

Notes
Article history
The contractual start date for this research was in July 2017. This article began editorial review in February 2023 and was accepted for publication in April 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Global Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Bhatta et al. This work was produced by Bhatta et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Bhatta et al.
Background
Road traffic crashes (RTCs) are the 12th leading cause of mortality globally, resulting in 1.3 million deaths and over 50 million injuries annually. 1,2 More than 90% of global road traffic injuries (RTIs) and deaths are in low- and middle-income countries (LMICs), where rapid economic growth has been accompanied by increased motorisation and new road development. 3 The road user groups most likely to be involved and injured in traffic crashes, such as pedestrians, cyclists and motorcyclists, make up half of these deaths in LMICs. 3–5
In Nepal, the number of RTCs is increasing rapidly, resulting in many deaths and injuries. 6 Police data in Nepal show an increase in RTCs in recent years, particularly among two-wheeled vehicles such as motorcycles, three-wheeled vehicles such as autorickshaws and four-wheeled vehicles such as cars, buses and autorickshaws. A total of 8890 RTCs were reported in the fiscal year 2011–2, which rose to 15,554 in 2019–20. 7 Nepal traffic police data also show that the mortality rate due to RTIs almost doubled from 4 per 100,000 population in 2001 to 7 per 100,000 population in 2012. 8 However, these figures are likely to underestimate the actual number of casualties occurring in Nepal because only those crashes with severe injuries or property damage, or those involving disputes, are generally reported and recorded in the traffic police office. 9
Road traffic crashes were estimated to be the 10th leading cause of death in Nepal in 2019, with a rate of 16.3 deaths per 100,000 population. 10,11 The main causes are reported to be related to driver behaviour, including ‘carelessness’ (83%), ‘speeding’ (10%), ‘using alcohol’ (2%) and ‘overtaking’ (2%). 11–13 There is incomplete analysis of RTIs in Nepal in the last three World Health Organization (WHO) global status reports on road safety, with an absence of reporting of crashes and crash casualties by vehicle type or type of road user3–5 – essential information to inform preventive action.
Aims
To better understand the gap in the evidence relating to the epidemiology of RTCs and injuries in Nepal, this study aimed to critically analyse routinely collected traffic police data in one district to identify the road user groups most likely to be involved and injured in traffic crashes in this part of the country. The study was part of a broader body of research to improve injury prevention and prehospital injury care in Nepal, funded through a NIHR Global Health Research Group award to establish the Nepal Injury Research Centre in Kathmandu (NIHR award reference: 16/137/49).
Methods
In Nepal, traffic police officers keep the record of RTC in a paper register. Once notified of a crash, local traffic police officers are dispatched to manage the scene, support the care of victims and enable the resumption of traffic flow. At the scene, the officer sketches or photographs the crash site and makes notes about the crash from witnesses and their own observation. These details are then entered into a paper register at the local traffic police station/posts. The local traffic police stations/posts send the details to the local, or Ilaka Traffic Police Office (ITPO). The ITPO keeps the records and sends a copy to the District Traffic Police Office (DTPO). The DTPO maintains all the records of the crashes within the district. The crash details include information such as the registration number of the involved vehicles; vehicle travel direction; number of passengers in each vehicle; number of injured people; their age; details about the injury and the name of the hospital where they have been sent for treatment. We conducted a retrospective analysis of secondary data from the DTPO, Makwanpur, covering two periods: April 2017–March 2018 and May 2019–April 2020. Analysis of two periods enabled a comparison over time. Data from the second period were also used in a separate study. 9 The study location was chosen because it contains two major highways in Nepal: the East–West Highway and the North–South Road between Kathmandu and the Indian border. 13 These highways serve a significant portion of Nepal’s freight and passenger traffic. The traffic police crash register cannot be removed from the DTPO because it is the only hard copy of the data and it contains personally identifiable information. Therefore, we developed a paper-based data extraction form to capture data, in Nepali, from the District Traffic Police records. The data extraction form was based on the road accident reporting form used by the traffic police at the scene of a crash. We piloted the data extraction form on 20 RTC records from the fiscal year 2016–7. Following piloting, adjustments were made to the form to ensure data were extracted consistently and accurately. Two data collectors were trained to extract the data. Identifiable information, such as name, caste and vehicle registration number, was not collected. The data were entered into an electronic database [Research Electronic Data Capture, (REDCap)] by a data entry clerk. REDCap is a secure web application for both offline and online data collection for research studies. 14 Both numbers and free-text data were translated into English by the clerk during data entry. A field supervisor checked 20% of the data records to ensure the accuracy, completeness and consistency of the data during transcription from paper to electronic formats. The final set of data were stored in password-protected computers and backed up on a computer hard drive. Statistical analysis was performed using the Statistical Package for the Social Sciences version 24.0. Descriptive statistics such as frequencies and percentages were used to describe the patterns of RTCs by time, age and sex of victims; cause of crash and type of vehicle involved in the crash. Crash rates (crashes per kilometre per year) were calculated using published traffic flow data for the East–West highway. 15
Results
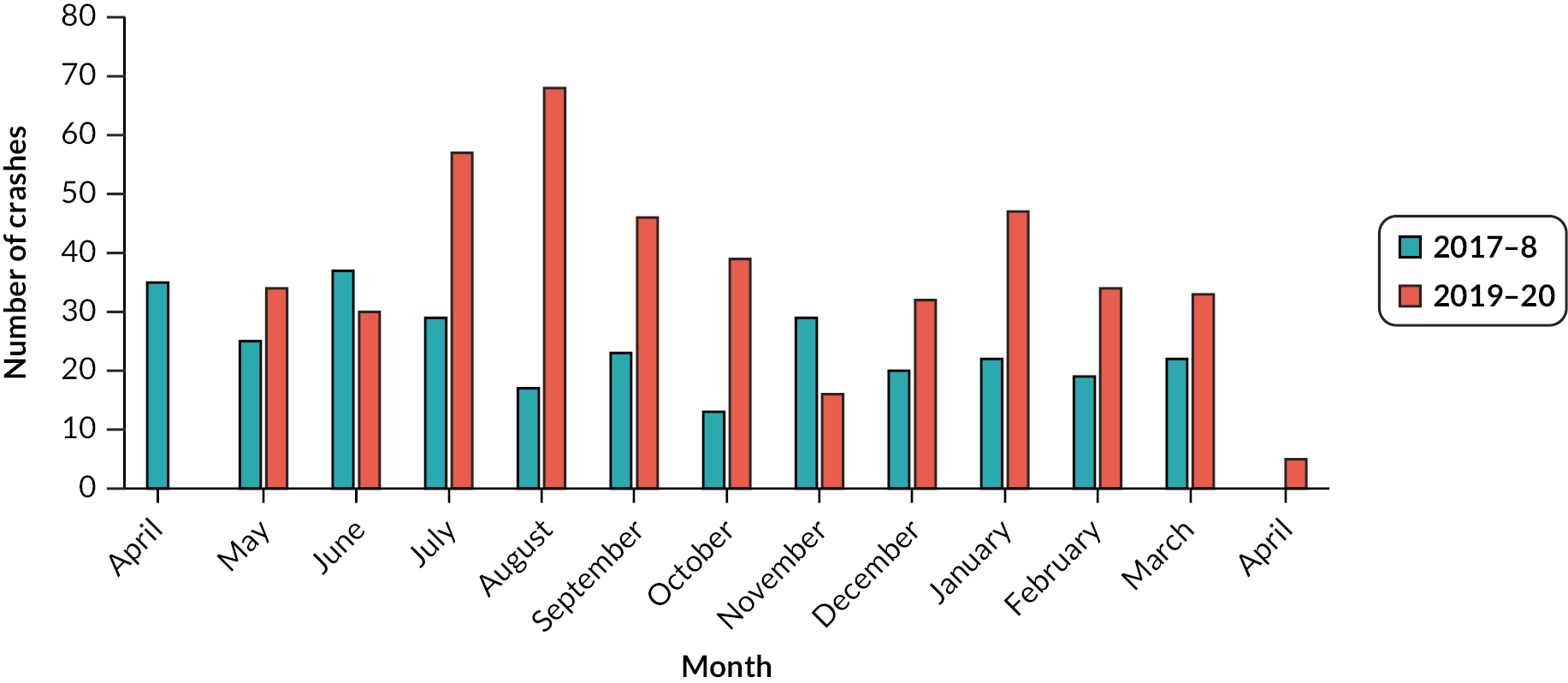
There were 291 and 435 crashes documented in the traffic police records in the years 2017–8 and 2019–20, respectively. Figure 1 shows the distribution by month for both years. The frequency of crashes varied by month, and no clear seasonal pattern was observed.
FIGURE 1.
Road traffic crashes in Makwanpur district, by year and month. Note: Number of crashes decreased in late March–April 2020 due to the COVID-19 pandemic and the nation-wide lockdown that prohibited unnecessary travel.
Over the two data collection periods, there were a total 1215 casualties (both fatal and non-fatal) resulting from the 726 crashes; 423 casualties were drivers, 670 were passengers and 122 were pedestrians. The sex of casualty victims was known for 88% of cases, and age was recorded for 80% of cases. Most victims were male (66.9%), and the largest age group was 18–29 years (34.7%), as shown in Table 1.
| Driver | Passenger | Pedestrian | Overall | |
|---|---|---|---|---|
| A ge (years) | ||||
| Median (interquartile range) | 28 (13) | 26 (16) | 34 (37) | 27 (17) |
| Minimum–maximum | 12–86 | 1–76 | 2–87 | 1–87 |
| Age in groups (years) | n (%) | n (%) | n (%) | n (%) |
| 1–4 | 0 (0.0) | 9 (1.3) | 3 (2.5) | 12 (1) |
| 5–17 | 8 (1.9)a | 78 (11.6) | 32 (26.2) | 118 (9.7) |
| 18–29 | 193 (45.6) | 212 (31.6) | 17 (13.9) | 422 (34.7) |
| 30–50 | 146 (34.5) | 171 (25.5) | 35 (28.7) | 352 (29) |
| > 50 | 17 (4.0) | 32 (4.8) | 28 (23.0) | 77 (6.3) |
| Not recorded | 59 (13.9) | 168 (25.1) | 7 (5.7) | 234 (19.3) |
| Total | 423 (100) | 670 (100) | 122 (100) | 1215 (100) |
| Sex | n (%) | n (%) | n (%) | n (%) |
| Male | 381 (90.3) | 362 (54) | 70 (57.4) | 813 (66.9) |
| Female | 13 (3.1) | 200 (29.9) | 44 (36.1) | 257 (21.2) |
| Not recorded | 28 (6.6) | 108 (16.1) | 8 (6.6) | 144 (11.9) |
| Total | 422 (100) | 670 (100) | 122 (100) | 1214 (100) |
Of the 1215 casualties, details of the severity of the injuries, as assessed by the traffic police, were recorded for only 813 (66.9%). Using the available data, Table 2 shows that most of the injuries were categorised as minor to severe, with 124/813 (15.3%) cases recorded as fatal. Out of 124 fatalities, 47 (37.9%) people died at the scene, 3 (2.4%) on the way to a health facility, and 71 (57.3%) died at a health facility. The location of death was not reported for three people (2.4%).
| Injury severity | Driver | Passenger | Pedestrian | Total |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Minor | 109 (42.7) | 243 (51) | 11 (13.4) | 363 (44.6) |
| Severe | 99 (38.8) | 187 (39.3) | 40 (48.8) | 326 (40.1) |
| Fatal | 47 (18.5) | 46 (9.7) | 31 (37.8) | 124 (15.3) |
| Total | 255 (100) | 476 (100) | 82 (100) | 813 (100) |
| Not recorded | 119 | 188 | 40 | 347 |
Most crashes (164 in 2017–8 and 255 in 2019–20) occurred on the East–West highway as opposed to other local roads. The total length of the East–West highway through the Makwanpur district is 46.35 km, giving a crash rate of 4.2 crashes/km/year. There are two main sections of the highway through Makwanpur; one is south of Hetauda city towards the Indian border and the other west, towards Chitwan. Data on traffic flow are available in the Department of Roads’ Status Paper on Road Safety in Nepal. 15 Table 3 gives the average daily traffic flow and estimates of the number of crashes per million vehicle kilometres. In the first year studied, the crash rate was higher on the highway south of Hetauda city, but in the second period studied, it was similar in both sections (see Table 3).
| East–West highway section South of Hetauda city (6.19 km length) | East–West highway section West of Hetauda city (40.16 km length) | |||
|---|---|---|---|---|
| 2017–8 | 2019–20 | 2017–8 | 2019–20 | |
| Number of crashes in traffic police recordsa | 29 | 29 | 110 | 169 |
| Annual average daily trafficb,15 | 11,249 | 15,380 | 13,540 | 14,056 |
| Crashes per million vehicle km | 1.14 | 0.83 | 0.55 | 0.82 |
Considering data for the whole of Makwanpur district, rather than just the East–West highway, there were 1172 vehicles involved in the 726 crashes recorded by the traffic police. Table 4 shows the types of vehicles involved in crashes across both data periods. Powered two-wheelers (motorcycles and scooters) were the vehicles most commonly involved and represented 35% of all vehicles recorded by the police; the categories ‘car, jeep, sumo’ and ‘pickup, van, jeep, minibus’ represented 15–16% of vehicles involved, respectively. Trucks and tippers represented around 20% of vehicles involved.
| Types of vehiclesa | N | % |
|---|---|---|
| Motorcycle/scooter | 417 | 35.6 |
| Truck/tipper | 235 | 20.1 |
| Car/jeep/sumo | 189 | 16.1 |
| Pickup/van/jeep/minibus | 174 | 14.8 |
| Bus | 80 | 6.8 |
| Others | 55 | 4.7 |
| Non-motorised vehicle (cart/bicycle) | 12 | 1 |
| Not recorded | 10 | 0.9 |
| Total | 1172 | 100 |
The Nepal traffic police use a specific set of categories to record the type of crash and the cause of the crash. Of 726 crash events, the most common type of crash recorded over the 2-year period was ‘collision’ (339, 46.7%), followed by ‘hit pedestrian’ (109, 15.0%), and ‘fell off the road’ (85, 11.7%) (Figure 2).
FIGURE 2.
Type of crashes (n = 726). a, Fell off the road is the traffic police category used when a vehicle left the carriageway. b, Fell on the road is the traffic police category used when a vehicle remains on the carriageway after the crash.
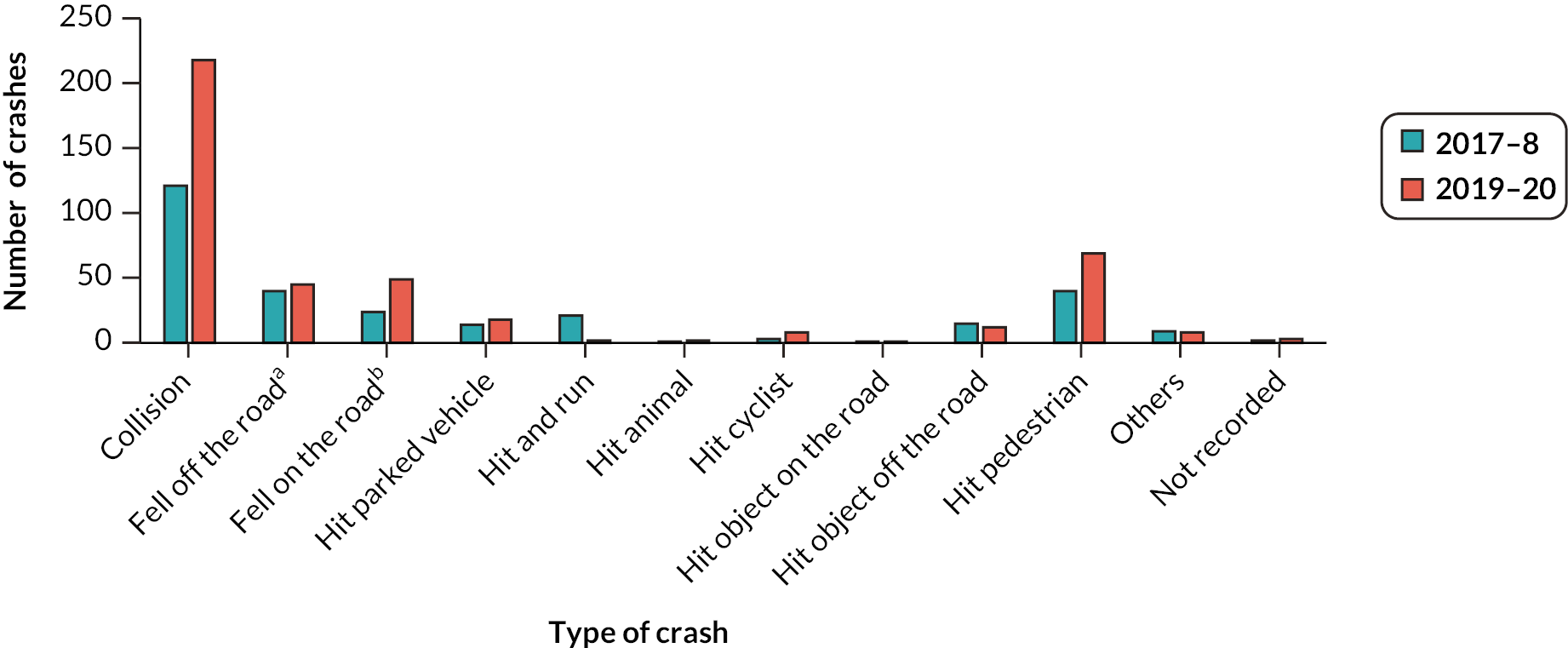
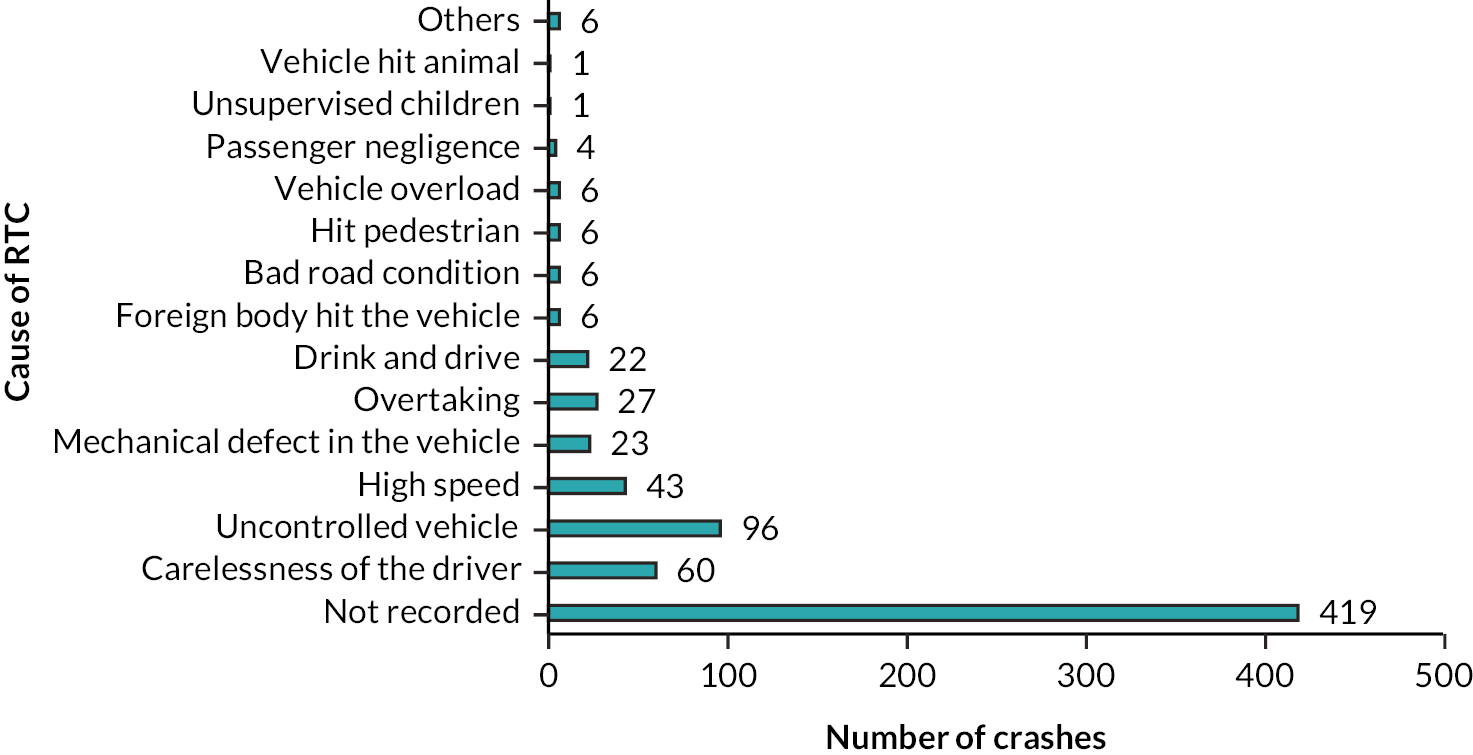
Figure 3 shows the frequency of different causes of crashes, using the classification system for crashes currently in use by the Nepal traffic police. The data for cause of the crash were missing in 58% (419/726) of the cases (i.e. not available in the traffic police record). Where data were available, the most commonly reported causes were ‘uncontrolled vehicle’ (96, 13.2%) and ‘carelessness of driver’ (60, 8.3%).
FIGURE 3.
Cause of RTCs (n = 726).
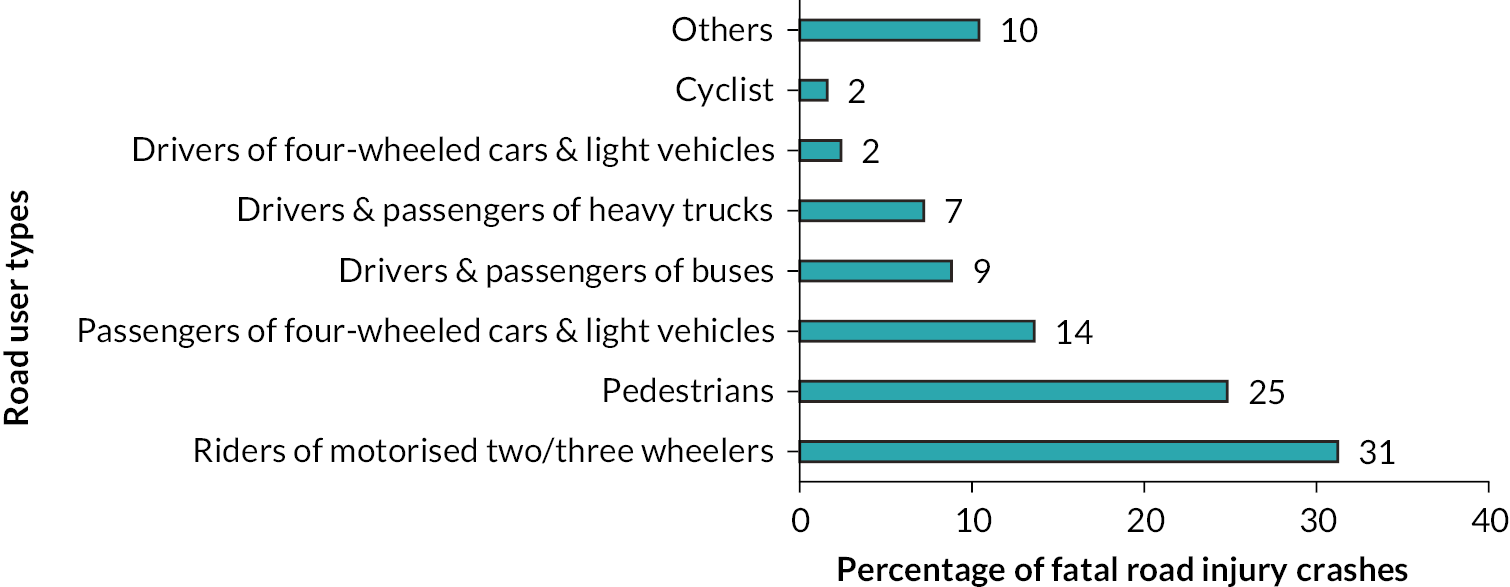
There were 1129 people involved in the 726 crash events. Applying the WHO classification of types of road users, as published in the global status reports on road safety,3 to these data, one-third of victims were riders of motorised two- or three-wheelers (377/1129, 33.4%) (Figure 4). Figure 5 shows the types of road user who were killed in these crashes. The most common road users who were killed were the riders of motorised two- or three-wheelers (39/125, 31.2%), followed by pedestrians (31/125, 24.8%).
FIGURE 4.
Traffic crashes over 2 years, by road user type (WHO classification) (n = 1129). Note: The category ‘Riders of motorised two-/three-wheelers’ includes both riders and passengers.
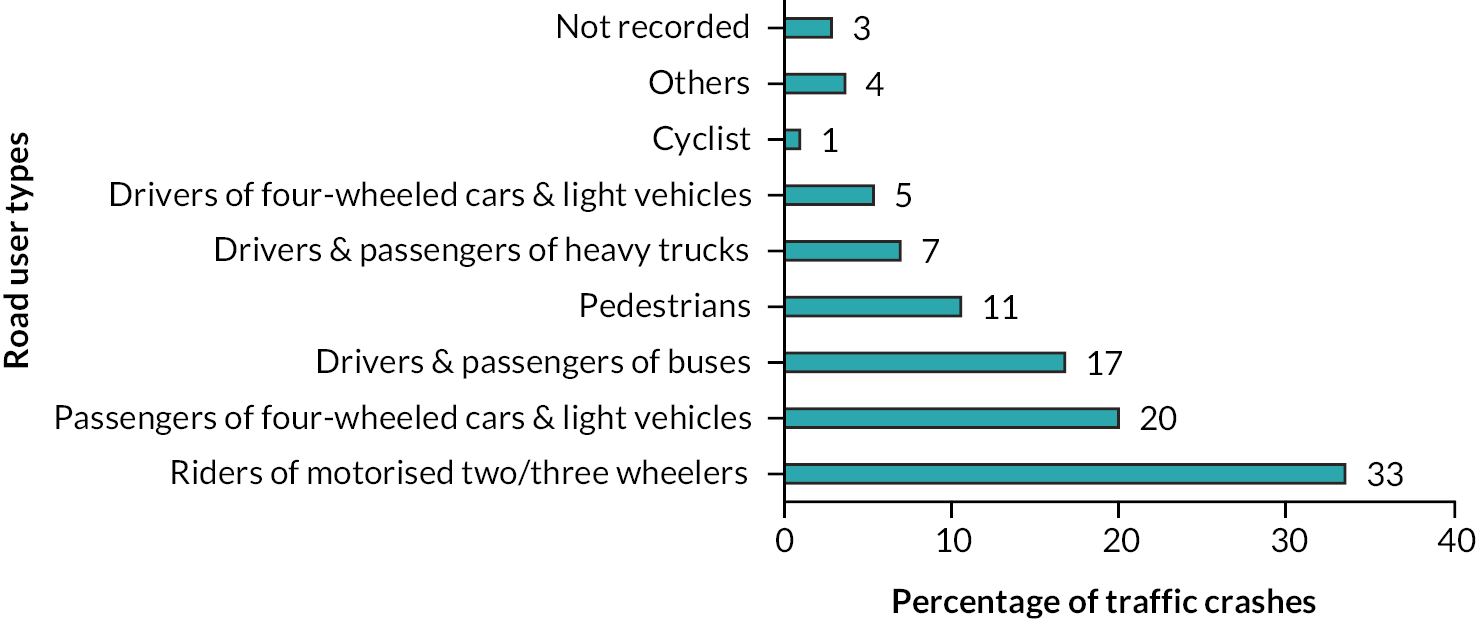
FIGURE 5.
Fatal road injury crashes over 2 years, by road user type (WHO classification) (n = 125). Note: The category ‘Riders of motorised two-/three-wheelers’ includes both riders and passengers. The road traffic fatality for this study included any person who died as a result of a road traffic crash either at the crash site, on the way to health facility, or at the health facility.
Discussion
We analysed secondary data from the DTPO, Makwanpur, covering the periods April 2017–March 2018 and May 2019–April 2020. The number of crashes increased by a factor of two from the first year to the second year of data. In contrast over the same period, there has only been an approximate 10% increase in traffic on the East–West highway, where the majority of crashes occurred. The increase in the number of crashes may partly be explained by the increase in traffic flow, or better crash reporting and recording in the second of the 2 years. However, the scale of the increase in numbers also suggests the potential for an increase in the rate of crashes per vehicle kilometres.
A study conducted in Nepal, where shopkeepers recorded RTCs close to their premises over a 12-month period, found a higher proportion of total crash events occurred than were reported by the traffic police for the same duration and in the same locations. While shopkeepers were estimated to have reported 94% of RTCs (110 of 117, 95% CI 88.1 to 97.0), the police were found to have reported only 19.7% (23 of 117, 95% CI 13.4 to 27.7) of crashes. 9 A similar study conducted in Bangladesh, where local shop keepers were trained to record and report RTCs, found that only one in five collisions were reported by the traffic police. 17 These studies suggest that traffic police records are likely to significantly underestimate the true burden of RTCs.
As enhanced data quality is required to understand the reasons for crashes,8 the Department of Transport Management of Nepal has recently initiated a web-based Road Accident Information Management System (RA-IMS) which is intended to replace the existing paper-based road accident recording system used by the traffic police. 18 The new system will enable electronic collection, verification, storage and dissemination of crash data. In the first stage, it has been implemented with traffic police offices in Kathmandu Valley and along the Kathmandu–Birgunj Highway Corridor, with plans to extend across the entire road network in Nepal. 13 This system has the potential to improve the quality of the data collected by the traffic police (e.g. through the use of mandatory fields) but will not address the issue of collisions not being reported to the police, or traffic police capacity to attend all reported collisions.
In our study, around 15% (124) of the road casualties were fatal, which is lower than fatal crash rates reported from India19 and Bangladesh17 but higher than that from Sri Lanka. 20 This disparity might be because of differences in quality and availability of healthcare services as well as data reporting.
On the highways included in this study, there is a significant difference in size and speed of vehicles ranging from powered two- and three-wheelers, to cars, light vehicles and trucks or trippers. While the type of traffic on the East–West Highway is fairly evenly spread across these different categories of vehicles,15 powered two-wheelers (motorcycles and scooters) were the vehicles most commonly involved in the crashes, and riders of motorised two- or three-wheelers represent 31% of fatalities, followed by pedestrians at 25% and drivers and passengers of cars and light vehicles at 23%. The findings in our sample are similar to those reported for India and Bangladesh in the WHO’s Global Status Report on Road Safety,3 and also in national reports from India19 and Bangladesh,17 where riders of two-wheelers represented more than one-third of the road fatalities. Riders of two- and three-wheelers and pedestrians are less protected than those travelling in cars or light vehicles. 3,10,15 This suggests that interventions to prevent RTCs for motorcycle and scooter riders in other South Asian countries may be generalisable to Nepal where the level of the problem is similar.
The majority of casualties over the 2 years of study were between 18 and 50 years of age and were predominantly male, and this finding is similar to the hospital-based studies where men are at a higher risk of becoming a victim of a RTC than women, and that most victims were young adults (15–40 years). 10,21 Young adults are more likely to be exposed to the risks of RTIs due to increased road travel for work-related purposes and may engage in driving behaviours that increase their crash risk. The most commonly reported causes of crashes were ‘carelessness of driver’ and ‘uncontrolled vehicle’, which is similar to the findings from studies conducted in other parts of Nepal, where 83% of crashes are reported as being due to driver ‘carelessness’. While this points to driver behaviour as being an important causal factor, a more detailed classification system that describes the act or behaviour leading to the crash would be more useful to indicate issues for intervention. 6,16 For example, the data available in this study do not allow an analysis to determine what proportion of crashes involved one or more vehicles travelling at a speed in excess of the limit or too fast for the road conditions. We know from other global road safety research that excess speed is the most common cause of RTCs globally. 3
The large number of crashes in our study where the cause of the crash was not reported (58%) means that we cannot be certain of the true distribution of causes. The categories used by the Nepal police for reporting the cause of crashes are ambiguous; a number of categories may overlap each other (e.g. overtaking and speeding), and there could be crashes with multiple causes, but only one is recorded. Some reported causes appear to be descriptions of what happened (such as ‘hit pedestrian’), rather than the reason why the pedestrian was hit. The descriptions of the type of collision are also quite general; for example, the collision category could be subdivided into head-on collision, rear-end shunt or side impact. The lack of use of recognised classification systems for reporting RTCs makes international comparison difficult. Our findings therefore support the ongoing reforms in the national traffic police crash reporting system which currently, by default, blames the driver for the crash rather than assessing and reporting the circumstances of the crash event.
Future research
This study supports WHO statements calling for more research on RTIs in LMICs. More research is required in Nepal because of the limited information on such injuries and their causes, and government’s commitment to doing its part to achieve Sustainable Development Goal target 3.6 of halving the global number of deaths and injuries from road traffic accidents. 22 Further studies to explore the road user groups most likely to be injured or killed using routinely collected electronic RA-IMS data over a larger geographical area would generate more robust evidence to inform decision-making and could be used for international comparisons with inclusion in future WHO Global Status Reports on road safety.
Lessons learnt
The findings of this study illustrate the importance of collecting data that is complete and well coded, to provide evidence that is better able to inform in-country and partner decision-making, including the development and implementation of road safety policy and legislation. The findings of the study highlight the need to roll out the RA-IMS and to ensure that it is collecting high-quality evidence to inform transport strategy and health service planning, including prehospital care/first response, and the availability of trauma care services at district level. Localised studies provide crucial insights into the nuanced and context-specific factors contributing to RTIs and fatalities. These insights are often overlooked in national-level analyses. Hence, the results are likely to be of interest to stakeholders at the district level, who have to design and implement effective local road safety interventions and develop local road safety policies.
Our data suggest the need for targeted interventions for vulnerable road users, such as pedestrians and motorcyclists, to prevent fatal and non-fatal injuries. While the data on the cause of the crash are incomplete, improved enforcement of existing legislation (such as compulsory wearing of helmets for both rider and pillion passengers) and implementing infrastructure changes to support pedestrian safety (e.g. segregation of pedestrians from other road users, availability of safe crossing points) are evidence-based interventions known to reduce traffic injuries and deaths. Any such interventions would need to be implemented alongside context-appropriate awareness raising campaigns, the provision of adequate and sustained financial support, and with multisector agreement across government authorities, non-governmental organisations and community leaders.
Limitations
The main strength of this paper is that it contributes towards filling the gap in WHO’s Global Status Report on Road Safety by including the crashes and mortality according to the road user category. The paper highlights the road user groups most likely to be involved and injured in traffic crashes at a district level, though these findings may not be generalisable to the national level. When extracting and transcribing data from paper records, there is a risk of transcription and coding errors. We used a data field supervisor to oversee the process and minimise this risk. We analysed data over 2 years to explore the causes and consequences of RTCs in Nepal using routinely collected data and temporal changes. The data give an indication of an increase in crash frequency, but to understand the factors behind this, an analysis over a longer period and a larger geographical area would be necessary. At the end of the second period of study, the COVID-19 pandemic occurred. Local movement restrictions associated with COVID-19 lockdown limited the traffic on the roads, resulting in fewer crashes in March and April 2020. 23 In the majority of crash records, there were missing data, limiting our ability to determine contributory factors with confidence. Of particular note was the absence of a record of the cause of the crash in 58% of police reports.
Conclusions
Traffic police records are helpful to identify which road users should be prioritised for road safety interventions. The study indicates that young male drivers and passengers, particularly of motorised two- and three-wheeled vehicles, are most likely to be involved in RTCs in this district of Nepal. Limitations in the quality of the data mean that the findings in this study should not be overinterpreted but used as evidence of the requirement to strengthen the quality of road traffic crash data across Nepal. The findings indicate that targeted road safety interventions should be considered for population groups most at risk, though further research will require improved data quality to confidently monitor trends over time.
What this study adds
-
All three of the most recent WHO global status reports on road safety contain incomplete data on traffic crashes in Nepal. The study contributes to filling this gap by describing crashes and mortality according to road user categories.
-
The study identifies the road user groups that are most likely to be involved in and injured in traffic accidents at the district level, which may not be reflected when data are aggregated to the national level.
-
The study highlights the need to roll out the RA-IMS and to ensure that it is collecting high-quality evidence to inform transport strategy and health service planning, including prehospital care/first response, and the availability of trauma care services at district level.
Additional information
CRediT contribution statement
Santosh Bhatta (https://orcid.org/0000-0001-6393-2495): Conceptualisation (equal), Methodology (equal), Data curation (equal), Formal analysis (supporting), Writing – original draft (supporting), Writing – reviewing and editing (lead).
Pratiksha Pathak (https://orcid.org/0000-0002-3582-147X): Formal analysis (lead), Writing – original draft (lead).
Anish Khadka (https://orcid.org/0000-0003-4432-7198): Data curation (equal), Formal analysis (supporting), Writing – original draft (supporting).
John Parkin (https://orcid.org/0000-0002-6084-4569): Formal analysis (supporting), Writing – original draft (supporting).
Paul Pilkington (https://orcid.org/0000-0002-5408-361X): Formal analysis (supporting), Writing – original draft (supporting).
Sunil Kumar Joshi (https://orcid.org/0000-0002-2704-5060): Conceptualisation (equal), Methodology (equal), Formal analysis (supporting), Writing – original draft (supporting).
Julie Mytton (https://orcid.org/0000-0002-0306-4750): Conceptualisation (equal), Methodology (equal), Formal analysis (supporting), Writing – original draft (supporting), Writing – reviewing and editing (supporting).
Acknowledgements
We acknowledge the support of Mother and Infant Research Activities in hiring the data collectors and with the collection of traffic police data. We are thankful to the District Traffic Police, Makwanpur, for their cooperation and the Hetauda Municipality for their permission to conduct the study.
Data-sharing statement
The data that support the findings of this study are available from the corresponding author upon request.
Ethics statement
Written permission to access and analyse the data was obtained from the District Traffic Police Office, Makwanpur, and Nepal Police Headquarters, Kathmandu. We obtained ethical approval from the Ethical Review Board (ERB) of Nepal Health Research Council (Reg. no. 217/2018), which was ratified by the Faculty of Health and Applied Sciences Research Ethics Committees (FREC) at the University of the West of England, UK (HAS.18.05.171) prior to the study beginning.
Information governance statement
The University of the West of England, Bristol (UWE Bristol), is committed to ensuring that all personal information is handled in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under Data Protection legislation, UWE Bristol is the Data Controller and the Nepal Injury Research Centre is the Data Processor, who process personal data in accordance with their instructions. The data governance strategy applied in this study used the ‘five safes’ framework. This is a systematic approach to good data governance, commonly used in government data management systems. The framework breaks data management and governance into five broad issues which need to be addressed: (1) safe projects, (2) safe people, (3) safe settings (which are all amenable to managerial controls), (4) safe data and (5) safe outputs (which are amenable to statistical controls). More information on the data governance strategy used in this study is available from the authors on request.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/DWTR9883.
Primary conflicts of interest: None of the authors have competing interests to declare, apart from Julie Mytton who was a member of the NIHR HTA MNCH Panel from 2008 to 2015 and Sunil Kumar Joshi who is an Editorial Board Member for the BMJ Injury Prevention.
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the Global Health Research programme or the Department of Health and Social Care.
Funding
This article presents independent research funded by the National Institute for Health and Care Research (NIHR) Global Health Research programme as award number 16/137/49 using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the UK government. Research is published in the NIHR Global Health Research Journal. See the NIHR Funding and Awards website for further award information.
This article reports on one component of the research award Injury risks for different road users in Nepal: a secondary analysis of routinely collected crash data. For more information about this research please view the award page (https://fundingawards.nihr.ac.uk/award/16/137/49)
About this article
The contractual start date for this research was in July 2017. This article began editorial review in February 2023 and was accepted for publication in April 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Global Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
This article was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Copyright
Copyright © 2024 Bhatta et al. This work was produced by Bhatta et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
List of abbreviations
- DTPO
- District Traffic Police Office
- ITPO
- Ilaka Traffic Police Office
- LMICs
- low- and middle-income countries
- RA-IMS
- Road Accident Information Management System
- REDCap
- Research Electronic Data Capture
- RTCs
- road traffic crashes
- RTIs
- road traffic injuries
- WHO
- World Health Organization
References
- Mohammed AA, Ambak K, Mosa AM, Syamsunur D. A review of traffic accidents and related practices worldwide. Open Transp J 2019;13:65-83. https://doi.org/10.2174/1874447801913010065.
- World Health Organization . Global Health Estimates: Deaths by Cause, Age, Sex, by Country and by Region 2000–2019 2020. www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed 21 September 2022).
- World Health Organization . Global Status Report on Road Safety 2018: Summary 2018.
- World Health Organization . WHO Global Status Report on Road Safety 2013: Supporting a Decade of Action 2013.
- World Health Organization . Global Status Report on Road Safety 2015 2015.
- Pant PR, Banstola A, Bhatta S, Mytton JA, Acharya D, Bhattarai S, et al. Burden of injuries in Nepal, 1990–2017: findings from the Global Burden of Disease Study 2017. Inj Prev 2020;26:i57-66. https://doi.org/10.1136/injuryprev-2019-043309.
- Atreya A, Shrestha DB, Budhathoki P, Nepal S. Epidemiology of road traffic accidents in Nepal from 2009/10 to 2019/20: a 10 year study. J Nepal Health Res Counc 2021;19:343-8. https://doi.org/10.33314/jnhrc.v19i2.3432.
- Karkee R, Lee AH. Epidemiology of road traffic injuries in Nepal, 2001–2013: systematic review and secondary data analysis. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2015-010757.
- Khadka A, Parkin J, Pilkington P, Joshi SK, Mytton J. Completeness of police reporting of traffic crashes in Nepal: evaluation using a community crash recording system. Traffic Inj Prev 2022;23:79-84. https://doi.org/10.1080/15389588.2021.2012766.
- Mytton JA, Bhatta S, Thorne M, Pant PR. Understanding the burden of injuries in Nepal: a systematic review of published studies. Cogent Med 2019;6. https://doi.org/10.1080/2331205X.2019.1673654.
- Central Bureau of Statistics . National Population and Housing Census 2011 (Population Projection 2011–2031) 2014.
- Central Bureau of Statistics . National Population and Housing Census 2011 (National Report) 2012.
- Department of Transport Management . Establishment and Operation of Road Accident Information Management System (RA-IMS) 2020.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-81. https://doi.org/10.1016/j.jbi.2008.08.010.
- Thapa A. Status Paper on Road Safety in Nepal. DDG, Department of Roads. Kathmandu, Nepal: Government of Nepal; 2013.
- McGee K, Sethi D, Peden M, Habibula S. Guidelines for conducting community surveys on injuries and violence. Inj Control Saf Promot 2004;11:303-6. https://doi.org/10.1080/156609704/233/327505.
- van der Horst ARA, Thierry MC, Vet JM, Rahman AFMF. An evaluation of speed management measures in Bangladesh based upon alternative accident recording, speed measurements, and DOCTOR traffic conflict observations. Transp Res Part F Traffic Psychol Behav 2017;46:390-403. https://doi.org/10.1016/j.trf.2016.05.006.
- Bhatta S, Bhatta S, Mytton J, Joshi SK. Improving estimates of injury burden in Nepal: a qualitative study. J Nepal Health Res Counc 2022;20:339-46. https://doi.org/10.33314/jnhrc.v20i02.3929.
- Arora YK, Kumar S. Computing in Engineering and Technology. Singapore: Springer; 2020.
- Lakmal M, Ekanayake E, Kelum S, Gamage B, Jayasundara J. Hospital-based case series analysis of road traffic trauma patients in Sri Lanka. Indian J Surg 2021;83:120-5. https://doi.org/10.1007/s12262-020-02473-8.
- Bhatta S, Magnus D, Mytton J, Joshi E, Bhatta S, Adhikari D, et al. The epidemiology of injuries in adults in Nepal: findings from a hospital-based injury surveillance study. Int J Environ Res Public Health 2021;18. https://doi.org/10.3390/ijerph182312701.
- Government of Nepal . Nepal’s Sustainable Development Goals, Status and Roadmap: 2016–2030 2017.
- Sedain B, Pant PR. Road traffic injuries in Nepal during COVID-19 lockdown. F1000Res 2020;9. https://doi.org/10.12688/f1000research.26281.3.