

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number NIHR134931. The contractual start date was in April 2021. The final report began editorial review in February 2022 and was accepted for publication in July 2022. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2023 Blank et al. This work was produced by Blank et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2023 Blank et al.
Introduction
Definitions of home, remote and tele working
In its broadest sense, working from home involves the practice of conducting paid occupational work in the home. Various terms have been used to describe working from home, including ‘teleworking’, ‘telecommuting’, ‘e-working’ and, more recently, ‘new ways of working’. Teleworking and telecommuting were terms coined in 1973 by Jack Nilles,68 and refer to the direct substitution of travel to a workplace for telecommunication (e.g. telephone calls, email, videoconferencing), and apply generally to managerial and office work. 68 The emphasis was on reducing travel (and thus traffic, particularly at peak times), and therefore Nilles68 considered that working for home-based businesses would not be considered as telecommuting, since there was no commuting to be substituted. In contemporary times, the focus is on internet connectivity, and the term ‘remote e-working’ is also used to describe this, with some suggestion that this is a preferred term in Europe,12,69 and again relates to traditional office work.
Nowadays, working from home can be positioned as one type of ‘flexible working arrangement’ (alongside part-time work and flexible hours), with the flexibility arising in the location of the work. 70 Messenger and Gschwind70 refer to three generations of telework as mobile technology advanced over time and locate these in a conceptual framework. The first generation (the ‘home office’) located telework in the home, the second generation (the ‘mobile office’) located telework additionally in third spaces (anywhere where work can be done regularly away from the workplace and home aided by information communication technologies, e.g. trains, airports, the client’s premises) and the third generation (the ‘virtual office’), referred to as ‘new ways of working’, located telework additionally in intermediate spaces (those that fall between the workplace, home and third spaces, e.g. car parks, lifts, pavements). Thus, working from home and telework/e-working overlap to a large extent, as telework can be undertaken in the home (but in other places too, under the most recent definition); however, not all work from home (WFH) is telework (e.g. running a small business, such as small-scale manufacture, or childcare). Working from home also includes work that is temporally flexible as well as temporally constrained by the employer.
Originally, telework was conceptualised as a complete substitution for traditional office work,68 mainly due to technological constraints at the time, for instance, the need to use a fixed-location desktop computer and telephone. With advances in technology and reconceptualisation of telework as ‘new ways of working’, it is possible for employees to engage in ‘hybrid working’ (i.e. working from home on some days and working in the workplace on others). Thus, contemporary definitions refer to telework as working away from the employer’s premises ‘for a portion of the work week while keeping in contact via information and communications technology’ (p. 511). 71
Initially, working from home (mainly via telework, among office workers), based mainly on a hybrid working model, was conceptualised as beneficial to both employees, who could benefit from the flexibility it afforded, and employers, who could benefit from more satisfied employees and lower turnover. 71,72 However, the prevalence of teleworking did not rise as rapidly as initially expected, due to resistance from management and a lack of trust, with the most famous example being Yahoo’s decision to abandon its working from home policy in 2013. 70 More recently, the widespread adoption of working from home due to the COVID-19 pandemic has also revealed many disadvantages, which may counteract the advantages that previously drove arguments for its uptake. 72
Prevalence of home working
Various data sources report data on the prevalence of working from home. According to the Chartered Institute of Personnel and Development (CIPD),73 in pre-pandemic times 18% of the UK workforce worked from home occasionally, and just over 2% worked mostly from home. The UK Office for National Statistics (ONS)74 reported that, in 2019, 5.2% of people in employment reported working mainly from home, 12.3% reported working from home at some point in the week prior to the interview and 26.7% people reporting ever having worked from home. These rates were highest in the information and communication sector (14.8%, 32.8% and 53.1%, respectively), the professional and scientific sector (12.8%, 26.3% and 46.3%, respectively) and the real estate sector (12.3%, 18.4% and 40.3%, respectively), and lowest in the accommodation and food services sector (2.1%, 4.4% and 10.0%, respectively), the transport and storage sector (1.8%, 3.4% and 11.0%, respectively), and the wholesale, retail and vehicle repair sector (3.2%, 6.2% and 13.4%). The ONS data show a clear social gradient in home working, with the highest rates among managers, directors and senior officials (10.0% mainly worked from home, 24.3% worked from home in the week prior to the interview and 46.7% ever worked from home), followed by professional occupations (5.8%, 20.3% and 45.0%, respectively) and associate professional and technical occupations (8.1%, 19.3% and 36.5%, respectively), intermediate levels in administrative and secretarial occupations (6.9%, 10.5% and 19.9%, respectively), skilled trades occupations (2.4%, 5.5% and 17.9%), and caring, leisure and other service occupations (4.5%, 5.3% and 14.1%), and the lowest rates found among elementary occupations (0.5%, 0.9% and 4.2%, respectively), process plant and machine operatives (1.2%, 2.1% and 6.5%), and sales and customer service occupations (1.6%, 3.1% and 8.7%, respectively). 74
The COVID-19 pandemic caused a rapid increase in working from home across many sectors and occupational types. The CIPD73 report that employers estimated that around 54% of their workforce were working continuously at home (with 35% of employers reporting that up to a quarter were, over 40% reporting that 75–99% were and 21% reporting that all of their workforce were working continuously from home). This was highest in the business and financial services sector (75–80%) and the public administration sector (67%), but lower in education, healthcare and other services (between 40% and 46%) and lowest in distribution (31%) and production (39%).
The ONS reports similar figures. In April 2020 specifically, towards the start of emergency pandemic control measures in the UK, 46.6% of people in employment did some work at home, with 86.0% reporting that they worked at home as a result of the COVID-19 pandemic. 75 As with pre-pandemic data there was a social gradient in home working; the highest proportions of those who did some work at home were among managers, directors and senior officials (67.3%), those who worked in professional occupations (69.6%) and associate professional and technical occupations (63.7%), although those working in administrative and secretarial occupations were not far behind (57.2%), perhaps because of the prevalent use of ICTs in those roles, and the lowest proportions of those who did some work at home were process plant and machine operatives (5.4%), those who worked in sales and customer service occupations (15.9%), caring, leisure and other service occupations (14.9%), and skilled trades occupations (18.9%). 75
In 2020, 35.9% of those employed did some work in the home (9.4 percentage points higher than in 2019). 76 Similar to pre-pandemic figures, the highest proportions of people mainly, recently and occasionally working from home in 2020 worked in the information and communication sector (21.9%, 32.3% and 7.8%, respectively), professional and scientific sector (17.4%, 29.2% and 9.6%, respectively), and the financial services and real estate sector (13.3%, 33.3% and 7.5%, respectively), with the lowest proportions in the accommodation and food services sector (2.7%, 3.2% and 6.4%, respectively), transport and storage sector (3.3%, 8.4% and 6.9%, respectively) and wholesale, retail and vehicle repair sector (5.0%, 7.4% and 7.4%, respectively). 76 As with pre-pandemic data, the social gradient in working from home in 2020 is reflected in educational qualifications; the highest proportions of people working from home mainly, recently and occasionally had a higher degree (11.7%, 29.2% and 13.4%, respectively), or a degree or equivalent (10.9%, 25.0% and 11.0%, respectively), with intermediate proportions among those educated to A-level or equivalent (8.0%, 17.0% and 10.1%, respectively) and GCSE or equivalent (6.4%, 12.7% and 9.4%, respectively), and the lowest proportions among those with no qualifications (4.0%, 3.2% and 6.7%, respectively) and entry-level qualifications (5.9%, 9.4% and 6.9%, respectively). 76
Looking to the future, the CIPD73 reports that employers expect 37% and 22% of their workforce to WFH after the COVID-19 pandemic on a regular basis and all the time, respectively, with many companies preparing for hybrid working, where people would either WFH 1–2 days a week or work from the workplace 1–2 days a week. Employees surveyed also preferred a hybrid approach overall. Thus, with a shift towards working from home for at least part of the working week over the medium to long term, evidence on the impact of working from home takes on greater importance than in previous times.
Guidance for the health of home workers
The current review is also timely in the sense that while there is a plethora of guidance on workplace health for other types of workplace, supported by an extensive range of workplace health programmes and specific interventions, there is a dearth of appropriate evidence-based workplace health guidance that specifically relates to the home as the workplace. The transition to wide-scale working from home at the start of the COVID-19 pandemic was rapid and unprecedented, and many organisations lacked the infrastructure and systems to support employees with these changes, at least initially. 77 Schall and Chen78 argue that specific challenges to occupational safety and health inherent in working from home can arise from a lack of face-to-face supervision, a lack of information and support relating to ergonomics, increased isolation from colleagues, and blurred boundaries between work and home. Such occupational safety and health risks may include musculoskeletal issues resulting from a sub-optimal workstation (potentially also combined with long work hours) and mental health issues resulting from isolation, blurred boundaries, overwork and work–home conflict. 78
Since the COVID-19 pandemic and associated emergency measures began, a large volume of survey data has been collected, which has raised concerns about the impact of working from home on health, wellbeing and inequalities. 79 Health and wellbeing are undeniably important among workers. As well as being important as outcomes in their own right, the health and wellbeing of workers can play an important role in the functioning of organisations, since those with higher levels of health and wellbeing are likely to have greater job satisfaction and organisational commitment and lower absenteeism and turnover intention. 69,71 Any potential detriment to health and wellbeing due to working from home is likely to have been magnified at a population level during the pandemic, because of the increased prevalence of home working and the crisis situation. Following the crisis, large numbers of people are expected to continue to WFH, at least some of the time, as discussed earlier.
Inequalities
Wide-scale working from home has also highlighted inequalities. Women with children have faced disproportionate challenges in working from home without childcare support during the pandemic. 80 Disproportionate challenges have also been experienced by those with a smaller living space and more people in the home. The Royal Society for Public Health42 reported that 26% of people working from home were working from a sofa or bedroom, and a greater proportion of people (41%) were more likely to think that working from home was worse for their health and wellbeing if they lived with multiple housemates compared with those who lived on their own (29%) or just with a partner (24%). Social gradients in the proportions of people able to WFH documented in pre-pandemic times have persisted during the more widespread use of working from home during the pandemic, as discussed earlier, with higher rates of home working reported among higher-grade professions and those with more advanced educational qualifications. The ONS76 reported that ‘The average gross weekly pay of employees who had recently worked from home was about 20% higher in 2020 than those who never worked from home in their main job, when controlling for other factors; this continues a long running trend’ (p. 3).
Thus, the issue of the impact of working from home on health and wellbeing is highly topical and of great interest to employers and employees alike, with a strong need for up-to-date guidance. There is therefore a need to formally and systematically synthesise evidence from both before and during the COVID-19 pandemic to understand the potential impact of current trends in home working and hybrid working and how negative impacts might be mitigated. Previous reviews examining this issue either predate the pandemic (and therefore did not consider the mass home working of recent times), or were conducted rapidly and/or focused on a specific aspect of working from home (e.g. virtual teams, teleworking), a specific timeframe (e.g. since the start of the pandemic) or a specific outcome (e.g. psychological distress, lived experience). There is currently a dearth of comprehensive systematic reviews on this topic, and the current review aims to fill this gap to provide evidence that can inform recommendations and guidance on working from home. This could inform decision-making by employers and workers about future patterns of home and hybrid working and about how employers can support workplace health, when the workplace is the worker’s home, and aim to mitigate inequalities brought about or exacerbated by working from home.
Methods
Review methodology and approach
We undertook a systematic review synthesising qualitative, quantitative and observational data. As the review was time-constrained, we employed elements of rapid review methodology as outlined by Kelly et al. (2016)81 and described in the methods sections below (for example limiting the number of papers which were formally double extracted, and not routinely contacting included authors for additional references).
Aims and objectives
The overall aim of this review was to identify, appraise and synthesise existing research evidence that explores the impact of home working on health and wellbeing outcomes for working people. We aimed to gain a better understanding of the factors that influence the physical health, mental health and overall wellbeing of home workers (including hybrid working where some time is spent working at home and some in the office or traditional place of work) as well as the potential for the wider impacts of home working on health inequalities.
The objectives in order to achieve this aim were:
-
to conduct a systematic review drawing on relevant, qualitative, quantitative and observational studies on the factors which influence the impact of home working (on the health of people working at home)
-
to describe the evidence for the potential impact of these factors in relation to health inequalities
-
to co-produce with stakeholders, a conceptual model to represent the factors that influence the health and wellbeing of home workers, and including the impact of home working on health inequalities
-
to identify the implications of the findings for developing evidence-based recommendations for policy and practice, including guidance to employers, and for future research priorities.
Search strategy
The searches were informed by a literature mapping exercise which was undertaken to scope out the volume and type of potentially relevant literature available. 3
We began by conducting searches in relevant databases. The search, which comprised subject headings and free-text terms, was initially developed on MEDLINE before being adapted for the other databases (see Supplementary Material: Search strategies). The following databases were searched: MEDLINE, EMBASE, Web of Science (Science Citation Index and Social Science Citation Index), Applied Social Sciences Index and Abstracts (ASSIA), International Bibliography of Social Sciences (IBSS), PsycINFO and LabourDiscovery.
The search was restricted to papers in English from Organisation for Economic Co-operation and Development (OECD)4 published from 2010 to current.
Database searching was accompanied by the following additional search methods:
-
scrutiny of reference lists of included papers and relevant systematic reviews (within search dates)
-
searches for UK grey literature
-
search of relevant key websites
-
citation searching of key included papers.
Authors were not routinely contacted to source additional papers. However, one study author was contacted to clarify a point in their paper.
Due to the rapidly expanding nature of the evidence on this topic, more citation searching was conducted than anticipated in order to identify papers published within the timeframe of the review. Citation searches were continued until no further new factors (not previously included in the analysis) were identified. Previous systematic reviews of relevant studies identified during the searches were not included, but their reference lists were checked to identify potentially relevant primary studies (within our search dates) that had not been identified by other methods.
Inclusion criteria
Population
The population included anyone in the working population who spends all or some of their working time at home. Papers which look at students, and those studying, rather than undertaking paid employment at home, are excluded from this review. Studies which looked at the impact of temporary remote teaching on teachers (where that was not their normal mode of teaching) as a result of COVID-19 lockdown measures were also excluded from the main review (these studies are discussed separately; see Supplementary Material: Full paper excluded studies).
Exposure
This included hybrid models of home working where some time is spent working at home and some in the office or other traditional place of work. Other aspects of flexible and remote working which do not relate directly to home working, for example studies about flexible office hours or specifically about working in remote locations away from the home, along with the impact of work accessibility (e.g. the impact of remote access to emails on home life), were considered to be outside the scope of this review.
Context
The extent to which people have been asked to work at home has escalated dramatically in response to the COVID-19 pandemic and much of the recent evidence relates to the specific circumstances of home working during the pandemic. The review and model take steps to take account of this by considering evidence from both before and during the pandemic and also considering the implications for future research and policy directions.
Outcomes
Any factor that has been shown to be associated with the health of people working at home was included. An association is defined as the link between two variables (often an exposure and an outcome) where no causal relationship between the variables can be defined. This included all measures of physical health (including self-reported outcomes) and mental health (including clinical indicators such as diagnosis and treatment and/or referral for depression and anxiety alongside self-reported measures). All measures associated with wellbeing including but not limited to wellbeing, happiness, mood and stress-related outcomes were included. Work satisfaction, along with all other employment-related outcomes such as job performance and work-life balance, is outside the scope of this review.
Studies
We included quantitative, qualitative, mixed-method and observational studies. Studies with and without a comparator group were included. Books and dissertations were excluded (but references were checked for relevance in specific cases). Case studies were considered on an individual basis in terms of their study design and risk of bias. Studies from OECD4 countries only were included in the review.
Study selection
Title and abstract screening
Search results were downloaded to a reference management system (EndNote). The title and abstract of each reference were screened against the inclusion criteria by one reviewer, and checked for agreement by a second reviewer. Keyword tags were used to identify the reviewer who had screened the record and to determine whether each record should be retained for consideration at the full paper stage. Full papers of potentially included studies were download as the pdf version and linked to the EndNote record for that reference. Where reviewers disagreed on the potential inclusion of a paper (i.e. one tagged the paper to be considered at the next stage and the other did not) the full paper was obtained to clarify the relevance of the work to the inclusion criteria. This was agreed by consensus between the three reviewers.
Full paper screening
The full paper of all potentially relevant papers was read by one reviewer. Where a decision to exclude the paper (due to lack of relevant data) was made the reason for this decision was tabulated and checked by a second reviewer. Uncertainties were resolved by discussion between the three reviewers and among the wider review team as required until a definitive list of included papers was obtained.
Data extraction
A data-extraction form was devised based on forms used successfully in previous reviews of public health topics using similar approaches undertaken by the review team. The extraction form was piloted by each of the three reviewers and any suggested revisions discussed and agreed.
We extracted and tabulate key data from the included papers. This included the study first author and year, country of origin, study design and methods of analysis, study population, outcome measures, study aims, summary of results, key messages and conclusions, and any study limitations.
Data extraction was performed by one reviewer, with a 10% sample formally checked for accuracy and consistency by a second reviewer. The lead reviewer (LB) also re-read all papers and extractions in order to be as familiar as possible with the evidence base. The data-extraction process for this review focused on identifying the links between factors reported in the papers. We included quantitative measures of any associations where these were reported. For qualitative papers we extracted data from both the authors’ findings and from raw data within the published paper. The descriptions of factors was recorded exactly as defined by the study authors; definitions were not manipulated nor was any attempt to classify or group factors attempted at this stage. In practice, the included papers were revisited and the extraction-table data checked on several occasions throughout the data-synthesis and report-writing stages.
Quality appraisal
Quality (risk of bias) assessment was undertaken using appropriate tools for the types of study designs included in the review (see Table 1. Quality appraisal tools). Quality assessment was performed by one reviewer, with a 10% sample checked for accuracy and consistency by a second reviewer. Mixed-methods studies were quality appraised for each type of method and data included in the study. Where there was not enough information contained in the paper to do this, the study was quality appraised with respect to the main focus of the data and approach.
| Study type | QA tool | Accessed via |
|---|---|---|
| Crosssectional studies | CEBMa | Center for Evidence-Based Management (2014). Critical Appraisal Checklist for Cross-Sectional Study. Retrieved (month, day, year) from www.cebma.org |
| Qualitative studies | CASP | CASP-Qualitative-Checklist-2018_fillable_form.pdf (b-cdn.net)https://casp-uk.net/casp-tools-checklists/ |
| Cohort studies | CASP | CASP Cohort Study Checklist 2018_DRAFT.docx (b-cdn.net)udy Checklist 2018_DRAFT.docx (b-cdn.net) |
| Quasi-experimental studies | JBI Systematic Reviews | https://jbi.global/sites/default/files/2020-07/Checklist_for_Quasi-Experimental_Appraisal_Tool.pdf |
| Grey literature | AACODS checklist | http://dspace.flinders.edu.au/dspace/ |
The overall quality of the evidence base and its impact on the review findings was also considered in order to describe the volume, quality and degree of consistency in the evidence, and where there are gaps requiring primary research.
Data synthesis
The extracted data were synthesised narratively due to the diverse nature of the evidence. 1 The variance in reported outcomes precluded any meta-analytical approaches to the data. We aimed to summarise all of the factors reported in the included papers to develop an overall picture of the how working from home affected health.
Once we had extracted data from the papers a meeting was held with the reviewers to construct mind maps and summary tables of the factors reported in the papers. We did this by tabulating the factors reported by the authors and noting whether the factor had a positive or negative influence (or no influence) on the association between working from home and health. Consensus was obtained within the review team as to where the factors reported could be effectively grouped together (for example different measures of stress or anxiety were grouped together). The grouping of factors was further discussed and validated by our patient and public involvement (PPI) group in order to ensure that they made sense in relation to their experiences.
As well as including qualitative studies in the above analysis, an additional thematic analysis of these studies was also undertaken to establish whether any further insights could be gathered by considering the depth of analysis presented in these types of studies. As our research question was very specific, and the qualitative research identified rarely had the same aim (findings were usually much broader), we chose to focus on data relating to working from home and its impact on health and wellbeing. We synthesised studies from before and during the COVID-19 pandemic separately, due to differences in context and implications for future home and hybrid working. Rather than coding extracted data line-by-line, we coded units of meaning, in the form of text extracts, which could have been a line, or a larger passage of text, to retain contextual information within each code. 82,83 Direct quotations from participants were coded where possible, and where an illustrative quotation was not provided then the interpretations of study authors were coded (i.e. a second-order interpretation84). The codes were then organised into categories, which were organised into themes and subthemes for each set of studies (pre-pandemic and during-pandemic) by looking for similarities and differences between the codes and text extracts,85 using tables in Microsoft Word. This process was undertaken by one author (EH) and checked by another (LB).
Developing a model to visualise the results
Prior to this work we development an a priori model of potential links between working from home and health-related outcomes. 3 Contextual and background factors for the model were identified through recent reviews and grey literature publications summarising the factors which have contributed to the increases in home working seen both prior to and as a result of the COVID-19 pandemic. The a priori model also defined the main outcomes as outlined by the research questions for this review. However, this did not provide information about the factors which influence the relationship between working from home and health-related outcomes. This systematic review allowed us to develop a more informed, evidence-based model to detail what is known about these factors and the relationships between them.
The first step to build on the a priori model was to use the factors which influence the associations reported in the literature to construct mind maps to visualise the extent and complexity of the relationships reported. We used our extracted data from the included papers which detailed the reported factors which influence the relationship between home working and the health and wellbeing outcomes as defined in the individual papers. Any interim factors which shape the pathways between variables were noted. We recorded the factors as they were reported by the authors and did not change or interpret any wording used.
Due to the volume of evidence and the complexity of the relationships and factors reported, we divided the evidence into studies published before the COVID-19 pandemic (where no reference to COVID-19 was made) and those published during the pandemic (where specific reference to COVID-19 was made in the paper). We also divided the studies into those reporting physical health, mental health and wellbeing and/or overall health outcomes, again to help with data presentation and understanding. The reported factors were tabulated from the data in the extraction tables, and then transferred to the mind maps (with a box and line to represent each reported factor and the outcome it was linked to) to give a summary of the overall volume, direction and consistency of the reported factors. Where a variety of factors and outcomes were reported, studies were included in more than one mind map to reflect this. The colours we selected for the mind maps were chosen in order to be accessible to those with colour-blindness.
The following colours are used in the mind maps and tables to attempt to give an overall visual statement regarding the influence of working from home on health:
-
blue: factor which positively influences the health of those working at home
-
orange: factor which negatively influences the health of those working at home
-
black: factor which has no influence on the health of those working at home.
Due to the high volume of studies reporting mental health and wellbeing outcomes published during the COVID-19 pandemic we developed a summary mind map for these outcomes as the original mind map was too complex to be clear. Studies reporting similar research findings were grouped together to generate a summary typology of factors which influence the associations between home working and health. This grouping occurred, for example, where studies reported on similar factors, or where the same factor is discussed but in more or less detail. In all cases we were confident that the authors were essentially reporting on the same factor, even if the terminology and wording used was different. This approach to grouping factors was validated by two reviewers independently grouping factors and then comparing grouping and making alterations where necessary to reach consensus. This approach is further described in the results section of this report.
The findings from our review were combined with the a priori model which was validated in consultation with stakeholders.
Patient and public involvement and stakeholder involvement
To ensure that the review was informed by, and useful to, all stakeholders who have an interest in the evidence base for home working, we have taken into account the views and recommendations of diverse stakeholders. Stakeholders have contributed to the review in the following ways:
-
consultation with members of the public prior to and during the review
-
consultation with employer representatives prior to and during the review
-
consultation with union bodies representing employees.
Three online discussion meetings were held with members of the public with experience of working from home. Potential participants were recruited via the People in Research website,86 which advertises opportunities for public involvement in NHS, public health and social care research. These discussion meetings were undertaken prior to starting the review (to comment on the scope and focus of the review), in the initial stages of the review (to comment on inclusion criteria and search terms), and at the end of the review process (to comment on the review finding and interpretation). In total eight people contributed to these online sessions. The individuals involved varied by demographic characteristics and their length and amount of experience of working at home. They also represented several different industries and occupations and included people who were self-employed as well as employees. As we had a significant response to our call for participants, we were able to select those we invited to the discussion based on these characteristics to ensure that they were sufficiently diverse in experience and viewpoints.
In each discussion meeting (which took place on line) members of the group were presented with up-to-date information regarding the progress and findings of the research and asked to comment and raise questions in order to ensure that the data presented made sense from their perspective. In the final meeting the participants were presented with the mind maps and final model and discussed their understanding of the data presented and whether anything did not reflect their experience. Minor changes to wording within the final model were made as a result.
Emails were sent to employer and union representatives in the initial stages of the review to ask for comments on the scope of the review and suggestions of evidence which should be considered for inclusion in the review. Towards the end of the review process respondents were re-contacted to ask for their comments on the main findings of the review (see Appendix 1: PPI and stakeholder participants for a full list of participants).
Results
Study selection
After de-duplication, the initial database searches generated 2514 records, of which 135 were retrieved as full papers and 23 found to meet the inclusion criteria for the review. A further 635 papers were identified via citation searching; of these, 42 were found to meet the inclusion criteria. An additional 20 papers were identified from checking the reference lists of the included studies and previous systematic reviews. Therefore, 85 peer-reviewed articles were included in the review. Grey literature searches identified a further 50 sources of which 11 were found to meet the inclusion criteria and were included in the review. Although 12 pieces of research were suggested by stakeholders, these were all found to have been already identified through the searches process, or to be beyond the scope of the review.
In total, 96 pieces of relevant evidence were identified and included. These have been summarised (see Figure 1. Study selection; and Table 2. Summary table of included studies) and are also presented as full extractions for each included study (see Supplementary Material: Full extraction tables).
| ID no. |
Study | Covid yes/no | Country Population |
Study design | Primary outcomes | Factors Work from home |
|---|---|---|---|---|---|---|
| 1. | Allen 202147 | Y | UK Workers |
Survey Cross-sectional |
Psychological wellbeing, Anxiety, depression Loneliness, insomnia |
No factors associated with working from home/wellbeing. Self-isolation (β = −0.162, p = 0.004) and loneliness scores (β = −0.596, p < 0.001) were the only significant predictors of wellbeing. |
| 2. | Alpers 202187 | Y | Norway Adults |
Survey Cross-sectional |
Health worries Alcohol consumption |
Increased alcohol consumption more common in those working from home. Self-assessed increased alcohol consumption during the lockdown period was more frequently reported by people working or studying from home (OR 1.4, 95% CI 1.3 to 16). |
| 3. | Anderson 201413 |
N | USA Workers |
Survey Cross-sectional |
Job-related affective wellbeing scale | The relationship between telework and positive affect is moderated by one’s social connectedness outside of the workplace such that the relationship becomes more positive as social connectedness increases (γ = 0.75, p < 0.001), also individuals experience less negative affect while teleworking as social connectedness increases; γ = −0.73, p < 0.01). |
| 4. | Argus 202140 | Y | Estonia Office workers |
Survey Cross-sectional |
Musculoskeletal pain (MSP)PA: BPAQ | Self-reported PA was significantly lower during than before the (mean change in BPAI −0.41, SD 1.37, 95% CI −0.62 to −0.19, p < 0.001, Cohen’s d = 0.26 (small effect)), but not leisure-time PA (mean change in BPAQ −0.07, SD 0.59, 95% CI −0.16 to 0.02, p = 0.15, Cohen’s d = 0.11), and work-related PA significantly increased (mean change in BPAQ0.18, SD 0.54, 95% CI 0.10 to 0.26, p < 0.001, Cohen’s d = 0.50 (medium effect)). Negative correlation between change in self-reported sports-related PA and change in the numbers of body regions with MSP during the lockdown (r = −0.206, p < 0.01). The number of body regions with MSP onset during the lockdown was also negatively correlated with change in workplace comfort score (r = −0.262, p < 0.001) and change in workplace ergonomics score (r = −0.231, p < 0.01). |
| 5. | Bennett 202188 | Y | USA Workers (range of industries) |
Survey Cross-sectional |
Video conference fatigue (Profile of Mood States scale) | Muting the microphone (γ = −0.09,p = 0.02) and perceptions of group belongingness (γ = −0.21, p = 0.003) were negatively related to fatigue (i.e. were associated with lower fatigue, whereas turning the webcam off, attention during the meeting, and videoconference meeting duration were not significantly related to post-meeting fatigue. Muting and perceptions of belongingness were significantly negatively correlated with each other (−0.45, p < 0.05). |
| 6. | Bentham 202148 | Y | UK CAMHS Services staff |
Survey Cross-sectional |
Wellbeing: Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) | Proportion of hours working from home not related to wellbeing: An independent samples Kruskal-Wallis H-test showed no statistically significant differences in wellbeing score based on the proportion of hours worked remotely during the pandemic (χ2 (4) = 4.45; p = 0.349). No difference with and without dependents. |
| 7. | Bentley 201614 | N | New Zealand Teleworkers |
Survey Cross-sectional |
Psychological strain | Organisational social and teleworker support resulted in increased job satisfaction (t = 10.02, 7.81; p < 0.001) and reduced psychological strain (t = 6.09, p < 0.001; t=2.06, p < 0.05). Social isolation mediated the relationship between organisational social support and the two outcome variables. Some differences in the structural relationships for hybrid and low-intensity teleworker sub-samples. |
| 8. | Bevan 202089 | Y | UK Home workers |
Survey Cross sectional |
Mental health Wellbeing Physical health |
Mental health is poorer for: younger workers, looking after elderly relatives (but parents are no different to non-parents), living with parents or renting, new home workers, working more than contracted hours, reduced contact with boss. Significant decline in musculoskeletal health. Poor sleep and increased fatigue a concern. Alcohol, diet & exercise declining for many. Emotional concerns over finance, isolation, energy, work-life balance and family health. |
| 9. | Boncor 202090 |
Y | UK Lone researcher |
Qualitative Ethnography |
‘Living and working during the COVID-19 pandemic’ | Openness to new ways of living linked to coping with COVID (and working at home wellbeing). Assumed link to wellbeing. |
| 10. | Burstyn 202191 | Y | USA General population |
Survey Cross-sectional |
Anxiety Depression |
Anxiety and depression negative link to concerns about return to work, childcare, lack of sick leave, and loss/reduction in work. Patterns differed by sex. Men (but not women) who identified as essential workers (RR 1.16, 95% CI 0.96, 1.40), had one-on-one contact with people at work (RR 1.14, 95% CI 0.98 to 1.34), including known or suspected cases of COVID-19 (RR 1.30, 95% CI 0.97 to 1.74), who were hourly employees (RR 1.24, 95% CI 0.96 to 1.60), and did not have access to disability/sick leave through work (RR 1.22, 95% CI 0.93 to 1.60) were more anxious. |
| 11. | Chakrabarti 201892 | N | USA Telecommuters |
Survey Cross-sectional |
PA | Working from home increased walking, cycling; PA decreased driving. Both frequent and occasional telecommuters engaged in 8–9 minutes more per day of PA than non-telecommuters, on average; 31% frequent, 27% occasional and 21% non-telecommuters met or exceeded the 30 minutes per day activity target. |
| 12. | Charalampous 202112 | N | UK Male workers |
Qualitative. Interviews | Wellbeing | Working from home had better work life balance and were happier. But were lonely and bored due to lack of social interaction. No impact on psychosomatic health, but increased sedentary behaviours. Stress linked to issues with technology. |
| 13. | Chung 202093 | Y | UK UK employees |
Survey Cross sectional |
Wellbeing (some assumed links) | Positive effects were the ability to: take care of children, do housework and spend more time with their partners. Negative aspects included: blurred boundaries between work/home, missing interactions with colleagues. Increased workload and conflict between work and family negatively impacted parents’ mental wellbeing, especially for mothers. Almost half of all mothers felt rushed and pressed for time, more than half of the time during the lockdown. In addition, 46% of mothers felt nervous and stressed more than half of the time. |
| 14. | CIPD 202149 | Y | UK Working population |
Online survey Interviews |
Wellbeing | Increased wellbeing through avoiding the commute, greater flexibility of hours, reduce distractions, normalising use of technology (helped disabled). The most frequently mentioned benefit of working at home was increased wellbeing through avoiding the commute (46% of survey participants), followed by enhanced wellbeing because of greater flexibility of hours (39%). Reduced wellbeing: isolation, unsuitable home circumstances, increased health anxiety, home-schooling. |
| 15. | Clark 202160 | Y | Ireland Working mothers |
Qualitative interviews | Psychological wellbeing | Increased levels of psychological distress as a result of the pandemic and working from home. Mediated by increased childcare and domestic duties. |
| 16. | Collins 201615 | N | UK Local authority workers |
Qualitative. Semi-structured interviews | Wellbeing Social support relationships with colleagues. |
Social relationships only with workers known face to face. Personal phones used for social support. Pressure (from self) to achieve expectations in order to maintain tele working. |
| 17. | Cotterill 202050 | Y | UK Water sector |
Survey Cross-sectional |
General wellbeing since lockdown. | More women saw a decrease in wellbeing (39%) than men (32%), although this was not statistically significant, and there were no significant difference between the median wellbeing values for men and women (U = 27 030, z = −1.472, p = 0.141). Essential workers had largest improvement in wellbeing. |
| 18. | Daniel 201816 | N | England Online home businesses |
Qualitative. Semi-structured interviews | Mobility, isolation and paradox. | Positive: feeling more fulfilled by having more time and mental space, and the inherent autonomy of scheduling from working from home. Negative: loneliness, isolation (professional and social). Fear of equipment/internet failure. |
| 19. | De Sio 202151 | Y | Italy Teleworkers |
Survey Cross-sectional |
Psychological distress and perceived wellbeing | Poor wellbeing was associated with having a higher job demand during pandemic (OR 2.61; 95% CI 1.10 to 6.19), with feeling not ‘sheltered at home’ (OR 8.80; 95%CI 2.60 to 29.75), with smoking more cigarettes during pandemic (OR 2.47; 95%CI 1.13 to 5.59), and with experiencing psychological distress (OR 8.01; 95% CI 2.57 to 24.97). |
| 20. | Delanoeije 202094 | Y | Belgium Employees |
Quasi-experimental | Stress | Working from home associated with lower stress, lower work-to-home conflict, higher work engagement and higher job performance. Univariate F tests showed there was a significant interaction effect between time and group for stress (F(1,62) = 4.21, p = 0.04, ηp2 = .06)’; however, the decrease in stress among the teleworking group could be accounted for by pre-existing differences in commuting time. For daily stress, ‘the standardized estimate of teleworking day on daily stress (γ = −0.20, p < 0.001) was negative and significant’. |
| 21. | Delfino 202152 | Y | Italy Professional services |
Qualitative. Semi-structured interviews |
Wellbeing, and factors affecting wellbeing | Employees experienced stress in relation to increased demands from working from home. Increased monitoring and expectation to all always be available (and increased video calling) reduced wellbeing. |
| 22. | Deloitte 202195 | Y | UK National population sample |
Survey Cross-sectional |
Wellbeing | Lockdown negative impact on wellbeing. After lockdown most office workers would prefer to work at home more often. |
| 23. | Di Tecco 202135 | Y | Italy Public admin workers |
Prospective cohort study | General health Wellbeing Job satisfaction, work-life balance, psychosocial factors |
Working from home (smart working) one day per week had no effect on wellbeing. Predictors of wellbeing were work demands, management of change. Demands and higher education significantly predicted general health. There was no significant change in general health (p = 1.00) and wellbeing (p = 0.247) as evaluated by t-tests. In the regression models, significant predictors of wellbeing were demands (−0.703, p = 0.027) and effective management of change (1.461, p = 0.003), and demands (−1.00, SE 0.048, p = 0.037) and higher education (0.238, SE 0.100, p = 0.018) significantly predicted general health. |
| 24. | Docka‐Filipek 202161 | Y | USA University workers |
Survey Cross-sectional |
Self-reported mental health (depression and state anxiety) | Gender accounted for unique variance in both depression (β = 0.17, p ≤ 0.01) and anxiety (β = 0.17, ss ≤ 0.01) risk. Higher financial concern accounted for unique risk for both depression (β = 0.30, p < 0.001) and anxiety (β = 0.26, p < 0.001), and having more dependents accounted for unique risk for anxiety (β = 0.13, p < 0.05). |
| 25. | Dunatchik 202153 | Y | USA Adults |
Survey Cross-sectional |
Altered responsibilities for domestic labour | The rise of remote work during the COVID-19 pandemic has not appreciably altered the domestic division of labour. 66% mothers and 65% fathers reported feeling ‘some’ or ‘a lot’ of pressure regarding children’s home learning. |
| 26. | Evans 202196 | Y | UK Remote workers |
Longitudinal survey | Wellbeing | Burnout, no effect overall. Extroversion and conscientiousness became a risk during the pandemic. |
| 27. | Felsted 202017 | Y | UK Workers |
Survey Cross sectional |
Wellbeing | Those who worked mainly at home reported greater difficulties in enjoying normal day-to-day activities compared to those not working at home, (48.2/49.3% vs. 38.5%) and more often felt constantly being under strain and unhappy with life (36.0/33.9 vs. 31.2). |
| 28. | Fukumura 202197 | Y | USA General population |
Survey Cross-sectional |
Wellbeing | Wellbeing: time use, working in home space, work-life balance, temporality. |
| 29. | Galanti 202198 | Y | Italy Public and private employees |
Survey Cross-sectional |
Stress due to working from home | Stress was positively correlated with family-work conflict (r = 0.50, p < 0.01), social isolation (r = 0.62, p < 0.01), distracting working environment (r = 0.36, p < 0.01), and negatively correlated with productivity (r = −0.39, p < 0.01) and work engagement (r = −0.47, p < 0.01). |
| 30. | Gao 202061 | Y | UK Female academics |
Qualitative Ethnography |
‘Living and working during the COVID-19 pandemic’ | Both women experienced social isolation as a result of being physically distanced from their workplace and colleagues, even if working alone was previously sought/preferred. Technology and silence were challenges. |
| 31. | Gijzen 202054 | Y | Netherlands Workers |
Survey Cross-sectional |
Mental health and wellbeing | Working from home was reported as a positive outcome of the COVID-19 pandemic for 17% (n = 142) participants. Others negative – so no effect overall. |
| 32. | Grant 201318 | N | UK e-workers |
Qualitative. Semi-structured interviews | Wellbeing | Communication and support from colleagues critical success factors for successful remote working and to balance the psychological aspects of wellbeing. Wellbeing enhancing: Fewer days lost through absenteeism, relieve stress from travel and child-care issues. Wellbeing detracting: Social interaction limited to family and local friends, Office grapevine and important information missed. Sitting behaviours may increase. |
| 33. | Hall 201917 | N | UK Employees |
Survey Cross-sectional |
How home working makes people feel | Home working can increase employee engagement, job satisfaction and wellbeing (no data presented). |
| 34. | Hallman 202197 | Y | Sweden Office workers |
Mixed: Survey Diary and accelerometer data |
PA (proxy to physical health), standing, sedentariness and sleep | Sedentariness, standing and movement did not differ significantly between working from home and working at the office. Time spent sleeping (relative to time spent awake) was significantly greater on working from home days than for days working at the office. Days working from home were associated with more time spent sleeping relative to awake, and the effect size was large (F = 7.4; p = 0.01; ηp2 = 0.22). The increase (34 min) in sleep time during WFH occurred at the expense of a reduction in work and leisure time by 26 min and 7 min, respectively. |
| 35. | Hayes 202199 | Y | USA (and global) Home workers |
Survey Cross-sectional |
Stress and work-related burnout | There was a significantly greater increase in perceived stress score from pre-COVID (retrospectively rated) to the current time among those whose job typically did not provide opportunities to WFH (mean increase 3.9, SD 6.4) than those whose did (mean increase 2.4, SD 5.3) (t(290) = 2.23, p = 0.03). Conversely, those who previously had flexibility to WFH before the pandemic had higher work-related burnout scores at data collection (mean 57.9, SD 21.5) than those without the flexibility to WFH (mean 41.0, SD 21.6) (t(284) = −16.84, p < 0.0001). Although women had lower pre-COVID and during-COVID perceived stress scores than men, the mean increase in stress scores was higher for females (4.2, SD 6.0) than males (2.4, SD 5.8) (t(294) = 2.59, p = 0.01). Women had significantly lower mean work-related burnout scores (43.3, SD 20.8) than men (53.0, SD 24.6) (t(299) = −3.82, p < 0.0002). |
| 36. | Heiden 2021100 | Y | Sweden University staff |
Survey Cross-sectional |
Perceived health, stress, recuperation, work-life balance and intrinsic work motivation | Those who teleworked several times per week or more reported more stress relating to indistinct organisation than those who teleworked less than once a month. There were no significant pairwise differences for fatigue. None of the outcomes were significantly predicted by the amount of telework per week in regression analyses but did show significant differences on fatigue (F = 3.47; p = 0.032) and work stress relating to indistinct organisation and conflicts (F = 4.80; p = 0.009). |
| 37. | Henke 201620 | N | USA Finance employees |
Retrospective cohort study | Telecommuting intensity and selected health indicators | Telecommuters were less likely to be at risk for most health risks studied (alcohol abuse, physical inactivity, tobacco use, depression, Edington risk scores) or stress risk; the predicted probability of being at risk appeared to increase with increasing telecommuting intensity. |
| 38. | Hislop 201521 | N | UK Self-employed home workers |
Qualitative. Semi-structured interviews | Experiences of work and isolation | Positive: spacio-temporal flexibility Negative: isolation, sense of perpetual contact |
| 39. | Hoffman 202119 | Y | USA Workers (hybrid) |
Survey Cross-sectional |
Wellbeing (positive and negative affect) Companion animals |
Neither the presence of dogs or cats nor the presence of other humans in the household predicted where participants preferred to work. For participants who worked from home, neither PAWB scores nor NAWB scores were associated with the presence of dogs or cats in the home. Paired samples t-tests indicated that neither positive or negative wellbeing scores differed significantly by workplace location (PAWB: t = 1.17, df = 453, p = 0.24; NAWB: t = −1.74, df = 453, p = 0.08). |
| 40. | Hornung 20095 | N | Germany Public admin workers |
Survey Cross-sectional |
QoL | There were small but statistically significant positive effects of telecommuting intensity on QoL mediated via both autonomy (βindirect = 0.02, z = 2.56, p < 0.01) and work-family conflict (βindirect = 0.11, z = 5.96, p < 0.01). |
| 41. | Hubbard 202163 | Y | UK Adults of working age |
Survey Cross-sectional |
Satisfaction with working from home | Women reported less satisfaction than men (chi-square 7.011, df = 3, p = 0.071), as did people with children (chi-square 7.299, df = 3, p = 0.063) – especially young children aged 0–4 years (chi-square 8.01, df = 3, p = 0.046). A significant predictor of dissatisfaction with home working was caring for a responsible adult (chi-square = 7.837, df = 3, p = 0.049). |
| 42. | Ignacio Gimenez-Nadal 202064 | Y | USA Employees |
Survey Cross-sectional |
Wellbeing (happiness, sadness, fatigue and stress) | Among males, teleworkers reported lower levels of sadness, stress and tiredness compared with commuters. Among females, teleworkers had significantly higher happiness levels than commuters. |
| 43. | Ingusci 202156 | Y | Italy Remote workers |
Survey Cross-sectional |
Behavioural stress | Behavioural stress was found to be positively related to work overload (β1 = 0.48, p = 0.015) and negatively related to job crafting (β3 = −0.38, p < 0.000), with a significant and negative indirect effect of work overload on behavioural stress through the intervention of job crafting (βa×b = −0.07, p = 0.029). |
| 44. | Jacukowicz 202022 | N | Poland Office and online workers |
Survey Cross-sectional |
Satisfaction with work-life balance | Working online significantly predicted lower satisfaction with work-life balance (β = –0.17, p < 0.01) but greater quality of social life (β = 0.13, p < 0.05). |
| 45. | Janssen 202065 | Y | Netherlands Adolescents and caregivers |
Ecological study | Positive and negative affect | Working from home was not related to the increase in parents’ negative affect during the COVID-19 pandemic, as compared with pre-pandemic data. |
| 46. | Kaduk 20196 | N | USA IT workers |
Survey Cross-sectional |
Wellbeing: work family conflict, job satisfaction, burnout, perceived stress, psychological distress | Involuntary WFH associated with greater work-to-family conflict, stress, burnout, turnover intentions, and lower job satisfaction (p < 0.10) Voluntary WFH is protective, and associated with greater job satisfaction, lower turnover intentions, and less stress (p < 0.10). |
| 47. | KCL 2021101 | Y | UK Large employers |
Survey Cross sectional |
Wellbeing | Increased anxiety and stress due to lockdown. Wellbeing poorer in organisations not supporting alternative ways of working. Disproportionally negative impact on parents/carers. |
| 48. | Koehne 201223 | N | USA,UK, Estonia, Spain, Mexico Workers |
Qualitative. Semi-structured interviews | Personal experiences of working from home, and coping strategies. Wellbeing | A lack of possibility for person-to-person social interaction could negatively impact on remote workers’ wellbeing. |
| 49. | Kotera 2020102 | Y | UK Working population |
Ecological | Wellbeing | Working from home: increase blurred work-home boundaries, fatigue and mental demands. |
| 50. | Kroll 2019103 | N | Germany Employees |
Longitudinal Survey |
Perceived health | Working from home did not have a significant effect on health when controlling for individual heterogeneity (b = 0.02, SE = 0.05, ns). There was also no statistically significant effect of working from home on leisure satisfaction, however (b = −0.01, SE = 0.10, ns). |
| 51. | Kubo 202136 | Y | Japan Workers |
Survey Cross-sectional |
Diet | Working from home had a negative effect on diet. The odds ratios (95% CI) for those who telecommuted at least 4 days per week relative to those who rarely telecommuted were: Skipping breakfast: 1.15 (1.03 to 1.29); Solitary eating: 1.44 (1.28 to 1.63); Lower meal frequency: 2.39 (1.66 to 3.44); and Meal substitution: 1.26 (1.04 to 1.51). |
| 52. | Lal 2021104 | Y | UK Working from home |
Qualitative interviews | Social interactions | Working from home had a negative effect on social interactions. The findings highlight the difficulty in maintaining social interactions via technology such as the absence of cues and emotional intelligence. |
| 53. | Limbers 202066 | Y | USA WFH mothers |
Survey Cross-sectional |
QoL, parenting stress, PA | Moderate intensity PA may attenuate the negative impact of parenting stress on social relationships and satisfaction with one’s environment in home working mothers during the COVID-19 pandemic. Greater levels of parenting stress were associated with lower physical health QoL (r = −0.42, p < 0.001), lower psychological QoL (r = −0.28, p < 0.001), lower social relationships QoL (r = −0.21, p < 0.01) and lower environment QoL (r = −0.19, p < 0.01). |
| 54. | Lundberg 200224 | N | Sweden White-collar government workers. |
Observational field study | Psychophysiological reactivity (blood pressure plus urine and saliva samples) Self-rated health/wellbeing |
No significant difference in self-ratings of stress between telework and office work. Blood pressure was significantly higher during work at the office than when teleworking at home, and men had significantly elevated epinephrine levels in the evening after telework at home (p < 0.01). |
| 55. | Magnavita 2021105 | Y | Italy Workers |
Survey Cross-sectional |
Happiness Anxiety Depression |
Intrusive leadership and overtime work were associated with reduced happiness, anxiety and depression in teleworkers (hybrid workers) (p < 0.001 for all the parameters). |
| 56. | Mann 200325 | N | USA Journalists |
Mixed: Survey cross-sectional Qualitative. Semi-structured interviews |
Physical health Mental health |
Higher levels of emotional ill health for the teleworkers. No significant difference for physical health. But, reduced stress at home due to: no office politics and transport and no travel to work perception of having control over their work (environment and work schedules). Negative effects of working from home: irritability, loneliness, lack of social support, insecurity/lack of confidence. Intrinsic rewards of working from home motivate to overcome negative emotions. |
| 57. | Mari 2021106 | Y | Italy Practitioners, managers, executives, teachers |
Survey Cross-sectional |
Stress Coping |
There were no significant differences between professional groups on the PSS (perceived stress), nor on the perceived self-efficacy subscale. For the perceived helplessness subscale, teachers had a higher mean score (11.07, SD 3.90) than managers (9.79, SD 3.81). |
| 58. | Mellner 201726 | N | Sweden Professional workers |
Survey Cross-sectional |
Psychological detachment | Working at several different places (hybrid) was inversely associated with weekly work hours and had no association with psychological detachment. |
| 59. | Molino 2020107 | Y | Italy Workers |
Survey Cross-sectional |
Technostress | Remote working reduces stress. Significant positive correlations were found between behavioural stress and work-family conflict (r = 0.23), the three techno-stress creators (techno-overload, techno-invasion and techno-complexity; r = 0.22, r = 0.24 and r = 0.23, respectively), and workload (r = 0.19) (all p < 0.01). Work-family conflict was also positively correlated with the three techno-stress creators (r = 0.35, r = 0.48 and r = 0.19, respectively) and workload (r = 0.47) (all p < 0.01). Remote working was positively correlated with techno-overload (r = 0.29), techno-invasion (r = 0.25), and workload (r = 0.13) (all p < 0.01), but not behavioural stress (r = −0.07), work–family conflict (r = 0.03) or techo-complexity (r = 0.01). |
| 60. | Moretti 202041 | Y | Italy Admin officers |
Survey Cross-sectional |
Work-related stress and musculoskeletal issues | Working from home increased risk of mental health and musculoskeletal problems, particularly affecting the spine. Neck pain worsened in 50%, improved in 8.3% and was the same in 41.7% of participants, whereas lower back pain worsened in 38.1%, improved in 14.3% and was the same in 47.6% of participants. |
| 61. | Parry 202157 | Y | UK Newly working from home |
Mixed: Survey Cross-sectional Interviews |
Wellbeing Physical health |
Working from home: experiencing worse symptoms of musculoskeletal pain, higher levels of fatigue, poor sleep, and higher levels of eye strain. Wellbeing score low compared to previous rounds of survey. Wellbeing scores lower for introverts – maybe due to video conferencing |
| 62. | Perry 20187 | N | USA Full time workers |
Longitudinal survey Additional cross sectional survey |
Emotional stability Strain Autonomy |
[Study 1]: Remote work was only correlated with ‘disengagement aspect of strain’. Moderated by emotional stability. [Study 2]: Remote work was not significantly correlated with strain outcomes or forms of need satisfaction. Positive ‘remote work-exhaustion slope’ among employees reporting low autonomy. Those with high autonomy and high emotional stability exhibited the lowest overall level of strain. There was a significant remote work × autonomy interaction for exhaustion, such that there was ‘a positive remote work–exhaustion slope among employees reporting low autonomy (0.82; t = 2.12, p < 0.05) but no significant relationship among those reporting high autonomy (slope = −1.20; t = − .68, p = 0.10).’ |
| 63. | PWC 202058 | Y | Malta Workers |
Survey Cross-sectional |
Wellbeing | Mostly positive experience on wellbeing. Negatively affected by loneliness (lack of social interactions and feeling detached from the office). |
| 64. | Ray 202127 | N | USA National sample |
Retrospective cohort | Wellbeing Work flexibility |
Working from home was associated with an increase in job stress and an increase in job satisfaction. In regression analyses, working from home was associated with a 22% increase in job stress and a 65% increase in job satisfaction (p < 0.01). Stress and non-healthy days increased in women, non-whites, lower income, lower health status, living with spouse, family interfering with work, and more hours worked. |
| 65. | Restrepo 2020108 | Y | USA Working age |
Survey Cross-sectional |
Sleeping Food prep Eating |
Those working from home the previous day had significantly more minutes of sleep than those who worked away from home the previous day. Assumed link to wellbeing. |
| 66. | Reuschke 201928 | N | UK Working age |
Retrospective cohort | Life satisfaction | Home working did not have an impact on overall life satisfaction overall, not among men or women, not by type of employment. Home working was found to be significantly positively related to leisure time satisfaction (men and women). |
| 67. | Ripoll 202137 | Y | Spain Adults |
Survey Cross-sectional |
Mental health and psychological wellbeing | Working from home associated with increased depression symptoms during early COVID-19 pandemic. Working from home (compared with other working arrangements) was not associated with increased consumption of psychotropic drugs between weeks 1 and 4 (consumed by 6.5% and 7.1%, respectively, p = 0.306) or weeks 1 and 8 (consumed by 8.4% and 8.9%, respectively, p = 0.952), nor consultations to improve mood/anxiety between weeks 1 and 4 (undertaken by 27.3% and 26.9%, respectively, p = 0.918) and weeks 1 and 8 (undertaken by 28.0% and 31.5%, respectively, p = 0.388). |
| 68. | Rodriguez 2020109 | Y | Spain General population |
Survey Cross-sectional |
Stress: Perceived Stress Scale | Lowest stress response those who combined teleworking and commuting (in-person working). Highest stress response (and lowest stress control) those who were dismissed during lockdown. Teleworking reported the highest stress control (a very slight increase), followed by those who were both teleworking and commuting. Working situation (during COVID-19 lockdown confinement) was related to stress response (F(4,918) = 4.914; p < 0.01; ηp2 = 0.020) and control of stress (F(4,928) = 4.017; p < 0.01; ηp2 = 0.016). |
| 69. | RSPH 202142 | Y | UK Newly working from home |
Survey Cross-sectional |
Wellbeing Physical health |
Working from home: less connected to colleagues (67%), taking less exercise (46%), developing musculoskeletal problems (39%) and disturbed sleep (37%). Feeling isolated. Working from sofa or bedroom increased musculoskeletal problems. Women more likely to feel isolated and to develop musculoskeletal problems. Poorer mental health if shared with many housemates. |
| 70. | Russo 2021110 | Y | Denmark Software professionals |
Longitudinal survey | Wellbeing Stress: Perceived Stress Scale. |
Quality of social contacts predicted positively, and stress predicted negatively an individual’s wellbeing. At Wave 1, stress negatively affected social contacts and daily routines predicted stress at α = 0.05. At Wave 2, need for competence and autonomy, stress, quality of social contacts, and quality of sleep uniquely predicted wellbeing at a = 0.05. No evidence that any predictor variable causal explained variance in wellbeing. |
| 71. | Sardeshmukh 20128 | N | USA Telecommuters (large company) |
Survey Cross-sectional |
Exhaustion Hours of telework |
Telework is negatively related to both exhaustion and job engagement, and job demands ((time pressure, role ambiguity, role conflict) and resources mediate these relationships. |
| 72. | Sato 2021a111 | Y | Japan General population |
Survey Cross-sectional |
Depressive symptoms | Working from home was negatively associated with depressive symptoms. In the logistic regression model, shifting to WFH was negatively associated with depressive symptoms (OR 0.83, 95% CI 0.69 to 0.99). |
| 73. | Sato 2021b38 | Y | Japan General population |
Survey Cross-sectional |
Diet | Working from home was more clearly associated with increased intake of vegetables, fruits and dairy products and decreased alcohol intake among women than men. Working from home was associated with increased intake of vegetables (1.02, 1.004- 1.03), fruits (1.06, 1.03–1.09), dairy products (1.03, 1.01–1.06) and snacks (1.04, 1.02–1.06) but decreased intake of seaweeds (0.94, 0.91–0.97), meats (0.98, 0.96–0.999) and alcohol (0.93, 0.86–0.997). |
| 74. | Schifano 202159 | Y | France, Italy, Germany, Spain and Sweden General population |
Prospective cohort Survey |
Wellbeing Life satisfaction |
Working from home was associated with lower wellbeing on all five variables – life satisfaction (coefficient = −0.09, p < 0.01), worthwhile (coefficient = −0.07, p < 0.05), not lonely (coefficient = −0.08, p < 0.05), not depressed coefficient = (−0.09, p < 0.01) and not anxious (coefficient = −0.09, p < 0.01), although not working had a greater negative impact. Switching to working from home reduced anxiety (coefficient = 0.05, p < 0.10) but also reduced the sense of a worthwhile life (coefficient = −0.07, p < 0.05), with no significant impact on other wellbeing variables. |
| 75. | Shockley 202129 | Y | USA Married couples with children |
Prospective cohort Survey |
Psychological distress Sleep quality |
In the latent class analysis, for health outcomes (psychological distress and sleep quality), those adapting the strategy of ‘alternating days’ fared the best (mean PD score 1.54 and 1.58 for wives and husbands, respectively). |
| 76. | Smith 2021112 | Y | Canada | Survey Cross-sectional |
Wellbeing Anxiety and depression: Generalised Anxiety Disorder (GAD-2); Patient Health Questionnaire (PHQ-2) |
Anxiety and depression scores significantly lower than onsite workers. Among those working remotely, the adjusted proportion of respondents with GAD-2 scores of ≥3 was 35.3% (95% CI 27.1 to 43.5) and the adjusted proportion of respondents with PHQ-2 scores ≥3 was 27.4% (95% CI 20.1 to 34.8), both of which were significantly lower than among site-based workers or those no longer employed. |
| 77. | Song 202030 | N | USA General population |
Survey Cross-sectional |
Subjective wellbeing | Telework on weekdays or weekends/holidays is associated with more stress. Parents, especially fathers, report a lower level of subjective wellbeing when working at home on weekdays but not weekends. Childless females feel more stressed teleworking instead of working in the workplace. |
| 78. | Stitou 201831 | N | Canada Homebased childcare workers |
Qualitative. Semi-structured interviews | Wellbeing proxy measures | Factors affecting health and wellbeing were reported as the absence of contact with other adults during working hours, a lack of external help during working hours (i.e. working alone, without breaks), difficulty filling spots, noise, interference with personal and family life, low and precarious remuneration, and incomplete or no benefits. |
| 79. | Taser 2022113 | Y | Turkey Financial services employees |
Survey Cross-sectional |
Mental experiences (flow) | Working from home positive effect on the flow (mental experiences related to concentration and satisfaction at work). Technostress and loneliness mediated the relationship between WFH and flow. Those who had a good remote e-working experience tended to have lower levels of technostress (b = - 0.17, SD = 0.06, p < 0.01). Those experiencing technostress were likely to feel lonely (b = 0.23, SD = 0.06, p < 0.001). |
| 80. | Thulin 201932 | N | Sweden Workers |
Survey Cross-sectional |
QoL and social sustainability | Advantages of teleworking included being able to work more undisturbed, work more efficiently, avoid commuting, and facilitate everyday life. In the logistic regression model for time pressure, never teleworking (β = −0.644, p < 0.05), only teleworking within regular hours (β = −0.866, p < 0.01), age (being older; β = −0.032, p < 0.01), working full time (β = −0.806, p < 0.05) and using a smartphone for private purposes often (β = −1.115, p < 0.05) or all the time (β = −1.089, p < 0.05) were associated with experiencing less time pressure, whereas having children at home (β = 0.406, p < 0.01) was associated with experiencing more time pressure. |
| 81. | Tietze 201129 | N | UK Home workers |
Qualitative. Semi-structured interviews and focus groups | Wellbeing | Home workers felt less stressed and more relaxed. Participants also reported being better able to combine their work and domestic responsibilities and be better parents. New working procedures were a source of stress. |
| 82. | Toscano 2020114 | Y | Italy Employees |
Survey Cross-sectional |
Social isolation Stress |
Social isolation was significantly correlated with stress (0.50, p < 0.01), perceived remote work productivity (−0.43, p < 0.01), remote work satisfaction (−0.50, p < 0.01) and COVID-19 concern (0.32, p < 0.01). Stress was significantly correlated with perceived remote work productivity (−0.35, p < 0.01), remote work satisfaction (−0.54, p < 0.01) and COVID-19 concern (0.16, p < 0.05). |
| 83. | Travers 2020115 | Y | UK/Worldwide General population |
Qualitative Ethnography | Demands of home working | Working from home new and excessive demands creating worry, stress and pressure, but also opportunities afforded by a lack of commute and spending more time with the family, also the opportunity to exercise. |
| 84. | Trent 199434 | N | USA Private-sector companies |
Survey Cross-sectional |
Stress Perceived social support |
No differences in perceived stress score between telecommuters, those who worked from home, those who worked from the office. Isolation scores were highest among the work-at-home group (mean 3.1, SD 1.1), higher than the office group (mean 2.4, SD 0.9), and lowest in the telecommuting group (mean 1.7, SD 1.0), and the ANOVA showed a significant difference of group (F = 5.82, p = 0.007). |
| 85. | University of Exeter 2020116 | Y | UK Working from home |
Survey Cross-sectional |
Wellbeing | Working from home: loneliness, increased demands to juggle work and domestic responsibilities (incl. child care) – negative effect on wellbeing. More anxious, less enthusiastic about job due to pandemic. Also lower wellbeing due to increased job insecurity, the unpredictability of future workloads, new ways of working and a lack of support from employers. |
| 86. | Virick 20109 | N | USA Employees |
Survey Cross-sectional |
Life satisfaction | Relation between extent of telecommuting and life satisfaction, with worker type (work drive and work enjoyment) moderating that relation. |
| 87. | Vitterso 200310 | N | Europe (UK, Norway, Iceland, Portugal) Workers |
Mixed: Survey Cross-sectional Qualitative Semi-structured interviews |
QoL | Employees’ sense of belonging increased with a greater number of days working from home (β = 0.30, p < 0.001). There were no significant impacts of WFH on control, flexibility or concentration in this model. |
| 88. | Waizenegger 202043 | Y | Worldwide | Qualitative. Semi-structured interviews | Experiences of home workers | Impact of working from home during COVID: no choice, health concerns, spaces shared with others. Participants’ mental and physical wellbeing was (equally) affected by a lack of PA, due to sports facilities being closed and minimal contact with others being allowed. |
| 89. | Weitzer 202139 | Y | Austria General population |
Survey Cross-sectional |
QoL | Working from home: positive effect on QoL, negative effect on perceived productivity. Older participants, men, university educated and persons not working from home were most likely to report no changes in QoL. Those who worked from home all the time were more likely to report an increased QoL compared with those who were not working from home (OR 3.69, 95% CI 1.86 to 7.29). Working part of the time from home was also associated with an increased QoL compared with not working from home (OR 2.07, 95% CI 1.09 to 3.91). |
| 90. | Wickens 2021117 | Y | Canada Adults |
Survey Cross-sectional |
Depressive symptoms | Working from home depressive symptoms lower than laid off / not working. After adjusting, from home was not a significant predictor of depressive symptoms (adjusted OR 1.16, 95% CI 0.75 to 1.77). |
| 91. | Wilke 202144 | Y | Worldwide Adults |
Survey Cross-sectional |
Mental wellbeing | Working outside the home vs. working remotely was associated with clinically relevant reductions in mental wellbeing (OR 1.29, 95% CI 1.16 to 1.44), as was working both outside the home and remotely vs. working remotely (OR 1.35, 95% CI 1.23 to 1.47). No factors associated with physical wellbeing (bodily pain) were found for work mode (p = 0.76). |
| 92. | Wöhrmann 202111 | N | Germany White-collar workers |
Survey Cross-sectional |
Wellbeing Psychosomatic health complaints |
No significant correlations were found between telework and psychosomatic health complaints. |
| 93. | Wood 202110 | Y | UK University staff |
Qualitative. Diary study | Wellbeing | Autonomy and social support associated with wellbeing. Loneliness was associated with working from home. Wellbeing was affected by the enforced nature of home working. |
| 94. | Xiao 202145 | Y | USA Newly WFH |
Survey Cross-sectional |
Physical and mental wellbeing | Compared with pre- working from home, mean ratings were decreased for overall physical and mental wellbeing. Compared with pre- working from home, mean ratings were decreased for overall physical (2.84, SD .87) and mental (2.70, SD 0.93) wellbeing. Overall PA and physical exercise decreased, and overall food intake increased (although this was the same for ‘healthy’ and ‘junk’ food). |
| 95. | Xue 202139 | Y | UK Working parent couples |
Prospective cohort Survey |
Unpaid care work Psychological distress |
Increased housework and childcare/home-schooling hours were (weakly) associated with higher levels of psychological distress (assessed on the General Health Questionnaire) among women (and lone parent women more so). Adapting work patters due to childcare/ home-schooling was associated with 1.39 (95% CI 0.403 to 2.382) higher GHQ scores in women and 1.16 (95% CI 0.296 to 2.015) higher GHQ scores in men. Being the only member of the couple to adapt working pattern to accommodate childcare was associated with 1.82 higher GHQ scores (95% CI 0.669 to 2.973) in women and 2.48 higher GHQ scores (95% CI 1.367 to 3.601) in men. Lone mothers who adapted work patterns to accommodate childcare/ home-schooling had on average 3.93 higher GHQ scores (95% CI 1.639 to 6.223; p = 0.001) than lone mothers who did not adapt work patterns. |
| 96. | Yoshimoto 202146 | Y | Japan Workers |
Survey Cross-sectional |
Pain conditions, PA psychological stress | Starting or increasing telework was significantly associated with pain augmentation in a logistic regression analysis (OR 2.32, 95% CI 1.79 to 3.02), including after adjustment for confounding factors (adjusted OR 2.27, 95% CI 1.68 to 3.06). Decreasing PA strengthened this association. |
FIGURE 1.
Study selection.

For reasons of clarity, due to the large number of studies excluded at the full paper stage the reasons for exclusion of each individual paper are provided in the Supplementary Material. These included: WFH not a focus (n = 70), not clear that the samples were WFH (n = 4), not examining association between WFH and health/wellbeing (n = 44), comparison of those WFH with another population (n = 6), no health or wellbeing outcomes (n = 89), population students (n = 4), population teachers (n = 22), non-OECD country (n = 17), language not English (n = 15), not a study/no data (n = 21), unpublished thesis or presentation (n = 5).
Typology of included studies
Of 96 studies which were found to meet the inclusion criteria for the review, 30 studies were published before the COVID-19 pandemic (or using data from before the COVID-19 pandemic, without making particular reference to it) and a further 66 were published during the pandemic (and made specific reference to COVID-19 and the pandemic influence on home working). This demonstrates the significant increase in the evidence base throughout 2020–2021 as a result of working from home in the pandemic.
Most of the included literature was published in 2020/21 (a total of 70 studies). Again, this reflects the substantial increase in relevant evidence as a result of the COVID-19 pandemic. One included study was a pre-print with a 2022 publication date. The remaining 25 studies were published between 2019 (five studies) and 1994 with only 13 studies published prior to 2016.
Quality of evidence
Overall, the quality of evidence was limited by the study designs employed by the authors, with the largest majority of studies being cross-sectional surveys (n = 59), mostly conducted online during the COVID-19 pandemic (see Table 3. Study designs of included studies) where remote methods such as online surveys were particularly common. These studies are limited by nature of their lack of follow-up data and the fact that they mostly used convenience sampling. Qualitative and mixed-method studies (which collected data via surveys and interviews) were the second most common type of research method employed, and these were more frequent prior to the pandemic. A small number of both prospective and retrospective cohort studies were also identified, along with a few ecological/observational studies (variably described by authors). Most studies scored reasonably on the quality appraisal tools for their study type. No studies were excluded on the basis of quality. The quality appraisals for each study are given in Appendix 2: Quality appraisals of included studies.
| Study design | Number of studies |
|---|---|
| Survey cross-sectional | 59 |
| Survey cross-sectional plus diary and accelerometer data |
1 |
| Longitudinal survey | 4 |
| Mixed: survey and qualitative | 5 |
| Qualitative interviews / focus groups | 12 |
| Qualitative ethnography | 4 |
| Prospective cohort study | 4 |
| Retrospective cohort | 3 |
| Quasi-experimental | 1 |
| Ecological/observational study | 3 |
For the most part, for studies which collected quantitative data, measures were self-reported. A small number of studies used validated scales to measure specific outcomes such as wellbeing, quality of life (QoL), general health, anxiety and depression. Therefore, overall due to the study designs identified, causation could not be inferred and only associations between factors are considered.
Country of origin
The countries with the highest number of included studies were the UK (n = 27 including grey literature), USA (n = 25) and Italy (n = 10), although overall there was a broad spread of countries, with 21 individual countries mentioned in the populations of included studies. Four studies described their population as ‘worldwide’ or recruited from a large list of countries. The full list of included study countries is given in Table 4. Location of included studies. Some non-OECD countries are listed where studies recruited from several countries and the majority of the sample came from within the OECD.
| Country of study | Total |
|---|---|
| UK | 27 |
| USA | 25 |
| Italy | 11 |
| Sweden | 6 |
| Spain | 4 |
| Japan | 4 |
| Germany | 4 |
| Worldwide/many | 4 |
| Canada | 3 |
| Austria | 1 |
| Turkey | 1 |
| Portugal | 1 |
| Norway | 2 |
| Estonia | 2 |
| Poland | 1 |
| Netherlands | 2 |
| Mexico | 1 |
| Ireland | 1 |
| France | 1 |
| Denmark | 1 |
| Belgium | 1 |
| New Zealand | 1 |
Most authors described their population as ‘workers’ or ‘employees’, limited their recruitment to ‘home workers’ or ‘e-employees,’ or surveyed the population in general. One study specifically considered those who were self-employed and working at home (Hislop et al. 201521), with a second conducted with home-based childcare workers (Stitou et al. 201831). Both these studies dated from before the COVID-19 pandemic.
Some studies limited their populations to particular employment sectors or occupations, including the financial sector (Henke et al. 2016,20 Taser et al. 2022113), public sector workers (Hornung et al. 2009,5 Di Tecco et al. 202135, Moretti et al. 202041), the IT sector (Kaduk et al. 2019,6 Russo et al. 2021110), journalists (Mann et al. 200325), private-sector companies (Trent et al. 199434), ‘white-collar workers’ (Wöhrmann et al. 2021,11, Mari et al. 2021,106 Lundberg and Lindfors 200224), office workers (Argus et al. 202140), the water sector (Cotterill et al. 202050), ‘professional services’ (Delfino and van der Kolk 2021,52 Mellner et al. 201726), university employees (Docka‐Filipek et al. 202,61 Gao and Sai 2020,62 Heiden et al. 2021,100 Wood et al. 202110) and mental health service staff (Bentham et al. 202148). It is likely that some of these populations were chosen due to convenience (e.g. university employees) rather than a strategic judgement that they were a population of particular interest or at greatest risk of poor health outcomes.
Six studies limited the population under study by other variables, including home working mothers (Clark et al. 2021,60 Limbers et al. 202066), female academics (Gao and Sai 202062), care-givers (Janssen et al. 202065) and couples with children (Shockley et al. 2021,29 Xue et al. 202139). These were all studies conducted during the COVID-19 pandemic. One study using data collected prior to the pandemic looked at men only (Charalampous 202112).
Related literature
A further 14 studies [not included in the above numbers] considered the impact of the COVID-19 pandemic on classroom (school or further/higher education) teachers teaching online during school closures as a result of COVID-19 restrictions, where they had not experienced this before. Six additional studies looked at differences in health-related outcomes for people working at home compared to those who had retired or lost their jobs. These studies are provided in the supplementary material, but are not included in the analysis of this report. This decision was taken so as not to bias the review findings towards studies which were not directly relevant to the research question, or studies which focused on a particular COVID-19 lockdown situation (online teaching as a result of lockdown home schooling) which would not be relevant beyond that particular context.
Factors and relationships identified in the included studies
To aid analysis, the papers were categorised in terms of those published prior to and during the COVID-19 pandemic, and separated into those relating to overall health and physical health, or mental health and wellbeing. This was done in order to begin to categorise the data available. The factors reported in the papers were also developed into mind maps to give a visual representation of the volume, direction and consistency of the reported association for each group of outcomes. Factors which have a positive impact on the primary outcome are coloured blue on the mind maps, with negative factors (where there is a negative impact on the primary outcome) represented in orange, and where the authors specifically report no association between the factors black boxes and lines are used. The primary factors in each mind map (e.g. working from home and wellbeing) are highlighted in bold text. Where associations between the primary factors were inferred by the authors rather than directly measured in their study, the relationship has been added to the mind map using a dotted line. Solid lines represent directly reported factors. The identification numbers for each study used in the mind maps are given in the summary table (see Table 2. Summary table of included studies). For the final summary mind map of the factors which influence the associations between working from home and wellbeing in the COVID-19 papers, the assumed lines were removed as the intention here was to provide as much clarity as possible on the reported factors given the huge complexity of the initial mind map for those studies.
Pre-COVID studies
General health
Prior to the COVID-19 pandemic, the evidence base for the impact of working from home on overall health was limited. We identified only seven studies which considered these factors (Hornung et al. 2009,5 Vitterso et al. 2003,10 Virick et al. 2010,9 Kaduk et al. 2019,6 Sardeshmukh et al. 2012,8 Perry et al. 2018,7 Wöhrmann et al. (2021)11). The factors reported in these studies are summarised in Table 5. Reported factors which influence the associations between working from home and general health (pre-COVID-19 papers), and Figure 2. Mind map of factors which influence the associations between working from home and physical or general health (pre-COVID-19 papers).
| WFH factor | Linked to outcome | Direction | Moderators | Study ID |
|---|---|---|---|---|
| QoL (increased) | Overall health | Positive effect | Autonomy Work family conflict Hybrid work Isolation |
40, 87 |
| Life satisfaction (increased) | Overall health | Positive effect | Work drive and work enjoyment | 86 |
| Psychosomatic health | Overall health | No effect | 92 | |
| Exhaustion | Overall health | Negative effect | Job demands | 71 |
| 62 | ||||
| Strain | Overall health | Negative effect | 62 | |
| Burnout, stress, conflict | Overall health | Negative effect | 46a |
FIGURE 2.
Mind map of reported factors which influence the associations between working from home and physical or general health (pre-COVID-19 papers). Key: Positive effect, Negative effect, No effect. See Table 2 for index of studies.
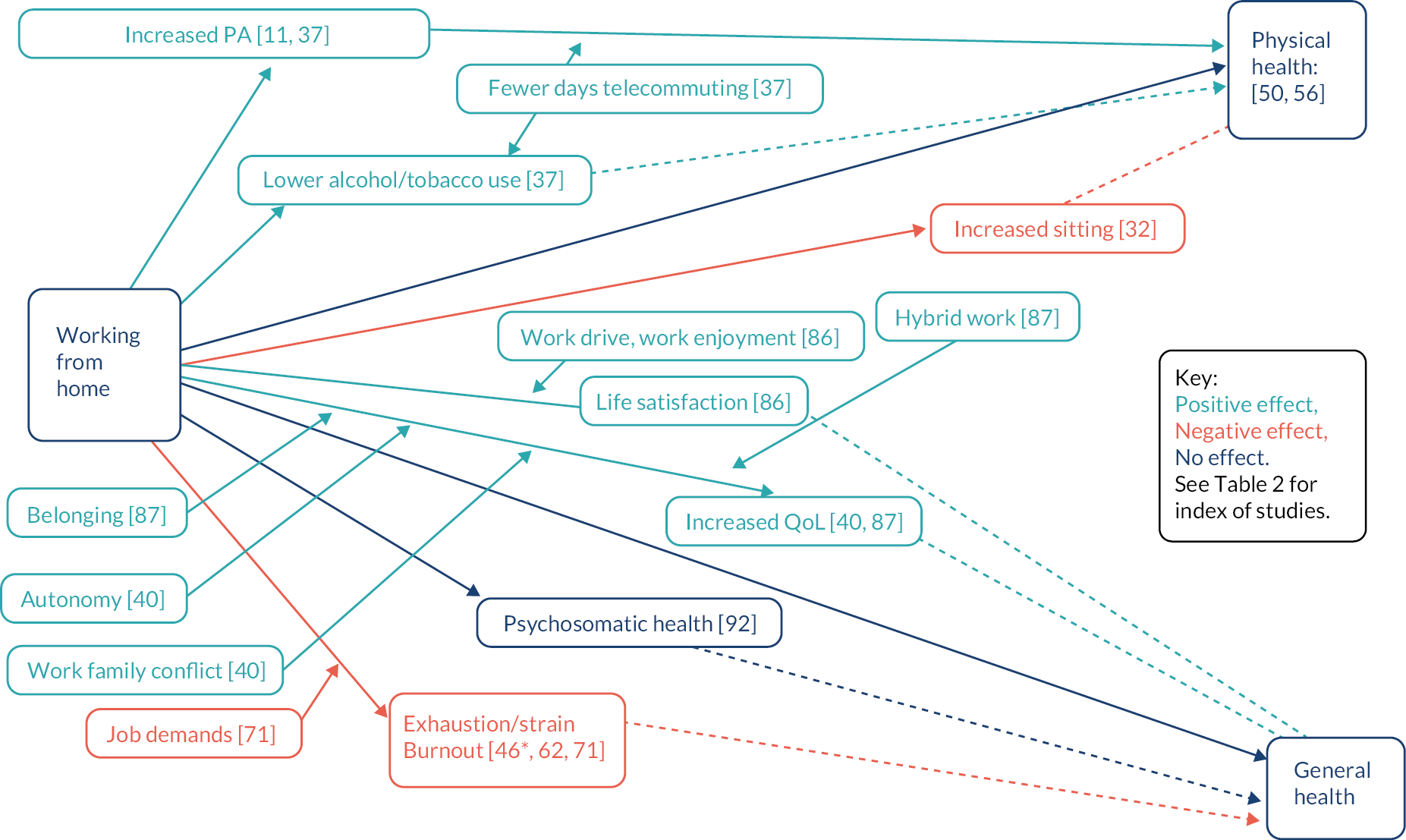
Two cross-sectional survey studies (Hornung et al. 20095, Vitterso et al. 200310) both demonstrated a positive effect on QoL from working at home, although factors which mediate this effect included autonomy and work–family conflict (Hornung et al. 20095), along with a sense of belonging versus isolation (Vitterso et al. 200310). The intensity of telecommuting was also considered, with hybrid working arrangements being seen to be most positive in both studies.
Hornung et al. (2009)5 conducted their study with German public administrators (including teleworkers and non-teleworkers). Their postal survey (n = 1008) had a response rate of 67% and was analysed using structural equation modelling. The workers were 27.5% female with a mean age 43.6 (SD 8.8); 62.6% had a teleworking arrangement (1–4 days per week, mean 1.7 (SD 1.1) days). QoL was assessed using the WHOQOL-BREF, and autonomy, work–family conflict and job satisfaction were also measured. There were small but statistically significant positive effects of telecommuting intensity on QoL mediated via both autonomy (βindirect = 0.02, z = 2.56, p < 0.01) and work–family conflict (βindirect = 0.11, z = 5.96, p < 0.01).
Vittersø et al. (2003)10 conducted their survey in Europe (UK, Norway, Iceland, Portugal) via self-administered questionnaires with a response rate of 41%. A subset of qualitative interviews on a more focused set of issues were also undertaken but there were no details on the collection or analysis of qualitative data. Workers (n = 217) were selected from companies where ‘teleworking seemed possible / likely’ (including those who did and did not telework). The sample means age was 38.25 years. Subjective QOL was assessed using the CHP’s QoL Profile, measuring four dimensions (three of human growth and one of overall life satisfaction) on a 5-point scale. Employees’ sense of belonging increased with a greater number of days working from home (β = 0.30, p < 0.001). There were no significant impacts of WFH on control, flexibility or concentration in this model. Those who had worked for a whole week at home described it as an ‘isolating experience’.
A positive effect on life satisfaction was observed with working at home by one further cross-sectional survey study, again mediated in the same way by the hybrid working approach (Virick et al. 2010)9. Virick et al. (2010)9 conducted an online survey with 85 telecommuters working for a large telecoms organisation in the USA. They were mostly male (75% male) with a mean age of 41.5 (SD 9.15) years. Life satisfaction was assessed using a four-item validated scale. The extent of telecommuting was assessed using an item asking respondents to estimate the average number of days worked from home (1–6 scale). They also assessed job satisfaction, worker types, perceived performance outcome orientation and control variables (tenure and gender). A ‘curvilinear relationship was identified’, whereby ‘for employees with high drive and low enjoyment, life satisfaction is low when there is a moderate amount of telecommuting. However, with other employees, the relation is the opposite. Life satisfaction is high when there is a moderate amount of telecommuting’. Therefore drive and enjoyment moderate the relationship between telecommuting and life satisfaction.
Exhaustion, strain and the risk of burnout were reported as negative effects of working at home by three cross-sectional surveys, one of which also included a longitudinal element for some participants (Kaduk et al. 2019,6 Sardeshmukh et al. 2012,8 Perry et al. 20187) The associations were made worse by high job demands (Sardeshmukh et al. 20128). Importantly, Kaduk et al. (2019)6 were the only authors to consider the difference between voluntary and involuntary working from home in the pre-COVID era. In addition, Wöhrmann et al. (2021)11 found no significant correlations between telework and psychosomatic health complaints. Their study was based on data collected in 2015.
Kaduk et al. (2019)6 conducted an in-person survey of IT workers (Fortune 500 companies) in the US (n = 758) with a 69.6% response rate. Six wellbeing outcomes of work–family conflict, job satisfaction, turnover intentions, emotional exhaustion (burnout), perceived stress and psychological distress were considered. Over 95% of employees reported doing some work at home; 31% do at least 20% of working time at home (‘substantial remote work’) voluntarily and 14% involuntarily. They reported that involuntary variable schedules are associated with greater work-to-family conflict, stress, burnout and turnover intentions, and lower job satisfaction in models that adjust for personal characteristics, job, work hours, family demands and other factors. Voluntary remote work was found to be protective, and associated with less stress (although this relationship was attenuated in the full models).
Sardeshmukh et al. (2012)8 surveyed telecommuters working for a large supply-chain-management company in the Midwestern USA (n = 417) with a 37.9% response rate. The sample were 29% female, with mean age 26–35 years. They had spent at least 1 year teleworking on average, spending 8–40 hours a week teleworking and most telecommuting less than 4 days per week. Exhaustion was assessed using the Maslach and Jackson validated scale. They also assessed time pressure, role ambiguity, role conflict, autonomy, feedback, social support and job engagement. They found that telework is negatively related to both exhaustion and job engagement. Job demands and resources (time pressure, role ambiguity, role conflict) partially mediated the relationship between the extent of telework and exhaustion.
Wöhrmann et al. (2021)11 reported on a telephone survey (described as large-scale, population-level) undertaken in 2015 in Germany with highly qualified white-collar workers aged below 65 years who reported the use of modern information and communication technology for their work. The sample were 49% female, with mean age 46.2 (SD 10.2) years. Of these, 18% teleworked, with an average of 1.92 days per week. Psychosomatic health complaints were assessed by aggregating into an index and included headache; fatigue, weariness or lassitude, stomach and digestion complaints, tension and irritability, sleep disorders, dejection, physical exhaustion and emotional exhaustion. Participants rated whether they occurred frequently in the last 12 months on work days. No significant correlations were found between telework and psychosomatic health complaints. They note that generalisability may have been limited by the disproportionately small numbers of teleworkers in Germany at the time of the survey (in comparison with international numbers).
Perry et al. (2018)7 conducted an online cross-sectional survey (with a longitudinal second-wave survey at 3 months for some participants) of full-time professional employees from three southern USA organisations. The overall response rate was not reported. Their sample (n = 258) were 55% female, with mean age 55 years. Emotional stability was assessed by to 10-item subscale of the IPIP Big Five personality scale and strain was assessed by the Oldenburg Burnout Inventory (8 items) to measure exhaustion and disengagement. There was a significant remote work × autonomy interaction for exhaustion, such that there was ‘a positive remote work-exhaustion slope among employees reporting low autonomy (0.82; t = 2.12, p < 0.05) but no significant relationship among those reporting high autonomy (slope = −1.20; t = −1.68, p = 0.10)’ Those with high autonomy and high emotional stability exhibited the lowest overall level of strain compared with other combinations of these predictor variables.
Physical health
The effect of working at home on measures of, or with direct links to, physical health were reported in five studies prior to the COVID-19 pandemic, again, reflecting a limited evidence base for these measures. The factors reported in these studies are summarised in Table 6. Reported factors which influence the associations between working from home and physical health (pre-COVID-19 papers), and Figure 2. Mind map of reported factors which influence the associations between working from home and physical or general health (pre-COVID-19 papers).
| WFH factor | Linked to outcome | Direction | Moderators | Study ID |
|---|---|---|---|---|
| Overall physical health | Physical health | No effect | 56 | |
| Perceived health | Physical health | No effect | 50 | |
| Physical inactivity (decreased) | Physical health | Positive effect | Telecommute intensity (less) | 37 |
| 11 | ||||
| Sitting (increased) | Physical health | Negative effect | 32 | |
| Alcohol use (abuse) (decreased) | Physical health | Positive effect | Telecommute intensity (less) | 37 |
| Tobacco use (decreased) | Physical health | Positive effect | Telecommute intensity (less) | 37 |
The impact on overall physical health (using perceived health / self-reported measures) was neutral for the two studies which considered it (Kroll and Nuesch 2019,103 Mann et al. 200325). These consisted of longitudinal survey data from 1999 and 2009 (Kroll and Nuesch 2019103) and a cross-sectional mixed-methods survey which included semi-structured interviews and a survey (Mann et al. 200325).
Kroll and Nuesch (2019)103 selected a representative sample (n = 6132) of those living in private households in Germany, limited to those aged 20–60 and employees (not self-employed). The analyses of working from home are based on data from the 1999 and 2009 waves, but were analysed as cross-sectional. Perceived health was assessed by the question ‘How would you describe your current health?’, with response options being very good, good, satisfactory, poor, bad. Job satisfaction and leisure satisfaction were each assessed by the question ‘How satisfied are you today with your job/your leisure time?’ Working from home did not have a significant effect on health when controlling for individual heterogeneity (b = 0.02, SE = 0.05, ns). There was also no statistically significant effect of working from home on leisure satisfaction, however (b = −0.01, SE = 0.10, ns).
Mann et al. (2003)25 conducted a study in the USA consisting of qualitative interviews (comparing the emotional impact of work patterns on teleworking and office-based journalists) and a quantitative questionnaire (comparing the occupational stress and health symptoms of office-workers and teleworkers). The study population consisted of eight males and four female (study 1) and 17 males and 15 females (study 2). Teleworking participants followed this working pattern (minimum of 3 days per week) from 3 months to 10 years (average 3 years 2 months) out of a total average working time of 17 years 11 months. Physical health was measured by self-reported frequency of physical symptoms associated with occupational stress. Mental health was measured by the feelings and behaviours that were perceived to be affected by the pressure of the job. There was no significant difference between the physical health scores for the teleworkers and office-workers (t = 1.05, df = 60, ns).
The effect on physical inactivity was mixed, with two studies (a retrospective cohort study and a national cross-sectional travel survey) reporting a positive effect on physical inactivity including increased walking and cycling (i.e. becoming more active) (Henke et al. 201620, Chakrabarti et al. 201892) and one further qualitative (interview) study reported increased sitting as a result of working at home (Grant et al. 201318). Henke et al. (2016)20 also considered the impact on alcohol and tobacco use and reported a decrease in both as a result of working at home. This was moderated by ‘telecommute intensity’, that is, the predicted probability of being at risk appeared to increase with increasing number of telecommuting days.
Chakrabarti et al. (2018)92 conducted a cross-sectional analysis of a national dataset in the USA. Their sample consisted of employed people aged 18–64 (n = 123,810) of whom 62.1% reported telecommuting (‘working at home for an entire work day’). Physical activity (PA) was assessed using the Day Trip File (one-day travel diary) calculated into minutes of PA, assumed to be at least moderate intensity. Telecommuters were classified into ‘frequent’ (more than 4 days over the past month or once per week on average) and ‘occasional’ (1–3 days over the past month). Both frequent and occasional telecommuters engaged in 8–9 minutes more per day of PA than non-telecommuters, on average; 31% frequent, 27% occasional and 21% non-telecommuters met or exceeded the 30 minutes per day activity target.
Grant et al. (2013)18 conducted in-depth interviews (n = 11) with UK e-workers, across five organisations and three sectors. All participants worked remotely using technology independent of time and location for several years. The focus of this study was on wellbeing. However, amongst the many wellbeing outcomes measures (discussed elsewhere in this report), it was noted that sitting behaviours may increase as a result of working from home.
Henke et al. (2016)20 conducted a longitudinal cohort study (retrospective) of employee data at one USA insurance firm from 2010 to 2011 (n = 3703). The sample were 62% female, 88% aged less than 55 years, 58% were prime-time telecommuters, 20% were off-hour telecommuters and 22% were non-telecommuters. The physical health outcome considered was ‘high risk for physical inactivity’ (reported less than 3 days of cardiovascular exercise per week). In 2011 a greater proportion of non-telecommuters were at risk of obesity, poor nutrition, physical inactivity (not statistically significant) and tobacco use. ‘Prime-time telecommuters’ (described as those with at least 51% of remote hours during prime work hours of 06.00–18.00) working at least 73 hours per month (very high intensity) had a significantly lower risk of alcohol abuse compared with non-telecommuters (1.8% vs. 2.9%). Prime-time telecommuters working 9 to 32 hours per month (medium intensity) had a significantly lower risk of physical inactivity compared with non-telecommuters (35% vs. 41%). Prime-time telecommuters working 33 to 72 hours per month (high intensity) had a significantly lower tobacco risk compared with non-telecommuters (4.5% vs. 7.2%).’
Mental health and wellbeing
A more substantial volume of evidence exists which consists of 24 studies considering the effects of working at home on a broad range of wellbeing and mental health-related measures prior to the COVID-19 pandemic. The factors reported in these studies are summarised in Table 7. Reported factors which influence the associations between working from home and wellbeing and mental health (pre-COVID-19 papers) and Figure 3. Mind map of reported factors which influence the associations between working from home and wellbeing or mental health (pre-COVID-19 papers).
| WFH factor | Linked to outcome | Direction | Moderators | Study ID |
|---|---|---|---|---|
| Wellbeing (increased) | Wellbeing | Positive effect | 33 | |
| Control over workspace/time (increased) | Wellbeing | Positive effect | 38, 56, 80, 81 | |
| Work undisturbed (increased) | Wellbeing | Positive effect | 80 | |
| Happier | Wellbeing | Positive effect | 12 | |
| Fear of tech failure (increased) | Wellbeing | Negative effect | 18 | |
| Stress | Wellbeing | Positive effect | 12, 46, 56, 77, 81 | |
| Less office politics | 37,56 | |||
| No travel to work | 56 | |||
| More control over work | 56 | |||
| Telecomm intensity (less) | 37 | |||
| Negative effect | Increased blood pressure, urine and saliva measures | 71 | ||
| 46a, 64 | ||||
| More hours worked | 64 | |||
| Family interference | 64 | |||
| Female | 64 | |||
| Non white | 64 | |||
| Low income | 64 | |||
| Low health status | 64 | |||
| Spouse in home | 64 | |||
| No effect | 84 | |||
| Childcare stress (decreased) | Wellbeing | Positive effect | 32 | |
| Travel stress (decreased) | Wellbeing | Positive effect | 32 | |
| Depression (decreased) | Wellbeing | Positive effect | 37 | |
| Positive affect (increased) | Wellbeing | Positive effect | Better coping | 3 |
| Openness to experience | 3 | |||
| Greater social connectedness | 3 | |||
| Emotional ill health (increased) | Wellbeing | Negative effect | 56 | |
| Psychosomatic health | Wellbeing | No effect | 12 | |
| Psychological strain (decreased) | Wellbeing | Positive effect | Reduced social isolation | 7 |
| Psychological detachment | Wellbeing | No effect | 58 | |
| Fulfilment (increased) | Wellbeing | Positive effect | Autonomy | 18 |
| Interference with family life (increased) | Wellbeing | Negative effect | 12, 78 | |
| Sense of perpetual contact (increased) | Wellbeing | Negative effect | 38 | |
| Self-imposed pressure to perform (increased) | Wellbeing | Negative effect | 16 | |
| Adult contact (decreased) | Wellbeing | Negative effect | 78 | |
| Social life (improved) | Wellbeing | Positive effect | 44 | |
| Social interaction (decreased) | Wellbeing | Negative effect | 16, 48, 12 | |
| Communication with colleagues | Wellbeing | Positive effect | 32, 12 | |
| Support from colleagues | Wellbeing | Positive effect | 32, 56 | |
| Office grapevine (decreased) | Wellbeing | Negative effect | 32 | |
| Life satisfaction | Wellbeing | No effect | Gender (no effect) | 66 |
| Type of employment (no effect) | 66 | |||
| Leisure time satisfaction (increased) | Wellbeing | Positive effect | 66 |
FIGURE 3.
Mind map of reported factors which influence the associations between working from home and wellbeing or mental health (pre-COVID-19 papers). Key: Positive effect, Negative effect, No effect. See Table 2 for index of studies.

There was no clear overall pattern to the factors which influence the associations reported between working at home and the broad range of wellbeing measures investigated by study authors prior to the COVID-19 pandemic. This lack of clarity highlights the complexity in the relationships being considered, and indicates how people are likely to experience working at home differently depending on their circumstances. A range of factors relating to overall wellbeing, depression and other mental health measures, measures of stress, control over the workspace (including ability to work undisturbed, interference with family life in the home, and fears associated with technology failure), social contact, communication with colleagues, and measures of satisfaction and fulfilment were considered. The evidence was from self-reported data collected via surveys, qualitative interview studies and retrospective cohort studies.
Wellbeing and mental health measures
Wellbeing as a result of working at home was reported by one survey to have increased overall (Hall et al. 201917) as rates of depression were reportedly reduced for some telecommuters in a further retrospective cohort study (Henke et al. 201620). Positive affect was also shown to increase with working at home and this was furthered by having better coping skills, being more open to new experience and having greater social connectedness (Anderson et al. 201413), as was a decrease in ‘psychological strain’ further enhanced by reduced social isolation (Bentley et al. 2016)14. However, Mann et al. (2003)25 conversely reported that emotional ill health increased for those working at home (survey and semi-structured interviews). Further, Mellner et al. (2017)26 found no effect on ‘psychological detachment’, and Charalampous et al. (202112) found no effect on psychosomatic health for home workers.
Hall (2019)19 in their online survey of UK employees who work two or more days a week from home (n = 897) stated that ‘homeworking can increase employee engagement, job satisfaction and wellbeing’. However, their research question was not clear and the paper contained very little detail. Henke et al. (2016)20 conducted a longitudinal cohort study (retrospective) of employee data at one USA insurance firm from 2010 to 2011 (n = 3703). The sample were 62% female, 88% aged less than 55 years, 58% were prime-time telecommuters, 20% were off-hour telecommuters and 22% were non-telecommuters. They reported that those who telecommuted for less than 8 hours per month (low-intensity telecommuters) were likely to reduce their rate of depression at a greater rate than non-telecommuters over time.
Anderson et al. (2014)13 in their survey of a ‘large US federal agency’ (n = 102) measured outcomes on the ‘Job-Related Affective Well Being Scale’. They also measured openness to experience, trait rumination and sensation-seeking, and social connectedness outside the workplace. They report that the relationship between telework and positive affect is moderated by one’s social connectedness outside of the workplace such that the relationship becomes more positive as social connectedness increases (γ = 0.75, p < 0.001); also individuals experience less negative affect while teleworking as social connectedness increases (γ = −0.73, p < 0.01). In addition, Bentley et al. (2016)14 in their online survey of ‘knowledge workers’ in New Zealand (n = 804, 47% female, mean age 30.9 (SD 11.4) found that psychological strain was significantly predicted by organisational social support (this did not differ significantly between hybrid and low telework (1–7 hours) and teleworker support (although this was only significant in the whole sample and not in the hybrid and low telework sub-samples)). Mann et al. (2003),25 described above, found there was a significant difference between the mental health scores of home and office workers f (t = 1.85, df = 60, p < 0.05), indicating higher levels of emotional ill health for the teleworkers.
Charalampous et al. 202112 conducted semi-structured interviews with 40 (23 male) remote e-workers working for a British IT company (mean age of 46.86 (SD = 8.43)) to explore the impact of the remote e-working experience on employees’ wellbeing. Regarding individuals’ psychosomatic health, they report that ‘it appeared that none of the employees reported serious and exaggerated health conditions resulting from remote e-working’. However, increased sedentary behaviours combined with the absence of breaks was a prominent risk factor for psychosomatic health. Regardless of the risk of not taking enough breaks, and not having appropriate ergonomics, interviewees suggested that a healthier lifestyle was available to them. Mellner et al. (2017)26 conducted an online survey with Swedish professionals working in one of four large organisations (n = 3846, 62% male, mean age 48 years). Working from home was negatively related with sleep duration: This is reported as follows: ‘In this context [of boundaryless working conditions], not being able to free oneself from work-related feelings and thoughts during leisure may be interpreted as the dark side of freedom as employees run the risk of working “anytime – all the time”, and as such, of “always being on” resulting in disturbed sleep.’
Stress
A significant number of studies considered how stress influences the association between working at home and health, with a similar number of studies reporting positive and negative effects. Working at home was reported to have a positive association with self-reported stress (i.e. stress was reduced as a result of working from home) in six studies (including cohort and survey and qualitative studies) (Henke et al. 2016,20 Kaduk et al. 2019,6 Mann et al. 2003,25 Song et al. 2020,30 Tietze et al. 201129). These positive relationships were further enhanced by having less office politics (Henke et al. 201620 and Mann et al. 200325), no travel to work (Mann et al. 200325), more control over work (Mann et al. 200325) and by reduced telecommute intensity (hybrid working) (Henke et al. 201620). A reduction in specific stress related to childcare and travel was also reported in one final qualitative study (Grant et al. 201318). Conversely perceived stress was negatively associated with working at home in two studies (survey and retrospective cohort) (Kaduk et al. 2019,6 Ray et al. 202127). Kaduk et al. (2019)6 reported that the negative association was made worse by working more hours, family interference in work and having a spouse in the home, being female or non-white, and having low income or low health status. Stress was linked to issues with technology by Charalampous et al. (2021)12. In addition Trent et al (1994)34 found no association between working from home and stress in their survey study.
In addition, one further observational study objectively measured levels of physiological stress response by taking blood pressure readings along with urine and saliva samples (Lundberg and Lindfors 200224). They reported no significant difference in self-rated stress between telework and office work; however, blood pressure was significantly higher during work at the office than when teleworking at home, and men had significantly elevated epinephrine levels in the evening after telework at home.
Ray et al. (2021)27 reported on a USA-based, face-to-face nationally representative survey (n = 7400, mean age 42.8 years, 52% female). The proportion working from home increased from 29% in 2002 to 33% in 2018 (remaining stable from 2010 onwards). In regression analyses, working from home was associated with a 22% increase in job stress and a 65% increase in job satisfaction (p < 0.01). This was modified by sex (women were 38% more likely to report job stress and 5% less likely to report healthy days than men), ethnicity (compared with non-Hispanic Whites, Hispanic workers were 32% less likely to report job stress, 5% more likely to report healthy days and 39% less likely to report days with activity limitations; Black workers were 40% less likely to report job stress and 4% more likely to report healthy days; and Asian workers were 36% less likely to report job stress and 4% more likely to report healthy days).
Song et al. (2020)30 conducted telephone interviews and time use survey with workers in the USA (n = 3962). Telework on weekdays or weekends/holidays was associated with more stress (p < 0.005) than working only in the office. Tietze et al. (2011)29 conducted interviews and focus groups with people working in local authorities in the UK. Pre-implementation, participants expected to gain better personal wellbeing form working from home, particularly in relation to being calmer and less stressed. Post-implementation, this expectation was realised for many participants, who felt less stressed and more relaxed. Some attributed it to escaping ‘bickering and gossiping’ in the office.
Trent et al. (1994)34 conducted a mailed survey with people working at private-sector companies in the USA (n = 38; 15 telecommuters, mean age 46.3 (SD 7.0); 9 people who worked exclusively from home, mean age 33.8 (SD 6.0); 14 people who worked exclusively from the office, mean age 41.7 (SD 8.6) years). Stress was assessed as perceived social support, assessed using the Social Support Index. There were no differences in perceived stress score between the three groups (telecommuters, those who worked from home, those who worked from the office), although the authors suggest this may be due to the sample size. Isolation scores were highest among the work-at-home group (mean 3.1, SD 1.1), higher than the office group (mean 2.4, SD 0.9), and lowest in the telecommuting group (mean 1.7, SD 1.0), and the ANOVA showed a significant difference of group (F = 5.82, p = 0.007).
Lundberg and Lindfors (2002)24 conducted a ‘repeated measures observational field study’ of white-collar workers at a Swedish government authority who worked 3 days at the office and 2 days per week at home (n = 26, 46% female, mean age 41.7 (SD 11.2) years). Psychophysiological reactivity, using an automatic ambulatory blood pressure monitor on three separate days, was undertaken. Urinary catecholamines and salivary cortisol were also measured at regular intervals during this period. Participants also reported self-rated health and wellbeing (Ryff’s Psychological Well-Being Scales). Women had significantly higher daytime systolic blood pressure (SBP) at the office than during telework or relaxation, but no differences between telework and relaxation. Men had significantly higher daytime SBP at the office than during relaxation at home, but no significant differences between office work and telework, or between telework and relaxation. Women, but not men, had significantly higher daytime DBP during work at the office than during telework. Women had significantly higher daytime epinephrine levels during telework than relaxation, and during office work than relaxation. Men had significantly higher daytime epinephrine levels during office work than relaxation, but not during telework. There were no significant effects of session for cortisol at any time period.
The remaining five studies have been described above. In terms of measures of stress: Henke et al. (2016)20 (longitudinal cohort study, n = 3703) reported that prime-time telecommuters had the highest risk of stress (but this was not statistically significant). Kaduk et al. (2019)6 (in-person survey n = 758) found that involuntary variable home working schedules were associated with greater stress. Voluntary remote work was found to be protective, and associated with less stress (although this relationships was attenuated in the full models). Mann et al. (2003)25 found a significant difference in mental health scores f (t = 1.85, df = 60, p < 0.05), indicating higher levels of emotional ill health for the teleworkers. Grant et al. (2013)18 (described above: in-depth interviews n = 11) reported that working from home can relieve stress from travel and child-care issues. Charalampous et al. (2021) 12 (semi-structured interviews, n = 40) reported that feelings of anger, frustration and stress were mainly linked to issues with technology, or not being able to get hold of colleagues when needed.
Life satisfaction
Factors which influence the associations between working at home wellbeing with measures of life satisfaction were reported in two studies. In a retrospective cohort study, Reuschke et al. (2019)28 reported no effect of working from home on life satisfaction overall, and no mitigation of that relationships by gender or type of employment. However, they did report a positive association between working at home and leisure-time satisfaction. Daniel et al. (2018) 16 reported a positive association between fulfilment and working at home, an association which was further increased by having greater autonomy at work.
Reuschke et al. (2019)28 analysed a large UK longitudinal dataset of people of working age (18–64 years) in either paid employment or self-employment (n = 33,719, 53.7% female); 11.1% (n = 3738) mainly worked from home in at least one wave. Home working was found to be positively associated with health satisfaction in men, but not in women (although this was not significant in their final model). The authors explain this in terms of both home working and self-employment having common elements, namely autonomy and control, and hypothesised that men ‘value these things’ – although this is a clearly subjective viewpoint. For women, both home working and self-employment (as an employer and solo) were significantly positively related to job satisfaction, and home working has an ‘additional’ benefit to the advantages gained from being self-employed. No data are presented in this discursive paper. Daniel et al. (2018) 16 conducted qualitative interviews with online home-based business owners in the UK (n = 23, 65% female). Participants described feeling more fulfilled by having more time and mental space for creativity and creative work, by working online and thus being ‘freed’ from daily face-to-face workplace interactions, which they saw as a distraction. Participants also enjoyed the autonomy of scheduling inherent in working from home (particularly with their own business), for example alternating working patterns to fit around preferences for each day, such as taking an extended lunch break and catching up in the evening.
Social interactions
More links to wellbeing were reported through changes to level of social interactions, with four studies reporting a negative association due to a decrease in social interaction and adult contact as a result of working at home (Charalampous et al. 2021,12 Collins et al. 2016,15 Koehne et al. 2012,23 Stitou et al. 201831). Conversely one study reported improvements in people’s social lives from working at home (Jacukowicz et al. 202022). Communication with and support from colleagues were also reported as critical success factors for working at home (Grant et al. 2013,18 Charalampous et al. 202112). This was further supported by Mann et al. (2003)25.
Collins et al. (2016)15 conducted semi-structured interviews with staff in a local authority in the UK (n = 33, demographics not reported). Teleworkers only had social relationships with office workers whom they already knew and had already met face-to-face. They did not know nor get to know new office staff. There was no social network functionality set up to facilitate interaction between teleworkers. Koehne et al. (2012)23 conducted interviews with individuals working primarily from home, or who worked in the office but had colleagues working from home in the USA, Estonia, UK, Spain and Mexico (n = 17, 29% female). They report that social isolation was an issue for 10/17 participants. Remote workers would counteract this by seeking social interaction in their home communities. Stitou et al. (2018)31 also conducted interviews with female, home-based childcare workers in Canada (n = 11). Factors affecting health and wellbeing were reported as the absence of contact with other adults during working hours, a lack of external help during working hours (i.e. working alone, without breaks), difficulty filling spots, noise, interference with personal and family life, low and precarious remuneration, and incomplete or no benefits.
Jacukowicz et al. (2020)22 conducted an online survey of traditional office workers (n = 200, 60% female) and online workers (n = 189, 82% female) in Poland. Quality of social relationships was assessed using one subscale of the WHOQOL-BREF questionnaire. Working online significantly predicted lower satisfaction with work-life balance (β = –0.17, p < 0.01) but greater quality of social life (β = 0.13, p < 0.05).
Charalampous et al. (2021)12 (semi structured interviews, n = 40) reported that numerous remote e-workers said that it was easy to feel lonely, bored and sad when the social interaction was reduced or eliminated when working at home. Grant et al. (2013)18 coducted in-depth interviews (n = 11), reporting that home working was ‘wellbeing detracting’ as social interaction may be limited to family and local friends. Mann et al. (2003)25 (qualitative interviews) reported that teleworkers emphasise the lack of social support available to talk things through which could produce other negative emotions such as feelings of insecurity and lack of confidence in their abilities.
Control
In terms of the home working environment, positive impacts on wellbeing were reported as a result of having more control over the workspace and times of work (Hislop et al. 2015,21 Mann et al. 2003,25 Thulin et al. 2019,32 Tietze et al. 201129), and having the ability to work undisturbed (Thulin et al. 201932). However, Stitou et al. (2018)31 reported an increase in interference with family life as a result of working from home. Hislop et al. (2015)21 reported a negative association with wellbeing due to a ‘sense of perpetual contact’ arising from working at home and the report of ‘self-imposed pressure to perform’. In addition, ‘fears of technical failure’ and the subsequent negative impact on wellbeing reportedly increased with working from home (Daniel et al. 2018)16.
Hislop et al. (2015)21 conducted qualitative interviews with self-employed home workers undertaking IT-based office support / administrative work in the UK (n = 14, gender/age not reported). The home workers reported being happy with their work, with the main benefit being the ‘spacio-temporal flexibility inherent in homeworking’, They could structure their own time and work location to balance their work with domestic commitments such as shopping and childcare. The negative aspects of home working included increasing people’s sense of ‘perpetual contact’, creating a sense that work was difficult to escape from.
Thulin et al. (2019)32 conducted an online survey in Sweden (n = 456, 70.6% female, mean age 43.2 (SD 10.9) years) with a response rate of 40%. In the logistic regression model for time pressure, never teleworking (β = −0.644, p < 0.05), only teleworking within regular hours (β = −0.866, p < 0.01), age (being older; β = −0.032, p < 0.01), working full time (β = −0.806, p < 0.05) and using a smartphone for private purposes often (β = −1.115, p < 0.05) or all the time (β = −1.089, p < 0.05) were associated with experiencing less time pressure, whereas having children at home (β = 0.406, p < 0.01) was associated with experiencing more time pressure.
Mann et al. (2003)25 (qualitative interviews) reported that teleworkers may experience a decrease in stress attributable to the perception of having control over their work (environment and work schedules). Tietze et al. (2011)33 (interviews and focus groups) reported that working from home made it easier for participants to manage their own workloads and consequently address equity issues and experience improved wellbeing. However, Stitou et al. (2018)31 (interviews, n = 11) reported that factors affecting health and wellbeing included interference with personal and family life. Daniel et al. (2018) 16 (qualitative interviews, n = 23) reported that fear of the IT equipment/online connection failing was ‘pervasive and driven by a fear of being completely cut off’.
COVID studies
As a result of the COVID-19 pandemic and work-at-home orders given as part of lockdown restrictions in many countries, the evidence base on the health impacts of working from home has developed rapidly in the last two years. However, the focus on wellbeing over physical health persists and most studies consisted of cross-sectional survey data with self-reported outcomes.
General health
Even as a result of increased working from home due to COVID-19 the volume of literature linking working at home with general health outcomes has not increased substantially. A further five studies linking the outcomes of QoL, higher demands and lifestyle factors (diet and alcohol intake) show a mixed picture in terms of their impact on the associations with working at home. These associations reported in these studies are summarised in Table 8. Reported factors which influence the associations between working from home and general health (COVID-19 papers) and Figure 4. Mind map of reported factors which influence the associations between working from home and general health (COVID-19 papers).
| WFH factor | Linked to outcome | Direction | Moderators | Study ID# |
|---|---|---|---|---|
| Higher demands | General health | Negative association | Lower education level, higher work demands, management of change | 1 |
| Drug use [no change WFH] | General health | No association | 65 | |
| Diet (improved; more fruit and veg) | General health | Positive association | Gender (women) | 74 |
| Diet (worse) | General health | Negative association | 39 | |
| Alcohol intake (reduced) | General health | Positive association | Gender (women) | 74 |
| QoL | General health | Positive association | Older participants, men, university educated | 50 |
FIGURE 4.
Mind map of reported factors which influence the associations between working from home and general health (COVID-19 papers). Key: Positive effect, Negative effect, No effect. See Table 2 for index of studies.

Quality of life was shown to be positively associated with working at home in a survey by Weitzer et al. (2021)39. Weitzer et al. (2021)39 conducted an online survey of the general population is Austria (n = 1007, 55% female, age 18–65); 29.3% were working from home part of the time and 21.0% were working from home all of the time. Those who worked from home all the time were more likely to report an increased QoL compared with those who were not working from home (OR 3.69, 95% CI 1.86 to 7.29). Working part of the time from home was also associated with an increased QoL compared with not working from home (OR 2.07, 95% CI 1.09 to 3.91). Likewise, not working from home appeared to be associated with decreased QoL compared with working part or all of the time from home. The positive association was strongest for older participants, men, and those who were university educated.
Conversely, general health was shown to be negatively associated with working from home in a prospective cohort study by Di Tecco et al. (2021)35. The association was also negatively affected by lower education level, higher work demands and poorer management of change. Di Tecco et al. (2021)35 conducted a prospective cohort study to investigate the impact of a ‘smart working pilot’ (flexible home working) in Italy (n = 187, 78.6% female, mean age 50.7 (SD 6.8) years). There was no significant change in general health (p = 1.00) or wellbeing (p = 0.247) as a result of the pilot as evaluated by t-tests. In the regression models, significant predictors of wellbeing were demands (−0.703, p = 0.027) and effective management of change (1.461, p = 0.003), and demands (−1.00, SE 0.048, p = 0.037) and higher education (0.238, SE 0.100, p = 0.018) significantly predicted general health.
In terms of lifestyle measures of health, factors which influence the associations between working from home and both an improved diet and reduced alcohol consumption were reported in a survey by Sato et al. (2021b38). These positive associations were seen more strongly in men than women. However, Kubo et al. (2021)36 reported negative associations between working from home and food behaviours including increased solitary eating and lower meal frequency (with more days of telecommuting increasing the negative associations). In considering drug use, Ripoll et al. (2021)37 found no association with working from home (survey study).
Sato et al. (2021b)38 conducted an online survey in Japan (n = 5929, 69% female, mean age 44.0 (SD 13.8)) Working from home was associated with increased intake of vegetables (1.02, 1.004–1.03), fruits (1.06, 1.03–1.09), dairy products (1.03, 1.01–1.06) and snacks (1.04, 1.02–1.06) but decreased intake of seaweeds (0.94, 0.91–0.97), meats (0.98, 0.96–0.999) and alcohol intake (0.93, 0.86–0.997). Among women, time spent on childcare was associated with reduced intakes of vegetables and fruits.
Kubo et al. (2021)36 also conducted an online survey of office workers who telecommuted in Japan (n = 13,468, 48.8% female, age 20–65). Those who telecommuted more frequently tended to have more unfavourable eating habits. Among workers who hardly telecommuted, 25.5% missed breakfast, 25.9% ate all meals alone, 1% ate less than two meals a day, and 6.6% adopted meal substitution. The corresponding proportions among workers who telecommuted in excess of four days per week were 28.7%, 37.0%, 2.5% and 8.4%, respectively. The odds ratios (95% CI) for those who telecommuted at least 4 days per week relative to those who rarely telecommuted were: skipping breakfast: 1.15 (1.03 to 1.29); solitary eating: 1.44 (1.28 to 1.63); lower meal frequency: 2.39 (1.66 to 3.44); and meal substitution: 1.26 (1.04 to 1.51).
Ripoll et al. (2021)37 conducted an online survey in Spain (n = 681, 77% female, age 18 and above). Working from home (compared with other working arrangements) was not associated with increased consumption of psychotropic drugs between weeks 1 and 4 (consumed by 6.5% and 7.1%, respectively, p = 0.306) or weeks 1 and 8 (consumed by 8.4% and 8.9%, respectively, p = 0.952), or consultations to improve mood/anxiety between weeks 1 and 4 (undertaken by 27.3% and 26.9%, respectively, p = 0.918) and weeks 1 and 8 (undertaken by 28.0% and 31.5%, respectively, p = 0.388).
Physical health
The COVID-19 pandemic has also resulted in a slight increase in the number of studies reporting factors which influence the associations between working at home and physical health measures. These factors reported in these studies are summarised in Table 9. Reported factors which influence the associations between working from home and physical health (COVID-19 papers) and Figure 5. Mind map of reported factors which influence the associations between working from home and physical health (COVID-19 papers). Notably all the factors reported had a negative effect on the relationships (or no change in the association was found). This entirely negative framing of the research is not seen in any of the other sets of data considered in this report. In total seven studies considered a range of physical health measures such as physical wellbeing, physical function, physical limitations, musculoskeletal problems, pain, PA and sedentariness and reduced work comfort.
| WFH factor | Linked to outcome | Direction | Moderators | Study ID |
|---|---|---|---|---|
| PA reduced (lockdown) | Physical health | Negative effect | 4 | |
| Reduced work comfort (lockdown | Physical health | Negative effect (musculoskeletal pain) | 4 | |
| Musculoskeletal problems (esp. spine) | Physical health | Negative association | 60 | |
| Working from sofa or bedroom Women |
69 | |||
| Bodily pain | Physical health | No association | 91 | |
| Physical wellbeing | Physical health | Negative association | mental wellbeing, overall PA, physical exercise, ‘healthy’ food intake, and ‘junk’ food intake. | 94 |
| Minimal contact with others Lack of sports facilities open |
88 | |||
| Pain augmentation | Physical health | Negative association | Decreasing PA | 96 |
FIGURE 5.
Mind map of reported factors which influence the associations between working from home and physical health (COVID-19 papers).

A negative association between physical wellbeing and working from home was reported in two studies (survey and qualitative) (Waizenegger et al. 202043 and Xiao et al. 202145). The negative relationship was mediated by poor mental wellbeing, low PA, low ‘healthy’ food intake and high ‘junk’ food intake (Xiao et al. 202145) along with having minimal contact with others due to the lack of sports facilities open during COVID-19 lockdowns (Waizenegger et al. 202043).
Waizenegger et al. (2020)43 conducted a ‘qualitative interpretive study’ of knowledge workers who were previously working in office spaces and worked from home during COVID-19 lockdowns in various countries (n = 33, 39.4% female, aged 20–50). They report that ‘participants’ mental and physical wellbeing was (equally) affected by a lack of PA, due to sports facilities being closed and minimal contact with others being allowed’.
Xiao et al. (2021)45 conducted an online survey in the USA of office workers who had transitioned to WFH during the COVID-19 pandemic (n = 988, 56.6% female, mean age 40.9 (SD 13.1) years). Compared with pre- working from home, mean ratings were decreased for overall physical (2.84, SD 0.087) and mental (2.70, SD 0.93) wellbeing. Overall PA and physical exercise decreased, and overall food intake increased (although this was the same for ‘healthy’ and ‘junk’ food).
In three studies, musculoskeletal problems (especially in the spine) were associated with working from home (Moretti et al. 202041) and starting or increasing telework was significantly associated with pain augmentation (Yoshimoto et al. 202146) which was made worse by decreasing PA, working from a sofa or bedroom and being female (RSPH 202142). Working from home was also associated with a reduction in PA and work comfort, which was further associated with musculoskeletal pain (as a result of lockdown) (Argus et al. 202140). However in one further study, no association between working from home and general body pain was found (Wilke et al. 202144).
Moretti et al. (2020)41 conducted a cross-sectional survey of Italian administrative officers who moved to work online during the COVID-19 pandemic (n = 51, 56.9% female, mean age 46.7 (SD 11.3) years). In relation to health problems, 70.5% of participants reported MSK pain (41.2% back, 23.5% neck, 7.8% shoulder, 7.8% hip, 7.8% knee, 5.9% thigh and 3.9% elbow). Low back pain and neck pain were more severe and interfered more with everyday activities. Neck pain worsened in 50%, improved in 8.3% and was the same in 41.7% of participants, whereas lower back pain worsened in 38.1%, improved in 14.3% and was the same in 47.6% of participants. Home workers without pain reported significantly higher job satisfaction than those with pain.
Yoshimoto et al. (2021)46 conducted an online survey of workers in Japan (n = 1941, 29.5% female, median age 43 (IQR 33, 52)). Starting or increasing telework was significantly associated with pain augmentation in a logistic regression analysis (OR 2.32, 95% CI 1.79 to 3.02), including after adjustment for confounding factors (adjusted OR 2.27, 95% CI 1.68 to 3.06).
Argus et al. (2021)40 conducted an online survey of office workers in Estonia (n = 161, 64.6% female, mean age 38.2 (SD 9.5) years). PA was assessed by the Baecke Physical Activity Questionnaire (BPAQ). Self-reported PA was significantly lower during than before the lockdown, in terms of sport-related PA (mean change in BPAQ −0.52, SD 0.98, 95% CI −0.67 to −0.37, p < 0.001, Cohen’s d = 0.42 (small effect)) and total PA (mean change in BPAI −0.41, SD 1.37, 95% CI −0.62 to −0.19, p < 0.001, Cohen’s d = 0.26 (small effect)), but not leisure-time PA (mean change in BPAQ −0.07, SD 0.59, 95% CI −0.16 to 0.02, p = 0.15, Cohen’s d = 0.11), and work-related PA significantly increased (mean change in BPAQ 0.18, SD 0.54, 95% CI 0.10 to 0.26, p < 0.001, Cohen’s d = 0.50 (medium effect)). There was a significant negative correlation between change in self-reported sports-related PA and change in the numbers of body regions with MSP during the lockdown (r = −0.206, p < 0.01). The number of body regions with MSP onset during the lockdown was also negatively correlated with change in workplace comfort score (r = −0.262, p < 0.001) and change in workplace ergonomics score (r = −0.231, p < 0.01).
Wilke et al. (2021)44 conducted an online survey of people aged 18 plus in 14 countries worldwide with confinement measures limiting movement in public spaces (n = 14,975, 58.1% female, mean age 38 (SD 15) years). Physical wellbeing, assessed using the bodily pain subscale of the SF-36, two items on musculoskeletal pain (6-point scale) and the resulting disability (5-point scale).No associations with physical wellbeing (bodily pain) were found for work mode (p = 0.76).
Mental health and wellbeing
The largest volume of evidence identified consisted of studies conducted during the COVID-19 pandemic which looked at factors which influence the associations between working from home and measures relating to mental health and wellbeing. The factors reported in these studies are summarised in Table 10. Reported factors which influence the associations between working from home and wellbeing or mental health (COVID-19 papers) and Figure 6. Mind map of summary factors which influence the associations between working from home and wellbeing or mental health (COVID-19 papers). A broad range of measures relating to wellbeing were used by study authors including direct measures of wellbeing, and measures of mental health (including negative affect, anxiety, depression, psychological distress), and stress (including perceived stress, perceived self-efficacy, ‘stress, worry and pressure’, burnout, ‘cognitive worsening’ and specific stress including parenting stress and occupational stress). Measures linked to wellbeing included the lifestyle behaviours sleep (sleep quality time sleeping and fatigue), alcohol use and PA (opportunity to exercise, sedentariness, standing and movement, lack of sports facilities open). Increased health concerns were also reported, as were factors linked with social interaction (social isolation, loneliness, minimal contact with others and social support). Satisfaction with working from home (including sense of worthwhile life) and QoL measures were also reported. Lack of choice over whether to WFH along with work autonomy and measures linked to videoconferencing (videoconference fatigue and technostress) were also considered in respect to wellbeing. Further measures linked to the home work environment and wellbeing included feeling in control of time, lack of commute, more time with the family, lower work/family conflict, and spaces shared with others. Openness to new ways of living was also included.
| WFH factor | Linked to outcome | Direction | Moderators | Study ID |
|---|---|---|---|---|
| Wellbeing | Wellbeing | No association | 1, 17, 23 | |
| Presence of dogs or cats in home | 39 | |||
| Dependents in home | 6 | |||
| 31 | ||||
| Domestic labour | 25 | |||
| Negative association | Higher job demand during pandemic Not feeling ‘sheltered at home’ Smoking more cigarettes during pandemic More psychological distress. |
19 | ||
| Increased monitoring Expectation to always be available Increased video calling |
21 | |||
| Work overload | 43 | |||
| Hybrid working | 91 | |||
| Overall PA, physical exercise, and distractions while working | 94 | |||
| 74 | ||||
| Positive association | Essential worker | 17 | ||
| Negative affect | Wellbeing | No association | 45 | |
| Mental health | Wellbeing | Negative association | ||
| 60 | ||||
| Perceived stress | Wellbeing | No association | Professional group | 57 |
| Perceived self-efficacy | Wellbeing | No association | Professional group | 57 |
| Stress, worry and pressure (increased) | Wellbeing | Negative association | New and excessive demands | 83 |
| Stress (increased) | Wellbeing | Negative association | Increased demands | 21 |
| Family-work stress, Social isolation, Distracting working environment, | 29 | |||
| 70 | ||||
| Stress relating to indistinct organisation Fatigue |
36 | |||
| Reduced stress | Wellbeing | Positive association | 20, 35, 59 | |
| Hybrid working | 68 | |||
| Male | 42 | |||
| Parenting stress (increased) | Wellbeing | Negative association | Lower PA | 53 |
| Alcohol use (increased) | Wellbeing | Negative association | 2 | |
| Video conference fatigue (increased) | Wellbeing | Negative association | Having camera on Low sense of belonging |
5 |
| Openness to new ways of living | Wellbeing | Positive association | ‘Coping with COVID’ | 9 |
| Psychological distress (increased) | Wellbeing | Negative association | Increased childcare Increased domestic duties |
15 |
| Graduate educational Not feeling ‘sheltered at home’ |
19 | |||
| Increased housework and childcare/ home schooling hours [women] Only member of couple of adopt working pattern for childcare |
95 | |||
| Positive association | Alternative office/home working days | 75 | ||
| Anxiety | Wellbeing | No association | 90 | |
| Positive association | 76 | |||
| Negative association | Female Financial concern More dependents |
24 | ||
| Intrusive leadership and overtime work | 55 | |||
| Concerns about return to work, childcare, gender | 10 | |||
| Depression | Wellbeing | Negative association | Female Financial concern |
24, 42 |
| 72 | ||||
| Reduced social contact Change physical health |
20 | |||
| Intrusive leadership and overtime work | 55 | |||
| Concerns about return to work, childcare, gender | 10 | |||
| Changes in physical health Social contact (reduced) |
7 | |||
| Positive association | 76 | |||
| Sleep quality (increased) | Wellbeing | Positive association | Alternative days at home/office | 75 |
| Time sleeping (increased) | Wellbeing | Direction unclear | 34 | |
| Fatigue | Wellbeing | No association | 36 | |
| Male | 116 | |||
| Sedentariness, standing and movement | Wellbeing | No association | 34 | |
| Social isolation (decreased) | Wellbeing | Negative association | Technology Silence |
45 |
| 52 | ||||
| Perceived remote work productivity and remote work satisfaction | 82 | |||
| Loneliness (increased) | Wellbeing | Negative association | 79, 93 | |
| Burnout (increased) | Wellbeing | Negative association | 35 | |
| No effect overall | Extroversion, conscientiousness | 26 | ||
| Satisfaction with working from home | Wellbeing | No association | Female | 41 |
| Caring responsibility | 41 | |||
| Lack of space | 41 | |||
| Sense of worthwhile life (reduced) | Wellbeing | Negative association | 74 | |
| In control of time | Wellbeing | Positive association | 28 | |
| Lack of commute | Wellbeing | Positive association | 57 | |
| more time with the family | Wellbeing | Positive association | 57 | |
| Lower work/family conflict | Wellbeing | Positive association | 20, 28 | |
| More opportunity to exercise | Wellbeing | Positive association | 57 | |
| Lack of choice whether to WFH (enforced) | Wellbeing | Negative association | 88, 93 | |
| Health concerns (increased) | Wellbeing | Negative association | 88 | |
| Spaces shared with others | Wellbeing | Negative association | 28, 88 | |
| Lack of sports facilities open | Wellbeing | Negative association | Reduced PA | 88 |
| Minimal contact with others | Wellbeing | Negative association | Reduced PA | 88 |
| Autonomy (increased) | Wellbeing | Positive association | 93 | |
| Social support (increased) | Wellbeing | Positive association | 70, 93 | |
| QoL (increased) | Wellbeing | Positive association | Hybrid working and WFH full time. | 89 |
FIGURE 6.
Mind map of summary of factors which influence the associations between working from home and wellbeing or mental health (COVID-19 papers).
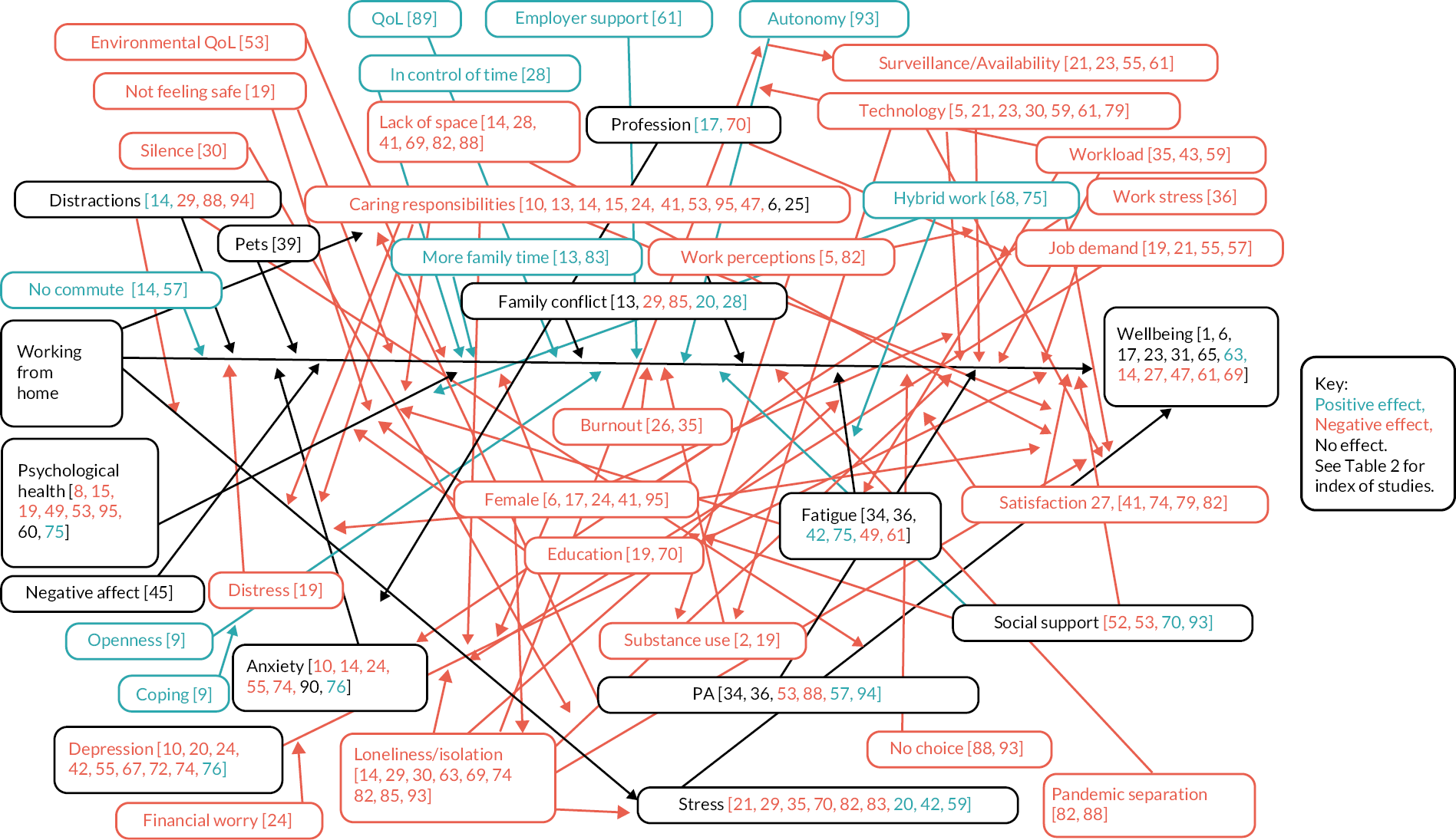
Wellbeing no associations
Direct measures of wellbeing were reported in 24 studies, with seven papers reporting no overall association between working from home and wellbeing (Allen et al. 2021,47 Cotterill et al. 2020,50 Di Tecco et al. 2021,35 Gijzen et al. 2020,54 Hoffman et al. 2021,55 Bentham et al. 2021,48 Dunatchik et al. 202153). The potentially relevant variables of having a pet or dependents in the home (Hoffman et al. 2021,55 Bentham et al. 202148) and division of domestic labour (Dunatchik et al. 202153) were also found to not be associated with wellbeing when working from home.
Allen et al. (2021) 47 undertook an online survey (recruited through social media and university courses) in the UK (n = 200, mean age 24.7 (SD 7.2) years, 86% female); 47.0% reported working from home. Psychological wellbeing was assessed using the PWB18 measure. Participants working from home did not significantly differ on wellbeing-related outcome measures. They report that a ‘linear regression model with self-isolation predicting PWB18 scores was significant [F(1,186) = 20.53, p < 0.001]; however, self-isolation (β = −.162, p = 0.004) and UCLA3 (loneliness) scores (β = −.596, p < 0.001) were the only significant predictors’. Cotterill et al. (2020)50 conducted an online survey of water-sector employees in the UK (n == 502, 60.6% male, 84.2% worked from home). One question related to wellbeing: ‘My general wellbeing has improved since lockdown’, and was rated on a Likert scale. More women saw a decrease in wellbeing (39%) than men (32%), although this was not statistically significant, and there were no significant differences between the median wellbeing values for men and women (U = 27 030, z = −1.472, p = 0.141).
Di Tecco et al. (2021)35 conducted a prospective cohort study to investigate the impact of a ‘smart working pilot’ (flexible home working) in Italy (n = 187, 78.6% female, mean age 50.7 (SD 6.8) years). There was no significant change in general health (p = 1.00) or wellbeing (p = 0.247) as a result of the pilot as evaluated by t-tests. Gijzen et al. (2020)54 conducted an online survey in the Netherlands (n = 1519, mean age 53 (SD 16) years (range 18 to 91), 52% female). They aimed to investigate the mental health and wellbeing of adults in the Netherlands 10 weeks after the start of COVID-19. However, although working from home was reported as a positive outcome of the COVID-19 pandemic for 17% (n = 142) participants this was not directly linked to wellbeing.
Hoffman et al. (2021)55 conducted an online survey in the USA with individuals who had experience working from home and from their employer’s office. (n = 454, 231 female, mean age = 41.3 years, SD = 11.5 years). They aimed to ‘Explore perceptions regarding how companion animals factor into the teleworking Experience’. Paired-samples t-tests indicated that neither positive nor negative wellbeing scores differed significantly by workplace location (PAWB: t = 1.17, df = 453, p = 0.24; NAWB: t = −1.74, df = 453, p = 0.08). When analyses were restricted to when participants worked from home, neither positive nor negative wellbeing scores were associated with the presence of dogs or cats in the home.
Bentham et al. (2021)48 completed a survey of people working in a UK mental health service (n = 51, 72.5% female, 29.4% aged 35–44, 23.5% aged 45–54, 15.7% aged 55–64 and 2% aged ≥65 years). Wellbeing was assessing using the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS). An independent-samples Kruskal–Wallis H-test showed no statistically significant differences in wellbeing score based on the proportion of hours worked remotely during the pandemic (χ2 (4) = 4.45; p = 0.349). Dunatchik et al. (2021)53 conducted an online survey with a nationally representative sample in the USA (478 partnered parents and 151 single parents). The authors report wellbeing in terms of pressure on working parents, and 66% mothers and 65% fathers reported feeling ‘some’ or ‘a lot’ of pressure regarding children’s home learning during the pandemic. However, no further indication of the impact on wellbeing is presented.
Wellbeing negative associations
However, 11 studies (including a number of grey literature sources) reported a negative association between working at home and wellbeing (Schifano et al. 2021,59 Xiao et al. 2021,45 Ingusci et al. 2021,56 De Sio et al. 2021,51 Wilke et al. 2021,44 Delfino and van der Kolk 2021,52 CIPD 2021,49 Felsted et al. 2020,17 KCL 2021,101 Parry et al. 2021,57 RSPH 202142). A variety of variables were identified which also had a negative effect on the relationship between working at home and wellbeing. Interruptions and distractions as a result of a lack of private space also impacted negatively on wellbeing when working at home (Xiao et al. 202145), as did increased monitoring (by the employer), including an expectation to ‘always be available’, and increased video calling (Delfino and van der Kolk 2021,52 Di Tecco et al. 202135). Higher job demands during the pandemic and work overload also impacted negatively on the work at home / wellbeing relationship (Ingusci et al. 2021,56 De Sio et al. 202151). Further factors which negatively moderated the relationship between working at home and wellbeing included hybrid working (Wilke et al. 202144) along with not feeling ‘sheltered at home’, smoking more cigarettes during the pandemic, and experiencing more psychological distress (De Sio 202151).
CIPD (2021) 49 conducted interviews with 32 senior managers and directors and an online survey with a total sample size of 2133 senior decision-makers in UK organisations, presented as a report and linked web page (grey literature). The most frequently mentioned benefit of working at home was increased wellbeing through avoiding the commute (46% of survey participants), followed by enhanced wellbeing because of greater flexibility of hours (39%).
Delfino and van der Kolk (2021)52 conducted semi-structured interviews with employees from professional service firms in Italy (n = 15, 9 female, 6 male). Management control practices and employees’ responses to these (including wellbeing, and factors affecting wellbeing) were considered ‘to investigate how remote working impacted the use of management control in professional service firms and explore how these changes affected employees’. Negative impacts on wellbeing were mentioned by respondents in terms of monitoring employees’ online/offline status, meaning employees felt they should always be available.
De Sio et al. (2021)51 conducted a web-based cross-sectional survey with Italian teleworkers (n = 348 (60.52%) females and 227 (39.48%) males, median age of 40 years (IQR: 33–49)). Perceived wellbeing was assessed using GHQ-12. Poor wellbeing was associated with having a higher job demand during the pandemic (OR 2.61; 95% CI 1.10 to 6.19), with feeling ‘not sheltered at home’ (OR 8.80; 95% CI 2.60 to 29.75), with smoking more cigarettes during the pandemic (OR 2.47; 95% CI 1.13 to 5.59), and with experiencing psychological distress (OR 8.01; 95% CI 2.57 to 24.97).
Felstead et al. (2020)17 completed three online survey of UK workers (April, May, June 2020). Wellbeing was assessed using GHQ-12 wellbeing questions. Those who worked mainly at home reported greater difficulties in enjoying normal day-to-day activities compared to those not working at home, (48.2/49.3% vs. 38.5%) and more often felt constantly being under strain and unhappy with life (36.0/33.9 vs. 31.2).
Ingusci et al. (2021)56 conducted an online survey of Italians who experienced remote working or working from home (n = 530, 60.4% female, mean age 39.0 (SD 11.2)). Behavioural stress was assessed using a seven-item validated scale. In a structural model with good fit indices (CFI = 0.96, TLI = 0.95, AGFI = 0.91, RMSEA = 0.05 (90% CI 0.05 to 0.06), SRMR = 0.06), behavioural stress was found to be positively related to work overload (β1 = 0.48, p = 0.015) and negatively related to job crafting (β3 = −0.38, p < 0.000), with a significant and negative indirect effect of work overload on behavioural stress through the intervention of job crafting (βa×b = −0.07, p = 0.029).
KCL (2021)101 conducted an online survey of 254 large employers in the UK. Their report states that organisations who reported improved morale compared to this time six months ago are considerably more positive about the support provided, particularly for parents and carers. This suggests that offering such support can contribute towards improved morale and wellbeing overall.
Parry et al. (2021)57 analysed 1035 survey responses of an UK online worker wellbeing survey. Using the World Health Organisation Five Wellbeing Index (WHO-5) to measure wellbeing, on average respondents scored 47 out of 100, relatively low compared to previous UK and Europe-wide surveys. Key determinants of wellbeing included fewer physical health symptoms, higher levels of satisfaction with work-life balance and identifying as extroverts.
RSPH (2021)42 reported on the mental and physical health impacts of home working during COVID-19. Overall, more people felt working from home was better for their health and wellbeing (45%), compared to around one-third (29%) who thought working from home was worse for their health and wellbeing. Home working was said to be having an impact on people’s mental health, with 67% saying they felt less connected to their colleagues and 56% saying they found it harder to switch off.
Schifano et al. (2021)59 conducted a longitudinal online survey in France, Italy, Germany, Spain and Sweden (n = 9700 observations). Wellbeing was assessed in terms of five variables: life satisfaction and life worthwhile, loneliness, depression, anxiety, and working from home. Working from home was associated with lower wellbeing on all five variables – life satisfaction (coefficient = −0.09, p < 0.01), worthwhile (coefficient = −0.07, p < 0.05), not lonely (coefficient = −0.08, p < 0.05), not depressed coefficient = (−0.09, p < 0.01) and not anxious (coefficient = −0.09, p < 0.01), although not working had a greater negative impact. Switching to working from home reduced anxiety (coefficient = 0.05, p < 0.10) but also reduced the sense of a worthwhile life (coefficient = −0.07, p < 0.05), with no significant impact on other wellbeing variables.
Wilke et al. (2021)44 conducted an online survey in 14 countries worldwide (n = 14,975, 58.1% female, mean age 38 (SD 15) years). Mental wellbeing was assessed using the World Health Organization Well-Being Index (WHO-5). Working outside the home vs. working remotely was associated with clinically relevant reductions in mental wellbeing (OR 1.29, 95% CI 1.16 to 1.44), as was working both outside the home and remotely vs. working remotely (OR 1.35, 95% CI 1.23 to 1.47).
Xiao et al. (2021)45 conducted an online survey in the USA of those who had transitioned to WFH during the COVID-19 pandemic (n = 988, 56.5% female, mean age 40.9 (SD 13.1) years). Physical and mental wellbeing were rated overall, relative to their wellbeing prior to WFH on a Likert scale. Compared with pre-WFH, mean ratings were decreased for overall physical (2.84, SD 0.87) and mental (2.70, SD 0.93) wellbeing. Mental wellbeing was significantly correlated with overall PA (r = 0.36, p < 0.01), physical exercise (r = 0.33, p < 0.01), and distractions while working (r = −0.30, p < 0.01). Mean mental wellbeing was lower for those who adjusted their work hours (2.65, 0.95) than those who did not (2.86, SD 0.87, p < 0.01), those who needed to schedule their work hours around others (2.59, SD 0.95) than those who did not (2.77, SD 0.92, p < 0.01), and those who reported somebody in the same workspace while WFH (2.64, SD 0.95) than those who reported a solitary work environment (2.78, SD 0.90, p = 0.04).
Wellbeing positive associations
Three additional studies reported improved wellbeing for those working at home (Cotterill et al. 2020,50 Xiao et al. 2021,45 PWC 202058). These relationships were moderated by a number of factors, including being an essential worker (amongst employees in the water sector; Cotterill et al. 202091) and having higher levels of overall PA and physical exercise (Xiao et al. 202145).
Xiao et al. (2021),45 described above, reported that improved mental wellbeing (F(38, 351) = 5.306, p < 0.001, R2 = 0.371) was predicted by increased physical exercise, increased communication with co-workers, and decreased junk food intake, along with being positively affected by having an infant in the home and negatively affected by increased distractions while working. Cotterill et al. (2020),50 described above, reported that essential workers had the largest improvement in wellbeing (29%). PWC et al. (2020)58 produced a web report to provide insights on the remote working experience of 875 workers in Malta (mean 36–45). The largest percentage of those who viewed the experience as having a positive impact on their wellbeing were those who lived alone and were aged 24–35.
Mental health
Two studies reported a negative association between working at home and a person’s overall mental health (Bevan et al. 2020,89 Kotera 2020102). A number of factors further impacting on the mental health of those working at home included those who were younger workers, looking after elderly relatives (but parents were no different from non-parents in this study), living with parents or renting, new home workers, working more than contracted hours, and reduced contact with their boss (Bevan et al. 2020)89. In one further study a negative association between working at home and experiencing negative affect was described (Janssen et al. 202065).
Bevan et al. (2020)89 in their online survey of UK home workers (n = 500) reported that mental health is poorer for younger workers, those looking after elderly relatives (but parents were no different to non-parents), those living with parents or renting, and those new to home working. Kotera (2020)102 in an opinion piece on new ways of working discusses how more attention needs to be paid to the negative impacts of blurred work–home boundaries, fatigue and increased mental demands.
Janssen et al. (2020)65 conducted an ‘ecological momentary assessment’ (n = 101 (34 adolescents, 67 caregivers), parents: 56.7% female, mean age 48.2; adolescents: 64.7% female, mean age 16.0). Working from home was not related to an increase in parents’ negative affect during the COVID-19 pandemic, as compared with pre-pandemic data.
Anxiety and depression
Anxiety and/or depression and their relationship to work at home wellbeing were considered by nine studies. For anxiety, no factors associated with home working were reported in one study (Wickens et al. 2021117), a positive association was reported in a second study (Smith et al. 2021112), but factors with negative associations for home workers were reported in three further studies (Docka‐Filipek et al. 2021,61 Magnavita et al. 2021105, Burstyn et al. 202191). There were additional negative impacts on wellbeing for females compared to males, and those with financial concerns and/or more dependents (Docka‐Filipek et al. 202161), where people experienced intrusive leadership and overtime work (Magnavita et al. 2021105), and where home workers had concerns about return to work and childcare (particularly for females) (Burstyn et al. 202191).
Five studies on depression reported factors with negative associations between working at home and wellbeing which were moderated by being female and/or having financial concerns (Docka‐Filipek et al. 2021,61 Sato et al. 2021a111), where people experienced intrusive leadership and overtime work (Magnavita et al. 2021105), and where home workers had concerns about return to work and childcare (particularly for females) (Burstyn et al. 202191). Only one study reported a positive association between depression and home working (i.e. home working was association with reduced levels of depression) during the pandemic (Smith et al. 2021112).
Burstyn et al. (2021) 91 conducted an online survey of workers in the USA (n = 911). Anxiety and depression were assessed using the HADS. They report that ‘starting or substantially increasing telecommuting appeared to be associated with increased anxiety and depression in both sexes as well, with the effect more prominent among men’. Men (but not women) who identified as essential workers (RR 1.16, 95% CI 0.96 to 1.40), had one-on-one contact with people at work (RR 1.14, 95% CI 0.98 to 1.34), including known or suspected cases of COVID-19 (RR 1.30, 95% CI 0.97 to 1.74), who were hourly employees (RR 1.24, 95% CI 0.96 to 1.60), and did not have access to disability/sick leave through work (RR 1.22, 95% CI 0.93 to 1.60) were more anxious.
Docka-Filipek et al. (2021)61 conducted an online survey of university faculty working from home at the start of the coronavirus pandemic in the USA (n = 345, 77% female, mean age 42.84 (SD 9.23)). Self-reported mental health (depression and state anxiety) was assessed using a shortened version of the Center of Epidemiologic Studies Depression scale and the state anxiety subscale of the six-item version of the State Trait Anxiety Inventory. Two multiple regression models were run, which accounted for significant variance in depressive symptoms (F(6, 322) = 7.29, p < 0.001) and state anxiety (F(6, 322) = 5.93, p < 0.001). Gender accounted for unique variance in both depression (β = 0.17, p ≤ 0.01) and anxiety (β = 0.17, p ≤ 0.01) risk, after covarying for ethnicity, academic position, teaching load, number of dependents in the home, and financial concerns at separate steps. Higher financial concerns accounted for unique risk of both depression (β = 0.30, p < 0.001) and anxiety (β = 0.26, p < 0.001), and having more dependents accounted for unique risk of anxiety (β = 0.13, p < 0.05).
Magnavita et al. (2021)105 conducted a survey of people working for trade and service-sector companies in Italy who telecommuted part time (n = 905, 36.6% male, mean age 45.93 (SD 11.39)). Common mental health issues were assessed using the Goldberg Anxiety and Depression Scale. They report that anxiety increased with intrusive leadership, workaholism and age, and was higher in females. Depression decreased with off-time work, was higher in females, and increased with workaholism and age.
Smith et al. (2021)112 conducted an online survey with non-healthcare workers in Canada (n = 3305, 61% female, 15.4% aged <34, 23.7% aged 35–44, 29.6% aged 45–54, and 30.3% aged above 55 years). Anxiety and depression were assessed by the Generalised Anxiety Disorder (GAD-2) and the Patient Health Questionnaire (PHQ-2) measures. Among those working remotely, the adjusted proportion of respondents with GAD-2 scores of ≥3 was 35.3% (95% CI 27.1 to 43.5) and the adjusted proportion of respondents with PHQ-2 scores ≥3 was 27.4% (95% CI 20.1 to 34.8), both of which were significantly lower than among site-based workers or those no longer employed.
Wickens et al. (2021)117 conducted an online survey with Canadian workers (n = 1002, 49.7% female, 13.2% aged 18–29, 26.1% aged 30–39, 23.9% aged 40–49, 17.7% aged 50–59, 30.4% aged over 60 years). Depressive symptoms were assessed by a single item from the Center for Epidemiologic Studies Depression Scale. In the regression analysis, after adjusting for demographic variables, working from home was not a significant predictor of depressive symptoms (adjusted OR 1.16, 95% CI 0.75 to 1.77) (the odds of experiencing depressive symptoms were higher among whose with a job at high risk of exposure to COVID-19 and who experienced financial worry due to COVID-19).
Sato et al. (2021a)111 conducted an online survey in Japan (n = 2846, 60% female, mean age 43.0 (SD 12.0) years for females and 50.3 (SD 10.2) years for males). The association of changes in work and life patterns with depressive symptoms was examined in users of the health app CALO mama, which records diet, exercise, mood and quality of sleep and provides feedback to users. Depressive symptoms were assessed by two validated items (‘During the past month, have you often been bothered by feeling down, depressed, or hopeless?’ and ‘During the past month, have you often been bothered by little interest or pleasure in doing things?’). In the logistic regression model, shifting to WFH was negatively associated with depressive symptoms (OR 0.83, 95% CI 0.69 to 0.99).
Other mental health measures
Mental health was also reported as psychological distress. One study reported a positive association with psychological distress (i.e. less distress) for those working at home which was further improved by hybrid working arrangements (alternative office/home working days) (Shockley et al. 202129). However, three studies reported factors with negative associations with working from home, which were moderated by increased childcare (including home schooling) and domestic duties particularly for mothers and lone parents (Clark et al. 2021,60 Xue et al. 202167), and being the only member of couple to adopt their working pattern for childcare (Xue et al. 202167). In addition, increased health concerns were also reported to negatively impact on the mental health of those working at home (Waizenegger et al. 202043)
Clark et al. (2021)60 conducted qualitative interviews in working mothers in Ireland (n = 30). Most participants reported increased levels of psychological distress as a result of the pandemic and resultant changes to the dynamic of work and family life. An additional challenge was managing the psychological welfare of their children during the pandemic, and helping them to cope.
Shockley et al. (2021)29 conducted a longitudinal online survey in the USA of heterosexual married couples where both spouses worked full-time (n = 274 at T1, 133 at T2, mean age at T2: 35.2 (SD 3.4) years for wives and 36.3 (SD 7.0) years for husbands). Psychological distress was assessed by the Kessler et al. (2002) 10-item measure. In the latent class analysis, for health outcomes (psychological distress and sleep quality), those adapting the strategy of ‘alternating days’ fared the best (mean PD score 1.54 and 1.58 for wives and husbands, respectively).
Waizenegger et al. (2020),43 outlined above, report that ‘participants’ mental and physical wellbeing was (equally) affected by a lack of PA, due to sports facilities being closed and minimal contact with others being allowed’.
Xue et al. (2021)67 conducted a longitudinal survey in a nationally representative survey of >100,000 individuals from 40,000 households in the UK (n = 14,150: 8291 women, 5859 men) to describe how men and women divided childcare and housework demands during the height of the first COVID-19 lockdown in the UK. Adapting work patters due to childcare / home schooling was associated with 1.39 (95% CI 0.403 to 2.382) higher GHQ scores in women and 1.16 (95% CI 0.296 to 2.015) higher GHQ scores in men. Being the only member of the couple to adapt a working pattern to accommodate childcare was associated with 1.82 higher GHQ scores (95% CI 0.669 to 2.973) in women and 2.48 higher GHQ scores (95% CI 1.367 to 3.601) in men. Lone mothers who adapted work patters to accommodate childcare / home schooling had on average 3.93 higher GHQ scores (95% CI 1.639 to 6.223; p = 0.001) than lone mothers who did not adapt work patterns. There was no effect of adapting work patterns on GHQ in couple mothers.
Stress
Stress, and its assumed impact on wellbeing, was measured by 13 studies which considered the impact of working from home. Stress was reported as perceived stress, perceived self-efficacy, ‘stress, worry and pressure’, burnout, and as specific stresses including parenting stress and occupational stress. Overall, more papers reported that working from home in the COVID-19 era increased stress than reported reduced stress or no impact on stress from working at home.
No change in perceived stress or perceived self-efficacy was reported with working from home in one survey study, even when differences by professional group (practitioners, managers, executives and teachers) were considered (Mari et al. 2021106). However, factors with negative associations between working at home and stress were reported by five studies (Russo et al. 2021,110 Travers et al. 2020,115 Delfino and van der Kolk 2021,52 Galanti et al. 2021,98 Heiden et al. 2021100). An increase in stress, worry and pressure as a result of working from home was made worse by new and excessive work demands according to Travers et al. (2020). 115 The same relationships were also reported by Delfino and van der Kolk (2021). 52 Negative relationships were also reported in a further three studies with the working from home / stress association mediated by family–work stress, social isolation, and a distracting working environment (Galanti et al. 202198), ‘indistinct organisation’ and fatigue (Heiden et al. 2021100).
Delfino and van der Kolk (2021)52 (qualitative field study) found that employees experienced stress in relation to increased demands and fear of management, which led them to miss breaks to increase their availability, decreased their motivation for their job (and subsequently looked for other work), and had a serious impact on mental health. Galanti et al. (2021)98 conducted an online survey of Italians working from home full time, in public and private organisations (n = 209, 71.3% female, mean age 49.8 (SD 9.4) years (range 25 to 65)). Stress was assessed using four items designed to measure workers’ perception of exhaustion and fatigue due to WFH. Stress was positively correlated with family–work conflict (r = 0.50, p < 0.01), social isolation (r = 0.62, p < 0.01) and distracting working environment (r = 0.36, p < 0.01), and negatively correlated with productivity (r = −0.39, p < 0.01) and work engagement (r = −0.47, p < 0.01).
Heiden et al. (2021)100 conducted an online survey of teaching and research staff at Swedish public universities (n = 392, 63% female, mean age 48.9 (SD 9.9) years). Separate ANOVAs for each outcome variable did not show any significant differences in health (or GHQ subscales), work stress related to individual demands and commitment, and influence at work, or rest, but did show significant differences on fatigue (F = 3.47; p = 0.032) and work stress relating to indistinct organisation and conflicts (F = 4.80; p = 0.009). Post hoc tests revealed that those who teleworked several times per week or more reported more stress relating to indistinct organisation than those who teleworked less than once a month. There were no significant pairwise differences for fatigue.
Mari et al. (2021)106 conducted an online survey in people doing ‘smart work’ (working from home only) (n = 628, 78% female, mean age 42.3 (SD 10.5), age range 21–70). Coping with stress was assessed using the Coping Orientation to Problems Experienced. There were no significant differences between professional groups on the PSS (perceived stress), or on the perceived self-efficacy subscale. For the perceived helplessness subscale, teachers had a higher mean score (11.07, SD 3.90) than managers (9.79, SD 3.81). Russo et al. (2021)110 undertook an international longitudinal survey (mainly UK, USA and countries in Europe) of software professionals working from home during COVID lockdown (n = 192, mean age 36.65 (SD 10.77) years, 20% female). Stress was assessed using a four-item version of the Perceived Stress Scale. At Wave 1, stress negatively affected social contacts, and daily routines predicted stress at α = 0.05. At Wave 2, need for competence and autonomy, stress, quality of social contacts, and quality of sleep uniquely predicted wellbeing at α = 0.05.
Travers et al. (2020)115 conducted an ‘internet-based ethnography’, although little methodology is given (n = 211), of people working at home during the COVID-19 pandemic in the UK. Working from home during lockdown was interpreted as ‘a time of contradictions and transitions’, with new and excessive demands creating worry, stress and pressure, but also opportunities afforded by a lack of commute and spending more time with the family.
Conversely, reduced stress was reported as a positive outcome of home working in four studies (Hayes et al. 2021,99 Molino et al. 2020,107 Delanoeije et al. 2020,94 Rodriguez et al. 2020109), with hybrid working arrangements further reducing stress beyond full-time working at home (Rodriguez et al. 2020109). Ignacio Gimenez-Nadal et al. (2020)64 also reported reduced stress for male teleworkers only.
Delanoeije et al. (2020)94 conducted a quasi-experimental study in Belgium of employees at a large construction and property-development firm allocated teleworking (at least 2 days per week) or control (no home working (n = 78, 75.6% male)). The univariate F tests showed there was a significant interaction effect between time and group for stress (F(1,62) = 4.21, p = 0.04, ηp2 = 0.06)’, whereby stress decreased among the teleworking group but not the control group – once commuting time was included as a covariate, there was no group by time interaction effect for stress, suggesting that the decrease in stress among the teleworking group could be accounted for by pre-existing differences in commuting time. For daily stress, ‘the standardized estimate of teleworking day on daily stress (γ = −0.20, p < 0.001) was negative and significant’, supporting the hypothesis that the intervention group would have less daily stress on a teleworking day compared with a non-teleworking day.
Hayes et al. (2021)99 conducted an online survey of people working from home due to COVID-19 restrictions in the USA (n = 326, 52.2% female, 30.7% aged 18–34, 38.3% aged 35–54 and 31.0% aged over 55 years). Stress was assessed by the Perceived Stress Scale (PSS). There was a significantly greater increase in perceived stress score from pre-COVID (retrospectively rated) to the current time among those whose job typically did not provide opportunities to WFH (mean increase 3.9, SD 6.4) than those whose did (mean increase 2.4, SD 5.3) (t(290) = 2.23, p = 0.03). Conversely, those who previously had flexibility to WFH before the pandemic had higher work-related burnout scores at data collection (mean 57.9, SD 21.5) than those without the flexibility to WFH (mean 41.0, SD 21.6) (t(284) = −16.84, p < 0.0001). Although women had lower pre-COVID and during-COVID perceived stress scores than men, the mean increase in stress scores was higher for females (4.2, SD 6.0) than males (2.4, SD 5.8) (t(294) = 2.59, p = 0.01). Women had significantly lower mean work-related burnout scores (43.3, SD 20.8) than men (53.0, SD 24.6) (t(299) = −3.82, p < 0.0002).
Molino et al. (2020)107 conducted an online questionnaire in Italy of home and traditional working (n = 749, 59% female, mean age 38.7 (SD 11.3) years, 63% working from home for a mean 4.7 (SD 1.3) days per week). Technostress creators were measured by the validated 11-item brief Italian technostress creators scale. Behavioural stress was measured by eight items from the Copenhagen Psychological Scale. Significant positive correlations were found between behavioural stress and work–family conflict (r = 0.23), the three techo-stress creators (techno-overload, techno-invasion and techno-complexity; r = 0.22, r = 0.24 and r = 0.23, respectively), and workload (r = 0.19) (all p < 0.01). Work–family conflict was also positively correlated with the three techno-stress creators (r = 0.35, r = 0.48 and r = 0.19, respectively) and workload (r = 0.47) (all p < 0.01). Remote working was positively correlated with techno-overload (r = 0.29), techno-invasion (r = 0.25) and workload (r = 0.13) (all p < 0.01), but not behavioural stress (r = −0.07), work-family conflict (r = 0.03) or techo-complexity (r = 0.01).
Rodriguez et al. (2020)109 conducted an online survey of people living in Spain during the COVID-19 lockdown (n = 1269, 18% male, mean age 38.8 (SD 10.6) years). Stress was assessed by the 14-item Perceived Stress Scale. Working situation (during COVID-19 lockdown confinement) was related to stress response (F(4,918) = 4.914; p < 0.01; ηp2 = 0.020) and control of stress (F(4,928) = 4.017; p < 0.01; ηp2 = 0.016).
Ignacio Gimenez-Nadal et al. (2020)64 conducted a face-to-face survey of employee workers in the USA (n = 5401, 47.9% female, mean age 43.8 (SD 10.7) for males and 43.9 (11.0) years for females). This consisted of recording a daily diary where pain, happiness, sadness, fatigue and stress were each rated 0–6. They report that among males, teleworkers reported lower levels of sadness, stress and tiredness compared with commuters. Among females, teleworkers had significantly higher happiness levels than commuters. There were no other significant differences.
In terms of specific stressors, parenting stress (made worse by lower PA) was negatively associated with working from home (Limbers et al. 202066). Evans et al. (2021)96 reported that those who scored highly for the personality measures of extroversion and conscientiousness were more likely to experience burnout while working from home as the pandemic progressed.
Limbers et al. (2020)66 conducted an online survey in the USA with females with at least one child who would normally work outside the home but were working from home during the COVID-19 pandemic (n = 200, mean age 33.5 (SD 6.25) years). Parenting stress was assessed using the Parental Stress Scale. Greater levels of parenting stress were associated with lower physical health QoL (r = −0.42, p < 0.001), lower psychological QoL (r = −0.28, p < 0.001), lower social relationships QoL (r = −0.21, p < 0.01), and lower environment QoL (r = −0.19, p < 0.01). Evans et al. (2021)96 conducted an online survey in UK remote workers (n = 974, 61% female, mean proportion of time WFH 91%). Burnout was assessed over the preceding month using five items. At the first wave, those scoring high on extroversion and conscientiousness were less likely to experience burnout, whereas those high in extraversion reported higher levels of burnout over time.
Satisfaction
Satisfaction with working from home (including sense of worthwhile life) and QoL measures were also reported. Measures of life satisfaction, along with a sense of having a worthwhile life, were reduced with working from home in four studies (Hubbard et al. 2021,63 Toscano et al. 2020,114 Taser et al. 2022113). Satisfaction with working from home was lower for females (Hubbard et al. 202163), those with caring responsibility (Hubbard et al. 202163) and those who had a lack of suitable space to work in the home (Hubbard et al. 202163). Low enjoyment of activities as a result of working from home was also reported (Felsted et al. 202017). Openness to new ways of living was positively associated with a positive view of working from home (Boncori 202090).
Boncori (2020)90 wrote an auto-ethnography on the experiences of living and working during the COVID-19 pandemic (early stages). She wrote of how openness to new ways of living was positively associated with a positive view of working from home. Felstead et al. (2020)17 (online survey) found that those who worked mainly at home – always or often – reported greater difficulties in enjoying normal day-to-day activities compared to those not working at home (48.2/49.3% vs. 38.5%) and more often felt constantly being under strain and unhappy with life (36.0/33.9 vs. 31.2).
Hubbard et al. (2021)63 conducted a cross-sectional survey (online) including 501 adults of working age currently working in the UK. Ratings of satisfaction with working from home were sought. Women reported less satisfaction than men (chi-square 7.011, df = 3, p = 0.071), as did people with children (chi-square 7.299, df = 3, p = 0.063) – especially young children aged 0–4 years (chi-square 8.01, df = 3, p = 0.046). A significant predictor of dissatisfaction with home working was caring for a responsible adult (chi-square = 7.837, df = 3, p = 0.049). No other predictors were listed.
Toscano et al. (2020)114 conducted an online survey of Italian employees working exclusively from home (n = 265, 63% female, 42% aged 26–35, 21% aged 36–45, 17% aged 46–55, 11% aged <25 and 8% aged over 56 years). Perceived remote working productivity, remote job satisfaction, concern about COVID-19, and experience with remote work were also assessed. Social isolation was significantly correlated with stress (0.50, p < 0.01), perceived remote work productivity (−0.43, p < 0.01), remote work satisfaction (−0.50, p < 0.01) and COVID-19 concern (0.32, p < 0.01). Stress was significantly correlated with perceived remote work productivity (−0.35, p < 0.01), remote work satisfaction (−0.54, p < 0.01) and COVID-19 concern (0.16, p < 0.05).
Taser et al. (2022)113 conducted an online survey of Turkish financial services sector employees, working from home during the pandemic (n = 202, 51.5% female, 2.4% aged 18–25, 25.7% aged 26–35, 42.2% aged 36–45, and 29.7% aged over 46 years). Technostress was assessed using the Tarafdar scale. Those who had a good remote e-working experience tended to have lower levels of technostress (b = −0.17, SD = 0.06, p < 0.01). Those experiencing technostress were likely to feel lonely (b = 0.23, SD = 0.06, p < 0.001).Technostress and loneliness mediated the relationship between remote e-working and flow at work.
Lifestyle behaviours
Lifestyle behaviours including sleep (and fatigue), alcohol use and PA (or sedentariness) were considered in seven studies. Sleep (sleep quality, time sleeping and fatigue) increased as a result of working from home in two studies (Shockley et al. 2021,29 Hallman et al. 2021118); however, it was not entirely clear whether an increase in sleep duration (rather than sleep quality) was considered to be positive. However, the impact of working from home on sleep was described as most positive for hybrid workers (alternative days at home/office) (Shockley et al. 202129). There was a negative association between levels of fatigue and working from home (Heiden et al. 2021100) and fatigue increasing whilst working from home reported in a further two studies (Kotera 2020,102 Parry et al. 202157). Ignacio Gimenez-Nadal et al (2020)64 reported reduced fatigue for male teleworkers only.
Hallman et al. (2021)118 conducted a cross-sectional online survey, with diary and accelerometer data, comparing activity between working in the office and working from home in Sweden (n = 27, 81.5% female, mean age 43.4 (SD 9.9)). Accelerometer-assessed PA (proxy for physical health), standing, sedentariness and sleep were assessed. Sedentariness, standing and movement did not differ significantly between working from home (WFH) and working at the office (WAO). Time spent sleeping (relative to time spent awake) was significantly greater on working-from-home days than for days working at the office. Days working from home were associated with more time spent sleeping relative to awake, and the effect size was large (F = 7.4; p = 0.01; ηp2 = 0.22). The increase (34 min) in sleep time during WFH occurred at the expense of a reduction in work and leisure time by 26 min and 7 min, respectively.
Five studies have been discussed previously: Heiden et al. (2021)100 (online survey) found home workers did show significant differences on fatigue (F = 3.47; p = 0.032). Kotera 2020102 (opinion piece) reported that new ways of working increase blurred work–home boundaries, fatigue and mental demands. Parry et al. (2021)57 (online survey) found higher levels of fatigue in home workers. Ignacio Gimenez-Nadal et al. (2020)64 (face-to-face survey) report that among males, teleworkers reported lower levels of tiredness compared with commuters. Shockley et al. (2021)29 (longitudinal online survey), in their latent class analysis, found that for health outcomes (psychological distress and sleep quality), those adapting the strategy of ‘alternating days’ fared the best (mean PD score 1.54 and 1.58 for wives and husbands, respectively).
The impact of PA levels on wellbeing whilst working from home were considered in a couple of different ways. Levels of sedentariness, standing and movement were not associated with wellbeing in one study (Hallman et al. 2021118), which included validating self-reported outcomes with accelerometer data. However, having more opportunity to exercise whilst working at home was positively associated with wellbeing (Travers et al. 2020115) and the lack of sports facilities open during lockdown was negatively associated with wellbeing due to reduced PA levels (Waizenegger et al. 202043). Greater alcohol use was associated with reduced wellbeing for those working at home in one study (Alpers et al. 202187).
Alpers et al. (2021)87 conducted an online survey in a random sample of adult residents in Norway (n = 25,708, 56% female, 13% aged 18–29, 16% aged 30–39, 18% aged 40–49, 21% aged 50–59, 18% aged 60–69, 14% aged 70 plus). Alcohol consumption was assessed through the AUDIT-C. Self-assessed increased alcohol consumption during the lockdown period was more frequently reported by people working or studying from home (OR 1.4, 95% CI 1.3 to 16) (as well as those reporting economic worries and in quarantine).
Hallman et al. (2021)118 (previously described: cross-sectional online survey) found that sedentariness, standing and movement did not differ significantly between working from home (WFH) and working at the office (WAO). Time spent sleeping (relative to time spent awake) was significantly greater on working from home days than for days working at the office. Travers et al. (2020)115 and Waizenegger et al. (2020)43 have also been previously described.
Social interaction
Social interactions were reported as social isolation, loneliness, minimal contact with others and social support. Social isolation was reported as more likely for those working at home (Lal et al. 2021104) and the relationship was mediated by technology and silence (Gao and Sai 202062), perceived remote work productivity and remote work satisfaction (Toscano et al. 2020114). Loneliness also increased during working from home, as was noted in four studies (Wood et al. 2021,119 Taser et al. 2022,113 RSPH 2021,42 University of Exeter 2020116), and minimal contact with others was made worse by reduced PA (Waizenegger et al. 202043). Conversely, the participants of two studies reported that their social support increased as a result of working at home (Wood et al. 2021119, Russo et al. 2021110).
Lal et al. (2021)104 conducted an exploratory, interpretive qualitative diary-keeping study of people who had recently transitioned to WFH during the pandemic mostly in the UK (n = 48% female, 69% had previously worked from home). Maintaining interaction while working remotely was also an issue, with a lack of face-to-face interaction leading to worries about colleagues: some people missed the small daily social interactions that they usually had at work. Gao and Sai (2020)62 completed an auto-ethnography (personal reflections of three researchers) in the UK. No details of the analysis were given. Both women experienced social isolation as a result of being physically distanced from their workplace and colleagues, even if working alone was previously sought. This was also explored in the context of possible regret for choosing to live alone (e.g. rather than starting a family), as one thing that added to the sense of isolation was not being able to see other people or to hug them.
Wood et al. (2021)119 reported a 4-week diary study over two time periods among UK university staff (n = 784 (20% response)). The Warwick–Edinburgh Mental Well-being Scale (WEMWBS) was used to assess the impact of home working on home worker wellbeing. Of the predictors tested at the between-person level, loneliness was associated (negatively) with all wellbeing measures for both phases.
The University of Exeter (2020)116 report a weekly survey during COVID-19 lockdown on their webpage of university employees working from home (n = 85). They state that the loneliness of working in a home environment and increased demands to juggle work and domestic responsibilities caused a decline in employee wellbeing. Nearly one in five (17%) remote workers reported feeling lonely,
In previously described studies: in Toscano et al. (2020)114 (online survey) social isolation was significantly correlated with stress (0.50, p < 0.01); Taser et al. (2022)113 (online survey) reported that technostress and loneliness mediated the relationship between remote e-working and flow at work; in RSPH (2021)42 (online report) nearly half (48%) of people who worked from a sofa or bedroom said they had developed musculoskeletal problems and nearly two-thirds (59%) said they felt more isolated from their colleagues; Waizenegger et al. (2020)43 (qualitative) reported that ‘participants’ mental and physical wellbeing was (equally) affected by minimal contact with others being allowed’; and Russo et al. (2021)110 (longitudinal survey) reported stress negatively affected social contacts.
Home environment
Measures linked to the home-work environment and wellbeing included feeling in control of time, lack of commute, more time with the family, lower work/family conflict, and spaces shared with others. The lack of a daily commute was positively associated with wellbeing for home workers (Travers et al. 2020115). A feeling of being in control of time was also positively associated with wellbeing,115 as was more time with the family (Travers et al. 2020115) and lower work/family conflict (Fukumura et al. 202197). However, having to work in home spaces shared with others was negatively associated with wellbeing (Waizenegger et al. 202043, Fukumura et al. 202197).
Fukumura et al. (2020)97 conducted an online survey of individuals who transitioned to WFH during the pandemic in the USA (n = 988, mean age 41.7 years (SD 12.9), 65.4% female). Physical and mental wellbeing were assessed using ‘Likert-type categorical response questions’. Some people preferred the spatial arrangements at home, for instance those with internal offices in the workplace, and no natural light, where they could work at home in a more comfortable space and take breaks in the garden. However this varied between people, with some describing the home environment less conducive to work, due to the presence of others including children, a lack of privacy and a lack of appropriate technology. Others reported wellbeing benefits in not having to speak to colleagues that they didn’t want to speak to, or be distracted by other people’s conversations in the office.
In previously described studies: Travers et al. (2020)115 (‘internet-based ethnography’) reported that the availability or lack of availability of suitable work space at home also impacted on people’s wellbeing. Working in unsuitable spaces (e.g. landing, blocking fridge door) and competing for space with other family members (e.g. children, pets) could cause problems, but people also expressed warmth for their children and pets; and Waizenegger et al. (2020)43 (qualitative) discussed how participants often worked in a space shared with other occupants of the household, and this caused distraction and difficulty in focusing on work tasks.
Work-related outcomes
Lack of choice over whether to WFH was explicitly stated as a negatively associated with wellbeing in two studies (Waizenegger et al. 202043, Wood et al. 2021119). However, this factor is implicit in all of the studies conducted during the COVID-19 pandemic and as such, although not frequently considered and reported, is likely to be one of the key factors impacting on wellbeing of those working at home. Along with this, increased work autonomy was positively associated with wellbeing for those working at home (Wood et al. 2021119).
Waizenegger et al. (2020)43 (qualitative) note that findings should be interpreted in the context that no-one had a choice about working from home, it was a requirement, and that most of the company’s workforce needed to WFH. Wood et al. (2021)119 (qualitative diary study) state that factors pertaining to the enforced nature of home working and the COVID-19 factors pertaining to increases in deaths and the interaction effect of this with age had some bearing on wellbeing.
Measures linked to videoconferencing including video conference fatigue, further negatively impacted by having camera on, and low sense of belonging as a result of remote interactions (Bennett et al. 2021)88 were all negatively associated with wellbeing for home workers.
Bennett et al. (2021)88 conducted an online survey with closed (quantitative) and open-ended (qualitative) questions with individuals working in a range of industries in the USA (n = 55, 58% male, 73% White, mean age 33.6 years (SD 9.1)). Videoconference fatigue was measured using the fatigue item from the Profile of Mood States scale, scored on a 6-point scale. In qualitative data, participants reported being particularly fatigued by multiple (including consecutive) videoconference meetings. Muting the microphone (γ = −0.09, p = 0.02) and perceptions of group belongingness (γ = −0.21, p = 0.003) were negatively related to fatigue (i.e. were associated with lower fatigue), whereas turning the webcam off, attention during the meeting, and videoconference meeting duration were not significantly related to post-meeting fatigue. The authors tested the interaction between muting and perceptions of belongingness (which were significantly negatively correlated with each other; −0.45, p < 0.05) in a multilevel regression, and the interaction was significant: ‘mute levels do not impact fatigue at high levels of group belongingness, indicating the importance of group belongingness to reduce videoconference fatigue’.
Qualitative studies: thematic analysis of findings
An additional analysis of the themes reported in the included qualitative papers was undertaken to ensure that meaning was not lost in the factors analysis reported above. A summary of the identified themes is provided with full extraction data included in the supplementary material.
Pre-COVID-19 studies
Qualitative data from pre-COVID working from home research revealed an intricate interplay of benefits and detriments (see Figure 7). Participants described positive impacts on their emotions, which stemmed from being more satisfied with their jobs (or even making a job that they didn’t enjoy bearable; Tietze 201133), attaining a better balance between work and other aspects of their lives, and having the mental space for creativity in their jobs, without the distractions of a workplace (Charalampous 2021,12 Daniel et al. 201816). In some cases, working from home brought more autonomy and control in terms of not just the time and place of work but also workloads, and this sense of control helped people to manage stress by fitting work in flexibly around other commitments and interests, and keeping workloads manageable (Daniel et al. 2018,92 Hislop 2015,21 Mann et al. 2003,25 Tietze 201133). Avoiding negative aspects of the workplace, such as negative interactions like ‘backbiting’, ‘bitching’, ‘bickering’ and ‘gossiping’ (and the resultant stress experienced), contributed to home workers’ wellbeing (Collins et al. 2016,15 Tietze 201133).
However, the flipside to this was that people working from home experienced isolation, frustration and stressors relating to the job role of specific WFH occupations. People working from home experienced isolation and loneliness as a result of the lack of social interaction, including not having day-to-day contact with co-workers, not getting to know new office staff, and no-one to help with problem-solving and ‘bounce ideas off’ (Charalampous 2021,12 Collins et al. 2016,15 Daniel et al. 2018,92 Hislop 2015,21 Mann et al. 2003,25 Stitou 2018,31 Vitterso 2003,10). This was exacerbated by extraversion (Koehne et al. 201223), working long and irregular hours (Daniel et al. 201892) and a longer duration of and/or more time spent working from home (Collins et al. 2016,15 Daniel et al. 2018,92 Vitterso 200310). This isolation could result in poor mental health (Stitou 201831) and in a feeling of insecurity and lack of confidence (Mann et al. 200325), and was even felt when the home-worker was working in home-based childcare and had daily contact with young children, but not other adults (Stitou 201831). People would counteract this isolation by finding ways to maintain communication and/or social contact, whether with their colleagues or in the community around their home, and some people reported that the lack of a commute gave them more time to spend with family and friends (Grant et al. 2013,18 Koehne et al. 2012,23 Tietze 2011,33 Vitterso 200310).
Another detriment to working from home was the feelings of irritation and frustration due to work factors outside the home-worker’s control that impacted on their ability to work. These included frustration with technological issues, not being able to get hold of colleagues when needed, and the intrusion of family members into work time (Charalampous 2021,12 Mann et al. 200325). The nature of the types of work that are amenable to a home-based setting could also cause stress and poor mental and physical wellbeing. For instance, home-based childcare work was perceived as mentally and emotionally draining, due to having to maintain concentration for long periods of time, deal with children with behavioural conditions, maintain relationships with parents, and ensure that regulations were being adhered to in case an inspector called unannounced, all while being (self-)employed precariously with no or little benefits such as sick pay, healthcare or pensions (Stitou 201831). In some types of office work where only a proportion of the workforce worked from home, staff were worried that they may be called back into the office if they were perceived as not performing to a certain standard, which had a negative emotional impact (Collins et al. 2016,15 Tietze 201133). Organisational culture could also impact on the wellbeing of people working from home. In some cases there was a possibility that working from home could impact on career progression and development due to missing out on opportunities and training, and thus being part of an organisation that embraced working from home was seen as being important by workers (Charalampous 202112) (Figure 7).
FIGURE 7.
Thematic structure tree diagram for pre-COVID studies.

COVID-19 studies
A wide variety of issues were reported through qualitative data analysis in relation to working from home during the COVID-19 pandemic. Again, there was a balance of benefits and detriments to working from home during the pandemic, although in this case there seemed to be more detriments (see Figure 8 and Figure 9). This could be due to the emergency situation, where people felt less control overall in their work circumstances, and this was reflected in the difficulty of finding appropriate working space in the home (Fukumura et al. 2020,97 Travers et al. 2020115), particularly having to share the space with other members of the household, including partners, housemates and children (Clark 2021,60 Fukumura et al. 2020,97 Travers et al. 2020,115 Waizenegger et al. 202043). Home workers spoke about the forced situation, and how it blurred boundaries between work and home life (Boncori 2020,90 Clark 202160), with new demands that included having to get used to an unusual situation, excessive work demands (including an expectation from employers of business as usual) and family demands, overlaying a backdrop of general worry and anxiety relating to the pandemic (Fukumura et al. 2020,97 Travers et al. 2020115). The change in routine was something that some people found a struggle; others adapted by introducing new routines (e.g. exercise regimes), but described these as unsustainable over the longer term (Travers et al. 2020115). As with the pre-OVID studies, isolation was experienced while working from home, but this was potentially more intense than pre-COVID due to the duration of homeworking and the lack of possibility for other forms of social interaction (Clark 2021,60 Gao and Sai 2020,62 Lal et al. 2021104).
With all interaction being online, videoconference fatigue was reported as a phenomenon, with symptoms including anxiety and tiredness (Boncori 2020,90 Lal et al. 2021,104 Waizenegger et al. 202043), as well as musculoskeletal pain from having to sit on video calls for long periods (Boncori 202090). There was also an element of occupational work invading the home space (Boncori 202090). Having to try and translate work online was a source of stress, and this was reported among those who had to try and manage the change among a number of employees (Boncori 202090). Additional pandemic-related concerns were silence and awkwardness in online interactions (Gao and Sai 202062) and concern and worry about colleagues and how they were coping, in the absence of visual cues (Lal et al. 2021104). Negative emotional responses such as ‘brain fog’, anxiety and fear were also reported (Travers et al. 2020115).
One thing that seemed more prevalent among the COVID qualitative data than among the pre-COVID data was increased monitoring of staff by managers, to the point where it became excessive and intrusive; people felt under pressure to be available and responsive at all times, and were under almost constant contact and scrutiny in some cases, which caused stress and fear (Delfino and van der Kolk 2021,52 Fukumura et al. 2020,97 Lal et al. 2021104). There was also an element of occupational work invading the home space (Boncori 202090). As with the pre-COVID studies, isolation was experienced while working from home, all the more so because of the duration of homeworking and the lack of possibility for other forms of social interaction (Clark 2021,60, Gao and Sai 2020,62 Lal et al. 2021104). The change in routine was something that some people found a struggle; others adapted by introducing new routines (e.g. exercise regimes), but described these as unsustainable over the longer term (Travers et al. 2020115).
Benefits included improved wellbeing, including through avoiding commuting and some of the negative aspects of office life (Fukumura et al. 202097), increased flexibility (Travers et al. 2020115), and, for some people (e.g. those with internal offices in the workplace), more optimal working conditions, with natural light and the possibility of spending breaks in the garden (Fukumura et al. 202097). To counteract isolation, some people created social interactions with friends, relatives and colleagues, for instance through ‘virtual coffees’, with some employers deliberately implementing these (Boncori 2020,90 Travers et al. 2020,115 Waizenegger et al. 202043). Others appreciated spending more time with family (Lal et al. 2021104). A beneficial side effect of the pandemic among those who were already working from home is that, in some cases, bonding between the whole team improved, and existing remote workers were included in social events for the first time (which would previously have been arranged as ‘in-person’) (Waizenegger et al. 202043).
Some inequalities were highlighted, for instance those with smaller or more crowded living space found working from home more stressful, particularly as pandemic conditions meant the space became crowded (Fukumura et al. 202097). The need to juggle work with childcare/home-schooling seemed to fall primarily onto women (Clark 202160), highlighting a potential gender inequality in working from home during the pandemic. This was exacerbated by a lack of consideration of childcare from male partners’ workplaces (Clark 202160).
Certain elements of organisational culture were found to impact negatively on wellbeing, for instance treatment of fathers vs. mothers, and micro-management. In considering potential childcare responsibilities of female but not of male workers, organisations inadvertently perpetuated gender inequality, which could disproportionately negatively impact women in terms of high stress levels and depression experienced by mothers who have to work at home (Clark 202160). Increased monitoring of staff by managers seemed more of a salient concern among the COVID qualitative data than among the pre-COVID data, to the point where it became excessive and intrusive. This often took the form of increased messages or phone calls from a supervisor and increased numbers of video calls (from the usual number of face-to-face meetings prior to the pandemic) (Delfino and van der Kolk 2021,52 Fukumura et al. 2020,97 Lal et al. 2021104). Staff felt under pressure to be available and responsive at all times, and were under almost constant contact and scrutiny in some cases, which caused stress and fear (Delfino and van der Kolk 2021,52 Fukumura et al. 2020,97 Lal et al. 2021104). This seemed to be born out of a lack of trust (Delfino and van der Kolk 202152), perhaps because of a lack of control over the work situation.
Inequalities and studies which consider subpopulations
A total of 15 studies considered the potential for working at home to have different effects for different subgroups of the population. A combination of studies which recruited specific sections of the population and those who included subgroup analyses within their reported results suggested overall that working at home may have more negative consequences during the COVID-19 pandemic for women and, in particular, mothers. However, it was impossible to tell whether this was primarily as a result of lockdown-related childcare responsibilities and home-schooling or related to other aspects of home working during the pandemic. There was very little evidence on age, ethnicity, education or income in terms of moderating home working effects, and very limited evidence from before the COVID-19 pandemic.
The evidence suggests that inequalities are essentially related to an individual’s socioeconomic circumstances, for example, appropriate space to work at home. There are likely to be other factors (not reported in these papers), in particular factors related to home environment and nature of job, especially control and autonomy over work, and the need to be accessible to colleagues when working at home, which will also have an impact.
Six studies, all conducted during the COVID-19 pandemic, recruited specific subpopulations of workers to look at the effects of working from home on them. These included mothers (Clark et al. 2021,60 Limbers et al. 202066), females (Gao and Sai 202062), parent couples (Shockley et al. 2021,29 Xue et al. 202167), and adolescents and caregivers (Janssen et al. 202065).
For mothers, increased levels of psychological distress as a result of the pandemic and working from home were reported in a qualitative study by Clark et al. (2021)60. These factors were negatively affected by increased childcare and domestic duties. In addition, one survey study reported that the negative impact on parenting stress on social relationships and satisfaction with one’s environment in home working mothers could be affected by moderate-intensity PA (Limbers et al. 202166). Gao and Sai (2020)62 described the female experience of social isolation due to working at home during the COVID-19 pandemic in an ethnographic study.
Xue et al. (2021)67 conducted a prospective cohort study with home working parents during the COVID-19 pandemic and found that increased housework and childcare/home-schooling hours were (weakly) associated with higher levels of psychological distress (assessed on the GHQ) among women (and lone parent women more so). Being the only member of the couple to adapt working patterns to accommodate childcare was associated with poorer GHQ scores in women and men. This was supported by Shockley et al. (2021),29 who reported those parent couples adapting the strategy of ‘alternating days’ fared the best in terms of the impact on psychological distress due to home working. In comparison, working from home was not related to the increase in parents’ negative affect during the COVID-19 pandemic, as compared with pre-pandemic data, according to Janssen et al. (2020)65.
A further eight studies of general populations reported subgroup analysis of specific population groups considering how factors which influence the associations between working at home and health measures varied by demographic variables within the populations studied.
Pre-COVID, one study reported that home working did not have an impact on overall life satisfaction, nor among men or women individually (Reuschke et al. 201928). However, a second study (Song et al. 202030) reported that parents (especially fathers), report a lower level of subjective wellbeing when working at home on weekdays but not weekends. They also found that childless females felt more stressed teleworking instead of working in the workplace (Song et al. 202030). Finally Charalampous et al. (202112) looked at the impact on working remotely on men and found mixed effects for wellbeing-related measures including happiness, loneliness, psychosomatic health, sedentary behaviour and stress due to technology issues.
COVID-19 studies
Seven COVID-19 studies reported on variable outcomes by gender, caring responsibilities, age, ethnicity, education and income.
Gender
Five studies reported negative impacts of working at home for women compared to men during the COVID-19 pandemic. Hubbard et al. (2021)63 said that women reported less WFH satisfaction than men during the COVID-19 pandemic. Further, Docka-Filipek et al. (2021)61 found that gender accounted for unique variance in both depression and anxiety (with rates for females higher in both cases). Stress and ‘non-healthy days’ increased in women but not men (Ray et al. 202127) and women were more likely to feel isolated and report developing musculoskeletal problems (RSPH 202142). Cotterill et al. (2020)50 reported that more women perceived that their wellbeing decreased in lockdown than men but found no difference in median wellbeing values. However, one study reported positive outcomes in women compared to men. Sato et al. (2021b38) found a greater increased intake of vegetables, fruits and dairy products and decrease in alcohol intake among women than men. Finally, Ignacio Gimenez-Nadal et al. (2020)64 reported that, compared with commuters, male teleworkers (but not females) reported lower levels of sadness, stress and tiredness and female teleworkers (but not males) reported higher happiness levels.
Burstyn et al. (2021)91 found that anxiety and depression were negatively linked to concerns about return to work, childcare, lack of sick leave, and loss/reduction in work. They reported that these ‘patterns differed by sex’ but the direction of differences was not clear. Finally Weitzer et al. (2021)39 reported that men were more likely to report no changes in QoL than women.
Caring responsibilities
Three studies looked at caring for children. Chung et al. (2020)93 reported that increased workload and conflict between work and family negatively impacted parents’ mental wellbeing, especially for mothers: ‘almost half’ of all mothers felt rushed and pressed for time, more than half of the time during the lockdown, and 46% of mothers felt nervous and stressed more than half of the time. A study by the University of Exeter (2020)116 also reported that increased demands to juggle work and domestic responsibilities (including childcare) had a negative effect on wellbeing. Having more dependents also accounted for ‘unique risk for anxiety’ (Docka-Filipek et al. 2021)61. Two further studies considered caring for adults. Hubbard et al. 202163 reported that a significant predictor of dissatisfaction with home working was having caring responsibilities for an adult. Mental health was found to be poorer among those who were looking after elderly relatives (but parents were no different to non-parents) (Bevan et al. 202089).
Age
Two studies considered age as a variable factor and reported that older participants were most likely to report no changes in QoL from working at home (Weitzer et al. 202139), and also that mental health was generally poorer for younger home workers compared to older age groups (Bevan 202089).
Ethnicity
Only one study considered the potential impact of ethnicity and found that reports of stress and ‘non-healthy days’ increased in ‘non-whites’ (Ray et al. 202127).
Education and income
The same two studies reported that those who were ‘university educated’ were most likely to report no changes in QoL (Weitzer et al. 202139), and that stress and non-healthy days increased in those of lower income and lower health status (Ray et al. 202127) (Figures 8 and 9).
FIGURE 8.
Thematic structure tree diagram for COVID-era studies – Benefits theme.
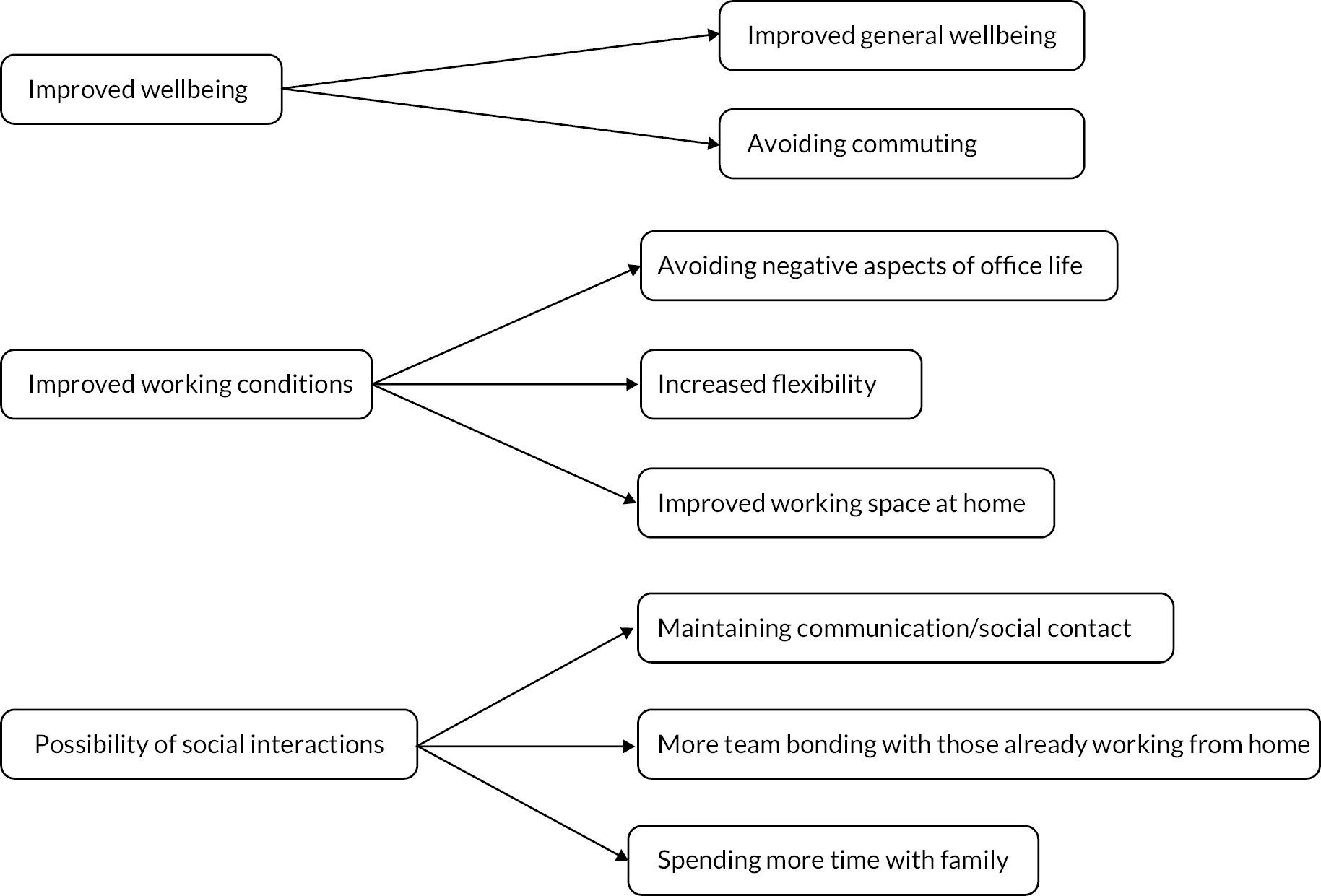
FIGURE 9.
Thematic structure tree diagram for COVID-era studies – Detriments theme.

The impact of COVID-19 on working from home
In order to consider whether any definitive statements could be made about the variation in outcome measures reported before and during the COVID-19 pandemic, a comparison table of outcomes reported and whether they were positively or negatively associated with working from home for studies completed in each time period was developed (see Table 11. Comparisons of working from home factors which influence the associations reported by studies conducted before and during the COVID-19 pandemic).
| Factor | Author descriptions | COVID study IDs | Pre-COVID study IDs |
|---|---|---|---|
| Choice | |||
| No choice | Enforced / no choice | 88, 93 | 46 |
| Home environment | |||
| Control | Control over workspace/time | 88 | 38, 56, 80, 81 |
| Commute | Lack of commute | 14, 83 | |
| No travel to work | 56 | ||
| Travel stress reduced | 32 | ||
| Silence | Silence (in virtual spaces as well as the home) | 30 | |
| Distractions | Increased distractions/interruptions while working | 29, 88, 94 | |
| Fewer distractions | 14 | ||
| Spouse in home | 64 | ||
| Work undisturbed | 80 | ||
| Lack of space | Lack of space / unsuitable home environment | 14, 28, 41,69, 82, 88 | |
| Environment | Lower environmental health QoL | 53 | |
| Pets | Presence of dogs or cats in home | 39 | |
| Caring responsibilities | Increased childcare | 14, 15, 95 | |
| Caring for a responsible adult | 41 | ||
| Being only parent to adapt working pattern to accommodate childcare | 95 | ||
| More dependants at home | 24 | ||
| Parent (stress) | 13, 47, 53 | ||
| Increased domestic duties | 15, 95 | ||
| Childcare stress reduced | 32 | ||
| Family conflict | Interference with family life | 64, 78 | |
| Family–work conflict | 13, 26, 28, 29, 85 | ||
| 20 | |||
| Time with family | More time with family | 57, 13 | |
| Safety | Not feeling ‘sheltered at home’ | 19 | |
| Work/job-specific factors | |||
| Professional group | Public vs private sector | 70 | |
| Being an essential worker | 17 | ||
| Type of employment | 66 | ||
| Work stress | Increased stress relating to indistinct organisation | 36 | |
| Less office politics | 37, 56 | ||
| Office grapevine decreased | 32 | ||
| Workload | Increased burnout | 26, 35 | |
| Work overload / increased workload | 43, 59 | ||
| More hours work | 56 | ||
| Work demands | New and excessive demands | 21, 57, 55 | |
| Higher job demand | 19 | ||
| Surveillance/availability | Increased (work) monitoring | 21, 23 | |
| Expectation to always be available | 21, 23, 61 | ||
| Sense of perpetual contact | 55 | 38 | |
| More control over work | 56 | ||
| Autonomy | Autonomy | 93 | 18 |
| Technology | Increased video calling | 21, 23, 61 | |
| Increased videoconference fatigue | 5 | ||
| Having camera turned on | 5 | ||
| Techno-overload / stress | 26, 59, 79 | ||
| Techno-invasion | 59 | ||
| Fear of tech failure | 18 | ||
| Hybrid working | Working alternative home and office days | 68, 75 | |
| Telecommute intensity (less) | 37 | ||
| Work perceptions | Low perceived remote work productivity | 82 | |
| Self-imposed pressure to perform | 16 | ||
| Low perceived remote work satisfaction | 82 | ||
| Low sense of belonging | 5 | ||
| Employer support | Low support for WFH | 61 | |
| Support from colleagues (increased) | 32,56 | ||
| Communication with colleagues (decreased) | 32 | ||
| Individual factors – wellbeing and mental health | |||
| Wellbeing | Wellbeing | 1, 6, 17, 23, 65, 63, 14, 27, 47, 61, 69 | 33 |
| Loneliness | Loneliness/isolation | [14, 26, 29, 30, 63, 69 74, 79, 82, 85, 93 | |
| Social support | Social support | 93, 70 | |
| Lower social relationship QoL | 53 | ||
| Social life (improved) | 44 | ||
| Social connectedness | 3 | ||
| Adult contact (less) | 78 | ||
| Social interaction (less) | 52 | 16, 48 | |
| Anxiety | Higher anxiety | 10, 14, 24, 55, 74, | |
| Anxiety | 90 | ||
| Lower anxiety | 76 | ||
| Depression | Depression | 76 | 37 |
| Higher depression | 10, 20, 24, 42, 55, 72, 74 | ||
| Psychological health | Mental health | 8, 49 | |
| Lower psychological health QoL | 53 | ||
| Increased psychological distress | 15, 19, 95 | ||
| Low levels of psychological distress | 75 | ||
| Emotional ill health | 56 | ||
| Coping | Coping | 3 | |
| Coping with COVID-19 | 9 | ||
| Affect | Negative affect | 45 | |
| Positive affect | 3 | ||
| Stress | Stress | 84, 37,46,56,77,81 [46a, 56, 64 | |
| Reduced stress | 20, 59 | ||
| Increased stress/worry/fear/ pressure | [21, 26, 29, 35, 42, 70, 82, 83 | 62, 71 | |
| Sleep | Good sleep quality | 75 | |
| Longer sleep duration (more sleep – unclear if considered positive) | 34 | ||
| Fatigue | 36, 31, 49, 61 | 62, 71 | |
| Demographics | Graduate education | 19, 70 | |
| Gender (female) | 17, 24, 41, 95 | 64 66 |
|
| Non-white | 64 | ||
| Health status | Low health status | 64 | |
| PA | More opportunity to exercise | 83 | |
| Increased PA | 94 | ||
| Decreased PA | 12, 53, 88 | ||
| Sedentariness, standing and movement | 34, 36 | ||
| Satisfaction | Fulfilment | 18 | |
| Life satisfaction | 66 | ||
| Worse life satisfaction | 74 | ||
| Worse satisfaction with WFH | 41, 79, 82 | ||
| Life less worthwhile | 74 | ||
| Low enjoyment of activities | 27 | ||
| Leisure time satisfaction | 66 | ||
| Openness | Openness to new ways of living | 9 | |
| Open to experience | 3 | ||
| Financial worry | Greater financial concerns | 24 | |
| Low income | 64 | 4, 94, 96 | |
| Overall physical health | 56 | ||
| Physical inactivity decreased | 11, 37 | ||
| Sitting increased | 32 | ||
| Lack of sports facilities open | 88 | ||
| Minimal contact with others | 88 | ||
| General health | General health | 23 | |
| Psychosomatic health | 92 | ||
| Perceived health | 50 | ||
| Physical health | Physical wellbeing | 94 | |
| Burnout | Burnout | 46a, 62 | |
| Quality of life | 12 | 40, 87 | |
| QoL satisfaction | 86 | ||
| Pain | Reduced work comfort (lockdown) musculoskeletal pain | 4 | |
| Spine problems | 60 | ||
| No association with bodily pain | 91 | ||
| Pain augmentation | 96 | ||
| Diet | Healthy food intake decreased. Junk food intake increased | 73, 94, 51 | |
| Substances | Drug use | 67 | |
| Tobacco use reduced | 37 | ||
| Alcohol use reduced | 73 | 37 | |
| Increased alcohol consumption | 2 | ||
| Increased cigarette consumption | 19 | ||
Wellbeing measures
A notable omission from the evidence is that the concept of enforced working from home and having ‘no choice’ was reported in only one paper prior to the pandemic and two papers reporting on working from home as a result of COVID-19 and the associated lockdown measures. However, the concept of lack of choice around working from home was implicit in much of the literature published during COVID-19 – even though it was not directly measured.
Prior to COVID-19 one study considered the difference of working from home on a voluntary basis compared to where it was enforced. Involuntary working from home was associated with greater work-to-family conflict, stress, burnout, turnover intentions, and lower job satisfaction whereas voluntary WFH was protective, and associated with greater job satisfaction, lower turnover intentions, and less stress (Kanduk et al. 2019). Two COVID-19 studies reported having no choice but to WFH as negatively impacting on wellbeing (Waizenegger et al. 2020,43 Wood et al. 2021119). The concept of choice was also implicit in many of the other COVID-19 papers, although it was not directly measured. It seems that allowing employees some flexibility over whether they choose to work at home in the future, and beyond the COVID-19 pandemic, will be a key factor in determining whether the home working experience is positive or negative, particularly for mental health and wellbeing-related outcomes.
Home environment
In terms of the home working environment, for factors which were reported both before and during the COVID-19 pandemic, there was no change of direction for any of the measures considered (with the exception of one study). Positive factors reported prior to COVID-19 which were also reported as being positively associated with wellbeing during the pandemic included having control over the workspace and the times worked, not having to commute (and the associated reduction in stress) and experiencing fewer distractions and disturbances whilst working at home, usually due to fewer people in the household (12 studies in total). The association which remained almost entirely negative with respect to wellbeing was family conflict as a result of home working and interference with family life (although one COVID-19 study did report a positive association with family conflict). No other measures relating to the home working environment were considered by studies conducted before or during the pandemic.
Job-related outcomes
Job-related factors which remained positively associated with better wellbeing both before and during the pandemic included hybrid working arrangements (three studies), having high autonomy over work (three studies) and receiving support from the employer to work at home (four studies). High work stress (four studies), high workload (six studies), work demands (four studies), surveillance (including an expectation to always be available) (six studies), low work perceptions (five studies) and problems associated with technology (seven studies) were consistently associated with poorer wellbeing-related outcomes for home workers. There were no consistent patterns in relation to professional group or type of employment.
Individual outcomes
There were consistently positive associations for better wellbeing both before and during the pandemic in terms of having good social support (10 studies), and a personality type which meant an individual had high ‘coping’ (two studies) and ‘openness to new experience’ (two studies). Having financial worries was unsurprisingly consistently associated with poorer WFH wellbeing (two studies). For depression, associations with health outcomes were mostly negative for studies conducted during the pandemic (resulting in poorer health) (seven studies), but positive before COVID-19 (resulting in better health) – although this was only reported by one study prior to the pandemic. All other outcomes were mixed in terms of the direction of association with wellbeing; or were not reported by studies conducted both before and during the pandemic.
Therefore, perhaps surprisingly there were no clear patterns of wellbeing measures which changed from positive to negative association (or vice versa) during the pandemic. This is of course determined by what authors chose to measure and report, and the paucity of evidence on wellbeing measures prior to the pandemic, so should in no way be taken to suggest that pandemic home working did not have an effect on wellbeing overall. Further it is impossible to separate out the effects of COVID-19 lockdown and uncertainties on wellbeing from the direct impacts of home working during this time on wellbeing, particularly for studies conducted during the early stages of the pandemic.
Physical and overall health measures
In terms of physical and overall health measures, the significantly smaller number of studies measuring these types of association both before and during the COVID-19 pandemic made it even more challenging for any potential patterns to be identified. However, there is some indication that the association between working at home and PA measures became more negative during COVID-19 pandemic, with five studies reporting reduced PA (compared to a more mixed picture before the pandemic of two studies reporting factors with positive associations, one negative, and one reporting no effect). This is unsurprising given the lockdown measures in which home working was implemented, during which time sports facilities, leisure centres and gyms were closed.
All other measures did not appear to be affected to any measurable extent by the COVID-19 pandemic (most likely due to the low number of studies identified). Better QoL and life satisfaction remained positively associated with working from home (in one COVID-19 study and two from before the pandemic); studies reporting on general/physical health and burnout all reported factors with negative associations with working from home (two studies from before COVID-19, including one of enforced home working, and three COVID-29 studies). Studies on pain-related outcomes during COVID-19 (four studies) reported factors with negative (less pain) or no association (with no pre COVID-19 studies identified). Studies measuring diet (four COVID-19 studies) showed factors with mixed positive and negative associations, as did studies on substance use, which were mostly positive (one measuring tobacco use during COVID-19, two measuring alcohol use; one before and one during COVID-19), with one final COVID-19 study reporting no association between drug use and working from home.
Evidence-based model – combining the findings
The a priori model3 developed at the outset of the project included information on contextual factors and outcome measures, as well as the expectation that the impact on health outcomes was likely to be moderated by factors relating both to the individual and their job, and to the home environment.
A number of key contextual factors identified through recent reviews and grey literature publications have contributed to the increases in home working seen both prior to and as a result of the COVID-19 pandemic. These can be summarised as:
-
changing preferences (employers and employees) – shift to home working (CIPD 2020) 73 and more generally to flexible work/multi-career work
-
technology development
-
increased commuting times
-
COVID-19 pandemic
-
environmental concerns.
Changing preferences
Even prior to the COVID-19 pandemic, more people were choosing home working for some or all of their working hours. Between 1999 and 2019 working mainly from home increased by 80% to reach 5.3% of workers (CIPD 2020). 73 However, prior to COVID-19 the majority of home workers did so only occasionally. A key determinant of working from home is age, with older workers more likely to be in the ‘mainly work from home’ category and the ageing workforce a reason for the increase in the number of people working from home (CIPD 2020). 73 Home working also varies by level of skill and experience and by industry, with ‘managers, directors and other senior officials and people in professional occupations’ most commonly working from home, and ‘process, plant and machine operatives and those in elementary occupations’ least likely to do so (CIPD 2020). 73 Flexible work and multi-career approaches have become more mainstream in recent years, with the UK Government now offering guidance that all employees have the right to request flexible working (working in a way of working that suits an employee’s needs, for example having flexible start and finish times, or working from home), with employers having to provide a ‘good business reason’ for refusing an application for flexible working (GOV.UK 2021120).
Technology
A key driver enabling working from home is technological development, with the transition to digital tasks and communication having a profound effect on the number and types of jobs which can be done from home. For most jobs the use of a computer is essential for at least some aspects of the work, and the huge increase in household internet access over the last two decades has enabled many more people to WFH (CIPD 202073).
Commuting
Increased commuting time is another driver, with people who occasionally worked from home prior to COVID-19 having a nine-minute longer journey time than those who do not (CIPD 202073). However, it is not clear whether longer commutes were leading people to WFH, or the ability to WFH was facilitating longer commutes for those with hybrid working arrangements.
COVID-19
Clearly the impact of the pandemic has had a significant effect on increasing the number of people working at home (at least for the present time). As a result, 35.9% of employees did some work at home in 2020, an increase of 9.4 percentage points compared with 2019 (ONS 202176).
Environmental concerns
With the COVID-19 pandemic lockdown causing a measurable decrease in carbon dioxide emissions as a result, in part, of decreased road and air-traffic journeys (including journeys made to and from places of work) (Sikarwar et al. 2021121) the awareness of the impact of commuting and travelling for work on contributing to the global climate emergency has been raised.
The results of our systematic review allowed us to build on the a priori model3 in order to develop an evidence-informed model and to add the huge variety of additional factors reported in the literature which are associated with the pathway between working at home and health-related outcomes. As a result of this analysis we have separated the factors into those related to the home working environment, those related to the job and employer behaviours, and those relating to the individual. Also implicit in the literature identified is the concept that having choice over whether to work at home or not is key to determining whether the experience is likely to be positive or negative for the individual. This extends to the notion that for many, a hybrid working situation (some time at home and some time in the office or usual place of work) can be of greatest benefit. Our final evidence-based model (see Figure 10. Final evidence-informed model of the factors which influence the associations between working from home and health outcomes) therefore draws together the result of our systematic review (and previous mapping review) along with our PPI and stakeholder consultation exercises to provide an overall summary of the reported factors which influence the associations between working from home and health (and related) outcomes.
FIGURE 10.
Final evidence-informed model of the factors which influence the associations between working from home and health outcomes.

Discussion
Summary
There has been a significant increase in the available evidence base for the factors which influence the associations between working from home and health-related outcomes as a result of the COVID-19 pandemic and working at home during lockdown measures and beyond. Previous reviews examining this issue either predate the pandemic (and therefore did not consider the mass home working of recent times), or were conducted rapidly and/or focus on a specific aspect of working from home (e.g. virtual teams, teleworking), a specific timeframe (e.g. since the start of the pandemic) or a specific outcome (e.g. psychological distress, lived experience). The current review aimed to fill this gap to provide evidence that can inform recommendations and guidance on working from home.
Our searches identified 96 studies which reported on the factors which influence the associations between working from home and health (and related) outcome measures; 30 published prior to the COVID-19 pandemic and 66 conducted in the last two years since the onset of COVID-19 and the compulsory WFH measures imposed in the UK as a result.
The largest volume of literature focused on measures of wellbeing and the associations with working at home which were conducted during the COVID-19 pandemic, with a relatively small evidence base relating to physical and overall health measures. The majority of studies identified (especially those published during the pandemic) were cross-sectional surveys and, as such, the limitations of the evidence base must be noted. It is only possible therefore to indicate the factors which were reported by the study authors and not to make any comment on factors which were not reported, nor on the relative strength of one association over another. Therefore, the results of this review should be taken as an indication of the effect that working at home can have on health-related outcomes, but not a definitive statement on those effects or any statement on the causality of the reported associations. The studies we have included, however, can give us an indication of the factors that might be important to consider if working at home is to continue at a significantly increased level in the future, in order to ensure that the potential benefits to impact on both physical health and mental wellbeing in the working population are maximised whilst potential risks to health and wellbeing are addressed.
The studies published before COVID-19 which looked at measures of physical and overall health suggested factors associated with better QoL and life satisfaction, and alcohol and tobacco use, factors associated with increased burnout and no association with ‘psychosomatic health’. Mixed relationships between factors associated with PA and working at home were reported. Overall, the small number of studies identified prior to the pandemic means these findings should be interpreted with caution. A slightly larger volume of literature on wellbeing and mental health-related outcomes was identified, but there was no clear overall pattern to the reported factors associated with the relationship between working at home and the broad range of wellbeing measures investigated by study authors. Overall, there were suggestions for factors associated positively with overall wellbeing, having control over the workspace, and having good communication with colleagues. Negative factors included fears associated with technology failure, including ability to work undisturbed, and interference with family life in the home. There was a mixed picture in terms of measures of stress, depression and other mental health measures, social contact, and measures of satisfaction and fulfilment.
The literature published during the COVID-19 pandemic, although more substantial in terms of volume, was mostly limited to cross-sectional survey data with self-reported outcomes, again limiting the conclusions which can be drawn. Studies considering general health were again limited but suggested positive factors associated with QoL and alcohol use, negative factors associated with high work demands, mixed factors associated with diet and no association with drug use. For physical health, all reported factors were negative associated and included reduced PA, reduced work comfort, pain measures and physical wellbeing. Mixed associations were reported for measures of wellbeing, stress (including perceived stress, perceived self-efficacy, ‘stress, worry and pressure’, burnout, ‘cognitive worsening’ and specific stress including parenting stress and occupational stress) and measures of mental health (including negative affect, anxiety, psychological distress). Measures linked to wellbeing including sleep (sleep quality, time sleeping and fatigue) also reported mixed factors associated with working from home. Nearly all reported factors associated with depression were negative (depression increased), as were factors associated with social interaction (social isolation, loneliness, minimal contact with others and low social support) along with increased health concerns, and having a lack of choice over whether to work at home. However, measures linked to the home work environment and wellbeing, including feeling in control of time, lack of commute, more time with the family, lower work/family conflict, work autonomy, and a measure QoL, were all reported as positive factors.
Based on the available qualitative evidence there was again a balance of benefits and detriments related to working from home, although in this evidence there seemed to be more detriments during the pandemic than prior to it. In this way the additional qualitative analysis serves to validate the overall patterns displayed in the mind maps.
There is some evidence that the impacts of home working on health are differentially distributed and that there may be some groups of workers particularly at risk of more negative outcomes associated with home working. Although a small number of studies limited their populations to particular employment sectors, or specific subgroups of the population, most authors recruited their samples from the working population in general and therefore it is also difficult to say anything definitive about differential effects of working from home for different groups within the population. Six studies did consider the impact on females, working mothers, couples with children and those with adult caring responsibilities and this evidence suggests the potential for the negative impacts of working from home to weigh most heavily on these population groups. However, as these were conducted during COVID-19 lockdown measures it is difficult to generalise their findings to the wider context and more information is needed to judge the impact on these subgroups.
Arguably the most important factor (at least for employee wellbeing) is choice over work location and the extent to which hybrid working options are available. A notable omission from the evidence is that the concept of enforced working from home and having ‘no choice’ was reported in only one paper prior to the pandemic and two papers reporting on working from home as a result of COVID-19 and the associated lockdown measures. However, the concept of lack of choice around working from home was implicit in much of the literature published during COVID-19 without being a factor that was routinely measured. It is important to acknowledge that both employer (providing the offer of home/hybrid working) and employee (acting on both the choice and ability to WFH) factors are key to influencing whether working from home is a positive or negative experience in terms of its association with health outcomes.
Perhaps surprisingly there were no clear patterns of wellbeing measures which changed from positive to negative association (or vice versa) as a result of the pandemic. This is of course determined by what authors chose to measure and report, and the paucity of evidence on health measures prior to the pandemic, so should in no way be taken to suggest that pandemic home working did not have any negative effect on wellbeing. In terms of physical and overall health measures, the significantly smaller number of studies measuring these types of association both before and during the COVID-19 pandemic made it even more challenging for any potential patterns to be identified. However, there is some indication that the associations between working at home and decreased PA measures were greater during COVID-19. This is unsurprising given the lockdown measures in which home working was implemented. All other measures did not appear to be affected to any measurable extent by the COVID-19 pandemic (most likely due to the low number of studies identified). QoL and life satisfaction remained positively associated with working from home, and studies on substance use were mostly positive. Studies reporting on general/physical health and burnout all reported negative factors associated with working from home. Factors associated with pain were only reported for pandemic-era studies, which was also the case for diet-related outcomes and drugs use.
Limitations
Due to the rapidly expanding nature of the evidence on this topic, it is possible that new studies were published after the final citation searches were conducted (November 2021) and before completion of this synthesis (mid-December 2021). However, although the final round of citation searches identified new papers, the impact on the developing models in terms of new factors was minimal. The additional papers identified at this stage strengthened the factors already identified rather than identifying completely new factors and did not identify new linkages which would alter the findings of the review. Given the unprecedented explosion of literature on working from home as a result of the COVID-19 pandemic it is necessary to acknowledge that new evidence will continue to be published beyond the final date of citation searching at a volume greater than would usually be expected whilst conducting a systematic review of this type.
The quality of the evidence base was very much limited by study designs, particularly for studies published during the COVID-19 pandemic, with the majority of studies consisting of data collected by cross-sectional surveys (often online). Most survey samples consisted of volunteers rather than a representative population of workers. The latter would have been more beneficial to minimise bias. Also, retrospective estimations of pre-pandemic values (inherent in many of the cross-sectional designs) will further have contributed to the potential for bias in the findings. Given the complexity of casual pathways and importance of context, appropriate designs would ideally include more qualitative or mixed-methods studies that collected much more detailed information on the context of home working and were not limited to self-reported outcomes.
Understanding the factors and relationships reported by authors and the impact of further sub-factors on these is challenging. In some instances, an association is described, and then additional factors are reported which further moderate this association. However, to some extent this appears dependent on what the primary interest of the authors was and therefore what they have chosen to measure. Where there are clear moderating factors reported on the pathway between the key variables of the paper, especially related to health inequality variables, we have included these in the tables, mind maps and narrative discussions. However, this evidence is not robust enough to separate these factors out in the final model. As so much of the evidence comes from cross-sectional surveys, most often direction of potential causality is unknown. There is also a high risk of potential response bias when participants are invited to share their experience of working from home, as those who feel it has had health impacts may be more likely to respond.
There are challenges in interpreting a number of the reported factors in terms of separating out the effects of the COVID-19 pandemic and enforced working from home, particularly on the reported stress, anxiety and changes to wellbeing when working at home. Understanding the balance will be a key challenge for both research and employers. What is COVID-19-specific and what will be important post-pandemic is difficult to judge whilst working from home is once again part of the pandemic response (at least at the time of writing). Thought needs to be given in order to determine whether we can judge this in any meaningful way whilst the pandemic is still in progress, and what research is needed to answer that question in the future. This is important in order to identify issues that will need more research to understand future public health implications of home working trends post-pandemic.
The study was limited to English-language publications only, which may have implications in terms of missing studies published in other languages.
Conclusions
The evidence base for the factors which influence the association between home working and health-related outcomes has expanded significantly as a result of the need for those whose work could be done from home to work at home during the COVID-19 pandemic. However, it remains limited in terms of study quality and is focused on mental health and wellbeing-related measures at the expense of measures of physical and overall health.
The current evidence base is not strong enough to determine whether certain individual factors are most important in the pathway between home working and health outcomes and there is a further lack of evidence to determine which groups within a population might be at greatest risk of negative outcomes. However, the findings of our systematic review and resulting model of factors which influence the association between working at home and employee health suggest that there are factors relating to the external context, the role of employers, and the circumstances of the employee which contribute to determining whether someone works at home and what the associated impacts on health and wellbeing may be. External drivers and current trends, as well as the COVID-19 pandemic, contribute to the contextual factors. The employer response is determined by their capacity and willingness to allow and/or mandate home working and hybrid options. If those choices are offered, then the individual factors relating to the employee, their job and their home environment (including their exposure to health inequalities) determine whether they are enabled to choose to work at home, and ultimately whether their experience is positive or negative in respect to the impact on their health and wellbeing. Learning from the COVID-19 lockdown experience will be important to inform future policy on home working.
Implications for employers
-
A key action for employers to support the health and wellbeing of their employees is likely to be the offer of choice over work location. Allowing employees some flexibility over whether they choose to work at home in the future and beyond the COVID-19 pandemic is likely to be a key factor in determining whether the home working experience is positive or negative, particularly for mental health and wellbeing-related outcomes. Hybrid working options appear to have the potential to be particularly positive.
-
Employers should seek to provide support to staff working at home so that they feel included and empowered, whilst ensuring that they are able to maintain autonomy over their work and do not feel subjected to excessive surveillance.
-
Organisations that have a culture of monitoring workers’ progress on projects may need to be aware that excessive monitoring can lead to anxiety, stress and fear among staff while working from home during an emergency situation, where this monitoring takes the form of constant contact and an expectation to always be available.
-
Employers should be aware of the potential for the health impact of working at home to differ between individuals (with the potential for more negative outcomes for females, mothers, parents, and others with caring responsibilities). Employers should consider providing specific support for females, parents and those with caring responsibilities. This may include support to combat isolation, improve mental health and prevent musculoskeletal problems (e.g. through a better workstation and ergonomic support), particularly where there is less choice in where to work.
Research recommendations
-
There is a need for better-quality studies of the health impact of home working, in particular studies which recruit a range of participants who are representative of the working population and are designed to minimise sampling/recruitment biases and response biases.
-
More longitudinal cohort studies would provide evidence for potentially causal relationships and direction of causality in the pathway between home working and health-related outcomes.
-
More in-depth qualitative research would be beneficial to explore the underlying factors which influence the association between home working and health related behaviours, particularly where the direction of change appears to be context-, individual- or job-specific (e.g. alcohol consumption, PA and sedentary behaviour).
-
Further research is needed on the impact of home working on different sections of the population and the potential for inequalities in outcome for different population groups, job roles and employment sectors.
-
Consideration could be given as to whether the factors which appear to remain relatively consistent despite COVID-19 and lockdown might be the most important to consider in terms of facilitating a positive work-at-home experience.
Acknowledgements
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
Contributions of authors
Lindsay Blank (https://orcid.org/0000-0002-8765-3076) (Research Fellow): Lead reviewer, protocol development, study selection, data extraction, report writing.
Emma Hock (https://orcid.org/0000-0002-8617-8875) (Senior Research Fellow): Study selection, data extraction, report writing.
Anna Cantrell (https://orcid.org/0000-0003-0040-9853) (Research Associate): Information retrieval.
Susan Baxter (https://orcid.org/0000-0002-6034-5495) (Senior Research Fellow): Patient and public involvement.
Elizabeth Goyder (https://orcid.org/0000-0003-3691-1888) (Professor): Methodological adviser, protocol development, guarantor of the review.
All authors commented on drafts of the protocol and report.
Ethical approval
This review did not involve the collection or analysis of any data that was not included in previously published research in the public domain. Therefore it was exempt from formal ethical review by the University of Sheffield Ethics Committee.
Data-sharing statement
Data extracted from the included papers is provided in full in the supplementary material provided with this report.
Equality, diversity and inclusion
As a secondary data study our review did not include any research participants. We were however, inclusive in the studies we selected and reported where demographic and socio-economic factors were considered by the studies we included. We also selected our PPI group to be as inclusive as possible in reference to underserved groups.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
Appendix 1 Stakeholder participants: PPI and stakeholders
-
NHS Midlands and Lancashire Commissioning Support group (n = 1)
-
PHE workplace health and wellbeing group (n = 1)
-
Strategy employers, health and inclusive employment – DWP (n = 1)
-
CIPD: Chartered Institute of Personnel and Development (n = 1)
-
PPI representatives with experience of home working (n = 8)
Appendix 2 Quality appraisals of included studies
Appendix 2.1. Quality appraisals of included cohort studies
-
Did the study address a clearly focused issue?
-
Was the cohort recruited in an acceptable way?
-
Was the exposure accurately measured to minimise bias?
-
Was the outcome accurately measure to minimise bias?
-
Have the authors identified all important confounding factors / taken account of them in the design and analysis?
-
Was the follow-up of subjects complete enough?
-
What are the results of the study?
-
How precise are the results?
-
Do you believe the results?
-
Can the results be applied to the local population?
-
Do the results of the study fit with other available evidence?
-
What the implications of the study for practice?
| First author / year | Design | N= | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Summary |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Di Tecco 202135 |
Longitudinal interventional cohort study | 187 | Y | Y | Y | Y | Y | Y | ? | Y | Y | Y | Y | ? | High response / completion rates. |
| Hallman 202197 |
Observational within-subject study – diary and accelerometer | 27 | Y | U | Y | Y | Y | N | ? | ? | Y | U | U | ? | Within-subjects design reduced confounding. Many participants did not have complete accelerometer data. Unclear if results are applicable elsewhere. |
| Henke 201620 |
Retrospective cohort (from employee database) | 3703 | Y | Y | Y | Y | N | Y | ? | N | Y | Y | Y | ? | One company’s data so may not be representative of other sectors or companies. Possibly other confounders. |
| Janssen 202065 |
Longitudinal ecological momentary assessment study | 101 | Y | Y | U | Y | Y | N | ? | N | Y | Y | Y | ? | Drop-out rate for the follow-up seemed high. WFH was not a main focus. |
| Lundberg 200224 |
Repeated measures observational field study | 26 | Y | Y | Y | Y | N | Y | ? | Y | Y | Y | Y | ? | Possibility of confounders, small sample size. |
| Perry 20187 (Study 1) |
2-wave online survey | 258 | Y | Y | N | Y | N | U | ? | Y | Y | Y | Y | ? | WFH assessed via recall of percentage of time (rather than calculated), possibility of confounders, follow-up unclear as only n of those who completed both waves was reported. |
| Reuschke 201928 |
Longitudinal dataset (7 waves) | 33,719 | Y | Y | Y | U | Y | U | ? | Y | Y | Y | Y | ? | Most confounders accounted for. Completeness of follow-up unclear. |
| Russo 2021110 |
Online survey (longitudinal) | 192 | Y | Y | Y | Y | Y | Y | ? | Y | Y | Y | Y | ? | Longitudinal study, used validated measures and assessed a large number of factors. |
| Schifano 202159 |
Longitudinal online survey | 9700 observations | Y | Y | Y | Y | P | N | ? | Y | Y | Y | Y | ? | Some confounders may have been missed. Follow-up data not complete. |
| Shockley 202129 |
Longitudinal online survey (2 timepoints) | 133 | Y | N | Y | Y | N | N | ? | ? | Y | Y | Y | ? | Potential for selection bias, potential for confounders. |
| Wood 202110 |
Diary study – two time points | 784 | Y | Y | Y | Y | Y | Y | ? | Y | Y | Y | Y | ? | 20% of invited participants recruited. |
Appendix 2.2. Quality appraisals of included qualitative studies
-
Was there a clear statement of the aims of the research?
-
Is a qualitative methodology appropriate?
-
Was the research design appropriate to address the aims of the research?
-
Was the recruitment strategy appropriate to the aims of the research?
-
Were the data collected in a way that addressed the research issue?
-
Has the relationship between researcher and participants been adequately considered?
-
Have ethical issues been taken into consideration?
-
Was the data analysis sufficiently rigorous?
-
Is there a clear statement of findings?
-
How valuable is the research?
| First author / year | Design | N= | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Summary |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boncori 202090 |
Auto-ethnography / personal reflection | 1 | Y | Y | Y | NA | U | NA | NA | U | Y | This research makes a valuable contribution as it presents insights from a particular (under-represented) population. | No detail on data collection and analysis. |
| Clark 202160 |
IPA interview study | 30 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Valuable | The paper mentioned that analysis was reflexive but I can’t see explicit reflexivity. |
| Collins 201615 |
Qualitative case study approach | 11 | Y | Y | Y | U | Y | N | Y | Y | Y | Valuable in relation to organisations where some people WFH and some don’t. | No detail on recruitment, no reflexivity. |
| Daniel 201816 |
Inductive, semi-structured interviews | 23 | Y | Y | Y | Y | Y | N | Y | Y | Y | Valuable as range of participants and an under-researched community. | Very little reflexivity. |
| Delfino 202152 |
Qualitative field study using semi-structured interviews | 15 | Y | Y | Y | Y | Y | N | Y | Y | Y | Valuable. | There is little in the way of reflexivity. |
| Fukumura 202097 |
Online survey (open-ended responses) | 988 | Y | Y | N | Y | Y | N | N | Y | Y | Complementary to existing evidence. | No reflexivity, little consideration of ethics, research design not optimal. |
| Gao 202061 |
Auto-ethnography / personal reflection | 2 | Y | Y | Y | Y | U | NA | NA | U | Y | This research makes a valuable contribution as it presents insights from a particular (under-represented) population. | No detail on data collection and analysis. |
| Grant 201318 |
In-depth interviews | 11 | Y | Y | Y | Y | Y | NR | Y | Y | Y | Only partial focus on wellbeing. | No reflexivity. |
| Hislop 201521 |
Open-ended interview study, content analysis | 14 | Y | Y | Y | Y | Y | N | Y | Y | Y | Valuable. | There is little in the way of reflexivity. |
| Koehne 201223 |
Semi-structured interviews | 17 | Y | Y | Y | Y | Y | N | N | Y | Y | Valuable for pre-COVID, though less of a focus on wellbeing. | Very little reflexivity. |
| Lal 2021104 |
Diary study | 29 | N | Y | Y | N | Y | N | N | Y | Y | Provides support to other findings. | Research question not clear, recruitment could have been more representative, no reflexivity. |
| Mann 200325 |
Semi structured interviews | 8 | Y | Y | Y | Y | Y | NR | Y | Y | Y | Valuable as wellbeing focused. | No reflexivity. |
| Stitou 201831 |
Semi-structured interviews | 11 | Y | Y | Y | Y | Y | N | Y | Y | Y | Unclear – may be different to other types of home working. | Little reflexivity (none reported). |
| Tietze 201133 |
Case study (interpretive, short-term longitudinal) | 7 | Y | Y | Y | Y | Y | N | Y | Y | Y | Valuable. | There is little in the way of reflexivity. |
| Travers 2020115 |
Netnography (internet ethnography) | 211 | Y | Y | Y | U | Y | N | U | U | Y | Useful insights. | Little reflexivity, very little detail on data collection and analysis methods. |
| Vittersø 200310 |
In-depth interviews (as part of a mixed methods) | 89 | Y | Y | Y | U | U | N | U | U | Y | It complements the quantitative data in this study. | No detail on collection or analysis of data. |
| Waizenegger 202043 |
Qualitative interpretive study | 33 | Y | Y | Y | Y | Y | N | Y | Y | Y | Valuable for examining some issues relating to pandemic WFH. | Limited reflexivity. |
Appendix 2.3. Quality appraisals of included cross-sectional studies
-
Did the study address a clearly focused question/issue?
-
Is the research method (study design) appropriate for answering the research question?
-
Is the method of selection of the subjects (employees, teams, divisions, organizations) clearly described?
-
Could the way the sample was obtained introduce (selection) bias?
-
Was the sample of subjects representative with regard to the population to which the findings will be referred?
-
Was the sample size based on pre-study considerations of statistical power?
-
Was a satisfactory response rate achieved?
-
Are the measurements (questionnaires) likely to be valid and reliable?
-
Was the statistical significance assessed?
-
Are confidence intervals given for the main results?
-
Could there be confounding factors that haven’t been accounted for?
-
Can the results be applied to your organisation?
| First author / year | Design | N= | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Summary |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Allen 202147 |
Online survey | 200 | Y | Y | Y | Y | N | N | U | Y | Y | N | Y | U | Potential for selection bias due to recruitment through social media and through university for course credit. May not be representative as 74% were students. Potential confounders. Results probably not generalisable. Poor quality. |
| Alpers 202187 |
Online survey | 25,708 | Y | Y | Y | N | Y | N | U | Y | Y | Y | Y | U | Potential selection bias due to being online and in Norwegian. |
| Anderson 201413 | Online survey | 102 | Y | Y | Y | N | Y | U | U | Y | Y | N | Y | Y | Possibility of confounders. |
| Argus 202140 |
Online survey | 161 | Y | Y | P | Y | N | N | U | Y | Y | Y | Y | Y | Little detail on recruitment, possibility of selection bias. Possibility of confounders. |
| Bennett 202188 |
Online survey | 55 | Y | Y | Y | N | Y | N | Y | Y | Y | NA | Y | Y | No sample size calculation. |
| Bentham 202148 |
Online and paper survey | 51 | Y | Y | Y | N | U | N | U | Y | Y | N | Y | Y | Unclear response rate, unclear if representative, possibility of confounders. |
| Bentley 201614 |
Online survey | 804 | Y | Y | Y | N | U | N | U | Y | Y | N | Y | Y | Unclear response rate, unclear if representative, possibility of confounders. |
| Burstyn 202191 |
Online survey | 911 | Y | Y | Y | Y | U | N | N | Y | Y | Y | Y | Y | Possibility of selection bias, unclear if representative, possibility of confounders. |
| Chakrabarti 201836 |
National dataset (cross-sectional) | 123,810 | Y | Y | Y | N | Y | U | U | Y | Y | N | N | Y | Large nationally representative survey, response rate unclear from this paper. |
| Cotterill 202041 |
Online survey | 502 | N | Y | Y | N | Y | N | U | N | Y | N | Y | N | Potential for selection bias and confounders. Sample may not be generalisable as just one sector. |
| De Sio 202143 | Web survey | 575 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Well conducted and reported survey. |
| Docka‐Filipek 202148 |
Online survey | 345 | Y | Y | Y | Y | N | N | N | Y | Y | N | Y | Y | Possibility of selection bias, findings may not be representative, possibility of confounders. |
| Dunatchik 202153 | Online survey | 2200 | Y | Y | N | U | Y | N | U | Y | N | N | Y | Y | Recruitment not clearly described, potential for selection bias unclear. Items not validated but have face validity. No statistical analysis of results. |
| Galanti 202198 | Online survey | 209 | Y | Y | N | Y | N | N | U | Y | Y | N | Y | Y | No detail on recruitment, possibility of selection bias due to online administration, results may not be representative. Possibility of confounders. |
| Gijzen 202054 | Online survey | 1519 | Y | Y | Y | N | Y | N | U | Y | N | N | Y | Y | Response rate NR. Possibility of confounders. |
| Hall 201919 | Online survey | 897 | N | U | N | U | U | N | U | N | N | N | Y | N | No detail on recruitment, possibility of selection bias due to online administration, measures not validated, results may not be representative. Possibility of confounders. |
| Hayes 202199 | Online survey | 326 | Y | Y | P | Y | Y | N | U | Y | Y | N | Y | Y | Little detail on recruitment, possibility of selection bias. Measures validated but pre-COVID ratings subject to recall bias. Possibility of confounders. |
| Heiden 2021100 | Online survey | 392 | Y | Y | Y | Y | N | N | N | Y | Y | N | Y | Y | Possibility of selection bias, findings may not be representative, possibility of confounders. |
| Hoffman 202163 | Online Survey | 454 | Y | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | Quota sample. No sample size calc or response rate reported. |
| Hornung 200964 | Mailed survey | 1008 | Y | Y | Y | N | U | N | Y | Y | Y | N | Y | Y | Unclear if sample representative, possibility of confounders, generally well conducted. |
| Hubbard 202165 | Online survey | 501 | N | Y | N | U | N | N | U | U | Y | N | Y | Y | No sample size calculation, response rate not reported, unclear how samples were obtained or if measures were validated, and confounding factors not mentioned. |
| Ingusci 202156 | Online survey | 530 | Y | Y | N | Y | N | N | U | Y | Y | Y | Y | Y | Little detail on recruitment. May not be representative. Possibility of confounders. |
| Ignacio Gimenez-Nadal 202064 | Face-to-face survey | 5401 | Y | Y | Y | N | Y | U | U | U | Y | N | Y | Y | Unclear response rate, unclear if measures validated, possibility of confounders. |
| Jacukowicz 202022 | Online survey | 389 (189 online) | Y | Y | N | Y | Y | N | U | Y | Y | NA | Y | Y | Some parts of recruitment are clearly described but others are not. Possibility of selection bias due to self-selection. Response rate not reported (probably not known). |
| Kaduk 20196 | In-person survey | 758 | Y | Y | Y | N | Y | N | Y | Y | Y | Y | Y | Y | No sample size calc. |
| Kroll 2019103 | Panel survey | 6132 | Y | Y | N | N | Y | N | U | N | Y | N | N | Y | Little detail on recruitment but should be available elsewhere. Measures not validated. |
| Kubo 202136 | Online survey | 13,468 | Y | Y | Y | Y | Y | N | N | U | Y | Y | Y | Y | Potential for selection bias as used sample registered to a survey company, very low proportion of those contacted responded, unclear if measures validated, potential for confounders. |
| Limbers 202066 | Online survey | 200 | Y | Y | Y | Y | N | N | U | Y | Y | N | Y | Y | Possibility of selection bias due to recruitment methods. Response rate NR. Possibility of confounders. |
| Magnavita 2021105 | Face-to-face survey | 905 | Y | Y | Y | N | Y | N | Y | Y | Y | N | Y | Y | Possibility of confounders, no power calculation. |
| Mari 2021106 | Online survey | 628 | Y | Y | N | Y | N | N | U | Y | Y | N | Y | Y | Selection process not clear, possibility of selection bias, findings may not be representative, possibility of confounders. |
| Mellner 201726 | Online survey | 3846 | Y | Y | Y | N | U | N | N | N | Y | N | Y | Y | Unclear if representative, low response rate, sleep duration not validated, possibility of confounders. |
| Molino 2020107 | Online survey | 749 | Y | Y | N | U | Y | N | U | Y | Y | Y | Y | Y | Recruitment not clearly described. Response rate not reported. There are some confounders that have not been considered. |
| Moretti 202041 | Survey (?online) | 51 | Y | Y | N | Y | Y | N | U | Y | Y | N | Y | Y | Little detail on recruitment, possibility of selection bias due to organisations being selected. Possibility of confounders. |
| Perry 20187 (Study 2) | Online survey | 145 | Y | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | Possibility of selection bias due to online administration, low response rate, possibility of confounders. |
| Ray 202127 | Face-to-face survey | ~7400 | Y | Y | Y | N | Y | N | Y | Y | Y | Y | Y | Y | Nationally representative survey, but with uncontrolled-for potential confounders. |
| Restrepo 2020108 | Face-to-face survey | 1784 | Y | Y | Y | N | Y | U | Y | Y | Y | N | Y | Y | Possibility of confounders. |
| Ripoll 202137 | Online survey (longitudinal) | 681 (week 1) | Y | Y | N | Y | N | N | U | Y | Y | N | Y | Y | Selection process not clear, possibility of selection bias, findings may not be representative, possibility of confounders. |
| Rodriguez 2020109 | Online survey | 1269 | Y | Y | N | Y | Y | N | U | Y | Y | N | Y | Y | Recruitment not clearly described, potential for selection bias. Response rate not reported. |
| Sardeshmukh 20128 | Survey (no further details) | 417 | Y | Y | N | U | U | N | N | Y | Y | N | Y | Y | Little detail on recruitment (or survey administration), unclear if representative, low response rate, possibility of confounders. |
| Sato 2021a111 | Online survey | 2846 | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | U | Potential selection bias (app users), not representative. Possibility of confounders as could not adjust for some covariates. |
| Sato 2021b38 | Online survey (with app data) | 5929 | Y | Y | Y | Y | N | N | Y | Y | Y | N | Y | Y | Possibility of selection bias, findings may not be representative, possibility of confounders. |
| Song 202030 | National web survey | 3962 | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Data from national survey. |
| Taser 2022113 | Online survey | 202 | Y | Y | N | U | U | N | N | Y | Y | Y | Y | Y | Selection not clearly described, unclear if representative, low response rate, many confounders not accounted for. |
| Thulin 201932 | Online survey | 456 | Y | Y | N | Y | N | N | U | N | Y | N | Y | Y | Little detail on recruitment, possibility of selection bias due to online administration. Possibility of confounders. |
| Toscano 2020114 | Online survey | 265 | Y | Y | Y | Y | N | N | U | Y | Y | N | Y | Y | Possibility of selection bias, findings may not be representative, response rate not clear, possibility of confounders. |
| Trent 199434 | Mailed survey | 38 | N | Y | Y | Y | U | N | N | Y | Y | N | Y | Y | Low response rate, unclear if sample representative, possibility of confounders. |
| Virick 20109 | Online survey | 85 | Y | Y | N | U | U | N | Y | Y | Y | N | Y | Y | Unclear if selection bias as used previous survey, unclear if representative, possibility of confounders. |
| Vittersø 200310 | Self-administered survey (as part of mixed-methods study) | 217 | Y | Y | Y | Y | U | N | N | N | Y | N | Y | Y | Possible selection bias (convenience sample), relatively low response rate, representativeness not known, measures not validated, possibility of confounders. |
| Weitzer 202039 | Online survey | 1007 | Y | Y | Y | N | Y | N | U | N | Y | Y | Y | Y | Response rate not clear, measures not validated, possibility of confounders. |
| Wickens 2021117 | Online survey | 1002 | Y | Y | Y | Y | U | N | U | N | Y | Y | Y | Y | Possibility of selection bias due to recruitment methods, possibility of non-response bias, may not be representative. Possibility of confounders. |
| Wilke 202144 | Online survey | 14,975 | Y | Y | N | Y | U | N | U | Y | Y | Y | Y | Y | Possibility of selection bias, unclear if findings are representative, possibility of confounders. |
| Wöhrmann 202111 | Telephone survey | 9165 | Y | N | Y | N | N | U | U | Y | Y | N | Y | Y | Findings may not be representative, possibility of confounders. |
| Xiao 202145 | Online survey | 988 | Y | Y | Y | Y | N | N | U | U | Y | N | Y | Y | Possibility of selection bias, findings may not be representative, response rate not clear, measures not validated, possibility of confounders. |
| Xue 202167 | Online survey | 15,426 (April); 14,150 (May) | Y | Y | Y | N | Y | N | ? | Y | Y | Y | ? | Y | No sample size calculation as participants were recruited from a national survey. |
| Yoshimoto 202146 | Online survey | 1941 | Y | Y | Y | Y | N | U | Y | N | Y | Y | Y | Y | Possibility of selection bias, findings may not be representative, measures not validated, possibility of confounders. |
Appendix 2.4. Quality appraisals of included quasi-experimental studies
-
Is it clear in the study what is the ‘cause’ and what is the ‘effect’ (i.e. there is no confusion about which variable comes first)?
-
Were the participants included in any comparisons similar?
-
Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest?
-
Was there a control group?
-
Were there multiple measurements of the outcome both pre and post the intervention/exposure?
-
Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analysed?
-
Were the outcomes of participants included in any comparisons measured in the same way?
-
Were outcomes measured in a reliable way?
-
Was appropriate statistical analysis used?
| First author / year | Design | N= | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Summary |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Delanoeije 202094 | Quasi-experimental study | 78 | Y | Y | Y | Y | Y | Y | Y | Y | Y | One company’s data so may not be representative of other sectors or companies. Possibly other confounders. Outcome measure not validated. |
Appendix 2.5. Quality appraisals of included grey literature
| Authority | Identifying who is responsible for the intellectual content. Individual author:
|
| Accuracy |
|
| Coverage | All items have parameters which define their content coverage. These limits might mean that a work refers to a particular population group, or that it excluded certain types of publication. A report could be designed to answer a particular question, or be based on statistics from a particular survey.
|
| Objectivity | It is important to identify bias, particularly if it is unstated or unacknowledged.
|
| Date | For the item to inform your research, it needs to have a date that confirms relevance
|
| Significance | This is a value judgment of the item, in the context of the relevant research area
|
| Author / year | Type of source | Authority | Accuracy | Coverage | Objectivity | Date | Significance | Comments |
|---|---|---|---|---|---|---|---|---|
| Bevan 202089 |
Web-based presentation | Y Institution named |
Y Not peer-reviewed |
Y Population: UK home workers |
Y | Y | Y | Limited. |
| Chung 202093 |
Report | Y Authors and institutions named |
Y Not peer-reviewed |
Y Population: UK employees |
Y | Y | Y | Non-peer-reviewed report from reputable author/institution. Basic data, limited methodology. |
|
CIPD 202149 |
Web-based presentation | Y Institution named |
Y Not peer-reviewed |
Y Population: UK home workers |
Y | Y | Y | Substantial report with quantitative and qualitative data. |
| Deloitte 202095 |
Web page Infographic | Y Organisation named No ref list |
N Sample size only |
Y Population: UK employees |
Y | Y | Y | Brief data on infographic only. No link to report or full data. |
| Felstead 202017 |
Report | Y Authors and institutions named |
Y Not peer-reviewed |
Y Population: UK employees |
Y | Y | Y | Non-peer-reviewed report from reputable author/institution. |
| KCL 2021101 |
Web page | Y Institution named |
Y Not peer-reviewed |
Y Population: UK employees |
Y | Y | Y | Non-peer-reviewed report from reputable institution. Basic data, limited methodology. |
| Kotera 2020102 |
Web page | Y Authors and institutions named |
Y Not peer-reviewed |
Y Population: UK employees |
Y | Y | Y | Discussion based on SR – check original paper. |
| Parry 202157 |
Report | Y Authors and institutions named |
Y Not peer-reviewed |
Y Population: UK employees in 2 sectors |
Y | Y | Y | Non-peer-reviewed report from reputable author/institution. |
| PWC 202058 |
Web-based report | Y Institution named |
Y Not peer-reviewed |
Y Population: Maltese employees |
N Employer market research |
Y | Y | Market research from major employer. Basic data, limited methodology. |
| RSPH 202142 |
Web page | Y Institution named |
N Very limited information |
Y Population: UK employees working from home. |
Y | Y | Y | Brief data on web page only. No link to report or full data. |
| Uni of Exeter 2020116 |
Web page | Y Authors and institutions named |
N Very limited information |
Y Population: university employees working from home. |
Y | Y | Y | Full article to follow. No link to data here. |
List of abbreviations
- BPAQ
- Baecke Physical Activity Questionnaire
- CIPD
- Chartered Institute of Personnel and Development
- OECD
- Organisation for Economic Co-operation and Development
- ONS
- Office for National Statistics
- PA
- physical activity
- PPI
- patient and public involvement
- QoL
- quality of life
- WFH
- work from home
Notes
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/AHFF6175).