
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 10/3002/03. The contractual start date was in May 2012. The final report began editorial review in August 2013 and was accepted for publication in July 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Segrott et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Parts of this text are reproduced with permission from Segrott et al. 1
This report describes an exploratory trial of Kids, Adults Together (KAT), a primary school-based, universal programme to promote prosocial family communication about alcohol, with the aim of preventing alcohol misuse in young people. This chapter summarises the literature on early preventative interventions for alcohol misuse, and describes the background and theoretical basis of KAT and the aims and objectives of the trial.
Scientific background and rationale
Public health context
Alcohol misuse has high personal, social and economic costs, and widens inequalities in health. 2 Harmful drinking has risen steeply in the UK during the last 20 years3 and the annual cost of alcohol misuse in the UK has been estimated at £25B, of which £1B was spent in Wales. 4,5 Misuse of alcohol by young people has raised particular concerns about the number who initiate alcohol consumption at a young age, and the high levels of regular and harmful alcohol use. 6,7 For example, 5% of 11-year-old boys in Wales report drinking alcohol at least once a week; the proportion increases to 35% at 15 years, by which age nearly half report having been drunk at least twice. 8 Alcohol misuse in young people has a range of health and social impacts, including disorderly and violent behaviour, risky sexual behaviour,9 accidental injury, and poor school attendance and achievement. 10,11 In the longer term, early initiation of alcohol consumption increases the risk of alcohol-related problems in later life. 12–15 There is also evidence to suggest that alcohol misuse in young people clusters with other risk behaviours. For instance, the 2011 survey of drug use, smoking and drinking among 11- to 15-year-olds in England found strong associations between past-year drug taking and alcohol use, while people who smoked were roughly twice as likely to have consumed alcohol in the previous 7 days. 16
Interventions to prevent alcohol misuse in children and young people
Schools have long been considered an important setting for delivering health behaviour interventions to young people, including those addressing alcohol misuse. In May 2013, four electronic databases [MEDLINE, Allied and Complementary Medicine (AMED), EMBASE and PsycINFO] were searched from 2010–13 to identify recent evaluations of school-based alcohol misuse programmes for children and young adolescents (see Appendix 1). Search terms for alcohol misuse (alcohol, alcoholic, binge drinking) were combined with a term for school based (school*) and terms for programme (interven*, prevent*, promot*, program*), with results limited to English-language publications. Evaluations identified by the search, including those that were community rather than school based, are presented in Appendix 1 and illustrate the breadth of approaches being investigated and the scarcity of programmes focused on younger children. Rather than focusing exclusively on individual behaviour, school-based interventions provide an opportunity to draw on the socioecological health promotion framework, thereby acknowledging and exploiting the wider influences on health behaviours, such as friendship groups and organisational (school) system influences. 17,18 Furthermore, schools have near-to-complete coverage of the target population, and so intervention reach is potentially very high, and they also have an expanding function as health-promoting institutions. 19–21 Health-promoting schools work within a framework based on the World Health Organization’s Ottawa Charter for Health Promotion22 and promote health through the whole school environment, not just through health education curricula. 23 Health-promoting schools, therefore, strive to integrate their curriculum teaching with the school’s physical, social and policy environment, and the wider school community including parents.
Teaching about alcohol is a component of the personal and social education (PSE) curriculum from Key Stage 2 (8- to 11-year-olds) onwards in Wales,24 and so classroom-based alcohol misuse interventions do not necessarily place additional strain on the curriculum and can help to fulfil key requirements. Since 2003, the All-Wales School Liaison Core Programme, funded by the Welsh Government,25 has provided lessons on alcohol and other drugs to pupils at Key Stages 1–4, delivered by police school liaison officers. While the programme has been well received by pupils and schools26,27 and is currently delivered in approximately 97% of schools in Wales,28 it has not been subjected to a rigorous outcome evaluation. Many studies of similar classroom-based programmes suggest that preventing alcohol misuse requires an approach which may be more complex than that used to teach subjects in which students are required to demonstrate knowledge, rather than to adopt and observe a behavioural principle. 29–34 Such complex interventions might have multiple interacting components and target different levels of the socioecological framework. 35 Effective alcohol-misuse prevention programmes for young people have been found to share characteristics which generally fall into one or more of three main themes outlined below: (1) use of a clear theoretical basis in programme design; (2) interactive delivery style; and (3) community (including family and parental) involvement. 29–34 We summarise each in turn.
Theory-based programme and design
Health-promotion research and practice have been criticised for being poorly theorised,36,37 but recent and influential guidance on the development and evaluation of complex health interventions has clarified the importance of identifying and developing the theory/theories upon which interventions are based. 35 The explication of programme theory, namely the assumptions of how and why an intervention will produce specified outcomes, is essential for meaningful programme evaluation and intervention development, and can be visually presented in a logic model. 38
Nation et al. 39 distinguish aetiological theory, which focuses on the causes of behaviour, from intervention theory, which focuses on how to address aetiological factors associated with the behaviour, and say that both are required to drive effective programmes. Aetiological theory around problem behaviours in adolescence has centred on risk factors and protective influences. 40 Risk factors, however, are often common to several problem behaviours, and so effective programmes addressing the aetiology of alcohol misuse will share many characteristics of interventions addressing other behaviours arising from the same risk factor(s), for example tobacco and other substance use. This is significant because interventions aimed at addressing one health behaviour may also have effects on other behaviours that share common antecedents. The development of KAT has, therefore, drawn on evidence about the prevention of antisocial behaviour in children and adolescents generally, as well as that specific to alcohol-prevention programmes.
The social influence model has been recommended as the most suitable intervention theory for school-based programmes which address risk and protective factors. 41 The model posits that children can be ‘inoculated’ against social pressure to adopt undesirable behaviours such as drug and alcohol use. 42 Social pressure can be active, for example explicit offers of drugs from peers, or passive, such as overestimating alcohol consumption among peers. The model suggests various programme mechanisms that can help children counter social pressures, for example resistance and refusal training, public pledges, critiques of tobacco and alcohol advertising, learning about real and perceived norms, and the use of peer leaders. 42–44
Interactive delivery style
Most of the mechanisms through which the social influence model is operationalised are highly compatible with an interactive delivery style, and programmes that employ such a style are more effective than those using more didactic, non-interactive methods. 43 According to the social influence model, interactive teaching and learning methods (e.g. role play) might increase programme effectiveness by providing opportunities for communication and social interaction and enhancing young people’s critical awareness of social norms and pressures around substance use. 41,45 Effective interactive learning strategies also enhance children’s negotiation skills and let them rehearse problem-solving strategies. 45 Involvement of peer leaders can make programmes highly interactive and participatory and can increase engagement of young people who feel more comfortable talking to peers than to teachers. Young people may also talk more openly with peers and find it more fun. 44
Community and family involvement
Engaging the wider community beyond the school strengthens the effects of school-based programmes41 and, like interactive delivery, is consistent with the social influence model. Community involvement increases young people’s opportunities for communication and social interaction, including opportunities to develop positive relationships with adults, be they parents, teachers or other community members. 39 Where parents or other community members are actively involved in programmes, they are exposed to the same health-behaviour messages as younger participants and, if they accept those messages, can reinforce them through their own actions, behaviours and attitudes. The consistency of what children learn in school with their experiences outside school may, therefore, increase,46 for example in the rules their parents set around drinking or the vigilance of alcohol vendors. 47
Involvement of pupils’ families in school life is part of schools’ core business48,49 and may be more important than other aspects of community engagement in alcohol misuse programmes. 50 In the UK, the National Institute for Health and Care Excellence (NICE) recommends that schools involve families in alcohol education initiatives. 34,51 Dimensions of family functioning such as parenting operate as key protective and risk factors for later alcohol misuse by young people. 29,31,32,52–54 The family environment plays an important role in shaping young people’s attitudes and behaviour towards alcohol, including the timing of first use. 29,55,56 Parental norms and examples may encourage children’s early alcohol use through providing models of alcohol consumption56 or easy access to alcoholic drinks. Parental rules relating to alcohol are also an important factor,57 but the sharing of values within a trusting parent–child relationship is more effective in preventing antisocial behaviour than formal rule-setting and surveillance by parents. 58
Despite the importance of parent participation being widely noted, programmes continue to be designed with no parent component (see Appendix 1). Meanwhile, those that do try to involve parents, be they community or school based, have experienced significant challenges in recruiting and retaining parents. Community-based interventions commonly seek to strengthen parenting skills, for example the Chicago Parent Programme for low-income parents of 2- to 4-year-olds. This programme recruited parents through day-care centres, but only 31% of those eligible in intervention centres enrolled; the most frequent reasons for not enrolling were being unaware of the programme, being too busy or the programme conflicting with work/school schedules. 59 Retention often proves equally problematic. When Incredible Years, a parenting programme for parents of 2- to 10-year-olds, was implemented in one English city, 38% of enrolled families never attended a session, and even after efforts to improve retention this only fell to 30%. 60 School-based programmes have experienced similar problems and low levels of engagement are common. 31,61 Even when school-based programmes have been modified to increase levels of parental involvement, poor engagement has persisted. 62–64 In the Blueprint Programme for drug prevention in English secondary schools, for example, attendance of parents at the programme launch in phase 1 schools was only 16% of those invited and, despite revised and more intensive recruitment strategies, attendance fell to < 10% in phase 2 schools. 62
Factors which affect parent participation in community and school-based prevention programmes include practical barriers such as programme timing and travel arrangements;65,66 programme length and location;67 parent beliefs about their child’s susceptibility to problematic behaviours;67 and sociodemographic characteristics such as educational background. 68,69
While reaching families at higher risk of alcohol misuse problems is important, accurate identification of such families is often challenging, and programmes targeted at families on the basis of risk may stigmatise attendance, thus affecting take-up. 70,71 Universal programmes are less likely than targeted interventions to deter parents, and, ideally, will reach families at higher risk from alcohol misuse while avoiding stigmatisation. Because alcohol consumption is a part of everyday life in the UK, a universal programme is relevant to everyone because they either drink alcohol themselves or are exposed to the effects of others’ alcohol consumption. From near-abstinence to alcohol dependence, drinking is associated with a continuum of alcohol-related risk. A universal programme can potentially significantly reduce the overall prevalence of alcohol-related harm by shifting the distribution of risk. 72 Patterning of take-up is a possibility, however, and care is needed to ensure that universal programmes fully cover the spectrum of risk. In terms of implementation in schools, a programme delivered to a whole class or year group is likely to cost no more than identifying and targeting a smaller group.
In addition to being consistent with the social influence model, parent participation in alcohol misuse programmes is also compatible with the social development model (SDM), a theory of antisocial behaviour upon which KAT draws.
The social development model
In terms of aetiological theory, the SDM supports the view that parental involvement should be a key principle of intervention theory. In addition to the general model, the SDM incorporates four key age periods, showing how social influences expand over time beyond the family environment to include school and peer influences and legal sanctions through the preschool period and (US) elementary, middle and high school periods. 73 By high school, peer norms, classroom management, school policies and legal sanctions are influential in addition to the family.
The SDM has predicted alcohol misuse in young people74 and interventions such as the Seattle Social Development Project in the USA and Preparing for the Drug Free Years, which operationalise the model, have achieved reductions in alcohol misuse. 75,76 The SDM proposes that young people learn social behaviour through interactions with others, resulting in the formation of attachments which, if strong, can have a lasting effect on behaviour through supporting the acquisition of skills and influencing norms and values. 77 Attachment to others who offer opportunities for and reward prosocial behaviour is a protective factor against antisocial behaviour. 73,78,79 Thus, involvement of both parents and children in interventions may increase the quality and frequency of parent–child interactions.
Pre-adolescent children who are still highly dependent on their parents will usually have more opportunities for interacting with and forming attachments to their parents than when they enter adolescence and develop a social life outside the home. Social influences expand over time beyond the family environment to include school and peer influences and legal sanctions. 73 Thus, a further implication of the SDM for intervention theory is that programmes involving parents and children will be more likely to succeed if they are based in primary rather than secondary schools. Intervention earlier in the life course is also supported by evidence that programme effectiveness is enhanced by involving young people who have not yet adopted the targeted behaviour(s). 39,53
The SDM also explains why interactive delivery methods and other features of the social influence model have been identified as elements in more effective preventative programmes. According to the SDM, initiation of social interactions depends on people perceiving that there is an opportunity for them to get involved with someone or some activity around them. That is, they see that interactions are relevant to, and intended for, themselves, and that they are competent to take part. Prevention programmes using interactive methods will boost opportunities for prosocial interaction. Perception of opportunities for social interaction is influenced by social structural factors (socioeconomic status, age, sex and race78), suggesting that programmes should include features which are acceptable to all social groups in the target population and which enhance participants’ confidence and skills.
Strength of the evidence base
Gaps remain in the knowledge base for alcohol misuse prevention, particularly in countries outside the USA, where most programme development and evaluation has been conducted. This was borne out in a recent Cochrane Library systematic review of school-based programmes which identified 53 randomised trials, 41 of which were conducted in North America and none in the UK. 50 Promising programmes from the USA may require adaptation and further evaluation when used elsewhere,80,81 to ensure that both aetiological and intervention theories are appropriate for participants with different cultural values and customs. While reviewers are clear that several programme components are needed and that components work together to increase effectiveness, the large number and variety of programmes, the relative rarity of long-term outcome evaluation (e.g. see the range of interventions and follow-up periods in Appendix 1) and systematic adaptation complicate efforts to understand the essence of effective prevention. 50 Lastly, most evidence relates to older age groups because relatively few interventions have been based in primary schools,31,82 despite the SDM indicating that programmes for younger children may be efficacious. Furthermore, most primary school programme evaluations use aggressive behaviour as a precursor to alcohol use as their primary outcome, as their follow-up of participants is not long enough to measure impact on alcohol use in adolescence. 82
An urgent priority in improving the evidence base is to identify and develop effective methods of engaging parents in prevention programmes. As outlined above, while the importance of family-based protective factors for alcohol misuse is widely recognised,29,32,52 knowledge remains limited regarding effective mechanisms for engaging parents in prevention programmes, particularly those that are school based, and differences in programme reach and acceptability between different socioeconomic groups. 83–86
Kids, Adults Together
Anecdotal evidence that some prevention programmes have attracted large numbers of parent participants is not well supported by detailed accounts of percentages or mechanisms of engagement. One such programme was the Parents, Adults, Kids Together (PAKT) programme in Victoria, Australia. 87 PAKT was designed as a family drug education forum prepared by children aged 10–12 years in class and presented to their parents after school. The forum was delivered in addition to existing school drug-education work. A police community safety officer from Wales visited Australia to see PAKT in action and subsequently adapted it for use in south-east Wales, specifically for prevention of alcohol misuse. An advisory group developed a teacher’s pack for the classroom work and Gwent police commissioned a digital versatile disc (DVD) for distribution to participants. The adapted programme was called Kids, Adults Together Family Forum, subsequently shortened to Kids, Adults Together or KAT, and piloted in two primary schools in Gwent, with the police officer presenting the family events.
Kids, Adults Together integrates specially designed classroom activities with a family education evening and a DVD to promote prosocial communication. The programme design addresses key factors affecting parental engagement and is promoted to parents as an opportunity for them to learn about the work their children have been doing in class, rather than as an educational evening about alcohol misuse. To encourage take-up by schools and parents, KAT is of much shorter duration and intensity than other such interventions; the Strengthening Families Programme 10–14 (SFP10–14), for example, requires parents to attend seven weekly 2-hour sessions. 88 A shorter approach is supported by evidence that brief interventions can be as effective as longer interventions in older adolescents. 89
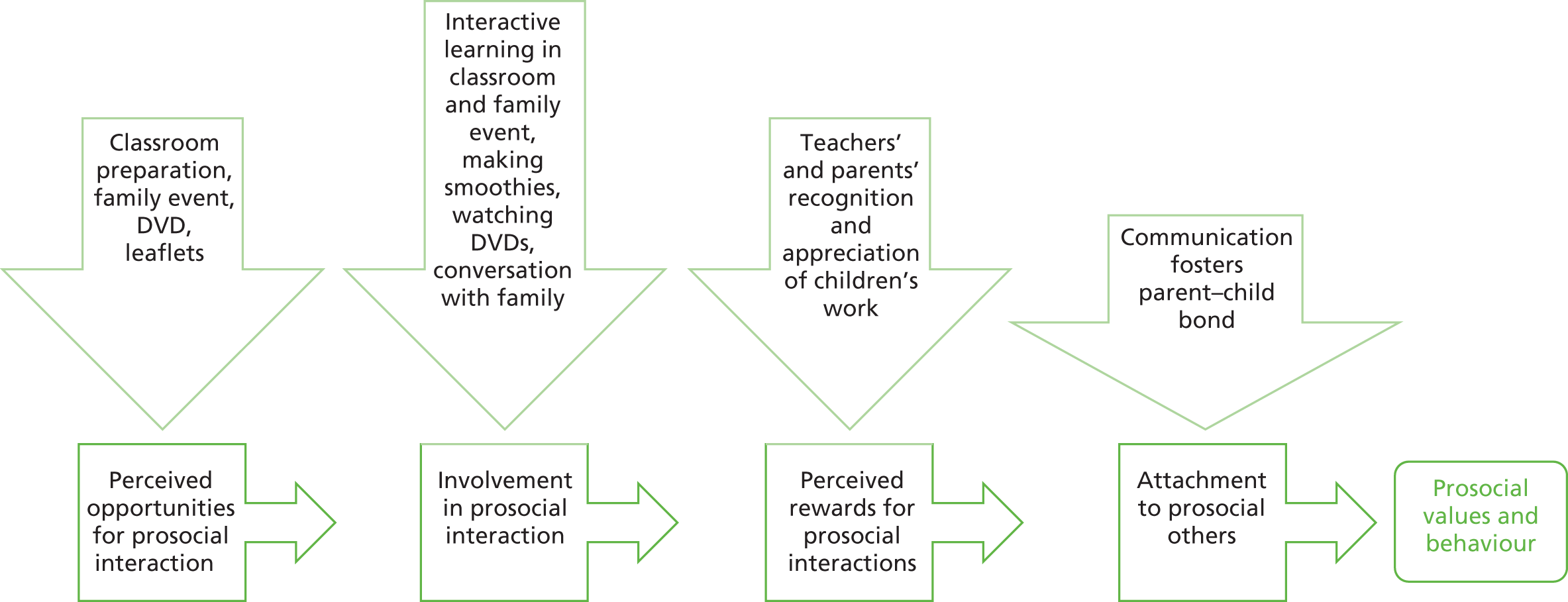
An evaluation at the development stage90 found that KAT had important features previously identified in more effective interventions. Interactive delivery methods are used throughout, and it is based in primary schools, where most children have not yet become regular drinkers. The early timing of programme delivery and the programme content were acceptable to parents, children and school staff. Figure 1 illustrates how KAT incorporates three crucial aspects of the causal pathways to prosocial behaviour contained within the SDM: (1) the creation of opportunities for prosocial interaction between and within families; (2) the strengthening of the necessary skills which parents and young people need to communicate about alcohol-related issues; and (3) the encouraging of parents to reward and reinforce prosocial behaviour and attitudes in relation to alcohol. 91 Crucially, the programme succeeded in involving 40–50 adult family members in the family events at both schools.
Aims and objectives
Findings from the evaluation at the development stage were promising,90 but questions remained about the acceptability and feasibility of KAT across a larger number of schools; its reach across social groups; and its effectiveness in preventing alcohol misuse. In line with the Medical Research Council (MRC) evaluation framework for complex interventions,35 it was, therefore, appropriate to move forward to an exploratory trial, the aim of which was to further develop and evaluate KAT in a larger number of schools in order to determine the value and feasibility of conducting a definitive effectiveness trial.
Specific objectives are listed below and pertained to the level of the individual participant, the family, the cluster or all three:
-
to refine the theoretical model and outcome pathways of the intervention (all)
-
to assess the feasibility and acceptability of the intervention (all)
-
to establish intervention participation rates and reach, including equality of engagement across socioeconomic groups and localities (all)
-
to assess trial recruitment and retention rates (individual and school)
-
to identify potential effect sizes that are likely to be detected as part of a definitive trial and an appropriate sample size (individual and school)
-
to determine the feasibility and cost of the proposed methods for measurement of the primary and secondary outcomes (individual and school)
-
to identify the costs of delivering KAT, and to pilot methods for assessing cost-effectiveness as part of a future definitive trial (school); and
-
to determine whether or not to proceed with a definitive trial (individual and school).
This exploratory trial was, therefore, not assessing the effectiveness of KAT, but testing the feasibility of the intervention and the trial methods. The logic model for the exploratory trial is shown in Table 1.
| Inputs | Outputs | Study outcomes | |||
|---|---|---|---|---|---|
| Actions | Participants | Short term | Medium term | Long term | |
|
|
|
|
|
|
The objectives are those of a Phase II trial described in the MRC framework for evaluation of complex interventions92 as:
-
acceptability and feasibility, including optimising the intervention and study design
-
defining the control: in this study, examining the acceptability of ‘usual practice’ in control-group schools
-
designing the main trial: in this study, noting the relevance of findings to the design of any future effectiveness trial and estimating sample size
-
outcomes: piloting measures which could be used in the main trial.
The study presented an opportunity to scrutinise two pertinent methodological issues:
-
family communication measures appropriate for 9- to 11-year-olds; and
-
criteria for progressing to an effectiveness trial.
Measures of both general family communication and family communication about alcohol were required for the study. While validated measures for both exist,93–102 they have been developed with adolescents (usually 12 years and/or older) and their acceptability and validity for younger children and their parents is unclear. The lack of communication measures likely reflects the fact that programmes targeting the late primary school years are less common. An opportunity, therefore, arose in KAT to use some of the measures developed for older children in 9- to 11-year-olds, to evaluate their acceptability and, if appropriate, to suggest adaptations.
The MRC guidance on developing and evaluating complex interventions recommends a systematic and phased approach which moves through literature review and theory development to pilot studies, exploratory trials and finally definitive (effectiveness) evaluations. 35 While the guidance is a welcome acknowledgement of the role and importance of exploratory trials, it neither provides comprehensive advice on how to conduct such trials nor describes the hallmarks of a ‘good’ exploratory trial. Detailed reports of exploratory trials of complex interventions in public health are beginning to emerge and these provide valuable insights,103–105 but detailed guidance on the design, analysis and reporting of exploratory trials remains absent.
One crucial area yet to be addressed in the literature is the decision that arises at the end of an exploratory trial on whether or not to recommend proceeding to a full effectiveness trial. This is a core purpose of exploratory trials, yet there are no precedents in the literature to guide the development of criteria upon which to make an objective decision. There were three key areas to consider in relation to KAT. First, whether or not structures and capacity were in place in schools and among the practitioners (police) who would support schools (through training and compering the family events) to implement the programme on a wide scale. Second, whether or not a randomised controlled trial (RCT) design using the piloted measures of family communication and pupil alcohol consumption would be an appropriate and acceptable method to evaluate KAT in an effectiveness trial. Finally, whether or not the intervention appeared to work as planned in schools (in a range of socioeconomic settings) (and in line with its logic model), and the extent to which it was acceptable to school staff, pupils and parents/carers. Criteria had to be developed to ensure that an objective and transparent decision was made at the end of this study. Reporting this process addresses an important gap in the literature and will possibly be of value to others conducting exploratory trials of complex interventions. Chapter 2 includes a description of how the criteria were developed and assessed (see Health economics).
Study design
An exploratory cluster RCT was used to evaluate KAT. A RCT is the most robust design available to obtain an unbiased estimate of a potential effect size, even with a complex intervention in a ‘real-world’ setting such as schools. 106 As an intervention delivered in the classroom, randomisation at the level of the individual child was not appropriate, and so schools were chosen as the unit of randomisation.
Because it was originally anticipated that programme delivery as part of the trial would need to take place before the outcome of a funding decision on our grant application, we did not request funding to cover recruitment of schools, parents and pupils, or baseline data collection. Recruitment and baseline data collection, therefore, took place before the start of the funded study. While the main trial was funded by the National Institute for Health Research (NIHR), a nested process evaluation was conducted by a PhD student from the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer). The process evaluation assessed implementation processes, fidelity and acceptability to families and schools. Qualitative methods, described in Chapter 2, were used to capture the experiences and perspectives of those delivering and receiving the intervention. A summary of key findings from an interim analysis is presented in Chapter 3.
Public and stakeholder involvement
The involvement of children, and stakeholders from the police, education, public health and national government has been integral to both KAT and this exploratory trial. Their involvement has included the development and piloting of KAT and development of the pupil questionnaires. Public and stakeholder involvement is fully described in Chapter 2.
Chapter 2 Methods
Parts of this text are reproduced with permission from Segrott et al. 1
Research design
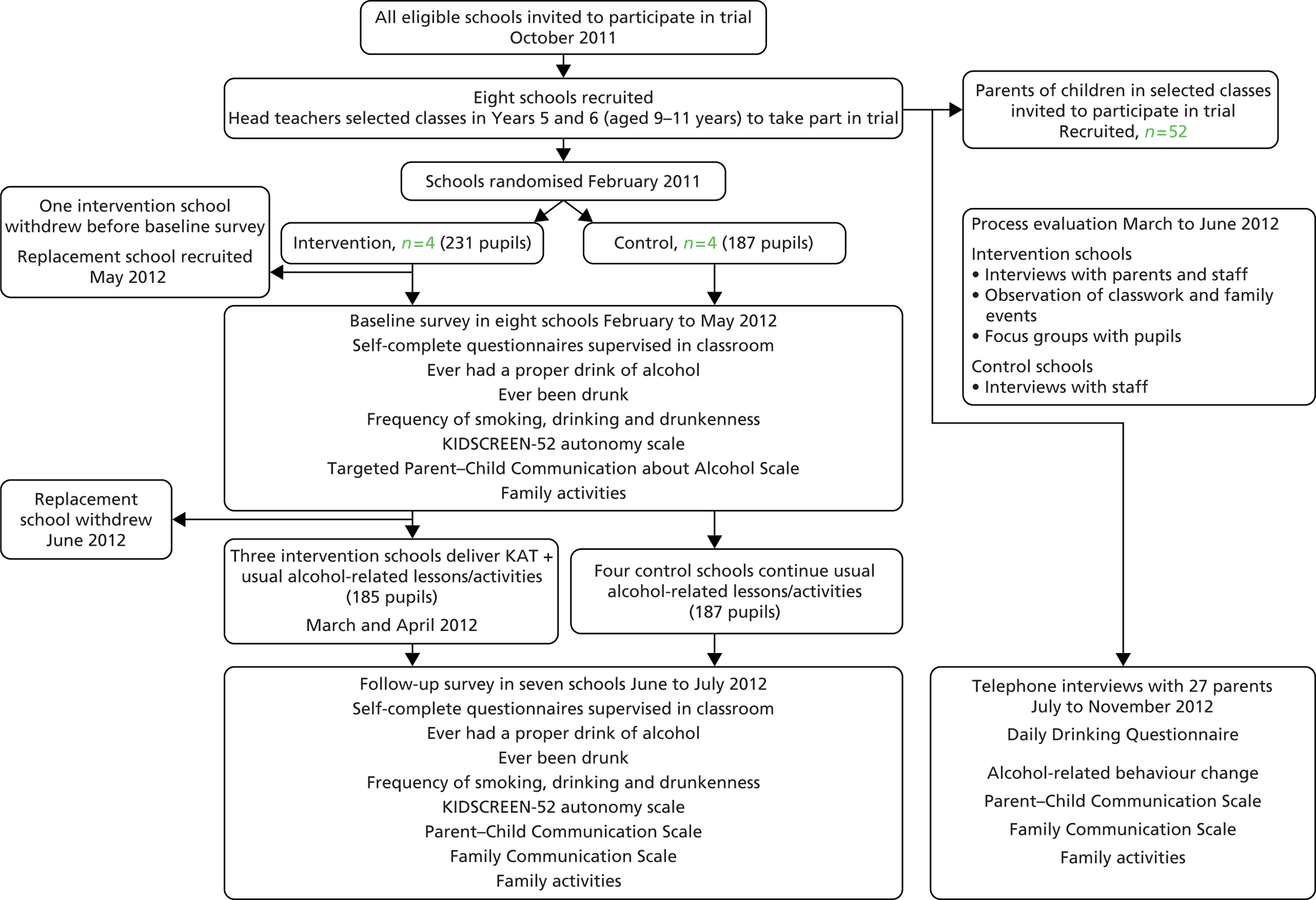
The study is a parallel-group cluster exploratory trial, with an embedded process evaluation. Schools were the unit of randomisation and were randomly assigned to intervention and control in a 1 : 1 ratio. Figure 2 provides a summary of the study.
FIGURE 2.
Research design.
The funded study lasted 14 months. Each child in the study was asked to complete two questionnaires: one at baseline and another approximately 4 months past baseline. Programme delivery in intervention schools took place immediately after baseline data collection. Children in intervention schools were also invited to take part in focus groups following the family events. Parents/carers who took part in the study participated in one telephone interview approximately 6 months post baseline, and parents of children in intervention-group schools also participated in interviews as part of the study’s process evaluation.
Ethical approval was given by the Cardiff School of Social Sciences Research Ethics Committee (SREC reference SREC/697). Amendments to the protocol were approved by the Trial Management Group; recorded; and communicated to the NIHR programme manager and the chair of the Research Ethics Committee. Because of delays in school recruitment, the interval between baseline and follow-up pupil questionnaires was changed from 6 months (stated in the original protocol) to 4 months, so that follow-up data collection could be carried out before the end of the summer term, when Year 6 pupils would be leaving their primary schools. Although this change was made for pragmatic reasons, it did not present a barrier to assessing the feasibility of measuring outcomes, which was a central aim of the evaluation. Process evaluation gives a detailed account of process evaluation methods.
The intervention
Kids, Adults Together has three main components: (1) classroom work (delivered by teachers) on the effects of alcohol consumption, and preparation for a family event; (2) the family event, delivered in school, and involving children and parents in activities addressing key health messages around alcohol; and (3) a ‘goody bag’ to take home, containing fun items, educational leaflets and an educational DVD for families to watch together.
Development
The first pilot study90 theorised the function of each KAT component using Valente’s framework of exposure, knowledge and attitudes, and practice. 107 There was evidence that each component had set off family communication which could mediate later drinking behaviour through parental regulatory practices (Figure 3). Viewing the DVD at home (and, as originally intended, on national television) had the potential to sustain, over a longer period, the immediate impacts of a short intervention. All of the components were thought to be necessary because of their cumulative effect: the classroom preparation led into the family event; the goody bags with the KAT badging and contents were physical reminders of the programme in children’s homes; and the DVD was particularly important for impact in the longer term.
FIGURE 3.
How KAT is expected to achieve its long-term aim. TV, television.

The first pilot study also established the importance of the classwork component in attracting parents to the family events. Children’s eagerness to show parents their work and parents’ status at the family events as proud supporters of their children were powerful factors in securing parental participation in the programme and were likely to be constant across different school contexts.
A further pilot study in 2011 focused on refining the materials provided to schools. An independent health education consultant employed by the research team modified the teachers’ handbook which had been developed for the earlier pilot study, clarifying the aims, learning outcomes and links to the curriculum for each lesson/activity and providing supporting information such as a timetable for the family event and a list of suggested questions for a quiz. As part of this work, the programme was implemented in two schools outside the trial area (one school which had previously implemented the programme, and one with no prior involvement) and feedback from staff, pupils and parents drawn upon. The number of suggestions for classroom activities in the teachers’ handbook was reduced and teachers were encouraged to choose their own way of achieving programme aims. That is, they had freedom (within limits) to alter the form of the activities, as long these still performed the same function. 108 The handbook included contact details of alcohol support services, and schools were encouraged to request one of them to attend the family event to facilitate contact between agencies and families needing support.
Implementation
The intervention was administered at cluster level (schools) and consisted of the KAT programme in addition to any existing alcohol-related lessons/school activities.
Kids, Adults Together requires approximately 1 week’s total classroom contact time (or around 20 hours). Classroom preparation for children was planned to take place over at least 1 week, with flexibility for schools to take longer according to, for example, the timing of the family event and the needs of the class. The KAT family event lasts about 1 hour and the contents of the ‘goody bag’ may be used by children and their families over an indefinite period.
Following baseline data collection in all schools, the health education consultant asked to visit all intervention schools to train teachers whose classes would be involved and to provide information about the programme to any other relevant members of staff. Staff training covered the key points in the KAT handbook and staff were also given a Microsoft PowerPoint (Microsoft Corporation, Redmond, WA, USA) presentation for use at the family event; appropriate information from websites, downloaded and photocopied; and Tacade’s Keys to Alcohol for Children Aged 7 to 11 Years Old resource. 109 Teachers were asked to ensure that support would be available for children who might be distressed by the topic (although this should usually have been in place to back up the usual alcohol-related curriculum content).
Evidence gathered during the pilot110 suggested that school staff would modify KAT in order to achieve programme aims and objectives in ways they thought would be more appropriate in the context of their own schools. The process evaluation included observation of classroom work so that analysis of any such adaptations could inform future programme development and evaluation.
The four schools randomised to the control group did not receive KAT, but continued with their usual activities, including any classroom work/school activities on alcohol. Process evaluation interviews with staff in control schools identified normal practice in relation to both substance education and structures for involving parents in school life.
Recruitment of schools
All English-medium primary schools (n = 39) in Newport County with Year 5/6 classes were invited to participate in the trial. Letters were sent to all 39 schools, inviting them to participate in the research, and telephone calls were then made to each school until eight schools had agreed to participate. The letter (see Appendix 2) sent to schools was drafted with input from the education consultant and the Healthy Schools Team in Newport. A member of staff from the Healthy Schools Team also accompanied the research team at some of the initial meetings with interested schools.
Recruitment of pupils
In each school, a member of the research team visited the classes which it had been agreed would participate in the trial. The researcher explained the study to the pupils, described the proposal to involve them in the study and answered any questions they had. All pupils in the class were provided with age-appropriate participant information sheets (see Appendix 3). Teachers were asked to ensure that pupils who were absent on the day of the visit received a copy of the participant information sheet.
Recruitment of parents/carers
Owing to data protection regulations, it was not possible for the research team to access names or any contact details of parents/carers of pupils who had been invited to participate in the trial. We therefore prepared a letter (which began ‘Dear parent/carer’) which we asked schools to send by Royal Mail to all parents/carers of pupils in those classes which were participating in the trial (see Appendix 4). This letter was accompanied by a participant information sheet (see Appendix 4). The letter asked parents/carers to return a reply slip to the research team if they were interested in participating in the research.
A follow-up letter to parents/carers was sent home via ‘pupil post’ (i.e. pupils were asked to take the letter home and show it to their parent/carer) approximately 1 week after the initial letter.
Parents who returned reply slips indicating that they would like to take part in the research telephone interviews were contacted by a member of the research team to check contact details and ascertain the best time to conduct a telephone interview.
Consent
Consent from head teachers for school participation was obtained before randomisation, and consent from children and parents as individual participants was sought after randomisation, with allocation revealed to both cluster and individual participants. Each head teacher signed a formal commitment form (see Appendix 5) for their school to take part in the study. The commitment form described the roles and responsibilities of the school and the research team, respectively, during the research period at the school.
The study tested the feasibility and acceptability to schools of using ‘opt-out’ parental consent to develop recruitment and data collection systems which would maximise response rates and minimise selection bias. 111,112 The use of ‘opt-out’ consent methods is more effective than ‘opt-in’, which often results in sample sizes which are too small to power a RCT. 112–114 Approval for the use of ‘opt-out’ consent was obtained from the ethics committee which had reviewed our study. At each school, we explained our preference to use ‘opt-out’ parental consent, but head teachers were able to stipulate that ‘opt-in’ consent should be used, and schools could participate in the study regardless of their preferences concerning parental consent. None of the schools raised any objections to us using ‘opt-out’ consent procedures, and this method was, therefore, used in all participating schools.
Approximately 1 week after the second letter was sent to parents, a member of the research team visited the class and asked those pupils who were willing to participate to complete a written questionnaire. An assent form for completion by pupils was attached to the front of each questionnaire.
Each potential parent participant was sent an information sheet, a booklet to assist them during telephone interviews and a consent form (see Appendix 6). They were requested to complete the consent form and return it in a prepaid envelope to the research team.
Individual teachers were asked to give informed consent to take part in the research. School and individual participants could withdraw at any time, without giving a reason, by informing the principal investigator or study manager that they did not wish to continue.
Inclusion/exclusion criteria
Primary schools which included Years 5 and 6 and taught through the medium of English were eligible to take part in the research. Welsh-medium schools and those with infant classes only were excluded. In each participating school, all children in Year 5 and Year 6 classes were eligible. Head teachers were encouraged to involve as many classes as possible, but were allowed to select which classes should take part, because we were interested in understanding how schools’ preferences would shape the likely cluster sizes as part of a future effectiveness trial. Table 2 gives details of numbers of classes taking part in intervention and control schools. A number of the schools had mixed year-group classes, and we allowed those with Year 4/5 classes to participate in the trial.
| School | Trial arm | Classes selected, n | Total classes selected, n | Total classes eligible, n | Eligible classes taking part, % | Reason for selection | |||
|---|---|---|---|---|---|---|---|---|---|
| Year 4/5 | Year 5/6 | Year 5 | Year 6 | ||||||
| 3 | I | 1 | 1 | 0 | 0 | 2 | 2 | 100 | All eligible classes involved |
| 4 | I | 0 | 0 | 0 | 2 | 2 | 5 | 40 | All Year 6 involved; Year 5 not selected because of impending inspection and demands on staff time |
| 6 | I | 1 | 0 | 1 | 1 | 3 | 3 | 100 | All eligible classes involved |
| 8 | I | 0 | 0 | 2 | 0 | 2 | 4 | 50 | All Year 5 involved; Year 6 not selected (reasons unknown) |
| Total (%) in intervention group | 2 | 1 | 3 | 3 | 9 | 14 | 64 | ||
| 1 | C | 0 | 0 | 2 | 0 | 2 | 4 | 50 | All Year 5 involved; Year 6 not participating as have already done SM work this year, and also practical considerations |
| 2 | C | 0 | 1 | 0 | 0 | 1 | 1 | 100 | All eligible classes involved |
| 5 | C | 0 | 3 | 0 | 0 | 3 | 3 | 100 | All eligible classes involved |
| 7 | C | 0 | 0 | 1 | 0 | 1 | 2 | 50 | Year 6 not included – reasons unknown |
| Total (%) in control group | 0 | 4 | 3 | 0 | 7 | 10 | 70 | ||
| Total (%) in both trial arms | 2 | 5 | 6 | 3 | 16 | 24 | 67 | ||
Where parents/carers or children refused consent for children’s participation, these children did not participate in the trial. Children who were absent at both baseline and follow-up data collections and parents who were unable to communicate in English or who did not return their contact details did not participate in the trial. In intervention schools, all children in participating classes received KAT whether or not they participated in the trial. KAT programme activities were integrated into their normal classroom work and their parents/carers were invited to attend the KAT family events. Head teachers in all participating schools, and parents and teachers of children in the relevant classes at intervention schools, were invited to take part in process evaluation interviews. Children in intervention schools also took part in focus groups.
Confidentiality
The chief investigator and the research team protected the confidentiality of participants in accordance with the Data Protection Act 1998. 115
All focus-group participants were asked to treat the discussion as strictly confidential. In reporting the results of the process evaluation, care has been taken to use quotations which do not reveal the identity of respondents. Individual teachers at participating schools were assured that if they decided not to participate, their decision would be handled confidentially.
All data collected as part of the trial were treated as confidential and accessed only by members of the trial team; anonymised data have been used wherever possible. However, all participants were informed that if they disclosed information about neglect, abuse, serious suicidal thoughts or self-harm, we would pass this information on to an appropriate agency: their assent for this was sought prior to data collection. The study adhered to the Cardiff University policy on safeguarding children and vulnerable adults and to schools’ own child protection policies. In each school, we also asked for guidance on which member of staff we could speak with if any children became upset during questionnaire completion or focus groups, and what procedures we should follow.
Measures
Key outcomes were the quality of programme implementation; recruitment and retention of research participants; and the acceptability and feasibility of research processes, including data collection methods. The study also assessed the feasibility and acceptability to children of providing demographic data and of answering questions measuring potential primary and secondary outcomes of any future effectiveness trial.
Table 3 lists outcome measures used with parents and children, and their function within the exploratory trial.
| Measure (potential primary outcomes in bold) | Children | Parents | Rationale | ||
|---|---|---|---|---|---|
| Baseline | Follow-up | Assess feasibility and acceptability | Assess potential effect sizes | ||
| Ever had a proper drink | ✓ | ✓ | ✓ | ||
| Ever drunk | ✓ | ✓ | ✓ | ||
| Drinking frequency | ✓ | ✓ | ✓ | ||
| Drunkenness frequency | ✓ | ✓ | ✓ | ||
| Smoking frequency | ✓ | ✓ | ✓ | ||
| KIDSCREEN-52: parent relationship and home-life dimension | ✓ | ✓ | ✓ | ✓ | |
| Targeted Parent–Child Communication about Alcohol Scale | ✓ | ✓ | |||
| Family Activities Scale | ✓ | ✓ | ✓ | ✓ | ✓ |
| Parent–Child Communication Scale | ✓ | ✓ | ✓ | ✓ | |
| Family Communication Scale | ✓ | ✓ | ✓ | ✓ | |
| Change in alcohol-related behaviour | ✓ | ✓ | |||
| Daily Drinking Questionnaire | ✓ | ✓ | |||
Questionnaire piloting
The MRC guidance on complex interventions encourages researchers to include user involvement in key phases of intervention development and evaluation, so as to maximise the relevance of research and the opportunities to implement findings. 116 Further still, the involvement of the public in research has been advocated to ensure that research is relevant, reliable and understandable. 117,118 Although the previous documents recommend involvement, they do not advise how to conduct public involvement and what issues should be covered.
As part of the trial, it was deemed most important to capture children’s views on the questionnaires, particularly as some of the measures had been taken from studies of older young people (≥ 11 years old) (e.g. an ongoing trial of the SFP10–14).
Prior to baseline data collection, the pupil questionnaire was piloted in a school not involved in the study. A group of pupils from Year 6 (five boys and four girls) were asked to read through the questionnaire and to use a highlighter pen to indicate any questions, response categories or other text which was unclear or difficult to understand, and to mark with an ‘X’ any question that they thought people in their class might feel uncomfortable or unhappy about answering. The pupils were then asked to discuss their thoughts about the questionnaire.
In general, the pupils felt that the questionnaire content was acceptable and accessible. In response to pupils’ comments about the sensitivity of questions concerning family structure and ethnicity, we made a number of changes to the baseline questionnaire. For example, in relation to questions on who participants lived with, we changed the closed questions with tick-box responses to an open question and invited participants to describe, using free text, who they lived with all or most of the time.
Children’s follow-up questionnaires were piloted with 36 children in Year 5 at a school outside the study area. The children were divided into small groups, each of which commented on a different part of the questionnaire. Children were asked about the meaning of questions and answers, and the acceptability and difficulty of the questions. Any questions children did not understand were explained by the researchers, and children were further asked to give examples of how we should word the questions. In this second round of piloting, we specifically asked the pupils to explain to us what they thought individual questions meant so that we could ascertain that participants were likely to derive the correct meaning from them. Amendments were made to the questionnaire; for example, the majority of children did not understand the term ‘peer pressure’, so this was changed to ‘pressure to use alcohol from other children who are about my age’.
The pilot was conducted during the school day, with each group spending about half an hour away from their class. Parents at the same school were invited to pilot the questions for telephone interviews but there were no volunteers.
Feedback to schools
Schools were offered a presentation on the KAT study at the end of the summer term in 2013. Two schools, both from the intervention group, accepted the offer. Presentation topics included information about research generally, the number of schools, children and parents who had taken part and some of the key findings. Parents were invited to both presentations but only two (both in the second school) attended.
Feasibility and acceptability of primary outcomes
The primary outcome for any future effectiveness trial was likely to be drinking initiation (at age 11–13 years). The age at which young people start drinking alcohol is strongly associated with later alcohol-related harm, and greater harm is related to earlier initiation. 119 An intervention which delayed drinking initiation, therefore, could reduce the prevalence of alcohol-related health and social problems in the long term. At the exploratory stage described here, the aim of asking children about alcohol consumption was to understand its acceptability and feasibility for this age group. Drinking initiation was assessed by adapting a question from the Survey of Smoking, Drinking and Drug Use Among Young People in England in 2008. 120
Measures of two other key alcohol initiation behaviours, namely alcohol consumption frequency and drunkenness frequency, were also used. The relevant questions from the 2009 Health Behaviour in School-aged Children (HBSC) survey were used as measures in this study. 121 The original item incorporates three questions measuring frequency of smoking cigarettes, drinking and drunkenness over the previous 30 days. The item on smoking was retained, in case any effectiveness trial might examine the intervention’s impact on more than one risk behaviour.
These three measures were adapted from an earlier HBSC survey and the European School Survey Project on Alcohol and other Drugs (ESPAD) for the HBSC 2009 survey. The alcohol items had previously been used in the HBSC 2005–6 optional package. The alcohol questions have good consistency with other HBSC measures of alcohol use but the smoking question has not been validated. The wording of the questions was:
On how many occasions (if any) have you done the following things in the last 30 days?
-
smoked cigarettes
-
drunk alcohol
-
been drunk.
(Never/1–2 times/3–5 times/6–9 times/10–12 times/20–39 times/40 or more.)
During baseline data collections, many children did not understand the term ‘occasions’; the concept of ‘30 days’ was troublesome for many; and those with low literacy had difficulty in linking the items in the list to the core question. Therefore, at follow-up the wording and response categories were adapted and a separate question was asked for each behaviour:
On how many days (if any) have you drunk alcohol in the last month?
On how many days (if any) have you been drunk in the last month?
On how many days (if any) have you smoked cigarettes in the last month?
(Never/1–2/3–5/6–9/10–12/13–19/20–29/every day.)
We also asked pupils a single question about whether or not they had ever been drunk, and adapted this question from the HBSC international survey of 11- to 15-year-old schoolchildren. 121 The original question (p. 282) asked, ‘Have you ever had so much alcohol that you were really drunk?’ (no, never/yes, once/yes, 2–3 times/yes, 4–10 times/yes, more than 10 times). It has been used in six HBSC surveys and found to be correlated with other measures of alcohol consumption. In this study, because the prevalence of drunkenness is generally low among 9- to 11-year-olds, it was not considered useful to distinguish between different frequencies of drunkenness; and as the term ‘really drunk’ may not be commonly used by children in this age group, they were thought likely to question the term ‘really’. Therefore, the question and response categories were simplified to read:
Have you ever had so much alcohol that you were drunk? (Yes/no)
Data on past-month frequency of drinking and frequency of drunkenness from 11- to 13-year-old pupils in the 2009 HBSC study in Wales were used to estimate prevalence of drinking in this age group as a basis for estimation of the sample size required for a potential future effectiveness trial. Data on rates of drinking among 11- to 13-year-olds from an ongoing trial of the SFP10–14 were also examined.
Feasibility and acceptability of secondary outcomes for a future effectiveness trial
We have proposed that the SDM73 can explain how KAT is expected to prevent alcohol misuse through improving adult–child communication and, thus, promote the formation of attachments to parents or other influential adults. Adult–child communication appears to be an important secondary outcome and appropriate measures would be needed to test programme theory. Measures of opportunities for communication and the quality and quantity of interaction were therefore used in this study.
The SDM postulates that perception of opportunities for communication is a preliminary to communication taking place. The KIDSCREEN-52 subscale on parent relations and home life was used as a measure of children’s perceptions of such opportunities at home. The Family Activities Scale and questions about the degree of involvement in KAT classwork and attendance at the family event were used to measure involvement in prosocial activity, assuming these also to be measures of the minimum number of participants who perceived such activities as opportunities which were relevant to them. We accept that there may have been some people who perceived KAT as a social opportunity but were prevented by other commitments from taking part.
Measures of family communication and of parent–child communication specifically about alcohol which could assess the quantity and quality of interaction taking place were also used. No measure of attachment was used because KAT is not aimed directly at increasing parent–child attachment but focused on earlier stages of the model. We speculate that in any future effectiveness trial, changes in scores for measures used at baseline (opportunities for, quality and quantity of communication in families) might be regarded as indicators of increased or decreased potential for attachment to a parent/caregiver. However, a more direct measure of attachment might be desirable for use in any effectiveness trial in which measures would be used to test the theoretical pathways hypothesised in the model. Figure 4 illustrates the relationship of the measures to the KAT logic model and the SDM.
FIGURE 4.
Kids, Adults Together programme activities and measures and their relationship to the SDM.

The main aim of this trial is to assess the feasibility of the communication measures, and they were expected to provide some indication of short-term differences between the groups which might be detected at follow-up in an effectiveness trial, probably falling short of statistical significance. We describe each of the measures below.
The Family Activity Scale formed part of the HBSC international survey of 11- to 15-year-old schoolchildren. 121 There are eight items in the scale, which was used in baseline and follow-up questionnaires for children and parents. Participants are asked ‘How often do you and your family usually do each of the following things?’ followed by the list of potential activities, for example watching television (TV) or a video together (every day/most days/about once a week/less often/never).
The context for family communication was assessed with the KIDSCREEN-52122 Parent Relation and Home Life dimension, which measures the quality of children’s home life, including parent/child interaction. KIDSCREEN-52 is a generic measure of children’s health-related quality of life across 10 dimensions, each of which has been independently validated with European children aged 8–18 years and their parents. The parent and home life subscale includes items on the home atmosphere and the child’s feelings towards parents/carers, each scored on a five-point scale (never/not very often/quite often/very often/always). In this study, question wording was adapted to facilitate responses from children who lived with adults other than parents, so, for example, ‘Have your parent(s) understood you?’ became ‘Has at least one of the grown-ups at home understood you?’
The Targeted Parent–Child Communication about Alcohol Scale (TPCCAS)123 measures general openness, frequency and, specifically, alcohol-related content of parent–child communication. Development of the measure was based on evidence that parent–child communication which was more protective against substance misuse not only involved open and frequent general communication but also specifically addressed the topic of substance misuse. As with the KIDSCREEN-52 measure, the wording was adapted by us to facilitate responses from children who lived with adults other than parents by substituting ‘the grown-ups at home’ for ‘parents’. The scale was validated with US children aged 11–13 years, and, to facilitate responses from the younger children in this study, a separate question was asked for each item instead of presenting the scale as one question followed by a list. In addition, children were asked whether they agreed or disagreed with each statement instead of being asked to indicate the extent of agreement on a five-point scale, for example ‘At least one of the grown-ups at home has warned me about the dangers of drinking alcohol’ (agree/disagree); ‘At least one of the grown-ups at home has talked to me about how to handle offers of alcoholic drinks’ (agree/disagree), etc. Nevertheless, the questions presented difficulties for a substantial number of children at baseline and the scale was not used at follow-up.
The Parent–Child Communication Scale (PCCS),101 which was used at follow-up in place of the TPCCAS, has been developed for use with parents and children to assess the nature of alcohol-related content in parent–child communication during the previous 6 months. Ten items are parallel in both questionnaires but the parent version has an eleventh question asking whether or not parents check the child’s room or clothes for evidence of alcohol use, and measures frequency of communication. The scale was used in telephone interviews with 537 parent–adolescent pairs in a US longitudinal study across 48 states. Adolescents in the sample were aged from 12 to 15 years. This was not the first choice for the KAT study because of the three types of communication identified by the US researchers – relating to rules, consequences and media examples – rule-related communication appeared to be associated with a small increase in adolescent alcohol misuse and there was no evidence that the other types of communication were predictive of later alcohol-related behaviour. However, Ennett et al. 101 point out that the timing of communication in relation to adolescent drinking initiation is likely to be an important influence on the impact of parent–child communication, and this factor was not accounted for in their study. More generally, imposition of rules by parents in the absence of reciprocity in the parent–child relationship has been found to be ineffective in preventing children’s antisocial behaviour. 58 Thus, the scale was judged likely to be satisfactory when used with younger children, of whom a larger proportion would not have initiated alcohol use, and when combined with measures of the home context and more general qualities of communication, as in this study.
With parents participating in the KAT study, the scale was used in an unmodified form. In the children’s questionnaire, the wording of six items was revised in line with guidance from children who piloted the questionnaire; in addition, the format was changed from a single question followed by a list to a series of discrete statements. References to parents were removed as for other questionnaire scales and the 6-month recall period was not specified. For example, the questions in the original scale were:
During the last 6 months, how many of the (n) other people living in your house
. . . encouraged you not to use alcohol?
. . . talked to you about how they would discipline you if you used alcohol?
These became:
At least one of the grown-ups at home has said I should not use alcohol (true/not true).
At least one of the grown-ups at home has talked to me about what they would do if they found out that I had used alcohol (true/not true).
Response categories ‘true/not true’ were preferred to ‘agree/disagree’ following advice from a teacher present at a baseline data collection who said that some children might feel reluctant to ‘disagree’ because the word held strong oppositional connotations for them.
The Family Communication Scale (FCS)95 evaluates respondents’ satisfaction with communication processes between family members. It was included in parent and pupil follow-up questionnaires to supplement the PCCS (see above), which covered only the alcohol-related content of communication. It is uncertain whether KAT would work through alcohol-specific or more general communication, and so measures of both were piloted.
The FCS was developed from the Parent–Adolescent Communication Scale124 which has previously been used to assess the role of parent–child communication in the pathways to adolescent drinking. 97 The FCS is briefer (10 items) and includes only the more predictive of the two subscales included in the earlier measure. It has been validated for use with both adolescents and their parents. In the parent interviews, the scale was used unchanged, for example ‘Family members are satisfied with how they communicate with each other’ (strongly disagree/generally disagree/undecided/generally agree/strongly agree). Scores are summed. Very high scores indicate that ‘family members feel very positive about the quality and quantity of their family communication’ and very low scores indicate that they ‘have many concerns about the quality of their family communication’.
Children who piloted the follow-up questionnaire suggested some changes to the wording to facilitate responses from 9- to 11-year-olds. ‘Family members’ in the original was changed to ‘the people in my family’ throughout, and the vocabulary was simplified; for example, ‘When angry, family members seldom say negative things about each other’ became ‘Even when they are angry, the people in my family hardly ever say nasty things about each other’. Following guidance from the children who piloted it, responses in the children’s questionnaire were changed from the original five-point scale to ‘true/not true’ except for two items, for which the option ‘sometimes true’ was added.
Effect sizes detected in previous studies
We undertook a search for previous studies which had used these selected outcome measures, to identify what size of effect had been detected in evaluations of interventions comparable with KAT. We present the results of this search in Chapter 3 [see Effect sizes detected in previous studies (secondary outcomes)].
Feasibility and acceptability of measuring changes in alcohol-related behaviour (parent telephone interviews)
Because evidence from our previous research on KAT110 suggested that adults might change their behaviour after participating in KAT, the following two questions were included to assess their feasibility and acceptability:
Thinking now about the last six months, has there been any change in your drinking habits (yes/no/don’t know/rather not say)?
How have your drinking habits changed (drink more than I used to/drink less than I used to/drink a different kind of alcohol/drink in a different place/take measures to ensure drinking does not cause harm)?
We also used the Daily Drinking Questionnaire in our telephone interviews with parents/carers. This measure asks for details of a typical week, rather than exact quantities for the last 7 days, to ensure that it reflects habitual drinking. Although it has been developed for, and used mainly with, student populations125,126 we decided to assess its acceptability to parents because of its proven ability to detect post-intervention changes.
Demographic information
Measures of sex, age, ethnicity, socioeconomic status and (for parents) qualifications and employment were used to assess their acceptability to participants and comparability between intervention and control groups. For children, the Family Affluence Scale127,128 was used as a measure of socioeconomic status.
Holstein et al. 129 point out that the Family Affluence Scale measures family consumption rather than occupation, education and income, which are usually considered to constitute a more accurate measure of socioeconomic status. However, the scale has been developed for use in HBSC surveys because younger children had difficulty in answering questions about parents’ occupations and because it measures more than one dimension of socioeconomic status. It was considered the best available measure for use with the children in our sample, some of whom are younger than the youngest taking part in the HBSC surveys and so may be considered even less likely to provide accurate data on parental occupation. The scale’s validity and the suitability of the items are subject to continual review, and in our study the scoring used in the 2009–10 survey was used. 121 The scale is composed of four items:
-
Does your family own a car, van or truck?
-
[no (0); yes, one (1); yes, two or more (2)]
-
-
Do you have your own bedroom for yourself?
-
[no (0); yes (1)]
-
-
During the past 12 months, how many times did you travel away on holiday with your family?
-
[not at all (0); once (1); twice (2); more than twice (3)]
-
-
How many computers does your family own?
-
[none (0); one (1); two (2); more than two (3)]
-
Participation in Kids, Adults Together
To assess reach, parents and children in the intervention group were asked about their own and other family members’ participation in KAT. The process evaluation also examined this issue in order to provide information about parents’ and children’s motivation to participate and their response to the programme.
Scale scores
Methods for calculating scores for the following scales are described in Appendix 7:
-
Family Activity Scale
-
Quality of parent relations and home life KIDSCREEN-52 subscale
-
PCCS
-
TPCCAS
-
FCS
-
Family Affluence Scale.
Data collection
In addition to piloting the acceptability and feasibility of measures, the study aimed to identify optimal data collection methods and to assess their costs.
At baseline and 4-month follow-up, measures were collected through self-completion questionnaires by children who were present on the day of data collection in all classes participating in KAT, subject to their own assent and parents not refusing permission. Questionnaires were completed in classroom time, supervised by members of the research team. Researchers and school staff assisted children who had difficulties in reading or writing English. Some children who were absent at baseline completed follow-up questionnaires.
The original study protocol stated that the follow-up data collections in schools would be conducted at 6 months after baseline. However, delays in the early stages of the project meant that the interval between baseline and follow-up data collection was reduced to ensure that the latter took place before the school summer holidays, and before Year 6 pupils left their primary school. This change would be significant in a trial which aimed to measure effects. However, in the current exploratory phase it has not been a barrier to achieving the aims of establishing recruitment and retention rates (for intermediate outcomes), and has resulted in some learning about time scales to be considered in the design of any future effectiveness study.
Contact details of parents who volunteered to participate in the research were forwarded to trained telephone interviewers at Cardiff University, who conducted the interviews approximately 6 months post baseline. Personal interviews would not be a practical method to collect data from larger numbers of parents who would participate in any future effectiveness trial, and so the feasibility and acceptability of telephone interviews were assessed by staff at the Participant Resource Centre (PRC) at Cardiff University. Calls were recorded (with the knowledge of interviewees) and responses were recorded on paper schedules during the interviews. Parents who completed interviews were given £15 gift vouchers.
Following baseline data collection, each participant was allocated a numerical identifier stored in an index list of study participant numbers and names held separately from the project data. At follow-up data collection, we gave each pupil a questionnaire which had their unique participant ID pre-printed on it. Pupils who had not completed baseline questionnaires (because either they had been absent from school/class or they did not want to complete the questionnaire) but wished to complete follow-up questionnaires were allowed to do so. All files were stored in secure password-protected folders with restricted access. Data from completed questionnaires and interviews were encrypted at the point of entry and stored in anonymised form, using participant identification numbers. PASW 18 (SPSS Inc., Chicago, IL, USA) software was used to store pupil questionnaire data, and parent data were stored in Excel (Microsoft Excel, Microsoft Corporation. Redmond, WA, USA). Ten per cent of questionnaires were selected at random from the electronic files and checked against the original paper questionnaires. The error rate was < 0.4% and the files were passed to the trial statistician for analysis.
During the study, we followed the Cardiff University Child Protection Guidelines. 130 As our data collection included issues relating to young people’s alcohol consumption, and family relationships, it was important for us to be prepared for responses that indicated that a child (or other person) was at risk of harm or abuse. In such cases, as data were collected in schools, Cardiff University policy dictated that any child protection concerns should be communicated to the head teacher of the school in question. A number of questionnaire responses (as can be seen in Chapter 3) indicated that child participants had consumed alcohol or been drunk – either in the last 30 days or in their lifetime. This presented us with a challenge in terms of how to respond to such information. It was important that we preserved confidentiality wherever possible, but also shared any information that might indicate risk of harm with schools. In the case of alcohol use, it was not appropriate or ethical to simply report all cases of children’s alcohol consumption to school staff. The law permits parents to provide alcohol to children aged ≥ 5 years within the family home, and so the consumption of alcohol by a child aged 9–11 years (as in this study) does not necessarily indicate illegality or parental irresponsibility. The measuring of alcohol consumption also raises challenges, in that, for instance, a child reporting having had a drink of alcohol could be referring to a whole drink or just a sip. The notion of drunkenness is subjective, and we, as adult researchers, and participants, being children, might have had very different understandings of the term. There was also clear evidence in our data (see Chapter 3) of inconsistent responses by pupils to alcohol-related questions. For instance, some participants reported drinking in the last month but also reported that they had never had an alcohol drink, and their responses also contradicted each other across data collection points. The ability to assess these reports was also made more difficult due to the fact that, unlike face-to-face interviews (where participants provide a response to the researcher), our questionnaire data were via written reports from pupils which were entered into the project database some time later. In many cases, children had moved schools, transferring to secondary schools at age 11 years.
Our approach to this issue was that reports of frequent drunkenness during the last month would constitute concern regarding the potential for an individual to experience harm, and would be shared. During data entry, significant concerns were raised regarding the responses of one child who answered ‘yes’ at both baseline and follow-up to the question ‘Have you ever had so much alcohol that you were drunk?’ Although this child answered ‘yes’ at baseline and ‘no’ at follow-up to the question ‘Have you ever had a proper alcoholic drink – a whole drink, not just a sip?’, they also reported in both questionnaires having drunk alcohol during the previous 30 days: on 3–5 occasions (baseline) and 6–9 days (follow-up). We complied with Cardiff University’s Child Protection Guidelines130 by following the policy of the relevant school and informing the teacher responsible for child protection.
Sample size
As this was an exploratory cluster randomised trial, no formal sample size calculation was carried out. However, in order to collect enough data to validate the outcome measures being tested and to calculate intracluster correlation coefficients (ICCs), eight schools were anticipated to equate to approximately 640 families, which with an estimated consent rate of 50% at baseline would achieve a sample of 320 families: 160 per group. No interim analyses or stopping guidelines were implemented.
Randomisation
The schools were stratified by size and free school meal (FSM) entitlement and these variables were used to balance the randomisation. The method of optimal allocation was used to determine the randomisation sequence. Here, a balance algorithm was used to provide a predefined sequence, and all schools were randomised jointly. 131,132 The method was implemented in R statistical software (The R Foundation for Statistical Computing, Vienna, Austria) in the South East Wales Trials Unit (SEWTU) and the allocation was concealed until after recruitment and the start of the intervention. An independent statistician within SEWTU assigned schools to the intervention arm. During recruitment of schools in the autumn term of 2011, a pragmatic decision was made to randomise in advance of baseline data collection so that schools allocated to the intervention group would have time to plan for programme delivery in the spring term of 2012. As explained earlier (see Chapter 1, Study design), recruitment and baseline data collection took place before the start of the funded study and there was no capacity to finalise children’s baseline measures until early 2012, by which time all schools in the study would have embarked upon their scheduled activities for the spring term.
Individual participants within schools were included according to complete class lists for Year 5 and 6 irrespective of attendance at KAT events and completion of group work. Pupils who were at school on the day of data collection were included in the study. Return visits to collect missing pupil data were not conducted owing to lack of capacity.
Statistical methods
In the context of an exploratory study, the main purpose of the statistical analysis was to assess the feasibility and acceptability of the measures used. Thus, an essential function of the analysis was to look for any pattern in the missing responses which might indicate respondents’ unwillingness or inability to answer certain questions. Some of the measures of potential secondary outcomes which were tested in this study had previously been used with different populations (e.g. older children than the KAT sample, data collected in countries other than the UK), and in some cases we used subscales which belonged to larger measures. It was, therefore, important to assess the reliability of the scales, including those which it was necessary to adapt. For some of the scales, the scoring methods previously used also needed to be adapted.
Assessment of the reliability of questionnaire measures
Assessment of reliability was carried out using Cronbach’s alpha for internal consistency and factor analysis for unidimensionality. Summed scores were created for each outcome scale. With previously validated scales, the outcome was used as directed in the manuals or scale references – either categorical (using validated cut-offs) or used as a continuous score. Where no guidance was given, the continuous data were used in the primary analysis and, if necessary, the categorical outcome was examined as a secondary analysis.
Analysis of future primary outcomes
All analyses were on an intention-to-treat (ITT) basis using all randomised participants in the groups to which they were randomised, regardless of the intervention received. However, missing data were not imputed, and so all analyses were carried out on complete cases. The primary outcomes were alcohol consumption and levels of harmful drinking and drunkenness at follow-up. Alcohol outcomes were analysed using two-level generalised logistic models. Responses from pupils were nested within schools fitted using models adjusting for baseline data where appropriate. The distribution of frequency of drinking and drunkenness in the last month was examined and it was determined that these ordinal categorical data were most appropriately collapsed into binary outcomes due to sparse data in higher categories. Covariates included in the models were those that were used to balance the randomisation (school size and FSM entitlement). While we acknowledge that a household-level cluster is present (siblings within a school), the number of these per school was very small and was not incorporated. As well as any differences between trial arms, estimates of ICCs at school level were reported.
Analysis of future secondary outcomes
Questionnaire outcome score data from pupils were analysed using two-level generalised linear models, with responses from pupils nested within schools fitted using models adjusting for baseline data. Covariates included in the model include those that were balanced on at randomisation (school size and FSM entitlement). As well as any differences between trial arms, estimates of ICCs and an indication of effect sizes are reported.
Outcome measures from parents were also collected but only a small number of parents returned data and, therefore, only descriptive analyses of these are provided.
No formal subgroup analyses were carried out; however, as there were differences in the ratio of Year 5 and 6 pupils between arms, the effects of age were investigated further, as it was important to identify any patterns in the data relating to these groups which might be present in a future effectiveness trial.
Process evaluation
Schools and families are complex systems within which KAT aims to achieve change. A process evaluation is vital to understand how these systems may influence intervention delivery in ways which support or obstruct the intended change. A process evaluation was conducted throughout the implementation of KAT with the following objectives:
-
to assess quality of delivery and fidelity
-
to develop and refine the programme logic model
-
to develop and refine the programme’s theory of behaviour change
-
to assess programme reach, particularly in relation to hard-to-reach and high-risk families.
Methods
This study used classroom observations, semistructured interviews and focus groups to develop the theoretical framework and explore implementation fidelity and acceptability of KAT. Semistructured schedules allowed the researcher to probe and explore key themes and issues while allowing participants to discuss issues, experiences and opinions about KAT that had not been anticipated by the interviewer. Observation, and interview and focus-group schedules are included in Appendix 8.
Observation
Non-participant observations were conducted during the KAT classroom delivery and fun evenings in order to gain a deeper insight into implementation fidelity and an understanding of contextual influences on implementation. Observation as a qualitative approach is useful to observe a phenomenon in its natural state. 133 Observers typically take extensive field notes which can be coded and analysed. In non-participant observation, the researcher endeavours to be as unobtrusive as possible because increased participant awareness of the researcher’s presence may affect participants’ behaviour (i.e. produce a Hawthorne effect). Observational data tend to be more valid and reliable than self-report data as they provide better understanding of the phenomenon and context under study. 134 However, combining observation with other data collection methods, such as interviews, will further strengthen the validity of the methods used135 and observational data can develop questions or emergent themes to be addressed by other methods and subsequent analyses. Moreover, observers may not always be present when program delivery takes place, and so it is important that information on implementation is also obtained through other methods. An example of a completed observation schedule is included in Appendix 8.
Classroom preparations for the KAT fun evening and the fun evening itself were observed in order to gain insight into the delivery of KAT and pupil and parent engagement in the programme. A total of 11 hours of observation took place in school 1 (over eight observations), 7 hours in school 2 (over four observations) and 6 hours in school 3 (over three observations). Notes were taken during observations and written up as soon as possible. The observations were used to inform interview questions and analysis. Table 4 shows the number of hours of observation and the estimated proportion of classwork observed in each intervention school.
| School | Classwork (estimateda total duration in hours) | Duration of observation (hours : minutes) | Percentage of classwork observed |
|---|---|---|---|
| 3 | 40 | 3 : 30 | 8.7 |
| 4 | 40 | 8 : 25 | 21.0 |
| 6 | 60 | 3 : 55 | 6.5 |
| 8 | Not completed | 2 : 25 | Not known |
Focus groups
The views and experiences of the pupils were captured through focus groups. Focus-group research involves organised discussion with a selected group of individuals to gain information about their views and experiences of a topic. 136 It was decided that a focus group would be a more suitable approach to use with children than individual interviews because children may be more comfortable expressing their attitudes, feelings and beliefs towards KAT in a peer-group setting than directly to an adult. This may be particularly pertinent in a school context where there may be considerable power imbalance in adult–child relationships. Reducing power dynamics may discourage children from providing responses they think the interviewer wants to hear. 137 Furthermore, in focus groups children may feel less pressure to answer questions they may not feel comfortable with or know the answers to, reducing the chance of false answers being given. 138
Focus groups with children were held in three schools. They were held by researchers away from the children’s classrooms so that teachers could not overhear the discussion. Pupils were asked about their experiences of participating in the KAT activities and about whether or not they had talked about KAT with family members or friends. Focus groups with children who received KAT took place in three schools (two focus groups with four children in each group at school 2, and one focus group with six children each at school 1 and school 3). A total of 17 parents took part in interviews: seven at school 1 (three of whom were fathers), four at school 2 and six at school 3. Lengths of interviews with parents ranged from 10 minutes to 30 minutes.
Interviews
One-to-one interviews with parents, programme deliverers and head teachers were chosen as the most effective methods for obtaining detailed information about individual participants’ thoughts and experiences of KAT. The privacy of an individual interview was felt to encourage frank responses from both junior and senior members of school staff139 and from parents who might be affected by sensitive family issues. The aim was for all interviews and focus groups to take place within a week of the KAT fun evening so that the programme would be fresh in the interviewees’ minds. Telephone and face-to-face interviews were used and have yielded similar qualitative results. 140
Teachers were asked about their experiences of delivering KAT, school contextual influences, acceptability and implementation. Teachers and head teachers could choose to have their interview at their workplace or somewhere more convenient to them. Three head teachers participated in interviews lasting between 10 and 15 minutes, with interviews with the heads at school 4 and school 3 taking place over the telephone. All teachers who delivered KAT took part in face-to-face interviews in school, each averaging around 20–30 minutes. This totalled nine teacher interviews (two at school 4 where one was also the head teacher, two at school 3, four at school 6 and one at school 8).
Interviews with parents explored family communication and their experiences of the fun evening. Parents were given a choice of interview location or telephone interview in order to suit their convenience and encourage participation.
Validity
Maxwell141 describes validity in relation to qualitative research as ‘the correctness or credibility of a description, conclusion, explanation, interpretation, or other sort of account’ (p. 87). The validity of qualitative research in the present study was maintained by following the recommendations of Ratcliff. 142 First, a reflective journal of personal notes was kept in order to capture and recognise data that diverged from initial expectations. This journal included initial assumptions, and identification of potential bias was noted. Second, different sources of data – observation notes, interviews and focus groups – were triangulated and their degree of convergence was estimated. Third, extensive quotations from interview transcripts and observation notes were used in order to create ‘think descriptions’ of themes from the data and to represent participants’ voices. Fourth, emerging findings from the process evaluation were regularly compared with the findings of other comparative studies, both empirical work on alcohol misuse prevention interventions and the broader theoretical literature. Finally, independent checks were made, with transcriptions and emerging themes shared with supervisors in order for discussion of key themes and interpretation to take place.
Although Table 4 shows small proportions of observed class work, it should be noted that on many occasions, two or more classes were delivering KAT at the same time and, consequently, the ’observable hours’ total is likely to have been considerably smaller than the estimated total number of hours of classwork delivered. Despite many requests, teachers at school 4 did not always inform the researcher of when the work was going to be carried out, and so in those instances the researcher arrived at the classroom only to find that children had already completed their work on KAT for that day. Two periods of observation were carried out at each of the other three schools. Table 5 provides a summary of the interviews with parents and teachers, focus groups and classroom observation conducted in intervention schools as part of the process evaluation. In addition, interviews with the head teachers of schools 3 and 6 and observation of family events at schools 3, 4 and 6 were carried out.
| Data collection method | School | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 4 | 3 | 6 | 8 | |||||||||
| Class | Year 6 (class 1) | Year 6 (class 2) | Not known | Year 4/5 | Year 6 | Not known | Year 4/5 | Year 5 | Year 6 | Not known | Year 5 (class 1) | Year 5 (class 2) |
| Parent interviews | 1 | 6 | 1 (two children) | 3 | 2 | 1 | 2 | 1 | 0 | 0 | ||
| Teacher interviews | 1 (acting head) | 1 | 0 | 1 | 1 | 0 | 1 | 1 (joint with teacher and deputy head) | 1 | 0 | 1 | 0 |
| Focus groups | 1 (seven pupils) | 0 | 1 (four pupils) | 1 (four pupils) | 0 | 1 (six pupils) | 0 | 0 | 0 | |||
| Class observation records | 4 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 |
Qualitative data were coded using Atlas.ti (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany). The process evaluation was funded separately from the main trial, and its reporting timeline is behind that of the mainevaluation. In this report, we have, therefore, provided an interim analysis of the findings from the process evaluation, concentrating on the extent to which key programme-related progression criteria have been met.
Health economics
To enable a cost-effectiveness study to be conducted as part of a potential definitive trial, we mapped key cost and consequence domains, and tested the feasibility of data collection as part of a definitive trial. We sought to identify all inputs, including staff time, materials, equipment and facilities, that were used during the delivery of KAT. This included all relevant inputs and contributions by young people, parents, schools and other agencies to all aspects of the intervention and its processes and procedures. The extent to which these inputs could be translated into financial costs was examined. The primary and secondary outcomes were considered for their suitability as measures of output and outcomes for an economic evaluation, and to inform the nature of the evaluation to be conducted.
Criteria for recommending an effectiveness trial of Kids, Adults Together
Between February and April 2013, a set of criteria were developed through discussions among the Trial Management Group in order to assess and inform a decision on whether or not to proceed with a proposal to evaluate KAT in an effectiveness trial. Tables 6 and 7 show the criteria developed relating to the value, feasibility and acceptability of implementing the KAT programme; and of conducting a RCT in schools; and their relationship to the study objectives outlined above (see Chapter 1, Aims and objectives) and set out in the study protocol.
| Criteria | Basis for assessment | Secondary objectives stated in study protocol |
|---|---|---|
| 1. KAT can be implemented successfully in primary schools | Process evaluation findings indicate that at least two of the intervention schools delivered key elements of KAT classroom work and family events in line with the teachers’ handbook; AND it is reasonable to expect that any significant problems identified can be overcome | Assess the feasibility of the intervention (objective 2) |
| 2. KAT is acceptable to children in the target age group (9–11 years) | Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of pupil participants in each school | Assess the acceptability of the intervention (objective 2) |
| 3. KAT is acceptable to parents of children aged 9–11 years | Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of parent participants in each school | |
| 4. KAT is acceptable to school staff involved in implementation (head teachers, teachers of Year 5 and 6 classes, and support staff) | Process evaluation findings indicate that a majority of school staff in each school support the concept of primary school education about alcohol; feel competent to deliver KAT; and think that KAT has potential benefits for families and school; AND that it is reasonable to expect that any significant problems identified can be overcome | |
| 5. KAT attracts high rates of participation from children aged 9–11 years | Process evaluation findings and pupil questionnaires from intervention schools suggest that all pupils in participating classes take part in classroom work (if present in school) and few if any objections from parents are received; AND that a minimum 50% of pupils attend KAT events | Establish intervention participation rates (objective 3) |
| 6. KAT attracts high rates of participation from parents of children aged 9–11 years | Pupil questionnaire data (intervention group) and process evaluation findings suggest that parents/caregivers or other adults from families of a minimum 25% of pupils attended KAT events | |
| 7. KAT can be implemented in schools serving a range of socioeconomic groups and localities | Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that, of schools which implemented KAT, some were above and some below median FSM for the county | Establish intervention reach, including equality of engagement across socioeconomic groups and localities (objective 3) |
| 8. KAT can engage parents and children from a range of socioeconomic groups and localities | Ethnicity and Family Affluence Scale data from pupil questionnaires; deductions about families from FSM rates and demographics of school area; and process evaluation interviews with school staff demonstrate inclusion of families from a range of social groups and localities that reflects the local population | |
| 9. KAT delivery costs can be recorded in a way which facilitates assessment of cost-effectiveness | Systems developed in current project can be used to monitor costs of larger-scale implementation | Identify the costs of delivering KAT and pilot methods for assessing cost-effectiveness as part of a future effectiveness trial (objective 7) |
| 10. Sufficient support exists in terms of policy and resources at school, LEA and national levels, to allow successful delivery of KAT on a large scale | Stakeholder group judge that structures and resources for further implementation can be put in place | Identify optimal delivery structures and systems for the KAT programme post trial (objective 2) |
| Criteria | Basis for assessment | Secondary objectives stated in study protocol 2 |
|---|---|---|
| 11. KAT is consistent with a theoretical basis which suggests that short-term impacts on parent–child communication may shape longer-term alcohol-related behaviours | Process evaluation findings and comparison of intervention and control group scores for intermediate outcomes (communication measures) indicate that participation in KAT is associated with an increase in parent–child communication | Refine the theoretical model of the intervention (objective 1) |
| 12. It is feasible to conduct a trial of KAT in schools serving a range of socioeconomic groups and localities | Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that schools within each trial arm varied in terms of social, demographic and geographic characteristics and that at least two were in areas above the county median for deprivation | Assess trial recruitment and retention rates (objective 4) |
| 13. The sample required to demonstrate a significant effect of KAT is achievable | Recruitment records indicate that we were able to recruit eight schools as per protocol; project records demonstrate that schools in both trial arms are retained in the study; questionnaire returns indicate that at least 80% of pupils in a majority of eligible classes provide data at each time point | Assess trial recruitment and retention rates (objective 4) Identify potential effect sizes that are likely to be detected as part of an effectiveness trial and an appropriate sample size (objective 5) |
| 14. Methods for measurement of primary and secondary outcomes are feasible and the cost of measurement can be estimated | Measures were understood by, and acceptable to, more than 75% of Year 5 and 6 pupils in each school | Determine the feasibility and cost of the proposed methods for measurement of the primary and secondary outcomes (objective 6) |
| 15. Promising effect sizes are achieved for key outcomes | After adjusting for baseline differences, comparison of intervention and control group pupil scores at follow-up shows that intervention group average scores are higher than control for at least one of the following measures: KIDSCREEN-52 autonomy dimension PCCS FCS Family Activities Scale AND that intervention group average scores are not lower than control group average scores for any of the other scales |
We structure our discussion chapter around these criteria, and assess the evidence for each of them individually before providing an overall assessment of the evidence.
Involvement of practice and policy stakeholders
A crucial aspect of any further evaluation is the availability of systems for the wider-scale programme implementation required for an effectiveness study. A stakeholder group was convened in February 2013 which included relevant individuals and representatives of key policy, health and education agencies. Membership comprised:
-
Head of Substance Misuse Policy and Finance, Welsh Government
-
Representative of Pupil Wellbeing Branch, Department for Education and Skills, Welsh Government
-
Consultant in Public Health, Public Health Wales
-
Retired head teacher of a school which piloted KAT
-
Chief Superintendent, Gwent Police (chairperson, Gwent Substance Misuse Area Planning Board)
-
Welsh Network of Healthy School Schemes Programme Manager
-
Health education consultant responsible for KAT development and training
-
National Co-ordinator, All-Wales Schools Liaison Core Programme.
Members of the group advised on the likely value of the programme to schools in Wales and the feasibility of implementation and funding on a wider scale. The principal investigator held separate discussions with the Chief Superintendent of Gwent Police to ascertain ownership rights to the programme and the extent to which Gwent Police wished to be involved in further implementation and evaluation.
Chapter 3 Findings
Parts of this text are reproduced with permission from Segrott et al. 1
Data analysis was similar to that which would be carried out in an effectiveness trial, but the objectives and interpretation which flow from this analysis are different. For example, important functions of the statistical analysis of primary and secondary outcome measures were to identify and interpret patterns of missing data and to estimate the sample size for an effectiveness trial. Recruitment rates, and aspects of data collection, which would ordinarily form part of the methods section in an effectiveness trial, are key findings in this exploratory trial because they help to determine the feasibility of the research design and procedures. The process evaluation was intended to examine feasibility of implementing KAT in different schools and whether or not the programme could be further developed in ways which would facilitate implementation and acceptability. Learning points for a future effectiveness trial are examined in Chapter 4.
Chapter overview
This chapter begins by describing the implementation and fidelity, acceptability, participation rates and perceived impacts on communication of KAT class work and family event components. For the trial, we describe recruitment and retention rates, feasibility of potential primary and secondary outcome measures, and estimation of the sample size required for any future effectiveness trial. The chapter finishes with a summary of financial costs of implementing and evaluating KAT.
Programme implementation and fidelity
Of the five schools allocated to the intervention group, one withdrew from the study before baseline data collection (school A) and another (school 8) withdrew after baseline data collection, shortly after beginning the KAT classwork. The following findings are based on data collected from the three schools (schools 3, 4 and 6) which completed programme delivery and follow-up data collections, with some additional information from school 8 on acceptability.
Training and roles and responsibilities
Training was offered to staff in intervention schools but some teachers in school 6 did not attend training sessions, mostly due to pressure of other work or because it was impossible for the school to bring together all relevant staff at one time. Consequently, the Year 6 teacher and Year 5 deputy head did not appear to be familiar with the contents of the handbook or to be aware of other information they would have received through training. In addition, although school staff arranged the date and venue for the family event and contacted parents, they did not get the hall ready or take charge of the activities. Teachers in the other two schools were on the whole satisfied that the KAT handbook provided ‘a good basis to work from’ (Year 6 teacher, head, school 4), but it was apparent that the success of the intervention was dependent on senior manager buy-in and support.
Classwork component
The programme handbook identified five key elements which teachers were asked to deliver as part of the classroom work:
-
establish pupil knowledge
-
emphasise healthy use of alcohol (not negatives)
-
develop responsible attitudes to alcohol use
-
improve communication skills – group/pair work
-
produce work for the family event including:
-
posters to advertise event
-
personal invitations
-
take work home to finish.
-
Classroom observation suggested that the majority of these elements were implemented with high fidelity in all three schools. Observation and interviews showed teachers followed the handbook closely, including the suggestions for assessing children’s knowledge. Interviews with teachers and focus groups with pupils demonstrated a good understanding of the ’not too much, not too soon’ healthy approach to alcohol, with teachers highlighting that in order for children to develop enough confidence to raise the topic at home, it was important for them to realise that alcohol was not ’all bad’ and that parents who drank alcohol were not doing wrong. However, it was recognised by some teachers and parents that in families where there was significant alcohol misuse, the balanced message might not reflect children’s experiences. In these cases, it was thought that children would benefit from more intensive support outside the family. If such children do talk to school staff or other adults, then KAT could maintain its reach to high-risk families, with children forming an attachment to a teacher or other supportive adult.
Group/pair work had high levels of fidelity and was something that pupils responded positively to, with clear examples of how interactive teaching and learning could be used to good effect in encouraging responsible attitudes to alcohol use, for example the ‘drinkers and thinkers’ role play rehearsal at school 4:
The drinkers were calling the thinkers ‘un-cool’, ‘boring’, ‘chicken’ etc., for not drinking. The thinkers were saying things like, ‘they had an exam tomorrow, they didn’t want smelly breath’, ‘didn’t want to get into trouble with police’, or ‘be ill’. The drinkers were being sick and falling over.
Observation 4, class 1
Group work was also thought to play a significant role in helping children to talk about alcohol at home because they had ‘almost practised saying it’ (Year 4/5 teacher, school 3).
Finally, while all classes prepared work for display or performance at the family event, including posters (though it is not clear that these were used to advertise the event), personal invitations were produced at only one school and there was no evidence from any school that children, parents or teachers thought that they were particularly important. Homework activities also had poor implementation, with school policies or existing practices resulting in low fidelity.
Kids, Adults Together family events
Key elements of KAT family events were identified from the manual as:
-
a presentation by pupils
-
a non-judgemental approach
-
an emphasis on healthy use of alcohol, not negatives
-
an aim for all pupils to take part in the event.
The handbook suggested how the event could be organised, with details of a suggested format and instructions on how to run two activities aimed at encouraging communication about alcohol: a quiz/treasure hunt and an activity called ‘Agree or Disagree’. This information, together with answers to the quiz, was repeated in a PowerPoint presentation which accompanied the handbook. The three intervention school events included both activities suggested in the handbook, alongside presentations by the children. Table 8 lists the presentations children made at each school.
| School | Presentation |
|---|---|
| School 3 | Role play |
| Mock TV game show | |
| School 4 | Role play |
| Talk by children about KAT classwork | |
| Animation including poems written and read out by children | |
| School 6 | Role play |
| Rap | |
| PowerPoint presentation |
Observation at all three schools found that they achieved a non-judgemental approach, and, overall, parents who participated in research interviews agreed with this. Interviews with teachers also suggest that they tried to ensure that the approach was ’light-hearted’ and humorous. There was evidence from all three schools that the family events promoted a healthy approach to alcohol use, with only a minority of parents indicating that their children were more focused on the dangers of alcohol than healthy use. There was less success in involving all children in the event, with two of the schools not appearing to have followed the guidance in the handbook.
Acceptability of the Kids, Adults Together intervention
Parents/carers
Initially, there were a very small number of objections to KAT from parents/carers (schools 3 and 4) and these were withdrawn after discussions with school staff. In all three schools, parents/carers were positive about the topic of alcohol being addressed at primary school, with parents generally seeing it as the ’perfect age I think, 10. I wish I had it when I was in school’ (parent interview 6).
All parents interviewed across all schools said they had enjoyed the family event, and this was confirmed by children’s focus groups who reported positive feedback from their family and observations. Teachers at all three schools also reported having received positive feedback from parents about the event, directly and/or through the children.
In the school which withdrew from the study after baseline (school 8), it is not clear how big a part KAT’s acceptability to predominantly Muslim parents played in the circumstances leading to the school’s withdrawal. The teacher of one class made it clear that he did not think KAT would benefit either the school or the children in his class and had expressed concern from the outset about delivering KAT to children from mostly Muslim families. Because the school decided to withdraw completely from the study, we were not able to conduct interviews with parents/carers in this school in order to ascertain to what extent the programme was acceptable to them.
Children
Observation suggested that the vast majority of pupils enjoyed KAT and were fully engaged in it. There was no evidence that large numbers of children had been bored or alienated by the project. This was supported by focus groups, with the participants stating that they had enjoyed the classwork and the family events; parents and teachers at all three schools also reported that the children had enjoyed KAT.
A few small issues were noted which slightly impaired the overall acceptability of the programme for children. Although KAT is intended for children in Years 5 and 6, Year 4 children were involved because they were in mixed classes, and they found the group work and writing tasks challenging. Observation records of the family event at school 6 where the school staff took no responsibility for organising or introducing activities showed some levels of boredom and restlessness among pupils. However, three parents from school 6 said that their own children had enjoyed the events, and general feedback from teachers and children was positive.
School staff
The vast majority of teachers thought that the intervention was age-appropriate, the ’perfect age’ to deal with this topic. Teachers were also pleased with the way KAT fitted into the curriculum and there was no evidence that teachers lacked the confidence or skills to deliver the classroom work. The Year 6 teacher at school 3 said that children had disclosed sensitive issues in class and it was not a problem for her: ’At this age they need to be talking about stuff like that’. Staff in all schools liked the way KAT facilitated parent–school contact (although there was some disquiet among teachers at the level of organisation at school 6), with some head teachers keen to use the same format for other topics.
Rates of intervention participation
Follow-up questionnaires completed by pupils in intervention schools included questions on whether or not pupils had done the KAT classroom work (all, part or none), whether or not they had attended the KAT family event, if any adult member of their family had attended and how many adult members from their family attended. The findings in the following sections are based on data from the recruited sample of pupils. Whole school classes undertook the KAT classroom work and were invited to the KAT family event. Participation rates, and their social patterning, may have differed for the classes as a whole.
Classwork
Table 9 shows that the majority (70.9%) of pupils who completed follow-up questionnaires reported covering KAT classroom work in full, and most of the remaining pupils (22.8%) had done part of it. These patterns held true across all three intervention schools which completed KAT, although there was significant variation in the proportion of pupils who completed KAT in full or in part. A greater proportion of pupils in school 4 had completed all the work (86%) than in schools 3 and 6 (64.7% and 63%, respectively).
| School | Did you do the KAT work in school? [n (%)] | |||
|---|---|---|---|---|
| All | None | Part | Not answered | |
| 3 (34 pupils) | 22 (64.7) | 1 (2.9) | 10 (29.4) | 1 (2.9) |
| 4 (51 pupils) | 44 (86.3) | 0 | 7 (13.7) | 0 |
| 6 (73 pupils) | 46 (63.0) | 6 (8.2) | 19 (26.0) | 2 (2.7) |
| Total (158 pupils) | 112 (70.9) | 7 (4.4) | 36 (22.8) | 3 (1.9) |
Family event
Table 10 shows the participation rates at the family event reported by pupils. An average of 59% of pupils reported attending the family events and 50% with their parents/carers. For the individual schools, the proportions of pupils whose families were represented by at least one adult member were 45.1%, 46.6% and 65.7%. For attendance by pupils themselves, the figures were 47.1%, 58.9% and 79.4%.
| School | Did any of your family go to the KAT event? [n (%)] | Did you go to the KAT event? [n (%)] | |||||
|---|---|---|---|---|---|---|---|
| Yes | No | Not answered | Total family members attending, N | Yes | No | Not answered | |
| 3 (34 pupils) | 22 (65.7) | 12 (34.3) | 0 | 47 | 27 (79.4) | 6 (7.6) | 1 (2.9) |
| 4 (51 pupils) | 23 (45.1) | 28 (54.9) | 0 | 36 | 24 (47.1) | 26 (51.0) | 1 (2.0) |
| 6 (73 pupils) | 34 (46.6) | 39 (53.4) | 0 | 51 | 43 (58.9) | 28 (38.4) | 2 (2.7) |
| Total (158 pupils) | 79 (50) | 79 (50) | 0 | 134 | 94 (59.5) | 60 (38.0) | 4 (2.5) |
Reach across socioeconomic groups and localities
Table 11 provides the KAT attendance rates categorised by Family Affluence Scale score (low, medium and high). When Family Affluence Scale scores are taken into account, pupils with high scores were more likely to have an adult member of their family present at the family event than pupils who had low/medium scores (56.6% vs. 41.4%). However, there was no such pattern in relation to whether or not pupils themselves attended (59% vs. 60.3%).
| Family Affluence Scale score | Did any of your family go to the KAT event? [n (%)] | Did you go to the KAT event? [n (%)] | |||||
|---|---|---|---|---|---|---|---|
| Yes | No | Not answered | Total family members attending, N | Yes | No | Not answered | |
| Low/medium (58 pupils) | 24 (41.4) | 34 (58.6) | 0 | 43 | 35 (60.3) | 20 (34.5) | 3 (5.2) |
| High (83 pupils) | 47 (56.6) | 36 (43.4) | 0 | 76 | 49 (59) | 33 (39.8) | 1 (1.2) |
| Unknown (17 pupils) | 8 (47.1) | 9 (52.9) | 0 | 15 | 10 (58.8) | 7 (41.2) | 0 (0) |
| Total (158 pupils) | 79 (50) | 79 (50) | 0 | 134 | 94 (59.5) | 60 (38.0) | 4 (2.5) |
Table 12 displays rates of participation in the family event for pupils and parents/carers for each school, and includes the FSM rate for each school. It shows clearly that the school with the highest FSM score (37.3.%) also had the highest proportion of families represented by at least one adult (65.7%). The school with the lowest FSM had the lowest proportion of families represented, and the school with the middle-ranking representation rates also had the middle-ranking FSM score.
| School | School FSM, % | Did any of your family go to the KAT event? [n (%)] | Did you go to the KAT event? [n (%)] | |||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Not answered | Total family members attending, N | Yes | No | Not answered | ||
| 3 (34 pupils) | 37.2 | 22 (65.7) | 12 (34.3) | 0 | 47 | 27 (79.4) | 6 (17.6) | 1 (2.9) |
| 4 (51 pupils) | 2.3 | 23 (45.1) | 28 (54.9) | 0 | 36 | 24 (47.1) | 26 (51.0) | 1 (2.0) |
| 6 (73 pupils) | 27.9 | 34 (46.6) | 39 (53.4) | 0 | 51 | 43 (58.9) | 28 (38.4) | 2 (2.7) |
| Total (158 pupils) | 79 (50) | 79 (50) | 0 | 134 | 94 (59.5) | 60 (38.0) | 4 (2.5) | |
At schools 3 and 4, staff reported that attendance by parents was higher than usual, with one teacher (school 3) ‘shocked’ when he or she saw the queue waiting to get in. At school 6, parental attendance was ‘on a par’ with the turnout for class assemblies. This appeared to be a positive assessment because the Year 5 deputy head said that the school had been making a special effort to get parents involved with their children in events at the school and that attendance at the KAT event had followed the recent trend.
Analysis of the process evaluation data suggested that there were three key reasons why parents/carers attended the family events: to support their children, to support the school and to satisfy children who put pressure on them to go. Also mentioned frequently by parents and children was that parents wanted to see their children’s work; and some had a general rule of always attending school events (school 4, parent 5, 6 and 7; school 6, parent 3). At school 3, the free tea and coffee may also have been influential (Year 4 focus group, Year 6 teacher, school 3).
Children whose parents do not attend the family event
Organising the event for family groups could be difficult for children whose parents do not attend. It was possible to count the number of children who had gone to the family event unaccompanied by members of their family using two questions from the children’s follow-up questionnaire: ‘Did you go to the KAT fun event at your school?’ and ‘Did any of your family go to the KAT fun event at your school?’. Table 13 shows that out of 94 children who said they had attended, 18 (19%) had gone without a member of the family.
| Did you go to the KAT fun event at your school? | Did any of your family go to the KAT fun event at your school? | ||
|---|---|---|---|
| No | Yes | Total | |
| No | 58 | 2 | 60 |
| Yes | 18 | 76 | 94 |
| Not answered | 3 | 1 | 4 |
| Total | 79 | 79 | 158 |
Schools 3 and 6 held their family events immediately following on from the school day, which might have led to more children staying on for the event without an adult. School 4 had started their event later so that children would have returned home after school and come back to school later in the evening. Responses for each school from the 18 unaccompanied children are shown in Table 14.
| Did you go to the KAT fun event at your school? | Did any of your family go to the KAT fun event at your school? | |||
|---|---|---|---|---|
| No | Total | |||
| School 3 | School 4 | School 6 | ||
| Yes | 5 (18%) | 4 (17%) | 9 (21%) | 18 (19%) |
| Total children attending | 27 | 24 | 43 | 94 |
Although proportions of unaccompanied children are slightly higher in the schools which ran the events straight after the school day, there is not much difference between the three schools. It should also be noted that children may have attended the events without having completed questionnaires, and so total rates of attendance by unaccompanied children could be higher or lower than described above.
Programme theory
Although this study is not designed to estimate the effect of KAT, it provides an opportunity to assess whether or not KAT has the potential to encourage more communication among family members – which is thought to be a precursor of the eventual intended reduction in alcohol misuse. Participants in the study’s process evaluation were, therefore, asked about the specific effects of classwork and the family event on communication about alcohol.
Classwork
In each school, both parents and children reported that children told their parents about what they were doing in class. Topics included the kinds of work they were doing (posters, etc.); the physical effects of alcohol; dangers of alcohol; safe drinking; parental alcohol use; the nature of the KAT project; reasons why people drink; and units of alcohol. There were a few reports that children had not talked about it (focus-group participants A and C, school 4; parent 5, school 4; parent 1, school 6) and two children withheld information so that their parents would have a surprise at the family event (focus-group participant school 3, parent 6, school 6).
Homework
The KAT programme manual encourages teachers to ensure that there are opportunities for pupils to take some of the classroom work home to finish, ‘to generate interest amongst family members’. No homework was set in school 6, but at school 4 and school 3 two teachers set homework with the specific aim of stimulating conversation between parents and children (second Year 6 teacher, school 4; Year 6 teacher, school 3). In both schools, there were more reports that parents helped with homework than not. Topics covered included support groups (parent 1, school 4), physical harm (parent 2 Year 4, school 3) and consequences of misuse (parent 3, school 4). This teacher thought that girls were more willing than boys to take work home and talk to their parents.
Family event
Parents at school 4 and school 3 enjoyed talking to other parents at the events (parent 5 and parent 7, school 4; parent 1, school 3). Most parents maintained that they were ’quite open’ about alcohol, that they talked about it at home anyway, and that attending the family event had not made any difference to that. However, some went on to say things which suggested that there had actually been at least small changes: one said that their child would ’chip in’ more when alcohol was discussed (parent 1, school 4); another parent had been shocked at some of the information and had become more aware of the implications of her own drinking behaviour (parent 7, school 4). Parent 4 (school 4) seemed to reflect that the KAT project as a whole had led to more conversation, and parent 5 (school 4) said that while there possibly had been more conversation after the family event, this was just repeating what had been said at home before.
A significant number of children at each school said that they had discussed alcohol with their families after the event, though it was not clear (except for boy D, Year 6, school 3) whether or not families had discussed it more than usual. At all schools, some parents and children had told other members of their family and friends about the KAT activities and what they had learnt. Teachers at all of the intervention schools said that KAT provided an opening for discussions, or more serious discussions, about alcohol, and drew on evidence of children having conversations not only with their parents but also with friends, classmates, siblings and other relatives, and suggested that during the project, other children became informed and informative participants in a wide-ranging dialogue about alcohol.
Trial recruitment and retention
One of the study objectives was to assess trial recruitment and retention rates (to help determine if an effectiveness trial would be feasible) and key design parameters. This section describes numbers of schools, children and parents recruited and retained in the research trial (i.e. those individuals who provided questionnaire data), and the issues arising during recruitment and data collection processes. The latter are dealt with here because in an exploratory context they constitute findings about the feasibility of conducting the evaluation rather than a simple account of methods.
Schools
All 39 eligible schools were contacted by letter, and invited to participate in the study, and telephone calls were made to all schools until sufficient schools were recruited. Meetings were held with nine schools which expressed an interest in the study. One head teacher was willing for the school to participate but only if it was not in the intervention group because there was no capacity within the school timetable to deliver KAT. The school was not, therefore, eligible to participate in the trial. However, they offered to assist with the piloting of the study questionnaires. The other eight schools with whom the principal investigator had meetings all went on to participate in the trial (a participation rate of 20.5%). Of the 31 eligible schools which did not participate at this point, 19 did not respond to letters or telephone calls, six indicated to the research team that they were not interested, four were too busy and two schools declined because they were already delivering projects similar to KAT.
Table 15 shows the number of pupils and percentages entitled to FSM in each of the recruited schools, alongside the average, median and range for all 39 eligible schools. It can be seen that the FSM rates in the recruited schools ranged from 1% to 37.2%. Six schools were above the county median, and three below.
| Schools | Pupils, n | FSM entitlement, % |
|---|---|---|
| KAT intervention schools | ||
| 3 | 188 | 37.2 |
| 4 | 264 | 2.3 |
| 6 | 312 | 27.9 |
| 8 (withdrew) | 384 | 21.6 |
| A (withdrew) | 205 | 1 |
| KAT control schools | ||
| 1 | 483 | 11.4 |
| 2 | 69 | 31.9 |
| 5 | 196 | 23.5 |
| 7 | 188 | 25.5 |
| All eligible schools (N = 39) | ||
| Average | 283 | 21.8 |
| Median | 211 | 18.4 |
| Range | 69–653 | 1–48.3 |
Figure 5 summarises the recruitment process. One intervention school (school A) withdrew from the study before baseline data collection. The school’s main reason for withdrawing from the study was parents’ concern about the research topic, and appeared to be linked to the fact that, due to an administrative error, main information letters and reminder letters were switched in order. However, given the fact that the reminder letter explained how parents could access the original letter if for some reason they had not received a copy (and a link to the information online was also provided), there may also have been other reasons. We were not able to obtain more detailed information from the school, though we requested this on several occasions.
FIGURE 5.
Recruitment of schools. White, recruitment activities; pale green, intervention group; dark green, control group.
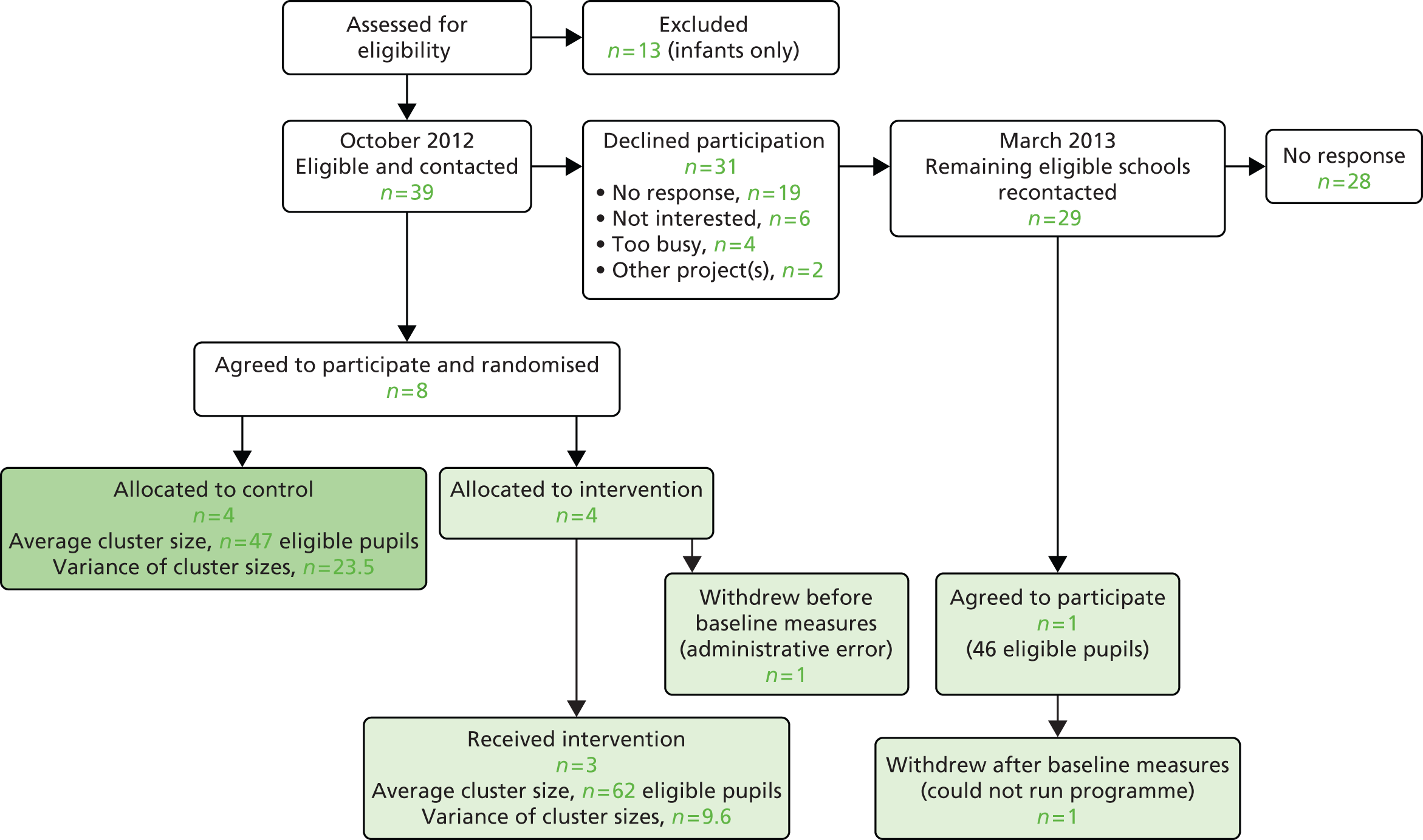
Following the withdrawal of this school, we wrote again in March 2012 to all eligible schools which were not already participating in the trial (n = 29) inviting them again to participate in the trial as an intervention school, but indicating that to take part they would need to be able to deliver the programme in the summer term of 2012. One school responded to this letter and agreed to participate in the trial. This school withdrew from the trial after baseline data collection had taken place, and shortly after programme delivery had commenced. Although the required timing and workload associated with the programme had been clearly explained to the school before they agreed to participate (see Appendix 9), their main reason for withdrawing from the study concerned these issues, and was mostly related to programme implementation and the need for multiple members of the study and programme support team to contact the school. However, it would appear that other issues, including one of the teacher’s concerns about the appropriateness of KAT for Muslim families, also played a part.
In total, therefore, we recruited nine schools from the 39 eligible (participation rate of 23.5%). We retained all four control group schools for the life of the trial, and three of the intervention schools, with two withdrawing as described above.
Pupils
Determining research trial participation rates
We originally aimed to recruit 50% of eligible children into the research trial order to achieve the sample size target (though this was based on using ‘opt-in’ parental consent for children’s participation, whereas we eventually used ‘opt-out’ parental consent). Table 16 shows the proportion of eligible pupils (at baseline) who provided questionnaire data. At baseline, this was 74% (intervention group) and 81% (control group). At follow-up, these figures were 68% and 74% respectively.
| Time point | Intervention | Control | |||||
|---|---|---|---|---|---|---|---|
| n | % eligible, four schools | % eligible, three schools | % present | n | % eligible, four schools | % present | |
| Baseline | 172 | 74 | N/A | 78 | 152 | 81 | 88 |
| Follow-up | 158 | 68 | 85 | 92 | 138 | 74 | 77 |
Table 16 also shows response rates using two other denominators. First, the proportion of children present in class on the day when questionnaires were completed, which in every case was higher than the proportion of eligible children (which included those absent from school). Second, for the intervention group schools, we provide the response rate at follow-up based only on the three schools which were still in the study (we could not collect any follow-up data in the school which withdrew). Using this calculation, the proportion of children eligible at baseline who went on to complete follow-up questionnaires was 85% (compared with 68% when the school which withdrew is included in this figure).
All eight schools at which data collections were conducted were asked to confirm numbers of pupils on the registers of classes involved, in order to ensure that participant information sheets were distributed to all parents/carers and pupils, and to allow preparation of sufficient copies of the questionnaire. We also asked schools for information on numbers of parental refusals (to ensure that no data were collected from the relevant pupils), and pupils present on the day we visited. Some of the information supplied by the schools appeared to be inaccurate; for example, the number of questionnaires completed was greater than the number of pupils that schools said were on the register. Where discrepancies were identified, we contacted schools to check the information.
Figure 6 displays the participation rates in the intervention and control groups, and reasons for non-completion of questionnaires. Absence from school or the classroom were the most likely reasons for non-completion, and rates of parental refusal for participation were very low. In one intervention school, a large number of children came from families who did not speak English as a first language, and were from Muslim families. When we visited the school to collect baseline data, some of the children were unsure whether or not their parents were happy for them to take part (though their parents had not contacted the school to refuse permission). To make absolutely sure that we did not collect any data from pupils whose parents were not happy for them to participate, we advised 15 children at this school not to complete a questionnaire. There were no other possible/definite parental refusals in the intervention schools, and only two in the control group schools, indicating that the vast majority of parents were happy for their child(ren) to participate in the trial and intervention.
FIGURE 6.
Kids, Adults Together participation rates: percentage of children eligible at baseline who completed questionnaires. a, All of these pupils were from one school where many pupils and their families did not speak English as a first language, and many came from Muslim homes. When we spoke to the children at the baseline visit, some were uncertain whether or not their parents would be happy for them to take part, and so we advised that these children should not complete questionnaires; b, uncertainty over the exact number. Reproduced with permission from Segrott et al. 1
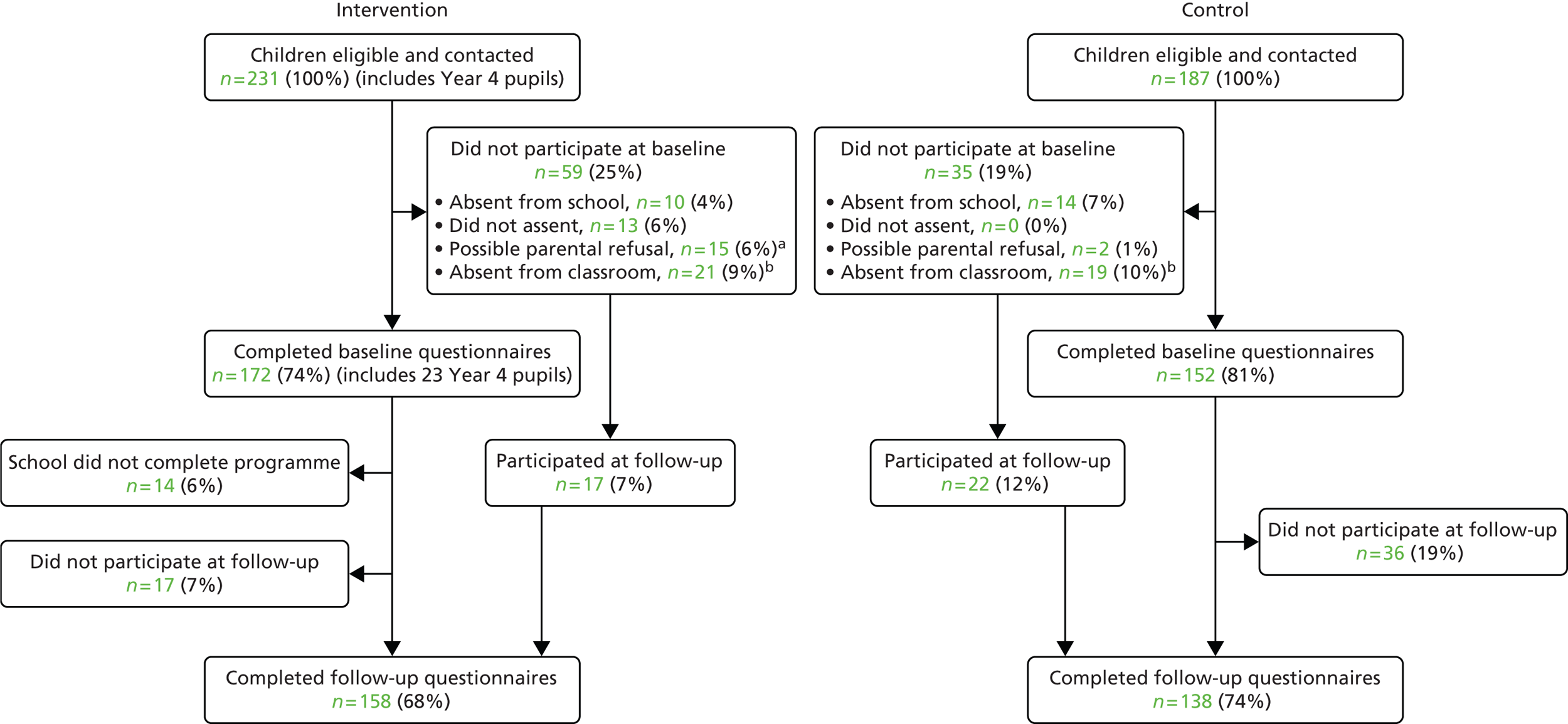
The pupils shown in as ‘Absent from classroom’ are those we cannot reasonably account for. This is the difference between the total number reportedly on the register, and the sum of those who completed questionnaires; absentees from school; and those who did not assent or whose parents withheld consent. In the intervention group, this number was 21 pupils (from 231 who were eligible), while in the control group 19 pupils (from 187 eligible) fell into this category. Figure 7 shows questionnaire completion rates as a percentage of those present in school on the day of data collection. Participation rates for the intervention group were 78% (baseline) and 92% (follow-up). For the control group, the figures were 88% and 77% respectively. The intervention school which withdrew after baseline (school 8) included a large number of pupils from ethnic minority groups, many belonging to Muslim families, and recent immigrants who did not speak or understand English very well. Letters and information sheets for parents and children were translated but because of the late recruitment of the school and the short time remaining for programme delivery, we did not adapt the information-giving process as completely as we would have liked, and school staff were unable to accept our proposals for providing extra information and explanations for participants. Consequently, when we spoke to the children at the data collection visit, we said that those who were at all uncertain about their parents’ wishes should not take part, although their parents had not actually contacted the school to refuse consent. This partly accounts for the lower numbers participating in this school and the impact on the overall recruitment rate.
FIGURE 7.
Kids, Adults Together participation rates: percentage of children present at baseline and follow-up who completed questionnaires. a, All of these pupils were from one school where many pupils and their families did not speak English as a first language, and many came from Muslim homes. When we spoke to the children at the baseline visit, some were uncertain whether or not their parents would be happy for them to take part, and so we advised that these children should not complete questionnaires; b, uncertainty over the exact number.

Figure 7 shows that 21 pupils in the intervention group are recorded as ‘Absent from classroom’ at baseline. If all of these had provided data on return visits, the percentage of those present who completed questionnaires at baseline would have been a little higher than the response rate of 92% at follow-up. In the control group, returning to recruit the 19 (baseline) and 25 (follow-up) pupils recorded as possibly absent from the classroom could also have increased response rates.
Figure 8 gives details of participation for only the three intervention schools which completed the programme, showing that 85% (baseline) and 85% (follow-up) completed questionnaires. In an effectiveness trial using an ITT analysis, the participants in school 8 would have been followed up.
FIGURE 8.
Kids, Adults Together participation rates: percentage of children eligible at baseline in intervention schools who completed questionnaires, excluding the school which withdrew after baseline. a, Uncertainty over the exact number.
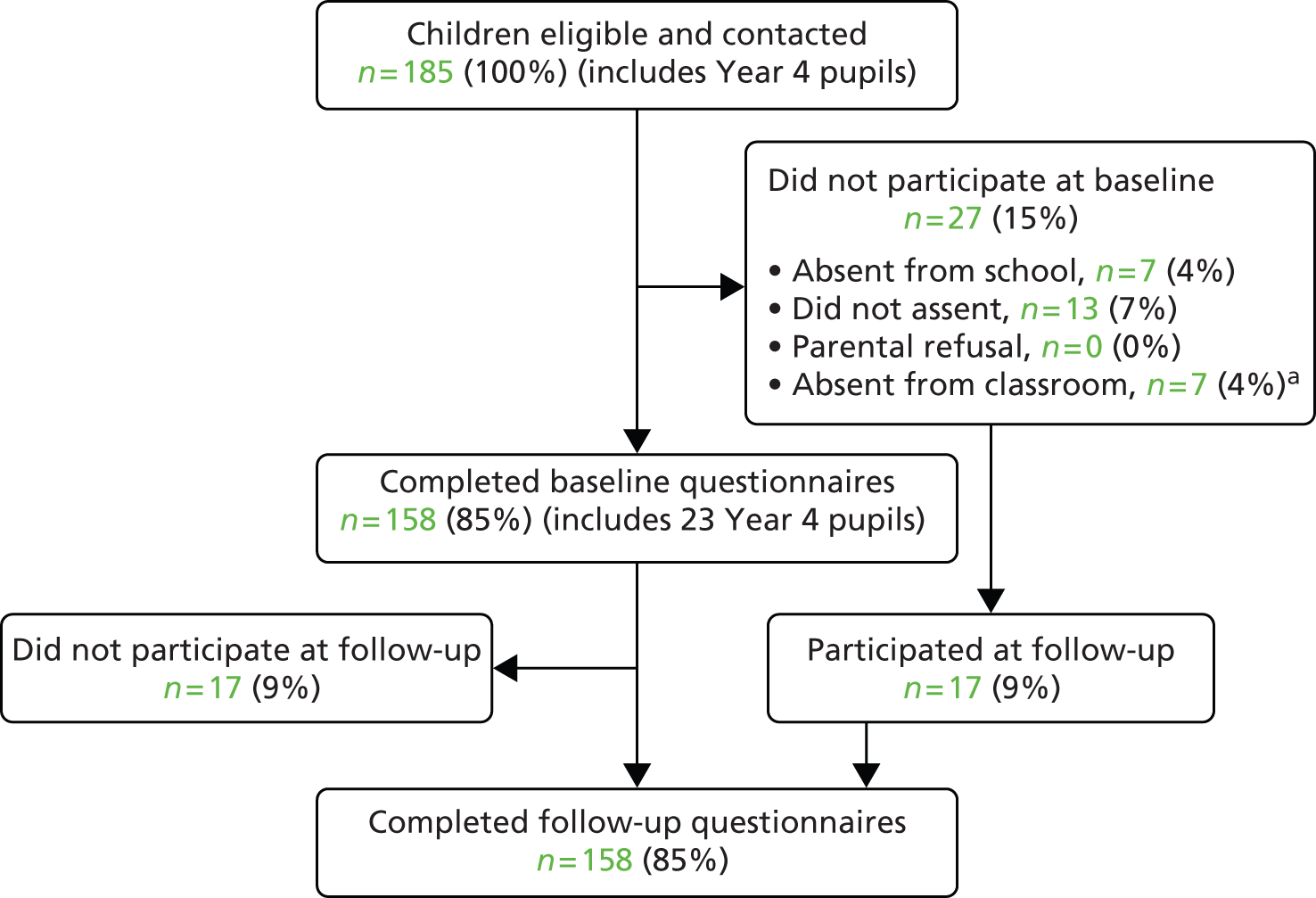
Table 17 shows the proportion of pupil participants with low, medium and high Family Affluence Scale scores in each school, and also shows each school’s FSM rate. Participants with high Family Affluence Scale scores formed the majority of participants in each school. It is not possible to determine to what extent the distribution of Family Affluence Scale scores among the recruited sample reflects the total eligible population of classes.
| School | Family Affluence Scale | Total | |||
|---|---|---|---|---|---|
| Low | Medium | High | Missing | ||
| 3 (FSM = 37.2%), n (%) | 8 (18.6) | 9 (20.9) | 16 (37.2) | 10 (23.3) | 43 (100) |
| 4 (FSM = 2.3%), n (%) | 0 (0) | 12 (21.1) | 43 (75.4) | 2 (3.5) | 57 (100) |
| 6 (FSM = 27.9%), n (%) | 5 (6.3) | 31 (38.8) | 38 (47.5) | 6 (7.5) | 80 (100) |
| 8 (FSM = 21.6%), n (%) | 0 (0) | 6 (42.9) | 7 (50.0) | 1 (7.1) | 14 (100) |
| Total, N (%) | 13 (6.7) | 58 (29.9) | 104 (53.6) | 19 (9.8) | 194 (100) |
Retention of children
Three hundred and twenty-four pupils completed the baseline questionnaire (152 control and 172 intervention), while 296 pupils completed the follow-up questionnaire (138 control and 158 intervention). An additional 39 pupils (22 control and 17 intervention) who did not complete baseline questionnaires completed follow-up questionnaires. The study retention rate in the control arm is, therefore, (138 – 22)/152 or 76.3% and that in the intervention arm is (158 – 17)/172 or 82.0%, an overall retention rate of 79.9%. Figure 9 displays these figures in the form of a flow chart.
FIGURE 9.
Pupil flow chart.
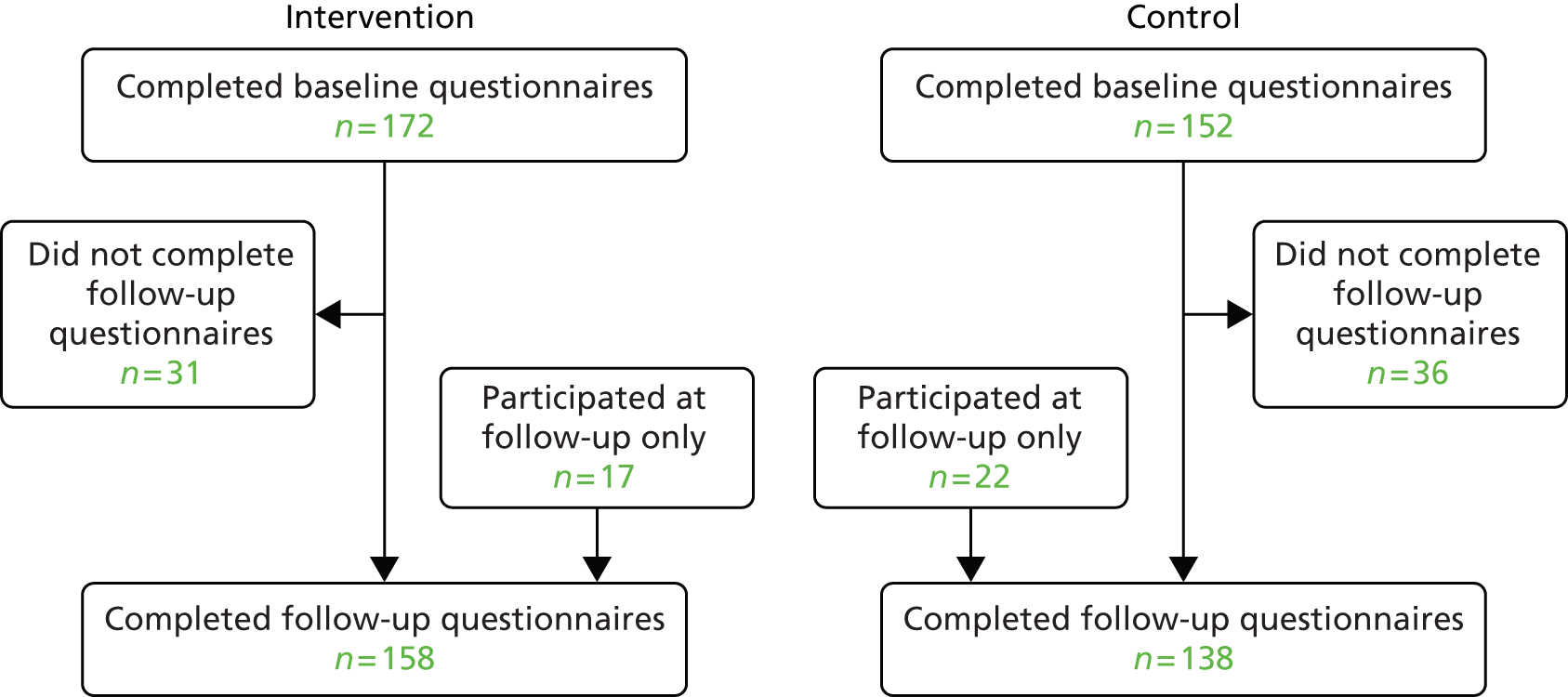
Demographic characteristics of children allocated to intervention and control groups
Of the 363 pupils (324 participating from baseline, 39 at follow-up only), 358 provided their demographic information. These figures were 169 in the control arm and 189 in the intervention arm.
The balance of the trial arms with regard to the demographic variables collected is given in Table 18. Sex, year of birth, nationality and family affluence were well balanced. However, there were more Year 5 pupils in the control group than in the intervention group, and slightly more Caucasian pupils in the intervention group. Pupils in the intervention group were generally older, with almost twice as many in Year 6 (10–11 years) than in the control group. Older children might be more competent to understand and complete questionnaires, and so this was examined in the analysis.
| Characteristics | Pupils (N = 358) | ||
|---|---|---|---|
| Control, n (%) | Intervention, n (%) | Overall, n (%) | |
| Sex | |||
| Boy | 81 (47.9) | 90 (47.6) | 171 (47.8) |
| Girl | 87 (51.5) | 99 (52.4) | 186 (51.9) |
| Missing | 1 (0.6) | 0 (0.0) | 1 (0.3) |
| Year of birth | |||
| 2000 | 17 (10.1) | 34 (18.0) | 51 (14.2) |
| 2001 | 76 (45.0) | 87 (46.0) | 163 (45.5) |
| 2002 | 76 (45.0) | 55 (29.1) | 131 (36.6) |
| 2003 | 0 (0.0) | 10 (5.3) | 10 (2.8) |
| Missing | 0 (0.0) | 3 (1.6) | 3 (0.8) |
| Year group | |||
| Year 4 | 1 (0.6) | 27 (14.3) | 28 (7.8) |
| Year 5 | 119 (70.4) | 60 (31.7) | 179 (50.0) |
| Year 6 | 48 (28.4) | 100 (52.9) | 148 (41.3) |
| Missing | 1 (0.6) | 2 (1.1) | 3 (0.8) |
| UK-born | |||
| Yes | 158 (93.5) | 176 (93.1) | 334 (93.3) |
| No | 10 (5.9) | 12 (6.3) | 22 (6.1) |
| Missing | 1 (0.6) | 1 (0.6) | 2 (0.6) |
| Ethnicity | |||
| White | 129 (76.3) | 162 (85.7) | 291 (81.3) |
| Black or black British | 5 (3.0) | 3 (1.6) | 8 (2.2) |
| Mixed race | 9 (5.3) | 6 (3.2) | 15 (4.2) |
| Chinese | 0 (0.0) | 1 (0.5) | 1 (0.3) |
| Asian or Asian British | 15 (8.9) | 11 (5.8) | 26 (7.3) |
| Other | 5 (3.0) | 4 (2.1) | 9 (2.5) |
| Missing | 6 (3.6) | 2 (1.1) | 8 (2.2) |
| Family Affluence Scale score | |||
| Low | 11 (6.5) | 12 (6.3) | 23 (6.4) |
| Medium | 59 (34.9) | 59 (31.2) | 118 (33.0) |
| High | 85 (50.3) | 104 (55.0) | 189 (52.8) |
| Missing | 14 (8.3) | 14 (7.4) | 28 (7.8) |
| Language | |||
| English | 152 (89.9) | 173 (91.5) | 325 (90.8) |
| Not English | 15 (8.9) | 16 (8.5) | 31 (8.7) |
| Missing | 2 (1.2) | 0 (0.0) | 2 (0.6) |
It can be seen from Table 19 that more boys than girls had missing follow-up data (58.2% and 40.3%, respectively). Year 5 pupils, and those born in 2001, were also more likely to have missing follow-up data. There appeared to be little variation in rates of missing data at follow-up by country of birth or Family Affluence Scale.
| Characteristics | Pupils (N = 324) | |
|---|---|---|
| Baseline and follow-up (n = 257) | Baseline only (n = 67) | |
| n (%) | n (%) | |
| Sex | ||
| Boy | 117 (45.5) | 37 (58.2) |
| Girl | 140 (54.5) | 29 (40.3) |
| Missing | 0 (0.0) | 1 (1.5) |
| Year of birth | ||
| 2000 | 40 (15.6) | 7 (10.4) |
| 2001 | 112 (43.6) | 34 (50.7) |
| 2002 | 96 (37.4) | 24 (35.8) |
| 2003 | 7 (2.7) | 2 (3.0) |
| Missing | 2 (0.8) | 0 (0.0) |
| Year group | ||
| Year 4 | 21 (8.2) | 5 (7.5) |
| Year 5 | 123 (47.9) | 40 (59.7) |
| Year 6 | 110 (42.8) | 22 (32.8) |
| Missing | 3 (1.2) | 0 (0.0) |
| UK-born | ||
| Yes | 241 (93.8) | 63 (94.0) |
| No | 14 (5.4) | 4 (6.0) |
| Missing | 2 (0.8) | 0 (0.0) |
| Ethnicity | ||
| White | 211 (82.1) | 50 (74.6) |
| Black or black British | 5 (1.9) | 2 (3.0) |
| Mixed race | 11 (4.3) | 3 (4.5) |
| Chinese | 1 (0.4) | 0 (0.0) |
| Asian or Asian British | 15 (5.8) | 10 (14.9) |
| Other | 7 (2.7) | 2 (3.0) |
| Missing | 7 (2.7) | 0 (0.0) |
| Family Affluence Scale score | ||
| Low | 17 (6.6) | 5 (7.5) |
| Medium | 86 (33.5) | 23 (34.3) |
| High | 134 (52.1) | 33 (49.3) |
| Missing | 20 (7.8) | 6 (9.0) |
Parents/carers
When schools were recruited (October 2011 to February 2012 and April 2012), we invited all parents/carers of children in participating classes to take part in telephone interviews (to collect outcome measure data at 6-month follow-up), and 52 volunteered. Interviews commenced in July 2012, and in an attempt to increase the number of participants, each participant was asked at the end of the interview if any other adult in the household would like to take part. One additional participant was recruited using this method. All interviews were completed by the end of September 2012 but interviewers continued their attempts to contact the remaining volunteers until the end of November 2012. Using an estimate that each eligible pupil would have only one parent/caregiver, the number of eligible parents was 418, of whom 12% volunteered to take part.
Figure 10 shows that numbers of parents from intervention schools who expressed interest in the research were much larger than in control schools. However, the larger drop-out rate from the intervention arm meant that approximately equal proportions of parents from each group provided data. Demographic data supplied by the 41 respondents were examined in case they were all alike in one or more respects but this was not the case (see Appendix 10). As the data set was so small, no further analyses were conducted.
FIGURE 10.
Parent recruitment for telephone interviews.

Numbers analysed (pupil data)
All analyses are ITT in the groups to which they were randomised using complete data for baseline and follow-up. In intervention schools, all trial participants’ data were included in the analyses, regardless of the extent of their engagement with the KAT programme. Numbers for each analysis are given in all results tables. p-values in the tables are indicative only and should not be interpreted as a definitive result. Confidence intervals are more useful to interpret the data at this stage.
Feasibility of primary outcome measures
Summary data for the alcohol questions in the baseline and follow-up questionnaires are given in Table 20. Data are given for all 324 pupils at baseline, irrespective of whether or not they were followed up, as well as data for all pupils at follow-up irrespective of baseline assessment.
| Question | Response, n (%) |
|---|---|
| Baseline (324 pupils) | |
| Ever had an alcoholic drink? | |
| Yes | 45 (13.9) |
| No | 268 (82.7) |
| Missing | 11 (3.4) |
| Ever been drunk? | |
| Yes | 9 (2.8) |
| No | 308 (95.1) |
| Missing | 7 (2.2) |
| Drinking frequency in the last 30 days | |
| Never | 252 (77.8) |
| 1–2 times | 46 (14.2) |
| 3–5 times | 13 (4.0) |
| 6–9 times | 2 (0.6) |
| Missing | 11 (3.4) |
| Drunk frequency in the last 30 days | |
| Never | 304 (93.8) |
| 1–2 times | 8 (2.5) |
| 3–5 times | 1 (0.3) |
| Missing | 11 (3.4) |
| Smoking frequency in the last 30 days | |
| Never | 312 (96.3) |
| 3–5 times | 3 (0.9) |
| 6–9 times | 1 (0.3) |
| Missing | 8 (2.6) |
| Follow-up (296 pupils) | |
| Ever had an alcoholic drink? | |
| Yes | 48 (16.2) |
| No | 246 (83.1) |
| Missing | 2 (0.7) |
| Ever been drunk? | |
| Yes | 10 (3.4) |
| No | 279 (94.3) |
| Missing | 7 (2.4) |
| Drinking frequency in the last 30 days | |
| Never | 255 (86.1) |
| 1–2 days | 27 (9.1) |
| 3–5 days | 6 (2.0) |
| 6–9 days | 2 (0.7) |
| 20–29 days | 2 (0.7) |
| Missing | 4 (1.4) |
| Drunk frequency in the last 30 days | |
| Never | 289 (97.6) |
| 1–2 days | 3 (1.0) |
| 10–12 days | 1 (0.3) |
| Missing | 3 (1.0) |
| Smoking frequency in the last 30 days | |
| Never | 292 (98.6) |
| 1–2 days | 1 (0.3) |
| Missing | 3 (1.0) |
Table 20 shows that rates of missing data for all of the questions were low, ranging from 0.7% to 3.4%. Reported rates of ever having consumed alcohol were 13.9% at baseline and 16.2% at follow-up. Rates of ever-drunkenness were 2.8% and 3.4%. It can be seen that at both baseline and follow-up there are some inconsistencies in the data. For example, at baseline 45 participants said that they had had a drink at some point in their lives, but 61 indicated that they had consumed alcohol at some point during the last month. The question about smoking was included to assess its feasibility in case an effectiveness trial should examine the effect of KAT on multiple risk behaviours, but responses were not analysed. The findings reported below focus on the alcohol-related questions.
The categories used for drinking frequency were changed between baseline and follow-up. For this reason, as well as the sparse data in the drinking categories, the data were recoded into binary responses of never/once or more, for further analysis, and this is shown in Table 21. The majority of pupils reported not having either consumed alcohol or been drunk in the last 30 days at both data collection points (e.g. 77.8% and 93.8% at baseline).
| Question | Baseline (324 pupils), n (%) | Follow-up (296 pupils), n (%) |
|---|---|---|
| Drinking frequency in the last 30 days | ||
| Never | 252 (77.8) | 255 (86.1) |
| Once or more | 61 (18.8) | 37 (12.5) |
| Missing | 11 (3.4) | 4 (1.4) |
| Drunk frequency in the last 30 days | ||
| Never | 304 (93.8) | 289 (97.6) |
| Once or more | 9 (2.8) | 4 (1.4) |
| Missing | 11 (3.4) | 3 (1.0) |
| Smoking frequency in the last 30 days | ||
| Never | 312 (96.3) | 292 (98.6) |
| Once or more | 4 (1.2) | 1 (0.3) |
| Missing | 8 (2.5) | 3 (1.0) |
Prevalence and odds ratios in the following tables are given for only those pupils who provided both baseline and follow-up outcomes as baseline drinking was used as a covariate. Table 22 gives the proportion of pupil responses for each of the drinking variables alongside the intervention effects. School size and FSM entitlement have been included as school-level covariates in the model as they were used to balance the randomisation, but were not statistically significant. The ICC values for each outcome demonstrate that up to 11% of the variation in outcomes is due to clustering by school and that the majority of the variation is at the pupil level. Baseline levels of alcohol consumption were also included in each model as pupil-level covariates to provide baseline adjusted odds ratios for the intervention effects. The zero ICC value (drunk, last 30 days) may be due to sparse data leading to an inability to estimate ICCs for these outcomes, rather than an indication of no school-level variation.
| Question | Control | Intervention | Intervention effect adjusted for baseline consumption level, FSM and school size | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Baseline, n (%) | Follow-up, n (%) | N | Baseline, n (%) | Follow-up, n (%) | ICC | Odds ratio and 95% CI | p-value | |
| Ever had an alcoholic drink? | 117 | 14 (12.0) | 9 (7.7) | 130 | 24 (18.5) | 31 (23.8) | 0.112 | 5.3 (1.2 to 23.9) | 0.030 |
| Ever been drunk? | 114 | 1 (0.9) | 0 (0.0) | 131 | 7 (5.3) | 8 (6.1) | 0.000 | 1.7 (0.5 to 6.8) | 0.423 |
| Had drink in the last 30 days? | 115 | 15 (13.0) | 14 (12.2) | 131 | 34 (26.0) | 19 (14.5) | 0.077 | 0.7 (0.2 to 2.5) | 0.558 |
| Been drunk in the last 30 days? | 117 | 3 (2.6) | 0 (0.0) | 129 | 6 (4.7) | 4 (3.1) | 0.000 | 1.5 (0.4 to 5.8) | 0.564 |
Overall, the levels of alcohol consumption at baseline in both groups are low, especially for those reporting drinking enough alcohol to be drunk. For the ‘ever had an alcoholic drink’ question, in the control group at baseline 14 of the 117 (12%) pupils said yes, which reduces to 9 out of 117 (7.7%) at follow-up. In the intervention group, the proportion reporting ‘ever had a drink’ was higher than in the control group at baseline (18%) and increased to 23.8% at follow-up. The intervention effects are given as odds ratios corrected for baseline drinking, FSM and school size. They can be interpreted as intervention group pupils being 5.3 times more likely to have ever had a drink at follow-up and 1.7 times more likely to have ever been drunk than those in the control group. Baseline rates of past-month drinking were higher in the intervention group [34 (26%)] than in the control group [15 (13%)]. At follow-up, the rates were 19 (14.5%) for the intervention group, and 14 (12.2%) for the control group.
Again, it can be seen that there are inconsistencies in pupils’ responses. For instance, at follow-up more children in the control group said that they had consumed alcohol in the last 30 days than reported ever having consumed alcohol. Another example is that the same type of discrepancy was also present for the intervention group at baseline.
To investigate the issue of changing responses, a cross-tabulation of baseline versus follow-up response was performed. Table 23 shows that for ‘ever had a drink’, eight pupils in the control group gave their answer as ‘yes’ at baseline and ‘no’ at follow-up. This also occurred in the intervention group, where six pupils answered ‘yes’ at baseline and ‘no’ at follow-up. For the question ‘have you ever been drunk?’ the data are extremely sparse, with only one pupil in the control group reporting that they had been drunk; moreover, this pupil answered ‘no’ at follow-up. There were seven pupils in the intervention group who answered ‘yes’ at baseline, two of whom answered ‘no’ at follow-up.
| Response | Question | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | Ever had an alcoholic drink?, n | Ever been drunk?, n | Frequency of drinking in last month/last 30 days?, n | Frequency of drunkenness in last month/last 30 days?, n | ||||
| C | I | C | I | C | I | C | I | ||
| Never | Never | 100 | 93 | 113 | 121 | 94 | 93 | 114 | 122 |
| Never | Yes | 3 | 13 | 1 | 3 | 6 | 4 | 0 | 1 |
| Yes | Yes | 6 | 18 | 0 | 5 | 8 | 15 | 0 | 3 |
| Yes | Never | 8 | 6 | 1 | 2 | 7 | 19 | 3 | 3 |
Because there was a small imbalance in age between the trial arms, the influence of the difference in age between the trial arms on the main outcomes was examined. Of the 358 pupils who provided their demographic variables, three failed to give their year group. Among the other 355 pupils, 28 were in Year 4, 179 in Year 5 and 148 in Year 6. Table 24 gives the data for year group and alcohol consumption. It can be seen that it is difficult to discern a clear pattern in the data.
| Question | Year 4 | Year 5 | Year 6 | |||
|---|---|---|---|---|---|---|
| Baseline, n (%) | Follow-up, n (%) | Baseline, n (%) | Follow-up, n (%) | Baseline, n (%) | Follow-up, n (%) | |
| Ever had an alcoholic drink? | ||||||
| Yes | 3 (10.7) | 5 (17.9) | 23 (12.8) | 19 (10.6) | 17 (11.5) | 23 (15.5) |
| No | 19 (67.9) | 18 (64.3) | 136 (76.0) | 117 (65.4) | 112 (75.7) | 104 (70.3) |
| Missing | 6 (23.4) | 5 (17.9) | 20 (11.2) | 43 (24.0) | 19 (12.8) | 21 (14.2) |
| Ever been drunk? | ||||||
| Yes | 1 (3.6) | 2 (7.1) | 3 (1.7) | 3 (1.7) | 5 (3.4) | 5 (3.4) |
| No | 23 (82.1) | 20 (71.4) | 156 (87.2) | 131 (73.2) | 126 (85.1) | 121 (81.8) |
| Missing | 4 (14.3) | 6 (21.4) | 20 (11.2) | 45 (25.1) | 17 (11.5) | 22 (14.9) |
| Drink frequency in last 30 days | ||||||
| Ever | 8 (28.6) | 5 (17.9) | 26 (14.5) | 18 (10.1) | 25 (16.9) | 14 (9.5) |
| Never | 16 (57.1) | 17 (60.7) | 131 (73.2) | 120 (67.0) | 104 (70.3) | 111 (75.0) |
| Missing | 4 (14.3) | 6 (21.4) | 22 (12.3) | 41 (22.9) | 19 (12.8) | 23 (15.5) |
| Drunk frequency in last 30 days | ||||||
| Ever | 1 (3.6) | 0 (0.0) | 4 (2.2) | 1 (0.6) | 4 (2.7) | 3 (2.0) |
| Never | 23 (82.1) | 22 (78.6) | 153 (85.5) | 136 (76.0) | 125 (84.5) | 123 (83.1) |
| Missing | 4 (14.3) | 6 (21.4) | 22 (12.3) | 42 (23.5) | 19 (12.8) | 22 (14.9) |
To investigate any effect of school year group on the results shown in Table 22, school year group was included as a covariate in the model. Results are shown in Table 25.
| Question | Control | Intervention | Intervention effect | Year 4 and 5 effect | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Baseline, n (%) | Follow-up, n (%) | N | Baseline, n (%) | n (%) | ICC | Effect and 95% CI | p-value | Effect and 95% CI | p-value | |
| Ever had an alcoholic drink? | 117 | 14 (12.0) | 9 (7.7) | 130 | 24 (18.5) | 31 (23.8) | 0.122 | 3.3 (0.9 to 25.0) | 0.067 | 2.0 (0.6 to 5.0) | 0.264 |
| Ever been drunk? | 114 | 1 (0.9) | 0 (0.0) | 131 | 7 (5.3) | 8 (6.1) | 0.000 | 1.7 (0.4 to 10.0) | 0.436 | 0.9 (0.2 to 5.0) | 0.915 |
| Drink frequency in last 30 days | 115 | 15 (13.0) | 14 (12.2) | 131 | 34 (26.0) | 19 (14.5) | 0.077 | 0.9 (0.4 to 2.5) | 0.802 | 0.7 (0.2 to 2.0) | 0.440 |
| Drunk frequency in last 30 days | 117 | 14 (12.0) | 9 (7.7) | 130 | 24 (18.5) | 31 (23.8) | 0.122 | 3.3 (0.9 to 25.0) | 0.067 | 2.0 (0.6 to 5.0) | 0.264 |
Table 25 shows that adding the year group to the models for drinking outcomes does not have a statistically significant impact. However, the significant difference in ‘ever had an alcoholic drink’ between the trial arms in Table 22 is no longer significant, indicating that some of the difference observed between the trial arms has been explained by a difference in ages between the intervention and control groups. Tables 22 and 25 also indicate that the intervention group participants are less likely than those in the control group to report drinking alcohol in the last 30 days. Again, this highlights the mixed, and sometimes contradictory, patterns in the data.
Of the 358 pupils who provided their demographic variables, eight failed to provide information on their ethnic group. Among the 350 pupils who did, 291 were white and 59 were from another ethnic group.
Table 26 shows the responses and missing data rates for the alcohol-related questions for those participants who described themselves as white, compared with all other participants. We used this classification mainly because the numbers for individual ethnic groups were very small. There does not appear to be a clear difference between these two groups at baseline in terms of rates of missing data. At follow-up, the rates of missing data appear to be higher among non-white participants.
| Question | White | Others | ||
|---|---|---|---|---|
| Baseline, n (%) | Follow-up, n (%) | Baseline, n (%) | Follow-up, n (%) | |
| Ever had an alcoholic drink? | ||||
| Yes | 42 (14.4) | 43 (14.8) | 3 (5.1) | 3 (5.1) |
| No | 210 (72.2) | 195 (67.0) | 52 (88.1) | 40 (67.8) |
| Missing | 39 (13.4) | 53 (18.2) | 4 (6.8) | 16 (27.1) |
| Ever been drunk? | ||||
| Yes | 8 (2.7) | 8 (2.7) | 1 (1.7) | 1 (1.7) |
| No | 247 (84.9) | 228 (78.4) | 55 (93.2) | 40 (67.8) |
| Missing | 36 (12.4) | 55 (18.9) | 3 (5.1) | 18 (30.5) |
| Drink frequency (past month) | ||||
| Ever | 53 (18.2) | 31 (10.7) | 8 (13.6) | 6 (10.2) |
| Never | 202 (69.4) | 207 (71.1) | 45 (76.3) | 37 (62.7) |
| Missing | 36 (12.4) | 53 (18.2) | 6 (10.2) | 16 (27.1) |
| Drunk frequency (past month) | ||||
| Ever | 8 (2.7) | 3 (1.0) | 1 (1.7) | 1 (1.7) |
| Never | 247 (84.9) | 235 (80.8) | 51 (86.4) | 42 (71.2) |
| Missing | 36 (12.4) | 53 (18.2) | 7 (11.9) | 16 (27.1) |
Feasibility of secondary outcomes
Secondary outcomes validation
There were five secondary outcomes in the pupils’ questionnaire: the Family Activity Scale, KIDSCREEN-52, TCPPAS, PCCS, and the FCS. All outcomes were modified and/or adapted for KAT, and therefore needed validation. For the outcomes measured at baseline and follow-up (Family Activity Scale, KIDSCREEN-52, TCPPAS), validation was carried out using baseline data, while the outcomes used only at follow-up (PCCS and FCS) were validated using the follow-up data set.
Table 27 shows that the reliability of the secondary outcomes was demonstrated using Cronbach’s alpha values. All were greater than 0.7, indicating high internal consistency of items. Factor analysis confirmed that each scale consisted of one factor, indicating that using a summed score for each is a valid interpretation of the data. Summed responses were investigated for normality and demonstrated negative skew. Positively skewed data can be log-transformed so that they become normally distributed before analysis. However, negatively skewed data are difficult to normalise using transformation. We have, therefore, left the data untransformed, as analysis of variance (ANOVA) and analysis of covariance (ANCOVA) are relatively robust to non-normality and the extension to two-level linear models should not invalidate the interpretation of the likely intervention effects. However, caution should be exercised when examining these data and reanalysing these scales as categorical outcomes rather than continuous scores may be preferable for investigating these data in a larger definitive trial.
| Secondary outcome | Cronbach’s alpha |
|---|---|
| Family Activity Scale | α = 0.807 |
| KIDSCREEN-52 | α = 0.752 |
| TCPPA | α = 0.775 |
| PCCS | α = 0.758 |
| FCS | α = 0.731 |
Two-level generalised linear modelling
Secondary outcome scores were analysed using two-level generalised linear models, with responses from pupils nested within schools using models adjusting for baseline data (if available). Covariates included in the model were school size and FSM entitlement. As TCPPA was captured only in baseline questionnaires and was replaced by the PCCS in the follow-up questionnaire, we did not conduct two-level modelling for TCPPA. Models for secondary outcomes were adjusted for school size and FSM. Neither covariate was statistically significant but they remained in the final model due to their use as balancing variables in the randomisation.
Rates of missing data
Of the 358 pupils who provided their demographic variables, three failed to provide their year group. Among the other 355 pupils, 28 were in Year 4, 179 in Year 5, and 148 in Year 6. Table 28 shows how many pupils in each year provided data for secondary outcome measures.
| Outcome measure | Year 4 | Year 5 | Year 6 | |||
|---|---|---|---|---|---|---|
| Baseline, n (%) | Follow-up, n (%) | Baseline, n (%) | Follow-up, n (%) | Baseline, n (%) | Follow-up, n (%) | |
| Family Activity Scale | ||||||
| Calculated | 26 (92.9) | 22 (78.6) | 158 (88.3) | 137 (76.5) | 129 (87.2) | 124 (83.9) |
| Missing | 2 (7.1) | 6 (21.4) | 21 (11.7) | 42 (23.5) | 19 (12.8) | 24 (16.1) |
| KIDSCREEN-52 | ||||||
| Calculated | 26 (92.9) | 23 (82.1) | 162 (90.5) | 137 (76.5) | 126 (85.1) | 127 (85.8) |
| Missing | 2 (7.1) | 5 (17.9) | 17 (9.5) | 42 (23.5) | 22 (14.9) | 21 (14.2) |
| PCCS | ||||||
| Calculated | N/A | 22 (78.6) | N/A | 134 (74.9) | N/A | 125 (84.5) |
| Missing | N/A | 6 (21.4) | N/A | 45 (15.1) | N/A | 23 (15.5) |
| FCS | ||||||
| Calculated | N/A | 16 (57.1) | N/A | 104 (58.1) | N/A | 108 (73) |
| Missing | N/A | 12 (42.9) | N/A | 75 (41.9) | N/A | 40 (17) |
Excluding the FCS, rates of missing data ranged from 14.1% to 23.5%. Rates of missing data were, thus, higher for the secondary outcomes than for the alcohol-related questions discussed above. For the measures used at both baseline and follow-up (the Family Activity Scale and KIDSCREEN-52 subscale), rates of missing data were higher at follow-up than at baseline, except for KIDSCREEN-52 in Year 6, where there was a small decrease in the rate from 14.9% at baseline to 14.2% at follow-up. For the FCS, there was a much lower rate of missing data in Year 6, 17%, compared with 41.9% in Year 5 and 42.9% in Year 4. One factor contributing to the highest rates of missing data found for the FCS (42.9% for Year 4) is that on 28 questionnaires, one item was accidentally omitted from the scale; otherwise, there was no discernible pattern to the unanswered items. Another possible reason is that the FCS was counted as missing if any one item out of 10 was not answered because the score for this measure is summed from the individual responses. However, we cannot rule out the possibility that the questions may have been unsuitable for children in all year groups. For the other scales, comparisons of rates across year groups do not support an age-related explanation for any differences, and the very small numbers of Year 4 pupils limit the scope for interpretation.
Table 29 shows the scores for the secondary outcomes. At follow-up, the average scores on the Family Activity Scale and PCCS were marginally higher for the intervention group. There was no difference between the average scores for the two groups on KIDSCREEN-52. The average score for the control group was marginally higher for the control group on the FCS. None of these effects reaches levels of conventional statistical significance and confidence intervals are wide. Of the four measures, two (the FCS and the PCCS) were used only at follow-up, while the other two were used at both baseline and follow-up.
| Outcome measure | Control | Intervention | Intervention effect | |||||
|---|---|---|---|---|---|---|---|---|
| n | Baseline, mean (SD) | Follow-up, mean (SD) | n | Baseline, mean (SD) | Follow-up, mean (SD) | Coefficient and 95% CI | p-value | |
| Family Activity Scale | 118 | 2.6 (0.8) | 2.55 (0.77) | 132 | 2.6 (0.8) | 2.7 (0.7) | 0.1 (–0.1 to 0.3) | 0.182 |
| KIDSCREEN-52 | 118 | 81.9 (18.2) | 82.5 (17.6) | 134 | 82.0 (15.7) | 81.7 (17.6) | 0.0 (–6.0 to 6.1) | 0.993 |
| PCCS | 136 | Not measured | 1.3 (0.3) | 153 | Not measured | 1.4 (0.3) | 0.1 (–0.1 to 0.3) | 0.314 |
| FCS | 117 | Not measured | 9.1 (1.4) | 118 | Not measured | 8.8 (1.8) | –0.2 (–1.1 to 0.6) | 0.610 |
Effect sizes detected in previous studies (secondary outcomes)
We identified previous studies which have used our selected secondary outcome measures, to identify what size of effect had been detected in evaluations of interventions comparable with KAT. However, this search yielded only limited information. For the FCS, we could find no trials which had used this measure, and the studies which had used it had done so with older children than KAT participants, and only at one time point. All of these studies were in countries other than the UK. Typical scores on the FCS appeared to be relatively high (around 35–45 out of a possible total score of 50). In our study, we replaced the five-point Likert scale with yes/no responses (to aid question comprehension), meaning that the total possible score was 10. Scores were 9.11 (intervention) and 8.81 (control). It is, therefore, not possible to make direct comparisons between our data and previous studies using the FCS. However, our scores appear to fit within the broad range of scores reported by previous studies. 143–145
Previous studies which have used KIDSCREEN (or only its parent relation and home life dimension as we did) have found relatively small changes in these scores; however, the studies identified were all observational,146–148 with the exception of Karasimopoulou et al. 149 They used KIDSCREEN-52 with 10- to 12-year-olds in Greece as part of an evaluation of a health education/social skills programme (possible scores ranged from 6 to 30). The experimental group had a mean [± standard deviation (SD)] parent relation/home life score of 23.81 (± 6.46) before the intervention and 25.54 at follow-up (± 4.09). The control group’s baseline score was 24.66 (± 4.20) and 24.3 (± 4.45) at follow-up. As with the FCS above, it is difficult to make direct comparisons with our study because we used a score of 0 (rather than 1) for the ‘not at all’ response on the Likert scale and linearly transformed scores to a 0–100-point scale. The control group in KAT had a baseline score of 81.87 (± 18.23) and a follow-up score of 82.47 (± 17.56). The respective figures for the intervention group were 81.98 (± 15.66) and 81.74 (± 17.56).
For the Family Activity Scale, we were unable to identify any previous RCTs or longitudinal studies which had used the scale. In our study, we created a single mean score based on all eight items in the scale (follow-up scores were 2.55 (intervention) (SD 0.77) and 2.70 (control) (SD 0.70). These appear to be broadly comparable with scores reported in previous studies, though they are mainly for the individual questions within the measure (in all cases, 1 = never and 5 = every day). For instance, Garmiene’s study55 of children aged 10 in Lithuania found mean scores which ranged from 2.62 for playing sports (± 1.24) to 4.57 for watching TV together (± 1.16).
For the PCCS, we were unable to identify any studies which reported baseline and follow-up scores from RCTs, and there were no studies of any design which had used the measure in the UK, or with the same age group as in the current study. It is, therefore, very difficult to assess what magnitude of effect a programme such as KAT might potentially have on alcohol-related parent–child communication using this scale. In Mares et al. ’s study,99 baseline means (11- to 12-year-olds) for communication frequency were 2.09 (± 0.85) (intervention) and 2.19 (± 0.91) (controls), while in Van der Vorst et al. ’s study150 of 13- to 16-year-olds, the mean report for younger siblings was 1.75 (± 0.67). In our study, the follow-up means were 1.25 (SD 0.26) (intervention) and 1.38 (SD 1.79) (control).
Estimation of sample size needed for an effectiveness trial of Kids, Adults Together
Determining the primary outcome for an effectiveness trial
Our data suggest some problems with the reliability of pupils’ recall of lifetime drinking. These may have related to the young age of the children, or heightened awareness of alcohol issues as a result of questionnaire completion/intervention receipt, though we do not have evidence to confirm or refute this. If follow-up took place at 2 years past baseline in a future trial, the participants would be 2 years older than they were in this study. Age-related issues around comprehension might, therefore, be less of a problem. However, basing the primary outcome on whether or not participants have had a drink in the last 30 days would provide a good indicator of recent drinking behaviour, and may avoid the problems described above concerning recall over a child’s entire life. Our sample size calculations for an effectiveness trial are, therefore, based on detecting differences in past-month drinking (as a binary outcome) between intervention and control. However, should any future trial be planned it would also aim to measure other aspects of alcohol behaviour (lifetime drinking, and aspects of drunkenness) as key secondary outcomes.
Rates of drinking behaviours in the Health Behaviour in School-aged Children survey and randomised controlled trial of the Strengthening Families Programme 10–14
To estimate the prevalence of past-month drinking rates, we examined the 2009 HBSC survey, which collected data on this outcome. We also examined baseline data from an ongoing trial of another alcohol misuse prevention programme (SFP10–14). That trial does not collect data on past-month drinking at baseline, but we were able to use the other alcohol-related data to provide some additional context on drinking behaviours among 11- to 13-year-olds (the age which participants would be at main follow-up in an effectiveness trial of KAT). The SFP10–14 trial is using past-month drinking as one of its twin primary outcomes, and these data will be available in 2014 (and, therefore, could aid further work on developing a sample size for any future effectiveness trial of KAT). 8
Table 30 shows data from the HBSC for participants born in 1997, 1998 and 1999 (i.e. 11- to 13-year-olds at the time of data collection) relating to the number of times that they consumed alcohol during the last 30 days.
| Birth year | Frequency, n (%) | Total, N (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| Never | 1–2 times | 3–5 times | 6–9 times | 10–19 times | 20–39 times | 40 times or more | ||
| 1997 | 1412 (73.31) | 356 (18.48) | 83 (4.31) | 34 (1.7) | 20 (1.04) | 9 (0.47) | 12 (0.62) | 1926 (100) |
| 1998 | 962 (78.98) | 182 (14.94) | 43 (3.53) | 12 (0.99) | 7 (0.57) | 5 (0.41) | 7 (0.57) | 1218 (100) |
| 1999 | 4 (57.14) | 1 (14.29) | 1 (14.29) | 1 (14.29) | 0 | 0 | 0 | 7 (100) |
The data in Table 30 show an overall prevalence rate for past-month drinking of 24.5% (773/3151 = 24.5%), and the majority of those who have consumed alcohol have done so on only a few occasions.
Table 31 shows data from the baseline questionnaire used in the SFP10–14 trial. It indicates that for the 13-year-olds in the sample, around 21% drink alcohol monthly or more frequently. This is slightly lower than, but broadly comparable to, the HBSC data.
| Age in years | How often do you usually have an alcoholic drink? | |||||
|---|---|---|---|---|---|---|
| Two or three times a week | About once a week | About once a month | Only a few times a year | I never drink alcohol now | Total | |
| 9 | ||||||
| n (% total in age group) | 0 | 0 | 1 (25.0) | 2 (50.0) | 1 (25.0) | 4 (100) |
| % all answers in this category | 0 | 0 | 2.8 | 1.1 | 2.2 | 1.4 |
| 10 | ||||||
| n (% total in age group) | 0 | 0 | 1 (4.5) | 15 (68.2) | 6 (27.3) | 22 (100) |
| % all answers in this category | 0 | 0 | 2.8 | 8.2 | 13.0 | 7.8 |
| 11 | ||||||
| n (% total in age group) | 0 | 0 | 2 (5.7) | 22 (62.9) | 11 (31.4) | 35 (100) |
| % all answers in this category | 0 | 0 | 5.6 | 12.1 | 23.9 | 12.4 |
| 12 | ||||||
| n (% total in age group) | 0 | 0 | 4 (7.8) | 41 (80.4) | 6 (11.8) | 51 (100) |
| % all answers in this category | 0 | 0 | 11.1 | 22.5 | 13.0 | 18.0 |
| 13 | ||||||
| n (% total in age group) | 1 (1.1) | 6 (6.6) | 12 (13.2) | 57 (62.6) | 15 (16.5) | 91 (100) |
| % all answers in this category | 25.0 | 40.0 | 33.3 | 31.3 | 32.5 | 32.2 |
| 14 | ||||||
| n (% total in age group) | 3 (3.8) | 9 (11.2) | 15 (20.0) | 45 (56.2) | 7 (8.8) | 80 (100) |
| % all answers in this category | 75.0 | 60.0 | 44.4 | 24.7 | 15.2 | 28.3 |
| Total | ||||||
| N (%) | 4 (1.4) | 15 (5.3) | 36 (12.7) | 182 (64.3) | 46 (16.3) | 283 (100) |
| % answers in each category | 100 | 100 | 100 | 100 | 100 | 100 |
Table 32 below displays data for the question on whether or not participants in the SFP10–14 trial had ever had a drink of alcohol. At age 11, only 15.2% of participants report ever having had a drink of alcohol, but this increases to 52% by age 13.
| Age in years | Have you ever had a proper alcoholic drink – a whole drink, not just a sip? | ||
|---|---|---|---|
| Yes | No | Total | |
| 9 | |||
| n (% in age group) | 4 (18.2) | 18 (81.8) | 22 (100) |
| % answers from children this age | 1.4 | 2.8 | 2.4 |
| 10 | |||
| n (% in age group) | 23 (11.0) | 187 (89) | 210 (100) |
| % answers from children this age | 8.0 | 29.3 | 22.7 |
| 11 | |||
| n (% in age group) | 35 (15.2) | 196 (84.8) | 231 (100) |
| % answers from children this age | 12.2 | 30.7 | 25.0 |
| 12 | |||
| n (% in age group) | 51 (30.2) | 118 (69.8) | 169 (100) |
| % answers from children this age | 17.8 | 18.5 | 18.3 |
| 13 | |||
| n (% in age group) | 92 (52.0) | 85 (48.0) | 177 (100) |
| % answers from children this age | 32.2 | 13.3 | 19.1 |
| 14 | |||
| n (% in age group) | 81 (69.8) | 35 (30.2) | 116 (100) |
| % answers from children this age | 28.3 | 5.5 | 12.5 |
| Total | |||
| N (%) | 286 (30.9) | 639 (69.1) | 925 (100) |
| % answers | 100 | 100 | 100 |
Sample size calculation
Our sample size calculations use the prevalence rate of 24.5% for past-month drinking, derived from the HBSC data above. Tables 33 and 34 present sample size calculations based on KAT reducing past-month drinking by 2.5%, 5% and 7.5% respectively, using the ICC of 0.021 from the HBSC data for 11- to 13-year-olds’ drinking in the last 30 days. We are not able to specify with precision what effect KAT would achieve, and have therefore included a range of sample size calculations (based on 2.5%, 5% and 7.5% reductions in past-month drinking). However, the brief duration of the KAT intervention and the evidence from this study, including the lack of evidence of effect on hypothesised mediators, suggest that any effect would be small, and a 2.5% reduction may be the most appropriate of the three we present below.
| Difference to detect | Control group proportion | Intervention group proportion | Significance | Power | OR | n per group | Total, N |
|---|---|---|---|---|---|---|---|
| 2.5% | 24.5% | 22% | 5% | 80% | 0.869 | 4481 | 8962 |
| 5% | 24.5% | 19.5% | 5% | 80% | 0.746 | 1077 | 2154 |
| 7.5% | 24.5% | 17% | 5% | 80% | 0.631 | 458 | 916 |
| Difference to detect | ICC | Average cluster size | DE | CV | DE (adjusted for CV) | Drop out/absent | Total sample size | Number of schools required | Pupils per school to recruit |
|---|---|---|---|---|---|---|---|---|---|
| 2.5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 9849 | 263 | 38 |
| 5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 4734 | 127 | 38 |
| 7.5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 2013 | 54 | 38 |
The total sample size estimated from Table 33 must then be inflated for clustering. It should also be inflated for varying cluster size and pupil drop out.
Table 34 shows that for an effectiveness trial designed to detect a 2.5% difference between the two trial arms, the necessary sample size would be 9849 participants, and 263 schools. To detect a difference of 5% and 7.5% would require 127 and 54 schools, respectively.
The estimated sample sizes with 90% power for the same range of differences in drinking prevalence are given in Tables 35 and 36.
| Difference to detect | Control group proportion | Intervention group proportion | Significance | Power | OR | n per group | Total, N |
|---|---|---|---|---|---|---|---|
| 2.5% | 24.5% | 22% | 5% | 90% | 0.869 | 5998 | 11,996 |
| 5% | 24.5% | 19.5% | 5% | 90% | 0.746 | 1441 | 2154 |
| 7.5% | 24.5% | 17% | 5% | 90% | 0.631 | 613 | 916 |
| Difference to detect | ICC | Average cluster size | DE | CV | DE (adjusted for CV) | Drop out/absent | Total sample size | Number of schools required | Pupils per school to recruit |
|---|---|---|---|---|---|---|---|---|---|
| 2.5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 13,183 | 351 | 38 |
| 5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 6335 | 169 | 38 |
| 7.5% | 0.021 | 30 | 1.61 | 0.487 | 1.76 | 20% | 2695 | 72 | 38 |
The total sample size estimated from Table 35 must then be inflated for clustering (see Table 36). It should also be inflated for varying cluster size and pupil drop-out.
Table 36 indicates that based on 90% power, a total of 351 schools would be needed to detect a 2.5% reduction in drinking in the intervention group. For 5%, the figure would 169 schools, and for 7.5% a total of 72 schools would need to be recruited.
Table 37 shows the total number of eligible schools (English-medium primaries) in each of the 22 local authorities in Wales, and the number of schools which could be recruited from each of these areas if 23% agreed to participate an effectiveness trial (the same proportion as in the current study). Using these calculations, it can be seen that if all eligible schools across Wales were invited to participate in the trial using the methods employed in the current study, 198 schools could be recruited, assuming that 23% agreed to participate. Presuming that a future effectiveness trial would use 80% power and would seek to detect a reduction of 2.5% in past-month drinking, this figure falls well short of the 263 schools which would be needed.
| Name of local authority area | Number of eligible schoolsa | Number of schools recruited if 23% agreed to take part |
|---|---|---|
| Isle of Anglesey | 2 | 0 |
| Gwynedd | 1 | 0 |
| Conwy | 36 | 8 |
| Denbighshire | 29 | 7 |
| Flintshire | 62 | 14 |
| Wrexham | 51 | 12 |
| Powys | 75 | 17 |
| Ceredigion | 7 | 2 |
| Pembrokeshire | 45 | 10 |
| Carmarthenshire | 39 | 9 |
| Swansea | 68 | 16 |
| Neath Port Talbot | 6 | 1 |
| Bridgend | 43 | 10 |
| Vale of Glamorgan | 39 | 9 |
| Rhondda Cynon Taf | 85 | 20 |
| Merthyr Tydfil | 20 | 5 |
| Caerphilly | 57 | 13 |
| Blaenau Gwent | 24 | 6 |
| Torfaen | 25 | 6 |
| Monmouthshire | 29 | 7 |
| Newport | 39 | 8 |
| Cardiff | 81 | 19 |
| Totals | 863 | 198 |
Exploratory work to facilitate an economic evaluation
Key cost domains
To enable an economic evaluation to be conducted as part of any future effectiveness trial, we sought to map, in as much detail as possible, the key cost domains.
The costs associated with running KAT can be mapped on to three levels, namely families, schools, and external organisations. We deal with each in turn. For families, the main costs incurred relate to the opportunity cost of attending the family event and the expenses incurred through travelling to and from school. Some parents/carers might also incur childcare costs for young siblings of children involved in KAT, though the family events are open to all family members.
Schools’ costs fall into three clear categories. First, there is the cost of staff time devoted to the programme. This comprises teaching staff, teaching assistants, and non-teaching staff such as caretakers. Second, there is a cost attached to the production of materials for the family event. These are mainly paper and stationery – there is no requirement for schools to buy equipment as part of their classroom preparation. Third, by delivering KAT, schools incur an opportunity cost – i.e. the time spent on the programme by staff and pupils could have been utilised for other curricular or non-curricular activities.
During this exploratory trial we were also able to map out which external organisations were involved in programme delivery, the nature and extent of their input, and how this might evolve as part of the systems and structures established for any future effectiveness trial. In the current study, the following agencies supported the implementation of KAT:
-
A Healthy Schools Scheme officer, who assisted with recruitment of schools, and also attended some of the training events for school staff and the family events.
-
An educational consultant who provided training and support for school staff and also assisted with the running of the family events. The cost of her employment was covered by a grant from the Welsh Government.
-
A local drugs agency which provided an information stand at all of the KAT events.
-
A local secondary school which loaned its ‘smoothie bike’ free of charge for use at the family event in all of the intervention schools.
A number of non-staff costs were also covered by external agencies (principally, by a grant from the Welsh Government). These were the updating and printing of the programme manual and the purchase of additional educational resources; the cost of providing refreshments at all three schools which ran family events; the purchase of additional display boards (which were used in multiple schools); and the cost of van hire to transport the ‘smoothie bike’ between schools. The ‘goody bags’ and their contents (including the DVD) had already been produced and paid for by Gwent Police before the start of the trial as part of the earlier phase of programme delivery; Gwent Police made these items freely available.
Questionnaires completed by pupils in this study included questions on whether or not they completed the KAT classroom work, and rates of attendance at the family event (for pupils, families, and the number of adults present from each family). This information on programme reach could be used alongside data on programme costs to ascertain the cost per participant/family.
Translating inputs into financial costs
Based on our experience in this exploratory trial, we believe that it should be possible to translate all of the key inputs into financial costs which could then be used as part of an economic evaluation. A section of the programme handbook could be used to ask staff to record (in a pro forma in the book) how many hours they spend on KAT (pupil contact time and other preparation time). It should be possible for a process evaluation within any future effectiveness trial to record total pupil contact time in a subsample of the intervention schools, so that teacher self-reports and researcher observations can be compared.
Although we did not ask schools to calculate the cost of teacher input into the programme, we believe that it would be feasible to ask head teachers either to provide this information or to share sufficient information for us calculate an hourly cost.
In this exploratory trial, the cost of refreshments, transportation of the ‘smoothie bike’, and other non-staff costs were paid directly by the research team from a centrally held programme grant. In any future effectiveness trial, we would expect schools to organise and pay for refreshments at their family event, and to submit invoices for these and other costs (such as those associated with the use of ‘smoothie bikes’) to a central programme co-ordinator. These data could, therefore, be used to provide accurate information on the non-staff costs which schools need to recoup.
Process evaluation observation of classroom preparation activities allowed us to generate an overall impression of the amount of consumable materials (e.g. paper, pens and posters) that schools used. Given the difficulty of producing exact costs for these materials, the most efficient way of estimating the costs would be to ask each school to provide an estimate of all of the non-staff expenditure items they provide. This information could be requested at the same time as schools submit invoices for reimbursement of costs paid by a central programme grant. It was feasible to separate research-related and programme delivery-related costs in this exploratory trial. A health economic evaluation as part of any effectiveness trial would also need to ensure that all costs could be allocated to the research process or the delivery of the KAT programme.
Suitability of primary and secondary outcomes for an economic evaluation
In a future effectiveness trial it should be possible to analyse primary outcomes (relating to alcohol consumption) and secondary/tertiary outcomes (relating to family communication) alongside data on costs relating to programme delivery. We would be likely to adopt a similar approach to that currently being used in an ongoing trial of the SFP10–14, in which a cost–consequences analysis is being used. However, given the problems experienced with recruitment of parents into the current trial, it is unlikely that we would be able to access data from parents on service utilisation, which is a component of the data collection from parents in the SFP10–14 trial. Traumatic, rather than medical, problems are common consequences of adolescent alcohol misuse, and so estimating service use would focus on accident and emergency admissions 2 years post intervention (or after other specified follow-up intervals).
Feasibility of the data collection instruments
Our experience in this exploratory trial suggests that it is feasible to collect comprehensive and reliable data concerning programme delivery costs, and intervention reach and engagement. Low rates of missing data for the questionnaire items in this study which would form the primary and secondary outcomes in any future effectiveness trial suggest that it would be feasible to link these data with programme cost data. However, it is unlikely that we could collect service utilisation data from large numbers of parents using the methods employed in this exploratory trial, given the low recruitment rates encountered.
Chapter 4 Discussion
Parts of this text are reproduced with permission from Segrott et al. 1
Introduction
In this chapter, we discuss our key findings. We begin by outlining the study’s main limitations. The chapter then discusses the study’s findings, structured around our progression criteria – starting with those relating to programme implementation, followed by the criteria concerned with a future effectiveness trial of KAT. For each criterion we provide a summary of the evidence generated by the study, and also map this onto the study’s objectives. This is followed by an overall assessment of our programme- and trial-related progression criteria. We then situate our findings in relation to the existing literature on school-based alcohol misuse prevention programmes.
Study limitations
In this exploratory trial we assessed the feasibility and acceptability of an effectiveness trial of KAT, and also aimed to identify systems and structures which would be required for such an effectiveness trial. The study was therefore designed to generate learning that could inform the decision about whether or not to proceed with an effectiveness trial, and optimising its design and implementation. For instance, we tested strategies for recruiting parents/carers into the trial, and the low rates of involvement are an important finding concerning the feasibility of these strategies, rather than a weakness in the design or implementation of the research. However, the current study does have a number of limitations. Although these have generated important learning, which would be incorporated into any future research we conduct on KAT, they should also be borne in mind when interpreting the results presented in this report.
Systems for identifying eligible pupils
Although we asked schools for accurate and up-to-date information on numbers of pupils eligible to participate in the trial, and the number present in school on the days when data collection took place, we could have developed better systems for capturing and managing this information. To some extent, this weakness in our systems happened because recruitment and baseline data collection took place before the funded trial, and when there were no dedicated resources. However, we could have developed more accurate and comprehensive systems for determining total numbers of eligible pupils, how many pupils were present in school, and present in class, during data collections. More attention should have been given to this aspect of recruitment and data collection during initial discussions with schools, and accurate class lists should have been obtained at the earliest point possible.
Withdrawal of two schools from the study
During the trial we lost two intervention group schools, which decided to withdraw. The first of these did so because parents raised objections after main information and follow-up letters were mixed up in error. It is difficult to identify to what extent the parents’ objections were based on the nature of the study, or the switching of the letters, but this experience underlines the critical importance of systems to ensure that nothing is done by the research team which might unnecessarily cause concern to parents.
The second school withdrew on the basis of two main issues: the timing of, and the workload generated by, the KAT programme, and the burden created by contact from multiple members of the research team. In this case it is harder to identify ways in which we could have managed the process better, given that we spelled out very clearly on multiple occasions the timing and workload which participation in the trial would involve. In this second school, at least one member of staff appeared to have concerns about the applicability and acceptability of the KAT programme to Muslim families, though the school did not present this as a reason for their withdrawal. We knew that implementation of the programme and research in a school with large numbers of ethnic minority families, including a number in which adults did not speak English, was likely to be challenging. However, we discussed these issues in depth with the school, who felt they would not be problematic, and, because the school met our inclusion criteria and a key aim of the study was to assess the feasibility of the trial in different school contexts, we felt it was right to include them in our study. However, there may have been ways in which we could have reduced the perceived burden of multiple contacts from the research team.
Our data on the acceptability and feasibility of KAT to schools, parents/carers and pupils need to be viewed in the context of the withdrawal of these two schools. In particular, there are two specific limitations which should be noted. First, we are not entirely clear on the precise reasons why the two schools which withdrew did so, and the extent to which their withdrawals related to (1) the general acceptability of the research/KAT; (2) the manner in which we carried out the research; and (3) characteristics of the school, and the population of parents/carers which it served. Second, it must be acknowledged that for key aspects of programme implementation, we have data from only the three schools which remained in the study. It is possible that the balance or content of the themes present in the data might have been different had these two schools remained in the study, or if we had been able to collect more data subsequent to their withdrawal from the study.
Feasibility of collecting follow-up data in secondary schools
In our application for funding we did not plan to conduct long-term follow-up of pupils (as would happen in a future effectiveness trial), as this would be unfeasibly costly for an exploratory trial, and would delay any decision on the future of the programme beyond that which was likely to be acceptable to policy and practice partners. Our focus in this trial was on the overall acceptability of the KAT programme to schools, parents and pupils, and participation in a randomised trial, and the feasibility of implementing KAT as part of such a trial.
During recruitment of primary schools we decided to test the acceptability of using ‘opt-out’ parental consent for pupils’ involvement in the research component of the trial. We did this so that we would know whether or not such an approach would be feasible in a future effectiveness trial. All schools (including those which later withdrew from the study) were happy for us to use this method. However, the use of ‘opt-out’ parental consent at recruitment does have important implications for our ability to follow up children 2 years later, and after they have moved to secondary schools. In another ongoing trial, we have been able to successfully engage secondary schools in allowing the research team to conduct follow-up interviews in school with young people who were recruited either in the community or via primary schools. However, in that trial we have explicit written consent from parents (collected at baseline) for all aspects of the data collection involving their child(ren), including follow-up interviews.
Secondary schools may be less likely to provide assistance to us if we do not have written consent from parents. Therefore, although we have relatively strong data on rates of recruitment for primary schools and pupils at baseline, there is still significant uncertainty about the extent to which we could achieve adequately high response rates at long-term follow-up via secondary schools. In retrospect, we should have included some exploratory work with secondary schools to assess the acceptability to them of collecting follow-up data from pupils, and what requirements they were likely to have.
Assessment of cost-effectiveness
This study has provided a description of key cost and outcomes domains, and the feasibility of monitoring them on a wider scale. Based on our experience in this exploratory trial, we believe that it should be possible to identify all key costs and to translate programme inputs into financial costs which could then be used as part of an economic evaluation in any future effectiveness trial. Low rates of missing data in pupil questionnaires mean that it in any future effectiveness trial it should be possible to use primary and secondary outcomes alongside programme cost data. Given the low rates of parental recruitment into the trial, it would probably not be possible to collect service utilisation data from parents/carers, though it could be feasible to access data for young people on alcohol-related harms (e.g. A&E attendance). We recognise that our exploratory work for a future cost-effectiveness evaluation has some limitations, and that a more detailed economic evaluation setting programme costs against potential future savings would have provided a better basis for decisions about investment in any future RCT.
Key findings: programme implementation
Implementation feasibility
Three schools completed programme delivery. One intervention school withdrew without delivering any part of the intervention, and one withdrew from the study after starting programme delivery, but had only done a small part of the classroom component (and had not held a family event). The three schools which completed programme delivery appeared to deliver most or all of the main components, and to retain the main underlying messages of KAT. In at least one class, there was a tendency for the negative aspects of alcohol to dominate rather than a more balanced set of messages on the healthy use of alcohol (‘not too soon, not too much’). Schools appeared to be generally happy with the KAT programme manual and the training provided by the health education consultant. However, some teachers had not read the programme manual, or were not aware of key guidance/instructions in it, and a number of teachers suggested that the manual could provide more detailed guidance. Of the three schools which completed programme delivery, only one asked pupils to write invitations to the family evening for their parents/carers. In one of the schools, the teaching staff appeared to believe that the health education consultant and research team would lead the KAT family event. This highlights the importance of ensuring that senior managers and other staff in schools take ownership and support the implementation of the programme (Table 38).
| Progression criterion 1 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT can be implemented successfully in primary schools Addresses study objective 2:a Assess the feasibility of the intervention |
Process evaluation findings indicate that at least two of the intervention schools delivered key elements of KAT classroom work and family events in line with the teachers’ handbook; AND it is reasonable to expect that any significant problems identified can be overcome | Three of the five intervention group schools delivered most or all of the main components of KAT. One intervention school withdrew before delivering any part of the programme. A second intervention school withdrew shortly after programme delivery had commenced There are ways in which the challenges encountered in the three schools which completed KAT could be addressed, particularly through optimising staff training, and ensuring that the roles and responsibilities are clear from the outset |
Intervention acceptability
The three schools which completed delivery of the KAT programme were happy with its content and structure, and were willing to deliver all of the main components. In these schools, very few parents objected to the study or intervention, or refused permission for their children to take part because they objected to the alcohol-related content. Most pupils enjoyed undertaking the KAT programme and few, if any, issues were raised about the content (Table 39). Process evaluation data support the idea that most parents who attended the KAT fun evening or who discussed the programme with their children found it acceptable (Table 40). In the first school which withdrew from the study, parents did raise concerns about the topic of the research/KAT programme to the school. It is difficult to ascertain whether this was mainly because the information and follow-up letters sent to parents/carers had been switched in order; as a result of particular aspects of the school population; a combination of these reasons; or due to another set of factors of which we were unaware. One of the reasons given by the second school which withdrew from the study was the time commitment needed by the programme and the timing of intervention delivery. However, one of the class teachers tasked with delivering the programme had concerns about its acceptability to the large number of Muslim parents in the school. Although process evaluation data indicated that some parents had asked questions about the KAT programme, we were not able to determine whether or not there were widespread concerns among parents at the school about either the research or the KAT intervention (Table 41).
| Progression criterion 2 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT is acceptable to children in the target age group (9–11 years) Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of pupil participants in each school | Process evaluation findings indicated that children enjoyed doing the KAT classroom work and taking part in the family event. Few, if any, concerns were raised about the programme content |
| Progression criterion 3 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT is acceptable to parents of children aged 9–11 years Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of parent participants in each school | All parents who participated in process evaluation research interviews identified high levels of acceptability. This was supported by data from researcher observations at the family events School A reported that parents had raised concerns about the topics covered in the research study/KAT programme |
| Progression criterion 4 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT is acceptable to school staff involved in implementation (head teachers, teachers of Year 5 and 6 classes, and support staff) Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings indicate that a majority of school staff in each school support the concept of primary school education about alcohol; feel competent to deliver KAT; and think that KAT has potential benefits for families and school; AND that it is reasonable to expect that any significant problems identified can be overcome | The majority of school staff supported the concept of KAT, were able to deliver its core components, and identified potential benefits for their school and families. Some of the challenges which arose during implementation related to training systems, and clarifying roles and responsibilities, and could be addressed in future implementation of the programme Parents at one school raised concerns about the topic being covered by the research study/KAT programme and the school withdrew from the study. A second intervention school also withdrew from the study. Dissatisfaction with the timing of and workload created by delivering the programme were some of the reasons given by this school |
Although we were not able to interview parents in school 8 (which withdrew after baseline data collection), the interview with one of the class teachers involved indicated that they had concerns about the relevance and acceptability of KAT to Muslim families. This was mainly related to the fact that because these families did not drink, an intervention which examined healthy behaviours and positive family communication in the home concerning alcohol would not be relevant. However, the programme does not assume that all families will drink alcohol, or that its content will be applicable only to those who do. The programme recognises that children will be exposed to alcohol-related behaviours, advertising and media portrayals, all of which take place outside the home setting. The programme aims to promote positive communication within families about alcohol, but the exact content of this communication is not intended, necessarily, to be based on family drinking. If KAT was to be run in schools with similar populations it would be important to fully address these issues.
Programme reach
The KAT programme demonstrated high levels of reach among both pupils and parents (Tables 42 and 43). In the three intervention schools which delivered KAT, 70.9% of pupils reported doing all of the KAT work in school, and a further 22.8% said that they had done part of it; 59.5% of pupils reported having attended the KAT fun evening at their school. For the three intervention schools as a whole, an average of 50% of children reported that at least one adult member of their family had attended the family event. While in two of the schools the figures were just below 50%, in the third school 65.7% of those families invited were represented by at least one adult. The ability of KAT to engage half of all the families invited to participate in the intervention is a significant achievement. When the three schools are ranked in order of the proportion of the families that attended, there is a positive association with FSM levels (Table 44). In the intervention group as a whole, pupils with higher Family Affluence Scale scores were more likely to have a parent who attended, suggesting that there is social patterning of family attendance at the school level. However, when rates of pupil attendance at the family event are examined, the proportions of pupils reporting low/medium and high Family Affluence Scale scores who attended the family event were almost identical (Table 45). A significant minority of pupils reported attending the KAT family event without a member of their family. It may be that these children remained in school (particularly where the fun evening was directly after the end of the school day) and were supervised by school staff, or that they came with other children’s parents. It is also possible that some children provided incorrect responses to the questions on attendance. Although the process evaluation researcher observed the family events, it was not possible to accurately identify the total number of pupils from the specific classes involved in the programme, and the precise number of families which were represented. In summary, KAT was able to engage with families from a range of socioeconomic backgrounds, and there is evidence to suggest that the programme could operate in a variety of school contexts.
| Progression criterion 5 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT attracts high rates of participation from children aged 9–11 years Addresses study objective 3: Establish intervention participation rates |
Process evaluation findings and pupil questionnaires from intervention schools suggest that all pupils in participating classes take part in classroom work (if present in school) and few if any objections from parents are received; AND that a minimum 50% of pupils attend KAT events | Questionnaire responses indicated that the majority of pupils had done either all or part of the KAT classroom work. An average of 59% of pupils reported attending the KAT family events |
| Progression criterion 6 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT attracts high rates of participation from parents of children aged 9–11 years Addresses study objective 3: Establish intervention participation rates |
Pupil questionnaire data (intervention group) and process evaluation findings suggest that parents/caregivers or other adults from families of a minimum 25% of pupils attended KAT events | Pupils reported that on average, 50% of those families invited to the family events were represented by at least one adult. In the three schools which delivered family events the rates were 45.1%, 46.6% and 65.7% |
| Progression criterion 7 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT can be implemented in schools serving a range of socioeconomic groups and localities Addresses study objective 3: Establish intervention participation rates |
Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that of schools which implemented KAT, some were above and some below median FSM for the county | Rates of FSM entitlement for the three schools which completed programme delivery were 37.2%, 2.3%, and 27.9% (county median = 18.4%). The two schools which withdrew from the study had rates of 1% (first school) and 21.6% (second school) |
| Progression criterion 8 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT can engage parents and children from a range of socioeconomic groups and localities Addresses study objective 3: Establish intervention participation rates |
Ethnicity and Family Affluence Scale data from pupil questionnaires; deductions about families from FSM rates and demographics of school area; and process evaluation interviews with school staff demonstrate inclusion of families from a range of social groups and localities that reflects the local population | KAT was delivered in schools with a range of FSM scores, and rates of parental engagement with the programme were particularly high in the school which had the highest FSM score. The programme engaged with pupils with both low/medium and high Family Affluence Scale scores. Rates of attendance for parents/carers were higher for those whose children had higher Family Affluence Scale scores |
There was some evidence from the study’s process evaluation that the ‘balanced approach’ advocated by KAT did not necessarily fit well with the experiences of families who had experienced alcohol-related problems. Although the training given to teachers as part of the KAT implementation dealt with this issue, the findings from the process evaluation may need to be further explored if KAT is implemented in the future. Although much of KAT’s content maps closely onto the school curriculum, some children may need additional support during the programme. Family communication processes are central to the programme’s intended mechanism of action. Children’s experiences of the programme may be negative if their parents/carers are not willing to engage in the intended prosocial communication, or do so in ways which are at odds with the core values of the programme.
Data from the study’s process evaluation – particularly from focus groups with pupils – highlighted that children were more likely to want to attend the family evening if their parents accompanied them. Ensuring that as many parents/carers as possible attend the family event would appear to be very important in ensuring that both pupils and parents receive the majority of the intervention, and that key intended family communication processes are set in motion. Were we recommending a future trial, we would need to maximise rates of participation by parents/carers, rather than aim for figures comparable with those achieved in this exploratory trial. As discussed above, a small but significant minority of pupils attended the KAT family event unaccompanied by members of their own families. It is not clear whether these pupils were with other participants’ families (and, therefore, may have directly experienced some of the key communication processes intended to occur) or if they sat by themselves or with friends.
Assessing whether or not policy and practice support exists for future implementation of Kids, Adults Together, and identifying optimal delivery systems
An important component of our work has been to identify whether or not there is support among key policy and practice organisations for future implementation of KAT. We also aimed to identify what might be the most effective systems and structures to develop KAT. We were able to engage key organisations to become members of a stakeholders group, whose advice we initially sought on the value and appropriateness of our draft progression criteria. The group supported the criteria which we had developed, subject to some minor modifications. We then shared our key findings with this group to identify whether or not they had value and importance for them, and if the constituent members would support further development of KAT.
Our discussions identified that all organisations were supportive of further development of the KAT programme. Some of the key reasons for their support included the fact that KAT had succeeded in engaging large numbers of parents; the way in which the programme had relevance and might contribute to other existing initiatives (e.g. the Healthy Schools Scheme, schools’ work on applying for Investors in Families Awards, the All-Wales School Liaison Core Programme); and the importance of alcohol misuse prevention.
We were unable to identify an organisation with the resources to fund and lead the next phase of development of KAT, although the national Healthy Schools Scheme in Wales was willing to assist with the training of teachers to deliver KAT. Gwent Police – who originally developed the KAT programme – were also willing for the next phase of programme implementation to be wholly within a RCT. However, without dedicated funding, no effectiveness trial of KAT could be contemplated (Table 46).
| Progression criterion 1 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| Sufficient support exists in terms of policy and resources at school, LEA and national levels, to allow successful delivery of KAT on a large scale Addresses study objective 2: Assess the feasibility of the intervention |
Stakeholder group judge that structures and resources for further implementation can be put in place | The stakeholder group supports further development of the KAT programme. The national Healthy Schools Team in Wales has agreed in principle to assist with training school teachers to deliver KAT, as part of an effectiveness trial. However, no organisation is presently able to fund the remaining intervention costs or to lead programme delivery as part of an effectiveness trial |
Trial recruitment and retention
Schools
This study tested the feasibility of recruiting schools for a future effectiveness trial and assessed the acceptability of randomisation to schools. From a total of 39 eligible schools, nine were recruited into the study (23%), though the recruitment process took longer than initially anticipated beacuse of delays in identifying the final school needed prior to randomisation. We purposefully selected recruitment strategies which could be scaled up as part of a future effectiveness trial, and tested their feasibility. We wrote to all schools in the study county inviting them to take part, and then made follow-up calls to all schools, until sufficient schools had been recruited. Therefore, we can be reasonably confident that the schools recruited into this exploratory trial might be broadly comparable with those likely to participate in a future effectiveness trial, and that the recruitment rates achieved in the current study could be achieved across multiple counties.
School recruitment could probably have been improved by inviting schools to participate during the academic year preceding a trial when it would have been easier for schools to include KAT in planning. However, evidence from two UK reports suggests that school staff generally may feel that their core function of delivering high-quality education to pupils may be compromised because they are overwhelmed with new initiatives. 151,152 Thus, it may not be realistic to expect better timing to result in a big increase in schools willing to participate in any further evaluation. McCrone et al. 151 note that involving staff is important to bringing about and maintaining change, suggesting a possible explanation for school 8’s withdrawal from the study.
Although KAT required input and commitment from head teachers, it also depended on the engagement of individual members of teaching staff, who were asked to deliver the intervention and facilitate data collection. Our findings, and those of our previous evaluation of KAT’s implementation,90 suggest that the quality and completeness of delivery of the intervention does depend to a large extent on the commitment and enthusiasm of individual teaching staff. A key issue here is perhaps the need to ensure that programmes such as KAT, which have a primary focus on health and well-being, can demonstrate how they might address educational outcomes for pupils, and thus help teachers to deliver their core role as educators. If such teachers can see the direct relevance and value of KAT, and its suitability for the pupils and families they work with, they may be more likely to fully engage with it. Individualised on-site coaching involving demonstrations, which show how interventions can be delivered in the ‘real world’ of the classroom, may be more effective ways of gaining teachers’ understanding of and commitment to an intervention than simply providing initial training alongside a handbook and support on request. 153 In this study, we sometimes found it very difficult to involve class teachers in initial meetings to discuss participation in KAT, and subsequent training and briefing sessions. Had we been able to achieve their involvement across all schools at initial programme set-up meetings, it might have been possible to identify and deal more effectively with some of the challenges which arose, in relation to both delivery of the intervention (e.g. the failure to include child invitations to parents in some schools), and teachers’ concerns about the appropriateness of the programme for families from ethnic minority backgrounds.
We recruited schools with a range of FSM entitlement rates, suggesting that, were we recommending a future trial, it would be possible to reach schools with families from a range of different socioeconomic backgrounds. In Newport, FSM rates range from 1% to 48.3% (median 18.4). FSM rates of the schools which participated in the trial were 1%, 2.3%, 21.6%, 27.9% and 37.2% (intervention), and 11.4%, 23.5%, 23.5% and 31.9% (control schools). The support of the local Healthy Schools Team (one of whose officers accompanied the research team on visits to schools to seek formal agreement to take part in the study) appeared to help communicate the value and importance of the study (Table 47).
| Progression criterion 12 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| It is feasible to conduct a trial of KAT in schools serving a range of socioeconomic groups and localities Addresses study objective 4: Assess trial recruitment and retention rates |
Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that schools within each trial arm varied in terms of social, demographic and geographic characteristics and that at least two were in areas above the county median for deprivation | Schools varied in terms of key demographic factors. Nine schools were recruited. Six had FSM scores above the county median, and three below |
From a small sample of nine schools, it is difficult to ascertain to what extent the recruitment and withdrawal rates in this trial might be replicated in a much larger effectiveness trial. For a larger effectiveness study, greater resources would be needed to recruit schools and develop better systems from the start, including contacting schools well in advance of the planned programme delivery period (thus minimising barriers to engagement in the trial). Because follow-up data would be collected from pupils in secondary schools, the loss of primary schools after baseline data collection (as happened in one of the cases in this study) would not have a major impact on the ability to collect follow-up data.
Although some of the schools which participated in the study expressed a clear preference to receive the KAT programme, randomisation was acceptable to all schools, and all those in the control group remained in the study and facilitated all data collection. Were we recommending a future trial, we would plan to collect baseline data before randomisation of schools took place, so it is unlikely that randomisation allocation would create significant risks to the viability of the trial. However, as noted above, the main follow-up data collections would take place in secondary schools, and not in the primary schools in which pupils were initially recruited. We did not include this aspect of data collection in our exploratory trial. If an effectiveness trial were to be considered in future, it would be important to undertake further work to assess the feasibility and acceptability of collecting follow-up data in secondary schools which had not been involved in the study from the start. In the trial itself, it would be important to engage with these secondary schools early in the research process, probably at the same time as the initial recruitment of feeder primary schools in which the study was taking place. As part of a current RCT of the SFP10–14, we have successfully engaged with secondary schools (most of whom have not had any role hitherto in the trial or the programme being evaluated) in order to conduct questionnaire completion with pupils in school. In these schools, we have written to the parents of the pupils concerned to inform them that we would like to conduct follow-up interviews with their child in school, and have given them the option to refuse permission. This system has been acceptable to most schools and enabled a significant number of interviews to be conducted in school, with very few parents refusing permission. Similar methods could be adopted for other school-based trials and also draw upon the network of contacts developed as a result. For instance, in our trial of SFP10–14, we have engaged the services of a retired head teacher, who has helped to negotiate entry into a large number of secondary schools. However, in the SFP10–14 study, ‘opt-in’ parental consent is being collected at baseline. Were we recommending a future trial of KAT, we would need to be clear right from the start about how many schools would be willing to allow follow-up interviews to take place with children without this ‘opt-in’ consent in place. Because pupils in KAT are recruited exclusively through the schools we would also be likely to need to interview more pupils per school at follow-up than is the case for the SFP10–14 study.
Pupil recruitment
Of those pupils eligible to participate in the study at baseline, response rates were 74% for the intervention group and 81% for the control group. Follow-up rates were 68% for the intervention group and 74% for the control group. If the school which completed baseline data collection but then withdrew from the study is removed (and from whose pupils no follow-up data could be collected) from the completion rates at follow-up, the figure for the intervention group rises from 68% to 85%. The main reason for non-completion of the questionnaires was absence from school or the classroom. In the control group, no eligible participants refused to complete questionnaires at baseline, and in the intervention group only 13 did so.
For both baseline and follow-up data collection, we paid a single visit to each school to collect data. At baseline, there were a total of 24 pupils absent from school on the day of data collection, and a further 40 who may have been present in school but not present in the classroom during data collection. Of those present in the classroom at baseline, 78% (intervention) and 88% (control) completed questionnaires – higher than the completion rates if the denominator used is those eligible. At follow-up, completion rates as a proportion of those present were 92% (intervention) and 77% (control). Had we made a second visit to each school to collect questionnaire data from pupils who were previously absent from school/their classroom, our recruitment and retention rates could have been increased. It should also be possible to optimise provision of support for pupils with low literacy levels, and we were able to achieve this to some extent when we conducted follow-up data collection. Literacy levels, rather than the questionnaire content, appeared to be the main reason for pupils refusing to complete questionnaires at baseline in at least one of the schools, based on feedback from teaching staff. A total of 39 pupils who did not complete questionnaires at baseline went on to complete follow-up questionnaires. Although we cannot be certain of the reasons for this, we feel it may be due in part to the provision of more members of research staff at follow-up data collection, and asking schools in advance how many pupils were likely to need assistance with reading questions. One suggestion made in one of the stakeholder group meetings (attended by key practice and policy collaborators) is that the use of online computer-based questionnaires could be considered. Internet-based activities and use of laptops is increasingly common in primary schools, though these might not be available in all schools. An internet-based questionnaire might be able to incorporate support for pupils with low literacy or offer questionnaires in languages other than English, and could also provide a means for pupils who were absent during data collection visits to complete the questionnaire at a later time point.
Our response rates also show some patterning according to sex and year group. More boys, and pupils in Year 5, completed questionnaires at baseline only. This may relate to differences in the proportion of girls and boys reaching expected literacy levels,154 but we cannot be certain as to the exact reasons. Were we recommending a future trial, it might be useful to consider in more detail whether there are aspects of data collection which are less appealing or more off-putting to boys, and how these could be modified. There were also sex differences in completion rates for our secondary outcomes (see Feasibility and acceptability of secondary outcomes).
Although rates of recruitment of pupils are important, the use of a cluster RCT design means that they need to be considered alongside rates of school recruitment (which is the unit of randomisation). Were we recommending an effectiveness trial, rates of school recruitment and retention would be very important in achieving the necessary statistical power.
Parents/carers
The number of eligible parents/carers who agreed to complete questionnaires was very low. Only 6.5% of eligible parents/carers participated in the questionnaire aspect of the study, and this is based on an assumption that there was only one adult in each household, so the true figure may be even lower. There are a number of factors which may explain this low rate. First, owing to data protection regulations, the research team was not able to access the names and contact details of eligible parents/carers from schools. We were only able to send a standard letter (which began ‘Dear parent/carer’) to parents via schools, and there was no way of identifying recipients who had not expressed an interest in participating in the research. Second, in this letter we asked parents to contact the school if they did not wish their child(ren) to participate in the study. If they were content for their child to participate, they did not need to make contact with school. In the same letter, parents were asked to complete a reply slip and return it to the research team if they themselves wished to take part in the study. It is possible that having two different consenting methods for children and parents in the same letter created confusion, or that, having established that no action was required of them in relation to their child’s participation, parents/carers were less inclined to respond to the remaining information. The method of providing parents with the option to withdraw their child from the study, rather than asking them to give explicit consent for their participation, is likely to have increased the rates of pupil involvement, and we chose this strategy deliberately as in an effectiveness trial primary outcome data would be collected from children. However, the relatively high rates of pupil questionnaire completion may have been at the expense of parental involvement. Third, in this exploratory trial we sought to use the best recruitment strategies which would be feasible and affordable if scaled up as part of a large effectiveness trial. With investment of more resources we could potentially have increased the rate of parental involvement in questionnaire completion (e.g. through holding information events, and spending more time in school, and placing less emphasis on letters). However, these procedures would be hard to sustain if an effectiveness trial involved a large number of schools. We were also concerned that a significant package of parental engagement work by the study team in schools could influence parental engagement in the KAT programme and school work, making it hard to disentangle programme processes from the research recruitment strategies. It is unlikely that we would be able to resolve all of these key challenges, and we return to this issue in our conclusion to suggest ways in which parents could be involved in effectiveness research.
Ethical issues raised by the study
A study such as this one, which involved collecting data from children on alcohol consumption and aspects of family communication in relation to alcohol, has the potential to encounter ethical challenges in relation to determining whether or not certain disclosures might amount to evidence of an individual being at risk of harm of abuse. We followed the Cardiff University policies and guidelines on child protection, part of which stipulated that because data collection had taken place in an external organisation, any child protection concerns should be shared with that institution (schools, in our case). One particular challenge we faced was to decide what frequency or type of alcohol consumption by young people might be considered an indication of a child being at risk of harm. The law permits parents to provide alcohol to children from the age of 5 years, and it was difficult to know whether some reports of drinking were based on whole drinks or on sips, and if children’s understanding of drunkenness corresponded with our own as adult researchers. The interval between data collection and data entry, the difficulties which some pupils experienced in understanding the questionnaires, the inconsistent responses within the data and the lack of personal contact with the child all added to the difficulties we faced.
Our approach as a Trial Management Group was to consider frequent drunkenness among child participants to be a possible indicator of harm, and in such cases our concerns would have to be shared with schools. One pupil’s questionnaire responses raised concerns which led to our contacting the school’s teacher who had responsibility for child protection. The recent Unicef guidance on researchers’ ethical responsibilities155 emphasises that guidelines can never be comprehensive enough to cover all possible contexts and individuals; this means that critical reflection on practice is always necessary. We sought to maintain the confidentiality of participants’ identities wherever possible, while ensuring that we followed good practice in relation to child protection procedures.
Sample size calculation
Basing the primary outcome on whether or not participants have had a drink in the last 30 days might provide a good indicator of recent drinking behaviour. Current practice in the field of alcohol misuse prevention intervention evaluation appears to vary widely, with studies using measures of current alcohol consumption frequency, past-week, past-month, past-year and lifetime drinking. 156 Our sample size calculations for an effectiveness trial are, therefore, based on detecting differences in past-month drinking (as a binary outcome) between intervention and control.
Based on data from the HBSC survey (using the ICC of 0.021 found in that survey for past-month drinking, and with 90% power), an effectiveness trial would require at least 351 schools, and 38 pupils per school, to be able to detect a 2.5% reduction in drinking rates in the intervention group. With 80% power to detect a 2.5% difference between groups, the total sample size would be 263 schools. If we were to invite all eligible schools across Wales (n = 863) to participate in the trial, and 23% participated (this is the same proportion as we achieved in the current study), then we would be able to recruit 198 schools. This would be challenging and costly to achieve, and would still fall well short of the 263 schools needed for a trial with 80% power. Retention of a large number of schools over a wide geographical area would also be a significant undertaking. The sample size calculations are our best current estimates, rather than final numbers, but it seems reasonable to expect that any intervention effects on alcohol-related behaviours are likely to be small (based on our findings in this trial which demonstrated no evidence of effects or a trend towards them on intermediate outcomes which hypothesised to prevent alcohol consumption) (Table 48).
| Progression criterion 13 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| The sample required to demonstrate a significant effect of KAT is achievable Addresses study objective 5: Identify potential effect size and appropriate sample size |
Recruitment records indicate that we were able to recruit eight schools as per protocol; project records demonstrate that schools in both trial arms are retained in the study; questionnaire returns indicate that at least 80% of pupils in a majority of eligible classes provide data at each time point | Nine schools were recruited (23% of those eligible), two of which (both intervention arm) withdrew from the study, one of which did so after baseline data collection Overall questionnaire completion rates at follow-up rates were 71% of those eligible at baseline. If the school which withdrew from the trial after baseline data collection is removed from the denominator the figure is 79.5% Our best estimate for the sample size needed to detect a 2.5% reduction in past-month drinking at 2-year follow-up is 351 schools (90%) power or 263 schools (80% power). To recruit this number of schools would be challenging and require significant resources |
Acceptability to schools of pupil recruitment methods
As part of the initial contact with interested schools, we tested the acceptability of methods for recruiting pupils into the study, and in particular our preference to offer parents/carers the opportunity to refuse permission for their children to participate in the study rather than asking them to provide written consent for their children’s participation (though in each school we included pupils in the study only if they were happy to participate and provided written assent). All nine schools which participated in the trial were happy to use this method, and it appeared to have a good fit with the approach they normally used when parents were consulted on activities which pupils would be involved with in school. The uniform acceptability of this approach is important, because it suggests that, if we were recommending an effectiveness trial, we would be able to at least replicate the pupils’ response rates at baseline achieved in this study. The method which we used for parental consent thus helped to maximise rates of pupil involvement in the study, and to avoid potential response bias which might occur using parental opt-in. 112 However, before undertaking any further study, we would have needed to investigate the extent to which pupils could be followed up in secondary schools, particularly in the absence of written consent from parents/carers.
Acceptability and feasibility of chosen measures
Alcohol-related questions
Were we recommending an effectiveness trial, the primary outcome would be based on alcohol consumption. Thus, in this exploratory trial, we were concerned with assessing the acceptability and feasibility of collecting these data from primary school age children. Low rates of missing data (maximum 3.4%) suggest that most pupils felt comfortable with answering questions on alcohol consumption and understood their meaning. Rates of missing data were slightly lower at follow-up than at baseline.
There was, however, some evidence of misclassification, with pupils providing inconsistent answers. The main example of this was that a number of pupils answered ‘yes’ to having ‘ever had a drink’ at baseline, but answered ‘no’ to the same question at follow-up. It may be that children in this age group find it difficult to accurately remember such events over their entire life, especially if they do not have strong salience for the individual concerned,157 or that the measures are unreliable in other ways. Another possibility is that the baseline/follow-up questionnaires, the KAT intervention, or a combination of the two caused pupils to change their perception of their past drinking behaviours, or created a desire to provide socially acceptable answers. There were discrepancies between rates of ‘ever drinking’ and ‘past-month’ drinking at individual data collection points (i.e. there were more reports of ‘past-month’ drinking than ‘ever drinking’). The wording of the questions on past-month drinking was modified at follow-up based on feedback from pupils at baseline that the original phrasing was confusing, but this did not appear to improve the reliability of the data.
Our findings suggest that in effectiveness studies with children of a similar age, it may be preferable to measure past-month drinking rather than lifetime drinking as a primary outcome, and to use ’ever use’ as a marker of reliability. Past-month drinking should provide a relatively accurate picture of whether or not children have started to drink regularly. Were we recommending an effectiveness trial of KAT, additional secondary outcomes related to drinking (e.g. age of first drink, ever drink, drunkenness) would have formed important aspects of the overall design and analysis as well as the choice of a primary outcome (on which to base sample sizes and other statistical calculations).
In this study, data on alcohol-related behaviours were collected from young people at a point when most of them had yet to start drinking. Thus, for some of our data points (particularly past-month and lifetime drunkenness), prevalence rates are very low. Were we recommending an effectiveness trial, these data would have been collected after an interval of several years (at age 11–13 years for most participants). Because the children would be older, issues of questionnaire comprehension might be less apparent; it is also likely that rates of drinking and drunkenness would be higher (given the normal increase in drinking behaviours as children grow older), meaning that any issues with sparse data present in this trial would not be present. Clearly, age adjustment would be important and assessment of drinking trajectories between intervention and control group might be required.
In this exploratory trial, we did not aim to assess the effectiveness of KAT on alcohol-related behaviours, and there were a number of methodological and theoretical reasons for this. First, the focus of the trial was to examine the feasibility of an effectiveness trial of KAT, rather than to conduct a ‘mini trial’ of the intervention’s effectiveness. Second, especially given its delivery to children of primary school age in order to prevent early alcohol consumption, and among whom rates of drinking are very low, any impacts of KAT on alcohol behaviours would need to be measured several years later once the natural prevalence of such behaviours had increased. Third, the logic model for KAT clearly hypothesises that prevention of alcohol misuse is mediated via the strengthening of family communication and attachment, and, thus, any short-term assessment of the programme should focus on these intermediate outcomes. In this trial, we collected alcohol-related data mainly to assess potential completion rates, reliability, and the acceptability of the individual questions to participants. The trial was not, therefore, designed or statistically powered to detect differences in alcohol-related behaviours between trial arms. Given these caveats, it is not possible to use the data presented in Chapter 3 to draw conclusions as to the effectiveness of KAT in preventing alcohol misuse. Our data on rates of drinking and drunkenness at follow-up are mixed, and there is evidence of inconsistent reporting by pupils. However, taking into consideration the above caveats, some of our results suggest that KAT may have potentially harmful effects (particularly whether or not pupils report ever having had a drink of alcohol). There may be a number of reasons for these results, including actual harmful effects of the intervention, the imbalance in the trial arms at baseline in terms of age, etc., or the reliability of the measures used for this age group. It is also possible that the intervention content may have influenced how children answered questions at follow-up, though we do not know if this is the case.
Existing research provides numerous examples of alcohol, drug and other prevention interventions which have produced iatrogenic effects (including increasing substance use), even when carefully designed and well implemented. 158,159 It is important to understand whether such effects arise from a particular intervention component (or negative effects for a particular subgroup), an overall failure of intervention theory, or inadequate implementation which undermines the intervention’s theoretical basis. 159
Feasibility and acceptability of secondary outcomes
We faced considerable difficulties in identifying suitable and validated measures of family communication which were designed for children aged 9–11 years, and this was particularly the case for measures of family communication in relation to alcohol. These difficulties have significance beyond our particular study, as many other researchers may potentially need to measures outcomes similar to ours among primary school-aged children. Given the emphasis on delivering family-based prevention interventions to children before they start drinking, and while parents are still a primary point of attachment (i.e. prior to the teenage years),31,53,73 we were surprised at the paucity of validated measures in this area for primary school-aged children.
From the very small number of candidate measures that we identified, most were aimed at older age groups of children (and outside the UK), and were not always easily understood by participants in our study. Another weakness of many of the measures we considered using was that they assumed that children lived with either one or two parents at home, and were difficult to answer for some pupils who spent time with different non-cohabiting parents, or lived with other adult figures. While the measures we eventually used had strong internal consistency, it was not always possible to determine how the measures had originally been validated by their authors. In most cases, the measures had been used in cross-sectional or longitudinal studies, and there were few examples of their use in trials, and, thus, of what kinds of effect sizes might be expected from interventions similar to KAT.
The measures used were validated on our data set and showed good levels of internal reliability. Factor analysis showed that single summed scores were an appropriate way to summarise the data. However, the distributions of the scores indicated that linear modelling may not be the most appropriate method of analysis for these scores if used in an effectiveness trial, and that categorising the scores and using ordinal or logistic methods would be more appropriate.
Rates of missing data for secondary outcomes were higher than for the alcohol-related questions. For the Family Activity Scale, KIDSCREEN-52 and the PCCS, the completion rates all lay between approximately 75% and 90%. The FCS had higher rates of missing data than the other secondary outcome measures, particularly for Year 4 and 5 participants, but this is probably due to the way in which missing data were categorised, rather than because there were more questions unanswered. For all of these measures, missing data rates were higher for boys than for girls. Missing data rates appeared to be higher at follow-up than at baseline in Years 4 and 5, though there was no clear pattern for Year 6 pupils. The reasons for non-completion of the measures (or individual questions within them) could relate to their acceptability, the phrasing of the questions not being clear, or the fact that participants found them hard to answer. Analysis of the patterning of missing data suggested that ‘missingness’ was broadly equal across individual questions within the measures, rather than due to a small number of questions consistently being left unanswered (Table 49).
| Progression criterion 14 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| Methods for measurement of primary and secondary outcomes are feasible and the cost of measurement can be estimated Addresses study objective 6: Determine feasibility and cost of measuring primary and secondary outcomes |
Measures were understood by and acceptable to > 75% of Year 5 and 6 pupils in each school | Rates of missing data were very low for the alcohol-related questions (maximum 3.4%). However, there was evidence that reports of alcohol consumption were unreliable, especially in relation to lifetime drinking Rates of missing data for secondary outcomes on family communication lay between 10% and 25%. We were not able to identify measures that had been developed for the age group included in this study, and those that we used required adaptation. The secondary outcome measures used in this exploratory trial would have required further testing and adaptation, or replacement with more suitable measures, had we been recommending an effectiveness trial We were able to determine the number of staff which would be needed to collect questionnaire data as part of an effectiveness trial, and the cost of employing them |
Identifying potential effect sizes
In this exploratory trial, our main aim in collecting data on alcohol-related behaviours was to assess the acceptability and feasibility of doing so in a future effectiveness trial, and we used data from 11- to 13-year-olds in the HBSC data set to calculate the sample size which would be needed for a 2-year follow-up.
As an exploratory trial, this study did not aim to measure the effectiveness of the KAT programme on predicted short-term outcomes. It is important to note that the trial was not powered to detect differences between the two groups, nor was it designed to ensure that intervention and control groups were equivalent in relation to key dimensions at baseline. In an exploratory trial such as this one, effect sizes provide only a broad estimation of what might be expected in an effectiveness trial in relation to intermediate outcomes on family communication. Analysis of these secondary outcomes indicated no evidence of any intervention effect (Tables 50 and 51). There are a number of possible explanations for these results. One is that KAT simply does not work, and that the results accurately reflect a lack of intervention effect. A second possibility is that KAT does, or may, have small short-term effects, but that our study has not detected them. This could be due to the imbalance of the intervention groups in important respects, the fact that the study was not large enough and not powered to detect effects, the unreliability of the measures used, or a combination of these factors. As noted above, we faced considerable difficulty in identifying suitable measures of family communication, and, even after adaptation by us, they were not always easily understood by participants, which may have influenced how they were completed. A third possibility is that our logic model for the programme (and, therefore, the dimensions we chose to measure) is incorrect or incomplete, and KAT operates through processes which we did not assess.
| Progression criterion 15 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| Promising effect sizes are achieved for key outcomes Addresses study objective 2: Assess the feasibility of the intervention Addresses study objective 5: Identify potential effect size and appropriate sample size |
After adjusting for baseline differences, comparison of intervention and control group pupil scores at follow-up shows that intervention group average scores are higher than control for at least one of the following measures: KIDSCREEN-52 autonomy dimension PCCS FCS Family Activities Scale AND that intervention group average scores are not lower than control group average scores for any of the other scales |
There were no significant difference between intervention and control groups for any of the secondary outcomes, and no evidence of promising effect sizes It was not possible to identify previous RCTs which had used any of these outcome measures to evaluate comparable interventions, and with comparable study populations (country, age group, etc.) |
| Progression criterion 11 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT is consistent with a theoretical basis which suggests that short-term impacts on parent–child communication may shape longer-term alcohol-related behaviours Addresses study objective 1: Refine the intervention’s theoretical model |
Process evaluation findings and comparison of intervention and control group scores for intermediate outcomes (communication measures) indicate that participation in KAT is associated with an increase in parent–child communication | There was some evidence from the process evaluation findings that KAT promoted parent–child communication There was no evidence from the scores for intermediate outcomes to indicate any increase in parent–child communication |
There were very few examples of previous studies which had used our secondary outcome measures. None were directly comparable to the current study, as they had used the measures with older age groups, in countries other than the UK, and had not used the measures to compare trial arm outcomes in RCTs. However, the average scores in our study sat within the range of scores previously recorded for these measures (see Table 50).
Assessment of Kids, Adults Together delivery costs
In this trial, we were able to identify key cost domains relating to the delivery of KAT and to capture the financial costs of most of these domains. Had we been recommending an effectiveness trial, it should have been possible to measure the cost of programme delivery, including those costs (such as staff time) incurred by schools. However, our inability to recruit parents/carers into this exploratory trial means that it would have been difficult to capture data on variations in service utilisation between trial arms. This would be a significant barrier to conducting a cost-consequence analysis (Table 52).
| Progression criterion 9 | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| KAT delivery costs can be recorded in a way which facilitates assessment of cost-effectiveness Addresses study objective 7: Identify programme costs and pilot methods for measuring them |
Systems developed in current project can be used to monitor costs of larger-scale implementation | It was possible to identify key cost domains for KAT programme delivery, and systems developed in this study could be used in a larger effectiveness trial to monitor implementation costs. Low rates of parental recruitment into the current study mean that it is unlikely that an effectiveness trial could capture data on variations in service utilisation |
Criteria for progression to effectiveness trial
Tables 53 and 54 display all of the progression criteria, the basis for their assessment (and what outcome would be needed to proceed to an effectiveness trial), and a summary of the evidence relating to them. They also map each criterion onto the study’s objectives.
| Progression criterion | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| Progression criterion 1 KAT can be implemented successfully in primary schools Addresses study objective 2:a Assess the feasibility of the intervention |
Process evaluation findings indicate that at least two of the intervention schools delivered key elements of KAT classroom work and family events in line with the teachers’ pack; AND it is reasonable to expect that any significant problems identified can be overcome | Three of the five intervention group schools delivered most or all of the main components of KAT. One intervention school withdrew before delivering any part of the programme. A second intervention school withdrew shortly after programme delivery had commenced. There are ways in which the challenges encountered in the three schools which completed KAT could be addressed, particularly through optimising staff training, and ensuring that the roles and responsibilities are clear from the outset |
| Progression criterion 2 KAT is acceptable to children in the target age group (9–11 years) Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of pupil participants in each school | Process evaluation findings indicated that children enjoyed doing the KAT classroom work and taking part in the family event. Few, if any, concerns were raised about the programme content |
| Progression criterion 3 KAT is acceptable to parents of children aged 9–11 years Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings from intervention schools suggest that KAT was acceptable to the majority of parent participants in each school | All parents who participated in process evaluation research interviews identified high levels of acceptability. This was supported by data from researcher observations at the family events School A reported that parents had raised concerns about the topics covered in the research study/KAT programme |
| Progression criterion 4 KAT is acceptable to school staff involved in implementation (head teachers, teachers of Year 5 and 6 classes, and support staff) Addresses study objective 2: Assess the feasibility of the intervention |
Process evaluation findings indicate that a majority of school staff in each school support the concept of primary school education about alcohol; feel competent to deliver KAT; and think that KAT has potential benefits for families and school; AND that it is reasonable to expect that any significant problems identified can be overcome | The majority of school staff supported the concept of KAT, were able to deliver its core components, and identified potential benefits for their school and families. Some of the challenges which arose during implementation related to training systems, and clarifying roles and responsibilities, and could be addressed in future implementation of the programme Parents at one school raised concerns about the topic being covered by the research study/KAT programme and the school withdrew from the study. A second intervention school also withdrew from the study. Dissatisfaction with the timing of, and workload created by, delivering the programme were some of the reasons given by this school |
| Progression criterion 5 KAT attracts high rates of participation from children aged 9–11 years Addresses study objective 3: Establish intervention participation rates |
Process evaluation findings and pupil questionnaires from intervention schools suggest that all pupils in participating classes take part in classroom work (if present in school) and few, if any, objections from parents are received; AND that a minimum 50% of pupils attend KAT events | Questionnaire responses indicated that the majority of pupils had done either all or part of the KAT classroom work. An average of 59% of pupils reported attending the KAT family events |
| Progression criterion 6 KAT attracts high rates of participation from parents of children aged 9–11 years Addresses study objective 3: Establish intervention participation rates |
Pupil questionnaire data (intervention group) and process evaluation findings suggest that parents/caregivers or other adults from families of a minimum 25% of pupils attended KAT events | Pupils reported that an average of 50% of those families invited to the family events were represented by at least one adult. In the three schools which delivered family events, the rates were 45.1%, 46.6% and 65.7% |
| Progression criterion 7 KAT can be implemented in schools serving a range of socioeconomic groups and localities Addresses study objective 3: Establish intervention participation rates |
Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that of schools which implemented KAT, some were above and some below median FSM for the county | Rates of FSM entitlement for the three schools which completed programme delivery were 37.2%, 2.3%, and 27.9% (county median = 18.4%). The two schools which withdrew from the study had rates of 1% (first school) and 21.6% (second school) |
| Progression criterion 8 KAT can engage parents and children from a range of socioeconomic groups and localities Addresses study objective 3: Establish intervention participation rates |
Ethnicity and Family Affluence Scale data from pupil questionnaires; deductions about families from FSM rates and demographics of school area; and process evaluation interviews with school staff demonstrate inclusion of families from a range of social groups and localities that reflects the local population | KAT was delivered in schools with a range of FSM scores, and rates of parental engagement with the programme were particularly high in the school which had the highest FSM score. The programme engaged with pupils with both low/medium and high Family Affluence Scale scores. Rates of attendance for parents/carers were higher for those whose children had higher Family Affluence Scale scores |
| Progression criterion 9 KAT delivery costs can be recorded in a way which facilitates assessment of cost-effectiveness Addresses study objective 7: Identify programme costs and pilot methods for measuring them |
Systems developed in current project can be used to monitor costs of larger-scale implementation | It was possible to identify key cost domains for KAT programme delivery, and systems developed in this study could be used in a larger effectiveness trial to monitor implementation costs Low rates of parental recruitment into the current study mean it is unlikely that an effectiveness trial could capture data on variations in service utilisation |
| Progression criterion 10 Sufficient support exists in terms of policy and resources at school, LEA and national levels, to allow successful delivery of KAT on a large scale Addresses study objective 2: Assess the feasibility of the intervention |
Stakeholder group judge that structures and resources for further implementation can be put in place | The stakeholder group supported further development of the KAT programme. The national Healthy Schools Team in Wales agreed in principle to assist with training school teachers to deliver KAT, as part of an effectiveness trial. However, no organisation was able to fund the remaining intervention costs or to lead programme delivery as part of an effectiveness trial |
| Progression criterion | Basis for assessment | Summary of assessment evidence |
|---|---|---|
| Progression criterion 11 KAT is consistent with a theoretical basis which suggests that short-term impacts on parent–child communication may shape longer-term alcohol-related behaviours Addresses study objective 1: Refine the intervention’s theoretical model |
Process evaluation findings and comparison of intervention and control group scores for intermediate outcomes (communication measures) indicate that participation in KAT is associated with an increase in parent–child communication | There was some evidence from the process evaluation findings that KAT promoted parent–child communication There was no evidence from the scores for intermediate outcomes to indicate any difference in parent–child communication between intervention and control schools |
| Progression criterion 12 It is feasible to conduct a trial of KAT in schools serving a range of socioeconomic groups and localities Addresses study objective 4: Assess trial recruitment and retention rates |
Details of FSM entitlement and school demographics (from Estyn school inspection reports) show that schools within each trial arm varied in terms of social, demographic and geographic characteristics and that at least two were in areas above the county median for deprivation | Schools varied in terms of key demographic factors. Nine schools were recruited. Six had FSM scores above the county median, and three below |
| Progression criterion 13 The sample required to demonstrate a significant effect of KAT is achievable Addresses study objective 5: Identify potential effect size and appropriate sample size |
Recruitment records indicate that we were able to recruit eight schools as per protocol; project records demonstrate that schools in both trial arms are retained in the study; questionnaire returns indicate that at least 80% of pupils in a majority of eligible classes provide data at each time point | Nine schools were recruited (23% of those eligible), two of which (both intervention arm) withdrew from the study, one of which did so after baseline data collection Overall questionnaire completion rates at follow-up were 71% of those eligible at baseline. If the school which withdrew from the trial after baseline data collection is removed from the denominator the figure is 79.5% Our best estimate for the sample size needed to detect a 2.5% reduction in past month drinking at 2-year follow-up is 351 schools (90% power) or 263 schools (80% power). To recruit this number of schools would be challenging and require significant resources |
| Progression criterion 14 Methods for measurement of primary and secondary outcomes are feasible and the cost of measurement can be estimated Addresses study objective 6: Determine feasibility and cost of measuring primary and secondary outcomes |
Measures were understood by, and acceptable to, more than 75% of Year 5 and 6 pupils in each school | Rates of missing data were very low for the alcohol-related questions (maximum 3.4%). However, there was evidence that reports of alcohol consumption were unreliable, especially in relation to lifetime drinking Completion rates for secondary outcomes lay between 75% and 90%. We were not able to identify measures that had been developed for the age group included in this study, and those that we used required adaptation. The secondary outcome measures adapted for use in this exploratory trial were not well suited to children aged 9–11 years We were able to determine the number of staff which would be needed to collect questionnaire data as part of an effectiveness trial, and the cost of employing them |
| Progression criterion 15 Promising effect sizes are achieved for key outcomes Addresses study objective 2: Assess the feasibility of the intervention Addresses study objective 5: Identify potential effect size and appropriate sample size |
After adjusting for baseline differences, comparison of intervention and control group pupil scores at follow-up shows that intervention group average scores are higher than control for at least one of the following measures: KIDSCREEN-52 autonomy dimension PCCS FCS Family Activities Scale AND that intervention group average scores are not lower than control group average scores for any of the other scales |
There were no significant difference between intervention and control groups for any of the secondary outcomes, and no evidence of promising effect sizes It was not possible to identify previous RCTs which had used any of these outcome measures to evaluate comparable interventions, and with comparable study populations (country, age group, etc.) |
The summary of the criteria and their assessment above indicates that some of them have been met, at least in part. KAT was successfully implemented in three schools, and achieved high rates of engagement and acceptability in relation to both pupils and parents. Although pupils with higher Family Affluence Scale scores were more likely to have been accompanied to their family event by an adult member of their family, the overall rates of family engagement were highest in the school with the highest FSM score. The programme was implemented in schools with very different socioeconomic catchment areas. Against these findings must be balanced the fact that two schools withdrew from the study, and this may have been due in part to the feasibility and acceptability of the intervention. While key policy and practice partners are supportive of the future development of KAT, no agency was able to fund the cost of delivering it in the number of schools, which would have been needed in an effectiveness trial.
Table 54 shows that, in relation to the trial-related criteria, there is considerable uncertainty about the extent to which these have or have not been met. The process evaluation findings suggest that some of the KAT programme’s key processes appeared to be operating as intended in relation to family communication. The trial succeeded in engaging schools which served a range of groups and socioeconomic localities, and overall, it was feasible to collect key outcome data from pupils (though not from parents), although two schools withdrew from the study. Either a number of the criteria have not been met, or there is not sufficient evidence to fully assess this. There was no evidence of any effect for the intermediate outcomes relating to family communication, although we cannot be certain that this indicates the absence of an effect. Rates of missing data were very low for the alcohol-related questions, but there are clear indications of unreliability in pupils’ reports, and we had difficulty in identifying suitable measures of family communication for children aged 9–11 years. Although our sample size calculation is not final, it suggests that a large number of schools would be required for an effectiveness trial, which raises issues of both feasibility and affordability.
A strength of the current study is that it developed a clear set of progression criteria based on the study aims and objectives, and these were shared with key policy/practice stakeholders whose input was sought on their value and appropriateness. We identified very few examples of guidance in the literature on how to design and conduct exploratory trials, and were unable to locate detailed guidance from previous studies on how researchers should identify, specify and assess progression criteria. We also identified considerable variation in the designs, aims and terminology employed by exploratory trials. We hope that the process we followed in this study to identify and evaluate our progression criteria might form a useful resource for future studies seeking to assess the feasibility of conducting a RCT of complex interventions.
Comparison with the existing literature
School-based alcohol misuse prevention programmes
Our review of recent studies identified that, while schools are generally acknowledged to be an important setting for the delivery of alcohol misuse prevention interventions and activities, there are a number of significant gaps in the literature. The majority of research on school-based alcohol misuse prevention interventions has been conducted in the USA, and the evidence base for UK programmes is, therefore, limited. 50 There is relatively little research on prevention interventions for primary school-age children,31,82 despite the recognition that this age group is the most appropriate development point for family-based programmes. 31 Long-term follow-up of participants is relatively rare. Although the involvement of parents and other community members has been shown to enhance intervention effectiveness, many school-based alcohol misuse prevention do not include them.
Our exploratory trial of KAT, therefore, makes an original contribution to the evidence base in these areas. KAT demonstrates features which have been shown to characterise effective prevention interventions: a theory-based design, interactive delivery styles and community involvement. 29–34 We deal with each of these in turn.
The importance of a strong theoretical design
Kids, Adults Together addresses key risk and protective factors for young people’s use of alcohol, particularly family relationships and communication. 29,31,32,52–54 The programme’s intended change processes are well explained by the SDM, which emphasises the critical role played by children’s attachment to prosocial adults in preventing later risk behaviours, and the important roles played by opportunities for prosocial interaction, the perceived availability of these opportunities, reinforcement of prosocial behaviour, and skill development in forming prosocial attachment. 73 The goals and activities within the KAT programme map very clearly onto this theoretical framework. For instance, the family evening provides clearly articulated opportunities for prosocial interaction (through encouraging children and parents to work together on quizzes), reinforcement of the achievements of children (through parental interest in pupils’ displays of work, and applause for pupils’ presentations), while the classroom component seeks to build children’s knowledge about the key health aspects of alcohol and develop their skills in discussing these issues with others.
Our findings suggest that within this overarching theoretical framework there are a number of key processes which may help KAT to achieve acceptability and engagement. For instance, findings from the process evaluation suggest that the mechanisms used by teachers to present a balanced view of alcohol, rather than focus solely on its negative health effects, were designed to allay concerns children might have about the appropriateness of moderate alcohol consumption by parents, and to ensure that communication between children and parents on the topics raised by KAT was not inhibited. Similarly, the attendance by parents at the KAT evening was mainly motivated by a desire to support their children, and children’s expressed desire that their parents should attend.
Interactive delivery
Interactive activities form an important aspect of all KAT components (classroom work, family event and the programme DVD). Teachers appeared to be comfortable with the interactive nature of the KAT classroom work, and there was evidence that interactive teaching methods were used consistently across the three intervention schools which completed intervention delivery. Pupils enjoyed the group-based work that they did as part of the KAT classroom work.
Rates of parental engagement in the programme
Involvement of parents/carers in school-based prevention programmes is important, as it can strengthen effectiveness through creating opportunities for prosocial interactions within families. Family and community engagement, more generally, is an important aim for many schools. However, previous studies have highlighted the challenges of engaging parents/carers in school-based prevention programmes. Rates of engagement are typically low, even when programmes have been modified to promote involvement. 62–64 There are also significant gaps in the literature, with relatively little written about why some strategies to engage parents/carers appear to work, while others do not. 110
The high rate of parental engagement in the KAT programme is, therefore, one of its key strengths, and create important opportunities for prosocial communication in families to take place. The rates of engagement compare favourably with those of other school-based programmes and appear to be achieved consistently across a range of school contexts. An important strength of the current study (and our previous research on KAT) is that we have been able to identify some of the key engagement processes and the ways in which they may be operating. In this way, it should be possible to identify aspects of programme implementation which contribute to these processes, and which need to be emphasised in future training activities and manuals. Two key processes were identified in our process evaluation. First, pupils were keen to go to the family event with their parents, and this may have encouraged family members to attend. Second, the family event was largely promoted and framed around parents/carers coming to school to see their children’s work and to support their children. The importance of this is that the event was not primarily marketed or understood as being about alcohol education. It may be that the opportunity to see the work that their children have done in school is a stronger draw for parents/carers than a more generic focus on a particular health issue or message, which has less of a personal connection. These insights should be generalisable to other similar interventions which seek to engage parents/carers in school-based health education activities.
Chapter 5 Conclusion
Parts of this text are reproduced with permission from Segrott et al. 1
Recommendations for future research
Our findings suggest that it would not be appropriate to undertake an effectiveness trial of KAT at this point. They have raised doubts or uncertainties about the potential effects of KAT; suitability of measures; feasibility of follow-up in secondary schools; and programme implementation and theory. While the KAT programme has a number of strengths, including its ability to engage with significant numbers of families and the way in which it can integrate with schools’ curricular activities, important trial-related progression criteria have not been met. Intermediate outcomes on family communication showed no evidence of intervention effectiveness, and it is also possible that KAT had negative impacts on certain aspects of family communication or alcohol-related behaviours. In essence, our findings indicate that KAT is likely either to be ineffective or to produce small changes in family communication which would require a very large sample size to be able to detect, and based on this it is likely that its effects on alcohol-related behaviour are also potentially small. Such a large trial could not be justified given the concerns identified regarding measurement of outcomes and the unknown feasibility of following up pupils after their transition to secondary school. 160
In this concluding chapter, we identify key issues for study design and implementation which may have broader methodological relevance for others conducting school-based trials. Finally, we outline a number of points for consideration in relation to the delivery of the KAT programme.
Issues requiring further research
Although we do not propose to proceed to an effectiveness trial at this point, we have identified a number of issues which would require additional research should any such trial take place in the future. Some of the methodological issues identified here also have broader relevance for researchers undertaking studies on family communication with primary school-age children.
-
For both primary and secondary outcomes, further work would be needed to identify valid, reliable, sensitive and precise measures suitable for children aged 9–11 years. This could involve additional searches of the literature for suitable measures, qualitative work and piloting of measures with children in the target age group, and validation of the measures.
-
The study has highlighted the challenges of asking primary school-age children to answer questions about alcohol consumption. Alcohol-related questions may require adaptation of wording or presentation in order to avoid the inconsistencies identified in this study.
-
The measures of family communication would need to be reviewed carefully. Ideally, measures designed for, and validated with, children aged 9–11 years should be used to assess intermediate outcomes. Alternatively, existing measures might need to be adapted and validated.
-
Methods are required for collecting information on family structure which would be acceptable to children in this age group, and which would yield useful responses.
-
-
The feasibility and acceptability of collecting follow-up data from pupils in secondary schools, and the response rates which would be achieved, should be assessed. Schools should be asked if they would require evidence of written consent from parents, which would have implications for the use of ‘opt-out’ parental consent at baseline.
Given the low costs of implementation, and its high levels of reach, KAT may be a worthwhile and cost-effective programme, but the size of effect is likely to be so small that a very large sample would be needed to estimate a statistically significant effect, and any trial would, therefore, be prohibitively expensive. In addition, issues concerning accurate measurement of primary and secondary outcomes described in this study would need to be resolved.
Issues which may have general relevance for school-based trials
-
Although rates of parent/carer involvement in the KAT programme were very high, we were not able to engage large numbers in the research element of the trial, and questionnaire completion rates were very low. Based on these findings, it would not be feasible to collect data on secondary outcome and service utilisation from parents in an effectiveness trial using the methods employed in this exploratory trial. Given that data for primary outcomes would be collected from children only, and that secondary outcomes would also be measured in children’s questionnaires, one option would be to remove all parent-based data collection from the trial. Another option would be to invest significant resources into increasing parent questionnaire completion rates, for example by offering a range of alternative response modes. However, the cost of this would probably be prohibitive and, for studies such as KAT that try to promote parental engagement, could have the effect of mimicking some of the intermediate processes, which would be problematic. It would also be very important not to alter parent recruitment methods in ways which could reduce the number of children who take part in the study. A study’s process evaluation could be designed in such a way that sufficient interviews with parents were included to explore potential intervention pathways. These data collection strategies would not provide an estimate of differences between the trial arms in relation to parent-derived outcomes, but they would allow greater understanding of potential mechanisms of action and provide information about the characteristics of parents who engaged with the programme.
-
In designing school-based trials, our findings suggest that it would be essential to build in sufficient time to recruit schools, and to approach them early in the life of the trial, so that intervention group schools had sufficient time to plan for programme delivery. However, while contacting schools well in advance may reduce the likelihood of schools refusing to take part because of time constraints or other projects, it could increase the risk of post-agreement/randomisation drop-out.
-
School recruitment was aided by having the support of a Healthy Schools Team practitioner. Recruitment and retention in school-based trials is likely to be increased by identification of influential figures such as healthy schools practitioners who can encourage schools to participate and remain in a study.
-
Offering incentives to schools to compensate them for the staff time and general inconvenience/disruption caused by trial participation (and staging these throughout a school’s involvement in the research process) may help to increase recruitment and retention rates.
Development and future implementation of the Kids, Adults Together programme: points for consideration
Our findings have indicated that KAT is unlikely to achieve large effect sizes in relation to alcohol-related behaviours, and that it would be unfeasible and poor value to conduct a RCT of the programme, given the large number of schools which would need to be recruited. However, the study has also shown that KAT has valuable assets: in terms of the RE-AIM framework160 it has good reach; challenges in implementation are surmountable; through the stakeholder group we identified a route for adoption and maintenance; and it would be easy to integrate with existing programmes. It is inexpensive to implement and could be cost-effective with a small effect, despite the fact that it is not cost-effective to conduct a trial to detect this effect. Even if the programme is not taken forward in its current form, there are a number of its constituent mechanisms which could be employed in other school-based prevention programmes and activities, particularly those relating to family engagement.
In general, the programme appears to have been delivered as intended in those schools which completed delivery, with the key components implemented, and the core messages conveyed with fidelity. However, there are a number of aspects of the programme manual and its implementation with teachers which could be further enhanced:
-
Although in each school we attempted to run an in-service training (INSET) session for the staff who would be delivering the intervention (and other school staff, where possible), some school staff either had not read all of the programme manual content, or had missed key guidance on how to deliver the intervention which it contained.
-
In at least one of the intervention schools, school staff expected the research team to organise and lead the family fun event, even though we had sought to clearly map out roles and responsibilities at the start of our discussions with school staff.
-
The KAT manual appeared, in general, to provide teachers with a relatively clear guide as to how to deliver the intervention. Some teachers felt that more information and guidance was needed in the manual, but not all staff shared this view.
-
KAT is designed to be relevant to families regardless of whether or not they drink; it promotes prosocial communication about alcohol, but it does not assume that this will always be based on rules and norms relating to drinking at home. However, in at least one school a teacher felt that the programme did not have relevance to Muslim families because they did not drink at home. The programme manual and the INSET training could have given greater guidance in this respect.
-
More generally, the trial has highlighted the challenges of delivering and evaluating an alcohol misuse prevention intervention such as KAT in schools with large numbers of families from ethnic minority backgrounds, in relation to both cultural acceptability and the availability of project materials in multiple languages.
-
The KAT programme achieved high rates of parental involvement. Our findings suggest that the involvement of parents in the intervention is very important because (1) children may be more likely to want to prepare for and attend the family event if they know that their family members will be present; and (2) some of the intended family communication processes may not take place if children attend the family events without their family.
Acknowledgements
Kids, Adults Together study participants
We are grateful to the staff and children, and parents/carers of children, in all schools who took part in the study.
Other assistance
The project benefited from funding provided for implementation of KAT by the Welsh Government and from the expertise of Mrs Ana Koleva-Thompson and Ms Maggie Gregory and their team at the Participant Resource Centre, Cochrane Institute of Primary Care and Public Health.
Thanks to Dr Rebecca Cannings-John, Senior Statistician, South-East Wales Trials Unit, who provided statistical expertise to the project during the absence on leave of the Trial Statistician; Dr Sara Jones (DECIPHer Centre Manager) for assistance with project budget management and accounting; Mrs Cheryl Briscombe (DECIPHer Centre Support Officer) for administrative support and assistance with data collection and input; Mrs Julie Hayward and Miss Elen Jones (fieldworkers, DECIPHer) for assistance with data collections.
Contribution of authors
Dr Jeremy Segrott (Research Fellow in Public Health, DECIPHer) was the lead applicant and chief investigator for the KAT trial. Substantial contributions were made to the overall design of the study; management and conduct of data collections; process evaluation supervision; the statistical analysis plan; and the writing of the background, methods, results and discussion sections of the report.
Mrs Heather Rothwell (Research Associate, DECIPHer) was the study manager; analysed the process evaluation data; and contributed to the conduct of data collections, the statistical analysis plan and the writing of the background, methods, results and discussion sections of the report.
Dr Gillian Hewitt (Research Associate, DECIPHer) updated the literature search and contributed to the writing of the background section of the report.
Dr Rebecca Playle (Senior Statistician, South East Wales Trials Unit) was a co-applicant and lead trial statistician; contributed to the study design; designed and carried out the randomisation; led the writing of the statistical analysis plan; supervised the statistical analysis of the trial data; and contributed to the methods, results and interpretation of the study and report.
Dr Chao Huang [Research Associate (Statistician), South East Wales Trials Unit] undertook the analysis of trial data.
Professor Simon Murphy (Professor in Public Health Improvement, DECIPHer) was a co-applicant; process evaluation supervisor; and contributed to the overall design of the study; and the writing of the background, methods, results and discussion sections of the report.
Professor Laurence Moore [Director, MRC/Chief Scientist Office (CSO) Social and Public Health Sciences Unit] was a co-applicant and contributed to the overall design of the study and the writing of the results and discussion sections of the report.
Professor Matthew Hickman (School of Social and Community Medicine, University of Bristol) was a co-applicant and contributed to the overall design of the study and the writing of the results section of the report.
Mrs Hayley Reed (Involving Young People Research Officer, DECIPHer) contributed to the piloting of the follow-up questionnaire and to the writing of the methods section of the report.
Other contributors
Professor Ceri Phillips (co-applicant, Swansea Centre for Health Economics): Professor Phillips acted as an advisor to the project and provided guidance on key elements of a health economics evaluation which would need to be included an effectiveness trial, which data collection procedures it would be helpful to pilot at exploratory trial stage, and key cost information which needed to be collected.
Mrs Joan Roberts (Health Education Consultant).
Ms Anna Flicker (PhD student, DECIPHer).
Independent members of the study steering committee
Dr Marion Henderson, Chair (Senior Investigator Scientist, MRC/CSO Social and Public Health Sciences Unit, Glasgow), Dr John Foster (Reader, Principal Lecturer, Family Care & Mental Health, University of Greenwich), Mr Chris Roberts (Knowledge and Analytical Services, Welsh Government) and Professor Harry Sumnall (Centre for Public Health Liverpool John Moores University).
Independent members of the stakeholder group
Dr Julie Bishop (Consultant in Public Health, Public Health Wales and DECIPHer), Mrs Gill Crandon (Head Teacher, KAT pilot school), Mr Gareth Hewitt (Head of Substance Misuse Policy & Finance, Welsh Government), Chief Superintendent Julian Knight (Gwent Police), Mrs Angela Latimer (Healthy School Scheme Co-ordinator, Swansea), Mrs Mary MacDonald (National Co-ordinator, Welsh Network of Healthy School Schemes), Mrs Joan Roberts (Health Education consultant), Mrs Linda Roberts (National Co-ordinator, All-Wales Police School Liaison Programme), Ms Alison Thomas (Substance Misuse Policy Division, Welsh Government), Ms Emma Toshack (Pupil Wellbeing Branch, Education and Skills Department, Welsh Government) and Mr Lyn Webber, KAT programme developer (Regional Drug Interventions Commissioner, Torfaen County).
Publication
Segrott J, Rothwell H, Pignatelli I, Playle R, Hewitt G, Huang C, et al. Exploratory trial of a school-based alcohol prevention intervention. Health Educ 2015; in press.
Data sharing statement
Requests to access available data should be made to the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Segrott J, Rothwell H, Pignatelli I, Playle R, Hewitt G, Huang S. Exploratory trial of a school-based alcohol prevention intervention. Health Educ 2015.
- Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009;373:2223-33. http://dx.doi.org/10.1016/S0140-6736(09)60746-7.
- Booth A, Meier P, Stockwell T, Sutton A, Wilkinson A, Wong R. Independent Review of the Effects of Alcohol Pricing and Promotion. Part A: Systematic Reviews. Sheffield: ScHARR, University of Sheffield; 2008.
- BMA Board of Science . Reducing the Affordability of Alcohol: A Briefing from the BMA Board of Science 2012.
- Reducing Alcohol Harm: Health Services in England for Alcohol Misuse. London: The Stationery Office; 2008.
- Smith L, Foxcroft DR. Drinking in the UK: An Exploration of Trends. York: Joseph Rowntree Foundation; 2009.
- Bellis M, Hughes K, Morleo M, Tocque K, Hughes S, Allen T, et al. Predictors of risky alcohol consumption in schoolchildren and their implications for preventing alcohol-related harm. Subst Abuse Treat Prev Policy 2007;2. http://dx.doi.org/10.1186/1747-597X-2-15.
- Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Robert C, et al. Social Determinants of Health and Well-Being Among Young People. Health Behaviour in School-aged Children (HBSC) Study: International Report from the 2009/2010 Survey. Copenhagen: WHO Regional Office for Europe; 2012.
- Arria A, Kuhn V, Caldeira K, O’Grady K, Vincent K, Wish E. High school drinking mediates the relationship between parental monitoring and college drinking: a longitudinal analysis. Subst Abuse Treat Prev Policy 2008;3. http://dx.doi.org/10.1186/1747-597X-3-6.
- The Alcohol Harm Reduction Group . No Half-Measures: A Report on the Impact of Alcohol Misuse on the Work of Emergency Service and Emergency Healthcare Workers 2003.
- Wynn SR, Schulenberg J, Kloska DD, Laetz VB. The mediating influence of refusal skills in preventing adolescent alcohol misuse. J Sch Health 1997;67:390-5. http://dx.doi.org/10.1111/j.1746-1561.1997.tb07183.x.
- Ward B, Snow P. The role of families in preventing alcohol-related harm among young people. Prev Res Q 2008. www.druginfo.adf.org.au/attachments/345_PRQ05Jun08_final.pdf (accessed 19 January 2015).
- Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Arch Pediatr Adolesc Med 2006;160:739-46. http://dx.doi.org/10.1001/archpedi.160.7.739.
- Hawkins JD, Graham JW, Maguin E, Abbott R, Hill KG, Catalano RF. Exploring the effects of age of alcohol use initiation and psychosocial risk factors on subsequent alcohol misuse. J Stud Alcohol 1997;58:280-90.
- Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev 1993;100:674-701. http://dx.doi.org/10.1037/0033-295X.100.4.674.
- Fuller E. Smoking, Drinking and Drug Use Among Young People in England in 2011. London: NatCen Social Research; 2012.
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Behav 1988;15:351-77. http://dx.doi.org/10.1177/109019818801500401.
- Moore L, de Silva-Sanigorski A, Moore SN. A socio-ecological perspective on behavioural interventions to influence food choice in schools: alternative, complementary or synergistic?. Public Health Nutr 2013;16:1000-5. http://dx.doi.org/10.1017/S1368980012005605.
- Velleman R. Influences on How Children and Young People Learn About and Behave Towards Alcohol. A Review of the Literature for the Joseph Rowntree Foundation (Part One). York: Joseph Rowntree Foundation; 2009.
- Jones L, Sumnall H, Burrell K, McVeigh J, Bellis MA. Universal Drug Prevention. Liverpool: National Collaborating Centre for Drug Prevention; 2006.
- Bryan H, Austin B, Hailes J, Parsons C, Stow W. On track multi-agency projects in schools and communities: a special relationship. Child Soc 2006;20:40-53. http://dx.doi.org/10.1111/j.1099-0860.2005.00003.x.
- World Health Organization . Ottawa Charter for Health Promotion 1986.
- Langford R, Campbell R, Magnus D, Bonell CP, Murphy SM, Waters E, et al. The WHO Health Promoting School framework for improving the health and well-being of students and staff (Protocol). Cochrane Database Syst Rev 2011;1. http://dx.doi.org/10.1002/14651858.CD008958.pub2.
- Personal and Social Education Framework for 7 to 19-Year-Olds in Wales. Cardiff: Welsh Assembly Government; 2008.
- Social Justice Regeneration Committee . The All Wales Police School Liaison Programme – National Progress Report n.d. www.cynulliad.cymru/Committee%20Documents/SJR%2009-05%20%28p.3%29%20Review%20of%20All%20Wales%20Schools%20Programme%20-%20Annex%20A-15062005-15524/n0000000000000000000000000032247-English.pdf (accessed 19 January 2015).
- Thomas N. The All Wales School Liaison Core Programme 2008. http://swanseapse.blogspot.com/2008/05/all-wales-school-liaison-coreprogramme.html (accessed 8 September 2008).
- School of Education . Evaluation of the All Wales School Liaison Core Programme 2011. www.ed.ac.uk/schools-departments/education/rke/centres-groups/creid/projects/eval-all-wales-school (accessed 19 January 2015).
- Gwent Police . Introduction to the All Wales School Liaison Core Programme 2012. http://corporate.gwent.police.uk/fileadmin/documents/general/AWSLCPReport2012.pdf (accessed 15 December 2014).
- Petrie J, Bunn F, Byrne G. Parenting programmes for preventing tobacco, alcohol or drugs misuse in children < 18: a systematic review. Health Educ Res 2007;22:177-91. http://dx.doi.org/10.1093/her/cyl061.
- Marlatt GA, Witkiewitz K. Harm reduction approaches to alcohol use: health promotion, prevention, and treatment. Addict Behav 2002;27:867-86. http://dx.doi.org/10.1016/S0306-4603(02)00294-0.
- Lloyd C, Joyce R, Hurry J, Ashton M. The effectiveness of primary school drug education. Drug Educ Prev Policy 2000;7:109-26. http://dx.doi.org/10.1080/713660098.
- Dishion TJ, Kavanagh K. A multilevel approach to family-centered prevention in schools: process and outcome. Addict Behav 2000;25:899-911. http://dx.doi.org/10.1016/S0306-4603(00)00126-X.
- Cuijpers P. Three decades of drug prevention research. Drug Educ Prev Policy 2003;10:7-20. http://dx.doi.org/10.1080/0968763021000018900.
- Stigler MH, Neusel E, Perry CL. School-based programs to prevent and reduce alcohol use among youth. Alcohol Res Health 2011;34:157-62. http://dx.doi.org/SPS-AR&H-31.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and Evaluating Complex Interventions: New Guidance. London: Medical Research Council; 2008.
- van den Broucke S. Theory-informed health promotion: seeing the bigger picture by looking at the details. Health Promot Int 2012;27:143-7. http://dx.doi.org/10.1093/heapro/das018.
- Stokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promot 1996;10:282-98. http://dx.doi.org/10.4278/0890-1171-10.4.282.
- Logic Model Development Guide. Battle Creek, MI: W.K. Kellogg Foundation; 2004.
- Nation N, Crusto C, Wandersman A, Kumpfer KL, Seybolt D, Morrissey-Kane E, et al. What works in prevention. Principles of effective prevention programs. Am Psychol 2003;58:449-56. http://dx.doi.org/10.1037/0003-066X.58.6-7.449.
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull 1992;112:64-105. http://dx.doi.org/10.1037/0033-2909.112.1.64.
- Cuijpers P. Effective ingredients of school-based drug prevention programs: a systematic review. Addict Behav 2002;27:1009-23. http://dx.doi.org/10.1016/S0306-4603(02)00295-2.
- Donaldson SI, Sussman S, MacKinnon DP, Severson HH, Glynn T, Stone EJ. Drug abuse prevention programming: do we know what content works?. Am Behav Scientist 1996;39:868-83. http://dx.doi.org/10.1177/0002764296039007008.
- Tobler NS, Roona MR, Ochshorn P, Marshall DG, Streke AV, Stackpole KM. School-based adolescent drug prevention programs: 1998 meta-analysis. J Prim Prev 2000;20:275-336. http://dx.doi.org/10.1023/A:1021314704811.
- Black DR, Tobler NS, Sciacca JP. Peer helping/involvement: an efficacious way to meet the challenge of reducing alcohol, tobacco, and other drug use among youth?. J Sch Health 1998;68:87-93. http://dx.doi.org/10.1111/j.1746-1561.1998.tb03488.x.
- Midford R, Cahill H, Ramsden R, Davenport G, Venning Lynne, Lester L, et al. Alcohol prevention: what can be expected of a harm reduction focused school drug education programme?. Drug Educ Prev Policy 2012;19:102-10. http://dx.doi.org/10.3109/09687637.2011.639412.
- Flay BR. Approaches to substance use prevention utilizing school curriculum plus social environment change. Addict Behav 2000;25:861-85. http://dx.doi.org/10.1016/S0306-4603(00)00130-1.
- Rowland B, Toumbourou JW, Osborn A, Smith R, Hall JK, Kremer P, et al. A clustered randomised trial examining the effect of social marketing and community mobilisation on the age of uptake and levels of alcohol consumption by Australian adolescents. BMJ Open 2013;3. http://dx.doi.org/10.1136/bmjopen-2012-002423.
- Goodall J, Vorhaus J. Review of Best Practice in Parental Engagement. London: Department for Education; 2011.
- Good Practice in Parental Involvement in Primary Schools. Cardiff: Estyn; 2009.
- Foxcroft DR, Tsertsvadze A. Universal alcohol misuse prevention programmes for children and adolescents: Cochrane systematic reviews. Perspect Public Health 2012;132:128-34. http://dx.doi.org/10.1177/1757913912443487.
- Interventions in Schools to Prevent and Reduce Alcohol Use Among Children and Young People. London: NICE; 2007.
- Velleman RDB, Templeton LJ, Copello AG. The role of the family in preventing and intervening with substance use and misuse: a comprehensive review of family interventions, with a focus on young people. Drug Alcohol Rev 2005;24:93-109. http://dx.doi.org/10.1080/09595230500167478.
- Perry CL, Williams CL, Veblen-Mortenson S, Toomey TL, Komro KA, Anstine PS, et al. Project Northland: outcomes of a communitywide alcohol use prevention program during early adolescence. Am J Public Health 1996;86:956-65. http://dx.doi.org/10.2105/AJPH.86.7.956.
- Jackson C, Ennett ST, Dickinson DM, Bowling JM. Attributes that differentiate children who sip alcohol from abstinent peers. J Youth Adolesc 2013;42:1687-95. http://dx.doi.org/10.1007/s10964-012-9870-8.
- Spoth RL, Redmond C, Trudeau L, Shin C. Longitudinal substance initiation outcomes for a universal preventive intervention combining family and school programs. Psychol Addict Behav 2002;16:129-34. http://dx.doi.org/10.1037/0893-164X.16.2.129.
- Garmiene A, Zemaitiene N, Zaborskis A. Family time, parental behaviour model and the initiation of smoking and alcohol use by ten-year-old children: an epidemiological study in Kaunas, Lithuania. BMC Public Health 2006;6. http://dx.doi.org/10.1186/1471-2458-6-287.
- De Looze M, Van den Eijnden R, Verdurmen J, Vermeulen-Smit E, Schulten I, Vollebergh W, et al. Parenting practices and adolescent risk behavior: rules on smoking and drinking also predict cannabis use and early sexual debut. Prev Sci 2012;13:594-60. http://dx.doi.org/10.1007/s11121-012-0286-1.
- Stattin H, Kerr M. Parental monitoring: a reinterpretation. Child Dev 2000;71:1072-85. http://dx.doi.org/10.1111/1467-8624.00210.
- Garvey C, Julion W, Fogg L, Kratovil A, Gross D. Measuring participation in a prevention trial with parents of young children. Res Nurs Health 2006;29:212-22. http://dx.doi.org/10.1002/nur.20127.
- Axford N, Lehtonen M, Kaoukji D, Tobin K, Berry V. Engaging parents in parenting programs: lessons from research and practice. Child Youth Serv Rev 2012;34:2061-71. http://dx.doi.org/10.1016/j.childyouth.2012.06.011.
- Faggiano F, Vigna-Taglianti FD, Versino E, Zambon A, Borraccino A, Lemma P. School-based prevention for illicit drugs’ use. Cochrane Database Syst Rev 2005;18.
- Stead M, Stradling B, MacKintosh AM, MacNeil M, Minty S, Eadie D, et al. Delivery of the Blueprint Programme. Stirling: Institute for Social Marketing; 2007.
- Faggiano F, Vigna-Taglianti F, Burkhart G, Bohrn K, Cuomo L, Gregori D, et al. The effectiveness of a school-based substance abuse prevention program: 18-month follow-up of the EU–Dap cluster randomized controlled trial. Drug Alcohol Depend 2010;108:56-64. http://dx.doi.org/10.1016/j.drugalcdep.2009.11.018.
- Van Der Kreeft P, Wiborg G, Galanti MR, Siliquini R, Bohm K, Scatigna M, et al. ‘Unplugged’: a new European school programme against substance abuse. Drug Educ Prev Policy 2009;16:167-81. http://dx.doi.org/10.1080/09687630701731189.
- Coombes L, Allen D, Marsh M, Foxcroft DR. Implementation of the Strengthening Families Program (SFP)10–14 in Barnsley: The Perspectives of Facilitators and Families. Oxford: Oxford Brookes University; 2006.
- Mihalic S, Irwin K. Blueprints for Violence Prevention. From research to real-world settings – factors influencing the successful replication of model programs. Youth Violence Juv Justice 2003;1:307-29. http://dx.doi.org/10.1177/1541204003255841.
- Spoth R, Redmond C. Research on family engagement in preventive interventions: toward improved use of scientific findings in primary prevention practice. J Prim Prev 2000;21:267-84. http://dx.doi.org/10.1023/A:1007039421026.
- Redmond C, Spoth R, Trudeau L. Family- and community-level predictors of parent support seeking. J Community Psychol 2002;30:153-71. http://dx.doi.org/10.1002/jcop.10002.
- Guyll M, Spoth R, Redmond C. The effects of incentives and research requirements on participation rates for a community-based preventive intervention research study. J Prim Prev 2003;24:25-41. http://dx.doi.org/10.1023/A:1025023600517.
- Wiggins M, Bonell C, Sawtell M, Austerberry H, Burchett H, Allen E, et al. Health outcomes of youth development programme in England: prospective matched comparison study. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b2534.
- Bayer JK, Hiscock H, Morton-Allen E, Ukoumunne OC, Wake M. Prevention of mental health problems: rationale for a universal approach. Arch Dis Child 2007;92:34-8. http://dx.doi.org/10.1136/adc.2006.100776.
- Rose G. Sick individuals and sick populations. Int J Epidemiol 2001;30:427-32. http://dx.doi.org/10.1093/ije/30.3.427.
- Catalano RF, Hawkins JD, Hawkins JD. Delinquency and Crime: Current Theories. Cambridge: Cambridge University Press; 1996.
- Lonczak HS, Huang B, Catalano RF, Hawkins JD, Hill KG, Abbott RD, et al. The social predictors of adolescent alcohol misuse: a test of the social development model. J Stud Alcohol 2001;62:179-89.
- Spoth RL, Guyll M, Day SX. Universal family-focused interventions in alcohol-use disorder prevention: cost-effectiveness and cost-benefit analyses of two interventions. J Stud Alcohol 1999;63:219-28.
- Hawkins JD, Catalano RF, Kosterman R, Abbott R, Hill KG. Preventing adolescent health-risk behaviors by strengthening protection during childhood. Arch Pediatr Adolesc Med 1999;153:226-34. http://dx.doi.org/10.1001/archpedi.153.3.226.
- Cleveland MJ, Feinberg ME, Bontempo DE, Greenberg MT. The role of risk and protective factors in substance use across adolescence. J Adolesc Health 2008;43:157-64. http://dx.doi.org/10.1016/j.jadohealth.2008.01.015.
- Catalano RF, Park J, Harachi TW, Haggerty KP, Abbott RD, Hawkins JD, et al. Integrated Developmental and Life-Course Theories of Offending. Piscataway NJ: Transaction Publishers; 2005.
- Schor EL. Adolescent alcohol use: social determinants and the case for early family-centered prevention. Family-focused prevention of adolescent drinking. Bull N Y Acad Med 1996;73:335-56.
- Castro FG, Barrera M, Martinez CR. The cultural adaptation of prevention interventions: resolving tensions between fidelity and fit. Prev Sci 2004;5:41-5. http://dx.doi.org/10.1023/B:PREV.0000013980.12412.cd.
- Ferrer-Wreder L, Sundell K, Mansoory S. Tinkering with perfection: theory development in the intervention cultural adaptation field. Child Youth Care Forum 2012;41:149-71. http://dx.doi.org/10.1007/s10566-011-9162-6.
- Spoth R, Greenberg M, Turrisi R. Preventive interventions addressing underage drinking: state of the evidence and steps towards public health impact. Pediatrics 2008;121:S311-S36. http://dx.doi.org/10.1542/peds.2007-2243E.
- Miller BA, Aalborg AE, Byrnes HF, Bauman K, Spoth R. Parent and child characteristics related to chosen adolescent alcohol and drug prevention program. Health Educ Res 2012;27:1-13. http://dx.doi.org/10.1093/her/cyr109.
- Quinn WH, Hall DB, Smith EP, Rabiner D. Predictors of family participation in a multiple family group intervention for aggressive middle school students. J Community Psychol 2010;38:227-44. http://dx.doi.org/10.1002/jcop.20361.
- Bruzzese J-M, Gallagher R, McCann-Doyle S, Reiss PT, Wijetunga NA. Effective methods to improve recruitment and retention in school-based substance use prevention studies. J Sch Health 2009;79:400-7. http://dx.doi.org/10.1111/j.1746-1561.2009.00427.x.
- Heinrichs N, Bertram H, Kuschel A, Hahlweg K. Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: barriers to research and program participation. Prev Sci 2005;6:275-86. http://dx.doi.org/10.1007/s11121-005-0006-1.
- Erebus International . Review of the Effectiveness of the Parents, Adults, Kids Together (PAKT) Program: Draft Final Report 2007.
- Riesch SK, Brown RL, Anderson LS, Wang K, Canty-Mitchell J, Johnson DL. Strengthening families program (10–14): effects on the family environment. Western J Nurs Res 2012;34:340-76. http://dx.doi.org/10.1177/0193945911399108.
- Tripodi SJ, Bender K, Litschge C, Vaughn MG. Interventions for reducing adolescent alcohol abuse: a meta-analytic review. Arch Pediatr Adolesc Med 2010;164:85-91. http://dx.doi.org/10.1001/archpediatrics.2009.235.
- Rothwell H, Segrott J. Preventing alcohol misuse in young people aged 9–11 years through promoting family communication: an exploratory evaluation of the Kids, Adults Together (KAT) programme. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-810.
- Hawkins JD, Weis JG. The social development model: an integrated approach to delinquency prevention. J Prim Prev 1985;6:73-97. http://dx.doi.org/10.1007/BF01325432.
- Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. BMJ 2000;321:694-6. http://dx.doi.org/10.1136/bmj.321.7262.694.
- Barnes HL, Olson DH. Parent-adolescent communication and the circumplex model. Child Dev 1985;56:438-47. http://dx.doi.org/10.2307/1129732.
- Olson DH, Gorall DM. FACES IV & the Circumplex Model. St. Paul, MN: University of Minnesota; 2006.
- Olson DH, Barnes H. Family Communication 2012. www.facesiv.com/pdf/4.communication.pdf (accessed 19 January 2015).
- Armsden G, Greenberg MT. Inventory of Parent and Peer Attachment (IPPA) 2009. www.prevention.psu.edu/media/prc/files/IPPAManualDecember2013.pdf (accessed 25 February 2015).
- Nash SG, McQueen A, Bray JH. Pathways to adolescent alcohol use: family environment, peer influence, and parental expectations. J Adolesc Health 2005;37:19-28. http://dx.doi.org/10.1016/j.jadohealth.2004.06.004.
- Health Behaviour in School-aged Children: A WHO Cross-National Collaborative Study (HBSC International Report from the 2001/02 Survey). Copenhagen: World Health Organization; 2004.
- Mares SHW, Van Der Vorst H, Vermeulen-Smit E, Lichtwarck-Aschoff A, Verdurmen JEE, Engels RCME. Results of the ‘in control: no alcohol!’ pilot study. Health Educ Res 2012;27:214-25. http://dx.doi.org/10.1093/her/cyr081.
- Litrownik AJ, Elder JP, Campbell NR, Ayala GX, Slymen DJ, Parra-Medina D, et al. Evaluation of a tobacco and alcohol use prevention program for hispanic migrant adolescents: promoting the protective factor of parent–child communication. Prev Med 2000;31:124-33. http://dx.doi.org/10.1006/pmed.2000.0698.
- Ennett ST, Bauman KE, Foshee VA, Pemberton M, Hicks KA. Parent-child communication about adolescent tobacco and alcohol use: what do parents say and does it affect youth behavior?. J Marriage Fam 2001;63:48-62. http://dx.doi.org/10.1111/j.1741-3737.2001.00048.x.
- Wills TA, Gibbons FX, Gerrard M, Murry VM, Brody GH. Family communication and religiosity related to substance use and sexual behavior in early adolescence: a test for pathways through self-control and prototype perceptions. Psychol Addict Behav 2003;17:312-23. http://dx.doi.org/10.1037/0893-164X.17.4.312.
- Watt RG, Draper AK, Ohly HR, Rees G, Pikhart H, Cooke L, et al. Methodological development of an exploratory randomised controlled trial of an early years’ nutrition intervention: the CHERRY programme (Choosing Healthy Eating when Really Young). Matern Child Nutr 2014;10:280-94. http://dx.doi.org/10.1111/mcn.12061.
- Watt RG, Hayter AKM, Ohly HR, Hynek P, Draper AK, Crawley H, et al. Exploratory and Developmental Trial of a Family Centred Nutrition Intervention Delivered in Children’s Centres n.d.
- Lloyd JJ, Wyatt KM, Creanor S. Behavioural and weight status outcomes from an exploratory trial of the Healthy Lifestyles Programme (HeLP): a novel school-based obesity prevention programme. BMJ Open 2012;2. http://dx.doi.org/10.1136/bmjopen-2011-000390.
- Bonell C, Fletcher A, Morton M, Lorenc T, Moore L. Realist randomised controlled trials: a new approach to evaluating complex public health interventions. Soc Sci Med 2012;75:2299-306. http://dx.doi.org/10.1016/j.socscimed.2012.08.032.
- Valente TW, Rice RE, Atkin CK. Public Communication Campaigns. Thousand Oaks, CA: Sage Publications Inc.; 2001.
- Hawe P, Shiell A, Riley T. Complex interventions: how ‘out of control’ can a randomised controlled trial be?. BMJ 2004;328. http://dx.doi.org/10.1136/bmj.328.7455.1561.
- Keys to Alcohol for Children aged 7 to 11 Years Old. Manchester: TACADE; 2010.
- Rothwell H, Segrott J. Preventing alcohol misuse in young people aged 9–11 years through promoting family communication: an exploratory evaluation of the Kids, Adults Together (KAT) Programme. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-810.
- Junghans C, Jones M. Consent bias in research: how to avoid it. Heart 2007;93:1024-5. http://dx.doi.org/10.1136/hrt.2007.120113.
- Junghans C, Feder G, Hemingway H, Timmis A, Jones M. Recruiting patients to medical research: double blind randomised trial of ‘opt-in’ versus ‘opt-out’ strategies. BMJ 2005;331. http://dx.doi.org/10.1136/bmj.38583.625613.AE.
- Berry JG, Ryan P, Gold MS, Braunack-Mayer AJ, Duszynski KM. Vaccine Assessment Using Linked Data Working Group . A randomised controlled trial to compare opt-in and opt-out parental consent for childhood vaccine safety surveillance using data linkage. J Med Ethics 2012;38:619-25. http://dx.doi.org/10.1136/medethics-2011-100145.
- Treweek S, Mitchell E, Pitkethly M, Cook J, Kjeldstrøm M, Taskila T, et al. Strategies to improve recruitment to randomised controlled trials. Cochrane Database Syst Rev 2010;1. http://dx.doi.org/10.1002/14651858.MR000013.pub4.
- Data Protection Act 1998. London: The Stationery Office; 1998.
- Medical Research Council. Developing and Evaluating Complex Interventions: New Guidance 2008. www.mrc.ac.uk/documents/pdf/complex-interventions-guidance/ (accessed 19 January 2015).
- Best Research for Best Health. London: Department of Health; 2006.
- Research Governance Framework for Health and Social Care. London: Department of Health; 2005.
- Foxcroft DR, Ireland D, Lister-Sharp DJ, Lowe G, Breen R. Longer-term primary prevention for alcohol misuse in young people: a systematic review. Addiction 2003;98:397-411. http://dx.doi.org/10.1046/j.1360-0443.2003.00355.x.
- Fuller E. Smoking, Drinking and Drug Use Among Young People in England in 2008 2009. www.hscic.gov.uk/pubs/sddo8fullreport (accessed 19 January 2015).
- Griebler R, Molcho M, Samdal O, Inchley J, Dür W, Currie C. Health Behaviour in School-Aged Children: A World Health Organization Cross-National Study. Research Protocol for the 2009/2010 Study. Vienna and Edinburgh: LBIHPR and CAHRU; 2010.
- The Kidscreen Group Europe . KIDSCREEN Questionnaire 2013. www.kidscreen.org/english/questionnaires/kidscreen-52-long-version/ (accessed 25 February 2015).
- Miller-Day M, Kam JA. More than just openness: developing and validating a measure of targeted parent–child communication about alcohol. Health Comm 2010;25:293-302. http://dx.doi.org/10.1080/10410231003698952.
- Barnes H, Olson D, Olson D, McCubbin H, Barnes H, Larsen A, et al. Family Inventories. St Paul, MN: University of Minnesota; 1982.
- Collins RL, Parks GA, Marlatt GA. Social determinants of alcohol consumption: the effects of social interaction and model status on the self-administration of alcohol. J Consult Clin Psychol 1985;53:189-200. http://dx.doi.org/10.1037/0022-006X.53.2.189.
- Neighbours C, Dillard AJ, Lewis MA, Bergstrom RL, Neil TA. Normative misperceptions and temporal precedence of perceived norms and drinking. J Stud Alcohol 2006;67:290-9.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc Sci Med 2008;66:1429-36. http://dx.doi.org/10.1016/j.socscimed.2007.11.024.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indicat Res 2006;78:473-87. http://dx.doi.org/10.1007/s11205-005-1607-6.
- Holstein BE, Currie C, Boyce W, Damsgaard MT, Gobina I, Kökönyei G, et al. Socio-economic inequality in multiple health complaints among adolescents: international comparative study in 37 countries. Int J Public Health 2009;54:S260-70. http://dx.doi.org/10.1007/s00038-009-5418-4.
- Cardiff University’s Child Protection Procedures – Interim Guidance for: Researchers Working with Children and Young People. n.d.
- Raab GM, Butcher I. Balance in cluster randomized trials. Stat Med 2001;20:351-65. http://dx.doi.org/10.1002/1097-0258(20010215)20:3<351::AID-SIM797>3.0.CO;2-C.
- Carter B, Hood K. Balance algorithm for cluster randomized trials. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-65.
- Trochim WM. The Research Methods Knowledge Base. New York, NY: Cornell Custom Publishing; 1999.
- Resnicow K, Davis M, Smith M, Lazarus-Yaroch A, Baranowski T, Baranowski J, et al. How best to measure implementation of school health curricula: a comparison of three measures. Health Educ Res 1998;13:239-50. http://dx.doi.org/10.1093/her/13.2.239.
- DeWalt KM, DeWalt BR. Participant Observation: A Guide for Fieldworkers. Oxford: AltaMira Press; 2002.
- Powell RA, Single HM. Focus groups. Int J Qual Health Care 1996;8:499-504. http://dx.doi.org/10.1093/intqhc/8.5.499.
- Heary CM, Hennessy E. The use of focus group interviews in pediatric health care research. J Pediatr Psychol 2002;27:47-5. http://dx.doi.org/10.1093/jpepsy/27.1.47.
- Lewis A. Group child interviews as a research tool. Br Educ Res J 1992;18:413-21. http://dx.doi.org/10.1080/0141192920180407.
- Reed J, Payton VR. Focus groups: issues of analysis and interpretation. J Adv Nurs 1997;26:765-71. http://dx.doi.org/10.1046/j.1365-2648.1997.00395.x.
- Sturges JE, Hanrahan KJ. Comparing telephone and face-to-face qualitative interviewing: a research note. Qual Res 2004;4:107-18. http://dx.doi.org/10.1177/1468794104041110.
- Maxwell JA. Qualitative Research Design: An Interactive Approach. Thousand Oaks, CA: Sage; 1996.
- Ratcliff D. Validity and Reliability in Qualitative Research 1995. http://qualitativeresearch.ratcliffs.net/Validity.pdf.
- Laghi F, Baiocco R, Lonigro A, Capacchione G, Baumgartner E. Family functioning and binge drinking among Italian adolescents. J Health Psychol 2012;17:1132-41. http://dx.doi.org/10.1177/1359105311430005.
- Poff RA, Zabriskie RB, Townsend JA. Modeling family leisure and related family constructs: a national study of U.S. parent and youth perspectives. J Leis Res 2010;42:365-91.
- Smith KM, Freeman PA, Zabriskie RB. An examination of family communication within the core and balance model of family leisure functioning. Fam Relat 2009;58:79-90. http://dx.doi.org/10.1111/j.1741-3729.2008.00536.x.
- Gillison F, Standage M, Skevington S. Changes in quality of life and psychological need satisfaction following the transition to secondary school. Br J Educ Psychol 2008;78:149-62. http://dx.doi.org/10.1348/000709907X209863.
- Gillison F, Skevington S, Standage M. Exploring response shift in the quality of life of healthy adolescents over 1 year. Qual Life Res 2008;17:997-1008. http://dx.doi.org/10.1007/s11136-008-9373-y.
- Palacio-Vieira JA, Villalonga-Olives E, Valderas JM, Espallargues M, Herdman M, Berra S, et al. Changes in health-related quality of life (HRQoL) in a population-based sample of children and adolescents after 3 years of follow-up. Qual Life Res 2008;17:1207-15. http://dx.doi.org/10.1007/s11136-008-9405-7.
- Karasimopoulou S, Derri V, Zervoudaki E. Children’s perceptions about their health-related quality of life: effects of a health education–social skills program. Health Educ Res 2012;27:780-93. http://dx.doi.org/10.1093/her/cys089.
- van der Vorst H, Engels RCM, Meeus W, Deković M, Van Leeuwe J. The role of alcohol-specific socialization in adolescents’ drinking behaviour. Addiction 2005;100:1464-76.
- McCrone T, Teeman D, Featherstone G, Rudd P, Ahmad S, Thompson H. Change Engagement Comparative Study: Final Report. Slough: NFER; 2008.
- The National Strategies: A Review of Impact. Manchester: OFSTED; 2010.
- Wanless SB, Patton CL, Rimm-Kaufman SE, Deutsch NL. Setting-level influences on implementation of the responsive classroom approach. Prev Sci 2013;14:40-51. http://dx.doi.org/10.1007/s11121-012-0294-1.
- Machin S, McNally S. The Literacy Hour. London: Centre for the Economics of Education, London School of Economics; 2004.
- Graham A, Powell M, Taylor N, Anderson D, Fitzgerald R. Ethical Research Involving Children. Florence: UNICEF Office of Research – Innocenti; 2013.
- Foxcroft DR, Ireland D, Lowe G, Breen R. Primary prevention for alcohol misuse in young people. Cochrane Database Syst Rev 2002;3.
- Funch DP, Marshall JR. Measuring life stress – factors affecting fall-off in the reporting of life events. J Health Soc Behav 1984;25:453-64. http://dx.doi.org/10.2307/2136382.
- McCord J. Cures that harm: unanticipated outcomes of crime prevention programs. Ann Am Acad Polit Soc Sci 2003;587:16-30. http://dx.doi.org/10.1177/0002716202250781.
- Werch CE, Owen DM. Iatrogenic effects of alcohol and drug prevention programs. J Stud Alcohol 2002;63:581-90.
- Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health 1999;89:1322-7. http://dx.doi.org/10.2105/AJPH.89.9.1322.
- Bodin MC, Strandgerg AK. The Örebro prevention programme revisited: a cluster-randomized effectiveness trial of programme effects on youth drinking. Addiction 2011;106:2134-43. http://dx.doi.org/10.1111/j.1360-0443.2011.03540.x.
- Brody GH, Chen Y-F, Kogan SM, McBride Murry V, Brown AC. Long-term effects of the strong african american families program on youths’ alcohol use. J Consult Clinl Psychol 2010;78:281-5. http://dx.doi.org/10.1037/a0018552.
- Caria MP, Faggiano F, Bellocco R, Galanti MR. EU-Dap Study Group . Effects of a school-based prevention program on european adolescents’ patterns of alcohol use. J Adolesc Health 2011;48:182-8. http://dx.doi.org/10.1016/j.jadohealth.2010.06.003.
- Conrod PJ, O’Leary-Barrett M, Newton N, Topper L, Castellanos-Ryan N, Mackie C, et al. Effectiveness of a selective, personality-targeted prevention program for adolescent alcohol use and misuse. JAMA Psychiatry 2013;70:334-42. http://dx.doi.org/10.1001/jamapsychiatry.2013.651.
- D’Amico EJ, Tucker JS, Miles JNV, Zhou AJ, Shih RA, Green HD. Preventing alcohol use with a voluntary after school program for middle school students: results from a cluster randomized controlled trial of project CHOICE. Prev Sci 2012;13:415-25. http://dx.doi.org/10.1007/s11121-011-0269-7.
- Eddy JJ, Gideonsen MD, McClaflin RR, O’Halloran P, Peardon FA, Radcliffe PL, et al. Reducing alcohol use in youth aged 12–17 years using the strategic prevention framework. J Community Psychol 2012;40:607-20. http://dx.doi.org/10.1002/jcop.21485.
- Evers KE, Paiva AL, Johnson JL, Cummins CO, Prochaska JO, Prochaska JM, et al. Results of a transtheoretical model-based alcohol, tobacco and other drug intervention in middle schools. Addict Behav 2012;37:1009-18. http://dx.doi.org/10.1016/j.addbeh.2012.04.008.
- Fang L, Schinke SP, Cole KCA. Preventing substance use among early asian–american adolescent girls: initial evaluation of a web-based, mother–daughter program. J Adolesc Health 2010;47:529-32. http://dx.doi.org/10.1016/j.jadohealth.2010.03.011.
- Gabrhelik R, Duncan A, Miovsky M, Furr-Holden CDM, Stastna L, Jurystova L. ‘Unplugged’: a school-based randomized control trial to prevent and reduce adolescent substance use in the Czech Republic. Drug Alcohol Depend 2012;124:79-87. http://dx.doi.org/10.1016/j.drugalcdep.2011.12.010.
- Hodder RK, Daly J, Freund M, Bowman J, Hazell T, Wiggers J. A school-based resilience intervention to decrease tobacco, alcohol and marijuana use in high school students. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-722.
- Koning IM, van den Eijnden RJ, Verdurmen JE, Engels RC, Vollebergh WA. Long-term effects of a parent and student intervention on alcohol use in adolescents: a cluster randomized controlled trial. Am J Prev Med 2011;40:541-7. http://dx.doi.org/10.1016/j.amepre.2010.12.030.
- Kovach Clark H, Ringwalt CL, Hanley S, Shamblen SR. Project ALERT’s effects on adolescents’ prodrug beliefs: a replication and extension study. Health Educ Behav 2010;37:357-67. http://dx.doi.org/10.1177/1090198109353283.
- Kupersmidt JB, Scull TM, Weintraub Austin E. Media literacy education for elementary school substance use prevention: study of media detective. Pediatrics 2010;126:525-31. http://dx.doi.org/10.1542/peds.2010-0068.
- Kupersmidt JB, Scull TM, Benson JW. Improving media message interpretation processing skills to promote healthy decision making about substance use: the effects of the middle school media ready curriculum. J Health Comm 2012;17:546-63. http://dx.doi.org/10.1080/10810730.2011.635769.
- Morgenstern M, Wiborg G, Isensee B, Hanewinkel R. School-based alcohol education: results of a cluster-randomized controlled trial. Addiction 2009;104:402-12. http://dx.doi.org/10.1111/j.1360-0443.2008.02471.x.
- Newton NC, Teesson M, Vogl LE, Andrews G. Internet-based prevention for alcohol and cannabis use: final results of the Climate Schools course. Addiction 2010;105:749-59. http://dx.doi.org/10.1111/j.1360-0443.2009.02853.x.
- O’Donnell L, Myint-U A, Duran R, Stueve A. Especially for Daughters: Parent education to address alcohol and sex-related risk taking among urban young adolescent girls. Health Promot Pract 2010;11:70S-8S. http://dx.doi.org/10.1177/1524839909355517.
- Pettersson C, Özdemir M, Eriksson C. Effects of a parental program for preventing underage drinking – The NGO program strong and clear. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-251.
- Schinke SP, Schwinn TM, Fang L. Longitudinal outcomes of an alcohol abuse prevention program for urban adolescents. J Adolesc Health 2010;46:451-7. http://dx.doi.org/10.1016/j.jadohealth.2009.11.208.
- Spaeth M, Weichold K, Silbereisen RK, Wiesner M. Examining the differential effectiveness of a life skills program (IPSY) on alcohol use trajectories in early adolescence. J Consult Clin Psychol 2010;78:334-48. http://dx.doi.org/10.1037/a0019550.
- Spoth R, Redmond C, Shin C, Greenberg M, Feinberg M, Schainker L. PROSPER community–university partnership delivery system effects on substance misuse through 6 1/2 years past baseline from a cluster randomized controlled intervention trial. Prev Med 2013;56:190-6. http://dx.doi.org/10.1016/j.ypmed.2012.12.013.
- Spradley JP. Participant Observation. New York, NY: Holt, Rinehart & Winston; 1980.
Appendix 1 Recently published trials and evaluations of programmes to address alcohol misuse in young people
| Programme name and reference | Age group | Setting, location and focus | Intervention and parental involvement | Theoretical basis | Alcohol or communication outcomes |
|---|---|---|---|---|---|
| Örebro Prevention Programme; Bodin and Strandberg, 2011161 | 13–16 years | School based; Sweden; alcohol only | Six 20-minute presentations during termly teacher-parent meetings. No additional incentives described. Parents encouraged to make written agreements on how to prevent their child drinking. No child component. Parent response rates to evaluation 75%, 70%, 67.6% over 3 years | Not specified | Drunkenness frequency by self-report. No effect at 2-year follow-up |
| Strong African American Families Programme; Brody et al. 2010162 | 11 years | Community based; Georgia, USA; alcohol only | Family-centred programme. Seven consecutive weekly meetings with separate parent and child skill-building curricula and a family curriculum. Sixty-four per cent of families invited to participate did so and 85% of recruited families completed the trial (5.4 years). Recruitment was undertaken by AA community members, not researchers, and AA community members and AA students did the home visits for data collection. Families were paid US$100 at each data collection point | Informed by other family-centred programmes and based on a developmental model of processes through which programme participation might protect rural AA youths from the initiation and escalation of alcohol use | Self-report of ever drinking alcoholic drinks and frequency of consumption in the last month At 65-month follow-up, youths in intervention arm drank 0.68 times in the previous month and youths in control arm drank 1.41 times |
| Unplugged (EU-Dap);64 Caria et al. 2011163 and Faggiano et al. 201063 | 12–14 years | School based; Austria, Belgium, Germany, Greece, Italy, Spain, Sweden; alcohol, tobacco and drugs | Interactive curriculum with knowledge, life skills and normative education components. Delivered in the classroom across 12 weekly lessons. Parents were involved in one of three formats of the programme (5). Three evening workshops 2–3 hours long on parenting skills, substance misuse information and skills to enhance parents’ confidence. Personal invitation signed by study co-ordinator/college principal sent to parents of all students involved. No incentives described. Maximum 28% students’ parents attended any one workshop (average 12 per workshop) (6). Student data were pooled across three intervention groups for analysis | Social influence model | Frequency of alcohol consumption, drunkenness and problem behaviours due to alcohol After 18 months, programme did not modify the risk of being a current or frequent drinker, and a lower prevalence of problem behaviours was seen in only some children, e.g. those who were not drinking at baseline and girls ≤ 12 years. Frequency of drunkenness episodes significantly reduced in intervention arm |
| Adventure; Conrod et al. 2013164 | 13–14 years | School based; London, UK; alcohol and other substances | No parent involvement. Two 90-minute group sessions for each of four high-risk groups of students (sessions differ according to risk group). Sessions focused on personality traits, not problem behaviours so alcohol was a minor focus. Used workbooks and goal setting. High-risk students identified from baseline survey | Personality is a risk factor for alcohol use. Selective preventions targeting specific risk profiles provide coping skills before the onset of drinking behaviours | Alcohol use in last 6 months, binge drinking in last 6 months and severity of alcohol problems in last 6 months After 24 months, risk intervention students drank less and their growth in quantity drunk and binge drinking frequency was lower. Positive herd effects in low-risk students (who attended intervention schools but did not receive the intervention) were observed |
| CHOICE; D’Amico et al. 2012165 | 11–14 years | Middle-school based, but after school; California, USA; alcohol and other drugs | No parent involvement. Voluntary programme; students met once a week after school; 5 × 30-minute sessions that rotate over 12 months; used motivational interviewing to present the curriculum | Social Learning Theory, Decision-making Theory and Self Efficacy Theory | Lifetime and past-month frequency of alcohol use and intention to drink in the next 6 months. Effect seen on lifetime alcohol use only OR = 0.7 |
| Eddy et al. 2012166 Note: before-and-after design, not a trial; repeat cross-sectional surveys |
12–17 years | School, family and community based; Wisconsin, USA; alcohol only | Two family-strengthening programmes were selected for use – Guiding Good Choices (parents with 9- to 14-year-olds) and Staying Connected With Your Teen (parents with 12- to 17-year-olds); both teach parenting strategies for setting and enforcing standards and strengthening family bonds. Rates of participation not provided. No incentives to participate described. All Stars implemented in schools and community settings for sixth to eighth graders (no parent involvement) | Used the Strategic Prevention Framework, a tool for communities seeking to use evidence-based programmes | Self-report age of first alcohol use, past-month alcohol use, ease of obtaining alcohol, binge drinking and perceived parental disapproval of alcohol use. Over 8 years, first use increased from 12.3 to 13.1 years and monthly alcohol use dropped by 8.6% |
| Evers et al. 2012167 | 10–14 years | School based; USA; alcohol, tobacco and other drugs | No parent involvement other than some substance information by post. Pupils did an individualised, interactive computer/internet intervention with three sessions over 3 months | Transtheoretical model of behaviour change | Self-report of lifetime and past-month alcohol use and past-month binge drinking. All substances combined in results. Significant impact at 3 months disappeared by 14 months |
| Fang et al. 2010168 | 10–14 years | Home based; USA; alcohol and other drugs | Nine internet-based sessions which Asian American mothers and daughters did together interactively. Recruitment via a ‘noticeboard’ website and mailings to Asian community services agencies. Eighty-two per cent of those coming forward were eligible and, of those, 64% were entered into the trial. Ninety-six per cent of participants completed the trial. Gift vouchers worth US$20 and US$25 were given at the two data collection points | Family interaction theory | Self-report of alcohol use in last month and intention to use in future; questionnaire items on mother–daughter closeness and communication (Iowa Family Interaction Rating Scale), maternal monitoring and rules At 3 months effect seen on alcohol use, closeness, communication, monitoring and rules |
| Unplugged; Gabrhelik et al. 2012169 | 11–13 years | School based; the Czech Republic; alcohol, tobacco, inhalants and other drugs | No parental involvement. Twelve 45-minute sessions delivered by teachers over a school year; each pupil has their own workbook; interactivity unclear | Comprehensive social influence model | Self-report frequency of drunkenness in past month. No effect |
| Hodder et al. 2011170 Note: before-and-after design, not a trial |
12–16 years | School based; New South Wales, Australia; alcohol, tobacco and marijuana | Interventions tailored to each school and had elements addressing all Health Promoting School areas, including initiatives to increase parent engagement with school. Parents were involved in intervention planning workshops. No information on number of parents involved or incentives provided | Resilience theory | Alcohol use in past 3 months, binge drinking in last month, resilience (empathy, help seeking, self-esteem, communication and cooperation, self-awareness, goals and aspirations) and protection (family connection, prosocial peers, autonomy experience, community connection, school connection, prosocial group) Resilience and protection went up and percentage of students reporting drinking behaviours decreased |
| Koning et al. 2011171 | 11–13 years old | School based; the Netherlands; alcohol only | Parent intervention to encourage restrictive rule setting delivered at a parents’ meeting at the start of the school year with a 20-minute presentation, consensus building around alcohol rules and a leaflet (no additional incentives described); pupil intervention to increase self-control and attitude towards alcohol delivered through four digital lessons (four-arm trial). Parent response rates to the evaluation were 86.1% at the first follow-up and 72.6% at the second | Theory of planned behaviour and Social Cognitive Theory | Self-report onset of weekly drinking in non-drinkers at baseline At 34 months, fewer students had started to drink or drink heavily on a weekly basis in combined intervention group. No effects in pupil/parent-only arms |
| Project Alert; Kovach Clark et al. 2010172 | 11–13 years | School based; USA; alcohol, tobacco and marijuana | No parent involvement. Eleven core lessons in 6th grade and three booster lessons in 7th grade delivered by teachers | Integrates several models of health promotion and behaviour change, including the health belief model and the self-efficacy theory of behaviour change | Self-report of intention to use alcohol in next 6 months, beliefs about alcohol use consequences, normative beliefs, and resistance self-efficacy No effects after 1 year |
| Media Detective; Kupersmidt et al. 2010173 | 7–13 years | School based; North Carolina, USA; alcohol and tobacco | No parent involvement. Ten 45-minute lessons culminating in pupils creating a ‘counter-advert’ | Based on the MIP model designed to increase children’s critical thinking around media messages; MIP draws on social cognitive theory, dual process theories of attitude change and the theory of reasoned action | Self-report of intention to use alcohol after 2 weeks. Results not presented separately from tobacco |
| Media Ready; Kupersmidt et al. 2012174 | 11–14 years | School based; North Carolina, USA; alcohol and tobacco | No parental involvement. Ten 45-minute lessons culminating in pupils creating a ‘counter-advert’ | Based on the MIP model, as above | Self-report of intention to use alcohol in the next year and before age 21 years after 2 weeks. Impact seen on boys only |
| In control: no alcohol! Mares et al. 201299 | 10–13 years | Home based; South Holland, the Netherlands; alcohol only | Focus on alcohol-specific communication, rules (drinking contracts) and monitoring; intervention was five monthly magazines sent to the home with activities for the child and mother to do together, also a website with more information and more games. Two hundred and eighteen out of 892 (24%) mothers returned consent forms and 213 entered the trial. One hundred and ninety (89%) completed the trial. No incentives reported | Based on socialisation and communication theories, namely that parent–child communication is a powerful tool in the socialisation of young adolescents so programme aimed to improve conversation quality; derived from social cognitive theory | Alcohol-specific communication (frequency and quality), alcohol specific rules, non-drinking contract after 5 months (immediately post intervention). Effect seen on frequency of communication, especially in mothers with alcohol problems. Quality of communication only improved in mothers who drank more than average |
| Drug Education in Victorian Schools; Midford et al. 201245 | 13–15 years | School based; Victoria, Australia; alcohol and other drugs | No parental involvement. 12 year 8 and 10 year 9 interactive lesson plans which addressed issues around alcohol, tobacco, marijuana and other drugs | Drew on earlier research and development projects on drug education in Australia. Incorporated elements of effective practice from the literature | Alcohol and other drug use knowledge, attitudes and harms; annual consumption of alcohol, drinking to get drunk, drinking more than planned, drinking in a manner that risks acute harm, communication with parents about alcohol At 20 months, improvements in knowledge, communication with parents, annual consumption, drinking to get drunk and alcohol harms |
| Morgenstern et al. 2009175 | 12–15 years | School based; Schleswig-Holstein, Germany; alcohol only | Four interactive classroom teaching units, a booklet for students and a booklet for parents. Parents therefore not actively recruited to programme and not involved in evaluation | Based on addressing social influences and enhancing motivation to avoid substance use | Alcohol use and alcohol knowledge, attitudes and intentions At 12 months, impact on knowledge, but not attitudes nor intentions. Only positive change in alcohol use was for lifetime binge drinking (OR 0.74) |
| Climate Schools Alcohol and Cannabis Course; Newton et al. 2010176 | 13 years | School based; Sydney, Australia; alcohol and marijuana | No parental involvement. Internet-based intervention with 12 × 40-minute lessons over 6 months; 20 minutes on the computer completed individually and then 20 minutes of teacher-led interactive activity | Consistent with the harm reduction approach and based on the social influence approach, derived from social learning theory | Alcohol knowledge and expectancies, weekly alcohol consumption, frequency of drinking to excess and alcohol-related harms At 12 months, impact seen on alcohol knowledge, weekly consumption and drinking to excess |
| Especially for Daughters; O’Donnell et al. 2010177 | 11–13 years | Home based; New York City, NY, USA; alcohol and sex initiation | Four audio CDs posted to homes every 6 weeks, each containing a drama for parent to listen to. No child component. Recruitment of parents through pupil post. Six hundred and six families expressed an interest, of whom 75% were eligible for the trial. Sixty per cent of eligible families consented. Parents given a portable CD player as an incentive after baseline data collection. Project staff telephoned all parents at least once during the study | Grounded in multiple theories: social development model, theory of planned behaviour, behavioural learning theory, sex theories; parents asked about alcohol-related communication in the evaluation | Alcohol use At 3 months, impact seen on reported alcohol use (OR 0.38) |
| Strong and Clear; Pettersson et al. 2011178 Note: not a randomised control group |
13–16 years | Home based with some meetings held in school; Värmland County, Sweden; alcohol focus | Four types of group and self-administered activities – parent meetings, family dialogues, friend meetings, family meetings (13 activities in all); children involved in some of the activities. Parent response rates to evaluation questionnaires were 69%, 54% and 46% at baseline and two follow-ups. No incentives mentioned | Not well described | Alcohol consumption Suggestion that intervention delayed alcohol debut, but no difference between groups by 27 months. Less drunkenness in intervention group |
| Rowland et al. 201347 | 12 years | School and community based; Australia; alcohol only | Community mobilisation to reduce sale of alcohol to minors and social marketing interventions delivered through schools but targeting parents too, e.g. mail-outs and parents nights. Parents not directly involved in the evaluation | Based on the Communities that Care approach and grounded in social ecological theory. Also integrated behavioural model, a more developed version of the theory of planned behaviour and the theory of reasoned action | Alcohol use Trial ongoing |
| Schinke et al. 2010179 | 9–11 years | Community agency and home based; New York City, NY, USA; alcohol only | Two intervention arms, one with parent involvement on top of computer-based, 10 × 45-minute CD-ROM session intervention for children (interactive exercises, puzzles and games); parent involvement via parallel, reinforcing supplemental materials (printed and video, then CD-ROM and iPod recordings) and a workshop. Both parent and child interventions had booster elements. Parent adherence rates ranged from 50% workshop attendance to 78% digital audio recording. No evaluation data collected from parents | Informed by social learning theory | Alcohol consumption in past 30 days, binge drinking, intentions to drink and alcohol refusal skills At 7 years, interventions had positive impact on the alcohol measures, but there was no additional benefit of the parent component |
| IPSY life skills programme; Spaeth et al. 2010180 | 10–13 years | School based; Thuringia State, Germany; alcohol and tobacco | No parent involvement: teachers deliver 15 interactive classroom sessions in 5th grade with seven booster lessons in 6th and 7th grades | Based on the model for life skills education, developmental psychological models and empirical findings | Alcohol use At 2 years, the intervention decreased the likelihood of drinking and the quantity drunk at each drinking occasion |
| Prosper; Spoth et al. 2013181 | 11–13 years | Family-focused and school-based interventions; Iowa and Pennsylvania, USA; alcohol, tobacco and drugs | School–community–university partnership; communities (including parent representatives) chose their own evidence based interventions and these included SFP10-14, Life Skills Training, Project Alert and All Stars; SFP10-14 involved parents, the other three are delivered in the classroom. Parents not involved in evaluation and participation in intervention not reported. Parent incentives not mentioned | Interventions were theory and evidence based | Past-month and frequency of drunkenness and drink driving After 6.5 years effects observed for drunkenness but not drink driving. Impact for both was greater in higher-risk students |
Appendix 2 Letter to all eligible schools
Appendix 3 Participant information for pupils
Appendix 4 Documents sent to parents in intervention schools
Appendix 5 Commitment form for head teachers
Appendix 6 Documents sent to potential parent interviewees
Appendix 7 Calculation of scores for scales used in questionnaires for Kids, Adults Together research participants
Family Activity Scale: from Health Behaviour in School-aged Children international survey of 11- to 15-year-old schoolchildren121
The scale was included as an optional package in the 2001–2 HBSC survey but we were unable to obtain information on validity, how to create a single summary score for the scale or how deal with missing data for this scale. Therefore, we used only those questionnaire responses where more than half of the items on the scale are filled in. An average score was calculated from the remaining items if validation indicates a single scale. If validation indicated more than one scale, then average scores were calculated for the subscales. Coding was reversed so that higher scores were interpreted as increased family activities.
Quality of parent relations and home life: KIDSCREEN-52 subscale
The scores for this dimension were calculated as the mean of the ratings for the six items. However, no score was computed if there was no response on two or more items. The score was transformed linearly to a 0–100-point scale, with 100 indicating the best quality of life and 0 the worst. The percentages of missing values, mean scores with standard deviation, range of scores and Cronbach’s alpha were calculated. High scores indicate that children feel secure, supported and loved, well understood and well cared-for, and that they feel that parents are available and fair; lower scores indicate the absence of some or all of these qualities in their parents and home.
Targeted Parent–Child Communication about Alcohol Scale
No information about how to score the scale or how to handle missing data was found and it was, therefore, handled in the same way as the Family Activity Scale.
Parent–Child Communication Scale
Validation was carried out on this scale to confirm the three factors previously identified, and summary scores for these factors were calculated as average scores over valid responses. Any questionnaires with missing responses for any single item on this scale were excluded from the validation but included in the score calculation using the valid responses.
Family Communication Scale
Parents:
-
Add all items of the FCS.
-
The sum of these items is the total score.
-
The range of scores is from 10 to 50.
As the score for this scale is summed, rather than averaged over the items, any questionnaires with missing items on this scale had the score set as missing.
| Level | Family communication | Score ranges |
|---|---|---|
| Very high | Family members feel very positive about the quality and quantity of their family communication | 44–50 |
| High | Family members feel good about their family communication and have few concerns | 40–43 |
| Moderate | Family members feel generally good about their family communication, but have some concerns | 36–39 |
| Low | Family members have several concerns about the quality of their family communication | 30–35 |
| Very low | Family members have many concerns about the quality of their family communication | 10–29 |
Pupils:
-
Add all items of the FCS.
-
The sum of these items is the total score.
-
The range of scores is 0–10.
The scoring in the pupils’ questionnaire has been changed from 1–5 to 0–1, which means that total score range is reduced to 0–10. As the score for this scale is summed, rather than averaged over the items, any questionnaires with missing items on this scale will have the score set as missing. Any responses coded 2 to question 8 will be recorded as 1 (true). Score ranges have been adjusted to a 0–10 scale for interpretation.
| Level | Family communication | Score ranges |
|---|---|---|
| Very high | Family members feel very positive about the quality and quantity of their family communication | 9–10 |
| High | Family members feel good about their family communication and have few concerns | 8 |
| Moderate | Family members feel generally good about their family communication, but have some concerns | 7 |
| Low | Family members have several concerns about the quality of their family communication | 6 |
| Very low | Family members have many concerns about the quality of their family communication | 0–5 |
In the follow-up questionnaires for pupils who did not complete baseline questionnaires, only nine questions are included (question 6, ‘The people in my family discuss their ideas and beliefs with each other’, was left out). For these questionnaires, the answers to question 6 were treated as missing data.
Family Affluence Scale
A composite Family Affluence Scale score was calculated (summed) for each child based on his or her responses to these four items. For analysis, we used a three-point ordinal scale, where Family Affluence Scale low (score = 0–2) indicates low affluence, Family Affluence Scale medium (score = 3–5) indicates middle affluence, and Family Affluence Scale high (score = 6–9) indicates high affluence. The Family Affluence Scale score was used as a covariate in the models of alcohol consumption and also for descriptive analysis across socioeconomic status levels. As summary scores for this scale are simply summed, any missing responses to any single items were set to missing for the scale composite summary score.
Appendix 8 Process evaluation tools
Appendix 9 Letter to schools, March 2012
Appendix 10 Demographic data from parents (N = 27) who completed the telephone questionnaire
| Characteristics | Control | Intervention | Overall | |||
|---|---|---|---|---|---|---|
| n | Mean (SD) or % | n | Mean (SD) or % | n | Mean (SD) or % | |
| Sex | ||||||
| Male | 1 | 9.1% | 3 | 18.8% | 4 | 14.8% |
| Female | 10 | 90.9% | 13 | 81.3% | 23 | 85.2% |
| Missing | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% |
| Year of birth | 10 | 38.6 (5.8) | 16 | 44.3 (7.6) | 26 | 42.1 (7.4) |
| Place of birth | ||||||
| Abergavenny | 0 | 1 | 1 | |||
| Bristol | 1 | 0 | 1 | |||
| Caerphilly | 1 | 0 | 1 | |||
| Cardiff | 0 | 1 | 1 | |||
| Essex | 0 | 3 | 2 | |||
| Margate, Kent | 0 | 1 | 1 | |||
| Newport | 7 | 5 | 12 | |||
| North Wales | 0 | 1 | 1 | |||
| Pentaeg | 1 | 0 | 1 | |||
| Pontypool | 0 | 1 | 1 | |||
| Reading | 1 | 1 | 1 | |||
| Somalia | 1 | 0 | 1 | |||
| West Africa | 0 | 1 | 1 | |||
| Missing | 0 | 1 | 1 | |||
| Education | ||||||
| A-level | 1 | 0 | 1 | |||
| Degree level | 1 | 3 | 4 | |||
| GCSE | 1 | 3 | 4 | |||
| Higher education | 1 | 1 | 2 | |||
| No formal qualification | 0 | 1 | 1 | |||
| O-level | 3 | 6 | 9 | |||
| ONC | 3 | 1 | 4 | |||
| Postgraduate degree | 1 | 1 | 2 | |||
| Marriage status | ||||||
| Civil partnership | 0 | 2 | 0 | |||
| Divorced | 2 | 2 | 4 | |||
| Married and living with husband/wife | 6 | 10 | 16 | |||
| Single, never married, in relationship | 1 | 0 | 1 | |||
| Single, never married, not in relationship | 2 | 2 | 4 | |||
| Ethnicity | ||||||
| African | 0 | 1 | 1 | |||
| White and black African | 1 | 0 | 1 | |||
| White British | 10 | 15 | 25 | |||
| Employment | ||||||
| In full-time education | 2 | 0 | 2 | |||
| In full-time paid work | 4 | 3 | 7 | |||
| In part-time paid work | 4 | 6 | 10 | |||
| Out of labour force | 0 | 2 | 2 | |||
| Unemployed | 1 | 3 | 4 | |||
| Missing | 0 | 2 | 2 | |||
List of abbreviations
- CSO
- Chief Scientist Office
- DECIPHer
- Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement
- DVD
- digital versatile disc
- FCS
- Family Communication Scale
- FSM
- free school meal
- HBSC
- Health Behaviour in School-aged Children
- ICC
- intracluster correlation
- INSET
- in-service training
- ITT
- intention to treat
- KAT
- Kids, Adults Together
- MRC
- Medical Research Council
- NIHR
- National Institute for Health Research
- PAKT
- Parents, Adults, Kids Together
- PCCS
- Parent–Child Communication Scale
- RCT
- randomised controlled trial
- SD
- standard deviation
- SDM
- social development model
- SEWTU
- South East Wales Trials Unit
- SFP10–14
- Strengthening Families Programme 10–14
- TPCCAS
- Targeted Parent–Child Communication about Alcohol Scale
- TV
- television