

Notes
Article history
The contractual start date for this research was in February 2019. This article began editorial review in June 2022 and was accepted for publication in April 2023. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Health Technology Assessment editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2023 Uthman et al. This work was produced by Uthman et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2023 Uthman et al.
Introduction
Cardiovascular disease (CVD) is a term that describes a family of diseases with a common set of risk factors that result from atherosclerosis (furring or stiffening of artery walls), particularly coronary heart disease (CHD), stroke and peripheral arterial disease. 1 As a major cause of disability and premature death throughout the world, CVD contributes substantially to the escalating costs of health care. 2 CVD affects around seven million people in the UK and is a significant cause of disability and death, affecting individuals, families and communities. Although rates have been reducing recently, CVD is responsible for one in four premature deaths in the UK. 1
Most CVD cases are preventable. Risk factors, such as high blood pressure, smoking, high cholesterol, diabetes, physical inactivity, obesity, poor diet and excessive drinking can all be reduced through lifestyle or medical interventions to reduce a person’s risk of CVD. 3 However, there is a strong consensus amongst public health communities about the powerful role of population-level policies. These are suggested to be more effective, cost saving and more equitable when compared with individual-level interventions. 3 Determining the best population-level intervention modality, delivery method and resource allocation, is complex because although they tend to cut across traditional government department boundaries, health policy and decision-makers must weigh the costs and benefits of structural interventions. Furthermore, such interventions often cannot be tested in clinical trials because of multiple environmental, sociocultural and health system factors that negate the feasibility and safety of trials. Researchers and decision-makers have increasingly relied on simulation models to evaluate structural interventions for primary prevention of CVD. Simulation models have been applied to a broad range of areas in health care to predict outcomes, unintended consequences and costs of proposed interventions, thereby offering an invaluable decision aid for policy-makers and health-care leaders. 4–6 The extent to which simulation modelling has provided decision-makers with evidence to facilitate decision-making in CVD prevention is unknown. 7 Simulation modelling has the potential to provide strong evidence for multiple aspects of informed decision-making at the policy and health system level, including a proposed intervention’s resource utilisation, cost-effectiveness, feasibility, sustainability, potential impact and acceptance among stakeholders. 8,9
No systematic review has investigated simulation models developed to comprehensively assess the impact of structural interventions on prevention of CVD. The most recent systematic reviews have addressed bans on individual topic areas, such as smoking in public places10 and policies to reduce trans-fat consumption. 11 Therefore, in this systematic review we aim to evaluate the potential impact of structural interventions for preventing CVD.
This publication on the systematic review of effectiveness of policies and structural interventions in reducing CVD and mortality is part of a series of publications on ‘Determining optimal strategies for primary prevention of CVD: systematic review, network meta-analysis and cost-effectiveness review (NIHR/HTA: 17/148/05)’. Other publications in this series include:
-
Interventions for primary prevention of cardiovascular: umbrella review of systematic reviews.
-
Increasing Comprehensiveness and Reducing Workload in the preparation of a Systematic Review of Complex Interventions using Automated Machine Learning.
-
Determining optimal primary prevention interventions for major CVD events and all-cause mortality – findings from systematic review and hierarchical network meta-analysis of randomised controlled trials (RCTs).
-
How conclusive is the evidence for interventions in primary prevention of CVD: a trial sequential analysis?
-
Mind the gap! A multilevel analysis of factors associated with variation in published CVD primary prevention interventions effect estimates within and between countries.
-
Determining optimal strategies for primary prevention of CVD: Systematic review of cost-effectiveness analyses in the UK.
The findings from all the workstreams, including those from the systematic review of modelling studies, will be summarised in a synopsis paper to be published alongside this series.
Methods
This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the following number: CRD42019154836. We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 12
Eligibility criteria
Type of population
Adult populations (≥ 18 years of age), where interventions may or may not be targeted at moderate/high CVD risk groups (such as hypertension, obesity, hyperlipidaemia, type 2 diabetes or a combination of these).
Type of interventions
Any form of structural and policy-based interventions (population-wide interventions) aimed at the primary prevention of CVD, including, but not limited to: taxation and subsidies, mass media campaigns, food and menu labelling, local food environment, worksite wellness programmes, marketing restrictions, quality standards, healthy local environment or addressing air pollution.
Study design
Studies that used any form of simulation model, including but not limited to system dynamics, Monte Carlo, Markov chain model, agent-based model or discrete event, to investigate the perceived value and efficacy of policy-level interventions for the prevention of CVD. Simulation and modelling studies are important tools in supporting evidence for the effectiveness of primary prevention of CVD. These types of studies allow researchers to investigate the potential impact of interventions on population health, without having to conduct large, costly and time-consuming randomised controlled trials (RCTs). However, we excluded other observational studies. Observational studies are often excluded in systematic reviews of primary prevention of CVD due to their inherent limitations, such as potential for bias and measurement errors, and the high volume of evidence to go through. These limitations make it challenging to draw valid conclusions from observational studies, and they are considered less informative than RCTs.
Comparator
There was no restriction on the comparator. The model or simulation could compare the results of all feasible options in relation to each other and/or to current practices.
Types of outcomes
All-cause mortality [deaths prevented or postponed (DPP)], CVD DPP, major cardiovascular events (MACEs) [defined as fatal and non-fatal myocardial infarction (MI), sudden cardiac death, revascularisation, fatal and non-fatal stroke and fatal and non-fatal heart failure], CHD (fatal and non-fatal MI and sudden cardiac death, excluding silent MI).
Information sources and search strategy
A systematic search was performed to identify all relevant studies that satisfied our selection criteria within the following databases from inception to March 2021: Medline, Embase, Web of Science and the Cochrane Library. Additionally, we checked the reviews that we identified for further studies. The search strategy is included as Report Supplementary Material 1.
Selection process
After removing duplicates, two authors independently screened titles and abstracts followed by full-text articles. Any disagreements between the two reviewers were resolved through discussions. However, if a disagreement persisted, it was resolved through consultations involving a third author.
Data extraction
Two reviewers independently extracted data using these forms. Disagreements were resolved through discussions between the two reviewers, and in cases in which no agreement was reached, a third author intervened.
Data items
The following data were extracted from each study: (1) overview of study characteristics, (2) model structure and (3) sources of evidence for model parameters.
Risk of bias in individual studies
The validation of a simulation model is an important determinant of the risk of bias and applicability of a simulation model. All models were assessed in accordance with the guidelines of the International Society for Pharmacoeconomics and Outcomes Research-Society for Medical Decision Making report. 7 For each study, we assessed face validity (wherein experts evaluate model structure, data sources, assumptions and results), verification or internal validity (check accuracy of coding), cross validity (comparison of results with other models analysing the same problem), external validity (comparing model results with real-world results) and predictive validity (comparing model results with prospectively observed events). 7
Data synthesis
We performed a systematic narrative synthesis to present a critical appraisal of the methodological quality and risk of bias of the selected modelling studies and of their results.
Results
Study selection and characteristics
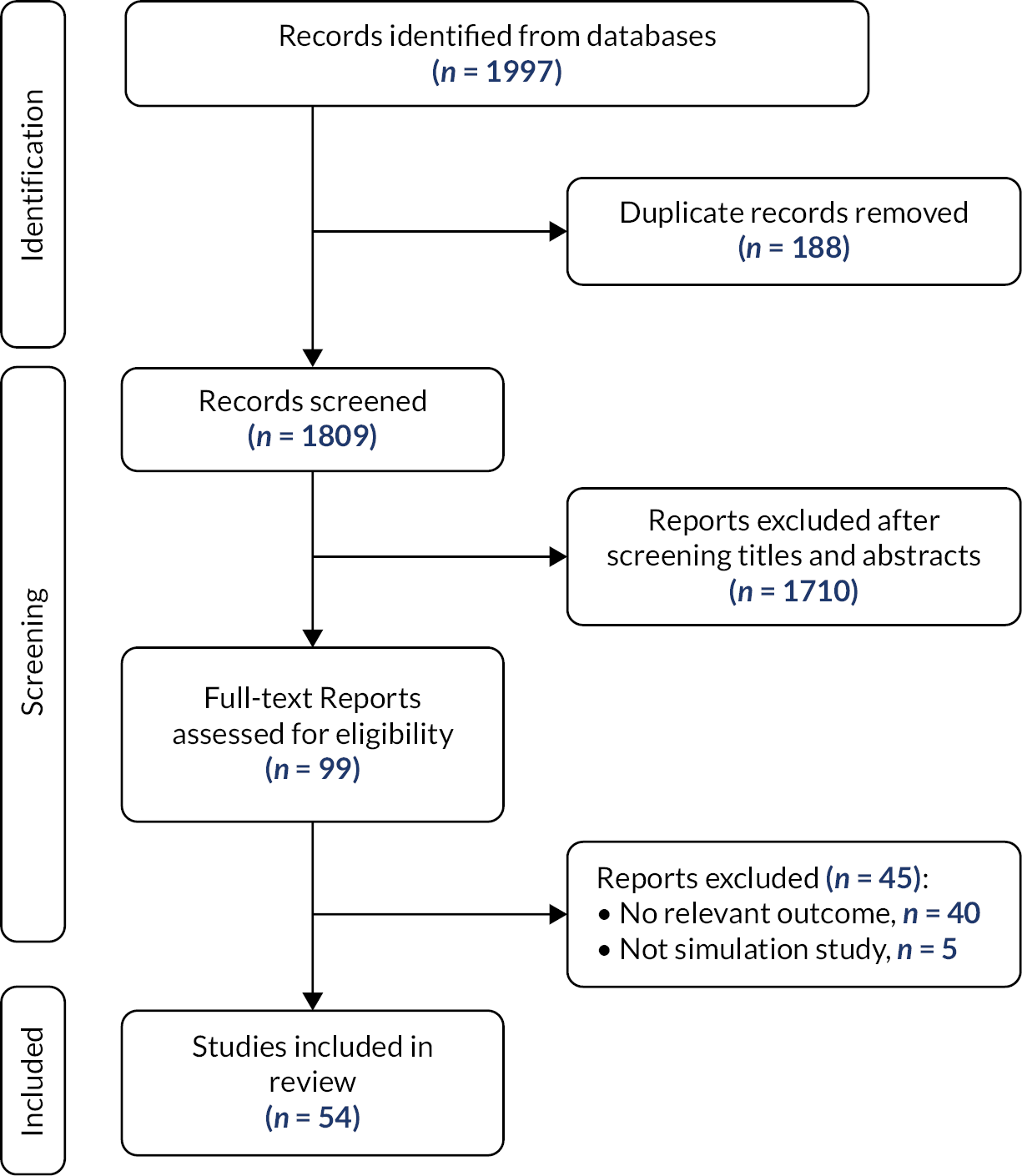
Figure 1 shows the study selection flow diagram. The literature search yielded 1997 articles. After review, 99 articles were selected for critical reading. Forty-five studies did not meet the inclusion criteria and were excluded. The other 54 studies were included. Table 1 presents the characteristics of the included studies. The studies were published between 2007 and 2021. Most of the studies were from the USA (n = 23, 42.6%), followed by the UK (n = 10, 18.5%). Most of the studies were based on the USA the Cardiovascular Disease Policy Model for Risk, Events, Detection, Interventions, Costs, and Trends (CVD PREDICT)13–17 and the UK Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT) Coronary Heart Disease (CHD) Policy Model. 18–24 The majority of the studies were full-text articles (n = 48, 88.9%), and only six were conference abstracts. When reported, the time horizon ranged from 3 years to as much as 50 years. Microsimulation (n = 32, 59.3%) was the most frequently used method for developing the policy simulation models, followed by Markov chain models (n = 11, 20.4%). Most studies conducted probabilistic sensitivity analysis (PSA) (n = 30, 56%). Fourteen studies conducted one-way sensitivity analysis. The policy simulation models can be broadly categorised into diet and nutrition, tobacco and alcohol control initiatives and other initiatives. Diet and nutrition initiatives included: national salt reduction initiatives, fruit and vegetable subsidies, sugar-sweetened beverage (SSB) taxes, elimination of industrial trans-fatty acids, food taxes and subsidies, healthy food and lifestyles policies, palm oil taxes, processed meat taxes, reduction in ultra-processed foods, a supplementary nutrition assistance program, stricter food policy and subsidised community-supported agriculture. Tobacco and alcohol control initiatives included smoking and alcohol, smoke-free policies, national tobacco control initiatives and alcohol pricing policies. Other initiatives included the NHS Health Check, the WHO 25 × 25 initiative and air quality management policies.
FIGURE 1.
Study selection flow.
| Study | Country | Year | Model name | Type of publication | Time period | Horizon | Type of model | Type of policy | Setting | Measurements | Sensitivity analysis | Validation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asaria25 | Multicountry | 2007 | – | Full-text article | 2006–15 | 10 | Microsimulation | National Salt Reduction Initiative, National tobacco control initiative | Adult population | Deaths averted | One-way | – |
| Basu26 | USA | 2020 | – | Full-text article | Microsimulation | Subsidised community-supported agriculture | Adult | DALYs | One-way | Longitudinal US cohort data sets | ||
| Basu27 | India | 2013 | – | Full-text article | 2014–23 | 10 | Microsimulation | Palm oil tax | Adult, nationally representative population | mortality due to myocardial infarction and stroke | One-way | Externally validated the model |
| Basu28 | India | 2013 | – | Full-text article | 2013–22 | 10 | Microsimulation | National tobacco control initiative | Adult population | Overall mortality trend for myocardial infarctions | One-way | The model’s predictions of deaths were validated against Global Burden of Disease estimates for myocardial infarction, stroke and other deaths for the years 2004 and 2008 |
| Bibbins-Domingo29 | USA | 2010 | CHD Policy Model | Full-text article | 2010–19 | 10 | Markov chain model | National Salt Reduction Initiative | US residents 35 years of age or older | Rates and costs of CVD in subgroups defined by age, sex and race | Monte Carlo simulations | |
| Choi30 | USA | 2016 | – | Full-text article | 2015–24 | 10 | Microsimulation | National Salt Reduction Initiative | US population aged 18–85 years | Myocardial infarction and stroke, as well as associated mortality | One-way | National Health and Nutrition Examination Survey (NHANES) |
| Choi31 | USA | 2017 | – | Full-text article | 2015 | Microsimulation | Supplementary nutrition assistance program | US population, Americans aged 0–85 years | Incidence of major cardiovascular events | Monte Carlo simulation | Centers for Disease Control and Prevention estimates | |
| Cobiac32 | UK | 2017 | PROMISE | Full-text article | 2013–20 | 8 | Dynamic population modelling | WHO 25 × 25 initiative | UK Population | Mortality and morbidity (years lived with disability) from non-communicable diseases (NCDs) that are averted or delayed | - | - |
| Collins18 | England | 2014 | IMPACT CHD | Full-text article | 2010–20 | 10 | Microsimulation | National Salt Reduction Initiative | UK population | Life-year gain | PSA | Calibrated for the English population |
| Dehmer33 | USA | 2020 | – | Full-text article | 2018–20 | 3 | Microsimulation | National Salt Reduction Initiative | US Population | Major cardiovascular events | One-way | representative of U.S. population and scaled to the US population aged ≥35 years |
| Dilley34 | USA | 2012 | Full-text article | 2000–9 | 10 | Linear regression | National tobacco control initiative | Washington State’s Behavioral Risk Factor Surveillance System from 1990 to 2009 to describe the state prevalence of adult cigarette smoking | Hospitalisations | – | National Health Interview Survey from 1990 to 2008 | |
| Gillespie19 | England | 2015 | IMPACT SEC (Socieconomic differentials) | Full-text article | Microsimulation | National Salt Reduction Initiative | England, population | CHD Death | Monte Carlo simulation | Validated | ||
| Han35 | Republic of Korea | 2018 | Full-text article | 2005–14 | 10 | Interrupted time series | Air quality management policy | CVD mortality | One-way | – | ||
| Homer36 | USA | 2010 | – | Full-text article | 1990–2040 | 50 | Systems dynamics | Multicomponent interventions | US population | MACE | One-way | – |
| Hurley37 | Australia | 2008 | Full-text article | 1997–2000 | 4 | Markov chain model | National tobacco control initiative | Major cardiovascular events | One-way | – | ||
| Kheirbek37 | USA | 2014 | – | Full-text article | Microsimulation | Air quality management policy | New York City | Premature deaths, hospital admissions for respiratory and CVD | – | – | ||
| Konfino38 | Argentina | 2013 | Full-text article | 2013–23 | 10 | Markov chain model | National Salt Reduction Initiative | Argentina | Major cardiovascular events | – | – | |
| Konfino39 | Argentina | 2014 | CHD Policy Model | Full-text article | 2012–20 | 9 | Markov chain model | National tobacco control initiative | Population of Argentina aged 35–84 years in the year 2010 | Major cardiovascular events | Monte Carlo simulations | – |
| Kypridemos21 | England | 2017 | IMPACT-NCD | Full-text article | 2016–30 | 15 | Microsimulation | National Salt Reduction Initiative | Non-institutionalised population of England | CVD mortality | Probabilistic sensitivity analyses | Model validated well against observed CVD and gastric cancer incidence and mortality in real populations, even when multiply stratified |
| Kypridemos20 | UK | 2018 | IMPACT NCD | Full-text article | 2017–40 | 25 | Microsimulation | NHS Health Check | Liverpool population | CVD cases | Second-order Monte Carlo simulation | Validated S1 |
| Lee13 | USA | 2020 | CVD-PREDICT | Full-text article | Microsimulation | Sugar-sweetened beverage tax | US adults 35–80 years of age | CVD cases | Probabilistic sensitivity analyses | Validated microsimulation model | ||
| Liu14 | USA | 2020 | CVD-PREDICT | Full-text article | 2018–23 | 5 | Microsimulation | National menu calorie labelling law | US adults aged 35–80 years | CVD cases | Probabilistic sensitivity analyses | Validated microsimulation model |
| Lloyd-Williams40 | EU | 2008 | – | Full-text article | – | Spreadsheet | Subsidized Community Supported Agriculture | EU population | CVD cases | Probabilistic sensitivity analyses | – | |
| Manyema41 | South Africa | 2016 | – | Full-text article | 20 years | 20 | Markov chain model | Sugar-sweetened beverage tax | Adult population | CVD cases | Probabilistic sensitivity analyses | – |
| Marklund42 | Australia | 2020 | – | Full-text article | 10 years | 10 | Markov chain model | Eliminating industrial trans-fatty acids | Adult population | CVD cases | Probabilistic sensitivity analyses | Outcomes were compared between a reference population with TFA intake of the Australian population before the intervention and an intervention population with identical characteristics |
| Mason43 | Multicountry | 2014 | IMPACT-CHD | Full-text article | 10 years | 10 | Microsimulation | National Salt Reduction Initiative | Four Eastern Mediterranean Countries | Life years gained | One-way | – |
| Mekonnen44 | USA | 2013 | CVD Policy Model | Full-text article | 2013–22 | 10 | Microsimulation | Sugar-sweetened beverage tax | All Californians and California subpopulations | CVD cases | One-way | NHANES and California Health Interview Survey (CHIS) for participants whose self-report of race and ethnicity and family income |
| Moreira22 | UK | 2015 | IMPACT Food Policy model | Full-text article | 2010–30 | 20 | Microsimulation | Reduction in ultra-process foods | UK | CVD cases | Probabilistic sensitivity analyses | UK population |
| Mozaffarian15 | USA | 2018 | CVD-PREDICT | Full-text article | 2013–18 | 5 | Microsimulation | Supplementary nutrition assistance program | NHANES, US adults aged 35–80 years | CVD cases prevented | Probabilistic sensitivity analyses | Validated microsimulation model |
| Mhurchu45 | NZ | 2015 | – | Full-text article | 2006–10 | 5 | Markov chain model | Food tax and subsidy | NZ (2.3 million adults, aged 35+ years) | Deaths prevented or postponed (DPP) | One-way | – |
| Nilson46 | Brazil | 2020 | – | Full-text article | 2017 | Markov chain model | National Salt Reduction Initiative | Brazilian population was 30 years of age or older | CVD mortality | Probabilistic sensitivity analyses | – | |
| Nnoaham47 | UK | 2009 | – | Full-text article | - | Spreadsheet | Food tax and subsidy | UK population | CVD mortality | – | – | |
| O’Flaherty48 | UK | 2012 | – | Full-text article | Spreadsheet | Stricter food policy | Adults aged 25–84 years | CVD mortality | Probabilistic sensitivity analyses | – | ||
| O’Keeffe23 | Ireland | 2013 | IMPACT Food Policy Model | Full-text article | - | Microsimulation | Food tax and subsidy | Irish adults aged 25–84 years | CVD mortality | Probabilistic sensitivity analyses | Validated IMPACT Food Policy Model | |
| Pearson-Stuttard49 | USA | 2017 | US IMPACT Food Policy Model | Full-text article | 2015–30 | 15 | Microsimulation | Fruit and vegetable subsidy | The US population was stratified by age (10-year age groups, 25 to ≥85 years) and sex | CVD death | Probabilistic sensitivity analyses | validated IMPACT methodology |
| Pearson-Stuttard50 | USA | 2017 | US IMPACT Food Policy Model | Full-text article | 2015–30 | 15 | Microsimulation | Food tax and subsidy | (Involving 44.5 million individual adults and children) nationwide | CVD mortality | Probabilistic sensitivity analyses | Validated model |
| Eom51 | USA | 2020 | SHINE CVD Model | Abstract | - | Microsimulation | Fruit and vegetable subsidy | New York City (NYC) population, NYC Health and Nutrition Examination Survey | CVD cases | – | – | |
| Garney52 | USA | 2019 | – | Abstract | 10 years | 10 | Agent-based model | Smoke-free policy | Arlington and Mesquite, Texas population | CVD cases averted | – | – |
| Wilde17 | USA | 2018 | CVD-PREDICT | Abstract | Microsimulation | Sugar-sweetened beverage tax | US adults 35+ years | CVD cases | Probabilistic sensitivity analyses | Validated | ||
| Sy53 | USA | 2018 | - | Abstract | 2015–35 | 20 | Microsimulation | Food tax and subsidy | US, 35-year olds | CVD death | – | – |
| Pearson-Stuttard54 | USA | 2018 | US IMPACT Food Policy Model | Abstract | Microsimulation | Food tax and subsidy | Entire US population | DPP | Probabilistic sensitivity analyses | Validated | ||
| Mejia55 | Argentina | 2011 | CHD Model | Abstract | Microsimulation | National Salt Reduction Initiative | Adult population | CVD cases | – | – | ||
| Pearson-Stuttard56 | USA | 2018 | US IMPACT Food Policy Model | Full-text article | 2017–36 | 20 | Microsimulation | National Salt Reduction Initiative | US population | CVD cases | Probabilistic sensitivity analyses | Previously validated US IMPACT Food Policy Model |
| Peñalvo57 | USA | 2017 | – | Full-text article | Comparative risk assessment | Food tax and subsidy | Nationally representative data | Cardiometabolic diseases | – | – | ||
| Purshouse58 | England | 2010 | – | Full-text article | – | Epidemiological mathematical model | Alcohol pricing policy | General Household Survey | Illness prevented | One-way | Validation against historical data | |
| Sahan59 | Turkey | 2016 | IMPACT model | Full-text article | 2008–25 | 18 | Microsimulation | Healthy food and lifestyles policy | Projected population in 2025 (aged 25–84) of 54 million in Turkey | CVD death | Probabilistic sensitivity analyses | Validated by comparing the model-predicted CHD death rates in 2008 with observed CHD deaths (ICD-10 codes I20–I25) in 2008, stratified by age and gender |
| Salgado60 | Argentina | 2020 | CVD Policy Model-Argentina | Full-text article | 2015–24 | 10 | Microsimulation | Sugar-sweetened beverage tax | Adult population | CVD deaths | Probabilistic sensitivity analyses | Validated for use in Argentina |
| Sanchez-Romero61 | Mexico | 2016 | CVD Policy Model–Mexico | Full-text article | Markov chain model | Sugar-sweetened beverage tax | Mexican adults aged 35–94 years | CVD cases | Probabilistic sensitivity analyses | Validated CVD simulation model adapted to describe the population of Mexico, using multiple Mexican national data sources | ||
| Schönbach62 | Germany | 2018 | DYNAMO-HIA | Full-text article | 10 years | 10 | Dynamic population modelling | Process meat tax | Adult population | CVD cases | Probabilistic sensitivity analyses | – |
| Seferidi24 | England | 2018 | IMPACT Food Policy model | Full-text article | Microsimulation | Sugar-sweetened beverage tax | Adults aged 25 years or older. | CVD deaths | Probabilistic sensitivity analyses | Validated | ||
| Smith-Spangler63 | USA | 2010 | Full-text article | Markov chain model | National Salt Reduction Initiative | US adults aged 40–85 years | CVD cases | One-way | – | |||
| Vega-Solano64 | Costa Rica | 2021 | PRIME | Full-text article | – | Microsimulation | National Salt Reduction Initiative | Costa Rican population | CVD cases | Probabilistic sensitivity analyses | – | |
| Wang65 | China | 2016 | – | Full-text article | 2010–19 | 10 | Markov chain model | National Salt Reduction Initiative | Chinese adults | CVD cases | Probabilistic sensitivity analyses and one way | Validation is detailed in S1 File |
| Wilde16 | USA | 2019 | CVD-PREDICT | Full-text article | – | Microsimulation | Sugar-sweetened beverage tax | US adults aged 35–85 years | CVD cases | Probabilistic sensitivity analyses | Validated microsimulation model |
Percentage reduction in cardiovascular disease mortality
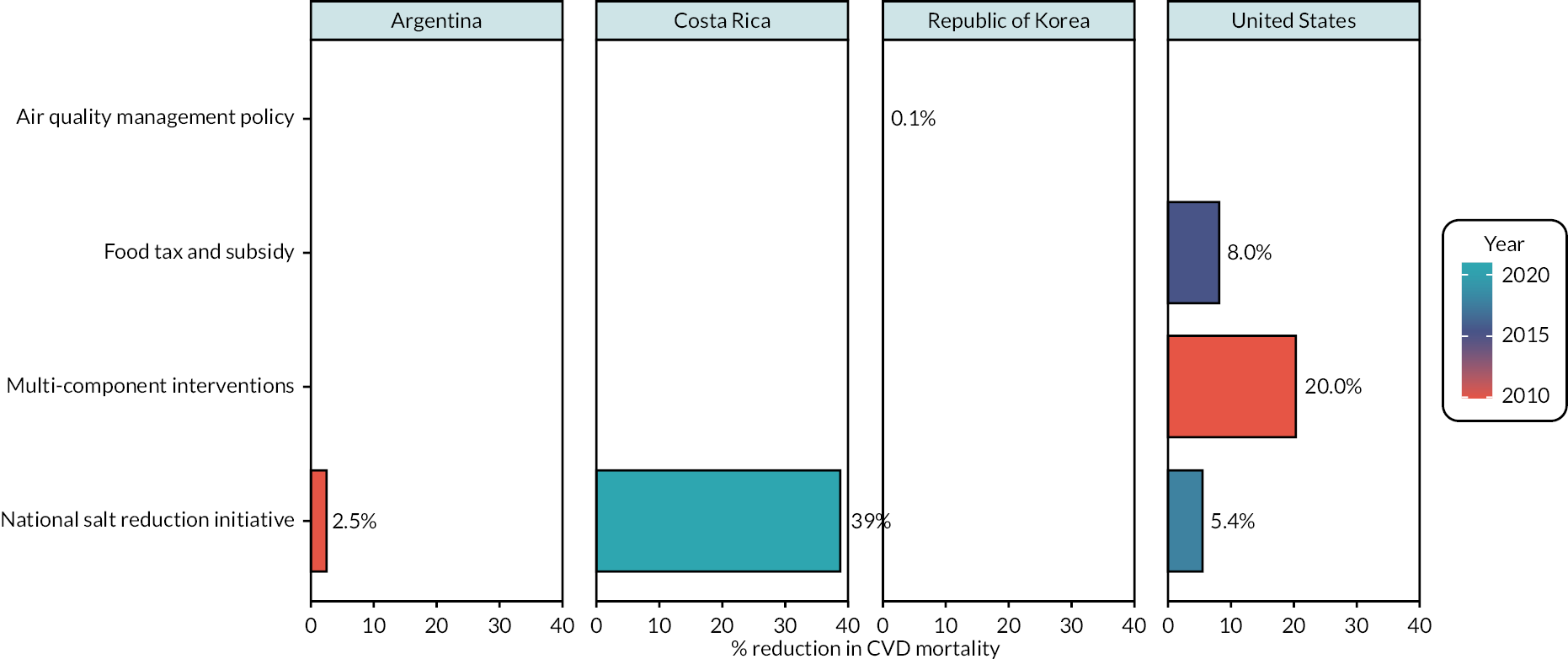
Six studies reported a percentage reduction in CVD mortality (see Figure 2). 30,35,36,53,55,64 Three studies were from the USA, one each from the Republic of South Korea, Argentina and Costa Rica. Face validation was adequate for all the studies. Internal validation was adequate in four studies and unclear in the remaining two studies (see Table 2). None of the studies reported cross-validation. External validation of the models was performed in only study and none of the studies did not perform predictive validation. The studies were published between 2010 and 2018 and the following policy-level interventions were modelled: national salt reduction initiatives (n = 3), air quality management policy (n = 1), food and tax subsidy (n = 1) and one multicomponent intervention (n = 1). The reported potential percentage reduction in CVD mortality varied across interventions modelled, from 0.1% for air quality management policy in the Republic of Korea to 39% for a national salt reduction initiative in Costa Rica. The potential benefit of a national salt reduction initiative varied across countries and periods, from a 2.5% reduction in CVD mortality in Argentina to a 39% reduction in Costa Rica. Three studies modelled different interventions among the US population. 30,36,53 Multicomponent interventions demonstrated the largest percentage reduction in CVD mortality (20%),36 followed by food tax and subsidy (8.0%)53 and a national salt reduction initiative (5.4%). 30
| Study | Year | Face validation | Internal validation | Cross-validation | External validation | Predictive validation |
|---|---|---|---|---|---|---|
| Asaria25 | 2007 | Yes | Yes | No | No | No |
| Basu26 | 2020 | Yes | Yes | No | Yes | No |
| Basu27 | 2013 | Yes | Yes | No | Yes | No |
| Basu28 | 2013 | Yes | Yes | No | Yes | Yes |
| Bibbins-Domingo29 | 2010 | Yes | Yes | No | Unclear | No |
| Choi30 | 2016 | Yes | Yes | No | Yes | No |
| Choi31 | 2017 | Yes | Yes | No | Yes | No |
| Cobiac32 | 2017 | Yes | Yes | No | Unclear | No |
| Collins18 | 2014 | Yes | Yes | No | Yes | No |
| Dehmer33 | 2020 | Yes | Yes | No | Yes | No |
| Dilley34 | 2012 | Yes | Unclear | No | Unclear | No |
| Gillespie19 | 2015 | Yes | Yes | No | Yes | No |
| Han35 | 2018 | Yes | Yes | No | Unclear | No |
| Homer36 | 2010 | Yes | Yes | No | Unclear | No |
| Hurley37 | 2008 | Yes | Yes | No | No | No |
| Kheirbek66 | 2014 | Yes | Unclear | No | No | No |
| Konfino38 | 2013 | Yes | Yes | No | No | No |
| Konfino39 | 2014 | Yes | Yes | No | Unclear | No |
| Kypridemos21 | 2017 | Yes | Yes | No | Yes | Unclear |
| Kypridemos20 | 2018 | Yes | Yes | No | Yes | Unclear |
| Lee13 | 2020 | Yes | Yes | Unclear | Yes | No |
| Liu14 | 2020 | Yes | Yes | No | Yes | No |
| Lloyd-Williams40 | 2008 | Yes | Yes | No | Unclear | No |
| Manyema41 | 2016 | Yes | Yes | No | Unclear | No |
| Marklund42 | 2020 | Yes | Yes | No | Yes | No |
| Mason43 | 2014 | Yes | Yes | No | Unclear | No |
| Mekonnen44 | 2013 | Yes | Yes | No | Yes | No |
| Moreira22 | 2015 | Yes | Yes | No | Yes | No |
| Mozaffarian15 | 2018 | Yes | Yes | No | Yes | No |
| Mhurchu45 | 2015 | Yes | Yes | No | Unclear | No |
| Nilson46 | 2020 | Yes | Yes | No | Unclear | No |
| Nnoaham47 | 2009 | Yes | Yes | No | No | No |
| O’Flaherty48 | 2012 | Yes | Yes | No | Unclear | No |
| O’Keeffe23 | 2013 | Yes | Yes | No | Yes | No |
| Pearson-Stuttard49 | 2017 | Yes | Yes | No | Yes | No |
| Pearson-Stuttard50 | 2017 | Yes | Yes | No | Yes | No |
| Eom51 | 2020 | Yes | Unclear | No | Unclear | No |
| Garney52 | 2019 | Yes | Unclear | No | Unclear | No |
| Wilde17 | 2018 | Yes | Yes | No | Yes | No |
| Sy53 | 2018 | Yes | Unclear | No | Unclear | No |
| Pearson-Stuttard54 | 2018 | Yes | Yes | No | Yes | No |
| Mejia55 | 2011 | Yes | Unclear | No | Unclear | No |
| Pearson-Stuttard56 | 2018 | Yes | Yes | No | Yes | No |
| Peñalvo57 | 2017 | Yes | Yes | No | No | No |
| Purshouse58 | 2010 | Yes | Yes | No | Yes | No |
| Sahan59 | 2016 | Yes | Yes | No | Yes | No |
| Salgado60 | 2020 | Yes | Yes | No | Yes | No |
| Sanchez-Romero61 | 2016 | Yes | Yes | No | Yes | No |
| Schönbach62 | 2018 | Yes | Yes | No | Unclear | No |
| Seferidi24 | 2018 | Yes | Yes | No | Yes | No |
| Smith-Spangler63 | 2010 | Yes | Yes | No | Unclear | No |
| Vega-Solano64 | 2021 | Yes | Yes | No | Unclear | No |
| Wang65 | 2016 | Yes | Yes | No | Yes | No |
| Wilde16 | 2019 | Yes | Yes | No | Yes | No |
FIGURE 2.
Effects of policies and structural interventions on percentage reduction in CVD mortality.
Percentage reduction in cardiovascular disease cases
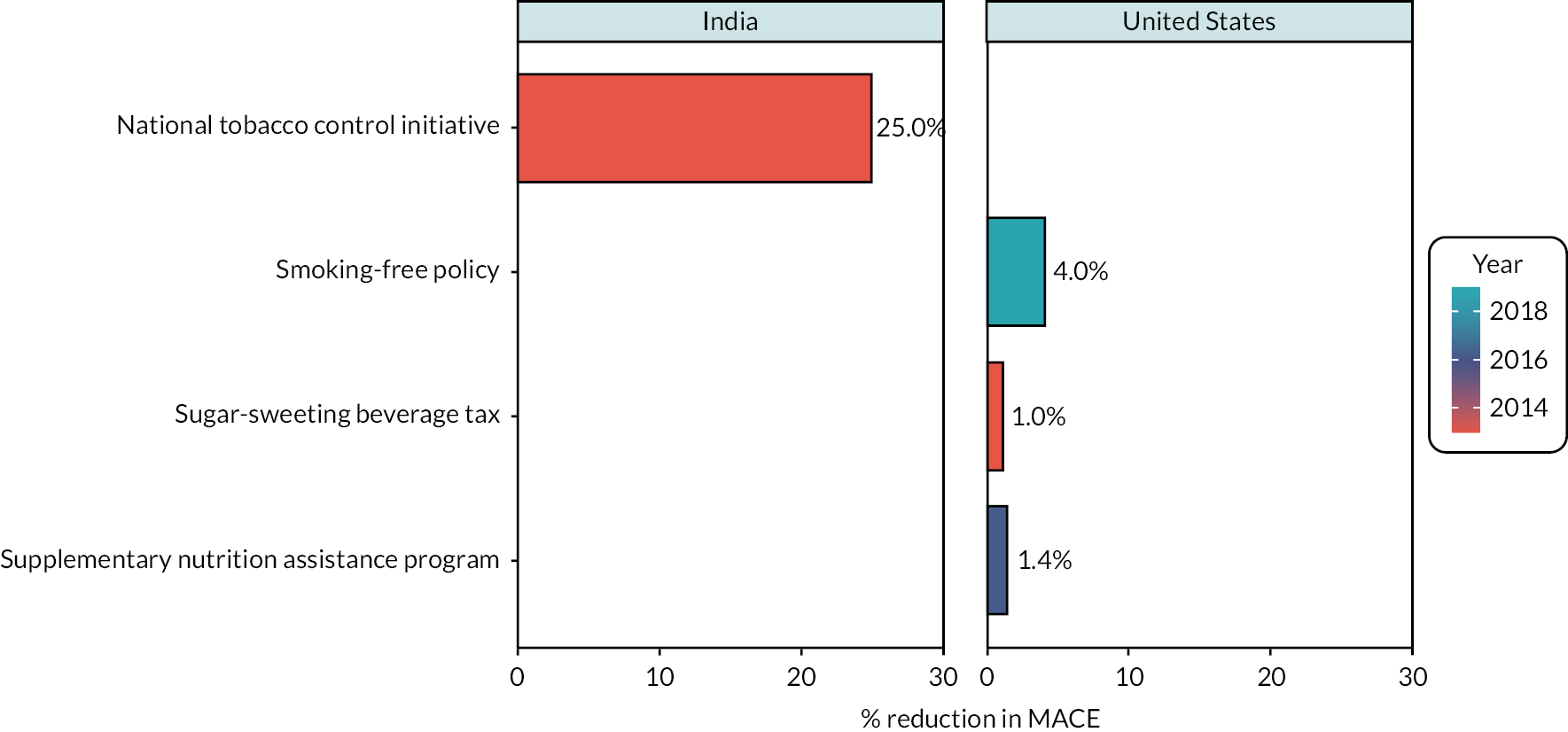
Four studies reported a percentage reduction in CVD cases (see Figure 3). 28,31,44,52 Three studies were from the USA31,44,52 and one from India. 28 Face validation was adequate for all the studies. Internal validation was adequate in three studies and unclear in one study (see Table 2). None of the studies reported cross-validation. External validation of the models was performed in three studies and none of the studies did not perform predictive validation. The studies were published between 2013 and 2019 and the following policy-level interventions were modelled: national tobacco control initiative (n = 1), smoking-free policy (n = 1), SSB tax (n = 1) and supplementary nutrition assistance programme (n = 1). The reported potential percentage reduction in CVD cases ranged from 1% for a SSB tax in the USA to 25% for a national tobacco control initiative in India. Three studies modelled different interventions among the US population. 31,44,52 A smoke smoking-free policy demonstrated the largest percentage reduction in CVD cases (4%),52 followed by a supplementary nutrition assistance programme (1.4%)31 and a SSB tax (1.0%). 31
FIGURE 3.
Effects of policies and structural interventions on percentage reduction in MACE cases.
Number of deaths prevented or postponed per year
Twenty-six studies reported the number of DPP per year (see Figure 4). 19,21–24,27,29,32,33,38–42,45–50,54,57,59,60,65,66 There were seven studies each from the USA and the UK, three from Argentina, and one each from Australia, Brazil, China, India, Ireland, New Zealand, South Africa and Turkey. One was a multicountry study. Face validation was adequate for all the studies. Internal validation was adequate in most studies (n = 25, 96%) and unclear in one study (see Table 2). None of the studies reported cross-validation. External validation of the models was performed by 14 studies (54%), not performed by 4 studies (15%) and unclear in the remaining 8 studies (31%). Most of the studies did not perform predictive validation (n = 24, 92%). The studies were published between 2008 and 2020, and the following policy-level interventions were modelled: food tax and subsidy (n = 7), national salt reduction initiative (n = 7), food and beverage tax (n = 3), air quality management policy (n = 1), eliminating industrial trans-fatty acids (n = 1), fruit and vegetable subsidy (n = 1), healthy food and lifestyle policy (n = 1), national tobacco control initiative (n = 1), palm oil tax (n = 1), reduction in ultra-processed foods (n = 1), stricter food policy (n = 1), Subsided Community Supported Agriculture (n = 1) and WHO 25 × 25 initiative (n = 1).
FIGURE 4.
Effects of policies and structural interventions on number of deaths prevented or postponed per year.
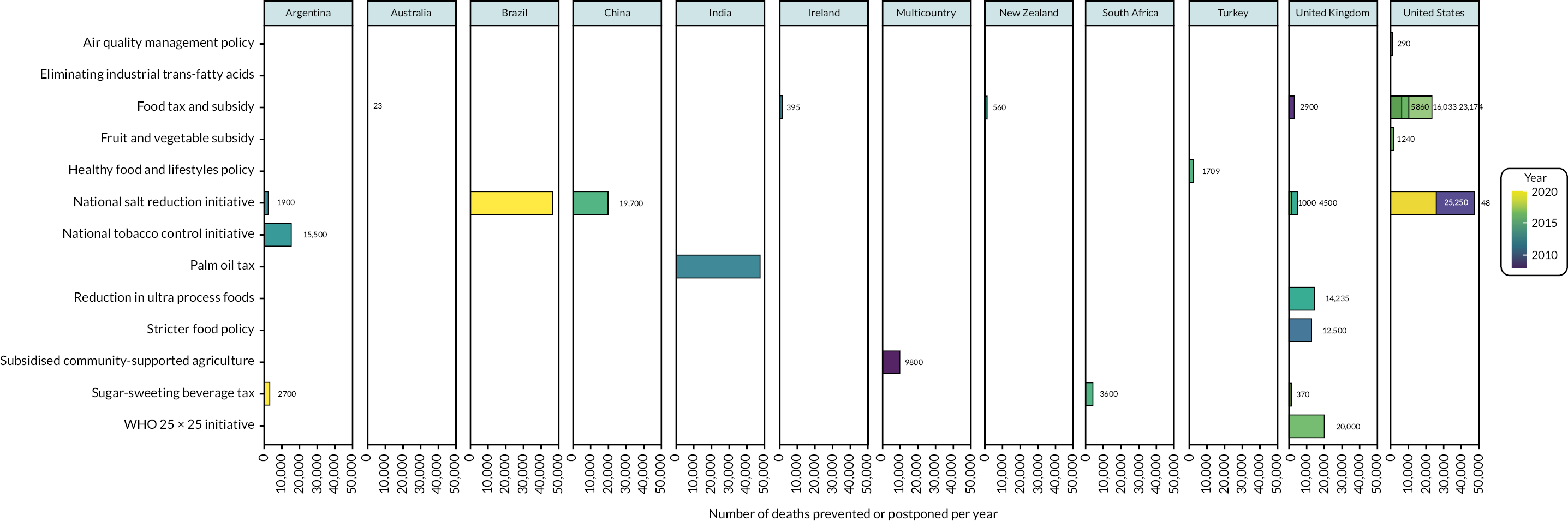
The number of DPP depended on the size of population affected but ranged from just 23 per year for eliminating industrial trans-fatty acids in Australia42 to as many as 48,000 per year for a national salt reduction initiative in the USA. 29 Evidence from Argentina38,39,60 showed that a national tobacco control initiative could prevent or postpone the largest number of deaths (15,500 deaths per year), followed by a SSB tax (2700 deaths per year) and a national salt reduction initiative (1900 deaths per year). Evidence from the USA29,33,49,50,54,57,66 showed that a national salt reduction initiative could prevent or postpone the largest number of deaths (48,000 deaths per year), while air quality management could prevent or postpone the least number of deaths (290 deaths per year). Evidence from the UK19,21,22,24,32,47,48 showed that the WHO 25 × 25 initiative could prevent or postpone the largest number of deaths (20,000 deaths per year), while a SSB tax could prevent or postpone the least number of deaths (370 deaths per year).
Number of CVD cases prevented or postponed per year
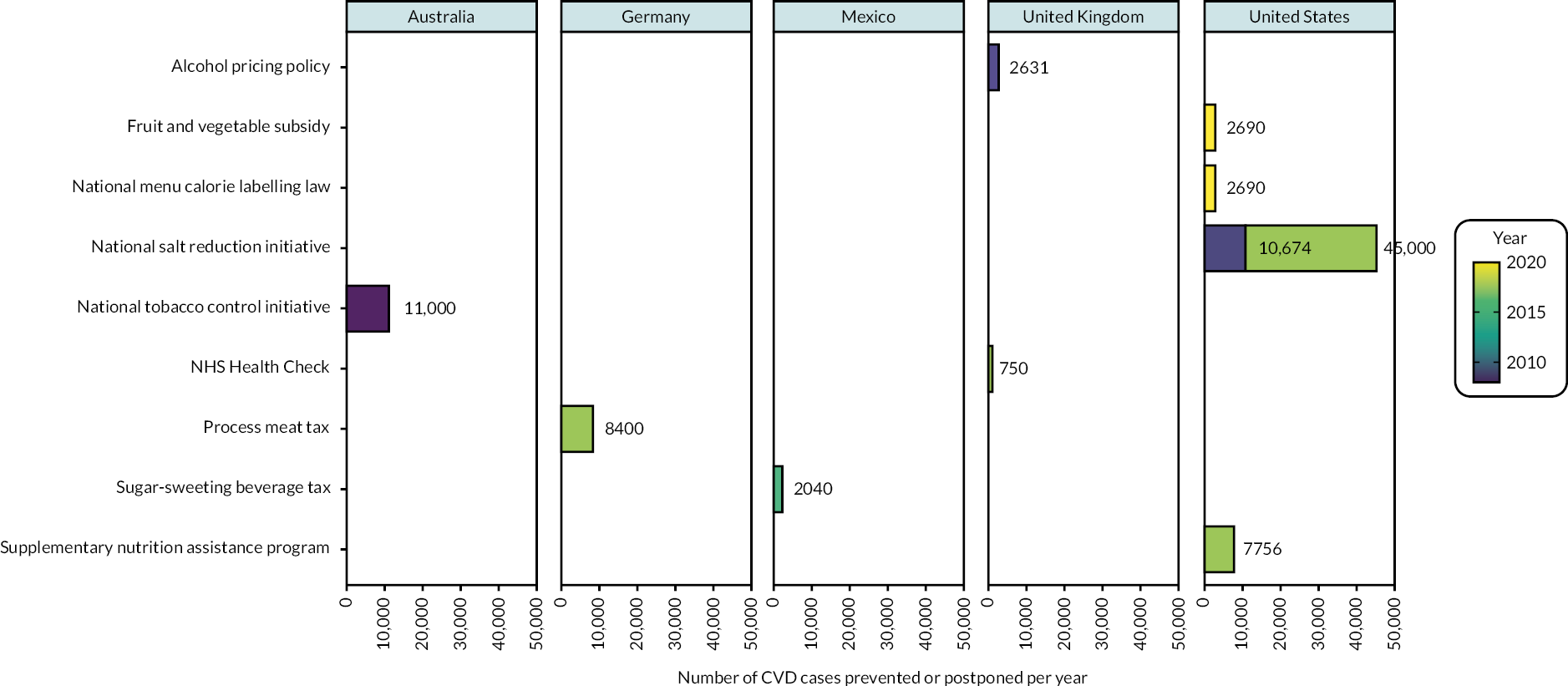
Ten studies reported the number of CVD cases prevented or postponed per year (see Figure 5). 14,15,20,37,51,54,58,61–63 Five studies were from the USA, two from the UK, and one each from Australia, Germany and Mexico. Face validation was adequate for all the studies. Internal validation was adequate in most studies (n = 9, 90%) and unclear in one study (see Table 2). None of the studies reported cross-validation. External validation of the models was performed by six studies (60%), not performed by one study (10%) and unclear in the remaining three studies (30%). Most of the studies did not perform predictive validation (n = 9, 90%). The studies were published between 2008 and 2020, and the following policy-level interventions were modelled: national salt reduction initiative (n = 2), alcohol pricing policy (n = 1), fruit and vegetable subsidy (n = 1), national menu calorie labelling law (n = 1), NHS Health Check (n = 1), processed meat tax (n = 1), SSB tax (n = 1) and supplementary nutrition assistance program (n = 1). The number of CVD cases prevented or postponed ranged from just 750 per year for the NHS Health Check in the UK20 to as many as 45,000 per year for the national salt reduction initiative in the USA. 54 Five studies modelled different interventions among the US population. 14,15,51,54,63 The national salt reduction initiative demonstrated the largest number of CVD cases prevented or postponed per year (45,000 CVD cases per year prevented), followed by supplementary nutrition assistance programmes (7756 CVD cases per year prevented), fruit and vegetable subsidies (2690 CVD cases per year prevented) and the national menu calorie labelling law (2690 CVD cases per year prevented). In the UK, a larger number of CVD cases could be prevented by alcohol pricing policy than through NHS Health Check (2631 vs. 750 CVD cases per year prevented).
FIGURE 5.
Effects of policies and structural interventions on number of CVD cases prevented or postponed per year.
Discussion
Main findings
The importance of population-level policies is becoming more widely recognised in the public health community. 67 When compared to individual-level interventions, they are more effective, cost-effective and equitable. 67 Policy-makers and the public health community must make further efforts towards shifting the focus of prevention away from individuals and towards populations. 67 Evidence about the potential benefits of a particular intervention is frequently available from a variety of sources. We included well-conducted simulation studies to examine the potential impact of structural and policy interventions at the national level. We identified 54 simulation-based studies finding that there is good evidence that population‐wide strategies could reduce the burden of CVD. The modelling studies we included suggest that these interventions could bring population‐wide reductions in the burden of CVD.
Diet and nutrition, tobacco and alcohol control, and other programmes are among the policy simulation models explored. The diet and nutrition initiatives included food taxes and subsidies, healthy food and lifestyles policies, palm oil tax, processed meat tax, reduction in ultra-processed foods, supplementary nutrition assistance programmes, stricter food policy and subsidised community-supported agriculture. Initiatives to reduce tobacco and alcohol use included a smoking ban, a national tobacco control initiative and a tax on alcohol. The other programmes we identified included the NHS Health Check, WHO 25 × 25 and air quality management policy. Our review shows that taxation on tobacco, salt, sugar and alcohol is the most potential impactful structural intervention to reduce CVD events and mortality at the population level.
Simulation and modelling studies are important tools in supporting evidence for the effectiveness of primary prevention of CVD. 68–71 These types of studies allow researchers to investigate the potential impact of interventions on population health, without having to conduct large, costly and time-consuming RCTs. 72 One advantage of simulation and modelling studies is that they can be used to estimate the potential impact of an intervention on a population level. 68–71 For example, a simulation study could be used to estimate the number of CVD cases that would be prevented by increasing physical activity levels in a population. This information can be used to inform public health policy and decision-making. Another advantage of simulation and modelling studies is that they can be used to investigate the impact of interventions in subpopulations that may be difficult to study in RCTs. For example, a modelling study could be used to investigate the impact of a dietary intervention on CVD risk in older adults. Simulation and modelling studies also can combine multiple interventions and assess their joint effect on population health; this is a critical aspect for primary prevention of CVD as it often involves multifactorial interventions. Overall, simulation and modelling studies are an important complementary tool to RCTs in providing evidence for the effectiveness of primary prevention of CVD. 68–71
Strengths and limitations
This systematic review has several advantages. Firstly, our study’s main strength was that we conducted a thorough up-to-date overview of the status of policy-level intervention models internationally, using search of the published literature to undertake a comprehensive review of their potential impact on primary prevention of CVD. Second, using appropriate validated tools, two reviewers independently checked all papers and assessed quality. Third, we documented the effect size used in each modelling paper, as well as the source reference. Finally, the studies included a wide range of interventions across a wide range of countries, providing highly useful estimates of potential impact and information to design future policies and action.
This review however has some limitations. Simulation and modelling studies are important tools in supporting evidence for the effectiveness of primary prevention of CVD, but they also have limitations that should be considered. 73–77 One limitation of simulation and modelling studies is that they rely on assumptions and estimates. For example, a simulation study may assume that a certain percentage of the population will respond to an intervention in a certain way. If these assumptions are not accurate, the results of the simulation may not be valid. Additionally, the accuracy of the simulation is dependent on the quality and availability of data used to input the model. Another limitation of simulation and modelling studies is that they may not capture all the complex interactions that occur in real-world settings. Additionally, simulation and modelling studies are mostly based on observational data, which is subject to the same limitations as observational studies. Observational studies are often excluded in systematic reviews of primary prevention of CVD due to their inherent limitations. One of the main limitations is the potential for bias, such as selection bias and confounding variables, which can make it difficult to determine causality between the intervention and the outcome. 73–77 This can make it challenging to draw valid conclusions from observational studies and make them less informative compared to RCTs which have a higher level of evidence. Moreover, observational studies are often subject to measurement errors, which can lead to inaccurate results. This can further decrease the validity and generalisability of the results.
We have been unable to undertake a formal meta-analysis because the studies were so diverse. Publication bias is still a possibility, which could lead to an overestimation of the real effects of some interventions. Furthermore, the positive effects of policy changes may appear to be greater when favourable underpinning secular trends are not formally considered. There is significant heterogeneity in simulation models, making output data significantly incomparable between models; thus, the studies in the analysis may not be necessarily comparable. While policy interventions typically include a variety of strategies, none of the models considered interrelations between multiple policies and potential interactions. Different aspects of these policies may have varying effects.
Another important limitation of the studies reviewed is that they primarily reported on major cardiovascular events, such as heart attacks and strokes, but did not report on other CVD outcomes such as cardiomyopathies. By not reporting on these outcomes, the studies may not provide a comprehensive understanding of the impact of the interventions on CVD. Furthermore, it may make it difficult to draw conclusions about the effectiveness of the interventions in preventing different types of CVD. This limitation should be taken into consideration when interpreting the results of the studies and considering the implications for public health policy and clinical practice.
Implications for future research and policy
Our research uncovered a number of evidence gaps that merit additional investigation. First, no real-world policy impact studies were uncovered. Though we discovered that policies and structural interventions aimed at reducing CVD could reduce the burden of CVD and save money if implemented over time, the feasibility of implementing policy changes also warrants further investigation. Many elements, including political feasibility and stakeholder engagement, can help or hinder successful policy formulation.
In a number of other areas, more research is required. Longitudinal studies, for example, are required to increase the evidence base and to aid in the identification of precise combinations of interventions that have the greatest impact on deaths avoided or postponed. These longitudinal studies need to be broader and more representative of target populations likely to benefit. In addition, the adoption of common measures to compare different initiatives and communities would help to boost such evaluation efforts. A standardised evaluation system across various policy-level interventions would be immensely valuable and might serve as a policy lever at the regional or national levels, inspiring greater action. Future study on the effectiveness of policy-level interventions in various populations and settings, as well as intervention effectiveness among different communities or populations with differing demography, would be beneficial. Finally, research that investigates dose–response and interactions between numerous modifications as well as longer-term clinical outcomes can help us better understand the potential impact of policy-level interventions.
Patient and public involvement
Drawing on INVOLVE guidance and support for best practice, we worked closely with three dedicated patient and public involvement advisors, and we welcomed guidance and support from our advisors during the preparatory phase of the project.
Conclusion
We found from simulation studies that there is evidence that population‐wide strategies could reduce the burden of CVD. There was no RCT evidence to support effectiveness of multifactorial ‘high-risk’ strategies for reducing stroke and CVD incidence and mortality. Policy-makers, politicians and public health professionals should continue to work to prioritise these population-wide strategies for CVD prevention.
Acknowledgements
Contributions of authors
Olalekan A. Uthman (https://orcid.org/0000-0002-8567-3081) (Professor, Evidence Synthesis) contributed to the protocol, study selection, data extraction, validity assessments and synthesis of the included studies. He developed the classifiers and undertook the analyses. He also contributed to the interpretation of the results and the writing of the report and had overall responsibility for the project.
Rachel Court (https://orcid.org/0000-0002-4567-2586) (Information Specialist) contributed to the protocol development, developed the search strategies, and wrote the sections of the report relating to the literature searches. She also contributed to the protocol and interpretation of the results and commented on drafts of the report.
Seun Anjorin (https://orcid.org/0000-0003-0187-6410) (Research Associate) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. He also contributed to the interpretation of the results and the writing of the report.
Jodie Enderby (https://orcid.org/0000-0002-1446-7512) (Research Associate) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. She also contributed to the interpretation of the results and the writing of the report.
Lena Al-Khudairy (https://orcid.org/0000-0003-0638-583X) (Associate Professor, Evidence Synthesis) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. She also contributed to the interpretation of the results and the writing of the report.
Chidozie Nduka (https://orcid.org/0000-0001-7031-5444) (Senior Research Fellow, Evidence Synthesis) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. He also contributed to the interpretation of the results and the writing of the report.
Hema Mistry (https://orcid.org/0000-0002-5023-1160) (Associate Professor, Health Economics) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. She also contributed to the interpretation of the results and the writing of the report.
G. J. Melendez-Torres (https://orcid.org/0000-0002-9823-4790) (Professor, Evidence Synthesis) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. He also contributed to the interpretation of the results and the writing of the report.
Sian Taylor-Phillips (https://orcid.org/0000-0002-1841-4346) (Professor, Evidence Synthesis) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. She also contributed to the interpretation of the results and the writing of the report.
Aileen Clarke (https://orcid.org/0000-0001-8299-3146) (Professor, Evidence Synthesis) contributed to the protocol, study selection, validity assessments and synthesis of the included studies. She also contributed to the interpretation of the results and the writing of the report.
Ethics statement
This work is a systematic review of accessing, processing and analysing data that has already been published and is available to the public. As a result, no patient data were processed; and patient consent and/or registration via human research ethics committees were, therefore, not relevant.
Data-sharing statement
No new data have been created in the preparation of this article and therefore there is nothing available for access and further sharing. All queries should be submitted to the corresponding author.
Consent for publication
Not applicable.
This article
The contractual start date for this research was in February 2019. This article began editorial review in June 2022 and was accepted for publication in April 2023. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Health Technology Assessment editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Disclaimer
This article presents independent research funded by the National Institute for Health and Care Research (NIHR) Health Technology Assessment programme as award number 17/148/05. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the Health Technology Assessment programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the Health Technology Assessment programme or the Department of Health and Social Care.
This article reports on one component of the research award The potential impact of policies and structural interventions in reducing cardiovascular disease and mortality: a systematic review of simulation-based studies. For more information about this research please view the award page [https://www.fundingawards.nihr.ac.uk/award/17/148/05]
References
- BHF . Facts and Figures 2022. https://www.bhf.org.uk/what-we-do/news-from-the-bhf/contact-the-press-office/facts-and-figures#:~:text=Heart%20and%20circulatory%20diseases%20cause,men%20and%203.6%20million%20women (accessed 20 January 2023).
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol 2020;76:2982-3021. https://doi.org/10.1016/j.jacc.2020.11.010.
- Feigin VL, Brainin M, Norrving B, Gorelick PB, Dichgans M, Wang W, et al. What is the best mix of population-wide and high-risk targeted strategies of primary stroke and cardiovascular disease prevention?. J Am Heart Assoc 2020;9. https://doi.org/10.1161/jaha.119.014494.
- Freebairn L, Atkinson J, Kelly P, McDonnell G, Rychetnik L. Simulation modelling as a tool for knowledge mobilisation in health policy settings: a case study protocol. Health Res Policy Syst 2016;14. https://doi.org/10.1186/s12961-016-0143-y.
- Salleh S, Thokala P, Brennan A, Hughes R, Booth A. Simulation modelling in healthcare: an umbrella review of systematic literature reviews. PharmacoEconomics 2017;35:937-49. https://doi.org/10.1007/s40273-017-0523-3.
- Xue H, Slivka L, Igusa T, Huang TT, Wang Y. Applications of systems modelling in obesity research. Obes Rev 2018;19:1293-308. https://doi.org/10.1111/obr.12695.
- Eddy DM, Hollingworth W, Caro JJ, Tsevat J, McDonald KM, Wong JB. ISPOR−SMDM Modeling Good Research Practices Task Force . Model transparency and validation: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force–7. Value Health 2012;15:843-50. https://doi.org/10.1016/j.jval.2012.04.012.
- Hanney SR, Gonzalez-Block MA, Buxton MJ, Kogan M. The utilisation of health research in policy-making: concepts, examples and methods of assessment. Health Res Policy Syst 2003;1. https://doi.org/10.1186/1478-4505-1-2.
- Moberg J, Oxman AD, Rosenbaum S, Schünemann HJ, Guyatt G, Flottorp S, et al. GRADE Working Group . The GRADE Evidence to Decision (EtD) framework for health system and public health decisions. Health Res Policy Syst 2018;16. https://doi.org/10.1186/s12961-018-0320-2.
- Meyers DG, Neuberger JS, He J. Cardiovascular effect of bans on smoking in public places: a systematic review and meta-analysis. J Am Coll Cardiol 2009;54:1249-55. https://doi.org/10.1016/j.jacc.2009.07.022.
- Downs SM, Bloem MZ, Zheng M, Catterall E, Thomas B, Veerman L, et al. The impact of policies to reduce trans fat consumption: a systematic review of the evidence. Curr Dev Nutr 2017;1. https://doi.org/10.3945/cdn.117.000778.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021;10. https://doi.org/10.1186/s13643-021-01626-4.
- Lee Y, Mozaffarian D, Sy S, Liu J, Wilde PE, Marklund M, et al. Health impact and cost-effectiveness of volume, tiered, and absolute sugar content sugar-sweetened beverage tax policies in the United States: a microsimulation study. Circulation 2020;142:523-34. https://doi.org/10.1161/circulationaha.119.042956.
- Liu J, Mozaffarian D, Sy S, Lee Y, Wilde PE, Abrahams-Gessel S, et al. FOOD-PRICE (Policy Review and Intervention Cost-Effectiveness) Project . Health and economic impacts of the National Menu Calorie Labeling Law in the United States: a microsimulation study. Circ Cardiovasc Qual Outcomes 2020;13. https://doi.org/10.1161/circoutcomes.119.006313.
- Mozaffarian D, Liu J, Sy S, Huang Y, Rehm C, Lee Y, et al. Cost-effectiveness of financial incentives and disincentives for improving food purchases and health through the US Supplemental Nutrition Assistance Program (SNAP): a microsimulation study. PLOS Med 2018;15. https://doi.org/10.1371/journal.pmed.1002661.
- Wilde P, Huang Y, Sy S, Abrahams-Gessel S, Jardim TV, Paarlberg R, et al. Cost-effectiveness of a US national sugar-sweetened beverage tax with a multistakeholder approach: who pays and who benefits. Am J Public Health 2019;109:276-84. https://doi.org/10.2105/ajph.2018.304803.
- Wilde P, Huang Y, Sy S, Abrahams-Gessel S, Jardim TV, Paarlberg R, et al. Abstract P229: cost-effectiveness of a US national sugar-sweetened beverage tax using a multi-stakeholder approach. Circulation 2018;137. https://doi.org/10.1161/circ.137.suppl_1.p229.
- Collins M, Mason H, O’Flaherty M, Guzman-Castillo M, Critchley J, Capewell S. An economic evaluation of salt reduction policies to reduce coronary heart disease in England: a policy modeling study. Value Health 2014;17:517-24. https://doi.org/10.1016/j.jval.2014.03.1722.
- Gillespie DO, Allen K, Guzman-Castillo M, Bandosz P, Moreira P, McGill R, et al. The health equity and effectiveness of policy options to reduce dietary salt intake in England: policy forecast. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0127927.
- Kypridemos C, Collins B, McHale P, Bromley H, Parvulescu P, Capewell S, et al. Future cost-effectiveness and equity of the NHS Health Check cardiovascular disease prevention programme: Microsimulation modelling using data from Liverpool, UK. PLOS Med 2018;15. https://doi.org/10.1371/journal.pmed.1002573.
- Kypridemos C, Guzman-Castillo M, Hyseni L, Hickey GL, Bandosz P, Buchan I, et al. Estimated reductions in cardiovascular and gastric cancer disease burden through salt policies in England: an IMPACTNCD microsimulation study. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-013791.
- Moreira PV, Baraldi LG, Moubarac JC, Monteiro CA, Newton A, Capewell S, et al. Comparing different policy scenarios to reduce the consumption of ultra-processed foods in UK: impact on cardiovascular disease mortality using a modelling approach. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0118353.
- O’Keeffe C, Kabir Z, O’Flaherty M, Walton J, Capewell S, Perry IJ. Modelling the impact of specific food policy options on coronary heart disease and stroke deaths in Ireland. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2013-002837.
- Seferidi P, Laverty AA, Pearson-Stuttard J, Guzman-Castillo M, Collins B, Capewell S, et al. Implications of Brexit on the effectiveness of the UK soft drinks industry levy upon CHD in England: a modelling study. Public Health Nutr 2018;21:3431-9. https://doi.org/10.1017/s1368980018002367.
- Asaria P, Chisholm D, Mathers C, Ezzati M, Beaglehole R. Chronic disease prevention: health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 2007;370:2044-53. https://doi.org/10.1016/s0140-6736(07)61698-5.
- Basu S, O’Neill J, Sayer E, Petrie M, Bellin R, Berkowitz SA. Population health impact and cost-effectiveness of community-supported agriculture among low-income US adults: a microsimulation analysis. Am J Public Health 2020;110:119-26. https://doi.org/10.2105/ajph.2019.305364.
- Basu S, Babiarz KS, Ebrahim S, Vellakkal S, Stuckler D, Goldhaber-Fiebert JD. Palm oil taxes and cardiovascular disease mortality in India: economic-epidemiologic model. BMJ 2013;347. https://doi.org/10.1136/bmj.f6048.
- Basu S, Glantz S, Bitton A, Millett C. The effect of tobacco control measures during a period of rising cardiovascular disease risk in India: a mathematical model of myocardial infarction and stroke. PLOS Med 2013;10. https://doi.org/10.1371/journal.pmed.1001480.
- Bibbins-Domingo K, Chertow GM, Coxson PG, Moran A, Lightwood JM, Pletcher MJ, et al. Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med 2010;362:590-9. https://doi.org/10.1056/NEJMoa0907355.
- Choi SE, Brandeau ML, Basu S. Expansion of the national salt reduction initiative: a mathematical model of benefits and risks of population-level sodium reduction. Med Decis Making 2016;36:72-85. https://doi.org/10.1177/0272989x15583846.
- Choi SE, Seligman H, Basu S. Cost effectiveness of subsidizing fruit and vegetable purchases through the supplemental nutrition assistance program. Am J Prev Med 2017;52:e147-55. https://doi.org/10.1016/j.amepre.2016.12.013.
- Cobiac LJ, Scarborough P. Translating the WHO 25 × 25 goals into a UK context: the PROMISE modelling study. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-012805.
- Dehmer SP, Cogswell ME, Ritchey MD, Hong Y, Maciosek MV, LaFrance AB, et al. Health and budgetary impact of achieving 10-year U.S. sodium reduction targets. Am J Prev Med 2020;59:211-8. https://doi.org/10.1016/j.amepre.2020.03.010.
- Dilley JA, Harris JR, Boysun MJ, Reid TR. Program, policy, and price interventions for tobacco control: quantifying the return on investment of a state tobacco control program. Am J Public Health 2012;102:e22-8. https://doi.org/10.2105/ajph.2011.300506.
- Han C, Lim YH, Yorifuji T, Hong YC. Air quality management policy and reduced mortality rates in Seoul metropolitan area: a quasi-experimental study. Environ Int 2018;121:600-9. https://doi.org/10.1016/j.envint.2018.09.047.
- Homer J, Milstein B, Wile K, Trogdon J, Huang P, Labarthe D, et al. Simulating and evaluating local interventions to improve cardiovascular health. Prev Chronic Dis 2010;7.
- Hurley SF, Matthews JP. Cost-effectiveness of the Australian National Tobacco Campaign. Tob Control 2008;17:379-84. https://doi.org/10.1136/tc.2008.025213.
- Konfino J, Mekonnen TA, Coxson PG, Ferrante D, Bibbins-Domingo K. Projected impact of a sodium consumption reduction initiative in Argentina: an analysis from the CVD policy model–Argentina. PLOS ONE 2013;8. https://doi.org/10.1371/journal.pone.0073824.
- Konfino J, Ferrante D, Mejia R, Coxson P, Moran A, Goldman L, et al. Impact on cardiovascular disease events of the implementation of Argentina’s national tobacco control law. Tob Control 2014;23. https://doi.org/10.1136/tobaccocontrol-2012-050599.
- Lloyd-Williams F, O’Flaherty M, Mwatsama M, Birt C, Ireland R, Capewell S. Estimating the cardiovascular mortality burden attributable to the European Common Agricultural Policy on dietary saturated fats. Bull World Health Organ 2008;86:535-41a. https://doi.org/10.2471/blt.08.053728.
- Manyema M, Veerman LJ, Tugendhaft A, Labadarios D, Hofman KJ. Modelling the potential impact of a sugar-sweetened beverage tax on stroke mortality, costs and health-adjusted life years in South Africa. BMC Public Health 2016;16. https://doi.org/10.1186/s12889-016-3085-y.
- Marklund M, Zheng M, Veerman JL, Wu JHY. Estimated health benefits, costs, and cost-effectiveness of eliminating industrial trans-fatty acids in Australia: a modelling study. PLOS Med 2020;17. https://doi.org/10.1371/journal.pmed.1003407.
- Mason H, Shoaibi A, Ghandour R, O’Flaherty M, Capewell S, Khatib R, et al. MedCHAMPS project team . A cost effectiveness analysis of salt reduction policies to reduce coronary heart disease in four Eastern Mediterranean countries. PLOS ONE 2014;9. https://doi.org/10.1371/journal.pone.0084445.
- Mekonnen TA, Odden MC, Coxson PG, Guzman D, Lightwood J, Wang YC, et al. Health benefits of reducing sugar-sweetened beverage intake in high risk populations of California: results from the cardiovascular disease (CVD) policy model. PLOS ONE 2013;8. https://doi.org/10.1371/journal.pone.0081723.
- Ni Mhurchu C, Eyles H, Genc M, Scarborough P, Rayner M, Mizdrak A, et al. Effects of health-related food taxes and subsidies on mortality from diet-related disease in New Zealand: an econometric-epidemiologic modelling study. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0128477.
- Nilson EAF, Metlzer AB, Labonté ME, Jaime PC. Modelling the effect of compliance with WHO salt recommendations on cardiovascular disease mortality and costs in Brazil. PLOS ONE 2020;15. https://doi.org/10.1371/journal.pone.0235514.
- Nnoaham KE, Sacks G, Rayner M, Mytton O, Gray A. Modelling income group differences in the health and economic impacts of targeted food taxes and subsidies. Int J Epidemiol 2009;38:1324-33. https://doi.org/10.1093/ije/dyp214.
- O’Flaherty M, Flores-Mateo G, Nnoaham K, Lloyd-Williams F, Capewell S. Potential cardiovascular mortality reductions with stricter food policies in the United Kingdom of Great Britain and Northern Ireland. Bull World Health Organ 2012;90:522-31. https://doi.org/10.2471/blt.11.092643.
- Pearson-Stuttard J, Bandosz P, Rehm CD, Penalvo J, Whitsel L, Gaziano T, et al. Reducing US cardiovascular disease burden and disparities through national and targeted dietary policies: a modelling study. PLOS Med 2017;14. https://doi.org/10.1371/journal.pmed.1002311.
- Pearson-Stuttard J, Bandosz P, Rehm CD, Afshin A, Peñalvo JL, Whitsel L, et al. Comparing effectiveness of mass media campaigns with price reductions targeting fruit and vegetable intake on US cardiovascular disease mortality and race disparities. Am J Clin Nutr 2017;106:199-206. https://doi.org/10.3945/ajcn.116.143925.
- Eom H, Yi SS, Bu D, Russo R, Bellows B, Zhang Y, et al. Abstract MP76: assessing the impact of the ‘Health Bucks’ program on cardiovascular disease in New York city: a modeling study. Circulation 2020;141. https://doi.org/10.1161/circ.141.suppl_1.MP76.
- Garney WR, Garcia KM. Abstract P003: evaluating comprehensive smoke free policy at the community level using systems modeling. Circulation 2019;139. https://doi.org/10.1161/circ.139.suppl_1.P003.
- Sy S, Peñalvo J, Abrahams-Gessel S, Alam S, Pandya A, Mozaffarian D, et al. Abstract P280: changes in food prices improve Cardiovascular Disease (CVD) outcomes. Circulation 2016;133. https://doi.org/10.1161/circ.133.suppl_1.p280.
- Pearson-Stuttard J, Kypridemos C, Collins B, Mozaffarian D, Huang Y, Bandosz P, et al. Estimating the health and economic effects of the proposed US Food and Drug Administration voluntary sodium reformulation: Microsimulation cost-effectiveness analysis. PLOS Med 2018;15. https://doi.org/10.1371/journal.pmed.1002551.
- Mejia R, Ferrante D, Perez-Stable EJ, Bibbins-Domingo K, Coxson P, Goldman L, et al. Projected effect of dietary salt reductions on future cardiovascular disease in Argentina Conference: 34th Annual Meeting of the Society of General Internal Medicine. Phoenix, AZ, United States. Conference Publication: (var. pagings). J Gen Intern Med 2011;26. https://doi.org/10.1007/s11606-011-1730-9.
- Pearson-Stuttard J, Bnadosz P, Rehm CD, Afshin A, Penalvo J, Whitsel L, et al. Abstract P281: comparing the impact of price change and mass media campaigns in reducing cardiovascular disease mortality and disparities in the US. Circulation 2016;133. https://doi.org/10.1161/circ.133.suppl_1.p281.
- Peñalvo JL, Cudhea F, Micha R, Rehm CD, Afshin A, Whitsel L, et al. The potential impact of food taxes and subsidies on cardiovascular disease and diabetes burden and disparities in the United States. BMC Med 2017;15. https://doi.org/10.1186/s12916-017-0971-9.
- Purshouse RC, Meier PS, Brennan A, Taylor KB, Rafia R. Estimated effect of alcohol pricing policies on health and health economic outcomes in England: an epidemiological model. Lancet 2010;375:1355-64. https://doi.org/10.1016/s0140-6736(10)60058-x.
- Sahan C, Sozmen K, Unal B, O’Flaherty M, Critchley J. Potential benefits of healthy food and lifestyle policies for reducing coronary heart disease mortality in Turkish adults by 2025: a modelling study. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2016-011217.
- Salgado MV, Penko J, Fernandez A, Konfino J, Coxson PG, Bibbins-Domingo K, et al. Projected impact of a reduction in sugar-sweetened beverage consumption on diabetes and cardiovascular disease in Argentina: a modeling study. PLOS Med 2020;17. https://doi.org/10.1371/journal.pmed.1003224.
- Sánchez-Romero LM, Penko J, Coxson PG, Fernández A, Mason A, Moran AE, et al. Projected impact of Mexico’s sugar-sweetened beverage tax policy on diabetes and cardiovascular disease: a modeling study. PLOS Med 2016;13. https://doi.org/10.1371/journal.pmed.1002158.
- Schönbach JK, Thiele S, Lhachimi SK. What are the potential preventive population-health effects of a tax on processed meat? A quantitative health impact assessment for Germany. Prev Med 2019;118:325-31. https://doi.org/10.1016/j.ypmed.2018.11.011.
- Smith-Spangler CM, Juusola JL, Enns EA, Owens DK, Garber AM. Population strategies to decrease sodium intake and the burden of cardiovascular disease: a cost-effectiveness analysis. Ann Intern Med 2010;152:481-7. https://doi.org/10.7326/0003-4819-152-8-201004200-00212.
- Vega-Solano J, Blanco-Metzler A, Madriz-Morales K, Fernandes-Nilson EA, Labonté ME. Impact of salt intake reduction on CVD mortality in Costa Rica: a scenario modelling study. PLOS ONE 2021;16. https://doi.org/10.1371/journal.pone.0245388.
- Wang M, Moran AE, Liu J, Coxson PG, Penko J, Goldman L, et al. Projected impact of salt restriction on prevention of cardiovascular disease in China: a modeling study. PLOS ONE 2016;11. https://doi.org/10.1371/journal.pone.0146820.
- Kheirbek I, Haney J, Douglas S, Ito K, Caputo S, Matte T. The public health benefits of reducing fine particulate matter through conversion to cleaner heating fuels in New York City. Environ Sci Technol 2014;48:13573-82. https://doi.org/10.1021/es503587p.
- Salgado MV, O’Flaherty M, Mejía R. The role of computer simulation models in the design of public policies. Medicina (B Aires) 2020;80:681-4.
- Egger M, Moons KGM, Fletcher CG. GetReal: from efficacy in clinical trials to relative effectiveness in the real world. Res Synth Methods 2016;7:278-81. https://doi.org/10.1002/jrsm.1207.
- Eichler H-G, Abadie E, Breckenridge A, Flamion B, Gustafsson LL, Leufkens H, et al. Bridging the efficacy-effectiveness gap: a regulator’s perspective on addressing variability of drug response. Nat Rev Drug Discovery 2011;10:495-506. https://doi.org/10.1038/nrd3501.
- Garnett GP, Cousens S, Hallett TB, Steketee R, Walker N. Mathematical models in the evaluation of health programmes. Lancet 2011;378:515-25. https://doi.org/10.1016/s0140-6736(10)61505-x.
- Weinstein MC, Toy EL, Sandberg EA, Neumann PJ, Evans JS, Kuntz KM, et al. Modeling for health care and other policy decisions: uses, roles, and validity. Value Health 2001;4:348-61. https://doi.org/10.1046/j.1524-4733.2001.45061.x.
- Victora CG, Habicht JP, Bryce J. Evidence-based public health: moving beyond randomized trials. Am J Public Health 2004;94:400-5. https://doi.org/10.2105/ajph.94.3.400.
- Boyko EJ. Observational research–opportunities and limitations. J Diabetes Complications 2013;27:642-8. https://doi.org/10.1016/j.jdiacomp.2013.07.007.
- Gueyffier F, Cucherat M. The limitations of observation studies for decision making regarding drugs efficacy and safety. Therapie 2019;74:181-5. https://doi.org/10.1016/j.therap.2018.11.001.
- Lipsitch M, Tchetgen Tchetgen E, Cohen T. Negative controls: a tool for detecting confounding and bias in observational studies. Epidemiology 2010;21:383-8. https://doi.org/10.1097/EDE.0b013e3181d61eeb.
- Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al. American Heart Association Strategic Planning Task Force and Statistics Committee . Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic impact goal through 2020 and beyond. Circulation 2010;121:586-613. https://doi.org/10.1161/circulationaha.109.192703.
- Metelli S, Chaimani A. Challenges in meta-analyses with observational studies. Evid Based Ment Health 2020;23:83-7. https://doi.org/10.1136/ebmental-2019-300129.
List of abbreviations
- CHD
- coronary heart disease
- CVD
- cardiovascular disease
- DPP
- deaths prevented or postponed
- IMPACT
- infliximab multinational psoriatic arthritis controlled trial
- MACE
- major cardiovascular event
- MI
- myocardial infarction
- PSA
- probabilistic sensitivity analysis
- RCT
- randomised controlled trial
- SSB
- sugar-sweetened beverage
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/NMFG0214).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.