use these to help the construction of practical tools and resources. 32,38
Alongside these varied approaches, and the accompanying research effort to tease out their roles and contributions, we can see a growing number of local initiatives that deploy embedded researchers. The distinctive features of this approach are elaborated on in Box 5. 158,184 For those who judge the conventional research approach to be a distant and tardy process, insufficiently focused on utility, embedding researchers is intuitively appealing; consequently, the approach is growing in popularity in many health sectors. Indeed, we found around 50 such schemes in the UK NHS (see Chapter 3). Nevertheless, even prior to this most recent work, it was clear that challenges remain, chief of which were the problems of dual identity or affiliation, the potential for conflicting objectives between multiple institutions and the challenge for the embedded researcher of retaining a ‘critical’ academic perspective. 158
Embedded researchers, or ‘researchers-in-residence’:
-
are affiliated to both an academic institution and a service-based host organisation, spending considerable time in the latter
-
try to develop long-term relationships with staff in the host organisation, and are seen as members of the service team capable of bringing new expertise and experience to group discussions
-
import and interpret research-based knowledge and/or co-produce with local teams new research-based knowledge that responds to the needs of the host organisation
-
help to build research capacity and capability in the host organisation.
Adapted with permission from Vindrola-Padros et al. 158 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The box includes minor additions and formatting changes to the original box.
Recognising that embedded researcher initiatives were gaining traction in the UK and elsewhere, this project placed such schemes at the centre of its research focus. Before recapping on the study aims and objectives, and then setting out the key findings of the work, we first briefly rehearse the logic of knowledge co-production that lies at the heart of such embedded models.
From knowledge transfer to embedded co-production
The increase in interest in embedding researchers reflects, at least in part, a recognition of the importance of ‘co-producing knowledge in context’ as a means of crafting more applicable research knowledge that is more likely to be actioned. Rather than research and practice being construed as separate processes operating sequentially (research fed ‘into’ practice), the production and utilisation of research evidence are seen as complex, interdependent and situated activities (research ‘in and with’ practice). 11 The emphasis is on dialogue about how research-informed knowledge is shaped and understood, on encouraging productive ongoing relationships, and on creating environments conducive for change. 14
This reframing suggests that researchers need to be willing to actively negotiate knowledge among managers, practitioners and (crucially) patients and service users; they need to recognise and accommodate power differentials in who dictates how knowledge is defined; and they must adopt a pluralistic orientation to knowledge to achieve change. 26,195 Co-production models of knowledge mobilisation are based on the assumptions that research knowledge usually needs to be adapted if it is to have impact, and that all participants need to be involved in its creation, interpretation and use.
Participatory approaches, such as co-production through embedded research, attempt to mobilise knowledge by encouraging greater interaction and dialogue between researchers, practitioners and people who use health services. Beyond these basic principles, there is great diversity over, for example, the individuals involved, the academic interests or disciplines engaged, the level of embeddedness of individuals in the practice setting, the structural arrangements for such embedding, the nature and degree of co-production, and the type of activities that take place. Until recently, there has been little in the way of systematic examination of either the nature or the impact of the different approaches to embedding, and this study was an attempt to address such knowledge gaps.
Study aims and objectives
As detailed in Chapter 1, the Embedded project aimed to increase the influence of health services research on decisions about the improvement and redesign of NHS services by:
-
developing insights and understanding about the nature, challenges and effectiveness of co-production initiatives in which researchers are embedded within service settings
-
producing practical guidance on the design and implementation of embedded models of co-production for managers and clinicians in the NHS, their academic partners and people who use services.
In addressing these aims, the project focused on the following specific objectives:
-
to review the theoretical and empirical health services, management and organisational literature relevant to embedded research initiatives and knowledge co-production, and identify the relationship(s) between the two (workstream 1)
-
to gather examples of embedded models in operation around the UK’s health services and public health sectors, focusing on examples where embeddedness and co-production co-exist, and to describe the features of these models, including their history, context, participants, scale, scope and content (workstream 2)
-
to undertake in-depth case studies in four of the examples identified, in order to understand their mechanisms, effectiveness and challenges (workstream 3)
-
to provide resources aimed at assisting the recruitment of embedded researchers, alongside recommendations and guidance for their training and development, customisable for the different ways in which embedded co-production may be framed and specified, to allow those interested in developing and using such approaches to understand the design choices they face (workstream 4).
Progress against objectives
All of the aims and objectives as set out previously were met in full, with one exception covered shortly. Chapters 2 and 3 provide a full account of the two literature reviews (on knowledge co-production and on embedded research initiatives, respectively). The findings from the scoping review of UK health-related embedded research initiatives were used to augment and enrich the literature-based accounts of such schemes, and, as such, feed into the derivation of the 10 domains that were used to characterise embedded initiatives (see Chapter 3). The four in-depth case studies are presented descriptively in Chapter 4, and analytically in Chapter 5. Finally, findings from across all four workstreams are brought together in Chapters 6 and 7 to provide the promised practical guidance on the design, implementation and management of embedded initiatives in UK health settings. Subsequent sections in this chapter reflect on these findings in more depth.
The one aspect of the overall aims to which we were able to make only indirect contributions was on the issue of scheme effectiveness. As expected, published data (in the literature reviews) and systematic analyses (in the scoped extant initiatives) were very scant. Thus, we were much more able to provide rich accounts of the nature and challenges of embedded co-production than we were to provide robust evidence on their effectiveness (or otherwise). That said, the more structured ways of describing and analysing embedded co-production enabled by our analysis point to many areas where scheme rationale and coherence can be assessed, as well as contributing to the capacity for shared goals and understandings across diverse stakeholders. Such indirect assessments of effectiveness are likely to prove of great utility while we await further robust studies of scheme outputs, impacts and outcomes.
Deviations from the original proposal
Deviations from the funded protocol were minimal, and all workstreams unfolded largely to plan. There were some minor methodological adjustments to the case study data gathering, including less reliance on diary methods, but these were inconsequential (see Chapter 4 and Appendix 3). It also became clear that the extent of knowledge co-production in the embedded schemes was often difficult to discern, and so our focus tilted more towards embeddedness per se, rather than co-production (although obviously these two are often linked). Finally, there were some adjustments to the tools, resources and templates developed to support practical scheme development: recognising the sheer diversity of schemes in operation and planned, these now provide guides and customisable resources rather than definitive items (see Chapters 6 and 7).
One area where progress was limited was our goal of creating an active network for those engaged in developing or running embedded research initiatives. In general, this proved relatively muted in operation, for what appeared to be two main reasons: first, the sheer diversity of approaches to embedding researchers sometimes precluded shared interests, terminology and concerns; and, second, potential network participants consistently noted that interactions depended largely on saliency (i.e. engagement was sporadic depending on what participants needed to know at specific points in time). Despite initial enthusiasm from participants, and several attempts to create and facilitate the network, including experimenting with different technologies (e-mail discussion lists, Google Groups and WhatsApp chats), it never reached self-sustaining status.
The only other significant deviation from the original proposal occurred towards the end of the project (March 2020), when some of the engagement activities (notably, the final workshop) had to be reworked in the light of the COVID-19 crisis. However, it proved possible to achieve the aims of these activities through other means, for example by tapping into professional networks, having virtual conversations with the more active members of the embedded network and attendees at prior workshops, and drawing on the materials produced at workshop 2. Hence, the COVID-19 disruptions did not hamper the overall achievement of the project objectives.
Reflections on the findings
In the following sections, we reflect on the findings in the light of the aims and objectives as set out previously. The two literature reviews (augmented by data from the scoping review) provided clear and structured language that has allowed us to describe and disentangle diverse approaches to both knowledge co-production and the nature of embedded research initiatives. In addition, the scoping review provided a snapshot of the landscape of health-related embedded research initiatives in the UK in 2018, and contributed to a deeper understanding of their design contours and operational challenges. The in-depth case study work that followed, in four divergent examples of embedded researcher schemes, provided additional insights into the dynamics and life cycles of such initiatives. Finally, integration between the emergent findings from each strand of the research and the engagement and influencing work of workstream 4 led to a range of tools and resources for embedded scheme designers. Each of these sets of findings is now elaborated in turn, with a concluding discussion on the role of PPI in embedded research initiatives.
A language for knowledge co-production
In recent years, attention has turned to how closer relationships and partnerships can be assembled that enable researchers and non-researchers (including policy-makers, practitioners, service users, carers, the public) to create knowledge collectively. For those crafting policies, designing and managing services and delivering care, co-productive relationships around knowledge offer the prospect of more relevant, timely, contextually sensitive (and, therefore, usable) knowledge directly applicable to organisational needs. 33,196 For researchers, knowledge co-production is seen to offer easier access to research sites; stronger and more effective research collaborations; more engaged scholarship;167 and greater engagement, influence and reward for their work. In addition, there is the possibility of achieving and evidencing ‘impact’ with academic work, neatly fitting with the increasing rhetoric and use of metrics around this topic. 197 For similar reasons, knowledge co-production also clearly holds some attractions for funding bodies. 127
Co-production, then, has risen quickly to prominence as an approach to knowledge-making. Promising to address many well-worn problems of creating actionable knowledge that is fit for purpose, it is invested with great hopes, alongside some emerging fears and disputation,82,198 across many disciplines. Our review and synthesis of the burgeoning literature (see Chapter 2) offers a means of exploring and disambiguating the conceptual underpinnings in a way that also provides practical tools and resources for collaborative conversations.
What we found, from reading across the literature and developing a framework analysis (see Chapter 2), was that issues and approaches in knowledge co-production could be thought of in five main domains of meaning: politics, knowledge, identity, space–time and aesthetics. Drilling down, each of these domains yielded two subthemes to provide a finer-grained analysis of the issues. Furthermore, we found that each of these domains could be overlaid with a graded spectrum of co-production ‘styles’, from relatively conventional research processes, through provisional, moderate and committed, to, finally, radical knowledge co-production. The exploration of meanings in each of these domains and across these spectrums, and the surfacing of very divergent exemplifications of co-production, provide some clear conceptual guidance and more precise language to aid in the disambiguation of both the rhetoric and the practice of knowledge co-production.
Disentangling distinct conceptual concerns in this way will, we hope, lead to further discussion and insights on the nature and role of co-production processes, helping to prompt more focused empirical and evaluative work. More pragmatically, we hope that the framework we have presented will be used by those involved in embedded initiatives (and, indeed, in knowledge co-production achieved through other means) to articulate their understandings of their own and each other’s approaches. This, in turn, may help to clarify, and support discussion of, the implications of their respective stances, and so facilitate better communication around the difficulties and challenges of such collaborations.
As well as aiding conceptual clarity and being of practical use, our analysis moves to forestall a growing risk that knowledge co-production could become unattractive as a result of its complexities, ambiguities and difficulties, which can all be germinal points for misunderstandings, disappointments and disillusionment. 198 Debates about knowledge for practice and policy are, we think, well rehearsed,4 and new grounds for conversation are needed if we are collectively to create a more progressive and enlightened culture around knowledge production and use. In short, we must be able to make the most of different possibilities for co-producing knowledge, and the first step to capitalising on them is to find ways to think and speak about them with greater clarity. 198 The work presented in Chapter 2 begins the task of arraying these different possibilities so that they can be systematically and transparently explored. All of this has great relevance to embedded research initiatives, many of which have co-production at their heart (at least rhetorically, if not always so obviously in practice).
Crucially, our work in the review and synthesis was not an attempt to solve the problems of co-production, or even necessarily to promote its application (although it is clear that we think it has some potential). In exploring the growing literature, we were acutely aware of the frequently aspirational and rhetorical uses of language in this field. During our analysis, we sought to lay out constellations of ideas and themes, with their associated tensions, overlaps and consequences, without lapsing into judgement or advocacy. The value of this analysis lies, we believe, in its capacity to provide a useful framework for more thorough conceptual work and better communication over practices in this area.
Overall, knowledge co-production can take many and diverse forms, from approaches more akin to conventional collaboration to those with much more radical intent. To date, many embedded research initiatives do not appear to have fully understood or engaged with this diversity and there may be advantages in doing so using the conceptual groundwork we have laid out in Chapter 2.
The landscape of embedded research initiatives in the UK
Embedding researchers in service delivery, public health or service commissioning settings is a key means of developing knowledge co-production. Knowing that embedded research initiatives (or ‘researcher-in-residence’ schemes) were springing up in UK health settings made an analysis of such schemes a timely proposition. The combination of literature review and scoping of extant schemes allowed us to develop a bounded account of what constitutes embedding and a structured way of describing the components of such schemes (see Chapter 3), even when the contours of these components in practice are more implicit than explicit (such as addressing power dynamics).
Reading across the 45 embedded researcher schemes uncovered in the UK (those that met our criteria as set out in Chapter 3), a number of features of this landscape became clear. First, schemes were in place across the UK, and were located in primary, secondary and community settings. It was clear that this approach to the knowledge–practice puzzle held some wide and enduring attractions. Second, the scale of embedded research initiatives was highly variable, ranging from single short-term projects to longer-term programmes of work or strategic partnerships, sometimes involving multiple embedded researchers. Relatedly, some of these initiatives were funded for fixed periods, some had secured sequential funding as they evolved, and others were in receipt of more stable ongoing support. Third, around half of the schemes used university-held contracts for their embedded researchers, around one-quarter used NHS contracts, and joint appointments were relatively unusual (only about 10% of schemes). Finally, it was clear that some initiatives were carefully planned from the start, but many more were evolving and emergent, with changing intentions, structures and processes.
The formalised accounts in the published literature (which tend to focus on a relatively established or successful subset of schemes) were usefully enriched by the intelligence gathered on the wider hinterland of schemes in the UK. From the scoping work, we gained sight of internal scheme documents, and interviewed embedded researchers and scheme managers, to gain insights into the intricacies of scheme design and delivery. This work, when combined with the literature review, led to the exposition of 10 domains (grouped under the headings of scheme intents, structures and processes) that provided a comprehensive way of articulating the contours of embedded researcher initiatives (see Chapter 3). What was clear from this analysis was that there were many different ways of constructing embedded research initiatives, and that there was real diversity of approach across the field, as well as a frequent reshaping of approach in ostensibly a single initiative over time.
This research provides then, for the first time, a robust theoretically and empirically informed tool to describe and analyse embedded research initiatives. Such a tool can be used for various purposes: for research, to delineate embedded researchers as interventions that can be compared and evaluated; for practice, as a design aid to the development of new schemes (see the extended account of such a development in Chapter 6, and later discussion in this chapter); and for management of extant schemes, by aiding dialogue between stakeholders. It was also clear from the later case study work that significant tensions could arise between and within stakeholders in embedded research initiatives; the tool described here can provide a useful framework for exploring (if not always resolving) such tensions.
Finally, the work in understanding the landscape of embedded research in UK health settings underpinned the workstream 3 case studies in various ways. It aided the identification of potential study sites: the scoping work enumerated all the sites known to exist and provided sufficient information on the intent, structure and processes of those sites to allow for purposeful selection (see Chapter 4). Moreover, the 10 domains surfaced through the literature review and scoping interviews provided a means for structured engagement with stakeholders: shaping the interview schedules (see Appendices 4 and 5), the use of the partner identification tool (see Appendix 1) and the focus of site observations (see Report Supplementary Material 4). Ultimately, the data analysis of the case accounts (both descriptive and analytic) drew on and expanded the insights articulated in the earlier workstreams; it is to this that we now turn.
The dynamics of embedded research initiatives
We purposively selected four embedded researcher initiatives (denoted as Bridgetown, Coxheath, Porter and Evansville). These showed marked differences in the embedded researchers’ backgrounds, motivations and practices, yet a common thread was a desire to ‘make a real-world difference’, to get research ‘out of the ivory tower’ and to improve local services. Using the design domains surfaced in workstreams 1 and 2, we also saw much diversity in the scheme intentions, structures and processes. Taken together, these provided many insights into the wide range of embedded tasks and activities undertaken in the roles.
There were common themes across the schemes in their basic intentions. The embedded researchers (and members of their networks) aimed at mediating between different forms of knowledge, negotiating organisational, cultural and epistemic boundaries to promote co-produced, shared and actionable understandings. There were also significant differences between schemes (indeed, sometimes within schemes, e.g. in Porter). The degree to which knowledge co-production was evident varied considerably: even though these cases were all selected in search of co-production, the approaches deployed were more usually provisional or moderate (see Chapter 2) with more radical intents towards knowledge co-production largely absent. The degree to which active co-production figured was often dependent on the framing and structuring of the embedded researchers’ roles: less bounded roles usually offered greater scope than those roles with narrow and concrete goals.
Often there was no single or sustained intent, at least explicitly. Intentions evolved or fluctuated over time, sometimes only crystallising as the scheme matured. The intents/purposes were also influenced by key partners, not only at the design stage, but as schemes unfolded. The individual skills and motivations of the embedded researcher were also influential, especially in shaping some of the changing goals and increasing ambitions of the schemes.
Most intentions (as articulated by the embedded researchers, but also by their service partners and associated networks) were related to creating situated knowing by brokering external knowledge and combining that with locally collected data, building research capacity (to shift capabilities from academic institutions to front-line staff), and enhancing a reputation for research-informed care. Because of this range, the embedded researchers were often left to juggle, prioritise or reconcile competing and changeable expectations about what being embedded actually entailed. As a result, embedded initiatives (and especially their embedded researchers) needed advocacy at strategic levels: people who could ‘see the big picture’, shape the narrative and influence expectations. Embedded researchers also needed support (from academic partners) to maintain critical distance and objectivity, with local ‘capture’ being an occupational hazard.
A common theme under ‘intentions’, often raised obliquely, was the need to address power dynamics. The issue of power was seen as a potential minefield and was rarely addressed directly in the articulation of scheme intents. Nevertheless, a restructuring or rebalancing of power across different stakeholders was often implicit, not just in scheme intentions, but also in how these intentions were put into operation. However, understandings of power were, perhaps unsurprisingly, fairly rudimentary, and this remains an underdeveloped aspect of embedded research initiatives and of knowledge co-production in general.
Looking across these insights, it is clear that the intentions of embedded research schemes are far more complex than initially might be assumed. The diverse and dynamic nature of these goals makes for very different schemes under the broad rubric ‘embedded research’, and this diversity is seen equally often in the assembled structures through which embedded research is to be delivered.
Core to the operationalisation of an embedded research scheme is the creation of opportunities for sustained interaction between the embedded researcher and actors in the non-academic setting. Practical matters such as contractual arrangements, line management and physical location all contribute to proximity, visibility and perceived contributions. Such structural arrangements also have implications for more nebulous concerns, such as a sense of belonging or the maintenance or blurring of professional identities. There was much ‘hidden labour’ by embedded researchers in negotiating these concerns, and a real necessity to draw on wider networks and senior advocates to help achieve ‘buy-in’, ‘open doors’ or ‘provide air cover’.
The structural arrangements, and the softer consequences of these noted previously, often went through a recognisable trajectory: an initial incubation period exploring the possibilities; a degree of formalisation as the embedded researcher came into post; developmental work to ‘flex’ the arrangements as the scheme bedded in and responded to local contingencies (not least of which are the skills and aptitude of the embedded researchers themselves); and, finally, some consolidation and addressing of sustainability issues, or (for fixed-term initiatives) a managed completion and attention to legacy issues.
The dynamic and contingent nature of these structural arrangements, although a key element of the model, poses real challenges: when schemes are (explicitly or implicitly) in a process of ‘becoming’, there is a real need for ongoing dialogue among all stakeholders to keep coherence and alignment. Changes of personnel in the service setting, and evolving knowledge needs, reinforce the necessity of structured engagement and shared understandings. The insights gleaned from the literature reviews and the empirical work, and the tools and resources laid out in Chapters 6 and 7 (to be discussed shortly), could be seen to assist such processes.
Whatever the structural arrangements, embedded research initiatives delivered value through the activities and processes that they pursued. These varied dramatically, but included (to different degrees) activities aimed at research capacity development, activities related to research itself and activities in support of knowledge utilisation and service improvement. Either directly related to these ‘goal-supporting’ activities, or more indirectly necessary to build visibility and support for the initiative, were diverse activities aimed at creating, maintaining or strengthening networks, communications and relational bonds. Such relational processes were at multiple levels, including the strategic (securing senior management and clinician buy-in), cross-professional (building support for new research or improvement projects) and peer to peer (maintaining academic support networks and searching for informal support from people in similar roles).
The wide range of supporting processes and the emphasis on relationship-building often placed significant strains on embedded researchers. This draws attention to an apparent paradox at the heart of embedded research schemes: the relatively simple idea of placing research expertise at the sites where research-informed knowledge is most needed is gainsaid by the complexity of the structural and processual arrangements needed to support such placements. This further reinforces the need for training to support an embedded researcher’s own capacity development, and organisational strategies to ensure that appropriate support functions are in place. Again, the tools and supporting materials described in Chapters 6 and 7 may have a productive role to play.
Given the wide-ranging (and sometimes implicit) nature of embedded scheme intentions, and the varied and sometimes nebulous nature of the processes used to achieve these, it is unsurprising that most schemes struggled to articulate or evidence success. Although the enthusiasm for, and belief in the potential of, such schemes was widely evident (and there is a strong theoretical rationale based on critiques of ‘knowledge transfer’), systematic (as opposed to perceptual or anecdotal) evidence of effectiveness was harder to come by. Moreover, the scope for assembling such evidence varied as a function of the boundedness and definitional clarity of the schemes. Initiatives that were relatively narrowly defined (in terms of scope, activities, skill set, expectations, etc.) tended to have concrete deliverables that were more easily achieved and acknowledged. Embedded roles with more ambition and broader goals (such as increasing absorptive capacity or changing the culture around knowledge and collaboration) had more ambiguity and fewer boundaries, and, therefore, were much harder to assess, monitor and manage.
Overall, the case accounts and the insights drawn from them add nuance and depth to the 10 domains of embedded research uncovered through the literature work and scoping review. By themselves though, such insights sit more in the research domain, perhaps not so readily accessible to scheme protagonists. A core plank of the Embedded project was to ensure that robust insights rigorously derived through research were made widely available through practical tools and resources, and it is to these that we now turn.
Tools and resources to support embedded research schemes
As befits a project concerned with knowledge co-production, we adopted a collaborative, creative and engaged approach to translating the research insights into practical tools and resources (see the account of the overall engaging and influencing strategy in Chapter 1, the specific account of tools and resources creation in Chapters 6 and 7, and the recruitment resources pack in Chapter 7 and on the project web page [www.journalslibrary.nihr.ac.uk/programmes/hsdr/165221/#/ (accessed 18 February 2021)]. This led to a design framework (with visual metaphors, dialogic questions and interactive web resources) and various other supporting materials (e.g. an introductory animation, case studies of existing schemes and a recruitment resources pack). We anticipate that, collectively, these tools and resources will support the development of new embedded research schemes, their ongoing management and evolution, and (importantly) renewed efforts to examine their effectiveness both formatively (as part of within-scheme learning) and summatively (as part of a wider research effort to assess impacts).
In terms of developing new schemes, much of the literature on embedded research highlights the importance of agreeing and communicating the intention, structure and processes of initiatives early and clearly. 65,162 Such calls tend to be born of the frustrating experiences of embedded researchers who are often faced with the need to manage competing demands and expectations and respond to the differing needs, priorities and values of the individuals and organisations involved. These dynamics were also readily seen in our case studies. We suggest that many of these frustrations and tensions stem from the difficulty of identifying and discussing the multiple features of an embedded research initiative, especially at its inception. A further layer of tension is introduced by the difficulty of reconciling some aspects of embedded research with one another (e.g. an initiative premised on disrupting power dynamics will need to pay particular attention to the contractual arrangements, as these may work with or against existing power relations). We propose that our framework provides a way of assessing the internal coherence of planned initiatives and the extent to which the various features have been considered and discussed sufficiently by those involved.
Moreover, because many embedded schemes evolve over time, the framework provides a means of revisiting design considerations in an ongoing manner, hopefully contributing to better communication and alignment across stakeholders. By focusing not just on the main design parameters (intentions and structures), but also on the more dynamic array of processes (what embedded researchers actually do), it should allow better dialogue between embedded researchers and other stakeholders as schemes mature or become reconfigured. Local learning too may be facilitated.
Many embedded research initiatives appear to lack clear mechanisms for learning and evaluation. This is perhaps unsurprising, given that the difficulty of evaluating such complex and relational knowledge/practice initiatives is well documented. 199,200 It is, however, becoming increasingly accepted that evaluating complex social initiatives depends on the ability to articulate and link the intended outcomes, activities and resources associated with the initiative. 199,201 This can inform, not only summative, but also developmental approaches to evaluation, which may be particularly valuable given the fluid and emergent nature of embedded research initiatives. We suggest, therefore, that our tools, resources and supporting materials can provide a basis for articulating an embedded research initiative’s intended outcomes, activities and resources and for building a coherent logic model to guide evaluation and learning. Such evaluative work is needed not only to support scheme evolution, but also to create an evidence base to underpin the selection of embedded approaches in the first place.
In these ways, we hope that our tools and resources can make a substantial contribution to the maturation of the field. Moreover, all the tools and resources described in Chapters 6 and 7 (and discussed here) will remain available67 hosted through the Research Unit for Research Utilisation179 at the University of St Andrews (project co-applicants and report authors VW and HD are co-directors of this long-established research unit). In this way, we hope to ensure the enduring accessibility and ongoing application of the insights detailed in this project report.
Reflections on patient and public involvement in embedded research
Data from the scoping of UK embedded research initiatives, the findings from the literature review, and the detailed work in the four case studies presented a picture of very patchy PPI. There was a wide range of PPI activity in the initiatives that we explored, ranging from a ‘patient panel’ supporting the overarching initiative (seen in Evansville; see Chapter 4) through to minimal involvement, with PPI described as not needed or not useful. In general, PPI was most often seen at project level (consistent with current research norms), but was rarely seen at the level of the embedded initiative itself. That is, patients and the public were far less likely to be involved in conversations about the overall design of embedded co-production than they were to be engaged in specific research or improvement projects. Even when PPI was seen, there were many different approaches to the role of lay representation, including drawing on existing NHS arrangements or using local charities to act as liaison. Moreover, the style of engagement also varied, from active participation in project work to more passive engagement, such as simple consultation about patient information.
Throughout the Embedded project, and as they learned about existing PPI arrangements in embedded schemes, our own project PPI group met to explore what a more effective and comprehensive set of arrangements for PPI in embedded research initiatives might look like. This group (see Acknowledgements) had wide and diverse experience of PPI in health services.
First, the group explored and differentiated active from passive PPI, under the three headings of intent, structure and process surfaced by the review and scoping exercise (see Chapter 3). As shown in Table 17, a spectrum of PPI arrangements can be envisaged from more passive to more active. Relating these features of PPI to the design concerns for embedded research initiatives allows us to see how building in more active PPI begins at the design stage. Thus, the passive/active ‘anchors’ in Table 17 provide a framework for integrating PPI concerns into the design discussions.
| Broad design concerns | PPI | |
|---|---|---|
| Passive | Active | |
| Intentions | Neutral | Influential |
| Little status | Legitimated | |
| Consulted | Involved/co-producing | |
| Retrospective | Prospective | |
| Structural components | One-off | Ongoing |
| Fragile | Sustainable | |
| ‘Usual suspects’ | Diverse representation | |
| Work for nothing | Payments and expenses | |
| Process issues | Knowledge reinforcers | Knowledge challengers |
| Benign engagements | Challenging/constructive | |
| Medical profession benefit | Patient and public benefit | |
| Self-interest | Alliances | |
Discussions in the Embedded project PPI group concluded that the limited and patchy engagement of lay perspectives in many embedded research initiatives was a missed opportunity, but that there were few easy answers and no ‘off-the-shelf’ models. In particular, the group recognised the complexity and challenge of bringing together researcher perspectives with health service perspectives, and acknowledged the essentially relational nature of embedded co-production. This challenge can be encapsulated as that of building more complex and multifaceted relationships that include patients and lay representatives in equal dialogue with embedded researchers and service actors. That will require firm commitment as an intent, with redesigned structures and clearly set-out processes: using Table 17 in tandem with the embedded design framework (see Chapter 6) to build in deeper PPI. In addition, the group identified the need for more innovative recruitment to PPI roles to ensure that those participating truly reflect the diverse populations beings served.
These discussions in the Embedded PPI group led to the sketching out of a more radical vision for PPI in embedded research initiatives (Table 18). Again, drawing on the design framework (see Chapter 6), this sets out some core presumptions that would underpin more radical and embedded PPI. These could be seen as touchstones for discussions, or as more concrete goals for redesigned PPI in embedded initiatives.
| Broad design concerns | Radical redesign of PPI in embedded initiatives |
|---|---|
| Intentions | Broader cultural change, bringing patient/lay perspectives to the fore |
| Seeing health care as an integral part of wider social and community care | |
| Knowledge co-production explicitly across academic, service and lay perspectives | |
| Structural components | Established PPI personnel, resources and support |
| Formal assessment of training needs for PPI leads and partners | |
| Structural arrangements for dialogue in the embedded initiative reflect the importance and relevance of PPI | |
| Process issues | Organisational awareness of PPI to the fore |
| Shared training and support in place and routinely accessed | |
| PPI integral to operational processes and learning mechanisms |
In conclusion, the lack of nationally available models of PPI for embedded co-production has led to diversity of practice and sometimes a lack of focus on this crucial part of knowledge co-production. The work of the Embedded PPI group and the insights generated from the research data have been combined to sketch out a more radical vision for PPI in embedded initiatives, with Tables 17 and 18 offering a route map through discussions for implementing that more radical vision.
Future research
As befits the pragmatic intent of this project (supporting the development of embedded knowledge co-production), we have focused here on the practical insights and outputs from this project, and their potential application in the field, especially in the NHS. However, it is also clear that there are more academic contributions to be made emerging from the extensive empirical work. These will probably explore issues such as identities, power and liminality, as well as the means of accommodating across diverse epistemologies. That is, the material gathered across this project has the potential to contribute to academic and service innovation debates much broader than those limited to embedded research initiatives.
There is also an important future empirical research agenda. In order of importance to the overall aim of increasing the impact of health services research, we propose the following:
-
How effective are different models of embedded research in achieving their aims? The Embedded study explicitly aimed to shine a light on the theory and current practice of embedded research, rather than to formally evaluate the outputs, outcomes, value for money and impact of embedded initiatives. The effectiveness and cost-effectiveness questions either are, or should be, asked by those responsible for initiating, funding and maintaining embedded research initiatives on the ground. There are many ways of addressing effectiveness. Given the complex, multifaceted nature of embedded research highlighted in this study, it is probable that a realist-type evaluation approach will be more useful than an experimental one.
-
How does embedded research work in practice? This study has highlighted both the choices available to those who wish to use the embedded research model, and the possible ways in which embedding researchers in practical settings might add value. But more detailed process unpacking is required; for example, to unpick the role of embedded researchers in mediating different epistemic, cultural and political boundaries, such as the way stakeholders make sense of knowledge needs in different ways, and the divergent assumptions about what counts as valid knowledge and how knowledge might be used. Part of any embedded researcher’s role is to build connections between parties in ways that lay the foundations for more partnership-working, collaboration and co-production, leading to more sustainable collaborative communities. Exploring the accomplishment of these complex tasks is both necessary and valuable and could be achieved by further developing the methods used in workstream 3 of this study.
-
What is the relative effectiveness of investing in the embedded research model, in comparison with investing in other ways of increasing the impact of health services research? The embedded research model is just one approach to increasing the impact of health services research. Some localities are investing in research partnership infrastructures such as local R&D units or learning systems. Others are funding placements for practitioners to spend time in academic settings, rather than placing researchers in service delivery settings. We do not currently know the relative effectiveness of these different investment decisions. Starting with comparative case study designs, this is an important research question for those investing in initiatives to increase the impact of research on practice.
-
What role can patients and members of the public play in co-designing, implementing and evaluating embedded research initiatives? This study describes the significant challenges that we experienced in identifying the role of patients and members of the public in embedded research, despite our commitment to and investment in developing the PPI agenda. We developed a radical vision of what effective PPI in embedded research might look like. There is an urgent need to evaluate the implementation of different practical models of this vision, initially, at least, using an in-depth case study approach.
-
What needs to be done to maximise the attractiveness to researchers of contributing to embedded research, and to minimise the risks? This study has clearly described the challenges and risks to researchers, especially early-career ones, of engaging in what is not currently a valued mainstream academic career path. Recruitment of researchers to embedded posts will remain challenging until we have a better understanding from a researcher and academic institutional perspective of the associated challenges and solutions. A qualitative case study approach would most likely add greatest value.
-
Are the tools and resources developed as part of this study being used and are they useful? The purpose of this study was not only to deepen our understanding of the theory, evidence and practice of embedded research, but also to make a practical contribution to those wanting to establish embedded research schemes through the development of the tools and resources described in Chapters 2, 3, 6 and 7. Although these tools and resources were co-created with practitioners and researchers and were, in many cases, based on materials that have a track record of use in health and care settings, we do not have a systematic understanding of their use in practice. A multimethod evaluation of the tools and resources would help to maximise their contribution to embedded initiatives.
-
To what extent are embedded research initiatives being used in the health and care sectors? This study identified a large number of initiatives across the country that satisfied our criteria for embedded research. We also identified the lack of infrastructure and sustained funding to support these initiatives beyond short-term projects. An ongoing assessment of the scale and scope of embedded research initiatives would build helpfully on the findings of workstream 2 in this study and enable policy-makers and research funders to maintain a strategic view of the field.
Taken together, there is a large and fascinating research agenda that opens up as a result of our preliminary attempt to gain some clarity and place some structure on the field of embedded knowledge co-production.
Concluding remarks
Embedded co-production initiatives have sprung up across the NHS in many different settings: acute care, primary care, community care and public health. There is considerable enthusiasm for such schemes, among service personnel and embedded researchers alike, and there is a robust logic that underpins their use. However, we found considerable diversity as to the nature and understandings of embedded research and knowledge co-production, a diversity and complexity that belies the apparently simple precepts.
By definition, embedding research means deploying a person (or people) to build connections between the world of research and that of practice. We found that beyond this simple and seemingly straightforward idea lies a tangled web of possibilities and challenges that have much to do with the structures, cultures and social institutions within which individual capacities and experiences are nested. A researcher may be embedded, but, in a broader sense, they also facilitate embedding by establishing connections between people, ideas, knowledge and action, with potential dividends in terms of social and institutional change. Judgements about, and measures of, successful embeddedness are likely to be highly variable between particular contexts and projects. Understandings about embeddedness and co-production are not yet at the stage that would allow detailed recommendations to be made that cut across contexts. Rather, every embedded research initiative is an opportunity to learn more about the gains that are possible and the challenges to be faced.
The insights and resources from this project are intended to support the NHS and other partners to develop such learning. These focus on providing practical support to the dialogue needed for more thoughtful schemes, and we hope that this more structured way of describing and delineating schemes will also allow for more concerted research efforts to assess scheme impacts where they count: on the service.
Acknowledgements
Our thanks go to Joe Langley and Rebecca Partridge from the Lab4Living team at Sheffield Hallam University for designing and facilitating the co-production workshop that developed our design framework, and to Chris Redford for designing the visual landscape (workstreams 1 and 2). We are also extremely appreciative of the enthusiastic participation of embedded researchers and their managers during our scoping work (workstream 2). In addition, we are very grateful to the four case study sites (and the additional pilot site) for their unwavering support and enthusiasm. In particular, we are extremely appreciative of each of the embedded researchers who went above and beyond to help us with our study (workstream 3).
The Embedded project was supported in the design and delivery of workshops, digital events and practical resources (workstream 4) by Kaleidoscope Health and Care. Kaleidoscope Health and Care is a social enterprise that brings people together to improve health and care through the creation of engaging events, fostering collaboration, providing strategy advice and supporting research and evaluation, and we are grateful for its contribution to this project.
The Embedded project had a PPI group that consisted of Karen Bollan, Tessa Holmes, Richard Parnell and David Woodcock, and we are very thankful for their many contributions to this programme.
We also received excellent advice and welcome challenge from our steering group: Mike Cooke (chairperson), Andrew Bindman, Kevin Orr, John Ovretveit, Barbara Riley, Martin Utley and Lesley Wye. We are very grateful for their ongoing interest and support.
Finally, Emily Bellshaw at University College London provided excellent project management and administrative support throughout, keeping the various strands of the work on track and properly documented, and Nic Barnard provided hugely appreciated subediting skills during the compilation of this final report. Their extremely valuable contributions are noted with sincere thanks.
Contributions of authors
Martin Marshall (https://orcid.org/0000-0001-8575-5442) (Professor of Healthcare Improvement) was principal investigator and oversaw all aspects of project delivery. He was also co-lead for workstream 4.
Huw Davies (https://orcid.org/0000-0002-2653-3695) (Professor of Healthcare Policy and Management) was co-lead for workstreams 1 and 2, and led on assembling the final report with Martin Marshall.
Vicky Ward (https://orcid.org/0000-0001-8684-0403) (Reader in Management, Director of Impact and Co-director of the Research Unit for Research Utilisation) was co-lead for workstreams 1 and 2.
Justin Waring (https://orcid.org/0000-0003-1459-5896) (Professor of Medical Sociology and Healthcare Organisation) was co-lead for workstream 3.
Naomi J Fulop (https://orcid.org/0000-0001-5306-6140) (Professor of Healthcare Organisation and Management) was co-lead for workstream 3.
Liz Mear (https://orcid.org/0000-0001-5523-0338) (Managing Director, Leeds Academic Health Partnership; formerly chief executive, Innovation Agency) was co-lead for workstream 4.
Breid O’Brien (https://orcid.org/0000-0002-3647-895X) (Director of Digital Transformation) was co-lead for workstream 4.
Richard Parnell was independent PPI lead on the project team.
Katherine Kirk (Research Fellow, School of Social Policy) was research fellow on workstream 3.
Benet Reid (https://orcid.org/0000-0002-4408-8791) (Associate Lecturer, School of Management) and Tricia Tooman (https://orcid.org/0000-0002-1227-2033) (Research Fellow, School of Management) were research fellows on workstreams 1 and 2.
All authors were involved in the programme conception, design, methods, analysis and interpretation. All authors contributed to delivering the programme and to the drafting, revision and approval of the final report.
Publications
Mear M, Fulop N. How the ‘lonely ones’ can drive meaningful change. 2019. URL: https://hsj.co.uk/service-design/how-the-lonely-ones-can-drive-meaningful-change/7025001.article (accessed 22 January 2021).
Ward V, Tooman T, Reid B, Davies H, Marshall M. Embedding researchers into organisations: a study of the features of embedded research initiatives [published online ahead of print 19 April 2021]. Evid Policy 2021.
Ward V, Tooman T, Reid B, Davies H, O’Brien B, Mear L, et al. A framework to support the design and cultivation of embedded research initiatives [published online ahead of print 19 April 2021]. Evid Policy 2021.
Presentations on embedding and knowledge co-production
Marshall M. Increasing Research Impact: The Researcher-in-Residence Model. Keynote address at the NIHR School for Primary Care Research research showcase, London, 13 November 2018.
Marshall M. On the Role of General Practice-Based Primary Care in Challenging the Traditional Medical Model of Care and Promoting One that More Effectively Addresses the Social Determinants of Ill Health in Our Communities. Primary Care Forum, Singapore, 25 October 2018.
Fulop N. Learning from Embedded Research. AcademyHealth (U.S. national health services research network) annual conference. Washington, DC, 2–4 June 2019.
Marshall M. On Improvement Science. National Healthcare Group Polyclinics, Singapore, 29 March–6 April 2019.
Mear L. How to Embed Research. Royal College of Physicians Research Effect Conference, Liverpool, 28 November 2019.
Mear L. The Potential of Embedded Research. AHSN Chief Officers Meeting (online meeting), 10 December 2019.
Reid B, Ward V, Davies H, Tooman T. Knowledge Co-Production: A Vocabulary of Concepts. Presentation at Researching Knowledge Co-production: What Do We Know and Where Do We Go Next? Research Unit for Research Utilisation, University of St Andrews, St Andrews, 8 October 2019.
Reid B, Ward V, Tooman T, Davies H. The Design Features of Embedded Research Initiatives. Poster presentation at the UK Knowledge Mobilisation Forum, Newcastle, 20–21 March 2019.
Ward V. The Features of Embedded Research Initiatives and a Framework to Support Their Design and Operationalisation. Presentation at a Local Authority Champions of Research (LACoR) project workshop, London, 19 September 2019.
Kirk K, Waring J, Ward V, Fulop N, Mear L. Embedding Researchers into Organisations: Studying the Features of Embedded Research Initiatives. Health Services Research UK, online conference, 1–3 July 2020.
Various other events for which the team had submissions accepted for presentation were cancelled because of COVID-19 (e.g. the Institute for Healthcare Improvement Research Symposium; the NHS ConfedExpo; the Organisational Learning, Knowledge and Capabilities conference).
Webinars on embedded research
The project webinars and ‘melting pot lunches’ are listed in the Resources section of the Embedded Research project website. 67
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HSDR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HSDR programme or the Department of Health and Social Care.
References
- Lomas J. Essay: using ‘linkage and exchange’ to move research into policy at a Canadian foundation: encouraging partnerships between researchers and policymakers is the goal of a promising new Canadian initiative. Health Aff 2000;19:236-40. https://doi.org/10.1377/hlthaff.19.3.236.
- Rycroft-Malone J, Wilkinson J, Burton CR, Harvey G, McCormack B, Graham I, et al. Collaborative action around implementation in Collaborations for Leadership in Applied Health Research and Care: towards a programme theory. J Health Serv Res Policy 2013;18:13-26. https://doi.org/10.1177/1355819613498859.
- Davies HT, Powell AE, Nutley SM. Mobilising knowledge to improve UK health care: learning from other countries and other sectors – a multimethod mapping study. Health Serv Deliv Res 2015;3. https://doi.org/10.3310/hsdr03270.
- Boaz A, Davies H, Fraser A, Nutley S. What Works Now? Evidence-informed Policy and Practice. Bristol: Policy Press; 2019.
- Mitton C, Adair CE, McKenzie E, Patten SB, Waye Perry B. Knowledge transfer and exchange: review and synthesis of the literature. Milbank Q 2007;85:729-68. https://doi.org/10.1111/j.1468-0009.2007.00506.x.
- Greenhalgh T, Wieringa S. Is it time to drop the ‘knowledge translation’ metaphor? A critical literature review. J R Soc Med 2011;104:501-9. https://doi.org/10.1258/jrsm.2011.110285.
- Engebretsen E, Sandset TJ. Ødemark J. Expanding the knowledge translation metaphor. Health Res Pol Syst 2017;15. https://doi.org/10.1186/s12961-017-0184-x.
- Ferlie E, Crilly T, Jashapara A, Peckham A. Knowledge mobilisation in healthcare: a critical review of health sector and generic management literature. Soc Sci Med 2012;74:1297-304. https://doi.org/10.1016/j.socscimed.2011.11.042.
- Nutley S, Walter I, Davies H. Using Evidence: How Research Can Inform Public Services. Bristol: Policy Press; 2007.
- Soper B, Hinrichs S, Drabble S, Yaqub O, Marjanovic S, Hanney S, et al. Delivering the aims of the Collaborations for Leadership in Applied Health Research and Care: understanding their strategies and contributions. Health Serv Deliv Res 2015;3. https://doi.org/10.3310/hsdr03250.
- Salter KL, Kothari A. Knowledge ‘translation’ as social learning: negotiating the uptake of research-based knowledge in practice. BMC Med Educ 2016;16. https://doi.org/10.1186/s12909-016-0585-5.
- Bullock A, Morris ZS, Atwell C. A Formative Evaluation of the Service Delivery and Organisation (SDO) Management Fellowships. Final Report 2012.
- Currie G, Waring J, Finn R. The limits of knowledge management for UK public services modernization: the case of patient safety and service quality. Public Adm 2008;86:363-85. https://doi.org/10.1111/j.1467-9299.2007.00705.x.
- Best A, Greenhalgh T, Lewis S, Saul JE, Carroll S, Bitz J. Large-system transformation in health care: a realist review. Milbank Q 2012;90:421-56. https://doi.org/10.1111/j.1468-0009.2012.00670.x.
- Martin GP, Williams O, Boaz A, Davies H, Fraser A, Nutley S. What Works Now?: Evidence-Informed Policy and Practice. Bristol: Policy Press; 2019.
- Kitson A, Brook A, Harvey G, Jordan Z, Marshall R, O’Shea R, et al. Using complexity and network concepts to inform healthcare knowledge translation. Int J Health Policy Manag 2018;7:231-43. https://doi.org/10.15171/ijhpm.2017.79.
- Beckett K, Farr M, Kothari A, Wye L, le May A. Embracing complexity and uncertainty to create impact: exploring the processes and transformative potential of co-produced research through development of a social impact model. Health Res Policy Syst 2018;16. https://doi.org/10.1186/s12961-018-0375-0.
- Reed MS, Stringer LC, Fazey I, Evely AC, Kruijsen JHJ. Five principles for the practice of knowledge exchange in environmental management. J Environ Manage 2014;146:337-45. https://doi.org/10.1016/j.jenvman.2014.07.021.
- Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift. BMC Med 2018;16. https://doi.org/10.1186/s12916-018-1089-4.
- Greenhalgh T. What is this knowledge that we seek to ‘exchange’?. Milbank Q 2010;88. https://doi.org/10.1111/j.1468-0009.2010.00610.x.
- Wehrens R. Beyond two communities – from research utilization and knowledge translation to co-production?. Public Health 2014;128:545-51. https://doi.org/10.1016/j.puhe.2014.02.004.
- Jackson CL, Greenhalgh T. Co-creation: a new approach to optimising research impact?. Med J Aust 2015;203:283-4. https://doi.org/10.5694/mja15.00219.
- McCabe KE, Wallace A, Crosland A. A model for collaborative working to facilitate knowledge mobilisation in public health. Evid Policy 2015;11:559-76. https://doi.org/10.1332/174426415X14298767491657.
- Clarke J, Waring J, Timmons S. The challenge of inclusive coproduction: the importance of situated rituals and emotional inclusivity in the coproduction of health research projects. Soc Policy Admin 2019;53:233-48. https://doi.org/10.1111/spol.12459.
- Duijn M, Rijnveld M, van Hulst M. Meeting in the middle: joining reflection and action in complex public sector projects. Public Money Manag 2010;30:227-33. https://doi.org/10.1080/09540962.2010.492183.
- Beebeejaun Y, Durose C, Rees J, Richardson J, Richardson L. Public harm or public value? Towards coproduction in research with communities. Environ Plan 2015;33:552-65. https://doi.org/10.1068/c12116.
- Ostrom E. Crossing the great divide: coproduction, synergy, and development. World Dev 1996;24:1073-87. https://doi.org/10.1016/0305-750X(96)00023-X.
- Boyle D, Harris M. The Challenge of Co Production: How Equal Partnerships between Professionals and the Public Are Crucial to Improving Public Services. London: New Economics Foundation; 2009.
- Osborne SP, Strokosch K. It takes two to tango? Understanding the co-production of public services by integrating the services management and public administration perspectives. Br J Manag 2013;24:S31-S47. https://doi.org/10.1111/1467-8551.12010.
- Orr K, Bennett M. The politics of co-produced research: editorial. Public Money Manag 2010;30:199-203. https://doi.org/10.1080/09540962.2010.492171.
- Orr K, Bennett M. Public administration scholarship and the politics of coproducing academic–practitioner research. Public Adm Rev 2012;72:487-95. https://doi.org/10.1111/j.1540-6210.2011.02522.x.
- Heaton J, Day J, Britten N. Collaborative research and the co-production of knowledge for practice: an illustrative case study. Implement Sci 2016;11. https://doi.org/10.1186/s13012-016-0383-9.
- Rycroft-Malone J, Burton CR, Bucknall T, Graham ID, Hutchinson AM, Stacey D. Collaboration and co-production of knowledge in healthcare: opportunities and challenges. Int J Health Policy Manag 2016;5:221-3. https://doi.org/10.15171/ijhpm.2016.08.
- Brandsen T, Verschuere B, Pestoff V, Pestoff V, Brandsen T, Verschuere B. New Public Governance, the Third Sector, and Co-Production. London: Routledge; 2012.
- Verschuere B, Brandsen T, Pestoff V. Co-production: the state of the art in research and the future agenda. VOLUNTAS 2012;23:1083-101. https://doi.org/10.1007/s11266-012-9307-8.
- Durose C, Needham C, Mangan C, Rees J. Generating ‘good enough’ evidence for co-production. Evid Policy 2017;13:135-51. https://doi.org/10.1332/174426415X14440619792955.
- Hewison A, Gale N, Shapiro J. Co-production in research: some reflections on the experience of engaging practitioners in health research. Public Money Manag 2012;32:297-302. https://doi.org/10.1080/09540962.2012.691311.
- Flinders M, Wood M, Cunningham M. The politics of co-production: risks, limits and pollution. Evid Policy 2016;12:261-79. https://doi.org/10.1332/174426415X14412037949967.
- Crompton A. Inside co-production: stakeholder meaning and situated practice. Soc Policy Admin 2019;53:219-32. https://doi.org/10.1111/spol.12466.
- Bell DM, Pahl K. Co-production: towards a utopian approach. Int J Soc Res Methodol 2018;21:105-17. https://doi.org/10.1080/13645579.2017.1348581.
- Weiss CH. Research for policy’s sake: the enlightenment function of social research. Policy Anal 1977;3:531-45.
- Kothari A, Wathen CN. Integrated knowledge translation: digging deeper, moving forward. J Epidemiol Community Health 2017;71:619-23. https://doi.org/10.1136/jech-2016-208490.
- Miles S, Renedo A, Marston C. ‘Slow co-production’ for deeper patient involvement in health care. JHD 2018;3:57-62. https://doi.org/10.21853/JHD.2018.39.
- Pollard K, Moule P, Evans D, Donald C, Donskoy A, Rice C. User Engagement in the Co-production of Knowledge for Knowledge Exchange in Health and Social Care. Bristol: University of the West of England Bristol; 2020.
- Kislov R, Wilson PM, Knowles S, Boaden R. Learning from the emergence of NIHR Collaborations for Leadership in Applied Health Research and Care (CLAHRCs): a systematic review of evaluations. Implement Sci 2018;13. https://doi.org/10.1186/s13012-018-0805-y.
- Boaz A, Hanney S, Borst R, O’Shea A, Kok M. How to engage stakeholders in research: design principles to support improvement. Health Res Policy Syst 2018;16. https://doi.org/10.1186/s12961-018-0337-6.
- Gradinger F, Elston J, Asthana S, Martin S, Byng R. Reflections on the researcher-in-residence model co-producing knowledge for action in an integrated care organisation: a mixed methods case study using an impact survey and field notes. Evid Pol 2019;15:197-215. https://doi.org/10.1332/174426419X15538508969850.
- Gagliardi AR, Berta W, Kothari A, Boyko J, Urquhart R. Integrated knowledge translation (IKT) in health care: a scoping review. Implement Sci 2016;11. https://doi.org/10.1186/s13012-016-0399-1.
- Graham ID, Kothari A, McCutcheon C. Integrated Knowledge Translation Research Network Project Leads . Moving knowledge into action for more effective practice, programmes and policy: protocol for a research programme on integrated knowledge translation. Implement Sci 2018;13. https://doi.org/10.1186/s13012-017-0700-y.
- Bailie J, Cunningham FC, Bainbridge RG, Passey ME, Laycock AF, Bailie RS, et al. Comparing and contrasting ‘innovation platforms’ with other forms of professional networks for strengthening primary healthcare systems for Indigenous Australians. BMJ Glob Health 2018;3. https://doi.org/10.1136/bmjgh-2017-000683.
- Kanani N, Hahn EE, Gould MK, Brunisholz KD, Savitz LA, Holve EC. Academy Health’s Delivery System Science Fellowship: training embedded researchers to design, implement, and evaluate new models of care. J Hosp Med 2017;12:570-4. https://doi.org/10.12788/jhm.2776.
- Ghaffar A, Langlois EV, Rasanathan K, Peterson S, Adedokun L, Tran NT. Strengthening health systems through embedded research. Bull World Health Organ 2017;95. https://doi.org/10.2471/BLT.16.189126.
- Glegg SM, Hoens A. Role domains of knowledge brokering: a model for the health care setting. J Neurol Phys Ther 2016;40:115-23. https://doi.org/10.1097/NPT.0000000000000122.
- Hoens AM, Reid WD, Camp PG. Knowledge brokering: an innovative model for supporting evidence-informed practice in respiratory care. Can Respir J 2013;20:271-4. https://doi.org/10.1155/2013/121654.
- Ward V, Smith S, House A, Hamer S. Exploring knowledge exchange: a useful framework for practice and policy. Soc Sci Med 2012;74:297-304. https://doi.org/10.1016/j.socscimed.2011.09.021.
- Wright N. First-time knowledge brokers in health care: the experiences of nurses and allied health professionals of bridging the research-practice gap. Evid Pol 2013;9:557-70. https://doi.org/10.1332/174426413X13836462527470.
- Chew S, Armstrong N, Martin G. Institutionalising knowledge brokering as a sustainable knowledge translation solution in healthcare: how can it work in practice?. Evid Pol 2013;9:335-51. https://doi.org/10.1332/174426413X662734.
- Frost H, Geddes R, Haw S, Jackson CA, Jepson R, Mooney JD, et al. Experiences of knowledge brokering for evidence-informed public health policy and practice: three years of the Scottish Collaboration for Public Health Research and Policy. Evid Pol 2012;8:347-59. https://doi.org/10.1332/174426412X654068.
- Booth A. Bridging the ‘Know–Do Gap’: a role for health information professionals?. Health Info Libr J 2011;28:331-4. https://doi.org/10.1111/j.1471-1842.2011.00960.x.
- Dobbins M, Greco L, Yost J, Traynor R, Decorby-Watson K, Yousefi-Nooraie R. A description of a tailored knowledge translation intervention delivered by knowledge brokers within public health departments in Canada. Health Res Policy Syst 2019;17. https://doi.org/10.1186/s12961-019-0460-z.
- Marshall MN. Bridging the ivory towers and the swampy lowlands; increasing the impact of health services research on quality improvement. Int J Qual Health Care 2014;26:1-5. https://doi.org/10.1093/intqhc/mzt076.
- Marshall M. Researchers-in-residence: a solution to the challenge of evidence-informed improvement?. Prim Health Care Res Dev 2014;15:337-8. https://doi.org/10.1017/S1463423614000310.
- Marshall M, Eyre L, Lalani M, Khan S, Mann S, de Silva D, et al. Increasing the impact of health services research on service improvement: the researcher-in-residence model. J R Soc Med 2016;109:220-5. https://doi.org/10.1177/0141076816634318.
- Eyre L, George B, Marshall M. Protocol for a process-oriented qualitative evaluation of the Waltham Forest and East London Collaborative (WELC) integrated care pioneer programme using the researcher-in-residence model. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-009567.
- Vindrola-Padros C, Eyre L, Baxter H, Cramer H, George B, Wye L, et al. Addressing the challenges of knowledge co-production in quality improvement: learning from the implementation of the researcher-in-residence model. BMJ Qual Saf 2019;28:67-73. https://doi.org/10.1136/bmjqs-2017-007127.
- Langley J, Wolstenholme D, Cooke J. ‘Collective making’ as knowledge mobilisation: the contribution of participatory design in the co-creation of knowledge in healthcare. BMC Health Serv Res 2018;18. https://doi.org/10.1186/s12913-018-3397-y.
- Embedded Research . Embedded Research: Increasing the Influence of Health Services Research on Decisions about the Improvement and Redesign of NHS Services. What Is Embedded Research? n.d. www.embeddedresearch.org.uk (accessed 1 March 2021).
- Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Health Care 2006;15:307-10. https://doi.org/10.1136/qshc.2005.016527.
- Snape D, Kirkham J, Preston J, Popay J, Britten N, Collins M, et al. Exploring areas of consensus and conflict around values underpinning public involvement in health and social care research: a modified Delphi study. BMJ Open 2014;4. https://doi.org/10.1136/bmjopen-2013-004217.
- Sunderji N, Nicholas EA, Polaha J, Gao C. Why and how to use patient-oriented research to promote translational research. Fam Syst Health 2019;37:1-9. https://doi.org/10.1037/fsh0000405.
- Boaz A, Locock L, Ward V. Whose evidence is it anyway?. Evid Pol 2015;11:145-8. https://doi.org/10.1332/174426515X14313738355534.
- Lancaster K, Seear K, Treloar C, Ritter A. The productive techniques and constitutive effects of ‘evidence-based policy’ and ‘consumer participation’ discourses in health policy processes. Soc Sci Med 2017;176:60-8. https://doi.org/10.1016/j.socscimed.2017.01.031.
- Kouri D. Knowledge exchange strategies for interventions and policy in public health. Evid Pol 2009;5:71-83. https://doi.org/10.1332/174426409X395420.
- Ward V. Why, whose, what and how? A framework for knowledge mobilisers. Evid Pol 2017;13:477-97. https://doi.org/10.1332/174426416X14634763278725.
- Glasziou P, Haynes B. The paths from research to improved health outcomes. Evid Based Nurs 2005;8:36-8. https://doi.org/10.1136/ebn.8.2.36.
- Dopson S, Locock L, Gabbay J, Ferlie E, Fitzgerald L. Evidence-based medicine and the implementation gap. Health 2003;7:311-30. https://doi.org/10.1177/1363459303007003004.
- Davies H, Nutley S, Walter I. Why ‘knowledge transfer’ is misconceived for applied social research. J Health Serv Res Policy 2008;13:188-90. https://doi.org/10.1258/jhsrp.2008.008055.
- Fitzgerald L, Harvey G. Translational networks in healthcare? Evidence on the design and initiation of organizational networks for knowledge mobilization. Soc Sci Med 2015;138:192-200. https://doi.org/10.1016/j.socscimed.2015.06.015.
- Filipe A, Renedo A, Marston C. The co-production of what? Knowledge, values, and social relations in health care. PLOS Biol 2017;15. https://doi.org/10.1371/journal.pbio.2001403.
- Holmes B, Best A, Davies H, Hunter D, Kelly M, Marshall M, et al. Mobilising knowledge in complex health systems: a call to action. Evid Pol 2016;13:539-60. https://doi.org/10.1332/174426416X14712553750311.
- Palmer VJ, Weavell W, Callander R, Piper D, Richard L, Maher L, et al. The Participatory Zeitgeist: an explanatory theoretical model of change in an era of coproduction and codesign in healthcare improvement. Med Humanit 2019;45:247-57. https://doi.org/10.1136/medhum-2017-011398.
- Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research?. Health Res Pol Syst 2019;17. https://doi.org/10.1186/s12961-019-0432-3.
- Nicholas G, Foote J, Kainz K, Midgley G, Prager K, Zurbriggen C. Towards a heart and soul for co-creative research practice: a systemic approach. Evid Pol 2019;15:353-70. https://doi.org/10.1332/174426419X15578220630571.
- Smith S, Ward V. The role of boundary maintenance and blurring in a UK collaborative research project: how researchers and health service managers made sense of new ways of working. Soc Sci Med 2015;130:225-33. https://doi.org/10.1016/j.socscimed.2015.02.023.
- Torraco RJ. Writing integrative literature reviews: guidelines and examples. Hum Resour Dev Rev 2005;4:356-67. https://doi.org/10.1177/1534484305278283.
- Barnett-Page E, Thomas J. Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol 2009;9. https://doi.org/10.1186/1471-2288-9-59.
- Dixon-Woods M. Using framework-based synthesis for conducting reviews of qualitative studies. BMC Med 2011;9. https://doi.org/10.1186/1741-7015-9-39.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Jabareen Y. Building a conceptual framework: philosophy, definitions, and procedure. Int J Qual Methods 2009;8:49-62. https://doi.org/10.1177/160940690900800406.
- Lövbrand E. Co-producing European climate science and policy: a cautionary note on the making of useful knowledge. Sci Public Policy 2011;38:225-36. https://doi.org/10.3152/030234211X12924093660516.
- Jull J, Giles A, Graham ID. Community-based participatory research and integrated knowledge translation: advancing the co-creation of knowledge. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0696-3.
- Rowley E, Morriss R, Currie G, Schneider J. Research into practice: Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Nottinghamshire, Derbyshire, Lincolnshire (NDL). Implement Sci 2012;7. https://doi.org/10.1186/1748-5908-7-40.
- Hutchins K, Lindenfeld LA, Bell KP, Leahy J, Silka L. Strengthening knowledge co-production capacity: examining interest in community-university partnerships. Sustainability 2013;5:3744-70. https://doi.org/10.3390/su5093744.
- Martin S. Co-production of social research: strategies for engaged scholarship. Public Money Manag 2010;30:211-8. https://doi.org/10.1080/09540962.2010.492180.
- Greenhalgh T, Jackson C, Shaw S, Janamian T. Achieving research impact through co-creation in community-based health services: literature review and case study. Milbank Q 2016;94:392-429. https://doi.org/10.1111/1468-0009.12197.
- Klenk N, Meehan K. Climate change and transdisciplinary science: problematizing the integration imperative. Environ Sci Policy 2015;54:160-7. https://doi.org/10.1016/j.envsci.2015.05.017.
- Brown MB. Politicizing science: conceptions of politics in science and technology studies. Soc Stud Sci 2015;45:3-30. https://doi.org/10.1177/0306312714556694.
- Olesen BR, Nordentoft HM. Walking the talk? A micro-sociological approach to the co-production of knowledge and power in action research. Int J Action Res 2013;9:67-94.
- Anderson L, Ellwood P, Coleman C. The impactful academic: relational management education as an intervention for impact. Brit J Manag 2017;28:14-28. https://doi.org/10.1111/1467-8551.12202.
- Wall TU, McNie E, Garfin GM. Use-inspired science: making science usable by and useful to decision makers. Front Ecol Environ 2017;15:551-9. https://doi.org/10.1002/fee.1735.
- Scaratti G, Galuppo L, Gorli M, Gozzoli C, Ripamonti S. The social relevance and social impact of knowledge and knowing. Manag Learn 2017;48:57-64. https://doi.org/10.1177/1350507616680563.
- Antonacopoulou EP. Beyond co-production: practice-relevant scholarship as a foundation for delivering impact through powerful ideas. Public Money Manag 2010;30:219-26. https://doi.org/10.1080/09540962.2010.492182.
- Pain R, Kesby M, Askins K. Geographies of impact: power, participation and potential. Area 2011;43:183-8. https://doi.org/10.1111/j.1475-4762.2010.00978.x.
- Cherney A. Academic–industry collaborations and knowledge co-production in the social sciences. J Sociol 2015;51:1003-16. https://doi.org/10.1177/1440783313492237.
- Bremer S, Meisch S. Co-production in climate change research: reviewing different perspectives. Wiley Interdiscip Rev Clim Change 2017;8. https://doi.org/10.1002/wcc.482.
- Durose C, Beebeejaun Y, Rees J, Richardson J, Richardson L. Towards Co-production in Research with Communities. Manchester: Arts and Humanities Research Council, The University of Manchester; 2012.
- Rossi F, Rosli A, Yip N. Academic engagement as knowledge co-production and implications for impact: evidence from knowledge transfer partnerships. J Bus Res 2017;80:1-9. https://doi.org/10.1016/j.jbusres.2017.06.019.
- Campbell LK, Svendsen ES, Roman LA. Knowledge co-production at the research–practice interface: embedded case studies from urban forestry. Environ Manage 2016;57:1262-80. https://doi.org/10.1007/s00267-016-0680-8.
- Kitson AL, Harvey G. Methods to succeed in effective knowledge translation in clinical practice. J Nurs Scholarsh 2016;48:294-302. https://doi.org/10.1111/jnu.12206.
- Kothari A, Hovanec N, Hastie R, Sibbald S. Lessons from the business sector for successful knowledge management in health care: a systematic review. BMC Health Serv Res 2011;11. https://doi.org/10.1186/1472-6963-11-173.
- Nowotny H. Democratising expertise and socially robust knowledge. Sci Public Policy 2003;30:151-6. https://doi.org/10.3152/147154303781780461.
- Kothari A, Wathen CN. A critical second look at integrated knowledge translation. Health Policy 2013;109:187-91. https://doi.org/10.1016/j.healthpol.2012.11.004.
- Phillips LJ. Analysing the dialogic turn in the communication of research-based knowledge: an exploration of the tensions in collaborative research. Public Underst Sci 2011;20:80-100. https://doi.org/10.1177/0963662509340092.
- Pohl C, Rist S, Zimmermann A, Fry P, Gurung GS, Schneider F, et al. Researchers’ roles in knowledge co-production: experience from sustainability research in Kenya, Switzerland, Bolivia and Nepal. Sci Public Policy 2010;37:267-81. https://doi.org/10.3152/030234210X496628.
- Schuttenberg H, Guth HK. Seeking our shared wisdom: a framework for understanding knowledge coproduction and coproductive capacities. Ecol Soc 2015;20. https://doi.org/10.5751/ES-07038-200115.
- Jagosh J, Macaulay AC, Pluye P, Salsberg J, Bush PL, Henderson J, et al. Uncovering the benefits of participatory research: implications of a realist review for health research and practice. Milbank Q 2012;90:311-46. https://doi.org/10.1111/j.1468-0009.2012.00665.x.
- Rycroft-Malone J, Langley J. Re-framing the knowledge to action challenge through NIHR knowledge mobilisation research fellows; comment on “CIHR Health System Impact Fellows: Reflections on ‘Driving Change’ within the health system”. Int J Health Policy Manag 2020;9:531-5. https://doi.org/10.15171/ijhpm.2020.02.
- O’Hare P, Coaffee J, Hawkesworth M. Managing sensitive relations in co-produced planning research. Public Money Manag 2010;30:243-50. https://doi.org/10.1080/09540962.2010.492188.
- Burns D, Hyde P, Killett A, Poland F, Gray R. Participatory organizational research: examining voice in the co-production of knowledge. Br J Manag 2014;25:133-44. https://doi.org/10.1111/j.1467-8551.2012.00841.x.
- Klenk NL, Wyatt S. The design and management of multi-stakeholder research networks to maximize knowledge mobilization and innovation opportunities in the forest sector. For Policy Econ 2015;61:77-86. https://doi.org/10.1016/j.forpol.2015.06.008.
- Fenge L-A, Fannin A, Hicks C. Co-production in scholarly activity: valuing the social capital of lay people and volunteers. J Soc Work 2012;12:545-59. https://doi.org/10.1177/1468017310393796.
- Arancibia F. Rethinking activism and expertise within environmental health conflicts. Sociol Compass 2016;10:477-90. https://doi.org/10.1111/soc4.12374.
- Orr K, Bennett M. Down and out at the British Library and other dens of co-production. Manag Learn 2012;43:427-42. https://doi.org/10.1177/1350507612440409.
- Pinfold V, Szymczynska P, Hamilton S, Peacocke R, Dean S, Clewett N, et al. Co-production in mental health research: reflections from the People Study. MHRJ 2015;20:220-31. https://doi.org/10.1108/MHRJ-09-2015-0028.
- Lehmann U, Gilson L. Action learning for health system governance: the reward and challenge of co-production. Health Policy Plan 2015;30:957-63. https://doi.org/10.1093/heapol/czu097.
- Miszczak S, Patel Z. The role of engaged scholarship and co-production to address urban challenges: a case study of the Cape Town Knowledge Transfer Programme. S Afr Geogr J 2018;100:233-48. https://doi.org/10.1080/03736245.2017.1409649.
- Campbell H, Vanderhoven D. Knowledge that Matters: Realising the Potential of Co-production. Manchester: N8 Research Partnership; 2016.
- Polk M. Transdisciplinary co-production: designing and testing a transdisciplinary research framework for societal problem solving. Futures 2015;65:110-22. https://doi.org/10.1016/j.futures.2014.11.001.
- Bremer S, Funtowicz S. Negotiating a place for sustainability science: narratives from the Waikaraka Estuary in New Zealand. Environ Sci Policy 2015;53:47-59. https://doi.org/10.1016/j.envsci.2014.11.006.
- Ospina S, El Hadidy W, Hofmann-Pinilla A. Cooperative inquiry for learning and connectedness. Action Learn Res Pract 2008;5:131-47. https://doi.org/10.1080/14767330802185673.
- Kernick D, Mitchell A. Working with lay people in health service research: a model of co-evolution based on complexity theory. J Interprof Care 2010;24:31-40. https://doi.org/10.3109/13561820903012073.
- Borg M, Karlsson B, Kim HS, McCormack B. Opening up for many voices in knowledge construction. Article 1. Forum Qual Soc Res 2012;13.
- Edelenbos J, Van Buuren A, van Schie N. Co-producing knowledge: joint knowledge production between experts, bureaucrats and stakeholders in Dutch water management projects. Environ Sci Policy 2011;14:675-84. https://doi.org/10.1016/j.envsci.2011.04.004.
- Chesters G. Social movements and the ethics of knowledge production. Soc Mov Stud 2012;11:145-60. https://doi.org/10.1080/14742837.2012.664894.
- Jasanoff S, Jasanoff S. States of Knowledge. Oxford: Routledge; 2004.
- Castree N. Coproducing global change research and geography: the means and ends of engagement. Dialogues Hum Geogr 2015;5:343-8. https://doi.org/10.1177/2043820615613265.
- Cunliffe AL. Reflexive inquiry in organizational research: questions and possibilities. Hum Relat 2003;56:983-1003. https://doi.org/10.1177/00187267030568004.
- Bekker M, van Egmond S, Wehrens R, Putters K, Bal R. Linking research and policy in Dutch healthcare: infrastructure, innovations and impacts. Evid Pol 2010;6:237-53. https://doi.org/10.1332/174426410X502464.
- Pols J. Enacting appreciations: beyond the patient perspective. Health Care Anal 2005;13:203-21. https://doi.org/10.1007/s10728-005-6448-6.
- Ewert B, Evers A. An ambiguous concept: on the meanings of co-production for health care users and user organizations?. VOLUNTAS 2014;25:425-42. https://doi.org/10.1007/s11266-012-9345-2.
- Nunn N. Emotional and relational approaches to masculine knowledge. Soc Cult Geogr 2017;18:354-70. https://doi.org/10.1080/14649365.2016.1180705.
- Maclean K, Cullen L. Research methodologies for the co production of knowledge for environmental management in Australia. J R Soc N Z 2009;39:205-8. https://doi.org/10.1080/03014220909510581.
- Gillard S, Simons L, Turner K, Lucock M, Edwards C. Patient and public involvement in the coproduction of knowledge: reflection on the analysis of qualitative data in a mental health study. Qual Health Res 2012;22:1126-37. https://doi.org/10.1177/1049732312448541.
- Frantzeskaki N, Kabisch N. Designing a knowledge co-production operating space for urban environmental governance – lessons from Rotterdam, Netherlands and Berlin, Germany. Environ Sci Policy 2016;62:90-8. https://doi.org/10.1016/j.envsci.2016.01.010.
- Klenk N, Fiume A, Meehan K, Gibbes C. Local knowledge in climate adaptation research: moving knowledge frameworks from extraction to co-production. Wiley Interdiscip Rev Clim Change 2017;8. https://doi.org/10.1002/wcc.475.
- Ward V, Tooman, Reid B, Davies H, Marshall M. Embedding researchers into organisations: a study of the features of embedded research initiatives. Evid Policy 2021. https://doi.org/10.1332/174426421X16165177580453.
- World Health Organization (WHO) . Changing Mindsets: Strategy on Health Policy and Systems Research 2012.
- Koon AD, Rao KD, Tran NT, Ghaffar A. Embedding health policy and systems research into decision-making processes in low- and middle-income countries. Health Res Policy Syst 2013;11. https://doi.org/10.1186/1478-4505-11-30.
- Wolfenden L, Yoong SL, Williams CM, Grimshaw J, Durrheim DN, Gillham K, et al. Embedding researchers in health service organizations improves research translation and health service performance: the Australian Hunter New England Population Health example. J Clin Epidemiol 2017;85:3-11. https://doi.org/10.1016/j.jclinepi.2017.03.007.
- Eyre L, Farrelly M, Marshall M. What can a participatory approach to evaluation contribute to the field of integrated care?. BMJ Qual Saf 2017;26:588-94. https://doi.org/10.1136/bmjqs-2016-005777.
- Marshall M, Pagel C, French C, Utley M, Allwood D, Fulop N, et al. Moving improvement research closer to practice: the Researcher-in-Residence model. BMJ Qual Saf 2014;23:801-5. https://doi.org/10.1136/bmjqs-2013-002779.
- Cheetham M, Wiseman A, Khazaeli B, Gibson E, Gray P, Van der Graaf P, et al. Embedded research: a promising way to create evidence-informed impact in public health?. J Public Health 2018;40:i64-i70. https://doi.org/10.1093/pubmed/fdx125.
- Cunliffe AL, Scaratti G. Embedding impact in engaged research: developing socially useful knowledge through dialogical sensemaking. Br J Manag 2017;28:29-44. https://doi.org/10.1111/1467-8551.12204.
- Wong S. Tales from the frontline: the experiences of early childhood practitioners working with an ‘embedded’ research team. Eval Program Plann 2009;32:99-108. https://doi.org/10.1016/j.evalprogplan.2008.10.003.
- Duggan JR. Critical friendship and critical orphanship: embedded research of an English local authority initiative. Manag Educ 2014;28:12-8. https://doi.org/10.1177/0892020613510118.
- Rowley H. Going beyond procedure: engaging with the ethical complexities of being an embedded researcher. Manag Educ 2014;28:19-24. https://doi.org/10.1177/0892020613510119.
- Booth A, Harris J, Croot E, Springett J, Campbell F, Wilkins E. Towards a methodology for cluster searching to provide conceptual and contextual ‘richness’ for systematic reviews of complex interventions: case study (CLUSTER). BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-118.
- Vindrola-Padros C, Pape T, Utley M, Fulop NJ. The role of embedded research in quality improvement: a narrative review. BMJ Qual Saf 2017;26:70-8. https://doi.org/10.1136/bmjqs-2015-004877.
- Bate P. Synthesizing research and practice: using the action research approach in health care settings. Soc Policy Admin 2000;34:478-93. https://doi.org/10.1111/1467-9515.00205.
- Cheek J, Denzin N, Lincoln Y. The SAGE Handbook of Qualitative Research. Thousand Oaks, CA: SAGE Publications Ltd; 2005.
- Hackett EJ, Rhoten DR. Engaged, embedded, enjoined: science and technology studies in the National Science Foundation. Sci Eng Ethics 2011;17:823-38. https://doi.org/10.1007/s11948-011-9307-x.
- Wye L, Cramer H, Beckett K, Farr M, le May A, Carey J, et al. Collective knowledge brokering: the model and impact of an embedded team. Evid Pol 2019;16:429-52. https://doi.org/10.1332/174426419X15468577044957.
- Crowe S, Grieco L, Vindrola-Padros C, Elkhodair S. Multidisciplinary embedded research to identify solutions to emergency department overcrowding. Int J Qual Health Care 2017;29:55-6. https://doi.org/10.1093/intqhc/mzx125.89.
- Jenness V. Pluto, prisons, and plaintiffs: notes on systematic back-translation from an embedded researcher. Soc Probl 2008;55:1-22. https://doi.org/10.1525/sp.2008.55.1.1.
- Lewis SJ, Russell AJ. Being embedded: a way forward for ethnographic research. Ethnogr 2011;12:398-416. https://doi.org/10.1177/1466138110393786.
- Wye L, Cramer H, Carey J, Anthwal R, Rooney J, Robinson R, et al. Knowledge brokers or relationship brokers? The role of an embedded knowledge mobilisation team. Evid Pol 2019;15:277-92. https://doi.org/10.1332/174426417X15123845516148.
- Van de Ven AH, Johnson PE. Knowledge for theory and practice. Acad Manage Rev 2006;31:802-21. https://doi.org/10.5465/amr.2006.22527385.
- Gibbons M. The New Production of Knowledge: The Dynamics of Science and Research in Contemporary Societies. London: SAGE Publications Ltd; 1994.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. https://doi.org/10.1093/intqhc/mzm042.
- Carlile PR. A pragmatic view of knowledge and boundaries: boundary objects in new product development. Organ Sci 2002;13:442-55. https://doi.org/10.1287/orsc.13.4.442.2953.
- Waring J, Clarke JM, Vickers R. A comparative ethnographic study of collective knowledge brokering across the syntactic, semantic and pragmatic knowledge boundaries in applied health research. Evid Pol 2021;17:111-30. https://doi.org/10.1332/174426420X15825348594538.
- Stake RE. The Art of Case Study Research. London: SAGE Publications Ltd; 1995.
- Flyvbjerg B. Five misunderstandings about case-study research. Qual Inq 2006;12:219-45. https://doi.org/10.1177/1077800405284363.
- Yin RK. Case Study Research: Design and Methods. London: SAGE Publications Ltd; 2009.
- Knoke D, Yang S. Social Network Analysis. Thousand Oaks, CA: SAGE Publications Ltd; 2008.
- Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. London: SAGE Publications Ltd; 2014.
- Clarke V, Braun V, Hayfield N, Smith JA. Qualitative Psychology: A Practical Guide to Research Methods. London: SAGE Publications Ltd; 2015.
- Ward V, Tooman T, Reid B, Davies H, O’Brien B, Mear L, et al. A framework to support the design and cultivation of embedded research initiatives. Evid Policy 2021. https://doi.org/10.1332/174426421X16165177707227.
- University of St Andrews . Welcome to the RURU Website! n.d. www.ruru.ac.uk (accessed 10 March 2021).
- Contandriopoulos D, Lemire M, Denis JL, Tremblay E. Knowledge exchange processes in organizations and policy arenas: a narrative systematic review of the literature. Milbank Q 2010;88:444-83. https://doi.org/10.1111/j.1468-0009.2010.00608.x.
- Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf 2016;25:986-92. https://doi.org/10.1136/bmjqs-2015-004411.
- Walshe K, Davies HT. Health research, development and innovation in England from 1988 to 2013: from research production to knowledge mobilization. J Health Serv Res Policy 2013;18:1-12. https://doi.org/10.1177/1355819613502011.
- Ovretveit J, Hempel S, Magnabosco JL, Mittman BS, Rubenstein LV, Ganz DA. Guidance for research-practice partnerships (R-PPs) and collaborative research. J Health Organ Manag 2014;28:115-26. https://doi.org/10.1108/JHOM-08-2013-0164.
- Gould MK, Sharp AL, Nguyen HQ, Hahn EE, Mittman BS, Shen E, et al. Embedded research in the learning healthcare system: ongoing challenges and recommendations for researchers, clinicians, and health system leaders. J Gen Intern Med 2020;35:3675-80. https://doi.org/10.1007/s11606-020-05865-4.
- Nyström ME, Hansson J, Garvare R, Andersson-Bäck M. Locally based research and development units as knowledge brokers and change facilitators in health and social care of older people in Sweden. Evid Pol 2015;11:57-80. https://doi.org/10.1332/174426514X14098428292539.
- Greene SM, Reid RJ, Larson EB. Implementing the learning health system: from concept to action. Ann Intern Med 2012;157:207-10. https://doi.org/10.7326/0003-4819-157-3-201208070-00012.
- Antil T, Desrochers M, Joubert P, Bouchard C. Implementation of an innovative grant programme to build partnerships between researchers, decision-makers and practitioners: the experience of the Quebec Social Research Council. J Health Serv Res Policy 2003;8:35-43. https://doi.org/10.1258/135581903322405153.
- Walter I, Davies H, Nutley S. Increasing research impact through partnerships: evidence from outside health care. J Health Serv Res Policy 2003;8:58-61. https://doi.org/10.1258/135581903322405180.
- Chafe R, Dobrow M. Health services researchers working within healthcare organizations: the intriguing sound of three hands clapping. Healthc Policy 2008;4:37-45. https://doi.org/10.12927/hcpol.2008.20266.
- Bammer G, Michaux A, Sanson A. Bridging the ‘Know–Do’ Gap: Knowledge Brokering to Improve Child Wellbeing. Canberra, ACT: ANU Press; 2010.
- Mitchell P, Pirkis J, Hall J, Haas M. Partnerships for knowledge exchange in health services research, policy and practice. J Health Serv Res Policy 2009;14:104-11. https://doi.org/10.1258/jhsrp.2008.008091.
- Campbell DM, Redman S, Jorm L, Cooke M, Zwi AB, Rychetnik L. Increasing the use of evidence in health policy: practice and views of policy makers and researchers. Aust New Zealand Health Policy 2009;6. https://doi.org/10.1186/1743-8462-6-21.
- Lomas J. The in-between world of knowledge brokering. BMJ 2007;334:129-32. https://doi.org/10.1136/bmj.39038.593380.AE.
- Phipps D, Morton S. Qualities of knowledge brokers: reflections from practice. Evid Pol 2013;9:255-65. https://doi.org/10.1332/174426413X667784.
- Bevir M, Needham C, Waring J. Inside co production: ruling, resistance, and practice. Soc Policy Admin 2019;53:197-202. https://doi.org/10.1111/spol.12483.
- Cooke J. Building research capacity for impact in applied health services research partnerships; comment on “Experience of Health Leadership in Partnering With University-Based Researchers in Canada – A Call to ‘Re-imagine’ Research”. Int J Health Pol Manag 2020;10:93-7. https://doi.org/10.15171/ijhpm.2020.11.
- Cruz Rivera S, Kyte DG, Aiyegbusi OL, Keeley TJ, Calvert MJ. Assessing the impact of healthcare research: a systematic review of methodological frameworks. PLOS Med 2017;14. https://doi.org/10.1371/journal.pmed.1002370.
- Williams O, Sarre S, Papoulias SC, Knowles S, Robert G, Beresford P, et al. Lost in the shadows: reflections on the dark side of co-production. Health Res Policy Syst 2020;18. https://doi.org/10.1186/s12961-020-00558-0.
- Morton S, Wilson S, Inglis S, Ritchie K, Wales A. Developing a framework to evaluate knowledge into action interventions. BMC Health Serv Res 2018;18. https://doi.org/10.1186/s12913-018-2930-3.
- Fazey I, Bunse L, Msika J, Pinke M, Preedy K, Evely AC, et al. Evaluating knowledge exchange in interdisciplinary and multi-stakeholder research. Global Environ Chang 2014;25:204-20. https://doi.org/10.1016/j.gloenvcha.2013.12.012.
- Patton MQ. Developmental Evaluation: Applying Complexity Concepts to Enhance Innovation and Use. New York, NY: The Guildford Press; 2011.
- Silverman D. Qualitative Research. London: SAGE Publications Ltd; 2016.
- Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. London: SAGE Publications Ltd; 1994.
Appendix 1 Partner identification tool
What this tool does
This tool can help you to identify and think about the main relationships you have with partners and collaborators in your embedded role.
How to use the tool
Think about yourself as an embedded researcher working at the centre of a network of relationships with people from different organisations. We want to understand these relationships.
Some people will be more important to your embedded role. You may interact with some more regularly than others. Some may be trusted or help you reflect on problems. Some may be from particular organisations or settings.
We will explore the character of these relationships with you through our interviews. Completing this activity will help you think about these people and their contributions to your work.
We would like you to:
-
Put your name at the centre of the diagram (Figure 13).
-
Think about the three or four people who are most important to your embedded role (for whatever reason) and allocate them to the inner ring.
-
If these people are based in particular organisations and settings, try to allocate them in a quadrant.
-
Then identify the next most important three or four individuals and allocate them to the middle ring, replicating the quadrants if these people are based in similar settings.
-
Finally, identify those individuals who are perhaps less integral to your work.
-
Throughout the activity, consider how these people might be separated by particular boundaries, for example university/NHS.
FIGURE 13.
Blank template for partner identification tool.
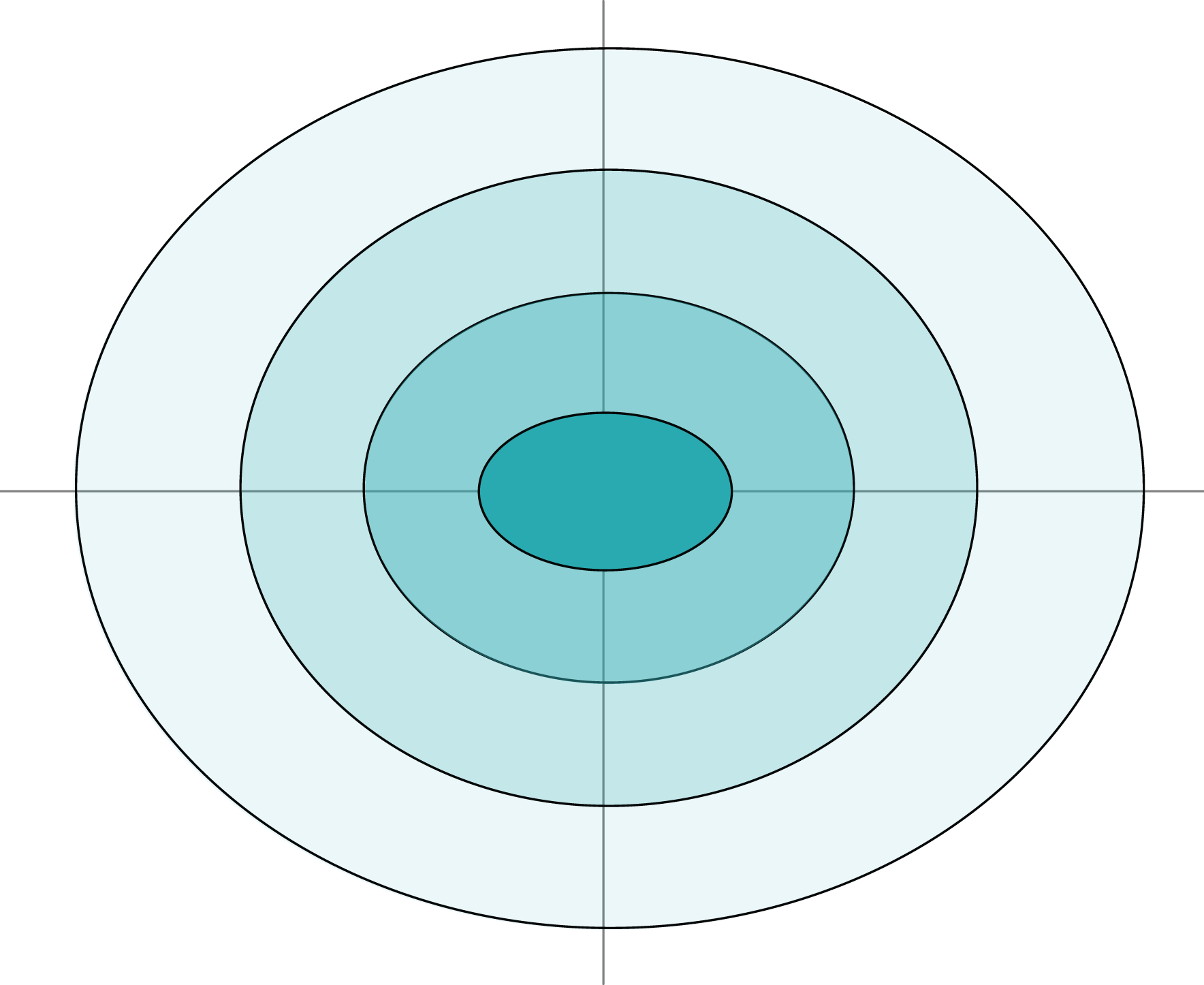
Appendix 2 Study participants (anonymised)
Table 19 lists the study participants interviewed in each of the four case sites and in the pilot site, Ferland. It notes the numbers of interviews, and durations thereof, when multiple engagements were held.
| Site, initiative details, description | Interview details | ||
|---|---|---|---|
| Participant pseudonym | Overview of role | Duration | |
| Ferland, pilot case, acute | Carrie | NHS England manager | 45 minutes |
| Adam | Academic professor | 57 minutes | |
| Lucy | Embedded researcher | 43 minutes | |
| Bridgetown, case study, acute | Anna | Embedded researcher | 1 hour 52 minutes, 48 minutes, 57 minutes |
| Jill | Nursing academic | 1 hour 52 minutes, 48 minutes | |
| Karen | Associate dean of research | 33 minutes | |
| Mark | PhD student and podiatrist | 31 minutes, 26 minutes | |
| Hannah | AHP lead | 40 minutes | |
| Joanne | Occupational therapy team lead | 40 minutes | |
| Gillian | AHP lead | 29 minutes, 27 minutes | |
| Belinda | AHP director | 45 minutes | |
| Coxheath, case study, acute | Jane | Embedded researcher | 51 minutes, 29 minutes, 46 minutes, 44 minutes |
| Sally | PhD student and chief nurse | 40 minutes | |
| Clare | NHS trust director of nursing and quality, and chief operating officer (retired) | 42 minutes | |
| Josephine | PhD student, previously nurse education lead | 57 minutes | |
| Violet | Local collaborator, GP | 51 minutes | |
| Olivia | Fellowship candidate | 38 minutes | |
| Porter, case study, community | Rachel | Embedded researcher: capacity-building focus | 1 hour 37 minutes |
| Carol | Head of R&D, NHS | 46 minutes | |
| Victoria | Embedded researcher | 36 minutes, 20 minutes, 38 minutes | |
| Katrina | Embedded researcher: service evaluation focus | 39 minutes, 21 minutes | |
| Bev | Embedded researcher: service evaluation focus | 39 minutes, 21 minutes | |
| Bill | Research development manager (NHS) | 44 minutes | |
| Karla | Embedded researcher: service evaluation focus | 46 minutes, 1 hour 8 minutes | |
| Lorraine | Community health director | 32 minutes | |
| Peggy | Nursing professor and NHS director | 48 minutes | |
| Evansville, retrospective case study, acute | Bella | Embedded researcher | 41 minutes, 39 minutes |
| Julie | Academic professor | 41 minutes, 41 minutes | |
| Janet | NHS manager | 39 minutes | |
| Mike | NHS manager | 38 minutes | |
| Tim | Embedded researcher | 48 minutes | |
Actual (at May 2020)
-
Total number of interviews: 46.
-
Total number of participants: 31.
Appendix 3 Workstream 3: detailed methodology
Introduction
Informed by the findings of preceding workstreams, workstream 3 involved in-depth qualitative research with four purposively selected cases of embedded research to understand the contribution such initiatives can make to the co-production and translation of research. As shown in Chapter 3, embedded research initiatives can vary considerably in terms of intent, structure and processes, and so the intention of this in-depth work was to understand how such factors, together with other unanticipated factors, might relate to differences in how knowledge is co-produced and translated into everyday practice. The specific research objectives addressed in workstream 3 were to:
-
purposively select four exemplar embedded research initiatives reflecting anticipated typographical differences, for example in their affiliations, project characteristics, relational networks and funding
-
describe the embedded researchers’ career histories, motivations and networks of research (university) and practice (NHS) partners, including changes over time in relationships, tasks and activities, and pattern of interactions
-
understand how embedded researchers and members of their networks mediated different forms of knowledge and cultural and social boundaries to promote co-production
-
appraise the contribution of embedded researchers and their networks to knowledge co-production, including detailed case examples in selected NHS settings.
Study methods
In addressing the study objectives, workstream 3 adopted a qualitative comparative case-study design. Qualitative case studies afforded in-depth descriptive and explanatory understanding of each embedded initiative, whereas comparative case analysis facilitated conceptual and theoretical elaboration by exploring common and distinct features.
Selection of in-depth cases
The workstream 3 sampling strategy aimed to identify and select exemplar cases of embedded initiatives that were ‘most likely’ to co-produce knowledge, while taking into account key differences in their configuration that might explain how and why such co-production varied. The selection of in-depth cases was informed by the learning of workstream 2 (see Chapter 3), especially the national review of current initiatives and the emerging typology of co-production initiatives for embedded research.
The initial selection process focused on the following criteria:
-
the intent of the embedded initiative (the purpose of the initiative)
-
the structure of the initiative (including setting, project scale, employment contract, and time frame and the maturity of the project)
-
the processes/outcomes of the initiative.
Guided by these conceptual and empirical sources, the sampling process first involved reviewing and shortlisting initiatives identified during workstream 2 (n = 45). Katherine Kirk and Justin Waring independently reviewed and categorised the initiatives according to the aforementioned criteria.
Further review considered the importance of the time frame and maturity of each initiative, especially whether or not the initiative was early stage, mature or had ended. This factor was seen as important in addressing the objective of understanding how embedded research initiatives might change over time and face particular challenges at different stages of their life cycle. Given the time constraints of the Embedded study, it was not feasible to carry out fieldwork with an initiative over a sustained period in excess of 18–24 months; therefore, the decision was made to select cases that were at different stages of their life cycle to compare the experiences of mature cases with those of cases in their early stages.
Next, initiatives were reviewed according to their espoused approach to co-production, seen as a core conceptual precept of an embedded research initiative. This included prioritising initiatives that took a ‘moderate’ or ‘committed’ approach over those initiatives that appeared to be carrying out more instrumental co-production or orthodox research.
Finally, we considered whether or not the initiatives focused on a particular service sector (primary, acute or community), the contractual or employment position of the embedded researchers, and whether the initiatives were primarily led from the NHS or university setting. An additional consideration in the shortlisting was the extent to which a basis of comparisons could be realised, in as much that initiatives could be compared as similar on one dimension, such as their approach to co-production, but different on another, such as service setting.
Justin Waring and Katherine Kirk independently identified a total of seven potential cases, of which there was agreement on six. In consultation with Vicky Ward, this list was reduced on the basis of the relatively low levels of involvement of potential cases during workstream 2 (Weedon and Usk) or their direct association with members of the Embedded research team (Sherwood Park). The selection process was then independently reviewed by Naomi J Fulop to question and confirm the shortlist, resulting in the four shortlisted cases (Table 20). E-mail invitations were sent to Porter, Bridgetown, Coxheath and Fulford cases with positive replies received from all except Fulford. Subsequent meetings were held with the lead from each of the three remaining cases [via Skype™ (Microsoft Corporation, Redmond, WA, USA) or in person] to discuss the possibility of becoming a case study site. Following these meetings, all three sites were keen to take part in the study.
| Site: researcher(s) | Approach to knowledge | Primary outcome | Secondary outcome | Other outcomes | Setting | Scale | Employment | Time (years) | Maturity | Location |
|---|---|---|---|---|---|---|---|---|---|---|
| Bridgetown: Anna, previously Jill | Moderate co-production | Capability/capacity | Formal academic knowledge | Local practice insights | Multiple | Portfolio | Joint | 4+ | Emerging | Scotland |
| Coxheath: Jane | Committed co-production | Local practice insights | Capability/capacity | Formal academic knowledge, prestige/credibility | Acute | Portfolio | Joint | 8+ | Established | South East |
| Porter: Rachel, Bev, Katrina, Karla and Victoria | Moderate co-production | Capability/capacity | Formal academic knowledge | Prestige/credibility, local practice insights | Primary | Portfolio | NHS | 10+ | Established | Midlands |
| Evansville: Bella and Tim | Provisional co-production | Formal academic knowledge | Local practice insights | – | Acute | Portfolio | University | 4 | Ended | South East |
After further discussion with the Embedded team, the decision was made to include two additional cases. The first of these was a pilot case to be recruited explicitly for the purpose of testing and refining the research methods. The primary basis of sampling the pilot was opportunistic access via established university–NHS research links. The other additional case study site (Evansville) was selected on the basis of the initiative being concluded for at least 1 year, thereby allowing us to investigate the longer impact and sustainability of embedded research, for example whether or not relationships were sustained beyond the specific project or portfolio, and how learning became adopted or sustained over time. Evansville was selected as the retrospective case; although this limited our data collection to more reflective forms of interviewing, rather than real-time observation or shadowing, it was seen as offering important insights about legacy and sustainability.
Within-case sampling considerations
In the first instance, we contacted the lead or main identified embedded researchers from each initiative on the basis that these people would be the primary focus and point of contact for in-case sampling. For Porter, contact was made via a gatekeeper (the head of R&D).
Through preliminary discussions with each individual, and by using the partner identification tool (see Appendix 1), additional stakeholders for each initiative were identified, with a focus on the main or key people involved. Ultimately, we sought to identify those practitioners, managers, commissioners and patients who, in different ways, supported, worked with and interacted with the embedded researcher: those people who the embedded researchers saw as important to their role. Appendix 2 offers a detailed view of the participants from each site. These people were contacted by e-mail and invited to participate in the study.
Data collection
In line with the research objective and methodological position, the study used a range of qualitative research methods to enable data collection and analysis, including semistructured interviews, focused observation and reflective diaries. It also made use of less common techniques, derived from stakeholder analysis and social network analysis, to facilitate discussion with individual embedded researchers about the key contacts or people they engage with as part of their activities. In practical terms, these were organised with each participating case through a series of site visits over 12 months, with the intention of studying changes over time.
The initial site visit involved introducing the research to key study partners, carrying out initial interviews with the embedded researcher and key partners, observing aspects of day-to-day practice, and/or observing one or more planned meetings. On subsequent visits, follow-up interviews were carried out with the embedded researcher and additional partners, identified through the use of the partner identification tool, as well as additional observations and shadowing of embedded research activities. During the intervening period, additional short telephone interviews were carried out with each embedded researcher to discuss ongoing and planned embedded research activities. The research methods are detailed below.
Interviews
Semistructured qualitative interviews were the primary method of data collection for workstream 3. These were designed to explore with participants their views and experiences of each embedded research initiative, focusing on key stages and activities in the development and function of each initiative, investigating the contribution of key people, meetings or activities, and discussing participants’ views about the types of knowledge or evidence co-produced and how it was translated into practice.
The interviews were semistructured through the use of two topic guides (see Appendices 4 and 5), and the more structured partner identification tool (see Appendix 1). One interview schedule was developed for use with the embedded researcher(s) to understand their particular career biography, profile of activities, relationship-building and management issues, and views about co-production. As outlined previously, each embedded researcher was interviewed on at least two occasions, to understand changes in their role over time, the development of their project and their reflections of the Embedded study. The second interview guide was designed to explore the views and experiences of those individuals who and groups that worked with the embedded researcher or as part of the wider initiative, to understand their views of the initiative. Given the diversity of people interviewed, this topic guide was much more open and relied on the researchers to respond to issues and topics in situ.
Although interviews followed a topic guide, each was relatively open, enabling participants to develop rich narratives of their experiences, as well as opportunities to raise in-depth, emotive and personal experiences; as mentioned previously, all interviews relied on the researchers to actively listen and respond to issues and topics. Given the longitudinal approach to data collection, and the time demands placed on participants, it was important to build strong rapport and positive relationships. For example, one embedded researcher was interviewed on five separate occasions, totalling > 4 hours.
Most researcher interviews were undertaken face to face at a location that was most convenient for them. We held periodic follow-up telephone conversations to clarify issues. Interviews with members of the wider network were often undertaken by telephone, again working around their schedules and resources.
Partner identification tool
The partner identification tool (see Appendix 1) was informed by social network analysis to help participants reflect and identify people they worked with through also thinking about the extent of their proximity or closeness of their relationship, and also whether people aligned or were based in different sectors. The model therefore comprised concentric rings, with the inner rings representing more proximal relationships and the outer rings representing more distal relationships. The tool was also designed with four unlabelled quadrants, with the expectation that participants could reflect on the grouping of their connections and determine the best way to label them.
The tool prompted participants to first identify people they engaged or related with around a given issue or activity, to think about the quality or frequency of these relationship, and to consider ways in which this ‘alternate’ person might be categorised. For workstream 3, therefore, the use of this tool served two key purposes: it helped the team to identify potential participants related to the work of each embedded researcher, and it helped them to understand the participants’ reflections or views of these relationships.
In practice, the field researcher introduced this tool as part of the introductory interview with each embedded researcher. The tool was completed as part of the relatively free-flow dialogue between researcher and participant, which enabled the researcher to seek clarification of the answers given, and for participants to explain their answers. Once completed, the embedded researcher was asked to further explain their choices for the allocation of individuals and groups, the nature of the interaction and communication with them, how they related to one another, how boundaries between the groups were negotiated, any sources of conflict, and knowledge-sharing across boundaries.
Observations
The study was designed with the goal of carrying out a series of relatively focused observations with each embedded researcher during each site visit. The primary purpose of these observations was to deepen insight into the embedded researchers ‘at work’, including the types of activity carried out and the relationships developed. This included observations of project meetings, staff consultation events, training workshops and research seminars. Report Supplementary Material 4 describes the range and number of activities and events observed in fieldwork for each case study.
We also shadowed the individual embedded researchers on their day-to-day activities. This was often difficult to organise owing to the variable and diffuse nature of participants’ work patterns. For example, during site visits, it was common to convene a one-to-one meeting, carry out a semistructured interview and observe an event or meeting, but then the embedded researcher would need to dedicate ‘quiet time’ to answering e-mails, which offered little utility in terms of observation.
Although much of the observation was undertaken with ease, observation at Porter was considerably more challenging to facilitate. Despite observing a large quality improvement conference hosted by Porter, we experienced difficulty accessing other opportunities. The main concern held by the embedded researchers related to potentially sensitive organisational data (based on recent reports and findings from regulatory bodies). Therefore, with this case, the study relied more on interview data to develop its analysis.
Reflective diaries
Given that site visits could be organised several months apart, the study was designed to make use of reflective diaries for embedded researchers to record reflections on their work, thus capturing data and also informing subsequent interviews. Initially, pen-and-paper diaries were proposed, but, after discussion with the wider Embedded team, we decided that a voice-recorded diary (for later transcription) was more likely to be user friendly. A short guide was produced outlining the purpose of the diary method, which asked the embedded researchers to describe their activities and tasks, the types of knowledge employed, the relationships involved and any challenges or issues faced (a flexible, semistructured approach was adopted from the outset). During the initial site visit and introductory meeting, each participant was invited to use a voice-recorder, and given a short instructional guide on the purpose and use of the diaries. All agreed to participate in the diaries, with six using the recorder provided by the research team, and one using their personal phone. The recordings were collected before or during subsequent site visits.
Despite our efforts, some researchers found the diaries difficult to engage with because of excessive workload. Engagement was partial and somewhat superficial, and we recognised that the data from the diaries were likely to be of limited use. To maintain and continue to grow the warm relationships with the researchers, we focused our attention on methods that supported generation of the best-possible data. Despite these difficulties, Victoria and Bev (Porter) and Jane (Coxheath) completed diary entries that informed subsequent interviews with these participants.
Data analysis
Data analysis took an interpretative and abductive approach. The abductive approach seeks to combine inductive (grounded) data analysis with elements of more deductive (proposition-driven) analysis, with the goal of fostering close empirical–theoretical dialogue and ultimately proposition (theory) refinement. Empirically induced codes and concepts derived through standard coding processes are then systematically related back to heuristic concepts and theories derived from the literature to look for opportunities to confirm, clarify and challenge these thematic concepts as a basis of empirically informed theoretical elaboration.
In practice, the process started by uploading the transcribed interview transcripts, observational field notes and reflective diary entries to the electronic data management software. There was then a substantial familiarisation period, in which the data were read and re-read. Interpretive coding then began with the emergence of inductive initial codes, in line with established qualitative traditions. 202,203 Two members of workstream 3 undertook the coding of transcripts separately; the themes/codes were then amalgamated and refined. The codes were extensively reviewed, compared and reflected on before a final set of codes and subcodes was honed. These codes informed the development of individual and comparative case analyses. Comparison between cases allowed for further interpretation based on understanding of the common and divergent experiences, which were then thematically analysed according to the analytical heuristic outlined previously, with subsequent questions asked of the individual and comparative cases to refine explanatory understanding. As analysis progressed, a framework approach was utilised, with fields derived from the aforementioned heuristic model.
Appendix 4 Interview topic guide for embedded researchers
| Aim of workstream 3 | Related discussion topics | Potential research questions |
|---|---|---|
| Describe each embedded researcher’s career history and motivations | Career background |
|
| Job details and tasks |
|
|
| Motivations |
|
|
| Network of research (university) and practice (NHS) partners, including changes over time in relationships, tasks and activities, and pattern of interactions | Promoting co-production |
|
| Perceptions of ‘embedded’ |
|
|
| Relationships and networks |
[Fill out partner identification tool]
|
|
| Boundary negotiation |
|
|
| Challenges in knowledge exchange and production |
|
Appendix 5 Interview topic guide for other stakeholders
| Aim of workstream 3 | Related discussion topics | Potential research questions |
|---|---|---|
| Describe each embedded researcher’s career history and motivations | Career background |
|
| Job details and tasks |
|
|
| Motivations |
|
|
| Network of research (university) and practice (NHS) partners, including changes over time in relationships, tasks and activities, and pattern of interactions | Promoting co-production |
|
| Perceptions of ‘embedded’ |
|
|
| Relationships and networks |
|
|
| Boundary negotiation |
|
|
| Challenges in knowledge exchange and production |
|
Appendix 6 Case studies coding table
| Bridgetown | Coxheath | Porter | Evansville | Subcode | Family code | Overarching theme | Workstream 2 category |
|---|---|---|---|---|---|---|---|
| Anna’s very, very visible. She’s very easy to talk to. And she’s approachable . . . Anna makes it . . . now part of the conversation . . . [research is] more and more becoming a part of the daily conversations at work I would sayMarkKaren:I think the embedded part, the difference it makes is that, it’s a little bit related to what I said before about the being, being there . . .Interviewer:Physically?Karen:Yeah, you’re not going looking for the lengths, you’re not going looking for the partnership, you’re already there, you’re in it, you know, so the co-production is natural and real because if you’re embedded, then what’s happening is coming out of the fact that you’re there | Olivia:So she was visible around the hospital, she was seen by staffInterviewer:And is that important?Olivia:I think so because, so the world of academia is over there, the world of health is over here . . . the world of academia is a mystery sometimes, isn’t it, to some, particularly if . . . they’ve not had any more further dealings in terms of research . . . | . . . the majority of the time I spend over at [place] because that’s where our base is . . . I like to be in the thick of things and that’s what I really, really enjoy about my role because through writing these narrative reports I’ve started to get a really . . . good understanding of the service . . .KarlaShe provides a level of security for people, that they’ll say about her being there because she’s employed by the trust, she gets the red pay packet and holidays that they do. She walks in the same door they do. So she’s not scary, she has that level of being around all the time. So she . . . and she belongs, she has that level of belonging. And she also . . . she’s good at, err, I don’t know almost how to put it really. But it’s . . . people want to be acknowledged that their work is hard and tough and we’re asking them to do extra. And because she’s there all the time, because they know her, because she’s doing things for them and with them all the time, they understand and feel that she is with them and on their sidePeggy | . . . there’s this thing of running into people in a hallway or in the kitchen and striking up a conversation or, you know, walking with a member of staff who comes across another member of staff and says ‘oh, have you met [deleted]? She’s an embedded researcher’ . . . there’s that type of dynamic that you can only get if you’re there . . . even if you’re sitting answering e-mails but people are seeing you working with the team and you know they have a quick question about something that we’re doing together you know, they can come up. So it’s completely different than them sending you an e-mail and you reply, you know, it’s that type of dynamic . . .Bella | Visibility | Home/location | Logistics | Structure |
| . . . the first part for me was getting [name] an introduction to, to the chair of that, and for [name] then to create that space for herself within that environment . . .. . . who’s going to be your allies . . . you know, because it can be a very lonely place for a person, if they didn’t have thatKaren | These posts are so dependent on having people at very senior level who can appreciate what you do . . .Interviewer:That process of getting your contract sorted . . . that negotiation?Jane:It was done by my colleague, so she achieved that when she was Head of the Faculty of Nursing . . . she’s very good at networking and getting money . . .Interviewer:. . . the development, and its sustainability, seems very dependent upon people, individuals and relationships?Jane:Yes | I really think that making, err, those key relationships work is an important thing to be able to do. I do think it is all down to your relationship. You’ve got to find the . . . at the university you’ve got to find the professor who is willing to work with you, who’s willing to be open-minded. Who’s willing to be helped and guided to work within the NHS and that’s not everybody by any means . . .PeggyLorraine:[Name] was working entirely in the medical research field in, in a portfolio of services that, when I joined the trust, trust, fell into my portfolio. And, and I didn’t know anything about her probably for the first 3 or 4 years that I was in post because she was hidden with the medical consultants supporting medical research in the trust. And then there was a bit of a, there was a bit of a dispute I think one day, over who funded her post. I can’t recall the detail of it but I think the university used to recharge us for her time or somethingInterviewer:RightLorraine:And her budget disappeared as a few things have a habit of doingInterviewer:MmmLorraine:A consultant wrote then and her job was at risk and a consultant wrote to me and said it’s absolutely terrible, blah, blah, blah, you can’t possibly leave somebody with [name]’s skills and expertise, you know the trust, the trust, our research programme will fall to pieces without her. Can you do anything? . . . so I went to meet with her . . . to hear her side of the story and what was going on. And I felt when I met her that she had so much more to offer the trust, in addition, in, in addition to the support that she gave to the consultants | What happened to us at [deleted] is we had two people who were really engaged but then they left the organisation, which is a major setback for us . . . So that also became quite an important lesson to say ‘OK, yes you have to have champions and sponsors, but also you need to spread’ . . .BellaSo the origin of that study was that the clinical leaders of the changes in [deleted] and [deleted] were old friends and over a coffee or beer or whatever at some point they said, and they were implementing as it happened different ways of doing this reorganisation of centralising acute stroke care and they said gosh, wouldn’t it be good to get some research funding to study these changes to see if they make any difference and if, you know, the difference between our two models. So they came to us and said are you interested in doing this and so from the very beginning we had buy-in to this research from the senior clinical leaders who then, and then we had buy-in from, you know, people involved . . .Julie | Relationships | Role creation and sustainability | Logistics | Structure |
| RES: Yeah, so I’d say that one of the quadrants definitely would be about [name] and the . . . director, would be one of the inner circle. But then I guess you’ve kind of like . . . she’s not my line manager, she’s my kind of equivalent, if you like, in the NHS. So she’s the Head of the . . . Directorate. . . she’s the person that I report to if you likeAnna:I guess she’s the person who I kind of report to [in academia] And also I collaborate closely with [Jill], because our research interests are similar. But also because [name] was the person who used to do this job, or something similar to this job, a few years agoInterviewer:What is . . . what is [name]’s title now?Anna:So she is Leader in Rehabilitation Research . . . we’re going through a bit of structural in management team, the way universities do . . . | Peggy:Sometimes I can have a voice where she can’t again just because of my role. Erm, so . . . and I can say things that perhaps she can’t because of my role. So I think on a personal level I’m a sort of mentor and supporter of her, erm of a . . . on a work level I can enable her, sometimes, to do things that . . . erm, to get things happening that she wants to get happening . . . So what I can do is I can go and I can say I understand that that post is difficult at the moment to this. But you know [university] are paying half of it and as such I think you should be looking at what you can do to support that because I represent [university] and we are paying for half of this and we want to see it happenInterviewer:YeahPeggy:[Name] can’t say that but [name] can let me know what needs to be said | I think I supported the team as in once they had a project and they had a project lead, they worked with them and I really only saw them at our regular steering group meetings or I think they called them steering groups, but equally, they would contact me if they were having any challenges or things we as a trust weren’t, you know, moving things on . . . or if they felt their resource wasn’t being used well enough . . . my role was to try to make sure, you know, I suppose it was just making sure things, that everyone was clear on what they needed to do and it was never a problem because it was often people just busy at the frontline and needed a bit of a prod to think ‘oh yeah, I mustn’t forget I’ve got to do that’ . . .. I would say ensure that you build up your support mechanisms within academia before you start . . . you’ve got that peer support or a good line manager, you know, somebody that you can really, a mentor, coach, whatever, in the academic world. I would say at the beginning of your tenure as an embedded researcher be willing to commit quite a lot of time on relationship-building because that is what will get you through difficult times in the projectJanetBella:. . . one of the projects that we worked on . . . we had to go and tell them ‘your service is not fit for purpose, it’s not well designed’ . . .Interviewer:What was that like?Bella:So we had to go in and talk to him about it . . . this is the evidence and this is our role and we are critical friends . . . and if we didn’t share these findings, then we wouldn’t be doing our job . . . you need to constantly remind yourself that, you know, you are there to do a particular job. You are not like any other staff member within that organisation, you’re there as a researcher and there is that . . . academic layer to the work that you’re doing where you need to maintain that critical point really. . . . [T]here is that risk of, you know, of your, of creating potentially, you know, working really well with the service . . . becoming . . . subsumed into that and that affecting the way in which we’re doing research; there is always that risk . . . one of the key things that helped us a lot . . . is to have people in the team like [deleted] for instance. So a chief investigator on a professor level, someone senior in academia as well who is kind of part of the team but she’s not an embedded researcher . . . she would always be like the bad boss . . . she would be the person who said ‘no we’re not doing that’ . . . and she does that at a very senior level and we use that on purpose. So for me . . . as a researcher who has to go into the trust on a daily basis and has to build relationships . . . | Managerial/senior support | Support systems | Logistics | Structure Process | |
| Which . . . So they’re the people that actually probably understand my role better than everyone else, so I mean [name] who I share an office with, is a really experienced researcher, but has never done anything like in her research, in trials, for this, so in terms of our similarity in that way is small and she’s not likely to have a connection with anyone in any of the other quadrants of the NHS but she’s probably the person that understands my role the best ’cause I come in and I talk about what I’ve been doing or I moan about it, or I’m facing some sort of challenge, so actually the boundary’s really good I think because it’s those wee people that are my support unitAnna | So another person that I get, kind of have quite a bit of contact with, but I don’t know, I don’t know how to put her in terms of influence, is [name] . . . Talking to her she spans across the trust and [place]. So yeah, I suppose she’s, she’s very much like a partner, partner in crime I guess. So between us we run the quality improvement group for the directorate . . . She was brought in as the strategic lead to basically get research on people’s agendas. So she is, in terms of the pecking order, very high up within the organisation, and it was her job to integrate research into people’s day jobs . . . I’d say peer support to be honest, because we meet every couple of months, and we just chew the fat about life in the different organisations and things . . . Because [name] is still quite active in actually doing research, doing evaluation. So it’s kind of peer support that she’s done a PhD, I’ve done a PhD, and there aren’t many of us, what are we doing with that now? So with that one it is more peer support I guess, and thinking about and talking about the development of the quality improvement agendaKarla | There was one group that was created by some of the other researchers working under [name] work. I think you’ve talked to [name] already, so he’s had two embedded researchers at the time and they created a little support group and I think [name] who worked with [name] was part of that. [Name] in my department was the project lead and basically we got together and talked about the problems and things we were facing and trying to find out what the strategy that other people were using. It was a really good groupBella | Informal/peer support | Support systems | Logistics |
|
|
| Those who have come into our organisation in the last 3 years, erm have welcomed the opportunity and they have someone with that dedicated role. And because our ethos and our approach is an excellent in trying to build the . . . build that internal enquiry into [name] and into staff about saying actually how am I contributing to the four pillars? And so from a clinician and individual trail, from a service manager, how am I creating the conditions and giving staff the time to undertake evidence-based practice?Gillian | Sometimes these things are a question of timing and when, when you’re talking about you know, about much more transformation of leadership styles and more compassionate leadership styles, then, then I think you know, these sorts of ways of working, would, will be able to flourish much more, because it, it inverts the organisation. So it gives power to the frontline staff really. And it sort of, it fits with all the you know, I’m sort of showing my age really but you know, all the stuff around shared governance and you know, we map the history of some of this stuff. I think some of these things are just sort of points in time and I think it’s just when things need to converge to get the right ingredients to enable something like this to flourish. But I, I still believe that you, you have to try, even if, because it’s, it’s a long process to change the culture I thinkClare | Peggy:I’ve got my master’s and he said ‘that’s really good [name], if you were to apply for your job now’, bearing in mind I was a staff nurse, ‘I wouldn’t give you it because you’re overqualified’Interviewer:Oh my goodnessPeggy:And I thought I’ve got to get out, I have got to get out. This isn’t . . . this is not a place that is going to embrace me or people like me . . . that is an important bit of story because that really, for me, is the trigger for why I’m supporting people like [name]. . . But there were no opportunities when I was a girl at that time, for me to do what I would have loved to have done, which was be a clinical academic and to have that sort of mixture of erm a foot in both camps. And it was very evident that the culture wouldn’t have been there, even if I’d have created that, or had the power to create that I wouldn’t have got anywhere, as you can tell with attitudes like that, I really wouldn’t have got anywhere at allInterviewer:RightPeggy:So from then obviously, err I just . . . I spent 10 years at the [university] erm my job went from being a 1-year contract to, erm doing . . . made a permanent post. And from [university] I went up to [place], from [place] I went to [place] and from [place] I came here to [university] as a chair. So that’s obviously over a career of research in research time. But that is . . . my personal experience has always been like wanting the support embedded researchers or research . . . or clinicians that want to do research, erm and that’s really where my background comes from and where that influence is, how I feel, strongly I feel about embedded researchers | So in a way, my involvement was by chance because somebody suggested this as an opportunity and I just thought well actually this makes a lot of sense because if you’re involved in quality improvement, embedded research just seems like so naturally sits with it, but to be fair, I didn’t quite, it was a bit like, it just seemed natural to me rather than I was really ‘oh, my God this is the best thing ever’; it just made sense . . .. It was sort of by chance but actually made more sense to me and I’m really interested in research the sort of idea that we don’t wait for an end point, that was for me the sort of idea that this was translating and people working alongside actually you know, you’re learning as you do as well as [unclear-0:03:10.2] at the end, that for me was the biggest drawJanet | Leadership style (empowering others) | To support | Motivations | Intent |
| . . . and I just said . . . ‘If research was only about being more efficient, then first of all we’re never going to motivate staff to be more involved in research and second of all, I wouldn’t be a researcher if that was what it was all about’, you know, ‘I’m not driven by money and by savings, um, and actually I do genuinely perceive research as being crucial to improving people’s lives and improving the care that we deliver’ . . .AnnaHannah:. . . she’s quite focused on understanding what the clinical issues and clinical priorities are and has been using that to shape the research that she’s involved in . . .. There is that buy-in from the services that actually this is something that we said we’d like . . . people have really engaged with that . . . they understand the drive and the purpose behind it, so there’s a definite link between clinical practice and her role . . .Interviewer:Would it be fair to say you’re almost striving for a change in culture?Hannah:Yes absolutely . . . her focus is about undertaking research or undertaking research that actually will have an impact on practice, because it actually makes a difference to people and their outcomes . . . that’s one of the reasons why Anna is such a strong candidate for us . . . we’ve got people who are working so hard to deliver services, that unless for the majority of people, they would be undertaking and participating in research or applying research that they know it’s going to have an impact . . . | . . . no disrespect but she’s got a better understanding of the health-care arena and the constraints of the health-care arena, more so than perhaps somebody who’s got an academic research background but has never actually encountered a health-care setting. So the potential for Jane to pick up on things that somebody who’s not had that background is increased because she understands more, because she’s been embedded she understands more about the challenges . . .Sally | I did my PhD in [topic], and I got to the end of that, and I thought I don’t want to be a full-time ivory tower academic that does research that’s philosophical or abstract or metaphysical or any of those kind of things, I wanted to do research that had some applied meaning, that would mean something to [patients and their families] . . .Victoria | . . . one thing that keeps you going is the idea that what you’re doing has benefit beyond just you, social benefit rather than just private benefit.. . . Applied, particularly Health and Applied Research I would say it’s such an immediate social benefit, relative to something more theoreticalTim | Superiority (patient care focus) | To do/support | Motivations | Intent |
| Researcher:. . . when you meet with someone, and they’re like ‘Oh no, I would never be a researcher, like that is just so boring’ [chuckling], which happens all the time, it does happen, it’s happened to me in, in this job as well, I mean that is a personal insult to all of us, who have chosen um research as a career. Err and that it does happen at err different levels, so um there’s NHS [place] are developing that, err Nursing Midwifery [name] Health Strategy and I was asked to be in a group to um, contribute to how research should be included within this strategy and it went through various iterations, then went up to kind of the managers above us and it came back and research was only connected to the bit that was about better value and efficiency. So they had both sections about better patient care, better umInterviewer:Oh there’s no research involved in that, is there?Researcher 1:Yeah about better workforce and work satisfaction, um, better outcomes for people and research wasn’t in any of them, and err, I got err, fed back through and just said you know, ‘If research was only about being more efficient, then first of all we’re never going to motivate staff to be more involved in research and second of all, I wouldn’t be a researcher if that was what it was all about’, you know, ‘I’m not driven by money and by savings, um, and actually I do genuinely perceive research as being crucial to improving people’s lives and improving the care that we deliver’Anna and Jill | Jane:Key motivations, one is, erm, I, I’m passionate about growing a workplace culture where everyone can grow and flourish, I think that’s really vital, and the second, erm, the second one is about being person-centred and being person-centred with each and with our patients and staff and modelling those valuesInterviewer:’Cause when we say person-centred, people often, I would automatically go to that, being in terms of the patient, but you’re talking about that in a different way, aren’t you?Jane:Yes, about recognising the person, and the patient, recognising their choices as an individual and using those principles with each staff member as well | I am a strong believer that research should be driven by practice and the results should return to practice and if it doesn’t happen, then it’s not worth doing. So very much my work is very implied, so we don’t have any issues with that, you know; do you see what I mean? It’s like that’s almost a given for both [name] and I and our stance and where we . . . our philosophical view on what research is about. If it should be about, erm improving patient and family care experiences and staff experiences of care as wellSo I think that’s a shared . . . and that’s perhaps where, erm, where I benefit [name] is because she doesn’t have to make that argument with me, it’s given, it’s a given with me. Whereas some . . . if she’d have got these close associations with perhaps some other professors who were less from a practice background she might have had to have more conversations about well that might be very interesting technically but in terms of patients it’s not that interesting and therefore the trust won’t be as interested in driving it forwardPeggy | So kind of from early stages quite a direct interest in using research findings in a way that they can, you know, inform changes and practice in policy . . .It appealed to me the fact that there was an applied focus, definitely . . .Bella | ||||
| I think that . . . the hybrid role, whatever the terminology, is hard; you’re always going to have competing priorities from both sides of your role . . . I think it’s just about being really, really clear and open about your role. Anna is really good at that; she will say to people and just signpost people to other places if that doesn’t sit within her role it’s not something that’ll be appropriate but she’ll make sure they get the support and advice from elsewhere . . . she’s just that kind of link and that conduitHannah | Jane:The two halves do integrate with each other, erm, in a funny way, ’cause it is also about practice, so what I do in the university I try always get involved in the trust, and benefit the trust wherever possible. What I do in the trust also benefits the wider research as wellInterviewer:So you’re kind of ticking everyone’s box?Jane:Yeah, that’s right, and kind of, and synthesising | . . . help clarify boundaries if that’s required but also . . . I feel at times with Rachel, I’m helping her frame her boundaries so that she has a visibility and clarity as to what role she will take in different places . . .. . . so it depends on what the demand of the job role is . . . what she could do and what she has to do and what she needs to do may at times be different . . . she could run a project, she could design, develop . . . a project and some clinical staff would love her to do that . . . but she knows that that’s not, she can’t do that because that’s not what we need her to do except in an area that we have pre-agreedCarol | . . . if you’re gonna set up a team like this, it needs to have support right from the top of the shop and it needs to have [pause] I suppose there’s something that, and I even reflected on how we could’ve done this. So something about building in, building in so that it’s not individual people . . . so, you know, if you’ve got somebody who is the sponsor and they leave, it won’t make a differenceJanet | Role boundaries | Competing research priorities and two roles | Perceived/potential challenges |
|
| I think the support networks within the university is crucial and the team that she works within erm but I think having leadership-level support in practice is crucial, it doesn’t really matter much about everyone else, it’s got to be supported at senior level. You know, they’ve got to believe in it as a useful approach rather than just agreeing to it, I think it needs the belief that it’s actually important and why it’s worth investing in . . . the person who’s in that leadership role, you know, if they’re motivated and interested and keen to support it it’s very opportunistic, but if it’s not there, if that support isn’t there the person who’s leading that furthest for example, if they’re not interested then you can’t do it. It also needs, you need support on the, at erm lower management levels as well because people, in my experience senior charge nurses, for example, are very powerfulKarenI think the leadership role part of that being acknowledged and appreciated by the team so she’s actually included, that part of the role has made a huge difference to erm the engagement and buy-in and the impact that they’ve had on the clinical service. I know for example perhaps with the nursing we have some clinical academic research posts erm and I don’t think they’re as well embedded into setting the direction and the drive and the purpose of the directory as [name] is because it has that leadership role. . . . because she has the visible support and buy-in at that level that helps the role become accepted by the managers, the clinicians and everyone else that sits thereHannah | I think the important thing for me and I, I think there’s still learning around this, is how you win the hearts and minds of other people that aren’t really very aware of what the capability of this sort of approach is and definitely have to have executive sponsorship. I mean I happened to be working with a chief executive who, at the time, was very, I mean he didn’t particularly understand it, or hadn’t experienced it, but he was very tolerant of actually us trying different things.I think I would say, on reflection, that I wasn’t really able to necessarily completely win the hearts of, of all the executive team, and I, I know that you know, my colleague that I handed the button . . . over to, who was my deputy, who became Director of Nursing, continued with, with [name]. But I know that they, they, you know, they had some challenges I think along the way with changes in executive team members and that sort of thing. So it, it’s one of those things that, you know, it has to become culturally the norm to the organisation and that takes time, and it takes a lot of time, and people don’t always, you know, aren’t always appreciative of what it, what, what how important it is, and I think if they took it away from [place] now, I think they would really understand what the impact wasClareIn another 5 years they would realise or wish they’d continued doing this sort of thing and you get the full cycle again, probably that’s what will happen, but do you know these posts are so dependent on having people at very senior level who can appreciate what you do.The previous Chief Nurse, [name], she was, she got a PhD so she’s not, you know, she’s a clever person, she’s got a PhD in decision-making, she wasn’t really using that ’cause it’s such a complex organisation and she was very supportive to me, she was very operational, her whole focus is on operations, it’s not about being proactive, being excellent, leading the way, which is what I’m used to doing and so, erm, she said to me when you explain to the interim chief nurse what you do, you’re going to have to translate what I do for her to understand, but actually I didn’t find that at all because of this point I mentioned which is, I don’t think the trust has used me strategically, erm, strongly enough. She understood all of that, so I’m thinking well maybe it is about somebody with the strategic visionJane[Name] knows, to really make change, takes a lot longer than some flash old boss, you know, we all know that, but for some CEOs, that’s how they operate. They get their mates in, and they know they won’t be there forever.Whereas I think [name] has really invested . . . I think because, from what I can see, I don’t know the trust that well, but the CEO has gone, the Head of Nursing is . . . who was very . . . you know, they’re not so much friends, but they’re just respected colleagues, who believe in her, and believe in her programmeJosephine | Where we have services that are, that have a supportive leading manager or a driving manager that sees the value, it’s transformative to the roles of people being able to engage in research. Where that doesn’t exist, it’s almost like, well let’s take our backpacks and go home, it’s not going to happen there. If the management don’t see the value in it, they will actively conspire and I will use that word advisedly, conspire against it happening and that’s despite what might be high-level imploring from trust boards which may or may not be there, then the reality of having to meet performance metrics of commissioned service delivery mean that few managers are prepared to take the punt and see research as a way of being able to both meet that target and improve at the same timeBillSo to me it’s, I’m absolutely delighted we’ve got them, I think they have a fantastic role to provide us with, they’re great and I think they’re right for us as an organisation where we’re at now . . . but I’m not sure that our senior management, for example, would understand why on earth would I want more of them rather than upskilling our clinical colleagues moreCarol | Bella:So what happened to us at [deleted] is we had two people who were really engaged but then they left the organisation, which is a major setback for us . . . So that also became quite an important lesson to say OK, yes you have to have champions and sponsors but also you need to do a lot of work to kind of spread some of that . . .Interviewer:So it’s putting a lot of emphasis on, the importance of individuals getting it, if you like?Bella:Yeah, yeah. . . So the way in which the team was designed was we had one kind of lead sponsor who was a really senior trust member so he led the whole kind of, so [deleted] is divided into kind of three parts, medicine wards, specialist hospital and surgery and cancer. So he led medicine wards just to give you an idea of that and he was like, yes, the person who was fighting for us to be thereThe day to day of trying to help these projects it was down to particular individuals on those projects and the degree to which they bought into usTim[Senior buy-in] is necessary but not sufficient. So you need it, but then you also need to do the really hard work on the ground, which, you know, I can talk about but I haven’t done for quite a long time. So it’s people like [deleted] who do that of building the relationships on the ground to do the work you know, erm but with that kind of backstop of the senior people whose supporting it, if you don’t have senior people supporting it, you won’t get the funding to go forwardJulie | Buy-in | Perceived/potential challenges |
|
|
| The huge challenge with sustainability is that we’re a small, you know, we’re a small board, we have limited you know, internal resourceGillian | Josephine:It’s a different relationship nowInterviewer:Between academia and clinical practice?Josephine:Yeah. It’s still an important relationship, and sometimes it’s very close and works brilliantly, but it used to be like Director of Nursing would have a chat and a coffee with Director of . . . Director of Nursing trust would have, you know, maybe a regular meeting with Director of Education, and they’d say ‘well, we need someone for this’. And they’d say ‘well, we’ve got a little bit of money for the . . .’, they’d engineer somethingBut nowadays those things are more difficult, not because they don’t get on, it’s just financial issues on both sides, lots of reasons I think. Philosophical . . . so I think they’re rarer than they were, much rarerInterviewer:When you say philosophical, do you mean . . .?Josephine:Well, because I think education is the prime aspect of the university, and the students, and their student journey, and in the trust, pre reg[istration] and post reg[istration], the student is not the . . . the patient is the main reason they’re there. And things like 4-hour targets, and their financial pressures, so . . .Interviewer:Different priorities?Josephine:Different priorities and things are much tighter and . . . there’s not loose bits of money and stuff now, on both sides | I managed to push the trust to pay for me full time, but it had an academic arm, but with the financial crisis back whenever it was, the trust couldn’t really afford to keep me full time, but only have me as a part time. So even though I was part time for the trust, they were paying my full time salary, and that wasn’t deemed fair or they couldn’t afford to sustain that. So I went to the university and got the university to sort out the funding, and now the university pay 3 days and the trust pay 2Victoria | Generating knowledge in applied health research that we like to do is to have comparators and so that raises the issue about well then, how do you generate that research? Do you do that in an embedded way as well? So if you are looking at a particular change, for example, so that raises a question and the other is if you’re trying to look at different, a number of different sites. Because that same organisational case studies, I wouldn’t say the gold standard, but ideally one likes to look at the number of different sites where one is conducting the research to kind of enhance generalisability and different types of context where one is looking at the same thing. Or, comparators for the change one is looking at. And that is difficult, challenging in using the embedded research model because you’d have, it is potentially very costly. . . So that is, that is an important point about it that it is resource intensive and it limits, it can therefore limit you in comparison, either with places not undergoing that change or with other places undergoing those same set of changes to compare themJulie | Funding | Resources | Perceived/potential challenges |
|
| Mark:I’ve also had conversations with one manager who, who would like to try and use my research skills, in a way that provides direct benefit to the serviceInterviewer:MmmMark:That’s not in terms of developing things like interventions, which is what I’ve done before. To give you an example, what she’s interested in is looking at things like population trajections. So what, what are going to be the needs of our podiatry patients in 10, 15, 20 years’ time? What’s the evidence to support that? And she wants to use that to create business cases for service development and so on. So I think there’s a, there is an appreciation of the skills, but they want quick wins from it | Key part of the getting research underway in the NHS is understanding the time pressures that staff have and trying to be flexible around that because they ask people what the barriers are for them to doing research and the first one that most people mention is time, they just don’t have the timeRachelRachel:. . . it’s not just one person on their own, they have to have the support network around them to make that possible . . .Interviewer:UmRachel:. . . erm, and that’s part of the culture change I think that we’re trying to gain momentum is that, erm, er, middle and upper managers understand the need to be flexible and, erm, recognise the value of research and supporting staff who are interested to do research . . . so that, you know, they can make allowances, maybe, you know, give a staff member a couple of hours off to go to some meeting about research or you know whatever, erm, can all make the differenceInterviewer:Yeah, that senior support buy-in, if you like?Rachel:Yeah, um | Tim:I was on a number of others that fit that sort of paradigm, which was rush, rush, rush, meet every 2 weeks, change something, barely able to evaluate what it was before, let alone afterwards and then just keep going and then do that again and then again and then again. I can hardly do anything. We were asked to write a report at the end of the year, but after 2 weeks any report we would have written would be out of date, you know . . .Interviewer:MmmTim:. . . I got very frustrated. And another different one where I submitted a final report after our, our year’s time was up, and I don’t think they looked at it. I’m pretty sure they didn’t look at it. But even if they had, a lot of it was out of date anyway, in the sense that it probably would have changed and I was speculating a lot. . . I was familiar with the research paradigm, I could do that, I could . . . you know, I, I understood my role, I understood their role, it all fit together and the timelines in particular really, really matched up with the ongoing sort of, let’s call it service development stuff. I didn’t really understand my role, I didn’t, I cou– . . . the timelines between different teams or you know, with the embedded research timeline and the ongoing service timeline didn’t gel at all | Incompatible time frames and time | Resources | Perceived/potential challenges |
|
|
| . . . if I make my research relevant to more strategic stuff . . . then it becomes valued . . . if I was doing this work and it was just sitting in the abstract with no perceived elements to clinical work, then I don’t think . . . there’d be so much buy-in and support from NHS as I’ve actually received. So they can, they can see the value that that bringsMark | I think the main challenge for me is to get strategic uptake. When I don’t have a, I don’t have a . . . That’s what I want to do next, when I finish this I want to go and be a non-exec[utive] director in this trust, that’s what I’d like to do, because they don’t seem to understand, the trust board don’t seem to understand the values that they need to live, to achieve the changes that are required.. . . often the findings are so ahead of the time people can’t understand what they need to do with it, so 5 years down the line they begin to realise if only we’d done that 5 years ago we’d be in a different position [laughing]Jane | Bill:. . . research roles are not always seen as, how can I put this delicately, they’re not always seen as worthy of investment by people who commission services as those in the services who value themInterviewer:Why do you think that is?Bill:I would have to say that for a large part, and there are some notable exceptions, the commissioning process is an evidence-free zone . . . I do think that commissioning is driven by anecdote and financial pressures rather than that is necessarily best for the health system as a whole . . . | As our time was coming to an end, I think we should’ve done more work from the beginning to demonstrate what we were doing and the impact of what we were doing. So we didn’t do a lot of the communications, the kind of PR [public relations] like this is our team, this is what we’ve accomplished in our first year, this is what we need doing. So we didn’t do that and I think that was a missed opportunity because then when we had to go to the trust to say ‘can you send our funding?’ they, they, we tried different routes and they said no, they didn’t see the value of that team. They were under great, financial pressures and they felt that they wanted to invest that money elsewhere and, but I think the big thing is that they, they couldn’t really conceptualise, you know, why would I invest in the team, what is it giving me, what is it giving my clinicians. I mean, you know, maybe we could’ve done that brilliantly as a trust, would they have still said no? I don’t know, just because of their priorities, but I think as part of the, you know, the blame is also on us because I don’t think we did that properly from the start. So I think it’s a lesson for, for other teams to, you need to think about dissemination right at the beginning and hopefully that will come laterBella | Value of knowledge/research | Strategic/organisational | Perceived/potential challenges |
|
| Gillian:Because we have a huge pressure on us in the system to keep people as clinically active as possible, you know, lots and lots of clinics, you know, and therefore, there’s, there’s not the same potential to, you know, the non-verses, it’s described as non-direct activity, so that research is better, doesn’t get the same level of support within the organisationGillian:. . . obviously within the health service there is a focus on quality improvement and improvement cultureInterviewer:Yeah, yeahGillian:And our board invested it, has invested very, very heavily in that over the last well 10 years, and one of the things that working alongside [name] and colleagues, colleagues at university in this, is around that understanding of the continuum that improvement isn’t the only answer, and about how we . . ., because there’s a, there was, obviously there was, care . . . and, and an unspoken attitude, that you didn’t need to do research in the health service, all you needed to do was the quality improvement and because actually that was how you were going to bring about quick change, you know, but the balance, I’m much more committed to the balance of that and, and research, and then, and that skillset we’d like to, as an approach, we’d like to instil on our staff | I think people, people are very suspicious of things that they don’t quite understand, and because I, I mean, you know, I haven’t really had this conversation with [name] but my, my reflections on it is that I mean it may be some things that, that we’ve got to reflect on professionally, but I do think that sometimes the way we use language, might sometimes act as a bit of an obstacle. We, we know what it means and we’re quite comfortable with it, but I think it’s, it’s a new language for other people and culturally I mean I’m very passionate about the NHS actually but, but culturally we’ve been in a situation where, you know, what trumps all is you know a top-down performance-type regime, which, you know, you and I and others would know actually is not very empowering for people, and did ask them . . . and actually doesn’t value what frontline staff really, who knows the business intimately and what they’re trying to achieve. It, it, it’s, you know, completely wrong, but that has been the culture of the NHS and has been driven really by this top-down stuff from the Department of Health, NHS England over timeClare | Rather than an initiative that, that seconds two people into a university and we never see them again, this was wholly about how do we work with the universities to, to give some of our staff an opportunity to, to practise and develop some academic research skills and bring that back into practice. And, and because, I suppose because it was sold as a, as an opportunity that was going to be meaningful they could see what the outputs were going to be in terms of the care that we deliver to patients on the, on, on the wards. Their, their ears pricked up a little bit I thinkLorraine | Now the other thing is, I think I talked to you about before was that the funding for the [hospital name] wasn’t renewed and the feedback I had about that was informally was that they knew chief executives wanted to focus the trust energies on clinical research rather than the applied health research or health services researchJulie | ||||
| So what the managers want to look atInterviewer:UmResearcher 2:Is something very, very differentResearcher 1:Yeah I mean it is much, it is exactly like you say, that it’s about umResearcher 2:The floor and service delivery and uh huhResearcher 1:Service delivery and um yeah that’sResearcher 2:It’s a very different modelResearcher 1:Uh huh yeahResearcher 2:Which againResearcher 1:And a lot about value and efficiency that’s what their, um interest inResearcher 2:Yes, value for money, efficiency, throughput, flowInterviewer:Um, aligned with governmental . . . targets and stuffResearcher 1:YeahResearcher 2:ExactlyResearcher 1:Whereas the practitioners, what they want to know is ‘oh we’ve developed a, a new intervention’Researcher 2:That’s rightAnna and Jill | Rachel:So it’s very much, erm, you know those tangible benefits, erm, but I think valued by the staff considering doing the research, but also the managers and the service around them in terms of supporting the research. If they can be told ‘well, if we do this piece of research, it might mean that we can make a cost saving or a more . . .’Interviewer:UmRachel:‘. . . efficient service’, then they’re much more likely to get that supportInterviewer:Onboard?Rachel:YeahInterviewer:So it’s a, I guess it’s . . . speaking a specific language to kind of, er, meet the broader organisational . . .Rachel:Yeah, yeah and sometimesInterviewer:. . . direction?Rachel:Yeah, I mean our trust has come out with nine prioritiesRachel:. . . so we’re realising, you know if you’re proposing to do a project, use these priorities, you know, mention them when you’re trying to describe what you’re proposing to do . . .Interviewer:UmRachel:. . . then you’re much [more] likely to get buy-in from the senior management to support you to do that because they will see that it’s working towards . . .Interviewer:UmRachel:. . . one of the key priorities . . . that have been identified | So the board would say ‘oh I think such and such a unit in this area of the organisation’, you know, . . . ‘they’ve got a challenge around x’, it would be really helpful. Anyway so the team then went to this unit and they went ‘no, that’s not the issue we’ve got here, it’s something completely different’Julie | Misalignment (front line/management) | Research priorities | Perceived/potential challenges | Intent | |
| Interviewer:You said about [name] being a bridge?Gillian:YesInterviewer:Can you tell me a bit more about that?Gillian:. . . for her to have that contemporary knowledge around the research and the research community and to make those connections, erm again to understand what is active elsewhere, what we’ve got an opportunity to become involved in | I think the essence of this is the connectivity . . .. . . it’s working in that liminal zone, it’s the bridging, it’s the knowing who to go to as well as the actual insight that you gain, so that you can transfer knowledge and you can transfer skills, and I think [name] is a conduit in a similar way, she can bring her expertise and mesh it with the messy reality of the workplace and similarly the, the workplace . . .. I’ve been able to say to other people, ‘Well actually, there’s this work and there’s this person’, and if, it sort of connects the system. I’m very much one for permeating boundaries and . . . trying to bridge those gapsViolet | You know I think that people like [name], it’s a conduit . . .You know [she] can face me with the realities of . . . when I’m saying, ‘oh let’s do this’, ‘let’s do that’, ‘why don’t we do this?’, [name] can very much say to me, ‘mm but we have to be aware of x, y and z’. She very much is a bridge, negotiator, she is a diplomatPeggy | . . . the steering group that I have in that second circle, that wouldn’t exist without us because we created those groups at those trusts, so we know people might get together for different reasons and the health organisation, but for the purposes of this, we’ve put them together and we’ve built that infrastructure . . .Bella | Bridge | Facilitating connection | Qualities/strengths of researcher and role | Process |
| . . . she allows clinicians to see that they could potentially be a, a researcher within a health-care setting, but at the same time demystifying it all. Because it’s a little bit of a black box to those who aren’t in that world . . . She’s very easy to talk to. And she’s approachable and she’s done a good job going on all sorts of staff groups around the NHS here . . . The idea being research-active has become far less nebulous and out-there, as it might have been 5 to 10 years ago . . . more and more becoming a part of the daily conversationsMark | . . . when I talk to non-registered staff . . . when you say to them about doing a module at university to advance, ‘oh God, I couldn’t possibly go to university; I couldn’t cope with research or anything like that’. So they already have this negative perception of it and that’s a huge shame because they could come up with some of the answers to the challenges that we face.Jane’s very approachable, she doesn’t make you feel stupid, she listens, she’s an active listener and then she helps you assimilate it. So she’s, she’s got that, that, her communication skills are brilliant and she is . . . approachable and obviously the knowledge is there . . .Sally | . . . some people initially contact me saying, ‘oh, can you come and meet with us because I don’t know where to start with this form?’ . . . I think they’ve just seen it and initially been like, ‘oh, it’s academic, I can’t do it’, but then by the time I’ve met with them . . . I really tried to break it down for them, sort of really understandable language . . .. . . it’s that translation between academia and NHS which is massive that terrifies some people . . . I think it’s that experience of working with people to understand actually at what level you need to pitch things . . . because there’s definitely a fine balance between being really patronising and actually putting it in a way that everybody’s going to understand . . .Karla | Having the skills, you know, to, to be able to work well with other people, to be able to recognise the different contributions people can make to a project regardless of where they come from, you know. If they’re clinicians, if they’re managers, if they’re, you know, statisticians, you know, to be able to have, to really open, to have a way of dealing with people and to foster collaboration; I think it requires that, it requires a knowledge of context . . . understand how the context and the workings . . . ultimately shape your experience, people’s perceptions of you, your perceptions of other people . . . it’s that kind of really dynamic relationship between individuals in contextBella | Interpersonal skill | Making research accessible and inclusive | Qualities/strengths of research/role | Process |
| I think trying to humanise researchers in the university world is quite an important part in breaking down that barrier, which I suppose is something that I try to do . . .. I think the split with the university thing helps, because they see me as being both part of the NHS but also out with those hierarchical structures. I actually think a big part of it comes down to social interaction and personality because I, I do, I think it’s happening less now because people are more aware of me but certainly initially when I would go along to meet with people I could te–, I could feel that they were anxious and that they were intimidated by me being a researcher and being from the university or being new in the directorate because there is such a big gulf. So, like, [laughs] I’ve had lots of feedback from people who say now, ‘just, you’re such a normal person’, which I guess we should take as a compliment but I don’t know what they expect . . .Anna. . . it was a difficult meeting, because the starter session was really scary but, but it was such a positive meeting, because I came away from there, much, much more clued in to what exactly I was going to do and how, what questions I needed to ask . . . I think the person . . . have to have insight and understanding . . . she’s a very good communicator, she’s very good at facilitating, and encouraging things . . . I think that’s a real quality that she has, and she feels approachable . . . If somebody comes into post and they are too academic, it’ll just put people offJoanne | I always work to diminish that, and oh, yes, there are some people who I could, there is one or two people who, especially in health, human resources, ’cause I do a lot of work around workforce and they see themselves as the experts, but I’ve always worked with them, always collaborative, mind you we get the odd challenge, er, but because I’m collaborative, I’m always happy to see the world with their eyes, it’s just having the dial up. The people I can’t, I don’t like working with are the ones who are not authentic, or who are top down, top down in their approaches ’cause we know from all the evidence and the research, that that doesn’t work, but OK, I appreciate that’s what you’ve got to do, I will help you to be more effective in the ways that you work, even if you are taking a top-down approach . . .. I know I’m not intimidating but yes, I do appreciate thatJane | Karla:I’m really conscious again with that sort of, I don’t want to say, yeah I would say stigma, academic stigma, but I don’t want people to think that, ‘oh, an academic’s coming to talk to me’. Like, for example, as an example, yesterday one of the ladies on reception, she got really confused about my wage slip because she said, she came up to me and she said I’ve worked there for 2 years now, she said ‘are you a doctor?’, I was like ‘yes’, she was like, ‘oh, I had no idea’ and she didn’tInterviewer:That’s interestingKarla:Yeah, because I don’t tell people because when I go and meet with people I won’t, and when I, on my e-mail signature I won’t put doctor on most occasions because I don’t want people to think, ‘oh, she’s an academic, she knows lots’, I don’t want to engage in that, I kind of want to meet people first and you know if it comes up I will tell people, like if I feel like I have to clarify my sort of expertise in the area, but other than that I won’t say it because I don’t want people to have that sort of association | I think we were fortunate that most of the members in our team had worked in the NHS before, so I think that helped in terms of navigating the organisation and then problem-solving, and the other skills is, there’s a communication skill and that’s especially important for us qualitative researchers who, you know, if you look at our stereotype we tend to be quite worthy, well not worthy but, you know, to need lots of pages to transmit a message for instance or, you know, we, yeah I think it’s in terms of being able to communicate things in a simple way, a direct wayBellaThey need to, people need to see that they know what they’re talking about and it’s quite important I think in the NHS and from a, from a how they interact and work within the trust they need the [pause] good team players and if we pull that apart, you know, they need to have good communication skills, good listeners. Being able to constructively challenge in a, you know, in a friendly way that would, you know, but equally be quite resilient because their personal resilience is quite important . . .Julie | Relatable/adaptable | Interpersonal | Qualities/skills of researcher/role | Process |
| They were funny, because they’re . . . they’re both people who are . . . I think they were quite anxious about reviewing it at first. They were really keen to, I don’t know, they talked a lot at me, and they’re the people that were probably the earliest to give me like feedback, because they said then, you’re just a normal person, which I think was [unclear – 18:31], but I don’t know what they were expecting. If they thought I was, I don’t know, be like stern or talking in a completely different language to them, or . . . there was a lot of our meetings were kind of starting and ended with general chitchat about their daughter’s wedding, or weight loss or you know, just general chitchat . . . I’m perfectly normal(!) I think that helped, after the first few times. The first few meetings they just seemed really anxious, waiting for whatever piece of wisdom was going to come out of my mouth. I think they thought I was going to come in, tell them they were doing it all wrongAnna | You do need to have that sort of integrity, you know, and that thought, so you know, all these things that you talk about now, about thought leadership and integrity and trust and that sort of thing, so it doesn’t matter how much knowledge you’ve got, if you bring people together and you’re not being integral yourself, you’re not being seen as somebody who works in that way and also you’re not honouring them. So you need to be very, you need to be able to respect everything that people bring to you and be able to say ‘yeah that’s really worthwhile and really useful’ or even when they’ve seen quite negative things . . .Olivia | Karla:I’ll go over and just say, ‘oh’, you know, ‘are you on your own today? Do you want, I’m going to the kitchen, do you want me to get you a tea or a coffee? Oh, by the way I’m blah-blah-blah’, so then I’ve kind of connected with them, so then if they see me on an e-mail or whatnot, they know who I am, they know, they can approach me if, because I think that’s a big thing in work especially if we’re wanting them to sort of do extra, do this quality improvement, do service evaluation . . .Interviewer:YeahKarla:. . . I think it’s about them knowing that they’ve got someone that they can talk to about it and it’s that relational thing that if I embark in this I know I’ve got someone that’s friendly and supportive and whatnot, so I try and make that impression when I see people, just to kind of help them engage in the process and because I think sometimes that support that you can get can either help or hinder people in going forward in the first place and asking for the help . . . | Julie:She is absolutely superb at building relationships and getting in there and you know and all of that, oh, and that’s another thing about who you recruit to do these roles. . . what I’d say is you need that senior buy-in and it’s necessary but not sufficient. So you absolutely need it but no, it’s now you don’t . . .Interviewer:OK, OK I was going to say is that it?Julie:No, no absolutely not, no it’s not; so it’s necessary but not sufficient. So you need it but then you also need to do the really hard work on the ground which you know, I can talk about but I haven’t done for quite a long time. So it’s people like [deleted] who do that, of building the relationships on the ground to do the work you know . . . | Relationship-building/trust and respect | Interpersonal skill | Qualities/skills of researcher/role | Process |
| Joanne:It’s made it easier for me and it feels like she’s an ally because it’s very, very daunting and I think it would have been easier just to not do it, but part of me feels I have to do it, because it, the potential of coming up with some answers and that, you know, we’ve invested a lot so far in the literature research and that, we can’t just turn around and walk away, but sometimes it feels really overwhelming and I think especially because you’ve got your clinical remit and your, like I’ve got my team leader and my clinical remit, on top of it, which it would have just been easier just to not do it, but I think that knowing that [name] there, and it will make that process a lot easierInterviewer:You said you called [name] an ‘ally’, can you tell me a bit more about that?Joanne:Yes well I think that’s probably my expression of where I’m at with . . . governance . . . in a sense that they’ve, this, they’re the gatekeepers and the process that you have to go through is very daunting and the form that I’ve just sort of tried to fill out, has, it’s not the easiest of forms to do. So feeling like you’re on your own again, a barrier that you’ve got to overcome, whereas [name], she feels, well she’s definitely is on my, because she had e-mailed a quick reply, I was reading it one time, she said ‘Be careful how you word such and such or this will happen’, and she helped us a lot, you know, so she’s always there, sort of watching that I don’t trip myself upI’m just glad that she’s here, to be honest, [chuckling], like I said it has made a huge difference to me and my ability just to think, no we’re OK, we’re doing this and it doesn’t matter how long it takes, in fact, if it takes longer, the process of, of getting all our permissions, means that we actually have more data to look at, because we’re going back in a way, which is a good thing, but yeah, I, I, I would be struggling to sustain my energy and enthusiasm if it wasn’t for that I know that I’ve got [name], I can e-mail her, I can lift the phone and she has encouraged me | What she did was she gave ownership to the staff, the staff felt engaged, the staff felt empowered and if people feel that they’re more likely to take it forwards, they’re more likely to embrace it because actually they have developed it. Whereas if your managers come along and say ‘right, you do that’, you know, you’re not going to be as enthusiastic as it’s been done unto you and if you don’t agree with it that’s even more of a reason to drag your heels and implement itSally | I think my role is much more about helping them realise that they can do it, you know, just because they’ve not done any research before, or they haven’t done any for years, it, it always surprises me slightly, even though I’ve been in the job for such a long time, how frightened clinicians can be . . . of doing research, they don’t think they’ve got the skills to do it, they don’t think they, they don’t know where to begin, the whole NHS ethic thing terrifies them, because they hear stories and of course those stories are all true [chuckling], which doesn’t help, because you can’t dispel the myths, you can’t say ‘Oh no, no that’s nonsense’, because it’s like ‘Well actually yes that’s true’, but it’s about fostering an environment where it doesn’t feel so scary, where they know they’re supported, where they’ve got someone they can come to and go ‘Actually I just want to do this little project’, and it is, you know, or this great big world-changing project, and be supported in thatVictoria | There’s still something around having the skills you know to, to be able to work well with other people, to be able to recognise the different contributions people can make to a project regardless of where they come from, you know. If they’re clinicians, if they’re managers, if they’re, you know, statisticians, you know, to be able to have, to really open, to have a way of dealing with people and to foster collaboration I think it requires that, it requires a knowledge of context. I think knowing how to not only just list potential factors, because anyone can do that, but to understand how the context and the workings out ultimately shaping your experience, people’s perceptions of you, your perceptions of other people, you know, it’s that kind of really dynamic relationship between individuals in context . . .Bella | Harnessing potential in others | Interpersonal skill | Qualities/skills of researcher/role | Process |
| We wanted them to have a track record of interdisciplinary and interagency working, and also that they’ve been successful at securing funding, so they knew exactly all the challenges around funding you know and, and with regard to that in seeking funding and things, having that resilience around, so a tenacious person, because I, I know now that working with and I can see how important that is, is that with [name], quite often they’ll go in, and it’ll get rejected and have to be rewritten you know, and, and the time and the effort and the attention to that detail, you knowGillian | Anyway, so I followed up this idea of studentships, and then the money . . . they didn’t get studentships in the end, but I just had a chat with them, and then a telephone interview, and they were very supportive. She’s quite nurturing, she’s quite tough, she’s brought in life challenge, life support, which is what all her literature’s about. She’s quite tough . . .Josephine | I have to say, despite the extra stress, despite the extra hours, and despite the constant juggling and despite the fact that I have to live my life with a pair of trainers and a rucksack, because I’m never in one building long enough to just be able to settle, I have to, I run round [place], you know, I walk up to [name] which is where you’re going in a bit, and, and the CAMHS site is right over the other side of the city and I walk there, and the university campus is all spread out over here, and in one day I can be in four or five different buildings, I still love itVictoria | You’re not in an academic institution, you’re in, you know, somewhere that people, if people are having a bad day sometimes in the NHS, you know, it’s not the most welcoming place. So you know, you get to a meeting where this is your project and you are so interested in it and you’re so focused and the people around you have got operational roles and something has happened and they’re all a bit stressed and that does make it quite hard. So I think personal resilience and a very clear ability to work through quite a lot of thinkingJanet | Resilience | Committed/driven | Qualities/skills of researcher/role | Process |
| Anna:We’ve got this governance priority, which . . .Interviewer:It doesn’t sound very excitingAnna:Yeah, we’ve got about like information management, and regulatory bodies, and different things. And one of the groups is quality and effectivenessInterviewer:RightAnna:So when I started, that group were kind of, I guess, floundering a little bit, so it lead by an OT and a physio[therapist]. They are both very senior, they’re both service managers. And . . . but really, I mean, they knew that research was one of the standards that they were supposed to be looking after, but they didn’t have a clue at all. So I got paired up, put with them, as a critical strength, they were calling itAnd I think they were really, really, well at first I think they were very intimidated, they were a bit concerned about me turning up speaking about it, but then we just had a look at kind of defining well, what do we mean by research, and how is that different from quality improvement? How do we make sure that you’ve written your standards in a clear way, that’s about people using research evidence, or the fact that . . . and also that we’re doing research, at best as the option comes up.. . . So I’d been working with them . . . so I would say that yeah, the governance group set with the . . . Lead in that outside circle, but that certain individuals, as I start to work with them, they move a bit closer | I’ve used [name] as a critical friend, and our paths obviously still cross, because one of the areas of overlap is around the notion of facilitators in the workplace. We use lots of different language and we may sometimes be talking about the same thing but with a different language and these system leaders for me, need to be expert facilitators and that fits with a lot of the work that [name] has done and her team. So we’ve also linked with her recently around the piece of work that we’re doing, with the help of the Darzi Fellow, that I managed to recruit and that’s around the learning environment. So we’re doing a specific piece of work, looking at what will make an interprofessional learning environment in a PCN . . .VioletOlivia:Have you heard the phrase ‘critical friend’ before, because you just said that’s an interesting phrase?Interviewer:Well I’ve heard lots of people use it, but I imagine everyone’s using it in a different way, so your version would be goodOlivia:Yes I would imagine so. So the way that [name] described it to me at the time was that you would meet and it would be for mutual benefit, so I would talk about anything, that I felt I needed to talk about, that I either needed help with or just needed to reflect on, or think about and then she would do the same and the idea is that the other person would offer you, high support, but high challenge, in order to challenge your thinking, but support you to develop | Victoria:Yeah first started talking about evidence-based research, they talked about the importance of combining science with clinical judgement and decision-making, and, and people’s opinions and narratives and ideas, and that was a really sound definition of evidence, and we’ve moved away from that with this whole dominance of the RCT being the only possible way of doing research, but that misses all that real-world stuff. So I prefer, what I call naturally occurring data and ethnographic data, where you combine natural data with interviews and things like that, and I actually think it’s the clinicians who make the world go round, and to just disregard their views and opinions and favour testing drug A, in this sterile, unnatural environment, against drug B. It’s got a place, we need that kind of, I call it, I guess, proper science, we need that proper science, but we seem to have forgotten the value of people, in that, and we’re seeing a shift with qualitative research again being disregarded as being less important or not mattering, not being so relevant to clinical practice, but actually I would say it’s more relevant to clinical practice, than it ever has been before. So I think those partnerships between social scientists, scientists and clinicians, are really crucial, because I think if you just get a group of scientists, it risks all their natural biases coming into play and likewise if you just have a group of clinicians, all their natural biases. People, like-minded people come together and they agree with each other and if you haven’t got anybody in the room that says ‘Oh actually have you thought about X?’, no one will ever think about XInterviewer:Are you that person?Victoria:In some situations, yes, and in some situations, I’m just the person who facilitates another person to do thatPeggy:The benefit that [name] has, if I work in a R&D department it means that she’s always in research, even in the trust. Are you with me? So she never loses that. Unlike some of my other colleagues who are doing research and clinical practice. So the matrons, they’re very much driven by what service requirements areInterviewer:YeahPeggy:So very much research comes second, even though they’re excellent, it has to come second to what’s required for service . . . for the service side | So and I, I know [name] particularly is interested in what is embedded and what is embeddedness. I think she’s done a number of papers . . .. Or at least she’s . . . a lot of, certainly a lot of thinking on that thing and I did as well, so and I describe, you know, my colleague, the anthropologist by trade who wanted to very much observe and not affect her subject matter . . . don’t affect the natives. So she probably felt even more outside than I did but also just because if I was within that structure or if I felt more within that structure, I probably would have been much more hesitant to raise all these things . . . and to flag all these problems.So that’s what I mean is that people are up for it in theory except when actually you want to do some research to uncover. And we are not trying to make them look stupid or failing or, that’s not the point of the research but we do want to understandJulieInterviewer:So having the academic link? I’m using the word ‘link’ . . .Bella:Yeah, yeah it gives you the opportunity to say from an academic point of view and if we are doing rigorous research what you’re proposing, so if you’re proposing a design that you know will ultimately show improvements in terms of you know, will ultimately show that your service is actually improving quality of care, let’s say. So we know that that’s flowed from the start, but we can’t really do it that way, you know, we want to do proper evaluation of whatever it is that you’re doing or you know [unclear-0:33:06.3] and we will do it this way, we’ll do it together but there might be a possibility that the findings are not something that you will like. So we need to share and publish, that was a big one, we need to publish them anywayInterviewer:So that time you’re physically spending in your university setting or desk or whatever, environment, is that helping that process?Bella:Yeah definitely and it brings you back to reality as well. So it helps from a physical point of view of having connections with other academics and you can talk through things | Critical friend | Independent from team/NHS | Qualities/strengths of researcher/role |
|
| Researcher 1:Therapeutic radiographers, we had OTs, physio[therapists]s, we had dietitians and so on, and really, I think from that point of view, it really did boil down, it boiled down to the arguments, and it boiled down to the methods, and it was, it, it, it was kind of being able to talk about things at that level, that wasn’t about the detail of theInterviewer:Uh huhResearcher 1:Professional content or the clinical content, and that, that’sInterviewer:YeahResearcher 2:That’s where the skill comes in, I think, with this and it takes a while for you to get confident about that, but it is about the inherent knowledge, that we bring as a researcherAnna and Jill | I mean obviously it goes without saying, but the person probably needs a, a very deep understanding of research and the nature of research and methodologies, and so it needs to be able to be comfortable in working in both academic ways as well as actually in practice, and alongside [name]. They have to be able to cope with ambiguity, with messiness, with, you know, not having to control confounding variables, because that’s not possible, you know, so they have to be able to understand that you might start out with a question or a direction of travel, but it, it might meander a bitClare | Rachel:I think we might get some people who say, ‘oh, I want to look at this topic’ and not have a particular methodology in mind, in which case we can, erm, perhaps explore it with them as to which methodology would actually . . .Interviewer:UmRachel:. . . be sufficient to answer their question. So my role, so when I was, I was thinking about you know, this embedded researcher title, I’m thinking well I’m not actually doing much, any research myself anymore. When I worked for the university I did my own research and I did a master’s and a PhD, my own research . . .Interviewer:UmRachel: . . erm, but now I’m very much a kind of facilitator and signposter and that side of my role and the trust-funded part of my role . . .Interviewer:UmRachel:. . . is very much, erm, kind of guiding other people through the process . . . | Bella:Think in terms of think creative by the team, I don’t think that would exist without us. I mean I think the leads for each of the projects they would probably continue and they would have carried out essentially their own stuff either or without us thereInterviewer:How would that have been different, do you think?Bella:Well I don’t think they would have evaluated without us, for instance, because most of the cases and evaluation designs were not built into their intervention designs. We actually did that with them when we came in and a lot of the experts that the teams needed were around evaluation, so what might have happened is they might have rolled out the intervention without then having data required to evaluate . . .Interviewer:I seeBella:. . . which is a bit problematic | Methodological/research expertise | Knowledge | Qualities/strengths of researcher/role | Process |
| We also thought it was important that we understood, because obviously the post for us is that current health and social care research priority, so they understood, you know, they understood about the environment and they had some line of sight, and what they thought was important for future health and social careGillianShe has an understanding of the clinical world and that’s the other thing . . . It’s about understanding how strong . . . our research to be orientated into what makes it different to clinical practice and how to construct . . . people. And just what’s . . . what are our current priorities, helping, you know, give direction to the research that, erm . . . in other people [unclear 00:08:24]. But also, erm how to inform the research community about actually what matters, you know, to servicesGillian | Additionally the universities have not reached out into the workplace in primary care at all, and it’s, it’s working in that liminal zone, it’s the bridging, it’s the knowing who to go to as well as the actual insight that you gain, so that you can transfer knowledge and you can transfer skills, and I think [name] is a conduit in a similar way, she can bring her expertise and mesh it with the messy reality of the workplace and similarly the, the workplace. So OK well that doesn’t make sense, that’s not going to work, you, you, you then build it together by understanding one another’s needs and perspectives, because you’re living them as well. Not in exactly the same way, but you’re both sharing some of the journey and you’re both living some of the same tensions and at a very healing level, you, you get to know people, and you make the connections, it’s the networking approach as well. So through knowing [name] and understanding her work back when I was on the urgent care board, I’ve been able to say to other people, ‘Well actually, there’s this work and there’s this person’, and if, it sort of connects the system. I’m very much one for permeating boundaries and seeing the gaps and trying to bridge those gapsViolet | Karla:Yeah, I like to be in the thick of things and now that’s what I really, really enjoy about my role because through writing these narrative reports I’ve started to get a really, really good understanding of the service, I understand a lot more about how it works, what they deliver, how they deliver on it, how they collect information, what information they collect, so now when I kind of, I feel like I can be quite effective when I go into meetings that aren’t about research or evaluation because someone might say ‘well I think we do this and this’, whereas I can, because I’ve been in the thick of it, I can really . . . help themInterviewer:So that contextual knowledge . . .Karla:YeahInterviewer:. . . background of how the service is run is really important too?Karla:Really important and actually, I think, do you know, if they could have similar roles across the organisation within each directorate, I think that would be really, useful because then you’ve got someone that’s got a really good understanding of that service . . . that helps no end | So, I think the main way, or one of the main ways, they’re different, it is different is that if the researcher is really embedded, working really closely with the team, unit, organisation, where they’re doing research, and that sort of begs the question about what we mean by really embedded. Perhaps I’ll come back to that. OK, so they have, the researcher has, or through, over time, by being embedded, they have a very deep understanding of that team, unit, organisation, the way it works, the challenges, sort of warts-and-all look, if you like. So that, by its nature, is gonna be different from other ways of doing research where even if you sort of go into maybe for a week or if even a few weeks to an organisation, you just won’t get that level, that deep level of understanding. And I guess it’s modelled on the kind of old, or not old but old as in not old-fashioned, traditional anthropological type of research where researchers went and lived with [unclear: 0:03:00] for several years in order to have that really deep level of understanding. And through that understanding, asks different kinds of questions and interprets data in a different kind of a way than, shall we say, traditional, several other ways of generating knowledge . . .Julie | NHS contextual knowledge | Knowledge | Qualities of researcher/role | Process |
List of abbreviations
- AHP
- allied health professional
- AHSN
- Academic Health Science Network
- ARC
- Applied Research Collaboration
- CEO
- chief executive officer
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- CLUSTER
- Citations, Lead authors, Unpublished materials, Google Scholar, Theories, Early examples and Related projects
- MoU
- memorandum of understanding
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- PhD
- Doctor of Philosophy
- PPI
- patient and public involvement
- R&D
- research and development
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/HFUU3193).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.