
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 09/169/07. The contractual start date was in October 2011. The draft report began editorial review in October 2014 and was accepted for publication in July 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Resulting from this work, a manual has been written by Barry Wright and Chris Williams in conjunction with Carol Gray on the writing of Social Stories™ for children in mainstream schools in the UK.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Wright et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
Autism spectrum disorders and challenging behaviour
Children with autism spectrum disorders (ASDs) are less able to learn social rules, conventions and behaviours by intuition compared with their typically developing peers. This may impact upon social interaction, social integration, learning and mental health and on occasions may lead to high levels of anxiety and or challenging behaviours. 1 Both parents and teachers report more behaviour problems in children with ASD than in typically developing children. 2 Many children with ASD therefore need additional support to understand and adopt social behaviours that are helpful to them. Social Stories™ (Carol Gray) are a non-intrusive, child-focused intervention designed to fill in the gaps of the child’s social understanding with the intention of helping them develop constructive behaviours and coping strategies.
Social Stories
Social Stories are short stories characterised by 10 predefined criteria developed by their original creator, Carol Gray. 3 These criteria both define and guide story development. They ensure that the story structure and content is descriptive, meaningful and safe for its audience. In particular, the content is tailored to the specific needs of each individual child, which can usually be incorporated into the story.
For the purposes of this study we are referring to Social Stories (using upper case letters) when these 10 criteria are adhered to (described more fully in the next section). A wider literature exists using stories in a range of ways to support children’s learning (e.g. generic stories about starting school or going to the dentist) but without adhering to these principles and we will refer to these as social stories (using lower case letters).
The ten criteria of Social Stories
Gray’s 10 criteria must be adhered to for a story to be considered a Social Story™. 3 The criteria give clear guidance on the elements that make a Social Story what it is and the process of researching, writing and formatting or illustrating one. They lead a Social Story to be developed and delivered in a certain way and consider the specific qualities of children with ASD. To give the later chapters the appropriate context, each of these criteria is described below using Gray’s original terminology as headings. 3
One goal
The first criterion emphasises the main purpose and overall tone of Social Stories. It states that the goal of a Social Story is to share accurate, socially meaningful information in a positive and reassuring way. Although they are often used in response to challenging behaviour, the focus of the content of the story would not be on that particular behaviour. The focus of the Story is usually provision of social information with the expectation that it will bring about changes in behaviour that benefit the child. Having one clear and shared goal enables those around the child to support them in a co-ordinated and supportive way.
Two-step discovery
This criterion emphasises the importance of gathering information before developing the story. This is an essential, non-negotiable part of developing a Social Story. It is the process by which the child and their needs are better understood. For example, ‘why is the child frustrated?’ or ‘what is it they do not understand?’. It is suggested that people who know the child best will be the best source of information for this stage. This criterion discourages ‘off the peg’ stories being used that are only partially suitable to the situation or the child.
Three parts and a title
The third criterion simply states that a Social Story is a story and needs a title describing the content, a beginning (introduction), a middle (body) and an end (conclusion). A good title should be clear to the child and easy to understand. It describes what the story is about.
Four-mat
The fourth criterion details four characteristics of the child which should be considered to ensure the story is appropriate for their cognitive ability. This criterion emphasises the importance of tailoring the Social Story to the child. The factors to be considered are their learning style, attention span, comprehension level and reading ability.
Five factors define voice and vocabulary
This criterion recognises the importance of the use of language and how the story is told. It details five separate rules when selecting the language used that are important in providing the story with the appropriate tone. The main emphasis is for the language to be positive and for the information presented to be accurate. The five rules are:
-
Write sentences in the first (I, we) and/or third person (she, it, they). Gray3 argues that ‘you’ statements are too directive and/or may be misunderstood by a child with ASD.
-
Use a positive and patient tone. The tone of the story needs to be positive, non-judgemental and non-authoritarian. An example of an unhelpful sentence in a Social Story would be: ‘I should not interrupt the head teacher when she is speaking in assembly’. An example of an alternative sentence to use would be ‘Children try to listen when the head teacher is talking to the group in assembly’. This constructive language is an important central feature of a Social Story.
-
Use information from the past in Social Stories. Past information can be useful in building self-esteem and remind people about previous positive events and outcomes.
-
Social Stories are literally accurate. Each word, phrase or sentence can be interpreted literally without changing the intended meaning. Children with ASD often have difficulty understanding complex, metaphorical phrases or words (e.g. ‘pull your socks up’) or phrases that might have multiple meanings (e.g. ‘take your seats’).
-
It is important to be accurate in meaning, especially when using verbs. For example, instead of ‘Jane will get the food from the supermarket’, a better sentence would be ‘Jane will buy the food from the supermarket’.
Six questions guide story development
The sixth criterion ensures that the appropriate content and information relevant to the situation is presented in the story. It encourages the writer to ask the six questions (who, what, where, when, why and how) about the situation that provides in-depth information about the child, and what needs to be explained in the Story to help the child. The questions are intended to explore the gaps in information for the child as the story is developed. For example, where and when does the issue occur? Who does it involve?
Seven types of sentences
The seventh criterion describes how the information included in a story should be presented by detailing seven types of sentence. Each sentence type has a different function in a story. The following are the common different types of sentences used.
-
Descriptive sentences: these are sentences that describe the situation factually and objectively. They may also describe the context and the information that we often assume everybody knows.
-
Perspective sentences: these sentences attempt to give the perspectives of different people. They can describe a person’s thoughts, feelings, beliefs, internal states and opinions. They can also describe a person’s sensations or physical health.
-
Coaching sentences (previously called directive sentences): this category of sentence accounts for three of Gray’s3 sentence types. These sentences gently guide or coach behaviour or suggest a more effective response. They often begin with ‘I will try to . . .’ or ‘I may choose to . . .’ or they list possible responses. There are three types of coaching sentences. Those which:
-
describe or suggest responses for the child (e.g. ‘I may choose to work on a table where there is no tinsel’ for a child who is so distressed by the presence of tinsel that they often tip the work tables over)
-
describe or suggest responses for the care-giver (e.g. ‘The teacher will try to set up some tables with tinsel and some tables without tinsel’).
-
are developed by the child themselves [e.g. ‘I may choose to . . .’ (the child chooses). . .]
-
-
Affirmative sentences: these are used to reinforce the meaning of other types of sentence. They may reinforce a point about safety or a positive statement. For example, ‘Children take turns going down the slide. This is very important.’ or ‘Sometimes I may lose the game. This is OK’.
-
Partial sentences: a partial sentence is one in which there are blanks that can be filled in by the child as they read.
A gr-eight formula
The eighth criterion defines the structure of the story by examining the balance of sentence types. It states that for something to be considered a Social Story, coaching sentences must amount to less than one-third of the total number of sentences in the story.
Nine makes it mine
This criterion emphasises the importance of using the child’s interests (e.g. trains or superheroes) in the story. A story should be written with knowledge of the child’s personal interests and preferences in an effort to make Stories more interesting and fun to read.
Ten guides to editing and implementation
The tenth criterion details the best practice for finalising and delivering the intervention. It emphasises the need to monitor and edit the story when necessary and the importance of having a quiet safe place to deliver it.
Evidence for the effectiveness of Social Stories
Social Stories can be effective in tackling challenging behaviour when they set out to explicitly teach social skills. 4 Until recently, research exploring efficacy and outcome has been confined to single-case studies. These case reports in children with ASD have suggested improvements in social interactions,5,6 choice making in an educational setting,6 voice volume in class7 and meal time skills. 8 Success has also been reported in addressing disruptive behaviours, including reducing tantrums9,10 and behaviours associated with frustration. 11 Non-comparative research has examined Social Story use in special education,12 mainstream education settings13 and within the home. 14
Two previous systematic reviews of Social Story effectiveness4,15 identified largely single-case designs and a paucity of good quality, comparative evidence on Social Stories. Both suggest further research, especially with the use of randomised controlled trials (RCTs) to evaluate whether or not positive outcomes seen in case series can be replicated.
Although Social Stories have much potential to improve behaviour, the comparative evidence base is limited and attributed levels of effect are based mostly on single-case research. A well-designed RCT is required to address this important gap in our knowledge, and a feasibility RCT is required to plan the appropriate experimental design. Evidence suggests that Social Stories delivered in a general education setting produced significantly larger effect sizes on behaviour than those implemented at home or in self-contained settings, such as separate schools or self-contained classrooms. 4 Therefore, this study specifically focuses on the feasibility of assessing Social Stories delivered within a mainstream schooling system.
Overview
Social Stories for children with ASD represents a complex, individualised intervention. With this in mind the feasibility of conducting a full RCT must be examined. Our aim in this study was to develop a UK-accessible, manualised Social Stories training intervention for teachers of children with ASD in mainstream schools and to explore the effect of this on reducing challenging behaviour or other social difficulties. We conducted a feasibility study to inform the design of a full RCT, including a justification and description of appropriate costs, outcomes and parameters to include cost-effectiveness. The study was carried out in three phases, following the guidelines set out by the Medical Research Council in their framework for development and evaluation of RCTs for complex interventions to improve health. 16
Theoretical phase
The initial pre-clinical phase was to conduct a systematic review of the current literature on social stories (including stories following Gray’s criteria). Chapter 2 details the findings of this systematic review. It included studies using social stories in all settings but paid particular attention to those used in mainstream schools. The review had two broad aims: firstly to provide a comprehensive description of how they have been used in education and clinical practice, and secondly to provide a quantitative estimate of the effectiveness of these interventions.
Phase 1
Chapters 3 to 6 detail phase 1 of the study. The aim of this phase was to develop a toolkit for writing Social Stories more accessible to a UK audience. It included a qualitative element to help develop the intervention and a small pilot study to refine it. This process was informed by patient and public involvement (PPI) on the study team who gave in depth advice for the qualitative interviews including assistance in the development of the topic guides and in supporting the research team in understanding the family perspective. Chapter 3 gives an overview of the development process as a whole. This process had strong PPI, including parent and teacher involvement and interviews with young people on the autism spectrum. Chapter 4 details the qualitative element in which interviews and focus groups were conducted with people with experience of using Social Stories. The aim of this process was to gather information relating to the optimum design and use of Social Stories, and to explore whether or not the intervention can feasibly be delivered in this particular context. Chapter 5 describes the progress at each stage of the developmental process for the intervention to be used in the feasibility study. Finally, Chapter 6 details the final stage of development of the intervention; a pilot study conducted with a small number of participants to examine the acceptability of the intervention before using it in the feasibility study.
Phase 2
Chapters 7 to 9 detail phase 2 of the study, the feasibility trial. Chapter 7 reports on the findings of the feasibility RCT and the considerations for conducting a full-scale trial. Chapter 8 details the health economic component of the study. Finally, Chapter 9 describes the findings of an additional qualitative component which consisted of interviews with the participating parents, teachers and children after they had completed their involvement with the feasibility trial. This additional component was suggested by our PPI representatives to give a richer quality of information to inform a fully powered trial.
Discussion
Chapter 10 attempts to bring together the conclusions from the previous chapters into a general discussion that critically evaluates the findings against the proposed objectives and makes recommendations for a future trial.
Objectives
-
To carry out a systematic review examining the use of social stories and other social stories for children with ASD, with particular reference to mainstream school-aged children and challenging behaviour.
-
To conduct a qualitative analysis of interviews and focus groups, to gather information relating to the optimum design and use of Social Stories in children with ASD in a mainstream school setting.
-
To form an expert writing panel and develop a manualised toolkit (including a training package) for writing and delivering Social Stories for use in mainstream schools.
-
To conduct a feasibility RCT comparing the developed manualised Social Stories training intervention with an attention control on challenging behaviour, demonstrating the feasibility of recruitment and delivery of the intervention and follow-up.
-
To establish the acceptability and utility of the developed manualised Social Stories intervention and trial to teachers, parents and children.
-
To identify parameters, outcomes and cost-effectiveness from the feasibility study in order to inform a future full-scale RCT.
Chapter 2 Theoretical phase: use of social stories in practice and evaluation of effectiveness – systematic review
Background
As discussed in Chapter 1, there have been a number of single-case studies on the use of social stories as an intervention for children diagnosed with ASD. It is currently unclear, however, how they have been used in education and clinical practice. There is also a lack of clarity about how closely the intervention used in the studies followed Gray’s criteria (if they could be considered Social Stories). Furthermore, although there are previous systematic reviews of the clinical effectiveness of this intervention, there is no comprehensive review in this area. The current chapter seeks to close these evidence gaps.
Patient and public involvement representatives gave advice to systematic reviewers to help them to understand the issues facing children with ASD and on elements that were important to families. This informed the development of the review methodology and content. In particular the decision to carry out more in-depth assessments of the single-case designs was driven by PPI advice that rich information could be found in single-case reports.
While social stories are widely referred to in education and clinical practice their precise definition is malleable. On the other hand Social Stories (with capitals) have a clear definition and structure. 3 This phase aimed to obtain comprehensive information about the available research on how social stories (including those that follow the criteria and those that do not) are written and used, and how faithful this is to current theories on what makes them effective. The review had two broad objectives.
Objectives
-
To provide a comprehensive description of how social stories have been used in education and clinical practice as reported in the literature (overview of practice).
-
To provide a quantitative estimate of the clinical effectiveness of this intervention (overview of effectiveness).
Method
The protocol for the review is registered on the PROSPERO database (registration number CRD42011001440).
Databases and additional resources
A wide range of databases and additional resources were searched to identify relevant information, including databases of peer-reviewed studies and sources of grey literature. The use of social stories spans the health and educational literature. Therefore, we sought to search databases that covered, health, mental health, education and social care. The full list of databases searched included:
-
Applied Social Sciences Index and Abstracts
-
Australian Education Index
-
British Education Index
-
British Library integrated catalogue
-
British Nursing Index
-
Campbell Library
-
Cumulative Index to Nursing and Allied Health Literature
-
ClinicalTrials.gov
-
Cochrane Central Register of Controlled Trials
-
Cochrane Database of Systematic Reviews
-
Conference Proceedings Citation Index – Science
-
Conference Proceedings Citation Index – Social Science & Humanities
-
Database of Abstracts of Reviews of Effects
-
EMBASE
-
Health Technology Assessment (HTA) database
-
Index to Theses
-
International Clinical Trials Registry Platform
-
Library of Congress catalog
-
MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations
-
NHS Economic Evaluation Database
-
OAIster
-
PsycINFO
-
Social Care Online
-
Science Citation Index
-
Social Science Citation Index
-
Social Policy & Practice
-
Social Services Abstracts
-
Zetoc.
The searches were not limited by date range, language or publication status. Each database was searched from inception to July 2011. Additional searches for dissertations/theses were undertaken using Google Scholar (advanced) (Mountain View, CA, Google).
The following organisation websites were also searched (accessed July 2011):
-
American Psychiatric Association (www.psych.org)
-
Asperger’s Syndrome (www.aspergerssyndrome.org)
-
Autism Education Trust (www.autismeducationtrust.org.uk)
-
Autism-Europe (www.autismeurope.org)
-
Autism Independent UK (www.autismuk.com)
-
Autism in Mind (www.autism-in-mind.co.uk)
-
Autism Research Centre (www.autismresearchcentre.com/arc/default.asp)
-
Autism Research Institute (www.autism.com)
-
Autism Society of America (www.autism-society.org)
-
Autistica (Autism Speaks) (www.autismspeaks.org.uk)
-
Mental Health Foundation (www.mentalhealth.org.uk)
-
MIND (www.mind.org.uk)
-
National Autistic Society (www.autism.org.uk)
-
National Collaborating Centre for Mental Health (NCCMH) (www.nccmh.org.uk)
-
National Institute of Mental Health (www.nimh.nih.gov)
-
Research Autism (www.researchautism.net/pages/welcome/home.ikml)
-
Royal College of Psychiatrists (www.rcpsych.ac.uk)
-
Scottish Society for Autism (www.autism-in-scotland.org.uk)
-
The Autism Acceptance Project (www.taaproject.com)
-
The Gray Center (www.thegraycenter.org)
-
UK Autism Foundation (www.ukautismfoundation.org).
We used a number of additional strategies to ensure the search was as comprehensive as possible. This included a hand search of reference lists of all studies included in the overview of practice stage and previously conducted systematic reviews in the area. It also included a reverse citation-search, conducted in ISI Web of Science Citation Databases and Google Scholar, for the same papers (i.e. those included in overview of practice and previous systematic reviews).
Search terms
The search terms were devised using a combination of subject indexing terms, such as medical subject headings in MEDLINE, and free text search terms in the title and abstract. The search terms covered two broad constructs, autism spectrum and social stories. They were developed through discussion between the research team and members of the PPI group, by scanning background literature and by browsing database thesauri. Full details of the specific search strategies for PsycINFO, MEDLINE and EMBASE are given in Appendix 1.
De-duplication
As a number of databases were searched, some degree of record duplication resulted. To manage this issue, the titles and abstracts of bibliographic records were downloaded and imported into EndNote version 7 (Thomson Reuters, CA, USA) bibliographic management software and duplicate records were removed.
Screening of citations
Two researchers independently examined the titles and abstracts of all identified citations using a pre-piloted, standardised screening form based on the population, intervention, comparator, outcome (PICO) criteria for the overview of practice and the evaluation of clinical effectiveness described below. Full papers were obtained for any citations that passed this first sift; these were again independently examined by two researchers using a pre-piloted, standardised forms. At both stages, any disagreements were resolved through consensus and referred to a third reviewer if necessary.
Inclusion–exclusion criteria
Detailed PICO criteria were developed to guide the screening of citations. PICO criteria for the participant and intervention criteria were the same for both the overview of practice and evaluation of clinical effectiveness reviews, but differed for the remaining criteria (comparator, outcome and study design). The PICO criteria are summarised below. Full criteria are given in Appendix 2.
Participants
Criteria for overview of practice and effectiveness
The sample must be aged between 4 and 15 years. The study must have included a participant or participants with a diagnosis on the autism spectrum [e.g. autism, atypical autism, pervasive developmental disorder – not otherwise specified (PDD-NOS), Asperger syndrome]. The diagnosis could be established by any method; a gold standard assessment such as the use of the Autism Diagnostic Observation Schedule17 was not required.
Intervention
Criteria for overview of practice and effectiveness
Any intervention described as a social story was included, as was any study that used an intervention with similar characteristics to a social story. This did not include sensory stories. If the term social story was used it was not required that the term was trademarked.
Comparator
Overview of practice
For the overview of practice, any comparator, including no comparator, was included.
Overview of effectiveness
For between-groups designs (e.g. RCTs or non-RCTs), studies with any comparator were included (e.g. other active treatment including psychological or medication, placebo, attention control, treatment as usual, waiting list, etc.); however, a comparator had to be present. For single-case designs, any within-participant (e.g. alternative treatment or no treatment phase) or between-participant (e.g. small N design with counterbalancing across participants) comparator was included; a baseline phase of an AB design met the criterion for a within-participant comparator.
Outcome
Overview of practice
There were no specific outcome criteria for ‘overview of practice’.
Overview of effectiveness
Any study was included that used a standardised, numerical measure of behavioural outcomes or non-standardised, numerical measure of behaviour. For single-case designs, studies had to report repeated measurement of the target behaviour. Challenging behaviour was defined as any target behaviour that the author sought to reduce. To ensure the review was as comprehensive as possible, studies were not excluded if beneficial behaviours were measured.
Study design
Overview of practice
For ‘overview of practice’ any type of study design was included. This included RCTs, non-RCTs and quantitative single-case studies. It also included non-quantitative case studies, narrative descriptions of the use of an intervention and pre–post designs. Book reviews, guidance on using social stories for parents/carers, teachers or clinicians and actual social stories were excluded.
Overview of effectiveness
Single-case studies were defined as using repeated measurements of quantifiable (numerical) data on a single clinical case. 18 The approach may involve replicating the basic design over several people to form a single-case series. Examples of single-case designs include AB designs, reversal/withdrawal designs, changing criterion methods, multiple baseline, small N designs that use counterbalancing across participants and alternating treatment designs (ATDs). 18 Single-case studies that relied solely on pre- and post-treatment measurements were excluded. Narrative, non-quantitative case studies were also excluded. The decision to include a study was made on the actual design used not on the design the authors reported using. For example, if a design was described as a single-case study or single-case series but the design did not meet the definition given above, the study was excluded.
For between-groups designs, both RCTs and non-RCTs were included.
Data extraction
A coding manual was developed by the research team with guidance from Gray and PPI representatives to guide data extraction. This was piloted and refined before use. Two researchers independently extracted data. Disagreements were resolved through consensus and if necessary discussion with a third reviewer. Data on descriptive characteristics included setting and participants (e.g. setting in which the study was conducted, country, numbers of participants, age, gender, diagnosis or cognitive functioning), characteristics of the social story (e.g. number of stories per child, sentence length, delivery format, timing, who developed the story or who delivered the story) and details of the behavioural category targeted, including how it was measured and if it were challenging or beneficial. Additional information was extracted for particular study designs. For example, for the single-case studies, details were extracted about the design used (e.g. AB, reversal or alternating treatment) and for between-groups designs details of the comparator were coded. Data were also extracted on the extent to which the development and delivery of the social stories adhered to best practice guidance. To determine this, Gray’s3 10 criteria were used as a base, but the reviewers added five additional component parts, developed from criteria five and ten, for more detail. A description of these fifteen criteria and how they map onto Gray’s original ten is displayed in Table 1. The table also includes a final category, criteria statement, which indicates whether the study reported following Gray’s criteria. The researchers assigned to extract this data were experienced in writing Social Stories and their use.
| Concordance item | Description | Gray’s criterion |
|---|---|---|
| Positive goal | The story has a positive goal that is safe for the child | Criterion 1 |
| Information gathered | Information is gathered preceding story selection | Criterion 2 |
| Structured story | The story has a title, introduction, body and conclusion | Criterion 3 |
| Tailored for ability/attention | The story is tailored for ability and attention span | Criterion 4 |
| Tailored for interests | The story is tailored for interests | Criterion 9 |
| ‘Wh’ questions answered | The story answers ‘wh’ questions and clearly explains the situation to the child | Criterion 6 |
| Listed sentence types | The story uses the listed sentence types (e.g. coaching, descriptive, perspective). The story should not combine different sentence types within the same sentence | Criterion 7 |
| Balance of sentence types | The story follows the Social Story formula for the balance of sentence types: no more than one-third of the sentence types should be ‘coaching’ sentences | Criterion 8 |
| First/third person statements | The story contains only first and third person statements | Criterion 5 |
| Non-authoritarian | The story has a non-authoritarian tone | Criterion 5 |
| Avoids should/must | The story avoids the use of words such as should and must, etc. | Criterion 5 |
| Literally accurate | The story is accurate in a literal sense | Criterion 5 |
| Story edited | The story has been edited after the first draft | Criterion 10 |
| Appropriate setting | There is a plan for reading the story in a quiet, comfortable setting | Criterion 10 |
| Introduced appropriately | There is a plan for introducing the story in a positive manner | Criterion 10 |
| Criteria statement | The authors state that they followed the Social Story criteria in developing and delivering the story |
For the single-case designs, data on clinical effectiveness were extracted from graphs or comparably reported data of the target behaviour at different time points. For between-groups designs, information was extracted on the sample size of each group, post-treatment means and standard deviations (SDs).
Quality assessment
For single-case designs, the Single-Case Experimental Design (SCED) scale was used. 19 This is a quality assessment tool designed specifically for the evaluation of single-case studies. The SCED has 11 items, 10 of which evaluate key threats to the validity of single-case designs. An eleventh item, ‘specification of clinical history’, rates the extent to which the clinical history of the participant is described in sufficient detail to permit the assessment of whether or not the intervention may be relevant to other individuals. In the original recommendations for the SCED, items were scored a 1 if the validity criterion was met and a 0 if not met. We differentiated between a score of 0 if the criterion was clearly not met and ‘not reported’ if there was insufficient detail given to rate the criterion. This helped to distinguish between methodological limitations and reporting limitations. Table 2 provides a description of the items used in the SCED.
| SCED item | Description |
|---|---|
| Clinical history | The study provides critical information regarding demographic and other characteristics of the research participant that allows the reader to determine the applicability of the treatment to another individual |
| Target behaviours | The paper identifies a precise, repeatable and operationally defined target behaviour that can be used to measure treatment success |
| Design | The study design allows for the examination of cause and effect relationships to demonstrate treatment efficacy |
| Baseline | To establish that sufficient sampling of behaviour had occurred during the pre-treatment period to provide an adequate baseline measure |
| Sampling behaviour during treatment | To establish that sufficient sampling of behaviour during the treatment phase has occurred to differentiate a treatment response from fluctuations in behaviour that may have occurred at baseline |
| Raw data record | To provide an accurate representation of the variability of the target behaviour |
| Inter-rater reliability | To determine if the target behaviour measure is reliable and collected in a consistent manner |
| Independent assessment | To reduce assessment bias by employing a person who is otherwise uninvolved in the study, to provide an evaluation of the patients |
| Statistical analysis | To demonstrate the effectiveness of the treatment of interest by statistically comparing the results over the study phases |
| Replication | To demonstrate that the application and results of the therapy are not limited to a specific individual or situation (i.e. that the results are reproduced in other circumstances – replicated across subjects, therapists or settings) |
| Evidence for generalisation | To demonstrate the functional utility of the treatment in extending beyond the target behaviours or therapy environment into other areas of the individual’s life |
We used the Cochrane risk of bias tool to assess the methodological quality and potential sources of bias for RCTs. 20 This measure contains a number of domains, such as random sequence generation, that relate to potential biases in a randomised trial. Each item was rated as high, low or unclear. Table 3 provides a description of the items used in this measure.
| Risk of bias item | Description |
|---|---|
| Selection bias: random sequence generation | Does the study describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether or not it should produce comparable groups? |
| Selection bias: allocation concealment | Does the study describe the method used to conceal the allocation sequence in sufficient detail to determine whether or not intervention allocations could have been foreseen in advance of, or during, enrolment? |
| Performance bias: blinding of participants and personnel | Does the study describe all measures used, if any, to blind study participants and personnel from knowledge of which intervention a participant received? |
| Detection bias: blinding of outcome assessment | Does the study describe all measures used, if any, to blind outcome assessors from knowledge of which intervention a participant received? |
| Attrition bias: incomplete outcome data | Does the study describe the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis? |
| Reporting bias: selective reporting | Does the study state how the possibility of selective outcome reporting was examined and what was found? |
| Other sources of bias | Are there other important concerns about bias not addressed in the other domains in the tool? |
For both the SCED19 and the Cochrane risk of bias tool,20 two researchers independently rated the quality of the studies. Disagreements were resolved through consensus and, when necessary, by referral to a third reviewer.
Data synthesis
There is as yet no agreement in the literature about how the effects from single-case designs should be quantified and collated. We therefore chose two estimates of effect rather than relying on a single one. The first, the percentage of non-overlapping data (PND),21 is the percentage of phase B (i.e. intervention phase) data that exceeds the highest point (or lowest depending on the direction of scoring) for the phase A data (i.e. baseline phase). There are potential problems with such an index of effectiveness; it relies, for example, on a single data point from the phase A, a data point that may in fact be a single, unrepresentative outlier of the index of behaviour during the baseline phase. It is, however, widely used and so was included as one estimate of effectiveness. Scruggs and colleagues21 recommend the following guidelines when interpreting PND values: a PND of ≥ 90% indicates that an intervention is highly effective, of ≥ 70 to < 90% indicates moderate effectiveness and of < 70% indicates questionable effectiveness or that the intervention is not effective. These guidelines were used here. The second estimate of effect was the percentage of data points exceeding the median (PEM). 22 The PEM involves calculating the median for the baseline phase and then identifying the proportion of data points in the intervention phase that exceed this value. Ma22 used the same guidelines to quantify improvement as used by Scruggs and colleagues21 and these were used to facilitate the interpretation of this calculation.
Results were grouped on the basis of four broad categories of target behaviours, three relating to the difficulties typically experienced by children diagnosed with ASD, corresponding to the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV) criteria (social; communication; and restricted and repetitive behaviours/interests) and a fourth miscellaneous category. 23 With the exception of restricted behaviours, in which all of the identified studies in this category examined similar target behaviours, the categories were further divided into subcategories. For each subcategory, a single study may have included more than one participant, and in some cases a participant may have contributed data on more than one target behaviour within a subcategory. Data were summarised at the level of the target behaviour for each subcategory.
For the between-groups designs, the standardised mean difference (Hedges’ g) was calculated. Where insufficient data were reported to make this calculation, the results in the original paper are given. A number of the studies used a design in which the comparator group went on to receive treatment. In these designs, data were analysed up to the point at which the distinction between the treatment and comparator groups was maintained. There were an insufficient number of studies that were comparable in terms of the comparator and the target behaviour to conduct a meta-analysis.
Results
Figure 1 summarises the results of the search. The database searches identified 1072 records; an additional nine were identified through other sources. After the records were de-duplicated, this left 646 records for screening. In total, 135 met first-sift inclusion criteria, of which 99 met the final inclusion criteria for the overview of practice. Of this 99, 77 used single-case designs and seven used between-groups designs and so were included in the overview of clinical effectiveness. The reasons for exclusion for each of the 36 studies that passed the first sift, but were subsequently excluded are summarised in Appendix 3.
FIGURE 1.
Results of the literature search.

Overview of practice
Single-case studies
As we have described above, the first aim of the review was to provide an overview of how social stories have been used in clinical and educational practice. We did this first for the 77 single-case designs, then for the seven between-groups designs and finally for the 15 other designs. Table 4 provides a summary of this information for the single-case studies and, related to this aim, Table 5 provides a summary of the extent to which the use of the social stories adhered to the criteria set out by Gray. 3
| Study | Setting and participants | Social story intervention | Single-case design | Outcome |
|---|---|---|---|---|
| Abraham (2004)27 | Setting: general education, USA | Story characteristics: two stories, 14 and 16 sentences; written story | Design: ACBD | Category: social ability, social communication, other |
| n = 4 | Timing: once a day, three times a week, over 17 days | Subcategory: various | ||
| Age (years): 7–14 | Developed by: research team | Measure: % of intervals | ||
| Gender: four males | Delivered by: teachers (mixed) | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: NR | ||||
| Adams (2004)11 | Setting: home, USA | Story characteristics: one story, 24 sentences; NR | Design: reversal (ABAB) | Category: other |
| n = 1 | Timing: once a day, four times a week, over 12 weeks | Subcategory: emotional development | ||
| Age (years): 7 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: parents | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR | ||||
| Agosta (2004)28 | Setting: general education, USA | Story characteristics: two stories, six sentences; written story and illustrations | Design: reversal (ABCA) | Category: social ability, other |
| n = 1 | Timing: at least three times a day, at least five times a week, over 28 days | Subcategory: social awareness, emotional development | ||
| Age (years): 6 | Developed by: research team | Measure: frequency – unclear | ||
| Gender: male | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Antle (2007)76 | Setting: home, USA | Story characteristics: one story, nine sentences; written story and photographs | Design: AB | Category: social ability, other |
| n = 1 | Timing: once a day, seven times a week, over 11 days | Subcategory: social awareness, life skills | ||
| Age (years): 5 | Developed by: research team and parents | Measure: frequency – unclear | ||
| Gender: male | Delivered by: parents | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Bailey (2008)56 | Setting: special education, USA | Story characteristics: one story; written story and illustrations | Design: ACABADAD | Category: social communication, other |
| n = 2 | Timing: over 36–38 days | Subcategory: various | ||
| Age (years): 10–15 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: two males | Delivered by: research team and target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Barry (2004)6 | Setting: special education, USA | Story characteristics: more than two stories; written story and photographs | Design: ABCD | Category: restricted behaviours |
| n = 2 | Timing: once a day, five times a week, over 14 days | Subcategory: restricted, repetitive patterns of behaviour/interests | ||
| Age (years): 7–8 | Developed by: NR | Measure: other | ||
| Gender: one male, one female | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Beh-Pajooh (2011)57 | Setting: special education, Iran | Story characteristics: NR | Design: AB | Category: other, social ability |
| n = 3 | Timing: once a day, over 21 days | Subcategory: emotional development, social awareness | ||
| Age (years): 8–9 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: three males | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Bell (2005)58 | Setting: special education, USA | Story characteristics: one story, 10 sentences; written story and illustrations | Design: ABCD | Category: restricted behaviours, social ability |
| n = 3 | Timing: once a day, over 27 days | Subcategory: various | ||
| Age (years): 5–10 | Developed by: NR | Measure: % of intervals | ||
| Gender: three males | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Bernad-Ripoll (2007)77 | Setting: home, USA | Story characteristics: two stories; written story and photographs | Design: ABC | Category: other, social ability |
| n = 1 | Timing: over 10 days | Subcategory: emotional development, social awareness | ||
| Age (years): 9 | Developed by: NR | Measure: % of correct responses | ||
| Gender: male | Delivered by: research team | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: high | ||||
| Bledsoe (2003)8 | Setting: special education, USA | Story characteristics: one story, eight sentences; NR | Design: reversal (ABAB) | Category: other |
| n = 1 | Timing: at least once a day, at least five times a week, over 13 days | Subcategory: life skills | ||
| Age (years): 13 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: male | Delivered by: research team | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: low | ||||
| Brownell (2002)29 | Setting: general education, USA | Story characteristics: one story, seven sentences; written story and illustrations, musical format | Design: reversal (ABAC) | Category: social communication, social ability |
| n = 4 | Timing: once a day, over 20 days | Subcategory: unusual voice modulation, social interest | ||
| Age (years): 6–9 | Developed by: teacher (special education), research team | Measure: frequency – event recording | ||
| Gender: four males | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Chan (2005)78 | Setting: home, China | Story characteristics: one story; written story and illustrations, musical format | Design: reversal (ACAB) | Category: social ability, social communication, other |
| n = 4 | Timing: once per day, over 5 days for each format | Subcategory: various | ||
| Age (years): 4–12 | Developed by: research team | Measure: duration, frequency – event recording | ||
| Gender: two males, two females | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Chan (2008)30 | Setting: general education, USA | Story characteristics: more than two stories; written story | Design: multiple baseline, reversal (ABA) | Category: social ability, social communication |
| n = 2 | Timing: 10–20 minutes, once a day, one to four times a week, over 5 weeks | Subcategory: various | ||
| Age (years): 5–6 | Developed by: NR | Measure: frequency – event recording, % of correct responses | ||
| Gender: two males | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Chan (2009)89 | Setting: general education, USA | Story characteristics: one story; written story and photographs, computer media, audio format | Design: AB | Category: other, social ability, restricted behaviours |
| n = 6 | Timing: once a day, over 34 days | Subcategory: various | ||
| Age (years): 7–9 | Developed by: teacher (special education) | Measure: % of intervals, frequency – event recording, % of correct responses | ||
| Gender: five males, one female | Delivered by: target student | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: average | ||||
| Cihak (2012)31 | Setting: general education, USA | Story characteristics: one story, seven sentences; DVD format | Design: ATD followed by BAB | Category: social ability |
| n = 4 | Timing: 30–35 seconds for 23 sessions | Subcategory: social awareness | ||
| Age (years): 11–14 | Developed by: teacher (special education and mainstream) and research team | Measure: % of intervals | ||
| Gender: four males | Delivered by: target student | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: average | ||||
| Crozier (2005)32 | Setting: general education, USA | Story characteristics: one story, eight sentences; written story and illustrations | Design: reversal (ABACA) | Category: social ability |
| n = 1 | Timing: once a day, five times a week, over 26 days | Subcategory: social awareness | ||
| Age (years): 8 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Crozier (2007)12 | Setting: general education, USA | Story characteristics: one story, 10 sentences; written story and illustrations | Design: reversal (ABABA) | Category: restricted behaviours |
| n = 1 | Timing: 5 minutes, once a day, three times a week, over 17 days | Subcategory: restricted, repetitive patterns of behaviour/interests | ||
| Age (years): 5 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: high | ||||
| Cullain (2000)90 | Setting: general education, home, USA | Story characteristics: one story, 5–17 sentences; written story | Design: AB | Category: all categories represented |
| n = 5 | Timing: twice a day, over 5 days | Subcategory: various | ||
| Age (years): 6 | Developed by: parents, teacher (special and mainstream education) and research team | Measure: frequency – event recording | ||
| Gender: four males, two females | Delivered by: teachers (both) and parents | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Daneshvar (2006)79 | Setting: community setting, USA | Story characteristics: two stories; four sentences; written story | Design: AB | Category: social communication |
| n = 4 | Timing: over 46–78 days | Subcategory: various | ||
| Age (years): 5–10 | Developed by: research team | Measure: % of correct responses | ||
| Gender: two males, two females | Delivered by: NR | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Delano (2006)13 | Setting: general education, USA | Story characteristics: one story; written story and illustrations | Design: reversal (ABCDA) | Category: social ability |
| n = 3 | Timing: once a day over 45 days | Subcategory: general communication skills | ||
| Age (years): 6 | Developed by: clinical workers/other professionals and research team | Measure: duration, frequency – interval recording | ||
| Gender: three males | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Demiri (2004)33 | Setting: home, general education, USA | Story characteristics: NR, NR; written story | Design: AB | Category: all categories represented |
| n = 5 | Timing: once a day | Subcategory: various | ||
| Age (years): 5–7 | Developed by: research team, teacher (special education) and parents | Measure: % of correct responses | ||
| Gender: five males | Delivered by: parents and teacher (mainstream education) | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: average | ||||
| Dodd (2008)80 | Setting: home, USA | Story characteristics: two stories, 15–17 sentences; written story and photographs | Design: multiple baseline (ABC) | Category: social ability |
| n = 2 | Timing: once a day, none to three times a week, over nine days | Subcategory: social awareness | ||
| Age (years): 9–12 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: two males | Delivered by: parents | |||
| Diagnosis: PDD-NOS | ||||
| Cognitive functioning: high | ||||
| Eckelberry (2007)34 | Setting: general education, USA | Story characteristics: one story, 15 sentences; written story and illustrations | Design: AB | Category: social ability |
| n = 1 | Timing: at least once a day, at least five times a week, over 15 days | Subcategory: social awareness | ||
| Age (years): 6 | Developed by: research team and teacher (mainstream education) | Measure: frequency – event recording | ||
| Gender: male | Delivered by: NR | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Gilles (2008)81 | Setting: home, USA | Story characteristics: one story; written story | Design: ABCD | Category: other |
| n = 9 | Timing: 8 weeks but only 8 days with social story | Subcategory: life skills | ||
| Age (years): 5–9 | Developed by: research team | Measure: other, sleep behaviours | ||
| Gender: seven males, two females | Delivered by: parents | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: mixed | ||||
| Graetz (2003)59 | Setting: special education, USA | Story characteristics: one story, eight sentences; written story, illustrations and photographs | AB | Category: social ability, social communication, other |
| n = 5 | Timing: once a day, over 40 days | Subcategory: various | ||
| Age (years): 10–14 | Developed by: research team and teacher (special education) | Measure: % of correct responses, % of intervals | ||
| Gender: four males, one female | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Hagiwara (1999)60 | Setting: special education, USA | Story characteristics: more than two stories; computer media | Design: multiple baseline (AB) | Category: other |
| n = 3 | Timing: once a day, over 19 days | Subcategory: life skills, sustained attention | ||
| Age (years): 7–9 | Developed by: research team and teacher (mainstream education) | Measure: % of correct responses, duration | ||
| Gender: three males | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Hanley (2008)35 | Setting: general education, USA | Story characteristics: one story, 21 sentence; written story | Design: reversal (ABA) | Category: social communication |
| n = 4 | Timing: < 15 minutes, four times per week, over 38 days | Subcategory: various | ||
| Age (years): 6–12 | Developed by: research team | Measure: frequency- event recording | ||
| Gender: three males, one female | Delivered by: teacher (special education) | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: group mix | ||||
| Hobbs (2003)24 | Setting: general education, UK | Story characteristics: one story, 13 sentences; written story and photographs | Design: AB | Category: social ability, restricted behaviours, other |
| n = 7 | Timing: once a day, over 10 days | Subcategory: various | ||
| Age (years): 6–10 | Developed by: teacher (special education) and research team | Measure: other | ||
| Gender: seven males | Delivered by: teacher (special education) | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: NR | ||||
| Holmes (2007)36 | Setting: general education, USA | Story characteristics: more than two stories, 13 sentences; written story and illustrations | Design: reversal (ABAB) | Category: social ability, social communication |
| n = 1 | Timing: three times a day, over 4 weeks | Subcategory: social awareness, general communication skills | ||
| Age (years): 11 | Developed by: research team and target student | Measure: frequency – event recording | ||
| Gender: male | Delivered by: target student | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: NR | ||||
| Hung (2011)37 | Setting: general education, Taiwan | Story characteristics: one story; written story | Design: reversal (ABAB) | Category: social ability |
| n = 1 | Timing: once a day, over 24 days | Subcategory: social awareness | ||
| Age (years): 6 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: male | Delivered by: teacher (mainstream education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Hutchins (2006)82 | Setting: home, USA | Story characteristics: one story, 18 sentences; written story | Design: AB | Category: other |
| n = 2 | Timing: once a day, three times a week, over 6 weeks | Subcategory: emotional development | ||
| Age (years): 6–12 | Developed by: parents and research team | Measure: other | ||
| Gender: one male, one female | Delivered by: NR | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR | ||||
| Ivey (2004)14 | Setting: home, USA | Story characteristics: more than two stories; written story, illustrations and photographs | Design: reversal (ABAB) | Category: restricted behaviours |
| n = 3 | Timing: once a day, five times a week, over 12 weeks | Subcategory: restricted, repetitive patterns of behaviour/interests | ||
| Age (years): 5–7 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: three males | Delivered by: parents | |||
| Diagnosis: PDD-NOS | ||||
| Cognitive functioning: mixed | ||||
| Keyworth (2004)38 | Setting: general education, USA | Story characteristics: one story, nine sentences; written story and illustrations | Design: ABCBCD | Category: social ability, social communication, restricted behaviours |
| n = 3 | Timing: 5 minutes, once a day, over 21 sessions | Subcategory: various | ||
| Age (years): 7–12 | Developed by: parents, teacher (mainstream education) and research team | Measure: % of correct responses | ||
| Gender: three males | Delivered by: teacher (mainstream education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Kuoch (2000)39 | Setting: general education, Canada | Story characteristics: one story, 22 sentences; written story and illustrations | Design: reversal (ABA) | Category: restricted behaviours, other |
| n = 2 | Timing: 3–4 minutes, over 44 days | Subcategory: various | ||
| Age (years): 5–6 | Developed by: parents, research team and teacher (mainstream education) | Measure: other | ||
| Gender: two males | Delivered by: teacher (mainstream education) | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: NR | ||||
| Kuttler (1998)10 | Setting: special education, USA | Story characteristics: two stories, 5–7 sentences; written story and illustrations | Design: reversal (ABAB) | Category: other |
| n = 1 | Timing: once a day, over 19 days | Subcategory: emotional development | ||
| Age (years): 12 | Developed by: parents, teacher (special education) and research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Lorimer (2002)9 | Setting: home, clinic/hospital, USA | Story characteristics: two stories, 9–11 sentences; written story and illustrations | Design: reversal (ABAB) | Category: social communication, other |
| n = 1 | Timing: 5 minutes, at least once a day, over 14 days | Subcategory: turn-taking, emotional development | ||
| Age (years): 5 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: male | Delivered by: parents and clinician/other professional | |||
| Diagnosis: autism | ||||
| Cognitive functioning: high | ||||
| Mancil (2009)62 | Setting: special education, USA | Story characteristics: one story, seven sentences; written story and photographs, computer media | Design: reversal (ACACBCBD) | Category: other |
| n = 3 | Timing: 5 minutes, once a day, five times a week, over 35 days | Subcategory: emotional development | ||
| Age (years): 6–8 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: two males, one female | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Mandasari (2011)61 | Setting: special education, Malaysia | Story characteristics: more than two stories; written story, computer media, illustrations and photographs | Design: ABC | Category: social communication |
| n = 3 | Timing: 10–15 minutes, two to three times a day, over 28 days | Subcategory: general communication skills | ||
| Age (years): 10–11 | Developed by: research team | Measure: other | ||
| Gender: three male | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Hsu (2009)40 | Setting: general education, USA | Story characteristics: one story, 11 sentences; written story and illustrations | Design: ABCB | Category: other |
| n = 1 | Timing: 10 minutes, once a day, four times a week, for 14 sessions | Subcategory: sustained attention | ||
| Age (years): 7 | Developed by: research team | Measure: % of intervals | ||
| Gender: male | Delivered by: teacher (mainstream education) | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: NR | ||||
| Norris (1999)5 | Setting: general education, USA | Story characteristics: more than two stories; written story, illustrations and photographs | Design: AB | Category: social ability, social communication |
| n = 1 | Timing: 10 minutes, at least once a day, at least five times a week, over 18 days | Subcategory: social awareness, unusual voice modulation, social interest | ||
| Age (years): 8 | Developed by: research team and teacher (mainstream education) | Measure: % of intervals | ||
| Gender: female | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: average | ||||
| Okada (2008)63 | Setting: special education, Japan | Story characteristics: one story; written story, illustrations and photographs | Design: ABCD | Category: other |
| n = 2 | Timing: once a day | Subcategory: emotional development, life skills | ||
| Age (years): 12–13 | Developed by: teacher (special education) and research team | Measure: frequency – event recording | ||
| Gender: two males | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Okada (2010)64 | Setting: special education, Japan | Story characteristics: more than two stories, 10–13 sentences; written story, illustrations and photographs | Design: ABCDE | Category: other |
| n = 1 | Timing: once a day, five times a week, over 41 days | Subcategory: life skills | ||
| Age (years): 14 | Developed by: research team | Measure: % of intervals | ||
| Gender: male | Delivered by: research team and target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Ozdemir (2008)41 | Setting: general education, USA | Story characteristics: one story, computer media | Design: reversal (ABCDA) | Category: social ability |
| n = 3 | Timing: once a day, three times a week, over 45 days | Subcategory: social interest | ||
| Age (years): 6 | Developed by: research team | Measure: % of intervals | ||
| Gender: three males | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Ozdemir (2008)7 | Setting: general education, USA | Story characteristics: one story, eight sentences, written story, illustrations and photographs | Design: reversal (ABCDA) | Category: social communication, other |
| n = 3 | Timing: at least once a day, at least five times a week, over 51 days | Subcategory: unusual voice modulation, life skills, emotional development | ||
| Age (years): 7–9 | Developed by: NR | Measure: % of intervals | ||
| Gender: three males | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Pasiali (2004)83 | Setting: home, USA | Story characteristics: one story, eight sentences, written, musical format | Design: reversal (ABAB) | Category: social ability, social communication, Restricted behaviours |
| n = 3 | Timing: 15 minutes, once a day, over 28 days | Subcategory: various | ||
| Age (years): 7–9 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: two males, one female | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Powell (2009)84 | Setting: home, USA | Story characteristics: two stories, 18 or 19 sentences, written | Design: multiple baseline (ABCD) | Category: social communication |
| n = 1 | Timing: NR | Subcategory: general communication skills | ||
| Age (years): 7 | Developed by: NR | Measure: % of intervals | ||
| Gender: female | Delivered by: family members | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Quilty (2007)42 | Setting: general education, USA | Story characteristics: one story, written story and photographs | Design: ABC | Category: social ability |
| n = 3 | Timing: 27 days | Subcategory: social awareness | ||
| Age (years): 6–10 | Developed by: teacher (special education), research team | Measure: frequency – event recording | ||
| Gender: two males, one female | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Reichow (2009)43 | Setting: general education, USA | Story characteristics: one story, written, illustrations and photographs | Design: reversal (ABABC) | Category: social communication |
| n = 1 | Timing: once a day, over 35 days | Subcategory: initiations and requests | ||
| Age (years): 11 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: average | ||||
| Reynhout (2007)65 | Setting: special education, Australia | Story characteristics: one story, written story and photographs | Design: ABC | Category: restricted behaviour |
| n = 1 | Timing: at least once a day, at least five times a week, over 70 days | Subcategory: restricted, repetitive patterns of behaviour/interests | ||
| Age (years): 8 | Developed by: teacher (special education), research team and clinical workers/other professionals | Measure: % of intervals | ||
| Gender: male | Delivered by: teacher (special education) and research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Reynhout (2008)66 | Setting: special education, Australia | Story characteristics: one story, four sentences, written story and photographs | Design: ABCD | Category: other |
| n = 1 | Timing: at least once a day, at least four times a week, over 38 days | Subcategory: sustained attention | ||
| Age (years): 8 | Developed by: parent, teacher (special education) and research team | Measure: frequency – interval recording | ||
| Gender: female | Delivered by: teacher (special education), research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Sansosti (2006)44 | Setting: general education, USA | Story characteristics: one story, 12 sentences, written story and illustrations | Design: reversal (ABA) | Category: social ability, social communication |
| n = 3 | Timing: twice a day, 10 times a week, over 36 days | Subcategory: social awareness, general communication skills | ||
| Age (years): 9–11 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: three males | Delivered by: parents | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: average | ||||
| Sansosti (2008)45 | Setting: general education, USA | Story characteristics: one story, written story and illustrations, computer media | Design: ABCD | Category: social ability, social communication |
| n = 3 | Timing: once a day, five times a week, over 30 days | Subcategory: social interest, general communication skills | ||
| Age (years): 6–9 | Developed by: research team | Measure: % of intervals | ||
| Gender: three males | Delivered by: target student | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: mixed | ||||
| Scapinello (2009)85 | Setting: home, Canada | Story characteristics: one story, nine sentences; written story, illustrations and photographs | Design: AB | Category: social ability, social communication, other |
| n = 8 | Timing: over 24 days | Subcategory: various | ||
| Age (years): 4–7 | Developed by: research team and parents | Measure: various | ||
| Gender: eight males | Delivered by: parents | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR | ||||
| Scattone (2002)67 | Setting: special education, USA | Story characteristics: one story, 10 sentences; written story | Design: AB | Category: social ability, social communication, other |
| n = 3 | Timing: once a day, over 22 days | Subcategory: social awareness, unusual voice modulation, life skills | ||
| Age (years): 7–15 | Developed by: NR | Measure: % of intervals | ||
| Gender: three males | Delivered by: teacher (mainstream education) and target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Scattone (2006)68 | Setting: special education, USA | Story characteristics: one story, 26 sentences, written | Design: AB | Category: social communication |
| n = 3 | Timing: once a day, over 33 days | Subcategory: general communication skills | ||
| Age (years): 8–13 | Developed by: research team | Measure: % of intervals | ||
| Gender: three males | Delivered by: target student | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: low | ||||
| Scattone (2008)86 | Setting: Clinic/hospital, home, USA | Story characteristics: more than two stories, 10 or 11 sentences, written, DVD format | Design: multiple baseline (AB) | Category: social ability, social communication |
| n = 1 | Timing: at least once a week, at least seven times a week, over 22 days | Subcategory: social attention, initiation and requests | ||
| Age (years): 9 | Developed by: research team | Measure: % of intervals | ||
| Gender: male | Delivered by: research team and parents | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: average | ||||
| Schneider (2010)46 | Setting: general education, USA | Story characteristics: one story; written story and illustrations | Design: AB | Category: social ability, restricted behaviours |
| n = 3 | Timing: once a day, five times a week, over 71 days | Subcategory: social awareness, restricted, repetitive patterns of behaviour/interests | ||
| Age (years): 5–10 | Developed by: clinical workers/other professionals and research team | Measure: % of intervals | ||
| Gender: three males | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Scurlock (2008)47 | Setting: general education, USA | Story characteristics: one story, 21 sentences; written story | Design: AB | Category: other |
| n = 1 | Timing: 5 minutes, once a week, five times a week, over 2 weeks | Subcategory: emotional development | ||
| Age (years): 10 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: target student | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: high | ||||
| Smith (2004)48 | Setting: general education, USA | Story characteristics: two stories, five sentences; written story | Design: reversal (ABA) | Category: social communication |
| n = 3 | Timing: 5 minutes, three times a week, over 23 days | Subcategory: initiations and requests | ||
| Age (years): 4 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: three males | Delivered by: NR | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Staley (2001)69 | Setting: special education, USA | Story characteristics: two stories, nine sentences; written story | Design: ABCDCD | Category: other |
| n = 1 | Timing: once a day, over 85 days | Subcategory: life skills | ||
| Age (years): 14 | Developed by: NR | Measure: other, frequency – event recording | ||
| Gender: male | Delivered by: teacher (special education) and research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Styles (2009)25 | Setting: general education, UK | Story characteristics: one story, 11 sentences; written story | Design: ABC | Category: social ability |
| n = 6 | Timing: once a day, over 6 weeks | Subcategory: social awareness | ||
| Age (years): 7 | Developed by: research team | Measure: % of intervals | ||
| Gender: five males, one female | Delivered by: teacher (mainstream education) | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: NR | ||||
| Swaggart (1995)70 | Setting: special education, USA | Story characteristics: two stories; written story and photographs | Design: AB | Category: social communication, other |
| n = 3 | Timing: once a day | Subcategory: various | ||
| Age (years): 7–11 | Developed by: research team | Measure: % of correct responses, frequency – event recording | ||
| Gender: two males, one female | Delivered by: teacher (special education) | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: NR | ||||
| Swaine (2004)49 | Setting: general education, Canada | Story characteristics: two stories, 16–20 sentences; written story and illustrations | Design: ABCDEFDG | Category: social communication |
| n = 2 | Timing: twice a day, two times a week, over 4 weeks | Subcategory: various | ||
| Age (years): 11 | Developed by: research team | Measure: % of correct responses | ||
| Gender: two males | Delivered by: research team | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: low | ||||
| Tarnai (2009)87 | Setting: Social skills service, USA | Story characteristics: one story, 20 sentences; written story | Design: AB | Category: social ability, social communication, other |
| n = 6 | Timing: 2–3 minutes, twice a week, for eight sessions | Subcategory: various | ||
| Age (years): 9–13 | Developed by: research team and other agency staff | Measure: frequency – interval recording | ||
| Gender: five males, one female | Delivered by: other agency staff | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: NR | ||||
| Tarnai (2011)88 | Setting: social skills service, USA | Story characteristics: one story, 32 sentences, written story and illustrations | Design: AB | Category: other |
| n = 6 | Timing: once a day, for four sessions | Subcategory: life skills | ||
| Age (years): 9–11 | Developed by: teachers (special and mainstream education), research team | Measure: % of correct responses | ||
| Gender: six males | Delivered by: other agency staff and target student | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: NR | ||||
| Taylor (2009)50 | Setting: general education, USA | Story characteristics: one story, 13 sentences; written story | Design: AB | Category: social communication |
| n = 4 | Timing: once a day, over 10 days | Subcategory: turn-taking | ||
| Age (years): 6–8 | Developed by: teacher (special education) and research team | Measure: other | ||
| Gender: four males | Delivered by: teacher (special education) | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR | ||||
| Thiemann (2001)51 | Setting: general education, USA | Story characteristics: more than two stories; written, illustrations and photographs | Design: multiple baseline (ABA) | Category: social communication |
| n = 4 | Timing: 10 minutes, once a day, seven times a week, over 30–38 days | Subcategory: various | ||
| Age (years): 6–12 | Developed by: NR | Measure: frequency – event recording | ||
| Gender: four males | Delivered by: parents | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Travis (2006)71 | Setting: special education, USA | Story characteristics: one story, 12 sentences; musical format | Design: AB | Category: social communication, restricted behaviours |
| n = 2 | Timing: once a day, over 1 week | Subcategory: various | ||
| Age (years): 4 | Developed by: research team | Measure: frequency – unclear | ||
| Gender: one male, one female | Delivered by: research team | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR | ||||
| Vanderhoek (2004)52 | Setting: general education, China | Story characteristics: more than two stories, variable length; written story and photographs | Design: AB | Category: social ability, social communication |
| n = 1 | Timing: once a day, over 5 days | Subcategory: social awareness, unusual voice modulation | ||
| Age (years): 8 | Developed by: teacher (mainstream education) and research team | Measure: frequency – event recording | ||
| Gender: male | Delivered by: teacher (mainstream education) | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: NR | ||||
| Voges (2009)26 | Setting: general education, UK | Story characteristics: one story, five sentences; written story and photographs | Design: reversal (ABA) | Category: other |
| n = 1 | Timing: twice a day, 10 times a week, over 14 days | Subcategory: life skills | ||
| Age (years): 8 | Developed by: research team | Measure: % of correct responses | ||
| Gender: male | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Washburn (2006)53 | Setting: general education, USA | Story characteristics: one story, 30 sentences; written story | Design: reversal (ABCDA) | Category: social communication |
| n = 4 | Timing: 10 minutes, once a day, three times a week, over 9 weeks | Subcategory: turn taking | ||
| Age (years): 12–14 | Developed by: research team | Measure: % of intervals | ||
| Gender: four males | Delivered by: target student | |||
| Diagnosis: Asperger | ||||
| Cognitive functioning: average | ||||
| Washburn (2006)72 | Setting: special education, USA | Story characteristics: one story, 21 sentences; written story and illustrations | Design: reversal (ABA) | Category: social ability, restricted behaviours, other |
| n = 2 | Timing: less than 30 minutes, twice a week, over 8 weeks | Subcategory: various | ||
| Age (years): 8–11 | Developed by: research team and teacher (special education) | Measure: frequency – event recording, frequency – interval recording | ||
| Gender: two males | Delivered by: research team | |||
| Diagnosis: ASD mixed | ||||
| Cognitive functioning: average | ||||
| Watts (2008)73 | Setting: special education, USA | Story characteristics: one story, 11 sentences; written story and illustrations | Design: AB | Category: social ability, social communication |
| n = 6 | Timing: 3–5 minutes, once/day, three times/week, over 23 days | Subcategory: various | ||
| Age (years): 6–9 | Developed by: teacher (special education), research team, clinical workers and other professionals | Measure: frequency – event recording | ||
| Gender: four males, two females | Delivered by: research team | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Wheeler (2005)74 | Setting: special education, USA | Story characteristics: one story, 16 sentences; written story, illustrations and photographs | Design: AB | Category: social communication, other |
| n = 2 | Timing: over 4 weeks | Subcategory: various | ||
| Age (years): 8 | Developed by: NR | Measure: frequency – event recording, duration | ||
| Gender: two males | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: low | ||||
| Wilkinson (2010)54 | Setting: general education, USA | Story characteristics: more than two stories, 9–11 sentences; written story and photographs | Design: multiple baseline (ABCDE) | Category: social ability |
| n = 2 | Timing: twice a day, over 47 days | Subcategory: social attention | ||
| Age (years): 7–9 | Developed by: NR | Measure: % of correct responses | ||
| Gender: one male, one female | Delivered by: target student | |||
| Diagnosis: autism | ||||
| Cognitive functioning: high | ||||
| Wright (2007)55 | Setting: general education, USA | Story characteristics: one story, 10 sentences; written story, illustrations and photographs | Design: ABCD | Category: social ability |
| n = 4 | Timing: once a day, five times a week, over 38 days | Subcategory: social interest | ||
| Age (years): 4–5 | Developed by: research team | Measure: frequency – event recording | ||
| Gender: four males | Delivered by: teacher (special education) | |||
| Diagnosis: autism | ||||
| Cognitive functioning: NR | ||||
| Xin (2011)75 | Setting: special education, USA | Story characteristics: one story, eight sentences; written story, photographs, computer media and audio format | Design: AB | Category: social ability, social communication |
| n = 2 | Timing: at least once a day, over 13 days | Subcategory: various | ||
| Age (years): 9 | Developed by: teacher (special education), target student | Measure: frequency – event recording | ||
| Gender: one male, one female | Delivered by: teacher (special education) | |||
| Diagnosis: ASD | ||||
| Cognitive functioning: NR |
The majority of the single-case data are based on interventions conducted in the USA. Eighty-one per cent of the single-case studies were conducted in the USA, with only three studies24–26 (4%) conducted in the UK. Approximately one-half (48%) of the studies5,7,12,13,24–55 provided the intervention in a general education setting and just over one-quarter6,8,10,56–75 (29%) used a special education setting. The remainder of the studies9,11,14,76–88 used a home or other setting.
In terms of the study participants of the single-case studies, the majority were male and under the age of 10 years. Only 18% of the single-case studies8,10,31,36,43,47,49,56,59,61,63,64,69,72 had participants who were all aged 10 years or above; in only three studies8,64,69 (4%) were all the participants aged 13 years or above. Over two-thirds7–14,24,26–34,36–41,43–53,55–58,60,61,63–65,67–69,72,74,76,77,80,85,86,88 (71%), had samples that were entirely male, three studies5,66,84 (4%) were all female, and the remaining studies1,6,25,35,42,54,59,62,70,71,73,75,79,81–83,87,89,90 (25%) had a mixed sample. Over half of the studies5–7,9,10,12,13,26,28–30,32,34,37,38,41–43,46,48,51,54–67,69,73,74,76,78,79,83,84,90 had participants who were diagnosed with autism (58%). A small percentage8,24,27,36,40,44,47,52,68,72,77 (14%) had participants diagnosed with Asperger syndrome and just two14,80 (3%) with PDD-NOS. There were a mix of diagnoses in 18% of the studies25,31,33,35,39,45,49,53,68,70,81,87–89 and a small number11,50,71,75,82,85 (6%) stated that the sample were on the autistism spectrum but did not provide further details. The cognitive functioning of participants was not reported in over half (55%) of the studies,6,7,10,11,13,24–30,32,34,36,38–40,42,46,48,50–52,55,57,58,61,63,64,69–71,75,76,78,82–85,87,88,90 but when it was reported approximately half8,37,41,49,56,58–60,62,65–68,73,74,79 stated that participants had low functioning and half5,9,12,31,33,43,44,47,53,54,77,80,86,89 reported either average or above average functioning.
There was substantial variation in the characteristics of the social stories. Two-thirds of studies7,8,11–13,24–26,29,31,32,34,35,37–47,50,53,55,56,58,59,62,63,65–68,71–76,78,81–83,85,87–90 used one story per child, approximately equal numbers used two stories9,10,27,28,48,49,69,70,77,79,80 (17%) or more than two stories5,6,14,30,36,51,52,54,60,61,64,86 (16%) per child. The stories ranged in length from four to 32 sentences; the median sentence length was 11 [interquartile range (IQR) 8–16]. Over half (55%) of the studies5,6,9,10,12–14,24,26,28,29,32,34,36,38–46,51–56,58,59,63–66,70,73–78,80,85,88,89 used stories combining a written format with either illustrations or photographs, and one-quarter25,27,30,33,35,37,47–50,67–69,72,79,81–84,87,90 used a written format alone. Of the remainder, 12% of the studies41,45,60–62,75,86,89 used some form of electronic media (e.g. computer, DVD or audio) either alone or in combination with other media and 5% used a musical format,29,71,78,83 again either alone or in combination with other formats. In the studies that reported data on duration, the length of the intervention ranged from 5 to 85 days with a median duration of 28 days (IQR 16–39 days).
The researchers developed the stories alone in over one-third (36%) of studies11–14,25–28,32,35,40,41,43–45,47,49,55,56,61,64,68,70–72,78,79,81,83,86 and in the same number of studies5,10,13,24,29,31,33,34,36,38,39,42,46,50,52,59,60,63,65,66,72,73,76,82,85,87,88,90 (36%) the researchers worked with others (e.g. parents, teachers) to develop the story. In only three studies36,75,89 (4%) was the study developed by teachers without researcher input. The researchers alone delivered the story in 18% of the studies8,12,13,29,46,49,57,58,71,72,73,77,78,83 and in combination with others (e.g. researchers and teachers) in 8% of the studies. 56,64–66,69,86 Teachers alone delivered the story in 29% of the studies6,10,24–28,35,37–42,50,52,55,59,63,70,74,75 and family members alone in 12%. 11,14,44,51,76,80,81,84,85 In 19% of the studies,5,30,31,36,41,43,45,47,53,54,60–62,68,89 the story was self-administered by the child. Other combinations were used in 9% of the studies9,33,67,87,88,90 and in 5% of the studies34,48,79,82 the information was not reported.
The next stage of the overview of practice evaluated the extent to which the authors had adhered to the Social Story guidance in the development and delivery of the Social Story. Tables 5 and 6 summarise the extent to which the 77 single-case studies adhered to this guidance (see Table 1 above for a description of the Social Story guidance criteria).
| Study | Positive goal | Information gathered | Structured story | Tailored for ability/attention | Tailored for interest | ‘Wh’ questions answered | Listed sentence types | Balance of sentence types |
|---|---|---|---|---|---|---|---|---|
| Abraham (2004)27 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Adams (2004)11 | ✗ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✗ |
| Agosta (2004)28 | ✗ | ✓ | NR | NR | NR | ✓ | ✓ | ✓ |
| Antle (2007)76 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Bailey (2008)56 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Barry (2004)6 | NR | ✓ | NR | NR | NR | NR | NR | NR |
| Beh-Pajooh (2011)57 | NR | ✓ | NR | NR | NR | NR | NR | NR |
| Bell (2005)58 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Bernad-Ripoll (2007)77 | ✗ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Bledsoe (2003)8 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Brownell (2002)29 | ✗ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Chan (2005)78 | ✗ | ✓ | ✗ | NR | NR | NR | ✓ | ✓ |
| Chan (2008)30 | NR | ✓ | NR | NR | NR | NR | NR | NR |
| Chan (2009)89 | ✗ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✗ |
| Cihak (2012)31 | ✗ | ✓ | NR | NR | NR | NR | ✓ | ✗ |
| Crozier (2005)32 | ✗ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✗ |
| Crozier (2007)12 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Cullain (2000)90 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Daneshvar (2006)79 | ✓ | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Delano (2006)13 | NR | ✓ | NR | ✓ | NR | NR | ✓ | ✓ |
| Demiri (2004)33 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Dodd (2008)80 | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Eckelberry (2007)34 | ✗ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Gilles (2008)81 | NR | ✓ | NR | NR | NR | NR | NR | NR |
| Graetz (2003)59 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Hagiwara (1999)60 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✗ |
| Hanley (2008)35 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Hobbs (2003)24 | ✗ | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Holmes (2007)36 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✗ | ✗ |
| Hung (2011)37 | ✗ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Hutchins (2006)82 | ✗ | ✓ | ✓ | ✓ | NR | ✓ | ✗ | ✓ |
| Ivey (2004)14 | ✓ | ✓ | NR | NR | NR | ✓ | ✓ | ✓ |
| Keyworth (2004)38 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Kuoch (2000)39 | ✓ | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ |
| Kuttler (1998)10 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✗ |
| Lorimer (2002)9 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ |
| Mancil (2009)62 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Mandasari (2011)61 | NR | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Hsu (2009)40 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Norris (1999)5 | NR | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ |
| Okada (2008)63 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Okada (2010)64 | ✓ | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Ozdemir (2008)41 | NR | NR | NR | NR | NR | NR | NR | NR |
| Ozdemir (2008)7 | ✗ | NR | NR | NR | NR | ✓ | ✓ | ✓ |
| Pasiali (2004)83 | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Powell (2009)84 | ✗ | NR | ✓ | NR | ✓ | ✓ | ✓ | ✗ |
| Quilty (2007)42 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Reichow (2009)43 | NR | NR | NR | NR | NR | ✓ | NR | NR |
| Reynhout (2007)65 | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ |
| Reynhout (2008)66 | ✓ | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Sansosti (2006)44 | ✗ | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ |
| Sansosti (2008)45 | NR | ✓ | NR | NR | NR | NR | ✓ | ✓ |
| Scapinello (2009)85 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ |
| Scattone (2002)67 | ✗ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Scattone (2006)68 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✗ |
| Scattone (2008)86 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Schneider (2010)46 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Scurlock (2008)47 | ✗ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Smith (2004)48 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Staley (2001)69 | ✓ | NR | ✓ | NR | NR | NR | ✓ | ✓ |
| Styles (2009)25 | ✓ | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ |
| Swaggart (1995)70 | ✗ | ✓ | ✗ | NR | NR | ✗ | ✓ | ✗ |
| Swaine (2004)49 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Tarnai (2009)87 | ✗ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Tarnai (2011)88 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Taylor (2009)50 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Thiemann (2001)51 | ✓ | NR | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Travis (2006)71 | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Vanderhoek (2004)52 | ✗ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Voges (2009)26 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ |
| Washburn (2006)53 | ✗ | ✓ | ✓ | NR | NR | NR | ✓ | ✓ |
| Washburn (2006)72 | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Watts (2008)73 | ✗ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Wheeler (2005)74 | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ |
| Wilkinson (2010)54 | ✓ | NR | NR | NR | NR | ✓ | ✓ | ✗ |
| Wright (2007)55 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Xin (2011)75 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ |
| Study | First/third person statements | Non-authoritarian | Avoids should/must | Literally accurate | Story edited | Appropriate setting | Introduced appropriately | Guideline statement |
|---|---|---|---|---|---|---|---|---|
| Abraham (2004)27 | ✓ | ✓ | ✗ | ✗ | NR | NR | ✓ | ✓ |
| Adams (2004)11 | ✓ | ✗ | ✗ | ✓ | NR | NR | NR | ✗ |
| Agosta (2004)28 | ✓ | ✗ | ✓ | ✗ | ✓ | NR | NR | ✓ |
| Antle (2007)76 | ✓ | ✓ | ✗ | ✓ | NR | NR | NR | ✓ |
| Bailey (2008)56 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | ✓ |
| Barry (2004)6 | NR | NR | NR | NR | NR | NR | NR | NR |
| Beh-Pajooh (2011)57 | NR | NR | NR | NR | NR | NR | NR | NR |
| Bell (2005)58 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Bernad-Ripoll (2007)77 | ✓ | ✗ | ✗ | ✓ | NR | NR | NR | ✓ |
| Bledsoe (2003)8 | ✓ | ✓ | ✓ | NR | NR | NR | NR | NR |
| Brownell (2002)29 | ✓ | ✗ | ✓ | ✓ | NR | ✓ | NR | NR |
| Chan (2005)78 | ✓ | ✗ | ✓ | NR | NR | ✓ | NR | ✓ |
| Chan (2008)30 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Chan (2009)89 | ✓ | ✗ | ✗ | ✓ | NR | ✗ | NR | ✓ |
| Cihak (2012)31 | ✓ | ✗ | ✓ | ✗ | NR | NR | NR | ✓ |
| Crozier (2005)32 | ✓ | ✗ | ✓ | ✗ | NR | ✓ | ✓ | ✗ |
| Crozier (2007)12 | ✓ | ✗ | ✓ | ✓ | NR | NR | ✓ | ✓ |
| Cullain (2000)90 | ✓ | ✓ | ✓ | ✗ | NR | NR | NR | ✓ |
| Daneshvar (2006)79 | ✓ | ✓ | ✓ | ✗ | NR | NR | NR | ✓ |
| Delano (2006)13 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Demiri (2004)33 | ✓ | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ |
| Dodd (2008)80 | ✗ | ✗ | ✓ | ✓ | NR | NR | NR | ✓ |
| Eckelberry (2007)34 | ✓ | ✗ | ✗ | ✓ | NR | NR | NR | ✓ |
| Gilles (2008)81 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Graetz (2003)59 | ✓ | ✓ | ✓ | ✗ | ✓ | NR | NR | ✓ |
| Hagiwara (1999)60 | ✓ | ✗ | ✓ | ✗ | NR | NR | NR | ✓ |
| Hanley (2008)35 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Hobbs (2003)24 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | NR |
| Holmes (2007)36 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | NR |
| Hung (2011)37 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | ✓ |
| Hutchins (2006)82 | ✓ | ✗ | ✓ | ✓ | ✓ | NR | NR | ✗ |
| Ivey (2004)14 | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | NR | ✓ |
| Keyworth (2004)38 | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | NR |
| Kuoch (2000)39 | ✓ | ✓ | ✓ | ✗ | ✓ | NR | NR | ✓ |
| Kuttler (1998)10 | ✓ | ✓ | ✓ | ✗ | NR | NR | NR | ✓ |
| Lorimer (2002)9 | ✓ | ✗ | ✓ | ✗ | NR | ✓ | NR | NR |
| Mandasari (2011)61 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Mancil (2009)62 | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | ✓ |
| Hsu (2009)40 | ✓ | ✓ | ✗ | ✓ | NR | NR | NR | ✓ |
| Norris (1999)5 | NR | NR | NR | NR | NR | ✓ | NR | ✓ |
| Okada (2008)63 | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ |
| Okada (2010)64 | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | ✓ |
| Ozdemir (2008)41 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Ozdemir (2008)7 | ✓ | ✗ | ✓ | ✗ | NR | NR | NR | ✓ |
| Pasiali (2004)83 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | NR |
| Powell (2009)84 | ✓ | ✗ | ✗ | ✓ | NR | ✓ | NR | NR |
| Quilty (2007)42 | ✓ | ✓ | ✓ | ✗ | NR | NR | ✓ | ✓ |
| Reichow (2009)43 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Reynhout (2007)65 | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | NR | ✓ |
| Reynhout (2008)66 | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | ✓ |
| Sansosti (2006)44 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | ✓ |
| Sansosti (2008)45 | NR | NR | NR | NR | NR | NR | NR | ✓ |
| Scapinello (2009)85 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | NR |
| Scattone (2002)67 | ✓ | ✗ | ✗ | ✓ | NR | NR | NR | ✓ |
| Scattone (2006)68 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Scattone (2008)86 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Schneider (2010)46 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Scurlock (2008)47 | ✓ | ✗ | ✓ | ✗ | NR | NR | NR | ✓ |
| Smith (2004)48 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Staley (2001)69 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | ✓ |
| Styles (2009)25 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ |
| Swaggart (1995)70 | ✓ | ✗ | ✓ | ✗ | NR | NR | NR | NR |
| Swaine (2004)49 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Tarnai (2009)87 | ✓ | ✗ | ✗ | ✗ | ✓ | ✓ | ✓ | ✓ |
| Tarnai (2011)88 | ✗ | ✗ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ |
| Taylor (2009)50 | ✓ | ✓ | ✓ | ✗ | NR | ✓ | NR | ✓ |
| Thiemann (2001)51 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | NR |
| Travis (2006)71 | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | ✓ |
| Vanderhoek (2004)52 | ✓ | ✗ | ✗ | ✗ | NR | NR | ✓ | ✓ |
| Voges (2009)26 | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | ✓ |
| Washburn (2006)53 | ✓ | ✗ | ✗ | ✗ | NR | ✓ | NR | ✓ |
| Washburn (2006)72 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ |
| Watts (2008)73 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | ✓ |
| Wheeler (2005)74 | ✓ | ✓ | ✓ | ✗ | NR | NR | NR | NR |
| Wilkinson (2010)54 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | NR |
| Wright (2007)55 | ✓ | ✗ | ✗ | NR | NR | NR | NR | ✓ |
| Xin (2011)75 | ✓ | ✗ | ✗ | ✗ | NR | NR | NR | ✗ |
For just under half of the concordance items, the studies tended to meet criteria. These included information gathered5,6,8,9,11–14,24–34,36,37,39,40,42,44–47,49,52,53,55–61,63–66,70–72,74–83,85,87–90 (74% of studies met the criterion), structured story8–12,24–27,29,32–40,42,44,46–53,55,56,58–69,71–77,79,80,82–84,86–90 (79%),’wh’ questions answered5,7–12,14,26–29,32–38,40,42,43,46–52,54–56,58–60,62,63,67,68,71–77,80,82–90 (73%), listed sentence types5,7–14,24–29,31–35,37–40,42,44–56,58–80,83,84,86–90 (88%), balance of sentence types5,7,8,12–14,24–29,33–35,37–40,42,44–53,55,56,58,59,61–67,69,71–74,76–80,82,83,85–88,90 (75%) and use of first and third person statements7–12,14,24–29,31–40,42,44,46–56,58–60,62–79,82–86,88–90 (84%). Over half of the studies7–10,12,14,25,26,28,29,31–33,35,36,38,39,42,46–51,56,58–60,62–66,68,69,71,72,74,78–80,82,83,85,86,88,90 (62%) met the criterion for avoiding the use of ‘should’ and ‘must’, although a sizeable minority11,24,27,34,37,40,44,52–55,67,73,75–77,84,87,89 (25%) did not meet this criterion.
For five of the criteria, the majority of studies were rated as unclear. Categories in which only a small proportion of studies were coded as meeting the criteria included tailored for ability5,9,12,13,25,27,29,35,39,42,44,55,59,62,63,65,73,75,76,82,85,87–90 (32%), tailored for interest5,9,27,64,65,71,72,74–77,80,83–85 (19%), story edited14,25,28,39,49,51,59,63,65,72,82,87,88 (17%), appropriate setting5,9,14,25,29,32,35,36,46,48–51,53,56,58,63,65,68,69,71,72,78,83–88 (38%) and introduced appropriately12,27,32,33,42,48,49,52,63,87,88 (14%). For the remaining three criteria (positive goal, non-authoritarian and literally accurate), approximately equal numbers of studies did and did not meet criteria.
A minority of studies either stated they did not adhere to the Social Story criteria in developing and delivering the intervention (5%)11,32,75,82 or did not report if they adhered to them (20%). 6,8,9,24,29,36,38,48,51,54,57,70,74,83–85 However, 52 studies7,9–12,14,24,27–29,31,32,34–37,39,40,42,44,46,47,50,52–55,58–60,63,65,67,68,70,73–80,82–90 (68%) were rated as not meeting at least one of the criteria. Of the remaining studies, only 1025,26,33,48,49,51,56,62,71,72 were rated as meeting 10 or more of the 15 criteria. No study met all 15 criteria.
Between-groups designs
Although the vast majority of studies used a single-case approach, we identified seven studies91–97 that used a between-groups design, of which four92–95 used some form of randomisation. Table 7 summarises the descriptive characteristics of the four randomised studies92–95 and Table 8 does the same for the non-randomised studies. 91,96,97
| Study | Setting and sample | Intervention | Comparator | Outcomes |
|---|---|---|---|---|
| Andrews (2004)92 | Setting: experimental conditions, USA | Story characteristics: one story/child, written story | Story characteristics: story with no social loading | Social skills related to playing a game |
| Age (years): 8–12 | Timing: five times a day, over 1 day | Timing: five times a day, over 1 day | ||
| Gender: NR | Developed by: NR | Developed by: NR | ||
| Diagnosis: autism | Delivered by: research team | Delivered by: research team | ||
| Cognitive functioning: low | n = 10 | n = 10 | ||
| Bader (2006)93 | Setting: experimental conditions, USA | Story characteristics: one story per child; written story and photographs | Story characteristics: story with no social loading | Learning of facial emotion |
| Age (years): 6–13 | Timing: over 1 day | Timing: over 1 day | ||
| Gender: NR | Developed by: research team | Developed by: research team | ||
| Diagnosis: autism | Delivered by: research team | Delivered by: research team | ||
| Cognitive functioning: low | n = 10 | n = 9 | ||
| Feinberg (2001)94 | Setting: experimental conditions, USA | Story characteristics: one story per child, written | Story characteristics: story with no social loading | Social skills related to playing a game |
| Age (years): 10.2 (SD 1.8) | Timing: five times a day, over 1 day | Timing: five times a day, over 1 day | ||
| Gender: 73.5% male | Developed by: research team | Developed by: existing story | ||
| Diagnosis: autism | Delivered by: research team | Delivered by: research team | ||
| Cognitive functioning: low | n = 17 | n = 17 | ||
| Quirmbach (2009)95 | Setting: NR, USA | Story characteristics: one story per child, 25/34 sentences (standard/directive); written story | Story characteristics: one story per child, 28 sentences; written, control story | Social skills related to playing a game |
| Age (years): 7–14 | Timing: four times a day, over 1 day | Timing: four times a day, over 1 day | ||
| Gender: 93.3% male | Developed by: research team | Developed by: NR | ||
| Diagnosis: ASD mixed | Delivered by: research team | Delivered by: research team | ||
| Cognitive functioning: low | n = 15 (standard story), n = 15 (directive story) | n = 15 |
| Study | Setting and sample | Intervention | Comparator | Outcomes |
|---|---|---|---|---|
| Ali (2010)91 | Setting: general education, Egypt | Story characteristics: NR | Story characteristics: NR | Scale for communication skills |
| Age (years): 5–10 | Timing: 20–30 minutes, over 14 teaching sessions | Timing: NR | ||
| Gender: NR | Developed by: NR | Developed by: NR | ||
| Diagnosis: autism | Delivered by: NR | Delivered by: NR | ||
| Cognitive functioning: NR | n = 15 | n = 15 | ||
| Ricciardelli (2006)96 | Setting: special education, USA | Story characteristics: > two stories per child; written story and photographs | Story characteristics: standard school curriculum (no control story) | The Children’s Institute Social Skills Rating Scale |
| Age (years): 8–11 | Timing: 10 minutes, two times a day, over 1 month | Timing: N/A | ||
| Gender: 100% male | Developed by: NR | Developed by: N/A | ||
| Diagnosis: autism | Delivered by: teacher (special education) | Delivered by: N/A | ||
| Cognitive functioning: low | n = 3 | n = 3 | ||
| Romano (2002)97 | Setting: special education, USA | Story characteristics: > two stories per child; written story and photographs | Story characteristics: no social story | Frequency of behaviours |
| Age (years): 4–8 | Timing: 50 times per week, over 30 days | Timing: N/A | ||
| Gender: 50% male | Developed by: NR | Developed by: N/A | ||
| Diagnosis: ASD mixed | Delivered by: teacher (special education) | Delivered by: N/A | ||
| Cognitive functioning: NR | n = 5 | n = 5 |
With the exception of one study91 conducted in Egypt, all of the studies were conducted in the USA. Three of the four randomised studies92–94 conducted the social story under experimental conditions; the remaining randomised between-group study95 did not report details of the setting. The three non-randomised designs91,96,97 were conducted in educational settings.
The gender of the participants was not reported in three studies. 91–93 In the remaining four, three94–96 of the samples were predominantly or entirely male, one study97 had an equal balance. The studies were conducted in a range of age groups. Five of the studies91–94,96 were conducted with children diagnosed with autism and two95,97 had a mix of ASD diagnoses. The participants were coded as having low cognitive functioning in all of the studies in which this was reported.
In terms of the characteristics of the social stories, all four of the randomised designs92–95 used one story per child. Two96,97 of the non-randomised designs used more than two stories per child (details not reported in the third study91). Three studies92,94,95 used a written format alone and three93,96,97 used a combination of written story and photographs (data not reported in one study91). The stories were all delivered over 1 day in the four randomised designs;92–95 this is in contrast to two of the non-randomised designs,96,97 which used interventions over 1 month. In the four randomised designs92–95 the research team developed the stories and delivered the stories. Information about who developed the stories was not given in the three non-randomised designs;91,96,97 teachers delivered the story in two96,97 of the three non-randomised studies (details were not given in the third study91).
The comparator used in the randomised designs was a story without a social loading. In the non-randomised designs, two studies96,97 did not use any form of story and details were not reported in the third. 91
Table 9 summarises the extent to which the between-group randomised designs adhered to Social Story criteria; Table 10 summarises the same for the non-randomised designs. For the randomised designs, all four studies92–95 met the criteria for at least 10 of the 15 items. For three items, the information was coded as not reported in all four studies. For the remaining criteria, the studies varied in the extent to which the criteria were met. All four studies stated that they followed Gray’s criteria; however, two of these studies94,95 did not meet the criterion for avoiding ‘should’ and ‘must’, and one study92 did not meet the criteria for correct balance of sentences.
| Study | Positive goal | Information gathered | Structured story | Tailored for ability/attention | Tailored for interest | ‘Wh’ questions answered | Listed sentence types | Balance of sentence types | First/third person statements | Non-authoritarian | Avoids should/must | Literally accurate | Story edited | Appropriate setting | Introduced appropriately | Guideline statement |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andrews (2004)92 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | ✓ |
| Bader (2006)93 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ |
| Feinberg (2001)94 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | NR | ✓ |
| Quirmbach (2009)95 | ✓ | NR | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | NR | ✓ | NR | ✓ |
| Study | Positive goal | Information gathered | Structured story | Tailored for ability/attention | Tailored for interest | ‘Wh’ questions answered | Listed sentence types | Balance of sentence types | First/third person statements | Non-authoritarian | Avoids should/must | Literally accurate | Story edited | Appropriate setting | Introduced appropriately | Guideline statement |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ali (2010)91 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Ricciardelli (2006)96 | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✗ | NR | NR | NR | NR |
| Romano (2002)97 | NR | NR | ✓ | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | NR | NR | NR | NR | NR | ✓ |
For the three non-randomised designs,91,96,97 the level of reporting was not as clear. One of these studies91 provided little detail of the story, so all criteria were rated as not reported. For the Romano study97 the majority of items were also rated as not reported, although for the remainder the criteria were met. For the remaining study,96 the picture was more mixed.
Other studies
The remaining 15 studies described the use of a social story, but did not use either a single-case design or a between-groups design. Table 11 summarises the descriptive characteristics of these studies. Unlike the other designs, the majority of the remaining studies were not conducted in the USA and approximately half98–104 were conducted in the UK. In four studies98,101,105,106 the intervention was delivered at home and in seven100,102–104,107–109 in an educational setting. One study110 used a dental setting and three studies99,111,112 did not provide these details.
| Study | Setting and sample | Details of social story | Outcome |
|---|---|---|---|
| Backman (1999)110 | Setting: dental setting, Sweden | Story characteristics: one story per child, written | Category: other |
| n = 1 | Timing: NR | Subcategory: emotional development | |
| Age (years): 9 | Developed by: NR | ||
| Gender: male | Delivered by: NR | ||
| Diagnosis: Asperger | |||
| Cognitive functioning: average | |||
| Botha (2009)98 | Setting: home, UK | Story characteristics: one story per child; written story and photograph | Category: social communication |
| n= 3 | Timing: NR | Subcategory: initiations and requests | |
| Age (years): 8–10 | Developed by: research team | ||
| Gender: three males | Delivered by: parents | ||
| Diagnosis: ASD | |||
| Cognitive functioning: NR | |||
| Bracke (2008)107 | Setting: general education, USA | Story characteristics: one story per child, nine sentences; written story and illustrations | Category: social ability |
| n = 1 | Timing: 5 minutes, twice a day | Subcategory: social awareness | |
| Age (years): NR | Developed by: teacher (general education) | ||
| Gender: male | Delivered by: teacher (general education) | ||
| Diagnosis: Asperger | |||
| Cognitive functioning: NR | |||
| Camire (2011)105 | Setting: home, France | Story characteristics: one story per child, written story, photographs, illustrations and computer media | Category: restricted behaviours, other |
| n = 2 | Timing: once per day | Subcategory: restricted, repetitive patterns of behaviour/interests, emotional development | |
| Age (years): 14–15 | Developed by: research team, parents | ||
| Gender: one male, one female | Delivered by: research team, parents | ||
| Diagnosis: PDD-NOS | |||
| Cognitive functioning: NR | |||
| Chapman (2000)99 | Setting: NR, UK | Story characteristics: one story for each day; written story and illustrations | Category: restricted behaviours |
| n = 1 | Timing: approximately two times per day | Subcategory: restricted, repetitive patterns of behaviour/interests | |
| Age (years): 14 | Developed by: NR | ||
| Gender: male | Delivered by: NR | ||
| Diagnosis: ASD | |||
| Cognitive functioning: NR | |||
| Choi (2008)108 | Setting: general education, Australia | Story characteristics: written story | Category: social communication |
| n = 1 | Timing: once per day, over 4 weeks | Subcategory: general communication skills | |
| Age (years): 8 | Developed by: teacher (general education) | ||
| Gender: male | Delivered by: NR | ||
| Diagnosis: Asperger | |||
| Cognitive functioning: NR | |||
| Dentato (2006)109 | Setting: special education, USA | Story characteristics: > two stories per child, 10–12 sentences; written story | Category: social communication |
| n = 1 | Timing: NR | Subcategory: general communication skills | |
| Age (years): 12 | Developed by: teacher (special education) | ||
| Gender: male | Delivered by: teacher (special education) | ||
| Diagnosis: autism | |||
| Cognitive functioning: NR | |||
| Moffatt (2001)100 | Setting: general education, UK | Story characteristics: one story per child, 7–12 sentences; written story and illustrations | Category: other |
| n = 2 | Timing: once per day | Subcategory: life skills | |
| Age (years): 8–14 | Developed by: teacher (general education) | ||
| Gender: two males | Delivered by: NR | ||
| Diagnosis: ASD | |||
| Cognitive functioning: NR | |||
| Moore (2004)101 | Setting: home, UK | Story characteristics: one story per child, 16 sentences; written story and illustrations | Category: other |
| n = 1 | Timing: two times per day | Subcategory: life skills | |
| Age (years): 4 | Developed by: NR | ||
| Gender: male | Delivered by: parent | ||
| Diagnosis: ASD | |||
| Cognitive functioning: low | |||
| O’Connor (2009)102 | Setting: general education, UK | Story characteristics: one story per child, DVD and printed format of DVD | Category: social communication |
| n = 1 | Timing: three times per week | Subcategory: turn-taking | |
| Age (years): NR | Developed by: teacher (general education) | ||
| Gender: NR | Delivered by: target student | ||
| Diagnosis: autism | |||
| Cognitive functioning: low | |||
| Rogers (2001)111 | Setting: NR, USA | Story characteristics: two stories per child, 6–8 sentences; written story and illustrations | Category: restricted behaviours |
| n = 1 | Timing: once a day | Subcategory: restricted, repetitive patterns of behaviour/interests | |
| Age (years): 14 | Developed by: teacher (special education), research team | ||
| Gender: male | Delivered by: target student | ||
| Diagnosis: Asperger | |||
| Cognitive functioning: NR | |||
| Rowe (1999)103 | Setting: general education, UK | Story characteristics: one story per child, 13 sentences; written story | Category: social ability |
| n = 1 | Timing: NR | Subcategory: social interest | |
| Age (years): NR | Developed by: NR | ||
| Gender: male | Delivered by: NR | ||
| Diagnosis: Asperger | |||
| Cognitive functioning: NR | |||
| Sotelo (2010)112 | Setting: NR, USA | Story characteristics: NR | Category: social ability |
| n = 18 | Timing: NR | Subcategory: various | |
| Age (years): 4–6 | Developed by: NR | ||
| Gender: NR | Delivered by: NR | ||
| Diagnosis: ASD | |||
| Cognitive functioning: NR | |||
| Thorne (2005)104 | Setting: special education, UK | Story characteristics: 10 stories, interactive white board | Category: social ability, restricted behaviours, other |
| n = 5 | Timing: three times per week, over 8 weeks | Subcategory: various | |
| Age (years): NR | Developed by: teacher (special education) | ||
| Gender: males | Delivered by: teacher (special education) | ||
| Diagnosis: ASD | |||
| Cognitive functioning: NR | |||
| Vitale (2007)106 | Setting: home, USA | Story characteristics: one story per child, written | Category: social communication |
| n = 1 | Timing: once a day, over 10 days | Subcategory: general communication skills | |
| Age (years): 8 | Developed by: research team | ||
| Gender: male | Delivered by: research team | ||
| Diagnosis: PDD-NOS | |||
| Cognitive functioning: NR |
The participants that received the intervention ranged in age from 4 to 15 years. The majority of the participants were male. The participants had a diagnosis of autism in two studies,102,109 Asperger syndrome in four103,107,108,110 and PDD-NOS in two. 105,106 In six studies98–101,104,112 the participants were described as having an ASD, but no further details were given. Few of the studies provided details of the level of cognitive functioning of the participants.
In terms of the characteristics of the Social Stories, the majority (nine) of the studies98,100–103,105–107,110 had one story per child. Five of the studies103,106,108–110 used a written format, six98–101,107,111 used a combination of written story and photographs or illustrations, and three102,104,105 used an electronic medium either alone or in combination with another format (details not reported in one study108). Details of the timing of the Social Stories were not reported in five studies. 98,103,109,110,112 In the remaining studies, the stories were read once a day in five,100,105,106,108,111 more than once a day in three99,101,107 and fewer times than once a day in two studies. 102,104 Few studies provided information on how many days the stories were read to the child, although when this was reported it was for at least a week (10 days, 4 weeks and 8 weeks). The story was developed by the research team in two studies,98,106 the research team in combination with others in two studies105,111 and teachers alone in six studies. 100,102,104,107–109 Details about the delivery of the social story were not given in six studies. 99,100,103,108,110,112 In three studies,104,107,109 a teacher delivered the stories and parents alone in two studies. 98,101 Researchers delivered the story in one study106 and the research team and others in one study. 105 In the remaining studies, the story was delivered by the child themselves. 102,111
Table 12 summarises the extent to which the 15 studies classified as other designs adhered to the Social Stories guidance. Most of the studies met the six following criteria: positive goal98–101,103–105,107,112 (67%), information gathered98,101–105,107–109,111 (67%), structured story98,100,101,103–105,107,109,112 (60%), ‘wh’ questions answered98–101,103–105,107,109,110 (67%), listed sentence type98–101,103–105,107,109,111,112 (73%) and first and third person used98–101,103–105,107,109–111 (73%). For a further four concordance items, approximately half of the studies met the criteria: balance of sentence types98,100,101,103,104,107,109,111 (53%), non-authoritarian98–101,103–105,107 (63%) and avoids should/must99,101,103–105,107,109,112 (53%).
| Study | Positive goal | Information gathered | Structured story | Tailored for ability/attention | Tailored for interest | ‘Wh’ questions answered | Listed sentence types | Balance of sentence types | First/third person statements | Non-authoritarian | Avoids should/must | Literally accurate | Story edited | Appropriate setting | Introduced appropriately | Guideline statement |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Backman (1999)110 | NR | NR | NR | NR | NR | ✓ | NR | NR | ✓ | NR | NR | NR | ✓ | NR | NR | NR |
| Botha (2009)98 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | NR | NR | ✓ | NR |
| Bracke (2008)107 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | NR | ✓ |
| Camire (2011)105 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Chapman (2000)99 | ✓ | NR | ✗ | NR | NR | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | NR |
| Choi (2008)108 | ✗ | ✓ | NR | NR | NR | NR | NR | NR | NR | ✗ | NR | NR | NR | NR | NR | NR |
| Dentato (2006)109 | ✗ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | NR | NR | ✓ |
| Moffatt (2001)100 | ✓ | NR | ✓ | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | NR | ✓ | NR | ✓ |
| Moore (2004)101 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | NR | ✓ | NR | NR |
| O’Connor (2009)102 | NR | ✓ | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | ✓ | NR | NR | ✓ |
| Rogers (2001)111 | ✗ | ✓ | NR | NR | NR | NR | ✓ | ✓ | ✓ | ✗ | ✗ | ✗ | ✓ | NR | NR | ✓ |
| Rowe (1999)103 | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | NR | NR | NR | ✓ |
| Sotelo (2010)112 | ✓ | NR | ✓ | NR | NR | ✗ | ✓ | ✗ | ✗ | ✗ | ✓ | ✗ | NR | NR | NR | NR |
| Thorne (2005)104 | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | NR | NR | ✓ |
| Vitale (2007)106 | NR | NR | NR | NR | ✗ | NR | NR | NR | NR | NR | NR | NR | NR | ✓ | NR | NR |
For another five criteria, the majority of studies were rated as not reported; these were tailored for ability98–100,102–104,108,110–112 (67%), tailored for interest98,99,102,103,108–112 (60%), story edited98–101,103,104,106–108,112 (67%), appropriate setting98,99,102–104,108–112 (67%) and introduced appropriately99–104,106,108–112 (87%). For the final criterion, literally accurate, four studies98,103,111,112 did not meet this criterion, six studies99,100,104,105,107,109 did and the remainder were coded as not reporting the information.
Just over half of the studies100,102–105,107,109,111 made a statement that Gray’s criteria were followed (53%). However, similar to the findings on the concordance of the other study designs to the criteria, only five studies101,102,105,107,110 (33%) had no ratings of ‘not meeting the criteria’ in any category and only three101,105,107 of these (20% of the total number of studies) were rated as meeting 10 or more of the 15 criteria. No study met all criteria.
Summary of overview of practice
Many of the included studies were conducted in the USA. Few studies that used either a single-case or between-groups design were based in the UK. The majority of studies were conducted in educational settings across the designs. The randomised between-groups studies were the exception; these were conducted predominantly under experimental conditions, which may limit the extent to which the findings from these can be generalised to clinical or educational settings.
Across the study designs the participants were predominantly male and included a range of ages. Autism was the most common diagnosis in both the single-case and between-groups designs. The level of cognitive functioning was commonly not reported in studies, but when it was reported a substantial proportion of the participants were described as having low levels of functioning.
There was substantial variation in the characteristics of the social stories used within and across designs, although some commonalities do exist. Many studies used one story per child and a written format was by far the most frequent, although often this was supported by either photographs or illustrations. The median length of the intervention in the single-case studies was 28 days; this was comparable to the duration in the non-randomised between-groups designs. The other designs, when duration was reported, all used the stories over a week. This contrasts with the between-group randomised designs in which the intervention was conducted in a single day. Again, this reflects the experimental nature of these study designs, as does the development and delivery of the story. In the four randomised between-groups designs the stories were developed and delivered by the researchers alone. 92–95 In these four studies, a standard story was delivered to all children rather than developing one tailored to the children, a potential major limitation of these designs given that this tailoring is seen as a key component of an effective social story and one of Gray’s criteria. In the single-case designs, the majority of the studies were not developed by the researchers alone or delivered by the researchers alone. For the other designs and the non-randomised between-groups designs researchers did not dominate the development and delivery in this way either. This may further indicate limits in external validity for the four randomised designs.
The second part of the overview of practice examined the extent to which the development and delivery of the social stories adhered to best-practice guidance. Within and across the different study designs, there was substantial variation in the extent to which these criteria were met, although some general themes can be discerned. For only a small number of the guidance items are the criteria met by the majority of the studies across the designs (e.g. structured story, listed sentence types or first and third person used) and for a small additional number the criteria are predominantly met for single-case designs, which contributes by far the largest number of studies, although the pattern is less clear for the remaining designs. A lack of detail about the development and delivery of the social stories meant that a coding of not reporting was common, in particular for some items for which it made up the majority of coding across designs (i.e. tailored for interest, story edited and introduced appropriately). The findings across designs indicate that although most studies report following Gray’s3 criteria a majority of studies were rated as not meeting at least one of the criteria and only a small proportion of these studies meet the majority of criteria.
Evaluation of clinical effectiveness
The second phase of the review examined the clinical effectiveness of those studies that used a single-case or between-groups design. This included an assessment of the methodological quality of the studies to contextualise the observed effects of the intervention followed by an examination of the effectiveness.
Single-case designs
Quality assessment of single-case design studies
Table 13 summarises the results of the quality assessment of the 77 single-case design studies5–14,24–90 using the SCED. 19 For four of the items, most studies (over 90%) met the quality assessment criteria. Most studies provided sufficient information on the demographic and other important characteristics of the research participants so that a judgement could be made about the applicability of the treatment to other people (clinical history item). Studies also typically had sufficient sampling of behaviour during the pre-treatment phase to establish an adequate baseline (baseline item) and did the same during the treatment phase (sampling behaviour during treatment item). Most studies also met the replication criterion in that they established that the results of the intervention are not limited to a specific individual or situation.
| Author | Clinical history | Target behaviours | Design | Baseline | Sampling during treatment | Raw data record | Inter-rater reliability | Independent assessment | Statistical analysis | Replication | Evidence for general |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abraham (2004)27 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | ✓ |
| Adams (2004)11 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✗ | NR |
| Agosta (2004)28 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✗ | ✗ |
| Antle (2007)76 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | ✗ | ✗ | ✓ | NR |
| Bailey (2008)56 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | ✓ |
| Barry (2004)6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Beh-Pajooh (2011)57 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Bell (2005)58 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Bernad-Ripoll (2007)77 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | ✗ | ✗ | ✗ | NR |
| Bledsoe (2003)8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✗ | NR |
| Brownell (2002)29 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Chan (2005)78 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Chan (2008)30 | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Chan (2009)89 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Cihak (2012)31 | ✓ | ✓ | ✗ | ✗ | ✗ | ✗ | ✓ | NR | ✗ | ✓ | NR |
| Crozier (2005)32 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✗ | NR |
| Crozier (2007)12 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Cullain (2000)90 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | ✗ | ✗ | ✓ | NR |
| Daneshvar (2006)79 | ✗ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Delano (2006)13 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Demiri (2004)33 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Dodd (2008)80 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Eckelberry (2007)34 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | NR | ✗ | ✓ | NR |
| Gilles (2008)81 | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ | NR | NR | ✓ | ✓ | ✓ |
| Graetz (2003)59 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Hagiwara (1999)60 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Hanley (2008)35 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Hobbs (2003)24 | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ | NR | NR | ✓ | ✓ | ✓ |
| Holmes (2007)36 | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | NR | NR | ✗ | ✗ | NR |
| Hung (2011)37 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✗ | NR |
| Hutchins (2006)82 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | ✗ | ✗ | ✓ | NR |
| Ivey (2004)14 | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Keyworth (2004)38 | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Kuoch (2000)39 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Kuttler (1998)10 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Lorimer (2002)9 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✗ | NR |
| Mandasari (2011)61 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Mancil (2009)62 | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ | NR | NR | ✗ | ✓ | NR |
| Hsu (2009)40 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Norris (1999)5 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | ✗ | ✗ | ✗ | NR |
| Okada (2008)63 | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Okada (2010)64 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | ✗ | ✗ | ✓ | NR |
| Ozdemir (2008)41 | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Ozdemir (2008)7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Pasiali (2004)83 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | NR |
| Powell (2009)84 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Quilty (2007)42 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Reichow (2009)43 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✗ | NR |
| Reynhout (2007)65 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✗ | ✓ |
| Reynhout (2008)66 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | NR | ✓ | ✗ | NR |
| Sansosti (2006)44 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Sansosti (2008)45 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ |
| Scapinello (2009)85 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Scattone (2002)67 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Scattone (2006)68 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Scattone (2008)86 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✗ | ✓ |
| Schneider (2010)46 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | NR |
| Scurlock (2008)47 | ✓ | ✗ | ✗ | ✓ | ✓ | ✓ | NR | NR | ✗ | ✗ | NR |
| Smith (2004)48 | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | ✓ |
| Staley (2001)69 | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Styles (2009)25 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Swaggart (1995)70 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | NR | NR | ✗ | ✓ | NR |
| Swaine (2004)49 | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | ✓ | NR | ✗ | ✓ | ✓ |
| Tarnai (2009)87 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Tarnai (2011)88 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ |
| Taylor (2009)50 | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ | NR | NR | ✗ | ✓ | ✓ |
| Thiemann (2001)51 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | NR |
| Travis (2006)71 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | ✓ | NR | ✓ | ✓ | NR |
| Vanderhoek (2004)52 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | NR | ✗ | ✗ | NR |
| Voges (2009)26 | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | ✗ | ✗ | ✗ | NR |
| Washburn (2006)53 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Washburn (2006)72 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | NR | ✗ | ✓ | NR |
| Watts (2008)73 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | NR |
| Wheeler (2005)74 | ✓ | ✗ | ✗ | ✗ | ✓ | ✗ | NR | NR | ✗ | ✓ | NR |
| Wilkinson (2010)54 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✗ | ✓ | ✓ |
| Wright (2007)55 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ✓ | ✓ | NR |
| Xin (2011)75 | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | NR | NR | ✗ | ✓ | NR |
For a further four items, approximately three-quarters of studies met the criteria. These included the identification of a precise, repeatable and operationally defined behaviour that can be used to measure treatment success (target behaviour), the use of a design that permits a causal inference (design), the reporting of an accurate representation of the variability of the target behaviour (raw data record) and the reliable assessment of the target behaviour (inter-rater reliability).
For the remaining three items, the majority of studies did not meet criteria or the study did not provide sufficient detail to rate the item. Data on the independence of assessment, the use of an observer who is independent of the study to carry out assessments, was coded as not reported for approximately two-thirds (64%) of the studies; the other third did not meet this criterion. Eighty-two per cent of the studies did not report a suitable analysis to compare the results over the study phases (statistical analysis criterion). Finally, approximately three-quarters (77%) of the studies were coded as not reported for the evidence for generalisation criterion, which assesses whether or not the study has established if the utility of treatment extends to other areas of the child or young person’s life.
Single-case studies: clinical effectiveness
Of the 77 single-case designs studies,5–14,24–90 data could not be extracted from five24,50,61,69,81 because of poor reproduction of graphs. There were an additional 23 graphical summaries that could not be used to make a calculation of effect because the studies did not report either a baseline or an intervention phase. Of the remaining 307 behaviour graphs, only 144 (47%) examined a challenging behaviour as defined in the method section; however, all graphs were included to give a comprehensive measure of effect.
Table 14 provides a summary of the clinical effectiveness. As described under the data synthesis section, results were grouped on the basis of four broad categories of target behaviours (social, communication, restricted behaviours, other) and, when necessary, further divided into subcategories. Within each of the subcategories, a study may have included more than one participant, and in some cases a participant may have contributed data on more than one target behaviour within a subcategory. Data are summarised at the level of the target behaviour within each subcategory.
| Category | Subcategory | Number of studies, participants and target behaviours | % of target behaviours meeting effectiveness criteria using PND (n/N) | % of target behaviours meeting effectiveness criteria using PEM (n/N) |
|---|---|---|---|---|
| Social | Social attention and non-verbal communication | Five studies | Highly effective: 15% (2/13) | Highly effective: 46% (6/13) |
| Eight participants | Moderately effective: 15% (2/13) | Moderately effective: 15% (2/13) | ||
| 13 target behaviours | ||||
| Social awareness | 29 studies | Highly effective: 19% (11/58) | Highly effective: 39% (23/58) | |
| 41 participants | Moderately effective: 17% (10/58) | Moderately effective: 21% (12/58) | ||
| 58 target behaviours | ||||
| Social interest | Nine studies | Highly effective: 5% (1/22) | Highly effective: 23% (5/22) | |
| 16 participants | Moderately effective: 23% (5/22) | Moderately effective: 32% (7/22) | ||
| 22 target behaviours | ||||
| Communication | General communication skills | 12 studies | Highly effective: 19% (6/32) | Highly effective: 38% (12/32) |
| 27 participants | Moderately effective: 16% (5/32) | Moderately effective: 25% (8/32) | ||
| 32 target behaviours | ||||
| Initiation and requests | 13 studies | Highly effective: 49% (18/37) | Highly effective: 68% (25/37) | |
| 26 participants | Moderately effective: 8% (3/37) | Moderately effective: 8% (3/37) | ||
| 37 target behaviours | ||||
| Turn-taking | Five studies | Highly effective: 29% (4/14) | Highly effective: 57% (8/14) | |
| 10 participants | Moderately effective: 14% (2/14) | Moderately effective: 14% (2/14) | ||
| 14 target behaviours | ||||
| Unusual voice modulations and vocalisations | 11 studies | Highly effective: 14% (3/21) | Highly effective: 62% (13/21) | |
| 18 participants | Moderately effective: 38% (8/21) | Moderately effective: 14% (3/21) | ||
| 21 target behaviours | ||||
| Restricted behaviours | Restricted, repetitive patterns of behaviour/interests | 14 studies | Highly effective: 13% (4/32) | Highly effective: 50% (16/32) |
| 20 participants | Moderately effective: 13% (4/32) | Moderately effective: 19% (6/32) | ||
| 32 target behaviours | ||||
| Other | Emotional development | 20 studies | Highly effective: 28% (9/32) | Highly effective: 63% (20/32) |
| 24 participants | Moderately effective: 16% (5/32) | Moderately effective: 9% (3/32) | ||
| 32 target behaviours | ||||
| Life skills | 13 studies | Highly effective: 9% (3/32) | Highly effective: 50% (16/32) | |
| 25 participants | Moderately effective: 31% (10/32) | Moderately effective: 31% (10/32) | ||
| 32 target behaviours | ||||
| Sustained attention | Eight studies | Highly effective: 0% (0/11) | Highly effective: 9% (1/11) | |
| Nine participants | Moderately effective: 9% (1/11) | Moderately effective 9% (1/11) | ||
| 11 target behaviours |
Two estimates of effectiveness are reported: the PND21 and the PEM. 22 These are described in greater detail in the method section. As also described in that section, Scruggs and colleagues21 recommend that a PND of ≥ 90% indicates that an intervention is highly effective and a PND of ≥ 70% to < 90% indicates moderate effectiveness. Others22 have applied the same criteria to the interpretation of PEM values and this approach was also used here.
As Table 14 indicates, the assessment of effectiveness based on PND criteria indicates substantial variability between subcategories, although predominantly less than half of the target behaviours met the criteria for highly effective or moderately effective. In contrast, the assessment based on PEM presents a largely positive picture with many target behaviours meeting the criteria for highly or moderately effective, the sole exception being sustained attention.
Quality assessment of between-groups designs
The four between-group studies92–95 that used some form of randomisation procedure scored similarly on the Cochrane risk of bias quality assessment tool,20 as summarised in Table 15. Although all four reported using randomisation, none provided further details of the method used, so it was not possible to determine whether or not the study used an appropriate randomisation technique that would minimise the likelihood of selection bias. For this reason, all were rated as unclear on this quality criterion. None of the studies reported on the use of allocation concealment methods, so again all were rated as unclear. Blinding of participants and personnel is typically impossible in studies of psychological interventions, so all were rated as at risk of bias on this criterion. Blinding of outcome assessment, however, is possible, and all of the studies,92,94,95 with the exception of Bader93 reported the use of appropriate methods to ensure such blinding. All of the studies92–95 appeared to report on all or the vast majority of the children and young people assigned to either the experimental or control condition, so met the quality criterion for complete reporting of outcome data. All were rated as at unclear risk of bias for selective outcome reporting, because none reported a pre-published protocol in which all outcomes were specified or provided a clear statement to this effect in the text.
| Study | Selection bias: random sequence generation | Selection bias: allocation concealment | Performance bias: blinding of participants and personnel | Detection bias: blinding of outcome assessment | Attrition bias: incomplete outcome data | Reporting bias: selective reporting | Other sources of bias |
|---|---|---|---|---|---|---|---|
| Andrews (2004)92 | ? | ? | ✗ | ✓ | ✓ | ? | ✓ |
| Bader (2006)93 | ? | ? | ✗ | ? | ✓ | ? | ✓ |
| Feinberg (2001)94 | ? | ? | ✗ | ✓ | ✓ | ? | ✓ |
| Quirmbach et al. (2009)95 | ? | ? | ✗ | ✓ | ✓ | ? | ✓ |
The three non-randomised studies91,96,97 were also assessed using the Cochrane risk of bias tool, as summarised in Table 16, although it was not possible, given the nature of their study designs, to evaluate the studies on random allocation and allocation concealment. All three studies met the criterion for complete reporting of outcome data. However, the studies were rated as either not meeting the criterion or as unclear for the two questions related to blinding and selective reporting.
| Study | Selection bias: random sequence generation | Selection bias: allocation concealment | Performance bias: blinding of participants and personnel | Detection bias: blinding of outcome assessment | Attrition bias: incomplete outcome data | Reporting bias: selective reporting | Other sources of bias |
|---|---|---|---|---|---|---|---|
| Ali (2010)91 | N/A | N/A | ✗ | ? | ✓ | ? | ✓ |
| Ricciardelli (2006)96 | N/A | N/A | ✗ | ✗ | ✓ | ? | ✓ |
| Romano (2002)97 | N/A | N/A | ✗ | ✗ | ✓ | ? | ✓ |
Between-groups designs: clinical effectiveness
Effect sizes estimates could be calculated for only two93,94 of the four randomised designs. One study92 reported sufficient data to make the calculations, but the data were substantially non-normal, so effect sizes were not estimated. In the Andrews study92 participants were randomised to a social story condition or a control condition that used a story with no social loading to examine the impact on social skills related to game playing. Results for this study are based on the statistical analysis reported by the author, although caution is needed given the use of a parametric test [analysis of variance (ANOVA)] when assumptions of normality are likely to be violated. The study used a two (condition) by six (time) repeated measures ANOVA and reported a significant trial by condition interaction for four of the five outcome measures (game playing, initiation of game playing, turn taking and enjoyment in game playing), the exception being continued desire for interaction.
A further study95 did not report sufficient data on the control condition to estimate effect sizes. This study compared three conditions (standard story, directive story, control story) and, as with Andrews study,92 examined the impact on social skills related to playing a game. Again, the results are based on those reported by the authors, because it was not possible to calculate effect sizes. A three (condition) by four (time) repeated measures ANOVA was conducted with total game playing skills as the dependent variable. The ANOVA indicated a significant condition by time interaction with both social story groups (standard and directive) demonstrating greater improvement in game-playing skills than those who received the control story.
Feinberg94 also examined the effect of social stories on game-playing abilities and again compared a social stories intervention with a story that had no social loading. For this study it was possible to calculate an effect size. For the total social skills score, the effect size (Hedges’ g) was 1.21 [95% confidence interval (CI) 0.48 to 1.94]. The final randomised between-groups design93 examined the impact of social stories on the learning of facial emotions. Participants were randomised to either a social story or a story without a social loading. The effect size (Hedges’ g) for affect discrimination was 1.38 (95% CI 0.38 to 2.38), for emotion matching was 1.73 (95% CI 0.68 to 2.79) and for affect choice was 2.13 (95% CI 1.01 to 3.26).
It also proved difficult to calculate meaningful estimates of effects for the three between-group non-randomised designs. 91,96,97 Two of the studies96,97 had very small sample sizes. Ricciardelli96 had three participants in each of the two groups and Romano97 had five in each group, which is likely to make any standard method of quantifying a between-group difference difficult to interpret. Ricciardelli96 compared social stories combined with a social skills curriculum with the curriculum alone. Differences between the groups were not detected on most outcome measures, although it is difficult to interpret any between-group differences given the very small sample size. Differences were detected on one variable, maintaining attention, but again this is difficult to interpret given that the ratings were made by teachers who were not blind to the treatment conditions. The Romano study97 examined the impact of social stories on communication, socialisation and aggression, and reported benefits for those receiving the intervention. Again, the raters were not blind to the conditions making interpretation difficult. The study by Ali91 was larger (although only in relative terms; n = 15 in each condition), so is still likely to be substantially underpowered. The reporting in this study made it difficult to estimate effect sizes, although the author did report that the intervention had a significant effect on communication skills.
Discussion
Social stories have been used in a variety of settings and to help children and young people make a wide range of behavioural changes. The evidence is predominantly based in the USA; this places some limitations on the extent to which the results are generalisable to other countries such as the UK. Across all studies there was variation in the extent to which studies met Gray’s criteria.
Interpreting the results of the large number of single-case studies is difficult. A surprising finding was that the majority of the target behaviours were positive or pro-social in nature (53%) behaviours as opposed to challenging behaviours. Unlike between-groups designs, there is no commonly agreed metric for quantifying the results of single-case designs. The results differed according to whether the PND21 or PEM22 method was used, with substantially fewer target behaviours meeting the criteria for highly or moderately effective when the PND method was used. However, as described in the methodology section, the PND calculation relies on a single baseline data point, which may limit its usefulness in providing an accurate estimate of the effectiveness of an intervention. The PEM results broadly supported the effectiveness of the intervention, with the majority of target behaviours meeting criteria for highly or moderately effective. These broadly positive findings, however, need to be placed in the context of the assessment of single-case design quality, as assessed by the SCED. 19 The majority of single-case designs were either rated as not meeting the criterion or the information was not reported for the independence of assessment item. This item assesses whether or not an observer who is independent of the study was used to conduct outcome assessments. It is possible, therefore, that the observed effect of the single-case studies is artificially inflated because raters were not independent of the study and may, therefore, have an interest in finding a positive result.
There was only a small number of between-groups designs91–97 (n = 7) and only four92–95 of these used some form of randomisation procedure. Although these studies appear to provide broadly supportive evidence of an effect of the social stories interventions, the findings from the studies are compromised in a number of ways. There were gaps in the reporting of results, which made it difficult to quantify the level of effect of the intervention. There was also insufficient information to assess a number of important sources of potential bias as measured by the Cochrane risk of bias tool. 20 A further problem, particularly for the four randomised designs, is the use of experimental conditions for the intervention. While this may have benefits in limiting extraneous factors and so protect internal validity, the interventions used may be better considered as analogues of social stories rather than social stories as would be used in practice. In the randomised designs92–95 the interventions were often delivered over a much shorter time frame than was typically used in the single-case designs, and the intervention was a standard one, rather than individually tailored to the child or young person, a practice that breaches the criteria defining Social Stories.
There are a large number of single-case studies that provide some evidence for the effectiveness of social story interventions, although as described above, there are some caveats to this. In contrast, there are very few studies that use a between-groups design and what evidence there is has a number of substantial limitations. The implications of the findings of this review for the development of the intervention are discussed in Chapter 5.
Conclusions
-
The research into social stories is predominantly based in the USA.
-
Very few studies looked at the effectiveness of social stories on children over 12 years old.
-
There was very little collaboration recorded between researchers, teachers and parents in the studies.
-
Although a large proportion of studies claimed to use Social Stories and follow all of Gray’s criteria, there was variation in the extent to which the studies met them when stories used in the studies were examined by reviewers. Many studies did not give enough information to be clear the criteria were being used.
-
The majority of the target behaviours were positive or pro-social in nature (53%) as opposed to challenging behaviours. This suggests that an appropriate measure of effect for the trial should encompass both challenging behaviour and positive behaviours.
-
The review of the single-case studies broadly supported the effectiveness of the intervention. However, the majority of these studies were rated as not meeting the criterion for the independence of assessment item on the SCED.
-
The review of the between-groups studies appears to provide broadly supportive evidence of an effect of the social stories interventions. However, there were gaps in the reporting of results and insufficient information to assess a number of important sources of potential bias as measured by the Cochrane risk of bias tool.
-
The interventions in the randomised designs were often delivered over a much shorter time frame than was typically used in the single-case designs, and the interventions used were standard ones, rather than individually tailored to each child. In this and some other important regards, this meant that they were not fulfilling Gray’s criteria.
Chapter 3 Phase 1: the process of developing the intervention
Background
In this chapter, the characteristics, role and purpose of the three different groups involved in the development of the intervention are outlined. The process by which the views of each of these groups were integrated in the final version of the intervention is also described (see Figure 2).
Objectives
-
To develop a manual and training package for Social Stories that could be used in mainstream schools and could be evaluated in the feasibility study.
Component groups
User groups
These groups consisted of users of Social Stories whose views were obtained through a series of qualitative interviews and focus groups (see Chapter 4). Users in this context included parents (or carers), teachers, health professionals and young people with ASD. The role of these groups was to express to a qualitative researcher their experiences of and beliefs around the writing and delivery of Social Stories. There were two stages of this process. The objectives of each of these stages were:
-
to gather information relating to the optimum design and use of Social Stories for children with ASD
-
to explore the views of users on whether the intervention can feasibly be delivered in this particular context and to ensure the intervention is acceptable to service users and providers.
Expert panel
The expert panel comprised people with knowledge of Social Stories, training delivery in a Child and Adolescent Mental Health Service (CAMHS) setting, and ASD. It also consisted of three PPI representatives (two parents of children with ASD and a representative from the National Autistic Society) and the qualitative researcher who analysed the findings from the user groups (see Chapter 4). Their role was to support a writing group to develop a Social Stories training package including a manual by evaluating, marshalling and representing the evidence and information from the systematic review, user group feedback and the thematic analysis from the qualitative researcher. The objectives of the expert panel were:
-
to provide expert opinions on the creation and use of Social Stories
-
to synthesise and evaluate the information arising from the systematic review and user groups and present this to the writing group
-
to review drafts of the manual at regular intervals to ensure that the findings from the systematic review and the views of the user groups had been represented appropriately.
Expert writing group
The expert writing group comprised a subset of those on the expert panel. It had five members including Carol Gray and two PPI representatives. Their role was to take direct responsibility for the writing of the manual and assembling the training package from the recommendations of the expert panel. The objectives of the expert writing group were:
-
to produce a manual on writing and using Social Stories based on information gained from the systematic review, the expert opinions, user group feedback and the thematic analysis from the qualitative researcher
-
to produce a training package to teach how to write and use Social Stories which will also provide familiarisation with the manual.
The process
An iterative approach was used in which Social Story users in the user groups were interviewed and this information was fed back to the expert panel by the qualitative researcher. Once this information was considered by this panel they would ask the qualitative researcher to elicit more responses from the user groups and ask for feedback on drafts of the manual they had completed. The user group and expert panel were conducted separately at the request of PPI representatives as a mechanism for ensuring that their voices were not drowned out by clinicians or academics. The important need to bring the groups together was met by three mutually agreed meetings where two representatives of each user group, parents and professionals (see Chapter 5) were given opportunities to speak directly to the expert panel.
Once this process was complete, a final draft of the manual and training package was produced for use in a pilot study with a small number of participants (see Chapter 6). The feedback from this study was then considered by the expert panel and writing group, and subsequently represented in the final version of the manual and training package offered in the feasibility study. A graphical depiction of this process of development is shown in Figure 2.
FIGURE 2.
The process of development of the intervention.
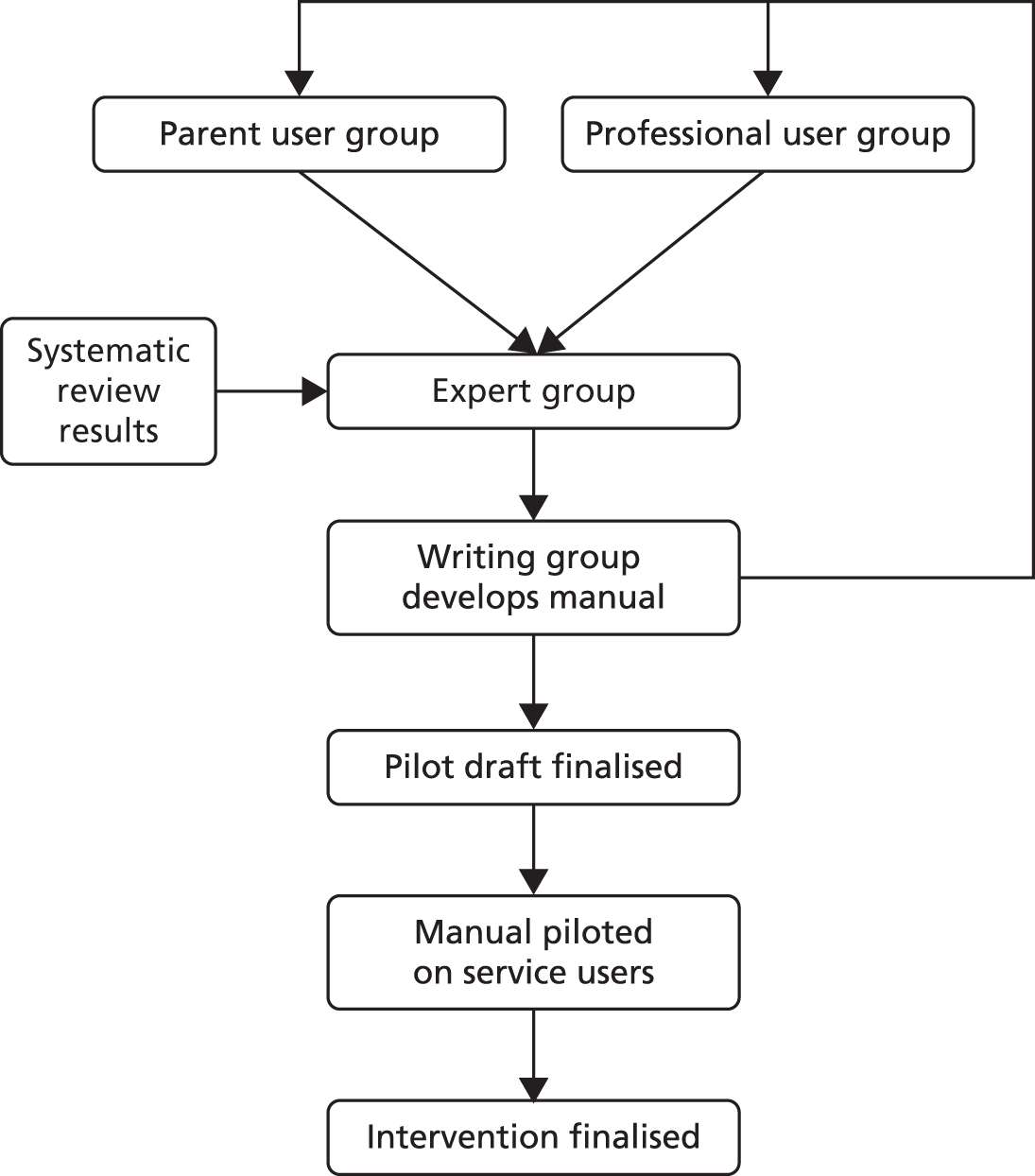
Chapter 4 Qualitative analysis of the views of Social Story users
Background
The findings of the systematic review (see Chapter 2) indicate that the research into Social Stories is predominantly based in the USA. This places some limitations on the extent to which the results are generalisable to other countries such as the UK, as there may be a cultural bias in the intervention. This phase of the development process used qualitative methods to take stock of current experience and elicit the views and experiences of various stakeholders to ensure that Social Stories could feasibly be delivered in this particular context and that they are acceptable to users and providers in the UK.
Objectives
The overall aims of the qualitative element of the research were:
-
to gather information relating to the optimum design and use of Social Stories for children with ASD
-
to explore the views of users on whether the intervention can feasibly be delivered in this particular context and to ensure the intervention is acceptable to service users and providers.
Methods
The qualitative research was conducted in two phases, built around the stages of the development of the Social Stories training manual (see Chapter 5).
Stage 1: preliminary data collection to inform the initial design and content of the Social Stories manual and training day (landscape interviews and focus groups).
Stage 2: feedback on content of draft chapters of the Social Stories training manual developed by the writing group (focus groups).
Stage 1: informing the design of the Social Stories manual
Landscape interviews
‘Landscape interviews’ were conducted with key informants in order to define and articulate the key concepts and ideas of relevance to the project113 and fill out the topic guide for the scheduled user focus groups. It was important that key stakeholders were represented – including parents/carers, clinicians, learning support workers and children with ASD. Participants were opportunistically selected from individuals known to two clinician members of the study team as having prior experience with the use of Social Stories. It was expected that a sample of five to ten participants would be sufficient to map out the key issues around the use of Social Stories, in order to familiarise the research team with the topic and to inform subsequent data collection in stage 1 of the qualitative research.
Semi-structured interviews were conducted, using a topic guide with adult participants (see Appendix 4). The interviews with children with ASD were more flexible which allowed the researcher to meet the individual needs of the child, and also focus on their areas of interest to aid responses.
Focus groups
In order to inform the development of the Social Stories training manual, focus groups were employed to gather information from key stakeholders. It was felt that two focus groups would be adequate to gain an understanding of participants’ experience with Social Stories and the features they would like included in a Social Stories manual. One group comprised key ‘professional’ stakeholders, the other parents and carers. From the outset it was felt that it would be preferential to separate professionals from parents, as this would allow for a range of discourse in which the parents felt more empowered to speak openly. This was suggested by PPI representatives on the steering group. Participants were purposively sampled to include representation from relevant professional groups (including psychology, teaching and speech and language therapy). For the parent group, it was important to include individuals with a range of expertise of Social Stories and with differing perceived outcomes.
Participants were not given anything to prepare, they were simply asked to come and talk about their experiences of Social Stories with others. A range of different activities broke up the focus group into distinct parts which focused around:
-
understanding of Social Stories
-
informing the content of the manual
-
informing the training package.
(See Appendix 5 for further details.)
Focus groups were held at a CAMHS unit, facilitated by the qualitative research fellow and supported by two members of the research team, one facilitating with the exercises and the other documenting turn taking of participants. A clinician who had been instrumental in the training and support groups and was familiar to the parents and professionals acted as a host to set attendees at ease and make them feel welcome. Food and drink was provided for those attending the focus groups.
Transcripts from the interviews and focus groups (including material from audio-recordings and exercises) were read and key points were coded according to a priori themes based on the topic guides using NVivo version 10 (QSR International, Warrington, UK) using a framework approach (see Appendix 6).
Stage 2: feedback on content of draft Social Stories manual developed by the writing group
Focus groups
The stage 2 focus groups followed a format similar to those in stage 1. As above, it was felt that two focus groups would elicit adequate information on the draft manual. One group comprised key ‘professional’ stakeholders, the other parents and carers. They were led by the same research team in the same location.
Stage 2 focus groups examined the following areas:
-
checking definitions and use of Gray’s3 criteria
-
discussing the different sentence types (criterion 7)
-
breaking down the manual into three components
-
considering what type of format, size and shape would be best for the manual
-
considering what types of example stories the manual needs to contain
-
discussing types of training and any issues the team need to consider.
The focus groups included similar exercises as before, such as discussion, written and oral feedback (see Appendix 7). They also incorporated a number of tactile exercises, which involved highlighting statements using stickers and using colour-coded highlighter pens, to elicit finer detail about constructing Social Stories.
The exercises and discussion invited comments on the newly created manual outline which had been developed by the writing team. In total, individuals were given three documents to comment and write on. The documents consisted of:
-
a one-page summary of the criteria for writing Social Stories
-
a seven-page synopsis of the new manual headings
-
a one-page flowchart explaining the process of creating writing and evaluating Social Stories.
The annotated sheets and transcripts from the focus groups were read, key points were coded and a number of key-word searches were conducted using NVivo using a framework approach (see Appendix 6). The key themes, based on the questions included in the topic guide, were collated and presented in a report, which was circulated and discussed amongst the writing team, in order to assist decisions about what to include in the final version of the manual.
Results
Stage 1: informing the design of the Social Stories manual (landscape interviews and focus groups)
Research participants
The landscape interviews were conducted with three parents of a child with ASD, one clinician, one learning support worker and three children with ASD.
Five people attended the teachers and professionals’ focus group: a clinical psychologist, a teaching assistant, two speech and language therapists and a specialist teacher for children with ASD. The professional group had three members who had written and used Social Stories regularly for a number of years: the teaching assistant, the specialist teacher and one of the speech and language therapists. The remaining two participants had only used Social Stories occasionally. A further five people were invited but were unable to attend.
The second focus group had five parents, two of whom had had a background in teaching. This group had two members that had used Social Stories extensively, two with some experience of their use and one who had tried them but did not feel they had been effective.
Understanding of Social Stories
Experience of Social Stories
The landscape interviews and focus groups revealed that parents, teachers and clinicians all had different levels of proficiency in using Social Stories. However, the general perception was that Social Stories were about putting into words and pictures the unwritten rules of society.
It’s what many of us would just take for granted, but it needs to be actually defined. It’s sort of the unwritten rules of society in some ways, or the expectations within a school environment.
Professionals’ focus group
It’s meant to define why you do something, what the expectation is around the behaviour.
Professionals’ focus group
Social Stories were generally regarded positively by children, parents and professionals alike. They were seen to help children understand social situations from their point of view and from the perspective of others. When used in the transcript excerpts, R refers to the researcher and INT to interviewee.
So . . . do you like them [Social Stories]?
Yes
Why do you like them?
They make things simple.
Male, primary school, child interview 2
I always think, you know, how normal children can learn from books and put themselves in them and learn from situations like that, I think autistic children sometimes, they can’t do that, so if you write them into the story and tell them what to do, then I think it’s easier.
Parents’ focus group
Social Stories were seen as a useful tool to ensure that all interested parties:
. . . have been consistent in what they are saying perhaps about a specific situation.
Professionals’ focus group
A benefit of a written Social Story is that multiple adults share a similar language, have the same ‘script’, when conveying the message and meaning to the child. It appeared to be taken for granted that Social Stories were linked with positive behaviour change.
I’m a little bit scared of writing them because I know that when they’re written well they’re very effective. So . . . when I’ve got to write a Social Story I really have to kind of whip up myself to get cracking with it.
Female, teaching assistant, landscape interview 2
Identifying behaviours to address
The focus groups identified five key areas of behaviour they felt were most important to address within school with the use of Social Stories.
-
Managing emotions to create ‘emotional calmness’: this reflects developing Social Stories which help students manage their emotions. Three main areas were identified: happiness, calmness and avoiding aggression.
-
Understanding conventional social behaviours: Social Stories help students understand conventional social behaviours and expectations relating to school activities, such as ‘listening to the teacher’ or ‘following instructions’, in addition to issues specific to certain parts of the curriculum, for example subjects for which a certain level of group interaction is required such as physical education or foreign languages.
-
Preparation for change: preparation for change needs to be present within a school environment as certain days or terms may be different. Changing routine may result in changes in behaviour. For example, changes in staff, especially teaching staff, can be problematic for a child with ASD.
-
Understanding routines: this can be further split into two main domains. Firstly, there is the school routine which includes Social Stories developed around ‘attending school’, ‘doing homework’ and ‘following timetables’. Secondly, there are personal routines, relating to managing personal care needs, such as toileting, particularly those that have an impact on school life.
-
Safety: safety will include both for the child and others around them.
These five main areas distil down many of the important areas for which Social Stories may be used within the school environment. They provide a useful way of thinking about appropriate areas for applying stories and a potential guide for the types of stories to be included in the manual.
Delivery of Social Stories
As Social Stories provide information about expectations relating to the social acceptability of behaviours, this makes them particularly suitable for use within schools, they were considered by professionals and parents alike as a useful teaching tool. The focus groups suggested there are a range of different people capable of delivering Social Stories. Examples include parents, teaching assistants, key workers or someone the child relates to contextually, such as child escort/transportation assistants. The view was that this would vary depending on which of the five behaviour areas were being addressed.
within mainstream schools it was suggested that the delivery of the Social Stories would generally be the responsibility of those who work closest with the child such as the teaching assistants.
. . . teaching assistants that work with your child on a daily basis and really got to know them really well.
Parents’ focus group
There was a strong suggestion that a quiet place within the school was best for delivering stories. The participants highlighted a number of logistical issues that need to be considered within a school which can impact on where Social Stories may be read. These include access to the child, access to a suitable quiet space without distractions and the time of day. The child participants also emphasised the need for a quiet place, as they had some concern over their peers overhearing their story.
Where is the best place to read them [Social Stories]?
I’m not sure as long as it’s not out in public.
Right . . . so . . . private?
Private.
Yeah . . . because these are your stories so you want to read them on your own.
hmmm.
. . . or with another person.
Yeah.
Female, primary school, child interview 1
the consensus was that the role of parents in the delivery of the intervention varies depending on their own resources and ability to deal with issues.
. . . teachers can want often you know, from my own sort of personal experience would like to meet with parents but again it’s not always possible [it] depends on which environment you work in. Some parents are more receptive to it and would do anything to help their child and other parents just don’t want to get involved so that’s really difficult isn’t it I think.
Parents’ focus group
Furthermore, it was suggested that the role of parents also vary depending what the Social Story is about. For example, a Social Story which is primarily located within a school (e.g. with nipping other students at playtimes) may not need to be reinforced at home. However, the professionals’ focus group suggested that a copy of the Social Story should be sent home as a matter of course, so that the parents know about possible interventions and are aware of any issues. The parents likewise would prefer information to be sent home.
I think that they should be sent out like with their homework books and things like that and ask for them to read them over again.
Parents’ focus group
I concur really, the thought of having it put in the homework book or so that our child can actually read it out to us so they can show us what they have done at school and we always like to know what they have done at school.
Parents’ focus group
Collaboration when writing Social Stories
Both groups highlighted the importance in parents having more than simply a consultative role and whenever possible have some involvement with writing stories that are to be used in school. The view was expressed that parents should be considered ‘experts’ on their own children. Indeed they may be ‘writers’ and ‘knowledgeable practitioners’ in their own right, who can build on the experiences of teachers. Information which can benefit the child can be passed from home to school and vice versa. This suggests that good communication channels need to be in place between home and school.
. . . parents do need to have the stories, they do need as well to be consulted on the input because problems are often going on at home as well, so they [children] are keeping calm, there might be strategies parents use at home that work that we can incorporate into Social Stories in a school setting.
Professionals’ focus group
Parents talked about the different people that they would be in contact with, within the school. They might not necessarily speak directly with the teaching assistant, but speak with the teacher or head teacher, especially in primary school settings. At secondary school there is likely to be a special educational needs co-ordinator (SENCO) whom they would be in dialogue with.
Informing the manual
Style and content
While participants had a range of different expectations of what the manual would look like and what it would contain, all parties wanted a manual that was easy to follow and that would make the writing of Social Stories feasible within the time constraints held by teachers, clinicians and parents. A number of general suggestions on the potential direction for the manual were provided including a section up front providing definitions of ASD and Social Stories including an introduction to their purpose and how they can be used.
I mean, one thing you could do is, like if you had success [using a story], if you showed some examples of how it’s worked . . . To make it seem as if, yeah, this is worthwhile doing. Because otherwise you’re just like, do I really need this? Whereas if you had examples of, this has helped . . . Just a few examples of how it can work, and they’ll say, oh right, well maybe we could use that because we’ve got a problem with such and such. If they can see that it works, then they’re more likely to bother.
Female, teaching assistant, landscape interview 5
An electronic manual was discounted, with preference given to something portable, short and ‘handbag’ size. A comb-bound version was suggested, as it would be easier to photocopy sections.
Examples
Given the individual nature of each child, their environment and the story writer, it was suggested that the manual should not publish a single, definitive ‘set’ of stories, applicable to the majority of identifiable situations; rather they could provide a range of examples. The compromise between having enough information to make story writing easy and the ability to allow for the individualisation of stories was very important. Parents were particularly keen to access examples of good stories that they could develop on and use with their own children.
. . . very broad categories, and within that you might have to expect that people would have guidance to develop more specific ones that tailored to individual children, so that you are flexible.
Parents’ focus group
This was echoed by professionals who thought exemplars of well-written Social Stories provide a good starting point from which to diverge and are particularly useful for inexperienced writers.
. . . and you think all that will do and I will change those bits or whatever but you could do it much quicker because it is hard sitting with a blank piece of paper even when you’re used to writing with them.
Professionals’ focus group
. . . everyday sort of common scenarios and then you can personalise them to a child and it saves you a lot of time.
Professionals’ focus group
It was highlighted that the examples should be well indexed and include range of different scenarios including classroom activities, personal care, examples for use with older children and examples from the UK.
Checklist
Checklists were suggested as a useful tool for helping authors check the stories against the criteria for a ‘good’ Social Story and a useful way of conveying the ‘rules of writing’ in retrospect.
. . . you have a checklist as well to say have I put something positive in have I done, is there any negative things in them or have I, have I understood the child’s feelings.
Parents’ focus group
One participant suggested following or using an already existing checklist.
Carol Gray does have a nice checklist actually yes, right to just check your story does it have x y z, it’s a tick list.
Professionals’ focus group
Simplicity
As stated in Chapter 1, Social Stories follow a range of rules based on 10 criteria parents felt these could be intimidating, there were some concerns about getting started in particular, writers sometimes were apprehensive about interpreting and using the criteria. The overriding message from parents was the need for the simplicity and that the manual should be easy to follow.
So in other words, try to debunk all this stuff and make it more followable, would be good for me. Anything like that . . . I mean, I need the idiot’s guide. The parents of an autistic child don’t have the energy for all of that.
Female, parent, landscape interview 3
No, I don’t want a rigid structure, I just want something that’s fairly broad, can give fairly clear instructions on how to begin it and sort of some sort of, not having to follow a set model.
Parents’ focus group
Informing the training
There was recognition that Social Stories need careful crafting to reflect the individual needs of child, often responding to environmental or social cues around them. Stories take time to develop as do the requisite skills needed to create them. People were willing to invest the time and effort (including getting proper training and advice) to apply the rules and get stories right. Most people were in agreement that the manual in itself was not enough. There needed to be an interactive workshops or training to support the use of the manual and help with the process of writing stories.
Stage 2: feedback on the draft Social Stories manual (focus groups)
Research participants
Two focus groups were conducted in stage 2, one with teachers and clinicians and one with parents and carers, focusing on the construction of stories; style and content of manual; and teaching, training and dissemination.
Five professionals attended the professionals’ focus group, one teaching assistant, one retired teacher, two autism specialist teachers and one speech and language therapist. Three of these had attended the previous group and these had the most experience of Social Stories (teaching assistant, autism specialist teacher and the speech and language therapist). The two new participants had both written and used Social Stories. There were three parents in the parents’ focus group, two of whom participated in the first parents’ focus group and had used Social Stories extensively. The new parent had some experience writing Social Stories with her child but still considered herself a novice. All participants were female.
Experiences of using Gray’s criteria
As described in Chapter 1, the criteria for the construction of Social Stories is formulated around 10 criteria. 3
-
one goal
-
two-part discovery
-
three parts and a title
-
four-mat
-
five factors define voice and vocabulary
-
six questions guide story development
-
seven types of sentences
-
a gr-eight formula
-
nine makes it mine
-
ten guides to editing and implementation.
The participants were asked to expand on their experience of using these criteria and how they would like them presented in a manual. While participants appreciated their comprehensive nature, several issues were raised with their operationalisation, for example some of the criteria use ‘Americanisms’ which might cause confusion for a UK audience.
Simplification of the criteria
The parents expressed many difficulties with the way the criteria were laid out by Gray. 3 They described finding it difficult to remember the component parts of the Social Story. Furthermore, parents found the text provided to explain the criteria difficult in places and were heavily reliant on the notes and questioning during the focus groups to make sense of them.
As a consequence of the perceived complexity of the criteria, none of the participants described using all of the criteria or their component parts. Some of the criteria had multiple parts which made them less likely to be used in their entirety. For example, criterion 10 has 10 parts, so it was less likely to be used fully than some of the shorter criteria, compared with criterion nine which was popular with everybody:
I think that’s the most important one . . .‘cos it’s got to be personal for it to be effective . . .
Parents’ focus group-2
In addition to having a focus on making stories individual, criterion nine was also one of the shortest criteria with the easiest explanation. Therefore, rather than always following the criteria in a strict fashion, respondents were more likely to work to rules of thumb based on previous experiences.
In particular, criterion seven (relating to seven types of sentences) was highlighted for simplification. Several participants across both focus groups said they were more likely to use some sentence types over others. It was felt that many of the sentence types could be simplified with more revealing titles which would make them easier to remember and apply when constructing Social Stories.
I think simply the simplification . . . of the sentences, ‘cos it’s the one thing that I mentioned before that people get very stressed about. Not so much the balance, but even what does each, just descriptive, perspective . . . what do they all mean?
Professionals’ focus group-2
With this in mind the group developed a series of taglines which go alongside the different types of sentences in order to make them easier to remember and use. Table 17 displays the consensus of the groups.
| Carol Gray sentences | New name | Tagline |
|---|---|---|
| Descriptive sentences | Descriptive sentences | Statement of fact sentences |
| Perspective sentences | Perspective sentences | ‘Understanding others’ sentences |
| Coaching sentences | Directive sentences | I will try sentences |
| Partial sentences | Interactive sentences | Sentences that involve the child |
| Affirmative sentences | Reassuring sentences | ‘It’s okay’ sentences |
Using positive language
A common theme that emerged was the importance of the writer to focus on positive aspects of the child and their behaviour rather than challenging behaviours. A central theme of Social Stories is that they have a positive, reassuring tone that intends to fill in the gaps of a child’s understanding in the hopes that this will indirectly change a behaviour. When the writer focuses on a challenging behaviour and the consequences of it, it is very likely for negative language to be used inadvertently. Both groups emphasised that while challenging behaviours often improve through Social Stories, this is not their true purpose. They stressed that the emphasis of the story should not be on a negative behaviour that is being targeted but rather on suggesting alternatives for that behaviour. One practitioner that had experience in training others in the use of Social Stories often read the stories back to the adult writing them to pick up on negative phrasing.
I think you do find people who write Social Stories who are unaware, when you read it through alongside them, that’s the adult, not the child, that actually they have put in negatives and they don’t, they don’t realise, you know, because it, it, it’s so difficult to get out of that habit, don’t do something or whatever . . .
Professionals’ focus group-2
Limiting Social Stories
Participants felt there was a need to limit both the content of created Social Stories (i.e. focus on one issue) and the number of Social Stories being used at any one time (creating under-absorption). One participant used the metaphor of digestion:
. . . you’ve got to give time for them to be digested and taken on board before you start to introduce others.
Professionals’ focus group-2
Feedback on the manual
The manual writing team had simplified the criteria to fall under three main headings: Stop, Look, Listen; Prepare; and Share. The focus groups were given an outline of the proposed new rules, which simplified and explained the existing ones used by Gray,3 using these headings. Two versions were supplied: a single sheet version with topics and main headings and a more in-depth version which provided brief explanations and examples. The focus groups made suggestions and small changes to these, mainly to help clarify and simplify.
Stop, Look, Listen
This heading encompasses criteria one and two. The idea of stopping first highlights the participants’ view that the initial process should be one of scoping the environment in which particular behaviours occur and confirming whether or not a Social Story is required. Through gathering information about the setting, the behaviours, the individuals involved and listening to the child and their carers, the story writer is able to understand the situation and provide the bulk of the information required for the story.
Prepare
This heading encompasses criteria three to nine. The next stage involves the preparing of the Social Story, in addition to consideration of the form and content; where possible the child should be involved in the early stages of writing. At this stage the manual should be useful in offering suggestions about writing and developing Social Stories.
Share
This heading encompasses criterion ten. The final stage of the process is sharing the story. The work of writing a Social Story is an ongoing process that may change and develop over time. Sharing may be undertaken by a range of people. For example, a teacher may share with a parent or with a consultant or clinician. Further, sharing the story with the child may bring up other issues, such as changes in images or clarification of text based on their preference.
Through a process of Stop, Look, Listen, Prepare and Share, the writer looks at the situation holistically. The writer assesses whether or not a story is required and then seeks to implement it in a way that is unique to the needs of the child. Finally, it is recommended that stories, the child and the situation are regularly monitored and reviewed, with changes being made as necessary.
Other factors informing the manual
Manual size and design
Preference was for A4 paper size with secure binder for ease of photocopying; with a folder space in the manual to hold paper, extra stories and note; and with a fold-out sheet which contains the simplified rules. It was also recommended that this sheet could be replicated within the manual so that it could also be photocopied and reused.
Example Social Stories
As highlighted in stage 1, the focus groups wanted the manual to include a wide selection of example Social Stories that they could use to borrow and adapt from. This was very important at all stages of their writing career, not just at the beginning. Having Social Stories which could be adapted was seen as different from having Social Stories which they could copy.
. . . and get that repetition of those phrases, like we’ve said, the beginning and the end, and, and then they start putting in their own bits.
Professionals’ focus group-2
These focus groups expanded on the previous discussions by suggesting they wanted to see examples which were split into the different (academic) key stages. This would allow them to navigate to example stories which relate to the cognitive abilities of the child they are working with. The professionals’ focus group suggested 3 to 4 stories in each of the key areas would be sufficient.
Other factors informing training
Overall, the groups suggested a half day maximum training session, which could cover basic to more advanced use of the manual and writing individualised Social Stories. Participants stated they would consider online training, but most discounted the use of a DVD. Importantly, the participants indicated that the training should include peer support throughout the process, focusing on making sure stories are right and ‘checked by others’.
Discussion
The qualitative research revealed that the Social Stories manual and training day needed to balance a number of competing demands. One of the main difficulties would be to express the relevant concepts without being overly theoretical and following the spirit of the original criteria which make Social Stories unique. The feedback suggested that the manual needs to be accessible, relatively small and get information across without ‘overloading’ the readers in a form that appeals to a UK audience.
Within the manual, participants suggested the need for definitions. An introduction to autism in general and on Social Stories in particular was considered to be useful. In addition, it may be useful for some readers to outline where Social Stories work well in the form of case studies. Any theoretical approaches/links and literature may be best placed at the back of the manual in a separate section for those who are interested and, indeed, to keep the manual short, websites may be employed for this type of information.
The evidence from the focus groups suggested that interest lies in three domains. Firstly, attendees suggested that they would like to have guidance on how to write Social Stories, secondly they would also like to have a manual which has examples of Social Stories and finally they would like confirmation and support through direct training to make sure they are writing well.
Conclusions
Stage 1: informing the design of the Social Stories intervention
-
Within mainstream schools it was suggested that teaching assistants who know the child well and have their trust would be best placed to support the development and delivery of the stories.
-
The intervention would be best delivered in a quiet place apart from the other children.
-
Focus groups highlighted the importance of parents being involved with writing (including school-based stories).
-
The focus of a Social Story is not on a challenging behaviour even when they are specifically targeted. As such it would be important not to limit a measure of effect to challenging behaviours but also socially appropriate behaviours.
-
Individualising the stories for each child was seen as important for them to be effective.
-
Groups indicated that they would prefer a manual that was short and simple.
-
Checklists were suggested as desirable in a manual.
-
Participants wanted access to examples of good Social Stories to help in their learning.
-
Most people were in agreement that the manual in itself would not be sufficient and wanted training to support its use.
Stage 2: feedback on the draft Social Stories manual
-
Participants recommended further alterations to tailor the writing to a UK audience.
-
The groups believed that the way the criteria were represented and explained were still quite complex and needed further simplification.
-
The groups wanted more emphasis on the importance of the Stories having a positive tone.
-
The groups were positive about the three stage model of presenting Gray’s 10 criteria.
-
Participants considered that a half-day training session, which could cover basic to more advanced use of the manual and writing Social Stories, would be sufficient.
Chapter 5 Developing the manual and training package
Background
Two expert groups were formed with the remit of producing a manual and training package for Social Stories for use in mainstream schools. They did this through evaluating information from the systematic review, qualitative interviews and user groups, and incorporating this into their work. The development of the intervention was an iterative process between these expert groups and the user groups which fed back to them on the work they produced. The process can roughly be divided into two stages in line with the stages of the qualitative work in Chapter 4. These stages had three objectives.
Objectives
-
To utilise an expert panel to identify and highlight findings from the theoretical phase (see Chapter 2) and the opinions of users (see Chapter 4).
-
To engage in an iterative process of feedback and development that made full use of the rich information coming from PPI and the user groups.
-
To develop a manual and training package that could be evaluated in a pilot study.
Methods
We formed two expert groups and gave them the remit of taking the information from the systematic review and user groups, synthesising it and ensuring that it was incorporated it into the Social Stories manual and training package for use in a feasibility study conducted in mainstream schools. As outlined in Chapter 3 the developmental work used an iterative process of information exchange between the user groups and expert groups. This process can be subdivided into two main stages.
Stage 1: this stage was to synthesise the findings from the systematic review and preliminary data collection from the first stage of user groups to inform the initial design and content of the Social Stories training manual.
Stage 2: this stage was to incorporate the feedback on the content of draft chapters of the Social Stories training manual developed by the writing group.
Expert panel
The role of the expert panel was to support a writing group to develop a Social Stories manual and training package by evaluating, marshalling and representing the evidence gathered from the systematic review, the user group feedback and the thematic analysis from the qualitative researcher.
The expert panel comprised:
-
three co-applicants, each with expertise in Social Stories and including an autism specialist teacher, a child psychiatrist with 25 years’ experience of working with children with ASD and a consultant clinical psychologist with 19 years’ experience of working with children with ASD
-
two PPI parents of children with ASD, one of whom had written an article on the use of Social Stories
-
a qualitative researcher who brought information from the user groups to the meetings
-
a researcher who was working on the systematic review and was up to date on its findings
-
two clinicians trained in the writing Social Stories by Carol Gray and with expertise in developing and delivering training packages for parents in a child mental health setting
-
Social Stories designer, Carol Gray.
Expert writing group
Their role was to take direct responsibility for writing the manual and putting together the training package from the recommendations of the expert panel. This expert writing group comprised a subset of the members of the expert panel and included:
-
two PPI parents
-
two people with expertise in developing and delivering training packages for parents in a child mental health setting
-
The Social Stories designer, Carol Gray.
Carol Gray
The original designer of Social Stories contributed at times to both the expert panel and writing group, although as a resident of the USA did not attend the meetings. She came to England on one occasion and met some members of both groups. She was also in regular e-mail contact and had some Skype™ (Microsoft Corporation, Redmond, WA, USA) and telephone contact. All minutes of meetings and reports from the focus groups and systematic review were e-mailed to her throughout the study, to ensure that she was fully informed. However, owing to her wealth of experience and knowledge of Social Stories, she often contributed points of view that none of the other groups had considered, and the team found this invaluable. She championed the importance of the criteria and how they were presented, and gave valuable insights into the ethos of Social Stories. In particular, she was keen to impart the central importance of getting to know the child, understanding their perspectives and generating empowering and positive interventions. The process of preparing the manualised intervention for this study needs to recognise her particular contributions.
Results
Stage 1: informing the design of the Social Stories intervention
Conclusions from the systematic review
-
The research into social stories is predominantly based in the USA.
-
Very few studies looked at the effectiveness of social stories on children over 12 years old.
-
There was very little collaboration recorded between researchers, teachers and parents in the studies.
-
Although a large proportion of studies claimed to use Social Stories and follow all of Gray’s criteria, there was variation in the extent to which the studies met them when stories were examined by reviewers, and many studies did not give enough information to be clear the criteria were being used.
-
The majority of the target behaviours were positive or pro-social in nature (53%) behaviours as opposed to challenging behaviours. This suggest that an appropriate measure of effect for the trial should encompass both challenging behaviour and more positive behaviours.
-
The review of the single-case studies broadly supported the effectiveness of the intervention. However, the majority of these studies were rated as not meeting the criterion for the independence of assessment item on the SCED. 19
-
The review of the between-groups studies appears to provide broadly supportive evidence of an effect of the social stories interventions. However, there were gaps in the reporting of results and insufficient information to assess a number of important sources of potential bias as measured by the Cochrane risk of bias tool. 20
-
The interventions in the randomised designs were often delivered over a much shorter time frame than was typically used in the single-case designs, and the interventions used were standard ones, rather than individually tailored to each child. In this and some other important regards, this meant that they were not fulfilling Gray’s criteria.
Conclusions from stage 1 user groups
-
Within mainstream schools it was suggested that teaching assistants who know the child well and have their trust would be best placed to support the development and delivery of the stories.
-
The intervention would be best delivered in a quiet place apart from the other children.
-
Focus groups highlighted the importance of parents being involved with writing (including school-based stories).
-
The focus of a Social Story is not on a challenging behaviour even when they are specifically targeted. As such it would be important not to limit a measure of effect to challenging behaviours but also socially appropriate behaviours.
-
Individualising the stories for each child was seen as important for them to be effective.
-
Groups indicated that they would prefer a manual that was short and simple.
-
Checklists were suggested as desirable in a manual.
-
Participants wanted access to examples of good Social Stories to help in their learning.
-
Most people were in agreement that the manual in itself would not be enough and wanted training to support its use.
Implications for the manual
Social Stories were developed originally in the USA. The finding that the majority of studies examining the effectiveness of social stories (and Social Stories) were also conducted in the USA suggested that it was important to make sure that the intervention was developed for the UK audience and culturally adapted for that audience. PPI representatives suggested discussion of this in the qualitative work. It was agreed early on that this was an important consideration. Considering the importance placed on individualising stories and collaboration when writing the stories by the service users, the expert panel wanted to place strong emphasis on the importance of involving the parent and child in the story development.
The expert panel believed that it was important that the manual reflected the wishes of the user groups for it to be short and simple. As discussed in Chapter 4, there was some discussion about the preferred structure and size of the manual as a result. This varied from a pocket-sized booklet that might fit on a key ring to an encyclopaedia of Social Stories, ‘a template for every possible situation’. There were several options in between these two extremes, which were guided by the groups’ views about the content. Owing to the lack of consensus on the best format for the manual, it was decided that more information would be needed before a final decision could be made.
In addition to the findings of the systematic review and user groups, the expert panel also wanted to place emphasis on how the process of gathering information and writing the stories is an important process in helping the writers to understand the context of the problem to be addressed.
Finally, the group wished to take on board the preferences of the user groups for the use of plain English where possible. The point was made that the heavy use of metaphor for example may be problematic for some parents, especially if they have an ASD themselves. The group also supported the suggestion of checklists and example Social Stories. It was decided that the language within the manual should be clear and easy to follow without reference to complex theoretical models. In addition, the creation of a checklist and example stories were considered as a good starting point for development work. As such, before work on the text itself began, priority was given to three tasks:
-
for the members of the expert panel to gather Social Stories for the manual with informed consent from previous users
-
for two members of the writing group (with the most experience of using Social Stories) to work with Carol Gray to put together a checklist that novices could use to help them evaluate how closely their stories fit the criteria
-
to write an outline for the structure of the manual.
Implications for training
The expert panel agreed that training and extra support would be important for teachers and parents to be able to prepare and deliver Social Stories effectively. They believed, however, that this training should closely mirror the structure and writing in the manual, so preparing a complete draft for review was given priority at this point.
Implications for intervention delivery
A series of decisions were made from the conclusions of the systematic review and stage 1 of the qualitative work. We would ensure that the Social Stories adhered to Gray’s criteria so that that the intervention was clearly defined and consistent across families and schools. In line with the HTA call, we would deliver the intervention in mainstream schools. It would be emphasised that the person who was to deliver the intervention should be well known to the child (e.g. their teaching assistant). The Social Story would be read in a quiet space and should minimise disruption to the child’s established routine. Finally, the intervention should take place over a period of time rather than being read to the child on a one-off basis, as was the case in previous between-groups design studies (see Chapter 2), as this is how they are recommended to be used in practice.
Implications for trial
Both the systematic review and the qualitative work indicated that a valid measure of effect for Social Stories should not focus solely on challenging behaviours. The goal of a Social Story is to enhance the child’s social understanding which in turn helps them to cope more effectively. The expert group recommended that all outcome measures on the trial should include a measurement of both challenging behaviours and more pro-social ones.
The systematic review highlighted that most studies in the area did not use independent or blinded assessors of the intervention. Considering the importance of the involvement of the child’s teachers and parents in the intervention, it would not be possible to blind them to the intervention in a large scale trial while maintaining external validity. The expert panel decided to examine the feasibility of including a behavioural frequency measure which could be blinded in a full-scale trial.
The first draft of the manual
The writing group put together the following outline for the first draft of the manual and this was agreed by the expert panel. There was strong input from the PPI representatives in these discussions. There was agreement about the need for six separate chapters in the manual that could be easily differentiated and navigated by a reader. These sections were then delegated to individual members of the writing group to prepare a draft manuscript for review by the members of the user groups. The first draft was 36 pages long and included the following chapter headings:
What is a Social Story?
This introductory chapter was three pages long and gave a brief description of the purpose and potential benefits of using Social Stories.
A guide to writing Social Stories
This chapter was six pages long and attempted to detail Gray’s criteria in a manner that was more accessible for a UK audience. The writing group attempted to simplify the criteria in line with the service users’ expectations, and to give examples and use language more in tune with UK readers. In an attempt to make the criteria more manageable for the reader, it also split the criteria into three categories based on the qualitative researcher’s findings from the stage 1 user groups
-
stop, look and listen
-
prepare
-
share and show care.
Worked examples of Social Stories
A number of different examples were prepared for review of the service users but these were not part of the main document.
A template for gathering information
In line with the importance that the writing group wished to place on the process of writing and individualising Social Stories, a two-page template was prepared to guide the writer in discovering information about the child.
Understanding autism
This chapter was ten pages long and attempted to explain the theories behind ASD and the strengths and challenges facing children with ASD. It was intended to help the reader better understand the perspectives of a child with ASD.
Other information
This was not really a chapter in itself but contained two draft versions of a checklist to help readers evaluate their stories once written and a flowchart of the process of writing Social Stories. An extended version of the checklist was provided for novices that included guidance throughout. There was also a shortened form for those with a bit more experience which left out this guidance but was otherwise the same.
On completion of the first draft of the manual by the writing group, copies were sent to all members of the user and expert panel for comments.
Stage 2: feedback on the draft Social Stories manual
Conclusions from stage 2 user groups
-
Participants recommended further alterations to tailor the writing to a UK audience.
-
The groups believed that the way the criteria were represented and explained were still quite complex and needed further simplification.
-
The groups wanted more emphasis on the importance of the Stories having a positive tone.
-
The groups were positive about the three-stage model of presenting Gray’s 10 criteria3 but suggested alternative ways of presenting or expressing this.
-
Participants considered that a half day training session, which could cover basic to more advanced use of the manual and writing Social Stories would be sufficient.
Implications for the manual
It is important to re-emphasise that the process of development was an iterative one and this section encompasses more than just the feedback from the second stage of focus groups. Aside from the conclusions from the qualitative reviewer, three additional meetings of the expert group were held with representatives from the user groups attending. Within these meetings clarifications and direct feedback on drafts were made. The comments from this less formal contact with users (PPI) were very important to producing the draft at the end of this stage.
The main focus of the feedback was on the guide to Social Stories section of the manual which detailed the 10 criteria, seeking clarity, further simplification and headings that were more intuitive. A greater range of examples was also provided and it included two step-by-step guides to creating example stories reflecting each stage of the process. Examples of case studies were also included to better reflect the practicalities of creating stories and what situations they could be used in.
Implications for training
The two-day training course for Social Stories used by Gray in the USA was considered. The expert panel expressed the view that while this course was excellent, the two-day format would make it inaccessible to many parents and teachers. Schools often found it difficult to release teachers and teaching assistants and parents would find attendance very difficult. Both the PPI representatives and the qualitative interview feedback suggested a 5-hour course in the middle of the day (9–2 p.m.) as the most popular option. The groups therefore worked around this to plan training sessions to be tested in the feasibility study.
A short training day was designed with two parts. The first part was a presentation which closely followed the structure of the manual and detailed the background and writing of Social Stories. The second part was designed to take account of the users’ requests for support in writing stories. For this part of the training, the presenters aided the participants in putting together their own stories through direct support and guidance.
The second full draft of the manual
A draft was completed in September 2012 which consisted of 54 pages. This draft had been approved by the representatives of the user groups and the expert panel with the exception of Carol Gray who could not be present at the meeting. The chapter structure was as follows:
-
Prologue: this was a two-page prologue written by one of the parent members (PPI) which highlighted the ethos of those who wrote the manual.
-
Social Stories: this introductory chapter was extended to four pages but was not substantially different from the original version.
-
How to write a Social Story: this chapter was eleven pages long and differed substantially from the first version. In particular, criteria four, seven, eight and nine were substantially altered to reflect the service users’ desire for language more appropriate to a UK audience and greater simplicity. For example, when describing criterion eight, Gray’s formula for the correct balance of sentence types the description read. ‘Coaching sentences are usually less than a third of the total number of sentences and usually a lot less! This is to avoid the Story having a directive tone’. This was paired with the original criterion description for clarity.
-
Gathering information: in line with the a request from the focus groups, a two-page template was constructed as an aide memoire for gathering information to better understand the child and the current issue being addressed.
-
Understanding autism: this section was 13 pages long and was given more detail but did not otherwise differ substantially from the original version.
-
Putting it all together: this chapter was eight pages long and detailed a practical, stepwise approach with worked examples for writing Social Stories.
-
Appendix: included in the appendix was the template for gathering information, a short and a long version of both of the finalised both checklists (for checking all 10 criteria for Social Stories were met), and a more detailed flowchart of the process of writing a Social Story.
Carol Gray’s comments
Before this draft of the manual was piloted, a copy was sent to Carol Gray to ensure its consistency with her original design. She felt that it was important to retain her original named headings for the 10 criteria, as this was what would allow users to cross-check with other publications that had used these headings. We therefore paired the original headings with the new headings chosen by our user and writing groups.
After discussions it was also decided that a new section would be added to the manual written by Carol Gray, which detailed her original version. This resulted in a much longer manual (80 pages) providing detailed information that could be tested in further study.
Discussion
Based upon initial findings from the systematic review, user group stages 1 and 2 and with input from the expert panel, the writing group developed a manualised intervention for use in the mainstream school setting with children with ASD and a training day for the development of Social Stories. This version of the manual was prepared for use in the final stage of the development process (see Chapter 6).
Chapter 6 Pilot of manual by users
Background
The manualised intervention and training day on Social Stories was prepared for use in a pilot study. The purpose of this aspect of the research was to pilot the manualised toolkit (including the training) with a small number of service users. This chapter describes that pilot work. The manual and training were developed with both teachers and parents/carers in mind (discussed further in Chapter 5).
Objectives
-
To identify facilitators and barriers to use of the intervention in the mainstream school context (both primary and secondary).
-
To ensure the intervention is acceptable to users and providers.
-
To elicit participants’ views on the intervention.
-
To pilot possible outcome measures to be used in the feasibility trial.
Methods
Setting
Goal-setting meetings (GSMs) were conducted either within a CAMHS setting or at the participating school depending on the preference of the participants. Professional educational and CAMHS clinical staff associated with the research team delivered the training in Social Stories in a CAMHS setting. The delivery of the Social Stories took place within the classroom.
Design
This was a small pilot study designed to walk six participant groups through the intervention. No comparator group was used.
Participants
As part of the study, questionnaires were administered to the teachers and parents of the children with ASD in addition to the children themselves. For ease of reference, the children on the study are referred to as participating children. For each participating child there was also a participating teacher and participating parent who completed questionnaires and delivered the intervention. Accordingly, a distinction is made between the participant groups, which include the participating child, parent and teacher, and the adult participants group, which refers only to the parent and teacher associated with each participating child. We use the term teacher to refer to any school staff member designated to work with the participating child in the study (encompassing teaching assistants and SENCOs as well as class teachers).
Inclusion criteria
The eligibility criteria for a participant group to take part in this aspect of the research were based on the child. They were that the participating child was:
-
aged between 5 and 15 years
-
attending mainstream school (this includes children who may have some mainstream lessons and some lessons in a ‘base’ or equivalent within a mainstream school)
-
diagnosed with ASD by the multi-disciplinary, multi-agency York Autism Spectrum Disorders Forum or other equivalent body using the International Statistical Classification of Diseases, Tenth Edition (ICD-10)114 or DSM-IV23 research diagnostic criteria
-
exhibiting challenging behaviour as reported by parents and teachers. The definition of challenging behaviour we used was behaviour that those close to the child wanted to see decrease and which they believed could result in social exclusion.
Exclusion criteria
The following criteria detail the conditions which mean a participant group would not be included in the study.
-
any child that had used Social Stories within the last 6 months was excluded
-
if either the parent or the teacher had already taken part in one of the user groups (see Chapter 4), they were excluded from taking part to ensure maximum data saturation.
Participant recruitment
Potential participants were identified through the user groups and expert panel, including clinicians identifying families whom they believed met the eligibility criteria. Local authority staff also identified schools where children meeting the eligibility criteria attended. Schools were approached through these existing relationships and through direct invitation by e-mail and post to the school.
Interested schools were provided with written information (see Appendix 9) about the research and were visited by the research team who explained the research and sought to answer any questions about taking part. Families were provided with written information about the research (see Appendix 9) either through their school or via the clinicians working with them. Interested families were encouraged to contact the research team for more information and to ask any questions.
The participating teacher was asked to sign a consent form. Parents signed a consent form on behalf of themselves and their child. Children gave their assent to take part.
Research procedures
Participant groups were asked to walk through the proposed package of care. This included the adult participants being invited to attend a GSM and a Social Stories training session.
Goal-setting meeting
This was an initial meeting with participating adults to establish a simple goal for the intervention to focus on. The rationale for establishing this in the methodology of the feasibility study came from PPI representatives. They were keen to point out that Social Stories could be used for a very wide range of difficulties. This was also exemplified by the systematic review (see Chapter 2). They therefore wished to include an outcome measure that could capture this wide diversity. After taking advice from the Team Management Group (TMG), it was agreed that an individualised goal-based outcome measure would be included in the feasibility study. It was therefore decided that for each participant group, a meeting to establish and agree a clear goal would be necessary before measurement could take place. The pilot phase allowed the opportunity to explore possible ways of helping participants to set and rate goals at the beginning of the study and rate these goals after the intervention period.
A secondary purpose for the GSM was to examine the feasibility of operationalising two target behaviours related to this goal which, in a full-scale trial, could be assessed by an independent observer. It was hoped that the teachers and parents could provide enough information by meeting with a clinician and a trained researcher to operationalise these behaviours. If it proved successful an independent observer could then arrange a baseline observation shortly afterwards without encumbering participant flow excessively.
Goal-setting was initially conducted as a two-step process. Participating teachers and parents were asked to identify two goals separately (a goal focused on a positive behaviour and a goal focused on a negative behaviour) and secondly, rate both their own and each other’s goals. The pilot phase demonstrated that this process was cumbersome, time-consuming and resulted in lengthy delays in return of data. After consultation with the TMG, we changed this to a one-step joint goal-setting process. Participating teachers and parents were encouraged to jointly identify one goal they would like to work on during the intervention period. They were also asked to identify a positive behaviour and a negative behaviour associated with this goal. The mechanisms for measuring this and other outcome measures are described below.
Intervention
Adult participants were invited to the next available training day and were given a copy of the Social Stories training manual to read through. The training day used in this pilot lasted approximately 5 hours and aimed to teach how to create and deliver Social Stories to the participants. The first half of the session consisted of a presentation detailing the theory behind Social Stories and the practicalities of writing and delivering them. The structure of the presentation closely mirrored that of the manual, making reference to it in places. The second half of the training session was devoted to creating the Social Story for the goals set in the GSM for each child. Participating teachers had the central role in creating the story. Participating parents when present were there in an advisory capacity to offer insight into their child’s world. Guidance was also provided on how to format the story to individualise it to the particular child’s needs [e.g. story book format, Microsoft PowerPoint® (Microsoft Corporation, Redmond, WA, USA) presentations or on a single sheet of A4 paper]. An example of an unformatted Social Story is provided in Appendix 10.
The intervention delivery period lasted 4 to 6 weeks. How often the intervention was delivered was left up to the participating teachers. This approach is consistent with the individualised nature of the Social Story intervention, which is driven by the child’s needs and ability. As a starting point, the researchers suggested that the intervention could be delivered three times a week for 2 weeks. However, adult participants were advised to use their judgement based on their knowledge of the child when deciding how much to present the story and for how long. Similarly, the participating teachers were not required to read the Social Story to children who would prefer to read it by themselves (as was the case with the older participants), as long as time was set aside for the child to have an opportunity to read it with the teacher present.
Qualitative interviews
Semi-structured interviews using topic guides were conducted with all participant groups after the intervention period. Interviews with participating parents lasted approximately 45 to 60 minutes. A short interview, ranging from 2 to 10 minutes, took place with the participating child, with their parent helping to facilitate the interview.
The participating teachers were also interviewed. The interviews aimed to elicit users’ thoughts and experiences of setting goals and completing the questionnaires. The interviews were an opportunity to get feedback on goal-setting, background information to the story, its implementation and impressions of how well it worked. The interview also considered the reading of the story and overall views on the presentation, structure and content of the manual.
Interviews were conducted by two qualitative researcher fellows, one acting as the main interviewer, and the second taking notes during the interview and picking up any outstanding questions or topics to probe. Following the interview a discussion between the two interviewers picked out the main issues and points in a recorded debrief. A brief two-page summary of the interview which included background information, brief comments and key points was made available to the writing team quickly after the interviews occurred. This made sure that up-to-date information was provided to allow iterative development of the training manual. Interviews were transcribed verbatim and imported into NVivo and thematically analysed.
During the intervention period teaching staff were also asked to complete a practitioner reflective diary (see Appendix 11). The diaries sought to capture information about facilitators and barriers to delivering Social Stories within existing service models and the participants’ perception of whether the intervention was or was not working well, including their views of why. Participants were asked to note experiences that highlight where Social Stories worked well and less well and to provide any perceptions of reasons for any discontinuation with the intervention.
Adult participants were encouraged to make any notes or suggestions on the manuals and these were collected in by the researchers at the end of the intervention period and fed into the writing groups to inform revisions to the manuals.
All participants were asked to complete outcome measure tools as designed for use in the feasibility trial. This included setting ‘goals’ and completing a questionnaire at 4 weeks post intervention start date. Space for comments and the opportunity to record the estimated questionnaire completion time was provided.
Outcome measures
The pilot provided the opportunity to pilot questionnaires to be used in the feasibility trial. Participants only completed the goal-based outcome measure at baseline. The full set of questionnaires (including the goal-based measure) were sent out 4 weeks after the intervention start date and consisted of:
-
The Strengths and Difficulties Questionnaire (SDQ). 115 The SDQ is a brief child mental health screening questionnaire. It was completed by the adult participants and older participating children (11–15 years).
-
The Social Responsiveness Scale-2 (SRS-2). 116 The SRS-2 identifies social impairment associated with ASD and quantifies its severity. It was completed by the participating teachers.
-
A goal-based outcome measure, designed by the research team (see Appendix 12) including operationalised behavioural measures. It was completed by all participants.
-
Bespoke resource-use questionnaires were developed by the health economist to capture the resource implications of the child’s behaviour at school and home see (see Appendix 13). These were completed by the adult participants.
-
The European Quality of Life-5 Dimensions (EQ-5D) proxy and the European Quality of Life-5 Dimensions youth questionnaire (EQ-5DY). 117 These are standardised instruments for use as measures of generic health outcomes recommended by National Institute for Health and Care Excellence (NICE). They were completed by the participating parents and children respectively.
-
The Health Utilities Index 2 (HUI2). 118 This is an alternative preference based generic health outcome measure to establish health states in children, and to report their health-related quality of life and produce utility scores. It was completed by the participating parents.
-
The Parental Stress Index (PSI-4). 119,120 The PSI-4 is designed to evaluate the magnitude of stress in the parent–child system. It was completed by the participating parents.
-
Spence Childhood Anxiety Scale (SCAS). 120 The SCAS is a 44-item questionnaire developed to assess the severity of anxiety symptoms broadly in line with the dimensions of anxiety disorder. It was completed by the children.
Results
Recruitment
Invitation letters were sent to all schools in York (excluding private schools). This included 32 schools known to have children with ASD attending which received invitations in September 2012. The 29 remaining schools in York received invitations in November 2012.
Schools expressing interest were visited by a member of the research team and invited to take part in the pilot work. Subsequent schools expressing interest were invited to take part in the feasibility trial. Full details on school recruitment strategies are given in the Chapter 7.
Ten children meeting the inclusion criteria were initially identified at five primary schools and one secondary school. One primary school (with two eligible children) subsequently chose not to participate because they were too busy and wanted to start using Social Stories with children immediately. Two further eligible children were excluded from the sample because in one case their teaching assistant had taken part in the user group and in the other their parent had taken part in the user group.
Six eligible and consenting participant groups remained from three primary schools and one secondary school. For school with multiple students, a separate participating teacher was recruited for each child. The sample is described in more detail in Tables 18–20.
| Participant group | School type | Background | Training date | Intervention start | Interview date | Interview number |
|---|---|---|---|---|---|---|
| PG 1 | Primary | Teaching assistant had previously received training and had used but not written Social Stories. Parent had written Social Stories in collaboration with local authority specialists, may have previously attended training. Child had not used Social Stories within last 6 months | Parent: 4 October 2012 | 12 November 2012 | Parent and child: 11 December 2012 | 1 |
| Teaching assistant: 4 October 2012 | Teaching assistant: 13 December 2012 | 2 | ||||
| PG 2 | Primary | Teaching assistant had had written social stories for this child during the last 6 months but they were not considered to be Carol Gray Social Stories | Parent: did not attend | 12 November 2012 | Parent and child: 14 December 2012 | 4 |
| Teaching assistant: 4 October 2012 | Teaching assistant: 13 December 2012 | 3 | ||||
| PG 3 | Primary | Teaching assistant knew about but had not used Social Stories. Parent and child had not used Social Stories, but parent had heard about them and very keen to use | Parent: 28 November 2012 | 28 November 2012 | Parent and child: 11 January 2013 | 6 |
| Teaching assistant: 28 November 2012 | Teaching assistant: 10 January 2013 | 5 | ||||
| PG 4 | Primary | Teacher knew about but had not used Social Stories. Parent and child had not used Social Stories | Parent: did not attend | 28 November 2012 | Parent × 2 and child: 21 January 2013 | 10 |
| Teacher: 28 November 2012 | Teacher: 24 January 2013 | 11 | ||||
| PG 5 | Secondary | Advanced teaching assistant had not used or received training on Social Stories. Parent and child had not used Social Stories | Parent: 28 November 2012 | 28 November 2012 | Parent and child: 11 January 2013 | 7 |
| Teaching assistant: 4 October 2012 | Teaching assistant: 18 January 2013 | 9 | ||||
| PG 6 | Secondary | Advanced teaching assistant had not used or received training on Social Stories. Parent very knowledge about Social Stories, had used with child when in primary school | Parent: 28 November 2012 | 28 November 2012 | Parent and child: 15 January 2013 | 8 |
| Teaching assistant: 4 October 2012 | Teaching assistant: 18 January 2013 | 9 |
| PG | School Type | Goal/s | Goal rating (0–10), baseline | Goal rating (0–10), 4-week questionnaire | 4-week questionnaire completion time (minutes) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Teacher/teaching assistant | Parent | Teacher/teaching assistant | Parent | Child | Teacher/teaching assistant | Parent | Child | |||
| PG 1 | Primary | Teaching assistant: positive behaviour – to stop and listen when my teacher asks me a question and then try to answer appropriately | 1 | 4 | 7 | Parent felt could not answer, as goals relate to school | 6 | 30 | 25 | Left blank |
| Teaching assistant: negative behaviour – to say ‘excuse me’ when I pump in class (to try not to do it in the first place) | 3 | 2 | 9 | Parent felt could not answer, as goals relate to school | 8 | |||||
| Parent: positive behaviour – replying/acknowledging his teacher | Parent identified same goal as teaching assistant, so parent and teaching assistant not asked to rate twice | |||||||||
| Parent: negative behaviour – farting in class | Parent identified same goal as teaching assistant, so parent and teaching assistant not asked to rate twice | |||||||||
| PG 5 | Secondary | Teaching assistant: positive behaviour – to increase his positive behaviour to include arriving to lesson on time, finding his seat and getting his equipment | Not returned | 3 | Left blank | 5 | 9 | 15 | 20 | 15 |
| Teaching assistant: negative behaviour – losing focus on task and becoming fixated on trivial issues | 2 | 6 | 5 | |||||||
| Parent: positive behaviour – increased positive interaction with members of staff | 4 | 7 | 7 | |||||||
| Parent: negative behaviour – stopping putting head in hands | 3 | 4 | 4 | |||||||
| PG | School Type | Joint goal | Goal rating (0–10), baseline | Goal rating (0–10), 4-week questionnaire | 4-week questionnaire completion time (minutes) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Teacher | Parent | Child | Teacher | Parent | Child | ||||
| PG 2 | Primary | Goal: to increase his ability to listen in maths lesson | 4 | Not returned | 7 (note: parent changed goal to ‘keep unkind thoughts to himself’) | 5 (note: parent changed goal to ‘keep unkind thoughts to myself’) | Not returned | 20 | 15 |
| Positive behaviour: calmer approach to tasks after instructions | |||||||||
| Negative behaviour: distracting other children during instructions | |||||||||
| PG 3 | Primary | Goal: understanding turn-taking | 1 | 3 | 6 | 8 | 10 | 40 | 10 |
| Positive behaviour: turn-taking | |||||||||
| Negative behaviour: talking or shouting at wrong times | |||||||||
| PG 4 | Primary | Goal: to talk to somebody, stay calm | 3 | 8 | 6 | 0 | 20 | 5 | 20 |
| Positive behaviour: calmer | |||||||||
| Negative behaviour: making less negative comments | |||||||||
| PG 6 | Secondary | Goal: interaction with other children | 1 (note: goals identified and rated by parent only) | Left blank | Not sent out | Not sent out | 15 | Not sent out | Not sent out |
| Positive behaviour: number of approaches/initiations | |||||||||
| Negative behaviour: repetition of lists, things read | |||||||||
Qualitative findings
Timing of intervention
The timing of the intervention was seen as problematic for many of the adult participants. Delivering the intervention during the lead up to the Christmas holiday was a problem as this period is a particularly busy time with all the activities that occur. In some cases the intervention was squeezed or abandoned as a result, with parents and teachers feeling they did not deliver it as much as they would have liked. This could mean planning around school ‘pinch points’ such as statutory assessment tests (SATs) and holidays. Participating teachers suggested that it would be better to start the intervention early in a term, that is, in September or January.
Goal-setting
Throughout the pilot a number of issues and challenges with setting and rating goals were identified:
-
A separate, two-step goal-setting process was not feasible.
-
It became clear that goal-setting needed to be carefully guided by a clinician (defined as a mental health professional with experience of working with children with ASD and their families) to ensure that suitable goals were identified.
-
Operationalising behaviours needed a large amount of time and the method needed refining.
-
Joint goal-setting was not always possible or feasible.
-
The goal identified at the outset did not always remain the goal of the Social Story actually written, or rated after 4 weeks of intervention delivery.
-
The goal-setting process leads naturally to participants trying to identify ways to achieve this goal. This could have implications for accurately measuring the frequency of a behaviour at baseline, for example interventions/strategies could be implemented before a baseline measurement has been made.
Goal-setting was seen as important, as was having both adult participants present. Some people found that they were able to work on goals during training. The GSM provided a space for parents and teachers to meet and discuss the child’s difficulties. They expressed comfort in their ability to gather information and also share ideas in a protected environment. It was logistically difficult, however, to find times that were suitable to all parties. Providing people with a range of dates was considered to improve accessibility. PPI representatives were also clear after reviewing the feedback that the dates would also need to span different days and times.
One of the biggest issues beyond having people attending the GSM was developing measurable goals. Adult participants sometimes were overambitious in what they were attempting to set as their goal. In the meeting, people negotiated and limited the scope of the goal, with the aid of a clinician or someone from the research team. One participating teacher described this process as follows:
[The goal-setting was] very useful, . . . it helped, well just trying to unpick it gets you to the root of what it is that you’re trying to, trying to sort out, I think that was really good. It’s almost like walking down a path and clearing bits out, things that don’t really matter . . . Filtering and then realising that it’s, it’s really getting to the nitty-gritty and then seeing it much more clearly.
Female, teacher, primary school
A few people commented that the manual needs to include more guidance about goal-setting.
. . . really focus or, possibly a bit more training on that to assist [them].
Female, parent, primary school
Having access to members of the research team such as the consultant or researcher was useful in helping determine the goals, suggesting that the manual by itself was insufficient for some in helping with goal-setting. The manual was used more as a reference tool by some.
Yeah, yeah, I think it was more about the training, really useful to start off with as a kind of coming in, you have the training and then the manual’s a reference point to back it up . . .
Female, teaching assistant, primary school
Although happy with the goals set, one participating teacher found that they were very difficult to implement and measure. Another participant group made changes to better reflect the needs of the child. Adult participants recorded a dichotomy between achieving goals at school and at home which can sometimes mean that goals set in one place will not be as appropriate for the other.
We had an hour set aside so we [parent and teacher] talked through some of the issues at home, issues at school and then we chose a target we thought would be good for both home and school. I think in hindsight actually it’s probably a better target for home and, and the issue that we’ve picked hasn’t cropped up an awful lot. He’s been quite good at managing himself in a way, so if I’d had the time I’d have loved to have done a second story to target some of the classroom behaviour that he’s come back from, after Christmas.
Female, teacher, primary school
Training
All six participating teachers and four participating parents attended a training day. The training day was on the whole well-received. Interviewees reported it as being positive and informative. For some attending this was their first exposure to Social Stories. One participating teacher would have preferred a teacher-orientated training session that contained less introductory material on autism, as this had been covered as part of their teacher training. Others found this element enlightening. One suggestion was to shorten the length of the session when a teaching assistant had to get time off to attend. This was offset by concerns by some PPI members that a ‘good enough’ training session was needed to enable the best possible intervention construction.
One consequence of the training session was having quality time with knowledgeable people who understand Social Stories. This was seen as very important. This helped define goals further and shape the stories that were written on the day. It was considered that the training helped make sense of the manual.
I think both is good but if you couldn’t get the training the manual would help because it’s the same thing, but actually I think when someone explains something in person you get a better thing.
Female, parent, primary school
The manual seemed to supplement the training rather than the other way around and many reflected that the training and manual would need to be used together for best effect.
[We] went through the training and everything, and once they’d gone through parts of the manual we went into a separate room to try and write the stories, so, which, to start with, was very daunting to try and write it, because seeing everything on the screen and what was the, what was a descriptive sentence, what’s an affirmative sentence, and all this lot, just seeing the words didn’t really, I didn’t really get it until I actually saw some story.
Female, parent, secondary school
Additional areas were identified for further training, beyond understanding, developing, implementing and writing Social Stories. One teaching assistant would have liked to learn skills in using ‘communicate and print’. Two other people mentioned that support developing the physical story, that is adding visuals, using Microsoft PowerPoint presentations, fonts and layouts would be useful.
Manual
Participants were very thorough in their feedback about the manual. Beyond the interviews, a number of people had made detailed comments in the margins of their copy, which were passed to the writing group. These included points for clarification and areas for improvement.
General content
One parent found the section that covered information on autism to be particularly useful for extended members of her family. Photocopying this section provided useful concise information for people who are unfamiliar with autism.
. . . family or friends get the gist about autism, so I think little things like this, very short but totally what it is, they can see what you’re seeing every day.
Female, parent, primary school
Another person felt this section was useful for people who had not attended the local course on autism.
The checklists and flowchart were considered useful, providing concise instructions on what to do. Teachers found the checklists and flowcharts useful. Overall, the manual provided a useful framework and memory aid for distinguishing between different types of sentences and also for phrases that were not useful.
Step-by-step guide is very useful, especially the examples of social stories and the type of language to use, i.e. descriptive, coaching, etc.
Female, teaching assistant, secondary school
One of the design issues with the manual was that it was seen as repetitive. There was considerable overlap between a section written by Gray (section 3) and the ‘How to write a Social Story’ section (section 2) written by the expert writing group with PPI representation.
There were a small number of practical issues with the format of the document such as sorting text boxes, adding more charts and diagrams and removing hash tags from headings. There was strong support for adding more visual elements throughout the manual. However, this needed to be balanced against the desire to not have a document which was too much like a textbook or too long.
Size
Size was an issue, with most people not wanting an increase in size of the manual and some considering it too long already.
. . . it’s good, like I say, it’s a lot of pages already you know, making it any bigger would be silly, it’s 84 pages anyway.
Female, parent, primary school
Writing style
There were some issues with the overall language in the section, with feedback suggesting that the language should be more inclusive, less academic.
. . . if I hadn’t have been on the course I think I might have struggled with some of it.
Female, parent, primary school
Similar feedback was given to other parts of the manual. Several found some abstract language difficult to follow in places and the original rules on sentence numbers and balance difficult to work out. One person commented that some sections with informality got in the way of explanations, making it harder to pick out information. Two people found the writing style ‘too positive’ in places, and requested information in a more plain English writing style. Others liked the use of images.
Example stories
Consistent feedback suggested providing more examples of Social Stories throughout the manual. People tended to hone in on the examples included. Suggestions included providing a variety of examples and case studies, which reflected common behaviours, with several mentioning how to cope with aggression, as well as provision of stories suitable for older children. Several participants suggested the use of examples requesting that they be peppered throughout the manual with case studies (breaking down the more difficult parts of writing). Participants suggested the need for clarification and felt that they would better identify with writing stories when they had examples that used and explained the context behind choosing the different types of sentences.
It’d be nice to know whether it was successful, if it wasn’t, did they change it? But they [sighs] I don’t know if you need to go into the whole detail of exactly what they changed because, for me, getting the examples there is to help me to write mine.
Female, parent, secondary school
Type of school
Primary school teachers reported an additional benefit from undertaking the pilot study in that they got to know their students better through the process of individualising the story and spending time with the child. They also reported an improved relationship with parents. This worked particularly well in primary schools.
The feedback from the participant groups in the secondary school was less positive about the study. The groups did not seem to have as effective a communication channel between parents and teachers working with the child in this setting. For example, one parent felt they had to ‘nudge the school’ to get them to take part. In addition, it was found that the structure of teaching is different in secondary schools, with one child often having multiple teaching assistants and less consistency of support from day to day. The secondary school teachers noted that it was difficult to implement Social Stories during the school day. They did not feel it was appropriate to use break times.
We were keen to learn from this point and reinforce to parents and teachers that a child should never be coerced or ‘forced’ to complete an intervention of this nature. This was seen as a learning point to reinforce the constructive and positive ethos of Social Stories.
Pupils at secondary school have a structured timetable there is little to no time to sit down with a pupil and really go through a social story. Pupils don’t tend to want to go through the stories in their break times and we feel that we can’t force them.
Female, teaching assistant, secondary school
Finding a quiet location without too many distractions was difficult, particularly in one school, as was finding time to make changes to the story. Teachers are very aware about potential stigma and discrimination with regard to the implementation of stories and considered carefully the best ways to implement them.
Teenagers are a lot more aware when they are different from their peers and therefore don’t like to stand out further.
Female, teaching assistant, secondary school
Outcome measures
Five participating parents and children were sent the 4-week follow-up questionnaire (the questionnaire was not sent to one parent and child, as by this point all changes had been made and submitted to the NHS Research Ethics Committee in preparation for the feasibility trial) and all returned them. Six participating teachers were sent the 4-week questionnaire and five returned them. Reported questionnaire completion time ranged between 5 and 40 minutes for the parents, 10 to 20 minutes for the child and 10 to 30 minutes for the teachers. Despite reminders and encouragement to complete questionnaires, it proved difficult in some cases to collect completed questionnaires.
Overall, the 4-week questionnaires were not fully completed with a wide variety of different questions and sections left blank in almost all questionnaires returned.
Some notable points are highlighted in the following sections:
Goal-based questionnaire
In general, all the participants struggled with questions related to the frequency of behaviours in the goal-based outcome measure at both baseline and 4-week follow-up, finding it difficult to estimate the number of times the behaviour occurred. This may be down to the process of operationalising the behaviours in the GSM which did not result in behaviours that were readily measurable.
In three cases participating parents did not fully complete the goal rating and behaviour frequency section, and in two cases they commented that the goal and behaviours related to school so they were not able to answer the questions. In one case the parent changed the goal and behaviours and therefore rated a different goal to that identified at baseline.
One participating teacher left the entire goals section blank in the 4-week questionnaires relating to two pupils, noting that this section was confusing. Another left questions related to behaviour frequency and to educational outcomes blank. This gave us a large amount of information about possible necessary adjustments to these measures. PPI representatives gave invaluable advice subsequently in their redesign.
Parent questionnaire
Three participating parents commented that they thought some questions were irrelevant and inappropriate, or difficult to answer. In particular, one noted that the questions related to income and questions within the PSI-4119 were inappropriate. They also disliked a question referring to a ‘problem’. Two further parents left questions relating to income blank and also left questions with the health and community service use sections blank.
Child questionnaire
In two cases, participating parents reported that they completed the child questionnaire on behalf of their child, with both noting they felt the questions were unsuitable for their children, one particularly mentioned questions within the Spence Children’s Anxiety Scale. 120 One parent commented that asking the child the questions caused a lot of confusion. In one case, parents noted that they did not agree with the rating of ‘0’ their child had given the goal at 4-week follow-up.
Discussion
The findings of the pilot study had implications for the manual, training and general implementation of the trial. The research team found the pilot invaluable in designing the feasibility trial to come. The consequences of these implications for the feasibility trial are detailed in the following sections.
Implications for the manual
The writing group made a number of changes to the manual as a result of the feedback received. Firstly, section 3 of the manual was deemed to contain too much duplication and was removed. The writing group incorporated any material from section 3 that was seen as essential into the section ‘How to Write a Social Story’. We had specific support from Gray in doing this to make sure that all essential items were presented faithful to the original criteria. 3 The language throughout the manual was also further clarified, simplified and refined. Finally, the examples chapter was expanded to include a range of different Social Stories and case studies.
Implications for the training
Training sessions were reduced to one 3-hour sessions by increasing efficiency and offering an optional lunch at the end of the session instead of in the middle. Training dates were set to have a greater range of times and days.
Implications for the feasibility trial
It was decided that participants would not be asked to run the intervention in the 2 weeks before a school term was to end. Although there appeared to be a number of issues with recruiting from secondary schools, we noted that all secondary school participants came from the same school in this pilot study. It was therefore decided that this may not be indicative of all secondary schools. As such, no modifications to recruitment strategy were made based on this feedback. However, it was decided that the difference between school types should be looked at separately when examining the feasibility for a full trial.
Based on participant feedback and questionnaire completion, revisions were made to all the questionnaires to be used in the feasibility trial. Most notably behaviour frequency questions included in the goals section were revised and the process by which researchers were to elicit operationalised behaviours in the GSM was better defined. In addition, a daily diary to capture frequency of behaviours was also designed for use in the feasibility trial to further elicit data on the feasibility of conducting a behavioural measurement in a large-scale trial. Although comments had been about some of the standardised tools included in the questionnaires, it was not possible to alter individual questions within standardised tools, although we noted these comments for the future feasibility work.
Conclusions
-
Delivering the intervention leading up to the Christmas holiday was problematic, as this period is a particularly busy time. Intervention delivery in the feasibility trial took account of this.
-
There was some difficulty arranging meetings and training. Providing people with a wider range of dates for training was deemed necessary.
-
The training session was said to be slightly too long. A shorter training session was recommended and developed.
-
The feedback on the training was positive. It was considered something that helped participants make sense of the manual.
-
There was strong support for adding more visual elements throughout the manual.
-
Most people did not want an increase in the size of the manual and some considered it too long already. Two sections where duplication of material was noted were conflated and this allowed space for newer requested content.
-
There were some issues with the overall language in the manual with feedback suggesting that the language should be straightforward, more inclusive and less academic. This was taken on board for the next iteration.
-
Consistent feedback suggested providing more example Social Stories throughout the manual. These were added for the next iteration.
-
The routine of reading Social Stories may be less appropriate in secondary schools or harder to implement. This suggested that special consideration should be made for evaluating the feasibility of the trial in secondary schools.
-
Participants struggled with questions related to the frequency of behaviours in the goal-based outcome measure. Outcome measures were altered accordingly.
Chapter 7 Phase 2: feasibility randomised controlled trial
Background
As discussed in Chapter 2, evidence has suggested that Social Stories can be effective in improving social behaviour in children with ASD. 5,6 Success has also been reported in addressing challenging behaviours, including reducing tantrums9,10 and behaviours associated with frustration. 11 However, the evidence highlighted in two previous systematic reviews of their effectiveness is limited. 4,15 The reviews identified largely single-case designs and a paucity of good quality, comparative evidence on Social Stories.
Our own systematic review (see Chapter 2) indicated that social stories have been used in a variety of settings, providing social information in a range of contexts, and help children to make a wide range of behavioural changes. In general, the review indicated social story research has largely been based in the USA. This places some limitations on the extent to which the results are generalisable to other countries such as the UK. The majority of studies have used single-case design methodology and very few studies have been conducted using between-groups designs.
With regard to the studies using single-case designs, the findings of the review broadly supported the effectiveness of the intervention, with the majority of target behaviours meeting criteria for highly or moderately effective. However, the majority were rated as not meeting the criterion for the independence of assessment item on the quality assessment measure indicating that the observed effect of the single-case studies may have been artificially inflated because raters were not independent of the study. Publication bias may also potentially inflate effectiveness ratings.
Similarly, the review of the between groups studies appears to provide broadly supportive evidence of an effect of the social stories interventions. However, there were gaps in the reporting of results and insufficient information to assess a number of important sources of potential bias as measured by the Cochrane risk of bias tool. 20 In addition, in the randomised designs the interventions were often delivered over a much shorter time frame than was typically used in the single-case designs, and the intervention was a standard one, rather than individually tailored to the child or young person, an important feature of Social Stories.
Therefore, although there are a large number of single-case studies that provide some evidence for the effectiveness of social story interventions, the findings are not conclusive. In contrast, there are very few studies that use a between-groups design and what evidence there is has a number of substantial limitations. These limitations provided a good rationale for conducting phase 2 of Autism Spectrum Social Stories in Schools Trial (ASSSIST) a feasibility trial (this chapter), including an economic evaluation (see Chapter 8) and a qualitative evaluation (see Chapter 9) with a view to testing the parameters for conducting a full-scale RCT in the UK.
Objectives
The main aim of phase 2 of ASSSIST was to assess the feasibility of delivering of a RCT comparing the manualised Social Stories intervention with an attention control for children with ASD in mainstream schools.
The objectives for this component of the exploratory trial were to:
-
assess the recruitment and retention of participants
-
assess the appropriateness of cluster randomisation
-
assess the process of delivering the intervention and the trial
-
assess the collection of outcome measures
-
select a primary outcome measure for a full-scale RCT
-
produce estimates of effect sizes to inform sample size estimation for a future trial.
The protocol for this feasibility study has been published in BMJ Open. 121
Methods
Trial design
The feasibility study was a single centre, unblinded, cluster RCT, comparing the effectiveness of Social Stories on altering the behaviour of children with ASD in a mainstream school setting with a comparator group using an attention control.
Setting
Goal-setting meetings were conducted either within a CAMHS setting or at the participating school depending on the preference of the participants. This flexibility was suggested by the PPI representatives. Professional educational and CAMHS clinical staff associated with the research team delivered the training in Social Stories in a CAMHS setting. The delivery of the Social Stories took place within the classroom.
Participants
Schools
Inclusion criteria
Schools were eligible for recruitment if they:
-
had at least one child on the school register who had been diagnosed with ASD
-
were located in York or its surrounding regions
-
were a mainstream school.
Exclusion criteria
Schools were excluded from the study if they:
Participants
As detailed in Chapter 6, for ease of reference, the children in the study are referred to as participating children. For each participating child there was also a participating teacher and participating parent (or carer) who completed questionnaires and delivered the intervention. Accordingly, a distinction is made between the participant groups, which include the participating child, parent and teacher, and adult participants, which refers only to the parent and teacher associated with each participant. We use the term ‘teacher’ to refer to any school staff member designated to work with the participating child on the study (encompassing teaching assistants and SENCOs as well as class teachers).
Inclusion criteria
Participant groups were included only if the child:
-
had a diagnosis of ASD given by the multidisciplinary, multiagency York Autism Spectrum Disorders Forum or other equivalent body using ICD-10114 or DSM-IV23 research diagnostic criteria
-
was between 5 and 15 years old
-
attended mainstream school (this includes children who may have some mainstream lessons and some lessons in a ‘base’ or equivalent within a mainstream school)
-
exhibiting challenging behaviour as reported by parents and teachers. The definition of challenging behaviour we used was behaviour or lack of a behaviour which those close to the child wanted to see decrease which they believed could result in social exclusion.
Exclusion criteria
Participant groups were excluded if:
-
the child had used Social Stories in the preceding 6 months
-
the child was likely to move schools in the following 4 months
-
either the parent or the teacher of the child had already taken part in the qualitative interviews or focus groups (see Chapter 4).
Sample size
We aimed to recruit a total of 50 participant groups, as we considered this number would be sufficient to address our objectives. As this is a feasibility study, a formal sample size calculation was not undertaken.
Participant recruitment
Three alternative recruitment procedures were used to identify potential participants: a school approach, direct contact with parents through local autism support groups such as the Autism Spectrum Conditions – Enhancing Nurture and Development (ASCEND) parent group122 and referrals from clinicians involved in the York Autism Spectrum Disorders Forum which is a multiagency, multidisciplinary forum for diagnosing and discussing provision of supporting interventions for all local children on the autism spectrum. PPI representatives were keen for families to have access to the study and recommended the range of routes to disseminate information about the study to maximise accessibility. Figure 3 indicates how these different methods of recruitment interacted with each other and participation in the feasibility trial.
FIGURE 3.
Outline of participation in the feasibility trial.

Direct recruitment of schools
Identification of schools within York and its surrounding areas was done through use of the Department of Education website. From this information a list of 131 schools (including those already contacted for the pilot study) was compiled with their contact details. Invitation letters were sent to all schools on this list in January 2013. This was followed up by a phone call inviting the school to participate. If schools were interested in taking part, a researcher would then visit the school to determine eligibility. If eligible, a researcher would invite them to pass on recruitment packs to parents of children who could potentially benefit from the intervention. The recruitment packs consisted of information about the study and consent forms together with the contact details of the study team. Once the parent contacted the study team requesting further information, a researcher would arrange to visit the parent to more fully explain the study and answer any questions. Once fully informed consent was obtained they were offered dates to attend a GSM and/or training.
Direct recruitment of parents
In addition to recruiting through schools, attempts were made to recruit parents directly. As a strategy to allow for this, the research team gave presentations and leaflets about the research to local autism support groups for parents of children with ASD such as the ASCEND group. 122 Recruitment packs were given to interested parents and the researchers collected their contact details and those of the child’s school. For interested parents of children that attended a school that met the eligibility criteria, a researcher would arrange to visit them to more fully explain the study, check eligibility, answer any questions and ask for permission to speak to their child’s school about taking part. The school would then be contacted to inform them that there was a child interested in taking part. If the school showed interest, the research team would follow the same recruitment procedure as in the direct recruitment of schools and check for other eligible children attending the school. For those schools that were unable to take part, the parents who had initially been in contact with the research team were offered to attend the free training sessions at a later date.
Recruitment through referrals
Four clinical members of the study team had access to the forum database of children diagnosed with ASD in the York area. These members contacted the parents of children that were potentially eligible and who attended eligible schools. The members were also able to inform us when new diagnoses were made to schools previously found to be ineligible because they had had no children with ASD on their register. Once a referral was made to the research team, researchers followed the same procedure as described under direct recruitment of parents.
Research procedures
Once participants were identified as eligible and contact details had been acquired for both their parents and a person responsible for them at their school, a researcher would arrange a time for a GSM for the adult participants. Baseline measures were distributed within this meeting and once all the questionnaires within a cluster were returned, participant groups were allocated to a condition by remote randomisation. Adult participants assigned to the intervention group were invited to the next available training day whereas those assigned to the comparator group were asked to choose a typical story of interest to the participating child and given guidance on reading it with them. Follow-up outcome measures were sent to all participants via post at 6 and 16 weeks after training (for those in the intervention group) or being informed of their allocation (for those in the comparator group). Adult participants allocated to the comparator group were invited to the next available training date once they had completed participation in the feasibility trial.
Goal-setting meeting
In accordance with the findings of the pilot study (see Chapter 6) and with advice from our PPI representatives, a single-step process for setting goals and behaviours was used. GSMs lasted approximately 90 minutes and were held either at the participant’s school or at a pre-booked room in a CAMHS outpatient setting. GSMs were initially held by a clinician with the aid of at least one researcher and both adult participants were invited to participate (see Figure 3). Over time the requirement to have a clinician present was dropped as researchers gained more training and experience and for pragmatic feasibility reasons.
The participation and randomisation processes were explained fully at the start of these sessions and the participants were given the opportunity to ask any questions they might have about the study. Consent forms were collected and checked before proceeding. The primary goals of the GSM were to:
-
set a unique goal by consensus for the participant to achieve
-
define and operationalise a specific behaviour related to the goal that they hoped to increase and one that they hoped to decrease as a result of achieving that goal.
The majority of the meeting was devoted to reaching this consensus. Baseline questionnaires were given to the participants near the end of the session and, if time allowed, participants could take some time to complete them in the presence of the researcher. A stamped addressed envelope was provided to return questionnaires that were not completed by the end of the session.
Randomisation and allocation concealment
After all baseline measures pertaining to a specific school had been returned, participants within that cluster were randomly allocated a group. A cluster randomisation approach by school was adopted to minimise the likelihood of participants in the intervention and comparator groups being affected by changes in teacher or school behaviour. School randomisation using minimisation was selected as an appropriate means to take into account the numbers of children with ASD, levels of support, the socioeconomic status of the school (as measured by the deprivation indices) and the school’s academic achievement (as measured by their value added measures). The cut-off points for each of these variables are described in Table 21. School Value Added Measure categories were determined by using the central value of 100 [on which KS1 to KS2 (Primary School) value added measures are based] and the central value of 1000 [on which KS2 to KS4 (Secondary School) value added measures are based].
| ASD Support | School deprivation score | School value added measure | Number of children with ASD |
|---|---|---|---|
| School has specialist autism unit | High deprivation: score equal to or greater than 13.8 | Scores between 95.00 and 99.99 | 1 or 2 |
| School has no specialist autism unit | Low deprivation: score less than 13.8 | Scores between 100.00 and 105.00 | 3 and above |
| Scores between 900.00 and 999.99 | |||
| Scores between 1000.00 and 1100.00 |
Allocation to groups was conducted by the York Clinical Trials Unit through use of a custom-made computer program which accounted for the stratification variables. The program did not contain any personal details but allocated participants by anonymous participant numbers. Once allocation was made, the school and all participants were informed of their allocation. Researchers attempted to inform adult participants of their group by phone or e-mail as soon as possible after allocation. A letter with this information and details on what their particular allocation involved was also sent out to all adult participants.
Intervention
Adult participants in the intervention group were invited to the next available training day and were given a copy of the Social Stories training manual to read through. The training day was a half-day group session including many parents and teachers (usually about 3 hours long) and taught the participants how to create and deliver the intervention. Times of training were designed to maximise attendance and were suggested with key input from PPI representatives. The first half of the session consisted of a presentation detailing the theory behind Social Stories and the practicalities of writing and delivering them. The structure of the presentation closely mirrored that of the manual, making reference to it in places. The second half of the training session was devoted to creating the Social Story for the goals set in the GSM for each participant. The adult participants constructed and revised their stories with support from the specialist trainers and other members of the research team to ensure that the finished product followed all of Gray’s criteria. 3 In this way, by the end of the session, the adult participants left with a fully constructed narrative for the Social Story for the particular goal to be measured for the participant. Guidance was also provided on how to format the story to individualise it to the particular child’s needs (e.g. story book format, Microsoft PowerPoint slides or on a single sheet of A4 paper). Most participating teachers did this at school in their own time, involving the child when possible.
The delivery of the intervention was left up to the adult participants with regard to how often and by whom the story was read. This approach is consistent with the individualised nature of the Social Story intervention, which is driven by the child’s needs and ability. As such, the adult participants were not required to read the story to children who would prefer to read it by themselves (as was the case with the older participants) as long as time was set aside for the child to have an opportunity to read the story with the adult participant present. As a starting point, the researchers suggested that the story could be read three times a week at school for 2 weeks by the participating teacher, but the adult participants were told to use their judgement based on their knowledge of the child as to how much to present the story and for how long. Adult participants were asked to record the frequency at which they read the stories using a behavioural diary. Guidelines were given to the adult participants in relation to the delivery of Social Stories including that it was not to be presented directly after a negative behaviour that they were hoping to reduce. This was to minimise the likelihood of the intervention being experienced as punitive.
Comparator group
Adult participants in the comparator group were asked to choose a typical age appropriate story of interest to the child and were given similar guidance on reading it to those in the intervention group. A letter detailing how to present this story was sent to the adult participants and this included a date to start delivering the attention control. Similar to the intervention group’s instructions, the adult participants were not required to read the story to children who would prefer to read it by themselves, as long as time was set aside for the child to have an opportunity to read the story with them present. They were advised that as a starting point, the story could be read three times a week for 2 weeks but were told to use their judgement based on their knowledge of the child as to how much to present the story and for how long. Adult participants were asked to record the frequency at which they read the stories using a behavioural diary.
Follow-up
Follow-up outcome measures were sent to all participants by post at 6 and 16 weeks after the training date for participants in the intervention group and an equivalent date for participants in the comparator group based on the date on which they were informed of their allocation. Stamped addressed envelopes were provided with the questionnaires but participants were also informed that researchers were available to collect them if this was more convenient.
The comparator group were offered a place on the next available training session after they completed participation on the feasibility trial. The PPI representatives were keen for this to occur to make sure that participating families gained skills and knowledge as acknowledgement for participation. For ethical reasons, we offered a place to anyone on a training session who had participated in the study even if they had not returned all questionnaires. Full details of participation are outlined in Figure 3.
Outcome measurement
Feasibility outcome measurement
The feasibility of participant recruitment was determined by examining the number of child participants assessed for eligibility; the number eligible; reasons for ineligibility; reasons for non-participation; and the number randomised. In addition, comparisons were made between recruitment techniques.
The feasibility and acceptability of data collection processes were investigated through the number of missing items and follow-up rates relating to the clinical outcome measurements likely to be used in a full-scale trial. The acceptability of the treatment was examined through assessing the reasons reported for withdrawal from treatment, qualitative interviews (see Chapter 9) and follow-up questionnaires.
Clinical outcome measurement
Potential primary outcome selection
The following measures were considered as potentially appropriate to be selected as the primary outcome in a full scale RCT. Consideration was given to outcome measures that included measurements of both challenging and more positive social behaviours.
-
The SDQ. 115 The SDQ is a brief child mental health screening questionnaire. It was completed by participating parents, teachers and older children (11–15 years).
-
The SRS-2. 116 The SRS-2 identifies social impairment associated with ASD and quantifies its severity. It was completed by the teachers.
-
A goal-based outcome measure, designed by the research team, to enable individualised goals and measured on an 11-point Likert scale (see Appendix 13). This was promoted by PPI representatives who were keen to capture parent or teacher goals rather than more general questionnaire-based measures. It was completed by the all participants.
-
Behavioural frequency measures, designed by the research team, to enable individualised goals and measured on a 5-point Likert scale. There were two of these scales: one of which measured a desired behaviour and one which assessed a challenging behaviour (see Appendix 14). They were completed by all participants.
-
A diary, designed by the research team to collect data on the frequency of use of the intervention and directly count the frequency of the behaviours across the school day (see Appendix 13). It was completed by adult participants.
Other potential outcomes
The following measures were considered as potentially appropriate to be selected as the secondary outcome measures in a full-scale RCT. The first three of these measures relate to health economics and are detailed in Chapter 8.
-
Bespoke resource-use questionnaires were developed by the health economist to capture the resource implications of child’s behavioural problems at school and home (see Appendix 16 and 17). These were completed by the adult participants.
-
The EQ-5D proxy and the EQ-5DY. 117 These are standardised instruments for use as measures of generic health outcomes recommended by NICE. They were completed by the participating parents and children respectively.
-
The HUI2. 118 This is an alternative preference-based generic health outcome measure to establish health states in children, and to report their health-related quality of life and related produce utility scores. It was completed by the participating parents.
-
The PSI-4. 119 The PSI-4 is designed to evaluate the magnitude of stress in the parent–child system. It was completed by the participating parents.
-
The Spence Children’s Anxiety Scale (SCAS). 120 The SCAS is a 44-item questionnaire developed to assess the severity of anxiety symptoms broadly in line with the dimensions of anxiety disorder. It was completed by the participating children.
Statistical analysis
We report the flow of participants through this study according to the CONSORT (Consolidated Standards of Reporting Trials) guidelines for non-pharmaceutical interventions. In line with recommendations about good practice in the analysis of feasibility studies,123 no comparisons of the outcomes between the two arms of the study were conducted. Descriptive statistics were calculated for recruitment rates, follow-up rates, attrition and for baseline characteristics. These are presented as means and SDs or 95% CIs, medians and IQR, or percentages. Descriptive statistics are also calculated for the outcome measures. We will use the data to develop estimates for a fully powered RCT taking into account attrition and follow-up rates. All analyses were undertaken on IBM Statistical Product and Service Solutions (SPSS) version 21 (IBM Corporation, Armonk, NY, USA).
Adverse events
Adult participants were provided with a contact telephone number to ring if they had any concerns about the study. Any concerns raised were either dealt with by members of the research team or referred to an appropriate clinician or services as per usual practice. This research team recorded details of all adverse events reported to them.
The trial manager informed the chief investigator/delegated clinician and two members of the TMG when an event was recorded, who jointly decided if it should be reported to the main research ethics committee. An occurrence was reported if it was suspected to be related to the intervention or an aspect of the research procedures (e.g. completion of follow-up questionnaires, participation in qualitative substudies or telephone contact). Related and unexpected serious adverse events were reported to the main research ethics committee within 15 days of the chief investigator/delegated clinician becoming aware of the event. The occurrence of adverse events during the study was monitored by an independent Data Monitoring Ethics Committee and the Trial Steering Committee. The Data Monitoring Ethics Committee/Trial Steering Committee immediately saw all serious adverse events thought to be treatment related and saw serious adverse events not thought to be treatment related by the TMG at the next scheduled meeting.
Results
Recruitment
Owing to overlap between the three different recruitment methods, participants within the same cluster were often recruited through different means. Therefore, for clarity, the recruitment breakdown is reported according to recruitment of schools and participants separately.
School recruitment
Thirty-eight schools were recruited within the 12-month period between February 2013 and January 2014; one of which withdrew from the study before participating. All three recruitment methods were successful in gaining school support for the feasibility trial.
The research team identified 131 schools in the York area through the school performance tables on the Department of Education website. Three additional schools that were not listed on the performance tables because they were private or independent schools were identified through contact with parents on the ASCEND122 course. This led to a total of 134 potentially eligible schools in the York area.
Of the schools initially identified, five were known to be ineligible as a result of taking part in phase 1 of the study in either the focus groups (see Chapter 4) or the pilot study (see Chapter 6). Through direct contact with some of the remaining schools, 25 were found to be ineligible because they had no students with ASD. Two additional schools that did have students with ASD were found to be ineligible, as they regularly used Social Stories with eligible children. Twenty-five further schools were not interested in taking part in the feasibility trial and their eligibility was not checked. No information is known on the remaining 39 schools, as no contact was made bar the initial invitation letter as the research team met recruitment targets before it was necessary.
Of the 38 schools recruited to the study, 27 were recruited through following up with the schools directly by phone after the initial invitation letter. However, one of these withdrew from the feasibility trial before baseline at the request of a parent. Eleven schools were recruited indirectly through contact with a parent of one of their students. This parental contact occurred through the ASCEND122 course in six cases. The remaining five cases were referred to the research team by clinicians and a specialist autism teacher. School recruitment is summarised in Figure 4. In the majority of these schools (34) separate teachers were recruited for each participating child. However, in three schools only one teacher was provided for multiple students (two students in two schools and three in one school). We allowed for this initially as part of the analysis of the trial’s feasibility, but it quickly became apparent that the quality of the data was being impacted on and we required a separate participating teacher for each child thereafter.
FIGURE 4.
Numbers of schools recruited through the three recruitment methods. SS, Social Story.

Participant recruitment
Including withdrawals before participation, 52 participant groups with ASD were recruited to the feasibility study. Two participants withdrew before baseline collection. In both of these cases the parents made this decision and stated that they did not feel the intervention would benefit their child. A full breakdown of recruitment follows and is summarised in Figure 5.
FIGURE 5.
Number of participant groups recruited by three different recruitment methods. SS, Social Story.
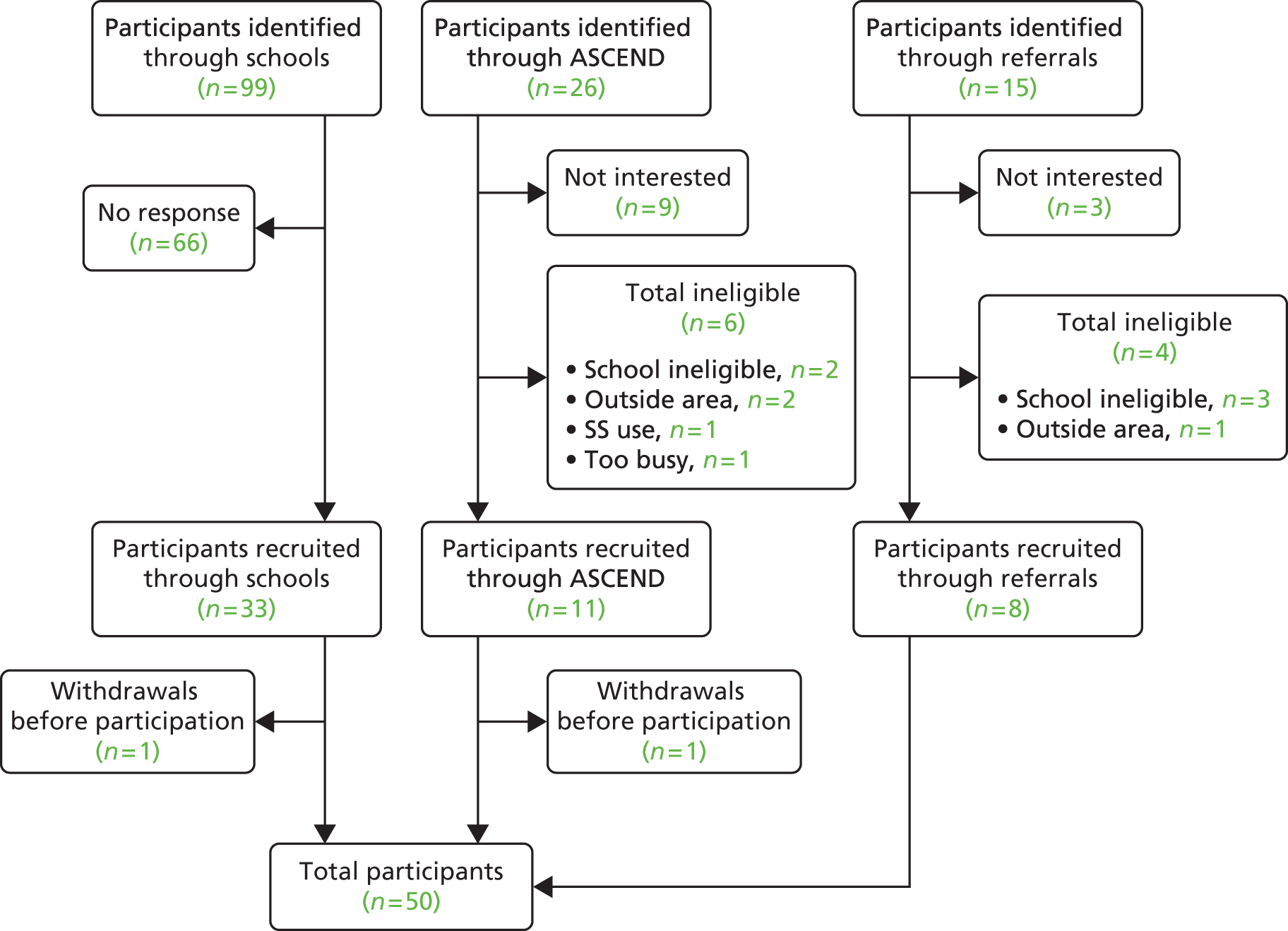
Direct recruitment of schools
Within the 38 schools recruited, teachers identified 99 children who met the eligibility criteria. As outlined in Chapter 7, Methods, schools were asked to pass on a recruitment pack to each of these children. Thirty-three participant groups were recruited through this method, although one group withdrew from the study before participation. As this withdrawal was the only eligible child participant within the school, the school also had to withdraw from the study.
Direct recruitment of parents
Twenty-six parents of children with ASD attending the ASCEND122 course expressed interest in the feasibility trial. Of these, nine decided not to participate after hearing full details on what the study involved. Six of the remaining 17 were found to be ineligible as the school their child attended was either not in the targeted area (one case), had already taken part in the study (two cases), had used Social Stories with the child (one case) or were too busy (one case). This left a total of 11 participants recruited through this method; however, one of these withdrew before participation.
Recruitment through referrals
Fifteen parents of children were referred to the research team either through clinicians connected to the ASD Forum or the specialist autism teacher. After contacting these parents, nine expressed interest in participating in the feasibility trial. Four of these were found to be ineligible, as the school their child attended was either not in the targeted area (one case) or had already taken part in the study (three cases). This left a total of eight participants recruited through this method.
Randomisation
All participants consented to random allocation. School randomisation was stratified using minimisation to take into account the number of ASD children attending the school, the levels of ASD support given, the socioeconomic status of the school (as measured by the deprivation indices) and the school’s academic achievement (as measured by their value added measures). Thirty-seven schools were allocated to either the intervention or the comparator arms of the study. Eighteen schools were allocated to the comparator group and 19 to the intervention group. As the average cluster size was higher in the schools allocated to the comparator group, this resulted in 27 participant groups being allocated to the comparator group and 23 to the intervention group.
In some cases there were delays to the randomisation process with participants waiting between 3 and 6 weeks to be allocated to a group. These delays were thought to be because of two factors, the requirement to record observations of the target behaviour over the course of a week and the cluster design methodology, which meant there were some instances in which participant groups that had completed their baseline measures had to wait for others in the same cluster to complete theirs.
To improve the logistics of the feasibility trial, the requirement to complete a diary was withdrawn for the last 12 participant groups. This alteration to the procedure led to shorter and less in-depth GSMs, subsequently allowing for more time within the meeting to complete baseline questionnaires. This impact of this change on the study logistics is discussed under Study logistics.
Characteristics of clusters
Table 22 shows the characteristics of the schools by allocated group. Clusters ranged in size from one to four participant groups with the majority containing only one. One participant group was recruited in 25 of the participating schools (71%). Two participant groups were recruited in eight of the participating schools (23%). Three participant groups were recruited in one participating school (3%). Finally, four participant groups were recruited in one participating school (3%).
| Characteristic | Intervention group | Comparator group | Total |
|---|---|---|---|
| School type breakdown | |||
| Primary schools | 13 | 12 | 25 |
| Secondary schools | 5 | 4 | 9 |
| Private/independent schools | 1 | 2 | 3 |
| Cluster size | |||
| Mean | 1.28 | 1.42 | – |
| Range | 1–2 | 1–4 | 1–4 |
| Cluster size breakdown | |||
| n = 1 | 12 | 13 | 25 |
| n = 2 | 5 | 3 | 8 |
| n = 3 | 0 | 1 | 1 |
| n = 4 | 0 | 1 | 1 |
Twenty-five of the recruited clusters were primary schools, nine were secondary schools and three were private/independent schools. Value added measure scores were found to be calculated differently for primary and secondary schools. Thus, these are reported on separately in Table 22.
Characteristics of participants
Table 23 summarises the characteristics of the child participants recruited to the feasibility trial. The majority of these participants were male (74%), which is consistent with the distribution of ASD in the population. Most of the participants were recruited from primary schools (62%). The participants assigned to the comparator group were slightly older on average, as more participants who attended secondary schools were assigned to it. This was a result of two clusters that were larger than the average, which were both assigned to the comparator group.
| Characteristic | Intervention group | Comparator group | Total |
|---|---|---|---|
| Gender | |||
| Male | 19 (83%) | 18 (67%) | 37 (74%) |
| Female | 4 (17%) | 9 (33%) | 13 (26%) |
| Age at study entry | |||
| Mean | 9.2 | 9.9 | 9.5 |
| SD | 2.67 | 2.46 | 2.63 |
| School type | |||
| Primary schools | 16 (70%) | 15 (56%) | 31 (62%) |
| Secondary schools | 6 (26%) | 10 (37%) | 16 (32%) |
| Private/independent schools | 1 (4%) | 2 (7%) | 3 (6%) |
Retention and completion of measures
The rates of completion of measures by participant groups according to allocation are shown in Table 24. Results differ markedly between questionnaire return rates and diary return rates. Differences were also noted between return rates of primary and secondary schools.
| Time point | Comparator | Intervention | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Teacher | Parent | Child | Teacher | Parent | Child | Teacher | Parent | Child | |
| Baseline | |||||||||
| Completed baseline questionnaire | 27/27 (100%) | 25/27 (93%) | 18/27 (67%) | 23/23 (100%) | 21/23 (91%) | 18/23 (78%) | 50/50 (100%) | 46/50 (92%) | 36/50 (72%) |
| Returned baseline diary | 12/19 (63%) | 11/19 (58%) | – | 13/19 (68%) | 11/19 (58%) | – | 25/38 (66%) | 22/38 (58%) | – |
| Intervention | |||||||||
| Commenced intervention | – | – | – | 23/23 (100%) | 17/23 (74%) | – | 23/23 (100%) | 17/23 (74%) | – |
| Completed intervention | – | – | – | 23/23 (100%) | – | – | 23/23 (100%) | – | – |
| 6 weeks | |||||||||
| Returned 6-week follow-up questionnaire | 24/27 (89%) | 21/27 (78%) | 15/27 (55%) | 21/23 (91%) | 16/23 (70%) | 12/23 (52%) | 45/50 (90%) | 37/50 (74%) | 27/50 (54%) |
| Returned 6-week diary | 13/19 (68%) | 8/19 (42%) | – | 15/19 (79%) | 7/19 (37%) | – | 28/38 (74%) | 15/38 (40%) | – |
| 16 weeks | |||||||||
| Returned 16-week follow-up questionnaire | 19/27 (70%) | 16/27 (59%) | 10/27 (37%) | 18/23 (78%) | 14/23 (60%) | 7/23 (30%) | 37/50 (74%) | 30/50 (60%) | 17/50 (34%) |
| Returned 16-week diary | 6/19 (32%) | 4/19 (21%) | – | 8/19 (42%) | 5/19 (26%) | – | 14/38 (37%) | 9/38 (24%) | – |
Questionnaire return rates
Teachers
With regard to baseline measurements, all 50 (100%) participating teachers returned the questionnaires. Forty five (90%) returned the 6-week follow-up questionnaires. Twenty four (89%) were returned from those in the comparator group and 21 (91%) from those in the intervention group. The response rates dropped for the 16-week follow-up questionnaires with 37 (74%) returning these questionnaires. This drop in rates was equivalent across groups with 19 (70%) being returned from those in the comparator group and 18 (78%) from those in the intervention group.
Parents
A slightly lower response rate was seen from participating parents at baseline, with 46 (92%) returning the questionnaires. Of the parent questionnaires that were not returned, two parents stated at the GSM before receiving them that although they were happy to take part in the study, they did not wish to fill out questionnaires because of time constraints. No explanation was given by the other two parents for not returning the questionnaires. Response rates were markedly lower at the 6-week follow-up point, with 37 (74%) returning their questionnaire. The drop seemed to be equivalent in both groups with 21 (78%) being returned from those in the comparator group and 16 (70%) from those in the intervention group. At the 16-week follow-up point questionnaire, response rate dropped further. Only 30 (60%) returned these questionnaires. Again the drop was equivalent for both groups 16 (59%) were returned from those in the comparator group and 14 (60%) from those in the intervention group. Reminder emails and a further questionnaire were sent or phone calls were made to those who did not respond but no further replies were received.
Children
The participating children had the lowest response rate. Thirty six (72%) of the children completed the questionnaires at baseline. This comparably low rate of returns for child questionnaires was unsurprising considering the range of ages and abilities of children with ASD in mainstream schools. This figure was taken as indicative of what proportion of this target population would be able to feasibly complete questionnaires.
These 36 participating children were sent a 6-week follow-up questionnaire and 22 (58%) were returned. As with the adult participants, this drop was equivalent across both groups, with 11 (58%) being returned from those in the comparator group and 11 (58%) being returned from those in the intervention group. At the 16-week follow-up point, 17 (34%) returned the questionnaires. As before, both groups had equivalent rates with 10 (37%) being returned from those in the comparator group and seven (30%) returned from those in the intervention group.
Owing to the vulnerable nature of this group of individuals, it was not considered ethical to send reminder emails or make phone calls either directly to these participants or indirectly to their parents or teachers, so unreturned questionnaires were not followed up by the research team for these participants.
Diary return rates
The rates of completion of diaries by the adult participants were markedly lower. The low rate of return of the diaries when compared with questionnaires led to them being removed for the last 12 participant groups to attempt to improve study logistics. Full details on the rationale behind their removal are provided in the Study Logistics section following. As such, percentage calculations are based on only the 38 participant groups who received the diaries and not on the total number of participants.
Rates of completion by participants according to allocated group are shown in Table 24. With regard to baseline diaries, 25 (66%) of the participating teachers and 22 (58%) of the participating parents completed the diaries.
Thirty-eight participating teachers were sent a 6-week follow-up diary and 28 (74%) returned these diaries. Of these, 13 (68%) were from those in the comparator group and 15 (79%) were from those in the intervention group. At the 16-week follow-up point, 15 (39.5%) returned the diaries. Of these, 8 (42.1%) were from those in the comparator group and 7 (36.8%) were from those in the intervention group. Reminder emails were sent and phone calls were made to those who did not respond but no further replies were received.
Thirty-eight participating parents were sent a 6-week follow-up diary and 19 (50%) returned these diaries. Of these, 8 (53%) were from those in the comparator group and 7 (46%) were from those in the intervention group. At the 16-week follow-up point, 9 (24%) returned the diaries. Of these, 4 (21%) were from those in the comparator group and 5 (26%) were from those in the intervention group. Reminder emails were sent and phone calls were made to those who did not respond but no further replies were received.
Comparison of questionnaire returns by school type
The rates of completion of follow-up questionnaires by teachers differed markedly by school type as shown in Table 25. For the purposes of this comparison, the three private/independent schools were re-categorised according to the age of the participating child.
| Time point | Primary (n = 34) | Secondary (n = 16) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Baseline measure | ||||
| Teacher | 34 | 100.0 | 16 | 100.0 |
| Parent | 31 | 91.2 | 15 | 93.8 |
| Child | 24 | 70.6 | 12 | 75.0 |
| 6-week follow-up | ||||
| Teacher | 32 | 94.1 | 13 | 81.3 |
| Parent | 25 | 73.5 | 12 | 75.0 |
| Child | 20 | 58.8 | 7 | 43.8 |
| 16-week follow-up | ||||
| Teacher | 26 | 76.5 | 11 | 68.8 |
| Parent | 20 | 58.8 | 10 | 62.5 |
| Child | 10 | 29.4 | 7 | 43.8 |
Despite the 100% completion rate at baseline, of the 16 participating teachers in secondary schools, only 13 (81.3%) returned their questionnaires at the 6-week follow-up point and 11 (76.5%) at the 16-week follow-up point. In comparison, of the 34 participating teachers in primary schools, 32 (94.1%) returned questionnaires at the 6-week follow-up point and 26 (76.6%) at the 16-week follow-up point. Similar differences were found when examining delays in questionnaire returns, as detailed in the next section.
Study logistics
Goal-setting
Goal-setting meetings were held for all 50 participant groups. Only the adult participants were invited to attend these meetings. Every effort was made to set a time when both participating teachers and parents could attend but, because of the conflicting nature of their respective timetables, this was not always feasible. When it became apparent that it would not be possible to arrange a convenient time for both adult participants, priority was given to the participating teacher because of the remit of the trial being an intervention for mainstream schools.
Of these 50 participant groups, 39 were held with both of the adult participants in attendance, 10 were held with just the participating teacher in attendance and one was held with just a participating parent in attendance. Of the 10 participating parents that could not attend, two had previously indicated that although they were comfortable participating in the research, they did not want to attend this meeting or complete the questionnaires. For the remaining eight participating parents, every effort was made to contact them by phone before the meeting to ask them if they had any views on what goals they would like to set for their child. For two of these parents, the research team was unable to do so but a researcher did arrange a meeting with them shortly afterwards to ensure they were comfortable with the goal set and to give them their baseline questionnaires. As previously indicated, there was one GSM for which only the participating parent could attend. This occurred as the participating teacher had to cancel on short notice because of bereavement. The teacher had been phoned prior to the meeting by a researcher to discuss goals and later met with them to ensure they were comfortable with the goal set.
The logistical issues for setting this meeting up due to conflicting timetables was impaired further by the availability of clinicians. Consequently, the time taken to set up this meeting once the participants agreed to attend was between 3 and 6 weeks. However, it was not considered appropriate for researchers to conduct the meeting alone, as clinicians often had to question the adult participants quite thoroughly to arrive at a goal that was measurable. The in-depth nature of the meeting also resulted in the participants not having time to complete the questionnaires within the meeting, leading to further delays with the randomisation process.
Owing to these difficulties, it was decided by the TMG that it was necessary to reduce the complexity and detail required in GSMs. This was done to both enable a researcher to conduct them at the school without requiring the presence of a clinician and allow for time to be set aside within the meeting to complete baseline questionnaires. This was achieved through the removal of the requirement for the completion of diaries for the last 12 participant groups.
Questionnaire retrieval time
Table 26 evidences the length of time taken to complete questionnaires after it was sent. When the date of completion was missing, it was replaced with the date received. There was no apparent difference between the control and intervention groups with regards to the length of time.
| Questionnaire | Comparator | Intervention | Total | |||
|---|---|---|---|---|---|---|
| Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | |
| Child | ||||||
| Baseline | 13.2 (12.1) | 18 | 10.2 (7.4) | 17 | 11.8 (10.1) | 35 |
| 16 weeks | 18.5 (29.8) | 10 | 18.1 (10.8) | 7 | 18.4 (23.3) | 17 |
| Teacher | ||||||
| Baseline | 11.2 (14) | 27 | 5.3 (8.5) | 23 | 8.5 (12.1) | 50 |
| 6 weeks | 19.8 (19.9) | 24 | 17.2 (12.3) | 18 | 18.6 (17) | 42 |
| 16 weeks | 13.7 (12.2) | 19 | 17.3 (19.5) | 18 | 15.5 (16) | 37 |
| Parent | ||||||
| Baseline | 10.8 (15.9) | 24 | 8.7 (9) | 21 | 9.8 (13.1) | 45 |
| 6 weeks | 16.3 (14.7) | 21 | 11.7 (7.7) | 16 | 14.3 (12.2) | 37 |
| 16 weeks | 19.6 (29.3) | 16 | 14.3 (9) | 12 | 17.4 (22.7) | 28 |
Effect of diary removal on retrieval times
There was some difficulty with receiving questionnaires back in good time despite reminder emails and phone calls. This was thought to be in part because of the requirement for the adult participants to complete a diary and also for baseline data because of the lack of time available in GSMs to complete questionnaires. The removal of the diaries for the final 12 participant groups allowed for a comparison of questionnaire response time as detailed in Table 27. Overall, the questionnaire response time for the final 12 participant groups compared with the first 38 was slightly shorter for adult participants and slightly longer for the participating child. However, the duration for retrieving the baseline measures from the adult participants was greatly improved. The mean retrieval time for the participating teachers’ questionnaires reduced from 10.4 days to 2.6 days with the SD also reducing. Similarly, retrieval time for the participating parents’ questionnaires reduced from 11.4 to 4.4 days.
| Questionnaire | First 38 participant groups | Last 12 participant groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparator | Intervention | Total | Comparator | Intervention | Total | |||||||
| Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | |
| Child | ||||||||||||
| Baseline | 14.9 (12.5) | 15 | 8.1 (6) | 14 | 11.6 (10.3) | 29 | 5.0 (6.2) | 3 | 20.0 (5.6) | 3 | 12.5 (9.8) | 6 |
| 6 weeks | 12.9 (10.3) | 13 | 10.8 (6.5) | 12 | 11.9 (8.6) | 25 | 3.5 (3.5) | 2 | – | – | 3.5 (3.5) | 2 |
| 16 weeks | 20.0 (31.2) | 9 | 15.5 (9) | 6 | 18.2 (24.3) | 15 | 5.0 (0.0) | 1 | 34.0 (0.0) | 1 | 19.5 (20.5) | 2 |
| Teacher | ||||||||||||
| Baseline | 15.2 (15) | 19 | 5.6 (9) | 19 | 10.4 (13.1) | 38 | 1.9 (3.6) | 8 | 4.0 (6.7) | 4 | 2.6 (4.6) | 12 |
| 6 weeks | 22.1 (20.7) | 17 | 18.3 (12.6) | 16 | 20.3 (17.1) | 33 | 14.0 (18.2) | 7 | 8.0 (4.2) | 2 | 12.7 (16.0) | 9 |
| 16 weeks | 10.9 (10) | 14 | 18.5 (20.3) | 16 | 15 (16.5) | 30 | 21.6 (15.5) | 5 | 8.0 (8.5) | 2 | 17.7 (14.7) | 7 |
| Parent | ||||||||||||
| Baseline | 14.4 (17.5) | 17 | 8.5 (8.7) | 18 | 11.4 (13.8) | 35 | 2.0 (5.3) | 7 | 10.0 (13.2) | 3 | 4.4 (8.5) | 10 |
| 6 weeks | 17.2 (15.5) | 15 | 9.8 (6.1) | 14 | 13.6 (12.3) | 29 | 14.2 (13.5) | 6 | 25.0 (1.4) | 2 | 16.9 (12.4) | 8 |
| 16 weeks | 23.9 (34.3) | 11 | 14.3 (9) | 12 | 18.9 (24.5) | 23 | 10.2 (10.7) | 5 | – | – | 10.2 (10.7) | 5 |
Comparison of questionnaire retrieval time between school types
It was also noted that, similar to the findings with respect to response rates, questionnaires from participating teachers from secondary schools were slower to arrive than those from primary schools. Table 28 displays the mean response time for questionnaires returned broken down by school type.
| Questionnaire | Primary | Secondary | Total | |||
|---|---|---|---|---|---|---|
| Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | |
| Child | ||||||
| Baseline | 12 (11.9) | 23 | 11.3 (5.5) | 12 | 11.8 (10.1) | 35 |
| 6 weeks | 10.1 (8.5) | 20 | 14.7 (8.4) | 7 | 11.3 (8.6) | 27 |
| 16 weeks | 14.5 (10.7) | 10 | 23.9 (34.9) | 7 | 18.4 (23.3) | 17 |
| Teacher | ||||||
| Baseline | 7.1 (10.8) | 34 | 11.6 (14.3) | 16 | 8.5 (12.1) | 50 |
| 6 weeks | 15.6 (12.1) | 29 | 25.5 (23.7) | 13 | 18.6 (17) | 42 |
| 16 weeks | 18.5 (17.7) | 26 | 8.5 (8.2) | 11 | 15.5 (16) | 37 |
| Parent | ||||||
| Baseline | 9.1 (11.4) | 30 | 11.2 (16.3) | 15 | 9.8 (13.1) | 45 |
| 6 weeks | 13.2 (10.8) | 25 | 16.7 (15) | 12 | 14.3 (12.2) | 37 |
| 16 weeks | 15.7 (18.9) | 18 | 20.3 (29.3) | 10 | 17.4 (22.7) | 28 |
Participant flow
There were some long delays in the flow of participants from expressing interest in the feasibility study through full enrolment (defined as participation in a GSM) to being allocated to a group. This would be unfeasible in a large pragmatic trial. In addition to the time taken to arrange a GSM described in the previous section, baseline data took between 2 and 8 weeks to be returned. Furthermore, although the randomisation process itself did not cause delays, it would then take between 2 and 4 weeks for adult participants to attend a training session. Consequently, it took between 6 and 14 weeks to be assigned a group and another 2 to 4 weeks after that for those in the intervention group to be trained. This was not deemed acceptable by the TMG for a full-scale trial. It was noted that the target behaviour could change in its severity or manifestation in the intervening period between setting the goal and receiving the intervention.
As already stated, it was decided that it was necessary to reduce the complexity and detail required in GSMs. This was to both enable a researcher to conduct them at the school without requiring the presence of a clinician and to allow for time to be put aside within the meeting to complete baseline questionnaires. The clinicians and researchers conducting these meetings reported that the thoroughness of questioning, required to establish a measurable target behaviour for the diaries, lengthened the meetings considerably. At this point, it had been ascertained that the response rate of the diaries was too low to be considered a feasible primary outcome measure and that they negatively impacted on baseline retrieval times. In addition, the quality of the data obtained was questionable because of the necessity for participants to complete the observations after a goal has been set, requiring them to not intervene throughout this time. With respect to their secondary purpose of examining the feasibility of operationalising behaviours that could be measured by an independent observer in a full-scale trial, we considered data from 38 participant groups sufficient to make this judgement. Consequently, they were removed to examine their effects on study logistics.
As discussed, it was decided to remove the diary requirement for the final 12 participant groups to see how it impacted the study logistics. The removal of the diaries reduced the time from agreement of participation to group allocation from 6 to 14 weeks down to 2 to 6 weeks. This was a substantial improvement that greatly increased the feasibility of the trial.
Delivery of the intervention
Training sessions were again well received (see Chapter 9). In order to take account of the feedback from teachers on the pilot study (see Chapter 6), sessions were reduced to a half-day slot by cutting down the introductory talk and providing lunch at the end rather than in the middle. To aid in the prompt delivery of the story, it was ensured that all participants left the training session with a completed narrative for the story and would just need to individualise the format for the child (through use of pictures, etc.).
To further test the feasibility of rolling out the study to a full-scale trial, a specialist autism teacher who had previously been involved in the user focus group (see Chapter 4) and an educational psychologist were trained to deliver the sessions by the clinicians. These sessions were monitored by the trial co-ordinator for consistency with the other trainers and were found to be successful in that regard.
With regard to the delivery of the Social Stories, no difficulties with implementing the intervention were reported to the researchers by participating teachers and parents. It was noted that, although the researchers requested a copy of the final story to be sent to the research team, only five (10%) of participant groups did so. This was not sufficient to examine treatment fidelity with regard to whether or not the stories themselves followed all Gray’s criteria. 3 This finding was considered an unexpected flaw with the current methodology and would need to be addressed in a future trial.
Adverse events
Only two adverse events were reported to the research team. Both were deemed to be unrelated to the intervention and not to be serious. One occurred in June 2013 when a child participant fell off swing and hurt his chest. A radiograph indicated no damage and he did not have to stay overnight at a hospital. The second event was reported in January 2014 when a child participant was reported to have tripped outside and fractured his wrist in November. The event had resolved itself by the time of discovery and did not require hospitalisation. The father indicated that the event was unrelated to treatment, as it occurred before they had received the training.
Outcome measurement
Completion rates and descriptive statistics for potential primary outcome measures
The following sections show the descriptive analysis and questionnaire completion rates for the appropriate outcome measures.
The Strengths and Difficulties Questionnaire
Completion rates for the teacher SDQ at baseline were 96% for the comparator group and 100% for the intervention group. At 6 and 16 weeks the completion rates were also high: comparator group (78% and 63%, respectively) and for the intervention group (91% and 74%, respectively).
Completion rates for the parent SDQ at baseline were 93% for the comparator group and 91% for the intervention group. At 6 and 16 weeks the completion rate was also high: comparator group (70% and 59%) and for the intervention group (70% and 61%).
The SDQ was only administered to participating children aged 11–15 years, of which there were 12 in the comparator group and seven in the intervention group. The completion rates for the SDQ at baseline were 75% for the comparator group and 57% for the intervention group. At 6 and 16 weeks the completion rates were 50% and 57%, respectively, for comparator group and 43% and 29%, respectively for the intervention group.
Table 29 shows the SDQ scores at each time point. The total difficulties score is based on 20 items in the questionnaire and results in a score ranging from 0 to 40 with a higher score indicating more difficulties. The pro-social score is based on five items in the questionnaire and results in a score ranging from 0 to 10 with a higher score indicating more pro-social behaviours. The overall distress and impairment scale generates an impact score that ranges from 0 to 10 for parent- and self-report, and from 0 to 6 for teacher-report, a higher score indicates higher impairment.
| Subscale | Comparator (n = 27) | Intervention (n = 23) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 Weeks | 16 Weeks | Baseline | 6 Weeks | 16 Weeks | |||||||||||||
| Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | |
| Teacher | ||||||||||||||||||
| Emotional symptoms | 3.2 (2.6) | 3 (1–6) | 26 | 3.1 (2.5) | 3 (1–5) | 21 | 3.2 | (2) 3 (2–4) | 17 | 3.8 (2.5) | 3 (1–6) | 23 | 3.7 (2.5) | 3 (2–6) | 21 | 3.8 (2) | 4 (2–5) | 17 |
| Conduct problems | 2.7 (1.4) | 2 (2–4) | 26 | 2.6 (1.1) | 2 (2–3) | 21 | 2.9 (1.5) | 3 (2–4) | 17 | 2.6 (1.3) | 2 (2–3) | 23 | 2.9 (1.4) | 3 (2–3) | 21 | 3.0 (1.5) | 3 (2–4) | 17 |
| Hyperactivity/inattention | 4.5 (1.8) | 5 (3–6) | 26 | 4.6 (1.4) | 5 (4–6) | 21 | 4.5 (1.4) | 5 (4–5) | 17 | 4.7 (1.5) | 5 (3–6) | 23 | 4.6 (1.3) | 5 (4–5) | 21 | 4.5 (1.4) | 4 (3–6) | 17 |
| Peer problems | 4.9 (1.0) | 5 (4–6) | 26 | 4.7 (1.5) | 5 (4–6) | 21 | 4.9 (1.1) | 5 (4–5) | 17 | 4.3 (1.3) | 4 (3–5) | 23 | 4.4 (1.2) | 4 (4–5) | 21 | 4.5 (0.9) | 4 (4–5) | 17 |
| Pro-social | 4.1 (2.6) | 4.5 (2–6) | 26 | 4.1 (2.8) | 5 (1–6) | 21 | 4.4 (2.8) | 4 (3–7) | 17 | 4.0 (2.3) | 4 (2–5) | 22 | 4.5 (2.6) | 5 (3–6) | 21 | 5.4 (1.5) | 6 (5–6) | 17 |
| Total difficulties | 15.2 (3.3) | 14.5 (12–17) | 26 | 15 (3.5) | 14 (13–17) | 21 | 15.4 (2.8) | 15 (13–17) | 17 | 15.3 (4.2) | 14 (13–18) | 23 | 15.6 (4.7) | 15 (12–18) | 21 | 15.9 (4.6) | 16 (11–20) | 17 |
| Impact | 2.5 (1.5) | 2 (1–4) | 26 | 0.5 (0.9) | 0 (0–1) | 17 | 0.8 (1.2) | 0 (0–1.5) | 12 | 2.6 (1.5) | 2 (1–4) | 23 | 0.6 (0.9) | 0 (0–1) | 18 | 0.2 (0.5) | 0 (0–0) | 16 |
| Parent | ||||||||||||||||||
| Emotional symptoms | 4.9 (2.7) | 6 (3–7) | 25 | 5.5 (3) | 6 (3–7) | 19 | 4.8 (2.7) | 5 (2.5–7) | 16 | 4.1 (2.5) | 4 (3–5) | 21 | 4.4 (2.7) | 4 (2–6.5) | 16 | 3.6 (2) | 3 (2–4) | 14 |
| Conduct problems | 3.6 (2.0) | 3 (2–4) | 25 | 3.4 (1.8) | 3 (2–4) | 19 | 2.9 (1.1) | 3 (2–3.5) | 16 | 3.0 (1.5) | 3 (2–4) | 21 | 3.1 (1.4) | 3 (2–4) | 16 | 3.0 (1.4) | 3 (2–3) | 14 |
| Hyperactivity/inattention | 4.7 (1.9) | 5 (4–6) | 25 | 4.5 (1.4) | 4 (3–6) | 19 | 3.9 (1.7) | 3.5 (3–5) | 16 | 4.6 (1.4) | 5 (4–6) | 21 | 4.0 (1.6) | 4 (3–5) | 16 | 4.9 (1.7) | 5 (4–6) | 14 |
| Peer problems | 5.5 (1.3) | 5 (5–6) | 25 | 5.5 (1.9) | 5 (4–6) | 19 | 5.7 (1.6) | 5.5 (5–6.5) | 16 | 5.9 (1.4) | 5 (5–7) | 21 | 5.2 (2) | 5 (3.5–7) | 16 | 5.6 (1.4) | 5 (5–7) | 14 |
| Pro-social | 4.1 (2.0) | 4 (3–5) | 25 | 4.3 (2.6) | 4 (3–7) | 19 | 4.6 (2.3) | 5 (3–6.5) | 16 | 4.9 (2.2) | 5 (4–6) | 21 | 5.4 (2.4) | 5.5 (4.5–6) | 16 | 6.1 (2.8) | 5.5 (5–9) | 14 |
| Total difficulties | 18.7 (4.3) | 19 (16–21) | 25 | 18.9 (5) | 18 (15–24) | 19 | 17.3 (3.7) | 17.5 (15–20) | 16 | 17.6 (3.9) | 18 (15–21) | 21 | 16.6 (4.2) | 15.5 (13–19.5) | 16 | 17.1 (4) | 16.5 (15–18) | 14 |
| Impact | 4.4 (2.7) | 4 (3–5) | 25 | 0.6 (1.1) | 0 (0–1) | 17 | 0.5 (1.1) | 0 (0–0.5) | 16 | 4.9 (2.6) | 5 (3–7) | 21 | 0.9 (1.5) | 0 (0–2) | 15 | 0.7 (1.5) | 0 (0–1) | 14 |
| Child | ||||||||||||||||||
| Emotional symptoms | 5.0 (3.2) | 4 (3–8) | 9 | 4.2 (3.5) | 3.5 (1–6) | 6 | 4.0 (2.8) | 5 (1–6) | 7 | 6.3 (2.2) | 6 (4.5–8) | 4 | 7.7 (2.5) | 8 (5–10) | 3 | 3.5 (3.5) | 3.5 (1–6) | 2 |
| Conduct problems | 3.3 (1.1) | 3 (3–4) | 9 | 2.2 (1) | 2 (2–2) | 6 | 2.3 (0.5) | 2 (2–3) | 7 | 2.8 (1) | 2.5 (2–3.5) | 4 | 4.3 (1.2) | 5 (3–5) | 3 | 3.5 (0.7) | 3.5 (3–4) | 2 |
| Hyperactivity/ inattention | 5.4 (1.2) | 5 (5–6) | 9 | 5.5 (1.6) | 5 (4–7) | 6 | 4.1 (1.9) | 3 (3–6) | 7 | 4.3 (1.5) | 4 (3–5.5) | 4 | 6.3 (3.2) | 5 (4–10) | 3 | 6.5 (3.5) | 6.5 (4–9) | 2 |
| Peer problems | 5.8 (1.6) | 5 (5–7) | 9 | 5.5 (1.6) | 5 (4–7) | 6 | 6.3 (1.4) | 7 (5–7) | 7 | 5.3 (1.3) | 5 (4.5–6) | 4 | 8.0 (1) | 8 (7–9) | 3 | 6.0 (1.4) | 6 (5–7) | 2 |
| Pro-social | 5.6 (2.9) | 7 (4–8) | 9 | 5.2 (3.1) | 5.5 (4–7) | 6 | 5.1 (3.4) | 4 (2–9) | 7 | 6.0 (3.7) | 6 (3–9) | 4 | 5.0 (2.6) | 6 (2–7) | 3 | 9.0 (0) | 9 (9–9) | 2 |
| Total difficulties | 19.6 (3.2) 19 | (17–21) | 9 | 17.3 (6) | 17 (12–22) | 6 | 16.7 (4.5) | 17 (15–19) | 7 | 18.5 (5.1) | 16.5 (15.5–21.5) | 4 | 26.3 (1.2) | 27 (25–27) | 3 | 19.5 (9.2) | 19.5 (13–26) | 2 |
| Impact | 2.4 (2.4) | 2 (1–3) | 9 | 0.2 (0.4) | 0 (0–0) | 5 | 0.1 (0.4) | 0 (0–0) | 7 | 6.0 (2.9) | 5.5 (4–8) | 4 | 0.7 (1.2) | 0 (0–2) | 3 | 0.0 (0) | 0 (0–0) | 2 |
As can be seen in the table, the scores in each group stay stable across time for all participant types. Despite the good completion rates, this stability indicates that the measure would not be suitable as a primary outcome measure as it does not capture any change in the behaviour of the child.
The Social Responsiveness Scale-2
Completion rates at baseline were 100% for the comparator group and 100% for the intervention group. At 6 and 16 weeks the completion rates were also high: 74% and 63%, respectively, for the comparator group and 91% and 74%, respectively, for the intervention group.
Table 30 shows the descriptive summary of the raw SRS-2 subscale and total scores. This is a 65-item questionnaire which can result in a score ranging from 0–195. Higher scores indicate more social and emotional difficulties. Raw scores can be converted to standardised t-scores which can be interpreted as follows: t-scores of 76 or higher are considered severe, t-scores of 66 through 75 are interpreted as indicating moderate deficiencies in reciprocal social behaviour that are clinically significant, whereas t-scores of 60 to 65 indicate mild deficiencies.
In the intervention group, the total mean scores fell over the time period of the study (baseline 103.1, 6 weeks 93.0 and 16 weeks 90.8), whereas in the comparator group the mean scores were more stable (baseline 90.8, 6 weeks 92.6 and 16 weeks 91.6). For the subscales, the same trends were observed. The high completion rates and positive trends in the scores indicate that this measure would be an effective primary outcome measure in a future trial.
| Subscale | Comparator (n = 27) | Intervention (n = 23) | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | |
| Social awareness | |||||||||
| Baseline | 11.5 (4.2) | 11 (8–15) | 27 | 13 (3.8) | 13 (10–15) | 23 | 12.2 (4.0) | 12 (9–15) | 50 |
| Social awareness 6 weeks | 10.7 (3.1) | 11 (9–13) | 20 | 10.9 (3.0) | 10 (9–13) | 21 | 10.8 (3.0) | 10 (9–13) | 41 |
| Social awareness 16 weeks | 11.6 (3.8) | 11 (10–13) | 17 | 11.5 (3.6) | 12 (10–13) | 17 | 11.6 (3.6) | 12 (10–13) | 34 |
| Social cognition | |||||||||
| Baseline | 17.9 (7.0) | 21 (11–24) | 27 | 19.8 (5.7) | 20 (15–24) | 23 | 18.8 (6.4) | 21 (13–24) | 50 |
| Social cognition 6 weeks | 17.3 (4.9) | 18 (15–20) | 20 | 18.9 (4.7) | 18 (16–20) | 21 | 18.1 (4.8) | 18 (15–20) | 41 |
| Social cognition 16 weeks | 17.1 (6.0) | 18 (14–21) | 17 | 17.8 (5.4) | 19 (15–21) | 17 | 17.4 (5.6) | 18 (14–21) | 34 |
| Social communication | |||||||||
| Baseline | 30.6 (10.8) | 29 (20–42) | 27 | 35.3 (10) | 35 (29–41) | 23 | 32.8 (10.6) | 34 (25–41) | 50 |
| Social communication 6 weeks | 31.8 (9.2) | 32 (26–40) | 20 | 30.3 (7.3) | 29 (26–32) | 21 | 31 (8.2) | 30 (26–34) | 41 |
| Social communication 16 weeks | 31.1 (10.6) | 29 (25–40) | 17 | 30 (9.9) | 27 (25–35) | 17 | 30.6 (10.1) | 28 (25–35) | 34 |
| Social motivation | |||||||||
| Baseline | 14.7 (4.7) | 15 (12–19) | 27 | 15.7 (5.6) | 16 (11–20) | 23 | 15.2 (5.1) | 15 (12–19) | 50 |
| Social motivation 6 weeks | 15.3 (4.9) | 15 (12–19) | 20 | 15.1 (4.5) | 15 (12–18) | 21 | 15.2 (4.6) | 15 (12–18) | 41 |
| Social motivation 16 weeks | 13.9 (6.7) | 14 (10–20) | 17 | 14.2 (5.0) | 14 (11–18) | 17 | 14.0 (5.8) | 14 (10–20) | 34 |
| Autistic mannerisms | |||||||||
| Baseline | 16.1 (6.3) | 16 (12–19) | 27 | 19.2 (6.5) | 18 (16–23) | 23 | 17.5 (6.5) | 17 (13–22) | 50 |
| 6 weeks | 17.6 (6.1) | 18 (13–22) | 20 | 17.8 (8.9) | 16 (11–25) | 21 | 17.7 (7.6) | 17 (12–24) | 41 |
| 16 weeks | 17.9 (6.1) | 18 (13–23) | 17 | 17.3 (8.3) | 15 (13–23) | 17 | 17.6 (7.2) | 17 (13–23) | 34 |
| Sum of four treatment subscales | |||||||||
| Baseline | 74.7 (23.8) | 75 (52–96) | 27 | 83.9 (21.8) | 83 (71–97) | 23 | 78.9 (23.2) | 81 (57–96) | 50 |
| 6 weeks | 75 (18.4) | 75 (61–89) | 20 | 75.2 (16.0) | 74 (66–81) | 21 | 75.1 (17.0) | 74 (64–86) | 41 |
| 16 weeks | 73.7 (24.1) | 74 (61–94) | 17 | 73.5 (21.8) | 69 (65–86) | 17 | 73.6 (22.6) | 72 (62–86) | 34 |
| Total raw score | |||||||||
| Baseline | 90.8 (28.2) | 90 (68–120) | 27 | 103.1 (26.3) | 101 (88–123) | 23 | 96.4 (27.8) | 97 (74–120) | 50 |
| 6 weeks | 92.6 (22.5) | 92 (76–110) | 20 | 93.0 (24.0) | 91 (78–107) | 21 | 92.8 (23) | 91 (78–108) | 41 |
| 16 weeks | 91.6 (29.1) | 87 (76–117) | 17 | 90.8 (29.2) | 88 (79–102) | 17 | 91.2 (28.7) | 88 (76–110) | 34 |
Table 31 shows the descriptive summary of the converted SRS-2 total raw scores converted to t-scores. A total t-score of 76 or higher is considered severe and strongly associated with a clinical diagnosis of ASD. A t-score of 60 through to 75 is interpreted as falling in the mild to moderate range and considered typical for children with mild or ‘high functioning’ ASD, while a t-score of 59 or fewer is regarded as being within typical limits. When the scores were converted, it was noted that eight of the participating children had scores that fell below this cut-off value (five in the comparator group and three in the intervention group). This suggests that 16% of the sample recruited may have had relatively limited social impairments, calling into question their need for intervention in this area. Further examination of the data for these children supported this assessment, as all eight either withdrew from the study or showed no change in scores at the follow-up points. This is an important consideration for screening participants in a future trial.
| Subscale | Control (n = 27) | Intervention (n = 23) | Total (n = 50) |
|---|---|---|---|
| Baseline | |||
| n | 27 | 23 | 50 |
| Mean (SD) | 72.2 (10.7) | 74.8 (9.6) | 73.4 (10.2) |
| Median (IQR) | 74 (62–81) | 74 (69–82) | 74 (67–81) |
| ≤ 59 | 5 (18%) | 3 (13%) | 8 (16%) |
| 60–75 | 11 (41%) | 9 (39%) | 20 (40%) |
| ≥ 76 | 11 (41%) | 11 (48%) | 22 (44%) |
| 6 weeks | |||
| n | 20 | 21 | 41 |
| Mean (SD) | 73.8 (10.1) | 71.5 (9) | 72.6 (9.5) |
| Median (IQR) | 75 (66–79) | 71 (65–75) | 71 (66–78) |
| ≤ 59 | 2 (10%) | 2 (9%) | 4 (10%) |
| 60–75 | 9 (45%) | 14 (67%) | 23 (56%) |
| ≥ 76 | 9 (45%) | 5 (24%) | 14 (34%) |
| 16 weeks | |||
| n | 17 | 17 | 34 |
| Mean (SD) | 72.3 (10.9) | 70.1 (10.7) | 71.2 (10.7) |
| Median (IQR) | 71 (64–80) | 71 (65–76) | 71 (64–78) |
| ≤ 59 | 1 (6%) | 3 (18%) | 4 (12%) |
| 60–75 | 10 (59%) | 9 (43%) | 19 (56%) |
| ≥ 76 | 6 (35%) | 5 (29%) | 11 (32%) |
Diaries
As stated earlier, the requirement for adult participants to complete diaries was removed part way through the feasibility study. This was in part to improve study logistics but also because of the delay in questionnaire retrieval times associated with diary completion, the comparably low rate of response for diary data particularly at follow-up points and the necessity for participants to complete the observations after a goal has been set which required them to not intervene despite this goal. Consequently, requiring participants to complete the diary was not considered feasible for use in a large pragmatic trial and their data were not analysed.
The inclusion of the diaries also had the secondary goal of examining the feasibility of using the GSM to operationalise individualised behaviours which an independent blinded observer could measure in a full-scale trial. To assess this, the resulting behaviours were examined and categorised by a researcher experienced in applied behaviour analysis and a researcher who had been present in the majority of GSMs. All 38 behaviours were categorised as measurable by a researcher trained in behavioural observation. However, of these, 13 were categorised as requiring a full day (low frequency, non-situational behaviours) for an accurate assessment rather than a set time period.
Goal-based outcome measure
There was an improvement in child scores in the intervention group with the mean scores increasing from baseline to 6 weeks and then a slight fall at 16 weeks (baseline 3.0, 6 weeks 7.9 and 16 weeks 7.6). In the comparator group there was a smaller increase in scores (baseline 3.9, 6 weeks 4.6 and 16 weeks 5.3).
Table 32 shows the descriptive summary of the question asking ‘How close are you to reaching your goal today’. This is rated on a scale from 0 (goal not met) to 10 (goal reached).
| Questionnaire | Comparator (n = 27) | Intervention (n = 23) | Total (n = 50) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | |
| Teacher | |||||||||
| Baseline | 2.8 (2.0) | 3 (1–4) | 27 | 1.9 (2.0) | 1.5 (1–2) | 22 | 2.4 (2.1) | 2 (1–3) | 49 |
| 6 weeks | 5.4 (2.7) | 5.5 (3–7) | 24 | 6.5 (2.9) | 7 (4–9) | 19 | 5.9 (2.8) | 7 (3–8) | 43 |
| 16 weeks | 5.4 (2.8) | 5 (3–8) | 19 | 7.3 (2.7) | 8 (6.5–9) | 16 | 6.3 (2.9) | 7 (4–9) | 35 |
| Parent | |||||||||
| Baseline | 2.5 (2.1) | 2 (1–3) | 25 | 2.1 (1.7) | 2 (1–3) | 20 | 2.3 (1.9) | 2 (1–3) | 45 |
| 6 weeks | 4.3 (2.9) | 5 (2–7) | 19 | 5.9 (2.4) | 5 (5–8) | 15 | 5.0 (2.8) | 5 (3–7) | 34 |
| 16 weeks | 4.0 (2.6) | 4.5 (2–6) | 14 | 7.2 (2.7) | 8 (6.5–8.5) | 12 | 5.5 (3.0) | 6 (3–8) | 26 |
| Child | |||||||||
| Baseline | 3.9 (2.4) | 4.5 (2–5) | 14 | 3.0 (2.8) | 2.5 (1–5) | 14 | 3.4 (2.6) | 3.5 (1–5) | 28 |
| 6 weeks | 4.6 (2.8) | 4.5 (2.5–7.5) | 12 | 7.9 (3) | 10 (6–10) | 10 | 6.1 (3.3) | 6.5 (3–10) | 22 |
| 16 weeks | 5.3 (2.3) | 6 (5–6) | 6 | 7.6 (2.1) | 8 (6–9) | 5 | 6.4 (2.4) | 6 (5–8) | 11 |
Completion rates for teachers at baseline were 100% for the comparator group and 97% for the intervention group. At 6 and 16 weeks the completion rate was also high: at 89% and 83%, respectively, for the comparator group and 83% and 70%, respectively, for the intervention group. There was an improvement in teacher scores in the intervention group with the mean scores increasing from baseline to 6 weeks and to 16 weeks (baseline 1.9, 6 weeks 6.5 and 16 weeks 7.3). In the comparator group, there was a smaller increase in scores (baseline 2.8, 6 weeks 5.4 and 16 weeks 5.4).
Completion rates for parents at baseline were 93% for the comparator group and 87% for the intervention group. At 6 weeks the completion rate was also high but rates reduced to approximately half the sample at 16 weeks: comparator group (70% and 52%) and for the intervention group (65% and 52%). There was an improvement in parent scores in the intervention group with the mean scores increasing from baseline to 6 weeks and to 16 weeks (baseline 2.1, 6 weeks 5.9 and 16 weeks 7.2). In the comparator group there was a smaller increase in scores (baseline 2.5, 6 weeks 4.3 and 16 weeks 4.0).
Completion rates for children at baseline were 52% for the comparator group and 61% for the intervention group. At 6 and 16 weeks the completion rates were much lower: at 44% and 22% for the comparator group and 43% and 22% for the intervention group. There was an improvement in child scores in the intervention group with the mean scores increasing from baseline to 6 weeks and then a slight fall at 16 weeks (baseline 3.0, 6 weeks 7.9 and 16 weeks 7.6). In the comparator group there was a smaller increase in scores (baseline 3.9, 6 weeks 4.6 and 16 weeks 5.3).
The high rates of return and positive trend in the results for the teacher questionnaires indicate that this would be an appropriate outcome measure for a large-scale trial.
Behavioural frequency Likert scales
Table 33 displays the ratings of behaviour by the parent for the target behaviour/social skill identified at the GSM that it was hoped would increase and Table 34 displays the target behaviour/social skill identified that it was hoped would decrease.
| Category | Response | Baseline | 6 weeks | 16 weeks | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparator | Intervention | Total | Comparator | Intervention | Total | Comparator | Intervention | Total | |||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Frequency on an average day | Never | 3 | 12 | 2 | 10 | 5 | 11 | 3 | 15 | 0 | 0 | 3 | 8 | 2 | 13 | 1 | 8 | 3 | 11 |
| Rarely | 7 | 28 | 10 | 48 | 17 | 37 | 5 | 25 | 1 | 6 | 6 | 17 | 4 | 27 | 1 | 8 | 5 | 18 | |
| Occasionally | 9 | 36 | 7 | 33 | 16 | 35 | 8 | 40 | 9 | 56 | 17 | 47 | 7 | 47 | 3 | 23 | 10 | 36 | |
| Frequently | 4 | 16 | 2 | 10 | 6 | 13 | 3 | 15 | 5 | 31 | 8 | 22 | 2 | 13 | 8 | 62 | 10 | 36 | |
| Very frequently | 2 | 8 | 0 | 0 | 2 | 4 | 1 | 5 | 1 | 6 | 2 | 6 | – | – | – | – | – | – | |
| Frequency on an average week | Never | 2 | 8 | 2 | 10 | 4 | 9 | 3 | 15 | 0 | 0 | 3 | 8 | 2 | 13 | 1 | 8 | 3 | 11 |
| Rarely | 5 | 20 | 5 | 24 | 10 | 22 | 4 | 20 | 1 | 6 | 5 | 14 | 2 | 13 | 1 | 8 | 3 | 11 | |
| Occasionally | 10 | 40 | 10 | 48 | 20 | 43 | 10 | 50 | 8 | 50 | 18 | 50 | 8 | 53 | 2 | 15 | 10 | 36 | |
| Frequently | 5 | 20 | 3 | 14 | 8 | 17 | 1 | 5 | 6 | 38 | 7 | 19 | 3 | 20 | 9 | 69 | 12 | 43 | |
| Very frequently | 3 | 12 | 1 | 5 | 4 | 9 | 2 | 10 | 1 | 6 | 3 | 8 | – | – | – | – | – | – | |
| Category | Response | Baseline | 6 weeks | 16 weeks | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparator | Intervention | Total | Comparator | Intervention | Total | Comparator | Intervention | Total | |||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Frequency on an average day | Never | 0 | 0 | 1 | 5 | 1 | 2 | 1 | – | 1 | – | 2 | – | 1 | 7 | 0 | 0 | 1 | 4 |
| Rarely | 2 | 8 | 4 | 19 | 6 | 13 | 3 | 16 | 2 | 13 | 5 | 15 | 3 | 21 | 3 | 25 | 6 | 23 | |
| Occasionally | 5 | 21 | 6 | 29 | 11 | 24 | 8 | 42 | 9 | 60 | 17 | 50 | 5 | 36 | 4 | 33 | 9 | 35 | |
| Frequently | 12 | 50 | 4 | 19 | 16 | 36 | 5 | 26 | 3 | 20 | 8 | 24 | 3 | 21 | 3 | 25 | 6 | 23 | |
| Very frequently | 5 | 21 | 6 | 29 | 11 | 24 | 3 | 16 | 1 | 7 | 4 | 12 | 2 | 14 | 2 | 17 | 4 | 15 | |
| Frequency on an average week | Never | 0 | 0 | 1 | 5 | 1 | 2 | 1 | – | 2 | – | 3 | – | 1 | 7 | 0 | 0 | 1 | 4 |
| Rarely | 2 | 8 | 4 | 20 | 6 | 14 | 2 | 11 | 2 | 14 | 4 | 12 | 1 | 7 | 3 | 25 | 4 | 15 | |
| Occasionally | 4 | 17 | 3 | 15 | 7 | 16 | 8 | 42 | 8 | 57 | 16 | 48 | 7 | 50 | 4 | 33 | 11 | 42 | |
| Frequently | 13 | 54 | 6 | 30 | 19 | 43 | 5 | 26 | 3 | 21 | 8 | 24 | 3 | 21 | 3 | 25 | 6 | 23 | |
| Very frequently | 5 | 21 | 6 | 30 | 11 | 25 | 4 | 21 | 1 | 7 | 5 | 15 | 2 | 14 | 2 | 17 | 4 | 15 | |
For the rating of behaviour by the parent for the target behaviour/social skill that it was hoped would increase, in the intervention group on an average day the proportion reporting never or rarely reduced from a baseline of 58% to 6% at 6 weeks and 16% at 16 weeks, whereas in the comparator group it remained at 40% for baseline, 6 weeks and 16 weeks.
For the rating of behaviour by the parent for the target behaviour/social skill that it was hoped would increase, in the intervention group on an average week the proportion reporting never or rarely reduced from a baseline of 34%, to 6% at 6 weeks and 16% at 16 weeks, whereas in the comparator group this was 28% at baseline, 35% at 6 weeks and 26% at 16 weeks.
For the rating of behaviour by the parent for the target behaviour/social skill that was hoped would decrease, in the intervention group on an average day the proportion reporting frequently or very frequently reduced from a baseline of 48% to 27% at 6 weeks and 42% at 16 weeks, whereas in the comparator group it was 71% at baseline, 42% at 6 weeks and 35% at 16 weeks.
For the rating of behaviour by the parent for the target behaviour/social skill that was hoped would decrease, in the intervention group on an average week the proportion reporting frequently or very frequently, reduced from a baseline of 60%, to 28% at 6 weeks and 42% at 16 weeks, whereas in the comparator group this was 66% at baseline, 47% at 6 weeks and 35% at 16 weeks.
Teacher behavioural frequency Likert scales
Table 35 displays the ratings of behaviour by the teacher for the target behaviour/social skill identified at the GSM that were hoped would increase and Table 36 displays the target behaviour/social skill identified that was hoped would decrease.
| Category | Response | Baseline | 6 Weeks | 16 Weeks | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparator | Intervention | Total | Comparator | Intervention | Total | Comparator | Intervention | Total | |||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Frequency on an average day | Never | 4 | 15 | 3 | 14 | 7 | 14 | 0 | 0 | 2 | 10 | 2 | 4 | 0 | 0 | 1 | 6 | 1 | 3 |
| Rarely | 11 | 41 | 8 | 36 | 19 | 39 | 5 | 21 | 4 | 19 | 9 | 20 | 4 | 21 | 3 | 18 | 7 | 19 | |
| Occasionally | 6 | 22 | 7 | 32 | 13 | 27 | 11 | 46 | 11 | 52 | 22 | 49 | 9 | 47 | 7 | 41 | 16 | 44 | |
| Frequently | 5 | 19 | 2 | 9 | 7 | 14 | 5 | 21 | 2 | 10 | 7 | 16 | 4 | 21 | 4 | 24 | 8 | 22 | |
| Very frequently | 1 | 4 | 2 | 9 | 3 | 6 | 3 | 13 | 2 | 10 | 5 | 11 | 2 | 11 | 2 | 12 | 4 | 11 | |
| Frequency on an average week | Never | 3 | 11 | 3 | 14 | 6 | 12 | 0 | 0 | 1 | 5 | 1 | 2 | 0 | 0 | 1 | 6 | 1 | 3 |
| Rarely | 8 | 30 | 6 | 27 | 14 | 29 | 5 | 21 | 3 | 14 | 8 | 18 | 3 | 16 | 2 | 12 | 5 | 14 | |
| Occasionally | 10 | 37 | 6 | 27 | 16 | 33 | 12 | 50 | 13 | 62 | 25 | 56 | 10 | 53 | 8 | 47 | 18 | 50 | |
| Frequently | 5 | 19 | 3 | 14 | 8 | 16 | 4 | 17 | 2 | 10 | 6 | 13 | 4 | 21 | 5 | 29 | 9 | 25 | |
| Very frequently | 1 | 4 | 4 | 18 | 5 | 10 | 3 | 13 | 2 | 10 | 5 | 11 | 2 | 11 | 1 | 6 | 3 | 8 | |
| Category | Response | Baseline | 6 Weeks | 16 Weeks | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparator | Intervention | Total | Comparator | Intervention | Total | Comparator | Intervention | Total | |||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Frequency on an average day | Never | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 9 | 2 | 10 | 4 | 9 | 2 | 11 | 1 | 6 | 3 | 9 |
| Rarely | 3 | 12 | 5 | 22 | 8 | 16 | 5 | 22 | 5 | 24 | 10 | 23 | 1 | 6 | 5 | 29 | 6 | 17 | |
| Occasionally | 9 | 35 | 4 | 17 | 13 | 27 | 10 | 43 | 8 | 38 | 18 | 41 | 9 | 50 | 5 | 29 | 14 | 40 | |
| Frequently | 12 | 46 | 5 | 22 | 17 | 35 | 5 | 22 | 6 | 29 | 11 | 25 | 6 | 33 | 5 | 29 | 11 | 31 | |
| Very frequently | 2 | 8 | 9 | 39 | 11 | 22 | 1 | 4 | 0 | 0 | 1 | 2 | 0 | 0 | 1 | 6 | 1 | 3 | |
| Frequency on an average week | Never | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 9 | 2 | 10 | 4 | 9 | 2 | 11 | 1 | 6 | 3 | 9 |
| Rarely | 2 | 8 | 3 | 14 | 5 | 10 | 4 | 17 | 4 | 20 | 8 | 19 | 1 | 6 | 4 | 24 | 5 | 14 | |
| Occasionally | 10 | 38 | 4 | 18 | 14 | 29 | 11 | 48 | 7 | 35 | 18 | 42 | 8 | 44 | 7 | 41 | 15 | 43 | |
| Frequently | 12 | 46 | 5 | 23 | 17 | 35 | 5 | 22 | 7 | 35 | 12 | 28 | 7 | 39 | 4 | 24 | 11 | 31 | |
| Very frequently | 2 | 8 | 10 | 45 | 12 | 25 | 1 | 4 | 0 | 0 | 1 | 2 | 0 | 0 | 1 | 6 | 1 | 3 | |
For the rating of behaviour by the teacher for the target behaviour/social skill that it was hoped would increase, in the intervention group on an average day the proportion reporting never or rarely, reduced from a baseline of 50%, to 29% at 6 weeks and 24% at 16 weeks, whereas in the comparator group this was 56% at baseline, 21% at 6 weeks and 21% at 16 weeks. On an average week the proportion in the intervention group reporting never or rarely reduced from a baseline of 41%, to 19% at 6 weeks and 18% at 16 weeks, whereas in the comparator group this was 41% at baseline, 21% at 6 weeks and 16% at 16 weeks.
For the rating of behaviour by the teacher for the target behaviour/social skill that it was hoped would decrease, in the intervention group on an average day the proportion reporting frequently or very frequently, reduced from a baseline of 61%, to 29% at 6 weeks and 35% at 16 weeks, whereas in the comparator group this was 54% at baseline, 26% at 6 weeks and 33% at 16 weeks. On an average week the proportion in the intervention group reporting frequently or very frequently, reduced from a baseline of 68%, to 35% at 6 weeks and 30% at 16 weeks, whereas in the comparator group this was 54% at baseline, 26% at 6 weeks and 39% at 16 weeks.
Secondary outcome measures
The Parental Stress Index, Fourth Edition Short Form
Table 37 shows the descriptive summary of the parental PSI-4 scores for each group at baseline, 6 weeks and 16 weeks.
| Subscale | Comparator (n = 27) | Intervention (n = 23) | Total (n = 50) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | |
| Parental distress | |||||||||
| Baseline | 56.3 (25.6) | 66 (34–80) | 24 | 67.6 (27.1) | 71 (50–92) | 21 | 61.6 (26.6) | 71 (46–82) | 45 |
| 6 weeks | 52.4 (34) | 51 (18–88) | 20 | 61.2 (33.4) | 64 (38–97) | 16 | 56.3 (33.6) | 59 (26–92) | 36 |
| 16 weeks | 47.5 (27.2) | 50 (27–68) | 15 | 51.1 (30.2) | 55 (36–68) | 14 | 49.3 (28.2) | 50 (27–68) | 29 |
| Difficult child | |||||||||
| Baseline | 85.7 (14.5) | 95 (76–98) | 24 | 84.6 (19.2) | 93 (81–99) | 21 | 85.2 (16.7) | 95 (76–98) | 45 |
| 6 weeks | 80.7 (20.8) | 87 (76–98) | 20 | 81.4 (21.7) | 85 (78–97) | 16 | 81 (20.9) | 86 (77–98) | 36 |
| 16 weeks | 81.1 (21.1) | 83 (81–97) | 15 | 76.4 (27.4) | 82 (76–96) | 14 | 78.8 (24) | 83 (76–96) | 29 |
| Parent–child dysfunctional interaction | |||||||||
| Baseline | 77.9 (17) | 83 (67–89) | 24 | 80.6 (15.8) | 83 (73–94) | 21 | 79.2 (16.3) | 83 (73–92) | 45 |
| 6 weeks | 76.2 (20.3) | 79 (67–93) | 20 | 79.1 (16.5) | 79 (70–95) | 16 | 77.4 (18.5) | 79 (67–95) | 36 |
| 16 weeks | 75.3 (20.2) | 80 (67–90) | 15 | 70.1 (22.8) | 78 (48–85) | 14 | 72.8 (21.3) | 80 (67–86) | 29 |
| Total stress | |||||||||
| Baseline | 76.4 (16.8) | 79 (65–89) | 24 | 79.1 (19.9) | 83 (74–92) | 21 | 77.6 (18.1) | 80 (67–91) | 45 |
| 6 weeks | 72.1 (25.4) | 78 (55–95) | 20 | 75.8 (21.2) | 76 (66–93) | 16 | 73.7 (23.4) | 76 (65–94) | 36 |
| 16 weeks | 71.1 (22.5) | 76 (58–91) | 15 | 66.9 (26.5) | 74 (61–79) | 14 | 69.1 (24.2) | 75 (61–87) | 29 |
| n/N (%) | n/N (%) | n/N (%) | |||||||
| Total stress (91st percentile or higher) | |||||||||
| Baseline | 6/24 (25) | 8/21 (38) | 14/45 (31) | ||||||
| 6 weeks | 7/20 (35) | 5/16 (31) | 12/36 (33) | ||||||
| 16 weeks | 4/15 (27) | 2/14 (14) | 6/29 (21) | ||||||
Completion rates at baseline were 89% for the comparator group and 91% for the intervention group. At 6 and 16 weeks the completion rate was also high: at 74% and 56% for the comparator group and 70% and 61% for the intervention group.
Total stress provides an overall level of stress that the parent is experiencing. In the intervention group the mean scores fell over the time period of the study (baseline 79.1, 6 weeks 75.8 and 16 weeks 66.9), whereas in the comparator group the mean scores were more stable (baseline 76.4, 6 weeks 72.1 and 16 weeks 71.1). For the subscales the same trends were observed (see Table 37).
Parents who obtain a total stress score in the 91st percentile or higher are deemed to be experiencing clinically significant levels of stress. 119 In the intervention group the percentage scoring in the 91st percentile or higher reduced over the period of the study (baseline 38%, 6 weeks 31% and 16 weeks 14%), whereas in the comparator group this remained more stable (baseline 35%, 6 weeks 35% and 16 weeks 27%). This analysis is limited because of missing data at 6 and 16 weeks, so these data were also investigated by just looking at the patients who had data both at baseline and at 6 weeks, and baseline and 16 weeks. In the comparator group (n = 20), the number who scored in the 91st percentile was 5 out of 20 (25%) at baseline and 7 out of 20 (35%) at 6 weeks. In the intervention group (n = 16), the number who scored in the 91st percentile was 5 out of 16 (31%) at baseline and 5 out of 16 (31%) at 6 weeks. At 16 weeks, in the comparator group (n = 15) the number who scored in the 91st percentile was 4 out of 15 (27%) at baseline and 4 out of 15 (27%) at 6 weeks. In the intervention group (n = 14) the number who scored in the 91st percentile was 3 out of 14 (21%) at baseline and 2 out of 14 (14%) at 16 weeks.
The high levels of completion and downwards trend in the scores indicate that this is an appropriate choice for a secondary outcome measure in a full-scale trial.
Spence Childhood Anxiety Scale
Completion rates out of those who returned the questionnaires at baseline were 59% for the comparator group and 70% for the intervention group. At 6 and 16 weeks the completion rates were much lower: at 48% and 30% for the comparator group and 48% and 30% for the intervention group.
This is a 38-item questionnaire which can result in a total score of 0–114. Higher totals indicate more anxiety. As can be seen in Table 38, in the intervention group the total SCAS mean scores fell over the time period of the study (baseline 38.3, 6 weeks 34.1 and 16 weeks 31.6). There were similar falls in the mean scores of the comparator group but they were more stable overall (baseline 34.8, 6 weeks 27.2 and 16 weeks 26.3). For the subscales the same trends were observed (see Table 38). The low rates of return for this questionnaire indicated it is not feasible to ask children with ASD to complete in a full-scale trial; however, the decreasing trend in the scores indicates a proxy measure may be an appropriate alternative for a secondary outcome measure.
| Subscale | Comparator (n = 27) | Intervention (n = 23) | Total (n = 50) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | Mean (SD) | Median (IQR) | n | |
| Baseline | |||||||||
| Total | 34.8 (14.1) | 35 (30–46) | 16 | 38.3 (20) | 39 (28–45) | 16 | 36.6 (17.1) | 36 (29–45) | 32 |
| Separation anxiety | 6.1 (4.1) | 6 (3–9) | 16 | 6.6 (3.7) | 7 (4–10) | 16 | 6.4 (3.9) | 7 (3–10) | 32 |
| Social phobia | 6.1 (3.3) | 6 (4–8) | 16 | 8.6 (3.8) | 10 (7–11) | 16 | 7.3 (3.8) | 7 (4–10) | 32 |
| Obsessive compulsive | 6.8 (3.9) | 6 (3–10) | 16 | 4.9 (4) | 4 (2–7) | 16 | 5.9 (4) | 5 (2–10) | 32 |
| Panic/agoraphobia | 4.2 (3.4) | 3 (2–8) | 16 | 5.6 (4.3) | 5 (3–6) | 16 | 4.9 (3.9) | 5 (2–7) | 32 |
| Physical injury fears | 4.4 (2.3) | 4 (3–6) | 16 | 5 (3.4) | 5 (3–7) | 16 | 4.7 (2.9) | 5 (3–6) | 32 |
| Generalised anxiety | 7.3 (3.8) | 8 (5–11) | 16 | 7.6 (4.4) | 7 (5–10) | 16 | 7.4 (4) | 7 (5–10) | 32 |
| 6 weeks | |||||||||
| Total | 27.2 (13.1) | 26 (19–37) | 13 | 34.1 (17.3) | 40 (15–44) | 11 | 30.4 (15.2) | 35 (17–43) | 24 |
| Separation anxiety | 5.0 (3.2) | 5 (3–6) | 13 | 6.5 (3.9) | 6 (3–10) | 11 | 5.7 (3.5) | 5 (3–9) | 24 |
| Social phobia | 5.3 (2.3) | 6 (4–7) | 13 | 7.3 (5.3) | 6 (3–14) | 11 | 6.2 (4.0) | 6 (4–8) | 24 |
| Obsessive compulsive | 4.4 (4.3) | 1 (1–8) | 13 | 5.1 (4.2) | 5 (1–9) | 11 | 4.7 (4.2) | 4 (1–9) | 24 |
| Panic/agoraphobia | 3.2 (3.2) | 3 (0–5) | 13 | 4 (3.9) | 3 (1–6) | 11 | 3.5 (3.5) | 3 (1–6) | 24 |
| Physical injury fears | 4.5 (2.3) | 4 (3–6) | 13 | 4.5 (2.5) | 5 (3–7) | 11 | 4.5 (2.3) | 4 (3–6) | 24 |
| Generalised anxiety | 4.8 (3.3) | 3 (3–8) | 13 | 6.7 (4.8) | 6 (2–12) | 11 | 5.7 (4.1) | 5 (3–10) | 24 |
| 16 weeks | |||||||||
| Total | 26.3 (13.0) | 24 (20–35) | 8 | 31.6 (14.3) | 34 (23–44) | 7 | 28.7 (13.4) | 24 (22–36) | 15 |
| Separation anxiety | 4.9 (4.1) | 4 (2–8) | 8 | 6.0 (3.4) | 6 (3–10) | 7 | 5.4 (3.7) | 4 (3–10) | 15 |
| Social phobia | 5.4 (3.1) | 5 (3–8) | 8 | 6.1 (3.5) | 7 (4–10) | 7 | 5.7 (3.2) | 5 (4–8) | 15 |
| Obsessive compulsive | 3.8 (2.8) | 4 (2–6) | 8 | 5.9 (4.2) | 3 (2–10) | 7 | 4.7 (3.6) | 3 (2–8) | 15 |
| Panic/agoraphobia | 3.0 (2.6) | 3 (1–5) | 8 | 3.9 (3.3) | 4 (1–6) | 7 | 3.4 (2.9) | 3 (1–5) | 15 |
| Physical injury fears | 4.0 (1.7) | 4 (3–5) | 8 | 3.7 (3.5) | 4 (1–6) | 7 | 3.9 (2.6) | 4 (2–5) | 15 |
| Generalised anxiety | 5.3 (3.7) | 5 (3–8) | 8 | 6.0 (3.7) | 6 (2–7) | 7 | 5.6 (3.6) | 6 (2–7) | 15 |
Power calculation for full-scale trial
We explored power based on two outcome measures, SRS score and teacher goal score. Both had face validity in terms of the study, in that they measure social responsiveness (the focus of the Social Story intervention) or the specific goal targeted. They both also had good completion rates because they were relatively easy to fill in.
Calculation based on Social Responsiveness Scale t-score total score
Calculations were undertaken based on the SRS-2 t-score total score using the change in score from baseline to 6 weeks. Table 39 showed the descriptive summary of the SRS-2 total scores. In the intervention group, the total mean scores fell over the 6 weeks from baseline (baseline 74.8 and 6 weeks 71.5), whereas in the comparator group the mean scores were slightly increased (baseline 72.2 and 6 weeks 73.8). When paired data were available, the scores showed similar trends (see Table 39). In the intervention group the total mean scores fell over the 6 weeks from baseline (baseline 77.30 and 6 weeks 72.28), whereas in the comparator group the mean scores were more stable (baseline 75.59 and 6 weeks 74.37). The intervention group’s scores changed by 5.28 (7.17 SD, n = 8) and 1.95 (6.79 SD, n = 19) in the comparator group from baseline to 6 weeks. Using the difference in the change in scores of 3.33 (i.e. 5.28 – 1.95), a sample size of 72 in each group would be required at 80% power to detect a difference of 3.33, assuming that the common SD is 6.975 using a two group t-test with a 5% two-sided significance level. At 6 weeks the completion rate was high: for the comparator group (74%) and for the intervention group (91%). So allowing for 80% response rate we require 90 participant groups, which is a total sample size of 180.
| Time point | Group | n | Mean | SD |
|---|---|---|---|---|
| Baseline | Comparator | 22 | 75.59 | 8.75 |
| Intervention | 20 | 77.30 | 7.53 | |
| 6 weeks | Comparator | 19 | 74.37 | 10.01 |
| Intervention | 18 | 72.28 | 8.84 | |
| Difference (6 weeks – baseline) | Comparator | 19 | –1.95 | 6.79 |
| Intervention | 18 | –5.28 | 7.17 |
A total t-score of 76 or higher is considered severe and strongly associated with a clinical diagnosis of autistic disorder. A t-score of 66 through 75 is interpreted as falling in the moderate range. We therefore saw the mean in the intervention group fall from 77.30 to 72.28, which is a fall from the severe range to the moderate range. Hence we were able to detect a clinically significant change.
Calculation based on teacher goal score
Table 32 showed the descriptive summary of the question asking ‘How close are you to reaching your goal today’. This is rated on a scale from 0 (goal not met) to 10 (goal reached). There was an improvement in child scores in the intervention group with the mean scores increasing from baseline to 6 weeks (baseline 3.0 and 6 weeks 7.9). In the comparator group there was a smaller increase in scores (baseline 3.9 and 6 weeks 4.6). When there was paired data, there was an increase from baseline to 6 weeks of 4.44 (2.81, n = 10) in the intervention group and 2.58 (2.30, n = 8) in the comparator group. To detect this difference, a sample size of 31 in each group will have 80% power to detect a difference in means of 1.86 assuming that the common SD is 2.53 using a two-group t-test with a 5% two-sided significance level. At 6 weeks, the completion rate for the goal was high: at 89% for the comparator group and 83% for the intervention group. So allowing for 80% response rate we require 39 participants per group, which is a 78 total sample size.
The goal-based score range is from 0 to 10, and we observed a difference in the change scores between groups of 1.86. As this is a subjective measurement, we cannot fully demonstrate if this is a clinically significant change.
Discussion
Summary of findings
We conducted a feasibility trial on the use of Social Stories to improve the behaviour of children with ASD attending mainstream schools. We sought to recruit 50 participant groups. We tested three methods of recruitment and all three showed a degree of success, with the school route being the most effective. We were able to recruit to target within the specified time frame of 12 months. All participants consented to randomisation and the resulting groups were equivalent in terms of their demographics. Retention and questionnaire return rates were high for adult participants although participating parents’ returns dropped sharply across follow-up points. We identified issues relating to study design, retention, intervention delivery and outcome measure selection to inform a future trial. No serious adverse events were reported.
Strengths of the feasibility study
Despite the challenges of attempting to involve both parents and teachers, who have very different availability, and the logistical delays described in this chapter, we have been able to fully recruit to this project on time and within budget. Multiple strategies of recruitment were used to determine the most appropriate method and establish networks to facilitate larger-scale recruitment were the study to be taken forward.
All participating teachers attended a training session, completed a Social Story and reported that they successfully delivered the intervention within the intervention period. We were able to improve the study logistics and speed up the process of participation through the removal of an outcome measure (the diaries) that required more time to administer, explain and complete than was feasible for a full-scale trial. Participant retention and completion of measures was also high on the feasibility trial with the notable exception of the children themselves although this is likely because of the range of abilities within this target population.
Two outcome measures, the SRS-2116 and the custom-made goal-based measure (see Appendix 14), both showed high levels of completion rates for participating teachers and a trend in the desired direction indicating that they would be suitable for use as primary outcome measures in a full-scale trial. Power calculations were conducted to give a total required sample size for this further trial.
A particularly important strength of this feasibility study has been the involvement of parent and teacher consultants. These have significantly informed our decision-making and also aided in recruitment through the ‘recruitment through referral’ strategy. These PPI consultants have attended the TMG and Trial Steering Committee meetings to offer advice and support throughout the study and have proved invaluable and a considerable asset to the study.
Limitations highlighted by the feasibility study
Participant flow was slow in some cases. This delay was found to be because of a combination of reasons such as the difficulty in arranging GSM, not enough time being set aside to complete measures, availability for training and waiting for all measures to be returned in a cluster before participants were randomly allocated to groups.
It was noted that 16% of the participating children recruited may not have had sufficient social impairments to warrant the intervention as measured by the SRS-2. 116 Change scores for these participants reflected this. This is an important consideration for a further trial.
Although the feasibility of using a behavioural frequency outcome measure which could be conducted by a blinded observer in a full-scale trial was assessed, an independent observer could not be employed on the feasibility study because of resource limitations.
Intervention fidelity was not assessed, as few participants sent the stories they had used to the research team to check against the criteria. A future trial should have a definitive time point at which these stories can be examined for fidelity.
Conclusions
The following points should be considered in the event of a full-scale trial on Social Stories in mainstream schools for children with ASD:
-
Recruitment is most effective when contacting schools directly. However, other strategies such as recruitment through parent support groups and professional referrals further augment this process.
-
Randomisation should take into account the age of the child and whether they are in primary or secondary school.
-
Cluster randomisation by school is not necessary for this sample because a low average cluster size.
-
Retention and questionnaire completion rates are highest for participating teachers, but also good for participating parents. The feasibility of collecting questionnaires from child participants is questionable.
-
Diary return rates were very low for both teacher and parents and these are considered not feasible to use in a full-scale trial.
-
Diaries revealed it was possible to operationalise behaviours for individual participants during the GSM but approximately one-third of the child participant’s resulting target behaviours required a full school day to measure effectively.
-
Two outcome measures, the SRS-2116 and the custom-made goal-based measure, showed both high levels of completion rates (for teachers), good face validity and a trend in the desired direction indicating that they would be suitable for use as primary outcome measures in a full-scale trial.
-
Delays in participant flow could be reduced by conducting less in-depth GSMs and removing the requirement to cluster by schools.
-
Power calculations suggest that a total sample size of 160 participant groups would be required for a full-scale trial using the SRS-2 or 78 participant groups using the goal-based measure.
-
It was not possible to assess the fidelity of the Social Stories to Gray’s criteria because of low rates of returns of the stories from participants. This is a methodological concern that needs to be addressed in future trials.
-
It was noted that although the researchers requested a copy of the final story used to be sent to the research team, only five (10%) of participant groups did so. This was not sufficient to examine treatment fidelity with regard to whether or not the stories themselves followed all Gray’s criteria. 3
-
Findings suggest that 16% of the sample recruited may not have had sufficient social impairments to warrant the intervention using the SRS-2. 116 Consideration could be given whether or not this could be used as an exclusion criterion.
Chapter 8 Feasibility of economic evaluation
Background
Cost-effectiveness analysis is an integral component of HTA. Given the cost of running fully powered RCTs, it is important to establish their feasibility to evaluate whether or not to conduct the trial and how to best to do so.
This part of the second phase of the ASSSIST study evaluated the feasibility of collecting data for economic analysis. More specifically, the economic study aimed to establish whether or not it was feasible to collect data on generic measures of health and relevant resource use in this population to allow estimation of costs associated with treatment delivery and associated health-care and societal costs (i.e. how various service usage changes given treatment and the costs associated with that change).
Health economic evaluations are commonly conducted using a UK NHS perspective which is in line with the recommendations of NICE. 124 However, recent UK evidence (2015) suggests that large proportions of the total costs of autism may be borne by the education system. 125,126
Given that Social Stories can be delivered by health and educational professionals, there may be health economic implications for both sectors. Therefore, an economic evaluation from an education system perspective may also be of relevance, given that the Social Stories intervention is usually implemented in schools. Moreover, challenging behaviour and social difficulties may have implications for social care, for voluntary services or youth justice services, or indeed for the productivity of carers of children with ASD (in the form of work absenteeism). Therefore, wider societal costs are likely to be relevant and it is important to establish feasibility of capturing resource information.
Objectives
The objectives of this economic evaluation were:
-
the feasibility of collecting data on outcome and resource use measures for cost-effectiveness analysis in a fully powered trial
-
the identification of relevant perspectives and related resource-use categories for cost-effectiveness analysis and evaluation of the feasibility and challenges of measuring costs and outcomes in the target population
-
the feasibility of conducting a within-trial cost-effectiveness analysis comparing Social Stories to treatment as usual for children with ASD.
Methods
This economic analysis is divided into two sequential stages:
-
evaluating response rates to establish feasibility of data collection for cost-effectiveness analysis
-
if data permits, conducting within-trial cost-effectiveness analysis of complete cases.
Exploration of outcome measures for the cost-effectiveness analysis
The first section of the feasibility evaluation aimed to explore outcome measures that are feasible to examine the impact of Social Stories on the child, on the parents (or carers) and within a school environment.
We evaluated response rates at follow-up; missing responses to conventional instruments used in economic evaluation (e.g. EQ-5D117, HUI2118 and resource-use questions) are evaluated over the study, including the degree of completion of instruments by various study participants. The feasibility of collecting data on condition-specific outcome measures of health (e.g. goal-based outcomes, SCAS120) may be considered as alternatives to generic measures. The feasibility of these measures has already been reported in Chapter 7. However, for the economic evaluation, generic quality-of-life instruments are preferred.
Within-trial cost-effectiveness analysis of complete cases
The second aim of the economic evaluation is to identify the relevant resource-use categories for the cost-effectiveness analysis. To demonstrate the feasibility of conducting a cost-effectiveness analysis, if a sufficient number of respondents provided complete responses, the second stage performed a within-trial cost-effectiveness analysis. To do so, the study conformed to guidelines for cost-effectiveness analysis by specifying an appropriate perspective, defining the outcomes of interest and indicating which categories of resource use are utilised to compare costs.
The evaluation was conducted from the UK societal perspective, taking account of the use of health services, education services and social and voluntary services over the study period.
Based on complete responses to the generic health measures and resource-use questionnaire, the feasibility of conducting a cost-effectiveness analysis of Social Stories was examined. The cost of Social Stories intervention was calculated using a bottom-up estimation of the time spent by professionals delivering the intervention, the cost of training and other resources used. Unit costs of health service use were obtained from the UK national database of reference costs. The cost of social services was calculated from the Unit Costs of Health and Social Care, produced by the Personal Social Services Research Unit, and the cost of other professional support was estimated from relevant salary scales. 127
Although the study was not powered to detect differences in outcome measures or resource use, the standard cost-effectiveness analysis utilised the available complete case data from the two measures of generic health (i.e. EQ-5D117 and HUI2118) to estimate quality-adjusted life-years (QALYs) and associated cost consequences from the resource-use questionnaire.
The analysis aimed to calculate the difference in costs (such as incremental costs), difference in effectiveness (i.e. incremental effectiveness) and the incremental cost-effectiveness ratio by taking a ratio of the incremental costs (C) and incremental effectiveness (E), formally denoted as:(1)ICER=ΔCΔE=C¯I−C¯CE¯I−E¯C.
Results
Feasibility of measuring generic health and resource use
In this feasibility aspect of the economic evaluation, we investigated the response rates of quality-of-life questionnaires (including item completion rates) which would allow health economic analysis to be conducted. The completion rate provides important information for design and data collection in relation to future full-scale trial. This section will review the response rates of economically relevant information, by whom this was reported and whether or not a cost-effectiveness analysis was feasible.
Feasibility of collecting data using European Quality of Life-5 Dimensions youth questionnaire and European Quality of Life-5 Dimensions proxy questionnaire117
Completions by participating children
The EQ-5D117 questionnaire is preferred by NICE124 as a means to estimate individuals’ preference for generic health states and thus to indicate the effectiveness of treatment in terms of QALYs. However, one important aim to assess feasibility for a study on children with autism was to understand how the children or their parents/carers report information on health status. To examine this, completion of the EQ-5D117 was requested for both participating children and parents.
Table 40 provides the completion rates at 6 and 16 weeks of children with ASD who are receiving Social Stories. This table shows that at 6 weeks, a total of 27 out of 50 questionnaires were returned. There were 12 out of 23 (52%) returned questionnaires in the Social Stories group and 15 out 27 (56%) returned in the comparator group. However, of the returned responses, the percentage of pupils who fully completed all items of EQ-5D117 questionnaires at 6 weeks was 83% in the Social Stories group compared with 87% in the comparator group. Of the returned questionnaires, the proportion of non-responders was high for the questionnaires self-completed by participating children compared with parents. Examining completion rates in participating children at 16 weeks, Table 40 shows that seven out of 23 returned the questionnaires from the Social Stories group (30%) and eight out of 27 in the control (30%) group. Of those who did return the questionnaire, all were able to complete the five items in the EQ-5D117 questionnaire.
| EQ-5D items | At 6 weeks | At 16 weeks | ||||||
|---|---|---|---|---|---|---|---|---|
| Social Stories (n = 23) | Comparator (n = 27) | Social Stories (n = 23) | Comparator (n = 27) | |||||
| Number of complete responses | % of all | Number of complete responses | % of all | Number of completes | % of all | Number of complete responses | % of all | |
| Mobility | 11 | 48 | 13 | 48 | 7 | 30 | 8 | 30 |
| Self care | 11 | 48 | 13 | 48 | 7 | 30 | 8 | 30 |
| Usual activities | 11 | 48 | 13 | 48 | 7 | 30 | 8 | 30 |
| Pain | 10 | 43 | 13 | 48 | 7 | 30 | 8 | 30 |
| Anxiety/depressed | 11 | 48 | 13 | 48 | 7 | 30 | 8 | 30 |
| Complete cases | 10 | 43 | 13 | 48 | 7 | 30 | 8 | 30 |
Completions by participating parents
Proxy respondents are used in health economics research when measurement is difficult or unreliable from the participants (such as patients with dementia or childhood conditions). Hence, as a potential alternative to obtaining a response about the child health state directly from the child, participating parents were asked to act as proxy to estimate the five items measured by the EQ-5D;117 proxy responses should, however, be examined carefully because psychometric tests of differential item functioning of EQ-5D117 suggest that proxies may be more likely to report health problems than the patients themselves in certain conditions. 128 However, this may prove to be an important strategy whereby it is established that children with ASD have a higher rate of non-response to questionnaires.
Table 41 provides the completion rates of the EQ-5D proxy117 at 6 and 16 weeks as completed and returned by the participating parents. The questionnaire return rates at 6 weeks showed a total of 37 out of 50 questionnaires returned, and at 16 weeks 30 out of 50. In the Social Stories group, 16 out of 23 (70%) of participants completed all items of the EQ-5D117 at 6 weeks and 14 out of 23 (61%) completed all items at 16 weeks. In the comparator group, 14 out of 23 (61%) participants completed all items of the EQ-5D117 at 6 weeks and 15 out of 27 (56%) completed all items at 16 weeks. Inspecting the overall sample available for cost-effectiveness analysis at 16 weeks, for complete-case analysis there would be 15 out of 23 (65%) in the intervention group and 13 out of 27 (48%) in the comparator group.
| EQ-5D items | At 6 weeks | At 16 weeks | ||||||
|---|---|---|---|---|---|---|---|---|
| Social Stories (n = 23) | Comparator (n = 27) | Social Stories (n = 23) | Comparator (n = 27) | |||||
| Number of complete responses | % of all | Number of complete responses | % of all | Number of complete responses | % of all | Number of complete responses | % of all | |
| Mobility | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Self care | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Usual activities | 16 | 70 | 21 | 78 | 14 | 61 | 15 | 56 |
| Pain | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Anxiety/depressed | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Complete cases | 16 | 70 | 21 | 78 | 14 | 61 | 15 | 56 |
Therefore, at 16 weeks there is a relatively high rate of non-responders. This suggests that if the full-scale trial is implemented, strong measures will need to be implemented to increase response rate. However, parents who returned the questionnaire had a high EQ-5D117 completion rate and almost always completed all items in the questionnaire.
To further explore the association between responses returned by the participating children and parents, Table 42 presents the correlation between completion rates of EQ-5DY and EQ-5D proxy117 by the participating parent. The EQ-5D117 was the only generic health questionnaire jointly piloted in both participating children and parents (who may be required to serve as proxy for the child with ASD in certain circumstances). Table 42 allows us to examine the relationship of the completion of questionnaires by the participating children to completion of questionnaires by the participating parents at both follow-up points (6 and 16 weeks, respectively).
| Number of unanswered items by parent | Number of unanswered items by child | ||||||
|---|---|---|---|---|---|---|---|
| 6 weeks | 16 weeks | ||||||
| 0 | 1 | 5 | Total | 0 | 5 | Total | |
| 0 | 21 | 1 | 15 | 37 | 15 | 14 | 29 |
| 1 | – | – | – | – | 0 | 1 | 1 |
| 5 | 2 | 0 | 11 | 13 | 0 | 20 | 20 |
| Total | 23 | 1 | 26 | 50 | 15 | 35 | 50 |
| Pearson χ2(2) | 7.5247; p = 0.023 | 15.5172; p = 0.000 | |||||
At 6 weeks, we observe that a total of 24 out of 50 children returned the EQ-5D117 questionnaire (one of whom missed one item out). In 22 of these 24, the participating parent provided a proxy version. In contrast (also at 6 weeks), when the child provided all five items, in most cases (21 out of 23) parents also provided the proxy version. Furthermore, a further 16 complete EQ-5D117 questionnaires were also available when participating children had partially or fully not completed the EQ-5D. 117 This means that, at 6 weeks from baseline, the parent proxy-version increased the number of complete cases from 23 to 39, a 68.6% increase of potential complete cases for economic analysis.
To further explore the association between the responses returned by the participating children and parents, Table 42 presents a cross-tabulation of completion rates of the EQ-5DY117 by the child and the EQ-5D-proxy117 by the parent. It shows that there is a clear relationship between child and parent responses in terms of having missing items (as shown by the χ2 test), that is when the parent returns the complete questionnaire, the child is also more likely to do the same. However, overall, participating parents were more likely to complete the quality-of-life questionnaire than children, who also have more missing items. For instance, at 16-week time point, 29 out of 50 (58%) parents returned complete questionnaire with no missing data compared with 15 out of 50 (30%) children in the study. Hence, we recommend that the EQ-5D proxy117 should be considered in a full-scale trial over the self-completed EQ-5D117 by children. However, further measures will need to be implemented to increase completion rates.
Whether or not child and parent proxy responses actually agree can only be tenuously explored. Using a Pearson product-moment correlation, these responses provisionally suggest only moderate correlation: baseline 0.5 (n = 30); 6 weeks 0.4 (n = 21); and 16 weeks 0.64 (n = 10). Consideration of the findings into psychometric research indicate that this is likely because of the parents’ tendency to report health issues. 128
Feasibility of Health Utilities Index: proxy version118
The HUI2118 is a multi-attribute health status classification system that provides an alternative method for measuring health-related quality of life. Studies using this measure provide UK-specific preference-based scoring systems to estimate QALYs. 118 HUI2118 has been deemed sensitive to characterise children with ASD129 and is generally preferable to EQ-5D117 in which research has a relation to cognition,130 as the questionnaire covers alternative attributes (sensation, mobility, emotion, cognition, self-care, pain and fertility) and up to five categorical levels per attribute. HUI2118 contains 16 questions and, to assess whether or not this is a feasible alternative proxy-questionnaire to the EQ-5D,117 the trade-off between increased questionnaire length and response rates have been explored.
Table 43 presents the completion rates of the HUI2118 questionnaire at the 6- and 16-week follow-ups. At the 6-week follow-up, 13 out of 23 (57%) of participants in the Social Stories group and 19 out of 27 (70%) in the control group provided fully complete HUI2118 questionnaires.
| Time points | 6 weeks | 16 weeks | ||||||
|---|---|---|---|---|---|---|---|---|
| Group | Social Stories (n = 23) | Comparator (n = 27) | Social Stories (n = 23) | Comparator (n = 27) | ||||
| HUI2 Items | Complete response | % of all (n = 23) | Complete response | % of all (n = 27) | Complete response | % of all | Complete response | % of all |
| Sight 1 | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Sight 2 | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Hearing 1 | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Hearing 2 | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Comprehension 1 | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Comprehension 2 | 15 | 65 | 20 | 74 | 14 | 61 | 16 | 59 |
| Happiness | 15 | 65 | 21 | 78 | 14 | 61 | 16 | 59 |
| Pain and discomfort 1 | 14 | 61 | 21 | 78 | 14 | 61 | 16 | 59 |
| Mobility | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Dexterity | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Memory | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Cognition | 16 | 70 | 21 | 78 | 14 | 61 | 15 | 56 |
| Daily living | 16 | 70 | 20 | 74 | 14 | 61 | 16 | 59 |
| Anxiety/depression | 16 | 70 | 21 | 78 | 14 | 61 | 15 | 56 |
| Pain and discomfort 2 | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Overall health | 16 | 70 | 21 | 78 | 14 | 61 | 16 | 59 |
| Complete cases | 13 | 57 | 19 | 70 | 14 | 61 | 15 | 56 |
At 16 weeks, 14 out of 23 (61%) participants in the Social Stories group and 15 out of 27 (56%) in the comparator group provided fully complete HU2118 questionnaires. Of those who completed the questionnaires, all items were completed in all cases in the Social Stories group and in 94% cases in the comparator group.
To examine whether or not there are patterns of responding based on specific items missed between the two follow-up time points, Table 44 presents a two-by-two table of the number of missing items at each time point. The main observation is that the majority of respondents who fully completed the HUI2118 at 6 weeks also completed questionnaire at 16 weeks, 54% of the total recruited sample. The second highest proportion are respondents who do not complete any of the 16 items of the HUI2118 at either 6 or 16 weeks, 24% of the recruited sample.
| Number of unanswered items at 6 weeks | Number of unanswered items at 16 weeks | |||
|---|---|---|---|---|
| 0 | 2 | 16 | Total | |
| 0 | 27 | 0 | 5 | 32 |
| 1 | 0 | 0 | 2 | 2 |
| 2 | 1 | 0 | 0 | 1 |
| 3 | 0 | 1 | 0 | 1 |
| 4 | 0 | 0 | 1 | 1 |
| 16 | 1 | 0 | 12 | 13 |
| Total | 29 | 1 | 20 | 50 |
| Pearson χ2 (5) | 5.9198; p = 0.314 | |||
The remaining 22% relates to parents who did not provide a complete HUI2118 questionnaire at either 6 or 16 weeks. The data specifically tell us that at 6 weeks, of the 37 participating parents who returned questionnaires, 32 fully completed them, two missed one item, one missed two items, one missed three items and one missed four items, creating a total of five respondents who attempted but did not fully complete the HUI2118 at one or more follow-ups. Examining this small group of partial HUI2118 completers, three out of five who omitted items at 6 weeks missed all items at 16 weeks. A possible explanation may be that some participants may have found the questionnaire lengthy; however, qualitative feedback from these individuals would help understand this better.
One possibility for not completing HUI2118 relates to specific items not being well understood. To explore this notion, Table 44 shows only one individual repeatedly missed items at consecutive time points, not answering two items on cognition (at 6 weeks), and omitting the same item on cognition again and one related to depression/anxiety at 16 weeks. This does not give sufficient evidence to make any reliable conclusions about specific items.
Feasibility of measuring resource consequences in adult participants
Aside from estimating the incremental health gains attributable to Social Stories (using the generic measures discussed in Feasibility of measuring generic health and resource use), to fully inform whether or not some other health-care intervention should be displaced (given the finite NHS budget), a cost-effectiveness analysis must appraise all costs associated with a new intervention (i.e. implementing Social Stories in schools).
The costs which must be considered are broadly divided into two groups, the cost of the new intervention (the inputs cost required) and resource-use consequences (resulting from change in service use following the new treatment). Both are important to consider when estimating the total cost associated with a new intervention.
Resource-use consequences (which translate into costs) are measured using resource-use questionnaires in this study. To consider the appropriate costs, it is important to state the perspective used to analyse cost consequences in the economic analysis. The most commonly used perspective is that of health-care services, which includes resource-use implications for primary and secondary care and community services. This perspective can be extended to include the resource use implications for the education sector because the Social Stories intervention is delivered by teachers and is likely to displace resources in schools. Finally, a wider societal perspective is also relevant and would include costs implications for social services and the criminal justice system. Moreover, cost of work absenteeism and lost productivity of parents with children with ASD are also relevant.
To assess resource use from these perspectives, we developed a bespoke resource-use questionnaire with advice from Professor Sarah Byford (an independent health economist with experience in mental health) for use with children on the autism spectrum where the intervention was taking place in school. Using this questionnaire, we evaluated the feasibility of collecting resource use data from the above perspectives. To primarily ascertain whether or not a fully powered RCT could capture such implications, a resource-use questionnaire was distributed to the adult participants.
Resource implication indicated by participating parents
Table 45 presents response rates to the first part of the bespoke questionnaire that was within the questionnaire booklet completed by participating parents. This tool is designed to estimate resource-use consequences, primarily from the health-care perspective (asking respondents to retrospectively indicate their use of primary, secondary and community services). It also considers relevant wider perspectives, such as education (e.g. absenteeism), social services (e.g. out of home placement or use of social services), and contact with justice services and parental productivity (e.g. income and absenteeism).
| Items of resource use | 6 weeks | 16 weeks | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Social Stories | Comparator | Social Stories | Comparator | |||||||||
| Number complete | % of returns (n = 16) | % of all (n = 23) | Number complete | % of returns (n = 21) | % of all (n = 27) | Number complete | % of returns (n = 14) | % of all (n = 23) | Number complete | % of returns (n = 16) | % of all (n = 27) | |
| Inpatient admission | 15 | 94 | 65 | 17 | 81 | 63 | 13 | 93 | 57 | 13 | 81 | 48 |
| Outpatient admissiona | 15 | 94 | 65 | 17 | 81 | 63 | 13 | 93 | 57 | 12 | 75 | 44 |
| Accident and emergency admissiona | 15 | 94 | 65 | 17 | 81 | 63 | 13 | 93 | 57 | 13 | 81 | 48 |
| Out of home placement | 7 | 44 | 30 | 4 | 19 | 15 | 2 | 14 | 9 | 1 | 6 | 4 |
| Prescribed medicationa | 14 | 88 | 61 | 11 | 52 | 41 | 12 | 86 | 52 | 13 | 81 | 48 |
| Use community health servicesa | 11 | 69 | 48 | 7 | 33 | 26 | 9 | 64 | 39 | 7 | 44 | 26 |
| Use counselling servicea | 14 | 88 | 61 | 14 | 67 | 52 | 11 | 79 | 48 | 11 | 69 | 41 |
| Use social service/support service | 10 | 63 | 43 | 12 | 57 | 44 | 9 | 64 | 39 | 9 | 56 | 33 |
| State another service | 9 | 56 | 39 | 14 | 67 | 52 | 8 | 57 | 35 | 10 | 63 | 37 |
| Criminal justices services | 15 | 94 | 65 | 14 | 67 | 52 | 12 | 86 | 52 | 12 | 75 | 44 |
| Parents accommodation | 16 | 100 | 70 | 20 | 95 | 74 | 14 | 100 | 61 | 15 | 94 | 56 |
| Child accommodation | 16 | 100 | 70 | 20 | 95 | 74 | 14 | 100 | 61 | 15 | 94 | 56 |
| Parent 1: employment status | 15 | 94 | 65 | 20 | 95 | 74 | 13 | 93 | 57 | 15 | 94 | 56 |
| Parent 2: employment status | 12 | 75 | 52 | 19 | 90 | 70 | 11 | 79 | 48 | 15 | 94 | 56 |
| Parent 1: income | 9 | 56 | 39 | 5 | 24 | 19 | 9 | 64 | 39 | 5 | 31 | 19 |
| Parent 2: income | 9 | 56 | 39 | 6 | 29 | 22 | 9 | 64 | 39 | 6 | 38 | 22 |
| Child absence from school | 15 | 94 | 65 | 19 | 90 | 70 | 14 | 100 | 61 | 15 | 94 | 56 |
| Parent 1: absence from work | 12 | 75 | 52 | 18 | 86 | 67 | 12 | 86 | 52 | 11 | 69 | 41 |
| Parent 2: absence from work | 9 | 56 | 39 | 17 | 81 | 63 | 11 | 79 | 48 | 10 | 63 | 37 |
| Parent 1: absence from work (ASD) | 15 | 94 | 65 | 18 | 86 | 67 | 12 | 86 | 52 | 13 | 81 | 48 |
| Parent 2: absence from work (ASD) | 11 | 69 | 48 | 16 | 76 | 59 | 10 | 71 | 43 | 10 | 63 | 37 |
| Complete cases | ||||||||||||
| Health perspective | 11 | 69 | 48 | 7 | 33 | 26 | 9 | 64 | 39 | 7 | 44 | 26 |
| Societal perspective | 7 | 44 | 30 | 4 | 19 | 15 | 2 | 14 | 9 | 1 | 6 | 4 |
Examining response rates to the resource questionnaire from parents at 6 weeks, six items relate to a health-care perspective. Overall, the percentages of all respondents completing these sections are 48% for Social Stories and 26% in the comparator group. At 16 weeks, the percentages are 39% for Social Stories and 26% in the comparator group.
We examined response completion rates of health-care use questions as a proportion of all returned questionnaires. We found that while most respondents completed questions about inpatient, outpatient and emergency care use, the response rates were low to medium for the use of community health services (between 33% and 69%). This may be because respondents who did not use community health services did not report ‘zero’ use in the questionnaire but left it blank instead. This gives some pointers towards design features. However, another explanation is that this item was not well understood and therefore should be revisited when the full-scale trial is designed. In the absence of further information, it is not possible to establish whether or not missing responses should be treated as zero.
To examine the implication for complete case analysis for health-care, Table 46 cross-tabulates the proportion of the sample with unanswered items at 6 and 16 weeks. This is under the assumption that missing responses do not represent zero resource use in a particular category. Under this scenario, 12% (6 out of 50) of the originally randomised sample would be available for a complete-case cost-effectiveness analysis with the perspective of the health-care system (specifically, Social Stories n = 3 and comparator n = 3).
| Number of unanswered items at 6 weeks | Number of unanswered items at 16 weeks | ||||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 5 | 6 | Total | |
| 0 | 6 | 2 | 1 | 0 | 0 | 4 | 13 |
| 1 | 3 | 4 | 0 | 1 | 1 | 2 | 11 |
| 2 | 2 | 4 | 1 | 0 | 0 | 1 | 8 |
| 4 | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| 6 | 1 | 0 | 0 | 0 | 0 | 16 | 17 |
| Total | 13 | 10 | 2 | 1 | 1 | 23 | 50 |
As indicated, a potential reason for missing data may be that zero resource use in a category is not reported by respondents (and instead appears as missing data). Under this assumption, if a respondent reports resource use for at least one category, then other categories with no response can be assumed to be zero. Using this scenario, 33 out 50 (66%) respondents will be available for analysis. However, with the current data set it is not possible to distinguish non-response because of zero use from non-response because of missing data. However, this highlights the importance of providing clear instructions to study participants and the potential need for supervised completion of questionnaire.
Education system perspective
Missed school days can have significant future costs, both in terms of missed education and longer-term impact on potential future earnings. The perspective of economic evaluation can be extended to consider cost of lost future earnings.
We evaluated the feasibility of collecting school absenteeism data using the following question in the resource-use questionnaire presented to parents: ‘How many days has your child been absent from school in the last 6 weeks?’, examining the proportion of the sample available to incorporate into a supplementary perspective, extending the economic analysis (i.e. available for complete-case analysis). Results suggest that 26 out of 50 (52%) participating parents provided complete information. Of the total number of participating parents who returned questionnaires, response rates were 94–100%.
Table 47 summarises statistics of the ‘number of school days reported as missed’ by parents. This illustrates that data on school absenteeism could feasibly be collected to be used to value changes in school attendance and potential association with the use of using Social Stories.
| Number of missed school days at 6 weeks | Number of missed school days at 16 weeks | ||||||
|---|---|---|---|---|---|---|---|
| 0 days | 1 days | 2 days | 3 days | 5 days | Missing | Total | |
| 0 | 17 | 2 | 0 | 2 | 0 | 5 | 26 |
| 1 | 1 | 2 | 0 | 0 | 0 | 2 | 5 |
| 2 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| 4 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| 7 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Missing | 1 | 1 | 0 | 0 | 0 | 14 | 16 |
| Total responses | 19 | 5 | 1 | 2 | 1 | 22 | 50 |
Consequences to the educational system were more comprehensively assessed in the questionnaire given to participating teachers (more detail is available in Feasibility of examining opportunity costs to education).
Wider societal perspectives
As was mentioned earlier in this chapter, challenging behaviours and social difficulties may have resource implications for the wider society. Accounting for these implications can inform an economic evaluation adopting a wider societal perspective and therefore offer additional information to support health-care and/or education decision-makers on the best use of limited resources. The feasibility of collecting data on social services (i.e. out of home placement, use of Social Services), contact with justice services and parental productivity (income and absenteeism) were evaluated.
The evaluation of implications to social services was based on two questions. The first related to out-of-home placement (‘Has your child stayed away overnight in any of the following places in the last 6 weeks?’) and the response rates were low (between 6 and 44% across all time points). The second question examines social service/support service use asking ‘Has your child used any of the following services in the last 6 weeks?’ with options such as ‘Family support worker’, ‘Social services youth worker’ or ‘none of the above’. Overall, the completion rates ranged from 56% to 64% across all time points. This response rate may be as a result of the design of the questionnaire and specifically the fact that this formed the last element in a long table (see Appendix 16).
There is some evidence to suggest that ASD has been linked to increased likelihood of contact with criminal justice services. 131 The questionnaire asked ‘Has your child been involved with the police/youth offending team in the last 6 weeks?’ and if answered ‘Yes’ to provide details. The response rate was variable, ranging from 67% to 94% of parents who returned questionnaires with this item completed. No participating parent who responded at follow-up indicated that their child had had any contact. While no indication of contact with criminal justice was noted in follow-up questionnaire, one report was provided at baseline which indicated that the child had contact with the police as the victim of crime; this potential consideration was overlooked and is a useful consideration.
Challenging behaviour or social difficulties in children with ASD may be associated with higher probability of work-related absenteeism or career breaks for parents to accommodate the needs of children. Firstly, respondents were asked to indicate their and their partner’s employment status. At 6 weeks, 70% of those who were sent questionnaires responded about themselves and 62% about their partners. At 16 weeks, 56% of those who were sent questionnaires responded about themselves and 52% about their partners. Out of the questionnaires returned, 94–95% responded about themselves and 75–94% about their partner across all follow-up time points.
To estimate parent’s forgone income, respondents were asked: ‘What is your/your partner approximate gross pay per year?’ While this was asked at every time point, an analysis would take the values provided at baseline. As a subgroup analysis, out of all those who indicated that they were employed, 23 out of 31 (74.2%) indicated their own income and 26 out of 35 (74.3%) their partners. Participants were also able to indicate if they were not in paid employment and whether or not they engaged in other productive activities, which (using various valuation methods in the economic literature) can indicate an opportunity cost or proxy-good value that is related to informal activities. 132
The final question related to productivity was ‘If applicable, how many DAYS have you (or your partner, if applicable) been absent from work to care for you son/daughter in the last 6 weeks?’ Directly reporting the specific subgroup of those who indicated their employment status at baseline, 15 out of 31 (48.4%) indicated how many days they had missed from work at 6 weeks, and 14 out of 31 (45.2%) at 16 weeks. Across the two follow-up points, the number of days reported absence by those in paid employment ranged from none (the most common) to 16 days of reported absence.
Of those respondents who indicated they were not in paid employment at baseline (n = 13), 23% did not respond to the question ‘number of days absent from work’ and the remainder (77%) indicated ‘zero’ days absent. This highlights the importance of considering the non-labour-force productivity of individuals. Measuring productivity (and applying associated value) is particularly pertinent when a large amount of informal care may be required, as may often be the case in families with a child with ASD. Overall, the response rate to the measurement of productivity suggests that the questions were well understood by those who returned questionnaire.
Feasibility of examining opportunity costs to education
While the use of cost-effectiveness analysis conducted alongside a clinical trial has become routine (to inform health-care decisions on the use of limited health-care budget to maximise health), there is a relative paucity of equivalent research to inform policy and decision-makers in the education system. 133 The preferred maxim in health economic evaluation in the UK are QALYs. This provides a metric of specific welfare gain from health-care perspective. The education system (as another public good) contributes to total social welfare in various ways, such as improving short-term outcomes of education (e.g. grade attainment) or meeting specific development needs through education services (e.g. services in which special educational requirements exist).
In this feasibility study, we assessed the feasibility of extending the perspective of within-trial economic evaluation beyond a health-care perspective by designing questions that considered consequences within the educational system. For this, a separate questionnaire was developed to be completed by participating teachers. While this health economic evaluation of Social Stories did not intend to fully estimate associated welfare change from what may be considered a special education intervention, the feasibility of measuring resource consequence within the education system has been examined.
Table 48 presents response rates to the second part of the bespoke questionnaire which was completed by participating teachers. The overall aim is to estimate cost consequences for the schools (by measuring the use of school support services), non-attendance rate to school (because of either absence or exclusion) and grade attainment as an indication of productivity while attending school. Potentially, the Social Stories intervention for challenging behaviour and social difficulties may influence such consequences and, when compared with an appropriate comparator, indicate the marginal difference associable with the intervention. Furthermore, some of the resource-use data, such as certain low-intensity health services (such as a school nurse) may be directly available within school which may otherwise not be directly captured elsewhere.
| Items of resource use | 6 weeks | 16 weeks | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Social Stories | Comparator | Social Stories | Comparator | |||||||||
| Number of complete responses | % of all returners (n = 21) | % of all (n = 23) | Number of complete responses | % of all returners (n = 24) | % of all (n = 27) | Number of complete responses | % of all returners (n = 18) | % of all (n = 23) | Number of complete responses | % of all returners (n = 19) | % of all (n = 27) | |
| Special educational requirements | 20 | 95 | 87 | 21 | 88 | 78 | 15 | 83 | 65 | 17 | 89 | 63 |
| Special school/unit attendance | 21 | 100 | 91 | 21 | 88 | 78 | 16 | 89 | 70 | 16 | 84 | 59 |
| Type | 1 | 5 | 4 | 4 | 17 | 15 | 0 | 0 | 0 | 3 | 16 | 11 |
| 1/2 days per week | 3 | 14 | 13 | 4 | 17 | 15 | 2 | 11 | 9 | 1 | 5 | 4 |
| Teaching assistant’s time | 17 | 81 | 74 | 18 | 75 | 67 | 14 | 78 | 61 | 13 | 68 | 48 |
| Teacher’s time | 11 | 52 | 48 | 8 | 33 | 30 | 7 | 39 | 30 | 7 | 37 | 26 |
| School support provided | 20 | 95 | 87 | 20 | 83 | 74 | 15 | 83 | 65 | 16 | 84 | 59 |
| Professional services observed within school | 12 | 57 | 52 | 10 | 42 | 37 | 7 | 39 | 30 | 8 | 42 | 30 |
| Report exclusion/suspension | 21 | 100 | 91 | 21 | 88 | 78 | 16 | 89 | 70 | 17 | 89 | 63 |
| Times excluded | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| School absences | 18 | 86 | 78 | 18 | 75 | 67 | 14 | 78 | 61 | 12 | 63 | 44 |
| Absences because of ASD | 16 | 76 | 70 | 13 | 54 | 48 | 13 | 72 | 57 | 10 | 53 | 37 |
| English performance | 17 | 81 | 74 | 18 | 75 | 67 | 12 | 67 | 52 | 12 | 63 | 44 |
| Maths performance | 16 | 76 | 70 | 18 | 75 | 67 | 11 | 61 | 48 | 12 | 63 | 44 |
| Science performance | 13 | 62 | 57 | 15 | 63 | 56 | 11 | 61 | 48 | 9 | 47 | 33 |
| Complete cases | 11 | 52 | 48 | 8 | 33 | 30 | 7 | 39 | 30 | 7 | 37 | 26 |
the first component of the school-level assessment relates to the use of school support services. Firstly, the questionnaire aims to ascertain specific educational needs asking whether or not a pupil had identified school requirements such as the School Action, School Action Plus or Statement of Special Educational Needs (1981 Education Act134). From the total sample of 50 participating teachers recruited to report outcomes, 63–100% responded across time points to indicate children’s requirements. The specific needs were reported as School Action (8%), School Action Plus (40%) and Statement of Special Educational Needs (1981 Education Act134) (52%).
The next category was whether or not the ‘pupil attended a special school or unit in the last 6 weeks’. At 6 and 16 weeks follow-up, respondents’ completion was 84% and 62% respectively (of the completed responses, participating teachers indicated that 90% of the children being referred did not attend special school/units). Of the remaining 10% who indicated that the child attended a special school or unit, all indicated the type of school as ‘Special Unit in mainstream school’; however, only 20% responded to the item asking to quantify the level of attendance (see question 2b in Appendix 17).
To evaluate the feasibility of collecting data on extra help from school staff, respondents were asked: ‘In the last 6 weeks how many hours extra help a week does this pupil receive from (1) a teaching assistant and (2) a teacher?’ The mean extra time reported for teaching assistants and teachers was (1) at baseline 14.24 hours/week and 2.41 hours/week, (2) at 6 weeks 15.32 hours/week and 1.82 hours/week, and (3) at 16 weeks 13.75 hours/week and 0.75 hours/week, respectively. However, response rates were variable over the study and the presentation of these statistics should be considered as purely illustrative of the potential of these questionnaires to capture variation.
To ascertain the types of additional support participating children may have received, the questionnaire asked: ‘In the last 6 weeks has this pupil received any of the following support?’ The potential answers were ‘Individual tuition at home provided by the Local Authority’, ‘Individual tuition at home provided privately’, ‘Individual tuition in a special unit’, ‘Help in a small group for classes (e.g. English/maths)’, ‘Individual help for classes (e.g. English/maths)’ or ‘Individual Education plan’. From the total number of questionnaires returned, response rates for this item ranged from 83% to 95% across follow-up time points.
To examine other potential professional services accessed through schools (including health care), participants were asked ‘Has this pupil seen any of the following people in school in the last 6 weeks due to their autistic spectrum disorder?’ and could answer ‘Education Psychologist’, ‘Welfare Officer’, ‘Special educational needs coordinator’, ‘Speech and language therapist’ or ‘Other, please state’. Overall, the response rate of questionnaires returned was relatively low for participating teachers, ranging from 39% to 57%. This might suggest that they have limited knowledge of such services.
participating teachers were asked about two potential issues causing non-attendance, namely exclusions and absences. Regarding exclusion, teachers were asked ‘Has this pupil been excluded or suspended in the last 6 weeks?’ In returned questionnaires, responses rates were high across follow-up time points (88–100%) but in all cases no pupil was excluded or suspended from school.
Teachers were then asked ‘How many days has this pupil been absent from school in the last 6 weeks?’ Responses rates by treatment group across all follow-up time points ranged between 44% and 70%. Table 49 indicates the mean, SD, minimum and maximum days absence at baseline, 6 weeks and 16 weeks.
| Variable | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|
| Baseline | 44 | 0.91 | 1.48 | 0 | 5 |
| 6 weeks | 30 | 1.03 | 2.25 | 0 | 12 |
| 16 weeks | 25 | 1.16 | 1.70 | 0 | 7 |
the final resource-related category relates more to the pupils’ grade achievements in English, maths and science. Participating teachers were asked to indicate the ‘pupil’s current teacher assessment SATs’ and the response rates ranged from 47% to 81% across all subjects and follow-up time points.
In conclusion, the data from this study suggest that it is feasible to collect resource-related information from the participating teacher. They are also found to provide a good indication of how often participating children may not attend school. Finally, the level of pupil productivity may be measured by assessing teacher SAT assessment. This study also found that, overall, participating teachers have lower rates of non-responses and may be a valuable resource for data collection to inform an extension beyond the health-care perspective.
Discussion
This study evaluates the feasibility of collecting data on outcomes and resource utilisation from the perspective of the health-care system, education system and the wider society. Second, this study evaluates the feasibility of collecting data from various sources, including children with ASD, their parents and their teachers/teaching assistants. Response rates for each item in the quality-of-life instruments and a bespoke resource-use questionnaire were evaluated at baseline and at two follow-up time points (i.e. 6 and 16 weeks).
The feasibility study found that parents were more likely to respond to the quality-of-life questionnaires compared with children with ASD. This was true for the overall response rates and item completion rates for EQ-5D117 and HUI2118 questionnaires (note: parents completed the proxy versions of these questionnaires). We find that 56% of parents completed the EQ-5D117 at all time points and 54% completed all items of the HUI2118 questionnaire at all time points. This would suggest that collecting data from parents on the child’s health-status may be more reliable than from the child. We also found that for those who do return questionnaires, it is highly likely that all items of the EQ-5D117 and HUI2118 questionnaires will be completed.
The analysis also enquired how likely it is that parent-proxies can substitute completion of the questionnaire when the child does not respond. The analysis revealed that parents are significantly more likely to respond (completion of all five times at the three time points was 2.8 times higher for parents than for children). Furthermore, it was found that the children completing the full EQ-5D117 were correlated with the parents who also responded in full. This means that parent responses can provide more complete data to indicate the child’s health that may not otherwise be available. A limited number of completed EQ-5D117 by both parents and children were available to assess correlation of aggregated utility score which indicated moderate correlation between utility estimates.
The HUI2118 is an alternative (preference-based) measure of generic health piloted in this feasibility study. The questionnaire contains 16 items and has been shown to be a sensitive instrument in children with ASD. The questionnaire was administered to parents, and 54% of parents returned all items at the three time points. This is comparable to the response rate for EQ-5D proxy. 117 However, the high rate of non-response to both quality-of-life instruments indicates that self-completion of questionnaires may lead to low response rates, and further methods (potentially involving interviewer-supported response recording) should be considered in the fully powered trial. The second component of economic evaluation was to assess resource use and indicate related cost consequences of an intervention. The ability to assess resource implications was piloted using a bespoke resource-use questionnaire for parents and teachers to record resources use which may be related to behavioural problems.
The primary perspective for a HTA is the health-care system. There were six items in the resource-use questionnaire presented to parents that assessed health service use. However, examining these items at baseline, 6 weeks and 16 weeks showed a high proportion of missing responses. Based on the current information, it is not possible to assess whether or not missing values represent no service utilisation in relation to particular items of resource use or missing response. Again, improved questionnaire guidance or interviewer-supported recording of responses may reduce missing responses.
As the pilot implementation of Social Stories involved schools and since social difficulties in ASD may affect provisions for education, supplementary perspectives for an economic analysis were considered in which both parents and teachers were asked to report educational outcomes. When parents were asked to report their children’s days of absence from school, 34% of parents reported at least 1 day of absence. This implies that Social Stories may have implications for the education system that can be feasibly recorded within a trial.
The feasibility of collecting resource-related information from the educational sector (i.e. from participating teachers) seemed promising and overall teachers provided the relatively thorough information required to inform this extended perspective. Teachers were also found to provide a good indication of how often participating children may not attend school. Finally, teachers had good reporting of school grades and the level of pupil productivity.
A wider societal perspective was also explored. It was found that parents gave information on social service use, contact with the criminal justice system and issues affecting their own productivity. It was found that most parents who were employed reported their annual income (74.3%) which can help capture implications of a child’s challenging behaviour or social difficulties on their parents’ income. Responses to the productivity questions suggest future research design should provide the option ‘full-time parent/carer’ in the questionnaire to capture data on parents who are not in employment. The results of the feasibility assessment of reported resource consequences from parents provide very important information for a prospective full-stage study.
Conclusions
-
Health economics data completion rates are good overall indicating they would be feasible to collect in a full-scale trial.
-
Parents are more likely to fill in proxy health-related quality of life measures than their children with ASD.
-
Suggestions for improvements in completion rates include improved guidance on filling in questionnaires (e.g. clarifying that it is important to use the score of zero rather than assuming that leaving a response blank means ‘zero’).
-
When children cannot fill in questionnaires, parent/carer proxies can be used to obtain supplementary information.
-
Participating teachers can provide useful information about education-related outcomes such as attendance and achievement (e.g. SATs).
-
A number of items were not completed on the resource-use questionnaire. This may be because respondents who did not use community health services did not report ‘zero’ use in the questionnaire but left it blank instead or it was not well understood.
-
The results of the feasibility assessment of reported resource consequences from parents provide very important information for a prospective full-stage study.
Chapter 9 Qualitative process evaluation
Background
There has been little previous qualitative work exploring issues of effectiveness and acceptability of Social Stories amongst this population. An in-depth appreciation of these issues will be essential for any future implementation of the manualised intervention. Therefore, the process of participation in the intervention and the feasibility study was explored using semistructured interviews with key stakeholders. This information was used to plan a fully powered RCT.
Objectives
-
To establish the acceptability and utility of the manualised Social Stories intervention among those delivering the intervention and the parents/children receiving the intervention.
-
To elicit information on the feasibility trial process in order to inform any future full-scale RCT.
Methods
Qualitative interviews have been used extensively to examine the acceptability of complex interventions (to both those delivering and in receipt of the intervention) and to inform the design of a full-scale RCT. 135 We purposively sampled parents (or carers) and their children in receipt of intervention (or comparator) from participants in the pilot RCT. We wanted this sample to include some parents who were actively involved in supporting the delivery of the intervention to their children at home. We felt a sample of ten parents/children from the intervention arm and five from the comparator arm should be sufficient to address the aims of the study, especially given that this component was building on the previous qualitative work outlined in Chapters 4 to 6. In addition, we purposively sampled from the group of professionals who were delivering the intervention (n = 5), where possible we attempted to sample the professionals who were delivering the intervention to the families recruited to the qualitative study in groups of parent/child and teacher. This was in order to achieve a rounded picture of the intervention delivery from all key stakeholders across a series of cases from the pilot RCT.
Interviews took place in the participants’ home or place of work. For the interviews with the children/parents, these generally took place together; the child was interviewed first (when appropriate in the presence of the parent) and, when data had been collected from the child, the parent interview was then conducted (when possible in the absence of the child). The interviews were conducted using a topic guide (see Appendix 18) with a focus on ascertaining information on the intervention itself including goal-setting, training, using the Social Stories manual in practice and the perceived utility of the intervention. In addition, the interviews included questions on the feasibility study process itself and sought to elicit information that would inform a future full-scale RCT. This included information on recruitment, communication within the study and outcome measurement.
Interviews were audio-recorded and fully transcribed. Transcripts were read and key points were coded according to a priori themes based on the aims of the process evaluation using NVivo using a framework approach (see Appendix 6).
Results
Findings from the qualitative interviews during the pilot study are described under two main subthemes:
-
lessons learnt about the intervention delivery
-
lessons learnt for a full scale RCT.
Lessons learnt about the intervention delivery
Goal-setting
Goal-setting meetings lasted approximately 90 minutes and were held either at the child participant’s school or at a pre-booked room in a CAMHS outpatient setting. GSMs were held by a clinician with the aid of at least one researcher and both adult participants were invited to participate. The primary goals of the GSM were to:
-
set a unique goal by consensus for the participant to achieve
-
define a specific behaviour that they hoped to increase (pro-social) and one that they hoped to decrease (challenging) as a result of achieving that goal.
In the feasibility trial GSMs were held, in most cases, with both the participating teacher and parent. However, priority was given to including the participating teacher if it was not possible to include both. It was seen as beneficial by both teachers and parents that the participating parent was present at these meetings. When feasible within the time frame, attempts were made to enable this and, if not, the research team attempted to contact them before the meeting for their input.
I said [to the researchers] ‘Can we tweak it a bit because [the child is] never going to get a piece finished if he doesn’t get started?’ because that was my issue.
Yes.
I mean if I had been at the meeting I maybe could have put that point forward.
Female, teaching assistant, primary school, intervention group
It was felt, by both teachers and parents, that having more information prior to the GSM would be beneficial:
I think if you had like an A4 sheet of what a Social Story is, some examples of Social Stories to kinda talk through, then gone to the goal-setting meeting, then you’d kinda followed up about how to write a Social Story at the training and things, yeah.
Female, teaching assistant, primary school, intervention group
She had as much as us.
Right so she pretty much had nothing?
Yes.
You’re all in the dark really?
We were all in the dark when we got there and we hadn’t been sort of primed to choose a target before we went.
Female, teaching assistant, primary school, intervention group
Goals which were considered easy to set were often ones that were ongoing or had been considered prior to the meeting. Difficulties with the GSM often focused around setting a goal which was measurable or which transcended the locations of home and school. For example, a goal about coping with winning or losing would work well both in classroom and home settings. Sometimes, however, goal-setting felt contrived to fit the purposes of the feasibility study (i.e. that it was measurable), rather than a goal more appropriate for a particular behaviour in that setting.
Goal-setting was seen as useful in that it encouraged people to meet around the table and ‘bounce’ ideas off each other and it was less intimidating than with just the researcher alone. However, with hindsight, a number of participants would have preferred to change their goals following the meeting, to reflect more closely the needs of the child.
Lessons for goal-setting
-
As the trial will focus on Social Stories as a school-based intervention, teachers should have the central role in goal-setting.
-
Clearer information about Social Stories and the aims of the GSM should be sent to participants prior to the meeting.
Training
The training day was a half-day session (usually about 3 hours long) which taught the participants how to create and deliver the intervention to the participants. The first half of the session consisted of a presentation detailing the theory behind Social Stories and the practicalities of writing and delivering them. The structure of the presentation closely mirrored that of the manual, making reference to it in places. The second half of the training session was devoted to creating the Social Story for the goals set in the GSM for each participant. The adult participants constructed and revised their stories with support from the specialist trainers and other members of the research team to ensure that the finished product followed all of Gray’s criteria. 3
Story writing an integral aspect of training
Participants felt a key aspect of the training provided was that plenty of time was allowed for story writing. Participants felt supported by the presence of clinicians and researchers to address any anxieties or uncertainties:
. . . because when we sat down to write it, between us, with the people being there to help, that, I think that was vital that they were there to help for that first sentence, that first story, but with their help I think we did OK.
. . . so almost you need the expert there, along with the training, to be able to achieve the stories quite well, by the sound of it?
Yeah. The morning was like the theory of it and then late morning and early afternoon was the actual sitting down and writing it, and then there was two people I think circulating.
Circulating and doing it. And how much did they help with your story?
We had lots of ideas but it was useful for them to be there, because when we were trying to get him to not swear in school, to write a story that doesn’t say not swearing.
So getting the positive.
To get the positive angle [R laughing] in that, it was pretty tricky.
Female, teaching assistant, secondary school, intervention group
I think we found it interesting, the only it was good but I would say the only criticism was they probably should have got us more at that stage before we walked out . . . But then it just sort of stopped too quickly they should have actually let us write the story whilst we were.
Female, teaching assistant, secondary school, intervention group
For those who had not undergone any previous training in Social Stories or who did not complete writing their story in the allotted time, they felt that a second follow-up session would have been useful to check the story’s progress and get further support to finalise it.
The manual was not necessarily regarded as a key feature of the training provided, especially compared with the hands-on support that was available for story writing within the training session:
Were the instructions that you were given in the manual straightforward really in delivering the story, setting it up or doing it?
Didn’t read it.
If you didn’t read it that’s OK. [INT laughs] You haven’t looked at the manual, so pretty much you just relied on the training?
No . . . just the training, yeah.
Female, teaching assistant, primary school, intervention group
‘You’ve got the Social Story,’ I thought, ‘Okay that’s fine. ‘And now you are going to write it come to the training,’ ‘Okay.’ And then they gave us a book which I thought, ‘Okay. Do I have to go and read this quite thick book before I do the Social Story,’ but they went through it all first, but I thought, ‘Well no if they are going to help us write it now, that is fine.’
Female, teaching assistant, primary school, intervention group
The overall perception was that the manual was useful in providing ancillary information, which would be particularly useful in the longer term, acting as an aide memoir for use beyond the training sessions, rather than use as a stand-alone item:
Yeah, I think the training was good ‘cos you need just to have all the professionals there to help you and say, oh no you can’t put that in it, and you, no, you can’t, shouldn’t, you can’t use that, that’s negative, no, you’ve got to use this. And that was helpful. I don’t think you could have just done it from a manual.
Female, teaching assistant, primary school, intervention group
Yeah, yeah, no, it was, it was, to, to write the Social Story, yes it was, yeah, it was clear and came away with a booklet, lots of examples in it of, you know, so if, if, we did the majority of it in the session which I think is really crucial.
Female, parent, primary school, intervention group
Like the months that follow on if I need to use Social Stories again then I will go straight back to that and use it as a guide.
Female, teaching assistant, primary school, intervention group
Lessons for goal-setting
-
Adequate time should be allowed for writing Social Stories within the training session.
-
Navigation to the key aspects of the manual should be provided in the training for future use.
Intervention delivery
For those randomised to the Social Story group, finding the time for reading the Social Story was important especially in a busy, fast-paced classroom. It was seen as important to create ‘protected time’. One way to do this was to make sure that there intervention was formally timetabled.
Within the secondary school there is an added complication of children moving from lesson to lesson and where and when to run the intervention.
Well if, say for instance, we picked the, us to do the reading during registration, there’s 1 day a week when there’s assembly so you can’t take them out of assembly. It’s quite important that they’re in the tutor group sometimes. It’s which lessons do you take them out of? Can’t take them out of English, Maths, Science. It’s quite, quite difficult. And then matching timetables, well when, when can you do this? That’s quite difficult.
Female, SENCO, secondary school, comparator group
Sometimes, however, the secondary school timetable provided additional flexibility.
[Child 1] just used to read in form in here, so either way just depending on where she was timetabled. With [child 2] it would be usually in here in literacy but he would read in his form time as well. And the English lessons they would have 10 minutes reading in that too. So we would adapt it accordingly . . .
Female, teaching assistant, secondary school, intervention group
The process of implementation differed depending on the child’s individual needs and age. A number of children particularly liked their story and the process was straightforward. Indeed one child fully identified with the story making implementation particularly easy.
Yes. I mean when he read the story first of all he turned to me and he went, ‘That’s me.’ It was just like that.
Just a small light bulb going on.
Yes.
Female, teaching assistant, secondary school, intervention group
On the other hand, a few children refused to take part in reading the Social Story.
His English teacher said that he’d been chosen to take part in some university research and he said ‘Thank you very much but I don’t think I’d like to’. And refused very politely to have anything to do with it. So that was our experience.
Female, parent, secondary school, comparator group
There was a concern for some that being told that they were involved in research would put the child off from participating in the Social Story intervention. This was particularly the case for older children.
I don’t know whether he would see it as a ploy . . . as if we are trying to get through to him, which we are but he might react; he might you know if we got that far he might react badly to it or think, ‘What is the underlying message here, what are they trying to do?’
Right.
Which might be a reaction of older children.
A bit more suspicious or?
Yes.
Female, SENCO, secondary school, comparator group
For younger children, it was easier to make the story reading more a matter of course, rather than something unique. For example, one teaching assistant used a less formal approach with reading stories, reading the story to a group of students, rather than just to the child in the intervention.
Yeah, it was, you know, obviously these children, sometimes they’re in the right frame of mind and sometimes they’re not. So I tried to make it exciting that it was her story and let’s read it together, and I didn’t make it, she never ever realised that it was to get her to actually do the next thing I was gonna try and get her to do [laughter]. So I tried to do it in a roundabout way, just let’s go and read the story, and made, just made it really exciting. So that helped. I think if, if I’d have said ‘Right, come on, we need to do the story before we do this task’ then I think she would have. . .Twigged and thought no.
Right. So you’ve almost had to do it quite subtly or quite subliminally almost?
Yeah, yeah, definitely. And that’s why reading it to the group that I was working with, with her, helped as well, ‘cos I said ‘Oh I know, we’ve got a few minutes, let’s just read the story’. But she didn’t then realise she was gonna have to go and do the task next. [laughs]
Do the task next?
Yeah.
Do you think the kids twigged on to that?
No.
They didn’t twig?
Not at all, no.
Female, teaching assistant, primary school, intervention group
The Social Story criteria describe the importance of tailoring the story to a specific child and treating the child with dignity when delivering the intervention. A question was raised in the team about whether or not there would be anything to stop other children from benefiting from hearing the Story if it was deemed helpful by the teachers. Through the process of reading the story to a class of peers, the aim was to reduce stigma and stop the child feeling ‘different’.
And I think it’s helped her to feel the same as the other children, not to feel singled out and different, ‘cos they are, they, I think she did feel different and she wasn’t as confident. She’d say ‘Oh it’s too easy, I can’t do it’ when it really, it wasn’t too easy, she needed help.
Female, teaching assistant, primary school, intervention group
As well as using different approaches to delivering the Social Stories, others described additional reinforcement they were using to try to support the story. For example, one participant group reported using class peers to reinforce positive behaviour. The child’s outbursts in class were found to be funny and were encouraged by other children, so by explaining to the class that the teachers were trying to stop the use of strange words and noises helped to control the behaviour, alongside the use of the Social Story.
. . . the story stands alone but what’s as important to the story is the, the fact that it’s about him using words with other children and the children not using noises back was just as critical as the story by itself.
Female, parent, secondary school, intervention group
Verbal reinforcement was another strategy used by those delivering the story, where the content of the story (rather than the story itself) would be shared, further reinforcing and reminding the child of the particular actions required. For example, one parent who provides 1-day-a-week home schooling discusses with the child first what will be happening before reading the story. She called this a pre-implementation phase.
. . . the pre-implementation, the, you talk, you read the story then you’ll talk about, OK now we’re going to do this task, what do we need to be clear about.
Female, parent, secondary school, intervention group
Other inducements or rewards included using multiple stories to stop boredom, being allowed to play computer games after completing work, providing additional breaks or giving an offer of toys.
Lessons for goal-setting
-
There is an added complication of deciding where to run the intervention within the secondary school and if necessary which lessons to take a child out of.
-
One teaching assistant used a less formal approach with reading stories, reading the story to a group of students, rather than just to the child in the intervention. This is indicative of a lack of treatment fidelity and needs to be addressed in a full-scale RCT.
Perceived impact of Social Stories
For the children who had participated in the reading of Social Stories, most of the teachers/parents felt the stories had achieved a positive outcome:
You could see the difference at the beginning of the week, at the end of the week.
Female, teaching assistant, primary school, intervention group
It went really well using the Social Story because she had to physically put her book away and then go and sit on the carpet. But before that she was sitting on the carpet with her book. So the social story worked for her to put the, to put the book away with no problem and to go and sit on the carpet, and she stayed on the carpet for, for fifteen minutes.
Female, teaching assistant, primary school, intervention group
Yeah, definitely, definitely. I can now use these stories to get her to do things that I could never get her to do things from before. And she’s realising, from the wording of, in these stories, that it’s OK to ask for this and it’s OK to do this now, whereas before she would put a, just a, a screen, almost a screen there, no, no way, not doing it, not doing it, not doing it. Now I can use these stories and she’ll listen, she takes it all in, and then takes on board what’s been said and, and seems to do it.
Female, teaching assistant, primary school, intervention group
For some they were happy to credit the perceived behaviour change to the story, rather than alternative explanations, for example one of the additional reinforcement strategies being implemented.
Yes it was yes because like I say he will now say, one day he would come home and he got his, which he would never do, he’s got his homework out, sat at the table, I says, ‘What you doing?’ He says, ‘I’m doing my homework, I can go on Minecraft[®, Mojang, Stockholm, Sweden] then’.
Female, parent, primary school, intervention group
However, for others it was difficult to tell what had attributed to any change. For example, one child had come back from holiday and their behaviour had improved. How much of this was related to the story was very hard for the teacher to pinpoint:
As a result, is this really though as a result of the stories or is it because of holidays, is it because of other things, what would you, what would you ascribe it to?
It’s difficult to say. I mean how can you say that this is cause and result of anything? But certainly it won’t have harmed and if he thinks that now if he sorta thinks, takes a deep breath and thinks before he opens his mouth or thinks before he does something or whatever, it’s going to help him, you know . . .
So you kinda sow the seed there almost by using the story?
Yeah, yeah, I think it’s been a vehicle for him to get to think about what he’s doing and to try and improve his behaviour.
And by the sound of it, also the chats and everything else. So it’s not just the story, it’s the whole package of intervention, if you like . . . you spending quality time with him, all these kinda things.
Yeah, yeah.
Female, teaching assistant, secondary school, intervention group
For some, the stories were ‘working’ however, under very limited circumstances or having a slightly different impact to that expected.
Well it’s working as in he’ll do some maths but every other subject during the day he chooses not to do.
Female, teaching assistant, primary school, intervention group
For example, one child had difficulty with people laughing at him rather than with him. Through a Social Story about laughter he now has adopted a ‘comic’ persona, using a joke book to tell jokes.
I think he understands, which is what I’ve said then actually that he likes making people happy so I think this is kind of reinforced for him if he tells a joke it makes somebody happy and I think that’s what he’s grasped really and the laughing around when he does that is okay. Probably what I would like to focus on a bit more is not, you know when you laugh, but he’s not actually said a joke but you’d laugh at something that he did . . . but you don’t mean it in a bad way, that he struggles with that.
So the kind of new onuses of laughter you still need to tweak out a bit more?
Yes. He still gets upset about things and I’m not I don’t mean it in a bad way, you know, it’s just what you did was funny, well he can take that in a wrong way and that’s what he has done and that is the little part of Asperger’s that he’s got he’s taken that literally so it’s all about jokes now.
Female, parent, secondary school, intervention group
The teacher further explains that the full goal was not met, but the story certainly is working in the right direction and nurturing positive responses from the child when other children laugh.
The fact that he’s now telling people jokes, I think, he’s maybe not got it completely but he is understanding that they are not just laughing at him and how he is.
Female, teaching assistant, secondary school, intervention group
Further, indirect positive results include developing a closer relationship with the child allowing better communication or in the extract below, developing special time which is individualised.
I read stories to her and she loved coming in here having a little sit, she likes the one-to-one attention . . . And so it was really good for her to have a story quietly and she’s all excited, so it was the 20 minutes that she loved, we did it three times a week . . . And to be honest if I had the time it would have been nice to carry it on for her to do that.
Female, teaching assistant, primary school, comparator group
Lessons learnt for full-scale randomised controlled trial
Recruitment into the trial
Three alternative recruitment procedures were used to identify potential participants: a school approach, direct contact with parents through local autism support groups and professional referrals from clinicians and education specialists. Most children were recruited through the first method, direct contact with schools. Maintaining this contact with schools could be problematic. A number of teachers highlighted that a good way to develop communication was through either specialist teachers that work across schools or SENCOs.
In order to conduct the intervention within a school, it is important to make the inclusion criteria clear to the school and that there should be a designated teacher who knows the child well. There is a possible drawback that schools agree to participate in the study in order to benefit from the Social Stories training even though they may not be able to fully take part.
I think, I think for me, because it seemed very last minute, yeah, very quick, as soon as I’d spoken then there was a meeting and things like that, and it seemed really, really quick. Whereas it didn’t really give me an awful lot of time to find out enough or to, to talk to other people to see whether there was somebody better to do it. And I think maybe I wasn’t the best person to do, to be part of it.
Why, why do you think that?
I didn’t, I didn’t know the student to start with, so I think that maybe it would’ve been better having somebody who knew the student. But it kind of just felt like it snowballed a little bit . . .
Would you have dropped out if you could of?
Yes. I probably. Because I didn’t feel like we could give it everything, or even find somebody that knew the student well enough to do it, to take over.
Female, SENCO, secondary school, comparator group
Within the ASSSIST study, recruitment was enhanced through strong links between the study team and the ASD infrastructure in the local area. For example, contact was made with people who have attended a local CAMHS course (called ASCEND) or through local autism events. This joined-up approach with events, calls and publicity material, means that information is not often arriving to families unsolicited. Participants were generally happy to be contacted through the child’s school, as a trusted institution.
Yeah I think it probably was [better that the teacher phoned] because we have a very good relationship with school, so from our point of view, if a complete stranger wrote a letter to us or somebody else, it needs to be somebody who we have a very good relationship with in order for us to trust it in the first place because you do get asked to do an awful lot of research projects.
Female, parent, secondary school, comparator group
Lessons for the full-scale trial
-
It was suggested that recruitment would benefit from the research team making more direct contact with schools via SENCOs.
-
It was suggested that more attempts to make families in the community aware of the study through networking within services for children with ASD.
Communication within the trial
Contact with those delivering intervention
The pilot study highlighted the importance of putting in place a contact plan with those directly involved with delivery of the intervention/comparator. Teaching assistants are busy during the day so they cannot receive calls and leaving messages was found to have varying degrees of success. Some mentioned calling to their mobile phones, although these numbers were not always given to or collected by the research team. Some suggested they were able to respond to or receive emails by phone and could do this in class. This would suggest the importance of setting up a firm communication plan at the outset, making it clear when the best times are to contact using which particular medium (resulting in calls out of office hours if necessary), tailored for the individual.
Contact with parents
Findings suggest that it would be useful to have a single dedicated study contact person with a specific phone number for each of the families involved in the trial. Parents found it confusing when contact was made from several different members of the study team and could not return calls when ringing from the university/NHS.
Yeah, yeah, because a lot of times as well [laughs] they would call me and they were using the [CAMHS] phone and it would just come up as blocked number or unknown . . . I couldn’t ring ‘em back and I, I don’t, ‘cos a block to me means it’s, it’s a cold call so I don’t answer. So that was also a bit of an issue.
So it’d almost have been better having a mobile number for you or something, or somebody?
If they’d just called me on, if they’d just, they, they didn’t realise that, I had to tell them, and I said ‘Well maybe if you just call me on the number that is not blocked I’ll know.’ . . .Yeah, so that did not help [laughs] because it would ring and I, I wouldn’t answer or, you know, it, I couldn’t ring them back if I genuinely hadn’t heard, because you can’t ring the numbers back, so.
Female, parent, primary school, intervention
Contact with the comparator arm
Obviously for those in the comparator arm, the intervention merely entailed reading a story with the child with ASD, indeed this could be a continuation of other reading that was already being undertaken. However, parents of children in the comparator arm spoke of feeling ‘out of the loop’:
It’s been really hard if I’m totally honest, I still haven’t really got a clue what we’re doing with this research because we’re in the comparator group so we set a goal and we still haven’t really done anything else from it so we’re a bit lost with this one if I’m honest . . .
Female, parent, secondary school, comparator group
Information about the trial
There is a balance between providing individuals with enough information to make an informed decision about the study and not overwhelming them with too much. Some teachers and parents did not feel they were sure about the commitment at the outset:
. . . at the beginning where it’s very nebulous on no one really knew, I think when it was very nebulous you weren’t sure about what you were going to give the parents, the parents then thought, ‘What are you signing up to?’ . . . I think especially that sort of preliminary time there just weren’t enough specifics.
Female, SENCO, secondary school, comparator group
What they said was they said it just Social Stories first. They didn’t say it was a study.
Right.
They said it was, ‘How to write a Social Story but you needed a child to write it for’. That’s what they said at first.
And you feel they could have done with giving you more information?
It would have been quite nice to find out before we got thrown in and then the paperwork put at us and we thought, ‘Okay!’
So pretty much you came on to it just thinking you were what, they were going to show you how to write a story?
How to write a Social Stories and you would write one with a child in mind, which obviously you need to really, and then go from there that you could write Social Stories.
So do you feel that they didn’t give you enough information early on?
I think it would have been nice to know what I was getting in to right from day one and how long it was going to take.
Female, teaching assistant, primary school, intervention group
Other issues that were mentioned by the staff in schools regarding contact with the researchers about the project included limited availability of research staff for meetings in schools, advanced warning about up-and-coming project meetings, the project timetable taking into account term times and key dates in the school calendar (e.g. SATs and the Christmas period):
. . . and then we weren’t given enough times to come and meet up either and for people that work, even part-time work, you need to have not just two slots you need maybe three or four slots.
Female, SENCO, secondary school, comparator group
Oh yes we know how long it’s going to be, but what worries me is the 6 weeks’ holiday that we’ve got in is counted in their 16 weeks or whatever it is and you can’t measure anything in there.
Female, teaching assistant, primary school, intervention group
. . . that was, I had to, we had to ask a teacher to do that out of their own time, when they were busy, you know, do, getting everything ready for SATs, marking SAT papers, getting all the information ready for report-writing.
Female, teaching assistant, primary school, intervention group
This suggests a simple time scale for the study would be a useful tool for schools and parents in order to highlight the different stages of the research in a relatively simply way and allow potential participants to appreciate key project milestones and what these would involve. This document could be kept for reference, allaying some of the current issues where people have been given information and have forgotten/not retained the information. Following recruitment into the study, the timeline could be individualised to reflect participants’ starting dates.
Resentful demoralisation
Generally, the participants entered the study with a vested interest to take part in the intervention. The possible impact of not being randomised to the intervention group was negated by the promise of the full training and manual at the end of the study:
I think the letter said that if you got picked for the other group I think you got more information and a pack or something, but if you got picked for the comparator group, at the end of the, at the end of study you got that pack as well, later, even if, even, you wouldn’t miss out; if you, if you were in the comparator group you still wouldn’t miss out.
Female, parent, secondary school, comparator group
Were, were you upset that you didn’t get into the intervention group, did that upset you or were you?
No, no, no, no, I just thought whichever one it is.
Didn’t really faze you at all?
No, whatever it is we get the training either way, it doesn’t matter.
Yeah. So you’re getting something at the end, I suppose?
Yes.
So not, not particularly disappointed?
No.
Female, parent, secondary school, comparator group
However, there was still a sense of frustration from some parents and teachers, as an intervention that they generally thought would be useful was withheld for an extended period of time.
We were . . ., you know, sort of impatient, oh yeah, we want to get him on this and we want to be on the, the first group so he’s getting in the help straight away and the more, and the more we can do for him the better to help him not get in as much trouble.
Female, teaching assistant, secondary school, intervention group
Given the preference to be allocated to the intervention arm (even though this was more work for time-pressured teachers) does indicate the information provided may not be clear enough about the genuine uncertainty relating to the effectiveness of the Social Stories as an intervention.
Lessons for the full-scale trial
-
It would be beneficial to require a participating teacher who knows the child well.
-
A pre-prepared individualised communication plan with the teachers delivering the intervention, highlighting their preferred communication method and time of contact, would be useful.
-
A single point of contact for parents would avoid confusion and make sure that the intervention was accessible.
-
It is advisable to offer the intervention to control arm at end of study period (if effective).
-
It is important to ensure communication with participants is clear about equipoise.
Outcome measurement
Parents and teacher questionnaire
While some people found the paperwork relating to outcome measurement (see Appendices 13–17) straightforward to fill out, most reported that they felt that too much information was being collected. Many were willing to complete the questionnaires because of the perceived benefits to the research, but there were common complaints about length, clarity and repetitive questions.
It’s good because you need to know the outcome of the story but I think it’s just too long.
Female, teaching assistant, primary school, intervention group
I would say a shorter one would be better from a family’s point of view. I would try and keep some in. You don’t mind just taking maybe half an hour three-quarters of an hour or so, but when it starts to take up to 2 hours it does sort of well we’ve touched it a couple of times where we fill in part and then went back.
Male, parent, primary school, intervention group
However, this was not universal, some respondents completed the outcome measures quickly and others finding additional benefits to the process. For example, the questions made them explore their relationship and interaction with the child. When thinking about and answering the questions, it affirmed what the parent had been told about their child’s condition:
I think so, yeah, and I, I quite like doing things like this because it makes you think, you know, it makes you focus on your child.
Oh right, of course. Yeah, yeah, focus on child.
Yeah, but . . .
And did you, did you have any insights as a result of filling it out . . .
No, but it just makes you, like this sort of thing, which is clearly . . .
That’s page three.
. . . you know, there’s a lot of that in there that applies to children like [child’s name], and it makes, it kinda affirms what you’ve been told about your child, but you know that this is, these are kind of standard behaviours. So it’s kind of reassuring in a way.
Female, parent, secondary school, comparator group
‘Oh wait a minute,’ you read a question and you take that little second and go, ‘Oh I never thought about that.’ I think when in applied it to my kids it was quite interesting looking over some of the questions and thinking, ‘Goodness I hadn’t thought about that before’.
Male, parent, primary school, intervention group
Questions could make people think about the child in a new way, or indeed make them consider issues that had not been apparent previously:
So the teacher questionnaire was helpful because it highlighted very specific issues for example one for us about teasing I think, ‘Was he teased?’. . . and that is something that he suffers from and that did help, yes ‘Gets teased a lot,’ number 57.
So it’s making you think about your practice . . .
And it did make me think that, ‘Yes this child is getting teased’. This is one of his big things, so just from point of view from a member of staff it did focus that it’s one thing he complains a lot about, sometimes it’s justified sometimes it isn’t but it did at least make me sit up and think about the teasing issue.
Isn’t that interesting? So you are actually getting something out of that filling out the forms is making you think about your own practice, your own . . .
Yes. It did because when I then put, ‘Yes almost always true. He gets teased a lot’. I thought yes we’ve got to do something about this, yes.
Female, SENCO, secondary school, comparator group
Parents and teacher diaries
Participants reported a number of difficulties and issues in completing the behaviour diaries. Some behaviours are relatively straightforward to measure, for example an action is achieved, books are opened for lessons or the child does homework. Such binary measures are easier to record than more subjective observations, such as ‘responds better’, ‘is less angry’ or ‘socialises more’. Equally, some behaviours are easier to observe, as they happen within a specific time scale which is very short or geographically defined (e.g. within the classroom), others happen over a longer period of time in multiple locations (e.g. the playground and classroom). In addition, some target behaviours are not particularly conducive to timing; therefore, they are open to a lot of interpretation, for example how long was the person angry for, how long did they sip water for.
The inherent difficulties in measuring certain behaviours may be additionally hindered by attempts to do this subtly and unobtrusively. For example, it may be inappropriate to follow a child (e.g. at a break to see how the child responds to others) or the behaviour may not exhibited during the lesson. Difficulty observing some behaviours resulted in guessing or creating scenarios to allow the behaviour to happen.
. . . it was all about winning and losing and with, with him, we thought, I kinda set up a little thing, so we were looking at, you know, the po, positive comments and negative comments and things and, you know, whether he was, whether he was winning and things, and also we had to, we had to set up some games which we wouldn’t normally have kind of played. So it was false in a way, but you had to do that so that you could do.
Female, teaching assistant, primary school, intervention group
In addition, the diaries were not found to be user friendly but were considered tiresome and difficult. From some of the interviews it was clear that the paperwork did not fit the specified behaviour goals. For example, in some contexts the forms were too generic, resulting in people interpreting the various boxes and making answers fit. Some activities may not run every day, so the form was filled out for sessions rather than weekdays. Rather than people instinctively knowing what to put down, they were being confused by the increased behaviours goal and the decreased behaviours goal and kept having to refer back to these.
Children with autism spectrum disorder
Some problems were encountered in completing the outcome measures aimed at children with ASD. Conceptually some children struggled with the content of some questions, requiring further explanation and therefore extending the time taken to complete the question or impacting on the accuracy of the response. Adult participants were unsure whether or not they were to edit the results provided by children, especially when they thought that these had been filled out inaccurately.
He didn’t mind the smiley faces but again I found this difficult with him because I said, ‘Did you like reading the Social Stories with your teachers?’ And he said he hadn’t read them, so oh right, so I didn’t know what to do there . . .
Female, parent, primary school, intervention group
Parents/teachers varied in their response to helping the child complete the outcome measures. Some allowing the children to fill in the results themselves, others copied the child’s answers onto the sheets verbatim, while others responded in proxy for the child:
So do you think she filled it out accurately? Did you change the answers that she gave?
No. I put down I described exactly the same on what she said and there were some funny answers, I can’t remember them now but I put ‘This is what [child’s name] said’, and I know she’s made up a couple of things because her mum says, ‘Well we haven’t got that, and we haven’t done that,’ and I was telling her afterwards. She lives in a bit of a dream world, but she was quite happy coming in. Again it’s the attention finding a little 10-minute slot, well it was about quarter of an hour one.
Female, teaching assistant, primary school, comparator group
It was hard because the young lady that I look after could not express herself. So basically I just did it on the day that we filled it out and I made.
Did you guess?
Yes, I guessed basically, yeah.
So you actually did, was she able to complete any bits?
No, none at all. But she sat next to me and I did read the questions to her, and sometimes she’d say sometimes, never or often, but if it was too way out I just made.
You changed it?
I changed it.
So you made changes based on, so how, how she was?
How she was feeling on that day.
Right.
Yeah, and also how much I know of her in school.
That’s all right. And do you think it was accurate again?
Yes, yeah, it was accurate too.
Right. So it was accurate because you did it?
For me, for her, yes.
Female, teaching assistant, primary school, intervention group
In addition, some parents felt the length of the questionnaires were too long.
Oh yes, I’d say it was time-consuming, definitely for a 5-year-old.
Right. How big do you think the form needs to be for a 5-year-old?
Oh def, half personally, I’d say half, half of what you’ve got here, for a 5-year-old.
Female, teaching assistant, primary school, intervention group
Lessons for the full-scale trial
-
Outcome measures were seen as too long, especially for child participants.
-
Many participants did not feel the diaries were useful or accurate.
-
The attempts at defining a target behaviour that was directly measurable by frequency counts were not seen as successful by participants.
-
Parents were confused about how to complete the child questionnaires, especially when children had severe autism.
Discussion
The qualitative process evaluation aimed to establish the acceptability and utility of the manualised Social Stories intervention and to elicit information on the feasibility trial process in order to inform any future full-scale RCT. A wide range of issues were covered by the qualitative interviews. The interviewees gave in-depth information from the perspective of participants about the workings of the study and views about the training materials and interventions, and the questionnaires. The feedback was used to compile a list of lessons learned which were discussed by the various groups. PPI feedback was very positive about the process by which researchers were open to hearing negative as well of positive feedback and take it on board in planning.
The participants felt that the GSM needed further refinement for two reasons. Firstly, some felt that not enough information was provided about the study beforehand and did not feel fully informed as a result. This is a concern as the research team had attempted to impart this information on at least two occasions for each participant before the GSM. This indicates that this information may be too complex and needs revision. Secondly, the process of goal-setting was made more difficult by the requirement of needing a goal applicable to both school and home. This requirement was to try and be as inclusive as possible to parents; however, it is recommended that in a future trial, unless there is an obvious goal applicable to both adult participants, priority should be placed on the needs of the participating teacher.
There were some reported issues with communicating with the research team once the participants were enrolled on the feasibility study. This was even more apparent with those in the comparator group. It would be of benefit in a full-scale trial to have a pre-prepared individualised communication plan, with each participant highlighting a preferred communication method and time of contact.
Outcome measures were seen as too long, especially for child participants. It is recommended that these be reduced for a future trial. The participants also reported confusion about how to complete the child questionnaires. If these are used in a future trial, clearer instructions should be given to parents and teachers about how to facilitate helping the children to complete these measures. Finally, participants did not feel the diaries were useful or accurate. These are unlikely to be feasible for a future trial.
Conclusions
Goal-setting
-
As Social Stories are going to be used as a school-based intervention, teachers should have a central role in goal-setting.
-
Interviewees indicated they did not always have a clear idea of what to expect at a GSM. Clearer information about Social Stories and aims of the GSM should be sent to participants prior to this meeting.
-
There was difficulty finding a goal applicable to both school and home in some cases, and this resulted in a less appropriate goal being set. It would improve the trial design if this consistency across settings was not required and the goal focused on the school, given that the HTA call was for interventions in ‘mainstream schools’.
Intervention
-
Adequate time should be allowed for writing Social Stories within the training session.
-
Navigation to the key aspects of the manual should be provided in the training for future use.
-
There is an added complication of deciding where to run the intervention within the secondary school and, if necessary, which lessons to take a child out of.
-
One teaching assistant used a less formal approach with reading stories, reading the story to a group of students, rather than just to the child in the intervention. This is indicative of a lack of treatment fidelity and needs to be addressed in a full-scale RCT
Full-scale trial
-
It was suggested that recruitment would benefit from the research team making more direct contact with schools via SENCOs.
-
It was suggested that there should be more attempts to make families in the community aware of the study through networking within services for children with ASD.
-
There were a small number of occasions when the participating teacher did not sufficiently know the child. In a full trial, it would be beneficial to require a participating teacher who knows the child well.
-
Communication with participants was difficult at times. It would be of benefit in a full-scale trial to have a pre-prepared individualised communication plan with teaching assistants delivering the intervention, highlighting preferred communication method and time of contact.
-
It would also be of benefit to have a single point of contact for parents to avoid confusion and to make sure that the intervention was accessible for parents.
-
Those in the comparator arm reported less effective contact from the research team. This could be improved by a communication plan and improved information.
-
There was confusion about the process among participants. This could be improved by using a generic timeline for the study including key contact points and milestones to help simplify the information given to parents/teachers at recruitment. Providing an individualised timeline for the study for each recruited participant taking into account key dates in the school calendar would also improve this.
-
Outcome measures were seen as too long, especially for child participants. It is recommended that these be reduced for a future trial.
-
Many participants did not feel the diaries were useful or accurate. These are unlikely to be feasible for a future trial.
-
The attempts at defining a target behaviour that was directly measurable by frequency counts was not seen as successful by participants.
-
Parents were confused about how to complete the child questionnaires, especially when children had severe autism. If these are used in a future trial, clearer instructions should be given to parents and teachers about how to facilitate helping the children to complete these measures.
Chapter 10 General discussion and conclusions
This chapter brings together the component sections of the study. In Summary of main findings, the outcomes of the systematic review, the intervention development process and feasibility study are summarised and discussed. In this section, we critically evaluate our achievements against the objectives we set at the start of the study. In Strengths and limitations, we present some short bullet points that we believe best summarise the impact of the study. In Implications for a future trial, we bring together the conclusions from each section of this report and discuss the implications these would have for a potential future RCT looking at Social Stories in mainstream schools.
Summary of main findings
Theoretical phase: systematic review
Objective: to conduct a systematic review examining the use of Social Stories and other social stories for children with ASD, with particular reference to mainstream school-aged children and challenging behaviour.
This objective was fully met. The systematic review was conducted in two stages. The first stage aimed to provide a comprehensive description of how Social Stories have been used in education and clinical practice. The goal of the second stage was to provide a quantitative estimate of the clinical effectiveness of this intervention.
Social stories have been used in a variety of settings to help children make a wide range of behavioural changes. The evidence is predominantly based in the USA and the majority of studies use single-case design methodology. Very few studies looked at the effectiveness of social stories on children over 12 years old. The results broadly supported the effectiveness of the intervention for both the single-case and the between-groups studies but there are some caveats to these findings.
Although a large proportion of studies claimed to use Social Stories and follow all of Gray’s criteria, there was variation in the extent to which the studies met them when the stories used in the studies were examined by reviewers. Many studies did not give enough information to be clear the criteria were being used. In addition, there was very little collaboration recorded among researchers, teachers and parents when writing the stories in the studies, an important element in their design.
The majority of single-case designs did not have (or did not report) having an observer independent of the study to conduct outcome assessments. It is possible, therefore, that the observed effect of the single-case studies may have been artificially inflated because raters had a vested interest in finding a positive result.
There was seven between-groups designs91–97 and only four92–95 of these used some form of randomisation procedure. There was insufficient information to assess a number of important sources of potential bias as measured by the Cochrane risk of bias tool. 20 In the randomised designs, the interventions were often delivered over a much shorter time frame than was typically used in the single-case designs and in practice, and the intervention was a standard pre-written story rather than individually tailored to the child, so therefore they did not qualify as Social Stories. None of these studies therefore adequately tested Social Stories in a RCT.
Phase 1: development of the intervention
Qualitative analysis of the views of Social Story users
Objective: to conduct a qualitative analysis, with user interviews and a user focus group, to gather information relating to the optimum design and use of Social Stories in children with ASD.
This objective was met according to timelines. There were two main aims for the qualitative element of the development of the intervention phase. These were first, to gather information relating to the optimum design and use of Social Stories in children with ASD. Second, this component was intended to explore whether or not the intervention could feasibly be delivered in this context and to ensure the intervention is acceptable to users and providers.
The evidence from the focus groups suggested that in general those who have used Social Stories thought they were an acceptable and effective intervention. They believed that the intervention would be best delivered in a quiet place apart from the other children and that individualising the story to the child was considered vital to their effectiveness. Teaching assistants who know the child well and have their trust would be best placed to support the development and delivery of the stories. The focus group also highlighted the importance of parents being involved with writing the stores and that the focus of a Social Story should never be on a challenging behaviour even when this is specifically being targeted.
The groups believed the development team needed to focus on three domains. Firstly, attendees suggested that they would like to have guidance on how to write Social Stories in a short, simple manual with an easy-to-use checklist. Secondly, they would like this manual to have examples of Social Stories. Finally, they would like confirmation and support through face-to-face training to make sure they are writing well. The feedback also suggested that the manualised component of the intervention needed to be accessible and relatively short, in a format that appeals to a UK audience.
Development and piloting of intervention
Objective: to form an expert writing group and develop a manualised toolkit (including a training package) for writing and delivering Social Stories for use in mainstream schools.
This developmental work was also completed within timelines. An iterative approach was used in which information from the user groups was fed back to the expert panel by the qualitative researcher. Once this information was considered by this panel, they would ask the qualitative researcher to elicit more responses from the user groups and ask for feedback on drafts of the manual they had completed. A complete draft of the manual was completed and a training day developed to be piloted with a small number of service users.
Findings from this stage of the research indicated a number of areas that needed further development before the feasibility trial could go ahead. The manual in particular needed refining. There was strong support for adding more visual elements and to remove some repetitive sections. There were some issues with the overall language, with feedback suggesting that it could be more straightforward and less academic. Consistent feedback suggested providing more example Social Stories throughout the manual. In response, the language throughout the manual was further clarified and refined. More example stories were included to provide a range of different stories and case studies.
Further findings indicated issues with the study logistics. Delivering the intervention leading up to the Christmas holiday was problematic, as this period is a particularly busy time. There was some difficulty arranging meetings and training. The training session was said to be slightly too long. In addition, participants struggled with questions related to the frequency of behaviours. Consequently, alterations were made to the study logistics and outcome measures based on participant feedback.
Phase 2: exploratory trial
Feasibility randomised controlled trial
Objective: to conduct a feasibility RCT comparing the developed manualised Social Stories intervention with an attention control (demonstrating the feasibility of recruitment, delivery of the intervention and follow-up).
This objective was completed. However, the feasibility work identified a number of logistical issues from the original proposal that needed to be resolved. All 50 participant groups were recruited within the proposed timescale of 12 months. We tested three methods of recruitment and all three showed a degree of success, with recruitment through direct contact with schools being the most effective. All participants consented to randomisation and the resulting groups were equivalent in terms of their demographics. Cluster randomisation by school was not deemed to have been necessary because of a low average cluster size.
Retention and questionnaire return rates were high for teachers and parents, although parent returns dropped sharply across follow-up points. Two outcome measures, the SRS-2116 and the custom-made goal-based measure, showed both high levels of completion rates (for teachers), good face validity and a trend in the desired direction indicating that they would be suitable for use as primary outcome measures in a full-scale trial.
We identified issues with the study design, retention of participants, intervention delivery and outcome measures that could be used to inform a future trial. No serious adverse events were reported.
Economic feasibility
Objective: to identify parameters, outcomes and cost-effectiveness from the feasibility study in order to inform a future full-scale RCT.
Response rates from the economic questionnaires in the feasibility study were broadly similar to other outcome questionnaires. The completion rates of the economic and resource use outcome measures indicate it would be feasible to collect them in a full-scale RCT. Parents/carers were more likely to fill in quality-of-life information than children, and when both completed them, there was a moderate correlation between the scores. Both the EQ-5D proxy117 and the HUI2118 had similar completion rates but contained much duplicated material.
Overall teachers/teaching assistances provided the relatively thorough information required to inform resource-related information. Teachers are also found to provide a good indication of how often pupils may not attend school. Finally, teachers had good reporting of school grades and the level of pupil productivity.
Parents gave good information on social service use, contact with criminal justice system and issues affecting their own productivity. Most employed parents reported their annual income (74.3%) which can help capture implications of a child’s behavioural problems on their parent’s lost income. Responses to the productivity questions suggested useful alterations to the questionnaire to capture data on parents who are not in employment.
Qualitative process evaluation
Objective: to establish the acceptability and utility of the developed manualised Social Stories intervention to teachers, parents and children.
Qualitative interviewing provided information to establish the acceptability and utility of the manualised Social Stories intervention to parents and carers. Overall, the intervention itself was received positively but there were a number of issues with the process which are important considerations for future work for a full-scale trial or any trials based on this population.
This is summarised in Chapter 9 and includes information to improve recruitment, to improve the satisfaction of users, to improve channels of communication and the utilisation of outcomes measures that were easy to fill in and not too time-consuming. Consideration was given to the involvement of children with ASD, as their outcome measures were seen as particularly long. It is recommended that these be reduced for a future trial. The participants also reported confusion about how to complete the child questionnaires. If these are used in a future trial, clearer instructions should be given to parents and teachers about how to facilitate helping the children to complete these measures. Feedback about GSMs has improved their implementation, making them more streamlined. While diaries appeared an accurate way of measuring specific behaviours related to goals, they did not work in practice; participants did not feel the diaries were useful or accurate. These are unlikely to be feasible for a future trial.
Strengths and limitations
-
The study had extensive PPI input and involved service users at all stages.
-
The study provided valuable information to inform a future trial design and methods.
-
The study recruited to target and within the proposed time frame.
-
We used a very wide definition of challenging behaviour to ensure the study included all children who could potentially benefit from the intervention.
-
The searches conducted for the systematic review were complete in July 2011 and are no longer current at the time of this publication. These were not updated, as the systematic review was conducted primarily as a backdrop to develop the intervention for the feasibility RCT alongside qualitative work. In this sense, the systematic review happened very early on in the study and was part of the planning for the feasibility work rather than a stand-alone piece of work.
-
The sample of participants was obtained from only one NHS Trust, resulting in the potential for minorities to be under-represented.
-
Blinding of participants to the intervention was not feasible because of the nature of the intervention. However, the feasibility of operationalising behaviours through use of the GSM that could be monitored by a blinded independent observer in a full-scale trial was examined.
-
Treatment fidelity with respect to how closely the finalised stories reflected Gray’s 10 criteria, was not assessed because of low levels of story return rates from participants.
Implications for a future trial
Study eligibility
The inclusion of secondary schools as eligible for the trial was problematic. Focus groups indicated that Social Stories weren’t always appropriate for older children (see Chapter 4). The participant groups from secondary schools in the pilot study highlighted a number of issues they had when participating in the trial (see Chapter 6). In addition, feedback suggested that the routine of reading Social Stories may be less appropriate in secondary schools and harder to implement. The findings from the feasibility study concur with this argument, as the quality of the data from this group was lower than for those from primary schools (see Chapter 7). Participant groups from secondary schools had lower response and retention rates. Those who did return the outcome measure usually did so much later than those from primary schools.
We found from our developmental work that it would have been unfeasible to recruit to the trial if a narrow definition of challenging behaviour had been used. Most teachers and parents report that the behaviours of concern are those which may result in the child’s isolation but that these are not always oppositional in nature. A definition of any behaviour that may result in social exclusion that those who care for the child wish to decrease was used for this trial.
It is likely that 16% of the sample recruited had a score within normal ranges on the SRS-2. 116 None of this subgroup showed any improvements in their scores over time, compared with significant improvements in the children with SRS-2116 scores above the threshold. This implies some recruited children may not have had sufficient social impairments to warrant the intervention, and also implies that those with higher scores are more likely to benefit from the Social Stories intervention.
Recommendations: only use participant groups from primary schools in a full-scale trial. Screen out children who have scores on the SRS-2 within normal ranges. Wide inclusion criteria should be set for challenging behaviour.
Recruitment
Recruitment was most effective when schools were contacted directly. However, other strategies augmented this process (see Chapter 7). The qualitative interviews (see Chapter 9) suggested other routes should be explored to further augment the primary strategy. Specifically, more attempts to make families in the community aware of the study through networking within services for children with ASD were suggested. Additional strategies such as advertising in general practitioner surgeries could also enhance recruitment.
Recommendation: for a full-scale trial, expanding the types of recruitment strategies to augment direct recruitment through schools.
Goal-setting
Goal-setting meetings were seen in a positive light by participants. Focus groups highlighted the importance of parents being involved with writing Social Stories even when the goal is a school-based one (see Chapter 4). However, some difficulties arose when involving them at this point. GSMs were difficult to set up because of conflicting timetables of the teachers and parents. There was difficulty finding a goal applicable to both school and home in some cases and this may have sometimes resulted in a compromised choice. Interviewees also indicated they did not always have a clear idea of what to expect at a GSM.
Recommendations: clearer information about Social Stories and the aims of the GSM should be sent to participants prior to it. As Social Stories are going to be used as school-based intervention, teachers should have the central role in goal-setting. Parents should be invited and encouraged to attend, but would their non-attendance would not prevent a school-based intervention taking place.
Randomisation
We used a cluster randomisation approach by schools but found that the majority of schools only had one or two eligible children (mean 1.35). Feedback from participants found very little contamination across teachers in primary schools. In addition, this approach brought an ethical dilemma, as the requirement to complete baseline measures with all participants at a school before randomisation led to some participants having to wait a number of weeks to be assigned to a condition and consequently were delayed in receiving the intervention.
Recommendation: use an individual remote randomisation process by participating teacher but stratify the randomisation by schools in order to overcome any potential clustering effect.
Training
Participants were very positive about the training days (see Chapter 9). Through increased efficiency, the length of these sessions was reduced from 5 to 3 hours. There was some difficulty arranging meetings and training. An important consideration training in a larger trial is that more trainers in different locations will be needed, increasing the likelihood of inconsistencies in its delivery.
Recommendations: providing people with a wider range of dates for training well in advance is deemed necessary for a full-scale trial. Consistency of training will need to be monitored by observations.
Contact with participants
Participant groups in the feasibility study indicated a desire for more communication with the research team. This was especially the case for those in the comparator group. Researchers running the feasibility study similarly reported difficulty in contacting participants. Possibly as a result of this, there was reported confusion about the process of the study among participants.
Recommendations: it would be of benefit in a full-scale trial to have pre-prepared individualised communication plans with teachers delivering the intervention, highlighting the preferred communication method and time of contact. Providing a generic timeline for participants in the study including key contact points and milestones would help simplify the information given to parents/teachers at recruitment.
Intervention delivery
User groups reported that the intervention would be best delivered in a quiet place apart from the other children. This is consistent with Gray’s tenth criterion. 3 However, qualitative interviews of participants indicated that this guideline was not always followed. One teaching assistant read the story to a group of students, rather than just to the child in the intervention. Delivering the intervention leading up to the Christmas holiday was a problem as this period is a particularly busy time.
Recommendations: stricter guidance on and monitoring of intervention delivery would benefit a full-scale trial. Providing an individualised timeline for the study for each recruited participant taking into account key dates in the school calendar would improve clashes with holiday periods. Qualitative interviewing to specifically assess fidelity and understand factors that could enhance it would also be of benefit.
Outcome measures
Retention and questionnaire completion rates were highest for participating teachers, but also good for participating parents. The feasibility of collecting questionnaires from child participants raised some difficulties, particularly where children appeared to be guessing responses and/or were not fully understanding the questionnaire. Many adult participants had to broker their child’s involvement and some admitted to guiding or adapting responses based on their knowledge of the child. Some parents were uncertain about how to complete the child questionnaires. If these are used in a future trial, clearer instructions should be given to parents and teachers about how to facilitate helping the children to complete these measures.
Outcome measures were also seen as too long especially for child participants. Health economics data completion rates are good overall, indicating they would be feasible to collect in a full-scale trial. The economic section showed good correlation between quality-of-life child and parent proxy measures with improved overall completion if both were filled in, but there seemed little extra to be gained from filling in two separate quality of life measures (EQ-5D117 and HUI2118).
Diary return rates were very low for both teachers and parents and these were considered not to be feasible to use in a full-scale trial. Participants did not feel the behaviours in the diaries were useful or accurate. However, when the resulting behaviours were examined and categorised by a researcher experienced in applied behaviour analysis, all 38 behaviours were categorised as measurable for someone trained in behavioural observation.
Two outcome measures, the SRS-2116 and the custom-made goal-based measure, showed both high levels of completion rates (for teachers) and they appeared to be capturing the social and behaviour skills that professionals and users felt would be most important to alter via the use of Social Stories. They also had the most face validity in that they were measuring social responsiveness or a very specific goal, the main focus of the Social Story intervention. The SRS-2116 is also a validated instrument for use in this group and is widely used.
One issue apparent in the studies highlighted by the systematic review (see Chapter 2) was that those who deliver the intervention were often the same people who rated the behaviours or completed the outcome measure leading to a potential vested interest in its success. This was also the case for the measures in this feasibility study and it would be of benefit to address this in full-scale RCT.
Recommendations: it is important that the length of the questionnaire is reduced and, if children are to receive questionnaires in a larger RCT, outcome measures need to be greatly simplified. Behavioural diaries are not feasible and should not be used in a full-scale trial. Outcome measures should be completed by a second teacher not involved in the development or delivery of the intervention in a full-scale trial. It could be feasible to include an additional observational measure through use of an independent researcher, blind to group allocation, observing the goal in a school setting.
Treatment fidelity
It was not possible to assess the fidelity of the Social Stories to Gray’s criteria3 because of low rates of returns of the stories from participants. This is a methodological concern that needs to be addressed in future trials as feedback from all parts of the study tell of the difficulty in conforming to these. This is also represented by the findings of the systematic review as, although a large proportion of studies claimed to use Social Stories and follow all of Gray’s criteria, there was extensive variation in the extent to which the studies met them when stories were examined by reviewers.
Recommendation: in a future trial, participants should be informed that stories will be collected at the first follow-up period.
Sample size
Power calculations were made based on the two outcome measures most appropriate to be used as primary outcomes for a full-scale trial (the SRS-2 and goal-based outcome).
Recommendation: a total sample size of 180 participant groups would be required for a full-scale trial.
Other recommendations for research
In a psychosocial intervention such as Social Stories, when it is not possible or desirable for the teaching staff, parents or the children involved to be blind to their group allocation, the question of whether or not a truly blinded outcome measure of effect can be achieved is a major issue. This is particularly true for studies on children with ASD, particularly young children, as because of their specific needs and idiosyncratic behaviours and language, proxy measure completed by those who know them well are necessary. Owing to resource limitations, we were not able to examine the feasibility of independent observers conducting blinded assessments of behaviours, although we did discover that it was feasible to operationalise behaviours through meeting with those who know the child. Despite this, findings indicate observations may take a full day and it would likely be very costly to conduct a measurement in this way. It would be of great benefit for research in this area for a more generic outcome measure to be developed for children with ASD that rated the child on observable social behaviours that could be completed by a researcher blind to allocation. This is a priority issue to be addressed which could be further examined in further small group comparison studies.
Conclusions
We have successfully developed and refined a Social Stories training package for use in mainstream school but also suitable for parents of children with ASD. This training package, which consists of a manual and a training day, has the potential to help children with ASD overcome some of the social difficulties they experience at school in a non–expensive, non-intrusive way, subject to its being shown to be effective and cost-effective in a future trial. Were this to be demonstrated, the intervention could be made widely available to educational and community settings across the country.
Some implications for clinical practice have been gleaned from the feasibility trial. It is clear that parents and teachers (at least in one part of the UK) are currently well disposed towards the Social Story intervention. Many regard it as effective in practice and are motivated to attend training. Many have also been enthusiastic in requesting accessible training materials for the UK setting. Further important implications will be generated by a full-scale RCT.
Acknowledgements
We would like to acknowledge the contributions of the following people:
Professor Stephen Morley for his advice on single-case studies in the systematic review.
Professor Sarah Byford for her help on the resource-use questionnaire in the health economic evaluation.
Anastasia Kokina for her assistance on the systematic review and data extraction.
Carol Gray for her invaluable advice and input regarding Social Stories development.
Lisa Dyson for helping with the interviews and providing input regarding the qualitative work.
Dr Sam Beeson, Dr Elizabeth Edgington and Emma Medford for their assistance on recruiting participants to the feasibility study.
Anne McKelvey and Claire Elsdon for their help with recruiting and training participants.
Danielle Varley, Jules Beresford-Dent and Jenny Sweetman for their help on the drafting of this report.
Catherine Arthurson for her administrative support throughout the study.
The attendees of the TMG, the Trial Steering Committee and the Data Monitoring Ethics Committee for their useful insight throughout the study.
The participant groups and their respective schools for their participation throughout the feasibility study.
Contributions of authors
Professor Barry Wright (Clinical Director) was chief investigator, designed and led the study, led the expert panel and writing group for the intervention and prepared the final report.
Dr David Marshall (Trial Coordinator) managed the daily running of the study, assisted with the systematic review and focus groups and co-ordinated the writing of the report.
Dr Joy Adamson (Deputy Director) led on the qualitative aspects of the study and provided methodological support throughout the feasibility trial.
Ms Hannah Ainsworth (Research Fellow) assisted in the management of the study, providing guidance and expertise to the study team, assisted with the qualitative work and analysis, took the lead on running the pilot study and led the team designing and selecting the outcome measures for the feasibility trial.
Dr Shehzad Ali (Research Fellow) assisted in developing the resource-use questionnaires and assisted in the preparation of the health economic parameters.
Dr Victoria Allgar (Senior Statistician) provided methodological and statistical support, facilitated preparation of and interpreted the quantitative data.
Ms Danielle Collingridge Moore (Research Fellow) assisted in data extraction for the systematic review and contributed to the original design of the study.
Ms Elizabeth Cook (Research Fellow) assisted in the coordination and running of the feasibility trial.
Dr Paul Dempster (Qualitative Research Fellow) managed the qualitative work and focus groups and prepared the qualitative chapters of the report.
Ms Lisa Hackney (Clinical Studies Officer) assisted in recruitment and to the running of the study, assisted in the data extraction of the systematic review and helped prepare Chapter 2 for the report.
Dr Dean McMillan (Senior Lecturer) led on the systematic review and provided methodological advice throughout the study
Dr Dominic Trepél (Research Fellow) led on the development of the resource-use questionnaires and assisted in the preparation of the health economic parameters.
Dr Chris Williams (Clinical Psychologist) provided expertise in ASD, Social Stories and recruitment, contributed to the expert panel and writing group, led on the delivery of training and prepared Chapter 3.
Publications
Moore D, Wright B, Williams C, Moore K, Dempster PG. The experiences of parents and teachers who use Social Stories for children with autism spectrum disorders. Clinical Psychology Forum 2014;255:10–13.
Wright B, Marshall D, Moore DC, Ainsworth H, Hackney L, et al. Autism spectrum Social Stories in schools trial (ASSSIST): study protocol for a feasibility randomised controlled trial analysing clinical and cost-effectiveness of Social Stories in mainstream schools. BMJ Open 2014;4:e005952.
Data sharing statement
Full information of all aspects of the trial is available on request from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Carbo BC. The Use of Social Stories with Individuals with Autism Spectrum Disorders. Newark, DE: University of Delaware; 2005.
- Macintosh K, Dissanayake C. Social skills and problem behaviours in school aged children with high-functioning autism and Asperger’s Disorder. J Autism Dev Disord 2006;36:1065-76. http://dx.doi.org/10.1007/s10803-006-0139-5.
- Gray CA. The New Social Story Book. Arlington: Future Horizons Inc.; 2010.
- Kokina A, Kern L. Social Story™ interventions for students with Autism Spectrum Disorders: a meta-analysis. J Autism Dev Disord 2010;40:812-26. http://dx.doi.org/10.1007/s10803-009-0931-0.
- Norris C, Dattilo J. Evaluating effects of a social story intervention on a young girl with autism. Focus Autism Other Dev Disabl 1999;14:180-6. http://dx.doi.org/10.1177/108835769901400307.
- Barry L, Burlew S. Using Social Stories to teach choice and play skills to children with autism. Focus Autism Other Dev Disabl 2004;19:45-51. http://dx.doi.org/10.1177/10883576040190010601.
- Ozdemir S. The effectiveness of social stories on decreasing disruptive behaviors of children with autism: three case studies. J Autism Dev Disord 2008;38:1689-96. http://dx.doi.org/10.1007/s10803-008-0551-0.
- Bledsoe R, Myles BS, Simpson RL. Use of a Social Story intervention to improve mealtime skills of an adolescent with Asperger syndrome. Autism 2003;7:289-95. http://dx.doi.org/10.1177/13623613030073005.
- Lorimer PA, Simpson RL, Myles BS, Ganz JB. The use of social stories as a preventative behavioral intervention in a home setting with a child with autism. J Posit Behav Interven 2002;4:53-60. http://dx.doi.org/10.1177/109830070200400109.
- Kuttler S, Myles BS, Carlson JK. The use of social stories to reduce precursors to tantrum behavior in a student with autism. Focus Autism Other Dev Disabl 1998;13:176-82. http://dx.doi.org/10.1177/108835769801300306.
- Adams L, Gouvousis A, VanLue M, Waldron C. Social story intervention: improving communication skills in a child with an Autism Spectrum Disorder. Focus Autism Other Dev Disabl 2004;19:87-94. http://dx.doi.org/10.1177/10883576040190020301.
- Crozier S, Tincani M. Effects of social stories on prosocial behavior of preschool children with Autism Spectrum Disorders. J Autism Dev Disord 2007;37:1803-14. http://dx.doi.org/10.1007/s10803-006-0315-7.
- Delano M, Snell ME. The effects of social stories on the social engagement of children with autism. J Posit Behav Interven 2006;8:29-42. http://dx.doi.org/10.1177/10983007060080010501.
- Ivey ML, Heflin L, Alberto P. The use of Social Stories to promote independent behaviors in novel events for children with PDD-NOS. Focus Autism Other Dev Disabl 2004;19:164-76. http://dx.doi.org/10.1177/10883576040190030401.
- Reynhout G, Carter M. Social Stories™ for children with disabilities. J Autism Dev Disord 2006;36:445-69. http://dx.doi.org/10.1007/s10803-006-0086-1.
- Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. BMJ 2000;321:694-6. http://dx.doi.org/10.1136/bmj.321.7262.694.
- Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, Dilavore PC, et al. The Autism Diagnostic Observation Schedule--Generic: a standard measure of social and communication deficits associated with the spectrum of autism. J Autism Dev Disord 2000;30:205-23. http://dx.doi.org/10.1023/A:1005592401947.
- McMillan D, Morley S, Barkham M, Hardy GE, Mellor-Clark J. Developing and Delivering Practice-Based Evidence. London: John Wiley & Sons, Ltd; 2010.
- Tate RL, McDonald S, Perdices M, Togher L, Schultz R, Savage S. Rating the methodological quality of single-subject designs and n-of-1 trials: introducing the Single-Case Experimental Design (SCED) Scale. Neuropsychol Rehabil 2008;18:385-401. http://dx.doi.org/10.1080/09602010802009201.
- Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343. http://dx.doi.org/10.1136/bmj.d5928 (accessed 18 October 2011).
- Scruggs TE, Mastropieri MA, Cook SB, Escobar C. Early intervention for children with conduct disorders: a quantitative synthesis of single-subject research. Behav Disorders 1986;11:260-71.
- Ma HH. An alternative method for quantitative synthesis of single-subject researches: percentage of data points exceeding the median. Behav Modif 2006;30:598-617. http://dx.doi.org/10.1177/0145445504272974.
- Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
- Hobbs AM. Facilitating the Inclusion of Pupils with Asperger’s Syndrome in Mainstream Schools. Southampton: Southampton University; 2003.
- Styles A. Using Mixed Methods of Analysis to Explain the Impact of a Social Stories Intervention for Children with Autism Spectrum Disorders in a Mainstream Primary School. Essex: University of Essex; 2009.
- Voges CM. Using a Social Story to Teach an Eight-Year-Old Girl with Autism a Socially Appropriate Way of Eating: A Case Study. Christchurch, NZ: University of Canterbury; 2009.
- Abraham JA. Generalization Effects of Social Story Interventions for Individuals with Asperger’s Disorder. Hattiesburg, MS: University of Southern Mississippi; 2009.
- Agosta E, Graetz J, Mastropieri M, Scruggs T. Teacher–researcher partnerships to improve social behavior through Social Stories. Interv Sch Clinic 2004;39:76-87. http://dx.doi.org/10.1177/10534512040390050401.
- Brownell M. Musically adapted social stories to modify behaviors in students with autism: four case studies. J Music Ther 2002;39:117-44. http://dx.doi.org/10.1093/jmt/39.2.117.
- Chan JM, O’Reilly MF. A Social Stories intervention package for students with autism in inclusive classroom settings. J Appl Behav Anal 2008;41:405-9. http://dx.doi.org/10.1901/jaba.2008.41-405.
- Cihak D, Kildare L, Smith C, McMahon D, Quinn-Brown. Using video Social Stories to increase task engagement for middle school students with Autism Spectrum Disorders. Behav Modif 2012;36:399-425. http://dx.doi.org/10.1177/0145445512442683.
- Crozier S, Tincani MJ. Using a modified Social Story to decrease disruptive behavior of a child with autism. Focus Autism Other Dev Disabl 2005;20:150-7. http://dx.doi.org/10.1177/10883576050200030301.
- Demiri V. Teaching Social Skills to Children with Autism using Social Stories: an Empirical Study. Hempstead, NY: Hofstra University; 2004.
- Eckelberry E. Using Social Stories with Children with Autism, Learning Disabilities and ADHD. Athens, Ohio: Ohio University; 2007.
- Hanley KP. Social Stories to Increase Verbal Initiations to Peers in Children with Autistic Disorder and Asperger’s Disorder. Mansfield, CT: University of Connecticut; 2008.
- Holmes CM. Using Social Stories to Increase Social Skills for a Student with Autism. Marshall, MN: Southwest Minnesota State University; 2007.
- Hung L-C, Smith CS. Autism in Taiwan: using social stories to decrease disruptive behaviour. Br J Dev Disab 2011;57:71-80. http://dx.doi.org/10.1179/096979511798967197.
- Keyworth P. The Effect of Social Stories on the Social Interaction of Students with Autism. Iowa city, IA: University of Iowa; 2004.
- Kuoch H. Social Story Interventions for Young Children with Autism Spectrum Disorders: A Comparative Study. PhD thesis. Vancouver, BC; 2000.
- Hsu N. The Effectiveness of Multicultural Based Social Stories to Increase Appropriate Behaviors of Children with Developmental Delay. El Paso, TX: University of Texas; 2009.
- Ozdemir S. Using multimedia social stories to increase appropriate social engagement in young children with autism. Turk Online J Educ Technol 2008;7:80-8.
- Quilty KM. Teaching paraprofessionals how to write and implement social stories for student with Autism Spectrum Disorders. Rem Spec Educ 2007;28:182-9. http://dx.doi.org/10.1177/07419325070280030701.
- Reichow B, Sabornie EJ. Brief report: increasing verbal greeting initiations for a student with Autism via a social story intervention. J Autism Dev Disord 2009;39:1740-3. http://dx.doi.org/10.1007/s10803-009-0814-4.
- Sansosti FJ, Powell-Smith KA. Using social stories to improve the social behavior of children with Asperger syndrome. J Posit Behav Interven 2006;8:43-57. http://dx.doi.org/10.1177/10983007060080010601.
- Sansosti FJ, Powell-Smith KA. Using computer-presented social stories and video models to increase the social communication skills of children with high functioning Autism Spectrum Disorders. J Posit Behav Interven 2008;10:162-78. http://dx.doi.org/10.1177/1098300708316259.
- Schneider N, Goldstein H. Using social stories and visual schedules to improve socially appropriate behaviors in children with autism. J Posit Behav Interven 2010;12:149-60. http://dx.doi.org/10.1177/1098300709334198.
- Scurlock M. Using Social Stories with Children with Asperger Syndrome. Athens, Ohio: Ohio University; 2008.
- Smith A. Increasing Social Initiations in Preschoolers with Autism using a Combination of Social Stories, Pictorial Cues and Role Play. Denver, CO: University of Denver; 2004.
- Swaine J. Teaching Language Skills to Children with Autism Through the Use of Social Stories. Halifax, NS: Dalhousie University; 2004.
- Taylor KM. The effects of Social Stories on Language and Social Appropriateness in Children with Autism Spectrum Disorders. Greenville, NC: East Carolina University; 2009.
- Thiemann KS, Goldstein H. Social stories, written text cues, and video feedback: effects on social communication of children with autism. J Appl Behav Anal 2001;34:425-46. http://dx.doi.org/10.1901/jaba.2001.34-425.
- Vanderhoek A, Fielding Barnsley R, Bartlett B, Bryer F, Roebuck D. Proceedings International Conference on Cognition, Language and Special Education Research Crown Plaza Surfers Paradise. Brisbane, SEQ: School of Cognition, Language and Special Education, Griffith University; 2004.
- Washburn KP. The Effects of a Social Story Intervention on Social Skills Acquisition in Adolescents with Asperger’s Syndrome. Gainesville, FL: University of Florida; 2006.
- Wilkinson L. The Effect of Social Stories and Peer Video Modeling to Increase Social Pragmatics in Children with Autism. Boston, MA: Northeastern University; 2010.
- Wright LA. Utilizing Social Stories to Reduce Problem Behavior and Increase Pro-social Behavior in Young Children with Autism. Columbia, MI: University of Missouri; 2007.
- Bailey DA. Analysis of a Social Story Intervention to Increase Appropriate Social Interactions in Children with Autism. Tallahassee, FL: Florida State University; 2008.
- Beh-Pajooh A, Ahmadib A, Shokoohi-Yektac M, Asgarya A. The effect of social stories on reduction of challenging behaviours in autistic children Procedia. Soc Behav Sci 2011;15:351-5. http://dx.doi.org/10.1016/j.sbspro.2011.03.100.
- Bell N. Using Social Stories to Improve Socially Appropriate Behaviours in Children with Autism. Florida, FL: Florida State University; 2005.
- Graetz JE. Promoting Social Behavior for Adolescents with Autism with Social Stories. Fairfax, VA: George Mason University; 2003.
- Hagiwara T, Myles BS. A multimedia social story intervention: teaching skills to children with autism. Focus Autism Other Dev Disabl 1999;14:82-95. http://dx.doi.org/10.1177/108835769901400203.
- Mandasari V, Lu MV, Theng LB, Theng LB. Assistive and Augmentive Communication for the Disabled: Intelligent Technologies for Communication, Learning and Teaching. IGI Global; 2011.
- Mancil GR, Haydon T, Whitby P. Differentiated effects of paper and computer-assisted Social Stories™ on inappropriate behavior in children with autism. Focus Autism Other Dev Disabl 2009;24:205-15. http://dx.doi.org/10.1177/1088357609347324.
- Okada S, Ohtake Y, Yanagihara M. Effects of perspective sentences in Social Stories™ on improving the adaptive behaviors of students with Autism Spectrum Disorders and related disabilities. Educ Train Dev Disab 2008;43:46-60.
- Okada S, Ohtake Y, Yanagihara M. Improving the manners of a student with autism: the effects of manipulating perspective holders in Social Stories™ – a pilot study. Int J Disab Dev Educ 2010;57:207-19. http://dx.doi.org/10.1080/10349121003750927.
- Reynhout G, Carter M. Social Story™ efficacy with a child with Autism Spectrum Disorder and moderate intellectual disability. Focus Autism Other Dev Disabl 2007;22:173-82. http://dx.doi.org/10.1177/10883576070220030401.
- Reynhout G, Carter M. A pilot study to determine the efficacy of a Social Story intervention for a child with autistic disorder, intellectual disability and limited language skills. Australas J Spec Educ 2008;32:161-75. http://dx.doi.org/10.1080/10300110802047210.
- Scattone D, Wilczynski SM, Edwards RP, Rabian B. Decreasing disruptive behaviors of children with autism using social stories. J Autism Dev Disord 2002;32:535-43. http://dx.doi.org/10.1023/A:1021250813367.
- Scattone D, Tingstrom DH, Wilczynski SM. Increasing appropriate social interactions of children with Autism Spectrum Disorders using Social Stories. Focus Autism Other Dev Disabl 2006;21:211-22. http://dx.doi.org/10.1177/10883576060210040201.
- Staley MJ. An Investigation of Social-Story Effectiveness Using Reversal and Multiple-Baseline Designs. Lawrence, KA: University of Kansas; 2001.
- Swaggart B, Gagnon E, Bock SJ, Earles TL, . Using social stories to teach social and behavioral skills to children with autism. Focus Autistic Behav 1995;10:1-16. http://dx.doi.org/10.1177/108835769501000101.
- Travis D. The Effect of Musical Social Stories™ on Target Behaviors of Preschool Children with Autism Spectrum Disorders: Three Case Studies. East Lansing, MI: Michigan State University; 2006.
- Washburn M. Using Social Stories to Teach On-Task Behavior and Participation Skills with Children on the Autism Spectrum. Rochester, NY: Rochester Institute of Technology; 2006.
- Watts KS. The Effectiveness of a Social Story Intervention in Decreasing Disruptive Behavior in Autistic Children. Columbus, OH: Ohio State University; 2008.
- Wheeler K. The Power of Social Stories: A Strategy for Students with Autism Spectrum Disorder. Fullerton, CA: California State University; 2006.
- Xin JF, Sutman FX. Using the smart board in teaching Social Stories to students with autism. Teaching Exceptional Children 2011;43:18-24.
- Antle ML. The Use of Social Stories to Teach Social and Behavioural Skills to Preschool Children with Moderate to Severe Autism. Bowling Green, KY: Western Kentucky University; 2004.
- Bernad-Ripoll S. Using a self-as-model video combined with Social Stories to help a child with Asperger syndrome understand emotions. Focus Autism Other Dev Disabl 2007;22:100-6. http://dx.doi.org/10.1177/10883576070220020101.
- Chan Y-M. Modifying Behaviors of Children with Autism: The Use of Musically Adapted Social Stories in Home-Based Environments. FL: Florida State University; 2005.
- Daneshvar SD. A Comparison of Steps to Social Success (SSS) and Social Stories for Teaching Social Skills to Children with Autism. Clarmont, CA: The Claremont Graduate University; 2006.
- Dodd S, Hupp SD, Jewell JD, Krohn E. Using parents and siblings during a social story intervention for two children diagnosed with PDD-NOS. J Dev Physical Disabil 2008;20:217-29. http://dx.doi.org/10.1007/s10882-007-9090-4.
- Gilles AA. Treatment of Sleep Disturbances in Children with Autistic Disorder: Utilization of Behavioral Intervention, Social Story, and Picture Activity Schedule. Orono, ME: University of Maine; 2008.
- Hutchins TL, Prelock PA. Using social stories and comic strip conversations to promote socially valid outcomes for children with autism. Semin Speech Lang 2006;27:47-59. http://dx.doi.org/10.1055/s-2006-932438.
- Pasiali V. The use of prescriptive therapeutic songs in a home-based environment to promote social skills acquisition by children with autism: three case studies. Music Ther Perspec 2004;22:11-20. http://dx.doi.org/10.1093/mtp/22.1.11.
- Powell JL. Using Social Stories and Behavior Skills Training Involving Family Members to Increase Social Skills for a Child with Autism. Tampa, FL: University of South Florida; 2009.
- Scapinello SS. Effectiveness of Social Stories™ for Children with Autism Spectrum Disorders. Windsor, ON: University of Windsor; 2009.
- Scattone D. Enhancing the conversation skills of a boy with Asperger’s disorder through Social Stories™ and video modeling. J Autism Dev Disord 2008;38:395-400. http://dx.doi.org/10.1007/s10803-007-0392-2.
- Tarnai B, Wolfe P, Rusch F, Lee D, Demir O, Celik C. Multimedia in Education and Special Education. Hauppauge, NY: Nova Science Publishers, Inc.; 2009.
- Tarnai B. Establishing the relative importance of applying Gray’s sentence ratio as a component in a 10-step social stories intervention model for students with ASD. Int J Spec Educ 2011;26:58-79.
- Chan JM. Pre-Service Teacher-Implemented Social Stories Intervention for Students with Autism Spectrum Disorders in General Education Settings. Austin, TX: University of Texas at Austin; 2009.
- Cullain R. The Effects of Social Stories on Anxiety Levels and Excessive Behavioral Expressions of Elementary School-Aged Children with Autism. Brattleboro, VT: The Union Institute; 2002.
- Ali M. Communication skills in children with autism: the effect of the Social Stories technique. Interven Sch Clin 2010;5:88-104.
- Andrews SM. Increasing Game Playing Skills and Social Comprehension in School-Aged Children with Autism using Social Stories. San Diego, CA: Alliant International University; 2004.
- Bader R. Using Social Stories to Increase Emotion Recognition and Labeling in School-Age Children with Autism. San Diego, CA: Alliant International University; 2006.
- Feinberg MJ. Using Social Stories to Teach Specific Social Skills to Individuals Diagnosed with Autism. San Diego, CA: California School Of Professional Psychology; 2001.
- Quirmbach LM, Lincoln AJ, Feinberg-Gizzo MJ, Ingersoll BR, Andrews SM. Social stories: mechanisms of effectiveness in increasing game play skills in children diagnosed with Autism Spectrum Disorder using a pretest posttest repeated measures randomized control group design. J Autism Dev Disord 2009;39:299-321. http://dx.doi.org/10.1007/s10803-008-0628-9.
- Ricciardelli D. A Social Skills Program Evaluation: Will Social Stories Combine with a Traditional Social Skills Curriculum Increase Pro-Social Behavior in Autistic Children?. Teaneck, NJ: Fairleigh Dickinson University; 2006.
- Romano J. Are Social Stories Effective in Modifying Behavior in Children with Autism?. Teaneck, NJ: Fairleigh Dickinson University; 2002.
- Botha N. Residential trips: using social stories to support children on the autism spectrum. Good Autism Pract 2009;10:79-87.
- Chapman L, Trowbridge M. Social Stories for reducing fear in the outdoors. Horizons 2000;121:38-40.
- Moffatt E. Social stories: a collection of three papers. 1. Writing social stories to improve students social understanding. Good Autism Pract 2001;2:12-5.
- Moore PS. The use of social stories in a psychology service for children with learning disabilities: a case study of a sleep problem. Br J Learn Disabil 2004;32:133-8. http://dx.doi.org/10.1111/j.1468-3156.2004.00278.x.
- O’Connor E. The use of Social Story DVDs to reduce anxiety levels: a case study of a child with autism and learning disabilities. Support Learn 2009;24:133-6. http://dx.doi.org/10.1111/j.1467-9604.2009.01413.x.
- Rowe C. Do social stories benefit children with autism in mainstream primary schools?. Br J Spec Educ 1999;26:12-4. http://dx.doi.org/10.1111/1467-8527.t01-1-00094.
- Thorne A. Using an interactive whiteboard to present social stories to a group of children with Autistic Spectrum Disorders. Good Autism Pract 2005;6:3-18.
- Camire S, Goupil G. The use of social stories: An elaboration of an intervention program and perceptions of adolescents with Autism Spectrum Disorder. Revue De Psychoeduc 2011;40:87-104.
- Vitale N. Social Stories and Social Behavior in Children within the Autism Spectrum Disorder. New York, NY: Wagner College; 2007.
- Bracke D, Therrien W. Using a social story to improve the recess behavior of a student with Autism Spectrum Disorder. ACEI Focus on Inclusive Educ 2008;6:1-8.
- Choi SH-J, Nieminen TA. Naturalistic intervention for Asperger syndrome – a case study. Br J Spec Educ 2008;35:85-91. http://dx.doi.org/10.1111/j.1467-8578.2008.00377.x.
- Dentato K. Effect of Sequential Social Stories Series on Social Register in Individual with Autism. Hempstead, NY: Hofstra University; 2006.
- Backman B, Pilebro C. Augmentative communication in dental treatment of a nine-year-old boy with Asperger syndrome. J Dent Child 1999;66:419-20.
- Rogers MF, Myles BS. Using Social Stories and Comic Strip Conversations to interpret social situations for an adolescent with Asperger syndrome. Interven Sch Clin 2001;36:310-13. http://dx.doi.org/10.1177/105345120103600510.
- Sotelo M. Improving Social Competence in Children with Autism Spectrum Disorders through a Combined-Strategy Group Intervention: A Pilot Study. Fort Lauderdale, FL: Nova Southeastern University; 2010.
- Kuzel A, Crabtree B, Miller W. Doing Qualitative Research. Thousand Oaks, CA: Sage Publications; 1999.
- The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: WHO; 1993.
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry 1997;38. http://dx.doi.org/10.1111/j.1469-7610.1997.tb01545.x.
- Constantino J, Gruber C. Social Responsiveness Scale. Los Angeles, CA: Western Psychological Services; 2012.
- The EuroQol Group . EuroQol – a new facility for the measurement of health-related quality of life. Health Pol 1990;16:199-208. http://dx.doi.org/10.1016/0168-8510(90)90421-9.
- Stevens K, McCabe C, Brazier J, Roberts J. Multi-attribute utility function or statistical inference models: a comparison of health state valuation models using the HUI2 health state classification system. J Health Econ 2007;26:992-1002. http://dx.doi.org/10.1016/j.jhealeco.2006.12.007.
- Abidin RR. Parenting Stress Index, Fourth Edition (PSI-4). Lutz, FL: Psychological Assessment Resources Inc.; 2012.
- Spence SH. Structure of anxiety symptoms among children: a confirmatory factor-analytic study. J Abnorm Psychol 1997;106:280-97. http://dx.doi.org/10.1037/0021-843X.106.2.280.
- Wright B, Marshall D, Collingridge Moore D, Ainsworth H, Hackney L, Adamson J, et al. Autism Spectrum Social Stories In Schools Trial (ASSSIST): study protocol for a feasibility randomised controlled trial analysing clinical and cost-effectiveness of Social Stories in mainstream schools. BMJ Open 2014;4. http://dx.doi.org/10.1136/bmjopen-2014-005952.
- Pillay M, Alderson-Day B, Wright B, Williams C, Urwin B. Autism Spectrum Conditions – Enhancing Nurture and Development (ASCEND): an evaluation of intervention support groups for parents. Clin Child Psychol Psychiatry 2011;16:5-20. http://dx.doi.org/10.1177/1359104509340945.
- Lancaster GA, Dodd S, Williamson PR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract 2004;10:307-12. http://dx.doi.org/10.1111/j. 2002.384.doc.x.
- Guide to the Methods of Technology Appraisal 2013. London: NICE; 2013.
- Barrett B, Byford S, Sharac J, Hudry K, Leadbitter K, Temple K, et al. Service and wider societal costs of very young children with autism in the UK. J Autism Dev Disord 2012;42:797-804. http://dx.doi.org/10.1007/s10803-011-1306-x.
- Barrett B, Mosweu I, Jones CR, Charman T, Baird G, Simonoff E, et al. Comparing service use and costs among adolescents with autism spectrum disorders, special needs and typical development. Autism 2015;19:562-9. http://dx.doi.org/10.1177/1362361314536626.
- Whynes DK, Sprigg N, Selby J, Berge E, Bath PM. Testing for differential item functioning within the EQ-5D. Med Dec Making 2013;33:252-60. http://dx.doi.org/10.1177/0272989X12465016.
- Curtis L. Unit Costs of Health and Social Care 2014. University of Kent, Canterbury: Personal Social Services Research Unit; 2014.
- Tilford JM, Payakachat N, Kovacs E, Pyne JM, Brouwer W, Nick TG, et al. Preference-based health-related quality-of-life outcomes in children with Autism Spectrum Disorders: a comparison of generic instruments. Pharmacoeconomics 2012;30:661-79. http://dx.doi.org/10.2165/11597200-000000000-00000.
- Oostenbrink R, HA AM, Essink-Bot ML. The EQ-5D and the Health Utilities Index for permanent sequelae after meningitis: a head-to-head comparison. J Clin Epidemiol 2002;55:791-9. http://dx.doi.org/10.1016/S0895-4356(02)00448-1.
- Haskins BG, Silva JA. Asperger’s disorder and criminal behavior: forensic-psychiatric considerations. J Am Acad Psychiatry Law 2006;34:374-84.
- Trépel D. Informal cost of dementia care – a proxy-good valuation in Ireland. Econ Soc Rev 2011;42:479-503.
- Haynes L, Service O, Goldacre B, Torgerson D. Test, Learn, Adapt: Developing Public Policy with Randomised Controlled Trials. London: Cabinet Office Behavioural Insights Team; 2012.
- Education Act 1981. London: The Stationery Office; 1981.
- O’Cathain A, Murphy E, Nicholl J. Why, and how, mixed methods research is undertaken in health services research in England: a mixed methods study. BMC Health Serv Res 2007;7. http://dx.doi.org/10.1186/1472-6963-7-85.
- Ritchie J, Spencer L. Qualitative Analysis for Applied Social Policy. London: Routledge; 2004.
- Pope C, Ziebland S, Mays N. Qualitative research in health care. Analysing qualitative data. BMJ 2000;320:114-16. http://dx.doi.org/10.1136/bmj.320.7227.114.
Appendix 1 Database searches
| Resource | Records identified |
|---|---|
| PsycINFO | 178 |
| MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations | 29 |
| EMBASE | 50 |
| Cumulative Index to Nursing and Allied Health Literature | 31 |
| British Nursing Index | 1 |
| Cochrane Database of Systematic Reviews | 2 |
| Database of Abstracts of reviews of Effects | 3 |
| Cochrane Central Register of Controlled Trials | 2 |
| HTA database | 0 |
| NHS Economic Evaluation Database | 0 |
| Education Resources Information Center | 123 |
| British Education Index | 11 |
| Australian Education Index | 9 |
| Applied Social Sciences Index and Abstracts | 23 |
| Social Policy & Practice | 26 |
| Social Services Abstracts | 8 |
| Science Citation Index | 57 |
| Social Science Citation Index | 207 |
| Conference Proceedings Citation Index – Science | 17 |
| Conference Proceedings Citation Index – Social Science & Humanities | 12 |
| Social Care Online | 8 |
| Campbell Library | 0 |
| OAIster | 32 |
| Index to Theses | 6 |
| Zetoc | 77 |
| British Library integrated catalogue | 4 |
| Library of Congress catalog | 10 |
| ClinicalTrials.gov | 0 |
| International Clinical Trials Registry Platform | 0 |
| Google Scholar – advanced (dissertations/theses) | 36 |
| Citation searches | 108 |
| Total | 1070 |
| Total after deduplication | 637 |
Example search strategies
PsycINFO (OvidSP)
Date range searched: 1806–2011/July week 4.
Date searched: 18 July 2011.
-
exp pervasive developmental disorders/ (19,541)
-
(autistic or autism or kanner$ or ASD).ti,ab. (22,378)
-
asperger$.ti,ab. (2262)
-
(pervasive adj2 develop$).ti,ab. (2052)
-
PDD.ti,ab. (1076)
-
or/1-5 (24,939)
-
storytelling/ (2951)
-
(social adj4 (story$ or stories$ or storytelling)).ti,ab,id. (584)
-
((individual$ or sensory) adj4 (story or stories or storytelling)).ti,ab,id. (712)
-
(comic$1 or comicstrip$).ti,ab,id. (946)
-
(social article$ or storymovies).ti,ab. (1)
-
or/7-11 (4912)
-
6 and 12 (158)
-
(social story$ or social stories$).ti,ab. (128)
-
13 or 14 (178)
MEDLINE and MEDLINE In-Process & Other Non-Indexed (OvidSP)
Date range searched: 1948–2011/July week 1.
Date searched: 18 July 2011.
-
exp Child Development Disorders, Pervasive/ (15,543)
-
(autistic or autism or kanner$ or ASD).ti,ab. (18,004)
-
asperger$.ti,ab. (1249)
-
(pervasive adj2 develop$).ti,ab. (1398)
-
PDD.ti,ab. (1710)
-
or/1-5 (22,321)
-
(social adj4 (story$ or stories$ or storytelling)).ti,ab. (96)
-
((individual$ or sensory) adj4 (story or stories or storytelling)).ti,ab. (142)
-
(comic$1 or comicstrip$).ti,ab. (249)
-
social article$.ti,ab. (0)
-
storymovies.ti,ab. (0)
-
or/7-11 (483)
-
6 and 12 (24)
-
(social story$ or social stories$).ti,ab. (23)
-
13 or 14 (29)
EMBASE (OvidSP)
Date range searched: 1980–2011/week 28.
Date searched: 18 July 2011.
-
exp autism/ (24,855)
-
(autistic or autism or kanner$ or ASD).ti,ab. (22,596)
-
asperger$.ti,ab. (1581)
-
(pervasive adj2 develop$).ti,ab. (1783)
-
PDD.ti,ab. (2182)
-
or/1-5 (32,043)
-
storytelling/ (288)
-
(social adj4 (story$ or stories$ or storytelling)).ti,ab. (131)
-
((individual$ or sensory) adj4 (story or stories or storytelling)).ti,ab. (171)
-
(comic$1 or comicstrip$).ti,ab. (268)
-
(social article$ or storymovies).ti,ab. (0)
-
or/7-11 (826)
-
6 and 12 (43)
-
(social story$ or social stories$).ti,ab. (37)
-
13 or 14 (50)
Appendix 2 Population, intervention, comparator, outcome, setting for systematic review
Sift one
This section describes the criteria for deciding whether or not a paper meets the criteria for sift one of the study. The decision about whether or not the criteria are met should be made on the basis of reading the title of the study and abstract if available.
In sift one the criteria for the two phases of the review (overview of practice and overview of effectiveness) are the same. All of the criteria need to be met for the paper to be selected. If the criteria are met, then the study should be marked appropriately in an EndNote file. If the criteria are not met, no further action should be taken.
Criterion 1: participants
The study must include a sample between 4 and 15 years of age. Studies which state that 90% or more of the participants or the mean age of participants are within these age bands will also be included. Studies which refer to children, adolescents or young people should be included at this stage of selection. If the paper refers to ‘school-aged children’ or any other ambiguous definition, but does not provide further information on the age range of participants, the citation should be included at this stage.
Participants in the sample must have a diagnosis on the autism spectrum. This could be stated as ASD, autism, atypical autism, PDD-NOS or Asperger syndrome. Studies which refer to participants with a mixture of developmental disabilities or learning disabilities will also be included at this stage providing that the sample includes at least one child with a diagnosis on the autism spectrum. Any comorbidities will be included at this stage. Studies which do not specifically discuss autism but meet all other criteria, for example age range and intervention, will not be included.
Criterion 2: intervention
The study must include a story-based intervention which is aimed at altering a behaviour. Studies which describe an intervention as a ‘social story’ will be included, as will any study which uses an intervention with similar characteristics to a Social Story. This does not include sensory stories. If the term social story is used it is not required that the term is trademarked for inclusion.
In addition, any study which uses an intervention as described above combined with or as part of other behavioural interventions will be included at this stage. Studies which provide a description of Social Stories but do not discuss a specific example of how a Social Stories have been used in practice will not be included.
Criterion 3: comparator
At this stage any comparator, including no comparator, will be included.
Criterion 4: outcome
There are no specific outcome criteria at this stage.
Criterion 5: study design
At this stage any type of study design will be included. This includes randomised trials, non-RCTs and quantitative single-case studies. It also includes non-quantitative case studies, narrative descriptions of the use of an intervention and pre–post designs. Book reviews, guidance on using social stories for parents/carers, teachers or clinicians and actual Social Stories will not be included.
Sift two
This section describes the criteria for deciding whether or not a citation that met sift one criteria (examining abstract and title) meets the sift two criteria based on examining the full paper. The decision about whether or not the criteria are met should be made on the basis of reading the full paper.
There are two sets of inclusion–exclusion criteria for sift two: papers that are included in the ‘overview for practice’ and papers that are included in the ‘overview of effectiveness’. All papers that meet criteria for the ‘overview of effectiveness’ automatically meet criteria for the ‘overview of practice’; however, some papers that meet criteria for ‘overview of practice’ will not meet criteria for ‘overview of effectiveness’. If the criteria are met, then the entire coding sheet should be completed. If the criteria are not met, only the basic information on the first page of the coding sheet and the inclusion–exclusion criteria need to be completed.
Criterion 1: participants
Overview of practice and overview of effectiveness
The study must include a sample of 90% or more participants between 4 and 15 years of age. If the mean age of the participants is within these age bands, then the study will be included. Studies that are based on adults will not be included, neither will studies in which more than 10% participants are outside the age range.
The study must include at least one participant with a diagnosis on the autism spectrum. This could be stated as ASD, autism, atypical autism, PDD-NOS or Asperger syndrome. The diagnosis of ASD does not need to have been established by a gold standard method. If a mixed group is used consisting of some people with and some people without autism, but data are reported separately for the participants with autism (e.g. a single-case series with separate data reported for each case or a group design but separate data reported on the group with autism) the study will be included. However, if the sample consists of a mixture of people with and without a diagnosis of autism (e.g. ‘The sample consisted of children attending a day centre, 40% of which met criteria for autism’) and separate data are not reported for the subgroup of children with autism, the study will not be included.
Criterion 2: intervention
Overview of practice and overview of effectiveness
As in sift one, studies which describe an intervention as a ‘social story’ will be included, as will any study which uses an intervention with similar characteristics to a Social Story. This does not include sensory stories. If the term social story is used, it is not required that the term is trademarked.
In addition, any study which uses an intervention as described above combined with or as part of other behavioural interventions will be included at this stage. Studies which provide a description of Social Stories, but do not discuss a specific example of how a Social Stories have been used in practice, will not be included.
Criterion 3: comparator
Overview of practice
For the overview of practice, any comparator, including no comparator, will be included.
Overview of effectiveness
For between group designs (RCTs, non-RCTs): studies with any comparator will be included (e.g. other active treatment including psychological or medication, placebo, attention control, treatment as usual, wait list, etc.); however, there must be a comparator present.
For single-case designs any within-participant or between-participant comparator will be included (e.g. alternative treatment or no-treatment phase); a baseline phase of an AB design meets the criterion for a within-participant comparator.
Criterion 4: outcome
Overview of practice
There are no specific outcome criteria for ‘overview of practice’.
Overview of effectiveness
Any standardised, numerical measure of behavioural outcomes or non-standardised, numerical measure of behaviour.
Criterion 5: study design
Overview of practice
For ‘overview of practice’ any type of study design will be included. This includes randomised trials, non-RCTs and quantitative single-case studies. It also includes non-quantitative case studies, narrative descriptions of the use of an intervention and pre–post designs. Book reviews, guidance on using social stories for parents/carers, teachers or clinicians and actual Social Stories will not be included.
Overview of effectiveness
For between-group designs, RCTs and non-RCTs will be included.
For single-case studies, any single-case study design that uses repeated numerical measurement, such as AB designs, reversal/withdrawal designs, changing criterion methods, multiple baseline, small N designs that use counterbalancing across participants and ATDs, will be included.
Note that not all studies that describe themselves as a case study or a single-case study will meet this definition (see below). Studies which use pre–post test designs or narrative non-quantitative case studies will not be included. The study must meet the definition of a quantitative single-case study given below.
Definition of a quantitative single-case study: a quantitative single-case study is one that uses repeated measurement of quantifiable (numerical) data on a single clinical case. Such an approach may involve replicating the basic design over several people to form a single-case series. Single-case series are also to be included (as long as there is repeated measurement of quantifiable numerical data).
Studies that describe the design used as a single-case study or single-case series but which do not meet the above definition should be excluded. The decision should be made on the design not the name used to describe the design.
Some studies describe the design used as a ‘case study’. This typically involves a non-quantitative, narrative description of the effects of an intervention, so would be excluded. However, studies described as case studies should be judged on the basis of the design used. If they meet the definition of a quantitative single-case study as described above they should be included; if not they should be excluded. Again, the decision should be made on the basis of the design not the name.
Pre–post designs, which use a single point of measurement before and after an intervention, do not meet the criteria of a quantitative single-case study because there is insufficient repeated measurement.
There are several types of single case design, such as AB designs, reversal or withdrawal designs, changing criterion methods, multiple baseline designs, small N designs with counterbalancing across participants and ATDs. All meet the criteria for a quantitative single-case study.
Appendix 3 Excluded studies with reasons
| Number | Reference | Reason for exclusion |
|---|---|---|
| 1 | Carbo BC. The Use of Social Stories with Individuals with Autism Spectrum Disorders. Newark, DE: University of Delaware; 2005 | Incorrect design |
| 2 | Chan JM, O’Reilly MF, Lang RB, Boutot A, Whiute PJ, Pierce N, et al. Evaluation of a Social Stories™ intervention implemented by pre-service teachers for students with autism in general education settings. Res Autism Spect Dis 2011;5:715–21 | Overlap in samples |
| 3 | Cifelli ME. The Effectiveness of Social Stories in a Young Child with Autism: a Single-Case Study. [Masters]. Scranton, PA: University of Scranton; 2009 | Age of participant/s outside range |
| 4 | Daly DA, Gill JM, Cullinane CG, Hourihane JO. Using Social Stories to prepare children with ASD for allergy testing. J Allergy Clin Immunol 2010;125(2 Suppl. 1):AB51 | Abstract only |
| 5 | Fisher K, Haufe T. Developing Social Skills in Children Who Have Disabilities Through the Use of Social Stories and Visual Supports. Chicago, IL: Saint Xavier University; 2009 | Age of participant/s outside range |
| 6 | Frew C. The Effectiveness of Using Social Stories to Modify Inappropriate Behaviours in Children with ASD. Sydney: University of Sydney; 2010 | Incorrect design |
| 7 | Glaeser BC, Pierson MR, Fritschmann N. Comic Strip Conversation: a positive behavioral support strategy. Teach Except Child 2003;36:14–19 | Incorrect design |
| 8 | Graetz JE, Mastropieri MA, Scruggs TE. Decreasing inappropriate behaviors for adolescents with autism spectrum disorders using modified social stories. Educ Train Dev Disabil 2009;44:91–104 | Overlap in samples |
| 9 | Gray CA, Garand JD. Social stories: improving responses of students with autism with accurate social information. Focus Autistic Behav 1993;8:1–10 | Incorrect design |
| 10 | Haggerty NK. Social stories and apron storytelling: the effects on self-managed coping strategies of a child that experienced chronic school difficulties. Manoa, HI: University of Hawaii at Manoa; 2003 | Not ASD |
| 11 | Haggerty NK, Black RS, Smith GJ. Increasing self-managed coping skills through social stories and apron storytelling. Teach Except Child 2005;37:40–7 | Not ASD |
| 12 | Hanley-Hochdorfer K, Bray MA, Kehle TJ, Elinoff MJ. Social stories to increase verbal initiation in children with ASD and Asperger’s disorder. Sch Psychol Rev 2010;39:484–92 | Overlap in samples |
| 13 | Hess L. I would like to play but I don’t know how: a case study of pretend play in autism. Child Lang Teach Ther 2006;22:97–116 | Incorrect intervention |
| 14 | Hodge JL. Social Story Instruction for Students with Autism Spectrum Disorders. Carbondale, IL: Southern Illinois University Carbondale; 2008 | Unavailable |
| 15 | Holland O. Teaching at Home: a New Approach to Tutoring Children with ASD and Asperger Syndrome. London: Jessica Kingsley Publishers; 2005 | Incorrect intervention |
| 16 | Johnson H, Phillips L, Iacono T, Hagiliassis N. Behavioral social stories to reduce behaviors of concern and restrictive practice: preliminary work. J Pol Pract Intellect Disabil 2009;6:117 | Abstract only |
| 17 | Kitchin E. The Use of Social Stories to Help Bedtime Resistance in a Sample of Young School-aged Children. Southampton: University of Southampton; 2009 | Not ASD |
| 18 | Kuoch H, Mirenda P. Social story interventions for young children with ASD spectrum disorders. Focus Autism Other Dev Disabil 2003;18:219–27 | Overlap in samples |
| 19 | Lee Y-F. The Effects of Concept Mapping Strategy Mediated Social Story Intervention on Peer Interactions of an Elementary School Child with Autism. Dissertation. Tainan, Taiwan: National University of Tainan; 2007 | Abstract only |
| 20 | Litras S, Moore DW, Anderson A. Using video self-modelled social stories to teach social skills to a young child with autism. Autism Res Treat 2010 | Age of participant/s outside of range |
| 21 | Poon P-lP. Social Story Intervention for Preschoolers with Autism. Hong Kong: Hong Kong Polytechnic University; 2006 | Incorrect design |
| 22 | Posselt M. The Effect of Animated Social Stories on Emotion Recognition and Social Functioning in Children with Pervasive Developmental Disorders. Adelaide: Flinders University; 2010 | Overlap in samples |
| 23 | Quirmbach LM. Social Stories: Mechanisms of Effectiveness in Increasing Social Skills, Social Skill Comprehension, Generalization and Maintenance of Newly Acquired Skills in School-Aged Children Diagnosed with Autism. San Diego, CA: Alliant International University; 2007 | Abstract only |
| 24 | Reynhout G, Carter M. The use of Social Stories by teachers and their perceived efficacy. Res Autism Spectr Dis 2009;3:232–51 | Incorrect design |
| 25 | Ravenhill J. Social stories for difficult situations. Communication 2002;36:37–8 | Age of participant/s outside of range |
| 26 | Richardson D. Evaluation and Needs-Based Assessment of Special Education Teachers’ Knowledge of Austism Interventions. Bowling Green, KY: Western Kentucky University; 2007 | Abstract only |
| 27 | Sanders DA. The Impact of Storytelling on the Social Development of Learners with Asperger’s Syndrome. Pretoria, South Africa: University of South Africa; 2007 | Incorrect design |
| 28 | Sansosti FJ. Effectiveness of Social Story Interventions for Children with Asperger’s Syndrome. Tampa, FL: University of South Florida; 2003 | Overlap in samples |
| 29 | Sansosti FJ. Using Video-Modeled Social Stories to Increase the Social Communication Skills of Children with High Functioning Autism/Asperger’s Syndrome. Tampa, FL: University of South Florida; 2005 | Overlap in samples |
| 30 | Scattone D. Increasing Appropriate Social Interactions of Children with Autistic Spectrum Disorders Using Social Stories. Hattiesburg, MS: University of Southern Mississippi; 2003 | Overlap in samples |
| 31 | Smith C. Social stories: a collection of three papers. 2. Using social stories with children with autistic spectrum disorders: an evaluation. Good Autism Pract 2001;2:16–25 | Incorrect design |
| 32 | Smith C. Using Social Stories to enhance behaviour in children with autistic spectrum difficulties. Educ Psychol Pract 2001;17:337–45 | Incorrect design |
| 33 | Toplis R, Hadwin JA. Using social stories to change problematic lunchtime behaviour in school. Educ Psychol Pract 2006;22:53–68 | Not ASD |
| 34 | Thompson RM. Social Stories as a Tool to Help Preschool Aged Children with ASD Spectrum Disorders Utilize Self-regulation Strategies to Promote Increased Functional Behaviors. Salt Lake City, UT: University of Utah; 2011 | Age of participant/s outside range |
| 35 | Walsh L, Barry M. A Multimedia Instruction to Enhance the Social Skills of the Young Learner with Autism. ALT-C, Leeds, UK, 9–11 September 2008 | Abstract only |
| 36 | Verheyden S. Effects of Social Story Intervention with Operant Conditioning on Toilet Training Children with ASD. Vancouver: University of British Columbia; 2007 | Age of participant/s outside range |
Appendix 4 Landscape interview topic guides
What are Social Stories?
Describe as neatly and succinctly as you can what Social Stories are:
-
When I say Social Stories what does that mean to you?
-
Can you describe for a complete outsider what is a Social Story?
Can you suggest what the main reasons for using Social Stories are?
-
What are the benefits of Social Stories? What are the negative aspects?
Your involvement in Social Stories
When did you get involved with using Social Stories? Why did you get involved?
Best use for Social Stories
In your experience, are there particular behaviours that are more suited to using Social Stories?
-
How do you know if a Social Story works?
Can you suggest the best ways we can involve children in the process of understanding how Social Stories work?
Can you suggest the best approaches to collecting information?
How do we monitor when things go wrong with Social Stories?
Best practice for developing Social Stories
What are the rules associated with developing Social Stories?
How closely do you follow the rules when you are developing your own Social Stories?
-
Have the rules (or main concepts/criteria) of Social Stories changed?
Which factors would you consider to be acceptable and unacceptable within Social Stories?
Developing the manual
What basic information would you provide to a novice for using Social Stories?
-
What would be the most important things that you could include within a basic manual on Social Stories?
-
Tell me how you envisage the manual looking
Would a manual be sufficient in itself?
-
What type of training do you think people will need to be able to use Social Stories?
Choosing the focus of the story
In general how do you go about choosing the focus of the story?
Appendix 5 Focus group 1 topic guide
Introduction
The protocol suggests that the overall aim of the focus groups is to ‘gather information relating to the optimum design and use of Social Stories in children and young people with autism spectrum disorders’.
The focus group aims include checking that the ‘intervention can feasibly be delivered in this particular context and to ensure the intervention is acceptable to users and providers’ so the following factors will be taken into consideration:
-
the helpful and unhelpful parts of the social story intervention
-
the characteristics of individuals best placed to deliver the intervention
-
determining which professional groups are best equipped to deliver and or support this package
-
mode of delivery including the role of parents or carers
-
the style and content of the manual
-
the construction of the social stories (for example the ratio of directive to descriptive sentences in the story, the use of pictures, etc.)
-
teaching in the social story theory, and dissemination.
Further, the writing group want qualitative information which will enable them to make informed decisions about what to include in the manual.
An initial focus group will cover eight main sections based on the factors highlighted above. The amount of attendees has meant that the questions have needed consolidating. I have taken on board the landscape interviews and further suggestions of colleagues and the writing group and have created a final synthesis. There is further space in the second focus group to pick up issues that arise in the first. Questions for the second round will be written in light of analysis and discussion with the team and writing group.
The format for the focus group will be mainly discussion but I have decided to include two Post-it® (Evernote Corporation 3M, Maplewood, MN, USA) exercises. The requirements for the focus groups will be name tags for participants, pens and post it notes. A board or wall space on which to put the top three behaviours will also be required. Table 52 shows the overall questions which may be asked of teacher/clinician focus groups. Text displayed in bold are prompts.
| Task | Teachers and clinicians | Time |
|---|---|---|
|
Shall we start with some introductions? | 8 |
| Can I have your full name, job title and organisation? | ||
| Clarify teacher or clinician? | ||
| If I say your name after any comments that you make this is for taping purposes | ||
|
What are the most important behaviours for autistic children to address within school? | 3 |
| How would you define social stories? | 7 | |
| How do you use social stories (in your work)? | 7 | |
| Does anyone do it in a different way? | ||
|
The trial will look at the success of using a manual for developing social stories within schools | 7 |
| Which of the behaviours already identified do you think may be suited to use in social stories within school? | ||
| Why? | 6 | |
| Why do social stories work well with these behaviours? | ||
| Which behaviours are least suited and why? | 2 | |
| Total | 15 | |
|
What characteristics do you need to have when delivering social stories? | 3 |
|
Who would be best placed to write and develop social stories in schools? | 3 |
| Does that ring true of the schools you are involved in? | ||
| Who is best placed to deliver/read them? Why? | 3 | |
| What different ways have you delivered social stories in the past? | 5 | |
| I.e. has it always been in picture book format/read? | ||
| Have you tried other formats? | ||
| How can parents support social stories that are being used in school? | 6 | |
| Where is the best location to deliver social stories within a school? | 3 | |
| Total | 20 | |
|
We want to produce a manual about writing and delivering social stories in schools | 20 |
| What should the manual contain (and anything to avoid)? | ||
| Use top example from earlier | ||
| How much theory should the manual contain? Is it how to do it . . . do you want the theory or just how to . . . | ||
| How much about autism? | ||
| Checklists for behaviours | ||
| In terms of presentation what style should the manual take that would best suit schools? | 5 | |
| DVD, written, how long, length, lists of links websites e.g. clip art, etc. | ||
| Total | 25 | |
|
What are the different components you use when putting together a social story? | 5 |
| E.g. pictures, descriptive text, text which instructs the child | ||
| What rules of thumb do you use? | ||
| Do you find some components work better than others? | 5 | |
| How do you know if a social story works? Which components? Why do they work better? Is there a ratio? | ||
| What tools do you use to help write social stories? | 5 | |
| Do you use the manual (Carol Gray’s)? | ||
| What other resources do you use? Websites, other books, etc. | ||
| Total | 15 | |
|
If you have been on any training sessions on social stories, what did you find useful? | 10 |
| What would you like future social story training to cover? | 5 | |
| In what format would you prefer the training?a | 5 | |
| Workbooks, workshops, scenarios, role-playing, case studies or vignettes | ||
| How long would you like the training to be?a | 4 | |
| E.g. half day/day | ||
| Is there a time and day that would be better for you?a | 3 | |
| Friday mornings? | ||
| Where is the best location for training?a | 3 | |
| Total | 30 |
Appendix 6 Details of framework analysis
Audio-recordings were fully transcribed and anonymised. The framework method of analysis136 was used to organise the data. This approach was developed specifically for applied qualitative research in which the objectives of the study are often known in advance. This method was particularly suited to the ASSSIST project, as specific questions were being addressed through the qualitative interviews and focus groups. Although the framework approach starts with pre-set aims (which were reflected in the ASSSIST topic guides), it retains some flexibility in order to reflect the experiences and views of the study participants based on a grounded and inductive approach. The stages of framework analysis followed were those detailed by Pope and colleagues. 137
Familiarisation
The main researcher (PD) was immersed in the data by listening to the recordings and reading transcripts to list key ideas and recurrent themes. Memos were used during initial stages of analysis to provide a visible ‘audit trail’ as the analysis moved from ‘raw’ data to the production of findings.
Thematic framework
The ideas and themes identified during the process of familiarisation were then developed into a thematic framework. This drew on the study objectives and the views and experiences raised by the participants. At significant points during the process of data analysis, the researchers most closely involved in data collection and the early stages of analysis (PB, HA, DM, LD and JA) discussed a priori and emerging codes. Through this process the data analysis drew on the combined insights of those ‘handling’ the data closely (PB and HA) and members of the team with a wider perspective of methodological issues (LD and JA) and Social Stories topic expertise (DM).
Indexing
The data in the transcripts were systematically indexed by annotating all the data with codes from the thematic framework. For the ASSSIST project this process was supported using NVivo. The indexing process included using the constant comparison method to check and compare each item with the rest of the data to establish appropriate analytical categories. This also ensured that any additional categories were added to reflect as many of the nuances or outlier views in the data as possible. Midway through the analysis of the qualitative data, a member of the qualitative research team (JA) examined three transcripts which had been coded by the lead qualitative researcher most closely involved in data collection and analysis (PD), as an independent check on the assignment of codes to data.
Charting
This process then organised the data according to the relevant part of the thematic framework to form charts. One chart per theme across participants was initially developed, containing summaries of the participant views and experiences and references to verbatim text in the transcript. This allowed for comparative analysis to be conducted in which data from individual participants and subgroups could be compared and contrasted within and across themes. Analysis included a search across the data set for ‘negative’ cases (evidence that contradicts, or appears to contradict, the explanations being developed) and alternative ways of explaining the data were considered.
Mapping and interpretation
This was used to examine the associations between themes and to present the results. Through supervision of the qualitative data collection and analysis in regular meetings (PD, LD and JA), the qualitative team was able to discuss all aspects of the coding and presentation of the qualitative data.
As a reflexive approach was taken to data analysis, it is important to consider the ways in which the interactions of researchers with participants might be influenced by their own professional background, experiences and prior assumptions. The main interviewer (PB) was an academic research fellow from non-clinical background, with experience as a youth worker but with no prior knowledge or experience of Social Stories. The other members of the qualitative team (HA, LD and JA) all have academic research backgrounds and also did not have previous knowledge or experience of Social Stories. None of the research team had a vested interest in the study, and none of them was the parent or close family member of a child with ASD. This placed the qualitative research team in a very neutral position relating to any prior expectations relating to the study intervention or interventions aimed at children with ASD. Those involved in data collection were known to the participants as researchers and not clinicians involved with the intervention training or Social Story writing. It is therefore unlikely that the background of those involved with data collection or analysis will have impacted on the participants’ willingness to talk openly about their experiences or bias the analysis.
Appendix 7 Focus group 2 topic guide
Appendix 8 Example pilot study topic guide (teacher)
Standard opening discussion
We are going to explore your experiences of using the Social Stories intervention. You have been working with a child/young person implementing, developing, writing or sharing a social story over a period of time.
We are interested in your experiences of this. There are no right or wrong answers, only your experience of how it went, what worked well, what did not etc. The aim of this part of the study is to try and work out what we need to develop further and also what does not need to change so that this intervention can be rolled out to other schools.
We value your opinions so speak honestly and openly. You are free at any time to withdraw from the study. Any information you give us is stored confidentially and will not be ascribed back to yourself.
Goal Setting
You were asked to set a number of goals.
-
What processes were involved in setting goals?
-
How were issues/goals identified?
-
Who was at meeting (i.e who was involved)?
-
Did you meet together or separately?
-
Where did you meet?
-
-
-
How straightforward was it setting goals?
-
How long did it take to decide on/write goals?
-
How useful did you find setting goals?
-
Were you happy with the outcomes of goal setting?
-
-
Did you find the manual useful in terms of goals?
-
If yes, why/if no why not?
-
-
Did the training link to setting the goals?
What was story about
-
Can you tell me about the social story(ies) that you worked on?
-
What were the story/ies?
-
Do you have copies?
-
-
What was reason behind writing the social story?
-
What was it trying to achieve, what behaviours was it trying to explore?
-
Did you manage to marry up the goals set within the story?
-
-
How long did it take you to write a social story?
-
Who was involved in writing?
-
How closely did you follow the manual when writing this social story?
-
How often did you refer back to the manual whilst developing the social story?
What about the parents: were they supportive? What was their input? Do you know if the stories were read at home?
Using the story
Was it read completely, how many times?
-
Over what sort of period?
-
Why was it read so frequently/infrequently?
-
When is a good time to withdraw it/reduce it, when is it phased out?
-
How is this planned for?
Using the manual
Did you write any comments on the manual for the authors?
If yes, collect in
Views on presentation of manual
Do you have any comments about presentation?
Was it the right format, shape?
-
Do you have any comments about the layout?
-
Was the type setting good, images?
-
Develop/change/keep the same?
Views on structure of manual
What are your views on the structure of the manual?
-
Are the sections laid out logically?
-
Were they in the right order for you?
-
Was it easy to navigate?
-
Anything you would change/develop/keep the same?
Views on content of manual
What were your views on the content of the manual?
How did you find the language in the manual?
-
I.e. was it pitched at the right level for you?
Was the content easy to understand?
-
Was there anything in the manual that you had to ask advice about or seek clarification?
-
Were there are bits of the manual that you skipped over? Why?
If you could speak to the authors, what would you like to be changed, developed or to stay the same?
Facilitators, barriers and experiences
In your experience, how pragmatic is the use of social stories in classroom settings?
-
Can you see any barriers? Also, what facilitates a social stories use?
-
Is it keen, skilled teachers, settings, supportive infrastructure?
-
Teacher experiences
How do you think it went?
-
Generally?
-
Overall?
Having read the manual how confident do you feel about preparing and delivering your own social story in future?
How useful was the manual in helping you to prepare and deliver your social story?
-
Is the training alongside the manual enough to support people in using social stories?
Child experiences
Initially did the child want to take part in the social stories?
-
Was this a new experience for them?
How did the child receive the social story?
-
Did reading social stories at school cause any distress?
-
Did they like it/adapt it/reject it?
Do you think the social story affected the child’s social skills and/or behaviour in any way?
Do you think the social story had any other impacts?
Prompt: home-school relations, understanding of child
Other than social stories, did you use any other interventions or types of support at school to help achieve the goals that were set?
Improving the intervention
Do you think there is anything that can be done within the classroom or outwith it that would give the social stories better impact/make them work better?
Is there anything else that could be done to make this intervention and the manual a success?
Exploring the quantitative domains
Did you complete the paperwork sent by Hannah?
-
Was there anything that you did not understand or was difficult to complete?
Which of these 9 titles would you hope would be improved using social stories? Is there anything else missing e.g. any others? (use a blank post it note)
-
Mobility
-
Self-care
-
Usual activities
-
Pain/discomfort
-
Anxiety/depression
-
Sensation
-
Emotion
-
Cognition
-
Fertility
Rank in order of importance (check which ones are most relevant/not relevant)
Which are the top 3 that would give the best measure of how child’s life would be improved?
Collect in social story, collect in diary, collect in paperwork.
Appendix 9 Example participant information sheets and consent forms in original formatting
Appendix 10 Example Social Story
Sometimes as part of my lesson I have to complete worksheets.
Most of the time I do this successfully without help from my TA or teacher.
Sometimes my TA or teacher may offer me extra help when I don’t really need it.
This is because I may look unsure but I am just concentrating and I need more time to process things.
It is really difficult for my TA or teacher to know when I need extra help and when I can manage on my own.
I like to do things on my own when I can, it makes me feel proud of myself and I learn better.
Woohoo!!
Sometimes to help me concentrate I put my head down and cover my ears.
I do this because I need to concentrate but people are still talking to me.
I will try to tell them that I can manage and need to concentrate and that I would like to try on my own.
This will mean that I can work independently and make my teachers proud.
Appendix 11 Practitioner diary for pilot study
Appendix 12 Goal-based measure for pilot study
Appendix 13 Bespoke outcome measures for feasibility trial (behaviour diary)
Appendix 14 Bespoke outcome measures for feasibility (goal-based)
Appendix 15 Bespoke outcome measures for feasibility (behavioural frequency measure)
Appendix 16 Bespoke outcome measures for feasibility (resource use: parents)
Appendix 17 Bespoke outcome measures for feasibility (resource use: teachers)
Appendix 18 Example Qualitative evaluation topic guide (teacher)
How many children are taking part in the trial from this school?
Experience of entering trial and randomisation
How were you approached and asked to take part in this trial?
-
Who spoke to you? How did they approach you? Was it by letter, phone, conversation?
-
What did they say? What did they tell you?
Do you think that was the best way to make contact?
-
Was it appropriate?
-
Is there anything that could have been done better?
How easy was it to communicate with parents/teachers and with researchers?
-
Probe: what can we do to improve communication? With each other?
As a school, why did you decide to take part in the trial?
Which group was your school assigned to?
-
Did it matter to you which group you are assigned to?
-
Probe issues/disappointment/how it affected them etc.
-
-
How long did it take to get assigned to a group?
-
Were there any issues with this, time, getting all paperwork back etc.
-
Any suggestions for improvement?
-
(If school is working with more than one child/young person).
Did that affect the way you worked?
-
Once your school was randomized, no further children from the school could take part – what did you think about this?
-
Any issues?
Is there anything that could have been done better?
Goal setting
How straightforward was it setting goals?
-
How useful did you find setting goals meeting?
-
What was parents involvement in the goal setting/did child have any role?
-
Were you happy with the outcomes of goal setting?
-
In what ways do they meet the needs of your child/children?
-
Did you use any (additional) strategies to try and achieve the goals?
-
Did you use anything, set anything up, what were responses to strategies? How were these approached? How did you know you were meeting the goals? What kind of feedback did you get from child?
Paperwork
What was the paperwork like that you were asked to complete?
Questionnaire
Diaries
-
(Bring examples and talk through any big issues) eg:
-
Did the questions ask for a lot of detail? Was it enough detail?
-
Were the types of questions you were being asked relevant to the child/you?
-
What was the diary like?
-
What problems did you encounter? Time, resource issues, layout etc.?
-
How straightforward was it to measure behaviour activity?
-
How accurate/time involved/appropriateness/did they comply?
-
Experience of delivery of Social Stories
-
Was the training suitable?
-
Did it provide enough information on delivering the intervention?
-
What is the best method for training given the busyness of teachers?
-
How did you find using the manual? What was helpful/unhelpful for developing and maintaining intervention
-
Control questions
-
Were the instructions clear for choosing and reading stories?
-
Did you manage to implement the story?
-
Were there any issues around this?
-
how straightforward was delivering stories?
Was the intervention straightforward to deliver?
(Particularly for secondary schools): were there any issues (e.g. around suitability of location, timing) logistics or any other factors that would have an impact on the trial?
Using the intervention
-
Overall how do you think the social story/*story went?
-
*Were the instructions straightforward?
-
How willing was the child/family to take part?
-
Did you encounter any problems? Also what did not work?
-
What worked for you and the child?
-
Did the story impact the child in any other ways?
-
-
Is this intervention suitable for your child? Is it suitable for staff to use in schools?
-
What changes would you make? What would you adapt, change or keep the same?
-
Was the intervention long enough?
-
Were you given enough time to prepare?
-
Did you have enough time to put resources in place?
-
Any issues about location, space, amount of staff etc.?
Do you think there is anything that can be done within the classroom or outwith that would give the social stories trial better impact/make it work better?
List of abbreviations
- ANOVA
- analysis of variance
- ASCEND
- Autism Spectrum Conditions – Enhancing Nurture and Development
- ASD
- autism spectrum disorder
- ASSSIST
- Autism spectrum Social Stories in schools trial
- ATD
- alternating treatment design
- CAMHS
- Child and Adolescent Mental Health Service
- CI
- confidence interval
- DSM-IV
- Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition
- EQ-5D
- European Quality of Life-5 Dimensions
- EQ-5DY
- European Quality of Life-5 Dimensions youth questionnaire
- GSM
- goal-setting meeting
- HTA
- Health Technology Assessment
- HUI2
- Health Utilities Index 2
- ICD-10
- International Statistical Classification of Diseases, Tenth Edition
- IQR
- interquartile range
- PDD-NOS
- pervasive developmental disorder – not otherwise specified
- PEM
- percentage of data points exceeding the median
- PICO
- population, intervention, comparator, outcome
- PND
- percentage of non-overlapping data
- PPI
- patient and public involvement
- PSI-4
- Parental Stress Index, Fourth Edition Short Form
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SAT
- statutory assessment test
- SCAS
- Spence Children’s Anxiety Scale
- SCED
- Single-Case Experimental Design
- SD
- standard deviation
- SDQ
- Strengths and Difficulties questionnaire
- SENCO
- special educational needs co-ordinator
- SRS-2
- Social Responsiveness Scale-2
- TMG
- Team Management Group