

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 14/184/02. The contractual start date was in April 2017. The final report began editorial review in January 2020 and was accepted for publication in July 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2021. This work was produced by Ponsford et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2021 Queen’s Printer and Controller of HMSO
Chapter 1 Background
This chapter includes material reproduced or adapted from Ponsford et al. 1 This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. The text includes minor additions and formatting changes to the original text.
Description of the problem
The UK has the highest rate of teenage births in western Europe, despite significant declines over the last 20 years and the success of the England Teenage Pregnancy Strategy. 2,3 Teenagers are the age group at highest risk of unplanned pregnancy, with around half of conceptions to those aged < 18 years ending in abortion. 4 Even after controlling for prior disadvantage, teenage parenthood is associated with adverse medical, social, educational and economic outcomes for both mothers5–7 and children. 8,9 Teenage childbearing is subject to and contributes to health inequalities. 10 In 2006, teenage pregnancy cost the NHS £63M per year. 11 In 2009–10, £26M was paid in benefits to teenage mothers on income support. 12 Other adverse sexual health outcomes also cost the NHS large sums. 13,14 Reducing rates of unintended teenage pregnancy in England, therefore, remains a priority. Existing systematic reviews suggest that traditional classroom-based relationships and sex education (RSE) may not be sufficient on its own to produce consistent, sizeable and sustained changes in the behaviours underlying teenage pregnancy and, therefore, population-level reductions in this outcome. 15–17
Description of the intervention
A recent systematic review of social-marketing interventions to reduce teenage pregnancy examined studies of interventions embracing social-marketing elements,18 regardless of whether or not these were explicitly termed ‘social marketing’. 19 Heterogeneity precluded meta-analysis, but narrative synthesis concluded that this was a promising approach. 19 We developed an intervention, Positive Choices, with the National Children’s Bureau’s (NCB’s) Sex Education Forum (SEF) and other stakeholders. This intervention was informed by selected components from two effective interventions included in the above review – ‘Safer Choices’ and the ‘Children’s Aid Society (CAS) Carrera’ programme – plus selected elements from the ‘Gatehouse Project’, which, although not included in the review, also embraced social-marketing principles and was effective in increasing the age at sexual debut.
Safer Choices is a school-based social-marketing intervention involving a school health promotion council (SHPC) co-ordinating intervention activities, a classroom–based RSE curriculum, student-led social-marketing campaigns and information for parents. A US randomised controlled trial (RCT) of this intervention reported reduced unprotected last sex and reduced numbers of partners with whom unprotected sex occurred, but did not measure effects on pregnancy. 20–22 Positive Choices was informed by all of the above elements of Safer Choices. The ‘CAS Carrera’ programme is an after-school intervention providing careers, academic, arts, sports and life-skills sessions, and sexual health services. A RCT of this intervention in New York City reported fewer pregnancies and delayed sexual debut among girls. 23 An attempted replication study in other US locations reported no such reductions, reportedly owing to poor fidelity. 24 Positive Choices was informed by the emphasis on general life skills as well as sexual health-specific skills within the CAS Carrera curriculum. The Gatehouse Project is a school-based intervention that includes a student needs survey and classroom-based curriculum addressing social and emotional learning. Although primarily addressing mental health, a RCT in Australian high schools reported participants’ increased age at sexual debut, but did not measure impacts on teenage pregnancy. 25 Positive Choices was informed by all of the above elements of the Gatehouse Project.
Rationale for the current study
Our optimisation, feasibility assessment and pilot RCT of Positive Choices was, to our knowledge, the first UK study of a whole-school social-marketing intervention to prevent unintended teenage pregnancy. The intervention involved multiple components. Those in years 9 and 10 (aged 13–15 years) would be targeted because proximal risk factors are manifesting,26 prevention is not too late, and RSE is acceptable. 21,27,28 Consultation with schools, which informed the proposal, suggested that provision to year 11 students would be unfeasible because of General Certificate of Secondary Education (GCSE) preparation. Although not aiming to replicate existing interventions, the intervention was informed by approaches and certain components used in the previous Safer Choices,20–22 CAS Carrera23 and Gatehouse interventions. 25 Optimisation refers to the elaboration of the intervention, developing it from a basic description of a new intervention, its theory of change and components, to a fully specified intervention with full materials.
Our study involved three elements: (1) optimising the intervention to elaborate its components and develop intervention materials in collaboration with SEF and one state secondary school; (2) assessing the feasibility of each component of the intervention by implementing, assessing and refining it in the secondary school involved in optimisation; and (3) undertaking a pilot RCT of the intervention across six other schools to assess the feasibility and value of conducting a future Phase III RCT of the effectiveness of the intervention.
Study aims and objectives
Aims
-
In collaboration with SEF, one secondary school and other stakeholders, to optimise Positive Choices, a school-based social-marketing intervention to promote sexual health, prevent unintended teenage pregnancies and address health inequalities in England.
-
To conduct a formative feasibility assessment and refinement of the intervention in collaboration with the secondary school involved in optimisation.
-
To conduct a pilot RCT (four intervention and two control schools) to determine the feasibility and utility of conducting a Phase III RCT of effectiveness and cost-effectiveness.
-
To answer the study’s research questions.
Objectives
-
To optimise Positive Choices in collaboration with SEF, the staff and students from one secondary school, and other stakeholders.
-
To assess the feasibility and acceptability of implementing each component of the intervention in the school involved in optimisation, and to make any necessary refinements in the light of this feasibility assessment.
-
To recruit six schools for the pilot RCT, undertake baseline surveys of students at the end of year 8 (age 12/13 years) and randomise schools.
-
To implement the intervention to students in year 9.
-
To conduct quantitative and qualitative elements of the process evaluation.
-
To undertake follow-up surveys at 12 months post baseline.
-
To link self-report data to routine administrative data on teenage pregnancies 18 months post baseline.
-
To conduct data analysis addressing all of the above research questions and draft a report of the pilot evaluation.
-
To disseminate findings and determine whether or not progression to a Phase III RCT is justified.
Study research questions
-
Is it possible to optimise Positive Choices in collaboration with SEF, a secondary school and other stakeholders?
-
Is it feasible and acceptable to implement each component of this intervention in the secondary school involved in optimisation, and what refinements are suggested?
-
In the light of a pilot RCT across six schools, is progression to a Phase III RCT justified in terms of prespecified criteria?
-
The intervention is implemented with fidelity in three or four out of four intervention schools.
-
Process evaluation indicates that the intervention is acceptable to a majority of students and staff involved in implementation.
-
Randomisation occurs and five or six out of six schools accept randomisation and continue within the study.
-
Student questionnaire follow-up rates are ≥ 80% in five or six out of six schools.
-
Linkage of self-report and routine administrative data on pregnancies is feasible.
-
-
Are secondary outcome and covariate measures reliable and what refinements are suggested?
-
At what rates are schools recruited to and retained in the RCT?
-
What level of student reach does the intervention achieve?
-
What do qualitative data suggest in terms of intervention mechanisms and refinements to programme theory and theory of change?
-
How do contextual factors appear to influence implementation, receipt and mechanisms of action?
-
Are any potential harms suggested and how might these be reduced?
-
What sexual health-related activities occur in and around control schools?
-
Are methods for economic evaluation in a Phase III RCT feasible?
Chapter 2 Methods
This chapter includes material reproduced or adapted from Ponsford et al. 1 This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. The text includes minor additions and formatting changes to the original text.
This chapter also includes material reproduced or adapted from the ISRCTN registry. 29 This material is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this registry, unless otherwise stated. The text includes minor additions and formatting changes to the original text.
Design
The study involved three phases with different designs: (1) a facilitated, systematic optimisation of the Positive Choices intervention using participative methods; (2) a formative feasibility assessment of intervention components in one secondary school and refinement using a case study design; and (3) an external pilot cluster RCT across six schools with integral process evaluation and economic evaluation feasibility study.
Optimisation
Key elements of the theory of change of the intervention, as well as the basic outline of its core components, had already been determined, informed by, but not directly replicating, selected elements from the Safer Choices, CAS Carrera and Gatehouse interventions. Further work was required to elaborate and optimise the intervention for the UK context, developing in detail the intervention components and intervention materials. The optimisation of the intervention was led by the research team and staff from SEF, and involved the staff and students from one secondary school plus other youth and policy and practitioner stakeholders. Optimisation occurred in phases. Elaboration of the intervention theory of change, logic model and overall approaches of the intervention occurred between April 2017 and June 2017. Development of the student needs survey, the manual guiding the SHPC and the staff training package occurred between June 2017 and August 2017. Development of the student curriculum occurred between September 2017 and December 2017. Development of guidance for the student-led social marketing and review of school sexual health services occurred between January 2018 and March 2018.
In each case, optimisation of the above resources occurred through a systematic process as follows:
-
review by researchers and SEF staff of existing systematic reviews and the evaluations of the Safer Choices, CAS Carrera and Gatehouse interventions, and materials from Safer Choices
-
drafting of resources by SEF staff and the research team
-
consultation with staff and students from one secondary school, as well as the Advice Leading to Public Health Advancement (ALPHA) group [a group of young people based at the Centre for Development and Evaluation of Complex Interventions (DECIPHer) Centre at Cardiff University who are trained to advise on public health research] and other stakeholders
-
refinement of these resources.
Review of existing literature and materials
The research team reviewed existing systematic reviews, Safer Choices, CAS Carrera and Gatehouse Project evaluation reports, and literature on school-based interventions to identify best practices and inform the intervention design and materials. SEF reviewed Safer Choices materials, as well as materials from other interventions and resource packages, to inform drafting of intervention materials with research team input. Staff from ETR Associates and CAS (originators of the Safer Choices and Carrera interventions, respectively) also contributed to intervention optimisation, advising on learning from their interventions.
Production of draft materials
The National Children’s Bureau led the drafting of intervention materials. These were reviewed by the research team, including to ensure these aligned with the intervention’s theory of change, and then redrafted.
Consultation
We consulted with students and staff from one London secondary school in June 2017. This school was purposively selected based on its location in south-east England, and it having a higher than median local Index of Multiple Deprivation and value-added GCSE attainment, suggesting a high level of need for the intervention, but with high organisational capacity to participate in optimisation and refinement. 26 The school was recruited via our existing contacts to ensure that the school had the capacity to participate.
The consultation session involved teachers and students from different year groups, focused on acceptability of the proposed intervention aims, components and delivery models (particularly the tasks of the SHPC); teacher preference for the format and content of the manual guiding the intervention and presentation of the needs data; students views on the curriculum content; and implementation of the SHPC. The data collection tools used for the session are in Report Supplementary Material 1. Further planned consultation on intervention materials was not possible because of school capacity. The consultation was facilitated by one researcher and one member of SEF staff. Following introductions, teachers and students worked separately in small groups. The session was audio-recorded. Field notes were also taken during and directly after the session. Because these optimisation activities were framed as co-design and not in-depth qualitative research, a summary was then prepared based on audio-recordings and field notes, but formal qualitative analysis was not carried out. Students and staff participating in focus groups were treated as research participants and provided with written information about the research 1 week beforehand, as well as orally just prior to the research. All students completed written opt-in consent/assent forms. Parents of participating students were also provided with information 1 week in advance and could opt out their children.
As part of the optimisation phase, we also consulted with the ALPHA group in July 2017 and in April 2018, to explore these young people’s perspectives on parent engagement in the Positive Choices intervention, and the acceptability and potential challenges of implementing student-led social-marketing campaigns in schools. These sessions were audio-recorded and summaries drafted by the group’s professional facilitator. ALPHA participants gave written, informed consent for their participation in the group.
In March 2018, we also convened a meeting of practitioners and policy-makers from governmental and non-governmental organisations working in education and health to inform optimisation. Following presentations by research staff on the intervention, participants provided feedback via small-group discussion on questions set by researchers, focusing on intervention design and practical challenges to implementation. Drawing on facilitator notes, researchers drafted an anonymised summary of the event, again with no formal qualitative analysis. Consultation with practitioners and policy-makers was treated as public engagement rather than research, so no ethics review was undertaken and no consent was sought. Participants were made aware of how their contributions would be used and received a summary of discussion to which they could suggest amendments.
Refinement of resources
The researchers and SEF staff discussed the summaries above, agreeing how these should inform elaboration of the interventions, models of delivery and materials.
The outcome for the optimisation phase was meeting the criterion for progression to feasibility testing: for the materials for the training, SHPC, social-marketing meetings, student curriculum and sexual health services review to be optimised in line with the theory of change and to the satisfaction, expressed in writing, of the research team, SEF, the participating secondary school and the Study Steering Committee (SSC).
Feasibility testing
Intervention components were implemented and assessed for feasibility and acceptability in the same secondary school that was involved in optimisation. This occurred over 1 school year, in phases, overlapping with optimisation:
-
term 1 (September–December 2017) – implementation of the student needs survey with year 9 students, staff training and SHPC
-
term 2 (January–March 2018) – implementation of the student curriculum
-
term 3 (April–July 2018) – implementation of the student-led social marketing and review of school sexual health services.
The feasibility-assessment involved a case study design with no comparator. Intervention components were assessed by the research team as they were implemented to inform phased refinements led by SEF staff as follows:
-
January–March 2018 – refinements of the survey, materials for SHPC and staff training
-
April–July 2018 – refinement of the student curriculum
-
June–August 2018 – refinement of the student-led social marketing and review of school sexual health services.
Data collection
In the feasibility-testing phase, our process evaluation aimed to collect data via audio-recording of SEF training for school staff; surveys of school staff trained by SEF; logbooks completed by school staff implementing the SHPC, curriculum and social-marketing meetings; structured observations of the SHPC, curriculum lessons and social-marketing meetings; and interviews with four SEF and four schools’ staff (purposive by role/seniority), and group interviews with eight year 9 students [purposive by sex and socioeconomic status (SES)].
Progression criteria and data analysis
Outcomes for the feasibility-testing phase were to meet the criteria for progression to the pilot RCT: according to audio recordings, diaries and researcher observations, the training, SHPC, social-marketing meetings, student curriculum and sexual health services review components were implemented with > 70% fidelity in the participating school; and interviews with students and staff conducted as part of the process evaluation indicated that the intervention was acceptable to at least 70% of students and staff involved in implementation.
Fidelity was assessed using data derived from audio-recordings, diaries and observations; the specific sources are reported for each aspect of fidelity in our results. Quantitative tick-box quality metrics were developed for each intervention component. Each training session was assessed against session-specific quality metrics relating to the number of participants, the topics covered, the exercises used and opportunities for discussion. Meetings of the SHPC were assessed against meeting-specific quality metrics relating to the agenda items covered, actions agreed and opportunities for discussion. The curriculum was assessed against lesson-specific metrics concerning the essential topics covered, exercises used and opportunities for discussion. The student-led social marketing was assessed against metrics concerning the items discussed, actions agreed and opportunities for discussion. The review of sexual health services was assessed against quality metrics concerning the review of existing services and actions taken to enhance these. The specific metrics used to assess each element are provided in Report Supplementary Material 2.
Acceptability of the optimised Positive Choices intervention was quantitatively assessed via two specific questions included in the interview and focus group schedule as a measure of intervention acceptability. These were:
-
Do you think your school should deliver the Positive Choices Programme again?
-
Do you think other schools should?
Our data analyses determined whether the study should proceed to the pilot RCT phase against the criteria described above. Findings were fed back to SEF staff, who were then responsible for refining the intervention ready for implementation in the pilot RCT.
Pilot randomised controlled trial
We then conducted a pilot RCT (four intervention and two control schools; different from those involved in the intervention optimisation), with an integral process evaluation and economic evaluation feasibility study. In this phase, the research and intervention teams were managed separately to ensure that the evaluation was independent and did not distort intervention delivery.
Pilot study population and inclusion/exclusion criteria
State secondary schools (including free schools and academies) in south-east England (maximum 1-hour rail journey from London) were eligible to participate. Private schools, pupil referral units or special schools for those with learning disabilities were excluded. Boys’ but not girls’ schools were also excluded from the pilot RCT as our primary outcome focused on unintended pregnancies among girls. In a Phase III RCT, the intervention would target students in years 9 and 10. In the pilot RCT, the intervention targeted year 9 students, reflecting the truncated timescales of the pilot compared with a Phase III RCT; therefore, students nearing the end of year 8 at the baseline survey (conducted in the term before the intervention was to begin) were eligible to participate. No student deemed competent by their teacher to consent was excluded from our study. Those with mild learning difficulties or poor English were supported to complete the questionnaire by fieldworkers.
Sample size
The pilot RCT focused on various aspects of feasibility and no power calculation was performed. Having four schools implementing the intervention in the pilot RCT combined with two schools acting as controls balanced the need to assess implementation in a diverse range of schools with ensuring that the pilot was small enough to be appropriate as a preliminary to a larger Phase III RCT. The planned analytic sample for outcome assessment in the pilot RCT was 1159 students at the end of year 8 (aged 12/13 years) at baseline, with follow-up at 12 and 18 months. Our pilot aimed to provide estimates for recruitment and retention rates that would allow us to estimate more accurately the sample size required for a Phase III RCT.
Recruitment
Six schools across south-east England were recruited (purposively varying by local deprivation and school-level GCSE attainment). Schools were recruited to the pilot RCT via e-mail mailouts. For the pilot RCT phase, we aimed to recruit only six schools spread across different parts of south-east England and did not want to focus recruitment on schools already known to us; therefore, our strategy aimed to be broad in geographical scope (to recruit a diverse range of schools) but not intense in how we communicated with schools (because we only needed to recruit six). We sent a single e-mail to schools’ general administrative e-mail addresses with no follow-on emails, no telephone calls and no targeting of head teachers or other named members of staff. Response rates were recorded, as were any stated reasons for non-participation.
Randomisation
After baseline surveys with students at the end of year 8, schools were randomly allocated to intervention/control remotely by London School of Hygiene & Tropical Medicine (LSHTM) clinical trials unit (CTU) on 9 July 2018, stratified by GCSE attainment, a key predictor of pregnancy. 26 Allocation was 2:1 favouring the intervention (compared with 1 : 1 in any future Phase III RCT).
Planned interventions
Below, we describe the Positive Choices intervention using the Template for Intervention Description and Replication (TIDieR) framework. 30
Theory of change
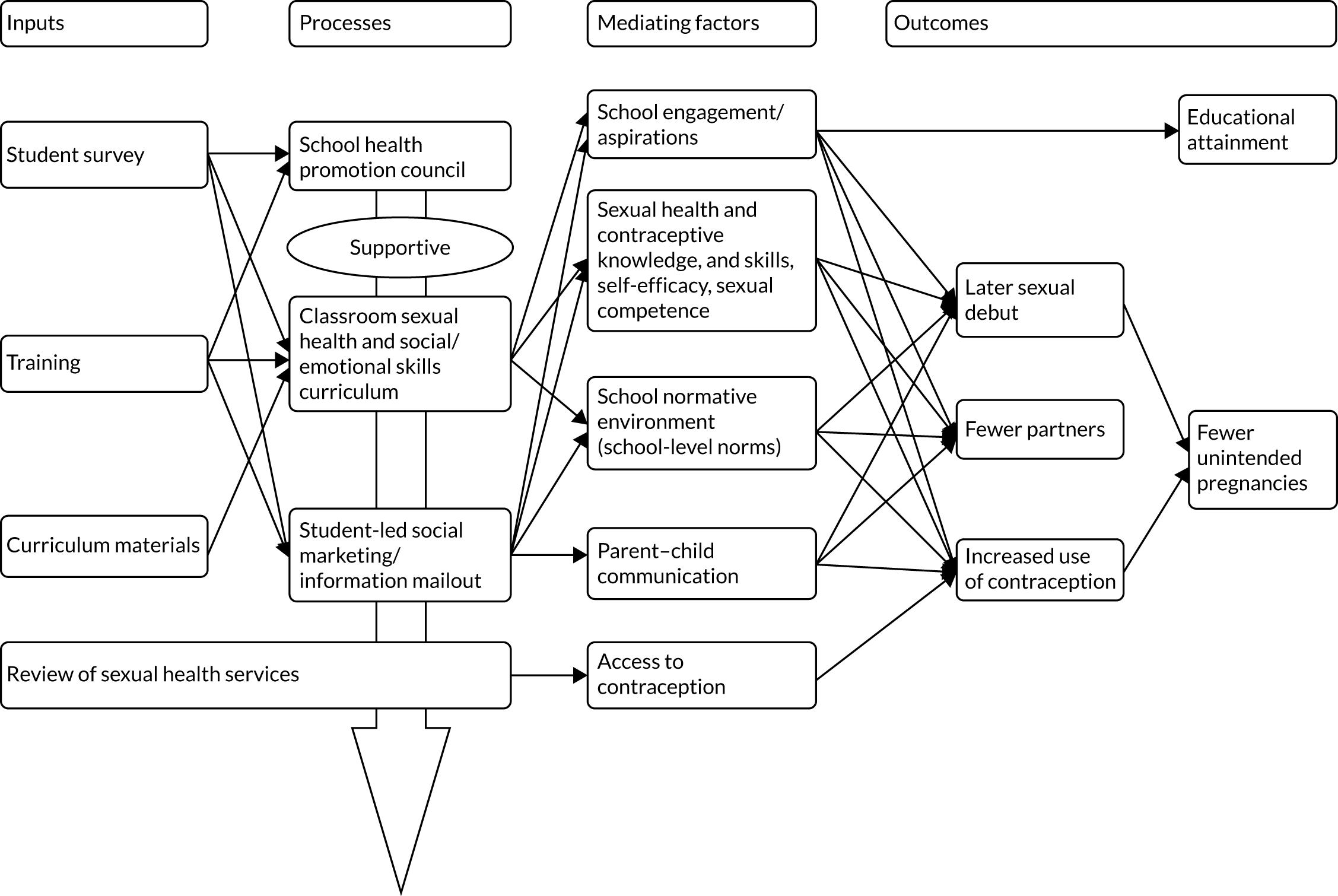
Positive Choice’s programme theory is informed by social-marketing principles and has been developed with experts in this field, addressing the ‘4Ps’: product, place, price and promotion. 31,32 The intervention aims to ‘sell’ consumers a product they want (education on emotions, relationships and sexual health) in an accessible place (school) at a low price (free to students), with promotion to peers and parents (campaigns, parent information),19,31 and to address competing influences from their peers, the media, etc. 33 The needs survey component enables SHPCs (with student involvement) to tailor provision in each school to local consumer priorities. The intervention’s theory of change has been informed by the Safer Choices20–22 intervention theory and models of school change,34 social influence35 and social cognitive theory36 to address the following determinants of unintended teenage pregnancy: sexual health and contraceptive knowledge; self-efficacy to communicate about sex; sexual health skills and competence; communication with parents; and school-wide social norms supporting positive relationships/sexual health. The curriculum was informed by the CAS Carrera intervention theory,23 in terms of the social development model,37 and by addressing additional protective factors: positive aspirations and school engagement. 38 Refined school sexual health services aim to provide advice and contraception in line with National Institute for Health and Care Excellence guidance. 39 The intervention is a universal intervention that has the potential for greater population-level impacts than targeted interventions while minimising the risk of ‘positive deviancy training’, which can be a problem in targeted interventions,10,26 as they bring together at-risk individuals to increase harm. 40 The logic model for the intervention is shown in Figure 1.
FIGURE 1.
Positive Choices Logic Model.
Materials
School staff are offered training in instituting and running a SHPC, delivering the classroom curriculum and facilitating student-led social marketing. Training materials consist of slides and handouts. Schools are provided with a manual to guide each component of the intervention. Schools are sent a report on student needs detailing the findings from a survey of year 8 students, aged 12–13 years, (drawing on baseline trial survey) about their sexual health needs, and attitudes to and experiences of school. Schools are provided with lesson plans and slides to guide delivery of the classroom curriculum. Schools send out parent information comprising three newsletters and two homework assignments per year addressing parent–child communication.
Procedures
Positive Choices is a manualised social-marketing intervention, delivered for one academic year to students in year 9 in this pilot trial, and for two academic years to years 9 and 10 in any future Phase III trial. Training comprises in-depth training for selected staff as in Materials. Guided by the manual, schools institute SHPCs comprising staff and students to review local needs data, and use this to tailor each intervention component, and then to co-ordinate delivery of the intervention. Schools deliver the curriculum in various lessons and/or tutor time to students in year 9 (13–14 years). The curriculum was designed as a set of 10 hours of learning modules to cover social and emotional skills, and relationships and sexual health. The social and emotional skills to cover were establishing respectful relationships in the classroom and the wider school; managing emotions; understanding and building trusting relationships; exploring others’ needs and avoiding conflict; and maintaining and repairing relationships. Sexual health topics to cover were healthy relationships, negotiation and communication skills, positive sexual health, sexual risk reduction, contraception and local services. The SHPCs select whether to deliver the curriculum in PSHE lessons, tutor groups or to integrate it into other lessons, and whether to use Positive Choices materials or existing materials (if these conform to the curriculum). Student-led social marketing is facilitated by trained teachers and led by teams of 12–18 students per school. Teachers actively promote recruitment among at-risk students based on the strongest evidenced risk factors for teenage pregnancy on which schools have data (i.e. free meals eligibility, persistent absenteeism and slower than expected academic progress26). This is not to target provision at those most at risk, but rather to ensure campaigns appeal to a diversity of students including those most at risk, of teenage pregnancy. When recruiting such students, teachers are open with them about this rationale. Campaigns can use social and other media, posters and events, and focus on healthy relationships, sexual and human rights, delayed sex and access to local services. Student social marketers were to use data from the student needs survey to segment the student population based on year group. The student social marketers use such information to design social-marketing campaigns that address the most important topics among the groups who needed the interventions the most. The review of school sexual health services was to involve SEF providing guidance to schools on how sexual health services in or around schools might be developed or promoted among students.
Training
Training is provided by trainers from SEF.
Delivery
All intervention components were to be delivered face to face on school premises. SEF trains school staff to implement SHPCs, implement the classroom curriculum and facilitate student-led marketing. SEF also provides guidance to schools to support refinement and promotion of existing sexual health services. In each school, a ‘product champion’ [senior leadership team (SLT) member] oversees the SHPC. SHPC members comprise at least six staff and at least six students from each school. Staff sitting on this council include those teaching the curriculum, those co-ordinating student-led social marketing and, where applicable, the school nurse. These staff attend the SHPC training and some also attend the curriculum and social-marketing training. The curriculum is delivered by trained teachers guided by lesson plans. Students sit on the SHPC and also lead social marketing to their peers guided by a teacher and a manual with clear milestones, including plans for ‘quick wins’ to build momentum and enthusiasm. 21
Dose
The SHPC and student-led social-marketing training comprises a half-day session. The curriculum training comprises a whole-day session. SHPCs meet six times per year. Students receive 10 hours’ teaching per year.
Planned adaptations
The optimisation phase led to some planned adaptations, reported in full in Chapter 3. The needs assessment was not used to determine in which lessons the Positive Choices curriculum would be taught, or whether or not to use existing or Positive Choices materials. It was used to inform the selection of add-on lessons to be taught in each school; build support for implementation of the intervention in schools; and inform the content of parent newsletters, and the focus of student-led social-marketing activities and the sexual health services review. The remit of the SHPC was refined to comprise launching the intervention in schools and promoting the intervention to parents; selecting the ‘add-on’ curriculum topics informed by the needs-assessment data; overseeing delivery of the curriculum; recruiting the social-marketing team; monitoring and voting on campaign activities; preparing and distributing parent newsletters; and carrying out the school sexual health services review. The curriculum was adapted to align with SEF-recommended comprehensive RSE, but with all of the topics included in the original protocol being addressed. Student-led social marketing was refined in line with Andreasen’s six characteristics of social marketing. 18 The student-led social marketing was also adapted so that this did not segment the student population based on cultural styles but rather only by year group, with the team comprising students from years 8 to 11. The review of school sexual health services was adapted to comprise SEF detailed guidance for the school to review and improve its own and local sexual health services, rather than SEF reviewing these services directly.
Unplanned modifications
There were no unplanned modifications.
Intervention funding
Intervention delivery in the feasibility assessment and pilot RCT phases was funded by the NCB, and by schools, which provided staffing for project oversight, the running of SHPCs, curriculum delivery and social-marketing teams.
Comparator
In the pilot RCT phase, two schools were randomised to the control group and did not receive the intervention, but continued with any existing sexual health-related provision, which was examined in our process evaluation. Retention of control schools was maximised with a £500 payment and feedback of survey data after RCT analyses.
Outcome and other measures
Outcome measures
The pilot RCT did not aim to assess intervention effects. The pilot primary outcomes were to meet the criteria for progression to Phase III, which were that the intervention was implemented with fidelity in three or four out of four intervention schools; process evaluation indicated that the intervention was acceptable to a majority of students and staff involved in implementation; randomisation occurred and five or six out of six schools accepted randomisation and continued in the study; student questionnaire follow-up rates were ≥ 80% in five or six out of six schools; and linkage of self-report and routine administrative data on pregnancies was feasible. Secondary outcomes addressed other research questions, including the feasibility of economic evaluation.
We did, however, pilot the primary outcome and other measures that we anticipated would be used in a future Phase III RCT. The primary outcome in such a RCT was anticipated to be routine data on births and abortions at 48 months (age 16/17 years) with secondary outcomes measured via self-reports at 24 months (age 14/15 years). Routine data on abortions minimise information bias and clearly indicate unintentional pregnancy; however, some unintended pregnancies will not result in abortion, and changes in abortion rates may also reflect variations in access;41 therefore, our indicative primary outcome measure piloted in this study also encompassed routine data on live births. Although it is recognised that around half of teenage pregnancies will, to some extent, be intended,42 this outcome measure was anticipated, nonetheless, to provide a better indication of the overall impact of the intervention.
We aimed to pilot indicative secondary outcome measures to examine broader intervention effects via survey self-reports:
-
pregnancy and unintended pregnancy for girls and initiation of pregnancy for boys using adapted versions of the Ripple measures41
-
diagnosed sexually transmitted infections (STIs), which focused on diagnosis with common infections, using an adapted version of the Ripple measure41
-
age at sexual debut, which focused on age at vaginal sexual debut with someone of the opposite sex using an adapted version of the Ripple measure41
-
number of sexual partners, which focused on vaginal sex partners using an adapted Ripple measure41
-
use of contraception at first and last sex, which focused on which common contraceptives, if any, were used in first and last vaginal sex, using an adapted Ripple measure41
-
non-volitional sex, which examined experience within the last 12 months of forced sex using an adapted version of the Conflicts in Adolescent Dating Relationships Inventory (CADRI) measure43
-
educational attainment, which is a plausible intervention effect and, for scale-up, a critical outcome of our intervention,44 but which was not possible to pilot in this study because the pilot RCT involved a shorter period of follow-up than would be the case in a Phase III RCT and so did not include the time when students took public examinations.
Mediators and covariates
Informed by our theory of change, we also piloted the following mediators using existing self-report measures:
-
school-level social norms supportive of positive relationships and sexual health, using an adapted measure from the Safer Choices study22
-
perceived behavioural norms about early sexual experience and use of condoms and contraception, using an adapted measure from the Safer Choices study22
-
sexual health knowledge, which used an adapted version of a measure from the Share trial27
-
sexual health and contraceptive skills and access, using a measure adapted from the Share study27
-
sexual health service access, using a measure adapted from the Share study27
-
sexual communication self-efficacy, using selected items appropriate for young people from the Sexual Communication Self-Efficacy scale45
-
sexual competence, using the Natsal measure46
-
communication with parents using a measure from the Ripple study41
-
school engagement using the Beyond Blue School Climate Questionnaire (BBSCQ) measure47
-
career/educational aspirations, using an adapted version of the measure from the Ripple study. 41
We did not pilot a measure of intentional self-regulation as originally planned because we determined that, given the intervention theory of change, it was sufficient to measure self-efficacy of sexual communication.
All of the above measures were assessed for reliability in our pilot, by reporting intracluster correlation coefficients (ICCs) for repeat measures over time and Cronbach’s alpha statistics at baseline and follow-up for scaled outcomes.
Potential confounders/moderators were SES, as measured using the Family Affluence Scale (FAS),48,49 sex and ethnicity, using standard Office for National Statistics (ONS) categories. 50 The FAS score was calculated by scoring item responses numerically, with the least affluent options being scored 0, and the item scores being summed to give a total scale score. We originally planned to pilot moderator analyses, but this was not done as these analyses would have been severely underpowered.
A detailed table describing key measures is provided in Report Supplementary Material 3.
Economic evaluation outcomes
Given the lack of previous economic evaluations in this area, the aim of the economic analysis was to examine whether or not it would be feasible to assess the cost-effectiveness of the Positive Choice intervention using a cost–consequences analysis within a Phase III trial. The objectives of the economic analysis were to estimate the costs of delivering this new intervention; collect data on health-related quality of life among students and examine response rates and data quality, and to undertake a pilot analysis of intervention impact; and make recommendations about the feasibility of undertaking a cost–consequences analysis alongside a Phase III RCT.
Within the pilot, study methods to measure the incremental cost of the intervention in a Phase III RCT study were developed and piloted. With use of a broad public and third-sector perspective, resources to be measured included those used by SEF, schools and the NHS. Within this, key interventional resources included SEF and school staff time, training events/workshops and consumables. Measures included standardised sessional checklists to monitor and document attendance, preparation and delivery time for key training events and SHPCs; logbooks e-mailed to school staff charged with intervention delivery, assessing time spent on tasks relating to intervention; and all intervention staff travel and other expenses relating to the intervention charged to a specific project grant code.
The Child Health Utility-9D (CHU9D) measure was used to assess students’ health-related quality of life. 51 The CHU9D is a validated, age-appropriate measure that was explicitly developed using children’s input and has been suggested to be more appropriate and function better than other health utility measures for children and adolescents. Student utility values were converted into utility scores using a UK valuation set. 52 CHU9D utility values are measured on a scale from 0 to 1, anchored at 1 for full health and 0 for dead. We calculated the completion rates for the CHU9D based on the number of students for whom it was possible to compute CHU9D utility scores at baseline and follow-up. We then observed the distribution of CHU9D scores at both time points, calculating summary statistics and drawing histograms showing the percentage of values at each CHU9D value. We assessed the inter-item reliability of the nine dimensions of the CHU9D using Cronbach’s alpha and the ordinal alpha.
Finally, we undertook a pilot analysis of intervention impact on CHU9D scores using unadjusted and adjusted regression analyses. We regressed (using ordinary least squares) student-level CHU9D utility scores at follow-up against whether the student was in an intervention school or not (1 = yes, 0 otherwise). We ran unadjusted and adjusted analyses. For the latter, we ran two models: the first controlled for baseline age, sex, ethnicity and SES as measured by the FAS, and the second controlled for these variables plus baseline CHU9D utility scores. Results were presented as marginal effects [mean difference (MD) in utility scores between students in intervention and those in control schools] and corresponding 95% confidence intervals (CIs).
Assessment of harms
It was considered unlikely that any harms would arise because of the intervention or the research. The pilot study was not powered to examine intervention effects (beneficial or harmful), but qualitative data were collected as part of the process evaluation to explore any potentially harmful mechanisms.
Data collection
Student surveys
Baseline surveys were conducted before randomisation as students neared the end of year 8 (age 12/13 years) in June 2018, collecting data on outcome measures and potential confounders and moderators. Around 1 week before completing the surveys, students were given an information sheet about the study and the survey. Immediately prior to completing the surveys, students were given an oral description of the study and had the chance to ask questions. Students were then invited to assent to participate in data collection. As is conventional with UK RCTs in secondary schools (including RCTs of sexual health interventions),41,53,54 parents/carers were sent a letter and a detailed information sheet around 1 week before data collection and asked to contact the school or research team should they wish for their child not to participate in the RCT. Paper questionnaires were completed confidentially in classrooms, supervised by fieldworkers, with teachers remaining at the front of the class to maintain quiet and order, but unable to see student responses. Absent students were surveyed by leaving questionnaires and stamped, addressed envelopes with schools for the students to complete.
Students were resurveyed 12 months later in June 2019 as they neared the end of year 9 (age 13/14 years), collecting data on outcomes and mediators using the same consent and fieldwork procedures. Fieldworkers were blind to allocation. Based on past experience, we expected 95% baseline survey participation and 90% at follow-up. 28,53
Data linkage
In the pilot, we sought to link our self-report data with administrative data on abortions and births up to 18 months after baseline surveys, in collaboration, respectively, with the Department of Health and Social Care (DHSC) and the ONS. This was to occur by linking data on female RCT participants to routine data on statutory abortion notifications and registration of births, by staff blind to allocation. Linkage of such data had been previously conducted for observational studies26 and initial discussion with ONS had established that data linkage was feasible despite the limited identifiers attached to abortion records, and was consistent with DHSC and ONS guidance and data protection law.
In the case of obtaining birth data from ONS, the research team aimed to implement the following procedures to ensure the anonymity and confidentiality of data. The fieldwork team would securely transfer a password-protected data set of female participants’ names, postcodes and dates of birth (DOBs), to which the CTU did not have access, linked to a unique identifier code for each participant (with the data set not including any self-report survey data). ONS would then prepare a data set containing unique identifier codes (but not other identifiers) linked to any births among trial participants. Having been accredited by the ONS, Elizabeth Allen would then attend the ONS secure data centre to access and carry out analysis of birth data with these having been imported into the main anonymised trial data set. A similar process was to occur to access abortion data, but, in this case, using only DOB and postcode information and not participant names (because routine records of abortion data do not contain patient names), and would involve the secure sending of each data set, rather than in-person visits. Although ONS initially committed to providing data on births up to 18 months after baseline surveys, in the course of the project it reported that it could provide such data up to only 11 months after baseline surveys (from July 2018 to June 2019) because of the time needed to undertake internal quality checks before releasing data.
Process evaluation
Approach to process evaluation
Integral process evaluation informed by existing frameworks54–56 had three purposes: first, to examine intervention feasibility, fidelity, reach and acceptability; second, to assess provision in control schools and potential contamination; and, third, to explore context and potential mechanisms of action, including potential harmful and other unintended effects, in order to refine the intervention theory of change and design.
Intervention feasibility, fidelity, reach and acceptability
Fidelity metrics were finalised once the intervention was fully optimised (August 2018) and approved by the SSC prior to their use (see Appendix 1, Tables 41–44 and Boxes 1–3). Fidelity was defined as:
-
≥ 70% delivery of defined essential elements for the SEF-delivered training
-
≥ 100% attendance of the target number of participants at all training and SHPCs
-
≥ 70% fidelity of defined essential items covered in at least one SHPC and student-led social-marketing meeting, and 70%+ fidelity of other defined essential items covered in every SHPC and every student-led social-marketing meeting
-
≥ 70% delivery of essential elements of eight core and two add-on lessons, including for two homework topics
-
≥ 70% fidelity of defined essential elements of sexual health services review processes.
Data were collected via observation and audio-recording of SEF training for school staff; logbooks of school staff implementing SHPCs, curriculum and social-marketing meetings; and structured observations of a randomly selected session per school of SHPCs, curriculum lessons and social-marketing meetings.
In addition to assessing feasibility and fidelity, we also examined reach and acceptability via qualitative research, as well as student questionnaire survey items at follow-up and surveys of trained staff. Qualitative research explored participants’ experiences to assess their engagement and satisfaction with the intervention and what factors influenced this. Our protocol indicated that we would examine how reach varied by sociodemographic, educational and neighbourhood characteristics; however, because we lacked information on students’ baseline educational attainment or postcode, we confined these analyses to an assessment by SES, ethnicity and sex.
Provision in control schools and potential contamination
We examined sexual health provision in and around control schools in order to describe our comparator. We examined the potential for contamination across arms to ensure that this would not be a threat to internal validity in a Phase III RCT. Data were collected via interviews with at least two members of staff per control school (purposive by seniority) and at least four year 9 students (purposive by sex and SES) per control school.
Context and mechanisms of action
In addition to piloting intermediate outcome variables required for mediator analyses in a subsequent Phase III RCT, we collected qualitative data and analysed these to explore potential mechanisms of action and how these might vary with context to refine and optimise the intervention’s theory of change. We also analysed qualitative data to explore any mechanisms that might give rise to unintended, potentially harmful consequences. Data were collected via individual or group interviews with SEF trainers, at least four staff per intervention school (purposive by seniority/activity involved in), and at least six year 9 students per intervention school (purposive by intervention involvement, risk status and gender).
Sources of data
We aimed to observe one randomly selected session per school of SHPCs, curriculum lessons and social-marketing meetings and to audio-record the SEF-delivered trainings in each intervention school.
After training, staff participants completed anonymous satisfaction surveys, which were an intrinsic part of the intervention.
Each school received a logbook for each school staff member leading the SHPC, or implementing the curriculum or social-marketing meetings. Logbooks contained lists of activities and staff were asked to mark those that were covered.
Interviews with school staff and students were conducted at schools by trained researchers using semistructured interview guides (see Report Supplementary Material 4). No staff were present at student interviews. Interviews were audio-recorded and transcribed in full. We note the student’s gender where it is identifiable in interview transcripts. We also conducted two interviews with SEF staff which explored their experiences and views of the different phases of the research.
Data analysis
Our main analyses aimed to determine whether or not the criteria for progression to a Phase III RCT were met. Descriptive statistics on fidelity drew on audio-recordings of training, diaries of providers and structured observations of intervention activities. Statistics on acceptability drew on surveys of students and trained staff, and interviews with staff and students. School randomisation and retention, and student response rates at baseline and follow-up were described using a CONSORT flow diagram. 57 We aimed to assess the precision of data linkage in association with DHSC and ONS researchers.
Other analyses addressed our additional research questions. Descriptive summaries of baseline and follow-up data by arm were tabulated. Item completion rates were calculated with the denominator being all students or, where appropriate, students who were routed to these items on the basis of earlier responses. We assessed the reliability of secondary outcome measures by reporting ICCs for repeat measures over time and Cronbach’s alpha statistics at baseline and follow-up for scaled outcomes.
We piloted intention-to-treat analyses of outcomes57 to ensure that these were feasible but, because such analyses were highly underpowered, did not aim to determine intervention effectiveness. In a deviation from protocol, we did not attempt to pilot moderator analyses (how effects vary by SES, sex, ethnicity and baseline risk) because our experience in an earlier study indicated that such analyses would be so severely underpowered as to be completely meaningless. 58 The analysis of the indicative primary outcome included data on pregnancies and abortions at follow-up only. All other outcomes included student-level covariates. For the secondary outcomes, no contraception at first and last sex, students were categorised as reporting this outcome if they reported vaginal sex and a lack of a reliable method of contraception at the sexual event in question. Students who reported no vaginal sex or use of a reliable method of contraception were categorised as not reporting this outcome. For the secondary outcome, non-volitional sex, students were categorised as reporting this outcome if they reported sex with a same- or opposite-sex partner and had experience of forced sex. Students who reported no sex or no forced sex were categorised as not reporting this outcome. Students not providing data to be able to categorise in this way were treated as missing.
As per our protocol, analyses of outcomes adjusted for baseline age, sex, ethnicity and SES as measured by the FAS, with these being imputed from follow-up data when missing at baseline. The protocol originally described the intended analysis as repeat cross-sectional; however, because of low rates of attrition in this pilot and to be able to adjust for baseline student-level covariates, we instead used a longitudinal approach to analysis. For binary outcomes, the fitted model was a mixed-effect logistic regression with random effect for school, reporting odds ratios (ORs). For continuous outcomes (i.e. age at sexual debut and number of partners), a linear mixed model was used, reporting MDs. Standard, rather than bootstrap, CIs were estimated because with these very small numbers more robust inference would represent misleading precision.
Qualitative data were subject to thematic content analysis using techniques drawn from grounded theory such as in vivo and axial codes, and constant comparison. 59 Although deriving themes inductively from the data, analyses were sensitised by realist approaches to evaluation60 and May’s implementation theory55 to examine potential mechanisms of action and of harm, and how contextual factors influence implementation and mechanisms; describe relevant activities in and around intervention and control schools; and refine our programme theory and theory of change.
Our economic feasibility study piloted collection of quality of life data and assessed the feasibility of methods to be used within a Phase III RCT, which, in line with National Institute for Health and Care Excellence guidance,39 would involve a wider cost–consequences analysis, comparing intervention costs with the full range of study outcomes.
Protecting against bias
Although the aim of this study was to optimise the intervention, assess feasibility and then pilot outcome measures and analyses, rather than estimate intervention effects, we piloted methods aimed at minimising bias. The investigator team and the intervention delivery team were separately managed. In the pilot RCT, outcome data were collected and analysed blind to allocation, and we examined effects adjusting for potential baseline confounders. We aimed to maximise response rates at each pilot RCT site at baseline and at follow-up to minimise non-response and attrition bias, for example following up those individuals not present during survey sessions. Response rates and qualitative data were analysed to refine data collection methods prior to a Phase III RCT examining effectiveness. Blinding of participants to allocation was not possible.
Consultation with public, policy and practice stakeholders
Positive Choices was optimised by the research team, SEF staff, and staff and students from one secondary school. Young people from the ALPHA group were consulted three times during the project: in July 2017, April 2018 and January 2019. Policy and practice stakeholders were consulted twice: in March 2018 and June 2019. The first two consultations with the ALPHA group and the first policy and practitioner stakeholder group focused on intervention optimisation and their methods are described in Optimisation, with the results presented in Chapter 3. The third meeting of the ALPHA group focused on refining sexual behaviour questions and consent materials for the pilot follow-up. Findings from this meeting, as well as findings from earlier consultations that focused on the research rather than the intervention, are reported in Chapter 4. The second meeting of the policy and practitioner stakeholder group provided a progress update to participants and shared some early findings from the ongoing process evaluation. A further meeting scheduled with the ALPHA group and one with the policy and practice stakeholder group will focus on interpreting the results and implications of the study, mechanisms for knowledge exchange and future research.
Registration
The study protocol was published online (https://pilotfeasibilitystudies.biomedcentral.com/track/pdf/10.1186/s40814-018-0279-3) and registered Current Controlled Trials ISRCTN12524938.
Revisions to the protocol
The protocol was revised a number of times between 23 May 2017 to 22 February 2018 (see Appendix 2, Table 45).
Deviations from the protocol
There were also a number of deviations from the protocol, which are listed in Chapter 6 and summarised in Table 40.
Socioeconomic position and inequalities
In the pilot RCT, six schools in south-east England were recruited (varying by local deprivation and school-level GCSE attainment) to ensure diversity and balance on key predictors of teenage pregnancy. 26 Our process evaluation aimed to assess how implementation and intervention mechanisms appeared to vary by student SES and gender.
Research governance
The principal investigator (PI), Chris Bonell, had overall responsibility for the conduct of the study. The day-to-day management of the study was co-ordinated by the trial manager, Ruth Ponsford, based in LSHTM. The PI (CB) chaired weekly Trial Executive Group meetings with the trial manager, statistician (EA) and, where appropriate, SEF, CTU and fieldwork staff. Chris Bonell also chaired a Trial Investigators’ Group, which included all co-investigators and members of the Trial Executive Group; the Trial Investigators’ Group met monthly during the early stages of the research (months 1–6), and every 3 months thereafter. An independent SSC was established and met three times throughout the life of the project to advise on the conduct and progress of the RCT, and on relevant practice and policy issues. Professor Angela Harden of the University of East London chaired the SSC. Because this was a pilot and not a Phase III RCT, the SSC undertook data monitoring and ethics duties and was informed of any serious adverse events (SAEs) as described in Ethics arrangements. The project employed standardised research protocols and prespecified progression criteria, which were agreed and monitored by the Trial Investigators’ Group and SSC.
Ethics arrangements
Ethics review
Ethics approval for the study was obtained from the LSHTM Ethics Committee on 21 March 2017.
Policies and checks
Any member of the research/fieldwork team visiting a school was required to have a full Disclosure and Barring Services check. All work was carried out in accordance with guidelines laid down by the Economic and Social Research Council, the Data Protection Act 1998, the latest Directive on Good Clinical Practice (2005/28/EC) and the General Data Protection Regulation 2018.
Informed consent/assent
Informed, written consent was sought from head teachers for random allocation and intervention. Informed written consent (for adults) and assent (for young people) was sought for participation in research activities from all research participants judged competent to provide this. We sought advice from Professor Richard Ashcroft, Professor of Medical Ethics at Queen Mary University of London, who is an expert on informed consent. He advised that in the case of secondary-school students, unless individuals were deemed not competent by teachers to provide it, assent for participation should be sought from the young people themselves.
For surveys, interviews and focus groups, observations and audio-recordings, participants were given an information sheet around 1 week before data collection. Just before data collection, participants also received an oral description of the study and had the chance to ask questions. Participants were advised that participation was voluntary and that they could withdraw at any point. All participants were advised that they were free to withhold consent and this matter would not be communicated to teachers or, in the case of staff participants, their managers. Students opting not to participate in surveys were offered alternative activities in the classroom. Those opting out of other data collection were free to continue with their normal activities.
The research also involved the piloting of the linkage of student survey data to administrative data on births and abortions with, respectively, the ONS and DHSC. Female survey participants were informed of this process as part of consent procedures for follow-up surveys, and their specific assent for this was sought.
In addition, students’ parents were contacted by letter 1 week prior to research activities, informing them about informed consent and providing them with the option of withdrawing their child by contacting the school or the research team. Parental consent for intervention was not required because this was a universal intervention delivered in schools as part of broader educational activities.
Confidentiality, safeguarding and serious adverse events
All participants, including students, were informed in the consent materials of the confidentiality with which the information they provided would be treated, as well as the circumstances in which we would need to breach confidentiality to ensure student safeguarding. In collaboration with a qualified social worker specialising in child protection, we developed a priori categories of abuse that, if reported through the research, would necessitate our breaching confidentiality to ensure that individuals were offered care and protection: if they reported sex at age ≤ 12 years or if they wrote anything on the questionnaire that would lead us to believe that they were at risk of ongoing serious harm. These criteria were established so that we could balance our ethical duty of promoting participant autonomy by respecting confidentiality and our ethical duty of safeguarding participant well-being when we determined that we needed to breach confidentiality to address abuse that appeared to be serious and ongoing. It was planned that where such abuse was reported through a questionnaire, we would contact the safeguarding lead at the school. Where such abuse was reported directly to research staff, we planned to first discuss the need for a response with the research participant prior to contacting the school safeguarding lead (see Appendix 3).
Qualitative research (i.e. interviews, focus groups and observations) did not ask staff or students about their experience of sex; however, if participants nonetheless described any sexual abuse, or otherwise became upset in any way, our researchers were trained in how to respond. In the case of focus groups, our researchers were trained to ensure that discussions did not move in the direction of personal disclosures of sexual behaviour since this was not the purpose of the groups and it would have been very difficult to ensure that all focus group participants did not talk about such disclosures outside the group. Our staff were trained to identify the potential for such disclosures, working to avoid them but then approaching participants immediately after the focus group to offer support and to assess whether or not any other response was needed, using the same procedures as described above.
In addition, we requested information on SAEs from participating schools and assessed the plausibility that any of the SAEs were related to intervention or research activities in collaboration with school safeguarding leads.
It was planned that the SSC and LSHTM Ethics Committee would be provided with anonymised reports of all disclosures of serious abuse and SAEs, categorised by type, circumstances and the extent of any possible connection with intervention or research activities.
In each school and within NCB, a senior member of staff was identified who was not directly involved with the intervention and whom staff or students could go to if they had complaints about any elements of the research study. This was communicated to students outside the research process to increase trust that this was truly independent.
Data anonymity and security
Quantitative and qualitative data were managed by project staff using secure data management systems and stored anonymously using participant identification numbers. Quantitative data were managed by LSHTM’s accredited CTU. Files containing participant identification numbers and corresponding participant names were held in password-protected files separate to files containing self-report survey data, which were attached only to student identification numbers. No single researcher had access to both sets of data. The names used in qualitative data were replaced with pseudonyms in interview/focus group transcripts. In reporting the results of the process evaluation, care was taken to use quotations that did not reveal the identity of respondents. The methods by which anonymity was maintained in relation to the linkage of survey data and routine data on births and abortions are described in Data linkage.
In line with Medical Research Council guidance on personal information in medical research, we will retain all research data for 20 years after the end of the study. This is to allow secondary analyses and further research to take place, and to allow any queries or concerns about the conduct of the study to be addressed. In order to maintain the accessibility of the data, the files will be refreshed annually and upgraded, if required.
Chapter 3 Results: optimisation and feasibility testing
This chapter includes material reproduced or adapted from Ponsford et al. 1 This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. The text includes minor additions and formatting changes to the original text.
Overview
The first phase of the Positive Choices study involved intervention optimisation in collaboration with SEF, one London secondary school and other youth, practitioner and policy stakeholders. As explained earlier, optimisation refers to the elaboration of the intervention, developing it from a basic description to a fully specified intervention with materials. Optimisation overlapped with feasibility assessment in the participating London secondary school, with the student needs survey, the manual guiding the SHPC and the staff training package being optimised June–August 2017 and tested September–December 2017; the student curriculum being optimised September–December 2017 and tested January–March 2018; and the student-led social marketing and sexual health services review being optimised January–March 2018 and tested April–July 2018. Feasibility testing was followed by further intervention refinement in preparation for the pilot. This part of the report presents the results from the optimisation and feasibility-testing phases.
Optimisation
Initial elaboration of Positive Choices
Initial elaboration of Positive Choices was carried out following a review by researchers of existing systematic reviews, Safer Choices, CAS Carrera and Gatehouse Project evaluations, and a review by SEF of materials from Safer Choices and other interventions and resource packages, as well as a telephone conversation with Karin Coyle of ETR Associates who led the Safer Choices RCT. Initial points of elaboration agreed between researchers and SEF prior to consultation with schools, other youth and practitioner and policy stakeholders are outlined below. Where these deviated from the specification in the original protocol, this is highlighted.
Needs survey to tailor intervention components
The original protocol had specified that a student needs survey of year 8 students (drawing on the baseline RCT survey) would be used to tailor Positive Choices to local priorities in each school. There was, however, a need for some elaboration of the content of the needs survey and how it would be used to inform the intervention. Regarding the curriculum, the protocol originally specified that, informed by the needs assessment data, SHPCs would select the order in which to deliver modules; whether to deliver them within personal, social, health and economic education (PSHE), tutor groups or by integrating them into other lessons; and whether to use materials from Positive Choices or existing materials, if these conformed to our curriculum. However, SEF advised that, in practice, not all of these things would be likely to be open to influence by the needs data or the SHPC. In which lessons the curriculum would be taught, for example, would probably already be determined by school leaders. Whether to use existing or Positive Choices materials would be determined through an assessment by SEF of the resources to which the school already had access. SEF also felt that there should be a logical order to lessons (e.g. understanding reproduction before contraception), which precluded SHPCs determining this.
It was agreed that the most useful way to use the student needs assessment was to inform the selection of curriculum lessons for each school. Students would be asked in the needs survey what RSE topics they had covered previously in school, how well they had been covered and what they wanted to cover in year 9. To ensure alignment with the intervention theory of change and that all basic SEF-recommended material was covered in a logical order, the curriculum was initially designed to include a set of five ‘essential’ lessons to be covered by all schools and a bank of 10 ‘add-on’ lessons, five of which could be selected by the SHPC based on the student needs data. This was a deviation from the protocol.
Questions on how well RSE topics had been covered in school, knowledge of conception, contraception and STIs, knowledge of services, parental communication, experiences of sending/receiving sexual imagery and sexual harassment at school were included in the needs survey (see Report Supplementary Material 5) to lend more general support for implementation of Positive Choices in schools and to inform the content of parent newsletters, the focus of student-led social-marketing activities and the review of sexual health services.
School health promotion council activities
Although the original protocol stated that the role of the SHPC would be to review local needs data and to use these to tailor each intervention component, and co-ordinate intervention delivery, the exact tasks of the SHPC (other than those set in relation to the student curriculum) were not specified. Based on a review of the Safer Choices materials and discussion between researchers and SEF, it was agreed that the main activities of the SHPC would involve reviewing the student needs data and identifying how the data could inform decisions about the implementation of each intervention component of Positive Choices; launching the intervention in schools and to parents; selecting the ‘add-on’ curriculum topics informed by the needs data; taking a role in recruiting the social-marketing team and monitoring campaign activities; preparing and distributing parent newsletters; and carrying out the school sexual health services review. These elaborations did not constitute a deviation from the protocol.
Topics covered by curriculum
Although the curriculum areas identified in the protocol reflected those recommended by SEF for inclusion in a comprehensive year 9 curriculum, they did not map exactly onto the SEF’s suggested curriculum structure and there were some additional topics such as ‘pornography and the law’, ‘female genital mutilation’ (FGM) and ‘body image’ that SEF wanted to ensure were covered for year 9. Inclusion of topics such as ‘the male/female body and reproduction’ were also considered to be essential, as these provided the building blocks for later learning, which many students may not have received in primary school or in years 7 or 8. It was agreed that the curriculum format and lesson titles suggested by SEF would be adopted, but that all topics referred to in the protocol would be embedded within the lessons to ensure alignment between the lessons and intervention theory of change. This did not constitute a deviation from the protocol.
The curriculum was initially designed within the optimisation and feasibility-testing phase to include the following five essential lessons: (1) the female/male body and reproductive organs; (2) reproduction, pregnancy and contraception; (3) STIs and safer sexual practices; (4) sexual response and pleasure; and (5) building blocks to good relationships to cover the core topics specified in the protocol. Five of the following 10 ‘add-on’ lessons were also to be selected, informed by the student needs data: (6) readiness for intimacy; (7) unsafe relationships; (8) love; (9) sexual identity, gender and orientation; (10) understanding consent; (11) pregnancy options; (12) FGM; (13) pornography and the law; (14) body image and the digital world; and (15) values in our community. However, the number of lessons and titles, and the balance between ‘essential’ and ‘add-on’ lessons were modified again when moving from the feasibility-testing to the pilot RCT phase of the study.
Student-led social marketing
The initial protocol specified the number of students that should be involved in developing student-led social-marketing campaigns (n = 12–18); that students from a range of backgrounds should be recruited to take part; the topics that campaigns should cover; and the kind of activities that the social marketing might involve. There was, however, a need to elaborate how student-led social marketing would be implemented in schools. Drawing on Andreasen’s six characteristics of social marketing,18 SEF developed the student-led social-marketing component of Positive Choices to include the following steps: selecting a campaign focus; carrying out new consumer research and/or reviewing student needs data to inform campaign messages; deciding on targeting of subgroups; selecting the marketing mix; considering the ‘exchange’/benefit to students; assessing barriers to achieving the behaviour change goal (the ‘competition’); pitching ideas to the SHPC and SLT; finalising a campaign plan; working on campaign development/implementation; and debriefing by reviewing the campaigns implemented in the school. Guidance materials were designed for each of these core steps. These elaborations did not constitute a deviation from the protocol.
The initial protocol had also stated that student social marketers would use data from the student needs survey to segment consumers based, for example, on cultural styles; however, SEF staff were not comfortable with targeting in this way as they judged that it might be offensive and stigmatising to some students. This was confirmed through consultation with Karin Coyle and with the ALPHA group (see Findings from consultation with the ALPHA group). Karin Coyle also advised that younger students might be less able to contribute to campaign activities, especially where independent work outside structured lessons was required.
Following discussions between SEF and researchers, it was agreed that segmentation and targeting would be considered only on the basis of year group and that the student-led social-marketing team should focus on including students from years 8 to 11. These decisions were reflected in the content of social-marketing materials, and questions on student ‘cultural styles’ were ultimately not included in the student needs survey. This was a deviation from the protocol.
Review of sexual health services
The protocol originally specified that SEF would review school sexual health services. However, SEF advised that the most efficient and sustainable approach to reviewing and improving local sexual health services was for SEF to develop an audit tool that schools could use to carry out their own reviews and make recommendations to improve and promote services on an ongoing basis. This was a deviation from the protocol.
Findings from consultation with one London secondary school
Participant characteristics
Five girls and four boys from year 8, and eight staff holding various roles (including one member of the school SLT, and the school’s marketing and communications manager), participated in an initial optimisation session held at the school in June 2017. Although we had intended to hold more optimisation sessions at the school to gather feedback on draft intervention materials, this proved impossible because of significant problems with the school’s capacity, which emerged in the course of the year and are in Qualitative findings on implementation. In this section, we describe the feedback received from the initial consultation, which focused on the overall acceptability of the proposed intervention aims, components and delivery models (particularly the tasks of the SHPC); teacher preference for the format and content of the manual guiding the intervention and presentation of the needs data; students’ views on the curriculum content; and implementation of the SHPC.
Views on intervention aims, components and delivery models
Staff and students generally confirmed the acceptability of intervention aims and components. Unintended teenage pregnancy was identified as a salient issue for young people in the local area. Students and staff recognised the need for improved RSE. The activities of the SHPC were perceived as feasible and appropriate by students and staff. Student involvement and the use of student needs data to tailor the intervention to local priorities were particularly welcomed. However, some teachers raised concerns about student responses being used to shape curriculum content as they felt that students might be unable to foresee what they needed to learn about relationships and sex. This feedback resonated with our planned approach (outlined in Topics covered by the curriculum) to ensure a core set of RSE topics were covered by all schools, while also providing some flexibility for schools to draw on student data to identify ‘add-on’ lessons.
Although staff appreciated that delivery by trained teachers was a more sustainable option for schools, they were unsure about whether students preferred teachers or external providers to deliver RSE. Based on observations of externally facilitated RSE at the school, one teacher felt that students would ask more personal or sensitive questions with external providers. Other staff, however, thought that students might be more comfortable talking to teachers who were already familiar to them. Some teachers proposed that outside specialists could usefully be involved to cover topics that teachers felt ill-equipped to teach, such as sexual violence and FGM, but this was not an option within Positive Choices. Some staff and students suggested that single-sex teaching was appropriate for more sensitive topics, such as FGM. Although this was not built into Positive Choices because single-sex provision was judged to hamper the sharing of perspectives and to introduce additional logistic complexities, it was retained as an option that schools could use if judged as locally appropriate.
Views on content format of intervention materials
Staff felt that the items proposed for inclusion in the needs survey (see Report Supplementary Material 5) were appropriate, and that analysis would provide valuable information to identify and address any gaps in student knowledge. Staff were particularly keen to assess the prevalence of sharing of sexual images and sexual harassment in schools as they felt these might be important issues to address, possibly through student-led social-marketing campaigns.
Staff reported that, as their time was often so stretched, the needs report and manual guiding intervention components should be comprehensive but concise. They suggested that key requirements, processes and milestones should be highlighted, and that detail on the evidence base and theory of change for the intervention should be relegated to appendices. Most staff also preferred to have reports and intervention materials provided in electronic format.
Students were asked open questions about the topics that they had learnt about previously in RSE and what they thought should be covered in year 9. Most reported that they had covered puberty and the female/male anatomy in primary school or year 7. Students were keen to learn more about STIs, sexual consent, hormones and how bodies worked, sexual pleasure and the sharing of nude pictures. The topics that students suggested broadly reflected those proposed by SEF and confirmed their relevance for inclusion in either essential or add-on lessons.
Table 1 provides an overview of the findings from this consultation and how these informed intervention design.
| Component/resource | Finding on views | How informed intervention design |
|---|---|---|
| Proposed intervention aims, components and delivery models | Staff and students felt that intervention aims were appropriate and relevant, and intervention components were appropriate, including the tasks of the SHPC | Confirmed planned approaches |
| Use of needs data | Teachers concerned that students should not have too much decision-making power over which lessons were taught as they may not have a clear sense of what is important for them to learn about at this stage | Resonated with plan to demarcate ‘essential’ and ‘add-on’ lessons, with only the latter being informed by student needs data |
| Teacher delivery | Teachers felt that external educators could bring expert knowledge to lessons that teachers feel ill-equipped to teach themselves | Intervention trains staff to be competent in teaching topics covered by the intervention and is a more sustainable option for schools. Budget also did not allow for the inclusion of external experts to deliver lessons for each school |
| Single-sex teaching | Some teachers and students felt that some sensitive topics should be taught in single-sex lessons | Not actively recommended for Positive Choices. Guidance for schools that, in general, lessons should be taught in mixed-sex groups to enable the sharing of ideas and discussion across genders. In addition, potential alienation of trans, non-binary or questioning students. Preferences to deliver in single-sex classes because of cultural or religious sensitivities to be discussed with individual schools on a case-by-case basis. But allow schools flexibility where locally appropriate |
| Needs report | Staff interested in all items suggested for inclusion in the needs report, particularly those relating to circulation of sexual imagery and sexual harassment in school | All items included for needs assessment report in optimisation and pilot phase |
| Manual format | Staff felt that manual materials should be concise and easily accessible for teachers with little time. Detail of evidence base and theory of change to be relegated to appendices | Materials designed with concise text, clear titles and subheadings, lots of bullet points, and clear timelines and milestones highlighted |
| Preference is to have electronic materials | Manual designed as an interactive portable document format (PDF) with all additional materials accessible online | |
| Format of needs report | Staff agreed that they would prefer the format of the needs report to be in tables rather than graphs; wanted something short that contained the headline facts and wanted electronic version | Incorporated into the design of the needs assessment for optimisation and pilot |
| Curriculum topics | Students indicated that topics selected for inclusion in the curriculum are appropriate and relevant | Confirmed list of topics to be covered by the curriculum and to be used to select ‘add-on’ lessons |
Findings from consultation with the ALPHA group
Participant characteristics
The first two consultations with the ALPHA group informed optimisation. Five boys and four girls took part in the first session in July 2017. Three boys and four girls took part in the second session in April 2018. Table 2 gives a breakdown of participants by age and gender.
| Session | Age (years) | Male, n | Female, n | Total, n |
|---|---|---|---|---|
| First session (July 2017) | 14 | 2 | 0 | 2 |
| 15 | 1 | 1 | 2 | |
| 16 | 0 | 1 | 1 | |
| 17 | 1 | 0 | 1 | |
| 18 | 1 | 2 | 3 | |
| Total | N/A | 5 | 4 | 9 |
| Second session (April 2018) | 14 | 0 | 1 | 1 |
| 15 | 2 | 1 | 3 | |
| 16 | 1 | 0 | 1 | |
| 17 | 0 | 0 | 0 | |
| 18 | 0 | 1 | 1 | |
| 19 | 0 | 1 | 1 | |
| Total | N/A | 3 | 4 | 7 |
Views on intervention content
In the first ALPHA session in July 2017, participants proposed possible activities for the launch of Positive Choices in schools that could be incorporated as suggestions into guidance materials. These included events for parents, presentations in assemblies or in tutor time, use of social media, communications to parents, updating the school website, running RSE-themed interactive performances, using promotional screens in schools and creating a graffiti wall for questions about sexual health.
In the second session in April 2018, participants reported that they were supportive of the parent component of the Positive Choices intervention, recognising the value of informing parents about the RSE being taught in school and involving them in supporting their children’s learning at home. Consultation with ALPHA on the most appropriate models of engaging parents revealed that schools had a variety of ways of communicating with parents. These included sending letters home with children; communicating via e-mail, text messages and, in fewer cases, via social media; posting information on school websites; and holding parent events.
Some participants were sceptical about whether or not homework assignments could prompt conversations at home, suggesting that many students would avoid such homework activities because of the risk of embarrassment or breaching existing child/parent boundaries. In line with SEF’s intended plan, homework activities were selected with these considerations in mind and aimed to ease into parent/child discussion at home, focusing initially on the less sensitive topic of ‘rites of passage’ before progressing to ‘abusive and healthy relationships’ in a later assignment. Participants also suggested that there was a need for the content of parent materials to be sensitive to different home cultures. Templates for parent newsletters were therefore included in intervention materials, but the precise content and mode of delivery was left to schools.
The ALPHA members were also generally supportive of the student-led social-marketing element of Positive Choices, on the grounds that student-led campaigns could ensure messaging was relevant to young people, complementing teacher-led lessons. Resonating with SEF concerns outlined above, ALPHA participants suggested that younger students might be less competent to participate fully in student-led social-marketing campaigns. They also agreed that targeting students on the basis of knowledge, cultural style or peer group affiliation could be stigmatising. Participants further raised the importance of ensuring flexibility in the programme so that campaigns could fit the context and resources available in each school. Campaigns being genuinely student led and messaging being consistent with programme aims were also highlighted as important issues. The latter informed our decision to ensure student-led social-marketing groups were accountable to SHPCs.
Table 3 outlines how feedback from the ALPHA meetings were incorporated during optimisation. A full summary of each of the ALPHA sessions is provided as Report Supplementary Material 6.
| Component/resource | Issue identified | Action taken to incorporate |
|---|---|---|
| Launch of Positive Choices (SHPC manual section) | ALPHA identified a number of ways that Positive Choices could be launched in schools including a separate parent event; different events approaches for different year groups; involving external people in presentations; assemblies or dedicated lesson time to run launch activities; using social media; sending communications home to parents including by e-mail and website; running RSE-themed role plays; and using promotional screens in schools | Many of these were incorporated into the SHPC manual section as ideas for the launch of Positive Choices |
| Parent materials | Ways of communicating with parents differ by school, so mode should be flexible. Participants also suggested that there was a need for the content of parent materials to be sensitive to different home cultures | Templates for parent newsletters were included in intervention materials, but the precise content and mode of delivery was left to schools |
| Homework with parents may be uncomfortable and breach usual parent/child boundaries | Confirmed planned approach ‘ease in’ to homework assignments, using universal, less sensitive topics initially | |
| Student-led social marketing | Campaigns should be delivered by older students as younger students may be less familiar with content | This suggestion has been incorporated into the manual guidance |
| Student involvement and control must be genuine to guarantee the authenticity of campaigns | Need for genuine student involvement is highlighted in all materials and activities to be overseen by SHPC to ensure this | |
| To ensure fit of campaign messages, social-marketing group should present ideas to the SHPC, including members of SLT | A presentation to a panel activity has been incorporated into the design so that members of the SHPC can assess and select campaign ideas and ensure their appropriateness. The trained facilitator will also help to ensure that messaging is appropriate | |
| Campaign messages should not be targeted as this may cause offence and be stigmatising for those groups | It was agreed that segmenting particular groups of students was not appropriate other than by year group | |
| Flexibility of campaign approach needs to be allowed as school context and what will work in each setting may differ significantly | This was incorporated so that schools choose activities appropriate for their school |
Findings from practice and policy stakeholder feedback
Twenty-three practitioners and policy-makers from governmental and non-governmental organisations in the field of education and health attended the first consultation event in March 2018, which focused on intervention optimisation. The timing of the event, however, meant that this consultation informed refinements for the pilot, rather than for the initial feasibility assessment.
Discussions focused on potential challenges to implementation in the pilot and how to overcome these. Participants highlighted that one of the major challenges to implementation would be ensuring that schools prioritised the intervention, given other pressures. Stakeholders made suggestions to address this, which included increasing engagement with head teachers and/or SLTs; disseminating programme information to all school staff to raise awareness of Positive Choices in schools; seeking ‘buy-in’ from school governors and parents; involving local partners with long-standing relationships with schools, such as those in public health departments or school networks; and maintaining regular contact with a named strategic lead with enough seniority to drive implementation.
Participants recommended that researchers should highlight what schools stood to gain from participating in Positive Choices including free staff training to support continued professional development; specialist-designed curriculum materials; improved safeguarding procedures; meeting statutory obligations to support students’ social and emotional well-being; contributing to meeting national school inspectorate criteria; and potential for improved pupil attendance and attainment. Stakeholders recommended signing service-level agreements with schools, highlighting expectations for intervention providers, schools and researchers.
Some stakeholders also expressed concern about how Positive Choices materials might fit with existing provision in schools, and were keen that they should not replace this where provision was already good. Stakeholders also cautioned that some schools might see Positive Choices as ‘the answer’ to RSE in their school, which could reduce the incentive to implement a comprehensive curriculum across the year groups. These findings informed our decision for SEF to carry out an assessment of how Positive Choices would be integrated with existing provision in each intervention school and whether existing or Positive Choices materials would be used for year 9 students. It was also emphasised to schools that they were to continue with any usual provision for other year groups.
Stakeholders also pointed to the importance of building flexibility into the curriculum to accommodate variability in the timetabling of lessons and existing provision, and suggested that a gradual approach to implementation might be necessary in schools where capacity was more limited.
Table 4 outlines how suggestions from the practice and policy stakeholder meeting were incorporated into the refined intervention for the pilot.
| Component/resource | Issue identified/stakeholder suggestion | How incorporated/addressed |
|---|---|---|
| Programme overview manual section (school engagement specifically) | Participants raised the challenges of ensuring school commitment, increasing engagement with SLT and disseminating information about the programmes to staff throughout the organisation. Gaining support from school governors and parents, and involving local partners with long-standing relationships, credibility and leverage with schools, such as those in public health departments or school improvement, as well as school networks or academy chains, was also perceived to be important. Participants suggested that it was important to maintain contact with a named strategic lead with authority to drive the intervention forward | Staff held face-to-face meetings with SLT members at all pilot schools to ensure commitment to the trial and capacity to deliver. Programme overview manual section was adapted to include clear instructions for nominating a dedicated member of SLT with overall responsibility and oversight for the programme as well as a day-to-day lead. A suggestion was included to brief all staff on the programme. A note to involve governors, parents and other local partners in the SHPC was included in the manual |
| Participants emphasised the importance of recognising and stressing to schools the value of what they are receiving in exchange for participation. This includes free, quality-assured staff training and materials and many potential benefits to the school, including in relation to safeguarding, meeting Ofsted judgements, and the potential for improved pupil attendance and attainment | The benefits to the school of being involved in the programme were highlighted more clearly in the programme overview section of the manual guiding the intervention and in initial communication with pilot schools | |
| Participants highlighted the need to have service level agreements and to be firmer with schools that are not meeting the obligations that they have signed up to | Service level agreements were devised and signed by both intervention and control schools for the pilot RCT. See Appendix 4 | |
| Curriculum materials | Some stakeholders expressed concern about how Positive Choices materials might fit with existing provision in schools, especially where provision was good | In the pilot, SEF to carry out an assessment of how Positive Choices would be integrated with existing provision and whether existing or Positive Choices materials would be used. Also emphasised to schools that they were to continue with any usual provision for other year groups |
| General | Stakeholders pointed to the importance of building flexibility into the curriculum to accommodate variability in the timetabling of lessons and existing provision, and that a gradual approach to implementation might be necessary in schools where capacity was more limited | Scope for flexibility in timetabling and gradual implementation was built into planned approaches |
Findings from interviews with Sex Education Forum staff on optimisation processes
We interviewed three SEF staff about the optimisation phase. They were positive about the optimisation process and felt that bringing together various stakeholders, a school and research evidence contributed to the production of high-quality intervention materials.
The SEF lead described how having a clear protocol was useful for focusing and pushing forward the development work and ensuring alignment with the theory of change:
It was like . . . a persistent extra voice that then forced me to think, ‘Right, I’ve got to look for different material and we’ve got to work within it’. And it probably did result in better quality curriculum materials . . . And I think, you know, [LSHTM] and I all agreed once we’d kind of pushed ourselves [both laugh], that it came out better and differently because of that aspect of the protocol.
Lead on intervention development, SEF
The student-led social-marketing element was described as being the most challenging to elaborate because there were no existing materials on which to build, and because it used a different vocabulary from that familiar to SEF staff. However, once understood in terms of student participation and voice, it was said to be more comprehensible and acceptable.
The multicomponent approach was highlighted as being the most exciting and innovative aspect of Positive Choices for SEF:
A multicomponent programme is a really interesting and worthwhile thing to look at . . . I think that is a really important contribution that it makes, to say we’re going to have all these bits working together . . . That could be quite a fundamental shift in the mindset of lots of people.
Lead on intervention development, SEF
The SEF staff were also pleased that, based on stakeholder feedback and their own experience in schools, the intervention could accommodate variation in school structures and processes:
The school health promotion council . . . you don’t know what the structure’s going to be in the school and you can’t just be creating lots of new structures. You don’t know what their time is going to be, or their resource constraints. So, you’ve got to have some flexibility built in and I think we’re all fairly agreed about the way we’re going about that now. The same with the parental stuff. We’ve given examples of how you can communicate with parents, but with an acceptance that every school is going to communicate with parents a different way and they’ve got to find a way that fits them. And that’s what the research needs to be looking out for, whether it’s successful.
Lead on intervention development, SEF
However, staff reported that a dilemma emerged concerning the level of flexibility that could be incorporated into the curriculum materials. The protocol called for, and consultation with schools supported, the need to provide teachers with detailed and prescriptive curriculum materials. Yet this did not resonate with SEF’s perception of a ‘gold-standard’ approach, whereby trained teachers develop their own curriculum:
We knew the kind of evidence that LSHTM were drawing on, but I think where the tension came up was the amount of flexibility in the design of the curriculum materials . . . What was needed . . . was quite a formulaic set of lessons with activities that are described. It’s just more manualised . . . But it wouldn’t be quite at that level of really competent teachers crafting an RSE lesson based on some guidance and some really good tools, and thorough training.
Lead on intervention development, SEF
After some discussion, however, researchers and SEF agreed that to ensure quality and fidelity of delivery it was important to use a directed approach.
Another issue was the focus on the year 9 curriculum. SEF recognised that for the purposes of trialling a discrete public health intervention to address unintended teenage pregnancy and sexual health, targeting the curriculum at year 9 students was appropriate. However, this was somewhat at odds with the widely recognised need for a curriculum that built across year groups:
One thing we were conscious of is that stakeholders were likely to criticise some of the rigidity in the programme design . . . I don’t think they could forget that question about . . . why is this just involving year 9 in the curriculum, what’s going to happen before, what’s going to happen after?
Lead on intervention development, SEF
Ultimately, SEF’s lead recognised that:
What you need to do to have a randomised control trial type model is different to everyday good practice that is holistic and runs over the long-term of children and young people’s education and that in the end collaboration between SEF, researchers and other youth and practice and policy stakeholders had led to something that everyone’s really happy with.
Lead on intervention development, SEF
Formative feasibility testing
Response rates
Student needs survey
The survey was completed by 127 (80%) year 8 students. Twenty-two students did not consent to participate, six were absent and three were considered not competent to give consent because of language difficulties or special educational needs and disabilities (SEND). No students were withdrawn by parents.
Researcher observations and teacher logbooks
All three SEF-delivered training sessions were audio-recorded and observed by a researcher. Six SHPC meetings and five student-led social-marketing meetings were observed. Owing to implementation challenges with the curriculum (see Quantitative findings on implementation, Fidelity of classroom curriculum), only one curriculum lesson was observed. Staff logbooks for curriculum delivery and SHPC meetings were not completed, but was completed for the student-led social-marketing meetings. The fidelity checklist for the sexual health services review was completed by researchers in consultation with students from the SHPC.
Table 5 outlines the data collection activities that were carried out.
| Data source | Feasibility testing school, n (% response rate) |
|---|---|
| Student needs survey | 127 (80) |
| Observation/recording of SEF SHPC training | 1 (100) |
| Observation/recording of SEF curriculum training | 1 (100) |
| Observation/recording of SEF student-led social-marketing training | 1 (100) |
| Observation of SHPC meetings | 6 (300) |
| Observation of curriculum delivery | 1 (50) |
| Observation of student-led social-marketing meetings | 5 (250) |
| SHPC meeting teacher logbooks | 0 (0) |
| Curriculum delivery teacher logbooks | 0 (0) |
| Student-led-social-marketing meetings teacher logbooks | 1 (100) |
| Sexual health services review fidelity checklist | 1 (100) |
Staff, student and Sex Education Forum interviews
Five school staff involved in the implementation were interviewed (three as individuals and two in a paired interview). Eight year 9 pupils (five girls and three boys) who received the Positive Choices curriculum, two of whom were also involved in the SHPC, participated in a focus group discussion about their experiences. Interviews were carried out with three SEF staff members: one involved in the initial development of the SHPC and curriculum components, and training students and staff on the SHPC; one leading on the development of the curriculum, parent and student-led social-marketing components, and training school staff on these; and one contributing to the social marketing and review of sexual health services. All interviews took place following the end of the optimisation and feasibility-testing phase.
Quantitative findings on implementation
Fidelity of staff training
All SEF trainings were delivered with > 70% fidelity overall (Table 6). Time limitations affecting the curriculum training reduced the fidelity of this element.
| Training | Number of attendees | Data source | Topics covered | Exercises used | Opportunities for discussion | Overall fidelity of implementation |
|---|---|---|---|---|---|---|
| SHPC training | 9 students, 4 staff | Audio-recording/researcher observation | 96% | 91% | 100% | 92% |
| Curriculum training | 11 staff | Audio-recording/researcher observation | 83% | 73% | 100% | 78% |
| Student-led social-marketing training | 12 students, 1 staff | Audio-recording/researcher observation | 100% | 71% | 100% | 81% |
Fidelity of school health promotion council meetings
Six SHPC meetings were held (two in term 1 and four in term 3). Although no teacher logbooks were received, according to researcher observations of all six meetings, implementation of the SHPC met fidelity across all measures, with overall fidelity of 72% (Table 7).
| Data source | Total number of meetings | Items discussed | Actions agreed | Opportunities for discussion | Overall fidelity of implementation |
|---|---|---|---|---|---|
| Researcher observations | 6 | 80% | 70% | 100% | 72% |
| Teacher logbooks | N/A | N/A | N/A | N/A | N/A |
Fidelity of classroom curriculum
Although Positive Choices included 10 hours of classroom curriculum for year 9 students, the collaborating school experienced a number of challenges to implementation (outlined in more detail in Curriculum delivery) and was only able to deliver the five lessons specified as ‘essential’ in the initial intervention design. These were the female/male body and functions of reproductive organs; fertility and contraception; STIs and safer sex; building blocks to good relationships; and consent.
Overall fidelity of the lesson that was observed by a researcher was poor, at only 54% (Table 8). Possible reasons for this are explored in more detail using qualitative data in Qualitative findings on implementation.
| Data source | Topics covered | Exercises used | Opportunities for discussion | Overall fidelity of implementation |
|---|---|---|---|---|
| Researcher observations | 62.5% | 50% | 0% | 54% |
| Teacher logbooks | N/A | N/A | N/A | N/A |
Fidelity of student-led social marketing
Fidelity of the student-led social-marketing meetings was high at 82% overall (Table 9). However, despite their investment in planning a campaign, students were unable to deliver their final production in school. The reasons for this are explored in more detail using qualitative data in Qualitative findings on implementation.
| Data source | Total number of meetings | Items discussed | Actions agreed | Opportunities for discussion | Overall fidelity of implementation |
|---|---|---|---|---|---|
| Researcher observations | 5 | 89% | 71% | 100% | 82% |
| Teacher log sheets | 5 | 89% | 71% | 100% | 82% |
Fidelity of school sexual health services review
The SHPC completed the review of school-based and other local sexual health services. According to the logbook completed with students, the overall fidelity for implementation of this component of the programme was 83% (Table 10).
| Data source | Steps 1–5: review of existing services | Step 6: actions taken to enhance existing services | Overall fidelity of implementation |
|---|---|---|---|
| Checklist | 100% | 0% | 83% |
Overall fidelity of implementation
Overall, the participating school implemented Positive Choices with 80% fidelity.
Acceptability
Staff and student acceptability of the optimised Positive Choices intervention was quantitatively assessed via two questions included in staff interviews and the focus group with year 9 pupils. These were:
-
Do you think your school should deliver the Positive Choices programme again?
-
Do you think other schools should?
In response to these questions, staff and students unanimously (100%) agreed that their school should deliver Positive Choices again and that it should be delivered in other schools.
Qualitative findings on implementation
Staff views on implementation and feasibility
Initial engagement
Although the participating school implemented Positive Choices with ≥ 70% fidelity, staff interviews were dominated by the discussion of challenges to implementation. These were attributed overwhelmingly to recent, repeated changes in school leadership that occurred as a result of a poor school inspection result, and which led to the programme no longer being prioritised, as the new leadership focused on teaching and behaviour:
September comes along and Ofsted did a little surprise visit . . . and . . . we went from having a ‘good’ rating to a ‘requires improvement’ rating. So, the focus was shifted . . . What is deemed as extra, they get cut . . . Unfortunately, because it wasn’t a school priority to make sure that RSE was getting delivered and to be committed to the project, I think that the leadership decided that they wanted to go another way.
SLT lead
The SLT lead at the school suggested that the lack of support from school leadership was compounded by the initial day-to-day lead stepping down from her role as RSE co-ordinator at the start of term 2, citing overwork and personal health issues. She was replaced by another member of the school inclusion team who was not a qualified teacher and was less experienced in teaching RSE:
I’m not the expert, I’ve been told so-and-so’s no longer doing this . . . I was told, ‘this is what you’re doing . . . I’ve gone from somebody who would possibly deliver a session around something that I felt comfortable, maybe the relationship part of it, alright, to actually being the man who’s upfront responsible for a programme.
Replacement day-to-day lead
This staff member managed the implementation of Positive Choices alongside his existing responsibilities as safeguarding lead for the school. He focused on co-ordinating curriculum delivery, but took little responsibility for overseeing other components.
Curriculum delivery
Co-ordinating the curriculum lessons was particularly challenging and the new lead reported that this resulted in conflict as he attempted to get staff released to deliver Positive Choices lessons.
This led to the school implementing only 5 of the 10 hours of curriculum teaching and the new lead delivering many lessons himself, sometimes to a hall of up to 90 year 9 students. The lead felt ill-equipped to deliver some of the lessons:
I felt that I was going into, um, situations with some of the topics where I thought [sighs] I hate not knowing this . . . I feel so bad delivering something that’s half-hearted and it’s unmeaningful as well, especially when it got to where I was delivering to like maybe three year groups, you’ve got 90 children, how do you go through the subtleties of some of the subjects that you’re covering?
Replacement day-to-day lead
Student-led social marketing
Although a number of meetings were held with students to develop their social-marketing campaigns, the staff facilitator reported that a lack of prioritisation of the programme at a senior level meant that they were unable to deliver what they had planned: a student drama sketch on the topic of sexual consent in a whole-school assembly:
So your three main halls are completely busy, and you’ve got nowhere to have an assembly and then it was last minute in fact like everyone was scrambling because nobody had known and it’s one of those things . . . no time for our clever skit.
Social-marketing facilitator
The social-marketing facilitator suggested that, had the work begun earlier in the year, they may have had a better chance of delivering the final performance.
Sexual health services review
With the support of SEF, the review of school and local sexual health services was completed by the SHPC. Although students were able to carry out the review of sexual health services, they were unable to present their recommendations to school leaders. Students and SEF staff also reported how the review was hampered by new discipline policies that did not allow students to be outside classrooms and in school corridors without a teacher present.
General feasibility of implementation
Despite the challenges experienced with implementation, staff remained positive about the feasibility of Positive Choices in secondary schools with the right level of support from a senior level:
Definitely a workable programme . . . it just needed . . . I don’t know whether management just don’t understand logistics or whatever, but yeah, it needed the full backing from them.
Initial day-to-day lead, optimisation and feasibility testing school
It is workable and it can work in other schools, absolutely yes. And I think with the correct support of leadership it can.
SLT lead
Staff highlighted the importance of staff dedicated to co-ordinating implementation, and the importance of selecting skilled teaching staff to deliver the curriculum.
But in the main I think for me the programme it was essential or it is essential, absolutely essential, but I just think the problem with people like me . . . I just didn’t feel I was the right person to be delivering some of the subject matter.
Replacement day-to-day lead
Views of Sex Education Forum staff on implementation and feasibility
Staff from the SEF were similarly concerned about the fact that teaching support staff rather than trained teachers were being selected by the school to be trained to deliver the curriculum:
It shouldn’t be taught by non-teaching staff, it’s got to insist on teachers coming on the training and not support staff, otherwise you’ll get support staff teaching, and if they don’t do that for other subjects they shouldn’t do it for Positive Choices.
SEF trainer
The trainer felt that this exemplified the low priority Positive Choices and RSE more generally were afforded in the school under new management. SEF staff felt that the change in management and crisis situation in the school had rendered it a poor site to test feasibility of the intervention, notwithstanding the fidelity results being good enough for progress to the pilot RCT.
Staff view on intervention acceptability
Staff were very positive about the intervention and saw the content as important and necessary for their students. Staff were particularly enthusiastic about the student participation element of the intervention, which they suggested had given students a sense of empowerment and ownership over the programme and made sure it was relevant to their experience:
I think it’s a good way of getting the students involved in it and making them feel like they are creating something for themselves. It’s all about empowering students, getting them to be in a leadership position, I think they feel that.
SLT lead
The social-marketing facilitator commented on the value of providing students who were usually less vocal or engaged with school with an alternative space to express themselves and flourish:
So, I think like for the boy who was very quiet but also quite astute . . . he came religiously to every meeting and would ask me about when the next one was. And this is a boy that’s very, you know, that was a shining example of someone who doesn’t get tapped up to be part of these groups and really flourished . . . And even one of the girls . . . who was reluctant to separate from her friend during the workshop but then eventually came to me afterwards and said how much she’d enjoyed it. So, I think it’s giving students who don’t always get tapped up to take part in things opportunity to express themselves and I thought they did really well overall.
Social-marketing facilitator
Staff reported that they thought Positive Choices had had an impact on student knowledge, with the lesson on sexual consent in particular increasing awareness and reporting of sexual harassment in school:
‘Yes, I would [link the increase in reporting] to Positive Choices because actually, the consent stuff was delivered in the April . . . And from that point the girls were actually making disclosures to counsellors . . . So I think it was giving them a little bit more self-confidence to say, well actually . . . you shouldn’t be doing that to me and I’m going to tell someone about that . . . So a positive impact on the girls and in theory, a positive impact on the boys because hopefully they now know what they can and can’t do’.
SLT lead
Student views on intervention acceptability
Students were enthusiastic about Positive Choices, reporting that the curriculum covered topics more comprehensively than most RSE delivered in schools:
What they [in other schools] learnt is basically just condoms, condoms, condoms, condoms . . . We’ve had conversations like with my friends from different schools, and then we was talking about like just sex ed[ucation] in general, and how it can be uncomfortable and it’s like, ‘The only thing we’ve learnt about is like condoms,’ I was like, ‘You haven’t learnt about sexual beliefs, none of that?’
Year 9 girl
Students generally appreciated the focus on relationships, not just sex. The content on different types of abuse in relationships was particularly powerful for some female students:
I learnt like that, like, I don’t know what the word’s called again, but like controlling, how you’re being controlling, that can count as a mental abuse. Because always wanting to know where someone is and stuff like that, I didn’t realise that before, that that could count as abuse, or any different things, so I learnt that there’s different . . . it was more of an eye-opener.
Year 9 girl
Most students felt that the curriculum content was appropriate and important to enable them to protect themselves and develop their own sense of what was right for them now or in the future:
I feel like the key messages was to prepare us for the future and like if you decide, OK you want to be in a relationship now, that’s your choice, but make sure you’re doing what’s right for you and your body and like know how, where the law fits in within it, and what’s legal for you to do and what’s illegal for you to do.
Year 9 girl
Students also appreciated the opportunity to discuss with their peers in lessons, exploring other students’ views. This represented a different pedagogical approach to that used in their other lessons. Some, nevertheless, felt that they wanted more time to explore issues with each other in class:
Compared to maths, it wasn’t as fast, but I feel like there still wasn’t enough time, to become in depth and understand the situation and anything that people go through, or what they can go through.
Year 9 boy
Underscoring the value of mixed-sex teaching, one student also reported that she valued the space for discussing and for challenging the opinions of male students in the class:
When the boys were there, there was a lot of . . . controversy, so it was a lot of arguing and disagreements, and it was good arguing . . .
Year 9 girl
Refinements made based on feasibility assessment in one London school
Although fidelity of implementation met the progression criteria, our observations, and staff and SEF accounts of implementation informed further refinements to the intervention. These are described in Table 11. In particular, our experience with the optimisation and feasibility school emphasised the need to assess the capacity of pilot schools for participation in the trial and ensure strong commitment from participating schools.
| Component/resource | Issue identified | Refinement made |
|---|---|---|
| General | Optimisation school faced challenges with implementation because the programme was not recognised as a priority for the school by the SLT and staff were not adequately supported to deliver | Implement existing stakeholder recommendations to increase SLT commitment and prioritisation. See Table 4 |
| Curriculum delivery | Issues with the confidence and quality of delivery of curriculum by non-teaching staff |
Refinements made to ensure that it is teaching staff who undertake curriculum training and delivery in pilot schools Refinements were also made to the lesson on STIs that staff found particularly tricky to teach Procedures for additional remote support from SEF via e-mail agreed for pilot |
| Social marketing | Staff reported it was challenging to fit the activities into the last term of the year | Flexibility included for schools to implement across the academic year |
To support implementation, it was also agreed that additional time in the SHPC training and space in the manual should be given to clarify the key tasks and activities of the SHPC, describe the timeline for activities and provide action planning for the SHPC.
Other refinements made prior to pilot
As the curriculum lessons were developed and tested, it also became necessary to increase the number of essential lessons from five to eight to ensure that all topics set out in the protocol were covered. The final set of essential lessons for the pilot were (1) the female/male body and reproductive organs, (2) fertility and contraception, (3) STIs and safer sex, (4) building blocks to good relationships, (5) consent, (6) sustaining relationships, (7) sexual response and pleasure and (8) pornography. It was also agreed that there was some unnecessary overlap in the remaining ‘add-on lessons’ so these were combined and reduced. The final agreed set of add-on lessons was (9) pregnancy options, (10) readiness for intimacy, (11) body image and the digital world, (12) FGM and (13) human rights, stigma and discrimination.
Safeguarding and adverse events
During the course of fieldwork at the feasibility school, no student disclosures met the criteria for reporting safeguarding concerns to a school safeguarding officer based on the safeguarding policy in place at the time. In line with our standard operating procedure (see Appendix 5), at the end of the implementation phase, the feasibility testing school reported to the research team on SAEs among the cohort of students taking part in Positive Choices. No SAEs were reported by school staff.
Progression to pilot randomised controlled trial
Despite challenges to implementation in the optimisation and feasibility testing school, overall implementation fidelity was 80%. Acceptability of the intervention was also high, with 100% of staff and students agreeing that the intervention should be implemented in their own and other schools again. Refinements to planned approaches and materials were made on the basis of school, ALPHA group and practitioner/policy stakeholders’ input and feasibility testing to improve implementation for the pilot. In July 2018, all members of the research team, SEF, the principal (head teacher) of the collaborating school and the SSC indicated that the Positive Choices intervention materials had been optimised to their satisfaction. Copies of SSC minutes and correspondence confirming this are provided as Report Supplementary Material 7. Progression to the pilot RCT was, therefore, recommended by the SSC and the National Institute for Health Research (NIHR) at the beginning of September 2018.
Chapter 4 Results: undertaking the pilot randomised controlled trial
Recruitment and participant flow
On 13 November 2017, 334 mixed-sex state secondary schools within 1 hour’s train journey from London were e-mailed with an invitation to participate in the pilot RCT. Eleven schools responded to indicate interest. These schools were sent a consent form for the head teacher to sign. Eight provided this consent, the first six of which were recruited to the study; however, on 18 May 2018, one of these six dropped out of the study. The mailshot was repeated, excluding schools already recruited. Nine schools expressed an interest and were sent a consent form for the head teacher to sign. The first school to respond was recruited as the sixth of our participating schools.
Baseline surveys were conducted in these six schools, with an overall response rate of 88.0%. Four schools were then randomised to receive the intervention and two to continue with usual activities. No schools withdrew from the study, and at 12 months follow-up surveys had an overall response rate of 87.1% (89.0% in the intervention group and 82.0% in the control group). Recruitment and participation are also illustrated in Figure 2.
FIGURE 2.
Participant flow.
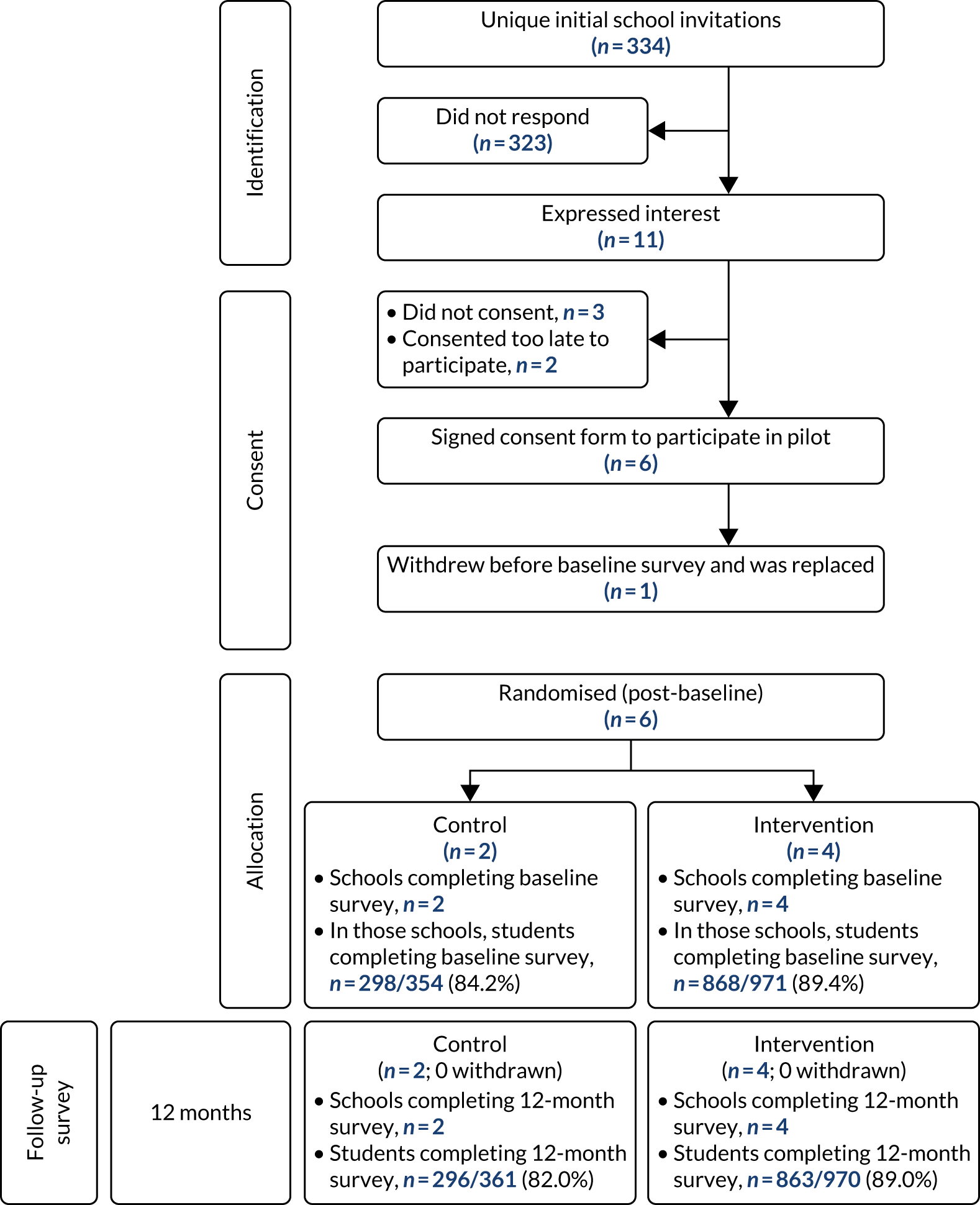
Baseline school and student characteristics
Unsurprisingly, given the small number of schools involved, there were baseline differences between those schools allocated to the control and intervention groups regarding student sociodemographic characteristics (Table 12). Schools looked different by arm in terms of school institutional type, but not by Ofsted rating at the time of recruitment. Schools were similar in terms of value-added educational attainment. Schools in the control group had a higher proportion of students entitled to free school meals and were slightly larger in terms of student numbers. Schools in each arm were in areas of similar deprivation. There was a slightly higher proportion of male students in control schools. There was a considerably lower proportion of white students and higher proportion of students of Asian/Asian British ethnicity in control schools, resulting from one control school being a faith school with predominantly Asian/Asian British students. A slightly lower proportion of students identified as gay or lesbian, bisexual, other or unsure/questioning in control schools. There was a higher proportion of Sikh students in control schools with correspondingly lower proportions of most other religious affiliations. A higher proportion of students reported living with two biological parents in control schools. Students in the control group also reported slightly higher family affluence. However, the groups were balanced in terms of self-reported secondary outcomes (sexual debut) at baseline (see Table 12).
| Characteristic | Intervention (4 schools) | Control (2 schools) | Overall (6 schools) | |
|---|---|---|---|---|
| School | ||||
| School type | Academy converter (mainstream) | 3 | 1 | 4 |
| Academy sponsor led (mainstream) | 0 | 1 | 1 | |
| Community school | 1 | 0 | 1 | |
| Ofsted ratinga | Good | 4 | 2 | 6 |
| 2017 attainment 8 score,a mean (SD) | 47.3 (6.80) | 51.1 (2.75) | 48.6 (6.03) | |
| Value-added score,1 mean (SD) | 0.16 (0.40) | 0.50 (0.15) | 0.17 (0.41) | |
| Proportion of students entitled to free school meals,a mean (SD) | 30.25 (4.64) | 23.2 (8.35) | 27.9 (6.98) | |
| School size (registered students),a mean (SD) | 1342 (355.22) | 1193 (390.50) | 1292 (374.08) | |
| IDACI score,b mean (SD) | 0.130 (0.04) | 0.183 (0.06) | 0.147 (0.05) | |
| Student characteristics (survey) | ||||
| Age (years), mean (SD) | 12.79 (0.41) | 12.81 (0.40) | 12.80 (0.40) | |
| Sex, n (%) | ||||
| Male | 428 (49.3) | 166 (55.7) | 594 (50.9) | |
| Female | 431 (49.7) | 131 (44.0) | 562 (48.2) | |
| Prefer not to say | 6 (0.7) | 1 (0.3) | 7 (0.6) | |
| Missing | 3 (0.3) | 0 (0.0) | 3 (0.3) | |
| Gender, n (%) | ||||
| Boy | 428 (49.3) | 166 (55.7) | 594 (50.9) | |
| Girl | 424 (48.8) | 129 (43.3) | 553 (47.4) | |
| Trans boy | 2 (0.2) | 0 (0.0) | 2 (0.2) | |
| Trans girl | 1 (0.1) | 0 (0.0) | 1 (0.1) | |
| Non-binary | 1 (0.1) | 1 (0.3) | 2 (0.2) | |
| Other | 2 (0.2) | 0 (0.0) | 2 (0.2) | |
| Unsure | 5 (0.6) | 1 (0.3) | 6 (0.5) | |
| Prefer not to say | 3 (0.3) | 0 (0.0) | 3 (0.3) | |
| Missing | 2 (0.2) | 1 (0.3) | 3 (0.3) | |
| Ethnicity, n (%) | ||||
| White | 538 (62.0) | 86 (28.9) | 624 (53.5) | |
| Mixed | 105 (12.1) | 29 (9.7) | 134 (11.5) | |
| Asian/Asian British | 97 (11.2) | 151 (50.7) | 248 (21.3) | |
| Black African/black Caribbean/black British | 90 (10.4) | 20 (6.7) | 110 (9.4) | |
| Other | 33 (3.8) | 8 (2.7) | 41 (3.5) | |
| Missing | 5 (0.6) | 4 (1.3) | 9 (0.8) | |
| Sexual identity, n (%) | ||||
| Straight or heterosexual | 773 (89.1) | 257 (86.2) | 1030 (88.3) | |
| Gay or lesbian | 7 (0.8) | 1 (0.3) | 8 (0.7) | |
| Bisexual | 19 (2.2) | 2 (0.7) | 21 (1.8) | |
| Other | 10 (1.2) | 2 (0.7) | 12 (1.0) | |
| Unsure/questioning | 35 (4.0) | 5 (1.7) | 40 (3.4) | |
| Prefer not to say | 19 (2.2) | 15 (5.0) | 34 (2.9) | |
| Missing | 5 (0.6) | 16 (5.4) | 21 (1.8) | |
| Religion, n (%) | ||||
| None | 466 (53.7) | 86 (28.9) | 552 (47.3) | |
| Christian | 213 (24.5) | 30 (10.1) | 243 (20.8) | |
| Jewish | 8 (0.9) | 0 (0.0) | 8 (0.7) | |
| Muslim/Islam | 64 (7.4) | 4 (1.3) | 68 (5.8) | |
| Hindu | 45 (5.2) | 18 (6.0) | 63 (5.4) | |
| Buddhist | 4 (0.5) | 1 (0.3) | 5 (0.4) | |
| Sikh | 2 (0.2) | 139 (46.6) | 141 (12.1) | |
| Unsure | 46 (5.3) | 13 (4.4) | 59 (5.1) | |
| Other | 10 (1.2) | 1 (0.3) | 11 (0.9) | |
| Missing | 10 (1.2) | 6 (2.0) | 16 (1.4) | |
| Family structure, n (%) | ||||
| Two parents | 589 (67.9) | 229 (76.8) | 818 (70.2) | |
| Lone mother | 192 (22.1) | 43 (14.4) | 235 (20.2) | |
| Lone father | 14 (1.6) | 1 (0.3) | 15 (1.3) | |
| Reconstituted | 57 (6.6) | 17 (5.7) | 74 (6.3) | |
| Other | 13 (1.5) | 4 (1.3) | 17 (1.5) | |
| Missing | 3 (0.3) | 4 (1.3) | 7 (0.6) | |
| FAS, mean (SD) | 7.93 (2.16) | 8.52 (2.08) | 8.08 (2.15) | |
| Sexual debut | ||||
| Yes | 7 (0.8) | 2 (0.7) | 9 (0.8) | |
| Missing | 69 (7.9) | 29 (9.7) | 98 (8.4) | |
Baseline student surveys
Fieldwork
Baseline surveys were conducted between 4 June 2018 and 6 July 2018. Initial consultation with the ALPHA group on 31 July 2017 informed refinements to the wording of some of the questions in the baseline questionnaire. A copy of the baseline survey and all information and consent materials were e-mailed to school liaison staff at least 2 weeks ahead of the survey date. School liaison staff added school safeguarding and local sexual health information to the student information sheet and distributed student and parent information via their usual means at least 1 week before the surveys. All schools provided individual class registers of year 9 pupils ahead of time and each student was allocated an individual student identity number to be linked to self-report data at baseline and follow-up. Data collection records were prepared for each class to record attendance and consent (see Appendix 6).
In intervention school 4 and control schools 1 and 2, the survey was administered in 1 day. Surveys in intervention school 1 involved five visits and in intervention school 3 involved two visits; in both cases this was so that surveys could be completed in PSHE lessons. In intervention school 2, initial problems with the accuracy of class lists necessitated a return visit.
Surveys were administered in classrooms of up to 30 students (often fewer) by members of the research team supported by a group of fieldworkers recruited and trained (including in safeguarding procedures) for this purpose. Fieldworkers were issued with standard operating procedures for data collection (see Appendix 7). Information about the study and the role of the teacher in data collection was also provided to staff (see Appendix 8). Consent procedures occurred as planned. Students who had opted out of the survey themselves or had been opted by their parents ahead of time were not present. At baseline, no students were identified by schools as being not competent to give consent. Control school 1 had a small class of four students with mild learning difficulties who required additional support from an experienced member of the research team.
While students completed consent forms, surveys in brown envelopes with student names attached as sticky labels were distributed by the class teacher or student assistants. Students were asked to remove the name label from the envelope, leaving only the student code attached to the survey. Students were asked to return questionnaires in the brown envelopes when they had finished. Surveys took approximately 45 minutes to complete, with a minority taking longer.
Very few students expressed discomfort with the questions, a few saying that they were ‘weird’ or ‘too explicit’. In the main, students appeared comfortable completing the questionnaire and rarely identified any questions as being problematic. No serious complaints or concerns were raised by students, teachers or parents at the time or afterwards, and no student indicated that they were distressed by the experience of completing the survey. Common questions recorded by fieldworkers included queries about how to answer some of the identity categories on the survey, such as ethnicity, sexuality and religion. Students who lived in two homes were sometime unsure of how to answer the FAS questions about the number of bedrooms or bathrooms in their home. Students also asked about the meaning of some terms used in the survey, such as conception, masturbation and genitalia, despite many of these being defined in the survey. Some found answering the contraceptive and sexual health skills questions challenging, suggesting an option for ‘I am not sure’ should be included. A few students wanted clarification whether items on contraceptive and sexual health skills, and sexual communication self-efficacy referred to them as they were ‘now’, as they had not yet had a relationship, or in the future. Some also said that they felt unable to answer the social norms questions as they were unsure what their friends thought about these items. Some students were puzzled by the questions in the FAS scale on dishwashers and bathrooms at home, commenting that they thought the questions were about hygiene or parental care. Over the course of fieldwork, researchers developed a list of frequently asked questions and model answers to support fieldworkers to respond to questions like these.
Once the surveys had been returned to the LSHTM offices, all consent forms were checked and found to be accurately completed. All completed surveys were sent for data entry. Scanned copies of surveys that were identified by the data enterers as including handwriting were checked by researchers but no safeguarding concerns were raised.
Response rates by school
Baseline response rates vary from 75.9% to 94.1% between schools (Table 13).
| Baseline student survey | Pilot intervention schools | Pilot control schools | Pilot total | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | ||
| Overall response rate, n/eligible (%) | 224/238 (94.1) | 234/274 (85.4) | 126/148 (85.1) | 284/311 (91.3) | 132/174 (75.9) | 166/180 (92.2) | 1166/1325 (88.0) |
| Absent on the day n (% eligible) | 23a (10) | 21 (8) | 14 (9) | 24b (8) | 15c (8.6) | 8 (4) | 105 (8) |
| Parent opt-out ahead n (% eligible) | 1 (0.5) | 1 (0.5) | 4 (3) | 3 (1) | 28 (16) | 2 (1) | 39 (3) |
| Student opt-out ahead n (% eligible) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Student opt-out on day n (% eligible) | 2 (1) | 18 (7) | 4 (3) | 12 (4) | 4 (2.2) | 4 (2) | 44 (3) |
| Ineligible n (% eligible) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Overall, 105 (8%) students were absent on the day of the survey, although a total 29 surveys were returned later across three of the six schools. The overall response rates in Table 13 reflect the total number of surveys completed, including those returned later. Most schools had few parental opt-outs ahead of the survey. In control school 1, however, 16% of students were opted out by parents. This accounts for the lower overall response rate in this school. Overall, only 3% of students opted out on the day of the survey and none was identified by schools as ineligible at baseline.
Randomisation
Following completion of the baseline surveys, schools were randomised by the CTU on 9 July 2018. All six schools accepted the results of the randomisation and continued with the study. Between 28 September 2018 and 14 November 2018, head teachers signed service level agreements concerning intervention activities.
Follow-up student surveys
Consultation and preparation
We consulted on the contents of the sexual behaviour questions added to the follow-up questionnaire with the ALPHA group of young people on 26 January 2019. The group consisted of 12 young people (five male and seven female) aged 14–19 years. The group commented that the draft survey was clear and appropriate. Participants had reservations about the appropriateness of question wording about forced sex, but the wording was retained as these were standard measures. The group also reviewed the information and consent materials, focusing on how we would seek consent from the girls to link survey data to routine data on births and abortions. As a result, we amended some wording, for example, referring to ‘routine medical data’ rather than ‘official government records’.
Fieldwork
Procedures largely mirrored those for the baseline survey. Surveys were implemented between 4 June 2019 and 9 July 2019. Schools were sent parent and student information and the follow-up survey by e-mail at least 2 weeks in advance of the survey taking place. Schools were asked to distribute the information sheets via their usual means at least 1 week in advance of the survey.
One complaint was raised by a parent from intervention school 1, stating that the time between receiving the information and the survey was only 2 days, and objecting to the questions on self-described gender identity. The PI wrote to the complainant apologising for the school’s delay in sending out information and explaining the rationale for inclusion of these questions.
Year 9 class registers were obtained from all schools in advance and the original individual student identity codes were matched to student names and added to surveys. Students not present at baseline were allocated new codes. Data-collection records were prepared as for the baseline, with an additional column to indicate if female students had consented to follow-up (see Appendix 9).
Surveys took place over 1 day for intervention schools 2 and 4 and both control schools, over 2 days in intervention school 3, and over repeated visits for intervention school 1. All surveys were administered in classrooms by trained fieldworkers, except in intervention school 4 where, because of timetabling challenges, the survey was conducted with all year 9 students in a school hall. The same school informed researchers on arrival that they also had a small group of six students who required reading support to complete the questionnaire, whom they separated and placed into a classroom. An experienced fieldworker was, therefore, allocated to support this class.
Following learning from baseline, information and consent forms were printed on different coloured paper so that students could easily distinguish them. As well as receiving the information sheet and consent form, students received a yellow form with their unique student identifier asking for DOB and postcode from female students consenting to data linkage.
Fieldworkers were briefed in detail about the data linkage process and instructed to explain clearly that the researchers would not link routine data to names or share births data with others, and that all data would be stored securely in line with data protection regulations. Fieldworkers were also instructed to check carefully whether or not consent to data linkage had been ticked on the main consent form and that, where appropriate, DOB and postcode data were complete. Fieldworkers were also provided with a revised standard operating procedure (see Appendix 10) for follow-up, and the frequently asked questions and responses compiled from baseline.
Few female students verbally objected to data linkage, but not all of those who completed the survey consented to follow-up. Those who did object usually cited concerns over confidentiality or the rationale for collecting such personal or, what they considered, useless (because they were not yet sexually active) data. Response rates for data linkage are described in more detail in Response rates by school.
Once all data had been returned to LSHTM offices, data collection records and consent forms were check and reconciled. All surveys and DOB and postcode collection forms were transferred to the data enterers. Scanned copies of surveys identified by the data enterers as including handwriting were checked by researchers individually, but no safeguarding concerns were raised. Two separate files, one containing the student identifier codes alongside the self-report survey data, and one containing student identifier codes, postcodes and DOB information for data linkage, were securely returned by the data enterers. The number of records on each file was accurately reconciled against the number of records sent.
Response rates by school
Follow-up response rates varied from 78.0% to 94.6% between schools (Table 14).
| Response | Pilot intervention schools | Pilot control schools | Pilot total | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | ||
| Follow-up student survey, n/eligible (%) | 214/239 (89.5) | 220/270 (81.5) | 133/148 (89.9) | 296/313 (94.6) | 142/182 (78.0) | 154/179 (86.0) | 1159/1331 (87.1) |
| Absent n (% eligible) | 20 (8) | 37 (14) | 13 (9) | 10 (3) | 20 (11) | 12 (7) | 112 (8) |
| Parent opt out ahead n (% eligible) | 1 (0.5) | 0 (0) | 1 (1) | 2 (1) | 12 (7) | 0 (0) | 16 (1) |
| Student opt out ahead n (% eligible) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 6 (3) | 0 (0) | 6 (0) |
| Student opt out on day n (% eligible) | 4 (2) | 13 (5) | 1 (1) | 4 (1) | 1 (0.5) | 13 (7) | 36 (3) |
| Ineligible n (% eligible) | 0 (0) | 0 (0) | 0 (0) | 1 (0.5) | 1 (0.5) | 0 (0) | 2 (0.2) |
| Consent to data linkage n (% eligible)a | 80 (70) | 83 (70) | 54 (81) | 127 (93) | 51 (73) | 58 (91) | 453 (79) |
Eight per cent of students were absent overall. As with baseline, in most schools there were few parental and no student opt-outs ahead of the survey, but, in control school 1, 10% of students were opted out by their parents or themselves in advance. This, again, accounts for the relatively lower overall response rate in this school. Two students were identified by school staff as being ineligible because of cognitive limitations and were not present when the survey was completed. Across all six schools, only 3% of students opted out of completing the survey on the day.
Across schools, consent to checking births and abortions records ranged from 70% to 93%.
Piloting of primary and secondary outcomes
Primary outcome measures
Primary outcomes were measured using routine data on births and abortions. A total of 453 (79%) female students responding to the survey provided postcode and/or DOB information at follow-up, of whom 9% provided incomplete or invalid data (Table 15).
| Completion of postcode and DOB data | n (%) |
|---|---|
| Records where postcode was valid and DOB was missing | 1 (0.2) |
| Records where postcode was valid and DOB was invalid | 12 (3) |
| Records where DOB was valid and postcode was missing | 12 (3) |
| Records where DOB was valid and postcode was invalid | 13 (3) |
| Records where postcode was missing and DOB was invalid | 1 (0.2) |
| Total | 39 (9) |
Births
Name, postcode and DOB data were matched to ONS births registration data for the period 1 July 2018–1 June 2019. There were no births among the trial cohort based on exact matching of name, DOB and postcode. Focusing on the subset of the births data where the mother’s year of birth was equivalent to that in the survey data (2004–5) produced 81 matches. Focusing separately on given/first and family/second names and running searches for matching values across both data sets resulted in 44 records that did not match to either a forename or a surname; 26 that matched to a forename only; 10 that matched to a surname only; and one to a surname and forename. For the one record that matched on surname and forename, neither the DOB nor the postcode matched the participant data. It was determined, therefore, that there were no probable matches in our cohort.
Abortions
Postcode and DOB information was matched by DHSC with abortions data in the Abortion Notification System (ANS) for the period from 1 June 2018 to 9 October 2019. There were no abortions among the trial cohort based on exact matching of DOB and postcode. There were 166 cases in our data set with an exact match on postcode only. Some of these matched more than once because there was more than one record with the same postcode in the ANS, giving a total of 235 individual matches on postcode only (Table 16).
| Matches | n |
|---|---|
| Exact match on postcode with one case in ANS | 115 |
| Exact match on postcode with two cases in ANS | 39 |
| Exact match on postcode with three cases in ANS | 6 |
| Exact match on postcode with four cases in ANS | 6a |
| Total matches | 235 |
However, none of these matches in the ANS had a birth year of 2004 or 2005, as was the case for all female students in our cohort, and none of the DOBs contained in our data set was considered close enough to those in the ANS to constitute a possible match. There were no matches on DOB alone.
A search of partial matches based on postcode sector, combining a postcode area, a postcode district and a single character indicating the location’s inward code (e.g. YO23 2), revealed 428 cases that matched at least one case in the ANS. There were a total of 9784 individual abortion records in the ANS database that matched on postcode sector. Thirty-eight cases (or 47 matches as a result of the same postcode sector appearing more than once in the ANS data) had a year of birth of either 2004 or 2005, for the female students in our cohort. Nineteen of these 47 matched our data on year of birth, but none matched on day or month. From this, we concluded that there were also no probable partial matches in our cohort.
Secondary outcome measures
Table 17 reports completion rates for secondary outcomes among students routed to the relevant questions, indicating rates were generally good. However, completion rates were lower for reporting number of heterosexual partners (38.3%) and contraception at last vaginal sex (59.6%) among students routed to these questions. The low rate of completion of the question on partner numbers reflects that students were required to write in a number.
| Secondary outcome | Completion rate | ICC test–retest baseline: follow-up | |
|---|---|---|---|
| Baseline | Follow-up | ||
| Pregnancy (girls) | N/A | 15 (100.0) | N/A |
| Unintended pregnancy (girls) | N/A | 1 (100.0) | N/A |
| Initiation of pregnancy (boys) | N/A | 25 (78.1) | N/A |
| Diagnosed STIsa | N/A | 1053 (90.9) | N/A |
| Sexual debuta | 1068 (91.6) | 1044 (90.1) | N/Ab |
| Number of heterosexual partnersa | N/A | 18 (38.3) | N/A |
| No contraception at first vaginal sexa | N/A | 46 (97.9) | N/A |
| No contraception at last vaginal sexa | N/A | 28 (59.6) | N/A |
| Non-volitional sexa | N/A | 47 (88.7) | N/A |
Table 18 reports the proportion of missing values for the secondary outcome measures at follow-up by arm. This indicates a low proportion of missing data for all measures except age at sexual debut (12.5% in the control group and 25.6% in the intervention group), number of sexual partners (62.5% in the control group and 53.8% in the intervention group) – again, probably reflecting the use of free-text responses for these items – and no contraception at last vaginal sex (37.5% in the intervention group and 41.0% in the control group), probably reflecting issues with question routing.
| Secondary outcome measure | Baseline | Follow-up | ||
|---|---|---|---|---|
| Control (N = 298), n (%) | Intervention (N = 868), n (%) | Control (N = 296), n (%) | Intervention (N = 863), n (%) | |
| Pregnancy (girls) | N/A | N/A | 0 (0.0) | 0 (0.0) |
| Unintended pregnancy (girls) | N/A | N/A | 0 (0.0) | 0 (0.0) |
| Initiation of pregnancy (boys) | N/A | N/A | 0 (0.0) | 0 (0.0) |
| Diagnosed STIs | N/A | N/A | 27 (9.1) | 79 (9.2) |
| Vaginal sexual debut with partner of opposite sex | N/A | N/A | 21 (7.1) | 64 (7.4) |
| Sexual debut with partner of same sex | N/A | N/A | 19 (6.4) | 70 (8.1) |
| Age at vaginal sexual debut with partner of opposite sex | N/A | N/A | 1 (12.5) | 10 (25.6) |
| Number of heterosexual partners (sexually active) | N/A | N/A | 5 (62.5) | 21 (53.8) |
| No contraception at first vaginal sex | N/A | N/A | 0 (0.0) | 1 (2.6) |
| No contraception at last vaginal sex | N/A | N/A | 3 (37.5) | 16 (41.0) |
| Non-volitional sex (Q51 only) | N/A | N/A | 0 (0.0) | 6 (13.3) |
Discrimination
Table 18 indicates that, at baseline, our measure of sexual debut did not allow us to discriminate well between a defined, sizeable, ‘at-risk’ group and lower-risk students, because the prevalence of sexual activity was so low. Table 18 indicates that this was similarly the case at follow-up and this was also the case for the other secondary outcome measures, probably reflecting the truncated period of follow-up and, therefore, the young age of participants in this pilot RCT in comparison with any future Phase III RCT. The relatively high prevalence of STI diagnoses considering the low prevalence of sexual debut suggests that some students either did not understand these questions or chose to answer them incorrectly.
Longitudinal reliability: intracluster correlation coefficient
Table 19 indicates that for most secondary outcomes, ICC for test–retest was not undertaken, reflecting these measures being assessed at follow-up but not at baseline. The ICC test–retest was not performed as planned for sexual debut. Although this was measured at both baseline and follow-up, the wording of the questions was not congruent: at baseline examining sexual debut regardless of whether partners were same sex or opposite sex, whereas at follow-up examining sexual debut separately by partner type. This represented a deviation from the protocol. However, this is a minor deviation given that the student cohort was mid-way through adolescence and thus, longitudinal inconsistency in measurement at an interval of 12 months would probably reflect adolescent development trajectories rather than limitations with measure reliability.
| Secondary outcome measure | Control | Intervention | Effect estimates and 95% CIs | |||
|---|---|---|---|---|---|---|
| Unadjusted | 95% CI | Adjusted | 95% CI | |||
| Pregnancy (girls), n (%) | 0 (0.0) | 1 (0.2) | – | – | – | – |
| Unintended pregnancy (girls), n (%) | 0 (0.0) | 1 (0.2) | – | – | – | – |
| Initiation of pregnancy (boys), n (%) | 1 (0.6) | 2 (0.5) | OR = 0.75 | (0.1 to 8.3) | OR = 0.51 | (0.0 to 6.8) |
| Diagnosed STIs, n (%) | 14 (4.7) | 38 (4.4) | OR = 0.93 | (0.5 to 1.7) | OR = 1.17 | (0.6 to 2.3) |
| Vaginal sexual debut with partner of opposite sex, n (%) | 8 (2.7) | 39 (4.5) | OR = 1.70 | (0.6 to 4.9) | OR = 2.06 | (0.6 to 7.2) |
| Sexual debut with partner of same sex, n (%) | 1 (0.3) | 11 (1.3) | OR = 3.81 | (0.5 to 29.6) | OR = 4.40 | (0.5 to 35.4) |
| Age at vaginal sexual debut with partner of opposite sex, mean (SD) | 13.7 (0.5) | 13.6 (0.5) | MD = –0.13a | (–0.5 to 0.3) | MD = –0.10a | (–0.5 to 0.3) |
| Number of heterosexual partners, mean (SD) | 0.03 (0.29) | 0.35 (4.78) | MD = 0.33 | (–0.7 to 1.3) | MD = 0.41 | (–0.7 to 1.5) |
| No contraception at first vaginal sex, n (%) | 0 (0.0) | 7 (0.9) | – | – | – | – |
| No contraception at last vaginal sex, n (%) | 1 (0.4) | 5 (0.6) | OR = 1.17 | (0.2 to 8.1) | OR = 1.77 | (0.2 to 17.3) |
| Non-volitional sex, n (%) | 0 (0.0) | 4 (0.5) | – | – | – | – |
Piloting intention-to-treat analyses
Despite the pilot RCT not aiming to assess intervention effectiveness, we piloted intention-to-treat analyses (see Table 19). As expected, given the small sample size, short period of intervention and relatively young age at follow-up in this pilot RCT, there were no secondary outcomes where CIs suggested significant benefits or harms in unadjusted or adjusted analyses. Some responses regarding sexual activity appeared dubious. Seven boys in the intervention schools and two in the control schools reported over 50 partners. Although these were not excluded in our analyses, it might be prudent for the statistical analysis plan for any future Phase III RCT to use fixed-response categories rather than free-text responses with a plausible upper limit informed by existing evidence on partner ranges for this age group.
Piloting of potential mediators
Completion rates and reliability
The completion and reliability of potential mediator measures are reported in Table 20. Response rates were high for all measures at baseline and/or follow-up. Unsurprisingly, the ICCs for test–retest reliability were low, probably reflecting that what was being measured was unlikely to be stable among young people in early adolescence. Cronbach’s alphas and ordinal alphas for the measures were generally high, suggesting good inter-item reliability. Alphas for perceived behavioural norms, sexual health knowledge and sexual health access were lower, probably reflecting that these measures included items focused on different phenomena. The negative ordinal alpha for perceived behavioural norms at follow-up arose because of negative correlations (after appropriate coding reversal, etc.) among some items. This may have arisen if students misunderstood the conditional logic or some other aspect of the question.
| Mediator | Completion rate, n (%) | ICC test–retest baseline–follow-up | Inter-item reliability at baseline | ||
|---|---|---|---|---|---|
| Baseline | Follow-up | Cronbach’s alpha | Ordinal alpha | ||
| Social norms supportive of positive relationships and sexual health | 1024 (87.8) | 1028 (88.7) | 0.41 | 0.73 | 0.77 |
| Perceived behavioural norms about early sexual experience and low use of condoms and contraception | 970 (83.2) | 1020 (88.0) | 0.33 | 0.61 | –0.15 |
| Sexual health knowledge | 1087 (93.2) | 1110 (95.8) | 0.13 | 0.63 | 0.78 |
| Sexual health and contraceptive skills | 950 (81.5) | 1008 (87.0) | 0.35 | 0.89 | 0.92 |
| Sexual health service access | 1078 (92.5) | 1102 (95.1) | 0.32 | 0.69 | 0.83 |
| Sexual communication self-efficacy | 974 (83.5) | 1009 (87.1) | 0.42 | 0.91 | 0.93 |
| Sexual competencea | N/A | 34 (72.3) | N/A | N/A | N/A |
| Engaging school climate | |||||
| Overall scale | 1027 (88.1) | 1027 (88.6) | 0.59 | 0.73 | 0.74 |
| Relationships | 1106 (94.9) | 1116 (96.3) | 0.57 | 0.89 | 0.92 |
| Belonging | 1101 (94.4) | 1085 (93.6) | 0.48 | 0.80 | 0.84 |
| Commitment | 1136 (97.4) | 1127 (97.2) | 0.48 | 0.74 | 0.85 |
| Participation | 1133 (97.2) | 1114 (96.1) | 0.59 | 0.84 | 0.88 |
| Communication with parents | |||||
| Mother/female carer | 1146 (98.3) | 1136 (98.0) | 0.47 | N/A | N/A |
| Father/male carer | 1145 (98.2) | 1131 (97.6) | 0.58 | N/A | N/A |
| Career/educational expectations | 1080 (92.6) | 1089 (94.0) | 0.31 | N/A | N/A |
Economic evaluation
Child Health Utility-9D
The CHU9D measure was used to assess students’ health-related quality of life at baseline and at follow-up. 61 Student utility values were converted into utility scores using a UK valuation set. 52 The CHU9D is valued on a scale from 0 to 1, anchored at 1 for full health and 0 for dead.
Completion rates and utility scores
Completion rate for the CHU9D was 1058 (81%) at baseline and 1056 (81%) at follow-up (Table 21). CHU9D data were available for 863 students at follow-up who had also completed the CHU9D at baseline. Mean [standard deviation (SD)] and median [interquartile range (IQR)] utility scores at baseline were 0.864 (SD 0.105) and 0.884 (IQR 0.808–0.952), respectively. At follow-up, these scores were 0.835 (SD 0.115) and 0.856 (IQR 0.768–0.921), respectively. The distributions of utility scores at baseline and follow-up were broadly similar (Figures 3 and 4, respectively). Minimum and maximum values were similar at both time points, as were the proportion of cases reporting maximum utility scores. The distributions of utility scores at baseline and follow-up were broadly similar, with few students reporting utility scores under 0.5, a right-skewed distribution with modal values of around 0.95, and 5–10% students reporting maximum utility scores (see Figures 3 and 4, respectively).
| Statistic | Baseline (all respondents) | Follow-up (all respondents) | Follow-up (respondents with baseline CHU9D scores) |
|---|---|---|---|
| Mean | 0.864 | 0.833 | 0.835 |
| SD | 0.105 | 0.117 | 0.115 |
| Minimum | 0.389 | 0.376 | 0.376 |
| 1st percentile | 0.533 | 0.490 | 0.495 |
| 5th percentile | 0.656 | 0.606 | 0.606 |
| 10th percentile | 0.723 | 0.669 | 0.677 |
| 25th percentile | 0.808 | 0.762 | 0.768 |
| Median | 0.884 | 0.853 | 0.856 |
| 75th percentile | 0.952 | 0.921 | 0.921 |
| 90th percentile | 0.979 | 0.952 | 0.952 |
| 95th percentile | 1.000 | 1.000 | 1.000 |
| 99th percentile | 1.000 | 1.000 | 1.000 |
| Maximum | 1.000 | 1.000 | 1.000 |
| Observations (% total) | 1058 (81) | 1056 (81) | 863 (74) |
| Missinga (% total) | 108 (9) | 103 (9) | 296 (26) |
FIGURE 3.
Distribution of baseline CHU9D utility scores among students: 1058 observations, all respondents.
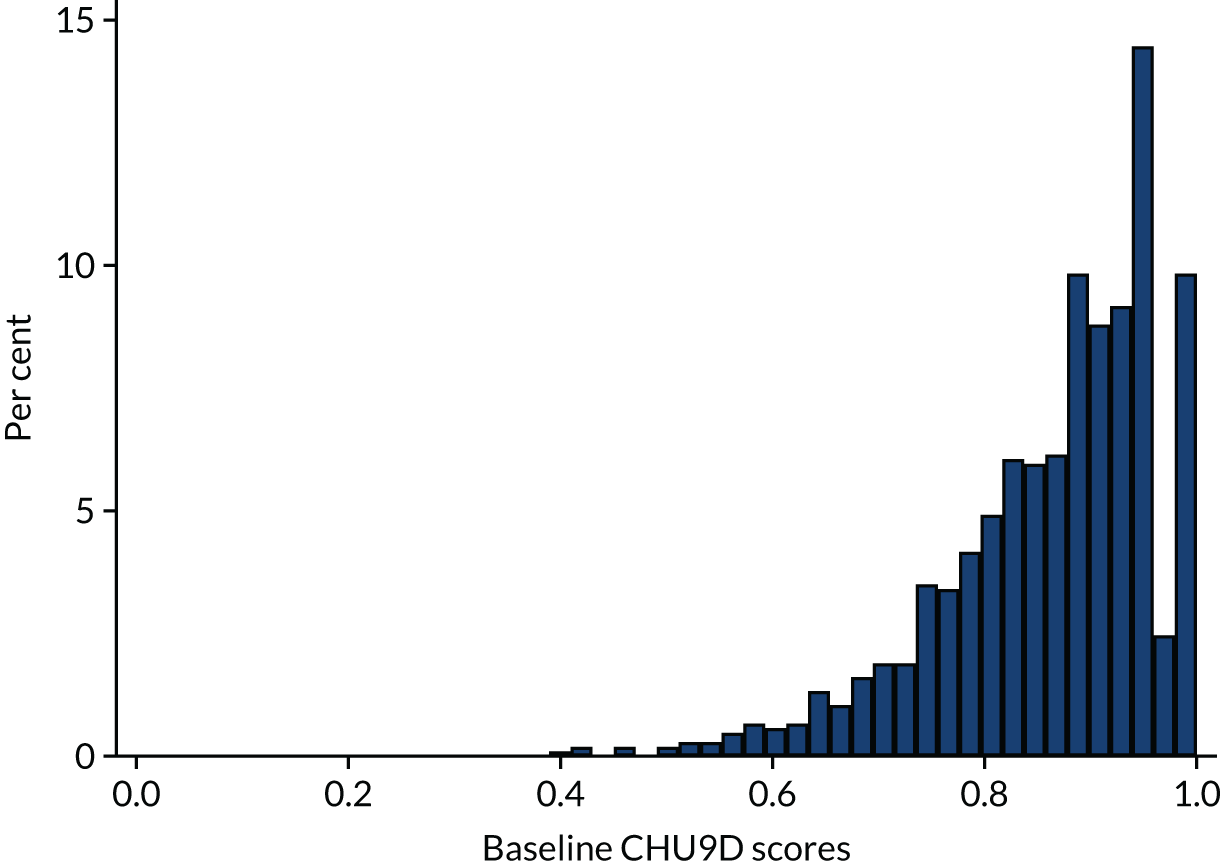
FIGURE 4.
Distribution of follow-up CHU9D utility scores among students: 1056 observations, all respondents.
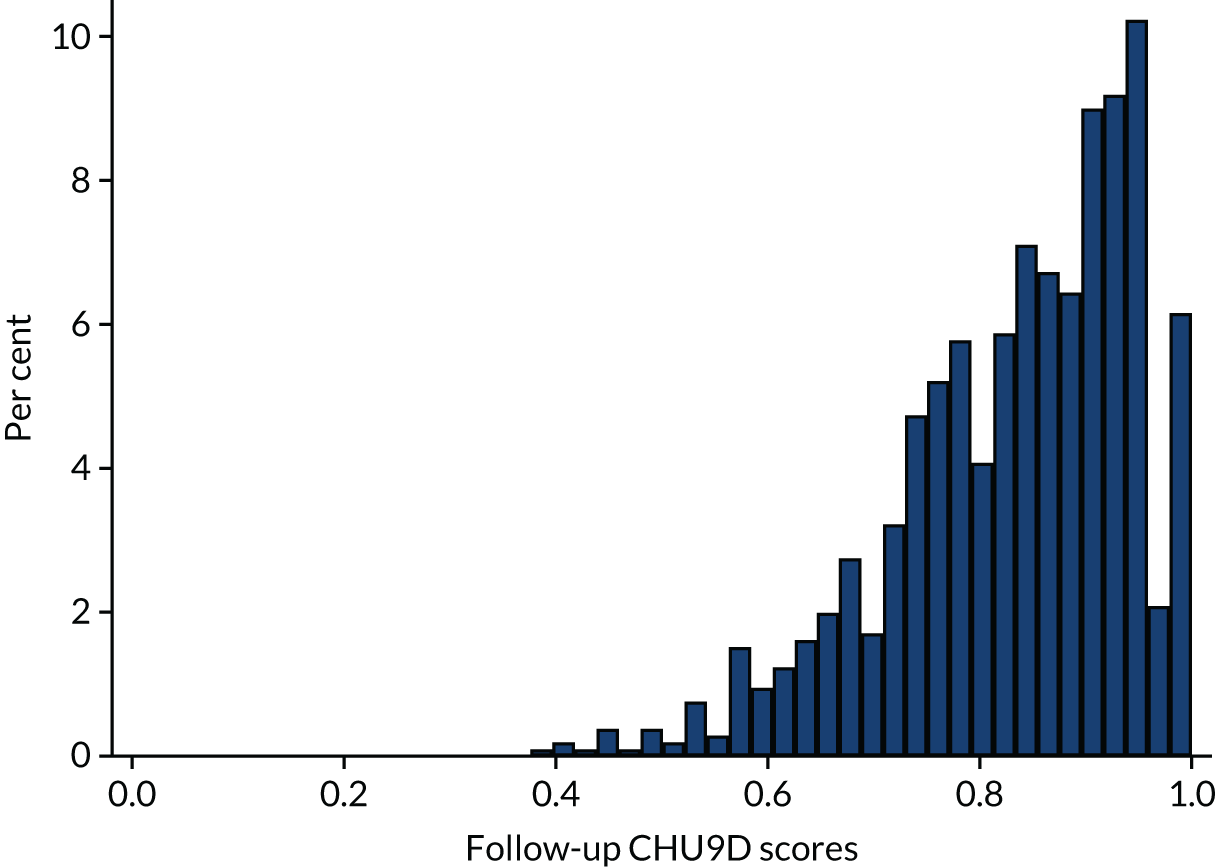
Reliability
Reliability of the nine CHU9D items was assessed separately at baseline and at follow-up using Cronbach’s alpha and the ordinal alpha. In every case, it was over 0.8; at baseline, it was 0.805 (Cronbach’s alpha) and 0.874 (ordinal alpha). At follow-up, it was 0.826 (Cronbach’s alpha) and 0.876 (ordinal alpha).
Pilot analysis of intervention impact on Child Health Utility-9D scores
In the unadjusted model, utility scores were significantly lower at follow-up among students in the intervention schools, although the difference was small [marginal effect –0.020 (95% CI –0.037 to –0.004); Table 22]. After adjustment, this effect was non-significant. We reran the unadjusted model on the smaller sample that was included in the second adjusted model (841 observations) and the difference in utility scores remained statistically significant [marginal effect –0.023 (95% CI –0.041 to –0.004)]; this suggests that the non-significance in the adjusted models was due to the adjustment, rather than the different sample.
| Outcome measure | Control, mean (SD) (observations) | Intervention, mean (SD) (observations) | Marginal effect (95% CI), unadjusted estimate | Marginal effect (95% CI), adjusteda estimate | Marginal effect (95% CI), adjustedb estimate |
|---|---|---|---|---|---|
| CHU9D | 0.848 (0.116) | 0.827 (0.117) | –0.020 (–0.037 to –0.004) | –0.011 (–0.030 to 0.008) | –0.003 (–0.020 to 0.013) |
| Observations | 265 | 791 | 1056 | 897 | 841 |
Safeguarding and adverse events
In the course of data collection, no student disclosures met the criteria for reporting safeguarding concerns to a school safeguarding officer based on the safeguarding policy in place at the time. In line with our standard operating procedure (see Appendix 5), schools annually reported to the research team on SAEs among the cohort of students taking part in Positive Choices (Table 23). Four SAEs were reported in intervention schools. Zero were reported in control schools, although one control school did not respond to requests for data. No reported SAEs were deemed to be plausibly linked to the intervention or research.
| Event | Intervention schools | Control schools | Overall | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | ||
| Death | 0 | 0 | 0 | 0 | 0 | Missing | 0 |
| Hospitalisation | 1 | 0 | 1 | 2 | 0 | Missing | 4 |
| Disability | 0 | 0 | 0 | 0 | 0 | Missing | 0 |
| Congenital abnormality | 0 | 0 | 0 | 0 | 0 | Missing | 0 |
| Life-threatening illness | 0 | 0 | 0 | 0 | 0 | Missing | 0 |
| Total | 1 | 0 | 1 | 2 | 0 | Missing | 4 |
Chapter 5 Results: piloting the intervention
Process evaluation
Response rates
All SEF training delivered at the four intervention schools was audio-recorded (and observed by a researcher) (Table 24). The student-led social-marketing training was delivered to all schools jointly via a conference call and slide show, and was audio-recorded and observed remotely by two researchers. Most staff completed satisfaction surveys following each training (range 75–100%), but as a result of time constraints for the curriculum training at intervention school 2 (discussed in more detail in Staff training), staff did not have time to complete the satisfaction survey after training. In intervention schools 1, 3 and 4, logbooks for those implementing the curriculum, SHPC and student-led social marketing were completed. However, in intervention school 2, logbooks were not returned because of constraints on staff time and issues with staff turnover, discussed in more detail in Staff training. Informal feedback from teachers suggested that those who did complete logbooks found them time-consuming and an unwanted burden on top of implementation.
| Data source | Intervention schools | Control schools | Total | |||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | |||
| Audio-recording of NCB training, n/target (% response) | SHPC | 1 (100) | 1 (100) | 1 (100) | 1 (100) | N/A | N/A | 4 (100) |
| Curriculum | 1 (100) | 1 (100) | 1 (100) | 1 (100) | N/A | N/A | 4 (100) | |
| Student-led social marketing | 1 (100) | 1 (100) | 1 (100) | 1 (100) | N/A | N/A | 4 (100) | |
| Trainee satisfaction surveys, n/eligible (% response) | SHPC | 3 (75) | 3 (100) | 1 (100) | 2 (100) | N/A | N/A | 9 (90) |
| Curriculum | 5 (100) | 0 (0) | 5 (100) | 4 (100) | N/A | N/A | 14 (61) | |
| Student-led social marketing | 1 (100) | 0 | 1 (100) | 1 (100) | N/A | N/A | 3 (75) | |
| Logbooks by teaching staff, n/eligible (% response) | Curriculum | 5 (100) | 0 | 5 (100) | 3 (100) | N/A | N/A | 13 (59) |
| SHPC | 1 (100) | 0 | 1 (100) | 1 (100) | N/A | N/A | 3 (75) | |
| Student-led social marketing | 1 (100) | 0 | 1 (100) | 1 (100) | N/A | N/A | 3 (75) | |
| Observations of one session per school, n/target (% response) | Curriculum | 1 (100) | 5 (500) | 1 (100) | 1 (100) | N/A | N/A | 8 (200) |
| SHPC | 2 (200) | 1 (100) | 0 | 3 (300) | N/A | N/A | 6 (150) | |
| Student-led social marketing | 1 (100) | 1 (100) | 1 (100) | 2 (200) | N/A | N/A | 5 (125) | |
| Interviews with two SEF Staff, n/target (% response) | N/A | N/A | N/A | N/A | N/A | N/A | 2 (100) | |
| Interviews with four staff per intervention school, n/target (% response) | 5 (125) | 4 (100) | 4 (100) | 5 (125) | N/A | N/A | 18 (113) | |
| Group interview with students per intervention school, n/target (% response) | 1 (100) | 1 (100) | 2 (200) | 1 (100) | N/A | N/A | 5 (125) | |
| Interviews with two staff members per control school, n/target (% response) | N/A | N/A | N/A | N/A | 3 (150) | 2 (100) | 5 (125) | |
| Group interviews with four students per control school, n/target (% response) | N/A | N/A | N/A | N/A | 1 (100) | 1 (100) | 2 (100) | |
Researchers observed one curriculum lesson in intervention schools 1, 3 and 4, and five lessons in school 2 on a one-off drop-down day. At least one SHPC meeting was observed in intervention schools 1, 2 and 4, but we were unable to observe any SHPC meetings in intervention school 3 as we were not notified of dates. Student-led social-marketing meetings were observed in all four of the intervention schools.
Interviews were conducted with two SEF staff at the end of the pilot. Individual or paired interviews were carried out with at least four staff in each intervention school and at least two staff in each control school. Mixed-gender group interviews with at least eight year 9 students were conducted in three of the four intervention schools. Only six students were able to attend the group interview in school 1 because of timetabling constraints. Group interviews with at least four year 9 students were carried out in each of the control schools. A more detailed breakdown of student participation in group interviews is provided in Table 25.
| Participants | Intervention schools | Control schools | Total | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | ||
| Boys | 4 | 2 | 5 | 6 | 3 | 3 | 23 |
| Girls | 2 | 6 | 12 | 5 | 4 | 4 | 33 |
| Total | 6 | 8 | 17a | 11 | 7 | 7 | 56 |
Quantitative findings on implementation
Fidelity
Student needs survey
The student needs survey was carried out in all four interventions schools as part of the baseline trial survey, with a response rate of > 85% (Table 26). A report summarising student needs data was provided to each intervention school at the start of the school year. A sample needs report is provided in Appendix 11.
| Intervention component | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Student needs survey: response rate (%) | 94.1 | 85.4 | 85.1 | 91.3 | 4 |
Staff training
All four intervention schools received the SEF training on setting up and running the SHPC, curriculum delivery and facilitating student-led social marketing. The SHPC training was delivered with fidelity in all four intervention schools in the first term of the school year, with a range of 86–100% of the essential elements delivered (Table 27).
| Intervention component: training | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| SHPC training | |||||
| Attendance, n (sheet) | 4 | 3 | 1 | 2 | N/A |
| % coverage of essential topics (researcher observation) | 91 | 100 | 100 | 88 | 4 (100) |
| % coverage of essential training activities (researcher observation) | 81 | 100 | 94 | 86 | 4 (100) |
| Opportunities for discussion (Y/N) | Y | Y | Y | Y | 4 (100) |
| Overall | 86 | 100 | 96 | 87 | 4 (100) |
| Curriculum training | |||||
| Attendance, n (sheet) | 5 | 9 | 5 | 4 | N/A |
| % coverage of essential topics (researcher observation) | 88 | 66 | 88 | 76 | 4 (100) |
| % coverage of essential training activities (researcher observation) | 80 | 44 | 88 | 71 | 4 (100) |
| Opportunities for discussion (Y/N) | Y | N | Y | Y | 4 (100) |
| Overall | 83 | 50 | 88 | 74 | 3 (75) |
| Student-led social-marketing training | |||||
| Attendance, n (sheet) | 1 | 1 | 1 | 1 | N/A |
| % coverage of essential topics (trainer diary) | 100 | 100 | 100 | 100 | 4 (100) |
| % coverage of essential training activities (researcher observation) | 89 | 89 | 89 | 89 | 4 (100) |
| Opportunities for discussion (Y/N) | Y | Y | Y | Y | 4 (100) |
| Overall | 94 | 94 | 94 | 94 | 4 (100) |
Intervention schools 1, 3 and 4 also received the curriculum training in the first term of the school year, with schools 3 and 4 receiving both SHPC training and curriculum training on the same day. In all three of these training sessions, > 70% of essential elements were delivered, with a range of 74–88% (see Table 27).
In intervention school 2, owing to a change in headship and leadership of the programme at the start of the school year, the curriculum training was delayed until the end of the second term, with lessons scheduled to be delivered to students in the final term of the year. Time constraints imposed by the school meant that essential elements of the curriculum training were delivered to 50% fidelity overall (see Table 27). SEF, however, provided additional support remotely to this school in June 2019 to troubleshoot any issues that staff were encountering with curriculum delivery.
All four intervention schools jointly received the training on facilitating student-led social marketing via a conference call and slide show in February 2019. According to audio-recording and researcher observation, 94% of essential elements were delivered in this training (see Table 27).
School health promotion council
According to the staff logbooks received, intervention schools 1, 3 and 4 each held three SHPC meetings during the school year, with the majority taking place in the first term (Table 28). All schools achieved above the 70% fidelity threshold for implementation of the SHPC meetings, with a range of 83–87% of essential elements covered.
| Intervention component: SHPC | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Number of meetings (staff logbooks) | 3 | 2 | 3 | 3 | N/A |
| Topics covered (staff logbooks) | 90 | Missing | 88 | 100 | 3 (75) |
| % completion of actions (staff logbooks) | 73 | Missing | 81 | 73 | 3 (75) |
| % opportunities for discussion (staff logbooks) | 100 | Missing | 100 | 100 | 3 (75) |
| Overall | 83 | Missing | 81 | 87 | 3 (75) |
We observed two SHPC meetings at intervention school 1, one meeting at school 2 and three meetings at school 4 to compare researcher-reported coverage of essential elements with self-report data in teacher logbooks. For school 1, in both meetings there was 100% agreement on essential items covered. Agreement for school 2 could not be calculated as no logbook data were received from this school. For school 4, there was 86% (in one meeting) and 100% (in two meetings) agreement between teacher logbooks and researcher observations. For one meeting, one item was reported in the staff logbook but not in the observation, whereas a further item was reported by the researcher and not the staff member. The disagreement concerned two very similar items on parental communication and might indicate a need for clearer distinction between the two items. For full details, see Appendix 12, Tables 46–50. No SHPC meeting was observed at school 3, so agreement could not be calculated.
Curriculum delivery
According to staff logbooks from the three schools that completed them, fidelity of delivery of the student curriculum was high, with all three reporting implementation of > 70% of essential elements across the 10 lessons, ranging from 96% to 100% (Table 29). Intervention school 1 delivered the eight essential lessons and three ‘add-on’ lessons on pregnancy options, readiness for intimacy and body image (although only two ‘add-ons’, to give a total of 10 lessons, are reported in Table 29). School 3 completed eight essential lessons and two ‘add-ons’: readiness for intimacy and body image. As agreed in advance with SEF, intervention school 4 did not complete the first essential lesson on the female/male body and functions of the reproductive system, as this material had already been covered when students were in year 8 using similar SEF-produced materials. This school completed seven essential lessons (although did not provide teacher logs for one of these) and three ‘add-on’ lessons: pregnancy options, readiness for intimacy and FGM. At this school, the lessons were also taught in a slightly different order based on what had already been covered in years 7 and 8. In all three of these schools, lessons were delivered in regularly scheduled PSHE lessons.
| Intervention component: curriculum | Intervention school | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| % coverage of essential topics across classes (logbooks) | |||||
| Core lesson 1 | 97 | Missing | 100 | N/Aa | 3 (75) |
| Core lesson 2 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 3 | 99 | Missing | 100 | 100 | 3 (75) |
| Core lesson 4 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 5 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 6 | 100 | Missing | 100 | Missing | 2 (50) |
| Core lesson 7 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 8 | 97 | Missing | 100 | 100 | 3 (75) |
| Additional lesson 1 | 100 | Missing | 100 | 77 | 3 (75) |
| Additional lesson 2 | 100 | Missing | 100 | 100 | 3 (75) |
| Overall % of topics covered | 99 | Missing | 100 | 98 | 3 (75) |
| % coverage of essential activities (logbooks) | |||||
| Core lesson 1 | 80 | Missing | 100 | N/Aa | 3 (75) |
| Core lesson 2 | 97 | Missing | 100 | 100 | 3 (75) |
| Core lesson 3 | 84 | Missing | 100 | 89 | 3 (75) |
| Core lesson 4 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 5 | 100 | Missing | 100 | 77 | 3 (75) |
| Core lesson 6 | 100 | Missing | 100 | Missing | 2 (50) |
| Core lesson 7 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 8 | 96 | Missing | 100 | 100 | 3 (75) |
| Additional lesson 1 | 96 | Missing | 100 | 79 | 3 (75) |
| Additional lesson 2 | 97 | Missing | 100 | 100 | 3 (75) |
| Overall % of activities covered | 95 | Missing | 100 | 93 | 3 (75) |
| Opportunities for discussion (%) | |||||
| Core lesson 1 | 100 | Missing | 100 | N/Aa | 3 (75) |
| Core lesson 2 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 3 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 4 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 5 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 6 | 100 | Missing | 100 | Missing | 2 (50) |
| Core lesson 7 | 100 | Missing | 100 | 100 | 3 (75) |
| Core lesson 8 | 100 | Missing | 100 | 100 | 3 (75) |
| Additional lesson 1 | 100 | Missing | 100 | 100 | 3 (75) |
| Additional lesson 2 | 100 | Missing | 100 | 100 | 3 (75) |
| Overall opportunities for discussion (%) | 100 | Missing | 100 | 100 | 3 (75) |
| Homework one set? | Y | Missing | Y | N | 2 (50) |
| Homework two set? | Y | Missing | Y | N | 2 (50) |
| Overall curriculum delivery (%) | 98 | Missing | 100 | 96 | 3 (75) |
In intervention school 2, as a result of challenges with time frames for delivery after the staff training, the first three curriculum lessons were delivered in science classes while a one-off ‘drop-down’ day to cover the remaining seven lessons (in 45-minute rather than 60-minute slots) was implemented. Although this school did not return any teacher logbooks for the curriculum component, researcher observation of the ‘drop-down’ day indicated that these lessons were delivered to 88% fidelity.
Only intervention schools 1 and 3 set the two compulsory homework assignments. School 4 was unable to do so as school policy dictated that homework could not be set in PSHE. School 2 did not report on this.
We observed delivery of one lesson each in intervention schools 1, 3 and 4, and delivery of five lessons on a one-off drop-down day in school 2 to compare researcher-reported coverage of essential topics with the self-reported data in teacher logbooks. In schools 1 and 3 there was 90% agreement on essential items covered between teacher logbooks and researcher observations. In both cases, one item was recorded by the staff member completing the logbook, but not the researcher observing the lesson (for full details see Appendix 12, Tables 51 and 52). Agreement could not be calculated for schools 2 and 4 as logbook data were not received for the lessons observed by a researcher.
Student-led social marketing
According to the teacher logbooks received from schools 1, 3 and 4, all of the schools implemented the student-led social-marketing meetings above the 70% fidelity threshold, ranging from 71% to 100% (Table 30).
| Intervention component | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Student-led social marketing (staff logbooks) | |||||
| Number of planning meetings | 3 | Missing | 3 | 8 | N/A |
| Topics covered (%) | 100 | Missing | 78 | 67 | 3 (75) |
| Actions completed (%) | 100 | Missing | 56 | 67 | 2 (50) |
| Opportunities for discussion (%) | 100 | Missing | 100 | 100 | 3 (75) |
| Overall (%) | 100 | Missing | 71 | 74 | 3 (75) |
Intervention school 1 focused its campaign on accessing local services and delivered presentations in assemblies and ran quizzes and competitions based on this topic. School 3 focused on healthy relationships and delivered a poster campaign and planned to deliver presentations informed by the Positive Choices curriculum to year 7 and year 8 students in assemblies before the end of term. School 4 incorporated student-led social marketing into the existing year 9 performing arts curriculum, and delivered a performance on unhealthy relationships to students, staff and parents at their summer showcase.
Although no staff logbooks were returned from school 2, researcher observation and interviews with school staff and students revealed that several student-led social-marketing meetings were held. A researcher observed a meeting in which a campaign was planned, focusing on social norms supportive of sexual health, specifically in relation to reducing spreading of rumours about sexual activity among students. This was to be delivered before the end of term 3.
We observed delivery of one student-led social-marketing meeting in each of the four intervention schools to compare researcher-reported coverage of essential elements with the self-reported data in teacher logbooks. In intervention school 1, there was 67% agreement on coverage of essential elements between teacher logbooks and researcher observation. The disagreement was rooted in school staff reporting more topics and actions covered than the researcher (for full details, see Appendix 12, Table 53). No logbook data for social-marketing meetings were received for school 2, therefore, agreement could not be calculated for this school. Although intervention schools 3 and 4 did provide logbook data, they did not include information on the meetings observed by researchers, therefore, agreement could not be calculated for these schools either.
Communication with parents
Only two schools (intervention schools 1 and 4) implemented parent newsletters (Table 31). In both cases, information about Positive Choices was integrated into regular school newsletters that were available to students and parents. Intervention school 1 included information about Positive Choices in two school newsletters and, in the first article, reported on data from the student needs survey. Intervention school 4 included information about Positive Choices in a general school newsletter at the start of the school year to introduce the programme. Supported by the research team, intervention school 1 also held a parent meeting to introduce and discuss Positive Choices and its content.
| Intervention component: parental information | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Number of parent newsletters | 2 | Missing | 0 | 1 | 2 (50) |
Information about the delivery of parent communication materials was not received from intervention schools 2 or 3, although the lead staff member at school 2 stated in an interview that a parent newsletter was to be sent out. Intervention school 1 sent two parent newsletters and school 4 sent one.
Sexual health services review
According to staff logbooks, intervention schools 1, 3 and 4 carried out the sexual health services review, implementing > 70% of essential elements, ranging from 83% to 100% (Table 32).
| Intervention component: review of school sexual health services (logbooks) | Intervention schools | Total (%) (N = 4) | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Topics covered (%) | 83 | Missing | 100 | 83 | 3 (75) |
All three schools providing logbooks reported that they carried out the review of local and school-based sexual health services, and acted to improve promotion of these services in school. Schools 3 and 4 also reported acting to improve school-based services.
Overall fidelity of implementation
The SHPC training and student-led social-marketing training were implemented with fidelity in all four schools. The curriculum training, the SHPC meetings, the curriculum lessons, student-led social-marketing meetings and the sexual health services review were implemented with fidelity in three out of four schools. Overall, the fidelity target of 70%+ implementation of essential elements in three schools was met. There was generally good agreement between teacher logbooks and researcher observation of intervention activities. Limited data received from implementation school 2 meant that a rigorous assessment of overall fidelity for this school could not be made.
Intervention reach and acceptability: students
Students in intervention and control schools were asked about their awareness of new RSE provision in their school. Those in control schools were asked about this as a check on the rate of over-reporting of awareness where no new programme had been implemented. Students in intervention schools were more likely to report that their school had recently been running a new programme (Table 33). But of those reporting a new programme, large majorities in both arms reported that this was a good thing and that it included a new curriculum. Of students reporting a new intervention, those in the intervention group were more likely to report that it included parental information and help for students seeking sexual health services, but were actually less likely to report that it involved student involvement in decisions. Much higher proportions of students in intervention schools than in control schools reported coverage of various topics in RSE at school. A majority of students in intervention schools reported coverage of all topics except ‘masturbation’ and ‘love’.
| Measure | Control, n (%) | Intervention, n (%) |
|---|---|---|
| Report this school has recently been running a new RSE programme | 96 (37.6) | 458 (59.2)a |
| Of students reporting new programme, report that it is a good thing that the school is involved in this programme | 77 (80.2) | 361 (80.0) |
| Of students reporting new programme, report that it includes a new RSE curriculum | 82 (85.4) | 400 (87.3) |
| Of students reporting new programme, report that it includes student-led campaigns to promote sexual health | 15 (15.6) | 71 (15.5) |
| Of students reporting new programme, report that it includes information for parents | 18 (18.8) | 135 (29.5)a |
| Of students reporting new programme, report that it includes help for students to access sexual health services | 45 (46.9) | 268 (58.5)a |
| Of students reporting new programme, report that it includes student involvement in decisions | 33 (34.4) | 116 (25.3)a |
| Sex education covers well/very well | ||
| Body | 151 (56.6) | 556 (69.6)a |
| Parts of genitalia | 135 (50.6) | 543 (68.0)a |
| Conception | 154 (57.7) | 638 (79.8)a |
| Contraception options | 160 (59.9) | 670 (83.9)a |
| Diagnosed STIs | 99 (37.1) | 586 (73.3)a |
| Condom use | 69 (25.8) | 548 (68.6)a |
| Safer sex | 31 (11.6) | 347 (43.4)a |
| Abusive relationships | 73 (27.3) | 549 (68.7)a |
| Help for abuse | 129 (48.3) | 508 (63.6)a |
| Sexual consent | 166 (62.2) | 662 (82.9)a |
| Sexual pleasure | 66 (24.7) | 480 (60.1)a |
| Masturbation | 40 (15.0) | 379 (47.4)a |
| Law on pornography | 78 (29.2) | 543 (68.0)a |
| Law and naked image sharing | 122 (45.7) | 551 (69.0)a |
| Resisting pressure | 143 (53.6) | 600 (75.1)a |
| Media and body image | 115 (43.1) | 495 (62.0)a |
| FGM | 21 (7.9) | 435 (54.4)a |
| Love | 66 (24.7) | 395 (49.4)a |
| Managing conflict | 67 (25.1) | 431 (53.9)a |
| Pregnancy options | 61 (22.8) | 483 (60.5)a |
| Readiness for intimacy | 55 (20.6) | 412 (51.6)a |
| Sexual rights | 69 (25.8) | 431 (53.9)a |
Among the intervention group, there were minimal differences in reported awareness of the intervention by sex or SES as measured by FAS, but significant differences by ethnicity, with a reduction in reported awareness when comparing white, black African/black Caribbean/black British, Asian/Asian British and mixed ethnicity subgroups (Table 34).
| Subgroup | Report this school has recently been running a new RSE programme, n (%) | p-value (significant difference among subgroups) |
|---|---|---|
| Sex | ||
| Male | 210 (56.0) | 0.067 |
| Female | 245 (62.5) | |
| Ethnicity | ||
| White | 316 (62.0) | 0.006 |
| Mixed | 32 (47.8) | |
| Asian/Asian British | 53 (51.0) | |
| Black African/black Caribbean/black British | 36 (55.4) | |
| Other | 20 (83.3) | |
| FAS | ||
| 0–8 | 261 (57.4) | 0.221 |
| > 8 | 197 (61.8) | |
Training acceptability: staff
Satisfaction surveys of staff undergoing training by SEF indicated that all three trainings were received very positively by participants, being rated as excellent or good by 100% of participants. All participants reported that they felt either confident or very confident to deliver the relevant intervention component after training. All participants reported that they would recommend the training to colleagues. Full results of the training satisfaction surveys are presented in Appendix 13, Tables 54–56.
Overall intervention acceptability: staff
Of the staff we interviewed who had been involved in implementing Positive Choices, almost all of them indicated positive views about the acceptability of the intervention in their school. Of the staff who expressed views on this (18 out of 19), 100% stated that Positive Choices was feasible and acceptable in their school. All four lead staff stated that they would use the Positive Choices teaching materials again. In all four schools, other aspects of the programme, such as the student-led social marketing and/or SHPC, were planned to continue the following year, albeit in adapted forms in three schools. Seventeen (94%) of the 18 classroom teachers interviewed stated that they enjoyed teaching most of the materials, but two (11%) expressed concerns that they were personally not best placed to have done so. Four (22%) also queried the age-appropriateness of the materials.
Qualitative findings on implementation
School context: staff and student views
Intervention school 1
School 1 is a large community school in inner London. It was described by the assistant head teacher as being very diverse by ethnicity and SES. Students described the school as hectic, loud and chaotic, but also hard-working and ‘good’. The assistant head teacher was responsible for PSHE, which the head teacher strongly supported. There is also a PSHE co-ordinator and a borough-wide nurse available for regular drop-in sessions. The school joined the study because it was aware of the need to develop its RSE programme. Staff delivering Positive Choices were chosen largely on the basis of their availability. There was a school nurse who held drop-in sessions on site.
Intervention school 2
School 2 is an academy in outer London that is part of a large chain. Early in the study, it had major changes to its SLT, following an inspection downgrading its status from ‘good’ to ‘requires improvement’. Students reported that they received little RSE in the school prior to the introduction of Positive Choices, although some students remembered covering puberty in year 7 and having a condom demonstration. Practice appeared to be inconsistent in different classes. Opinions about the degree of trust students had in teachers and tutors also varied.
Intervention school 3
School 3 is a relatively small academy in outer London, variously described by teachers as having both a middle-class and a working-class intake. Staff described the school as forward-thinking, kind, supportive and protective, accepting/including of its lesbian, gay, bisexual, transgender, queer or questioning (LGBTQ) students. Students also described the school as smart, helpful, welcoming, crowded and caring. The school has a head of spiritual, moral, social and cultural (SMSC) education. According to one teacher, the school was unusual locally in continuing to emphasise this aspect of education. It was school policy not to set homework in this subject, but for Positive Choices the homework was set. One teacher stated that the school had a ‘spiral’ curriculum for SMSC education (where topics are revisited in an age-appropriate manner across school years) covering topics such as puberty in year 7, healthy lifestyles and personal well-being in year 8, unhealthy relationships, and personal well-being and sex education in year 9, with year 11 focusing on exam stress and mental health. There was a school nurse who held drop-in sessions on site.
Intervention school 4
School 4 is a large school in outer London, part of a small academy trust, and described by staff as ‘happy’ and having the ‘feel’ of a community school. The pastoral aspects of the school’s mission are given high priority by the SLT; the school has an on-site counselling service. PSHE is taught by a specific department of those volunteering to teach the subject, timetabled in 55-minute lessons. A spiral curriculum aims to build on knowledge acquired in previous years. The long-standing head of PSHE leads its curriculum, revising materials regularly, while staff adapted materials to student needs. PSHE lessons regularly provide anonymous question boxes so that teachers are aware of students’ responses to the curriculum and any ongoing concerns. Staff describe their PSHE role as a privilege, involving different kinds of relationships with students and different pedagogies, which students appreciated. Students supported this perspective.
Implementation, feasibility and acceptability
Interviews with Sex Education Forum staff
The SEF lead delivered most of the training to schools herself. She commented that the training for school staff to run SHPCs was focused on procedures and hence somewhat dry. She felt that it may not be necessary to train all SHPC members. She suggested that, instead of this training, it might be more useful to have a set-up meeting with the PSHE and SLT leads co-ordinating Positive Choices in each school to ensure that they understand how the intervention is intended to work and can timetable and staff all the various activities:
Maybe there’s another way of kind of integrating the set-up kind of work with the school with a briefing on the [SHPC]. So, I don’t know, like a twilight briefing for the key members of staff that covers the [SHPC] and the considerations they need to have around being able to implement the curriculum.
SEF lead
The curriculum training was much more engaging, according to the SEF lead and another trainer. It was run in each school for a group of staff identified to teach the curriculum. In the feasibility-testing phase, there had been a problem of some of those identified to attend training not being qualified teachers. This problem did not recur in the pilot phase because it had been made a strict requirement for qualified teachers to do this work.
The SEF lead suggested that, given different levels of teacher experience, it might be that in a future trial there could be a ‘train-the-trainers’ model, where SEF staff train the teacher leading PSHE in a school, who then cascades this training to the other teachers identified to teach the curriculum. It was clear in the pilot that, in some schools, teachers did work together so that they offered support to each other and shared their learning. A train-the-trainers model could build on such approaches and mitigate the challenges of organising all-staff training. In intervention school 2, for example, the curriculum training was cancelled repeatedly at short notice and, as outlined in Curriculum delivery, ultimately the school did not allow sufficient time for staff to be released to receive the curriculum training:
[They] repeatedly cancelled training at the last minute, or kept dates in our diary kind of in, and you couldn’t get hold of them. They would decide the day before, they’d just say no we’re not doing it, when you’ve already built your diary around doing it. And that happened, you know, several times, it was infuriating.
SEF lead
The SEF trainer (who observed school 2’s drop-down day) commented that the problems with the training resulted in the curriculum being delivered suboptimally in some cases:
It felt to me very much as if the teachers were just given the lesson plans and told to get on with it. And so, some of the lessons went really well, and I’m assuming that those teachers were more experienced, and some of them did not go so well.
SEF trainer
However, the SEF trainer reported that, even in this school, she had heard positive feedback from students.
The SEF lead reported that the training for school staff facilitating student-led social marketing was via a Skype™ (Microsoft Corporation, Richmond, WA, USA) session involving staff across schools. This was highly acceptable to participants, and appropriate given that only one individual per school needed training, schools were from a wide geographical area and the training was more about processes than skills. The training was informed by findings from school needs assessments. The SEF lead felt that the student-led social-marketing component was highly promising in that it enabled students to get actively involved in actions, and outputs to be informed by student preferences:
The student-led social marketing . . . I kind of feel that it has such a lot of potential, when a school can invest a little bit in it. And it’s, you know, so pupil led, and linked to the local data, and can be a really creative, exciting element.
SEF lead
Overall, the SEF lead’s view was that Positive Choices was a feasible and acceptable intervention for schools, with implementation being strong in three of the four schools. The SEF trainer added that the intervention offered a coherent package that schools found highly feasible and acceptable to deliver:
I think the advantage of having a complete package of lessons, something that enables you to get your data from your students ready-made, other tools that can enhance the work through the parent contacts, the student-led social marketing, you know, it is already made for them.
SEF lead
The SEF lead suggested that the intervention also provided enough flexibility to engage with schools’ different needs and starting points. She stressed that the needs assessment report was a unique and key component of the intervention, which allowed appropriate local tailoring. Its findings aroused staff and students’ interest and encouraged them to think about how to address the needs identified:
When it worked well, and it generally did, getting the range of staff, whatever their job was going to be, excited about the data that had come from their school, and seeing how using that data could drive all the other processes, all the other components . . . [They could] see why the curriculum needed to happen . . . I think it’s quite a USP [unique selling point] of Positive Choices that it has that year 8 needs assessment. And it turns into a kind of report card for the school that then feeds into these multiple components.
SEF lead
She reported that it was helpful for schools to be able to benchmark themselves against other schools delivering the intervention.
The SEF lead suggested that the extent to which implementation was feasible and that fidelity was achieved in schools was related to the extent to which the school had strong leadership that supported the intervention. Where the intervention was led by the school’s PSHE lead with oversight and support from an SLT lead:
If there was a kind of supported lead for Positive Choices, whether they were the pre-existing PSHE lead or somebody else, and the senior leadership team was behind them having the space in the curriculum, and having staff released for training, it seemed to be fine.
SEF lead
This model enabled the curriculum to be timetabled, appropriate teachers to be identified as to teach this, and these staff to be released to attend training. Fidelity was also promoted by Positive Choices being a ready-made package and by SEF being aware of how important this was to the research team so that this was emphasised in their communications with schools.
The SEF lead suggested that the problems with releasing staff for training and the delivery of lessons in school 2 reflected wider management problems at the school, which resulted in limited commitment of the SLT to the intervention. The service-level agreement signed with the school was important, however, in ensuring the school’s, at least partial, engagement.
The SEF lead suggested that Positive Choices would be attractive to schools within a Phase III RCT, particularly with RSE becoming a statutory requirement from 2020:
I think with the policy contexts of statutory, RSE and HE [health education], you know, it is going to fulfil quite a lot of that content. And you know, that’s quite a neat solution for schools to just say, well we’re running Positive Choices, and doing some additional health education to create our PSHE package, job done!
SEF lead
However, the SEF trainer commented that the curriculum targets only students in years 9 and 10 in a full trial might deter some schools from buying into the intervention unless materials could also be offered for students in other years.
The SEF lead and trainer both commented that the intervention should be made more inclusive for students with SEND, for example, in terms of lessons and participation on the SHPC.
The SEF lead also suggested that it would be useful to construct case studies of successful activities that schools ran in the pilot, and to use these to offer examples for schools in the full trial. This could include, for example, case studies of the outputs arising from student-led social marketing. Schools would be interested in how these could be harnessed to give schools public relations opportunities.
Perhaps from the pilot schools, there’s enough to give them some little case studies about ways that other schools have organised it. Just to show them that there’s a variety of ways you can do it . . . I wonder if having more concrete examples of how other schools have done it, might have just made them think, ‘oh that would fit in our context, or that might, or a little bit of this’ . . . I wonder, this is, you know, partly speculation, but I wonder if they need to see almost photos of the finished product and get some kind of, sort of be inspired about the impact it can have and how it could then fit with things that are important to the school. To give them a bit of PR [public relations] value for it as well as knowing it’s going to help their pupils’.
SEF lead
The SEF lead commented that it would also be useful for the intervention to include elements aimed at encouraging schools to maintain momentum and fidelity. This might occur, for example, by sending regular newsletters or incorporating some form of online monitoring/tracking for each school’s activities. To help schools maintain the support of SLT and governors, it would also be useful for the intervention to include some internal evaluation, focused on how student-reported needs change over time, so that the school can see the benefits being derived from the intervention.
Interviews with staff
In the three schools where the curriculum training was delivered in full, staff who were interviewed reported that the training was acceptable and sufficiently prepared them to deliver lessons. The lead in school 3 suggested that the opportunity to understand the background as to how and why the lessons had been designed as they were and to anticipate how they might be delivered was particularly valuable. Two staff members, however, reported that the training was somewhat advanced for them as they were new to teaching RSE. One staff member in school 4 explained that the other teachers present at the training, who were highly experienced, had different needs and questions to those he had as a newly qualified teacher:
They just really zoomed in on very specific things and because I was new I was a bit kind of like, ‘I’ve never done this before’, don’t really know. So, it was kind of a bit more tailored to their experience and expertise.
School 4, lesson teacher and social-marketing lead
As a result of a lack of time and teacher availability, school 2 had to condense the training into a 1-hour face-to-face session covering the first three lessons, and a follow-up Skype session to support staff delivering the drop-down day. Staff did not feel this approach prepared them as well as it could have. However, since teachers each taught a single lesson seven times on the drop-down day, they generally expressed confidence in their delivery.
Staff reported that the student needs survey was acceptable to conduct and that they valued learning about the results, suggesting that this sensitised them to, sometimes shocking, gaps in student knowledge:
There’s so much knowledge that is just missing and it’s scary almost to think of what the kids think can and can’t, and even when I say it to them . . . ‘x amount of kids think that you can’t get pregnant standing up,’ they’re like, ‘what?’ But, actually, that came from them, you know, so it’s a bit worrying.
School 2, Positive Choices lead
The data was shared with all staff [. . .] and I think we got a lot of interesting conversations after that. [. . .] Like ‘I can’t believe some of them thought that!’ from . . . some of the head of years and . . . form tutors being like ‘that’s nuts!’ [. . .] We assume quite a lot [that] because it makes sense to us [. . .] it will then make sense to all the students, and it’s not always the case.
School 3, Positive Choices lead
Interviews suggested that the SHPC component was feasible, although school 4 found that SLT membership on the SHPC made scheduling difficult, and student engagement was variable. The assistant head teacher in school 1 reported that the school ‘did manage to progress [the SHPC] somewhat’ but struggled to find time to meet during the school day and achieve the attendance that they wanted. This individual thought that the SHPC and student-led social marketing would be important components once established:
My feeling is that both in terms of the Council and in terms of the social marketing notion behind Positive Choices, I feel that those are the vehicles through which you’re going to get the most open dialogue, if they work correctly, but it’s so difficult setting these things up and maintaining it so.
School 1, assistant head teacher
Schools enhanced feasibility by tailoring their approach to organising the SHPC according to their needs and existing school structures. For example, in school 2, where implementation began later in the year, the Positive Choices lead invited students whom they thought would be most engaged to launch the SHPC’s work as quickly as possible. In contrast, school 1 aimed to recruit and sustain the engagement of what the PSHE co-ordinator described as a ‘mix of students’, which required additional work:
So it was kind of trying to get a mix of students in there. And then the ones that did continue [to come to meetings] tend to be the goody-goody ones, and then the ones who were a bit naughty sometimes, I went to go and collect them during the break times and bring them into it all.
School 1, PSHE co-ordinator
School 1 also integrated the SHPC with a broader health improvement committee, which they had planned to cover other issues including transport and diet. Interviews suggested that, while the SHPC was generally thought to be acceptable and feasible, it could be better facilitated through integration with existing student groups and committees:
What I found as well was, doing the Health Council, we’ve got a Student Council at the school, so it felt like, in a way, we were kind of like doing the same thing in tandem, when, really, it would be nice to . . . put onto the School Council for them to look at as well. Because it makes sense to have a School Council looking at it rather than having . . . a separate group.
School 1, PSHE co-ordinator
By contrast, the lead in school 3 suggested that the SHPC was particularly welcome precisely because it fitted with the school’s existing ethos of student involvement and active learning:
Rather than just ‘this is what you’re learning’, actively involving them, again it’s a big thing in school. I think getting them to really think about what they thought and what potentially . . . their peers thought was . . . really good.
School 3, Positive Choices lead
The SHPCs drew on the needs-assessment survey and student members’ perceptions to inform the choice of ‘add-on’ lessons. Interviews suggest a benefit to this student-led approach, as staff were sometimes surprised by the lessons that students thought should take priority.
In school 1, following the departure of the teacher who was to teach PSHE, Positive Choices lessons were assigned mostly to social science teachers who had availability in their timetables, and who had no specialist training in PSHE or RSE. Lessons were around 1 hour in length. Where staff were uncomfortable delivering particular lessons, the PSHE co-ordinator or the head of department for social science delivered the lessons. In school 2, PSHE and citizenship lessons were normally delivered in tutor time; however, as some tutors felt uncomfortable delivering RSE, lessons with a biological focus were delivered in science lessons and the Positive Choices lead recruited volunteers to deliver the remaining lessons in 45-minute slots during a ‘drop-down’ day. As the Positive Choice lead commented:
Because I just didn’t have enough time to spend convincing and training and talking and all that stuff so I just thought, ‘OK right plan B, let’s get a new group of teachers that are willing to teach it and then go from there’.
School 2, Positive Choices lead
In school 3, Positive Choices lessons were delivered by humanities teachers in weekly 1-hour SMSC lessons. No staff at this school had previously been specially trained in PSHE or RSE, but most had delivered some SMSC lessons at the school before. In school 4, Positive Choices lessons were delivered in fortnightly 55-minute PSHE lessons. One staff member had been specifically recruited to teach PSHE and drama; other staff were selected based on aptitude and availability, but tended to be experienced and committed.
Most staff that were interviewed considered year 9 to be an appropriate point for teaching the content covered in Positive Choices. Some staff from schools 1 and 2 were, however, worried that this age group was not yet mature enough to handle some lesson content. Staff generally reported enjoying teaching the lessons:
At first I was really nervous about teaching sex and relationships and now I’ve actually asked for next year I was like, ‘Yes I’ll have loads of year 9 classes, I’ll do it again.’ I loved it, it was great.
School 4, lesson teacher and social-marketing lead
The interviews suggested that some staff in schools 1 and 2 resisted teaching RSE based on religious or cultural beliefs. A teacher in school 1 shared that although they did not oppose the lesson content per se, they personally felt uncomfortable teaching some of the topics:
Well me personally, a lot of it I wasn’t really comfortable with just in terms of culture and stuff like that. I see the importance of it so I’m not saying that it shouldn’t be delivered, but I think it should be delivered by someone who kind of fully understands it, fully kind of embraces it.
School 1, lesson teacher and social-marketing lead
The staff leading implementation navigated these diverse views by, for example, in school 1, swapping lessons so that other willing teachers delivered those that some teachers found more sensitive (such as on condom demonstration or pornography) or, in school 2, arranging delivery during a drop-down day with willing staff. Where teachers were uncomfortable with particular elements of a lesson, some made adaptations, as the Positive Choices lead in school 2 described:
They, some of them, did feel uncomfortable about the models of the penises and the vaginas but they took that, some of them took that out but explained it in a different way.
School 2, Positive Choices lead
Interview participants appreciated that lesson materials came ready to use and did not tend to find the curriculum burdensome:
If you said that we had to plan everything ourselves, then that’s slightly different. But the fact was that everything was given to us.
School 2, lesson teacher
Some highlighted particular areas where materials could have been more comprehensive, especially for teachers new to delivering RSE, such as a teacher in school 1:
With some of the [science] stuff the answers weren’t easily available from the materials that you provided and we had to, like there was one, the fertility one, it was only once I was going through it [in class] that I realised I didn’t have a clue what each of the bits was for even though I’d looked at the stuff for about half an hour the night before, and I was just like on the spot, I was like I don’t know, I’m going to have to look that up, in front of the kids which is not really [ideal].
School 1, lesson teacher
A key theme was that student needs varied and so materials were most usable when they were both comprehensive and adaptable. Lessons could be adapted by adding content, modifying activities or wording to better match student needs (including for SEND students), or tweaking materials to bring them in line with school policy or practice. Although this could be time-consuming and an added pressure for staff who already had full workloads, modifications were often viewed as a typical and acceptable element of a teacher’s role:
I think the lessons themselves were OK, what they were, I’m just thinking some parts . . . might need to be tweaked slightly, based on the class, but that’s the teacher’s job to do.
School 1, PSHE co-ordinator
In schools 3 and 4, the Positive Choices lead and head of SMSC undertook to go through the slides carefully to suit the school’s style and sometimes to include additional or different material on behalf of their colleagues, who could adapt the material further if they wished.
Staff disagreed about whether there were too many or too few activities and written elements to the curriculum. In school 3, a lesson teacher described how teachers could creatively adapt activities as appropriate for different classes:
Even with a discussion activity . . . you can turn that very easily into a writing task you know what I mean? So instead of them getting them to argue each way, you just get them to do a table for and against. And get them to write down the actual arguments for both. And then you can have a more structured class debate on that as well so there are ways of doing it both sides.
School 3, lesson teacher
Some staff advised that Positive Choices lessons should be more inclusive for LGBTQ students, for example in the contraception module, which addresses heterosexual reproduction but not how same-sex couples could have children. There was also a suggestion to add lesson content on the relationship between age and fertility. Some suggested using simpler language to make lessons more accessible for students and covering biological topics (for example, sections on hormones or stages of fetal development) in less detail.
Staff varied in their feelings about the atmosphere and interactions in Positive Choices lessons. They commonly described cultivating a more relaxed atmosphere, which they viewed as key to delivering RSE, and valuing the opportunity to interact with students in a less formal setting:
It’s nice because I get to see them in a different side from the necessary teaching science, I got to talk to them about real life stuff.
School 2, Positive Choices lead
Teachers’ reactions to students’ behaviour in Positive Choices lessons varied. Although students were often described as open and engaged during lessons, staff sometimes reported that students were ‘silly’ or ‘giggly’. Teachers described strategies for managing such behaviour:
I try to make it quite obvious that I’m not embarrassed to speak about this stuff because I think if you like, there times where I just laugh at some of the stuff they said and I thought, ‘If I have a go at them it’s just going to revert them, they’re not going to be interested.’ So I [insert] just, a little bit of light humour where appropriate because otherwise I think you’ve just lost them.
School 3, lesson teacher
Even using terminology like penis and vagina, like, I had to get them to say it. At the beginning, I was like, ‘Right, everyone say ‘penis’ and ‘vagina’ 50 times and then we can move on.’ And then once we’d said it, then it was fine, we could then.
School 2, lesson teacher
A minority found this behaviour among students less acceptable and interpreted it as an indication that their students were not yet mature enough for aspects of the curriculum, including a teacher in school 1 who said that their students were ‘literally in bits’ over pictures in the lesson on genital variation and suggested an approach such as anatomical models would be ‘a bit more appropriate’ for young people.
Social marketing was led by staff with different roles in different schools. For example, in school 2, the head of media and performing arts led the work whereas in school 4 a drama teacher led it, adapting this element to be incorporated into a year 9 student drama performance. Interviews suggest that the social-marketing component was highly acceptable to staff; for instance, the lead in school 3 expressed how impressed he had been by students’ original and innovative ideas about how to present material. In school 4, the focus on drama contributed to feasibility by allowing the teacher, who was new to RSE, to draw on his existing expertise and to work with students primarily in lesson time. However, campaigns were not always implemented fully by the end of the year, and some staff expressed a need for an extended time frame to ensure that enough time could be given to developing campaigns outside lesson time. Finding opportunities to integrate the student-led social marketing with existing school activities, as it was in school 4, was also highlighted as a means of enhancing the feasibility of this component.
Staff in schools 1 and 4 reported creating newsletters with Positive Choices content. This was ‘piggy-backed’ on the school newsletter. Staff reported little parental opposition to Positive Choices across schools. A letter sent home in school 4 introducing the new curriculum generated calls from some parents seeking more information, but mainly to support their child, with only three withdrawals from the programme. The notion of discussing pornography in school occasioned some concern from parents in school 3, but, across schools, staff reported few parents opting their children out of lessons.
The staff who were interviewed were less aware of the sexual health services review, but this was undertaken by the SHPC in schools 1, 3 and 4. Interviews with staff suggest that the sexual health services review was an acceptable and valuable exercise. The lead in school 3, for example, noted that the review revealed that many local services had closed, and made staff aware that spaces within the school that had previously displayed relevant information had been taken over for other purposes, meaning that the SHPC had to consider how to make sure information found its way to students.
Implementation of Positive Choices was influenced by the level of priority that school leaders accorded to the programme and to PSHE more broadly. For example, school 3 was said to be unusual in according importance to SMSC education compared with other schools in the borough; its existence as a timetabled and valued subject made it easier to embed Positive Choices there. Similarly, school 4 was able to integrate Positive Choices lessons within its existing, highly valued PSHE provision, delivering the curriculum during the school’s regular PSHE timetable slot to a student body who, staff reported, enjoyed PSHE and already viewed it as an important subject. The school’s head teacher valued PSHE and entrusted it to the head of PSHE, who had the power and autonomy needed to lead the programme effectively:
When [the PSHE/Positive Choices lead] decides we’re going to do something, then that’s what we’re doing and we’re all focused and we’re giving it 100%.
School 4, Positive Choices co-ordinator and lesson teacher
The Positive Choices co-ordinator in this school also explicitly attributed successful implementation to having a designated role co-ordinating the programme, and administrative time dedicated to this task. In contrast, in school 2, staff reported that PSHE had a low priority in the school and, as a result of poor handover following a change of roles, the staff member who became the Positive Choices lead was not fully up to speed with it until the second half of the school year. A lack of timetabled lessons and PSHE teachers meant that this individual had to rely on colleagues to agree to deliver the programme. Many such staff did not take the programme seriously until a new school head teacher came into the post and lent support to the programme:
It was the help from the senior leadership that didn’t really kick in until about April or after April and that was quite late in the curriculum . . . That was the main challenge. I think if the head teacher had got everybody on board from the beginning then it would be. I think people didn’t really take it as seriously as I took it and that frustrated me a little bit.
School 2, Positive Choices lead
Staff sometimes cited RSE’s forthcoming statutory status and acknowledged that Positive Choices would enable schools to meet this requirement. Interviews suggest that the anticipation of statutory RSE increased the salience of Positive Choices and, in some cases, contributed to schools’ openness to the programme; for example:
It’s a go-to, one-stop solution, ‘here you go . . . there’s your SRE [sex and relationships education] programme ready to go, you’re going to hit all the new requirements’ . . . It’s going to tick all your boxes, it’s here, it’s there, it’s ready.
School 4, lesson teacher and social-marketing lead
Commitment to implementation was enhanced where staff had strong feelings about the importance of delivering RSE, for example:
I personally am all for this type of thing, I really do think it’s something students need to know and I personally think that these days that they don’t find it out here, they find it watching porn and they find it doing other, places or speaking to their friends which might be incorrect.
School 3, lesson teacher
Another staff member described herself as perhaps ‘more passionate about it than most’ because she had a child in her teens and wished that she had received accurate RSE as a young person. Staff in school 4 attributed successful implementation of the programme to the personal commitment of the PSHE lead.
Several staff mentioned concerns in their schools about issues the programme addressed, such as teenage pregnancy in school 2, sexual harassment in school 1, and high rates of domestic violence in the community around school 4. Although they did not link these concerns directly to support for Positive Choices, these repeated references suggest that staff members’ awareness of these issues affecting students and their families might shape their thinking and their level of support for the programme.
Staff who were new to teaching (in general, or RSE specifically) sometimes reported discomfort and limited confidence in delivering programme lessons; for example, a social sciences teacher in school 1 felt that the lesson on biology required specialist knowledge and did not deliver that lesson because she ‘didn’t know any of that’. Where science teachers taught Positive Choices lessons, staff reported their background knowledge was a benefit for delivery.
Staff thought that the lessons worked best when delivered by teachers who had good relationships with their students, and who were confident and comfortable delivering the content, as described by a teacher in school 1:
I feel it’s about the confidence of the teacher and if you are not confident, you’re not going to be able to, you’re not going to create an environment for them that is going to be beneficial to them you know which is why some of the lessons I said I can’t, because I don’t want to do them a disservice, and it’s stuff that they need to know.
School 1, lesson teacher and social-marketing lead
Trusting relationships between school staff facilitated implementation. In school 4, the PSHE lead explained how the trust the head teacher placed in them facilitated Positive Choices:
He just gives me sole responsibility but that’s because we’ve got a very good working relationship. I think if it was somebody else, maybe he might’ve wanted to know a bit more about it. I mean in the first instance, he met with [name] and myself and then I gave him my breakdown of how I think it’s going to work and the confidence he has with me, he’s just let me go with it.
School 4, PSHE lead
These relationships were also important in schools without established PSHE programmes, where Positive Choices leads had to rely on their colleagues to co-operate and agree to deliver components of the programme. For example, when implementation started late in school 2, the Positive Choices lead described one colleague as key:
I started working with [colleague] and [she was] fantastic, I wish I was working with her from the beginning . . . She was kind of like somebody else, my go-to person . . . while I was trying to figure out everything in my head, [she] was there to kind of help.
School 2, Positive Choices lead
Good relations between staff enabled some teachers to take over from others at points where they were less confident delivering the materials, for example in school 1. Good relations enabled Positive Choices leads to successfully recruit colleagues based on knowledge about their strengths and preferences in school 2. In school 3, good relationships facilitated joint reflection on the materials, in between teaching lessons, and meant that less experienced or specialised teachers trusted the materials (and any adaptations of them) that they were given by the PSHE lead.
I trust [Positive Choices lead], [he] is a really good teacher so normally the changes he makes, I’ll normally have a flick through the lesson a couple of days before and then obviously if I have any issues with how to deliver certain things I’ll go and speak to [him], but on the whole normally I just teach it.
School 3, lesson teacher
According to staff, students and classes varied in their level of comfort, openness and maturity during lessons. Staff reported that students varied in their stages of sexual maturity and levels of sexual activity, with those at an earlier or less sexually active stage less able to engage with the lessons:
I’ve got some students in that class who in my mind are probably very aware of sex and how it works and have maybe already you know, tried it, but there were equally quite a few students in that same class, because they just mix, quite a few students in that same class who just looked like absolutely stunned and disgusted that these words were coming out of my mouth, like couldn’t even bring themselves to say the word sex in some lessons and were just sitting there looking at me like I don’t want to be here, or just literally couldn’t even look at the board, had to just look away.
School 3, lesson teacher
Engagement could also vary by gender, with teachers reporting that boys disengaged during certain topics including fetal development and contraception. Interviews present conflicting views on whether or not lessons were pitched appropriately for students of all academic abilities, including SEND students. Some staff reported making adaptations in this respect, where needed. Some teachers suggested that students of different academic abilities could engage in the lessons. Several staff said Positive Choices presented a valuable opportunity for less academically oriented students to engage in lessons:
More high attaining pupils in the higher-ability groups tend to be a little bit more shy and reserved . . . Whereas the more out-loud-and-proud ones who are a bit more like, you know the ones that where typically you might look to make sure that they’re on-task and not being disruptive . . . They’re the ones that were actually a bit more like, ‘shh, no I want to listen to this,’ and asking questions and being like, and being actually more engaged.
School 4, lesson teacher and social-marketing lead
Interviews with staff provided limited insight into programme mechanisms, but some staff discussed the importance of the programme’s multicomponent approach, the impact of cultivating a comfortable atmosphere for learning about RSE, and how the programme strengthened relationships and eroded boundaries between students and school staff.
With regard to Positive Choice’s multicomponent approach, staff in school 4 suggested that the components worked synergistically to contribute to their intended impact:
I think it was a really good concept to have the three [components] going on together . . . And that’s the thing that I think made it work, because there were different parts of it and the students could see, obviously the assemblies and the school health promotion council, and the drama and then coming to the lessons, so it all sort of fed into each other really, really well.
School 4, Positive Choices co-ordinator
Interviews suggest that Positive Choices presented opportunities for students and staff to interact in new ways, which strengthened relationships and eroded boundaries between them. In school 4, the programme lead described how the SHPC in that school created the opportunity for dialogue between students and the SLT:
It’s enabled [the SLT member attending the SHPC] to have a forum of our young people across each year group. And when things have come up she can directly [ask], ‘What do you think about that? Do you think we should include that in the curriculum?’ So, it’s given us a forum really where everyone’s happy to speak really, really openly, and the students, I think have been really open with the things that they’ve been happy to share.
School 4, Positive Choices co-ordinator
Several staff felt the opportunity to interact with students in a less formal setting enriched their relationships with students and their accounts suggested that through the programme students learned which staff members they could go to with questions:
The fact that they’re seeing me in a non-scientific teaching kind of role, I think that they’re, a lot of the students were being a little more open to actually sit down and hold a conversation with me. As opposed to thinking that I’m dishing out loads of detentions or homework . . . So I think that the fact that it was a little less formal, I think gave them an opportunity to open up a little bit.
School 2, lesson teacher
Interviews suggested limited potential for staff experiencing harm from the intervention. One teacher shared that she had difficulty teaching about fertility due to personal challenges she was experiencing at the time. Staff from school 1 swapped teaching with their colleagues for specific lessons that they were uncomfortable delivering, but acknowledged that in schools where this was not possible staff might feel distress:
If you’re a member of staff who isn’t necessarily confident at delivering and it’s a sensitive topic for yourself and you’ve not been told that you’re teaching it but you kind of have to, it might be a bit distressing for some.
School 1, lesson teacher
Staff did not identify any potential harms for students.
The interviews suggested that all schools intended to continue at least some aspects of Positive Choices in the next school year. Most schools planned to continue using the curriculum materials in full or in part. Most also planned to carry one or more of the whole-school components into the next year, including conducting a version of the student needs-assessment survey again in school 1. Students in school 4 were reportedly keen to continue with the SHPC in the next school year:
Yeah, they’re sort of asking, when’s the next meeting, and are we going to continue with this next year, and what’re we going to do. So I would like it to continue, just as that really, safe and open place for them to be able to share with people that they wouldn’t normally be able to share with really on a one-on-one basis, or part of a very small group. I think it worked really well.
School 4, Positive Choices co-ordinator and lesson teacher
The Positive Choices lead in school 2 suggested that implementation could be smoother if it were more deeply embedded in existing practices:
I think once it’s embedded and it’s known that it’s an expectation and it’s not really optional and everyone gets a bit more used to it, I think that’ll be fine.
School 2, social-marketing co-ordinator
Interviews with students
Students participating in the SHPC were positive about their roles and the impact it had. One student in school 4 recounted proudly the SHPC’s role in choosing additional lessons and having a say:
They came to us and said these are the lessons: which ones do you feel are most important?
School 4, year 9 girl
Students felt that their views were being acted on:
For the third meeting, they were talking about action plans and getting it into motion, like [teacher] is working on putting some posters around the school based on like Positive Choices, mental health – all the stuff we’ve been doing right now.
School 4, year 9 girl
This student also expressed appreciation of the range of experiences and opinions in the group, and the honesty that was possible:
It felt good because there were lots of variations . . . and we all kind of brought that to the table and it was nice to just collaborate on that together.
School 4, year 9 girl
Even in school 2, where there had been challenges to implementation, the students who were interviewed expressed a sense of agency in picking the subjects for the curriculum, writing to parents and ‘spreading it around school so people know’:
It just gets the word out more, yeah, because a few of our mates have been asking what we’re doing . . . then the word usually gets out from there. Yeah, it got out quite a bit because like a boy called [name], he’s quite popular in our year and he’s gone and told all his mates and then they’ve all asked questions about it.
School 2, year 9 boy
All students interviewed were supportive of RSE and most were supportive of the lessons they received:
It’s like compulsory stuff that you should know by the time of being an adult.
School 2, year 9 girl
Even when they personally found the lessons uncomfortable or awkward, students supported the idea of the curriculum being important and necessary:
We might have felt a bit awkward at first but I think that these lessons should be like shown more in class so there isn’t, it doesn’t feel uncomfortable and that it becomes more of an open thing. Because at the end of the day it’s like our bodies and it’s something that everyone has. So, like we should talk about it more instead of being so private and secretive.
School 3, year 9 girl
One student described the lessons as ‘brutally honest’, albeit in a way that she found appropriate or suited to her age, compared with the RSE that she had experienced in previous years:
I think it was definitely a lot more brutally honest because when we had lessons similar to this in year 7 or 8, I feel like we’re kind of sheltered a bit more, whereas when we came into year 9 . . . we were kind of surprised because of how much information they were sharing with us because we wouldn’t like expect to be taught that in school . . . I feel like because of our age they went in much more depth in it because they sort of, when we’re in year 7 and 8 they dodge the questions like about it and then as soon as we got into year 9 they let us know.
School 3, year 9 girl
In terms of who delivered the lessons, some students welcomed lessons being taught by teachers with whom they were already familiar:
I think we felt more comfortable with them since we know them before and obviously we kind of had a relationship with them before because of other lessons. So, I think it was good that it was a teacher that we knew and it wasn’t just a random teacher that came in and we didn’t know before because then we wouldn’t feel as comfortable kind of talking to them about it or opening up or sharing thoughts or experiences.
School 3, year 9 girl
Students valued teachers who were committed and skilled as well as open:
My teacher . . . she never made anything that she was saying awkward and she like made it clear that anyone in the class could share their opinions or experiences on it and they wouldn’t feel judged.
School 3, year 9 girl
In terms of content, opinions and memories differed, but students were largely positive about how the curriculum addressed topics such as pornography, sexual debut and pressure. Students mentioned topics that they would have liked to spend more time on, such as what to do about pregnancy, the emotional changes of puberty, FGM, how to build a relationship, sexuality and LGBTQ issues, in-vitro fertilisation, how to talk to parents, and how to access information without your parents knowing (some of this being dependent on which ‘add-on’ lessons were covered by their school).
Students noted and were grateful for the signposting to further resources:
I think it was good because like at the end they gave you like websites to go to if you needed help . . . They gave you websites if you needed extra help like.
School 3, year 9 girl
In terms of classroom activities, students appreciated the role of ground rules in establishing confidentiality and privacy:
We were also able to give our own opinions and stuff, and like we weren’t asked to share anything personal.
So yeah, it was very comfortable in the lessons.
[The teacher] made us feel relaxed and he said you can ask any questions, he kind of just made us feel confident in ourselves.
School 4, year 9 girls in focus group
Where classes were more active, collective or discussion based, students were noticeably positive:
You get to experience everyone in your class’s . . . opinions . . .
And it’s really interesting to see other people’s opinions instead of just focusing like on stuff that you think or you believe, it’s interesting to see what someone else believes and how that clashes or how it’s similar.
Yeah. It’s quite a nice space to be in.
School 4, year 9 boys and girls in focus group
One activity that students enjoyed involved students lining up opposite each other and moving towards each other only on receiving consent from their partner:
The lessons did help us to gain a tiny bit of more confidence and we kept continuing to talk about it . . . but if you think about it, like if you’re in a sexual relationship and you ask the question, like ‘Do you want to have sex?’ it will be kind of awkward but like I think this thing made us have like . . .
Confidence talking about it.
Confidence, yeah . . . and I know what I’m saying now, I know what I’m doing.
School 4, year 9 boys and girls in focus group
Students complained when lessons were focused on teachers’ presentations:
To be honest I think the lesson it was just kind of like teacher talking to you, telling you all the information. You couldn’t really take much out of the lesson. I didn’t really learn a lot in the lessons to be honest. I just kind of went with it.
We were waiting to do more tasks.
Because if it’s just the teacher speaking for an hour no-one takes it in. It’s like watching a documentary for an hour, you just get bored and don’t take anything in.
School 3, year 9 boys and girls in focus group
Many students expressed enjoyment of the discussion-based approaches used in Positive Choices. However, it appeared that classes needed to be both familiar and comfortable with such approaches for it to work well. Thus, students in school 4, which had a spiral curriculum of RSE from year 7 onwards, experienced teachers, and a strong commitment to reinforcing and following ground rules for discussion, seemed to be the ones who got most out of the discussion-based elements of Positive Choices. In school 1, where some teachers were less experienced and students were apparently less accustomed to free discussion, the more open-ended activities were reported to work less well.
A few students said that they talked to their parents about what they were learning, but it did not appear that the homework exercises had facilitated this. Two schools had explicit policies against setting homework in PSHE, and most students were sceptical of the potential of this intervention component:
What’s the point of giving information to parents because they’re not going to sit down with their kids and teach them because that’s more awkward to them?
I think part of the culture is to try and make parents talk to their children, so some people find that awkward and then they try to teach us it at school . . . but no one really took any notice.
School 2, year 9/10 boys and girls in focus group
Students involved in social marketing described a range of activities: assemblies, quizzes, surveys, newsletters, PowerPoint® 2016 (Microsoft Corporation, Richmond, WA, USA) and poster campaigns, and a bake sale. School 2, for example, planned a campaign about peer gossiping, confidentiality, trust and rape jokes, whereas school 4 pursued the social-marketing campaigns in year 9 drama lessons, focusing on domestic abuse and healthy/unhealthy relationships. School 1 raised awareness about access to sexual health services. Students reported enjoying running campaigns and were optimistic about their potential impact:
We sent PowerPoints out to every form class and we did put posters up around the school, we did raise awareness, I think we did like raise awareness.
I’ve seen the posters.
And I have, yes.
. . . You just can express how you feel . . . when you’re doing the team you have to plan everything yourself, and like present it as if a teacher was doing it . . . I guess since we relate to [students] more, like we know like what they would like take seriously and what they would find funny.
School 1, year 9 girls in mixed gender focus group
Students in schools in which PSHE and RSE already seemed to be valued by the school (e.g. in timetabled lessons and delivered by teachers volunteering for it) appeared to be the ones who also most valued Positive Choices. Students in school 2 were the most negative about Positive Choices. This may have reflected limitations with past and present provision at the school as well as the dynamics of the focus group, which was dominated by two vocal and negative students who may have inhibited other students from expressing different views. Their criticisms of lessons as being repetitious, too intense or with too little time to absorb learning may have reflected limitations with the curriculum being delivered largely as a single ‘drop-down’ day. Nonetheless, more positive feedback was filtered back to the research team, both in their conversations with students on the day itself and afterwards through parents and teachers.
Where Positive Choices built on a well-established programme of PSHE, such as in school 4, it seemed to be able to meet student needs more successfully. School 4 used suggestion boxes in its PSHE provision to understand students’ questions, and staff relished bringing in additional materials to supplement those provided as part of Positive Choices. Such elements may have boosted student satisfaction. In school 2, in contrast, there appeared to be less of a history of RSE provision; some tutors seemed uncomfortable with the pastoral aspects of their role and there was less time to involve students in shaping the provision. This may help explain the students’ complaints about the limitations of the curriculum delivered via a drop-down day.
Established processes for communication between staff and students, for example via student councils, may have made the SHPC and social marketing easier to set up and run in some schools. Nonetheless, in school 2, where relations within the school were less harmonious, the SHPC and student-led social marketing may have had an even stronger impact as a visible mark of students contributing to school improvement.
Some students reported that the lessons had brought students together, enabling them to learn together and have the confidence to have more open conversations about sexuality and sexual health:
It’s not like someone’s, like, telling you: ‘This is what it is’. Like, you’re learning with other people. Not, like, some people, like, know more than others. It’s like you’re learning with them. So, I feel like just . . . come together more.
School 3, year 9 girl
It’s become a much more open topic that people can talk about. And it’s also reassuring because, like, you know that if you’re going through, like, a personal problem, it’s reassuring to know that you’re not the only one, and like there’s other people your age that you can talk to about it and everyone feels more comfortable.
School 3, year 9 boy
It’s definitely helped with confidence over lessons. I notice more people putting their hands up, more people actually wanting to talk about it and get involved.
School 4, year 9 girl
Students identified similar mechanisms arising from the student-led social-marketing component:
It made me slightly more comfortable to talk to another student rather than just the teacher. So, you know like, they’re going to relate to you as well.
I think that it’s like changed and improved morals within, like, the students within the school. Because it’s more of an open thing that we talk about now. We just, like, know what’s right and like how to deal with like situations and things, and it’s something that’s openly spoken about with students and it’s not like a secretive or an uneducated thing anymore.
School 3, year 9 girls in mixed focus group
Some saw the intervention as providing ‘the basics’ of knowledge that could provide the foundation for broader transformations:
I think it’s good that they teach like the basics because in the end they’re the most important things . . . It’s obviously important to know the more like complicated and other important things but if you have the basics you can just work off that.
School 4, year 9 boy
Several students identified that lessons had raised awareness of their rights within relationships:
I think it made me more aware of, um, kind of like my rights. Like makes me more aware of my rights in a relationship and just like what’s acceptable and what’s not acceptable.
School 3, year 9 girl
Some stated that they felt better prepared to ‘say no’ and to talk in relationships:
After this like course, I think everyone knows how to say no if someone, like consent.
School 4, year 9 boy
However, some students were more doubtful about whether or not any intervention could impact on behaviour because this was down to individual agency:
I think the lessons were good and the education that they brought to the lessons was good but I don’t think anyone’s taken on the information that they said like properly.
School 3, year 9 girl
Such views on the limitations of mechanisms of impact were, however, most common in the context of school 2, which had experienced challenges with implementation and delivered the curriculum as a single drop-down day:
It’s like that day never happened and that we already knew all of that . . .
Yeah, I don’t really remember when it happened.
It’s really pointless.
Like everything’s just the same as it was before, no-one’s changed their perspective on anything.
School 2, year 9 students in mixed boy and girl focus group
No potential harms were suggested by students.
Control condition and potential contamination
Both control schools had recently revised their RSE programmes. The deputy head teacher of control school 1 reported that the school had over the last couple of years developed a curriculum for students from years 7 to 11, revisiting topics across years to provide age-appropriate learning.
According to the PSHE lead, control school 2 had minimal RSE teaching until recently, which covered biological aspects in science and forced marriage in religious education:
I do know that it wasn’t taught I believe because it was just lack of knowledge, lack of experience for staff. Could be taboo as well being a [faith] school, I think that’s probably the biggest worry, worrying what teachers think, worrying what the school views are, worrying what parents, so I know for a long time there wasn’t any RSE taught at the school . . .
Control school 2, PSHE lead
However, control school 2 had recently developed and piloted a new RSE programme for students in years 7–11 led by the PSHE lead with, according to the school’s PSHE lead and the SLT member leading on RSE, strong support from the head teacher and governors. The PSHE lead reported that she had attended a course at an external charity, reviewed externally produced resources and then led the development of the new programme.
In terms of consultation with parents and students about RSE provision, the deputy head teacher at control school 1 reported that student councils were consulted on students’ RSE needs, parental representatives on the governing body were informed about RSE provision and there were details on the school website. However, both the deputy head teacher and head of year 8 reported that broader parental views were not solicited. Students reported that there was little consultation with students about RSE. In control school 2, the PSHE lead reported that parents were consulted on the programme and were able to review some of the teaching materials:
Before we launched, it we spoke to parents. We invited parents in. We said to parents, ‘Look, we are going to teach this’. To be fair, all the parents are happy, there’s no concerns.
Control school 2, SLT lead
The SLT lead in control school 2 reported that implementation of the new RSE programme had been delayed to ensure that there was adequate time for consultation. The SLT lead and year 9 students agreed that student consultation had occurred through the student council, which offered strong support.
In terms of timetabling, staff in control school 1 reported that RSE lessons were delivered in 30-minute tutor-time sessions by form tutors, most of whom were teachers but some of whom, according to the head of year 8, were teaching assistants. RSE was provided via one or two sessions per fortnight. In control school 2, RSE was also taught in tutor time, comprising six sessions per year each of 25 minutes, according to the PSHE lead.
In control school 1, the deputy head teacher said that RSE was taught in tutor sessions because of the difficulty fitting PSHE into the school timetable. The head of year 8 also suggested that form tutors were more likely to engage students and be able to provide follow-up care for students when needed:
Generally, I would think yes, I suppose from the perspective of our mentors, the people the kids see every day, they tend to be people the kids trust.
Control school 1, head of year 8
Staff in control school 1 reported that teaching RSE was challenging and staff varied in their comfort teaching it. The deputy head teacher and head of year 8 both said that the quality of delivering RSE varied among staff, reflecting differences in values and aptitude. The deputy head teacher commented:
Any school that is having its PSHE programme delivered by form tutors or mentors has to acknowledge the fact that there is an inconsistency, there is a difference between your strongest and your weakest members of staff. Our responsibility as leaders is to narrow that gap through the quality of the resources that are in place, through the training the staff get and through exactly how you deliver it.
Control school 1, deputy head teacher
There was some training (according to the head of year 8, there was not very much), for example on handling disclosures of safeguarding issues and challenging inappropriate language. The deputy head teacher acknowledged that training for tutors was currently suboptimal:
And what sort of training is provided to those who are doing the RSE teaching?
At the moment, not enough, is the honest answer. A lot of the training is through their [line manager] and they meet weekly . . . And a lot of that will be as a year group training session. We do some work on our inset days that cover various bits and pieces, but we’ve identified this year that, actually . . . training needs to be, you know, a higher priority for us, especially with the SRE stuff coming in. Yeah, so it’s, it’s not bad, but it isn’t anywhere near what it could be.
Control school 1, deputy head teacher
Staff reported that, where form tutors did not feel comfortable delivering a specific lesson, more senior staff would do so. The head of year 8 reported that some teaching, for example about contraception, was taught in science and some, for example about relationships, was taught in religious education.
Control school 2 also delivered RSE primarily via form tutors. According to the PSHE lead, tutors were regarded as the best providers because of their existing relationships with students and their pastoral role:
They’ve already got that relationship with the students anyway and form tutors, you know, when you come in year 7 it’s always the first person they approach isn’t it when they’ve got a problem? The big problems of friendships and oh someone’s picking on me. And, and every time, you know, there’s messing around in lessons, the form tutors are informed about it so it’s always the central person that they come to.
Control school 2, SLT lead
Most tutors volunteered to teach RSE and received 2–3 hours of training from an external charity. The PSHE lead commented:
We invited staff and said ‘Look, if you want to become specialist teachers you are just going to teach those topics whatever time in the year, so probably once a year for 6 weeks, you’ll be teaching those topics and you’ll be trained and become a specialist RSE team.’ So, we’ve gone with that and it’s gone down quite well.
Control school 2, PSHE lead
Those staff who had opted out did so primarily because of religious objections or embarrassment. In these cases, their lessons were delivered by SLT members or science teachers who had previous experience teaching some aspects of RSE. The SLT lead commented that it was important for SLT to be involved to signal the priority given to RSE:
I think it’s good that the SLT are involved almost on a point of the students understand . . . it’s really, it’s actually really important maybe that they’re delivering it. But we want to show staff as well that it is important. So, it’s not just to the kids, it’s to staff as well to say that we should be involved with this. We’re not just telling you to do it, we see it as a significant part of students’ or young people’s lives, so you should be doing it too.
Control school 2, SLT lead
This individual added that some of the staff opting out sat in on the new lessons and some of these planned to opt in to teach RSE in future years:
There were some, well since then though, which has been a positive thing, some form tutors who were originally a little bit worried about it [but] have seen the lessons. Because they’ve observed lessons that have been going on and they’ve said ‘Actually, this next training session you’re having, can we be involved?’ Which is a good thing because we want teachers to feel comfortable about what they’re doing.
Control school 2, SLT lead
In terms of classroom activities and materials, most lessons in control school 1, according to the head of year 8, were structured around slides with some use of class surveys to assess knowledge and needs. Boys and girls were generally taught together, according to both the deputy head teacher and head of year 8, but there were some single-sex lessons, for example on consent. The deputy head teacher said that the curriculum aimed to be inclusive, for example in terms of LGBTQ identities. The deputy head teacher and head of year 8 both reported that the school used some externally produced RSE materials (the head of year 8, for example, referred to the ‘cup of tea’ video about consent), but, according to the deputy head teacher, these were of variable quality and could sometimes encourage staff to underprepare for lessons. According to the head of year 8, form tutors each led on developing materials for different PSHE topics, which were then collectively reviewed to ensure their quality.
In control school 2, RSE lessons typically involved a mix of information, whole-class and small-group discussion, videos (including the ubiquitous cup of tea/consent video) and student presentations with little written work. All RSE teaching was in mixed-sex groups, primarily for logistical reasons, according to the SLT lead. The PSHE lead produced an overview of the curriculum and the team of specialist teachers then planned lessons, with the PSHE lead providing some externally produced materials. According to the SLT lead, these were adapted for the school so that they met teachers’ individual needs and preferences. Each teacher planned and delivered lessons as they wished, depending on their preferences and what was most appropriate to each topic.
In terms of topics, year 7 students in control school 1 learnt about relationships (initially mostly focused on family and friendship relationships), consent, sexting, internet safety and grooming, self-esteem, and assertiveness, for example in challenging sexual harassment. Older students learnt about sexual health in more detail, such as safer sex, STIs, deeper learning about intimate relationships and consent (building on year 7 provision), pornography (in terms of exploitation in its production, its consequences for realistic understanding of sex and the legal status of revenge pornography). There was some RSE for year 11 students but, according to the deputy head teacher, this was limited by GCSE preparation. The head of year 8 and the school nurse reported that RSE tended to focus on ‘the basics’, for example safer sex, and did not engage more deeply with the emotional aspects of sexual relationships. The deputy head teacher reported that control school 1’s approach to RSE emphasised that sexuality was normal and healthy but did not address sexual pleasure. The RSE curriculum involved no homework.
In control school 2, year 7 students learnt about romantic relationships, family life, puberty, managing online and off-line relationships, unwanted contact and FGM. Year 8 covered sexuality, consent and contraception. Year 9 focused on healthy and unhealthy relationships, STIs, sexting and pornography. Year 10 covered different types of families, parenting skills, risk of STIs, sexting, pornography, tackling transphobia and homophobia, and managing romantic relationships. Year 11 students learnt about domestic abuse and forced marriage.
In both schools, there was also some RSE provided outside the classroom. Staff in control school 1 reported that some RSE learning was delivered via assemblies and off-curriculum days. Assemblies could involve external speakers, according to the school nurse. However, students in control school 1 reported that no external speakers came to assemblies for RSE. In control school 2, the SLT lead and year 9 students reported that an external charity came in to lead some assemblies, for example on gender identity and legal issues in sexual relationships.
In terms of student views, a focus group with students in control school 1 suggested that most sex education was actually taught in religious education (marriage, relationships, cheating, same-sex relationships) or science (anatomy, fertility and contraception, STIs). Students commented that provision varied greatly between teachers:
We haven’t really done much PSHE.
I don’t think it’s every week. I think it’s like every, once a term.
Yeah. Like we barely do it really. Like we did one the other day about like puberty and stuff but we haven’t really done, we’ve done about like three lessons on it.
I think we learn about growing up. We don’t learn about like sex education.
Control school 1, year 9 students in focus group
Students reported that some tutors appeared ill-informed and underprepared, and awkward teaching RSE and went rapidly through their slides asking students to copy down the information:
Like they go through slides and stuff but they go over like puberty and things like that but they don’t go through like sex education. And even if they do get like a slide show about it they just kind of go through the slides really quick.
Control school 1, year 9 student in focus group
Another commented:
They just, like they don’t really know about the topic before they teach it so they kind of just look at when the slides are up, they just look at it and then just say what’s on there. Like they need to know more about the situations and stuff.
Control school 1, year 9 student in focus group
Students complained about one teacher who told a student off for asking too many questions in RSE. However, students also reported that some teachers were good RSE educators. Such teachers were more confident and comfortable, and more prepared to engage in discussion and practical demonstrations (for example, of condom use). Students said of one particularly well-regarded teacher:
He like told us like everything.
He used to just tell us straight, like he didn’t sugar coat it or anything like.
He kept it real. He kept it like as a teacher like in the right boundaries but he told us straight up like.
Control school 1, year 9 student in focus group
Students in control school 2 were much more positive about RSE, and about their school and teachers in general. They reported that they had learnt about contraception, pornography, relationships, consent, STIs and LGBTQ rights, largely in weekly PSHE lessons in tutor time, but also with some learning in science (e.g. conception) and religious education lessons (e.g. different faiths’ teachings on sex and relationships). Students were particularly enthusiastic that those teaching them RSE had been trained, which they felt enhanced both their expertise and communication skills:
It’s trained.
There’s trained teachers that teach.
Trained teachers particularly like just teach us about these different things.
Control school 2, year 9 student in focus group
Some students preferred RSE to be taught by staff other than their form tutors because this enabled students to know there was an additional teacher from whom they could get support if needed. Other students preferred non-form tutors because they wanted RSE to be taught by someone not responsible for behaviour and other aspects of students’ lives at the school:
I feel like form tutors deal with our behaviour. So, say if someone’s messing about in lessons, they will talk about behaviour, they will talk about what you’re doing in school, your lessons. And I feel like if you’re going to talk about them, they’re still very open. Like my form tutor she’s like really, like she’ll talk to us about anything really. But something about like SRE, I just feel a bit awkward to talk to her about that kind of stuff, because we talk to our form tutors about different things. And then because SRE just is like a little bit of a different kind of subject, it’s a bit awkward talking to a teacher that you talk about with educational, other educational purposes, yeah.
Control school 2, year 9 student in focus group
However, some students were happy with RSE being provided by form tutors as long as the tutors were trained and comfortable with this role.
There were also some whole-school activities addressing sexual health in control schools. Control school 1 had posters and displays, for example about safeguarding and LGBTQ inclusion. The deputy head teacher said that there were some student-led campaigns that touched on some aspects of sexual health, such as transgender inclusion, but the deputy head teacher as well as the head of year 8 said that there were not, generally, student-led campaigns centrally focused on sexual health. In control school 2, the SLT and PSHE leads reported that their RSE programme included a survey of students to assess need and inform future provision:
There’s definitely elements, for example FGM, where lots of students said they don’t know about that. And that’s obviously something that we need to then obviously look at and incorporate. Well, we’re going to incorporate anyway but it’s interesting to know what they do and they don’t know.
Control school 2, SLT lead
Questions asked about personal hygiene, FGM, consent, contraception, LGBTQ identities, sexting, pornography and managing romantic relationships. Control school 2 had also engaged in work with teachers across the school to normalise the use of inclusive language, for example to recognise same-sex relationships, which was confirmed by students. The SLT lead also referred to the RSE programme enabling students to design leaflets and posters, and to lead assemblies on sexual health, including drama skits.
Sexual health services in both control schools were patchy. Control school 1 had a well-being centre staffed by a school nurse who also had safeguarding responsibilities. The nurse reported that students were generally referred to external services rather than providing STI testing and contraception on site. She reported that she initiated conversations with students who were in relationships at school:
I mean a lot of the students you know, we’re aware of them being in relationships with each other. We will often talk to them if we hear kids talk, you know, about that and make sure that they are practising safe sex, etc. and then pointing them in that direction.
Control school 1, school nurse
Students, however, reported that they were uncomfortable discussing sexual health or pregnancy with school staff, and would not access contraception or pregnancy tests via the well-being centre. They were concerned about the maintenance of confidentiality in the school and there were stories of students being visibly removed from classrooms as a result of safeguarding responses after students had disclosed sexual activity. Students commented:
I feel like if you were to go to them, it’s not really that confidential. So, like if you told them like ‘Oh, someone like did this’ then obviously they tell the other safeguarding, who tell like the well-being, who tell your parents. And then, before you know it, like everyone knows, which is like the last thing you want. And they pull you out of lesson in front of everyone. It’s just like . . . Like they just do it in front of everyone and then people like listen in on conversations. And it’s just like really like not confidential at all.
Control school 1, year 9 student in focus group
In control school 2, there was no sexual heath provision on site. Pregnancy tests, and routine or emergency contraception were not available at the school. There were sexual health services relatively nearby and these were advertised to students via assemblies led by the clinic, which year 9 students did recall. Staff reported that any disclosures of sex by students < 16 years would be shared with parents.
Economic evaluation
Intervention costs
Positive Choices comprises the following intervention components:
-
staff training delivered by SEF
-
in setting up and delivering the SHPC
-
in curriculum delivery
-
in facilitating student-led social marketing.
-
-
SHPC meetings
-
10 hours of classroom lessons comprising eight ‘essential lessons’ and two ‘add-on’ lessons chosen by each school
-
student-led social marketing
-
parent information
-
sexual health services review.
We undertook a detailed cost analysis of each component, focusing on the staff costs incurred. Costs were measured from the perspective of the public and voluntary sectors, and valued in 2018–19 Great British pounds. We estimated additional costs per school, over and above those of usual practice, and focused on opportunity costs (i.e. the cost of the resources used, irrespective of whether or not they were directly purchased for the study).
Staff training
For the SEF training of school staff, data were obtained from the trainers on time spent at each individual session on curriculum training and SHPC training. At two schools, curriculum and SHPC training were delivered on the same day. Using the data from the schools where it was delivered separately, the mean total trainer time per school to deliver curriculum training and SHPC training including preparation, travel and delivery time was 12 hours 52 minutes and 12 hours 15 minutes, respectively (Table 35). The daily rate per trainer was £610 plus VAT (Lucy Emerson, NCB, 2019, personal communication). Assuming an 8.5-hour working day, the hourly cost per trainer was £86.12, and the mean cost per school was £1108 for the curriculum training and £1055 for the SHPC training. In addition, on average. 4.5 members of school staff attended the curriculum training for an average of 3 hours 45 minutes and three attended SHPC training for an average of 1 hour 45 minutes. We did not collect data on the grade of each staff member attending training; assuming each staff attendee was paid at the maximum value of the upper pay range for classroom teachers (£39,406 per year)62 and worked 1265 hours per year of directed time,62 the hourly rate was £31.15. The mean cost per school for staff attendance for curriculum training was therefore £526; for the SHPC training, it was £164. Combining trainer and school staff costs, the mean cost per school was therefore £1634 for curriculum training and £1219 for SHPC training. The social-marketing training comprised a teleconference lasting 2 hours with the SEF trainer and one staff member from each school. Assuming 2 hours’ preparation time for the trainer, the trainer costs were £344.47; the school staff costs were £249.20, giving a total cost across the four schools of £593.67 and a mean cost per school of £148.42. The mean cost per school for all three types of training combined was therefore £3001.
| Activity | Intervention school | Total | Mean | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Curriculum training | ||||||
| Trainer preparation time (hours:minutes) | 2:00 | 2:30 | 4:30 | 2:15 | ||
| Trainer travel time (hours:minutes) | 7:00 | 6:45 | 13:45 | 6:52 | ||
| Trainer delivering training (hours:minutes) | 3:30 | 4:00 | 7:30 | 3:45 | ||
| Number of staff attending | 5 | 4 | 9 | 4.5 | ||
| SHPC training | ||||||
| Trainer preparation time (hours:minutes) | 2:30 | 2:00 | 2:00 | 6:30 | 2:10 | |
| Trainer travel time (hours:minutes) | 6:45 | 5:00 | 13:15 | 25:00 | 8:20 | |
| Trainer delivering training (hours:minutes) | 2:15 | 1:30 | 1:30 | 5:15 | 1:45 | |
| Number of staff attending | 4 | 3 | 2 | 9 | 3 | |
| Combined curriculum + SHPC training | ||||||
| Trainer preparation time (hours:minutes) | 2:00 | 2:00 | 2:00 | |||
| Trainer travel time (hours:minutes) | 10:15 | 10:15 | 10:15 | |||
| Trainer delivering training (hours:minutes) | 5:15 | 5:15 | 5:15 | |||
| Number of staff attending | 5 | |||||
School health promotion council
Costs were also included for each school implementing the SHPCs, using logbooks completed by teachers. Data were obtained from three intervention schools including staff preparation time (assuming preparation time involved a single staff member). Each school held three implementation meetings, with durations and numbers of staff present as shown in Table 36. Assuming an hourly cost for school staff of £31.15 (see Staff training), the costs of staff time in schools 1, 3 and 4 were £253, £132 and £548, respectively, giving a mean cost per school of £311.
| Resource use | Intervention school | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||||
| Meeting number | 1 | 2 | 3 | Mean | 1 | 2 | 3 | Mean | 1 | 2 | 3 | Mean |
| Staff preparation time (minutes) | 40 | 40 | 20 | 33 | 45 | 30 | 10 | 28 | 120 | 120 | 120 | 120 |
| Meeting duration (minutes) | 50 | 50 | 45 | 48 | 60 | 60 | 50 | 57 | 60 | 60 | 55 | 58 |
| Number staff present at meeting | 3 | 3 | 2 | 2.7 | 1 | 1 | 1 | 1 | 4 | 4 | 4 | 4 |
Curriculum delivery
The Positive Choices intervention also included 10 hours of lessons (eight ‘essential’ lessons and two ‘add-on’ lessons chosen by each school from a selection of topics). We calculated the cost of this component based on the amount of classroom teacher time required to prepare and deliver the lessons, as recorded in logbooks completed by teachers. Data were collected from three intervention schools on the number of times each session was run by a school, the planning time needed for each lesson by the classroom teacher and the mean duration of each session (Table 37). We assumed that the planning time for each lesson was only incurred once per individual teacher, irrespective of the number of times the lesson was taught by each teacher, and calculated the total teacher time per school for each of the essential lessons. The mean total teacher time per school was 596 minutes. Assuming an hourly cost for school staff of £31.15 (see Staff training), and that the two add-on lessons had the same mean duration and planning as the essential lessons, the mean total cost per school was £3096.
| Lesson | Mean number of times lesson runs per school | Planning time per lesson (minutes) | Mean number of teachers providing lessons | Mean duration per lesson (minutes) | Total teacher time per school (minutes) |
|---|---|---|---|---|---|
| 1 | 6 | 45 | 4 | 60 | 540 |
| 2 | 7 | 30 | 4 | 60 | 540 |
| 3 | 8 | 30 | 4 | 60 | 600 |
| 4 | 9 | 30 | 4 | 60 | 660 |
| 5 | 10 | 25 | 4 | 60 | 700 |
| 6 | 7.5 | 20 | 4 | 60 | 530 |
| 7 | 8 | 30 | 4 | 60 | 600 |
| 8 | 8 | 30 | 4 | 60 | 600 |
Student-led social marketing
Costs were also incurred by each school through implementing the student-led social marketing, measured using logbooks completed by teachers, because it involved school staff time. Data were obtained from three intervention schools, including staff preparation time. Each school held three sessions, with preparation and delivery time and numbers of staff present as shown in Table 38. Assuming an hourly cost for school staff of £31.15 (see Staff training), the costs of staff time in schools 1, 3 and 4 were £93, £187 and £179, giving a mean cost per school of £153.
| Resource use | Intervention school | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Number of meetings | 3 | 3 | 7 |
| Mean staff preparation per meeting time (minutes) | 30 | 20 | 15 |
| Mean duration per meeting (hours:minutes) | 0:30 | 1:40 | 1:35 |
| Mean number staff present at meeting | 1 | 1 | 1 |
Parent information
At each intervention school, three newsletters were sent home to parents to explain project progress. Data were not collected in the present study on the resources incurred by these activities. We assume that these were sent electronically at negligible cost, and that each newsletter took 1 hour to produce by a teacher. Assuming an hourly cost for school staff of £31.15 (see Staff training), the mean cost per school was estimated to be £93.
Sexual health services review
Using logbooks completed by teachers, schools were asked to record the amount of staff time used to facilitate each step of the sexual health services review, which was included in the intervention cost. Three schools returned data and the amount of staff time for each school was 2 hours 30 minutes, 2 hours 40 minutes and 7 hours 30 minutes, respectively. The mean staff time per school for the review was, therefore, 4 hours 13 minutes. Assuming an hourly cost for school staff of £31.15 (see Staff training), the mean cost per school was estimated to be £132.
Total intervention cost
Combining the costs of each intervention component, the mean intervention cost per school was estimated to be £6786 (Table 39); the two intervention components contributing the most to this total were the staff training (44%) and the curriculum delivery (46%).
| Intervention component | Mean cost per school, £ (% total) |
|---|---|
| Staff training | 3001 (44) |
| SHPC | 311 (5) |
| Curriculum delivery | 3096 (46) |
| Student-led social marketing | 153 (2) |
| Parent information | 93 (1) |
| Sexual health services review | 132 (2) |
| Total | 6786 (100) |
Additional findings from policy and practitioner consultation not related to intervention optimisation
At the policy and practitioner event held on 9 March 2018, as well as the information collected to inform intervention optimisation, broader feedback was collected on the study aims and approaches. Some participants raised concerns that the timeline between schools finding out if they were allocated to the intervention group and schools implementing the intervention would leave little time for planning for intervention schools. Although this could not be adjusted for the pilot, this is something to consider for a full trial.
Participants also expressed enthusiasm that the research ultimately would aim to use realist approaches within an RCT design to understand underlying mechanisms of action and how these varied with context, rather than merely to determine the overall effectiveness of the intervention. Participants suggested that the former was useful for developing transferable learning for other programmes. They also valued the focus on evaluating implementation and exploring how the intervention interacted with and was shaped by existing school practices, particularly in the light of new statutory RSE guidance for England from 2020. It was suggested that disseminating findings on the implementation of the Positive Choices intervention might usefully inform implementation of the new guidance.
Stakeholders also supported the inclusion of a different primary outcome in any future Phase III RCT because unintended teenage pregnancy was perceived as too narrow and less relevant in the current context of declining prevalence of teenage pregnancy and increasing concerns about other outcomes, such as non-volitional sex, and dating and relationship violence. Participants favoured more comprehensive sexual health measures, such as sexual competence and sexual well-being. Other possible secondary outcome measures such as school attendance and attainment were also suggested, which would be important evidence for schools in deciding whether to scale up the intervention after a Phase III trial. A full summary of this policy and practitioner event is provided in Report Supplementary Material 8.
A further policy and practitioner event was held on 14 June 2019 to disseminate interim findings from the study. A summary of this event is supplied in Report Supplementary Material 9. A further meeting scheduled with the policy and practice stakeholder group will focus on interpreting the results and the implications of the study, mechanisms for knowledge exchange and future research.
Chapter 6 Discussion
Summary of key findings
Our first research question was whether or not it is possible to optimise Positive Choices in collaboration with SEF, a secondary school and other stakeholders. Intervention optimisation involved the elaboration of the intervention, developing it from a basic description to a fully specified intervention with materials. Initial elaboration was informed by existing systematic reviews, Safer Choices, CAS Carrera and Gatehouse Project evaluations and materials from Safer Choices and other interventions and resource packages. Draft intervention materials were produced. The purpose of the needs survey came to focus on the selection of curriculum lessons for each school. The SHPC’s work was focused on reviewing student needs data to inform decisions, launching the intervention, selecting the ‘add-on’ curriculum topics, selecting staff to attend training, overseeing the social-marketing team and parent newsletters, and reviewing school sexual health services. The curriculum was broadened slightly to ensure that it was comprehensive while still addressing all of the topics in the protocol. The curriculum was initially designed to include a set of five ‘essential’ lessons to be covered by all schools plus a bank of 10 ‘add-on’ lessons, five of which could be selected by the school. The curriculum was later refined to include eight ‘essential’ lessons and a bank of five ‘add-on’ lessons from which two would be chosen. Social-marketing methods were elaborated and it was decided to avoid segmenting student audiences on factors other than age, informed by SEF and other advice. Sexual health review methods were elaborated, with this being reoriented to guided school self-review rather than SEF-led review to ensure efficiency and sustainability. Initial consultation with the collaborating secondary school, the ALPHA young researchers’ group and the other stakeholders demonstrated support for these decisions. School staff asked that materials be concise and easy to use. ALPHA participants suggested refinements to the wording of questions on the needs survey, and offered practical suggestions for the launch of Positive Choices in schools and other elements.
Our second research question was whether or not it is feasible and acceptable to implement each component of this intervention in the secondary school involved in optimisation, and what refinements are suggested. The school involved experienced a poor inspection which resulted in repeated changes in leadership and a refocusing on teaching and behaviour, leading to reduced SLT commitment to Positive Choices. However, overall implementation met fidelity targets and acceptability of the intervention was 100%, assessed via staff and student interviews. Only the curriculum element was delivered with suboptimal fidelity, reflecting challenges in identifying staff and time for lessons. The SSC and NIHR approved progression to the pilot RCT.
Our third research question was whether or not, in the light of a pilot RCT across six schools, progression to a Phase III RCT is justified in terms of prespecified criteria. The first criterion was that the intervention was implemented with fidelity in three or four out of four intervention schools. Limited data received from implementation school 2 meant that a rigorous assessment of overall fidelity for this school could not be made. Based on the data received, the target of 70%+ implementation of essential elements in three schools was achieved. The SHPC and student-led social-marketing training were implemented with fidelity in all four schools. The curriculum training, the SHPC meetings, the curriculum lessons, student-led social-marketing meetings and the sexual health services review were implemented with fidelity in three out of four schools. The second criterion was that the intervention is acceptable to a majority of students and staff involved in implementation. Of students reporting awareness of the programme, around 80% reported acceptability. Students in the intervention arm reported much more comprehensive coverage of RSE topics than did students in control schools. Interviews with staff and students involved in implementation indicated predominantly positive views. The third criterion, that randomisation occurs and five or six out of six schools accept this and continue within the study, was met, with all schools being randomised and retained. The fourth criterion, that student questionnaire follow-up rates are ≥ 80% in five or six out of six schools, was also met with overall responses > 80% in both arms at both surveys, and with only one school having a response rate < 80%. The fourth criterion, that linkage of self-report and routine administrative data on pregnancies is feasible, was also met. There were no births or abortions among the trial cohort based on exact or approximate matching.
Our fourth research question was whether or not secondary outcomes and covariate measures are reliable, and what refinements are suggested. Questions on secondary outcomes were included only at follow-up on the advice of the ethics committee, precluding analysis of test–retest reliability (which, in retrospect, would have been a poor test of reliability given rapid transitions in behaviour among early adolescents). Completion rates were high for all items, except for those on age at sexual debut and partner numbers (with lower completion for these items probably because of the use of free-text responses), and contraception at last vaginal sex (possibly because of issues with question routing). There was poor discrimination for these measures in the sense of identifying a sizeable subgroup of participants reporting certain outcomes. This probably reflected the truncated period of follow-up and, therefore, the young age of participants in this pilot RCT in comparison with any future Phase III RCT. Most potential mediators were assessed at baseline and follow-up (sexual competence only being assessed at follow-up on the advice of the ethics committee). Unsurprisingly, test–retest reliability was low for potential mediators; as indicated above, this probably reflected rapid transitions in early adolescence. Inter-item reliability was, however, generally high. Where this was not so, for perceived behavioural norms, sexual health knowledge and sexual health access, this probably reflected that these measures included items focused on different phenomena.
Our fifth research question was ‘At what rates are schools recruited to and retained in the RCT?’. We used a low-intensity recruitment strategy reflecting our need to secure the involvement of only six schools. Of the 334 schools invited, 11 expressed interest and eight provided consent, of which six were recruited with one dropping out and being replaced quickly. All six were then retained in the study.
Our sixth research question was ‘What level of student reach does the intervention achieve?’. Around two-thirds of students in the intervention arm reported awareness of the programme. Much higher proportions of students in intervention schools than in control schools reported coverage of RSE topics. Awareness was lower among students from ethnic minorities or of low SES.
Our seventh research question was ‘What do qualitative data suggest in terms of intervention mechanisms and refinements to programme theory and theory of change?’. Interviews with students suggested that the curriculum and social-marketing components had brought students together, enabling them to learn together and have more open conversations about sexuality and sexual health. Staff interviews similarly suggested that the intervention could enhance staff–student relationships and increase engagement among less academic students. Staff also highlighted synergies between the intervention components. Some students saw the intervention as providing ‘the basics’ of knowledge, which could provide the foundation for broader transformations in attitudes and behaviours. Several students indicated that the curriculum had raised awareness of their rights within relationships, particularly their right to say ‘no’ to unwanted sexual activities. These insights support the existing theory of change with its emphasis on sexual health knowledge and self-efficacy, and also suggest that the theory might be broadened to include improving relationships between and among students and staff as a potential mechanism for increasing engagement with intervention content and with school more broadly.
Our eighth research question was ‘How do contextual factors appear to influence implementation, receipt and mechanisms of action?’. Staff interviews suggested several factors as promoting good implementation: leadership commitment to PSHE and the intervention; RSE becoming statutory in English schools; personal commitment among staff responsible for implementation; and trusting relationships between staff delivering the intervention. Similarly, there was evidence from student accounts that schools in which PSHE and RSE already seemed to be valued by the school were more able to implement Positive Choices well. Where schools struggled to provide committed teachers for Positive Choices lessons, students felt that lessons were less successful, particularly where a school delivered the curriculum during one ‘drop-down’ day. Established processes for communication between staff and students, for example via student councils, may have made the SHPC and social marketing easier to set up and run in some schools. Schools struggled with the timetable imposed by the RCT. Schools learnt whether they were allocated to the intervention or control group in the summer term and were then expected to implement the intervention from the following autumn term. We found it unrealistic to expect schools to staff and timetable RSE lessons with so little lead-in time.
Our ninth research question was whether or not any potential harms are suggested and how might these be reduced. No harms to students were apparent from student or staff accounts. The possibility of increased stress for staff experiencing fertility issues or not comfortable teaching RSE were raised in staff interviews.
Our tenth research question was ‘What sexual health-related activities occur in and around control schools?’. Some aspects of sexual health provision in control schools resembled those offered in Positive Choices. In both schools, teachers delivered RSE largely in form time. However, in neither school did the total time devoted to RSE approach that offered in Positive Choices. Staff training in control schools was also less than in the intervention. The comprehensiveness, quality and acceptability to students of teaching appeared to differ between the two control schools. In one, actual provision appeared to fall short of what was aimed for in terms of the topics covered and classroom approaches used, with many teachers taking a cursory approach, which was largely rated badly by students. In the other school, lessons were much more comprehensive, addressing a breadth of topics similar to that in Positive Choices, with more participative teaching methods and greater acceptability to students. Neither school had a staff/student committee which co-ordinated sexual health activities, but there was some evidence that RSE was discussed at the student council in at least one of the schools. One school used a student survey similar to that used in Positive Choices to inform RSE planning. Neither school explicitly used student-led social marketing to promote sexual health across the school, but one school did include some student-led posters and assemblies. Both control schools had little or no on-site sexual health services. Both marketed local sexual health services to students, but with variable impact. Both schools had revised sexual health provision at around the time they were recruited into the trial and allocated to the control group.
Our eleventh research question was whether or not methods for economic evaluation in a Phase III RCT are feasible. We found that it would be feasible to conduct economic evaluation of the Positive Choices intervention, based on the idea that this would comprise a cost–consequences analysis from a public sector plus voluntary sector perspective. The evaluation should ideally include assessment of the potential consequences affected by the intervention, for example the primary and secondary outcomes associated with the intervention and health-related quality of life, and the potential costs associated with the intervention, including the mean cost of the intervention per school and the intervention impact on use of services and other costs relating to its consequences. This pilot study has shown that it would be feasible to collect a range of quantitative outcomes suitable for inclusion in a cost–consequences analysis including pregnancy (unintended and not) in girls; initiation of pregnancy in boys; incidence of STIs; vaginal sexual debut with partner of opposite sex; sexual debut with partner of same sex; age at sexual debut; number of heterosexual partners; contraception at first vaginal sex; contraception at last vaginal sex; non-volitional sex; and health-related quality of life measured using the CHU9D. Some of these measures (e.g. pregnancy) may not be informative for evaluating the intervention because of low and declining prevalence, but they are feasible to collect. Other measures identified as potentially relevant, but not tested in this study, are measures of dating violence and sexual well-being. We determined that it would be feasible to calculate the mean costs of the intervention per school, accounting for each of the main intervention components.
A full account of the net cost of the intervention would also include its impact on use of services and other costs, arising from the consequences associated with the intervention. Based on the data collected in the present study, these are likely to arise from impacts on teenage pregnancies, STIs, and dating and relationship violence, as well as costs associated with detriments to mental well-being arising from unhealthy relationships. There is UK evidence of the health and other public sector costs associated with some of these outcomes,63–65 but further work would be beneficial to quantify these costs.
Deviations from protocol
Deviations from the protocol are listed in Table 40. In terms of the intervention, the needs assessment data were not used by SHPCs to select in what order to deliver modules; whether to deliver within PSHE, tutor groups or integrate into other lessons; and whether to use materials from Positive Choices or existing materials if these conformed to our curriculum. This was because SEF advised that in practice not all of these things would be likely to be open to influence by the needs data or the SHPC. The needs assessment was instead used to inform the selection of the add-on curriculum lessons for each school. It was agreed that segmentation and targeting for student-led social marketing would only be considered on the basis of year group and that membership of the student-led social-marketing team should focus students from years 8 to 11. SEF did not themselves review school sexual health services to schools. A more efficient and sustainable approach was for SEF to develop an audit tool that schools could use to carry out their own reviews.
| Deviation | Rationale |
|---|---|
| Needs survey of year 8 students would not be used by SHPCs to select in what order to deliver modules; whether to deliver within PSHE, tutor groups or integrate into other lessons (e.g. English); and whether to use materials from Positive Choices or existing materials if these conformed to our curriculum | SEF advised that in practice not all of these things would be likely to be open to influence by the needs data or the SHPC |
| Needs data were used to inform the selection of five out of eight possible ‘add-on’ curriculum lessons for each school | To ensure that SHPCs still had flexibility to align learning with the needs of their students while maintaining intervention coherence and alignment with the theory of change |
| Social-marketing campaigns were not targeted based on consumer segmentation other than in terms of year group | Such segmentation was considered likely to be offensive and stigmatising to some students |
| Rather than themselves reviewing school sexual health services to schools, SEF developed an audit tool that schools could use to carry out their own reviews and make recommendations to improve and promote services on an ongoing basis | This was considered a more efficient and sustainable approach |
| The ICC test–retest was not performed as planned for sexual debut | Although this was measured at both baseline and follow-up, the wording of the questions was not congruent, at baseline examining sexual debut regardless of whether partners were same- or opposite-sex at baseline, whereas at follow-up examining sexual debut separately by partner type |
| We did not attempt to pilot moderator analyses (how effects vary by SES, sex, ethnicity and baseline risk) | Our experience in an earlier study indicated that such analyses would be so drastically underpowered as to be completely meaningless |
| Intention-to-treat analyses were longitudinal rather than repeat cross-sectional | This was to adjust for baseline student-level potential confounders (SES, sex, ethnicity, age) |
In terms of the research, the ICC test–retest was not performed as planned for sexual debut. Although this was measured at both baseline and follow-up, the wording of the questions was not congruent; however, this was a minor deviation given that the student cohort was mid-way through adolescence and longitudinal inconsistency in measurement at an interval of 12 months might reflect adolescent development trajectories rather than limitations in measure reliability. We did not attempt to pilot moderator analyses because our experience in an earlier study indicated that such analyses would be so drastically underpowered as to be completely meaningless. 58 Intention-to-treat analyses were longitudinal rather than repeat cross-sectional so that these could adjust for baseline student-level covariates. The original protocol’s reference to a cross-sectional analysis adjusting for student-level covariates was in error.
Other limitations
Optimisation and feasibility testing with the school collaborating on this phase was limited by a poor inspection report and repeated changes in school leadership leading to reduced commitment from the school. This meant that consultation was limited to one rather than three waves and feasibility testing was challenging.
In the pilot RCT, most elements of the evaluation had very good response rates but there were problems in one school, again reflecting management challenges experienced by the school, which did not return satisfaction surveys for one training event or staff logbooks for any intervention component. This hampered the assessment of intervention fidelity in this school.
In retrospect, our use of simple ‘stop’/‘proceed’ progression criteria was too crude. It would be more appropriate for external pilot studies such as this one to use criteria which allow for ‘stop’/‘proceed immediately’/‘proceed with refinements’, where the thresholds of success for ‘proceed with refinements’ might, for example, be lower than for ‘proceed immediately’.
Our pilot RCT was focused on questions of feasibility and acceptability. The small number of schools limited statistical power and baseline comparability. This and the reduced period of intervention and follow-up in comparison with that anticipated in a future Phase III RCT meant that the pilot should not be used to estimate intervention effects.
Conclusions
Implications for research
The criteria for progression to a Phase III RCT were achieved. In general, Positive Choices was well delivered, highly acceptable to staff and students, and distinctive from the provision in control schools, particularly in terms of the quality of training and materials, and in its whole-school components such as the SHPC and social marketing. Students in the intervention arm reported much more comprehensive coverage of RSE topics than those in control schools. Now is an auspicious time for a rigorous study of the effects of such a programme, with the advent of statutory RSE for all secondary schools in England from 2020.
Further work is needed to refine Positive Choices. Refinements should include the development of curriculum materials for year 10 students. Our original proposal and protocol made clear that the intervention that was to be subject to a Phase III RCT should include lessons for year 10, but that the pilot RCT was to focus only on year 9s to reduce costs and the time required for piloting. As suggested in interviews with SEF staff, it may also be necessary to provide curriculum materials for schools to use with students in years 7, 8 and 11 even though the intervention cohort in a trial would proceed through years 9 and 10 only. This is because, with the advent of statutory RSE, schools that might be interested in participating in the trial may be seeking comprehensive interventions that meet statutory requirements. Positive Choices could incorporate existing materials developed by SEF to address this. Further work is also required to build SLT commitment to the intervention and facilitate schools’ timetabling and staffing of curriculum delivery, which might take the form of start-up meetings with school leaders instead of the existing training for SHPCs, as suggested by SEF staff. A train-the-trainer model should be considered as an alternative to direct training of all staff involved in delivery on the basis of both efficiency and building schools’ capacity for intervention sustainability. Consideration should also be given to whether existing school meetings could be used to conduct SHPC business rather than necessarily convening a new structure of meetings. SEF staff also recommended revising the intervention so that materials include case studies of successful work from the pilot, and including elements aimed at ensuring schools maintain momentum (e.g. self-evaluation elements so that schools can assess progress). Our pilot suggested that the intervention theory of change was appropriate, but that this might be refined to encompass enhanced relationships among and between staff and students as a means of increasing school engagement among less academic students. These resonate strongly with the theory of human functioning and school organisation, which might, therefore, usefully inform the theory of change. 66 Further patient and public involvement with young people should explore ways of increasing awareness among students from ethnic minorities and of low SES.
The pilot study found that trial methods were feasible, but suggests several ways in which they could be refined for a Phase III RCT. Routine data on births and abortions, although feasible to collect (albeit with assent to data linkage slightly below 80% among female trial participants), do not make for an appropriate primary outcome. There were no births or abortions among the trial cohort drawing on routine data based on exact or approximate matching. Prevalence of teenage pregnancy is now so low nationally that powering a primary analysis based on births and abortions would require a very large sample size. The < 18 years conception rate in England and Wales has reduced by 62% since 1998. In 2017, the conception rate was 17.9 per 1000 women aged 15 to 17 years, a 14.7% decrease from 21.0 in 2015. This fall comprises reductions in births (decreased by 15.5%) and abortions (decreased by 13%) since 2015. 4 Focusing on births and abortions as the primary outcome is also inappropriate given the much broader aims of RSE, which include avoidance of STIs, as well as preparing young people, whatever their sexuality, for healthy, communicative and non-abusive relationships and consensual, safe and pleasurable sex at a point when individuals feel ready for this. Policy and practice stakeholders recommended lack of sexual competence at first sex, assessed using the Natsal measure, as the most appropriate primary outcome. Surveys should involve simpler question routing and use multiple-choice responses for questions on age at sexual debut and numbers of sexual partners. There should be a longer lead-in time between schools finding out that they have been allocated to the intervention group and being expected to start implementing the intervention. It was determined that an economic evaluation in the form of a cost–consequences analysis, as described, is likely to be feasible. However, further research is warranted, especially in terms of identifying the costs associated with the potential consequences of the intervention. Any Phase III trial should include boys-only schools (which were excluded from the pilot to enable it to assess the feasibility of linkage to administrative data on births and terminations among girls). The trial would assess health inequalities via assessing moderation by factors such as SES, gender, ethnicity and sexual orientation.
Implications for policy
In terms of broader learning about school-based sexual health interventions, the study provided a number of insights. To our knowledge, the pilot study provides the first evidence that a multicomponent, whole-school intervention to promote sexual health is feasible to deliver in secondary schools in England. Although such interventions have been delivered to address bullying,67 our previous study of a whole-school intervention to address dating and relationship violence suggested that this was not feasible because the topic was not sufficiently central to school priorities to ensure commitment. 58 Particularly with RSE becoming statutory in English schools, this study suggests that schools were sufficiently committed to the broader topic of sexual health to enable them to commit to implementing a whole-school intervention. Our results also suggest that delivery of RSE by existing teachers is potentially acceptable to students where teachers are committed and trained, in contrast to previous research suggesting that external providers are more acceptable in terms of expertise and boundaries. 68 However, our results also suggest that some teachers are unwilling to teach, or are uncomfortable teaching, RSE because this conflicts with some of their own values or they lack the confidence or skills to teach certain topics or use more discursive teaching styles that are suited to the subject matter.
Our findings about the contextual factors affecting implementation align with previous theory and research, which suggest the importance to implementation of processes of interventions becoming understood, committed to, worked on collectively and reflected on, as well as the importance of senior staff commitment. 55,69 Our results contribute to this literature by looking at factors that might be especially important for whole-school sexual health interventions in schools such as the broader status of RSE within a school and in government policy, and the personal commitment to sexual health education among staff responsible for implementation.
Acknowledgements
We would like to thank SEF for their work in developing and supporting implementation of the intervention. We would also like to thank the members of the SSC for their feedback on the study design and methods, and the ALPHA young researchers’ group as well as the stakeholder group of practitioners and policy-makers for their feedback on the intervention and methods. We are also grateful to Professor Karin Coyle of ETR Associates for her advice and guidance on intervention development and implementation. Finally, we would like to thank the students and staff at the schools taking part in optimisation, feasibility testing and the pilot trial for their contributions and support.
Contributions of authors
Ruth Ponsford (https://orcid.org/0000-0003-2612-0249) (Assistant Professor, LSHTM) and Sara Bragg (https://orcid.org/0000-0002-0377-5843) (Research Fellow, LSHTM) managed the trial and data collection.
Ruth Ponsford, Sara Bragg, Steve Morris (https://orcid.org/0000-0002-5828-3563) (RAND Professor of Health Services Research, University of Cambridge) and Chris Bonell (https://orcid.org/0000-0002-6253-6498) (Professor of Public Health Sociology, LSHTM) contributed to the initial drafting of the manuscript. The drafting was led by Ruth Ponsford.
Elizabeth Allen (https://orcid.org/0000-0002-2689-6939) (Professor of Medical Statistics, LSHTM), Charles Opondo (https://orcid.org/0000-0001-8155-4117) (Assistant Professor, LSHTM) and Diana Elbourne (https://orcid.org/0000-0003-3044-4545) (Professor of Healthcare Evaluation, LSHTM) developed the statistical analysis plan.
Elizabeth Allen oversaw the statistical analysis.
Nerissa Tilouche (https://orcid.org/0000-0002-2668-8881) (Administrative Officer, LSHTM) and Rebecca Meiksin (https://orcid.org/0000-0002-5096-8576) (Research Fellow, LSHTM) supported data collection and analysis.
Lucy Emmerson (Director, NCB SEF) advised on intervention design.
Laura Van Dyck (https://orcid.org/0000-0002-5720-8633) (Data Manager, LSHTM) and Joanna Sturgess (https://orcid.org/0000-0001-7312-4598) (Research Fellow, LSHTM) managed the student survey data.
Steve Morris designed and conducted the economic evaluation.
Elizabeth Brocklehurst (Analyst, DHCS) collaborated on data linkage.
Alison Hadley (https://orcid.org/0000-0002-1489-9825) (Director, Teenage Pregnancy Knowledge Exchange, University of Bedfordshire) advised and facilitated policy consultation.
GJ Melendez-Torres (https://orcid.org/0000-0002-9823-4790) (Professor of Clinical and Social Epidemiology, University of Exeter), Honor Young (https://orcid.org/0000-0003-0664-4002) (Senior Lecturer, Cardiff University), Maria Lohan (https://orcid.org/0000-0003-3525-1283) (Professor of Social Science and Health, Queen’s University Belfast), Catherine Mercer (https://orcid.org/0000-0002-4220-5034) (Professor of Sexual Health Science, University College London) and Rona Campbell (https://orcid.org/0000-0002-1099-9319) (Professor of Public Health Research, University of Bristol) advised on methods, and provided edits to and comments on drafts of the report.
Chris Bonell was the PI, conceived of the trial and led the trial design, overall analysis plan and funding application.
All authors contributed to the design of the trial and its procedures. All authors read and approved the final manuscript.
Data-sharing statement
Requests for access to survey data should be addressed to the corresponding author. Qualitative data generated are not suitable for sharing beyond that contained within the report. Further information can be obtained from the corresponding author.
The births analysis presented in Chapter 4 was produced using statistical data from ONS. The use of the ONS statistical data in this work does not imply the endorsement of the ONS in relation to the interpretation or analysis of the statistical data. This work uses research data sets that may not exactly reproduce National Statistics aggregates.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Ponsford R, Allen E, Campbell R, Elbourne D, Hadley A, Lohan M, et al. Study protocol for the optimisation, feasibility testing and pilot cluster randomised trial of Positive Choices: a school-based social marketing intervention to promote sexual health, prevent unintended teenage pregnancies and address health inequalities in England. Pilot Feasibility Stud 2018;4. https://doi.org/10.1186/s40814-018-0279-3.
- Office for National Statistics . Conceptions in England and Wales, 2012. Statistical Release 2014.
- Wellings K, Palmer MJ, Geary RS, Gibson LJ, Copas A, Datta J, et al. Changes in conceptions in women younger than 18 years and the circumstances of young mothers in England in 2000–12: an observational study. Lancet 2016;388:586-95. https://doi.org/10.1016/S0140-6736(16)30449-4.
- Office for National Statistics . Statistical Bulletin: Conceptions in England and Wales: 2016 Annual Statistics on Conceptions to Residents of England and Wales; Numbers and Rates, by Age Group Including Women Aged Under 18 Years 2019.
- Ashcraft A, Fernández-Val I, Lang K. The consequences of teenage childbearing: consistent estimates when abortion makes miscarriage non-random. Econ J 2013;123:875-90. https://doi.org/10.1111/ecoj.12005.
- Fletcher J, Wolfe B. Education and labor market consequences of teenage childbearing: evidence using the timing of pregnancy outcomes and community fixed effects. J Hum Resour 2009;44:303-25. https://doi.org/10.3368/jhr.44.2.303.
- Ermisch J. Does a ‘Teen-Birth’ Have Longer-term Impacts on the Mother? Suggestive Evidence from the British Household Panel Survey. Colchester: Institute for Social and Economic Research; 2003.
- Berthoud R, Ermisch J, Francesconi M, Liao T, Pevalin DJ, Robson K. Long-Term Consequences of Teenage Births or Parents and their Children. Teenage Pregnancy Research Programme Research Briefing, No. 1. London: Department of Health; 2004.
- Francesconi M. Adult outcomes for children of teenage mothers. Scand J Econ 2008;110. https://doi.org/10.1111/j.1467-9442.2008.00526.x.
- Kneale D, Fletcher A, Wiggins R, Bonell C. Distribution and determinants of risk of teenage motherhood in three British longitudinal studies: implications for targeted prevention interventions. J Epidemiol Community Health 2013;67:48-55. https://doi.org/10.1136/jech-2011-200867.
- Department for Education and Skills . Teenage Pregnancy Next Steps: Guidance for Local Authorities and Primary Care Trusts on Effective Delivery of Local Strategies 2006.
- UK Parliament . Hansard, 10 January 2011 n.d. www.publications.parliament.uk (accessed 1 November 2019).
- Health Protection Agency . Focus on Prevention: HIV and Other Sexually Transmitted Infections in the United Kingdom 2003. Annual Report 2004 2004.
- Independent Advisory Group on Teenage Pregnancy . Independent Advisory Group Response to Government White Paper Choosing Health 2004.
- DiCenso A, Guyatt G, Willan A, Griffith L. Interventions to reduce unintended pregnancies among adolescents: systematic review of randomised controlled trials. BMJ 2002;324. https://doi.org/10.1136/bmj.324.7351.1426.
- Kirby D. Emerging Answers 2007: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted Diseases. Washington, DC: The National Campaign to Prevent Teen and Unplanned Pregnancy; 2007.
- Mason-Jones AJ, Sinclair D, Mathews C, Kagee A, Hillman A, Lombard C. School-based interventions for preventing HIV, sexually transmitted infections, and pregnancy in adolescents. Cochrane Database Syst Rev 2016;11. https://doi.org/10.1002/14651858.CD006417.pub3.
- Andreasen AR. Marketing social marketing in the social change marketplace. J Public Policy Mark 2002;21:3-13. https://doi.org/10.1509/jppm.21.1.3.17602.
- Wakhisi AS, Allotey P, Dhillon N, Reidpath DD. The effectiveness of social marketing in reduction of teenage pregnancies: a review of studies in developed countries. Soc Mark Q 2011;17:56-90. https://doi.org/10.1080/15245004.2010.546941.
- Basen-Engquist K, Coyle K, Parcel GS, Kirby D, Banspach SW, Carvajal SC, et al. School wide effects of a multicomponent HIV, STD and pregnancy prevention program for high school students. Health Educ Behav 2001;28:166-85. https://doi.org/10.1177/109019810102800204.
- Coyle K, Basen-Engquist K, Kirby D, Parcel G, Banspach S, Collins J, et al. Safer choices: reducing teen pregnancy, HIV, and STDs. Public Health Rep 2001;116:82-93. https://doi.org/10.1093/phr/116.S1.82.
- Coyle K, Basen-Engquist K, Kirby D, Parcel G, Banspach S, Harrist R, et al. Short-term impact of safer choices: a multicomponent, school-based HIV, other STD, and pregnancy prevention program. J Sch Health 1999;69:181-8. https://doi.org/10.1111/j.1746-1561.1999.tb06383.x.
- Philliber S, Kaye JW, Herrling S, West E. Preventing pregnancy and improving health care access among teenagers: an evaluation of the children’s aid society-carrera program. Perspect Sex Reprod Health 2002;34:244-51. https://doi.org/10.2307/3097823.
- Kirby DB, Rhodes T, Campe S. Implementation of Multi-component Youth Programs to Prevent Teen Pregnancy Modelled After the Children’s AID Society – Carrera Program. Scotts Valley, CA: ETR Associates; 2005.
- Patton GC, Bond L, Carlin JB, Thomas L, Butler H, Glover S, et al. Promoting social inclusion in schools: a group-randomized trial of effects on student health risk behavior and well-being. Am J Public Health 2006;96:1582-7. https://doi.org/10.2105/AJPH.2004.047399.
- Crawford C, Cribb J, Kelly E. Teenage Pregnancy in England CAYT Impact Study: Report No. 6 2013.
- Henderson M, Wight D, Raab GM, Abraham C, Parkes A, Scott S, et al. Impact of a theoretically based sex education programme (SHARE) delivered by teachers on NHS registered conceptions and terminations: final results of cluster randomised trial. BMJ 2007;334. https://doi.org/10.1136/bmj.39014.503692.55.
- Stephenson JM, Strange V, Forrest S, Oakley A, Copas A, Allen E, et al. Pupil-led sex education in England (RIPPLE study): cluster-randomised intervention trial. Lancet 2004;364:338-46. https://doi.org/10.1016/S0140-6736(04)16722-6.
- ISRCTN registry . Pilot Study to Develop and Assess the Feasibility and Acceptability of Positive Choices: A School-Based Social Marketing Intervention to Improve Sexual Health and Reduce Unintended Teenage Pregnancies in England 2020. www.isrctn.com/ISRCTN12524938 (accessed 6 October 2020).
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Hastings G, McDermott L. Putting social marketing into practice. BMJ 2006;332:1210-12. https://doi.org/10.1136/bmj.332.7551.1210.
- Hastings G, Stead M, Macdowall W, Bonell C, Davies M. Health Promotion Practice. Maidenhead: Open University Press; 2006.
- Fletcher A, Harden A, Brunton G, Oakley A. Interventions addressing the social determinants of teenage pregnancy. Health 2008;108:29-3. https://doi.org/10.1108/09654280810842111.
- Marsh D, Brown E, Crocker P. Building Effective Middle Schools: A study of Middle School Implementation in California Schools. Los Angeles, CA: University of Southern California; 1988.
- Fisher JD. Possible effects of reference group-based social influence on AIDS-risk behavior and AIDS prevention. Am Psychol 1988;43:914-20. https://doi.org/10.1037//0003-066x.43.11.914.
- Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
- Hawkins JD, Weis JG. The social development model: an integrated approach to delinquency prevention. J Prim Prev 1985;6:73-97. https://doi.org/10.1007/BF01325432.
- Gavin LE, Catalano RF, David-Ferdon C, Gloppen KM, Markham CM. A review of positive youth development programs that promote adolescent sexual and reproductive health. J Adolesc Health 2010;46:75-91. https://doi.org/10.1016/j.jadohealth.2009.11.215.
- National Institute for Health and Care Excellence . Contraceptive Services With a Focus on Young People Aged up to 25 Overview 2014.
- Dishion TJ, McCord J, Poulin F. When interventions harm. Am Psychol 1999;54:755-64. https://doi.org/10.1037/0003-066X.54.9.755.
- Stephenson J, Strange V, Allen E, Copas A, Johnson A, Bonell C, et al. The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England. PLOS Med 2008;5. https://doi.org/10.1371/journal.pmed.0050224.
- Welligs K, Jones KG, Mercer CH, Tanton C, Clifton S, Datta J, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet 2013;382:1807-16. https://doi.org/10.1016/S0140-6736(13)62071-1.
- Chiodo D, Crooks CV, Wolfe DA, McIsaac C, Hughes R, Jaffe PG. Longitudinal prediction and concurrent functioning of adolescent girls demonstrating various profiles of dating violence and victimisation. Prev Sci 2012;13:350-9. https://doi.org/10.1007/s11121-011-0236-3.
- Durlak JA, Weissberg RP. The Impact of After-school Programs that Promote Personal and Social Skills. Chicago, IL: Collaborative for Academic, Social and Emotional Learning; 2007.
- Quinn-Nilas C, Milhausen RR, Breuer R, Bailey J, Pavlou M, DiClemente RJ, et al. Validation of the Sexual Communication Self-Efficacy Scale. Health Educ Behav 2016;43:165-71. https://doi.org/10.1177/1090198115598986.
- Palmer MJ, Clarke L, Ploubidis GB, Mercer CH, Gibson LJ, Johnson AM, et al. Is ‘sexual competence’ at first heterosexual intercourse associated with subsequent sexual health status?. J Sex Res 2017;54:91-104. https://doi.org/10.1080/00224499.2015.1134424.
- Sawyer MG, Pfeiffer S, Spence SH, Bond L, Graetz B, Kay D, et al. School-based prevention of depression: a randomised controlled study of the Beyond Blue schools research initiative. J Child Psychol Psychiatry 2010;51:199-20. https://doi.org/10.1111/j.1469-7610.2009.02136.x.
- Currie CE, Elton RA, Todd J, Platt S. Indicators of socioeconomic status for adolescents: the WHO Health Behaviour in School-aged Children Survey. Health Educ Res 1997;12:385-97. https://doi.org/10.1093/her/12.3.385.
- Torsheim T, Cavallo F, Levin KA, Schnohr C, Mazur J, Niclasen B, et al. FAS Development Study Group . Psychometric validation of the Revised Family Affluence Scale: a latent variable approach. Child Indic Res 2016;9:771-84. https://doi.org/10.1007/s12187-015-9339-x.
- Office for National Statistics . Ethnic Group, National Identity and Religion. Measuring Equality: A Guide for the Collection and Classification of Ethnic Group, National Identity and Religion Data in the UK 2019. www.ons.gov.uk/methodology/classificationsandstandards/measuringequality/ethnicgroupnationalidentityandreligion (accessed 31 October 2019).
- Stevens K. Assessing the performance of a new generic measure of health-related quality of life for children and refining it for use in health state valuation. Appl Health Econ Health Policy 2011;9:157-69. https://doi.org/10.2165/11587350-000000000-00000.
- Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Bonell C, Fletcher A, Fitzgerald-Yau N, Hale D, Allen E, Elbourne D, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE): a pilot randomised controlled trial. Health Technol Assess 2015;19. https://doi.org/10.3310/hta19530.
- Linnan L, Steckler A. Process Evaluation for Public Health Interventions and Research. San Francisco, CA: John Wiley; 2002.
- May C. Towards a general theory of implementation. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-18.
- Moore G, Audrey S, Barker M, Bond L, Connell C, Handeman W, et al. Process Evaluation of Complex Interventions UK Medical Research Council (MRC) Guidance. London: Medical Research Council; 2013.
- Campbell MK, Piaggio G, Elbourne DR, Altman DG. CONSORT Group . Consort 2010 statement: extension to cluster randomised trials. BMJ 2012;345. https://doi.org/10.1136/bmj.e5661.
- Meiksin R, Crichton J, Dodd M, Morgan GS, Williams P, Willmot MA, et al. A school intervention for 13- to 15-year-olds to prevent dating and relationship violence: the Project Respect pilot cluster RCT. Public Health Res 2020;8.
- Green J, Thorogood N. Qualitative Methods for Health Research. London: SAGE Publications Ltd; 2004.
- Pawson R, Tilley N. Realistic Evaluation. London: SAGE Publications Ltd; 1997.
- Stevens K, Ratcliffe J. Measuring and valuing health benefits for economic evaluation in adolescence: an assessment of the practicality and validity of the child health utility 9D in the Australian adolescent population. Value Health 2012;15:1092-9. https://doi.org/10.1016/j.jval.2012.07.011.
- Department for Education . School Teachers’ Pay and Conditions Document 2018 and Guidance on School Teachers’ Pay and Conditions 2018.
- Family Planning Association . Unprotected Nation 2015 – An Update on the Financial and Economic Impacts of Restricted Contraceptive and Sexual Health Services 2015.
- Oliver R, Alexander B, Roe S, Wlasny M. The Economic and Social Costs of Domestic Abuse: Research Report 107 2019.
- McCrone P, Dhanasiri S, Patel A, Knapp M, Lawton-Smith S. Paying the Price: The Cost of Mental Health Care in England to 2026. London: The King’s Fund; 2008.
- Markham WA, Aveyard P. A new theory of health promoting schools based on human functioning, school organisation and pedagogic practice. Soc Sci Med 2003;56:1209-20. https://doi.org/10.1016/S0277-9536(02)00120-X.
- Bonell C, Allen E, Warren E, McGowan J, Bevilacqua L, Jamal F, et al. Initiating change in the school environment to reduce bullying and aggression: a cluster randomised controlled trial of the Learning Together (LT) intervention in English secondary schools. Lancet 2018;392:2452-64. https://doi.org/10.1016/S0140-6736(18)31782-3.
- Pound P, Langford R, Campbell R. What do young people think about their school-based sex and relationship education? A qualitative synthesis of young people’s views and experiences. BMJ 2016;6. https://doi.org/10.1136/bmjopen-2016-011329.
- Pearson M, Chilton R, Wyatt K, Abraham C, Ford T, Woods HB, et al. Implementing health promotion programmes in schools: a realist systematic review of research and experience in the United Kingdom. Implement Sci 2015;10. https://doi.org/10.1186/s13012-015-0338-6.
Appendix 1 Fidelity metrics for pilot randomised controlled trial
Fidelity metrics for Sex Education Forum-delivered training
Drawing on researcher observation/audio-recording.
Fidelity defined as:
-
≥ 70% delivery on items indicated by *
-
100% of target number of participants for training.
| Topic | Exercise |
|---|---|
| *Introductions | *Trainer presentation: Why are we here today? |
| *Paired introductions and feedback to the group | |
| *Working together as a mixed student/staff group | *Whole group discussion on working as a mixed staff/student group |
| *Whole group activity: Produce a working agreement together | |
| *Introduction to Positive Choices | *Trainer presentation: Introduction to Positive Choices |
| *Role of the SHPC | *Trainer presentation: What is a school council? What is the purpose of the SHPC? |
| *The six programme components | *The six components ranking game |
| *Setting up and organising your council | *Trainer presentation: Setting up and organising your council |
| *Review action planning template | |
| *Launching Positive Choices in your school | *Group discussion of launch activities |
| *Using needs data to inform the launch of Positive Choices | *Group discussion of how data can be used as part of launch |
| *Using needs data in parent communications | *Group discussion of how data can be used as part of communicating with parents |
| *Using data to inform the year 9 curriculum | *Group discussion: How could this data be used to inform curriculum design? |
| *Whole group activity: sample needs data and how to select curriculum topics | |
| *Next steps for implementing the SHPC | *Whole group discussion: What makes a successful SHPC? |
| *Individual action planning for next steps of the SHPC when back at school | |
| *Were opportunities for discussion provided? (Y/N) | |
| Topics covered | Activities used |
|---|---|
| Introductions | Share personal experiences of RSE and how things have changed |
| *Learning agreements/ground rules | *Trainer presentation on the importance of learning agreements and different methods of creating them |
| *Group discussion of how learning agreements contribute to a safe and democratic learning space for both pupils and teachers | |
| *Statutory and non-statutory responsibilities | *Trainer presentation on statutory and non-statutory responsibilities |
| *Legislation and guidance review | *Trainer presentation on legislation and draft RSE guidance |
| *Introduction to Positive Choices | *Trainer presentation outlining programme principles, evidence base and components (essential and add-on lessons) |
| *Introduction to the curriculum | *Small group discussion of curriculum framework |
| *Twelve statements of good quality RSE | *Paired discussion of how far school meets statements |
| *The Year 8 Pupil Needs Survey | *Group discussion: why is it important to involve pupils in RSE? |
| *Quiz: RSE and Young People | |
| *Positive Choices lesson plans | *Trainer presentation outlining design of lesson plans |
| *Trainer presentation outlining how lesson plans are to be used, including homework and differentiation | |
| *‘Planning Your Lesson’ activity on lesson 1 focusing on correct terminology | |
| *Creating a safe learning environment | *Complete ‘Creating a Safe Learning Environment’ sheet for a lesson on sexual parts of the male/female body small group activity |
| *Practice and discuss warm-up activity from lesson 1 (distancing techniques) | |
| *Using the Positive Choices lesson plans | *Using lesson plan 2 ‘Fertility, conception and contraception’, carry out activity 4 ‘Contraception Choices’ |
| *Using lesson plan 3 ‘Safer Sex and STIs’ activity (including condom demonstration and distancing techniques) | |
| *‘Add-on’ lessons: using lesson 12 on FGM | *FGM activities discussion |
| *Homework activities | *Trainer presentation on homework activities |
| *Group discussion of value of homework activities aimed at parent–child communication | |
| *Signposting | *Group discussion on the lesson on consent and importance of signposting |
| *Group discussion of how to use signposting options | |
| *Skills development | *Discussion of relationships skills and assertive communication |
| *Activities about dealing with conflict | |
| Optional session: answering questions | Group activity discussing how to answer questions and ‘worst case scenario’ questions |
| Optional session: assessment | Discussion of different assessment strategies and why they matter |
| *Individual action planning | *Individual reflection and action planning – template; one action to take away |
| *Follow-up support | *Trainer presentation on follow-up support available |
| *Were opportunities for discussion provided? (Y/N) | |
| Topic | Exercise |
|---|---|
| *Introductions | *Trainer presentation: Why are we here today? |
| *Paired introductions and feedback to the group | |
| *Working together | *Whole group discussion of working agreement and how to use it |
| Whole group activity: Quick marketing challenge | |
| *Understanding how marketing works | *Whole group activity: Introduction to marketing |
| *Introduction to social marketing | *Trainer presentation: What are the main steps in social marketing? |
| *Choosing a topic of focus | *Trainer presentation: List of possible topics |
| *Whole group activity: Values continuum | |
| *Carrying out consumer research | *Trainer presentation: Carrying out consumer research |
| *Designing a social-marketing campaign | *Small group activity: Design your own social-marketing campaign using the six principles of social marketing |
| *Next steps for implementing student-led social marketing | *Trainer presentation: Recruitment and schedule of meetings |
| Individual reflection: What are you most looking forward to in terms of leading the social-marketing group? | |
| *Were opportunities for discussion provided? (Y/N) | |
Fidelity metrics for school health promotion council and student-led social-marketing meetings
Drawing on staff logbooks, with verification via researcher observation of at least one meeting.
Fidelity defined as:
-
≥ 70% delivery on items indicated by * covered in at least one meeting
-
≥ 70% delivery on items indicated by ** covered in every meeting
-
100% of target number of participants for meeting.
*Role and activities of the SHPC.
*Timeline of SHPC activities.
*Working agreement.
*Roles of committee members.
*Launch of Positive Choices.
*School needs assessment data and selection of ‘add-on’ topics.
*Parent communication/newsletters.
*Student-led social marketing.
*Review of school sexual health services.
School policies to support sexual health.
Actions taken*Timeline of SHPC activities.
*Working agreement.
*Roles of committee members.
*How to launch Positive Choices.
*Where to concentrate the curriculum based on needs assessment.
*How to deliver parent communication/newsletters.
*Content of parent newsletters.
*How to recruit the student-led social-marketing team.
*Which student-led social-marketing campaigns should be run in school.
*Who will carry out the review of school sexual health services.
*How the review of school sexual health services will be carried out.
Opportunities for discussion**Were opportunities for staff/student discussion provided at this meeting (Y/N)?
*Selecting campaign topics/focus.
*Review of needs assessment data on topic to inform ideas/key messages for campaigns.
Review curriculum materials on topic to inform ideas/key messages for campaigns.
Carrying out new consumer research on topic to inform ideas/key messages for campaigns.
Findings of new consumer research on topic to inform ideas/key messages for campaigns.
*Whether to target subgroups.
*Selecting campaign activities (the ‘marketing mix’).
*The benefit to students (the ‘exchange’).
*Barriers to achieving behaviour change goal (the ‘competition’).
*Date for group to attend SHPC to pitch ideas.
*Pitching ideas to the SHPC/SLT.
*Finalising a campaign plan.
Dates for further meetings of whole group or subgroup to enable campaigns.
Work on campaign development/implementation.
Debrief: review of campaigns implemented in school.
Actions taken*Topic or focus of campaign selected?
*How needs assessment data will inform campaign ideas/key messages.
Process for carrying out new consumer research on topic to inform campaign ideas/key messages.
*Key campaign messages identified?
*Whether to target subgroups.
*What campaign activities to use (the ‘marketing mix’).
*What the benefit of the campaign to students will be (the ‘exchange’).
*Plan to overcome barriers to achieving behaviour change goal (the ‘competition’).
*Date for group to attend SHPC to pitch ideas.
*Final campaign plan.
Dates for further meetings of whole or subgroup to enable campaigns.
Debrief: review of campaigns implemented in school.
Opportunities for discussion**Were opportunities for staff/student discussion provided at this meeting (Y/N)?
Fidelity metrics for curriculum lessons
Drawing on staff logbooks, with verification via researcher observation of at least one lesson.
Fidelity defined as:
-
≥ 70% delivery on items indicated by * for eight essential lessons and two add-on lessons.
This includes * for homework for topic 2 plus a homework for one other topic.
| Variable | Y/N |
|---|---|
| Year 9: topic 2. Fertility, conception and contraception (essential) | |
| Topics covered | Covered? |
| *Sperm and egg cells | |
| *The route from sperm/egg production to fertilisation | |
| *Sequence of processes from conception to birth | |
| *How contraception prevents pregnancy | |
| *Advantages and disadvantages of different contraception types | |
| *Emergency contraception | |
| *How to get information and advice about contraception | |
| *Why early detection of pregnancy is important for choices and good health | |
| Exercises used | Used? |
| *Activity 1: The egg and the sperm | |
| *Activity 2: Timeline – from conception to birth | |
| *Activity 3: Contraception brainstorm | |
| *Activity 4: Contraception choices | |
| Opportunities for discussion | Provided? |
| *Were opportunities for discussion provided? | |
| Homework activities | Set? |
| *Activity 1: Rites of passage (essential part of Positive Choices) | |
Fidelity metrics for review of school/local sexual health services
Drawing on log sheet completed school staff.
Fidelity defined as:
-
≥ 70% completion of items indicated by *.
*Step 1: review of what services pupils already know about, using the questionnaire provided.
*Step 2: learning walk.
*Step 3: desk research.
*Step 4: check for accuracy.
*Step 5: make recommendations.
*Step 6: take action.
Step 7: accountability and further action.
Appendix 2 Summary of amendments to protocol
| Amendment | Rationale | Date approved by SSC | Date approved by NIHR | Protocol version |
|---|---|---|---|---|
| ‘Intentional self-regulation’ removed as a mediator | This construct related more closely to initial plans to involve after-school activities but, because of concerns over feasibility, these were removed from the funding proposal. We did not consider that the revision would have a significant impact on this construct. The logic model was also amended accordingly | 23 May 2017 | 6 June 2017 | 3 |
| Removal of Neil Underwood as named advisor on safeguarding | This was an error noticed by SSC. NCB, not Neil Underwood, should have been included as advisors on safeguarding | 8 August 2017 | 17 October 2017 | 4 |
| Removal of text referring to Functional Assessment of Spiritual Well-Being (SP-12) measure to assess teachers’ health-related quality of life | This was a vestige of an earlier draft of the protocol when we had planned to do a staff survey, but the staff survey was dropped from the final proposal that was approved for funding | 22 February 2018 | 13 March 2018 | 5 |
| Change of construct to be measured as potential mediator from ‘self-efficacy’ to ‘sexual communication self-efficacy’ | ‘Sexual communication self-efficacy’ is a specific measure more pertinent to our study. We also located and used a validated measure of this construct | 22 February 2018 | 13 March 2018 | 5 |
Appendix 3 Safeguarding procedures for Positive Choices pilot randomised controlled trial phase
Appendix 4 Sample Positive Choices service level agreement
Appendix 5 Standard operating procedure for reporting serious adverse event and suspected unexpected serious adverse reactions
Appendix 6 Baseline data collection record
Appendix 7 Positive Choices student baseline survey fieldwork standard operating procedure
Appendix 8 Briefing for teachers about the Positive Choices student questionnaire
Appendix 9 Positive Choices follow-up data collection record
Appendix 10 Positive Choices student follow-up survey fieldwork standard operating procedure
Appendix 11 Sample needs report
Appendix 12 Agreement between teacher logbooks and researcher observation
| Variable | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Role and activities of the SHPC | Y | Y | Y | ||
| *Timeline of SHPC activities | |||||
| *Working agreement | Y | Y | Y | ||
| *Roles of committee members | Y | Y | Y | ||
| *Launch of Positive Choices | Y | Y | Y | ||
| *School needs assessment data and selection of ‘add-on’ topics | |||||
| *Parent communication/newsletters | Y | Y | Y | ||
| *Student-led social marketing | |||||
| *Review of school sexual health services | |||||
| School policies to support sexual health | |||||
| Actions | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | Y | Y | Y | ||
| *Roles of committee members | Y | Y | Y | ||
| *How to launch Positive Choices | |||||
| *Where to concentrate the curriculum based on needs assessment | |||||
| *How to deliver parent communication/newsletters | Y | Y | Y | ||
| *Content of parent newsletters | |||||
| *How to recruit student-led social-marketing team | |||||
| *Which student-led social-marketing campaigns should be run in school | |||||
| *Who will carry out the review of school sexual health services | |||||
| *How the review of school sexual health services will be carried out | |||||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 9 | 9 | 9 (100%) | 0 (0%) | 0 (0%) |
| Variable | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Role and activities of the SHPC | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *Launch of Positive Choices | Y | Y | Y | ||
| *School needs assessment data and selection of ‘add-on’ topics | Y | Y | Y | ||
| *Parent communication/newsletters | |||||
| *Student-led social marketing | |||||
| *Review of school sexual health services | |||||
| School policies to support sexual health | |||||
| Actions | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *How to launch Positive Choices | Y | Y | Y | ||
| *Where to concentrate the curriculum based on needs assessment | Y | Y | Y | ||
| *How to deliver parent communication/newsletters | |||||
| *Content of parent newsletters | |||||
| *How to recruit student-led social-marketing team | |||||
| *Which student-led social-marketing campaigns should be run in school | |||||
| *Who will carry out the review of school sexual health services | |||||
| *How the review of school sexual health services will be carried out | |||||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 5 | 5 | 5 (100) | 0 (0) | 0 (0) |
| Variable | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Role and activities of the SHPC | Y | Y | Y | ||
| *Timeline of SHPC activities | Y | Y | Y | ||
| *Working agreement | Y | Y | Y | ||
| *Roles of committee members | Y | Y | Y | ||
| *Launch of Positive Choices | Y | Y | Y | ||
| *School needs assessment data and selection of ‘add-on’ topics | Y | Y | Y | ||
| *Parent communication/newsletters | Y | Y | Y | ||
| *Student-led social marketing | Y | Y | Y | ||
| *Review of school sexual health services | |||||
| School policies to support sexual health | |||||
| Actions | |||||
| *Timeline of SHPC activities | Y | Y | Y | ||
| *Working agreement | Y | Y | Y | ||
| *Roles of committee members | Y | Y | Y | ||
| *How to launch Positive Choices | Y | Y | Y | ||
| *Where to concentrate the curriculum based on needs assessment | |||||
| *How to deliver parent communication/newsletters | Y | N | Y | ||
| *Content of parent newsletters | Y | N | Y | ||
| *How to recruit student-led social-marketing team | |||||
| *Which student-led social-marketing campaigns should be run in school | |||||
| *Who will carry out the review of school sexual health services | |||||
| *How the review of school sexual health services will be carried out | |||||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 14 | 13 | 12 (86) | 1 (7) | 1 (7) |
| Variable | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Role and activities of the SHPC | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *Launch of Positive Choices | |||||
| *School needs assessment data and selection of ‘add-on’ topics | Y | Y | Y | ||
| *Parent communication/newsletters | |||||
| *Student-led social marketing | |||||
| *Review of school sexual health services | |||||
| School policies to support sexual health | |||||
| Actions | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *How to launch Positive Choices | |||||
| *Where to concentrate the curriculum based on needs assessment | Y | Y | Y | ||
| *How to deliver parent communication/newsletters | |||||
| *Content of parent newsletters | |||||
| *How to recruit student-led social-marketing team | |||||
| *Which student-led social-marketing campaigns should be run in school | |||||
| *Who will carry out the review of school sexual health services | |||||
| *How the review of school sexual health services will be carried out | |||||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 3 | 3 | 3 (100) | 0 (0) | 0 (0) |
| Variable | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Role and activities of the SHPC | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *Launch of Positive Choices | |||||
| *School needs assessment data and selection of ‘add-on’ topics | |||||
| *Parent communication/newsletters | |||||
| *Student-led social marketing | |||||
| *Review of school sexual health services | Y | Y | Y | ||
| School policies to support sexual health | |||||
| Activities | |||||
| *Timeline of SHPC activities | |||||
| *Working agreement | |||||
| *Roles of committee members | |||||
| *How to launch Positive Choices | |||||
| *Where to concentrate the curriculum based on needs assessment | |||||
| *How to deliver parent communication/newsletters | |||||
| *Content of parent newsletters | |||||
| *How to recruit student-led social-marketing team | |||||
| *Which student-led social-marketing campaigns should be run in school | |||||
| *Who will carry out the review of school sexual health services | Y | Y | Y | ||
| *How the review of school sexual health services will be carried out | Y | Y | Y | ||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 4 | 4 | 4 (100) | 0 (0) | 0 (0) |
| Readiness for intimacy | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *Your own and others’ decision-making related to sex | Y | Y | Y | ||
| *Factors that may affect decisions to do with sex including alcohol | Y | Y | Y | ||
| *Factors that are important for a safe and comfortable sexual relationship | Y | Y | Y | ||
| *The ability to communicate about contraception and what is pleasurable are skills that will support good sexual health including enjoyable relationships | Y | N | N | Y | |
| *Personal concept of ‘readiness’ for sexual intimacy | Y | Y | Y | ||
| Activities | |||||
| *Activity 1: Decisions about sex – values activity | Y | Y | Y | ||
| *Activity 2: Ready or not? | Y | Y | Y | ||
| *Activity 3: Alcohol and other drugs | Y | Y | Y | ||
| *Activity 4: ‘Pass it on’ | Y | Y | Y | ||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 10 | 9 | 9 (90) | 1 (10) | |
| Consent | Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook |
|---|---|---|---|---|---|
| Topic | |||||
| *What consent means | Y | Y | Y | ||
| *Different ways of communicating non-consent | Y | Y | Y | ||
| *What sexual consent means, why it is different | Y | N | Y | ||
| *Why sexual consent is important | Y | Y | Y | ||
| *Consent requires choice, freedom, and capacity – responsibility lies with the person seeking consent | Y | Y | Y | ||
| *Factors that might affect the capacity to consent | Y | Y | Y | ||
| *The legal age of consent | Y | Y | Y | ||
| *The age at which most young people start having sex | Y | Y | Y | ||
| Activities | |||||
| *Activity 1: What is consent? | Y | Y | Y | ||
| *Activity 2: Parallel lines and personal boundaries | Y | Y | Y | ||
| *Activity 3: Sexual consent what’s the difference? | Y | Y | Y | ||
| *Activity 4: Sex and the law – quick quiz | Y | Y | Y | ||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 13 | 12 | 12 (92) | 1 (8) | |
| Covered in logbook | Covered in observation | Agreement between logbook and observation | Disagreement: covered in logbook, not observation | Disagreement: covered in observation, not logbook | |
|---|---|---|---|---|---|
| Topic | |||||
| *Selecting campaign topics/focus | Y | Y | Y | ||
| *Review of needs assessment data on topic to inform ideas/key messages for campaigns | Y | N | Y | ||
| *Whether to target subgroups | Y | Y | Y | ||
| *Selecting campaign activities (the ‘marketing mix’) | Y | Y | Y | ||
| *The benefit to students (the ‘exchange’) | Y | Y | Y | ||
| *Barriers to achieving behaviour change goal (the ‘competition’) | Y | Y | Y | ||
| *Date for group to attend SHPC to pitch ideas | |||||
| *Pitching ideas to the SHPC/SLT | |||||
| *Finalising a campaign plan | |||||
| Activities | |||||
| *Topic or focus of campaigns? | Y | Y | Y | ||
| *How needs assessment data will inform campaign ideas/key messages? | Y | N | Y | ||
| *Key campaign messages | Y | Y | Y | ||
| *Whether to target subgroups | Y | Y | Y | ||
| *What campaign activities to use (the ‘marketing mix’) | Y | Y | Y | ||
| *What the benefit of the campaign to students will be (the ‘exchange’) | Y | Y | Y | ||
| *Plan to overcome barriers to achieving behaviour change goal (the ‘competition’) | Y | N | Y | ||
| *Date for group to attend SHPC to pitch ideas | Y | N | Y | ||
| *Final campaign plan | |||||
| Opportunities for discussion? | Y | Y | Y | ||
| Total | 15 | 10 | 10 (67) | 5 (33) | |
Appendix 13 Acceptability of Sex Education Forum-delivered training
| Topic | Intervention schools | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Total | |
| Number of satisfaction surveys received | 3 (75) | 3 (100) | 1 (100) | 2 (100) | 9 (90) |
| Answering covered well or very well (n, %) | |||||
| Introduction to Positive Choices | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Introductions to each other | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| How to work together as a mixed student/staff group | 3 (100) | 3 (100) | 1 (100) | N/Aa | 7 (100) |
| Role of the SHPC | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| The six programme components | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| How to set up and organise your council | 2 (67) | 3 (100) | 1 (100) | 2 (100) | 8 (89) |
| Launching Positive Choices in your school | 3 (100) | 3 (100) | 1 (100) | N/Aa | 7 (100) |
| Using needs data to inform the launch of Positive Choices | 2 (66.6) | 3 (100) | 1 (100) | N/Aa | 6 (89) |
| Using needs data in parent communications | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Using needs data to select curriculum components | 2 (67) | 3 (100) | 1 (100) | 2 (100) | 8 (89) |
| Planning next steps for your SHPC | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Answering yes (n, %) | |||||
| Did the training provide sufficient opportunities for discussion? | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Answering good or excellent (n, %) | |||||
| Overall, how would you rate this training? | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Answering confident or very confident (n, %) | |||||
| How confident do you feel about putting into practice what you have learnt today? | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Answering yes (n, %) | |||||
| Would you recommend this training to other colleagues? | 3 (100) | 3 (100) | 1 (100) | 2 (100) | 9 (100) |
| Topic | Intervention schools | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Total | |
| Number of satisfaction surveys received | 5 (100) | 0 (0) | 5 (100) | 4 (100) | 14 (100) |
| Answering covered well or very well (n, %) | |||||
| Current legislation and new RSE guidance | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Statutory and non-statutory responsibilities for RSE | 5 (100) | Missing | 4 (80) | 4 (100) | 13 (93) |
| The 12 statements of good quality RSE | 2 (40) | Missing | 3 (60) | 4 (100) | 9 (64) |
| Developing learning agreements | 5 (100) | Missing | 4 (80) | 4 (100) | 13 (93) |
| The year 8 pupil needs survey: what pupils want from RSE | 4 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Overview of the Positive Choices programme, its principles and evidence base | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| The Positive Choices Curriculum Framework | 5 (100) | Missing | 4 (80) | 4 (100) | 13 (93) |
| Introducing the Positive Choices lesson plans | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Employing differentiation in the lesson plans | 0 (0) | Missing | 3 (60) | 3 (75) | 9 (64) |
| Practically using lesson 1 (male and female body) | 0 (0) | Missing | 2 (40) | 0 (0)a | 2 (14) |
| Ways to create a safe learning environment | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| The value of warm-up activities, and other distancing techniques | 0 (0) | Missing | 5 (100) | 3 (75) | 8 (57) |
| Practically using lesson 2 (fertility, conception and contraception) | 4 (80) | Missing | 5 (100) | 3 (75) | 12 (86) |
| Practically using lesson plan 3 (safer sex and STIs) | 4 (80) | Missing | 5 (100) | 4 (100) | 13 (93) |
| Using lesson plan 10 on FGM | 6 (60) | Missing | 0 (0)a | 4 (100) | 10 (71) |
| The Positive Choices homework activities | 4 (80) | Missing | 4 (80) | 4 (100) | 12 (86) |
| Signposting to further information and services | 2 (40) | Missing | 3 (60) | 4 (100) | 9 (64) |
| Developing skills in assertive communication and dealing with conflict | 4 (80) | Missing | 4 (80) | 3 (75) | 11 (78) |
| Answering questions in the classroom | 4 (80) | Missing | 3 (60) | 2 (50) | 9 (64) |
| Assessment strategies | 3 (60) | Missing | 2 (40) | 1 (25) | 6 (43) |
| Individual action planning | 4 (80) | Missing | 3 (60) | 1 (25) | 8 (57) |
| Sources of support to assist with curriculum delivery | 3 (60) | Missing | 3 (60) | 1 (25) | 7 (20) |
| Answering yes (n, %) | |||||
| Did the training provide sufficient opportunities for discussion? | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Answering good or excellent (n, %) | |||||
| Overall, how would you rate this training? | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Answering confident or very confident (n, %) | |||||
| How confident do you feel about putting into practice what you have learnt today? | 5 (100) | Missing | 5 (100) | 4 (100) | 14 (100) |
| Answering yes (n, %) | |||||
| Would you recommend this training to other colleagues? | 3 (60) | Missing | 5 (100) | 4 (100) | 12 (86) |
| Topic | Intervention schools | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Total | |
| Number of satisfaction surveys received | 1 (100) | 0 (0) | 1 (100) | 0 (0) | 2 (100) |
| Answering covered well or very well (n, %) | |||||
| Introduction to the day | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| Introductions to each other | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| Group agreement and its purpose | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| Introduction to marketing | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| Introduction to social marketing | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| How to choose a campaign topic | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| How to carry out consumer research | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| How to design a social-marketing campaign | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| Next steps for implementing the student-led social marketing in your school | 0 (0) | Missing | 1 (100) | Missing | 1 (50) |
| Answering yes (n, %) | |||||
| Did the training provide sufficient opportunities for discussion? | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| Answering good or excellent (n, %) | |||||
| Overall, how would you rate this training? | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| Answering confident or very confident (n, %) | |||||
| How confident do you feel about delivering the Positive Choices Classroom Curriculum? | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
| Answering yes (n, %) | |||||
| Would you recommend this training to other colleagues? | 1 (100) | Missing | 1 (100) | Missing | 2 (100) |
List of abbreviations
- ALPHA
- Advice Leading to Public Health Advancement
- ANS
- Abortion Notification System
- CAS
- Children’s Aid Society
- CHU9D
- Child Health Utility-9D
- CI
- confidence interval
- CTU
- clinical trials unit
- DHSC
- Department of Health and Social Care
- DOB
- date of birth
- FAS
- Family Affluence Scale
- FGM
- female genital mutilation
- GCSE
- General Certificate of Secondary Education
- ICC
- intracluster correlation coefficient
- IQR
- interquartile range
- LGBTQ
- lesbian, gay, bisexual, transgender, queer or questioning
- LSHTM
- London School of Hygiene & Tropical Medicine
- MD
- mean difference
- NCB
- National Children’s Bureau
- NIHR
- National Institute for Health Research
- ONS
- Office for National Statistics
- OR
- odds ratio
- PI
- principal investigator
- PSHE
- personal, social, health and economic education
- RCT
- randomised controlled trial
- RSE
- relationships and sex education
- SAE
- serious adverse event
- SD
- standard deviation
- SEF
- Sex Education Forum
- SEND
- special educational needs and disabilities
- SES
- socioeconomic status
- SHPC
- school health promotion council
- SLT
- senior leadership team
- SMSC
- spiritual, moral, social and cultural
- SSC
- Study Steering Committee
- STI
- sexually transmitted infection
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/phr09010).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.