
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 08/20/03. The contractual start date was in March 2011. The draft report began editorial review in January 2014 and was accepted for publication in August 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Rona Campbell receives personal fees from the Wellcome Trust for work as a member of an Expert Review Group. She is also Director of DECIPHer Impact Limited, a not-for-profit company that is wholly owned by the University of Bristol and Cardiff University.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Mezey et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
This chapter situates the necessity for developing effective interventions to reduce rates of teenage pregnancy in the context of recent shifts in policy discourses, outlines the rationale for mounting a peer mentoring intervention specifically to reduce rates of teenage pregnancy in looked-after children (LAC) and discusses research on peer mentoring, all of which have led to the aims and objectives of our study. The structure of the report is also outlined.
Teenage pregnancy in the UK
Teenage pregnancy rates in England (under 18 years and under 16 years) are compiled by the Office for National Statistics (ONS), combining information from birth registration and abortion notifications. Data for 2008 showed that there were 38,750 conceptions in the under-18 age group, a rate of 40.5 per 1000 girls aged 15–17 years. This is a fall of 13.3% in the under 18s and a fall of 11.7% in the under 16s since the start of the teenage pregnancy strategy in 1998. 1 The under-18 conception rate for 2011 was the lowest since 1969 at 30.9 per 1000 women aged 15–17 years. 2 However, rates of teenage pregnancy in the UK remain among the highest in Europe. 3 Data on births per 1000 population among women aged 15–19 years in countries of the Organisation for Economic Co-operation and Development in 19984 and from the United Nations Population Division5 in 1994 illustrate that rates of teenage pregnancy in the UK are more than three times higher than in Switzerland, the Netherlands, Italy and France. Teenage parenthood may be negotiated positively by some young people6,7 and early motherhood can be perceived as a means of rectifying early negative life experiences. 8 However, it is also associated with a wide range of adverse socioeconomic and health outcomes for them and their children. 9–16
Teenage pregnancy has been recognised as an important cause, and consequence, of social exclusion. 17 Women who give birth as teenagers are more likely to be living in poverty than women who delay becoming mothers. 9,11,15 Furthermore, the children of teenage parents are more likely to become teenage parents themselves, suggesting a continuing intergenerational impact. 12
The association between socioeconomic deprivation and teenage pregnancy is widely evidenced in the UK. 16,18–20 In response to the report that identified teenage pregnancy as both a cause and a consequence of social exclusion,17 the UK Government set up the Teenage Pregnancy Unit (TPU) in 1999. The unit embarked on a strategy aimed at halving the rate of conception in under 18s over the following 10 years. Risk factors for teenage pregnancy include educational disadvantage and low expectations for employment; a lack of accurate information about contraception and sexually transmitted infections (STIs); and sexualised images in the media combined with a lack of openness about sex. 17 Using multiple regression data from all local authorities in England, Bradshaw and colleagues21 found that deprivation explained about three-quarters of area variation in teenage conceptions and abortions. A systematic review of 10 controlled trials and five qualitative studies evaluating early childhood interventions or youth development programmes found that the main associations with early pregnancy were dislike of school, poor material circumstances and an unhappy childhood and low expectations for the future. 22
Teenage pregnancy and looked-after children
The term ‘looked-after children’ is used in England to refer to children who are in the care of the state. Children and young people can be subject to a care order (Section 31 of the Children Act 198923) but the term ‘looked-after children’ is also used to describe children and young people who are looked after on a voluntary basis at the request of, or by agreement with, their parents (Section 20 of the Children Act 198923). Children may also be removed from their parents and placed in care on a non-voluntary basis, for example under an assessment or an emergency protection order. The majority of LAC (75%) in England are placed with foster carers. 24
There is a strong link between teenage pregnancy and age of first intercourse. The third National Survey of Sexual Attitudes and Lifestyles (NatSAL) found that the median age of first sexual intercourse among young people (both males and females) aged 16–24 years in the UK is 16 years; however, 31% of young people report having had sex before the age of 16 years. 25 LAC generally become sexually active earlier than other groups of young people26 and between 20% and 50% of those aged 16–19 years with a background of care become parents compared with a rate of around 5% in the general population. 27–30 One recent study found that one-quarter of young women leaving care were pregnant or were young parents within a year of leaving care31 and, once pregnant, young women who have been in care are more likely to continue a pregnancy to term. 32
Looked-after children are more likely to have experienced several of the risk factors for social exclusion than children living at home. 27,33–39 They typically report disrupted and unstable family backgrounds and experience frequent placement moves, which threaten and undermine their emotional and physical security and which are associated with unplanned pregnancies and early motherhood. 16,40–44 LAC are at greater risk of disengaging from education, truancy and school exclusion than non-LAC,45 which are risk factors for and may be exacerbated by teenage parenthood. 46–48 Educational outcomes for LAC remain poor compared with those for other children. In 2012, only 15% of LAC achieved grades A* to C GCSEs (General Certificate of Secondary Education) in English and mathematics at Key Stage 4, compared with 58% of young people who were not looked after. 49
Disengagement and low educational attainment are risk factors for becoming NEET (not in education, employment or training) and LAC are around twice as likely to be identified as NEET at the age of 19 years as a non-looked-after group. 24 They also have higher rates of learning difficulties,39 which may impair their ability to understand and negotiate safe and stable sexual relationships and their knowledge and decision-making around contraceptive use and fertility.
Looked-after children are also much less likely to receive meaningful sex and relationships education (SRE) from their parents or carers than children living with their family of origin. 50 Following the establishment of the TPU, SRE was introduced in schools to help improve knowledge and awareness and to address the problem of teenage pregnancy. 51,52 However, high rates of truancy and school exclusion51,52 and frequent placement moves mean that LAC are more likely to miss out on curriculum-based SRE, as well as health interventions and other school-based interventions to reduce teenage pregnancy, than non-LAC. 36,37,53 Based on an investigation of the effect of the 1972 education reform, known as the Raising of School Leaving Age, a recent research study predicts that teenage fertility rates will fall in response to legislative changes from summer 2013 that will require 16- and 17-year-olds to participate in education or training. 54
Looked-after children are around three times more likely to run away or go missing than non-LAC. 55,56 This in turn puts them at risk of being physically or sexually abused or exploited. 57–60 Perhaps not surprisingly, therefore, a disproportionate number of sex workers are, or were previously, LAC. 61–64 In 2011, the Child Exploitation and Online Protection Centre gathered data on 2083 victims of sexual exploitation and found that 311 (34.7%) of 896 children whose living situation was known were looked after at the time of the exploitation. 28
Childhood abuse and neglect increase the risk of a young person becoming a teenage parent65–67 and can also give rise to long-term mental health problems. 68 Various studies have reported significantly higher rates of mental health problems among LAC than among other disadvantaged young people who lived in private households. 69,70 A national survey of the health of LAC by the ONS found that 45% had at least one type of mental disorder and two-thirds had at least one physical health complaint. 70 The same research found that, compared with children in private households, LAC were around three times more likely to drink regularly, four times more likely to smoke and four times more likely to be taking drugs. 70
The policy perspective
Teenage pregnancy
In the UK, policy discourses around the prevention of teenage pregnancy have changed in recent years. The Teenage Pregnancy Strategy71 resulted in various positive outcomes, such as an increased number of school- and college-based contraception and sexual health (CaSH) services and support for teenage parents through, for example, Care to Learn, which helps towards childcare costs for young people aged < 20 years who wish to study, and the Family Nurse Partnerships, which aim to improve pregnancy outcomes for first-time mothers. In some areas where there was effective implementation of the strategy the rate of under-18 conceptions fell by up to 45% from the 1998 baseline1 (under-18 conceptions in England as a whole fell by 13% from the 1998 baseline to 2008). Immediate challenges to maintaining the achievements of the Teenage Pregnancy Strategy were identified as public spending cuts, a lack of young person-friendly CaSH services and variation in provision and quality as well as unequal provision of SRE. 1
Since the change of government in 2010, the aim of reducing teenage pregnancy has come to be positioned within the remit of improving health inequalities. In 2012, the TPU was disbanded and responsibility for improving the quality of SRE in schools and colleges and integrating it within personal, social, health and economic education (PSHE) was taken over by the Department for Education. Subsequent initiatives included increasing the availability of young person-friendly CaSH services and targeted SRE advice for groups of young people at risk of teenage pregnancy. From April 2013, local authority (LA) health and well-being boards have had a statutory duty to improve the health and well-being of the local population and reduce health inequalities, through joint strategic needs assessments, as well as to support young people to prevent unhealthy lifestyle choices, which include risky sexual behaviour. 72 Reducing the rates of teenage pregnancy and STIs now forms a key part of the work of local areas to tackle child poverty and address health inequalities. 72 This reflects research evidence that illustrates the impact of socioeconomic disadvantage on rates of teenage pregnancy.
Looked-after children
In March 2012 there were just over 67,000 children and young people in England and Wales under the care of local authorities, designated as ‘looked after’. This is an increase of 13% compared with 31 March 2008. 24 The increase in care applications in recent years can, in part, be attributed to a number of high-profile cases involving the deaths of young children, which it was judged could have been prevented if they had been removed from their homes at an earlier stage. 73,74 In 2012 the Children and Family Court Advisory and Support Service (Cafcass), which safeguards the welfare of children involved in family court proceedings, received a record amount of care applications and they are expected to rise further as a result of changes to the benefits system. 75 Recent amendments to the Children and Families Bill76 have increased the age at which children in England can remain with their foster parents, from 18 years to 21 years, which it is hoped will encourage LAC to remain in education for longer.
Child protection policy in the UK is based on the Children Acts 198923 and 200477 and in the past decade a raft of major initiatives has been introduced to promote the rights and health and welfare of children and young people. In the wake of the enquiry into the death of Victoria Climbie in 2000, the government published the Keeping Children Safe report,73 the Every Child Matters programme78 and the Children Act 2004. 77 The 2010 Working Together to Safeguard Children guidance79 outlines statutory and non-statutory guidance on how organisations and individuals should ensure that services are ‘joined up’ and the National Healthy Care Standard [see www.ncb.org.uk/media/173813/healthy_care_standard_entitlements_and_outcomes.pdf (accessed 21 July 2015)] is intended to help LAC and young people achieve the five outcomes described in Every Child Matters. 78 In recent years, the Care Matters White Paper80 and the Children and Young Persons Act 200881 created independent reviewing officers to oversee the process of placement moves of young people in care and brought in higher education bursaries and other changes designed to encourage them to remain in education for longer.
Statutory and other guidance on promoting the health and well-being of LAC82,83 were brought in to improve collaborative working between local authorities, primary care trusts (PCTs) and strategic health authorities (SHAs) and to collect, monitor and share information more effectively. Following successful piloting of virtual school heads to promote the educational achievement of LAC,84 and in response to the latest statistics on educational GCSE outcomes for LAC,49 the government intends to enshrine in law a virtual head teacher for LAC in every council. 85 However, there is still a lack of consistent support and advocacy for LAC and care leavers. Various barriers to participation for LAC have been documented, including a lack of an advocate to take proactive action on their behalf, lack of meaningful and sensitive involvement in their education plans, lack of an effective voice at reviews and lack of confidentiality. 86–89
Rationale for developing a peer mentoring intervention to reduce pregnancy in looked-after children
Positive youth development and peer support
Although the TPU considered that the decline in the under-18 conception rate in some LA areas had occurred as a result of targeted work with LAC and care leavers,90 there has been no independent evaluation of the effectiveness of the various measures put in place to address this issue and none using an experimental design.
Positive youth development (PYD) programmes, focusing on the development of strong bonds with appropriate adults and maintaining regular involvement in positive activities, appear to be more successful at preventing young people from engaging in risky behaviours than programmes that focus on the ‘problem’ that has to be solved. 91 A systematic review including a statistical meta-analysis of controlled trials of early childhood interventions and youth development programmes showed that the teenage pregnancy rate was 39% lower amongst individuals receiving an intervention than amongst those receiving standard practice or no intervention [relative risk 0.61; 95% confidence interval (CI) 0.48 to 0.77]. 22 The interventions aimed to promote engagement with school and counter the effects of early adverse experiences through learning support, guidance and social support and to raise aspirations through career development and work experience.
One systematic review of PYD programmes in the USA, using experimental or quasi-experimental evaluation design,92 found 15 programmes that had led to an improvement in at least one sexual and reproductive health outcome for young people. However, a non-randomised UK study to evaluate the effectiveness of development programmes for young people at reducing teenage pregnancy, substance use and other outcomes93 found no evidence of effectiveness and some suggestion of an adverse effect. Methodological limitations of this study may have affected outcomes and it was recommended that any further implementation of PYD programmes in the UK should be randomised trials.
A number of studies have focused on peer support, which includes mentoring, befriending, counselling and other types of support provided by someone who has knowledge, or experience, relevant to their mentee. 94–97 The Randomised Intervention trial of PuPil-Led sex Education in schools (RIPPLE) project, which employed peer educators to provide sex education within schools, appeared to be effective in reducing self-reported pregnancies by the age of 18 years. 95 An informal, peer-led approach to adolescent smoking prevention has also been shown to be effective. 96 However, the only comprehensive systematic review of the effectiveness of peer-led health promotion interventions for young people, half of which were concerned with sexual health, concluded that, although a peer-led approach was promising, there were too few studies to be able to identify what constituted an effective model. 97
Mentoring and peer mentoring
‘Mentoring’ is a somewhat ambiguous concept that has been used as a broad term to describe a variety of interventions and practices. 98,99 A common thread linking all mentoring schemes is the development of a trusting relationship between an older, more experienced person and a younger, less experienced person over an extended period of time, with the aim of providing social support. 98 The UK-based Mentoring and Befriending Foundation (MBF) advises that mentoring usually involves some form of goal-oriented work in addition to building a relationship, which is the cornerstone of befriending. 98 Mentoring can take place in a formal or an ‘artificial’ context, in which the mentor is acting in a voluntary or paid capacity, involving an external organisation, or it can be naturally occurring, usually involving a non-familial adult who is already present in the young person’s life. 99,100
There has been an increase in ‘peer mentoring’ programmes in recent years101 and particularly in schools. 102 However, the definition of ‘peer mentoring’ varies widely across programmes. Over one-third of schools in England operate some form of peer mentoring/peer support scheme to reduce bullying and promote self-confidence and self-esteem, some of which have been effective. 102 The MBF review102 of peer mentoring programmes in schools demonstrated the interchangeable use of the terms ‘peer education’, ‘peer support’, ‘peer befriending’, ‘peer buddying’ and others. Most programmes characterise the ‘peer’ element in relation to mentors being slightly older than, or having had similar life experiences to, the young people who they are supporting. In relation to LAC, the Scottish Government’s report Peer Mentoring Opportunities for Looked After Children and Care Leavers103 identified the most important criterion for being a peer as having a shared experience of being in care.
Impacts of peer mentoring schemes have been variable. In 2006, the MBF conducted a national pilot of formalised peer mentoring schemes in 180 secondary schools in England. Self-report and qualitative data demonstrated some benefits; however, there was no clear impact on pupils’ behaviour, school attendance or educational attainment. 104 A study of year 10 students supporting year 7 pupils with the transition from primary to secondary school found that, following the mentoring, year 7 pupils reported increased self-esteem and confidence and less anxiety. 105
A US meta-analysis of 55 evaluations of mentoring programmes found small benefits in general from mentoring but greater benefits for disadvantaged youth. 106 Very few controlled evaluations of mentoring have been carried out in the UK. However, an evaluation of the Mentoring Plus programme found that mentoring had positive impacts on training, education and work engagement in disaffected young people. 107,108 There were no clear impacts on offending, which was a general aim of the programme rather than a goal set as part of the programme.
Peer mentoring and policy
The concept of peer mentoring for LAC is consistent with the coalition government’s key factors for success, particularly ‘aspirational personal and social development programmes, targeted SRE and sexual health advice for at risk groups of young people’ (p. 49) and the requirement on local areas to address child poverty and health inequalities. 73 There is little evidence for the effectiveness of using peer mentors, as opposed to adult mentors, for LAC and care leavers; however, non-peer mentoring for care leavers has been shown to increase confidence, self-esteem and aspirations. 109 One large-scale study, supported by the Department for Children, Schools and Families (DCSF), evaluated one-to-one mentoring relationships to increase educational engagement and performance for 449 LAC aged 10–15 years. 110 The programmes were managed mainly by voluntary organisations and the majority of mentors were adults, although some providers included peer mentors. The evaluation found marked improvements in school work, attendance and participation in hobbies and social activities, as well as in young people’s feelings about themselves, the future and relationships with others. Providers that were located within a LA were found to be the most successful at delivery.
Mounting an intervention
Given the available evidence, we believe that a system of peer mentoring and support, involving a young person whose experience of life post care has been positive, may be a promising approach to intervention with this group. Factors influencing decisions around pregnancy in LAC include low self-esteem, loneliness, mistrust of others, lack of assertiveness and lack of perceived choices or options in life. 44,111 The concept of resilience, associated with building self-esteem and self-efficacy, is increasingly seen as offering a framework for intervention with disadvantaged and vulnerable young people and has been shown to be protective in the context of care and teenage pregnancy. Resilience can be enhanced by the presence of positive role models and at least one secure attachment relationship. 112–114 Having access to a trusted confidant who provides care, respect and guidance, through and beyond the period of care, may go some way towards creating emotional security and improving self-esteem and confidence, as well as providing an opportunity to deliver important messages and information around relationships, sexuality and pregnancy. This approach has the potential to assist young people to develop new identities and make choices regarding their education and personal development, increase their self-confidence and self-esteem115–117 and provide real opportunities for alternative life choices. 48,118
Social support interventions119 involving trained volunteers have been shown to be effective in other areas of health care,120,121 with adolescents122 and in foster care. 123 There is some evidence that mentoring can help to increase the confidence, self-esteem and aspirations of young people in care109 and may also have a positive impact on training, education and work engagement. 107 Relatively less is known about the impact of peer mentoring as opposed to adult mentoring.
Potential pitfalls
We were aware of the potential challenges involved in accessing and engaging LAC,124 of finding positive role models125,126 and of sustaining such an intervention. We nevertheless considered that a peer mentoring approach would benefit from research, geared towards intervention refinement and experimental evaluation. In particular, we hoped to be able to explore the acceptability and feasibility of such an intervention; the need for and nature of rewards for the mentor; the training and support needs of the mentors; the means by which sustainability can be ensured; and the management of the post-intervention transition in a way that supports both mentor and mentee. From the available evidence we were convinced that not only was this a promising avenue to pursue given the aims of the project, but also the systematic and rigorous exploration of peer mentoring in this context would be generalisable and of benefit to a broader field.
Study aim and objectives
This study aimed to develop a peer mentoring intervention to reduce teenage pregnancy in LAC and to undertake an exploratory randomised controlled trial (RCT) to assess the feasibility of evaluating the effectiveness of the intervention in a definitive trial.
The objectives were to:
-
develop a complex intervention to reduce teenage pregnancy in girls and young women who are ‘looked after’
-
conduct an exploratory RCT of the intervention in three LAs in England, pilot recruitment, randomisation and consent procedures, examine recruitment and retention rates and the feasibility of collecting reliable and valid data on the primary and secondary outcome measures and estimate what might be feasible effect sizes and intervention costs for a future full-scale RCT
-
embed a process evaluation within the exploratory trial to assess the acceptability of the intervention and the trial procedures to LAC and those working as mentors and to document what constitutes usual care in this context for those LAC randomised to the control arm.
Chapter 2 Study methods
This chapter describes the study research design and methods used. The research aims and objectives are as set out in the previous chapter.
Research design
This was an intervention development and pilot study of peer mentoring for children and young people who have been in care, followed by an exploratory RCT, based on Phase I and Phase II of the MRC’s original framework for evaluating complex interventions. 127 We also looked at feasibility criteria and acceptability of the intervention to establish whether progression criteria for a Phase III trial could be met. The components of the peer mentoring intervention were based on existing evidence about mentoring interventions and discussions with key stakeholders; it was aimed to pilot this (Phase I) in one LA with six mentor–mentee dyads (actual n = 4). Phase II consisted of an exploratory RCT of the intervention in three LA areas. The target was to recruit 48 LAC mentees (young women aged 14–18 years) and 24 care leaver mentors (young women aged 19–25 years). The LAC mentees were individually randomised with half receiving the peer mentor intervention and half receiving ‘usual support’ (see Usual support condition). However, only 26 LAC were recruited and available for randomisation (see Chapter 5 for the reasons for this).
Selection of local authorities
Local authorities were selected on the basis of advice from the Advisory Group, in particular the TPU and the Who Cares? Trust. The team sought the involvement of two London-based and one non-London-based LA. The three LAs were selected because of their size and numbers of LAC in the areas that they covered and their perceived ability to support a research programme in this area. We looked for LAs with a previous track record, either in terms of peer mentoring or in terms of their interest in, and willingness and ability to engage in, the research.
An initial meeting was set up with the Director of Children’s Services (DCS) and key senior staff members in the three LAs for the Principal Investigator and team to present the project and provide an opportunity to ask any questions, to advise on any practical difficulties and to suggest changes. Following the first meeting, all three LAs agreed to participate. Further meetings were then held with the senior social workers from the LAs who had been identified as being able to take on the role of project co-ordinators (PCs). Following these meetings, the team, with the assistance of the LA staff, drew up an operational policy for the project, setting out in detail the roles and responsibilities of the LAs and specifically the PCs. The LAs received no reimbursement for participation in the project.
To preserve the anonymity of participants, the two London LAs are referred to as LA1 and LA2 and the non-London-based LA is referred to as LA3 in this report. The Phase I pilot was undertaken only in LA1. The exploratory trial mentoring was to be conducted in all three LAs. However, the non-London-based LA withdrew from the project before commencement of the exploratory trial and a replacement non-London-based LA (LA3) was then identified. However, LA3 experienced problems with recruiting and retaining mentors, which meant that no mentoring relationships could be established and LA3 had to withdraw from the project. This left only the two London LAs in the exploratory trial. Further details of the problems encountered and the reasons for mentor dropout are described and discussed later in this report (see Chapters 5 and 8).
Ethical approval and research governance
Ethical approval to conduct this research was granted in December 2010 by the Research and Ethics Committee based at the London School of Hygiene and Tropical Medicine (reference number 5866) (see Appendix 1). Local approval was obtained from the three LAs to ensure that the trial met their standards for research governance. Permission to conduct national surveys of social work staff was obtained from the Association of Directors of Children’s Services (see Appendix 2). The trial was registered with the Bristol Randomised Trials Collaboration [BRTC; see www.bristol.ac.uk/cobm/research/brtc.html (accessed 20 April 2015)], a UK Clinical Research Collaboration (UKCRC)-registered clinical trials unit. The BRTC provided a randomisation service for the exploratory trial and a trial database.
Developing the peer mentoring intervention (Phase I)
Existing evidence (see Chapter 1) suggested that peer mentoring would be an appropriate approach to reducing teenage pregnancy. However, a scoping exercise and targeted review of the literature was undertaken as part of Phase I to assist with the process of defining the intervention components, logic model and delivery plan.
Scoping exercise
Information was sought regarding local or national voluntary or statutory sector projects as well as published or unpublished reports, papers and web links relating to the following three types of intervention:
-
peer mentoring interventions for LAC
-
peer mentoring interventions to reduce teenage pregnancy
-
other interventions to reduce teenage pregnancy in LAC.
Directors of Children’s Services for England and Wales and virtual head teachers, teenage pregnancy co-ordinators, children’s and young people’s charities, mentoring organisations and members of the study Advisory Group were contacted (n = 457) between April and May 2012 to see if they were able to provide relevant information. Reminder e-mails were sent throughout the 2-month period. Initial responses were followed up by telephone or e-mail to explore professionals’ views on the components of existing interventions. Particular attention was paid to questions around the selection, training and support of mentors, the specification of the mentoring relationship (e.g. amount and types of contact and duration of relationships), exit strategies and views on contextual factors affecting the effectiveness of these interventions.
Targeted literature review
A targeted literature review was conducted at the same time as the scoping exercise. The following databases were searched between March and April 2011 for published and unpublished literature on peer mentoring for LAC with the aim of reducing teenage pregnancy: PsycINFO, Social Sciences Citation Index, MEDLINE, Database of Abstracts of Reviews of Effects, Education Resources Information Center (ERIC), System for Information on Grey Literature in Europe (SIGLE) and Cumulative Index to Nursing and Allied Health Literature (CINAHL). Studies pre-1992 were excluded. An initial search of these databases revealed only limited available literature and so the search strategy was broadened to include studies that used more traditional (i.e. adult to youth) mentoring methods. The literature review encompassed the following types of mentoring:
-
mentoring and peer mentoring for young people
-
mentoring and peer mentoring for LAC
-
mentoring and peer mentoring to increase positive sexual behaviours and/or reduce teenage pregnancy
-
mentoring and peer mentoring for pregnant and parenting adolescents.
For a detailed description of the search strategy used in the review, see Appendix 3.
A further database search was conducted in December 2012 to incorporate more recent literature into the review.
Intervention logic model
The behaviour–determinants–intervention (BDI) logic model63 is a standardised approach to theorising and informing the development of social interventions for community health problems, including sexual health and teenage pregnancy. Drawing on the literature review and scoping exercise, a BDI logic model was designed to describe and explain the intended causal mechanism of the intervention. The BDI logic model is presented in Chapter 3 of this report.
Piloting the peer mentoring intervention
A 3-month pilot of the methods for recruiting participants and the delivery of the intervention was undertaken in LA1. The recruitment target was six mentors and six mentees. The findings were used to refine the mentor training programme and other intervention components and to test the research methods and instruments to be used in the exploratory trial.
Methods used included observation of the training programme, a focus group with mentors on the last day of training and individual semistructured interviews with participants at the end of the 3-month period. Semistructured interviews were also held at the end of the 12-month intervention to explore the mentoring relationships and any impacts on mentors and mentees. These interviews were not included in the original protocol but were added because of the lower than planned level of recruitment in the exploratory trial.
Exploratory randomised controlled trial (Phase II)
A RCT was undertaken in LA1, LA2 and LA3 with 26 young women aged 14–18 years, randomised to receive the peer mentor intervention or the usual support provided to LAC. Randomisation was stratified by LA. Participants, both mentors and mentees, were interviewed 1 year post randomisation, at which time the mentoring had concluded. For details on the recruitment process see Chapter 5.
Components of the peer mentoring intervention
Mentor training and support
A 3.5-day training programme was designed by the research team in collaboration with the National Children’s Bureau (NCB) and Straight Talking, a teenage pregnancy organisation (see Chapter 6 for details). All potential mentors were offered the training, after which they were asked whether they were still willing to act as mentors and were consented. Only those who completed the training programme were permitted to work as peer mentors. We anticipated that pilot training would be delivered to 8–10 young people from LA1 and that the exploratory trial training would be delivered to 10–12 young people from each of LA1, LA2 and LA3. Training was delivered locally, in each of the LAs, to make attendance easier for participants, generally at a location arranged through the LA. Participants were paid £30 in shopping vouchers for attendance at training. The pilot training took place between 31 August 2011 and 5 September 2011. Exploratory trial training ran from 13 to 16 February 2012 in LA3, from 22 to 25 February 2012 in LA2 and from 20 to 23 March 2012 in LA1.
A booster training day, delivered by the NCB and Straight Talking, was held approximately 4 months into the intervention. This focused on discussing issues that had arisen for mentors within the mentoring relationship and problem solving.
Mentors were provided with ongoing support from the PC in each LA for the duration of the intervention, through monthly support groups and ad hoc troubleshooting and the provision of advice in-between these meetings on an individual basis. The PC role was refined during the pilot stage and is described later in this report (see Chapter 3).
Mentor role
It was agreed at the outset that each mentor should be required to take on only one mentee at a time, for a period of up to 1 year. Contact between the mentor and the mentee was by a variety of means (face-to-face meetings, e-mail, telephone conversations and texts). Mentors were provided with a mobile phone to facilitate communication with their mentee. Mentors received a monthly stipend in recognition of their work and contribution to the study, as well as money for activities with their mentees (described later in this chapter). They were also offered the opportunity to gain an accreditation for their peer mentoring through the Award Scheme Development and Accreditation Network (ASDAN). Mentors signed a mentoring ‘contract’ that outlined the responsibilities expected of them in terms of maintaining contact with their mentee, attending support group meetings and using the money and mobile phone appropriately. The mentor role was refined during the pilot phase and then further refined before commencement of the exploratory trial (see Chapter 3).
Study participants (Phases I and II)
Inclusion criteria
Participants aged 14–18 years
Young women were considered eligible to participate if they met the following criteria:
-
they were aged between 14 and 18 years
-
they were currently under the care of the LA in children’s homes or with foster carers or were care leavers. 128
An age of 14 years was specified as the lower limit because of the evidence suggesting that LAC are at risk of early sexual initiation. 28 This age was also chosen because ethical guidelines require additional consent to be sought when obtaining information on sexual behaviour below the age of 14 years. 129
The inclusion criteria did not specify whether the young women were sexually active or had previously been pregnant. However, these data were collected at baseline and follow-up.
Mentors
Young women were considered eligible to participate as mentors if they met the following criteria:
-
they were aged between 19 and 25 years
-
they had experienced the care system
-
they were deemed safe to work with children and vulnerable young people by having a satisfactory Criminal Records Bureau check [now referred to as the Disclosure and Barring Service (DBS)].
The scoping and peer mentoring literature review (see Chapter 3) identified the qualities and characteristics desired of peer mentors in previous work. These findings were relayed to PCs to assist them in the selection of suitable peer mentors.
Exclusion criteria
Young women (both mentors and mentees) were originally to be excluded if they were pregnant at the time they were approached to give consent, but they were not necessarily excluded if they already had a child (see Chapter 5 for details on exceptions to these criteria because of recruitment difficulties).
Recruitment
Pilot study recruitment was scheduled over a 2-month period between July and August 2011. Recruitment for Phase II was scheduled over a 3-month period between December 2011 and February 2012, although in practice we were unable to keep to these recruitment windows (see Chapter 5).
Recruitment leaflets and posters were designed by the research team in collaboration with a service user representative to ensure that they were appropriate. The leaflets summarised information about the study, explained confidentiality and anonymity procedures and included researcher contact details. To make the study accessible to young people and other stakeholders and for easy referral it was named ‘the Carmen study’ (derived from the words ‘care’ and ‘mentoring’). These materials were given to PCs to distribute to professionals and young people within their LA (see Appendix 4 for the written information included in the recruitment leaflets).
When a potential mentee indicated that they might be interested in participating, the researcher made an introductory telephone call and arranged to meet. The initial meeting with one or both of the researchers (DM and FC) was held on LA premises or at the participant’s home address if the participant preferred. At the meeting the researchers checked that the participant understood the nature of their involvement, details about the mentoring programme and the randomised nature of the trial (Phase II only). If the potential mentee was happy to enter the trial the researcher completed the consent procedures and baseline interview. Participants were given a £15 shopping voucher for completing this.
When a potential mentor indicated a willingness to participate, the researcher made an introductory telephone call and checked that potential mentor could attend the training. The potential mentor was then sent a letter with details of the training times and venue. If they were still interested in participating after completing the training course, a meeting was arranged with the researchers to complete the consent procedures and baseline interview. These meetings were held in the same locations as meetings with potential mentees. Participants were given a £10 shopping voucher for completing this.
Informed consent and safeguarding
Verbal and written consent was obtained from participants before completing the baseline interview (see Appendix 5 for consent forms). Baseline interviews were completed before randomisation. Young people aged < 16 years were invited to have their social worker or other LA individual present when obtaining consent. If they preferred to attend alone, the researchers spoke to their social worker to confirm their capacity to consent. Young people aged between 16 and 18 years could also elect to have a third person present if they wished. Fraser guidelines,129 which set out criteria for determining if a child is mature enough to make decisions around contraception and sexual matters, were followed. Participants were advised to direct initial queries about the research to the researchers and any other queries or concerns to the PC. A copy of the mentee consent form was sent to the mentee’s social worker, together with details of the PC.
We developed protocols for dealing with a disclosure of significant risk or ongoing harm involving a mentor or menteed young person. Before giving consent, all participants were informed of the limits of confidentiality in research interviews and that their social worker or another member of their care network would be informed if any such disclosures were made. Mentors were also advised to inform the PC if their mentee made any disclosures to them.
Randomisation
Mentees participating in the exploratory trial were individually randomised. Randomisation was stratified by LA using blocking and was undertaken using the BRTC automated randomisation service. After obtaining consent from the mentee, the researcher contacted the randomisation service to obtain the allocation. This information was then communicated to the mentee, their social worker and the PC.
Mentees were randomised to either the intervention arm of the trial or the usual support arm. Those in the intervention arm received a peer mentor in addition to their usual services.
Usual support condition
Those in the usual support arm received the services already available to them because of their status as a looked-after young person. These services aim to promote their educational achievement, physical health and social and emotional well-being. 83
Sample size
The sample size in the exploratory trial was not intended to have sufficient power to detect a significant difference in the primary outcome measure. However, the target sample size, 48, was sufficient to test whether the trial methods were robust and to provide sufficient data to check the reliability of the psychometric measures being used as secondary outcome measures.
Measures
Baseline measures
The following data were collected from LAC aged 14–18 years (see Appendix 6 for the baseline questionnaire):
-
sociodemographic data (age, ethnicity, etc.)
-
care history (current and previous)
-
forensic history and alcohol and drug use
-
educational attainment and achievement – attainment, school attendance, history of exclusions, truancy and suspensions, future educational/vocational intentions
-
sexual activity, contraception use, condom use to prevent STIs, history of pregnancy and STIs (some questions were adapted from the second NatSAL, a large UK study of sexual behaviour130)
-
physical and psychological health (see Explanatory variables for list of standardised measures used)
-
interpersonal and social functioning including number of confidants/close friends and engagement in leisure/sporting activities.
Additional information (including care history, sexual health and contact with other agencies) was collected from mentees’ social workers using a questionnaire (see Appendix 7). Consent for obtaining this information was obtained from mentees.
Outcome measures for mentees
Follow-up data collection took place when the peer mentoring intervention ended; this was scheduled at 12 months after the baseline interview. Follow-up interviews with Phase II mentors and mentees took place in June and July 2013. Participants were given a £20 shopping voucher for this.
Primary outcome measure
As the key purpose of the intervention is to reduce the rate of pregnancy, the ideal would be to have pregnancy as the primary outcome for this exploratory trial and in any subsequent definitive trial. However, this makes sense only if there is a reasonable chance of detecting a meaningful reduction in the rate of pregnancy between the intervention group and the control group in a Phase III trial. It is difficult to estimate accurately what the rate of pregnancy is for LAC and teenagers. Some studies have suggested that the rate may be as high as 40%. 131 However, data collected on live births to LAC in combination with routine data on teenage conceptions and abortions for the population as a whole in England suggest that the rate may be 10%. 72 If we assume that it would not be feasible to mount a Phase III trial with > 1000 LAC randomised to the intervention and control groups, Table 1 suggests that, if the pregnancy rate in LAC is between 20% and 40% and an effect size of 10% is deemed reasonable, using pregnancy as the primary outcome measure in a definitive trial would be possible. However, as the lower part of the table indicates, if the pregnancy rate for LAC is nearer to 10% then the intervention would have to have the effect of halving the pregnancy rate in the intervention group to have a reasonable chance of detecting this change.
| Pregnancy rate (%) | n required per arma | |
|---|---|---|
| Control | Intervention | |
| 40 | 35 | 1511 |
| 40 | 30 | 376 |
| 35 | 30 | 1417 |
| 35 | 25 | 349 |
| 20 | 15 | 945 |
| 20 | 10 | 219 |
| 10 | 8 | 3313 |
| 10 | 7 | 1422 |
| 10 | 6 | 771 |
| 10 | 5 | 474 |
| 10 | 4 | 316 |
Although data on live births to LAC are routinely recorded, routine data on abortions for women aged < 18 years do not distinguish between those who are looked after and those not in care. Thus, it is not possible to calculate a pregnancy rate for this group. Our estimate of a pregnancy rate of 10% rests on an assumption that the ratio of live births to termination of pregnancy in LAC is the same as that for all teenagers, even though there is some suggestion that this may not be the case. 28 An important function of this exploratory trial was to (1) conduct further analyses of routine data on births to LAC and conception and abortion rates in teenage women, to produce more robust estimates of the pregnancy rate in the subgroup of LAC that our intervention is designed for; (2) explore the feasibility of collecting pregnancy data from the young people themselves; and (3) consider in detail what other surrogate measure for pregnancy could be used as a primary outcome measure in a Phase III trial should it become clear that using pregnancy as the primary outcome is not feasible. Current candidate surrogate measures collected included age of first sexual intercourse, use of contraception compared with incidents of unprotected sex in the previous 3-month period and number/nature of sexual relationships and STIs. Of these, our primary surrogate markers were age of first sexual intercourse and use of contraception compared with incidents of unprotected sex in the previous 3-month period. We examined whether all of the effects of our intervention were mediated through and reflected in the surrogate measures as well as in the primary clinical outcome.
Secondary outcome measures
Secondary outcome data for mentees were collected using a questionnaire, measuring change to those feelings, thoughts and behaviours collected at baseline.
Explanatory variables
Data were collected on variables that may help to explain the mechanisms by which the intervention achieved its effect. These were informed by the development of the BDI model (see Chapter 3 for more details). The following psychological measures were self-completed by mentees at baseline and follow-up:
-
Self-Esteem Scale132 – 10-item self-report measure of global self-esteem. Answers are given on a 4-point scale ranging from ‘strongly agree’ to ‘strongly disagree’, with a higher score indicating greater self-esteem. This measure has demonstrated reliability and validity with young people.
-
General Health Questionnaire133 – 12-item scale to detect symptoms of anxiety or depression. A score of ≥ 4 defines common mental disorder with a maximum score of 12 indicating a high likelihood of psychiatric illness.
-
General Help-Seeking Questionnaire (GHQ)134 – 8-item scale, with each item identifying intentions to seek help from different sources. Good reliability and validity with young people.
-
Locus of control135 – This 29-item scale was shortened to a 10-item scale to ensure that it was appropriate for the young people participating. It measures generalised expectancies for internal compared with external control of reinforcement (internal locus of control characterises those seeing their own actions determining life events; external locus of control characterises those seeing events in life as generally outside their control). Scores range from 0 to 13, with a low score indicating internal control and a high score indicating external control.
-
Attachment style136 – Self-report questionnaire classifying four attachment styles: secure, fearful, dismissive and preoccupied. Good reliability and validity, including for use with adolescents.
Outcome measures for mentors
Mentors completed a baseline questionnaire prior to the commencement of the intervention (see Appendix 8). The questionnaire recorded:
-
sociodemographic data (age, ethnicity, etc.)
-
care history
-
education and employment status
-
physical health, alcohol use and pregnancy history
-
interpersonal and social functioning including number of confidants/close friends and engagement in leisure/sporting activities.
Mentors also completed three psychological measures – the Self-Esteem Scale, the GHQ and the locus of control – pre intervention and following completion of the intervention to assess change.
Economic evaluation
The first intention of the economic evaluation was to determine the costs of the intervention and develop a model of the running costs suitable for estimating the costs of a larger trial. Timesheets were provided for PCs to record the time that they spent delivering the scheme. They were also asked to record details of expenses associated with these activities. In the event, these methods were used infrequently by the co-ordinators and the project costs had to be estimated from the small number of data that they did return, qualitative remarks made during interviews and the time that the researchers had to commit to supporting the co-ordinator role. Mentors were also asked to record the time spent on activities with their mentee and retain records of all expenses incurred whilst undertaking the role.
The second intention was to develop a conceptual model to detail the connection between the value added by the intervention and the probabilities of various medium- to long-term outcomes for the young women and any children they may have, aimed at supporting the design of future interventions.
Process evaluation
A process evaluation was undertaken to examine implementation and receipt of the intervention and to assess feasibility and fidelity, accessibility, acceptability and contextual factors affecting implementation. The process evaluation was also used to gain insights into the mechanism of action of the intervention.
The process evaluation was informed by data from semistructured interviews with mentors, mentees and PCs and mentor diary data, focus groups, survey data and interviews with other professionals.
Follow-up semistructured interviews
At the end of the Phase II mentoring intervention (June 2013), follow-up semistructured interviews were conducted with mentors, mentees and PCs (see Appendix 9 for qualitative interview schedules). We originally intended to qualitatively interview a sample of mentors and mentees; however, low recruitment numbers resulted in us attempting to interview all participants at follow-up. The interviews explored their experiences of the mentoring relationship in terms of its acceptability, appropriateness and impact, their views of whether mentoring is effective, their views of how it effects change and their suggestions for how mentoring could be enhanced. With regard to the research, views were examined on the consent and randomisation procedures. Interviews were also sought with mentors or mentees who left the programme early, to understand their reasons for exiting the study. Interviews were conducted by the researchers (DM and FC) on LA premises or at participants’ home address, depending on their preference.
Assessing the feasibility of a Phase III trial
To assess the feasibility of delivering the peer mentoring intervention in a Phase III trial, the following domains were explored:
-
availability of eligible participants for a Phase III trial
-
feasibility of recruiting mentors and mentees
-
acceptability of the consent and randomisation procedures
-
participant retention
-
evidence of harm to participants
-
characteristics and appropriateness of proposed outcome measures
-
costs for a full trial
-
ability to manualise the intervention.
Training evaluation
The training sessions were observed to assess whether the specific components were being delivered and the appropriateness of the approaches used and the level of the mentors’ engagement with the training material presented/discussed. A semistructured checklist was used to guide the researchers’ observations and the observations were recoded qualitatively. Participants completed a questionnaire at the beginning of training and at the end of each day and participated in a focus group on the last day (see Appendix 10 for schedules), giving feedback to the researchers on the training provided. Further feedback regarding training delivery and the training process was provided by the trainers to the researchers.
Mentor diaries
Mentors were asked to keep a structured diary logging the frequency, nature and content of their communication with mentees, as well as their reflections about their mentoring experiences (see Appendix 11 for schedule). A mobile phone-based application known as Magpi [see www.magpi.com (accessed 21 April 2015)] was downloaded onto the mobile phones and used to capture the information. Mentors were also given an option of completing the diary online. Diary entries were sent electronically to the researchers and were held on a secure, confidential server. The researchers provided guidance on completing the diary at the mentor training. Mentors were asked to complete the diary after each contact with their mentee, as well as weekly, even if no contact had taken place that week.
During the Phase II exploratory trial, researchers collected information from mentors and mentees over the telephone, taking the form of a ‘snapshot’ diary at three time points – 3, 6 and 9 months into the intervention – asking about contact in the previous week (see Appendix 12 for schedules). The diaries were digitally recorded and transcribed verbatim.
Amendments introduced to the study
A number of additional elements (not originally included in the study protocol) were introduced to the study in May 2012. This was in response to recruitment difficulties that had resulted in target participant numbers not being met (see Chapter 5) to enable us to further explore the barriers to recruitment and assess the feasibility and acceptability of undertaking a Phase III definitive trial. These additional elements are described in Table 2.
| Title | Original protocol | Change made | Reason for change | Month in projecta |
|---|---|---|---|---|
| Inclusion criterion for ages of mentors | 18–25 years | 19–25 years | When possible, minimum 5-year age gap between mentees (age 14–18 years) and mentors | 1 |
| LAs | LA1, LA2, Southend | LA1, LA2, LA3 | Having initially indicated a willingness to participate, Southend LA subsequently decided not to take part in the research study | 1 |
| Inclusion criterion for number of mentee placements | Three or more placements | One or more placements | Low recruitment numbers within the first few weeks resulted in the inclusion criterion being widened | 2 |
| Payments for participant interviews | £10 for individual interviews and £20 for focus groups | Payments made in shopping vouchers – £15 for mentee baseline interviews, £15 for mentor baseline interviews, £20 for follow-up interviews | Feedback from social workers that payments should be made in vouchers rather than in cash | 4 |
| PC role | One PC per LA | Two PCs per LA | LAs felt that the PC role required too much time commitment for one person | 5 |
| Mentor training | 3-day course | 3.5-day course | The design of the intervention necessitated a longer training period for mentors than had originally been anticipated | 5 |
| Social worker questionnaire | Not included in the original protocol | Mentees’ social workers were sent questionnaires at baseline and follow-up | To compare self-report information with case records; to identify whether there had been any variation in contact with agencies at the 1-year follow-up | 5 |
| Mentor payments | £40 per month in recognition of their contribution to the study | Payments in recognition of role made in Love2Shop vouchers | Feedback from social workers that payments should be made in vouchers rather than cash | 12 |
| Additional £40 per month for activities with mentees | Activity payment costs for London boroughs increased to £60 per month | Feedback from pilot mentors/mentees that activity payments were insufficient | ||
| Mentor diary | Magpi technology used to collect data | Diary completed using Magpi or online | Feedback from pilot mentors/mentees that they would like to complete the diary online | 12 |
| Semistructured interviews with LA staff | Not included in the original protocol | 13 interviews with PCs, senior managers and social workers | To understand individual experiences of participant identification and referral to the study and also barriers to recruitment | 15 |
| Focus groups for refining the intervention | Four focus groups before the start of the pilot study | Focus groups conducted during Phase II – five focus groups with LA staff and two with LAC | To assess feasibility and explore views on the peer mentoring intervention | 15 |
| Surveys of LA staff and young people | Not included in the original protocol | National survey of LAC and care leavers; national survey of DCSs/social workers; local survey of social workers from LA1, LA2 and LA3 | To assess feasibility and explore views on the peer mentoring intervention | 15 |
| Interview with university student | Not included in the original protocol | Interview with a university student from St George’s, University of London | To assess feasibility and explore views on the peer mentoring intervention | 24 |
Semistructured interviews with professionals
In June and July 2012, 13 semistructured interviews were conducted with PCs, senior managers (referred to as SM in quotations) and social workers (referred to as SW in quotations) from LA1, LA2 and LA3 (see Appendix 13 for schedules). We interviewed all PCs and senior managers involved in the study and a sample of social workers, who were chosen because of their involvement in recruitment. A senior manager was defined as a person who had management responsibility within the field of LAC/care leavers and who did not have a caseload. The purpose of these interviews was to understand individual experiences of participant identification and referral to the study and also barriers to recruitment. Interviews were conducted either in person on LA premises (in a private office) or on the telephone and lasted from 30 minutes to 1 hour. All interviews were digitally recorded and transcribed verbatim.
Surveys of local authority professionals and female looked-after children and care leavers
The following surveys were conducted (see Appendix 14 for schedules):
-
A survey of social work staff in the three LAs (whose caseload included LAC or care leavers) explored their involvement with the study and barriers to recruitment. Senior managers were asked to distribute the survey, which was open from 11 January to 21 March 2013. In total, 22 responses were received (three from LA1, five from LA2, 14 from LA3).
-
A national survey of two groups of young women from the UK (LAC aged 14–18 years and care leavers aged 19–25 years) was open from 3 September to 14 December 2012. The purpose of the survey was to examine views on recruitment, randomisation and the peer mentoring intervention as well as young people’s experiences of other mentoring schemes. The survey was advertised through the Who Cares? magazine, produced by a national charity for LAC. Other organisations were contacted by e-mail and on Facebook and Twitter, including children’s charities, youth services and Children in Care Councils (CiCCs). Flyers were distributed during National Care Leavers’ Week in October 2012. In total, 27 responses were received to the 14–18 years survey [mean age 16.78 years, standard deviation (SD) 1.15 years]; 15 respondents lived in southern England, five lived in London, four lived in the Midlands and three lived in Northern England. For the 19–25 years survey, 37 responses were received (mean age 21.58 years, SD 2.13 years); 11 respondents lived in southern/eastern England, 10 lived in London, eight lived in the Midlands, five lived in northern England and two lived in Scotland (one response was missing).
-
Two surveys were e-mailed to DCSs in 152 LAs in England and Wales. One survey was completed by DCSs and/or senior managers within children’s services. This survey assessed the availability of eligible participants within their LA, their views on peer mentoring and randomisation and their interest in participating in a larger trial. The second survey was completed by social workers whose caseload included LAC aged 14–18 years or care leavers aged 19–25 years. This survey assessed respondents’ views on the peer mentoring intervention and randomisation. The surveys were open from 11 January until 21 March 2013. In total, 85 responses were received to the DCS survey (25 from LAs in London, 24 from LAs in northern England, 20 from LAs in southern/eastern England and 16 from LAs in the Midlands). For the social worker survey, 118 responses were received (47 from LAs in northern England, 29 from LAs in the Midlands, 29 from LAs in southern/eastern England and 13 from LAs in London).
The surveys were constructed using LimeSurvey [see www.limesurvey.com (accessed 21 April 2015)], a survey software tool, and were completed online. Recruitment was facilitated by the circulation of the survey URL. There was an opportunity to enter a prize draw in the surveys of young people and social workers, with one respondent in each survey winning a shopping voucher (£30 for young people and £50 for social workers).
Focus groups with female looked-after children and care leavers and local authority professionals
Focus groups with LAC/care leavers and professionals working with LAC were held to explore their views on the peer mentoring intervention (see Appendix 15 for focus group schedules). Two focus groups were held in an additional LA (referred to as LA4) with (1) two LAC aged 14–18 years and (2) five female care leavers aged 19–25 years. This LA was chosen because of its expression of interest when contacted during the scoping exercise. Recruitment flyers were provided to a LA4 Children’s Rights, Participation and Engagement Manager in May 2012, who distributed them to eligible young women. The groups were held at a local youth centre in July 2012. Participants were given a £20 shopping voucher for their participation.
In May 2012, managers were asked to distribute preliminary written information to their staff and to nominate individuals to participate in focus groups about the project. Following this, two additional groups were held in each of LA1 and LA2 consisting of (1) social workers working with LAC and care leavers and (2) health and education staff. One focus group was held with social workers in LA3. The groups were held on LA premises or in local education centres between August and November 2012. The number of participants in each group ranged from three to six. The length of the focus groups ranged from 1 hour to 90 minutes.
All focus group discussions were digitally recorded and transcribed verbatim.
Interview with university students
Following advice from the Trial Steering Committee that university students may be a fruitful avenue of recruitment in a future trial, because of their perceived status as aspirational role models for young people in care, we attempted to arrange a focus group with university students who had experience of the care system. The aim was to explore their interest in acting as peer mentors and the potential barriers that they may encounter. For ease of recruitment, students were selected from St George’s, University of London (SGUL) and Kingston University. Recruitment was conducted through the SGUL Student Centre, who contacted all eligible female students aged 19–30 years who had experience of the care system (the upper age limit was extended because of feedback from social work professionals that mentors could be older than 25 years). The head of the Student Centre reported that there were approximately 10 eligible participants. Two students expressed an interest in participating but only one of them subsequently presented for interview, in July 2013 (see Appendix 16). The participant was given a £20 shopping voucher for her participation. The interview was recorded and transcribed verbatim.
Data analysis
Qualitative data analysis
For the purpose of this report we adopted a pragmatic thematic approach to the analysis of qualitative data, seeking to provide a largely descriptive account137 of the peer mentoring process that would complement the analysis of quantitative data and enable further refinement of the intervention and research procedures. Although we borrowed analytical techniques of coding and comparing data from grounded theory,138 we used these tools to organise our data, rather than seeking to build theory about the processes underpinning the peer mentoring relationship (this approach will inform additional, in-depth qualitative outputs from the study).
Transcripts from the process evaluation interviews were read a number of times by researchers (DM and FC) to familiarise themselves with the data. Participant and LA area attributes were assigned to each transcript to allow analytical themes to be explored in relation to the experiences of different groups and to compare processes across areas.
An initial ‘open coding’ was undertaken of a selection of transcripts from different participant types and LAs. Coding involved assigning labels to data (passages of text) – where possible retaining language used in the transcripts – that indicated the relevance of that data to the research questions being addressed. In this study, the coding process was guided by the team’s key questions about the processes of mentoring and relationship building and the progress of the relationships between dyads, what made a relationship work and what did not. Questions asked of the data included how the mentor and mentee experienced the relationship; the expectations of mentors and mentees about the workings/dynamic of the relationship; what mentors and mentees thought was a safe and appropriate relationship; and the impact of this supportive relationship on their relationships.
Following open coding, researchers adopted an iterative process139 whereby they looked for patterns, similarities and differences, as well as silences, in the coded data. This process was used to coalesce codes into categories or themes that constructed our descriptive account of the mentoring process. The iteration was a reflexive process and was key to sparking insight and developing meaning. The researchers visited and revisited the data and connected them with emerging insights, progressively refining the themes. The themes emerging from the data were driven by the inquiries above but also by the researchers’ interpretations of what the data were telling them based on their experiences of having undertaken the interviews and of the fieldwork environment. The researchers undertaking the coding (DM and FC) presented the emerging analysis to members of the research team through regular meetings and to members of the Advisory Group on two occasions to validate themes from the wider team perspective.
Through the iterative process we developed an analytical framework – a comprehensive set of themes – that was applied to all semistructured interview and focus group data. Themes that made up the framework were created as ‘nodes’ in the NVivo qualitative analysis software package (version 10; QSR International, Warrington, UK) and all transcripts were coded to those nodes, that is, sections of text were assigned, using the software, to the themes to which they were relevant.
The resulting coded NVivo database was used to facilitate the management of the large qualitative data set. In undertaking the process evaluation ‘query’ functions within NVivo were used to collate data relating to particular themes that described the mentoring process and to enable comparisons between data from different types of participant (see Chapter 8).
As well as the process evaluation, qualitative data also explored the structure and components of the intervention (examined through follow-up interviews and mentors’ diaries). NVivo software was used to collate qualitative data from all sources to support and make comparisons with the quantitative data collected through baseline and follow-up interviews and survey data, that is, data sources were triangulated139 (see Chapter 7).
Quantitative data analysis
Because of the small sample size in this study no hypothesis testing has been conducted comparing the outcomes of the intervention and usual support groups. Baseline data have been presented for all participants (by randomised allocation) using descriptive statistics (see Chapter 5), frequencies and percentages for categorical variables, means, SDs and minimum and maximum values for continuous normally distributed variables and medians with minimum and maximum values for discrete count variables. The pilot study sample has been added to the Phase II sample for reporting of quantitative data in Chapters 5 and 7. For the follow-up data (see Chapter 7) descriptive statistics are again used to report the primary and secondary outcomes by randomised allocation. Individual data are presented for the pregnancy and sexual behaviour outcomes given their importance and paucity. Frequencies and percentages are reported for categorical variables and medians and minimum and maximum values for all quantitative variables (given the smaller sample size at follow-up). For the three psychological measures (GHQ, Self-Esteem Scale and locus of control) mean changes from baseline to follow-up with 95% CIs are presented. All analysis was conducted using IBM SPSS Statistics version 20 (IBM Corporation, Armonk, NY, USA).
Chapter 3 Phase I: development and piloting of the intervention
To inform the components of our intervention, a scoping exercise and literature review of peer mentoring interventions was conducted during the development phase. The first section of this chapter contains the results of the scoping exercise and literature review, including evidence on what constitutes ‘best practice’ in mentoring and peer mentoring and the way that the effectiveness of an intervention can be increased when particular features are adopted. The review was used to inform the design of the mentoring intervention, which is outlined later in the chapter.
Scoping review findings
The scoping review identified small-scale projects in Great Britain that were in the development stage or established. Information about peer mentoring for LAC and interventions to reduce teenage pregnancy was sought, with a specific focus on LAC. Fifty-two responses were received from 457 professionals contacted during the scoping exercise. The breakdown of responses by professional organisation is presented in Table 3. Many programme providers could not be contacted because of high staff turnover within organisations and, in some cases, the lack of response was due to a lack of relevant interventions. However, in some regions, professionals were more responsive and contacts in their area snowballed. From the responses, 19 relevant peer mentoring interventions were identified (Table 4).
| Organisation | Number of professionals contacted | Number of professionals who responded |
|---|---|---|
| Advisory Group | 12 | 6 |
| Children’s charities | 13 | 6 |
| Sexual health/teenage pregnancy organisations and teenage pregnancy co-ordinators | 45 | 11 |
| Mentoring organisations | 2 | 0 |
| LAC organisations | 32 | 11 |
| DCSs | 152 | 14 |
| Virtual head teachers | 201 | 4 |
| Total | 457 | 52 |
| Intervention type | Number of interventions identified | Regions |
|---|---|---|
| Peer mentoring for LAC, aiming to improve outcomes generally (six involve mentors with experience of the care system) | 7 | London (four boroughs), Cornwall, Central Bedfordshire, Wakefield |
| Peer mentoring for LAC to improve educational outcomes (four involve university students acting as mentors) | 5 | London (six boroughs), Bradford, Leeds, Lincolnshire, Walsall |
| Peer mentoring for LAC who were pregnant (mentors had experience of the care system and being a parent) | 1 | North Lincolnshire |
| Peer mentoring for teenage parents (not specifically LAC) | 4 | Hull, Leeds, Leicester, North Lanarkshire |
| Online peer mentoring for young people about sex, relationships and pregnancy | 1 | Nationwide |
| Peer mentoring course to train LAC to be school mentors | 1 | Wakefield |
The scoping review did not identify any interventions designed to reduce teenage pregnancy in LAC or other young people. Most interventions were focused on promoting positive outcomes for LAC, including raising educational outcomes and supporting them through their transition from care to independence (13 out of 19 interventions). Some of the interventions used mentors with experience of the care system but these were focused on goal-setting and promotion of independent living skills. Peer mentoring interventions with LAC aimed at improving educational attainment often employed university student mentors, who were not specifically required to have experience of care.
Initiatives to prevent teenage pregnancy
The scoping review did not identify any peer mentoring interventions for preventing teenage pregnancy; however, effective peer-led sexual health interventions do exist in England. 140 Several interventions were identified that aimed to support pregnant teenagers or teenage parents and increase their engagement in health and education services. Mentors were often teenage parents themselves, although they did not have to have been in care. We identified one scheme in North Lincolnshire that was in the process of being set up to support LAC who were already pregnant, using peer mentors who had experience of the care system and who were teenage parents.
Other interventions focused on equipping young people, including vulnerable groups such as LAC, with the knowledge and skills to negotiate safe sexual relationships. In areas with high teenage conception rates, teenage pregnancy was addressed by condom distribution services and fast-track access to CaSH services; sexual health outreach teams providing advice and support to young people; allowing young people to interact with toddlers in a nursery environment; and teaching parents skills to discuss sex and relationships with their children. Examples of peer education initiatives to reduce teenage pregnancy were peer-led SRE and teenage parents going into schools to discuss their experiences and the realities of being a teenage parent.
Based on these findings it would appear that peer-led education on sexual health and pregnancy is commonly used but peer mentoring has not been widely used as an approach to preventing teenage pregnancy either generally or in LAC specifically.
Recommendations from peer mentoring providers
At the time of scoping, some peer mentoring schemes had been running and expanding over a number of years, others no longer existed because of the various problems that they had encountered and a few were still in the development stage. Only a limited number of programmes had conducted any type of formal evaluation, although some had carried out internal audits. The dearth of independent, external evaluations meant that reports of benefits tended to be anecdotal or based solely on the individual practitioner’s experience, making it difficult to compare effectiveness across programmes. However, the problems encountered and the recommendations made by the providers were broadly consistent with those identified in the research literature.
Some of the key problems encountered by providers included:
-
Lack of funding for staff time and inadequate administrative and mentoring resource, which made it difficult for providers to carry out work effectively. Some programmes did not have their funding renewed to allow them to continue.
-
Concern over the ability of mentors and mentees to sustain appropriate boundaries in their relationship when mentoring is unsupervised. Providers advised caution over the exchange of personal mobile phone numbers.
-
Infrequent and inconsistent meetings between mentors and mentees, which therefore need to be carefully monitored.
-
Transport issues, especially in LAs that cover a large area. Some programmes had to fund taxis to transport mentors and mentees to sessions.
All established programmes offered some form of training and support for mentors. Providers considered that adequate training for mentors was essential and emphasised that a substantial amount of support may be needed for peer mentors who have left care to enable them to meet the demands of the role and cope with issues in their own lives.
Different approaches and criteria were adopted for matching mentors and mentees. Some providers reported matching on the basis of their professional knowledge of the young people, whereas others used specific criteria such as location, ethnicity or shared interests. A number of providers also based their matching on preferences expressed by the young people themselves.
The most common format for mentoring was weekly sessions, either one-to-one or in a group. Anecdotal evidence was provided for the benefits of mentoring for young people’s aspirations, education, self-esteem and confidence, but no formal evaluations had been carried out.
Literature review findings
Both the scoping exercise and the literature review found that fundamental to the success of any mentoring programme is the presence of a clear and structured organisational framework and strong management of the intervention, as well as training and support for mentors, the nature of the mentor–mentee relationship, the frequency of contact and the duration of the relationship and careful management of the ending of the relationship. These factors are described in more detail in the following sections.
Building a successful framework for mentoring
Research has shown that a crucial element in the success of mentoring programmes is a strong infrastructure,141–144 including adequate resources, staffing and management of programmes and also appropriate selection, training and ongoing support for mentors.
The role of the mentoring PC is to co-ordinate and manage the screening, training, matching, support and supervision of mentors, as well as to effectively integrate the mentoring into the organisational context and establish appropriate links with other services. 141 Co-ordinators need to be adequately inducted into the role and have the relevant skills and experiences and sufficient time to commit to the task. 145 Evaluation of the MBF peer mentoring scheme in 180 secondary schools in England104 found significant workload pressures – almost one-quarter of PCs had experienced a ‘major problem’ with managing their time, which impacted on their ability to perform this role effectively, and only a small percentage (6%) said that they had ‘no problems’ with managing their time.
Recruitment and selection of mentors and mentees
The literature also provides guidelines on risk management, to guide the recruitment of volunteer mentors. The MBF’s guide to risk management146 suggests that providers of mentoring schemes should ensure that all potential hazards and risks relating to mentors are identified, assessed and managed. The guide recommends that PCs should keep records relating to DBS checks for mentors, training attendance, supervision and contact with mentors and mentees and any incidents.
Most peer mentoring programmes employ a mentor recruitment and selection strategy, often involving a job description, a person specification and an application and interview process. 147 Careful selection of mentors is key, as mentors who cannot commit to the task or act as appropriate role models may undermine the effectiveness of the intervention. 148 For example, an effective mentor should be able to prioritise the young person’s emotional well-being. 149 An evaluation of 10 UK mentoring programmes working with hard-to-reach young people recommended ascertaining whether mentors’ motivations were primarily ‘instrumental’, namely a means to financial or other rewards, or ‘normative’ and primarily driven by the desire to help someone. 107
When mentoring is based within LAs it is also important for there to be a selection and referral process that is understood by all relevant social services teams. 141 Mentees need to fully understand the aims and purpose of the mentoring scheme to reduce the risk of misunderstandings or unrealistic expectations,145 and an orientation session for mentees, before they commit to the programme, could be beneficial. 150,151
Mentor training and support
Some form of initial training, ongoing support and supervision for mentors is essential. 106,144 The length of training varied across the mentoring programmes identified. The initial training among the 28 delivery partners for the DCSF mentoring and LAC pilot scheme141 ranged from 1 to 5 days, although most had a minimum 2-day training package and ongoing training. The Centre for Excellence for Looked After Children in Scotland’s (CELCIS) review of LA-led peer mentoring interventions in Scotland concluded that a minimum of 20 hours of training was necessary for peer mentors to feel fully equipped to undertake the role103 and, overall, it would appear that longer training times are associated with longer-lasting mentoring relationships. 152
The DCSF-funded mentoring and LAC pilot scheme141 recommended that mentor training should include introducing the role of the mentor, stages of the mentoring relationship, dealing with conflict, maintaining boundaries, confidentiality, child protection and health and safety. Mentors who are going to work with LAC should also receive training in relevant legislation, goal setting and action planning, communication skills and attachment and loss issues. It is important for programme providers and trainers to monitor mentors’ suitability on a continuing basis. Unsuitable mentors may need to be identified and deselected during the training. Evaluation of 20 Prince’s Trust mentoring projects for care leavers found that only 50–90% of volunteers completed the training and selection processes successfully. 109
The provision of ongoing support and supervision for mentors following initial training is important both to maximise the benefits for mentees and to reduce the risk of inappropriate or harmful contacts. 153 The National Children’s Home Cornwall pilot mentoring project (now known as Action for Children) found that, without proper supervision and support, unresolved issues in the mentors’ lives could impact on their commitment to mentoring. 141 There is some evidence the most failed matches are reported by programmes in which co-ordinators do not regularly contact mentors. 154 Rainer141 recommended that programmes offer group support for mentors every 4–6 weeks, as well as ad hoc or one-to-one-support every 2–3 months. Supervision serves a number of purposes for mentors: to record their contacts, reflect on their relationship and feedback concerns, submit work for accreditation if the programme offers this and identify additional training needs. Although it can be difficult to get mentors to attend group supervision, attendance may be increased by providing an advance schedule of meetings to mentors, ringing or texting mentors before each meeting to remind them, providing refreshments and adding a social element to the sessions. 141
Building the mentoring relationship
A great deal of the success of mentoring programmes depends on the quality of the relationship between mentor and mentee. 106,152,155
There is no consistent evidence on the benefits of matching mentors and mentees143,144,156 or on what attributes, if any, they should be matched on. 144,157 In practice, matching is most frequently based on geographical location, gender, race/ethnicity or shared interests. 106
Regular contact and clear expectations
It is important to provide mentors with some guidelines and expectations regarding their roles and responsibilities and some structure with regard to mentoring sessions. The DCSF-funded mentoring and LAC pilot scheme141 found that most providers delivered an introductory session facilitated by the mentoring co-ordinator. With regard to timing, content, frequency, etc., there is also evidence that mentees value the opportunity for regular but also flexible contact and the mentor being available on an impromptu basis.
Characteristics of the mentor
Mentors who have high relational qualities such as empathy, engagement, authenticity and empowerment appear to be the most effective in bringing about positive change in their mentees,158 including the formation of constructive relationships with others in the future. 159,160 Focusing on the mentee’s preferences and interests is also important for establishing and maintaining a good mentoring relationship. 161
Building rapport and trust and maintaining a strong emotional connection may be particularly difficult for LAC, many of whom will have experienced relationship breakdowns in the past,111 and this in turn may affect the motivations of the mentors. 162
Frequency of contact and length of the mentoring relationship
Different mentoring programmes adopt different arrangements for the frequency and length of contact between mentors and mentees. A Canadian review of the literature144 recommended that adult mentors and young people spend between 2 and 5 hours together every week over a minimum of 12 months. There is strong evidence to suggest that the most positive improvements for young people occur among those whose mentoring relationships last for a year or longer. 152,155,163–165 However, mentoring providers in the DCSF-funded mentoring and LAC pilot scheme141 found that 12 months of mentoring may not be sufficient for LAC and young people with multiple and complex needs. However, LAC are at risk of becoming overdependent on their mentors, which means that care has to be taken to encourage them to move gradually from a state of dependency to growing autonomy and agency. 155,163
Sustaining the mentoring relationship
When mentoring programmes are goal focused, establishing mutually agreed short- and long-term goals can be helpful, as can providing mentees with opportunities to reflect on their goals and progress within the mentoring relationship. 166
Some estimates suggest that around 50% of mentoring relationships will fail in the initial months167 and failure rates may be even higher for young people with complex problems such as LAC. 168 In a RCT of a peer mentoring programme for first-time mothers aged 16–30 years, 22 of the 32 mothers who acted as mentors resigned during the intervention and 33% of their mentees declined the offer of a new mentor. 169 The reasons given for attrition by mentors included new employment, disillusionment and insufficient time. In the DCSF-funded mentoring and LAC pilot scheme,141 the most common reason cited for relationship termination was that the mentee no longer wished to engage.
Sometimes the mentor and mentee perceive their relationship differently. Philip and colleagues170 found that, although adult mentors tended to describe their relationship with their mentee as a ‘working’ one, their mentees largely viewed their mentor as being more like a confidant or a friend. It is therefore important for mentors to be clear about their role and to be able set this out at the start of the relationship.
Ending the relationship
Research emphasises the importance of ensuring that mentoring relationships end in a carefully planned and managed way. Premature or unplanned endings may have a detrimental impact on mentees,171 especially for at-risk youth such as LAC. 144,152,155,168 Philip and colleagues170 argue that an over-reliance on the mentor may undermine the positive outcomes achieved through the intervention and lead to feelings of loss, abandonment and rejection by the mentee if endings are not managed sensitively. Conversations about ending the relationship should therefore form an integral part of the mentoring relationship from the outset. 141 This may be particularly relevant for LAC, who have often already experienced repeated rejections and losses in their lives.
Peer mentoring intervention design
The scoping exercise and the literature review were used to inform the design of the Carmen study peer mentoring intervention. This section of the chapter outlines the components of the Carmen study intervention, which were subsequently piloted.
Mentor selection process
Individual qualities most likely to be associated with being a successful mentor were being non-judgemental, empathetic and a good listener, being able to act as an appropriate and positive role model, being committed and able to meet the demands of the role. LA staff were asked to select young people who they felt were appropriate based on these criteria and professional knowledge. PCs were asked to ensure that there was enough time for DBS checks to be completed on potential mentors.
Mentor training
In spring/summer 2011 the research team met with NCB training staff and managers to discuss and finalise the content of the 3.5-day mentor training course. Following discussion with the research team it was agreed that the NCB would produce the training material. Key aspects to be covered during training were the expectations of the mentoring role, confidentiality and safeguarding, maintaining boundaries, facilitating help-seeking behaviour and dealing with difficulties (see Chapter 4 for further details).
Matching
Because of the lack of consistent evidence on attributes that mentors and mentees should be matched on, PCs were advised, as a minimum, to match mentors and mentees on the basis of geographical proximity. A 5-year age differential between mentor and mentee was specified, on the basis that mentors might experience more difficulty in maintaining an appropriate emotional distance in the relationship if they were too close in age to their mentee.
Managing the mentoring relationships
The PCs were given responsibility for recruiting mentors and mentees, managing the contacts and providing support to mentors through monthly group meetings. PCs were asked to commit a minimum of 3 hours a week to the role. It was felt that one-to-one support for mentors, in addition to monthly support groups, would be too much of a burden for PCs. The monthly support group meetings with the mentors were created for the purposes of monitoring relationships, identifying concerns, signing off work for ASDAN accreditation, giving out monies for activities and identifying additional training needs. PCs were asked to facilitate a three-way meeting with the mentor and mentee at the start of the intervention, to ensure that the aims, roles, responsibilities, length and boundaries of the relationship were clearly understood. A detailed PC role description can be found in Appendix 17, which was provided to all PCs when they commenced the role.
Mentor–mentee contact
Mentors were asked to spend at least 1 hour of face-to-face contact time per week with their mentee over a 12-month period. They were also encouraged to contact their mentee on an ad hoc basis, by telephone, e-mail or text message. Mentors were advised to give mentees the number of the mobile phone provided to them by the research team, rather than their personal contact details. They received a monthly stipend from the PC of up to £40 a month to pay for any leisure, social or other activities with their mentee and to cover travel expenses.
In relation to the intervention’s primary outcome, reducing teenage pregnancy, mentors were asked to discuss issues relating to sexual health and relationships when they felt that this was appropriate or if raised by the mentee. Mentors were advised to encourage their mentees to seek help for troubling issues (e.g. sexual health, substance use, criminal activity, mental health) using knowledge of local services or by asking professionals and, if required, to accompany their mentee to any subsequent appointments (see Appendix 17 for a detailed description of the mentor role).
Exit strategy
Mentors were asked to end the relationship in a carefully planned and managed way, to ensure that the mentee was clear about the length of the relationship from the outset and to ensure that the mentee was able to identify a support network post mentoring relationship. Towards the end of the mentoring period, mentors were asked to identify any additional or unmet support needs for their mentee and to discuss these with the PC.
Behaviour–determinants–intervention logic model: the theoretical basis for the peer mentoring intervention
The BDI logic model in Figure 1 describes the intended causal mechanism of the intervention.
FIGURE 1.
Behaviour–determinants–intervention logic model for the intended causal pathway. GP, general practitioner.
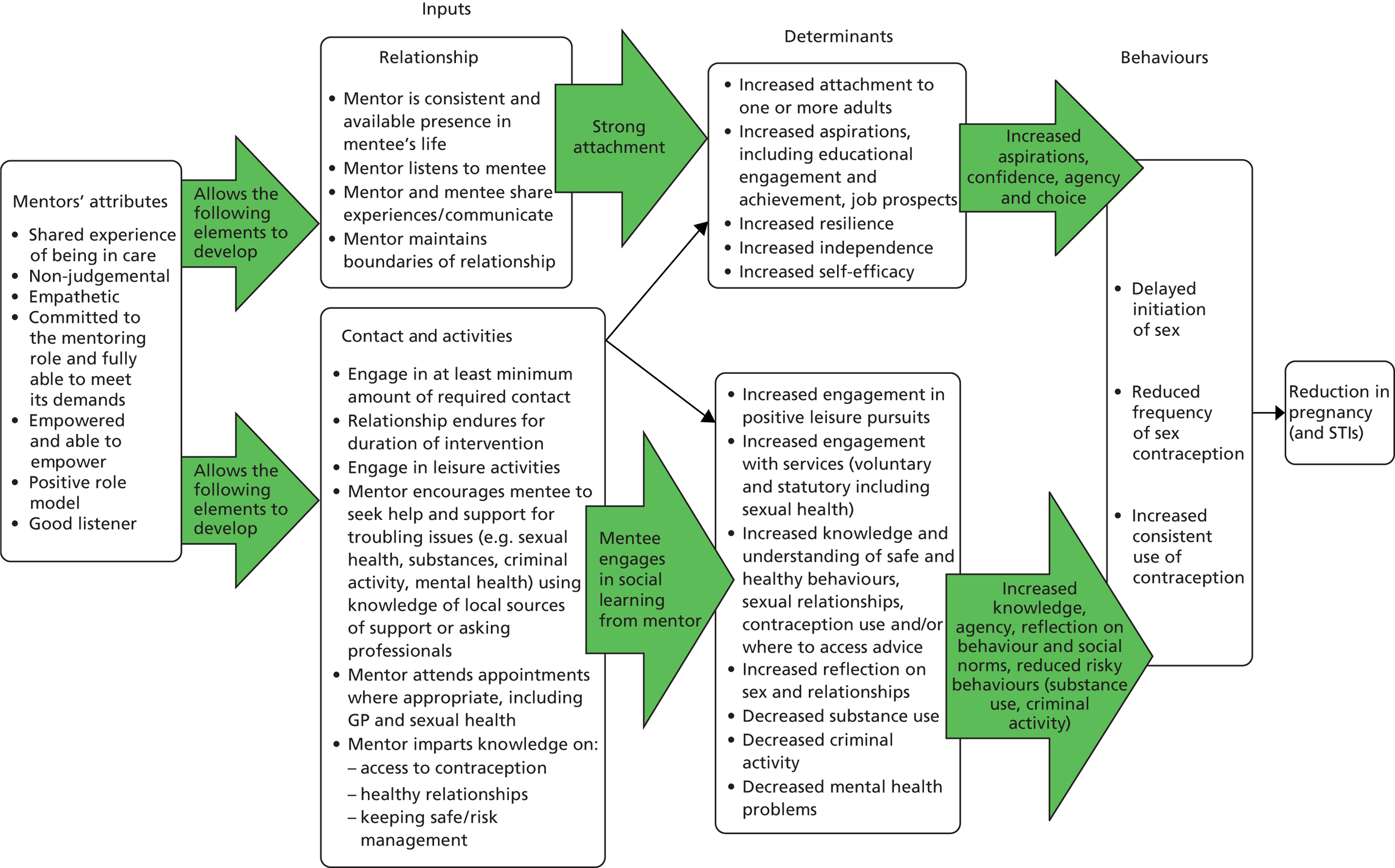
The BDI model is informed by a theory of change drawing on social learning theory and attachment theory. Bandura’s172 social learning theory posits that most human behaviour is learned observationally through modelling. From observing others, one forms an idea of how new behaviours are performed, and on later occasions this coded information serves as a guide for action. Social learning theory explains human behaviour in terms of continuous reciprocal interaction between cognitive, behavioural, and environmental influences. Necessary conditions for effective modelling are as follows:
-
Attention – various factors increase or decrease the amount of attention paid. Includes distinctiveness, affective valence, prevalence, complexity and functional value.
-
Retention – remembering what you paid attention to.
-
Reproduction – being able to reproduce the image.
-
Motivation – having a good reason to imitate.
Learning is most likely to occur if there is a close identification between the observer and the model and if the observer also has a good deal of self-efficacy.
Social learning theory could explain the following aspects of the logic model:
-
increased engagement in positive leisure pursuits
-
increased engagement with services
-
increased knowledge and understanding of safe and healthy behaviours
-
increased reflection on sex and relationships
-
decreased substance use
-
decreased criminal activity.
Attachment theory conceptualises attachment as an affectional bond, or tie, between an individual and an attachment figure. The theory was developed by Bowlby173 in relation to infant attachments but has since been applied to older children and adolescents and adults. 174 Infants form attachments to any consistent caregiver who is sensitive and responsive in social interactions with them. The quality of the social engagement is more influential than the amount of time spent. There is an extensive body of research demonstrating a significant association between children’s attachment and functioning across multiple domains. 175 Interventions informed by attachment theory posit that secure attachments are required for the development of self-esteem and social skills in adolescents. 176
Thus, attachment theory could explain the following aspects of the logic model:
-
increased attachment to one or more adult
-
increased aspirations
-
increased resilience
-
increased self-efficacy/assertiveness/confidence
-
increased independence
-
increased self-worth/self-esteem.
Furthermore, attachment theory might explain how the development of a close connection between mentor and mentee and the development of self-efficacy in the latter enables social learning to occur within the mentoring relationship.
Following the development of the BDI logic model and the components of the peer mentoring intervention, we then tested the intervention in a 3-month pilot study in LA1. The process and results of the pilot study are described in Chapter 4.
Chapter 4 Phase II: piloting the Carmen study intervention
This chapter describes recruitment and delivery of the pilot peer mentoring intervention in LA1, using researcher observations as well as individual interviews with young people and the PC at the end of the 3-month piloting period. The mentor training was also piloted and discussion about this is presented later (see Chapter 6). Further interviews were conducted with the pilot mentors and mentees at the end of the 12-month mentoring period. The discussion and outcomes data from these interviews are combined with the data from Phase II in later chapters of this report (see Chapters 7 and 8).
Recruitment criteria
The following criteria were used by senior managers and the PC for the selection of mentors: young women aged 19–25 years who were currently, or who had been, looked after. Following the recruitment stage, the researchers asked PC1 about the characteristics of the young women she had approached to take part in the mentor training. PC1 commented:
I don’t think they necessarily have to be at university or anything like that, or even working, as long as they’re . . . emotionally stable . . . it doesn’t matter how old they are, they still have their hang ups.
LA1 PC1
The three criteria stipulated by the team for mentee recruitment were being female, looked after and aged 14–18 years. It became clear following a meeting with the PC that it had been targeting only the most vulnerable and disengaged young women, as they were considered to be ‘more at risk of becoming pregnant’ (LA1 SM). This misunderstanding of the inclusion criteria had contributed to the delay in recruitment. Even after the criteria were clarified, however, the recruitment rate remained slow.
Recruitment process
The recruitment strategy was for LA1 to recruit six mentees and at least eight mentors, to allow for the possibility of up to two mentors dropping out before being matched to a mentee. LA1 was asked to recruit mentees and mentors concurrently.
The research team designed a recruitment poster containing contact details for PC2, which was distributed in LA1 buildings, to invite expressions of interest from young people who wished to be considered as mentors or mentees. One young woman made contact with the PC after seeing the poster and ended up attending the mentor training. However, others lacked the confidence to refer themselves to the study:
I saw the leaflet first, all over the place . . . yeah the poster, and you have to take one of those things, yeah and call up. So I didn’t because, I didn’t know [PC2]. I didn’t know what it’s going to be like, like talking to PC2.
Pilot mentor 3
Recruitment of mentors was aided by the existence of an established, structured, education-focused mentoring scheme within the LA. One mentor for this study was identified and recruited using this existing network:
I was already a mentor on another programme and I had resigned, quit on that programme ‘cos I wanted to join a programme that was hands on but it’s – I wanted to do more . . . so [PC1] thought this would be a good project for me to be on. And then she asked me and I said yes.
Pilot mentor 2
By June 2011, social workers from LAC teams had been informed about the project and it had been discussed in team meetings. Recruitment materials had been distributed in the Education and Achievement Centre and Leaving Care buildings. In July 2011 the research team met with the PC and several social work professionals, who reported that 12 individuals had been identified as potential mentors. However, at the end of July 2011, LA1 reported that only eight potential mentors remained, of whom six agreed to attend mentor training.
Mentor training took place at the end of August 2011 and five participants attended. Researchers made various attempts to contact the sixth individual who had expressed an interest in participating, but with no success. Following training, all five participants agreed to take part in the study and were consented, but delays in obtaining DBS clearance and in mentee recruitment meant that the intervention would not commence straight away.
Project co-ordinator 1 encountered even more difficulties with the recruitment of mentees than with the recruitment of mentors and she expressed frustration at the lack of response from social workers to her requests for the names of young people who met the inclusion criteria and the amount of time she was having to spend on chasing this up:
Despite sending out a number of e-mails to both teams, I have not heard back from any social workers as yet and the deadline I gave them was last week. I am still working on it; however, my other work has taken precedence this week.
LA1 PC1
She considered that the lack of response she encountered may have been because she was not perceived as having any particular authority within the LA. This improved, however, after a team manager (PC2) was brought in to assist her with recruitment. To try and encourage recruitment and raise awareness of the study, the researchers set up face-to-face meetings with social work teams and individuals responsible for working with young people in care. This approach appeared to be more successful in eliciting a response than the e-mail requests.
By July 2011, only one mentee (instead of the target six) had been identified. In September 2011, eight potential mentees had been identified by social work teams, but none had been informed about the study as a planned mail-out from PC1 inviting the young people to an information session about the project was not sent. Following repeated attempts by the researchers to contact the eight young women, four of them consented to take part in the study as mentees. The four who did not consent did so for various reasons, which included a wish to be a mentor rather than a mentee and reluctance to be told what to do by social workers.
Mentees and mentors were introduced to each other in November 2011. As five mentors had been recruited and only four mentees, one of the mentors was asked to delay mentoring until the Phase II trial, which she agreed to do.
Some mentors expressed frustration about the gap of 3 months between the end of training and being matched to a mentee:
That enthusiasm that I walked away with from here, it would have been nice if our relationship sort of started the following week . . . I personally felt there was too much of a gap for me to apply what I’ve learnt from the training into our relationship.
Pilot mentor 1
Communication between the team and PC1 and the LA1 social workers in the pilot phase was difficult and subject to misinterpretation. It was clear that, although the research team was operating to tight deadlines and regarded recruitment as a high priority, LA1 was unable to prioritise recruitment in the same way, largely because of the competing priorities and agendas they were operating to, which led to feelings of frustration on both sides.
The pilot recruitment process highlighted the importance of clear communication, both within the LA and in particular between the PC and social worker colleagues and between the PC and the research team. It also highlighted the importance of encouraging the LAs to recruit mentors and mentees concurrently in Phase II and the fact that this requires dedicated time from a PC, properly supported by management, which again would require adequate resourcing and financial reimbursement of the participating LA.
Consent and matching process
During consent meetings, the researchers tested out the acceptability of the baseline measures and questionnaires by examining young people’s understanding of the questions and any areas of concern for them. Three out of four participants said that they had no issue with answering questions about their sexual experiences.
With regard to matching, further data from the exploratory trial would be required to elucidate the need for and the correct basis for matching mentors and mentees. In general, mentees did not appear to feel that it was necessary for them to be able to choose their mentor, with one of them making a comparison with being at school:
You can’t choose teachers at school that you want, if you did they would all go for the same teacher you know, some teachers that are . . . would have no one in the class.
Pilot mentee 4
However, another mentee expressed appreciation at having been matched with a mentor from a similar background to herself:
I think like, if I had to pair people up, I would have to get to know the person so I could pair them with someone that’s quite like them . . . not too much like them ‘cos it causes too much argument and they clash but just enough so like, they feel comfortable . . . So, it’s like when I was talking about my mentor having certain traits ‘cos we’re both from the Caribbean . . . people might think, ok, so what? You’re both from the Caribbean but it’s just that certain factor, that, certain things we‘ve both been through together. It just makes it easier.
Pilot mentee 3
Initial meetings
Both mentors and mentees described feeling somewhat nervous before their first meeting, regardless of whether or not the PC was present. In one case this was picked up on by the mentee, who appeared to value her mentor’s lack of confidence and willingness to show her emotions:
Because when she, when I met her she wasn’t, like . . . I don’t know how to explain it but, she felt the same way as I did, so she was just as nervous and scared at meeting a new person that she’d never seen or known before, and she was very nice.
Pilot mentee 2
Project co-ordinator 1 had been asked to facilitate the initial meeting between each mentor and mentee, to discuss the frequency of the meetings, contingency planning in case of changes in circumstances or problems in the relationship and lines of communication. However, only one of these three-way meetings took place. The mentor involved in this meeting said that having the PC present at the first meeting had made her feel ‘watched’ and unable to direct the discussion as she wanted. Another mentor had requested that PC1 be present for the initial meeting but she had been unable to attend and so it had gone ahead without her. This mentor commented that the meeting had gone well although she would have liked the PC to have been present:
The main thing is just in case some people are overly nervous like me with meeting new people just someone to definitely be there to support them . . . ’cos it can be really intense.
Pilot mentor 5
The mentors made various suggestions about how the first meeting could have been made less anxiety provoking. All four mentors considered that some sort of group session, attended by all four mentor–mentee pairs and facilitated by a PC, would have been a helpful introduction to the intervention:
My education project [a mentoring project delivered at the Education and Achievement Centre], what we do every single year, at the start of the year September, the mentees and the mentors all come in the drop-in centre, what they do is like a cooking session for the whole of the 2 hours, they do a cooking session. That’s just to get them talking.
Pilot mentor 2
When you’re meeting together for the first time and you could work on teamwork and stuff like that. And that would really help you to sort of get on with mentee through that day so you can work on the relationship outside, after that.
Pilot mentor 1
Project co-ordinator 1 agreed that a group session would be a good way to introduce the mentors and mentees to each other and ‘break the ice’, which she would be happy to facilitate.
Initial stages of the relationships
The pilot mentoring phase began in November 2011. For the first 10–12 weeks of the relationships, contact between the four mentor–mentee pairs was fairly infrequent. One pair met three times, one pair met twice, the third pair met once and the fourth pair did not meet at all. This was because the mentor had gone abroad for several weeks and her mentee had then cancelled the first arranged meeting because of college commitments. One mentor said that her mentee had been very shy at their first meeting, which had discouraged her from getting in contact again:
She comes across as a very shy girl to me. She just says yes to everything and I find that very awkward to work with that ‘cos I’m a very open and blunt person, I’ll say it how it is sort of thing. So, that’s something I’m going to have to probably work on.
Pilot mentor 1
Another mentor said that she had been unable to meet with her mentee on more than three occasions in the first 3 months as the mentee either did not respond to her text messages or failed to turn up when a meeting was arranged. She expressed frustration about the amount of time that she was spending having to chase her mentee:
And then so I go there, waiting for her and she call and cancel and say ‘I can’t make it until about an hour’. And then I wait and then she calls and say ‘oh you have to come and meet me here’.
Pilot mentor 3
This mentor had wanted to take this up with her mentee but also ‘didn’t want to turn her off and stuff so [I] let it slide for a bit’. When matters failed to improve she contacted the mentee’s semi-independent outreach (SOT) worker for help, who gave her a telephone number for the mentee’s residence, which made communication easier. In addition, the mentor spoke with PC1 about the problems she was having and was advised to ‘make clear to her that I’m not available the whole day and tell her the times I’m available and she needs to be there’.
Interestingly, this mentor’s frustration was not mirrored by her mentee, who viewed their relationship very positively:
Each time it’s been fun and different. Yeah and we went to the movies and then we went out for coffee and yeah, we were just talking. Yeah, I don’t know, she feels like a sister in a way, ‘cos I talk to her about random stuff and that, will just be troubling me . . . Yeah or I’ll be on my Blackberry talking to people and then there’ll be like a random issue and we’ll just start discussing it. And it just feels good to talk to someone who is older and while they are talking to you they are giving you advice at the same time and not just talking to you on the same level if you get what I mean like . . . If I was talk to some of my friends they would understand what I mean but they are not giving me no information about the subject. Yeah, so I think it’s really good so far.
Pilot mentee 3
The initial finding was that weekly face-to-face contact for 1 hour was not feasible. This was generally, although not always, because of the unreliability and disorganisation of the mentees rather than because they did not want to see their mentor or value their input:
Yeah, it’s supposed to be every week but some of my weeks have been quite occupied so I couldn’t get to see her but hopefully I will get to see her again . . . I think when I don’t meet her, like I am disappointed sometimes. But at the same time I just know there is going to be more to talk about the next time I meet her, ‘cos there’s more of a gap, and there’s more stuff going on, so . . .
Pilot mentee 3
Despite infrequent meetings during the first 3 months, some of the pairs began to build up a relationship, which allowed for discussion of personal issues, including sex and relationships. Initial findings from the pilot were that mentees appreciated having someone to talk to about their worries and taking time out of their week to go out and do something different:
Just going out somewhere, like sitting eating or I don’t mind where I go as long as I’m not stuck at home, sitting there doing nothing . . . I don’t mind whatever I do as long as I get fed and talk to someone if I’ve got anything I specially want to talk about.
Pilot mentee 4
It’s just a different environment; like . . . ’cos, how I would put it, like all my friends are hood like. We talk and we do the same thing day in day out. So just to have one day of the week where you do something completely different it’s just relaxing in a way and you get a lot off your chest at the same time.
Pilot mentee 3
Even though I haven’t met her that much at least I still know that I have someone that I could talk to, whenever I’m worried or stressed or have coursework to finish off.
Pilot mentee 2
Mentor diary entries
During the initial months, only two out of four mentors were filling in their contact Magpi diaries on a weekly or fortnightly basis. Frequent reminders were issued by the team, as well as by the PC, but with little improvement. One mentor said that, although she had filled in the details of her contact, she had failed to complete the process by pressing ‘send to server’. Although the failure to complete the diary on a regular basis did not seem to be the result of problems with using Magpi, the team introduced an online diary as an alternative way of recording contacts for the exploratory trial, following a suggestion by one of the mentors.
Payments for mentors and funding for mentoring activities
To enable participation in activities with their mentees, pilot mentors were initially provided with £40 cash per month. They were also given £40 per month in vouchers for themselves in recognition of their role. When asked about the adequacy of these payments, PC1 commented that mentors in the LA1 education mentoring programme received a £20 voucher per session for themselves (i.e. £80 per month). There was no reason to offer additional payments for activities in the community as all of the meetings took place within the centre. No additional payments were provided to the educational mentors as all of the meetings took place within the centre. PC1 felt that increased payments for mentoring activities and travel would be appropriate in a future trial.
Of the two mentors who claimed activity money over the first few weeks, one said that she had adequate money because of the infrequency of the meetings and was able to use it to go to the cinema with her mentee; however, another mentor had found herself £5 short because of the cost of travel in London:
The money is a big issue because if you want to go out and do anything, it will cost, depending on the time of day you want to meet, that £10 just barely cover your travel let alone anything else you want to do.
Pilot mentor 1
Mentors frequently forgot to obtain receipts for activities shared with their mentee, even though they were reminded by the PC and researchers of the need to present these each month at the support meeting. In no case was money withheld because of an individual’s inability to produce a receipt.
Support for mentors
Perceptions about the frequency and adequacy of the support received from the PC during the first 3 months of the mentoring were mixed. One mentor said that she had not contacted the PC for support but would have felt able to do so if required. Another said that both her mentee’s SOT worker and PC1 had been helpful after she contacted them for advice on difficulties that she was experiencing with setting up meetings with her mentee. The two other mentors felt that more involvement and communication from PC1 would have been helpful:
The project co-ordinator . . . I think they can do more, they can do more in terms of communication, just on a weekly basis you know phoning every single mentor, have you met up with your mentee? Are you doing your weekly diary?
Pilot mentor 2
Only one support meeting was delivered by PC1 during the first 3 months of the pilot and this was attended by only one mentor. The others could not attend because of other commitments, even though this meeting had been arranged by PC1 and agreed some time in advance. The mentor who did attend used the meeting to work on personal targets as well as to complete her ASDAN paperwork, although she expressed disappointment that none of the other mentors had been able to make it:
[I’d like to talk about] how things are going and if things are not going well then why and maybe do some targets, on things like how you can personally work on things. Because . . . I’m going to have to set myself some sort of targets to aim towards and least I’ve got at the back of my head that look, this is my weakness and I need to work on it to make it my strength.
Pilot mentor 1
Project co-ordinator 1 commented that guidance from the researchers on the format and content of the support meeting had been useful. However, she said that she had found it difficult to offer the resources required to deliver sufficient support to the mentors, given her other commitments:
At the moment, it feels like I got too many roles with the project . . . I think it’s the amount of time . . . I think a lot of that’s down to me as well, it’s like [pilot mentor 1 says] ‘can you ring me just to make sure I’m doing it?’ And because at the moment everything’s been up the air with my other work, I haven’t been concentrating too much on this. So once everything is all sorted and I’m able just to ring them and say have you met that young person? Are you doing the requirements? . . . and I think for me, reflecting on my practice I need to make sure they’re coming down to the meetings as well.
LA1 PC1
Despite the amount of additional work involved and the problems encountered, PC1 expressed optimism that, during the exploratory phase, she would be able to better support the mentors and encourage the formation of mentoring relationships. Towards the end of the pilot and before the start of Phase II, she informed us that, having discussed the time constraints she was experiencing with her manager, she had been given some dedicated time to carry out the PC role in the exploratory trial.
Summary
The pilot study identified a number of problems around the recruitment of mentors and mentees, in particular difficulties in recruiting target numbers and a delay in recruiting mentees, which resulted in a delay to the start of the mentoring intervention. There were different expectations and prioritisation of the research demands between the research team and the LA professionals. Mentors sometimes found it difficult to establish the mentoring relationship, which it was considered could be rectified by more support and guidance from the PC and group meetings involving all of the mentor and mentee pairs. Mentors and mentees failed to meet as regularly as stipulated, largely because of difficulties in establishing contact and mentees failing to respond to contacts or to turn up to prearranged meetings. The payment offered to mentors for activities with their mentee was considered insufficient by a number of participants and few of the mentors complied with the requirement to complete their Magpi diaries, detailing the timing and nature of contacts. The PC experienced difficulties in carrying out her role because of her other work commitments. Nevertheless, some of the relationships did begin to develop during the first 3 months of the pilot and mentees largely expressed appreciation of their mentor’s involvement. Table 5 summarises the issues identified in the pilot study and the changes that were introduced to address and rectify these problems for the exploratory trial.
| Issue | Amendments for the exploratory trial |
|---|---|
| Lack of regular (weekly) communication from the PC regarding progress on recruitment |
|
| E-mail requests for referral elicited a low response compared with delivery of face-to-face information sessions by researchers |
|
| Failure to recruit mentors and mentees concurrently |
|
| Delay between training and intervention start – loss of mentor motivation |
|
| PC1 encountered difficulties with contacting social workers and young people, creating delays in mentor–mentee relationship start dates |
|
| Too much focus on recruitment of ‘vulnerable’ young people aged 14–18 years slowed down rates of recruitment |
|
| Recruitment – self-referral may not be a fruitful method of recruitment for vulnerable young people |
|
| Consent meetings – three out of four participants said that they had no issue with answering questions about their sexual experiences directly |
|
| Consent meetings – piloting questions about experiences of non-consensual sex, self-harm and suicide attempts |
|
| Initial meetings were not attended by PC1 – initial evidence illustrates that this would have been valued by three out of four mentors |
|
| Mentor diary was not completed on a regular basis |
|
| £10 per week for activities inadequate (for mentor who met regularly with mentee) |
|
| Competing priorities for PC led to inadequate support |
|
Chapter 5 Phase II: recruitment
This chapter describes the recruitment process that took place between September 2011 and September 2012.
Recruitment process
Allocation of project co-ordinator roles
Allocation of the LA1 PC role was described as part of the pilot process (see Chapter 4). The same individual continued to act as PC in LA1 for Phase II.
In LA2, the PC role was divided between a sexual health outreach worker from the primary care trust (referred to as LA2 PC1) and an assistant team manager from the Leaving Care Team (referred to as LA2 PC2). Senior management identified a worker with sexual health knowledge to deliver the intervention and facilitate support groups for mentors. However, the fact that she was employed outside the LA limited her access to social workers and LAC. This resulted in a second PC being identified from social services, whose role was to assist with recruitment and deal with internal organisational issues, such as mentor DBS checks.
In LA3, the PC role was given to a manager within the LAC service, who volunteered for the role, supported by a team manager from the Leaving Care Service (referred to as LA3 PC1), who was chosen because of her background in research. However, in January 2012, following an organisational restructure, her post was relocated to a different service. The LA3 PC role was then split between two individuals: LA3 PC1 and a mental health co-ordinator in the Leaving Care Team (LA3 PC2). They divided the tasks so that LA3 PC1 focused on recruitment and LA3 PC2 assisted with supporting the mentors.
Promotion of the study within the local authorities
The recruitment strategy was modified after the pilot phase. The research team met with the PCs in August 2011 to explain the recruitment process, the numbers required and the milestones we were working to. Recruitment guidelines were then distributed to all PCs in September 2011 (see Appendix 19). PCs were requested to make contact with LA professionals to provide preliminary information about the study and to meet with social workers to explain the study and ask them to identify participants. Senior managers were encouraged to disseminate information to staff. Social workers were asked to pass on the details of potential mentees and mentors to the researchers. Mentors were then invited to attend the training and mentees were contacted by the research team and consent procedures were completed.
By October 2011, very few participants had been identified by social workers, despite regular prompts from the PCs and LA senior managers. To try and encourage recruitment, in LA1 and LA2 the researchers started attending social work team meetings, together with the PCs, to promote the study. However, because of an imminent reorganisation, LA3 did not accept the researchers’ offer to attend one of their meetings. Following advice received from a CiCC Participation Officer in LA3, the team distributed new social worker recruitment guidelines and information about the study, aimed at alleviating concerns related to the use of randomisation in the study and the safety of mentor–mentee relationships (see Appendix 20).
In February 2012, the research team had another meeting with the PCs to discuss progress in recruitment. Despite being requested to complete mentor and mentee recruitment concurrently, the PCs had mainly been focusing on ensuring that there were enough mentors to attend the training, which was due to commence imminently. Even so, only 15 potential mentors (as opposed to the hoped-for 30) attended the training, which took place throughout February and March 2012 (LA1: n = 5; LA2: n = 6; LA3: n = 4).
Mentee recruitment failed to progress, even after mentor training had taken place, largely because of competing time pressures and work constraints on the PCs. PCs felt that active and visible support and back-up for the study by senior managers would have improved the response of social workers to their requests for participants (also found in the pilot study). In LA2 and LA3, senior management had been active in sending out e-mails asking social workers to identify participants. However, in LA1, there was relatively little input or visible support for the study from senior management:
I think if [name of senior manager] had sent an e-mail out saying to all the social workers that, you know, they must do their best, I think that would have went a long way . . . there’s a lot more different teams out there that we don’t work with but we could’ve got young people from them.
LA1 PC2
As a result of the delay in recruiting mentees, the researchers had to become much more actively involved in recruitment than was originally planned or anticipated. We presented the study at social worker team meetings, followed up on leads and completed a ‘floor walk’ of offices with the PCs in LA2 and LA3, which involved approaching social workers at their desks and providing them with information about the study. However, team managers often turned down, or failed to respond to, our requests to attend team meetings and so this strategy met with only partial success. The researchers then resorted to publicising the study more widely to other professionals working with LAC within the LAs. A one-page flyer, advertising the study to LAC, was developed in response to the PCs’ observations that the recruitment leaflets were too wordy to appeal to young people. These were distributed at social worker meetings. In LA3, regular e-mails from senior management to social workers produced a list of potential mentees and the researchers then asked the relevant social workers in LA3 to discuss the study with the individuals identified. Finally, following advice from a Corporate Parenting Manager, LA1 and LA3 sent a letter to all eligible young women within the boroughs (see Table 12 for numbers of eligible women), inviting them to participate.
By June 2012, LA1 and LA3 had recruited sufficient numbers of potential mentees to be randomised to the intervention and control arms. By contrast, LA2, having recruited the largest number of mentors, completed mentee recruitment only in September 2012.
Recruitment sources
Young people aged 14–18 years (mentees)
In total, 26 LAC aged 14–18 years were recruited to the Phase II trial as potential mentees (10 from LA1, 12 from LA2 and four from LA3). Thirteen were allocated to the intervention arm and 13 to the usual support arm. In LA1, the majority of participants were recruited through the mail-out letter to eligible young women in the borough. The number recruited through social worker referrals was much lower in LA1, consistent with PC1’s perception that she did not have much senior management support when pushing for referral. This is highlighted in Table 6.
| Method | LA1 | LA2 | LA3 | Total |
|---|---|---|---|---|
| Number of mentees recruited by social workers | 1 | 6 | 2 | 9 |
| Number of mentees recruited by PCs | 2 | 4 | 0 | 6 |
| Number of mentees recruited by other methods/professionals | 7 | 2 | 2 | 11 |
In LA2, the majority of participants were identified by a combination of referrals from social workers and the PCs. PC1’s role as a sexual health outreach worker also enabled her to recruit LAC who were accessing sexual health services through her clinic. Two mentees were recruited by other professionals (youth offending team and clinical psychology services). In LA3, referrals increased following a direct request from senior managers.
These results show that different approaches were used to recruit mentees. In LA1 and LA2 the PCs used the existing contacts that they had with young people to identify potential participants. Although the mail-out approach in LA1 identified more potential participants than referrals from PC1, the fact that she was well known to young people and fellow social workers within the LA made the process of identification and communication more straightforward:
In LA1 we have a sort of you know quite good relationship with young people. So, it wasn’t because of the Carmen project, I knew them anyway and I had the relationships already established.
LA1 PC1
Young people aged 19–25 years (mentors)
Fourteen mentors were recruited to the Phase II trial (five from LA1, six from LA2 and three from LA3). One additional young woman who was pregnant attended the LA3 training. However, she gave birth shortly after this and did not proceed to mentoring. In all LAs, referrals were received from social workers, PCs and other professionals. In LA2, most mentors were recruited by the PC through a LA event for care leavers. Fewer mentors than mentees were recruited through social workers. This may be because of the decreased direct involvement of social workers with young people who have been in care after they reach the age of 18 years, unless they are still in full-time education. The recruitment method for mentors is illustrated in Table 7.
| Method | LA1 | LA2 | LA3 | Total |
|---|---|---|---|---|
| Number of mentors recruited by social workers | 2 | 1 | 2a | 5 |
| Number of mentors recruited by PCs | 1 | 4 | 1 | 6 |
| Number of mentors recruited by other professionals | 1 | 1 | 1 | 3 |
| Recruitment method not known | 1 | 0 | 0 | 1 |
The most effective strategy for recruiting young people aged 19–25 years to act as mentors was through existing networks of care leavers. Some were identified by social workers who already had some professional knowledge of the young person concerned:
I did the [name of other mentoring programme run in LA1] mentoring programme . . . I think they must have heard about it and then they need mentors for their research and you know, to reduce the teenage pregnancy, to see how it goes and I think they just chose people from the [name of other mentoring programme].
LA1 mentor 4
Selection criteria for mentors
Project co-ordinators and social workers targeted individuals who they thought would be good role models for young women in care – those who had engaged in education or work and who had aspirations and a sense of direction in life. They also considered individuals’ personality, level of maturity, reliability, commitment to taking on a mentoring role, level of self-awareness and communication and interpersonal skills:
You might have so-called successful university graduate . . . but they might not be as suitable as somebody . . . who’s just steady, calm and cheerful. In fact, sometimes if you’ve got that, that person that’s up there it’s going to be quite far away from that person . . . it’s almost like they’re in a different stratosphere from me.
LA2 SW
I would be looking for somebody that has a certain level of maturity, not necessarily that they haven’t got their issues but they’re aware of what their issues are and they’re working on them. That’s stable at the moment, making quite good life choices.
LA1 PC2
Personal or psychological problems, such as a history of substance misuse or past abuse, were not necessarily regarded as exclusion factors, provided that the young woman had overcome them:
Someone who has got life experiences, so I’m not saying they couldn’t have had issues with the police or issues with substance misuse in the past, I think in some ways that’s quite useful. But more that they are more settled in where they were. In the sense of ‘I’ve had that experience, this is what I’ve done and I’ve been stable for a period of time’. I think that was for me, just that they are emotionally in the right place to be able to offer someone else support.
LA3 PC1
Pregnancy, or having a young child, did not necessarily exclude a young person from acting as a mentor, although these had been exclusion criteria in the pilot study. The appropriateness and adequacy of the mentor selection criteria are explored in Chapter 8.
Participants in the trial
Figure 2 shows the Consolidated Standards of Reporting Trials (CONSORT) diagram for the flow of participants aged 14–18 years through the trial.
FIGURE 2.
Consolidated Standards of Reporting Trials 2010 flow diagram showing the flow of participants aged 14–18 years through the trial. a, For reasons stated earlier, that is, social services do not have an available network of care leavers to recruit from.

Figure 3 shows the CONSORT diagram for the flow of mentors through the trial.
FIGURE 3.
Consolidated Standards of Reporting Trials 2010 flow diagram showing the flow of mentors through the trial.

Baseline characteristics of mentees/usual support group participants
Table 8 shows the baseline characteristics of the 30 participants aged 14–18 years. The participants in the pilot study (n = 4) are included in addition to the 26 Phase II participants. This is because the outcome analyses (see Chapter 7) include the pilot study data because of the small number of participants recruited in Phase II. The data presented in Table 8 are based on participants’ self-reported history and current circumstances. To corroborate these baseline data we sought information from each participant’s social worker; however, only 12 out of 26 social workers returned the baseline questionnaire.
| Characteristic | Intervention group (n = 17)a | Usual support group (n = 13)a |
|---|---|---|
| Age (years) at baseline, mean (SD), min.–max. | 16.4 (1.4), 14.2–18.3 | 16.7 (1.4), 15.4–18.7 |
| Country of birth | ||
| England | 13 (77) | 11 (85) |
| Other country | 4 (24) | 2 (15) |
| Ethnicity | ||
| White/white British | 7 (41) | 4 (31) |
| Mixed ethnicity | 3 (18) | 2 (15) |
| Asian/Asian British | 4 (24) | 3 (23) |
| Black/black British | 3 (18) | 4 (31) |
| Age (years) on entering the care system, mean (SD), min.–max. | 11.6 (4.7), 0–17 | 12.1 (6.3), 0–17 |
| No. of care placements, median (min.–max.) | 2.5 (1–8) | 1 (1–15) |
| Living in care continuously | 12 (71) | 10 (77) |
| Living situation | ||
| Foster home | 9 (53) | 7 (54) |
| With relatives or friends | 1 (6) | 2 (15) |
| Hostel/YMCA | 5 (29) | 3 (23) |
| Other | 2 (12) | 1 (8) |
| Self-harmed in lifetime | 9 (53) | 6 (46) |
| Missing data | 1 (6) | 0 (0) |
| Attempted suicide in lifetime | 3 (18) | 3 (23) |
| Missing data | 2 (12) | 1 (8) |
| Truanted in lifetime | 11 (65) | 12 (92) |
| Missing data | 2 (12) | 0 (0) |
| Suspended/expelled in lifetime | 5 (29) | 9 (69) |
| Missing data | 2 (12) | 0 (0) |
| Contact with police in lifetime | 10 (59) | 8 (62) |
| Missing data | 1 (6) | 0 (0) |
| Engaged in sexual intercourse | 10 (59) | 9 (69) |
| Age (years) of first sexual intercourse, mean (SD), min.–max. | 14.8 (1.6), 13–17 | 13.8 (1.1), 12–15 |
Participants often gave more than one reason for having entered the care system. The main reasons cited for being taken into care were emotional abuse (n = 6 intervention group, n = 6 usual support group), breakdown of relationship with family carer (n = 3 intervention group, n = 5 usual support group), sexual abuse (n = 3 intervention group, n = 1 usual support group), neglect (n = 2 intervention group, n = 1 usual support group), unaccompanied minor (n = 1 participant in each group) and physical abuse (n = 1 intervention group). Four participants (n = 3 intervention group, n = 1 usual support group ) stated that they did not know why they had been taken into care.
Participants reported high rates of self-harm (50%), truancy (76%), suspension/expulsion from school (50%), contact with the police (60%) and episodes of going missing from home (40%). Over half of participants had already engaged in sexual intercourse (63%), with a mean age of first intercourse of 14.3 years.
With regard to the primary outcome variable, one-fifth of participants (n = 3 in each group) had been pregnant. Four participants had been pregnant once (n = 2 in each group), one participant (in the intervention group) had been pregnant twice and one participant (in the usual support group) had had three previous pregnancies. No participants were pregnant at baseline. Out of the total of nine pregnancies, three had resulted in a live birth (n = 2 intervention group, n = 1 usual support group), four had ended in spontaneous miscarriage/stillbirth (n = 2 in each group) and two had resulted in a termination (n = 1 in each group). Only one of the nine pregnancies had been intended. Of the eight unintended pregnancies, contraception had been used on only two occasions.
Before the start of the intervention, participants were asked to state the youngest age at which they thought it would be acceptable to have a baby. The mean age reported was 17.2 (SD 3.4) years, ranging from 11 to 29 years. In total, 22 participants (73%) reported that they would feel scared/nervous if they found out that they were pregnant now, with only 2 (7%) participants stating that they would feel happy/excited. Sixteen (53%) would give birth and keep the baby, six (20%) would have a termination and two (7%) would give birth and have the baby adopted or fostered.
At baseline, seven of the intervention group (41%) and five of the usual support group (42%) scored ≥ 4 on the 12-item General Health Questionnaire (GHQ-12) (Table 9).
| Measure | Intervention group (n = 17)a | Usual support group (n = 12)a,b |
|---|---|---|
| GHQ-12 | 3.9 (3.0), 0–10 | 2.9 (3.1), 0–8 |
| Self-Esteem Scale | 14.8 (6.0), 3–30 | 18.3 (3.1), 12–23 |
| Locus of control | 3.7 (2.2), 0–9 | 4.1 (1.8), 1–7 |
A similar distribution of attachment styles was reported across the two groups, with 10 out of 29 participants (34%) indicating a secure attachment style. Eleven (38%), two (7%) and six (21%) participants indicated a fearful, preoccupied and dismissing attachment style respectively. Participants were asked to rate the likelihood that they would seek help from a variety of sources, first, if they had a personal or emotional problem and, second, if they were feeling desperate and having thoughts about suicide. The most popular source of help for a personal or emotional problem was a friend, from whom 17 (57%) participants reported that they would be extremely or very likely to seek help. The least popular sources of help were religious leaders, helplines and doctors, from whom 24 (80%), 22 (73%) and 19 (63%) participants, respectively, reported that they would be extremely or very unlikely to seek help. Only four (13%) participants reported that they were likely or more than likely to seek help from no one for personal or emotional problems. A similar pattern occurred in the second scenario. However, nine (30%) participants reported that they were likely or more than likely to seek help from no one when feeling desperate and having thoughts about suicide.
Baseline characteristics of mentors
Table 10 shows the baseline characteristics of mentors, including the pilot participants, based on self-reported history and current circumstances. All of the mentors in the study had educational qualifications. At baseline, three had already received a degree and a further four were studying at university. Of the remaining 11, six had a level 3 qualification (equivalent to A level) and five had level 1 or level 2 qualifications. Ten of the mentors had been pregnant at least once and eight were already mothers at baseline. One additional participant was pregnant at baseline.
| Characteristic | Mentors (n = 18)a |
|---|---|
| Age (years) at baseline, mean (SD), min.–max. | 21.97 (1.64), 17.71–23.81 |
| Country of birth | |
| England | 11 (61) |
| Other country | 7 (39) |
| Ethnicity | |
| White/white British | 4 (22) |
| Black/black British | 10 (56) |
| Other | 4 (22) |
| Age (years) on entering the care system, mean (SD), min.–max. | 12.17 (3.13), 17.71–23.81 |
| Educational qualifications | |
| Level 1(GCSEs D–G grades) | 2 (11) |
| Level 2 (GCSEs A*–C grades) | 3 (17) |
| Level 3 (A level or equivalent) | 10 (56) |
| Level 6 (degree or equivalent) | 3 (17) |
| Living situation | |
| Renting | 16 (89) |
| Living with family | 2 (11) |
| Occupation | |
| Full-time education | 11 (61) |
| Part-time education and part-time work/government training scheme | 2 (11) |
| Full-time work | 2 (11) |
| Unemployed and receiving benefit | 3 (17) |
| History of pregnancy (n = 10) | |
| One pregnancy | 6 |
| Two pregnancies | 3 |
| Three pregnancies | 1 |
| Age (years) at first pregnancy, mean (SD), min.–max. | 17.70 (2.62), 15–23 |
Data were missing for all psychological measures for one pilot participant. Two out of 17 mentors (12%) scored ≥ 4 on the GHQ-12 (Table 11).
Phase II matching process
Project co-ordinators were asked to match participants based on their professional knowledge of the young people, while also giving consideration to geographical proximity. PCs were asked to record the reasoning behind their decisions.
In LA1, it took > 2 months for the matching process to be completed (between June and August 2012). This was because of changes in the participants’ circumstances (one mentor had given birth; one mentor was temporarily residing outside the area; there were concerns over one mentee’s mental health issues; and one mentee moved placements) and resulted in matches being made on a staggered basis throughout the summer of 2012. LA1 PC1 tended to make matches based on her professional knowledge of the young people and their personal circumstances, for example, ‘Mentor 15 . . . has emotional well-being issues . . . and so does mentee 1001, so I thought it might be easier for them to talk to each other’ (LA1 PC1).
If LA1 PC1 did not know the individuals, she tended to match them based on geographical proximity.
In LA2, because of mentee recruitment significantly over-running, the research team advised PC1 to stagger the matching process so that mentees already randomised to the intervention arm could begin to receive mentoring. However, it took several months for participants to be matched and the process was completed only in October 2012. LA2 PC1 struggled with matching because her role was based outside social services and she therefore had less access to information about the young people. Also, by this stage, PC2 was giving little support to PC1 because of competing commitments. The research team therefore became involved by forwarding relevant information, and matching decisions were eventually based on mentors and mentees having shared interests (three pairs), shared religion (one pair), shared ethnicity (one pair) and geographical proximity to each other (one pair).
In LA3, the matching process also took over a month (between June and July 2012) because LA3 PC1 was waiting for the results of the mentor DBS checks. These had not been undertaken earlier because PC1 said that she wanted to wait until all of the mentees had been recruited. Matches in LA3 were based on geographical proximity, probably because of the large size of this LA (however, LA3 subsequently dropped out of the study before any meetings took place between mentors and mentees).
This process highlighted the length of time it took LAs to match the pairs, which added to delays in the mentoring commencing and resulted in the intervention being shortened by a number of months. Consistent with the findings from the literature review, the matching criteria were diverse; however, shared backgrounds or experiences and geographical proximity were considered important. Chapter 7 explores whether the PCs’ matching strategy was effective and makes recommendations for the process in a future trial.
Factors impacting on recruitment
To understand the barriers to recruitment, interviews with PCs, social workers and senior managers were conducted towards the end of the recruitment period. We also conducted a national survey to examine views on the feasibility of recruitment in a future trial. In the following sections we explore the factors impacting on recruitment with regard to motivations to participate in the trial, the resources available to social workers and social workers’ understanding of the inclusion/exclusion criteria and of randomisation, as well as describing, more generally, some of the difficulties encountered by researchers and social workers in attempting to engage LAC in this research.
Mentors’ motivations to participate
Mentors mostly gave altruistic reasons for becoming a mentor. These included wanting to ‘make a difference’ to another young person’s life and help them to achieve their aspirations, wanting to help them to make more informed choices about relationships and using their shared care experience to act as a positive role model.
Personal development, such as the acquisition of new skills and increasing future employability by being able to add this experience to their curriculum vitae (CV), was also cited as a reason to become a mentor:
I’d like to become a peer mentor to help young women who have been in a similar situation to myself and because I’d like to help young people in my future career and this project will give me some experience [of that].
LA3 mentor 12
A number of mentors said that they would have valued the support of a peer mentor themselves when they were younger.
Several mentors from LA1 had already been involved in an established group peer mentoring scheme run within the borough and therefore had experience of mentoring young people in care:
The first thing that came to my mind was that it would be good for me anyway ‘cos I wanted something that could be hands on, like properly get into the actual work . . . of mentoring, not being supervised all the time . . . having that free time to just, you know, talk . . . so I was interested in that.
Pilot mentor 2
The national survey similarly found that wanting to help a young person in care (28/37 responses; 76%) and being able to share their own experiences (24/37 responses; 65%) were the most frequent reasons given for wanting to be a mentor amongst care leavers aged 19–25 years.
In return for their participation, mentors were offered a £40 voucher per month and the option of completing a level 1 ASDAN qualification. At follow-up interviews, mentors were asked for their views on the adequacy of these incentives. Most said that they would have taken part in the study even without a financial reward; however, they agreed that the vouchers added an extra incentive to participate. This particularly resonated with mentors who were mothers:
Having it there is handy . . . especially like being a single mum it’s like okay, I can go and buy the nappies with this if I’m kind of short on money that week or something. So it is a bit like . . . it is quite a big incentive.
LA1 mentor 15
The mentors were undecided on the adequacy of the £40 voucher. One mentor commented: ‘I think that was reasonable . . . ‘cos it’s a volunteer position I wasn’t really expecting anything – that’s a lot – so I’m quite happy with that £40’ (pilot mentor 3).
Another mentor thought that more money should have been offered, given the amount of effort needed. She was not in education or employment and therefore financial remuneration may have been more important to her. Others, who recognised that their commitment had not been as much as expected, felt that £40 was more than sufficient (see Chapter 7 for an analysis of the reasons why mentors did not fulfil their responsibilities). Three mentors said that they may have been more committed to the role if they had been paid more, with one commenting that ‘if it was a job, I think yeah, maybe the focus would have been there a bit more’ (LA1 mentor 18).
Twenty-five out of 29 (86%) respondents in the national survey of care leavers aged 19–25 years said that they would take part in the study even if they were not paid and 21 out of 33 (63%) rated the incentives offered as 4 or 5 on a satisfaction scale (1 being ‘unsatisfactory’ and 5 being ‘satisfactory’). Only two respondents rated the incentives as ‘unsatisfactory’.
In terms of the ASDAN qualification on offer, mentors had initially valued the opportunity to pursue this. However, those mentors who already had, or who were pursuing, a university degree felt that a level 1 qualification was quite low. Some with lower-level or no qualifications welcomed the chance to obtain the ASDAN qualification whereas others said that they were too busy to complete the paperwork. By the end of the study, however, none of the mentors had obtained this qualification (see Chapter 7 for reasons why).
These findings suggest that a future trial could offer the option of a qualification for mentors; however, it would need to be managed effectively with consideration given to ensuring that the qualification being offered reflected the educational and vocational needs of the participants.
Mentees’ motivations to participate
Having the opportunity to be in a mentoring intervention, to meet new people with similar experiences to their own and to form a network were the main reasons given by mentees for participating. Several young people also expressed the desire to talk to someone who they could relate to, someone similar in age, whose role was separate and distinct from that of their social worker, who ‘didn’t know my situation, and wasn’t involved in it basically’ (LA1 mentee 1009).
I thought . . . well if I had got a mentor then I thought that would really be like really good, ‘cos I didn’t really have someone my age that I could tell completely everything to. So, it was nice to have someone like old enough to understand and relate rather than someone like my age that hasn’t been through the same things.
LA2 mentee 2008
Because I wanted someone that I could see like every week or something. Seeing the social worker’s two different things. Seeing a mentor is like, someone you bond with. And might have some kind of connection with like, for example, past experiences and stuff like that.
LA2 mentee 2002
Participants often found it difficult to differentiate between their participation in the research and the mentoring intervention; however, some did express positive views about the research, including the opportunity to be involved in a project aimed at helping young people in care and also being able to express their opinions in a research interview:
Being able to speak out about more things . . . and express the way I feel and, yeah, so if someone could get an understanding of how I am as well . . . ‘Cos most of the time I wasn’t really asked questions, like these kind of questions [referring to research interview] that I will be asked from my social worker.
LA2 mentee 2002
Local authority structural barriers
Lack of time to commit to this research was the most common reason given by social workers preventing their effective participation in this study. Despite the fact that most social workers saw the value in what the study was trying to achieve, they were unable to prioritise it because of competing work commitments and deadlines. LA1 PC2 commented that social workers’ large caseloads and time pressures meant that they often prioritised ‘reactive knee-jerking stuff’ rather than preventative work. This had a detrimental impact on recruitment to this study. Furthermore, during the recruitment period, all three LAs were subject to a number of reorganisations, inspections and cutbacks, which tended to push the requirements of this project further down the agenda:
I think on some level the team managers is maybe where there’s been a bit of a . . . blockage. Yeah, they’ve not really followed it up. And I say that, bearing in mind the environment, the climate we are all in. Consultations, inspections, Ofsted, health. These are massive things not to be considered lightly. So . . . the information may have gone out but it then slips very quickly through the list of priorities, which is understandable.
LA2 PC1
I think you get people who think well that person may or may not be interested, but it’s about trying to continue to get social workers to prioritise it. Because they are constantly getting other needs, other issues, child protection . . . I think the general concept has been received well and most people think it’s a good idea but it’s then the effort it needs to actually translate that into something active and meaningful.
LA2 SM
In LA1, PC1’s role was integrated into her existing workload. However, in other LAs, the PC role was in addition to the PCs’ existing role, which meant that they constantly had to juggle a number of competing priorities. All PCs felt that the role required a greater time commitment than originally anticipated, especially during the busy recruitment period: ‘Somebody’s got to have the time to devote that . . . I think the downside has been the consistency and you know it hasn’t been there’ (LA2 PC1).
Within all three LAs there was a lack of clear communication about the study from the PCs to social workers, despite the standardised recruitment guidelines designed for this purpose. Of the 19 social workers who responded to our survey of social workers across the three LAs, only eight said that they had been informed about the study. The focus group discussions also highlighted some confusion amongst social workers over the purpose of the study; not all social workers realised that this was a study aimed at reducing teenage pregnancy.
Given the problems encountered with recruitment, we conducted interviews with LA professionals towards the end of the recruitment period, exploring their suggestions for management in a future trial. Most suggestions complemented those from the pilot study. These included PCs adopting a face-to-face approach with social workers (rather than e-mail exchanges); having consistent support from senior management, who can use their authority to filter information down through the organisational structure; and wide advertising of the study across the borough with clear communication amongst professionals:
[It] means everybody working together consistently, sort of singing from the same hymn sheet basically. So that if you’ve got the IROs [Independent Reviewing Officers] chairing reviews that it’s featured there. If you go to a stat medical where, you know, things like sexual health, all the things that the project is trying to promote is actually discussed so it’s featured there. In schools they also have a curriculum so it’s featured there. So it’s in everybody’s face.
LA2 PC2
Professionals were united in expressing the view that a dedicated PC role should be built into a future project. This would allow PCs to persist with encouraging social workers to recruit without the constraints of competing priorities:
If you seriously wanted to take peer mentoring forward then I think you’d need to have someone who is dedicated to doing it even if it’s a 0.5 of a post, but that would be what they do. They actually support, they actually recruit because it is a process where I think you’ve got to keep on going at it, you’ve got to follow up the leads . . . it’s about that follow-up and I think the project’s shown that, that as soon as you begin to lose that focus, lose that emphasis on it, things begin to slide back and stuff doesn’t get followed up. It’s competing with other priorities and you need someone who’s really focused on it.
LA3 SM
Based on this suggestion we explored further the characteristics of the PC role, including the amount of time needed to deliver the intervention and the professional role best placed to co-ordinate it. This is discussed in Chapters 8 and 9.
Availability of eligible participants
In our national surveys of DCSs (n = 39) and social workers (n = 103), the DCSs reported that on average, LAs had 31 young women who fitted the mentee recruitment criteria and were placed in the borough (SD 26.6, range 0–160) and social workers reported an average of six young women fitting the mentee recruitment criteria per social worker’s caseload (SD 9.4, range 0–75). In theory, therefore, the pool of young people who would meet the criteria for inclusion in this and any future study is large enough to support a Phase III trial.
However, it was not considered feasible, or reasonable, to expect mentors to travel long distances to see a mentee and this placed a geographical limitation on the numbers of eligible participants, which impacted on recruitment rates. In LA3, which covered a very large mainly rural area, the professionals had to limit their recruitment to only one region, further reducing the number of potential participants (Table 12).
| Females in care | LA1 | LA2 | LA3 |
|---|---|---|---|
| Number aged 14–18 years | 101 | 102 | 269 |
| Number aged 14–18 years out of borough | 47 | 80 | 66 |
| Number aged 14–18 years living in borough | 54 | 22 | 203 |
| Totalb | 54 | 75c | 47d |
Social workers in the local and national surveys were asked for suggestions for increasing the pool of potential participants. Nearly one-third of respondents (31/91) thought that the minimum age for mentees should be younger than 14 years, to encourage them to engage in safe behaviours and to make better choices around their sexuality and relationships before they became sexually active. The suggested minimum age was around 12–13 years, although some thought that the intervention could start even earlier, at age 10–11 years:
What my belief is it needs to start at a much younger age group. I think if there is anything, it’s a process . . . in terms of positive sexual health you need to educate before they are sexually active. Sometimes by the time they are sexually active, the horse has kind of bolted.
LA2 PC1
With regard to recruiting mentors, PCs experienced a great deal of difficulty in accessing them, because looked-after young people mostly leave care at 18 years of age. LAs remain in contact with young people until the age of 25 years only if they are in education. This meant that recruitment of mentors had to be focused on care leavers who were currently in education or who had kept in contact with the LA:
I don’t know whether or not that’s just about young people moving on and disengaging with social services ‘cos they don’t want the stigma of us being involved in their lives you know, some young people simply move on and don’t stay in touch with anyone . . . perhaps they feel they’ve had so much kind of social services involvement that that’s sort of enough for them.
LA1 PC1
After we were alerted to this issue we endeavoured to explore the possibility of recruiting care leavers directly from universities, by conducting a focus group with students from universities in south-west London. However, as discussed in Chapter 2, on speaking to the head of the Student Centre it was apparent that there were very few students across the two universities in the right age range and who had self-identified as being a care leaver (and it was unclear what proportion of these were female). This suggests that recruiting care leavers directly from universities may not prove to be any more successful than recruiting them from LAs.
Randomisation
From the interviews and survey data there were mixed views about, and understandings of, the need for randomisation. In the DCS survey, over two-thirds of respondents (34/48 responses) stated that they would not have concerns about randomisation in a study of this kind and most respondents recognised the need for randomisation as a method of measuring effectiveness:
I think randomisation is a vital part of research and is a must. It is an excellent way to possibly rule out any confounding factors early on in the study that could potentially impact the study.
DCS survey respondent
Similarly, some social workers said that randomisation would not, in itself, deter them from approaching young people to participate, ‘as long as they fully understood what they were making a decision about’ (LA3 SW).
However, several senior professionals and social workers were uneasy about failing to offer a service that might be beneficial to all young people and thought that the randomisation process potentially conflicted with their role as a service provider. Many of them felt that it was unethical to raise expectations in vulnerable young people that could not be met and thought that the young people should automatically receive the mentoring if they showed any interest in the study. Concerns were expressed that young people who had agreed to participate would feel let down and disappointed if they were allocated to the usual support group and that this could affect their willingness to engage in services more generally. These concerns may have deterred some social workers from approaching young people to participate in the study or from passing on their names to the PC:
If they are going through this and then they feel that they are going to have a mentor how do they respond to that, being told well you haven’t been allocated one after they’ve gone through that process. And sometimes it’s really hard for them to accept or say to themselves that you know, I do need a mentor and once they’ve made that step, how crushing is that to then to say they haven’t got one?
LA2 health and education professionals focus group
I think for some social workers they may have identified a young woman who definitely needed a mentor . . . and the idea that they may be put forward a name and then they may not get a mentor, this may have stopped them.
LA2 PC1
The national survey of social workers came up with similar findings to the interviews: 40 out of 80 social workers said that only young people who could ‘manage rejection’, who needed less specialist support and who did not have learning difficulties could be considered for a study involving randomisation.
Finally, the interview and survey data highlighted some confusion over what exactly was meant by randomisation. Research equipoise was an alien concept to many and, for some, this extended to a deep-rooted mistrust of academic research. One social worker in particular was vocal about this:
To me it’s blatantly obvious that having a mentor is going to be a positive beneficial effect, so it’s almost like saying, well how many people think that letterbox is red? Yes everybody’s going to nearly think it’s red because it’s blatantly obvious . . . so I actually think it’s an incredible waste of money and resources.
LA2 SW
And then usually what’ll happen after all that wasted money and resource [spent on academic research], they’ll bring out some paper or form for us to do something else, which’ll just clog up 85, 95% of our work doing something that’s not necessary. So I find it . . . it’s just a waste of time, waste of money. I understand the need for a little bit of research, because that’s how things come out, but I think we’ve gone research bureaucracy mad at the moment.
LA2 SW
By contrast, evidence from the national LAC survey suggested that randomisation is not a deterrent for the young people concerned. Over three-quarters of respondents (16/21) stated that they would take part in the study knowing that they had only a 50% chance of receiving a mentor. Only one of the five respondents who said that they would not take part cited randomisation as the reason. The other reasons were all related to not wanting support from a mentor at that time in their life.
The study participants themselves had mixed understandings of randomisation, even though this was explained to them when they were consented. Data from the follow-up interviews confirmed that, although some of them were able to recall the purpose of randomisation, others could not remember or had misconceptions about it. For example, some believed that they had been allocated on the basis of their personal characteristics or behaviours, or that it was a resource issue, that is, there were not enough mentors available, or that receiving a mentor was based on ‘luck’. One mentee thought that the study was a ‘competition . . . to win a mentor’ (LA1 mentee 1007).
Of the 13 young people interviewed directly after they were allocated to the usual support group, 10 reported that they were ‘OK’ with not having a mentor or ‘didn’t mind’ and three said that they were ‘disappointed’. However, it was clear that the majority had gone into the study hoping to receive a mentor, as expressed in the following quote:
I was hoping that I did get one and I was thinking that I hope I do actually get one. I think I hoped too much though. So it was, I was fine about it afterwards, ‘cos I understood, but it was just like that fact I really wanted one.
LA2 mentee 2002
Ten out of 26 participants aged 14–18 years (n = 6 intervention group, n = 4 usual support group) did not complete follow-up interviews. For those participants in the usual support group, we do not know whether their decision to disengage from the research was influenced by the fact that they were not allocated a mentor.
Lack of understanding about recruitment criteria
Despite being given clear recruitment guidelines, social workers remained unclear about the inclusion/exclusion criteria: whether males could be included, whether potential mentees had to be sexually active and whether potential mentees could be children ‘in need’ (Section 17 of the Children Act 198923), a lower threshold than those under LA care:
‘Cos initially we didn’t know whether it was male and, we did think it was male and female and that came up in the team meeting and it’s just been, obviously with it being teenage pregnancy it didn’t filter through straight away.
LA3 SW
This lack of clarity led to social workers adopting opposing recruitment strategies: LA1 approached ‘at-risk’ young women (for further details see Chapter 4) whereas LA2 PCs approached less chaotic individuals. Although they felt that the mentoring would be particularly beneficial for the most troubled, isolated young people, they also wanted to protect them from harm or potential risk:
I think probably the ones who possibly are completely off the rails and maybe have so much issues going on . . . even though I must say you would consider all young people, because it may be even somebody in that remit would benefit from a mentor – but it would have to come at possibly at a different stage . . . it’s about is it the right time to introduce a mentor? Or would you wait until that person is a little bit more settled?
LA2 PC2
Many professionals acknowledged that it was easier to select young people who they knew would engage with services, although they also felt that hard-to-reach young people would benefit the most from the intervention:
Two of the young people that you’ve been working with . . . those two were selected because they’re here [attending the Education and Achievement Centre]. Because they’re here, they come to everything, and you can engage them. And because they’re known to us, it’s almost like ‘right well we’ll use them then for this’ whereas actually there are a lot needier young people who are incredibly hard to reach and it’s them that need it.
LA1 health and education professionals focus group
Within LA3, social workers still seemed to be adopting a targeted approach, with one social worker reporting that she chose young women who she felt would ‘potentially be vulnerable to, you know, to pregnancy in itself’.
Engaging looked-after children in this study
It was very difficult for the researchers to set up the consent meetings with the mentees; numerous contacts were usually necessary before a date and place could be agreed. In many instances these then had to be rearranged because the young person concerned did not turn up to the meeting.
Our experiences were consistent with those of the LA professionals, who reported that it can be extremely difficult to engage this group of young people in services. Some social workers wondered whether the young people’s reluctance could be related to the negative connotations of being singled out for a pregnancy prevention intervention, or the fact that this was perceived as ‘just another process that they have to go through that makes them feel different’ (LA3 SW):
I think by that stage some young people are really suffering from professional burnout, so, they just don’t want to . . . ‘I don’t want to hear . . . don’t tell me about another person that you’re going to refer me to. I’ve already got a youth offending officer, a probation officer, a social worker, a keyworker, I’ve got somebody from children looked after health . . . my teacher, my school nurse’. You start potentially going into double figures.
LA2 PC1
The LAC population often have difficulty in establishing trusting relationships because of early experiences of rejection, neglect and abuse by adults. Professionals reported that it can take a long time for LAC to build positive relationships and this was supported by some young people, who expressed suspicion that the research was being run by social services and was yet another service they were being forced to engage with:
I thought it was gonna be like time wasted and like, like how the social workers do it; like ask a load of things – I just thought it was the random things that the social workers just have to do.
LA1 mentee 1003
Although there were difficulties with accessing and engaging the young people, it was also apparent that the opportunity to participate appealed to some. Seventeen out of 22 respondents to the survey of mentee-aged LAC reported that they would want a peer mentor if they were offered one.
For care leavers aged 19–25 years, the main barrier to participation was fitting the mentoring around existing commitments. Many were in education or work and some had decided against participation because they were concerned about their ability to do the mentoring role justice. There was also a problem in making the time to attend the 3-day training event. One PC commented:
Because these guys are at school or colleges and stuff like that, it’s about trying to find an appropriate time for the training which suits everybody . . . I think you would have, you would’ve been inundated . . . you would’ve had more than 10 if we did it, the training, at a time when they all could attend.
LA1 PC1
The young people’s survey supported this. In total, 30 out of 34 (88%) young people said that they would be interested in becoming a mentor for young people in care. Of the four respondents who said that they would not consider becoming a mentor, the most cited reason was education/work commitments (four responses), as well as issues in their own lives (three responses) and family commitments (two responses).
Given these barriers, we again explored professionals’ and young people’s suggestions for promoting the study to young people in the future. Most professionals felt that a direct approach, contacting young people face-to-face, would be the best method of recruitment. They suggested accessing networks of young people in care, such as CiCCs or youth centres, as well as promoting the study at events where they would be present.
Data from the survey of young people aged 14–18 years indicated that many young people would prefer e-mail contact to other means of communication (12/18 responses). Several participants in the study also recommended wider advertising through posters and leaflet distribution, possibly because this would feel less pressurised than a face-to-face approach. As discussed in Chapter 4, however, it is not clear whether young people would have the confidence to actively put themselves forward; the survey results showed that only 30% of the 14–18 years age group felt able to call the PC after seeing a poster compared with 65% of the 19–25 years age group.
Most professionals felt that the initial approach regarding the study should be made by a professional known to the young person (i.e. a member of their care network). However, the young people who were surveyed did not have a preference as to who they received the initial information from (Table 13). Most participants in the trial had no problems with the way that they were recruited to the study. However, their willingness to engage was clearly influenced by whether or not they had a good relationship with the professional who made the initial approach:
I think sometimes with young people they may not want to listen to what their social worker says. Because social workers they really drive people mad. What I thought it could be . . . if you contacting them, contact them yourself, and say that we’d like to meet you.
LA2 mentee 2011
So I think maybe next time, as well as using the social worker . . . maybe trying to go through . . . we have like a Foster Carer’s Forum where a big percentage of our LA2 carers go – and if you tell them ‘cos they direct[ly], they know the children better than social workers, better than anybody. And I think carers have a better way of being able to talk to and persuade young people as well.
LA2 mentor 11
| Type of professional | 14–18 years age groupa | 19–25 years age groupa |
|---|---|---|
| Social worker | 4 (15) | 2 (5) |
| Another professional known to the young person | 1 (4) | 3 (8) |
| Researcher | 1 (4) | 1 (3) |
| Carmen study PC (even if not known to the young person) | 2 (7) | 10 (27) |
| Carmen study mentor | 2 (7) | NA |
| Carer/family member | 3 (11) | NA |
| Do not mind who they receive information from | 7 (26) | 16 (43) |
| Missing responses | 7 (26) | 5 (14) |
It was also suggested that a mentoring scheme that was run by an organisation external to social services, such as a voluntary sector organisation, might increase young people’s engagement with the service:
If it was sort of independent from CYPS [Children and Young People’s Services] the response may actually be sort of different. So, for example, if it was a service we had to buy into or we had to sort of refer young people to ourselves, rather than be directly from CYPS, that may be a better option and young people would probably be more welcoming to it as opposed to a bit more dubious about it.
LA2 PC2
These suggestions are considered in further detail in the discussion chapter of this report and are used as a basis for making recommendations for future recruitment (see Chapter 10).
Summary
This is a hard-to-reach population in terms of recruiting for a study of this nature. On examining the extent to which the actual recruitment process reflected the proposed one it is clear that some elements were adopted by PCs but others were ignored. Initial efforts were concentrated on recruiting mentors, resulting in potential mentors being trained before mentees were available. As in the pilot, this resulted in a delay between the end of training and the start of the intervention, which many mentors found discouraging and which is addressed in later chapters.
The reason for the PC role being split in two out of the three LAs was to avoid any single individual being burdened with an unmanageable workload. However, splitting the roles created more scope for miscommunication with regard to the specific responsibilities of each individual. Further, when the PC was placed outside Children’s Services, as in LA2, it was more difficult for the PC to access the social work individuals and networks, which were necessary to identify and recruit participants.
Senior management support was not consistent across all three LAs but appeared to make a significant difference in terms of boosting recruitment efforts and underlining the importance of the task. Although the PCs initially attempted face-to-face meetings with social workers to identify study participants, this soon tailed off as their other duties took precedence.
Overall, the recruitment process highlighted difficulties over the capacity of social workers to prioritise the study. The original intention was for the LAs to manage recruitment in-house. Although the research team was keen to retain its independence from the LA care providers, it became clear quite early on that recruitment would not have been completed without the active input of the researchers. This suggests that, in a future trial, more dedicated protected time would be needed for PCs to be able to persist in their approaches to social workers and meet the recruitment targets.
Chapter 6 Mentor training
Development and delivery of the pilot training
The training programme was developed by the NCB in consultation with the research team. It was agreed that each LA should have a separate training programme for its mentors and that the training location would be located within the LA or at a LA building to facilitate access for the mentors. The training programme was designed to last for 3.5 days and mentors were provided with a training resource pack (consisting of information on the mentor role, key messages from topics covered in training and a list of useful contacts including sexual health services – see Appendix 21). Key topics to be included in the training were derived from the literature and from advice received from members of the Advisory Group, which were then refined through further discussions with our trainers. The areas included in the pilot training were expectations of the mentoring role, confidentiality and safeguarding, maintaining boundaries, facilitating help-seeking behaviour and dealing with difficulties. Mentors also received a sex education module and learnt about risk factors for teenage pregnancy, including being a looked-after child. They were provided with information to enable them to advise mentees about where to seek sexual health advice and they were asked to accompany mentees to appointments and check-ups, etc. if invited by them.
The emphasis of training was on empowering the young person and encouraging self-reliance. We tried to discourage the development of excessive dependence within the relationship by being clear about the time-limited nature of the intervention as well as managing the ending in a sensitive and planned way. The two trainers had considerable experience in delivering training and education to young people, specifically around sex and relationships. One of the trainers was a NCB consultant and the other was a consultant for Straight Talking (a specialist teenage pregnancy organisation). The pilot training was delivered in a comfortable young person-friendly space, in the LA Education and Achievement Centre. Five participants attended and completed the training. One member of the research team observed the training on each day and conducted a focus group on the last day, to ascertain participants’ perceptions and views of the training. This feedback, as well as feedback from the trainers, was subsequently used to modify the training for the exploratory trial.
The pilot phase ‘booster’ or ‘refresher’ training was delivered in April 2012. All five mentors attended. The booster training provided mentors with an opportunity to come together, discuss their relationships and deal with difficulties that had arisen. Some of this material was then used to modify the training. However, the trainers were unable to obtain detailed feedback from the PC about the support groups or individual feedback from pilot mentors, particularly with regard to items that might helpfully be added to the exploratory phase training.
Feedback from Phase I mentor training
All participants said that they had enjoyed the training and found it relevant and useful, although many said that they would have liked there to have been more role play:
I think we could have brought a bit of drama into it . . . could have been another way of reflecting sort of thing on what we’ve learnt, rather than jotting everything down on paper . . . maybe do a little bit of role play, that would have been good I thought.
Pilot mentor 1
There was a lack of consensus in the pilot about whether mentors would prefer training to take place during the week or at weekends. One participant said that it would not have been possible to attend training during the week as she had so little annual leave; another said that she preferred training to be during the week as she appreciated having free time at weekends. There was general agreement, however, that the short and intensive training course had encouraged a positive group formation, which might not have been possible if training had been less intensive and spread out over a longer period. Interviews with pilot mentors at 3 months found that some had found the early stages of their relationship, and in particular the first meeting with their mentee, rather challenging. Many mentors lacked confidence in knowing how to approach the first meeting and also found it difficult to persevere with their approach if their mentee appeared to be reluctant or disinterested in meeting:
I think a lot more needs to be done around the first session. Because it’s not as easy as it sounds. And that’s your first initial point and if you can’t get that right then the whole relationship is more likely to just break down and not work. The other stuff will come right in the middle towards the ending of your relationship. And that’s your foundation that you need to build quite strong. And if that doesn’t exist then there’s no point to that.
Pilot mentor 1
Some of the mentors were unclear about the basic steps that they should be taking to keep themselves and their mentee safe during meetings. One mentor had been unsure about whether she should be meeting her mentee at her hostel, until she was reassured by the mentee’s SOT worker and the PC that this would be appropriate.
Development and delivery of training for the exploratory trial
Adaptations to the pilot training
Based on the feedback from the pilot, the Phase II training programme was adapted as follows:
-
more discussion about how to approach the first meeting with the mentee, including consideration of mentees’ feelings and how to respond to these
-
emphasis on the need to persevere with contacting the mentee during the initial stages of the relationship
-
an additional module on risk awareness and management, with examples and advice on what mentors should do if there were concerns about the mentee and ensuring that meetings take place in a safe setting and that the PC is made aware when meetings are set up and are taking place
-
increased use of role play, including potential scenarios that could occur in mentoring relationships
-
the need to identify and draw on outside sources of advice and support, including from professionals within their mentee’s and their own care network.
The Phase II training agenda can be found in Appendix 22.
Phase II training took place in all three LAs between January and March 2012. Five mentors attended in LA1, six in LA2 and four in LA3. All participants completed the training course, although there were varying degrees of attendance throughout the 4 days, with some participants arriving late and others leaving early because of other commitments. A minimum of 80% attendance was required to commence mentoring. The same data collection methods were used as in the pilot study.
Overall, the training was received well by participants across the three delivery sites. Feedback forms, completed at the end of each day and using a rating scale from 1 (‘very poor’) to 5 (‘excellent’), showed that the overwhelming majority of modules (16/18) were rated as 4 or 5 by participants who completed them. Participants described the training as a useful learning experience – all either agreed or strongly agreed that they had gained additional knowledge as a result of the training.
Preferred learning modules
Participants preferred the modules that allowed them to reflect on their own lives and experiences, as well as those that provided them with new knowledge. Across all sites, participants most enjoyed the modules on sex education, contraception and STIs, both because of the content and because of the interactive learning methods used. Participants were also generally positive about being given the opportunity to learn about risk factors for teenage pregnancy. One young woman in LA3 valued listening to the perspectives of other participants in the group who had become teenage parents. With regard to the module on healthy and unhealthy relationships, one participant said:
I didn’t really think of sex as in a very major thing, but obviously it opens your eyes up to a lot of things . . . because you could get yourself into a lot of trouble with that like herpes and stuff I didn’t realise you can’t get rid of it . . . and I’m thinking oh my God.
Pilot mentor 1
Other popular modules included those about child rights and building trust among the peer mentor group and a module entitled the ‘three P’s’, in which participants were asked to consider professional, personal and private boundaries in relationships and what they would be willing to share with a mentee. Mainly these modules were valued because of the combination of practical and reflective elements:
And I really enjoyed . . . the trust thing, with the eyes closed . . . I’m used to doing things all by myself and taking control of things. And what I really enjoyed was that I had to trust her to take control of, not my actions, but my steps and get me to the right place. And I think that helps in terms of trust.
LA2 mentor 19
Was it the ‘three P’s’ . . . there should be boundaries . . . on what you talk to your mentee about, plus to some extent you have to be very professional. And there will be some certain situations where you have to talk about your personal experience. So it’s about balancing everything.
LA2 mentor 10
Information relating to safeguarding and confidentiality was less positively received, largely because a few participants felt that, because of their ‘lived experiences’ as a child in care, they already knew about, or had learnt about, these issues:
Sometimes I drift off ‘cos it was a bit slow for me personally. Sometimes we go over the same thing a few times and I’ve either done it before in other training stuff or . . . not that I’m saying I know everything, I don’t know everything but sometimes I’d be like ‘come on’.
LA3 mentor 12
However, most participants were able to recognise that the reiteration of safeguarding procedures was important within the context of mentoring relationships and tried to view it as a ‘refresher’ of their existing knowledge.
Delivery methods
The emphasis of training was on discussion and reflection coupled with practical activity sessions:
The reason why I liked case studies, because you’re given a situation and then you’re asked questions which make your brain think a bit and it’s asking like what are your concerns and what would you say and what else might you do, so it’s getting you to be like placing you in the mentoring role . . . so it’s kinda like equipping you with the skills that you’re gonna need.
Pilot mentor 3
Group learning was viewed as important as participants valued the opportunity to share their experiences and opinions with their peers and the trainers:
When we split up into groups and we had our pieces of paper and pens on the floor and we were all putting in our ideas. I enjoyed that. And then coming together afterwards and both saying and sharing and putting it all together.
LA1 mentor 11
Pilot study participants suggested that role-play of potential scenarios in mentoring relationships would be a helpful tool for future training. In Phase II, role-play was implemented only in LA1 because in LA2 the participants were more reserved and in LA3 there were too few participants for role-play to be effective. When role-play was used in Phase II, participants were generally positive because it ‘gives you the experience of being in the situation and how you’re feeling’ (LA1 mentor 11).
PowerPoint slides were used infrequently by trainers and only to deliver factual information. However, this mode of delivery was the least preferred by participants. One mentor commented, ‘when you sit and listen it’s really hard to focus’ (LA2 mentor 7).
The dynamics of the group also impacted on the way that the participants engaged with the training. LA2 mentors were very different to those in LA1 and LA3. They were initially very quiet and reluctant to engage in discussion or to share personal experiences, unlike LA1 and LA3 mentors, who had been more open and cohesive as a group. The different group dynamics required the trainers to be flexible in their approach and to be willing to adapt delivery methods to the needs of each group.
Across all sites, participants expressed appreciation for the fact that the trainers were non-judgemental and encouraged them to express their views, as well as making time to speak to them individually outside the session if they needed additional support or input. Many of them referred to the importance of a safe and supportive environment, which helped their learning and also gave them the confidence to ask questions: ‘because of the environment that we’re in there’s like no one’s judging you, no one’s laughing at you or anything like that, I feel more comfortable speaking out’ (pilot mentor 3).
Factors influencing the effectiveness of training
In Phase II we had originally anticipated that around eight participants would attend the training programme in each of the three LAs. However, far fewer attended: five in LA1, six in LA2 and four in LA3. Having fewer participants meant that the two trainers were able to provide more individual support to the mentors throughout the course of the training. However, it was sometimes difficult to organise the 4-day programme around their availability. Mentors also found it difficult to fit the training in with their other commitments, including childcare, work and education. Participants sometimes arrived late or left before the end of the day, which disrupted the training and meant that it was often difficult for the trainers to cover all of the material within the time available. Some activities had to be adapted because there were so few participants present. However, participants in two of the three LAs said that they appreciated the small group size because it enabled them to gain confidence more quickly and to ‘bond as a group as well, if it was bigger you’d get little small groups I think’ (LA3 mentor 12).
Participants’ attention and concentration were affected by practical considerations such as the physical environment. LA2 had no appropriate facilities available within the LA, which meant that a small and rather airless room in a local Young Men’s Christian Association (YMCA) building had to be booked. One of the participants described it as being like a ‘prison’. Participant energy levels and enthusiasm tended to decline during the afternoon sessions; however, the use of ‘energiser’ activities were quite effective at combating these dips and were a worthwhile component of the programme:
We had to stand in a circle holding hands and we had to pass the rope over each other without using our hands. That was a good one ‘cos everyone was just . . . like it was just . . . laughter.
Pilot mentor 5
The researchers informed participants on the first day that they would be observing the training and the reasons for this. In LA1 and LA3, participants had no issue with being observed. However, in LA2, participants felt uncomfortable being observed whilst talking about themselves, which led to the researchers discontinuing observation of the LA2 mentors on the final day of the training:
I can be a bit shy in groups with delivering what I want to say . . . I could see that you lot was looking to see what I was going to say and I was a bit conscious of what to say and how I was going to say it just in case your facial expression was going to change.
LA2 mentor 8
What we actually did in this group is build up a relationship and trust, and you guys weren’t part of that. You were just on one side of the room taking notes.
LA2 mentor 7
Because of the difficulties in recruiting sufficient mentees for the exploratory trial, there was a long time gap between the training programme ending and the mentoring commencing. During follow-up interviews, participants reported that they had been excited and enthusiastic about starting the mentoring but that this had ‘fizzled out’ for many of them and they had been nervous about returning to the mentoring after such a long wait:
It did un-nerve you a little bit because you really geared yourself up for starting and then you’ve got to sort of wait . . . and then like waiting takes away the buzz of starting . . . so when you leave it and you have to come back to it it’s like ‘oh my God, like I’m gonna be in this situation again’.
LA1 mentor 18
Feedback from the booster training
The Phase II booster-training day was delivered 3 months after the start of the mentoring interventions (November 2012 in LA1 January 2013 in LA2). Because there was a long delay between the initial training and commencing the mentoring, the booster training was delivered 8 and 11 months, respectively, following the initial training. There was a consensus that the booster training should have been delivered earlier to refresh mentors’ enthusiasm and learning.
A recommendation from the pilot was that PCs should provide trainers with detailed information about the emerging issues in the mentoring relationships in advance of the booster training, to ensure that issues of relevance to the mentors could be covered in the follow-up session. However, trainers were unable to obtain this information from the PCs (see Chapters 5 and 8).
Mentors in both the pilot and Phase II reflected that they found the booster training day helpful as a reminder of what they needed to be doing and in terms of renewing their motivation and enthusiasm:
It recapped your mind really a little bit of what you are actually supposed to be doing and stuff, ‘cos half-way through I think we had all lost track of what we . . . not what we were supposed to be doing but in terms of the oomph that we all started in with, you know I think it was fading a little bit. And you know some of us was getting tired of the mentees not responding back. So that little booster training is like, you know gave us back our confidence.
Pilot mentor 2
Impact of training
Follow-up interviews were conducted with training participants at the end of the mentoring period to ask them whether they had found the training relevant and helpful, what would have made the training better and what had not been helpful or effective. There was general agreement that the training had been relevant and ‘fit for purpose’. Most felt that the training had increased their confidence in talking to young people and that they had been better able to pass on relevant and accurate information to their mentees:
I felt more confident and at the same time I was shy . . . I was thinking like how it would be the first time I see . . . I will meet my mentee, how would she react, will she be talkative, like asking questions and you feel like it’s more serious or things like that.
LA2 mentor 9
Loads of the things that I’ve learnt I didn’t know before. Like, back to the diseases, sexually transmitted diseases and safeguarding and healthy unhealthy relationships.
Pilot mentor 3
What I pretty much gained, just knowledge and being able to help young people that are looking for help really . . . and just confidence to be able to talk to them and stuff.
Pilot mentor 5
I think it’s helped me to come back to this place [Education and Achievement Centre] because I, I’ve never really use this . . . it’s helped me now to come back and then maybe use the services that are useful to me.
Pilot mentor 1
Summary
The training was largely acceptable to, and viewed positively by, participants, as evidenced by their feedback and observation by the researchers and trainers. Most of the suggestions from the pilot training were taken on board by the trainers and integrated into the Phase II training programme. However, the training did not in itself appear to prevent problems from arising when the mentoring actually commenced, as will be described later (see Chapter 8). Overall, the feelings of mentors at follow-up suggest that, although the training gave them the initial building blocks to take on a mentoring role, ongoing support was crucial to them to enable them to manage the demands of the role in the longer term.
Chapter 7 Impacts
This chapter presents descriptive quantitative data on the primary and secondary outcome measures for mentees and mentors. It also describes the qualitative data on potential impacts, collected through follow-up interviews and a ‘snapshot’ survey of participants in the pilot and exploratory trial.
Follow-up interviews were conducted with 19 out of 30 (63%) participants from the intervention and usual support groups [n = 11 intervention (three from the pilot study), n = 8 usual support; see Figure 2 for details of the flow of participants through the trial]. The interviews were conducted between June and July 2013; this was 11 months into the mentoring intervention in LA1 and 9 months into the mentoring intervention in LA2. However, the staggered starts in both LAs meant that many relationships were much shorter and therefore follow-up interviews were conducted earlier in the relationships (see Chapter 8 for a full description of the length of all mentoring relationships).
Primary outcome measure: prevention of teenage pregnancy
None of the participants became pregnant in the year between baseline and the 1-year follow-up. One participant subsequently discovered that she had been pregnant when she was interviewed at baseline.
Surrogate measures of teenage pregnancy
It is important to note that the study was not designed to identify differences between arms in any quantitative outcomes. First, the study was not powered to detect significant differences and thus all estimates have very wide CIs and the point estimates described in the following sections are not meaningful. Second, as might be expected in an exploratory trial randomising only 26 participants, there were marked differences at baseline (see Chapter 5).
Delayed age at first intercourse
At the baseline interview, 19 out of 30 participants reported that they had previously had sexual intercourse. Of the remaining 11, follow-up data were available for seven (n = 4 intervention group, n = 3 usual support group). None of the four from the intervention group reported first intercourse during the study year whereas one out of the three in the usual support group reported first intercourse during this time.
Contraceptive use
Of 19 participants followed up, 12 had sexual intercourse during the study year. They were asked to report the number of sexual partners they had had and to distinguish between contraceptive use to prevent pregnancy and use of condoms (as the only method to prevent against STIs).
Table 14 illustrates that, at follow-up, 10 out of 12 were using contraceptives to prevent against pregnancy. One-third (n = 4) were using condoms as an additional form of contraception. In the 3 months prior to follow-up, although six young women had sex without using a condom, only two of them were not using any other form of contraception against pregnancy. Three young women who were not using contraception at baseline were using it at follow-up. Interestingly, the contraceptive implant was the most popular choice of contraceptive (n = 4) followed by the injection (n = 2). Others used the patch, the contraceptive pill and the coil.
| Sexual behaviour and contraceptive use | Interventiona | Usual supporta | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID1 | ID2 | ID3 | ID4 | ID5 | ID6 | ID7 | ID8 | ID9 | ID10 | ID11 | ID12 | |
| Number of sexual partners | 1 | 7 | 1 | 2 | 1 | 10 | 1 | 1 | 1 | 3 | 3 | 1 |
| Using contraception at baseline | Yes | No | Yes | No | Yes | Yes | Yes | Yes | No | Yes | No | NAb |
| Using contraception at follow-up | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sex without a condom in the 3 months before follow-up | Yes | Yes | No | Yes | Yes | No | NAc | No | Yes | NAc | Yes | No |
| Use of emergency contraception in the last year | Yes | No | Yes | No | Yes | No | NAc | No | Yes | No | No | No |
| Tested for STIs in the last year | No | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Contracted a STI in the last year | Unknown | No | No | No | No | No | Unknown | No | No | No | No | No |
Attitudes to pregnancy
At follow-up, participants were asked to state the youngest age at which they thought it would be all right to have a baby. The mean age reported by the intervention group was 17.0 (SD 2.8) years, ranging from 14 to 24 years, whereas the usual support group gave a mean of 17.8 (SD 1.8) years, ranging from 15 to 20 years.
At follow-up, three (27%) in the intervention group reported that they would feel happy/excited if they found out they were pregnant now whereas none of the usual support group said that they would feel happy or excited. Seven (64%) in the intervention group reported that they would have negative feelings (scared/nervous/sad/depressed) if they found out that they were pregnant now compared with eight (100%) in the usual support group. In the intervention group, six (55%) said that they would give birth and keep the baby, one (9%) would give birth and have the baby adopted/fostered, two (18%) would have a termination and two (18%) would make some ‘other’ choice. In the usual support group, five (63%) said that they would give birth and keep the baby and one (13%) said that she would have a termination (two participants did not respond).
Secondary outcomes
Health and well-being
At follow-up, five of the 11 (45%) in the intervention group scored ≥ 4 on the GHQ-12 compared with three out of six (50%) in the usual support group. The vast majority of participants self-rated their emotional and physical health as ‘OK’ or better. Four participants in the intervention group reported self-harming during the study year and one reported a suicide attempt, whereas none of the usual support group reported these behaviours. Over one-third of the participants reported using at least one substance. Seven reported using cannabis and one a hallucinogen. Five of the 19 (26%) participants reported drinking at least fortnightly in the last year. Nearly half of the participants (47%) reported episodes of drinking six or more units on at least one occasion during the study year (Table 15).
| Health, self harm and substance misuse | Interventiona | Usual supporta |
|---|---|---|
| Physical health – rated OK or better | 8 (73) | 8 (100) |
| Emotional health – rated OK or better | 10 (91) | 7 (88) |
| GHQ-12 score, median (min.–max.) | 2 (0–11) | 2 (0–9) |
| Self-harmed | 4 (40) | 0 (0) |
| Suicide attempt | 1 (11) | 0 (0) |
| Used at least one substance in the last year | 4 (36) | 3 (38) |
| Drank alcohol fortnightly or more often in the last year | 4 (36) | 1 (13) |
| Anyone raised concerns over drinking | 2 (18) | 0 (0) |
| Drank six or more units on at least one occasion in the last year | 5 (45) | 3 (38) |
| Currently smoke regularly | 3 (27) | 2 (25) |
| Seen sexual health practitioner | 6 (55) | 5 (71) |
| Seen doctor more than six times in the last year | 2 (18) | 5 (63) |
Eleven young women had attended an appointment with a sexual health practitioner during the study year. Two of them had not had sex during this period. As shown in Table 14, 10 out of 12 young women who had had sex during the study year also had a STI test. Fewer participants in the intervention group than in the usual support group had seen their doctor more than six times in the last year.
Educational engagement and criminal justice involvement
At follow-up, the majority of the sample was still in full-time education; however, over one-third in both groups had truanted in the previous year. More participants in the intervention group than in the usual support group reported police involvement, had been cautioned/convicted or had had contact with a youth offending team, with none in the usual support group reporting these outcomes (Table 16).
| Education, employment and criminal justice involvement | Interventiona | Usual supporta |
|---|---|---|
| Educational/vocational status | ||
| Full-time education or training | 8 (73) | 6 (75) |
| Part-time work | 1 (9) | 1 (13) |
| Other | 2 (18) | 1 (13) |
| Truanted in the last year | 4 (36) | 3 (38) |
| Suspended/expelled in the last year | 3 (27) | 1 (13) |
| Had contact with the police in the last year | 4 (36) | 0 (0) |
| Been cautioned/convicted | 3 (27) | 0 (0) |
| Had contact with the YOT in the last year | 2 (18) | 0 (0) |
Interpersonal and social functioning
There was an increase in self-esteem of three points between baseline and follow-up in the intervention group (Table 17). There was no change in the locus of control measure. About one-third of the participants reported a secure relationship style. Six of the 11 young women (55%) in the intervention group had made a significant new friendship in the past year compared with five (63%) in the usual support group. Five of 11 (45%) in the intervention group reported feeling unable to trust anyone compared with three (38%) in the usual support group. At follow-up, 14 (82%) were unlikely, or more than unlikely, to seek help from no one for a personal or emotional problem (82% in the intervention group vs. 83% in the usual support group). The most popular source of help was friends [three (27%) in the intervention group and five (83%) in the usual support group responded that they were very or extremely likely to seek help from friends]. The corresponding numbers for seeking help when feeling desperate or thinking about suicide were 10 (59%) overall, six (55%) in the intervention group and four (67%) in the usual support group; 11 (65%) reported being unlikely or very unlikely to seek help from no one when feeling desperate or thinking about suicide, seven (63%) in the intervention group, four (67%) in usual support.
| Measure | Interventiona | Usual supporta |
|---|---|---|
| Locus of control, median (min.–max.) | 4 (0–8) | 4 (2–5) |
| Change in locus of control, mean (95% CI) | 0.4 (–1.4 to 2.2) | 0.3 (–3.0 to 3.7) |
| Self-esteem, median (min.–max.) | 18 (5–28) | 20 (14–25) |
| Change in self-esteem, mean (95% CI) | –3.0 (–6.2 to 0.2) | –0.3 (–4.4 to 3.7) |
| Relationship style | ||
| Secure | 4 (36) | 2 (33) |
| Fearful | 3 (27) | 3 (50) |
| Dismissing | 4 (36) | 1 (17) |
Qualitative follow-up interviews with mentees
The primary, thematic analysis of qualitative data is presented as part of the process evaluation (see Chapter 8). In this chapter we present qualitative data that further elucidate the outcomes data presented earlier in this chapter. The data presented in this section were collected from interviews with mentees at 12 months’ follow-up and were coded to the themes of increased mentee confidence and improved mentee decision-making. These findings have relevance to informing the logic model underpinning the intervention (see Chapter 3) and are briefly discussed here.
Mentoring and increased mentee confidence
Several of the mentees felt that having a mentor amounted to gaining a ‘friend’:
I feel a bit more confident about deciding – like making decisions . . . as a mentor, they don’t really see you as a teacher to student thing, they see you as a friend, so somebody you can relate with, have just a talk, or just hang out with.
Pilot mentee 2
One mentee had entered the care system as an unaccompanied minor 6 months previously. She spoke very little English and she had been nervous about meeting her mentor because of this. However, she reported that her mentor had encouraged her and helped her to feel more confident about speaking: ‘When I want to say something and, you know, she could understand [my English] and she say to me “say it” . . . so yeah, I can say anything to her’ (LA2 mentee 2001).
One mentee reported that she had felt confident about discussing her sexual orientation because of her mentor’s empathic and non-judgemental approach when they had first started to discuss sex and relationships:
She kind of taught me don’t let people judge me like, just be who I want to be. If they don’t like it then obviously they are not my true friends . . . I’ve gossiped about my sexuality with her, because I think . . . when I was younger . . . at the time I had a group of friends which was proper anti-gay and anti-lesbian, so I couldn’t really play on it. But now I’ve got older and I don’t really care what people say. I’m just me, if you like me, you like me. I’ve learned to open it and I’ve spoken to her about it. I think that’s the first time I actually spoke about it properly and actually decided like d’you know what? Actually I do like girls, and if you don’t like the fact that I like girls then you don’t have to be my friend.
Pilot mentee 3
Another mentee described feeling more confident about asserting herself appropriately with boys, rather than just becoming angry, as a result of her conversations with her mentor:
Well she used to say to me, ‘you can’t always beat your boy up, you have to like let them look but they’re not allowed to like come to you, because obviously if you don’t want to be talking to them and you don’t like them, you don’t have to’ . . . I still hit them [boys], but I’m a bit kinder.
LA1 mentee 1007
Another mentee felt that spending time with her mentor had broadened her mind and encouraged her to be more open, which had reduced her stress levels. At follow-up she believed that she was less likely to get angry with people:
I don’t know whether it’s just me growing up, or in a way . . . while she was there I think maybe I was like opening up myself . . . opening up did kind of release certain stress. Because I’m used to just bottling everything up, and then one day I’ll just have a meltdown and that’s when I’ll overdose myself. And that’s when I’ll go out and then I’ll sleep with like 10 different men or do something stupid, to harm myself.
Pilot mentee 3
Nowadays people could step on my foot and I’ll just blow it off, like literally because I think just life’s too short. And this time last year I would have probably got arrested for someone stepping on my foot because I would just turn around and get mad.
Pilot mentee 3
Mentoring and improved mentee decision-making
Mentees reported benefits from being able to engage in positive leisure pursuits with their mentor, including being able to make more positive decisions and ‘good choices’. For example, one mentee said that her mentor had helped her to realise that that she tended to be somewhat judgemental of other people, which had limited her social interactions and engagement. She had learnt that it was important ‘not to judge a book by its cover’ and to try to be a bit less judgemental, which had in turn begun to open up her social network:
It’s like if you see my set of friends . . . it’s like I need to stop – what’s it called? Not stereotyping . . . I need to stop having a type basically. Like because, to be honest, like my next-door neighbour she’s more into her jobs and stuff so I wouldn’t really be her friend because she’s . . . like they say a ‘nerd’ init? She’s more of a nerd and I’m more of I dunno, a problem, because it’s me that’s bad. So I wouldn’t really be her friend . . . so I think now I’m gonna start like making friends no matter what they are like . . . I should just be friends with everyone.
Pilot mentee 3
Another mentee reported that her mentor had helped her to realise that she needed to broaden her horizons, which had previously largely been focused on impressing the opposite sex:
I think that it should be for most girls now in care, living by themselves – I think this would be good for them . . . because I know a lot of depressed people and I think they just need someone, not from the area, to take them out, to show them that, look, you don’t have to get ready, put on make-up and go meet a boy, it’s not all about that. ‘Cos that’s what I used to do. You don’t have to do that.
Pilot mentee 3
Mentees also reported feeling more confident in being able to make the right choices in other important areas, including education and family life:
When I was younger, thinking I don’t care about my future, I’ve still got a long time to go, but then it comes quite quick and you’ve got to think about what you’re gonna do; so you should know from a long-off . . .’cos before I was choosing my GCSEs and like she was saying, ‘go for what you enjoy for’ and stuff so I went for that, I enjoyed what I was going to, like I hopefully want to go into . . . like when I leave school and get a job.
Pilot mentee 4
She tried encouraging me to see my family more and everything like that . . . it was just general encouragement to be honest. But there was a time where she said you need to take a step back because like my family problem was getting to like an extent that I couldn’t handle.
LA1 mentee 1006
Mentors
Impact of mentoring: quantitative findings
Twelve mentors (63%) completed follow-up interviews at 1 year. Table 18 indicates that there was little change in their general health (GHQ-12), locus of control and self-esteem between baseline and follow-up. Four of 12 (33%) mentors at follow-up scored ≥ 4 on the GHQ-12.
Impact of mentoring: qualitative findings
Although there were no significant changes in quantitative outcomes for mentors, the qualitative data suggest that some mentors experienced benefits in terms of increased confidence and self-efficacy. Our logic model did not attempt to theorise change for mentors, but these findings do suggest that mentors’ experience of the intervention might impact on implementation. This is discussed further in the following sections.
Mentoring and increased mentor confidence
The majority of mentors said that being a mentor had given them a sense of responsibility and had also helped them to feel more confident, in terms of their social interactions and when required to tackle new and unfamiliar situations. One mentor said that through having a mentee she came to realise that her anxiety in social situations ‘just means this person is new to me’ and was something that she could overcome (LA1 mentor 15):
I feel a bit more confident. Like before like, I’m not gonna lie, before if I used to see a teenager I’d be like oh my gosh, like what do I say to them . . . whereas now I’m a bit more like open. Like before I’d think, oh I bet they’re up to no good . . . whereas now I’m a bit more like, I wonder what’s going on for them, I wonder . . . how they’re feeling?
LA1 mentor 15
Another mentor said that she had applied that confidence to more practical challenges:
Whereas before I would, I would try and get someone else to ring for me, like, or, or even other calls like housing, I’d always try and get someone else to ring, ‘cos I’m not really . . . but from that [mentoring] like I had to ring the girl myself. Like I ring people now, like I’ll ring them and be like, I need . . .
LA1 mentor 18
Mentoring and increased mentor self-efficacy
A number of mentors talked about a sense of satisfaction in having been able to persevere with the mentoring in spite of things having been difficult. Pilot mentor 3 referred to how telephoning her mentee, organising meetings and encouraging her mentee to meet her had given her a new-found ‘sense of responsibility’:
I’ve learned how to interact more with young people and seen the difficulties that staff face when trying to get hold of the young people and stuff like that; ‘cos they are not very committed and not very consistent . . . But even myself I wasn’t very consistent, but I learnt . . . I want to get more involved, like to build a relationship more, I want to see in the start and then finish.
Pilot mentor 3
Mentoring and change in mentor attitudes
Improved attitudes and interactions with others were frequently attributed to the experience of mentoring, including the development of patience, tolerance and understanding and open-mindedness in speaking to younger people. One mentor explained:
It helped me to be more patient, because I’m so impatient . . . I’m still impatient but I’m working on it . . . I’m more tolerant now. Before I weren’t tolerant. I’m surprised I didn’t quit . . . it helped me now, in this job that I’m at now, the Children’s Home, you know I look back and I think [mentee 1007]’s a saint, even though she’s difficult . . . working with [mentee 1007] was a foundation of building my speaking skills a bit more, dealing with challenging behaviour a bit more and . . . having patience and being tolerant . . . try and get people to listen, you know try to, you know advocate, empower people to like change or whatever.
LA1 mentor 4
Mentors gained an understanding that people have different needs, work at their own pace and, with support, must make their own decisions:
It’s very difficult in terms of education because I’ve sort of been there, done that sort of thing and it’s very hard for me to step out of the box and think this is her life and she’s got to decide . . . and you’ve got to take it at their pace. Okay you might be an expert but they’re an expert in their own sort of background and their own, whatever is happening in their life.
Pilot mentee 1
One mentor talked about how her experience had made her decide to seek further experience, carrying out advocacy work with young people:
With pilots you know that everything isn’t airbrushed out and . . . so it’s not gonna be perfect . . . I think the positive that I can take from it is that it’s made me even more eager to kind of get out there and do something, which was . . . kind of how I come across the whole advocacy thing.
LA2 mentor 11
Summary
The qualitative data were indicative of the impacts of peer mentoring for mentees and mentors that had been anticipated in the model (see Chapter 3 for the BDI model) although, also as anticipated, this study could not demonstrate any significant changes. Mentees reported increased confidence and improved decision-making skills, especially around social networks and life choices such as education. Mentors also reported increased confidence and increased self-efficacy. These findings usefully inform the design of any future evaluation.
Chapter 8 Process: peer mentoring relationships
This chapter outlines the process of creating, sustaining and ending the mentoring relationships. It explores facilitators of and barriers to engagement, unintended consequences, safeguarding issues and the support provided to participants. These data will form the basis for investigating the feasibility domains described in Chapter 2, particularly in relation to a future full trial of a peer mentoring intervention in a social care context. The process of the mentoring relationships will be considered in six sections: nature of contact, factors affecting engagement with the mentoring process, mentor role, safety concerns, undesirable effects of the mentoring intervention and support for mentors. Within each section, when appropriate, national survey data will be used to reflect on the wider validity of interview data from participants and professionals directly involved in the study.
Nature of contact
Duration and frequency of contacts
The original timetable for the duration of mentor relationships was September 2011 to August 2012 in the pilot study and May 2012 to April 2013 for the exploratory phase. However, because of the over-running of recruitment, the relationships began later and some ended later than planned. Exploratory trial pairs had until the end of June 2013 to complete their relationships.
Tables 19 and 20 show the approximate length of each mentoring relationship calculated using mentor diary entries and self-report interview data. The tables show the approximate number of face-to-face contacts that occurred by month. All four relationships in the pilot phase (see Table 19) lasted between 5 and 11 months, although not all relationships were consistent in their level of contact. The maximum number of contacts per month was two (i.e. fortnightly contact).
| Pair | 2011 | 2012 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| September | October | November | December | January | February | March | April | May | June | July | August | September | October | |
| 1 | 1 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | |||
| 2 | 0 | 1 | 0 | 2 | 0 | 0 | 1 | 1 | 0 | |||||
| 3 | 2 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 1 | |||||
| 4 | 1 | 1 | 1 | 1 | 0 | |||||||||
| Pair | 2012 | 2013 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| April | May | June | July | August | September | October | November | December | January | February | March | April | May | June | July | |
| LA1 | ||||||||||||||||
| 5 | 3 | 4 | 3 | 3 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | |||||
| 6 | 2 | 2 | 2 | 2 | 1 | 2 | 3 | 1 | 3 | 1 | ||||||
| 7a | 1 | 1 | 1 | 0 | 0 | 1 | ||||||||||
| 8a | 2 | 0 | 0 | |||||||||||||
| 9b | 0 | |||||||||||||||
| 10b | 1 | 1 | 1 | |||||||||||||
| 11 | 0 | |||||||||||||||
| 12 | Mentor dropped out following consent and matching because at late stage of pregnancy | |||||||||||||||
| 13 | Mentor dropped out following consent and matching because of birth of child | |||||||||||||||
| LA2 | ||||||||||||||||
| 14 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | |||||||
| 15 | 1 | 0 | 1 | 1 | 1 | |||||||||||
| 16 | 1 | 1 | ||||||||||||||
| 17 | 0 | |||||||||||||||
| 18 | 0 | |||||||||||||||
| 19 | Mentor dropped out following consent and matching because of personal issues | |||||||||||||||
| LA3 | ||||||||||||||||
| Pair 20 | Mentor dropped out following consent and matching because of personal issues | |||||||||||||||
| Pair 21 | Mentor dropped out following consent and matching because of university commitments | |||||||||||||||
Table 20 shows the length of relationships during the exploratory phase. In four cases no face-to-face contact took place because the mentees were unresponsive to the mentors’ calls or were non-contactable or the mentor did not put in enough effort to ensure contact. Seven relationships lasted for ≥ 3 months, with the longest three relationships lasting for 9, 10 and 11 months. Weekly contact was not feasible. Mentors and mentees were more likely to meet once or twice a month because they were busy with education, work or childcare commitments; although mentees were more likely than mentors to desire a weekly meeting, a couple of them said that they were also too busy.
Two-thirds of survey respondents aged 14–18 years (14/21) said that meeting once a week would be ‘just right’ whereas over one-quarter (6/21) said that it would be too much. Participants aged 14–18 years in the usual support group also thought that weekly meetings would be feasible.
Tables 19 and 20 show that contact tended to be fairly consistent over the first 3–4 months of relationships but it then became less regular. Following their initial meeting in December 2011, pair 1 did not have any face-to-face contact until 2 months later. Initially, the mentee had been somewhat shy and unforthcoming, which the mentor had found difficult. However, they had maintained their relationship over 7 months, only ending then because of commitments in the mentor’s life and difficulties in finding suitable times to meet. The mentor in pair 2 found it difficult to make contact with her mentee and she often requested support from professionals in the mentee’s network. In spring 2012, the mentee in pair 3 was tagged and had a curfew imposed by the courts as a result of an offence she had committed, which impacted on her availability to see her mentor. Pair 5 began by seeing each other once a month and the relationship seemed strong, but it tailed off to no contact by April 2012.
During the exploratory trial, the mentor in pair 5 maintained a relationship with her mentee for > 11 months, with monthly contact for around 6 months supplemented by telephone conversations. Despite living furthest from her mentee, the mentor in pair 6 had one of the longest and most consistent relationships with her mentee. She was the only mentor to see her mentee at least once a month for the duration of her relationship, occasionally arranging two or three meetings a month.
In addition to face-to-face contact, pair 14 held long conversations over the telephone (usually around 30 minutes), particularly as the mentor said that she felt that she needed to save up activity money to participate in activities with her mentee. In general, however, the mentors’ research telephones were just used for the purpose of setting up meetings with their mentee, rather than providing the intervention.
Initial meetings between the mentor and the mentee
In LA1, the majority of mentors and mentees met up for their initial meeting without anyone else being present, although two pairs had meetings facilitated by the PC. Three pairs held their initial meeting in the education centre, which meant that the PC or other staff were available if needed. In general, mentors and mentees appreciated the presence of the PC at the initial meeting:
‘Cos it was the first like additional meeting with anyone it was kind of like, it was a bit nice to have that support, like from [PC1], so like, you know like every now and again I could just give that look like ‘am I saying everything right, am I doing?’ . . . and just get that little reassurance like okay you’re doing alright.
LA1 mentor 15
In LA2, the PC organised a group meeting for the mentors and mentees to get acquainted with each other in an informal atmosphere. All of the mentors attended, but none of the mentees turned up, despite being reminded several times about the day and location. As a result, the introductory meetings between mentors and mentees had to be arranged on an individual basis over the following weeks. It was clear that both mentors and mentees were somewhat nervous about the initial encounter:
I was a bit worried that we wouldn’t get on. Or if we just didn’t like each other . . . so I was worried that I wouldn’t be able to even talk to her . . . it was . . . like when we first talking to each other it was just a bit like getting to know each other, but we got comfortable with each other, like over time.
LA2 mentee 2008
Her mentor was somewhat more positive about their first meeting: ‘My first meeting was excellent, me and my mentee got on like we’d met before’ (LA2 mentor 8).
Contact during the mentoring period
Activities
During the mentoring period the most popular shared activities were eating in fast food restaurants, drinking in coffee shops and going shopping together. In addition, three pairs had some form of beauty treatment (e.g. manicure/eyebrow threading). Other activities included going to the cinema and going bowling and in LA1 two pairs made use of the education centre where they participated in activities such as table tennis.
Topics of conversation
Data from the mentor diaries show that the most discussed issues, in order of frequency, were family/carers, school/education and relationships with boys and friends. Many of the mentees had exams during the year and wanted to talk about the future and transitions from care, as illustrated in the following quotes:
We talked about college; we talked about someone helping her with some of her work. Talked about her home life, we touched about boyfriends and stuff like that as well.
LA1 mentee 1001
She knew the situation with my mum so she felt that she would be able to call me and ask about that. So when, like if I’d call her she’d call me and I told her there was something wrong then we’d have conversations about that.
LA1 mentee 1008
I spoke to her about me moving and everything and told her I felt really lonely and everything ‘cos obviously I’m living in a flat on my own.
LA1 mentee 1006
Some mentees wanted to discuss problems that they were having in their relationships, which in turn allowed mentors to introduce the subject of healthy relationships:
I was talking to her about him . . . ‘cos he was acting kind of weird, like putting up girl’s pictures and stuff on BBM [Blackberry Messenger]. I would talk to her about I don’t know what to do, whether I should play his game or if I should just act like I don’t care about it, when it does [bother me]. And she will be like I should talk to him, like just be like ‘Look, you do not do this if you’re with me kind of thing’ . . . I did take her advice, and it went alright, for a while, then he went back to the same stupid things.
Pilot mentee 3
Four mentees were not interested in talking about sex or contraception at all, either because they did not have a boyfriend or because they thought that their education or other issues were more important. However, there were several examples of mentors ensuring that their mentees were aware of local sexual health clinics and encouraging them to attend:
My understanding is that she doesn’t have a boyfriend at the moment. But obviously it never hurts to pass on the information anyway . . . And when she said she doesn’t have one I thought okay I’ve already given her the information that she needs to know, so now we can move away from that subject, unless she, you know, she then says she’s got one.
LA1 mentor 6
Young women we questioned in the usual support group also said that they regarded issues around their schooling and education as more of a priority than relationships, sex and contraception:
No . . . ‘cos I think of school and education first and studying; that’s the . . . like the last thing on my mind.
LA2 mentee 2002
I was going the study centre [she was kicked out of school], so we did talk about sex, like once or twice but it wasn’t the main thing.
LA1 mentee 1005, who had a professional mentor at the study centre
Mentor 9 stated that she would have felt uncomfortable speaking to her mentee about safe sex and thought that her mentee would not have wanted to broach the subject with her. She considered that it would be best to discuss neutral topics at the beginning of the mentoring relationship, before moving on to more personal and intimate issues, including sexual relationships, once the mentee indicated that she felt comfortable with this:
It’s better when it’s general because you can start from school and end up in sex. You see because when you talk about school you are gonna have a topic where it’s gonna drive you into a different topic and so on.
LA2 mentor 9
Two mentors spoke to their mentees about safe sex and healthy relationships, despite finding it somewhat embarrassing, with one mentor persisting in checking whether her mentee felt safe in her relationship and was not being forced to engage in anything she did not want to and advising her to seek advice from a clinic if necessary.
Relationship endings
Four pairs, one during the pilot and three during the exploratory phase, participated in a planned final meeting. One mentor said that her mentee had ‘seemed shocked’ by the ending, despite the fact that she had been expecting it. Mentor 18 had not reminded her mentee about the ending, as she had not seen her for 2 months, but she did arrange a final meeting to say goodbye. She felt that it would have been better to have had this last meeting as a group meeting, involving all of the mentors and mentees:
End it how it kind of started with everybody, like you know? Bring it all back to one again, like and not just everyone finish separately . . . I think maybe a little gathering at the end.
LA1 mentor 18
Some of the mentors arranged shopping or restaurant trips with their mentee for their final meeting. Mentor 4 used the last meeting as an opportunity to reminisce about the things that they had done together and clearly found the experience valuable and rewarding:
It was lovely, it was so nice. We did . . . her favourite, which is restaurant and cinema in one . . . and we were reminiscing all the like highlights and what happened and [when] we was out and about, like little situations we got into . . . we just talked about the good times, the bad times and she let me know how she felt . . . she said she was gonna miss me, she really loved working with me, she thinks I’m a really lovely person and she goes if you go on to be a social worker or whatever you will be so good at it . . . oh and I go shocking you are saying all this after how many times I had a go at you. And then she just went like ‘even though you had a go at me . . . it’s not like you was like being horrible’, she goes at least you cared or whatever.
LA1 mentor 4
Two of the four mentees were openly disappointed when the relationship ended:
I wouldn’t mind talking to her again actually yeah . . . I wouldn’t mind her being my tutor for college actually – that’d be really helpful ‘cos I’m going to do animal care.
LA1 mentee 1007
I’m sad. I thought it would have lasted longer so I could see her a bit more. But hopefully I’ll see her again anyway.
LA2 mentee 2008
However, another mentee said that she was ‘okay’ about the mentoring ending, as her mentor had informed her she could keep in touch with her by phone if she wanted to talk. One of the mentors expressed disappointment at ending the relationship, which she thought had been ‘strong’, and worried about the impact of ending on her mentee: ‘I kept saying all the way through that it’s ending now. So I think she was ready. She mentioned that every time she gets close to someone they go away’ (LA2 mentor 8).
A number of pairs had no definite ending because their contact tailed off. Some of the mentees expressed disappointment that the relationship had ended prematurely, even though they had often failed to respond to their mentor’s calls/texts and requests to meet up: ‘It’s like knitting a scarf and not completed it, you just feel like why did you start it . . . I don’t know me personally I didn’t want it to end’ (pilot mentee 3).
Following concerns raised by professionals that ending the relationships after 12 months could leave mentees feeling disappointed, mentors were asked to ensure that their mentee was aware of the official month of the relationship ending from the outset and to identify any follow-up needs for their mentee before ending the relationship.
Focus group participants aged 14–18 years in the other London borough (LA4) were concerned that if a mentee remained in need of support but was unable to continue seeing her mentor, any benefits from the mentoring could be cancelled out:
Because I’ve been so used to that support, if I was happy and was willing, I don’t need no more support. But if I felt like I needed support and they just dropped it then it’d be I’d just gone back to square one again . . . I wouldn’t wanna to do that support for a year and then I’ve achieved everything and then I’ve just gone back downhill again.
LA4 age 14–18 years focus group
The national survey of young women aged 14–18 years and 19–25 years also provided examples of young people who had felt let down and disappointed following the end of a mentoring relationship:
I was gutted because it was really helpful and made a difference for the right reasons.
Age 14–18 years national survey respondent
I felt fortunate to of even had a mentor who helped me so much, however I was a little sad because I had no one to go to for advice when difficulties arose.
Age 19–25 years national survey respondent
Factors affecting engagement with the mentoring process
In this section we explore the factors that affected engagement with the mentoring process, together with preferred mentoring styles and matching considerations. We also identify some of the barriers that young people experienced in establishing, developing and maintaining mentoring relationships.
From the analysis of the qualitative data, seven themes emerged, which highlight attitudes, skills and personal qualities that enabled mentors to effectively engage in a mentoring relationship, regardless of whether this was a short or long relationship. These were the basic building blocks for trust to develop, which is a vital element for establishing and sustaining mentoring relationships. The seven themes were:
-
non-judgemental attitude
-
active listening and advising
-
sharing personal experiences
-
advocacy and signposting to support
-
maintaining confidentiality
-
offering new opportunities
-
persistence.
Non-judgemental attitude
Because many of these young people were very used to being judged or criticised by others, the idea of having someone to talk to from outside their friendship or social network who would not judge them was very appealing:
I would have them [friends], but then I wouldn’t talk to them as much . . . because they’re close to me, so I wouldn’t really talk to them . . . because I’m scared in case they judge me. I thought if I had a mentor they wouldn’t really judge me ‘cos they don’t really know me.
LA1 mentee 1006
Mentee 1006 valued the fact that her mentor did not simply tell her off or panic after she disclosed that she might be pregnant, but offered her help and practical advice to deal with the situation:
She tried helping me out saying do you want me to come [to a clinic] and everything. I was like okay. And then like I found out I wasn’t [pregnant] anyway . . . it was really calm. Like if I told my friends, my friends would panic; they would be like ‘oh my God, you’re pregnant’ da-da-da, they wouldn’t, they wouldn’t stop and kind of go you might not be.
LA1 mentee 1006
Active listening and advising
Mentees in the study said that they appreciated being able to ‘offload’ to a mentor and to feel that they were being listened to. They also appreciated that a mentor would only offer advice after listening to them and taking their views and concerns seriously: ‘When I see her I get things off my chest and that. So it helps, a lot. Because I’m the type to not really say a lot’ (LA1 mentee 1006).
Mentees appeared to differentiate between talking to their mentor and talking to their friends or to an adult in a position of authority:
‘Cos she’s really down to earth and she just says it how it is, like, she says it straight. Like, she don’t use these big political words and stuff like that . . . She just makes me feel really comfortable, like I’m talking to one of my home girls. But at the same time she’s not ‘cos you know she has that professional side to her . . . it feels good.
Pilot mentee 3
Sharing personal experiences
During the training, mentors were encouraged to think about the aspects of themselves that they would like to keep private and those that they would be happy to discuss. Limited self-disclosure by mentors of personal information was often quite useful in facilitating difficult conversations:
I’ll be like ‘So tell me about your love life?’ and then I just like mention something minor about mine or whatever, or ‘mine’s dead boring’ and then I realise it makes her talk a bit more.
LA1 mentor 4
Because it wasn’t just me opening up, it’s not like someone’s asking questions and I’m answering, it was both – like she’ll tell me stuff about her current life and I’ll tell her something about mine, so it’s like we are both really trusting each other, and I saw that she trusted me, when like she told me stuff about her and her boyfriend and I think her son . . . so I thought okay, then I’ll tell her stuff about me.
Pilot mentee 3
Advocacy and signposting to support
An important part of the mentor role was the mentors using their knowledge and experience of the care system to support mentees with their issues in care:
And then we were talking about getting my passport done and she got in contact with my social worker and pushed him to do it – that got done.
Pilot mentee 2
I even said to her . . . advised her like did she know places like Children Right‘s Officer, things like that . . . ‘Cos, honestly, myself, I never knew about all that, until, you know . . . when I start learning about all those services it was a bit too late really . . . I was trying a little bit just to put her into that, and say to her ‘We can meet those kind of people, they can explain things to you if you don’t understand’.
LA2 mentor 9
Maintaining confidentiality
Mentees appeared to appreciate the fact that whatever they told their mentor would be kept confidential, but they also understood the limits of that confidentiality. It was also important that the mentor was located outside their usual social network in terms of facilitating disclosure of sensitive information:
It’s good . . . because I know . . . things that I told her and if I told like my other friends – I’m not trying to say they will tell other people – but somehow it always ends up coming out – but I know for a fact ‘cos she don’t know no one that I know, no one that I know would come back to me and be like ‘Well I heard she said this’ because it can’t happen . . . So that’s why I liked her.
Pilot mentee 3
Offering new opportunities
Some mentees felt that having a mentor had given them opportunities to do new and exciting things or to have new experiences:
She’s just so different. And like, you know whereas I’ll wake up and I’ll ping [call/text] my friend and be like, ‘So what’s the motive?’ and she’ll be like, ’Can we go link [hook up with] a boy’ – she’ll [my mentor] be like, ‘Can we go shopping?’ . . . I mean my usual group of friends it will be like a special occasion. Like for us [friends] to go ice skating it would be like ‘oh my God we’re going ice skating’ but for me and her it will just be like ‘Yeah, it’s just ice skating’.
Pilot mentee 3
Persistence
It was difficult to assess why some mentor–mentee pairs were able to sustain a relationship over a period of time whereas others fell by the wayside at a relatively early stage. Some mentors withdrew from the intervention when faced with a difficult or reluctant mentee; however, others remained enthusiastic and adopted various strategies to engage their mentee and persevered with the relationship:
I say let’s do something different, but she keeps on wanting to go cinema . . . I said we can do other things you know? I go if you wanna go to a show or do you wanna do something that’s involved with sexual health? Sometimes you can go [to a] clinic and book an activity . . . I said to her we could do ice skating. I go we can do anything; it can be sport – to get fit or whatever . . . It helps you find her a little hobby. But, no, she seems to just like cinema.
LA1 mentor 4
It would appear that the personal qualities of the mentors, in particular openness, dedication, persistence and good problem-solving skills, were important determinants of a sustainable mentoring relationship, as illustrated by the following case study examples:
Case study: pilot mentor 1 and pilot mentee 2
Mentor 1’s motivations for becoming a mentor had been to gain work experience. However, she was very enthusiastic about the task and her motivations had become increasingly altruistic as the mentoring went on. At follow-up she said:
Even though I didn’t think of it at that time, it’s good to see another young person’s point of view in terms of the care system and how things are going – from their perspective ‘cos obviously things are different from my own.
Pilot mentor 1
She had reported difficulties in the first few months of the relationship because her mentee was very reserved. She admitted that she had been discouraged by her mentee’s response and this had deterred her from making further contact with the mentee for a couple of months. However, after contacting PC1 to ask for support, she decided to persevere and introduced her mentee to activities such as bowling and going to the education centre. Through participating in these activities, the mentee met new people and started feeling more confident about voicing her opinion:
We went to Pizza Hut and she was so scared about whether she could eat with her hands and things. And I just said to her ‘You can do what you want, it’s okay’. ‘Cos she was so looking around the environment, trying to fit in to try and please other people – that other people who eat with a knife and fork – and she goes to me, ‘Can I eat with my hand?’ I go ‘Yeah, go for it’.
Pilot mentor 1
This mentor also acted in the role of advocate for the mentee who was applying for her passport.
It was clear that the mentee had enjoyed having someone to listen to her and her mentor kept encouraging her to make decisions, which had a positive impact: ‘ I feel a bit more confident about deciding – like making decisions . . . I know what I want to do next . . . what I have to do next year in order for me to be able to do nursing’ (pilot mentee 2).
Pilot mentor 1 was able to manage her time around other commitments, including her child, who was looked after by family members, and her college work. As a result of her persistence, she and her mentee met up at least once a month on a Saturday. The mentee ended up visiting her friend who lived near the mentor on Saturdays and she would meet her mentor afterwards. The mentor expressed a sense of satisfaction at having persisted with the relationship with her mentee, despite the initial difficulties:
I stuck by it, it’s a very good thing. ‘Cos normally I don’t like talking to people that are like that . . . becomes a very judgemental sort of thing from my perspective ‘cos she’s not open and she’s not talking. That’s a can’t be bothered . . . that’s the kind of attitude I’ve sort of had. So the fact that I’ve actually stuck by it and she kept at it as well made it a good relationship . . . and we’re still in touch now.
Pilot mentor 1
Case study: mentor 4 and mentee 1007
Mentor 4 was faced with some challenging behaviour from her mentee (1007) from the outset and dealt with this by sharing her concerns with the mentee’s carer. She also explained to her mentee that her behaviour was unacceptable and decided not to meet with her during the holiday period to show her that there were consequences to bad behaviour: ‘Like I say to her this is voluntary work so I’m volunteering to be here with you, don’t disrespect that. And then I think that’s when she’ll calm down’ (LA1 mentor 4).
At times, mentee 1007 would become angry or frustrated about issues in her life and would vent her frustrations by being rude to her mentor or by discontinuing calls (the researchers also experienced this when contacting this mentee). As a result, mentor 4 began to send mentee 1007 a text message before attempting to call her, to test the water:
When she’s annoyed like she gets stroppy with me. And I always have a go at her about this. I go you need to stop acting like that . . . and I go, to top it off, if you continue acting like this I will turn around and say I don’t want to work with you no more, [because] I said to her this is voluntary . . . I go you’re acted like a spoilt brat, and you acted selfish. Then I go, ‘I’m not saying this to be rude or hurtful, I’m just letting you know because like I say you’re 16 – you’re soon gonna be 18 – life gets harder for us’ . . . I just told her the truth.
LA1 mentor 4
When the mentor reprimanded her mentee or refused to see her there appeared to be a temporary improvement in her mentee’s behaviour. The mentor acknowledged that, although she felt guilty about reprimanding her mentee and was concerned that she would not want to engage with her any more, her mentee continued to send her text messages and she remained engaged, appearing to appreciate the consistent messages and boundaries that were being put around her behaviour. When asked what qualities she valued in a mentor, this mentee responded: ‘[Be] confident, open to speak their minds, friendly, and not too over the top. Not scared to speak their minds when it comes to anything. Tell me where I’m going wrong’ (LA1 mentee 1007).
This mentee did not consider that she had experienced any significant difficulties or arguments with her mentor, in spite of the firm approach adopted, although she did recognise that on occasions her mentor was ‘peed off’ by her behaviour. She spoke only in positive terms about her mentor and her mentoring experience, including the last late-night meeting when she said ‘I was safe ‘cos I was with her’.
Mentor 4 was hoping to work with young people in the future, which she felt had helped her to maintain the contact, despite her frustrations. She also acknowledged that she was generally not very good at seeing things through to the end, which had made her more determined to make the relationship work:
When you work with vulnerable people, you are always gonna get difficulties, that’s just normal. It’s just helping you to gain the skills so when you have challenging situations, gain the skills and learn how to handle it, deal with it and overcome it in different ways . . . She is a nice person as well.
LA1 mentor 4
Shared experience of care
The majority of mentees said that they would rather speak to a mentor than to their social worker about personal issues, as social workers were often too busy fulfilling statutory requirements to listen to them or to support them with emotional issues. At the end of the mentoring period, when the mentees were asked if there was any more support that they required, one said:
Having someone like her . . . a mentor that isn’t a social worker, who I can talk to about problems, and then yeah, just to get a bit of space away – like with someone that’s older . . . so she could give me advice.
LA2 mentee 2008
Social workers also felt that they would be less effective than peers at engaging the young people in conversations around intimate issues, both because of the age gap and because they tend to be viewed rather negatively and mistrusted by the young people they work with:
I think it’s really difficult for looked-after young people to talk to social workers. I think that although social workers are skilled in communication, I think they know that if they share too much information that social workers might have to act on that if they feel it’s a child protection issue.
LA1 SM
This view was echoed by the mentors:
This is what I thought, ‘Anyone who’s working with me, they’re going to report back to my social worker ‘cos that’s their job’ . . . when I speak to a lot of young people they said the exact same thing.
LA1 mentor 4
The majority of those aged 14–18 years (seven of the 11 who spoke about it) considered that it was important that their mentor had some experience of care, as it made it easier to relate to them:
Someone was actually in your situation so they knew what they’ve also been through and what you had been through, instead of saying ‘Ah, I know how you feel’ when actually they don’t know nothing how you feel . . . it’s like teachers say ‘Yeah, I know what you’re going through’ and it’s like, no you don’t, shut up [laughs].
Pilot mentee 4
One of the mentors also considered that her experience of care had helped her to empathise with and build up a relationship with her mentee:
There was one girl that come up to me, and she was like ‘I just miss my mum, I don’t understand’ . . . and she just broke down crying. One of the other members of staff she come over and she was like ‘Oh it’s alright, it’s alright’ and the girl flipped out. And then I went over and I was like ‘Look, I’ve been there, I’ve come through now, like look at me’ . . . and I kind of explained a little bit of my story without trying to traumatise her and by the end she was like ‘Oh’, she was like ‘You went through that?’ and I was like ‘Yeah’. And she was like, ‘And you’re like this now?’ and I was like ‘Yeah’ and she was like ‘Oh’. And then she kind of went off and toddled and carried on.
LA2 mentor 11
However, mentees also considered that it was important for their mentor to have a genuine interest in them and to support them, regardless of whether they had been through the care system themselves:
You’re more likely to open up to someone who has been through what you’ve been through, but at the same time, she [a previous mentor] was the one who invested in my life the most, and you know, she came from like a really good background . . . and she had a lot to offer me.
LA1 mentee 1009
With regard to the survey findings, 10 out of 22 (45%) LAC aged 14–18 years said that they would prefer a mentor aged 19–25 years and a further six (27%) said that they should be aged 26–30 years. Only one person said that they would like a mentor aged ≥ 40 years, whereas four (18%) said that they would not mind what age they were.
More than half of respondents (12/22) stated that they would like their mentor to have had experience of care. Just under one-quarter said that they would like to be mentored by a professional who already worked with LAC, such as a participation worker or advocate, and the same number said that it would not matter whether the mentor had any experience of working with LAC. No one felt that it would be appropriate to have a mentor who had no experience of the care system, as either provider or recipient.
Matching
Mentors and mentees tended to value having some common background or interests. Three pairs with a shared Caribbean background and one pair from Central Africa commented about the importance of this:
It’s like when I was talking about my mentor having certain traits ‘cos we’re both from the Caribbean, like, it’s like one simple thing. People might think, ok, so what? You’re both from the Caribbean but it’s just that certain factor, that, certain things we’ve both been through together. It just makes it easier.
Pilot mentee 3
She’s just really good; she understands me . . . she’s like Caribbean as well. And obviously I’m half Caribbean as well so we are like get on very well.
LA1 mentee 1007
One of the mentors had attended the same college as her mentee, which they had been able to discuss. Another pair discovered a shared interest in fashion.
Professionals also identified location as an important matching consideration, although one of the most successful relationships involved the mentor having to travel across London, from her university, to meet up with her mentee:
You think if people have got a gym, if the gym is right by your house 10 minutes away, you’re going to go. If the gym means that you have to get a bus or train, you’re not going to go.
LA2 SW
Survey findings of young people aged 14–18 years indicated that it was more important for mentors and mentees to have some shared interests than shared ethnicity.
Information sharing
Of the 76 social workers who responded to the national survey, 65 (86%) thought that a mentor should have some information about a mentee before they start mentoring whereas 11 (14%) felt that they should not have any information.
When this issue was discussed at a focus group, social workers were concerned about historical information about a mentee being disclosed, as the situation for the mentee may have changed. However, they also agreed that sometimes it would be in the best interests of the young person to share certain sensitive information with a mentor:
When you read some of our young people’s files there could be something that happened, what 6–7 years ago, and you look at them and you just judge them sometimes before you’ve even met them. So sometimes it’s better to not know anything.
LA3 SW
I suppose, I was just thinking about one of my young people and I was thinking she’s been sexually abused, and I just . . . wonder if somebody goes bowling in there talking about pregnancy and sex and all thoughts of things, they’re not aware of some of the issues of the young people. How it might cause more harm than good.
LA3 SW
Overall, there was a consensus amongst professionals that mentors should be given any relevant information about a mentee that might impact on their ability to mentor that they should be alerted to issues that could potentially arise during mentoring.
Format of meetings
Mentors and mentees were asked for their views on the format of the mentoring sessions. Eight out of 12 mentors, as well as three mentees, expressed a preference for group mentoring in addition to one-to-one meetings. Mentors and mentees felt that group mentoring would accelerate the bonding process between pairs, encourage a more relaxed atmosphere and open dialogue, increase confidence, widen their social networks and encourage additional one-to-one meetings to take place:
I think what we can do once a month at least . . . have a meeting where both mentees and mentors come together; like you know at the [LA1 mentoring project] they come every single . . . you know Monday 5 pm – all of them in one place . . . once a month you all come in, you know and do an activity together . . . at least then you can guarantee that once a month they’ve actually met . . . and then from then onwards see whether it’s actually going on, you know after that meeting . . . and if that doesn’t work I think you should just make it to be that every single week they all come in – like you know how the [LA1 mentoring project] does? ‘Cos they all come in, every single week.
LA1 mentor 6
One of the mentors in LA2 recalled group meetings that she had participated in on the CiCC, which she felt would be a helpful model to adopt in the mentoring project:
In [CiCC] we used to have meetings once a month . . . when we meet we just sit around the table talking about everything concerning young people in care, law, everything. But when we speak about that we get to know each . . . even when we meet each other on the street, it’s like . . . that’s your family . . . we know each other for other things than the world outside, because we all come from the same background . . . so it’s kind of our secret you see?
LA2 mentor 9
One of the mentors thought that a group setting would be useful for SRE and another felt that it would encourage mentees to engage with other LAC of a similar age, thereby increasing their social network:
I would like to do a group thing like and teaching them like sexual health . . . but they can talk about other stuff that’s on their mind as well, ‘cos er, a lot of teenagers do need that – as they tell me.
LA1 mentor 4
In a situation where she [mentee] is really happy and things are settled for her so she’s not seeing you, so she’s only using you for like crisis points, could we not all do something where we all met and then we all sort of know that we’re all in a similar boat.
Pilot mentor 1
Barriers to engagement
Mentees would often agree to attend a meeting with their mentor but then would alter the time or place of the meeting, without notice, or simply fail to turn up. Reasons given for not turning up included too much school work, seeing friends and ‘bad weather’. This led to some mentors themselves feeling let down and demoralised:
I initiated contact and I spoke to her, everything seems fine, she was willing to meet me and everything. But when it comes to meeting up it’s . . . either she cancels or she never shows.
LA1 mentor 20
You do get young people that will be like yeah yeah and that meeting would be their number one priority and then someone else, like a friend will come round oh let’s go here so, it will always just change.
Pilot mentor 5
One mentor said that she ended up feeling ‘like a teacher trying to find a, you know a primary school kid, chasing them around the playground’ (pilot mentor 2).
Even when mentees were not required to travel far to meet their mentor, they were often unmotivated to make the effort:
‘Cos sometimes like I’ll have one of them lazy days when I’ll just . . . don’t want to go nowhere and I just want to stay in my house and . . . It’s like if she came to get me – I know it sounds lazy, but if she came to get me then obviously I wouldn’t mind going, but I don’t really . . . I like travelling but sometimes I don’t.
Pilot mentee 3
To address the issues of non-attendance, mentors usually had to go to where their mentee was, rather than expect the mentee to come to them.
As some young people said that they did not like having to engage with social workers, it is perhaps unsurprising that one of the barriers to engagement was the mistaken belief by mentees that the mentors were part of social services provision:
That made me feel like oh maybe, they don’t want to meet us, because for myself I know like sometime[s] you don’t really want to talk to someone . . . they were all scared . . . maybe they thought like we were part of social services.
LA2 mentor 9
It is perhaps not surprising that mentees find it difficult to build up trusting relationships and are likely to regard any new people introduced into their social orbit with a degree of suspicion, particularly if they themselves have not chosen them: ‘It takes me a while to get close to someone and become friends with someone or, until I trust someone. I thought it’d be hard for me to do that’ (LA1 mentee 1001).
Pilot mentee 3 started off from a position of mistrust and suspicion; however, her position later started to shift, particularly in response to her mentor disclosing information about herself: ‘I will never fully trust someone innit, but I do trust them to a certain point – but you can never really give anyone your full trust can you?’ (pilot mentee 3).
It may be that the mentees in those relationships that did not last long, or that were inconsistent, never got to the point of trusting their mentor enough to be able to talk about things that were important to them.
Even when a mentee appeared to have engaged well with a mentor at one meeting, this did not mean that they would necessarily turn up for the next one, which often left the mentors questioning their judgement and whether they might have done or said something wrong:
I mean on the first day she was quite open . . . ‘cos we did have some sort of similarity in terms of education ‘cos she went to the same college as I did. So I mean from the word first go I mean we was chatting from start to end. That’s why I think she felt comfortable . . . but I think, the problem is . . . It’s just about getting her here . . . I mean I’ve told her many times I don’t mind going to obviously where she [lives] . . . it’s just about obviously getting that time. ‘Cos when we did get that time it was quite nice.
Pilot mentor 2
Overall, non-engagement of mentees appeared to reflect their ambivalence about the intervention. The researchers also encountered a lack of motivation and ‘mixed messages’ regarding engagement and often had to rearrange meetings with mentees after they failed to show up, without providing an explanation or an excuse. One PC expressed the view that LAC may find it hard to express their opinion about whether or not they want to participate, possibly because they feel so disempowered, and so they end up voting with their feet, by not turning up or not responding to phone calls. Some mentees may have found the mentoring encounters too anxiety provoking and therefore withdrew, or they may not have appreciated the importance of not letting other people down. Professionals also considered that these young people may experience difficulties in planning ahead and organising, or taking control over their lives, so that if something better comes along they will simply go with whatever seems easiest.
Mentor role
This section explores how the mentors undertook their role, the difficulties that they experienced and how they overcame them. It also explores the extent to which LA professionals’ concerns about one-to-one mentoring were substantiated.
Personal lives and communication
Some mentors acknowledged that, despite their best intentions, personal and work-related issues impacted on their ability to fulfil commitments. Mentees reported that mentors did not always communicate with them when other commitments made it difficult for them to keep up with their mentoring role:
She said she is busy in Christmas and everything and I was like ok, just contact me like when do we want to meet and stuff, and then after there was no contact for . . . a couple of months and then yeah we got back in contact again and then she was, she just kept saying oh it’s busy and everything . . . and then afterwards, yeah, we was in contact and then it just fell back again.
LA1 mentee 1006
One mentor failed to inform her mentee that she had a job interview and could no longer make the arranged meeting. This frustrated her mentee who, when asked for her views on what an ideal mentor should do, responded ‘just turn up’.
Many LA professionals expressed concerns about the vulnerability of the mentors and the extent to which they would be able to separate their own issues from the mentees’ issues. Some of them also had to deal with family issues, domestic violence and/or mental health issues. Moreover, a number of the mentors were juggling other commitments during the mentoring period, including college, work and childcare responsibilities:
With any study that you do, when you’re working with looked-after young people, it’s whatever’s going on for them is gonna always take precedent because that’s how they’ve been growing up; you know because they are in the care system.
LA1 PC1
There was evidence from the national survey that competing commitments and life stresses would prevent some care leavers from volunteering as mentors in the first place. Four young women aged 19–25 years (12%) indicated that this was the case.
Managing money and mentor diary entries
Although there were several examples of mentors who fulfilled the responsibilities of the mentoring role, there were a greater number who, in some form, breached the terms in the mentor contract (see Appendix 23). Issues included not collecting receipts for money spent, running up large phone bills on calls not related to the project and keeping money for their own use:
I know that she wasn’t spending all that money on that ’cos I was getting the receipts and like I’m thinking look at this baby stuff on it . . . I was like ‘did you actually go out with your young person?’ [she said] yeah, and then she was like but I forgot the receipt, so I just gave you one that I had.
LA1 PC1
In one case a mentor confided in her mentee that she felt irritated that other mentors were spending money on themselves and not spending it on the mentees. The mentee believed that this was ‘out of order’ but was also content in the knowledge that her mentor ‘would never do that’.
In relation to excessive phone usage, the PCs felt that it was difficult for them to challenge the mentors about what had occurred and, without proof of any wrongdoing, they were reluctant to take action:
And if it turns out that actually I get the bill and it’s like ‘hang on’– right? . . . there’s a mismatch here right? Then that’s a different conversation yeah? . . . but without evidence . . . I’ll ask the question and I’ll challenge and I’ll look at you hard – but if you’re sticking to your guns what . . . where’s my proof?
LA2 PC1
Anecdotal evidence suggested that one or two mentors were attending the support group meeting solely for the purpose of collecting vouchers as a reward for their role, even if they were no longer making attempts to meet regularly with their mentees:
Some of the mentors – I think they know the loopholes of the whole mentoring programme . . . they know that every single month PC1 is going to send a text saying, ‘Ladies, let’s meet up soon’, as long as they say ‘oh I’ve been trying to call, they haven’t picked up’, PC1 will say – you know, she’ll say why haven’t you done this, why haven’t you done . . . but after that they’ll still get their payment, and that’s all they want – really and truly.
LA1 mentor 6
There was a clear indication from social work professionals that, when mentors were not fulfilling their role, they should not receive the full £40 voucher payment. Yet, in LA1, the PC took a more lenient approach:
I never did tell them they couldn’t have their money . . .‘cos I do think there’s a conflict of interest. Because they will, no matter what they’ll take it out on you. You know, and I’ve got to continue working with them after the study has finished. So I just gave it to them, but for me it’s about working with them to empower them to do their role . . . it would be different if I was running it. If it was my project . . . I would tell ‘em straight, you know, ‘you’re not getting paid if you’re not doing your work’. But you know, it isn’t my project.
LA1 PC1
This PC acknowledged that ‘they all knew what they were doing wrong . . . and all said what they had to do, and they all did nothing’.
Only two of the mentors made regular diary entries, despite weekly text message reminders from the researchers. LA1 PC1 noted that, apart from the monthly support group meetings (which some mentors did not attend), she lacked information about how often mentors were seeing their mentees and this made it difficult to impose penalties. The PCs and one mentor thought that it would have been helpful for data from the diaries on the frequency of contacts to be made available to the PCs and that they should give the full voucher payment only to mentors who had completed the diary.
Undertaking a dual role: motherhood and peer mentoring
Five out of 10 mentors who met with their mentee had a child and most of them were single mothers. For the majority of mentors, childcaring responsibilities had a negative impact on their ability to give time to a mentee:
I wouldn’t have minded to see her continuously ‘til it finished, but it was literally just that I had so many things to do, for myself, being a single mum which was a bit difficult. Yeah, I think that was the most difficult thing.
LA1 mentor 18
She had a child and she had her job to do as well, so it kind of depended on both of us, and it’s like most of the times she’ll be busy when I’m free and then when I’m free, she’ll be busy . . . and even in phone calls I will hear how busy she is with her child, so it’s like sometimes I’ll have to be like, ‘D’you know what, deal with your family and then ring after or call tomorrow or something’.
Pilot mentee 3
Clearly, in any future study, there would need to be proper thought given to whether it is appropriate to recruit peer mentors who are pregnant or who have young children unless they are sure that they will have the time to give to the task.
Prerequisites for the peer mentor role
In LA3, where professionals experienced difficulties recruiting mentors to the study and retaining them, professionals believed that care leavers needed to have sufficiently ‘left the system‘ to be effective mentors:
It’s far too early and life events are still happening for these 18-, 19-, 20-year-olds you know? And I think, you know, even beyond 25 we’re still asking quite a lot for somebody who needs to establish themselves. Chronologically they’re not the age we think we [they] are, you know, with our teams. I don’t think those young people are where they should be yet and I think it takes a lot of life and a lot of sorting out to get to a place where you do feel comfortable about a 13 – or whatever age – coming at you and asking very difficult questions.
LA3 PC2
The PCs in LA1 and LA2 believed that care leavers should be given an opportunity to mentor, despite the difficulties highlighted earlier. However, they were clear that, in a future study, PCs would require additional time to work one-to-one with each mentor to ensure that they had the required skills to fulfil the mentor role and to explore their ability to manage their time and emotions over the mentoring period:
At the entry point, we need to really be firm in terms of their availability and getting them to think about even looking forward, about the possibility that may have certain things, like courses starting, movement – they might be going through a transition stage, ‘cos of moving, etc. Looking forward, there’s a number of things that maybe, I think we need to consider in terms of what could possibly change that mentor’s circumstances.
LA2 PC1
Similarly, nearly three-quarters (65/88) of survey respondents from the national and local social workers survey thought that care leavers aged 19–25 years were capable of acting as mentors, provided that they were mature enough and were given sufficient training and support. However, nearly one-fifth of respondents (16/88) thought that the mentors should be older (e.g. in their early to mid-20s) and that the upper age limit should be extended to around 30 years.
Safety concerns
This section highlights the concerns expressed in relation to the nature and content of the peer mentoring and the extent to which they were substantiated.
Boundaries
Local authority professionals believed that there was a potential for boundaries between mentor and mentee to become blurred, unless they were well defined by the project and monitored by the PC:
I was in a meeting and they were setting up a meeting of her and her mentor and swapping telephone numbers. And I sort of asked well are there any sort of boundaries around the relationship and it didn’t seem as if there . . . they had talked about boundaries, but it didn’t seem as if there was any clear kind of guidelines around that.
LA2 SW
Concerns revealed in the national surveys mirrored this:
Young people in distress could contact their mentor relentlessly if appropriate boundaries are not established . . . what if the YP [young person] is texting/calling constantly or disclosing issues of a safeguarding nature? Mentors will need considerable training/support to manage these sorts of difficulties.
SW survey respondent
Although some professionals had expressed concerns about mentees becoming over-reliant on their mentor, there was no evidence of this or indeed of any inappropriate or excessive contact. However, because of the rather chaotic nature of some of the mentees’ lives and their difficulty with time management, some mentees appeared to expect their mentor to be able to drop everything and see them at a moment’s notice, rather as a friend would do:
You know she doesn’t plan. She keeps on calling me up last minute, like ‘Hey girl how are you? Yeah, d’you wanna come and meet up?’. . . ‘I’m busy’ I said to her and I go, ‘I have a very busy schedule’ and everything has to be planned with you I’m sad to say.
LA1 mentor 4
Disclosures
Mentors were told during their training that, if they had any concerns about the health or welfare or safety of their mentee, they should immediately pass on the information to the PC, after first informing their mentee. Some professionals thought that mentors would find it difficult to make decisions in relation to sharing information, because of the potentially damaging effect that it could have on their relationship, and that they would need a lot of guidance and support around responsible information sharing to ensure that the best interests of the child are met. However, within this study, a number of mentors were able to report concerns to the PC without this impacting negatively on their relationship with their mentee.
Unsupervised meetings
Many professionals expressed some concerns about meetings being set up between vulnerable young women, without supervision or without sufficient communication between professionals in the mentee’s network. In one focus group it was suggested that allegations of misconduct could be made against a mentor by a mentee. However, the main risk identified in the exploratory trial was of mentors failing to inform the PC where and when they were meeting with their mentee, which was in clear breach of the mentor contract. LA1 PC1 admitted that only one of her mentors regularly informed her of when and where she was meeting her mentee.
Undesirable effects of the mentoring intervention
For some, particularly when relationships were inconsistent or ended prematurely, there was the potential for the intervention to be harmful to the mentee. One mentee (1001) lost her first mentor, who dropped out for ‘personal’ issues’, and had to be allocated to a different mentor, who also failed to see her regularly:
It made me feel a bit upset and then like it did make me sometimes feel like, I didn’t see the point in me doing it; I just felt like giving up. ‘Cos I’ve had two [mentors] and they haven’t really worked out so well. But then, it kind of questions me, like maybe it’s something I’m doing wrong.
LA1 mentee 1001
During training, mentors were told that if they were unable to continue a relationship they should make sure that their mentee did not blame herself or feel responsible for the failure of the relationship. However, this did not happen in the case of mentee 1001.
Local authority 1 PC1 said that, although she would not go as far as calling the process damaging, because she could ‘rectify some of the stuff’, she was concerned about the consequences of having an unreliable mentor for vulnerable young women and, in this study, for mentee 1001 specifically:
When someone says they’re gonna see you, they need to see you. And when someone like mentee 1001 – she was really upset with this whole process and so basically the stuff going on in her brain – it stopped firing.
LA1 PC1
Apart from this case, in the main, mentees appeared accepting of infrequent contact and/or unreliable mentors, possibly because this represented a repetition and re-enactment of past experiences of rejection and abandonment that they had come to anticipate.
Several mentors also admitted feeling frustrated or let down when their mentee failed to turn up to meetings or show sufficient acknowledgement of their efforts. One mentor found it difficult that the other mentors had been successful at making initial contact with their mentee whereas she had not:
I liked the challenge of it but the thing I got really annoyed about – I don’t know if annoyed was really the word – is that I knew I could help if given the chance for her to receive my help d’you know what I mean? ‘Cos I’m . . . it’s like fighting with a wall really – that’s how I felt like. I felt like okay I could really help her but if she’s not willing to meet me halfway then I can’t really help.
LA1 mentor 3
Professionals were concerned that the study could bring up difficult feelings for mentors and that the mentors were not being provided with adequate support to help them deal with these feelings. Many sensitive issues were covered in the training, which also encouraged reflection on personal issues. One participant admitted to her group that she had drunk a bottle of alcohol because she felt overwhelmed by the discussion the previous day. Another mentor said that meeting her mentee, who was experiencing similar issues to those that she had faced when she was younger, had reminded her of her past, but that she had been able to ‘deal with it’ by seeking support from the PC.
Local authority 1 PC2 reflected that the study had enabled some participants to come to terms with their past:
Volunteering for the Carmen project, it made her re-evaluate her own life . . . it’s thought-provoking, it has allowed young people to do the reflection, reflective stuff. A lot of them weren’t able really to tap in to that emotional need and then sort of articulate that to worker . . . But I’ve seen the change, and it might have only been a tiny change. For one particular person . . . it’s had quite a massive impact, she’s going back to university, and she’s actually going to do the therapeutic work. Because she suffered sexual abuse, horrific sexual abuse . . . she’s started to talk about her experiences, her experience of violence, of being raped, sexual exploitation . . . And I truly believe that if it had not been for this project and her involvement, we had always guessed that something had gone on for her but we did not know to what degree.
LA1 PC2
Support for mentors
This section explores the extent to which the mentors were supported by, and felt able to contact, the PCs and the extent to which support for mentors was sufficient.
Individual support
Following training, mentors in both LAs faced a long wait whilst the mentees were recruited and matched to mentors, which tended to decrease their motivation. In LA1 there was little pre-emptive communication from the PC to the mentors about this, but in LA2 the PC’s communicative approach was particularly appreciated by the mentors: ‘She’d be saying, ‘okay, we haven’t forgotten about you’ like just to remind us that she hasn’t like forgotten about us but she was doing whatever she needed to do at the time’ (LA2 mentor 11).
In general, mentors felt able to contact the PC in their LA to discuss issues that were preventing them from seeing their mentee, concerns about their mentee’s welfare and difficulties with making contact. Mentors said that the advice that they received was helpful. However, in LA1, mentors said that the PC was difficult to contact and too busy to support them:
To be honest I could have had more support. And um, but whenever I did manage to get hold of her, ‘cos she’s a very difficult person to get hold of, when I did manage to get hold of her, and um, I did like contact her to let her know anything that’s going on, she will give advice, I’ll give her tops for that. But I still think I could have had a bit more support.
LA1 mentor 4
Regarding the direction of communication, several mentors believed that the PC should have been more proactive in contacting them:
I would like somebody to just chase because there are so many other things going on in my life, if somebody was on my case sort of thing, like ringing up to find out . . . how did your thing go you are more likely to think oh . . . I need to go and meet her . . . there is not any of that support going on. So I know that PC1 is really busy so I can’t blame her for that.
Pilot mentor 1
I think they need to be more active towards the role in a weekly sense of basis, because all the communications I’ve had with PC1, it was me making the communication – all the calling up instead of actually her calling me up and giving me some information.
Pilot mentor 2
As she was often in the education centre, it was easy for one of the mentors to make face-to-face contact with LA1 PC1 on an informal basis, outside the support meetings. She reiterated, however, that it was often difficult to get through to the PC by telephone.
In LA2 there was less evidence from the mentors about how supported they felt. However, the PC often contacted her mentees by text message. One mentor said:
I do feel like she was quite supportive, yeah. Because, every time that I called her, apart from when her phone had a problem, yeah, I was able to get through to her. Yeah. And she always motivated us as well. Sometimes . . . it’s not even a call, she will text and stuff like that, you know to let us know that we are doing a great job and stuff like that. And if we do need to speak to her about anything, we shouldn’t waste time; we should just call her.
LA2 mentor 10
However, LA2 PC1 described feeling guilty that she had been unable to give as much attention to the mentors as she felt they required:
They’d be like oh I know you’re busy and I’d be like ‘ahh’ and I felt really bad that I’d given that impression that they were taking up my time. But in a way they were . . . but I owed them a duty of care . . . it was conflicting for me . . . I’m out on the street and I can’t speak properly so [I said] can I call you back? And sometimes I didn’t call them back until maybe 7 o’clock in the evening or the following day . . . and it would just be nice to know that that’s who I’m committed to.
LA2 PC2
In both LAs, the consensus amongst the mentors was that a weekly phone call from the PC to motivate them would have been helpful in keeping them focused and motivated. LA1 PC1 recognised the importance of calling mentors every week and admitted that she had not done enough of this, although she thought that mentors could have contacted her when they experienced problems. The extent to which this is true is unclear. One of the mentors in the pilot said that she was ‘put off’ calling the PC because she seemed too busy.
The national social worker survey asked respondents about the type of support they believe mentors require. As well as telephone calls and monthly support group meetings, 67 out of 118 (57%) social workers said that there should be individual, face-to-face support with a PC and 37 of them (56%) believed this should be provided monthly. A further 17 (26%) said this should be every two weeks and the rest (18%) every week. One of the mentors in the study thought one-to-one meetings with a PC should occur every two months, or quarterly, because group meetings had been poorly attended.
Monthly support meetings
In both LAs the PCs struggled to deliver a support group every month, and even when they did occur few mentors attended. The main difficulty in arranging meetings appeared to be around scheduling a date and time that suited all of the mentors:
It was something to do with the mentor availability. The dates, time, so some agree with the dates, some don’t agree with the time, some agree with the time, some don’t agree with the dates, so that’s why everything was just being pushed. Okay let’s, let’s find another date for next month and so on.
LA2 mentor 9
One of the mentors in the pilot believed that LA1 PC1 was simply too overworked to be expected to deliver a monthly meeting and suggested that someone with dedicated time should deliver the support. She commented:
She’s got so many other things that she’s doing. And then she knackered by the end of the day. She’s been here since 9 o’clock and then [at] 6–7 [pm] we’re expecting her to do a support session. Come off of it, she must be physically and emotionally knackered. So I think somebody else should be employed and that person works specifically with the mentors and mentees. I think that person will be able to relate better to the mentors and mentee because they have that specific knowledge about this project in itself.
Pilot mentor 1
During the pilot, the PC role in LA1 was formally integrated into her existing role by management, meaning that she had slightly more time to devote to the role during Phase II. One of the mentors involved in both the pilot and the exploratory trial said that she felt better supported by the PC during the exploratory trial. However, the data suggest that only two or three mentors regularly attended the support meetings and problems persisted. For those mentors who attended regularly and saw their mentee, it was frustrating and demoralising to be let down by their fellow mentors:
I don’t think they was monthly or an appointment to the month. And, um, I think like that more of the girls could turn up, like the girls didn’t turn up as well, so sometimes we’d be sitting there and there’s about three girls that’s actually turned up to the support groups and things like that, so yeah.
LA1 mentor 18
Despite the low turnout, in both LAs mentors who attended felt that the meetings were useful for talking about their experiences and comparing these and getting support from both the PC and other mentors to deal with issues:
We’d talk about our experiences that we’d had so far with young people . . . say for instance one of them was like ‘ah my young person’s really shy’, we’d all work and like talk about things that we . . . like come up with ideas just off the top of our head, like ooh try this and – maybe if you’d start with this and start with an ice-breaker.
LA2 mentor 11
It was quite good actually because you start to realise that actually I’m not the only one that’s having issues, like other people are having issues too; even if they’re not the same issues that you are suffering with, it’s still nice to know that . . . you don’t feel as bad, like you don’t feel as guilty or like oh my gosh. Like, so it, it is nice so that everyone can kind of share their views and experiences.
LA1 mentor 15
Support group meetings were also designed to enable PCs to sign off ASDAN award paperwork for accreditation. However, it became clear that most of the mentors were not prepared or perhaps simply did not understand that they were expected to do the work in their own time to achieve accreditation:
I couldn’t even get the ASDAN qualification – because not everybody was here and then if I wanted to answer a question I have to be on my self-initiative, it wouldn’t be like oh PC1 will sit down and then she’ll help me go through it – none of that. But I think if it would have been other people then people could have helped each other, but nobody came.
Pilot mentor 1
I even came a couple of times for the ASDAN, like there hasn’t really been much focus and really sit down and make, like help, and get on with this ASDAN.
LA1 mentor 18
The PCs admitted that they felt ill equipped in terms of having information from the training partners and researchers about how to implement and sign off work for the ASDAN qualification and believed that additional training would be required in a future intervention.
Overall, the PCs felt that they had been unable to commit sufficient resources or emotional support to the mentors and considered that to deliver the work effectively a dedicated PC would be required. In LA1, the PC believed that mentor support groups could have been delivered more effectively by going back over training material and that delivery of group mentoring sessions would ensure that the PCs have a better grasp of communication and knowledge of the status of the mentoring relationships. PCs in LA2 and LA3 thought that the support package should also include one-to-one support meetings.
Alternative support for mentors
Social workers/semi-independent outreach workers
In both LAs, mentors were supported by additional professionals, usually as a result of referral by the PC. These were either SOT workers in LA1 (working from the education centre) or social workers. As a result of the PC’s recommendation, one mentor formed a working relationship with her mentee’s SOT worker, who helped her to contact the mentee at her hostel. She considered that, if all mentors had contact with a mentee’s key worker or a social worker, it would make their role easier:
Again we planned to meet up. Didn’t happen the way we planned it. And then I called [SOT worker name] and [SOT worker name] told me where she was staying. And [SOT worker name] called the hostel and asked if she was there. And then she called her and she asked [her] if I could come and wait for her there. So I went to the hostel.
Pilot mentor 3
The existence of the education centre in LA1 was clearly a help to the mentors and enabled them to signpost their mentees to other support workers:
It’s helped me realise half of the roles ‘cos I didn’t know half of the people who work here, so you realise what different people, what different roles people are doing . . . that will help with your mentee . . . you can go and point them in their direction.
Pilot mentor 1
Forming a positive relationship with her mentee’s carer was extremely helpful for one mentor, enabling her to adapt her mentoring around her mentee’s needs and weekly routine. The carer preferred the pair to meet every 2 weeks as the mentee was studying for her GCSEs and, according to the mentor, because the mentee was becoming too attached to her.
Mentors also appreciated other mentors as a source of support, talking to them both on their mobile phones outside of the mentoring meetings and within meetings: ‘I used to talk to a few others of the mentors, some outside [support group] and some just in . . . but sometimes you used to ask like, oh what, have you been with your mentee this week?’ (LA1 mentor 18).
Support for mentees
The research team had assumed that, during the mentoring, mentees would be well linked in with their social workers and would raise any issues with regard to the mentoring with them or with the PC. PCs were not expected to routinely contact the mentees. This was a mistaken assumption because many of the mentees were left for periods of time without contact from their mentors and not all of them asked for support. Those who had an existing relationship with their PC did ask for help or advice: ‘She did try and get in contact with her but if [mentor 15] didn’t pick up her phone or answer to any of the letters or anything’ (LA1 mentee 1001).
However, one or two mentees said that they would not have known who to contact in the event of difficulties. One mentee said that she wanted to speak to someone about the fact that she was not seeing her mentor, but she would not speak to her social worker as she did not want the social worker involved in her life. Another mentee said that, when she lost her phone and lost contact with her mentor, she thought about asking her social worker but did not as she ‘was enrolling for colleges and thinking about my birthday’.
Allocation of support
The DCS and national social workers survey asked professionals to consider who would be best placed to take on a PC role.
There was a clear indication that the PC role should be separate from the social care role, with many stating that the responsibility should be shared between someone able to offer therapeutic input to mentors and someone with experience of teaching PSHE/sexual health, to drive the prevention of teenage pregnancy agenda:
I think sexual health expertise is critical to the project and so the person must first and foremost be an expert, from medical perspective. I think the other roles can be provided to support the medical expert or be learnt.
DCS survey respondent
I think the programme will be best placed to carry out by two project coordinators, a child and adolescent mental health clinician as well as a sexual health worker. The clinician will be able to address and offer knowledge on the emotional and developmental support while the sexual health worker could offer advice on the sexual health impact.
DCS survey respondent
Responses from the DCS survey highlighted the importance of health professionals and youth workers rather than social workers offering emotional support (Table 21). One-quarter of national social worker respondents also felt that graduate mentors could work alongside a health practitioner to deliver the role, or that ‘lead’ mentors could assist with the recruitment of new mentors, encouraging mentors to attend meetings and lead some of the group sessions. A social worker in LA2 said:
I run a group for care leavers, and I have a care leaver co-facilitator that runs the group with me. And I find that the young people will ask him questions quite often and I’ll just kind of stand back and listen . . . it works really well having young people guiding young people ‘cos they are more likely to listen to the young person.
LA2 SW
| Professional | DCS (n = 41)a | Social workers (n = 69)a |
|---|---|---|
| Youth worker/participation worker/personal advisor from the LA | 14 (34) | 22 (32) |
| A mentor who has graduated from the programme | 5 (12) | 17 (25) |
| Health professional from the LA (e.g. sexual health worker) | 15 (37) | 13 (19) |
| Independent worker, e.g. from a charity | 6 (15) | 9 (13) |
| Social worker | 1 (2) | 8 (12) |
The existing educational mentoring model in LA1 involves mentors in leading the sessions. In addition, one mentor from LA2 described a system of ‘lead’ mentors, which, from her experience on the CiCC, is an effective way to drive attendance:
A lot of people never used to come [to CiCC], sometime only five, six people come in the meeting and we are meant to be 12 of us – no more motivation and everything. So [the PC would] nominate a chair, within the group, yeah and maybe a co-chair within the group. Because it’s a group of mentors, you should have a chair. And that chair will nominate herself within the group, like okay I want to be the chair. Her role would be more like to contact the others to motivate them. So it needs to be someone who is more motivated.
LA2 mentor 9
Role of the researchers
From the outset, the researchers offered to assist mentors with research-related issues. However, some mentors seemed to regard the researchers as a source of emotional support. This was in part because of a misunderstanding of the role of the researchers, but in LA1 it was also because of the perceived lack of capacity of the PC to provide this support. For example, one of the mentors telephoned the research team after discovering that her mentee had a diagnosis on the autistic spectrum. She had assumed that both the researchers and the PC knew about it but had simply failed to inform her. The researchers advised her to discuss her concerns with the PC, who was also unaware of the mentee’s diagnosis; the PC said to the mentor that ‘if anything I would have thought the Carmen study would know about it’. Having promised to look into the mentee’s situation, the mentor reported that the PC then failed to get back to her. She subsequently stated that, in relation to the research team, ‘Me personally it just felt like we were just being used for research and they didn’t really care – as long as you guys got your data that’s all you care about’ (LA1 mentor 4).
She felt that the research team should have been more directly involved in supporting her and troubleshooting difficulties as and when they arose:
Yeah, come down and see us more, I think talk to us more as well and if . . . the concerns we have or whatever, like proper take it on board and just like help us out and stuff. I know that it’s [PC1]’s job to do that, but it would be nice if like the people above did it as well, yeah.
LA1 mentor 4
The researchers (DM and FC) were constantly being required to overstep the boundaries of their research and to take on a more active management and even counselling role, which was difficult to resist and not always appreciated by participants or social work professionals.
Summary
This chapter has outlined the nature and content of the mentoring relationships and explored engagement and barriers to engagement. Through the data we have illustrated the basic requirements for successful relationships, including the formation of trust as well as determination and persistence on the part of mentors, safety guidelines and adequate support. The implications of these findings, particularly in terms of the feasibility of delivering a future trial of a peer mentoring intervention, are discussed in Chapter 10.
Chapter 9 Economic analysis
An economic analysis was undertaken to determine the costs of the peer mentoring intervention components and, separately, the costs of the outcome assessment and process evaluation. This will allow appropriate costing of a Phase III trial.
An approach is suggested for modelling the connection between the value added by the intervention and the probabilities of various medium- to long-term outcomes for the young women and any children they may have.
Cost of the intervention
The first element of this study was to measure the cost to the LAs of implementing a mentor programme for LAC and to use these data to develop a general model for costing interventions on any scale and in different areas. Most of the cost was expected to be staff time and a spreadsheet was designed to allow staff to record their time input every week, as the project progressed. An example of the time recording sheet is provided in Appendix 24.
It soon became apparent that the staff were finding it difficult to record their time because work on the project had to be fitted into whatever gaps arose in their already busy working week. Attempts to obtain the information during interviews also failed for the same reason. We did, however, obtain some heavily qualified estimates from the staff. These figures are shown in Appendix 24. A different approach to fulfilling the costing requirement was required.
As we could not measure a definitive ‘did take’ cost, we used the experience of observing the process of setting up and running the project to construct a model for how the project could be implemented in a tightly structured way. We used this, with some assumptions, to calculate a theoretical ‘should take’ cost. Figure 4 provides the model, showing the essential elements of the project.
FIGURE 4.
Overview of the steps involved in setting up and running a mentor scheme for looked-after girls and young women.

The quantitative model is constructed by unpacking each of the boxes in the diagram, asking what actions are required under each of those headings and then asking how much staff time and of what staff grade each action would be expected to take. The principal drivers for the time required are:
-
the size of the pools of potential mentees and mentors, which determine the size of the recruitment task
-
the proportions in each pool likely to express an interest, which determines both the size of the training task and the number of mentor–mentee pairs to be supported
-
the numbers of mentees and mentors likely to drop out once the mentoring process has started, which determines the effort required to debrief the ex-participants and find a new mentor if required.
Some data obtained from the study can be used in this model. For example, in one of the LAs the PC recruited seven mentees by writing to all eligible young women. National statistics show that, in LA1, 145 children between the ages of 10 and 15 years and 95 aged > 16 years were looked after, including adoption. 24 Approximately 46% of these are girls. If one assumes that about one-third of the first group (n = 48) are aged > 14 years, then there are 0.46 × (49 + 95) = 66 eligible girls. This means that 10.6% responded positively to the recruitment letter.
For the most part, however, the model is theoretical, albeit with what are believed to be realistic estimates for the time taken by LA staff to perform the various activities. The model is written in Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA, USA) and is available to any LA wishing to adapt it to its own circumstances by changing the assumptions or indeed the structure.
The model
The assumptions that the model currently uses are listed in Appendix 25. It is designed to cost the first year of operation of the intervention in a ‘greenfield’ LA. Some of the costs are largely non-recurring and we also make an estimate of the costs as they would appear in future years.
The following sections describe the content of each of the blocks shown in Figure 4.
Inception and preparation
This element of the project was one of the most opaque in terms of what went on and the resources consumed, but it is also one of the most critical elements to its success. Accordingly, the model envisages a formal approach to consideration of the project by senior management, including preparation of a detailed, costed plan that is submitted for approval and backing to an assistant director. This process assumes the creation of a steering group, which nominates a working group to develop the project. The steering group is considered necessary to ensure the direct involvement of senior management.
The final output of this stage is a package containing a list of things to be done; who is expected to do those things; and materials to make these tasks easier, including standard draft letters, explanatory leaflets, posters and training provision already negotiated with providers. The list is based on experience with the present exercise.
An important part of the preparation is the recognition that problems may arise during the course of the project that require intervention from management. To allow for this, the management group will meet twice during the year and once after the trial is over. Of course, these meetings may be cancelled if there are no problems requiring intervention. The burden of ‘ongoing management’ is likely to be lighter beyond the first year.
Awareness raising
The model envisages that the project being launched has the strong backing of senior management, but there will still be a need to repeat the message on a more personal basis. This is seen as the responsibility of the PC, who will arrange presentations to various groups of staff. The most important of these groups includes the social workers dealing with looked-after girls, not least because the model assumes that they will bear the main responsibility for recruitment.
Recruitment of mentors and mentees
Experience in the pilot and the exploratory trial found that recruitment was a particular problem. It took a lot of time and progress chasing by the PC and the researchers to identify potential mentors and mentees.
The solution envisaged in this model was to require social workers to write to all of the young women on their caseload, through their carers, to outline the project and ask anyone who was interested to contact them to discuss the project further. The social workers would then pass any likely candidates to the PC, along with a summary of their case file.
A similar procedure would be followed for the mentors. Social workers would write to the last known address of women who met the inclusion criteria and who they considered would be appropriate mentors. Anyone expressing an interest would speak to the social worker in the first instance and then, if they were still interested and considered appropriate, their names would be passed on to the PC.
The model assumes that social workers and the PC have some administrative support for sending letters and extracting case file summaries, etc.
Training of mentors
This section of the model also includes the DBS checks for potential mentors. As it is a relatively simple section of the model, the detailed list of actions and assumptions about staff time required to perform them is presented in Table 22 as an illustration of the nature of the whole approach.
| Task | Type of cost | Time/cost | Basic salary cost (£) | Notes |
|---|---|---|---|---|
| Communicate to each potential mentor what ID papers are needed for DBS check | PC | 10 minutes per potential mentor | 88.89 | Assumes all 30 mentors in pool are to be checked |
| Assemble papers for each potential mentor | PC | 3 minutes per potential mentor | 26.67 | Assumes all 30 mentors in pool are to be checked |
| Pass papers to clerical officer who handles DBS checks for the LA | PC | 3 minutes | 0.89 | |
| Clerical officer initiates check procedure with the DBS | Clerical officer | 15 minutes | 2.78 | |
| Write to potential mentors when DBS checks are returned | PC | 5 minutes per potential mentor | 44.44 | Assumes all 30 mentors in pool are to be checked |
| Cost of DBS check | Other | £44.00 | Per check | |
| Select 20% more mentors than expected mentees for training | PC | 5 minutes per potential mentor | 44.44 | Assumes six mentees so seven mentors are selected |
| Write to selected potential mentors to inform of training dates | PC | 5 minutes per potential mentor | 19.95 | See above |
| Contact training providers to arrange training | PC | 30 minutes | 8.89 | |
| Cost of training a mentor | Other | £500 per potential mentor |
The activities required are listed in an intermediate level of detail. For the DBS check, the basic requirements would have been communicated to the potential mentors in the recruitment letter sent by the social worker seeking expressions of interest, but it is assumed here that this would need repeating probably in a telephone conversation. The material required for the DBS check would be sent to the PC, who would assemble it for the set of mentor applicants and then hand it over to the administrator who handles DBS checks for the LA. The DBS results, when received, would be passed on to the PC, who would send the appropriate standard letter back to each mentor applicant.
At this point the PC would have a list of cleared potential mentors and some idea of how many mentees to expect. To allow for contingencies, the PC would arrange training for 20% more mentors than there are mentees.
Matching mentors and mentees
At this point the PC has a pool of trained mentors and a pool of mentees. The aim is to match a mentor to each mentee. Once this is achieved, the PC has to organise and attend a meeting between the members of each pair. This could be a lengthy process, with the potential for more than one attempt being necessary, and there is a possibility that the relationship will fail at this first meeting. A judgemental allowance is made for these possibilities.
Support/maintain relationships
Over the course of the next 12 months the PC will remain in contact with the mentors through regular group meetings, as well as dealing with expenses, payments and any contingencies arising, including a mentor or mentee dropping out.
Normal terminations
Towards the end of the 12 months, the PC will take steps to smooth the termination of the relationship. This entails finding someone to take responsibility for supporting the mentee through the withdrawal process and arranging a three-way meeting with that person, the mentor and the mentee. The model also assumes that there will be a standard end of relationship debrief of the mentor by the PC and of the mentee by her social worker.
Review
After running for 12 months the model assumes that there will be a review of procedures and outputs. This will take the form of a report compiled by the PC with the support of the management group and delivered to the steering group. The report will cover the whole process, with particular emphasis on the views of the mentors and mentees as expressed during the debrief sessions on ending the intervention and the views of the social workers on the effect of the process on the girls and young women.
Results
As indicated in the previous section, the model covers all of the main actions and is believed to be complete. It is, however, based on best estimates for the time taken to perform the component activities. These are believed to be plausible but it is of course open to others to make their own assessments. The spreadsheet is available for this purpose. The ‘bottom-line’ results are set out in Table 23 and Figures 5 and 6 and are based on the assumptions in Appendix 25.
| Task | Cost (£) | Staff hours | Notes |
|---|---|---|---|
| Inception and preparation | 6017 | 177 | |
| Ongoing management | 684 | 20 | |
| Initial awareness raising | 1085 | 32 | |
| First recruitment round | 1714 | 75 | |
| Training | 5283 | 11 | Includes DBS and training costs |
| Matching | 227 | 7 | |
| Supporting/maintaining pairs | 8345 | 142 | Includes payments to mentors |
| Normal terminations | 266 | 8 | |
| Review | 791 | 24 | |
| Total cost over the whole project | 24,412 | 496 | |
| Cost breakdown | |||
| Set-up costs | 7102 | Largely non-recurring | |
| CRB and training costs | 5283 | An element may be non-recurring | |
| Payments to mentors | 3600 | £40 stipend + £10 phone vouchers | |
| Remaining costs (largely staff plus overheads) | 8427 | = Total – set-up costs – DBS/training costs – payments to mentors | |
| In terms of total staff time, the remaining costs are equivalent to | 14% of a social worker | ||
| The support and maintenance function costs are equivalent to | 8% of a social worker, which rounds up to around 3 hours per week | ||
FIGURE 5.
Analysis of modelled staff time for the first year of an intervention.

FIGURE 6.
Cumulative project costs for the trial.
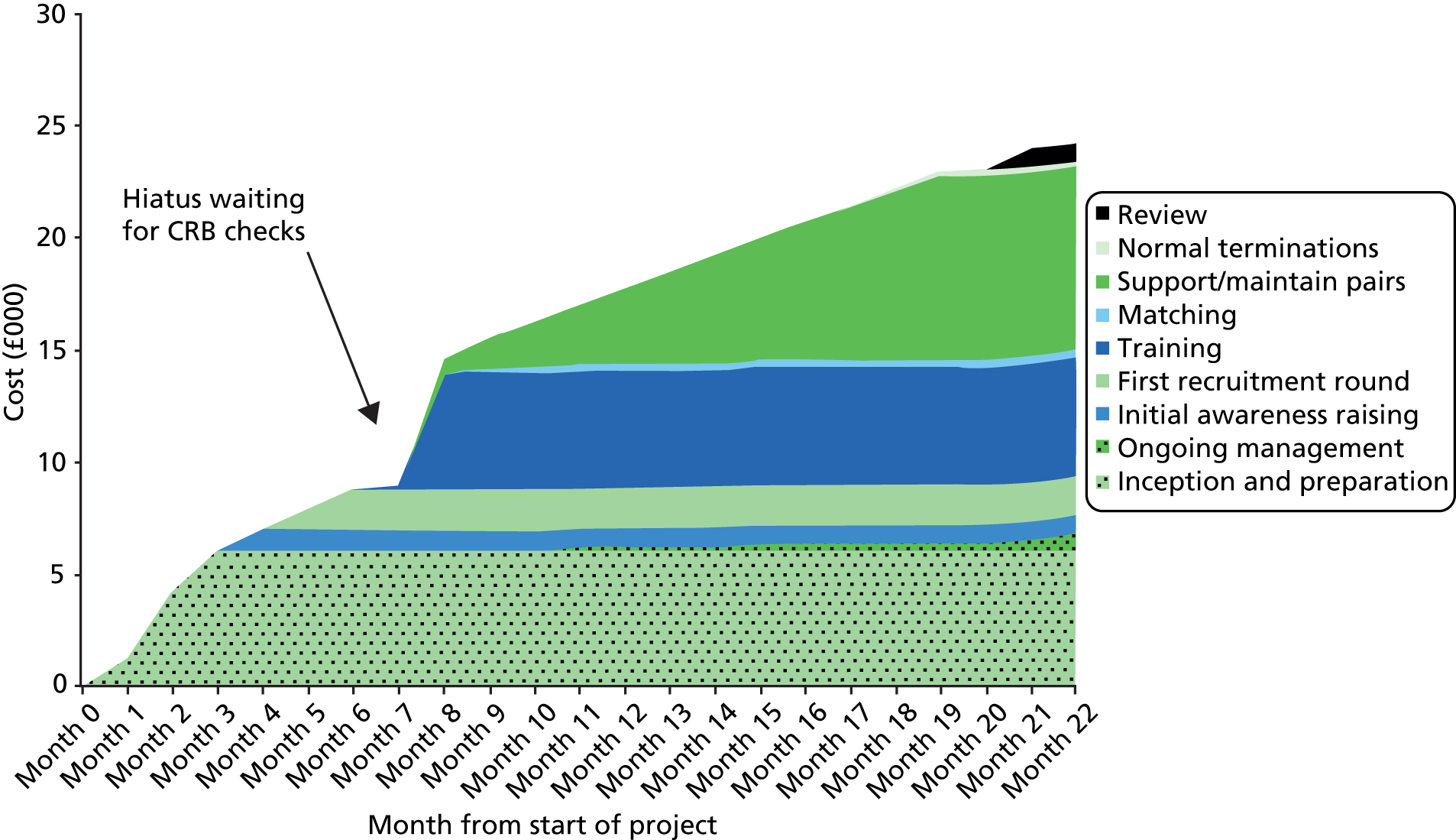
The total staff time estimated by the model is 496 hours. The costs in money terms are based on staff time, converted into staff salaries, and reflect the mix of staff expected to be involved. The basic salary figures (appropriate for London) are factored up to include national insurance contributions and pension contributions and are further factored up to include allowances for direct overheads (office space, equipment, etc.) and indirect overheads (e.g. personnel and finance functions). These cost factors are published by the Personal Social Services Research Unit (PSSRU)177 and amount to an 87% overhead on the basic salary.
Critique
There are few data available to reality check these results. However, one observation that was made by a PC with some certainty was that the demand on her time during the support/maintenance stage was 3 hours per week, which squares quite well with the last row of Table 23.
The same person also estimated that recruiting mentors and mentees each took 56 hours of her time (112 hours in total). These figures were recalled during an interview some time later and cover only the PC’s own time. The model results give an estimate of 80 hours of total staff time for recruitment and DBS checks combined. As both the PC’s estimate and the model’s estimate are subject to some uncertainty we are assuming that the model gives a better estimate of the time required by the recruitment phase in a tightly managed project.
Implications for the longer-term running of a peer mentoring scheme
The cost estimates presented in the previous section are for a 1-year trial. If it were decided to continue the scheme indefinitely, the annual costs would certainly be lower. Table 24 shows the costs revised for the longer-term running of a peer mentoring scheme (still using the assumption of six mentor–mentee pairs).
| Task | Cost (rounded) (£) | Notes |
|---|---|---|
| Recruitment round | 1200 | |
| Training staff cost | 2500 | Includes training fees |
| Matching | 800 | |
| Supporting/maintaining pairs | 8500 | Includes mentor payments of £80 per month |
| Normal terminations | 250 | |
| Review | 800 | |
| Total cost over the whole year | 14,000 |
The initial set-up and steps to raise awareness would not be needed. The recruitment would be of the same scale as before but the response rate of potential mentees and mentors would vary depending on how the project was perceived after 1 year of live running. However, the recruitment round would probably be better targeted and so we assume that the overall recruitment cost would be down to two-thirds of that in the first year. The training cost would depend on the number of trained mentors still available from the previous round, but it would be reasonable to assume that longer-term training costs would be half those in the first year. The matching, support, termination and review costs would remain the same. The end-of-trial review may also find ways to reduce the remaining costs still further. Using these assumptions, a programme on this scale (six mentor–mentee pairs) could be run for around £14,000 per annum, with about £3600 of this cost being payments to mentors.
Cost of the evaluation in terms of researcher time
The time that the researchers put into the evaluation was recorded in considerable detail from the beginning up to July 2013. The purpose of this section is to describe how these data will be used to estimate the researcher time required for a larger study on the same lines as this but with a rigid policy of non-participation in the implementation of the initiative.
We begin with categorising the work carried out by the researchers, as follows:
-
work whose outputs can be carried over to a new project and thus either not repeated or needing only some updating
-
work carried out by the researchers that should properly have been carried out by the LA and which will therefore not be a burden on researchers in some future exercise
-
work that is proportional to the scale of the exercise as measured by the target number of mentees.
Analysis of the research team data
Figure 7 shows the aggregate effort expended on the whole project by the researchers. In total, over the duration of the project, just under 7600 hours were logged under the five headings shown. The first Phase I mentor–mentee pair met in November 2011 (week 52 in Figure 7).
FIGURE 7.
Cumulative cost of the evaluation in hours.
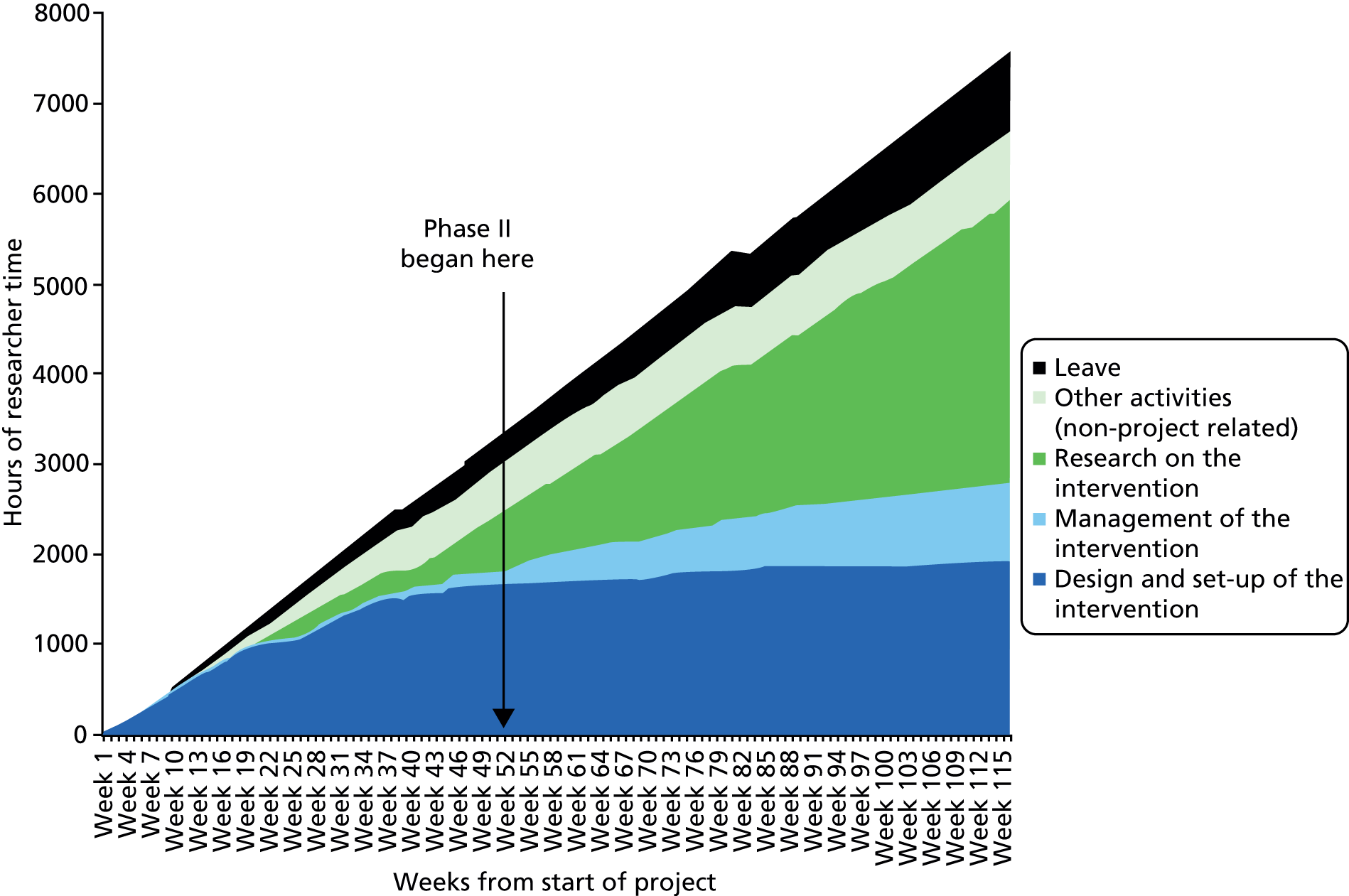
Other activities (non-project related) are basically staff development. Research on the intervention and design and set-up of the intervention take up 1925 and 3080 hours of researcher time respectively. Project management, which takes up 876 hours, largely consists of management meetings within the team and communication with outside interested parties. It also includes a relatively small amount of time spent carrying out actions that in a strictly ‘hands-off’ exercise would be left to the LA staff.
Each of the three main components in Figure 7 are examined in greater detail in Figures 8–10.
FIGURE 8.
Analysis of the researcher time put into the design and development of the project.
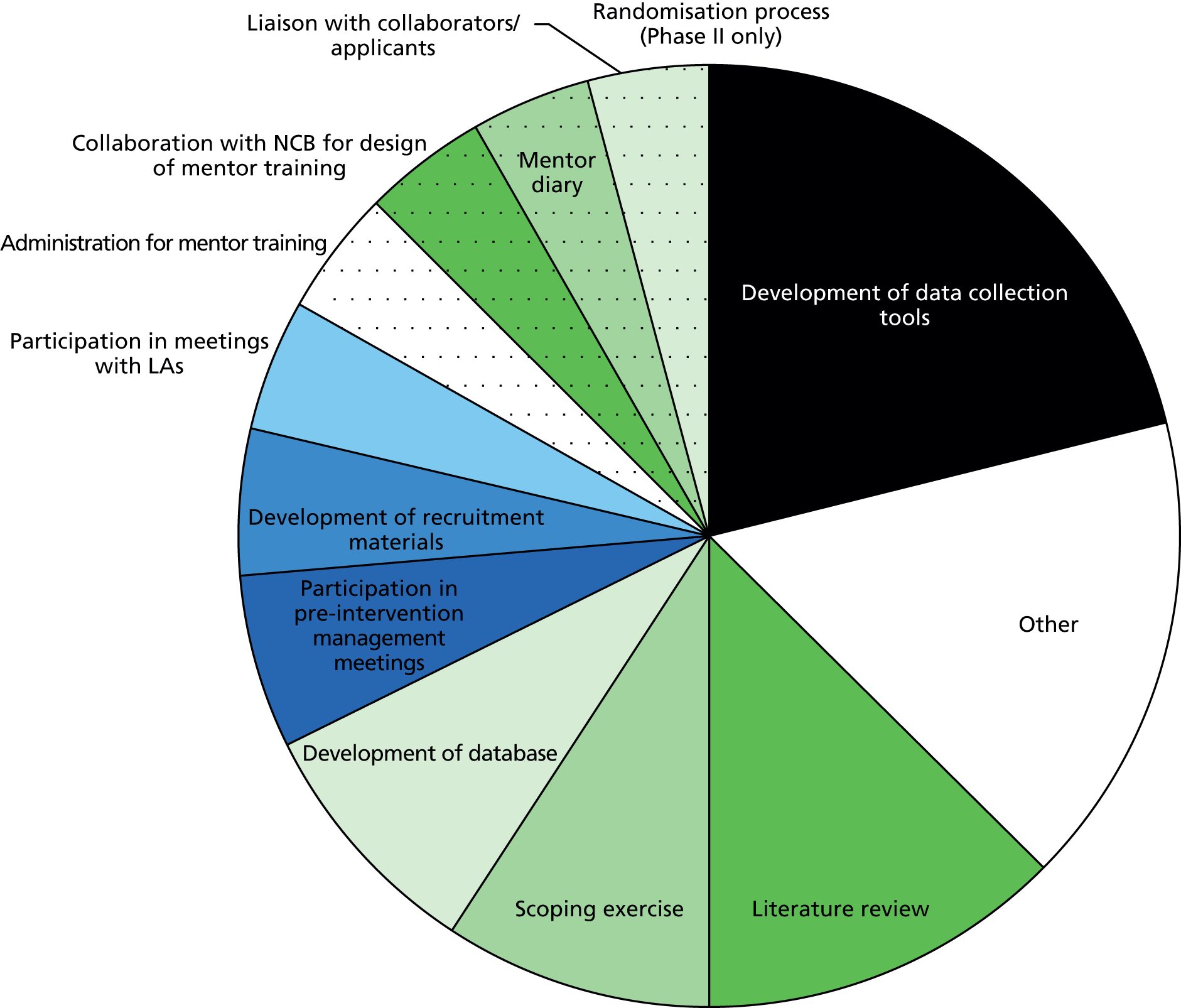
FIGURE 9.
Analysis of the researcher time put into the management of the project. HTA, Health Technology Assessment.
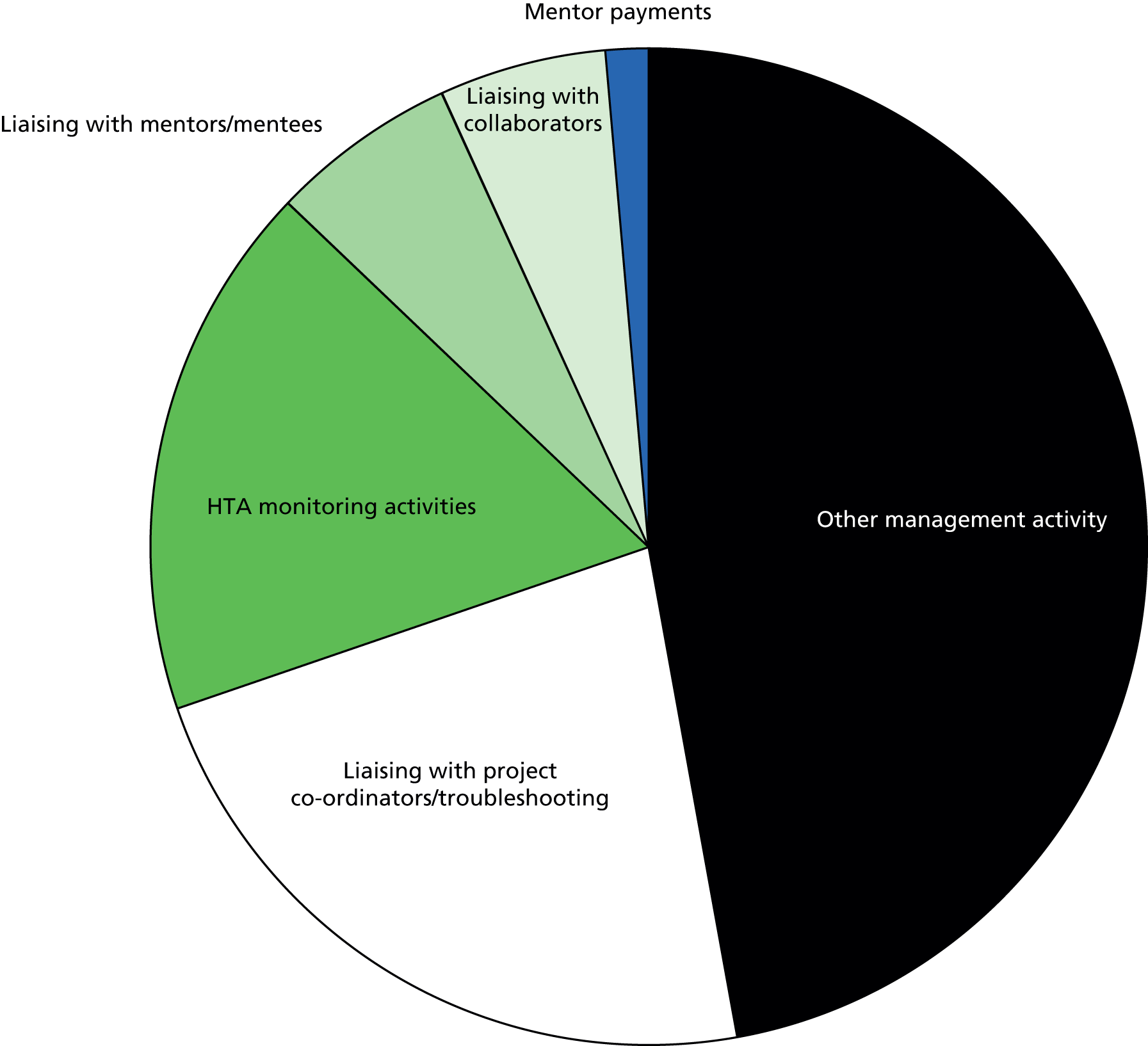
FIGURE 10.
Analysis of the researcher time put into the research activities of the project. HTA, Health Technology Assessment.

Figure 8 shows an analysis of the time spent on design and set-up of the intervention. The items concerned with recruitment materials and mentor training might fairly be considered as work that would have to be carried out by the LAs if the research team had not been available and these items could therefore be excluded from any research effort on a completely hands-off basis. In addition, examination of the researchers’ comments (attached to their data returns) suggests that some 104 hours logged under ‘other’ could similarly be considered work that the LAs could do for themselves.
Figure 9 shows an analysis of the time spent on management of the intervention. Three blocks of time contain tasks that are properly for the LAs. The block marked ‘troubleshooting’ is almost entirely concerned with chasing up recruitment of mentors and mentees and accounts for 200 hours. Examination of the free-text comments under ‘other’ shows that this block contains a number of similar activities, adding up to 29 hours. Also, examination of the element labelled ‘liaising with mentees and mentors’ shows another 40 hours dealing with problems that could be considered work that the LAs could do for themselves.
Figure 10 shows an analysis of the time spent on research activity. As an aid to costing the evaluation of a larger project, each element of the analysis is expected to be either independent of the project size or proportional to the number of one or other of the mentees, mentors or LA staff.
Using the data to estimate research costs for a Phase III evaluation
The figures in the previous section show the finest level of analysis of the researchers’ logged time that is possible given the nature of the data. Table 25 shows each component and the total associated hours recorded.
| Activity | Hours | Scaling factor |
|---|---|---|
| Design and set-up of the intervention | ||
| Development of data collection tools | 408 | 0.25 – tools already developed but may need adapting |
| Other | 209 | Proportional overhead on the number of researcher hours calculated for the exercise |
| Literature review | 244 | 0.25 – will need updating |
| Scoping exercise | 177 | 0.25 – will need adapting |
| Development of a database | 163 | 0.25 – database already developed but may need adapting |
| Participation in pre-intervention management meetings | 114 | 1.0 – will be about the same for any study regardless of scale |
| Development of recruitment materials | 97 | 0 – this is left to the LAs involved |
| Participation in meetings with LAs | 86 | Proportional to the number of LAs involved in the study |
| Administration for mentor training | 84 | 0 – this is left to the LAs involved |
| Collaboration with the NCB for design of mentor training | 82 | 0 – this is left to the LAs involved |
| Mentor diary | 78 | 0.25 – diary already developed but may need adapting |
| Liaison with collaborators/applicants | 75 | Proportional to the size of the study as measured by the number of mentees |
| Randomisation process (Phase II only) | 6 | Will not be significantly different from that in Phase II |
| Management of the intervention | ||
| Other management activity | 382 | After removal of the work best carried out by the LAs, proportional to the number of LAs |
| Liaising with PCs/troubleshooting | 198.5 | 0 – this would not be carried out by researchers in a hands-off exercise |
| HTA programme monitoring activities | 152 | Proportional to the scale of the exercise as measured by the number of mentees |
| Liaising with mentors/mentees | 12 | Proportional to the number of mentees |
| Liaising with collaborators | 47 | Proportional to the size of the study as measured by the number of mentees |
| Mentor payments | 12 | 0 – this would not be carried out by researchers in a hands-off exercise |
| Research on the intervention | ||
| Data collection, handling and interpretation | 1929 | Proportional to the size of the study as measured by the number of mentees |
| Drafting the final report | 411 | 1.0 – not directly related to the size of the exercise |
| Other research-related activity | 291 | Proportional overhead on the number of researcher hours calculated for the exercise |
| Research management meetings during the intervention | 250 | |
| Attendance at mentor training | 157 | Proportional to the number of mentors trained |
| Travel time | 99 | Proportional to the number of LAs and to the average journey length |
As discussed earlier, the researchers spent some time actually helping to manage the intervention. Corrections have been made to the figures shown in the table to remove this element of work. The table also shows how each remaining element of time is to be scaled to estimate the cost of a Phase III exercise. A spreadsheet has been constructed to carry out the scaling, including the calculation of an overhead for the research managers and steering group. It is available for use by any interested party.
Savings and benefits of the project
The previous sections estimate the cost of setting up and running the intervention and the cost of evaluating it. This leaves the question of how we determine whether or not the costs are justified in terms of the results achieved.
On the basis of a Phase II study we can make only a general assessment of outputs against costs. We know that, for the effort expended, 17 matched pairs were created, of whom eight pairs met at least once and three lasted through the full year. If we assume that the average duration of the five partial successes was 6 months, the cost model provides the estimated costs for the whole exercise, assuming that it was conducted in just one LA (Table 26). In practice, the duplication of set-up costs by two LAs would increase the costs. It appears that the cost of delivering 66 months of mentor–mentee contact in a tightly managed exercise would be £32,000. The efficiency of the process would undoubtedly improve with practice.
| Output | Cost of delivery (£)a |
|---|---|
| Setting up the exercise (independent of numbers) | 7000 |
| Getting 17 pairs to the starting point (includes cost of training) | 14,500 |
| Running five pairs for 6 months | 4000 |
| Running three pairs for 12 months | 5000 |
| Ongoing management (including end-of-year review) | 1500 |
| Total | 32,000 |
We cannot take the comparison of costs and benefits any further as there were no measurable differences between the intervention group and the control group beyond a slight increase in self-esteem in the intervention group. Two open questions remain. The most important is whether there are any longer-term effects in the mentored group. It may well be that the relevance of some of the ideas planted during mentoring will not become apparent to the mentees until much later. The second open question is whether any effect of the mentoring is ‘dose dependent’. In other words, is 6 months of mentoring half as effective as 12 months of mentoring? Looking ahead to a Phase III study, the above questions are noted for further exploration.
Assuming that a Phase III study would show clearer differences between the intervention group and the control group, how would these differences be evaluated? We could concentrate solely on teenage pregnancies averted or, more accurately, postponed and measure the costs saved (postponed) in terms of medical costs and social security. However, that may miss some longer-term benefits.
It is generally assumed that teenage pregnancies have a negative impact, which can be manifested in a number of ways:
-
through the health of the mother and the baby in both the short and the long term
-
through the education and employability of the mother in both the short and the long term, with a consequent reduction in income and dependence on social security
-
through a greater probability of the child and any future children being low achievers, with a greater tendency towards antisocial or criminal behaviour
-
through a greater probability of entering into a violent relationship with further negative impacts on the health of the mother and on the child’s health and emotional stability.
It is true that there do appear to be short-term health consequences but they are not huge and there is still controversy over how far they are related to maternal age and how far they are related to socioeconomic status. Relatively little is known about the longer-term impacts. A recent review of research evidence178 found that:
Current econometric studies suggest that effective interventions to prevent teenage pregnancies will not eradicate the poorer long term socioeconomic outcomes. Additional econometric analyses around the mothers’, fathers’ and children’s long term socioeconomic and health-related outcomes would be valuable.
Because averting a teenage pregnancy is actually a postponement perhaps by only 1–3 years, the short-term benefits of doing so are relatively slight. It is to the longer term that one must look for more substantial benefits. By offering guidance and a role model, a mentoring programme is likely to have a greater impact than simply addressing the issue of pregnancy through, say, contraception. We suggest a way to develop a longer-term model of teenage pregnancy outcomes, which offers a basis for an evaluation of prevention approaches. If this problem can be successfully addressed it will have value in evaluating any change to policies concerning LAC.
Proposal
Suppose that we have a group of young women leaving care, approximately half of whom have been mentored. The first question is whether the pregnancy rate in each group is different. If yes, we need to assess the benefits in the short and long term; if no, do we expect that there will be any delayed effects of mentoring that will prove beneficial in the longer term? If yes, we need to follow the intervention group further to discover what they are; if no, we can stop at this point. Assuming that we have a case for assessing the benefits, how do we go about this?
The study population can be divided into six groups:
-
group 1 – mentored and not pregnant
-
group 2 – mentored and became pregnant and miscarried or terminated the pregnancy
-
group 3 – mentored and became pregnant and carried the pregnancy through
-
group 4 – not mentored and not pregnant
-
group 5 – not mentored and became pregnant and miscarried or terminated the pregnancy
-
group 6 – not mentored and became pregnant and carried the pregnancy through.
A full evaluation of the mentoring requires a comparison of the future life course of girls in group 1 with those in group 4, those in group 2 with those in group 5 and those in group 3 with those in group 6. The comparison could be made in a range of ways but here we are interested primarily in the costs incurred by the six groups and the economic contribution that they make to society.
It would be possible to construct a probabilistic model of the kind used in other evaluations, but these rapidly become mired in conditional probabilities and have to be simplified. A better course would be a longitudinal study of a cohort of treated and untreated girls. However, that is not practicable.
An intermediate approach is to draw on existing cohort studies and use them to fill out a likely future for each of the young women in the Phase III trial. One would do this by selecting a longitudinal study (e.g. the 1970 birth cohort study179) and looking at how the girls in that study were categorised at age 16 years. 13 One would ensure that data were collected from the subjects in Phase III that would allow them to be matched to young women in the longitudinal study (ideally but not exclusively to girls who were in care).
One would then construct a range of futures for each young woman, based on the experience of her matched group. That experience may need to be modified using other data pertaining to broad social change, for example changes in relationship patterns, social security and treatment for health conditions. The aim would be to estimate the costs incurred by any family unit that the young women find themselves in during every future year and the share of those costs incurred by the young women and their children.
The cohort study would, in effect, provide a framework onto which one could map data from other studies in a disciplined and progressive manner and thus accumulate knowledge of the impact of ‘care’ policies on children. Cohort studies have previously been used to study long-term effects of teenage pregnancy and it would be very useful to draw on those studies; however, none, as far as we are aware, has attempted to build a general economic evaluation tool as envisaged here.
Summary
The direct measurement of the costs of implementing and running the project proved difficult as staff found that the work was interleaved with pressing normal duties and was not undertaken in easily measurable blocks. However, the study did allow us to specify a methodology for undertaking the work in a more coherent fashion and that model implementation has been broken down into constituent tasks that have been costed using our estimates of the time that they would take in a tightly managed project. The detailed assumptions and calculations are in the form of a spreadsheet, which is available for examination and further development. The costs of the research in terms of researcher time were much easier to determine and a spreadsheet is available to scale them up to a larger exercise.
We can make only a general assessment of outputs against costs. Focusing on Phase II, we know that, for the effort expended, 17 matched pairs were created of whom eight pairs met at least once and three lasted through the full year. If we assume that the average duration of the five partial successes was 6 months, then the cost model provides the estimates, shown in Table 26, for the whole exercise.
It appears that the cost of delivering 66 months of mentor–mentee contact in a ‘greenfield LA’ would be £32,000. The efficiency of the process would undoubtedly improve with practice.
There were no measurable differences between the intervention group and the control group beyond a slight increase in self-esteem in the intervention group. Two open questions remain. The most important is whether there are any longer-term effects on the mentored young women. It may well be that the relevance of some of the ideas planted during mentoring will not become apparent to the young women until much later. The second open question is whether any effect of the mentoring is ‘dose dependent’. In other words, is 6 months of mentoring half as effective as 12 months of mentoring?
Were the exercise to be extended to a larger, Phase III trial, the evaluation would ideally be extended to follow the intervention group and the control group beyond the end of the study to look for longer-term effects of mentoring. As an alternative, if a larger study reveals clear differences between the intervention group and the control group, we would seek to estimate longer-term benefits by projecting the longer-term life paths of the two groups using core data from cohort studies and drawing data from other studies into that framework.
Chapter 10 Discussion and conclusions
Summary of the findings
A summary of the key findings and recommendations can be found in Table 27.
| Key findings | |
|---|---|
| Participant recruitment and retention |
|
| Training |
|
| Randomisation |
|
| Matching |
|
| Peer mentoring intervention |
|
| Outcomes |
|
| Economic analysis |
|
| Because of the difficulties encountered in recruitment and management of the intervention, the small sample size and the inability to demonstrate significant change in the outcome variables, we would not recommend progressing to a Phase III trial. We recommend that a further small-scale exploratory trial is conducted in one LA, using the findings gained from this study as a basis for implementing the intervention: |
|
| Recruitment and management of the intervention |
|
| Peer mentoring intervention |
|
This exploratory trial was not able to demonstrate significant change in the primary outcome of reducing teenage pregnancy in looked-after young women. There was also no significant change in the secondary outcomes, although qualitative data were indicative of some positive impacts for mentees and mentors. We found that delivery of the intervention, although challenging, was feasible and the intervention did not cause harm to participants. There were considerable challenges to conducting a RCT with a vulnerable population in a social care setting, although data were indicative of approaches to improve trial design and conduct. These findings are discussed in detail below.
The intervention, as designed, was inappropriate for the context. Difficulties were encountered in meeting the recruitment target, with only 54% of target recruitment reached in Phase II. Thirteen out of 20 mentors (65%) and 19 out of 30 participants aged 14–18 years (63%) (recruited during Phases I and II) were retained for the research. The training programme for mentors was acceptable and could be manualised and replicated in a future Phase III trial. There would be a sufficient pool of potential participants for a future Phase III trial. However, LAs lacked the infrastructure, or resources, to be able to manage the intervention effectively; there was variable understanding and acceptance of the research methodology and inclusion criteria and a varying ability, or perception of need, to prioritise the research alongside other generic work.
Social workers tended to act as informal gatekeepers, which limited access to potential participants. Randomisation was acceptable to the young people, although less so to the social care professionals. Mentees appeared to value the intervention, but often failed to make scheduled meetings, either with their mentors or with the researchers. Similarly, mentors frequently failed to deliver, either in terms of the intervention or in terms of the research requirements, for example completing contact diaries, providing receipts and taking appropriate precautions around safety. Sex and relationships tended not to be the main focus of the mentoring. Weekly meetings were not feasible and only one in four of the relationships continued for the full year. Mentors and social workers considered that more individual and group support for mentors would need to be provided in any future trial. There was a slight increase in self-esteem in the mentored group compared with the care as usual group at the end of the intervention; however, between baseline and follow-up there was no evidence of any shift in attitudes regarding the acceptability of teenage pregnancy in either group.
The data do not allow us to address the primary question, which is whether a peer mentoring programme is effective in reducing rates of teenage pregnancy in LAC. The measures used were acceptable and appropriate although, given the size of the sample, we are unable to comment on the impact of the intervention on help seeking, attachment or other psychological measures related to general anxiety, self-esteem and locus of control. Young people were happy to answer questions related to sexuality and relationships and there was no evidence of harm. Different perceptions and assumptions about teenage pregnancy were found in the participants and the providers of the intervention, in particular the fact that the young people themselves did not regard teenage pregnancy as a problem, which may have undermined their motivation and engagement in the project.
Various changes would be recommended for a future Phase III trial. Peer mentoring should be delivered in an individual and a group format, with SRE best delivered in a structured format within a group setting. The project would need to be managed internally although delivered in combination with an external agency, such as a charity or the voluntary sector. LAs would need to receive research support costs to be able to provide dedicated PC time to support the recruitment of participants to the study and their retention and to manage the project effectively. Mentors would also require more support to be able to deliver the intervention. A future trial should consider lowering the age of mentees to 12 years (instead of 14 years), based on the fact that many of them were already sexually active by the age of 14 years, and should raise the age of mentors (to 21–28 years), based on the relative vulnerability and immaturity of young women who have been in care. Formalised structures for recruiting, selecting and supporting mentors and ensuring that they have the capacity, as well as the willingness, to deliver the mentoring in a consistent and responsible way and to monitor their mentoring contacts would need to be introduced.
Economic analysis
The direct measurement of the costs of implementing and running the project proved difficult as the staff found that the work was interleaved with pressing normal duties and was not undertaken in easily measurable blocks. To fill the gaps in the sparse data returned, using the experience of the study we constructed a model of implementation, specifying the actions to be taken by staff at each stage. By making realistic assumptions about the staff time required for each component action we were able to make estimates of the total staff time required to develop, implement and run a tightly managed exercise in one LA. The spreadsheet developed for this purpose is available to any LA wishing to examine or develop it.
In Chapter 9 we used the model to make an estimate of the cost of the actual Phase I/II experiment, but, for the purposes of looking forward, it is more useful to ask what would be the cost of the mentoring scheme were it to be developed in a greenfield site using the lessons learned in this exercise. On this basis we estimate the first-year cost of a scheme that mentors six people to be just over £24,000, reducing to around £14,000 in future years. The next question to ask is whether the benefits of the scheme justify this level of expenditure.
The study groups were very small and no measurable differences were found between the intervention group and the control group beyond a slight increase in self-esteem in the intervention group. From this study we cannot obtain a sound estimate of the benefits arising. However, we can ask what the benefits would have to be to justify the expenditure. This requires an estimate of the benefits to be expected from averting a teenage pregnancy.
A recent study180 of the costs and benefits of dispensing contraceptives and contraceptive advice to teenagers concluded that the most significant saving in averting pregnancy was from reduced benefit expenditure. This far outweighed any medical cost savings. The benefit savings, tracked up to the subjects reaching 35 years of age, were around £19,000 per teenage pregnancy averted. If we set this potential saving alongside the estimate of between £14,000 and £24,000 for mentoring six teenage girls in an established mentoring scheme, the benefits would be similar to the costs if the scheme averted roughly one pregnancy for every six girls treated.
There may be further benefits from averting teenage pregnancy that were not considered in the above study, including the effect on the future families of the people involved and interruption of a familial cycle of early pregnancy. The value of £19,000 should be considered a lower limit, although future changes in social security policy may reduce this further.
There are still some open questions. The most important is whether there are any longer-term effects of the intervention on the mentored young women. It may well be that the relevance of some of the ideas planted during mentoring will not become apparent to the young women until much later. This could generate benefits both in subjects who became pregnant in their teens and in those who did not. The second unanswered question is whether any effect of mentoring is ‘dose dependent’, that is, whether 6 months of mentoring is half as effective as 12 months of mentoring.
Feasibility and acceptability of the trial
The following domains were explored to assess the feasibility of delivering the peer mentoring intervention:
-
availability of eligible participants for a Phase III trial
-
recruitment of mentors and mentees
-
consent and randomisation
-
participant retention
-
evidence of harm to participants
-
characteristics and appropriateness of the proposed outcome measures.
Availability of eligible participants for a Phase III trial
As has been found in a number of RCTs based in social care181 and trials of peer mentoring,162 we experienced considerable difficulties in achieving the target recruitment, which delayed the start of the intervention. Determining the reasons for non-participation amongst young women aged 14–18 years was difficult as social workers provided only the names of the young women who they felt were suitable and who had agreed to be contacted by the researchers. We were unable to obtain detailed information from the social workers or the PCs on how many approaches had been made to the young women or how many of the young women had then declined to be referred on. There would appear to be a sufficient number of eligible young people at a national level for a future Phase III trial. Our survey of young people in care elicited a positive response with regard to participating in a mentoring intervention in the future, either as a mentor or as a mentee. Given adequate information, participants were generally willing to take part in the study and none of the young women who we approached subsequently declined to give consent once the study had been explained to them. There is some evidence that, when recruitment can be carried out directly by researchers, recruitment rates appear to be higher; however, this also carries considerable ethical challenges in such a vulnerable population. 182
Oakley and colleagues183 have suggested that, to successfully implement randomisation in social care settings, the issue being addressed should be considered a priority issue by the participants. One of the problems that we encountered in this study was the fact that, although teenage pregnancy in LAC was, at the time of developing this programme, a priority issue for government and arguably for health and social care providers, it was not viewed as such by the young people themselves, in contrast, for example, to educational outcomes.
A second prerequisite for mounting a RCT in a social care setting is that there needs to be a clear scientific and policy rationale for using random allocation and sufficient consideration given to ensuring that stakeholder groups are fully signed up to, and understand, this approach. 183 We found that stakeholders were not entirely in agreement with, nor fully understanding of the need for, randomisation. Indeed, many social workers were extremely uneasy about the principle of randomisation on the basis that they considered it unethical to deprive the care as usual group from an intervention that they considered would benefit them.
Project co-ordinator and social worker understandings and expectations of the trial, its methodological approach and effective intra- and interagency communication were crucial for its success. However, many social workers in the participating LAs viewed the study as an additional burden that had been imposed on them by their managers and external researchers, which meant that they lacked a sense of ownership of or commitment to the project. PCs were also frustrated by the lack of recognition and support of their role by senior management or by social worker colleagues.
If this trial had taken place within a health-care setting, payment would have been made for PCs on the basis that they constituted an excess treatment cost. In health-care settings there is a culture of NHS trusts supporting the cost of providing an experimental intervention and, under the terms of the new clinical commissioning groups’ mandate, commissioners are committed to providing the funding to support National Institute for Health Research-funded research (updating and strengthening previous similar agreements). No such culture or provision exists in social care, resulting in a situation in which senior management in the LAs agreed to participate in the study but could not commit additional resources to the teams implementing the intervention.
Had the trial taken place in a health-care setting, mechanisms would have been in place to cost for health-care professionals’ time to recruit participants (research support costs), enabling the host trust to backfill that time. No equivalent system is in place in social care settings, which meant that PCs were required to support the trial in addition to their other duties, which, more often than not, had to take priority.
To improve recruitment and retention rates in any future trial, additional research support costs would need to be provided to participating LAs to cover the costs of recruitment and retention and any additional research-related tasks. In addition, social workers would need to be fully informed about the need for the research and the specific research approach being taken, with additional input and support from senior managers, to encourage internal management and ownership of a future trial.
The process cannot be successful without adequate backing from senior management to disseminate information about the trial, throughout the organisation and borough wide, to the teams and groups that work with LAC: children’s social work teams, leaving care teams, fostering teams, virtual school teams, independent reviewing officers, LAC nurses and foster carers.
Recruitment of mentees and peer mentors
The vulnerability of children and young people in the care system is well recognised. Participants in this study exhibited emotional and behavioural problems, consistent with the literature,49 including self-harm (52%), truancy (82%), suspension or expulsion from school (50%), contact with the police (62%) and running away (40%). Over half of participants had already engaged in sexual intercourse (63%), the mean age of first intercourse was 14.3 years and one-fifth of participants (n = 3 in each group) had been pregnant. A recent national survey of sexual behaviours and attitudes in the UK found that the average age reported by young people for first sexual intercourse was 16 years. 25 The same survey also reported that 29% of women had had sexual intercourse before the age of 16 years. This group would therefore appear to be more sexually active and at a younger age than the national average. Several professionals in the study suggested that any future intervention to reduce the rate of teenage pregnancy in LAC should target a younger age group, those aged 12–16 years, before they become sexually active. They also recommended ‘front loading’ data on eligible young people in a future trial, in which senior management, working with their data management officers, would identify eligible young people, who would be approached in the first instance by the professional who has the closest relationship with them regarding their interest in participating. Networks of young people in care could be accessed in alternative ways, for example through CiCCs or youth centres, events for young people in care and specialist publications such as the Who Cares? Trust newsletters.
When obtaining consent, LAC aged 14–18 years were told by researchers that they wanted to look at the effects of peer mentoring on general well-being, as well as work, social life relationships, attitudes to sex and thoughts about early pregnancy. We found no evidence that being informed of the aims of the programme deterred anyone from taking part, although young people may have been more engaged and motivated had the approach been to focus on developing positive behaviours skills and opportunities rather than avoiding the ‘problem’ of teenage pregnancy, as advocated in the PYD model (see Chapter 1).
Because of the difficulties that we encountered in recruiting sufficient numbers of young women to act as mentors, we ended up essentially accepting onto the training all those who met the age criterion. This included young women who were pregnant or who had young children, none of whom were able to complete, or in some cases even commence, mentoring. Social workers were simply given the following as inclusion criteria: young people aged 19–25 years who were currently, or who had recently been, in care and who they considered would be suitable as a mentor. There was otherwise no independent assessment of a mentor’s motivation, capability or commitment to the role or any exploration of personal issues that might affect a mentor’s ability to perform this role. Any future trial would need to adopt a more formalised approach to mentor recruitment whereby social workers ensure that relevant information about potential participants is passed on to the PC and that mentors are subjected to a rigorous selection and screening procedure, both before and post training. It would also be important to use the training process to screen, and if necessary exclude, individuals who may not be suitable as a mentor.
Despite the qualities identified by social workers as desirable for good mentoring, we were unable to predict from the training who out of the young people who participated would go on to form a successful mentoring relationship and who would drop out, simply based on their personal qualities or characteristics. However, one of the factors that did appear to predict failure to take up mentoring, or early discontinuation, was the mentor being pregnant; therefore, in any future trial this should be added to the exclusion criteria.
Although some of the mentors were conscientious and assiduous in fulfilling all of the components of their role and took their responsibilities towards their mentee very seriously, a large number did not commit themselves to the task, with high rates of dropout and disappearing from contact without warning, misuse of the mobile phone, failure to attend support sessions, failure to record contacts and non-contact with their mentee. We underestimated the vulnerability of our mentor group; there was evidence of significant psychological, emotional and social problems in this group, despite the fact that over two-thirds of them were in further education. Based on our findings, we consider that only the most resilient of young people should be recruited to act as a mentor in any future trial. Raising the lower and upper age limits for mentors from 19–25 years to 21–28 years may help to ensure that applicants are sufficiently mature and emotionally stable to take on this work. However, it might also make it more difficult to identify potential candidates, as most of them will no longer have any formal contact with social services.
Training and matching
The 3-day training course for mentors was judged to be acceptable and relevant by the young people who participated. Both trainers had experience of working with young people in care, skills in group work and a willingness to be open, were non-judgemental and flexible in their approach and adopted a range of non-didactic training methods including role play. A high trainer to participant ratio was important to enable trainers to provide individual support to mentors if required.
Post-training interviews with the participants would help to assess the commitment and ability of would-be mentors to deliver the intervention and any personal or structural barriers that might get in the way of their effective participation or lead to early dropout. Effective communication between the referrer and the PC would ensure that mentors are provided with any information about their mentee in advance that might impact on their ability to build a relationship and provide support. No clear evidence was found to support the need for matching, apart from the tactical consideration of geographical location.
The delay between training mentors and recruitment of sufficient numbers of young women aged 14–18 years to act as mentees meant that the momentum and motivation of mentors waned, again highlighting the importance of a more stringent recruitment process in the future to ensure that recruitment of mentors and mentees takes place concurrently.
Randomisation
Amongst the young women we consented to be randomised to the intervention arm or the control arm, and from our national survey of young people in care, we found no evidence that randomisation, that is, the prospect of having only a 50% chance of receiving the intervention, was a deterrent to participation.
Participants randomised to the control arm reported minimal levels of distress, despite having hoped for a mentor. By contrast, there was considerable unease expressed by social workers about the harmful and even unethical aspects of randomisation when dealing with such a vulnerable population and some evidence that these concerns deterred some from approaching or referring eligible young people. Similar findings have been reported by other researchers in relation to research in social care settings. 181,184
Content of mentoring sessions
In this study, weekly face-to-face contact between mentors and mentees was not feasible; fortnightly contact would appear to be more realistic, in terms of what actually happened but also based on feedback from the participants, social work professionals and young people in the national survey. Many young people expressed a preference for group meetings held at monthly intervals, which they felt would be less intimidating and would encourage mentees to be more open, both within and outside the group setting. The mentors rarely used the mobile phones provided except for the purpose of arranging appointments with their mentee. However, some mentors did abuse the privilege by using the phone for unrelated calls and texts and running up large phone bills.
The content of the mentoring sessions was left to the mentor and the mentee to decide on. Many of the mentors lacked confidence to structure the sessions and similarly many of the mentees were unwilling, or unable, to express a preference as to how they wanted to use this time together. The findings illustrate the importance of creating some structure to the mentoring whilst not being overly prescriptive. There is an abundance of materials that charities give to mentors to use to address healthy relationships, which were discussed with mentors during the training but not provided or used during the sessions. In a future study such materials could be provided as an alternative way for mentors to address these issues on an individual basis. A goal-oriented approach, providing mentees with a clear sense of purpose for mentoring as a whole and for each meeting, might encourage more regular attendance. In a future trial, mentoring sessions would need more of a focus on the issues that are of relevance to these young women – education, transitions from care and future aspirations – to try to ensure that they remain engaged with the programme.
Although the intervention was designed with the aim of reducing rates of teenage pregnancy, it is unclear to what extent this aim was fully understood, or endorsed, by participants. We found from our interviews that, although a reduction in teenage pregnancy may have been a desired outcome for policy-makers, professionals and the research team, it was not necessarily an aspiration that was fully embraced by the young people themselves. This clearly contrasts with the education mentoring scheme, which young people chose to attend because they wanted to perform better educationally (see Chapter 8). Despite the training, many mentors felt somewhat reticent about discussing sex and relationships with their mentee and felt that they lacked the personal resources, or confidence, to be able to do this effectively. SRE could be delivered by a trained practitioner, as part of group mentoring sessions, to ensure that mentees and their mentors receive sufficient and accurate information. It is likely that delivery of this material in a group setting would increase mentors’ confidence to discuss these issues further during individual sessions with their mentee.
Retention
Thirteen out of 20 mentors (65%) and 19 out of 30 participants aged 14–18 years (63%) were retained for the research. We overestimated the resilience and independence of the young women who were recruited as mentors, which meant that many of them struggled to deliver the intervention as specified. Perhaps not surprisingly, given the fact that they were drawn from the same pool as the mentees and shared many of their characteristics, they were a vulnerable group with limited problem-solving skills, which meant that some of them were overwhelmed by the emotional as well as practical demands of the role. The 3.5-day training was not in itself sufficient to sustain the mentors, or keep them motivated, particularly when problems arose in the mentoring relationship. Providing additional support in a future trial would be expected to improve retention rates of mentors.
The role of the PC is crucial in terms of running the monthly support groups and offering ad hoc advice and support to mentors for the duration of the intervention, as well as monitoring their contacts, facilitating communication with other involved social care professionals and providing crisis management. However, this requires a significant investment of time and energy and without additional resources for a dedicated PC is not realistically achievable.
If funding could be made available in a future trial, PCs would need to be contacting mentors with weekly phone calls as well as providing monthly group support meetings. Mentors would benefit from a one-to-one review with a PC on a quarterly basis, allowing mentors the opportunity to reflect on the mentoring relationship and PCs to assess progress and consider whether the work carried out warrants payment for input and activities. It remains to be seen whether the level of support that would be required from LA professionals to make a future peer mentoring intervention feasible would be economically viable.
Although mentors and the PCs said that the monthly group support meetings had helped them to reflect on the progress of their mentoring and discuss problems that they might be having, the mentors did not attend these meetings on a regular basis or they sometimes turned up only to collect their activity money and shopping vouchers. It is therefore unclear whether simply offering more support would fully address issues around mentor compliance and retention.
In a future trial, an alternative model to address problems around mentor recruitment and retention would be to recruit mentors from outside the care system altogether, for example through universities. This would certainly increase the potential pool of applicants; however, it would also mean losing one aspect of the ‘peer’ support, that is, the shared experience of care, which appeared to help mentors to empathise with mentees, act as advocates and raise concerns with social workers, which mentees appeared to value (see Chapter 8).
Evidence of harm to participants
Beyond the fact that there were no examples brought to our attention of inappropriate or risky contacts between mentors and mentees, it is difficult to determine the extent of any harm associated with participation in the study. The research team was very aware of the highly vulnerable population involved in the study. We were particularly aware of the potential for harm to the mentors, possibly as a result of being asked to deal with situations that they were poorly equipped to deal with, feeling out of their depth and becoming emotionally overwhelmed. We were also concerned about the potential for excessively dependent relationships to develop and the risk of personal versus professional roles becoming blurred, particularly given the synergy between the mentee and the mentor in terms of age and life experience. We attempted to address these issues through the training and the ongoing support meetings and by emphasising the need for clear lines of responsibility and accountability and channels of communication within the mentees’ care networks. In spite of this, however, some of the contacts between mentors and mentees took place without PCs or social workers being informed.
All participants had given informed consent to participate in the trial knowing that they had a 50% chance of not being allocated a mentor and all were deemed Gillick competent. 129 Although those participants who were randomised to the care as usual arm of the trial expressed some disappointment at not being allocated a mentor, there was no evidence of any lasting harm, or damage, to these individuals. Equally, a number of mentees expressed feelings of rejection or disappointment if their mentor dropped out prematurely or failed to match up to their expectations. It is not clear to what extent these feelings were severe or persistent or to what extent they might impact on the mentees’ willingness to engage with carers or seek help in the future. However, any future trial would need to mention mentor dropout as a possibility when obtaining informed consent from would-be mentees, particularly when working with such a vulnerable group whose past experiences may have made them particularly sensitive to rejection and loss.
Characteristics and appropriateness of the proposed outcome measures
The outcome measures were acceptable to the young people and appropriate; however, given the low numbers recruited to the study, there was necessarily more emphasis on the qualitative data than on the quantitative data. Measuring pregnancy as a primary outcome was not possible given the low numbers recruited and retained. Equally, the proxy measure, initiation of sexual activity, was not particularly illustrative given the high baseline levels of sexual contact and pregnancy (one-fifth of the young people had been pregnant on at least one occasion at baseline). The low numbers of mentees recruited prevented us from being able to interpret any changes in the quantitative measures around psychological health, attachment and help seeking. This is not to say that these measures would not provide a useful insight into the mechanism of action of any future intervention. The logic model (see Chapter 3) supports the relevance of self-esteem, self-efficacy and decision-making capacity in teenage pregnancy in this group, which our qualitative data would appear to support.
There was some qualitative evidence for an increase in self-esteem and sense of control in the mentees. Similarly, mentors reported feeling more confident and competent as a result of their mentoring experience. Therefore, in a future trial, there is sufficient qualitative evidence to support the continuing use of the locus of control measure and a self-esteem measure for mentees and a measure of self-efficacy for mentors. Similarly, although there was no evidence in this trial for a reduction in feelings of general anxiety and depression, the GHQ is a sensitive measure of clinical distress and of change over time and was acceptable to this population.
Strengths and limitations
Although we recruited only around half the target group for both mentors and mentees, this is similar to findings of other RCTs with vulnerable groups. 182 The reasons for this reflected difficulties with engaging young people in care as well as working with LAs:
-
LA staff lack time to prioritise recruitment and awareness of the study was patchy
-
informal gatekeeping by social workers
-
lack of exposure to and experience in research and research concepts such as equipoise and lack of research infrastructure to support this project within LAs
-
concerns about the project aims and variable interpretations about the recruitment criteria
-
the overall aim of the research project may not have been fully shared with or accepted by the young people concerned or viewed by them as a priority.
The non-London site that we recruited (LA3) had to withdraw from the intervention because of problems recruiting and retaining mentors. This limits the generalisability of our findings somewhat as LA1 and LA2 were both based within London, although it is not entirely clear how this may have affected our results.
One of the strengths of this trial is the fact that the intervention has been embedded within the LAs that would be required to deliver the intervention in the real world. However, this strength has also proved to be one of its limitations. Many of the problems that we encountered are representative of a fundamental clash of professional philosophies and values as well as divergent professional cultures that make cross-agency research collaboration so difficult. 185
Some have suggested that there is a fundamental incompatibility between social work practices and the science of evidence-based practice,183,185–190 which has resulted in an evidence base that lags behind current social work policy and practice. 191 Opposition to RCTs by social scientists has been based around feasibility, science and ethics, particularly in relation to the use of randomisation. 183 As a result of this, research evidence in social care often falls short of what is considered to be the gold standard for health and clinical research – the RCT. 188
In social work, research and development runs at about 0.3% of total spend compared with 5.4% in health. 189 Within social work there is considerable disagreement as to what constitutes current best practice and, although there may be a lot of support for the idea of research, in practice social workers lack training compared with health workers, as well as skills in critical appraisal, and tend instead to follow a type of practice wisdom or intuition. 185,186 It has been noted that the fact that a study may receive approval from official gatekeepers will not necessarily guarantee the co-operation of the informal gatekeepers and participants or professional commitment to the study. 181,190 This observation certainly replicates the experiences of the researchers in this trial.
The difficulties that we have encountered in this trial are similar to those described in many other studies of hard-to-reach and hard-to-engage populations. 181,182,187,191 The staging of a RCT within, and in collaboration with, LAs was undermined by different understandings of research methodology; the lack of a research infrastructure within the LAs; our inability to provide LA research support costs; the absence of a dedicated in-house project manager, which meant that competing generic commitments took priority; frequent LA reorganisations, economic cutbacks and demoralisation amongst social workers; and a tendency of social workers to act as informal gatekeepers.
Feasibility of a Phase III trial
A number of key uncertainties around conducting a RCT of the intervention have been addressed by this study: randomisation is acceptable to participants; measures of outcomes and process used are largely acceptable and appropriate (and have been refined when necessary); and inclusion and exclusion criteria have been refined. As such, there is no requirement to conduct a further pilot study of the trial processes. Outstanding feasibility issues are linked to implementation of the intervention in a social care context. The issue of recruitment of participants to the study (mentees) and of mentors to deliver the intervention, and the retention of both mentees and mentors, is a function of processes and resources within participating LAs, as discussed earlier. Modifications to the intervention protocol, as it would be delivered by LAs, would need to be made to the content of mentor training, the processes for selecting mentors and the provision of appropriate support for mentors. Ideally, a small-scale peer mentoring programme could be mounted in a single LA, incorporating changes recommended from the Phase II study, to test the modifications indicated in this study. This would provide a further opportunity to establish an accurate cost of delivering the intervention.
Successful trials involving health and social care require that all parties understand the roles and responsibilities of those involved at an individual and a strategic level; all professionals understand and agree to the aims and objectives of the project; strong management and professional support; strategic commitment at an executive level; and adequate resources. 185 These elements would have to be put in place in a future Phase III trial.
With regard to the recruitment of mentors and mentees, the age of prospective mentees would be changed to 12–16 years and the age of mentors would be changed to 21–28 years. Several professionals suggested ‘front-loading’ data on eligible young people in a future trial so that senior management, working with their data management officers, would identify eligible young people, who would be approached in the first instance by the professional who has the closest relationship with them regarding their interest in participating. Networks of young people in care could be accessed in alternative ways, for example through CiCCs or youth centres, events for young people in care and specialist publications such as the Who Cares? Trust newsletters.
Any future trial would need to adopt a more formalised approach to mentor recruitment whereby social workers ensure that relevant information about potential participants is passed on to the PCs and that mentors are subjected to a rigorous selection and screening procedure, both before and post training. It would also be important to use the training process to screen and if necessary exclude individuals who may not be suitable as mentors. Pregnancy would be an exclusion criterion for mentoring in any future trial as this appeared to predict dropout and early discontinuation.
To improve retention and fidelity to the intervention in a future trial, more support at an individual and a group level would need to be provided to mentors, particularly if the mentors continue to be drawn from the looked-after population.
To improve recruitment and retention rates in any future trial, additional research support funds would need to be provided to participating LAs to cover the costs of recruitment and retention and any additional research-related tasks and social workers would need to understand and accept the rationale for the research approach being taken, with additional input and support from senior managers, to encourage internal management and ownership. An alternative model would be for LAs to commission a charity or other specialist organisation with expertise in sexual health and/or youth work to deliver the intervention in partnership with the LA.
In a future trial, mentoring should include both individual sessions and group meetings, each held at approximately monthly intervals. SRE would best be delivered in a group context, supplemented by individual sessions outside the group meetings. Mentors would need more direction and support in terms of the structure and content of their meetings. Mentoring sessions that have more of a focus on the issues that are of relevance to looked-after young children and young women – education, transitions from care and future aspirations – will be necessary to increase mentees’ levels of engagement with, and retention to, the intervention. Individual meetings between mentors and mentees could be arranged at the monthly group session, without recourse to a phone. Alternative means of communication outside of group sessions should be considered, such as Freephone messaging services (e.g. WhatsApp, Blackberry Messenger) and e-mail. In addition, for the purposes of privacy and maintaining boundaries, mentors could consider using an alternative phone number (SIM card only) purely for contacting their mentee. PCs would need to monitor contacts when possible to ensure adherence to the above.
An interesting question is whether there might be any longer-term effects of this intervention on the girls and young women who were mentored. The apparent lack of difference between the intervention group and the care as usual group may reflect not only the small numbers but also the fact that we were able to follow up fewer of the care as usual group than the intervention group, who remained more engaged with the study. It could be suggested that young women in the care as usual group who had the highest level of social and health-related problems and who were the most chaotic and disorganised were the most likely to have dropped out at an early stage, leaving the more stable and compliant individuals in the study. This would have masked any remaining differences between the two groups at follow-up.
A second unanswered question is whether any effect of the mentoring is ‘dose dependent’, that is, whether 6 months of mentoring is only half as effective as 12 months of mentoring. Were the exercise to be extended to a larger Phase III study, the evaluation would ideally involve following up the intervention and control group participants beyond the end of the study to look for longer-term effects of mentoring. As an alternative, if a larger study revealed clear differences between the intervention group and the control group, we would seek to estimate the longer-term benefits by projecting the longer-term life paths of the two groups using core data from cohort studies and drawing data from other studies into that framework.
Recent reductions in teenage pregnancy rates in the UK have been largely attributed to education-based initiatives introduced over the last decade. There is currently a lack of a formal evidence base supporting this hypothesis, as would be expected if one was to support new clinical guidance in a health-care context. However, the National Institute for Health and Care Excellence (NICE) Collaborating Centre for Social Care Guidance, delivered by the Social Care Institute for Excellence (SCIE), indicates a desire at policy level to see trial methodology informing service delivery in social care. However, we have demonstrated both structural (including funding infrastructure) and cultural problems (including differing expectations between senior management and the workforce around prioritising research), which may prove a barrier to achieving this aspiration.
Acknowledgements
The trial was funded by the Health Technology Assessment programme (project number 08/20/03) of the National Institute for Health Research. We would like to thank participating local authorities and in particular the project coordinators, senior managers and directors of children’s services who lent their support to this project; all of the young people who participated in the project; our Advisory Group and Trial Steering Committee for their constructive feedback and support throughout; the National Children’s Bureau and Straight Talking for providing the mentor training; and Ros Hampton for providing administrative support to the project.
Through Rona Campbell’s involvement the work was undertaken with the support of the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer), a UKCRC Public Health Research Centre of Excellence. Funding from the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council (RES-590–28–0005), the Medical Research Council, the Welsh Government and the Wellcome Trust (WT087640MA), under the auspices of the UKCRC, is gratefully acknowledged.
Advisory group
Ravinder Barn (Professor of Social Policy).
Ann Phoenix (Professor of Social and Developmental Psychology).
Geraldine McCormick (Lambeth PCT).
Khatija Hafesji (service user).
Natasha Finlayson (the Who Cares Trust).
Sheryl Burton (National Childrens Bureau).
Sara Brookes (Bristor University).
Michael Allured (Department of Education).
Trial steering committee
External
Professor Geraldine Macdonald (Queens University) (Chairperson).
Dr Kristin Liabo (Institute of Education).
Professor Janet Peacock (King’s College London).
Internal
Professor Gillian Mezey (Principal Investigator SGUL).
Khatija Hafesji (user representative).
Professor Rona Campbell (Bristol University).
Contribution of authors
Gillian Mezey (Reader in Forensic Psychiatry) conceived and designed the intervention and study alongside members of the Advisory Group, provided overall management and direction and contributed to drafting and editing of the report.
Deborah Meyer (Research Trial Manager) was the Project Manager, supported the data collection process, facilitated the involvement of young people and contributed to data analysis and the writing of the report.
Fiona Robinson (Research Assistant) supported the data collection process, facilitated the involvement of young people and contributed to data analysis and the writing of the report.
Chris Bonell (Professor of Sociology and Social Policy) advised on the design of the trial and intervention, with particular regard to the BDI model, and contributed to and commented on drafts of the final report.
Rona Campbell (Professor of Public Health Research) contributed to the design of the intervention and the trial and commented on draft chapters of the final report.
Steve Gillard (Senior Lecturer in Social and Community Mental Health) co-led on the qualitative data analysis and contributed to the design of the intervention and study and writing of the report.
Peter Jordan (Health Economist) led on the economic evaluation and the preparation of the health economic aspects of the study.
Nadia Mantovani (Postdoctoral Research Fellow) led on the qualitative data analysis and contributed to the design of the intervention and study and writing of the report.
Kaye Wellings (Professor of Sexual and Reproductive Health Research) contributed to the development of the study, including questionnaire development, and commented on drafts of the final report.
Sarah White (Biostatistician) led on the analysis and interpretation of the quantitative data and contributed to the design of the trial and report writing.
Data sharing statement
All available data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Teenage Pregnancy: Past Successes – Future Challenges. London: Department for Education; 2010.
- Office for National Statistics . Conceptions in England and Wales, 2011 2013. www.ons.gov.uk/ons/rel/vsob1/conception-statistics--england-and-wales/2011/2011-conceptions-statistical-bulletin.html (accessed 13 August 2015).
- Avery L, Lazdane G. What do we know about sexual and reproductive health of adolescents in Europe?. Eur J Contracept Reprod Health Care 2008;13:58-70. http://dx.doi.org/10.1080/13625180701617621.
- A League Table of Teenage Births in Rich Nations. Florence: Innocenti Research Centre; 2001.
- Nationmaster.com . Health Statistics: Teenage Pregnancy (Most Recent) by Country 1994 n.d. www.nationmaster.com/graph/hea_tee_bir_rat-health-teen-birth-rate (accessed December 2013).
- Duncan S. What’s the problem with teenage parents? And what’s the problem with policy?. Crit Soc Policy 2007;27:307-34. http://dx.doi.org/10.1177/0261018307078845.
- Duncan S, Edwards R, Alexander C. Teenage Parenthood: What’s the Problem?. London: Tufnell Press; 2010.
- McMahon M. Engendering Motherhood: Identity and Self-Transformation in Women’s Lives. New York, NY: Guilford Press; 1995.
- Dickson R, Fullerton D, Eastwood A, Sheldon T, Sharp F. Preventing and reducing the adverse effects of unintended teenage pregnancies. Effect Health Care 1997;3:1-12.
- Moffitt T. E-Risk Study Team . Teen-aged mothers in contemporary Britain. J Child Psychol Psychiatry 2002;43:727-42. http://dx.doi.org/10.1111/1469-7610.00082.
- Hobcraft K, Kiernan K. Childhood Poverty, Early Motherhood and Adult Social Exclusion 1999. http://sticerd.lse.ac.uk/dps/case/cp/CASEpaper28.pdf (accessed December 2012).
- Botting B, Rosato M, Wood R. Teenage mothers and the health of their children. ONS Popul Trends 1998;93:19-28.
- Ermisch J, Pevalin DJ. Who Has a Child as a Teenager?. London: Institute for Social and Economic Research; 2003.
- Ermisch J. Does a ‘Teen-Birth’ Have Longer-Term Impacts On The Mother? Suggestive Evidence from the British Household Panel Survey. London: Institute for Social and Economic Research; 2003.
- Mayhew E, Bradshaw J. Mothers, babies and the risks of poverty. Poverty 2005;121:13-6.
- Swann C, Bowe K, McCormick G, Kosmin M. Teenage Pregnancy and Parenthood: A Review of Reviews. London: Health Development Agency; 2003.
- Teenage Pregnancy. London: The Stationery Office; 1999.
- McLeod A. Changing patterns of teenage pregnancy: population based study of small areas. BMJ 2001;323:199-203. http://dx.doi.org/10.1136/bmj.323.7306.199.
- Smith T. Influence of socioeconomic factors on attaining targets for reducing teenage pregnancies. BMJ 1993;306. http://dx.doi.org/10.1136/bmj.306.6887.1232.
- Diamond I, Clements S, Stone N, Ingham R. Spatial variation in teenage conceptions in south and west England. J R Stat Soc Series A (Stat Soc) 1999;162:273-89. http://dx.doi.org/10.1111/1467-985X.00135.
- Bradshaw J, Finch N, Miles J. Deprivation and variations in teenage conceptions and abortions in England. J Fam Plan Reprod Health Care 2005;31:15-9. http://dx.doi.org/10.1783/0000000052973022.
- Harden A, Brunton G, Fletcher A, Oakley A. Teenage pregnancy and social disadvantage: systematic review integrating controlled trials and qualitative studies. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b4254.
- Children Act 1989. London: The Stationery Office; 1989.
- Children Looked After in England (Including Adoption and Care Leavers) Year Ending 31 March 2012. London: Department for Education; 2012.
- Mercer C, Tanton C, Prah P, Erens B, Sonnenberg P, Clifton S, et al. Changes in sexual attitudes and lifestyles in Britain through the life course and over time: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal). Lancet 2013;382:1781-94. http://dx.doi.org/10.1016/S0140-6736(13)62035-8.
- McGlone F. Families. Res Matters 2000;9:32-4.
- Brodie I, Berridge D, Beckett W. The health of children looked after by local authorities. Br J Nurs 1997;6:386-90. http://dx.doi.org/10.12968/bjon.1997.6.7.386.
- Corylon J, McGuire C. Young Parents in Public Care: Pregnancy and Parenthood among Young People Looked after by Local Authorities. London: National Children’s Bureau; 1997.
- Biehal N, Clayden J, Stein M, Wade J. Moving On: Young People and Leaving Care Schemes. London: Her Majesty’s Stationery Office; 1995.
- Garnett L. Leaving Care and After. London: National Children’s Bureau; 1992.
- Dixon J. Young people leaving care: health, well-being and outcomes. Child Fam Soc Work 2008;13:207-17. http://dx.doi.org/10.1111/j.1365-2206.2007.00538.x.
- Hobcraft J. Intergenerational and Life-Course Transmission of Social Exclusion: Influences and Childhood Poverty, Family Disruption and Contact with the Police. London: Centre for Analysis of Social Exclusion, London School of Economics; 1998.
- Schofield G, Ward E, Biggart L, Scaife V, Dodsworth J, Larsson B, et al. Looked after Children and Offending: Reducing Risk and Promoting Resilience. Norwich: University of East Anglia; 2012.
- Francis J. Investing in children’s futures: enhancing the educational arrangements of ‘looked after’ children and young people. Child Fam Soc Work 2000;5:23-3. http://dx.doi.org/10.1046/j.1365-2206.2000.00141.x.
- Polnay L, Ward H. Promoting the health of looked after children. Government proposals demand leadership and a culture change. BMJ 2000;320:661-2. http://dx.doi.org/10.1136/bmj.320.7236.661.
- Ward H, Jones H, Lynch M, Skuse T. Issues concerning the health of looked after children. Adopt Foster J 2002;26:8-18. http://dx.doi.org/10.1177/030857590202600403.
- Williams J, Jackson S, Maddocks A, Cheung WY, Love A, Hutchings H. Case control study of the health of those looked after by local authorities. Arch Dis Child 2001;85:280-5. http://dx.doi.org/10.1136/adc.85.4.280.
- Viner RM, Taylor B. Adult health and social outcomes of children who have been in public care: population-based study. Pediatrics 2005;115:894-9. http://dx.doi.org/10.1542/peds.2004-1311.
- Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Pyschiatry 2007;190:319-25. http://dx.doi.org/10.1192/bjp.bp.106.025023.
- Wellings K, Nanchahal K, Macdowall W, McManus S, Erens B, Mercer C, et al. Sexual behaviour in Britain: early heterosexual experience. Lancet 2001;358:1843-50. http://dx.doi.org/10.1016/S0140-6736(01)06885-4.
- Stone N, Ingham R. Factors affecting British teenagers’ contraceptive use at first intercourse: the importance of partner communication. Perspect Sex Reprod Health 2002;34:191-7. http://dx.doi.org/10.2307/3097729.
- Bonell C, Strange V, Stephenson J, Oakley A, Copas A, Forrest S, et al. Effect of social exclusion on the risk of teenage pregnancy: development of hypotheses using baseline data from a randomised trial of sex education. J Epidemiol Community Health 2003;57:871-6. http://dx.doi.org/10.1136/jech.57.11.871.
- Social Care Institute for Excellence . Preventing Teenage Pregnancy in Looked After Children 2004. www.scie.org.uk/publications/briefings/briefing09/ (accessed 13 August 2015).
- Haydon D. Teenage Pregnancy and Looked after Children/Care Leavers. London: Barnardo’s; 2003.
- Daniels H, Cole T, Sellman E, Sutton J, Visser J, Bedward J. Study of Young People Permanently Excluded from School. Nottingham: DfES Publications; 2003.
- Selman P, Richardson D, Hosie A. Monitoring of the DfES Standards Fund Teenage Pregnancy Grant. Newcastle upon Tyne: University of Newcastle; 2001.
- Dawson N, Hosie A. The Education of Pregnant Young Women and Young Mothers in England 2005. http://webarchive.nationalarchives.gov.uk/20130401151715/http://www.education.gov.uk/publications/eOrderingDownload/RW40.pdf (accessed December 2013).
- Bonell C, Allen E, Strange V, Copas A, Oakley A, Stephenson J, et al. The effect of dislike of school on risk of teenage pregnancy: testing of hypotheses using longitudinal data from a randomised trial of sex education. J Epidemiol Community Health 2005;59:223-30. http://dx.doi.org/10.1136/jech.2004.023374.
- Outcomes for Children Looked after by Local Authorities in England, as at 31 March 2012. London: Department for Education; 2012.
- Turnbull T, Van Wersch A, Van Schaik P. A review of parental involvement in sex education: the role for effective communication in British families. Health Educ J 2008;67:182-95. http://dx.doi.org/10.1177/0017896908094636.
- Sex and Relationships Education. London: Department For Children, Schools and Families; 2009.
- Emmerson L. Parents and SRE: a Sex Education Forum Evidence Briefing. London: National Children’s Bureau; 2011.
- Payne I, Butler H. Improving the health care process and determining health outcomes for children looked after by the local authority. Ambulat Child Health 1998;4:165-72.
- Wilson T. Compulsory Education and Teenage Motherhood. London: Royal Holloway; 2012.
- Statutory Guidance on Children Who Run Away or go Missing from Home or Care. London: Department for Education; 2013.
- Make Runaways Safe. London: The Children’s Society; 2011.
- Report from the Joint Inquiry into Children Who Go Missing from Care. London: Department for Education; 2012.
- Out of Mind, Out of Sight: Breaking Down the Barrier to Understanding Child Sexual Exploitation. London: CEOP; 2011.
- Missing Children and Adults: A Cross Government Strategy. London: Home Office; 2011.
- Tackling Child Sexual Exploitation: Action Plan. London: Department for Education; 2011.
- Jago S, Arocha L, Brodie I, Melrose M, Pearce J, Warrington C. What’s Going On to Safeguard Children and Young People from Sexual Exploitation?. Bedford: University of Bedfordshire; 2011.
- Puppet on a String: The Urgent Need to Cut Children Free from Sexual Exploitation. London: Barnardo’s; 2011.
- Pearce J, Campbell R, O’Neill M. Sex Work Now. Cullompton: Willan Press; 2006.
- Friedberg M, Radford J, Friedberg M, Harne L. Women, Violence and Strategies for Action. Buckingham: Open University Press; 2000.
- Blinn-Pike L, Berger T, Dixon D, Kuschel D, Kaplan M. Is there a causal link between maltreatment and adolescent pregnancy? A literature review. Perspect Sex Reprod Health 2002;34:68-75. http://dx.doi.org/10.2307/3030209.
- Noll J, Shenk C, Putnam K. Childhood sexual abuse and adolescent pregnancy: a meta-analytic update. J Pediatr Psychol 2009;34:366-78. http://dx.doi.org/10.1093/jpepsy/jsn098.
- Rainey D, Stevens-Simon C, Kaplan D. Are adolescents who report prior sexual abuse at higher risk for pregnancy?. Child Abuse Neglect 1995;19:1283-8. http://dx.doi.org/10.1016/0145-2134(95)00088-P.
- Gilbert R, Widom C, Browne K, Fergusson D, Webb E, Janson S. Burden and consequences of child maltreatment in high-income countries. Lancet 2009;373:68-81. http://dx.doi.org/10.1016/S0140-6736(08)61706-7.
- Blower A, Addo A, Hodgson J, Lamington L, Towlson K. Mental health of ‘looked after’ children: a needs assessment. Clin Child Psychol Psychiatry 2004;9:117-29. http://dx.doi.org/10.1177/1359104504039176.
- Meltzer H, Gatward R, Corbin T, Goodman R, Ford T. The Mental Health of Young People Looked after by Local Authorities in England. London: Her Majesty’s Stationery Office; 2003.
- Teenage Pregnancy Strategy: Beyond 2010. London: Her Majesty’s Stationery Office; 2010.
- Positive for Youth: A New Approach to Cross-Government Policy for Young People Aged 13 to 19. London: Her Majesty’s Stationery Office; 2011.
- Keeping Children Safe: The Government’s Reponse to the Victoria Climbie Inquiry Report and Joint Chief Inspectors’ Report Safeguarding Children. London: Her Majesty’s Stationery Office; 2003.
- Macleod S, Hart R, Jeffes J, Wilkin A. The Impact of the Baby Peter Case on Applications for Care Orders. Slough: National Foundation for Educational Research; 2010.
- Cassidy S, Duggan O, Milmo C. Benefit cuts ‘will see more children taken into care’. Warning of economic impact on struggling households. The Independent 2013. www.independent.co.uk/news/uk/home-news/benefit-cuts-will-see-more-children-taken-into-care-8440235 (accessed January 2013).
- Children and Families Bill. London: Her Majesty’s Stationery Office; 2013.
- Children Act 2004. London: The Stationery Office; 2004.
- Every Child Matters. London: Her Majesty’s Stationery Office; 2003.
- Working Together to Safeguard Children: A Guide to Inter-Agency Working to Safeguard and Promote the Welfare of Children. London: Her Majesty’s Stationery Office; 2010.
- Care Matters: Time for Change. London: Her Majesty’s Stationery Office; 2007.
- London: The Stationery Office; 2008.
- Mooney A, Statham J, Monck E. Promoting the Health of Looked after Children: A Study to Inform Revision of the 2002 Guidance. London: Department for Children, Schools and Families; 2009.
- Promoting the Quality of Life of Looked-After Children and Young People. London: SCIE/NICE; 2010.
- Berridge D, Henry L, Jackson S, Turney D. Looked after and Learning. Evaluation of the Virtual School Head Pilot. Bristol: School for Policy Studies, University of Bristol; 2009.
- Help for Children in Care to Achieve Better School Results. London: Department for Education; 2012.
- Munro J. Empowering looked-after children. Child Fam Soc Work 2001;6:129-37. http://dx.doi.org/10.1046/j.1365-2206.2001.00192.x.
- Hayden C. More than a piece of paper? Personal education plans and ‘looked after’ children in England. Child Fam Soc Work 2005;10:343-52. http://dx.doi.org/10.1111/j.1365-2206.2005.00364.x.
- After Care: Young People’s Views on Leaving Care. Manchester: Ofsted; 2012.
- Dickson K, Sutcliffe K, Gough D. The Experiences, Views and Preferences of Looked After Children and Young People and their Families and Carers about the Care System. London: Institute of Education; 2009.
- Hadley A, Baker P, Guthrie K, Hutchinson C, Kane R, Wellings K. Teenage Pregnancy and Reproductive Health. London: Royal College of Obstetricians and Gynaecologists; 2007.
- Catalano R, Berglund M, Ryan J, Lonczak H, Hawkins J. Positive youth development in the United States: research findings on evaluations of positive youth development programs. Ann Am Acad Polit Soc Sci 2004;591:98-124. http://dx.doi.org/10.1177/0002716203260102.
- Gavin L, Catalano R, David-Ferdon C, Gloppen K, Markham C. A review of positive youth development programs that promote adolescent sexual and reproductive health. J Adolesc Health 2010;46:S75-91. http://dx.doi.org/10.1016/j.jadohealth.2009.11.215.
- Wiggins M, Bonell C, Sawtell M, Austerberry H, Burchett H, Allen E, et al. Health outcomes of youth development programme in England: prospective matched comparison study. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b2534.
- Hutson N, Cowie H. Setting up an email peer support scheme. Pastoral Care Educ 2007;25:12-6. http://dx.doi.org/10.1111/j.1468-0122.2007.00420.x.
- Stephenson J, Strange V, Allen E, Copas A, Johnson A, Bonell C, et al. The long-term effects of a peer-led sex education programme (RIPPLE). PLoS Med 2008;5. http://dx.doi.org/10.1371/journal.pmed.0050224.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. http://dx.doi.org/10.1016/S0140-6736(08)60692-3.
- Harden A, Weston R, Oakley A. A Review of the Effectiveness and Appropriateness of Peer-Delivered Health Promotion Interventions for Young People. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 1999.
- Philip K, Spratt J. A Synthesis of Published Research on Mentoring and Befriending. Manchester: Mentoring and Befriending Foundation; 2007.
- Philip K. Young People and Mentoring: A Literature Review for the Joseph Rowntree Foundation. Aberdeen: University of Aberdeen; 1999.
- Hall J. Mentoring and Young People: A Literature Review. Glasgow: Scottish Council for Research in Education (SCRE) Centre, Faculty of Education, University of Glasgow; 2003.
- Karcher M. Cross-age peer mentoring. Research in Action Series 2007;7.
- Peer Mentoring In Schools. Manchester: Mentoring and Befriending Foundation; 2010.
- Middleton S. Peer Mentoring Opportunities for Looked after Children and Care Leavers. Edinburgh: Scottish Government; 2012.
- Parsons C, Maras P, Knowles C, Bradshaw V, Hollingworth K, Monteiro H. Formalised Peer Mentoring Pilot Evaluation. London: Department for Children, Schools and Families; 2008.
- Nelson A. Peer mentoring: a citizenship entitlement at Tanfield School. Pastoral Care Educ 2003;21:34-41. http://dx.doi.org/10.1111/j.0264-3944.2003.00276.x.
- DuBois D, Holloway B, Valentine J, Cooper H. Effectiveness of mentoring programs for youth: a meta-analytic review. Am J Commun Psychol 2002;30:157-97. http://dx.doi.org/10.1023/A:1014628810714.
- Shiner M, Young T, Newburn T, Groben S. Mentoring Disaffected Young People. York: London School of Economics, Joseph Rowntree Foundation; 2004.
- Newburn T, Shiner M. Young people, mentoring and social inclusion. Youth Justice 2006;6:23-41. http://dx.doi.org/10.1177/1473225406063450.
- Clayden J, Stein M. Mentoring Young People Leaving Care: ‘Someone for Me’. York: Joseph Rowntree Foundation; 2005.
- Final Evaluation Report of the DCSF Funded National Mentoring Pilot for Looked after Children. London: Department for Children, Schools and Families; 2008.
- Knight A, Chase E, Aggleton P. Teenage pregnancy among young people in and leaving care: messages and implications for foster care. Adopt Foster J 2006;30:58-69. http://dx.doi.org/10.1177/030857590603000108.
- Daniel B. The value of resilience as a concept for practice in residential settings. Scot J Resident Child Care 2003;2:6-15.
- Gilligan R. Enhancing the resilience of children and young people in public care by mentoring their talents and interests. Child Fam Soc Work 1999;4:187-96. http://dx.doi.org/10.1046/j.1365-2206.1999.00121.x.
- Masten A, Coatsworth J. The development of competence in favorable and unfavorable environments: lessons from research on successful children. Am Pyschol 1998;53:205-20. http://dx.doi.org/10.1037/0003-066X.53.2.205.
- Kidger J. Young Mothers As Peer Educators in School Sex Education: A Beneficial Approach 2002.
- Thomson R, Holland J, McGrellis S, Bell R, Henderson S, Sharpe S. Inventing adulthoods: a biographical approach to understanding youth citizenship. Sociol Rev 2004;52:218-39. http://dx.doi.org/10.1111/j.1467-954X.2004.00466.x.
- Karcher M, Kuperminc G, Portwood S, Sipe C, Taylor A. Mentoring programs: a framework to inform program development, research, and evaluation. J Commun Psychol 2006;34:709-25. http://dx.doi.org/10.1002/jcop.20125.
- Allen E, Bonell C, Strange V, Copas A, Stephenson J, Johnson AM, et al. Does the UK government’s teenage pregnancy strategy deal with the correct risk factors? Findings from a secondary analysis of data from a randomised trial of sex education and their implications for policy. J Epidemiol Commun Health 2007;61:20-7. http://dx.doi.org/10.1136/jech.2005.040865.
- Hogan B, Linden W, Najarian B. Social support interventions: do they work?. Clin Psychol Rev 2002;22:381-440. http://dx.doi.org/10.1016/S0272-7358(01)00102-7.
- Norbeck J, DeJoseph J, Smith R. A randomized trial of an empirically-derived social support intervention to prevent low birthweight among African American women. Soc Sci Med 1996;43:947-54. http://dx.doi.org/10.1016/0277-9536(96)00003-2.
- Watt R, Tull K, Hardy R, Wiggins M, Kelly Y, Molloy B, et al. Effectiveness of a social support intervention on infant feeding practices: randomised controlled trial. J Epidemiol Commun Health 2009;63:156-62. http://dx.doi.org/10.1136/jech.2008.077115.
- Malgady R, Rogler L, Costantino G. Hero/heroine modeling for Puerto Rican adolescents: a preventive mental health intervention. J Consult Clin Psychol 1990;58. http://dx.doi.org/10.1037/0022-006X.58.4.469.
- Yancey A. Building positive self-image in adolescents in foster care. Adolescence 1998;33:253-67.
- Heptinstall E. Gaining access to looked after children for research purposes: lessons learned. Br J Soc Work 2000;30:867-72. http://dx.doi.org/10.1093/bjsw/30.6.867.
- Teitler J. The Impact of the Los Angeles Neighbourhood Variation in Youth Sexual, Fertility and Educational Outcomes. Princeton: Bendheim-Thoman Center for Research on Child Wellbeing, Office of Population Research; 1998.
- Burton L, Jarrett R. In the mix, yet on the margins: the place of families in urban neighbourhood and child development research. J Marriage Fam 2000;62:1114-35. http://dx.doi.org/10.1111/j.1741-3737.2000.01114.x.
- A Framework for Development and Evaluation of RCTs for Complex Interventions to Improve Health. London: MRC; 2000.
- The Quality Protects Programme: Transforming Children’s Services. London: Department of Health; 1999.
- Gillick v . West Norfolk and Wisbech Area Health Authority 3 All ER 402 n.d.
- Johnson A, Mercer C, Copas A, McManus S, Wellings K, Fenton K, et al. Sexual behaviour in Britain: partnerships, practices and HIV risk behaviours. Lancet 2001;358:1835-42. http://dx.doi.org/10.1016/S0140-6736(01)06883-0.
- Barn R, Andrew L, Mantovani N. Life after Care: the Experiences of Young People from Different Ethnic Groups. London: Joseph Rowntree Foundation; 2005.
- Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press; 1965.
- Goldberg D, Williams P. A User’s Guide to the General Health Questionnaire. London: NFER Nelson; 1991.
- Wilson C, Deane F, Ciarrochi J, Rickwood D. Measuring help-seeking intentions: properties of the General Help-Seeking Questionnaire. Can J Counsel 2005;39:15-28.
- Rotter J. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr 1966;80:1-28. http://dx.doi.org/10.1037/h0092976.
- Bartholomew K, Horowitz L. Attachment styles among young adults: a test of a four-category model. J Pers Soc Psychol 1991;61:226-44. http://dx.doi.org/10.1037/0022-3514.61.2.226.
- Richie J, Lewis J. Qualitative Research Practice: a Guide for Social Science Students and Researchers. London: Sage; 2003.
- Strauss A, Corbin C. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. London: Sage; 1998.
- Patton M. Qualitative Evaluation Methods. Beverley Hills, CA: Sage; 1980.
- Stephenson J, Strange V, Forrest S, Oakley A, Copas A, Allen E, et al. Pupil-led sex education in England (RIPPLE study): cluster-randomised intervention trial. Lancet 2004;364:338-46. http://dx.doi.org/10.1016/S0140-6736(04)16722-6.
- Mentoring for Looked after Children: Dissemination Manual. Westerham: Rainer; 2008.
- Sipe C, Baldwin Grossman J. Contemporary Issues in Mentoring. Philadelphia, PA: Public/Private Ventures; 1999.
- Foster L. Effectiveness of Mentor Programs: A Review of the Literature from 1995 to 2000. Sacramento, CA: California State Library, California Research Bureau; 2001.
- Satchwell K, Waring S, Walters R. Mentoring Literature Review. Alberta, AB: Alberta Children’s Services; 2006.
- Knowles C, Parsons C. Evaluating a formalised peer mentoring programme: student voice and impact audit. Pastoral Care Educ 2009;27:205-18. http://dx.doi.org/10.1080/02643940903133888.
- A Guide to Effective Risk Management for Providers of Mentoring and Befriending Services. Manchester: Mentoring and Befriending Foundation; 2007.
- National Peer Mentoring Pilot Dissemination Manual. Manchester: Mentoring and Befriending Foundation; 2008.
- Yoo S, Johnson CC, Rice J, Manuel P. A qualitative evaluation of the Students of Service (SOS) program for sexual abstinence in Louisiana. J School Health 2004;74:329-34. http://dx.doi.org/10.1111/j.1746-1561.2004.tb06623.x.
- Jones K, Doveston M, Rose R. The motivations of mentors: promoting relationships, supporting pupils, engaging with communities. Pastoral Care Educ 2009;27:41-5. http://dx.doi.org/10.1080/02643940902733167.
- Tierney J, Branch A. College Students as Mentors for At-Risk Youth: A Study of Six Campus Partners in Learning Programs. Philadelphia, PA: Public/Private Ventures; 1992.
- Kendrick A, Hunter L, Cadman M. Evaluation of Fostering Network Scottish Care Leavers Mentoring Projects. Glasgow: Glasgow School of Social Work/Fostering Network; 2005.
- Jekielek S, Moore K, Hair E, Scarupa H. Mentoring: A Promising Strategy for Youth Development. New York, NY: Springer; 2002.
- Karcher M. The effects of developmental mentoring and high school mentors’ attendance on their younger mentees’ self-esteem, social skills, and connectedness. Psychol Schools 2005;42:65-77. http://dx.doi.org/10.1002/pits.20025.
- Tebb K. The Effectiveness of Mentoring for Adolescent Mothers and Their Infants: A Comparative Study Between Sister Friend and Cal Learn 1999.
- Goldner L, Mayseless O. The quality of mentoring relationships and mentoring success. J Youth Adolesc 2009;38:1339-50. http://dx.doi.org/10.1007/s10964-008-9345-0.
- Garraway H, Pistrang N. ‘Brother from another mother’: mentoring for African-Caribbean adolescent boys. J Adolesc 2010;33:719-29. http://dx.doi.org/10.1016/j.adolescence.2009.10.011.
- Nash C. Development of a mentoring system within coaching practice. J Hospitality Leisure Sport Tourism Educ 2003;2. http://dx.doi.org/10.3794/johlste.22.37.
- Liang B, Tracy A, Taylor C, Williams L. Mentoring college-age women: a relational approach. Am J Commun Psychol 2002;30:271-88. http://dx.doi.org/10.1023/A:1014637112531.
- Dallos R, Comley-Ross P. Young people’s experience of mentoring: building trust and attachments. Clin Child Psychol Psychiatry 2005;10:369-83. http://dx.doi.org/10.1177/1359104505053755.
- Munson M, Smalling S, Spencer R, Scott L, Tracy E. A steady presence in the midst of change: non-kin natural mentors in the lives of older youth exiting foster care. Child Youth Serv Rev 2010;32:527-35. http://dx.doi.org/10.1016/j.childyouth.2009.11.005.
- Morrow K, Styles M. Building Relationships with Youth in Program Settings: A study of Big Brothers/Big Sisters. Philadelphia, PA: Public/Private Ventures; 1995.
- Bogat G, Liang B, Rigol-Dahn R. Stages of mentoring: an analysis of an intervention for pregnant and parenting adolescents. Child Adolesc Soc Work J 2008;25:325-41. http://dx.doi.org/10.1007/s10560-008-0130-4.
- Rhodes J, DuBois D. Mentoring relationships and programs for youth. Curr Direct Psychol Sci 2008;17:254-8. http://dx.doi.org/10.1111/j.1467-8721.2008.00585.x.
- Spencer R, Collins M, Ward R, Smashnaya S. Mentoring for young people leaving foster care: promise and potential pitfalls. Soc Work 2010;55:225-34. http://dx.doi.org/10.1093/sw/55.3.225.
- Rhodes J, Spencer R, Keller T, Liang B, Noam G. A model for the influence of mentoring relationships on youth development. J Commun Psychol 2006;34:691-707. http://dx.doi.org/10.1002/jcop.20124.
- Byington T. Keys to successful mentoring relationships. J Extens 2010;48.
- Rhodes J. Stand by Me: The Risks and Rewards of Mentoring Today’s Youth. Cambridge, MA: Harvard University Press; 2009.
- Grossman J, Rhodes J. The test of time: predictors and effects of duration in youth mentoring relationships. Am J Commun Psychol 2002;30:199-21. http://dx.doi.org/10.1023/A:1014680827552.
- Cupples M, Stewart M, Percy A, Hepper P, Murphy C, Halliday H. A RCT of peer-mentoring for first-time mothers in socially disadvantaged areas (the MOMENTS study). Arch Dis Child 2011;96:252-8. http://dx.doi.org/10.1136/adc.2009.167387.
- Philip K, Shucksmith J, King C. Sharing a Laugh? A Qualitative Study of Mentoring Interventions with Young People. Aberdeen: University of Aberdeen, Joseph Rowntree Foundation; 2004.
- Downey G, Lebolt A, Rincón C, Freitas A. Rejection sensitivity and children’s interpersonal difficulties. Child Dev 1998;69:1074-91. http://dx.doi.org/10.1111/j.1467-8624.1998.tb06161.x.
- Bandura A. Social Learning Theory. Morristown, NJ: General Learning Press; 1977.
- Bowlby J. Attachment and Loss. Volume 3 – Sadness and Depression. Harmondsworth: Penguin; 1980.
- Bond L, Thomas L, Coffey C, Glover S. Long-term impact of the gatehouse project on cannabis use of 16-year-olds in Australia. J School Health 2004;74:23-30. http://dx.doi.org/10.1111/j.1746-1561.2004.tb06597.x.
- Pearce JW, Pezzot-Pearce TD. Psychotherapy of Abused and Neglected Children. New York, NY: Guilford Press; 2007.
- Patton G, Bond L, Carlin JB, Thomas L, Butler H, Glover S, et al. Promoting social inclusion in schools: group-randomized trial of effects on student health risk behaviour and well-being. Am J Public Health 2006;96:1582-7. http://dx.doi.org/10.2105/AJPH.2004.047399.
- Curtis L. Unit Costs of Health and Social Care 2012. Canterbury: PSSRU, University of Kent; 2012.
- Squires H, Hernández Alava M, Payne N, Blank L, Baxter S, Preston L. How Much Does Teenage Parenthood Affect Long Term Outcomes? A Systematic Review. Sheffield: University of Sheffield, School of Health and Related Research (ScHARR); 2010.
- Centre for Longitudinal Studies . 1970 British Cohort Study n.d. www.cls.ioe.ac.uk/page.aspx?sitesectionid=795sitesectiontitle=Welcome+to+the+1970+British+Cohort+Study+(BCS70) (accessed 14 August 2015).
- Pilgrim H, Payne N, Chilcott J, Blank L, Guillaume L, Baxter S. Modelling the Cost-Effectiveness of Interventions to Encourage Young People, Especially Socially Disadvantaged Young People, To Use Contraceptives and Contraceptive Services. Sheffield: University of Sheffield, School of Health and Related Research (ScHARR); 2010.
- Dixon J, Biehal N, Green J, Sinclair I, Kay C, Parry E. Trials and tribulations: challenges and prospects for randomised controlled trials of social work with children [published online ahead of print 4 March 2013]. Br J Soc Work 2013. 10.1093/bjsw/bct035.
- Howard L, de Salis I, Tomlin Z, Thornicroft G, Donovan J. Why is recruitment to trials difficult? An investigation into recruitment difficulties in an RCT of supported employment in patients with severe mental illness. Contemp Clin Trials 2009;30:40-6. http://dx.doi.org/10.1016/j.cct.2008.07.007.
- Oakley A, Strange V, Toroyan T, Wiggins M, Roberts I, Stephenson J. Using random allocation to evaluate social interventions: three recent UK examples. Ann Am Acad Polit Soc Sci 2003;589:170-89. http://dx.doi.org/10.1177/0002716203254765.
- McDonald A, Knight R, Campbell M, Entwistle V, Grant A, Cook J, et al. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials 2006;7. http://dx.doi.org/10.1186/1745-6215-7-9.
- Gray M, Joy E, Plath D, Webb S. Opinions about evidence: a study of social workers’ attitudes towards evidence-based practice. J Soc Work 2014;14:23-40. http://dx.doi.org/10.1177/1468017313475555.
- Burke A, Early T. Readiness to adopt best practice among adolescents’ AOD treatment providers. Health Soc Work 2003;28:99-105. http://dx.doi.org/10.1093/hsw/28.2.99.
- MacDonald G, Davies H, Nutley S, Smith P. What Works? Evidence-Based Policy and Practice in Public Service. Bristol: Policy Press; 2000.
- Guyatt G, Oxman A, Kunz R, Vist G, Falck-Ytter Y, Schunemann H. What is quality of evidence and why is it important to clinicians?. BMJ 2008;336:995-8. http://dx.doi.org/10.1136/bmj.39490.551019.BE.
- Marsh P, Fisher M. Developing the Evidence Base for Social Work and Social Care Practice. London: Social Care Institute for Excellence; 2005.
- Morrow V, Richards M. The ethics of social research with children: an overview. Child Soc 1996;10:90-105. http://dx.doi.org/10.1002/(SICI)1099-0860(199606)10:2<90::AID-CHI14>3.0.CO;2-Z.
- Cameron A, Lart R, Bostock L, Coomber C. Factors that Promote and Hinder Joint and Integrated Working Between Health and Social Care Services. London: Social Care Institute for Excellence; 2012.
- Curtis L. Unit Costs of Health and Social Care 2012. Canterbury: PSSRU, University of Kent and London School of Economics and Political Science; 2012.
Appendix 1 Ethical approval from the London School of Hygiene & Tropical Medicine
Appendix 2 Ethical approval from the Association of Directors of Children’s Services for national surveys of social care professionals
Dr Gill Mezey and Deborah Meyer
St George’s University of London
Department of Mental Health – Division of PHSE
Cranmer Terrace
London
SW17 ORE
By email
9 January 2013
Dear Deborah and Dr Mezey,
Request for ADCS research approval – St George’s University of London – Developing and piloting a peer mentoring intervention to reduce teenage pregnancy in Looked After Children (LAC) and Care Leavers
ADCS ref: RGE130103
I write on behalf of Sue Wald, Chair of the ADCS Research Group regarding your request for research approval for the above named project.
The Research Group has considered your request and given its approval believing that the results of the project will be useful to local authorities. We would be grateful if when contacting local authorities you would quote the reference above.
The group would like the following issue(s) to be considered alongside their approval:
Any future contact with local authorities should be made to the target audience of Service Managers/Head of Service for services to Looked After Children/care leavers, rather than the Director of Children’s Services (DCSs). It is unlikely that the DCS will directly have the information required.
The Group’s encouragement to respond to the survey will be communicated to ADCS members in local authorities in England in the next edition of the ADCS weekly e-bulletin which is produced and circulated on Friday afternoons. A list of approved research projects can be found on the ADCS website. The Research Group wishes you well with the project.
As mentioned in the ADCS Guidelines for Research Approvals, please send the Research Group a copy of the full report and the summary of your main findings when the research is complete.
If you have any queries about this feedback, please contact me in the first instance.
Yours sincerely
Gary Dumbarton, on behalf of Sue Wald, Chair of the ADCS Research Group
Appendix 3 Targeted literature review search strategy
A search strategy was developed to enable identification of the most relevant published and unpublished literature. This involved searching for literature based around concepts of mentoring, teenage pregnancy and LAC. A variety of alternative terms for these concepts were identified:
| 1. Teenage pregnancy | 2. LAC | 3. Mentoring |
|---|---|---|
| Teen*pregnan* Teen* mother* Young parent* Youth pregnan* Young pregnan* Young mother* Adolescen* mother* Adolescen* parent* Adolescen* pregnan* Juvenile pregnan* Sexual health |
Looked After Child* Looked after young people Child* in Care Young people in Care Youth in Care Adolescen* in Care Juvenile in Care Teen* in Care Residential Care Foster Care Girl* in Care Care leav* |
Mentor* Peer-Mentor* Peer Mentor* Youth Mentor* Coach* Buddy* Cross-Age Peer Mentor* Cross Age Peer Mentor* Child Mentor* Adolescen* mentor* Teen* mentor* |
The following databases were searched:
-
PsycINFO
-
Social Sciences Citation Index
-
MEDLINE (via Ovid and EBSCOhost)
-
Database of Abstracts of Reviews of Effect (free access via The Cochrane library)
-
ERIC
-
SIGLE
-
CINAHL.
To enter these concepts into databases, the following search strings were used:
-
Mentoring and LAC – 2 and 3
(Looked After Child* OR Looked after young people OR “Child* in Care” OR “Young people in Care” OR “Youth in Care” OR “Adolescen* in Care” OR “Juvenile in Care” OR “Teen* in Care” OR Residential Care OR Foster Care OR “Girl* in Care” OR Care leav*) AND (Mentor* OR Peer-Mentor* OR Peer Mentor* OR Youth Mentor* OR Coach* OR Buddy* OR Cross-Age Peer Mentor* OR Cross Age Peer Mentor* OR Child Mentor* OR Adolescen* mentor* OR Teen* mentor*)
-
Mentoring and teenage pregnancy (in general) – 1 and 3
(Teen*pregnan* OR Teen* mother* OR Young parent* OR Youth pregnan* OR Young pregnan* OR Young mother* OR Adolescen* mother* OR Adolescen* parent* OR Adolescen* pregnan* OR Juvenile pregnan* OR Sexual health) AND (Mentor* OR Peer-Mentor* OR Peer Mentor* OR Youth Mentor* OR Coach* OR Buddy* OR Cross-Age Peer Mentor* OR Cross Age Peer Mentor* OR Child Mentor* OR Adolescen* mentor* OR Teen* mentor*)
-
Mentoring and teenage pregnancy for LAC – 1, 2 and 3
(Teen*pregnan* OR Teen* mother* OR Young parent* OR Youth pregnan* OR Young pregnan* OR Young mother* OR Adolescen* mother* OR Adolescen* parent* OR Adolescen* pregnan* OR Juvenile pregnan* OR Sexual health) AND Looked After Child* OR Looked after young people OR “Child* in Care” OR “Young people in Care” OR “Youth in Care” OR “Adolescen* in Care” OR “Juvenile in Care” OR “Teen* in Care” OR Residential Care OR Foster Care OR “Girl* in Care” OR Care leav* AND (Mentor* OR Peer-Mentor* OR Peer Mentor* OR Youth Mentor* OR Coach* OR Buddy* OR Cross-Age Peer Mentor* OR Cross Age Peer Mentor* OR Child Mentor* OR Adolescen* mentor* OR Teen* mentor*)
Following the completion of the database searches using the above strategy, a coding framework and inclusion/exclusion criteria were designed to determine the most relevant studies for inclusion in the review.
Coding framework
Relevance to the primary research question
Empirical studies
Include all types of mentoring interventions (peer, one-to-one, group, e-mentoring) that focus on prevention for young people at risk, who are pregnant or who are parents. Exclude studies in which mentoring is just a result or recommendation.
-
4 = mentoring interventions and LAC
-
4 = mentoring interventions and teenage pregnancy.
Empirical studies in which mentoring is one part of the intervention strategy
-
3 = interventions with LAC in which mentoring is one part
-
3 = teenage pregnancy interventions in which mentoring is one part.
Descriptive pieces/literature reviews on mentoring
Include descriptions/reviews of mentoring programmes for all young people (not limited to at-risk or pregnant youth etc.).
-
2 = descriptive pieces about mentoring interventions for LAC or mentoring interventions for teenage pregnancy
-
2 = literature reviews of mentoring interventions for LAC or mentoring interventions for teenage pregnancy.
Mentoring theme only
-
1 = empirical or descriptive studies.
Exclude if mentoring is only one part of the intervention strategy.
No relevance
-
0 = mentoring is one part of the intervention strategy but no mention of LAC
-
0 = mentoring is one part of the intervention strategy but no mention of teenage pregnancy
-
0 = no relevance to LAC, mentoring or teenage pregnancy
Publication type
-
3 = journal articles
-
2 = published reports, books or chapters
-
1 = dissertations, internal reports, classroom guides
-
Publication date – exclude studies pre 1992.
-
Language – exclude studies that are not written in the English language.
-
Type of participants:
-
Care history – include studies involving young people who are currently in care or who have left care.
-
Age – between 13 and 25 years.
-
At risk – include studies involving young people aged 13–25 years who are ‘at risk’ or showing behaviour that would constitute risk. ‘At risk’ is defined as the presence of individual or ecological characteristics that increase the probability of teenage pregnancy. Ecological characteristics include family and parenting influences on behaviour, residence in a neighbourhood with high levels of poverty or crime or exposure to gangs. For the mentoring and teenage pregnancy search, include studies focusing on at-risk and pregnant young women and teenage mothers only, and mentoring that aims to improve sexual health/behaviour generally.
-
Scoring
As well as taking into account publication date, language and participant type, inclusion/exclusion was based on the following scoring system.
Included articles
-
Any article that scores 4 on relevance
-
Relevance 3 + publication type 3
-
Relevance 3 + publication type 2
-
Relevance 2 + publication type 3
-
Relevance 2 + publication type 2
-
Relevance 1 + publication type 3
-
Relevance 1 + publication type 2
Excluded articles
-
Relevance 3 + publication type 1
-
Relevance 2 + publication type 1
-
Relevance 1 + publication type 1
-
Any article that scores 0 on relevance
Appendix 4 Recruitment leaflets for participants aged 14–18 years and 19–25 years
Appendix 5 Consent forms for participants aged 14–18 years and 19–25 years
Appendix 6 Baseline questionnaire for participants aged 14–18 years
Appendix 7 Baseline questionnaire sent to social workers of participants aged 14–18 years
Appendix 8 Baseline questionnaire for mentors
Appendix 9 Follow-up qualitative interview schedules for participants aged 14–18 years, participants aged 19–25 years and project co-ordinators
Appendix 10 Training evaluation forms and focus group schedule
Appendix 11 Mentor diary questions
Survey name: e-mail
No. of questions: nine
-
This form should be completed after each e-mail conversation between you and your mentee (label).
-
Who sent the first e-mail? (multi)
-
Possible responses:
-
I sent the first e-mail
-
my mentee sent the first e-mail.
-
-
-
Why did you e-mail your mentee today? (multi)
-
Possible responses:
-
I wanted to be in touch with them today
-
someone had asked me to get in touch with them today.
-
-
-
Why did your mentee e-mail you today? (multi)
-
Possible responses:
-
my mentee wanted to get in touch with me
-
someone had asked my mentee to contact me.
-
-
-
What were the topics of discussion today? Tick all that apply (label).
-
We discussed . . . (multi)
-
Possible responses:
-
arrangements for next meeting
-
general, e.g. getting to know you
-
family/carers
-
friends
-
sexual relationships/boyfriends/girlfriends
-
contraception
-
school/education
-
training/work
-
alcohol/drugs
-
directing mentee to other support/help
-
relationship between you and your mentee
-
other.
-
-
-
If other, please specify (text).
-
Are there any thoughts or comments you want to tell us about your e-mail conversation today? (text)
-
Thank you for completing this form today (label).
Survey name: face-to-face
No. of questions: 13
-
This form should be completed after each face-to-face contact made with the mentee (label).
-
Roughly how long did you meet for today? (multi)
-
Possible responses:
-
up to 30 minutes
-
30 minutes to 1 hour
-
1–2 hours
-
more than 2 hours.
-
-
-
Where did you meet today? (text)
-
What did you do together? Tick all that apply (multi).
-
Possible responses:
-
talk
-
leisure activity
-
attend an appointment
-
other.
-
-
-
What were the topics of discussion today? Tick all that apply (label).
-
We discussed . . . (multi).
-
Possible responses:
-
arrangements for next meeting
-
general, e.g. getting to know you
-
family/carers
-
friends
-
sexual relationships/boyfriends/girlfriends
-
contraception
-
school/education
-
training/work
-
alcohol/drugs
-
directing mentee to other support/help
-
relationship between you and mentee
-
other.
-
-
-
If ‘other’, please specify (text).
-
The next questions are about how much it cost to meet with the mentee. Please enter as xx.xx (label).
-
How much did the activity cost? (number)
-
How much did it cost you to travel to the meeting? (number)
-
How much did it cost your mentee to travel to the meeting? (number)
-
Are there any thoughts or comments you want to tell us about your contact today? (text)
-
Thank you for completing this form today (label).
Survey name: phone call
No. of questions: 10
-
This form should be completed after each phone call between you and your mentee (label).
-
Roughly how long was your phone call today? (multi)
-
Possible responses:
-
up to 15 minutes
-
15–30 minutes
-
30 minutes to 1 hour
-
more than 1 hour.
-
-
-
Who made the phone call? (multi)
-
Possible responses:
-
I made the call
-
my mentee made the call.
-
-
-
Why did you call your mentee today? (multi)
-
Possible responses:
-
I wanted to be in touch with them today
-
someone had asked me to get in touch with them today.
-
-
-
Why did your mentee call you today? (multi)
-
Possible responses:
-
my mentee wanted to get in touch with me
-
someone had asked my mentee to contact me.
-
-
-
What were the topics of discussion today? Tick all that apply (label).
-
We discussed . . . (multi)
-
Possible responses:
-
arrangements for next meeting
-
general, e.g. getting to know you
-
family/carers
-
friends
-
sexual relationships/boyfriends/girlfriends
-
contraception
-
school/education
-
training/work
-
alcohol/drugs
-
directing mentee to other support/help
-
relationship between you and your mentee
-
other.
-
-
-
If ‘other’, please specify (text).
-
Are there any thoughts or comments you want to tell us about your phone conversation today? (text)
-
Thank you for completing this form today (label).
Survey name: text message
No. of questions: nine
-
This form should be completed after each text message exchange between you and your mentee (label).
-
Who sent the first text? (multi)
-
Possible responses:
-
I sent the first text
-
my mentee sent the first text.
-
-
-
Why did you text your mentee today? (multi)
-
Possible responses:
-
I wanted to be in touch with them today
-
someone had asked me to get in touch with them today.
-
-
-
Why did your mentee text you today? (multi)
-
Possible responses:
-
my mentee wanted to get in touch with me
-
someone had asked my mentee to contact me.
-
-
-
What were the topics of discussion today? Tick all that apply (label).
-
We discussed . . . (multi)
-
Possible responses:
-
arrangements for next meeting
-
general, e.g. getting to know you
-
family/carers
-
friends
-
sexual relationships/boyfriends/girlfriends
-
contraception
-
school/education
-
training/work
-
alcohol/drugs
-
directing mentee to other support/help
-
relationship between you and your mentee
-
other.
-
-
-
If ‘other’, please specify (text).
-
Are there any thoughts or comments you want to tell us about your text conversation today? (text)
-
Thank you for completing this form today (label).
Survey name: weekly non-contact
No. of questions: 7
-
Please complete this form if there has been no face-to-face contact or lengthy phone call this week (label).
-
Has the mentee initiated any contact with you either by phone/text or e-mail? (multi)
-
Possible responses:
-
yes
-
no.
-
-
-
Did you initiate contact with your mentee by phone/text or e-mail? (multi)
-
Possible responses:
-
yes
-
no.
-
-
-
If ‘no’, please comment (text).
-
Why did a face-to-face meeting not go ahead this week? (multi)
-
Possible responses:
-
mentee said they did not have time
-
mentee cancelled the arranged meeting
-
mentee did not turn up to arranged meeting
-
I did not have time
-
I had to cancel the arranged meeting
-
other.
-
-
-
If ‘other’, please specify (text).
-
Please make any comments about this (text).
Survey name: weekly reflective diary
No. of questions: 15
-
Please complete this form if you have had face-to-face contact or a lengthy phone conversation with your mentee this week (label).
-
This week I had a . . . (multi).
-
Possible responses:
-
face-to-face meeting with my mentee
-
lengthy phone conversation lasting more than 30 minutes.
-
-
-
On what date did your face-to-face meeting or lengthy phone call take place? (date)
-
What time of day did it take place? (multi)
-
Possible responses:
-
morning
-
afternoon
-
evening
-
-
-
Is there anything you think worked particularly well with your mentee this week? Please tell us about this and why you think it worked well (text).
-
Is there anything you think did not work well with your mentee? Please tell us about this and why you think it may not have worked well. What steps did you take to overcome the problem? (text)
-
On a scale of 1–5, where 1 is least confident and 5 is very confident, how confident did you feel that you had the skills needed to deal with the issues raised by your mentee? (number)
-
Are there any comments you want to make about this? (text)
-
Did your mentee tell you about anything significant that happened to them this week? It could be a positive thing (e.g. a good grade/comment from school) or a negative thing (e.g. a bad argument, moving placement, etc.) (text).
-
On a scale of 1–5, where 1 is not helpful and 5 is very helpful, please rate how helpful you think the mentoring has been to your mentee this week? (number)
-
Are there any comments you want to make about this? (text)
-
This week, during contact with your mentee, is there anything that made you feel your mentee may be at significant risk of harm? (i.e. from someone else or from themselves) (multi)
-
Possible responses:
-
yes
-
no
-
unsure.
-
-
-
If ‘yes’ or ‘unsure’, please comment (text).
-
Please comment on anything else with regards to your contact with your mentee in the last week. For example, this could be about the relationship with your mentee, your time management, how you feel about the mentoring or the topics you discussed (text).
-
Thank you for completing your weekly diary. Remember, your local project co-ordinator is available to answer any questions or talk to you about any concerns you may have (label).
Appendix 12 Mentor and mentee snapshot diary interview schedules
Appendix 13 Feasibility interview schedules for project co-ordinators, senior managers and social workers
Appendix 14 Online survey questions
Appendix 15 Feasibility focus group schedules
Appendix 16 Interview schedule for university student care leaver
-
Welcome the participants and thank them for participating.
-
Provide preliminary information about the study.
-
Purpose of the interview – to assess feasibility for a larger trial.
-
Explain the structure of the interview.
-
Confidentiality and recording.
Name:
Age:
Course details:
Length of time in care:
1. Views about mentoring
-
What is a mentor (i.e. meaning for you)?
-
What do you think of the idea of mentors (in general) for people in care?
-
Probe:
-
Is there any value?
-
What makes a good mentor?
-
What kind of young people would benefit?
-
-
-
What sort of things might young people in care want and/or need a mentor for?
-
Did you have a mentor when you were aged 14–18 years? If so, what can you remember about them?
-
Probe:
-
Important attributes: good/bad – age, gender, etc.
-
-
2. Task: creating a mentoring scheme for young people in care
You have decided you want to be a mentor for young people who are in care. You are thinking of setting up a new mentoring programme for young people who have left care, which will involve identifying a project manager and a trainer for the mentors. You will participate in the training to become a mentor.
Based on your own experiences of the care system, please decide:
-
What do the young people in care need support with?
-
What is the aim of your peer mentoring intervention for looked-after children/young people? What do you hope to achieve? (Please outline the reasons for your choices)
-
Based on the aim, who will the mentoring intervention be for (i.e. males/female)? What age are the young people?
-
How long will the mentoring last for?
Selection of mentors
-
How will you select mentors? (How might you access them?)
-
What characteristics would they have? What knowledge/skills would they need?
-
Do you think there would be any issues with mentors being aged 19–25 years and having been in care? How old should they be and why?
Training
The training would last for a minimum of 2–3 days.
-
What days of the week and at what times would your training be held? (What might you have to consider in your decision?)
-
What difficulties might you have in attending training? How could these be overcome?
Contact
-
Based on the aims of your programme, will you be meeting your mentee in the community (e.g. café) or in a young person’s centre? Why?
-
How often would you have time to meet with your mentee? Would you like it to be the same day/time each week or would you like it to be flexible?
-
What are your other commitments? How would you manage your time around them?
-
What will you do during your meetings with your mentee (based on the aims of your mentoring programme)?
-
What difficulties might you have with meeting your mentee? How would you overcome the difficulties?
-
Probe:
-
Travel – car/public transport.
-
Other commitments – childcare expenses.
-
-
-
What would you think about when it was nearing the end of the relationship? (How would you end the relationship?)
Support
-
What support do you think you would need to be an effective mentor? (Who would provide it? How often? In what location?)
Incentives
-
Do you think mentors should receive anything in return for mentoring? (What would that be?)
Carmen study
The Carmen peer mentoring intervention is managed and run by a project co-ordinator within the local authority. The role of the project co-ordinator is to recruit mentors and mentees and to provide support to mentors.
Recruiting mentors
-
Mentors in the Carmen study are aged 19–25 years. When you were aged 19–25 years what contact did you have with social services? What other organisations/services did you have contact with?
-
Based on the above, what do you think is the best organisational context for recruiting mentors aged 19–25 years who have left care?
-
Probe:
-
Social services, universities, other organisation mentioned above.
-
-
Contact with mentee
-
Mentors in the Carmen study were asked to meet with their mentee once a week, face-to-face, for 1 year. What do you think about this?
-
Probe:
-
Is it too much, too little, just right?
-
-
-
Mentors were asked to complete a diary of their contact for the researchers. They are able to complete the diary using an application on their mobile phone or by completing it online, through a confidential server. What do you think about completing a diary on a phone/online? The mentors have not completed the diary consistently – what do you think would be a better system for them to feed back their contacts to a project co-ordinator?
-
What do you think about 1 year as the amount of time for the mentoring relationship?
Support
-
What do you think of the idea of a monthly support group? This would be to discuss how things are going with other mentors and the project co-ordinator and to try and resolve any issues.
-
What kind of professional do you think should provide the support?
-
Probe:
-
Attributes and role, i.e. a social worker?
-
Incentives
-
Mentors in the Carmen study receive a £40 voucher per month and can gain a level 1 ASDAN qualification. What is your view on these incentives?
-
Mentors receive £60 per month for paying for activities with their mentee and for travel for both of them. What do you think about this amount of money for activities (£15 per week)?
Any other questions/comments? (recruitment, difficulties we’ve experienced).
Appendix 17 Project co-ordinator, mentor and research team role description
| PC role | Mentor role (note: PC is first point of contact for mentor) | Research team role |
|---|---|---|
Mentor recruitment and training:
|
Training and support:
|
This will involve: Mentor recruitment and training:
|
Appendix 18 Guidance given to project co-ordinators on conducting monthly support group meetings
Guidance for mentor support and supervision
On introduction to the session remind mentors of confidentiality within the group, that is, not discussing any of the issues or mentees outside of the group. The project co-ordinator will ensure confidentiality except in instances when it is in the best interests of a mentee for a social worker/other professional to be informed (e.g. child protection or access to services).
The purpose of the supervision sessions is:
-
To allow mentors to:
-
reflect on their relationship with the mentee
-
feed back any concerns to the project co-ordinator
-
consider and monitor important ‘milestones’ in their relationship
-
verify and submit work for their accreditation if applicable
-
identify any additional training needs
-
receive any up-to-date information about agency policies and continue to adhere to these, e.g. safeguarding.
-
-
To allow project co-ordinators to:
-
be aware of and continue to monitor potential difficulties that may arise in mentoring relationships (including non-engagement and boundaries being crossed)
-
give consideration to the specific needs of mentors who are care leavers, monitor any issues in their lives and provide additional support when necessary to enable them to meet the demands of the role
-
troubleshoot difficulties
-
sign off mentors’ work for accreditation
-
distribute money for activities and voucher payments
-
communicate any relevant updates/information on agency policies to mentors.
-
-
Project co-ordinators should increase the likelihood of mentors attending group supervision sessions by:
-
providing a yearly schedule of meetings to mentors from the outset
-
ringing/texting mentors before each meeting to remind them about the meeting
-
providing refreshments and adding a social element to the sessions
-
being flexible and ensuring that the supervision sessions are compatible with demands on the mentors’ time (e.g. working arrangements).
-
Appendix 19 Project co-ordinator recruitment guidelines
Appendix 20 Social worker recruitment guidelines
Appendix 21 Mentor training handbook
Appendix 22 Phase II training agenda
| Time | Session title | Learning aim | Details | Materials | Who |
|---|---|---|---|---|---|
| Day 1 | |||||
| 1000 | Introduction to the research study | To understand the background to the Carmen study, why peer mentoring is being tested and the methods to be used; to clarify what the aim of this project is and what role researchers/research participants have in the study | Also, explanations of support and guidance available for mentors from PCs and the research team | Deborah and Fiona | |
| 1015 | Welcome, introductions | To give participants an opportunity to find out about each other | Paired introductions – participants pair up with someone they don’t know very well and obtain answers to the following four questions: name, a bit about who they are, what they hope to gain from the course and something interesting/surprising about them that no one else in the room is likely to know about Energy barometer: explain that every day we will be checking on the level of energy that people have today – thumbs up, midway, down |
Trainer 1 | |
| 1045 | Introduction to training | To let participants know what is in store for the next 3.5 days | Give an overview of the training days using slides, emphasising that valuing and working with diversity is not a separate element but permeates throughout. Potential mentors make a decision whether they want to become a peer mentor after the training so that they are making an informed decision PPP outlining learning methods and give an overview of training, stressing open dialogue, challenge by choice, confidentiality ‘Parking lot’ – if questions arise that don’t fit with the session, participants can write them down on a Post-it note and place it on a flip chart entitled ‘Parking lot’. The question/issue will be dealt with at a later stage; parking it means that we won’t forget it ASDAN accreditation, explanation of units and support available |
Handbook, PPP slides | Trainer 1 |
| 1115 | Break | ||||
| 1130 | Building the peer mentor team | To give the participants the opportunity to have a little fun together while at the same time experiencing what it is like to be guided through direction and then through support | Facilitator sets out an obstacle course with chairs, etc. in the room. Participants pair up: one partner is blindfolded and the other has to guide them through the obstacle course as quickly and safely as possible to the other side of the room. Facilitator checks understanding of the task among participants 1. 5 minutes to prepare, then the participants stand at opposite ends of the room with one guided and the other communicating what needs to happen 2. Discuss between the pair how to improve the experience – 5 minutes preparation and then repeat the exercise This should take about 20 minutes |
Blindfolds, flipchart, pens | Trainer 1 |
| 1150 | Reflection | To give participants an understanding of professional reflection and how important it is for peer mentoring | Reflection: first explain that reflection is an essential part of being a mentor so we will be doing lots of it on the course. Also, that every experience is useful, whether good or bad, and that through reflection our aim is to find learning, not to blame or ridicule – reflecting on successes and mistakes are a good way of learning. Write responses on a flip chart under following headings: Facts – what happened – without going into feelings, only the facts Feelings (emotional effects, physical effects, social effects) – how did it feel to be guided? What made it good/not so good? How did it feel to be guiding? What made it feel good/not so good? Influences – what influenced your experience during the activity? Guided person first and then the guide Learning – what, if anything, would you do differently? What is it important to remember when supporting someone? What values and behaviours underpin supporting and guiding people? Using the flip chart, facilitator divides participant contributions into: Values – e.g. respect, participation, empowerment, trust, empathy Behaviours – e.g. positive support and encouragement, listening, clear communication This reflection is likely to take about 30 minutes |
Trainer 1 | |
| 1220 | Peer mentor role | To clarify the role and expectations | The role of the mentor – what will be expected of you Exploration of the role as stated in the leaflet – what this means in practice Personal qualities and practicalities PPP: explore the meaning of each bullet point in the large group, adding the clarifications to the flip chart and encouraging the participation of all. Issues that must be covered at some point during the year: contraception, healthy/unhealthy relationships and keeping safe. Reassure the mentors by adding that they will have had training on this and will not be expected to talk about relationships right away |
PowerPoint presentation | Trainer 1 |
| 1245 | Lunch | ||||
| 1330 | Energiser | To connect the group, connect left and right sides of the brain and raise energy levels | Finger grab | Trainer 1 | |
| 1340 | Getting started – what mentees value in the relationship with mentors | To identify what kinds of attitudes and behaviours mentees are likely to value in the relationship with the mentor | Individually, think of a time when you have had a positive, supporting/guiding relationship – could be with a family member, carer, social worker, teacher. What did you value in your relationship with them? Jot your memories down on a sheet of paper. If you can’t think of anyone, consider what you would value in a hypothetical positive supportive relationship (3 minutes) In small groups (three to four people): discussion on what young women mentees are likely to value in the relationship with the mentor. Participants share their experiences. Split flip chart into three columns. Look at one thing from each person: what they are likely to value? (e.g. enthusiasm), how would they know you value it too? (e.g. you show up on time with a smile and some ideas), why is this important? (e.g. because life in care can be miserable and the relationship needs mentors to be positive and to have thought about what they could do with the mentee). Feed back responses and link to how the value base guides the mentor, adding to the previously generated values and behaviours as necessary (15 minutes) Links to empowerment; emphasis on supporting and enabling the young woman to make informed choices, especially about sex and relationships; developing self-esteem and self-confidence; encouraging self-reliance; developing social networks Use quotes from pilot |
Trainer 1 | |
| 1430 | Break | ||||
| 1445 | Energiser | Star dance | To illustrate the difficult link between theory and practice | Trainer 1 | |
| 1500 | Ethics and accountability | To provide an opportunity to explore ethics and accountability | Ethics – what are ethics? Relate to current issues in the news – News International seems like a good one – also to the ethics of providing training for this research study Slide on ethics – present and discuss Mentors are the adults in the relationships; you are responsible for your actions – group discussion – what does this mean to and for you? |
Slide | Trainer 1 |
| 1515 | Boundaries | To explain and explore what professional boundaries are, why we need them and how to use reflection to think about them | PPP presentation and group discussion Professional – what guides you: values, law, theory, policy Personal – what you bring of yourself into the relationship to support the mentee Private – what you keep private and don’t share with the mentee; your private feelings Group discussion – what does this mean in practice? Link to what the mentee is likely to value in a relationship with you. What personal attributes can you bring to the relationship with the mentee? What are you good at, do you enjoy, do you want to explore further/develop? What could you do together in your first meeting? Depending on group size, small group or whole group discussion: scenario – your mentee wants to know about your own care history; your mentee wants to know about your boyfriend Private – how do you feel about being asked these questions? Can you name your feelings? Are your feelings influencing you? If so how? What do you not want to tell her? Personal – what information about your own experiences will be helpful for her to know and what is your motivation for telling her? Are you comfortable about this information now being ‘public’ (you can’t ask her to keep it secret but you can ask her to treat it with sensitivity)? Professional – what are the underpinning values when answering a question like this? Reflection on what PPP means for each participant |
Slide | Trainer 1 |
| 1600 | Reviewing learning and feedback | To consolidate the learning and find out how the participants experienced the day and whether there is anything that trainers need to do to make it a better experience | Spider chart – ask participants what they have done today, write it up on a flip chart and place it on the wall – too little, too much, just right amount? | Trainer 1 | |
| 1630 | End | ||||
| Day 2 | |||||
| 1000 | Starting the day | Welcome – introduce trainer 2 Recap and questions/queries from day 1 Energy barometer – traffic lights Introduce the day |
Flip chart and pens Red, amber and green cards |
Trainer 1 | |
| 1015 | Confidentiality | To explain and discuss confidentiality in the peer mentoring context | Mutual trust and confidentiality are central to the success of any mentoring relationship. It is essential that mentors respect the confidentiality of what is discussed within the relationship. However, there are exceptions, which can normally be divided in three categories: (1) the disclosure of information with the explicit agreement of the mentee (this will include the information that you agree to pass on to the researchers); (2) when the mentor believes that there is convincing evidence of serious danger to the mentee or others if the information is withheld (e.g. mentee revealing that her friends are planning to stab someone tonight); (3) when disclosure is required by law, for example when it concerns child protection issues (e.g. when the mentee reveals that her boyfriend is in his 30s and she is 14 years old) (safeguarding will be discussed in more detail after this session) Exercise in pairs: (1) think back to when you were in care – how did/does it feel to have lots of information about you held by your carers and/or social worker? What would reduce your anxieties about someone holding your private information? (2) Discuss what kinds of information should be kept confidential and what should not Group reflection: discuss what confidentiality means in this relationship, including at the start of the relationship. Discuss how information about the mentee’s personal life, including sexual activity, will be treated. Any written information is kept safe and locked away. Any break in confidentiality is discussed with the mentee first. Deciding to break confidentiality after discussing it with another professional if there is a risk of harm or harm has occurred |
Trainer 1 | |
| 1045 | Safeguarding children and child protection | To give a basic overview of safeguarding and child protection responsibilities | Overview of safeguarding policy Definitions of abuse and neglect, relating specifically to risks for adolescent young women, including self-harm Confidentiality in child protection |
Safeguarding procedures | Trainer 1 |
| 1115 | Break | ||||
| 1130 | Energiser | ||||
| 1140 | Safeguarding | To provide an opportunity to think about what you would do if something worries you and examine some case studies | What to do if your mentee discloses or does something that worries you Disclosures: group discussion on what to do and what not to do during (while the mentee is talking), immediately after (with the mentee and with other professionals) and following up - write up group responses on the flip chart, adding or modifying when necessary Case studies: in small groups consider what are your concerns about this situation? What do you say to the mentee in the case study? What else do you do? Structured reflection: facts, feelings, influences, learning |
Case studies | Trainer 1 |
| 1245 | Lunch | ||||
| 1315 | Energiser | Gordian knot | |||
| 1325 | Healthy/unhealthy relationships | To examine what constitutes a healthy and an unhealthy relationship | What makes a healthy/unhealthy friendship? In pairs, design a job description for a friend – personal qualities and attributes. Then, promote this person to being in an intimate relationship. Redesign the job description for an intimate relationship on a separate flip chart, keeping the friendship job description for tomorrow. Now you want to fire the person in your relationship – list 10 things that would give you grounds to fire them Group discussion and reflection |
Trainer 2 | |
| 1400 | Sex | To explore the emotional aspects of sexual relationships For participants to feel confident about the general rules about confidentiality and how to access services (e.g. U16s seeking support and their protection) |
Why do we do it? In two groups the participants need to be given a sheet of flip chart paper and pens. Ask them to come up with as many reasons why people have sex as they can think of. After 5–10 minutes, when a number of reasons have been written down, give each group a green and a red pen. The groups then circle each reason with green if they feel that the experience of sex would be emotionally fulfilling or with red if they think that the experience would be negative or leave them feeling unfulfilled afterwards. One group will present the ‘red’ examples and the other group will present the ‘green’ examples. Both groups will be given time to add and explore examples that they could not circle as they felt that they could be either red or green Sex and the law quiz |
Prizes | Trainer 2 |
| 1445 | Break | ||||
| 1500 | Contraception and STIs | To gain a greater awareness of the types of contraception available and how to use them; to understand the prevalence of STIs/sexually transmitted diseases; to learn about where to get more information/help and the clinics available locally | Modules 1–3 Trainer 2 will add government guidance on testing although it must be noted that it is not recommended to be tested every year or before starting a new sexual relationship as per feedback suggestion. This is unrealistic, especially for young women in care, and provides no protection; condoms are the best form of prevention |
Game board, dummy contraceptives, information handbook, lottery ticket | Trainer 2 |
| 1600 | Reviewing learning | ||||
| 1630 | End | ||||
| Day 3 | |||||
| 1000 | Welcome, recap and outline of the day | Recap and questions Energy levels Outline of the day |
Trainer 1 | ||
| 1015 | Teenage pregnancy and parenthood | To learn the prevalence of teenage pregnancy in England and Wales and the perceived problems related to this; to gain an ability to recognise some of the key causes of teenage pregnancy; to be able to recognise the challenges faced by teenage parents; to explore the impact of teenage pregnancy on both the parent and the child; to learn where to get more information and advice | Also discuss mental health and domestic abuse; presentation and group discussion relating to teenage pregnancy and parenthood | Trainers 1 and 2 | |
| 1130 | Break | ||||
| 1145 | Keeping safe and minimising risk | To examine how young women can keep themselves safer and minimise risks | Case studies: aspects of keeping safe and minimising risk – for mentors and for mentees; small group/paired work Mentee Your mentee is planning to go out and meet some friends tonight. What can you advise to help her keep safe? Your mentee is meeting up with her new boyfriend tonight. What can you advise to help her keep safe? Mentor You are planning to meet your mentee in a café in an area of town that you are not familiar with. What will you do to keep yourself and the mentee safe? Your mentee wants you to meet her new boyfriend. What will you do to keep yourself and the mentee safe? Group reflection: what are the common themes for keeping safe? |
Trainers 1 and 2 | |
| 1215 | Empathic listening skills | To understand and experience empathic listening skills | Presentation/group discussion on empathic listening skills (10 minutes) Activity: in pairs sit opposite each other. One of each pair has 2–3 minutes to tell the other about their time with someone who supported them really well. The partner has to listen without asking questions and then has a minute to repeat how she or he has heard the story. The pair then swap so that the listener tells their partner about their time with someone who supported them really well Reflection on skills used and how they felt for both giver and receiver and on how they felt during and after telling a positive story – use this for reflection on building trusting relationships |
Trainer 1 | |
| 1300 | Lunch | ||||
| 1330 | Energiser | Hoola hoop chase | |||
| 1335 | Building trusting mentoring relationships | To examine how to build a trusting relationship; first meetings | Re-look at job description for friendship and agree what modifications are needed for a mentoring relationship (30 minutes) How to engage well with your mentee on first meetings: Find an actor in the group. Their role is to play the mentee, who is experiencing a combination of the following feelings (get them to overplay if possible): nervous (what’s going to happen?), suspicious (who is this mentor anyway, what’s in it for her), excited (at last, a friend! or this could be really helpful), worried (is she going to tell me not to have a boyfriend?), relieved (phew, I can finally find some stuff out!), reluctant (my carer and social worker want me to do this but I’m not so sure), disinterested (I was interested when they asked me but now I’m not) Ask the rest of the group to shout ‘freeze frame!’ when they can think of the emotion and any questions the mentee might have; look at hopes vs. fears. Then, get the whole group to think of things to ask, say or do that could address the difficulty. Add the responses to the flip chart If group is not large enough or there are no potential actors, in small groups ask the following questions: how would you expect the mentee to be feeling and how might they behave? (10 minutes), what could you do to lessen any difficult/problematic/negative feelings? (10 minutes) Acknowledge that their feelings may be mixed and talk about your feelings about starting the relationship (demonstrate that you are prepared to talk about your own difficult feelings; talk about your own nervousness maybe): assure her that you will not launch straight into the difficult stuff; think of something to do or a game to play with each other (think of the Personal element of PPP); talk about boundaries and confidentiality; discuss and agree how often, for how long, when and how you will mentor her; tell her about why you wanted to be a mentor and the stuff you like to do and a bit about your background; tell her about what you know about her from the information shared with you before you started; ask her questions about how she would like the relationship to work, what she wants to get out of it and how she would like you to be; ask her about the things she likes – easy(ish) questions; bring a small (low-cost) present to give to her at the end of the first session (object association, leaving the child with something they can look at when you are apart and that will remind them of you) 30 minutes of feedback and a summary of the key messages |
Mentee emotions Blue monkey |
Trainer 1 |
| 1445 | Break | ||||
| 1500 | Dealing with difficulties | To explore what kinds of difficulties may occur, the reasons behind this and what to do about it | In trios, each person takes a role: mentor, mentee or observer Mentee only is given background information. The mentor and mentee agree what the context of the meeting is and then have about 5 minutes to role play while the observer takes notes of what she notices. Each trio could role play to the whole group or just to each other. Could ask the group for more examples if there is time How did that feel (mentor, mentee in role)? What did the observer notice? What are the key messages from this scenario? Add the key messages to the flip chart |
Mentee roles | Trainer 1 |
| 1600 | Ending the mentoring relationship | To examine creating positive endings | Trainers get a call and have to end the training without warning – leave the room with bags, etc. so that it looks real. Stay out for 1 minute. Return and ask how that felt Small group exercise looking at how we can make ending the relationship positive, what to do and what to avoid (15 minutes) Group reflection |
Trainer 1 | |
| 1630 | Reviewing learning | Trainer 2 | |||
| 1645 | End | ||||
| Day 4 | |||||
| 1000 | Welcome back | Energy levels Outline of the morning |
Everyone writes their name on a piece of paper, folds it and puts it in a hat. Participants then draw a name at random, keeping the name secret until the end of the morning, when we will have a celebration ceremony | Trainer 1 | |
| Record keeping and communication | To ensure that participants are clear about their recording and communication responsibilities | Deborah and Fiona | |||
| 1020 | Reviewing learning Q&A |
To provide an opportunity to go over the training and answer questions | Trainer 1 | ||
| 1130 | Break | ||||
| 1145 | Support group | To give PCs time to explain how mentors will be supported | PCs | ||
| 1215 | ASDAN award | To explain the award in more detail and sign mentors up if they want to | Trainer 1 | ||
| 1230 | Ending ceremony | Each person says something positive about and to the person whose name they picked out of the hat at the start of the day and chooses a gemstone for them. Trainer 1/Deborah/Fiona give participants their certificates and a final toast is made to the mentors and the project with bubbly (non-alcoholic!) | Gemstones, Shloer-type drinks, certificates | ||
| 1245 | Lunch | ||||
| 1330 | Feedback focus group | Deborah and Fiona | |||
| 1500/1530 | End | ||||
Appendix 23 Mentor contract
Appendix 24 Time sheet for project co-ordinators to record their time once a week during the project
Year: mid-July 2011–mid-September 2012 (exactly 14 months).
| Activity | Hours | Comments |
|---|---|---|
| Familiarisation | 15 | Attending meetings and reading a lot of e-mails |
| Setting up the intervention | ||
| Recruit mentors | 56 | Attending meetings, talking to young people, writing letters and making phone calls |
| Arrange training for mentors | 7 | |
| Recruit mentees | 56 | |
| Attend mentor training session | 7 | |
| Arrange initial mentor–mentee contact | 7 | |
| Other activities | ||
| Running of the intervention | ||
| Meetings with mentors (i.e. group meetings or individual supervision) | 33 | |
| Phone calls with mentors | 14 | |
| Additional support for mentors/mentees, e.g. contacting/liaising with social workers, etc. | 7 | |
| Mentors’ expenses (distributing monies and/or queries) | Included in mentor supervision | |
| Read and approve mentors’ work for ASDAN accreditation | Included in mentor supervision | |
| Replace mentors as/when necessary | NA | |
| Replace mentees as/when necessary | NA | |
| Other activities | ||
| Research project | ||
| Co-ordination/assistance to researchers | 7 | |
| Total | 209 | |
| Co-ordinators’ expenses/organisational overheads | ||
| Specific personal overheads | ||
| Travel/subsistence | £7.50 | Cost of one meeting that I attended |
| General overheads | ||
| Administrative overheads | ||
| Mobile phones | ||
| IT equipment | ||
| Photocopying | ||
| Office space | ||
| Other | ||
Appendix 25 Assumptions made in the spreadsheet model which estimates the costs to a local authority of setting up and running a mentoring programme
The basic assumptions are:
-
The model begins from the point at which it has been decided to proceed with a trial:
-
a Steering Group (SG) will oversee the broad design and purpose of the project and evaluate it on completion
-
a smaller Management Group (MG) will oversee the detailed design and day-to-day management of the project, referring issues upwards as necessary
-
most of the development work will be carried out by a project development officer (PDO)
-
a PC will take responsibility for running the project, with other staff being called on as necessary.
-
-
The SG consists of three senior social workers (SSW) and three social workers (SW) (or approximately equivalent grades).
-
The MG consists of one SSW, one SW, the PDO and PC. The PDO will undertake the work of designing the project. The PC will take over when the project goes live.
-
The staffing suggestions above are flexible both in terms of numbers and grades. They are offered as a starting point for any LA wishing to make and cost its own plans. It must be emphasised again that they, and all assumptions in this appendix, are, in the absence of solid cost data from the study, plausible guesses that should not be used for any other purpose without this understanding being clearly acknowledged.
General input assumptions
| Item | Assumption | Notes |
|---|---|---|
| Number of social workers dealing with LAC | 24 | |
| Number of geographical centres from which they work | 4 | |
| Number of potential mentees | 66 | |
| Number of potential mentors | 200 | |
| Number of working days | 240 | |
| Number of working hours per day | 7.5 | |
| Second class postage (£) | 0.33 | |
| Cost of criminal record check (DBS) (£) | 44.00 | |
| Average length of SG meetings (minutes) | 60 | |
| Average length of MG meetings (minutes) | 60 | |
| Salaries, per hour/per year (£) | ||
| Assistant director | 61.11/110,000 | Source: 2012 job advertisements for Lambeth (includes London weighting) |
| Clerical officer | 11.11/20,000 | |
| PC | 17.78/32,000 | |
| PDO | 17.78/32,000 | |
| SSW | 20.56/37,000 | |
| SW | 17.78/32,000 | |
| Salary oncosts for national insurance and pension (%) | 29 | Source: PSSRU 2012192 |
| Direct overheads for office and supplies (%) | 29 | |
| Indirect overheads for support services (%) | 16 | |
‘Inception and preparation’ and ‘ongoing management’ assumptions
| Item | Assumption | Notes |
|---|---|---|
| PDO familiarisation (minutes) | 900 | |
| Drafting proposal for first meeting of the SG (minutes) | 900 | PDO |
| SG to read proposal (minutes) | 120 | SG |
| Number of SG meetings | 3 | In months 1, 2 and 3 |
| Number of MG meetings | 3 | In months 1, 2 and 3 |
| MG team to prepare fully costed plan (minutes) | 900 | WG |
| Revise plan (minutes) | 900 | PDO |
| Submit plan to assistant director for approval (minutes) | 30 | SSW |
| Assistant director to read papers and approve (minutes) | 30 | Assistant director |
| Choose PC (minutes) | 30 | SSW |
| Brief PC (minutes) | 60 | SSW and PC |
| PC familiarisation (minutes) | 450 | PC |
| Draft initiation letter for assistant director (minutes) | 60 | PDO |
| Draft brief guidance notes for SWs (minutes) | 900 | PDO |
| Draft standard letters for SW recruitment of mentees (minutes) | 60 | PDO |
| Draft standard letters for SW recruitment of mentors (minutes) | 60 | PDO |
| Draw up posters for recruitment purposes (minutes) | 120 | PDO |
| Negotiate training provision (minutes) | 900 | PDO |
| Negotiate provision of mobile telephones (minutes) | 450 | PDO |
| Average length of MG meetings (minutes) | 60 | MG |
| Amend draft of fully costed plan (minutes) | 240 | PDO |
| Sign off amended plan as suitable for assistant director (minutes) | 30 | SSW, chairperson of SG |
| Send draft plan to assistant director (minutes) | 10 | SSW |
| Assistant director to approve sending to SWs (minutes) | 10 | AD |
| Clerical officer to send plan to SWs (minutes) | 5 | Clerical officer |
| Ongoing MG meetings | 3 | MG |
Awareness-raising assumptionsa
| Item | Assumption | Notes |
|---|---|---|
| Social workers to become familiar with the papers (minutes) | 60 | All SWs involved in care |
| Number of presentation meetings in first couple of months | 4 | One in each geographical centre including one SSW and six SWs plus the PC |
| Duration of meetings (minutes) | 60 |
Assumptions regarding recruitment of mentees and mentorsa
| Item | Assumption | Notes |
|---|---|---|
| Mentee recruitment | ||
| General management of process (minutes) | 45 | SSW; SSW manages this to ensure compliance from SWs |
| Management of clerical officer by SSW (minutes) | 45 | SSW and clerical officer |
| Setting up mentee recruitment mailshot (minutes) | 10 | Clerical officer; per potential mentee (find their name, the names and addresses of their carers and the name and contact details of their SW) |
| Stuffing envelopes (minutes) | 2 | Clerical officer; per eligible girl |
| Percentage of girls responding positively within first month | 6.00 | Of ‘number of potential mentees’ |
| Percentage of girls responding positively within second month | 4.60 | Of ‘number of potential mentees’ |
| Dealing with further queries in response to letters (minutes) | 10 | SW; per response (telephone call, e-mail) |
| Logging names of potential candidates (minutes) | 1 | SW; per response |
| Looking out file summaries of potential candidates (minutes) | 5 | Clerical officer; per case file |
| Passing names and summaries over to PC (minutes) | 15 | Clerical officer |
| Mentor recruitment | ||
| General management of process (minutes) | 45 | SSW; SSW manages this to ensure compliance from SWs |
| Management of clerical officer by SSW (minutes) | 45 | SSW and clerical officer |
| Setting up mentor recruitment mailshot (minutes) | 10 | Clerical officer; personalising the standard letters, finding the names and last known addresses of potential mentors |
| Stuffing envelopes (minutes) | 2 | Clerical officer; per eligible girl |
| Percentage of recipients responding positively within first month | 10 | Of ‘number of potential mentors’ |
| Percentage of recipients responding positively within second month | 5 | Of ‘number of potential mentors’ |
| Dealing with further queries in response to letters (minutes) | 10 | SW; per response (telephone call, e-mail) |
| Logging names of potential mentors (minutes) | 1 | SW; per name |
| Looking out file summaries of potential mentors (minutes) | 10 | Clerical officer; per case file |
| Passing names and summaries over to the PC (minutes) | 15 | Clerical officer; minutes in total |
Training assumptionsa
| Item | Assumption | Notes |
|---|---|---|
| Communicate to each potential mentor what ID papers are needed (minutes) | 10 | PC; telephone conversations |
| Assemble papers for each potential mentor (minutes) | 3 | PC |
| Pass papers to the clerical officer who handles DSB checks for the LA (minutes) | 3 | PC |
| Clerical officer initiates check procedure with the DSB (minutes) | 15 | Clerical officer |
| Write to potential mentors when DSB checks are returned (minutes) | 5 | PC; standard letters |
| Percentage of potential mentors failing the DSB check | 10 | PC |
| Select 20% more mentors than mentees for training (minutes) | 5 | PC; per cleared mentor |
| Write to potential mentors to arrange training dates (minutes) | 10 | PC |
| Contact training providers to arrange training (minutes) | 30 | PC |
| Cost of training a mentor (£) | 500 |
Pairing assumptionsa
| Item | Assumption | Notes |
|---|---|---|
| Pair mentor and mentee (minutes) | 5 | PC |
| Arrange first meeting between mentor and mentee | 30 | PC; minutes of telephone calls |
| Length of first mentor–mentee meeting | 30 | PC |
| Percentage of first meetings showing incompatibility | 5 | Means PC must choose another mentor and arrange another meeting |
Assumption regarding supporting/maintaining pairsa
| Item | Assumption | Notes |
|---|---|---|
| Pay mentor expenses (minutes) | 20 | PC; per active mentor per month |
| Expenses: stipend (£) | 40.00 | Per month per mentor |
| Expenses: telephone vouchers (£) | 10.00 | Per month per mentor |
| Arrange monthly group meetings with mentors (minutes) | 60 | PC; in total |
| Occasionally rearrange monthly group meetings (minutes) | 120 | PC |
| Percentage of monthly meetings needing to be rearranged | 20 | |
| Attend monthly group meetings (minutes) | 140 | PC; per month |
| Individual contact with active mentors on ad hoc matters | 40 | PC; per active mentor per month |
| Individual contact with inactive mentors on ad hoc matters | 5 | PC; per active mentor per month |
| Mentee dropout probability | ||
| Proportion of mentees expected to drop out over 12 months (%) | 33 | |
| Report dropout to responsible social worker (minutes) | 10 | PC |
| Debrief mentee after dropping out (minutes) | 30 | SW |
| Report to PC on reasons for dropout (minutes) | 10 | Responsible SW |
| Debrief mentor after mentee dropout (minutes) | 30 | PC |
| Mentor dropout probability (minutes) | ||
| Proportion of mentors expected to drop out over 12 months (%) | 33 | |
| Report to social worker (minutes) | 10 | PC |
| Debrief mentee after mentor dropout (minutes) | 30 | SW |
| Report to PC (minutes) | 10 | SW |
| Pair with replacement mentor (minutes) | 65 | PC |
Assumptions regarding normal terminationsa
| Item | Assumption | Notes |
|---|---|---|
| Contact mentor to get views on who best to come to termination meeting (minutes) | 5 | PC |
| Contact SW to get views on who best to come to termination meeting (minutes) | 5 | PC |
| Contact SW to get views on who best to come to termination meeting (minutes) | 5 | SW |
| Resolve any differences (minutes) | 10 | PC |
| Contact chosen person, social worker and mentor to arrange time for the termination meeting (minutes) | 5 | PC |
| Debrief mentor (minutes) | 10 | PC |
| Debrief SW after the meeting (minutes) | 10 | PC |
| Debrief SW after the meeting (minutes) | 10 | SW |
| Draft report on that matching (minutes) | 20 | PC |
Review assumptionsa
| Item | Assumption | Notes |
|---|---|---|
| Draft report on the project (minutes) | 450 | PC |
| Meeting of MG (minutes) | 60 | MG |
| Amend draft report (minutes) | 225 | PC |
| Submit draft report to SG (minutes) | 15 | SSW |
| Meeting of SG (minutes) | 60 | SG; outcome is a decision on the value of the project and how to proceed |
Glossary
- Award Scheme Development and Accreditation Network
- An awarding body providing qualifications related to learning, employment and life skills (see www.asdan.org.uk/).
- Mentee
- A participant aged 14–18 years who was allocated to the intervention arm of the trial (and therefore received a mentor).
- Mentor
- A participant aged 19–25 years who mentored a young person.
- Usual support group participant
- A participant aged 14–18 years who was allocated to the usual support arm of the trial and who received the services that she usually has access to as a looked-after child.
List of abbreviations
- ASDAN
- Award Scheme Development and Accreditation Network
- BDI
- behaviour–determinants–intervention (model)
- BRTC
- Bristol Randomised Trials Collaboration
- CaSH
- contraception and sexual health
- CI
- confidence interval
- CiCC
- Children in Care Council
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CONSORT
- Consolidated Standards of Reporting Trials
- DBS
- Disclosure and Barring Service
- DCS
- Director of Children’s Services
- DCSF
- Department for Children, Schools and Families
- ERIC
- Education Resources Information Center
- GCSE
- General Certificate of Secondary Education
- GHQ
- General Help-Seeking Questionnaire
- GHQ-12
- 12-item General Health Questionnaire
- LA
- local authority
- LAC
- looked-after children
- MBF
- Mentoring and Befriending Foundation
- NatSAL
- National Survey of Sexual Attitudes and Lifestyles
- NCB
- National Children’s Bureau
- NEET
- not in education, employment or training
- NICE
- National Institute for Health and Care Excellence
- ONS
- Office for National Statistics
- PC
- project co-ordinator
- PSHE
- personal, social, health and economic education
- PYD
- positive youth development
- RCT
- randomised controlled trial
- SD
- standard deviation
- SGUL
- St George’s, University of London
- SIGLE
- System for Information on Grey Literature in Europe
- SM
- senior manager
- SOT
- semi-independent outreach (worker)
- SRE
- sex and relationships education
- STI
- sexually transmitted infection
- SW
- social worker
- TPU
- Teenage Pregnancy Unit
- UKCRC
- UK Clinical Research Collaboration