
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1002/02. The contractual start date was in July 2010. The final report began editorial review in January 2013 and was accepted for publication in July 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors:
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Ward et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
Health and well-being services, in common with many public services, cannot be delivered by a single organisation. Weight loss, exercise, smoking cessation and other programmes require the co-ordination of services delivered by several organisations in a locality. There is some evidence, mostly from other sectors, that middle managers play pivotal roles in this co-ordination. They have to find ways of co-ordinating services, such that organisations are able to meet their own objectives while working together, and issues raised by cultural and other differences can be overcome. In doing so, they have to find ways of explaining what they do, and what they need to get done, to one another. This study focuses on the knowledge creation processes that underpin these activities, in the context of health and well-being services.
Aims and objectives
Our objectives in this study were to develop a better understanding of the way that knowledge is created within and between health-care organisations, across different managerial levels, and of the role played by informal networks in those processes. We aimed to understand:
-
how health-care managers exchange knowledge to bring about changes in health-care delivery and organisation
-
the role played by the connections between the managers who are responsible for bringing about those changes.
In relation to (a), our specific questions were:
-
To what extent is the exchange of knowledge based on the identification of a specific organisational need?
-
What are the different types and sources of information which influence the exchange of knowledge?
-
How do the organisational circumstances surrounding the manager influence the exchange of knowledge?
-
What activities are undertaken by managers to share and exchange knowledge?
-
To what extent is the exchange of knowledge based on an assessment of the potential influence of that knowledge?
In relation to (b), our specific questions were:
-
What is the role of informal networks in exchanging knowledge across different organisational settings and boundaries?
-
How does the density of networks influence the process of exchanging knowledge?
-
Does the centrality of individual managers within an informal network influence the knowledge exchange process?
-
How do directional relationships within informal networks facilitate or constrain the exchange of knowledge within and between settings?
Study rationale and decisions
We set out our study design and methods in full in Chapter 2. Before we get to them, however, it is useful to be clear about the rationale for our approach. As in any field study, we had to identify methods for addressing the research questions, taking into account the characteristics of the sites, a number of conceptual issues and the ways in which the findings would be used. These three considerations – sites, concepts and uses – substantially influenced the study design and selection of methods. Specifically, they influenced decisions about the focus of the research, the way we thought about knowledge creation, and the nature of networks that link individuals and organisations to one another.
The focus of the research
Our research questions prompted us to look for settings where we would be able to separate out formal and informal relationships in order to expose, or reveal, the latter as far as possible. By formal relationships we mean those found in any large bureaucracy – line management, financial accountability and so on. Informal relationships, in contrast, are typically based on trust and often established over months and years. These are the relationships that people rely on, on a day-to-day basis, to get work done, and are not reflected in any organisation chart.
We took the view that we should look outside the main bureaucratic structures of the NHS and of local authorities, where formal relationships would be well developed. Health and well-being services seemed, to us, to fulfil our requirement. No single organisation can realistically hope to provide a full range of weight loss, exercise, smoking cessation and other programmes, and in any given locality health and well-being services have, for some time, been provided by several agencies working together. Indeed, some services are provided by combinations of public, private and voluntary organisations. While the organisations involved were likely to have formal meetings, successful co-ordination was likely to depend on managers liaising informally with one another, and it would be easier to observe informal relationships in these settings. Moreover, health and well-being matters. As we will see in Chapter 3, successive governments have placed great emphasis on the need to improve the health and well-being of populations. In recent years there has been a particular focus on populations in less advantaged areas, where people are more likely to have, or to develop, long-term health conditions.
Each service would have middle managers, working in offices in different locations, sometimes several miles apart. For much of the time, managers would be based in their home organisations, enmeshed in work with immediate colleagues. They would attend formal meetings, but were also likely to liaise in ways that could not readily be observed (e.g. by telephone). Moreover, some were likely to have established relationships with one another long before the fieldwork started, and it would be difficult to tell from meetings alone how these relationships shaped discussions. The challenge was to identify methods that allowed us to observe how managers were collectively creating knowledge (or, if they were doing so), even though relationships between them were likely to span organisational boundaries and geographies.
In the early part of the study we observed managers at formal meetings with one another. It became apparent that no single meeting would be attended by all, or even most, of the health and well-being managers of interest in any of our study sites. There was no straightforward way of knowing who was involved in health and well-being services in any one site, how their relationships with one another were created and sustained, and what kinds of knowledge they were able to create collaboratively. We would, therefore, have to establish ‘who’ and ‘how’ – who was involved and how they were interacting – as well as characterising knowledge creation processes.
The nature of knowledge
There are many different conceptions of knowledge creation and mobilisation. A review by Ferlie and colleagues1 emphasises the diversity of conceptualisations and methods used in both the health services research and broader management literatures. We had to decide, therefore, which conceptualisation to use in our study design. Flyvbjerg2 argues that most social researchers observe the production of one or three kinds of knowledge, namely universal scientific knowledge, technical knowledge and prudence.
Scientific knowledge is generally taken to be value-free universal knowledge, which exists independently of any observer. Today it is the dominant form of knowledge sought in health service research, and the primary type of knowledge that researchers seek to produce and disseminate in implementation science. Technical knowledge concerns ‘know-how’, the skills needed to undertake a task, whether it is mending a tap or liaising effectively with local communities. It does not claim universality: knowledge is embedded in people’s skills, and is used to understand and solve problems in particular contexts. Technical knowledge is often tacit: it is integral to the way that people do their work, and when asked how they solve problems they can find it difficult to explain how they do so. Prudence, or practical wisdom, refers to value-based – rather than analytical or instrumental – rationality. Experienced managers and clinicians are able to draw on their experience in arriving at judgements about the course of action to be taken.
Given our research questions, and our focus on health and well-being services, we sensed that managers might draw on all three types of knowledge. That is, they might draw on all three in the process of collectively creating the knowledge needed to solve problems.
The nature of networks
The third decision concerned the way we thought about networks. In one way, networks are very simple – they are arrangements of things linked together with one another. The challenge is that, as with knowledge, there is an array of different ways of conceptualising networks, and many methods for studying them. To give just three examples here, networks can be physical, with wires and wi-fi connections linking servers, tablets and smartphones; they can be composed of individuals, working in different organisations on shared programmes; or they can link people, objects and ideas.
In this study, we found that it was useful to make a broad distinction between analytically rational and narrative accounts of networks. The analytically rational view is that social and organisational networks are essentially like networks in nature. As Crossley3 puts it, analytical rationalists believe that networks are structures of something – neural connections in the brain, communication networks, or the interactions of genes and proteins. A key assumption is that the configuration of a network, and the interactions between its components, can help to explain its behaviour. Thus, individuals linked in a network interact with one another, and the interactions produce some behaviour of interest, such as the spread of a communicable disease.
The alternative, narrative, view is that networks reveal something useful about the underlying properties of social relationships. In narrative accounts social and organisational phenomena are irreducibly complex, and hence impossible ever to describe completely. Knowledge creation processes are therefore social processes, involving dynamic interactions between a number of people, and with those processes being open to influences from the environments that people work in.
Taking these three arguments together, about focus, knowledge and networks, we concluded that we should study knowledge creation principally as a social, or narrative, phenomenon. For the reasons given above, however, it was also important to be confident that we could characterise the networks that linked the individuals and organisations in our field sites. Accordingly, we also undertook a quantitative network analysis, nestled within the broad context of a narrative case study design.
Changes to our protocol
In our original research proposal, we planned an initial phase of work which would involve developing and sharing ‘tailored messages’ about vascular disease prevention with health and well-being managers at our study sites. These messages were to be drawn from a research project on improving the prevention of vascular disease (IMPROVE-PC) being undertaken within the National Institute of Health Research Collaboration for Leadership in Applied Health Research and Care for Leeds, York and Bradford. 4 The messages would be developed in collaboration with senior health and well-being managers at our study sites who, we believed, would be able to advise us about what they needed to know in order to help them to address local vascular disease prevention issues. This would provide us with valuable insights into the challenges sites had identified, and the scientific knowledge that might help them to address them.
As we began to undertake this phase of the project, we discovered that our plan to engage with the sites in this way was not practicable. They had considerable difficulty specifying their challenges in preventing vascular disease, and they were unable to suggest ways in which the scientific knowledge identified by the IMPROVE-PC project could be useful to them. As a result it proved impossible to identify information which our study sites might find useful. In taking stock and deciding how to proceed, we also realised that we would be in danger of influencing the naturally occurring problem-solving processes and networks that we were hoping to observe.
These insights led us to rethink our approach, and to make two substantive changes. First, we developed a ‘landscape mapping’ phase of work to help us situate our fieldwork in the context of specific vascular disease prevention issues at each study site and provide a focus for our observations. This work replaced the development element of the tailored messages. It was set out in an interim report submitted to the National Institute for Health Research’s (NIHR) Health Services and Delivery Research (HSDR) programme in August 2011. Further details of the landscape mapping method are presented in Chapter 2. Second, we moved the production of tailored messages to the end of our fieldwork, proposing to organise interactive engagement events, where we would provide structured feedback from our research to local health and well-being managers. This phase of the work is reported in Chapter 8. These changes preserved the integrity of the project, enabling us to remain focused on observing the ways in which middle managers create knowledge, while still providing our study sites with an opportunity to benefit directly from our research.
Organisation of the report
Chapter 2 will set out our study design and methods: a case study design employing both quantitative and qualitative methods, with data collected at three sites. Chapter 3 will provide the national policy context for the study. In Chapter 4 we will present a focused review of the knowledge creation literature. The empirical results in this literature have, in large part, been obtained in other settings – in industrial firms in Japan and the USA, for example. One of the issues in this study was, therefore, to establish whether or not the theoretical insights in that literature are useful in the context of health and well-being services in England.
Chapters 5 and 6 will set out our empirical results. Chapter 5 will present the qualitative findings from each of the three study sites. They illustrate the ways in which middle managers were able to use their relationships with one another to get useful work done. Chapter 6 presents the findings from our network analyses. Chapter 7 is the main discussion chapter and will draw together material from the preceding chapters. Chapter 8 will describe the interactive feedback events that were run at the three sites in the late autumn of 2012, where we used videos and graphs to convey our provisional interpretations of our findings. Chapter 9 will set out our conclusions.
Chapter 2 Study design and methodology
Introduction
This chapter sets out the study design and methods. The next section briefly outlines the overall design, a case study design, and the section after that describes the process of selecting the three study sites. The following sections describe the strategy used to undertake a focused literature review on knowledge creation, and the field methods that were used – landscape mapping, structured data collection for network analysis and latent cluster analysis, and semi-structured interviews for qualitative analysis. The analytical strategies used in the empirical components of the study are then outlined before we finally describe the three feedback events that were held at the end of the study, where we presented our provisional findings to each of the study sites.
Case study design
We used a case study design, focused on our case, or main phenomenon of interest, namely collective knowledge creation. 5,6 There are a number of different case study strategies, each of which is motivated by the need to study a case in detail, and in its broad social context. We might, in principle, have chosen to identify a number of hypotheses, or theories, about knowledge creation by middle managers, and gathered evidence in order to support or undermine each hypothesis. 7 As we note below, however, a review by Ferlie and colleagues1 highlighted significant gaps in our understanding, and the published literature was not robust enough to allow us to identify appropriate theories with any confidence.
An alternative strategy would have been to pursue a more naturalistic strategy, with features in common with ethnography, which has been used to investigate the long-term effects of health policies. 8 This strategy is feasible when all of the data sources are qualitative, but not – as here – when there is a quantitative component, and the case study requires the use of both qualitative and quantitative data.
We developed a case study design that allowed us to draw on both qualitative and quantitative data. It was based on a broad theoretical base, derived from a review of the knowledge creation literature (see Literature review section below), which allowed us make theoretical generalisations at the end of the study. The study design had two distinctive features. On the basis of our literature review, and of our own experiences early in the study, it became apparent to us that knowledge creation processes unfold over substantial periods of time, measured in months and – as we will see – years. If we relied solely on prospective data collection, we would run the risk of having to stop observing processes before they had run their course. We therefore opted for a retrospective approach to our analyses, and used process tracing to construct accounts of projects and programmes which had been running for some time. 9
The second feature follows from a point made in Chapter 1, about the importance of collecting both narrative and network analytical data. Having collected two very different types of data, we had to address methodological questions about ways in which they could be used together, in our quest to describe and explain knowledge creation activities at our study sites. The following sections set out our strategy, respecting the distinctive contributions of narrative and analytical data on the one hand, and using them both to shed light on knowledge creation processes on the other.
Site selection and recruitment
Health and well-being services pose major, novel co-ordination challenges to the NHS, social care and other services. It was clear from the start of the project that we would need to study the work of people in a number of different organisations in any locality we studied. On the basis of the time and resources available to us, we judged that we would be able to study three sites in depth over an 18-month period.
We discussed our research plans with senior regional public health managers. They helped us to identify localities in northern England where the development of health and well-being services was high on local agendas, and provided us with introductions to directors of public health in three localities, each of whom had a joint primary care trust (PCT)/local authority appointment. It became clear in the course of discussions that organisations had different boundaries, and it would therefore be important to identify the geographical boundaries for each study site. We decided, pragmatically, that the sites would be defined by PCT boundaries.
The three study sites had a number of general features in common. Their local authorities were all metropolitan boroughs, each including a number of towns and more rural districts. None of them was in the list of 20 most deprived local authority areas, as measured using the Index of Multiple Deprivation. 10 However, each had more than one Lower Layer Super Output Area that was in the bottom 10% of areas nationally; as we will see in Chapter 5, a number of projects and programmes were focused on these areas.
All three directors of public health who were approached approved the involvement of their own services, and also agreed to act as local sponsors for the research. As we explain in the sections below, the process of selection of participants was a key feature of the study design. The focus throughout the study was on middle managers, and our interviewees were selected on the basis that they fulfilled a basic definition of middle manager, that is they were not frontline service providers or board-level managers but sat between the two in their host organisations. As we will discuss in Chapter 7, the term middle manager proved, in practice, to cover a wide range of roles, some very close to frontline practitioners, and others working directly to senior managers (e.g. directors of public health) and not having daily contact with frontline workers.
We applied for NHS ethics approval to cover the whole study, and research and development (R&D) approval for the PCTs covering the three geographical areas. Research ethics approval was granted in December 2010, and NHS R&D approvals were granted in early 2011. Ethics and R&D documents are included in Appendices 1–4. We also complied with R&D processes in non-NHS organisations where we expected health and well-being managers to be working.
The approvals process was complicated by changes in NHS services, which saw NHS community service providers moving out of PCTs around the time that the study was beginning, and the move of public health to local authorities being planned for and then executed during the fieldwork. We dealt with the issues pragmatically, and applied for R&D permissions in some organisations only at the points where it became clear where health and well-being managers were based at the time that we needed to interview them.
Literature review
Ferlie and colleagues1 published a valuable, broad-based review of the literatures on knowledge mobilisation for the NIHR Service Delivery and Organisation programme, before the start of this study. They found that the literatures are fragmented, and contain important gaps, for example an absence of evidence about the effects of organisation design on knowledge mobilisation. The review saved us a great deal of effort at the start of the study and, in particular, confirmed that there was no single literature on which we should base our thinking. We would need to select a theoretical framework, and a supporting literature, from among the many options available. Given our research questions, we looked for a relevant literature which would help us to link together key elements of our study – knowledge mobilisation, network relationships and the roles of middle managers. We identified the knowledge creation literature, stemming from Nonaka and Takeuchi’s The Knowledge Creating Company,11 as the most comprehensive literature that did so.
The volume of publications in the knowledge creation literature in the last 20 years is substantial. 12 Initial searches, using the cited reference search facility on the Web of Science database, revealed almost 4000 articles or reviews which cited our chosen text. The annual rate of citation increased constantly until a peak of nearly 600 was reached in 2008–9, implying that the relevance or intellectual currency of the theory has not declined over time. Owing to our dual focus on knowledge creation and networks, we filtered the results using the search terms ‘network’ and ‘knowledge’ (recognising that the term ‘network’ is itself broad), for the period covered by the calendar years 1995 to 2011. This resulted in the identification of 554 potentially relevant papers. Abstracts from each paper were read and 135 relevant papers were selected. These papers covered a range of disciplines and topics, including organisational studies, communication studies, knowledge management, knowledge transfer, implementation science, communities of practice, professions, regional studies, leadership, innovation and entrepreneurship, and social psychology.
We then performed a further selection based on three considerations, namely:
-
Some papers were excluded on the basis of quality criteria.
-
Some papers were excluded owing to minimal engagement with the concept of knowledge creation or adoption of a non-relational understanding of knowledge creation.
-
Organisational studies were prioritised as the most relevant discipline, leading us to select a higher proportion of papers from organisational studies than from the other disciplines.
Our final selection comprised 34 key papers and 35 more papers which we felt had some conceptual relevance to the study, but which did not deal centrally with organisational knowledge creation. The results of the literature review are set out in Chapter 3.
Landscape mapping
Health and well-being is a broad topic, increasingly seen as ‘everyone’s business’, involving many agencies in any given locality. Our initial challenge, therefore, was to identify the organisations and the people that we should focus on in our fieldwork, in each of our study sites. That is, we needed to identify a sampling strategy (Figure 1).
FIGURE 1.
Study design: sampling strategy.
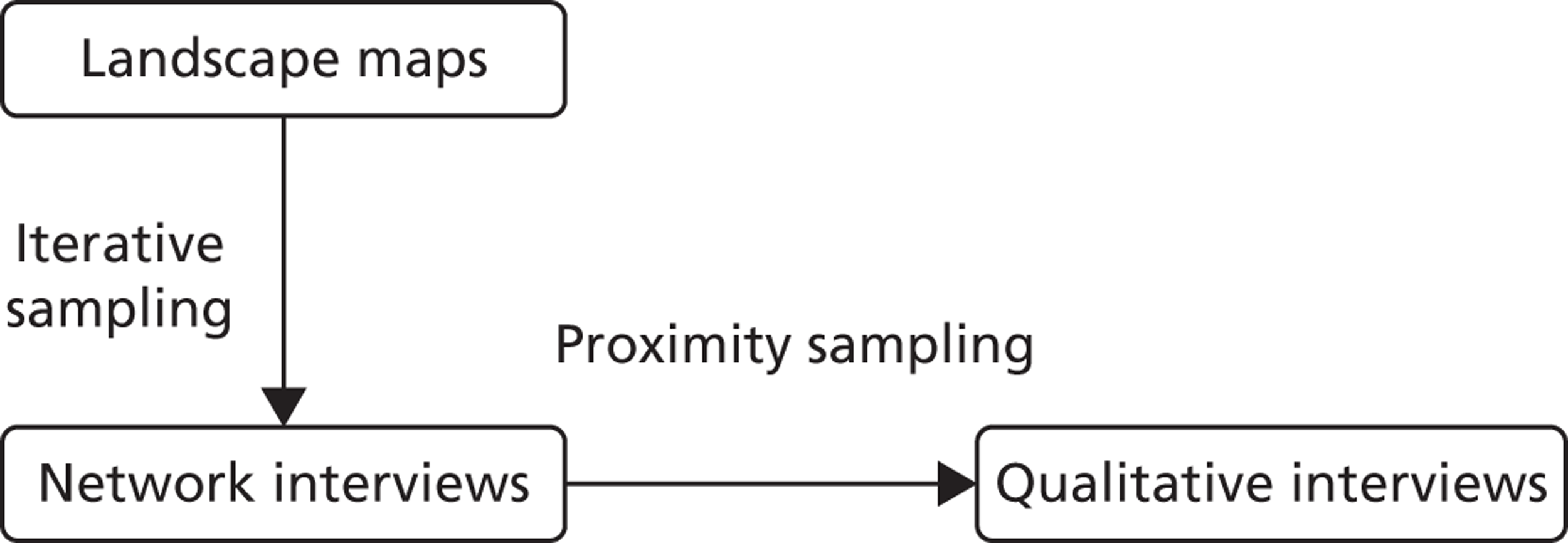
One option was to follow the lead of several other network studies and identify the core and periphery of our network, by taking a relatively restrictive definition of our target population, for example everyone who was invited to key meetings. 13–15 A second option was to compile a complete list of actors which represented the entire study population. 16 These options were unsuitable for two reasons: one practical and one methodological. The practical reason was that there was no authoritative list, at any of the sites, which we could use to identify meetings that we could observe, or middle managers that we should interview. The methodological problem was that the approaches inevitably introduce artificial boundaries, which either follow pre-existing organisational contours or flow from assumptions made by the research team, which cannot subsequently be tested. 17
A third option for identifying the population was to use snowballing, where researchers begin with a small number of actors and ask them to nominate others who are involved in the network. Each of their nominees is then asked for further nominees. The process generally ends when there are very few, or no, new nominees. 16 Snowball sampling approaches have been widely criticised because they potentially lead to bias in the analysis, where the resulting network is substantially determined by the connections of the first few actors. 17
We were concerned to avoid some of the pitfalls of these sampling strategies. Our solution was to develop a method which we called landscape mapping. The essence of the method is to interview people who are not in our target group (i.e. middle managers of health and well-being services), but who nevertheless know who they are and where they work. Landscape mapping interviews were undertaken with senior managers at each of the three sites, who we judged would have a good overview of the people and organisations involved in managing health and well-being services across each PCT area18 and could help us to identify a pressing local health and well-being issue, which would frame our subsequent data collection. At least one of the interviewees at each site was a director or deputy director of public health.
Each mapping interview lasted 60–90 minutes (two were undertaken at two sites, and three at the third), and involved populating an A3 sheet of paper with the names of all of the organisations and people that interviewees told us were involved in managing health and well-being services relevant to a pressing local issue. 19,20 This allowed us to mitigate the biases associated with snowball sampling because – for sampling purposes – the senior managers were independent of the people they named.
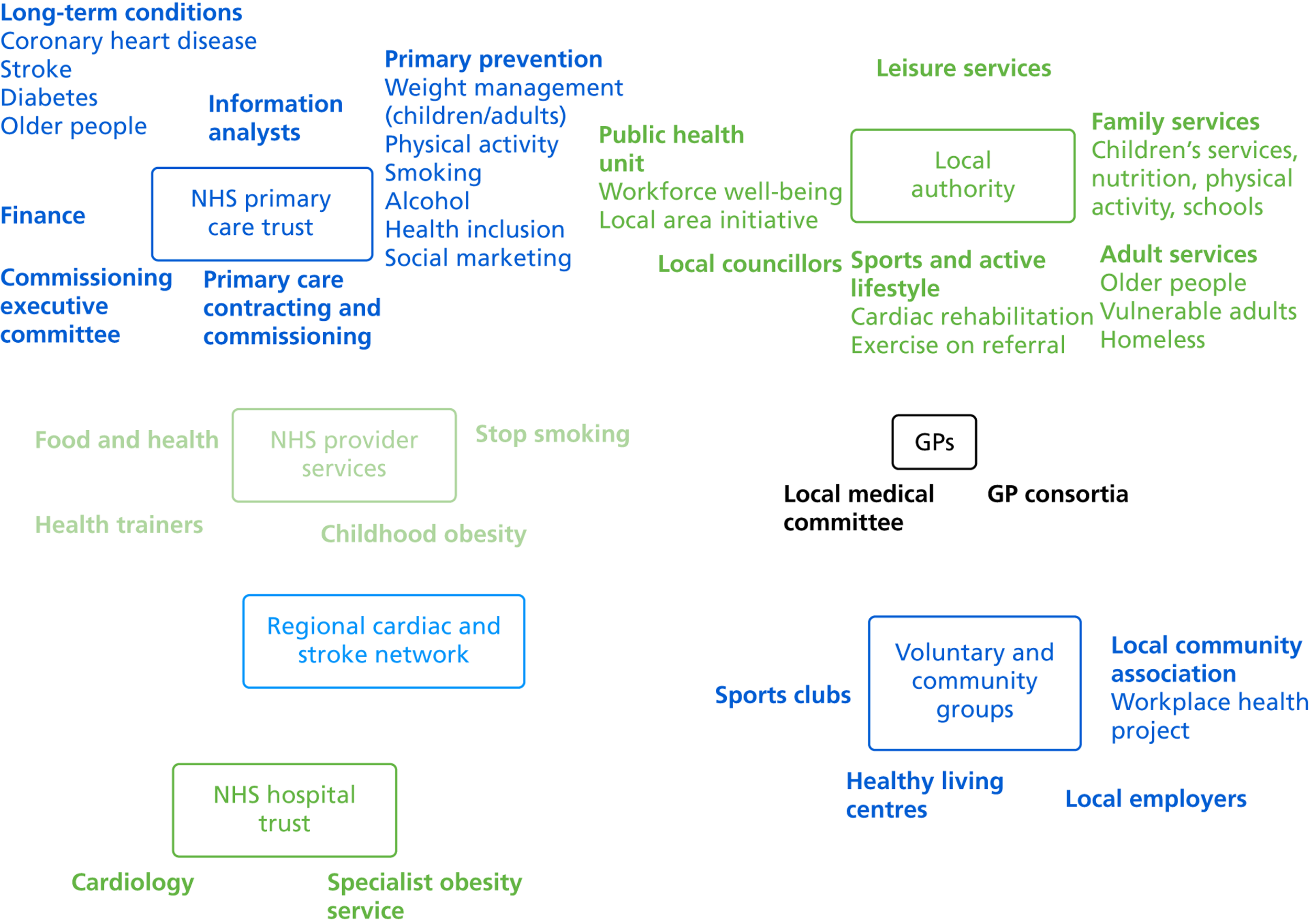
Interviewees provided information about managers involved in health and well-being services within their local PCT boundaries. We recorded job titles and responsibilities (e.g. smoking or weight loss). We did not explicitly ask interviewees to draw any links between individuals or organisations, but interviewees sometimes added connections to the map to emphasise particular relationships. Figure 2 is an example of a composite map from two interviews at one of the study sites.
FIGURE 2.
Landscape map. GP, general practitioner.
Network study: iterative sampling
The results of the landscape mapping interviews were used to identify an initial sample of four middle managers at each study site. We selected them on the basis that they covered key areas of the local landscape between them; for example, we ensured that PCTs and local authorities were included, and that they were reported as working across organisations and/or professional groups.
We used structured network interviews: the data collection form is in Appendix 6. Other commonly used data collection techniques such as postal questionnaires were considered but we judged that structured, face-to-face interviews were most likely to ensure data quality and participation. Face-to-face interviews have also been used successfully in study designs similar to ours. 21,22 Interviews combined free recall and fixed-choice strategies;16,23 that is, we asked interviewees to name people in response to our two questions, but allowed them to list only up to five people. Our reasoning was that although we had defined a loose boundary for our network, we were most interested in identifying the core of the network, which would best be revealed by asking people to nominate their most important relationships rather than all relationships.
Although we focused on the ‘core’ of each network, we were also aware of the need to gain sufficient coverage of the landscape. This posed a practical challenge as the potential size of our networks (as revealed through the landscape mapping exercise) was large. Owing to resource constraints, we would not be able to interview all of the managers identified on the landscape maps. We had to find an economic approach to collecting data about relationships across the landscapes at our three sites. Our solution was to gather ‘secondary data’ by asking interviewees to name people who their nominees talked with or went to. This method has been validated in the context of criminal networks, where research showed that the relational knowledge of a few informants compensated for the lack of objective knowledge arising from low response rates. 24 If we subsequently interviewed someone for whom we had secondary data from other respondents, we used their actual responses when constructing our data set.
We took the view that two types of relationships would be of particular interest in relation to knowledge mobilisation. The first was ‘talks with’, which involved asking participants, ‘Who do you talk with about [the pressing local topic/problem]?’ The second was ‘goes to’, which involved asking participants, ‘Who do you go to get things done about [the pressing local topic/problem]?’ These questions broadly correspond to the sociological concepts of speech and action. We also asked interviewees to provide further details (organisation or role/job title) about each of the people they named.
Having completed these initial interviews, we needed a strategy for sampling further interviewees without resorting to snowball sampling (for the reasons discussed above). Our solution was to select further interviewees by modelling the data from the first sample (hence the term ‘iterative sampling’ for this section). Because we were particularly interested in the collective thoughts and actions of middle managers, we modelled these partial networks using a method specifically designed to reveal clusters – latent cluster analysis. We judged that identifying clusters would help to identify any ‘holes’ in the networks – gaps between groups within a network. In order to identify clusters, we used an approach which uses the concepts of latent position network models25 and cluster latent position models. 26 Further details about our modelling methods can be found in Network analysis: latent clusters, below.
We also referred back to our landscape maps, in order to ensure that our sampling achieved the most extensive coverage of the landscapes possible with the resources available to us. Our selection was made using the following criteria:
-
Actors near the centres of the clusters are sufficiently well specified in terms of their network links and need not be selected for interview (i.e. we knew enough about them already).
-
Those near the edges of clusters had network links which might be less well specified, and could, therefore, reveal links with parts of the landscape that were not yet covered. These actors should be selected for interview.
-
Individuals ‘outside’ clusters may be isolates, on the periphery of the network, or beyond our loosely defined boundary, but they could still be a key link to other parts of the landscape. They should be selected for interview if other sources (e.g. documents, observations or local knowledge) suggested that this might be the case.
Having identified, and collected network data from, the second phase sample, we modelled the network again. At this stage, we found that saturation of some parts of the landscape was already apparent. Equally, it was sometimes difficult to identify middle managers who would link to areas of the local landscape not yet covered. For our third and final phase of sampling, therefore, we focused on sampling individuals who had already been identified as particularly well connected in order to collect primary data in place of secondary, and to establish whether or not the managers identified in the landscape maps were linked to one another in practice.
We were aware, throughout, that there are always questions about the location of the boundaries of a network. Network and system theorists both emphasise that social systems are open, in the sense that they do not have well-defined boundaries with their ‘environments’, and are continuously subject to external influences. 3,27,28 As some of the preceding points suggest, we addressed the problem in two ways. First, we felt that it was reasonable to assume that interviewees would name people who were the most important members of a network and, by implication, not located close to any boundaries. Second, some of our interviewees were selected on the basis that they spanned the landscape (in our landscape maps), and this selection strategy gave us some confidence that we were able to achieve reasonable coverage within boundaries that were defined by our interviewees.
The network interview process was repeated approximately 8 months after the initial round of network interviews. For the second round of interviews, we did not develop the sample iteratively, but rather reinterviewed all round 1 participants. Where this was not feasible (e.g. owing to interviewees having left their posts), interviewees were replaced with individuals who were currently performing the same or a similar role within the organisation.
Qualitative study: proximity-based sampling
We also needed to identify a sampling strategy for the qualitative interview programme at each site. The networks we identified were large, with at least 70 members at each site. We did not have the resources to interview this number of people, and we therefore needed to identify a manageable number, such that an interview programme would still allow us to address our study questions. For the first round, in the summer of 2011, we identified middle managers who were positioned close to the centre of each of the clusters in the ‘Goes To’ and ‘Talks With’ networks (n = 6 at each of our three sites). We undertook semi-structured interviews, lasting 60–90 minutes. We decided that we could not ask interviewees how they created or mobilised knowledge – the question would not have made any sense, however we phrased it. (If our chosen literature was correct, interviewees would have a tacit understanding of many of their own work practices and would not be able to articulate the knowledge underpinning them.) Our strategy was, instead, to ask interviewees about their work with other middle managers. Their accounts of particular projects, or problems that they had to solve, would, we judged, allow us to infer any knowledge creation that had occurred.
The initial sampling strategy was only partially successful and, for the second round of interviews, conducted in the early summer of 2012, we focused on interviewees who were close to the centre of a single cluster, had a high degree of connection within a cluster, and who connected the cluster of interest to other clusters. The topics covered in the interviews were the same as in the first round; a topic guide is in Appendix 7.
Because these interviews marked the end of the fieldwork phase of the study, we were able to share some of our initial findings with interviewees without jeopardising the quality of data collected earlier. Drawing on the experiences of other network researchers,24,29,30 we showed interviewees the ‘goes to’ latent cluster diagrams from the second round of network interviews, for their own site. Data protection considerations meant that we could not reveal the names of individuals in each diagram, but we were able to show each interviewee where he or she was located. This process provided us with the opportunity to assess the face validity of the results of the network analysis, and fed into our interpretation of the network data, presented in Chapter 6.
Analysis: qualitative to quantitative relationship
As noted earlier, we used a process tracing method9 to analyse the qualitative data. The framework for the analyses of our qualitative and network data is shown in Figure 3. This is the point where the arguments set out in the section Analysis: Qualitative to Quantitative Relationship in Chapter 1 have had the greatest influence on our study design. If we were working in an analytical rational tradition, we would place the greatest weight on our network analyses, taking the view that the network structures corresponded to relationships ‘in the real world’ – if we can understand the networks, we will understand something of this interesting part of the world. The qualitative data might embellish any structural explanations we produced but would play second fiddle to the network data. The reader would expect to see the network analysis first, followed by the qualitative analysis.
FIGURE 3.
Study design: analysis.
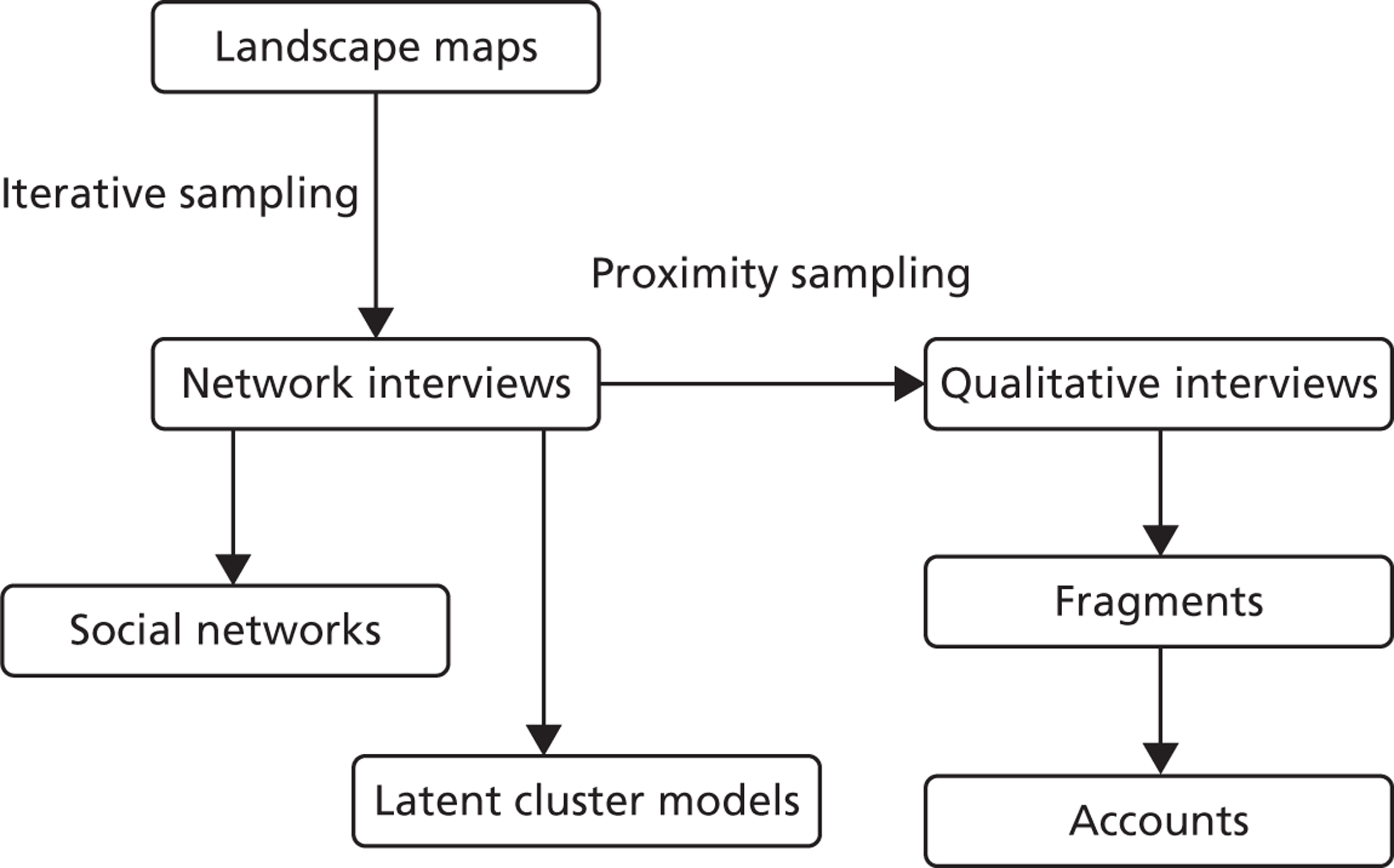
We took the alternative, narrative, view in this study. The key point is that network data, of the kind we collected, indicate underlying patterns of relationships at our study sites. They are useful abstractions and representations, but are embedded in complex webs of relationships, where trust, legitimacy and other social and organisational phenomena matter – and which are not captured by ‘talks with’ and ‘goes to’ questions. The practical effect of this approach was that, when we came to the analysis, we considered the qualitative data first. Thus, the sampling strategy took us from networks to qualitative results but the logic of the analysis is the other way around, starting with qualitative findings and then considering ways in which the network data help us to interpret, and refine our understanding of, the qualitative interviews.
Qualitative analysis
In the round 1 qualitative interviews, in 2011, we had two objectives – to begin to shed light on middle managers’ knowledge creation at the study sites and to inform the design of the second phase of the study in 2012. Two members of the research team read the interview transcriptions and post-interview notes, and produced detailed thematic summaries using a flexible template that covered service priorities, the purpose and structure of networks, knowledge exchange and networking activities, networking problems and network effectiveness, while allowing for the emergence of further themes that were often specific to particular interviewees. The summaries were then shared and discussed among the research team, focusing particularly on comments shedding light on knowledge creation. We concluded that the interviews, taken together, did not allow us to shed light on knowledge creation processes. We changed our data collection strategy for Phase 2 of the study.
In Phase 2 we interviewed middle managers who, on the evidence of our ‘goes to’ network data, occupied similar positions in our graphs (i.e. were located in a single cluster). We produced accounts of knowledge creation relating to particular activities, such as organising a health promotion event, drawing on Greimas’s conceptualisation of speech act theory. 31 The approach is based on the premise that the language we use provides important clues about the way we think about problems – the way we make sense of them and work out how to tackle them. The approach has previously been used in studies of technology implementation32 and of public discussion,33 as well as of organisational routines, important in this study. 34
Three members of the research team undertook the analysis, which proceeded as follows:
-
Using Qualitative Data Analysis (QDA) Miner (v.2.0, Provalis Research, Montreal, QC, Canada), a qualitative data mining and visualisation tool,35 we searched all of the interviews at one site, and identified passages of text which referred to specific activities at that site,34,36 for example using central government funding to launch a new local service.
-
Using the framework function in NVivo version 9.2 (QSR International, Victoria, Australia), we grouped the passages referring to each activity into framework tables, and then analysed them. For each one, we looked for evidence about participants’ intentions and actions, on the basis that these would help us to identify the knowledge creation processes underpinning them. We coded text which indicated managers’ obligation and desire (‘have to’, ‘want to’), and their competence and know-how (‘able to’, ‘know how to’). 31 This process was repeated for activities at each of the three study sites.
-
We summarised the material in the framework tables in accounts of projects and programmes. 37 At this stage of the analysis, we also selected accounts to focus on in the subsequent phases of our analytical work using the following criteria: participants attributed significance to the activities, the accounts were told from at least two perspectives, they contained evidence about peoples’ intentions and actions, and we could describe the nature of the knowledge being created. This resulted in three accounts at each of the three sites, presented in Chapter 5.
Network analysis: latent clusters
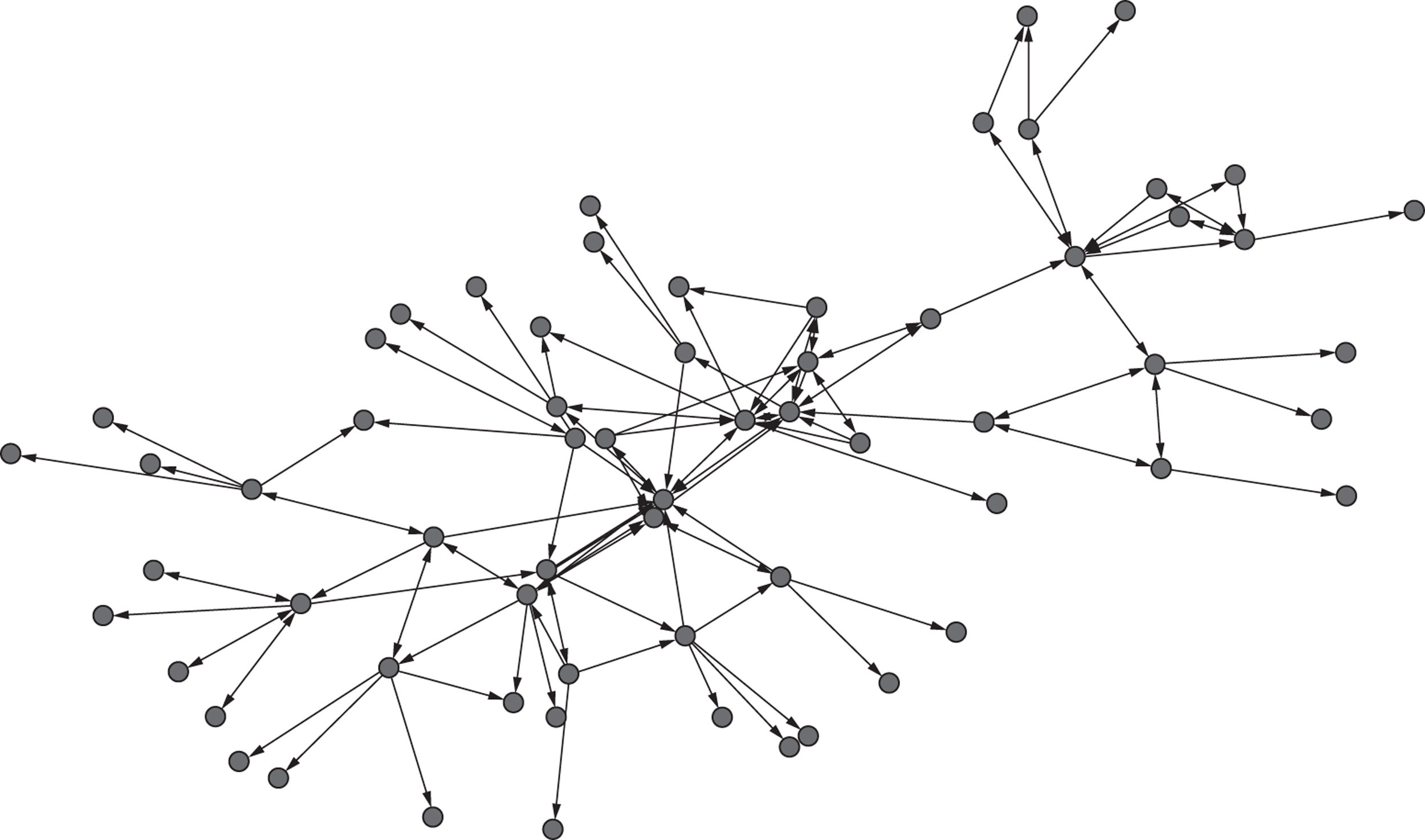
The most common approach to network analysis makes use of graph theory to express the pattern of connections between actors. Diagrams, or sociograms, such as that shown in Figure 4, are usually used to visualise relations in networks. The positioning of the actors on the page and the relative length of their connections is not important, meaning that sociograms are drawn with lines of equal length wherever possible. 17
FIGURE 4.
Sociogram of a network with 64 nodes and 134 links.
It is also usual to generate measures of a network to show the importance of actors within it, for example by establishing the degree or number of connections with others, for members of the network. For our study, identifying degrees was of limited value, because we had limited the number of connections named by participants to five: the method must have influenced the degree statistics. We therefore used other summary network statistics defined as below.
Eigenvalue centrality: This aims to measure the influence of an individual actor within a network. An actor’s centrality, or influence, becomes greater if he or she has more influential alters, that is if he or she is connected to more influential people. As the influence of the alters is defined by the influence of their alters, the calculation of the measure is not straightforward and involves an eigenvalue decomposition. Numerically, this involves recursive calculation and is not difficult for the size of networks encountered in this project. A value is assigned to each actor in the network describing their influence based on all of the connections within the network.
Betweenness: This aims to measure the dependence of the connectedness of a network on the links identified by each actor. An actor will have high betweenness if many paths (through multiple actors) pass through him or her. Then removal of that actor from the network will impact on the overall connectedness. As with eigenvalue centrality, betweenness is defined recursively and is expressed as a numerical calculation based on the connection matrix (i.e. adjacency matrix). An actor who helps to link groups of people to one another will have high betweenness. 16
These network measures focus on the roles of individual actors within a network. However, our research questions in Chapter 1, and the literature on knowledge creation in Chapter 3, suggest that groups or teams are important. We therefore agreed with Crossley,3 who argues that a number of important network phenomena sit between the two poles of structure and agency – in clusters. In addition, we felt that clusters would be easier for managers at the study sites to interpret: they might make more intuitive sense than conventional network diagrams (see Interactive feedback workshops, below).
Our network modelling approach used the concepts of latent position network models25 and cluster latent position models. 26 We used these models to identify clusters of people within networks, and people who acted as bridgers between clusters. It also helped us to identify any ‘holes’ in the networks; that is, social gaps between groups within a network. Krivitsky and Handcock38 have provided software tools for the necessary analyses. During the course of the project, new software was released with much improved convergence properties. This is the variational Bayes latent position cluster model (VBLPCM) R package. 39
The key aspects of the method are:
-
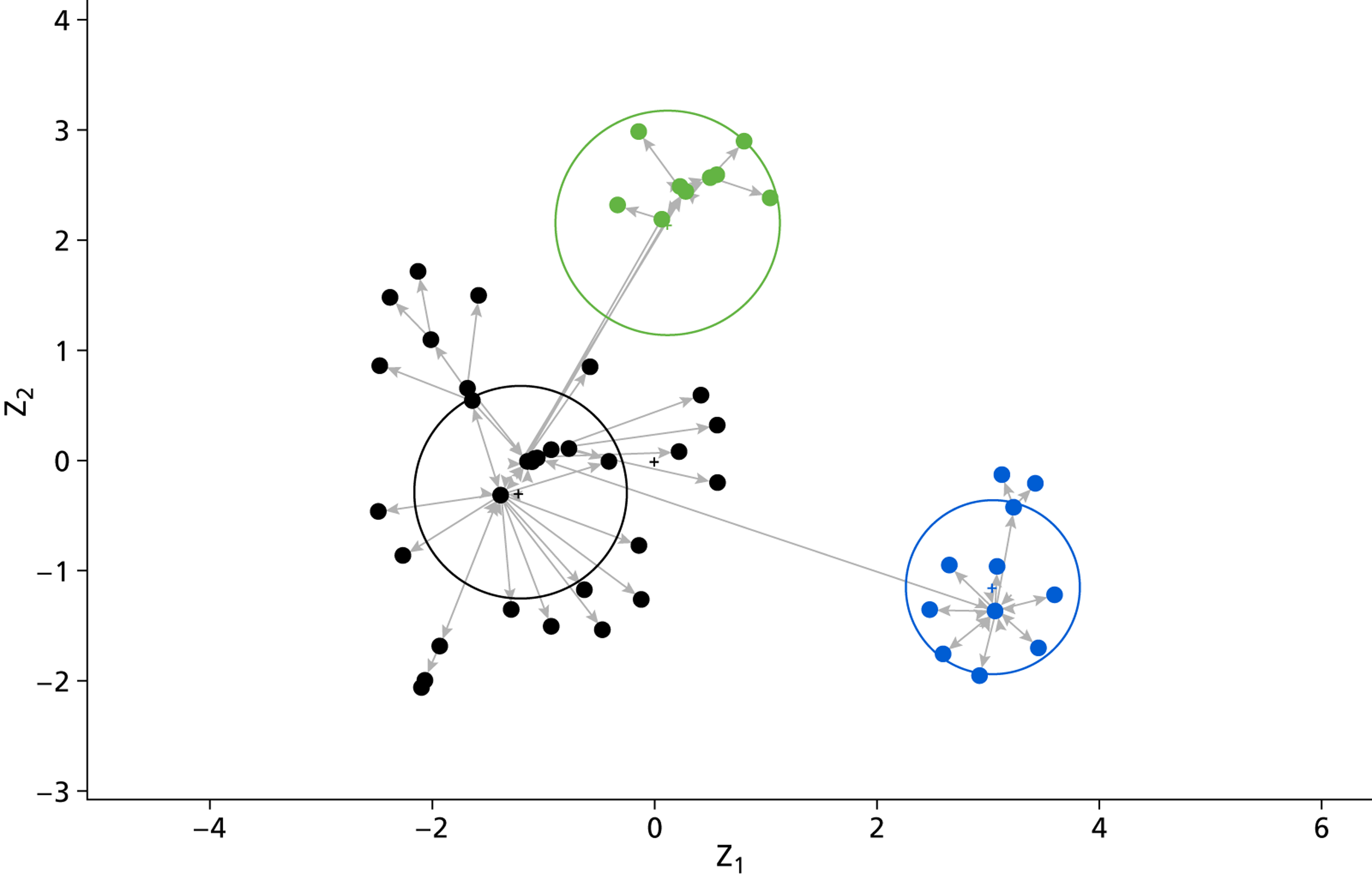
Data from the network interviews were used to model the relationship (tie) between two individual actors. Ties are represented by lines in the diagrams and actors are represented by small filled circles (Figure 5).
-
A two-dimensional latent social space was used such that individuals were more likely to be connected when placed close together.
-
An additional condition was imposed such that individuals were associated with clusters. In the diagrams, individuals were coloured according to the cluster with which they were most strongly associated. Within the latent social space, a cluster has a centre indicated by a small coloured cross and surrounded by a large open circle representative of the spread of the cluster in the social space.
-
The model with clusters in social space was fitted using a Markov chain Monte Carlo method. Details of the method can be found in the references above and software is available for the R statistical software package (The R Foundation for Statistical Computing, Vienna, Austria).
-
The number of clusters was initially determined by calculating a Bayesian information criterion for an increasing number of clusters, starting with one large cluster. The idea here was that we wanted to minimise the information lost by the model representation of the network. This was achieved by increasing the value of the likelihood function, indicating a better fit, as more clusters were permitted but penalised by the greater number of parameters needed for a more complex model. The Bayesian information criterion provided a mathematical strategy for achieving a practical balance between fit and complexity. The smallest value of the Bayesian information criterion suggests the optimum fit, least information lost relative to the complexity, and indicates the strongest candidate for the number of clusters. In all cases, further support for the initial candidate was found in the form of practical explanation, and that number of clusters adopted as best representing the structure within the network.
-
When the representative circles for the most likely number of clusters did not overlap in the social space plot, as in Figure 5, there was support for the possibility that individuals belonged to distinct clusters. The circle radii were equal to one standard deviation, so that when circles did not overlap, the clusters were well separated (by ‘two = one plus one’ standard deviations). Although not constituting a formal hypothesis test (achieved otherwise through the information criterion), this was, at the least, a useful visual guide.
-
The clustering clearly identified limitations of influence. Most influence from an actor was within the cluster to which he or she was assigned. Owing to these limitations, concerns regarding boundary influences (actors not identified and included in the network but influencing from just beyond the observed network) were much reduced, as clusters could be seen to be mostly complete.
-
The diagrams output from the VBLPCM software package were further enhanced. The small circles representing actors were replaced by circular symbols indicating the organisation to which the actor belonged. For each actor, the probability of being assigned to each cluster was calculated. For the purposes of the enhanced diagrams, actors were assigned to the most probable cluster: that is, they were modally assigned. To make the representation comprehensible, coloured regions were extended around the actors belonging to the same cluster (all diagrams in Chapter 6 are coloured in this way).
-
Once we had produced cluster diagrams, we sought a finer-grained understanding of the network models by focusing on the attributes of individual actors. To do this we used the details collected during network interviews and membership lists from key meetings (which we also collected in the course of the fieldwork), focusing on seniority (senior manager, middle manager or frontline worker), organisation, role/area of work and meetings attended. This allowed us to focus in more depth on the organisational membership of each cluster and the official roles and responsibilities of actors in relation to health and well-being services.
FIGURE 5.
Latent position cluster model showing three distinct clusters.
Leximancer: a bridge between paradigms?
One of the obvious features of our study design is that it is based on two distinct pillars, with their foundations in different research paradigms. We looked for ways of creating an ‘empirical bridge’ between the two, so that it would be possible to link the qualitative and network analyses at each site in some way. The most promising approach, we felt, was likely to be based on an analysis of the network-like patterns contained in the qualitative interviews: it might be possible to compare these patterns with the patterns generated by the cluster analyses.
We used Leximancer (Leximancer, Brisbane, QLD, Australia), a computer software package that conducts quantitative content analysis on text files, using a machine learning technique, to analyse the set of qualitative interviews at each site. We concluded that, while Leximancer produced some interesting results, it did not fulfil our objective for it: that is, enabling us to link the qualitative and network findings empirically. The details of the method, and the outputs, are presented in Appendix 8. While Leximancer did not produce the results we hoped for, it was nevertheless important in shaping our thinking about what we could do to maximise the value of our two sets of findings. Our approach is set out in the next section.
Addressing our study questions
The final stage in the study design is represented in Figure 6. Our experiences with Leximancer, while producing some interesting results, led us to conclude that we could not construct an empirical bridge between the two main components of our study. We could, however, identify recurring patterns in both sets of findings and use them to address our study questions. The first of our two questions concerns the nature of knowledge creation by middle managers, and the qualitative findings shed light on that question. The second question concerns the relationships between managers, and that question can be addressed – in different but complementary ways – by both the qualitative and network analytic findings.
FIGURE 6.
Study design: interpretation.
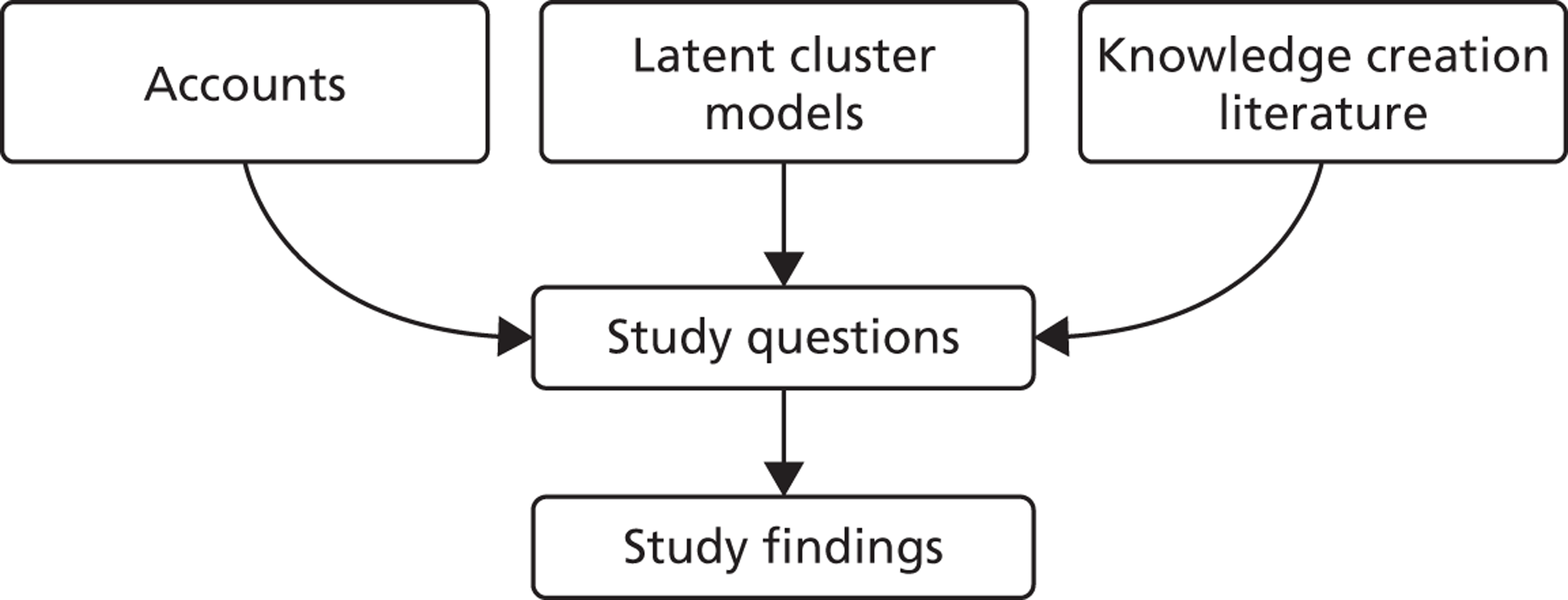
In addressing the study questions, we draw on the knowledge-creation literature, described in Chapter 3. We are able to use the literature to help to interpret our findings, and conversely use our findings to reflect on the extent to which the knowledge-creation literature is relevant to our chosen settings, in health and well-being services.
Interactive feedback workshops
Towards the end of the study, in the late autumn of 2012, we presented our provisional findings at each study site, at events that they organised for their own purposes (e.g. to review a local strategy or to discuss the setting up of a formal public health network). For us, the events had two purposes. The first was that we wanted to ‘road test’ a method for feeding back the findings of our study that went beyond the standard methods of written reports and presentations. Second, we were tasked with identifying ‘actionable findings’. We reasoned that, if managers at the study sites thought that the findings were valuable, this would provide suggestive evidence that they might be valuable to managers in other localities.
The local organisers identified and invited colleagues, including senior and middle managers. Between 15 and 25 people attended each event, in each case representing a wide range of local organisations.
At each event, we presented selected qualitative and network material. Qualitative material was presented in video monologues where individual actors, filmed in advance of the events, ‘told the story’ of selected projects at a site. That is, although a number of people were involved in each account, the videos presented each account as a monologue. The accounts were fictionalised and embellished, in small ways, by the actors in order to protect the identities of the managers who were involved. Three monologues were used at each event. The first was an account from one of the other sites, used to ‘set the scene’ and introduce attendees to the focus of our study. Then, two videos based on accounts at that site were shown. Our network material was presented in professionally produced diagrams.
Chapter 3 Literature review
Introduction
The review undertaken by Ferlie and colleagues1 provides a valuable overview of the literatures on knowledge mobilisation. It emphasises that the literatures are diverse and contested, and that there is no unified theory which covers the whole field. It also identifies important gaps in our understanding, notably in relation to the role of organisational form in shaping knowledge mobilisation, and knowledge mobilisation involving managers. This study was designed to contribute to the literature in both of those gaps.
It was clear at the start of the project, therefore, that there would be little merit in undertaking a further wide-ranging review of knowledge mobilisation. It was also clear that we would be working in a topic area with relatively limited published evidence and argument to guide us. More positively, however, we were able to identify a coherent subliterature that we could use in this study. This was the literature on organisational knowledge creation, whose foundational work is Nonaka and Takeuchi’s The Knowledge Creating Company. 11 The literature links three of the four key topics in our research questions: namely, knowledge creation, the work of groups or teams, and middle managers. It does not deal with networks in the way that we do in this study, but we are not aware of any literature that combines knowledge mobilisation/creation with quantitative network analysis. As in many studies, we might have alighted on a different subliterature, for example theories of practice, but our judgement was that the knowledge creation literature would provide a useful, if general, theoretical context for our study.
The work of Nonaka and Takeuchi, and those who have followed them, is based on the argument that knowledge creation involves tapping the tacit, and often highly subjective, insights of employees about their working environments. Tacit knowledge consists partly of technical skills – the informal skills often referred to as ‘know-how’. Experienced individuals, who have spent years developing their skills, typically find it difficult to explain to anyone else how they do what they do. The challenge is to make tacit knowledge explicit, in order that it can be discussed with colleagues and acted upon – used to work out a new way of delivering a service, for example.
In the knowledge creation literature this involves people with different backgrounds working together on shared problems. The process requires everyone to find ways of explaining what they know to colleagues, often by using metaphors on the basis that metaphors can be grasped by everyone, even though they do not have – and cannot ever have – a detailed understanding of their colleagues’ working practices. Nonaka and Takeuchi also argue that middle managers are singularly well placed to foster knowledge creation, because their roles naturally involved co-ordination across traditional organisational boundaries. Middle managers are the glue, often invisible to outsiders, that binds organisations together.
The main themes
The method for the literature review is described in Chapter 2. In the following section we briefly summarise the main themes that we identified in the literature. The papers are summarised in Table 1. The table has five columns, covering the main conceptual insight(s), the main empirical findings, and then the theoretical, methodological and managerial implications for our study. By managerial implications, we mean the ways in which authors think about the roles and actions of middle managers.
| Paper | Main insight on organisational knowledge creation | Main empirical findings | Conceptual implications | Methodological implications | Managerial implications |
|---|---|---|---|---|---|
| Locus of knowledge creation: group | |||||
| Brown and Duguid 200140 | Tradability of knowledge not a function of explication but of social–epistemic bonds created through common practice: challenge for organisations is to mobilise the dynamism of communities that make them up by facilitating intercommunal negotiation. Network of practice concept deals with knowledge flows beyond organisational boundaries | Focus on knowledge disembedding and re-embedding circumstances | |||
| Erden et al. 200841 | Typology of intra- or interorganisational groups based on quality of group tacit knowledge: higher levels provide ‘collective mind’ or ‘collective intuition’ but incur higher opportunity costs | Model claims practical relevance for selection, specification and management of project groups | |||
| Nonaka and von Krogh 200942 | Reaffirms individualism by appealing to a biographical perspective, which enables analysis to account for broader historical trajectories and fuzzy organisational boundaries. Concedes inadequate consideration of roots of knowledge creation in social practice, i.e. scope for combination with communities/networks of practice perspective | Cites numerous studies offering empirical corroboration of key contentions | Be explicit about normative assumptions, e.g. what kind of knowledge processes you are trying to explain: we require different kinds of theory to grasp conservation of tacit knowledge or innovation | Focus on network clusters with high internal diversity of experience and background, where (according to the theory) knowledge conversions are likely to be more frequent | |
| Nonaka et al. 200643 | Stock-take of progress in development of ‘organisational knowledge creation theory’ sees two waves of take-up: defining the facilitating conditions, and implications for the nature of the firm as a social institution. Defence of individualism as attempt to leverage insights from cognitive psychology overlooked by management theory, while insisting the individual–social axis remains an ‘open problem’ for the theory | Knowledge-creation theory understood in relation to context (facilitating context). More research needed on how organisations can manage context | Call for longitudinal studies exploring trajectories and processes and relations between knowledge assets (the past), knowledge creation (the present) and knowledge visions (the future) | ||
| von Krogh 200944 | Locus of organisational knowledge creation in the group; individual heterogeneity seen as vital to organisational creativity. Information systems research highlights declining costs of participation and new patterns of reuse of collective knowledge | Individual mobility and diversity of career paths revives traditional concerns of individualist perspectives on organising | |||
| Locus of knowledge creation: project ecologies | |||||
| Grabher 200245 | A project ecology distributes knowledge and design, responsibility and accountability ‘across professional domains and across organizational boundaries’, but lacks a strong organisational memory and the conventions that underlie trust in other kinds of knowledge network (e.g. professions) | Does organisational culture evaporate in a project environment? What project models are utilised in a particular setting (e.g. studio, agency, consultancy, partnership)? | |||
| van Wijngaaarden et al. 200646 | Learning can occur in interprofessional project teams via process and professional practice alignment even if structures are not conducive | Network learning transpired spontaneously when project teams had access to performance data for collective evaluation | Provide groups with performance data to stimulate network learning | ||
| Locus of knowledge creation: individual agents including managers | |||||
| Akiyama 201047 | Middle managers act as boundary spanners | Top managers lacked a strong enough interface with employees to act as ‘moral managers’ | |||
| Alin et al. 201148 | Knowledge exchange viewed as interpersonal, and organisational knowledge embedded in work practices | Outcome of dialogue across boundaries more likely to be altered knowledge when there is diversity with aligned interests, but new (synthesised) knowledge where interests also diverge | Diversity plus conflict necessary to stimulate new knowledge creation | It is at the level of sequences of speech acts that knowledge transformation was observable | Benchmarking-like settings for people of similar background from different organisations help alter individuals’ knowledge; tightly-scoped context-specific innovations call for cross- specialisation settings; uncertain goals call for settings where both boundaries are crossed |
| Collinson and Wilson 200649 | Knowledge management as the management of interactions between knowledgeable specialists within and beyond the firm | Stable networks disincentivised organisational knowledge search, and were affected by labour market trends | Do not make network stability a fetish | ||
| Currie et al. 200650 | Organisations risk exclusion from professional knowledge exchange, which is increasing in significance with the growth of boundary-less careers | Middle managers were pivotal in organisational knowledge processes | Consider how to retain knowledge in the face of occupational mobility | ||
| Kuk 200651 | Deals with participation equality in knowledge creation networks (online) | A certain degree of participation inequality facilitates knowledge reuse, recombination and self-expression | Pay attention to ephemeral microstructures of knowledge creation | Do not intervene correctively unless participation highly unequal | |
| Lindsay et al. 200352 | Individual agency is central to knowledge creation; middle managers as knowledge entrepreneurs | Middle managers in peripheral network positions (e.g. overseas subsidiaries) had to contend with indifference from the centre to local knowledge, using informal contacts, often pre-dating current employment, in knowledge strategies | |||
| Locus of knowledge creation: the organisation | |||||
| Nahapiet and Ghoshal 199853 | Seminal contribution to knowledge-based theory of the firm, arguing that organisations are institutions for developing social capital, which in turn facilitates knowledge creation, but there are costs as well as benefits to this process | ||||
| Spender 199654 | Attempt to bring collective knowledge centre-stage as a public good for holding together the firm as a semi-autonomous field | Proposes a four-way matrix for studying knowledge: tacit-explicit and individual-social, arguing different knowledge-based theory of the firm needed for each type | Calls for longitudinal, case study and novelistic analysis of organisational knowledge dynamics | ||
| Locus of knowledge creation: external context (public sector) | |||||
| Hartley and Benington 200655 | Relational approach to interorganisational knowledge creation | Macro-contextual constraints: UK government policy favourable to collaborative knowledge creation but also source of barriers, notably the audit culture | Organisational knowledge-creation theory may need adapting for public sector, e.g. more fluid organisational boundaries, internalisation of competing interests | ||
| Kim and Lee 200656 | Individualist assumption that employees are the drivers of knowledge creation, through partially self-organising structures within organisations | Public and private sector knowledge sharing compared: public sector managers face more organisational constraints; hierarchy did not prevent sharing but work experience encouraged it | |||
| Rashman et al. 200912 | Practice-based conception of knowledge creation. Qualifies the transferability of organisational learning and knowledge creation theories from private to public sector contexts, arguing that there are specific features of external and internal organisational context in public services | Public sector has complex interorganisational links and strong professional subcultures, multiplex group belongings, and is subject to conflicting demands regarding outcomes | Social practice perspective and network governance theory seen as especially relevant/applicable to public sector (knowledge networks that span organisational boundaries, learning through collaboration) | Crucial to describe context-specific factors and to clarify authority of group membership | |
| Locus of knowledge creation: space/geography | |||||
| Amin and Roberts 200857 | Different modes of ‘knowing in action’ have differing organisational forms and geographies of knowledge creation | Professional mode of knowing in action characterised by two-phase learning (co-location important for induction but updating skills often virtual) and significant intersections between professions | |||
| Araujo 199858 | Knowledge practices develop in locales that are ‘momentary interaction settings embedded in a wider network of relations’ | ‘Situated’ does not mean immobile; mediation and propagation connect locales: focus on how knowledge is repeatedly re-embedded | |||
| Cohendet et al. 199959 | Multiscaled model of knowledge creation involving nested network clusters. Specific sequences of knowledge conversions may be important for bridging cultural boundaries | Measure similarity and difference within and between network clusters, and look for a correlation between intranetwork breadth and diversity | |||
| Goodall and Roberts 200360 | If knowledge is socially embedded and presumes intersubjective communication, distance is a problem for knowledge-creation theory. Knowledge-ability (hyphenated to capture active dimension) needs to be continually repaired through reputational work, since participation conditional on being recognised as ‘someone who might create valid knowledge’ | Onus for maintenance of knowledge-ability fell disproportionately on those in peripheral network positions | Knowledge-ability deteriorates without co-presence | ||
| Rutten 200461 | Critical of overemphasis on stability to network learning (the social capital argument). More confident about agency and effectiveness of design choices | Long-term relations were not necessary for trust and openness to emerge in an interorganisational network | Emphasises content and process design over structure in knowledge creation networks | Difficult question in network studies is: What is actually embedded? Rutten’s answer: ‘understand the process of knowledge creation first and then look at how this process is embedded in various layers of social and organisational context’ | Deliberately layer networks so that knowledge can flow freely at operational level |
| Locus of knowledge creation: politics/conflict/networks of power | |||||
| Argote and Miron-Spektor 201162 | Knowledge creation is a subprocess of organisational learning. Members, tools and tasks combine to form knowledge-creation networks | Member turnover less detrimental to knowledge retention in hierarchical organisations or strong procedural rules | Call for more research on the characteristics of knowledge-creating teams | Procedural rules may mitigate negative effects of turnover | |
| Bogenrieder 200263 | Organisational learning produced from constructive sociocognitive conflict. Knowledge creation typology starts from different problem situations (degree of goal and technical uncertainty). Structural embeddedness of networks more important than tie strength alone except when both types of uncertainty high | Define problem situations, e.g. those with clear goals but high technical uncertainty make tacit knowledge central to participation legitimacy and network structure important to ‘force’ interaction | |||
| Rodan and Galunic 200464 | Knowledge diversity seen as critical to innovation, but enrolling political support and buy-in from advocates also important, especially in early stages | Relational content at least as important as network structure in explaining innovation but structural factors may protect nascent ideas from ‘sceptical scrutiny’ | Assess knowledge heterogeneity alongside network structure when studying knowledge creation | Do not pursue networking for its own sake: network maintenance is costly, and it is not the only way to access diverse knowledge | |
| Swan and Scarbrough 200565 | Posits generative relationship between power, knowledge integration and network formation, highlighting co-ordinating power of key actors to recruit network members with diverse knowledge assets and co-ordinate interaction | Innovation champions were able to overcome weak organisational positions through process power and meaning power | Structural features of networks can matter less than other types of power | ||
| Locus of knowledge creation: tacit knowledge processes | |||||
| Breschi and Lissoni 200166 | Tacitness relates to knowledge flows not stocks | Knowledge externalities often mediated by local labour markets | Need to study career mobility to understand regional knowledge spillovers | ||
| Doak and Assimakopoulos 200767 | Tacit knowledge embedded in collective social arrangements | Hierarchies determined by belonging to communities of practice outlasted organisational changes/transfers | Look at knowledge creation network dynamics over different time scales | ||
| Siemsen et al. 200968 | Examines psychological factors in knowledge sharing, highlighting two: willingness to take reputational risks and confidence that own tacit knowledge justified and accurate | Communication frequency was important to tacit knowledge sharing | Study of knowledge sharing incidents within dyads can reveal important features of knowledge networks | Encourage frequent communication if tacit knowledge exchange important | |
| Locus of knowledge creation: content of relational ties | |||||
| Cross et al. 200169 | Organisations are transactive knowledge systems, producing meaning interactively | Diversity in sourcing of information support, emphasising friendship and trust over organisational status. Organisational affiliation explained networking for legitimacy support, but not for more practical exchanges of advice | If knowledge production is highly distributed (specialised) indexing is important so that individuals can find one another | Go beyond the usual questions asked in analyses of work-based advice networks (e.g. ‘who do you usually go to for advice on work-related matters?’) and inquire after the content of each relation | |
| Obstfelt 200570 | Deals with the relationship between types of knowledge creation and two different social networking mechanisms/logics | Co-ordinating and introducing behaviour produced dense knowledge exchange networks | Collaboration associated with incremental innovation, competition with radical innovation | ||
| Locus of knowledge creation: activity systems | |||||
| Blackler et al. 200071 | The organisation is a network of overlapping activity systems (Vygotski, Engestrom): what people do, how and with whom, and how they shape the context of knowledge practices are central concerns | Study practices as transformative activity, located in history, looking for disturbances that stimulate learning | Analysis needs to be multilayered: explore relations between communities of activity | ||
| Macpherson 200572 | Knowledge is an activity structured by systems of knowing such as organisational routines, which are in turn shaped by the agency of managers though negotiation, persuasion and rhetoric to build collective understandings of legitimate action | If knowledge is a social process, research on knowledge creation should incorporate member checking | |||
Most of the papers focus on knowledge creation as a collective process, taking place in groups or teams. This includes work by Nonaka and his collaborators41–44 as well as authors adopting a social practice perspective. 40 Authors concerned with knowledge creation in ‘project ecologies’,45,46 with project teams working in parallel, also treat the locus of knowledge creation as a team or group. Most papers report groups as being relatively fluid entities that co-ordinate the knowledge flows between individuals and higher levels of organisations. As we will see in Chapters 6 and 7, this fluidity turned out to be a feature of our study sites.
In contrast, some authors emphasise the roles of agency and individual ‘knowledge assets’, either in general48–51 or by attributing a special role to (middle) managers. 47,52 This appears to reflect the diversity in the wider field of organisation studies, where some authors emphasise the roles of individuals (or agency) while others emphasise the importance of institutions and the ways in which they shape (and are shaped by) the behaviour of individuals.
There is also a literature on the institutional contexts within which knowledge-creating organisations operate. Two papers on knowledge-based theories of firms53,54 emphasise the importance of collective knowledge creation, contrasting this stance with more market-based or contractual theories of the firm. Three papers12,55,56 focus on the influence of the wider context for organisational knowledge creation, arguing that there are substantive differences in the contexts within which teams in private and public sector organisations work. A distinct spatial perspective is offered by a number of authors, whose interest is in regional science initiatives, demonstrating how knowledge practices develop in distinct locales or exhibit particular geographies. 57,58,60,61
Several authors discuss the nature of knowledge created, focusing either on the particular role of tacit knowledge66–68 or on the nature of relational ties in knowledge networks. 69,70 These papers point to the range of information and ideas that can be integrated into collective problem-solving processes, echoing the points made in Chapter 1.
The remaining papers include some which focus on the politics of knowledge creation, suggesting that knowledge networks can reflect power relationships62,64,65 or can involve constructive sociocognitive conflict as problems are debated by people with different skills and viewpoints. 63 Conflicts of interest across professional and organisational boundaries are accentuated by Alin et al. 48 Finally, a distinctive approach is taken by two papers which apply Vygotskian activity theory to the study of organisational knowledge creation. 71,72
Relevance to the study
We agree with Ferlie and colleagues’ observations about the status of the academic literature. 1 The consequence, for our study, was that it was reasonable to draw on the knowledge-creation literature for general theoretical insights, but we did not expect a ‘close fit’ between our findings and the literature. For example, we took the view that the roles of middle managers at the study sites were likely to be important, and focused our empirical work on them. We also started with the view that knowledge creation would be a collective process, involving people with different backgrounds and skills, but we did not make any particular assumptions about the ways in which middle managers would work with one another or with other colleagues. By extension, we did not make assumptions about who would be involved in knowledge-creation processes or what kinds of knowledge would be created. In summary, the knowledge-creation literature was helpful in developing our study design, but prompted us to make as few assumptions as possible about what we might find. We comment on the extent to which the literature resonates with our findings in Chapter 7.
Chapter 4 Policy context
Introduction
In this chapter we review the recent history of public health policies for England, in order to place the work of the three study sites in context. We make two main points, namely: (1) smoking, diet and other policy areas have their own distinct histories, although they have begun to overlap with one another in recent years, and (2) there are continuing debates about the objectives of public health programmes and the appropriate strategies for achieving them. In the next section we briefly summarise public health-related policies from the last 20 years. In subsequent sections we argue that there are three broad classes of policy, each based on a different way of thinking about risk, and identify the main policy responses to those risks.
Three approaches
Historically, there have been at least three distinctive approaches to public health problems. The first approach is exemplified by policies on smoking, and focuses on health promotion and prevention. There is clear evidence of the harmful effects of smoking on individuals, and a range of strategies have been developed and are used in parallel, including education, restrictions on advertising, taxation and the provision of NHS services to help people to stop smoking. The second approach focuses on the major causes of disease and disability. This approach can be traced back to Health of the Nation, published in 199273 in response to the World Health Organization’s Health For All programme. It listed five priority areas for work to improve population health. Four were clinical [cancer, human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), stroke and mental health] and the fifth was accidents. Saving Lives: Our Healthier Nation74 was published in 1999 by the New Labour administration and also focused principally on acute services and major diseases.
The third approach focuses on households and communities rather than on specific behaviours or on diseases and disabilities, and is characterised by initiatives aimed at poorer families and communities, including Health Improvement Programmes, SureStart, Health Action Zones and New Deal for Communities. It also published a new review of health inequalities, the Acheson Report. 75
The key point, in the context of our study, is that each approach has different origins. Towards the middle of the last decade, though, there were signs of overlap. The Wanless report76 on population health, commissioned by HM Treasury, was published in 2004. It linked medical and social models of public health in a single analysis, pointing out that a number of health problems were on the increase. It urged closer working between the NHS and local authorities to tackle these problems by focusing resources on promoting health and preventing illness. It recommended that the NHS would need to:
. . . shift its focus from a national sickness service, which treats disease, to a national health service which focuses on preventing it. The key threats to our future health such as smoking, obesity and health inequalities need to be tackled now.
Wanless report, p. 183
The Choosing Health White Paper, also published in 2004, accepted some of the Wanless arguments, and smoking, diet, exercise, health inequalities and the need for ‘healthy communities’ were presented in a single document. The NHS contribution to policies to stop people smoking was boosted, and the need to address the health problems associated with obesity were emphasised.
This said, Choosing Health also stressed the need for individuals to take responsibility for their own health, and downplayed the role of the social determinants of health, that had underpinned arguments about health inequalities since the 1970s. This appeared to go against the earlier rash of community-based initiatives. The government also continued to publish guidance in discrete policy areas, including smoking and diet, continuing practices established over many years. That is, policies in these areas continued to have distinct identities, but from this point on were presented as being part of a broader family of policies, and drawing on both medical and social models of public health.
Viewed in this context, the Healthy Lives, Healthy People White Paper, published by the Coalition Government in 2010, continues with much of the thinking of Choosing Health 6 years earlier. As before, smoking, diet and other topics are discussed in the same document. In common with Wanless and Choosing Health, the urgency of tackling problems, particularly problems associated with obesity, is emphasised. The importance of healthy communities is discussed, but given less emphasis than in 2004. The major point of departure from earlier policies is that Healthy Lives, responding to the Marmot Report of 201077 (see below), reintroduces health inequalities as a key policy driver. The NHS Future Forum’s report, which was accepted by the government in January 2012, continues with the broad approach of Choosing Health and Healthy Lives. The report talks about health and well-being rather than inequalities, but does not suggest that this marks another point of departure from previous policies.
Finally here, the NHS Health Checks programme was announced in Putting Prevention First in 2008. 78 General practitioners (GPs) screen adults between the ages of 40 and 74 for clinical signs of risks of heart disease, stroke, kidney disease and type 2 diabetes. The policy focuses on the implementation of checks by GPs, and on modifying individual patients’ behaviours, rather than (for example) on the ways in which families and wider communities might influence an individual’s behaviour. This policy sits squarely in the second, medical public health, tradition of policy-making. As far as we can tell, there are no significant links at policy level between health checks and other policies discussed here (e.g. there is no mention of health checks in the 2010 tobacco control plan for England, published alongside Healthy Lives).
Three classes of risk
The brief summary helps to make the point that there is not a single set of public health policies, which managers in localities can use to identify clear policy objectives or practical interventions. However, some common themes can be identified, and in order to characterise them we note three main classes of public health risks which have been identified consistently over the last decade. The work undertaken at the study sites, described in Chapters 5 and 6, is usefully understood as a response to one or more of these risks.
The first class of risks focuses on the lifestyle choices made by a substantial minority of people in England. The argument that many of us need to change our lifestyles is straightforward: too many of us are smoking, do not take enough exercise, abuse alcohol and so on. This reduces the quality of our lives, and some of our behaviours can reduce life expectancy. It also places strains on the public purse, increasing expenditure on benefits and on NHS and local authority services. Policy prescriptions are concerned with changing individuals’ behaviour – stopping smoking, taking more exercise and drinking alcohol more sensibly.
The second class of risks focuses on health, and in particular on the large number of people who live with chronic health problems. The Department of Health estimates that some 15 million people are living with at least one long-term condition such as asthma, diabetes or a neurological problem. The distinction between this and lifestyle risk is that some people have a predisposition to certain diseases and illnesses, or may simply be unlucky, and become ill even though they are fit and eat healthily. Policy prescriptions focus on ways in which individuals can play active roles in managing their problems, on the contributions of informal carers, and on the need to improve the co-ordination of statutory and independent services, so that they provide effective treatment and care.
The third type of risk is concerned with the health and well-being of populations. The main ‘diagnoses’ of population ills focus on the wide variations in illness, disability and life expectancy between different communities. People living in poorer communities are more likely to get ill, to be disabled in some way, and to have shorter life expectancy. This type of account is exemplified by the Marmot Report of 2010,77 which argues that health inequalities are substantially determined by our social circumstances, and are largely preventable. The report advocates a ‘life course’ approach, on the basis that:
Disadvantage starts before birth and accumulates throughout life . . . Action to reduce health inequalities must start before birth and be followed through the life of the child. Only then can the close links between early disadvantage and poor outcomes throughout life be broken . . . Meanwhile, there is much that can be done to improve the lives and health of people who have already reached school, working age and beyond . . . Services that promote the health, well being and independence of older people and, in so doing, prevent or delay the need for more intensive or institutional care, make a significant contribution to ameliorating health inequalities.
Marmot Report 2010, p. 20
Policy responses and organisational learning
National policies do not comment on the kinds of knowledge that are needed to co-ordinate successfully, or the means by which the knowledge needed to achieve effective co-ordination might be created. 79 There are, however, a number of policy instruments that might, in principle, play a role. Two examples are noted here by way of illustration. First, some forms of legally binding contract may have the potential to promote interorganisational learning. The organisations contracting with one another – such as a local authority and a private firm providing sports and leisure services – can use the contract to regulate their relationships with one another. 80 If, for example, it becomes clear that part of a contract cannot be fulfilled, then the two sides can negotiate and agree a new way of spending resources that satisfies both sides. That is, the two parties can learn about one another, and about what can and cannot be delivered, over time.
Second, the Department of Health has emphasised the importance of the Quality, Innovation, Productivity and Prevention (QIPP) agenda. 81 QIPP is a term that is more familiar in the NHS than outside it, but its logic extends beyond the boundaries of the NHS: other public services, and private and voluntary organisations, are in a position to help the NHS to tackle the individual and population risk factors set out in the previous section. The opportunities for learning lie in the challenges of designing services that effectively target people ‘at risk’, and simultaneously finding ways of reducing the costs and improving the quality of those services. These services, as pointed out in Chapter 1, can only be solved by a number of organisations working together and solving problems collectively. As our findings in the next two chapters show, designing and implementing effective health and well-being services poses substantial conceptual and practical challenges.
Finally in this chapter, we note the changes that have occurred in the wake of the financial crisis of 2007–8. In the first decade of this century some public services, and in particular the NHS, received substantial real-terms increases in budgets. This was not true of all services; social services experienced flat budget settlements during the decade. In the period since 2010 there has been a greater focus, in all public services, on reducing costs. Comparatively, there has been less emphasis on inequalities and other themes highlighted in earlier sections of this chapter.
Chapter 5 Qualitative accounts of knowledge creation
Introduction
This chapter presents the results of our qualitative analyses. As discussed in Chapter 2, the findings of this component of the study are drawn from the second round of interviews at each of the three study sites, supplemented in some instances with documentary material from the sites. Our approach was to ask interviewees to describe how they had identified and solved particular problems, on the basis that these accounts would help us to address our research questions: the accounts would reveal who was involved, and how their joint efforts had created knowledge.
We identified 30 accounts in total across the three sites, but many of these were described by only one or two of our interviewees. Here, we present three accounts about knowledge creation from each site, selected on the basis that several interviewees gave us their accounts of the same processes. This meant that we had sufficient detail about events to reconstruct them. Cross-matching the different accounts gave us confidence in the validity of each account.
For each account, we outline the collective problem that was being addressed, identify the key episodes – the fragments identified in the analysis – and comment on the nature of the knowledge-creation processes revealed. That is, the accounts set out what one might call resource mobilisation – how managers were able to acquire and use resources – and the inferences we made about knowledge creation linked to the activities described. At the end of each site section we note commonalities between the three accounts. Figure 7 shows a timeline for the nine accounts, indicating the points during the accounts when fieldwork took place.
FIGURE 7.
Timeline of stories of knowledge creation. T1/T2 indicate approximate times of first and second interviews.
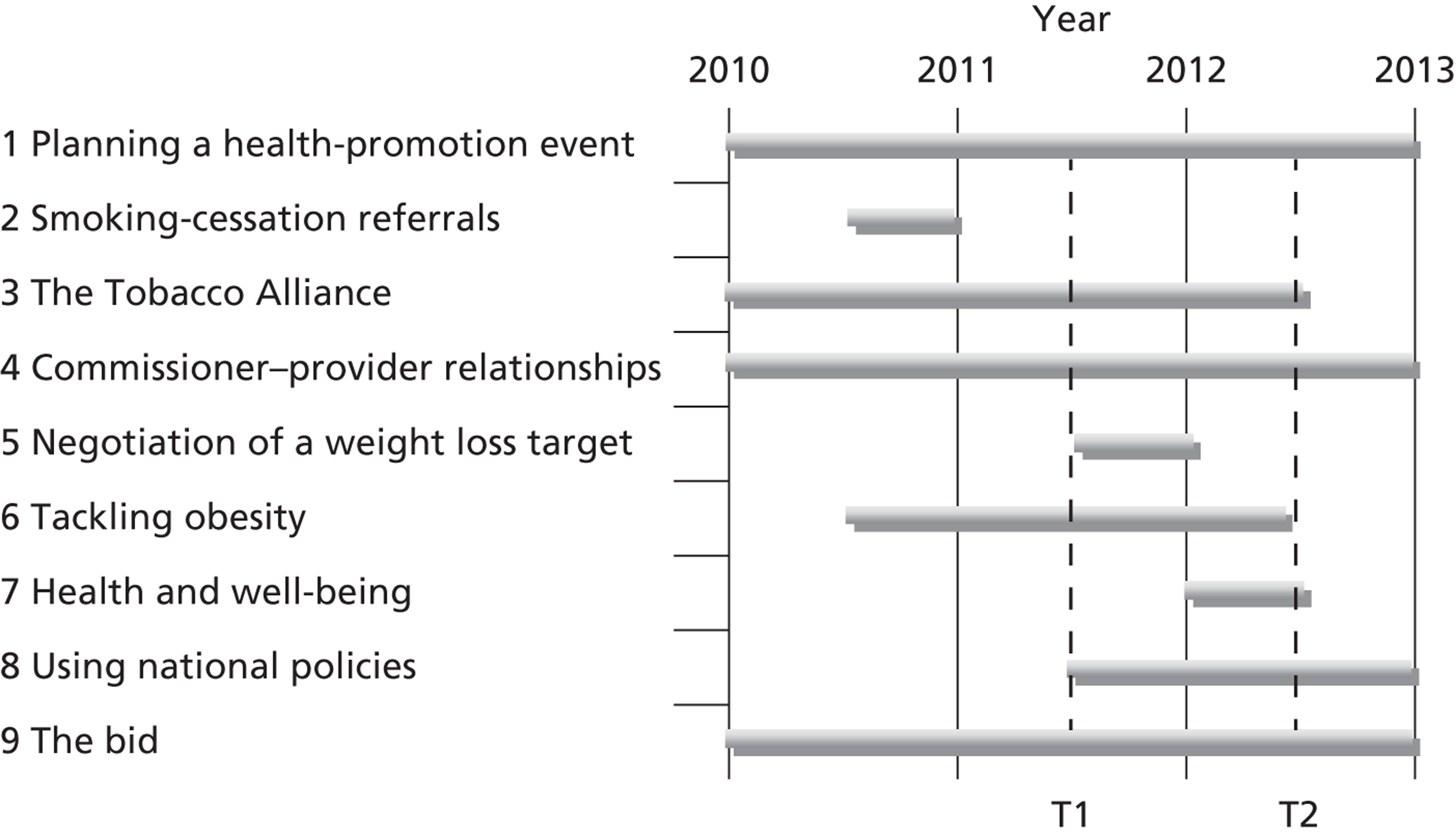
Site 1 accounts
The pressing local health and well-being issue at site 1 was tobacco control. Site 1 accounts describe the planning of a health promotion event, setting up a smoking cessation referral service, and working together in a Tobacco Alliance.
Planning a health promotion event
This account concerns the planning of a health promotion event, to coincide with National No Smoking Day in 2012. The account is compiled from six interviews and augmented by material from meeting minutes. It has a wide-ranging cast of characters including public health managers from the PCT, and managers from the smoking cessation service, NHS acute trust, health trainers, professional groups such as pharmacists and probation officers, several council services including trading standards and the communications team, and the local professional football club. Figure 8 presents the key fragments in a tellable sequence.
FIGURE 8.
Planning a health promotion event story flow chart.
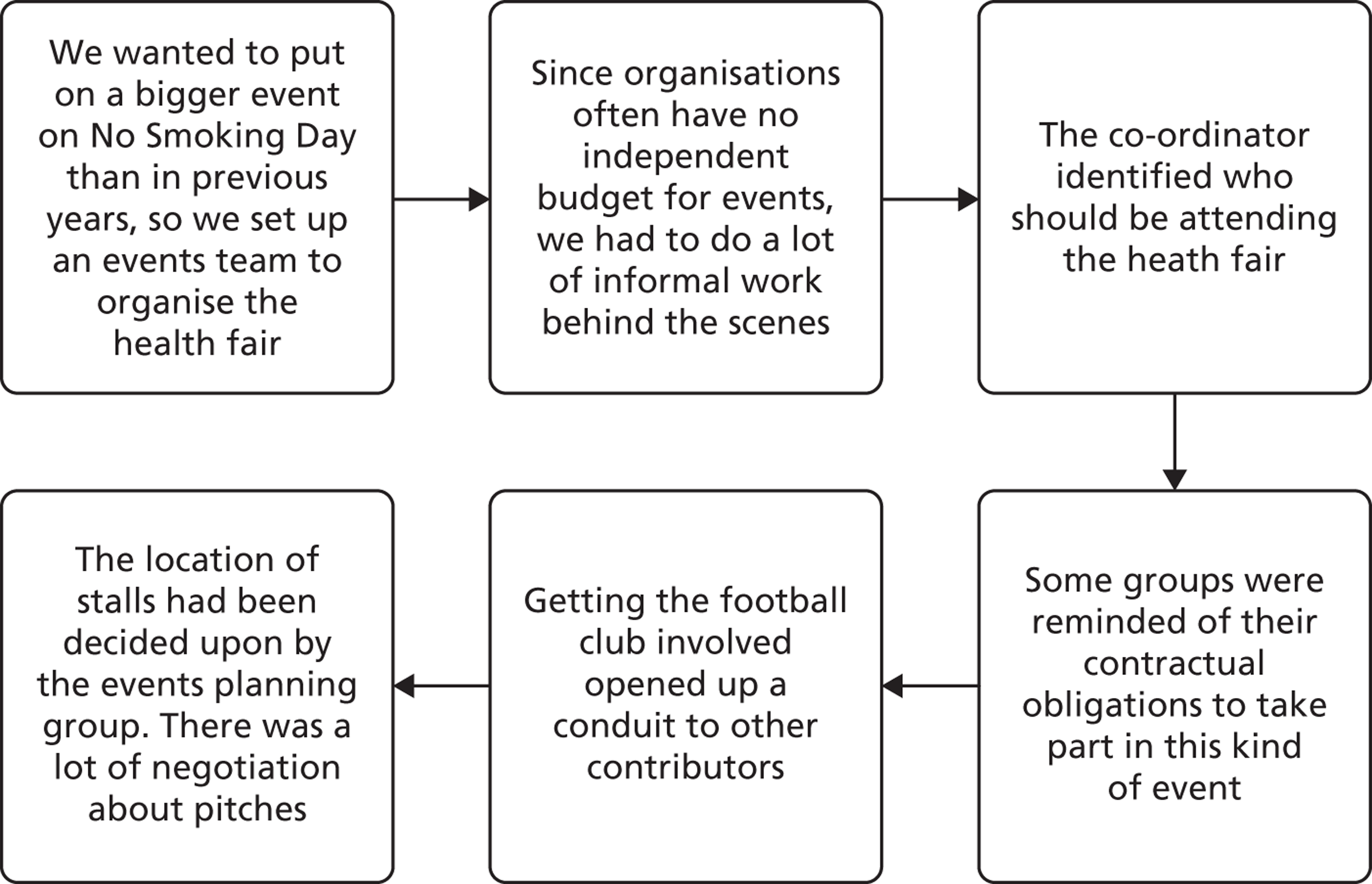
Managers in the lead team had organised health promotion events before, but wanted to organise a larger event than in previous years. They decided to hold a ‘health fair’. This would involve a number of local organisations providing stalls in different places in the town’s main shopping area to maximise exposure and make it possible to approach members of the public and offer them advice on healthy lifestyles (e.g. stopping smoking).
They set up an events team to organise the health fair and appointed a project manager. They looked for ways of publicising the fair:
. . . public health were looking at an idea that we had when the legislation came in: we had big daisies that people could ring into the local radio station if they saw them across the town centre, so we were looking to do something similar, so they were involved for how we’d go about planning that.
Manager
Relationships with a number of organisations were already well established. Some of them had targets for contacts with members of the public, and the health fair would help them hit those targets. This prompted the need to negotiate over the locations of individual stalls, with some plots being deemed superior to others. Conversely, some organisations did not have events budgets, and managers from the lead team spent time persuading them to be involved and to then commit money and/or personnel. The result was a series of discussions and negotiations with a range of stakeholders:
But I think they’ve changed the idea completely now, so they [environmental health] were involved I think for maybe the planning and the booking side of things . . . trading standards were there because we know we’ve got a big issue with illicit and illegal tobacco, so they’ve got some resources where they’ve got some counterfeit tobacco that looks so genuine you wouldn’t know the difference. So we were seeing if they could get involved and maybe have a stall there . . . [The communications team] were there to look at ideas of how we could communicate the different events, I was there as a representation from the [lead team] to see what’s worked in the past and what ideas I could take forward.
Manager
Looking back, managers believed that the health fair had brought together a number of different organisations, and had demonstrated that they could put on a significant event with limited resources.
This account suggests that managers can use established relationships to mobilise resources across a number of organisations. The project team had a limited budget and, while there were a number of planning meetings, the setting up of the event relied largely on those involved having meetings and informal conversations with potential stallholders. Put another way, knowledge creation was intimately linked with negotiations between the various parties. The account also emphasises the point that middle managers have to co-ordinate people with discrete skills, in this instance including project management, publicity and teams with specific content knowledge. This was an account where conscious efforts were made to draw on the experience of participants, either repeating activities that had worked before or capturing ideas generated elsewhere (e.g. the daisies that were used to publicise the fair).
Smoking cessation referrals
This account is compiled from four interviews and focuses on the introduction of a new referral system for people caught smoking in public places, targeted at taxi drivers. It involves actors from the council’s environmental health team and the smoking cessation service as well as public health managers from the PCT, other members of the local Tobacco Alliance and the target group of the proposed intervention – taxi drivers. Figure 9 shows the key fragments in sequence.
FIGURE 9.
Developing a smoking cessation referral system story flow chart.
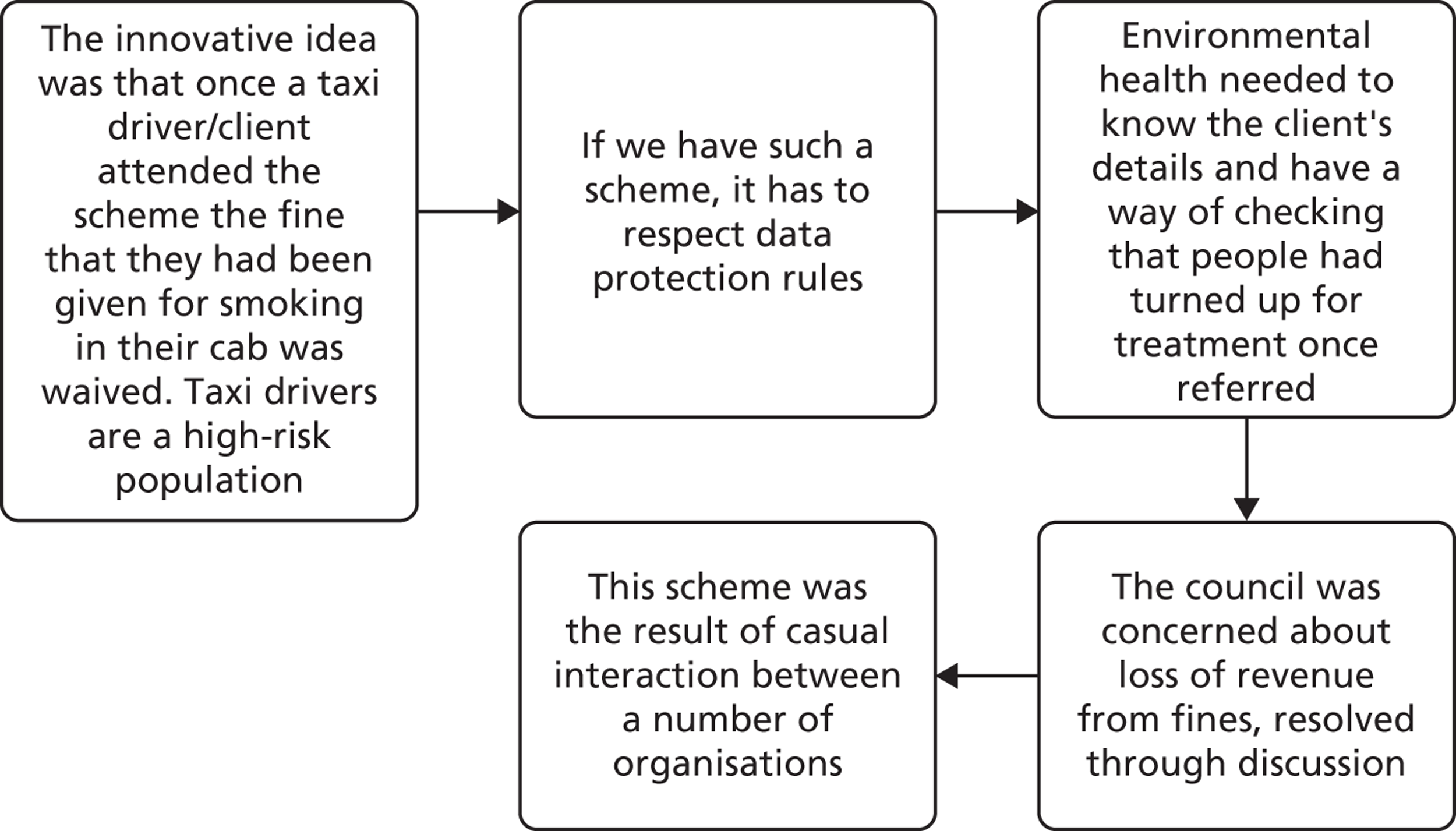
This account started with an imaginative leap made by one of the middle managers in site 1:
Mrs J**** has been on a speed awareness course. She’s actually been on a few speed awareness courses, and as you probably know if you get caught speeding up to a certain level, instead of taking your penalty points and getting the fixed penalty notice, you can pay a lower fee and go on a half day awareness course.
Middle manager
The insight was that a similar scheme could be introduced to tackle smoking in public places using a relatively new legal provision, whereby fines could be issued when people were caught. The idea was discussed at a Tobacco Alliance meeting, which included people from the smoking cessation and environmental health services. A manager recalled:
If we find you having a cigarette you’re normally liable to a fixed penalty notice, so instead of giving you the fixed penalty notice we’ll give you a referral to smoking cessation. As long as you take that up in the month we’ll forget about the fixed penalty notice.
Manager
Through discussion, it was agreed that the scheme would focus, in the first instance, on local taxi drivers. Under the scheme, any taxi driver found smoking in his or her car would be referred to a Stop Smoking scheme as an alternative to getting a fixed penalty notice.
While there was enthusiasm for the scheme, details had to be negotiated. For example, there was concern at the council about the possible loss of income streams from waiving fixed penalty notices. The loss of income would only be in the order of hundreds of pounds, but a loss was a loss:
. . . that took quite a lot of discussion, because of course that means we are not getting the fine. But actually it was agreed, A**** eventually agreed that actually the cost long term to the council of people smoking in the community was lower.
Manager
Similarly, concerns about sharing personal information among agencies caused some headaches.
One of the things that might have influenced things, and slowed it down, was data protection . . . If I remember rightly, [the NHS] didn’t want to do it by patient name, it had to be a reference number.
Manager
The details of those caught smoking would have to be passed from the environmental health team in the council to the NHS Stop Smoking service. They would then need to tell the environmental health enforcement officers whether or not people were attending courses. This problem was also resolved through discussion.
The Tobacco Alliance
This story is compiled from five interviews. It centres on the activities of the local Tobacco Alliance and the operational Stop Smoking team, and the cast is their membership. GPs feature as peripheral players, whose marginality is the source of debate among other actors. Figure 10 shows the key fragments in sequence.
FIGURE 10.
Tobacco Alliance story flow chart. ops, operational; PH, public health.
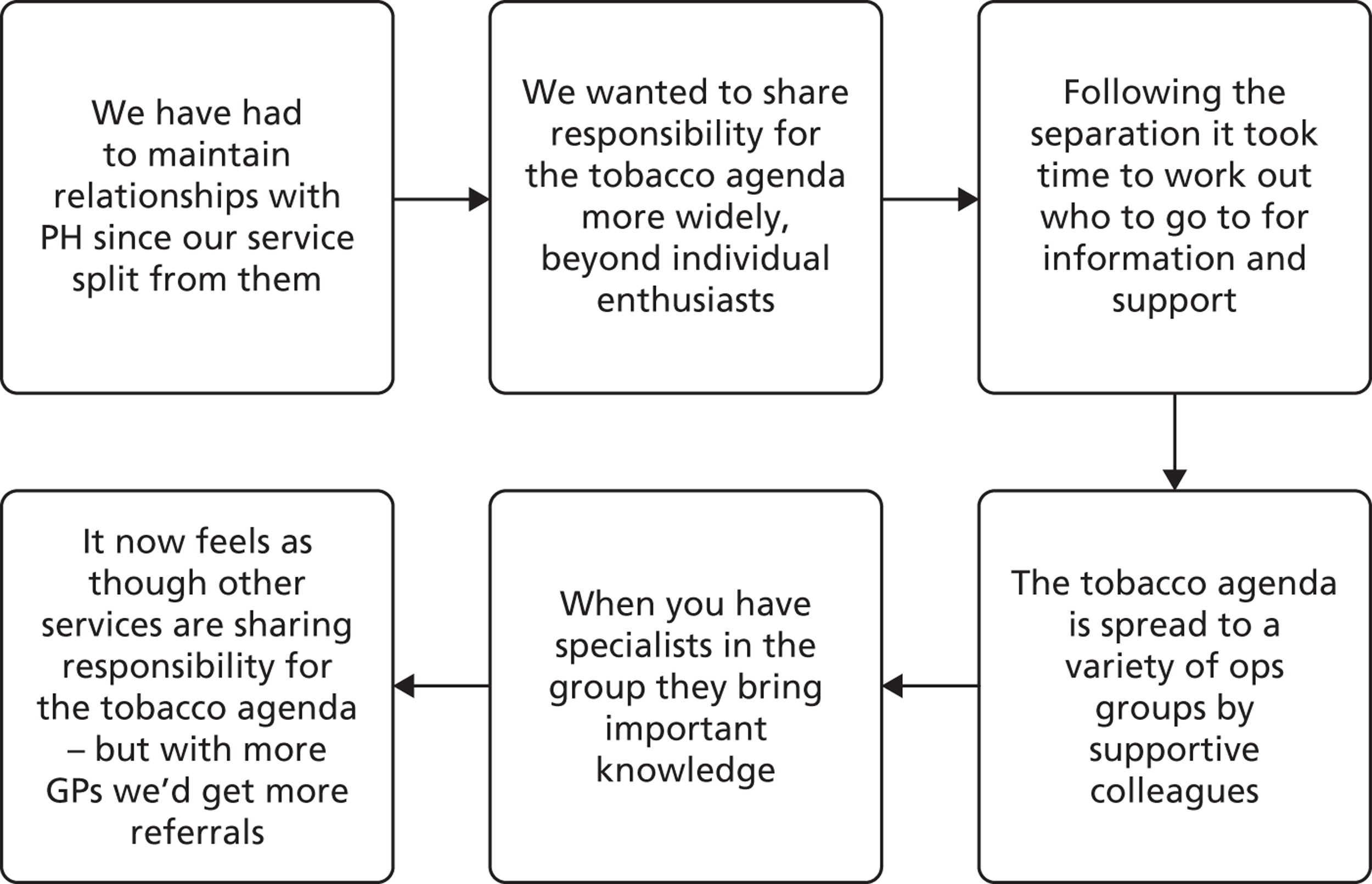
In common with many other PCTs in England, the local PCT separated its commissioner and provider functions. In order to mitigate negative effects of the separation, the cross-organisational Tobacco Alliance was created to support smoking cessation and related services. This was deemed important:
It was never that things weren’t getting done, or nothing was happening . . . we didn’t know where to go with things . . . that’s sort of merged back together really with the help of things like the [operational service] group and the Tobacco Alliance that has been set up since that split, so that feels like those relationships have built on and are strong again.
Manager
Another manager observed that effective relationships had been established, with teams contributing in different ways:
Previously we felt that we had been on our own with the tobacco agenda . . . [now] public health take some responsibility for tobacco as a whole in the Borough, and also . . . environmental health, we need that support, whether it’s brief interventions that their enforcement officers are doing and referring in, or if it’s looking at bigger projects like the taxi project.
Manager
The Alliance was viewed by some managers as a solid base that could be used to widen participation. One manager outlined the philosophy:
How do we start to make smoking everybody’s business? And that’s our baseline, really . . . we’re not talking to a lot of people outside of the health community, and actually this is still very primary care [oriented]. Where is maternity, where is the acute, where is the Mental Health Trust?
Manager
Another manager suggested that they should exploit networks of service providers to ‘spread the word’:
We can’t do it in isolation, so what we attempt to do is to speak to lots of people to raise awareness of our service so that they can tell others, by word of mouth, about what we do. So it’s almost like an ant, isn’t it, where you live in this colony but actually if we all work together we can get somebody else doing our job for us, the word of mouth bit, and then we can increase our referrals without having to keep sending our health trainers out doing promotional events.
Manager
It was suggested that there was some evidence that this approach could work:
If you looked at the web where tobacco control business is played out there might be a children’s centre operational group, but smoking’s on the agenda. . .
Manager
Equally, progress was slow with some groups, notably GPs. People providing services had regular contacts with GPs, but one-to-one meetings might not be effective. Managers were thinking about ways of involving GPs more directly, because they would be able to refer many people:
. . . if we can speak to the GPs, say there’s 50 GPs in the area, they have contact with thousands of people, and if we can sell them our idea and if they buy into it, they will start referring in.
Manager
Managers were clear that each of the main organisations made an important, but different, contribution:
. . . public health, I suppose they drive it from a figures perspective, don’t they? And from apportioning money. And then health improvement drive it from on the ground, helping people to quit. And then you’ve got environmental that are there to make sure that where public health and health improvement are unable to make an impact they can go in, I suppose, with a heavy hand.
Manager
Reflections on the site 1 accounts
The three site 1 accounts highlight two common themes, under the broad headings of knowledge creation and network relationships. In relation to knowledge creation, middle managers were able to identify a novel way of achieving a policy goal. In doing so they drew on, and created, both technical and prudential knowledge – knowledge of how to design and deliver services, and of populations that could be targeted, and how to mobilise support for the new service. They were also able to co-ordinate distinctive contributions, particularly in the preparations for the Health Fair, ranging from the communications team to the local football club. The accounts suggest that a common understanding of a particular problem – ‘tobacco is everybody’s business’ – can play an important role in the co-ordination of services.
Second, relationships spanned public, private and voluntary organisations. A formal arrangement, the Tobacco Alliance, provided a solid basis for co-ordinating activities, and allowed ‘core’ members to reach out and involve other individuals and organisations when the need arose. Relationships between managers, notably those between commissioner and provider managers, were underpinned by (often long-established) trust. The accounts also suggest that relationships can be simultaneously stable and fluid. Stable relationships included those based on ‘old PCT’ relationships. More fluid, or tactical, relationships were established for particular projects, for example involving the football club in the Health Fair. As above, managers believed that their informal relationships had proved to be resilient, helping them to maintain services in a period of substantial organisational change. Here, though, the resilience was also attributed to the formal structure: the Tobacco Alliance.
Site 2 accounts
The pressing health and well-being issue at site 2 was health improvement. The three accounts concern the regulation of commissioner–provider relationships, negotiations surrounding a weight loss target, and a programme to tackle obesity.
Commissioner–provider relationships
This account is compiled from eight interviews. It focuses on the relationships between managers who had worked in the same organisation, but who were now in separate commissioning and provider organisations. It involves actors involved in commissioning health improvement services, including the public health team, the council’s health inequalities team, a health improvement team from a NHS trust and service providers in the areas of weight management, smoking cessation and midwifery. Figure 11 shows the key fragments in a tellable – rather than strictly chronological – sequence, distinguishing commissioner and provider perspectives.
FIGURE 11.
Commissioning services story flow chart.
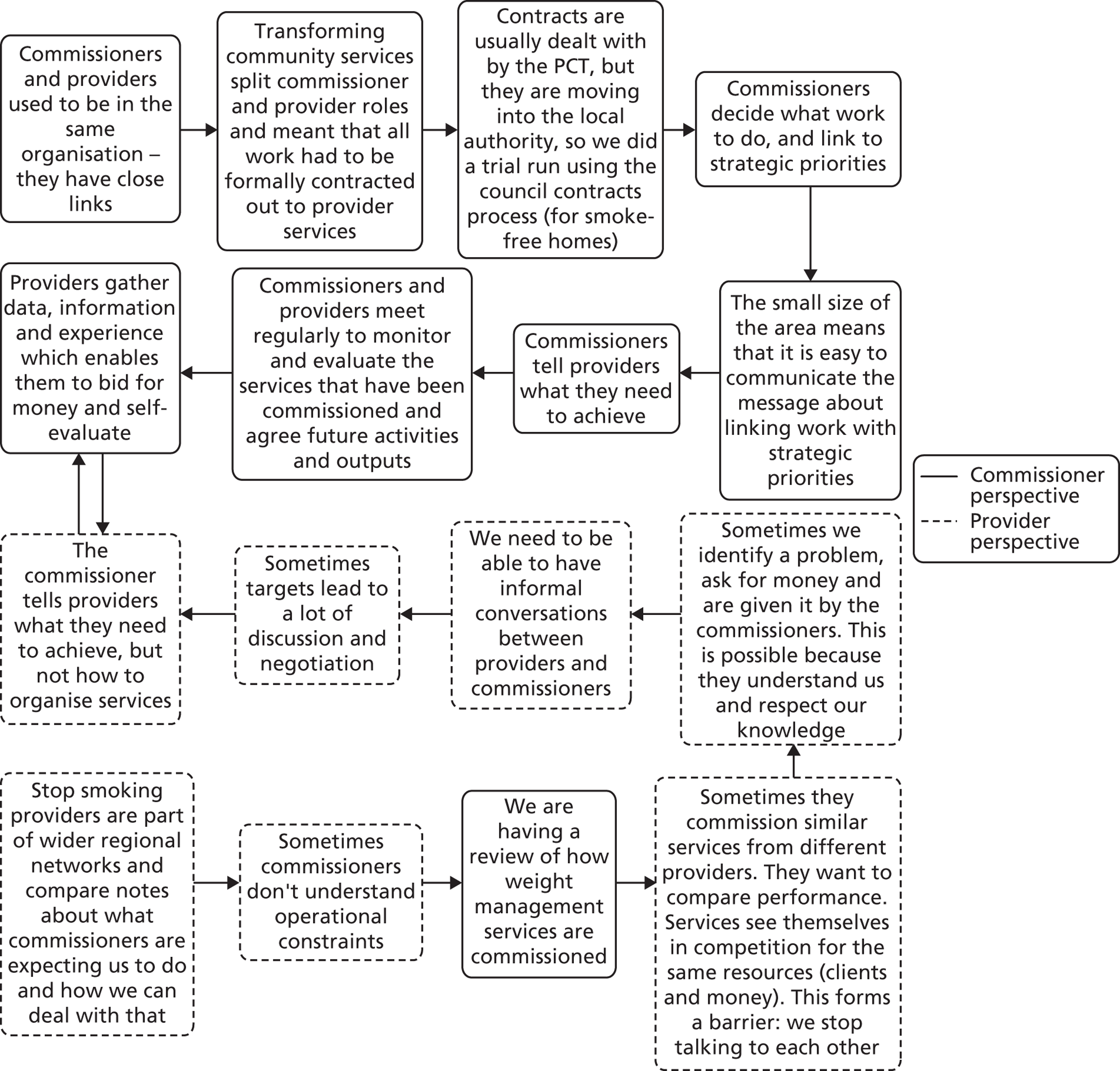
Whenever they discussed services with providers, commissioners needed to take account of local strategic priorities and the need to make the best use of resources in a period of fiscal austerity. They needed to ‘commission smart’. One manager argued that contracts could be used to encourage co-ordination between providers:
What we are now getting this provider organisation to do is to try and embed smoke-free homes work within the everyday work of midwives and health visitors and children’s centres etcetera, to make it part of midwives’ and health visitors’ everyday business . . . when we want that sort of work doing we have to contract with [the health improvement service].
Manager
Both sides described the commissioning process as communication-intensive. Discussions between people who had worked together could be more formal than in the past:
We’ve worked in a different culture where our commissioners have been in the same buildings, have been in the same jobs, so they have often felt they could just come and ask us for information, and we’ve always been very proactive in giving them that information, whereas within [a provider organisation] there’s a lot more formal structures and procedures to go through which I think has its benefits. . .
Manager
Regular meetings were held, where contracts were negotiated, monitored and evaluated, and contract variations – including new activities – discussed. At the same time, however, interviewees reported that informal relationships were important; commissioning involved continuous dialogue. Three provider managers gave these examples:
We have a really good working relationship with [a commissioner] where we can go back and say ‘well look we thought this but it didn’t really work can we tweak it like this?’ And nine times out of ten she’ll say, ‘yeah as long as you get me results, crack on with it’. And it’s nice to be able to do that. . .
. . . we’ll also share good practice. So for example [a manager has] had an excellent smoke-free homes campaign in [a town] . . . We’ve just been commissioned to do that in our area, so we would talk to [the manager] about smoke-free homes, ‘cause we know that they’ve got evidence of good practice.
We often felt that they [overweight people] didn’t really put the effort in to try and lose weight through healthy lifestyle changes, because they just saw surgery as being the way to do it, and couldn’t really see beyond that. So we identified that, went back to the commissioners and said ‘look this isn’t working, how can we make it work?’ . . . They came back and gave us some more money so we could target more specifically those patients.
Colleagues in other localities undertaking similar work could also be a source of ‘how to’ knowledge. Provider managers reported that they compared notes with peers in neighbouring areas, and collected and evaluated data to reassess their own performance and the value of the service contract to their organisation.
Less positively, some of the information gleaned from other localities was valuable in bidding for contracts, and for this reason was not usually shared with potential competitors. Competition – or at least the prospect of competition – influenced the extent to which knowledge was passed on to other organisations. Additionally, NHS provider staff were apprehensive that the transfer of commissioning roles to the local authority could upset their relationships with former PCT colleagues:
The local authority provides services very much like we provide, and how will that sit in the new way of working? . . . I feel personally the relationships we used to have have become a little bit more precious, because we’re very aware of, we’re not sharing quite as much as we would have done because they could then take those ideas and present them to a commissioner as, ‘we can provide this service’.
Provider manager
Managers’ accounts suggest that their informal networks had been resilient in the face of organisational change. Continuity and familiarity with colleagues were viewed as important network resources that helped managers to cope better with changes.
The accounts suggest that useful information could be identified in a number of places, including managers drawing on their own or others’ experiential knowledge, from formally reviewing their own performance, and in informal discussions with colleagues in other localities. It also suggests that knowledge creation – here, the practical process of integrating the information, using it to understand ‘what works’ and negotiating new service models – did not have to involve everyone in a network. If commissioners trusted colleagues in provider organisations, they felt that they did not need to review proposals in any detail.
Negotiation of a weight loss target
This account is based on seven interviews, and focuses on the negotiations surrounding a service designed to achieve a weight loss target. It involves actors from the public health team at the PCT, a subgroup of the local strategic partnership and weight management provider services from the public, private and voluntary sectors. Figure 12 shows the key fragments in sequence.
FIGURE 12.
Negotiating a weight loss target story flow chart.
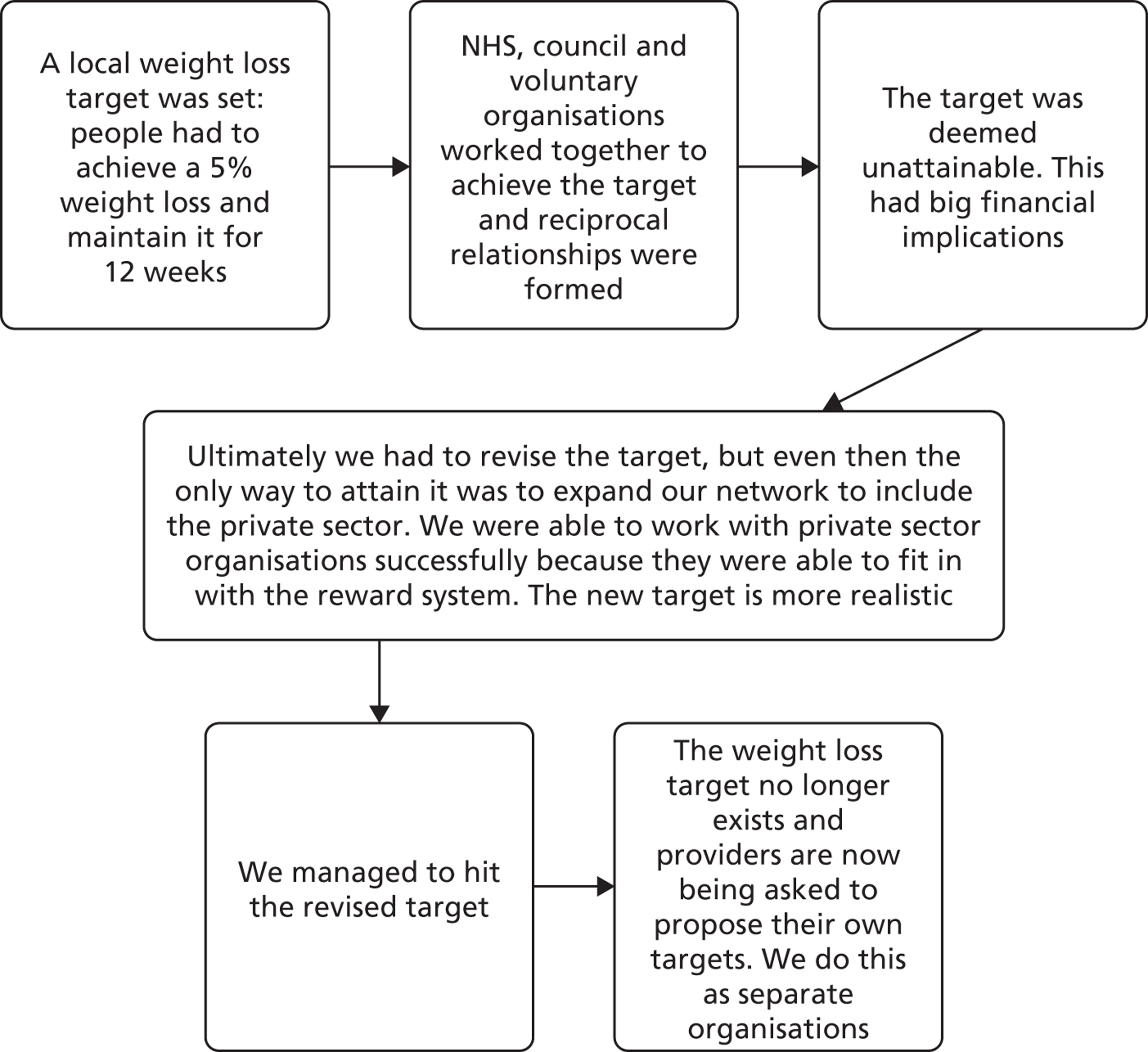
The local strategic partnership set a weight loss target to be implemented across the locality. It specified that a number of people who were seriously overweight had to lose 5% of their body weight and maintain the new weight for 12 weeks. Services would receive outcome-based payments for hitting the targets. The target was applicable to organisations running weight loss services across the locality, which at the time included services in both the council and PCT. The partnership negotiated support from other organisations, including free access to local leisure facilities to help people to maintain their weight loss.
Both organisations found that the original target could not be achieved. This could have resulted in them not being paid for their work, and this prompted them to renegotiate the target with the partnership. The commissioners agreed to change the target, and once it had been changed the organisations were able to meet it, although they needed to involve other provider organisations in order to do so. Some of this widening of involvement was viewed positively, some less so. Said a provider manager:
. . . working with the gyms, Weight Watchers and Slimming World worked really well. The voluntary sector was more difficult because there seemed to be different rules around what payments they would get for their activity . . .
The locality-wide target was later dropped. Provider organisations were invited to propose targets, which provided the basis for contract negotiation with the partnership. This change of approach is attributed to a more competition-oriented approach locally. It was felt that this militated against the more integrated approach that had prevailed previously:
We’re all competing for pots of money separately . . . and we’ve all got different targets, so you tend to pursue your own area at the expense of your colleagues’ areas, which as a team we’re trying to stop, because if somebody overachieves at the expense of another team it will impact on us all eventually.
Provider manager
This account emphasises the role of formal relationships, underpinned by legally binding contracts. Viewed positively, it suggests that targets can be used to encourage the creation of new relationships, as occurred with the private firms. Less positively, in network terms, managers believed that competition discouraged the sharing of intelligence. When the target was changed, the principal sources of information were quantitative data on the performance of the provider organisations and the practical experience of the managers working in both the commissioning and the providing organisations. The account implies that a number of managers shared a mental model of the ideal situation, which was one where services were integrated across the locality.
Tackling obesity
This story is compiled from two interviews, supplemented with documentary material including meeting minutes. It concerns the use of a central government grant to develop innovative ways of tackling obesity, and involves actors from the public health commissioning team and voluntary and private sector providers. Figure 13 shows the key fragments in sequence.
FIGURE 13.
Tackling obesity story flow chart.
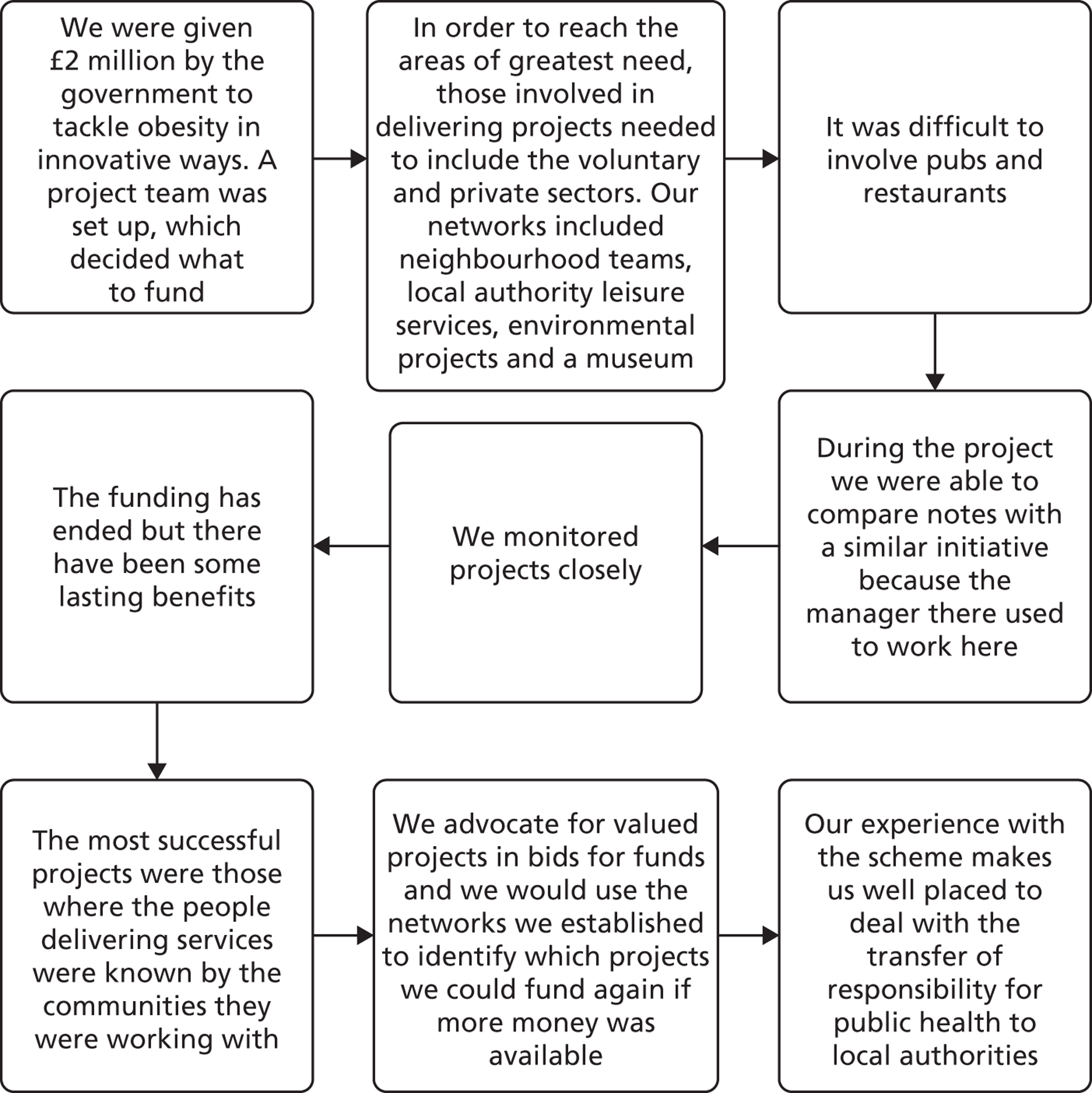
In the early phase of the programme, the public health team decided to focus on the four wards which had the highest incidence of obesity in the locality. They also identified suitable projects, based partly on fitting the criteria set by central government, and partly on the basis that they would be sustainable once the programme funding ran out. They believed that local credibility was particularly important:
Two of the projects were run by the neighbourhood management team . . . they had people who lived in the community who knew everybody, who knew every street, whose children went to the schools, who had that interaction with parents.
Manager
The programme involved building relationships with a range of providers. Experiences were mixed:
The public and voluntary sector organisations I feel are quite easy to get your foot in the door and deal with it, it’s when you want to deal with the restaurants or the pubs . . .
. . . we just couldn’t manage the pubs, and it took three visits to a pub until they would sign up to do what you wanted them to do, you know. We wrote to them, we rung them, we went in and saw them, then you have to see the manager, who then has to then ring head office . . .
Manager
During the programme, managers in the public health team and in teams providing services gathered, and integrated, information from a variety of sources, including routine performance reports and regular informal conversations. Colleagues in other localities were a valuable source, too:
So we have that sort of little link that we were able to talk about [central programme] things with [her], ‘Have you heard from the Department, have they given you your money yet?’ or, ‘Have they asked for this quarter, have they asked you for this form?’, you know we were able to have that sort of informal . . .
Manager
The programme had finished when the second round of interviews was conducted. Managers believed that there were positive long-term effects:
. . . we’ve still got a lot of links with [an activity centre] and you know we laid the foundations with the [centrally funded] programme but that has then given them the platform . . . to call on other people who they hadn’t had the contact with before. But because we’re here they’ve come to us and said ‘who would I go to for this?’ and that’s opened the door for them.
Manager
This account shows that middle managers acquire, and then integrate, information from a range of sources, including colleagues in other localities. It also hints at the importance of an ‘organising idea’, a coherent way of thinking that can facilitate co-ordination of ideas and actions. Here, the organising idea was that resources should be targeted on the geographical areas where the problem was most common, and that the programme would work best if community workers were based with, and known to, local residents.
Reflections on the site 2 accounts
The three accounts have a number of features in common. They can be grouped under three broad headings – knowledge creation, relationships and the wider context. First, middle managers drew upon different types of information from a range of sources, including routine data about local populations and services, and ‘comparing notes’ with colleagues in other localities. They synthesised the information in the course of knowledge creation. They used different kinds of knowledge in their discussions and negotiations, including both technical and prudential knowledge (using the terminology introduced in Chapter 1).
Second, relationships spanned public, private and voluntary organisations. They were simultaneously formal and informal: formal contracts were managed in a context of ongoing conversations. Relationships between managers, notably those between commissioner and provider managers, were underpinned by (often long-established) trust. The accounts suggest that a common understanding of a particular problem, such as those outlined in the accounts, can play an important role in the co-ordination of services. The accounts also suggest that relationships can be simultaneously stable and fluid. Stable relationships included those based on ‘old PCT’ relationships, outlasting the commissioner–provider split. More fluid, or tactical, relationships were established for particular projects, for example involving Weight Watchers in the weight loss account. The tackling obesity account suggested that the latter, while tactical in the first instance, could lead to longer-lasting relationships.
Third, the view was expressed that competition could limit the sharing of information, and hence opportunities for knowledge creation. This said, managers believed that their informal networks had proved to be resilient, helping them to maintain services in a period of substantial organisational change.
Site 3 accounts
The health and well-being issue at site 3 was vascular disease prevention and the three accounts concern a neighbourhood health and well-being intervention, using national policies instrumentally to get initiatives off the ground, and bidding for project funding.
Health and well-being
This story is compiled from six interviews. A team was tasked with designing and co-ordinating a complex neighbourhood-based health and well-being intervention, for which funding had been made available. The account spans managers from the council, including adult services, sports divisions and councillors, a joint commissioning board and a joint public health team, PCT data analysts, community groups and voluntary organisations. Figure 14 shows the key fragments in sequence.
FIGURE 14.
Health and well-being project story flow chart.
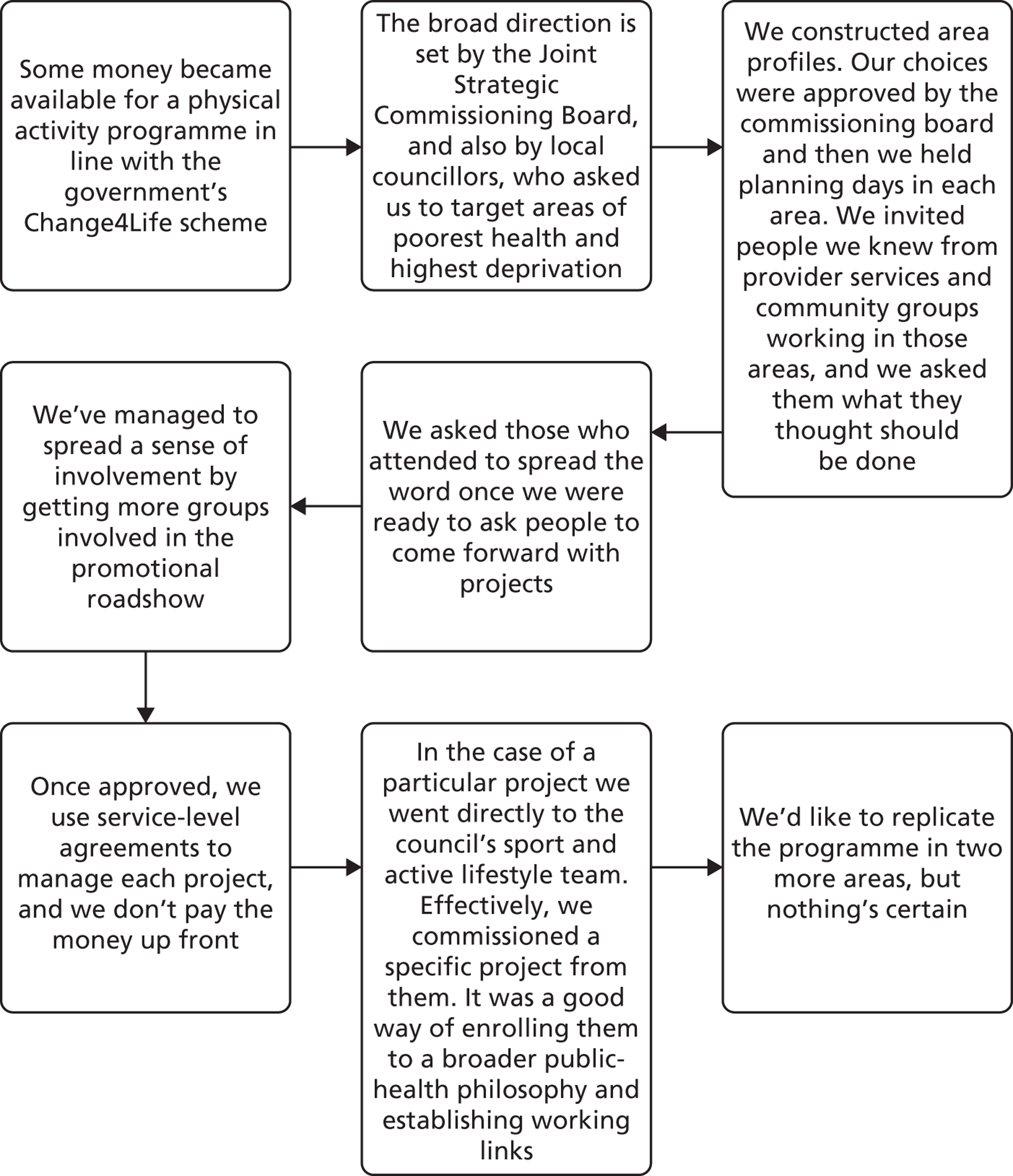
Once the funding had been secured, managers responsible for the new programme drew on the expertise of data analysts from the PCT to construct profiles for different neighbourhoods in the locality. These were used to decide which neighbourhoods should be included. The choices were approved by a commissioning board of senior managers from the council and the PCT. Said a middle manager:
We wanted to base it on evidence, look at the information around physical activity and nutrition, prevalence of heart disease, diabetes, deaths from those conditions, and . . . look at which areas seem to appear to be the worst . . . although I could access that information, I had asked the team to produce that information.
Then planning days were organised. The invitees included people from community groups and organisations who provided physical activity services (including voluntary, public and private organisations) in the selected neighbourhoods. The aim was to identify local priorities – activities that would have the greatest impact. One of the managers involved recalled that:
We then went into those three areas and asked people who worked in those areas what they thought needed to be delivered there . . .
and
We asked community development to make sure that they spread it amongst their networks as well, so that we weren’t missing any small or third sector organisations. We did get criticised to a certain extent that we didn’t take that as wide as we possibly could have done, but again time’s always an issue.
The programme team then issued a call for proposals: local service providers were invited to bid for money for specific physical activity projects.
We were asked to go away and do some further consultation . . . about who would be best placed to deliver the physical activity elements . . . so we went back into the communities and asked some people who were already doing physical activity . . . it was decided that the best people would be Sport and Active Lifestyles within the Council, so we asked them to develop a project proposal.
Manager
The commissioning board approved projects, and in so doing ensured that projects supported local strategic priorities:
The Joint Strategic Commissioning Board made the decision as to which projects would be funded to meet the objectives of the project, which were around preventing or reducing obesity and promoting healthy lifestyles.
Manager
Projects were managed using outcomes-based contracts:
Each project’s got a service level agreement that says this is what you will deliver and this is how much you will get paid, and you will get paid quarterly providing you are delivering on these things. If you stop delivering we’ll stop paying you, and that’s been very effective . . .
Manager
The contracts provided the basis for relationships between commissioners and service providers, but a broader, less formal set of relationships was created in the course of the programme:
A**** is the actual manager. We commission part of it from S***’s team. B*** and C**** work very closely with A**** on it. D**** does a lot of the intelligence around that particular project. We have been out to E****’s team and spoken to F**** and E**** about how he can give us some of their information . . . I could say yes definitely that we all come together.
Manager
Some groups felt excluded from the planning and bidding processes; it has been possible to involve them in a road show and by supporting them with in-kind resources. Equally, the projects have helped to create new relationships:
There’s quite good links there with a lot of different people just through one element of the [local] project.
Manager
This account starts with middle managers who had established relationships with one another being able to undertake initial analysis and gain approval for a particular type of intervention targeted on specific neighbourhoods. As the programme developed, managers were able to develop new relationships in the neighbourhoods, and then use the commissioning mechanism to ensure that the activities they wanted were delivered. The sources of knowledge included quantitative evidence about neighbourhoods, the views of neighbourhood residents, and the experience of providers in putting together bids and delivering services. These activities were couched within networks of informal relationships, involving regular exchanges of information about progress with contracts.
Using national policies
This story is compiled from six interviews. It concerns the implementation of elements of national stroke policies, and involves actors from the PCT, the council and a joint public health division accountable to both. Figure 15 shows the key fragments in sequence.
FIGURE 15.
Using national policies story flow chart.
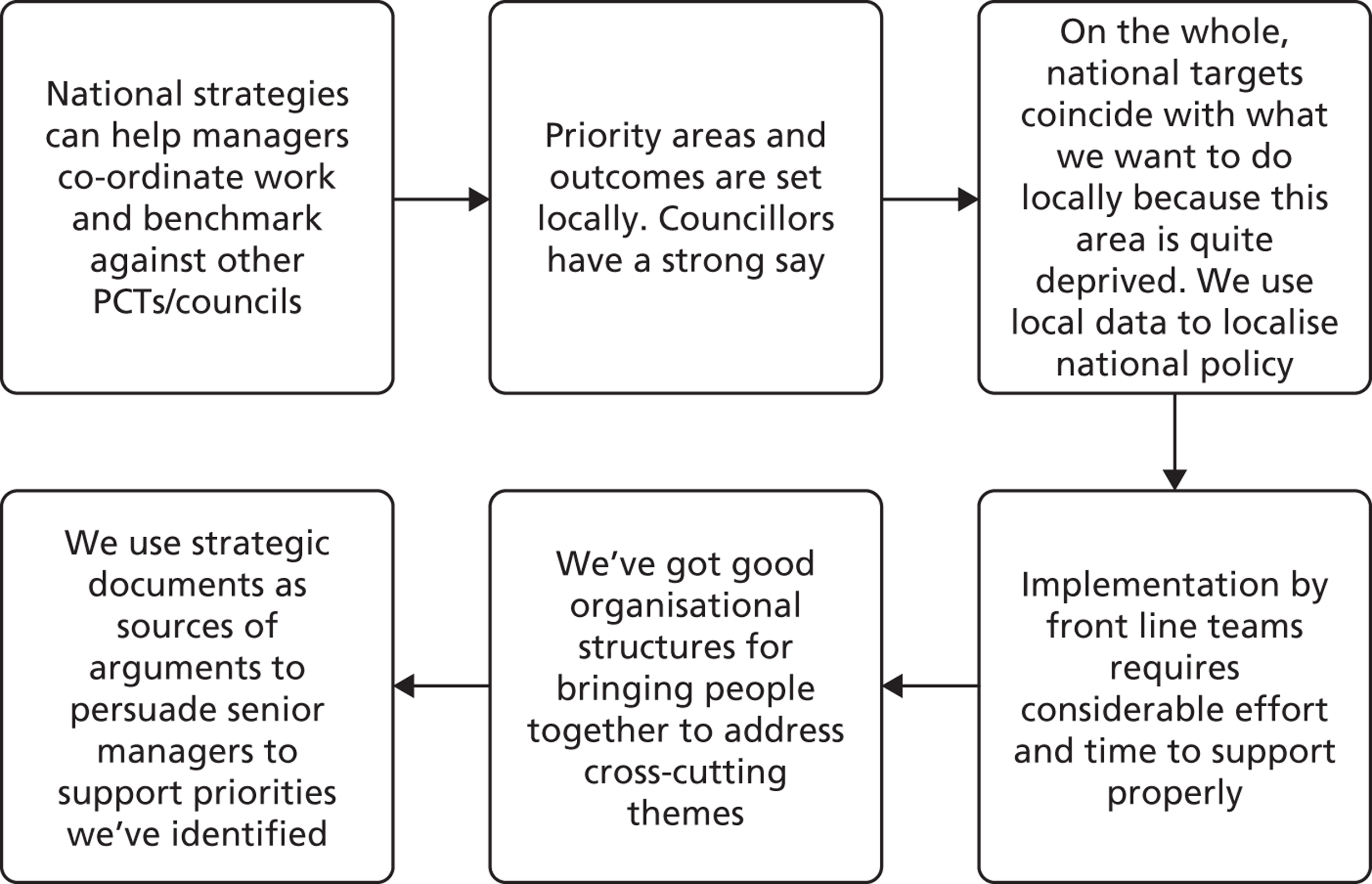
Site 3 has a number of wards with high deprivation scores. As a result, a number of national public health and social care policies in recent years have been helpful, insofar as they have encouraged targeting of resources on deprived areas. Local managers reported that, when they coincide with local needs, national policies could be useful in legitimising particular activities. If you have good working relationships with colleagues in other organisations, and regular meetings where opportunities can be discussed, it is possible to use national policies to mobilise around them. In those meetings:
I would maybe pitch it around something that is quite important. So ‘the Joint Strategic Needs Assessment has identified this’ or ‘the Health and Wellbeing Board are doing a piece of work around this’. Or ‘one of the corporate priorities is this’ . . .
Local manager
A manager observed that:
I think I know everybody, I can say ‘this piece of work needs x, y and z’ and they will come, you know, they’ll come to me and we’ll work together and we’ll get the piece of work done . . . the reason stroke has come to the forefront is because it’s been nationally driven, so all we’ve really done is just got the national policies and guidance and made it happen . . .
The involvement of council services requires a slightly different approach. Activities have to have more of a local feel because councillors need to be satisfied that a particular piece of work needs doing:
The council operates slightly differently . . . the councillors have more of a say about how things are done locally. But between the councillors and the directives that we are given from the Department of Health, there is the director level, that filters down into the teams . . . At least it shows we work together . . .
Manager
This account suggests that national policies can be used instrumentally by middle managers in localities, and as a source of information about good practice as well as legitimacy. Regular meetings are helpful: they are forums where new pieces of work can be discussed. Managers stressed the considerable amount of work needed to get new programmes off the ground: knowledge creation drew on a mix of evidence, including routine quantitative data and the experience of middle managers, who know how to ‘get things done’.
The bid
This account is compiled from three interviews with middle managers. It focuses on the preparation of a bid for funding for a project, co-ordinated by a middle manager from the public health team. It involves actors from the public health team, then still in the PCT, the council and a national charity. Figure 16 shows the key fragments in sequence.
FIGURE 16.
The bid story flow chart. DPH, Director of Public Health
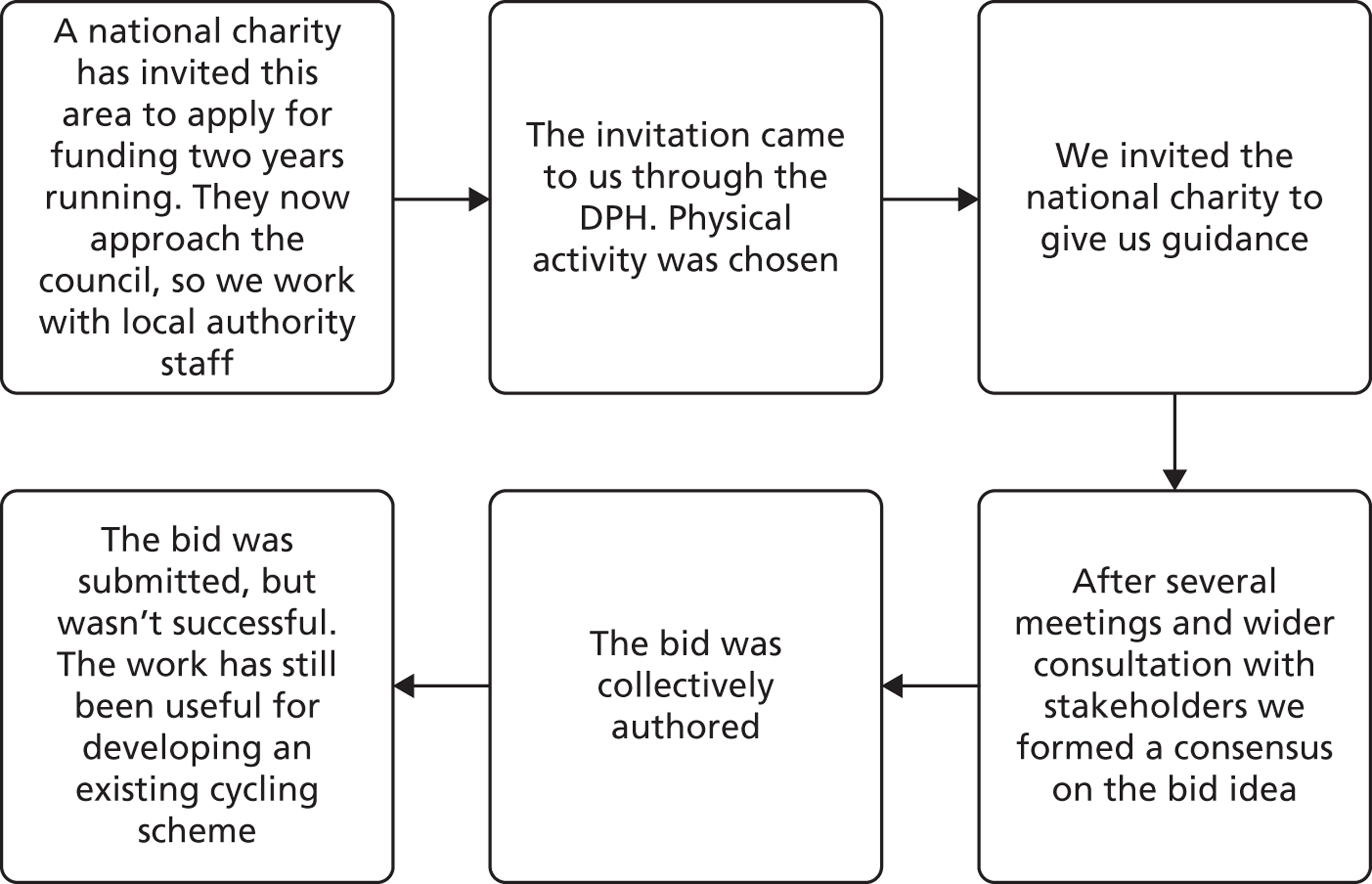
A national charity sometimes identifies localities where it wants to commit resources, and invites local public health teams to bid for them. Site 3 was invited to prepare such a bid. The timescale was tight, and this was therefore a test of local relationships:
[A middle manager] co-ordinated a bit of a subgroup to start with, to see if we had any plans or ideas that we could put forward . . . several meetings later we formulated an application . . . there was a number of local authority and PCT staff [involved].
We pulled in one or two other people to come to the group once we’d got more of a firmed up idea of the direction of travel that we wanted to go.
Manager
Reflecting on the preparation of the bid, one manager observed that the quality of the co-ordinator’s relationships had been important:
She’s obviously got the contacts got the networks, myself included, and obviously several others . . .
Manager
The topic for the bid was scoped and then further narrowed on the basis of the information and skills available to the working group. In the event the bid was not successful and the project group was disbanded. However, managers involved in the bid felt that it had been a valuable exercise, not least because they had been able to use some of the learning in another local scheme.
This account suggests that relationships developed in relatively short periods of time can have lasting value. Managers were able to transfer knowledge created collectively during the preparation of the bid to an unrelated topic area: a cycling scheme. That is, their relatively abstract ‘thinking through’ of ideas was translated into practical action in another context.
Reflections on the site 3 accounts, and overall
The three site 3 accounts have a number of features in common. As in sites 1 and 2, middle managers drew upon different types of information, including routine quantitative data, and synthesised the information in the course of knowledge creation. They were also able to reconcile national and local strategic priorities with operational realities. They used different kinds of knowledge in their discussions and negotiations, including both technical and prudential knowledge. The site 3 accounts highlight the importance of agency – individuals playing key roles – particularly in the funding bid, but once again collective working relationships were emphasised.
Again as in sites 1 and 2, relationships spanned public, private and voluntary organisations. They were simultaneously formal and informal: formal contracts were managed in the context of ongoing conversations. Relationships between managers, notably those between commissioner and provider managers, were based on trust, but in site 3 the legitimising and mobilising role of national policies was also emphasised.
Looking ahead
This chapter has presented nine accounts, three from each of our study sites. As discussed in Chapter 2, our study design has two main pillars – these accounts and network analysis. It is to the network analysis that we will now turn, before considering what the two together tell us in Chapter 7.
Chapter 6 Network modelling and analysis
Introduction
This chapter presents the results of the network analysis and modelling for our three study sites. For each site, we describe the networks and compare them with the initial landscape mapping results. We present summary network measures and more comprehensive modelling results.
As described in Chapter 2, the diagrams illustrate the results of our latent space cluster modelling. It is useful to recap what the diagrams in this chapter will show. A symbol within a small circle represents a person and shows which organisation they work for. A dashed line (link) between two symbols indicates a relationship: it shows that one person has identified the other as someone that they talk with or go to in order to get things done. People are placed closer together if they are more likely to be linked.
Our modelling was also designed to reveal clusters which represent the joint action and interaction within groups of people. Clusters of people are represented by the shaded areas which are separated by white space. People are shown as belonging to a single cluster. The closer they are positioned to the centre of the cluster, the more strongly they are associated with that cluster. People at the fringes are more weakly associated with that cluster.
Site 1 results
As described in Chapter 5, the health and well-being issue for site 1 was tobacco control, and we asked interviewees who they talked with/went to about reducing the prevalence of smoking across the local area. Individuals from the following organisations were named:
-
NHS PCT
-
NHS community service provider (providing community-based health improvement services)
-
NHS acute hospital trust
-
local government authority
-
regional trading standards
-
fire service
-
probation trust
-
police
-
private sector organisations licensed to provide goods and services (taxis, pubs, clubs)
-
a voluntary sector organisation (providing training to parents on the harms of second-hand smoke).
The majority of these organisations were included in our landscape maps, with the exception of regional trading standards, the voluntary sector organisation, police and the private sector organisations. This suggests that the relevance of these organisations to tobacco control was hidden from our landscape interviewees. By referring back to our landscape maps, we are also able to note the absence of the long-term conditions department of the PCT from our network data and the absence of GPs from our ‘Goes To’ network data. This suggests that these organisations/groups play lesser roles in exchanging and creating knowledge about tobacco control than our landscape interviewees supposed.
The ‘Talks With’ network generated from data collected at time 1 is in Figure 17. The network comprised 61 people with 124 connections between them. A total of three clusters represent the situation well, as the clusters are well separated. Each cluster has a core of strong connections with fewer connections between clusters.
FIGURE 17.
’Talks With’ network for site 1 time 1.
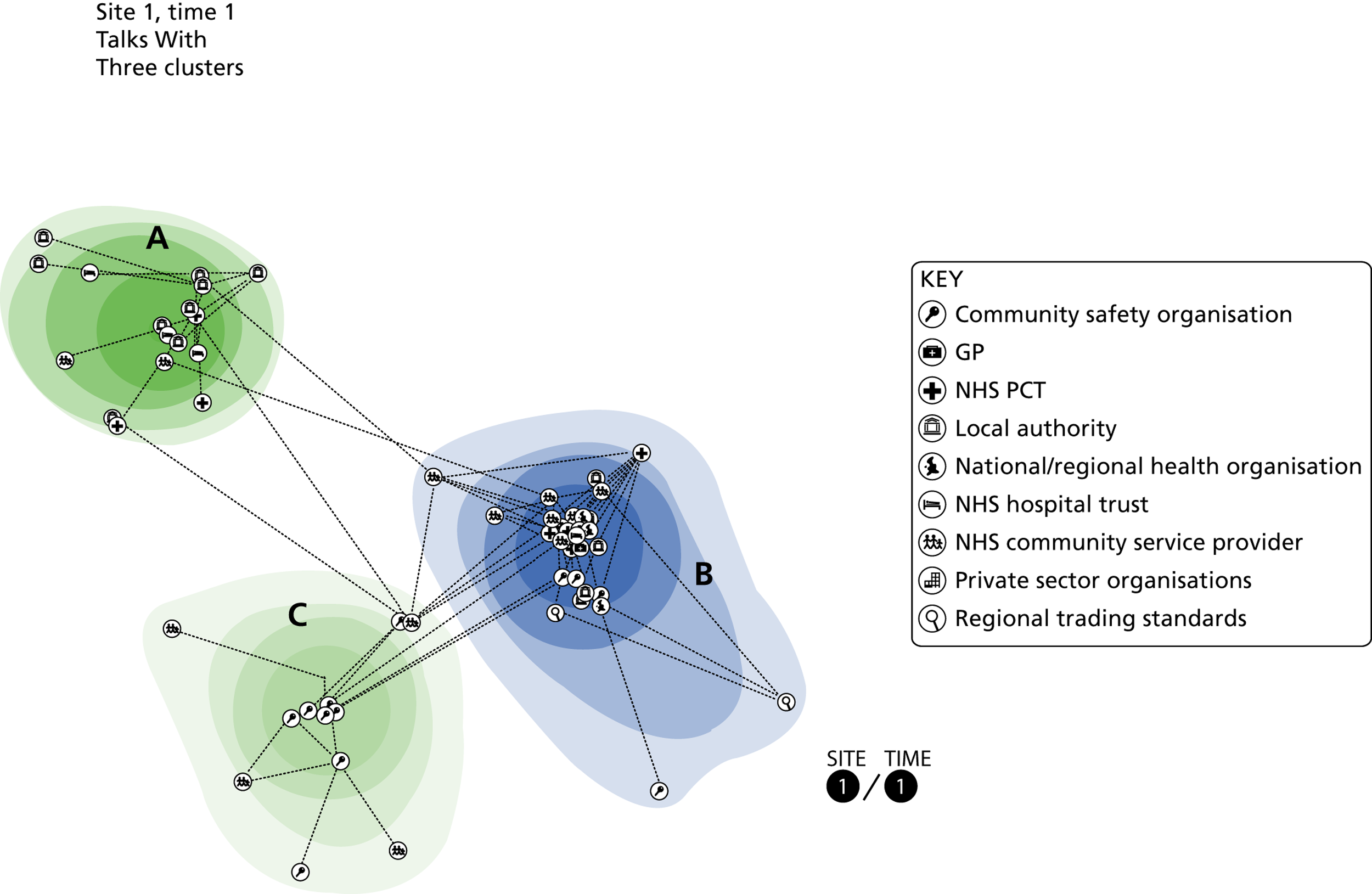
The ‘Talks With’ network for site 1 generated from data collected at time 2 is in Figure 18. The network comprised 68 people with 165 connections between them. Four well-separated clusters can be identified, each of which has a core of strong connections with fewer between clusters.
FIGURE 18.
’Talks With’ network for site 1 time 2, showing four clusters.
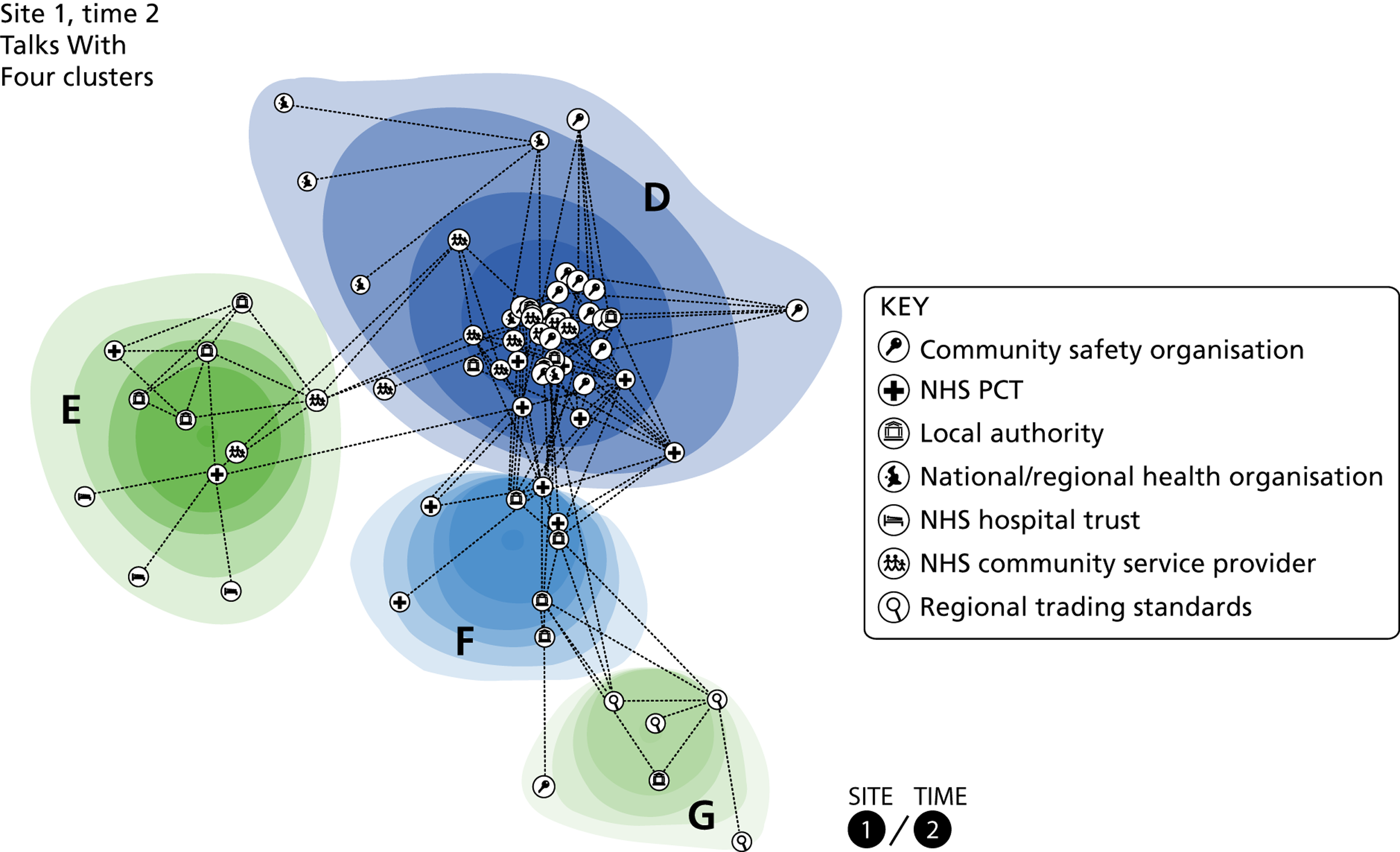
Table 2 shows key individuals, identified by their betweenness and centrality scores (their rank within the network is shown in brackets). This shows that while some individuals (actors 2 and 3) are key bridges at both time points, others are prominent at only one time point. Similarly, some individuals are central to the network at both time points (actors 1 and 2), while the centrality of others changes between time points.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | Community services | 379.96 (6) | 1033.291 (1) | 0.278 (4) | 0.381 (2) |
| 2 | PCT | 415.831 (4) | 726.981 (2) | 0.333 (2) | 0.389 (1) |
| 3 | Community services | 691.967 (1) | 526.25 (3) | 0.213 (10) | 0.14 (14) |
| 4 | Local authority | 234.422 (7) | 436.559 (4) | 0.272 (6) | 0.198 (9) |
| 5 | PCT | N/A | 358.801 (5) | N/A | 0.287 (4) |
| 6 | Local authority | 641 (2) | 51.917 (8) | 0.037 (30) | 0.038 (38) |
| 7 | PCT | 638.227 (3) | 241.206 (22) | 0.465 (1) | 0.262 (5) |
The ‘Talks With’ network changed substantially between time 1 and time 2 – Table 2 tracks the movement of people from clusters A, B and C at time 1 to D, E, F and G at time 2. The numbers of actors and links were similar but the cast of actors changed, with 37 leaving and 44 new actors entering (Table 3). Only 24 individuals appear in both networks and 12 of these were necessarily included because they were interviewed.
| Cluster | D | E | F | G | Exit | Total |
|---|---|---|---|---|---|---|
| A | 2 | 3 | 0 | 0 | 12 | 17 |
| B | 9 | 1 | 3 | 2 | 16 | 31 |
| C | 4 | 0 | 0 | 0 | 9 | 13 |
| Enter | 27 | 8 | 5 | 4 | 44 | |
| Total | 42 | 12 | 8 | 6 | 37 | 105 |
It helps to provide further details about the make-up of the clusters with respect to the organisations, roles and seniority of cluster members. Table 4 shows that, at time 1, both the network as a whole and each cluster are dominated by middle managers. Cluster B contains the majority of senior managers, suggesting that senior people tended at that time to talk more with their peers. Further consideration of the membership of each cluster shows that:
-
Cluster A comprises managers and frontline staff from a range of organisations who have an identifiable focus on child and maternal health (e.g. children’s centres or school nursing).
-
Cluster B is dominated by individuals from a range of organisations with an identifiable role in tobacco control (e.g. members of the local Tobacco Alliance, local operational smoking cessation group or regional tobacco control groups).
-
Cluster C is dominated by individuals from community safety organisations (fire service and probation service).
| Time 1 | A | B | C | Total | Time 2 | D | E | F | G | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 1 | 10 | 0 | 11 | Senior manager | 5 | 1 | 4 | 0 | 10 |
| Middle manager | 11 | 20 | 9 | 40 | Middle manager | 24 | 4 | 3 | 3 | 34 |
| Frontline staff | 5 | 1 | 4 | 10 | Frontline staff | 13 | 7 | 1 | 3 | 24 |
| Total | 17 | 31 | 13 | 61 | Total | 42 | 12 | 8 | 6 | 68 |
At time 2, membership lists for each cluster show that:
-
Cluster D comprises those with an identifiable role in tobacco control (as members of the local Tobacco Alliance and local operational smoking cessation group) as well as those who work in the areas of environmental health or community safety (fire service or probation service).
-
Cluster E comprises frontline staff and middle managers from a range of organisations who have an identifiable focus on child and maternal health (e.g. children’s centres or school nursing.)
-
Cluster F is dominated by managers from the local authority and PCT.
-
Cluster G comprises frontline staff and middle managers with an identifiable focus on illicit and illegal goods and activity (trading standards or police).
These descriptions show that, while the cast of actors in the network and across clusters has substantially changed, there is temporal stability of the activities attributed to clusters.
The ‘Goes To’ network generated from data collected at time 1 is shown in Figure 19. The network comprised 64 people with 127 connections between them and is best represented as three clusters. The ‘Goes To’ network at time 2 is shown in Figure 20. This comprised 71 people with 142 connections between them. Again, this is best represented as three clusters.
FIGURE 19.
’Goes To’ network for site 1 time 1, showing three clusters.
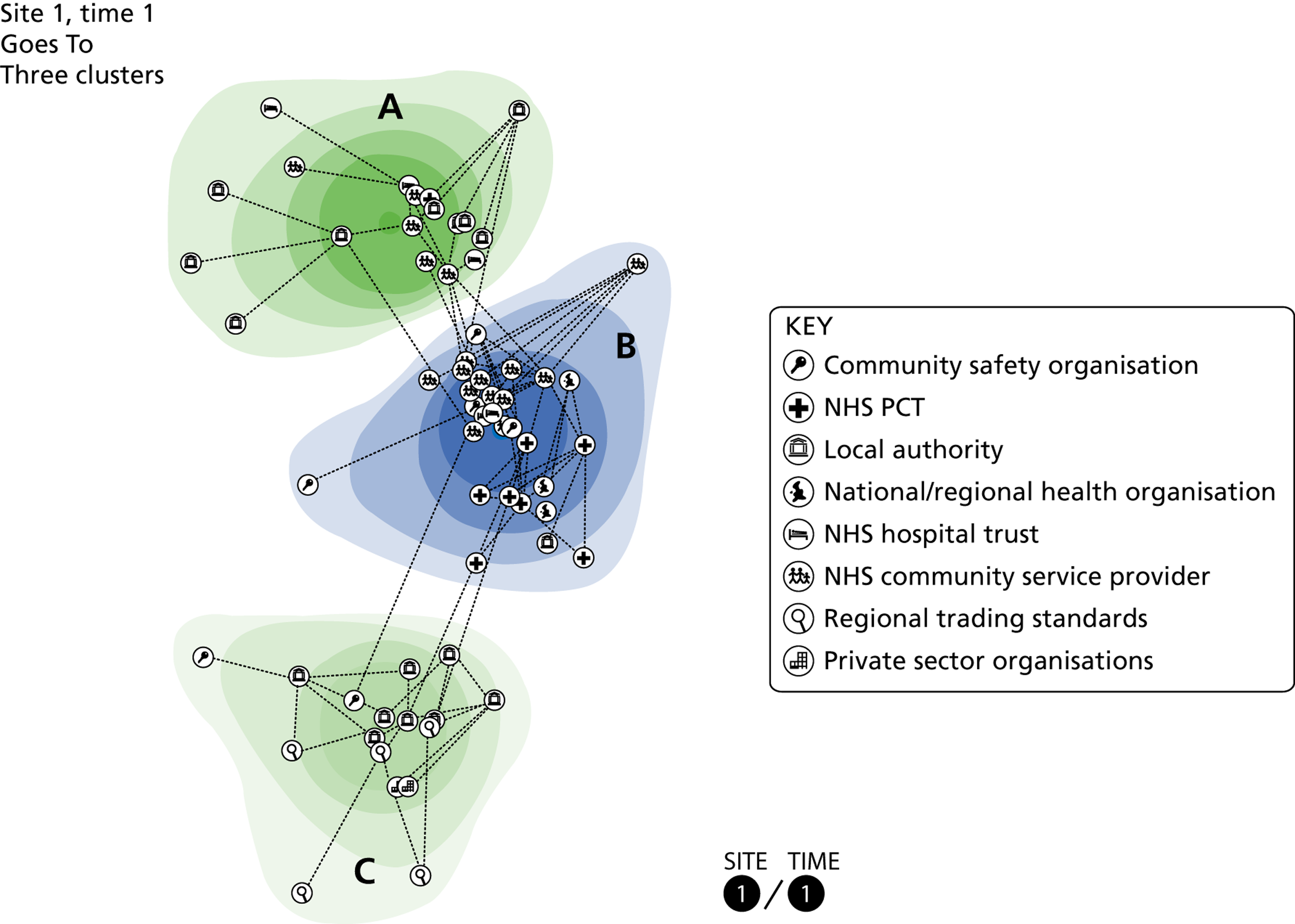
FIGURE 20.
’Goes To’ network for site 1 time 2, showing three clusters.
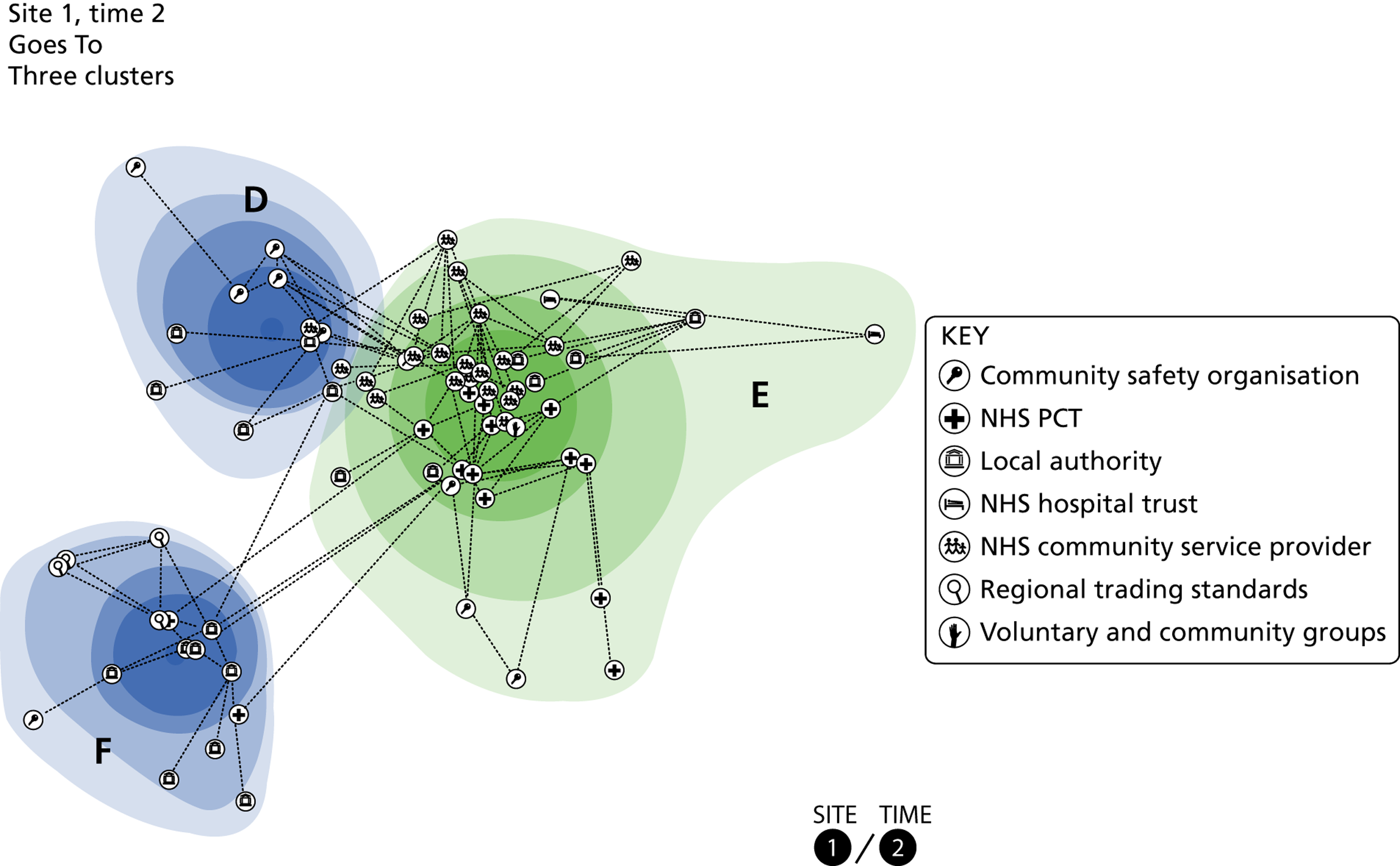
Table 5 below shows that the actors who act as bridges within the ‘Talks With’ network also act as important bridges in the ‘Goes To’ network. Their roles as bridges also remain fairly consistent over time, and centrality scores are also consistent.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | Community services | 839.835 (1) | 1044.415 (1) | 0.452 (1) | 0.453 (1) |
| 2 | PCT | 769.279 (2) | 785.83 (2) | 0.375 (2) | 0.336 (3) |
| 3 | Community services | 368.383 (5) | 635.522 (4) | 0.147 (16) | 0.149 (14) |
| 4 | Local authority | 515.5 (3) | 676 (3) | 0.031 (34) | 0.052 (30) |
| 5 | PCT | 473 (4) | 313 (8) | 0.111 (17) | 0.1 (18) |
| 6 | Local authority | 245.3 (7) | 352.022 (6) | 0.075 (22) | 0.035 (34) |
Table 6 shows that there was a substantial change of actors between time 1 and time 2, along with a substantial flow of actors between clusters. Of 105 people listed in the two networks, only 30 appear at both time points. There have also been substantial changes to the links between individuals in the network, with only 20 of the 128 links between consistent network members remaining at time 2. This shows that not only have the individuals involved in the network changed, but the relationships between actors have also changed.
| Cluster | D | E | F | Exit | Total |
|---|---|---|---|---|---|
| A | 0 | 5 | 0 | 13 | 18 |
| B | 1 | 14 | 0 | 14 | 29 |
| C | 4 | 0 | 6 | 7 | 17 |
| Enter | 7 | 26 | 8 | 41 | |
| Total | 12 | 45 | 14 | 34 | 105 |
Examining the make-up of the clusters with respect to organisations, roles and seniority shows that the number and spread of managers and frontline staff are remarkably similar at each time point (Table 7). At time 1, middle managers dominate clusters A and C with cluster B (which acts as a link between clusters A and C) containing a mix of seniorities. Further consideration of cluster membership shows that:
-
Cluster A comprises managers and frontline staff involved with child and maternal health (e.g. children’s centres, school nursing or midwifery).
-
Cluster B is dominated by individuals from a range of organisations with an identifiable role in tobacco control and smoking cessation (e.g. members of the local Tobacco Alliance, smoking cessation service or regional tobacco control groups).
-
Cluster C comprises middle managers and frontline staff with a focus on illicit and illegal goods and activity (trading standards or police) and the enforcement of health-related legislation (environmental health) along with those licensed to provide goods and services (taxis, pubs or clubs).
| Time 1 | A | B | C | Total | Time 2 | D | E | F | Total |
|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 2 | 7 | 0 | 9 | Senior manager | 1 | 8 | 0 | 9 |
| Middle manager | 10 | 12 | 13 | 35 | Middle manager | 6 | 25 | 8 | 39 |
| Frontline staff | 6 | 10 | 4 | 20 | Frontline staff | 5 | 12 | 6 | 23 |
| Total | 18 | 29 | 17 | 64 | Total | 12 | 45 | 14 | 71 |
At time 2, middle managers dominate cluster E (which acts as a link between clusters D and F). The majority of senior managers are also included within this central cluster. Membership lists for each cluster show that:
-
Cluster D comprises managers and frontline staff dealing with the enforcement of health-related legislation (environmental health) and individuals from the fire service. Note that the former are positioned very close to cluster E.
-
Cluster E includes individuals from a range of organisations with an identifiable role in tobacco control and smoking cessation (e.g. members of the local Tobacco Alliance, smoking cessation service or regional tobacco control groups) along with those involved with child and maternal health.
-
Cluster F has managers and frontline staff with an identifiable focus on illicit and illegal goods and activity (trading standards or police).
Despite the high turnover of actors, there is temporal stability of activities attributed to clusters. Our descriptions of the clusters also suggest that there is equivalence match between clusters across the two networks in terms of the activities attributed to them. Table 8 and Table 9 examine this relationship. At time 1, most of the common actors from the cluster B ‘Talks With’ network match to cluster B in the ‘Goes To’ network. Similarly, actors from cluster A in the ‘Talks With’ network match to cluster A in the ‘Goes To’ network.
| Goes To | ||||||
|---|---|---|---|---|---|---|
| Talks With | Cluster | A | B | C | Exit | Total |
| A | 5 | 0 | 0 | 12 | 17 | |
| B | 1 | 14 | 7 | 9 | 31 | |
| C | 0 | 3 | 0 | 10 | 13 | |
| Enter | 12 | 12 | 10 | 34 | ||
| Total | 18 | 29 | 17 | 31 | 95 | |
At time 2 we see a similar pattern. Actors from clusters D and F in the ‘Talks With’ network match to cluster E in the ‘Goes To’ network. They are joined by actors from cluster E in the ‘Talks With’ network. Actors from cluster G in the ‘Talks With’ network match to cluster F in the ‘Goes To’ network.
| Goes To | ||||||
|---|---|---|---|---|---|---|
| Talks With | Cluster | D | E | F | Exit | Total |
| D | 8 | 16 | 1 | 17 | 42 | |
| E | 0 | 4 | 0 | 8 | 12 | |
| F | 0 | 3 | 2 | 3 | 8 | |
| G | 0 | 0 | 6 | 0 | 6 | |
| Enter | 4 | 22 | 5 | 31 | ||
| Total | 12 | 45 | 14 | 28 | 99 | |
Summary of findings for site 1
Both the ‘Talks With’ and ‘Goes To’ networks maintained a similar size at the second time point. This disguises the fact that for both there was a very considerable change in the people nominated by the interviewees. Despite this, the ‘Talks With’ network contained a cluster associated with child and maternal health and a cluster associated with tobacco control at both times. The ‘Goes To’ network had clusters associated with tobacco control and with illicit and illegal tobacco at both times. GPs are missing from the ‘Goes To’ network at both times.
Site 2 results
The health and well-being issue for site 2 was health improvement, and we asked interviewees who they talked with/went to about planning lifestyle interventions which would be relevant to the needs of local communities. Individuals from the following organisations were named:
-
NHS PCT
-
NHS community service provider (providing community-based health improvement services)
-
NHS acute hospital trust [providing acute services and community-based services for adults and children (e.g. health visiting or school nursing)]
-
local government authority
-
schools
-
NHS regional health authority
-
voluntary and community groups working with specific populations/areas (e.g. minority ethnic groups or areas of high deprivation)
-
private sector organisations including the local press and specialist consultants.
There were few differences between our landscape maps and network data: our landscape interviewees had a relatively good overview of the different organisations involved in exchanging and creating knowledge locally. The exception was the private sector organisations not included in our landscape maps. This suggests that our landscape interviewees might not have appreciated the relevance of these organisations to their local knowledge creation efforts.
The ‘Talks With’ network generated from data collected at time 1 is shown in Figure 21. The network comprised 91 people with 183 connections between them. A total of three clusters represent the situation well.
FIGURE 21.
‘Talks With’ network for site 2 time 1, showing three clusters.
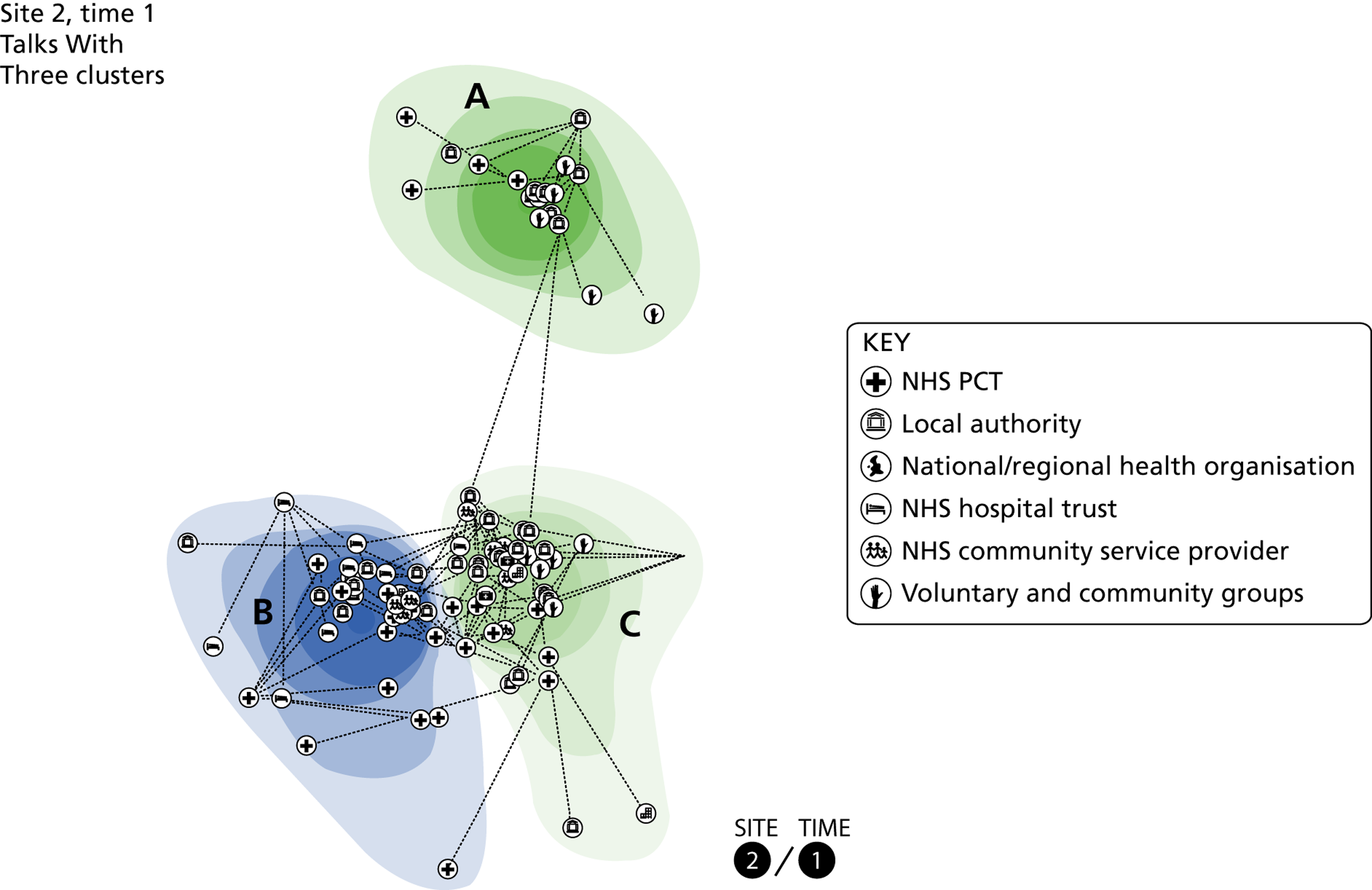
Figure 22 shows the ‘Talks With’ network generated from data collected at time 2. This comprised 83 people with 207 connections between them. Four well-separated clusters can be identified.
FIGURE 22.
‘Talks With’ network for site 2 time 2, showing four clusters.
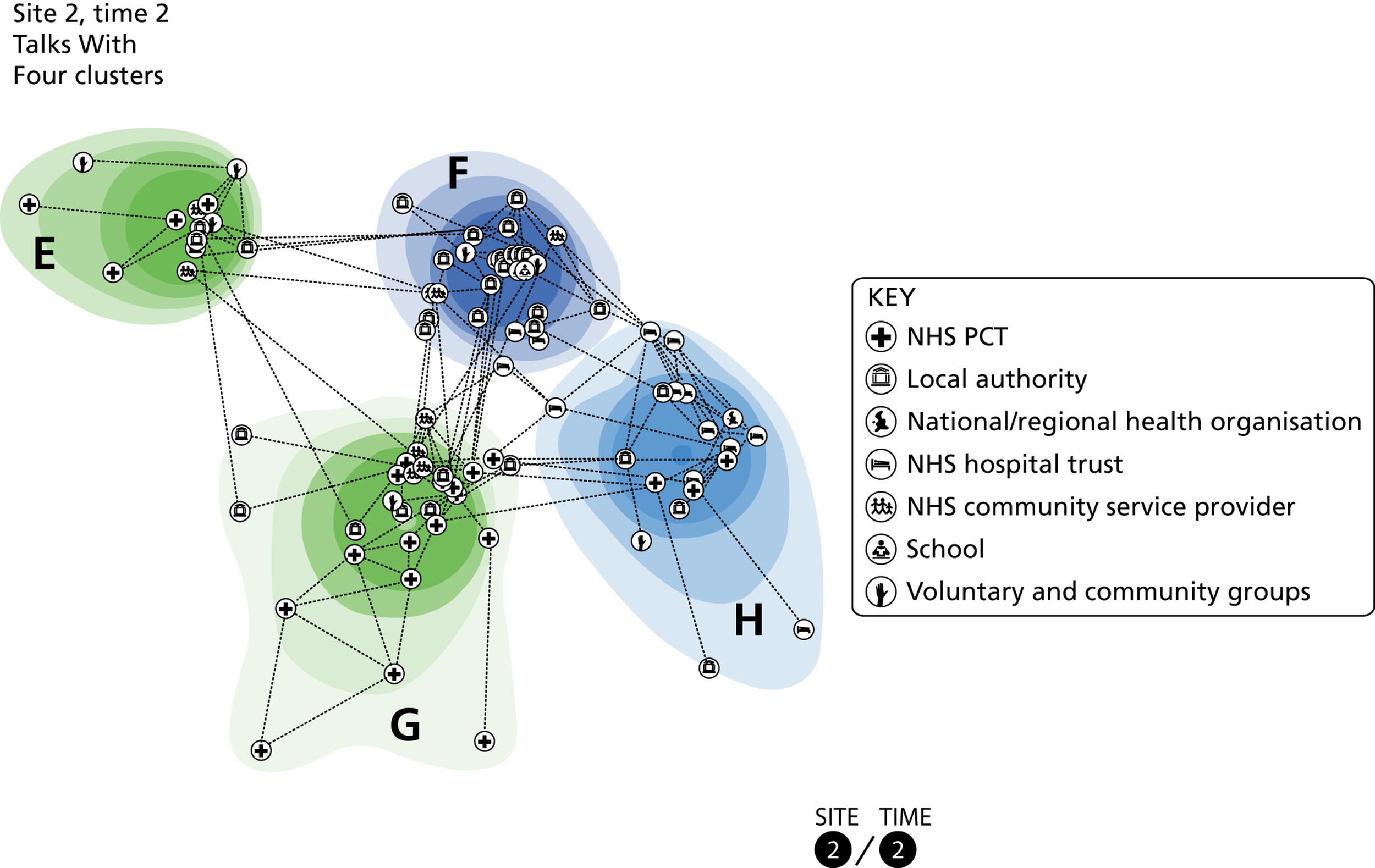
Table 10 below shows that some actors retain their key role as bridges between times, while others do not. Some also have similar centrality at both times, while others do not.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | PCT | 786.653 (1) | 990.277 (1) | 0.365 (1) | 0.438 (1) |
| 2 | Local authority | 435.815 (7) | 888.977 (2) | 0.2071 (10) | 0.172 (11) |
| 3 | PCT | 778.862 (2) | 665.889 (3) | 0.364 (2) | 0.35 (2) |
| 4 | Hospital | 304.567 (12) | 573.997 (4) | 0.036 (40) | 0.157 (12) |
| 5 | Local authority | 244.5 (20) | 410.761 (6) | 0.0341 (42) | 0.033 (52) |
| 6 | Local authority | 338.133 (8) | 401.876 (7) | 0.244 (6) | 0.248 (6) |
| 7 | Local authority | 649.232 (4) | 147.209 (19) | 0.135 (13) | 0.04 (41) |
Although the number of actors decreased at the second time, the number of connections between actors increased, resulting in a significant increase in density. As with site 1, the cast of actors in the network has substantially changed, with 45 actors leaving the network and 37 actors entering the network at time 2 (Table 11).
| Cluster | E | F | G | H | Exit | Total |
|---|---|---|---|---|---|---|
| A | 5 | 0 | 2 | 0 | 11 | 18 |
| B | 1 | 0 | 6 | 11 | 15 | 33 |
| C | 0 | 11 | 9 | 1 | 19 | 40 |
| Enter | 7 | 12 | 11 | 7 | 37 | |
| Total | 13 | 23 | 28 | 19 | 45 | 128 |
Seniority by cluster is provided by Table 12.
| Time 1 | A | B | C | Total | Time 2 | E | F | G | H | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 8 | 16 | 12 | 36 | Senior manager | 3 | 4 | 13 | 8 | 28 |
| Middle manager | 7 | 13 | 17 | 37 | Middle manager | 4 | 8 | 9 | 9 | 30 |
| Frontline staff | 3 | 4 | 11 | 18 | Frontline staff | 6 | 11 | 6 | 2 | 25 |
| Total | 18 | 33 | 40 | 91 | Total | 13 | 23 | 28 | 19 | 83 |
Further detail about the role and make-up of each cluster is:
-
Cluster A is well separated from the other two clusters and is dominated by managers commissioning adult health and social care services. There also appears to be a focus on disability.
-
Cluster B comprises senior managers from the PCT and local authority (e.g. chief executive or finance director) and managers with an identifiable focus on child and maternal health (e.g. children’s community health services or midwifery).
-
Cluster C links clusters A and B. It comprises individuals from a wide range of organisations (including voluntary and community groups), many of whom have a focus on health improvement, public health or sport and physical activity.
-
Cluster E is well separated from the others and contains individuals with a mixture of roles, including those who commission adult health and social care services, provide disability services and commission and provide cardiology and stroke services.
-
Cluster F comprises managers with a focus on health improvement and sport and physical activity.
-
Cluster G is well connected to cluster F, and together they link clusters E and H. The cluster comprises managers focused on public health, and senior managers from the PCT and local authority.
-
Cluster H comprises managers with an identifiable focus on child and maternal health.
FIGURE 23.
‘Goes To’ network for site 2 time 1, showing four clusters.
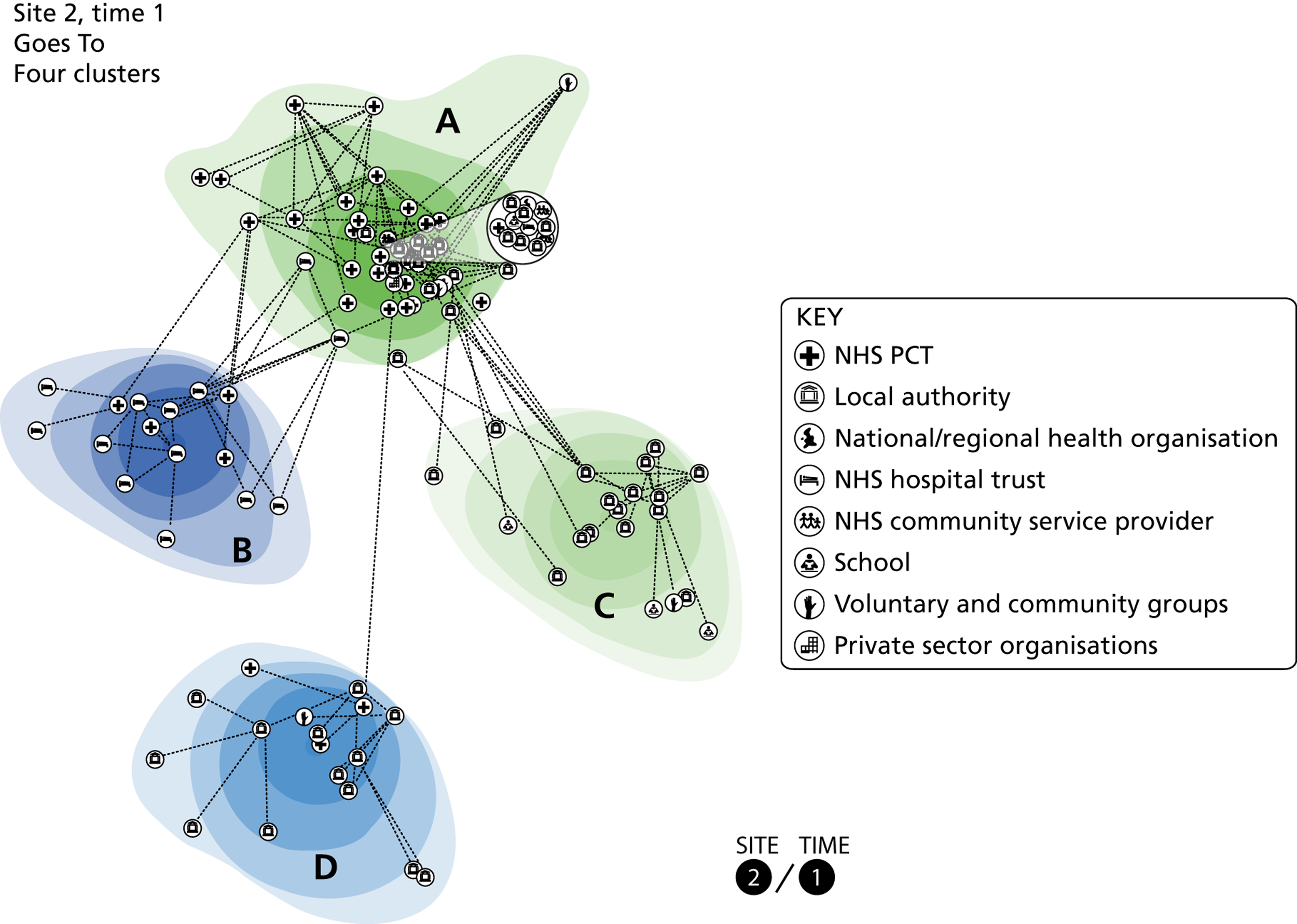
The ‘Goes To’ network generated from data collected at time 1 is shown in Figure 23. The network comprised 108 people with 215 connections between them and is best represented as four clusters. The ‘Goes To’ network at time 2 is shown in Figure 24. This comprised 91 people with 162 connections between them and is also best represented as four clusters. Both numbers and density of connections decrease.
FIGURE 24.
‘Goes To’ network for site 2 time 2, showing four clusters.
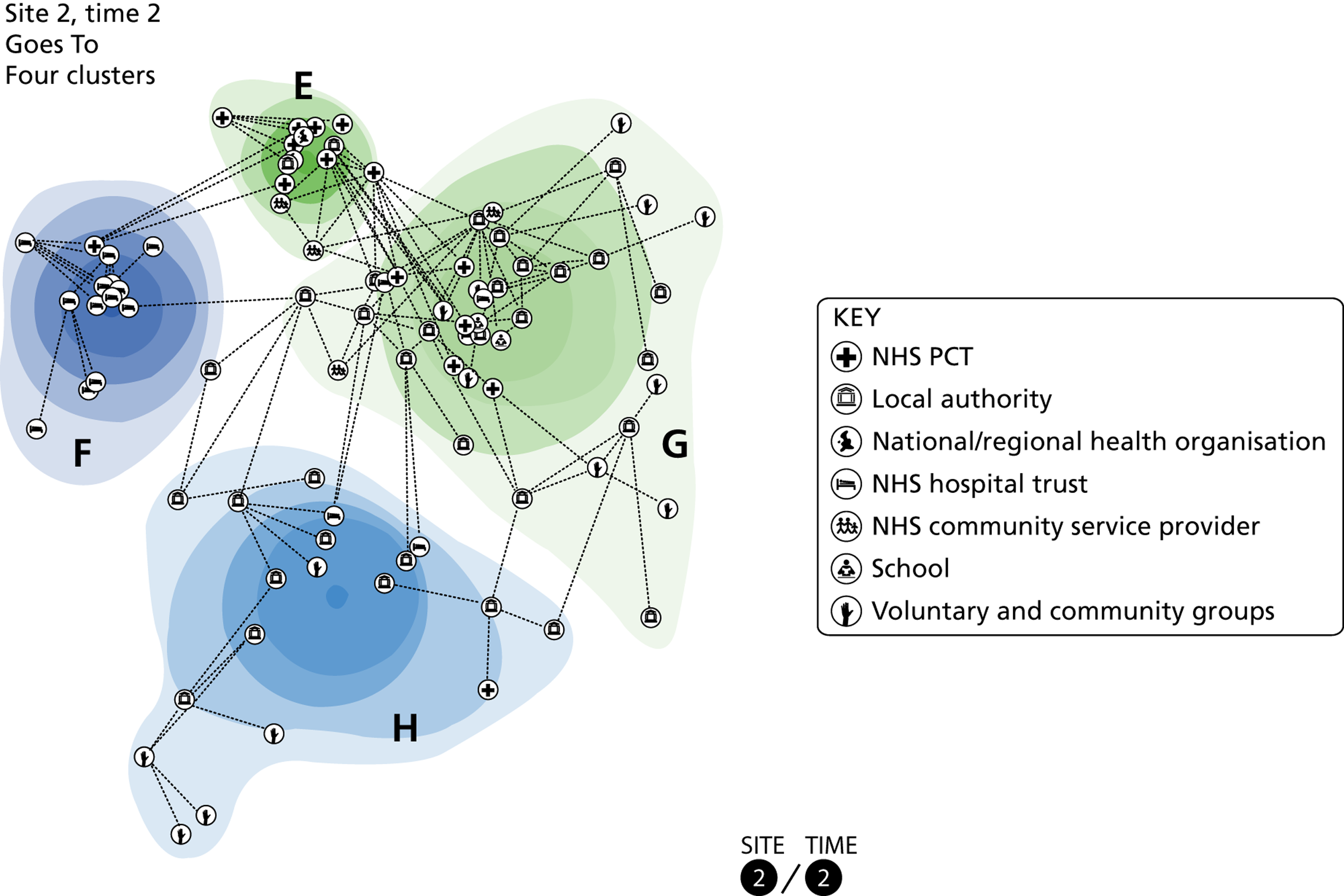
Table 13 shows that individuals who played a key role as bridges within the ‘Talks With’ network play a lesser role within the ‘Goes To’ network. Some continue to possess high centrality (which persists across networks and time), while others do not.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | PCT | 524.968 (9) | 693.694 (3) | 0.4572 (1) | 0.426 (1) |
| 2 | Local authority | 535.543 (7) | 97.528 (34) | 0.101 (20) | 0.1571 (10) |
| 3 | PCT | 568.996 (5) | 705.125 (2) | 0.278 (3) | 0.4 (2) |
| 4 | Hospital | 0 | 238.173 (20) | 0.003 (84) | 0.026 (37) |
| 5 | Local authority | 269 (21) | 627 (5) | 0.0021 (87) | 0.036 (33) |
| 6 | Local authority | 416.418 (14) | 220.055 (22) | 0.0971 (21) | 0.2911 (6) |
| 7 | Local authority | 655.294 (3) | 289.481 (14) | 0.114 (15) | 0.0431 (31) |
Table 14 shows that there has been a substantial change of actors between time 1 and time 2: 54 people exit the network and 37 enter. While there is flow between the clusters at time 1 and time 2, this mainly affects cluster A (whose members disperse between clusters E, G and H or exit the network) and cluster D (who mainly exit the network). The majority of cluster B remain together in cluster F and the majority of cluster C remain together in cluster G.
| Cluster | E | F | G | H | Exit | Total |
|---|---|---|---|---|---|---|
| A | 9 | 1 | 9 | 6 | 31 | 56 |
| B | 1 | 10 | 0 | 1 | 3 | 15 |
| C | 0 | 0 | 11 | 1 | 8 | 20 |
| D | 0 | 0 | 1 | 4 | 12 | 17 |
| Enter | 4 | 6 | 18 | 9 | 37 | |
| Total | 14 | 17 | 39 | 21 | 54 | 145 |
Table 15 shows that at time 1 the majority of senior managers are situated in cluster A. At time 2 they constitute the largest group in cluster E, suggesting some attribute matching between these clusters. Similarly, frontline staff dominate clusters C and G, suggesting matching between these clusters.
| Time 1 | A | B | C | D | Time 2 | E | F | G | H | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 19 | 6 | 2 | 7 | 34 | Senior manager | 8 | 8 | 3 | 7 | 26 |
| Middle manager | 24 | 7 | 6 | 9 | 46 | Middle manager | 6 | 7 | 16 | 8 | 37 |
| Frontline staff | 13 | 2 | 12 | 1 | 28 | Frontline staff | 0 | 2 | 20 | 6 | 28 |
| Total | 56 | 15 | 20 | 17 | 108 | Total | 14 | 17 | 39 | 21 | 91 |
As there is some matching between clusters in terms of their membership at the two times, it is useful to examine the role and make-up of the clusters further.
-
Cluster A is a central cluster in that it is the only cluster to which the remaining clusters link. The cluster comprises actors from a range of organisations, many of whom have a focus on health improvement and health inequalities (e.g. community weight management services and community groups from deprived areas). The NHS and local authority public health managers included in the network are also included.
-
Clusters B and F comprise managers and frontline staff involved with child and maternal health (e.g. children’s community health services or midwifery).
-
Cluster C is dominated by managers and frontline staff in sport-related roles (e.g. leisure facility managers or school sport development officers).
-
Cluster D comprises managers with an identifiable focus on providing and commissioning adult social care services (e.g. disability services).
-
Cluster E comprises senior and middle managers who have come from cluster A, the majority of whom have an identifiable focus on public health.
-
Cluster G comprises actors from a range of organisations, with the largest identifiable group sharing a common focus on sport and physical activity. The cluster is similar to cluster C, but also includes managers with a specific focus on obesity and weight management.
-
Cluster H comprises managers and frontline staff with a focus on adult social care services and community initiatives.
In addition to the stability of attributed action between clusters across time within each network, our descriptions of each cluster also suggest that there may be strong similarities between the clusters across the two networks. Table 16 and Table 17 add to this interpretation. There are matching clusters for adult health and social care and for child and maternal health at time 1. At time 2, clusters match for action in sport and physical activity and for managers involved with public health.
| Goes To | |||||||
|---|---|---|---|---|---|---|---|
| Talks With | Cluster | A | B | C | D | Exit | Total |
| A | 1 | 0 | 1 | 9 | 7 | 18 | |
| B | 11 | 8 | 0 | 0 | 14 | 33 | |
| C | 25 | 0 | 1 | 0 | 14 | 40 | |
| Enter | 19 | 7 | 18 | 8 | 52 | ||
| Total | 56 | 15 | 20 | 17 | 35 | 143 | |
| Goes To | |||||||
|---|---|---|---|---|---|---|---|
| Talks With | Cluster | E | F | G | H | Exit | Total |
| E | 0 | 0 | 4 | 4 | 5 | 13 | |
| F | 1 | 1 | 14 | 2 | 5 | 23 | |
| G | 9 | 0 | 7 | 3 | 9 | 28 | |
| H | 1 | 7 | 0 | 4 | 7 | 19 | |
| Enter | 3 | 9 | 14 | 8 | 34 | ||
| Total | 14 | 17 | 39 | 21 | 26 | 117 | |
Summary of findings in site 2
The ‘Talks With’ network decreases a little in size at time 2 but increases the density of connections. There is also a decrease for the ‘Goes To’ network together with a decrease in density. There is a high turnover of actors.
For the ‘Talks With’ network, clusters associated with adult health and social care and with sport and physical exercise are seen at both time 1 and time 2 with consistency of participants. For the ‘Goes To’ network, the persistent clusters are associated with health improvement, with child and maternal health, and with sport and physical exercise.
Site 3 results
The health and well-being issue for site 3 was vascular disease prevention, and we asked interviewees who they talked with/went to about identifying people at risk of vascular disease. The resulting networks comprised individuals from the following organisations:
-
GPs (including members of the local medical committee and emerging clinical commissioning groups)
-
NHS PCT
-
local government authority
-
NHS community service provider (providing community-based health improvement services)
-
NHS acute hospital trust
-
regional cardiac and stroke network
-
NHS regional health authority
-
Department of Health
-
voluntary and community groups working with specific populations/areas (e.g. neighbourhood groups in areas of high deprivation)
-
private sector organisations including specialist consultants and therapists.
The majority of the organisations listed by our landscape interviewees were named during network interviews, with the exception of the private sector organisations. Landscape interviewees had named local employers and sports clubs among those thought to play an important role in preventing vascular disease, but network interviewees named individuals providing informatics consultancy and physical therapy. Perhaps the role of these individuals in creating and exchanging knowledge was hidden from our landscape interviewees.
The ‘Talks With’ network generated from data collected at time 1 is shown in Figure 25. The network comprised 105 actors with 208 connections between them. A total of three clusters represent the situation well. Figure 26 shows the ‘Talks With’ network generated from data collected at time 2, which comprised 74 people with 164 connections between them. Again, three clusters can be identified. Although at both time points the three clusters are well separated, there are multiple connections between them.
FIGURE 25.
‘Talks With’ network for site 3 time 1, showing three clusters.
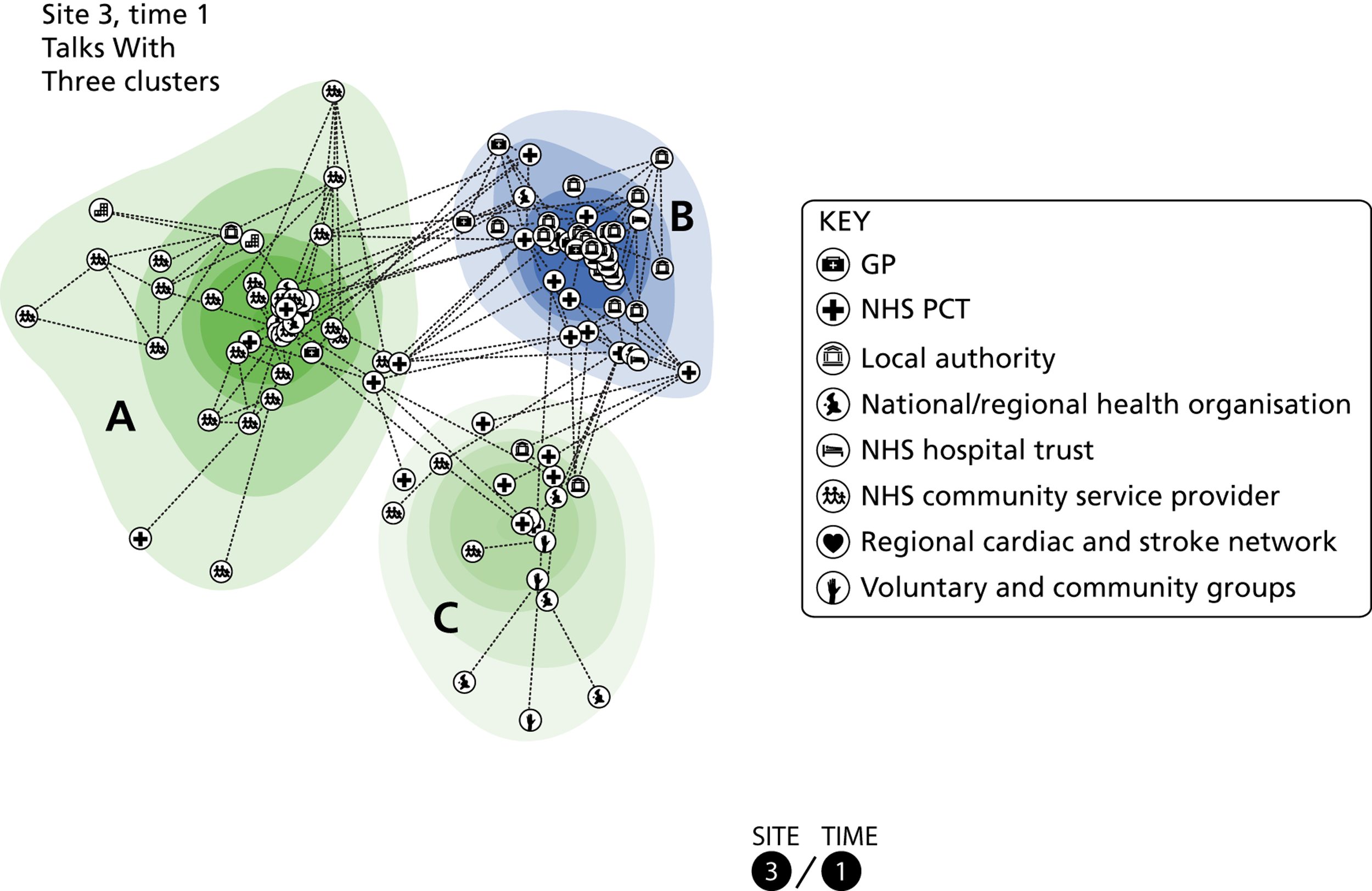
FIGURE 26.
‘Talks With’ network for site 3 time 2, showing three clusters.
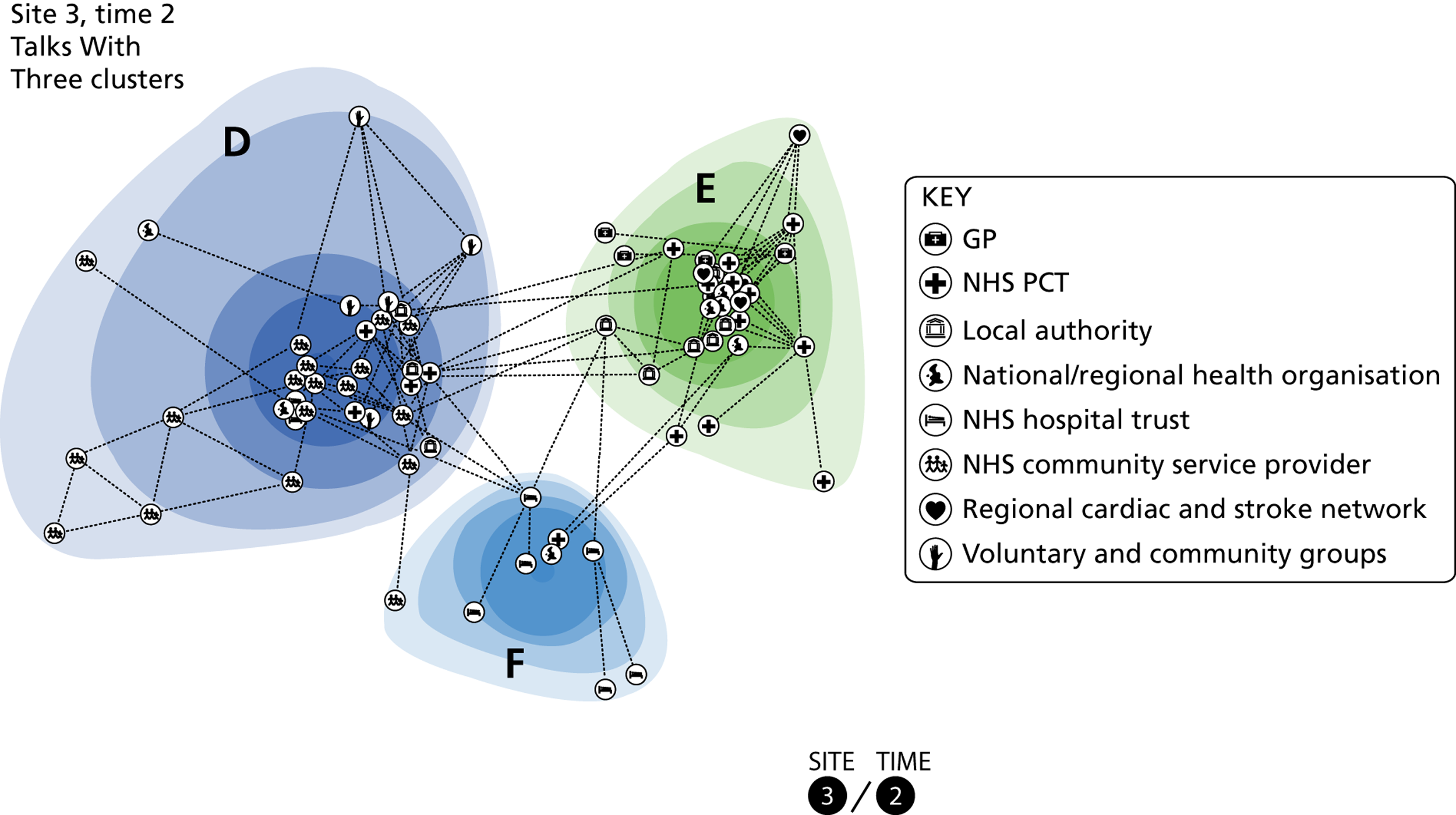
Table 18 shows that some actors retain their key role as bridges between times (actors 2 and 3) but most do not. Some have similar high centrality at both times but most do not.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | Community services | 156.503 (30) | 690.107 (1) | 0.0621 (26) | 0.111 (19) |
| 2 | PCT | 850.607 (3) | 687.577 (2) | 0.323 (2) | 0.297 (5) |
| 3 | PCT | 982.222 (1) | 458.227 (3) | 0.4361 (1) | 0.311 (2) |
| 4 | PCT | 84.145 (39) | 428.592 (4) | 0.2501 (4) | 0.299 (4) |
| 5 | Community services | 860.303 (2) | 387.865 (5) | 0.1491 (14) | 0.228 (8) |
| 6 | Local authority | 681.782 (5) | 298.377 (11) | 0.178 (10) | 0.327 (1) |
| 7 | Voluntary | 526 (6) | 101.942 (19) | 0.061 (27) | 0.088 (24) |
There has clearly been a drastic reduction in the number of actors in this network. Table 19 below shows that 67 actors have exited the network and 36 have entered between the two time points. Actors have exited from all three clusters, but clusters A and C have both lost the majority of their members.
| Cluster | D | E | F | Exit | Total |
|---|---|---|---|---|---|
| A | 8 | 3 | 1 | 32 | 44 |
| B | 4 | 14 | 2 | 21 | 41 |
| C | 4 | 2 | 0 | 14 | 20 |
| Enter | 18 | 12 | 6 | 36 | |
| Total | 34 | 31 | 9 | 67 | 141 |
Table 20 below shows that, at both time points, middle managers constituted the largest group within the network. They are also the largest group in each cluster, with the exception of cluster A, with many frontline staff.
| Time 1 | A | B | C | Total | Time 2 | D | E | F | Total |
|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 5 | 15 | 2 | 22 | Senior manager | 4 | 9 | 1 | 14 |
| Middle manager | 17 | 20 | 11 | 48 | Middle manager | 16 | 16 | 5 | 37 |
| Frontline staff | 21 | 6 | 7 | 34 | Frontline staff | 11 | 5 | 3 | 19 |
| Missing | 1 | 0 | 0 | 1 | Missing | 3 | 1 | 0 | 4 |
| Total | 44 | 41 | 20 | 105 | Total | 34 | 31 | 9 | 74 |
Further detail about the make-up of each cluster is provided below:
-
Cluster A is dominated by actors with a focus on the commissioning and provision of community health-improvement services (e.g. health trainers, business development managers or contracting managers).
-
Cluster B is dominated by managers from a range of organisations with an identifiable focus on public health (e.g. regional and local public health managers focusing on long-term conditions or health improvement/prevention) and includes all of the GPs listed in the network.
-
Members of cluster C include those with a focus on healthy eating, workplace health, and analysing population data.
-
At time 2, the focus of cluster E is similar to that of cluster B, and includes managers with an identifiable focus on long-term conditions and GPs. There are fewer actors with a focus on health improvement/primary prevention.
-
At time 2, cluster D is similar to cluster A at time 1, but includes actors with a focus on workplace health, healthy eating and physical activity. Actors in this cluster appear to share an identifiable focus on primary prevention and health improvement.
-
At time 2, cluster F comprises actors with an identifiable focus on cardiac rehabilitation.
The ‘Goes To’ network generated from data collected at time 1 is shown in Figure 27. The network comprised 123 people with 200 connections between them and is best represented as four clusters. The ‘Goes To’ network at time 2 is shown in Figure 28. This comprised 58 people with 115 connections between them and is best represented as three clusters.
FIGURE 27.
‘Goes To’ network for site 3 time 1, showing four clusters.
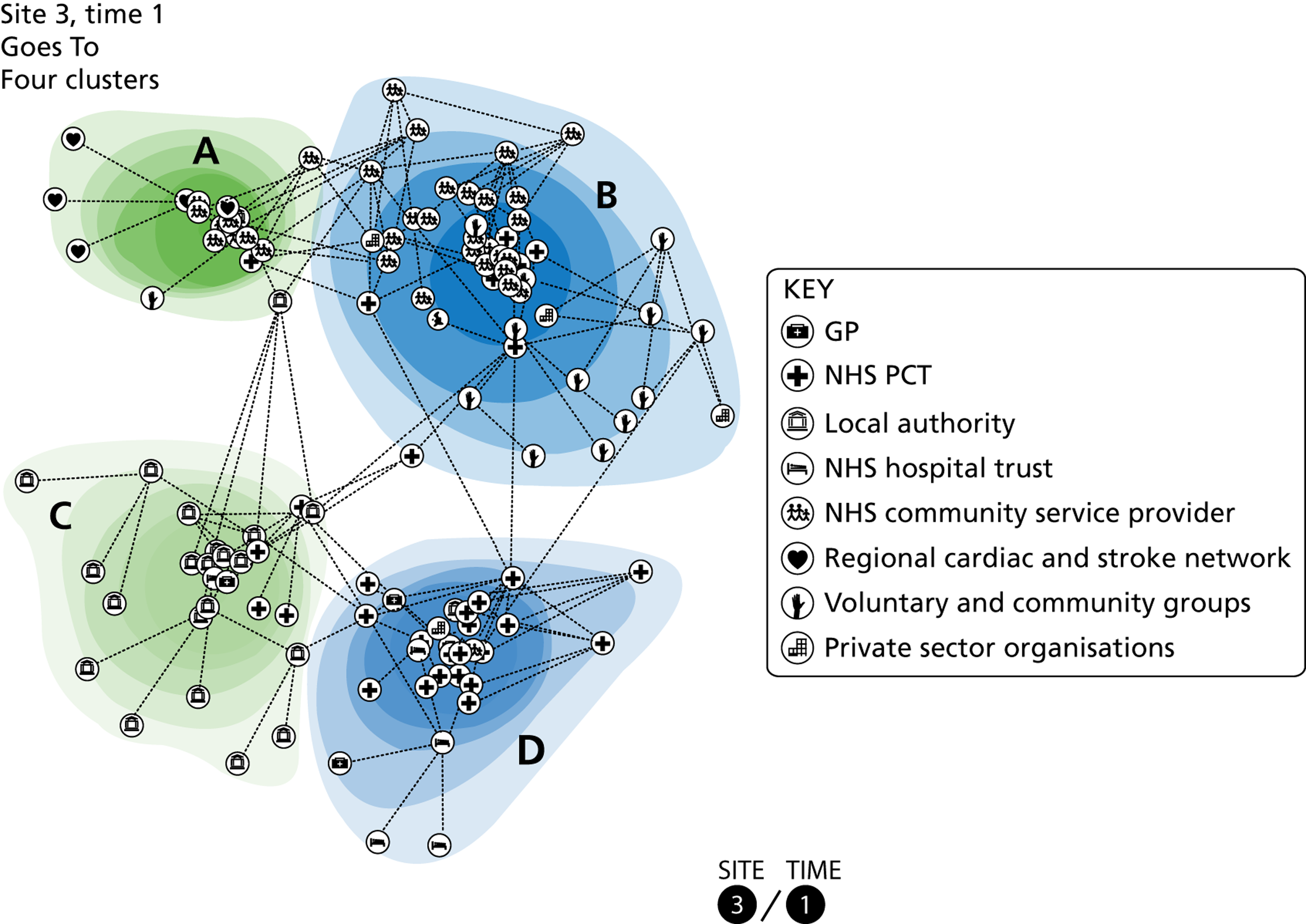
FIGURE 28.
‘Goes To’ network for site 3 time 2, showing three clusters.
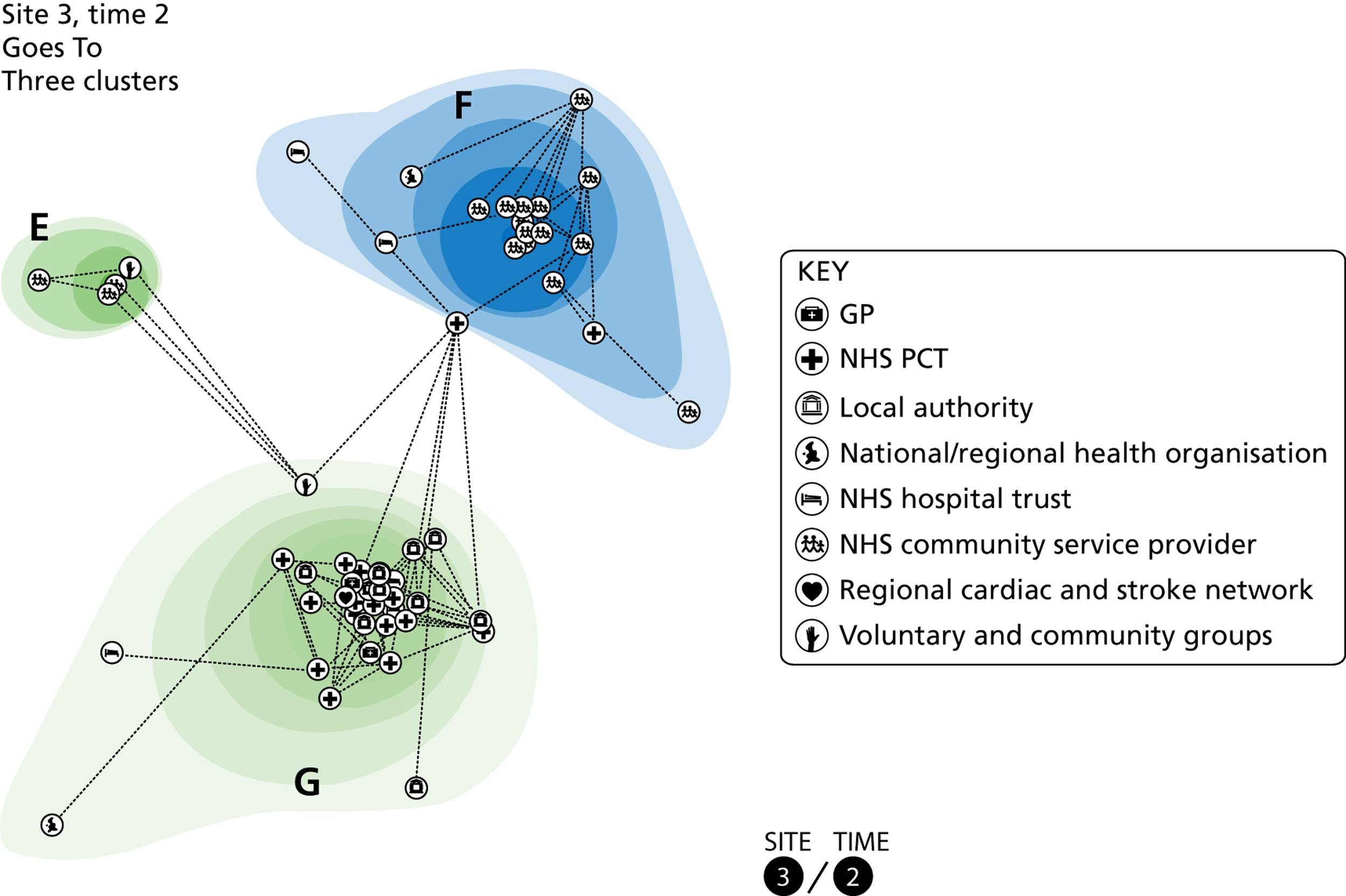
Table 21 below shows that some individuals who played a key role as bridges within the ‘Talks With’ network play a similar role within the ‘Goes To’ network, which persists across time. Some also continue to possess high centrality, while others do not.
| Actor | Organisation | Betweenness | Centrality | ||
|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 1 | Time 2 | ||
| 1 | Community services | 552.276 (8) | 255 (5) | 0.2181 (5) | 0.019 (37) |
| 2 | PCT | 370.724 (20) | 398.883 (3) | 0.165 (11) | 0.359 (2) |
| 3 | PCT | 864.587 (4) | 170.3 (6) | 0.3902 (1) | 0.275 (4) |
| 4 | PCT | 726.682 (6) | 736.75 (1) | 0.2632 (4) | 0.253 (6) |
| 5 | Community services | 646.922 (7) | 667 (2) | 0.2712 (2) | 0.064 (21) |
| 6 | Local authority | 960.473 (2) | 31.65 (22) | 0.171 (9) | 0.256 (5) |
| 7 | Voluntary | 32 (46) | 8 (25) | 0.0991 (26) | 0 |
At time 2, the size of the network has significantly decreased and the configuration of the network and relationships between the clusters has also substantially altered. As Table 22 shows, 89 actors exit the network and 24 enter between the two time points. Clusters A and D have largely disbanded, while members of cluster B have dispersed across the network. A high proportion of cluster C members remain together in cluster G, suggesting some temporal stability.
| Cluster | E | F | G | Exit | Total |
|---|---|---|---|---|---|
| A | 0 | 0 | 3 | 15 | 18 |
| B | 3 | 8 | 2 | 37 | 50 |
| C | 0 | 0 | 11 | 14 | 25 |
| D | 0 | 0 | 7 | 23 | 30 |
| Enter | 1 | 11 | 12 | 24 | |
| Total | 4 | 19 | 35 | 89 | 147 |
Further changes to the network and the clusters can be seen from Table 23, which shows the seniority of network actors.
| Time 1 | A | B | C | D | Total | Time 2 | E | F | G | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Senior manager | 0 | 6 | 7 | 8 | 21 | Senior manager | 0 | 0 | 10 | 10 |
| Middle manager | 11 | 21 | 10 | 12 | 54 | Middle manager | 0 | 9 | 16 | 25 |
| Frontline staff | 7 | 23 | 8 | 10 | 48 | Frontline staff | 4 | 9 | 8 | 21 |
| Total | 18 | 50 | 25 | 30 | 123 | Missing | 0 | 1 | 1 | 2 |
| Total | 4 | 19 | 35 | 58 |
Examining the membership of cluster further, we can see that:
-
Cluster A comprises middle managers with a focus on stroke and frontline staff who are health trainers.
-
Cluster B comprises middle managers and frontline staff with a focus on health improvement services (e.g. healthy weight advisors or smoking cessation), workplace health, and those with a role to play in commissioning and contracting these services.
-
Cluster C is dominated by actors from the local authority, including those with specific roles in public health and physical activity.
-
Cluster D comprises managers and frontline staff with a focus on cardiac disease and analysing population data; it also includes GPs.
-
Cluster E comprises actors with an identifiable focus on workplace health.
-
Cluster F comprises actors with a specific role in providing health improvement services (e.g. healthy weight advisors or health trainers).
-
Cluster G comprises actors from a range of organisations with an identifiable focus on public health (e.g. data analysts or public health managers); GPs are included in this cluster.
Tables 24 and 25 show that there is some equivalence between clusters A and B at time 1, and between clusters E and G, and D and F at time 2.
| Goes To | |||||||
|---|---|---|---|---|---|---|---|
| Talks With | Cluster | A | B | C | D | Exit | Total |
| A | 3 | 18 | 0 | 5 | 18 | 44 | |
| B | 3 | 2 | 8 | 7 | 21 | 41 | |
| C | 0 | 4 | 2 | 3 | 11 | 20 | |
| Enter | 12 | 26 | 15 | 15 | 68 | ||
| Total | 18 | 50 | 25 | 30 | 50 | 173 | |
| Goes To | ||||||
|---|---|---|---|---|---|---|
| Talks With | Cluster | E | F | G | Exit | Total |
| D | 4 | 11 | 5 | 14 | 34 | |
| E | 0 | 0 | 17 | 14 | 31 | |
| F | 0 | 2 | 0 | 7 | 9 | |
| Enter | 0 | 6 | 13 | 19 | ||
| Total | 4 | 19 | 35 | 35 | 93 | |
Summary of findings at site 3
There are dramatic reductions in the size of both the ‘Talks With’ and ‘Goes To’ networks. This occurred despite the consistent manner of data collection. The interviewees were the same in rounds 1 and 2 but there was a change in interviewers. Despite the changes in individuals within each network, there was some consistency of clusters associated with health improvement and clusters associated with public health and physical activity.
Chapter 7 Discussion
Introduction
Chapters 5 and 6 presented the main empirical results of the study. In this chapter, we will discuss the qualitative and network results, drawing out the common findings from our three study sites. We will also comment on the extent to which the results are consistent with the main themes in the knowledge-creation literature. That is, we comment on whether or not the literature helps us to describe and explain the results in our chosen settings of health and well-being services in England. Conversely, we will make some observations about ways in which the knowledge-creation literature might be refined and extended in the light of our results. In the final section, we will set out the main strengths and weaknesses of our study design and methods.
Qualitative themes
This section summarises the themes, derived from the nine accounts, that are common across our three study sites. They are presented under three subheadings – middle managers, knowledge creation and networks of relationships.
Middle managers are synthesisers
Over time, middle managers developed an understanding of their managerial colleagues, and the organisations they worked for. In the process of working with one another, they came to understand colleagues’ perspectives, and the priorities and targets that govern their actions. This allowed them to be synthesisers, in three different senses of the term.
First, they drew on different types of information, from a range of sources – quantitative routine data about populations and services, reports on progress against contractual targets, research evidence, and intelligence from colleagues in other localities.
Second, middle managers were able to link national policies and local priorities, and reconcile them with local operational realities. They were able to integrate the different approaches and working practices of NHS, local authority, private and voluntary organisations. They were not always successful, but the accounts suggest that sector boundaries were not, of themselves, barriers to collaborative working.
Third, they were able to link ideas, negotiation and action. For example, they were able to identify the possibility of a new referral service as an alternative to fixed penalty notices for smoking, negotiate the details of the new service, and implement it.
Knowledge creation
We can make three observations about knowledge creation.
First, as noted above, middle managers drew on different types of information. That is, they took a broad view of knowledge, and were prepared to use research evidence (i.e. scientific knowledge), as well as localised or situated knowledge, relying on the judgements of colleagues in several of the accounts. Knowledge creation, therefore, involved the synthesis of different knowledge claims.
Second, organising ideas – ‘tobacco is everybody’s business’, ‘healthy communities’ – can play an important role in collective knowledge creation. Organising ideas, by their nature, do not develop over short periods of time. In our accounts, relatively small numbers of managers had acted as advocates for particular, collective, ways of thinking about services over a number of years.
Third, knowledge creation is embedded in institutional contexts, and cannot be separated from other phenomena. The accounts emphasised the importance of trust. In some of the accounts, commissioners trusted providers to do what they said they would: they were prepared to rely on providers’ technical and prudential knowledge. The accounts also highlighted the interweaving of knowledge creation and negotiation (the smoking cessation account at site 1 is perhaps the clearest example). Additionally, they suggest that formal arrangements – contracts and targets – can help or hinder knowledge creation.
Network of relationships
Middle managers were working in webs of informal relationships, rather than in the teams that one would expect to find in an acute trust or, indeed, on a car assembly line. In the site 1 account about the health fair, for example, middle managers were able to work in a ‘loose’ network, where different teams made their contributions without all having to co-ordinate directly with one another.
Relationships spanned public, private and voluntary organisations. They were simultaneously formal and informal: formal contracts were managed in a context of ongoing conversations and negotiations. Some of the accounts suggested that a ‘core’ of managers provided a solid basis for co-ordinating new projects and programmes when opportunities arose. For example, the Tobacco Alliance in site 1 – a formal strategy for maintaining relationships – provided a base from which core members were able to reach out and involve other individuals and organisations when the need arose.
The accounts suggest that relationships can be simultaneously stable and fluid. Stable relationships included those based on ‘old PCT’ relationships, outlasting the commissioner–provider split. More fluid, or tactical, relationships were established for particular projects, for example involving Weight Watchers in the weight loss account, or the football club at the Health Fair. The tackling obesity account suggested that the latter example, while tactical in the first instance, could lead to longer-lasting relationships.
At site 2 and site 1, in particular, managers believed that the combination of formal and informal relationships had proved to be resilient, helping them to maintain services in a period of substantial organisational change. Conversely, some of the accounts suggested that competition could limit the sharing of information and, hence, opportunities for knowledge creation.
Network themes
Our analysis has revealed several findings regarding knowledge mobilisation that are common across all three sites. These can be classified by the level at which they hold: either at the individual level relating to people involved in providing services or at the cluster level where groups of people act together to create knowledge or act upon it. At the individual level, we observed that the ‘Talks With’ network involved different actors to the ‘Goes To’ network. Although the networks were of similar sizes, the individuals included in them differed substantially. We also observed that the networks changed markedly over time. Both the actors in the networks and the configuration of links between them differed between the two time periods.
We found that the data produced more meaningful representations when we used clusters to explain the relationships between actors. That is, the clusters corresponded to activities at the sites that we observed in the accounts. More generally, they corresponded to the work of groups – teams, clans, alliances – that are reported in organisation theory and in new institutional theories. Actors within clusters had common attributes, and as a result we were able to interpret the broad purpose of each of the clusters in the graphs for each site. For example, there were clusters comprising people concerned with child services at site 1, at both time periods, and for ‘Talks With’ and ‘Goes To’ networks. This increased our confidence that cluster modelling was a valid, and valuable, method. (Equally, though, there were some clusters that did not match across network type not over time. We did not have sufficient data, from either part of the study, to allow us to investigate this issue in any greater detail.)
The most useful number of clusters was three or four for both network types, and for both sampling periods, at each of the three sites. This may reflect the mathematical formulation of our models, or may relate to something more fundamental, for example the numbers of people who can effectively co-ordinate with one another for a given activity. Clusters typically included around 20–40 people: too many to manage at regular, formal meetings, but perhaps a realistic number of people who can maintain informal relationships with one another.
Looking ahead to the next sections, which consider the relevance of the knowledge creation literature, we were struck by the fact that the clusters, at all three sites, all had a mix of organisations represented within them. The clusters were the opposite of teams working in traditional bureaucracies – where teams specialise in particular functions, and middle managers co-ordinate across functions. They were a little more like Lean organisations, where teams with a range of skills are responsible for products or services, and where managers operate more tactically (and typically also less formally).
The relationships we observed, revealed by the cluster arrangements, seemed to us to have two distinctive features that are not like Lean or other learning/improvement governance arrangements and have not been reported elsewhere. First, there were several clusters at each site that comprised combinations of organisations. (In some clusters, one organisation dominated, but even here other organisations were represented.) That is, the results hint at a distributed, but multiorganisational, pattern of co-ordination of health and well-being services. It may be stretching a point, but if we combine the observations about the fluidity and the distributed nature of the clusters, then the three sites had developed arrangements with the capacity to respond to opportunities and new challenges – new projects, good ideas – as they came up.
Second, there was a mix of seniorities in all clusters. In the ‘Talks With’ networks the more senior participants tended to group together, but in general there was a marked mixing of seniorities. The knowledge-creation literature emphasises the important role that middle managers play in many organisational contexts. In our three sites, in contrast, the cluster arrangements suggest that co-ordination between people at different levels of organisations is important.
Reflections on the knowledge-creation literature
As we noted in Chapter 3, much of the knowledge-creation literature is based on studies in industrial settings, far removed from the health and well-being services that we studied. We took the view that the literature could provide us with some broad steers, for example focus on middle managers. We have, in the end, been pleasantly surprised by the extent to which the literature resonates with our findings. There appear to be four particular points of connection – the key roles played by middle managers, the fluidity of groups involved in knowledge creation, the use of a range of sources of information and ideas, and the reliance on situated, or localised, knowledge.
At the same time, our findings failed to shed light on two issues. Our accounts shed limited light on two topics, namely the reported differences in the contexts of publicly and privately owned organisations,12,55,56 and the ways in which power relations influence knowledge creation. 62,64,65
Two arguments in the literature were not supported, concerning the role of agency48–51 and the superiority of organisational co-ordination over relational contracts. 53,54 On agency, we are only in a position to observe that only one of our nine accounts indicated that an individual had played a crucial role; in any case, it seems reasonable to note that the bulk of the literature emphasises collective actions rather than agency. On the merits of organisational and contractual co-ordination, our accounts offer suggestive evidence that both can underpin knowledge creation. It is worth pointing out here that other literatures, notably in sociolegal studies, focus on ways in which contracts can be the basis for organisational learning, though contractual relations can disappoint as well as fulfil expectations in practice. 79
Reading the other way, from our findings out to the literature, we have two observations. The first is that, in common with the great majority of papers in the (wider) knowledge mobilisation literature, papers in the knowledge-creation literature assume the presence of network relationships. However, we think importantly, they do not offer any direct evidence about the nature of those networks – who is in them, who is in the core and who on the periphery, how particular relationships and networks as a whole change over time, and so on. Put simply, groups, teams and the wider networks within which they sit are deemed to be important, but the networks of relationships are not described. The network element of our study has shown that it is possible to reveal useful information about network configurations, both at a given point in time and over time.
Second, as just noted, the knowledge-creation literature draws a distinction between public and private organisations. This is understandable, given the organisations studied in that literature. It is worth noting, though, that in this study the boundaries between public, private and voluntary services were not clear-cut. This is not surprising when one takes account of the dominant ideas in policy making over the last 20 or so years, with New Public Management policies leading to a blurring of the distinction between public and private organisations. 82 However, it suggests that the ownership status of organisations may play less of a role than reported elsewhere in the knowledge-creation literature.
This brings us to the final point in this section, about the extent to which our findings might be generalised. We can address the point in two ways. First, following Ragin,83 we can ask: what population are we generalising to? Our instinct is to be conservative, extending the relevance of our findings only to other localities in England co-ordinating health and well-being services. All localities have health and well-being services, are funded in similar ways, and have to respond to the same national policies. Many of the ideas and practices observed at our study sites are likely to be ‘in the air’ in other localities, for example health and well-being services involve the co-ordination of several services, and there is merit in focusing efforts on particular neighbourhoods.
The second response reflects the scope for theoretical generalisation, and here we can be more confident. The resonances with the knowledge-creation literature, set out in this section, suggest that our findings are broadly consistent with studies conducted in a wide range of settings, both in other sectors and in other countries. They contribute to the view that knowledge creation is a ubiquitous phenomenon that can be observed in the many settings where managers have to co-ordinate with one another across organisational boundaries, using a combination of formal and informal relationships.
Strengths and weakness of the study design and methods
In this section we will set out the main strengths and weaknesses of our study design and methods.
Strengths
In this study we faced two main methodological challenges. The first concerned the ‘dual’ nature of knowledge creation, which sits on a fault line between narrative and analytically rational perspectives. The qualitative accounts were important, in this study, because we were principally concerned with situated knowledge. The network analyses were important because organisations were geographically dispersed: there was no other way of observing the networks of relationships. We identify some of the problems created by the ‘duality’ below but, overall, we found that the narrative and network findings complemented one another. Each provided us with insights that the other could not.
The second challenge concerned sampling. We set out the challenges, and our responses to them, in Chapter 2. At the end of the study we can say that landscape mapping proved to be an effective strategy for minimising some known sources of bias. In the network analyses, our sampling regime enabled us to visualise networks of 100+ members with good accuracy from just 10–12 interviews. This is an efficient strategy for generating a network, which we have not seen used elsewhere in health services research. Further, we found that we could use the clusters in the latent cluster graphs to identify qualitative interviewees. This sequence, from landscape maps to clusters to accounts, is a novel sampling strategy for observational studies.
On our choice of methods, we felt that each of our main methods had advantages. The latent cluster graphs allowed us to visualise networks. The membership and configuration of networks are typically implied, or just absent, in most published studies. We are not aware of other health services research studies which have used latent cluster modelling. As we will see in Chapter 8, the visualisations also appear to be meaningful to our target audience. The accounts, at least in the second round of interviews, shed light on both of our main study questions, concerning knowledge creation and networks of relationships, both formal and informal.
Finally, as discussed in the previous section, the study findings allow us to identify points in common with the knowledge-creation literature. Our findings were consistent with key themes in the literature, and this allows us to argue that our findings might be generalisable to a wide range of settings, where managers have to co-ordinate with colleagues in other organisations in order to deliver a service.
Weaknesses
We have noted a number of the weaknesses and limitations of our methods in preceding chapters, notably in Chapters 2, 5 and 6. Starting with the case study design, we used a novel design and have produced plausible findings about knowledge creation. We were not, however, able to integrate the nine accounts and the network analyses successfully within our design. The technical challenges stem both from the very different ontological bases of our methods and from practical issues, such as the different sizes of the populations described, so that we could not simply ‘map’ the nine accounts onto the graphs presented in Chapter 6.
In the network analyses, while we observed that there were substantial changes in the networks between the two periods, suggesting fluidity of membership, it should be noted that each round of interviews required a few weeks to complete in practice. It was simply not possible to complete the interviews in a shorter time period – people were on leave, off sick, etc. As a result, we cannot be confident that we observed a true ‘snapshot’, which we should ideally have captured.
On the interpretation of our network results, there are three important reservations. First, although our sampling represented an efficient use of resources, we cannot be certain that the specification of the network is perfect without interviewing all actors. As noted in Chapter 2, this was not a practical option. Second, our network information consisted of answers to simple questions (‘talks with’ and ‘goes to’) and, if further resources had been available, we could have addressed other aspects of the relationships between managers. Third, one of the strengths of our method, our ability to describe a large social network based on a relatively small number of interviews, might also be viewed as a weakness.
Our qualitative results also come with reservations. In the knowledge-creation literature, some of the best papers are based on close observation of managers working collectively to address and solve problems. In this study, for the reasons set out in Chapter 2, it was not possible to ‘get close’ to managers in the same way. When they did get together, and we could therefore observe them, they were in formal meetings, which were important for monitoring activities rather than for generating ideas and actions. As a result, our accounts are based to a substantial extent on events that we were not able to observe directly. We were able to use the process tracing method to produce accounts, but we were not able to make the fine-grained observations reported in some other studies.
Our aspirations for the Leximancer software were not fulfilled. Given the experiences reported in Chapter 8, where site managers found the cluster graphs helpful, we are still of the view that visualisations can be important aids to presenting findings from technically challenging studies. But, on this occasion, we were not able to obtain the outputs we had hoped to, and more work is needed on generating useful visualisations from qualitative data.
The knowledge-creation literature proved to be valuable in some ways, but at the same time key themes in the literature were not supported. In the last section we noted that our findings did not offer much support for the role of agency, or for the opposition of contractual and non-contractual relationships. We also noted two ways in which our findings lay outside the knowledge-creation literature, in our emphasis on rendering network relationships explicit and in the effects of New Public Management policies, which have tended to dissolve distinctions between public, private and voluntary services in England.
Finally, there is a broader question, about the extent to which our interpretation of our empirical findings has been shaped by the knowledge-creation literature. While we still believe that it was an appropriate choice given our research questions, we have to accept than other knowledge mobilisation literatures might have produced different interpretations. For example, as Ferlie and colleagues’ review emphasises,1 some authors emphasise the institutional impediments to innovation, and if we had followed their lead we might have given greater weight to the difficulties that managers encountered.
Chapter 8 Interactive feedback events
Introduction
As described in Chapter 2, we cohosted an interactive event at each of our three study sites with managers who had been involved in our study. Although other teams report findings at the end of studies, our interactive approach was relatively novel. We aimed to move beyond disseminating our findings and offering advice or guidance to managers about knowledge creation. Instead, we aimed to use our materials and emerging insights to prompt discussion and reflection about local managers’ ability to mobilise knowledge which could inform their discussions about how to address a pertinent local health and well-being issue.
In this chapter we will begin by describing the focus of each event and presenting the site-specific insights about knowledge mobilisation which were generated. We will then draw these together into some general insights about knowledge mobilisation and networks from the perspective of health and well-being managers. Finally, we will reflect on the interactive engagement process itself, drawing on our own experiences and feedback from attendees, and offer some insights for other research teams about the potential value of this approach.
This chapter describes the feedback events that were held at each of the study sites in the late autumn of 2012, at the tail end of the study period. It is common to feed back the findings of research studies in one of two ways, namely by sending written site reports and by presenting findings to participating sites. Both methods have merits, not least in allowing sites to check that researchers’ versions of events ring true.
Health Service and Delivery Research requires research teams to identify ‘actionable findings’ from their studies. It was difficult to imagine that the standard methods would help us to identify actionable findings – findings that we could be confident were meaningful to managers at the sites, and which they found helpful. We needed to find a way of presenting our results that allowed us to gauge their value to managers. By extension, we reasoned, findings valued by managers at our sites were more likely to be relevant to their opposite numbers in other localities.
We asked our three sites whether or not it would be helpful to them to present our findings to them in person, giving them the opportunity to discuss them with us – and giving us the opportunity to identify possible actionable findings. Our liaison managers at all three sites responded positively, and through discussion we arrived at a common format. The events were organised by the sites themselves. They were focused on local needs, for example discussion of strategic objectives for health and well-being services. In the course of the planning for the events, it became clear that managers at two of the sites – site 1 and site 2 – did not know one another very well. Accordingly, we ran ‘speed dating’ sessions on behalf of the sites early on in the workshops, where participants introduced themselves to one another sequentially, for 1 minute at a time.
We presented our findings at or near the start of each event, so that the findings and any discussion they generated could feed into the sites’ own discussions. A range of local organisations was invited to each event, including but not limited to the organisations covered in our network and narrative studies.
Event materials
In order to encourage discussion of our findings at the events, we created two types of visual representation of our findings. The first were videos, based on our narratives (see Chapter 5). Even though both accounts involved several people, for clarity of presentation the accounts in the videos are presented as if a single manager had taken the lead. The second type of representation was based on our cluster graphs (see Chapter 6). Selected graphs were edited by a graphic designer in order to make them easier to explain in a workshop setting. In the process, we ensured that the locations of particular managers within the graphs could not be identified, on the basis that this was personal information that should not be published in a workshop.
The events: October and November 2012
The three workshops were well attended, and many of the people we had interviewed in 2011 and/or 2012 were in the audience for our presentations. The principal investigator introduced the research study and then outlined the study objectives, our rationale for presenting at this particular event, and what participants would see in the following 30–40 minutes. At each workshop we showed three videos. The first was an account from one of the other sites, designed to familiarise participants with the medium. Then, we showed videos of two accounts from that site, and after each video one of us offered our interpretation of the events described. We invited comments on the videos and on our own provisional interpretation, and took notes of comments made. Then, one of us presented the graphs, highlighting the ways in which the membership and the cluster configurations changed between the two time periods. One of the graphs shown, which is the same as Figure 17 in Chapter 6, is reproduced below as Figure 29. Again, comments were invited and notes taken.
FIGURE 29.
‘Talks With’ network for site 1 time 1.
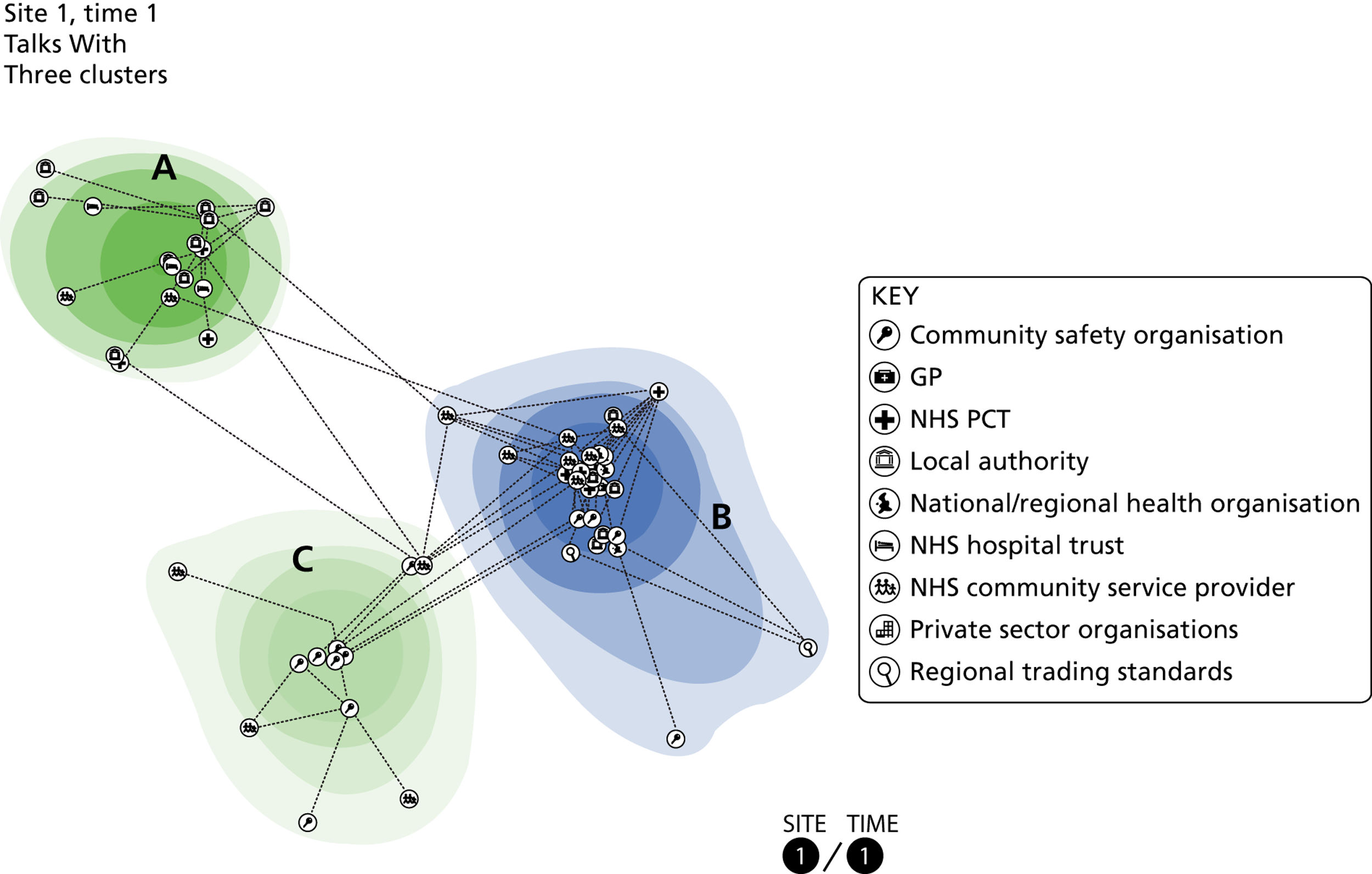
The responses of participants to our material are summarised in the following three sections, which are presented in the order in which the workshops were held – site 1, site 3, site 2. At the first event, in site 1, we realised that we had not provided sufficient information about the graphs, with the result that participants found them difficult to understand. We provided more information about the clusters in site 3 and site 2, and there were richer discussions at their workshops. The remaining time in the workshops was focused on the sites’ own priorities, was not part of this research study, and accordingly is not reported here.
The site 1 workshop
The workshop was a tobacco strategy ‘refresh’, organised in the context of work that had been taking place over in the locality over many years. Participants responded to the videos in four ways.
First, they were able to ‘get things done’ when there was a clear objective that different organisations understood and could support. The creation of the smoking cessation referral system was a good example. Second, some participants were struck by the fact that, although they knew the names of most of the people at the workshop, they had never met before. They may have exchanged e-mails, or occasionally been at the same meetings, but had not sat down and discussed Tobacco Alliance work. Third, the accounts reminded managers of successful initiatives, and of the relationships that they were based on: ‘other local authorities and PCTs don’t have the relationships we have’. Fourth, and conversely, there was considerable scope to learn practical lessons – ‘how to’ lessons – from other organisations based in site 1, and from other localities. There were also opportunities to make imaginative links between services. One participant suggested that similar people could be targeted for smoking cessation and discarding chewing gum at the same time.
Participants found it difficult to interpret the graphs that they were shown. This may well be because we gave limited information about the graphs, on the basis that we might inadvertently reveal the names of individual member of the networks. It may also be that participants did not all know one another particularly well – a situation which had been anticipated, and which prompted the ‘speed dating’ exercise.
The site 2 workshop
The site 2 workshop was organised to consider ‘where next?’ for health and well-being services in the locality. The videos prompted discussion of ‘then and now’. Some 18 months ago, cross-organisational working relationships had been good. Today, in large part owing to diminishing resources, organisations were tending to work in relative isolation, fulfilling bilateral contracts with commissioners. It was now difficult to know where to go, outside one’s own organisation, to find help to get something done.
There was a sense that targets, whether set by central government or in local contracts, could be used to encourage integration or separate working. Targets and performance measures were not going to go away, because they were necessary for organisations to demonstrate that they were having positive effects on local communities. Interpreted defensively, targets had to be met to protect one’s colleagues’ jobs and make it possible to win the next contract. Interpreted more positively, targets could be used to encourage effective co-ordination (e.g. in the case of the weight loss account in Chapter 5).
Following our experience at site 1, where we felt that we had not explained the network diagrams properly, at site 2 we provided more information, while still taking care to preserve the anonymity of members of the networks. The network diagrams generated two main lines of discussion. The first concerned the possibility that they depicted a ‘core’ of stable relationships, with changes between the two time periods reflecting changes in active projects outside the core. One particularly large project had finished between the two time periods, and it was suggested that some of the change could be attributed to the presence, and subsequent absence, of project-based relationships. The second line of discussion focused on the possible deleterious effects of competition, set against a background of diminishing resources. This may have led to a reduction in the number of connections between the two periods: people competing against one another were less likely to share information or to rely on one another to get things done.
The site 3 workshop
The workshop was convened by the public health team to consider the creation of a formal public health network, engaging with a wide range of organisations in the locality. The videos prompted a number of observations. Two main themes emerged. First, there were comments that teams tended to work in silos. There was scope to co-ordinate work more effectively, and work together towards locality-wide outcomes, for example a reduction in the incidence of chronic diseases. To achieve this, it would be necessary to involve more people earlier in new initiatives. Second, there was discussion of different ways of communicating, given that the proposed network was likely to be large in terms of the numbers of organisations and of individuals involved. E-mail is easy and allows people to communicate between organisations, but equally real work gets done when people meet face to face.
The diagrams prompted a lengthy discussion, which focused on three features – the nature of the clusters, links between the clusters, and changes in cluster configurations over time. Participants asked questions in order to clarify what the clusters in the diagrams represented – not separate organisations, but people from several different organisations linked by some activity or common objective. The suggestion was made that separate clusters might be desirable. It is not feasible to have everybody connected to everybody else when there are dozens of people in a network. Having discrete groups of people working on particular topics or projects makes sense. On links between clusters, it was observed that links could be traced to one or two individuals. That is, relationships between otherwise discrete teams depended on just one or two people.
Participants speculated about possible explanations for the changes between the 2011 and 2012 network diagrams. The changes might reflect wider organisational changes in the locality, for example organisations were more inclined to ‘look after their own’ than they had been a few years before. It might be that, in a period of substantial organisational change, interviewees in the research study were ‘going to’ a relatively small number of people that they knew well when they needed to get something done.
Reflections on the workshops
We can reflect back on the three workshops in two ways – as a method for disseminating research findings, and as a method for helping to identify findings that might be relevant to managers in other localities.
We cannot make strong claims, because we have not tested our approach against more conventional feedback methods. It seems reasonable, however, to observe that the videos and network diagrams both worked, in the sense that they prompted the discussions we hoped for at the workshops. Our own subjective reflections are that:
-
The videos help to avoid the ‘death by PowerPoint’ problem of feeding back any research findings. The professional actors were, we felt, able to convey messages in ways that we would have struggled to match ourselves.
-
The network diagrams worked – at site 3 and site 2 – because it was possible to explain the clusters and the links between them. The diagrams were not easy to present, not least because we could not identify the locations of individuals at the workshops, but the idea that people work in multiorganisational and/or multidisciplinary associations seemed to be intuitively reasonable to participants. We speculate that it would have been more difficult to explain more conventional network analysis diagrams, based solely on agent-to-agent links.
Finally, the workshop discussions give us some confidence that at least some of our findings were understood by middle managers at our sites, and prompted a number of thoughtful comments. The workshop discussions, therefore, feed usefully into our ‘implications for practitioners’ observations in the next chapter – and are our attempt to produce actionable findings.
Chapter 9 Conclusions
Introduction
In this chapter we will discuss our study questions. We will draw on the material presented in the preceding chapters, including the empirical findings in Chapters 5 and 6, the literature review from Chapter 3, and the policy context in Chapter 4. We will also comment on the implications of our findings for researchers and for managers of health and well-being services. Our reflections on the interactive feedback events, set out in Chapter 8, inform this last set of comments.
From knowledge exchange to knowledge creation
We set out in this study to address two main questions. The first was: how do health-care managers exchange knowledge to bring about changes in health-care delivery and organisation? Related to this question, we asked five more detailed questions. We will make two general observations, and then give our answers to the detailed questions, before returning to the main question.
Reflections
First, if we were able to have our time on the study over again, we would phrase the first question differently. The term ‘knowledge exchange’ implies that the study is concerned with universal scientific knowledge – with concrete knowledge picked up and passed from person to person. However, as the preceding chapters have demonstrated, this study highlights the importance of very different types of knowledge – what we termed technical and prudential knowledge in Chapter 1, and might also be referred to as ‘know-how’ or ‘the wisdom that comes with experience’. We would instead have asked a question about knowledge mobilisation or knowledge creation. Second, we would also have emphasised the social processes that produce them: knowledge creation is a collective act, and occurs in particular places and at particular times. This way of thinking resonates with key writers on case studies – our chosen study design – such as Flyvbjerg,2 and with leading writers on knowledge creation, including Nonaka and Takeuchi. 11 These thoughts should be borne in mind in our responses to the five questions below.
Knowledge exchange questions
1. To what extent is the exchange of knowledge based on the identification of a specific organisational need?
Evidence from the accounts, presented in Chapter 5, suggests that managers at the three sites had priorities in common, notably in relation to channelling resources towards communities with the greatest needs. Beyond this, however, our results suggest that managers were opportunistic, seizing on programme funding when it became available and navigating from an imaginative idea to a new service. As we note below in our responses to the second question, health and well-being services in our sites were not goal-oriented. There were, rather, loose but also robust networks, with the capacity to mobilise in different ways to opportunities and challenges.
2. What are the different types and sources of information which influence the exchange of knowledge?
Middle managers drew on different types of information. They took a broad view of the sources and nature of the information that would help them, and were prepared to use research evidence (including scientific evidence) as well as localised or situated knowledge. The accounts show that managers were often prepared to rely on the judgements of their colleagues. Knowledge creation, therefore, involved the synthesis of different types of information and of different knowledge claims.
We also note that organising ideas – ‘tobacco is everybody’s business’, ‘healthy communities’ – can play an important role in collective knowledge creation. Organising ideas, by their nature, do not develop over short periods of time. In our qualitative accounts, relatively small numbers of managers had acted as advocates for particular, collective, ways of thinking about services over a number of years.
3. How do the organisational circumstances surrounding the manager influence the exchange of knowledge?
Our results confirmed those found in the knowledge-creation literature, and in the wider knowledge mobilisation literature – knowledge creation is not something that managers achieve in isolation. This said, we can make three comments in response to this question.
First, middle managers are synthesisers. That is, they are the actors who make sense of their contexts, and tie together otherwise unconnected policies, ideas and practices. One might say that they internalise their contexts, and draw on their understanding when they act.
Second, knowledge creation is embedded in institutional contexts, and cannot be separated from other phenomena. The accounts emphasised the importance of trust. In some of the accounts, commissioners trusted providers sufficiently to rely on their (technical and prudential) knowledge. The accounts also highlighted the interweaving of knowledge creation and negotiation (the smoking cessation account at site 1 is perhaps the clearest example). Additionally, they suggest that formal arrangements – contracts and targets – can either help or hinder knowledge creation, depending on the local context.
Third, we found some evidence that competition may limit knowledge creation. While it seemed clear that the use of legally binding contracts was not a barrier to collaboration in some of the accounts, it was also clear that some managers decided not to share intelligence with potential competitors.
4. What activities are undertaken by managers to share and exchange knowledge?
Over and above the comments about the acquisition of information above, managers used a combination of formal and informal strategies for co-ordinating with one another. While the activities captured in the accounts all involved several organisations, they used recognisable bureaucratic strategies to co-ordinate their work with one another, most obviously by setting up regular, minuted, meetings. At the same time, they relied heavily on informal relationships, both to maintain key relationships over time and to mobilise support for specific activities and programmes.
5. To what extent is the exchange of knowledge based on an assessment of the potential influence of that knowledge?
In general, it is not. Managers were concerned to spread collective approaches to thinking about problems, on the basis that shared thinking would positively influence the behaviour of colleagues, and beyond them the organisations in which they worked. One possible exception is related to the competition point made above: some managers opted not to discuss potentially valuable information with potential competitors, and wanted to limit its effects.
How do health-care managers exchange knowledge to bring about changes in health-care delivery and organisation?
Our main question concerned managers exchanging knowledge to bring about changes in health-care delivery and organisation. One response would be to say that, strictly speaking, we have not been able to link managers’ knowledge creation with substantive changes in the delivery of services. We have shown how managers mobilised both knowledge and resources in projects and programmes, but not how they led to long-term changes in the organisation and delivery of services. More constructively, we can say that our findings support key arguments in the knowledge-creation literature. Knowledge creation is a collective act, involving a number of people working together over a period of time. It involves addressing and solving problems in particular local contexts, and the creation of technical and prudential knowledge. Over longer time periods, key managers maintain relationships, and in so doing conserve common objectives and approaches.
Networks: from individuals to clusters
The second main question was: what role is played by the connections between the managers who are responsible for bringing about changes in health-care delivery and organisation? As in the last section, we will make general observations, address the detailed questions, and then return to the main question.
Reflections
This research question was framed at a time when we assumed that individual level analysis would be fruitful. In the event, as set out in Chapters 2 and 6, we found that focusing on relations was more fruitful for our sampling and analysis and for feedback to the three sites.
Network questions
1. What is the role of informal networks in exchanging knowledge across different organisational settings and boundaries?
Informal relationships play a crucial role in knowledge creation, and in particular in maintaining shared ideas over time, during a period of considerable organisational change. Our network analyses do not discriminate between formal and informal relationships, but as noted above we found that relationships were intertwined, or braided, with one another.
The composition of networks and of clusters indicates that knowledge mobilisation involves people of different seniorities and from different organisations. We were able to establish, in the qualitative analysis, that they were not all attending regular meetings with one another. Indeed, there were simply too many people in the networks to imagine that formal meetings could underpin many of the relationships reported. We conclude that informal relationships can be maintained, in health and well-being services, across organisational boundaries and across localities.
2. How does the density of networks influence the process of exchanging knowledge?
There is not substantial variation in density between sites, or between network types (‘Talks With’ or ‘Goes To’). We cannot usefully comment upon density, other than to say that it appears not to have a strong influence on our findings.
3. Does the centrality of individual managers within an informal network influence the knowledge exchange process?
At an individual level, fluidity of relationships was observed. With the exception of a small number of highly influential people (one or two per site), the measure of centrality that we considered (eigenvalue centrality) was very variable. Similarly, our measure of betweenness varied appreciably by time and by network type. The identification of highly influential actors within a network – the top 2% – may be made in this way. Our interest, however, was in knowledge creation throughout the network and for this purpose the cluster analysis was more informative.
4. How do directional relationships within informal networks facilitate or constrain the exchange of knowledge within and between settings?
Although we noted the direction of relationships – who talks with whom and who goes to whom in order to get things done – our network analysis had very little dependence on direction. As a result, we have not emphasised direction in the analysis, producing diagrams without adding arrows to indicate direction. The relationships are a combination of formal and informal, and in both circumstances directionality may not be crucial. Our resources did not permit detailed enquiry.
What role is played by the connections between the managers who are responsible for bringing about changes in health-care delivery and organisation?
We observed clusters at two time points. Some consistency was observed, in parallel with marked changes. We suspect that, had we captured data at more time periods, we would have seen actors moving into and out of clusters.
Established relationships within a cluster that persist over time are clearly useful for continuity of action of groups of managers. On the other hand, some movement from one cluster to another (seen in our tables in Chapter 6) also has advantages – know-how and experience are transferred where they may be needed, and perhaps movement encourages the injection of new ideas and methods for getting things done.
We observed the three sites during a period of organisational change which included the move of public health teams from the NHS to local authorities. We were not in a position to capture the effects of NHS and other public service reforms with the methods available to us. However, we note the importance of continuity of relationships in a time of organisational turbulence.
Implications for research
Turning to our research findings, we can evaluate the implications against the gaps in the research literature identified by Ferlie and colleagues. 1 They listed six priorities for further research, three of which were theoretical and three about ‘end users’ of knowledge mobilisation. Our study does not shed any light on two of the six, relating to the resource-based view of the firm and the roles of information technologies. We are, though, in a position to comment on the other four.
Theoretical research gaps
1. Organisational form and design – there is currently an absence of high-quality literature in this area.
Two of our findings may be relevant to questions about organisational form and design. The first is that mainstream literatures, including many papers in organisation theory as well as in knowledge mobilisation, typically emphasise the importance of managers who work informally in the ‘gaps’ between formal organisational structures. In this study, in contrast, formal and informal relationships are closely entwined, or braided. Managers, at least in the health and well-being services that we studied, were not working in the gaps, but rather working within formal and informal governance arrangements. Indeed, while we have commented elsewhere on the possible negative effects of competition on knowledge creation, we also note that several of our accounts weave informal relationships around legally binding contracts and quantified targets.
The second finding concerns clusters. As we noted in Chapter 7, the results hint at a distributed, cross-organisational, pattern of co-ordination of health and well-being services. We emphasised that we may be stretching a point, but if we combined the observations about the fluidity and the distributed nature of the clusters, then we might say that the three sites had developed arrangements with the capacity to respond to opportunities – new projects, good ideas – as they came up. In a word, they were resilient. One might also say that they have some of the characteristics associated with complex adaptive systems. 84
2. Conceptual epistemological questions, for example ‘what is evidence?’, are fundamental and underpin all enquiries into knowledge mobilisation in the NHS.
As discussed in Chapters 1 and 2, we had to think hard about the nature of knowledge before we started the fieldwork. At the end of the study we can report that these fundamental terms are still causing us to think hard about our methods and our findings. On the methodological front, it not realistic to ask direct questions about knowledge – ‘what knowledge have you created recently?’ – and expect to obtain sensible answers. We found that we had to observe knowledge creation ‘out of the corners of our eyes’. That is, we asked interviewees to help us to construct accounts about activities that they had undertaken, and which were likely to have involved knowledge creation. Knowledge creation had to be inferred from the accounts. Similarly, the ‘Goes To’ and ‘Talks With’ questions in the network interviews are not questions about knowledge, or indeed about collective acts – they capture more general patterns of relationships. However, the latent cluster modelling provides suggestive evidence about the relationships that make knowledge creation possible – the core actors, and their seeming ability to mobilise resources when needed.
Moving on to our findings, we feel comfortable using terms such as technical and prudential knowledge, which have a venerable lineage that can be traced back to Aristotle’s Nicomachean Ethics. 85 However, we are struck by the fault-line in health services research, with evidence-based medicine and implementation science on one side and narrative accounts on the other. The findings do not support the view, favoured in some strands of health services research, that scientific knowledge is the only legitimate type of knowledge.
End user research gaps
3. Models of knowledge transfer, innovation and diffusion – we have identified several models. Empirical work is needed to evaluate those that have greatest application to the NHS.
This study has drawn only on one model – or more accurately one theory – of knowledge mobilisation. As discussed in Chapter 7, our findings are consistent with key arguments in the knowledge-creation literature, even though much of that literature is based on evidence and argument produced in other sectors on other continents.
4. Barriers and facilitators – there is a considerable body of work in this area. It is underpinned by an assumption that managers have power and autonomy to deliver knowledge mobilisation. This needs to be tested through empirical research, given the presence of powerful professional groups.
This study has not used the language of barriers and facilitators, and the medical profession has been largely absent from health and well-being services in this study. It is worth noting, though, that our findings support the assumption that managers are able to ‘deliver’ knowledge mobilisation. It is a moot point whether or not they are able to deliver because they have the necessary power and autonomy. It is also moot whether or not they would have the same discretion were GPs to extend their work beyond vascular checks and colonise health and well-being services.
Research priorities
Our findings, and our reflections in this chapter, suggest four priorities for further research:
-
The dynamics of networks with respect to knowledge mobilisation.
-
Establishing the value of latent cluster modelling in understanding the work of groups and teams in other health and social care settings.
-
Knowledge mobilisation in the context of the interorganisational co-ordination of services by clinicians, as opposed to co-ordination by managers.
-
The nature of knowledge. Where is the common ground between the scientific and narrative paradigms?
Implications for managers
Our research highlights four implications for middle managers. The comments in this section are informed by the findings set out in Chapter 7 and by our experiences at the feedback events reported in Chapter 8.
-
Middle managers play important co-ordinating roles in health and well-being services. In the 1990s, the fashion for re-engineering and delayering led to the elimination of middle managers. It had the paradoxical effect of highlighting the importance of middle managers in a wide range of organisational settings. This study contributes to the view that they still matter: they are able to absorb, and synthesise, many competing priorities, secure resources, and work out how to allocate them. It is difficult to imagine how health and well-being services could be co-ordinated without them.
-
Managers working in health and well-being services are able to co-ordinate work across boundaries – across public, private and voluntary organisations, and across geographical areas. In doing so, informal relationships play a vital role. While formal meetings are clearly important, the extensive relationships required to co-ordinate health and well-being services could not be co-ordinated through meetings alone.
-
It is helpful to think about services as being co-ordinated clusters. Managers at the feedback events were struck by the idea that separate clusters may have important advantages; distributed arrangements make sense, given the project-driven nature of much health and well-being work. The importance of one or two people within a site was also noted; it was appreciated that this was a potential source of fragility, and if those people left then clusters might lose their links with one another.
-
Knowledge creation requires those involved to trust one another. In this regard formal instruments – contracts and targets – are double-edged. Used constructively they can encourage collective working, but they can also discourage it, with organisations retreating into silos when their viability is perceived to be threatened.
Acknowledgements
We could not have undertaken the research without the considerable good will and – at times – forbearance of the staff at the three sites we studied. We are particularly grateful to the managers who acted as primary points of contact throughout the study, and to the managers and administrators who helped us with the interactive feedback events.
The members of our study advisory group gave us invaluable advice and support in the course of the project:
Ruth Boaden (chair), Professor of Service Operations Management, Manchester Business School and Deputy Director – NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Greater Manchester.
Laura Hibbs, Associate Director for Innovation and Improvement, NHS Yorkshire and the Humber.
Lucy Jackson, Consultant in Public Health, NHS Airedale, Bradford and Leeds.
Jenny Lewis, Professor of Public Administration and Public Policy, Roskilde University, Denmark.
Janet Ratcliffe, Network Director, Greater Manchester & Cheshire Cardiac and Stroke Network.
We also acknowledge the hard work and dedication of a wider team of people who contributed to the production of this report and the study as a whole through data collection, administrative support, video production and graphic design:
Paul Dempster.
Amy Russell.
David Brennan.
Emma Yeomans.
Matt Wilson.
Delia Muir.
Martina McClements.
Chris Orton.
Daphne Franks.
Becky Edlin (Magpie Communications).
Contributions of authors
Vicky Ward Principal investigator, field research, analysis, preparation of final report.
Robert West Analysis of network interview data, preparation of final report.
Simon Smith Field research, analysis of qualitative interviews using NVivo.
Steven McDermott Field research, analysis of qualitative interviews using NVivo, Leximancer and QDA Miner.
Justin Keen Study design, analysis, preparation of final report.
Ray Pawson Study design, advice on field research and analysis.
Allan House Advice on field research and analysis.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Ferlie E, Crilly T, Jashapara A, Peckham A. Knowledge mobilisation in healthcare: a criticial review of health sector and generic management literature. Soc Sci Med 2012;74:1297-304. http://dx.doi.org/10.1016/j.socscimed.2011.11.042.
- Flyvbjerg B. Making social science matter: Why Social Inquiry Fails and How it Can Succeed Again. Cambridge: Cambridge University Press; 2001.
- Crossley N. Towards Relational Sociology. London: Routledge; 2011.
- House A, Forster A, Lewin R, Watt I, Gilbody S, Farrin A. IMPROVE-PC: Improving Prevention of Vascular Disease in Primary Care, A Research Theme in Leeds York Bradford CLAHRC n.d.
- Campbell D, Brenner M, Marsh P. The Social Contexts of Method. London: Croom Helm; 1978.
- Hammersley M, Foster P, Gomm R, Gomm R, Hammersley M, Foster P. Case Study Method. London: Sage Publications Ltd; 2000.
- Yin RK. Case Study Research: Design and Methods. London: Sage Publications, Incorporated; 2008.
- Exworthy M, Peckham S, Powell M, Hann A. Shaping Health Policy: Case Study Methods and Analysis. Bristol: University of Bristol, Policy Press; 2011.
- George AL, Bennett A. Case Studies and Theory Development in The Social Sciences. Cambridge, MA: MIT Press; 2005.
- The English Indices of Deprivation 2010. Statistics on Relative Levels of Deprivation in England. London: Department for Communities and Local Government; 2011.
- Nonaka I, Takeuchi H. The Knowledge-Creating Company; How Japanese Companies Create the Dynamics of Innovation. Oxford: Oxford University Press; 1995.
- Rashman L, Withers E, Hartley J. Organizational learning and knowledge in public service organizations: a systematic review of the literature. Int J Manag Rev 2009;11:463-94. http://dx.doi.org/10.1111/j.1468-2370.2009.00257.x.
- Currie G, Starr T, White L, Dingwall R, Watson A, Trueman P. Comparative Evaluation of Children’s Services Networks: Analysing Professional, Organisational and Sector Boundaries in Paediatric Nephrology, Children’s Safeguarding and Cleft Lip and Palate Networks. London: NIHR SDO; 2010.
- Creswick N, Westbrook JI, Braithwaite J. Understanding communication networks in the emergency department. BMC Health Serv Res 2009;9. http://dx.doi.org/10.1186/1472-6963-9-247.
- Dyer J, Nobeoka K. Creating and managing a high-performance knowledge-sharing network: the Toyota case. Strateg Manag J 2000;21:345-67. http://dx.doi.org/10.1002/(SICI)1097-0266(200003)21:3%3C345::AID-SMJ96%3E3.3.CO;2-E.
- Wasserman S, Faust K. Social Network Analysis: Methods and Application. Cambridge: Cambridge University Press; 1994.
- Scott J. Social Network Analysis: A Handbook. London: Sage Publications Ltd; 2000.
- Crilly N, Blackwell AF, Clarkson PJ. Graphic elicitation: using research diagrams as interview stimuli. Qual Res 2006;6:341-66. http://dx.doi.org/10.1177/1468794106065007.
- Schiffer E, Hauck J. Net-Map: collecting social network data and facilitating network learning through participatory influence network mapping. Field Method 2010;22:231-49.
- Emmel N. Participatory Mapping: An Innovative Sociological Method. Manchester: ESRC National Centre for Research Methods; 2008.
- Lewis JM. A network approach for researching partnerships in health. Aus N Z Health Policy 2005;2.
- Krauss M, Mueller N, Luke D. Interorganizational relationships within state tobacco control networks: a social network analysis. Preventing Chronic Dis 2004;1.
- Waddington K, Fletcher C. Gossip and emotion in nursing and health-care organizations. J Health Organ Manag 2005;19:378-94. http://dx.doi.org/10.1108/14777260510615404.
- Chattoe E, Hamill H. It’s not who you know – It’s what you know about people you don’t know that counts – extending the analysis of crime groups as social networks. Brit J Criminol 2005;45:860-76.
- Hoff PD, Raftery AE, Handcock MS. Latent space approaches to social network analysis. J Am Stat Assoc 2002;97:1090-8. http://dx.doi.org/10.1198/016214502388618906.
- Handcock MS, Raftery AE, Tantrum JM. Model-based clustering for social networks. J R Stat Soc 2007;170:301-54. http://dx.doi.org/10.1111/j.1467-985X.2007.00471.x.
- Mina A, Braha D, Bar-Yam Y. Complex Engineered Systems: A New Paradigm. Complex Engineered Systems: Science Meets Technology. Berlin: Springer; 2006.
- Teisman G, Gerrits L, van Buuren A, Teisman G, van Buuren A, Gerrits L. Managing Complex Governance Systems Dynamics, Self-Organization and Coevolution in Public Investments. London: Routledge; 2009.
- Pope J, Lewis JM. Improving partnership governance: using a network approach to evaluate partnerships in Victoria. Aust J Publ Admin 2008;67:443-56. http://dx.doi.org/10.1111/j.1467-8500.2008.00601.x.
- Provan K, Veazie M, Staten L, Teufel-Shone N. The use of network analysis to strengthen community partnerships. Public Admin Rev 2005;65:603-13. http://dx.doi.org/10.1111/j.1540-6210.2005.00487.x.
- Greimas A-J. Sémantique Structurale. Recherche de Méthode. Paris: Larousse; 1966.
- Groleau C, Cooren F. A socio-semiotic approach to computerization: bridging the gap between ethnographers and systems analysts. Commun Rev 1999;3:125-64. http://dx.doi.org/10.1080/10714429909368576.
- Robichaud D. Textualization and organizing: illustrations from a public discussion process. Commun Rev 1999;3:103-24. http://dx.doi.org/10.1080/10714429909368575.
- Cooren F, Fairhurst G. Speech timing and spacing: the phenomenon of organizational closure. Organization 2004;11:793-824. http://dx.doi.org/10.1177/1350508404047252.
- Lewis RB, Maas SM. QDA Miner 2.0: Mixed-model qualitative data analysis software. Field Methods 2007;19:87-108. http://dx.doi.org/10.1177/1525822X06296589.
- Cooren F. Translation and articulation in the organization of coalitions: the Great Whale River case. Commun Theor 2001;11:178-200. http://dx.doi.org/10.1093/ct/11.2.178.
- Pentland BT, Feldman M. Narrative networks: patterns of technology and organization. Organ Sci 2007;18:781-95. http://dx.doi.org/10.1287/orsc.1070.0283.
- Krivitsky PN, Handcock MS, Raftery AE, Hoff PD. Representing degree distributions, clustering, and homophily in social networks with latent cluster random effects models. Soc Networks 2009;31:204-13. http://dx.doi.org/10.1016/j.socnet.2009.04.001.
- Salter-Townshend M, Murphy TB, Lausen B, van del Poel D, Ultsch A. Algorithms from and for Nature and Life Studies in Classification, Data Analysis, and Knowledge Organization. Heidelberg: Springer; 2012.
- Brown JS, Duguid P. Knowledge and organization: a social-practice perspective. Organ Sci 2001;12:198-213. http://dx.doi.org/10.1287/orsc.12.2.198.10116.
- Erden Z, von Krogh G, Nonaka I. The quality of group tacit knowledge. J Strategic Inf Syst 2008;17:4-18. http://dx.doi.org/10.1016/j.jsis.2008.02.002.
- Nonaka I, von Krogh G. Tacit knowledge and knowledge conversion: controversy and advancement in organizational knowledge creation theory. Organ Sci 2009;20:635-52. http://dx.doi.org/10.1287/orsc.1080.0412.
- Nonaka I, von Krogh G, Voelpel S. Organizational knowledge creation theory: evolutionary paths and future advances. Organ Stud 2006;27:1179-208. http://dx.doi.org/10.1177/0170840606066312.
- von Krogh G. Individualist and collectivist perspectives on knowledge in organizations: implications for information systems research. J Strategic Inf Syst 2009;18:119-29.
- Grabher G. Fragile sector, robust practice: project ecologies in new media. Environ Plan 2002;34:1911-26. http://dx.doi.org/10.1068/a35256.
- van Wijngaarden JDH, de Bont AA, Huijsman R. Learning to cross boundaries: the integration of a health network to deliver seamless care. Health Policy 2006;79:203-13. http://dx.doi.org/10.1016/j.healthpol.2006.01.002.
- Akiyama T. CSR and inter–organisational network management of corporate groups: case study on environmental management of Sekisui House Corporation Group. Asian Bus Manag 2010;9:223-43.
- Alin P, Taylor JE, Smeds R. Knowledge transformation in project networks: a speech act level cross-boundary analysis. Project Manag J 2011;42:58-75. http://dx.doi.org/10.1002/pmj.20254.
- Collinson S, Wilson DC. Inertia in Japanese organizations: knowledge management routines and failure to innovate. Organ Stud 2006;27:1359-87. http://dx.doi.org/10.1177/0170840606067248.
- Currie G, Tempest S, Starkey K. New careers for old? Organizational and individual responses to changing boundaries. Int J Hum Resour Man 2006;17:755-74. http://dx.doi.org/10.1080/09585190600581733.
- Kuk G. Strategic interaction and knowledge sharing in the KDE developer mailing list. Manage Sci 2006;52:1031-42. http://dx.doi.org/10.1287/mnsc.1060.0551.
- Lindsay V, Chadee D, Mattsson J, Johnston R, Millett B. Relationships, the role of individuals and knowledge flows in the internationalisation of service firms. Int J Serv Ind Manag 2003;14:7-35. http://dx.doi.org/10.1108/09564230310465976.
- Nahapiet J, Ghoshal S. Social capital, intellectual capital, and the organizational advantage. Acad Manag Rev 1998;23:242-66. http://dx.doi.org/10.2307/259373.
- Spender JC. Making knowledge the basis of a dynamic theory of the firm. Strateg Manage J 1996;17:45-62.
- Hartley J, Benington J. Copy and paste, or graft and transplant? Knowledge sharing through inter-organizational networks. Public Money Manage 2006;26:101-8. http://dx.doi.org/10.1111/j.1467-9302.2006.00508.x.
- Kim S, Lee H. The impact of organizational context and information technology on employee knowledge-sharing capabilities. Public Admin Rev 2006;66:370-85. http://dx.doi.org/10.1111/j.1540-6210.2006.00595.x.
- Amin A, Roberts J. Knowing in action: beyond communities of practice. Res Policy 2008;37:353-69. http://dx.doi.org/10.1016/j.respol.2007.11.003.
- Araujo L. Knowing and learning as networking. Manage Learn 1998;29:317-36. http://dx.doi.org/10.1177/1350507698293004.
- Cohendet P, Kern F, Mehmanpazir B, Munier F. Knowledge coordination, competence creation and integrated networks in globalised firms. Cam J Econ 1999;23:225-41. http://dx.doi.org/10.1093/cje/23.2.225.
- Goodall K, Roberts J. Repairing managerial knowledge-ability over distance. Organ Stud 2003;24:1153-75. http://dx.doi.org/10.1177/01708406030247007.
- Rutten R. Inter-firm knowledge creation: a re-appreciation of embeddedness from a relational perspective. Eur Plan Stud 2004;12:659-73. http://dx.doi.org/10.1080/0965431042000220002.
- Argote L, Miron-Spektor E. Organizational learning: from experience to knowledge. Organ Sci 2011;22:1123-37. http://dx.doi.org/10.1287/orsc.1100.0621.
- Bogenrieder I. Social architecture as a prerequisite for organizational learning. Manage Learn 2002;33:197-212. http://dx.doi.org/10.1177/1350507602332003.
- Rodan S, Galunic C. More than network structure: how knowledge heterogeneity influences managerial performance and innovativeness. Strateg Manage J 2004;25:541-62. http://dx.doi.org/10.1002/smj.398.
- Swan J, Scarbrough H. The politics of networked innovation. Hum Rel 2005;58:913-43. http://dx.doi.org/10.1177/0018726705057811.
- Breschi S, Lissoni F. Localised knowledge spillovers vs. innovative milieux: knowledge “tacitness” reconsidered. Pap Reg Sci 2001;80:255-73. http://dx.doi.org/10.1007/PL00013627.
- Doak S, Assimakopoulos D. How forensic scientists learn to investigate cases in practice. R&Amp;D Manage 2007;37:113-22. http://dx.doi.org/10.1111/j.1467-9310.2007.00467.x.
- Siemsen E, Roth AV, Balasubramanian S, Anand G. The influence of psychological safety and confidence in knowledge on employee knowledge sharing. M&Amp;Som-Manuf Serv Op 2009;11:429-47. http://dx.doi.org/10.1287/msom.1080.0233.
- Cross R, Borgatti SP, Parker A. Beyond answers: dimensions of the advice network. Soc Networks 2001;23:215-35. http://dx.doi.org/10.1016/S0378-8733(01)00041-7.
- Obstfeld D. Social networks, the Tertius lungens and orientation involvement in innovation. Admin Sci Quart 2005;50:100-30.
- Blackler F, Crump N, McDonald S. Organizing processes in complex activity networks. Organization 2000;7:277-300. http://dx.doi.org/10.1177/135050840072005.
- Macpherson A. Learning how to grow: resolving the crisis of knowing. Technovation 2005;25:1129-40. http://dx.doi.org/10.1016/j.technovation.2004.04.002.
- The Health of the Nation: A Strategy for Health in England. London: Department of Health; 1992.
- Saving Lives: Our Healthier Nation. London: The Stationery Office; 1999.
- Acheson SD. Independent Inquiry Into Inequalities in Health Report. London: The Stationery Office; 1998.
- Wanless D. Securing Good Health for the Whole Population. London: The Stationery Office; 2004.
- Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M. Fair Society, Healthy Lives: The Marmot Review; Strategic Review of Health Inequalities in England Post-2010. London: Marmot Review; 2010.
- Putting Prevention First – Vascular Checks: Risk Assessment and Management. London: Department of Health; 2008.
- Levy C. Making the Most of Public Services: a Systems Approach to Public Innovation. London: The Work Foundation; 2011.
- Vincent-Jones P. The New Public Contracting: Regulation, Responsiveness, Relationality. Oxford: Oxford University Press; 2006.
- Quality, Innovation, Productivity and Prevention (QIPP). NICE; 2013.
- Bockaert G, Pollit C. Public Management Reform: A Comparative Analysis. Oxford: Oxford University Press; 2011.
- Ragin CC. Introduction: Cases of “What is a Case?”. What is a Case. Cambridge: Cambridge University Press; 1992.
- Axelrod R, Cohen MD. Harnessing Complexity: Organizational Implications of a Scientific Frontier. New York, NY: Basic Books (AZ); 2000.
- The Nicomachean Ethics. London: Penguin; 2004.
- Smith AE, Humphreys MS. Evaluation of unsupervised semantic mapping of natural language with Leximancer concept mapping. Behav Res Meth 2006;38:262-79. http://dx.doi.org/10.3758/BF03192778.
- Rooney D. Knowledge, economy, technology and society: the politics of discourse. Telematics Inform 2005;22:405-22. http://dx.doi.org/10.1016/j.tele.2004.11.007.
- Zappavigna M, Patrick J. Eliciting tacit knowledge about requirement analysis with a Grammar-targeted Interview Method (GIM). Eur J Inf Syst 2010;19:49-5. http://dx.doi.org/10.1057/ejis.2010.1.
- Halliday M, Matthiessen C. Introducing Functional Grammar. New York, NY: Edward Arnold; 2004.
- Sternberg RJ. Beyond IQ: A Triarchic Theory of Human Intelligence. Cambridge: Cambridge University Press; 1984.
- Sternberg RJ, Forsythe GB, Hedlund J, Horvath JA, Wagner RK, Williams WM, et al. Practical Intelligence in Everyday Life 2000.
- Linde C. Narrative and social tacit knowledge. J Knowledge Manag 2001;5:160-71. http://dx.doi.org/10.1108/13673270110393202.
- Nonaka I, Takeuchi H. The Knowledge-Creating Company: How Japanese Companies Create the Dynamics of Innovation. Oxford: Oxford University Press; 1995.
- Rose D, Veel JR, Martin R. Reading Science: Critical and Functional Perspectives on Discourses of Science. London: Routledge; 1998.
- Halliday MAK, Matthiessen C. Construing Experience Through Meaning: A Language-Based Approach to Cognition. London: Continuum; 2006.
Appendix 2 Information sheet – interviews

Academic Unit of Primary Care
Leeds Institute of Health Sciences
Charles Thackrah Building
101 Clarendon Road
LEEDS LS2 9LJ
We would like to invite you to take part in our research study. Before you decide whether to take part we would like you to understand why the research is being done and what it would involve for you. Please do not hesitate to contact us if anything is not clear or you have any questions. One of our research team will be very happy to go through the information sheet with you and answer any questions. Our contact details can be found at the end of this information sheet.
This research is designed to help us understand more about how knowledge spreads within and between organisations to develop potential solutions to challenging vascular risk prevention and reduction problems across a local area. It is being carried out by a team of researchers at the University of Leeds, funded by the National Institute for Health Research Service Delivery & Organisation Programme (SDO).
Background to the research
Gathering, exchanging and combining knowledge and information is a key part of developing, altering and implementing healthcare. This implies a process which involves a network of more than one manager or decision maker. The development of solutions to location-wide disease prevention/health promotion issues is also likely to involve individuals working in different organisations who are linked in a number of different ways. Although we know that this process is related to the networks of connections between individuals, we do not know enough about the role that they play.
By studying how the networks of connections between individual and groups of managers influence the development of solutions to vascular risk prevention and reduction problems, we are likely to have a better idea about how they could be manipulated to bring about innovative changes to healthcare delivery.
Purpose of the study
The purpose of the study is to build a better understanding of how managers develop potential solutions to the challenge of preventing and reducing people’s risk of vascular disease at both an individual and population level within a local area. We will be particularly focusing on a) how managers exchange knowledge and ideas and b) how managers are connected to each other.
The nature of our work
Our work will involve observing how individual and groups of managers come together to develop solutions to vascular risk prevention and reduction challenges.
We will be particularly looking at who is talking to whom and what they are talking about.
We will be using three methods to collect our data:
-
Face-to-face interviews with managers who are developing solutions to the challenge of preventing and reducing people’s risk of vascular disease across the local area
-
Observation of meetings where vascular risk prevention and reduction challenges are discussed and potential solutions are developed.
-
Analysis of administrative documents (e.g. researchers will examine meeting minutes, agendas, working papers, reports)
Invitation to participate
You are being invited to participate in this research because you are involved in making decisions about vascular risk prevention and reduction in your local area. Your organisation has kindly agreed to take part in this research study and you are one of the professionals and managers we wish to include in the interview stage of the project.
We would be grateful if you would be willing to be interviewed about your involvement in making decisions about vascular risk prevention and reduction. We will need to interview you twice. We would like to schedule the first interview between April and June 2011. This will last for up to an hour and take place at a time and work location convenient to you. The second interview would take place at the end of our research, between March and May 2012. This will last for up to 90 minutes and would again take place at a time and work location convenient to you. With your permission, we would like to audio record the interviews as it makes analysis more reliable.
It is up to you to decide whether to take part and your involvement in the research is entirely optional. If you agree to be interviewed you will be asked to sign a consent form, but you will be free to withdraw at any time during the interview or during the study without giving reason. We will always respect your choice, and anyone who does not wish to take part can ask the researcher not to record information about themselves.
What will happen to the information
All the information collected during the course of the research will be kept confidential and personal details will be anonymised. The anonymised data will be stored on a secure University server, password and firewall protected and accessible only to the research team and at the end of the project will be securely archived to a maximum of five years and then destroyed.
We will write a report based on the findings of the study and send it to the organisations involved and to the SDO/Department of Health. We also aim to publish our findings in health service journals. Organisations and individuals will not be named in any reports or publications.
Who has reviewed the study
The design of the study has been reviewed by Leeds West NHS Research Ethics Committee.
Complaints
If you have a concern about any aspect of this study, please speak to the researcher (see numbers below) who will do their best to answer your questions. If you remain unhappy and you wish to complain formally, you can do this by contacting Leeds University sponsor representative, Clare Skinner, Head of Research and Support, Faculty of Medicine and Health at governance-ethics@leeds.ac.uk or telephone 0113 343 4897.
Further information
If you have any further questions about the study please contact the research team:
Dr Vicky Ward, Academic Unit of Primary Care, Leeds Institute of Health Sciences, Charles Thackrah Building, 101 Clarendon Road, Leeds LS2 9LJ; 0113 343 0848; v.l.ward@leeds.ac.uk.
Appendix 3 Consent form – interviews
Academic Unit of Primary Care
Leeds Institute of Health Sciences
Charles Thackrah Building
101 Clarendon Road
LEEDS LS2 9LJ
Site number:
Name of Researcher: Dr Paul G Dempster/Dr Vicky Ward
Staff member identification number for this study:
The role of informal networks in spreading knowledge between healthcare managers
CONSENT FORM
Please consider each of the statements below and initial each box to signify your consent. Please add your name and date to the end of the sheet.
Please initial box
| 1. I confirm that I have read, and that I understand, the Participant Information Sheet, for the above study | |
| 2. I agree that I have had the opportunity to consider the information, ask questions and have had these answered satisfactorily | |
| 3. I understand that my participation is voluntary and that I am free to withdraw at any time from the interview, without giving any reason | |
| 4. I agree to take part in the study which will involve taking part in two interviews | |
| 5. I consent to the interview being audio-taped and the data collected to be stored at the university for 5 years, then destroyed | |
| 6. I understand that any quotations used in writing up the study findings will not be identifiably attributed to me | |
| 7. I understand that the data collected for the study may be looked at by authorised persons from the organisation sponsoring the research (NIHR SDO) to check that the study is being carried out correctly. All will have a duty of confidentiality to you as a research participant and we will do our best to meet this duty |
I agree to take part in the study.
_________________________ ________________ ____________________
Name of Participant Date Signature
_________________________ ________________ ____________________
Name of Person taking consent Date Signature
(if different from researcher)
_________________________ ________________ ____________________
Researcher Date Signature
1 copy for participant; 1 for researcher.
Appendix 4 Information sheet – observation
Academic Unit of Primary Care
Leeds Institute of Health Sciences
Charles Thackrah Building
101 Clarendon Road
LEEDS LS2 9LJ
This research is designed to help us understand more about how knowledge spreads within and between organisations to develop, alter and/or implement vascular risk prevention services. It is being carried out by a team of researchers at the University of Leeds, funded by the National Institute for Health Research Service Delivery & Organisation Programme (SDO).
Background to the research
Gathering, exchanging and combining knowledge and information is a key part of developing, altering and implementing healthcare services. This implies a process which involves a network of more than one manager or decision maker. The development of disease prevention/health promotion initiatives is also likely to involve individuals working in different organisations who are linked in a number of different ways. Although we know that the development and alteration of healthcare services is related to the networks of connections between individuals, we do not know enough about the role that they play.
By studying how informal, day to day connections influence the development, alteration or implementation of vascular risk prevention services, we are likely to have a better idea about how they could be manipulated to bring about innovative changes to healthcare delivery.
Purpose of the study
The purpose of the study is to build a better understanding of the way that knowledge spreads within and between organisations and of the role played by informal networks. We aim to understand a) how knowledge is exchange to bring about changes in vascular risk prevention services and b) the role that is played by the connections between the managers who are responsible for bringing about those changes.
The nature of our work
Our work will be divided into two phases. The first phase involves sharing some information about vascular risk prevention with individuals who are involved in making decisions about vascular risk prevention services in your organisation. This information will be drawn from a range of sources and packaged so that it is useful for the development or alteration of vascular disease prevention services. The second phase involves observing what happens next in terms of any development or alteration of vascular disease prevention services. We will observe how any changes come about and will look at how individuals and groups of staff exchange information to bring about those changes. We will be particularly looking at who is talking to whom and what they are talking about.
We will using three methods to collect our data:
-
Face-to-face interviews with staff involved in developing, altering or implementing vascular risk prevention services
-
Observation of meetings
-
Analysis of administrative documents (e.g. meeting minutes, agendas, working papers, reports)
Invitation to participate
You are being invited to participate in this research because you are responsible for convening meetings where decisions about vascular risk prevention services in your local area are made. Your organisation has kindly agreed to take part in this research study and we would like to attend the meetings that you convene as part of the observation stage of the project.
We would be grateful if you would be willing for us to observe the meetings which you convene. We will not need to participate in the meetings, but will need to take brief notes during each meeting. Due to one member of our team having RSI we may also need to record each meeting. This will enable him to make notes afterwards using audio software.
It is up to you to decide whether you will allow us to observe the meetings which you convene. If you do agree to take part, we will ask you to confirm this in writing to us by completing a consent form. We would also like to send information about our research to all of the individuals who attend the meetings and gain their consent. We will liaise with you to work out the best way of sending this information to them. If anyone who is attending the meeting does not wish to take part, their details and actions during the meeting will not be recorded.
We will introduce ourselves at the first meeting that we attend. At this or any future stage, you or any of the attendees will be free to ask us to leave a meeting without giving reason. We will always respect your choice. Anyone who does not wish to take part can ask the researcher not to record information about themselves.
What will happen to the information
All the information collected during the course of the research will be kept confidential and personal details will be anonymised. The anonymised data will be stored on a secure University server, password and firewall protected and accessible only to the research team and at the end of the project will be securely archived to a maximum of five years and then destroyed.
Any recordings made during meetings will be used to make observational fieldnotes within 7 days of the meeting. Recordings will then be destroyed.
We will write a report based on the findings of the study and send it to the organisations involved and to the SDO/Department of Health. We also aim to publish our findings in health service journals. Organisations and individuals will not be named in any reports or publications.
Who has reviewed the study
The design of the study has been reviewed by Leeds West NHS Research Ethics Committee.
Complaints
If you have a concern about any aspect of this study, please speak to the researcher (see numbers below) who will do their best to answer your questions. If you remain unhappy and you wish to complain formally, you can do this by contacting Leeds University sponsor representative, Clare Skinner, Head of Research and Support, Faculty of Medicine and Health at governance-ethics@leeds.ac.uk or telephone 0113 343 4897.
Further information
If you have any further questions about the study please contact the research team:
Dr Vicky Ward
Academic Unit of Primary Care Leeds Institute of Health Sciences Charles Thackrah Building 101 Clarendon Road Leeds LS2 9LJ 0113 343 0848 v.l.ward@leeds.ac.uk
Dr Paul Dempster
Academic Unit of Primary Care Leeds Institute of Health Sciences Charles Thackrah Building 101 Clarendon Road Leeds LS2 9LJ 0113 343 0848 p.dempster@leeds.ac.uk
Appendix 5 Consent form – observation
Academic Unit of Primary Care
Leeds Institute of Health Sciences
Charles Thackrah Building
101 Clarendon Road
LEEDS LS2 9LJ
Site number:
Name of Researcher: Dr. Paul G Dempster/Dr Vicky Ward
Staff member identification number for this study:
The role of informal networks in spreading knowledge between healthcare managers
CONSENT FORM
Please consider each of the statements below and initial each box to signify your consent. Please add your name and date to the end of the sheet.
Please initial box
| 1. I confirm that I have read, and that I understand, the Participant Information Sheet, for the above study | |
| 2. I agree that I have had the opportunity to consider the information, ask questions and have had these answered satisfactorily | |
| 3. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving any reason | |
| 4. I agree to take part in the study which will involve recording my details and participation in meetings | |
| 5. I consent to the data collected to be stored at the university for 5 years, then destroyed | |
| 6. I understand that any details or actions recorded by the researchers and used in writing up the study findings will not be identifiably attributed to me | |
| 7. I understand that the data collected for the study may be looked at by authorised persons from the organisation sponsoring the research (NIHR SDO) to check that the study is being carried out correctly. All will have a duty of confidentiality to you as a research participant and we will do our best to meet this duty |
I agree to take part in the study.
__________________________ ________________ ____________________
Name of Participant Date Signature
__________________________ ________________ ____________________
Name of Person taking consent Date Signature
(if different from researcher)
__________________________ ________________ ____________________
Researcher Date Signature
1 copy for participant; 1 for researcher.
Appendix 6 Network data collection sheets
| Interview code no: | Name | Organisation, department & role | Meetings | |||
|---|---|---|---|---|---|---|
| Name | Organisation, department & role (note any changes since previous interview) | Meetings attended | ||||
| Network 1: Who do you talk with? | ||||||
| Q1 – who do you talk with about [site specific topic]? Name up to five (white boxes) Q2 – who do they talk with about [site specific topic] Name up to five (green boxes) Q3. What meetings do they go to? | ||||||
| Name | Organisation, department & role | Meetings | Name | Organisation, department & role | Meetings | |
| Interview code no: | Name | Organisation, department & role | Meetings | |||
|---|---|---|---|---|---|---|
| Network 2: Who do you go to? | ||||||
| Q1 – who do you go to to get things done about [site specific topic]? Name up to five (white boxes) Q2 – who do they go to to get things done about [site specific topic] Name up to five (green boxes) Q3. What meetings do they go to? | ||||||
| Name | Organisation, department & role | Meetings | Name | Organisation, department & role | Meetings | |
Appendix 7 Interview 2 topic guide
Narrative interview schedule
A. Understanding the network diagram
Timescale = the present
-
[Show network diagram and give brief explanation that the diagrams have been generated from data provided by a number of people. Pointing to the cluster the interviewee is involved in]. What do you do together? What kinds of things is this cluster involved in?
-
Tell me what you do or what role you play within the cluster?
-
Network structure – How/why does this thing/activity involve the people you have told us about (in network interviews)?
-
Knowledge creation activities – How would you characterise the cluster’s style of working – its approach? Why are you doing it like that?
Question to self at end of this section – do I understand the diagram (cluster and network) any better?
B. Story about an example of recent activity/problem situation
Timescale = the recent past
-
(In the context of the cluster) Can you tell me about any specific activity that people in your cluster were recently involved in? [focus on the level of the whole cluster, not just a few people]
-
Tell me a story about the planning that was involved?
-
How did involvement spread through the cluster – who enrolled whom?
-
Please describe a problem or challenge that the cluster faced during this activity and what steps you took to overcome the problem?
Question to self at end of this section – do I have a good story which illustrates the cluster as a whole
C. History of the cluster
Timescale = the past
-
Does the cluster have a longer history than the example you’ve described? [If so] What keeps relationships ticking over when there’s not a project to work on?
-
How did you get here? Can you recall how it was decided to focus on this thing/activity? How much did the decision involve the people in the cluster?
-
Can you help me understand the context of your activity: to what extent do national or local policies influence/constrain what you do and how you go about it?
Question to self at end of this section – do I know how they got here?
D. Values and skills: commonalities and diversity
Timescale = the present
-
What do people in this cluster have in common? – Are there shared values, idea, attitudes? Would you say you make similar distinctions and judgements about what’s important/relevant?
-
Would you say the people in the cluster have the same sorts of knowledge and skills or are you a highly diverse group? If so, do you feel the knowledge and skills people bring complement one another well?
-
What about the other clusters? Can you tell me anything about what they do together, what their focus is etc? How is your cluster different to the others?
Question to self at end of this section – do I understand the ‘culture’ of the cluster? Do I know anything about the other clusters?
E. Difference between networks/other
-
[Show interviewee the second network diagram and briefly explain the differences, including their own position within clusters] What is the difference between the ‘talks with’ and ‘goes to’ networks?
-
Missing people – [draw the interviewee’s attention to the list of agencies who are represented in the whole network diagram] Are any groups of people missing for what you are trying to do? Why are they missing? What’s stopping you bringing in the missing people?
Appendix 8 Leximancer analysis
Background: Leximancer
Leximancer is computer software that conducts quantitative content analysis using a machine learning technique. It learns what the main concepts are in a text and how they relate to each other. It conducts a thematic analysis and a relational (or semantic) analysis of the interview data. Leximancer provides word frequency counts and co-occurrence counts of concepts present in the transcripts of the narrative interviews. It is:
[A] Method for transforming lexical co-occurrence information from natural language into semantic patterns in an unsupervised manner. It employs two stages of co-occurrence information extraction—semantic and relational—using a different algorithm for each stage. The algorithms used are statistical, but they employ nonlinear dynamics and machine learning.
Smith and Humphreys, p. 2686
Once a concept has been identified by the machine learning process, Leximancer then creates a thesaurus of words that are associated with that concept giving the ‘concept its semantic or definitional content’. 87
We are made aware of the larger context of all the narrative interviews of the cluster and the prominence of certain concepts. It ensures that we do not become fixated on some concepts to the detriment of others. Leximancer uses a combination of techniques such as Bayesian statistics that record the occurrence of a word and connects it to the occurrence of a series of other words. It then quantifies those outputs by coding the segments of text, from one sentence to groups of sentences. As the data set presented here is relatively small, we are looking at the data sentence by sentence. Each word or concept is associated with a subset of related terms. The next step involves the machine learning from the concepts already uncovered and linked to other concepts creating a ‘concept space’. It then iteratively creates a thesaurus around a group of seed concepts. This information is visualised using network analysis.
Emergent themes are then visible to the user, and are expandable using the map visualisation that links directly to the areas of the data in which the concept occurs. The themes map enables a quick reading of the narrative interviews. It lets us see what the dominant themes are, rather than imposing our own interpretations on the data. The proximity of two concepts indicates how often or not they appear in similar conceptual contexts. So, when two concepts are placed at a distance from each other, it indicates that they are not used in the same context. The themes are the coloured circles around clusters of concepts. The lines or pathways navigate the most likely path in conceptual space between concepts in order to aid reading the map. The connectivity score reflects the degree (equivalent to degree score in network analysis) to which the theme is connected to the other concepts in the map.
Re-presenting narrative interviews
We focus here on results from one of our sites, site 1, to illustrate our methods. A thematic analysis looking at the ranked ordering of the concept list was created and then a thesaurus for each concept was collected. The thesaurus list for each concept, presented in Table 26, shows the most strongly connected – either directly or indirectly – related words to the concept they are defining. 87
At site 1, of the top 20 most important concepts, two – smoke/smoking and tobacco – are the focus of the cluster selected from the sociograms for the ‘Goes To’ network in round 2. This is the specific problem identified by the cluster. They are more generally concerned with health of people; however, they have focused on smoking as the main hindrance to achieving public health. As the cluster is involved in public health, this is not surprising. The focus is on smoking.
The clusters’ values and preferences are related to the urgency with which a working solution is required and, looking at the concept of time in Table 26 with an absolute count of 67 and a relative count of 20%, it is present in the clusters cognition. The source of that urgency is thematically related to meetings, issue, year, local, working, person, services, public and support.
The value present in the cluster is that of public or more specifically public health. There is a level of uncertainty surrounding the problem of smoking as the suppose (absolute count of 99, relative count of 29%) and probably (absolute count of 96, relative count of 28%) concepts are prominent for this cluster, with obviously (absolute count of 91, relative count of 27%) less prominent.
| Top 20 word-like concepts | Absolute count | Relative count | Thesaurus |
|---|---|---|---|
| People | 337 | 100% | smoke, probably, working, trying, services, time, talk, group, prevalence, suppose |
| Smoking | 273 | 81% | prevalence, service, services, smoke, working, somebody, talk, team, meeting, support |
| Health | 243 | 72% | public, management, issue, support, look, team, services, smoke, service, coming |
| Work | 200 | 59% | tobacco, public, trying, health, smoke, time, things, issue, probably, doing |
| Service | 159 | 47% | spec, management, provider, year, smoking, look, working, public, health, doing |
| Cause | 156 | 46% | stuff, smoke, management, things, involved, meetings, level, saying, work, talk |
| Public | 126 | 37% | health, management, working, probably, team, smoke, year, issue, service, different |
| Things | 121 | 36% | tobacco, different, issue, prevalence, look, cause, support, suppose, meetings, trying |
| Doing | 121 | 36% | spec, somebody, year, stuff, look, service, probably, provider, work, used |
| Suppose | 99 | 29% | trying, services, prevalence, smoke, talk, issue, things, money, meetings, probably |
| Probably | 96 | 28% | thought, public, person, services, talk, people, coming, management, doing, trying |
| Group | 96 | 28% | tobacco, person, trying, suppose, people, team, public, local, terms, support |
| Different | 93 | 28% | working, things, support, role, tobacco, look, public, meetings, level, service |
| Team | 91 | 27% | support, public, health, smoking, level, involved, services, different, group, thought |
| Obviously | 91 | 27% | management, provider, spec, prevalence, smoking, services, public, local, involved, role |
| Terms | 85 | 25% | support, level, look, person, different, probably, tobacco, stuff, coming, work |
| Services | 81 | 24% | smoking, probably, suppose, management, health, person, time, prevalence, team, tobacco |
| Tobacco | 77 | 23% | things, group, coming, different, trying, work, smoke, issue, services, terms |
| Time | 67 | 20% | used, meetings, issue, year, local, working, person, services, public, support |
| Look | 66 | 20% | prevalence, spec, provider, role, things, health, service, different, doing, terms |
| Name-like | Absolute count | Relative count | Thesaurus |
| Tobacco Alliance | 45 | 13% | person, prevalence, group, probably, meeting, tobacco, suppose, look, time, smoke |
| Site 1 | 40 | 12% | prevalence, trying, provider, coming, team, year, group, public, tobacco, services |
| PCT | 40 | 12% | year, role, money, doing, different, cause, time, prevalence, provider, people |
The range of activities which can be used to share and exchange knowledge related to the specific problem of smoking are within the cluster. These activities are situated within the context that the cluster is in. After a 20-year period of market-inspired organisational reform (managerialism, or the New Public Management), concepts such as, service (absolute count of 159 and relative count 47%) and public (absolute count of 126 and relative count of 37%) could be indicative of a social policy-orientated outlook rather than a managerial one. The thesaurus list does contain the more market inspired concept of management. However, management does appear, with a low absolute count of 30 and a relative count of 0.9%.
It appears that the cluster is social policy orientated. However, this is not unambiguously so. The concept of service is related to spec, management, provider, year, smoking, look, working, public, health and doing. The concept of public is related to health, management, working, probably, team, smoke, year, issue, service and different. So, the concept of service is orientated towards management rather more so than public, health, and public relates to health, and management more than service. What this highlights is the level of ambiguity around the concept of management for the cluster.
How the concepts are semantically contextualised can be seen in the Leximancer concept map below (Figure 30). The map is a re-presentation of the relational or semantic characteristics of the concepts presented in Table 1. To paraphrase Rooney,87 the direct co-occurrence between concepts is extracted from the data and these direct links are based on the strength of relations between the concepts. The more often two concepts appear together in the same sentence the more likely they are to be linked together. Leximancer then compares each concepts thesaurus and creates indirect links between them, meaning that even when concepts do not appear in the same sentence together there can still be an indirect connection between them. So, Leximancer rank orders concepts and presents them according to the strength of association and semantic similarity. So,
Concepts that are directly related but not necessarily strongly semantically linked can be far apart on the concept map while concepts that are strongly semantically related will be close to each other on the concept map . . . concepts that occur in similar semantic contexts tend to form clusters (or gather together).
Rooney, p. 41087
FIGURE 30.
Leximancer map of the 11 site 1 narrative interviews combined. General concepts are in black with themes in colour.
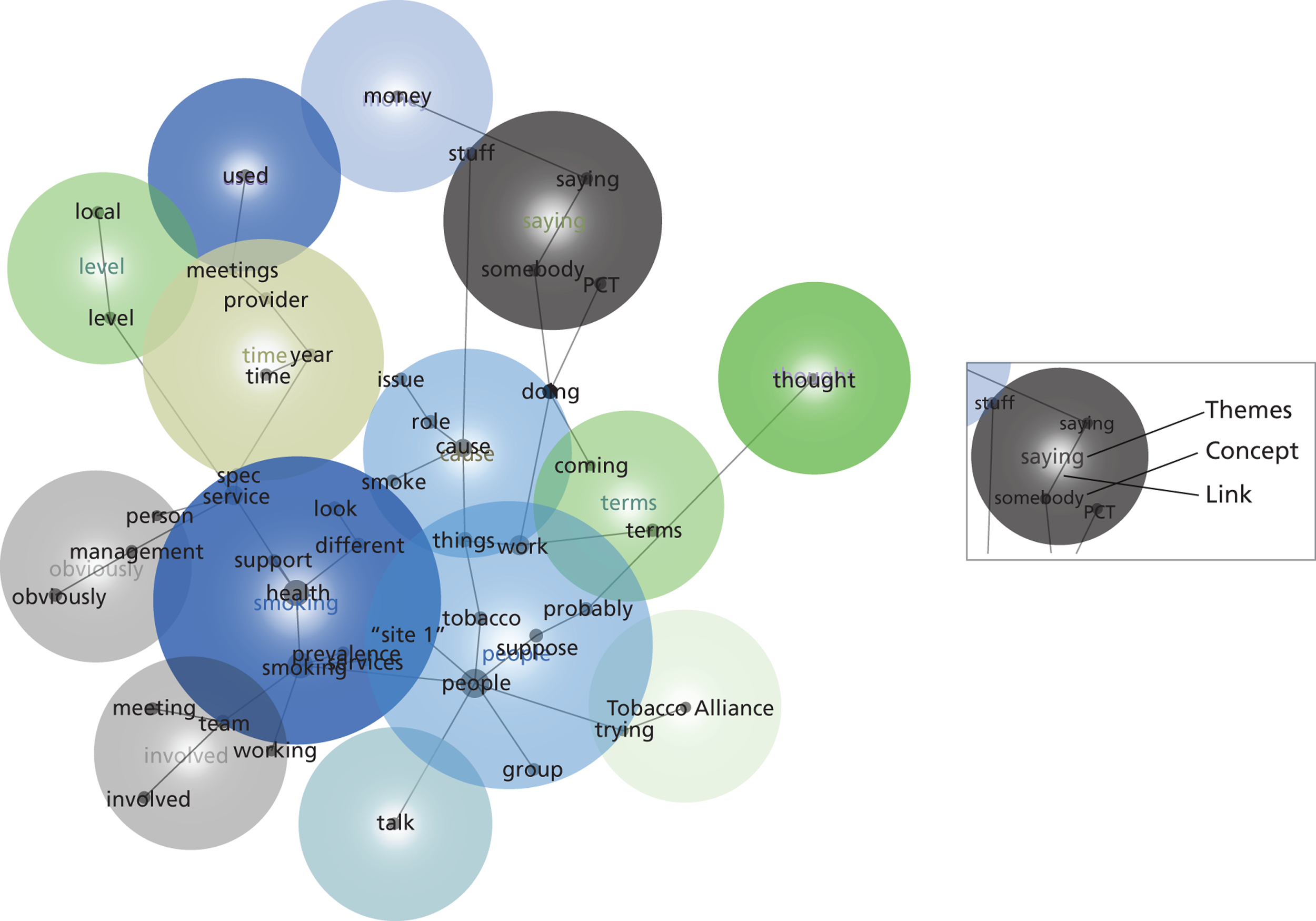
The coloured circles indicate the thematic space of a theme with the label of that theme at the centre. The words in black are the concepts and the lines between are links that tell us which concepts are semantically linked. When two or more circles overlap it indicates that the themes are semantically related to each other.
Figure 31 shows for the cluster the most dominant theme is SMOKING, followed by PEOPLE, CAUSE, TIME, SAYING, OBVIOUSLY, INVOLVED, GROUP, TERMS, LEVEL, TALK, TOBACCO, ALLIANCE, MONEY, THOUGHT and USED. The proximity of SMOKING, PEOPLE, CAUSE, TIME, OBVIOUSLY and INVOLVED themes indicate that they are related to each other in a chain-like manner. GROUP, TERMS, LEVEL, TALK, TOBACCO, ALLIANCE, MONEY, THOUGHT and USED are semantically isolated. The name like concepts of Tobacco Alliance and PCT are not directly connected to the dominant theme of SMOKING, while site 1 is within the SMOKING theme. Therefore, site 1 resides in the same semantic space and is connected to SMOKING, while Tobacco Alliance and PCT are not.
Focusing on the theme of SMOKING (see Figure 31), it is associated and linked with smoking, health, services, prevalence, support, spec, site 1, different and look. However, smoking is not linked directly but indirectly to management, team or working. SMOKING is also semantically associated with management, as the two themes overlap slightly.
FIGURE 31.
Close-up of the SMOKING theme from site 1.
We tell more than we realise we know
Taking Polanyi’s concept of ‘knowing more than we can tell’, we can reformulate it to read ‘we tell more than we realise we know’, to paraphrase Zappavigna (p. 298). 88
This is the position that speakers express what they tacitly know through grammatical patterns without being aware they are doing so. By carefully analysing the grammatical patterns of ‘under-representations’88 in texts, we can bring to the fore the tacit knowledge assertions of our interviewees.
The next phase of the analysis of the interview texts makes explicit that which is tacit by looking at the function of the grammatical choices the interviewees are making.
Systemic Functional Linguistics (SFL) is an analytical method from Halliday89 which is concerned with grammar’s functionality or, rather, how it creates and expresses meaning. It regards grammar as a system of explaining things by referring to other things. Each system of the interconnected words construct the ‘meaning potential’ shaped by the semantic choices being made and the activity in the brain. SFL’s position is that when text is analysed it brings to the fore the meaningful choices made at the expense of the choices that were not made. This analysis goes beyond the usual procedures employed by others who typically look at scenarios90,91 and narratives92 and then deliver a running commentary on the text.
The functionality in language is central to language or rather the function of language is to convey experience and to generate interaction with others. With the construction of experience and interaction needing cohesion and continuity of text, a second function of language emerges – that experience and interaction require text. According to SFL, language has three ‘metafunctions’, ideational, interpersonal and textual, with the term ‘metafunction’ being used to ensure that function is regarded as an integral component of the interaction of the three terms.
The texts collected during the narrative interviews are ways of being that allows the relationship between the text and persons involved to bring in the ‘below-view patterning in language’. 88 SFL allows us to bring out the ‘tacit assumptions and ideological assumptions’ that characterise certain domains of discourse. This corresponds with Halliday’s interpersonal function of language. So when analysing the texts this accounts for social practices that are being realised in the texts.
Language is an abstract social structure that defines what is and is not possible. Orders of discourse are linguistic practices that select which linguistic elements are included and excluded, and texts or social events are the products of the mediation by orders of discourse. Focusing on analysing the use of nominalisations, modality, generalisation and agency in what people commit themselves to when they make statements, ask questions, make demands or offers in texts we are able to categorise the tacit knowledge assertions that are being made during the narrative interviews. 88
The following descriptions are taken from Zappavigna. 88 Her approach is also based on the ideas of Nonaka and Takeuchi93 – that middle managers are knowledge engineers. When they are involved in creating mid-level business and product concepts they mediate between ‘what is’ (epistemic modality; is, are, was, were . . .) and ‘what should be’ (deontic modality; should, would, will, ought to be, can . . .). They remake reality, or engineer new knowledge assertions, according to the ideas they have received from meetings and documents from more senior or external inputs. ‘They facilitate all four varieties of knowledge conversion and engineer knowledge spirals between organisational levels (cross-levelling). Their essential skills are in project coordination, formulating hypotheses, integrative methodologies, facilitating dialogue, use of metaphor, ability to engender trust, and ability to envision the future based on an understanding of the past’ (Nonaka and Takeuchi). 93
According to Zappavigna,88 these attempts at project co-ordination, formulating hypotheses, integrative methodologies, facilitating dialogue, use of metaphor, ability to engender trust, and ability to envision the future based on an understanding of the past are evident in the choices they make when talking about what they do. Analysing the specific words they use can highlight for us when they are facilitating knowledge.
Zappavigna argues that ‘the central linguistic process of tacit knowing is ‘under-representation’. The under-representation of meaning is how tacit knowledge is indicated in language.’88
Nominalisation
The use of nominalisation in speech indicates an ongoing project. By looking at when the interviewees use nominalisation, we are seeing where the interviewee is presenting an ambiguous or unambiguous relationship with the statement they are making.
When they refer to processes as things such as ‘health improvement’, which is an ongoing project that they are co-ordinating, they in fact see is it as a project and they refer to it as an entity in its own right. The meaning of ‘a person’s need to do something’ (i.e. improve health) has become condensed with the use of ‘ment’ in improvement.
Nominalisations are demarcated by the use of suffixes (able, ad, age, agogy, al, ality, ative, ment, to name only a few) which are placed at the end of words.
Processes become things that act on other processes as things, then this relation of ‘acting upon’ itself becomes a thing. The unfolding of activity sequences are finally re-expressed as parts of composition taxonomies, as criteria for classifying the abstract entities they modify. Instead of a sensually experienced world of unfolding processes involving actual people, things, places and qualities, reality comes to be experienced virtually as a generalised structure of abstractions.
Rose, pp. 263–494
Modality
The use of modality in speech indicates the formulating of hypotheses [is, are, were] – ability to envision the future [should, would, will].
Examples of modality are can, could, should, would, might, must and probably (this list is not exhaustive). They are an indicator of the level of certainty or uncertainty that the speaker has in regard to the assertion being made.
Modality contains meaning by embedding the agent motivating the opinion expressed. The use of modality in text under-represents agency or cause. For example, an IT professional might say ‘I should reassess this requirement’.
The use of the modal verb should is masking the ‘who’ or ‘what’ motivating the process of reassessing. It could be a command from a senior and not from the interviewee.
Generalisations
Rather than saying that something is a fact, speakers make generalisations in order to sound less direct and allow for uncertainty in the statement that they are making. Generalisations indicate to us the cognitive process and contents of the statement.
Generalisation contains meaning through underspecifying a concept and pattern. Examples of words that demarcate generalisations are some, a bit, a few, any, part of, complete, entire, none, no one, nothing and zero (again to name only a few). The generalisation usually follows these words.
General terms are not necessarily more abstract; a bird is no more abstract than a pigeon. But some words have referents that are purely abstract – words like cost and clue and habit and strange; they are construing some aspect of our experience, but there is no concrete thing or process with which they can be identified.
Halliday and Matthiessen, p. 61595
Generalisation underspecifies meaning and highlights assumptions; examples are system and programme.
Cognitive analysis
Within Leximancer, there is a pre-set ability to conduct sentiment analysis. Simply put, sentiment analysis measures the attitude of a speaker or writer towards a concept, whether they express something positively or negatively. In order to conduct cognitive analysis, we have combined sentiment, nominalisation, generalisation and modality. By doing so we focus on what the interviewee holds to be pre-supposed or tacit knowledge, thereby enabling us to answer two questions: what do they know, and what do they not know?
Cognitive analysis using sentiment analysis settings
What types of knowledge is the cluster concerned with? Taking each concept as highlighted by Leximancer and extracting the complete thesaurus of all words related to that concept by Leximancer, we then count the number of uses of nominalisation, modality, generalisation and agency in relation to each concept (see Table 27).
It is clear from Table 27 and Figure 32 that the cluster is predominantly involved in the use of nominalisations; this indicates ongoing projects being perceived as entities in their own right rather than processes. What Table 27 and Figure 32 do not tell us, however, is whether the cluster perceives these projects are ongoing or finished, whether they are making claims with epistemic certainty or uncertainty and whether there assertions are based on assumptions or ‘fact’.
| Concept | Nominalisation: project coordination | Modality: formulating hypotheses | Generalisations | Agency | |
|---|---|---|---|---|---|
| 1 | People | 119 | 54 | 30 | |
| 2 | Smoking | 119 | 54 | 30 | |
| 3 | Health | 119 | 54 | 30 | |
| 4 | Work | 119 | 54 | 30 | |
| 5 | Service | 56 | 54 | 30 | |
| 6 | Cause | 119 | 54 | 30 | |
| 7 | Public | NA | NA | NA | |
| 8 | Things | 111 | 54 | 30 | |
| 9 | Doing | 101 | 54 | 30 | |
| 10 | Suppose | 64 | 54 | 30 | |
| 11 | Probably | 55 | 54 | 30 | |
| 12 | Group | 31 | 31 | 30 | |
| 13 | Different | 55 | 54 | 30 | |
| 14 | Team | 48 | 48 | 30 | |
| 15 | Obviously | 50 | 50 | 30 | |
| 16 | Terms | 41 | 41 | 30 | |
| 17 | Services | 56 | 54 | 30 | |
| 18 | Tobacco | 58 | 53 | 30 | |
| 19 | Time | 53 | 48 | 30 | |
| 20 | Look | 48 | 54 | 30 | |
| TOTAL | 1422 | 973 | 570 | ||
| Name-like | Nominalisation: project coordination | Modality: formulating hypotheses | Generalisations | Agency: power | |
| 21 | Tobacco Alliance | 13 | 13 | 13 | |
| 22 | Site 1 | 45 | 45 | 30 | |
| 23 | PCT | 28 | 28 | 28 | |
| TOTAL | 86 | 86 | 71 |
FIGURE 32.
Nominalisation, modality and generalisation frequency for each concept of site 1 interviews.
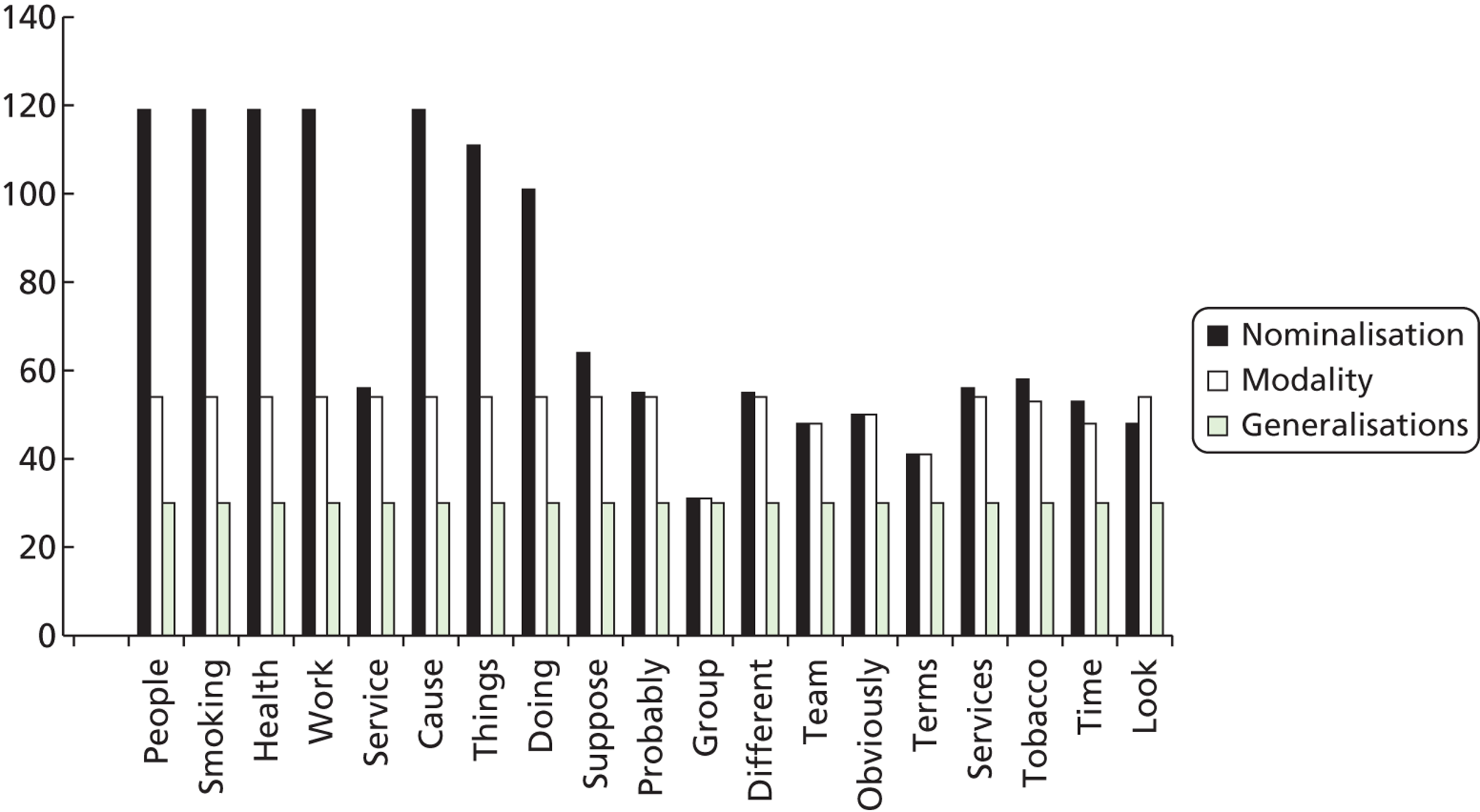
What follows is an automated report generated by limiting the number of concepts to 23 listed in Figure 30, above, plus 2 GPs, and Public Health, as they were highlighted by Leximancer as potential names. The categories of interest are the interviewee data files. So, what we get is an analysis of each interviewee’s use of the top concepts for the cluster.
As well as that, the technology within Leximancer that analyses positive and negative sentiment has been altered to include categorisation of terms that indicate nominalisation, generalisation and modality. The results are presented in a high-level, visual chart displayed in a ‘magic quadrant’ format. The axes are relative frequency, which is a measure of the conditional probability of the concept given the categories of Sentiment, Nominalisation, Generalisation and Modality (cognitive analysis – positive or negative). We are looking at the occurrence of positive or negative words when ‘health’ is mentioned. The axes labelled ‘strength’ is a measure of the conditional probability of the category cognitive analysis – positive or negative given the particular concept (e.g. how often is ‘service’ mentioned with positive or negative cognition?).
There are four areas to the quadrant, and the different colours of concepts refer to different interviewees’ accounts. Concepts in quadrant one (bottom left) are weak and less prevalent within the interviewee’s data – this is where negative Sentiment, Nominalisation, Generalisation and Modality manifest. Concepts in quadrant four (top right) are strong, prominent and more likely to co-occur with the category. This is where positive Sentiment, Nominalisation, Generalisation and Modality sit.
Figure 33 indicates a low frequency for the majority of concepts except for terms and obviously and these are both from one interviewee. A majority of the concepts are also viewed negatively on the negative cognition scale.
FIGURE 33.
Cognitive analysis quadrant of top 20 concepts: frequency and strength results for site 1.
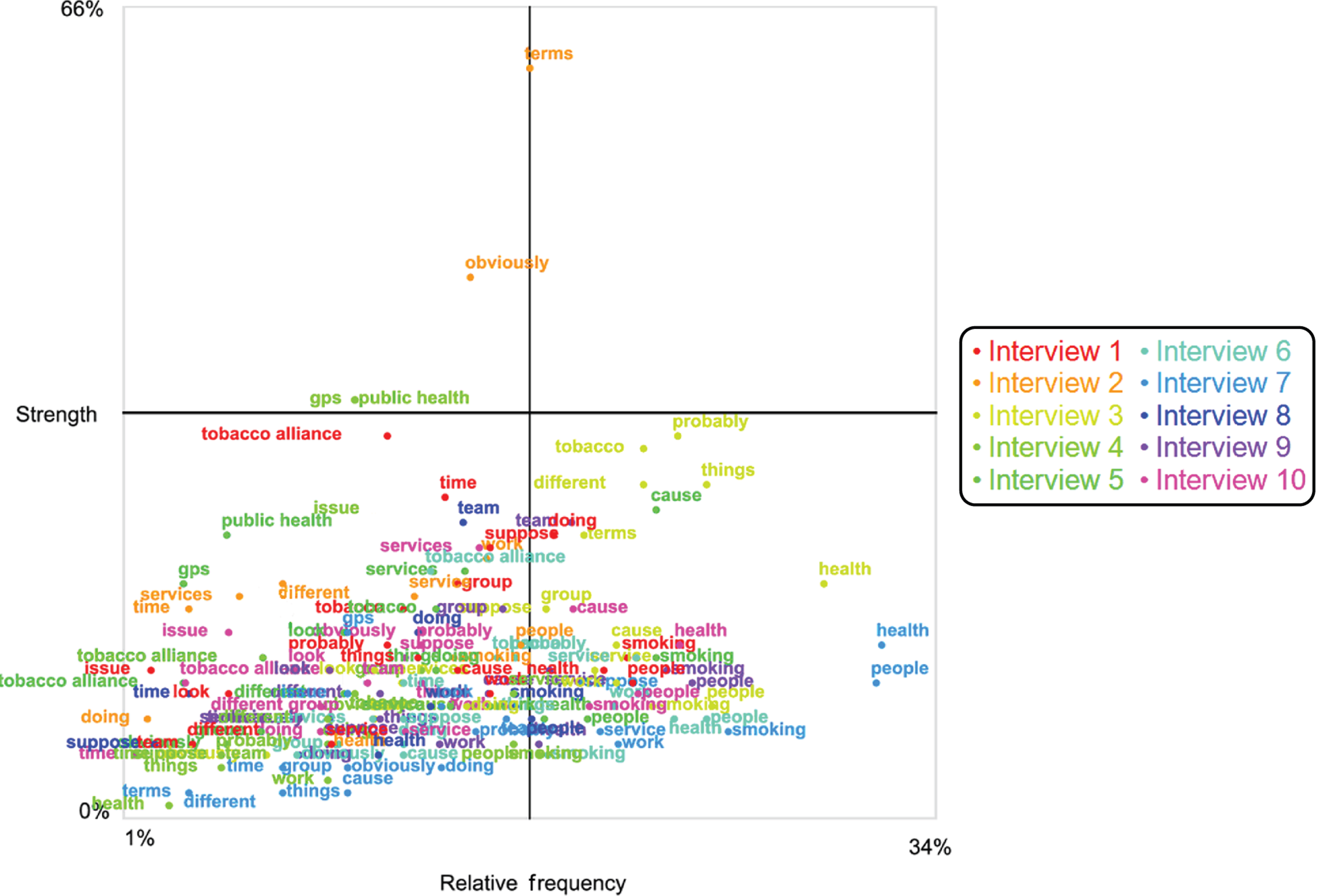
When the data from Figure 33 are compared with the cognition scale frequency and strength results of the cluster, this generates Figure 34 (presented below). The concepts cause, service, health, smoking, people and work are viewed moderately positively on the cognition scale. They have also scored highly for cognition scale for each concept of site interviews in Figure 33.
FIGURE 34.
Cognitive analysis quadrant of top 20 concepts: frequency and strength compared with cluster results for site 1.
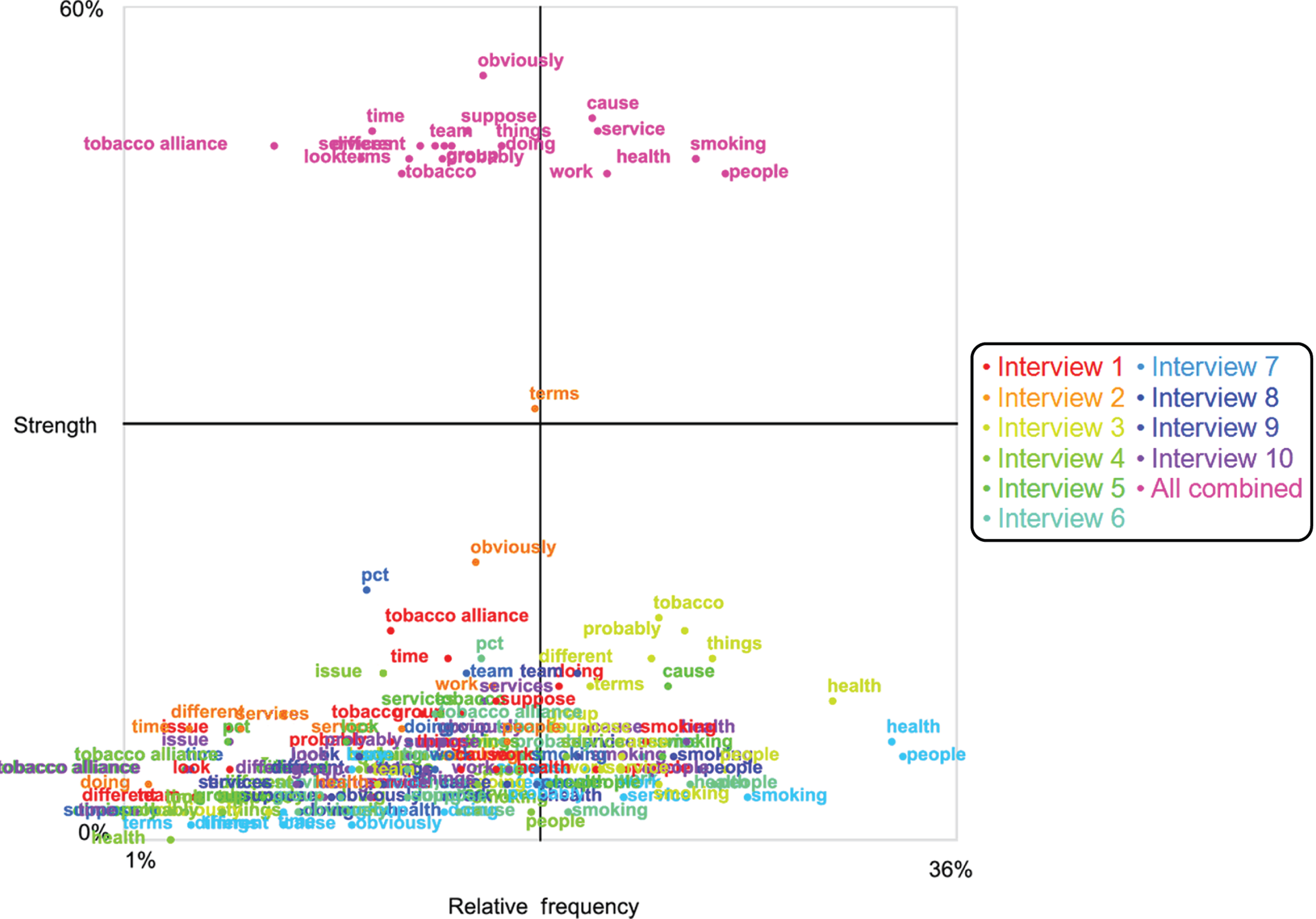
The most striking aspect of Figure 34, which shows all interviews combined as well as the individual interviews, is that the Tobacco Alliance, which has a high frequency score, also has a negative or weak cognition score, meaning that the concept Tobacco Alliance is used in a manner that indicates that the cluster does not know what the Tobacco Alliance is, or what it intends to do. Work, cause, smoking, people, health and service are all within the positive quadrant of the scale, indicating that these terms are used positively and that the cluster knows what these things are. For the cluster, the concepts public, things, doing, suppose, probably, group, different, team, obviously, terms, tobacco, time, look, Tobacco Alliance, site 1 and PCTs fall into the negative, high-frequency quadrant.
Site 1 documents results
Figure 35 shows that for the cluster the most dominant theme is TOBACCO, followed by SMOKING, LOCAL, SUPPORT, GROUPS, SMOKEFREE, SCHOOL, ENSURE, SMOKING, YEAR, TOBACCO, CIGARETTES and PROJECT. The proximity of TOBACCO, LOCAL and GROUPS are overlapping. This indicates that they are related to each other in a chain-like manner. YEAR, SCHOOL and PROJECT are semantically isolated. The concepts of council, control, products, public, communities and inequalities are directly connected to the dominant theme of TOBACCO (Figure 36). The theme of SCHOOL is semantically isolated from the dominant theme of TOBACCO.
FIGURE 35.
Leximancer default positions map of the documentation for site 1. General concepts are in black with themes in colour.
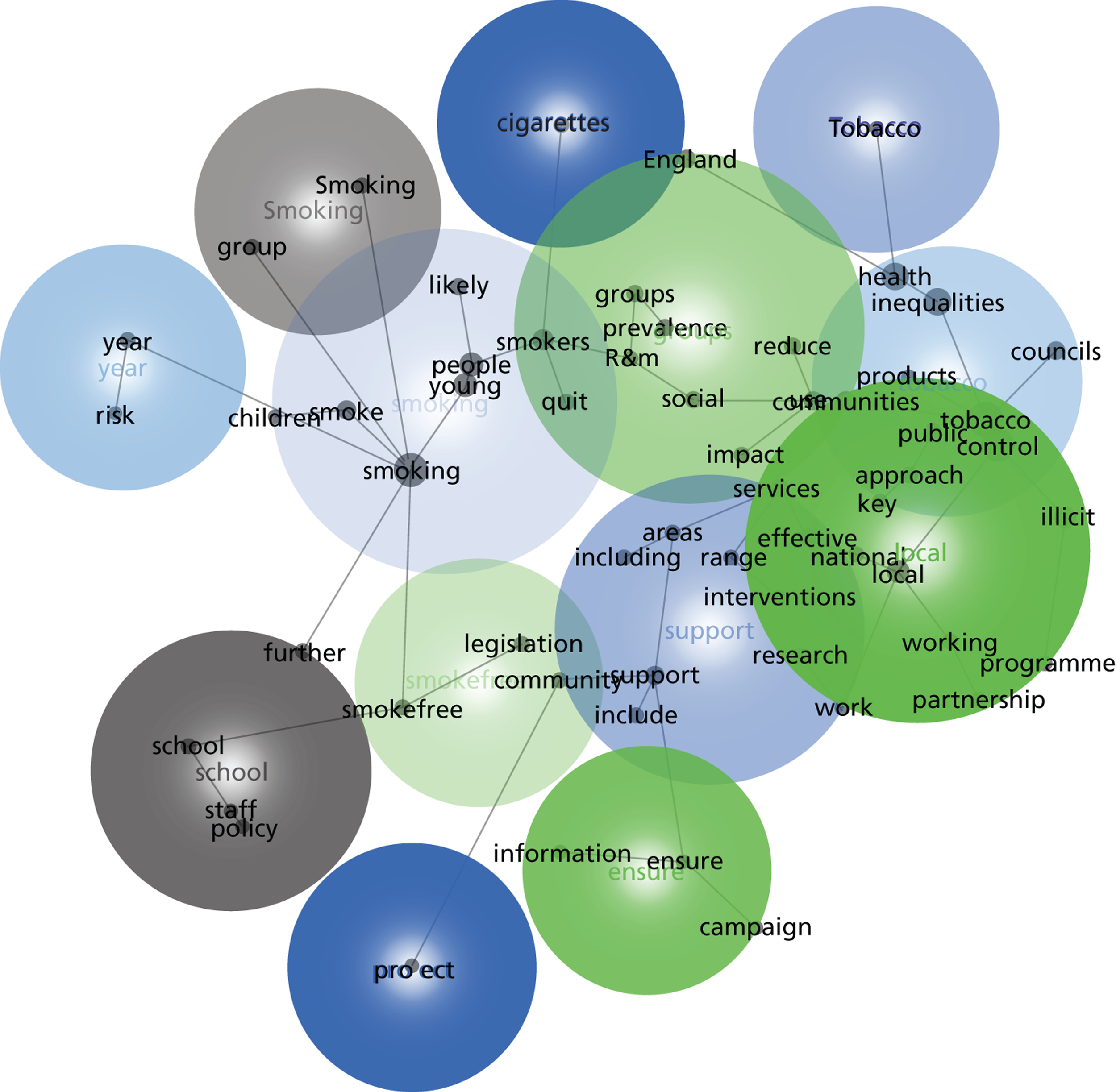
FIGURE 36.
Close-up of the TOBACCO theme from documents for site 1.
| Top 20 word-like concepts | Count | Relevance | Thesaurus |
|---|---|---|---|
| smoking | 797 | 100% | prevalence, quit, risk, children, smokers, likely, reduce, social, groups, service |
| tobacco | 774 | 97% | products, control, illicit, councils, use, communities, key, public, local, reduces |
| control | 650 | 82% | councils, illicit, products, tobacco, use, key, communities, reduce, national, programme |
| inequalities | 458 | 57% | health, councils, public, use, approach, communities, reduce, control, services national |
| health | 446 | 56% | inequalities, councils, public, reduce, use, approach, communities, services control, social |
| people | 405 | 51% | young, children, social, likely, smokers, quit, groups, products, smoke, use |
| young | 393 | 49% | people, children, social, likely, smokers, quit, groups, smoke, products, group |
| local | 327 | 41% | services, effective, national, areas, communities, approach, public, partnership, community, use |
| smokers | 267 | 34% | quit, likely, groups, communities, services, impact, cigarettes, year, range prevalence |
| illicit | 253 | 32% | products, programme, control, tobacco, partnership, reduce, working, impact, communities, key |
| smoke | 247 | 31% | children, risk, likely, smoke-free, legislation, cigarettes, smokers, people, year, young |
| support | 229 | 29% | services, effective, local, staff, areas, quit, legislation, ensure, national, research |
| use | 177 | 22% | reduce, social, communities, impact, national, range, products, areas, interventions, councils |
| work | 158 | 20% | partnership, legislation, effective, national, working, public, local, including, programme, reduce |
| communities | 157 | 20% | key, approach, councils, partnership, public, effective, social, use, local, reduce |
| groups | 157 | 20% | social, likely, smokers, key, range, group, services, areas, research, communities |
| school | 151 | 19% | policy, staff, smokefree, ensure, legislation, including, support, community, children, smoking |
| public | 149 | 19% | approach, legislation, communities, inequalities, health, working, reduce, local, partnership, work |
| councils | 149 | 19% | inequalities, key, communities, health, approach, control, use, tobacco, services, range |
| prevalence | 136 | 17% | reduce, areas, national, smoking groups, smokers, further, year, services, likely |
| Name-like | Count | Relevance | Thesaurus |
| England | 123 | 15% | year, public, prevalence, reduce, young, people, national, children, control, research |
| Smoking | 86 | 11% | risk, prevalence, groups, social, smoking, interventions, further, including, year, smokers |
| R&M | 71 | 9% | groups, smokers, communities, group, key, likely, impact, social, councils, quit |
| Tobacco | 56 | 7% | products, control, use, tobacco, smoke, cigarettes, public, social, people, young |
Comparison of site 1 documents against cluster (Figure 37)
FIGURE 37.
Cognitive analysis quadrant of top 20 concepts: frequency and strength results for site 1 with comparison with all interviewee data for the same site.
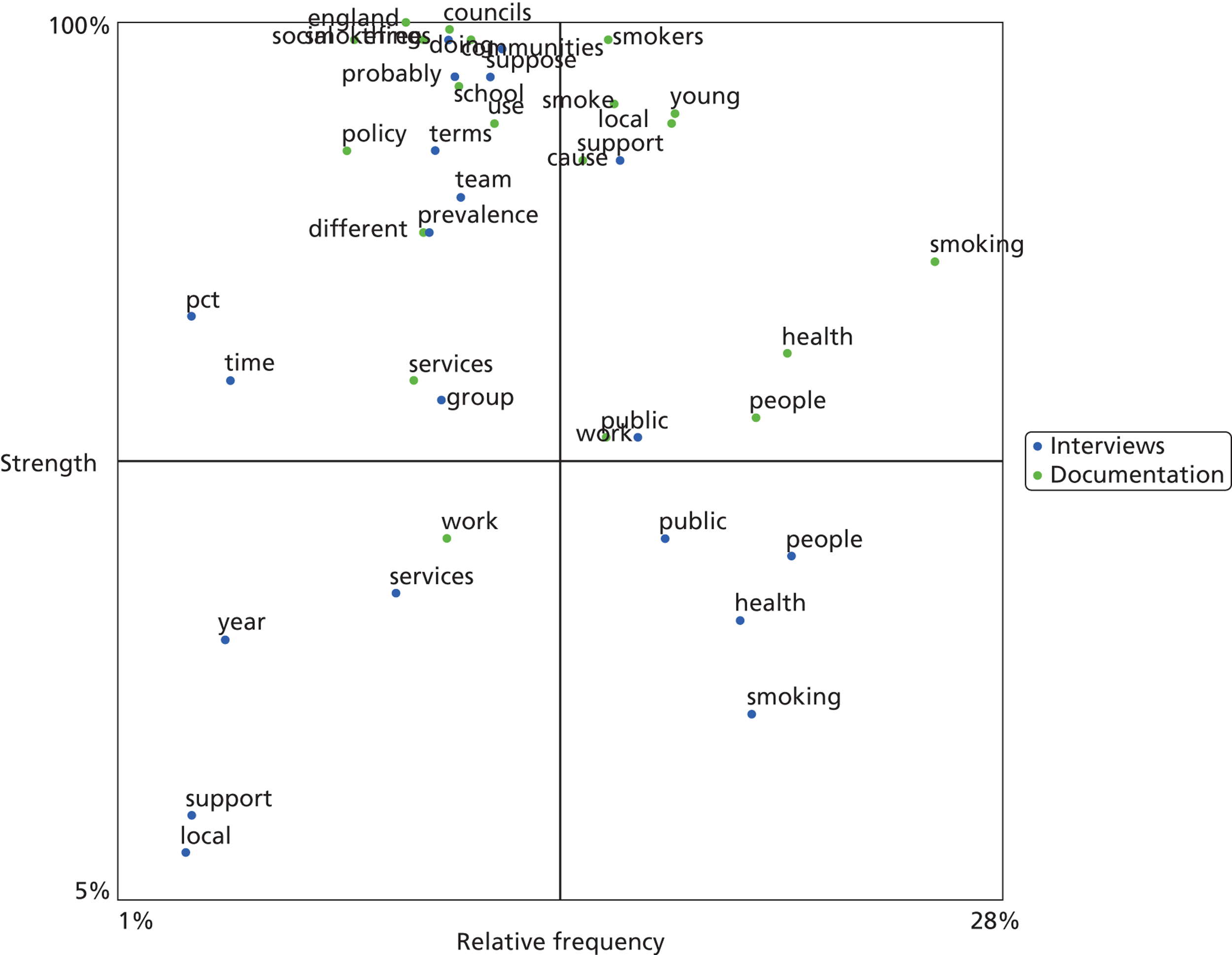
List of abbreviations
- GP
- general practitioner
- HSDR
- Health Services and Delivery Research
- IMPROVE-PC
- Improving the Prevention of Vascular Disease
- NIHR
- National Institute for Health Research
- PCT
- primary care trust
- QDA Miner
- Qualitative Data Analysis Miner
- QIPP
- Quality, Innovation, Productivity and Prevention
- R&D
- research and development
- R&M
- routine and manual
- SDO
- Service Delivery and Organisation
- SFL
- Systemic Functional Linguistics
- SOC
- Standard Occupational Classification
- VBLPCM
- variational Bayes latent position cluster model