

Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 16/53/03. The contractual start date was in February 2018. The final report began editorial review in August 2019 and was accepted for publication in January 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Keen et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Just 25 years ago, most commentators assumed that health services were generally safe. Then, in 2000, the Institute of Medicine in the USA published a report on patient safety: To Err is Human: Building a Safer Health System. 1 The evidence presented in the report suggested that rates of adverse events – events that resulted in harm to patients – were far higher than anyone had realised. It proved to be a landmark report, not just in the USA but around the world. Ever since, policy-makers around the world have been acutely aware that treatment and care need to be safer.
The NHS in England has committed considerable resources to improving patient safety in the intervening 20 years. Overall, however, the rate of adverse events remains high and it is widely accepted that there is still considerable scope for improvement. 2 A range of interventions have been proposed by policy-makers, including quality improvement initiatives, the use of performance targets and comparative audits. A series of government policies and official reports published over the last 20 years have argued that health information technologies (HITs) can also improve patient safety. 3–5 This report investigates this argument. We have undertaken a realist synthesis of evidence about an important class of HITs, namely interoperable networks. These are networks that link the information technology (IT) systems of different organisations in a health economy, so that a professional based in one organisation can access data about a patient held in another organisation during the course of treatment and care. There is a continuum of technical solutions. At one end is a network that allows a user to access a remote patient database using a separate log-in, so that the user has to accept the layout and content of that database. At the other end is an integrated solution in which a user logs on once and sees a patient record that has a single consistent layout and for which data from all sources are easily accessed.
The effects of health information technologies on patient safety
When we bid for this evidence synthesis, we were aware of two systematic reviews that usefully summarised what we knew about HITs and patient safety, and helped us to pinpoint what we did not. Black and colleagues6 undertook a ‘review of reviews’ of a number of HITs that have been available for many years, including telehealth, electronic health records (EHRs) (used within organisations), decision support systems and hospital e-prescribing systems. Black and colleagues6 focused initially on experimental and quasi-experimental studies, but then broadened their searches to include a selection of observational studies of implementation. The majority of reported studies were conducted in hospital settings, with the main exception being studies of telehealth applications. Some of the studies reported positive results, notably for electronic medicines reconciliation, whereas others found mixed and negative results, including for telehealth. The authors commented on the poor overall quality of the literature and, in particular, on the small numbers of high-quality randomised controlled trials in the domain.
Second, Brenner and colleagues7 identified 31 systematic reviews that focused on HITs and patient safety. The authors7 reported on a range of systems, including computerised physician order entry (CPOE), order entry alerts (e.g. for contraindicated drugs), EHRs, clinical decision support systems, electronic medicines reconciliation and electronic clinical pathways software. They used a broad definition of patient safety, and the end-point measures included mortality, adverse drug events and infection rates. Twenty-five out of 69 included studies reported a statistically significant positive effect on the patient safety measure assessed. Overall, however, the authors concluded that, ‘many areas of health IT application remain understudied and the majority of studies have non-significant or mixed findings’. 7
These reviews led us to identify two significant gaps in the applied health research literature. First, we did not find any systematic reviews of the effects of interoperable networks on patient safety outside hospitals. There was evidence about telehealth, but a large England-based trial showed that telehealth was not cost-effective and systematic reviews of international evidence were, at best, inconclusive. There was no case for another systematic review. The one published review that shed light on interoperable networks focused on effects on resource use rather than on patient safety. 8
This state of affairs was a surprise, given that government policies in many countries had promoted investments in interoperable networks – or, to use the preferred US term, health information exchanges (HIEs) – for some years. In particular, the Barack Obama administration in the USA had allocated US$35B to HIT investments from 2009. A substantial proportion of the money was to be spent on information exchanges, linking hitherto separate IT systems in hospitals, family physicians’ offices, pharmacies and elsewhere. The benefits claimed initially included improvements in patient safety, cost savings and productivity improvements.
Information technology policies in England had also promoted investments in interoperable networks from 2015 onwards, although the central monies allocated were initially modest. 9 We were also aware of developments on the ground in a number of health economies. For example, health and social care organisations in the city of Leeds had been developing an IT platform, or information infrastructure, linking their various systems together for a number of years. Nurses, doctors and other professionals working in one organisation could already access patients’ records held in others’ systems. There was a gap, then, between investments in this sort of development and the evidence about their value, particularly in relation to patient safety.
The second gap concerned the ‘how and why’ of the deployment and use of HITs. We were struck by the effectiveness evidence: why was it so mixed and why were effect sizes so modest? Mobile phones and other consumer technologies have transformed the way we search for information, shop and communicate with one another. Why were no similar effects found in health and social care settings? We did not expect effectiveness studies to answer these questions, but we were aware of other literatures that might help us to do so. For example, a comprehensive review of evidence from the field of human–computer interactions revealed that, in contrast with applied health research, there was a long history of empirical studies stretching back to the 1980s. The review suggested that health professionals often found systems difficult to access and use. A range of problems was cited, including poor interface designs and the unreliability of hardware. 10 There was, again, more evidence about hospital than extra-hospital systems, but some evidence about the latter was presented. Similarly, sociological studies reported problems with integrating IT systems into routine clinical practice. 11–13
These literatures were consistent with reports that HITs could increase patients’ risks. A 2011 Institute of Medicine report neatly summarised the problem:
. . . some case reports suggest that poorly designed health IT can create new hazards in the already complex delivery of care. Although the magnitude of the risk associated with health IT is not known, some examples illustrate the concerns. Dosing errors, failure to detect life-threatening illnesses, and delaying treatment due to poor human–computer interactions or loss of data have led to serious injury and death.
A realist synthesis
Putting these lines of argument together, we decided to focus on interoperable networks that link organisations across health economies, and their effects on patient safety. Furthermore, we agreed with the Institute of Medicine that there were risks, as well as benefits, associated with HITs. It would therefore be important to go further than identifying the effects associated with interoperable networks, and explain how and why the networks produced these effects.
We needed, then, to identify an evidence synthesis method that would allow us to investigate the ‘how and why’ of interoperable networks, as well as their effects on patient safety. We would also need to be able to assimilate both narrative and quantitative evidence into the synthesis. Pope and colleagues15 have reviewed the methods that are available for the synthesis of ‘mixed’ health evidence, including narrative reviews and thematic analyses. Pope and colleagues15 emphasise that each method has strengths and weaknesses, and that each one is better suited to some topics and research questions than others. Following Pope and colleagues’ analysis,15 and drawing on our own experience, we judged that a realist synthesis would be appropriate. It would allow us to identify how and why interoperable networks led to particular outcomes, in our case how and why they led to changes in patient safety. As we show in Chapters 2 and 3, we took the caution about the weaknesses of the method seriously and actively sought to mitigate them in this review.
Aims and objectives
The aim of the study was to establish how and why networked, interorganisational HIT services improve patient safety, fail to do so or increase safety risks. We undertook a realist synthesis. The method involved identifying (1) programme theories that capture the chains of reasoning that lead from an intervention to its use and subsequent effects, and (2) reasons why the intended improvements are, or are not, achieved in practice, or indeed increase safety risks.
The objectives of the study were to:
-
identify initial programme theories and prioritise theories to review
-
search systematically for evidence to test the theories
-
undertake quality appraisal, and use included texts to support, refine or reject programme theories
-
synthesise the findings
-
disseminate the findings to a range of audiences.
Protocol change
One change was made to the protocol for this evidence synthesis. The intention was to run three nominal groups to consult with policy-makers, senior informatics managers and front-line clinicians in the theory development stage. We were able to organise the first two nominal groups but not the third, principally because front-line staff were not able to obtain permission for time off to attend the initial meeting. We used a different method, eliciting the views of seven health and social care professionals based in two localities in the north of England in semistructured telephone interviews. This method is described in Chapter 3.
Structure of this report
Chapter 2 provides an overview of the study design of the realist synthesis and shows how we made key decisions about the design. Chapter 3 describes our literature review, nominal group and interview methods. Chapter 4 sets out the findings of the theory development phase of the synthesis. The next four chapters present evidence search findings. Chapter 5 presents the findings for the co-ordination of services for older people. Chapter 6 presents the findings for searches on medication reconciliation undertaken in the course of care of older people. Chapter 7 presents the co-ordination of child protection services. Chapter 8 presents the evidence about economies of scope and scale resulting from the deployment and use of networked HITs. In Chapter 9 overall synthesis of the findings is presented and discussed, and the conclusions and recommendations are listed.
Chapter 2 Study design
Introduction
This chapter sets out the study design for the realist synthesis. The next section (see Theory development and programme theories) outlines the key features of a ‘standard’ realist syntheses, reported in many published accounts. Core elements of our study design are consistent with those accounts. We then note the diversity of study designs and methods reported in the literature. 16 Realist syntheses have common characteristics, notably in the development and testing of programme theories that investigate the relationships between interventions and outcomes. However, they also vary in the ways in which theories are developed and in which they are tested, and teams therefore need to make choices about their synthesis designs. The last section (see Mid-range theory) sets out the choices that we made and the ways in which they influenced our study design. The synthesis is registered with PROSPERO CRD42017073004.
Theory development and programme theories
The realist synthesis review method was first described in detail by Pawson in Evidence-Based Policy17 in 2006. The first stage, which we refer to as theory development in this report, involves the development of a programme theory. 18,19 A programme theory is a representation of the way in which an intervention is intended to work. It typically involves a sequence of decisions and actions that lead to a defined outcome, underpinned by reasoning about how those decisions and actions follow one another. A number of programme theories may initially be developed, reflecting different ways in which an intervention might lead to an outcome. Sources of programme theories can include government and other policy documents, and accounts by opinion leaders in journal editorials and elsewhere. It has become usual, in the last few years, for stakeholder consultation to be used as another source of information for developing programme theories.
Sometimes, established theories have already been published, and these can be used by the review team. On other occasions, no plausible, published sequences can be found. When this happens, review teams can instead identify potentially useful fragments, covering partial sequences of events, which are pieced together by the review team. Evidence is then identified and evaluated. This is to establish the actual sequence of events that links an intervention and an outcome, and whether or not the underlying reasoning is supported by empirical evidence. (Putting this a slightly different way, a rationalist approach to identifying an intended sequence of events is followed by empirical assessment of that sequence.)
Most realist syntheses present evidence reviews in three distinct stages (Figure 1). First, key concepts are identified from the review question and used to design the literature searches. Inclusion and exclusion criteria are defined and used to identify articles for full-text review. The second stage involves close scrutiny of the full text of the included articles, which are assessed for rigour and relevance, with data and relevant theory extracted. Third, the data and theory in the included articles are synthesised and compared with the initial programme theories. Any one theory might be supported, refined or rejected. Pawson points out that the conduct of realist syntheses is typically iterative. Empirical evidence might, for example, suggest that there is evidence to support a proposed sequence of events, but there may be additional steps in the sequence that were not identified in initial programme theories. As a result, evidence has not been sought for these steps, and further searches need to be designed and conducted.
FIGURE 1.
Study design.

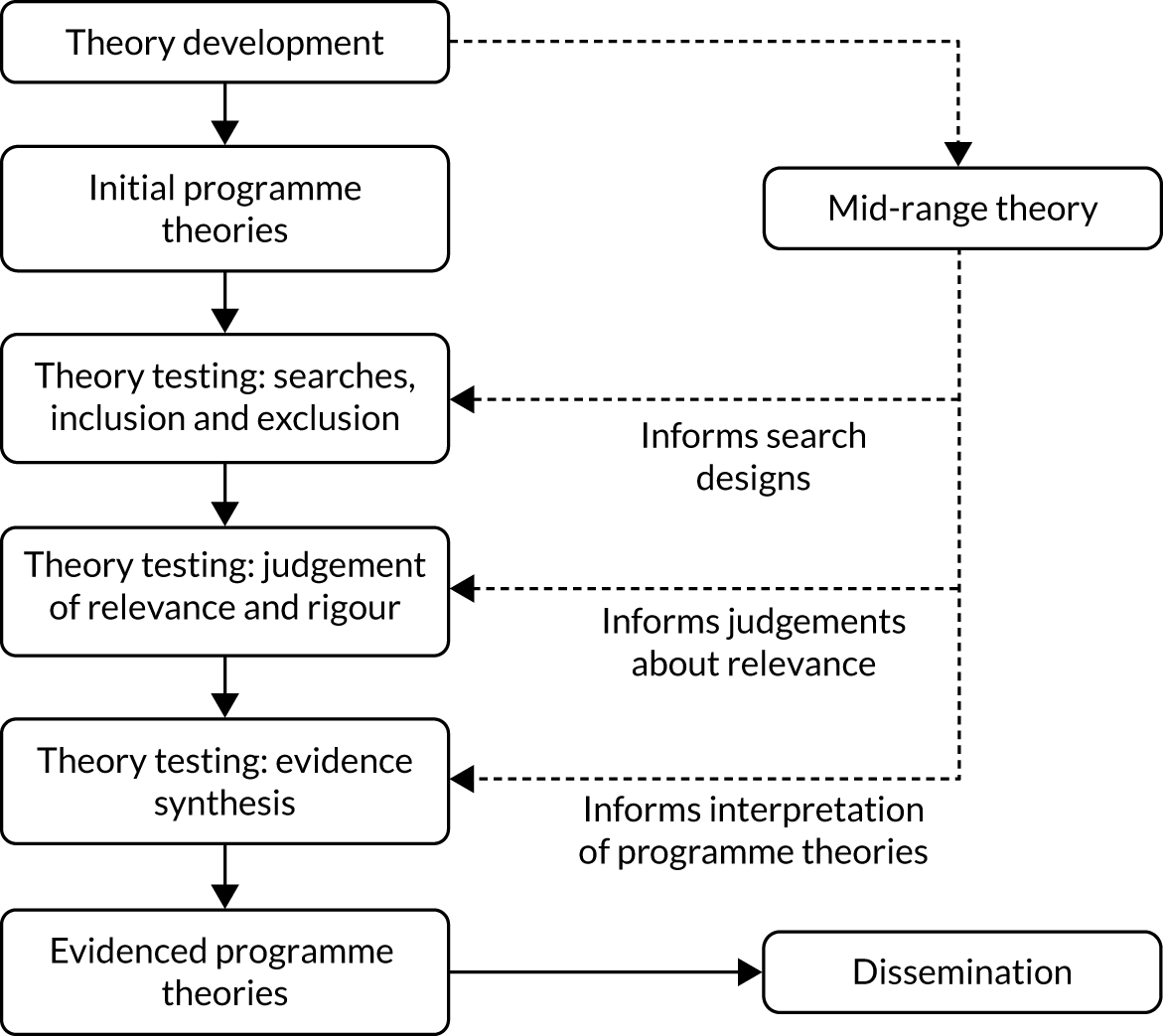
The design of our realist synthesis is consistent with the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) guidance. The left-hand column in Figure 2 illustrates the flow of methods. The first stage involved developing initial programme and mid-range theories. These represented the intended changes and effects associated with the intervention (i.e. the use of interoperable networks). The methods used include literature searches and consultation with stakeholders, the latter using nominal groups and semistructured telephone interviews. The next three stages were designed to identify evidence about actual changes and effects. The evidence reviews comprised carrying out literature searches, screening reports against inclusion and exclusion criteria, assessing relevance and rigour, data extraction and synthesising evidence. The methods are described in Chapter 3.
FIGURE 2.
Study design, including mid-range theory.
Mid-range theory
As we have noted, there is also variation in published study designs, particularly in relation to the role of theory. The RAMESES guidelines on the conduct and reporting of syntheses provide general, rather than prescriptive, guidance, offering flexibility to each research team. 20 It can be argued that this state of affairs is reasonable: it gives teams the space to develop a still-new methodology and evaluate different ways of conducting one. It also means, however, that a team undertaking a realist synthesis today has to make some choices about its preferred study design and methods.
The right-hand column in Figure 2 represents a distinctive feature of our study design and reflects our thinking about the role of theory. Our starting point is the observation that programme theories are not neutral, for the straightforward reason that researchers from different backgrounds (psychology, sociology, geography and so on) might develop different programme theories about the same intervention. That is, they think about, or frame, their theories in different ways, reflecting the beliefs and assumptions of their host disciplines. It is therefore important, as a minimum, to know what beliefs and assumptions have framed any given programme theory.
In 2013, Pawson21 noted the diversity of ways in which theories are incorporated into study designs. Our reading of the realist synthesis literature in the course of this study supports this point; we found that published accounts offer three main options. One is to use concepts derived from classical systems theories, typically referred to as context–mechanism–outcome configurations. The key idea is that the course of a given sequence of events (i.e. the events represented in a programme theory) is directly influenced by the context in which those events occur. Evidence searches might show that an intervention that works in one context may not work in another; the differences between the two can shed light on how and why the sequences of events work, or fail to do so. We decided not to use this approach, because in this study interoperable networks seemed to be the context for behaviour change across a locality. That is, it seemed that interoperable networks were both contexts and mechanisms.
The second option, which appears to be the most popular in practice, is to rely solely on programme theories; a psychological, sociological or other theory is embedded in the programme theories (implying that the nature of the theory should be stated explicitly by the research team). We decided not to rely on programme theories alone for the reason given above: we felt that it was important to make any conceptual framing of theories explicit in the study design.
The third option is for a research team to identify a relevant theory, typically referred to as a mid-range theory. The theory used might be based on the team’s prior knowledge of a domain or on the initial reading in the course of the study, or a combination of the two. We decided to pursue this option. In doing so, we were able to draw on the work of authors who have identified and used mid-range theories to inform their deliberations. 22–24 We also drew on Pawson’s17 account of mid-range theories as ‘reusable conceptual platforms’ (they are reusable in the sense that the same underlying reasoning can underpin a number of programmes). 17
The mid-range theory needed to be integrated into the study design and we were not able to find published accounts that made it clear how this could be done. We took the view that mid-range theory performs different functions (represented by the dotted lines in Figure 2): informing the design of searches, serving as a source of criteria for judging the relevance of articles and facilitating the synthesis of evidence. Following the synthesis of findings, the theory was used to inform the generalisation outwards from programme theories across populations, interventions or settings. Overall, it acted as a sort of ‘glue’, helping to bind the stages of the synthesis together.
The decision to use a mid-range theory influenced other design decisions. One decision concerned the assessment of rigour and relevance, which we discuss in Chapters 2 and 3. Additionally, at the start of the study, we assumed that there would be both similarities and differences in the ways in which interoperable networks influenced processes and outcomes. We were already aware of relevant literatures, including the human–computer interaction literature and the sociological literature on the development of large-scale IT systems. Our initial reading and deliberation confirmed that a theoretical framework that might account for large-scale change, spanning organisational and professional boundaries, would be appropriate. As we will see in Chapter 4, our mid-range theory (our reusable conceptual platform) drew principally on the literature on information infrastructures. This is an example of an institutional theory: published realist syntheses have used institutional frameworks and we followed their example in this study. 25,26
Finally, the decision about mid-range theory influenced our thinking about programme theories. They are used in different ways, for example to characterise causal relationships between activities or to capture the underlying inferential logic of an intervention. 27 Our choice here was to develop programme theories that represented contingent sequences of concrete decisions and actions, ending in a defined outcome. In this synthesis the outcome was a change in patients’ or clients’ risks, consistent with arguments about outcomes made by Pawson and colleagues. 28,29 We sought to strengthen our confidence in findings about these contingent sequences by undertaking searches focusing on different functions of interoperable networks (e.g. supporting professionals co-ordinating care for older people and reconciling medication lists for older people) and different populations (older people, at-risk children). Comparing across functions and populations provided us with a means of identifying and interpreting any similarities and differences that we found between functions and populations.
Chapter 3 Methods
Introduction
In Chapter 2 we described the overall design of the realist synthesis and explained the rationale for key design decisions. In this chapter we describe our methods. The next section introduces the literature search methods, including the common features of methods used throughout the study. The following sections set out screening and selection, and data extraction and quality appraisal. The final section describes the stakeholder consultation that we undertook in the course of the review.
Literature search methods
We took the approach of conducting a number of literature searches throughout the review, rather than relying on a single ‘big bang’ search that could be used to address a number of questions. This allowed us to identify separate literatures that were pertinent to identifying theories and theory fragments in the theory development phase or to identifying empirical evidence in the theory testing reviews. 16 The following 19 information resources were searched:
-
Association for Computing Machinery (ACM)’s Digital Library (full text)
-
Agency for Healthcare Research and Quality’s PSNeT Patient Safety Network
-
Applied Social Sciences Index and Abstracts (via ProQuest)
-
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
-
The Cochrane Library (via Wiley Online Library), including Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Health Technology Assessment Database
-
Criminal Justice Abstracts (via EBSCOhost)
-
EMBASE Classic and EMBASE (via Ovid)
-
Epistemonikos (Epistemonikos Foundation, Santiago, Chile)
-
Google (Google Inc., Mountain View, CA, USA)
-
Google Scholar (Google Inc., Mountain View, CA, USA)
-
Health Management Information Consortium (via Ovid)
-
Health Systems Evidence (McMaster University, Hamilton, ON, Canada)
-
Inspec (via EI Village)
-
Ovid MEDLINE®, including Epub Ahead of Print and Ovid MEDLINE® In-Process & Other Non-Indexed Citations
-
PsycINFO (via Ovid)
-
Research Papers in Economics (EconPapers; Örebro University Business School, Örebro, Sweden)
-
Scopus® (Elsevier, Amsterdam, the Netherlands)
-
Sociological Abstracts (via ProQuest)
-
Web of Science™ Core Collection (Clarivate Analytics), including Arts and Humanities Citation Index, Book Citation Index – Social Sciences and Humanities, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Sciences Citation Index, Social Sciences Citation Index and Emerging Sources Citation Index.
Appendix 1 provides a detailed listing of databases, sources and search strategies used for each individual search.
The databases and sources used for each search were selected based on the type of study or publication being sought (e.g. policy document, systematic review) and the question posed for each search (e.g. the nature of co-ordination problems, users’ experiences of interoperable networks). Populations, interventions, comparators, outcomes and settings (PICOS) were identified before some of the theory development and all of the evidence searches to aid search strategy development. All of the searches were performed and peer-reviewed by information specialists (NK and JW). Search terms and synonyms were identified by the project team and from known relevant papers. Structured search strategies were developed using free-text words, synonyms and subject index terms, organised into search concepts. Further complementary searches, including forwards and backwards citation searches, were undertaken by both the information specialists and the reviewers; the team members who undertook the searches are stated in each instance.
Searches that were designed to retrieve particular study types, such as systematic reviews or narrative research articles, used one of three strategies, namely (1) database ‘limit’ features (e.g. systematic reviews publication type limit in Ovid MEDLINE), (2) a ‘study type’ search strategy developed by the University of Leeds information specialists, or (3) a published search strategy. Each of the three options was tried and tested before it was decided which was the most appropriate for each search.
Theory development
In February and March 2018 we undertook five types of search to identify programme and mid-range theories. We aimed to find literature that, taken together, captured the sequences of events that policy-makers and other stakeholders believe link the deployment of interoperable networks to effects on patient safety. An update search for systematic reviews was conducted in July 2019 to identify any new theoretical explanations for the effectiveness or lack of effectiveness of interoperable networks on patient safety. Appendix 1 provides a detailed listing of databases, sources and search strategies used for each search.
Government policies and official reports
We were aware at the start of the study of policies and reports that might contain programme theories or theory fragments. We collected all of the policies and reports for England and the USA that had been cited in our research proposal, plus additional reports that we were aware of, and traced further reports via references and through pragmatic Google searches.
Structured subject searches
Two searches were conducted in three health databases for studies that presented theories or theory fragments associated with terms that identified relevant HIE-type technologies and either ‘patient safety’ terms or ‘interoperability’ terms (see Chapter 1 for definitions of HIE and interoperability).
Named author searches
Searches were undertaken to identify articles by or citing two opinion leaders, Robert Wachter (author of an influential 2016 report30 on IT in the NHS in England) and David Bates (the most highly cited author in the academic health informatics literature). Slightly different search methods were used owing to the large volume of literature authored by Bates compared with that by Wachter. We searched three health databases and one multidisciplinary database (Web of Science Core Collection) for both. In addition, we identified studies by Wachter on the Agency for Healthcare Research and Quality Patient Safety Network Portal. The Bates search in Web of Science involved a further search using the ‘usage count’ search feature, which identifies the most prominent or popular articles by ranking those that are accessed the most. This was to ensure that we had captured and reviewed key papers by Bates that may have had valuable insights but had not been found by the standard ‘Bates AND HIT terms’ search. We looked at (1) articles authored by Bates mentioning HIT terms and (2) any article he authored or any article in which he was mentioned with a usage count ≥ 20 (at least 20 records or full-text downloads).
Systematic review searches
We searched seven health databases for systematic reviews that included theories or theory fragments linking HITs, including, but not limited to, interoperable networks and patient safety. We were not at this stage, concerned with the evidence in the reviews, but rather the discussion sections that offered explanations that could help with theory development.
‘Usage count’ search
In the Web of Science Core Collection, usage counts measure the level of interest in a specific record since a given date (e.g. 1 February 2013). This is calculated by users either downloading it into reference management tools or linking to the article’s full text. The usage count demonstrates current activity and interest in a record and can help identify recently published articles that may not register using traditional citation counts, which tend to favour older publications. We searched for interoperable systems or HIEs, selecting results with a usage count of ≥ 50 since 2013. We also used this technique to identify key articles by Bates, which were detailed and recorded in the author searches above.
Evidence review
The co-ordination of services for older people living at home
We identified three linked search questions that between them, were designed to provide evidence about the main programme theory (presented in Figure 9). The intuition here was that we needed to identify empirical evidence about the nature and extent of co-ordination problems. Were problems amenable to IT-based solutions or were they problems of a different kind (e.g. attributable to differences in objectives and values between the different professionals who care for older people)? If some problems were amenable, then this might help us to focus later searches. If, on the other hand, there was a mismatch between the proposed solution (interoperable networks) and the nature of co-ordination problems, we would want to investigate the reasons for the mismatch. For each search we tested subject headings and search terms iteratively until we agreed on a search strategy that identified a representative evidence base and that we were also able to screen in the time available to us. We used a modified version of the DeJean and colleagues31 qualitative search filter to identify qualitative studies and our internally validated reviews of search strategies to identify systematic reviews. 31
What is the nature and extent of care co-ordination problems for frail older people living at home?
Five health and social science databases were searched in August 2018 for either reviews or qualitative studies describing the care co-ordination for frail older people. Engineering databases were not searched as we were not concerned with technical aspects of care co-ordination systems. We also hand-searched the Integrated Care topic page and the Integrated Care and Partnership Working reading list from The King’s Fund. 32
What are the experiences of professionals using interoperable networks in the course of care co-ordination?
We searched initially for studies of experiences gained in the course of treating and caring for frail older people living at home. This produced a small number of papers that, on screening, seemed unlikely to shed any useful light on the question. In September 2018, we revised the search to cover services for older people, rather than focus on frail older people. At the same time, we restricted the search to review articles. Seven health, social science, engineering and multidisciplinary databases were searched.
We also undertook a forwards citation search of the four databases and search engines of Fitzpatrick and Ellingsen’s10 2013 review of 25 years of computer-supported co-operative work in health care. This was in our personal library at the start of the study, and at the end of the theory development phase it was still the most relevant review that we were aware of on the topic of users’ experiences.
Do interoperable networks improve patient safety outcomes for frail older people living at home?
In March 2019 we conducted structured database searches in six health, social science, engineering and multidisciplinary databases to identify evaluation studies of interoperable networks or HIE and care co-ordination.
We undertook additional forwards and backwards citation searches using Google Scholar for three included studies. 33–35
Medicine reconciliation for older people living at home
We identified three search questions.
What is the nature and extent of the medicine reconciliation problem among older people?
In December 2018, we conducted structured database searches of three health databases and one multidisciplinary database to identify reviews or qualitative studies investigating medicine reconciliation for older people living at home. Two further searches were conducted in Google Scholar.
What are professionals’ experiences of using interoperable networks in medicine reconciliation for frail older people?
In November and December 2018, we searched for users’ experiences of interoperable networks in medicine reconciliation processes. Our initial search and screening was not fruitful. We consulted with colleagues in the study team and, through them, with colleagues with specialist knowledge of the literatures on medicine reconciliation. This led to the pragmatic identification of a book chapter, which we used as the basis for a cluster search that identified a further two relevant articles. 119,120,124 Structured database searches were then designed using terms found in the two articles to identify studies of medicine reconciliation and cognitive reasoning. We ran the search in two health databases and one multidisciplinary database.
What are the patient outcomes of using interoperable networks in medicine reconciliation?
In December 2018, we conducted structured database searches in four health databases and one multidisciplinary database to identify any reports of medicines reconciliation, prescription errors and HIE (or interoperable health records). The searches were not limited by study type.
The co-ordination of services for at-risk children
The searches were designed to address three questions.
What is the nature and extent of the co-ordination problem in services for at-risk children?
In May 2019, we conducted structured searches of four health databases for literature reviews of care co-ordination in child protection services.
What are clinicians’ and other professionals’ experiences of using interoperable health information technology to co-ordinate the care of children at risk and what are the effects of interoperable networks on outcomes for at-risk children?
In March 2019, we conducted searches to cover the second and third questions (i.e. to retrieve any type of study on HIE or interoperable records and child protection services). We searched four health databases, one social science database, one engineering database, one criminal justice database and one multidisciplinary database.
Economies of scope and scale in health economies
In June 2019, structured searches were conducted of three health databases, one economics database and two multidisciplinary databases to identify studies of HIE (or networked IT) and economies (or efficiencies) of scope or scale.
Records management and tracking
All database search records were downloaded and stored in an EndNote library (version 9.2; Clarivate Analytics), the same library used in the theory development searches. Duplicates were removed from the EndNote library every time a new set of searches (for a new review subquestion) was added. Records were clearly labelled with the review subquestion for which they had been identified. Some records were found and screened several times for different review subquestions.
We were unable to download the results of some website and complementary searches into EndNote. In these cases, we screened the search results for potentially relevant report records during the search and manually created EndNote records from the selected results.
The details of all search activities were recorded in a summary spreadsheet, so that we had an evolving overview of the number and nature of searches that we conducted. The spreadsheet included the date of the search, the information resource, the purpose of the search and the numbers of records found.
Screening and study selection methods
Inclusion and exclusion criteria were identified for screening for programme theory development and evidence reviews. The following inclusion criteria were common to all searches:
-
written in the English language
-
published in 2000 or later (following the publication of the Institute of Medicine’s To Err is Human: Building a Safer Health System;1 see Chapter 1).
Inclusion and exclusion criteria for the specific searches are described in the following section (see Evidence review: the co-ordination of services for older people living at home). Throughout the study we adopted a cautious approach to inclusion and exclusion, preferring to include or ‘provisionally include’ articles until we were confident about our judgements.
Theory development
Screening was performed by three members of the review team (MA, JK and JG). Initially, 20% of the records from all the searches were double screened by two reviewers. Following this, all of the titles and abstracts were screened by one reviewer. The remaining records were categorised as clearly included or potentially included, and these were then independently assessed by a second reviewer. Any disagreements were resolved through discussion.
Evidence review: the co-ordination of services for older people living at home
As noted above, the searches were designed to address three questions about the co-ordination of services for older people and the effects of interoperable networks. Screening in this and the next two sets of searches (medicine reconciliation and at-risk children) was undertaken by three members of the review team (MA, JK and JG).
The nature of co-ordination problems
We identified separate inclusion and exclusion criteria for systematic reviews and individual narrative studies. We included systematic reviews if they were:
-
articles that described and explained the nature of care co-ordination problems across health and social care organisations in frail older people (later expanded to all older people)
-
literature reviews of any type that searched at least two academic databases.
We excluded:
-
non-peer-reviewed reviews
-
studies that were condition or disease specific (as opposed to studies focusing on services for frail older people in the round).
For individual studies we included:
-
narrative or mixed-method studies that described care co-ordination problems for frail older people
-
studies published from at least 1 year earlier from the date of the most recent review of evidence of care co-ordination problems in elderly patients (this was identified later as 2016–present).
We excluded:
-
studies that focused on single conditions or diseases
-
surveys and intervention studies.
Users’ experiences of interoperable networks
We included articles if they were:
-
reviews or studies that included evidence about users’ experiences of interoperable networks
-
focused on older people or on the general adult population (i.e. did not specify an age limit)
-
literature reviews of any kind, or individual observational studies.
We excluded:
-
studies that described professionals’ experiences of using single databases
-
surveys.
Patient safety outcomes
Studied were included if they met the following criteria:
-
study design – literature reviews, observational and interventional studies
-
population – older people living at home
-
outcomes – any measurable change in patient risk, defined in the article.
We excluded studies if they were:
-
reports of tools and technologies based on single patient databases or in other settings (e.g. within-hospital networks)
-
studies that did not include evidence about the effects of interoperable networks
-
studies of condition- or disease-specific outcomes
-
implementation studies or surveys.
Evidence review: medication reconciliation for older people living at home
We defined medicine reconciliation as the process by which any two or more lists of medications are reconciled with one another, or two or more lists that are reconciled with an assessment of a patient, to identify the appropriate medication list. Some definitions allow for reconciliation of a single medication lists against a patient’s assessed need, but in this study our interest was in the reconciliation of two or more lists, on the basis that interoperable networks might have roles in their reconciliation, not least because two or more patient records linked in the network would be available to professionals.
The nature and extent of medicine reconciliation problems
We included studies that were:
-
observational studies that explored the nature of the medicine reconciliation problem (independent of any given technology)
-
focused on services for frail older people (later expanded to adult populations) living at home
-
literature reviews or single observational studies.
We excluded:
-
studies that focused solely on IT-related problems, or were studies of technologies, including applications, for single users
-
studies evaluating the impact of medicine reconciliation on patient outcomes
-
quantitative studies of patient-related risk factors for medication discrepancies
-
studies based in other settings (e.g. hospitals or care homes)
-
surveys.
Users’ experiences of interoperable networks
We included studies that:
-
explored networked IT-supported medicine reconciliation across health and social care organisations
-
described the cognitive process of professionals (pharmacists, doctors, nurses) in medicine reconciliation
-
explored these processes in the context of services for older people living at home (later expanded to the adult population).
We excluded:
-
studies of medicine reconciliation in single organisations
-
studies of medicine reconciliation for patients who were not living at home (e.g. in a care home)
-
surveys.
Patient safety outcomes
Our inclusion criteria were:
-
study design – literature reviews, observational and interventional studies
-
population/setting – older people living at home who may have experienced a care transition (e.g. from hospital back home)
-
intervention – interoperable networks
-
outcomes – any measurable change in patient risk, defined in the article.
We excluded:
-
studies that reported on tools and technologies based on single patient databases or in other settings (e.g. within-hospital networks)
-
studies that did not include evidence about the effects of interoperable networks
-
studies of condition- or disease-specific outcomes
-
surveys.
Evidence review: the co-ordination of services for at-risk children
As with earlier searches, we undertook searches to establish the nature and extent of co-ordination problems, users’ experiences and outcomes.
The nature and extent of co-ordination problems
We included studies that met the following criteria:
-
literature reviews (of any kind)
-
studies that described care co-ordination problems for at-risk children living at home.
We excluded studies if they:
-
discussed children receiving routine services, including children in accident and emergency departments who were not deemed to be at risk
-
described only IT-related problems
-
were experimental studies of individual patient records systems or IT applications
-
were quantitative studies of patient-related risk factors.
Users’ experiences of interoperable networks and patient safety outcomes
Inclusion and exclusion criteria were developed for both questions. We included studies if they satisfied the following criteria:
-
described users’ experience of interoperable networks or patient safety outcomes (with outcomes defined in the articles)
-
included at-risk children (aged < 18 years) living in their own home.
Excluded were studies that:
-
focused on children living in settings other than their own home (e.g. in institutional care)
-
described professionals’ experiences of using single patient databases.
Economies of scope and scale in health economies
One member of the team (SN) screened all of the abstracts, and two members of the team (SN and JK) read seven of the full-text articles and together made the final selection. Data extraction and quality appraisal methods were not required, as there were no relevant full-text papers to synthesise.
Inclusion and exclusion criteria
We included studies that satisfied the following criteria:
-
Interoperable networks that linked two or more organisations outside (but possibly including) hospitals in a health economy.
-
Interoperable networks supported direct treatment and care.
-
Studies that included empirical evidence about the added value of interoperable networks, as measured by economies of scope and scale.
We excluded studies if they:
-
described hospital-only IT systems
-
described systems that did not link two or more distinct organisations in a health economy
-
focused on IT systems that supported secondary uses of data (e.g. for service planning, research).
Data extraction and quality assessment
Theory development
For each included article, we recorded the details of studies (authors, publication year) and text that described potential programme theories or theory fragments. As can be seen in Chapter 4, we did not find any complete programme theories, but we identified a substantial number of theory fragments. As noted in Chapter 2, we were looking for theory fragments, and so either copied all of the relevant text, which might be a few sentences, or recorded the location of larger sections of text for later analysis. Similar fragments that dealt with a particular topic, such as users’ experiences of interoperable networks, were grouped together. The groups of fragments were then pieced together so that initial programme theories could be developed both in text form and as visual representations. When possible the representations were annotated with claims about the reasons why programmes succeeded or failed in practice. The programme theories were used as the basis for consultation with three groups of stakeholders: (1) policy-makers, (2) senior IT managers and (3) front-line clinicians.
We undertook two broad types of evidence search. One focused on components of programme theories (e.g. users’ experiences of using interoperable networks) and the other focused on evidence of the outcome (which in this review was a change in patients’ risks of harm). For the former, data extracted included the study identifiers (author, publication year and country), information about study methods (the methods used and the numbers and types of participants), the evidence itself and information about the theoretical approach used. In this study, most of the evidence identified was narrative and extracted wholesale from papers (i.e. it was not summarised before synthesis), in part to retain the relationship between data and theoretical frameworks. Data extraction was undertaken by one researcher and checked by a second researcher (one MA, JG or JK).
For evidence about outcomes, a customised data extraction spreadsheet was designed for the recording of study identifiers, objectives, settings and a description of the intervention. Information that allowed us to judge the rigour of the study, including study design, participants, duration and theoretical framework, was also extracted. Finally, we extracted the findings of the study in terms of safety-related outcomes in quantitative studies, and quotations and comments in narrative studies. Critical Appraisal Skills Programme quality assessment checklists were used to appraise the rigour of systematic reviews and narrative and cohort studies.
Rigour and relevance
Most published accounts of realist syntheses include the assessment of the rigour and relevance of included articles. Rigour is concerned with the technical quality of the methods used in an article. In realist syntheses and any other review method that incorporates a range of experimental and observational methods, the approach is to judge technical quality against accepted standards appropriate for the methods used. In this review, we drew on the approaches used by other teams. 36,37
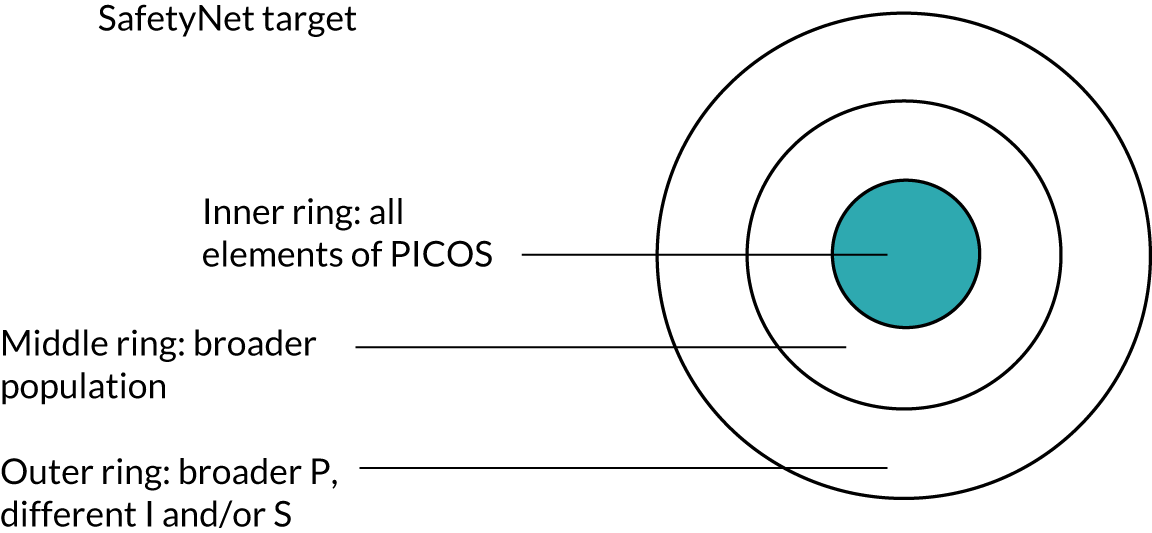
One consequence of the decision to use a mid-range theory (see Chapter 2) was in the ways in which judgements were made about the relevance of articles. Clear accounts of judgements about relevance are less common than those of judgements about rigour, but our approach was similar to that taken by Greenhalgh and colleagues38 in their review of patient-reported outcome measures. We took the view that the judgement criteria should be independent of, not derived from, the articles being assessed, and of the methods used to identify and assess them. We extended the method by developing a pragmatic ‘target’ akin to an archery target (Figure 3). Articles that clearly met the inclusion criteria were placed in the bullseye. Those that met most of the criteria, but not the population (e.g. all adults, rather than older people) criteria, were placed in the next ring. Articles that did not strictly meet the population, intervention or setting criteria, but were nevertheless deemed potentially relevant, were placed in the third ring. The use of the two outer rings is consistent with the view in realist syntheses that evidence can be included as long as it sheds useful light on a programme theory (i.e. articles were included if they shed light on the processes that linked an intervention and an outcome).
FIGURE 3.
Relevance ‘target’ diagram. I, interventions; P, populations; PICOS, populations, interventions, comparators, outcomes and settings; S, settings.
The ‘target’ was not used in the theory development searches. These were satisficing searches, which means that we did not conduct exhaustive searches, but rather we made practical judgements about the points for which we had identified sufficient evidence to answer the search question.
Stakeholder consultation
Alongside gathering literature to inform theory development, we consulted with stakeholders.
Nominal groups
We originally intended to use nominal groups with representatives of three groups of people: (1) policy-makers, (2) senior IT managers and (3) front-line clinicians. In the event, we ran nominal groups with the first two and conducted semistructured telephone interviews with front-line clinicians. The telephone interviews are described below (see Telephone interviews).
The nominal group technique involves an initial meeting with stakeholders at which a topic of interest is discussed and initial agreement or consensus is reached. The extent of agreement is then tested in one or two rounds of electronic consultation, typically e-mail or web based. Nominal groups were appropriate in this study because the underlying mechanisms linking interoperable networks and patient safety are poorly understood. We developed initial visual representations of programme theories, supported by text. Participants were sent the visual representations and text in advance of the meeting (see Appendix 2). The first meeting was with three senior NHS IT managers, all of whom were responsible for interoperable networks. It was held in May 2018 and was audio-recorded. At the meeting participants were asked to:
-
comment critically, on the basis of their knowledge and experience, on the initial programme theories
-
develop and then prioritise theories, or particular sequences of decisions and action within theories, for detailed study.
The prioritisation took account of the types of networked health and care systems that the participants were responsible for. That is, they were encouraged to identify questions that they were asking about their own networks (e.g. concerning the functions that appeared to be most closely associated with safety risks or improvements).
The second meeting was held with five managers from NHS Digital and NHS England in June 2018, and was also audio-recorded. As with the first group the participants were sent the initial programme theories in advance and were asked to comment critically on them, and to prioritise theories, or elements of theories, for detailed study.
In July 2019, both groups were sent a paper that summarised the findings of the evidence searches and the implications for our programme and mid-range theories (see Appendix 3).
Telephone interviews
It was not possible, in practice, to convene a nominal group of front-line clinicians. We spoke to a number of clinicians who explained that it was very difficult to obtain permission for time away from clinical duties. We consulted with our Steering Group, who advised us to conduct interviews instead. We obtained ethics approval to include a short topic guide for the telephone interviews (see Appendix 4). In common with the nominal group meetings, we sent the initial programme theories and supporting text in advance, and asked the clinicians to comment critically on the proposed programme theories and to prioritise the theories that they would like us to test. Potential interviewees were approached in two ways: via a short article in the Clinical Human Factors Group’s newsletter (circulated in October 2018) and through personal contacts in two cities that had interoperable networks routinely used by clinical staff. Seven interviews were conducted in November 2018.
Analysis
The nominal group meetings and interviews were audio-recorded and transcribed. Open coding was used to identify broad themes, on the basis that we were interested in insights into our programme theories, rather than the meaning inherent in anyone’s comments. Implications for our programme theories were identified pragmatically by members of the study team (MA and JK). The outputs of the nominal groups were summarised, and possible implications were noted and shared with the patient and public involvement (PPI) panel and the Steering Group. The comments of the nominal groups, PPI panel and Steering Group were all taken into account when refining the initial programme theories. The interview programme was undertaken later; the study team used the interviews to feed into thinking about the framing of the programme and mid-range theories.
Chapter 4 Theory development
Introduction
This chapter presents the findings of the systematic and grey literature searches undertaken to support the development of programme and mid-range theories. The searches identified 1302 records to be screened, of which 46 were included in the synthesis [see the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram39 in Figure 4].
FIGURE 4.
Theory development PRISMA flow diagram.

Government policies and official reports
We were aware of a number of relevant government policies and official reports at the start of the study (these are recorded as being in our personal library in Chapter 3). These were reviewed first for statements about the nature and role of interoperable networks, or patient safety or, ideally, both together. We identified additional documents via two routes: (1) references made to them in our initial reading and (2) informal means (e.g. in conversations with colleagues and in incidental ‘finds’ in the course of other searches). These additional documents were not identified in formally structured searches and were therefore added to our personal library as we came across them.
At this early stage, we included any relevant statements irrespective of the settings described, and so included statements about hospital IT systems as well as interorganisational networks. For reasons of time, we did, however, focus on documents about the NHS in England and national health-care policies in the USA. Interoperable networks have been an important element of current IT policies in England in the last 5 years and attracted considerable federal investment in the USA after 2009.
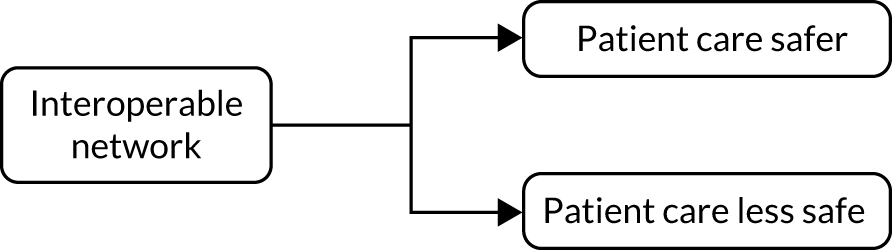
Taking US policies first, we noted in Chapter 1 that the Institute of Medicine published To Err is Human: Building a Safer Health System in 2000. 1 The report focused principally on ways in which the overall design of a health-care system makes errors and adverse events more or less likely. The report took a measured view of the role of HITs in helping to improve system design and hence patient safety. On the one hand, it observed that all technologies introduce new risks and hence the possibility of harm to patients. On the other, it recognised that technologies have the potential to support better clinical processes and decision-making. It recommended that research was needed to establish where and how that potential could be realised. The report provided us with a very simple initial programme theory: the deployment of HITs might lead to safer care or might increase patients’ risks, or both (Figure 5).
FIGURE 5.
Official policy and report programme theory.
A great deal has been written about the HIT policies during the era of US President Barack Obama. We reviewed a substantial number of reports but did not find any detailed accounts of ‘how and why’ interoperable networks were expected to improve patient safety. Rather, the reports commented on ongoing problems with achieving interoperable networks. Typical of the documents we reviewed is an Institute of Medicine report14 that stated that:
Lack of interoperability is a barrier to improving clinical decisions and patient safety, as it can limit data available for clinical decision making.
The report referred to the role of human–computer interaction and its impact on clinical working practices:
The process of implementing software is critical to optimizing value and mitigating patient safety risks. A constant, ongoing commitment to safety – from acquisition to implementation and maintenance – is needed to achieve safer, more effective care.
Similarly, a 2016 report for the Office of the National Coordinator for Health Information Technology, Report of the Evidence on Health IT Safety and Interventions,40 argued that:
Interoperable health information exchange (HIE) . . . can improve . . . safety by improving the timelines and completeness of important patient health information.
Graber and colleagues, p. 11. 40
The report then went on to argue that interoperability was desirable, but that a number of hurdles still had to be overcome, including a lack of data standards and of interfaces that avoided overloading clinicians with patient data. In practice, limited progress with implementation meant that clinicians encountered problems with access to patient data held on IT systems in other organisations.
Turning to English reports and policies, the 2001 Bristol Inquiry report into the deaths of adults and children in cardiac surgical services argued that ‘The need to invest in world-class IT systems must be recognised . . .’ (recommendation 154, p. 456; © Crown copyright). 5 Similarly, the 2003 Bichard41 report into the murders of two girls in Soham recommended the implementation of a national IT system to monitor sex offenders. It was initially envisaged that the system would link police forces, but later iterations expanded the scope of the system to include a range of agencies. The NHS National Programme for IT was launched in parallel with these reports in 2002, with significant funding that eventually totalled > £10B. At the outset it was claimed that this would drive a transformation of NHS services, including improvements in patient safety. 42 None of the authors of these reports and policies elaborated on why they believed that HITs would improve safety.
The numbers of incidents and complaints remained large throughout the 2000s. The problems were highlighted most dramatically by the scandal at Mid Staffordshire NHS Foundation Trust. 43 Sir Robert Francis’ second report on the trust in 2013 made a number of recommendations about HITs, including that all provider organisations should:
. . . develop and maintain systems which give them:
effective real-time information on the performance of each of their services against patient safety and minimum quality standards
effective real-time information of the performance of each of their consultants and specialist teams in relation to mortality, morbidity, outcome and patient satisfaction.
Francis, Recommendation 262. 43
These recommendations were accepted by the government in its formal response to the report in November 2013. 44 The government also commissioned a report from the respected US clinician and analyst Donald Berwick. 45 The Berwick report also identified a potential role for HITs:
Most health care organisations at present have very little capacity to analyse, monitor, or learn from safety and quality information. This gap is costly, and should be closed.
Berwick, p. 27. 45
Again, the statements in the reports were general. They did not specify how HITs would improve patient safety, or the clinical settings in which the improvements were most likely to be achieved.
A number of HIT policies that included relevant statements were published from 2012 onwards. The Power of Information: Putting All of Us in Control of the Health and Care Information We Need was published in 2012. 3 It set out a 10-year framework for information and IT investments in the NHS in England. The report stated that current information systems were disjointed and that paper records could get lost. It gave examples of services that could be improved if professionals had access to information from other organisations:
The Accident and Emergency doctor does not always have the information needed, such as details of important allergies or information about vulnerable children at risk, to be able to treat the sick person in front of them safely. On discharge to a care home, the busy care worker has inconsistent paper medication records to interpret.
Department of Health and Social Care, p. 43 ©
The report3 also made the first explicit statement that we found about the value of interoperable networks in the NHS, particularly for people with complex care needs:
Connected information and new technology can help health care professionals to make informed decisions and provide safe patient care through faster access to test results in hospitals or by ensuring a care worker gives the right medicines to the right person in a care home.
Department of Health and Social Care. 3
The policy also argued that failing to share information had the potential to do more harm than sharing it.
NHS Digital is responsible for two clinical safety standards, which were first published in 2013. 46,47 They mark a departure from earlier English policies in echoing To Err Is Human1 and emphasising both the risks and the benefits associated with HITs:
[HITs] . . . can deliver substantial benefits to NHS patients through the timely provision of complete and correct information to those healthcare professionals that are responsible for administering care. However, it must be recognised that failure, design flaws or incorrect use of such systems has the potential to cause harm . . .
The next policy document was Personalised Health and Care 2020: Patient, Carers and Service User Vision, published in 2014. 4 It pledged an ‘information revolution’, with the aim of putting people first and providing what it called ‘transparent’ care. It observed that most hospital information systems could not be accessed by care professionals outside hospitals, including those in nursing homes and hospices. It identified the lack of interoperability as a major problem. 4 The policy also noted a number of barriers to the more effective use of HITs, including lack of consideration of the clinician’s working practices in their design.
Making IT Work: Harnessing the Power of Health Information Technology to Improve Care in England – Report of the National Advisory Group on Health Information Technology in England,30 often called the Wachter Report after the chairperson of the group, was published in 2016. 30 It made recommendations about many aspects of HITs, including education and training. One of them was that the NHS should:
. . . ensure interoperability as a core characteristic of NHS Digital ecosystem – to support clinical care and to promote innovation and research.
National Advisory Group on Health Information Technology in England. 30 ©
The report suggested that the end goal of interoperability is not solely exchanging digital data, but enabling integrated workflow, service redesign and clinical decision support. There were, further, general statements about how digital systems could improve patient care. Implicitly, at least, the statements assumed that patient information would be widely available, presumably via interoperable networks:
We cannot emphasise enough that the purpose here is not to computerise . . . The purpose is to radically improve the chances that important information will be available when and where it is needed, because no health system or clinician can perform at the top of their potential if it is not . . .
National Advisory Group on Health Information Technology in England. 30 ©
The most recent policy document is The Future of Healthcare: Our Vision For Digital, Data and Technology in Health and Care, published in 2018. 48 It picked up, and greatly expanded on, the interoperability theme in Personalised Health and Care4 and Making IT Work. 30 In a section headed ‘Infrastructure’, it states that:
The ability to share records between hospitals, GPs [general practitioners], community pharmacies and care providers is inconsistent and people are frequently discharged from hospital without sufficient or accurate information about their care needs.
Department of Health and Social Care, Section 1. 48
The policy emphasises the extent to which successful deployment of interoperable networks will require NHS organisations and suppliers to adhere to common data and technical standards, and meet users’ needs. Once again, however, there is no account of the ways in which networks will improve patient safety (or other desired outcome). As things stand, therefore, it seems reasonable to summarise the official reports and policies by saying that, (1) interoperability has become increasingly important in the last 5 years, but (2) they do not spell out in any detail how they, or HITs more generally, might improve patient safety. Figure 5 therefore represents current thinking, as represented in the documents discussed in this section.
Structured subject searches
We tested a number of search terms, and combinations of terms, and found that two terms that described our technology of interest produced distinct and useful results. These terms were HIE and ‘interoperability’, which we discuss in turn.
We came to understand, through these searches, that the term HIE is used in two ways in the literature. The first of these is general in nature, particularly in the USA, where it is used as a shorthand for the major Obama-era IT investment programme. One reason to use HIE as a search term was, indeed, to identify articles discussing that programme. The second is more technical, and refers to the ability to move data between any two or more IT systems. HIE’s are therefore necessary for interoperability, which we discussed in Chapter 1, which refers both to technology and to the use of data. Put another way, interoperability is a broader term than HIE.
Health information exchange structured subject search
We did not find any articles that set out a detailed programme theory. We therefore sought to identify theory fragments and identified three types of fragment in 13 articles49–61 (Table 1). The first type concerned the value of HIE, one centred on access to remotely held patient data. HIE could provide health-care professionals with a more comprehensive view of a patient’s information and thereby avoid or decrease medication-related errors. In the second type, HIEs could be used to facilitate communication between professionals. This might avoid delays in clinical decisions or facilitate improved co-ordination of care.
| Study | Topic | Theory fragment(s) |
|---|---|---|
| Alvarez49 | Canada Health Infoway, part of a pan-Canadian interoperable EHR solution | Discussion article. Argued that co-ordinated national EHR initiative would cost less, save lives and prevent reduce harm. It then described Infoway, a Canadian initiative intended to improve electronic access to accurate and timely health information, which would improve safety, quality, accessibility, cost-efficiency and the sustainability of the health-care system. Patient safety was described as a cornerstone of Infoway’s activities |
| Bowden and Coiera50 | Impact of accessing primary care records during unscheduled care | Review article. It concluded that:no study reported on clinical outcomes or patient safety, and no economic studies of shared electronic record access during unscheduled care were available. Design factors that may affect utilization included consent and access models, shared electronic record content, and system usability and reliability50 |
| Cotter51 | Benefits of HIT | Opinion article. Argued that the creation and implementation of a comprehensive clinical information system would entail many difficulties, particularly in regard to patients’ privacy and control of their information, standardisation of EHRs, cost of adopting IT, unbalanced financial incentives and the varying levels of preparation across providers of care. There will also be potential effects on the physician–patient relationship |
| Fontaine et al.52 | Survey of primary care practices regarding plans and motivation to invest in HIE | Primary research article. This was an original article describing the use of HIE in primary care practices in Minnesota, USA. Internal ‘motivators’ to use were anticipated cost savings, quality, patient safety and efficiency. The most frequently cited barriers were lack of interoperability, cost, lack of buy-in for a shared HIE vision, security and privacy, and limited technical infrastructure and support |
| Foley53 | Confidentiality and shared clinical records | Letter. Author expressed concerns about the risks to confidentiality associated with shared patient records |
| Goroll et al.54 | Experiences of Massachusetts eHealth Collaborative | Case report. The authors reported that, despite initial enthusiasm, progress with implementation was impeded by a range of challenges, including lack of technical standards, costs of converting paper to electronic records, and concerns about privacy and confidentiality |
| Gottlieb et al.55 | Policy and regulatory barriers to successful clinical data exchange project in Massachusetts, USA | In this article, the authors described a number of barriers and lessons learned from piloting the use of data exchange project in emergency departments in Massachusetts, USA. This included privacy concerns, accessibility, data quality and technical issues with the software, which led to challenges in use and uptake of the project by the clinicians |
| Hawking56 | Medicolegal issues with shared electronic records | Letter. GP voiced concerns about the use of shared EHRs in primary care, including problems with functionality and governance. He had particular concerns about data entry errors and responsibility for updating medication information in a shared record environment |
| Hillblom et al.57 | Impact of HIE on pharmacy practices | Opinion article. Argued that HIEs will knit together unrelated information sources to provide health-care professionals with a more comprehensive view of a patient’s medical information |
| Hopf et al.58 | Health-care professionals’ views on linking patient data | Systematic review. Facilitators of use of a network included having trust in the system, including in its reliability. Barriers included costs and information governance and technical issues. Possible effects on the physician–patient relationship and on workload were also identified as barriers. Health-care professionals supported the idea that an integrated system would improve patient safety |
| Ishikawa et al.59 | Proposals for an integrated, networked EHR | Primary research article: survey. The authors argued that a system should be designed to share information among all professionals, which would promote team practices and, in turn, improve patient safety. System security and reliability were acknowledged to be risks |
| Traynor60 | Commentary on Institute of Medicine report1 | Opinion article. The author noted a lack of robust evidence that HITs can improve patient safety. There is also limited evidence about the harms resulting from HITs |
| Zimlichman and Bates61 | National priorities in the patient safety agenda in the USA and Canada | Opinion article. Argued that harnessing HIT to promote patient safety was ‘pivotal’ because it extended to all providers |
For the third type, some articles commented on the potential risks arising from poor data quality and consequent risks to accurate diagnosis and treatment. Authors mentioned system reliability and poor user interface design, and the implications of these for patient safety. Privacy and confidentiality were also mentioned; Foley,53 for example, argued that:
Workers in hospitals or general practice surgeries might seek inappropriate access to medical records because of curiosity or malice, commercial gain, or simple errors.
Foley53
Interoperability structured subject search
We also used interoperability (replacing HIE) as a key search term. Seven articles were included, and these are described in this section.
Most of the theory fragments were general in nature. The most commonly cited theory fragment concerned access to additional patient data via an interoperable network. A report commissioned by the European Union argued that access to patient records would lead to more accurate diagnosis and better-quality treatment and care delivery, as well as potential for improved patient safety through:
-
improved knowledge of the patient’s health, social status, family and personal history
-
improved care co-ordination between health-care professionals
-
more and higher-quality communication between health-care professionals and patients
-
avoidance of errors, including prescribing and medication administration errors. 62
Huckvale and colleagues63 reviewed the role of IT systems in general in patient safety, citing roles for clinical decision support and for linking and sharing patient data. They argued that HIE would improve safety by reducing clinical errors, preventing data loss and ensuring that information was available when needed. Huckvale and colleagues63 noted a ‘fragmented theoretical framework’, which limited the scope for the understanding of the issues involved in promoting safer care using HIE to evolve.
Some authors argued that interoperability could offer a solution to the fragmentation of health care. For example, Font and colleagues64 described a number of case studies in which interoperable systems were implemented, and argued that these offered evidence of the value of those systems. Similarly, Foisey,65 based in New Zealand, argued that patient journeys can involve many health-care professionals. Data exchange and easy access to complete patients’ health information could reduce patients’ risks. In a similar vein, Hutchison66 outlined the benefits of pharmacy interoperability: the ability for physicians to securely and electronically exchange prescription information with pharmacies. It would reduce the time staff spent on filling prescriptions and would reduce medical errors. More broadly, it would allow licensed prescribers and pharmacists to access securely the drug history of any patient in an emergency, anywhere in the country.
Conversely, a family physician who also worked as a part-time emergency physician at a local hospital in the USA expressed his frustration at not being able to access the patient hospital record in his clinic and the patient’s clinic record from the emergency department. 67 Finally, two studies identified concerns about privacy and confidentiality. 68,69 There were, the authors argued, important legal and ethical considerations associated with sharing patient records across different professionals and organisations.
Summing up our insights from the articles identified in the structured searches, we can say that we were cautious about excluding potentially useful observations and insights early in the synthesis but, even so, found relatively few articles that could contribute to the development of programme theories. We found more comments on the nature of possible barriers or risks than on the nature of the processes that might be affected. We were not much further forward than we were at the end of our analysis of government policies and official reports.
Named author searches
Robert Wachter’s and David Bates’ literature typically discusses HITs in general, rather than focusing on interoperable networks.
One title by Wachter, The Digital Doctor: Hope, Hype and Harm at the Dawn of Medicine’s Computer Age, was included. 70 Few passages commented, directly or indirectly, on interoperable networks, but three theory fragments were identified, on information sharing in medical emergencies, the safety implications of information sharing and the design of interoperable networks. Regarding the last of these Wachter commented on Epic (Verona, WI, USA), a major US-based IT supplier:
The company also worries about the safety implications of trying to cobble together mismatched parts, particularly in complex clinical environments like hospitals. The company is ‘religious’ about not mixing and matching components in areas where integration is critical to safety.
Wachter70
More generally, Wachter was sceptical about the US Federal programme, arguing that there was little to show for an investment of almost US$30B.
Bates is co-author of five articles that include observations about the relationship between HITs and patient safety. In a 2003 article71 he argued that HITs could reduce errors resulting from inadequate access to clinical data, and could rapidly communicate important results, monitor adverse events and provide decision support. Barriers to the adoption of HITs Bates identified included cultural issues and high implementation costs. In 2007, Kaelber and Bates72 suggested ways in which HITs could improve patient safety. Some ways were related to improving the processing of laboratory information, radiology information and medication information. Others were concerned with improving communication among providers, and among patients and providers and, finally, the role of HIE in public health information processing.
Panjamapirom and colleagues73 were more sceptical about HITs in a 2010 article noting growing concerns about the privacy and security of personal data, and the lack of incentives for making use of data. The authors referred to problems of data ownership (i.e. who owns a patient’s data) and the lack of standards and legal frameworks for the use of personal data. Similarly, Kushniruk and Bates74 commented on US federal efforts to improve the safety of HITs (i.e. ensuring that HITs do not themselves increase patients’ risks). They described the growing body of evidence about the unintended consequences of using HITs and consequent risks to patient safety. They produced a simple framework for thinking about improving safety, involving:
-
recognition of the problem and of the role of safety and regulation influences
-
usability and design considerations, which influence
-
implementation issues, which influence
-
post-implementation issues and error reporting.
In 2015, Bates75 described a previous study on the role of EHRs in co-ordinating the care of elderly people in nursing homes. Four ‘domains’ were identified: (1) reconciling medication, (2) tracking laboratory tests, (3) communicating across settings and (4) managing care planning, referrals and consultations. 75 Finally, Rudin and colleagues76 argued that HITs could be used to improve the co-ordination of treatment and care, in part by making it easier for professionals to identify and communicate with one another.
We can make similar observations about the named author search to those we made about the structured database search. There are useful theory fragments that offer more detail about risks than about clinical processes, so that the risks were presented without any useful context; and fragments were general, rather than specific, in nature.
Systematic reviews search
By their nature, most systematic reviews focus on evidence rather than theory. However, they served three purposes in the theory development phase of the review. First, we needed to check whether or not we had missed any systematic reviews in our chosen topic area at the proposal stage, and whether or not any had been published in the period between the research award and the start of the study. Second, systematic reviews might help to identify empirical evidence that we could use in later evidence searches. Third, a systematic review might not cover exactly the same ground as ours, but might include useful interpretations of evidence that are relevant to one or more programme theories.
We did not find any systematic reviews using a realist, narrative or other method that covered the same review aims and objectives as ours. We did, however, identify reviews that covered aspects of topics that we might be interested in, for example process measures of the effects of interoperable networks. 8,77–79 Many reviews noted the paucity of research into the processes that led to changes in quality of care and patient safety.
Four reviews78,80–82 were included on the basis that they went beyond the data they presented and sought to explain how and why clinical processes were influenced by interoperable networks and had subsequent effects on patient safety. Bassi and colleagues78 presented a general sequence of events in medicine management: obtain medication information (from a computer system), compare medications, clarify discrepancies and then, in parallel, communicate medication information to relevant clinical colleagues and track discrepancies.
The other three reviews highlighted the importance of what they termed the unintended consequences of HITs. Back in 2004, Ash and colleagues80 presented two categories of such consequences, errors associated with entering and retrieving information, and errors associated with communication and co-ordination. An example of the former might occur if interfaces are not suitable for working environments in which professionals are regularly interrupted. An example of the second might occur if the HIT itself leads to ‘cognitive overload’, perhaps by overemphasising the need for structured and ‘complete’ information entry or retrieval.
Zheng and colleagues81 published a review in 2016 of the unintended consequences of interoperable networks and observed that:
. . . a widely held consensus has been reached that unintended adverse consequences brought by health IT implementation are almost inevitable, even if their effects may be temporary and the magnitude of the impact may be small. 81
Zheng and colleagues81
They did not, however, provide any detail about the processes that might be involved in producing unintended consequences, and noted that more research was needed into ‘root causes and remedies’. Similarly, Jones and colleagues82 found that hospital IT systems reduced medication management errors and, conversely, that ‘alert fatigue’ and ‘incongruent workflows’ were barriers to the successful use of systems. The authors also observed that:
. . . the health IT literature is expanding rapidly but failing to produce a commensurate amount of useful knowledge . . .
Jones and colleagues82
In addition, they stated that:
. . . insufficient reporting of implementation and context of use makes it impossible to determine why some health IT implementations are successful and others are not.
Jones and colleagues82
The pattern that emerges is one of relatively little detailed information about clinical working practices, but rather more about the unintended consequences of deploying interoperable networks.
Usage count search
Usage count searches limit search results to articles in the academic literature that are most frequently accessed and downloaded. We identified two articles that included theory fragments. Kalra and colleagues83 presented the outcomes of three workshops held with domain experts on interoperable networks in the USA and Europe. The main action suggested was to urgently ensure access to high-quality interoperable information resources that:
. . . (1) provide clinical context, (2) be mapped to interoperability standards for EHR data, (3) be linked to well specified multi-lingual terminology value sets, and (4) be derived from high quality ontologies.
Kalra and colleagues83
That is, the paper argued that the fundamental computing issues involved were far from straightforward, and a number of problems had to be solved if sophisticated interoperable networks were to become a reality.
Adjerid and colleagues84 evaluated the impact of privacy regulation on the development of interoperable networks, comparing legislative frameworks and consent policies in different US states. The authors argued that networks could foster the co-ordination of patient care across the fragmented US health-care system, but that evidence suggested that the uptake of interoperable networks depended on frameworks and policies. The more the policies incentivised citizens, the more the networks were likely to be used.
Although this search resulted in a small number of included articles, it reminded us of some of the wider issues that interoperable networks raise. Once again, however, there was little detail about the effects of networks on clinical working practices and, hence, on patient safety.
Initial programme theories and nominal groups
All five searches described in the previous sections were undertaken in the first 2 months of the study. In month 4 we prepared materials outlining the initial programme theories for the two nominal group meetings (see Appendix 2). One of the programme theory diagrams is reproduced for convenience in Figure 6, and Table 2 summarises some of our thinking about patient safety. The diagrams and text could be described, in accordance with Shearn and colleagues,23 as initial rough programme theories.
FIGURE 6.
One of the initial programme theories presented to nominal groups.
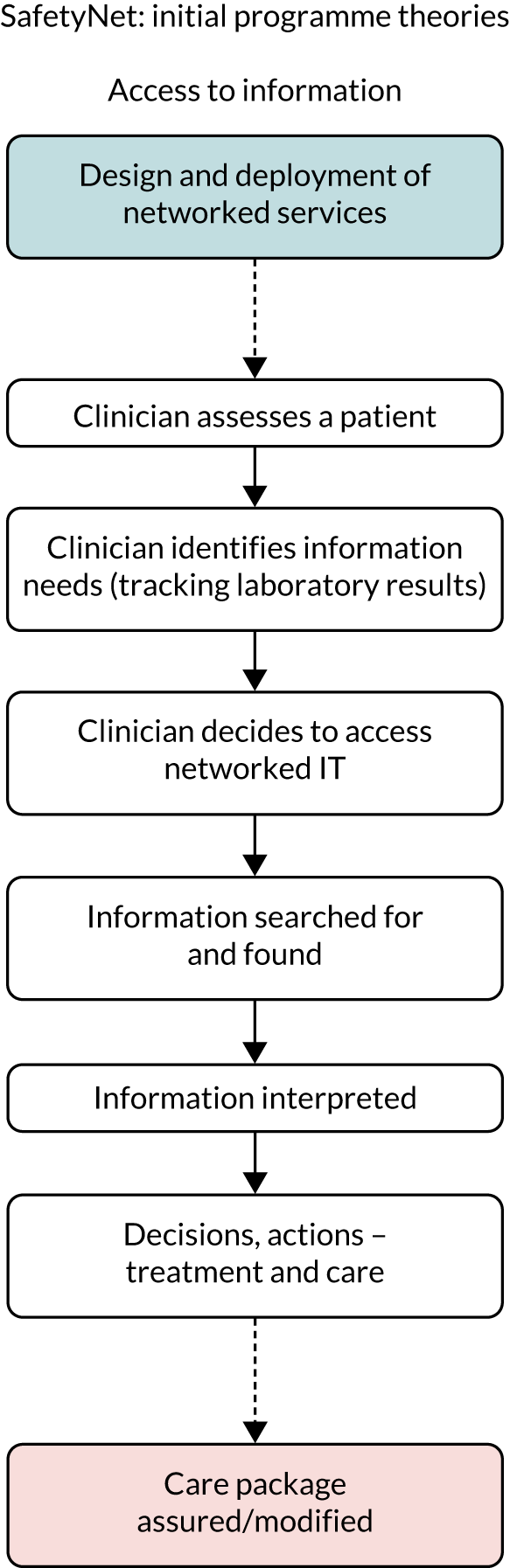
| Theme | Key feature | Example | Managing or avoiding risk |
|---|---|---|---|
| Co-ordination | Clinicians use records and networks to co-ordinate with one another | Community nurse reviews elderly person’s care package, contacts services that have not been attending | Managing |
| Non-standard patterns of care/alerts | Systems provide data to alert clinicians | Safeguarding | Managing |
| Reconciliation | Clinicians access data from ‘remote’ systems | Medicines reconciliation | Managing and avoiding |
| Design to eliminate risks | ‘Whole-system’ approach to the role of networked IT services | Comprehensive redesign of services | Avoiding |
Figure 6 and Table 2 capture two key, early, lines of thinking. The first was that we represented clinical working practices in simple terms, reflecting the lack of detailed theories resulting from any of the searches. The second was that we noted articles that resonated with two of the themes in our proposal – the possible effects of deployment on the use of networks, and privacy and confidentiality – but decided not to pursue either theme. We decided against studying deployment on pragmatic grounds: the lack of detail about programme theories of professionals’ working practices would have required us to speculate about the effects of deployment on them. This seemed to us to be a risky strategy. We decided against focusing on privacy and confidentiality because we had established, in during another study that one of the authors (JK) was involved in [URL: https://gow.epsrc.ukri.org/NGBOViewGrant.aspx?GrantRef=EP/N013980/1 (accessed 25 February 2020)], that there was a limited empirical literature in relation to HITs in general, and none that we could find in relation to interoperable networks. We judged that we would find it difficult to link elements of programme theories on privacy and confidentiality to elements representing clinical working practices.
Table 2 draws on one of the publications in our personal library, Vincent and Amalberti’s85 three-way classification of approaches to managing risks in health-care systems: embracing, managing and avoiding risks. We focused on the last two of these, describing them in the following way in the text provided to the nominal groups:
[Managing risks] . . . involves actively managing patients’ risks. The key idea here is that much health and social care is inherently uncertain, so that it’s never going to be possible to know when any particular patient falls ill, or deteriorates. The appropriate response is to set the care system up so that clinicians can respond to patients’ problems as they arise.
The [avoiding risks] approach involves eliminating risks. The Virginia Mason model, currently being piloted in five English NHS hospitals, is an example of this approach (improvement.nhs.uk/resources/virginia-mason-institute/). The starting point is that, although some aspects of care are inherently uncertain, much can be done to eliminate uncertainty for many patients. Our question is, do you think that networked IT services can be designed and deployed in support of an inherently safer care system?
By way of illustration, medicines reconciliation can be interpreted as an example of this approach (as well as of actively managing risks). By providing the means to check current medications, and contraindicated medication, IT systems can be part of a comprehensive approach to eliminating patients’ risks.
The nominal groups did not offer detailed comments on our initial rough theories, but instead provided four key insights. First, the health and social care IT managers stressed that very few localities in England could currently provide health and social care staff with ‘seamless’ or ‘click through’ access to patients’ records held by several organisations (general practices, community NHS services, social services and so on). Indeed, most of the leading localities offered access to records on an organisation-by-organisation basis, typically by clicking on an icon to access each one. Systems were designed this way at least in part because doctors (in particular) could not be persuaded to do more than access patients’ remote records on a tactical basis, when they really needed information. There was little incentive to provide more integrated solutions. Thus, although it would be theoretically interesting to focus searches on fully (semantically) interoperable solutions, the results would not reflect current realities on the ground, and the value to the staff who procured, built and maintained networks would be limited. Second, although the initial programme theories were of some interest, there was a more specific challenge, namely to establish the value of interoperable networks. It would be helpful to know how and why interoperable networks worked, but it was more important to identify and, ideally, quantify the outcomes associated with their deployment. Third, the meetings confirmed the intuition, arising from the initial searches, that those responsible for IT systems did not themselves think through the ways in which systems might influence patient safety. Fourth, and finally, we asked about the patient groups or services that we should focus on. At both meetings, the suggestions included services for a frail elderly person living at home who has a fall (or some other event), an adult with mental health problems who needs urgent treatment and care, and an at-risk child who attends a general practice or an urgent care service.
Revised programme theories 1
We used the nominal groups’ observations to revise the initial programme theories. The changes were reflected in papers prepared for the first Steering Group and PPI panel meetings, both held in June 2018. Figure 7 was our attempt to represent the insights gained from the nominal group meetings, with each band representing events unfolding over time in a different domain: patient records systems, the technologies professionals use to initiate an encounter with a patient, clinical actions and patient experiences. The comments at both meetings suggested that although the representations had some merit they were simply too abstract to be of real value; we determined to rethink them rather than revise them.
FIGURE 7.
Programme theories presented to the PPI panel. (a) Draft programme theory 1; (b) draft programme theory 2; and (c) draft programme theory 3.
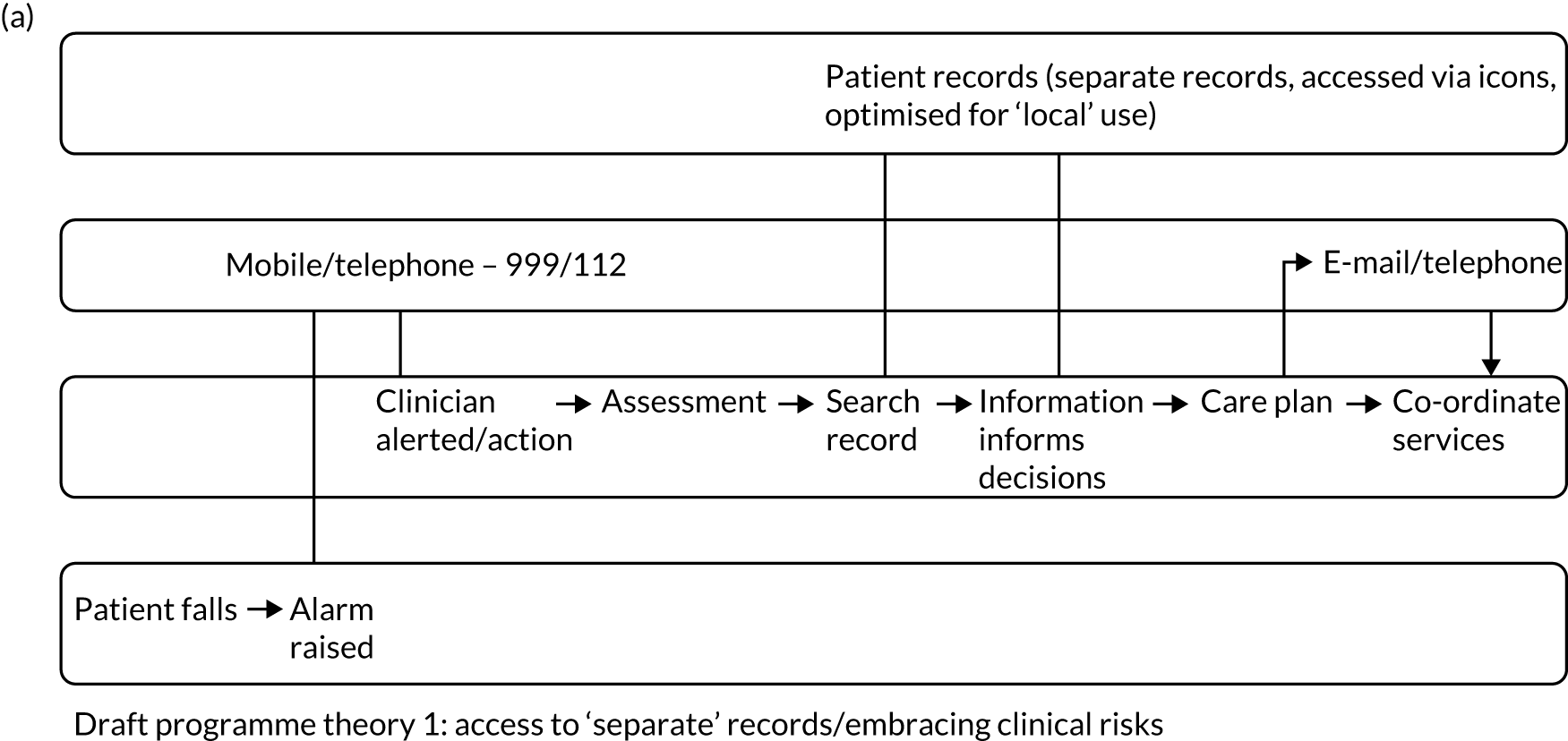
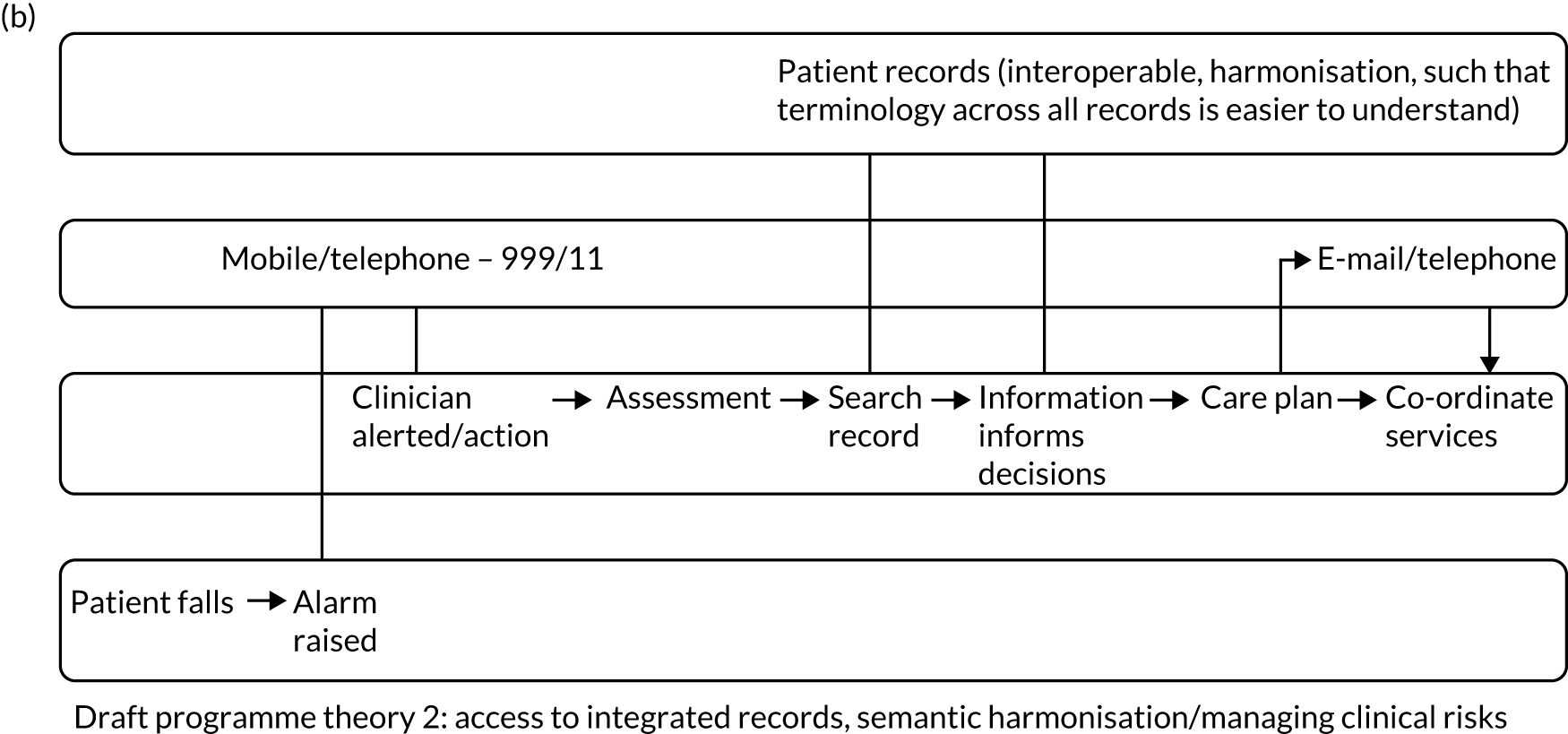

We also asked the PPI panel for guidance on the population(s) that we should focus on in our literature searches, setting out some of the suggestions made by the nominal groups to ‘seed’ the discussion. The panel gave us clear steers. Support was strongest for focusing on the support of frail older people, including people with dementia. More generally, it was suggested that we focus on people who need support from a number of health and social care services, and who may not be able to organise that support for themselves. Other possible groups mentioned included children who are safeguarding risks and patients who take a number of medications (polypharmacy). Broadly, then, the PPI panel supported the nominal groups’ suggestions.
Revised programme theories 2
Following the PPI and Steering Group meetings, we sought to think in different ways about programme theories. Our first output is in Figure 8, which illustrates ways in which care processes, which are not represented, could go wrong. Although this did not, in itself, represent a plausible programme theory, it did help to consolidate our thinking about many of the theory fragments that we had identified in the literature searches. This led us on to Figure 9, which is in effect an amalgamation of, and simplification of, Figures 6 and 8. Figure 9 was the main programme theory that we used to guide our evidence searches, reported in the next four chapters.
FIGURE 8.
How might things go wrong?
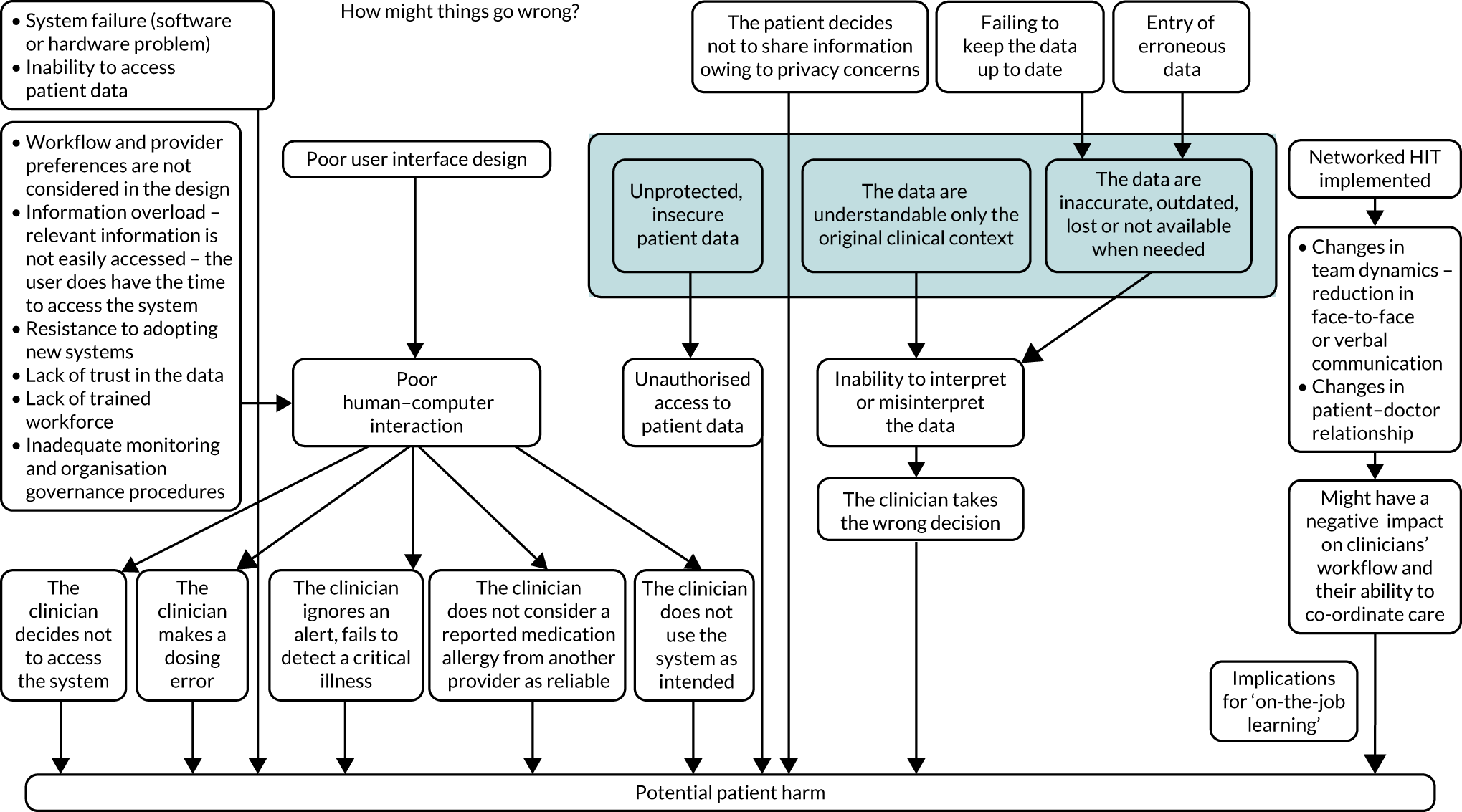
FIGURE 9.
Main programme theory.
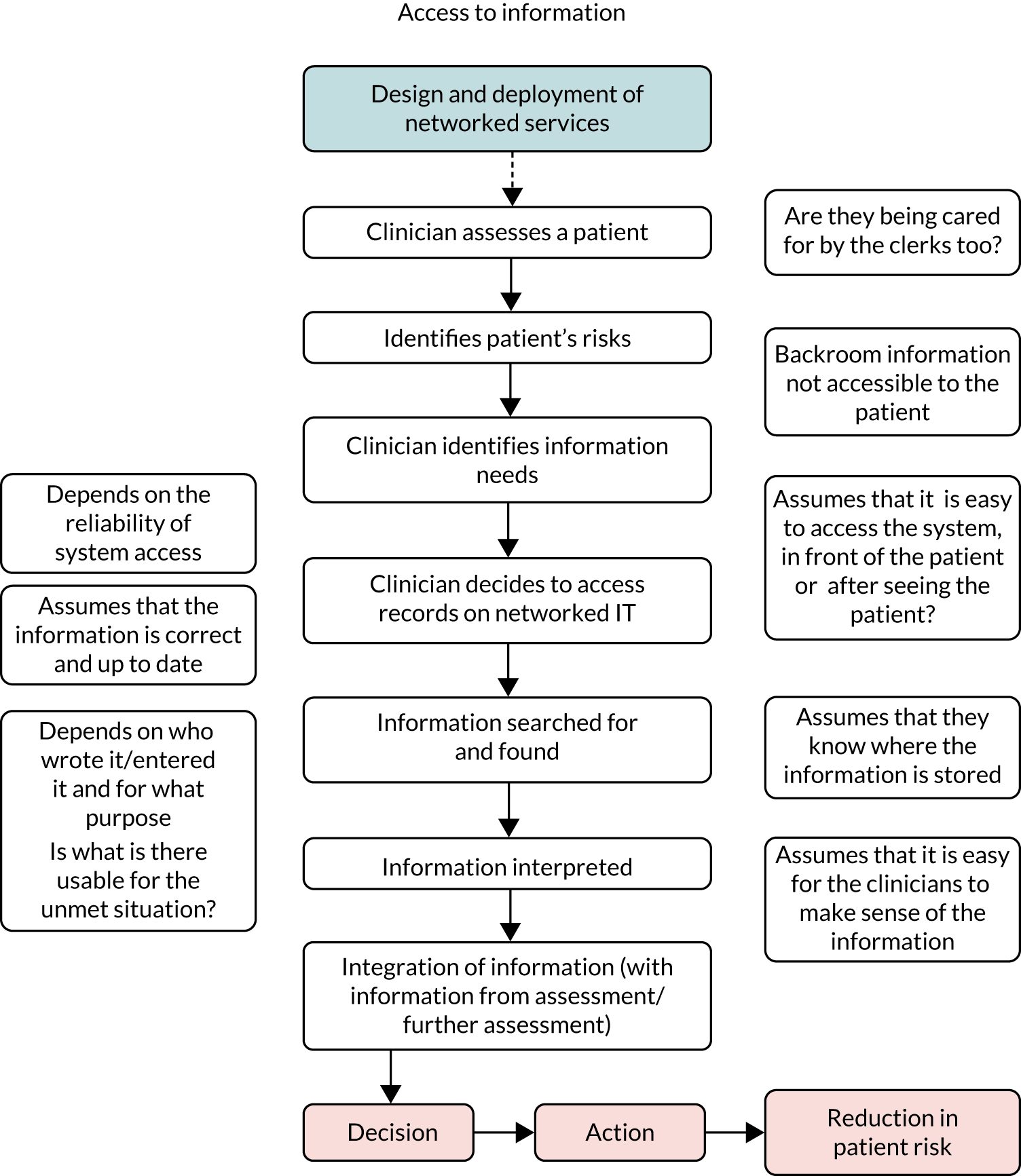
We draw attention to three features of the main programme theory in Figure 9. First, in representing the intended effects we assume that an interoperable network is available for use. We were not concerned in this review with the implementation of a network or with the details of its architecture. The programme theory focused, instead, on the use of networks, and the decisions and actions that might follow. Second, Figure 9 focuses on access to information held on other organisations’ systems, but we were interested in evidence about any possible function of an interoperable network, which (on the basis of our theory fragments) included communicating with colleagues in other organisations and comparing (reconciling) information about a patient held on two or more systems. Third, we clarified our thinking about the outcomes of interest in the synthesis. In the early months, we used the umbrella term ‘patient safety’ in our discussions, but realised that this was too broad a description of an end point in a programme theory. We settled on ‘changes in patients’ risks’ as the end point of each theory.
Finally, in this section, we also settled on the domains of interest for our evidence searches. These closely followed the advice we received from the nominal groups and PPI panel, as shown in Table 3.
| Population | Topic | Interoperability | Main programme theory |
|---|---|---|---|
| Frail older people | Co-ordination of care | Functional | Access to information |
| Frail older people | Medicine reconciliation | Functional or semantic | Medicine reconciliation |
| At-risk children | Co-ordination of child protection | Semantic | Access to information and communication |
Second programme theory and mid-range theory
In our proposal we identified a distinct economic programme theory concerning economies of scope and scale. We hypothesised that there might be ‘global’ effects associated with the deployment of an interoperable network when the costs and benefits were distributed across the network and, hence, across a health economy. This contrasts with the more individualistic programme theory in Figure 9. Our searches and consultation had not given us any reason to either include or exclude this theory; we retained it for the evidence searches and discuss the results in Chapter 8.
As we noted in Chapter 2, we developed a mid-range theory, as well as programme theories. The general form of the mid-range theory was identified at the end of the theory development phase of the study. Given the study protocol, and the steers from the nominal groups, the theory selected needed to address the issues associated with large-scale networks, spanning organisational and professional boundaries to shed light on the relationships between interorganisational networks and changes in clinicians’ working practices; and to have a solid evidence base. This ruled out a number of frameworks that have been found to be useful in other settings. This included normalisation process theory, which is well suited to studies of interventions in single settings (as opposed to studies of interventions spanning many settings). 86 Other sociological and sociotechnical theories have been used fruitfully over the last two decades, but they tend to focus more on implementation failures than on successes, and our concern here was to explain, if possible, both successes and failures. One framework that does this, and meets the three listed criteria, is a sociotechnical theory concerned with the development of information infrastructures. 87 The initial form of the mid-range theory was as follows:
-
Older people with complex needs are supported by care professionals who have different backgrounds and training, and who often work in different organisations. Networked IT systems are embryonic information infrastructures that over time are likely to become more interoperable (in the sense that an engineer would use this term). Information infrastructures span a number of professionals and organisations. The long-run intention is that professionals will integrate the use of the IT systems into their work so that the systems effectively become invisible. Professionals will not think about if or how to use them; they will be just part of ‘the way we do things here’.
-
When infrastructures become invisible, they contribute to overcoming co-ordination challenges that naturally arise in these institutional arrangements. The resulting improvements in the effectiveness of co-ordination will, in turn, lead to reductions in patients’ risks.
-
This positive account is qualified by evidence about the practical difficulties that professionals can face when using IT systems. Far from becoming invisible, and part of usual working practices, the systems can be difficult to use. The difficulties can stem from poor-quality interfaces and the fact that IT systems can create additional work compared with paper systems, notably in the time it can take to input data.
Interview programme findings
The interview programme with front-line health and social care professionals who were using interoperable networks was undertaken in November 2018, after the initial programme and mid-range theories had been settled. The interviews could not, therefore, influence the development of the theories. As we noted in Chapter 3, however, following consultation with our Steering Group we decided that consultation with professionals was important for two reasons. First, any insights generated could still be used, notably in helping us to frame our thinking about the evidence we found. Second, there was still time to modify our search plans if the professionals highlighted an important issue that we had not thought of or had undervalued earlier in the study.
A community nurse, a general practitioner (GP), a social worker, two pharmacists and two physiotherapists were interviewed. Professionals valued their local interoperable networks. In both localities, the networks could be described as functionally or partially interoperable, allowing access to patient information held in other organisations’ systems, each accessed via a separate web page. Interviewees stressed the value of access to a ‘wealth’ of data, which allowed some of the professionals to ‘follow their stories in detail’. Some were able to log on to other systems easily (e.g. just by clicking on an icon) and to keep two or more systems open at the same time on separate web pages (on a laptop or tablet). They could check current medications (which was particularly helpful to pharmacists, but was also useful for other professionals), access information about a recent hospital stay, look up who is visiting whom at home and check whether or not a particular patient is on a waiting list for a hospital appointment.
Some interviewees contrasted these facilities with the situation a few years earlier, when they would have had to call a general practice or hospital to request information. If they needed to know what was written in patient notes, they would have had to wait to receive a fax. The overall sense was that the networks reduced patients’ risks; even if professionals had access to incomplete information, they had better, more readily available information than would have been the case in the past and were, therefore, more likely to make better decisions. Two of the interviewees noted that it was possible to post alerts on their network; for example, new information about an at-risk child could be placed on that child’s home screen and the information would appear to anyone who accessed that child’s records.
At the same time, more mixed experiences were reported. Several interviewees lamented that they did not have access to mental health services’ systems. Some professionals did not have access to particular information they needed and so could end up repeating tests, which they felt did not promote patient safety.
Some interviewees also reported multiple, ‘clunky’ log-ons. Different professionals had different permissions, and some could access remote systems more easily than others. There was a view that networks were designed more around the needs of GPs than those of other professionals; for example, procedure or diagnostic codes for important and frequently occurring issues were not available to nurses and therapists (e.g. for pressure ulcers). GPs were able to choose which IT systems they used in their practices, which created issues for professionals in other organisations, as they might have access to one system but not to the other. When other professionals did not have access, they still had to telephone practices for information about a patient they were visiting that day.
Nurses and therapists took longer to complete assessments than they had done when paper assessment forms were used. One estimate was 60–70 minutes via a network, compared with 40 minutes using paper assessment forms. Standardised forms, which had to be completed in an order determined by the network managers, increased time costs. Social workers could refer someone to an NHS service, but they had no way of finding out, via the local network, whether or not an NHS colleague had actually followed up. Discharge letters often did not include full details of medications prescribed at hospital discharge, so that pharmacists had to call the hospital for more information. On one of the networks, take-out medication information was not uploaded until midnight on the day of discharge, which could exacerbate the problem of medicine reconciliation post discharge.
Finally, it was suggested that the networks were part of a larger HIT ecosystem. The combination of the networks, e-mail, Skype™ (Microsoft Corporation, Redmond, WA, USA) and other HIT services meant that co-ordinating treatment and care was easier than in the past. The fact that some of these services were separate from one another was not a problem. Several interviewees did, however, agree with the suggestion that semantic or seamless interoperability was desirable and might, in principle, make treatment and care safer.
The interviews confirmed views expressed in the nominal groups and by our PPI panel, not least about the combination of the potential of and the risks associated with interoperable networks and about the importance of medicine reconciliation. They did not change our views about our programme and mid-range theories.
Nominal group feedback
We sent the two nominal groups a summary of our findings in July 2019 (see Appendix 3). The response from the groups was brief. The groups were surprised and disappointed that the available evidence was so limited. They did not have anything to add to these comments.
Systematic review update
We updated the systematic review search in July 2019 to identify any new (evidence-based) theory fragments that might influence our thinking about our programme or mid-range theories and to check if any new reviews had been published in our domain. None of the reviews was included. We note, however, that two reviews gave us a little more confidence in our findings. The first was by Bowden and Coiera,50 who reviewed evidence about the use of primary care records, shared with local hospitals, during episodes of unscheduled care. We had found this study before, but re-read it in the light of our own results. Bowden and Coiera,50 like us, found little high-quality evidence and concluded that:
[Shared EHRs] should in principle be capable of improving the efficiency, quality and safety of unscheduled care, but at present the evidence for such benefits is weak, largely because it has not been sought.
Bowden and Coiera50
We had not previously identified Devine and colleagues’ review,88 even though it was published in 2017. They focused on evidence about the rates of deployment and use of interoperable networks up to 2015. They concluded that the availability of networks had increased substantially, particularly in the 10 years prior to 2015. The functionality of those systems had improved in that period, in that users had access to more services (e.g. to laboratory test results), to remotely held patient records and to secure communication with clinical colleagues. They also observed, however, that there was little evidence that localities, both in the post-Obama administration environment in the USA and in other countries, had developed semantically interoperable networks. As we will see in later chapters, all of the evidence we found was about what one might term ‘basic’ functionality in the interoperable networks studied.
Commentary
This chapter has set out the process of developing programme and mid-range theories. We were struck by the absence of theories that directly linked interoperable networks, and indeed HITs in general, to patient safety. As a result, we had to work harder than we expected to develop the theories ourselves. These theories did, however, provide a basis for the evidence searches that are described in Chapter 3 and, hence, the evidence presented in the next four chapters.
Chapter 5 The co-ordination of services for older people
Introduction
This chapter presents the findings of the first evidence review described in Chapter 3. The next section discusses the nature of problems with the co-ordination of services for older people and, by extension, whether or not any of them might benefit from the deployment of interoperable networks. The following sections focus on users’ experiences of interoperable networks and on evidence about the outcomes associated with the deployment of such networks.
What are the problems with the co-ordination of services?
The searches identified 619 records for screening, 10 of which were eligible for inclusion (Figure 10).
FIGURE 10.
A PRISMA flow diagram: care co-ordination – nature of the problem.
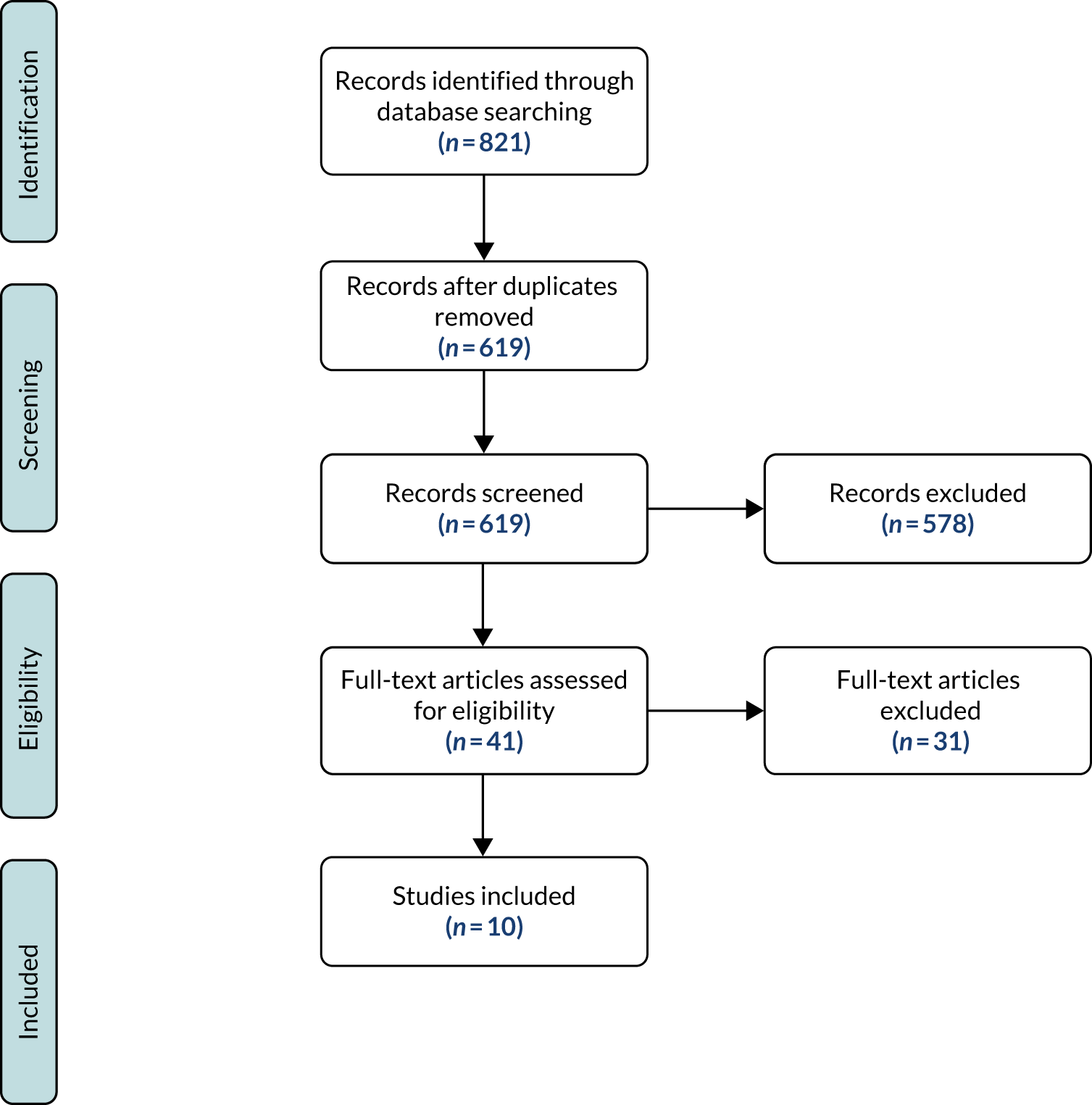
The nature of co-ordination problems
This section presents summaries of five review articles (Table 4) and of primary research articles published after the reviews and the results of hand-searching The King’s Fund reports, which yielded two further references. We highlight two broad themes: one is the nature of co-ordination problems in general and the other is a particular problem, namely communication between professionals.
| Study | Country | Method | Topic | Data type | Rigour | Relevance | Processes | Outcomes/errors |
|---|---|---|---|---|---|---|---|---|
| Auschra89 | Systematic review | Barriers to integrated care | Qualitative | 1 | 1 | Range of interpersonal and institutional issues | ||
| Threapleton et al.90 | Scoping review | Barriers to and facilitators of co-ordination | Quantitative (E & O) and qualitative | 2 | 1 | Organisational and cultural features of co-ordination | ||
| Allen et al.91 | Narrative review | Transition from hospital to home | Qualitative | 1 | 1 | Negotiation and navigation of service user independence | ||
| Kirst et al.92 | Realist review | Conditions for effective team integration | Quantitative (E & O) and qualitative | 1 | 1 | Service use, patient and provider experience | Patient health status | |
| Hudson et al.93 | Narrative review | Transition from hospital to home | Quantitative (O) and qualitative | 2 | 3 | Range of organisational and interprofessional issues | Re-admission rates, user satisfaction with transition | |
| Goodwin et al.94 | Seven countries | Synthesis of case study evidence | Models of integrated care | Qualitative | 2 | 1 | Range, including flexibility of team working, effective communication, focus on users’ needs | Effective integration associated with improved user satisfaction |
| Goodwin et al.95 | England | Multisite case study | Evaluation of care co-ordination programmes | Qualitative | 2 | 1 | Range, including organisational models, team cultures, engagement |
Review articles
Auschra89 undertook a review of barriers to the integration of care in interorganisational settings. 89 She argued that health care is delivered to many people by a number of professionals at any one time, and that integrated care is desirable as it leads to better outcomes. Similarly, Auschra89 identified a number of barriers to integration. The strongest evidence (i.e. the largest number of papers) was about problems arising from the differences in the professional backgrounds of care providers, problems with leadership across professional and organisational boundaries and the conflicting goals of those providing care. There was also evidence suggesting problems due to lack of trust and shared understanding between professionals.
Auschra89 also found evidence that a lack of communication and a failure to share information between professionals were barriers to integration. Confidentiality concerns were mentioned in relation to the latter. A lack of IT standards and the consequent inability to share information were also found to be barriers to integrated care.
Threapleton and colleagues90 reviewed evidence about integrated care for elderly people. The authors identified eight ‘components’ of integrated services: (1) care continuity, (2) the policy context, (3) shared values and goals, (4) person-centred care, (5) multidisciplinary teams, (6) effective communication, (7) case management and (8) needs assessment. The study cites evidence of co-ordination problems between primary and secondary health services, and health and social care services. Threapleton and colleagues90 argued that some of the prerequisites for integrated care are functional (e.g. funding, having multidisciplinary teams, having effective communication between service managers and between care providers) and others are more concerned with social and cultural issues (e.g. leadership, common values, problems posed by risk-averse or permission-based cultures).
Communication was one of the components of integrated care. Threapleton and colleagues90 cited evidence about the value of different modes of communication, including team meetings. They also cited papers that found evidence of a role for integrated electronic record management, suggesting that a common database (i.e. shared patient records helping the flow and exchange of information) was also deemed desirable.
Allen and colleagues91 reviewed evidence about care integration and the experiences of older people in the transition from hospital to home. They focused on the co-ordination of hospital and home-based services on the basis that problems with home-based services can affect decisions about an older person leaving hospital. The authors found evidence of inconsistent co-ordination of services. They suggested that this could be because the organisation was fragmented and/or because some services were not available in a given locality. They noted evidence of conflicting messages about care plans from different providers and practical difficulties at home (e.g. with personal hygiene, and with shopping, cleaning and other household tasks). Older people and their carers wanted information about their health problems, care plans or details of self-care, including how to access community services, but this was typically limited.
Allen and colleagues91 presented what they termed a social constructivist account of communication as embedded in the processes of patients and carers negotiating with community-based providers, and of providers negotiating with one another. Communication problems were evident in many of the papers that the authors cited. To take just one example, failure to discuss an older person’s needs could translate into missed opportunities to meet those needs, and to enable an older person to live independently.
Kirst and colleagues92 undertook a realist review of the implementation of integrated care programmes for older people with complex needs. They identified evidence that supported two inter-related context–mechanism outcome configurations. The first concerned trust in multidisciplinary team relationships. Programmes were successful when cross-sector multidisciplinary teams that spanned different organisations trusted each other, were clear about their roles and could rely on each other to perform their roles. These teams collaborated closely, communicated effectively and shared knowledge about their work and patient information effectively, which allowed for continuity of care and better co-ordination of care. They also identified what they described as contextual factors that helped to build trust. These included team collaboration, leadership, and an organisational culture that encouraged team participation.
The second context mechanism outcome configuration emphasised provider commitment to, and understanding of, an intervention. The contextual factors that influenced provider commitment included strong leadership and strong organisational culture, provider expertise and training, provider incentives, flexibility in implementation (to respond to patients’ needs) and time to build infrastructure. The last of these included building relationships across organisations and establishing management information systems.
Kirst and colleagues92 did not emphasise communication to the same extent as the first three reviews. It is, however, strongly implied in both configurations that teams cannot build relationships, or arrive at a shared understanding of an intervention, without effective communication. The authors were less sure about the role of HITs, finding that common IT solutions across partnering organisations facilitated effective team communication and collaboration, but that this was not a necessary condition for successful co-ordination.
Hudson and colleagues93 reviewed evidence about transitions in (what they termed) wicked environments for people aged ≥ 65 years (a broader group than in the other reviews). The authors identified six challenges that involved community-based services: (1) communication between professionals, and between professionals, patients and carers; (2) interprofessional relationships, including power differentials; (3) the primacy of the medical model; (4) role confusion, due in part to professionals not understanding one another’s roles and working circumstances; (5) having sufficient resources available to provide services; and (6) leadership. Again, communication is one of the themes the authors identified. This included evidence of colleagues failing to send information to one another and of a patient’s social history not being valued by medically qualified professionals involved in their care.
The King’s Fund publications
The King’s Fund has published a series of reports on the co-ordination of care for both older people and other groups that stretches back more than 10 years. We screened report titles and abstracts for relevance and then assessed 19 full texts. Two reports were included. 94,95 Given the evidence found in the five systematic reviews89–93 reported above, our focus here was evidence about the role of interoperable networks, or HITs more generally, to compensate for the relative lack of focus on this in the reviews.
The first report,95 published in 2013, was a comparative analysis of five UK-based case studies of care co-ordination programmes for people with long-term and complex chronic conditions. The report did not focus on a specific age group, but sections did discuss evidence of problems with the co-ordination of care for older people. The authors concluded that care co-ordination is a multifactorial problem. They created a framework that included > 30 characteristics of successful approaches to care co-ordination. The characteristics were divided into four ‘levels’ (system, organisational, clinical and professional, and service integration), with change needed at all four levels for effective co-ordination. System-level characteristics included universal health coverage, community- or primary care-led health care, emphasis on long-term and chronic conditions, and development of workforce skills in teamwork and care co-ordination. Integrated EHRs were reported to be facilitators of care co-ordination, along with strong leadership, common values and a shared mission, aligned finance and governance structures, and a focus on continuous quality measurement and improvement. Shared clinical records were also mentioned in the context of clinical and professional services. At the service integration level, multidisciplinary teamwork and the development on interprofessional networks were deemed important, as were co-location of services and shared accountability.
The second report94 was a synthesis of evidence from seven international case studies, from a number of countries, of integrated health and social care programmes for elderly patients with complex health needs. The authors collected key documents and conducted key informant interviews, evaluating the case studies against criteria identified in the previous report. 95 With regard to information management, the authors found that none of the case study programmes had developed fully shared electronic patient records that were accessible by all professionals involved in patient care. The authors94 concluded that the case studies showed that it was possible to deliver integrated care using older technologies, such as telephone and fax. Greater use of shared EHRs was potentially an important enabler of integrated care but did not appear to be a necessary condition for it.
Post-review individual studies
This search was designed to identify papers that had been published after the review by Threapleton and colleagues. 90 Three papers were included after full-text screening. These are summarised in Table 5.
| Study | Theme | Focus |
|---|---|---|
| Hainstock et al.96 | Information-seeking and knowledge gaps, navigating roles, regulations and procedures (staff turnover, lack of continuity of care), advocacy | How family caregivers navigate and make sense of the transition from home care to residential care for a family member |
| Jeffs et al.97 | Components of successful nurse-led care transitions | Nurse-led care transition intervention |
| Larsen et al.98 |
To collaborate is to feel trust or mistrust between health-care providers To collaborate is to have a sense of security or insecurity |
Interprofessional collaboration |
Hainstock and colleagues96 conducted interviews with family caregivers of older people to explore the challenges and needs of older patients when they transfer from one care environment to another. They interviewed 16 caregivers recruited from a ‘diverse health region’ in western Canada. During the transition of care, participants noted that communication between health-care professionals was problematic, and that it was complicating information flows and related caregiving efforts. Participants additionally described a perceived lack of empathy, compassion and continuity of care. The participants described experiences of receiving services from several health and social care professionals, and how they were not always informed about who was doing what and when. Other challenges were system related, including issues with funding and transport. The article mentioned issues with information transfer and effective communication, but did not explicitly mention interoperable networks.
Jeffs and colleagues97 studied a transition intervention for older people with complex needs in Canada. They used a modified Delphi consensus technique, asking 23 panellists (clinicians, managers and caregivers) to rank intervention components and contextual factors identified in an earlier realist review. 99 The results suggested that patient involvement and engagement in transitions was ranked highest, followed by improving communication, professional practices and strategic leadership. The facilitation of information transfer, enhancement of clinical information systems and use of integrated person-centred health records was ranked eighth by the panel.
Larsen and colleagues98 conducted an interview study with health-care professionals involved in providing care for older people living at home in Sweden. The study aimed to illustrate and describe how various health-care professionals experience collaboration in caring for older people living at home. The results suggested that a combination of clinicians’ personalities and professional boundaries may affect the quality of teamwork and, hence, the quality of care patients receive. The authors argued that the keys to successful collaboration were building trust and a sense of security, and not drawing boundaries between primary and specialist care.
Taking the papers as a group,96–98 the main themes identified were similar to those identified in the literature reviews.
Commentary
The literature reviews and other articles confirm that there is empirical evidence of co-ordination problems in the care of older people. Services are provided by people with different professional backgrounds, typically working for different organisations. Service providers have to co-ordinate their work, spanning professional and organisational boundaries, to provide integrated (or effectively co-ordinated, or person-centred) care. The evidence suggests that there is broad agreement about the nature of those problems. Reviews conducted in different academic traditions, and using different review methods, have produced broadly similar findings. The reviews indicate that this is an ongoing challenge: it is structural, it is not going to change and it is difficult. It makes sense that a great deal of work has to go into creating, and sustaining, multidisciplinary teams.
The articles89–98 all stress the fundamentally social nature of team working across professional and organisational boundaries: the importance of leadership, culture, trust and other qualities of teams. They also convey the point that co-ordination problems cannot be separated from one another. That is, it is not possible to solve one issue – say, a culture that does not encourage team working – separately from others. The question that follows, for this review, is whether or not any of the themes is amenable to solutions that involve interoperable networks. Most of the themes are not, by their nature, ones that an interoperable network – however designed – can obviously help to address. Their contribution to leadership or trust problems will be indirect, at best.
Our interpretation is that there might be a role for interoperable networks in addressing communication problems, but the communication problems can be addressed only in concert with addressing other problems.
Users’ experiences of interoperable networks
The searches identified 463 records to be screened, of which six100–105 were eligible for inclusion (Figure 11). All articles included are in the outer ring of the relevance ‘target’ described in Chapter 2.
FIGURE 11.
A PRISMA flow diagram: care co-ordination – users’ experiences.
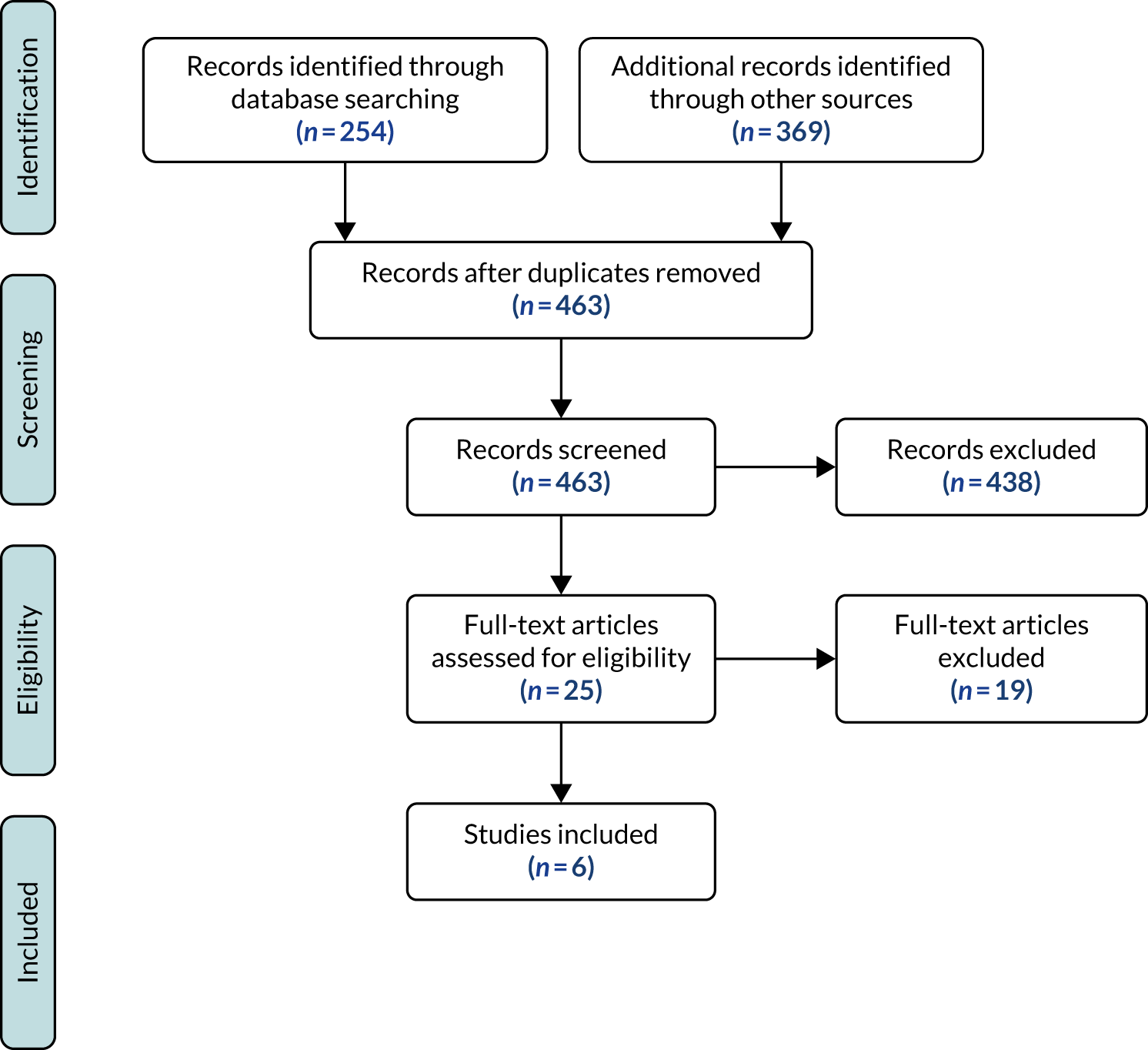
Literature reviews
We included four literature reviews and two primary research articles (Table 6). All four reviews100–103 were general in nature, and did not focus specifically on the experiences of users in the course of the treatment and care of frail older people, or of older people more broadly. The reviews reported that there was generally little information about the nature of the interoperable networks studied, including their user interfaces.
| Study | Country | Methods | Topic | Rigour | Relevance |
|---|---|---|---|---|---|
| Eden et al.100 | Systematic review | HIE barriers and facilitators | 1 | 3 | |
| Azarm-Daigle et al.101 | Systematic review | Cross-organisational data sharing | 1 | 2 | |
| Hoerbst and Schweitzer102 | Systematic review | Critical success factors for clinical information systems in integrated care | 1 | 2 | |
| Wu and LaRue103 | USA | Systematic review | HIE barriers and facilitators | 1 | 3 |
| Nicolaisen and Berg104 | Norway | Primary qualitative: interviews | Perceptions of messaging system | 1 | 2 |
| McMurray et al.105 | Canada | Primary qualitative: ethnographic study | Impact of partial interoperability | 1 | 1 |
Hoerbst and Schweitzer102 undertook a review of barriers to and critical success factors of HITs in integrated care settings. They identified 43 success factors, which they classified under five headings (organisational, technical level and user-related factors, and data and functionality of an IT system). For example, in relation to organisational success, they stated that the most important factor (cited in 24 studies) was project and IT management. The second most commonly cited success factor was active user participation in training and availability for IT support. Our interest was in user experiences. The most commonly cited success factors were perceived usefulness of a system and the active involvement of clinicians in the design process (24 studies). The engagement of managers with users’ feedback or concerns was cited in 11 studies. Less frequently cited factors included previous users’ experience and readiness to use these systems (seven studies), and availability of and easy access to computers (three studies).
Most of the evidence about barriers was focused on users’ working practices and on interface issues. The most cited barrier was increased clinician time spent on using IT (19 studies). Lack of involvement of clinicians in design and implementation was reported in 12 studies. Perceived negative impact of IT systems on the doctor–patient relationship was mentioned in 11 studies. The disruptive impact of systems on workflow was cited in nine studies.
Azarm-Daigle and colleagues101 conducted a literature review of studies that explored cross-organisational information sharing. Most of the evidence addressed implementation challenges rather than end-user experiences, so that evidence about information sharing was indirect. The authors did, however, cite evidence that might contribute to problems with information sharing. For example, they noted gaps in understanding between IT developers and health professionals, and the misconception that technology alone could solve all problems, both which might lead to suboptimal software solutions being implemented.
Wu and LaRue103 conducted a review of the barriers to and facilitators of adopting HIE in USA. They identified a number of challenges, many organisational, hindering the adoption of HIE. The review discussed five articles that focused on users’ experiences. The evidence suggested that overall usage rates were very low, with physicians using HIE the least and nurses using it more frequently. HIE varied by hospital department and user role. Reasons given for low usage rates included a lack of trust in data generated in other places, the disruptive effect of HIE on workflow, the redundancy or inaccuracy of information, time constraints and costs. Health professionals also commented on the need for more user-friendly designs, for automated single log-in (to interoperable networks) and for automated notification of the availability of new patient data.
Eden and colleagues100 conducted a review of barriers to and facilitators of using HIE (as distinct from Wu and LaRue’s103 focus on adoption). The review comprised 19 studies that used range of study designs, most of which were conducted in the USA. The most common perceived barriers to using HIE were incomplete information and the fact that the available information did not meet the needs of the users. Users were cited as saying that there was not enough information in the system to warrant use. Studies showed that users were frustrated because of the time they spent searching for information, which did not always lead to them finding anything clinically useful. Users also voiced concerns about the legality of sharing data.
The impact of HIE use on workflow was also found to be important. The review found that users struggled with separate log-ins and too many mouse clicks to get to information. In common with Wu and LaRue,103 the authors100 found that the role of the user affected when and how frequently they used systems, with nurses tending to use them more often than doctors. Facilitators of improving workflow included having single log-ins, training and IT support and, more generally, addressing the need for changes in working practices.
User experiences of interoperable networks: single studies
We found two studies that were not included in the four reviews reported in the last section. McMurray and colleagues105 interviewed 24 health-care professionals and 19 family members and caregivers involved in the transition of older patients in Canada. There was a combination of paper and digital records, with limited interoperability between the digital records held by different organisations. The two key themes emerging from the interviews were:
-
Partial interoperability between electronic information systems has complicated, rather than eased, the ability to communicate across settings and disciplines.
-
Although some information is more accessible and communications are more streamlined, the use of parallel paper and electronic systems has increased staff administrative time.
A physician was quoted as saying:
If the hospital doesn’t send the paperwork with the patient then I’ll never know the answer . . . who did you see while in hospital . . . why did you see a breathing type doctor while in hospital? . . . I don’t have that ability.
McMurray and colleagues105
Health professionals observed that one issue was a lack of trust that patient information would be accurate and up to date. These health professionals also raised concerns about the ease of looking for and finding information in electronic records, the structure and design of the records, and the impact on their autonomy in recording practices.
Nicolaison and Berg104 evaluated a national message exchange system in a sample of hospitals and primary care centres in Norway. The findings were based on interviews and a literature review. The interviews revealed differences in system use between hospitals and primary care settings. Hospital users saw the system as an ‘additional task’ that was used in parallel with other modes of communication. They reported finding message structures confusing. On the other hand, GPs and other professionals in primary care used and trusted the system. It was seen as a time-saving alternative method of cross-organisational asynchronous communication.
Fitzpatrick and Ellingsen forwards citation search
We did not find any articles that met our inclusion criteria in the forwards citation search of Fitzpatrick and Ellingsen’s 2013 review10 of computer-supported co-operative work literature.
Commentary
The evidence indicates that interoperable networks are difficult to use. We found limited evidence directly relating to the use of networks in the course of treatment and care of older people, but it seems reasonable to infer that some of the evidence in the literature reviews will include services for older people. There is a lack of studies involving direct observation of working practices; many studies were based on interviews. We did not find evidence about the use of interoperable networks when they are embedded in routine use (when implementation has been deemed a success).
Caution in interpretation of these findings is needed given that key details are missing from most reports, notably about the characteristics of the interfaces and other characteristics of interoperable networks. This said, the evidence casts doubt on the normative assumption underlying a section of the main programme theory. That is, users can access information to inform their decisions and actions.
The effectiveness of interoperable networks
The searches identified 977 records for screening, of which eight33–35,79,106–109 were eligible for inclusion (Figure 12).
FIGURE 12.
A PRISMA flow diagram: care co-ordination – outcomes.

Main search results
Three studies were included, all in the outer ring of the relevance ‘target’ described in Chapter 2. They used interviews as the main source of data (Table 7). None of the studies included quantitative data on patients’ risks, but all three studies did include perceptions of outcome changes.
| Study | Country | Methods | Topic | Rigour | Relevance |
|---|---|---|---|---|---|
| King et al.35 | Scotland | Interviews | Electronic shared assessment tool | 1 | 3 |
| Waterson et al.34 | England | Interviews, observations of meetings | e-health supported care pathway | 2 | 3 |
| Vimarlund et al.33 | Sweden | Interviews | Virtual health record tool | 3 | 3 |
| Health Quality Ontario106 | Systematic review | e-tools, HIE and care co-ordination | 1 | 2 | |
| Sadoughi et al.107 | Systematic review | HIE, quality of care | 1 | 2 | |
| Hersh et al.79 | Systematic review | Effectiveness of HIE | 1 | 2 | |
| Reis et al.108 | Review of systematic reviews | Cost–benefit of records, HIE, interoperability | 1 | 2 | |
| Menachemi et al.109 | Systematic review | HIE and service changes | 1 | 2 |
Vimarlund and colleagues33 report a case study of Old@home, a ‘virtual health record’ tool in Sweden. It allowed health-care professionals making home visits to access patient information from remote records systems and record new information at the point of care. The tool also allowed different parties to view the current services for a patient and was perceived to have reduced duplication or repetition of documentation. The team both developed and evaluated the tool.
The researchers33 conducted six semistructured interviews with project stakeholders, including system users. Overall, Old@home was perceived to improve team working, reduce pressures and reduce waiting time for the delivery of services. Access to real-time information was believed to improve relationships between various health-care professionals, was considered an important factor in improving work routines and was perceived as ‘a gain in efficiency’ for health-care staff.
Participants reported struggling to get used to the new system. Once they were familiar with it, however, they believed that it improved the transparency of work activities and also served to ‘reduce the constraints related to geographical locations and organizational cultural differences’. 33 The authors33 also argued that the new tool played a role in improving teamwork.
Waterson and colleagues34 reported on a 3-year project that aimed to design and implement an ‘e-health-supported’ care pathway for frail older patients in two NHS trusts in England. 34 The authors used a number of methods to collect the data, including 40 semistructured interviews with health-care professionals and observations of project meetings.
The findings were mixed. On the positive side, interviewees said that it was helpful to be able to see which other care professionals were involved in the care of patients and what the latest blood test results were. Community health-care professionals logged into the system when they received a referral for a frail older person. One nurse commented that ‘You have all the jigsaw puzzle pieces together’. 34 Accident and emergency staff used the system to send an alert to community nurses if a known frequent attender was at the hospital. Less positively, care co-ordinators reported that the system resulted in rushed arrangements for people being cared for in their own homes. 34
The system was also limited in that it did not allow nurses to access GP records. Social workers had limited access to the system. Many challenges were reported in being able to access patient information while working in the community (e.g. during home visits). Health-care professionals had to collect all of the data and then enter them into the system after they completed home visits, which increased their workload. Participants described how they worked around this and attempted to visit family practices while on the road to access the system. The paper concluded that the implementation of networked IT system was patchy and that further enhancements were needed.
King and colleagues35 undertook a case study of the implementation of an electronic version of the Single Shared Assessment (e-SSA) in three different health board regions in Scotland. The authors interviewed 30 health and social care workers across three study sites. They found that staff did not actively share e-SSA forms. An interviewee commented that:
I’d give it about 1 out of 10. I don’t think it has helped in the slightest. We don’t share a lot of them . . . they’re probably not a particularly good assessment either. In terms of a joint document it’s pretty pointless really.
King and colleagues35
Health information technology infrastructure was different between health boards and local authorities. Social workers were familiar with a mobile IT device and needed training only for the new application. Health-care workers had rarely used a mobile IT device to support their work and found it challenging. The authors also reported connectivity and IT infrastructure issues when the e-SSA was used in remote and rural locations. Participants also commented that the e-SSA document was lengthy and time-consuming. 35
The authors35 reported on broader issues. Professional boundaries between health and social care staff was a significant theme. There was evidence that different professionals had different views, roles and expectations. Overall, the authors found that the e-SSA did not meet professionals’ expectations.
Broader search results
The findings of the first search, which did not yield any direct evidence of outcome changes, prompted us to undertake a broader search. We searched for reviews relating to a broader population of adults and older people (i.e. relaxing the constraint of services for older people). Five reviews79,106–109 were included.
A systematic review106 and meta-analysis by Health Quality Ontario examined the impact of e-tools for HIE in the context of care co-ordination for individuals with chronic disease in the community. The review comprised 11 studies. Only one, a randomised controlled trial, reported on the impact of such tools on adverse events, with no statistically significant findings. The authors concluded that ‘the findings from this evidence-based analysis raise doubts about the ability of e-tools with care co-ordination capabilities to independently improve the quality of outpatient care’. 106
Sadoughi et al. 107 conducted a systematic review on the impact of HIE on quality of care, cost-effectiveness and use. The authors found 32 studies that satisfied their inclusion criteria. Medical error rates were reported in three studies; two reported reductions in rates and one reported no significant change.
Hersh et al. 79 undertook a systematic review of effectiveness of HIE. They included 34 studies, but none reported patient mortality or morbidity outcomes. Most of the evidence looked at hospital utilisation outcomes, such as use of investigations, hospital admissions and hospital re-admissions.
Reis and colleagues108 conducted a review of reviews to investigate the evidence base for ‘cost–benefits’ of EHRs, standards and interoperability. Six reviews were included, none of which included measures of cost-effectiveness.
Menachemi and colleagues109 published an updated systematic review of studies of the relationship between HIE and health-care outcomes. The authors109 reported substantial numbers of quantitative papers that included evidence of process measures, including hospital readmission rates and laboratory and radiology request rates. In relation to quality of care, 9 out of 10 included papers reported a positive impact of HIE on medicine reconciliation, immunisation and medical record completeness, and a reduction in care disparities and measures specific to HIV (human immunodeficiency virus). Of these, the most relevant is the report on medicine reconciliation, which we turn to in the next chapter.
Commentary
We did not find any useful evidence about the effects of interoperable networks on patient outcomes. The evidence in the articles is, at best, indirect and relatively weak. The wider evidence is barely more positive.
Conclusions
There is good evidence about the nature of co-ordination problems in the care of older people living at home. There is also good evidence about users’ experiences of interoperable networks, which suggests that users find such networks difficult to use. There was no evidence about the effectiveness of interoperable networks on the outcomes of older people. There was some more and better evidence about wider adult and older populations, but this too suggests that interoperable networks may not have substantial effects on patient outcomes.
In relation to the main programme theory, the evidence supports the contention that there may be problems that interoperable networks play a role in solving – communication problems. However, there is also evidence that undermines the programme theory, which assumes that users can access networks and find information – there is good evidence that this is not the case. Finally, we are struck by the lack of strong evidence from well-designed experimental or observational studies about patient outcomes.
Chapter 6 The co-ordination of medicine reconciliation
Introduction
This chapter presents the evidence about the role of interoperable systems in medicine reconciliation for older people. Our nominal groups and PPI panel identified medicine reconciliation as a priority. Medicine reconciliation involves the reconciliation of two or more lists of medications, or the reconciliation of a medication list with a patient’s assessed needs (or both). Barnsteiner110 defined this aspect of reconciliation as:
The process of obtaining and documenting a complete and accurate list of current patient medications and comparing this list with medication orders at each point of care transition to identify and rectify any discrepancies.
Barnsteiner110
Medicine reconciliation offers an appropriate ‘test case’ for interoperable systems. Interoperable systems might be a source of increased patient risks or they might be part of a strategy to reduce those risks. An interoperable network allows professionals to access medication lists both in their own patient record systems and in remote systems. Lists therefore need to be reconciled before systems can be used safely, and clinical risks may be associated with a failure to reconcile lists or with errors made in the process of reconciliation. Equally, there is the prospect that interoperable systems can be designed to support the accurate reconciliation of medication lists, contributing to the assurance of safe treatment and care.
There are three main sections, reflecting the questions set out in Chapter 3:
-
What is the nature and extent of problems with medication reconciliation?
-
What evidence is there about the experiences of the use of interoperable systems in medicine reconciliation in care transitions?
-
What evidence is there about the safety-related effects of interoperable systems?
The nature of the medication reconciliation problem
The search identified 1194 records for screening; of these, 22 studies were eligible for inclusion (Figure 13 and Table 8).
FIGURE 13.
A PRISMA flow diagram: medicine reconciliation – nature of the problem.
| Study | Country | Method | Topic | Data type | Rigour | Relevance | Processes | Outcomes/errors |
|---|---|---|---|---|---|---|---|---|
| Godfrey et al.111 | Scoping review | Medication management | Quantitative (E & O) and qualitative | 2 | 1 | Time costs, responsibility for reconciliation, communication problems | Polypharmacy, potentially inappropriate prescribing | |
| Tommelein et al.112 | Europe | Systematic prevalence survey | Potentially inappropriate prescribing | Quantitative (O) | 2 | 3 | Polypharmacy, patient characteristics, including advanced age | |
| Hernandez113 | USA | Interviews (community nurses) | Co-ordination of services | Qualitative | 1 | 1 | Interprofessional co-ordination, communication problems | Polypharmacy, medication errors, adverse events |
| Kennelty et al.114 | USA | Interviews (pharmacists) | Reconciliation post hospital discharge | Qualitative | 1 | 1 | Resources, communication, interprofessional relationships |
We noted in Chapter 4 that there was suggestive evidence that interoperable networks were associated with improvements in process measures relevant to our main programme theory. 77,78 One systematic review, one other review and three observational studies were included. Godfrey and colleagues111 conducted a systematic review of studies exploring the safety of medicine management among older adults living at home. The authors111 included 36 studies, 24 from the USA and 12 from other countries, the majority of which (28 studies) were observational. The most commonly cited problem was the large number of medications prescribed (polypharmacy): if medicines were prescribed by more than one provider, this was as predictor of inappropriate prescribing and, hence, of adverse events.
The authors111 argued that responsibility for medication management has shifted over the years. The earlier studies showed that doctors took responsibility, and nurses and pharmacists were not closely involved. More recent studies described the active involvement of pharmacists and nurses. The review did not mention HITs as an issue in medicine management.
Fernandes and Shojania115 reviewed evidence about the ‘what, why, when, who and how’ of medication reconciliation. The article is described as a combination of a literature review and the authors’ personal experiences. It does not describe the literature review method in any detail; it would be excluded from a conventional systematic review but is included here on the basis that it provides a useful summary of empirical evidence. The review found that few studies have examined medication reconciliation in ambulatory (i.e. community) care. Most studies have been conducted in hospitals, and for elective rather than emergency admissions. This said, the authors115 make two relevant points about transitions in care, notably hospital discharge to home. First, reconciliation practice is typically different from the normative ideal. In the ideal case, reconciliation is an interprofessional process that leads to active medication management. This is not always reflected in actual working practices, as reconciliation may be viewed as an administrative task (rather than a safety-promoting one) and community-based clinicians have to contact hospital staff post discharge. The authors argued that there was no clear consensus in the literature on who should be responsible for reconciliation. Second, they cite evidence that reconciliation can be used to reduce clinically important discrepancies during care transitions. That is, the review offers evidence of both a co-ordination problem and the possibility of addressing it.
Hernandez113 conducted interviews with 15 registered nurses in the USA to explore their experiences of medicine management for older patients. All participants practised in rural or urban clinics. Two relevant themes were identified. The first theme concerned communication between professionals to avoid the prescription of unnecessary medication and to avoid the ‘prescription cascade’ (when one drug is prescribed to manage to the side effect of another drug). One interviewee was quoted as saying that ‘I think it takes a very skilled clinician to be able to piece everything together; piece all the specialists’ work together; piece all the transitions of care together’. 113 The second theme focused on the problems of polypharmacy and avoidable drug–drug interactions. In relation to interoperable networks, an interviewee was quoted as saying of patients and carers that, ‘If we had access to medical records . . . we’d be better able to support them’. 113
Kennelty and colleagues114 conducted face-to-face interviews with 10 community pharmacists in USA, focusing on the pharmacists’ understanding of medicine reconciliation and its barriers and facilitators following hospital discharge. Interviewees reported a number of challenges, including a lack of clarity about roles and responsibilities and difficulties in communicating across organisational boundaries. The authors114 also reported that pharmacists were frustrated with not having access to patients’ (hospital) electronic medical records. One pharmacist stated that trying to confirm a prescription following a patient’s hospital discharge was ‘almost impossible’. When they did try, they encountered problems:
. . . we get transferred all around the hospital . . . And any time that [the hospital doctor] is not there, they always tell us, refer your questions to the primary care physician. Nine times out of ten, the primary care physician doesn’t even know that this patient was in the hospital . . .
Kennelty and colleagues114
Commentary
The systematic review by Godfrey and colleagues111 provides the strongest evidence about the nature of co-ordination problems in medicine reconciliation. The review by Fernandes115 has to be treated with more caution, but it is consistent with the results of the systematic review. These reviews,111,115 together with the individual studies,112–114 paint a picture that is broadly similar to that for the co-ordination of services in Chapter 5. Communication problems are a clear theme, which we interpret as offering a possible role for interoperable networks, hinted at in some of the articles. These problems are, however, embedded in others, notably uncertainty about roles and responsibilities for medicine reconciliation between doctors, nurses and pharmacists.
Cognitive processes in medicine reconciliation
The searches identified 436 records for screening, of which a total of eight114,116–123 were eligible for inclusion (Figure 14).
FIGURE 14.
A PRISMA flow diagram: medicine reconciliation – users’ experiences.
As explained in Chapter 4, we came across a book chapter by Cook124 that suggested that there might be an additional source of evidence about the nature of medicine reconciliation problems. The chapter summarised psychological research into the cognitive processes involved in reconciling lists of medications. We took the view, taking our cue from the World Health Organization,125 that cognitive processes involving professionals’ ability to reason and judge can have effects on patients’ clinical risks.
Cluster search findings
We found three studies, reported in four articles116–119 (Table 9). They all involved essentially theoretical, laboratory-type experiments, designed to reveal some aspect of the cognitive processes involved in medicine reconciliation (either matching medications to a clinical condition or matching medication lists). As a result, all are in the outer ring of the relevance ‘target’ described in Chapter 2. In Table 9, a relevance score of 1 indicates that the article is in the centre of the target, a 2 that it is in the middle ring, and a 3 in the outer ring. Rigour scores were assigned on the basis of judgements by the team, with 1 being most and 3 being least rigorous use of methods. A broad objective was to understand how best to present data on computer and tablet screens in putative future applications.
| Study | Country | Methods | Main findings | Rigour | Relevance |
|---|---|---|---|---|---|
| Horsky et al.116 | USA | Clinical scenario | Better-designed tools associated with more accurate reconciliation | 2 | 3 |
| Bitan et al.117 | USA | Clinical scenario | Insights into cognitive processes in reconciliation | 3 | 3 |
| van Stiphout et al.118 | USA and Netherlands | Interviews | Insights into cognitive processes in reconciliation | 1 | 3 |
| Vashitz et al.119 | USA | Clinical scenario | Insights into cognitive processes in reconciliation | 3 | 3 |
| Vashitz et al.120 | USA | Clinical scenario | Insights into cognitive processes in reconciliation | 3 | 3 |
| Foged et al.121 | Denmark | Observation of working practices, focus groups | E-messaging system did not meet nurses’ needs | 1 | 1 |
| Fanizza et al.122 | USA | Descriptive statistics | HIE data insufficient for pharmacists to perform reconciliation | 2 | 2 |
| Hohmeier et al.123 | USA | Mixed quantitative and qualitative methods | Pharmacists able to perform reconciliation | 2 | 2 |
| Kennelty et al.114 | USA | Interviews | Pharmacists found reconciliation difficult and time-consuming | 2 | 2 |
Vashitz and colleagues120 undertook a simulation experiment, based on a real case from a US anaesthesiology department of a 66-year-old woman presenting for resection of a base-of-tongue lesion. The authors120 used an affinity diagram method. Twenty-four clinicians were given paper cards, each with a disease (grey background) or medication (white background) printed on it. The task was to sort the cards into a pattern that made sense to them clinically; the performance of the task was video-recorded. Post-task interviews were also undertaken and recorded. The final patterns of cards were measured and their spatial relationships were analysed statistically. The results indicated that anaesthetists with different levels of training demonstrated a common tendency: they organised the disease cards by relevant organ system and then matched the medication cards to them. The interview data confirmed that participants used medical conditions as ‘anchors’, and then arranged cards by organ system and then medication. In a second paper,119 Vashitz and colleagues undertook a reanalysis of the same data. The authors119 argued that they found further evidence that organ-based information was central to the cognitive sorting task.
Bitan and colleagues117 also undertook a card sorting experiment. The design was similar to that used by Vashitz and colleagues120 using the same clinical scenario, although it involved 130 hospital clinicians and the experiment was undertaken on a tablet screen, with cards represented on the screen. Bitan and colleagues117 found that clinicians used one of three strategies to sort the ‘cards’. In the most popular, ‘most conditions first’, clinicians first sorted conditions and then matched medications by condition. In the second, ‘crossover’, they sorted a few cards from either the condition or the medication list, matched them and then moved on to the remaining ‘cards’. A third group used an ‘alternating’ strategy, in which clinicians chose a condition, matched a medication to it and then moved on to another condition. The authors argue that there was no ‘one size fits all’ cognitive strategy and that this should be taken into account in the design of future software solutions. 117
Horsky and colleagues116 also developed a clinical scenario but in this case involving reconciliation of two lists containing 16 medications each. Discrepancies were designed into the scenario, so that participants would have to make clinical judgements, rather than simply verify that a medication was appropriate. Eleven clinicians performed reconciliation on each of two different hospital EHRs, in alternating order. They were all familiar with one EHR, having used it for at least 4 months. Medication lists were presented on a single screen, with one above the other, so that users had to scroll up and down between the two lists. None of the participants had used the second EHR, in which medication lists were presented side by side. A research administrator was present throughout and fulfilled the role of the patient, answering questions about the scenario condition, including whether or not they had taken a medication, and also provided information about the listed medications. Participants were also interviewed after completing the tasks.
The error rates observed were higher for the first, familiar EHR (1.29 vs. 0.37 errors per participant). There were between zero and three errors per task per clinician for both EHRs. The difference in mean number of errors between systems was not significant (p < 0.057). The most common error made was a dosing error. The authors argue that the presentation of medication lists influenced the observed error rates. 116
Structured database search findings
Once we had identified the book chapter and journal article in the cluster search, we were able to design a structured database search, which included experiences of using interoperable networks. After full-text screening, one study was included. The ecological validity of the studies in this and the last section was judged as low or medium, using a simple set of categories devised by us (low, medium and high) (see Table 9). All of the studies were in the outer ring of the relevance ‘target’.
Van Stiphout and colleagues118 sought to identify the procedural, cognitive and macrocognitive skills needed for medication management using interoperable networks. 118 They used a formal task analysis method. This involved developing a general description of the medication management process based on a combination of relevant literature and exploratory interviews. In-depth interviews were then conducted with 20 domain experts in the Netherlands and the USA. The study made three observations that are relevant to this synthesis:
-
Medication reconciliation is a task that involves both cognitive and procedural skills.
-
There was no agreement among health-care professionals about what constitutes an adverse event.
-
Current IT systems did not support specific prescription actions, such as taking a medication at different doses per day or medication tapering schemes.
The authors concluded that:
Educating physicians in the cognitive skills of IT mediated medication management could be one of the missing links of patient safety.
Van Stiphout and colleagues118
Commentary
The articles in this section report laboratory-style experimental rather than observational studies, and so offer limited direct evidence about the nature of reconciliation. However, it is enough to allow us to sketch the nature of the cognitive processes involved. The evidence suggests that cognitive errors can be made in reconciliation, but we note that the error rates are relatively low: reconciliation was completed successfully more often than not. Insofar as this sheds light on our main programme theory, it contributes to our understanding of the nature of medicine reconciliation problems.
Clinicians’ experiences of interoperable networks and patient outcomes
The searches identified 289 records for screening, of which seven114,121–123,126–128 were eligible for inclusion (Figure 15). In the course of the screening and selection we identified articles on the accuracy and completeness of data, which are also presented (Table 10).
FIGURE 15.
A PRISMA flow diagram: medicine reconciliation – outcomes.
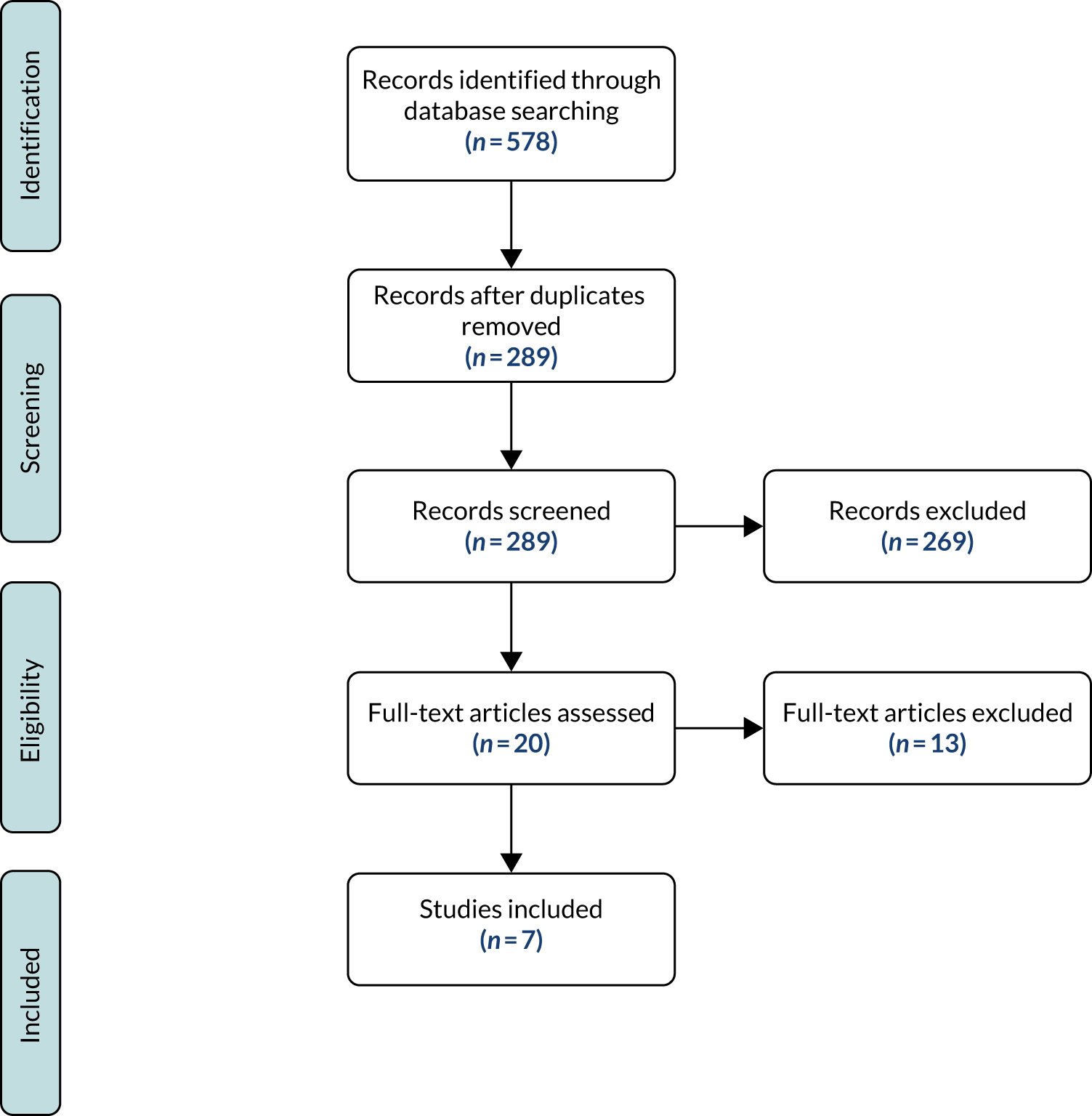
| Study | Country | Methods | Main findings | Rigour | Relevance |
|---|---|---|---|---|---|
| Foged et al.121 | Denmark | Participant observation and focus groups | System did not support medicine reconciliation; problems with professional responsibility for reconciliation | 1 | 2 |
| Fanizza et al.122 | USA | Quasi-experiment: access to medication lists | Problems accessing medication lists | 2 | 2 |
| Hohmeier et al.123 | USA | Pharmacist reconciliation of 25 patients’ medication lists | Problems with use of network; all lists had at least one ‘discordant’ medication; time constraints in pharmacies | 3 | 2 |
| Kennelty et al.114 | USA | Interviews | Reconciliation time-consuming; time pressures for pharmacists | 2 | 3 |
| Moniz et al.126 | USA | Before-and-after study of electronic transmission on dispensing errors | Incomplete system implementation; dispensing error rates halved following electronic transmission of prescription data | 2 | 2 |
| Pfoh et al.127 | USA | Retrospective review of medication data in three databases | Reconciliation improved accuracy and completeness | 1 | 2 |
| Pourrat et al.128 | France | Observational: comparison of medication lists, interviews | High incidence of medication list discrepancies | 3 | 3 |
Experiences of interoperable networks
The article by Foged and colleagues121 is in the inner ring of the relevance ‘target’, and the others are in the middle ring. Foged and colleagues121 reported on a study of Danish nurses’ working practices, and their perceptions of their working practices, in relation to an e-messaging system. The e-messaging system linked a university hospital and community-based services in 10 municipalities, six of which participated in the study. The system had been developed locally and had five modules: (1) admission report, (2) care plan, (3) discharge report, (4) discharge notification and (5) a ‘message platform’ that enabled users to exchange messages. Each of the organisations had an electronic patient record, but none of them was integrated with any other. Two methods were used: participant observation and focus groups.
Three main themes related to the e-messaging system were identified. 121 First, the e-messaging system did not support safe medication reconciliation. The authors found that the exchange of electronic data about medication in relation to both admission and discharge was limited. For example, automatic admission reports were sent from municipalities when a patient was admitted to hospital, which included a medication list alongside other service information. Reports were rarely read by hospital nurses, and some nurses were not aware of the availability of medication lists. Interface issues were also reported (e.g. it was not clear when medication information in the reports had been uploaded).
Home care nurses reported that information needed for safe medication post discharge was often missing. Patients’ printouts of medications were often the only source of information available, and these did not include any reasons for changes in medication, information that was important to the nurses.
Second, nurses bypassed the e-message system to assure medication-related safety. Home care nurses reported that accurate information about patients’ medications were a priority. The nurses did not trust the hospital medication lists and compared dispensed medications against the lists. If there was a discrepancy in the numbers of tablets or doses, they checked each affected tablet issued. It was also usual for them to telephone hospital nurses or sometimes to send an e-message list to a GP for an assessment. The nurses explained that this reflected a belief that hospital colleagues’ workloads were onerous and mistakes were therefore inevitable. Home care nurses also reported that they did not use the message platform as they were worried that messages would not be read. They also expressed frustration with the alternative namely telephoning hospital nurses. This could be time-consuming, and some home care nurses said that hospital nurses were not always helpful.
Third, nurses often assumed responsibility for medication reconciliation. Responsibility for medications was not always clear. Home care nurses reported that formal responsibility post discharge lay with GPs, but discharge medication information could be delayed and GPs could be reluctant to take responsibility for medication prescribed by a hospital doctor. GPs usually asked nurses to contact the relevant hospital doctor for information. Hospital doctors could, in turn, be reluctant to take responsibility for medication after discharge. Hospital nurses, who could also be contacted, reported that they could often do little more than check a patient’s hospital records. There was, then, typically extensive communication between nurses and hospital staff to ensure that patients received the correct post-discharge medication. Nurses reported that the result was that, in practice, they often found themselves taking responsibility for patients’ medications.
Fanizza and colleagues122 undertook a study of the use of interoperable networks by three pharmacies in a supermarket chain in Kansas, USA. They accessed (all) patients’ hospital discharge information from a hospital EHR, including discharge medication lists (a broader population than older people). The three pharmacies offered a free ‘transitions of care’ service to all members of a local community who were identified as having been discharged from hospital within the previous 14 days. Forty patients were screened in a 4-month study period in 2016/17, and all 40 were included in the study. Eighteen patients were assigned to the intervention group and 22 patients were assigned to a control group. Pharmacists could access EHRs via the network for 85% (n = 34) of patients. However, they could only access medication lists for only 12.5% (n = 5) of patients.
Hohmeier and colleagues123 reported a pilot study of the use of an interoperable network in a community pharmacy in east Tennessee, USA. A study of medication reconciliation was one component of the larger study. Pharmacists accessed the hospital discharge records of 25 patients and, when the records were available, reconciled their discharge medications with pharmacy medication lists. The average number of prescription medications per patient was 14. All 25 patients had at least one ‘discordant’ medication. The wider study found problems with the use of the network, including delays in the availability of hospital discharge summaries and time constraints in pharmacies, the latter meaning that reconciliation did not always occur in practice.
Kennelty and colleagues114 undertook an interview programme focusing on medicine reconciliation following hospital discharge with 10 community pharmacists in the Midwest of the USA. Interviews focused on two broad topics: (1) their experiences of medication reconciliation for patients recently discharged, and (2) their preferences for the content and presentation of information about medications. None of the pharmacies had access to hospital or clinical patient records.
Interviewees stressed the importance of medicine reconciliation post discharge to ensure that patients received the right medication and to avoid any potential errors. The interviewees noted that local care co-ordination teams alerted them, usually by telephone, when a patient was about to be discharged, and that this was helpful. Discharge medication lists would often be faxed to them. All interviewees reported that the process was time-consuming; they felt that having access to patient records would facilitate reconciliation and save time. The interviewees also believed that staffing was an issue; there were not enough staff and this increased time pressures on them. All interviewees said that electronic information transfer and/or access to electronic records would be helpful.
Accuracy and completeness of data
We found three papers126–128 that shed light on the accuracy and completeness of data in interoperable systems. These are included on the basis that they enhance understanding, albeit indirectly, on the main programme theory. All of the studies in this section were judged to be in the outer ring of the relevance ‘target’.
Pfoh and colleagues127 reported a retrospective study of the accuracy and completeness of medication data held in three databases in a health system in north-eastern USA. The three databases were the organisation’s EHR, a commercial medication database and a community-wide HIE web portal. The EHR was a commercial system that spanned two hospitals and seven ambulatory care clinics in the health system. The commercial database was used to validate medication history records in the EHR. The community portal provided access to patient information held by physician practices, home health agencies, nursing homes and other organisations.
Records were reviewed for 858 patients who were aged ≥ 18 years and who were admitted to one of the two hospitals (the mean age of patients was 65 years). A research pharmacist reviewed the three data sources. Data in each source were validated against a ‘gold standard’, a validated list of patients’ medications taken at home (i.e. post discharge). The completeness data are shown in Table 11. The authors assessed the incremental value of combining the different data sources. Pooling all three sources increased the proportion of patients with complete data to 85% (n = 726). The combination of hospital and community system produced 80% of essential medications (n = 682).
| Database | Number of patients with complete data (out of 858) | Percentage of patients with complete data (n/858) |
|---|---|---|
| EHR | 611 | 71 |
| Commercial medication database | 400 | 47 |
| Community HIE web portal | 312 | 36 |
Accuracy data are shown in Table 12. Twenty-three per cent of medications were found in all three sources and 9% were found in none of them. When all three sources were pooled, accuracy was 91% (n = 6997). The hospital EHR plus the community portal yielded an accuracy of 87%.
| Database | Number of medications with complete data (out of 7731) | Percentage of medications with complete data (n/7731) |
|---|---|---|
| EHR | 6152 | 80 |
| Commercial medication database | 3464 | 45 |
| Community HIE web portal | 2838 | 37 |
Pourrat and colleagues128 undertook a prospective study of 278 orthopaedic inpatients (average age 72 years) in a French hospital. They evaluated non-intentional discrepancies between home and hospital medication records for the inpatients, their potential clinical impact, and the effects of communication between community and hospital pharmacists on prevention of adverse medication-related events. Hospital pharmacists compared lists of medications at admission with lists of home medications for the previous 3 months provided by community pharmacists. Researchers also conducted interviews with patients’ GPs and reviewed their medication lists. These were used, together, to identify patients’ appropriate medications. When discrepancies were identified, researchers telephoned both GPs and community pharmacists, and on some occasions also checked with patients. Remaining non-intentional discrepancies were evaluated by a hospital pharmacist and physician, and rated on Bayliff’s scale (a 0–3 scale, ranging from no impact to life-threatening). The researchers also identified which non-intentional discrepancies were identified and by what type of clinician. Finally, they retrospectively compared their reconciled medication lists with medications prescribed and administered during hospital stays.
A total of 1532 prescription lines were analysed and 471 discrepancies at admission identified. The authors reported that 34.2% of patients had at least one non-intentional discrepancy at admission and 18.3% had a potentially harmful discrepancy. Clinical staff identified 69% of the discrepancies, thus reducing the numbers of potential adverse events in practice.
Moniz and colleagues126 reported on a before-and-after study designed to measure the effect of transmitting electronic prescription data to pharmacies on dispensing errors. 126 It was conducted in a health system in Massachusetts, USA, where all clinics used a CPOE. The intervention, in one clinic, was a new ‘electronic prescription transmission functionality’. 126 Two clinics were used as controls. Data were collected for 2 months before the new system and 2 months afterwards. In the intervention clinic, prescriptions recorded in the CPOE were reconciled with dispensed prescription data from participating pharmacy chains, linked via a national pharmacy information exchange network.
The systems were not ‘seamlessly’ interoperable: the majority of pharmacies printed electronically transmitted prescriptions and then re-entered it into the pharmacy system. A large proportion of prescriptions were not, in practice, transmitted electronically. Dispensing errors were defined as discrepancies between the CPOE data and dispensed prescriptions. A total of 41,022 prescriptions were studied: 29,575 from the intervention clinic and 11,447 from the control clinics. The authors found the following:
-
control clinics – no significant difference in dispensing error rates between baseline and intervention
-
intervention clinic – no significant difference in dispensing error rates between baseline and intervention for prescriptions that were not transmitted electronically
-
intervention clinic – dispensing error rates were significantly lower, reduced by about half, in the intervention than during the baseline period.
The most common errors involved prescription strength, dose and frequency of administration.
Interoperable networks and patients’ risks
We did not find any quantitative evidence about changes in patients’ risks relating to interoperable networks and medicine reconciliation.
Commentary
We found evidence, including high-quality articles,121–128 about the effects of interoperable networks, with a range of different characteristics, on medicine reconciliation. Taking the articles as a group, it seems reasonable to say that evidence about the effects of interoperable networks on reconciliation is mixed.
We were surprised not to find any empirical evidence about the effects of interoperable networks on patients’ risks, given the importance of medication errors as a source of adverse events and the possible contribution of reconciliation errors to event rates.
Discussion
We found evidence confirming that there are problems with medicine reconciliation that suggests that they are similar to those reported for care co-ordination in Chapter 5. That is, communication is reported to be a problem, but one entangled with wider cultural and organisational issues, notably uncertainty about the roles and responsibilities of doctors, nurses and pharmacists. The cognitive evidence contributes to this view.
We also found evidence about users’ experiences of interoperable networks with different functionality, which was mixed but suggested that users can experience problems with accessing networks and finding the information they need. Finally, as just highlighted, we were surprised at the lack of evidence of effects on patients’ risks. Given the importance of medication errors in health systems around the world, and the amounts of money invested in interoperable networks in recent years, we expected to find evidence, but we did not.
Chapter 7 The co-ordination of services for at-risk children findings
Introduction
This chapter reports on the searches conducted on the co-ordination of services for at-risk children. The next three sections, mirroring the structure of earlier chapters, present evidence about the nature of co-ordination problems, experiences of using interoperable networks and patient safety outcomes.
The nature of co-ordination problems
The searches identified 476 records for screening, of which three129–131 were eligible for inclusion (Figure 16).
FIGURE 16.
A PRISMA flow diagram: at-risk children – nature of the problem.
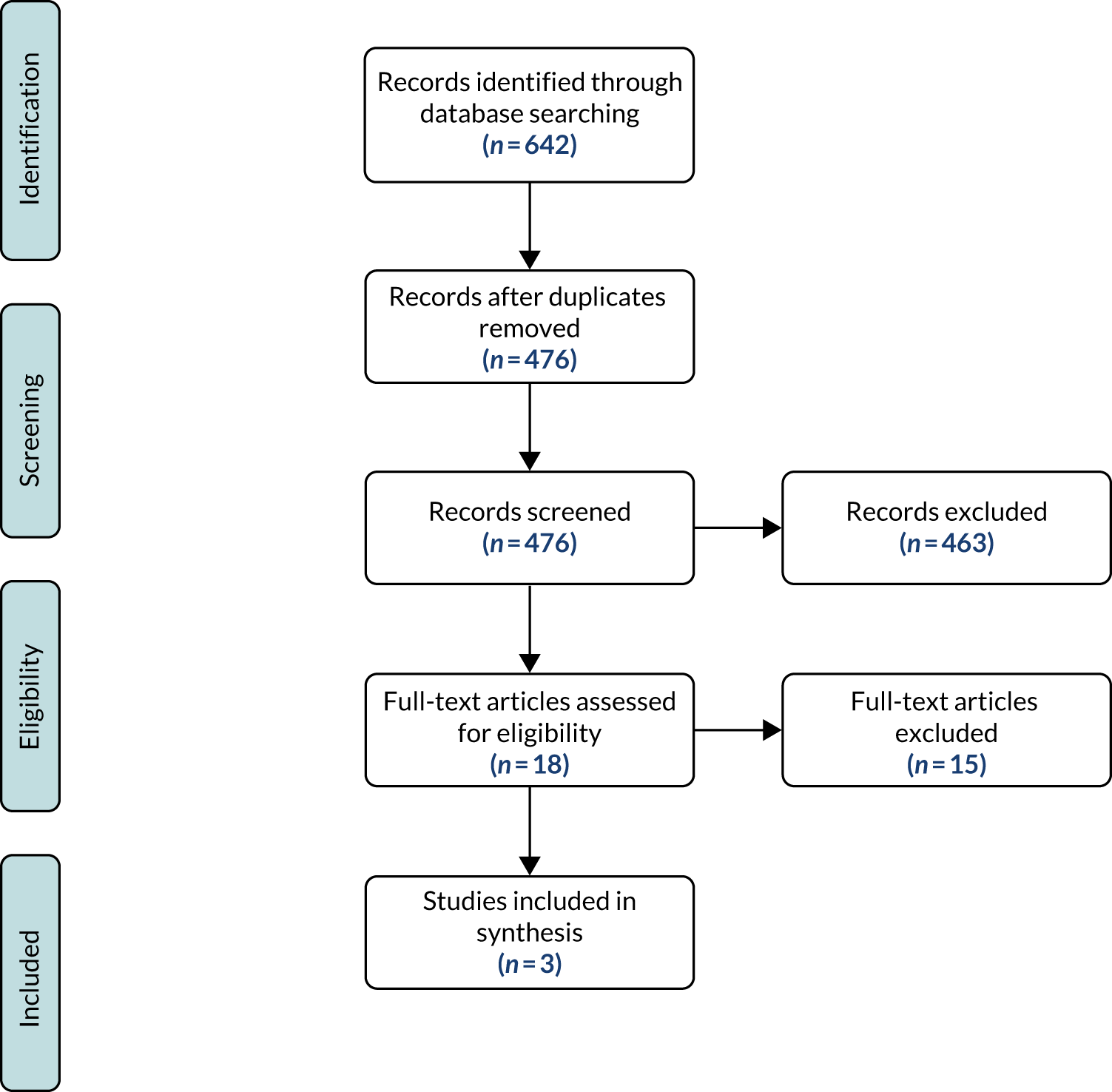
We identified good evidence about the nature of co-ordination problems. Table 13 lists three literature reviews129–131 and three primary observational studies132–134 that were not cited in the reviews. The three reviews129–131 used different methods and focused on different topics. Between them, they provide evidence about the nature of co-ordination problems in services for at-risk children and of those between child protection and domestic violence services.
| Study | Article type | Focus | Rigour | Relevance |
|---|---|---|---|---|
| Macvean et al.129 | Scoping review | Interface between child protection and specialist domestic violence services | 2 | 1 |
| Herbert and Bromfield130 | Review | Effectiveness of multidisciplinary teams | 1 | 1 |
| Bunting et al.131 | Narrative review | Professional barriers to reporting child maltreatment concerns | 2 | 1 |
| Lees132 | Observational study | Case study of three teams in one local authority in England: interviews and document analysis | 2 | 1 |
| Hwang et al.133 | Observational study | Interviews and focus groups | 2 | 1 |
| Thompson134 | Observational study | Observation of referrals, semistructured interviews | 1 | 1 |
Macvean and colleagues129 undertook a scoping literature review and identified 24 collaborative models, each one intended to promote the effective co-ordination of services. They identified five themes, which they termed ‘enablers’: shared vision (across providers of services), formalisation of a service model (involving formal contracts between agencies), and a culture where collaboration, leadership and information sharing was encouraged.
Herbert and Bromfield130 reviewed evidence of the effectiveness of multidisciplinary teams, focusing on the extent to which these teams improved child protection (i.e. reduced children’s risks of abuse). The authors130 stress that, even in included papers, there was often a lack of detail about the composition and working practices of a multidisciplinary team, and a corresponding lack of detail about the co-ordination challenges that had (or had not) been successfully addressed. This said, the authors concluded that (1) much of the research focused on criminal justice outcomes, with studies finding differences in both process measures and (higher) conviction rates, and (2) studies of mental health services found that the presence of a team led to increased service use. Putting this another way, the review provided evidence both that there were co-ordination problems involving criminal justice and mental health agencies, and that it was possible to design interventions to address these.
Bunting and colleagues131 reviewed evidence about information sharing and reporting systems. Their principal concern was with mandatory reporting of concerns about child abuse and the reasons why reporting did not occur. They found evidence of under-reporting. There were a number of reasons why it occurred, including the characteristics of a case, professionals perceiving that they had insufficient grounds to report it and the confidence that professionals themselves had to report more generally. The authors131 also found evidence about wider institutional considerations, including that reporting was less likely in some types of school (including Catholic and primary schools) than in others, and that training in reporting procedures needed to be improved.
As was the case for the co-ordination of care for older people, as discussed in Chapter 5, there is no obvious role for interoperable networks in relation to the social and organisational issues raised in these reviews. There might, however, in principle, be a role to support information sharing. On the one hand, Macvean and colleagues129 argue for greater standardisation of behaviour across professions. On the other hand, however, several authors reported in the reviews argue that their evidence points in a different direction, for example towards closer interpersonal relationships between professionals.
Primary studies
Each of the three individual studies focused on information sharing and related activities, including recording (see Table 11). Lees132 undertook observations of teams, 32 semistructured interviews and document analysis in three children and family social work teams in one local authority in England. Lees132 identified the dual nature of what she termed ‘information work’. Lees emphasised the distinction, in practice, between the recording and communication of information across teams and the emotional nature of child protection work. Information-related work was guided by rigid organisational protocols. This was recognised by interviewees as important: the acts of recording and communicating were essential to ensuring children’s safety. On the other hand, it led to a tension. Family circumstances were often messy and had to be ‘tidied up’ for recording and communication to other team members. As Lees put it, the circumstances had to be presented as rational and evidence based. One of the responses to the tension was to maintain interpersonal communication in the course of cases, so that team members could be clear about, and help to interpret, recorded information.
Hwang and colleagues133 undertook 13 interviews and nine focus groups with mental health professionals, social workers, other child welfare professionals and foster parents. They reported:
-
Problems with missing or incomplete information in referrals, assessments and case notes (the use of paperwork, faxes and e-mail was mentioned) and, thus, also concerns about the accuracy of information.
-
Problems being couched in contexts in which there was a lack of clarity about professionals’ roles, which led to confusion about policies on information sharing across agency boundaries. There were reports of decisions either not to share information with other agencies, or only to share partial information about a case.
Thompson134 undertook an observational study of referrals to local authorities. In common with Lees,132 Thompson found that there was a distinction between the situations on the ground and the formal recorded accounts that were required in children’s services. Thompson characterised the distinction in terms of different ways of thinking about a jigsaw. Lord Laming, in the Climbie Inquiry, had argued that professionals needed a ‘full picture’ of a child’s circumstances, implying that the picture was static, like a conventional jigsaw. However, Thompson134 argues that, in practice, professionals have pictures that are constantly in flux and open to ongoing interpretation. For example, the interpretation of the significance of a small scar on a child’s face might change over time, leading at one time to a belief that it resulted from an accident and at another that it was evidence of abuse. Thompson134 used her evidence to critique what she believed was the prevailing rational, bureaucratic approach to recording and information sharing.
Users’ experiences of using interoperable networks
The searches identified 832 records for screening, of which four were eligible for inclusion (Figure 17).
FIGURE 17.
A PRISMA flow diagram: at-risk children – users’ experiences and outcomes.
Four papers135–138 described experiences of using networks (Table 14). In terms of relevance, all four articles135–138 were in the outer ring: the interventions were those that we were interested in, but they were focused on both broader populations and limited settings, the latter typically covering just two organisations. The papers were heterogeneous in terms of methods, populations, interventions studied and settings. Our identification of common themes is therefore necessarily tentative, but the articles indicate a state of affairs similar to those reported in Chapters 5 and 6.
| Study | Study design/methods | Population | Intervention | Setting |
|---|---|---|---|---|
| Drinkwater et al.135 | Interviews | GPs and practice nurses regarding domestic violence and abuse/child safeguarding | Documenting practices in electronic patient records | Six localities in England |
| Baker et al.136 | Case study: document analysis, interviews | Broad population, including children and families | ‘IT infrastructure’ | Nine primary care organisations: Canada and New Zealand |
| Dellor et al.137 | Case study: interviews, observation, user feedback | Case worker referrals to social services for children and families | Needs portal | Families and children’s services/social services: Los Angeles, CA, USA |
| Vest et al.138 | Analysis of HIE user logs, linked to characteristics of paediatric emergency department encounters | Patients aged < 18 years attending paediatric emergency departments | HIE for ICC | Paediatric emergency departments in an ICC: central Texas, USA |
Drinkwater and colleagues135 relied principally on interviews (on subjective judgements rather than direct observation of systems in use). The authors135 reported problems accessing and using HIT infrastructures, which were reported to be ‘underdeveloped’ and ‘limited’. The authors also undertook field observations. The findings were broadly consistent with the interview data. Variation in users’ confidence in using the intervention (an electronic records system) were emphasised, as were variations in the ways in which caseworkers used the portal. Baker and colleagues136 drew attention to concerns about the role of HITs, particularly electronic patient records, in the wider context of co-ordinating services. Dellor and colleagues137 noted tensions between different objectives for records, and by implication for interoperable networks, including supporting continuity of care, facilitating information sharing, serving as a legal document and being an entity ‘owned’ by patients.
Vest and colleagues138 reported a different type of evidence, concerning the frequency of accessing an interoperable network. They found that the network was accessed in 8.7% of encounters (15,568/179,445) during a 42-month period (2006–9). The network was accessed more often for patients with more comorbidities, and less often if a patient had not been to that location in the previous 12 months or if department staff faced time constraints. This paper138 did not shed direct light on users’ experiences, but it is included on the basis that it complements the findings in the other three articles.
Patient safety outcomes
We did not find any evidence about the effectiveness of interoperable networks on the safety of at-risk children.
Commentary
Given the importance attached to co-ordinating the care of at-risk children, and the current funding of interoperable systems in England and elsewhere, we expected to find evidence in this domain. We also hoped to find evidence of the use of semantically interoperable networks, given the long history of initiatives in the domain. In the event, however, we found good evidence about the nature of co-ordination problems, which are rooted in institutional challenges and particularly evident at professional and organisational boundaries. We also found evidence that users experience problems with using interoperable networks. As in earlier chapters, we did not find any studies of professionals using embedded interoperable networks (i.e. embedded information infrastructures implied by our mid-range theory).
The absence of evidence about safety-related outcome changes is, we think, striking. The result for this study is that we cannot use the example of children’s services to assess our main programme theory.
Chapter 8 Economies of scope and scale searches and results
Introduction
This chapter focuses on the economies of scope and scale associated with interoperable networks, and presents methods and results. The topics arises from the second programme theory discussed at the end of Chapter 4. The key idea behind the programme theory is that interoperable networks can generate a ‘network externality’. An externality is a cost or benefit incurred by a third party. Air pollution is often used as an example: you and I do not control most air pollution, but we may suffer from high levels of contaminants and may benefit from policies that reduce those levels.
In the case of interoperable networks, economists have predicted that the benefits of being a member of a network will increase with the number of users. You and I do not control the numbers of people who use Facebook (Facebook, Inc., Menlo Park, CA, USA; www.facebook.com), but may benefit more as the number of users grows (e.g. because it is easier to communicate with our friends if they all use Facebook as well). The benefits might be of two kinds. Economies of scope might be achieved because a network makes it cheaper, on average, to produce a wider range of services (in part because they all share a common infrastructure). Economies of scale might be achieved because the cost of providing a service is shared between larger numbers of users, so the cost of each user reduces with increasing scale.
At the start of the study we were not aware of any evidence about interoperable networks in health and social care. As we have noted in earlier chapters, however, the numbers of digital data in the sector are growing rapidly and many governments are encouraging interoperability, so, in principle, at least economies of scope and scale might be generated. 139,140 It has also been suggested that interoperable networks might lead to the redesign of professionals’ working practices, which in turn could produce better patient outcomes. 141 There might, then, be system-wide improvements in patient safety that are attributable to a network as a whole rather than to the actions of single teams of professionals, discussed in the last six chapters. Equally, health and social care may face high transaction costs, partly due to information asymmetries (e.g. when one clinician cannot interpret another’s records). Such issues require careful consideration given the complexity of relationships that span organisational and professional boundaries, as highlighted in Chapters 5 and 6. 142
Results and commentary
The search found 117 records for screening; however, no studies met the inclusion criteria (Figure 18). As a result, we are not in a position to comment on the second programme theory. Many of the articles we screened and the full-text articles we reviewed did not focus on patient safety, focusing instead on broader quality or process measures that were outside the scope of this review. Other studies simply did not present any data or were in the wrong setting (e.g. hospital).
FIGURE 18.
A PRISMA flow diagram: economies of scope and scale.

By way of illustration of what we hoped to find, the most promising study was the retrospective study by Plantier and colleagues. 143 The researchers evaluated the impact of EHR use on the quality of care management in acute care hospitals in France. This was done using four quality indicators: (1) quality of patient record, (2) delay in sending information at hospital discharge, (3) pain status evaluation and (4) nutritional status evaluation. These indicators were derived by the French National Authority for Health from three national databases. The results revealed that EHR use had a significant positive impact on the four quality indicators. The results also found that this impact varied according to the EHR functionality (e.g. the quality of patient records was affected more by the computerisation of drug prescriptions than by the computerisation of patient records). Unfortunately, the focus on hospitals and on a single patient records system meant that this study was out of the scope of our review. Nevertheless, the article indicates the kind of study that might be undertaken in the future.
Chapter 9 Discussion and conclusions
Introduction
We have presented our empirical findings in the last five chapters. In this chapter, we draw the findings together and discuss their implications. The next section briefly summarises the findings from each domain, and then reviews the aims and objectives set out in Chapter 1. We assess the extent to which they have been met. The following sections reflect on our study design and methods and comment on their strengths and limitations. We then discuss our findings under three cross-cutting headings: Programme theory: issues and concerns, Programme theory: implications and Mid-range theory.
Summary of findings
In the theory development phase of the synthesis, we did not find any detailed accounts of the ways in which interoperable networks are intended to work and improve patient safety. There were many statements to the effect that they will improve patient safety, improve quality more generally and reduce health-care costs, but the majority did not attempt to explain in any detail how or why they would achieve these effects. We were, however, able to identify a substantial number of theory fragments, and used these to develop initial rough programme theories and to derive a mid-range theory.
The co-ordination of services for older people
We found substantial evidence about the nature and extent of care co-ordination problems. Most of the problems were essentially social or cultural. For example, there were several evidenced-based reports of difficulties due to different health-care professionals having incompatible working assumptions about the kinds of support that older people need. There was no obvious role for interoperable networks in most of these problems. There was one exception, which concerned difficulties associated with communication problems. The problems were attributed to a combination of interprofessional issues not directly related to technology, as well characteristics of the networks (such as multiple log-ons) and the difficulty of locating patient information held on other organisations’ servers. We did not find any countervailing studies reporting the ‘seamless’ use of interoperable networks.
There was limited, and weak, evidence about the effectiveness of interoperable networks in reducing older people’s risks. The evidence was for limited networks typically involving a single application (such as a shared assessment process) and was based on the subjective views of users. We did not find any quantitative evidence of effectiveness.
The co-ordination of medication reconciliation
We found evidence of co-ordination problems with medication reconciliation. The evidence suggested that responsibility for reconciliation was not clear on the ground and fell between professionals (principally pharmacists, doctors and nurses).
The second set of searches focused on the nature of problems encountered in reconciliation when using interoperable networks. We found one observational study114 and seven further ‘offline’ simulation studies116–123 about the nature of clinicians’ cognitive processes and the error rates associated with them. These studies suggested that errors could occur in both types of reconciliation. There was less field-based evidence about users’ experiences in this domain than in services for older people or child protection services.
The third set of searches produced seven articles121–128 with reasonable-quality, rather than high-quality, mixed results. Some articles indicated that the use of an interoperable network was associated with a (quantitative) reduction in reconciliation errors. Others reported problems with using systems that resulted in interoperable networks having no effects on reconciliation error rates.
The co-ordination of services for at-risk children
We found evidence of co-ordination problems in child protection services. There is a debate in the academic literature about the nature of those problems. In the context of this synthesis, the key difference is that some commentators interpret the problems in mechanistic terms (i.e. as communication failures), whereas others argue that the problems reflect deeper interprofessional and interorganisational problems.
In common with the first two searches, there was evidence that users find interoperable networks difficult to use in the course of the care of at-risk children. There was, however, no evidence about outcomes, defined as changes in children’s risks of harm.
Economies of scope and scale
We did not find any empirical evidence about the ‘global’ effects of interoperable networks on patient safety (or any other outcome). None of the excluded articles reported any evidence of economies of scope or scale: they were excluded because they were not relevant, rather on grounds of rigour.
Aims and objectives
The aim of the study was to establish how and why interoperable networks improved patient safety, failed to do so or increased safety risks. Our main conclusion is that there is insufficient evidence about the effectiveness of interoperable systems to allow us to establish how and why they affect patient safety. We searched for evidence across three distinct domains, (1) the care of older people, (2) medication reconciliation and (3) child protection, which increases our confidence that the paucity of evidence is real and not an artefact of our search strategies. The absence of evidence about economies of scope and scale further tends to increase our confidence in our conclusion.
This synthesis has, however, identified evidence that sheds useful light on two other substantive issues. First, there is good evidence of problems with the co-ordination of services in each of the three domains studied. In common with other authors, we take the view that these problems have deep institutional roots. 144,145 Second, there is evidence across the domains that professionals have found interoperable networks difficult to use. We have not found countervailing accounts: there were no accounts of the kind of high-quality interactions with laptops and other devices that we are used to in our private lives.
The objectives of the study were defined in terms of the stages of a realist synthesis: to identify programme theories, prioritise one or more theories and then evaluate them using relevant empirical evidence. We achieved these objectives in that we were able to complete the synthesis and to produce findings that we are able to describe and explain. This said, we are aware of the limitations as well as the strengths of our study design and methods.
Patient and public involvement
The PPI panel met three times during the study and contributed to its design and conduct on each occasion. At the first meeting, we presented the early findings of our theory development searches and the nominal group meetings. The PPI panel provided valuable comments, in particular in helping us to set priorities for the populations and settings for the evidence searches. It was their comments, taken in tandem with the views of the nominal groups, that led us to focus on services for frail older people living at home (later broadened, pragmatically, to older people in general). The PPI panel also noted the importance of medication reconciliation and expressed the view that the next most important population to study would be at-risk children. As this report shows, we acted on all three of these comments.
At the second meeting, we presented the interim findings of the first two sets of searches, namely on the co-ordination of services for older people and on medication reconciliation. The group gave their comments on, and interpretations of, those findings. The third meeting was used to comment on a draft of this chapter. Members also commented on a draft of the Plain English summary.
Strengths and limitations
We set out our study design and methods in Chapters 2 and 3. Having completed the synthesis, we have arrived at the view that the strengths and limitations of our synthesis are, to a large extent, mirror images.
There were three key strengths and limitations. First, we developed a study design that was suited to addressing our aims and objectives. It emphasised breadth, seeking evidence across different populations and settings rather than depth of evidence about specific aspects of programme theories for a single population and setting. The approach allowed us to compare and contrast evidence for those different populations, and the commonalities gave us confidence in our results. The approach may only work, however, for broadly based questions: the study design is pragmatic and will not suit all realist syntheses. Moreover, some of the searches, namely the three designed to characterise the nature and extent of co-ordination problems, were not exhaustive. The searches relied principally on published systematic reviews. This suited our purposes, as we needed only to establish that there were problems, but we cannot claim that we identified all of the available evidence from these three searches.
Second, we used a mid-range theory. The theory provided the single, independent statement against which relevance could be judged. It also provided a means for making our own theoretical assumptions explicit and, hence, open to wider scrutiny. A disadvantage of the mid-range theory, we found, is that it risked locking us into those same assumptions. It would have taken a great deal of time and intellectual effort to move to another theoretical framework. We are confident that the mid-range theory can be used to interpret our data, but another framework might, in principle, do equally well, and we have not tested alternative theories for their ‘fit’ with the data.
Third, we are aware that we deliberately biased our choice of domains in favour of services for which we were most likely to find evidence of effects. The advantage, if the strategy had been successful, is that a synthesis would have produced valuable insights into how and why interoperable networks influence patient safety. To set against this, the bias built into our choices means that we have to be particularly cautious about generalising from any of our findings to other HITs and settings. Furthermore, it is worth noting that we have focused on professionals’ use of interoperable networks. We are aware, through some of the literature we came across9,30 and our stakeholder consultation, that many localities are developing networks that patients and clients can also access and use. Our results cannot be used to generalise to patients’ and clients’ experiences.
Programme theory: issues and concerns
A realist synthesis should, ideally, identify a range of outcomes associated with an intervention, and use programme and mid-range theories to explain the outcome differences. A fully fledged programme theory should ideally have two characteristics. First, it should be underpinned by coherent reasoning: it should have a clear ‘internal logic’. Second, it should represent a solidly evidence-based sequence of decisions and actions, showing how an intervention leads to process changes and outcomes. As we noted in Chapter 2, teams undertaking realist syntheses might reasonably expect to find coherent, and possibly partially evidenced, programme theories in articles or reports.
We were struck by the absence of fully developed programme theories and, indeed, by a more general failure to consider how and why interoperable networks might improve patient safety (or any other outcome). As we found in Chapter 4, there has been a tendency to assume that desired outcomes would be achieved, without examining the assumption. Two of the most thoughtful accounts are relatively old: in To Err is Human: Building a Safer Health System in 20001 and in Bates and Gawande’s 2003 article. 71 It is not clear what has happened in the intervening period, as there has been no shortage of journal articles and official reports. 1,71 We are not aware of analyses that explain this state of affairs.
The result, for us, was that we found ourselves piecing together our programme theories from ‘fragments’. The iterations of our programme theories are set out in Chapter 4 and reflect our efforts to create a coherent account based on the fragments. The end result was a simple, initial, main programme theory. It should be stressed that we thought that the initial theory was highly provisional (and recognise that another team might interpret the fragments differently). The advantage, in principle, of the evidence testing in our case was that it might lead to a substantially different final programme theory. As the last four chapters have shown, however, this is not what happened.
These issues were compounded by the fact that we found very little evidence about patient outcomes in this synthesis. As we have noted, this means that it is not possible to evaluate our main programme theory. Without outcome evidence, we cannot know whether or not any given sequence of decisions and actions leads to a reduction in patients’ risks.
The paucity of evidence sits in sharp contrast with the emphasis around the world on integrating IT systems across organisational and professional boundaries. We were surprised, for example, that the multibillion-dollar Obama-era initiative in the USA did not lead to more high-quality studies of the effectiveness of interoperable networks. 146,147
We do not have a good explanation for the lack of evidence. It is not just that there were few high-quality studies – there were hardly any studies. One possible reason is methodology. Applied health researchers have preferences for studies based in single settings (such as hospital wards and departments) and are less interested in studying networks, or believe that such studies cannot produce valid findings. Another possibility is that funders have been reluctant to fund studies, perhaps believing that the value of networks is self-evident. Whatever the reason, we believe that there is a major evidence gap, given that interoperable networks are being actively promoted in current policies in England and many other countries.
Programme theory: implications
These issues notwithstanding, we can make two useful observations on the basis of our findings. The first concerns the evidence that there are co-ordination problems in all three domains studied. Perhaps the most significant aspect of this finding is that most of the problems are institutional in nature, and can be traced to interprofessional and interorganisational differences in objectives and values. If there are genuine differences of opinion between two professionals, say a nurse and a social worker, about the best course of action for a particular patient or client, it is difficult to see how any interoperable network can play a major role in resolving these differences.
We noted in Chapters 5–7 that one finding, concerning communication problems, suggested a possible role for interoperable networks. If we take a mechanistic view here, then we might say that an interoperable network can provide access to all of the records held about a patient across several organisations. This is the assumption of policy-makers and opinion leaders, captured in our initial programme theories. Wachter70 and other opinion leaders argue that current IT solutions are simply not very good. When the technologies improve, they believe that improvements in care and outcomes will follow. 148
Our findings suggest a rather different framing: the problems are institutional in nature and embedded in professionals’ working practices. Taking this view, changing the functional characteristics of HIT solutions will not, of itself, change professionals’ working practices. If the institutional problems are not addressed – and it seems that they have not been, at least in the places where the studies have been undertaken – then interoperable networks cannot by themselves improve patient safety. There may be an important conceptual gap here between proponents’ beliefs about the way in which HIT solutions, including interoperable networks, work, and evidence about the ways in which these solutions actually work.
We have also found evidence across all three domains that users find interoperable networks difficult to use. As far as we are able to tell, all of the reported studies were conducted on functionally interoperable networks: networks that allowed users to access patients’ records remotely, but did not link those records together in any way. Users had to interrogate each part of a patient’s record separately. If proponents of interoperable networks are right, then the development of more integrated solutions will eventually lead to more positive user experiences. We did not find any evidence that could shed light on this assumption and either support or refute it. As things stand, the argument that greater network integration will lead to improved co-ordination and, hence to safer care is not proven.
Mid-range theory
We argued in Chapter 2 that a mid-range theory can perform two roles. One role is to provide an explicit basis for judgements about the relevance of articles and the synthesis of evidence in the course of evidence searches. The other role is to provide a basis for generalising our findings. We noted above that care needs to be taken when generalising from our chosen domains to others. We are also aware of Campbell and colleagues’ classic work149 on external validity, which places strict limits on the extent to which any findings can be generalised. These points made, however, we feel that it is possible to make two observations.
The first observation follows from the end of the last section. Our mid-range theory emphasised the institutional nature of the challenge of designing and deploying interoperable networks, or, more generally, information infrastructures, in health and social care. We can say that the evidence is consistent with the mid-range theory. This is not at all the same as saying that it proves that the theory is right, but similar findings across three domains encourage us to have confidence in the mid-range theory. We can also suggest that proponents of HITs, whose views were highlighted in Chapter 4, should review the bases of their claims. Mechanistic assumptions about the effects of HITs once the problems have been ‘ironed out’ are not supported by the evidence in this synthesis.
Second, and finally, we are struck by the fact that patient safety has rarely been in our line of sight in the last few chapters. One of the implications of our mid-range theory is that, in practice, the various actors (doctors, nurses, informatics teams and others) develop ways of working with one another, and of using interoperable networks to co-ordinate with one another, over long periods of time. The absence of critical reflection about the ways in which interoperable networks affect patient safety, over a period of almost 20 years, suggests that key actors do not believe that the case needs to be made. It is not clear to us why this is the case. The evidence suggests that the embedding of interoperable networks in clinicians’ working practices is clearly important, and, to date, partial but effective use of networks has risked becoming the end rather than the means. That is, in focusing on implementation we may lose sight of the outcomes, including safer patient care, that have provided the basis of claims for investing in networks in the first place. Viewed from a different part of the terrain, that occupied by clinicians and others dedicated to improving patient safety, those interested in interoperable networks currently have little to offer.
Implications for practice
In the light of our findings, practitioners may wish to take account of the:
-
lack of evidence about reductions in patients’ risks associated with interoperable networks (and could take steps to monitor the effects of local programmes themselves)
-
negative evidence about users’ experiences of interoperable networks (and could take steps to engage with patients and other stakeholders in the design and deployment of new services)
-
extent to which institutional arrangements and, in particular, the challenges of working across professional and organisational boundaries influence the deployment and use of interoperable networks.
Implications for research
We have identified the following topics for future research:
-
Primary empirical studies of effectiveness will help to shed light on the value of current and future investments in interoperable networks.
-
Primary empirical studies of economies of scope and scale associated may, similarly, shed light on the value of investments in interoperable networks.
-
The findings indicate that there may be a broader research agenda into the development of information infrastructures in health and social care.
-
Given the current focus of IT investments in systems and networks outside hospitals, there may also be a case for evidence syntheses that shed light on the process changes associated with other community-based applications, such as patient portals.
-
A wide range of study designs and methods are used in realist syntheses. It is not obvious, in a burgeoning literature, which of them produce the most robust findings. There may be value in revisiting the RAMESES guidance on the design and conduct of realist syntheses to identify and highlight the best of current research practices.
Conclusions
We conclude that there is good evidence of problems with the co-ordination of services in each of the three domains studied. There is also evidence across the domains that professionals have found interoperable networks difficult to use. We found no evidence about economies of scope and scale. There is insufficient evidence about the effectiveness of interoperable networks to allow us to establish how and why they affect patient safety.
Acknowledgements
We are indebted to the participants in the nominal groups and to our interviewees for giving us their time and their insights. We are grateful to the members of our PPI panel for their steers on the study design and interpretation of findings: Mike Bush, Richard Cleverley, Peter Dransfield, Jean Gallagher, Jan Speechley, Andy Taylor and Matthew Wright. We are also grateful to the members of our Steering Group, who gave us strong nudges in the right direction at crucial moments: Alastair Cartwright, Sonia Dalkin, Michaela Graham, Tim Kelly and Roy Ruddle.
Contributions of authors
Justin Keen (https://orcid.org/0000-0003-2753-8276) (Professor of Health Politics) developed the proposal for the study; undertook screening and data extraction; identified the topic for the economies of scope and scale search, undertook screening and drafted Chapter 8; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Maysam Abdulwahid (https://orcid.org/0000-0002-4316-8589) (Research Officer) undertook screening and data extraction; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Natalie King (https://orcid.org/0000-0002-4215-2323) (Information Specialist) designed and undertook structured database searches; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Judy Wright (https://orcid.org/0000-0002-5239-0173) (Senior Information Specialist) developed the proposal for the study; designed and undertook structured database searches; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Rebecca Randell (https://orcid.org/0000-0002-5856-4912) (Professor in Digital Innovations in Healthcare) developed the proposal for the study; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Peter Gardner (https://orcid.org/0000-0002-8799-0443) (Professor of Healthcare Quality and Safety) developed the proposal for the study; provided specialist input for the design and interpretation of specific searches; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Justin Waring (https://orcid.org/0000-0003-1459-5896) (Professor of Medical Sociology and Healthcare Organisation) developed the proposal for the study; provided specialist input for the design and interpretation of specific searches; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Roberta Longo (https://orcid.org/0000-0002-9379-1627) (Lecturer in Health Economics) developed the proposal for the study; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; identified the topic for the economies of scope and scale search, and undertook screening and drafted Chapter 8; and drafted, or commented on drafts of, this report.
Silviya Nikolova (https://orcid.org/0000-0002-6922-5115) (Lecturer in Health Economics) contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; identified the topic for the economies of scope and scale search, and undertook screening and drafted Chapter 8; and drafted, or commented on drafts of, this report.
Claire Sloan (https://orcid.org/0000-0002-5324-8275) (Research Assistant) contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; identified the topic for the economies of scope and scale search, and undertook screening and drafted Chapter 8; and drafted, or commented on drafts of, this report.
Joanne Greenhalgh (https://orcid.org/0000-0003-2189-8879) (Associate Professor) developed the proposal for the study; undertook screening and data extraction; contributed to the detailed study design set out in Chapter 2, and to the interpretation of overall findings; and drafted, or commented on drafts of, this report.
Publications
Keen J, Greenhalgh J, Randell R, Gardner P, Waring J, Longo R, et al. Networked information technologies and patient safety: a protocol for a realist synthesis. Syst Rev 2019;8:307.
Keen J, Abdulwahid MA, King N, Wright JM, Randell R, Gardner P, et al. Effects of interorganisational information technology networks on patient safety: a realist synthesis. BMJ Open 2020;10:e036608.
Data-sharing statement
This is a qualitative study and therefore the data generated are not suitable for sharing beyond those contained within the report. Further information can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care.
References
- Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington, DC: The National Academies Press; 2000.
- Shojania KG, Thomas EJ. Trends in adverse events over time: why are we not improving?. BMJ Qual Saf 2013;22:273-7. https://doi.org/10.1136/bmjqs-2013-001935.
- Department of Health and Social Care (DHSC) . The Power of Information: Putting All of Us in Control of the Health and Care Information We Need 2012.
- Department of Health and Social Care (DHSC) . Personalised Health and Care 2020: Patient, Carers and Service User Vision 2014.
- Kennedy I. The Report of the Public Inquiry into Children’s Heart Surgery at the Bristol Royal Infirmary 1984–1995: Learning from Bristol 2001.
- Black AD, Car J, Pagliari C, Anandan C, Cresswell K, Bokun T, et al. The impact of eHealth on the quality and safety of health care: a systematic overview. PLOS Med 2011;8. https://doi.org/10.1371/journal.pmed.1000387.
- Brenner SK, Kaushal R, Grinspan Z, Joyce C, Kim I, Allard RJ, et al. Effects of health information technology on patient outcomes: a systematic review. J Am Med Inform Assoc 2016;23:1016-36. https://doi.org/10.1093/jamia/ocv138.
- Rudin RS, Motala A, Goldzweig CL, Shekelle PG. Usage and effect of health information exchange: a systematic review. Ann Intern Med 2014;161:803-11. https://doi.org/10.7326/M14-0877.
- Stocker R, Bamford C, Brittain K, Duncan R, Moffatt S, Robinson L, et al. Care home services at the vanguard: a qualitative study exploring stakeholder views on the development and evaluation of novel, integrated approaches to enhancing healthcare in care homes. BMJ Open 2018;8. https://doi.org/10.1136/bmjopen-2017-017419.
- Fitzpatrick G, Ellingsen G. A review of 25 years of CSCW research in healthcare: contributions, challenges and future agendas. J Collab Comput 2013;22:609-65. https://doi.org/10.1007/s10606-012-9168-0.
- Andreassen HK, Kjekshus LE, Tjora A. Survival of the project: a case study of ICT innovation in health care. Soc Sci Med 2015;132:62-9. https://doi.org/10.1016/j.socscimed.2015.03.016.
- Greenhalgh T, Wherton J, Papoutsi C, Lynch J, Hughes G, A’Court C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res 2017;19. https://doi.org/10.2196/jmir.8775.
- Williams R. Why is it difficult to achieve e-health systems at scale?. Inf Commun Soc 2016;19:540-50. https://doi.org/10.1080/1369118x.2015.1118521.
- Institute of Medicine . Health IT and Patient Safety: Building Safer Systems for Better Care 2011.
- Pope C, Mays N, Popay J. Synthesizing Qualitative and Quantitative Health Evidence: A Guide to Methods. Maidenhead: Open University Press; 2007.
- Booth A, Briscoe S, Wright JM. The ‘realist search’: a systematic scoping review of current practice and reporting. Res Synth Methods 2020;11:14-35. https://doi.org/10.1002/jrsm.1386.
- Pawson R. Evidence-Based Policy. London: SAGE Publications Ltd; 2006.
- Bunn F, Goodman C, Russell B, Wilson P, Manthorpe J, Rait G, et al. Supporting shared decision making for older people with multiple health and social care needs: a realist synthesis. BMC Geriatr 2018;18. https://doi.org/10.1186/s12877-018-0853-9.
- Greenhalgh T, Wong G, Westhorp G, Pawson R. Protocol – realist and meta-narrative evidence synthesis: evolving standards (RAMESES). BMC Med Res Methodol 2011;11. https://doi.org/10.1186/1471-2288-11-115.
- Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: meta-narrative reviews. BMC Med 2013;11. https://doi.org/10.1186/1741-7015-11-20.
- Pawson R. The Science of Evaluation: A Realist Manifesto. London: SAGE Publications Ltd; 2013.
- Salter KL, Kothari A. Using realist evaluation to open the black box of knowledge translation: a state-of-the-art review. Implement Sci 2014;9. https://doi.org/10.1186/s13012-014-0115-y.
- Shearn K, Allmark P, Piercy H, Hirst J. Building realist program theory for large complex and messy interventions. Int J Qual Methods 2017;16. https://doi.org/10.1177/1609406917741796.
- Brennan N, Bryce M, Pearson M, Wong G, Cooper C, Archer J. Towards an understanding of how appraisal of doctors produces its effects: a realist review. Med Educ 2017;51:1002-13. https://doi.org/10.1111/medu.13348.
- Jagosh J, Pluye P, Wong G, Cargo M, Salsberg J, Bush PL, et al. Critical reflections on realist review: insights from customizing the methodology to the needs of participatory research assessment. Res Synth Methods 2014;5:131-41. https://doi.org/10.1002/jrsm.1099.
- Best A, Greenhalgh T, Lewis S, Saul JE, Carroll S, Bitz J. Large-system transformation in health care: a realist review. Milbank Q 2012;90:421-56. https://doi.org/10.1111/j.1468-0009.2012.00670.x.
- Westhorp G, Stevens K, Rogers PJ. Using realist action research for service redesign. Evaluation 2016;22:361-79. https://doi.org/10.1177/1356389016656514.
- Pawson R, Wong G, Owen L. Known knowns, known unknowns, unknown unknowns: the predicament of evidence-based policy. Am J Eval 2011;32:518-46. https://doi.org/10.1177/1098214011403831.
- Pawson R, Tilley N. Realistic Evaluation. London: SAGE Publications Ltd; 1997.
- National Advisory Group on Health Information Technology in England . Making IT Work: Harnessing the Power of Health Information Technology to Improve Care in England: Report of the National Advisory Group on Health Information Technology in England 2016.
- DeJean D, Giacomini M, Simeonov D, Smith A. Finding qualitative research evidence for health technology assessment. Qual Health Res 2016;26:1307-17. https://doi.org/10.1177/1049732316644429.
- The King’s Fund . Reading List: Integrated Care and Partnership Working 2014. www.kingsfund.org.uk/sites/default/files/field/field_pdf/Library-reading-list-integrated-care-and-partnership-working-Dec2014.pdf.
- Vimarlund V, Olve NG, Scandurra I, Koch S. Organizational effects of information and communication technology (ICT) in elderly homecare: a case study. Health Informatics J 2008;14:195-210. https://doi.org/10.1177/1081180X08092830.
- Waterson P, Eason K, Tutt D, Dent M. Using HIT to deliver integrated care for the frail elderly in the UK: current barriers and future challenges. Work 2012;41:4490-3. https://doi.org/10.3233/WOR-2012-0750-4490.
- King G, O’Donnell C, Boddy D, Smith F, Heaney D, Mair FS. Boundaries and e-health implementation in health and social care. BMC Med Inform Decis Mak 2012;12. https://doi.org/10.1186/1472-6947-12-100.
- Greenhalgh J, Dalkin S, Gibbons E, Wright J, Valderas JM, Meads D, et al. How do aggregated patient-reported outcome measures data stimulate health care improvement? A realist synthesis. J Health Serv Res Policy 2018;23:57-65. https://doi.org/10.1177/1355819617740925.
- Booth A, Harris J, Croot E, Springett J, Campbell F, Wilkins E. Towards a methodology for cluster searching to provide conceptual and contextual ‘richness’ for systematic reviews of complex interventions: case study (CLUSTER). BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-118.
- Greenhalgh J, Dalkin S, Gooding K, Gibbons E, Wright J, Meads D, et al. Functionality and feedback: a realist synthesis of the collation, interpretation and utilisation of patient-reported outcome measures data to improve patient care. Health Serv Deliv Res 2017;5. https://doi.org/10.3310/hsdr05020.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000097.
- Graber ML, Johnston D, Bailey R. Report of the Evidence on Health IT Safety and Interventions 2016.
- Bichard M. The Bichard Inquiry Report 2004.
- Keen J, Margetts H, Perri 6, Hood C. Paradoxes of Modernisation: Unintended Consequences of Public Policy Reform. Oxford: Oxford University Press; 2010.
- Francis R. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry: Executive Summary 2013.
- Department of Health and Social Care (DHSC) . Hard Truths: The Journey to Putting Patients First. Volume One of the Government Response to the Mid Staffordshire NHS Foundation Trust Public Enquiry 2014.
- Berwick D. A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England. London: Department of Health and Social Care; 2013.
- NHS Digital . Clinical Safety Standards. Clinical Risk Management: Its Application in the Manufacture of Health IT Systems 2013.
- NHS Digital . Clinical Risk Management: Its Application in the Deployment and Use of Health IT Systems 2013.
- Department of Health and Social Care (DHSC) . The Future of Healthcare: Our Vision for Digital, Data and Technology in Health and Care 2018.
- Alvarez R. The electronic health record: a leap forward in patient safety. Healthc Pap 2004;5:33-6. https://doi.org/10.12927/hcpap.2004.16862.
- Bowden T, Coiera E. The role and benefits of accessing primary care patient records during unscheduled care: a systematic review. BMC Med Inform Decis Mak 2017;17. https://doi.org/10.1186/s12911-017-0523-4.
- Cotter CM. Making the case for a clinical information system: the chief information officer view. J Crit Care 2007;22:56-65. https://doi.org/10.1016/j.jcrc.2007.01.005.
- Fontaine P, Zink T, Boyle RG, Kralewski J. Health information exchange: participation by Minnesota primary care practices. Arch Intern Med 2010;170:622-9. https://doi.org/10.1001/archinternmed.2010.54.
- Foley M. To opt in or opt out of electronic patient records? Electronic patient record is incompatible with confidentiality. BMJ 2006;333:146-7. https://doi.org/10.1136/bmj.333.7559.146-b.
- Goroll AH, Simon SR, Tripathi M, Ascenzo C, Bates DW. Community-wide implementation of health information technology: the Massachusetts eHealth Collaborative experience. J Am Med Inform Assoc 2009;16:132-9. https://doi.org/10.1197/jamia.M2899.
- Gottlieb LK, Stone EM, Stone D, Dunbrack LA, Calladine J. Regulatory and policy barriers to effective clinical data exchange: lessons learned from MedsInfo-ED. Health Aff 2005;24:1197-204. https://doi.org/10.1377/hlthaff.24.5.1197.
- Hawking M. The single shared electronic patient record (SSEPR): problems with functionality and governance. Inform Prim Care 2008;16:157-8. https://doi.org/10.14236/jhi.v16i2.687.
- Hillblom D, Schueth A, Robertson SM, Topor L, Low G. The impact of information technology on managed care pharmacy: today and tomorrow. J Manag Care Spec Pharm 2014;20:1073-9. https://doi.org/10.18553/jmcp.2014.20.11.1073.
- Hopf YM, Bond C, Francis J, Haughney J, Helms PJ. Views of healthcare professionals to linkage of routinely collected healthcare data: a systematic literature review. J Am Med Inform Assoc 2014;21:e6-10. https://doi.org/10.1136/amiajnl-2012-001575.
- Ishikawa K, Ohmichi H, Umesato Y, Terasaki H, Tsukuma H, Iwata N, et al. The guideline of the personal health data structure to secure safety healthcare. The balance between use and protection to satisfy the patients’ needs. Int J Med Inform 2007;76:412-18. https://doi.org/10.1016/j.ijmedinf.2006.09.005.
- Traynor K. Solid data lacking on HIT and patient safety. Am J Health Syst Pharm 2012;69:91-2. https://doi.org/10.2146/news120006.
- Zimlichman E, Bates DW. National patient safety initiatives: moving beyond what is necessary. Isr J Health Policy Res 2012;1. https://doi.org/10.1186/2045-4015-1-20.
- eHealth Stakeholder Group . Perspectives and Recommendations on Interoperability 2014.
- Huckvale C, Car J, Akiyama M, Jaafar S, Khoja T, Bin Khalid A, et al. Information technology for patient safety. Qual Saf Health Care 2010;19:i25-33. https://doi.org/10.1136/qshc.2009.038497.
- Font D, Escarrabill J, Gómez M, Ruiz R, Enfedaque B, Altimiras X. Integrated Health Care Barcelona Esquerra (Ais-Be): a global view of organisational development, re-engineering of processes and improvement of the information systems. The role of the tertiary university hospital in the transformation. Int J Integr Care 2016;16. https://doi.org/10.5334/ijic.2476.
- Foisey C. 4 Ways Technology Is Improving Patient Safety 2017. www.healthitoutcomes.com/doc/ways-technology-improving-patient-safety-0001 (accessed 3 March 2020).
- Hutchinson KD. Economics, errors, and emergencies: the case for e-prescribing and ‘pharmacy interoperability’. MedGenMed 2007;9.
- Jacob JA. On the road to interoperability, public and private organizations work to connect health care data. JAMA 2015;314:1213-15. https://doi.org/10.1001/jama.2015.5930.
- Blobel B, Davis M, Ruotsalainen P. Policy management standards enabling trustworthy pHealth. Stud Health Technol Inform 2014;200:8-21.
- Alkhaldi B, Sahama T, Huxley C, Gajanayake R. Barriers to implementing eHealth: a multi-dimensional perspective. Stud Health Technol Inform 2014;205:875-9.
- Wachter R. The Digital Doctor: Hope, Hype and Harm at the Dawn of Medicine’s Computer Age. New York, NY: McGraw Hill Education; 2015.
- Bates DW, Gawande AA. Improving safety with information technology. N Engl J Med 2003;348:2526-34. https://doi.org/10.1056/NEJMsa020847.
- Kaelber DC, Bates DW. Health information exchange and patient safety. J Biomed Inform 2007;40:40-5. https://doi.org/10.1016/j.jbi.2007.08.011.
- Panjamapirom A, Burkhardt JH, Volk LA, Rothschild JM, Bates DW, Glandon GL, et al. Physician opinions of the importance, accessibility, and quality of health information and their use of the information. AMIA Annu Symp Proc 2010;2010:46-50.
- Kushniruk AW, Bates DW, Bainbridge M, Househ MS, Borycki EM. National efforts to improve health information system safety in Canada, the United States of America and England. Int J Med Inform 2013;82:e149-60. https://doi.org/10.1016/j.ijmedinf.2012.12.006.
- Bates DW. Health information technology and care coordination: the next big opportunity for informatics?. Yearb Med Inform 2015;10:11-4. https://doi.org/10.15265/IY-2015-0020.
- Rudin R, Volk L, Simon S, Bates D. What affects clinicians’ usage of health information exchange?. Appl Clin Inform 2011;2:250-62. https://doi.org/10.4338/ACI-2011-03-RA-0021.
- Marien S, Krug B, Spinewine A. Electronic tools to support medication reconciliation: a systematic review. J Am Med Inform Assoc 2017;24:227-40. https://doi.org/10.1093/jamia/ocw068.
- Bassi J, Lau F, Bardal S. Use of information technology in medication reconciliation: a scoping review. Ann Pharmacother 2010;44:885-97. https://doi.org/10.1345/aph.1M699.
- Hersh WR, Totten AM, Eden KB, Devine B, Gorman P, Kassakian SZ, et al. Outcomes from health information exchange: systematic review and future research needs. JMIR Med Inform 2015;3. https://doi.org/10.2196/medinform.5215.
- Ash JS, Berg M, Coiera E. Some unintended consequences of information technology in health care: the nature of patient care information system-related errors. J Am Med Inform Assoc 2004;11:104-12. https://doi.org/10.1197/jamia.M1471.
- Zheng K, Abraham J, Novak LL, Reynolds TL, Gettinger A. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform 2016;1:13-29. https://doi.org/10.15265/IY-2016-036.
- Jones SS, Rudin RS, Perry T, Shekelle PG. Health information technology: an updated systematic review with a focus on meaningful use. Ann Intern Med 2014;160:48-54. https://doi.org/10.7326/M13-1531.
- Kalra D, Musen M, Smith B, Ceusters W, De Moor G. ARGOS policy brief on semantic interoperability. Stud Health Technol Inform 2011;170:1-15.
- Adjerid I, Acquisti A, Telang R, Padman R, Adler-Milstein J. The impact of privacy regulation and technology incentives: the case of health information exchanges. Manage Sci 2016;62:1042-63. https://doi.org/10.1287/mnsc.2015.2194.
- Vincent C, Amalberti R. Safer Healthcare: Strategies for the Real World. New York City, NY: Springer Publishing; 2016.
- May CR, Mair F, Finch T, MacFarlane A, Dowrick C, Treweek S, et al. Development of a theory of implementation and integration: normalization process theory. Implement Sci 2009;4. https://doi.org/10.1186/1748-5908-4-29.
- Pollock M, Williams R. Software and Organisations: The Biography of the Enterprise-Wide System or How SAP Conquered the World. London: Routledge; 2008.
- Devine EB, Totten AM, Gorman P, Eden KB, Kassakian S, Woods S, et al. Health information exchange use (1990–2015): a systematic review. EGEMS 2017;5. https://doi.org/10.5334/egems.249.
- Auschra C. Barriers to the integration of care in inter-organisational settings: a literature review. Int J Integr Care 2018;18. https://doi.org/10.5334/ijic.3068.
- Threapleton DE, Chung RY, Wong SYS, Wong E, Chau P, Woo J, et al. Integrated care for older populations and its implementation facilitators and barriers: a rapid scoping review. Int J Qual Health Care 2017;29:327-34. https://doi.org/10.1093/intqhc/mzx041.
- Allen J, Hutchinson AM, Brown R, Livingston PM. User experience and care integration in transitional care for older people from hospital to home: a meta-synthesis. Qual Health Res 2017;27:24-36. https://doi.org/10.1177/1049732316658267.
- Kirst M, Im J, Burns T, Baker GR, Goldhar J, O’Campo P, et al. What works in implementation of integrated care programs for older adults with complex needs? A realist review. Int J Qual Health Care 2017;29:612-24. https://doi.org/10.1093/intqhc/mzx095.
- Hudson R, Comer L, Whichello R. Transitions in a wicked environment. J Nurs Manag 2014;22:201-10. https://doi.org/10.1111/j.1365-2834.2012.1478.x.
- Goodwin N, Dixon A, Anderson G, Wodchis W. Providing Integrated Care for Older People with Complex Needs Lessons from Seven International Case Studies. London: The King’s Fund; 2014.
- Goodwin N, Sonola L, Thiel V, Kodner DL. Co-ordinated Care for People with Complex Chronic Conditions. London: The King’s Fund; 2013.
- Hainstock T, Cloutier D, Penning M. From home to ‘home’: mapping the caregiver journey in the transition from home care into residential care. J Aging Stud 2017;43:32-9. https://doi.org/10.1016/j.jaging.2017.09.003.
- Jeffs L, Kuluski K, Law M, Saragosa M, Espin S, Ferris E, et al. Identifying effective nurse-led care transition interventions for older adults with complex needs using a structured expert panel. Worldviews Evid Based Nurs 2017;14:136-44. https://doi.org/10.1111/wvn.12196.
- Larsen A, Broberger E, Petersson P. Complex caring needs without simple solutions: the experience of interprofessional collaboration among staff caring for older persons with multimorbidity at home care settings. Scand J Caring Sci 2017;31:342-50. https://doi.org/10.1111/scs.12352.
- Jeffs L, Saragosa M, Law M, Kuluski K, Espin S, Merkley J, et al. Elucidating the information exchange during interfacility care transitions: insights from a qualitative study. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-015400.
- Eden KB, Totten AM, Kassakian SZ, Gorman PN, McDonagh MS, Devine B, et al. Barriers and facilitators to exchanging health information: a systematic review. Int J Med Inform 2016;88:44-51. https://doi.org/10.1016/j.ijmedinf.2016.01.004.
- Azarm-Daigle M, Kuziemsky C, Peyton L. A review of cross organizational healthcare data sharing. Procedia Comput Sci 2015;63:425-32. https://doi.org/10.1016/j.procs.2015.08.363.
- Hoerbst A, Schweitzer ML. A systematic investigation on barriers and critical success factors for clinical information systems (CIS) in integrated care settings. Yearb Med Inform 2015;10:79-8. https://doi.org/10.15265/IY-2015-018.
- Wu HX, LaRue E. Barriers and Facilitators of Health Information Exchange (HIE) Adoption in the United States n.d.
- Nicolaisen K, Berg K. Electronic Communication Across Organizational Borders in Healthcare: an Empirical Study. Tromsø: UiT; 2015.
- McMurray J, Hicks E, Johnson H, Elliott J, Byrne K, Stolee P. ‘Trying to find information is like hating yourself every day’: the collision of electronic information systems in transition with patients in transition. Health Informatics J 2013;19:218-32. https://doi.org/10.1177/1460458212467547.
- Health Quality Ontario . Electronic tools for health information exchange: an evidence-based analysis. Ont Health Technol Assess Ser 2013;13:1-76.
- Sadoughi F, Nasiri S, Ahmadi H. The impact of health information exchange on healthcare quality and cost-effectiveness: a systematic literature review. Comput Methods Programs Biomed 2018;161:209-32. https://doi.org/10.1016/j.cmpb.2018.04.023.
- Reis ZSN, Maia TA, Marcolino MS, Becerra-Posada F, Novillo-Ortiz D, Ribeiro ALP. Is there evidence of cost benefits of electronic medical records, standards, or interoperability in hospital information systems? Overview of systematic reviews. JMIR Med Inform 2017;5. https://doi.org/10.2196/medinform.7400.
- Menachemi N, Rahurkar S, Harle CA, Vest JR. The benefits of health information exchange: an updated systematic review. J Am Med Inform Assoc 2018;25:1259-65. https://doi.org/10.1093/jamia/ocy035.
- Barnsteiner JH, Hughes RG. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
- Godfrey CM, Harrison MB, Lang A, Macdonald M, Leung T, Swab M. Homecare safety and medication management with older adults: a scoping review of the quantitative and qualitative evidence. JBI Database System Rev Implement Rep 2013;11:82-130. https://doi.org/10.11124/jbisrir-2013-959.
- Tommelein E, Mehuys E, Petrovic M, Somers A, Colin P, Boussery K. Potentially inappropriate prescribing in community-dwelling older people across Europe: a systematic literature review. Eur J Clin Pharmacol 2015;71:1415-27. https://doi.org/10.1007/s00228-015-1954-4.
- Hernandez J. Medication management in the older adult: a narrative exploration. J Am Assoc Nurse Pract 2017;29:186-94. https://doi.org/10.1002/2327-6924.12427.
- Kennelty KA, Chewning B, Wise M, Kind A, Roberts T, Kreling D. Barriers and facilitators of medication reconciliation processes for recently discharged patients from community pharmacists’ perspectives. Res Social Adm Pharm 2015;11:517-30. https://doi.org/10.1016/j.sapharm.2014.10.008.
- Fernandes O, Shojania KG. Medication reconciliation in the hospital: what, why, where, when, who and how?. Healthc Q 2012;15:42-9. https://doi.org/10.12927/hcq.2012.22842.
- Horsky J, Aarts J, Verheul L, Seger DL, van der Sijs H, Bates DW. Clinical reasoning in the context of active decision support during medication prescribing. Int J Med Inform 2017;97:1-11. https://doi.org/10.1016/j.ijmedinf.2016.09.004.
- Bitan Y, Parmet Y, Greenfield G, Teng S, Nunnally M. The cognitive task of medication reconciliation – clinicians’ approaches to the arrangement of medical condition and medication history information. Proc Hum Factors Ergon Soc Annu Meet 2016;60:538-40. https://doi.org/10.1177/1541931213601124.
- van Stiphout F, Zwart-van Rijkom JE, Maggio LA, Aarts JE, Bates DW, van Gelder T, et al. Task analysis of information technology-mediated medication management in outpatient care. Br J Clin Pharmacol 2015;80:415-24. https://doi.org/10.1111/bcp.12625.
- Vashitz G, Nunnally ME, Parmet Y, Bitan Y, O’Connor MF, Cook RI. How do clinicians reconcile conditions and medications? The cognitive context of medication reconciliation. Cogn Technol Work 2011;15:109-16. https://doi.org/10.1007/s10111-011-0189-0.
- Vashitz G, Nunnally ME, Bitan Y, Parmet Y, O’Connor MF, Cook RI. Making sense of diseases in medication reconciliation. Cogn Technol Work 2011;13:151-8. https://doi.org/10.1007/s10111-010-0162-3.
- Foged S, Nørholm V, Andersen O, Petersen HV. Nurses’ perspectives on how an e-message system supports cross-sectoral communication in relation to medication administration: a qualitative study. J Clin Nurs 2018;27:795-806. https://doi.org/10.1111/jocn.14109.
- Fanizza FA, Ruisinger JF, Prohaska ES, Melton BL. Integrating a health information exchange into a community pharmacy transitions of care service. J Am Pharm Assoc 2018;58:442-9. https://doi.org/10.1016/j.japh.2018.02.012.
- Hohmeier KC, Spivey CA, Boldin S, Moore TB, Chisholm-Burns M. Implementation of a health information exchange into community pharmacy workflow. J Am Pharm Assoc 2017;57:608-15. https://doi.org/10.1016/j.japh.2017.05.009.
- Cook RI, Smith P. Cognitive Systems Engineering. Boca Raton, FL: CRC Press; 2017.
- World Health Organization (WHO) . Human Factors and Patient Safety 2009.
- Moniz TT, Seger AC, Keohane CA, Seger DL, Bates DW, Rothschild JM. Addition of electronic prescription transmission to computerized prescriber order entry: effect on dispensing errors in community pharmacies. Am J Health Syst Pharm 2011;68:158-63. https://doi.org/10.2146/ajhp080298.
- Pfoh ER, Abramson E, Edwards A, Collins J, Nolin J, Momrow DS, et al. The comparative value of 3 electronic sources of medication data. Am J Pharm Benefits 2014;6:217-24.
- Pourrat X, Corneau H, Floch S, Kuzzay MP, Favard L, Rosset P, et al. Communication between community and hospital pharmacists: impact on medication reconciliation at admission. Int J Clin Pharm 2013;35:656-63. https://doi.org/10.1007/s11096-013-9788-6.
- Macvean ML, Humphreys C, Healey L. Facilitating the collaborative interface between child protection and specialist domestic violence services: a scoping review. Aust Soc Work 2018;71:148-61. https://doi.org/10.1080/0312407x.2017.1415365.
- Herbert JL, Bromfield L. Better Together? A review of evidence for multi-disciplinary teams responding to physical and sexual child abuse. Trauma Violence Abuse 2019;20:214-28. https://doi.org/10.1177/1524838017697268.
- Bunting L, Lazenbatt A, Wallace I. Information sharing and reporting systems in the UK and Ireland: professional barriers to reporting child maltreatment concerns. Child Abuse Rev 2010;19:187-202. https://doi.org/10.1002/car.1076.
- Lees A. Facts with feelings – social workers’ experiences of sharing information across team and agency borders to safeguard children. Child Fam Soc Work 2017;22:892-903. https://doi.org/10.1111/cfs.12309.
- Hwang SHJ, Mollen CJ, Kellom KS, Dougherty SL, Noonan KG. Information sharing between the child welfare and behavioral health systems: Perspectives from four stakeholder groups. Soc Work Ment Health 2017;15:500-23. https://doi.org/10.1080/15332985.2016.1252825.
- Thompson K. Multi-agency information practices in children’s services: the metaphorical ‘jigsaw’ and professionals quest for a ‘full’ picture. Child Fam Soc Work 2013;18:189-97. https://doi.org/10.1111/j.1365-2206.2011.00821.x.
- Drinkwater J, Stanley N, Szilassy E, Larkins C, Hester M, Feder G. Juggling confidentiality and safety: a qualitative study of how general practice clinicians document domestic violence in families with children. Br J Gen Pract 2017;67:e437-e444. https://doi.org/10.3399/bjgp17X689353.
- Baker GR, Gray CS, Shaw J, Denis JL, Breton M, Carswell P. Navigating the challenges of building integrated care models: findings from the iCoach project. Int J Integr Care 2016;16:1-2. https://doi.org/UNSP A375.
- Dellor E, Lovato-Hermann K, Wolf JP, Curry SR, Freisthler B. Introducing technology in child welfare referrals: a case study. J Technol Hum Serv 2015;33:330-44. https://doi.org/10.1080/15228835.2015.1107520.
- Vest JR, Jasperson ’S, Zhao H, Gamm LD, Ohsfeldt RL. Use of a health information exchange system in the emergency care of children. BMC Med Inform Decis Mak 2011;11. https://doi.org/10.1186/1472-6947-11-78.
- Friedman C, Rubin J, Brown J, Buntin M, Corn M, Etheredge L, et al. Toward a science of learning systems: a research agenda for the high-functioning Learning Health System. J Am Med Inform Assoc 2015;22:43-50. https://doi.org/10.1136/amiajnl-2014-002977.
- Liebowitz SJ, Margolis SE. Network externality – an uncommon tragedy. J Econ Perspect 1994;8:133-50. https://doi.org/DOI 10.1257/jep.8.2.133.
- Zeng X, Forrestal EJ, Cellucci LW, Kennedy MH, Smith D. Using Electronic health records and data warehouse collaboratively in community health centers. J Cases Inf Technol 2013;15:45-62. https://doi.org/10.4018/jcit.2013100104.
- Bech M, Pedersen KM. Transaction Costs Theory Applied to the Choice of Reimbursement Scheme in an Integrated Health Care System. Health Economics Paper #2. Odense: University of Southern Denmark; 2005.
- Plantier M, Havet N, Durand T, Caquot N, Amaz C, Biron P, et al. Does adoption of electronic health records improve the quality of care management in France? Results from the French e-SI (PREPS-SIPS) study. Int J Med Inform 2017;102:156-65. https://doi.org/10.1016/j.ijmedinf.2017.04.002.
- Mannion R, Davies H. Understanding organisational culture for healthcare quality improvement. BMJ 2018;363. https://doi.org/10.1136/bmj.k4907.
- Exworthy M, Powell M, Glasby J. The governance of integrated health and social care in England since 2010: great expectations not met once again?. Health Policy 2017;121:1124-30. https://doi.org/10.1016/j.healthpol.2017.07.009.
- Gold M, McLaughlin C. Assessing HITECH implementation and lessons: 5 years later. Milbank Q 2016;94:654-87. https://doi.org/10.1111/1468-0009.12214.
- Kellermann AL, Jones SS. What it will take to achieve the as-yet-unfulfilled promises of health information technology. Health Aff 2013;32:63-8. https://doi.org/10.1377/hlthaff.2012.0693.
- Gawande A. Why doctors hate their computers. New Yorker 2018.
- Campbell DT, Cook TD, Shadish WR. Experimental and Quasi-Experimental Designs for Generalized Causal Inference. Boston, MA: Houghton Mifflin Harcourt; 2002.
Appendix 1 Search strategies and databases and sources searched
| Number | Title |
|---|---|
| 1 | Theory development |
| 1.1a | Theory development: structured subject search – patient safety in networked IT |
| 1.1b | Theory development: structured subject search – interoperability and networked IT |
| 1.2a | Theory development: named author searches – David Bates and interoperable systems or HIE |
| 1.2b | Theory development: named author searches – Robert Wachter |
| 1.3 | Theory development: systematic reviews searches |
| 1.4 | Theory development: usage count search |
| Evidence reviews | |
| 2 | The co-ordination of services for older people living at home |
| 2.1 | The nature and extent of care co-ordination problems for frail older people living at home |
| 2.2 | What are the experiences of professionals using interoperable networks in the course of care co-ordination? |
| 2.3 | Do interoperable networks improve patient safety outcomes for frail older people living at home? |
| 3 | Medication reconciliation for older people living at home |
| 3.1 | What is the nature of the medicine reconciliation problem in frail older people population? |
| 3.2 | What are professionals’ experiences of using interoperable networks in medicine reconciliation for frail older people? |
| 3.3 | What are the patient outcomes of using interoperable networks in medicine reconciliation? |
| 4 | The co-ordination of services for at-risk children |
| 4.1 | What is the nature and extent of the co-ordination problem for services for at-risk children? |
| 4.2 and 4.3 (single strategy) |
What are clinicians’ and other professionals’ experiences of using interoperable HIT to co-ordinate the care of children at risk? What are the effects of interoperable networks on outcomes for at-risk children? |
| 5 | Economies of scope and scale of interoperable networks in health economies |
Theory development searches
Theory development: structured subject search – patient safety in networked information technology
EMBASE (via Ovid)
Search date: 10 March 2018.
Date range searched: 1996 to week 10 2018.
Search strategy
-
“Comment on”.ti. (16,738)
-
(letter* adj3 editor*).ti. (19,988)
-
opinion*.ti. (12,189)
-
(view or views).ti. (37,100)
-
(editorial or journal letter or journal note or letter or note or report editorial or report letter or trade journal letter or trade journal note).pt. (1,772,500)
-
or/1-5 [opinion pieces - hidden theories] (1,817,733)
-
(policy or policies or guideline* or recommendation* or position).ti. (171,688)
-
*practice guideline/ (54,860)
-
exp *public policy/or *policy/ (58,445)
-
(theor* or concep* or logic).ti. (110,842)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (52,231)
-
or/7-11 [Policy, Guideline or overt Theory] (383,366)
-
6 or 12 [Theories search] (2,155,076)
-
*safety/and (outpatient* or patient*).tw. (31,576)
-
exp medical error/and (outpatient* or patient*).tw. (51,726)
-
((patient or patients or outpatient*) adj2 (safety or harm* or adverse*)).tw. (54,275)
-
exp *patient safety/ (12,682)
-
*risk management/ (13,493)
-
exp *adverse event/ (53,911)
-
or/14-19 [patient safety] (196,559)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (2649)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (285)
-
*medical information system/ (6904)
-
21 or 22 or 23 (9433)
-
exp medical record/ (176,429)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (77,872)
-
medical informatics/or nursing informatics/ (18,665)
-
(electronic adj3 record*).tw. (46,895)
-
((health or medical or clinical) adj5 (information or record*)).tw. (300,330)
-
computer system/ (20,409)
-
or/25-30 [health records & systems] (462,934)
-
exp computer network/ (11,623)
-
information dissemination/ (17,918)
-
(network* or exchange* or data shar*).tw. (603,816)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (16,717)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (2683)
-
or/32-36 [networked systems] (641,855)
-
31 and 37 (30,994)
-
38 or 24 [Networked IT or HIEs] (36,767)
-
20 and 39 [safety in networked systems] (1353)
-
13 and 40 [Theory & Opinion networked IT safety systems] (94)
Health Management Information Consortium (via Ovid)
Search date: 10 March 2018.
Date range searched: 1983 to present.
Search strategy
-
Commentaries/ (18)
-
“Comment on”.ti. (29)
-
editorial.ti. (265)
-
letter.ti. (328)
-
opinion*.ti. (508)
-
(view or views).ti. (3538)
-
(letter* adj3 editor*).ti. (1)
-
or/1-7 (4667)
-
(evidence* adj8 (policy or policies)).tw. (1368)
-
policy/or health policy/or public policy/ (8823)
-
(policy or policies or guideline* or recommendation* or position).ti. (12,107)
-
exp guidelines/ (6653)
-
(theor* or concep* or logic).ti. (2774)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (1825)
-
or/9-14 [Policy, Guideline or overt Theory] (27,515)
-
8 or 15 [Theories] (31,886)
-
patient safety/ (3678)
-
adverse events/ (718)
-
exp Errors/or exp Medication errors/ (1165)
-
((patient or patients or outpatient*) adj2 (safety or harm* or adverse*)).tw. (2830)
-
risk management/or safety measures/ (2818)
-
or/17-21 [patient safety] (7784)
-
information exchange/ (345)
-
exp Medical information exchange/ (20)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw. (105)
-
(patient information adj5 (exchang* or shar* or network*)).tw. (38)
-
or/23-26 (485)
-
exp medical records/ (3144)
-
information technology/ (4796)
-
exp information systems/ (4895)
-
exp informatics/ (308)
-
(electronic adj3 record*).tw. (1319)
-
((health or medical or clinical) adj5 (information or record*)).tw. (9925)
-
exp computer systems/ (4522)
-
or/28-34 [health records] (21,052)
-
exp information transfer/ (1978)
-
exp computer networks/ (1667)
-
(network* or exchange* or data shar*).tw. (7125)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (1342)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (145)
-
or/36-40 [networked] (11,264)
-
35 and 41 (3305)
-
42 or 27 [networked IT, HIE] (3541)
-
22 and 43 [safety in networked systems] (67)
-
16 and 44 [Theory & Opinion networked IT safety systems] (3)
Ovid MEDLINE
Search date: 10 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
-
(policy or policies or guideline* or recommendation* or position).ti. (157,471)
-
guideline/or practice guideline/ (29,721)
-
policy/or public policy/or exp health policy/ (126,430)
-
(theor* or concep* or logic).ti. (140,361)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (44,188)
-
or/1-5 [Policy, Guideline or overt Theory] (445,038)
-
Comment/ (664,894)
-
Letter/ (926,791)
-
Editorial/ (405,400)
-
news/or newspaper article/ (190,273)
-
“Comment on”.ti. (16,286)
-
(letter* adj3 editor*).ti. (6376)
-
opinion*.ti. (11,812)
-
(view or views).ti. (43,579)
-
or/7-14 [Discussion papers Hidden Theory] (1,710,573)
-
6 or 15 [Theory Search] (2,103,940)
-
“Safety Management”/and (outpatient* or patient*).tw. (7050)
-
“Medical Errors”/and (outpatient* or patient*).tw. (7399)
-
patient safety/ (13,787)
-
((patient or patients or outpatient*) adj2 (safety or harm* or adverse*)).tw. (31,734)
-
*risk management/ (8572)
-
or/17-21 [Patient Safety] (53,654)
-
Health Information Exchange/ (562)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (2012)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (198)
-
23 or 24 or 25 (2551)
-
exp Medical Records/ (132,774)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (67,432)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (15,531)
-
exp Decision Making, Computer-Assisted/ (124,934)
-
(electronic adj3 record*).tw. (20,676)
-
((health or medical or clinical) adj5 (information or record*)).tw. (190,180)
-
Computer Systems/ (12,550)
-
or/27-33 [health records] (484,060)
-
community network/ (6385)
-
computer communication networks/or local area networks/ (13,961)
-
information dissemination/ (14,049)
-
(network* or exchange* or data shar*).tw. (492,792)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (12,562)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (2196)
-
or/35-40 [networking systems] (529,805)
-
41 and 34 (28,255)
-
42 or 26 [Networked IT systems] (28,641)
-
43 and 22 [safety in networked systems] (468)
-
16 and 44 [Theory & Opinion networked IT safety systems] (47)
Ovid MEDLINE Epub Ahead of Print
Search date: 8 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
Same strategy as Ovid MEDLINE.
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Search date: 8 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
Same strategy as Ovid MEDLINE.
Theory development: structured subject search – interoperability and networked information technology
EMBASE Classic and EMBASE (via Ovid)
Search date: 16 March 2018.
Date range searched: 1947 to 15 March 2018.
Search strategy
-
“Comment on”.ti. (20,221)
-
(letter* adj3 editor*).ti. (24,062)
-
opinion*.ti. (16,905)
-
(view or views).ti. (61,981)
-
(editorial or journal letter or journal note or letter or note or report editorial or report letter or trade journal letter or trade journal note).pt. (2,268,207)
-
or/1-5 [opinion pieces - hidden theories] (2,344,004)
-
(policy or policies or guideline* or recommendation* or position).ti. (222,165)
-
*practice guideline/ (56,643)
-
exp *public policy/or *policy/ (85,626)
-
(theor* or concep* or logic).ti. (182,117)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (60,995)
-
or/7-11 [Policy, Guideline or overt Theory] (533,584)
-
6 or 12 [Theories search] (2,821,744)
-
exp medical record/ (204,622)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (94,578)
-
medical informatics/or nursing informatics/ (19,599)
-
(electronic adj3 record*).tw. (47,862)
-
((health or medical or clinical) adj5 (information or record*)).tw. (333,516)
-
computer system/ (24,959)
-
or/14-19 [health records & systems] (534,936)
-
“data interoperability”/ (30)
-
interoperab*.tw,kw. (3422)
-
21 or 22 (3434)
-
23 and 20 and 13 [Theory interoperable health systems] (218)
Health Management Information Consortium
Search date: 16 March 2018.
Date range searched: 1983 to present.
Search strategy
-
Commentaries/ (18)
-
“Comment on”.ti. (29)
-
editorial.ti. (265)
-
letter.ti. (328)
-
opinion*.ti. (508)
-
(view or views).ti. (3538)
-
(letter* adj3 editor*).ti. (1)
-
or/1-7 (4667)
-
(evidence* adj8 (policy or policies)).tw. (1368)
-
policy/or health policy/or public policy/ (8823)
-
(policy or policies or guideline* or recommendation* or position).ti. (12,107)
-
exp guidelines/ (6653)
-
(theor* or concep* or logic).ti. (2774)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (1825)
-
or/9-14 [Policy, Guideline or overt Theory] (27,515)
-
8 or 15 [Theories] (31,886)
-
exp medical records/ (3144)
-
information technology/ (4796)
-
exp information systems/ (4895)
-
exp informatics/ (308)
-
(electronic adj3 record*).tw. (1319)
-
((health or medical or clinical) adj5 (information or record*)).tw. (9925)
-
exp computer systems/ (4522)
-
or/17-23 [health records] (21,052)
-
interoperab*.tw. (87)
-
16 and 24 and 25 (4)
Ovid MEDLINE
Search date: 16 March 2018.
Date range searched: 1946 to March week 2 2018.
Search strategy
-
(policy or policies or guideline* or recommendation* or position).ti. (157,588)
-
guideline/or practice guideline/ (29,719)
-
policy/or public policy/or exp health policy/ (126,529)
-
(theor* or concep* or logic).ti. (140,426)
-
((theor* or concep* or logic) adj (framework* or model* or analy* or evaluat*)).ab. (44,221)
-
or/1-5 [Policy, Guideline or overt Theory] (445,305)
-
Comment/ (665,509)
-
Letter/ (927,149)
-
Editorial/ (405,687)
-
news/or newspaper article/ (190,369)
-
“Comment on”.ti. (16,291)
-
(letter* adj3 editor*).ti. (6383)
-
opinion*.ti. (11,818)
-
(view or views).ti. (43,602)
-
or/7-14 [Discussion papers Hidden Theory] (1,711,671)
-
6 or 15 [Theory Search] (2,105,265)
-
exp Medical Records/ (132,810)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (67,435)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (15,539)
-
exp Decision Making, Computer-Assisted/ (125,028)
-
(electronic adj3 record*).tw. (20,720)
-
((health or medical or clinical) adj5 (information or record*)).tw. (190,394)
-
Computer Systems/ (12,552)
-
or/17-23 [health records] (484,384)
-
HEALTH INFORMATION INTEROPERABILITY/ (36)
-
interoperab*.tw,kw. (2537)
-
25 or 26 (2555)
-
16 and 24 and 27 [Theory interoperability records] (163)
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Search date: 15 March 2018.
Date range searched: 1946 to March week 2 2018.
Search strategy
Same search strategy as Ovid MEDLINE.
Ovid MEDLINE Epub Ahead of Print
Search date: 15 March 2018.
Date range searched: 1946 to March week 2 2018.
Search strategy
Same search strategy as Ovid MEDLINE.
Theory development: named author searches – David Bates and interoperable systems or health information exchange
EMBASE Classic and EMBASE (via Ovid)
Search date: 22 March 2018.
Date range searched: 1947 to 21 March 2018.
Search strategy
-
exp medical record/ (205,201)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (94,759)
-
medical informatics/or nursing informatics/ (19,627)
-
(electronic adj3 record*).tw. (48,101)
-
((health or medical or clinical) adj5 (information or record*)).tw. (334,714)
-
computer system /(24,988)
-
or/1-6 [health records & systems] (536,527)
-
“data interoperability”/ (31)
-
(interoperab* or inter-operab*).tw,kw. (3489)
-
8 or 9 (3502)
-
7 and 10 [interoperable systems] (2272)
-
*medical information system/ (7111)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (2874)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (301)
-
or/12-14 [health info exchange] (9873)
-
11 or 15 (11,761)
-
Bates, DW.au. (865)
-
(Bates adj2 David).ti,ab,kw. (9)
-
or/17-18 (873)
-
19 and 16 [Bates on HIE and interoperability] (59)
Health Management Information Consortium (via Ovid)
Search date: 22 March 2018.
Date range searched: 1983 to present.
Search strategy
-
exp medical records/ (3144)
-
information technology/ (4796)
-
exp information systems/ (4895)
-
exp informatics/ (308)
-
(electronic adj3 record*).tw. (1319)
-
((health or medical or clinical) adj5 (information or record*)).tw. (9925)
-
exp computer systems/ (4522)
-
or/1-7 [health records] (21,052)
-
(interoperab* or inter-operab*).tw. (95)
-
8 and 9 [interoperable systems] (78)
-
information exchange/ (345)
-
exp Medical information exchange/ (20)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw. (105)
-
(patient information adj5 (exchang* or shar* or network*)).tw. (38)
-
or/11-14 [health info exchange] (485)
-
10 or 15 (551)
-
Bates, D*.au. (17)
-
Bates.ti,ab. (12)
-
17 or 18 (29)
-
19 and 16 [Bates on HIE and interoperability] (1)
Ovid MEDLINE
Search date: 22 March 2018.
Date range searched: 1946 to March week 3 2018.
Search strategy
-
exp Medical Records/ (132,904)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (67,498)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (15,554)
-
exp Decision Making, Computer-Assisted/ (125,253)
-
(electronic adj3 record*).tw. (20,785)
-
((health or medical or clinical) adj5 (information or record*)).tw. (190,733)
-
Computer Systems/ (12,558)
-
or/1-7 [health records] (485,075)
-
(interoperab* or inter-operab*).tw,kw. (2582)
-
9 and 8 [interoperable systems] (1800)
-
HEALTH INFORMATION INTEROPERABILITY/ (36)
-
10 or 11 (1820)
-
Health Information Exchange/ (567)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (2018)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (199)
-
or/13-15 [health information exchange] (2561)
-
12 or 16 (4170)
-
Bates, DW.au. (696)
-
(Bates adj2 David).ti,ab,kw. (7)
-
or/18-19 (702)
-
20 and 17 [Bates on HIE and interoperability] (29)
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Date searched: 21 March 2018.
Date range searched: 1946 to March week 3 2018.
Search strategy
Same search strategy as Ovid MEDLINE.
Ovid MEDLINE Epub Ahead of Print
Date searched: 21 March 2018.
Date range searched: 1946 to March week 3 2018.
Search strategy
Same search strategy as Ovid MEDLINE.
Web of Science Core Collection (Clarivate Analytics)
Date searched: 21 March 2018.
Database searched (date range searched): Arts and Humanities Citation Index (1975 to present), Book Citation Index – Social Sciences and Humanities (2005 to present), Conference Proceedings Citation Index – Science (1990 to present), Conference Proceedings Citation Index – Social Science & Humanities (1990 to present), Sciences Citation Index (1900 to present), Social Sciences Citation Index (1900 to present) and Emerging Sources Citation Index (2015 to present).
Search strategy
-
# 14 #13 AND #3 3 [1 Bates and HIE/interoperability]** (28)
-
# 13 #12 OR #8 2 [HIE/interop] (3837)
-
# 12 #11 OR #10 OR #9 (2442)
-
# 11 TOPIC: ((“patient information” NEAR/5 (exchang* or shar* or network*))) (208)
-
# 10 TOPIC: (((“health information” or “medical information” or “clinical information”) NEAR/5 (exchang* or shar* or network*))) (2265)
-
# 9 TOPIC: (“health information exchange”) (694)
-
# 8 #7 AND #6 (1618)
-
# 7 TS = (interoperab* or inter-operab*) (25,500)
-
# 6 #5 OR #4 (212,986)
-
# 5 TOPIC: (((health or medical or clinical) NEAR/5 (information or record*))) (207,575)
-
# 4 TOPIC: ((electronic NEAR/3 record*)) (28,520)
-
# 3 #2 OR #1 [Bates as author]** (921)
-
# 2 TOPIC: (Bates NEAR/2 David) (27)
-
# 1 AUTHOR: (Bates DW) (894)
**Bates is a prolific author on HITs and patient safety so we looked at only (1) articles he authored on HIT (line #14), or (2) any article he authored or articles in which he was mentioned with a usage count ≥ 20 (line #3), which gave 74 references from the 921 identified.
Theory development: named author searches – Robert Wachter
EMBASE (via Ovid)
Search date: 10 March 2018.
Date range searched: 1996 to 2018 week 10.
Search strategy
-
wachter rm.au. (244)
-
wachter.ti,ab,kw. (40)
-
1 or 2 (284)
-
limit 3 to yr = “2015 -Current” (32)
Health Management Information Consortium (via Ovid)
Search date: 10 March 2018.
Date range searched: 1983 to present.
Search strategy
-
wachter r*.au. (12)
-
wachter.ti,ab. (3)
-
1 or 2 (14)
-
limit 3 to yr = “2015 -Current” (3)
Ovid MEDLINE
Search date: 10 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
-
wachter rm.au. (232)
-
wachter.ti,ab,kw. (45)
-
1 or 2 (277)
-
limit 3 to yr = “2015 -Current” (18)
Ovid MEDLINE Epub Ahead of Print
Search date: 8 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
Same strategy as Ovid MEDLINE.
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Search date: 8 March 2018.
Date range searched: 1946 to February week 5 2018.
Search strategy
Same strategy as Ovid MEDLINE.
Web of Science Core Collection (Clarivate Analytics)
Search date: 21 March 2018.
Database searched (date range searched): Arts and Humanities Citation Index (1975 to present), Book Citation Index – Social Sciences and Humanities (2005 to present), Conference Proceedings Citation Index – Science (1990 to present), Conference Proceedings Citation Index – Social Science & Humanities (1990 to present), Sciences Citation Index (1900 to present), Social Sciences Citation Index (1900 to present) and Emerging Sources Citation Index (2015 to present).
Search strategy
PUBLICATION YEARS: (2015 OR 2016 OR 2017) *Note there was no option for 2018
-
# 3 #1 OR #2 (41)
-
# 2 AUTHOR: (wachter rm) (27)
-
# 1 TOPIC: (wachter) (14)
Agency for Healthcare Research and Quality PSNeT Patient Safety Network
Search date: 28 February 2018.
Search strategy
Search term ‘Robert Wachter’ was entered in the search tab. This retrieved all publications that were authored or co-authored by Robert Wachter.
Theory development: systematic reviews searches
Cochrane Database of Systematic Reviews (via Wiley Online Library)
Search date: 5 February 2018 and 5 July 2019.
Issue 7 of 12, July 2019.
Search strategy
-
#1 MeSH descriptor: [Safety Management] explode all trees (164)
-
#2 MeSH descriptor: [Medical Errors] explode all trees (2865)
-
#3 #1 or #2 (3008)
-
#4 (outpatient* or patient*):ti,ab (864,355)
-
#5 #3 and #4 (1959)
-
#6 ((patient or patients or outpatient*) N2(safety or harm* or adverse)):ti,ab,kw (343)
-
#7 MeSH descriptor: [Risk Management] explode all trees (8736)
-
#8 MeSH descriptor: [Patient Safety] explode all trees (515)
-
#9 #5 or #6 or #7 or #8 (11,261)
-
#10 MeSH descriptor: [Medical Informatics] this term only (71)
-
#11 MeSH descriptor: [Medical Informatics Applications] this term only (23)
-
#12 MeSH descriptor: [Health Information Exchange] explode all trees (5)
-
#13 MeSH descriptor: [Medical Informatics Computing] explode all trees (0)
-
#14 MeSH descriptor: [Nursing Informatics] explode all trees (10)
-
#15 MeSH descriptor: [Public Health Informatics] explode all trees (1)
-
#16 MeSH descriptor: [Information Systems] explode all trees (2180)
-
#17 MeSH descriptor: [Decision Making, Computer-Assisted] explode all trees (5060)
-
#18 (“Information technolog*” or computer*):ti (4965)
-
#19 MeSH descriptor: [Technology] this term only (29)
#20 MeSH descriptor: [Biomedical Technology] explode all trees (21)
-
#21 MeSH descriptor: [Computer Systems] explode all trees (5149)
-
#22 #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 (15,121)
-
#23 #9 and #22 (640)
Database of Abstracts of Reviews of Effects (via Wiley Online Library)
Search date: 5 February 2018.
Issue 2 of 4, April 2015.
Search strategy
Same search strategy as Cochrane Database of Systematic Reviews (Wiley): Issue 7 of 12, July 2019.
EMBASE Classic and EMBASE (via Ovid)
Search date: 5 February 2018 and 5 July 2019.
Date range searched: 1947 to 3 July 2019.
Search strategy
-
*safety/and (outpatient* or patient*).tw. (32,312)
-
medical error/and (outpatient* or patient*).tw. (8475)
-
((patient or patients or outpatient*) adj2 (safety or harm* or adverse*)).tw. (66,683)
-
exp patient safety/ (112,296)
-
*risk management/ (15,976)
-
exp adverse event/ (591,775)
-
or/1-6 (774,080)
-
exp *information system/ (65,112)
-
medical information system/ (20,086)
-
medical informatics/ (19,591)
-
(“Information technolog*” or computer*).ti. (90,275)
-
*information technology/or *medical technology/or *technology/ (33,552)
-
*computer system/ (6527)
-
or/8-13 [IT systems] (211,487)
-
7 and 14 (5785)
-
limit 15 to “reviews (maximizes specificity)” (117)
Epistemonikos (Epistemonikos Foundation)
Two searches were conducted using the advanced search interface.
Search strategy
-
Search title: information technology OR search title/abstract health information exchange AND Search title/abstract: patient safety OR Medical error* OR Adverse event* (26 results)
-
Search title: information technology OR information exchange OR interoperability AND Search title/abstract: patient safety OR Medical error* OR Adverse event* (44 results)
Health Technology Assessment Database (via Wiley Online Library)
Search date: 5 February 2018.
Issue 4 of 4, October 2016.
Search strategy
Same search strategy as Cochrane Database of Systematic Reviews (Wiley): Issue 2 of 12, February 2018.
Health Systems Evidence (McMaster University)
Search date: 5 February 2018 and 5 July 2019.
Search strategy
The search terms “health information exchange” AND “patient safety” were entered into the basic search interface (12).
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 5 February 2018 and 5 July 2019.
Date range searched: 1946 to 3 July 2019 (includes MEDLINE 1946 to June week 5 2019).
Search strategy
-
“Safety Management”/and (outpatient* or patient*).tw. (7369)
-
“Medical Errors”/and (outpatient* or patient*).tw. (7856)
-
patient safety/ (17,099)
-
((patient or patients or outpatient*) adj2 (safety or harm* or adverse*)).tw. (42,840)
-
*risk management/ (8922)
-
or/1-5 [Patient Safety] (67,271)
-
medical informatics/ (11,141)
-
health information exchange/ (717)
-
medical informatics applications/ (2417)
-
medical informatics computing/or nursing informatics/or public health informatics/ (3347)
-
exp *information systems/ (82,805)
-
exp *decision making, computer-assisted/ (96,082)
-
(“Information technolog*” or computer*).ti. (74,167)
-
*technology/or *biomedical technology/ (8748)
-
exp *Computer Systems/ (89,894)
-
or/7-15 [IT systems] (319,910)
-
6 and 16 (3123)
-
limit 17 to “reviews (maximizes specificity)” (82)
Theory development: usage count search
Web of Science Core Collection (Clarivate Analytics)
Search date: 22 March 2018.
Database searched (date range searched): Arts and Humanities Citation Index (1975 to present), Book Citation Index – Social Sciences and Humanities (2005 to present), Conference Proceedings Citation Index – Science (1990 to present), Conference Proceedings Citation Index – Social Science & Humanities (1990 to present), Sciences Citation Index (1900 to present), Social Sciences Citation Index (1900 to present) and Emerging Sources Citation Index (2015 to present).
Search strategy
-
# 10 #9 OR #5 [HIE/interop]** (3837)
-
# 9 #8 OR #7 OR #6 (2442)
-
# 8 TOPIC: ((“patient information” NEAR/5 (exchang* or shar* or network*))) (208)
-
# 7 TOPIC: (((“health information” or “medical information” or “clinical information”) NEAR/5 (exchang* or shar* or network*))) (2265)
-
# 6 TOPIC: (“health information exchange”) (694)
-
# 5 #4 AND #3 (1618)
-
# 4 TS = (interoperab* or inter-operab*) (25,500)
-
# 3 #1 OR #2 (212,986)
-
# 2 TOPIC: (((health or medical or clinical) NEAR/5 (information or record*))) (207,575)
-
# 1 TOPIC: ((electronic NEAR/3 record*)) (28,520)
**We selected only those records with a usage count ≥ 50 accesses, which gave 56 records from the 3837 identified.
Evidence review: the co-ordination of services for older people living at home
The nature and extent of care co-ordination problems for frail older people living at home
Structured database searches
Applied Social Sciences Index and Abstracts (via ProQuest)
Search date: 6 August 2019.
Date range searched: 1987 to present.
Reviews search
((su(frail) OR (ti((function* NEAR/1 impair*) AND (old* OR elderly OR geriatric*)) OR ab((function* NEAR/1 impair*) AND (old* OR elderly OR geriatric*))) OR (ti((cognitive NEAR/1 impair*) AND (old* OR elderly OR geriatric*)) OR ab((cognitive NEAR/1 impair*) AND (old* OR elderly OR geriatric*))) OR (ti((complex NEAR/2 needs) AND (old* OR elderly OR geriatric*)) OR ab((complex NEAR/2 needs) AND (old* OR elderly OR geriatric*))) OR (ti(frail*) OR ab(frail*)))
AND
(su(Integrated care pathways) OR (ti((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*)) OR ab((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*))) OR su(continuity) OR su(Joint working) OR (ti((joint NEAR/1 (working OR care OR service*))) OR ab((joint NEAR/1 (working OR care OR service*)))) OR su(transition program) OR (ti((intermediate OR transition* OR transfer* OR team*) NEAR/3 care) OR ab((intermediate OR transition* OR transfer* OR team*) NEAR/3 care)) OR su(intercessional approach) OR su(multidisciplinary care) OR su(Interdisciplinary team work) OR su(Interdisciplinary approach) OR (ti((interinstitution* OR interagenc* OR interdisciplin* OR Interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)) OR ab((interinstitution* OR interagenc* OR interdisciplin* OR interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)))))
AND
(su(systematic review) OR ti(review OR meta-analysis OR synthesis))
n = 10
Qualitative search
((MAINSUBJECT.EXACT.EXPLODE(“Surveys”) OR MAINSUBJECT.EXACT.EXPLODE(“Interviews”) OR MAINSUBJECT.EXACT.EXPLODE(“Questionnaires”) ti(((purpos* NEAR/4 sampl*) OR (focus NEAR/4 group*)).) OR ab(((purpos* NEAR/4 sampl*) OR (focus NEAR/4 group*)).)) OR (ti((grounded NEAR/4 (theor OR study OR studies OR research OR analys?s))) OR ab((grounded NEAR/4 (theor OR study OR studies OR research OR analys?s)))) OR (ti(phenomenol*.) OR ab(phenomenol*.)) OR (ti(qualitative) OR ab(qualitative)) OR (ti(ethnolog* OR ethnograph* OR ethnonursing) OR ab(ethnolog* OR ethnograph* OR ethnonursing)) OR su(Observational research) OR su(qualitative methods) OR su(qualitative research))
AND
((su(frail) OR (ti((function* NEAR/1 impair*) AND (old* OR elderly OR geriatric*)) OR ab((function* NEAR/1 impair*) AND (old* OR elderly OR geriatric*))) OR (ti((cognitive NEAR/1 impair*) AND (old* OR elderly OR geriatric*)) OR ab((cognitive NEAR/1 impair*) AND (old* OR elderly OR geriatric*))) OR (ti((complex NEAR/2 needs) AND (old* OR elderly OR geriatric*)) OR ab((complex NEAR/2 needs) AND (old* OR elderly OR geriatric*))) OR (ti(frail*) OR ab(frail*)))
AND
(su(Integrated care pathways) OR (ti((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*)) OR ab((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*))) OR su(continuity) OR su(Joint working) OR (ti((joint NEAR/1 (working OR care OR service*))) OR ab((joint NEAR/1 (working OR care OR service*)))) OR su(transition program) OR (ti((intermediate OR transition* OR transfer* OR team*) NEAR/3 care) OR ab((intermediate OR transition* OR transfer* OR team*) NEAR/3 care)) OR su(intercessional approach) OR su(multidisciplinary care) OR su(Interdisciplinary team work) OR su(Interdisciplinary approach) OR (ti((interinstitution* OR interagenc* OR interdisciplin* OR Interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)) OR ab((interinstitution* OR interagenc* OR interdisciplin* OR interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)))))
n = 57
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
Search date: 6 August 2019.
Date range searched: 1981 to present.
Note: records downloaded from S30 (reviews search) and S44 (qualitative studies search).
Search strategy
-
S44 S18 AND S42 Limiters - Published Date: 20000101-20181231 (193)
-
S43 S18 AND S42 (202)
-
S42 S40 OR S41 (452,543)
-
S41 ((MH “Interviews+”) or (MH “Questionnaires+”)) OR ((MH “Grounded Theory”) or (MH “Research, Nursing”)) OR ((MH “Ethnographic Research”) or (MH “Ethnonursing Research”) or (MH “Ethnological Research”)) (376,306)
-
S40 S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 (184,864)
-
S39 TX narrative analys?s (1981)
-
S38 TX ((discourse* or discurs*) N3 analys?s (3857)
-
S37 TX content analys?s (29,365)
-
S36 TX observational method* (16,252)
-
S35 TX cluster sampl* (3625)
-
S34 TX ((purpos* N4 sampl*) or (focus N1 group*)) (53,728)
-
S33 TX (action research or cooperative inquir* or co operative inquir* or co-operative inquir*) (7632)
-
S32 TX participant observ* (8986)
-
S31 TX (emic or etic or hermeneutic* or heuristic* or semiotic*) (4619)
-
S30 TX data N1 saturat* (447)
-
S29 TX grounded N1 (theor* or stud* or research or analys?s) (13,658)
-
S28 TX Ethnonursing OR TX ethnograph* or TX ethnolog* (31,218)
-
S27 (MH “Phenomenology”) (2529)
-
S26 (MH “Field Studies”) (2264)
-
S25 (MH “Observational Methods+”) (16,978)
-
S24 (MH “Content Analysis”) (24,944)
-
S23 (MH “Discourse Analysis”) (3303)
-
S22 (MH “Focus Groups”) (28,512)
-
S21 (MH “Qualitative Studies+”) (96,870)
-
S20 S18 AND S19 (30)
-
S19 Limiters - Published Date: 20000101-20181231; Publication Type: Systematic Review (55,215)
-
S18 S6 AND S17 (784)
-
S17 S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 (72,963)
-
S16 TI (((interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) N6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)) (3115)
-
S15 TI ((intermediate or transition* or transfer* or team*) N3 care) (4346)
-
S14 (MH “Transitional Care”) (530)
-
S13 (MH “Interprofessional Relations+”) (20,004)
-
S12 (MH “Transfer, Discharge”) (3884)
-
S11 TI (joint N1 (working or care or service*)) OR AB (joint N1 (working or care or service*)) (524)
-
S10 (MH “Continuity of Patient Care+”) (12,923)
-
S9 (MH “Health Care Delivery, Integrated”) (6466)
-
S8 TI ((co-ordinat* or coordinat* or integrat* or continuity) N3 (care or service*)) (5770)
-
S7 (MH “Multidisciplinary Care Team+”) (28,652)
-
S6 S1 OR S2 OR S3 OR S4 OR S5 (15,529)
-
S5 TI frail* OR AB frail* (6412)
-
S4 TI ((complex* N2 needs) AND (old* or elderly or geriatric*)) OR AB ((complex* N2 needs) AND (old* or elderly or geriatric*)) (353)
-
S3 TI ((cognitive* N6 impair*) AND (old* or elderly or geriatric*)) OR AB ((cognitive* N6 impair*) AND (old* or elderly or geriatric*)) (5464)
-
S2 TI ((function* N6 impair*) AND (old* or elderly or geriatric*)) OR AB ((function* N6 impair*) AND (old* or elderly or geriatric*)) (2556)
-
S1 (MH “Frail Elderly”) OR (MH “Frailty Syndrome”) (5380)
Health Management Information Consortium (via Ovid)
Search date: 6 August 2019.
Date range searched: 1983 to present.
Note: records downloaded from line 46 (reviews search) and line 41 (qualitative studies search).
Search strategy
-
exp frail older people/or exp Frail elderly people/ (314)
-
((function* adj1 impair*) and (old* or elderly or geriatric*)).tw,hw. (48)
-
((cognitive* adj1 impair*) and (old* or elderly or geriatric*)).tw,hw. (265)
-
((complex* adj2 needs) and (old* or elderly or geriatric*)).tw,hw. (129)
-
frail*.tw. (989)
-
or/1-5 [frailty] (1444)
-
collaborative care/or integrated care/or interagency collaboration/or joint working/ (5576)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,hw. (6550)
-
(joint adj (working or care or service*)).tw,hw. (2667)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,hw. (4138)
-
patient transfer/ (348)
-
health care teams/ (137)
-
long term care /(1778)
-
exp Intermediate care/ (518)
-
exp interorganisational relations/ (5496)
-
((interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw. (1881)
-
or/7-16 [care coordination] (19,596)
-
6 and 17 (294)
-
limit 18 to yr = “2000 -Current” (223)
-
exp qualitative techniques/ (323)
-
mixed methods research/or qualitative research/ (1250)
-
qualitative.tw. (8732)
-
(ethnolog* or ethnograph* or ethnonursing).tw. (691)
-
phenomenol*.af. (457)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (687)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (745)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (774)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (3723)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (506)
-
cluster sampl*.mp. (40)
-
observational method*.af. (36)
-
content analysis.af. (1021)
-
((discourse* or discurs*) adj3 analys?s).tw. (146)
-
narrative analys?s.af. (48)
-
or/20-34 [adapted qualitasitve filter] (13,942)
-
qualitative research/ (1244)
-
interviews/ (952)
-
interviews.tw. (11,703)
-
or/35-38 [qual & interviews] (20,362)
-
18 and 39 (46)
-
limit 40 to yr = “2000 -Current” (43)
-
systematic reviews/or literature reviews/or meta analysis/ (6475)
-
((systematic or metaanalys* or meta-analys* or rapid or evidence or qualitative or realist) adj2 (review or synthesis)).tw. (4442)
-
42 or 43 (8119)
-
18 and 44 (15)
-
limit 45 to yr = “2000 -Current” (13)
Ovid MEDLINE
Search date: 6 August 2019.
Date range searched: 1996 to July week 4 2018.
Note: records downloaded from line 22 (reviews search) and line 48 (qualitative studies search).
Search strategy
-
Frail Elderly/or Frailty/ (9088)
-
“Aged, 80 and over”/and (frail* or complex).tw. (24,288)
-
((function* adj1 impair*) and (old* or elderly or geriatric*)).tw. (3174)
-
((cognitive* adj1 impair*) and (old* or elderly or geriatric*)).tw. (13,985)
-
((complex* adj2 needs) and (old* or elderly or geriatric*)).tw. (362)
-
frail*.tw,kw. (12,564)
-
or/1-6 [frailty] (49,873)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).ti,kw. (5599)
-
“Delivery of Health Care, Integrated”/ (10,714)
-
*”Continuity of Patient Care”/ (7808)
-
(joint adj (working or care or service*)).tw,kw. (418)
-
Patient Transfer/ (6188)
-
*Patient Care Team/ (18,406)
-
((intermediate or transition* or transfer* or team*) adj3 care).ti,kw. (3712)
-
Transitional Care/ (389)
-
Intermediate Care Facilities/ (365)
-
*interprofessional relations/or *interdisciplinary communication/ (18,983)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).ti,kw. (3305)
-
or/8-18 [Care co-ordination] (63,400)
-
7 and 19 [Care co-ordination in the frail] (837)
-
limit 20 to (meta analysis or systematic reviews) [1a Frailty care co-ordination reviews] (50)
-
limit 21 to yr = “2000 -Current” (50)
-
limit 20 to (yr = “2000 -Current” and “qualitative (maximizes specificity)”) (82)
-
exp qualitative research/ (40,247)
-
qualitative.tw,kf. (133,174)
-
Nursing Methodology Research/ (14,985)
-
observational study/ (50,230)
-
ethnolog*.mp. (124,547)
-
ethnograph*.mp. (7008)
-
ethnonursing.af. (85)
-
phenomenol*.af. (14,598)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (8093)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (14,268)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (2724)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (42,519)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (7793)
-
cluster sampl*.mp. (4726)
-
observational method*.af. (462)
-
content analysis.af. (16,341)
-
((discourse* or discurs*) adj3 analys?s).tw. (1529)
-
narrative analys?s.af. (810)
-
or/24-41 [qualitative] (383,980)
-
“Surveys and Questionnaires”/ (361,279)
-
INTERVIEW/ (17,657)
-
interviews.tw,kf. (112,381)
-
or/42-45 [qual & interviews] (759,992)
-
20 and 46 (191)
-
limit 47 to yr = “2000 -Current” (185)
Ovid MEDLINE Epub Ahead of Print
Search date: 3 August 2018.
Search strategy Same search strategy as Ovid MEDLINE 1996 to July week 4 2018.
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Search date: 3 August 2018.
Search strategy Same search strategy as Ovid MEDLINE 1996 to July week 4 2018.
PsycINFO (via Ovid)
Search date: 6 August 2019.
Date range searched: 1806 to July week 5 2018.
Note: records downloaded from line 17 (reviews search) and line 41 (qualitative studies search).
Search strategy
-
health impairments/ (2299)
-
*geriatric patients/or elder care/ (13,064)
-
((function* adj1 impair*) and (old* or elderly or geriatric*)).tw. (1987)
-
((cognitive* adj1 impair*) and (old* or elderly or geriatric*)).tw. (12,949)
-
((complex* adj2 needs) and (old* or elderly or geriatric*)).tw. (279)
-
frail*.tw. (4263)
-
cognitive impairment/and (old* or elderly or geriatric*).tw. (9247)
-
or/1-7 [frailty] (33,360)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).ti,id. (4237)
-
integrated services/ (3213)
-
interdisciplinary treatment approach/ (6866)
-
“continuum of care”/ (1628)
-
(joint adj (working or care or service*)).tw,id. (238)
-
((intermediate or transition* or transfer* or team*) adj3 care).ti,id. (1981)
-
((interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).ti,id. (3090)
-
or/9-15 (17,309)
-
8 and 16 [care coordination in the frail elderly] (516)
-
limit 17 to (“reviews (maximizes specificity)” and yr = “2000 -Current”) (19)
-
exp qualitative research/(7890)
-
qualitative.tw,id. (144,618)
-
survey*.mp. (301,041)
-
ethnolog*.mp. (2683)
-
ethnograph*.mp. (26,448)
-
ethnonursing.af. (138)
-
phenomenol*.af. (104,146)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (50,918)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (90,872)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (8286)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (57,965)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (13,865)
-
cluster sampl*.mp. (1382)
-
observational method*.af. (1952)
-
observation methods/ (5201)
-
or/19-33 [qualitative terms] (670,126)
-
interviews/ (8107)
-
questionnaires/ (17,252)
-
interview*.tw,id. (297,486)
-
questionnaire*.mp. (369,227)
-
or/34-38 [qual & interviews] (1,076,024)
-
17 and 39 (168)
-
limit 40 to yr = “2000 -Current” (154)
Complementary searches
The King’s Fund: hand-searched
The King’s Fund integrated care topic web page, publications list (URL: www.kingsfund.org.uk/topics/integrated-care?f%5B0%5D=type%3A5842).
The King’s Fund integrated care and partnership working reading list (URL: https://koha.kingsfund.org.uk/cgi-bin/koha/opac-shelves.pl?op=view%26shelfnumber=108%26sortfield=copyrightdate%26direction=desc).
n = 137
The Journal of Integrated Care: hand-searched
Titles in all issues from 2014 to present were screened for relevance and possibly included studies were downloaded.
n = 72
What are the experiences of professionals using interoperable networks in the course of care co-ordination?
Structured database searches
Association for Computing Machinery’s Digital Library full text collection (Association for Computing Machinery’s Guide to Computing Literature) – advanced search mode
Search date: 30 September 2018.
Date range searched: 1947 to present.
Search strategy
-
[any field – matches all] interoperab* record* AND [any field – any] health clinical medical patient AND [any field all] review = 5
-
[any field – matches all] [interoperab* AND [any field – any] metaanalysis = 0
-
[any field – matches all] interoperab* AND [any field – all] Coordinat* AND [any field all] review = 0
-
[any field – matches all] interoperab* AND [any field – all] communicat* AND [any field all] review = 2
-
[any field – matches all] interoperab* AND [any field – al] collaborat* AND [any field all] review = 0
-
[any field – matches all] interoperab* AND [any field – all] integrat* AND [any field all] review = 0
-
[any field – matches all] interoperab* AND [any field – all] transition* AND [any field all] review = 0
-
[any field – matches all] “health information exchange” [any field all] AND care [any field] AND [any field all] review = 6
-
[any field – matches all] “health information exchange” [any field all] AND record* [any field] AND [any field all] review = 9
-
[any field – matches all] “health information exchange” [any field all] AND coordinat* [any field] AND [any field all] review = 0
-
[any field – matches all] “health information exchange” [any field all] AND communicat* [any field] AND [any field all] review = 0
-
[any field – matches all] “health information exchange” [any field all] AND integrat* [any field] AND [any field all] review = 0
-
[any field – matches all] “health information exchange” [any field all] AND transition* [any field] AND [any field all] review = 0
-
[any field – matches all] “health information exchange” [any field all] AND [any field all] review = 14
Combined 14 searches (n = 36).
Applied Social Sciences Index and Abstracts (via ProQuest)
Search date: 30 September 2018.
Date range searched: 1987 to present.
Search strategy
(((((MAINSUBJECT.EXACT.EXPLODE(“Health records”) OR MAINSUBJECT.EXACT.EXPLODE(“Medical records”) OR MAINSUBJECT.EXACT(“Computerized medical records”)) OR MAINSUBJECT.EXACT(“Records”)) OR TI,AB(electronic NEAR/3 record*) OR TI,AB((health or medical or clinical) NEAR/5 (information or record)))
AND
TI,AB(interoperab*)) OR TI,AB(“health information exchange”))
AND
(TI,AB((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*)) OR ((MAINSUBJECT.EXACT(“Care”) OR MAINSUBJECT.EXACT(“Integrated care pathways”) OR MAINSUBJECT.EXACT(“Intermediate care”) OR MAINSUBJECT.EXACT(“Shared care”) OR MAINSUBJECT.EXACT(“Continuing care”) OR MAINSUBJECT.EXACT(“Home care”)) OR (MAINSUBJECT.EXACT(“Transition programmes”) OR MAINSUBJECT.EXACT(“Continuity”)) OR (MAINSUBJECT.EXACT(“Care coordinators”) OR MAINSUBJECT.EXACT(“Care management”) OR MAINSUBJECT.EXACT(“Care delivery”)) OR MAINSUBJECT.EXACT(“Joint working”)) OR Ti,AB(joint NEAR/1 (working OR care OR service*)) OR TI,AB((intermediate OR transition* OR transfer* OR team*) NEAR/3 care) OR (MAINSUBJECT.EXACT.EXPLODE(“Interdisciplinary team work”) OR MAINSUBJECT.EXACT(“Interdisciplinary approach”)) OR TI,AB((interinstitution* OR interagenc* OR interdisciplin* OR Interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)))
AND
at.exact(“Literature Review”) (1)
EMBASE (via Ovid)
Search date: 30 September 2018.
Date range searched: 1996 to week 40 2018.
Search strategy
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (42,958)
-
integrated health care system/ (9709)
-
transitional care/ (1675)
-
*patient care/ (49,167)
-
(joint adj (working or care or service*)).tw,kw. (790)
-
patient transport/ (19,866)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (35,683)
-
Intermediate Care Facilities/ (34,086)
-
interdisciplinary communication/ (10,573)
-
((interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw. (33,105)
-
interpersonal communication/ (124,500)
-
public relations/ (37,161)
-
or/1-12 [care-coordination] (345,988)
-
exp medical record/ (186,463)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (81,079)
-
medical informatics/or nursing informatics/ (19,364)
-
(electronic adj3 record*).tw. (52,350)
-
((health or medical or clinical) adj5 (information or record*)).tw. (321,597)
-
computer system/ (20,637)
-
or/14-19 [health records & systems] (489,700)
-
data interoperability/ (77)
-
interoperab*.tw,kw. (3660)
-
21 or 22 (3687)
-
20 and 23 [interoperable records - based on theory search 3 interoperability] (2396)
-
*medical information system/ (7112)
-
24 or 25 (9298)
-
13 and 26 [care coordination interoperability] (969)
-
limit 27 to yr = “2000 -Current” (956)
-
limit 28 to “reviews (best balance of sensitivity and specificity)” (141)
Inspec (EI Village)
Search date: 30 September 2018.
Date range searched: 1896 to present.
Search strategy
((($meta-analysis OR $review OR search*) WN ALL))
AND
((((((({health information exchange}) WN ALL))) OR ((((((((({electronic health records} WN CV) OR ({medical information systems} WN CV) OR ({information systems} WN CV))))) OR ((($electronic NEAR/3 record* OR $health NEAR/3 record* OR $medical NEAR/3 record* OR $clinical NEAR/3 record* OR $health NEAR/3 $information OR $medical NEAR/3 $information OR $clinical NEAR/3 $information) WN ALL))))
AND
((((((({open systems} WN CV)))))) OR (((interoperab*) WN ALL)))))))))
AND
((((((({patient care} WN CV) OR (1 WN CV) OR ({professional communication} WN CV)))))) OR ((continuity NEAR/3 care OR continuity NEAR/3 service OR integrat* NEAR/3 service OR integrat* NEAR/3 care OR Coordinat* NEAR/3 care OR Co-ordinat* NEAR/3 service)) OR ((({joint working} OR {joint care} OR {joint service}) WN ALL))) OR ((($intermediate NEAR/3 $Care OR transition* NEAR/3 $Care OR $transfer NEAR/3 $Care OR $team NEAR/3 $Care OR $shared NEAR/3 $Care) WN ALL)) OR (((($interinstitution OR $interagency OR interdisciplin* OR interprofession* OR multiprofession* OR multidisciplin* OR multiagenc*)
AND
(relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR $care OR service*)) WN ALL) AND (1896-2019 WN YR)))))
AND
(2000-2019 WN YR))
132 results.
Ovid MEDLINE
Search date: 30 September 2018.
Date range searched: 1946 to September week 3 2018.
Search strategy
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (28,296)
-
“Delivery of Health Care, Integrated”/ (11,146)
-
*”Continuity of Patient Care”/ (9463)
-
(joint adj (working or care or service*)).tw,kw. (551)
-
Patient Transfer/ (7453)
-
*Patient Care Team/ (25,367)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (20,298)
-
Transitional Care/ (414)
-
Intermediate Care Facilities/ (675)
-
*interprofessional relations/or *interdisciplinary communication/ (25,620)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw,kw. (19,897)
-
or/1-11 [care co-ordination] (121,977)
-
exp Medical Records/ (135,875)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (68,814)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (16,030)
-
exp Decision Making, Computer-Assisted/(129,591)
-
(electronic adj3 record*).tw. (22,494)
-
((health or medical or clinical) adj5 (information or record*)).tw. (199,314)
-
Computer Systems/ (12,730)
-
or/13-19 [health records] (501,264)
-
Health Information Interoperability/ (64)
-
interoperab*.tw,kw. (2744)
-
21 or 22 (2769)
-
23 and 20 [interoperable records - based on theory search 3 interoperability] (1927)
-
Health Information Exchange/ (638)
-
24 or 25 (2499)
-
12 and 26 [coordinated care and interoperable systems] (270)
-
limit 27 to yr = “2000 -Current” (267)
-
limit 28 to “reviews (best balance of sensitivity and specificity)” (17)
Ovid MEDLINE In-Process & Other Non-Indexed Citations
Date searched: 28 September 2018.
Search strategy Same strategy as Ovid MEDLINE 1946 to September week 3 2018.
Ovid MEDLINE Epub Ahead of Print
Date searched: 25 September 2018.
Search strategy Same strategy as Ovid MEDLINE 1946 to September week 3 2018.
Sociological Abstracts (via ProQuest)
Search date: 30 September 2018.
Date range searched: 1952 to present.
Search strategy
(((TI,AB(electronic NEAR/3 record*) OR TI,AB((health or medical or clinical) NEAR/5 (information or record))) AND TI,AB(interoperab*)) OR TI,AB(“health information exchange”))
AND
(TI,AB((co-ordinat* OR coordinat* OR integrat* OR continuity) NEAR/3 (care OR service*)) OR TI,AB(joint NEAR/1 (working OR care OR service*)) OR TI,AB((intermediate OR transition* OR transfer* OR team*) NEAR/3 care) OR (MAINSUBJECT.EXACT(“Cooperation”) OR MAINSUBJECT.EXACT(“Teamwork”) OR MAINSUBJECT.EXACT(“Interdisciplinary Approach”)) OR TI,AB((interinstitution* OR interagenc* OR interdisciplin* OR Interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)))
Narrowed by: Document type: Review
n = 0
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 30 September 2018.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 2000–18.
Search strategy
-
# 17 #16 OR #15 (17)
-
# 16 #14 AND #13 (9)
-
# 15 #12 AND #5 Refined by: DOCUMENT TYPES: (REVIEW) (10)
-
# 14 TS = (meta-analysis or search*) (758,107)
-
# 13 #12 AND #5 (297)
-
# 12 #11 OR #10 (2350)
-
# 11 TOPIC: (“health information exchange”) (766)
-
# 10 #9 AND #8 (1700)
-
# 9 TOPIC: ((interoperab* or inter-operab*)) (24,924)
-
# 8 #7 OR #6 (198,344)
-
# 7 TOPIC: ((((health or medical or clinical) NEAR/5 (information or record*)))) (193,461)
-
# 6 TOPIC: (((electronic NEAR/3 record*))) (30,013)
-
# 5 #4 OR #3 OR #2 OR #1 (87,790)
-
# 4 TOPIC: ((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) near/6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)) (25,278)
-
# 3 TOPIC: ((intermediate or transition* or transfer* or team*) near/3 care) (23,166)
-
# 2 TOPIC: (joint near/1 (working or care or service)) (2884)
-
# 1 TOPIC: ((co-ordinat* or coordinat* or integrat* or continuity) NEAR/3 (care or service*)) (44,446)
Complementary searches
Forward citation searches of Fitzpatrick G, Ellingsen G. A review of 25 years of CSCW research in healthcare: contributions, challenges and future agendas. CSCW Conf Comput Support Coop Work 2013;22:609–65. In the following sources:
-
ACM Digital Library (full text) – 1947 to present
-
Google Scholar
-
Scopus (Elsevier) – 1823 to present
-
Web of Science Core Collection: Citation Indexes (Clarivate Analytics) – 1900 to present.
Do interoperable networks improve patient safety outcomes for frail older people living at home?
Structured database searches
Search date: 30 September 2018 and updated 3 March 2019.
Applied Social Sciences Index and Abstracts (via ProQuest)
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1987 to present.
Search strategy
((((MAINSUBJECT.EXACT(“Care”) OR MAINSUBJECT.EXACT(“Integrated care pathways”) OR MAINSUBJECT.EXACT(“Intermediate care”) OR MAINSUBJECT.EXACT(“Shared care”) OR MAINSUBJECT.EXACT(“Continuing care”) OR MAINSUBJECT.EXACT(“Home care”)) OR (MAINSUBJECT.EXACT(“Transition programmes”) OR MAINSUBJECT.EXACT(“Continuity”)) OR (MAINSUBJECT.EXACT(“Care coordinators”) OR MAINSUBJECT.EXACT(“Care management”) OR MAINSUBJECT.EXACT(“Care delivery”)) OR MAINSUBJECT.EXACT(“Joint working”)) OR TI,AB(joint NEAR/1 (working OR care OR service*)) OR TI,AB((intermediate OR transition* OR transfer* OR team*) NEAR/3 care) OR (MAINSUBJECT.EXACT.EXPLODE(“Interdisciplinary team work”) OR MAINSUBJECT.EXACT(“Interdisciplinary approach”)) OR TI,AB((interinstitution* OR interagenc* OR interdisciplin* OR Interprofession* OR multiprofessional* OR multidisciplin* OR multiagenc*) NEAR/6 (relations* OR collaborat* OR co-ordinat* OR coordinat* OR communicat* OR care OR service*)))
AND
(((((MAINSUBJECT.EXACT.EXPLODE(“Health records”) OR MAINSUBJECT.EXACT.EXPLODE(“Medical records”) OR MAINSUBJECT.EXACT(“Computerized medical records”)) OR MAINSUBJECT.EXACT(“Records”)) OR TI,AB(electronic NEAR/3 record*) OR TI,AB((health or medical or clinical) NEAR/5 (information or record))) AND TI,AB(interoperab*)) OR TI,AB(“information exchang*”)))
AND
((MAINSUBJECT.EXACT.EXPLODE(“Evaluation”) OR (MAINSUBJECT.EXACT(“Clinical effectiveness”) OR MAINSUBJECT.EXACT(“Medical effectiveness research”) OR MAINSUBJECT.EXACT(“Effectiveness”) OR MAINSUBJECT.EXACT(“Organizational effectiveness”) OR MAINSUBJECT.EXACT(“Cost effectiveness”)) OR (MAINSUBJECT.EXACT(“Total quality management”) OR MAINSUBJECT.EXACT(“Impact analysis”))) OR Ti,AB(evaluat* or impact or effectiveness))
n = 21
EMBASE (via Ovid)
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1996 to week 9 2019.
Search strategy
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (45,502)
-
integrated health care system/ (9937)
-
transitional care/ (1940)
-
*patient care/ (50,706)
-
(joint adj (working or care or service*)).tw,kw. (813)
-
patient transport/ (20,362)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (37,753)
-
Intermediate Care Facilities/ (33,832)
-
interdisciplinary communication/ (10,818)
-
((interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw. (35,024)
-
interpersonal communication/ (126,578)
-
public relations/ (37,525)
-
or/1-12 [care-coordination] (355,713)
-
exp medical record/ (194,712)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (83,582)
-
medical informatics/or nursing informatics/ (19,674)
-
(electronic adj3 record*).tw. (56,327)
-
((health or medical or clinical) adj5 (information or record*)).tw. (337,393)
-
computer system/ (20,773)
-
*medical information system/ (7264)
-
or/14-20 [health records & systems] (510,028)
-
data interoperability/ (117)
-
interoperab*.tw,kw. (3928)
-
22 or 23 (3975)
-
21 and 24 [interoperable records - based on theory search 3 interoperability] (2515)
-
*health information exchange/ (3887)
-
information exchang*.tw,kw. (3829)
-
or/25-27 [info exchange or records interoperability] (9666)
-
13 and 28 (1558)
-
exp evaluation study/ (55,500)
-
total quality management/ (52,914)
-
(evaluat* or impact or effectiveness).tw,kw. (4,914,881)
-
*health care quality/ (55,418)
-
outcome assessment/ (458,167)
-
30 or 31 or 32 or 33 or 34 (5,284,599)
-
29 and 35 (563)
-
limit 36 to conference abstract (137)
-
36 not 37 (426)
-
limit 38 to (english language and yr = “2000 -Current”) (405)
Inspec (EI Village)
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1896 to present.
Search strategy
(((((((((evaluat* OR $impact OR $effectiveness) WN KY)) OR ((((({computer network performance evaluation} WN CV) OR ({performance evaluation} WN CV))))))) AND ((((((((((((({electronic data interchange} WN CV))))) OR (((interoperab*) WN KY))))
AND
((((($electronic NEAR/3 record* OR $health NEAR/3 record* OR $medical NEAR/3 record* OR $clinical NEAR/3 record* OR $health NEAR/3 $information OR $medical NEAR/3 $information OR $Clinical NEAR/3 $information) WN KY)) OR ((((({electronic health records} WN CV) OR ({medical information systems} WN CV)))))))))) OR ((({health information exchange}) WN KY))))
AND
((((($continuity NEAR/3 $care OR $Continuity NEAR/3 service* OR integrat* NEAR/3 $care OR integrat* NEAR/3 service* OR coordinat* NEAR/3 $care OR Coordinat* NEAR/3 service*) WN KY)) OR (((($interinstitution OR $interagency OR interdisciplin* OR interprofession* OR multiprofession* OR Multidisciplin* OR Multiagenc*) AND (relations* OR Collaborat* OR Coordinat* OR Coordinat* OR Communicat* OR $care OR service*)) WN KY)) OR (((($intermediate NEAR/3 $care OR transition* NEAR/3 $care OR transfer* NEAR/3 $care OR team* NEAR/3 $care OR $shared NEAR/3 $care)) WN KY)) OR ((((({patient care} WN CV) OR ({professional communication} WN CV))))) OR ((({joint care} OR {joint working} OR {joint service*}) WN KY)
AND
(1896-2019 WN YR)))))))) NOT ((1999 OR 1998 OR 1997 OR 1996 OR 1995 OR 1994 OR 1989) WN YR))
n = 258
Ovid MEDLINE
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1996 to February week 4 2019.
Search strategy
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (25,475)
-
“Delivery of Health Care, Integrated”/ (11,164)
-
*”Continuity of Patient Care”/ (7990)
-
(joint adj (working or care or service*)).tw,kw. (437)
-
Patient Transfer/ (6382)
-
*Patient Care Team/ (18,805)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (18,067)
-
Transitional Care/ (468)
-
Intermediate Care Facilities/ (360)
-
*interprofessional relations/or *interdisciplinary communication/ (19,479)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw,kw. (18,762)
-
or/1-11 [care co-ordination] (101,963)
-
exp Medical Records/ (86,564)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (50,023)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (14,946)
-
exp Decision Making, Computer-Assisted/ (120,599)
-
(electronic adj3 record*).tw. (23,090)
-
((health or medical or clinical) adj5 (information or record*)).tw. (179,423)
-
Computer Systems/ (8476)
-
or/13-19 [health records] (410,352)
-
Health Information Interoperability/ (74)
-
interoperab*.tw,kw. (2830)
-
21 or 22 (2859)
-
23 and 20 [interoperable records - based on theory search 3 interoperability] (1963)
-
Health Information Exchange/ (671)
-
information exchang*.tw,kf. (2539)
-
or/24-26 [HIE or interoperable records] (4727)
-
12 and 27 (635)
-
“quality of healthcare”/ (50,954)
-
Quality Improvement/ (19,241)
-
exp program evaluation/ (64,176)
-
evaluation studies/or exp evaluation studies as topic/ (949,715)
-
(evaluat* or impact or effectiveness).tw,kw. (2,878,224)
-
“Outcome Assessment (Health Care)”/ (62,896)
-
“Process Assessment (Health Care)”/ (4027)
-
Quality Indicators, Health Care/ (14,355)
-
or/29-36 [evaluation] (3,547,278)
-
28 and 37 [evaluating interoperable care coordination] (273)
-
limit 38 to (english language and yr = “2000 -Current”) (255)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1946 to 1 March 2019.
Search strategy
Same strategy as Ovid MEDLINE 1996 to February week 4 2019.
Sociological Abstracts (via ProQuest)
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1952 to present.
Search strategy
((MAINSUBJECT.EXACT(“Quality”) OR MAINSUBJECT.EXACT(“Quality of Health Care”)) OR (MAINSUBJECT.EXACT(“Evaluation”) OR MAINSUBJECT.EXACT.EXPLODE(“Program Evaluation”) OR MAINSUBJECT.EXACT.EXPLODE(“Technology Assessment”)) OR MAINSUBJECT.EXACT.EXPLODE(“Effectiveness”))
AND
(TI,AB (evaluat* or impact or effectiveness))
n = 34
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 30 September 2018 and updated 3 March 2019.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 1900–2019.
Search strategy
-
#18 #16 AND #13 SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, ESCI Timespan = 2000-2019 (247)
-
# 17 #16 AND #13 (251)
-
# 16 #15 OR #14 (7,450,991)
-
# 15 TOPIC: (quality NEAR/3 (improvement* or healthcare or “health care”)) (96,954)
-
# 14 TOPIC: ((evaluat* or impact or effectiveness)) (7,392,745)
-
# 13 #12 AND #5 (678)
-
# 12 #11 OR #10 (14,578)
-
# 11 TS = (“ information exchang*”) (12,854)
-
# 10 #9 AND #8 (1937)
-
# 9 TOPIC: ((interoperab* or inter-operab*)) (27,738)
-
# 8 #7 OR #6 (237,037)
-
# 7 TOPIC: ((((health or medical or clinical) NEAR/5 (information or record*)))) (231,092)
-
# 6 TOPIC: (((electronic NEAR/3 record*))) (33,877)
-
# 5 #4 OR #3 OR #2 OR #1 (103,553)
-
# 4 TOPIC: ((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) near/6 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)) (29,498)
-
# 3 TOPIC: ((intermediate or transition* or transfer* or team*) near/3 care) (27,214)
-
# 2 TOPIC: (joint near/1 (working or care or service)) (3593)
-
# 1 TOPIC: ((co-ordinat* or coordinat* or integrat* or continuity) NEAR/3 (care or service*)) (52,368)
Complementary searches
Search date: 10 April 2019.
Google Scholar forward citation searches of:
Vimarlund V, Olve NG, Scandurra I, Koch S. Organizational effects of information and communication technology (ICT) in elderly homecare: a case study. Health Informatics J 2008;14:195–210. 33
Waterson P, Soares MM, Jacobs K, Eason K, Tutt D, Dent M. Using HIT to deliver integrated care for the frail elderly in the UK: current barriers and future challenges. Work 2012;41:4490–3. 34
King G, O’Donnell C, Boddy D, Smith F, Heaney D, Mair FS. Boundaries and e-health implementation in health and social care. BMC Med Inf Decis Mak 2012;12:100. 35
Evidence review: medication reconciliation for older people living at home
What is the nature of the medicine reconciliation problem in frail older people population?
Structured database searches
EMBASE (via Ovid)
Search date: 14 December 2018.
Date range searched: 1996 to week 50 2018.
Note: records downloaded from line 38 (reviews search) and line 42 (qualitative studies search).
Search strategy
-
exp qualitative research/ (58,974)
-
exp questionnaire/ (582,556)
-
exp interview/ (224,600)
-
interview*.tw,kw. (355,209)
-
qualitative.tw,kw. (215,788)
-
nursing methodology research/ (13,443)
-
questionnaire*.mp. (766,883)
-
survey*.mp. (963,944)
-
ethnolog*.mp. (60,189)
-
ethnograph*.mp. (10,319)
-
ethnonursing.af. (90)
-
phenomenol*.af. (25,685)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (12,366)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (21,081)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (4349)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (61,811)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (40,560)
-
cluster sampl*.mp. (7667)
-
observational method*.af. (2041)
-
content analysis.af. (27,040)
-
((discourse* or discurs*) adj3 analys?s).tw. (2084)
-
narrative analys?s.af. (1180)
-
or/1-22 [Qualitative Filter] (2,047,405)
-
*medication therapy management/ (3526)
-
exp *medication error/ (7536)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).ti,kw. (12,898)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).ti,kw. (1089)
-
(inappropriate prescribing or inappropriate prescription*).ti,kw. (977)
-
exp *inappropriate prescribing/ (1670)
-
((medicine* or medication) adj3 (review or management)).ti,kw. (5754)
-
“drug utilization review”/ (304)
-
or/24-31 [meds rec] (25,664)
-
exp *aged/ (27,394)
-
(elderly or geriatric*).tw. (284,835)
-
(old* adj1 (age or adult* or person* or patient)).tw. (194,590)
-
or/33-35 [focussed older pt] (452,120)
-
32 and 36 (2462)
-
limit 37 to (english language and “systematic review” and yr = “2000 -Current”) (109)
-
23 and 32 and 36 (554)
-
limit 39 to (english language and yr = “2000 -Current”) (519)
-
limit 40 to conference abstracts (147)
-
40 not 41 (372)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 14 December 2018.
Date range searched: 1946 to 12 December 2018.
Note: records downloaded from line 37 (reviews search) and line 39 (qualitative studies search).
Search strategy
-
exp qualitative research/ (42,909)
-
qualitative.tw,kf. (197,303)
-
Nursing Methodology Research/ (16,190)
-
observational study/ (55,507)
-
ethnolog*.mp. (153,408)
-
ethnograph*.mp. (9570)
-
ethnonursing.af. (108)
-
phenomenol*.af. (23,694)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (10,307)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (20,663)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (3761)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (54,815)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (14,207)
-
cluster sampl*.mp. (6469)
-
observational method*.af. (675)
-
content analysis.af. (22,875)
-
((discourse* or discurs*) adj3 analys?s).tw. (1956)
-
narrative analys?s.af. (1061)
-
or/1-18 [qualitative] (515,468)
-
“Surveys and Questionnaires”/ (413,145)
-
INTERVIEW/ (28,252)
-
interviews.tw,kf. (150,544)
-
or/19-22 [qual & interviews] (970,120)
-
exp *Medication Errors/ (10,626)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).ti,kw. (6769)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).ti,kw. (670)
-
((medicine* or medication) adj3 (review or management)).ti,kw. (3580)
-
“Drug Utilization Review”/ (3575)
-
(inappropriate prescribing or inappropriate prescription*).ti,kw. (606)
-
*Inappropriate Prescribing/ (1676)
-
or/24-30 [tight meds rec] (21,474)
-
exp *aged/ (24,847)
-
(elderly or geriatric*).tw. (252,221)
-
(old* adj1 (age or adult* or person* or patient)).tw. (166,191)
-
or/32-34 (403,927)
-
31 and 35 (1803)
-
limit 36 to (english language and yr = “2000 -Current” and systematic reviews) (140)
-
23 and 31 and 35 (252)
-
limit 38 to (english language and yr = “2000 -Current”) (223)
PsycINFO (via Ovid)
Search date: 14 December 2018.
Date range searched: 1806 to December week 1 2018.
Note: records downloaded from line 33 (reviews search) and line 35 (qualitative studies search).
Search strategy
-
exp qualitative research/ (8015)
-
questionnaires/ (17,465)
-
interviews/ (8164)
-
interview*.tw,id. (302,732)
-
qualitative.tw,id. (148,364)
-
questionnaire*.mp. (375,718)
-
survey*.mp. (306,730)
-
ethnolog*.mp. (2690)
-
ethnograph*.mp. (26,946)
-
ethnonursing.af. (138)
-
phenomenol*.af. (106,332)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (52,076)
-
(emic or etic or hermeneutic* or heuristic* or semiotic*).af. or (data adj1 saturat*).tw. or participant observ*.tw. (92,483)
-
(action research or cooperative inquir* or co operative inquir* or co-operative inquir*).mp. (8457)
-
((purpos* adj4 sampl*) or (focus adj group*)).af. (59,543)
-
(life world or life-world or conversation analys?s or personal experience* or theoretical saturation).mp. (14,066)
-
cluster sampl*.mp. (1423)
-
observational method*.af. (1994)
-
content analysis.af. (51,663)
-
((discourse* or discurs*) adj3 analys?s).tw. (8505)
-
narrative analys?s.af. (6468)
-
or/1-21 [Qualitative Filter] (1,118,848)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).tw. (3188)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).tw. (270)
-
((medicine* or medication) adj3 (review or management)).tw. (3003)
-
(inappropriate prescribing or inappropriate prescription*).tw. (245)
-
or/23-26 [med Rec] (6414)
-
geriatric patients/ (12,889)
-
(elderly or geriatric*).tw. (71,023)
-
(old* adj1 (age or adult* or person* or patient)).tw. (72,103)
-
or/28-30 (130,504)
-
27 and 31 (732)
-
limit 32 to (english language and “reviews (maximizes specificity)” and yr = “2000 -Current”) (52)
-
22 and 27 and 31 (209)
-
limit 34 to (english language and yr = “2000 -Current”) (193)
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 14 December 2018.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 2000–18.
Note: records downloaded from line 40 (reviews search) and line 41 (qualitative studies search).
Search strategy
-
# 41 (#39 AND #36 AND #31) AND LANGUAGE: (English)Timespan = 2000-2018 (414)
-
# 40 (#39 AND #36) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Review) Timespan = 2000-2018 (274)
-
# 39 #38 OR #37 (556,063)
-
# 38 TOPIC: ((old* NEAR/1 (age or adult* or person* or patient)).) (310,703)
-
# 37 TOPIC: (elderly or geriatric*) (307,597)
-
# 36 #35 OR #34 OR #33 OR #32 (17,068)
-
# 35 TI = (((medicine* or medication) NEAR/3 (review or management))) (4894)
-
# 34 TS = ((“inappropriate prescribing” or “inappropriate prescription*”)) (1581)
-
# 33 TS = ((prescrib* or prescription*) NEAR/3 (safety or error* or discrepanc* or reconciliation)) (3536)
-
# 32 TI = (((drug* or medicine* or medication*) NEAR/3 (error* or discrepanc* or reconciliation* or safety))) (7839)
-
# 31 #30 OR #29 OR #28 OR #27 OR #26 OR #25 OR #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18 OR #17 OR #16 OR #15 OR #14 OR #13 OR #12 OR #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 (5,935,626)
-
# 30 TS = (narrative analys?s) (29,138)
-
# 29 TS = (discourse analys?s) or TS = (discurs* analys?s) (47,161)
-
# 28 TS = (constant comparative) (13,874)
-
# 27 TS = (content analysis) (429,822)
-
# 26 TS = observational method* (96,128)
-
# 25 TS = (cluster sampl*) (110,512)
-
# 24 TS = (lived experience*) OR TS = (life experience*) (227,063)
-
# 23 TS = (life world) OR TS = (conversation analys?s) OR TS = (theoretical saturation) (99,750)
-
# 22 TS = (open-ended account*) OR TS = (unstructured account) OR TS = (narrative*) OR TS = (text*) (693,982)
-
# 21 TS = (purposive sampl*) (8614)
-
# 20 TS = (theoretical sampl*) (72,461)
-
# 19 TS = (biographical method*) (1660)
-
# 18 TS = (human science) (134,004)
-
# 17 TS = (field stud*) OR TS = (field research) (1,361,559)
-
# 16 TS = (humanistic) OR TS = (existential) OR TS = (experiential) OR TS = (paradigm*) (295,094)
-
# 15 TS = (action research) OR TS = (co-operative inquir*) (111,334)
-
# 14 TS = (social construct*) OR TS = (postmodern*) OR TS = (post structural*) OR TS = (feminis*) OR TS = (interpret*) (1,047,850)
-
# 13 TS = (emic) OR TS = (etic) OR TS = (hermeneutic) OR TS = (heuristic) OR TS = (semiotic) OR TS = (data saturat*) OR TS = (participant observ*) (325,003)
-
# 12 TS = (life stor*) OR TS = (women’s stor*) (77,757)
-
# 11 TS = (grounded theor*) OR TS = (grounded stud*) OR TS = (grounded research) OR TS = (grounded analys?s) (392,859)
-
# 10 TS = (phenomenol*) (97,714)
-
# 9 TS = (ethnological research) (329)
-
# 8 TS = (ethnonursing) (61)
-
# 7 TS = (ethnograph*) (47,723)
-
# 6 TS = (questionnaire) (541,312)
-
# 5 TS = (nursing research methodology) (3099)
-
# 4 TS = (qualitative) (396,431)
-
# 3 TS = (thematic analysis) (30,065)
-
# 2 TS = (theme*) (143,321)
-
# 1 TS = (interview*) (457,600)
Complementary searches
Two Google searches were run; the first used the phrase ‘Nature of Medicine Reconciliation problem’ and second used the terms ‘medicine reconciliation, barriers, ethnography, qualitative’. The first 50 records were screened from each search. A total of 17 references were potentially relevant and included for further screening.
What are professionals’ experiences of using interoperable networks in medicine reconciliation for frail older people?
Structured database searches
These specific searches were designed to retrieve the Vashitz and colleagues papers119,120 and those with similar concepts.
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 29 November 2018.
Date range searched: 1946 to 27 November 2018.
Search strategy
-
exp Medication Errors/ (15,326)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).ti,kw. (6762)
-
(inappropriate prescribing or inappropriate prescription*).tw,kw. (1562)
-
Inappropriate Prescribing/ (2395)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).ti,kw. (670)
-
((medicine* or medication) adj3 (review or management)).ti,kw. (3567)
-
*”Drug Utilization Review”/ (2012)
-
or/1-7 [medicines reconciliation] (25,073)
-
*Clinical Decision-Making/ (1962)
-
Heuristics/ (297)
-
*decision making/ (37,627)
-
(cognit* adj3 (step* or task* or reason* or process* or analys* or error* or mistake*)).tw. (35,271)
-
thinking/ (15,151)
-
(diagnostic adj2 (knowledge or judgement or reasoning)).tw. (1002)
-
(clinical adj2 (knowledge or judgement or reasoning)).ti,kw. (1897)
-
heuristic*.tw. (10,382)
-
((prescrib* or prescription*) adj2 (choice* or decision* or process*)).ti,kw. (228)
-
or/9-17 [cognitive tasks] (100,525)
-
8 and 18 (170)
-
limit 19 to english language (164)
PsycINFO (via Ovid)
Search date: 29 November 2018.
Date range searched: 1806 to November week 4 2018.
Search strategy
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).tw. (3185)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).tw. (270)
-
(inappropriate prescribing or inappropriate prescription*).tw. (244)
-
((medicine* or medication) adj3 (review* or management)).tw. (3409)
-
or/1-4 [medicines reconciliation] (6805)
-
(cognit* adj3 (step* or task* or reason* or process* or analys* or error* or mistake*)).tw. (60,429)
-
*Decision Making/ (54,907)
-
*”Cognitions”/ (6786)
-
heuristics/ (3326)
-
(diagnostic adj2 (knowledge or judgement or reasoning)).tw. (434)
-
(clinical adj2 (knowledge or judgement or reasoning)).ti. (735)
-
heuristic*.tw. (14,130)
-
((prescrib* or prescription*) adj2 (choice* or decision* or process*)).ti. (56)
-
exp reasoning/ (24,798)
-
cognitive processes/ (70,647)
-
or/6-15 [cognitive tasks] (200,582)
-
5 and 16 (148)
-
limit 17 to english language (144)
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 29 November 2018.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 2000–18.
Search strategy
-
# 13 (#11 AND #5) AND LANGUAGE: (English) (78)
-
# 12 #11 AND #5 (80)
-
# 11 #10 OR #9 OR #8 OR #7 OR #6 (184,189)
-
# 10 TI = (((prescrib* or prescription*) NEAR/2 (choice* or decision* or process*))) (350)
-
# 9 TOPIC: (heuristic*) (114,793)
-
# 8 TI = ((clinical NEAR/2 (knowledge or judgement or reasoning))) (3348)
-
# 7 TOPIC: ((diagnostic NEAR/2 (knowledge or judgement or reasoning))) (2879)
-
# 6 TOPIC: ((cognit* NEAR/3 (step* or task* or reason* or process* or analys* or error* or mistake*))) (63,853)
-
# 5 #4 OR #3 OR #2 OR #1 (17,010)
-
# 4 TI = (((medicine* or medication) NEAR/3 (review or management))) (4879)
-
# 3 TOPIC: ((“inappropriate prescribing” or “inappropriate prescription*”)) (1565)
-
# 2 TOPIC: ((prescrib* or prescription*) NEAR/3 (safety or error* or discrepanc* or reconciliation)) (3528)
-
# 1 TI = (((drug* or medicine* or medication*) NEAR/3 (error* or discrepanc* or reconciliation* or safety))) (7818)
Complementary searches
We searched Google Scholar in December 2018 using the terms ‘medicine reconciliation’ and ‘clinicians cognition’ to identify key papers exploring clinicians’ rationalisation and making sense of the fragmented disjoint medication information. The first 50 records were screened. This led us to identify a book chapter: Cook RI. Medication Reconciliation is a Window Into ‘Ordinary’ Work. In Smith P, editor. Cognitive Systems Engineering. Boca Raton, FL: CRC Press; 2017. pp. 53–76. 124
We hand-searched the reference list in Cook,124 which led us to identify two further studies:119,120
-
Vashitz G, Nunnally ME, Parmet Y, Bitan Y, O’Connor MF, Cook RI. How do clinicians reconcile conditions and medications? The cognitive context of medication reconciliation. Cogn Technol Work 2011;15:109–16. 119
-
Vashitz G, Nunnally ME, Bitan Y, Parmet Y, O’Connor MF, Cook RI. Making sense of diseases in medication reconciliation. Cogn Technol Work 2011;13:151–8. 120
We conducted forward and backward citation searches in Web of Science for the above studies.
What are the patient outcomes of using interoperable networks in medicine reconciliation?
Structured database searches
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
Search date: 29 December 2018.
Date range searched: 1981 to present.
Search strategy
-
S23 S13 AND S21 Limiters - English Language; Published Date: 20000101-20190131 (115)
-
S22 S13 AND S21 (118)
-
S21 S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 (29,326)
-
S20 TI (inappropriate prescribing or inappropriate prescription*) OR AB (inappropriate prescribing or inappropriate prescription*) (1077)
-
S19 (MH “Inappropriate Prescribing”) (1790)
-
S18 TI ((medicine* or medication) N3 (review or management)) OR AB ((medicine* or medication) N3 (review or management)) (8238)
-
S17 TI ((prescrib* or prescription*) N3 (safety or error* or discrepanc* or reconciliation)) OR ((prescrib* or prescription*) N3 (safety or error* or discrepanc* or reconciliation)) (1364)
-
S16 TI ((drug* or medicine* or medication*) N3 (error* or discrepanc* or reconciliation* or safety)) OR AB ((drug* or medicine* or medication*) N3 (error* or discrepanc* or reconciliation* or safety)) (11,690)
-
S15 (MH “Medication Reconciliation”) (1336)
-
S14 (MH “Medication Errors+”) (14,014)
-
S13 S10 OR S11 OR S12 (6167)
-
S12 TI information exchang* OR AB information exchang* (2695)
-
S11 (MH “Electronic Data Interchange+”) OR (MH “Health Care Information Exchange (Iowa NIC)”) (3130)
-
S10 S8 AND S9 (1070)
-
S9 TI (interoperab* or inter-operab*) OR AB (interoperab* or inter-operab*) (1594)
-
S8 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 (229,710)
-
S7 (MH “Computer Systems”) (1802)
-
S6 TI ((health or medical or clinical) N5 (information or record*)) OR AB ((health or medical or clinical) N5 (information or record*)) (89,751)
-
S5 TI (electronic N3 record*) OR AB (electronic N3 record*) (16,641)
-
S4 (MH “Decision Making, Computer Assisted+”) (36,843)
-
S3 (MH “Health Informatics+”) (12,213)
-
S2 (MH “Information Systems”) OR (MH “Health Information Systems+”) (51,203)
-
S1 (MH “Medical Records+”) (88,785)
EMBASE (via Ovid)
Search date: 29 December 2018.
Date range searched: 1996 to week 53 2018.
Search strategy
-
exp medical record/ (192,230)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (82,903)
-
medical informatics/or nursing informatics.mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] (19,823)
-
(electronic adj3 record*).tw. (54,793)
-
((health or medical or clinical) adj5 (information or record*)).tw. (332,154)
-
computer system/ (20,765)
-
*medical information system/ (7209)
-
or/1-7 [health records and systems] (503,935)
-
data interoperability/ (102)
-
1interoperab*.tw,kw. (3839)
-
9 or 10 (3879)
-
8 and 11 (2479)
-
information exchange.tw,kw. (3484)
-
or/12-13 (5771)
-
medication therapy management/ (9126)
-
exp medication error/ (16,437)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).tw,kw. (33,640)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).tw,kw. (3812)
-
(inappropriate prescribing or inappropriate prescription*).tw,kw. (2523)
-
((medicine* or medication) adj3 (review or management)).tw,kw. (17,135)
-
“drug utilization review”/ (314)
-
or/15-21 [medicines reconciliation] (64,138)
-
14 and 22 (188)
-
limit 23 to (english language and yr = “2000 -Current”) (183)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 29 December 2018.
Date range searched: 1946 to 26 December 2018.
Search strategy
-
exp Medical Records/ (137,059)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (69,366)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (16,168)
-
exp Decision Making, Computer-Assisted/ (131,543)
-
(electronic adj3 record*).tw. (29,521)
-
((health or medical or clinical) adj5 (information or record*)).tw. (237,174)
-
Computer Systems/ (12,789)
-
or/1-7 [medical records] (543,132)
-
Health Information Interoperability/ (65)
-
interoperab*.tw,kw. (3561)
-
or/9-10 (3586)
-
8 and 11 (2208)
-
Health Information Exchange/ (661)
-
information exchang*.tw,kw. (3343)
-
or/12-14 [HIE or interoperability] (5754)
-
exp Medication Errors/ (15,389)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).tw,kw. (20,422)
-
(inappropriate prescribing or inappropriate prescription*).tw,kw. (1568)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).tw,kw. (2219)
-
((medicine* or medication) adj3 (review or management)).tw,kw. (10,587)
-
“Drug Utilization Review”/ (3582)
-
or/16-21 [medicines reconciliation] (45,032)
-
15 and 22 (130)
-
limit 23 to (english language and yr = “2000 -Current”) (128)
PsycINFO (via Ovid)
Search date: 29 December 2018.
Date range search: 1806 to December week 4 2018.
Search strategy
-
exp medical records/ (3506)
-
exp information systems/or decision support systems/ (36,629)
-
(electronic adj3 record*).tw. (3681)
-
((health or medical or clinical) adj5 (information or record*)).tw. (108,603)
-
or/1-4 [records] (144,480)
-
interoperab*.tw. (513)
-
5 and 6 [interoperable records] (202)
-
information exchang*.tw. (1778)
-
7 or 8 [HIE or interoperability] (1960)
-
((drug* or medicine* or medication*) adj3 (error* or discrepanc* or reconciliation* or safety)).tw. (3192)
-
((prescrib* or prescription*) adj3 (safety or error* or discrepanc* or reconciliation)).tw. (271)
-
(inappropriate prescribing or inappropriate prescription*).tw. (246)
-
((medicine* or medication) adj3 (review or management)).tw. (3008)
-
or/10-13 [medicines reconciliation] (6424)
-
9 and 14 (18)
limit 15 to (english language and yr = “2000 -Current”) (17)
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 29 December 2018.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 2000–18.
Search strategy
-
# 14 #13 AND #8 (135)
-
# 13 #12 OR #11 OR #10 OR #9 (39,463)
-
# 12 TOPIC: (“inappropriate prescribing” or “inappropriate prescription*”) (1471)
-
# 11 TOPIC: ((medicine* or medication) NEAR/3 (review or management)) (14,452)
-
# 10 TS = ((prescrib* or prescription*) NEAR/3 (safety or error* or discrepanc* or reconciliation)) (3277)
-
# 9 TOPIC: (((drug* or medicine* or medication*) NEAR/3 (error* or discrepanc* or reconciliation* or safety)).) (23,025)
-
# 8 #7 OR #6 (15,833)
-
# 7 TS = (“information exchang*”) (11,377)
-
# 6 #5 AND #4 (4806)
-
# 5 TOPIC: (interoperab* or inter-operab*) (25,504)
-
# 4 #3 OR #2 OR #1 (560,712)
-
# 3 TOPIC: ((information or computer* or clinical or health) NEAR/5 system*) (382,181)
-
# 2 TOPIC: ((health or medical or clinical) NEAR/5 (information or record*)) (199,473)
-
# 1 TOPIC: (electronic NEAR/3 record*) (31,329)
Evidence review: the co-ordination of services for at-risk children
What is the nature and extent of the coordination problem for services for at-risk children?
Structured database searches
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
Search date: 10 May 2019.
Date range searched: 1981 to present.
Search strategy
-
S27 S16 AND S24 Limiters - Published Date: 20000101-20191231; Clinical Queries: Review - Best Balance (159)
-
S26 S16 AND S24 Limiters - Clinical Queries: Review - Best Balance (171)
-
S25 S16 AND S24 (1611)
-
S24 S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 (68,118)
-
S23 TI (Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) N3 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*) OR AB (Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) N3 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*) (12,903)
-
S22 (MM “Cooperative Behavior”) (3065)
-
S21 (MM “Interinstitutional Relations”) (3762)
-
S20 (MM “Interprofessional Relations”) (9180)
-
S19 TI (intermediate or transition* or transfer* or team*) N3 care OR AB (intermediate or transition* or transfer* or team*) N3 care (20,674)
-
S18 TI (joint N1 (working or care or service*)) OR AB (joint N1 (working or care or service*)) (725)
-
S17 TI (co-ordinat* or coordinat* or integrat* or continuity) N3 (care or service*) OR AB (co-ordinat* or coordinat* or integrat* or continuity) N3 (care or service*) (27,033)
-
S16 S8 OR S15 (69,105)
-
S15 S11 AND S14 (6042)
-
S14 S12 OR S13 (1,015,355)
-
S13 TI ((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) OR AB ((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) (622,122)
-
S12 ((MH “Child+”) OR (MH “Adolescence+”)) (834,505)
-
S11 S9 OR S10 (26,844)
-
S10 (MM “Social Welfare”) OR (MM”Social Work”) (8896)
-
S9 TI (“complex needs” OR safeguard* OR “social care” OR “social worker*”) OR AB (“complex needs” OR safeguard* OR “social care” OR “social worker*”) (19,996)
-
S8 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 (65,337)
-
S7 (MH “Orphans and Orphanages”) OR (TI (children* adj home*) OR AB (children* adj home*)) (1102)
-
S6 TI ((foster N1 (care or home*))) OR AB ((foster N1 (care or home*))) (2595)
-
S5 TI ((foster* or “looked after”) and child*) OR AB ((foster* or “looked after”) and child*) (4284)
-
S4 (MM “Foster Home Care”) (2736)
-
S3 TI (((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N2 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) OR AB (((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N2 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) (40,960)
-
S2 TI (child* N3 (protect* or welfare)) OR AB (child* N3 (protect* or welfare)) (8766)
-
S1 (MM “Child Welfare+”) OR (MM “Child Abuse+”) OR (MM “Child Safety”) (24,370)
EMBASE (via Ovid)
Search date: 10 May 2019.
Date range searched: 1996 to week 18 2019.
Search strategy
-
exp *child welfare/ (6410)
-
exp *child abuse/ (15,215)
-
(child* adj3 (protect* or welfare)).tw,kw. (11,746)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj2 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,kw. (39,832)
-
(foster adj (care or home*)).tw,kw. (2215)
-
(Children* adj home*).tw,kw. (599)
-
foster care/or orphanage/ (4077)
-
((foster* or “looked after”) and child*).tw,kw. (6071)
-
or/1-8 (63,615)
-
(social care or social worker*).tw,kw. (17,754)
-
*social welfare/or *social work/or *social care/ (9667)
-
(“complex needs” or Safeguard*).tw,kw. (12,128)
-
or/10-12 (36,980)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (1,866,490)
-
exp juvenile/ (2,309,698)
-
13 and (14 or 15) (8069)
-
9 or 16 [child protection] (69,911)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (46,843)
-
(joint adj (working or care or service*)).tw,kw. (832)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (38,891)
-
*public relations/ (17,511)
-
*interdisciplinary communication/or *interpersonal communication/ (35,520)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj3 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw,kw. (27,479)
-
*cooperation/or *teamwork/ (14,872)
-
or/18-24 [care coordination] (161,347)
-
17 and 25 (2450)
-
limit 26 to “reviews (best balance of sensitivity and specificity)” (328)
-
limit 27 to (english language and yr = “2000 -Current”) (271)
Health Management Information Consortium (via Ovid)
Search date: 10 May 2019.
Date range searched: 1983 to present.
Search strategy
-
child welfare/or child abuse/ (2336)
-
child protection services/or foster care services/or youth services/ (1293)
-
(child* adj3 (protect* or welfare)).tw,hw. (3248)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj2 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,hw. (3324)
-
exp foster care/ (677)
-
((foster* or “looked after”) and child*).tw,hw. (1555)
-
(foster adj (care or home*)).tw,hw. (872)
-
(children* adj home*).tw,hw. (1072)
-
orphan*.tw,hw. (105)
-
children in care/or exp community homes/ (2417)
-
or/1-10 [child protection] (8916)
-
social care.tw,hw. (17,382)
-
exp social welfare/or exp social work/ (10,132)
-
social worker*.tw,hw. (6600)
-
(“complex needs” or safeguard*).tw,hw. (1906)
-
or/12-15 (32,104)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (38,826)
-
exp children/or exp young people/ (26,934)
-
16 and (17 or 18) (5708)
-
11 or 19 [child protection] (11,955)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,hw. (6749)
-
(joint adj (working or care or service*)).tw,hw. (2678)
-
collaborative care/or integrated care/or interagency collaboration/or joint working/ (5730)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,hw. (4181)
-
exp interorganisational relations/or exp interprofessional relations/ (5523)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj3 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw,hw. (6400)
-
or/21-26 [care coordination] (17,937)
-
20 and 27 (833)
-
((comprehensive* or integrative or systematic* or scoping) adj3 (bibliographic* or review* or literature)).tw,hw. (5548)
-
(meta-analy* or metaanaly* or “research synthesis” or “evidence synthesis”).tw,hw. (1912)
-
((information or data) adj3 synthesis).tw,hw. (207)
-
(data adj2 extract*).tw,hw. (1042)
-
(“Search filter*” or “search strateg*” or “literature search*”).tw. (1135)
-
((“mixed method*” or qualitative or realist) adj3 (synthesis or review)).tw,hw. (341)
-
or/29-34 [review types] (7391)
-
28 and 35 (5)
-
limit 36 to yr = “2000 -Current” (5)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 10 May 2019.
Date range searched: 1946 to 3 May 2019.
Search strategy
-
exp *Child Welfare/ (20,303)
-
exp *Child Abuse/ (22,657)
-
Child Protective Services/ (326)
-
(child* adj3 (protect* or welfare)).tw,kw. (11,695)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj2 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,kw. (37,761)
-
Foster Home Care/or orphanages/ (3861)
-
((foster* or “looked after”) and child*).tw,kw. (5720)
-
(foster adj (care or home*)).tw,kf. (2447)
-
(children* adj home*).tw,kf. (794)
-
or/1-9 (77,940)
-
“complex needs”.kw,tw. (1308)
-
safeguard*.tw,kf. (9604)
-
(social care or social worker*).tw,kw. (14,514)
-
exp *social welfare/or exp *social work/ (47,032)
-
or/11-14 (68,661)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (1,952,690)
-
exp Child/or Adolescent/or exp Infant/ (3,399,022)
-
15 and (16 or 17) (32,253)
-
10 or 18 [child protection] (87,460)
-
((co-ordinat* or coordinat* or integrat* or continuity) adj3 (care or service*)).tw,kw. (35,751)
-
(joint adj (working or care or service*)).tw,kw. (655)
-
((intermediate or transition* or transfer* or team*) adj3 care).tw,kw. (25,480)
-
*interprofessional relations/or *interdisciplinary communication/ (26,231)
-
((Interinstitution* or interagenc* or interdisciplin* or interprofession* or multiprofessional* or multidisciplin* or multiagenc*) adj3 (relations* or collaborat* or co-ordinat* or coordinat* or communicat* or care or service*)).tw,kw. (18,925)
-
*Interinstitutional Relations/ (4446)
-
*cooperative behavior/ (16,851)
-
or/20-26 [care coordination] (113,458)
-
19 and 27 (1708)
-
limit 28 to “reviews (best balance of sensitivity and specificity)” (259)
-
limit 29 to (english language and yr = “2000 -Current”) (207)
What are clinicians’ and other professionals’ experiences of using interoperable health information technology to co-ordinate the care of children at risk and what are the effects of interoperable networks on outcomes for at-risk children?
Structured database searches
Applied Social Sciences Index and Abstracts (via ProQuest)
Search date: 29 March 2019.
Date range searched: 1987 to present.
Search strategy
-
S1 (MAINSUBJECT.EXACT.EXPLODE(“Health records”) OR MAINSUBJECT.EXACT.EXPLODE(“Medical records”) OR MAINSUBJECT.EXACT(“Computerized medical records”)) OR MAINSUBJECT.EXACT(“Records”) (2591)
-
S2 TI,AB(electronic NEAR/3 record*) (2040)
-
S3 TI,AB((health or medical or clinical) NEAR/5 (information or record)) (16,105)
-
S4 S1 OR S2 OR S3 (17,410)
-
S5 TI,AB(interoperab*) (103)
-
S6 S4 and S5 (47)
-
S7 TI,AB(“information exchang*”) (440)
-
S8 TI,AB(information NEAR/2 shar*) (1784)
-
S9 S6 OR S7 OR S8 (2209)
-
S10 MAINSUBJECT.EXACT.EXPLODE(“Child welfare”) AND (MAINSUBJECT.EXACT.EXPLODE(“Child maltreatment”) OR MAINSUBJECT.EXACT.EXPLODE(“Child abuse”) OR MAINSUBJECT.EXACT.EXPLODE(“Child neglect”)) (431)
-
S11 MAINSUBJECT.EXACT.EXPLODE(“Child welfare”) OR (MAINSUBJECT.EXACT.EXPLODE(“Child maltreatment”) OR MAINSUBJECT.EXACT.EXPLODE(“Child abuse”) OR MAINSUBJECT.EXACT.EXPLODE(“Child neglect”)) (8967)
-
S12 MAINSUBJECT.EXACT.EXPLODE(“Child protection”) (2352)
-
S13 MAINSUBJECT.EXACT(“Orphanages”) OR MAINSUBJECT.EXACT.EXPLODE(“Foster care”) (3074)
-
S14 TI,AB(child* NEAR/3 (protect* or welfare)) (9194)
-
S15 TI,AB((child* or infant* or baby or babies or adolescen* or teen* or youth* or juvenile* or paediatric* or paediatric*) NEAR/4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) (23,383)
-
S16 TI,AB((foster* or “looked after”) and child*). (4957)
-
S17 TI,AB((foster or residential OR children*) NEAR/1 (care or home*)) (8895)
-
S18 TI,AB(orphan*) (1083)
-
S19 S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 (42,192)
-
S20 MAINSUBJECT.EXACT(“Social care”) OR MAINSUBJECT.EXACT(“Social welfare”) OR MAINSUBJECT.EXACT.EXPLODE(“Social work”) (28,099)
-
S21 TI,AB(“complex needs” OR safeguard* or “social care” or “social worker*”) (21,097)
-
S22 MAINSUBJECT.EXACT.EXPLODE(“Children”) OR MAINSUBJECT.EXACT.EXPLODE(“Adolescents”) (117,450)
-
S23 TI,AB(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) (256,581)
-
S24 (S20 OR S21) AND (S22 OR S23) (15,283)
-
S25 S9 AND (S19 OR S24) (145)
-
S26 TI,AB(“child* protection information”) (5)
-
S27 S25 OR S26 (148)
-
S28 (S25 OR S26) AND yr(2000-2019) (137)
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
Search date: 29 March 2019.
Date range searched: 1981 to present.
Search strategy
-
S35 s32 or s33 Limiters - Published Date: 20000101- (237)
-
S34 S32 OR S33 (247)
-
S33 TI “child* protection information” OR AB “child* protection information” (7)
-
S32 S13 AND S31 (243)
-
S31 S22 OR S30 (101,683)
-
S30 S26 AND S29 (8172)
-
S29 S27 OR S28 (1,002,488)
-
S28 ((MH “Child+”) OR (MH “Adolescence+”)) (826,514)
-
S27 TI ((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) OR AB ((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) (611,880)
-
S26 S23 OR S24 OR S25 (38,490)
-
S25 (MH “Social Welfare”) OR (MH “Social Work”) (15,525)
-
S24 (MH “Residential Facilities”) OR (MH “Assisted Living”) (6501)
-
S23 TI (“complex needs” OR safeguard* OR “social care” OR “social worker*”) OR AB (“complex needs” OR safeguard* OR “social care” OR “social worker*”) (19,726)
-
S22 S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 (97,180)
-
S21 (MH “Orphans and Orphanages”) (1095)
-
S20 TI (orphan*) OR AB (orphan*) (2476)
-
S19 TI (((foster or residential or children*) N1 (care or home*))) OR AB (((foster or residential or children*) N1 (care or home*))) (14,766)
-
S18 TI ((foster* or “looked after”) and child*) OR AB ((foster* or “looked after”) and child*) (4161)
-
S17 (MH “Foster Home Care”) (3974)
-
S16 TI (((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) OR AB (((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) (53,074)
-
S15 TI (child* N3 (protect* or welfare)) OR AB (child* N3 (protect* or welfare)) (8598)
-
S14 (MH “Child Welfare+”) OR (MH “Child Abuse+”) OR (MH “Child Safety”) (35,023)
-
S13 S9 OR S10 OR S11 OR S12 (8756)
-
S12 TI (information N2 shar*) OR AB (information N2 shar*) (4155)
-
S11 TI “information exchang*” OR AB “information exchang*” (1668)
-
S10 (MH “Health Care Information Exchange (Iowa NIC)”) OR (MH “Electronic Data Interchange”) (2755)
-
S9 S7 AND S8 (999)
-
S8 TI interoperab* OR AB interoperab* (1642)
-
S7 S1 OR S2 OR S3 OR S4 OR S5 OR S6 (182,082)
-
S6 (MH “Computer Systems”) (1824)
-
S5 TI ((health or medical or clinical) N5 (information or record*)) OR AB ((health or medical or clinical) N5 (information or record*)) (92,449)
-
S4 TI electronic N3 record* OR AB electronic N3 record* (17,310)
-
S3 ((MH “Health Informatics”) OR (MH “Nursing Informatics”) OR (MH “Medical Informatics”)) OR (MH “Decision Making, Computer Assisted”) (10,693)
-
S2 (MH “Information Systems”) OR (MH “Health Information Systems”) OR (MH “Management Information Systems+”) (11,550)
-
S1 (MH “Medical Records+”) (89,799)
Criminal Justice Abstracts (via EBSCOhost)
Search date: 29 March 2019.
Date range searched: 1830 to present.
Search strategy
-
S32 S29 OR S30 Limiters - Published Date: 20000101-20191231 (73)
-
S31 S29 OR S30 (88)
-
S30 TI “child* protection information” OR AB “child* protection information” (2)
-
S29 S11 AND S28 (86)
-
S28 S20 OR S27 (28,010)
-
S27 S23 AND S26 (2050)
-
S26 S24 OR S25 (89,604)
-
S25 (((ZU “children”) or (ZU “infants”)) or ((ZU “teenagers”))) or ((ZU “toddlers”)) (6417)
-
S24 TI (child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) OR AB (child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) (89,407)
-
S23 S21 OR S22 (7502)
-
S22 (ZU “social workers”) (3160)
-
S21 TI ((“complex needs” OR Safeguar* OR “social care” OR “social worker*”) OR AB ((“complex needs” OR Safeguar* OR “social care” OR “social worker*”) (6590)
-
S20 S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 (27,157)
-
S19 TI orphan* OR AB orphan* (236)
-
S18 TI (((foster or residential or children*) N1 (care or home*))) OR AB (((foster or residential or children*) N1 (care or home*))) (2820)
-
S17 ((((ZW “group homes”))) or ((ZU “orphanages”) or (ZU “orphans”))) or ((ZU “group homes for children”)) (145)
-
S16 TI ((foster* or “looked after”) and child*) OR AB ((foster* or “looked after”) and child*) (1952)
-
S15 ((ZW “foster care”) or (ZU “foster children”)) or ((ZW “looked after children”)) (695)
-
S14 TI ((((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”))) OR AB ((((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) N4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”))) (18,695)
-
S13 TI (child* N3 (protect* or welfare)) OR AB (child* N3 (protect* or welfare)) (6399)
-
S12 ((((((ZU “child protection services”)) or ((ZW “child protection”))) or ((ZW “child welfare”))) or ((ZU “child welfare”))) or ((ZU “child abuse”))) or ((ZW “child abuse”) or (ZW “child abuse & neglect”)) (10,957)
-
S11 S7 OR S8 OR S9 OR S10 (1407)
-
S10 TI “information exchang*” OR AB “information exchang*” (195)
-
S9 (ZU “information sharing”) (385)
-
S8 TI information N2 shar* OR AB information N2 shar* (1080)
-
S7 S5 AND S6 (31)
-
S6 TI interoperab* OR AB interoperab* (285)
-
S5 S1 OR S2 OR S3 OR S4 (7060)
-
S4 TI (“information system*” OR “information technolog*”) OR AB (“information system*” OR “information technolog*”) (2846)
-
S3 (((((ZU “electronic records”)) or ((ZW “electronic records”))) or ((ZU “medical records”))) or ((ZU “computer systems”))) or ((ZU “information technology”)) (2455)
-
S2 TI ((health or medical or clinical) N5 (information or record*)) OR AB ((health or medical or clinical) N5 (information or record*)) (2930)
-
S1 TI electronic N3 record* OR AB electronic N3 record* (377)
EMBASE (via Ovid)
Search date: 29 March 2019.
Date range searched: 1996 to week 12 2019.
Search strategy
-
exp medical record/ (195,666)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (83,862)
-
medical informatics/or nursing informatics/ (19,734)
-
(electronic adj3 record*).tw. (56,765)
-
((health or medical or clinical) adj5 (information or record*)).tw. (339,394)
-
computer system/ (20,815)
-
*medical information system/ (7280)
-
or/1-7 [health records & systems] (512,665)
-
data interoperability/ (123)
-
interoperab*.tw,kw. (3957)
-
9 or 10 (4009)
-
8 and 11 [interoperable records - based on theory search 3 interoperability] (2536)
-
*health information exchange/ (3903)
-
information exchang*.tw,kw. (3856)
-
(information adj2 shar*).tw,kw. (8172)
-
or/12-15 [HIE or interoperable records] (17,536)
-
exp child welfare/ (12,511)
-
exp child abuse/ (27,245)
-
(child* adj3 (protect* or welfare)).tw,kw. (11,587)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,kf. (48,251)
-
((foster or residential or children*) adj (care or home*)).tw,kw. (7168)
-
orphan*.tw,kw. (20,217)
-
foster care/or orphanage/ (4048)
-
((foster* or “looked after”) and child*).tw,kw. (5979)
-
or/17-24 (104,463)
-
assisted living facility/or residential care/or residential home/ (15,726)
-
social care.tw,kw. (6399)
-
social welfare/or social work/or social care/ (34,843)
-
social worker*.tw,kw. (11,096)
-
(“complex needs” or Safeguard*).tw,kw. (11,907)
-
or/26-30 (72,651)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (1,840,170)
-
exp juvenile/ (2,279,545)
-
31 and (32 or 33) (16,042)
-
25 or 34 [child protection] (116,436)
-
16 and 35 [HIE and child protection] (260)
-
child* protection information.tw,kw. [named system] (6)
-
36 or 37 (265)
-
limit 38 to yr = “2000 -Current” (261)
Health Management Information Consortium (via Ovid)
Search date: 29 March 2019.
Date range searched: 1983 to present.
Search strategy
-
exp medical records/ (3183)
-
information technology/or exp information systems/or exp informatics/ (8981)
-
(electronic adj3 record*).tw. (1347)
-
((health or medical or clinical) adj5 (information or record*)).tw. (10,035)
-
exp computer systems/ (4552)
-
or/1-5 [health records] (21,256)
-
interoperab*.tw,hw. (90)
-
6 and 7 (76)
-
exp information exchange/ (424)
-
information exchang*.tw,hw. (554)
-
(information adj2 shar*).tw,hw. (755)
-
or/8-11 [HIE or interoperable records] (1349)
-
child welfare/or child abuse/ (2336)
-
child protection services/or foster care services/or youth services/ (1293)
-
(child* adj3 (protect* or welfare)).tw,hw. (3248)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,hw. (3643)
-
exp foster care/ (677)
-
((foster* or “looked after”) and child*).tw,hw. (1555)
-
((foster or residential or children*) adj (care or home*)).tw,hw. (7430)
-
orphan*.tw,hw. (105)
-
or/13-20 (13,484)
-
exp residential care/or care homes/ (6848)
-
exp community homes/ (1015)
-
social care.tw,hw. (17,382)
-
exp social welfare/or exp social work/ (10,132)
-
social worker*.tw,hw. (6600)
-
(“complex needs” or safeguard*).tw,hw. (1906)
-
or/22-27 (37,980)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (38,826)
-
exp children/or exp young people/ (26,934)
-
28 and (29 or 30) (7670)
-
31 or 21 [child protection] (16,750)
-
12 and 32 [HIE and child protection] (100)
-
child* protection information.tw,hw. (2)
-
33 or 34 (101)
-
limit 35 to yr = “2000 -Current” (62)
Inspec (EI Village)
Search date: 29 March 2019.
Date range searched: 1896 to present.
Search strategy
((“child* protection information”) WN KY) OR (((((child* NEAR abuse* OR child* NEAR neglect* OR child* NEAR mistreat* OR child* NEAR maltreat* OR child* NEAR $vulnerable OR child* NEAR {at risk}) WN KY) OR ((($foster NEAR/2 $care OR $foster NEAR/2 home* OR $residential NEAR/2 $care OR $residential NEAR/2 home* OR children* NEAR/2 $care OR children* NEAR/2 home*) WN KY) OR (((foster* AND child*) WN KY) AND OR ((({Looked after} AND child*) WN KY) OR (((orphan*) WN KY) OR (((child* NEAR/3 protect* OR child* NEAR/3 $welfare) WN KY) OR (((((({complex needs} OR safeguard* OR 48 OR {social worker*}) WN KY) OR ((((({public administration} WN CV))))
AND
(((child* OR infant* OR $baby OR $babies OR toddler* OR adolescen* OR teen* OR youth* OR juvenile* OR pediatric* OR paediatric*) WN KY) AND (((((((((interoperab*) WN ALL))) OR ((((({electronic data interchange} WN CV)))) AND ((((((({electronic health records} WN CV) OR ({medical information systems} WN CV)))) OR ((($electronic NEAR/3 record* OR $health NEAR/3 record* OR $medical NEAR/3 record* OR $clinical NEAR/3 record* OR $health NEAR/3 $information OR $medical NEAR/3 $information OR $Clinical NEAR/3 $information) WN ALL) OR ((({health information exchange}) WN ALL) OR ((($Information NEAR/2 shar*) WN KY)
AND
(1896-2019 WN YR))))
Ovid MEDLINE
Search date: 29 March 2019.
Date range searched: 1996 to March week 4 2019.
Search strategy
-
exp Medical Records/ (87,257)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (50,239)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (15,021)
-
exp Decision Making, Computer-Assisted/ (121,476)
-
(electronic adj3 record*).tw. (23,413)
-
((health or medical or clinical) adj5 (information or record*)).tw. (180,921)
-
Computer Systems/ (8496)
-
or/1-7 [health records] (413,430)
-
Health Information Interoperability/ (82)
-
interoperab*.tw,kw. (2852)
-
9 or 10 (2886)
-
11 and 8 [interoperable records - based on theory search 3 interoperability] (1979)
-
Health Information Exchange/ (677)
-
information exchang*.tw,kf. (2554)
-
(information adj2 shar*).tw,kw. (4820)
-
or/12-15 [HIE or interoperable records] (9348)
-
exp Child Welfare/ (18,706)
-
exp Child Abuse/ (19,268)
-
Child Protective Services/ (305)
-
(child* adj3 (protect* or welfare)).tw,kf. (7880)
-
((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) adj4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)).tw,kf. (32,132)
-
Foster Home Care/or orphanages/ (2456)
-
((foster* or “looked after”) and child*).tw,kw. (3729)
-
((foster or residential or children*) adj (care or home*)).tw,kf. (4804)
-
orphan*.tw,kf. (12,712)
-
or/17-25 (78,067)
-
residential facilities/or assisted living facilities/or group homes/ (4561)
-
“complex needs”.kw,tw. (973)
-
safeguard*.tw,kf. (6491)
-
(social care or social worker*).tw,kf. (9286)
-
exp Social Welfare/or exp Social Work/ (42,897)
-
or/27-31 (60,795)
-
(child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*).tw. (1,143,084)
-
exp Child/or Adolescent/or exp Infant/ (1,934,185)
-
32 and (33 or 34) (30,454)
-
26 or 35 [child protection] (87,387)
-
36 and 16 [HIE and child protection] (145)
-
child* protection information.tw,kf. [named system] (3)
-
37 or 38 (148)
-
limit 39 to yr = “2000 -Current” (140)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 29 March 2019.
Date range searched: 1946 to 28 March 2019.
Search strategy same as Ovid MEDLINE.
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 29 March 2019.
Date range searched: 1900 to present.
Indexes: Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index – Science, Conference Proceedings Citation Index – Social Science & Humanities, Emerging Sources Citation Index.
Time span: 2000–19.
Search strategy
-
#20 #18 OR #17 (283)
-
#19 #18 OR #17 (298)
-
#18 TOPIC: (“child* protection information”) (5)
-
#17 #16 AND #8 (294)
-
#16 #15 OR #14 OR #13 OR #12 OR #11 OR #10 OR #9 (138,832)
-
#15 TS = ((“social care” OR “social worker*”) AND (child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) (4719)
-
#14 TOPIC: (orphan*) (23,566)
-
#13 TS = ((foster or residential or children*) NEAR/1 (care or home*)) (28,852)
-
#12 TOPIC: ((foster* or “looked after”) and child*) (12,765)
-
#11 TS = ((“complex needs” OR Safeguard*) AND (child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*)) (1968)
-
#10 TS = ((child* or infant* or baby or babies or toddler* or adolescen* or teen* or youth* or juvenile* or pediatric* or paediatric*) NEAR/4 (abuse* or neglect* or mistreat* or maltreat* or vulnerable or “at risk”)) (65,690)
-
#9 TOPIC: (child* NEAR/3 (protect* or welfare)) (20,386)
-
#8 #7 OR #6 OR #5 (42,439)
-
#7 TS = (information NEAR/2 shar*) (28,833)
-
#6 TS = (“ information exchang*”) (12,958)
-
#5 #4 AND #3 (1949)
-
#4 TOPIC: ((interoperab* or inter-operab*)) (27,947)
-
#3 #2 OR #1 (238,843)
-
#2 TOPIC: ((((health or medical or clinical) NEAR/5 (information or record*)))) (232,870)
-
#1 TOPIC: (((electronic NEAR/3 record*))) (34,280)
Evidence review: economies of scope and scale of interoperable networks in health economies
Structured database search
EMBASE Classic and EMBASE (via Ovid)
Search date: 10 June 2019.
Date range searched: 1947 to 7 June 2019.
Search strategy
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (3351)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (338)
-
*medical information system/ (7541)
-
data interoperability/ (152)
-
or/1-4 (10,865)
-
exp medical record/ (229,767)
-
information system/or exp decision support system/or exp hospital information system/or medical information system/or nursing information system/or exp computerized provider order entry/ (101,938)
-
medical informatics/or nursing informatics/ (20,881)
-
(electronic adj3 record*).tw. (59,998)
-
((health or medical or clinical) adj5 (information or record*)).tw. (381,886)
-
computer system/ (25,497)
-
or/6-11 [health records & systems] (597,968)
-
exp computer network/ (14,592)
-
information dissemination/ (19,867)
-
(network* or exchange* or data shar*).tw. (825,591)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (21,662)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (3662)
-
(interoperab* or inter-operab*).tw. (4017)
-
or/13-18 [networked systems] (874,650)
-
12 and 19 (40,184)
-
20 or 5 [Networked IT or HIEs] (46,456)
-
(econom* adj3 (scope or scale)).tw,kw. (1923)
-
(diseconom* adj3 (scope or scale)).tw,kw. (68)
-
(efficienc* adj3 (scope or scale)).tw,kw. (854)
-
or/22-24 (2779)
-
21 and 25 (28)
Health Management Information Consortium (via Ovid)
Search date: 10 June 2019.
Date range searched: 1983 to present.
Search strategy
-
information exchange/ (349)
-
exp Medical information exchange/ (20)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw. (110)
-
(patient information adj5 (exchang* or shar* or network*)).tw. (39)
-
or/1-4 (494)
-
exp medical records/ (3194)
-
information technology/ (4873)
-
exp information systems/ (4907)
-
exp informatics/ (311)
-
(electronic adj3 record*).tw. (1351)
-
((health or medical or clinical) adj5 (information or record*)).tw. (10,080)
-
exp computer systems/ (4553)
-
or/6-12 [health records] (21,324)
-
exp information transfer/ (2008)
-
exp computer networks/ (1684)
-
(network* or exchange* or data shar*).tw. (7273)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (1365)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (147)
-
(interoperab* or inter-operab*).tw. (98)
-
or/14-19 [networked] (11,518)
-
13 and 20 (3393)
-
21 or 5 [networked IT, HIE] (3632)
-
(econom* adj3 (scope or scale)).tw. (153)
-
(diseconom* adj3 (scope or scale)).tw. (8)
-
(efficienc* adj3 (scope or scale)).tw,kw. (20)
-
or/23-25 (172)
-
22 and 26 [Economy of scope in networked systems] (6)
Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily
Search date: 10 June 2019.
Date range searched: 1946 to May week 5 2019 and 7 June 2019.
Search strategy
-
health information exchange/ (705)
-
((health information or medical information or clinical information) adj5 (exchang* or shar* or network*)).tw,kw. (2816)
-
(patient information adj5 (exchang* or shar* or network*)).tw,kw. (269)
-
Health Information Interoperability/ (91)
-
or/1-4 (3587)
-
exp Medical Records/ (139,237)
-
information systems/or decision support systems, clinical/or health information systems/or exp management information systems/ (70,403)
-
medical informatics/or medical informatics applications/or medical informatics computing/or nursing informatics/or public health informatics/ (16,459)
-
exp Decision Making, Computer-Assisted/ (135,429)
-
(electronic adj3 record*).tw. (31,681)
-
((health or medical or clinical) adj5 (information or record*)).tw. (246,632)
-
Computer Systems/ (12,876)
-
or/6-12 [health records] (558,899)
-
community network/ (6666)
-
computer communication networks/or local area networks/ (14,149)
-
information dissemination/ (15,405)
-
(network* or exchange* or data shar*).tw. (681,622)
-
(information adj3 (shar* or distribut* or disseminat*)).tw. (16,912)
-
(record* adj3 (shar* or distribut* or disseminat*)).tw. (2981)
-
(interoperab* or inter-operab*).tw. (3757)
-
or/14-20 [networking systems] (726,237)
-
21 and 13 (34,476)
-
22 or 5 [Networked IT systems] (35,007)
-
(econom* adj3 (scope or scale)).tw,kw. (1438)
-
(diseconom* adj3 (scope or scale)).tw,kw. (60)
-
(efficienc* adj3 (scope or scale)).tw,kw. (702)
-
or/24-26 (2151)
-
23 and 27 [Economy of scope in networked systems] (23)
Research Papers in Economics (EconPapers, Örebro University Business School)
Search date: 12 June 2019.
Search strategy
JEL Code I* AND Keywords & title: Economies of scope AND free text: “health information exchange” 0
JEL Code I* AND Keywords & title: Economies of scope AND free text: “information exchange” 0
JEL Code I* AND Keywords & title: Economies of scope AND free text inter-operab* or interoperab*
JEL Code I* AND Keywords & title: Economies of scope AND free text “electronic record* 0 (also clinical record, patient record medical record
JEL Code I* AND Keywords & title: Economies of scope AND free text: information technology 0/7
JEL Code I* AND Keywords & title: Economies of scope AND free text network 0
Repeated above using “economies of scale”.
Scopus (Elsevier)
Search date: 11 June 2019.
Date range searched: 1823 to present.
Search strategy
((((TITLE-ABS-KEY (“health information exchange”)) OR (TITLE-ABS-KEY ((“health information” OR “medical information” OR “clinical information” OR “patient information”) W/5 (exchang* OR shar* OR network*)))) OR (((TITLE-ABS-KEY (electronic W/3 record*)) OR (TITLE-ABS-KEY ((health OR medical OR clinical) W/5 (information OR record*))) OR (TITLE-ABS-KEY (((medical OR nursing OR health) W/2 informatics))) OR (TITLE-ABS-KEY (“information system*” OR “decision support system*” OR “computer system*”)))
AND
((TITLE-ABS-KEY (network* OR exchang* OR “data shar*”)) OR (TITLE-ABS-KEY ((information W/3 (shar* OR distribut* OR disseminat*)))) OR (TITLE-ABS-KEY ((record* W/3 (shar* OR distribut* OR disseminat*)))) OR (TITLE-ABS-KEY (interoperab* OR inter-operab*)))))
AND
(TITLE-ABS-KEY ((econom* OR diseconom* OR efficienc*) W/3 (scope OR scale))))
AND
(TITLE-ABS-KEY (health* OR medical OR clinical OR patient OR hospital))
n = 48
Web of Science Core Collection: Citation Indexes (Clarivate Analytics)
Search date: 10 June 2019.
Date range searched: 1900 to present.
Search strategy
-
#21 #20 AND #16 (66)
-
#20 #19 OR #18 OR #17 (19,781)
-
#19 TOPIC: (efficienc* NEAR/3 (scope or scale)) (6998)
-
#18 TOPIC: (diseconom* NEAR/3 (scope or scale)) (374)
-
#17 TOPIC: (econom* NEAR/3 (scope or scale)) (13,011)
-
#16 #15 OR #4 (49,960)
-
#15 #14 AND #9 (49,815)
-
#14 #13 OR #12 OR #11 OR #10 (2,869,294)
-
#13 TOPIC: (interoperab* or inter-operab*) (28,397)
-
#12 TOPIC: (record* NEAR/3 (shar* or distribut* or disseminat*)) (11,454)
-
#11 TOPIC: (information NEAR/3 (shar* OR distribut* OR disseminat*)) (72,876)
-
#10 TOPIC: (network* OR exchang* OR “data shar*”) (2,791,494)
-
#9 #8 OR #7 OR #6 OR #5 (403,909)
-
#8 TOPIC: (“information system*” or “decision support system*” or “computer system*”) (170,763)
-
#7 TOPIC: ((medical or nursing or health) NEAR/2 informatics) (7345)
-
#6 TOPIC: ((health or medical or clinical) NEAR/5 (information or record*)) (237,499)
-
#5 TOPIC: (electronic NEAR/3 record*) (35,309)
-
#4 #3 OR #2 OR #1 (2910)
-
#3 TOPIC: (“patient information” NEAR/5 (exchang* or shar* or network)) (240)
-
#2 TOPIC: ((“health information” or “medical information” or “clinical information”) NEAR/5 (exchang* or shar* or network*)) (2710)
-
#1 TOPIC: (“health information exchange”) (854)
Appendix 2 Paper for nominal group meetings
Appendix 3 Feedback paper sent to stakeholders in July 2019
University of Leeds logo reproduced with permission.
Appendix 4 Interview topic guide
University of Leeds logo reproduced with permission.
List of abbreviations
- CPOE
- computerised physician order entry
- EHR
- electronic health record
- e-SSA
- electronic version of single shared assessment
- GP
- general practitioner
- HIE
- health information exchange
- HIT
- health information technology
- IT
- information technology
- MeSH
- medical subject heading
- PPI
- patient and public involvement
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RAMESES
- Realist And Meta-narrative Evidence Syntheses: Evolving Standards